
Hemorrhage After Manual Removal of the Placenta - Harvard ...
35
Hemorrhage After Manual Removal of the Placenta: Weighing Risk Factors and the Role of the Third Stage of Labor The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Perlman, Nicola. 2018. Hemorrhage After Manual Removal of the Placenta: Weighing Risk Factors and the Role of the Third Stage of Labor. Doctoral dissertation, Harvard Medical School. Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:36923348 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Hemorrhage After Manual Removal of the Placenta - Harvard ...
Hemorrhage After Manual Removal ofthe Placenta: Weighing Risk Factors
and the Role of the Third Stage of LaborThe Harvard community has made this
article openly available. Please share howthis access benefits you. Your story matters
Citation Perlman, Nicola. 2018. Hemorrhage After Manual Removal of thePlacenta: Weighing Risk Factors and the Role of the Third Stage ofLabor. Doctoral dissertation, Harvard Medical School.
Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:36923348
Terms of Use This article was downloaded from Harvard University’s DASHrepository, and is made available under the terms and conditionsapplicable to Other Posted Material, as set forth at http://nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#LAA

2
Abstract:Introduction:Manualremovaloftheplacenta,oftenduetouterineatonyoranabnormallyadherentplacenta,canbeaccompaniedbyseverematernalpostpartumhemorrhage.Theobjectiveofthisstudywastoidentifyriskfactorsforpostpartumhemorrhagethatwouldallowtriagingofmostmorbidpatientspriortomanualremoval.Methods:ThiswasaretrospectivecasecontrolstudyofpatientswhohadundergonemanualremovaloftheplacentaaftervaginaldeliveryatBrighamandWomen’sHospitalbetweenJanuary1,2007andMay29,2015.Weevaluatedriskfactorsforpostpartumhemorrhageindependentlyandbypresumedcausativerole.Causativegroups(andriskfactors)includedAtony(multiplegestation,prolongedsecondstageoflabor,birthweight>4000g,parity>4,orBMI>40kg/m2),AbnormalPlacentation(>2priorD&Es,suspicionforaccretaonultrasound,ART,age>40years,priorcesarean,prioraccreta,priorretainedplacenta,prioruterinesurgery,resolvedlowlyingplacenta,orAshermanssyndrome),orOtherPostpartumHemorrhageRiskFactors(preeclampsia,acuteabruption,fibroids>6cm,orpretermdelivery).Riskfactorswerealsoclassifiedaseithermajor(concernforaccretaonultrasoundorsignsofabruptionatadmission)orminor(anyothervariable),andweanalyzedwhetheranyonemajorortwominorriskfactors,regardlessofcausativegrouping,wereassociatedwithpostpartumhemorrhageaftermanualremoval.Lengthofthirdstageoflaborwasanalyzedinrelationtopatientcharacteristics.Allsignificantvariableswereputintoamultivariableanalysistotestforconfounding.Results:Ofthe997womenidentifiedwithmanualremovaloftheplacentaduringourstudyperiod,172experiencedseverepostpartumhemorrhageandwereone-to-onematchedwithcontrolswithouthemorrhage.CasepatientsweremorelikelythancontrolstohaveanyoneriskfactorineithertheAtony(49%vs.37%respectively,p=0.01)orAbnormalPlacentationriskgroup(58%vs.38%,respectively,p<0.01)andadditionallyweremorelikelytohaveanyonemajorortwominorriskfactors(51%vs.26%controls;p>0.01).Postpartumhemorrhagepatientshadmanualremovaloftheplacentalaterinthethirdstageoflabor(p<0.01).Characteristicsassociatedwithrapidmanualremovaloftheplacentawithin30minutesafterdeliveryoftheinfantincludedcordavulsionandepiduralanalgesia(p<0.01),whereaschorioamnionitiswasassociatedwithdelayuntilmanualremoval(p=0.03).Increasinglengthofthirdstageofdeliveryshowedstrongassociationwithpostpartumhemorrhageinourmultivariateanalysis,alongwithriskfactorsforabnormalplacentation.Thoughsignificantintheunivariateanalysis,chorioamnionitis,ariskfactorforuterineatony,showednoassociationwithpostpartumhemorrhageaftercontrollingforotherfactorsinourmultivariableregression.Conclusion:Patientswithconcernforuterineatonyshouldhaverapidremovaloftheplacenta,regardlessofchorioamnionitisandepiduralanalgesia,inordertominimizeriskofpostpartumhemorrhage.Patientswithriskfactorsforabnormalplacentationorplacentaaccretamaynothaveriskofhemorrhagemitigatedbyrapidmanualdelivery.

3
TableofContents:Contents: PageAbstract 2Glossary 4Introduction 5Methods 12Results 16Discussion 19Summary 24References 26Tables 29Figures 35
4
GlossarylistingabbreviationsthatappearinyourthesisMROP:ManualremovaloftheplacentaPPH:PostpartumHemorrhageACOG:AmericanCollegeofObstetriciansandGynecologistsMAP:MorbidlyadherentplacentaDilationandCurettage:D&CDilationandEvacuation:D&EBodyMassIndex:BMIInVitroFertilization:IVFAssistedReproductiveTechnology:ART
5
Introduction:
Postpartumhemorrhage(PPH),occurringinapproximately2-6%ofdeliveries,isamajor
causeofmaternalmortalityworldwide.(1-4)Inthelasttwodecades,therehasbeenan
observedincreaseinpostpartumhemorrhage,whichcurrentlyaccountsforoneofthe
mostcommonreasonsformaternalintensivecareunitadmission.(1,3)
Uterineatonyandretainedplacenta(includingplacentaaccreta)arethetwoleadingcauses
ofpostpartumhemorrhage.(1,3-6)Bothetiologiescanalsobeindicationsformanual
removaloftheplacenta(MROP),whichcanbefollowedbyseverebleeding.(1)While
studieshaveexaminedriskfactorsforPPH,rarelyhaveriskfactorsspecifictomanual
removalbeenproposed.Triagingpatientsaccordingtohemorrhageriskwithmanual
removaloftheplacentamayallowphysicianstoproactivelyavoidormanagethismorbid
complication.
Postpartumhemorrhage:
Postpartumhemorrhageisawidelyrecognizedcauseofmaternalmorbidityand
mortality.(4,7)AsoneoftheleadingcausesofIntensiveCareUnitadmissionfollowing
deliveryintheUnitedStates,thereisgreatinterestinexaminingriskfactorsandmethods
topreventmorbidityfromPPH.(7-10)ThetrendisparticularlyprescientintheUnited
States,butotherdevelopedcountrieshaveseenasimilarlyriseinPPH,notexplainedby
temporalchangesinriskfactors.(11,12)Andwhileevenindevelopedcountrieswith
resourcesandadequatepersonneltheriskofmorbidityfrommaternalhemorrhageishigh,
givingbirthindevelopingcountriesposesastaggeringriskofdeathduetocomplications.
Somereportscitematernalmorbidityratios(maternaldeathsper100,000livebirths)to
beashighasoneinsixforAfghanistanandSierraLeone,versusalowestestimateofonein
30,000inSweden.(13)
Theimportofpostpartumhemorrhageincontributingtomaternalmorbidityhascreateda
demandforbettersystemsforpredictingandtriagingmassivebloodlossatdelivery.(9)
Theepidemiologyofpostpartumhemorrhagehasbeenwellstudied.TheAmericanCollege
6
ofObstetriciansandGynecologists(ACOG)warnsphysiciansintheirPracticeBulletinthat
primaryPPH,definedbytheCollegeasgreaterthan1000ccofbloodloss(arecentincrease
from500cc),occursin4-6%ofallpregnancies,citinga1991studybyCombsetalthatlists
PPHasaleadingcauseofmaternalmorbidityworldwide.(1,4)ResearchbyCallaghanetal
hasnotablyemphasizedthatwhilePPHisincreasing,maternaldeathfromPPHis
decreasingduetoincreasedratesoftransfusionandperipartumhysterectomy.(14-16)
However,whiledeathduringlaborhospitalizationhasdecreased,severematernal
morbidityhasinturnbecomeupto50timesmorecommon.(16)Itiswidelyrecognized
thatPPHisdueprimarilytopoorcontractionoftheuterus,oratony,followingdeliveryof
theinfant,andsecondarilytoretainedorabnormallyadherentplacentaduringthethird
stageoflabor.(1,4)Otherrecognizedcausesincludeinheritedoracquiredcoagulopathies,
andobstetricalcomplications—suchascervicallacerationsepisiotomies,anduterine
inversion.(4)
InordertoeffectivelyandefficientlytreatseverePPH,hospitalsandhealthcaresystems
areseekingtodevelopnovelwaystotriageandprepareforthisadverseoutcome.(4,17)
Riskscoresandalgorithmsarebecomingincreasinglycommonplace,andoftenemploya
multidisciplinaryteamincludingobstetricians,anesthesiologists,nursing,andpossibly
surgicalorradiologicsubspecialists.Riskpredictionmaybeparticularlyusefulinsettings
wheretreatmentmusthappenquicklyandinvolvesmanyteammembersandtreatment
modalities.Forinstance,whenapatientrequiresmanualextractionoftheplacentawith
subsequenttransfertotheoperatingroomwithseverepostpartumhemorrhage,setupof
cross-matchedbloodandsurgicalequipment,andearlynotificationofamultidisciplinary
hemorrhageteamwouldbeuseful.
VaginalDeliverywithManualExtractionofthePlacenta:
Manualremovaloftheplacenta,ormanuallycreatingacleavageplanebetweenthe
placentaandtheuterus,isgenerallyperformedinabsenceofdeliveryoftheplacenta
duringthethirdstageoflabor,andtypicallyafterothermanagementoptions(oxytocin,
uterinemassage,andcordtraction)havebeenexhausted.
7
Accordingtotheliterature,retainedplacentarequiringmanualremovalisgenerally
assumedtobedueto(1)anatonicuteruswithpoorcontractiondisallowingnormal
contractileexpulsionoftheplacenta,(2)abnormalplacentationoraccreta,inwhichthe
placentahasinvadedintothematernalmyometrium,or(3)trappedorincarcerated
placenta,inwhichthecervixhasclosedpriortodeliveryoftheplacenta.(5,18)
Normalplacentationbeginswithblastocystimplantationintothematernalendometrium.
Inpreparationforthisimplantation,theendometriumdevelopsthedeciduaunderthe
influenceofprogesteroneandestrogenofearlypregnancy.Astheblastocystinvadesthis
decidua,thelayerofcellsformingthesurfaceoftheblastocystdevelopsintothechorionic
membrane.Cytotrophoblastcellsproliferatefromthechorionicmembraneandform
multinucleatedaggregatescalledsyncytiotrophoblastcells.Thesecellsformtheplacental
villi,withcytotrophoblastsatthecoreandsyncytiotrophoblastsformingtheepithelial
outerlayer,allowingfetal-maternalinterchangebetweenthevilli-decidualinteraction.
Afterthesecondstageoflabor,withdeliveryoftheinfant,bothahormonalcascadeaswell
asuterinecontractionsallowforseparationoftheselayersandexpulsionoftheplacenta.
Ifanypartofthisprocessisdisruptedthentheplacentamaynotdeliverspontaneouslyand
couldberetained.Forinstance,ifplacentalvillihaveinvadedbeyondthedeciduaandinto
thematernalmyometriumcausingadherentplacentaduetothisabnormalplacentation,
theplacentawillnotdetachinthethirdstage.Alternatively,inthesettingofpooruterine
contractionsduetoatony,theplacentamaynotbesubjecttoexpulsiveforcesrequiredfor
delivery.
Indevelopedcountries,retainedplacentaaffectsaround3%ofallvaginaldeliveries.(5,19).
RiskfactorsforretainedplacentarequiringMROPwereelucidatedbyEndlerand
colleaguesina2012casecontrolstudy.(20)Theauthorsshowedthattheseindependent
riskfactorsincludedpriorretainedplacenta,pretermdelivery,prolongeduseofoxytocin,
preeclampsia,twoormorepriormiscarriages,andoneormorepriorabortions.(20)The
authorsalsoshowedthatMROPwassignificantlyassociatedwithPPH.(20)Inafollowup
8
studyEndleretalconfirmedtheseriskfactorsusingalargenationalregistrydatabaseas
cohort.(21)Theirfindingsshowedaparticularlystrongrelationshipbetweenpreeclampsia
andretainedplacenta,leadingtheauthorstohypothesizethatdisordersofplacentation
maybepositivelyassociatedwithMROP.(21)
Aprolongedthirdstageoflabor,ortimebetweendeliveryoftheinfantanddeliveryofthe
placenta,isalsorecognizedasasignificantriskfactorforpostpartumhemorrhage,and
studieshaveshownthatreducingthelengthofthirdstageoflaborviamanualextractionof
theplacentareducestheriskofpostpartumhemorrhage.(22-24)Inordertominimizethis
risk,failureofdeliveryoftheplacentainatimelymanneristhereforeacommonindication
forMROP.
IntheUS,however,thereisnooneguidelineformanagingMROP.(25)WhileACOG
recognizestheincreasedriskofPPHwithalongthirdstageoflaborandthusrecommends
activemanagement(withoxytocin,cordtraction,andmaternalefforttoexpelplacenta),
theydonotsuggestafirmtimelineformanualremoval.(4)Whilemajorityofplacentasare
spontaneouslyexpelledwellbefore30minutes,mostofthesparseliteratureonMROP
suggestsremovalinabsenceofspontaneousdeliveryatthistime.(5,25)
EventhoughthegeneralconsensusisthatMROPshouldbeattemptedinabsenceof
spontaneousdeliveryoftheplacentawithin30minutesofdeliveryoftheinfantorearlier
inthepresenceofPPH,thereislittledatatosupportthisguideline.(5,19)Inastudyby
Deneux-Tharauxetal,surveysfrom14Europeancountriesexhibitedwidevariationsin
waittimepriortoMROP,largelybycountrybutalsobyhospital.(19)Incountriessuchas
FinlandandDenmark,obstetricianstendedtowait60minutesormorepriortoMROP,
versusincountriessuchasSpainandFrance,whereprovidersremovedtheplacentaafter
30minutes.(19)Practicesalsovariedconsiderablydependingonwhetherornotthe
patientinquestionhadpriorepiduralanesthesia.(19)Similarly,theNationalInstitutefor
HealthandClinicalExcellence(NICE)suggestsawaittimeof30minutesintheUnited
KingdompriortoMROP,(26)whiletheWorldHealthOrganizationguidelinesproposea
waittimeof60minutes.(13)

9
Ina1991studybyCombsetal,authorstriedtodefinehowdurationofthirdstageis
relatedtocomplications.(25)Inthestudytheyfoundthatthethirdstagehadalognormal
distribution,withameanlengthof6.8minutes,withonly3.3%ofdeliverieshavinggreater
agreaterthan30minutethirdstage.Interestingly,theauthorscalculatedthatthe
incidenceofPPH,transfusion,anddilationandcurettageremainedconstantduringthis
period,increasingonlyafter30minutesandplateauingat75minutesforbothmanually-
andspontaneously-deliveredplacentas.BecausePPHincidencedidnotincreaseuntilafter
30minutes,CombsetalrecommendedthistimingasguidanceforwhentoinitiateMROP.
AsubsequentstudybyDombrowskietalin1995triedtodeterminegestationalagespecific
dataforlengthofthirdstage,retainedplacenta,hemorrhage,andmanualremoval.(27)The
authorsfoundthatbothMROPandPPHdecreasedwithincreasinggestationalage,andthat
thetwowererelated.However,causalassociationcouldnotbedetermined.Alternatively,
whilenotstudyingmanualremovalperse,Rogersetal,in1998,foundthatactive
managementofthethirdstageresultedinsignificantlyreducedriskofPPH.(22)
LaterstudiesbyMagannetalsoughttostrengthentherelationshipbetweenlengthofthird
stageandPPH.In2005,Magannandcolleaguesundertookaprospectiveobservational
studyinwhichallwomendeliveringvaginallywereassessedforPPH.(24)Usingreceiver
operatingcharacteristiccurves,theauthorsshowedthatathirdstageoflaborlongerthan
18minuteswasassociatedwithasignificantriskofPPH.(24)Theauthorsfollowedupthis
paperin2012witharandomizedcontrolledtrialassigningvaginaldeliveriestomanual
removalateither10or15minutes(asopposedtothetraditional30)iftheplacentahad
notyetspontaneouslydelivered.(23)Thefindingssupportedtheauthors’initialstudy,
showingthatremovalat15minuteshadasignificantlygreaterlikelihoodofhemorrhage
comparedto10minutes,augmentingthediscussionofMROP’sappropriatetiming,and
indications.(23)
Intheir2014review,Urneretalemphasizethatguidelinesformanagementofretained
placentarequiringMROPdonotexist,asidefrompoorlydefinedtimelinesfor

10
intervention.(5)TheauthorscitesimilarriskfactorsasthosestudiedbyEndleretal,and
additionallylistriskfactorsforinvasiveplacentaincludingpriorcesareansectionand
uterinesurgery.(5)Urnerandcolleaguessuggestthatroutinemanagementofretained
placentashouldinclude(inadditiontoMROPat30minutes)ultrasoundandamulti-
specialistteamapproach,aswellasfuturedevelopmentofstrictguidelinesforthethird
stageinordertoreducecomplicationssuchasseverePPH.(5)Corvielloetal,usingalarge
retrospectivecohortfromtheUnitedStates,echoedtheaboveriskfactors,particularly
stressingstillbirthasanindependentriskfactor,andproposingthatsomeintrinsic
pathophysiologyofintrauterinefetaldemiseleadstoincreasedriskofretained
placenta.(28)Titizandcolleaguessupportthesefindingsinalargecohortfrom
Australia.(2)
Whileabnormalplacentation,suchasaccreta,incretaorpercreta,isaknownsignificant
riskfactorforadherentplacentaatcesareansection,verylittlehasbeenwrittenonits
contributiontoretainedplacentaatvaginaldelivery.Thisconditionisbestunderstoodin
thesettingofplacentapreviawithpriorcesarean.(29,30)Inthisclinicalscenario,itis
recognizedthatlowlyingplacentaoverlyingauterinescarandprioruterinesurgeryare
majorriskfactorsforhemorrhagemorbidityatcesareandelivery.Becauseofit’s
associationwithlowlyingplacentaandcesarean,radiographicevidenceandclinical
suspicionforaccretaareoftenlackinginpatientswhopresentwithoutplacentaprevia,
whichincludesallpatientsundergoingavaginaldelivery.
Interestingly,ina2017paperbyBjurstrometal,theauthorsreportsixcasesoffailed
manualremovalatvaginaldeliveryduetoclinicallyadherentplacenta—referredtoas
morbidlyadherentplacenta,orMAP—onlyoneofwhichhadhistopathologicevidenceof
accreta.(31)Additionallyin2017,Roecaetalreported339patientswhocompleteda
pregnancywithpathologicallydiagnosedplacentaaccretawithouthysterectomywith39
returningforsubsequentpregnancy.(32)Ofthe39returningpatients,16underwent
manualremovaloftheplacenta.ThissuggeststhatthecontributionofaccretatoMROP
maybeunderrecognized.

11
Themechanismsbehindandoutcomesofabnormallyadherentplacentaatvaginaldelivery
havenotbeenwellreported.Afewstudieshaveaddressedrelationshipsbetweenin
assistedreproductivetechnology(ART)andinvitrofertilization(IVF)anddisordersof
placentation,thoughitsrelationshiptoretainedplacentaandPPHhasnotbeenwell
defined.Firstreportedin2011,Esh-Broderetalshowedasignificantrelationshipbetween
IVFandplacentaaccreta,proposingenvironmentaldifferencesbetweentheendometrium
ofpatientsconceivingwithIVFandversusthosewithspontaneousconception.(33)In
2014,Ishiharaetalalsoconcludedviaretrospectiveanalysisthatcryopreservedblastocyst
transferwasassociatedwithbothaccretaandpregnancyinducedhypertension,though
theyhadlimitedabilitytocontrolforconfounding.(34)A2015studybyKaserand
colleaguesthat,aftercontrollingformultipleconfounders,cryopreservedembryotransfer
wassignificantlyassociatedwithplacentaaccreta,andproposedrelativelythinned
endometriumandlowerestradiollevelsaspotentialmechanisms.(3)
OthershaveevaluatedIVFwithrelationtothethirdstageoflabor.Elenisetal,ina2015
studyfromSweden,lookedspecificallyatoocytedonationIVFandtheriskofpoor
obstetricaloutcomesinotherwisehealthywomen.(35)Theauthorsfoundapositive
associationbetweenretainedplacentaandoocytedonation,aswellasbetweenPPHand
oocytedonation.(35)Finally,inarecent2016studybyAzizetal,seekingtodetermine
whetherornotlengthofthirdstagewasrelatedtoIVF,theauthorsconcludedthat
cryopreservedembryotransfer(donatedorautologous)withoutcontrolledovarian
hyperstimulationwasnotrelatedtolongerthirdstage,butdidsignificantlyincreasethe
riskforMROP.(36)
PurposeofInquiry:
WhileindividualriskfactorsforMROPhavebeenproposedandstudied,nostudyhas
determinedfactorsassociatedwithhemorrhagicmorbidityinthiscontext.Additionally,
becauseitismostlystudiedinthecontextofcesareanwithknownprevia,fewstudieshave
lookedatmorbidlyadherentplacentaandplacentaaccretariskfactors(particularly
resolvedlowlyingplacenta,prioruterinesurgery,historyofpreviousretainedplacenta,
priorcesareansection,andART)aspredictorsofPPHaftermanualextraction.Thegoalof
12
thisstudywastodeterminepredictorsofprimary,severepostpartumhemorrhageafter
MROP,definedasanestimatedbloodloss(EBL)greaterthanorequalto1500ccoccurring
withinthefirst24hoursafterdelivery,needfortransfusion,greaterthanorequaltoa10
pointdropinhematocrit.(37)
Wehypothesizedthatonemajorriskfactorormultipleminorriskfactorsforpostpartum
hemorrhagewillincreaseriskofseverehemorrhageaftermanualextraction.Indefining
riskfactors,wegroupedvariablesaccordingtotheirassociationwithatony,invasive
placentation,orpostpartumhemorrhageintheabsenceoftheseotherfactors(other).Due
toworldwideincreaseduseofIVFandpathologicplacentaaccreta,andthepaucityof
researchconnectingthisproceduretothirdstageabnormalities,wewereparticularly
interestedinthisetiologyasariskfactorforPPH.(3)Wesecondarilyhypothesizedthat
patientswithriskfactorsforabnormalplacentationwouldshowthestrongestassociation
withPPH,basedontheseverityofthisconditionandlackoftimelyrecognitionand
managementatvaginaldelivery.
Elucidatingindependentriskfactorsforpostpartumhemorrhagewillallowobstetriciansto
betterprepareforandrecognizeseveremorbidityatvaginaldelivery,withthegoalof
reducingmaternalmorbidityandmortalityinbothdevelopedanddevelopingcountries.
Methods
Thisretrospectivecase-controlstudyhasbeenapprovedbyPartners/Brighamand
Women’sHospitalInstitutionalReviewBoard.Weusedbilling(ICD-9andCPT)codesin
ordertoidentifyallpatientswithvaginaldeliveriesbetweenJanuary1,2007andMay29,
2015whounderwentmanualremovaloftheplacenta(MROP).Thiswassupplemented
withdatafromourhospital’sofficialelectronicdeliveryrecord,whichcategorizesplacental
deliveriesas“manual”or“spontaneous.”Patientdatawascollectedfromelectronicand
papercharts.MROPwasdefinedasneedformanualcreationofaseparationplanebetween
uterusandplacentapostpartumforaneitherpartiallyorundeliveredplacenta.Two
authors(NPandDC)reviewedallchartstoconfirmmanualremoval.
13
Whilepracticesvary,manualremovaloftheplacentaistypicallyattemptedifthepatient
hasnotdeliveredtheplacentawithin30minutes,ifadeliveredplacentaisvisually
incomplete,orifheavybleedingmandatesMROPsoonerthan30minutes.AtBrighamand
Women’sHospital,obstetriciansusetheirdiscretionindecidingwhentomanuallyextract
theplacenta.
Ourcasegroupincludedpatientsexperiencingseverehemorrhageaftermanualextraction.
Severepostpartumhemorrhagewasdefinedinthisstudyasestimatedbloodloss(EBL)
≥1500cc,hematocritdrop≥10percentagepoints,orbloodproducttransfusionforthe
indicationofhemorrhage.OurEBLdefinitionwasbasedontheliteratureshowingthat
patientswith>1500ccbloodlossexperiencethemostmorbidityandmortality
peripartum.(10)Ourcontrolgroupwasrandomlyselectedfromthosepatientswhodidnot
experienceseverepostpartumhemorrhage.Controlswereone-to-onematchedbasedon
yearofdeliveryinordertominimizebiasescausedbychangesinpracticeoverthecourse
ofthestudyperiod.Anypatientinthecohortwhodeliveredextramurally,priorto24
weeksgestationalage,orhaddelayedextractionoftheplacentaformorethan24hours
afterdeliverywasexcludedfromtheanalysis.
Wecollecteddetaileddemographic,medicalandhistoricaldataforeachsubject,including
age,bodymassindex(BMI)attheendofpregnancy,race,parity,numberofprior
spontaneousortherapeuticabortions(medicalorsurgical),priorhistoryofretained
placenta(placentarequiringmanualorsurgicalremovalinpriorpregnancy),andprior
historyofpathologically-confirmedplacentaaccreta.Surgicalhistoricalvariablesincluded
priorcesarean,dilationandcurettage(D&C)performedinthesettingofpregnancy
(spontaneousortherapeuticabortion,ortreatmentofpostpartumhemorrhageorretained
productsofconception),oruterinesurgicalprocedures(myomectomy,anyoperative
hysteroscopy,orendometrialablation).PriorD&Conanon-pregnantuterusoruterine
polypectomieswerenotconsidered.

14
Alongwithdemographicsandhistoryabove,wecollectedcharacteristicsassociatedwith
currentpregnancy.TheseincludedconceptionachievedwithAssistedReproductive
Technology(ART;definedaseitherinvitrofertilizationorintracytoplasmicsperm
injection),multiplegestationinthecurrentpregnancy,aprolongedsecondstageoflabor
(timebetweenfullcervicaldilationof10cmanddeliveryoftheinfant),birthweightgreater
than4000g,signsofaccretaonultrasound(vascularlakes,lossofboundarybetween
placentaandmyometrium,absenceofsonolucentzone,orsignsofdeeperinvasionsuchas
percreta),resolvedlowlyingplacenta(definedasaplacentathathadcomewithin2cmor
coveredthecervicalosduringpregnancyviaultrasonographyrecords),Asherman
syndromeoruterinesynechiae(intrauterineadhesionsorbandsasindicatedby
ultrasound,hysteroscopy,orasnotedbypatient’sproviderinprenatalrecords),
preeclampsia(asindicatedbypatient’sproviderinprenatalrecords),acuteplacental
abruption(asmentionedbythepatientsprovider,orbyabnormallyheavybleedingat
presentation),fibroidsgreaterthan6cmonpregnancyultrasound,andgestationalage
(withpretermdeliverydefinedasdeliverypriorto37weeksgestationalage).
Wealsocollectedlaborvariablesofpresentpregnancyincludingoperativevaginaldelivery
(vacuumassistedorforcepsassistedvaginaldelivery)lowergenitaltractlaceration,degree
ofperineallaceration(asindicatedbyproviderinelectronicdeliveryrecord),episiotomy,
cordavulsion(completeseparationoftheumbilicalcordpriortodeliveryofplacenta,as
notedbydeliveryprovider),andchorioamnionitis(fevergreaterthan100.4Ftreatedwith
antibioticsduringfirstorsecondstageoflabor).
Pregnancyoutcomesandinterventionscollectedincludedatony(providernotedatonyin
chartorusedgreaterthanorequaltotwouterotonics—misoprostol,methylergonovine,
prostaglandinF-2α,oroxytocin),clinicalaccreta(providerreportedsuspectedclinical
accretaornotedabnormaladherenceoftheplacentatotheuterinewallwithunusually
difficultseparation),uterineinversion,hysterectomy,intrauterineballoonplacement,
uterinearteryembolization,needfordilationandcurettageincurrentpregnancy,intensive
careunitadmission,postpartumreadmission,andanypathologicaccretadiagnosis

15
(definedasplacentalfibersadherenttothemyometriumwithabsentinterveningdecidua,
asindicatedbythepathologist).
Weanalyzedriskfactorsforhemorrhageaftermanualdeliverybothindividuallyand
groupedbasedontheirpresumedcausativeroleinPPHassociatedwithMROP.Thefirst
groupincludedvariablesassociatedwithatony,includingbirthweightgreaterthan4000g,
morbidobesity(BMIgreaterthan40kg/m2),chorioamnionitis,multiplegestations,high
parity(greaterthan4)andprolongedsecondstageoflabor(greaterthantwohours).The
nextgroupincludedvariablesassociatedwithabnormalplacentationorplacentaaccreta,
includingpreviouscesareandelivery,prioruterinesurgery,resolvedpreviaorlowlying
placentainthecurrentpregnancy,Ashermansyndromeoruterinesynechiae,historyof
pathologicaccreta,conceptionachievedviaART,ormorethan2priorD&Cproceduresas
definedabove.OurfinalgroupconsistedofotherPPHriskfactors,includinguterine
leiomyomagreaterthanorequalto6cm,acuteplacentalabruption,orpreeclampsia.(1,3,
20,37-43).
WealsoexaminedwhetheranyonemajorriskfactororanytwominorriskfactorsforPPH,
regardlessofgrouping,wereassociatedwithhemorrhage.Majorriskfactorsforsevere
hemorrhageweredefinedassignsofaccretaonantepartumradiographorpresenceof
acuteabruption.(40)Anyotherriskfactorwasconsideredminor.
Toanalyzetherelationshipbetweentimeandhemorrhage,werecordedeverysubject’s
durationofthirdstageoflabor,definedastimeinminutesbetweendeliveryoftheinfant
anddelivery(manuallyinourcohort)oftheplacenta,asofficiallyrecordedinthe
electronicdeliveryrecord.Toevaluatetherelationshipbetweenhemorrhageandduration
ofthethirdstage,wedividedtimeuntilplacentaldeliveryintothreecategories(</=30
minutes,30-60minutes,and>60minutes).Finally,tobetterunderstandtheroleoftimein
thedevelopmentofPPH,weexploredwhetherpatientandlaborcharacteristicswere
associatedwithvaryinglengthsofthirdstageviaourthreetimecategoriesabove.
16
ThedataanalysisforthispaperwasgeneratedusingSASsoftware,version9.4.Copyright
©2016,SASInstituteInc.ContinuousvariableswereanalyzedwithWilcoxontests,while
categoricalvariableswereanalyzedwithconditionallogisticregressionorFisherExact
testsifavariablehadanullentry.P-valueslessthan0.05wereconsideredsignificantwith
two-tailedtests.Finally,inordertotestforindependentassociationsandcontrolfor
confounding,weenteredriskfactorvariablesintoastepwiselogisticregressionmodel.Any
variableassociatedwithhemorrhagewithap-valueof≤0.2wasincludedinthemodel.
Variableswereexcludedfromthemodeliffinalp-valueswere>0.35.
Results:
BetweenJanuary1,2007andJune30,2015,997womenwithmanualremovalofthe
placentawereidentified.Ofthesesubjects,172patientswereidentifiedashavingamajor
postpartumhemorrhage.Anadditional172matchedcontrolpatientswithMROPbut
withoutmajorPPHwererandomlyselectedfromtheremainingpatients.
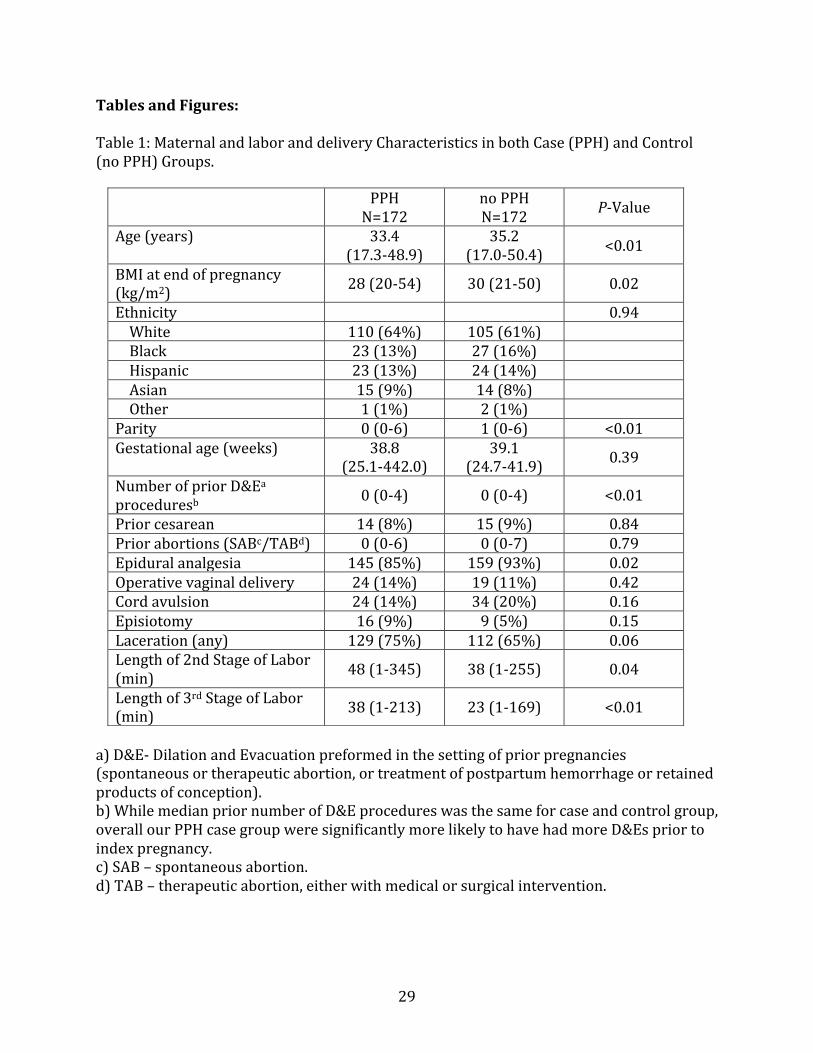
Characteristicsofcase(severePPH)andcontrol(noPPH)groupsareshowninTable1.The
casegroupshowedlowermedianBMI(33.4vs.35.2,p<0.01),longersecondstageoflabor
(48kg/m2vs.38kg/m2;p=0.04),andlongerthirdstageoflabor(38minutesvs.23
minutes;p<0.01).Thecasegroupwasslightlyyoungerthanthecontrols(33.4yearsvs.
35.2years;p<0.01),andthemediannumberofpriorpregnancieswasoneless(0vs.1,
p<0.01).Theyalsotendedtodeliverunderepiduralanalgesialessfrequentlythanthe
controlgroup(145(85%)vs.159(93%),respectively,p=0.02).Ethnicity,priornumberof
abortions(boththerapeuticandspontaneous),operativevaginaldelivery,cordavulsion,
episiotomy,laceration(includinghighdegrees),andgestationalagedidnotsignificantly
differbetweenPPHandnoPPHgroups.
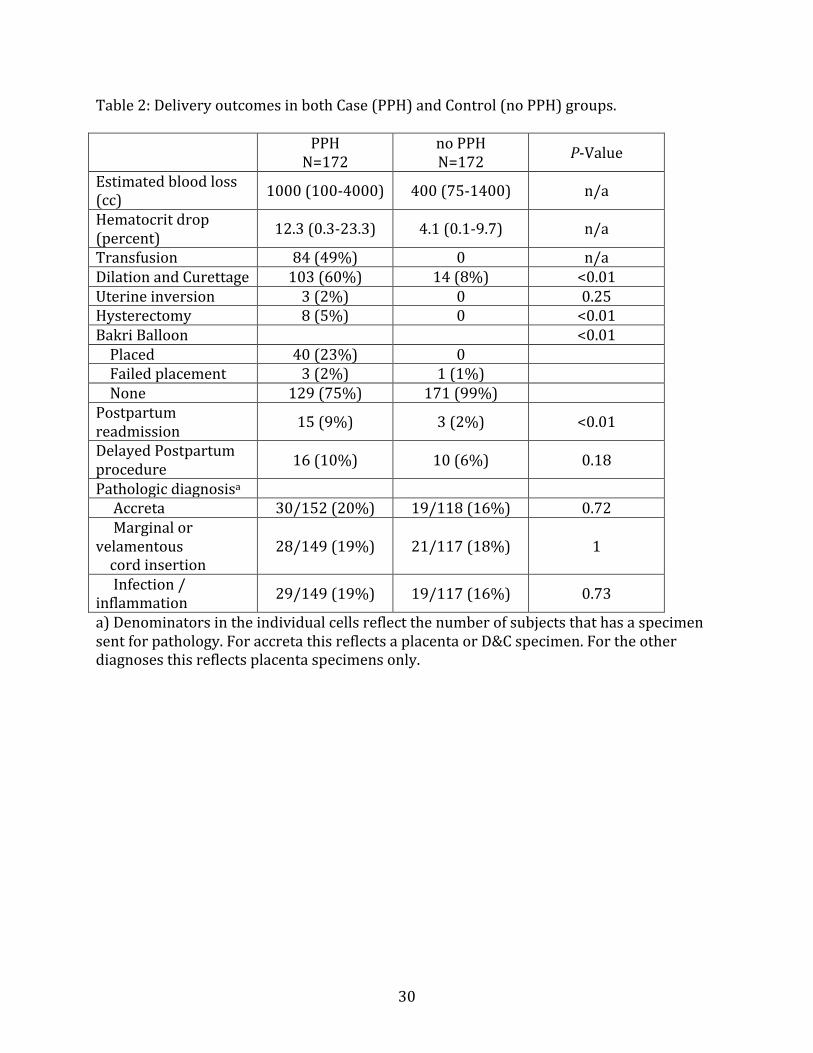
ObstetricaloutcomesforcaseandcontrolgroupsareshowninTable2.Averagebloodloss
inourseverePPHgroupwas1000cc(100-4000cc)andaveragehematocritdropwas
12.3%(0.3-23.3%).Inthecasegroup84patientsoutof173weretransfusedwithatleast

17
onebloodproduct.Averagebloodloosinourcontrolgroupwas400cc(75-1400cc),and
averagehematocritdropwas4.1(0.1-9.7)andnopatienthadatransfusion(percase
inclusioncriteria).Hematocritdropdatawasfrequentlyunavailable,particularlyforour
controlgroup,oftenduetonoblooddrawpostpartum.
Ofthe172patientswithsignificantPPH,51%ofourPPHgroupwasnotedtohaveuterine
atonybyobstetriciansorproviders,incomparisonto12%ofournon-PPHcontrolgroup
(p<0.01).ThePPHgroupandthecontrolgroupdidnotdifferinratesofpathologicaccreta
diagnosis(17%vs.11%;p=0.09).Similarly,thepercentageofPPHpatientswithclinically
adherentplacenta(20%)didnotdifferfromthecontrolgroup(19%;p=0.79),nordidthey
differwhentheclinicalandpathologicdiagnoseswerecombined(34%intheaccretagroup
versus29%inthecontrolgroup,p=0.36).
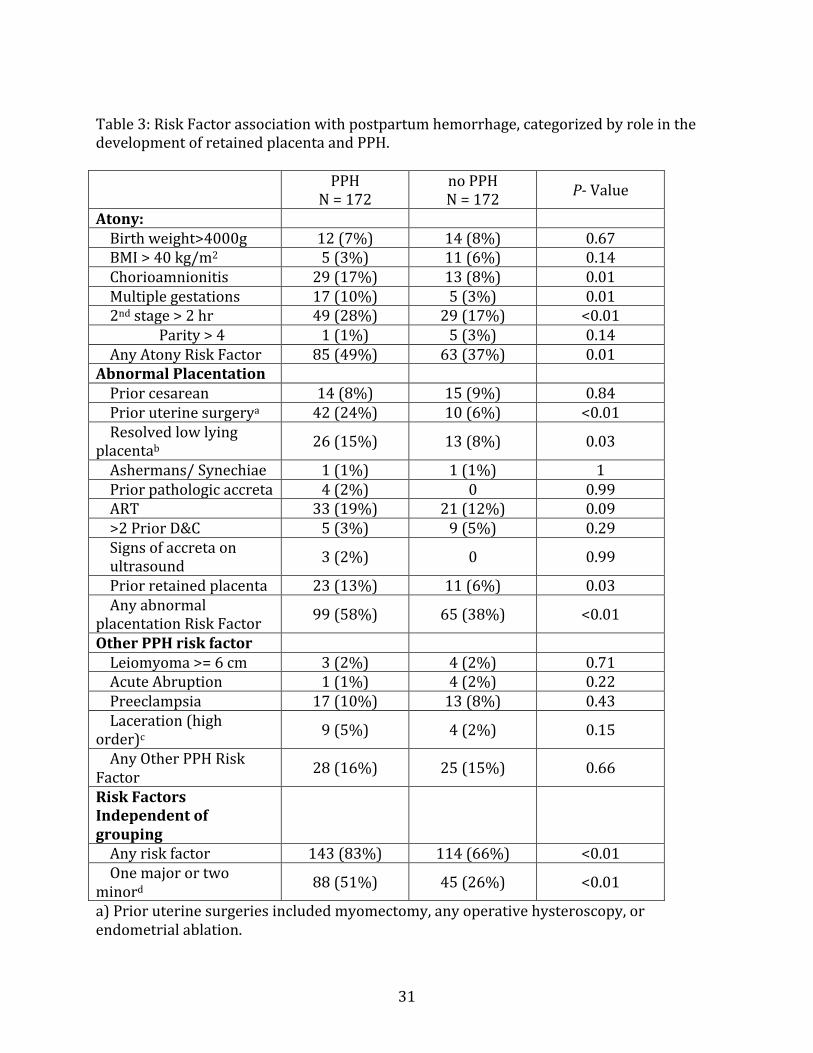
Individualpredictorswithinthethreehemorrhageriskfactorcategoriesandtheir
associationswithourMROPwithPPHandcontrolgroupsareshowninTable3.Withinthe
Atonycategory,17%ofPPHpatientsexperiencedchorioamnionitis,versusthecontrol
groupwhichhad8%withchorioamnionitis(p=0.01).Multiplegestation(10%PPHvs.3%
controls;p=0.01)andasecondstageoflaborlongerthantwohours(28%PPHcasesvs.
17%controls;p<0.01)werealsosignificantlyassociatedwithPPH.Highbirthweight,high
parity,andmorbidobesitywerenotsignificantlydifferentbetweenthecaseandcontrol
groups.
WithintheAbnormalPlacentationgroup,prioruterinesurgery(24%casesvs.6%controls;
p<0.01),historyofretainedplacenta(13%casesvs.6%controls;p=0.03)andresolved
low-lyingplacenta(15%casesvs.8%controls;p=0.03)weresignificantlyassociatedwith
PPHafterMROP.ThepercentageofourPPHcasegroupwhounderwentART(19%)didnot
differfromtherespectivepercentageofcontrols(12%;p=0.09).Inourcasegroupthere
werefourpatients(2%)whohadapriorpathologicaccretawithouthysterectomy,versus
noneinourcontrolgroup(NS).Similarlythreepatients(2%)ofourcasegrouphad
evidenceofaccretaonultrasound,versusnoneinourcontrolgroup(NS).Noneofthe
potentialriskfactorsintheOtherPPHRiskFactorsgroup(largefibroids,acuteabruption,

18
highorderlacerationorpreeclampsia)showedasignificantassociationwithPPHinthe
settingofMROP.
Casepatientsweresignificantlymorelikelythancontrolstohaveanyoneriskfactorin
eithertheAtony(49%vs.37%respectively,p=0.01)orAbnormalPlacentationriskgroup
(58%vs.38%,respectively,p<0.01,Table3).Similarly,PPHcasepatientswere
significantlymorelikelytohaveanyonemajor(signofaccretaonultrasoundorsignsof
abruptionatadmission)ortwominor(anyothervariable)riskfactors(51%vs.26%
controls;p>0.01)oranyriskfactorregardlessofgrouporseveritystratification(83%vs.
66%controls;p<0.01).
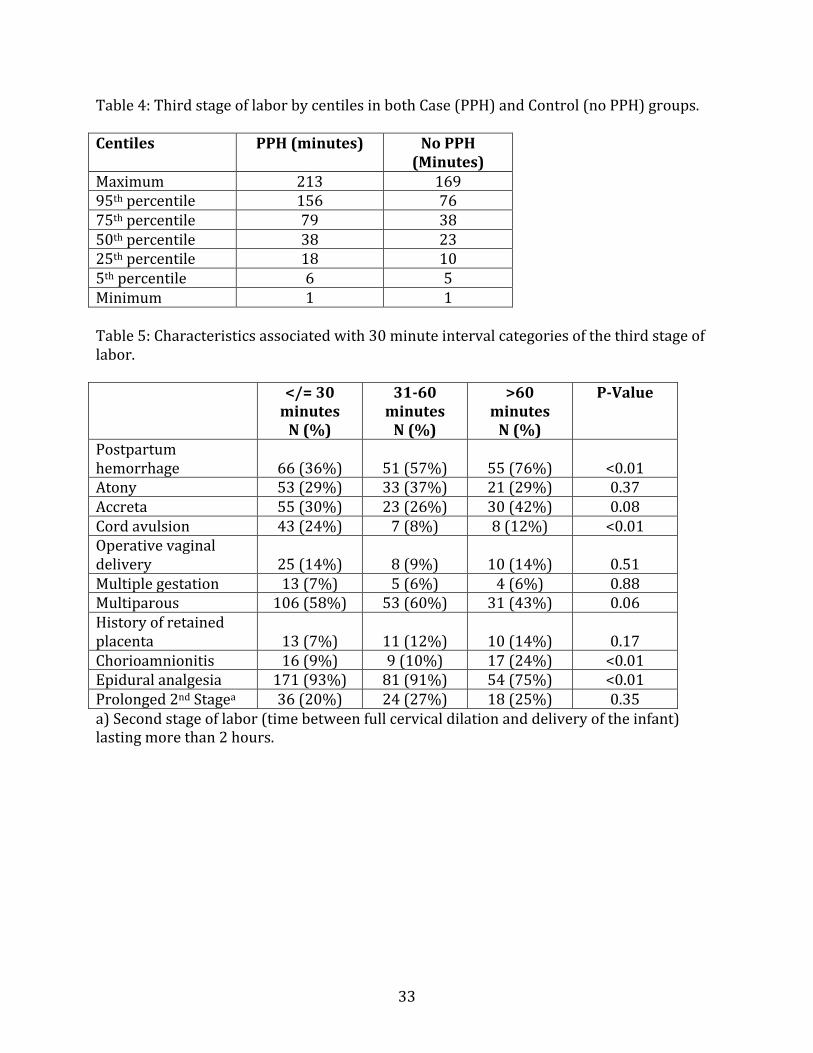
ThethirdstageoflaborbyquartileinourPPHcasegroupandournoPPHcontrolgroupis
showninTable4.WithinthePPHcasegroup,thirdstagerangedfrom1to213minutes,
with95%ofplacentaldeliveriesoccurringwithin2.5hoursandamedianof38minutes.
Thisvariedcomparedtothecontrolgroup,inwhich95%ofplacentasdeliveredwithin76
minutes,withamedianof23minutes.
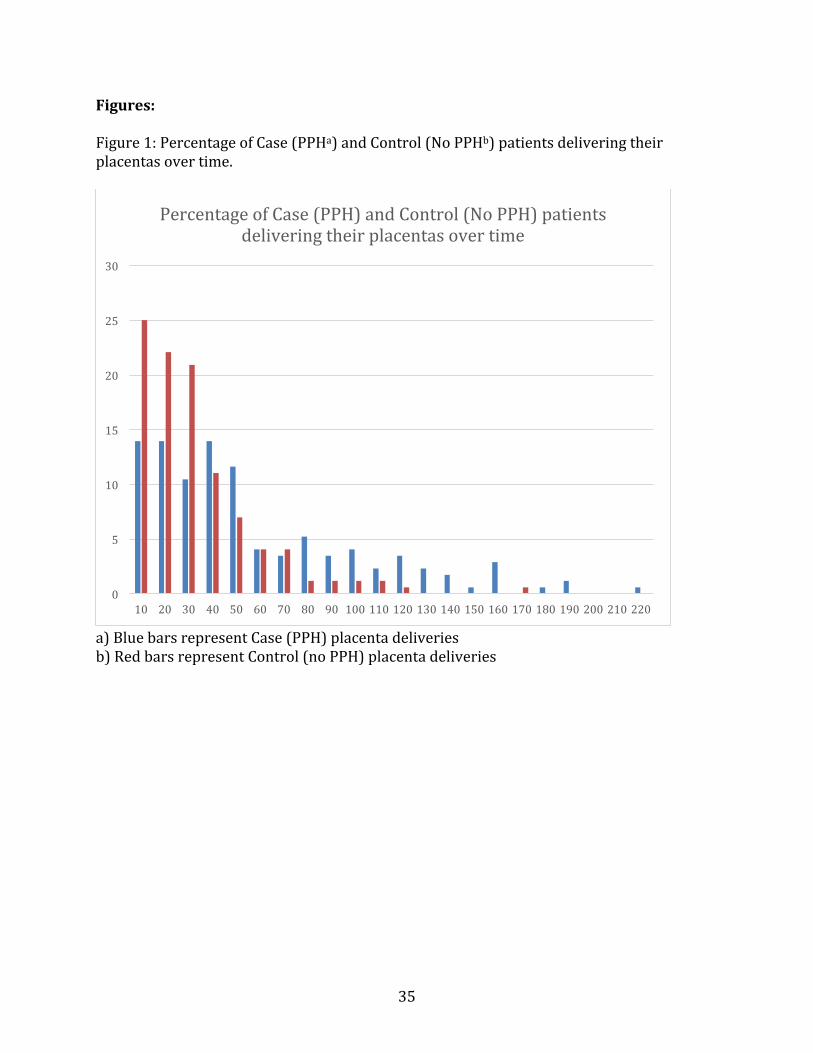
Table5alsoshowsthelengthofthirdstageoflaborbrokendownbytimecategory(</=30
minutes,31-60minutes,and>60minutes).PatientsinthePPHcasegrouphadtheir
placentasmanuallyremovedlaterthancontrols.Withinthefirst30minutes,38%ofour
PPHcaseshadMROPversus68%ofcontrols.Between31and60minutes,30%ofPPH
casesand22%ofcontrolshadMROP.Finally,afterwaiting60minutes,32%ofthePPH
casegrouphadtheirplacentasdeliveredduringthistime,asopposedto10%ofthe
controls(p<0.01)Figure1illustratesthepercentageofcaseandcontrolpatientsdelivering
theirplacentasovertime.
Characteristicsofpatientsdeliveringatdifferentintervalsofthird-stageareshowninTable
5.Patientsexperiencingcordavulsionhadsignificantlyshortertime-to-deliveryintervals,
with24%of</=30minutemanualextractionsduetocordavulsion(p<0.01)(versusother
timeintervals),asdidpatientswithepiduralanalgesiawith93%of</=30minutemanual
extractionshavinganepidural(versus75%of>60minutedeliveries;p<0.01).Incontrast,
19
chorioamnionitisduringlaborwassignificantlyassociatedwithalongerthirdstage,with
9%ofthe</=30minutedeliveries,10%ofthe31-60minutedeliveries,and24%ofthe>60
minutedeliveriesassociatedwithchorioamnionitisduringlabor(p=0.03).Ourthreetime
categoriesdidnotshowsignificantassociationwithatonyoraccreta,bothcharacteristics
tendedtohaveplacentaldeliveryearlierinourcohortsrangeofthirdstage.
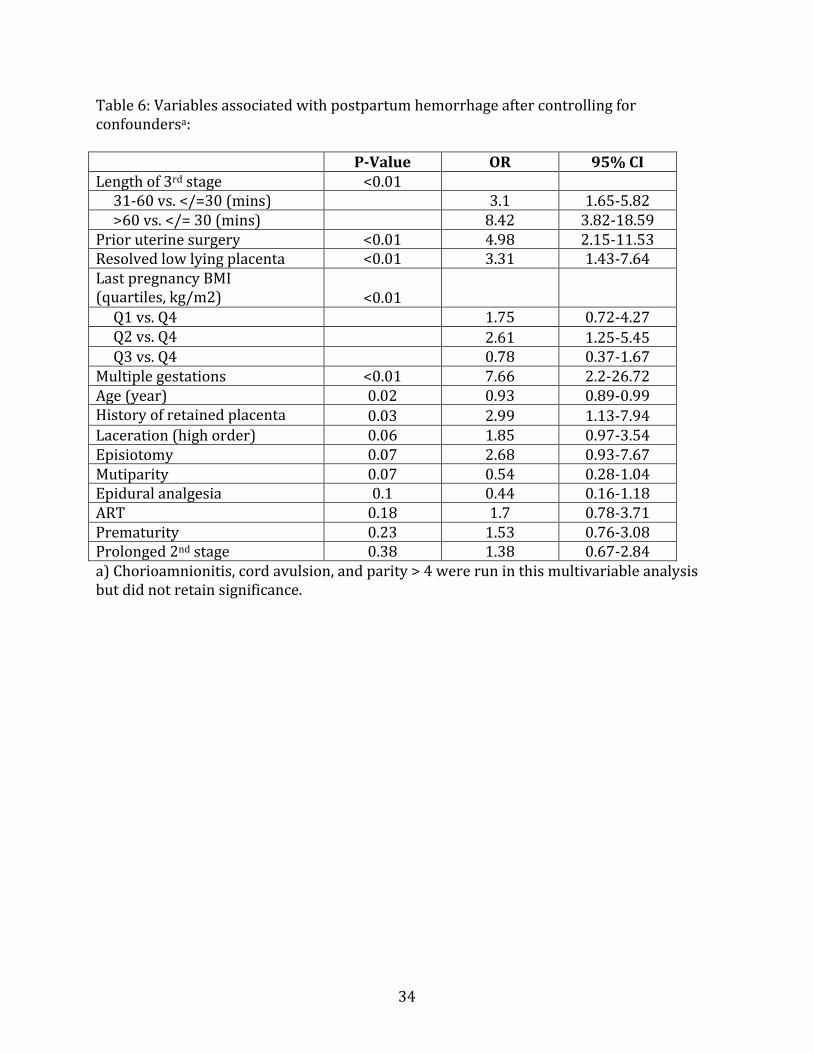
ResultsfromourstepwiselogisticregressionareshowninTable6,whichshowsall
variablesretainedinthefinalmodel.Afteradjustingforsignificantvariablesinthe
univariateanalysis(lengthofthirdstageoflabor,prioruterinesurgery,maternalageby
year,multiparity,multiplegestations,BMIbyquartile,lowlyingplacenta,historyof
retainedplacenta,episiotomy,laceration,epiduralanesthesia,ART,prematurity,second
stageoflabor>2hours,cordavulsion,chorioamnionitis,andparity>4),chorioamnionitis,
cordavulsion,andparity>4felloutofthemodel.Increasinglengthofthirdstageshowed
thestrongestassociationtoPPH(OR=3.1,95%CI1.65-5.8295%)for3rdstageof31-60
minutesvs.</=30minutes,andOR=8.42,CI3.82-18.5995%CIfor3rdstage>60minutesvs.
</=30minutes).Abnormalplacentationpredictorsremainedindependentlyassociated
withPPH.Theseincludedprioruterinesurgery(OR=4.98,CI2.15-11.52),resolvedlow-
lyingplacenta(OR=3.31,95%CI1.43-7.64),andhistoryofretainedplacenta(OR=2.99,
95%CI1.13-7.94).Incontrast,oftheAtonyriskfactors,onlymultiplegestationsremained
significantinthemultivariablemodel(OR=7.66,95%CI2.2-26.72),whilehighBMI
appearedprotectiveratherthanariskfactor,withthe2ndBMIquartile(28.5kg/m2-37
kg/m2)moreassociatedwithPPHthanthe4th(45.5kg/m2–54kg/m2;OR=2.61,95%CI
1.25-5.45).Secondstagedurationgreaterthan2hourswasalsonotassociatedwithPPHin
themodel.
Discussion:
Thepurposeofthisstudywastodefinecharacteristicsassociatedwithmajorhemorrhage
intheeventofmanualextractionoftheplacenta.Ourresultsledustoconcludethatlength
oftimeuntildeliveryoftheplacentaisofgreatestimportinpreventingpostpartum
hemorrhageinthesettingofpotentialuterineatony.Wealsoconcludedthatpatientswith

20
riskfactorsformorbidlyadherentplacentaareatriskofhemorrhagewithmanual
extraction,regardlessoflengthofthethirdstage.Thisinquiryisimportantfortriagingand
treatingmorbidpatientsonthelaboranddeliveryfloor.Ifcharacteristicsassociatedwith
massivehemorrhageareknownpriortoMROP,physicianscanadequatelyprepareby
transferringthemothertotheoperatingroom,callingfortypeandcrossedbloodproducts,
andnotifyingateamtrainedinsurgicalresponsetomassivebloodloss.
ThisstudyisuniqueinthatwecollectedbothhistoricalriskfactorsforPPHwithoutMROP
aswellasnovelriskfactorsrarelystudiedintheliterature,includingresolvedlowlying
placenta,priorhistoryofaretainedplacenta,andprioruterinesurgery.Wehypothesized
thatanyonemajorriskfactorormultipleminorriskfactorswouldbeassociatedwithan
increasedriskofsignificanthemorrhageaftermanualremovaloftheplacenta.This
hypothesisheldtruewithapproximatelyhalfofourseverepostpartumhemorrhage
patientshavinganyonemajorormultipleminorriskfactors,versusaboutafourthofour
controls.However,clinically,theseresultsshowthattriagingMROPpatientsviathese
criteriawillonlycatcharoundhalfofthepostpartumhemorrhagecases,andwillalso
incorrectlyidentifyatleastaquarterofpatientswhowillnotgoontohemorrhageafter
MROP.ThissuggeststhatinthesettingofMROP,mostpatients,regardlessofwhetherthey
experienceseverePPH,aremorbidapriori,andtraditionalriskstratificationforPPHmay
notbeasuseful.
Ofmoreusewasevaluatingtheroleoftimeinthethirdstageoflaborinrelationtorisk
factorsforthedevelopmentofatonyorabnormalplacentationandPPH.Weconfirmedthat
patientswithlongerthirdstagesoflabor—ordelayedmanualdeliveryoftheplacenta—
hadhigheroddsofexperiencingseverehemorrhage.Thisresultpersistedaftercontrolling
forpotentialconfounding.Wealsofoundthat,whenevaluatedcategorically,riskfactorsfor
atonyandabnormalplacentationwereassociatedwithPPH.However,withregardtoatony
riskfactors,onlymultiplegestationsremainedsignificantlyassociatedwithPPHinour
multivariableanalysis.Thesefindingssuggestthatatonyriskfactorsmaybemodulatedby
shorteningthetimeuntildeliveryoftheplacenta.Putanotherway,evenifapatienthas
exposuresassociatedwithatonyandPPH,timelydeliveryoftheplacentamaylessenor

21
eveneliminateapatient’sriskofhemorrhage.Thefactthatmultiplegestationsremained
significantinthecontrolledanalysissuggeststhatatonyduetouterineover-distention
behavesdifferentlythanthatrelatedtoinflammation(asseenwithchorioamnionitis),and
maybelesssensitivetothirdstageduration.Thesefindingsarenovelandunreportedin
theliterature.
Incontrasttoatonyriskfactors,multipleindividualriskfactorsformorbidlyadherent
placentahadastrongassociationwithPPHwhenanalyzedinthemultivariableanalysis.
Theseincludedresolvedlowlyingplacenta,prioruterinesurgery,orhistoryofretained
placentainapriorpregnancy,butnotuseofARTorpriorcesareansection.Thisimplies
that,unlikewithatony,timeuntilmanualdeliveryoftheplacentaisnotaconfounderinthe
settingofriskfactorsforabnormalplacentation.Thus,ourdatasuggeststhatshortening
thethirdstageoflaborwhenaphysicianplansMROPduetoconcernforabnormal
placentationmaynothelplessenthemother’sriskofPPH.Thisisnottosaythatproviders
shoulddelaymanualremovalinthesettingofabnormallyadherentplacenta.Instead,a
morerapidmanualremovalmaynothelptoavoidmaternalhemorrhage.
OurfindingssupportpriorstudiesbyMagannetal(2005)andCombsetal(1991)that
linkedprolongedthirdstageoflaborwithPPH(24).Ourresultsexpanduponthesestudies,
suggestingthatevenfordeliveriesinwhichtheobstetricianchoosestomanuallyremove
theplacentaasopposedtowaitingforspontaneousdeliverywithoutintervention,timely
removalmayparticularlyreducehemorrhageinpatientswithcertainriskfactors,andthat
perhapsourlimitedguidelinesontimingshouldbereconsidered.
GiventheobservedimportanceofthirdstagedurationwithregardstoPPHrisk,we
exploredclinicalfactorsthatwereassociatedwithashortorlongertimeintervalfrom
deliveryofinfanttomanualdeliveryoftheplacenta.Weobservedthatumbilicalcord
avulsionandepiduralanalgesiawereassociatedwithashorterthirdstage,and
chorioamnionitiswithalongerthirdstage.Thisobservedrelationshipmightsuggestthat
avulsionofumbilicalcord,disallowingitsuseastractionontheplacenta,isoftenusedas
anindicationforrapidMROP,whilechorioamnionitisisnot,despiteitsrelationshipto
22
atonyandPPH.Nootherriskfactorsinourstudywereindividuallyrelatedtoalongerthird
stageoflabor.
Therelationshipbetweenchorioamnionitisandalongerthirdstagemaybedueto
obstetricianswarinessofintroducingahandintotheuterusinthesettingofknown
intrapartuminfection,thusdelayingtimeuntilmanualremovalofaretainedplacenta.This
warinessmayexplainwhythisriskfactorforatonyaloneisrelatedtoprolongedthird
stageoflabor.Interpretingtheepiduralanalgesiarelationship,itispossiblethatphysicians
aremorelikelytoperformapotentiallyuncomfortableprocedurefaster(ratherthanwait
forpotentialspontaneousplacentaldelivery)underconditionsofanalgesia.Alternatively,
itmaybethatpatientswithoutanexistingepiduralmustwaitforeitherconscioussedation
orspinalanesthesiatobeplacedbeforeaphysiciancanattemptMROP,lengtheningtheir
thirdstageoflabor.
Whenconceivingofthisstudy,ARTwasavariableofparticularinterestduetoitsknown
associationwithplacentaaccreta,aconditionassociatedwithbothhemorrhagicmorbidity
andretainedplacentaduringdelivery.(3,33,34)WhilewefoundthatARTislikely
associatedwithMROP,asthe19%rateamongourpatientswithPPHand12%amongour
patientswithoutPPHreflectveryhighratesofARTinthisMROPpopulation.However,we
foundthatARTshowednosignificantrelationshiptoPPHinthisclinicalsetting.Thisis
likelybecausealthoughtheliteraturehasshownARTtobesignificantlyrelatedto
pathologicaccreta,ARTpregnanciesmaynotclinicallybemorelikelytohavehemorrhagic
morbidityduetoadherentplacenta.(3,33,34)Ofnote,standardizationofdefinitionsfor
placentaaccretadoesnotexist,andnotalladherentplacentasorpathologicaccretacause
massivehemorrhage,furtherconfusingthisrelationshipbetweenARTandmorbid
adherence.ThesefindingssupportAzizetal’sstudy,whichwhileshowinghigherratesof
MROPinARTpatients,alsoconcludedthatthereisnorelationshipbetweenARTand
hemorrhagiccomplicationsduringthethirdstageoflabor.(36)
AsopposedtoART,othervariableswithinourmorbidlyadherentplacentacategorywere
positivelyassociatedwithpostpartumhemorrhage.Thesesignificantexposuresincluded

23
resolvedlowlyingplacenta,priorretainedplacenta,andprioruterineprocedure—
variablesthatarenotgenerallyconsideredinstudiesofPPHriskintheliterature.A
clinicianplanningMROPinapatientwithanyoftheseriskfactorsforabnormal
placentationmaythuswanttoconsiderpreparingforhemorrhage.Interestingly,inthe
morbidlyadherentplacentacategory,priorcesareansectionwasnotassociatedwiththe
PPHgroup.Thisisstrikingincomparisontotheliterature,wherepriorcesareansectionis
associatedwithplacentaaccretainpatientswithprevia.Thissuggeststhatonlyinthe
settingofplacentalimplantationoveralowtransversecesareanscarispriorcesarean
associatedwithmorbidaccreta—generallynotthecasewithvaginaldeliveries.
Asecondaryfindingofinterestwasthehighrateofpathologicplacentaaccretainthe
cohort.Inourstudy,theoverallrateofplacentaaccretaonpathologyinboththecaseand
controlgroupswasaround20%.Thisismuchhigherthantherateinthegeneral
population(~0.2%)(44),andsuggeststhatthecontributionofabnormalplacentationto
manualextractionmaybehigherthanpreviouslyestimated.
Strengths,Limitations,andFurtherResearch
Ourstudydrawsstrengthfromouruseofdetailedchartreviewtocollectindividual
patients’data,whichallowedustoconfirmandconceiveofaccuratecriteriaforPPH
(>1500ccbloodloss,>/=10pointhematocritdrop,ortransfusion),ensuringthatourcase
groupcapturedtrueclinicalmorbidity.Ourdatacollectionadditionallyallowedusto
collectpreviouslyunstudiedexposures,sucharesolvedlow-lyingplacenta,prioruterine
surgery,andpriorretainedplacenta.ThisisincontrasttomostliteratureonPPHwhich
drawsriskfactorsfromlargenationaldatabasesanddischargecodingthatarenecessarily
limitedinavailablediagnoses.Additionally,ourrelativelylargenumberofcaseswith
severePPHinthesettingofmanualremovaloftheplacentaallowedustodetermine
significantrelationshipsbetweenmanyexposuresandPPH.
Amajorlimitationofourstudyisthatitwascompletedretrospectively,makingitdifficult
tofind,confirm,andstandardizealldata,andrestrictingchartreviewtowhatproviders
documented.Case-controlstudiesarealsolimitedbecausewhileexposuresandtheir

24
relationshipstooutcomescanbedetermined,PPHincidencecannot.Additionally,while
hematocritdropwasusedascriteriaforwhetherornotapatienthemorrhaged,notall
patientshadpostpartumblooddraws,meaningthathematocritdropcouldnotbe
calculatedforsomeofourstudysubjects.Thismayhaveunderestimatedournumberof
caseswithseverePPH,biasingourhypothesistothenull.Finally,theindicationformanual
removalwasoftennotindicatedinthechart;thereforeweareunabletodefinitivelystate
whyaplacentawasremovedatagiventime.
Futureresearchshouldfocusonvalidatingourpredictionvariableswithastandardized
protocolforplacentamanagementanddeliveryinaprospectivetrial.Aretrospectivestudy
fromanotherinstitutionvalidatingourcriteriaintheirMROPpatientswithPPHwouldbe
usefulaswell.Consideringthedelayinmanualremovalinthesettingofchorioamnionitis,a
prospectivestudyexaminingthebalanceofriskofpostpartumhemorrhageversusriskof
infectiousmorbiditymaybeusefulaswell.Additionally,wecouldevaluatetheuseofother
modalitiesforpredictingandtriagingpatientslikelytohemorrhage,suchasbedside
ultrasoundorquantitativebloodloss,inordertofurtherhelpphysicianscontemplating
morbidityaftermanualextractionoftheplacenta.
Summary:
Themostimportantpredictorofhemorrhageaftermanualremovaloftheplacentais
lengthofthethirdstageoflabor.Majorandminorriskfactorsgroupedbyatonyand
morbidlyadherentplacentaareclinicallyusefulinpredictinghemorrhageafterMROP.If
manualremovaloftheplacentaseemslikely,patientswithriskfactorsforatonyshould
havetheirplacentasremovedinatimelyfashion,eveninthesettingofintrapartum
chorioamnionitis.Whileprovidersmayhesitatetomanuallyremoveaplacentawithout
epiduralanalgesiaorinthesettingofchorioamnionitis,earlierplacentaldeliveryislikely
beneficialinordertolessenriskofhemorrhagicmorbidity.
Incomparison,inthesettingofpatientsundergoingmanualremovalwithriskfactorsfor
morbidlyadherentplacenta,hemorrhageriskdidnotappeartobemitigatedbyfaster
removaloftheplacenta.Thissuggeststhatobstetriciansshouldconsiderassemblyof

25
appropriateteammembersandtypeandcrossedbloodproducts,andrequesttransferto
anoperatingroombeforeperformingmanualremovaloftheplacentainapatientwith
concernforabnormalplacentation.Finally,whilepatientswithretainedplacentahavea
highrateofARTuse,thisfactordoesnotappeartopredicthemorrhageriskinthisspecific
clinicalscenario.
Whiletimeappearstobethemostimportantfactorintriagingpatientsatriskforsevere
postpartumhemorrhageaftermanualremovaloftheplacenta,patientswithmultiple
gestation,resolvedlowlyingplacenta,prioruterinesurgery,orhistoryofpriorretained
placentashouldbeconsideredatriskforseverepostpartumhemorrhageevenwithtimely
manualremovaloftheplacenta.
26
References1. CombsCA,MurphyEL,LarosRK,Jr.Factorsassociatedwithpostpartumhemorrhagewithvaginalbirth.Obstetricsandgynecology.1991;77(1):69-76.2. TitizH,WallaceA,VoaklanderDC.Manualremovaloftheplacenta--acasecontrolstudy.TheAustralian&NewZealandjournalofobstetrics&gynaecology.2001;41(1):41-4.3. KaserDJ,MelamedA,BormannCL,MyersDE,MissmerSA,WalshBW,etal.Cryopreservedembryotransferisanindependentriskfactorforplacentaaccreta.FertilSteril.2015;103(5):1176-84e2.4. AmericanCollegeofO,Gynecologists.ACOGPracticeBulletin:ClinicalManagementGuidelinesforObstetrician-GynecologistsNumber76,October2006:postpartumhemorrhage.Obstetricsandgynecology.2006;108(4):1039-47.5. UrnerF,ZimmermannR,KrafftA.Manualremovaloftheplacentaaftervaginaldelivery:anunsolvedprobleminobstetrics.JPregnancy.2014;2014:274651.6. BatemanBT,BermanMF,RileyLE,LeffertLR.Theepidemiologyofpostpartumhemorrhageinalarge,nationwidesampleofdeliveries.AnesthAnalg.2010;110(5):1368-73.7. KramerMS,BergC,AbenhaimH,DahhouM,RouleauJ,MehrabadiA,etal.Incidence,riskfactors,andtemporaltrendsinseverepostpartumhemorrhage.Americanjournalofobstetricsandgynecology.2013;209(5):449e1-7.8. MolinaRL,PaceLE.ARenewedFocusonMaternalHealthintheUnitedStates.TheNewEnglandjournalofmedicine.2017;377(18):1705-7.9. MahutteNG,Murphy-KaulbeckL,LeQ,SolomonJ,BenjaminA,BoydME.Obstetricadmissionstotheintensivecareunit.Obstetricsandgynecology.1999;94(2):263-6.10. ShieldsLE,WiesnerS,FultonJ,PelletreauB.Comprehensivematernalhemorrhageprotocolsreducetheuseofbloodproductsandimprovepatientsafety.Americanjournalofobstetricsandgynecology.2015;212(3):272-80.11. MehrabadiA,LiuS,BartholomewS,HutcheonJA,KramerMS,ListonRM,etal.TemporaltrendsinpostpartumhemorrhageandseverepostpartumhemorrhageinCanadafrom2003to2010.JObstetGynaecolCan.2014;36(1):21-33.12. JosephKS,RouleauJ,KramerMS,YoungDC,ListonRM,BaskettTF,etal.InvestigationofanincreaseinpostpartumhaemorrhageinCanada.BJOG:aninternationaljournalofobstetricsandgynaecology.2007;114(6):751-9.13. RonsmansC,GrahamWJ,LancetMaternalSurvivalSeriessteeringg.Maternalmortality:who,when,where,andwhy.Lancet.2006;368(9542):1189-200.14. CallaghanWM,KuklinaEV,BergCJ.Trendsinpostpartumhemorrhage:UnitedStates,1994-2006.Americanjournalofobstetricsandgynecology.2010;202(4):353e1-6.15. CreangaAA,BergCJ,KoJY,FarrSL,TongVT,BruceFC,etal.MaternalmortalityandmorbidityintheUnitedStates:wherearewenow?Journalofwomen'shealth.2014;23(1):3-9.16. CallaghanWM,MackayAP,BergCJ.Identificationofseverematernalmorbidityduringdeliveryhospitalizations,UnitedStates,1991-2003.Americanjournalofobstetricsandgynecology.2008;199(2):133e1-8.17. MainEK,GoffmanD,ScavoneBM,LowLK,BinghamD,FontainePL,etal.NationalPartnershipforMaternalSafety:ConsensusBundleonObstetricHemorrhage.Obstetricsandgynecology.2015;126(1):155-62.
27
18. GreenbaumS,WainstockT,DuklerD,LeronE,ErezO.Underlyingmechanismsofretainedplacenta:Evidencefromapopulationbasedcohortstudy.Europeanjournalofobstetrics,gynecology,andreproductivebiology.2017;216:12-7.19. Deneux-TharauxC,MacfarlaneA,WinterC,ZhangWH,AlexanderS,Bouvier-ColleMH,etal.Policiesformanualremovalofplacentaatvaginaldelivery:variationsintimingwithinEurope.BJOG:aninternationaljournalofobstetricsandgynaecology.2009;116(1):119-24.20. EndlerM,GrunewaldC,SaltvedtS.Epidemiologyofretainedplacenta:oxytocinasanindependentriskfactor.Obstetricsandgynecology.2012;119(4):801-9.21. EndlerM,SaltvedtS,CnattingiusS,StephanssonO,WikstromAK.Retainedplacentaisassociatedwithpre-eclampsia,stillbirth,givingbirthtoasmall-for-gestational-ageinfant,andspontaneouspretermbirth:anationalregister-basedstudy.BJOG:aninternationaljournalofobstetricsandgynaecology.2014;121(12):1462-70.22. RogersJ,WoodJ,McCandlishR,AyersS,TruesdaleA,ElbourneD.Activeversusexpectantmanagementofthirdstageoflabour:theHinchingbrookerandomisedcontrolledtrial.Lancet.1998;351(9104):693-9.23. MagannEF,NiederhauserA,DohertyDA,ChauhanSP,SandlinAT,MorrisonJC.Reducinghemodynamiccompromisewithplacentalremovalat10versus15minutes:arandomizedclinicaltrial.Americanjournalofperinatology.2012;29(8):609-14.24. MagannEF,EvansS,ChauhanSP,LanneauG,FiskAD,MorrisonJC.Thelengthofthethirdstageoflaborandtheriskofpostpartumhemorrhage.Obstetricsandgynecology.2005;105(2):290-3.25. CombsCA,LarosRK,Jr.Prolongedthirdstageoflabor:morbidityandriskfactors.Obstetricsandgynecology.1991;77(6):863-7.26. IntrapartumCare:CareofHealthyWomenandTheirBabiesDuringChildbirth.NationalInstituteforHealthandCareExcellence:ClinicalGuidelines.London2014.27. DombrowskiMP,BottomsSF,SalehAA,HurdWW,RomeroR.Thirdstageoflabor:analysisofdurationandclinicalpractice.Americanjournalofobstetricsandgynecology.1995;172(4Pt1):1279-84.28. CovielloEM,GrantzKL,HuangCC,KellyTE,LandyHJ.Riskfactorsforretainedplacenta.Americanjournalofobstetricsandgynecology.2015;213(6):864e1-e11.29. ThurnL,LindqvistPG,JakobssonM,ColmornLB,KlungsoyrK,BjarnadottirRI,etal.Abnormallyinvasiveplacenta-prevalence,riskfactorsandantenatalsuspicion:resultsfromalargepopulation-basedpregnancycohortstudyintheNordiccountries.BJOG:aninternationaljournalofobstetricsandgynaecology.2016;123(8):1348-55.30. MillerDA,CholletJA,GoodwinTM.Clinicalriskfactorsforplacentaprevia-placentaaccreta.Americanjournalofobstetricsandgynecology.1997;177(1):210-4.31. BjurstromJ,CollinsS,Langhoff-RoosJ,SundbergK,JorgensenA,DuvekotJJ,etal.Failedmanualremovaloftheplacentaaftervaginaldelivery.ArchGynecolObstet.2017.32. RoecaC,LittleSE,CarusiDA.PathologicallyDiagnosedPlacentaAccretaandHemorrhagicMorbidityinaSubsequentPregnancy.Obstetricsandgynecology.2017;129(2):321-6.33. Esh-BroderE,ArielI,Abas-BashirN,BdolahY,CelnikierDH.PlacentaaccretaisassociatedwithIVFpregnancies:aretrospectivechartreview.BJOG:aninternationaljournalofobstetricsandgynaecology.2011;118(9):1084-9.
28
34. IshiharaO,ArakiR,KuwaharaA,ItakuraA,SaitoH,AdamsonGD.Impactoffrozen-thawedsingle-blastocysttransferonmaternalandneonataloutcome:ananalysisof277,042single-embryotransfercyclesfrom2008to2010inJapan.FertilSteril.2014;101(1):128-33.35. ElenisE,SvanbergAS,LampicC,SkalkidouA,AkerudH,SydsjoG.Adverseobstetricoutcomesinpregnanciesresultingfromoocytedonation:aretrospectivecohortcasestudyinSweden.BMCpregnancyandchildbirth.2015;15:247.36. AzizMM,GuirguisG,MarattoS,BenitoC,FormanEJ.Isthereanassociationbetweenassistedreproductivetechnologiesandtimeandcomplicationsofthethirdstageoflabor?ArchGynecolObstet.2016;293(6):1193-6.37. CommitteeonPracticeB-O.PracticeBulletinNo.183:PostpartumHemorrhage.Obstetricsandgynecology.2017;130(4):e168-e86.38. MehrabadiA,HutcheonJA,LiuS,BartholomewS,KramerMS,ListonRM,etal.Contributionofplacentaaccretatotheincidenceofpostpartumhemorrhageandseverepostpartumhemorrhage.Obstetricsandgynecology.2015;125(4):814-21.39. WettaLA,SzychowskiJM,SealsS,MancusoMS,BiggioJR,TitaAT.Riskfactorsforuterineatony/postpartumhemorrhagerequiringtreatmentaftervaginaldelivery.Americanjournalofobstetricsandgynecology.2013;209(1):51e1-6.40. DillaAJ,WatersJH,YazerMH.Clinicalvalidationofriskstratificationcriteriaforperipartumhemorrhage.Obstetricsandgynecology.2013;122(1):120-6.41. AllenVM,BaskettTF,O'ConnellCM,McKeenD,AllenAC.Maternalandperinataloutcomeswithincreasingdurationofthesecondstageoflabor.Obstetricsandgynecology.2009;113(6):1248-58.42. PracticeACoO.ACOGCommitteeopinion.Number266,January2002:placentaaccreta.Obstetricsandgynecology.2002;99(1):169-70.43. EshkoliT,WeintraubAY,SergienkoR,SheinerE.Placentaaccreta:riskfactors,perinataloutcomes,andconsequencesforsubsequentbirths.AmericanJournalofObstetrics&Gynecology.2013;208(3):219.e1-7.44. CommitteeonObstetricP.ACOGcommitteeopinion.Placentaaccreta.Number266,January2002.AmericanCollegeofObstetriciansandGynecologists.Internationaljournalofgynaecologyandobstetrics:theofficialorganoftheInternationalFederationofGynaecologyandObstetrics.2002;77(1):77-8.
29
TablesandFigures:Table1:MaternalandlaboranddeliveryCharacteristicsinbothCase(PPH)andControl(noPPH)Groups.
a)D&E-DilationandEvacuationpreformedinthesettingofpriorpregnancies(spontaneousortherapeuticabortion,ortreatmentofpostpartumhemorrhageorretainedproductsofconception).b)WhilemedianpriornumberofD&Eprocedureswasthesameforcaseandcontrolgroup,overallourPPHcasegroupweresignificantlymorelikelytohavehadmoreD&Espriortoindexpregnancy.c)SAB–spontaneousabortion.d)TAB–therapeuticabortion,eitherwithmedicalorsurgicalintervention.
PPHN=172
noPPHN=172 P-Value
Age(years) 33.4(17.3-48.9)
35.2(17.0-50.4) <0.01
BMIatendofpregnancy(kg/m2) 28(20-54) 30(21-50) 0.02
Ethnicity 0.94White 110(64%) 105(61%) Black 23(13%) 27(16%) Hispanic 23(13%) 24(14%) Asian 15(9%) 14(8%) Other 1(1%) 2(1%) Parity 0(0-6) 1(0-6) <0.01Gestationalage(weeks) 38.8
(25.1-442.0)39.1
(24.7-41.9) 0.39
NumberofpriorD&Eaproceduresb 0(0-4) 0(0-4) <0.01
Priorcesarean 14(8%) 15(9%) 0.84Priorabortions(SABc/TABd) 0(0-6) 0(0-7) 0.79Epiduralanalgesia 145(85%) 159(93%) 0.02Operativevaginaldelivery 24(14%) 19(11%) 0.42Cordavulsion 24(14%) 34(20%) 0.16Episiotomy 16(9%) 9(5%) 0.15Laceration(any) 129(75%) 112(65%) 0.06Lengthof2ndStageofLabor(min) 48(1-345) 38(1-255) 0.04
Lengthof3rdStageofLabor(min) 38(1-213) 23(1-169) <0.01
30
Table2:DeliveryoutcomesinbothCase(PPH)andControl(noPPH)groups. PPH
N=172noPPHN=172 P-Value
Estimatedbloodloss(cc) 1000(100-4000) 400(75-1400) n/a
Hematocritdrop(percent)
12.3(0.3-23.3) 4.1(0.1-9.7) n/a
Transfusion 84(49%) 0 n/aDilationandCurettage 103(60%) 14(8%) <0.01Uterineinversion 3(2%) 0 0.25Hysterectomy 8(5%) 0 <0.01BakriBalloon <0.01Placed 40(23%) 0 Failedplacement 3(2%) 1(1%) None 129(75%) 171(99%) Postpartumreadmission 15(9%) 3(2%) <0.01
DelayedPostpartumprocedure 16(10%) 10(6%) 0.18
Pathologicdiagnosisa Accreta 30/152(20%) 19/118(16%) 0.72Marginalorvelamentouscordinsertion
28/149(19%) 21/117(18%) 1
Infection/inflammation 29/149(19%) 19/117(16%) 0.73
a)Denominatorsintheindividualcellsreflectthenumberofsubjectsthathasaspecimensentforpathology.ForaccretathisreflectsaplacentaorD&Cspecimen.Fortheotherdiagnosesthisreflectsplacentaspecimensonly.
31
Table3:RiskFactorassociationwithpostpartumhemorrhage,categorizedbyroleinthedevelopmentofretainedplacentaandPPH. PPH
N=172noPPHN=172 P-Value
Atony: Birthweight>4000g 12(7%) 14(8%) 0.67BMI>40kg/m2 5(3%) 11(6%) 0.14Chorioamnionitis 29(17%) 13(8%) 0.01Multiplegestations 17(10%) 5(3%) 0.012ndstage>2hr 49(28%) 29(17%) <0.01
Parity>4 1(1%) 5(3%) 0.14AnyAtonyRiskFactor 85(49%) 63(37%) 0.01AbnormalPlacentation Priorcesarean 14(8%) 15(9%) 0.84Prioruterinesurgerya 42(24%) 10(6%) <0.01Resolvedlowlyingplacentab 26(15%) 13(8%) 0.03
Ashermans/Synechiae 1(1%) 1(1%) 1Priorpathologicaccreta 4(2%) 0 0.99ART 33(19%) 21(12%) 0.09>2PriorD&C 5(3%) 9(5%) 0.29Signsofaccretaonultrasound 3(2%) 0 0.99
Priorretainedplacenta 23(13%) 11(6%) 0.03AnyabnormalplacentationRiskFactor 99(58%) 65(38%) <0.01
OtherPPHriskfactor Leiomyoma>=6cm 3(2%) 4(2%) 0.71AcuteAbruption 1(1%) 4(2%) 0.22Preeclampsia 17(10%) 13(8%) 0.43Laceration(highorder)c 9(5%) 4(2%) 0.15
AnyOtherPPHRiskFactor 28(16%) 25(15%) 0.66
RiskFactorsIndependentofgrouping
Anyriskfactor 143(83%) 114(66%) <0.01Onemajorortwominord 88(51%) 45(26%) <0.01
a)Prioruterinesurgeriesincludedmyomectomy,anyoperativehysteroscopy,orendometrialablation.

32
b)Lowlyingplacentawasdefinedasultrasonographicdiagnosisofplacentapreviaortheplacentacomingwithin2cmofthecervicalosduringthecurrentpregnancy.c)Highorderlacerationsincluded3rdand4thdegreevaginaltearsafterdeliveryoftheinfant.d)Majorriskfactorsincludeacuteabruptionandradiologicsignsofaccreta.Allotherriskfactorsareincludedasminor.
33
Table4:ThirdstageoflaborbycentilesinbothCase(PPH)andControl(noPPH)groups.Centiles PPH(minutes) NoPPH
(Minutes)Maximum 213 16995thpercentile 156 7675thpercentile 79 3850thpercentile 38 2325thpercentile 18 105thpercentile 6 5Minimum 1 1Table5:Characteristicsassociatedwith30minuteintervalcategoriesofthethirdstageoflabor.
</=30minutesN(%)
31-60minutesN(%)
>60minutesN(%)
P-Value
Postpartumhemorrhage 66(36%) 51(57%) 55(76%) <0.01Atony 53(29%) 33(37%) 21(29%) 0.37Accreta 55(30%) 23(26%) 30(42%) 0.08Cordavulsion 43(24%) 7(8%) 8(12%) <0.01Operativevaginaldelivery 25(14%) 8(9%) 10(14%) 0.51Multiplegestation 13(7%) 5(6%) 4(6%) 0.88Multiparous 106(58%) 53(60%) 31(43%) 0.06Historyofretainedplacenta 13(7%) 11(12%) 10(14%) 0.17Chorioamnionitis 16(9%) 9(10%) 17(24%) <0.01Epiduralanalgesia 171(93%) 81(91%) 54(75%) <0.01Prolonged2ndStagea 36(20%) 24(27%) 18(25%) 0.35a)Secondstageoflabor(timebetweenfullcervicaldilationanddeliveryoftheinfant)lastingmorethan2hours.
34
Table6:Variablesassociatedwithpostpartumhemorrhageaftercontrollingforconfoundersa:
P-Value OR 95%CILengthof3rdstage <0.01 31-60vs.</=30(mins) 3.1 1.65-5.82>60vs.</=30(mins) 8.42 3.82-18.59Prioruterinesurgery <0.01 4.98 2.15-11.53Resolvedlowlyingplacenta <0.01 3.31 1.43-7.64LastpregnancyBMI(quartiles,kg/m2) <0.01 Q1vs.Q4 1.75 0.72-4.27Q2vs.Q4 2.61 1.25-5.45Q3vs.Q4 0.78 0.37-1.67Multiplegestations <0.01 7.66 2.2-26.72Age(year) 0.02 0.93 0.89-0.99Historyofretainedplacenta 0.03 2.99 1.13-7.94Laceration(highorder) 0.06 1.85 0.97-3.54Episiotomy 0.07 2.68 0.93-7.67Mutiparity 0.07 0.54 0.28-1.04Epiduralanalgesia 0.1 0.44 0.16-1.18ART 0.18 1.7 0.78-3.71Prematurity 0.23 1.53 0.76-3.08Prolonged2ndstage 0.38 1.38 0.67-2.84a)Chorioamnionitis,cordavulsion,andparity>4wereruninthismultivariableanalysisbutdidnotretainsignificance.
35
Figures:Figure1:PercentageofCase(PPHa)andControl(NoPPHb)patientsdeliveringtheirplacentasovertime.
a)BluebarsrepresentCase(PPH)placentadeliveriesb)RedbarsrepresentControl(noPPH)placentadeliveries
0
5
10
15
20
25
30
10 20 30 40 50 60 70 80 90 100110120130140150160170180190200210220
PercentageofCase(PPH)andControl(NoPPH)patientsdeliveringtheirplacentasovertime




















