Height, Stunting, and Refractive Error Among Rural Chinese Schoolchildren: The See Well to Learn...
8
Height, Stunting, and Refractive Error Among Rural Chinese Schoolchildren: The See Well to Learn Well Project ABHISHEK SHARMA, NATHAN CONGDON, YANG GAO, YAOGUI LU, YANRU YE, JING WU, DENNIS S. C. LAM, LIPING LI, JIASI WU, YEE KIT TSE, MINGZHI ZHANG, YUE SONG, AND SIAN GRIFFITHS ● PURPOSE: To evaluate the hypothesis that changes in nutritional status could be partly responsible for observed increases in myopia prevalence among Chinese children. ● DESIGN: Cross-sectional cohort study. ● METHODS: Rural Chinese secondary school children participating in a study of interventions to promote spectacle use were randomly sampled (20% of children with uncorrected vision >6/12 bilaterally, and 100% of remaining children) and underwent cycloplegic refrac- tion with subjective refinement and measurement of height and weight. Stunting was defined according to the World Health Organization standard population. ● RESULTS: Among 3226 children in the sample, 2905 (90.0%) took part. Among 1477 children undergoing refraction, 1371 (92.8%) had height and weight mea- surements. These children had a mean age of 14.5 1.4 years, 59.8% were girls, and mean spherical equivalent refraction was 1.93 1.82 diopters. Stunting was present in 87 children (6.4%). While height was in- versely associated with refractive error (RE) (taller children were more myopic) among boys (r 0.147, P .001), this disappeared when adjusting for age, and no such association was observed among girls. Neither girls nor boys with stunting differed significantly in refraction from children without stunting, and neither stunting nor height was associated with RE when adjust- ing for age, height, and parental education. The power of this study to have detected a 0.75 diopters difference in RE between children with and without stunting was 0.96. ● CONCLUSION: Results from this cross-sectional study are not consistent with the hypothesis that nutritional status is a determinant of RE in this setting. (Am J Ophthalmol 2010;149:347–353. © 2010 by Elsevier Inc. All rights reserved.) E VIDENCE FROM STUDIES IN CHINA, 1–3 SINGAPORE, 4 Hong Kong, 5 Taiwan, 6 and Australia 7 suggests that children of Chinese descent have among the world’s highest prevalence of myopia. Furthermore, this already-high prevalence of myopia among Chinese children 8,9 and young adults 10 may be rising, though methodological questions remain about some studies of this phenomenon. 11 In order to explain the apparent rise in myopia preva- lence among children of Chinese ethnicity, a number of potential environmental causative factors have been ex- amined. These have included increased near-work ac- tivity, 12,13 higher levels of education, 14 decreased outdoor activity, 15,16 and increasing population density. 17 In China, improved nutrition in the two decades since the economic reforms of the early 1980s is believed to have resulted in increases in height among recent cohorts when compared to those born in previous years. 18,19 It has been theorized that a larger body habitus might be associated with a greater axial length (AL) simply as a function of larger overall body size. 20 This relationship between in- creased height and longer AL has been reported among Singaporean Chinese schoolchildren 21 and in a Singa- porean adult population. 22 The association of height with refractive error (RE) is likely to be more complex than that with AL, because of the process of vision-driven emmetropization. In fact, studies of height and RE have reported mixed results, including the finding of greater stature among myopic children, 21 of no association, 22,23 and of shorter heights among myopic individuals. 24 Nonetheless, some authors have proposed that nutritional differences might exist between myopic and nonmyopic individuals. 25–27 We sought to examine the basic plausibility of the hypoth- esis that nutritional changes might underlie observed in- creases in the myopia prevalence among Chinese children. Height and weight among children during the teenage years, when childhood myopia is most prevalent, may be assumed to reflect a variety of factors, including the stage of puberty and genetic inheritance. In order to focus on those aspects of stature most directly responsive to nutritional intake, we chose to study stunting, which is defined with reference to a standard population assembled by the World Health Organi- zation (WHO) 28 as height 2 standard deviations (SD) below the mean for gender and age in months, that is, at the 2.5th percentile or below. Stunting in children and teens is Accepted for publication Aug 13, 2009. From the Oxford University Department of Public Health, Oxford, United Kingdom (A.S.); Chinese University of Hong Kong Department of Ophthalmology and Visual Sciences, Hong Kong, China (N.C., D.S.C.L.); Joint Shantou International Eye Center of Shantou University and Chinese University of Hong Kong, Shantou, China (N.C., Jin.W., D.S.C.L., Jia.W., M.Z., Y.S.); Chinese University of Hong Kong School of Public Health, Hong Kong, China (Y.G., Y.K.T., S.G.); and Shantou University Faculty of Medicine, Shantou, China (Y.L., Y.Y., L.L.). Inquiries to Liping Li, Shantou University Medical College, Shantou, People’s Republic of China; e-mail: [email protected] © 2010 BY ELSEVIER INC.ALL RIGHTS RESERVED. 0002-9394/10/$36.00 347 doi:10.1016/j.ajo.2009.08.015
Transcript of Height, Stunting, and Refractive Error Among Rural Chinese Schoolchildren: The See Well to Learn...

●
ni●
●
pswrthW●
(rsyrpvcPngrsitR0●
asOI
A
UoDaDoU
P
0d
Height, Stunting, and Refractive Error Among Rural ChineseSchoolchildren: The See Well to Learn Well Project
ABHISHEK SHARMA, NATHAN CONGDON, YANG GAO, YAOGUI LU, YANRU YE, JING WU,DENNIS S. C. LAM, LIPING LI, JIASI WU, YEE KIT TSE, MINGZHI ZHANG, YUE SONG, AND
SIAN GRIFFITHS
Ehpar
lpata
trctwlcSp
ltsicahb
ecHwrgscszb
PURPOSE: To evaluate the hypothesis that changes inutritional status could be partly responsible for observed
ncreases in myopia prevalence among Chinese children.DESIGN: Cross-sectional cohort study.METHODS: Rural Chinese secondary school children
articipating in a study of interventions to promotepectacle use were randomly sampled (20% of childrenith uncorrected vision >6/12 bilaterally, and 100% of
emaining children) and underwent cycloplegic refrac-ion with subjective refinement and measurement ofeight and weight. Stunting was defined according to theorld Health Organization standard population.RESULTS: Among 3226 children in the sample, 2905
90.0%) took part. Among 1477 children undergoingefraction, 1371 (92.8%) had height and weight mea-urements. These children had a mean age of 14.5 � 1.4ears, 59.8% were girls, and mean spherical equivalentefraction was �1.93 � 1.82 diopters. Stunting wasresent in 87 children (6.4%). While height was in-ersely associated with refractive error (RE) (tallerhildren were more myopic) among boys (r � �0.147,
� .001), this disappeared when adjusting for age, ando such association was observed among girls. Neitherirls nor boys with stunting differed significantly inefraction from children without stunting, and neithertunting nor height was associated with RE when adjust-ng for age, height, and parental education. The power ofhis study to have detected a 0.75 diopters difference inE between children with and without stunting was.96.CONCLUSION: Results from this cross-sectional study
re not consistent with the hypothesis that nutritionaltatus is a determinant of RE in this setting. (Am Jphthalmol 2010;149:347–353. © 2010 by Elsevier
nc. All rights reserved.)
ccepted for publication Aug 13, 2009.From the Oxford University Department of Public Health, Oxford,nited Kingdom (A.S.); Chinese University of Hong Kong Department
f Ophthalmology and Visual Sciences, Hong Kong, China (N.C.,.S.C.L.); Joint Shantou International Eye Center of Shantou University
nd Chinese University of Hong Kong, Shantou, China (N.C., Jin.W.,.S.C.L., Jia.W., M.Z., Y.S.); Chinese University of Hong Kong Schoolf Public Health, Hong Kong, China (Y.G., Y.K.T., S.G.); and Shantouniversity Faculty of Medicine, Shantou, China (Y.L., Y.Y., L.L.).
2Inquiries to Liping Li, Shantou University Medical College, Shantou,
eople’s Republic of China; e-mail: [email protected]
© 2010 BY ELSEVIER INC. A002-9394/10/$36.00oi:10.1016/j.ajo.2009.08.015
VIDENCE FROM STUDIES IN CHINA,1–3 SINGAPORE,4
Hong Kong,5 Taiwan,6 and Australia7 suggests thatchildren of Chinese descent have among the world’s
ighest prevalence of myopia. Furthermore, this already-highrevalence of myopia among Chinese children8,9 and youngdults10 may be rising, though methodological questionsemain about some studies of this phenomenon.11
In order to explain the apparent rise in myopia preva-ence among children of Chinese ethnicity, a number ofotential environmental causative factors have been ex-mined. These have included increased near-work ac-ivity,12,13 higher levels of education,14 decreased outdoorctivity,15,16 and increasing population density.17
In China, improved nutrition in the two decades sincehe economic reforms of the early 1980s is believed to haveesulted in increases in height among recent cohorts whenompared to those born in previous years.18,19 It has beenheorized that a larger body habitus might be associatedith a greater axial length (AL) simply as a function of
arger overall body size.20 This relationship between in-reased height and longer AL has been reported amongingaporean Chinese schoolchildren21 and in a Singa-orean adult population.22
The association of height with refractive error (RE) isikely to be more complex than that with AL, because ofhe process of vision-driven emmetropization. In fact,tudies of height and RE have reported mixed results,ncluding the finding of greater stature among myopichildren,21 of no association,22,23 and of shorter heightsmong myopic individuals.24 Nonetheless, some authorsave proposed that nutritional differences might existetween myopic and nonmyopic individuals.25–27
We sought to examine the basic plausibility of the hypoth-sis that nutritional changes might underlie observed in-reases in the myopia prevalence among Chinese children.eight and weight among children during the teenage years,hen childhood myopia is most prevalent, may be assumed to
eflect a variety of factors, including the stage of puberty andenetic inheritance. In order to focus on those aspects oftature most directly responsive to nutritional intake, wehose to study stunting, which is defined with reference to atandard population assembled by the World Health Organi-ation (WHO)28 as height �2 standard deviations (SD)elow the mean for gender and age in months, that is, at the
.5th percentile or below. Stunting in children and teens isLL RIGHTS RESERVED. 347

gpsn
ptltns
T
rwipa
●
atPraiat
sfi
a9tof
●
T
rplesatmThhwsboilh
F
3
enerally held to reflect poor nutritional intake over arolonged period of time.29 To the best of our knowledge,tunting has not previously been examined as an index ofutrition in myopic children.Our hypothesis is that, if improved nutrition could
lausibly explain recent increases in myopia prevalence,hen children identified on a cross-sectional basis with veryow height attributable to poor nutrition (stunting) oughto have significantly less myopia than children withormal or above-normal (overweight or obese) nutritionaltatus.
METHODS
HE “SEE WELL TO LEARN WELL” PROJECT IS AN ON-GOING
andomized trial of interventions to promote spectacleear among 10 000 secondary school children in 3 towns
n the rural Chaoshan region of Southern China. Partici-ants are selected at random from Year 1 and Year 2 classest all junior and senior high schools in the area.
SUBJECTS: All Year 1 and Year 2 classes (average sizepproximately 60 children) in all 5 junior high schools andhe 1 senior high school of Fuyang Township, Guangdongrovince, were enumerated and classes were selected atandom from a list of all eligible classes at each school untiltotal of 600 children (usually 8 to 10 classes) had been
dentified in the sampling frame. Our pilot testing in therea had demonstrated that participation rates were on
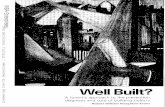
IGURE 1. Flow chart depicting the enrollment of rural Chin
he order of 80% to 85%, meaning that 600 children in the 2
AMERICAN JOURNAL OF48
ampling frame would be sufficient to guarantee a targetgure of 500 children examined at each school.Fuyang is located in the east of Guangdong province,
nd has a size of 38.5 square kilometers and a population of7 000 in 2004. It is located within 90 minutes’ drive ofhe city of Shantou (population 4.97 million at the endf 2006). The large majority of adults in Fuyang work inarming or agriculture.
MEASUREMENT OF VISUAL ACUITY AND REFRAC-
ION: Visual acuity (VA) with and without habitualefraction (if available) was measured by trained studyersonnel in well-lighted areas of the school during day-ight hours, at a distance of 5 meters, separately for eachye of each child. Children who did not have theirpectacles at school were asked to bring them for visionssessment on a separate day. Identical illuminated Snellenumbling E vision charts (Shantou City Medical Equip-ent Ltd, Shantou, China) were employed for all testing.he nontested eye was covered by the subject using aand-held occluder, with proper occlusion and neutralead position monitored by the examiner. The right eyeas tested first. A single optotype of each size was pre-
ented first, starting at 6/30. If a letter was failed, testingegan 2 lines above, with the child being asked to read allptotypes on the line sequentially. A subject had todentify correctly more than half of the letters on a givenine (eg, 3 out of 5, 4 out of 6) in order to be considered toave achieved that level of acuity.All subjects with vision of �6/12 in either eye, and a
choolchildren into a study of height, stunting, and myopia.
ese s0% sample of children with vision �6/12 in both eyes,
OPHTHALMOLOGY FEBRUARY 2010

uPbaLe(u
●
hsmCatcewois(sppBma
aa
●
ttntwiovpa
●
wnncPbdphpt
and
V
nderwent cycloplegic autorefraction (Potec PRK-5000;otec Co Ltd, Seoul, Korea) with subjective refinementy an ophthalmologist in each eye, at least 30 minutesfter receiving cyclopentolate 1% (Cyclogyl; Alconaboratories, Fort Worth, Texas, USA) 1 drop to bothyes every 5 minutes, for a total of 2 drops in each eye.Figure 1) The results of subjective refraction aretilized throughout.
MEASUREMENT OF HEIGHT AND WEIGHT: Theeight in centimeters and weight in kilograms of allubjects were measured (RGZ-120 analog height measure-ent unit and scale, Jiangsu Suhong Medical Instrumentso Ltd, Changzhou, Jiangsu, People’s Republic of China)
nd recorded by trained study personnel (physicians), withhe children dressed in stocking feet and their usual schoollothing. The scale was zeroed at the beginning and end ofach morning’s and afternoon’s testing session. Height andeight were used to calculate the body mass index (BMI)f each subject according to the following formula: (weightn kg)/(height in m)2. The following terms were defined forubjects by gender and age in months with regard to anon-Chinese) standard WHO reference population:28
tunting (height �2 SDs below the mean of the referenceopulation for gender and age in months, ie, at the 2.5thercentile or below); overweight (�1 SD above the meanMI by age and gender); and obese (�2 SD above theean BMI by age and gender). The latter 2 definitions
TABLE 1. Demographic Characteristics, Vision, and Visual Fuon Refraction,
Data Complete
(n � 1371)
Age (years), mean (SD) 14.5 (1.4)
Gender, n (%)
Male 551 (40.2%)
Female 820 (59.8%)
Parents’ highest education, n (%)
Primary or below 266 (19.4%)
Junior school 708 (51.6%)
High school 272 (19.8%)
College or above 46 (3.4%)
Missing 79 (5.8%)
Uncorrected vision in the better eye, n (%)
�6/12 753 (54.9%)
�6/12 618 (45.1%)
Presenting vision in the better eye, n (%)
�6/12 388 (28.3%)
�6/12 983 (71.7%)
Refractive error in the better eye, mean (SD) �1.93 (1.82)
Visual function score, mean (SD) 76.1 (16.0)
SD � standard deviation; VA � visual acuity.aP value for the comparison between children with normal vision
pproach the standard adult cut-offs of BMI �25 kg/m2 m
STUNTING AND REFRACTIOL. 149, NO. 2
nd BMI �30 kg/m2 respectively as the age of the childpproaches 19 years.30
INTERVIEW DATA: All study subjects were adminis-ered a Chinese-language questionnaire prior to being toldhe results of their vision assessment. The basic question-aire included questions on age, gender, highest educa-ional attainment by either parent, child’s history of glassesear, and reasons for glasses nonwear. The questionnaire
ncluded a Chinese translation of an instrument developedriginally by Fletcher and associates, to assess self-reportedisual function (VF) in rural Asia.31 This instrument hasreviously been validated for use in Chinese subjects,32
nd is described elsewhere in detail.31
STATISTICAL METHODS: A two-tailed Student t testas applied for group comparison if the data wereormally distributed. For skewed data, the Mann–Whit-ey U test was used. The �2 test was employed toompare group differences for categorical variables. Theearson correlation was used to evaluate the associationetween spherical equivalent (SE) and height by gen-er. Moreover, multiple linear regression analysis waserformed to examine the association between SE andeight and nutritional indicators, adjusting for age andarental education and stratifying by gender. Quantita-ive data were summarized either in mean (SD) or
for 1371 Rural Chinese Schoolchildren With Complete Datat, and Weight
Normal Vision
(VA �6/12 Both Eyes)
(n � 355, 25.9%)
Low Vision
(Uncorrected VA �6/12 Either Eye)
(n � 1016, 74.1%) P valuea
14.1 (1.1) 14.6 (1.4) �.001
184 (51.8%) 367 (36.1%) �.001
171 (48.2%) 649 (63.9%)
68 (19.2%) 198 (19.5%) .707
179 (50.4%) 529 (52.1%)
77 (21.7%) 195 (19.2%)
10 (2.8%) 36 (3.5%)
21 (5.9%) 58 (5.7%)
0 (0.0%) 753 (74.1%) �.001
355 (100.0%) 263 (25.9%)
1 (0.3%) 387 (38.1%) �.001
354 (99.7%) 629 (61.9%)
�0.48 (0.82) �2.44 (1.80) �.001
86.1 (13.0) 72.8 (15.5) �.001
low vision.
nctionHeigh
edian (interquartile range).
VE ERROR IN CHINA 349

Ca
A
sapdwrcutwc
1T
digc
w1a((a
nocog
snw
l chi
3
Statistical analyses were done using SPSS 14.0 (SPSS Inc,hicago, Illinois, USA). All statistical tests were two-sided,
nd a P value � .05 was considered statistically significant.
RESULTS
MONG 3,226 CHILDREN IN THE SAMPLE FRAME IN FUYANG
econdary schools, 2905 (90.0%) took part in the survey;mong those not taking part, 264 (8.2%) failed to obtainarental consent and 57 (1.8%) were absent from schooluring the survey period (Figure 1). Vision examinationsere completed on all but 0.2% of participants, while
efraction was carried out on a random 20% sample ofhildren with normal vision (n � 366) and 97% of those withncorrected VA �6/12 in either eye (n � 1,111). Amonghese 1477 children with refraction data, height and weightere measured for 1371 (92.8%) (Figure 1). These 1371hildren form the basis for the remaining analyses.
The mean age of children with complete data was4.5 � 1.4 years (range, 12 to 17 years), and 59.8% were girls.
TABLE 2. Analysis of Demographic Characteristics, Vision, Vi
Total Children
(n � 1364a)
Stunte
(n
Age (years), mean (SD) 14.5 (1.4) 14.7 (1.
Gender, n (%)
Male 549 (40.2%) 45 (51.7
Female 815 (59.8%) 42 (48.3
Height (cm), mean (SD) 155.7 (7.4) 144.4 (5.
BMI (kg/m2), median (interquartile
range) 18.0 (16.8 to 19.6) 17.0 (15
Parents’ highest education, n (%)
Primary or below 263 (19.3%) 23 (26.4
Junior school 705 (51.7%) 46 (52.9
High school 271 (19.9%) 11 (12.6
College or above 46 (3.4%) 4 (4.6%
Missing 79 (5.8%) 3 (3.4%
Presenting vision in the better eye,
n (%)
�6/12 386 (28.3%) 21 (24.1
�6/12 978 (71.7%) 66 (75.9
Child’s spherical equivalent in the
better, mean (SD) �1.93 (1.82) �1.91 (1
Visual function score, mean (SD) 76.1 (16.0) 76.9 (15
BMI � body mass index; SD � standard deviation.aOf the total 1371 subjects for whom height and weight m
overweight/obese were dropped from the analysis.bDefinition of stunting: height 2 SDs below the mean for age and gecDefinition of overweight: �1 SD above the mean BMI by age an
gender.dP value for the comparison between stunted children and overweP value for the comparison between stunted children and norma
he mean SE RE in the better-seeing eye was �1.93 � 1.82 g
AMERICAN JOURNAL OF50
iopters (D) (Table 1). Children with low vision (VA �6/12n either eye) were older, were significantly more likely to beirls, and had worse RE and self-reported visual function thanhildren with normal vision (Table 1).
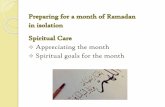
The mean height and BMI for children with complete dataere 156 � 7 cm and 18.0 kg/m2 (interquartile range, 16.8 to9.6 kg/m2) (Table 2). Height and RE were inversely associ-ted (that is, taller children were more myopic) among boysr � �0.147; P � .001) but not girls (r � �0.046,; P � .193)Figure 2). Height and RE were not significantly associatedmong boys (P � .46) or girls (P � .85) when adjusting for age.
The RE and presenting vision of stunted children didot differ significantly from those of either normal orbese/overweight children (Table 2). The lack of signifi-ant difference between stunted and normal or obese/verweight children persisted when data were stratified byender (data not shown).
In multivariate models predicting SE-RE in the better-eeing eye, when adjusting for age and parental education,either stunting nor height was significantly associatedith RE for the group of children as a whole, or for boys or
unction, and Refractive Error According to Nutritional Status
renbOverweight/Obese
Childrenc
(n � 79)
Normal Children
(n � 1,198)
P
valuedP
valuee
14.0 (1.30) 14.5 (1.3) .002 .260
39 (49.4%) 465 (38.8%) .762 .017
40 (50.6%) 733 (61.2%)
158.0 (6.4) 156.4 (6.8) �.001 �.001
18.6) 24.1 (23.2 to 25.9) 18.0 (16.8 to 19.3) �.001 �.001
14 (17.7%) 226 (18.9%) .106 .170
44 (55.7%) 615 (51.3%)
15 (19.0%) 245 (20.5%)
0 (0.0%) 42 (3.5%)
6 (7.6%) 70 (5.8%)
20 (25.3%) 345 (28.8%) .860 .352
59 (74.7%) 853 (71.2%)
�1.72 (1.88) �1.94 (1.82) .506 .883
75.6 (13.7) 76.0 (16.2) .590 .659
ements were available, 7 children who are both stunted and
according to the World Health Organization reference population.28
der. Definition of obese: �2 SD above the mean BMI by age and
/obese children.
ldren.
sual F
d Child
� 87)
4)
%)
%)
8)
.6 to
%)
%)
%)
)
)
%)
%)
.81)
.5)
easur
nder
d gen
eight
irls considered separately (Table 3).
OPHTHALMOLOGY FEBRUARY 2010

0w
D
ce
apptsaeb(
Fp
der; d
V
The power of the study to have detected a difference of.50 D in RE between stunted and normal children was 0.77,hile the power to detect a difference of 0.75 D was 0.96.
DISCUSSION
ATA FROM THIS COHORT OF RURAL SECONDARY SCHOOL
hildren suggests that stunting is unassociated with RE for
IGURE 2. The association of height and spherical equivalentarticipating in a study of height, stunting, and myopia in rura
TABLE 3. Association Between Spherical Equivalent and HEducation and S
Independent Variables
All (n � 1285a)
� value Standard Error P value
Model no.1: Nutritional status
Not stuntedb NA NA NA
Stunted �0.030 0.200 .880
Model no. 2: Nutritional status
Stunted NA NA NA
Overweight/obesec 0.013 0.284 .965
Normal 0.031 0.201 .876
Model no. 3: Height
Height (cm) �0.004 0.008 .599
BMI � body mass index; NA � not applicable.aOf the total 1371 subjects for whom height and weight m
overweight/obese were dropped from the analysis, as were 79 subjebDefinition of stunting: height 2 standard deviation (SD) below th
reference population.28
cDefinition of overweight: �1 SD above the mean BMI by age and gen
ither girls or boys. We chose to examine the plausibility of c
STUNTING AND REFRACTIOL. 149, NO. 2
link between nutrition and RE by investigating aopulation with a high prevalence of both myopia andoor nutrition, while focusing on children among whomhe influence of nutrition on height is expected to be mostalient: children with stunting. Although some childrenre naturally of short stature attributable to their geneticndowment, when this prevalence exceeds 2.5% (2 SDselow the mean), as in this cohort where 87 of 13646.4%) subjects were stunted, it is expected that many
ctive error in the better eye for male and female schoolchildrenina.
and Nutritional Indicators, Adjusting for Age and Parentalying by Gender
Male (n � 513a) Female (n � 772a)
alue Standard Error P value � value Standard Error P value
A NA NA NA NA NA
.191 0.263 .469 0.154 0.298 .605
A NA NA NA NA NA
.170 0.375 .651 �0.165 0.422 .697
.193 0.265 .467 �0.154 0.298 .607
.006 0.010 .531 �0.0004 0.014 .974
ements were available, 7 children who are both stunted and
ale � 36, female � 43) missing data for parents’ highest education.
n for age and gender according to the World Health Organization
efinition of obese: �2 SD above the mean BMI by age and gender.
refral Ch
eighttratif
� v
N
�0
N
0
0
�0
easur
cts (m
e mea
hildren have short stature as a result of poor nutrition.
VE ERROR IN CHINA 351

Obostopa
dcemdvTtcs
sndw
csdunaapn
tibvsol
malwhwus
smtbsfPw
ditcc
TCDpbP
3
ur failure to detect a difference in myopia prevalenceetween stunted children and those with normal stature,r children with overweight/obesity (thus eliminatingubjects with borderline nutritional status), is not consis-ent with a causative role for nutrition in the developmentf myopia in this population. This lack of an associationersisted when adjusting for age and parental educationnd stratifying by gender.
We considered the possibility that children of Chineseescent might naturally be of shorter stature than thehildren making up the WHO reference population. How-ver, when similar standard populations have been used toeasure ethnically Chinese children in economically less
isadvantaged areas, the prevalence of stunting has beenery low (for example, 0.2% in Singapore in 2000).33
hus, it would appear unlikely that a large proportion ofhe ethnically Chinese children classified as stunted ac-ording to the current study are in fact of shorter statureolely for genetic reasons.
Given the large number of children included in ourample and the relatively high prevalence of RE and poorutrition, the power to have detected visually significantifferences in RE between stunted and normal childrenas adequate.The results of this study must be understood within the
ontext of its limitations. Though a high prevalence oftunting as observed in this setting provides strong evi-ence of nutritional insufficiency among affected individ-als, we did not attempt to validate this with otherutritional indicators such as dietary recall or a record ofctual calories consumed. Height and weight measures asssessed by WHO cut-offs against the WHO standardopulation have been validated as robust indicators of
utritional status.34 y2888–2894.
AMERICAN JOURNAL OF52
Secondly, our study was cross-sectional, which meanthat the hypothesis that change in myopia status over times linked to longitudinal variations in nutriture could note directly examined. However, for this hypothesis to bealid, a minimum condition is that myopia and nutritionaltatus should be causally linked. Our cross-sectional datan stunting and myopia are not consistent with suchinkage.
Our sampling strategy over-sampled for children withyopia. Thus, it is possible that we failed to detect an
ssociation between myopia and stunting because of thearge number of myopic children included relative to thoseithout myopia. In order to reduce the chances of this,owever, we did include a 20% random sample of childrenith normal (�6/12) uncorrected vision in both eyes, andltimately obtained complete data on 355 such subjects,ome 26% of our total cohort.
Finally, our study design did not include an exhaustiveurvey of all potential environmental associations withyopia, potentially including near work,12,13 outdoor ac-
ivity,15,16 and population density.17 The possibility muste considered that an association might have been ob-erved between stunting and RE if these potential con-ounding factors had been measured and adjusted for.resumably, a strong association between stunting and REould have been detected with the current study design.Despite its limitations, this is one of the first studies to
irectly examine the association between stunting and REn a population at high-risk for both RE and poor nutri-ion. Our results do not appear consistent with a strongausative role for nutrition in determining the observedhanges in RE occurring among Chinese children in recent
ears.HIS STUDY WAS SUPPORTED BY A GRANT TO OXFORD UNIVERSITY FROM THE LI KA SHING FOUNDATION, HONG KONG,hina (the See Well to Learn Well Project). The authors indicate no financial conflict of interest. Involved in design and conduct of study (N.C., Y.G.,.S.C.L., L.L., M.Z., Y.S., S.G.); collection, management, analysis, and interpretation of data (A.S., N.C., Y.G., Y.L., Y.Y., Jin.W., Jia.W., Y.K.T.); andreparation, review, or approval of the manuscript (N.C., Y.G., Y.L., Y.Y., Jin.W., D.S.C.L., L.L., Jia.W., Y.K.T., M.Z., Y.S., S.G.). The protocol haseen approved in full by the Ethics Committees at the Chinese University of Hong Kong and the Joint Shantou International Eye Center, Guangdongrovince, China, and by the tenets of the Declaration of Helsinki.
REFERENCES
1. Zhao J, Pan X, Sui R, Munoz SR, Sperduto RD, EllweinLB. Refractive Error Study in Children: results fromShunyi District, China. Am J Ophthalmol 2000;129:427–435.
2. He M, Zeng J, Liu Y, Xu J, Pokharel GP, Ellwein LB.Refractive error and visual impairment in urban children insouthern China. Invest Ophthalmol Vis Sci 2004;45:793–799.
3. Congdon N, Wang Y, Song Y, et al. Visual disability, visualfunction, and myopia among rural Chinese secondary schoolchildren: the Xichang Pediatric Refractive Error Study(X-PRES) - Report 1. Invest Ophthalmol Vis Sci 2008;49:
4. Saw SM, Goh PP, Cheng A, Shankar A, Tan DTH, EllweinLB. Ethnicity-specific prevalences of refractive errors vary inAsian children in neighbouring Malaysia and Singapore. Br JOphthalmol 2006;90:1230–1235.
5. Fan DS, Lam DS, Lam RF, et al. Prevalence, incidence, andprogression of myopia of school children in Hong Kong.Invest Ophthalmol Vis Sci 2004;45:1071–1075.
6. Lin LL, Shih YF, Hsiao CK, Chen CJ, Lee LA, Hung PT.Epidemiologic study of the prevalence and severity of myopiaamong school children in Taiwan in 2000. J Formosa MedAssoc 2001;85:521–526.
7. Ip JM, Huynh SC, Robaei D, et al. Ethnic differences in theimpact of parental myopia: findings from a population-basedstudy of 12-year-old Australian children. Invest Ophthalmol
Vis Sci 2007;48:2520–2528.OPHTHALMOLOGY FEBRUARY 2010

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
V
8. Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopiain Taiwanese schoolchildren: 1983 to 2000. Ann Acad MedSingapore 2004;33:27–33.
9. Lin LL, Shih YF, Tsai CB, et al. Epidemiologic study ofocular refraction among school-children in Taiwan in 1995.Optom Vis Sci 1999;76:275–281.
0. Tay MT, Au Eong KG, Ng CY, Lim MK. Myopia andeducational attainment in 421,116 young Singaporean males.Ann Acad Med Singapore 1992;21:785–791.
1. Park DJ, Congdon N. Evidence for an “epidemic” of myopia.Ann Acad Med Singapore 2004;33:21–26.
2. Lu B, Congdon N, Liu X, et al. Associations between nearwork, outdoor activity and myopia among adolescent stu-dents in rural China: the Xichang Pediatric Refractive ErrorStudy report no. 2. Arch Ophthalmol 2009;127:769–775.
3. Saw S-M, Chua W-H, Hong C-Y, et al. Nearwork in early-onsetmyopia. Invest Ophthalmol Vis Sci 2002;43:332–339.
4. Mutti DO, Mitchell GL, Moeschbeger ML, Jones LA, ZadnikK. Parental myopia, near work, school achievement, andchildren’s refractive error. Invest Ophthalmol Vis Sci 2002;43:3633–3640.
5. Jones LA, Sinnott LT, Mutti DO, Mitchell GL, Moesch-berger ML, Zadnik K. Parental history of myopia, sports andoutdoor activities, and future myopia. Invest Ophthalmol VisSci 2007;48:3524–3532.
6. Rose KA, Morgan IG, Smith W, Burlutsky G, Mitchell P,Saw SM. Myopia, lifestyle, and schooling in students ofChinese ethnicity in Singapore and Sydney. Arch Ophthal-mol 2008;126:527–530.
7. Ip JM, Rose KA, Morgan IG, Burlutsky G, Mitchell P.Myopia and the urban environment: findings in a sample of12-year-old Australian school children. Invest OphthalmolVis Sci 2008;49:3858–3863.
8. Wang JJ, Study Group of Body Constitution and HealthStatus in Students Of Guangxi Zhuang Autonomous Region.Dynamic observations of their body constitution status inZhuang students of Guangxi from 1985 to 2000. ZhonghuaYu Fang Yi Xue Za Zhi 2002;36:84–88.
9. Yang XG, Li YP, Ma GS, et al. Study on weight and heightof the Chinese people and the differences between 1992 and2002. Zhonghua Liuxingbingxue zazhi 2005;26:489–493.
0. Weale RA. Epidemiology of refractive errors and presbyopia.Surv Ophthalmol 2003;48:515–543.
1. Saw SM, Chua WH, Hong CY, et al. Height and its relation-ship to refraction and biometry parameters in Singapore Chi-
nese children. Invest Ophthalmol Vis Sci 2002;43:1408–1413.STUNTING AND REFRACTIOL. 149, NO. 2
2. Wong TY, Foster PJ, Johnson GJ, Klein BEK, Seah SKL. Therelationship between ocular dimensions and refraction withadult stature: the Tanjong Pagar survey. Invest OphthalmolVis Sci 2001;42:1237–1242.
3. Ojaimi E, Morgan IG, Robaei D, et al. Effect of stature andother anthropometric parameters on eye size and refractionin a population-based study of Australian children. InvestOphthalmol Vis Sci 2005;46:4424–4429.
4. Rosner M, Laor A, Belkin M. Myopia and stature: findings ina population of 106,926 males. Eur J Ophthalmol 1995;5:1–6.
5. Edwards MH. Do variations in normal nutrition play a role inthe development of myopia? Optom Vis Sci 1996;73:638–643.
6. Cordain L, Eaton SB, Miller JB, Lindeberg S, Jensen C. Anevolutionary analysis of the aetiology and pathogenesis ofjuvenile-onset myopia. Acta Ophthalmol Scand 2002;80:125–135.
7. Matsumura H, Hirai H. Prevalence of myopia and refractivechanges in students from 3 to 17 years of age. Surv Ophthal-mol 1999;44:S109–115.
8. Growth Charts for Reference Population. Available at:http://www.who.int/growthref/en/. Accessed: October 28,2008.
9. Habicht JP, Pelletier DL. The importance of context inchoosing nutritional indicators [review]. J Nutr 1990;120:S1519–S1524.
0. Index of BMI by Age. Available at: http://www.who.int/growthref/who2007_bmi_for_age/en/index.html. Accessed:October 28, 2008.
1. Fletcher AE, Ellwein LB, Selvaraj S, Vijaykumar V,Rahmathullah R, Thulasiraj RD. Measurements of visionfunction and quality of life in patients with cataractsin Southern India. Arch Ophthalmol 1997;115:767–774.
2. He M, Xu J, Li S, Wu K, Munoz SR, Ellwein LB. Visualacuity and quality of life in patients with cataract in DoumenCounty, China. Ophthalmology 1999;106:1609–1615.
3. Under-nutrition and Stunting. Available at: http://www.childinfo.org/undernutrition_stunting.php. Accessed: November 5, 2008.
4. Lapidus N, Luquero FJ, Gaboulaud V, Shepherd S, Grais RF.Prognostic accuracy of WHO growth standards to predictmortality in a large-scale nutritional program in Niger. PLoS
Med 2009;6:e1000039.VE ERROR IN CHINA 353

Acfcm
3
Biosketch
bhishek Sharma, MBBS, is a medical doctor from Australia, graduating from University of Tasmania in 2004, andompleted a Masters in Medicine from University of Sydney in 2008. He is currently completing a DPhil in Public Healthrom the University of Oxford as a Rhodes Scholar, working on the Xichang Pediatric Refractive Error Study inonjunction with Chinese University of Hong Kong. He is interested in clinical science and public health research inyopia.
AMERICAN JOURNAL OF OPHTHALMOLOGY53.e1 FEBRUARY 2010