health - Western Cape Government
137
20 th Floor, 4 Dorp Street, Cape Town P O Box 2060, Cape Town, 8000 Tel: +27 21 483 3647 Fax: 086 276 4673 westerncape.gov.za OFFICE OF HEAD: HEALTH REF: 16/4 ENQUIRIES: DR K CLOETE TO ALL PROVINCIAL TOP MANAGEMENT SMS MEMBERS HEADS OF FACILITIES CIRCULAR H 67 OF 2020: PROVINCIAL PALLIATIVE CARE POSITION STATEMENT & PLAN FOR COVID-19 RESPONSE Purpose The purpose of this document is to clarify the Western Cape Government Health (WCGH) Palliative Care position statement and plan for the COVID-19 response. This will include the following categories of palliative care patients: Known Palliative Care patients who are COVID-19 negative Known Palliative Care patients who are diagnosed with COVID-19 COVID-19 diagnosed patients that will require Palliative Care Yours sincerely DR KEITH CLOETE HEAD: WESTERN CAPE DEPARTMENT OF HEALTH DATE: 11 MAY 2020
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of health - Western Cape Government
20th Floor, 4 Dorp Street, Cape Town P O Box 2060, Cape Town, 8000
Tel: +27 21 483 3647 Fax: 086 276 4673 westerncape.gov.za
OFFICE OF HEAD: HEALTH
REF: 16/4
ENQUIRIES: DR K CLOETE
TO ALL
PROVINCIAL TOP MANAGEMENT
SMS MEMBERS
HEADS OF FACILITIES
CIRCULAR H 67 OF 2020: PROVINCIAL PALLIATIVE CARE POSITION STATEMENT & PLAN FOR COVID-19
RESPONSE
Purpose
The purpose of this document is to clarify the Western Cape Government Health (WCGH) Palliative Care
position statement and plan for the COVID-19 response. This will include the following categories of palliative
care patients:
Known Palliative Care patients who are COVID-19 negative
Known Palliative Care patients who are diagnosed with COVID-19
COVID-19 diagnosed patients that will require Palliative Care
Yours sincerely
DR KEITH CLOETE
HEAD: WESTERN CAPE DEPARTMENT OF HEALTH
DATE: 11 MAY 2020

Page | 0
Provincial Palliative Care Position Statement & Plan
for COVID-19 Response
1. Purpose
The purpose of this document is to clarify the Western Cape Government Health (WCGH) Palliative Care
position statement and plan for the COVID-19 response. This will include the following categories of palliative
care patients:
• Known Palliative Care patients who are COVID-19 negative
• Known Palliative Care patients who are diagnosed with COVID-19
• COVID-19 diagnosed patients that will require Palliative Care
2. Palliative Care in the face of COVID-19
Palliative care is NOT only End of Life Care!!! Palliative care is an
interdisciplinary team approach that improves the quality of life of
patients (adults and children) and their families facing the problems
associated with life-threatening illness, through the prevention and
relief of suffering by means of early identification and impeccable
assessment and treatment of pain and other problems: physical,
psychosocial and spiritual. It begins when illness is diagnosed and
continues regardless of whether or not a person receives treatment
directed at the disease.
i) Known Palliative Care Patients who are COVID-19
negative
These patients have been assessed as eligible for palliation using the
SPICT (Supportive and Palliative Care Indicator Tool) or ACTS
(Association for Children with Life-Threatening & Life-Limiting
conditions) tools and are currently in care at any level within the
health system. The largest proportion of these patients are cared for
in their homes often by family members with support from
community health workers and the PHC clinical team, and hospice
staff if registered with hospice. These patients may be identified by
the purple ‘butterfly’ stamp on their folders or clinic cards; however,
it is notable that not all institutions use this stamp yet.
Page | 1
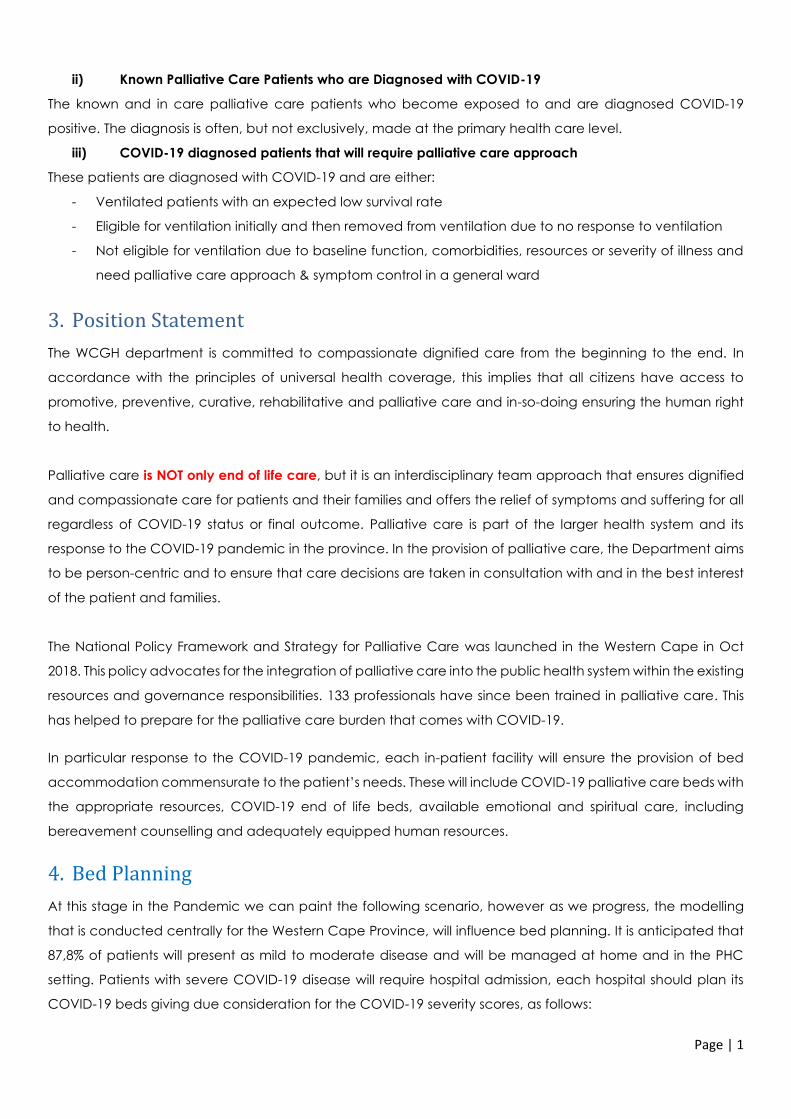
ii) Known Palliative Care Patients who are Diagnosed with COVID-19
The known and in care palliative care patients who become exposed to and are diagnosed COVID-19
positive. The diagnosis is often, but not exclusively, made at the primary health care level.
iii) COVID-19 diagnosed patients that will require palliative care approach
These patients are diagnosed with COVID-19 and are either:
- Ventilated patients with an expected low survival rate
- Eligible for ventilation initially and then removed from ventilation due to no response to ventilation
- Not eligible for ventilation due to baseline function, comorbidities, resources or severity of illness and
need palliative care approach & symptom control in a general ward
3. Position Statement
The WCGH department is committed to compassionate dignified care from the beginning to the end. In
accordance with the principles of universal health coverage, this implies that all citizens have access to
promotive, preventive, curative, rehabilitative and palliative care and in-so-doing ensuring the human right
to health.
Palliative care is NOT only end of life care, but it is an interdisciplinary team approach that ensures dignified
and compassionate care for patients and their families and offers the relief of symptoms and suffering for all
regardless of COVID-19 status or final outcome. Palliative care is part of the larger health system and its
response to the COVID-19 pandemic in the province. In the provision of palliative care, the Department aims
to be person-centric and to ensure that care decisions are taken in consultation with and in the best interest
of the patient and families.
The National Policy Framework and Strategy for Palliative Care was launched in the Western Cape in Oct
2018. This policy advocates for the integration of palliative care into the public health system within the existing
resources and governance responsibilities. 133 professionals have since been trained in palliative care. This
has helped to prepare for the palliative care burden that comes with COVID-19.
In particular response to the COVID-19 pandemic, each in-patient facility will ensure the provision of bed
accommodation commensurate to the patient’s needs. These will include COVID-19 palliative care beds with
the appropriate resources, COVID-19 end of life beds, available emotional and spiritual care, including
bereavement counselling and adequately equipped human resources.
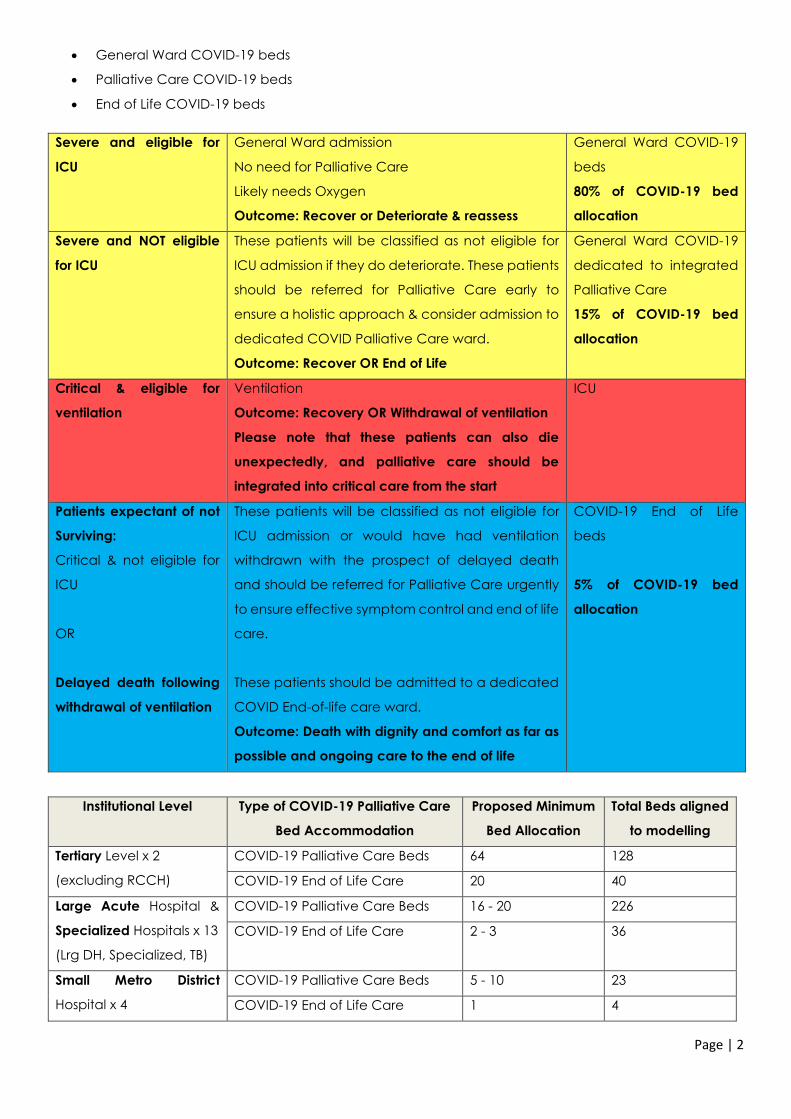
4. Bed Planning
At this stage in the Pandemic we can paint the following scenario, however as we progress, the modelling
that is conducted centrally for the Western Cape Province, will influence bed planning. It is anticipated that
87,8% of patients will present as mild to moderate disease and will be managed at home and in the PHC
setting. Patients with severe COVID-19 disease will require hospital admission, each hospital should plan its
COVID-19 beds giving due consideration for the COVID-19 severity scores, as follows:
Page | 2
• General Ward COVID-19 beds
• Palliative Care COVID-19 beds
• End of Life COVID-19 beds
Severe and eligible for
ICU
General Ward admission
No need for Palliative Care
Likely needs Oxygen
Outcome: Recover or Deteriorate & reassess
General Ward COVID-19
beds
80% of COVID-19 bed
allocation
Severe and NOT eligible
for ICU
These patients will be classified as not eligible for
ICU admission if they do deteriorate. These patients
should be referred for Palliative Care early to
ensure a holistic approach & consider admission to
dedicated COVID Palliative Care ward.
Outcome: Recover OR End of Life
General Ward COVID-19
dedicated to integrated
Palliative Care
15% of COVID-19 bed
allocation
Critical & eligible for
ventilation
Ventilation
Outcome: Recovery OR Withdrawal of ventilation
Please note that these patients can also die
unexpectedly, and palliative care should be
integrated into critical care from the start
ICU
Patients expectant of not
Surviving:
Critical & not eligible for
ICU
OR
Delayed death following
withdrawal of ventilation
These patients will be classified as not eligible for
ICU admission or would have had ventilation
withdrawn with the prospect of delayed death
and should be referred for Palliative Care urgently
to ensure effective symptom control and end of life
care.
These patients should be admitted to a dedicated
COVID End-of-life care ward.
Outcome: Death with dignity and comfort as far as
possible and ongoing care to the end of life
COVID-19 End of Life
beds
5% of COVID-19 bed
allocation
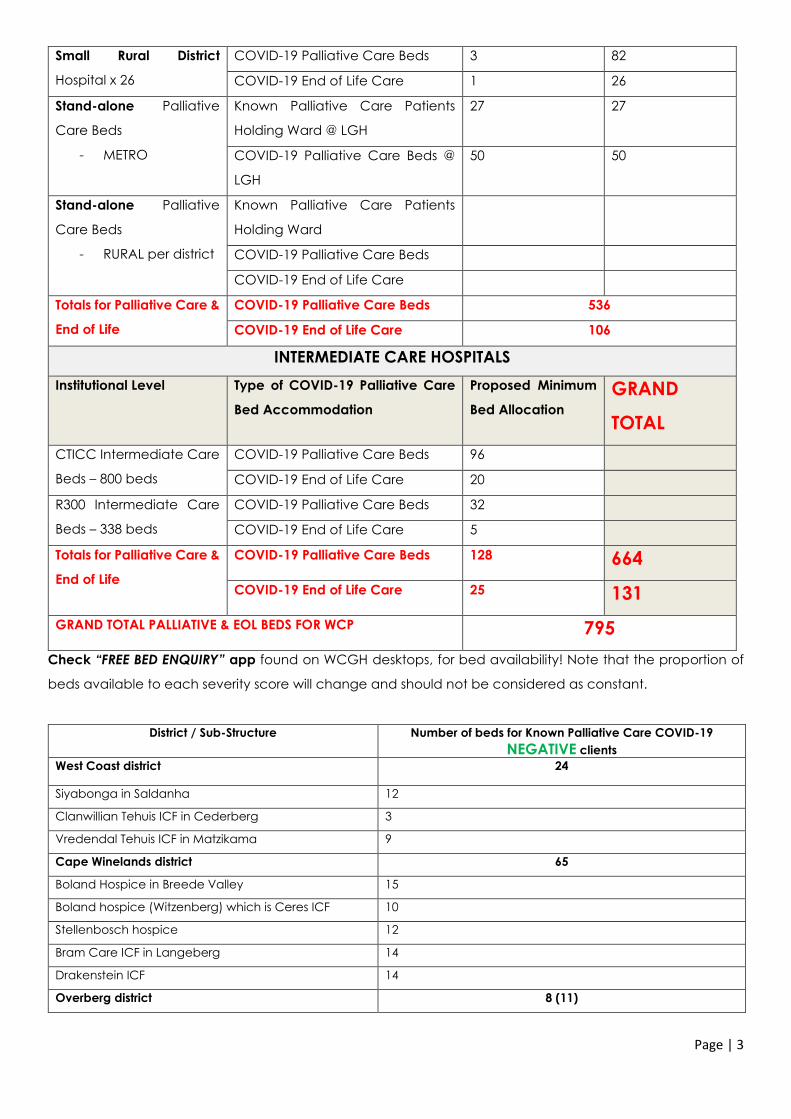
Institutional Level Type of COVID-19 Palliative Care
Bed Accommodation
Proposed Minimum
Bed Allocation
Total Beds aligned
to modelling
Tertiary Level x 2
(excluding RCCH)
COVID-19 Palliative Care Beds 64 128
COVID-19 End of Life Care 20 40
Large Acute Hospital &
Specialized Hospitals x 13
(Lrg DH, Specialized, TB)
COVID-19 Palliative Care Beds 16 - 20 226
COVID-19 End of Life Care 2 - 3 36
Small Metro District
Hospital x 4
COVID-19 Palliative Care Beds 5 - 10 23
COVID-19 End of Life Care 1 4
Page | 3
Small Rural District
Hospital x 26
COVID-19 Palliative Care Beds 3 82
COVID-19 End of Life Care 1 26
Stand-alone Palliative
Care Beds
- METRO
Known Palliative Care Patients
Holding Ward @ LGH
27 27
COVID-19 Palliative Care Beds @
LGH
50 50
Stand-alone Palliative
Care Beds
- RURAL per district
Known Palliative Care Patients
Holding Ward
COVID-19 Palliative Care Beds
COVID-19 End of Life Care
Totals for Palliative Care &
End of Life
COVID-19 Palliative Care Beds 536
COVID-19 End of Life Care 106
INTERMEDIATE CARE HOSPITALS
Institutional Level Type of COVID-19 Palliative Care
Bed Accommodation
Proposed Minimum
Bed Allocation
GRAND
TOTAL
CTICC Intermediate Care
Beds – 800 beds
COVID-19 Palliative Care Beds 96
COVID-19 End of Life Care 20
R300 Intermediate Care
Beds – 338 beds
COVID-19 Palliative Care Beds 32
COVID-19 End of Life Care 5
Totals for Palliative Care &
End of Life
COVID-19 Palliative Care Beds 128 664
COVID-19 End of Life Care 25 131
GRAND TOTAL PALLIATIVE & EOL BEDS FOR WCP 795
Check “FREE BED ENQUIRY” app found on WCGH desktops, for bed availability! Note that the proportion of
beds available to each severity score will change and should not be considered as constant.
District / Sub-Structure Number of beds for Known Palliative Care COVID-19
NEGATIVE clients
West Coast district 24
Siyabonga in Saldanha 12
Clanwillian Tehuis ICF in Cederberg 3
Vredendal Tehuis ICF in Matzikama 9
Cape Winelands district 65
Boland Hospice in Breede Valley 15
Boland hospice (Witzenberg) which is Ceres ICF 10
Stellenbosch hospice 12
Bram Care ICF in Langeberg 14
Drakenstein ICF 14
Overberg district 8 (11)
Page | 4
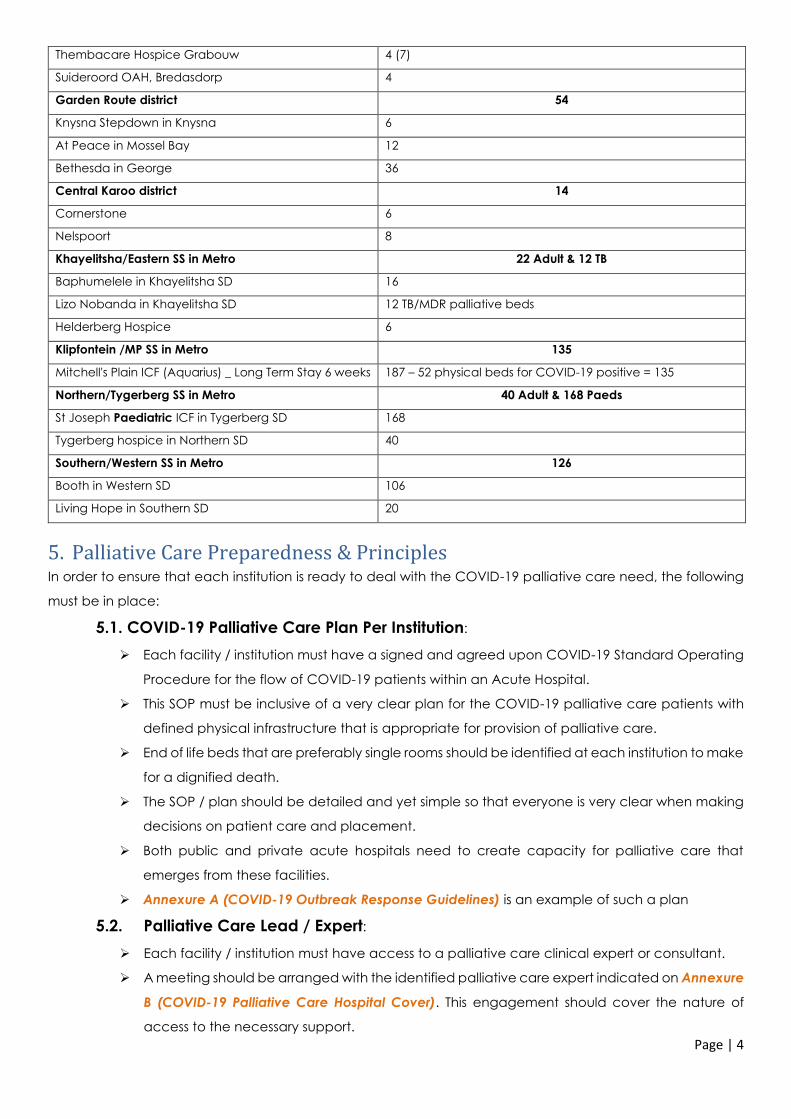
Thembacare Hospice Grabouw 4 (7)
Suideroord OAH, Bredasdorp 4
Garden Route district 54
Knysna Stepdown in Knysna 6
At Peace in Mossel Bay 12
Bethesda in George 36
Central Karoo district 14
Cornerstone 6
Nelspoort 8
Khayelitsha/Eastern SS in Metro 22 Adult & 12 TB
Baphumelele in Khayelitsha SD 16
Lizo Nobanda in Khayelitsha SD 12 TB/MDR palliative beds
Helderberg Hospice 6
Klipfontein /MP SS in Metro 135
Mitchell's Plain ICF (Aquarius) _ Long Term Stay 6 weeks 187 – 52 physical beds for COVID-19 positive = 135
Northern/Tygerberg SS in Metro 40 Adult & 168 Paeds
St Joseph Paediatric ICF in Tygerberg SD 168
Tygerberg hospice in Northern SD 40
Southern/Western SS in Metro 126
Booth in Western SD 106
Living Hope in Southern SD 20
5. Palliative Care Preparedness & Principles In order to ensure that each institution is ready to deal with the COVID-19 palliative care need, the following
must be in place:
5.1. COVID-19 Palliative Care Plan Per Institution:
➢ Each facility / institution must have a signed and agreed upon COVID-19 Standard Operating
Procedure for the flow of COVID-19 patients within an Acute Hospital.
➢ This SOP must be inclusive of a very clear plan for the COVID-19 palliative care patients with
defined physical infrastructure that is appropriate for provision of palliative care.
➢ End of life beds that are preferably single rooms should be identified at each institution to make
for a dignified death.
➢ The SOP / plan should be detailed and yet simple so that everyone is very clear when making
decisions on patient care and placement.
➢ Both public and private acute hospitals need to create capacity for palliative care that
emerges from these facilities.
➢ Annexure A (COVID-19 Outbreak Response Guidelines) is an example of such a plan
5.2. Palliative Care Lead / Expert:
➢ Each facility / institution must have access to a palliative care clinical expert or consultant.
➢ A meeting should be arranged with the identified palliative care expert indicated on Annexure
B (COVID-19 Palliative Care Hospital Cover). This engagement should cover the nature of
access to the necessary support.
Page | 5
➢ Each facility must sign a volunteer contract with the palliative care experts who are not in
employ within the WCGH and who are not covered by a bilateral or multilateral agreement.
5.3. Ethics Committees
The Provincial Clinical Ethics Committee has been established. Representatives include an
independent chairperson, reps from GSH, TBH, Private sector, and Legal. A representative for Palliative
care will be available to them. The Committee aims to support both clinicians in decision-making and
families where required.
5.4. Spiritual Care & Bereavement Counsellors
➢ Each District or Sub-Structure must actively recruit volunteers to provide spiritual care and grief
support. A database must be established from which each hospital and facility can access
support for patients and families
➢ The District or Sub-Structure must engage Department of Social Development to set up access
to additional social workers to support the WCGH. The DSD has established an SOP that
encourages collaboration.
➢ The social worker at each facility / institution must be able to access volunteer database and
continuously and actively recruit more volunteers to be trained in navigating grief and
engaging spirituality.
➢ Each social worker within the health system should also be trained in navigating grief and
engaging spirituality.
5.5. Training Programmes
It is imperative to ensure that staff providing care in the palliative care wards and environments are
adequately trained to holistically manage the client appropriately in a compassionate manner. Most
of the staff are not palliative care trained and will require further training. All training videos are easily
accessible on https://coronavirus.westerncape.gov.za/health-workers
5.5.1. Training Programmes on PalPrac Guidelines
The training programmes offered by PalPrac and based on Annexure C PALPRAC Guidelines is crucial
in order to be able to manage the palliative care client. The target audience is frontline clinicians, i.e.
Medical Officers and Professional Nurses. For those who did not attend the webinars, the 1 hr training
videos can be accessed online.
• Transitioning from Critical care to Palliative Care:
Addresses the spectrum of care for an in-patient palliative care patient and ranges from deciding on
eligibility for palliative care to withdrawal from ventilation to end of life care and appropriate
compassionate communication.
• Protecting, caring & supporting palliative care patients during COVID-19:
Addresses the process of rapid regression of a known palliative care patient who develops COVID-19
infection. There is constant and clear attention being drawn to providing compassionate care and
preserving the client’s dignity and managing challenging symptoms.
Page | 6
5.5.2. Training in Spiritual Care and Bereavement Support
Psycho-Social care, Spiritual care & Bereavement support training programmes are also crucial
components of palliative care. This gap within the public sector system will be closed as follows:
➢ Each district or sub-structure identifies a coordinator for spiritual care and bereavement support
➢ This coordinator will actively recruit and hold a database of counsellors, spiritual carers and
bereavement supporters. Target social workers, psychologists, other staff, NGOs, FBOs, religious
leaders, etc, within their geographic area to volunteer (use the standard process of acquiring
volunteers for COVID-19 for those who are not employed within the WCGH).
➢ For those who have not attended the two training webinars, the 1hour training videos are
available on the above link as well:
• Navigating Grief in Healthcare in the face of COVID-19:
Aimed at equipping healthcare professionals, faith leaders and lay counsellors with key skills to
support themselves and others through loss and grief in response to the pandemic
• Engaging Spirituality in Healthcare in the face of COVID-19:
Aimed at providing healthcare professionals, faith leaders and lay counsellors with the essential skills
for engaging spiritual matters in response to the pandemic
5.5.3. Breaking bad news
It is not second nature or simple for all clinicians to have difficult conversations with patients and their
family. Psychological and emotional work associated with dealing with clients at the end of life can
also have a negative impact on staff if self-care is not adequate and staff do not take a moment to
pause and process what they deal with daily. Training in Breaking bad news and Building Hope is
offered in the form of a 1-hour webinar and the video can be accessed on the above link.
5.6. Communication
➢ During this time can be extremely difficult and emotional burden will increase significantly. It is
however crucial that all relevant clinical and non-clinical staff are supported in acquiring the
necessary communication skills that are necessary to break bad news and build hope.
➢ In addition to this, managers and supervisors in these wards and units will be faced with various
scenarios that will require a degree of emotional maturity and clarity regarding what and how
to respond. Key communication tips are contained in the attached document:
(PalPrac 2020: p13 – 18). In addition, healthcare workers are encouraged to practice self-care and
to seek support if needed. (PalPrac 2020: p28-32).
➢ Communication with counsellors and family will require access to digital technology that is
adequate. Families will be saying goodbye to loved ones virtually with no touch. This will need
to be facilitated using tablets.
5.7. Procurement & Supply Chain
➢ Tablets: each hospital must ensure that they have at least 2 tablets to facilitate communication
between the patient and family as well as the spiritual & grief counsellor. The tertiary hospitals
and field hospitals will have to order proportionate to bed numbers for palliative care.
➢ Sub-cutaneous Syringe Drivers: administration of medicines related to pain management,
anxiety, etc requires a sub-cutaneous syringe driver

Page | 7
➢ Consider additional cost for items related to palliative care: i.e. ripple mattresses, urine bags,
adult diapers – see costing in section 8.
5.8. Referral processes
Referrals and carting confirmed COVID-19 cases across the service platform is not advisable due to
risk of transmission. However, should clients require referral due to bed constraints, the VULA APP will
be utilised to communicate such referrals once a bed has been located on the FREE BED ENQUIRY”
app.
6. The Patient Flow
Known Palliative Care Patients – COVID-19 NEGATIVE
Ensure continuity of care
during lock down.
Provide an extra medication kit:
- Symptom control
- Anticipatory symptoms
Morphine cannot be prescribed & issued on a repeat prescription. Should
the patient require more Morphine, a new prescription must be issued and
the primary health care (PHC) facility can liaise with a family member for
collection or send with the attending CHW.
Page | 8
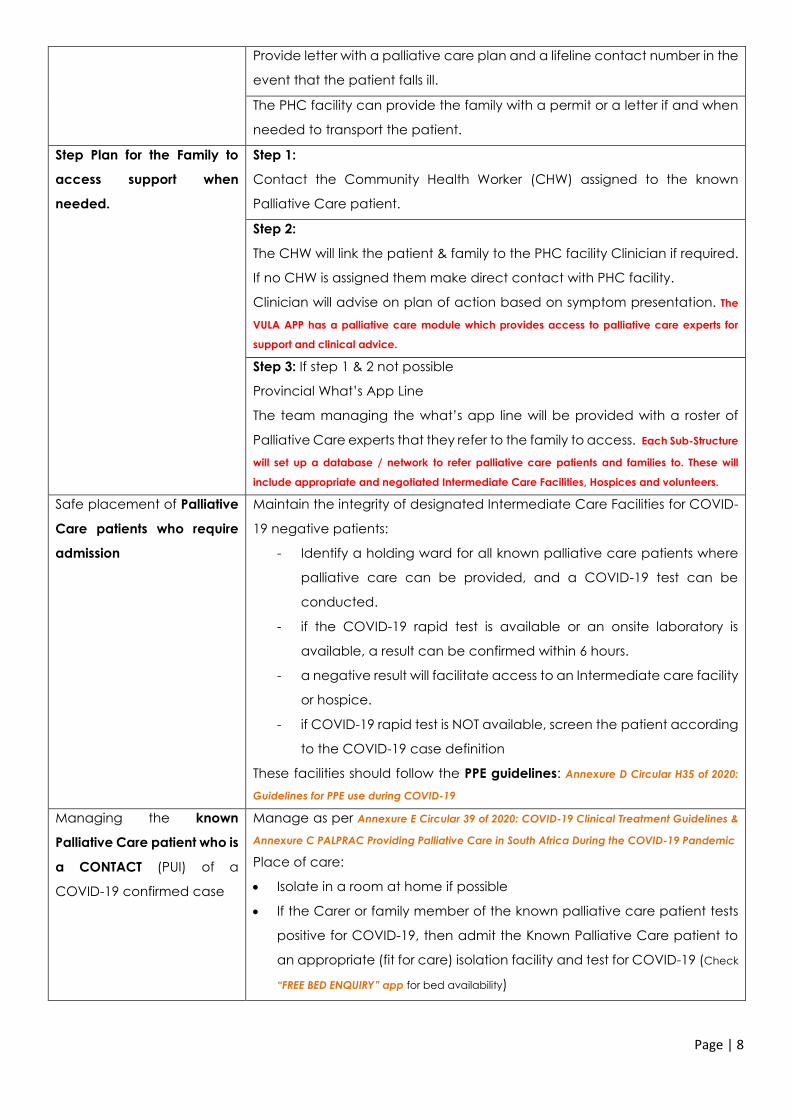
Provide letter with a palliative care plan and a lifeline contact number in the
event that the patient falls ill.
The PHC facility can provide the family with a permit or a letter if and when
needed to transport the patient.
Step Plan for the Family to
access support when
needed.
Step 1:
Contact the Community Health Worker (CHW) assigned to the known
Palliative Care patient.
Step 2:
The CHW will link the patient & family to the PHC facility Clinician if required.
If no CHW is assigned them make direct contact with PHC facility.
Clinician will advise on plan of action based on symptom presentation. The
VULA APP has a palliative care module which provides access to palliative care experts for
support and clinical advice.
Step 3: If step 1 & 2 not possible
Provincial What’s App Line
The team managing the what’s app line will be provided with a roster of
Palliative Care experts that they refer to the family to access. Each Sub-Structure
will set up a database / network to refer palliative care patients and families to. These will
include appropriate and negotiated Intermediate Care Facilities, Hospices and volunteers.
Safe placement of Palliative
Care patients who require
admission
Maintain the integrity of designated Intermediate Care Facilities for COVID-
19 negative patients:
- Identify a holding ward for all known palliative care patients where
palliative care can be provided, and a COVID-19 test can be
conducted.
- if the COVID-19 rapid test is available or an onsite laboratory is
available, a result can be confirmed within 6 hours.
- a negative result will facilitate access to an Intermediate care facility
or hospice.
- if COVID-19 rapid test is NOT available, screen the patient according
to the COVID-19 case definition
These facilities should follow the PPE guidelines: Annexure D Circular H35 of 2020:
Guidelines for PPE use during COVID-19
Managing the known
Palliative Care patient who is
a CONTACT (PUI) of a
COVID-19 confirmed case
Manage as per Annexure E Circular 39 of 2020: COVID-19 Clinical Treatment Guidelines &
Annexure C PALPRAC Providing Palliative Care in South Africa During the COVID-19 Pandemic
Place of care:
• Isolate in a room at home if possible
• If the Carer or family member of the known palliative care patient tests
positive for COVID-19, then admit the Known Palliative Care patient to
an appropriate (fit for care) isolation facility and test for COVID-19 (Check
“FREE BED ENQUIRY” app for bed availability)
Page | 9
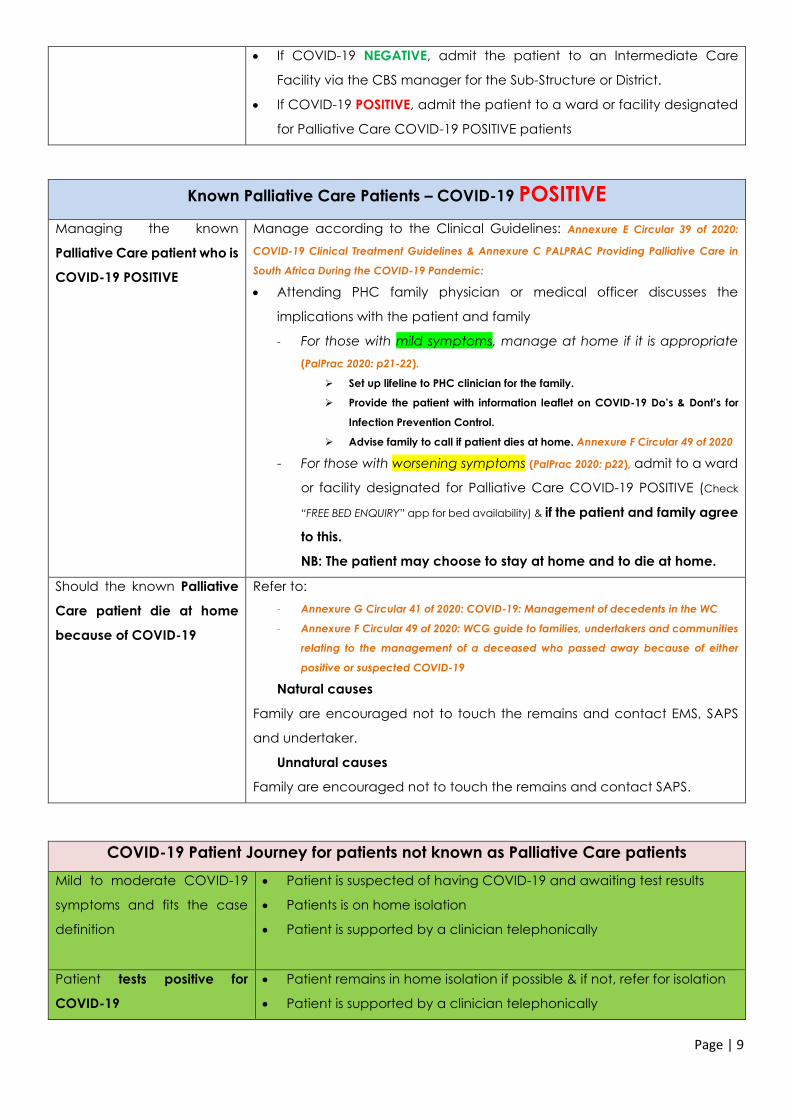
• If COVID-19 NEGATIVE, admit the patient to an Intermediate Care
Facility via the CBS manager for the Sub-Structure or District.
• If COVID-19 POSITIVE, admit the patient to a ward or facility designated
for Palliative Care COVID-19 POSITIVE patients
Known Palliative Care Patients – COVID-19 POSITIVE
Managing the known
Palliative Care patient who is
COVID-19 POSITIVE
Manage according to the Clinical Guidelines: Annexure E Circular 39 of 2020:
COVID-19 Clinical Treatment Guidelines & Annexure C PALPRAC Providing Palliative Care in
South Africa During the COVID-19 Pandemic:
• Attending PHC family physician or medical officer discusses the
implications with the patient and family
- For those with mild symptoms, manage at home if it is appropriate
(PalPrac 2020: p21-22).
➢ Set up lifeline to PHC clinician for the family.
➢ Provide the patient with information leaflet on COVID-19 Do’s & Dont’s for
Infection Prevention Control.
➢ Advise family to call if patient dies at home. Annexure F Circular 49 of 2020
- For those with worsening symptoms (PalPrac 2020: p22), admit to a ward
or facility designated for Palliative Care COVID-19 POSITIVE (Check
“FREE BED ENQUIRY” app for bed availability) & if the patient and family agree
to this.
NB: The patient may choose to stay at home and to die at home.
Should the known Palliative
Care patient die at home
because of COVID-19
Refer to:
- Annexure G Circular 41 of 2020: COVID-19: Management of decedents in the WC
- Annexure F Circular 49 of 2020: WCG guide to families, undertakers and communities
relating to the management of a deceased who passed away because of either
positive or suspected COVID-19
Natural causes
Family are encouraged not to touch the remains and contact EMS, SAPS
and undertaker.
Unnatural causes
Family are encouraged not to touch the remains and contact SAPS.
COVID-19 Patient Journey for patients not known as Palliative Care patients
Mild to moderate COVID-19
symptoms and fits the case
definition
• Patient is suspected of having COVID-19 and awaiting test results
• Patients is on home isolation
• Patient is supported by a clinician telephonically
Patient tests positive for
COVID-19
• Patient remains in home isolation if possible & if not, refer for isolation
• Patient is supported by a clinician telephonically

Page | 10
Symptoms worsen ➢ Supporting clinician refers patient to the PHC facility for
assessment
➢ Family Physician or Medical Officer clinically determines the
need for admission or further home care.
Patient requires admission ➢ Check “FREE BED ENQUIRY” app for bed availability
➢ Referral to COVID-19 general or field hospital based on bed
availability
On arrival at COVID-19
hospital
• Clinician conducts an assessment to determine the patient’s acuity.
Annexure E Circular 39 of 2020: COVID-19 Clinical Treatment Guidelines
➢ Patients are triaged or assessed by the clinical or emergency
medicine or critical care teams to determine ICU criteria and
palliative care needs.
Colour coded priority groups are assigned according to the critical
care guideline: Annexure H CSSA_Allocation of Scarce Critical Care Resources
during the COVID-19 Public Health Emergency in SA
Various tools can be used to identify a palliative care patient. Ultimately
the clinician makes the call and if this is not possible, a palliative care
expert can be consulted.
Patient not requiring
ventilation & eligible for
ventilation if deteriorates
Admission to a general ward for supportive therapy as per
Annexure E Circular 39 of 2020: COVID-19 Clinical Treatment Guidelines
Psychosocial support to patient and family
Patient eligible for ventilation Ventilation / critical care beds utilised
Integrate with palliative care as per relevant guidelines due to high risk of
death (PalPrac 2020: p7)
Psycho-social support to patient and family
Annexure H CSSA_Allocation of Scarce Critical Care Resources during the COVID-19 Public
Health Emergency in South Africa
Palliative care is impeccable care and not only end of life care. It is care that is intended to be
provided alongside standardised clinical care and all decisions will be made within the clinical
team with family involvement.
COVID-19 patient that may require Palliative Care approach
due to not being candidates for critical care or ventilation if deteriorates
Patient not requiring
ventilation or critical care, but
also not eligible for critical
care / ventilation if they
deteriorate – requires
palliative care
Allocated beds for COVID-19 palliative care are utilised & patient is
monitored. Oxygen Therapy & Pharmacological interventions as per
relevant guidelines (PalPrac 2020: p7-11 & Circular 39 of 2020: COVID-19 Clinical
Treatment Guidelines)
Patient outcome could be recovery or end of life.
Page | 11
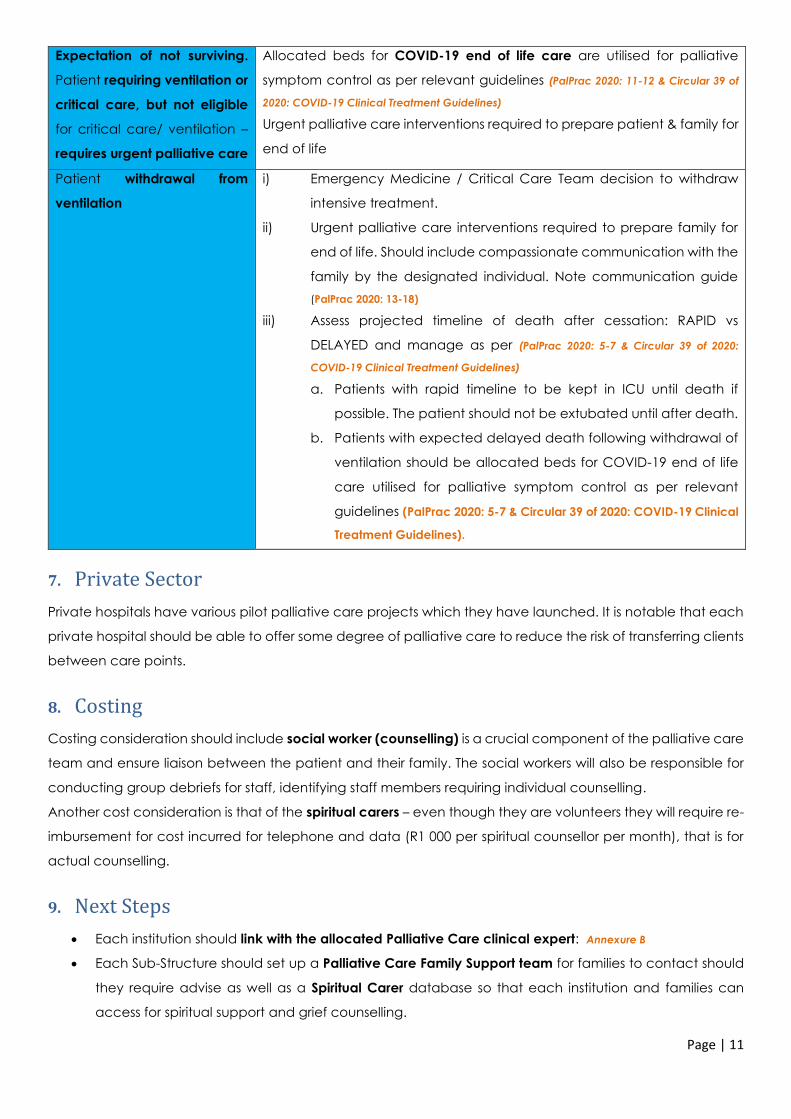
Expectation of not surviving.
Patient requiring ventilation or
critical care, but not eligible
for critical care/ ventilation –
requires urgent palliative care
Allocated beds for COVID-19 end of life care are utilised for palliative
symptom control as per relevant guidelines (PalPrac 2020: 11-12 & Circular 39 of
2020: COVID-19 Clinical Treatment Guidelines)
Urgent palliative care interventions required to prepare patient & family for
end of life
Patient withdrawal from
ventilation
i) Emergency Medicine / Critical Care Team decision to withdraw
intensive treatment.
ii) Urgent palliative care interventions required to prepare family for
end of life. Should include compassionate communication with the
family by the designated individual. Note communication guide
(PalPrac 2020: 13-18)
iii) Assess projected timeline of death after cessation: RAPID vs
DELAYED and manage as per (PalPrac 2020: 5-7 & Circular 39 of 2020:
COVID-19 Clinical Treatment Guidelines)
a. Patients with rapid timeline to be kept in ICU until death if
possible. The patient should not be extubated until after death.
b. Patients with expected delayed death following withdrawal of
ventilation should be allocated beds for COVID-19 end of life
care utilised for palliative symptom control as per relevant
guidelines (PalPrac 2020: 5-7 & Circular 39 of 2020: COVID-19 Clinical
Treatment Guidelines).
7. Private Sector
Private hospitals have various pilot palliative care projects which they have launched. It is notable that each
private hospital should be able to offer some degree of palliative care to reduce the risk of transferring clients
between care points.
8. Costing
Costing consideration should include social worker (counselling) is a crucial component of the palliative care
team and ensure liaison between the patient and their family. The social workers will also be responsible for
conducting group debriefs for staff, identifying staff members requiring individual counselling.
Another cost consideration is that of the spiritual carers – even though they are volunteers they will require re-
imbursement for cost incurred for telephone and data (R1 000 per spiritual counsellor per month), that is for
actual counselling.
9. Next Steps
• Each institution should link with the allocated Palliative Care clinical expert: Annexure B
• Each Sub-Structure should set up a Palliative Care Family Support team for families to contact should
they require advise as well as a Spiritual Carer database so that each institution and families can
access for spiritual support and grief counselling.

Page | 12
• Familiarise clinicians with the Palliative Care module on the VULA platform which is being expanded
beyond the pilot sites to include the entire Metro – palliative care experts will be on rotation to provide
support to clinicians regarding palliative care
• Each PHC and institution to check that known palliative care patients have access to extra
medication kit
• Check Palliative Care procurement needs and consider in planning and preparedness
• Access the Operational Guide to Implementing Palliative Care during COVID-19, guideline from sector
manager.
Contributors to this document
• Western Cape Palliative Care Task Team
• PALPRAC
• Clinicians, Managers, Public Health Specialists
• Partners
Annexures:
1. Annexure A: COVID-19 Outbreak Response Guidelines
2. Annexure B: COVID-19 Palliative Care Hospital Cover
3. Annexure C: PALPRAC_Providing Palliative Care in SA during the COVID-19 Pandemic
use the link below as the guideline will be updated https://palprac.org/for-healthcare-providers/palliativecarecovid-19/
4. Annexure D: Circular H35 of 2020: Guidelines for PPE use during COVID-19
5. Annexure E: Circular 39 of 2020: COVID-19 Clinical Treatment Guidelines
6. Annexure F: Circular 49 of 2020: WCG guide to families, undertakers and communities relating to the management of a deceased
who passed away because of either positive or suspected COVID-19
7. Annexure G: Circular H41 of 2020: Management of Decedents in the WC
8. Annexure H: CSSA_Allocation of Scarce Critical Care Resources during the COVID-19 Public Health Emergency in South Africa

1
WESTERN CAPE COVID-19 OUTBREAK
RESPONSE GUIDELINES
ACUTE HOSPITAL ADMISSIONS
Draft Document Version 4.1 - 30 April 2020
Annexure A

2
Acknowledgements:
1. WC Critical Care Forum - adapted from ICU – COVID-19 Response Guideline – 31 March 2020
2. Dr Neshaad Schrueder – Head: General Specialist Services – Tygerberg Hospital and Metro East
3. Dr Arifa Parker – Specialist Physician and Infectious Disease Specialist
4. Dr Mogamat Yazied Chothia – Specialist Physician and Nephrologist
5. Dr Abdurasiet Mowlana – Specialist Physician
6. Dr Sa’ad Lahri – Emergency Medicine Specialist
These guidelines are work in progress and are subject to change as the COVID-19 Pandemic unfolds in South Africa
3
Contents
Section A: Introduction
1. Executive summary
2. Fundamental issues in dealing with COVID-19
Section B: Planning and Preparedness
3. Legal, regulatory and ethical framework
4. Surge capacity
4.1. Isolation and critical care areas
4.2. Other patient care areas
4.3. Rapid discharges
4.4. Temporary transit lounges
4.5. Morgue capacity
5. Inter-hospital mutual aid agreements
6. Incident management structure
7. Roles and responsibilities
8. Infection prevention and control
9. Training
10. Safety and security
Section C: Operations
11. Proportionate response
11.1. Business continuity
11.2. Comorbidity
11.3. Critical care triage (assessment and escalation criteria)
12. Clinical Management of COVID-19 patients
12.1. Triage and Testing of Patients with suspected COVID-19
12.2. Admission of COVID-19 patients
12.3. Clinical care of COVID-19 patients
13. Implementation
14. Triggers and thresholds
15. Escalation
16. Contingency plans
17. De-escalation and return to normal function
18. Data collection, storage and protection
19. Communication
20. Event stages and activities
21. Staff support and debriefing
22. Annexure A Standard Operating Procedure for Triage and Testing Centre
23. Annexure B Standard operating procedure for flow of COVID-19 patients within Acute Hospital
24. Annexure C Patient Flow of COVID-19 cases
4
Section A: Introduction
1. Executive Summary
1.1.1. This document represents a consensus on the approach to managing the outbreak of SARS-CoV-2 in
the Western Cape.
1.1.2. There is currently little or no robust data on the management of patients with SARS-CoV-2 in the
literature. The content of this document has been put together based on the limited information
available, international recommendations and guidelines, the experience of international colleagues,
the participating clinicians and information that has come forth on the internet and through social
media.
1.1.3. It is proposed that 10 to 20 percent of all COVID-19 cases may need hospitalisation, including ICU care.
1.1.4. Depending on the success of mitigation efforts to contain the pandemic, there may be a demand for
inpatient care that outstrips resources available to deal with the load.
1.2. The main objectives of the guidelines contained in this document are to:
1.2.1. Maintain a standard of quality medical care
1.2.2. Direct scarce inpatient care resources as efficiently and efficaciously as possible
1.2.3. Provide a coordinated and consistent approach for public hospitals across the Western Cape
2. Fundamental issues in dealing with COVID-19
2.1. The recommendations of the World Health Organisation are to attempt to contain the spread of disease through isolation. This will be upheld as far as is reasonably possible.
2.2. It is desirable to keep the movement of confirmed cases to an absolute minimum both within and between healthcare facilities.
2.3. It is desirable to keep the exposure of all categories of healthcare workers, support personnel and the general public to an absolute minimum.
2.4. To successfully manage an outbreak, the combined efforts of all healthcare facilities is required. Each hospital will have to contribute to the mitigation of the disease outbreak.
2.5. Close communication between hospitals with respect to the demand for inpatient beds is likely to be crucial
in trying to ensure the best outcome for as many patients as possible.
Section B: Planning and Preparedness
3. Legal, regulatory and ethical framework
The guidelines in this document conform to the following:
• National Health Act 61 of 2003
• Disaster Management Act 57 of 2002
o Regulations issued in terms of Section 27(2) as published in volume 657 of the Government
Gazette on 18 March 2020
• Health Professions Act 56 of 1974
• Nursing Act 33 of 2005
• Occupational Health and Safety Act 85 of 1993, as amended by the Occupational Health and Safety Act
181 of 1993
• All guidelines of relevant Professional Councils
• The following ethical duties:
o Non-maleficence (duty to do no harm and to prevent harm)
o Distributive justice (fair distribution of benefits and burdens)
o Autonomy (the patient or their surrogate can make an informed decision to refuse critical care
treatment)
5
As seen in other countries where healthcare systems have been overwhelmed by COVID-19, it may happen that
medical and nursing personnel exceed their scope of practice out of necessity. These circumstances are
extraordinary and unprecedented. While every effort will be made by incident management teams, medical
personnel and nursing personnel to abide by legal, regulatory and ethical standards, there may be actions taken
that cannot be justified or that may lead to harm. The following actions will warrant immediate disciplinary
action:
3.1. Theft of medication or supplies
3.2. Sharing of patients’ photographs or other confidential information on social media
3.3. Physical altercations with colleagues, patients or other members of the public
3.4. Disobedience of a direct order that results in harm to the patient
3.5. The unauthorised release of information to the press
4. Surge capacity
COVID-19 will increase the number of patients requiring inpatient care and will place a significant burden on our
system. The current reality is that limited capacity to expand inpatient care services exists. Medical wards in
public hospitals are almost always operating at full capacity. The major stumbling block to the expansion of
capacity will likely be in the form of staff constraint, particularly nursing. With the progression of the outbreak,
staff illness, fear and truancy are likely to limit the ability to expand services. The secondment of staff from other
components of the service may be needed to support inpatient care units. Each hospital must develop a surge
plan including bed capacity, equipment requirements as well a human resource plan.
To prepare for this surge in admissions, the following actions are recommended:
4.1. Isolation and Cohort rooms
Hospitals are advised to find suitable areas to convert into COVID-19 inpatient care units provided that
there is sufficient equipment and trained personnel to care for patients in these areas. Isolation rooms must
be identified and equipped for patients who require testing or are awaiting test results for COVID-19.
Cohort rooms must be identified for the confirmed cases requiring hospitalisation.
4.2. Other patient care areas
Providing isolation rooms and additional cohort care rooms will impact on the space available for other
patient care areas. Each hospital must make a careful assessment of which services can be deferred to free
up space for isolation rooms and cohort care rooms.
4.3. Rapid discharges
If potential COVID-19 patients still need to be admitted, but all available space has been allocated, and
healthcare services have already been deferred, it will become necessary to discharge patients to free up
beds. A rapid discharge policy that lists specific criteria and guidelines should be in place so that patients are
not randomly discharged, possibly needing to be readmitted at a later stage.
4.4. Temporary transit lounges
Areas will need to be identified for patients who have been rapidly discharged but who are unable to leave
the hospital immediately.
4.5. Mortuary capacity
With the current mortality rates in the country, the average 3% mortality rate associated with COVID-19
could lead to insufficient space in hospital and state mortuaries. Protocols such as coordination with private
mortuaries must be in place as soon as possible.
6
The pathway to access these beds is indicated in Annexure C
5. Inter-hospital mutual aid agreements
Where possible hospitals may agree to assist each other with resources, procedures and information
Records should be kept when equipment is transferred between hospitals or when personnel are rerouted to
other hospitals as this may have financial implications that need to be addressed later
6. Incident management structure
6.1. This section only applies if a specific hospital does not already have an incident management team.
6.2. The response to this outbreak follows an incident management approach, allowing hospitals to maintain a
level of autonomy while still fitting into the provincial incident management structure. Each hospital must
be able to make decisions for its circumstances to provide the highest level of care according to the
guidelines of this document.
6.3. The functions of the management structure will include making decisions about whether or not to escalate
or de-escalate event stages regardless of thresholds and triggers, making decisions regarding the inpatient
care of patients and the operations of the inpatient care units and adjusting the hospital’s response plan
when necessary.
6.4. The recommended members of the incident management team are:
6.4.1. Hospital CEO
6.4.2. Clinical Manager / Head of Internal Medicine / Head of Family Medicine
6.4.3. Senior Nurse Manager or Deputy
6.4.4. Assistant Manager of Nursing: Emergency Unit
6.4.5. Assistant Manager of Nursing: Inpatient Wards
6.4.6. Representative for facility management rep
6.4.7. IPC team
6.4.8. Representative for EHS
6.4.9. Representative for support services
7. Roles and responsibilities
Roles and responsibilities that relate specifically to the COVID-19 outbreak should be established for all affected
departments and/or services and assigned to specific people for communication to their departments. Job cards
can be created for these roles so that, should certain responsibilities be assigned to specific people, someone
else can easily fill that role when the designated person is not available.
7.1. General management
7.2. Nursing management
7.3. Allied health management
7.4. Equipment distribution and tracking (clinical technicians and asset management)
7.5. Procurement (supply chain management and those responsible for ordering agency staff)
7.6. Security
7.7. Food, water, linen, hygiene, etc.
7.8. Support services

7
7.9. Bed management
7.10. Public and media liaison
7.11. Communications, information technology and information management
8. Infection prevention and control
All institutions must ensure that staff are adequately prepared and practised in the appropriate and rational use
of personal protective equipment and infection control.
It is suggested that staff that will be in contact with patients with SARS-CoV-2 have their infection control
practises scrutinised and checked.
The latest National Covid-19 Infection and Prevention Control Guidelines Version must be used for guiding the
necessary PPE requirements for the various clinical activities.
9. Training
Training, at this point, should already have been done for all hospital personnel. Hands-on refresher training will
be necessary and can be conducted by IPC or intensive care Operational Managers. Full training sessions for
agency personnel may be practical or feasible. It is recommended that only experienced agency personnel be
allowed to care for infected patients and that these agency workers be included in any refresher courses or
training conducted in the hospital.
10. Safety and security
Each hospital must adhere to the latest visitor policy. Security will be needed for intensive care units and
isolation units to assist with limiting inappropriate access by unauthorised persons to clinical areas.
A control measure must be implemented to control access for personnel who have been asked to assist during
this outbreak but who are not employed by the hospital or working through a registered agency.
Vigilance in the affected areas is needed to prevent the theft of medication or supplies.
Section C: Operations
11. Proportionate response
11.1. Business continuity
While it is of utmost importance to provide the highest level of care to patients infected with COVID-19,
the treatment and care of other patients in intensive care units and throughout the rest of the hospital
cannot be jeopardised. The additional requirement for critical care beds and inpatient beds will impact the
normal functions of a hospital, but this effect must be limited for as long as possible. Any plans for the
expansion of the inpatient units and the implementation of additional isolation areas must be done in
consultation with affected areas.
11.2. Comorbidity
Inpatient care resources are always in high demand, and this outbreak will increase that demand. Difficult
decisions will have to be made in allocating limited resources when demand exceeds availability, including
the expanded inpatient care units. The assessment criteria will include comorbidity. Patients and their
relatives must be made aware of this. There is currently not enough known about how COVID-19 affects
patients with HIV and TB, which are both widespread in the Western Cape. As more information is made
available, it may affect the triage assessment of these patients.
11.3. Acute care triage (assessment and escalation criteria)
At the outset, it must be appreciated that many patients will present as acute respiratory infection, of which
only a subgroup will have SARS-Cov-2 as an aetiologic agent. There is little need to alter the management of
this group of patients other than to include viral screening.
8
Patients presenting with acute respiratory infection and no diagnosis of COVID-19, who fit the case
definition for COVID-19, should receive the usual standard of care and then be isolated and discussed with
an specialist or infectious diseases expert.
Current evidence suggests that patients requiring admission and intensive care deteriorate 6-10 days after
presenting with symptoms of COVID-19, becoming progressively short of breath and developing signs of
multiple organ dysfunction.
For patients fitting the case definition of COVID-19 and presenting with late respiratory failure, the
following are noteworthy:
11.3.1. The late development of respiratory failure appears to carry a worse prognosis.
11.3.2. Elderly patients in other parts of the world have experienced higher mortality than younger
patients.
11.3.3. Patient comorbidity has an adverse impact on outcome. The comorbidities particularly associated
with a poor outcome are diabetes, hypertension and ischaemic heart disease.
11.3.4. The onset of other organ failures in addition to respiratory failure has a grave prognosis.
11.3.5. The need for acute dialysis, in combination with the need for ventilation, also carries a grave
prognosis.
11.3.6. With this in mind, the following recommendations are made:
11.3.6.1. Older patients (age more than 65 years) with comorbidity will not be considered for
ventilation.
11.3.6.2. Patients describe above and presenting with the need for ventilation or dialysis will be
offered palliative care.
11.3.6.3. Patients described above may be referred/admitted to intermediate care (field hospital)
setting to complete admission
12. Clinical management of COVID-19 patients
12.1. These guidelines must be used in conjunction with the latest NICD document: Clinical Management of
COVID-19 disease, Provincial Palliative Care Guidelines and Critical Care Guidelines.
12.2. The Triage and Testing of potential COVID-19 cases requires sorting of patients into PUIs and non-COVID
patients using an updated screening tool. The triage and testing activity should ideally be separate from the
usual Emergency Centre of a facility to limit the potential for nosocomial spread of the SARS Cov-2 virus.
(See TTC SOP Annexure A)
12.3. A symptomatic PUI or confirmed COVID-19 case must be triaged for admission using the Admission SOP
(Annexure B)
12.4. The inpatient management of COVID-19 patients with pneumonia requires the usual standard of care for
viral pneumonia with supplemental oxygen therapy, early awake proning but with stringent IPC practices.
12.5. High flow nasal oxygen, non-invasive ventilation and face mask CPAP may be considered in a patient
unresponsive to face mask oxygen. The risk of creating viral aerosols remains a concern and these
additional measures should ideally be applied in an isolation room with negative pressure ventilation.
12.6. Patients deemed suitable for critical care interventions must be monitored with pulse oximetry at regular
intervals to avoid the need for unprepared crash intubations. (Refer to latest Critical Care Guideline)
12.7. Patients requiring intubation must be discussed with the responsible Critical Care Service prior to
intubation to avoid unnecessary exposure of risk to Health Care Workers.
12.8. Patients with clinical deterioration but deemed not suitable for critical care interventions will be managed
as per the Provincial Palliative Care Guidelines for COVID-19. (refer to latest version)
13. Implementation
The guidelines are scalable to allow for the most effective response at each hospital whatever their current
situation may be. Due to the urgency of the situation, the guidelines in this document must be implemented
9
immediately. Circumstances will differ between hospitals, and they might be at different event stages. The
CEO/Incident Manager/Lead Clinician must assess the situation at the hospital to determine at which event stage
to implement these guidelines.
14. Triggers and thresholds
Each hospital, according to their resources, will set thresholds and triggers for escalating or de-escalating into a
different event stage. Moving from one event stage to another cannot happen randomly. The incident
management team must assess the situation before a decision is taken. Triggers and thresholds could be based
on:
• Admission numbers
• Demand for intensive care beds
• Availability of equipment, personnel or other resources necessary for treatment
Any escalation or de-escalation between stages must be communicated to all areas of the hospital.
15. Escalation
A phased approach allows for a planned and strategic increase and redirection of resources as it becomes
necessary. All personnel should be aware of their roles in each event stage. All personnel must be informed
when an escalation takes place so that they can adjust their tasks accordingly. Escalation should also be
communicated to other hospitals.
16. Contingency plans
There are a number of variables which can affect the care of patients during this pandemic. Personnel may
become infected and require isolation or treatment. Availability of equipment and medication could be affected
by stricter import protocols. Other incidents at the hospital, e.g. fires or power outages, could impact care. As far
as possible, there should be contingency plans for the incidents most likely to have a moderate to serious impact
on inpatient care.
17. De-escalation and return to normal function
As the outbreak is contained and fewer infections are reported, there will be a decrease in demand for critical
care treatment. It is advisable to delay the closure of expanded intensive care units and isolation areas until
assurance is received from the National Department of Health that there is little to no chance of sudden re-
emergence of large numbers of COVID-19 infections.
De-escalation must be strategic. Temporary inpatient cohort and isolation areas must be deep-cleaned before
being returned to normal use. Equipment must also be properly cleaned according to IPC principles before being
returned to use. De-escalation will most likely occur simultaneously with or shortly before the phased
reintroduction of services that were put on hold due to the outbreak. This transition process can be managed
between a member of the incident management team (or an appointed person) and the Operational Managers
of the areas being reopened.
18. Data collection, storage and protection
Throughout this outbreak, it is essential to collect as much data as possible and to maintain record-keeping
procedures. The knowledge and insight gained during this period will allow for better planning in preparedness
for future infectious disease outbreak scenarios.
Accurate data collection will make it easier for hospitals to compile the necessary reports once the outbreak is
declared resolved. Data will also be needed for financial reconciliations at a later stage when hospitals assess the
financial impact that this outbreak has had.

10
The coordinated and consistent approach taken by the hospitals in the Western Cape requires that certain
information be shared, within the hospital and between hospitals. An information system should be set up that
facilitates secure storage of and access to shared data and resources.
The patient’s right to privacy must still be respected, and any details pertaining to a patient’s identity and
treatment must be kept confidential.
19. Communication
The key to a coordinated and consistent response is effective communication. The incident management team
must keep personnel informed about any changes to the plan or any directives from the National or Provincial
Department of Health. Communication must be accurate and transparent. Personnel should also be able to
communicate their concerns, challenges and suggestions to the incident management team.
It is essential that hospitals remain in contact with each other to share information and resources as well as to
offer support.
General information regarding the nature and spread of COVID-19 and basic preventative and protective
measures should be posted on public noticeboards. Personnel should politely remind visitors about correct
hygiene procedures upon entering the facility and whenever lapses are noticed. Communication with patients
and their relatives must be timely, honest and direct, especially as it pertains to treatment. A certain amount of
frustration and possibly aggression is to be expected from patients or their relatives when being informed that
their conditions have declined or that they do not meet the criteria for critical care treatment. Personnel is
strongly advised to remain calm in these situations and to call a senior nurse or physician, or security if the
situation escalates.
Any requests from the press for information or access to the hospital must be addressed to public relations, and
the CEO must give permission. Liaising with the media is necessary to keep the public abreast of the situation.
Still, it must be done in a way that ensures the dignity of the patients and the safety of personnel and members
of the press. No member of staff may provide the media with any photographs, documents, copies of
photographs or documents or any information without authorisation from the CEO.
20. Event stages and activities
To be determined by each hospital in accordance with the National and Provincial Department of Health’s
response plan and guidelines.
21. Staff support and debriefing
It is expected that hospital personnel will, at some point, become overwhelmed by the daunting task of working
through this outbreak. There will be long hours, short tempers and not enough sympathy towards healthcare
workers, especially those who have to make decisions regarding refusal or withdrawal of treatment.
Healthcare workers are one of the most at-risk groups, and there will almost certainly be infections amongst
hospital personnel. It can be challenging to keep focused on the patients when healthcare personnel are seeing
their colleagues becoming ill. Personnel may also be worried about family members who are infected. This will
be a difficult period for South Africa as a nation, more so for those tasked with caring for the sick.
Hospital management is advised to provide support for personnel in any capacity that they can. The Western
Cape Government’s Employee Health and Wellness Programme can assist in this regard. If possible, hold regular
debriefings for personnel instead of waiting for a debriefing once the outbreak has been resolved. While patient
care is of great importance, the physical and psychological health of healthcare workers must be a priority.
11
22. Annexure A
Standard Operating Procedure for Triage and Testing Centre
Precautions:
All potential COVID-19 patients must be managed with utmost attention to adherence to IPC principles of Contact
and Droplet precautions:
a. Health Care Worker (HCW) must wear a surgical mask and plastic apron and keep a 1.5m distance from the
patient while interviewing the patient
b. A symptomatic patient must promptly receive hand hygiene and must don a surgical mask
c. The personal details must be captured without the patient completing any forms in person
d. The close quarters clinical evaluation must be kept to a minimum prior to the decision for admission
e. Health Technology Equipment must be cleaned and sanitised before and after use on a patient
f. All Airborne Generating Procedures (AGP) including swabbing and intubation must be done in a well-
ventilated area with full PPE (N95 mask, face shield, gown and gloves)
1. Streaming to single secured point of entry:
1.1. Clear signage from gate to TTC entry
1.2. Clear signage away from other entrances towards TTC
1.3. Clear signage away from TTC to other service points
1.4. Security to man the entry point to the TTC
1.5. Queue marshal must ensure adequate social distancing (clearly demarcated 2m distance markers)
2. Meet and greet HCW
2.1. HCW in basic PPE meets patient in screening area maintaining 2m distance
2.2. Patient is directed to a clean plastic chair spaced 2m apart from others
2.3. HCW interviews patient for COVID-19 to establish criteria for current case definition
2.4. Patient details and history is captured on a Screening Flow Chart (see below)
2.5. Determine patients case definition status
3. Risk assessment
3.1. Patient not at Risk is discharged home with educational material about COVID-19
3.2. Patient at Risk but not symptomatic is discharged home with educational material and contact numbers for
advice if develops symptoms and clear instructions to self-isolate for 14 days from date of contact
3.3. Patient at Risk with symptoms becomes a Person Under Investigation (PUI)
4. PUI management
4.1. Perform limited clinical assessment with minimal patient contact and determine if patient requires
admission. (see admission criteria below)
4.2. If patient needs admission then admit directly to PUI isolation room in a COVID ward or refer to Acute
Hospital if at PHC Facility
4.3. If patient does not require admission then move patient with their chair to the PUI cubicle in the TTC and
instruct not to move about or touch any surfaces
4.4. Prepare documents for opening a folder and the PUI NHLS/NICD form
4.5. Prepare specimens containers and label with patient details
5. Testing of PUI
5.1. Don full PPE for AGP(see above)
5.2. Ask patient to move with their chair from PUI cubicle to testing booth in TTC
5.3. Perform swab and place in specimen containers and double bag using an assistant outside the room
5.4. Doff PPE in testing booth

12
5.5. Perform hand hygiene and hand patient PUI documents and instructions
5.6. Educate the patient about the procedure for representing if symptoms worsen and emphasise need to self-
isolate for 14 days irrespective of result
5.7. Ask patient to leave testing booth with their chair and place at cleaning station
6. Follow up of PUI
6.1. Ensure that records and documents are filed in the patient folder
6.2. Ensure that the patient’s results are checked and recorded
6.3. Ensure that the patient is contacted with the result and appropriate advice is given about continued
quarantine or isolation
Criteria for mild disease - may be sent home to self isolate
1. Respiratory rate < 25 breaths per minute
2. Normal mental status
3. Normal mobility status
4. Peripheral O2 saturation SaO2 ≥ 95 % while breathing ambient air (optional)
5. Temperature 36-39OC (optional)
6. Pulse rate < 120 beats per minute (optional)
Support services essential for TTC
1. Patient admin clerk with IT equipment
2. Cleaning staff and equipment for chair and environmental cleaning
3. Security personnel for entry exit point control
4. Waste management
Supply Chain essentials
1. Stationery for screening
2. Educational material
3. PPE supplies
4. Hand hygiene supplies
5. Environmental Cleaning products and consumables
6. Biohazard Waste containers and consumables
This SOP is intended to be a guide for adaptation for local circumstances.
13
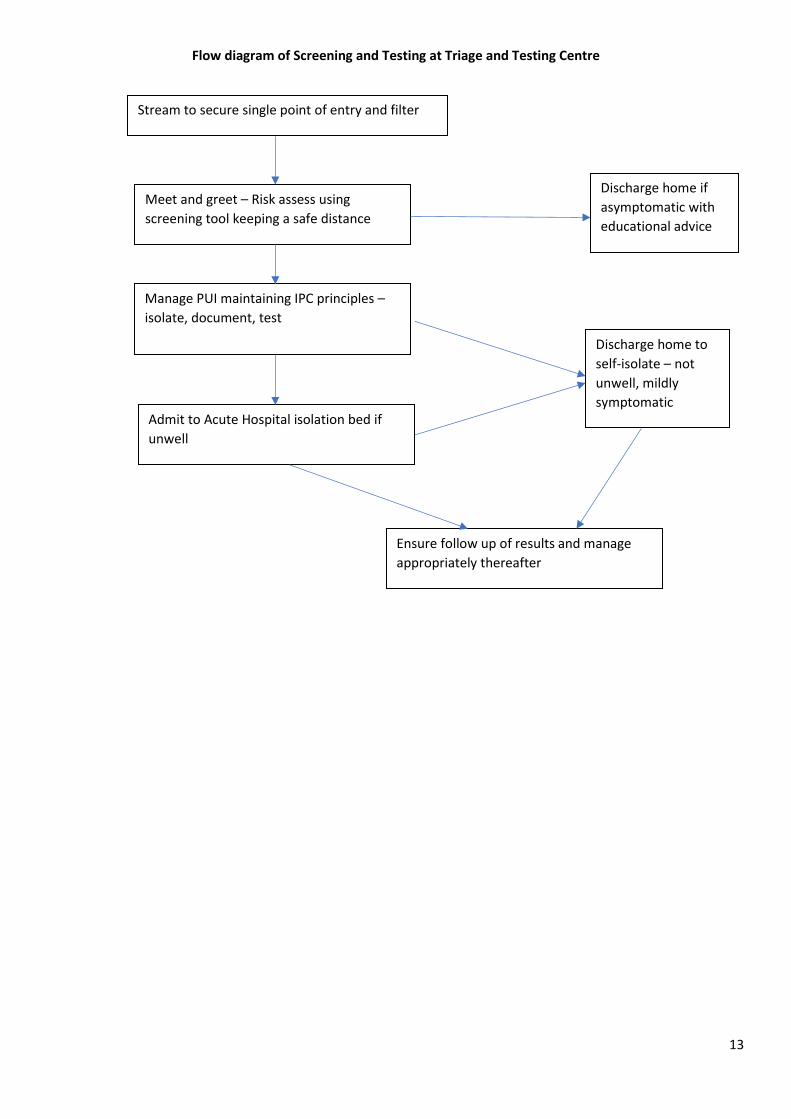
Flow diagram of Screening and Testing at Triage and Testing Centre
Stream to secure single point of entry and filter
Meet and greet – Risk assess using
screening tool keeping a safe distance
Discharge home if
asymptomatic with
educational advice
Manage PUI maintaining IPC principles –
isolate, document, test
Discharge home to
self-isolate – not
unwell, mildly
symptomatic Admit to Acute Hospital isolation bed if
unwell
Ensure follow up of results and manage
appropriately thereafter
14
23. Annexure B
Standard operating procedure for flow of COVID-19 patients within Acute Hospital
Objectives:
1. To achieve a clear guide on managing the rapid appraisal and management of a potential COVID-19
case referred for admission
2. To reduce unnecessary delay in decision-making about discharge to self-isolation or admission to
isolation facilities
3. To reduce the touch points in the care pathway to reduce the risk to staff and other patients in
Triage and Testing Centres and Emergency Centres
Precautions:
All potential COVID-19 patients must be managed with utmost attention to adherence to IPC principles of Contact
and Droplet precautions:
g. Health Care Worker (HCW) must wear a surgical mask and plastic apron and keep a 1.5m distance from the
patient while interviewing the patient
h. A symptomatic patient must promptly receive hand hygiene and must don a surgical mask
i. The personal details must be captured without the patient completing any forms in person
j. The close quarters clinical evaluation must be kept to a minimum prior to the decision for admission
k. Health Technology Equipment must be cleaned and sanitised before and after use on a patient
l. Use Respiratory Rate, Finger Oxygen Saturation Probe measurement for SaO2 and pulse and Temperature
m. All Airborne Generating Procedures (AGP) including swabbing and intubation must be done in a well-
ventilated area with full PPE (N95 mask, face shield, gown and gloves)
1. Any patient presenting to the Triage and Testing Centre or Emergency Centre with acute respiratory illness of
sudden onset of at least 1 of the following: cough, sore throat, shortness of breath AND the absence of an
alternative diagnosis, should be screened for COVID-19 (person under investigation – PUI).
1.1. Patients with criteria for “mild” disease should self-isolate at home or of unable to (e.g overcrowding at
home) the patient should be referred to a dedicated sponsored self-isolation facility while awaiting results
of testing
1.2. “Mild” disease criteria:
1.2.1. Respiratory rate < 25 breaths per minute
1.2.2. Peripheral O2 saturation SaO2 ≥ 95 % while breathing ambient air
1.2.3. Temperature 36-39C
1.2.4. Pulse rate < 120 beats per minute
1.2.5. Normal mental status
2. In PUIs presenting with evidence of severe acute respiratory syndrome (SARS), a decision to escalate support
with proning and enhanced oxygen delivery should be made. These patients should be managed as COVID-19
positive patients in a dedicated PUI room or area until the results of the SARS-CoV-2 PCR has become available.
2.1. Indications for escalation include:
2.1.1. Signs of SARS / severe hypoxaemic respiratory failure:

15
2.1.1.1. Respiratory rate > 40 breaths per minute
2.1.1.2. Pulse oximetry (SpO2) less than 90% or an arterial blood sample with PaO2 < 8.0 kPa (while using a
40% facemask)
2.1.1.3. Heart rate > 120 beats per minute
Patients deemed to be failing escalation measures may be considered for intubation and transfer to a Critical
Care Unit.
2.2. Palliative care (i.e. Patients not for intubation/ICU admission/), Priority 4 patients as outlined in the the latest
Critical Care Triage Tool
2.2.1. Acute irreversible multi-organ failure and anticipated poor prognosis
2.2.2. Chronic terminal and irreversible illness facing imminent death
2.2.3. Brain death in terms of legally defined criteria
2.2.4. Following a cardiac arrest AND:
2.2.4.1. does not re-establish a normal respiratory pattern or achieved a full level consciousness without
sedation OR
2.2.4.2. has fixed dilated pupils not due to medication OR
2.2.4.3. has a cause that is not immediately reversible OR
2.2.5. has irreversible brain injury.
2.2.6. End-stage renal disease (eGFR < 15 ml/min/1.73 m2) with or without chronic dialysis support
2.2.7. Chronic liver disease
2.2.8. End-stage congestive heart failure
2.2.9. Chronic debilitating pulmonary disease
2.2.10. Malignancies that are incurable/resistant to treatment
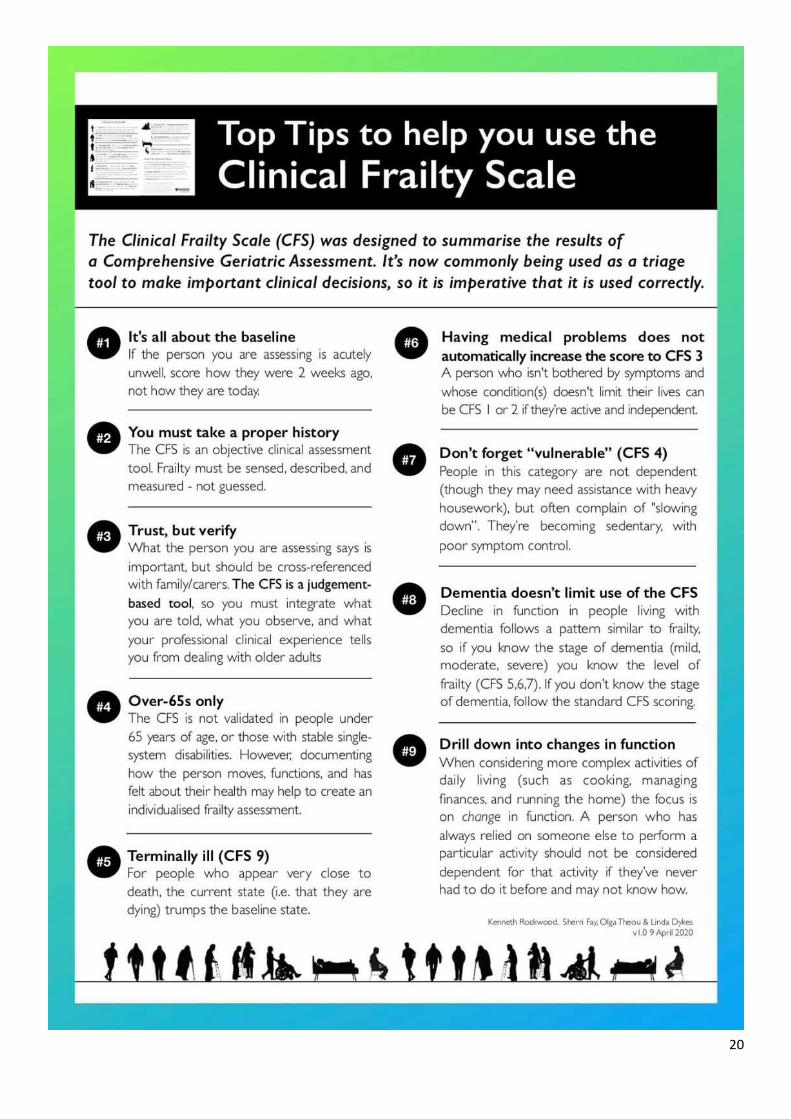
2.2.11. Clinical frailty score (CFS) of 5-9 (see attached).
2.2.12. Age > 70 years
2.2.13. HIV patients AND:
2.2.13.1. AIDS-defining illness
2.2.13.2. Viral load > 10 000 copies/mL despite antiretroviral therapy
2.3 Patients deemed unsuitable for critical care will be managed as per Provincial Palliative Care Guidelines for
COVID-19
CRITICALLY ILL PATIENTS
3. Critically ill PUIs requiring ICU admission:
3.1. Intubation should preferably be done within a designated area using appropriate personal protective equipment
(PPE), and a local intubation protocol.

16
3.2. PUIs already intubated, should be referred and admitted directly to ICU (unless COVID-19 consultant or ICU
team has decided on palliative care).
3.3. Patients should ideally be held in designated area for ventilation at the acute hospital of COVID-19 while
awaiting admission to ICU
3.4. PUIs testing positive for COVID-19 should continue receiving treatment with the designated ICU.
3.5. In PUIs initially testing negative:
3.5.1. If a high clinical index of suspicion remains for COVID-19, the patient should remain in the ICU and the
test should be repeated 72 hours later.
3.5.2. If the repeat test remains negative and/or an alternative diagnosis is made, the patient should be moved
to a non-COVID-19 ICU for further management. If the test remains negative but a high clinical index of
suspicion remains, a CT scan can be considered after discussion with an infectious diseases specialist.
3.5.3. If repeat test is positive for COVID-19, these patients should remain in the ICU and managed as outlined in
item 4 below.
4. Confirmed COVID-19 positive critically ill patients requiring ICU admission:
4.1. For patients within the Emergency Centre of the Acute Hospital:
4.1.1. A consultant and/or ICU consultant should decide on further escalation. Those for palliative care should
be moved to a COVID-19 ward.
4.1.2. Patients for intubation and ICU admission should preferably be moved to ICU and intubation performed
there or intubated in the ward following a local intubation protocol.
4.2. Patients already mechanically ventilated should be admitted directly to ICU unless COVID-19 consultant or ICU
team decides on palliative care.
NON-CRITICAL PATIENTS
5. Non-critically ill PUIs requiring hospital admission:
5.1. PUIs not meeting the criteria for SARS or critical illness requiring ICU admission will be admitted to PUI/COVID-
19 wards, in a single room with oxygen ports available. If no single rooms are available, then multi-bed rooms
may be used using the National IPC guideline for PUI Wards. Wards to be used include:
Phase 1: Wards (insert wards)
Phase 2: Wards (insert wards)
5.2. Once each ward reaches 50% capacity, sequential wards will be opened for PUI admissions.
5.3. PUIs testing positive for COVID-19 can be cohorted together in a COVID-19 room until either of the following
outcomes are reached:
5.3.1. Recovers and can be discharged. Criteria for discharge include symptom improvement AND SaO2 >94%
without oxygen for 24 hours
5.3.2. Requires admission to ICU.
5.3.3. Palliative care instituted.
5.4. PUIs initially testing negative for COVID-19:
17
5.4.1. If a high clinical index of suspicion remains for COVID-19, the patient should remain in the PUI ward and
the test should be repeated 72 hours later.
5.4.2. If the repeat test remains negative and/or an alternative diagnosis is made, the patient should be moved
to a non-COVID-19 ward for further medical management. If the test remains negative but a high clinical
index of suspicion remains, a CT scan can be considered after discussion with an infectious diseases
specialist. Patient should remain in PUI room.
5.4.3. If repeat test is positive for COVID-19, these patients should remain in the COVID-19 ward until an
outcome is reached as in 5.3 above.

18
Algorithm for the management of unconfirmed (PUI) cases of COVID-19
Continue Mx in
COVID-19 ward
Continue Mx in
non-COVID-19 ward
PCR +
Continue Mx in
COVID-19 ICU
PCR - or
alternative
Dx
Repeat PCR in 72 hrs
if NO alternative Dx
Indications for palliation? Yes
Refer to COVID-
19 ICU
PCR – and NO alternative Dx
Repeat PCR in 72 hrs PCR- and alternative Dx
PCR + PCR - Yes
Admit COVID-19
ward
Indications for
intubation?
No Yes
Person under investigation (PUI) with acute respiratory
illness
Critically ill?
Intubate
No
No
“Mild” disease
criteria met?
Yes No
Self-isolate at home
Or TPW Facility
Continue Mx in non-COVID-19 ICU

19
Algorithm for the management of confirmed COVID-19 cases at Acute Hospital
Indications for palliation?
Yes No
Refer to COVID-19 ICU
Yes No
Indications for
intubation?
No Yes
Confirmed COVID-19 case with acute
respiratory illness
Critically ill?
Intubate
Admit to COVID-19 ward
20

21
24. Annexure C
PATIENT FLOW DIAGRAM FOR COVID-19 CASES
Key:
PHC = Primary Health Center
TTC = Triage and Testing Center
ICB = Intermediate Care Beds for COVID-19 (Cape Town International Convention Center)
CCU = Critical Care Unit
HCU = High Care Unit
ICU = Intensive Care Unit
Acute hospital:
Isolation + cohort
TTC
PHC
TTC
Home
COVID ICB
(CTICC)
CCU
HCU + ICU
Palliative care
Palliative
care
Note:
1. COVID-19 POSITIVE test status required for transfer to COVID ICB
2. Palliative Care Beds will be required at Acute Hosp and COVID ICB Centre
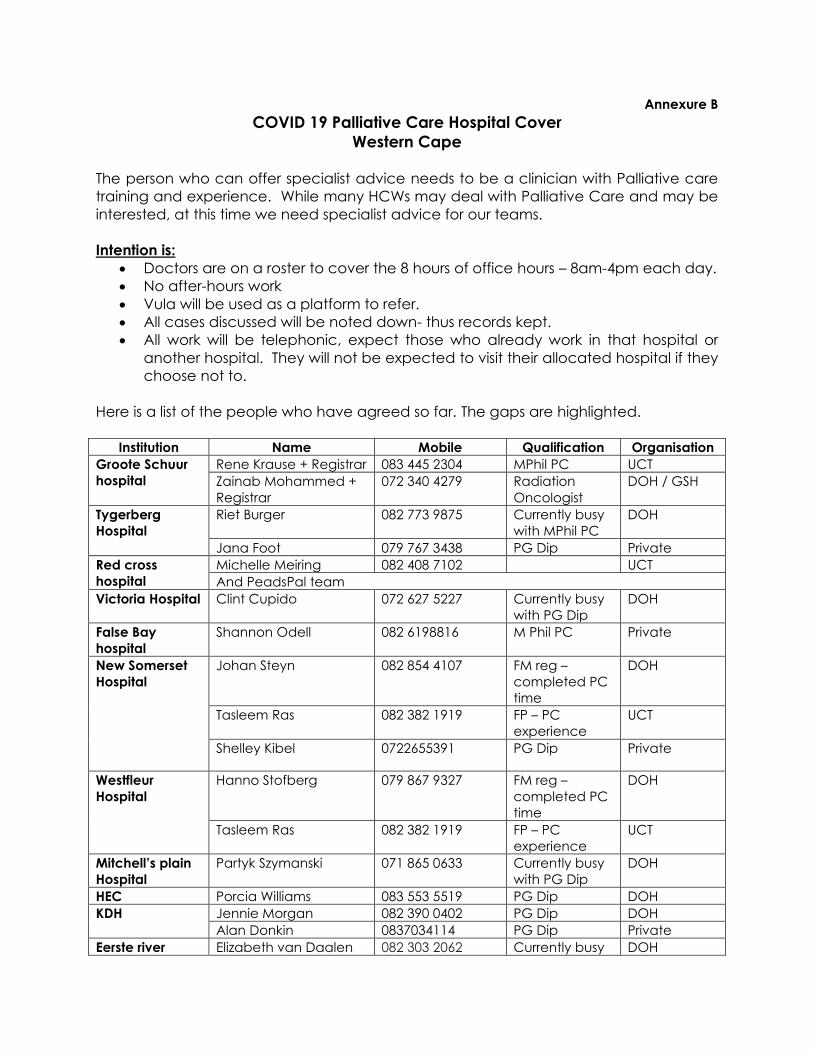
Annexure B
COVID 19 Palliative Care Hospital Cover
Western Cape
The person who can offer specialist advice needs to be a clinician with Palliative care
training and experience. While many HCWs may deal with Palliative Care and may be
interested, at this time we need specialist advice for our teams.
Intention is:
• Doctors are on a roster to cover the 8 hours of office hours – 8am-4pm each day.
• No after-hours work
• Vula will be used as a platform to refer.
• All cases discussed will be noted down- thus records kept.
• All work will be telephonic, expect those who already work in that hospital or
another hospital. They will not be expected to visit their allocated hospital if they
choose not to.
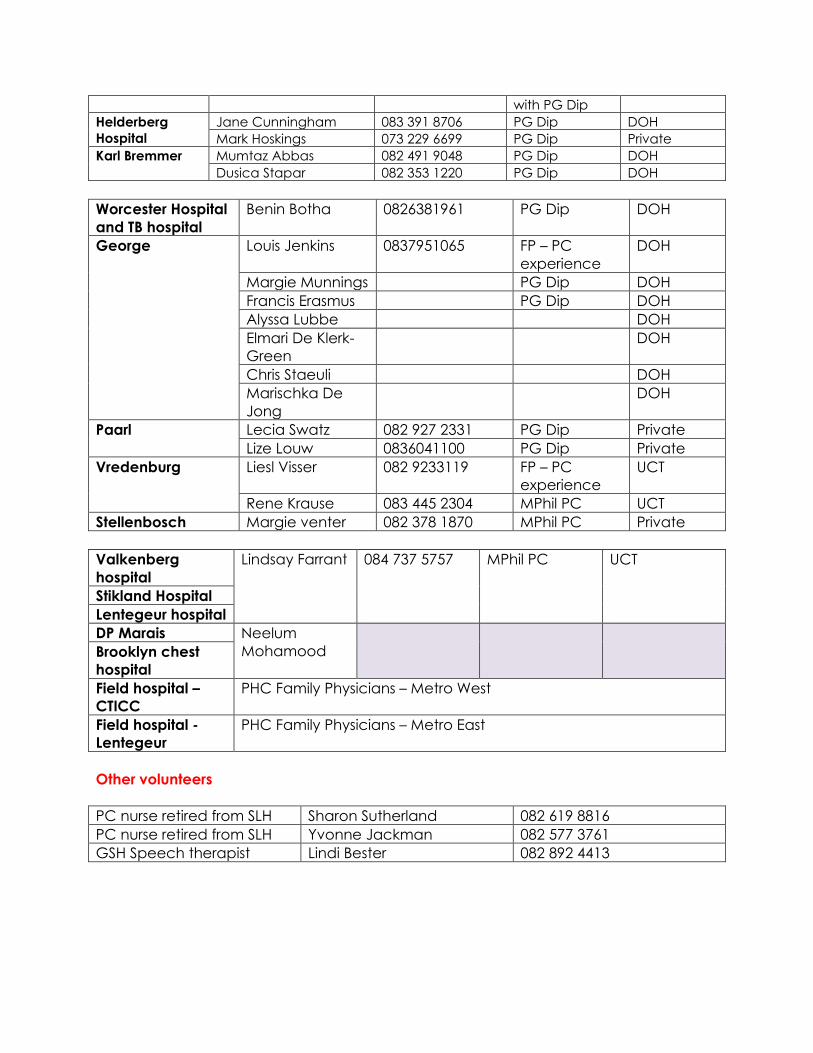
Here is a list of the people who have agreed so far. The gaps are highlighted.
Institution Name Mobile Qualification Organisation
Groote Schuur
hospital
Rene Krause + Registrar 083 445 2304 MPhil PC UCT
Zainab Mohammed +
Registrar
072 340 4279 Radiation
Oncologist
DOH / GSH
Tygerberg
Hospital
Riet Burger 082 773 9875 Currently busy
with MPhil PC
DOH
Jana Foot 079 767 3438 PG Dip Private
Red cross
hospital
Michelle Meiring 082 408 7102 UCT
And PeadsPal team
Victoria Hospital Clint Cupido 072 627 5227 Currently busy
with PG Dip
DOH
False Bay
hospital
Shannon Odell 082 6198816 M Phil PC Private
New Somerset
Hospital
Johan Steyn 082 854 4107 FM reg –
completed PC
time
DOH
Tasleem Ras 082 382 1919 FP – PC
experience
UCT
Shelley Kibel 0722655391 PG Dip Private
Westfleur
Hospital
Hanno Stofberg 079 867 9327 FM reg –
completed PC
time
DOH
Tasleem Ras 082 382 1919 FP – PC
experience
UCT
Mitchell’s plain
Hospital
Partyk Szymanski 071 865 0633 Currently busy
with PG Dip
DOH
HEC Porcia Williams 083 553 5519 PG Dip DOH
KDH Jennie Morgan 082 390 0402 PG Dip DOH
Alan Donkin 0837034114 PG Dip Private
Eerste river Elizabeth van Daalen 082 303 2062 Currently busy DOH
with PG Dip
Helderberg
Hospital
Jane Cunningham 083 391 8706 PG Dip DOH
Mark Hoskings 073 229 6699 PG Dip Private
Karl Bremmer Mumtaz Abbas 082 491 9048 PG Dip DOH
Dusica Stapar 082 353 1220 PG Dip DOH
Worcester Hospital
and TB hospital
Benin Botha 0826381961 PG Dip DOH
George Louis Jenkins 0837951065 FP – PC
experience
DOH
Margie Munnings PG Dip DOH
Francis Erasmus PG Dip DOH
Alyssa Lubbe DOH
Elmari De Klerk-
Green
DOH
Chris Staeuli DOH
Marischka De
Jong
DOH
Paarl Lecia Swatz 082 927 2331 PG Dip Private
Lize Louw 0836041100 PG Dip Private
Vredenburg Liesl Visser 082 9233119 FP – PC
experience
UCT
Rene Krause 083 445 2304 MPhil PC UCT
Stellenbosch Margie venter 082 378 1870 MPhil PC Private
Valkenberg
hospital
Lindsay Farrant
084 737 5757 MPhil PC UCT
Stikland Hospital
Lentegeur hospital
DP Marais Neelum
Mohamood
Brooklyn chest
hospital
Field hospital –
CTICC
PHC Family Physicians – Metro West
Field hospital -
Lentegeur
PHC Family Physicians – Metro East
Other volunteers
PC nurse retired from SLH Sharon Sutherland 082 619 8816
PC nurse retired from SLH Yvonne Jackman 082 577 3761
GSH Speech therapist Lindi Bester 082 892 4413
20th Floor, 4 Dorp Street, Cape Town, 8001 P O Box 2060, Cape Town, 8000
tel: +27 21 483 4473 fax: +27 21 483 5677 www.westerncape.gov.za
COVID-19 PROVIDING PALLIATIVE CARE
Purpose
This is an evolving document created to provide guidance to health care workers (HCW) on the integration of
palliative care (PC) into standard care in intensive care units, hospital wards, emergency departments, out-
patient clinics, intermediate care facilities, care homes and private homes.
It must be read in conjunction with, and aims to complement, the DOH Guidelines for the Clinical Management
of Suspected or Confirmed COVID-19 Disease (https://bit.ly/2wGFeQB).
It is aimed at ensuring that patients and families receive dignified, compassionate care during this pandemic.
Importantly, the term ‘palliative care’ does not only describe end-of-life care, but the relief of symptoms and
suffering for all, whatever their COVID status or final health outcome.
Palliative care intends not to hasten or prolong death and must be provided alongside standard care. It is
acknowledged that all South Africans currently do not have access to formal PC services in their communities.
However, this document aims to provide health care workers with the tools to limit the suffering of patients and
their families during COVID-19, aligning treatment decisions with patient and family values whilst also ensuring
that the community and health care workers are protected from infection. This type of care may require the
same level of intensity as that which is required in an intensive care unit. Palliative care is best provided by
interdisciplinary teams that may include palliative care physicians, as well as HCWs who usually focus on
standard medical care and psycho-social and spiritual carers in hospitals and in the community.
The purpose of this document is to improve patient outcomes by guiding the care from health care workers in
conjunction with mentorship from experienced palliative care providers. Patients with complex palliative care
problems and situations are best managed within experienced palliative care teams.
To find a palliative care provider close to you and access valuable resources for PC provision, follow this link to
the PALPRAC website: https://bit.ly/2UvLSC8
For further enquiries Professor Ivan Joubert may be contacted at [email protected]
Annexure C
Compiled for the Critical Care Forum of the Western Cape by PALPRAC – The Association of Palliative Care Practitioners of South Africa. The writing group comprised the following individuals – Riette Burger David Cameron Colleen Cox Jayne Cunningham Clint Cupido Charmaine de Blanchard Katya Evans Liz Gwyther René Krause Rebecca Lazarus Shannon Odell Patryk Szymanski John Turner Daleen van Jaarsveld Margie Venter Louise Walker Ivan Joubert Critical Care Forum chairperson 3 April 2020
2
Providing Palliative Care in South Africa
During the COVID-19 Pandemic
Table of Contents
Palliative care for patients who are suspected of having COVID-19 or who are COVID-19 positive ................. 4
Patients with hypoxemic respiratory failure and ARDS failing ventilation support: ................................................ 5
Procedure for withdrawal of ventilatory support: ............................................................................................................ 5 Death anticipated to occur rapidly after cessation of mechanical ventilation & inotropic support: ................................................................................................................................................................................................................. 6 Not anticipating rapid death after withdrawal of ventilatory support: ........................................................................ 6
Hospital-based care for patients with severe symptoms who are not candidates for critical care admission & ventilation if they deteriorate ................................................................................................................................... 7
Oxygen therapy: ............................................................................................................................................................................. 7
Pharmacological interventions: .............................................................................................................................................. 8 Oral route: ............................................................................................................................................................................................................ 8 Subcutaneous route (no syringe driver available) if patients are unable to swallow: .................................. 10
Non-pharmacological interventions: ................................................................................................................................... 11
End-of-Life Care ..................................................................................................................................................................................... 12
Communication in the time of COVID-19 .................................................................................................................................... 15
End-of-life care for COVID-19 patients at home ...................................................................................................................... 19
Management of COVID negative palliative care patients .................................................................................................... 21
Advance care planning ............................................................................................................................................................. 21
Palliative care patient who develops symptoms of COVID-19 ......................................................................................... 23
Protection for healthcare providers in the community ........................................................................................................ 25
Long-term care facilities ..................................................................................................................................................................... 25
Carer guidelines ..................................................................................................................................................................................... 27
The Wellbeing of Healthcare Professionals .............................................................................................................................. 27
Management of the deceased .......................................................................................................................................................... 32
Addenda ..................................................................................................................................................................................................... 33
Addendum 1: PATIENT AND CARER INFORMATION SHEET FOR WHEN END-OF-LIFE CARE WILL TAKE PLACE AT HOME ................................................................................................................................................. 33
Addendum 2: VIRTUAL SUPPORT ....................................................................................................................................... 37
Addendum 3: DRUG CONVERSION TABLES ................................................................................................................... 38 Addendum 4: ................................................................................................................................................................................................... 39
Addendum 5: MEET MY LOVED ONE ................................................................................................................................... 40

3
Introduction:
This is an evolving document created to provide guidance to health care workers (HCW) on the integration of palliative care (PC) into standard care in intensive care units, hospital wards, emergency departments, out-patient clinics, intermediate care facilities, care homes and private homes. It must be read in conjunction with, and aims to complement, the DOH Guidelines for the Clinical Management of Suspected or Confirmed COVID-19 Disease (https://bit.ly/2wGFeQB). It is aimed at ensuring that patients and families receive dignified, compassionate care during this pandemic. Importantly, the term ‘palliative care’ does not only describe end-of-life care, but the relief of symptoms and suffering for all, whatever their COVID status or final health outcome. Palliative care intends not to hasten or prolong death and must be provided alongside standard care. It is acknowledged that all South Africans currently do not have access to formal PC services in their communities. However, this document aims to provide health care workers with the tools to limit the suffering of patients and their families during COVID-19, aligning treatment decisions with patient and family values whilst also ensuring that the community and health care workers are protected from infection. This type of care may require the same level of intensity as that which is required in an intensive care unit. Palliative care is best provided by interdisciplinary teams that may include palliative care physicians, as well as HCWs who usually focus on standard medical care and psycho-social and spiritual carers in hospitals and in the community. The purpose of this document is to improve patient outcomes by guiding the care from health care workers in conjunction with mentorship from experienced palliative care providers. Patients with complex palliative care problems and situations are best managed within experienced palliative care teams. To find a palliative care provider close to you and access valuable resources for PC provision, follow this link to the PALPRAC website: https://bit.ly/2UvLSC8 This document covers the following topics: • Ventilatory withdrawal • Supportive care for patients suspected or diagnosed with COVID-19 • End-of-life care • Communication at the time of COVID-19 • Hospital-based care for patients with severe symptoms who are not
candidates for critical care admission & ventilation if they deteriorate • Communication in the time of COVID-19 • Care suggestions for long-term care facilities • Self-care and mental health for HCW
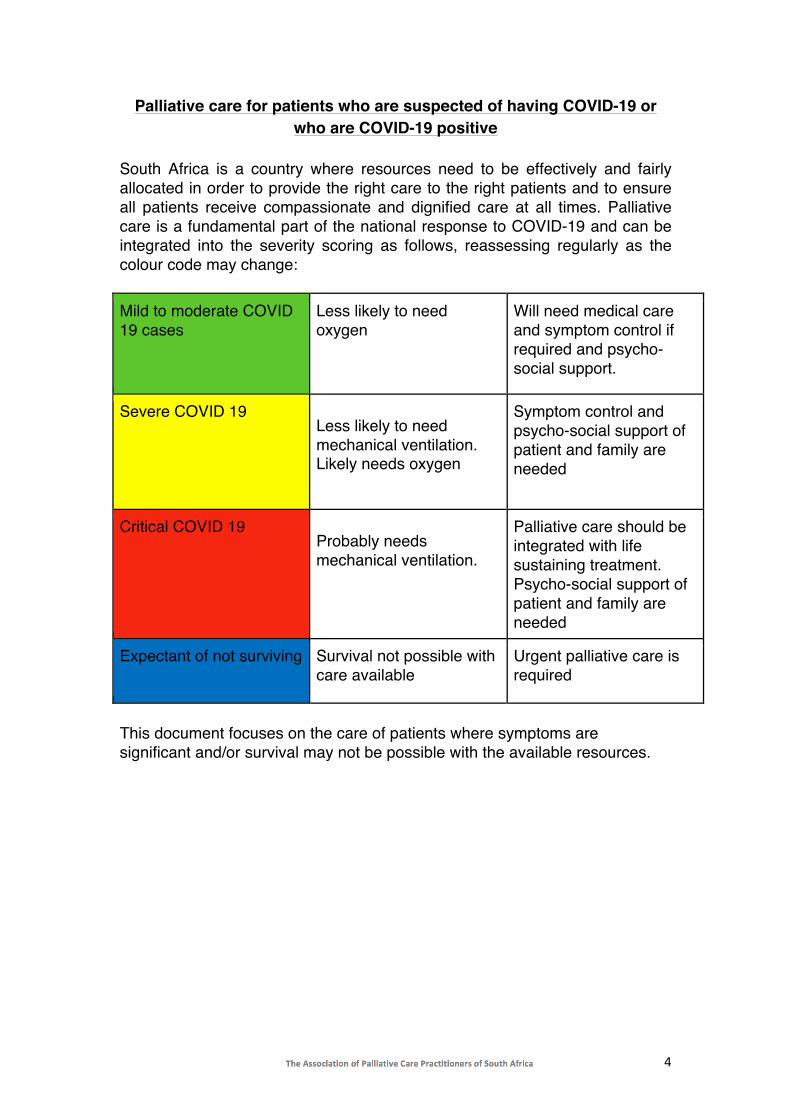
4
Palliative care for patients who are suspected of having COVID-19 or who are COVID-19 positive
South Africa is a country where resources need to be effectively and fairly allocated in order to provide the right care to the right patients and to ensure all patients receive compassionate and dignified care at all times. Palliative care is a fundamental part of the national response to COVID-19 and can be integrated into the severity scoring as follows, reassessing regularly as the colour code may change: Mild to moderate COVID 19 cases
Less likely to need oxygen
Will need medical care and symptom control if required and psycho-social support.
Severe COVID 19 Less likely to need mechanical ventilation. Likely needs oxygen
Symptom control and psycho-social support of patient and family are needed
Critical COVID 19 Probably needs mechanical ventilation.
Palliative care should be integrated with life sustaining treatment. Psycho-social support of patient and family are needed
Expectant of not surviving Survival not possible with care available
Urgent palliative care is required
This document focuses on the care of patients where symptoms are significant and/or survival may not be possible with the available resources.

5
Patients with hypoxemic respiratory failure and ARDS failing ventilation support:
Patients with hypoxemic respiratory failure and ARDS who were initiated on ventilatory support according to the DOH Guidelines for the clinical management of suspected or confirmed COVID-19 disease, but who fail to respond to intensive therapy may need to be considered for withdrawal of ventilatory support. The decision to withdraw ventilatory support is complex and emotive and must be done within the context of a team. Once the decision has been reached by the team, it must be clearly and compassionately communicated to the family. Psycho-social and spiritual support must be mobilised for the family and the HCW. It should be in place for the family and carers of all patients initiated on ventilation.
Procedure for withdrawal of ventilatory support:

6
Death anticipated to occur rapidly after cessation of mechanical ventilation & inotropic support:
Predictors - high PEEP & FiO2 or inotropic requirements or severe acidosis or obtunded. Approach summary:
1. Gradual scaling down of ventilatory support over 10-30 minutes to allow for the titration of medications to adequately control dyspnoea and anxiety, but not to allow for hastening or prolonging of death. The patient should not be extubated for staff safety.
2. Ensure neuromuscular blockade agents have worn off. 3. Turn off the multiparameter bedside monitor. Further monitoring and
management will be symptom-based and not based on vital sign measurement.
4. Stop inotropic infusions. 5. Decrease Pressure Support, PEEP, FiO2 every 5 minutes until at
0cmH2O & 0.21 (Room air - 21% oxygen). 6. If on an opiate infusion, continue the infusion to allow titration. 7. Reassess symptoms every 5 minutes whilst titrating down ventilatory
setting and administer additional boluses of intravenous morphine; increase the infusion rate if showing signs of breathlessness.
8. Administer bolus of available benzodiazepine if the patient develops restlessness/anxiety.
9. The patient should not be extubated until after death. Not anticipating rapid death after withdrawal of ventilatory support: Approach summary:
1. Gradual scaling down of ventilatory support over 10-30 minutes to allow for the titration of medications to adequately control dyspnoea and anxiety, but not to allow for hastening or prolonging of death.
2. Once comfortable, the patient will require palliative extubation. As this is an airway procedure, this poses a significant risk to staff and the procedure needs to be performed wearing the same PPE as per the Provincial PPE Guideline section on intubation procedure.
3. Ensure neuromuscular blockade agents have worn off. 4. Turn off the multiparameter bedside monitor. Further monitoring and
management will be symptom-based not based on vital sign measurement.
5. Stop inotropic infusions.

7
6. Administer Hyoscine Butylbromide (Buscopan) 20mg IVI or Robinul 200mcg IV.
7. Decrease Pressure Support, PEEP, FiO2 every 5 minutes until at 3cm H2O & 0.21 (Room air – 21% oxygen).
8. If on an opiate infusion, continue the infusion to allow for titration – to convert later to a subcutaneous infusion.
9. Reassess symptoms every 5 minutes whilst titrating down ventilatory setting and administer additional boluses of intravenous morphine; increase the infusion rate if showing signs of breathlessness.
10. Administer bolus of available benzodiazepine if the patient develops restlessness/anxiety.
11. Use patient head coverage at the hospital (same as per intubation procedure).
12. Suction airway using in-line closed suction if available; suction mouth; extubate the patient.
13. Convert to subcutaneous medication via bolus or infusion via syringe driver. See conversion in Addendum 2.
14. Provide oxygen via nasal cannula for comfort as required - patient to wear surgical mask over nasal cannula.
15. Move to the general ward or out of ICU/High Care. 16. Continue care as per detailed End-of-Life Guideline.
Hospital-based care for patients with severe symptoms who are not
candidates for critical care admission & ventilation if they deteriorate All patients with underlying chronic illnesses and severe COVID-19 symptoms should be considered for early supportive therapy (supplemental oxygen with or without empiric antimicrobials) as per the COVID-19 Clinical Guidelines section 4.2, unless resources do not allow for this or if the patient or their medical decision maker clearly states that they decline such therapy. Oxygen therapy: Oxygen therapy is likely to be the single most effective supportive measure in COVID-19 patients overall. Only a portion of patients with severe COVID-19 symptoms may require critical care and ventilation. The patient should be reassessed daily and triage repeated if the condition and/or circumstances change. As per the COVID-19 Clinical Guidelines, any patient with hypoxaemia (saturation <90%) should be given supplemental oxygen to achieve O2 saturation >90% (aim for >92% in pregnant women). • Nasal cannula: 21-40% oxygen (with surgical mask covering to prevent droplet spread); O2 dose 1-5L/min • Simple face mask:

8
40-60% oxygen; O2 dose 6-10L/min • Non-rebreather facemask: 60-95% oxygen; O2 flow rate of 10-15L/min; ensure proper fit, to reduce risk of aerosol spread.
Pharmacological interventions: Oral route:
This is the simplest and preferred route. Below are the starting doses for each symptom; COVID-19 symptoms might advance rapidly, needing dose escalation. • Fever: Paracetamol 1000mg 6hrly PO PRN • Anxiety: Lorazepam 1mg-2mg s/l q2h prn until patient has settled, then
6-12 hourly or alprazolam 0.5-1mg 8hrly PRN • Dyspnoea: Opioids will assist in respiratory distress - Morphine syrup
(Mist Morphine) 2.5-5mg PO 4hrly. Note: the amount of morphine syrup will vary depending on the strength at which it is mixed. This varies from pharmacy to pharmacy and region to region. Common strengths are 5mg/5mL (in which case give 2.5-5mL), 10mg/1mL (in which case give 0.25-0.5mL) or 20mg/5ml (in which case give 0.6-1.25ml).
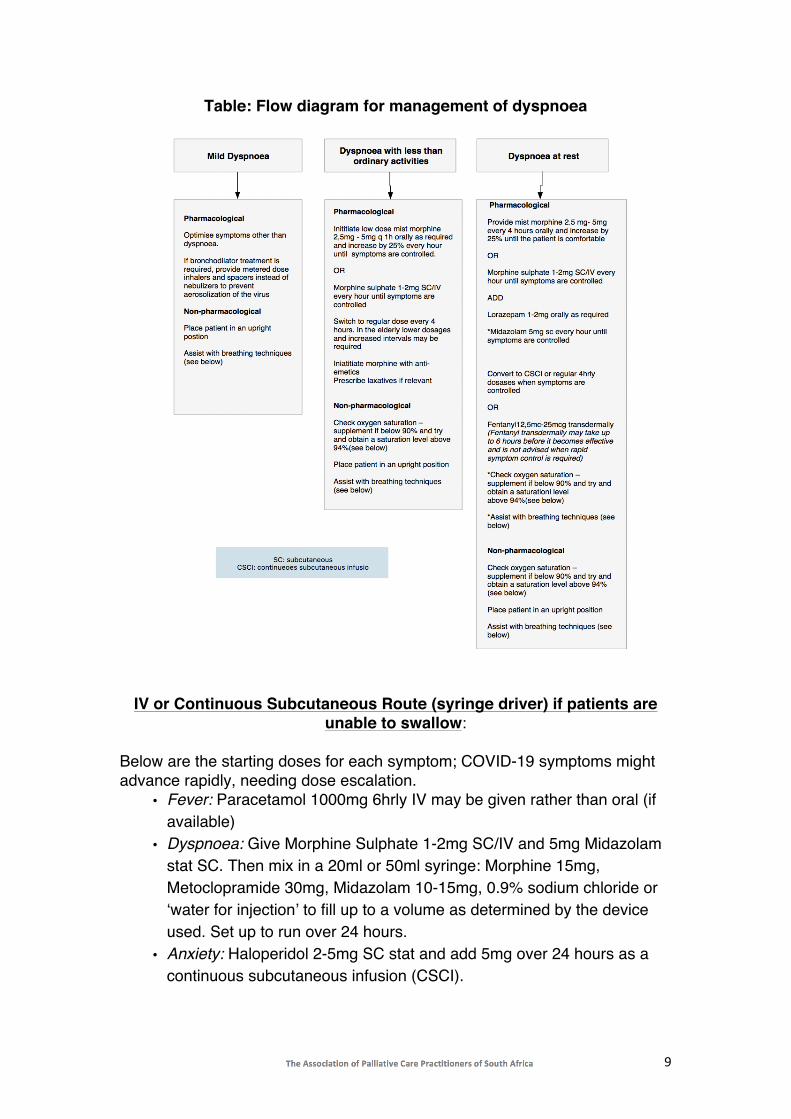
9
Table: Flow diagram for management of dyspnoea
IV or Continuous Subcutaneous Route (syringe driver) if patients are unable to swallow:
Below are the starting doses for each symptom; COVID-19 symptoms might advance rapidly, needing dose escalation.
• Fever: Paracetamol 1000mg 6hrly IV may be given rather than oral (if available)
• Dyspnoea: Give Morphine Sulphate 1-2mg SC/IV and 5mg Midazolam stat SC. Then mix in a 20ml or 50ml syringe: Morphine 15mg, Metoclopramide 30mg, Midazolam 10-15mg, 0.9% sodium chloride or ‘water for injection’ to fill up to a volume as determined by the device used. Set up to run over 24 hours.
• Anxiety: Haloperidol 2-5mg SC stat and add 5mg over 24 hours as a continuous subcutaneous infusion (CSCI).
10
Alternatives to morphine if available - Fentanyl patch 12mcg-25mcg/h every 72 hours (will need to give subcutaneous Morphine boluses for the first 12-24 hours). Reassess and adjust rate if the patient is not comfortable or give additional breakthrough doses (2.5mg morphine and 5mg midazolam stat SC or IV). In the elderly and those with renal failure, start at lower doses. Subcutaneous route (no syringe driver available) if patients are unable
to swallow: Below are the starting doses for each symptom; COVID-19 symptoms might advance rapidly, needing dose escalation. Subcutaneous bolus doses of medication can be given via an indwelling butterfly/cannula. It will need to be flushed with 0,9% saline after each use.
• Dyspnoea: Morphine 1-2mg SC q1h; increase dose by 25% if symptoms are not controlled; once controlled switch to regular 4-hourly dosing (typically 1.5-2.5mg 4hrly SC)
• Anxiety: Midazolam 5mg SC every hour until symptoms resolved • Nausea and vomiting: Metoclopramide 10mg 8hrly PRN
Alternative to Morphine if available: Fentanyl patch 12mcg-25mcg/h every 72 hours (will need to give SC Morphine boluses for the first 12-24 hours) Note: Paracetamol cannot be given via this route! One can also slowly drip mist morphine into the side of the mouth as a last resort.
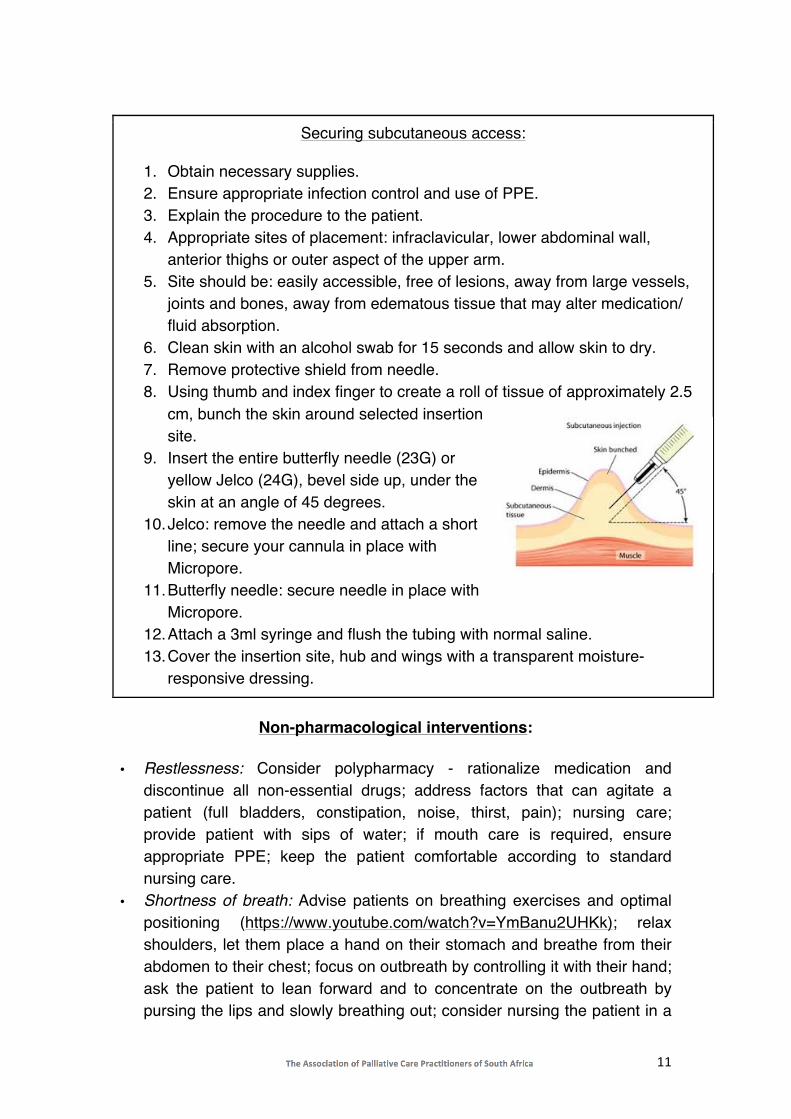
11
Securing subcutaneous access:
1. Obtain necessary supplies. 2. Ensure appropriate infection control and use of PPE. 3. Explain the procedure to the patient. 4. Appropriate sites of placement: infraclavicular, lower abdominal wall,
anterior thighs or outer aspect of the upper arm. 5. Site should be: easily accessible, free of lesions, away from large vessels,
joints and bones, away from edematous tissue that may alter medication/ fluid absorption.
6. Clean skin with an alcohol swab for 15 seconds and allow skin to dry. 7. Remove protective shield from needle. 8. Using thumb and index finger to create a roll of tissue of approximately 2.5
cm, bunch the skin around selected insertion site.
9. Insert the entire butterfly needle (23G) or yellow Jelco (24G), bevel side up, under the skin at an angle of 45 degrees.
10. Jelco: remove the needle and attach a short line; secure your cannula in place with Micropore.
11. Butterfly needle: secure needle in place with Micropore.
12. Attach a 3ml syringe and flush the tubing with normal saline. 13. Cover the insertion site, hub and wings with a transparent moisture-
responsive dressing.
Non-pharmacological interventions:
• Restlessness: Consider polypharmacy - rationalize medication and
discontinue all non-essential drugs; address factors that can agitate a patient (full bladders, constipation, noise, thirst, pain); nursing care; provide patient with sips of water; if mouth care is required, ensure appropriate PPE; keep the patient comfortable according to standard nursing care.
• Shortness of breath: Advise patients on breathing exercises and optimal positioning (https://www.youtube.com/watch?v=YmBanu2UHKk); relax shoulders, let them place a hand on their stomach and breathe from their abdomen to their chest; focus on outbreath by controlling it with their hand; ask the patient to lean forward and to concentrate on the outbreath by pursing the lips and slowly breathing out; consider nursing the patient in a
12
prone position for a part of the day if not contra-indicated or unnecessarily uncomfortable; stay calm with the patient and distract the patient with reassuring conversation; provide as much emotional and spiritual care as possible under the circumstances. See attached ‘What to Say’ guide for useful phrases when providing comfort.
Management of other commonly experienced symptoms (pain; nausea and vomiting) See HPCSA Clinical guideline
End-of-Life Care Patients can be defined as being terminal when there is irreversible decline in functional status prior to death. It is essential during this time to ensure the ethical management of the dying phase and to minimise distress for the patient, family and fellow health care professionals by using a bio-psycho-social and spiritual approach to care. General measures: Communication is at the centre of care. The following aspects should be addressed:
• Honest, direct, compassionate and culturally sensitive information about the prognosis (see Conversation Guide).
• Assessment of the patient and family resources and needs, especially spiritual needs.
• Place of death will be determined by the ability to maintain infection control.
• Emergency contact details, especially if the patient wants to go home. • Compassionate information about symptoms that might develop and how
to manage them (see Home Care Guide). • Nutrition and hydration. Provide sips of water and comfort feeding. • Discontinue all non-essential, non-beneficial procedures (which you will
not act on) and medication, e.g. 4-hourly blood pressure measurements and vitamin tablets.
• Ensure medications are prescribed for symptom management and prescribe, when needed, medication to pre-empt common symptoms during the terminal phase using the appropriate route:
o Pain: If the patient is on Morphine already, then continue; if the patient is unable to swallow, convert to Morphine Sulphate by dividing the total 24-hour dose by 3.
o Nausea and vomiting: see table below o Respiratory secretions: see table below
13
o Agitation/restlessness/delirium: see table below • Feeding and hydration - discuss with the family. If the decision is to
hydrate and/or feed, ensure gentle hydration and advise the family that hydration does not improve QOL, survival or symptom burden at the end of life and should not be given as routine management. Rather offer sips of water if the patient is able to swallow.
• Ensure impeccable nursing care. Source: NICD Environmental health guidelines: https://bit.ly/39vDWoS
Flow diagram of drug dosages for end-of-life care:
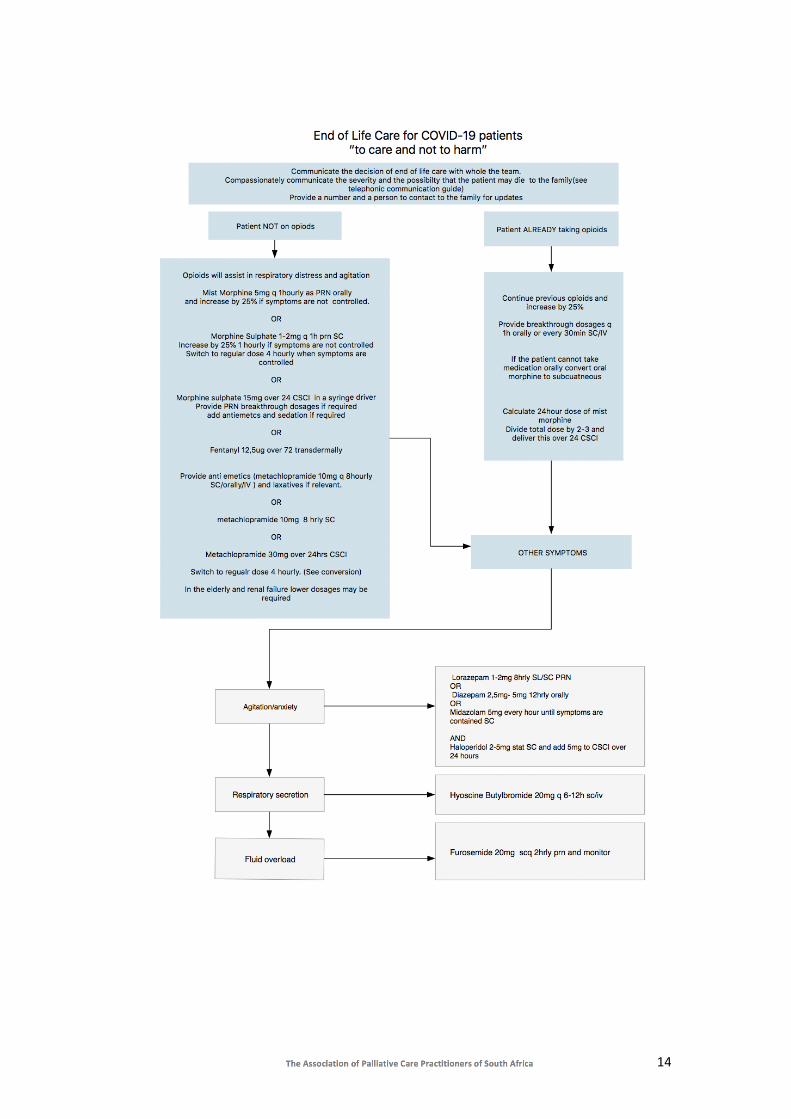
14

15
Communication in the time of COVID-19 Never more than in a time of high anxiety, great medical need and probable rationing of medical intervention, do we require skilled and compassionate communication with our patients, their families and each other. Important communication skills to remember: • Always start by checking the patient/family member’s understanding of the
situation and ask what they have been told before. There are often clues for you to use in order to take the conversation forward.
• Give information in small, digestible chunks, avoiding medical jargon. • Use silence- this allows people to absorb what was said and show
emotion. • Acknowledge emotion: NURSE acronym
Name emotion: ‘You seem to be upset/worried?’ Understanding: ‘Given what is going on, I can understand your concern.’ Respecting: ‘You have been really patient under difficult circumstances.’ Supporting: ‘I understand that this is very hard. We will be here to help.’ Exploring: ‘Tell me more, I would like to understand what you’re thinking.’
• Never say: ‘There is nothing more that we can do for you/your mother...’. Commit to excellent symptom management, compassionate communication and your presence.
• Consider linking family telephonically or online to say a final goodbye. • Consider arranging a tablet or phone in a wipeable pouch for the unit for
WhatsApp video calls or equivalent. Below are a number of communication tips for specific scenarios, adapted for the South African setting from VitalTalk and made freely available during the COVID crisis. You can find more information and the full guide on their website.

16
Admitting: When your patient needs to be transferred to hospital or the ICU
What they say What you say
[Patient] How bad is this? From the information I have now and from my exam, your situation is serious enough that you should be in the hospital. We will know more in the next day, and we will update you.
[Family] Is my grandfather going to make it?
I imagine you are scared. Here’s what I can say - because he is 90, and is already dealing with other illnesses, he is sick enough to die. Honestly, it is too soon to say for certain.
[Patient] Are you saying that no one can visit me?
I know it is hard to not have visitors. The risk of spreading the virus is so high that I am sorry to say we cannot allow visitors. They will be in more danger if they come into the hospital. I wish things were different. You can use your phone or request to use our portable phone, although I realize that is not quite the same.
[Family] How can you not let me in for a visit?
The risk of spreading the virus is so high that I am sorry to say we cannot allow visitors. We can help you be in contact electronically via video or phone call. I wish I could let you visit, because I know it’s important. Sadly, it is not possible now.
Admitting: When emotions are running high
What they say What you say
You people are incompetent! I can see why you are not happy with things. I am willing to do what is in my power to improve things for you. What could I do that would help?
I want to talk to your boss. I can see you are frustrated. I will ask my boss to come by as soon as they can. Please realize that they are juggling many things right now.
Do I need to say my good-byes?
I'm hoping that's not the case. And I worry time could indeed be short. What is most pressing on your mind?
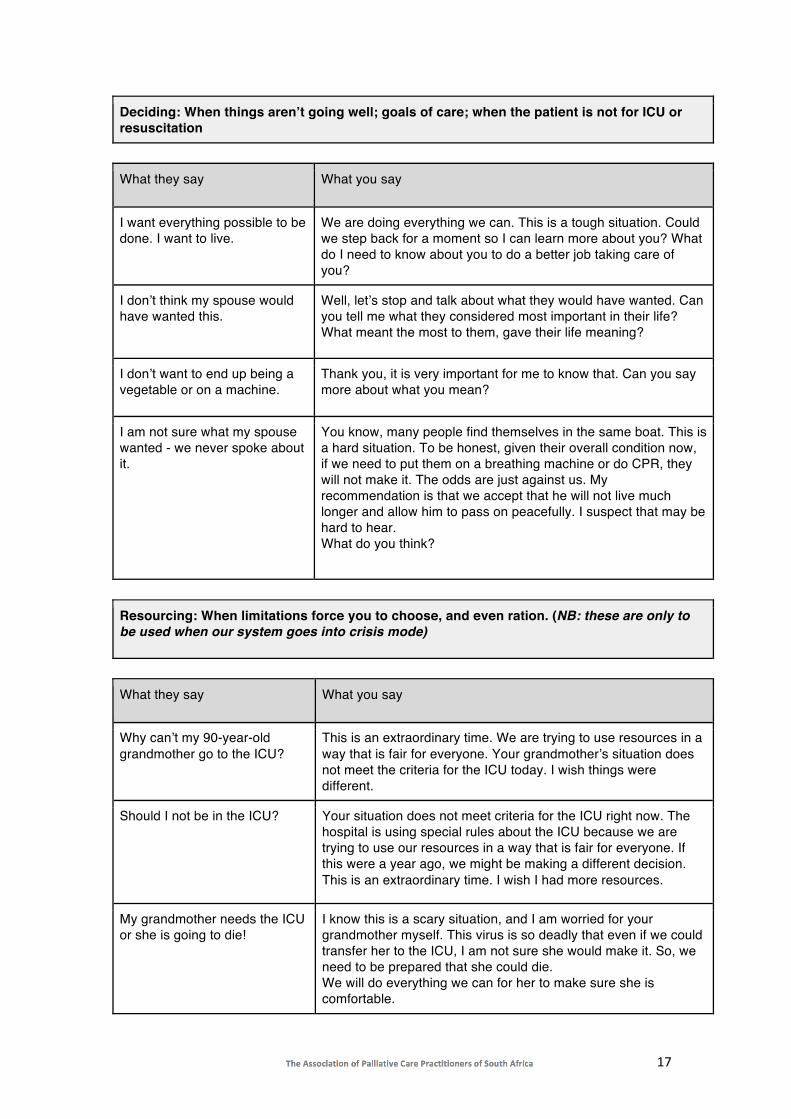
17
Deciding: When things aren’t going well; goals of care; when the patient is not for ICU or resuscitation
What they say What you say
I want everything possible to be done. I want to live.
We are doing everything we can. This is a tough situation. Could we step back for a moment so I can learn more about you? What do I need to know about you to do a better job taking care of you?
I don’t think my spouse would have wanted this.
Well, let’s stop and talk about what they would have wanted. Can you tell me what they considered most important in their life? What meant the most to them, gave their life meaning?
I don’t want to end up being a vegetable or on a machine.
Thank you, it is very important for me to know that. Can you say more about what you mean?
I am not sure what my spouse wanted - we never spoke about it.
You know, many people find themselves in the same boat. This is a hard situation. To be honest, given their overall condition now, if we need to put them on a breathing machine or do CPR, they will not make it. The odds are just against us. My recommendation is that we accept that he will not live much longer and allow him to pass on peacefully. I suspect that may be hard to hear. What do you think?
Resourcing: When limitations force you to choose, and even ration. (NB: these are only to be used when our system goes into crisis mode)
What they say What you say
Why can’t my 90-year-old grandmother go to the ICU?
This is an extraordinary time. We are trying to use resources in a way that is fair for everyone. Your grandmother’s situation does not meet the criteria for the ICU today. I wish things were different.
Should I not be in the ICU? Your situation does not meet criteria for the ICU right now. The hospital is using special rules about the ICU because we are trying to use our resources in a way that is fair for everyone. If this were a year ago, we might be making a different decision. This is an extraordinary time. I wish I had more resources.
My grandmother needs the ICU or she is going to die!
I know this is a scary situation, and I am worried for your grandmother myself. This virus is so deadly that even if we could transfer her to the ICU, I am not sure she would make it. So, we need to be prepared that she could die. We will do everything we can for her to make sure she is comfortable.

18
It sounds like you are rationing us.
What we are doing is trying to spread out our resources in the best way possible. This is a time where I wish we had more for every single person in this hospital.
How can you just take them off a ventilator when their life depends on it?
I’m so sorry that her condition has become worse, even though we are doing everything. Because we are in an extraordinary time, we are following special guidelines that apply to everyone here. We cannot continue to provide critical care to patients who are not getting better. This means that we need to accept that she will die, and that we need to take her off the ventilator. I wish things were different. We will make sure that she is comfortable, has no suffering and will make sure she is not alone.
Notifying: When you’re telling someone over the phone
What they say What you say
Yes, I’m his daughter. I am 5 hours away.
I have something serious to talk about with you. Are you in a place where you can talk?
What is going on? Has something happened?
I am calling about your mother. Are you in a place where you can talk? We are doing everything we can for her, and I am worried because she is getting worse.
What is going on? Has something happened?
I am calling about your mother. Are you in a place you can talk? We are caring for her in the best possible way and the breathing machine is not helping. (Silence) I know this is going to be hard to hear. We have to now have to take her off the machine and we are expecting that she might die within (insert timeline)… (Silence) I can imagine not seeing her makes it so much worse. Even though she is not fully awake, would be helpful if I held the phone to her ear so that you can say a few words or I can pass on a message to her.
What is going on? Has something happened?
I am calling about your father. I am afraid I have bad news for you. He was admitted to hospital diagnosed with COVID19. I am sorry to tell you that he died a short time ago.
Crying I am so sorry for your loss. (Silence) If you feel you must say something: Take your time. I am here.
I knew something was coming, but I didn’t realize it would happen this fast.
I can only imagine how shocking this must be. It is sad. (Silence - wait for them to restart).
19
Anticipating: When you’re worrying about what might happen
What you fear What you can do
That patient’s son is going to be very angry.
Before you go in the room, take a moment for one deep breath. What’s the anger about? Love, responsibility, fear?
I don't know how to tell this adorable grandmother that I can’t put her in the ICU and that she is going to die.
Remember what you can do: you can hear what she’s concerned about, you can explain what’s happening, you can help her prepare, you can be present. These are gifts.
Managing emotions in ourselves
What I am thinking What you say
I should have been able to save that person.
Notice: am I talking myself the way I would talk to a good friend? Could I step back and just feel? Maybe it’s sadness, or frustration, or just fatigue. Those feelings are normal. And these times are distinctly abnormal.
I cannot believe we don’t have the right equipment/how mean that person was to me/how everything I do is blowing up in my face.
Notice: am I letting everything get to me? Is all this analysing really about something else? Look how sad this is, how powerless I feel, how silly our efforts seem? Under these conditions, such thoughts are to be expected. We don’t have to let them drag us down. Can we just notice and feel/share them? Can I step into a less reactive, more balanced place as I move onto the next thing?
I am afraid of burnout, and of losing my heart.
Can you look for moments every day where you connect with someone, share something, enjoy something? It is possible to find little pockets of peace even in the middle of a maelstrom.
VitalTalk is a 501c3 non-profit social impact organization dedicated to making communication skills for serious illness part of every clinician’s toolbox.
End-of-life care for COVID-19 patients at home
Patients with COVID-19 who have become severely, critically ill and who may not qualify for crisis triaging of ICU or hospital beds or ventilation may be directed to stay at home and be cared for in their home setting.

20
These difficult decisions must be conveyed to the patient and family members in a compassionate manner by a senior clinician with ongoing home support offered. Patients and their caregivers should be given contact details of a local palliative care provider who would be available to guide them through this time. Palliative care providers must be informed of the discharged patient immediately via email or WhatsApp. These contact details are to be provided to the hospitals. Local hospitals should liaise with the designated palliative care provider, informing them of:
1. The patient’s COVID-19 status and laboratory results 2. Their clinical condition 3. Their medical information regarding relevant co-morbidities and
ethical decision-making 4. The patient and carer’s address and contact details 5. The patient’s contact tracing list.
See discharge form required (COVID-19 patient home discharge and palliative care referral) Supply the discharged patient with a tool kit for home:
• A care package with soap, masks, gloves, plastic refuse bags etc. • An education pack to be given to the family regarding symptom
control – available in all South African languages. • All palliative medication must be sent from the discharging hospital
or clinic; palliative care guidance to be given by the hospital doctor; script to include paracetamol, medication to manage symptoms and anticipatory symptoms.
• A phone number to contact if symptoms are not controlled. • A home-based care referral. • Pre-bereavement counselling/contact with a social worker or
psychologist on discharge from the hospital. • Guidance on financial matters e.g. a grant. • Guidance on childcare. • Guidance on wills.
Local epidemiology/ DOH authorities need to be informed of the patient returning to their community. At the same time, palliative care providers and home carers/nurses and family need to be adequately protected from contracting the virus.

21
Management of COVID negative palliative care patients
COVID-19 has been shown to affect the elderly and frail, as well as patients with underlying chronic diseases more severely than others. This may include patients with advanced cancer, end-stage organ failure, AIDS and degenerative neurological diseases. Many of these patients may already be part of palliative care programs or are candidates for palliative care (see guidelines for identifying patients with deteriorating health https://www.spict.org.uk). Unfortunately, in a severely resource limited setting like the current COVID pandemic, patients suffering from chronic diseases with no prospect of cure may not receive the care they deserve, due to patients with a better prognosis being prioritized above them. It is therefore imperative that we protect these vulnerable patients from being infected with COVID-19, whilst at the same time providing them with optimal symptom control for their existing conditions and ensuring ongoing palliative care according to their preferences and values. Consider the following aspects of care:
• Be proactive (protect, plan and support). • Encourage compliance with the strategies of hand hygiene and social
distancing. • Manage distressing symptoms of underlying disease as per the HPCA
Clinical Guidelines https://hpca.co.za/Resources/clinical-guidelines/. • Ensure more than one carer has been identified to help care for the
patient and a chain of care has been developed to ensure ongoing care if the main carer becomes infected and needs to self-isolate or be hospitalized.
• All carers and family members should be asked to report if they develop a fever or cough or other symptoms suggestive of COVID-19. This should be done before coming to work or visiting.
• Discuss what the family should do if they observe symptoms suggestive of COVID-19.
Advance care planning
Advance care planning (ACP) involves a dialogue between a healthcare provider and their patient about what might lie ahead with their illness and about how their personal goals, values and preferences can be respected and incorporated in the plan for their care. It is an integral part of caring for patients with serious illnesses or who are nearing the end of their lives, and healthcare providers should prioritize such discussions with their frail or chronically ill patients.

22
ACP has been shown to lead to care that is more aligned with patients’ wishes, reduce the rate of futile, aggressive interventions at the end of life and reduce complicated bereavement in family members. It also provides healthcare providers and family with valuable information when having to make healthcare recommendations and decisions in the future. In a time of limited healthcare resources like the COVID-19 pandemic such decisions can be particularly difficult to make, so we recommend the urgent implementation of ACP for all patients with serious illnesses or who are nearing the end of their lives. Guidance on ACP can be found on the PALPRAC website by following this link: https://bit.ly/2UPTjTF It might be important to specifically discuss what they would prefer to do (remain at home or go to hospital) if they should develop symptoms of COVID-19. Make a note of the decision and the name of their designated healthcare proxy (decision maker). Take note that a patient meeting the case definition for COVID-19, who chooses not to report to a healthcare facility or to get tested, is obliged to self-isolate and de-isolate strictly according to the clinical COVID-19 guidelines. The same applies to their carers. If such a patient should die before de-isolation, the body should be regarded as a COVID-19 infected body and be disposed of as per the COVID-19 environmental health guidelines. Medication, education and resources to ensure quality of life during isolation should be provided. Ensure patients have adequate medication at home to manage current symptoms, breakthrough symptoms and symptoms that might develop in the future Educate patient and families on:
• Pharmacological and non-pharmacological symptom control for current and future symptoms.
• Hand washing and hygiene • PPE (if needed) • Symptoms and signs of COVID-19 • Basic nursing care, if families have to provide this. • Resources - where to find help if symptoms are uncontrolled. • Link the patient telephonically to local clinic or hospital unit. • If possible, offer telemedicine. For basic advice on etiquette, follow
this link - Virtual Connection in an age of social distancing by Michael Fratkin.
• See the updated HPCSA guidelines on telemedicine during COVID: https://www.hpcsa.co.za/Uploads/Press%20Realeses/2020/Guidelines_to_telemedicine_in_South_Africa.pdf

23
• Provide patient and family with telephonic or online psycho-social and spiritual resources (it is best to link with local resources such as local churches and community organisations)
Palliative care patient who develops symptoms of COVID-19
Testing of palliative patients who are bedbound/housebound with possible COVID-19 infection: In patients with clinical suspicion and contact with a person either confirmed or under investigation for COVID, the NCID PUI form will need to be completed. However, many palliative care patients will not be able to visit testing sites. The need for further testing will need to be determined by health authorities. These are some suggestions for managing adult patients currently receiving palliative care outside of a hospital context during the COVID-19 epidemic:
• Discuss what the family should do if they observe symptoms suggestive of COVID-19.
• Explain that 80% will develop a mild illness, 15% will develop severe disease and 5% become critically ill and may die.
• The severity of COVID-19 infection increases with age and with the severity of any underlying medical co-morbidity.
• Symptoms of COVID-19 infection can escalate quickly, and decisions regarding escalation of care must be discussed early and are best not made in the midst of an escalating crisis.
For those with mild symptoms:
• Start symptomatic treatment with paracetamol for pain and fever. • Encourage appropriate fluid intake. • Do not use Ibuprofen or NSAIDs as they have been implicated in
aggravating the condition of some patients with COVID-191. • Explain that your patient should remain in one room until better and
have exclusive use of one bathroom, if possible. These rooms should be well ventilated (open windows and an open door). Limit the movement of the patient elsewhere in the house and ensure shared spaces e.g. kitchen and bathroom are well ventilated.
• Household members to maintain a distance of at least 1m (preferably 2m) from the ill patient. Limit the number of caregivers; ideally caregivers should be in good health with no underlying chronic or immunocompromising conditions. Non-essential visitors should not be allowed.
24
• Encourage hand washing, masks, appropriate disposal of tissues, dedicated crockery and cutlery, cleaning of surfaces with 0.1% hypochlorite or similar cleaning agent. Refer to the WHO guideline “Home care for patients with suspected COVID-19 infection”.
• Patients should be encouraged to wear a medical mask to contain respiratory secretions. If this is not feasible or not tolerated, cover the mouth and nose with disposable paper tissue when coughing or sneezing, and discard immediately after use. If handkerchiefs are used, wash after each use with soap and water.
• Arrange for a family member to report progress to you on a daily basis using WhatsApp.
• Warn of possible sudden deterioration. For those with worsening symptoms:
• Refer to hospital if the patient and family request this. Notify the hospital and follow their protocol for triage and admission. Keep up to date with the availability of beds in your local hospital and their admission criteria.
• If the patient wishes to remain at home, continue supportive palliative care: o low dose (5ml) oral morphine 4-hourly for dyspnoea if not already
on opioids. o consider home oxygen if this is feasible and practical in the home
environment. o consider an antibiotic if a secondary bacterial infection is suspected,
but only where this meets the goals of care. o sublingual Lorazepam (Ativan, Tranqipam) 1-2mg as required if
restless; repeat at 10-minute intervals until peaceful. o patients that are unable to swallow will need to be given medication
via a syringe driver or, if that is not available, via intermittent subcutaneous injection.
o Morphine and Midazolam should be given in appropriate doses, as discussed in the clinical management above.
• Refer for counselling and spiritual guidance if appropriate.
The dosages will vary depending on the patient’s current prescription and needs and discretion of the clinician. Throughout this time, provide appropriate information regarding your assessment and the possible future scenarios. We are in a time of great uncertainty and significant risk. Patients and families appreciate doctors who are willing to listen to their fears and provide adequate information and guidance.

25
• Download family guide to using oral morphine at home.
Protection for healthcare providers in the community Refer to the WHO guideline “Rational use of personal protective equipment for coronavirus disease (COVID-19)”. The recommendations differ according to the setting, personnel and type of activity involved. It is important to note that basic protection and excellent hand hygiene is all that is required in day to day interactions with asymptomatic patients. Wear a medical mask if you have respiratory symptoms. Here are some guiding principles around PPE for healthcare workers when caring for palliative patients in the home with known or suspected COVID-19:
1. Wear gloves, a surgical mask and perform hand hygiene after disposing of the mask. 2. Doctors and patients must stay at least 1m, and preferably 2m, apart except during examinations. 3. If tolerated, the patient needs to wear a surgical mask. Note: N95 masks, face-protectors, goggles and gowns are reserved for procedures where respiratory secretions can be aerosolized such as intubation in known or suspected cases of COVID-19.
What if you have been in contact with an infected person: Self-quarantine was advised in Hong Kong when contact was within 2m of a patient for >15 minutes; in Singapore that would be for >30 minutes. If exposure <15 minutes, but within 2m for >2 minutes, keep working but wear a surgical mask and have your temperature checked twice a day. If you have brief, incidental contact, you should monitor yourself.
Long-term care facilities Know your residents:
• Ensure all medical information is known to the staff and medical records are easily available.
• Ensure all residents have an advanced care plan in place. • Ensure family contact details are correct and available. • Ensure the highest standards of hygiene, sanitation, laundry and waste
management are in place. See the WHO Infection Prevention and Control guidance for Long-Term Care Facilities in the context of COVID-19 (interim guidance document, 21 March 2020) https://apps.who.int/iris/bitstream/handle/10665/331508/WHO-2019-nCoV-IPC_long_term_care-2020.1-eng.pdf
Prospective surveillance for residents and staff: Residents
• Assess each resident twice daily for fever >38C, cough and shortness of breath.

26
• Immediately report fever and respiratory symptoms to clinical staff. • Staff • Educate staff on signs and symptoms of COVID-19. • Staff should stay at home if they had close contact with a COVID-19
positive member. • Staff should stay home if ill and symptomatic (response to COVID-19
infection - see guideline above). General considerations for care:
• Older people, especially in isolation and those with cognitive decline, dementia, and those who are highly care-dependent, may become more anxious, angry, stressed, agitated and withdrawn during the outbreak or while in isolation.
• Provide practical and emotional support through informal networks (families) and health care providers.
• Regularly provide updated information about COVID-19 to residents, employees and staff.
Support for healthcare workers and caregivers:
• As much as possible, protect staff from stress both physically and psychologically so they can fulfil their roles, in the context of a high workload and in case of any unfortunate experience as a result of stigma or fear in their family or community.
• Regularly and supportively monitor all staff for their wellbeing and foster an environment for timely communication and provision of care with accurate updates.
• Consider rest and recuperation and alternate arrangements as needed. • Mental health and psychosocial support and psychological first aid
training can benefit all staff in having the skills to provide the necessary support in the LTCFs.
• Staff need to ensure that safety measures are in place to prevent excessive worries or anxiety within the LTCFs.

27
Carer guidelines
Download this carer handout in colour. Also see these links for guidelines:
• https://www.who.int/publications-detail/infection-prevention-and-control-during-health-care-when-novel-coronavirus-(ncov)-infection-is-suspected-20200125
• Western Cape DOH: https://www.westerncape.gov.za/department-of-
health/health-workers
The Wellbeing of Healthcare Professionals
When caring for patients with life-threatening illnesses or for those who are at the end-of-life, you as a health care practitioner are constantly faced with the suffering and distress that your patients and their families are experiencing. As members of a people-centred care profession we are constantly striving to
28
reduce our patients’ distress by giving them the best standard of health care that we can. Under normal circumstances we as healthcare professionals find that the demands of our work often exceed our inherent resources on the physical, emotional, psychological and spiritual levels.
In addition to this we have had limited formal training on how to practice self-awareness and to care for our own well-being. In fact, our training rewards characteristics like self-sacrifice, infallibility and not expressing our own emotions - be it anger, frustration or sadness. When pushed to the limits, these seemingly noble attributes can easily transform into feelings of resentment and deprivation. The consequences are self-entitlement, a conspiracy of silence around our shortcomings and errors and a sense of intense isolation and loneliness because our own emotions are never acknowledged.
Burnout is described as a ‘mental state that arises from prolonged interaction with the unrelenting demands of one’s work environment’ and is characterized by:
1. exhaustion, where you find yourself depleted of physical energy, emotional strength and spiritual resources
2. feelings of cynicism, depersonalization and indifference towards others 3. a loss of purpose and a sense of failure as a professional and as a
person
In healthcare practitioners, burnout has been linked to suboptimal patient care, medical error and reduced productivity, but more importantly it leads to reduced self-awareness, self-neglect, absence from work, depression and physicians leaving the profession. It is important to recognise that the presence of burnout itself is not a psychiatric disease. However, burnout may be associated with depression, substance abuse and suicidal ideation. Make sure that you are able to recognize your own signs of burnout and act on them.
Burnout in health care professionals can be caused by internal and external stressors as listed in the table below. It is possible to reduce some of our external stressors through careful analysis and re-organization of our workflow, work-environment and staff complement. Such changes require buy-in from employers and institutions and often take time to manifest. Some external and most internal risk factors for burnout can however only be mitigated through a personal commitment to self-awareness and self-care; recognizing the aspects of your work that drain you, knowing how to reduce their draining effect and making time to do the things that replenish your resources.
29
Internal
External
• Crossing of boundaries in doctor-patient relationships
• Compassion fatigue • Cumulative grief (Multiple losses or
deaths over a short time span) • Conversations that elicit emotion
(Breaking bad news, Advance care planning, conflict resolution)
• Countertransference • Lack of sense of control over events • Unable to access or utilize personal
support structures (life-partner, family, friends)
• Ethical dilemmas • Lack of sleep, exercise and a healthy
diet • Lack of experience, skills, knowledge
and mentorship • Attribution of achievement to chance
or others rather than one’s own abilities
• Passive, defensive approach to stress and conflict
• Lack of career fit or job dissatisfaction
• High expectations of self to transform institutional, clinical and social culture
• Inability to adapt to change
• Risk of personal physical harm
• Inadequate supervision • Red tape/ paperwork • Shift-work • Staff shortages • Limited resources • Excessive overtime • Conflict between
colleagues • Role blurring • Disorganized work
environment • Abuse in the workplace • Inconsiderateness
amongst colleagues • Inadequate remuneration • Workload
In the context of a global healthcare disaster like COVID-19, all these risk factors for burnout are amplified, but 3 of them bear special mention in the context of palliative care, namely cumulative grief, compassion fatigue and countertransference. Besides the medical care palliative care patients require, there is also a significant emotional component to their care – sometimes hidden and often disregarded in terms of its impact on the HCP.
Compassion fatigue:
A mental condition resulting from prolonged exposure to human suffering, particularly in persons working in people-orientated service professions who witness physical, emotional and mental pain on a daily basis as part of their job. It can manifest as exhaustion, irritability or emotional unavailability. In the setting of war and conflict, much like the current COVID pandemic, it is related to the witnessing of multiple deaths, senseless killing and seeing the

30
devastating often long-term effects that war has on surviving individuals and societies. Compassion fatigue evolves specifically from the relationship between the practitioner and patient or family. It has been seen as the cost of caring for those in emotional pain and is also known as vicarious or secondary traumatization.
Cumulative grief:
Defined as an intense form of grief resulting from experiencing multiple losses within a relatively short space of time without the opportunity to deal with each loss separately, thus leading to an individual suppressing their own grief response and simply carrying on. In the field of palliative medicine these losses are experienced at the death of a patient but also when children lose a parent, when we are unable to provide our patients with the kind of “good death” that they hoped for or when we see a family fall apart due to illness. And even though there may be recognition that we as doctors experience grief in response to these events, this is largely seen as an individual feeling which must be dealt with on a personal level. Not being afforded the time or space to express one’s own grief can lead to feelings of numbness, dehumanization and guilt. This type of silent mourning can become a source of chronic stress that leads to burnout and decreased effectiveness.
Countertransference:
Defined as the emotional reaction evoked in the carer, in response to the patient’s disease, problems, behaviour or feelings. This is individually determined by your unique history, your sense of self as a person, your role in your family or society or perhaps by how you came to work in this field. Caring for patients with life-threatening illnesses can force us to face our own mortality, deal with unexamined regrets or unresolved feelings from a previous experience of loss. Every dying patient can represent an opportunity to make up for past failure where we might have been unable to provide compassionate care for someone who was dying.
It can also manifest as having the need to have patients understand and experience the situation exactly as you do. It is not ‘wrong’ or bad to feel these feelings, on the contrary, they represent a very normal response to bearing someone else’s suffering. What is important is your awareness of the feelings, and the choices you have about what you do with them. If you are conscious of them, you will be less likely to feel guilty, criticize yourself, be angry or label the patient unnecessarily. Not recognizing these reactions as countertransference, will be unhelpful for the patient, and for yourself. Through self-awareness you can evaluate whether these reactions are your own uncomfortable feelings, or a clue to what the patient may be feeling. We are unsure of the duration of the COVID-19 ‘season’ and we need to ensure that we are going to be here at the start and the finish. We are expecting 20% of us to get infected and thus we are working on the premise
31
that only 80% of staff will be at work. Below are a number of things that you can do today to stay healthy, both in body, mind and soul.
Teamwork:
Working as part of a team can play a significant role in reducing the draining effect of these risk factors for burnout. The members of a team work together towards a common goal and each member, especially when the team consists of HCWs from different professional backgrounds, brings a different skill set to the table. These skills can be utilized to share the burden of decision-making, find creative solutions to complex patient and family problems and provide a safe space for confidential debriefing after a particularly draining event. Successful teams prioritize communication between its members and between the team and the patients and families they care for. They ensure a pragmatic balance between clear role-definition and the flexibility to take over or share tasks and leadership roles if the need arises. Team members provide emotional and psychological support for each other and monitor each other for signs of stress and burnout.
Learn to use the right words: Difficult conversations that involve emotions can be extremely draining on health care professionals. By teaching yourself a few skills your interactions with patients in families can become less daunting and more gratifying for all involved. See section on Communication in the time of COVID-19. Self-care and mental health: Physical Care:
• Eat a healthy diet (low in sugar) and drink sufficient fluids. • Sleep between 6-8 hours per day. • Exercise regularly. • Practice good personal hygiene at work and don’t forget on your way
home and at home. • Remove your second pair of clothes outside the house or in the
garage, leaving shoes outside. • Shower before spending time with your family. • Ensure you protect those at home, who are high risk.
Mental Health:
• Many of us are already suffering with Anxiety and Depression - DO NOT STOP your chronic medication.
• Be aware of your own stress levels and know your limitations.

32
• Be aware of your own losses (of normality; loss of free time) and be aware of your own grief for patients.
• Acknowledge that you are human and your experience of this pandemic.
• Take breaks from the work by spending time with family; make time for relaxation.
• Identify things that give your strength and enjoyment. • Seek help early if you need guidance or to talk to someone. There is
the Metropolitan Employee Health and Wellness program (0800 611 093) and find out about other mental health services available at this time at your facility.
• Seek professional help if you need it. Social Health:
• Do not emotionally isolate yourself during this time - communicate with colleagues, friends and family.
• Use WhatsApp, video calls and skype and check in on each other. • Communication is critical.
Spiritual Health: A pandemic like this often pushes one to the limits and we look within ourselves and search for meaning in all of this.
• Maintain your spirituality. • Know your values - what gives you meaning, purpose and hope • Practice gratitude and take time to reflect. • Keep in contact with your religious and cultural groups.
See these links for further guidelines: https://www.who.int/docs/default-source/coronaviruse/mental-health-considerations.pdf https://www.facebook.com/northbrisbanepsychologist/videos/2962907510419354/
Management of the deceased
Please see: Circular H 41 of 2020: COVID-19: Management of the deceased in the Western Cape.
33
Addenda
Addendum 1: PATIENT AND CARER INFORMATION SHEET FOR WHEN END-OF-LIFE CARE WILL TAKE PLACE AT HOME
We would like to give you some information to help you during this very difficult time. Your ongoing support and care are very important to us. You have been asked to care for someone who is very ill, but is also infected with a dangerous virus (Coronavirus) that could potentially cause you to become ill if safety precautions are not followed. General Health and Safety Precautions: • Wear a mask covering your mouth and nose. When your loved one coughs
or sneezes, the virus particles can spread through the air and will infect you if you breathe them in.
• Wear gloves (if available) or cover your hands with plastic packets and then dispose of them. If the virus gets on to your hands and you touch your eyes, nose or mouth, you will become infected.
• Wash your hands thoroughly with soap and water for 20 seconds after touching or being in the same room with your loved one.
• Wipe down all hard surfaces with a cleaning agent several times a day. The virus particles can settle and stay on surfaces for up to 9 hours. Touching these surfaces and then your eyes, nose or mouth might spread the virus to you and your other family members.
• It is best for the ill person to stay in a room by him- or herself and not be allowed to move around the house. Visitors should be strictly limited – only the person/s caring directly for the ill person and those closest to him/her should be exposed.
• Keep crockery, cutlery, linen and clothing that your loved one uses separate from the rest of the household. Clean them thoroughly with soap and water.
What to expect from the coronavirus: There is still no known cure or vaccine for this virus. Thus, as the virus continues, your loved one will become more ill and may display the following symptoms: • Ongoing high fevers with possible sweating and trembling. • They may be very thirsty initially; but will not be able to tell you this as they
become more unwell.
34
• Their mouth may become very dry, with their lips cracking, their tongue becoming fuzzy and their mouth smelling bad.
• Their cough may become more frequent and severe, preventing them from sleeping at night.
• They might cough up blood. • Worsening tiredness with inability to walk to the bathroom, sit up or move
around in bed. • They may be very short of breath, even too breathless to speak. The
slightest movement may make it worse, including going to the toilet or changing positions in bed.
• They are unlikely to be hungry and may refuse even small amounts of food and water.
• They will get thinner and weaker because the virus is attacking their bodies and also making them too sick to eat.
• They may develop constipation or even diarrhoea. • Their circulation will become poor, so their hands and feet may feel colder
and their skin will be more vulnerable to pressure sores. These will first appear as dark, pink to purplish areas and may form a blister. The skin will come off, leaving a moist yellowish area which will likely increase in size.
What you can do to help: • Try and rest when your loved one is sleeping, as their ongoing coughing is
likely to keep you awake as well. • Keep doing everything to prevent yourself from catching the virus. Follow
the Health and Safety Precautions above carefully. • If your loved one will tolerate wearing a mask/scarf/bandana please
encourage it. However, when they become more breathless this will be too restrictive and should be removed.
• Make sure there is a breeze in their room, coming from behind you and away from you, to disperse any virus in the air. A flow of air will also ease the breathlessness that your loved one may be experiencing.
For high fever: • ensure a breeze of fresh air • use a moist facecloth or sponge to gently wash over the body • take off unnecessary clothing or linen • give medicine (Paracetamol 500mg tablets – 2 tablets by mouth every 6
hours) For increasing shortness of breath, worsening cough or coughing up blood: • while they are coughing, stay well clear - it is essential to wear something
to cover your mouth and nose and even sunglasses over your eyes • continue to talk calmly to your loved one – try and soothe their anxiety

35
• inform your palliative care provider who will organize Morphine syrup (a strong painkiller) for your loved one - this will help to ease the breathlessness and cough
For fear and anxiety: • acknowledge their fears and reassure them that you will continue to
support and care for them • distract them with music or singing • try and ask about what is causing them to feel this way • contact people on the telephone if your loved one wants to talk to them –
estranged family or friends, their pastor etc. • if the breathlessness is causing anxiety, then more medication needs to be
given - contact your palliative care provider who would be able to give you another tablet for this anxiety with directions for its safe use.
Tablets will become more difficult to swallow. Crush them between two spoons and mix with a small quantity of water or juice to make them easier to swallow. What to expect towards the end: If you are struggling to cope with keeping your loved one calm and you feel he/she suffering, please contact your palliative care provider urgently. Be prepared for your loved one’s condition to worsen quickly and unexpectedly – have the contact numbers of support organisations and individuals that you can call close by. Try not to panic. You should not call an ambulance at this time as they won’t be able to help. If your loved one starts to show these signs, they may soon die: • Extreme difficulty breathing or breathing that becomes irregular and has a
rattling sound • Persistent pain or pressure in the chest • Increased confusion or sleepiness • Bluish lips or face What you can do:
• Continue to speak to your loved one - they can hear you, even if they do not respond
• Moisten their mouth with drops of water and try to position him/her comfortably
• Inform those that care about your loved one

36
Unfortunately, even after your loved one has died, you and everyone in your household will need to stay in quarantine for 14 days to prevent the virus from spreading to other people in your community. Download flyer.

37
Addendum 2: VIRTUAL SUPPORT
Offering know patients support via teleconference or telephone is encouraged during the COVID crises. • For advise on virtual consult etiquette - Virtual Connection in an age of
social distancing by Michael Fratkin. • See the updated HPCSA guidelines on telemedicine during COVID:
https://www.hpcsa.co.za/Uploads/Press%20Realeses/2020/Guidelines_to_telemedicine_in_South_Africa.pdf
38
Addendum 3: DRUG CONVERSION TABLES
Drug Conversion ratio from oral morphine
Equi-analgesic dose to 30mg of oral morphine
Mist Morphine (Morphine syrup)
1 30mg
Morphine sulphate (SC) 2 to 1 15 mg
Morphine sulphate (IV) 3 to 1 10 mg To convert Mist Morphine 60mg in 24 hours to Morphine subcutaneous, divide by 2 to give 30mg over 24hours. If the patient is in renal failure, use lower dosages. Syringe driver prescription for a patient who has not been on opioids: Morphine 15mg Metoclopramide 30mg Midazolam 10-15mg 0.9% sodium chloride or ‘water for injection’ to fill up the 20-50ml syringe Infusion rate settings For 20ml syringe: run @ 0.8ml/h continuously over 24 hours For 50ml syringe: run @ 2ml/h continuously over 24 hours
39
Addendum 4: ESSENTIAL EQUIPMENT
• Syringe drivers (Ambulatory syringe pumps) • Butterfly needles (23G) / yellow Jelcos (24G) • Webcols • Micropore • 50ml, 20ml and 3ml syringes • Short infusion set • Normal Saline UDVs for flushing lines

40
Addendum 5: MEET MY LOVED ONE During the COVID crises families are likely not able to visit their loved ones on hospital or a care facility. It is also important for the health care facility to have the correct contact details of family members. This flyer allows families to tell health care providers something of their loved ones as well as confirming relevant contact details. https://palprac.org/wp-content/uploads/2020/04/PALPRAC_MEET-MY-LOVED-ONE_BW.pdf here in black and white. https://palprac.org/wp-content/uploads/2020/04/PALPRAC_MEET-MY-LOVED-ONE.pdf here in colour.

Head of Department: Health
Reference: COVID-19
Enquiries: Dr G. Reagon
021 4835776
CD: Emergency & Clinical Support Services
Department of Health, 4 Dorp Street, Cape Town, 8000, P.O. Box 2060, Cape Town, 8000
Tel: 021-4835776 E-mail: [email protected]
Circular H35/2020
TO ALL SMS MEMBERS/ CHIEF DIRECTORATES / DIRECTORATES / REGIONAL / DISTRICT OFFICES, SUB-
STRUCTURES / ALL FACILITY MANAGERS/ CITY OF CAPE TOWN / HIGHER EDUCATION INSTITUTIONS /
PRIVATE SECTOR
Dear Colleagues
During this global COVID-19 pandemic it is heartening how everyone is working together to stop the
transmission and care for those who have contracted the disease. Our greatest asset in the battle is
you, all our health staff, and you must keep yourself healthy to enable you to look after our patients
and your families. To do this please wash your hands regularly, clean and disinfect surfaces, and
wherever possible keep a social distance of at least 1 metre from people. Of course, when caring
for patients we have to be in direct contact with them and it is in this situation that we must all wear
the correct personal protective equipment (PPE). Each situation staff may be placed in has a
different risk of exposure, so clear precise PPE guidelines have been developed to ensure that the
most appropriate and effective PPE is used by staff in each situation. The guidelines are attached.
Our second greatest asset is the actual PPE. Our stocks of PPE are sufficient if we use them carefully
and don’t waste any PPE. It is very important to conserve our PPE supplies and only use them in
situations where they are actually needed. We absolutely must wear PPE when we need to, but we
must wear the correct PPE for each situation we are in. We must not use PPE when it is unnecessary
to do so. PPE stocks will then be preserved to ensure the safety of everyone. Take care of yourselves
and we will beat COVID-19.
Yours Sincerely
DR E ENGELBRECHT
HEAD OF DEPARTMENT: HEALTH
DATE: 2020/03/26
Annexure D
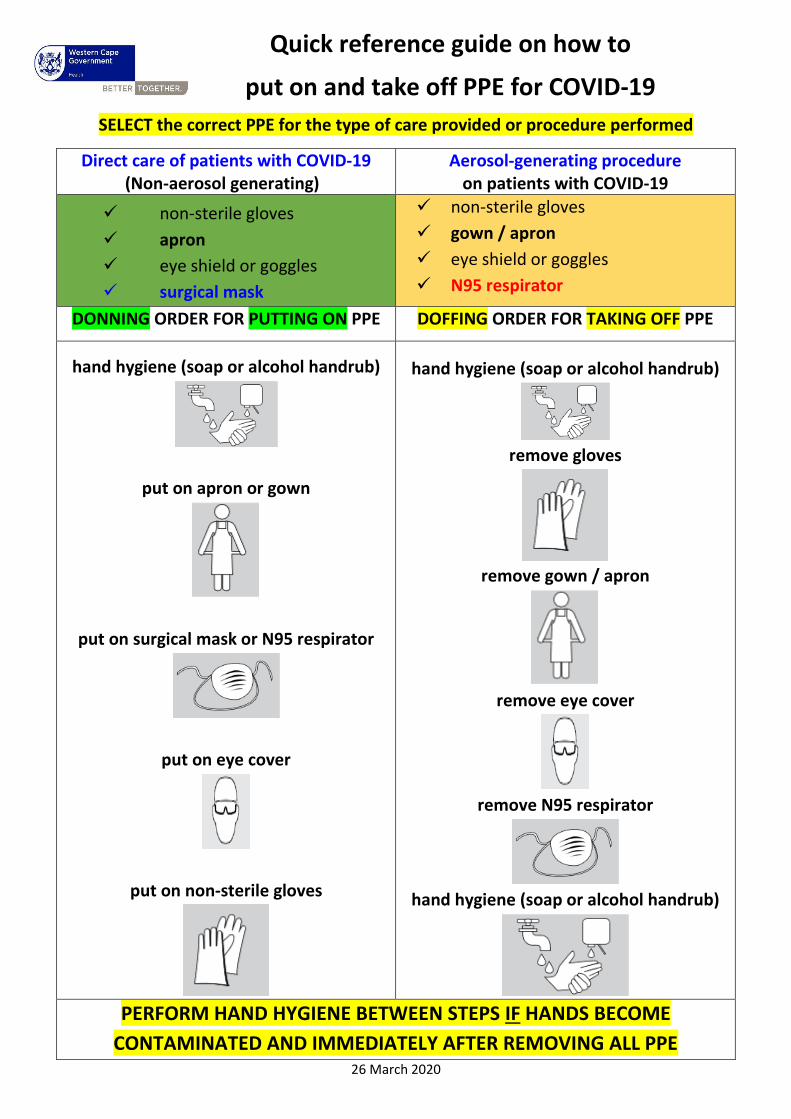
Quick reference guide on how to
put on and take off PPE for COVID-19
SELECT the correct PPE for the type of care provided or procedure performed
Direct care of patients with COVID-19 (Non-aerosol generating)
Aerosol-generating procedure on patients with COVID-19
✓ non-sterile gloves
✓ apron
✓ eye shield or goggles
✓ surgical mask
✓ non-sterile gloves
✓ gown / apron
✓ eye shield or goggles
✓ N95 respirator
DONNING ORDER FOR PUTTING ON PPE DOFFING ORDER FOR TAKING OFF PPE
hand hygiene (soap or alcohol handrub)
put on apron or gown
put on surgical mask or N95 respirator
put on eye cover
put on non-sterile gloves
hand hygiene (soap or alcohol handrub)
remove gloves
remove gown / apron
remove eye cover
remove N95 respirator
hand hygiene (soap or alcohol handrub)
PERFORM HAND HYGIENE BETWEEN STEPS IF HANDS BECOME
CONTAMINATED AND IMMEDIATELY AFTER REMOVING ALL PPE 26 March 2020
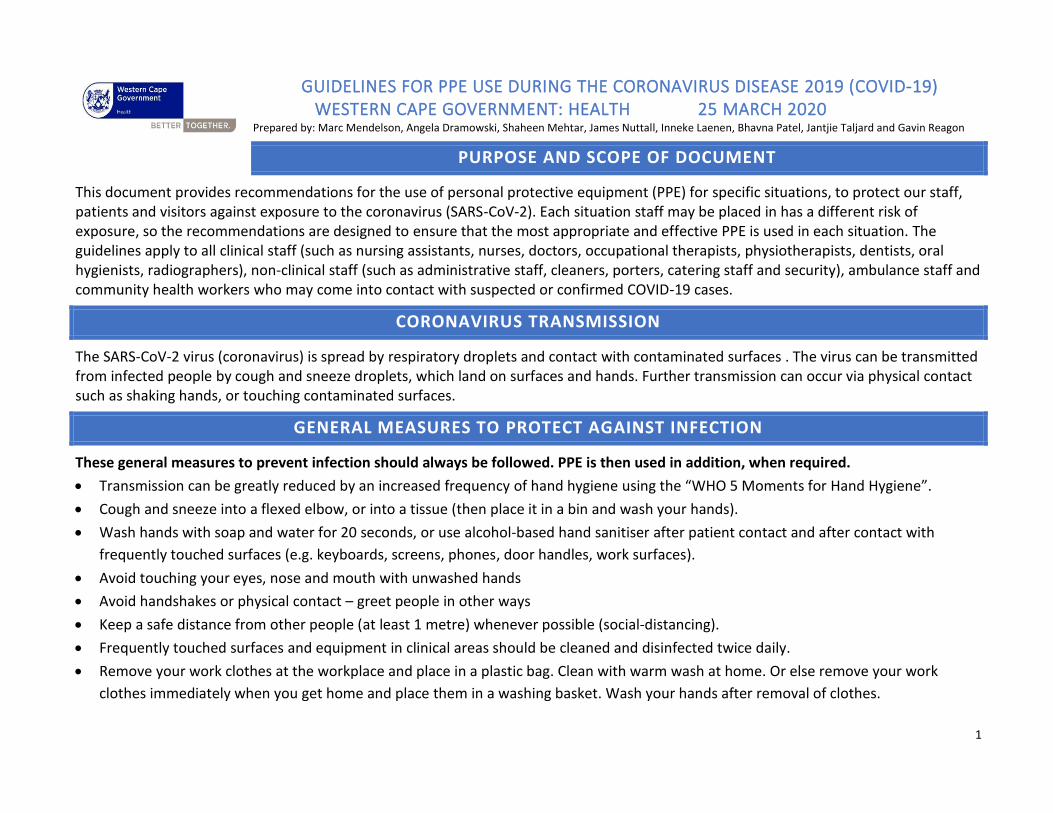
1
GUIDELINES FOR PPE USE DURING THE CORONAVIRUS DISEASE 2019 (COVID-19) WESTERN CAPE GOVERNMENT: HEALTH 25 MARCH 2020 Prepared by: Marc Mendelson, Angela Dramowski, Shaheen Mehtar, James Nuttall, Inneke Laenen, Bhavna Patel, Jantjie Taljard and Gavin Reagon
PURPOSE AND SCOPE OF DOCUMENT
This document provides recommendations for the use of personal protective equipment (PPE) for specific situations, to protect our staff, patients and visitors against exposure to the coronavirus (SARS-CoV-2). Each situation staff may be placed in has a different risk of exposure, so the recommendations are designed to ensure that the most appropriate and effective PPE is used in each situation. The guidelines apply to all clinical staff (such as nursing assistants, nurses, doctors, occupational therapists, physiotherapists, dentists, oral hygienists, radiographers), non-clinical staff (such as administrative staff, cleaners, porters, catering staff and security), ambulance staff and community health workers who may come into contact with suspected or confirmed COVID-19 cases.
CORONAVIRUS TRANSMISSION
The SARS-CoV-2 virus (coronavirus) is spread by respiratory droplets and contact with contaminated surfaces . The virus can be transmitted from infected people by cough and sneeze droplets, which land on surfaces and hands. Further transmission can occur via physical contact such as shaking hands, or touching contaminated surfaces.
GENERAL MEASURES TO PROTECT AGAINST INFECTION
These general measures to prevent infection should always be followed. PPE is then used in addition, when required.
• Transmission can be greatly reduced by an increased frequency of hand hygiene using the “WHO 5 Moments for Hand Hygiene”.
• Cough and sneeze into a flexed elbow, or into a tissue (then place it in a bin and wash your hands).
• Wash hands with soap and water for 20 seconds, or use alcohol-based hand sanitiser after patient contact and after contact with
frequently touched surfaces (e.g. keyboards, screens, phones, door handles, work surfaces).
• Avoid touching your eyes, nose and mouth with unwashed hands
• Avoid handshakes or physical contact – greet people in other ways
• Keep a safe distance from other people (at least 1 metre) whenever possible (social-distancing).
• Frequently touched surfaces and equipment in clinical areas should be cleaned and disinfected twice daily.
• Remove your work clothes at the workplace and place in a plastic bag. Clean with warm wash at home. Or else remove your work
clothes immediately when you get home and place them in a washing basket. Wash your hands after removal of clothes.
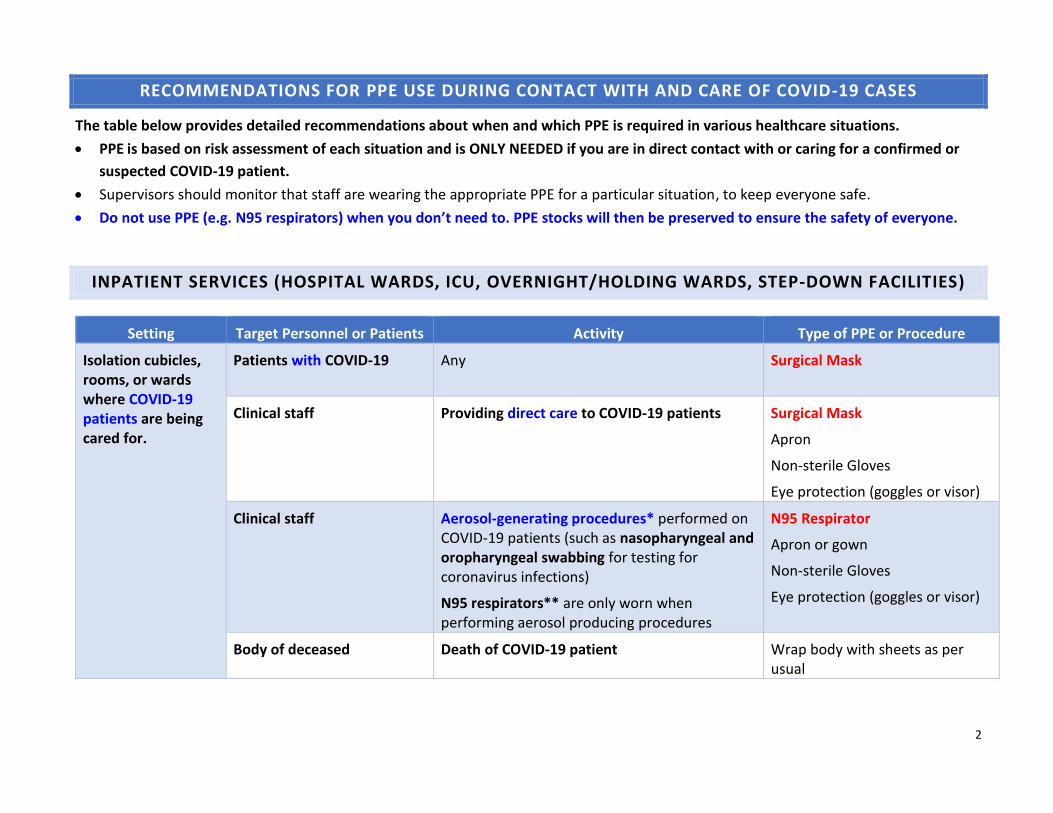
2
RECOMMENDATIONS FOR PPE USE DURING CONTACT WITH AND CARE OF COVID-19 CASES
The table below provides detailed recommendations about when and which PPE is required in various healthcare situations.
• PPE is based on risk assessment of each situation and is ONLY NEEDED if you are in direct contact with or caring for a confirmed or
suspected COVID-19 patient.
• Supervisors should monitor that staff are wearing the appropriate PPE for a particular situation, to keep everyone safe.
• Do not use PPE (e.g. N95 respirators) when you don’t need to. PPE stocks will then be preserved to ensure the safety of everyone.
INPATIENT SERVICES (HOSPITAL WARDS, ICU, OVERNIGHT/HOLDING WARDS, STEP-DOWN FACILITIES)
Setting Target Personnel or Patients Activity Type of PPE or Procedure
Isolation cubicles, rooms, or wards where COVID-19 patients are being cared for.
Patients with COVID-19 Any Surgical Mask
Clinical staff Providing direct care to COVID-19 patients Surgical Mask
Apron
Non-sterile Gloves
Eye protection (goggles or visor)
Clinical staff
Aerosol-generating procedures* performed on COVID-19 patients (such as nasopharyngeal and oropharyngeal swabbing for testing for coronavirus infections)
N95 respirators** are only worn when performing aerosol producing procedures
N95 Respirator
Apron or gown
Non-sterile Gloves
Eye protection (goggles or visor)
Body of deceased Death of COVID-19 patient Wrap body with sheets as per usual

3
Setting Target Personnel or Patients Activity Type of PPE or Procedure
Cleaners Entering the cubicle or room or ward of COVID-19 patients
Surgical mask
Apron
Long rubber utility cleaning gloves (ideally up to elbow) that can be washed
Eye protection (goggles or visor)
Closed work shoes
Porters and nurses Transport of COVID-19 patients Surgical Mask
Non-sterile Gloves
Catering staff Providing meals inside COVID-19 ward Surgical Mask
Non-sterile Gloves
Administrative personnel Administrative staff supporting COVID-19 ward services, who are not usually in direct contact with patients, but would enter the isolation ward.
Surgical mask
Non-sterile Gloves
Maintain spatial distance of at least 1 metre, where possible
Security personnel Any Surgical mask
Laundry workers Laundering of COVID-19 patient linen Linen to be bagged separate from other linen
Surgical mask
Apron
Long rubber utility cleaning gloves (ideally up to elbow) that can be washed
Eye protection (goggles or visor)
Closed work shoes

4
Setting Target Personnel or Patients Activity Type of PPE or Procedure
All types of wards where Non-COVID-19 Patients (i.e. patients who do NOT have COVID-19) are being cared for
Patients without COVID-19 Any No PPE required
Clinical staff Aerosol-generating procedures* performed on Non-COVID-19 patients*
Surgical mask
Apron
Non-sterile Gloves
Eye protection (goggles or visor)
All staff Any other activity besides Aerosol-generating procedures performed for Non-COVID-19 patients
No PPE required
Visitors Visiting patients without COVID-19 No PPE required
Other areas of the hospital where COVID-19 patients transit (e.g. corridors) but are not directly attended to.
All staff Any activity that does not involve contact with COVID-19 patients
No PPE required
* Aerosol-generating procedures are: collection of nasopharyngeal and oropharyngeal swabs for SARS-COV-2 testing, tracheal aspirate, bronchoalveolar lavage, manual bag-mask ventilation, non-invasive CPAP ventilation, tracheal intubation, open suctioning, tracheotomy, bronchoscopy, endoscopy, ENT procedures, dental procedures, maxillo-facial procedures and cardiopulmonary resuscitation.
**N95 respirator must still be used for all other Non-COVID-19 indications (e.g. when attend to a patient with confirmed or suspected TB)

5
SERVICES AT PHC FACILITIES, OUTPATIENTS, EMERGENCY UNITS AND TEMPORARAY FACILITIES
Setting Target Personnel or Patients Activity Type of PPE or Procedure
Triage at Clinics, CHC, OPD. Emergency Units and temporary facilities entrances
Clinical staff Triage: Preliminary screening of patients (via questions on symptoms and contact with COVID-19 cases) as they enter unit.
Maintain spatial distance of at least 1 metre
Surgical mask
Patients and escorts who screen positive
While waiting for testing Move patient to isolation room Provide Surgical mask
Patients and escorts who screen negative but have respiratory symptoms
While waiting for consultation Maintain spatial distance of
at least 1 metre.
Provide Surgical mask
Patients and escorts who screen negative but without respiratory symptoms
While waiting for consultation No PPE required
Administrative areas
All staff including reception, clerical and clinical staff
Administrative tasks that do not involve contact with COVID-19 patients
No PPE required
Clinic, CHC, OPD, Emergency Unit and Temporary facility Consultation rooms
Clinical staff Physical examination of suspected COVID-19 patients
Surgical Mask
Eye protection (goggles or visor)
Apron
Non-sterile Gloves
Clinical staff Aerosol-generating procedures performed on suspected COVID-19 patients (such as nasopharyngeal and oropharyngeal swabbing for testing for coronavirus infections)
Note that N95 respirators are only worn when performing aerosol-generating procedures
N95 Respirator
Apron or gown
Non-sterile Gloves
Eye protection (goggles or visor)

6
Setting Target Personnel or Patients Activity Type of PPE or Procedure
Clinical staff Physical examination of
patients without respiratory
symptoms.
No PPE required
Cleaners Cleaning the vacated room and areas used by a COVID-19 patient
Surgical mask
Apron
Eye protection (goggles or visor)
Long rubber utility cleaning gloves (ideally up to elbow) that can be washed
Closed work shoes
Body of deceased Death of COVID-19 patient Wrap body with sheets as per usual
Entrance to COVID-19 Area
Security personnel. Any Surgical mask
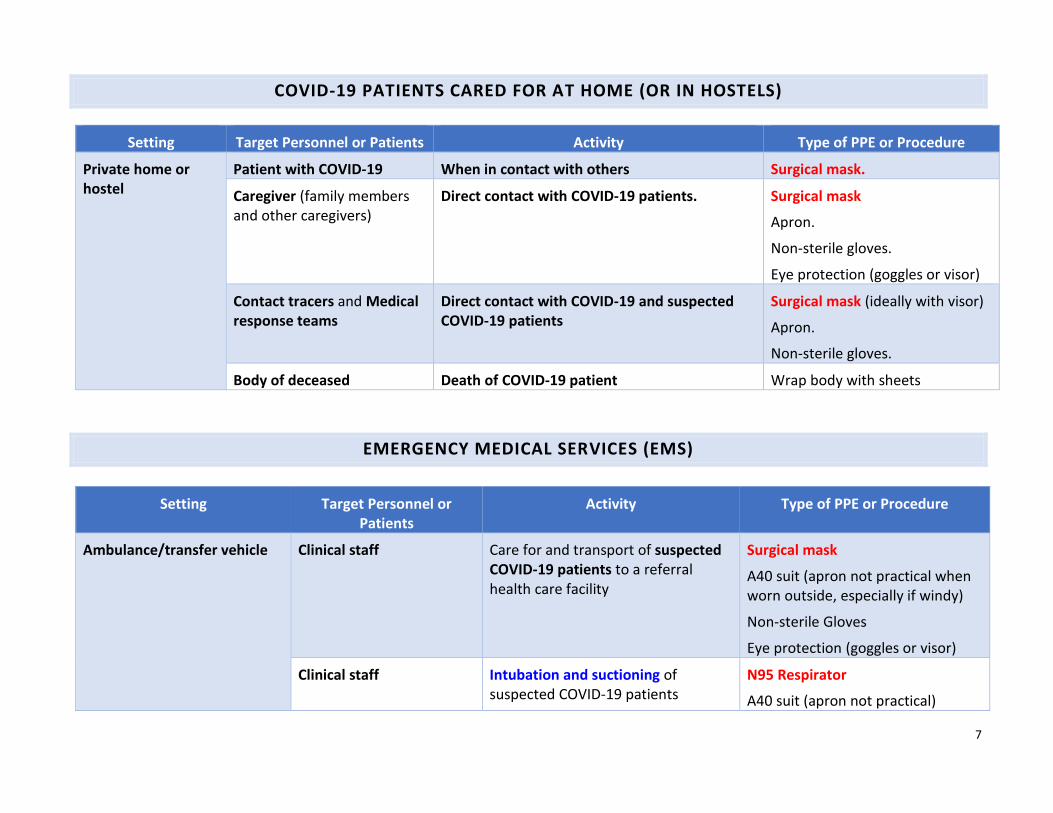
7
COVID-19 PATIENTS CARED FOR AT HOME (OR IN HOSTELS)
Setting Target Personnel or Patients Activity Type of PPE or Procedure
Private home or hostel
Patient with COVID-19 When in contact with others Surgical mask.
Caregiver (family members and other caregivers)
Direct contact with COVID-19 patients. Surgical mask
Apron.
Non-sterile gloves.
Eye protection (goggles or visor)
Contact tracers and Medical response teams
Direct contact with COVID-19 and suspected COVID-19 patients
Surgical mask (ideally with visor)
Apron.
Non-sterile gloves.
Body of deceased Death of COVID-19 patient Wrap body with sheets
EMERGENCY MEDICAL SERVICES (EMS)
Setting Target Personnel or Patients
Activity Type of PPE or Procedure
Ambulance/transfer vehicle Clinical staff
Care for and transport of suspected COVID-19 patients to a referral health care facility
Surgical mask
A40 suit (apron not practical when worn outside, especially if windy)
Non-sterile Gloves
Eye protection (goggles or visor)
Clinical staff Intubation and suctioning of suspected COVID-19 patients
N95 Respirator
A40 suit (apron not practical)
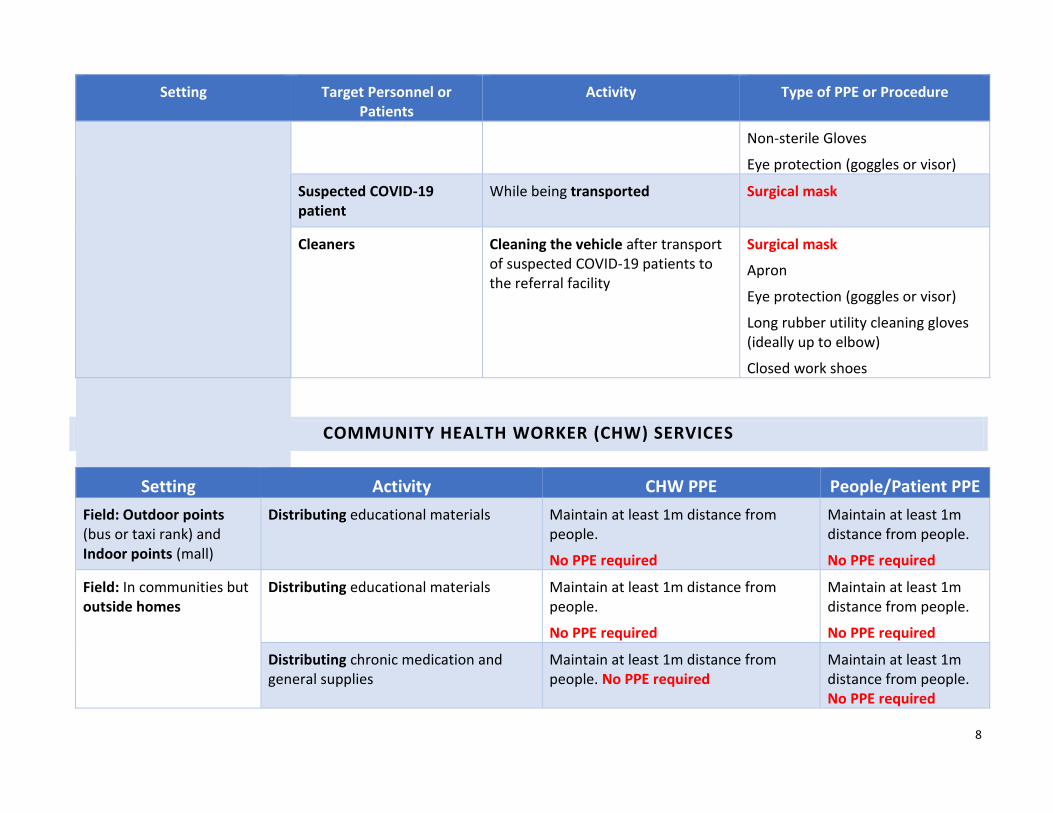
8
Setting Target Personnel or Patients
Activity Type of PPE or Procedure
Non-sterile Gloves
Eye protection (goggles or visor)
Suspected COVID-19 patient
While being transported
Surgical mask
Cleaners Cleaning the vehicle after transport of suspected COVID-19 patients to the referral facility
Surgical mask
Apron
Eye protection (goggles or visor)
Long rubber utility cleaning gloves (ideally up to elbow)
Closed work shoes
COMMUNITY HEALTH WORKER (CHW) SERVICES
Setting Activity CHW PPE People/Patient PPE
Field: Outdoor points (bus or taxi rank) and Indoor points (mall)
Distributing educational materials Maintain at least 1m distance from people.
No PPE required
Maintain at least 1m distance from people.
No PPE required
Field: In communities but outside homes
Distributing educational materials Maintain at least 1m distance from people.
No PPE required
Maintain at least 1m distance from people.
No PPE required
Distributing chronic medication and general supplies
Maintain at least 1m distance from people. No PPE required
Maintain at least 1m distance from people. No PPE required
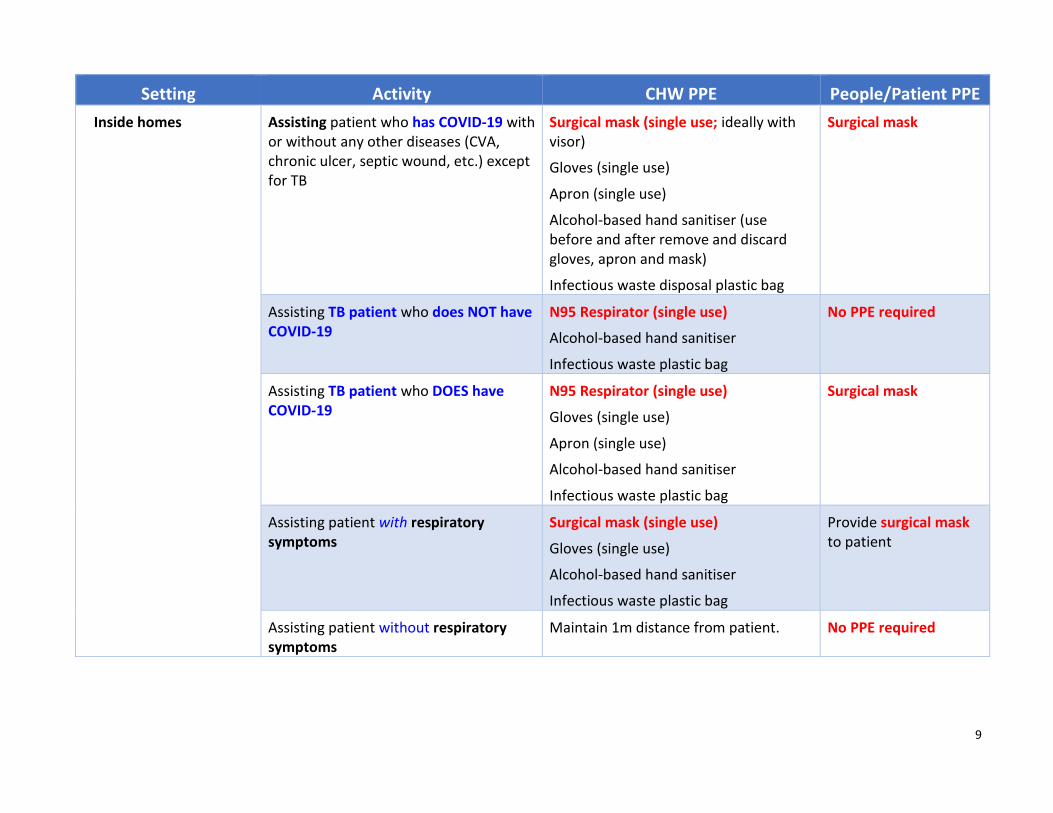
9
Setting Activity CHW PPE People/Patient PPE
Inside homes Assisting patient who has COVID-19 with or without any other diseases (CVA, chronic ulcer, septic wound, etc.) except for TB
Surgical mask (single use; ideally with visor)
Gloves (single use)
Apron (single use)
Alcohol-based hand sanitiser (use before and after remove and discard gloves, apron and mask)
Infectious waste disposal plastic bag
Surgical mask
Assisting TB patient who does NOT have COVID-19
N95 Respirator (single use)
Alcohol-based hand sanitiser
Infectious waste plastic bag
No PPE required
Assisting TB patient who DOES have COVID-19
N95 Respirator (single use)
Gloves (single use)
Apron (single use)
Alcohol-based hand sanitiser
Infectious waste plastic bag
Surgical mask
Assisting patient with respiratory symptoms
Surgical mask (single use)
Gloves (single use)
Alcohol-based hand sanitiser
Infectious waste plastic bag
Provide surgical mask to patient
Assisting patient without respiratory symptoms
Maintain 1m distance from patient. No PPE required

10
FORENSIC PATHOLOGY AND MORTUARY SERVICES
Setting Target Personnel or Patients Activity Type of PPE or Procedure
Private home, hostel or hospital
Caregivers, hospital staff, mortuary staff transporting and preparing the body and
Forensic Pathology staff transporting the body
Direct contact with deceased COVID-19 and suspected COVID-19 patients
Surgical Mask
Apron or gown
Non-sterile Gloves
Eye protection (goggles or visor)
Body of Deceased COVID-19 patients
Deceased body being removed Usual procedures for removing body
FPS vehicle used to transport deceased
Cleaner Cleaning of vehicle Surgical mask
Apron
Eye protection (goggles or visor)
Long rubber utility cleaning gloves (ideally up to elbow) that can be washed
Closed work shoes
Mortuary Forensic pathology staff Conducting autopsy (if required) N95 Respirator
Gown
Apron
Eye protection (goggles or visor)
Double gloves
Cut-proof synthetic mesh gloves
Closed work shoes

11
The tables above cover all the common scenarios in which PPE should be used. However, should a scenario arise which is not addressed above, then use the generic PPE principles below to decide on the appropriate PPE to use.
TYPE OF PPE CLINICAL STAFF
(nurses, doctors, EMS)
Providing direct care to COVID-19 patients or patients with
respiratory symptoms
NON-CLINICAL STAFF
(admin staff, catering staff) coming into distant contact with COVID-19 patients and
contaminated surfaces
NON-CLINICAL STAFF
(cleaners) coming into distant contact with
COVID-19 patients and contaminated surfaces
PATIENTS with RESPIRATORY
symptoms
PATIENTS without
RESPIRATORY symptoms
Gloves Non-sterile gloves.
Change between patients
Non-sterile gloves.
Change when leaving COVID-19 area
Reusable long rubber utility cleaning gloves (ideally up to elbow) Change after completed cleaning contaminated area
None None
Face cover type
Surgical Mask for general care of COVID-19 patients
N95 respirator for aerosol generating procedures on COVID-19 suspects/cases
Surgical mask when within <1m of a patient with respiratory symptoms (one per shift, if integrity maintained)
Surgical mask when within <1m of a patient with respiratory symptoms
Surgical mask worn when in contact with others
None
Aprons Change between patients Change when leaving COVID-19 area
After each work session (in absence of clinical contact)
None None
Face shields, or visors, or goggles, or other eye covers
Wash clean, disinfect and reuse None Wash clean, disinfect and reuse
None None
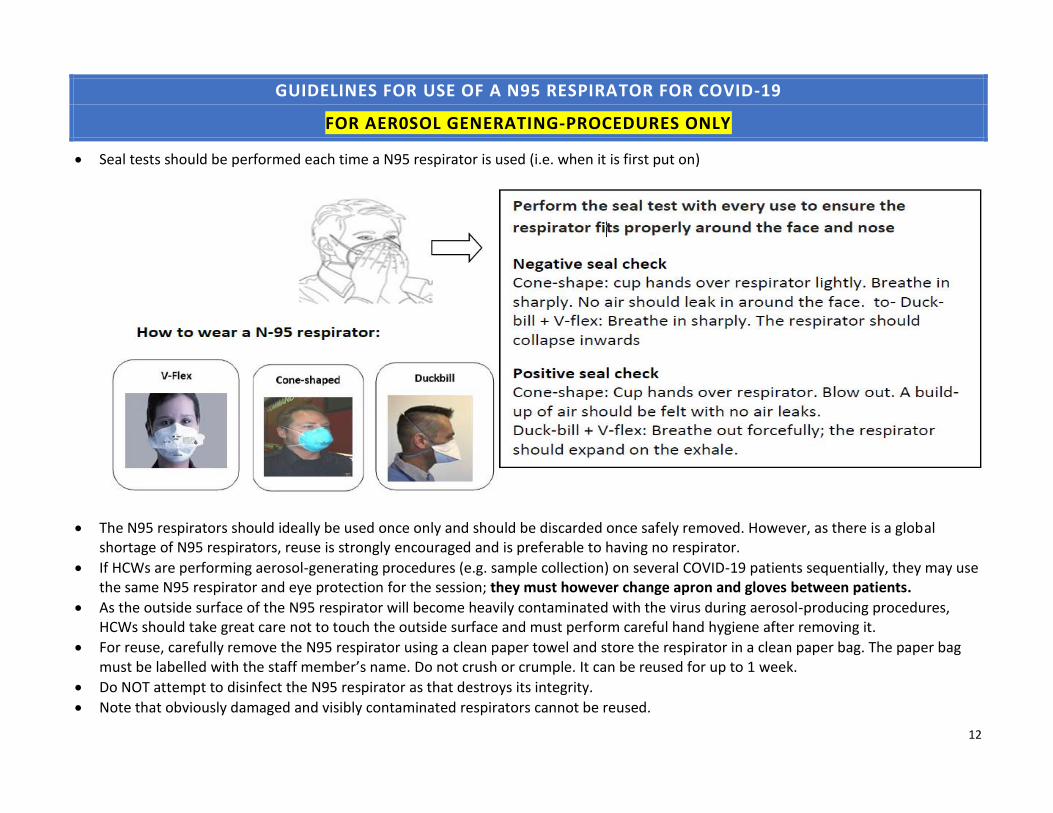
12
GUIDELINES FOR USE OF A N95 RESPIRATOR FOR COVID-19
FOR AER0SOL GENERATING-PROCEDURES ONLY
• Seal tests should be performed each time a N95 respirator is used (i.e. when it is first put on)
• The N95 respirators should ideally be used once only and should be discarded once safely removed. However, as there is a global shortage of N95 respirators, reuse is strongly encouraged and is preferable to having no respirator.
• If HCWs are performing aerosol-generating procedures (e.g. sample collection) on several COVID-19 patients sequentially, they may use the same N95 respirator and eye protection for the session; they must however change apron and gloves between patients.
• As the outside surface of the N95 respirator will become heavily contaminated with the virus during aerosol-producing procedures, HCWs should take great care not to touch the outside surface and must perform careful hand hygiene after removing it.
• For reuse, carefully remove the N95 respirator using a clean paper towel and store the respirator in a clean paper bag. The paper bag must be labelled with the staff member’s name. Do not crush or crumple. It can be reused for up to 1 week.
• Do NOT attempt to disinfect the N95 respirator as that destroys its integrity.
• Note that obviously damaged and visibly contaminated respirators cannot be reused.
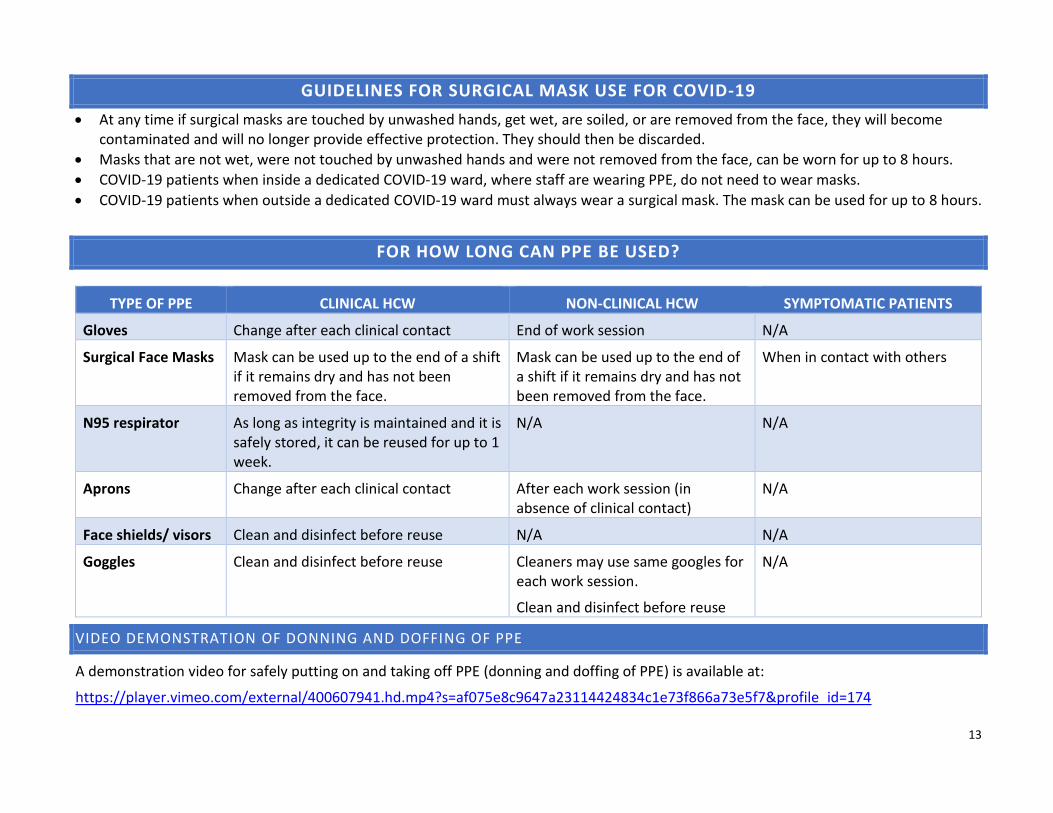
13
GUIDELINES FOR SURGICAL MASK USE FOR COVID-19
• At any time if surgical masks are touched by unwashed hands, get wet, are soiled, or are removed from the face, they will become contaminated and will no longer provide effective protection. They should then be discarded.
• Masks that are not wet, were not touched by unwashed hands and were not removed from the face, can be worn for up to 8 hours.
• COVID-19 patients when inside a dedicated COVID-19 ward, where staff are wearing PPE, do not need to wear masks.
• COVID-19 patients when outside a dedicated COVID-19 ward must always wear a surgical mask. The mask can be used for up to 8 hours.
FOR HOW LONG CAN PPE BE USED?
TYPE OF PPE CLINICAL HCW NON-CLINICAL HCW SYMPTOMATIC PATIENTS
Gloves Change after each clinical contact End of work session N/A
Surgical Face Masks Mask can be used up to the end of a shift if it remains dry and has not been removed from the face.
Mask can be used up to the end of a shift if it remains dry and has not been removed from the face.
When in contact with others
N95 respirator As long as integrity is maintained and it is safely stored, it can be reused for up to 1 week.
N/A N/A
Aprons Change after each clinical contact After each work session (in absence of clinical contact)
N/A
Face shields/ visors Clean and disinfect before reuse N/A N/A
Goggles Clean and disinfect before reuse Cleaners may use same googles for each work session.
Clean and disinfect before reuse
N/A
VIDEO DEMONSTRATION OF DONNING AND DOFFING OF PPE
A demonstration video for safely putting on and taking off PPE (donning and doffing of PPE) is available at:
https://player.vimeo.com/external/400607941.hd.mp4?s=af075e8c9647a23114424834c1e73f866a73e5f7&profile_id=174
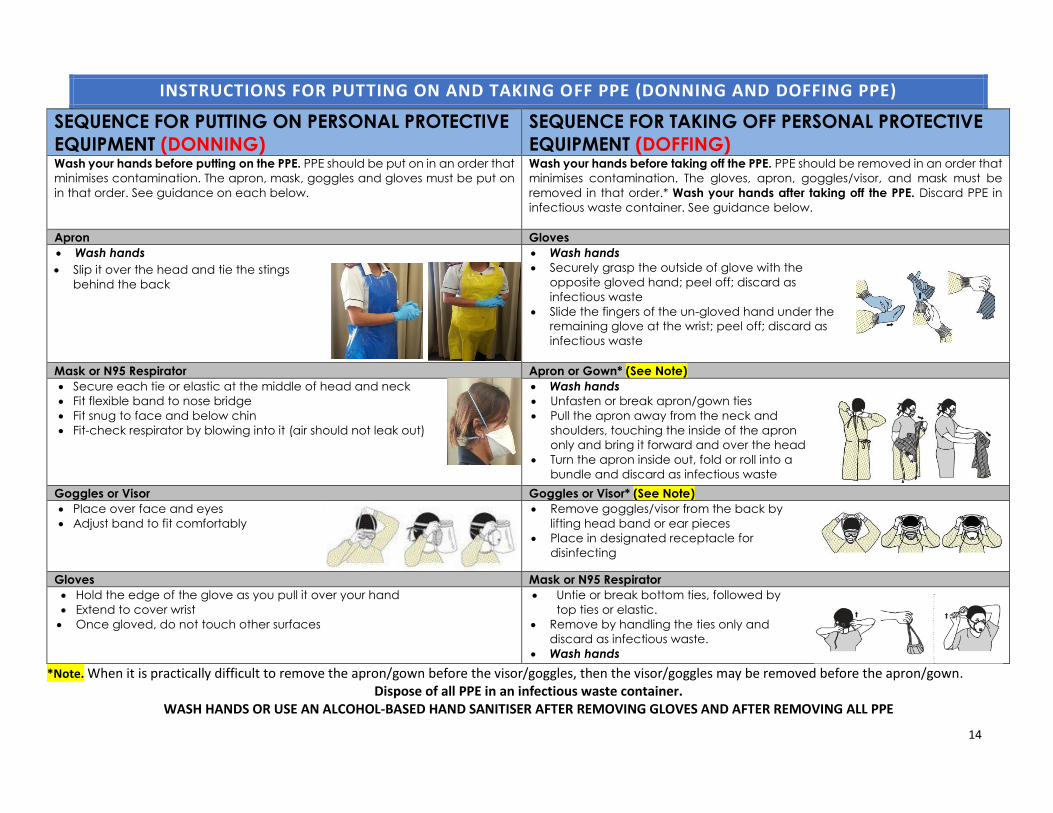
14
INSTRUCTIONS FOR PUTTING ON AND TAKING OFF PPE (DONNING AND DOFFING PPE)
SEQUENCE FOR PUTTING ON PERSONAL PROTECTIVE
EQUIPMENT (DONNING)
SEQUENCE FOR TAKING OFF PERSONAL PROTECTIVE
EQUIPMENT (DOFFING) Wash your hands before putting on the PPE. PPE should be put on in an order that
minimises contamination. The apron, mask, goggles and gloves must be put on
in that order. See guidance on each below.
Wash your hands before taking off the PPE. PPE should be removed in an order that
minimises contamination. The gloves, apron, goggles/visor, and mask must be
removed in that order.* Wash your hands after taking off the PPE. Discard PPE in
infectious waste container. See guidance below.
Apron Gloves
• Wash hands
• Slip it over the head and tie the stings
behind the back
• Wash hands
• Securely grasp the outside of glove with the
opposite gloved hand; peel off; discard as
infectious waste
• Slide the fingers of the un-gloved hand under the
remaining glove at the wrist; peel off; discard as
infectious waste
Mask or N95 Respirator Apron or Gown* (See Note)
• Secure each tie or elastic at the middle of head and neck
• Fit flexible band to nose bridge
• Fit snug to face and below chin
• Fit-check respirator by blowing into it (air should not leak out)
• Wash hands
• Unfasten or break apron/gown ties
• Pull the apron away from the neck and
shoulders, touching the inside of the apron
only and bring it forward and over the head
• Turn the apron inside out, fold or roll into a
bundle and discard as infectious waste
Goggles or Visor Goggles or Visor* (See Note)
• Place over face and eyes
• Adjust band to fit comfortably
• Remove goggles/visor from the back by
lifting head band or ear pieces
• Place in designated receptacle for
disinfecting
Gloves Mask or N95 Respirator
• Hold the edge of the glove as you pull it over your hand
• Extend to cover wrist
• Once gloved, do not touch other surfaces
• Untie or break bottom ties, followed by
top ties or elastic.
• Remove by handling the ties only and
discard as infectious waste.
• Wash hands
*Note. When it is practically difficult to remove the apron/gown before the visor/goggles, then the visor/goggles may be removed before the apron/gown. Dispose of all PPE in an infectious waste container.
WASH HANDS OR USE AN ALCOHOL-BASED HAND SANITISER AFTER REMOVING GLOVES AND AFTER REMOVING ALL PPE

39
Annexure E

2
Clinical management of suspected or
confirmed COVID-19 disease Version 3 (27th March 2020)
1. BACKGROUND 4
2. EPIDEMIOLOGY AND CLINICAL CHARACTERISTICS 4
3. MANAGEMENT OF SUSPECTED COVID-19 CASES 6
4. MANAGEMENT OF CONFIRMED COVID-19 CASES 10
5. INFECTION PREVENTION AND CONTROL (IPC) 16
6. RECORDING AND REPORTING 17
APPENDIX 1 – EXAMPLE OF A PATIENT INFORMATION SHEET 20
Writing committee (in alphabetical order): David Anderson, Lesley Bamford, Tom Boyles, Lucille
Blumberg, Cheryl Cohen, Andrew Gray, Ahmad Haeri Mazanderani, Tendesayi Kufa-Chakeza, Halima
Dawood, Fikile Mabena, Shaheen Mehtar, Natalie Mayet, Marc Mendelson, Jeremy Nel, Wolfgang
Preiser, Jantjie Taljaard
Version 2: What’s New?
• New de-isolation criteria for confirmed cases (section 4.5)
• Statement on therapeutics for hospitalized cases (section 4.3)
• Statement on the use of ACE-inhibitors, angiotensin receptor blockers, and nonsteroidal anti-inflammatory drugs (section 4.3).
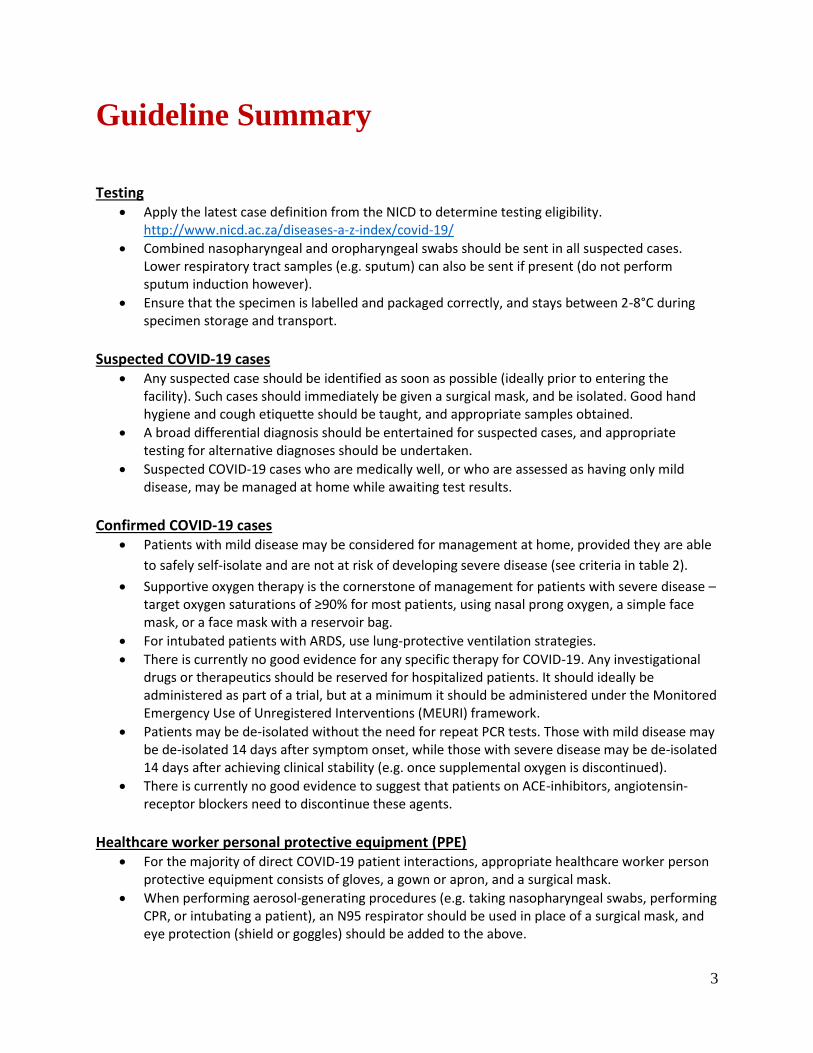
3
Guideline Summary
Testing
• Apply the latest case definition from the NICD to determine testing eligibility. http://www.nicd.ac.za/diseases-a-z-index/covid-19/
• Combined nasopharyngeal and oropharyngeal swabs should be sent in all suspected cases. Lower respiratory tract samples (e.g. sputum) can also be sent if present (do not perform sputum induction however).
• Ensure that the specimen is labelled and packaged correctly, and stays between 2-8°C during specimen storage and transport.
Suspected COVID-19 cases
• Any suspected case should be identified as soon as possible (ideally prior to entering the facility). Such cases should immediately be given a surgical mask, and be isolated. Good hand hygiene and cough etiquette should be taught, and appropriate samples obtained.
• A broad differential diagnosis should be entertained for suspected cases, and appropriate testing for alternative diagnoses should be undertaken.
• Suspected COVID-19 cases who are medically well, or who are assessed as having only mild disease, may be managed at home while awaiting test results.
Confirmed COVID-19 cases
• Patients with mild disease may be considered for management at home, provided they are able
to safely self-isolate and are not at risk of developing severe disease (see criteria in table 2).
• Supportive oxygen therapy is the cornerstone of management for patients with severe disease – target oxygen saturations of ≥90% for most patients, using nasal prong oxygen, a simple face mask, or a face mask with a reservoir bag.
• For intubated patients with ARDS, use lung-protective ventilation strategies.
• There is currently no good evidence for any specific therapy for COVID-19. Any investigational drugs or therapeutics should be reserved for hospitalized patients. It should ideally be administered as part of a trial, but at a minimum it should be administered under the Monitored Emergency Use of Unregistered Interventions (MEURI) framework.
• Patients may be de-isolated without the need for repeat PCR tests. Those with mild disease may be de-isolated 14 days after symptom onset, while those with severe disease may be de-isolated 14 days after achieving clinical stability (e.g. once supplemental oxygen is discontinued).
• There is currently no good evidence to suggest that patients on ACE-inhibitors, angiotensin-receptor blockers need to discontinue these agents.
Healthcare worker personal protective equipment (PPE)
• For the majority of direct COVID-19 patient interactions, appropriate healthcare worker person protective equipment consists of gloves, a gown or apron, and a surgical mask.
• When performing aerosol-generating procedures (e.g. taking nasopharyngeal swabs, performing CPR, or intubating a patient), an N95 respirator should be used in place of a surgical mask, and eye protection (shield or goggles) should be added to the above.

4
Clinical management of suspected or
confirmed COVID-19 disease
1. Background
On 31st December 2019, the World Health Organization (WHO) was alerted to a cluster of pneumonia of
unknown aetiology in patients in Wuhan City, Hubei Province of China. One week later the novel
coronavirus (severe acute respiratory syndrome coronavirus 2: SARS-CoV-2) was identified as the cause.
The resulting illness was named COVID-19 on the 11th February 2020. The clinical spectrum of COVID-19
ranges from an asymptomatic or mild flu-like illness to a severe pneumonia requiring critical care. These
guidelines describe the clinical management of cases of COVID-19 disease and covers clinical care in and
outside health care facilities. It is intended for health care practitioners taking care of symptomatic
patients with suspected or confirmed COVID-19.
2. Epidemiology and clinical characteristics
SARS-CoV-2 is a betacoronavirus closely related to SARS-CoV and MERS-CoV. It is an enveloped, non-
segmented, positive sense RNA virus. It is thought to have originated in bats but the animal that
mediated transmission to humans remains unknown.
2.1 Epidemiology
The median incubation period for COVID-19 is estimated to be 4-5 days, with an interquartile range of 2-
7 days.3,4 Transmission from asymptomatic patients has been postulated, but the extent of this is
unknown.5 The reproductive number for the virus is approximately 2.2 (meaning that on average each
person spread the infection to two others).3 In the early reported cases, the median age of reported
cases was 50 years with a male preponderance of cases (~60%). Very few severe cases which required
hospitalisation have been reported among children under the age of 15 years (~1%), although school
closures may have influenced this figure. Risk factors for severe disease include older age and
cardiopulmonary comorbidities.
2.2 Clinical characteristics – what to look for
80% of symptomatic patients develop mild disease, an estimated 15% develop severe disease (with
hypoxaemia, dyspnoea and tachypnoea) while 5% become critically ill (with respiratory failure, septic
shock and/or multiorgan dysfunction).6 The proportion of asymptomatic carriers is currently unknown.
The most common presenting symptom has been fever (~90%, but only present in 44% on admission).
Other common symptoms include cough (68%), fatigue (38%), sputum production (34%), shortness of
5
breath (19%), myalgia or arthralgia (15%), sore throat (14%), headache (13.6%) and chills (12%).4
Gastrointestinal symptoms such as nausea or vomiting (5.0%) and diarrhoea (3.8%) appear to be
uncommon.
Abnormalities are visible on chest X-ray in approximately 60% of COVID-19 patients, and on 85% of
patients’ chest CT scans.4 These are typically patchy ground glass opacities, though other patterns have
been described.4
2.3 Outcomes and prognosis
The vast majority of cases will make a full recovery, though this may take several weeks, particularly in
severe cases. In a minority of cases, COVID-19 has been associated with rapid progression to acute
respiratory distress syndrome (ARDS), multiple organ failure and sometimes death. The case fatality
ratio is currently unknown, but is estimated to be within the range of 0.5-4%.
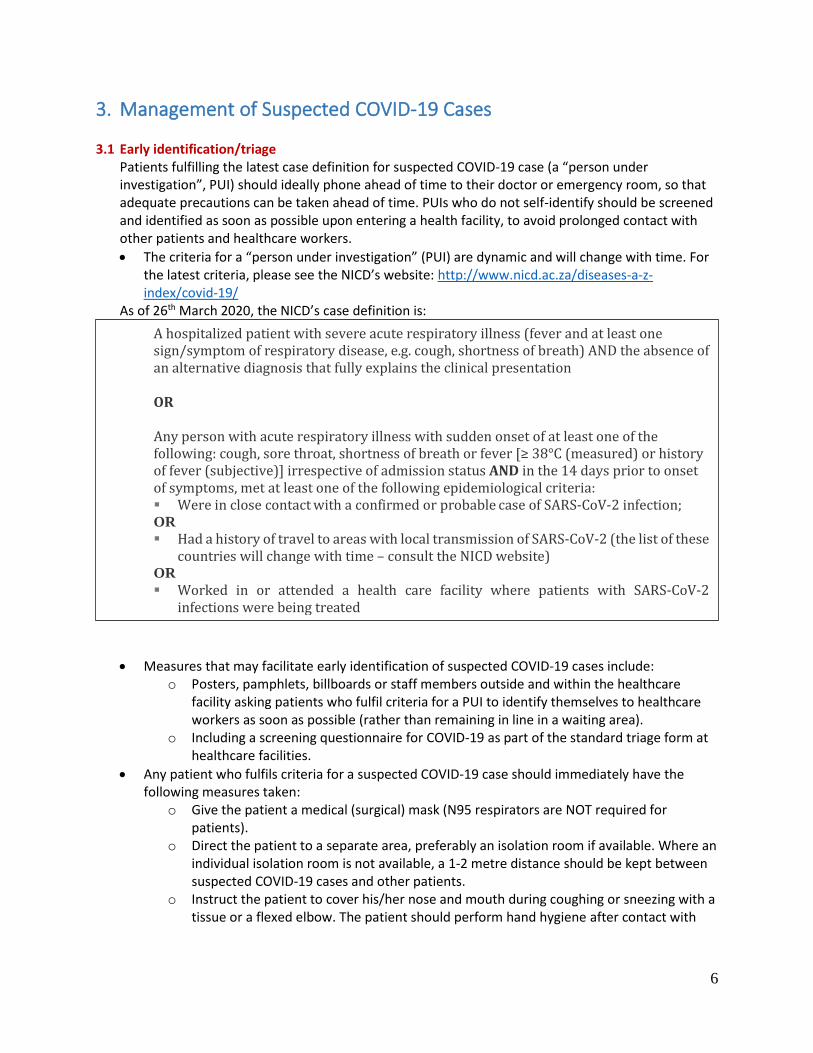
6
3. Management of Suspected COVID-19 Cases 3.1 Early identification/triage
Patients fulfilling the latest case definition for suspected COVID-19 case (a “person under investigation”, PUI) should ideally phone ahead of time to their doctor or emergency room, so that adequate precautions can be taken ahead of time. PUIs who do not self-identify should be screened and identified as soon as possible upon entering a health facility, to avoid prolonged contact with other patients and healthcare workers.
• The criteria for a “person under investigation” (PUI) are dynamic and will change with time. For the latest criteria, please see the NICD’s website: http://www.nicd.ac.za/diseases-a-z-index/covid-19/
As of 26th March 2020, the NICD’s case definition is:
• Measures that may facilitate early identification of suspected COVID-19 cases include: o Posters, pamphlets, billboards or staff members outside and within the healthcare
facility asking patients who fulfil criteria for a PUI to identify themselves to healthcare workers as soon as possible (rather than remaining in line in a waiting area).
o Including a screening questionnaire for COVID-19 as part of the standard triage form at healthcare facilities.
• Any patient who fulfils criteria for a suspected COVID-19 case should immediately have the following measures taken:
o Give the patient a medical (surgical) mask (N95 respirators are NOT required for patients).
o Direct the patient to a separate area, preferably an isolation room if available. Where an individual isolation room is not available, a 1-2 metre distance should be kept between suspected COVID-19 cases and other patients.
o Instruct the patient to cover his/her nose and mouth during coughing or sneezing with a tissue or a flexed elbow. The patient should perform hand hygiene after contact with
A hospitalized patient with severe acute respiratory illness (fever and at least one sign/symptom of respiratory disease, e.g. cough, shortness of breath) AND the absence of an alternative diagnosis that fully explains the clinical presentation OR Any person with acute respiratory illness with sudden onset of at least one of the following: cough, sore throat, shortness of breath or fever [≥ 38°C (measured) or history of fever (subjective)] irrespective of admission status AND in the 14 days prior to onset of symptoms, met at least one of the following epidemiological criteria: ▪ Were in close contact with a confirmed or probable case of SARS-CoV-2 infection; OR ▪ Had a history of travel to areas with local transmission of SARS-CoV-2 (the list of these
countries will change with time – consult the NICD website)
OR ▪ Worked in or attended a health care facility where patients with SARS-CoV-2
infections were being treated

7
respiratory secretions (wash hands or use alcohol-based hand rub, which should be readily available at the point of triage).
o Limit the movement of the patient (e.g. use portable X-rays rather than sending the patient to the X-ray department). If the patient has to be moved, ensure that (s)he wears a mask.
o The patient should have a dedicated bathroom (where this is possible).
• Patients should be quickly triaged in terms of clinical severity. Routine emergency department triage systems may be used. In the context of COVID-19, triaging is essential because:
o It allows for rapid initiation of supportive therapy (e.g. oxygen supplementation) o It has implications for whether or not the patient can be allowed home to await results
of the COVID-19 testing (see below). o It protects both patients and staff.
3.2 Testing
All persons under investigation require testing for SARS-CoV-2 by means of reverse transcriptase PCR (RT-PCR). Samples to be sent are:
• Upper respiratory tract samples – nasophargyngeal and oropharyngeal swabs (combined in the same universal transport medium tube) in all patients.
• Lower respiratory tract samples – may not be possible depending on the patient’s symptoms. Where available, send sputum, tracheal aspirates, or bronchoalveolar lavage fluid. Sputum induction should not be performed.
Appropriate personal protective equipment (PPE) should be worn by all healthcare workers when obtaining specimens (see IPC section below).
Obtaining samples for SARS-CoV-2 testing
• Healthcare workers obtaining respiratory samples require appropriate personal protective equipment, including those for contact, droplet and aerosol precautions (see infection prevention and control section below).
• Collecting a good quality specimen is vital. For details on how to properly obtain good quality specimens, please see Appendix 5 of the NICD’s COVID-19 guidelines for case-finding, diagnosis, management and public health response in South Africa: http://www.nicd.ac.za/wp-
The differential diagnosis of suspected cases includes influenza (remembering the seasonality in patients from the northern hemisphere differs from those of the southern hemisphere), both conventional and atypical bacterial pneumonias, and in patients with HIV and a CD4 count <200 cells/mm3 (or equivalent immunosuppression), Pneumocystis jirovecii pneumonia. Depending on the patient, appropriate samples may include:
▪ Full blood count + differential count ▪ Blood culture ▪ Nasopharyngeal swabs or aspirates and oropharyngeal swabs for detection of viral and
atypical pathogens ▪ Chest radiography ▪ Sputum for MCS and Mycobacterium tuberculosis detection (GeneXpert MTB/RIF Ultra). ▪ Urine for lipoarabinomannan (LAM) test if HIV positive

8
content/uploads/2020/02/Guidelines-for-case-finding-diagnosis-management-and-public-health-response-in-South-Africa.pdf
Transport of specimens
• Ensure that samples are kept between 2-8°C until they are processed.
3.3 Empiric treatment of other pathogens Where the patient fits the appropriate clinical syndrome, consider treatment of other pathogens such as:
• Conventional community-acquired pneumonia pathogens (or hospital-acquired pneumonia pathogens if appropriate) – e.g. ceftriaxone [see SA community-acquired pneumonia guidelines]
• Atypical pneumonia pathogens – e.g. azithromycin [see SA community-acquired pneumonia guidelines]
• Influenza (if influenza epidemiology fits and has severe illness or if patient is at risk of severe influenza) – oseltamivir [see NICD influenza guidelines]
• PJP (if appropriate risk factors present, e.g. HIV with low CD4 count)
3.4 Managing patients at home while awaiting COVID-19 test results Suspected COVID-19 cases who are medically well, or who are assessed as having only mild disease, may be managed at home while awaiting test results. Table 1 – Criteria for “mild” disease (for age >12 years)1
1For age 5-12, use respiratory rate <30, and heart rate <130. For younger ages, use age-appropriate normal values.
Such patients should be instructed to self-isolate at home and be given appropriate advice about reducing possible transmission to others:
•SpO2 ≥95%
•Respiratory rate <25
•Heart rate <120
•Temp 36-39°C
•Mental status normal
Criteria for "mild" disease
For samples sent to the NICD: Mark all samples as :
Suspected COVID-19 CRDM NHLS/NICD Centre for Respiratory Diseases and Meningitis (CRDM) Lower North Wing, SAVP Building 1 Modderfontein Road, Sandringham, Johannesburg, 2131
NHLS laboratories use usual overnight region courier service. Private labs should organise shipment using existing systems, or contact CRDM for assistance if shipping is unavailable.

9
• Patients should stay in a specific room and use their own bathroom (if possible). Patients should avoid unnecessary travel and unnecessary contact with other people.
• Where contact is unavoidable, the patient should wear a facemask, and maintain a distance of at least 1 metre (preferably 2 metres) from other people
• Patients should clean their hands with soap and water frequently. Alcohol-based sanitizers may also be used, provided they contain at least 70% alcohol.
• Patients should practice good cough and sneeze hygiene, by using a tissue, and then immediately discarding the tissue in a lined trash can, followed by washing hands immediately.
• Patients should not have visitors in their home. Only those who live in their home should be allowed to stay.
• At home, the patient should stay in a specific room and use his/her own bathroom (if possible). If they live in shared accommodation (university halls of residence or similar) with a communal kitchen, bathroom(s) and living area, they should stay in their room with the door closed, only coming out when necessary, wearing a facemask if they do so.
• Patients should avoid sharing household items like dishes, cups, eating utensils and towels. After using any of these, the items should be thoroughly washed with soap and hot water.
• All high-touch surfaces like table tops, counters, toilets, phones, computers, etc. should be appropriately and frequently cleaned.
• If patients need to wash laundry at home before the results are available, then they should wash all laundry at the highest temperature compatible for the fabric using laundry detergent. This should be above 60° C. If possible, they should tumble dry and iron using the highest setting compatible with the fabric. Disposable gloves and a plastic apron should be used when handling soiled materials if possible and all surfaces and the area around the washing machine should be cleaned. Laundry should not be taken to a laundrette. The patient should wash his/her hands thoroughly with soap and water after handling dirty laundry (remove gloves first if used).
• Patients should know who to call if they develop any worsening symptoms, so that they can be safely reassessed.
• In addition to being given the above advice, a patient information sheet can be given if possible (see Appendix 1 for an example).
See also the NICD’s self-isolation video available at: http://www.nicd.ac.za/how-to-self-isolation-at-home-everything-you-need-to-know/
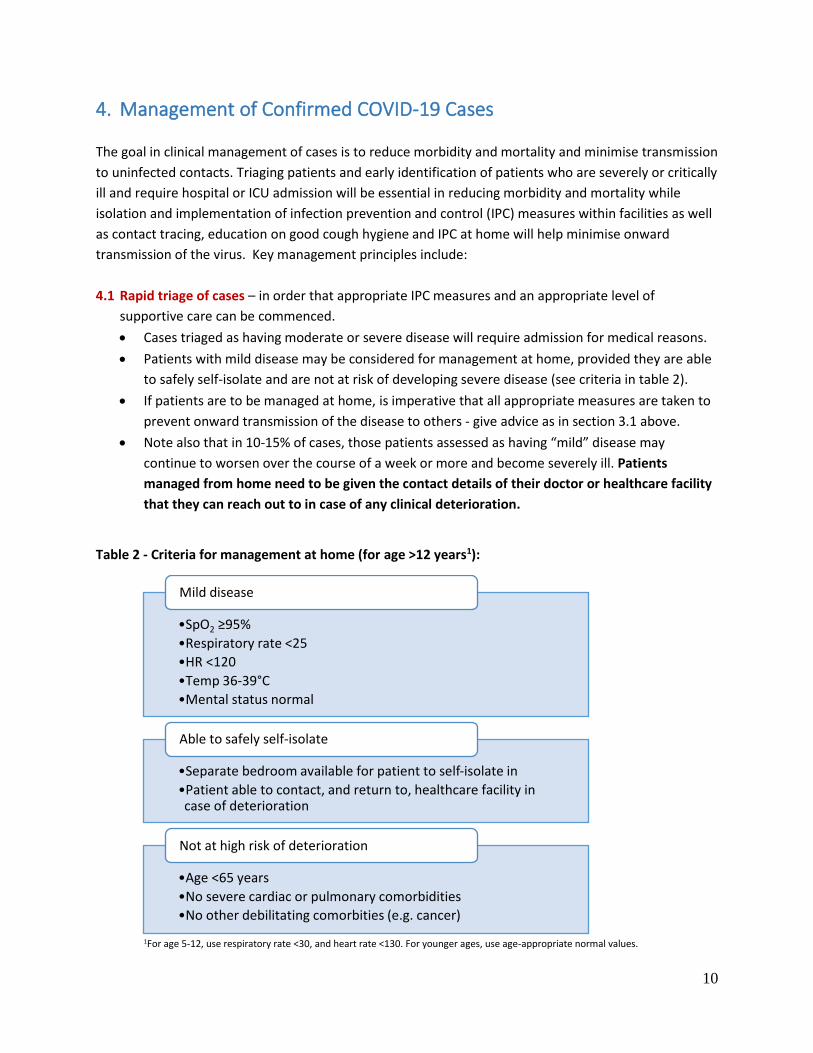
10
4. Management of Confirmed COVID-19 Cases
The goal in clinical management of cases is to reduce morbidity and mortality and minimise transmission
to uninfected contacts. Triaging patients and early identification of patients who are severely or critically
ill and require hospital or ICU admission will be essential in reducing morbidity and mortality while
isolation and implementation of infection prevention and control (IPC) measures within facilities as well
as contact tracing, education on good cough hygiene and IPC at home will help minimise onward
transmission of the virus. Key management principles include:
4.1 Rapid triage of cases – in order that appropriate IPC measures and an appropriate level of
supportive care can be commenced.
• Cases triaged as having moderate or severe disease will require admission for medical reasons.
• Patients with mild disease may be considered for management at home, provided they are able
to safely self-isolate and are not at risk of developing severe disease (see criteria in table 2).
• If patients are to be managed at home, is imperative that all appropriate measures are taken to
prevent onward transmission of the disease to others - give advice as in section 3.1 above.
• Note also that in 10-15% of cases, those patients assessed as having “mild” disease may
continue to worsen over the course of a week or more and become severely ill. Patients
managed from home need to be given the contact details of their doctor or healthcare facility
that they can reach out to in case of any clinical deterioration.
Table 2 - Criteria for management at home (for age >12 years1):
1For age 5-12, use respiratory rate <30, and heart rate <130. For younger ages, use age-appropriate normal values.
•SpO2 ≥95%
•Respiratory rate <25
•HR <120
•Temp 36-39°C
•Mental status normal
Mild disease
•Separate bedroom available for patient to self-isolate in
•Patient able to contact, and return to, healthcare facility in case of deterioration
Able to safely self-isolate
•Age <65 years
•No severe cardiac or pulmonary comorbidities
•No other debilitating comorbities (e.g. cancer)
Not at high risk of deterioration
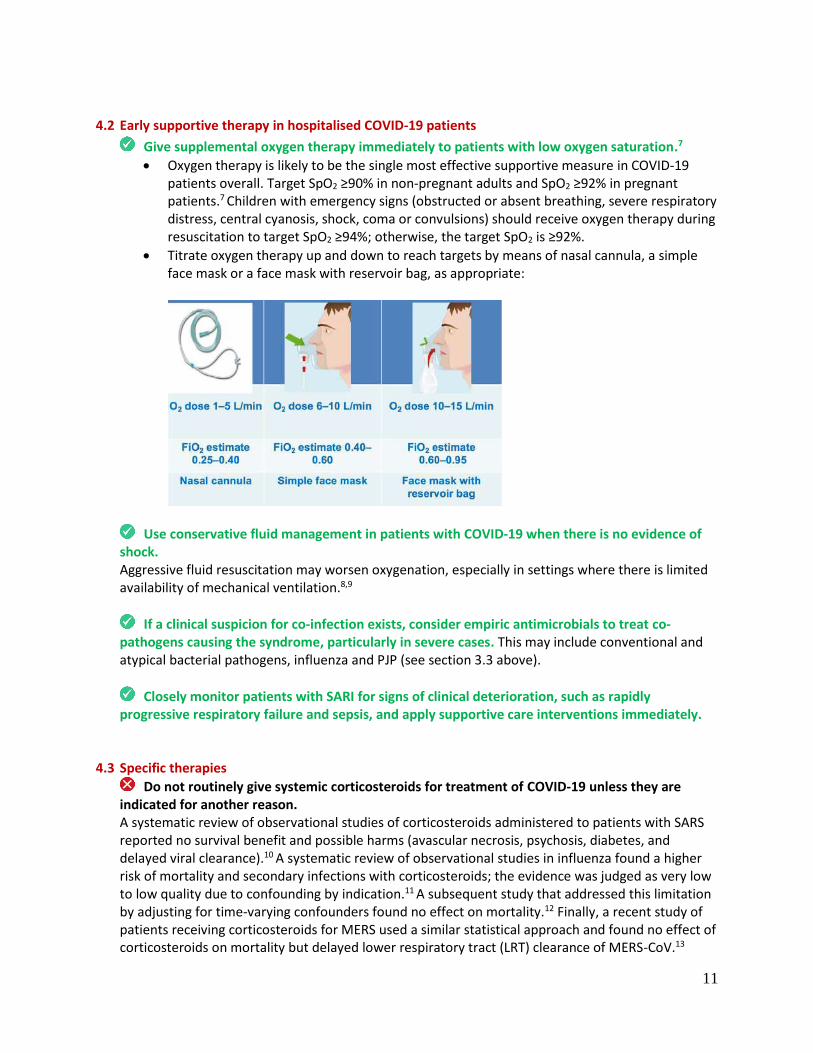
11
4.2 Early supportive therapy in hospitalised COVID-19 patients
Give supplemental oxygen therapy immediately to patients with low oxygen saturation.7
• Oxygen therapy is likely to be the single most effective supportive measure in COVID-19 patients overall. Target SpO2 ≥90% in non-pregnant adults and SpO2 ≥92% in pregnant patients.7 Children with emergency signs (obstructed or absent breathing, severe respiratory distress, central cyanosis, shock, coma or convulsions) should receive oxygen therapy during resuscitation to target SpO2 ≥94%; otherwise, the target SpO2 is ≥92%.
• Titrate oxygen therapy up and down to reach targets by means of nasal cannula, a simple face mask or a face mask with reservoir bag, as appropriate:
Use conservative fluid management in patients with COVID-19 when there is no evidence of shock. Aggressive fluid resuscitation may worsen oxygenation, especially in settings where there is limited availability of mechanical ventilation.8,9
If a clinical suspicion for co-infection exists, consider empiric antimicrobials to treat co-pathogens causing the syndrome, particularly in severe cases. This may include conventional and atypical bacterial pathogens, influenza and PJP (see section 3.3 above).
Closely monitor patients with SARI for signs of clinical deterioration, such as rapidly progressive respiratory failure and sepsis, and apply supportive care interventions immediately.
4.3 Specific therapies
Do not routinely give systemic corticosteroids for treatment of COVID-19 unless they are indicated for another reason.
A systematic review of observational studies of corticosteroids administered to patients with SARS reported no survival benefit and possible harms (avascular necrosis, psychosis, diabetes, and delayed viral clearance).10 A systematic review of observational studies in influenza found a higher risk of mortality and secondary infections with corticosteroids; the evidence was judged as very low to low quality due to confounding by indication.11 A subsequent study that addressed this limitation by adjusting for time-varying confounders found no effect on mortality.12 Finally, a recent study of patients receiving corticosteroids for MERS used a similar statistical approach and found no effect of corticosteroids on mortality but delayed lower respiratory tract (LRT) clearance of MERS-CoV.13

12
Given lack of effectiveness and possible harm, routine corticosteroids should be avoided unless they are indicated for another reason.
There is no current evidence from RCTs to recommend any specific treatment for patients with suspected or confirmed COVID-19 infection. This is an area of active study. Candidate drugs undergoing investigation include remdesivir, lopinavir/ritonavir, chloroquine, interferon, and toculizumab. To date, published clinical data on most of these agents consists largely of in vitro studies, with little or no human data. Hence we do not know whether these medicines benefit or cause harm to patients with COVID-19. One exception is lopinavir/ritonavir, which was studied in a recent randomized control trial of patients with severe COVID-19.14 No statistically significant benefit was seen with respect to viral load, time to clinical improvement, or mortality. Chloroquine has received considerable interest, given its relatively low cost, (limited) local availability, known side-effect profile (at registered doses), and some promising in vitro data. Published data from human trials is currently lacking.15 Given the state of evidence, we suggest consideration of the following:
• Where possible, consideration should be given to enroll hospitalized patients in clinical trials. This provides both adequate monitoring and ethics oversight, and affords the opportunity to contribute to the therapeutics evidence base for future patients.
• Where investigational therapeutics are given outside of a clinical trial, this should be done under the Monitored Emergency Use of Unregistered Interventions (MEURI) framework, whereby it can be ethically appropriate to offer individuals investigational interventions on an emergency basis in the context of an outbreak characterized by high mortality.16 The principles of this include:
o Data providing preliminary support for the intervention’s efficacy and safety are available, at least from laboratory or animal studies.
o The relevant human research ethics committee has approved the therapeutics’ use. o The patient’s informed consent is obtained. o Adequate resources are devoted to minimizing the therapeutics’ risk. o The results of the intervention are documented and shared with the wider medical and
scientific community.
• Where therapeutics are given to patients outside of a clinical trial, these should be reserved only for hospitalized patients (rather than given to mild cases, the vast majority of whom will recover fully without any intervention).
There is no evidence for the use of any drug or vaccine to prevent COVID-19 infection. Prevention consists of non-pharmaceutical interventions, such as good hand hygiene and social distancing.

13
4.4 Management of hypoxemic respiratory failure and ARDS
Recognize severe hypoxemic respiratory failure when a patient with respiratory distress is failing standard oxygen therapy. Patients may continue to have increased work of breathing or hypoxemia (SpO2 <90%, PaO2 <60 mmHg [<8.0 kPa]) even when oxygen is delivered via a face mask with reservoir bag. Hypoxemic respiratory failure in ARDS commonly results from intrapulmonary ventilation-perfusion mismatch or shunt and usually requires mechanical ventilation.
High-flow nasal oxygen (HFNO) or non-invasive ventilation (NIV) should only be used in selected patients with hypoxemic respiratory failure. The risk of treatment failure was high in patients with MERS treated with NIV, and patients treated with either HFNO or NIV should be closely monitored for clinical deterioration. In addition, HFNO and NIV carry the risk of aerosolization of viral particles against which adequate precautions need to be taken. Patients with hypercapnia (exacerbation of obstructive lung disease, cardiogenic pulmonary oedema), hemodynamic instability, multi-organ failure, or abnormal mental status should generally not receive HFNO, although emerging data suggest that HFNO may be safe in patients with mild-moderate and non-worsening hypercapnia.17 Patients receiving HFNO should be in a monitored setting and cared for by experienced personnel capable of endotracheal intubation in case the patient acutely deteriorates or does not improve after a short trial (about 1-2 hrs).
• Risks of NIV include delayed intubation, large tidal volumes, and injurious transpulmonary pressures. Limited data suggest a high failure rate when MERS patients receive NIV.13
• A single patient room and airborne precautions should be taken whenever HFNO and NIV is used.
For intubated patients with ARDS use lung-protective ventilation strategies. Always consult an expert intensivist if possible. Detailed recommendations on mechanical ventilation strategies are beyond the scope of the guideline. Nonetheless, the general principles in patients with ARDS include:
Statement on the use of angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARBs), and nonsteroidal anti-inflammatory drugs in COVID-19 patients
Recent work suggested that patients on ACEi or ARBs upregulate ACE2 receptors, the binding site for SARS-CoV-2, within tissues including the lung and heart, prompting concern that this might place patients at risk of worse outcomes with COVID-19.1 For the moment, this remains purely theoretical, with no evidence of a linkage to poor clinical outcomes. In addition, discontinuing or switching ACEi or ARBs to alternative agents may be deleterious to patient care. Pending further evidence we therefore do not recommend switching patients off ACEi or ARBs unless there are other medical reasons to do so. The evidence regarding nonsteroidal anti-inflammatory drugs (NSAIDs) in COVID-19 is similarly lacking. Nonetheless, where short-term fever or pain relief is required, it may be prudent to use drugs from other classes, such as paracetamol. For patients requiring NSAIDs for other indications however, the evidence is not definitive enough to recommend discontinuation. The South African Health Products Regulatory Authority (SAHPRA) has released a communication on the topic of NSAIDs and COVID-19.2
14
• Aim for an initial tidal volume of 6mg/kg.18 Higher tidal volume up to 8 ml/kg predicted body weight may be needed if undesirable side effects occur (e.g. dyssynchrony, pH <7.15).
• Strive to achieve the lowest plateau pressure possible. Plateau pressures above 30cm H20 are associated with an increased risk of pulmonary injury.18
• Hypercapnia is permitted if meeting the pH goal of 7.30-7.45.
• Application of prone ventilation >12 hours a day is strongly recommended for patients with severe ARDS.18
• In patients with moderate or severe ARDS, moderately higher PEEP instead of lower PEEP is suggested.18
• The use of deep sedation may be required to control respiratory drive and achieve tidal volume targets.
• In patients with moderate-severe ARDS (PaO2/FiO2 <150), neuromuscular blockade by continuous infusion should not be routinely used.19 Continuous neuromuscular blockade may still be considered in patients with ARDS in certain situations: ventilator dyssynchony despite sedation, such that tidal volume limitation cannot be reliably achieved; or refractory hypoxemia or hypercapnia.
• In settings with access to expertise in extracorporeal life support (ECLS), consider referral of patients with refractory hypoxemia despite lung protective ventilation.20-22
• Avoid disconnecting the patient from the ventilator, which results in loss of PEEP and atelectasis. Use in-line catheters for airway suctioning and clamp endotracheal tube when disconnection is required (for example, transfer to a transport ventilator). A high efficiency particulate filter on the expiratory limb of the ventilator circuit should be used.
4.5 De-isolation criteria
Patients can be de-isolated 14 days after the onset of their symptoms (mild cases), or 14 days after achieving clinical stability (moderate-severe cases). Most patients with mild COVID-19 infection continue to shed SARS-CoV-2 from their upper airways for approximately 7-12 days.23-25 The duration of shedding is longer in severe cases, though in both mild and severe cases, significant variation is seen.23,24,26 Viral shedding does not necessarily equate to infectiousness however. Viral shedding may decline to a level below the infectious threshold before it ceases completely, and/or non-viable virus may be shed. In a small cohort of mild COVID-19 cases from Germany (n=9), viral loads and viral cultures were performed on a variety of specimens simultaneously.27 The virus was readily culturable from specimens taken during the first week of symptoms, but no positive cultures were obtained from samples taken after day 8. Importantly, this was despite ongoing high viral loads being detected at the time. The authors estimated that there would be a <5% chance of successful culture by day 10. Given the very small sample size of the German cohort, we suggest a cautious approach of de-isolating patients with mild disease 14 days after symptom onset. Patients with severe disease (i.e. requiring admission due to clinical instability) may continue to shed virus at higher levels for longer periods. We therefore suggest de-isolating such patients 14 days after clinical stability has been achieved (e.g. after supplemental oxygen was discontinued).
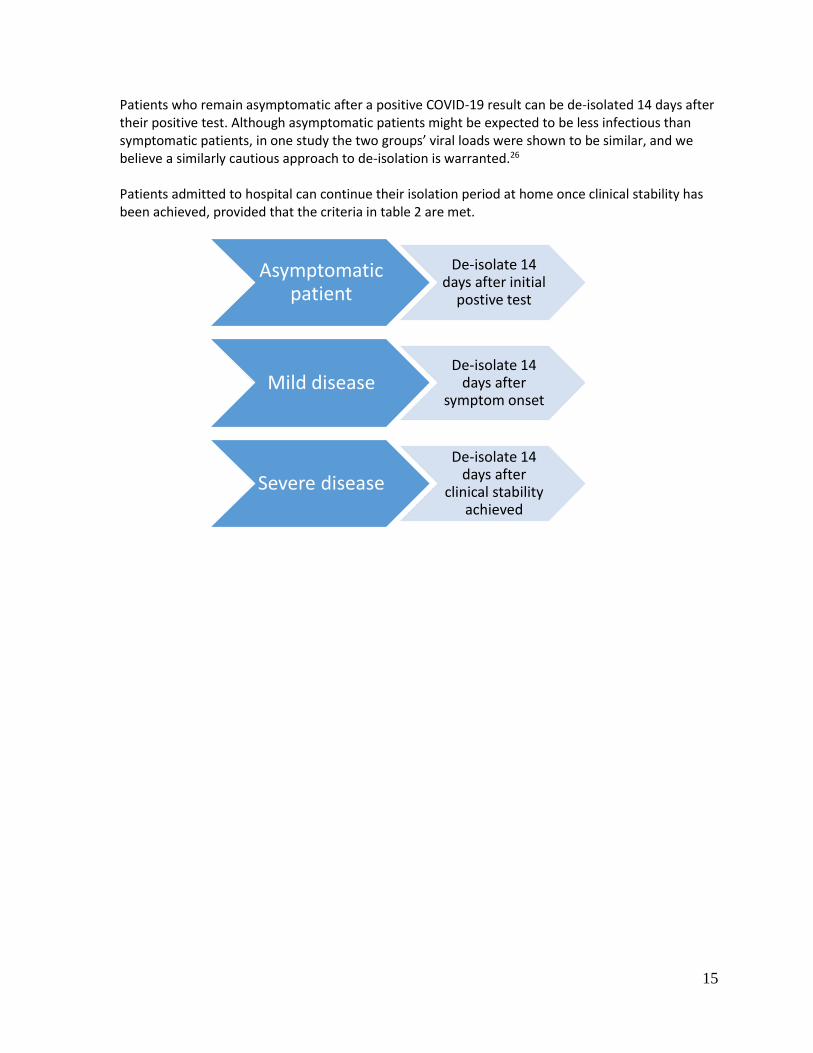
15
Patients who remain asymptomatic after a positive COVID-19 result can be de-isolated 14 days after their positive test. Although asymptomatic patients might be expected to be less infectious than symptomatic patients, in one study the two groups’ viral loads were shown to be similar, and we believe a similarly cautious approach to de-isolation is warranted.26 Patients admitted to hospital can continue their isolation period at home once clinical stability has been achieved, provided that the criteria in table 2 are met.
Asymptomatic patient
De-isolate 14 days after initial
postive test
Mild diseaseDe-isolate 14
days after symptom onset
Severe disease
De-isolate 14 days after
clinical stability achieved

16
5. Infection prevention and control (IPC)
IPC is a critical and integral part of clinical management of patients and should be initiated at the point
of entry of the patient to hospital (typically the Emergency Department). A combination of standard,
contact and droplet precautions should be practiced for all COVID-19 cases, and further precautions
when performing aerosol-generating procedures (AGP).
Standard precautions are used to prevent or minimize transmission of pathogens at all times, and
should be applied to all patients in healthcare facilities irrespective of their diagnosis or status. These
include hand hygiene, appropriate use of PPE, safe handling of sharps, linen and waste, disinfection of
patient care articles, respiratory hygiene, occupational health and injection safety.
Transmission-based precautions - droplet, and contact:
• Hand hygiene is the first and most essential aspect
• Healthcare worker PPE consists of gloves, gown (or apron), and a medical mask.
• Safe waste management
• Use either disposable or dedicated equipment (e.g. stethoscopes, blood pressure cuffs and thermometers). If equipment needs to be shared among patients, clean and disinfect between each patient use.
• Limit patient movement within the institution (e.g. where possible, use portable X-rays rather than sending the patient to the X-ray department), and ensure that patients wear medical masks when outside their rooms.
Aerosol-generating Procedures: Aerosol precautions are required when performing aerosol-generating procedures. These include taking respiratory tract samples for SARS-CoV-2 testing (such as nasopharyngeal and oropharyngeal swabs), intubation, bronchoscopy, open suctioning of the respiratory tract, and cardiopulmonary resuscitation. Aerosol precautions for healthcare workers:
• Healthcare worker PPE consists of gloves, gown (or apron), a fit-tested particulate respirator (N95 respirator), and eye protection (goggles or face shield).
• Use an adequately ventilated single room when performing aerosol-generating procedures, with spacing between beds of at least 1-1.5 metres.
For more details, refer to the World Health Organization IPC guidelines:
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/infection-
prevention-and-control

17
6. Recording and reporting
The goal of clinical management is to reduce morbidity and mortality from COVID-19 It is important to
record and report the cases of COVID-19 disease in order to track the size and severity of the epidemic,
the care received by patients in and out of hospital and identify areas for improvement in current and
future outbreaks. There different tools which will be needed to record and report clinical cases of
COVID-19.
Tool When to complete Comments
Person of interest form To be completed for all individuals suspected of COVID 19 disease and have a specimen taken
NMC case notification To be completed for all cases who meet the case definition for COVID-19
Can be completed online using NICD NMC mobile or web based app
Admission form (For inpatients)
To be completed for all confirmed patients admitted to a health care facility at admission or as soon as possible after admission
This form will document presence of co-morbidities, severity of illness at admission
Daily monitoring form (separate forms for inpatients and outpatients)
To be completed for all confirmed patients for each day until they are considered cured (by PCR criteria).
This form will document the daily symptoms, signs and severity of disease during admission
Discharge form (different forms for inpatients and outpatients)
To be completed for all confirmed patients
This form will document patient outcomes such as death, transfer or discharge.
Homecare form (for outpatients)
To be completed for all confirmed patients admitted with mild disease managed at home.
This form will document presence of co-morbidities, severity of illness at admission
The latest version of these forms are available from www.nicd.ac.za
18
References
1. Fang L, Karakiulakis G, Roth M. Are patients with hypertension and diabetes mellitus at increased risk for COVID-19 infection? Lancet Respir Med. 2020.
2. SAHPRA. The Use of Non-Steroidal Anti-Inflammatory Drugs in patients with Covid-19. Media release. 2020.
3. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med. 2020.
4. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N Engl J Med. 2020.
5. Yu P, Zhu J, Zhang Z, Han Y, Huang L. A familial cluster of infection associated with the 2019 novel coronavirus indicating potential person-to-person transmission during the incubation period. J Infect Dis. 2020.
6. Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA. 2020.
7. World Health Organization. Clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected 2020 [Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-suspected.
8. Schultz MJ, Dunser MW, Dondorp AM, Adhikari NK, Iyer S, Kwizera A, et al. Current challenges in the management of sepsis in ICUs in resource-poor settings and suggestions for the future. Intensive Care Med. 2017;43(5):612-24.
9. Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017;43(3):304-77.
10. Stockman LJ, Bellamy R, Garner P. SARS: systematic review of treatment effects. PLoS Med. 2006;3(9):e343.
11. Lansbury L, Rodrigo C, Leonardi-Bee J, Nguyen-Van-Tam J, Lim WS. Corticosteroids as adjunctive therapy in the treatment of influenza. Cochrane Database Syst Rev. 2019;2:CD010406.
12. Delaney JW, Pinto R, Long J, Lamontagne F, Adhikari NK, Kumar A, et al. The influence of corticosteroid treatment on the outcome of influenza A(H1N1pdm09)-related critical illness. Crit Care. 2016;20:75.
13. Arabi YM, Mandourah Y, Al-Hameed F, Sindi AA, Almekhlafi GA, Hussein MA, et al. Corticosteroid Therapy for Critically Ill Patients with Middle East Respiratory Syndrome. Am J Respir Crit Care Med. 2018;197(6):757-67.
14. Cao B, Wang Y, Wen D, Liu W, Wang J, Fan G, et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. New England Journal of Medicine. 2020.
15. Cortegiani A, Ingoglia G, Ippolito M, Giarratano A, Einav S. A systematic review on the efficacy and safety of chloroquine for the treatment of COVID-19. J Crit Care. 2020.
16. World Health Organization. Guidance For Managing Ethical Issues In Infectious Disease Outbreaks 2016. Available from:
https://apps.who.int/iris/bitstream/handle/10665/250580/9789241549837-eng.pdf;jsessionid=2C3A0BBB41D97192E283FF36FF1D7644?sequence=1.
17. Lee MK, Choi J, Park B, Kim B, Lee SJ, Kim SH, et al. High flow nasal cannulae oxygen therapy in acute-moderate hypercapnic respiratory failure. Clin Respir J. 2018;12(6):2046-56.
18. Fan E, Del Sorbo L, Goligher EC, Hodgson CL, Munshi L, Walkey AJ, et al. An Official American Thoracic Society/European Society of Intensive Care Medicine/Society of Critical Care Medicine

19
Clinical Practice Guideline: Mechanical Ventilation in Adult Patients with Acute Respiratory Distress Syndrome. Am J Respir Crit Care Med. 2017;195(9):1253-63.
19. National Heart L, Blood Institute PCTN, Moss M, Huang DT, Brower RG, Ferguson ND, et al. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. N Engl J Med. 2019;380(21):1997-2008.
20. Combes A, Hajage D, Capellier G, Demoule A, Lavoue S, Guervilly C, et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N Engl J Med. 2018;378(21):1965-75.
21. Goligher EC, Tomlinson G, Hajage D, Wijeysundera DN, Fan E, Juni P, et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome and Posterior Probability of Mortality Benefit in a Post Hoc Bayesian Analysis of a Randomized Clinical Trial. JAMA. 2018;320(21):2251-9.
22. Alshahrani MS, Sindi A, Alshamsi F, Al-Omari A, El Tahan M, Alahmadi B, et al. Extracorporeal membrane oxygenation for severe Middle East respiratory syndrome coronavirus. Ann Intensive Care. 2018;8(1):3.
23. World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19)2020. Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
24. Liu Y, Yan L-M, Wan L, Xiang T-X, Le A, Liu J-M, et al. Viral dynamics in mild and severe cases of COVID-19. Lancet Infect Dis [Internet]. 2020. Available from: https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30232-2/fulltext.
25. Young BE, Ong SWX, Kalimuddin S, Low JG, Tan SY, Loh J, et al. Epidemiologic Features and Clinical Course of Patients Infected With SARS-CoV-2 in Singapore. JAMA. 2020.
26. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020.
27. Woelfel R, Corman VM, Guggemos W, Seilmaier M, Zange S, Mueller MA, et al. Clinical presentation and virological assessment of hospitalized cases of coronavirus disease 2019 in a travel-associated transmission cluster. medRxiv. 2020:2020.03.05.20030502.

20
Appendix 1 – Example of a patient information sheet Example of a patient information sheet for use with suspected cases who are being sent home to await test results for SARS-CoV-2 (COVID-19). While awaiting test results for COVID-19 (the novel coronavirus), you have been assessed as being medically well enough to be managed at home. However, please consider yourself as potentially infectious until the final results are available. You will need to abide by the following:
• You should quarantine yourself at home. Don’t go to work, avoid unnecessary travel, and as far as possible avoid close interactions with other people.
• You should clean your hands with soap and water frequently. Alcohol-based sanitizers may also be used, provided they contain at least 60% alcohol.
• Do not have visitors in your home. Only those who live in your home should be allowed to stay. If it is urgent to speak to someone who is not a member of your household, do this over the phone.
• You should wear a facemask when in the same room (or vehicle) as other people.
• At home, you should stay in a specific room and use your own bathroom (if possible). If you live in shared accommodation (university halls of residence or similar) with a communal kitchen, bathroom(s) and living area, you should stay in your room with the door closed, only coming out when necessary, wearing a facemask if one has been issued to you.
• You should practice good cough and sneeze hygiene by coughing or sneezing into a tissue, discarding the tissue immediately afterwards in a lined trash can, and then wash your hands immediately.
• If you need to wash the laundry at home before the results are available, then wash all laundry at the highest temperature compatible for the fabric using laundry detergent. This should be above 60° C. If possible, tumble dry and iron using the highest setting compatible with the fabric. Wear disposable gloves and a plastic apron when handling soiled materials if possible and clean all surfaces and the area around the washing machine. Do not take laundry to a laundrette. Wash your hands thoroughly with soap and water after handling dirty laundry (remove gloves first if used).
• You should avoid sharing household items like dishes, cups, eating utensils and towels. After using any of these, the items should be thoroughly washed with soap and water.
• All high-touch surfaces like table tops, counters, toilets, phones, computers, etc. that you may have touched should be appropriately and frequently cleaned.
• Monitor your symptoms - Seek prompt medical attention if your illness is worsening, for example, if you have difficulty breathing, or if the person you are caring for symptoms are worsening. If it’s not an emergency, call your doctor or healthcare facility at the number below. If it is an emergency and you need to call an ambulance, inform the call handler or operator that you are being tested for SARS-CoV-2.
While awaiting the results, if your symptoms worsen:
• Call:
• Or come to:

21
For more information on COVID-19, see the NICD’s FAQ page: http://www.nicd.ac.za/diseases-a-z-index/covid-19/frequently-asked-questions/
20th Floor, 4 Dorp Street, Cape Town P O Box 2060, Cape Town, 8000
Tel: +27 21 483 3647 Fax: 086 276 4673 westerncape.gov.za
OFFICE OF HEAD: HEALTH
REF: 16/4
ENQUIRIES: DR K CLOETE
To All
SMS Members/ Chief Directorates/ Directorates / Regional / District Offices, Sub-Structures / All
Facility Mangers/ City of Cape Town / Higher Education Institutions / Private Sector
CIRCULAR H 49/2020: WESTERN CAPE GOVERNMENT (WCG) GUIDE TO FAMILIES, UNDERTAKERS AND
COMMUNITIES RELATING TO THE MANAGEMENT OF A DECEASED WHO PASSED AWAY BECAUSE OF
EITHER POSITIVE OR SUSPECTED COVID-19
Introduction
There is much that is unknown about the SARS-CoV-2 virus (COVID-19) but what is known is that
the virus most often spreads from person to person via respiratory droplets when people cough or
sneeze. These droplets end up on other objects or people and this is causing the transfer of the
virus.
The risk of infection from the deceased is therefore decreased because they do not cough or
sneeze, however, the risk is still high in terms of family members who may have been exposed to
the virus while the person was alive and in terms of direct handling of the body where the family
touches the body without the appropriate Personal Protective Equipment (PPE).
In South Africa, we have various cultural and religious beliefs which may have to be adapted in
the interest of protecting the population at large.
This guide is in accordance with current published National Health Environmental Health
guidelines (dated 27 March 2020) that may be amended as the pandemic progresses.
What to do when a person passes away at home
When a person dies at home of suspected or positive COVID-19, the family is encouraged not to
touch the remains and leave the remains in the room where the person passed away.
In cases where the death was due to any unnatural causes such as trauma caused by accidents,
murder and suicide for example, and the suspicion is that the individual also suffered from COVID-
19, the SAPS are to be notified. In cases where no foul play is suspected, it would be advisable to
contact an undertaker who is trained in managing such scenarios and who has the appropriate
PPE for removal.
While any form of contact is strongly discouraged, there are religious and cultural practices that
require that human remains be washed before burial. If families wish to perform these rituals, then
it is advised that this is done by members of the religious group who are properly trained in the
correct use of PPE.
Annexure F
It is advised that the deceased’s belongings be properly cleaned with a solution containing at
least 70% alcohol or 0.5% bleach. Any clothing should be washed with warm water at a
temperature of at least 60 to 90°C.
It is strongly advised that once the remains are prepared for the burial, that no further contact is
allowed. The deceased’s face may be shown at the funeral if there is no contact in the form of
kissing or touching of the deceased’s face.
People with respiratory diseases should not form part of the viewing process unless they wear a
medical face mask to prevent further transmission of possible disease.
It is advised that people who are older than 60-years and immunosuppressed should not have
contact with the body.
Funerals
Aside from the regulations relating to the funerals, the following information (guidelines) should
also be observed:
Human remains can be infectious on surfaces up to nine days, therefore it is important to
clean all surfaces that the body was in contact with.
Cremation is the preferred method for a funeral but if the family requires a burial then this
process should take no longer than two hours.
All attempts should be made to bury a deceased who passed away from confirmed or
suspected COVID-19 within three days if there is no indication for a post mortem
examination.
Yours sincerely
DR K CLOETE
HEAD: WESTERN CAPE GOVERNMENT HEALTH
DATE: 08 April 2020
Head of Department: Health
Reference: COVID-19 Enquiries: Ms Vonita Thompson
021 928 1501
1
TO ALL SMS MEMBERS/ CHIEF DIRECTORATES / DIRECTORATES / REGIONAL / DISTRICT OFFICES, SUB-
STRUCTURES / ALL FACILITY MANAGERS/ CITY OF CAPE TOWN / HIGHER EDUCATION INSTITUTIONS /
PRIVATE SECTOR
Circular H 41 of 2020: COVID-19: Management of decedents in the Western Cape
1 Introduction
1.1. This document serves to outline the functions of various role players in different settings in
response to a COVID-19 death in the Western Cape.
1.2. This document is a combination of various directives issued in the “Guidelines for case-
finding, diagnosis, management and public health response in South Africa”, the “COVID-
19 Environmental Guidelines” and the relevant National Health Act regulations and should
be read in conjunction with those documents.
2 Important notice
2.1. Deaths exclusively as a result of suspected or confirmed SARS-CoV-2/COVID-19 are NOT
unnatural deaths. These cases, therefore, do NOT require medicolegal autopsies.
2.2. Such cases should therefore NOT be referred to Forensic Pathology Service (FPS) mortuaries
by hospitals/clinics for medicolegal autopsies.
2.3. People that die of unnatural causes with suspected or confirmed SARS-CoV-2/COVID-19;
however, are still required by law to be referred for medicolegal examination by FPS.
3 Recommendation regarding swabbing of suspected COVID-19 deceased cases
3.1. In all the categories listed hereunder, where the case conforms to the criteria for a possible
COVID-19 diagnosis, it is recommended that throat and nasopharyngeal swabs be taken by
the responsible medical practitioner, and the swabs be dispatched according to the
accepted protocol to the designated NHLS laboratory in the prescribed way.
3.2. The taking of swabs is not indicated where the postmortem interval exceeds three days in
relation to deaths where there is a history consistent with COVID-19, where a patient was not
seen in a clinical setting and/or specimens retained.
Annexure G
2
4 Management of decedents that died in a Western Cape Government healthcare facility as a
result of COVID-19 where an undertaker serves as the designated mortuary
4.1. Healthcare facility staff to ensure that the human remains are appropriately double bagged
and sanitized to ensure safe transportation in line with that of a Biological safety Hazard level
3.
4.2. The healthcare facility shall contact the relevant Environmental Health Practitioner (EHP) in
the municipal district to ensure that the handling of the human remains is strictly monitored
by the EHP throughout the process.
4.3. The relevant contracted undertaker who serves as the undertaker for the removal of
decedents from the healthcare facility shall remove the human remains to the undertaker’s
premises.
4.4. The human remains must be transported in a manner that is compliant with the provisions of
the Regulations Relating to the Management of Human Remains.
4.5. Human remains can only be transferred from one designated facility to another designated
facility or from such to a cemetery or crematorium.
4.6. Direct handling of the human remains is strongly discouraged and if necessary, shall conform
to full Personal Protective Equipment (PPE).
4.7. Where it is feasible and acceptable to family culture and/or religion, it is strongly
recommended that the human remains be cremated.
4.8. In all cases, human remains should not be kept in households for a vigil or any purpose but
be kept in designated healthcare facility mortuary premises, and directly transported from
designated healthcare facility mortuary straight to the place of burial or cremation or the
home on the day of burial/cremation.
5 COVID-19 death in a Western Cape Government healthcare facility where the facility has a
mortuary
5.1. Healthcare facility staff to ensure that the human remains are appropriately double bagged
and the outer surface decontaminated to ensure safe transportation and further handling.
5.2. The healthcare facility shall contact the relevant EHP in the municipal district to ensure that
the handling of the human remains is strictly monitored by the EHP throughout the process.
5.3. The human remains are considered contagious and should be kept only in designated
health facilities’ mortuaries.
5.4. Human remains can only be transferred from one designated facility to another designated
facility or from such to a cemetery or crematorium.
5.5. Direct handling of the human remains is strongly discouraged and if necessary, shall conform
to full PPE.
5.6. Where it is feasible and acceptable to family culture and/or religion, it is strongly
recommended that the human remains be cremated.
5.7. In all cases, human remains should not be kept in households for a vigil or any purpose but
be kept in designated healthcare facility mortuary premises and directly transported from
the designated healthcare facility mortuary straight to the place of burial or cremation or
the home on the day of burial/cremation.
5.8. The human remains must be transported in a manner that is compliant with the provisions of
the Regulations Relating to the Management of Human Remains.

3
6 COVID-19 death at a private healthcare facility
6.1. Healthcare facility staff to ensure that the human remains are appropriately double bagged
and the outer surface decontaminated to ensure safe transportation and further handling.
6.2. The healthcare facility shall contact the relevant EHP in the municipal district to ensure that
the handling of the human remains is strictly monitored by the EHP throughout the process.
6.3. The undertaker contracted by the next of kin to collect the human remains.
6.4. The human remains must be transported in a manner that is compliant with the provisions of
the Regulations Relating to the Management of Human Remains.
6.5. Human remains can only be transferred from one designated facility to another designated
facility or from such to a cemetery or crematorium.
6.6. Direct handling of the human remains is strongly discouraged and if necessary, shall conform
to full PPE.
6.7. Where it is feasible and acceptable to family culture and/or religion, it is strongly
recommended that the human remains be cremated.
6.8. In all cases, human remains should not be kept in households for a vigil or any purpose but
be kept in designated healthcare facility mortuary premises and directly transported from
designated healthcare facility mortuary straight to the place of burial or cremation or the
home on the day of burial/cremation.
7 COVID-19 death in Emergency Medical Services (EMS) transport
7.1. If a patient dies in transit, the EMS provincial coordinator, provincial communicable disease
control coordinator (CDCC) and the standby forensic medical practitioner (in the case of
unnatural death) must be notified.
7.2. A decision on where to take the decedent must be communicated to the ambulance crew.
This should be the mortuary or undertaker which acts as the storage facility for the hospital
where the patient was on route to. In the case of unnatural deaths which is also a suspected
COVID–19, the human remains will be referred to the relevant FPS mortuary.
7.3. Provincial Environmental Health must be informed.
7.4. Under no circumstances will the decedent be removed from the ambulance other than at
an assigned facility that was communicated to the ambulance crew.
7.5. The decedent must be placed in double body bags that are fluid leak proof. The bags must
be wiped down with a 0.05% chlorine solution before leaving the ambulance by persons
with the appropriate PPE, either porters or crew.
7.6. The removal of a suspected COVID-19 decedent must be done under the directive of
Environmental Health. In FPS cases, the EHP must be informed but does not have to be onsite,
and this noted in the occurrence book.
8 COVID-19 natural death in a community
8.1. EMS performs the death declaration.
8.2. SAPS complete the SAPS 180 form.
8.3. The next of kin is instructed to contact an undertaker to facilitate collection of the human
remains.

4
8.4. During the initial phases of the health service response, FPS is dispatched on request of an
undertaker to assist in the double bagging and decontamination of the outer bag for the
safe transportation of the human remains. The undertaker is to be present whilst this occurs
and to take responsibility for all property and valuables. The deceased will be transported
from the scene in the undertaker’s vehicle.
8.5. The relevant EHP in the municipal district is dispatched to ensure that the handling of the
human remains is strictly monitored by the EHP throughout the process.
8.6. The undertaker collects the human remains under the supervision of the relevant EHP in the
district where the patient died.
9 Death where COVID-19 is suspected but results not available yet
9.1. The responsible medical practitioner is to proceed with notifying the death (e.g. lower
respiratory tract infection).
9.2. The body is to be sealed and removed by the designated undertaker.
9.3. The human remains are indicated as possible COVID-19 on the double bag and handled as
such.
10 Import and export of human remains who died of COVID-19
10.1. The human remains of a person who has died of a confirmed COVID-19 should be cremated.
10.2. Where cremation is not possible, the repatriation of human remains who died of confirmed
or suspected COVID-19 must be conducted in line with the Regulations Relating to the
Management of Human Remains (Regulation 363 of 22 May 2013).
10.3. A formal request for an import/export permit issued by the Director-General: Health must be
made by the Department of International Relations and Cooperation (DIRCO) or through
the embassies, prior to importation/exportation of the human remains.
10.4. The import/export permit, death certificate and written declaration by an institution
responsible for packaging the human remains; stating that the transportation of human
remains will not constitute a health hazard must always accompany the human remains. No
person must open the coffin or remove the human remains after they have been sealed
without prior approval from an EHP.
11 In the case of exportation of human remains who died of COVID-19
11.1. The human remains must be transported from the mortuary of a designated facility to the
point of entry by the relevant contracted undertaker in consultation with the embassy of
which the deceased holds residence.
11.2. The EHP at a municipal level must monitor the handling of the human remains at the
designated mortuary.
11.3. The EHP at a point of entry must monitor the removal of the human remains from the relevant
undertaker mortuary.
5
12 In the case of importation of human remains who died of COVID-19
12.1. The EHP at a point of entry must inform the relevant undertaker of the arrival of the human
remains for transportation.
12.2. The EHP at a point of entry must monitor the removal of the human remains from the
conveyance to the relevant undertaker vehicle.
12.3. The EHP at a municipal level must monitor the handling of the human remains after arrival at
the designated mortuary.
Yours Sincerely
DR E ENGELBRECHT
HEAD OF DEPARTMENT: HEALTH
DATE: 30/03/2020
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health
Emergency in South Africa
02 APRIL 2020
www.criticalcare.org.za
Email: [email protected]
Annexure H

2
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
Introduction
• The purpose of this document is to provide guidance for the triage of critically ill patients in the event that a public health emergency creates demand for critical care resources (e.g., ventilators, critical care beds) that outstrips the supply.
• These triage recommendations will be enacted only if: 1) critical care capacity is, or will shortly be, overwhelmed despite taking all appropriate steps to increase the surge capacity to care for critically ill patients; and 2) His Excellency, the President of South Africa has declared a public health emergency.
• This allocation framework is grounded in ethical obligations that include: o duty to care, o duty to steward resources to optimize population health, o distributive and procedural justice, and o transparency.
It is consistent with existing recommendations for how to allocate scarce critical care resources during a public health emergency.
• This document is based largely on The University of Pittsburgh, Pennsylvania guidelines from whom we have borrowed liberally with permission, with modifications as were deemed necessary.
• This document describes: I. The creation of triage teams to ensure consistent decision making;
II. Allocation criteria for initial allocation of critical care resources; and III. Reassessment criteria to determine whether ongoing provision of scarce critical care
resources are justified for individual patients.

3
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
Section 1. Creation of triage teams • The general recommendation in triage processes is that patients’ treating clinicians should not make
triage decisions. • The separation of the triage role from the clinical role is intended to promote objectivity, avoid
conflicts of commitments, and minimize moral distress. • Each hospital will designate an acute care physician triage officer, supported if resources allow by an
acute care nurse and administrator, who will apply the allocation framework described in this document.
• The triage team will use the allocation framework, detailed below, to determine priority scores of all patients eligible to receive the scarce critical care resource.
• The triage officer will also be involved in patient or family appeals of triage decisions, and in collaborating with the attending physician to disclose triage decisions to patients and families.
• An appeals process for individualized triage decisions needs to be in place. ***NOTE
The recommendation in terms of formation of triage teams as a formalized process will often be difficult in many of our settings. There is a limited number of critical care practitioners with the requisite experience to lead such triage teams. An alternate model may need to be sought where suitable team leaders and members are not available. In these situations, at an institutional level, any additional practitioners experienced in triage are encouraged to become involved in teams. Where possible, senior members of the critical care teams are encouraged to take on these roles. Where dedicated triage teams separate from clinical management teams cannot be formed, it is recommended that triage decisions are not left to individual managing clinicians, but are rather made by the managing clinical team. Additionally, consultative teams of experienced practitioners covering broader geographical areas may be necessary to provide an advisory role to local, institutional teams involved in triage.
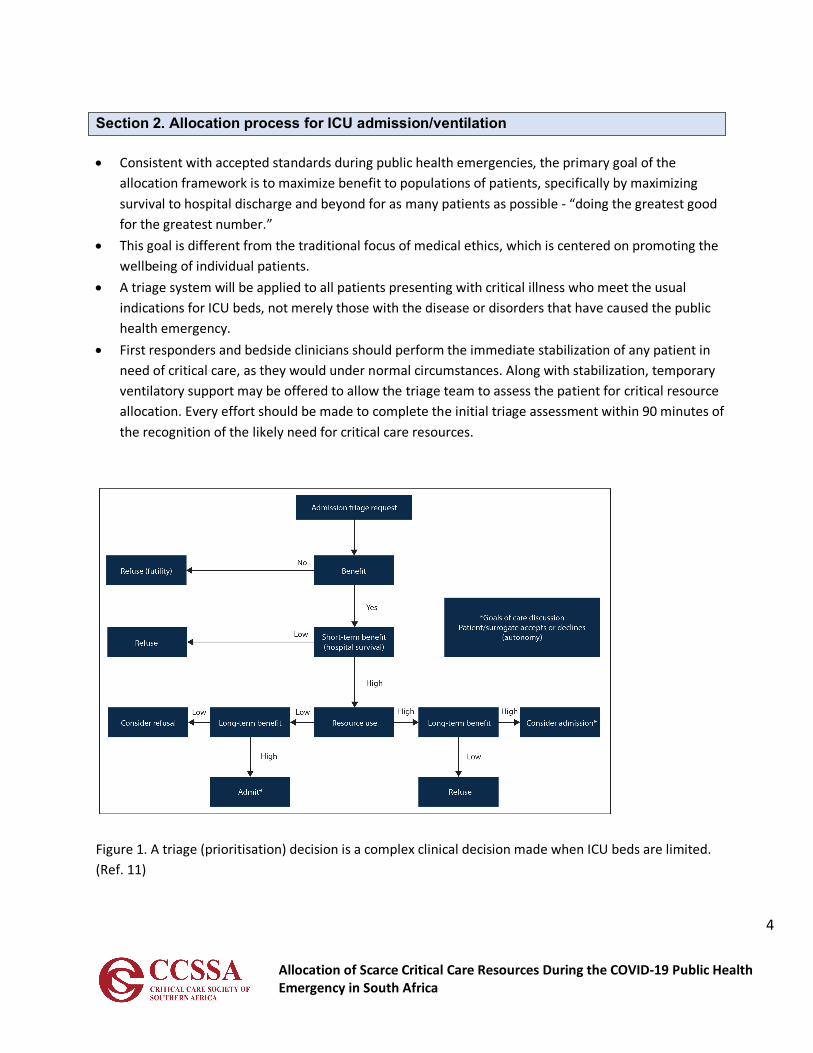
4
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
Section 2. Allocation process for ICU admission/ventilation
• Consistent with accepted standards during public health emergencies, the primary goal of the allocation framework is to maximize benefit to populations of patients, specifically by maximizing survival to hospital discharge and beyond for as many patients as possible - “doing the greatest good for the greatest number.”
• This goal is different from the traditional focus of medical ethics, which is centered on promoting the wellbeing of individual patients.
• A triage system will be applied to all patients presenting with critical illness who meet the usual indications for ICU beds, not merely those with the disease or disorders that have caused the public health emergency.
• First responders and bedside clinicians should perform the immediate stabilization of any patient in need of critical care, as they would under normal circumstances. Along with stabilization, temporary ventilatory support may be offered to allow the triage team to assess the patient for critical resource allocation. Every effort should be made to complete the initial triage assessment within 90 minutes of the recognition of the likely need for critical care resources.
Figure 1. A triage (prioritisation) decision is a complex clinical decision made when ICU beds are limited. (Ref. 11)
5
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
• The initial assessment of the referred patient focusses on whether the patient is critically ill needing
ICU admission for either ventilatory support or other organ support only available in ICU. If care, e.g. advanced monitoring is all that is needed, such patients should be managed at appropriate sites outside the ICU.
• Referred patients that are deemed not critically ill enough to be admitted to ICU will need to be monitored. In the event of a deterioration in their condition, such patients will be re-referred to the ICU team.
• Patients’ wishes in respect of ICU care need to be ascertained. The presence of e.g. advanced directives needs to be determined. If there is no clear indication of an expression by the patient to NOT be admitted, further evaluation of priority continues. If there is a clear expression of a wish to no be admitted to ICU, a further management plan excluding ICU is activated.
• An assessment is then made of the likelihood of care in the ICU being beneficial. Patients will not be considered for admission to critical care beds where further therapy is deemed to be futile. Futility is not necessarily related to the degree or pattern of acute organ dysfunction, but takes into account long term outcome. In general, ICU admission of the following examples of patients would be deemed non-beneficial (futile):
§ Brain death in terms of legally defined criteria § Chronic, terminal and irreversible illness, facing imminent death § Post cardiac arrest patients
o Resulting from a progressive decline in physiological function o In whom a normal respiratory pattern or full level of consciousness without sedation
is not achieved o Fixed dilated pupils not due to medication o Secondary to a cause that is not reversible
§ Irreversible severe brain damage § Acute, irreversible severe multi-organ failure and anticipated poor prognosis
• An assessment of the patient is then made on the Clinical Frailty Scale (CFS) (Figure 2) Patients with a CFS score ≥ 6 are to be offered a management plan excluding ICU. Patients with a CFS score < 6 are prioritized further.
• All patients who meet usual medical indications for ICU beds and services will be assigned a priority score using a 1-8 scale (lower scores indicate higher likelihood of benefit from critical care), derived from a multi-principle allocation framework (Table 1):
1) patients’ likelihood of surviving to hospital discharge, assessed with an objective and validated measure of acute physiology, the Sequential Organ Failure Assessment (SOFA); and 2) patients’ likelihood of achieving longer-term survival based on the presence or absence of comorbid conditions that may influence survival.
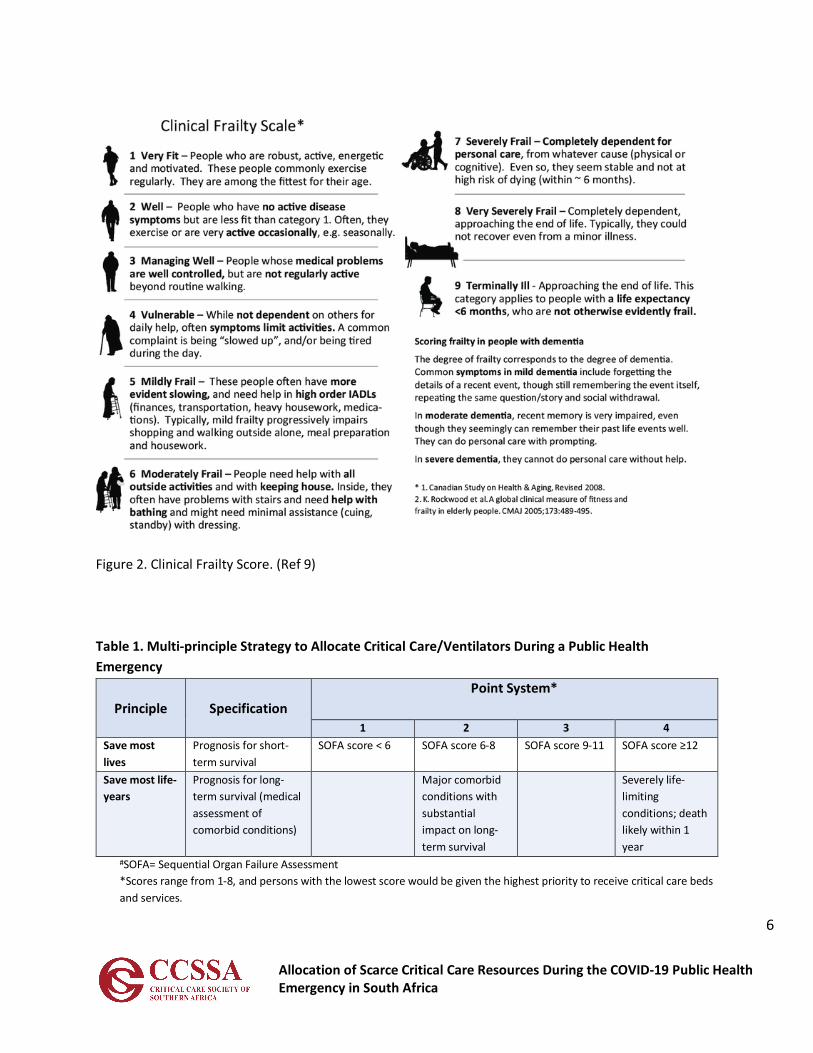
6
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
Figure 2. Clinical Frailty Score. (Ref 9) Table 1. Multi-principle Strategy to Allocate Critical Care/Ventilators During a Public Health Emergency
Principle
Specification
Point System*
1 2 3 4 Save most lives
Prognosis for short-term survival
SOFA score < 6 SOFA score 6-8 SOFA score 9-11 SOFA score ≥12
Save most life-years
Prognosis for long-term survival (medical assessment of comorbid conditions)
Major comorbid conditions with substantial impact on long-term survival
Severely life-limiting conditions; death likely within 1 year
#SOFA= Sequential Organ Failure Assessment *Scores range from 1-8, and persons with the lowest score would be given the highest priority to receive critical care beds and services.

7
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
• Points are assigned according to the patient’s SOFA score (range from 1 to 4 points) plus the presence or absence of comorbid conditions (1-4 points) See Table 2 for examples of comorbid conditions. These points are then added together to produce a total priority score, which ranges from 1 to 8. Lower scores indicate higher likelihood of benefiting from critical care, and priority will be given to those with lower scores.
• Priority Groups o This raw priority score is converted to three color-coded priority groups (e.g., RED=high,
ORANGE=intermediate, and YELLOW=low priority) to facilitate streamlined implementation in individual hospitals. (Figure 3)
o The priority group colour should be noted clearly on the patient chart. o Individuals in the red group have the best chance to benefit from critical care interventions
and should therefore receive priority over all other groups in the face of scarcity. o The orange group has intermediate priority and should receive critical care resources if there
are available resources after all patients in the red group have been allocated critical care resources.
o The yellow group has lowest priority and should receive critical care resources if there are available resources after all patients in the red and orange groups have been allocated critical care resources.
Table 2. Examples of Major Comorbidities and Severely Life Limiting Comorbidities*
Examples of Major comorbidities (associated with significantly decreased long-term survival)
Examples of Severely Life Limiting Comorbidities (commonly associated with survival < 1 year)
• Moderate Alzheimer’s disease or related dementia
• Malignancy with a < 10 year expected survival • New York Heart Association Class III heart
failure • Moderately severe chronic lung disease (e.g.,
COPD, IPF) • End-stage renal disease in patients < 75 • Severe multi-vessel CAD • Cirrhosis with history of decompensation
• Severe Alzheimer’s disease or related dementia • Cancer being treated with only palliative
interventions (including palliative chemotherapy or radiation)
• New York Heart Association Class IV heart failure plus evidence of frailty
• Severe chronic lung disease plus evidence of frailty
• Cirrhosis with MELD score ≥20, ineligible for transplant
• End-stage renal disease in patients older than 75 *This Table only provides examples.
• All patients will be eligible to receive critical care beds and services regardless of their priority score,
but available critical care resources will be allocated according to priority score, such that the availability of these services will determine how many patients will receive critical care.
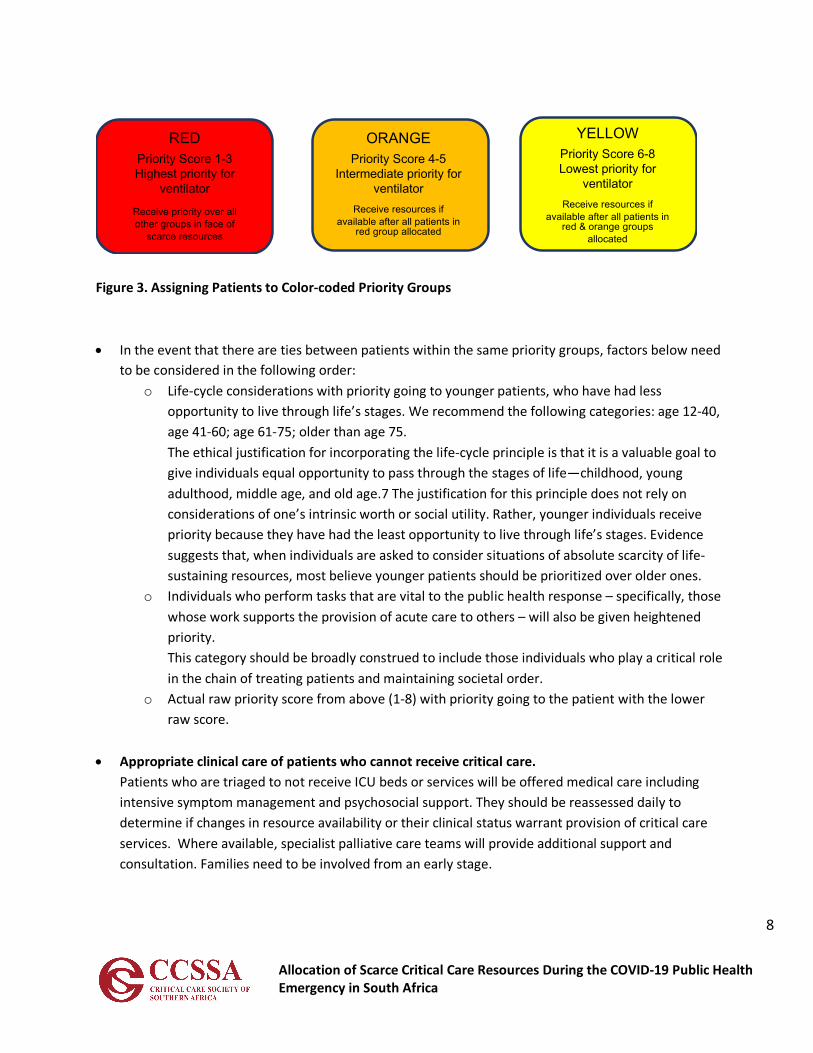
8
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
Figure 3. Assigning Patients to Color-coded Priority Groups • In the event that there are ties between patients within the same priority groups, factors below need
to be considered in the following order: o Life-cycle considerations with priority going to younger patients, who have had less
opportunity to live through life’s stages. We recommend the following categories: age 12-40, age 41-60; age 61-75; older than age 75. The ethical justification for incorporating the life-cycle principle is that it is a valuable goal to give individuals equal opportunity to pass through the stages of life—childhood, young adulthood, middle age, and old age.7 The justification for this principle does not rely on considerations of one’s intrinsic worth or social utility. Rather, younger individuals receive priority because they have had the least opportunity to live through life’s stages. Evidence suggests that, when individuals are asked to consider situations of absolute scarcity of life-sustaining resources, most believe younger patients should be prioritized over older ones.
o Individuals who perform tasks that are vital to the public health response – specifically, those whose work supports the provision of acute care to others – will also be given heightened priority. This category should be broadly construed to include those individuals who play a critical role in the chain of treating patients and maintaining societal order.
o Actual raw priority score from above (1-8) with priority going to the patient with the lower raw score.
• Appropriate clinical care of patients who cannot receive critical care. Patients who are triaged to not receive ICU beds or services will be offered medical care including intensive symptom management and psychosocial support. They should be reassessed daily to determine if changes in resource availability or their clinical status warrant provision of critical care services. Where available, specialist palliative care teams will provide additional support and consultation. Families need to be involved from an early stage.
YELLOWPriority Score 6-8Lowest priority for
ventilatorReceive resources if
available after all patients in red & orange groups
allocated
ORANGEPriority Score 4-5
Intermediate priority for ventilator
Receive resources if available after all patients in
red group allocated
REDPriority Score 1-3Highest priority for
ventilator
Receive priority over all other groups in face of
scarce resources

9
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
• During a public health emergency, clinicians should still make clinical judgments about the appropriateness of critical care using the same criteria they use during normal clinical practice.
• Make daily determinations of how many priority groups can receive the scarce resource. Regular (daily or twice daily) determinations to be made about what priority scores will result in access to critical care services. These determinations should be based on real-time knowledge of the degree of scarcity of the critical care resources, as well as information about the predicted volume of new cases that will be presenting for care over the near-term (several days). For example, if there is clear evidence that there is imminent shortage of critical care resources (i.e., few ventilators available and large numbers of new patients daily), only patients with the highest priority (lowest scores, e.g., 1-3) should receive scarce critical care resources. As scarcity subsides, patients with progressively lower priority (higher scores) should have access to critical care interventions.
10
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
Reassessment for ongoing provision of critical care/ventilation • The ethical justification for such reassessment is that, in a public health emergency when there are
not enough critical care resources for all, the goal of maximizing population outcomes would be jeopardized if patients who were determined to be unlikely to survive were allowed indefinite use of scarce critical care services. In addition, periodic reassessments lessen the chance that arbitrary considerations, such as when an individual develops critical illness, unduly affect patients’ access to treatment.
• The triage team will conduct periodic reassessments of all patients receiving critical care services during times of crisis (i.e., not merely those initially triaged under the crisis standards).
• The timing of reassessments should be based on evolving understanding of typical disease trajectories and of the severity of the crisis. It is recommended this occurs at 48 hours as a formality and thereafter every 24 hours.
• A multidimensional assessment should be used to quantify changes in patients’ conditions, such as recalculation of severity of illness scores, appraisal of new complications, and treating clinicians’ input.
• Patients showing improvement will continue to receive critical care services until the next assessment. • If there are patients in the queue for critical care services, then patients who upon reassessment show
substantial clinical deterioration as evidenced by worsening SOFA scores or overall clinical judgment and that portends a very low chance for survival, should have critical care withdrawn, including discontinuation of mechanical ventilation, after this decision is disclosed the patient and/or family.
• Appropriate clinical care of patients who cannot receive critical care. Patients who are no longer eligible for critical care treatment should receive medical care including intensive symptom management and psychosocial support. Where available, specialist palliative care teams will be available for consultation. Where palliative care specialists are not available, the treating clinical teams should provide primary palliative care. Families are to be intimately involved in these processes.
Special Acknowledgment: Writing Team CCSSA EXCO (Dean Gopalan, Ivan Joubert, Fathima Paruk, Brian Levy) Critical Care Teams from around South Africa for input Scott Halpern & Doug White - University of Pittsburgh, Pennsylvania on whose original document much of this guideline is based.

11
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
References
1. Halpern S, White D. Allocation of Scarce Critical Care Resources During a Public Health Emergency. Univ Pittsburgh, Pennsylvania. 23 March 2020
2. Childress JF, Faden RR, Gaare RD, et al. Public health ethics: mapping the terrain. J Law Med Ethics 2002;30:170-8
3. Gostin L. Public health strategies for pandemic influenza: ethics and the law. Jama 2006;295:1700-4. 4. Beauchamp TL, Childress JF. Principles of Biomedical Ethics. 6th ed. ed. New York, NY: Oxford University
Press; 2009 5. White DB, Katz MH, Luce JM, Lo B. Who should receive life support during a public health emergency?
Using ethical principles to improve allocation decisions. Ann Intern Med 2009;150:132-8. 6. Young MJ, Brown SE, Truog RD, Halpern SD. Rationing in the intensive care unit: to disclose or disguise?
Crit Care Med 2012;40:261-6. 7. Emanuel EJ, Wertheimer A. Public health. Who should get influenza vaccine when not all can? Science
2006;312:854-5. 8. COVID-19 rapid guideline: critical care. NICE guideline. 20 March 2020. www.nice.org.uk/guidance/ng159 9. Rockwood K, et al. CMAJ. 2005;173:489-495. 10. Emanuel EJ, Persad G, Upshur R, et al. Fair Allocation of Scarce Medical Resources in the Time of Covid-19.
NEJM. 2020. DOI: 10.1056/NEJMsb2005114 11. COVID-19 pandemic: triage for intensive-care treatment under resource scarcity. Swiss Med Wkly.
2020;150:w20229. doi:10.4414/smw.2020.20229 12. Joynt GM; Gopalan PD; Argent A; et al. The Critical Care Society of Southern Africa Consensus Statement
and Guideline on ICU Triage and Rationing (ConICTri). Joint publication. S Afr J Crit Care. 2019;35(1):36-65 and S Afr Med J 2019;109(8):613-642.
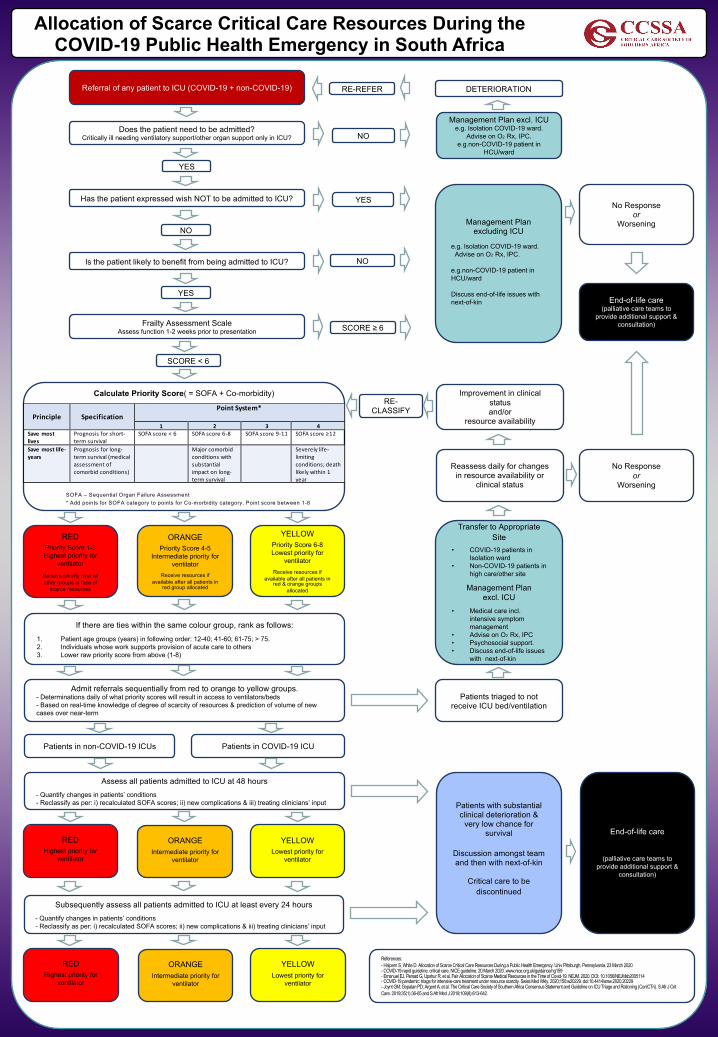
www.postersession.com
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
Does the patient need to be admitted?Critically ill needing ventilatory support/other organ support only in ICU?
Calculate Priority Score( = SOFA + Co-morbidity)
Has the patient expressed wish NOT to be admitted to ICU?
NO
YES
YES
NO
Referral of any patient to ICU (COVID-19 + non-COVID-19)
End-of-life care(palliative care teams to
provide additional support & consultation)
Management Plan excluding ICU
e.g. Isolation COVID-19 ward. Advise on O2 Rx, IPC.
e.g.non-COVID-19 patient in HCU/ward
Discuss end-of-life issues with next-of-kin
Transfer to Appropriate Site
• COVID-19 patients in Isolation ward
• Non-COVID-19 patients in high care/other site
Management Plan excl. ICU
• Medical care incl. intensive symptom management
• Advise on O2 Rx, IPC• Psychosocial support.• Discuss end-of-life issues
with next-of-kin
Patients triaged to not receive ICU bed/ventilation
Admit referrals sequentially from red to orange to yellow groups.- Determinations daily of what priority scores will result in access to ventilators/beds - Based on real-time knowledge of degree of scarcity of resources & prediction of volume of new cases over near-term
YELLOWPriority Score 6-8Lowest priority for
ventilatorReceive resources if
available after all patients in red & orange groups
allocated
ORANGEPriority Score 4-5
Intermediate priority for ventilator
Receive resources if available after all patients in
red group allocated
REDPriority Score 1-3Highest priority for
ventilator
Receive priority over all other groups in face of
scarce resources
If there are ties within the same colour group, rank as follows:1. Patient age groups (years) in following order: 12-40; 41-60; 61-75; > 75.2. Individuals whose work supports provision of acute care to others3. Lower raw priority score from above (1-8)
Assess all patients admitted to ICU at 48 hours - Quantify changes in patients’ conditions - Reclassify as per: i) recalculated SOFA scores; ii) new complications & iii) treating clinicians’ input Patients with substantial
clinical deterioration & very low chance for
survival
Discussion amongst team and then with next-of-kin
Critical care to be discontinued
Reassess daily for changes in resource availability or
clinical status
Improvement in clinical statusand/or
resource availability
RE-CLASSIFY
Is the patient likely to benefit from being admitted to ICU? NO
Management Plan excl. ICUe.g. Isolation COVID-19 ward.
Advise on O2 Rx, IPC.e.g.non-COVID-19 patient in
HCU/ward
YES
Frailty Assessment ScaleAssess function 1-2 weeks prior to presentation
SCORE < 6
SCORE ≥ 6
No Response or
Worsening
Principle
Specification
Point System*
1 2 3 4 Save most lives
Prognosis for short-term survival
SOFA score < 6 SOFA score 6-8 SOFA score 9-11 SOFA score ≥12
Save most life-years
Prognosis for long-term survival (medical assessment of comorbid conditions)
Major comorbid conditions with substantial impact on long-term survival
Severely life-limiting conditions; death likely within 1 year
SOFA – Sequential Organ Failure Assessment * Add points for SOFA category to points for Co-morbidity category. Point score between 1-8
Patients in non-COVID-19 ICUs Patients in COVID-19 ICU
No Response or
Worsening
Subsequently assess all patients admitted to ICU at least every 24 hours - Quantify changes in patients’ conditions - Reclassify as per: i) recalculated SOFA scores; ii) new complications & iii) treating clinicians’ input
YELLOWLowest priority for
ventilator
ORANGEIntermediate priority for
ventilator
REDHighest priority for
ventilator
End-of-life care
(palliative care teams to provide additional support &
consultation)
YELLOWLowest priority for
ventilator
ORANGEIntermediate priority for
ventilator
REDHighest priority for
ventilator
RE-REFER DETERIORATION
References:- Halpern S, White D. Allocation of Scarce Critical Care Resources During a Public Health Emergency. Univ Pittsburgh, Pennsylvania. 23 March 2020- COVID-19 rapid guideline: critical care. NICE guideline. 20 March 2020. www.nice.org.uk/guidance/ng159- Emanuel EJ, Persad G, Upshur R, et al. Fair Allocation of Scarce Medical Resources in the Time of Covid-19. NEJM. 2020. DOI: 10.1056/NEJMsb2005114- COVID-19 pandemic: triage for intensive-care treatment under resource scarcity. Swiss Med Wkly. 2020;150:w20229. doi:10.4414/smw.2020.20229- Joynt GM; Gopalan PD; Argent A; et al. The Critical Care Society of Southern Africa Consensus Statement and Guideline on ICU Triage and Rationing (ConICTri). S Afr J CritCare. 2019;35(1):36-65 and S Afr Med J 2019;109(8):613-642.
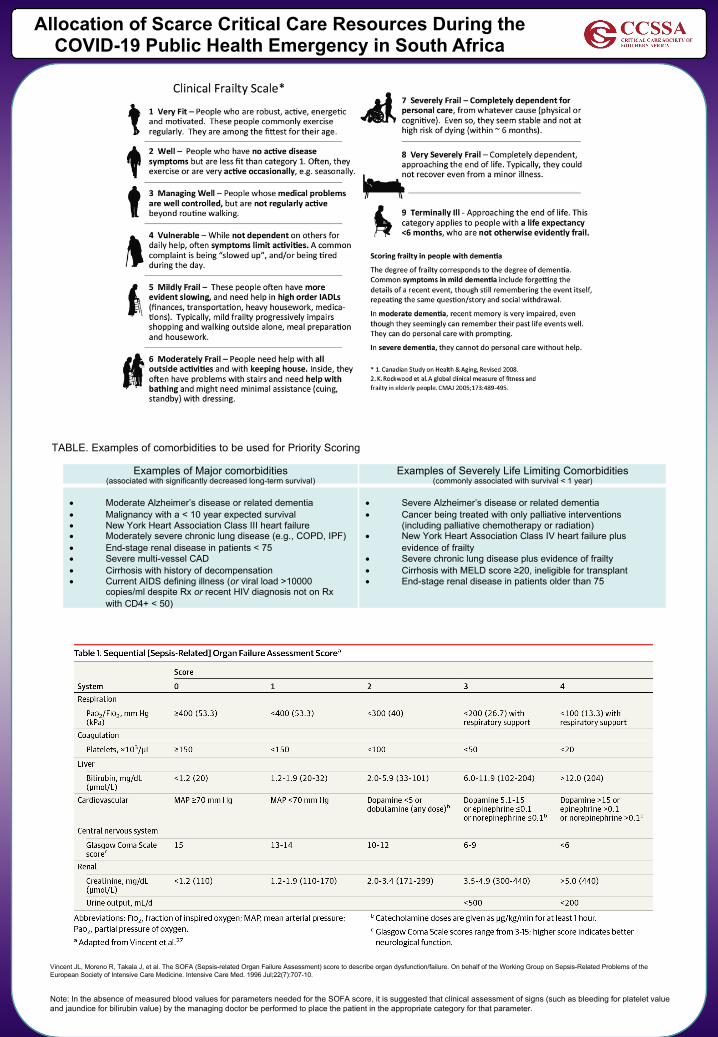
www.postersession.com
Allocation of Scarce Critical Care Resources During the COVID-19 Public Health Emergency in South Africa
Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996 Jul;22(7):707-10.
Examples of Major comorbidities (associated with significantly decreased long-term survival)
Examples of Severely Life Limiting Comorbidities (commonly associated with survival < 1 year)
• Moderate Alzheimer’s disease or related dementia• Malignancy with a < 10 year expected survival• New York Heart Association Class III heart failure• Moderately severe chronic lung disease (e.g., COPD, IPF) • End-stage renal disease in patients < 75• Severe multi-vessel CAD• Cirrhosis with history of decompensation• Current AIDS defining illness (or viral load >10000
copies/ml despite Rx or recent HIV diagnosis not on Rx with CD4+ < 50)
• Severe Alzheimer’s disease or related dementia• Cancer being treated with only palliative interventions
(including palliative chemotherapy or radiation)• New York Heart Association Class IV heart failure plus
evidence of frailty• Severe chronic lung disease plus evidence of frailty• Cirrhosis with MELD score ≥20, ineligible for transplant• End-stage renal disease in patients older than 75
TABLE. Examples of comorbidities to be used for Priority Scoring
Note: In the absence of measured blood values for parameters needed for the SOFA score, it is suggested that clinical assessment of signs (such as bleeding for platelet value and jaundice for bilirubin value) by the managing doctor be performed to place the patient in the appropriate category for that parameter.