
Health System of Canada
12
This article was originally published in the International Encyclopedia of Public Health, published by Elsevier, and the attached copy is provided by Elsevier for the author's benefit and for the benefit of the author's institution, for non- commercial research and educational use including without limitation use in instruction at your institution, sending it to specific colleagues who you know, and providing a copy to your institution’s administrator. All other uses, reproduction and distribution, including without limitation commercial reprints, selling or licensing copies or access, or posting on open internet sites, your personal or institution’s website or repository, are prohibited. For exceptions, permission may be sought for such use through Elsevier's permissions site at: http://www.elsevier.com/locate/permissionusematerial Marchildon G P Canada, Health System of. In: Kris Heggenhougen and Stella Quah, editors International Encyclopedia of Public Health, Vol 1. San Diego: Academic Press; 2008. pp. 381-391.
Transcript of Health System of Canada

This article was originally published in the International Encyclopedia of Public Health, published by Elsevier, and the attached copy is provided by Elsevier for the author's benefit and for the benefit of the author's institution, for non-commercial research and educational use including without limitation use in
instruction at your institution, sending it to specific colleagues who you know, and providing a copy to your institution’s administrator.
All other uses, reproduction and distribution, including without limitation commercial reprints, selling or licensing copies or access, or posting on open
internet sites, your personal or institution’s website or repository, are prohibited. For exceptions, permission may be sought for such use through
Elsevier's permissions site at:
http://www.elsevier.com/locate/permissionusematerial
Marchildon G P Canada, Health System of. In: Kris Heggenhougen and Stella Quah, editors International Encyclopedia of Public Health, Vol 1. San Diego:
Academic Press; 2008. pp. 381-391.

Canada, Health System of 381
Author's personal copy
Canada, Health System ofG P Marchildon, University of Regina, Regina, Saskatchewan, Canada
ã 2008 Elsevier Inc. All rights reserved.
Introduction
The Canadian health system reflects the inherent com-plexity and diversity of a country covering the secondlargest landmass in the world (Figure 1). In addition toits original Aboriginal inhabitants and official languagecommunities of French and English, the population ismade up of immigrants, many recent, from virtuallyevery part of the globe. Most live in large urban centersthat hug the southern border with the United States but
Figure 1 Source: Atlas of Canada, Natural Resources Canada.
International Encyclopedia of Public Hea
vibrant communities, some predating European coloniza-tion, are sprinkled throughout the ten provinces and threenorthern territories.
Not surprisingly, the Canadian health-care systemreflects the country’s complexity and diversity. Indeed, itis misleading to use the term ‘system’ when in fact therearemany health-care systems, sometimes operating simul-taneously, within the same country. For this reason, inter-governmental cooperation among the federal, provincial,and territorial governments – along with significant
lth, First Edition (2008), vol. 1, pp. 381-391

382 Canada, Health System of
Author's personal copy
nongovernmental health-care stakeholders – is so promi-nent in the financing, administration, and delivery of pub-lic health care in Canada. This article describes thepolitical and administrative organization of health care inCanada, including its intergovernmental dimensions forconventional as well as alternative medicine and publichealth, and the relationship of each with conventionalillness care. Since Canadians have played a major role inthe development of the determinants of health approach tohealth policy internationally, this history is brieflyrecounted.
Political and Administrative Organization
The provinces and northern territories of Canada cover aland area of about 10million km2. Under the constitutionof Canada, the provinces have the primary jurisdictionover health care. As a consequence, provincial govern-ments are mainly responsible for the financing andadministering of public health care in Canada. To enforceand uphold the Canada Health Act, the federal govern-ment makes cash transfers to the provinces, portions ofwhich it can deduct from the transfers to provinces if theypermit or encourage facilities or physicians to charge userfees for medically necessary and/or required services orbreach the five broad principles of public administration,comprehensiveness, universality, portability, and accessi-bility as defined in the Canada Health Act (Figure 2).
Singlepayer
hospital,and
medicalservices
Canadian Co
Regionalhealth
authorities
Ministries ofhealth
Mentalhealth and
publichealth
Homecare and
long-termcare
CHea
1
Provincial and territorialprescription drug subsidy
programs
Federal-provterritorial adv
committe
Transfer pa
CanHea
Infow(200
CanadianInstitute for
HealthInformation
(1994)
CanadianAgency forDrugs and
Technologies inHealth (1989)
Health Council
of Canada (2003)
Provincial and territorial governments
Figure 2 Political organization of the Canadian health-care system
International Encyclopedia of Public Healt
While provincial governments play a dominant anddirect role in the financing and administering of healthcare, they have a more arm’s-length role in the delivery ofmany public health-care services. Most physicians, forexample, are responsible for their own private practicesand clinics, and receive their remuneration through a feeschedule negotiated between these governments and theprovincial medical associations. Most of the health profes-sions are self-regulated under provincial government lawsthat set out a general framework under which the profes-sions operate. Many health facilities, including nursinghomes and other long-term care institutions, home careand community care organizations, medical laboratories,and diagnostic clinics are privately owned and adminis-tered. The majority are community-based not-for-profitorganizations but some are private for-profit enterprisesconducted on a commercial basis. Figure 3 illustrates theextent to which services are delivered privately in theCanadian system even when such services are publiclyfunded and administered.
Until recently, almost all hospitals in Canada wereowned and administered at the local level by municipali-ties or private not-for-profit corporations, including reli-gious-based organizations. However, some (but not all) ofthese hospitals have recently been subsumed by new pub-lic arm’s-length organizations known as regional healthauthorities (RHAs), which were established by the pro-vinces beginning in the late 1980s. This change, commonlyreferred to as regionalization in Canada, involved the
nstitution
Federal governmentCanadian Institutes
for HealthResearch
Statistics Canada
Minister of health
anadalth Act,984
HealthCanada
Public HealthAgency ofCanada
PatentMedicine
PricesReviewBoard
incial-isory
es
yments
adalthay1)
CanadianBlood
Services(1996)
CanadianPatientSafety
Institute (2005)
.
h, First Edition (2008), vol. 1, pp. 381-391

Funding Administration Delivery
Public Canada HealthAct services (hospital and physician services plus) and public health services
Public taxation, private insurance, and out-of-pocket payments
Private goods andservices including most dental and vision care as well as over-the-counter drugs and alternative medicines
Mixed goods andservice, including most prescription drugs, home care, and institutional care services
Public taxation
Privateinsurance and out-of-pocket payments including full payments, co-payments, anddeductibles
Public services that are generally welfare-based and targeted, private services regulated in the public interest by governments
Universal, single-payer provincial systems. Private self-regulating professions subject to provincial legislative framework
Private ownership and control; private professions, some self-regulating with public regulation of food, drugs, and natural health products
Privateprofessional, private not-for-profit and for-profit, and public arm’s-length facilities andorganizations
Privateprofessional, private not-for-profit, private-for-profit, and public arm’s-length facilities andorganizations
Privateproviders and private for-profit facilities andorganizations
Figure 3 Matrix of funding, administration, and delivery. Reproduced from Marchildon GP (2005) Health systems in transition: Canada, p. 120. Brussels: World Health Organization on
behalf of the European Observatory on Health Systems and Policies.
Canada,Health
System
of
383
International Encyclopedia of Public Health, First Edition (2008), vol. 1, pp. 381-391
Author's personal copy

384 Canada, Health System of
Author's personal copy
provincial governments carving up their respective terri-tories into geographic regions and then creating RHAs toadminister the delivery of a continuum of health services,from hospitals and nursing homes to home care and publichealth. As arm’s-length public organizations establishedunder provincial law, RHAs have a mandate to meet thehealth needs of the populations within their boundaries asboth purchasers and providers of services. The type andextent of services purchased from independent facilities orprofessionals vary considerably among RHAs and amongprovinces. As can be seen inTable 1, the population size ofRHAs varies considerably from province to province.
Although the provincial governments are responsiblefor administering most public health care in Canada, thefederal government nonetheless plays a critical role inhealth care beyond upholding the broad principles andconditions under the Canada Health Act. These otheractivities include: funding health research; collectinghealth data through Statistics Canada; financing andadministering health services for First Nations peopleand Inuit, inmates of federal penitentiaries, war veterans,and active members of the Canadian armed forces and theRoyal Canadian Mounted Police; as well as regulating thepharmaceutical and natural health products industries.
In 2000, the federal government replaced the MedicalResearch Council with the Canadian Institutes of HealthResearch (CIHR), which in turn, is made up of 13 fund-ing bodies supporting research on Aboriginal peoples’health, aging, cancer, circulatory and respiratory disease,gender, genetics, health services/policy, human develop-ment, children/youth, infection/immunity, metabolismand diabetes, neurosciences/mental health/addiction,and population and public health. Through CIHR fund-ing of both investigator-driven as well as more govern-ment-driven strategic research, the federal government’sobjective is to put Canada in the top five health researchnations in the world.
Table 1 Regionalization reforms in Canada, 1989–2005
Province or territoryTotal population(in thousands)
(Establi(year)
British Columbia 4196 (1997) 2
Alberta 3202 (1994) 2Saskatchewan 995 (1992) 2
Manitoba 1170 (1997–9
Ontario 12 393 2005
Quebec 7.543 (1989–9Nova Scotia 937 (1996) 2
New Brunswick 751 (1992) 2
Prince Edward Island 137 (1993–9
Newfoundland and Labrador 517 (1994) 2Northwest Territories 43 (1997–9
Reproduced fromMarchildon GP (2005) Health systems in transition:
of the European Observatory on Health Systems and Policies.
International Encyclopedia of Public Healt
Nonbiomedical Alternative Medicines andApproaches to Health
In Canada as in the United States, it has been customaryto include alternative nonbiomedical medicines andapproaches, including traditional Chinese medicines andacupuncture as well as native Canadian (Aboriginal) heal-ing practices, with less mainstream biomedical therapiessuch as chiropractic and psychological therapies in a singlecategory known as complementary and alternative medi-cine (CAM). The first category of therapies in particularshare four common characteristics: (1) they are presumedto work in conjunction with the body’s own self-healingmechanisms; (2) they are holistic in the sense that theytreat the whole person; (3) they try to involve the individ-ual as an active participant in the healing process; and(4) they tend to focus on prevention and well-being asmuch as on treatment (Achilles et al., 1999).
Most nonbiomedical treatments and approaches,including nutritional and herbal medicinal products andtherapies, are paid for and delivered privately, outside thepublic health-care system. The further west one travels inCanada, the more popular are nonbiomedical therapies.In addition, the intensity of their use is correlated withindividuals with higher income and higher education, andwith women more than men (McFarland et al., 2002). In2004, the federal government, through the Natural HealthProducts Directorate in Health Canada, began regulatingand approving traditional herb products, vitamins andmineral supplements, and homeopathic preparations.
Intergovernmental Collaboration in HealthRegulation, Planning, and Policy
Relative to Australia, Germany, and the United States,Canada is a relatively decentralized federation. As a
shed) changed Current numberof RHAs
Range in populationsize of RHAs (2005)
001 5 (16) 1 314 635! 285560
003 9 1 042855! 66005001–02 13 272195! 2125
8) 2002 11 622015! 955
14 1 356500! 234000
2) 2003 18 1 782835! 9600001 9 398038! 33 165
002 8 179840! 29 325
4) 2005 0 –
003–04 6/4/2 295 145! 40 5168) 2002 8 18115! 2441
Canada, p. 28. Copenhagen: World Health Organization on behalf
h, First Edition (2008), vol. 1, pp. 381-391

Canada, Health System of 385
Author's personal copy
consequence, Canadian governments at the federal andprovincial levels have been highly reliant on intergovern-mental collaboration to administer, deliver, and reconfigurepublic health care. At the apex of this collaboration is theConference of Federal-Provincial-Territorial Ministers ofHealth as well as a mirror committee of deputy ministersof health (O’Reilly, 2001). In addition to this committeestructure, intergovernmental organizations with specifichealth-care mandates and varying degrees of independencefrom their sponsoring governments have been establishedin recent years.
The federal government regulates the safety of foodand pharmaceutical products through Health Canada andthe Food and Drugs Act, and the prices of patented phar-maceutical products through the Patented MedicinePrices Review Board. Since the provincial governmentsoperate their own prescription drug programs, most ofwhich are categorical programs targeting seniors and thepoor, they in turn attempt to control cost by limiting thenumber and type of pharmaceuticals placed on provin-cial formularies. A minority of provinces have institutedreference-based pricing policies, in which only the lower-cost therapeutic alternative is subsidized in full by theprovincial drug plan. To manage the jurisdictional andpolicy overlaps in pharmaceutical regulation, the federaland provincial governments work through an intergovern-mental body known as the Canadian Agency for Drugs andTechnologies in Health (CADTH). Conducting clinical-and cost-effectiveness studies under a Common DrugReview, CADTH makes formulary listing recommenda-tions to all provincial governments with the exceptionof Quebec. Through the Canadian Optimal MedicationPrescribing and Utilization Service, CADTH promotesevidence-based best practices in pharmaceutical prescrib-ing and use. Finally, CADTH conducts a major healthtechnology assessment program for a broad range of pre-scription drugs, medical devices, and other similar healthtechnologies to assist all jurisdictions in decisions con-cerning the purchase of new health technologies on thebasis of both clinical and cost-effectiveness.
The Canadian Institute for Health Information (CIHI)was established in 1994 to coordinate the gathering anddissemination of health data previously done by jurisdic-tions in isolation of each other. CIHI’s core functionsinclude identifying national health indicators, coordinatingthe development and maintenance of national informa-tion standards, developing and managing health databasesand registries, as well as conducting and disseminating basicresearch and analysis. In its work, CIHI cooperates closelywith Statistics Canada, a federal government agency whichenjoys an international reputation for the gathering anddissemination of population health data.
Since the late 1990s, Canadian governments havecollaborated in the establishment of a number of newintergovernmental health organizations. These include
International Encyclopedia of Public Hea
Canadian Blood Services, which was set up by the pro-vinces and territories in response to a major ‘‘taintedblood’’ controversy surrounding the safety of the coun-try’s blood supply as then managed by the Canadian RedCross. Established in 2001, Canada Health Infowayemerged out of the desire of federal, provincial, andterritorial ministers of health to accelerate the devel-opment of electronic health records in all jurisdictions.In 2003, the Health Council of Canada was created toprovide both an assessment of progress in priority areas ofhealth reform, as identified by the prime minister and thepremiers of the provinces and territories, as well as makerecommendations for future health reform on a nationalbasis. Beginning its work in 2005, the Canadian PatientSafety Institute was established to provide systematicevidence on medical errors and initiate change to improvepatient safety throughout Canada.
Health Care Expenditures and Financing
As can be seen in Figure 4, approximately 70% of healthexpenditures are channeled through the public systemwhile a further 30% are funneled through the privatesector. Of the C$142 billion spent on health in 2005,approximately $99 billion was public health care financedand administered by the provincial and federal govern-ments. Of this sum, roughly $56 million was spent onmedically necessary or required hospital and physicianservices. As insured services under the Canada HealthAct, they are made universally available to all Canadianswithout user fees on the same terms and conditions.
Total health-care expenditures have now reached 10%of Canada’s gross domestic product. As can be seen inTable 2, much of this growth can be attributed to mixedand private (i.e., non-Canada Health Act) goods and ser-vices including prescription drugs, home care services,long-term institutional services including nursing homesfor seniors, dental services, vision care, as well as nonmed-ical goods and services. Whereas the first three categoriesof services may be subsidized by provincial governmentsfor some of their residents, the other categories of healthservices and products are largely provided through themarket and paid for through a combination of privateinsurance and out-of-pocket payments by consumers.
Almost all public health-care expenditures arefinanced through general government taxation at boththe provincial and federal levels of government. Privatehealth care is paid for out-of-pocket or through privateinsurance, the majority of which is employment-based.Unlike ‘voluntary’ health insurance in many othercountries, private health insurance in Canada is generallypart of a fixed (i.e., nonvoluntary) benefit package nego-tiated through a collective agreement between employersand employees. Private health insurance benefits generally
lth, First Edition (2008), vol. 1, pp. 381-391

Privatehealth insurance
12.2%
Other3.2%
Out-of-pocketexpenditures
14.4%
Commercialinsurance firms
Not-for-profitinsurance firms
Public sector69.6%
Hospitals
Long-term care
Other publicsector 6.3%
Federal direct4.2%
Municipal(public health)
0.7%
Community care
Social securityfunds 1.4%
Quebec druginsurance Fund
Provincial drugplans
Home care
Regional healthauthorities
Worker’scompensation
Private sector30.4%
Dental and vision care, complementary and alternative medicine, and some
long-term care and home care
Total health expenditures 2005 $142 billion
Provincial governmentsector 63.3%
Physicianremuneration
Figure 4 Overview of Canadian health care from an expenditure perspective, 2005. Reproduced from Canadian Institute for
Health Information (CIHI) (2005) National Health Expenditure Trends, 1975–2005. Ottawa: Canadian Institute for Health Information.
Table 2 Five-Year Trends in Canadian Health Expenditures, 1976–2005
Five-year averages 1976–1980 1981–1985 1986–1990 1991–1995 1996–2000 2001–2005
Total health expenditure (THE) as % of GDP 7.0 8.0 8.5 9.6 9.0 10.0
Canada Health Act (CHA) services as % of THE 58.1 56.7 55.4 51.7 46.2 43.3
CHA services as % of GDP 4.1 4.5 4.7 5.0 4.2 4.3
Non-CHA services as % of THE 41.9 43.3 44.6 48.3 53.8 56.7Non-CHA services as % of GDP 2.9 3.5 4.7 4.6 4.9 5.7
Mean annual growth rate in THE 12.8 12.4 8.9 4.0 5.8 7.7
Mean annual growth rate in CHA services 11.6 12.2 8.2 1.8 3.8 6.8Mean annual growth rate in non-CHA services 14.6 12.7 9.8 6.3 7.5 8.4
Mean annual growth rate in GDP 12.6 9.1 7.0 3.6 5.8 4.8
Mean real annual growth rate in THE 3.3 4.2 4.0 1.6 4.0 5.2
Mean real annual growth rate in CHA services 2.2 4.0 3.3 �0.5 2.1 4.3Mean real annual growth rate in non-CHA
services
4.9 4.5 4.8 3.9 5.7 5.9
Mean real annual growth rate in GDP 3.6 3.1 2.3 2.0 4.3 2.5
Reproduced fromMarchildon GP (2005) Health systems in transition: Canada, p. 55. Copenhagen: World Health Organization on behalfof the EuropeanObservatory onHealth SystemsandPolicies. Updated byCanadian Institute for Health Information (CIHI) (2005) National
Health Expenditure Trends, 1975–2005. Ottawa: Canadian Institute for Health Information; Organisation for Economic Co-operation and
Development (OECD) (2005) OECD health data 2005: A comparative analysis of 30 countries, 5th edn. Paris: Organisation for Economic
Co-operation and Development; Statistics Canada (2005). 1975 to 2005 national accounts. Ottawa, Canada: Statistics Canada.
386 Canada, Health System of
Author's personal copy
target dental care, vision care, and prescription drugs(Figure 5) (Marchildon, 2005).
Public Health in Canada’s Public HealthCare System
Public health can be defined as the science and art ofpromoting health, preventing disease, and prolonging life
International Encyclopedia of Public Healt
through policies and programs that focus on the popula-tion as a whole. The implicit contrast is with health-carepolicies, the main focus of which is on treating already illor injured individuals. Today, public health in Canada isgenerally identified with six discrete functions: (1) diseaseand injury control at the population level, (2) healthprotection at the population level, (3) emergency pre-paredness and response, (4) surveillance, (5) populationhealth assessment, and (6) health promotion.
h, First Edition (2008), vol. 1, pp. 381-391

Out of pocket14.4%
Private insurance12.2% Other
3.2%
Taxation70.2%
Figure 5 Revenue sources for total health expenditures in Canada, 2003. Reproduced from Canadian Institute for Health
Information (CIHI) (2005) National Health Expenditure Trends, 1975–2005. Ottawa: Canadian Institute for Health Information.
Canada, Health System of 387
Author's personal copy
Before the introduction of universal hospital insurancein the 1950s, and universal physician care insurance in the1960s – together referred to as Medicare – public healthprograms and services, at least those concerned withinfectious disease control and public health and safety,constituted the main health-care responsibilities of allgovernments in Canada. This was reflected in the namesof the departments that emerged in the early twentiethcentury – almost all were officially designated as depart-ments of public health. At the same time, however, thework of such departments was largely limited to treatingand preventing infectious diseases on a population basis aswell as recording vital statistics such as births and deaths.
With the introduction of Medicare, the responsibilitiesof departments and ministers of public health were greatlyexpanded. At the same time, the provincial departmentsof health, as they were renamed, increasingly assumedthe public health responsibilities of cash-strapped andtax-poor municipalities. Only larger urban centers inCanada were able to provide their inhabitants with publichealth services including infectious disease control andthe administration and enforcement of health and safetystandards.
The definition of public health, and along with it therole of government, did not change or expand fundamen-tally until the emergence of the determinants of healthapproach in the 1970s and 1980s, and the introduction ofregionalization in most provinces in the 1990s. Althoughhealth scholars and program decision makers were awareof the impact of living standards, education, employment,and healthy lifestyles on health outcomes, as well as theelimination of financial barriers to Medicare for all nec-essary treatment and the marginal influence of illness careon the ultimate health of a population, it took consider-able time for the full policy implications of this basicinsight to be systematically examined.
International Encyclopedia of Public Hea
The Lalonde Report and the OttawaCharter: New Approaches to HealthDeterminants?
In 1974, Marc Lalonde, the federal minister of the Depart-ment of National Health and Welfare, released a workingreport entitled A New Perspective on the Health of Canadians(Lalonde, 1974). Although it attracted little media attentionat the time, the four-quadrant health field concept at thecenter of the Lalonde report would prove to be exception-ally influential not only in Canada but throughout theworld, in large part because of its emphasis on the impactof lifestyle and environmental factors as major determi-nants of health alongside the long-emphasized factors ofhuman biology and health care. The Lalonde report wasthe product of a group of policy thinkers in the Long RangeHealth Planning Branch of the federal department ofhealth. For its eight-year existence, the branch operatedmore like a think tank than a bureaucratic unit withingovernment (McKay, 2000).
The reasoning behind the Lalonde Report was subse-quently used to support the federal government’s decisionto loosen the conditions on transfer funding in 1977 and toreduce the rate of growth of such transfers by the early1980s. At the same time, a new Health Promotion Direc-torate within the federal Department funded and super-vised cost-shared projects with citizen groups to pilot thenew approach to health determinants. Although the pro-jects at the local, regional, and national level initiallyfocused on encouraging lifestyle changes, they eventuallytargeted larger societal and structural changes. This workhad a profound impact on Health and Welfare Canada’sFramework for Health Promotion as well as the majorcontributions of Canada to the World Health Organiza-tion’s first international conference on health promotionand the release of the Ottawa Charter for Health
lth, First Edition (2008), vol. 1, pp. 381-391

Environment
Aspects of physical and socialenvironment over which individualhas little or no control
Human biology
Lifestyle
Personal decisions and risks overwhich individual has control
Health organizations
388 Canada, Health System of
Author's personal copy
Promotion, both of which appeared in 1986 (Epp, 1986;Boyce, 2002). Despite these advances, Canada’s more tra-ditional system of public health remained highly frag-mented, poorly coordinated, and poorly funded byfederal, provincial, and local governments. As a conse-quence, it did not fare well when faced with its firstmajor crisis of the twenty-first century.
Aspects of physical and mentalhealth that are a result of organicmake-up
The institutional arrangementsgoverning the provision of healthservices: access and quality
Figure 6 Health field concept from the Lalonde Report.
Reproduced from Lalonde M (1974) A new perspective on the
health of Canadians: A working document. Ottawa: Department
of Health and Welfare.
The SARS Crisis and the Establishmentof the Public Health Agency of Canada
In 2003, Canadians were caught by surprise with a majoroutbreak of severe acute respiratory syndrome, or SARS.By August of that year, there were 400 probable andsuspect SARS cases in Canada, as well as 44 deaths in thegreater Toronto area. Health-care workers were amongthe most vulnerable and three of the 100 SARS-infectedhealth-care workers ultimately died. As the hardest-hitcountry outside of the Asian continent, Canada becamethe focus of international attention, with the World HealthOrganization recommending against nonessential travelto Toronto for almost a month during the worst part ofthe crisis.
As a consequence of the problems of coordination andcommunication associated with the public health responseby the city of Toronto and the governments of Ontarioand Canada, Health Canada established a National Advi-sory Committee on SARS and Public Health chaired byDr. David Naylor of the University of Toronto. The man-date of the Naylor Committee went beyond recommenda-tions on how to organize responses to infectious diseasescrises in the future to providing directional recommenda-tions on the future of public health in Canada. Influencedby the coordinating function of the Centers for DiseaseControl and Prevention (CDC) in the United States, theNaylor Committee recommended the establishment of anational public health agency in Canada (Health Canada,2003). The federal government established the PublicHealth Agency of Canada (PHAC) in 2004. Althoughcreated as a government department separate fromHealthCanada, PHAC reports directly to the federal Minister ofHealth and is headed up by a Chief Public Health Officer.Although cities, provincial governments, and RHAs havelong had chief public health officers, this was the firstnational officer for the country as a whole.
PHAC’s internal organization is illustrated in Figure 6.The Scientific Director General is responsible for strength-ening the Agency’s scientific networks externally as wellas coordinating scientific research and scientific policythroughout the Agency.
The Infectious Disease and Emergency PreparednessBranch is responsible for enabling the prevention andcontrol of infectious diseases on a national basis as wellas improving the health of Canadian residents actually
International Encyclopedia of Public Healt
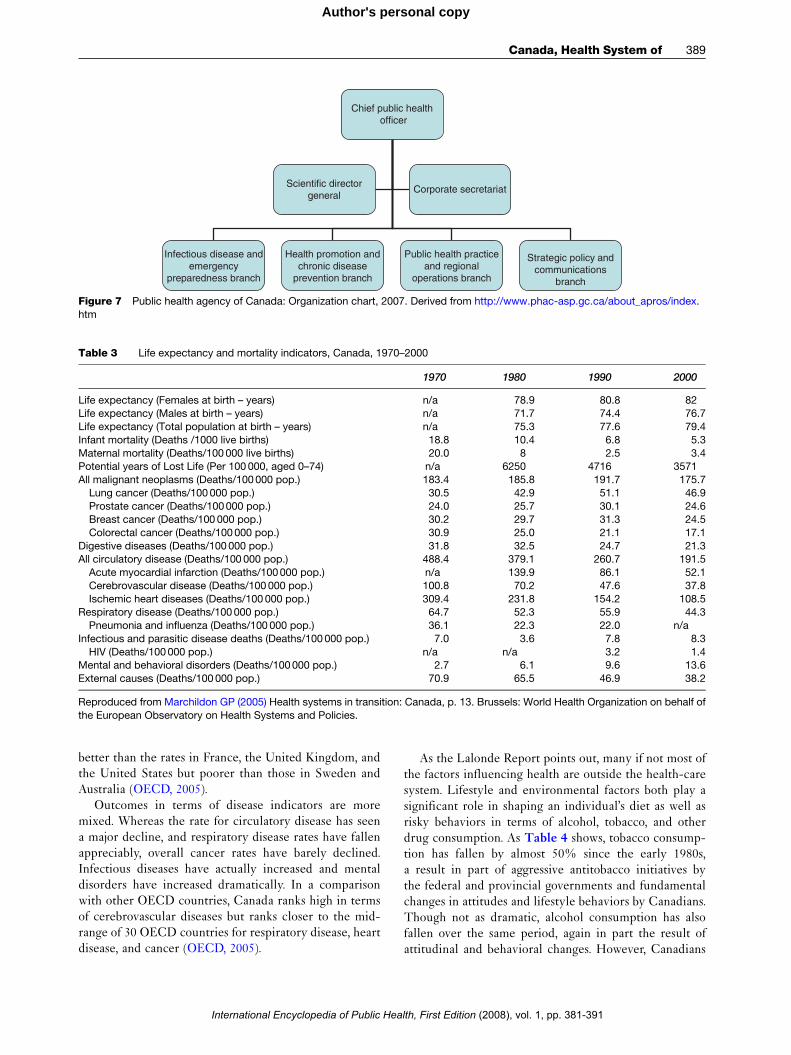
infected. This branch ensures that PHAC is ready torespond to public health emergencies including pan-demic influenza, HIV/AIDS, West Nile virus infection,Creutzfeldt-Jakob disease, food- or waterborne disease,and other diseases and outbreaks at all times. To meetPHAC’s emergency preparedness mandate, the Branchadministers five national laboratory and response centers:(1) Centre for Infectious Disease Prevention and Control;(2) Centre for Emergency Preparedness and Response;(3) National Microbiology Laboratory; (4) Laboratory forFoodborne Zoonoses; and (5) Pandemic PreparednessSecretariat (Figure 7).
The Health Promotion and Chronic Disease Preven-tion Branch works with numerous stakeholders to facili-tate leadership in health promotion, surveillance, chronicdisease control and preventions, and evaluation of existingprograms. To help achieve this objective, this branchadministers the Centre for Chronic Disease Preventionand Control and the Centre for Health Promotion. ThePublic Health Practice and Regional Operations Branchprovides strategic direction in public health surveillanceon a national basis while helping build public healthcapacity at the regional level.
Health Status and Health SystemOutcomes
Based upon a number of indicators,Table 3 illustrates thegrowing improvement in the health of the Canadian pop-ulation. Since 1970, life expectancy has risen dramaticallyfor both men and women and infant mortality has droppedsignificantly. In terms of two indicators – potential yearsof life lost and life expectancy at birth – Canada is rankedamong the very top of the Organisation for EconomicCo-operation and Development (OECD) nations. At thesame time, Canada’s perinatal mortality rate is more inthe middle of OECD countries: by way of illustration, it is
h, First Edition (2008), vol. 1, pp. 381-391
Chief public health officer
Infectious disease andemergency
preparedness branch
Health promotion andchronic disease
prevention branch
Public health practiceand regional
operations branch
Scientific directorgeneral
Corporate secretariat
Strategic policy andcommunications
branch
Figure 7 Public health agency of Canada: Organization chart, 2007. Derived from http://www.phac-asp.gc.ca/about_apros/index.
htm
Table 3 Life expectancy and mortality indicators, Canada, 1970–2000
1970 1980 1990 2000
Life expectancy (Females at birth – years) n/a 78.9 80.8 82Life expectancy (Males at birth – years) n/a 71.7 74.4 76.7
Life expectancy (Total population at birth – years) n/a 75.3 77.6 79.4
Infant mortality (Deaths /1000 live births) 18.8 10.4 6.8 5.3
Maternal mortality (Deaths/100000 live births) 20.0 8 2.5 3.4Potential years of Lost Life (Per 100 000, aged 0–74) n/a 6250 4716 3571
All malignant neoplasms (Deaths/100000 pop.) 183.4 185.8 191.7 175.7
Lung cancer (Deaths/100 000 pop.) 30.5 42.9 51.1 46.9
Prostate cancer (Deaths/100000 pop.) 24.0 25.7 30.1 24.6Breast cancer (Deaths/100 000 pop.) 30.2 29.7 31.3 24.5
Colorectal cancer (Deaths/100000 pop.) 30.9 25.0 21.1 17.1
Digestive diseases (Deaths/100000 pop.) 31.8 32.5 24.7 21.3All circulatory disease (Deaths/100 000 pop.) 488.4 379.1 260.7 191.5
Acute myocardial infarction (Deaths/100000 pop.) n/a 139.9 86.1 52.1
Cerebrovascular disease (Deaths/100 000 pop.) 100.8 70.2 47.6 37.8
Ischemic heart diseases (Deaths/100 000 pop.) 309.4 231.8 154.2 108.5Respiratory disease (Deaths/100000 pop.) 64.7 52.3 55.9 44.3
Pneumonia and influenza (Deaths/100 000 pop.) 36.1 22.3 22.0 n/a
Infectious and parasitic disease deaths (Deaths/100000 pop.) 7.0 3.6 7.8 8.3
HIV (Deaths/100000 pop.) n/a n/a 3.2 1.4Mental and behavioral disorders (Deaths/100000 pop.) 2.7 6.1 9.6 13.6
External causes (Deaths/100 000 pop.) 70.9 65.5 46.9 38.2
Reproduced from Marchildon GP (2005) Health systems in transition: Canada, p. 13. Brussels: World Health Organization on behalf of
the European Observatory on Health Systems and Policies.
Canada, Health System of 389
Author's personal copy
better than the rates in Fran ce, the United King dom, andthe United Stat es but poorer than tho se in Sweden andAustral ia (OECD, 2005 ).
Outcome s in ter ms of diseas e ind icator s are moremixed. Whereas the rate for circ ulatory diseas e ha s seena major dec line, and respira tory disea se rates have f allenapprecia bly, overall can cer rates have barely dec lined.Inf ectious diseas es have actu ally increas ed and men taldisor der s have increas ed dra matically. In a compar isonwith other O ECD countrie s, Canad a ranks high in te r msof cere brovascular diseas es but ranks c loser to the mid-range of 30 OECD countr ies for re spiratory diseas e, hear tdiseas e, and cancer ( OECD, 2005 ).
International Encyclopedia of Public Hea
As the Lalo nde Re por t points out, many if not mos t ofthe f actor s influ encing health are outsi de the health-c aresystem . Lif estyl e and environ mental f actor s both play asignifi cant role in shaping an individual’s diet as well asrisky behavior s in ter ms of alcohol, tobacco, and oth erdr ug consu mption. As Table 4 shows, tobacc o consump -tion has f alle n by almost 50% since the ear ly 1980s,a result in par t of aggressive ant itobacco initiatives bythe f ederal and provincial gover nments and fu ndamentalchanges in attitudes and lif estyl e behavior s by Canad ians.Though not as dr amatic, alco hol consu mption has alsof alle n over the same period , again in par t the re sult ofattitudi nal and behavioral changes. However, Canad ians
lth, First Edition (2008), vol. 1, pp. 381-391
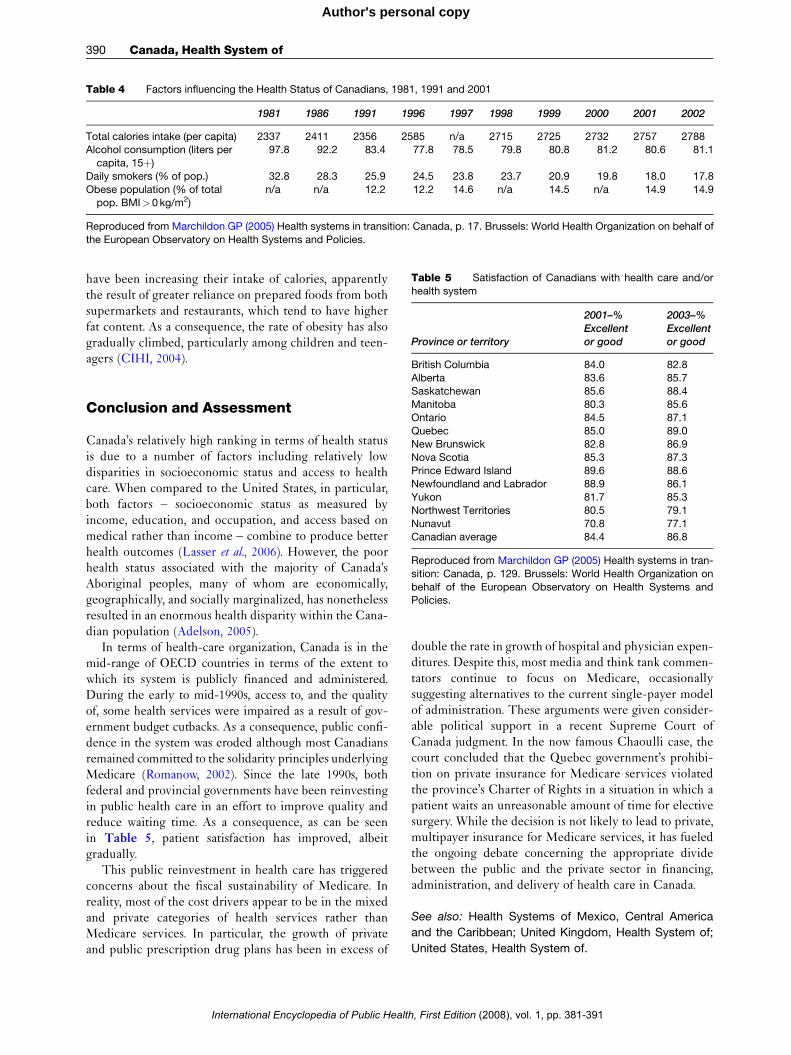
Table 4 Factors influencing the Health Status of Canadians, 1981, 1991 and 2001
1981 1986 1991 1996 1997 1998 1999 2000 2001 2002
Total calories intake (per capita) 2337 2411 2356 2585 n/a 2715 2725 2732 2757 2788Alcohol consumption (liters per
capita, 15þ)
97.8 92.2 83.4 77.8 78.5 79.8 80.8 81.2 80.6 81.1
Daily smokers (% of pop.) 32.8 28.3 25.9 24.5 23.8 23.7 20.9 19.8 18.0 17.8
Obese population (% of totalpop. BMI>0 kg/m2)
n/a n/a 12.2 12.2 14.6 n/a 14.5 n/a 14.9 14.9
Reproduced from Marchildon GP (2005) Health systems in transition: Canada, p. 17. Brussels: World Health Organization on behalf of
the European Observatory on Health Systems and Policies.
Table 5 Satisfaction of Canadians with health care and/or
health system
Province or territory
2001–%Excellentor good
2003–%Excellentor good
British Columbia 84.0 82.8
390 Canada, Health System of
Author's personal copy
have been increasing their intake of calories, apparentlythe result of greater reliance on prepared foods from bothsupermarkets and restaurants, which tend to have higherfat content. As a consequence, the rate of obesity has alsogradually climbed, particularly among children and teen-agers (CIHI, 2004).
Alberta 83.6 85.7Saskatchewan 85.6 88.4
Manitoba 80.3 85.6
Ontario 84.5 87.1
Quebec 85.0 89.0New Brunswick 82.8 86.9
Nova Scotia 85.3 87.3
Prince Edward Island 89.6 88.6Newfoundland and Labrador 88.9 86.1
Yukon 81.7 85.3
Northwest Territories 80.5 79.1
Nunavut 70.8 77.1Canadian average 84.4 86.8
Reproduced from Marchildon GP (2005) Health systems in tran-
sition: Canada, p. 129. Brussels: World Health Organization on
behalf of the European Observatory on Health Systems andPolicies.
Conclusion and Assessment
Canada’s relatively high ranking in terms of health statusis due to a number of factors including relatively lowdisparities in socioeconomic status and access to healthcare. When compared to the United States, in particular,both factors – socioeconomic status as measured byincome, education, and occupation, and access based onmedical rather than income – combine to produce betterhealth outcomes (Lasser et al., 2006). However, the poorhealth status associated with the majority of Canada’sAboriginal peoples, many of whom are economically,geographically, and socially marginalized, has nonethelessresulted in an enormous health disparity within the Cana-dian population (Adelson, 2005).
In terms of health-care organization, Canada is in themid-range of OECD countries in terms of the extent towhich its system is publicly financed and administered.During the early to mid-1990s, access to, and the qualityof, some health services were impaired as a result of gov-ernment budget cutbacks. As a consequence, public confi-dence in the system was eroded although most Canadiansremained committed to the solidarity principles underlyingMedicare (Romanow, 2002). Since the late 1990s, bothfederal and provincial governments have been reinvestingin public health care in an effort to improve quality andreduce waiting time. As a consequence, as can be seenin Table 5, patient satisfaction has improved, albeitgradually.
This public reinvestment in health care has triggeredconcerns about the fiscal sustainability of Medicare. Inreality, most of the cost drivers appear to be in the mixedand private categories of health services rather thanMedicare services. In particular, the growth of privateand public prescription drug plans has been in excess of
International Encyclopedia of Public Healt
double the rate in growth of hospital and physician expen-ditures. Despite this, most media and think tank commen-tators continue to focus on Medicare, occasionallysuggesting alternatives to the current single-payer modelof administration. These arguments were given consider-able political support in a recent Supreme Court ofCanada judgment. In the now famous Chaoulli case, thecourt concluded that the Quebec government’s prohibi-tion on private insurance for Medicare services violatedthe province’s Charter of Rights in a situation in which apatient waits an unreasonable amount of time for electivesurgery. While the decision is not likely to lead to private,multipayer insurance for Medicare services, it has fueledthe ongoing debate concerning the appropriate dividebetween the public and the private sector in financing,administration, and delivery of health care in Canada.
See also: Health Systems of Mexico, Central America
and the Caribbean; United Kingdom, Health System of;
United States, Health System of.
h, First Edition (2008), vol. 1, pp. 381-391

Cancer and Senescence 391
Author's personal copy
Citations
Achilles R (1999) Complementary and Alternative Health Practices andTherapies: A Canadian Overview. Toronto, Canada: York UniversityCentre for Health Studies.
Adelson N (2005) The embodiment of inequity: Health disparities inAboriginal Canada. Canadian Journal of Public Health 96: S45–S61.
Boyce WF (2002) Influence of health promotion bureaucracy oncommunity participation: A Canadian case study. Health PromotionInternational 17(1): 61–68.
Canadian Institute for Health Information (CIHI) (2004) Overweight andObesity in Canada: A Population Health Perspective. Ottawa,Canada: Canadian Institute for Health Information.
Epp J (1986) Achieving Health for all: A Framework for HealthPromotion. Ottawa, Canada: Health and Welfare Canada.
Health Canada (2003) Learning from SARS: Renewal of Public Health inCanada. Ottawa, Canada: Health Canada.
Jonas WB and Levin JS (eds.) (1999) Essentials of Complementary andAlternative Medicine. Philadelphia, PA: Lippincott, Williams &Wilkins.
Lalonde M (1974) A New Perspective on the Health of Canadians:A Working Document. Ottawa, Canada: Department of Health andWelfare.
Lasser KE, Himmelstein DU, and Woolhander S (2006) Access to care,health status, and health disparities in the United States and Canada:Results of a cross-national population-based survey. AmericanJournal of Public Health 96: 1300–1307.
Marchildon GP (2005) Health Systems in Transition: Canada.Copenhagen, Denmark: World Health Organization on behalf of theEuropean Observatory on Health Systems and Policies.
McFarland B, Bigelow D, Zani B, Newsom J, and Kaplan M (2002)Complementary and alternative medicine use in Canada and theUnited States. American Journal of Public Health 92(10): 1616–1618.
Cancer and SenescenceK Itahana, The University of North Carolina, Chapel Hill, NG P Dimri, Northwestern University, Evanston, IL, USA
ã 2008 Elsevier Inc. All rights reserved.
Increased Risk of Cancer Developmentwith Aging
The adult human body consists of approximately 60 trillioncells. The rate of proliferation and growth of this vastnumber of cells are under strict regulation and are highlycoordinated. However, in rare cases, a few cells in a partic-ular organ escape this tight regulation of growth, startuncoordinated proliferation, acquire invasive and meta-static properties, and become cancerous. The incidence ofcancer rises exponentially with age in humans (Ries et al.,2006). As shown in Fi gu re 1 , until age 35, the incidence ofcancer is 0.2% in the general population. This incidencerises to about 1.5% at ages 50–60. The maximum incidenceof cancer, which is close to 5%, occurs between ages 70 and80. Therefore, cancer tends to develop after 50 years ofage, which is halfway from the 100th year, the maximum
International Encyclopedia of Public Hea
McKay L (2000) Making the Lalonde Report: Background Paper.Ottawa, Canada: Canadian Policy Research Networks.
O’Reilly P (2001) The federal/provincial/territorial health conferencesystem. In: Adams D (ed.) Federalism, Democracy and Health Policyin Canada, pp. 107–129. Montreal and Kingston: McGill-Queen’sUniversity Press.
Organisation for Economic Co-operation and Development (OECD)(2005) OECD Health Data 2005: A Comparative Analysis of30 Countries, 5th edn. Paris, France: Organisation for EconomicCo-operation and Development.
Romanow R (2002) Building on Values: The Future of Health Care inCanada. Saskatoon, Saskatchewan: Commission on the Future ofHealth Care in Canada.
Further Reading
Canadian Institute for Health Information (CIHI) (2005) National HealthExpenditure Trends, 1975–2005. Ottawa, Canada: CanadianInstitute for Health Information.
Canadian Institute for Health Information (CIHI) (2006) Improving theHealth of Canadians: An Introduction to Health in Urban Places.Ottawa, Canada: Canadian Institute for Health Information.
Canadian Institute for Health Information (CIHI) (2006) How Healthy areRural Canadians: An Assessment of their Health Status and HealthDeterminants. Ottawa, Canada: Canadian Institute for HealthInformation.
Conference Board of Canada (2006) Healthy Provinces, HealthyCanadians: A provincial Benchmarking Report. Ottawa, Canada:Conference Board of Canada.
Ostry A (2006) Change and Continuity in Canada’s Health Care System.Ottawa, Canada: CHA Press.
C, USA
lifespan of humans. In addition, women tend to have twicethe incidence of cancer at age 30–50 than men, althoughthis trend reverses after age 50. After age 85, there tends tobe a slight decline in the incidence of cancer.
The genetic basis of this increased incidence of cancerwith age is unclear. Recent progress in aging and cancerresearch suggests that errors accumulated in DNA duringeach round of replication, together with several othergenetic and epigenetic factors, are involved in the increasedrisk of cancer with advanced age. In addition to geneticfactors such as the accumulation of mutations in DNA,epigenetic factors, such as methylation of DNA and acety-lation or deacetylation of histones, which do not affect DNAsequence per se, but change the expression of genes, alsocontribute to various diseases, including cancer (reviewedin Jones and Laird, 1999). Other factor s that may contributeto the age-dependent increase in cancer incidence areDNA
lth, First Edition (2008), vol. 1, pp. 381-391




















