
Health Communication in the Latino Community: Issues and Approaches
28
Health Communication in the Latino Community: Issues and Approaches John P. Elder, 1 Guadalupe X. Ayala, 1 Deborah Parra-Medina, 2 and Gregory A. Talavera 1 1 Graduate School of Public Health, San Diego State University, San Diego, California 92123; email: [email protected], [email protected], [email protected] 2 Institute for Health Promotion Research, Department of Epidemiology and Biostatistics School of Medicine, University of Texas Health Science Center, San Antonio, Texas, 78230; email: [email protected] Annu. Rev. Public Health 2009. 30:227–51 First published online as a Review in Advance on January 15, 2009 The Annual Review of Public Health is online at publhealth.annualreviews.org This article’s doi: 10.1146/annurev.publhealth.031308.100300 Copyright c 2009 by Annual Reviews. All rights reserved 0163-7525/09/0421-0227$20.00 Key Words Latinos, Hispanics, Hispanic Health Paradox, communication- persuasion model, acculturation Abstract With reference to the Communication-Persuasion model, we describe various research issues and challenges when considering the health of Latinos, and implications for designing and evaluating health commu- nication and behavior change efforts in this population. Latinos, collec- tively the nation’s largest minority group, vary substantially in terms of socioeconomic and legal status, their country of origin and the extent of ongoing contact with that country, their region of residence within the United States, their generation status and levels of acculturation, and psychosocial factors. Health communication efforts with Latinos need to focus on family, cultural traditions, and collectivism while attending to acculturation, language, generation and national origin. The most extensive intervention topic in Latino health promotion has been the application of the lay health advisor model. This and other fundamental communication approaches, as well as audience and population char- acteristics, need to be considered within the context of dynamic and complex societal changes. 227 Annu. Rev. Public. Health. 2009.30:227-251. Downloaded from arjournals.annualreviews.org by 68.101.165.183 on 03/28/09. For personal use only.
Transcript of Health Communication in the Latino Community: Issues and Approaches

ANRV370-PU30-13 ARI 15 February 2009 12:38
Health Communicationin the Latino Community:Issues and ApproachesJohn P. Elder,1 Guadalupe X. Ayala,1
Deborah Parra-Medina,2 and Gregory A. Talavera1
1Graduate School of Public Health, San Diego State University, San Diego, California92123; email: [email protected], [email protected], [email protected] for Health Promotion Research, Department of Epidemiology and BiostatisticsSchool of Medicine, University of Texas Health Science Center, San Antonio, Texas, 78230;email: [email protected]
Annu. Rev. Public Health 2009. 30:227–51
First published online as a Review in Advance onJanuary 15, 2009
The Annual Review of Public Health is online atpublhealth.annualreviews.org
This article’s doi:10.1146/annurev.publhealth.031308.100300
Copyright c© 2009 by Annual Reviews.All rights reserved
0163-7525/09/0421-0227$20.00
Key Words
Latinos, Hispanics, Hispanic Health Paradox, communication-persuasion model, acculturation
AbstractWith reference to the Communication-Persuasion model, we describevarious research issues and challenges when considering the health ofLatinos, and implications for designing and evaluating health commu-nication and behavior change efforts in this population. Latinos, collec-tively the nation’s largest minority group, vary substantially in terms ofsocioeconomic and legal status, their country of origin and the extent ofongoing contact with that country, their region of residence within theUnited States, their generation status and levels of acculturation, andpsychosocial factors. Health communication efforts with Latinos needto focus on family, cultural traditions, and collectivism while attendingto acculturation, language, generation and national origin. The mostextensive intervention topic in Latino health promotion has been theapplication of the lay health advisor model. This and other fundamentalcommunication approaches, as well as audience and population char-acteristics, need to be considered within the context of dynamic andcomplex societal changes.
227
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
PART I: LATINOS IN THEUNITED STATES
Many national health and social science studies,including the National Health Interview Sur-vey (NHIS) and other surveys, treat Latinos1 asthough they were a homogenous group. How-ever, as Modiano and colleagues (75) stated,
The aggregation of culturally distinct sub-groups, which have resided in the UnitedStates for different periods of time, into amore inclusive Latino category assumes thatall persons of Mexican, Cuban and PuertoRican origin have similar needs and experi-ence similar barriers in using health services.There is, however, no clear evidence for thisassumption. On the contrary, there is evidencethat each group has specific characteristics thatmake it different and independent from oneanother. . . . (p. 35)
Clearly, extraordinary diversity exists amongsubgroups of Latinos. The immigration and ac-culturation experiences of Mexican or CentralAmerican–descended Americans, South Ameri-cans, Puerto Ricans, and Cuban Americans varysubstantially from one another. The distinctionamong Latino subgroups can be traced back tohighly varied experiences not only with respectto encounters with the dominant American cul-ture but also extending back to Spanish colo-nization, which began to redefine the westernhemisphere 500 years ago. Indigenous groupsin the Caribbean Islands and coastal areaslargely succumbed to Iberian diseases and ag-gression and were replaced by Europeans andAfrican slaves. Although forced to adopt muchof the culture and religion of the conquista-dores, indigenous groups in central and high-land areas of Mexico and further south survived
1The field offers no consensus regarding the term to refer topersons of Latin American heritage who live in the UnitedStates. Both “Hispanic” and “Latino” are used extensively, al-though U.S. government documents, including the Census,use the term Hispanic. Given this mixed usage in the litera-ture, we use the term Latino to indicate, where possible, thespecific ethnic group in question.
to a great extent. Thus, the blends of European,African, and indigenous cultures find differentexpressions in the many regions and communi-ties of Latin America.
The historical and political interface of thevarious Latin American countries and regionswith the United States also manifests distinc-tive paths. The long, shared border betweenthe United States and Mexico among popula-tions in the southwestern states presents moreopportunity for Mexican immigrants to travelback and forth to their Mexican homeland. Alarge proportion of Mexican-derived inhabi-tants of Texas and New Mexico can still tracetheir roots to this region following its annexa-tion by the United States, which led to the warbetween the United States and Mexico (1846–1848). Puerto Rico has been part of the UnitedStates since the defeat of Spain in the Spanish-American War in 1898, and present-day inhab-itants of this island are American citizens. ManyCuban Americans trace their migration to theUnited States to the more recent conflict be-tween the American government and Cuba un-der Fidel Castro, a major element of the ColdWar and one of its last vestiges. Cuban migra-tion peaked in 1994. The history of Latino mi-gration into the United States is diverse and, inmany ways, brief. More importantly, the pop-ulation is growing. Heightened immigrationfrom Mexico and Central and South Amer-ica along with positive birth outcomes amongnative-born Latinos is transforming the demo-graphic and economic landscape of the UnitedStates dramatically. Over the past 30 years,the Latino population has grown more rapidly(337%) than the total U.S. population (41.9%)and accounted for 39% of the net populationgrowth in the United States (108). In general,Latino households are larger and younger thannon-Latino households in the United States,which suggests that the population growth islikely to continue (108).
Socioeconomic Realities
Upon arrival in this country, Latino immigrantsencounter vastly different socioeconomic
228 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
realities, some realizing middle-class statusfairly quickly, others finding themselves indef-initely at the lowest rung. These experiencesmay be a function of the structure of theirhome countries’ educational system, as wellas whether the immigrant is of European,African, or indigenous native ancestry. From aU.S. educational system perspective, Mexicansare disadvantaged before they arrive becausefewer individuals have access to a secondaryeducation compared with the opportunitiesto complete high school in the United States.Access to education, in turn, affects literacylevels. Along with Puerto Ricans and CentralAmericans, most Mexican immigrants to theUnited States end up as unskilled laborers(109). However, the premigration middle- orupper-class status of the first and largest waveof 1960-era Cuban immigrants contributedin part to their relatively strong economicstatus as Cubans living in the United States.Seventy-four percent of Cuban Americanshave graduated from high school, whereas50% of Mexican Americans and 67% of PuertoRicans have graduated from high school(90). Moreover, nearly one-fourth of CubanAmericans have graduated from college, whichis identical to the college graduation rateof the general U.S. population. In contrast,Mexican- and Puerto Rican–origin adultshave lower college graduation rates (7%and 11%, respectively). Despite educationaldisadvantages, recent unemployment figuresfor Latinos are relatively favorable, althoughthis appears to vary by generation status. First-and third-generation Latinos have approxi-mately the same employment-to-populationratio, both substantially higher than that ofsecond-generation Latinos. According to thePew Hispanic Research Center (87), age,geographic mobility, and family networksas sources of employment information allcontribute to the relatively better employmentpicture for foreign-born Latinos, even thoughwages lag behind those of white or AfricanAmerican workers. The variation observedamong Latino subgroups is arguably as great asthat which has existed among other American
subgroups, well before Latinos became thelargest American “minority.” The economicgains recently enjoyed by Latinos are threat-ened by low Latino educational achievementlevels.
Regional Issues
Economic, societal, and psychosocial factorsare in dynamic flux in Latino communitiesand, singly or in combination, may have animportant impact on Latino health. Johnsonet al. (49) proposed a classification system forunderstanding the diverse Latino communitiesin the United States that is based on the region’smigration history and which seems to have im-plications for health-promotion efforts. Maturemarkets include traditional immigrant gatewaystates, the largest markets being California,Arizona, Texas, Illinois, New York, and Florida.Emerging markets are states with little to noLatino migration prior to 1990 such as Geor-gia, Nevada, North Carolina, and Washington.Incipient markets are growing rapidly andneeds are changing (Iowa, Mississippi, RhodeIsland, South Dakota). The long history ofimmigration into mature markets has createdestablished communities that share a commonlanguage (Spanish) and culture (Mexican inCalifornia and Cuban in Florida), therebyreducing language and cultural barriers whenaccessing health care services, for example.Mature markets are also multigenerational, asreflected in the proportion of households withextended family members as compared withthe non-Latino population (14% versus 7.5%)(108). Thus, diverse sources of support andinfluence exist in these social environments.However, emerging and incipient markets aredominated by young adult males, many withwives and children in their home countries.These immigrant males demonstrate strongparticipation in the work force, with theconstruction industry accounting for morethan half of new Latino jobs (56). However,community and organizational needs changeas the families of these men join them in theUnited States and begin to access health and
www.annualreviews.org • Latino Community Health 229
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
education-related services, thus increasingthe demand for culturally competent servicesin environments with limited resources andcapacity to provide them. Most public healthresearch emerges from Latino populations inmature markets. A small but growing body ofresearch is available on public health inter-ventions in emerging and incipient markets.Given these differences, programs developedfor Latino populations in mature marketsmay not be directly transferable to Latinopopulations in other markets. These marketcharacteristics have implications for our ap-proach to intervention research. One area inwhich we have explored this issue is in the useof the promotor model (see Communities andPromotores, below).
Generation Status, Identity,and Language
First- and second-generation Latinos vary sub-stantially on their national identity. A smallpercentage of first-generation Latinos use theself-descriptor “American,” whereas more thanone-third of second-generation Latinos doso. One-fourth of both first- and second-generation Latinos use “Latino” or “Hispanic”as their primary term of self-identification.Twice as many third-generation as second-generation Latinos use “American” as at leastpart of their self-identity. The Pew HispanicCenter has studied important generational dif-ferences in demographics, identity, attitudes,and experiences. For example, first-generationLatinos are more socially conservative, as evi-denced by their attitudes toward divorce, abor-tion, and other social issues, which affects boththe context and the content of health messages.The Pew Hispanic Center employs the termGeneration 1.5 to identify a phenomenon typi-cal of many Latino immigrants. These immi-grants may be categorized as having arrivedin the United States by age 10. Therefore, al-though they are foreign born and may plan toreturn to their country of origin eventually, theymay be more similar to second-generation thanto first-generation immigrant Latinos because
most of their formative experiences are likely tohave taken place in the United States (87).
The Pew Hispanic Center (87) also pre-sented findings on bilingualism among Latinosin the United States. The 2000 census showedthat the number of Latinos speaking Spanishat home rose from ∼10.2 million in 1980 to24.7 million in 2000. Spanish is thus becomingan increasingly common language among U.S.Latino households. Despite the large propor-tion of immigrant and native-born Latinos inthe United States, language evolution amongthe Latino generations is largely similar to thatreported for other ethnic groups who have im-migrated to the United States. A small percent-age of second-generation Latinos speak mostlySpanish. By the third generation, knowledgeof Spanish effectively becomes extinct. In ad-dition, English remains the dominant languageof the United States in terms of commerce andtrade and dominates U.S. workplaces.
Language use drives the degree to which in-dividuals are acculturated to American society,which may influence not only how well theyrespond to our behavior change initiatives butalso their selection and use of media, in gen-eral. Acculturation may be defined as a processthrough which an individual’s attitudes and be-haviors shift from those of his or her cultureof origin toward those of the dominant culture.Changes that occur in attitudes, norms, and val-ues of individuals exposed to a new culture arean important part of this process (14) and mayprovide insight into the relationship betweenacculturation and health-related behaviors (60).
Addressing Health Disparities
The Healthy People 2010 objectives call for theelimination of health disparities among racial,ethnic, and other subgroups of the Americanpopulation (55, 110). Latino communities evi-dence some of the worst of these disparities (54),being challenged not only by chronic diseases,sexually transmitted diseases, tuberculosis, cir-rhosis, and exposure to particulate matter butalso by an even wider range of health risks andillnesses.
230 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
Health disparities are the product ofcomplex and only partly understood genetic,biological, psychosocial, and economic factors,compounded by discrimination and inequality(17, 58, 96, 118). Perceptions of stigmatizationand discrimination from the community atlarge and from the health care system arefrequently reported by Latinos (17, 95).The impact of discrimination against Latinoimmigrants may be compounded by language,legal status, and other bases for bias, furtherexacerbating their impact and resulting inconsiderably higher levels of stress amongminorities than among whites (58). Even forsecond-generation Latinos, the process ofmarginalization, disempowerment, and socialexclusion known as “othering” (43, 114) mayperpetuate the negative impact of discrimina-tion beyond the immigration experience.
Language use appears to have an impact onthe degree of disadvantage. Bilingual Latinoshave high-school graduation rates that are morethan twice that of Spanish-speaking Latinoadults. Given that English speakers are prizedmore greatly in the workplace, they also en-joy higher household incomes than do Span-ish speakers. Bilingual adults have incomesroughly equal to their English-only coun-terparts in terms of economic advancement(87).
In spite of socioeconomic challenges and avariety of disparities, Latinos, individuals andcommunities, evidence several positive healthoutcomes, a phenomenon that continues to in-terest and challenge epidemiologists and so-cial scientists. Relative to non-Hispanic whites,Latinos have a worse socioeconomic profile andless access to health care, but they have lowermortality and morbidity rates in crucial arease.g., low birth weight (40). In terms of specificchronic disease-related risk factors, for exam-ple, Latinos have been reported to have higherrates of obesity, elevated blood pressure, andserum lipids (62). Yet even with these risk fac-tors, studies have demonstrated lower rates ofboth coronary heart disease (CHD) and totalcardiovascular disease (CVD) (74). This epi-demiological phenomenon has been labeled the
Hispanic Health Paradox (39, 69, 84). Censusundercounts, the healthy migrant hypothesis(healthier individuals self-select to migrate tothe United States), and the salmon hypothe-sis (elderly immigrants or those with severe ill-nesses return to their native country to spendtheir last days) can partially (25) but not fully (2,77) explain this paradox. Other studies have notfound Latino ethnicity to serve as a protectivefactor (47), in part because of socioeconomicdifferences between whites and Latinos of Mex-ican origin (25) and the weaker relationshipbetween educational level and health amongLatino subgroups other than Puerto Ricans(42, 107).
A Framework for Latino HealthPromotion through Communication
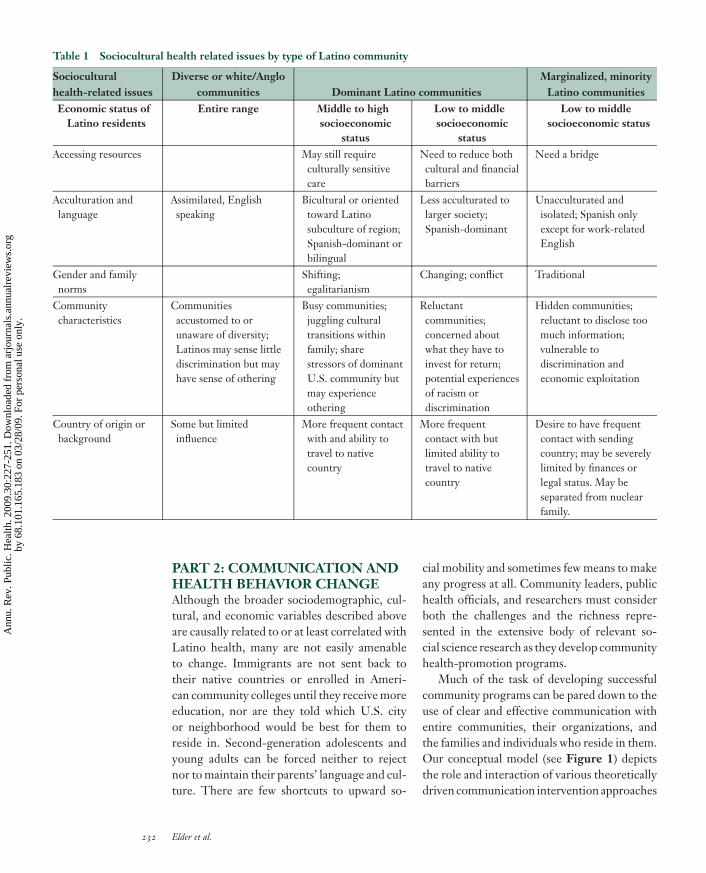
The primary themes and findings of sociode-mographic, cultural, and psychological influ-ences on Latino health are summarized inTable 1. The individuals and subgroups in theUnited States collectively labeled “Hispanics”or “Latinos” comprise the largest minority inthe country. Nevertheless, the variations withinthis group are nearly as great as those betweenthem and whites/Anglos or other subgroups.Latinos vary greatly with respect to nationalbackground and experience with immigration,their past and current socioeconomic status, thenature of the community in which they liveand their status within it, and acculturation andother cultural factors. In complex and some-times indirect ways, these factors protect or ad-versely impact health and contribute to narrow-ing or widening the Latino health disparitiesgap.
The growth of the Latino population in theUnited States, with the social and economicinequities they experience, demands contin-ued attention to their health care needs. Giventhe complexities identified, a framework fortargeting improvements in Latino health isneeded. Using a theoretically based model ofcommunication, the second part of this arti-cle presents a framework for promoting Latinohealth through families and communities.
www.annualreviews.org • Latino Community Health 231
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.
ANRV370-PU30-13 ARI 15 February 2009 12:38
Table 1 Sociocultural health related issues by type of Latino community
Socioculturalhealth-related issues
Diverse or white/Anglocommunities Dominant Latino communities
Marginalized, minorityLatino communities
Economic status ofLatino residents
Entire range Middle to highsocioeconomic
status
Low to middlesocioeconomic
status
Low to middlesocioeconomic status
Accessing resources May still requireculturally sensitivecare
Need to reduce bothcultural and financialbarriers
Need a bridge
Acculturation andlanguage
Assimilated, Englishspeaking
Bicultural or orientedtoward Latinosubculture of region;Spanish-dominant orbilingual
Less acculturated tolarger society;Spanish-dominant
Unacculturated andisolated; Spanish onlyexcept for work-relatedEnglish
Gender and familynorms
Shifting;egalitarianism
Changing; conflict Traditional
Communitycharacteristics
Communitiesaccustomed to orunaware of diversity;Latinos may sense littlediscrimination but mayhave sense of othering
Busy communities;juggling culturaltransitions withinfamily; sharestressors of dominantU.S. community butmay experienceothering
Reluctantcommunities;concerned aboutwhat they have toinvest for return;potential experiencesof racism ordiscrimination
Hidden communities;reluctant to disclose toomuch information;vulnerable todiscrimination andeconomic exploitation
Country of origin orbackground
Some but limitedinfluence
More frequent contactwith and ability totravel to nativecountry
More frequentcontact with butlimited ability totravel to nativecountry
Desire to have frequentcontact with sendingcountry; may be severelylimited by finances orlegal status. May beseparated from nuclearfamily.
PART 2: COMMUNICATION ANDHEALTH BEHAVIOR CHANGEAlthough the broader sociodemographic, cul-tural, and economic variables described aboveare causally related to or at least correlated withLatino health, many are not easily amenableto change. Immigrants are not sent back totheir native countries or enrolled in Ameri-can community colleges until they receive moreeducation, nor are they told which U.S. cityor neighborhood would be best for them toreside in. Second-generation adolescents andyoung adults can be forced neither to rejectnor to maintain their parents’ language and cul-ture. There are few shortcuts to upward so-
cial mobility and sometimes few means to makeany progress at all. Community leaders, publichealth officials, and researchers must considerboth the challenges and the richness repre-sented in the extensive body of relevant so-cial science research as they develop communityhealth-promotion programs.
Much of the task of developing successfulcommunity programs can be pared down to theuse of clear and effective communication withentire communities, their organizations, andthe families and individuals who reside in them.Our conceptual model (see Figure 1) depictsthe role and interaction of various theoreticallydriven communication intervention approaches
232 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
Communities and promotores
Behaviors
Diet
Physical activity
Sedentary behavior
Tobacco use
Sleep
Health care utilization
Medication use
Complimentary medicine
Acculturation and cultural influences
Schools and families
Clinics and health care providers
Figure 1A framework for promoting Latino health through communication.
to achieve health and environmental change inLatino communities. Our model is informed byBronfenbrenner’s socioecological framework,which illustrates the importance of interactionsamong various levels of influence from the mi-crosystem to the macrosystem (18). We focusspecifically on the interaction of places and peo-ple. Finally, our model reflects our collectiveexperience working primarily with Mexicans/Mexican American populations along the U.S.-Mexico border (8, 10, 11, 13, 28–33, 64) andalso in the U.S. Southeast region (12, 22, 36,53, 70, 100, 105), as well as our leadershipand participation in national Latino research ef-forts (see http://www.redesenaccion.org/ andhttp://www.cscc.unc.edu/hchs/).
Health Behavior Theories
In most cases, theories of behavior change growout of stable, middle-class societies, in turndriving the development of psychologicallyoriented interventions based on white/Anglonorms (59). These theories, to a large degree,
emphasize the role of the individual and his/herthought processes in the development and themaintenance of adaptive or high-risk health-related behaviors. However, the applicabilityof these theories to especially first-generationLatinos outside the dominant mainstreamAmerican culture can be questioned (28).First, the model of individuals as relativelyautonomous beings, who weigh potentialpersonal outcomes, their own self-efficacy,and their personal readiness to change, whilechoosing whether to listen to or ignore pres-sure from peers, may have limited relevanceto more traditional cultures. Instead, Latinosdemonstrate a strong sense of identificationwith and attachment to family members, bothnuclear and extended. The typical Latinowith traditional social values is someone whoprioritizes the needs of the group or family overhis or her own (68) and may not be influencedby messages that target only the individual. Forexample, in a study of Latino immigrants (1),perceived family approval and support morethan autonomous decision making influenced
www.annualreviews.org • Latino Community Health 233
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
an individual’s decision to participate in a heart-health-promotion program. This collectiveidentity must be calculated into the devel-opment of health communication targetingLatinos. Even when mainstream theories areused (e.g., 97), the design of health messagesmust acknowledge this attachment, which pro-motes loyalty, unity, reciprocity, and solidaritywithin the Latino community (93). Second, intraditional societies, the individual’s approachto health and illness is often fatalistic (98).Disease may be seen as an unavoidable crucibleor even as punishment for past sins and healthas a gift from God (79, 98). Because of this fa-talistic orientation, Western-style modificationof unhealthy lifestyle behaviors through anappeal to personal autonomy is less likely to besuccessful, as is Western medicine in general(61, 86).
Recent attempts in model development haveincluded application of the PEN3 model, whichemphasizes the importance of culture alongthree interrelated, interdependent dimensionsof health beliefs and behaviors: health educa-tion (person, extended family, neighborhood),educational diagnosis of health behavior (per-ceptions, enablers, and nurturers), and culturalappropriateness of health behavior (positive,exotic, and negative) (3–6, 48). PEN-3 incorpo-rates socioeconomic factors (e.g., income, ed-ucation, access to care), cultural beliefs, values,and attitudes concerning lifestyle behavior andpreventive health practices. Although PEN3was originally developed for use with AfricanAmericans, investigators have recently appliedit to research with Latinos that explored culturalfactors impacting health behaviors (41) and tothe development of culturally appropriate inter-ventions for cervical cancer (35). However, untilmodels such as PEN3 and more universallyapplicable theories can be developed, estab-lished functional models prescriptive of how tochange behavior (rather than how to explain it)may be more useful to reduce health disparities.McGuire’s (72) communication-persuasionmodel comprises one such functionalapproach.
The Communication-PersuasionModelThe communication-persuasion model (72)considers how various forms of public commu-nication change attitudes and behaviors. Theeffectiveness of a given communication effortwill depend on various inputs and their char-acteristics, as well as on the outputs of inter-est. Communication input variables applicableto Latino communities may vary substantiallyfrom those that appeal to the majority popu-lation. Input variables include the channel bywhich the message is sent, the source of themessage, the message itself, and the characteris-tics of the audience to whom it is sent. Channelfactors were initially thought to vary primarilybetween print (e.g., newspaper, pamphlets) andinterpersonal electronic (radio and television)media. Source variables focus on characteris-tics of the individual perceived as sending themessage. Sources vary in terms of the numbersof people sending the message, their credibil-ity, their physical attractiveness, and character-istics they have in common with the receiver.Messages themselves vary in their specific ap-peal (e.g., negative versus positive appeal), theinformation they present, what is included andwhat is omitted in the message, how the mes-sages are organized, and how frequently theyare repeated. Audience factors include the de-mographic, behavioral, and sociocultural char-acteristics of the people at whom the messagesare aimed, as well as their capacity to under-stand and assimilate the information. Finally,destination factors refer specifically to the tar-get behaviors the communication is expected toimpact.
How do these variables interact with thecomplex social, cultural, and economic factorsthat impact the health of Latinos and con-tribute to the diversity among them? Oetzelet al. (81) studied the influence of independenceand interdependence, ethnic identity (bicul-tural, assimilation, traditional, and marginal),and cultural health attributions (equity andbehavioral-environmental attributions) onsource, message, and channel preferences for
234 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
receiving breast health information by middle-aged or older Latinas. The researchers foundthat these three subjective cultural factorswere significantly related to a variety ofaudience preferences in terms of source ofcommunication, channels, and fear messages.For example, interdependence was positivelyassociated with preferences for significantother or family as a source of communication.This and related studies strongly imply theneed for tailoring health communication andcommunity interventions for Latinos (67, 119).
The next section presents an articulation ofMcGuire’s input variables with special charac-teristics of Latino communities. Specific atten-tion will be given to (a) the channel throughwhich the message is communicated; (b) sourceswithin settings; (c) the message itself, and(d ) audience factors.
Channels of Communication
Optimal exposure and attention to health-promotion messages require selection of an ap-propriate and popular channel for deliveringmessages at an appropriate time and place forthe target audience to attend to the message.Achieving this goal requires a very careful pro-cess because mistakes can be costly. The targetaudience must not only be exposed to the mes-sage, but also attend to it, as well. Health behav-ior communication is clearly at a disadvantagein competition with commercial marketing be-cause health messages by nature tend to be lessglamorous and the behavior more complicatedthan the simple purchase of a consumer prod-uct. When Latinos comprise the target audi-ence, exposing them and getting them to at-tend to the communication is complicated evenfurther.
Telephone interventions. Telephone coun-seling is convenient; inexpensive relative to in-person interventions; reduces the required timecommitment; overcomes geographic isolation;requires no travel, childcare, or parking; andcan easily be offered in Spanish. Neverthe-less, telephone information services using ei-
ther call-in information lines or proactive out-reach approaches are largely unexplored forLatino communities, but seem to demonstratesome promise. Findings from the Health Infor-mation National Trends Survey (HINTS) in-dicated that Latinos had the highest level ofawareness of the Cancer Information Service(CIS) language line among all racial and ethnicsubgroups studied (99). Furthermore, Latinopatients who called the CIS language line be-tween 2002 and 2003 were more likely to seekinformation about support services, referrals tomedical services, and psychosocial issues andless likely to request specific treatment infor-mation when compared with non-Latinos (99).Adios al Fumar (Goodbye to Smoking) was de-signed to increase the reach of the Spanish-language smoking cessation counseling serviceprovided by the National Cancer Institute’s CISand to evaluate the efficacy of a telephone-basedculturally adapted, proactive, behavioral treat-ment program for Spanish-speaking smokers(116). Participants were of very low socioeco-nomic status (SES), and more than 90% wereimmigrants. After targeted promotion, calls tothe CIS requesting smoking cessation help inSpanish increased from 0.39 to 17.8 per month,with a significant impact on smoking preva-lence among those who received the cultur-ally adapted counseling compared with callersreceiving standard counseling. This programdemonstrated that it is possible to reach, retain,and deliver an adequate dose of treatment to avery-low-SES population that has traditionallybeen viewed as difficult to reach and hard tofollow.
Print and mail interventions. The Secretos dela Buena Vida project was a randomized con-trolled trial targeting the diets of 357 Latinasusing a tailored communication approach. Ran-domly sampled and randomly assigned, thewomen participated in one of three conditions:12 weekly visits with a promotora (lay healthadvisor) and 12 weekly tailored, mailed infor-mation pieces; 12 weekly tailored, mailed in-formation pieces only; or (the control group)12 generic, mailed information pieces. The
www.annualreviews.org • Latino Community Health 235
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
content of the tailored print pieces includedculturally relevant behavioral strategies, tips onhow to eat healthier at a restaurant and selecthealthy snacks, a lifestyle column addressingcommon concerns among Latinas (e.g., timemanagement, finances), and a novela (story) de-picting a family dealing with nutrition-relatedchanges, as well as inspirational quotes, color-ful pictures, and other personalized informa-tion. Results at immediate postintervention in-dicated that the promotora condition achievedsignificantly lower levels of total fat grams andlower levels of energy intake, total saturated fat,total carbohydrates, glucose, and fructose (30).At the one-year follow-up, however, immedi-ate changes observed in the promotora conditiondid not persist and additional changes were ob-served in the tailored mailed condition (29).
In a similar fashion, Sauaia et al. (94) com-pared tailored print and promotora interven-tions in the Tepeyac Project, a church-basedproject to increase breast cancer screening ratesamong Latinas in Colorado. Culturally tailoredprint education packages were mailed to 209Colorado Catholic churches and contrasted topromotoras delivering the information to fourCatholic churches personally. The investigatorscompared biennial mammogram claims fromfive insurance plans covering these communi-ties over three years and found that, after adjust-ing for a variety of variables, women exposed tothe promotora intervention had a significantlyhigher increase in biennial mammograms thandid women exposed to the print alone. How-ever, the overall differences were modest, espe-cially given the far greater potential reach of aprint intervention.
Fox and colleagues (38) examined the ef-fects of a targeted low-cost mailed interventionon mammography rates among older women.Older, diverse, and disadvantaged women haveespecially low mammography and other can-cer screening rates, often because of financialconstraints. The intervention helped increasescreening rates among all elderly minoritywomen, and Latinas were more than twice aslikely to undergo screening relative to women
in a control condition. Thus, a mailed print in-tervention can effectively change behavior.
Mass media interventions: special case ofthe telenovela. Video interventions, in gen-eral, have proven effective at changing Latinopopulations’ knowledge, attitudes, and behav-iors on poison control (51), cancer screening(120), and condom use (80). The telenovela, aSpanish language version of a TV soap opera,is a popular form of mass entertainment formany Spanish-speaking households. Wilkinand colleagues (117) examined whether thischannel would be effective for providing healthinformation to Spanish-speaking viewers inthe United States if presented in a dramatic,narrative format. A breast cancer storylinewas developed for the telenovela Ladron deCorazones, and its effects on viewers’ knowledgeand behavioral intentions were assessed. Theapproach appeared effective. Calls placed to1-800-4-CANCER increased significantly;viewers demonstrated significant knowledgeincrements as measured through a nationalsurvey, and men who watched the show weresignificantly more likely to recommend thatwomen have a mammogram.
The Tu No Me Conoces (You Don’t KnowMe) social marketing campaign (82) promotedawareness of HIV risk and testing in Lati-nos living on the California-Mexico border.The eight-week campaign included Spanish-language radio, print media, a Web site, and atoll-free HIV-testing referral hotline. Twenty-eight percent of individuals who were sub-sequently tested at partner clinics specificallyidentified the Tu No Me Conoces campaign, indi-cating the potential for the effectiveness of mul-tiple mass media channels for even relativelyhigh-risk groups.
Given the size and diversity of Latino groupsthroughout society, there has been an increas-ing need to exploit both typical print and broad-cast channels, while shrinking the digital divideand expanding the use of computer-based massmedia (65) for addressing Latino health needs.This review suggests that interventions that do
236 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
not involve face-to-face contact can be effica-cious to achieve change.
Sources of Communication by Setting
Communities and promotores. Health careproviders may be ignored as message sources ifthey are perceived to be unaware of the impor-tance of the patient’s culture or even perceivedas siding with hostile law enforcement. Thisbarrier can be surmounted by the involvementof promotores, who come from the communitiesthey serve and yet are sufficiently acculturatedto the host culture to be able to understand andappreciate certain health-promotion and healthcare messages that need to be communicated torecent immigrants.
The promotor model is based on theassumption that every community has formaland informal social networks through whichhealth information is exchanged, and predis-posing interpersonal environments are created.Promotores are lay health advisors who generallyhave attributes of leadership, compassion, andfamiliarity with the community. Interpersonalcommunication via promotores addresses theweaknesses of impersonal mass media, which byitself may not result in sufficient exposure, at-tention, or comprehension. Promotores are oftenasked to communicate on a face-to-face basiswith Latino patients, reducing the likelihoodof misunderstanding of treatment or health-promotion communication while increasingthe acceptability of the communication. Thesepromotores in turn are accessible should patientsneed further follow-up regarding a specific issueor should they need to be referred for additionaltreatment. Through the promotor channel, in-formation is provided about the importance of amedical intervention, how the medical care sys-tem operates, eligibility requirements for var-ious health programs, and even how to fill outforms for participation. Promotores may be adeptat translating the need to alter health practicesthat are culturally bound, such as eatinghabits.
A recent literature review identified threeprimary roles for promotores: health education,
case management, and community outreach(101). Promotor roles range from informa-tion dissemination and health education to pol-icy and community advocacy and negotiatingagency services to providing preventive and cu-rative services (34, 50). In a 1994 report, theU.S. Centers for Disease Control and Preven-tion defined promotores as trusted communitymembers whose role was to provide informal,community-based, health-related services andto establish vital links between health providersand persons in the community (109). Withinthese roles, promotores have improved access tocare, various health behaviors and health out-comes, health status, and knowledge; they havealso improved cost-effectiveness. However, im-portant differences between established andnew immigrant–receiving communities seem towarrant attention in the design of promotor in-terventions. A systematic review currently un-derway (111) identified a uniform differencein the design of promotor-based interventionsin the United States based on where the study istaking place. Promotor-based interventions inthe Southwest were more likely to train pro-motores in traditional health education roles,whereas those in other regions of the countrywere more likely to train them to help bridgehealth services and other organizational sys-tems (see Figure 2). In these emerging and in-cipient markets, promotores are needed to serveas cultural brokers or intermediaries betweenthese larger predominantly English-speakingservice organizations and clients.
Unfortunately, as alluded to previously, thisinterpersonal channel suffers by comparisonwith mass media in terms of the scale or reach ofthe intervention effort. Promotores may be veryeffective but require a lot of professional timefor recruitment, training, and sustainability.High dropout rates, occasional errors in healthmessages, or eventual decay of acquired skillsmay all characterize a promotor-led program.Such risks are prevalent especially if the pro-gram is long term, which might require exten-sive new recruiting and retraining efforts. Aninteresting partial solution to the public healthchallenge of using promotores has been provided
www.annualreviews.org • Latino Community Health 237
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
Figure 2Geographic distribution of 47 lay health advisor ( promotores) studies with darker map zones depicting greater concentrations of Latinos(E = educator versus B = bridge).
by the A Su Salud program in southwesternTexas (7). Promotores working with A Su Saludare trained primarily to expose participants toa health-promotion effort (e.g., smoking ces-sation, lowering dietary fat) and to gain initialattention or cue patients to action by dissem-inating minimal information along with printmaterial and referring community members totune in to mass media messages. The more tech-nical details of the program are then offeredvia mass media channels. In this scenario, thepromotores recruit participants to join them inlistening to a particular radio show or televi-sion program that will convey the informationneeded. After the program is finished, the pro-motor conducts a discussion group with the par-ticipants and follows up with each of them ontheir own homework assignments. Using thisapproach, promotores can spend more of their
time recruiting an audience and less time train-ing to become risk factor experts.
Clinics and health professionals. A varietyof barriers exist to providing effective medi-cal and preventive care to Latinos, includinga lack of health insurance or a regular source ofhealth care and a lack of culturally and linguisti-cally proficient clinicians. Limited English pro-ficiency, low education, and low literacy lev-els can interfere with communications betweenLatino patients and the health care system.Improved provider/patient communication re-mains one of the biggest potentials for promot-ing health among Latinos, particularly immi-grants (26).
Improvements in communication, however,may require an extensive reorientation of pri-mary care providers and the health care delivery
238 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
system. Cooper et al. (24) proposed a modifi-cation of the Institute of Medicine frameworkto make it relevant to Latinos and other dis-advantaged groups. Health disparities could bereduced with changes in primary care provi-sion, including increased cultural and linguis-tic competency and more use of communityhealth workers and/or certified health inter-preters, improved access to care (including lo-cation, hours of operation, diversity of staff ),better marketing of services provided, and theinclusion of the family in care.
Brown et al. (19) put this proposal into actionin a study examining the effects of a culturallycompetent diabetes self-management interven-tion. Two hundred and fifty-six randomly se-lected persons with type 2 diabetes participatedin an intervention that consisted of 52 contacthours over 12 months delivered by bilingualMexican American nurses, dietitians, and com-munity health workers. The intervention wascomposed of weekly community-based instruc-tional sessions on nutrition, self-monitoring ofblood glucose, exercise, and other self-care top-ics, as well as biweekly support group sessions.The cultural competence of the program wasevidenced by its language, type of diet, socialemphasis, family participation, and incorpora-tion of cultural health beliefs. As a result, in-dividuals receiving the program showed sig-nificantly lower levels of HbA1c and fastingblood glucose at 6 months and at 12 months. At6 months, the mean HbA1c of the experimentalsubjects was 1.4% below the mean of the con-trol group, which indicated a modest yet im-portant effect.
One example of a comprehensive clinic-centered approach to health promotion is Vivala Vida (Live Life). Viva la Vida was developedto improve diabetes care among Latino Medi-care beneficiaries in four Southern Californiacounties. After researching barriers to gooddiabetes care among Latino seniors, Olson(83) designed a multifaceted program targetinghealth care providers and Medicare beneficia-ries through bilingual, low-literacy, and well-illustrated health education materials and tools,community and provider partnerships, and the
mass media. Program staff participated in liveinterviews on Spanish radio and television sta-tions and placed ads and articles in Spanishand bilingual community newspapers. Mediamessages emphasized the importance of proac-tive diabetes control and encouraged Latinosto discuss HbA1c testing with their physicians.Complementary messages were placed in physi-cian trade magazines. The project succeeded inhelping to reduce the disparity in glycosylatedhemoglobin testing between white and LatinoMedicare beneficiaries in the targeted region(83).
Schools and families. Sembrando Salud (Sow-ing the Seeds of Health) entailed the evaluationof an eight-week tobacco/alcohol use preven-tion program compared with a first aid/homesafety attention-control condition delivered toyouth and their parents in schools (33, 64). Sixhundred and sixty adolescents and one adultcaregiver per youth were recruited through thefederal Migrant Education Program in South-ern California. Random assignment to a condi-tion occurred at the school level in 22 schools.Seventy 8-week intervention groups (37tobacco/alcohol, and 33 first aid/home safety)were conducted by bilingual/bicultural col-lege undergraduates who served as older-to-younger peer educators. No between-groupdifferences in smoking or drinking followingthe intervention were significant: Thirty-daysmoking started and remained at very low levels,and the highest group prevalence at any mea-surement period was 4.7% and the lowest was2.5%. However, those considered susceptibleto smoking dropped by 50% in the interven-tion condition versus nearly 40% in the atten-tion control, from baseline to the final follow-up, with a statistically significant reduction atfinal follow-up. Of interest was the attention-control participants, who demonstrated signif-icantly higher first aid skills and home safetypractices at posttest: One adolescent appar-ently responded effectively to an emergencythat threatened the life of a toddler sibling (21).
Trevino et al. (106) studied a school-baseddiabetes mellitus prevention program on low
www.annualreviews.org • Latino Community Health 239
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
income, Mexican American fourth-grade chil-dren in San Antonio. The Bienestar Health Pro-gram entailed health and physical educationcurricula, a family program, a school cafete-ria program, and an after-school health club,all emphasizing a decrease in dietary saturatedfat intake, an increase in dietary fiber intake,and an increase in physical activity to favorablyimpact fasting capillary glucose level, percent-age of body fat, physical fitness level, dietaryfiber intake, and dietary saturated fat intake. Al-though body fat and dietary saturated fat intakedid not differ significantly between interventionand control children, fasting capillary glucoselevels decreased in intervention schools andincreased in control schools, whereas fitnessscores and dietary fiber intake significantly in-creased in intervention children and decreasedin control children.
The Message
Literacy issues. The U.S. Bureau of Censushas determined that more than 10% of adultAmericans are functionally illiterate in English(meaning they read at the fourth grade or lowerlevel), and another 70 million are marginallyilliterate (reading levels between the fifth andeighth grade) (108). More than half of the mi-nority population in the United States is classi-fied as functionally or marginally illiterate. Amajor aspect of the problem of low literacyin the United States is the fact that most re-cent immigrants, especially from Latin Amer-ica, know little or no English upon arrival in theUnited States. Their level of the English lan-guage is limited to what is required to functionin job training programs, the community, andthe workplace.
Although Guerra & Shea (44) point out thatfunctional health literacy may not be indepen-dently associated with perceived physical healthstatus or mental health status in ethnic minori-ties, economic and other vulnerabilities stem-ming from low literacy may in turn lead tohealth problems. For instance, current healthinstructional approaches and materials are typ-
ically designed for relatively educated individ-uals who are highly literate in English. Mate-rials available in Spanish or other non-Englishlanguages are largely direct translations fromEnglish and are often not culturally or even lin-guistically appropriate. Further, they tend to bewritten at a high Spanish (or other language)readability level, making them inappropriatefor low-level readers in the native languages(16, 115). Such barriers apply not only to healtheducation materials (73) but also to instruc-tions that go along with medication prescrip-tions (115) and even condom use (92). Illiteracymay negatively affect health through incorrectuse of medication and inability to comply withmedical directions or advice, high rates of acci-dents, and a lack of access to health informationand services.
Health messages that concurrently pro-mote literacy may comprise the ideal approachto health communication for immigrants. In“Language for Health,” Elder and colleagues(33) wove heart health and stress manage-ment information into English as a second lan-guage (ESL) courses for recent immigrants.While these immigrants were learning English,they were also successful in reducing dietaryfat and, at least for a short time period, im-proving HDL (total cholesterol levels). Alumnileft these classes with not only improved En-glish but improved health practices as well.Parra-Medina and colleagues (85) used a simi-lar approach to improve the ability of Latinoswith limited English proficiency to navigate theU.S. health care system in appropriate, cost-effective ways while improving their Englishlanguage skills. The Language for Health CareAccess educational intervention was deliveredby trained interventionists in 16 ESL classes;11 ESL classes served as controls. The interven-tion was effective in improving levels of knowl-edge about health care access, appropriate use,and the availability of language resources. Incomparison to the control group, the interven-tion also improved levels of self-efficacy relatedto both health care access and language (e.g.,using English to access and utilize services).
240 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
Language preference. A manifest tenet ofhealth communication is that messages must bepresented in the language of the audience. Yeta Pew Hispanic Center survey (87) showed that50% of all Latinos in the United States con-sider themselves to be bilingual, whereas 75%read in both Spanish and English. Thus, ap-propriate message language cannot be directlyinferred by the literacy or ethnicity of the tar-get audience or its overall acculturation level.Kelly et al. (52) studied 249 Mexican Americanmiddle-school youth from a U.S.-Mexico bor-der community to examine the effectiveness oflanguage and theme with respect to print to-bacco counter advertisements. Although a largeproportion of the students identified with theMexican American culture and spoke Spanish inselected contexts, readability was greater for adsin English, which were rated as more effective.
Collectivistic versus individualistic fearmessages. Murray-Johnson and colleagues(78) studied what they term “individualistic”and “collectivistic” cultural orientations by as-cribing these to African Americans and MexicanAmericans, respectively. Their results suggestthat Mexican American adolescent offspring ofimmigrant parents were more heavily influ-enced by AIDS fear messages that emphasizedharm that could come to the family of an in-fected person, especially through the loss offamily honor and the shame that would come tothem. African American teens, whom they char-acterized as relatively individualistic in orienta-tion, were in contrast more susceptible to mes-sages depicting individual harm (e.g., personalshame and fear of death). Although these resultsare not directly attributable to cultural orienta-tion nor to specific behavioral outcomes, theydo suggest that at a minimum the target audi-ence’s family orientation needs to be consideredin designing messages for Latino communities.
Multimedia vicarious learning. Ramirez andher colleagues (71, 89) designed a unique com-munication strategy to promote Pap screeningand other cancer control behaviors, using“diffusion acceleration’’ approaches in the
Texas-Mexico border region. The campaignincluded 82 television segments, 67 newspaperstories, and 48 radio programs featuring localrole models. Salud en Accion was conducted pri-marily in Spanish; many of the television, radio,and newspaper messages included stories abouthow and why women obtained Pap smears andother cancer screening services. Role models’stories were written to highlight how they cameto obtain a Pap smear. Some stories also showedhow husbands and children can help womenmake decisions and how to obtain free services.The campaign also included the participationof 175 volunteer peer educators, female home-makers who distributed educational leaflets ona monthly basis. The communication effortmet its goal of increasing cancer control, with atrend toward slightly more recent adherence inthe experimental community. The proportionof women in the highest level of Pap smearadherence showed a relative increase of ∼10%,whereas the proportion at the lowest level wasreduced by nearly 50%.
The Audience: A Family Focus
Effective health communication leads the targetaudience through behavior change once pre-requisite perceptual and cognitive factors areaddressed. For most Latino groups, that behav-ior change will occur in the context of the fam-ily. Families (and more globally, other house-hold members) are often the primary sources ofsocial support. This is true particularly amongnew Latino immigrants who may or may notengage in other social networks within the com-munity, given its immigrant receiving status asdescribed above. With longer residences in theUnited States, however, the structure and na-ture of this social support may change. An ex-ample of changes in nature is seen in the treat-ment of aging family members; they may berespected and obeyed in their home countrybut are paid less heed over time and as genera-tions progress in the United States. Aging fam-ily members may even spend their final yearsin a nursing facility rather than with offspring.Nevertheless, targeting interventions to the
www.annualreviews.org • Latino Community Health 241
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
entire family acknowledges this longstandingtradition of family connectedness.
From both ecological and sociological re-search on families, two themes have emergedconsistently as uniquely important among U.S.Latinos: respeto and familismo (20, 45, 112). Re-speto, or respect, refers to the importance ofteaching younger generations their obligationsfor proper levels of courtesy and decorum re-quired in various social contexts with peopleof a particular social status, sex, or age (espe-cially respeto a los padres, or respecting one’s par-ents). Familismo, or familism, refers to “feelingsof loyalty, reciprocity, and solidarity towardsmembers of the family, as well as the notion ofthe family as an extension of self ” (88, p. 249).This strong sense of family orientation, obliga-tion, and cohesion appears to protect Latinosagainst risk behaviors and improve their physi-cal and educational outcomes (15, 23, 27).
Family-based researchers need to considerthe cultural orientation of both the parentand child and the impact of acculturation ontheir relationship. Among immigrant families,clashes occur between parents and their chil-dren because children identify with the hostculture and parents are committed to the waysof their countries of origin. This divide exac-erbates the intergenerational gap in accultura-tion (23, 37, 102). Potential effects of this inter-generational gap include a family role reversal(because children have better English languagecapacity and are often placed in positions ofauthority over parents in family business mat-ters such as translating at the doctor, readingmaterials sent home from school, or businesscorrespondence) and increasing disengagementand rigidity in parent-child relationships thatpreviously had been flexible and cohesive(103, 113).
Health-promotion specialists must also de-termine the specific roles of each family mem-ber and help youth and parents understand oneanother as part of any health program or treat-ment regimen. Adherence to the regimen isunlikely to occur unless the family trusts theprovider and thinks that his or her recommen-dations are valuable and important. Such rec-
ommendations in the area of health behaviorchange may especially call for the involvementof the family, given that resistance to changewill occur if the targeted health behaviors arewidely accepted in the traditional culture (46).
Finally, despite the importance of involv-ing all family members, recent research high-lights the importance of the wife-mother, whooften serves as the primary target of health-promotion interventions given traditional gen-der norms and roles. This is normative withina largely patriarchal society and continues de-spite an increase in the proportion of womenemployed in the labor force. The primary fe-male often carries the brunt of change withinthe family, taking the lead in bringing aboutbehavior change among its members (76).
In one survey on food habits and attitudes,mothers served as the primary influence onmatters of nutrition and health (63). Researchalso indicates that parents’ eating behaviors di-rectly influence the child’s diet (i.e., model-ing the appropriate behavior), whereas parentknowledge and parent self-efficacy indirectlyinfluence dietary behavior among children (57).Similarly, targeting the adult woman and ad-dressing how her decisions on diet and physicalactivity influence the behaviors of the rest ofher family are consistent with the familial ori-entation of the Latino culture.
A family-based diabetes program on theU.S.-Mexico border helps illustrate the inte-gration of these points. In this study, familymembers were trained to collectively set health-behavior goals, to overcome obstacles hinder-ing healthy behaviors, and to develop a planto sustain behavior changes (104). The Famil-ias Unidas intervention targeted increases inprotective factors (e.g., familism, parental in-vestment, family cohesion, parent-adolescentcommunication, parental monitoring, and pos-itive parenting) and reductions in risk factors(e.g., family conflict resulting from differen-tial acculturation, and lack of parental moni-toring of adolescents, school, and peers). Theintervention was delivered in family-centered,multiparent groups that involved parents asagents of change by strengthening their sense of
242 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
responsibility and perceived control over theirlives and the lives of their children. Interventionmessages for the parents emphasized buildingcultural strengths to fortify culturally relevantprotective factors that exist within the individ-ual, family, and community, the importance ofthe family, cultural adaptation to American so-ciety, the marketing strategies of the alcohol andtobacco industries, and life issues experiencedwithin an economically disadvantaged environ-ment. The Familias Unidas approach focused onthe impact of deeply held values and beliefs onhealth (23). For example, respeto may engen-der family harmony. At the same time respetomay lead parents to view schools and teach-ers as the authority over their child’s educationand perceive and view parental interventions ontheir child’s behalf at school as inappropriateand overstepping their bounds. This conflictswith the mainstream American value that par-ents are important members of the educationalteam and with the expectation that they com-municate with schools. Thus, part of the in-tervention approach was in essence to redefinerespeto within the new and less familiar culturalcontext.
PART 3: DISCUSSION
We have described a framework for designingand evaluating health communication and be-havior change efforts in this large and diversepopulation. Latinos vary substantially on a vari-ety of overlapping and interactive dimensions.These include their socioeconomic and legalstatus, their country of origin or backgroundand the extent of ongoing contact with thatcountry, the nature of their receiving commu-nity or region of residence, their generation sta-tus and levels of acculturation, and psychosocialand demographic factors such as their expe-riences of racism or discrimination, familismo,collectivism, gender, and age-related issues.
In this article we have sought to bridgethe gap between this extensive and rich so-cial and behavioral science research tradi-tion with health communication and relatedbehavior-change efforts among Latinos resid-
ing in the United States. With reference tothe communication-persuasion model, Table 2summarizes how these broader social and cul-tural forces translate into the selection ofhealth communication channels, sources andsettings, messages and their design, and delimi-tations of target audiences. Programs presentedin recently published literature are describedin terms of these communication-persuasioninputs.
Much of the published literature on healthbehavior change in Latino communities repre-sents descriptions, program evaluations, or (insome cases) empirical studies of multicompo-nent communication efforts. In general, mul-tiple communication channels are employed,for example, with print materials accompaniedby face-to-face communication or mass media.Often, more than one source or setting is in-volved, such as when messages are presented byboth promotoras and providers in homes and alsoin clinics. Messages themselves may be multi-faceted, combining fear appeals with exhorta-tions to put personal health behavior in the con-text of family and culture. These combinationsof disparate elements are understandable, giventhat many studies describe earnest attempts toensure that community programs include allpotentially effective components. Nevertheless,in tandem they prevent adequate definition ofindependent variables.
Without well-specified independent vari-ables, the practice of community health promo-tion among Latinos cannot be refined, nor canthe empirical heritage be well established. Forexample, decade-old calls to close the digitaldivide (6) assume that Latinos and other disad-vantaged populations continue to have limitedaccess to the Internet. However, a recent PewHispanic Center report (87) showed that 78%of Latinos who are English dominant as well as76% of bilingual Latinos use the Internet. Al-though only 32% of Spanish-dominant Latinoadults do so as well, this proportion is certainto increase given the penetration of Internetcommunication into society and the prolifer-ation of Spanish-language Web sites. We needto be prepared for Internet delivery of written,
www.annualreviews.org • Latino Community Health 243
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
Table 2 Culture of origin issues and implications for communication interventions
Channel or medium Setting Source MessageCountry/culture oforigin
Mainstream versusLatin AmericanTV/radioprogramming
Dominant U.S.celebrations versusethnic or culturalfestivals (Dıa del Nino,Fiestas Patrias)
Idiomatic phrasingtailored to eachsending country’sculture
Socioeconomic and legalstatus
WIC and communityclinics or emergencyrooms versus regularproviders
Larger communitysettings versusapartment complexesand trailer parks(which are moreprivate social spheres)
Avoidance of use ofgovernment or theword American (e.g.,in “ACS”) as sourcefor communication tofirst-generation orundocumentedimmigrants
Where to find healthcare; adjustinghealth behaviormessages toeconomic reality
History of migration incommunity (mature,emerging, incipient)and acculturation
Mainstream versusface-face, sotto voceTV/print versusInternet and othernew media
Major malls, mobileconsulates, churchesand clinics versuslabor camps, tiendas,etc.
Community politicalleadership versusreligious or welfareworkers (or better yetpromotores)
Messages placed incontext of how onefits in the broadercommunity
Discrimination,perceived racism, andothering
Culturally competentcare versusinstitutional racism
Lawyers, activists,politicians
Health equalsfunction ofempowerment,rights
Familismo, collectivism Developmental orfamily specialist versusan abuela figure
Emphasis on impacton self versus largersocial group
Gender and age issues Equal rights
audio, and video formats, which have typicallybeen limited to traditional media channels inthis group. Additionally, 59% of Latinos havecell phones and half of these use text messaging,indicating further potential for this and othernew media.
Further limitations will then be placed onlinking existing intervention research back tothe Hispanic Health Paradox, acculturationand generational status, and other broader so-cial science-based themes. Ultimately, modifi-cations in or substitutions for Western healthbehavior theories cannot be achieved, leavingresearchers to choose between conceptual sys-tems predicated on research in other popula-tions or no theoretical base at all.
Target audiences are also not well definedat times. Some studies report only that “Lati-nos” or “Hispanics” were included without
reference to country of origin, and at timesthey are among other non-Latino participants.Generational status and length of time in theUnited States and the individual’s relationshipto his/her family and the broader communityare specified even less frequently (9). This in-adequate description may be accompanied bythe use of convenience samples and/or nonran-dom assignment in a comparison group designor even a single-group pretest/posttest. A lackof specification of audience/population factorsand a reliance on nonexperimental evaluationslimit the generalizability of existing findings.
These challenges face us even as the groundshifts rapidly beneath. America’s current de-mographic changes are the most pronouncedin more than a century. Latinos both defineand are defined by these changes, as is theirhealth. For example, as the debate continues
244 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
regarding the validity of the concept of theHispanic Health Paradox, the once-apparenthealth advantage of Latino ethnicity in theUnited States may be diminishing, even asrisks for chronic diseases accelerate rapidly inMexico and other sending countries. Althoughmany Latin American immigrants may live inisolated communities, most are increasingly ex-posed to diversity. Latinos of different genera-tions and national backgrounds intermarry, andyouth of mixed Latino and other backgroundscan be expected to join many in their age co-horts in self-identifying as multiracial. At thesame time, language, mass media, entertain-ment, religion, food preference, and other fun-damental cultural characteristics have an in-creasingly Latin American look to them in theUnited States, altering the very nature of theacculturative impetus.
Almost accepted as truisms for health com-munication with Latinos is the need to focuson family, cultural traditions, and collectivismwhile attending to acculturation, language, andgeneration status and national origin. The mostextensive intervention research topic in Latinocommunity health has been the application ofthe promotor model. Yet even this area needs farmore empirical treatment, as Rhodes and col-leagues (91) note in their extensive review of theuse of promotoras [which they label lay healthadvisors (LHAs)],
Given the long history of using LHAs asan approach to health promotion . . . andthe current emphasis of LHA approachesas a potential solution to health dispari-
ties . . . Latinos/Hispanics in particular, fewrigorous studies have been published that doc-ument the effectiveness of LHAs on a varietyof public health concerns. A stronger empiri-cal evidence base is clearly needed. (p. 418)
This lack of empirical documentation ofeffective community health-promotion effortswill continue to challenge researchers and pol-icy makers alike in the coming years anddecades. Such research, however, must be sit-uated in the context of broader social changeefforts to promote education and reduce dis-crimination, which can also promote individualhealth. Although these broader forces do not re-quire experimental evaluation, they inform rel-evant communication both to the Latino com-munity and to society as a whole.
IMPLICATIONS FOR PRACTICE
Community health-promotion practitionersworking with Latino communities must startwith a thorough knowledge of their audience,e.g., the sociocultural, economic, linguistic, andother characteristics of the members of thatcommunity. Specific variables to which practi-tioners should attend include country of origin,generation and acculturation, socioeconomicand legal status, and the interaction between thebroader community or region and the Latinopopulation. Whether programs are borrowedfrom elsewhere or developed from the groundup, this information will guide the selection ofchannels, messages, sources, and settings as wellas the implementation of such programs andwill help circumvent the one-size-fits-all pitfall.
DISCLOSURE STATEMENT
The authors are not aware of any biases that might be perceived as affecting the objectivity of thisreview.
ACKNOWLEDGMENTS
The authors thank Katherine Stewart for her extensive contributions to processing this manuscriptand current and former colleagues Amelie Ramirez, Nadia Campbell, Jeanette Candelaria, ElvaArredondo, Jo Anne Earp, Eugenia Eng, and Deanne K.H. Messias for their contributions to ourresearch program.
www.annualreviews.org • Latino Community Health 245
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
LITERATURE CITED
1. Apodaca X, Woodruff SI, Candelaria J, Elder JP, Zlot A. 1997. Hispanic health program participant andnonparticipant characteristics. Am. J. Health Behav. 21(5):356–63
2. Abraido-Lanza AF, Dohrenwend BP, Ng-Mak DS, Turner JB. 1999. The Latino mortality paradox: atest of the “salmon bias” and healthy migrant hypotheses. Am. J. Public Health 89(10):1543–48
3. Airhihenbuwa CO. 1995. Health and Culture: Beyond the Western Paradigm. Thousand Oaks, CA: Sage.152 pp.
4. Airhihenbuwa CO, Kumanyika SK, TenHave TR, Morssink CB. 2000. Cultural identity and healthlifestyles among African Americans: a new direction for health intervention research? Ethn. Dis.10(2):148–64
5. Airhihenbuwa CO, Obregon R. 2000a. A critical assessment of theories/models used in health commu-nication for HIV/AIDS. J. Health Commun. 5(Suppl.):5–15
6. Airhihenbuwa CO, Obregon R. 2000b. Toward a new communications framework for HIV/AIDS.J. Health Commun. 5(Suppl.):101–11
7. Amezcua C, McAlister AL, Ramirez A, Espinoza R. 1990. A Su Salud: health promotion in a Mexican-American border community. In Health Promotion at the Community Level, ed. N Bracht, pp. 257–77.Newbury Park, CA: Sage
8. Arredondo EM, Elder JP, Ayala GX, Campbell N, Baquero B, Duerksen S. 2006. Is parenting style relatedto children’s healthy eating and physical activity in Latino families? Health Educ. Res. 21(6):862–71
9. Ayala GX, Baquero B, Klinger S. 2008. A systematic review of the relationship between acculturation anddiet among Latinos in the United States: implications for future research. J. Am. Diet. Assoc. 108(8):1330–44
10. Ayala GX, Elder JP, Campbell NR, Slymen DJ, Roy N, et al. 2004. Correlates of body mass index andwaist-to-hip ratio among Mexican women in the United States: implications for intervention develop-ment. Women’s Health Issues 14(5):155–64
11. Ayala GX, Mueller K, Lopez-Madurga E, Campbell NR, Elder JP. 2005. Restaurant and food shoppingselections among Latinas in Southern California. J. Am. Diet. Assoc. 105:38–45
12. Ayala GX, Ornelas I, Rhodes SD, Amell J, Dodds J, et al. 2008. Determinants of dietary intake amongmen involved in the MAN for Health study. Am. J. Public Health. In press
13. Ayala GX, Rogers M, Arredondo E, Campbell NR, Baquero B, et al. 2008. Away-from-home food intakeand risk for obesity: examining the influence of context. Obes. Res. 16(5):1002–8
14. Berry J. 2003. Conceptual approaches to acculturation. In Acculturation: Advances in Theory, Measurement,and Applied Research, ed. K Chun, PB Organista, G Marin, pp. 17–37. Washington, DC: Am. Psychol.Assoc.
15. Bird HR, Canino GJ, Davies M, Zhang H, Ramirez R, Lahey BB. 2001. Prevalence and correlates ofantisocial behaviors among three ethnic groups. J. Abnorm. Child Psychol. 29(6):465–78
16. Boyd M, Feldman R. 1984. Health information seeking and reading and comprehension abilities ofcardiac rehab patients. J. Cardiac Rehab. 4:343–47
17. Brondolo E, Rieppi R, Kelly KP, Gerin W. 2003. Perceived racism and blood pressure: a review of theliterature and conceptual and methodological critique. Ann. Behav. Med. 25:55–65
18. Bronfenbrenner U. 1979. The Ecology of Human Development: Experiments by Nature and Design.Cambridge, MA: Harvard Univ. Press
19. Brown SA, Garcia AA, Kouzekanani K, Hanis CL. 2002. Culturally competent diabetes self-managementeducation for Mexican Americans: the Starr County border health initiative. Diabetes Care 25(2):259–68
20. Buriel R, Hurtado-Ortiz MT. 2000. Child care practices and preferences of native-and foreign-bornLatina mothers and Euro-American mothers. Hispanic J. Behav. Sci. 22(3):314–31
21. Campbell NR, Ayala GX, Litrownik AJ, Slymen DJ, Zavala F, Elder JP. 2001. Evaluation of a firstaid/home safety program for Hispanic migrant adolescents. Am. J. Prev. Med. 20(4):258–65
22. Cherrington A, Ayala GX, Sleath B, Corbie-Smith G. 2006. Examining knowledge, attitudes and beliefsabout depression among Latino adults with Type II Diabetes. Diabetes Educ. 32(4):603–13
23. Coatsworth JD, Pantin H, Szapocznik J. 2002. Familias Unidas: a family-centered ecodevelopmentalintervention to reduce risk for conduct problems and substance use among Hispanic adolescents. Clin.Child Fam. Psychol. Rev. 5:113–32
246 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
24. Cooper LA, Hill MN, Powe NR. 2002. Designing and evaluating interventions to eliminate racial andethnic disparities in health care. J. Gen. Intern. Med. 17(6):477–86
25. Crimmins EM, Kim JK, Alley DE, Karlamangla A, Seeman T. 2007. Hispanic paradox in biological riskprofiles. Am. J. Public Health 97(7):1305–10
26. Davidson JA, Moreno PR, Badimon JJ, Lopez-Candalas A, Maisonet Giachello AL, et al. 2007. Cardio-vascular disease prevention and care in Latino and Hispanic subjects. Endocr. Pract. 13(1):77–85 (Abstr.)
27. Dumka LE, Roosa MW, Jackson KM. 1997. Risk, conflict, mothers’ parenting, and children’s adjustmentin low-income, Mexican immigrant, and Mexican American families. J. Marriage Fam. 59(2):309–23
28. Elder JP, Apodaca JX, Parra-Medina D, Zuniga de Nuncio ML. 1998. Strategies for health education:theoretical models. See Ref. 66, pp. 567–86
29. Elder JP, Ayala GX, Campbell NR, Arredondo EM, Slymen DJ, et al. 2006. Long-term effects of acommunication intervention for Spanish-Dominant Latinas. Am. J. Prev. Med. 31(2):159–66
30. Elder JP, Ayala GX, Campbell NR, Slymen D, Lopez-Madurga ET, et al. 2005. Interpersonal and printnutrition communication for a Latino population. Health Psychol. 24(1):49–57
31. Elder JP, Campbell NR, Candelaria JI, Talavera GA, Mayer JA, et al. 1998. Project Salsa: developmentand institutionalization of a nutritional health promotion project in a Latino community. Am. J. HealthPromotion 12(6):391–401
32. Elder JP, Campbell NR, Litrownik AJ, Ayala GX, Slymen DJ, et al. 2000. Predictors of cigarette andalcohol susceptibility and use among Hispanic migrant adolescents. Prev. Med. 31:115–23
33. Elder JP, Candelaria JI, Woodruff SI, Criqui MH, Talavera GA, Rupp JW. 2000. Results of languagefor health: cardiovascular disease nutrition education for Latino English-as-a-second-language students.Health Educ. Behav. 27(1):50–63
34. Eng E, Parker E, Harlan C. 1997. Lay health advisor intervention strategies: a continuum from naturalhelping to paraprofessional helping. Health Educ. Behav. 24(4):413–17
35. Erwin DO, Johnson VA, Trevino M, Duke K, Feliciano L, Jandorf L. 2007. A comparison of AfricanAmerican and Latina social networks as indicators for culturally tailoring a breast and cervical cancereducation intervention. Cancer 109(Suppl.):368–77
36. Evenson K, Sarmiento O, Ayala GX. 2004. Acculturation and physical activity among North CarolinaLatina immigrants. Soc. Sci. Med. 59(2):2509–22
37. Felix-Ortiz M, Fernandez A, Newcomb M. 1998. The role of intergenerational discrepancy of culturalorientation in drug use among Latina adolescents. Subst. Use Misuse 33(4):967–94
38. Fox SA, Stein JA, Sockloskie RJ, Ory MG. 2001. Targeted mailed materials and the Medicare beneficiary:increasing mammogram screening among the elderly. Am. J. Public Health 91:55–61
39. Franzini L, Ribble JC, Keddie AM. 2001. Understanding the Hispanic paradox. Ethn. Dis. 11(3):496–51840. Fuentes-Afflick E, Hessol NA, Perez-Stable EJ. 1999. Testing the epidemiologic paradox of low birth
weight in Latinos. Arch. Pediatr. Adolesc. Med. 153(2):147–5341. Garces IC, Scarinci IC, Harrison L. 2006. An examination of sociocultural factors associated with health
and health care seeking among Latina immigrants. J. Immigrant Health 8:377–8542. Goldman N, Kimbro RT, Turra CM, Pebley AR. 2006. Socioeconomic gradients in health for white and
Mexican-origin populations. Am. J. Public Health 96(12):2186–9343. Grove NJ, Zwi AB. 2006. Our health and theirs: forced migration, othering, and public health. Soc. Sci.
Med. 62(8):1931–4244. Guerra CE, Shea JA. 2007. Health literacy and perceived health status in Latinos and African Americans.
Ethn. Dis. 17(2):305–12 (Abstr.)45. Harwood R, Leyendecker B, Carlson V, Asencio M, Miller A. 2002. Parenting among Latino families in
the U.S. In Handbook of Parenting: Social Conditions and Applied Parenting, ed. MH Bornstein, pp. 21–46.Mahwah, NJ: Lawrence Erlbaum
46. Horowitz C. 1998. The role of the family and the community in the clinical setting. See Ref. 66,pp. 163–82
47. Hunt KJ, Resendez RG, Williams K, Haffner SM, Stern MP, Hazuda HP. 2003. All-cause and cardio-vascular mortality among Mexican-American and Non-Hispanic White older participants in the SanAntonio Heart Study—evidence against the “Hispanic Paradox.” Am. J. Epidemiol. 158(11):1048–57
www.annualreviews.org • Latino Community Health 247
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
48. Jack LJ, Airhihenbuwa CO, Murphy F, Thompson-Reid P, Wheatley B, Dickson-Smith J. 1993. Canceramong low-income African-Americans: implications for culture and community-based health promotion.Wellness Perspect. 9(4):57–68
49. Johnson J, Sleath B, Ayala GX, Dardess M. 2006. A demographic profile of U.S. Hispanic markets. Rep.Glaxo-Smith-Kline, Univ. N. C., Chapel Hill
50. Kahssay H, Taylor ME, Berman PA. 1998. Community Health Workers: The Way Forward. Geneva: WorldHealth Organ.
51. Kelly KJ, Stanley LR, Comello ML, Gonzalez GR. 2006. Tobacco counter-advertisements aimed atbicultural Mexican American youth: the impact of language and theme. J. Health Commun. 11(5):455–76
52. Kelly NR, Huffman LC, Mendoza FS, Robinson RN. 2003. Effects of a videotape to increase use ofpoison control centers by low-income and Spanish-speaking families: a randomized, controlled trial.Pediatrics 111(1):21–26
53. Kepka D, Ayala GX, Cherrington A. 2007. Do immigrant Latinos link self-rated health with BMI andhealth behaviors? Am. J. Health Behav. 31:535–44
54. Keppel KG. 2007. Ten largest racial and ethnic health disparities in the United States based on HealthyPeople 2010 objectives. Am. J. Epidemiol. 166:97–103
55. Keppel KG, Pamuk E, Lynch J, Carter-Pokras O, Insun K, et al. 2005. Methodological issues in measuringhealth disparities. Vital Health Stat. 2(141):1–16
56. Kochhar R. 2005. Latino Labor Report 2004: more jobs for new immigrants but at lower wages. Rep.Pew Hisp. Cent. http://pewhispanic.org/reports/report.php?ReportID=45
57. Kratt PP, Reynolds KD, Shewchuk JM. 1998. Modeling family influence on the dietary intake of fourthgraders. Presented at Annu. Meet. Soc. Behav. Med., New Orleans
58. Krieger N. 2000. Discrimination and health. In Social Epidemiology, ed. LF Berkman, I Kawachi,pp. 36–75. Oxford: Oxford Univ. Press
59. Krumeich A, Weijts W, Reddy P, Meijer-Weitz A. 2001. The benefits of anthropological approaches forhealth promotion research and practice. Health Educ. Res. 16(2):121–30
60. Lara M, Gamboa C, Kahramanian MI, Morales LS, Hayes-Bautista DE. 2005. Acculturation and Latinohealth in the United States: a review of the literature and its sociopolitical context. Annu. Rev. PublicHealth 26(1):367–97
61. Latham CL, Calvillo E. 2007. A health protection model for Hispanic adults with type 2 diabetes.J. Clin. Nurs. 16(7B):186–96
62. Liao Y, Cooper FRS, Cao G, Kaufman JS, Long AE, McGee DL. 1997. Mortality from coronaryheart disease and cardiovascular disease among adult U.S. Hispanics: findings from the National HealthInterview Survey (1986 to 1994). J. Am. Coll. Cardiol. 30(5):1200–5
63. Litman TJ. 1974. The family as the basic unit in health and medical care: a social-behavioral overview.Soc. Sci. Med. 8:495–519
64. Litrownik AJ, Elder JP, Campbell NR, Ayala GX, Slymen DJ, et al. 2000. Evaluation of a tobacco andalcohol use prevention program for Hispanic migrant adolescents: promoting the protective factor ofparent-child communication. Prev. Med. 31:124–33
65. Lorence DP, Park H, Fox S. 2006. Racial disparities in health information access: resilience of the digitaldivide. J. Med. Syst. 30(4):241–49
66. Loue S, ed. 1998. Handbook of Immigrant Health. New York: Plenum67. Marın G. 1996. Perceptions by Hispanics of channels and sources of health messages regarding cigarette
smoking. Tob. Control 5(1):30–3668. Marın G, Triandis HC. 1985. Allocentrism as an important characteristic of the behavior of L.A. &
Latinos. In Cross-Cultural and National Studies of Social Psychology, ed. R Diaz-Guerrero, pp. 85–104.Amsterdam: North Holl.
69. Markides KS, Coreil J. 1986. The health of Hispanics in the southwestern United States: an epidemiologicparadox. Public Health Rep. 101:253–65
70. Mayo R, Parra-Medina DM, Messias D, Rhoades D. 2003. SC partnership for cancer prevention resultsfrom formative research with Latina women at risk for cervical cancer. J. Cancer Educ. 18(3):35–36
248 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
71. McAlister AL, Fernandez-Esquer ME, Ramirez AG, Trevino F, Gallion KJ, et al. 1995. Communitylevel cancer control in a Texas barrio: part II-base-line and preliminary outcome findings. J. Natl. CancerInst. Monogr. 18:123–26
72. McGuire WJ. 1989. Theoretical foundations of campaigns. In Public Communication Campaigns, ed. RERice, CK Atkin, pp. 43–65. Newbury Park: Sage
73. Mead C, Byrd J, Lee M. 1989. Improving patient comprehension of literature on smoking. Am. J. PublicHealth 79:1411–12
74. Mensah GA, Mokdad AH, Ford ES, Greenlund KJ, Croft JB. 2005. State of disparities in cardiovascularhealth in the United States. Circulation 111(10):1233–41
75. Modiano MR, Villar-Werstler P, Meister J, Figueroa-Valles N. 1995. Cancer in Hispanics: issues ofconcern. J. Natl. Cancer Inst. Monogr. 18:35–39
76. Moore J. 1994. The social fabric of the Hispanic community since 1965. In Hispanic Catholic Culture inthe U.S.: Issues and Concerns, ed. JP Dolan, AF Deck, pp. 6–49. Notre Dame, IN: Univ. Notre DamePress
77. Morales LS, Lara M, Kington RS, Valdez RO, Escarce JJ. 2002. Socioeconomic, cultural, and behavioralfactors affecting Hispanic health outcomes. J. Health Care Poor Underserved 13(4):477–503
78. Murray-Johnson L, Whitte K, Liu W, Hubbell AP, Sampson J, Morrison K. 2001. Addressing culturalorientations in fear appeals: promoting AIDS—protective behaviors among Mexican immigrant andAfrican American adolescents and American and Taiwanese college students. J. Health Commun. 6:335–58
79. Neff AJ, Hoppe SK. 1995. Race/ethnicity, acculturation and psychological distress: fatalism and religiosityas cultural resources. J. Comm. Psychol. 21:3–20
80. O’Donnell L, Sandoval A, Duran R, O’Donnell C. 1995. The effectiveness of video-based interventionsin promoting condom acquisition among STD clinic patients. Sex. Transm. Dis. 22(2):97–103
81. Oetzel J, De Vargas F, Ginossar T, Sanchez C. 2007. Hispanic women’s preferences for breast healthinformation: subjective cultural influence on source, message, and channel. Health Commun. 21(3):223–33(Abstr.)
82. Olshefsky AM, Zive MM, Scolari R, Zuniga M. 2007. Promoting HIV risk awareness and testing inLatinos living on the U.S.-Mexico Border: The Tu No Me Conoces Social Marketing Campaign. AIDSEduc. Prev. 19(5):422–35
83. Olson R, Sabogal F, Perez A. 2008. Viva La Vida: helping Latino medicare beneficiaries with diabeteslive their lives to the fullest. Am. J. Public Health 98(2):205–8
84. Palloni A, Morenoff JD. 2001. Interpreting the paradoxical in the Hispanic paradox: demographic andepidemiologic approaches. Ann. N. Y. Acad. Sci. 954:140–74
85. Parra-Medina DM, Wilcox S, Thompson-Robinson M, Sargent R, Will JC. 2004. A replicable processfor redesigning ethnically relevant educational materials. J. Womens Health 13(5):579–88
86. Pepitone A. 1995. Foreword. In Spirit Versus Scalpel, ed. LL Adler, BR Mukherji, pp. xiii–xiv. London:Bergin & Garvey
87. Pew Hispanic Cent. 2008. Statistical portrait of Hispanics in the United States, 2006. http://pewhispanic.org/files/reports/.pdf
88. Portes A. 1995. Segmented assimilation among new immigrant youth: a conceptual framework. InCalifornia’s Immigrant Children: Theory, Research, and Implications for Educational Policy, ed. RG Rumbaut,WA Cornelius, pp. 71–76. San Diego: Cent. U.S.-Mex. Stud., Univ. Ca.
89. Ramirez AG, McAlister A, Gallion KJ, Ramirez V, Garza IR, et al. 1995. Community level cancer controlin a Texas barrio: Part I—Theoretical basis, implementation, and process evaluation. J. Natl. Cancer Inst.Monogr. (18):117–22
90. Ramirez RR, de la Cruz P. 2003. The Hispanic population in the United States: March 2002, currentpopulation reports. U.S. GPO. Rep. 20–545, Washington, DC. http://factfinder.census.gov/
91. Rhodes SD, Foley KL, Zometa CS, Bloom FR. 2007. Lay health advisor interventions among Hispanics/Latinos: a qualitative systematic review. Am. J. Prev. Med. 33(5):418–27
92. Richwald G, Wamsley M, Coulson A, Morisky D. 1988. Are condom instructions readable? Results ofthe Readability Study. Public Health Rep. 103:355–63
www.annualreviews.org • Latino Community Health 249
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
93. Sabogal R, Marın G, Otero-Sabogal R, Marın BV, Perez-Stable EJ. 1987. Latino familism and accultur-ation: What changes and what doesn’t? Latino J. Behav. Sci. 9:397–412
94. Sauaia A, Min S, Lack D, Apodaca C, Osuna D, Stowe A, et al. 2007. Church-based breast cancerscreening education: impact of two approaches on Latinas enrolled in public and private health insuranceplans. Prev. Chronic Dis. 4(4):1–10
95. Schneider KT, Hitlan RT, Radhakrishnan P. 2000. An examination of the nature and correlates of ethnicharassment experiences in multiple contexts. J. Appl. Soc. Psychol. 85:3–12
96. Smedley BD, Stith AY, Nelson AR. 2002. Unequal Treatment: Confronting Racial and Ethnic Disparities inHealth Care. Washington, DC: Natl. Acad. Press
97. Smith C, Ryan A. 2006. Change for Life/Cambia Tu Vida: a health promotion program based on thestages of change model for African descendent and Latino adults in New Hampshire. Prev. Chronic Dis.3(3):A105–21
98. Spector RE. 1991. Cultural Diversity in Health and Illness. East Norwalk, CT: Appleton & Lange.490 pp. 2nd ed.
99. Squiers L, Finney-Rutten LJ, Treiman K, Bright MA, Hesse B. 2005. Cancer patients’ information needsacross the cancer care continuum: evidence from the cancer information service. J. Health Commun.10:15-34
100. Streng JM, Rhodes S, Ayala GX, Eng E, Arceo R, Phipps S. 2004. Realidad Latina: Latino adolescents,their school, and a university use photovoice to examine and address the influence of immigration.J. Interprof. Care 18(4):403–15
101. Swider SM. 2002. Outcome effectiveness of community health workers: an integrative literature review.Public Health Nurs. 19(1):11–20
102. Szapocznik J, Kurtines W. 1980. Acculturation, biculturalism and adjustment among Cuban Americans.In Acculturation: Theory, Models, and Some New Findings, ed. A Padilla, pp. 139–59. Boulder, CO: Praeger
103. Szapocznik J, Williams RA. 2000. Brief strategic family therapy: twenty-five years of interplay amongtheory, research and practice in adolescent behavior problems and drug abuse. Clin. Child Fam. Psychol.Rev. 3(2):117–34
104. Teufel-Shone NI, Drummond R, Rawiel U. 2005. Developing and adapting a family-based diabetesprogram at the U.S.-Mexico border. Prev. Chronic Dis. 2(1):1–9
105. Torres M, Parra-Medina D, Bellinger J, Johnson A, Probst JC. 2008. Rural hospitals and Spanish speakingpatients with limited English proficiency. J. Healthc. Manag. 53(2):107–19; discussion 119–20
106. Trevino RP, Yin Z, Hernandez A, Hale DE, Garcia OA, Mobley C. 2004. Impact of the Bienestar school-based diabetes mellitus prevention program on fasting capillary glucose levels: a randomized controlledtrial. Arch. Pediatr. Adolesc. Med. 158(9):911–17
107. Turra CM, Goldman N. 2007. Socioeconomic differences in mortality among U.S. adults: insight intothe Hispanic paradox. J. Gerontol. 62B(3):S184–92
108. U.S. Census Bur. 2005. Summary of social, economic, and housing characteristics. Rep. U.S. GPO,Washington, DC. http://factfinder.census.gov/
109. U.S. Dep. Health Hum. Serv. (USDHHS). 1994. Community Health Advisors: Models, Research, and Practice.Atlanta, GA: USDHHS, Public Health Serv., Cent. Dis. Control Prev.
110. U.S. Dep. Health Hum. Serv. (USDHHS). 2000. Healthy People 2010: understanding and improving health.http://www.healthypeople.gov/Document/tableofcontents.htm
111. Vaz L, Stoimenoff K, Ayala GX. 2003. Lay health advisors in Latino communities: A systematic review of theevidence. Am. Public Health Assoc. Conf., San Francisco, CA
112. Vega WA. 1990. Hispanic families in the 1980s: a decade of research. J. Marriage Fam. 52:1015–24113. Vega WA, Gil AG, Warheit GJ, Zimmerman RS, Apospori E. 1993. Acculturation and delinquent
behavior among Cuban American adolescents: toward an empirical model. Am. J. Community Psychol.21(1):113–25
114. Viruell-Fuentes E. 2007. Beyond acculturation: immigration, discrimination, and health research amongMexicans in the United States. Soc. Sci. Med. 65:1524–35
115. Vivian A, Robertson E. 1980. Readability of patient education materials. Clin. Ther. 3:129–36
250 Elder et al.
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

ANRV370-PU30-13 ARI 15 February 2009 12:38
116. Wetter DW, Mazas C, Daza P, Nguyen L, Fouladi RT, et al. 2007. Reaching and treatingSpanish-speaking smokers through the National Cancer Institute’s cancer information service. Cancer109(Suppl.):406–13
117. Wilkin HA, Valente TW, Murphy S, Cody MJ, Huang G, et al. 2007. Does entertainment educationwork with Latinos in the United States? Identification and the effects of a telenovela breast cancerstoryline. Health Commun. 21(3):223–33
118. Williams DR, Collins C. 1995. U.S. socioeconomic and racial differences in health: patterns and expla-nations. Annu. Rev. Sociol. 21:349–86
119. Yancey AK, Ortega AN, Kumanyika SK. 2006. Effective recruitment and retention of minority researchparticipants. Annu. Rev. Public Health 27:1–28
120. Yancey AK, Tanjasiri SP, Klein M, Tunder J. 1995. Increased cancer screening behavior in women ofcolor by culturally sensitive video exposure. Prev. Med. 24:142–48
www.annualreviews.org • Latino Community Health 251
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

AR370-FM ARI 15 February 2009 12:5
Annual Review ofPublic Health
Volume 30, 2009Contents
Epidemiology and Biostatistics
Adaptive Designs for Randomized Trials in Public HealthC. Hendricks Brown, Thomas R. Ten Have, Booil Jo, Getachew Dagne,Peter A. Wyman, Bengt Muthen, and Robert D. Gibbons � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1
Social Epidemiology. Social Determinants of Health in the UnitedStates: Are We Losing Ground?Lisa F. Berkman � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �27
The Behavioral Risk Factors Surveillance System: Past, Present,and FutureAli H. Mokdad � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �43
Geographic Life Environments and Coronary Heart Disease:A Literature Review, Theoretical Contributions, MethodologicalUpdates, and a Research AgendaBasile Chaix � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �81
Health Effects of Arsenic and Chromium in Drinking Water:Recent Human FindingsAllan H. Smith and Craig M. Steinmaus � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 107
Evidence-Based Public Health: A Fundamental Concept for PublicHealth PracticeRoss C. Brownson, Jonathan E. Fielding, and Christopher M. Maylahn � � � � � � � � � � � � � � � � 175
Prioritizing Clinical Preventive Services: A Review and Frameworkwith Implications for Community Preventive ServicesMichael Maciosek, Ashley B. Coffield, Nichol M. Edwards, Thomas J. Flottemesch,and Leif I. Solberg � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 341
Environmental and Occupational Health
Gene by Environment Interaction in AsthmaStephanie J. London and Isabelle Romieu � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �55
ix
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

AR370-FM ARI 15 February 2009 12:5
Geographic Life Environments and Coronary Heart Disease:A Literature Review, Theoretical Contributions, MethodologicalUpdates, and a Research AgendaBasile Chaix � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �81
Health Effects of Arsenic and Chromium in Drinking Water: RecentHuman FindingsAllan H. Smith and Craig M. Steinmaus � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 107
Health Effects of Combat: A Life-Course PerspectiveBarry S. Levy and Victor W. Sidel � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 123
Potential Health Impact of NanoparticlesTian Xia, Ning Li, and Andre E. Nel � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 137
Public Health Practice
Diffusion Theory and Knowledge Dissemination, Utilization,and Integration in Public HealthLawrence W. Green, Judith M. Ottoson, Cesar Garcıa, and Robert A. Hiatt � � � � � � � � � � � 151
Evidence-Based Public Health: A Fundamental Concept for PublicHealth PracticeRoss C. Brownson, Jonathan E. Fielding, and Christopher M. Maylahn � � � � � � � � � � � � � � � � 175
Public Health CertificationKristine M. Gebbie � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 203
Health Communication in the Latino Community:Issues and ApproachesJohn P. Elder, Guadalupe X. Ayala, Deborah Parra-Medina,and Gregory A. Talavera � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 227
The Delivery of Public Health Interventions via the Internet:Actualizing Their PotentialGary G. Bennett and Russell E. Glasgow � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 273
Social Environment and Behavior
A Crisis in the Marketplace: How Food Marketing Contributesto Childhood Obesity and What Can Be DoneJennifer L. Harris, Jennifer L. Pomeranz, Tim Lobstein, and Kelly D. Brownell � � � � � � 211
Health Communication in the Latino Community:Issues and ApproachesJohn P. Elder, Guadalupe X. Ayala, Deborah Parra-Medina,and Gregory A. Talavera � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 227
School-Based Interventions for Health Promotion and WeightControl: Not Just Waiting on the World to ChangeD.L. Katz � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 253
x Contents
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.

AR370-FM ARI 15 February 2009 12:5
The Delivery of Public Health Interventions via the Internet:Actualizing Their PotentialGary G. Bennett and Russell E. Glasgow � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 273
Social Epidemiology. Social Determinants of Health in the UnitedStates: Are We Losing Ground?Lisa F. Berkman � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �27
The Behavioral Risk Factors Surveillance System: Past, Present,and FutureAli H. Mokdad � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �43
Diffusion Theory and Knowledge Dissemination, Utilization,and Integration in Public HealthLawrence W. Green, Judith M. Ottoson, Cesar Garcıa, and Robert A. Hiatt � � � � � � � � � � � 151
Health Services
Cost-Sharing: A Blunt InstrumentDahlia K. Remler and Jessica Greene � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 293
Extreme Makeover: Transformation of the Veterans Health Care SystemKenneth W. Kizer and R. Adams Dudley � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 313
Prioritizing Clinical Preventive Services: A Review and Frameworkwith Implications for Community Preventive ServicesMichael V. Maciosek, Ashley B. Coffield, Nichol M. Edwards,Thomas J. Flottemesch, and Leif I. Solberg � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 341
Quality-Based Financial Incentives in Health Care: Can We ImproveQuality by Paying For It?Douglas A. Conrad and Lisa Perry � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 357
The Contribution of Hospitals and Health Care Systemsto Community HealthStephen M. Shortell, Pamela K. Washington, and Raymond J. Baxter � � � � � � � � � � � � � � � � � � 373
Untangling Practice Redesign from Disease Management:How Do We Best Care for the Chronically Ill?Katie Coleman, Soeren Mattke, Patrick J. Perrault, and Edward H. Wagner � � � � � � � � � � 385
Indexes
Cumulative Index of Contributing Authors, Volumes 21–30 � � � � � � � � � � � � � � � � � � � � � � � � � � � 409
Cumulative Index of Chapter Titles, Volumes 21–30 � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 414
Errata
An online log of corrections to Annual Review of Public Health chapters may be foundat http://publhealth.annualreviews.org/
Contents xi
Ann
u. R
ev. P
ublic
. Hea
lth. 2
009.
30:2
27-2
51. D
ownl
oade
d fr
om a
rjou
rnal
s.an
nual
revi
ews.
org
by 6
8.10
1.16
5.18
3 on
03/
28/0
9. F
or p
erso
nal u
se o
nly.




















