Benjamin Harrison And The American West - DigitalCommons ...
Upload
khangminh22Category
view
2download
0
Page 1 of 142
Conduct and Competence Committee
Substantive Hearing
2 May-8 June and 3-6 July 2017
Nursing and Midwifery Council, 2 Stratford Place, Montfichet Road, London, E20 1EJ
Name of registrant: Peter Harrison
NMC PIN: 88E1169E
Part(s) of the register: RN5, Registered Nurse (sub part 1)
Learning disabilities (16 July 1991)
Area of registered address: England
Type of case: Misconduct
Panel members: Hilary Nightingale (Chair, Lay member)
Caroline Healy (Registrant member)
Janet Leonard (Registrant member)
Legal Assessor: Lachlan Wilson (2-5 May, 16 May-8 June and
3-6 July 2017)
Jane Rowley (8-15 May 2017)
Panel Secretary: Nilima Ali
Representation:
Nursing and Midwifery Council (NMC): Represented by Greg Unwin, Counsel (2 May-
8 June 2017), and Neil Jeffs, Case Presenter

Page 2 of 142
(3-6 July 2017), instructed by the NMC
Regulatory Legal Team
Mr Harrison: Mr Harrison was not present in person and not
represented in his absence. He participated by
telephone on 24 May and 6 June 2017
No case to answer: 1.1 (paragraphs 1-12 of Schedule A only), 1.3
and 4.1 (paragraphs 1-32 of Schedule E only)
Facts found proved by admission: 1.1, 1.2, 1.4, 1.6.1, 1.8, 1.9, 1.10, 1.11, 1.12, 2
(in its entirety), 3 (in its entirety), 4 (in its
entirety), 5 (in its entirety), 6 (in its entirety) and
7 (in its entirety)
Facts found proved: 1.5, 1.6.2, 1.6.3 and 1.7
Facts found not proved: N/A
Fitness to practise: Impaired
Sanction: Striking off order
Interim Order: Interim suspension order: 18 months

Page 3 of 142
This was a multi-registrant hearing relating to Peter Harrison, Registrant A, Registrant C
and Registrant D. Separate determinations were produced for each registrant.
Determination on service – Tuesday 2 May 2017
The panel received information from Mr Unwin on behalf of the Nursing and Midwifery
Council (“NMC”) that the Notice of Hearing had been served in accordance with The
Nursing and Midwifery Council (Fitness to Practise) Rules 2004 (“the Rules”). The panel
accepted the advice of the legal assessor.
The Notice of Hearing was sent by first class post and the Royal Mail ‘signed for’
service on 29 March 2017 to Mr Harrison’s registered address as recorded on WISER,
the system supporting the NMC’s Register. The letter provided details of the allegations,
the times, dates and venue of the hearing and, amongst other things, information about
his right to attend, be represented and call evidence, as well as the panel’s power to
proceed in his absence.
The Notice of Hearing was signed for, as received, in the printed name of ‘HARRISON’
on 30 March 2017.
The panel concluded that service had been effected in accordance with Rules 11 and
34.
Determination on proceeding in the absence of Mr Harrison – Tuesday 2 May 2017
Mr Unwin invited the panel to proceed in the absence of Mr Harrison, pursuant to Rule
21(2)(b).

Page 4 of 142
Mr Unwin referred the panel to Mr Harrison’s completed ‘Standard Directions Form’,
signed 19 October 2014, in which Mr Harrison indicated that “I will not attend a hearing”.
Mr Unwin further referred the panel to an undated letter from Mr Harrison in which he
provided a response to the substance of the allegations. Mr Harrison concluded that
letter by stating “I hope that this information helps the NMC reach what they consider [a]
fair decision regarding my continued fitness to practise”. Mr Unwin informed the panel
that beyond that information, there had been no recent response from Mr Harrison in
relation to these proceedings.
In light of the above, Mr Unwin submitted that there was sufficient material before the
panel upon which it could be satisfied that Mr Harrison was aware of this substantive
hearing and his right to attend, be represented, or provide written representations. He
submitted that the panel could further be satisfied that Mr Harrison had chosen not to
attend or engage actively in this hearing, seeking rather to rely on previously submitted
written representations.
Mr Unwin submitted that there was no information to suggest that an adjournment of the
hearing at this stage would ensure Mr Harrison’s attendance on a future occasion, there
being no indication that he would attend a hearing on a future date.
Mr Unwin reminded the panel that it had a power to proceed in the absence of a
registrant. He invited the panel to have regard to the strong public interest in its
expeditious consideration of these historic and serious allegations. He contended that
the panel could properly adjudicate upon the charges, in the absence of Mr Harrison,
using its own discretion when assessing all the evidence and taking account of all
matters raised.
Mr Unwin informed the panel that the NMC sought to rely upon approximately 30
witnesses in this hearing, 15 of whom were due to attend in person to give evidence.
Page 5 of 142
In closing, Mr Unwin submitted that the panel could properly conclude that Mr Harrison
was aware of the times and dates of this hearing and that he had voluntarily absented
himself.
The panel considered whether to exercise its discretion to proceed in Mr Harrison’s
absence, in accordance with Rule 21(2)(b). The panel had regard to all the information
before it, including the submissions from Mr Unwin, and accepted the advice of the legal
assessor.
The panel, in considering this matter, had regard to the public interest in the expeditious
disposal of the case, the potential inconvenience caused to a party or any witnesses to
be called by that party, and fairness to Mr Harrison. The panel gave careful regard to
the judgment in the case of R. v Jones (Anthony William) (No.2) [2002] UKHL 5 and
exercised the “utmost care and caution” in coming to its decision, with close regard to
the overall fairness of proceedings. The panel was mindful that whilst a registrant has a
right to be present in regulatory proceedings, that registrant may also voluntarily absent
themselves such as to enable the panel to decide to proceed in their absence.
The panel took note that the Notice of Hearing, sent on 29 March 2017 to Mr Harrison’s
registered address, was signed for in the printed name of ‘HARRISON’ on 30 March
2017. It took further note that during the course of the NMC’s investigation into the
allegations against Mr Harrison, he had engaged with his regulator to the extent of
completing and returning various NMC correspondence and providing a letter in which
he responded to the allegations. In all of those circumstances, the panel was satisfied
that Mr Harrison was aware of this hearing and that he had voluntarily absented himself.
Moreover, there had been no request for an adjournment. In any event, the panel
considered that adjourning the hearing would serve no purpose as, on the basis of the
information before it, it would be highly unlikely to secure Mr Harrison’s attendance on a
future occasion.

Page 6 of 142
The panel was aware that there was some disadvantage to Mr Harrison in not being
present to give his account of events or challenge the evidence relied upon by the NMC,
and in relation to the personal and professional impact any adverse findings may have
against him. However, in the panel’s judgement, it could make allowance for the fact
that the NMC’s evidence would not be tested in cross-examination and, of its own
volition, could explore any inconsistencies in the evidence which the panel itself
identified, as well as any matters referred to by Mr Harrison in his written
representations to the NMC. Furthermore, the panel considered that any disadvantage
to Mr Harrison was as a result of his decision to absent himself from the hearing,
waiving his right to attend/be represented.
The panel was mindful of the public interest in the expeditious disposal of cases. There
were approximately 15 live witnesses, due to give evidence on behalf of the NMC, who
would be inconvenienced by an adjournment of these proceedings. The allegations in
this case dated back to 2008 and the panel was particularly mindful that any continued
delay in these matters could further impact upon the witnesses’ recollection of events.
In all of the circumstances, the panel concluded that it was reasonable, appropriate and
in the public interest to proceed today, and that it would not be unfair to Mr Harrison to
hear the case in his absence.
For all these reasons the panel determined to proceed in the absence of Mr Harrison.
The panel will draw no adverse inference from his absence in its findings of fact.
Charge read – Tuesday 2 May 2017
That you, whilst employed by Castlebeck Care (Teesdale) Limited as a Regional
Operations Director/ Regional Operations Manager between 2008 and June 2012:

Page 7 of 142
1 In relation to Winterbourne View:
1.1 Did not ensure that Winterbourne View met any or all of the national minimum
standards for independent healthcare, under the Care Standards Act 2000,
listed in Schedule A
1.2 Did not ensure that Winterbourne View was compliant with any or all of the
Health and Social Care Act 2008 essential standards listed in Schedule B
1.3 Did not apply to register with the Care Quality Commission as the accountable
officer at the hospital under Part 2 of The Controlled Drugs (Supervision of
Management and Use) Regulations 2006.
1.4 Did not ensure that an action plan was submitted to the Healthcare Commission
following an inspection on 24 March 2009
1.5 Did not ensure that Individual X was registered with the Care Quality
Commission as Manager of Winterbourne View at any time from January 2010
1.6 Following a whistle blowing complaint from Individual O on 11 October 2010:
1.6.1 Did not ensure that any or all identified staff were suspended;
1.6.2 Did not ensure that an investigation was promptly conducted;
1.6.3 Did not ensure that a Serious Untoward Incident Form was completed.
1.7 Did not ensure that one or more patients who were admitted to the Hospital
were suitable for admission;
1.8 Did not ensure that staff at Winterbourne View received sufficient training to
provide appropriate care

Page 8 of 142
1.9 Did not ensure that all staff at Winterbourne View received adequate
supervision and/or supervision records
1.10 Did not ensure that there were adequate systems in place for the analysis
and/or review of patient incidents at Winterbourne View
1.11 Did not ensure that there were adequate systems in place to prevent excessive
use of restraint
1.12 Did not ensure that patients at Winterbourne View were protected from verbal
and physical abuse by members of staff;
2 In relation to Rose Villa:
2.1 Did not ensure that Rose Villa was compliant with any or all of the Health and
Social Care Act 2008 essential standards listed in Schedule C
3 In relation to Croxton Lodge:
3.1 Did not ensure that Croxton Lodge was compliant with any or all of the Health
and Social Care Act 2008 essential standards listed in Schedule D
4 In relation to Arden Vale:
4.1 Did not ensure that Arden Vale met any or all of the national minimum
standards for independent healthcare, under the Care Standards Act 2000, for
independent healthcare listed in Schedule E

Page 9 of 142
4.2 Did not ensure that Arden Vale was compliant with any or all of the Health and
Social Care Act 2008 essential standards listed in Schedule F
5 In relation to Cedar Vale
5.1 Did not ensure that Cedar Vale met any or all of the national minimum
standards for independent healthcare, under the Care Standards Act 2000,
listed in Schedule G
5.2 Did not ensure that Cedar Vale was compliant with any or all of the Health and
Social Care Act 2008 essential standards listed in Schedule H
6 In relation to Willow House
6.1 Did not ensure that Willow House was compliant with any or all of the Health
and Social Care Act 2008 essential standards listed in Schedule I
7 In relation to The East Midlands Centre for Neurobehavioural Rehabilitation
7.1 Did not ensure that The East Midlands Centre for Neurobehavioural
Rehabilitation was compliant with any or all of the Health and Social Care Act
2008 essential standards listed in Schedule J
And light of the above your fitness to practise is impaired by reason of your misconduct.
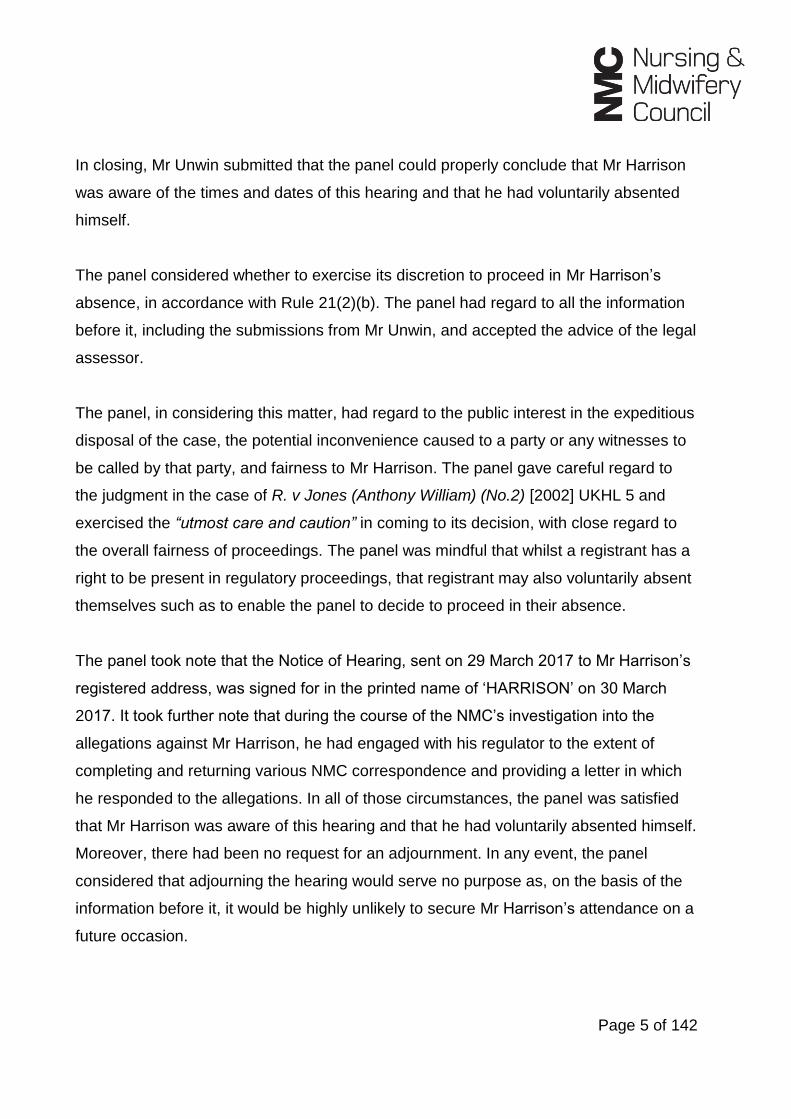
SCHEDULE A
No. Inspection date Standard
Private and Voluntary
Healthcare
Regulations 2001
Assessment
Outcome
Page 10 of 142
1. 1 December 2008 C24 Controlled
Drugs 15(5) Not met
2. 1 December 2008 M8 Suicide
Prevention 44(1)(c) Not met
3. 1 December 2008
C9 Human
Resources Policies
and Procedures
18(2)(a) Not met
4. 1 December 2008 M22 Patient's
Records 21(1)(a)(i)(ii) Not met
5. 1 December 2008 C14 Complaints
Process 23(5) Almost met
6. 1 December 2008
C15 Information
about Patient
Complaints
23(3)(a)(b) Not met
7. 1 December 2008 M10 Resuscitation
Procedures 15(2)(b) Not met
8. 1 December 2008 M27 Quality of Life
for Patients 16(4)(a) Not met
9. 1 December 2008
M42 The Rights of
the Patients under
the Mental Health
Act
47 Almost met
10. 1 December 2008 M44 Section 17
Leave 9(1)(e)(f) Not met
11. 1 December 2008 C17 Health Care
Premises 25(2)(a) and (d) Not met
12. 1 December 2008 C21 Health and
Safety Measures 25(5)(a) Not met
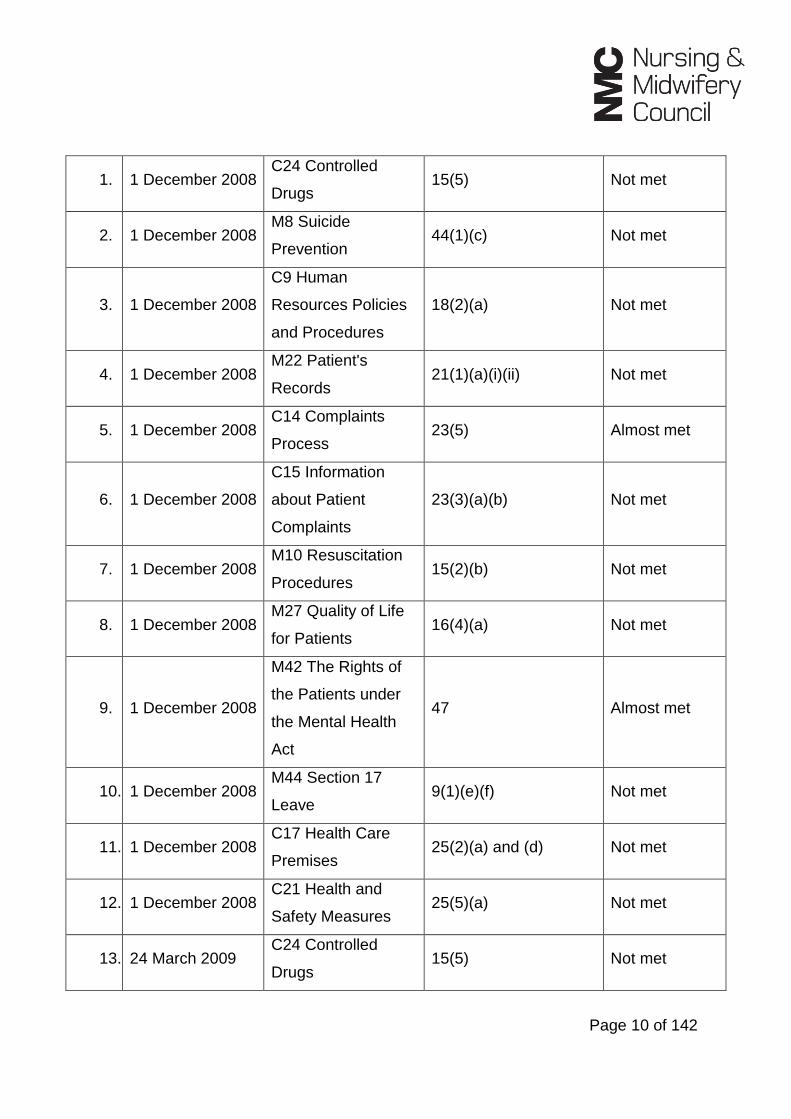
13. 24 March 2009 C24 Controlled
Drugs 15(5) Not met
Page 11 of 142
14. 24 March 2009 M8 Suicide
Prevention 44(1)(c) Not met
15. 24 March 2009 M22 Patient's
Records 21(1)(a)(i)(ii) Not met
16. 24 March 2009
C15 Information
about Patient
Complaints
23(3)(a)(b) Not met
17. 24 March 2009 M10 Resuscitation
Procedures 15(2)(b) Not met
18. 24 March 2009 M27 Quality of Life
for Patients 16(4)(a) Not met
19. 15 December
2009
C24 Controlled
Drugs 15(5) Almost met
20. 15 December
2009
C23 Ordering and
Storage of
Medicines
25(2)(d) Almost met
21. 15 December
2009 M6 Staff Training 18(2)(a) Almost met
22. 15 December
2009
C1 Information for
Patients 7 Almost met
23. 15 December
2009
A9 Health and
Safety 25(2)(d) Almost met
SCHEDULE B
No. Inspection dates Essential Standard Judgement
1. 17, 18 & 24 May and
2 June 2011
Outcome 4: Care and welfare of
people who use services Major Concerns
2. 17, 18 & 24 May and Outcome 7: Safeguarding people who Major Concerns

Page 12 of 142
2 June 2011 use services from abuse
3. 17, 18 & 24 May and
2 June 2011
Outcome 9: Management of
medicines Major Concerns
4. 17, 18 & 24 May and
2 June 2011
Outcome 12: Requirements relating
to workers Major Concerns
5. 17, 18 & 24 May and
2 June 2011 Outcome 14: Supporting workers Major Concerns
6. 17, 18 & 24 May and
2 June 2011
Outcome 16: Assessing and
monitoring the quality of service
provision
Major Concerns
7. 17, 18 & 24 May and
2 June 2011 Outcome 17: Complaints Major Concerns
8. 17, 18 & 24 May and
2 June 2011
Outcome 19: Notification of death or
unauthorised absence of a service
user who is detained or liable to be
detained under the Mental Health Act
1983
Major Concerns
9. 17, 18 & 24 May and
2 June 2011
Outcome 20: Notification of other
incidents Major Concerns
10. 17, 18 & 24 May and
2 June 2011 Outcome 21: Records Major Concerns
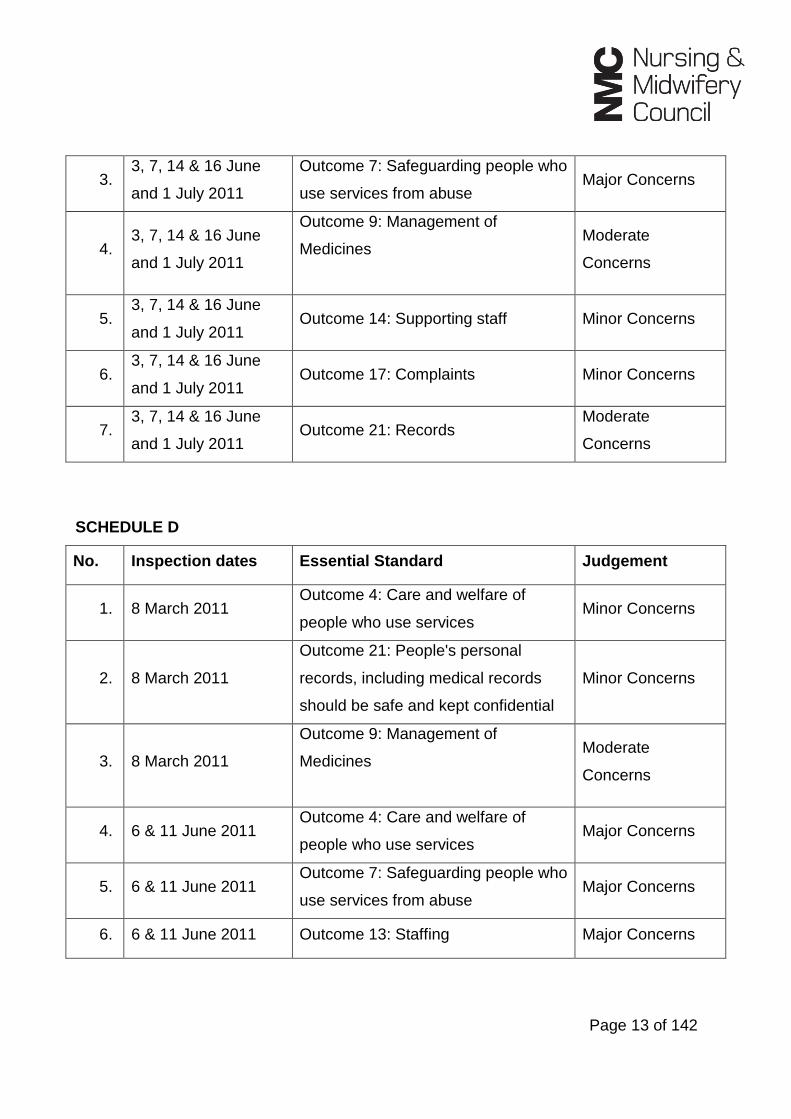
SCHEDULE C
No. Inspection dates Essential Standard Judgement
1. 3, 7, 14 & 16 June
and 1 July 2011
Outcome 1: Respecting and involving
people who use the services Major Concerns
2. 3, 7, 14 & 16 June
and 1 July 2011
Outcome 4: Care and welfare of
people who use services Major Concerns
Page 13 of 142
3. 3, 7, 14 & 16 June
and 1 July 2011
Outcome 7: Safeguarding people who
use services from abuse Major Concerns
4. 3, 7, 14 & 16 June
and 1 July 2011
Outcome 9: Management of
Medicines
Moderate
Concerns
5. 3, 7, 14 & 16 June
and 1 July 2011 Outcome 14: Supporting staff Minor Concerns
6. 3, 7, 14 & 16 June
and 1 July 2011 Outcome 17: Complaints Minor Concerns
7. 3, 7, 14 & 16 June
and 1 July 2011 Outcome 21: Records
Moderate
Concerns
SCHEDULE D
No. Inspection dates Essential Standard Judgement
1. 8 March 2011 Outcome 4: Care and welfare of
people who use services Minor Concerns
2. 8 March 2011
Outcome 21: People's personal
records, including medical records
should be safe and kept confidential
Minor Concerns
3. 8 March 2011
Outcome 9: Management of
Medicines
Moderate
Concerns
4. 6 & 11 June 2011 Outcome 4: Care and welfare of
people who use services Major Concerns
5. 6 & 11 June 2011 Outcome 7: Safeguarding people who
use services from abuse Major Concerns
6. 6 & 11 June 2011 Outcome 13: Staffing Major Concerns

Page 14 of 142
7. 6 & 11 June 2011 Outcome 21: Records Moderate
Concerns
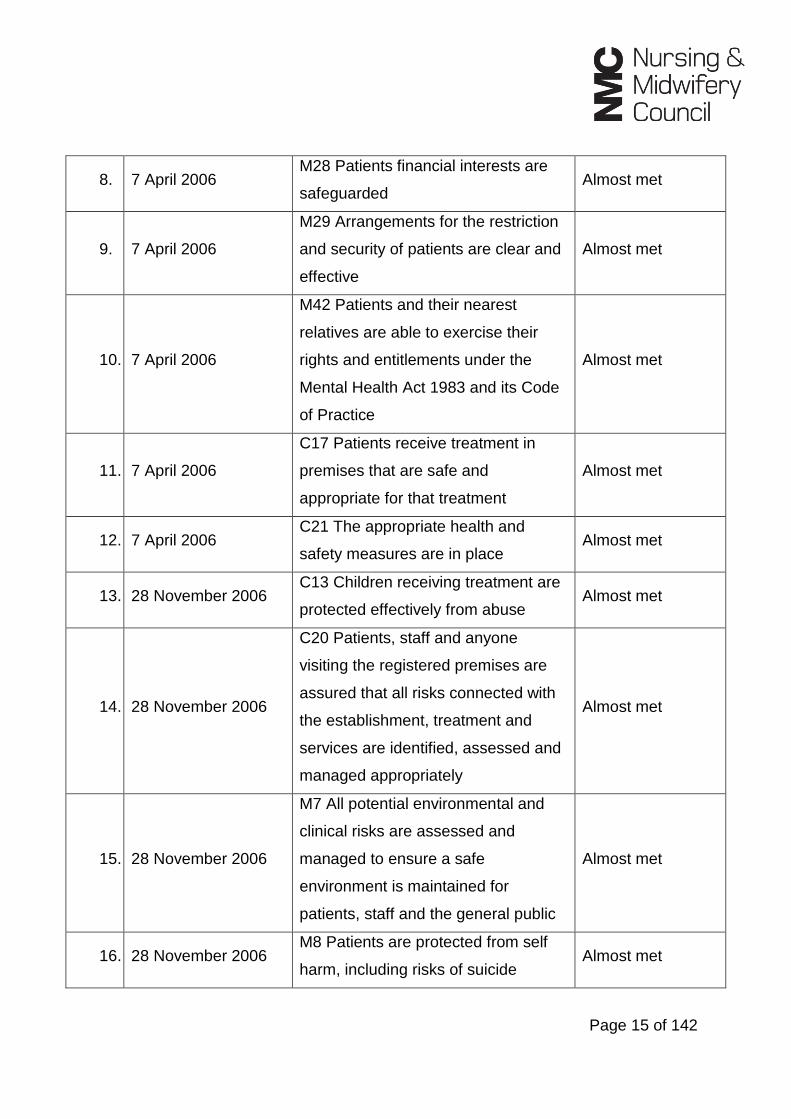
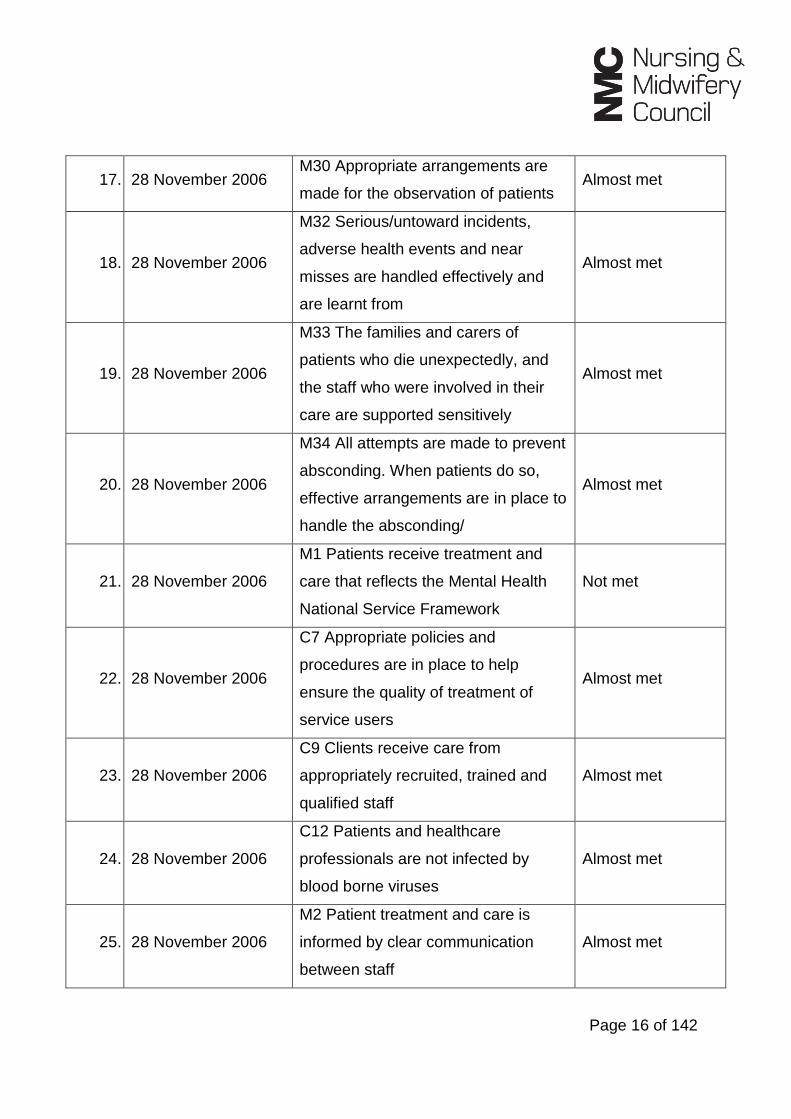
SCHEDULE E
No. Inspection dates Essential Standard Judgement
1. 7 April 2006
C20 Patients, staff and anyone
visiting the registered premises are
assured that all risks connected with
the establishment, treatment and
services are identified, assessed and
managed appropriately
Almost met
2. 7 April 2006
M32 Serious/untoward incidents,
adverse health events and near
misses are handled effectively and
are learnt from
Almost met
3. 7 April 2006 M35 Patients are restrained
appropriately and safely Almost met
4. 7 April 2006
C9 Clients receive care from
appropriately recruited, trained and
qualified staff
Almost met
5. 7 April 2006
M5 The numbers, type and skills of
clinicians ensure that patients are
appropriately treated and cared for at
all times
Almost met
6. 7 April 2006
M13 Each patient has a care plan
that addressed their needs
appropriately
Almost met
7. 7 April 2006 M27 The care provided recognises
the patients' personal needs Almost met
Page 15 of 142
8. 7 April 2006 M28 Patients financial interests are
safeguarded Almost met
9. 7 April 2006
M29 Arrangements for the restriction
and security of patients are clear and
effective
Almost met
10. 7 April 2006
M42 Patients and their nearest
relatives are able to exercise their
rights and entitlements under the
Mental Health Act 1983 and its Code
of Practice
Almost met
11. 7 April 2006
C17 Patients receive treatment in
premises that are safe and
appropriate for that treatment
Almost met
12. 7 April 2006 C21 The appropriate health and
safety measures are in place Almost met
13. 28 November 2006 C13 Children receiving treatment are
protected effectively from abuse Almost met
14. 28 November 2006
C20 Patients, staff and anyone
visiting the registered premises are
assured that all risks connected with
the establishment, treatment and
services are identified, assessed and
managed appropriately
Almost met
15. 28 November 2006
M7 All potential environmental and
clinical risks are assessed and
managed to ensure a safe
environment is maintained for
patients, staff and the general public
Almost met
16. 28 November 2006 M8 Patients are protected from self
harm, including risks of suicide Almost met
Page 16 of 142
17. 28 November 2006 M30 Appropriate arrangements are
made for the observation of patients Almost met
18. 28 November 2006
M32 Serious/untoward incidents,
adverse health events and near
misses are handled effectively and
are learnt from
Almost met
19. 28 November 2006
M33 The families and carers of
patients who die unexpectedly, and
the staff who were involved in their
care are supported sensitively
Almost met
20. 28 November 2006
M34 All attempts are made to prevent
absconding. When patients do so,
effective arrangements are in place to
handle the absconding/
Almost met
21. 28 November 2006
M1 Patients receive treatment and
care that reflects the Mental Health
National Service Framework
Not met
22. 28 November 2006
C7 Appropriate policies and
procedures are in place to help
ensure the quality of treatment of
service users
Almost met
23. 28 November 2006
C9 Clients receive care from
appropriately recruited, trained and
qualified staff
Almost met
24. 28 November 2006
C12 Patients and healthcare
professionals are not infected by
blood borne viruses
Almost met
25. 28 November 2006
M2 Patient treatment and care is
informed by clear communication
between staff
Almost met

Page 17 of 142
26. 28 November 2006
M5 The numbers, type and skills of
clinicians ensure that patients are
appropriately treated and cared for at
all times
Almost met
27. 28 November 2006 M6 Patients receive treatment and
care from appropriately trained staff Almost met
28. 28 November 2006
M23 Patients are informed about their
rights, their treatment and how to
obtain independent advocacy
Almost met
29. 28 November 2006 M26 Patients are not discriminated
against Almost met
30. 28 November 2006
M29 Arrangements for the restriction
and security of patients are clear and
effective
Almost met
31. 28 November 2006
C6 Patients' views are obtained by
the establishment and used to inform
the provision of treatment and care
and prospective patients
Not met
32. 28 November 2006
C17 Patients receive treatment in
premises that are safe and
appropriate for that treatment
Almost met
33. 18 October 2007 C20 Risk Management Policy Almost met
34. 18 October 2007 M7 Risk assessment and
management Almost met
35. 18 October 2007 M8 Suicide prevention Almost met
36. 18 October 2007 M1 Working within the Mental Health
National Service Framework Almost met
37. 18 October 2007 C7 Policies and Procedures Almost met

Page 18 of 142
38. 18 October 2007 C9 Human Resources Policies and
Procedures Almost met
39. 18 October 2007 C12 Healthcare workers and blood
borne viruses Almost met
40. 18 October 2007 M6 Staff Training Almost met
41. 18 October 2007 M13 CPA Care Planning and Review Not met
42. 18 October 2007 C6 Patient views Almost met
43. 18 October 2007 C17 Health Care Premises Not met
SCHEDULE F
No. Inspection dates Essential Standard Judgment
1. 3, 13 & 14 June 2011 Outcome 1: Respecting and involving
people who use the service Major concerns
2. 3, 13 & 14 June 2011 Outcome 2: Consent to care and
treatment Major concerns
3. 3, 13 & 14 June 2011 Outcome 4: Care and welfare of
people who use the service Major Concerns
4. 3, 13 & 14 June 2011 Outcome 7: Safeguarding people who
use services from abuse Major Concerns
5. 3, 13 & 14 June 2011 Outcome 9: Management of medicine Major Concerns
6. 3, 13 & 14 June 2011 Outcome 10: Safety and suitability of
premises Major Concerns
7. 3, 13 & 14 June 2011 Outcome 12: Requirements relating
to workers
Moderate
Concerns
8. 3, 13 & 14 June 2011 Outcome 13: Staffing Major Concerns

Page 19 of 142
9. 3, 13 & 14 June 2011 Outcome 14: Supporting workers Major Concerns
10. 3, 13 & 14 June 2011
Outcome 16: Assessing and
monitoring the quality of service
provision
Major Concerns
11. 3, 13 & 14 June 2011 Outcome 17: Complaints Major Concerns
12. 3, 13 & 14 June 2011 Outcome 21: Records Major Concerns
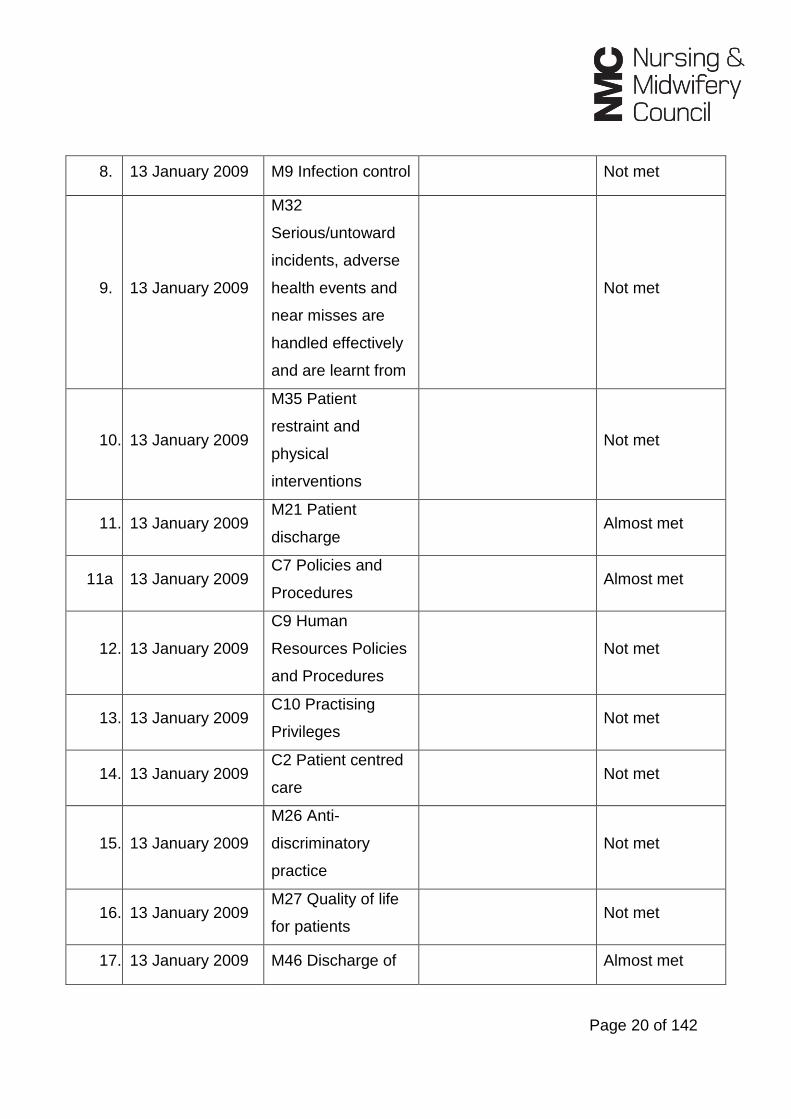
SCHEDULE G
No. Inspection date Standard
Private and
Voluntary Healthcare
Regulations 2001
Assessment
Outcome
1. 27 May 2008
M15 Patients with
Developmental
Disabilities
15(1)(a) Almost met
2. 27 May 2008 M6 Staff training 18(2)(a) Almost met
3. 27 May 2008
M13 CPA Care
Planning and
Review
21(1)(a)(i)(ii) Almost met
4. 27 May 2008 C6 Patient's views 16(3) & 17(2) Almost met
5. 13 January 2009 C20 Risk
Management Policy Not met
6. 13 January 2009 C25 Infection
Control Not met
7. 13 January 2009
M7 Risk
assessment and
management
Not met
Page 20 of 142
8. 13 January 2009 M9 Infection control Not met
9. 13 January 2009
M32
Serious/untoward
incidents, adverse
health events and
near misses are
handled effectively
and are learnt from
Not met
10. 13 January 2009
M35 Patient
restraint and
physical
interventions
Not met
11. 13 January 2009 M21 Patient
discharge Almost met
11a 13 January 2009 C7 Policies and
Procedures Almost met
12. 13 January 2009
C9 Human
Resources Policies
and Procedures
Not met
13. 13 January 2009 C10 Practising
Privileges Not met
14. 13 January 2009 C2 Patient centred
care Not met
15. 13 January 2009
M26 Anti-
discriminatory
practice
Not met
16. 13 January 2009 M27 Quality of life
for patients Not met
17. 13 January 2009 M46 Discharge of Almost met

Page 21 of 142
detained patients
18. 13 January 2009 C17 Health Care
Premises Not met
19. 1 & 2 June 2009 C20 Risk
Management Policy Not met
20. 1 & 2 June 2009
M7 Risk
assessment and
management
Not met
21. 1 & 2 June 2009
M30 Appropriate
arrangements are
made for the
observation of
patients
Not met
22. 1 & 2 June 2009 M31 Managing
disturbed behaviour Not met
23. 1 & 2 June 2009
M32 Management
of serious/untoward
incidents, adverse
health events and
near misses
Not met
24. 1 & 2 June 2009 C4 monitoring
quality Almost met
25. 1 & 2 June 2009 M4 Clinical Audit Not met
26. 1 & 2 June 2009 M20 Transfer of
patients Not met
27. 1 & 2 June 2009 C2 Patient Centred
Care Almost met
28. 1 & 2 June 2009 M13 CPA Care
planning and Almost met
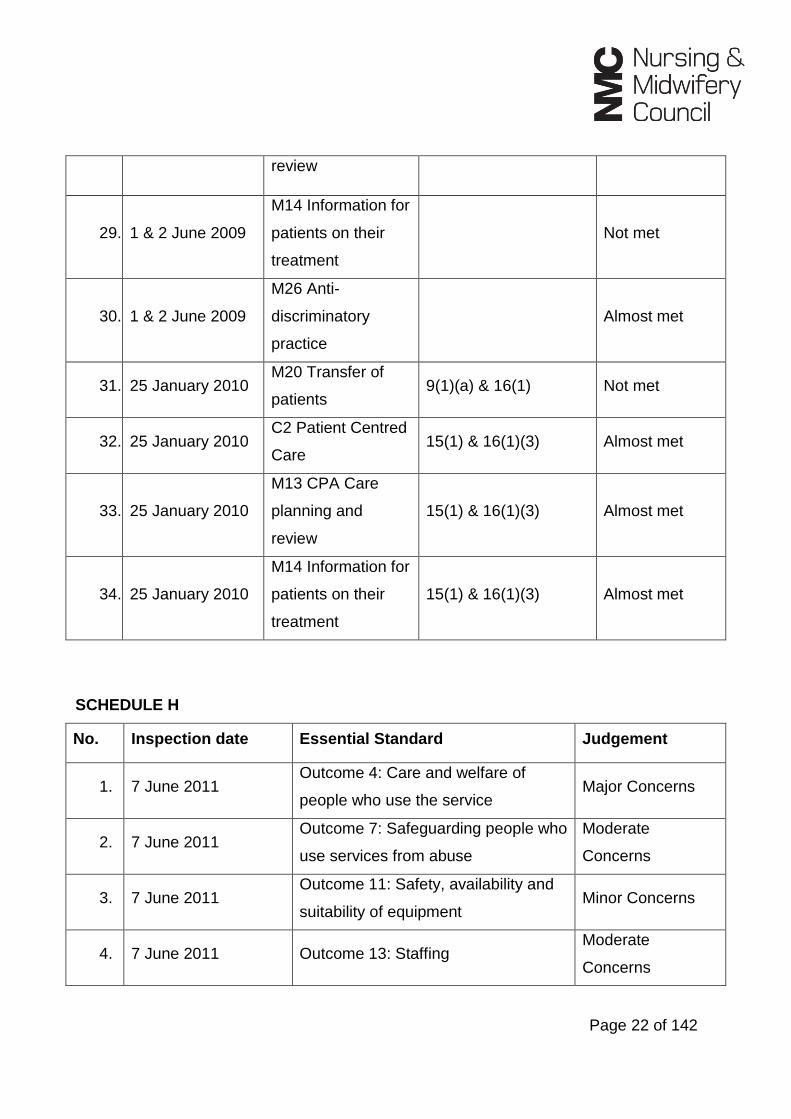
Page 22 of 142
review
29. 1 & 2 June 2009
M14 Information for
patients on their
treatment
Not met
30. 1 & 2 June 2009
M26 Anti-
discriminatory
practice
Almost met
31. 25 January 2010 M20 Transfer of
patients 9(1)(a) & 16(1) Not met
32. 25 January 2010 C2 Patient Centred
Care 15(1) & 16(1)(3) Almost met
33. 25 January 2010
M13 CPA Care
planning and
review
15(1) & 16(1)(3) Almost met
34. 25 January 2010
M14 Information for
patients on their
treatment
15(1) & 16(1)(3) Almost met
SCHEDULE H
No. Inspection date Essential Standard Judgement
1. 7 June 2011 Outcome 4: Care and welfare of
people who use the service Major Concerns
2. 7 June 2011 Outcome 7: Safeguarding people who
use services from abuse
Moderate
Concerns
3. 7 June 2011 Outcome 11: Safety, availability and
suitability of equipment Minor Concerns
4. 7 June 2011 Outcome 13: Staffing Moderate
Concerns

Page 23 of 142
5. 7 June 2011
Outcome 16: Assessing and
monitoring the quality of service
provision
Moderate
Concerns
6. 7 June 2011 Outcome 20: Notification of other
incidents
Moderate
Concerns
SCHEDULE I
No. Inspection date Essential Standard Judgement
1. 8 June 2011 Outcome 4: Care and welfare of
people who use the service Minor concerns
2. 8 June 2011 Outcome 7: Safeguarding people who
use services from abuse
Moderate
concerns
SCHEDULE J
No. Inspection date Essential Standard Judgement
1. 23 June 2011 Outcome 4: Care and welfare of
people who use services Minor concerns
2. 23 June 2011 Outcome 7: Safeguarding people who
use services from abuse Minor concerns
3. 23 June 2011 Outcome 13: Staffing Moderate
concerns
Mr Harrison’s response to the charges – Tuesday 2 May 2017
Mr Unwin informed the panel that Mr Harrison had, during the course of the NMC’s
investigation, submitted two separate written responses to the allegations (dated 19
Page 24 of 142
October 2014 and 10 June 2015). Mr Harrison made admissions to a number of the
allegations in his earlier response, however he denied all the allegations in his later
response.
In those circumstances Mr Unwin did not invite the panel to find any charges proved by
virtue of Mr Harrison’s earlier admissions, as it could not be said that Mr Harrison’s
admissions were unequivocal.
Background – Tuesday 2 May 2017
The background to the allegations was as follows:
Introduction
Winterbourne View was an independent purpose built hospital in South Gloucestershire
which opened in December 2006. It was owned and operated by Castlebeck Care
(Teesdale) Limited (“Castlebeck”). It was designed to accommodate 24 patients in two
separate wards. It was registered as a hospital with the stated purpose of providing
assessment and treatment and rehabilitation for adults with learning disabilities.
On 31 May 2011, BBC Panorama broadcast the documentary “Undercover Care: The
Abuse Exposed” which showed undercover footage by a reporter (Individual R, also
referred to as Witness 2) of staff (Nurses and Support Workers) abusing and mistreating
vulnerable Winterbourne View patients. After the transmission, staff were suspended,
the Care Quality Commission (“CQC”) inspected the Hospital, and patients were moved
to other locations. A Serious Case Review process was initiated. By the end of June
2011, Winterbourne View was closed.

Page 25 of 142
As a result of the police investigation, nine Support Workers and two Nurses involved at
Winterbourne View were prosecuted and convicted in 2012 for 38 offences of neglect
and abuse of patients.
The BBC had been contacted by a whistle-blower, Individual O (also referred to as
Witness 3), formerly a Charge Nurse at Winterbourne View, reporting to Registrant C. In
October 2010, Individual O raised in an email a number of concerns about the attitudes
of staff, the treatment of patients and the aggressive culture at Winterbourne View,
which foreshadowed some of the abuse captured in the documentary. No meaningful
action had been taken to address any of the concerns.
The four registrants in this case had management responsibilities in respect of
Winterbourne View during the time that abuse and mistreatment of patients was
undoubtedly taking place. Registrant A, a Senior Manager, was the Acting Manager,
then Registered Manager, of Winterbourne View from 2008 until 2010, and reported to
Mr Harrison. In 2010, Registrant A moved to act as Manager of another Home but
continued to offer support to Registrant C, who was appointed Manager of
Winterbourne View. Registrant A, however, remained the Registered Manager of
Winterbourne View with the CQC. Registrant D was appointed as Deputy Manager from
June 2010, reporting to Registrant C. Registrant C reported to Mr Harrison, the
Regional Director of Operations for South West England, who from 2009 had
responsibility for nine Castlebeck Units.
Reports and reviews of the systemic failures at Winterbourne were authored or
commissioned by Castlebeck, CQC, NHS South Gloucestershire Primary Care Trust (in
coordination with other involved Primary Care Trusts (“PCT”)) and Avon and Somerset
Police. Other Department of Health and agency reports also followed from the
Panorama broadcast.

Page 26 of 142
Of particular relevance to this hearing were the CQC Compliance Report published in
July 2011 and the Serious Case Review, commissioned by the South Gloucestershire
Adult Safeguarding Board, published in July 2012.
Many of the failings at Winterbourne View were a matter of record. It was not alleged by
the NMC that any of the registrants in this case played a direct role in the abuse or
mistreatment of patients. Nor was it alleged that they directly witnessed or necessarily
knew the full extent of the abuse that was occurring on their watch. The Panorama
documentary evidenced, for example, falsified reporting of restraint events by staff. The
Serious Case Review explored the complexity of the causes of, and failures to, prevent
institutional abuse of adults with learning difficulties.
The charges against the four registrants were intended to reflect actions and omissions
by them in their respective roles, in positions of responsibility as members of the senior
nursing and management team. These included issues around the recruitment,
management and disciplining of staff; training and supervision; the investigation and
reporting of incidents; and the lack of proactive steps to recognise and reduce the
excessive use of restraint. A number of allegations were brought to the attention of the
registrants, involving the individuals subsequently proven to be perpetrating abuse. In
several instances the responsibility was joint. The NMC alleged that these actions and
omissions were liable to contribute to missed opportunities and the failure to protect
vulnerable patients from harm.
Two registrants, Registrant A and Mr Harrison, faced charges in relation to their
responsibilities for other Castlebeck Units where there were management and
operational failings, some with similarity to those at Winterbourne View.
Before taking over as Acting Manager at Winterbourne View, Registrant A was the
Manager of Arden Vale, a Castlebeck learning disabilities hospital in Coventry. A
Healthcare Commission inspection report from October 2007 identified a number of
Page 27 of 142
shortcomings. After the BBC Panorama documentary, Individual Z (also referred to as
Witness 8), who had worked for a short time at Arden Vale while Registrant A was
Manager, contacted the helpline number with concerns she had raised at the time with
the then Manager about the frequent and unnecessary resort by staff to restraint of
patients.
From October 2010 Registrant A, although still the CQC Registered Manager for
Winterbourne View, became Acting Manager for Chesterholme, another Castlebeck
hospital in Northumberland. The CQC inspection in June 2011 identified major or
moderate concerns with eight essential standards.
When the abuse at Winterbourne View came to light, the CQC carried out reviews and
inspections of all the other Castlebeck services in England. Of the nine Units for which
Mr Harrison had responsibility, two were closed: Arden Vale and Rose Villa. Major
concerns were found with two: Croxton Lodge and Cedar Vale. Minor and moderate
concerns were identified with another two: Willow House and Warwick Lodge (the East
Midlands Centre for Neurobehavioural Rehabilitation).
Castlebeck Ltd
Castlebeck was registered with Companies House in 1986 and the Headquarters were
in Darlington. It was a specialist provider of healthcare and support for people with
learning disabilities, complex needs and behaviours that challenged services. It also
offered specialist support for people with mental health needs, people on the autistic
spectrum with and without a learning disability, and for people with acquired brain
injuries with associated challenging behaviour.
Castlebeck provided services in locations in the Midlands, North East England and in
Scotland. Winterbourne View and Rose Villa were the only two services that the
company had in the South West of England.

Page 28 of 142
Castlebeck went into administration in 2013 and its services were taken over by the
learning disability provider, the Danshell Group (“Danshell”).
Winterbourne View Hospital
Winterbourne View was a purpose built independent hospital in South Gloucestershire,
located in a business park in the northeast of Bristol. It was registered as a hospital with
the purpose of providing assessment and treatment and rehabilitation of people with
learning disabilities, many of whom had additional complex needs such as mental
health problems or conditions such as epilepsy or autistic spectrum disorders.
The people placed there were NHS patients, who were admitted through one of three
principal routes:
a. The patient had acute mental health needs which could not be met by local NHS
inpatient services, whether because they were assessed as too vulnerable,
challenging or otherwise unsuitable.
b. The patient had a learning disability but their mental health needs or challenging
behaviour meant they could no longer remain within their existing social care
service.
c. The patient was already placed in a specialist hospital but were being moved
closer to home, as a step down or step up in care, or as a court requirement.
During its five years of operation, services were commissioned at Winterbourne View for
48 patients, involving nine PCTs; 35 of these patients were admitted under a provision
of the Mental Health Act. Of the 13 admitted informally, six were detained following their
admission.

Page 29 of 142
The majority of patients were under the age of 50, with an equal number of men and
women. The average length of stay was 19 months. 13 admissions lasted for under six
months, but eight patients were at the Hospital for over three years, of whom two were
there for over four years. Some patients had particularly high care needs; for example,
Patient H who was admitted at an early stage, was only able to move one arm and her
head, and she required constant care. She could make sounds but was not able to
speak.
There were eighteen patients at the Hospital during the BBC Panorama filming.
Layout
The Hospital comprised three floors: Lower Ground, Upper Ground, and First. These
were variously referred to by witnesses as ground, middle and top, or first, second and
third.
On the Lower Ground Floor were the entrance, reception and public area, consultation
rooms, office shared by the Manager and Deputy Manager, the administrative team
office, kitchen and laundry.
The patient floors were accessed via a stairway near reception on the ground floor.
However, visiting family members (for example, Patient D’s mother, also referred to as
Witness 12), at some time, were told they were not allowed to visit the patient floors.
The Upper Ground Floor contained 12 patient bedrooms. This was considered as a
rehabilitation ward, intended for patients who might be considered ready for transition
back into the community. It was referred to by some patients as the ‘moving on’ ward.
Near the stairs were the dining room, a quiet lounge, an education room and activity
room. There was a medication room, which was locked when not in use. At the end of
the corridor, at the junction of the T-shaped layout, were a nursing office and a larger
Page 30 of 142
patient lounge, which opened to the garden area. The visibility of the patient floors from
the nursing office window was described as not particularly good.
The First Floor was a secure ward requiring a code or key to access, sometimes
referred to as the ‘Assessment Floor’, for patients requiring additional support and
assistance. Although the intention was that patients, after assessment, would move
down for rehabilitation and ultimately out of the service, in practice there were patients
who remained in Winterbourne View for years. The layout was similar to the Upper
Ground, with a dining room, activity room and quiet lounge near the stairs, and the
nursing office and lounge at the junction of the two corridors.
The patient lounges were the main focus for the patients, where they spent most of their
time during the day. They featured in the undercover footage.
Staffing and Organisation
Winterbourne View was intended to be a learning disability nurse-led service. The
Psychiatrist reported to the Clinical Director and had no management responsibility for
any of the staff working directly with patients.
Medication for all patients was prescribed by the local GP, and prescriptions dispensed
by the local pharmacy. Nurses were to complete the medicines administration record
sheets prepared by the Psychiatrist when they administered the medications.
Support Workers (also known as Healthcare Assistants) were responsible to the Nurse
in charge. Their duties were to support patients in developing daily living skills, follow
individual patient care regimes, maintain relevant documentation, and act as a Key
Worker when required or an escort for activities. They were required to be aware of
health and safety and safeguarding issues, and to bring all incidents to the attention of
the Nurse in charge.

Page 31 of 142
There were usually between three and five Support Workers on duty per floor, including
one Senior Support Worker. Staffing numbers would vary and sickness and
absenteeism was relatively high. Staff turnover was particularly high.
There would be one or sometimes two Nurses on duty per floor. Nurses mainly saw
each other during handover, for about 15 minutes at the start of the new shift. Many
staff members worked long shifts with day shifts running from 08:00 to 20:00 and night
shifts from 20:00 to 08:00. Witnesses suggested that Nurses would spend a lot of their
time in the office completing paperwork and dealing with medication.
Nursing staff reported to the Charge Nurses who were expected to have Registered
Nurse Learning Disability/Registered Nurse Mental Health qualifications. Charge Nurses
were responsible for the provision of nursing care, assessment of risk and care needs,
as well as all aspects of record keeping. Their responsibilities included assisting with the
induction of new staff; line managing Nurses; and a responsibility to escalate issues of
inappropriate attitudes or conduct by staff. The Charge Nurses were accountable to the
Manager and the Deputy Manager.
The Registrants
Registrant A was employed by Castlebeck as Senior Manager for the Midlands/South
West region. As Senior Manager she had responsibility, together with Mr Harrison, for
the delivery of care services and setting and maintaining acceptable operational
standards.
There was a pattern of Registrant A stepping in as Hospital Manager in different
locations, where failings had been identified. Prior to 2008 she was the Manager of
Arden Vale. She became Acting Manager of Winterbourne View in June 2008 following
an internal investigation into practices under the previous Manager, Individual AA, and
Page 32 of 142
Deputy Manager, Individual BB. Registrant A was formally registered as Manager of
Winterbourne View with the CQC on 5 May 2009. She remained the formally Registered
Manager until the closure of Winterbourne View in June 2011. However, she ceased to
act as the Unit Manager from January 2010 when Registrant C took on the role.
Registrant C had been employed as a Senior Staff Nurse at Winterbourne View from
January 2008 having previously worked as a Manager for the NHS. He was promoted to
Charge Nurse, and then to Deputy Manager, under Registrant A. He became the
Hospital Manager from January 2010 until his suspension after the Panorama
broadcast.
Between January 2010 and October 2010 Registrant A regularly visited Winterbourne
View and retained responsibility for supporting and supervising Registrant C, although
Registrant C had a formal reporting line to Mr Harrison. Registrant C commented in his
disciplinary hearing that he would call Registrant A if he had a problem. From October
2010 to February 2012 Registrant A was Acting Manager of Chesterholme and her line
management arrangements transferred from Mr Harrison to another Regional
Operations Director.
Registrant D was the Deputy Manager of Winterbourne View from June 2010 until May
2011, reporting to Registrant C. Registrant D became a Registered Nurse in 2004 and
this appeared to have been her first formal management position. The Castlebeck job
descriptions for Manager and Deputy Manager were almost identical. Both were
required to have Registered Nurse Learning Disability/Registered Nurse Mental Health
registration and a Registered Manager’s award. They were expected to be conversant
with relevant external requirements such as the CQC. Each was responsible for the
provision of nursing care, the coordination and distribution of staffing and other
resources. Registrant D was also responsible for dealing with any deficiencies in service
provision.

Page 33 of 142
The evidence suggested that Registrant D assumed particular responsibility for incident
forms, raising alerts and reporting on Serious Untoward Incidents (“SUI”). Witnesses
suggested that neither Registrant C nor Registrant D were proactive in spending time
on the patient floors. During his five weeks of filming, Individual R identified two
occasions on which Registrant D briefly attended the patient floors, on each occasion
when someone called down for a Manager’s assistance with a restraint. Registrant D
played a role in ongoing safeguarding procedures after the BBC documentary was aired
and was not subject to internal disciplinary proceedings.
Mr Harrison was the Castlebeck Regional Operations Director, responsible for nine
Castlebeck Units from 2009. The job description for Regional Operations Director
included ensuring that all Units complied with all appropriate statutory standards and
requirements as regulated by CQC (and others). He registered as Responsible
Individual for Arden Vale in 2005. Although he did not register as Responsible Individual
for Winterbourne View until February 2009, his responsibilities as Regional Operations
Manager, prior to 2009, were almost identical. In his Castlebeck interview he confirmed
that he was responsible for Winterbourne View at the time Registrant A was brought in
as Manager (June 2008). Mr Harrison usually visited Winterbourne View about once a
month. He stated that he was kept informed of serious incidents at Winterbourne View.
Mr Harrison also stated that the position of Responsible Individual for the Units was
taken over by the Managing Director, Individual CC, in 2010; however, he confirmed
that his remit remained to support the Managers of these Units. He was, according to
Castlebeck Human Resources (“HR”), the most senior member of staff with direct
responsibility for the nine Units, with responsibility to supervise, guide, support and
manage operational practices at a senior level, and ensure compliance with regulatory
standards. Mr Harrison was the CQC Registered Responsible Individual from 16
February 2009 onwards.
Winterbourne View: Charges

Page 34 of 142
Given the number of sub-charges against the registrants, the facts were grouped under
the following headings for the purpose of the NMC’s opening submissions:
Healthcare Commission Inspections 2008-2009 (Registrant A charges 2.1, 2.4; Mr
Harrison charges 1.1, 1.2, 1.4)
By June 2008 Registrant A was a Senior Manager and the Acting Manager responsible
for Winterbourne View. Mr Harrison had responsibility as the Regional Operations
Manager/Director.
On 1 December 2008 the Healthcare Commission completed an unannounced
inspection of Winterbourne View. A number of the Healthcare Commission national
minimum standards were not met, including concerns about ligature risks, signing for
controlled drugs, record keeping, training and appraisals. Following the inspection two
statutory notices were issued in relation to Health and Safety Measures and Health
Care Premises.
The Healthcare Commission completed a follow up inspection in March 2009 in order to
inspect the standards which had not been met during the previous inspection. The
Healthcare Commission were unable to inspect all of the standards due to patients
presenting with challenging behaviour. However, standards re-inspected were still not
being met and Winterbourne View was required to provide an action plan. There was no
record of this action plan being submitted.
The CQC conducted an announced inspection on 15 December 2009. There were
concerns about controlled drugs procedures and staff training.
Registration of Registrant C as Manager (Registrant A charge 2.7; Registrant C charges
5, 6; Mr Harrison charge 1.5)

Page 35 of 142
All of the registrants were required to be aware of regulatory requirements. The CQC
should have been notified of the new management arrangements at Winterbourne View
in January 2010. However, an application to register Registrant C as Manager was not
received until April 2011. The CQC replied stating that further documentation was
required for the application to be accepted. Registrant A was unable to register as
Manager of Chesterholme because she was still the Registered Manager of
Winterbourne View. In an email dated 5 May 2011 Individual CC asked Mr Harrison if
he had advised the CQC that Registrant A was no longer the Manager at Winterbourne
View. Mr Harrison replied that they had only been informed verbally at their last visit
(although this appeared to have been before Registrant C was appointed). Mr Harrison
said that sending the appropriate written notification had “completely slipped my mind”.
Registrant A was also the Accountable Officer under the Controlled Drugs Regulations.
Registrant C should also have applied to be appointed as the Accountable Officer.
Individual O’s whistle-blowing email (Registrant A charge 2.8; Registrant C charge 16;
Registrant D charge 4; Mr Harrison charge 1.6)
It was the NMC’s case that all four registrants were aware of the contents of the whistle-
blowing email sent by Individual O, which raised some 20 concerns about the culture
and treatment of patients including serious allegations about members of staff
subsequently shown to be involved in the abuse in the Panorama documentary. The
email was sent directly to Registrant C. Registrant D had a copy of the email in a senior
staff meeting a few days later. Individual O forwarded the email to Registrant A who
replied and forwarded it to Mr Harrison saying “this man is not going away. I will see him
Monday”. This meeting did not take place. Registrant C contacted SGC the following
month but “didn’t think there were safeguarding issues”. Around this time Individual O
resigned. The first meeting with Mr Harrison, Registrant C, the CQC and SGC was not

Page 36 of 142
until February 2011. Alerts were not raised until April 2011 and there was no SUI until
May 2011.
It was the NMC’s case that Registrant C should have considered suspending any of the
named staff. Registrant A and Mr Harrison should have provided Registrant C with
guidance and supervision to ensure that the issues were dealt with in a robust manner
and that appropriate action was taken to protect patient safety. Registrant C said in his
police interview that he was waiting for the Company to take the lead. Both Registrant A
and Mr Harrison sought to blame Individual O for not taking action, in their investigatory
interviews.
Suitability for admissions and staffing levels (Registrant C charges 18, 35, 41; Mr
Harrison charge 1.7)
Registrant C was responsible as Manager for ensuring appropriate staffing levels and
allocation of resources.
Individual T (Witness 10) recalled that she was placed on a night shift during her
preceptorship as the only Nurse on duty when she should have been supervised. She
further noted that Patients G, H and M, who were funded on a 2:1 or 1:1 basis, were not
in fact observed on that basis as there was insufficient staff.
The responsibility for admitting patients to Winterbourne View was with the Manager of
the service and Mr Harrison. Registrant C and Mr Harrison were aware of the difficulties
with staffing, resourcing and training, and the limitations of the service that
Winterbourne View was able to provide. Among the patients admitted when Registrant
C was Manager was Patient A, who needed 1:1 supervision as she would hit staff and
other patients. She would scream and cry and spit and, in the view of Witness 9,
needed to be looked after by staff with specialist training. Patient M had particularly
challenging behaviour, including faecal smearing and biting herself and staff. She

Page 37 of 142
needed 1:1 supervision at all times and had her meals separately. Patient F, who
featured in the BBC Panorama documentary, was also admitted when Registrant C was
Manager.
Registrant C said, in his interview, that he wanted to stop admissions and was not
satisfied that Patient F was suitable for Winterbourne View. He said that he had only
agreed to her admission under corporate pressure. There was no record of Registrant C
raising the issue in the minutes of regional meetings.
Mr Harrison stated, in his interview, that he was aware there were staffing issues,
especially in respect of enhanced observation levels. He said that he had requested
extra staff from Individual CC but that, when granted, it led to an increase in patient
numbers. Mr Harrison said he was not aware that Registrant C had refused to admit
patients due to staffing levels.
Staff training, supervision and induction (Registrant A charges 2.9, 2.10, 2.11;
Registrant C charges 37, 38, 42, 43; Registrant D charges 19, 20; Mr Harrison charges
1.8, 1.9)
Staff training was identified as out of date when Witness 19 attended in 2008, and in the
Healthcare Commission inspection report under the management of Registrant A.
The 2011 CQC inspection report identified numerous shortfalls in staff achieving training
requirements. It was the view of staff that there was insufficient specialist training for
patients with learning disabilities and mental health issues.
Individual H (Witness 11), Individual T and Individual O considered that the local
induction was inadequate and did not include specific information on how the Unit was
managed and the patients’ individual needs or care plans.

Page 38 of 142
The Castlebeck Supervision Policy required regular supervision of individual members
of staff with six sessions per year. The CQC inspection of staff records identified limited
or no supervision records for most staff. Annual medication competency checks had not
been completed at the time of inspection.
Analysis of incidents, excessive restraint, protection from abuse (Registrant A charges
2.11, 2.12, 2.13; Registrant C charges 40, 45, 46; Registrant D charges 23, 24; Mr
Harrison charges 1.10, 1.11, 1.12)
The ‘MAYBO’ training received by staff focused on restraint techniques, rather than de-
escalation and avoidance strategies. The numerous incident, alerts, and concerns
raised by Individual O and others, should have alerted members of the management
team that restraint was being resorted to far too readily and excessively by staff on the
patient floors. Incident reports recorded inappropriate methods, such as a patient being
restrained with a pillow over her mouth. Incident reports were provided to the
management team, but there was no recording or analysis of incidents to identify
whether there were patterns or high risk times of day. Individual O recalled that he
received a dismissive response from Registrant A when he suggested this.
The CQC inspection found that incidents in the daily care records did not correspond
with the incident reports. There was no analysis of the necessity and frequency of
restraints. The incidents summarised in the Serious Case Review and as depicted in the
Panorama footage demonstrated the failure to protect patients from abuse.
Arden Vale
Arden Vale was a purpose-built 31 bed hospital situated on the edge of Coventry, for
patients with a learning disability and challenging behaviour. Mr Harrison was the
Responsible Individual for Arden Vale from the time of its opening in October 2005.

Page 39 of 142
There was an unannounced inspection by the Healthcare Commission and the Mental
Health Act Commission in April 2006. 12 standards were ‘almost met’ and
recommendations were made.
The next unannounced inspection was on 28 November 2006. That inspection found
that not every employee had received safeguarding training; incidents were not being
reported in writing to the Commission; and staffing files did not reflect guidelines in
place at the time. 20 standards were ‘almost met’ or ‘not met’. Recommendations were
made and an action plan submitted.
According to Castlebeck HR, Registrant A was the Manager of Arden Vale from May
2007 until June 2008 (Items 1-32 of Schedule E did not therefore apply). She formally
became Registered Manager of Arden Vale in October 2007. There had previously
been a number of temporary Managers in place. The Healthcare Commission
conducted an unannounced inspection on 18 October 2007. 11 standards were ‘almost
met’ or ‘not met’ including issues not addressed from previous reports. There were no
local protocols and procedures on the prevention of suicide and homicide, as there
should have been. Fewer than 25% of staff had received an appraisal and not all staff
had received mandatory training.
Individual Z worked at Arden Vale for three weeks from the beginning of October 2007.
She was alarmed at the frequency of restraints being used. Staff informed her that they
were not aware of behavioural techniques and made inappropriate comments about
how they would respond to patients’ behaviour. She witnessed unnecessary restraints
during the time she was at Arden Vale. She also noted a common practice of staff
borrowing medication from another patient when a patient’s medication ran out.
Individual Z raised her concerns with the Deputy Manager and asked to see the
Manager. She wrote, and provided, a report of her concerns. She could not recall the

Page 40 of 142
name of the Manager; she said that this Manager had been brought in recently to get
Arden Vale ‘back into shape’: It could thus be reasonably inferred this was Registrant A.
Although Individual Z was told her concerns would be treated with the highest
importance, she was not provided with any information following the concerns she
raised. She asked to be transferred and then resigned because of her experiences at
Arden Vale.
There was a Healthcare Commission inspection of Arden Vale in 2009 (not in
evidence). Arden Vale remained within Mr Harrison’s responsibility.
Multiple concerns and incidents were brought to the attention of the CQC in the lead up
to the next inspection on 3 June 2011. From that visit, the CQC’s concerns were that
there was a closed regime with a culture of putting the needs of staff before the needs
of patients; relatives and commissioners were not given access to the patient floors;
incidents were not always recorded or reviewed; and inexperienced staff were working
long shifts in a challenging environment. There was a further visit which included a
review of staff files. The report published in July 2011 found major concerns with a wide
range of outcomes, including that patients did not experience safe and effective care,
and were not safeguarded from physical and emotional harm; that complaints were not
listened to; and that restraint was not proportionate. The Compliance Inspector, Witness
24, concluded that the abusive and detrimental regime at Arden Vale was significantly
related to management failures.
Following another inspection on 15 August 2011, all patients were moved to other
accommodation and Arden Vale was closed on 25 August 2011.
Rose Villa

Page 41 of 142
Rose Villa was registered as a nine bed care home with nursing for accommodation,
treatment and diagnostic procedures. It opened in Autumn 2009 and was not registered
to take detained patients. It was frequently used as a ‘step down’ facility for patients
from Winterbourne View. The CQC visited on five dates in June and July 2011.
Many essential standards were not being met. There were major concerns that the
Home operated a strict and controlled environment which was not respectful of patients’
individual needs. Furthermore, care was not person-centred and appropriate action had
not been taken following serious incidents. A warning notice was issued.
In September 2011 a further inspection of Rose Villa was completed. There were major
and moderate concerns with the outcomes reviewed. It appeared that there had been a
lack of communication between the Acting Manager and the Operations Director to
ensure a management presence on site so that patients and staff felt supported. Rose
Villa was subsequently closed by Castlebeck.
Croxton Lodge
Croxton Lodge was a learning disability hospital in Melton Mowbray which opened in
January 2007. It provided assessment, treatment and rehabilitation to adults with
learning disabilities, mental health needs and substance abuse problems. Mr Harrison
was registered as the Responsible Individual.
In a routine inspection in March 2011, only minor concerns were identified by the CQC.
However, in view of the incidents at Winterbourne View, further visits were conducted in
June 2011. There were major concerns in respect of a number of outcomes. Care plans
were out of date and conflicted with risk assessments. An unnecessary and
inappropriate restraint was witnessed. Nothing was done to review the information in
incident and accident forms. There were concerns about staffing and observation levels.

Page 42 of 142
A warning notice was issued. A follow up review was conducted on 5 September 2011
and the Unit was found to be compliant. The hospital is now operated by Danshell.
Cedar Vale
Cedar Vale was a 16 bedded hospital near Nottingham which opened in December
2004. It provided care to men with learning disabilities and autistic spectrum disorders.
In a Healthcare Commission inspection in May 2008, a number of standards were found
not to be met. A follow up inspection was conducted in January 2009, by which time
safeguarding concerns had been raised. The report found breaches of the following
regulations: not ensuring patients; privacy and dignity, poor standards of cleanliness
hygiene and maintenance of the building; failures in documentation; recording and
notification of serious incidents; and failure to achieve regular staff appraisals. A
statutory enforcement notice was sent to Mr Harrison as the Responsible Individual.
In a follow-up inspection in June 2009 a number of improvements were noted but the
hospital was still not meeting standards. Some standards were still not being met in the
following inspection in January 2010.
Cedar Vale was inspected in June 2011 as a result of the issues at Winterbourne View.
A number of moderate and minor concerns were identified, which included a concern
over staff following reporting procedures; the level of staffing support for outside
activities; and notifiable incidents that were not reported to the CQC. A warning notice
was issued, and in the follow up inspection in September 2011, the Unit was compliant.
Willow House
Willow House was a small residential home providing care and accommodation for up to
eight people with a disability. It opened in December 2006. It was inspected in June

Page 43 of 142
2011 and there were minor and moderate concerns in relation to two outcomes. The
major concern was that the service was implementing punitive measure, such that
patients were punished for displaying challenging behaviour rather than supported and
encourage for positive behaviour. The service was compliant with these outcomes in the
follow up inspection in November 2011.
Warwick Lodge
The East Midlands Centre for Neurobehavioural Rehabilitation (“Warwick Lodge”),
which opened in the summer of 2010, was a hospital providing a service for people who
had an acquired brain injury. It was inspected by the CQC in June 2011. There were
minor concerns about care records and training in restraint techniques. There were
moderate concerns about staffing levels given the high dependency needs of the
patients.
Determination on admissibility of evidence – Tuesday 2 May 2017
Ms Norris, on Registrant D’s behalf, raised an objection to the NMC seeking to put
before the panel, as part of its case, the BBC Panorama documentary “Undercover
Care: The Abuse Exposed”. She contended that viewing the documentary in this
substantive hearing would be highly prejudicial to all the registrants involved in this
case, who were not in fact seen in the footage at all. She submitted that, in cases of
abuse, it was ‘human nature’ to “look for someone to blame”; she expressed concern
that that ‘someone’ could be Registrant D.
Ms Norris argued that the documentary, which showed “horrific abuse”, made for
“deeply disturbing” viewing and did not take matters any further. She contended that the
documentary did not provide a balanced perspective of Winterbourne View, nor did it
depict instances of care that benefitted patients.
Page 44 of 142
Ms Norris went on to submit that the documentary demonstrated “a criminal conspiracy”
in which staff members were working together to abuse patients and conceal that
abuse. She argued that the management team were reliant on staff members correctly
recording incidents in incident forms.
Ms Norris submitted that the Serious Case Review summarised events as depicted in
the footage in any event and, thus, there was no need for the documentary to be
viewed.
Mr Unwin submitted that this was a professional panel, able to put aside any emotive or
prejudicial effect of watching the documentary. He submitted that the documentary
provided a far better understanding of conditions at Winterbourne View than that which
could simply be gleaned from reading summary descriptions. He further submitted that
the documentary provided “important” and “valuable” evidence as regards incidents that
took place at the time in contrast with information contained in incident forms and other
documentation before the panel.
Mr Unwin contended that the documentary was relied upon by the NMC in support of
specific allegations, for example the incident involving Patient F on 3 March 2011
(charge 24 as against Registrant C), the manner in which that incident was reported,
and whether the incident was reviewed. He further contended that there were particular
staff members, featured in the documentary, who formed the subject matter of specific
charges faced by all four registrants. The significance of this, he submitted, would be
made plain when the documentary was viewed. He went on to submit that the abuse
highlighted in the documentary spoke directly to the charges that related to the
widespread use of restraint and abuse; in that regard, he argued that the documentary
was the best available evidence of what had taken place in Winterbourne View at the
time and the staff members involved.

Page 45 of 142
As regards the relevance of the documentary, Mr Unwin submitted that it not only
depicted incidents of abuse and inappropriate restraints, it also provided an insight into
the importance of reviewing incident forms, and the degree to which management were
responsible for ensuring that such forms represented an accurate and satisfactory
account of what had taken place.
Mr Unwin made plain that it was not the NMC’s case that the registrants involved in this
case had witnessed the restraints/incidents depicted in the footage. He further
submitted that the documentary was not the sole and decisive evidence in respect of
any of the charges, nor was it required in order for the panel to adjudicate upon the
charges. That said, he submitted that it was relevant in understanding why the events
as shown in the footage were investigated and what in fact was taking place in
Winterbourne View at the time; in that regard, he submitted that it was key in
considering the extent to which the events were attributable to management failings, or
rather were the actions of unsupervised staff members. He further submitted that the
documentary depicted an incident, arguably of assistance as suggested by Ms Norris,
where a Support Worker had advised a colleague on how to complete an incident form
in order to conceal the true nature of the incident. To that extent, he submitted that the
footage was not disadvantageous to the registrants.
As regards any prejudicial effect of viewing the documentary, Mr Unwin informed the
panel that it was the NMC’s intention to present the documentary early on in the facts
stage of this hearing, as opposed to immediately prior to the panel deliberating on the
facts. In that regard, he submitted that the panel would have been presented with all the
evidence upon which the NMC sought to rely, and thus in possession of all the relevant
evidence, prior to its deliberations.
In reaching its decision on the application the panel considered the submissions of both
advocates. It accepted the advice of the legal assessor, who referred to Rule 31 of the
Rules:

Page 46 of 142
Evidence
31.—(1) Upon receiving the advice of the legal assessor, and subject only to the
requirements of relevance and fairness, a Practice Committee considering an allegation
may admit oral, documentary or other evidence, whether or not such evidence would be
admissible in civil proceedings (in the appropriate Court in that part of the United
Kingdom in which the hearing takes place).
The legal assessor further advised the panel that, as regards relevance, it was not the
NMC’s case that the documentary directly depicted management failings; rather, the
panel was being invited to infer that as instances of abuse had taken place, it must give
rise to management failings. It was, he advised, a matter for the panel to determine
whether this satisfied the “robustness” of the requirement of relevance.
The legal assessor also advised the panel to give careful consideration to the prejudicial
effect, if any, of viewing the documentary in respect of its consideration of the specific
allegations, the risk being that it may result in the panel reaching wrong conclusions in
this case.
As to the matter of relevance, the panel was mindful that the BBC Panorama
documentary was in fact the ‘starting point’ in this case; it was as a result of the
documentary that abuse at Winterbourne View was uncovered and subsequent
investigations undertaken. The panel took into account that the documentary was not
the sole and decisive evidence in respect of the allegations; rather, it provided useful
context as regards the working environment at the time, in addition to identifying specific
instances of abuse and particular staff members, which form the subject matter of some
of the allegations. The panel was mindful that the registrants did not have sight of the
documentary prior to it being aired; they thus relied on information provided by staff
members, upon which management decisions were based.

Page 47 of 142
The panel was satisfied, on the basis of the above, that the requirement of relevance
was met.
The matter for particular consideration was, therefore, the issue of fairness. This is an
experienced and professional panel. It considered that any unfairness, or prejudicial
effect of the documentary, would be mitigated by its duty to assess the evidence
appropriately and by its ability to attach what weight it deemed appropriate to the
footage. The panel was further satisfied that this course of action would accord with the
public interest in ensuring that the evidence in this case was explored fully.
Accordingly, the panel rejected Ms Norris’ application and thus determined to admit the
BBC Panorama documentary into evidence.
Determination on submission of offering no evidence in respect of charge 1.3 –
Wednesday 3 May 2017
On Tuesday 2 May 2017, after the charges were formally read into the record, Mr Unwin
informed the panel that the NMC did not intend to offer any evidence in respect of
charge 1.3 against Mr Harrison. He explained that this charge was relevant to
Registrant C who, it was the NMC’s case, ought to have applied to register with the
CQC as the Accountable Officer. Thus, the NMC did not seek to pursue this allegation
against Mr Harrison. Mr Unwin informed the panel that this proposed course of action
had been communicated to Mr Harrison.
For the purpose of expediency and efficient time management, particularly in light of the
NMC’s draft timetable of this substantive hearing, the panel was of the view that it was
not necessary to reach a decision on this matter until such time as it was deemed
appropriate. However, Ms Norris, on behalf of Registrant D, invited the panel to
Page 48 of 142
adjudicate upon the wider matter of the NMC offering no evidence, prior to hearing the
evidence of Witness 2 and viewing the BBC Panorama documentary (Wednesday 3
May 2017).
In reaching its decision on the matter, the panel had regard to the submissions made by
Mr Unwin and accepted the advice of the legal assessor.
The panel was mindful that the NMC had no jurisdiction to withdraw an allegation at a
substantive hearing. It took into account, however, Mr Unwin’s submission which made
plain that the NMC did not intend to offer any evidence in respect of charge 1.3.
The panel carefully considered all the documentation and was satisfied that, in light of
the NMC’s concession that it no longer sought to pursue this allegation against Mr
Harrison as it was not relevant to him, there was no longer a realistic prospect of charge
1.3 being found proved. The panel further had in mind that it is not in the public interest
to pursue a factual charge if there is no evidence to prove it.
Accordingly, Mr Harrison had no case to answer in respect of charge 1.3.
Determination on application to admit the witness statement and associated
exhibit of Witness 17 – Wednesday 3 May 2017
Mr Unwin made an application to admit into evidence the NMC witness statement of
Witness 17, Senior Associate Consultant at CPEA Ltd, and the Serious Case Review
(exhibited by her) which she completed following transmission of the BBC Panorama
documentary.
Mr Unwin told the panel that no objection to this course of action had been raised by
any of the four registrants in this case.

Page 49 of 142
In reaching its decision the panel had regard to the submissions made by Mr Unwin and
it accepted the advice of the legal assessor. In considering whether or not to admit into
evidence the documents in question, the panel had regard to the requirements of Rule
31 of the Rules and considered whether the evidence was relevant, whether it would be
fair to admit it and, if so, whether it would be appropriate to exercise its discretion in
favour of admitting it. The panel was mindful that the admission of the statement of an
absent witness should not be regarded as a routine matter.
The evidence of Witness 17 spoke not to the allegations directly, but rather assisted in
providing a useful contextual narrative to these matters. On that basis, the panel was
satisfied that the requirement of relevance was met.
Panels in regulatory proceedings perform an inquisitorial and investigatory role. In order
to perform this role, panels require the best evidence available. The panel accepted that
the best form of evidence is obtained by calling witnesses live before it. That being said,
the panel was mindful that the NMC’s proposal to admit into evidence the documents in
question, without calling Witness 17 to give evidence in this hearing in person, was not
objected to by the registrants in this case.
The panel bore in mind the disadvantage in not being able to assess a witness’
demeanour when giving evidence. However, it was mindful that Witness 17’s evidence
was contained within a written statement, supported by a signed statement of truth. Her
evidence, along with all other documentary evidence relied upon by the NMC, had been
served on Mr Harrison, in advance of and in preparation for this hearing.
The panel was satisfied that the admission of Witness 17’s witness statement and
associated exhibit would accord with the public interest in ensuring that the evidence in
this case was explored fully. Having considered this application with care, taking
account of the public interest in the expeditious disposal of this case and fairness in

Page 50 of 142
these proceedings, the panel determined that it would be fair to admit the documents. In
reaching this conclusion, the panel was mindful of the potential limitations of receiving
evidence in this manner and would, in due course, attach appropriate weight to the fact
that Witness 17’s written account could not be explored by way of oral evidence and
questions of clarification from the panel.
Determination on application to hear evidence by video link and to admit NMC
witness statements, and associated exhibits, into evidence – Monday 8 May 2017
Mr Unwin made an application, under Rule 31 of the Rules, to hear the evidence of
Witness 9, Witness 6 and Witness 13 by WebEx, an internal video link facility. In
support of his application, he submitted that the panel had a wide discretion to receive
evidence, in any format, subject to the requirements of relevance and fairness.
Mr Unwin referred the panel to the case of Nursing and Midwifery Council v Ogbonna
[2010] EWCA Civ 1216, which provided guidance in respect of the admissibility of
hearsay evidence. In particular, it was held that where a witness’ evidence spoke to
disputed matters, and that evidence was sole and decisive, panels should be slow to
receive that evidence as hearsay; in those instances, witnesses should be made
available in order for disputed matters to be put to them and for their evidence to be
tested.
Moreover, by way of background, Mr Unwin informed the panel that early on in these
proceedings, prior to each registrant’s case being considered by an Investigating
Committee, each registrant was provided with a list of witnesses upon whom the NMC
intended to rely. The registrants were invited to indicate whether the contents of the
witnesses’ statements were agreed and whether there was agreement to the
statements being ‘read’ as the witnesses’ evidence in chief. He referred the panel to the
responses provided by Mr Harrison and Registrant A in this regard.

Page 51 of 142
Mr Unwin further informed the panel that there had been additional communication
between the NMC and the registrants, not least for the purpose of this application,
indicating which witnesses the NMC intended to call as live evidence, and those
witnesses for whom it was intended their statements be ‘read’. He told the panel that no
response had been received from the absent registrants (Mr Harrison, Registrant A and
Registrant C). He did, however, remind the panel of Registrant A’s comments on day
one of these proceedings, in which she indicated that she did not wish to hear the NMC
witnesses’ testimonies and that she did not have any questions to put to them in cross-
examination.
Mr Unwin submitted that the video link facility relied upon was of an acceptable quality,
subject to the witness having the necessary technology and establishing a sufficient
connection. He submitted that receiving evidence by video link would enable the panel
to see the witness’ demeanour and ask any question of the witness which it would
otherwise do so in the presence of that witness. In that regard, he contended that no
unfairness would be caused to the registrants about whom the relevant witnesses would
give evidence, as the evidence could be tested in the usual manner.
Mr Unwin confirmed that the witnesses subject to this application had been provided
with all the relevant documentary evidence in advance of, and in preparation for, this
hearing.
[The positions recorded by the names of the witnesses below denoted the roles
undertaken by those witnesses at the material time]
Witness 9 (Support Worker, Winterbourne View)
Mr Unwin informed the panel that Witness 9, who resides in Bristol, had been warned to
attend the hearing in the first scheduled week, which she duly did. Following
Page 52 of 142
rearrangements to the provisional hearing timetable, Witness 9 did not give evidence as
scheduled.
Mr Unwin invited the panel to receive Witness 9’s evidence by video link. He submitted
that, from a case management perspective, receiving her evidence in this form allowed
for greater flexibility in respect of her availability. He submitted that whilst it was not
“impossible” for Witness 9 to return to London in order to give evidence in these
proceedings, the NMC was anxious not to request her attendance in person, given the
inconvenience already caused to her in the week prior.
Mr Unwin explained that Witness 9, a Support Worker in Winterbourne View at the
material time, spoke to a number of general issues including training and induction. She
was not, he submitted, a key or sole witness in respect of any specific incident or
allegation.
Mr Unwin informed the panel that no objection had been raised, in principle, by Ms
Norris as regards witnesses in general giving evidence by video link, as she would have
the opportunity to put Registrant D’s case to the witness and test the witness’ evidence
in cross-examination.
Witness 6 (Patient E’s mother)
Mr Unwin informed the panel that Witness 6 spoke to a discrete matter, namely an
alleged conversation she had had with Registrant A. Registrant A, in her signed NMC
‘Standard Directions Form’ dated 20 October 2014, indicated that she disagreed with
the evidence of Witness 6.
Mr Unwin told the panel that Witness 6 had limited availability in the coming weeks,
owing to work and other personal commitments. In those circumstances, she had
requested that she avoid making the journey to London, from Plymouth, in order to give

Page 53 of 142
evidence in person at the hearing. He submitted that, as this witness’ evidence was
confined to a specific incident, and as it was not reliant on significant documentation,
her evidence could properly be received by video link.
By way of information, Mr Unwin informed the panel that there was some scope for
Witness 6 to attend the hearing in person on Wednesday 10 May 2017, if deemed
necessary.
Witness 13 (Independent Consultant, subsequently employed as Group Director of
Nursing and Patient Safety, Danshell)
Mr Unwin informed the panel that Witness 13 had put the NMC on notice of health
issues that impaired her ability to travel to London. She therefore requested that she
give evidence remotely.
Mr Unwin submitted that Witness 13’s evidence did not speak directly to any specific
allegation. He explained that Witness 13’s role at the time was that of an Independent
Consultant, and she conducted a review (in 2011) of clinical safety and culture in
respect of 12 (non-Winterbourne View) Castlebeck Units. The report arising from that
review, as exhibited by her, was included in the evidence bundle before the panel and
was, as far as he was aware, a matter of public record. From October 2011, she was
appointed Group Director of Nursing, and played a role in Mr Harrison’s appeal hearing.
Mr Unwin submitted that decisions/findings made in local disciplinary proceedings would
not be relevant to these regulatory proceedings. That being said, any issues raised
during the course of such local proceedings may well be of some relevance to the
panel.
Mr Unwin informed the panel that whilst it was not “impossible” for Witness 13 to attend
the hearing in person, this course of action might present some difficulty to the witness.

Page 54 of 142
Mr Harrison, in his signed NMC ‘Standard Directions Form’ dated 19 October 2014,
indicated that he did not agree with the content of Witness 13’s statement. Registrant A,
in her signed NMC ‘Standard Directions Form’ dated 20 October 2014, indicated that
she agreed with the content of Witness 13’s statement.
Mr Unwin made a further application to admit into evidence the NMC witness
statements and associated exhibits of the following witnesses:
Witness 18 (Support Worker and subsequently Activities Coordinator, Monroe House)
Mr Unwin submitted that Witness 18’s evidence was not central to any disputed
allegation; rather he spoke of his general experience at Winterbourne View over a
period of two weeks in 2008. Witness 18 was, in the NMC’s view, a non-contentious
witness.
Registrant A, in her signed NMC ‘Standard Directions Form’ dated 20 October 2014,
indicated that she agreed with the content of Witness 18’s statement.
Witness 19 (Clinical Lead, Intensive Community Support Team, South Gloucestershire
Primary Care Trust)
Mr Unwin informed the panel that Witness 19’s evidence was relevant to charge 2.2 as
against Registrant A, which was admitted by her at the outset of this hearing. He
referred the panel to Registrant A’s signed NMC ‘Standard Directions Form’ dated 20
October 2014, in which she indicated that she agreed with the content of Witness 19’s
statement. Mr Unwin therefore submitted that as there was no suggestion that Witness
19’s evidence was contentious, his statement could properly be ‘read’ as his evidence in
chief.
Witness 20 (Senior Assessor, Healthcare Commission/CQC)

Page 55 of 142
Mr Unwin informed the panel that Witness 20 had recently experienced a significant and
serious personal event such that she was unable to attend the hearing.
Mr Unwin told the panel that Witness 20’s involvement in these matters was confined to
two unannounced Healthcare Commission inspections of Winterbourne View (1
December 2008 and 26 March 2009). In light of Registrant A’s signed NMC ‘Standard
Directions Form’, he submitted that it could properly be said that the substance of
Witness 20’s evidence was not in dispute by Registrant A. Whilst Mr Harrison did not
admit the charges about which Witness 20 gave evidence, he did not indicate any
specific challenges to her evidence. It was therefore unclear as to whether Mr Harrison
challenged the findings of Witness 20’s inspections or the degree of responsibility
attributable to him in the circumstances. In any event, Mr Unwin told the panel that
Witness 7 would give evidence about the specific responsibilities of each registrant in
this case, which might assist the panel in considering any contentious issues.
Mr Unwin invited the panel to conclude that Witness 20’s witness statement could be
‘read’ as her evidence in chief.
Witness 21 (Detective Constable, Avon and Somerset Constabulary)
Mr Unwin informed the panel that Witness 21’s witness statement related primarily to
the police investigation conducted into allegations of abuse and ill treatment of patients
in Winterbourne View. She exhibited material seized by the police during the course of
its investigation, as well as Registrant C’s police interview under caution in which he
responded to the allegations.
In the absence of any challenge to the authenticity of documents exhibited by Witness
21, Mr Unwin invited the panel to conclude that her witness statement could be ‘read’ as
her evidence in chief.

Page 56 of 142
Witness 22 (Interim Project Manager and subsequently Head of Governance, Danshell)
Mr Unwin told the panel that Witness 22 did not give direct factual evidence in respect
of any specific allegation, but rather she exhibited a number of Castlebeck policies.
Mr Unwin referred the panel to Registrant A’s signed NMC ‘Standard Directions Form’
dated 20 October 2014, in which she indicated that she agreed with the content of
Witness 22’s statement. In the absence of any challenge to her evidence, Mr Unwin
invited the panel to conclude that Witness 22’s witness statement could be ‘read’ as her
evidence in chief.
Witness 23 (Senior Assessment Manager, Healthcare Commission (2005-2009), CQC
Compliance Manager (2009)
Mr Unwin informed the panel that the NMC had initially intended on calling Witness 23
to give evidence in person at the hearing. For case management purposes, and in light
of ongoing issues with the hearing timetable, this position was reviewed.
By way of information, Mr Unwin explained that Witness 23 inspected Arden Vale in
April 2006, November 2006 and October 2007, and Croxton Lodge in June 2011.
Mr Harrison, in his signed NMC ‘Standard Directions Form’ dated 19 October 2014,
indicated that he agreed with the content of Witness 23’s statement and agreed to her
statement being ‘read’ as her evidence in chief. Registrant A, in her signed NMC
‘Standard Directions Form’ dated 20 October 2014, indicated that she agreed with the
content of Witness 23’s statement.
Mr Unwin submitted that whilst there might be general questions about CQC
methodologies which could be put to Witness 23, any such questions could properly be
Page 57 of 142
put to Witness 5, a witness who was due to give evidence in person. As no specific
factual dispute as regards Witness 23’s evidence had been raised by either Mr Harrison
or Registrant A, Mr Unwin invited the panel to conclude that her witness statement
could be ‘read’ as her evidence in chief.
Witness 24 (Compliance Manager, CQC)
By way of information, Mr Unwin told the panel that Witness 24 inspected Arden Vale in
June 2011. He referred the panel to Mr Harrison’s signed NMC ‘Standard Directions
Form’ dated 19 October 2014, in which he indicated that he agreed with the content of
Witness 24’s statement and agreed to her statement being ‘read’ as her evidence in
chief.
In the absence of any factual challenge to her evidence, Mr Unwin submitted that
Witness 24’s witness statement could properly be ‘read’ as her evidence in chief.
Witness 25 (CQC Compliance Inspector); Witness 26 (CQC Compliance Inspector);
Witness 27 (Healthcare Assessor for the Healthcare Commission and subsequently
CQC Compliance Manager); Witness 28 (CQC Compliance Inspector); and Witness 29
(CQC Compliance Inspector)
Each named witness was a CQC Compliance Inspector who carried out inspections of
non-Winterbourne View Units in 2011. In each case, Mr Harrison, in his signed NMC
‘Standard Directions Form’ dated 19 October 2014, indicated that he agreed with the
content of the witness’ statement and agreed to their statement being ‘read’ as their
evidence in chief.
In the absence of any factual challenge to their evidence, Mr Unwin submitted that each
witness’ statement could properly be ‘read’ as their evidence in chief. In any event, he
submitted that in their respective roles, each witness would subsequently have carried

Page 58 of 142
out a large number of inspections; in that regard, it was unlikely that their factual
recollection of relevant events would go above and beyond any documentation
exhibited by them.
Witness 30 (Castlebeck Interim Operations Director, September 2011)
Mr Unwin informed the panel that it was the NMC’s intention that Witness 30 attend the
hearing in person to give evidence; Witness 30 was not, however, able to attend on the
date proposed. Mr Unwin explained that Witness 30 could travel to London for the
purpose of the hearing, however, Registrant A, in her signed NMC ‘Standard Directions
Form’, dated 20 October 2014, indicated that she agreed with the content of Witness
30’s statement. Furthermore, Mr Harrison, in his signed NMC ‘Standard Directions
Form’ dated 19 October 2014, indicated that he agreed with the content of Witness 30’s
statement and agreed to his statement being ‘read’ as his evidence in chief.
Mr Unwin told the panel that Witness 30 chaired the disciplinary hearings held in
relation to Registrant C and Registrant A. Mr Unwin submitted that any decisions or
findings from the disciplinary hearings would not be relevant to the panel in adjudicating
upon the charges before it. That being said, Witness 30’s evidence was important
insofar as he referred to the registrants’ responses during the course of the disciplinary
hearings.
In the absence of any factual challenge to his evidence, Mr Unwin submitted that
Witness 30’s witness statement could properly be ‘read’ as his evidence in chief.
Panel’s decision
In reaching its decision, the panel had regard to the submissions made by Mr Unwin
and accepted the advice of the legal assessor, who referred the panel to Rule 31 of the

Page 59 of 142
Rules and to the NMC’s ‘Telephone evidence guidance’ (effective from 26 September
2016).
In respect of Mr Unwin’s application to hear the evidence of Witness 9, Witness 6 and
Witness 13 by video link, the panel carefully considered the following:
The panel took into account that neither Witness 9’s nor Witness 13’s evidence spoke
directly to any specific allegation, insofar as the panel’s ability to adjudicate upon the
charges. Witness 9 spoke of general matters arising from her experience as a Support
Worker at Winterbourne View, and Witness 13 exhibited a report she produced
following her review, in 2011, of 12 (non-Winterbourne View) Castlebeck Units. Witness
13 also played a role in Mr Harrison’s appeal hearing, the findings of which would not be
relevant for the purpose of this substantive hearing.
As regards Witness 6, the panel was mindful that her evidence was confined to a
discrete matter, namely an alleged conversation between herself and Registrant A in
around 2009. Registrant A, in her undated written response to the allegations, indicated
that she did not recall the alleged conversation, nor did she recall Witness 6.
On the information before the panel as to the substance of each witness’ evidence, the
panel was satisfied that the requirement of relevance was met.
Panels in regulatory proceedings perform an inquisitorial and investigatory role. In order
to perform this role, panels require the best evidence available. The panel accepted that
the best form of evidence is obtained by calling witnesses live before it. The panel was
satisfied that receiving evidence by video link would allow all parties to see the witness’
demeanour when giving evidence, and thus allow the panel to assess the witness’
credibility.

Page 60 of 142
The panel was mindful of its earlier decision to proceed in the absence of Mr Harrison.
With this in mind, the panel considered that any potential unfairness or disadvantage to
him in allowing this application would be as a result of his decision to absent himself
from the hearing and thus not be in a position to cross-examine the witnesses in any
event. That being said, the panel was acutely aware of its obligation to ensure fairness
in these proceedings. In that regard the panel, of its own volition, would explore any
inconsistencies in the NMC evidence which the panel itself identified, as well as any
matters referred to by Mr Harrison in his written representations to the NMC.
As at the time of the application, the panel had already read through all the
documentary evidence adduced by the NMC, as well as the written responses provided
by Mr Harrison. Whilst it was unclear, at this stage, the extent to which the witnesses’
credibility may be challenged by the absent registrants in this case, the panel was of the
view that any potential unfairness to Mr Harrison in acceding to Mr Unwin’s application
would be mitigated by their giving evidence by video link, because their evidence would
be subject to exploration and testing. Further, the panel would be able to put Mr
Harrison’s responses to the witnesses in question, to see their demeanour when giving
evidence and thus assess their credibility.
The panel was mindful that Witness 9’s, Witness 13’s and Witness 6’s evidence was
contained in written witness statements, supported by signed declarations of truth,
which, along with all other documentary evidence relied upon by the NMC, had been
served on Mr Harrison.
Having considered this application with care, taking into account the public interest in
the expeditious disposal of this case and fairness in these proceedings, the panel
considered that it was fair to allow Witness 9, Witness 13 and Witness 6 to give
evidence by video link.

Page 61 of 142
The panel wished to reaffirm the importance of each witness being provided with their
witness statements and associated exhibits in preparation for receiving their evidence
by video link.
In respect of Mr Unwin’s application to admit into evidence the witness statements and
associated exhibits of Witness 18, Witness 19, Witness 20, Witness 21, Witness 22,
Witness 23, Witness 24, Witness 25, Witness 26, Witness 27, Witness 28, Witness 29
and Witness 30, the panel considered the following:
The witnesses subject to this application were not relied upon by the NMC as principal
witnesses in respect of any specific allegation, but rather their evidence was ancillary
and would provide a contextual narrative in respect of some of the charges concerning
primarily Mr Harrison, and Registrant A. From the information before the panel as to the
substance of the witnesses’ evidence, the panel was satisfied that the requirement of
relevance was met.
As to fairness, the panel was mindful that no factual challenge had been raised by either
Registrant A or Mr Harrison in respect of the contents of the witnesses’ evidence. The
witnesses’ evidence was therefore non-contentious.
The panel bore in mind the disadvantage in not being able to assess the witnesses’
demeanour when giving evidence. However, it was mindful that the witnesses’ evidence
was contained within written statements, supported by signed declarations of truth.
Their evidence, along with all other documentary evidence relied upon by the NMC, had
been served on Registrant A and Mr Harrison, in advance of and in preparation for this
hearing.
The panel was satisfied that the admission of the witnesses’ statements and associated
exhibits would accord with the public interest in ensuring that the evidence in this case
was explored fully and that decisions were reached on the best available evidence.

Page 62 of 142
Having considered this application with care, taking account of the public interest in the
expeditious disposal of this case and fairness in these proceedings, the panel
determined that it would be fair to admit the documents. In reaching this conclusion, the
panel was mindful of the potential limitations of receiving evidence in this manner and
would, in due course, attach appropriate weight to the fact that the witnesses’ written
accounts could not be explored by way of oral evidence and questions of clarification
from the panel.
Submission on application to amend the header of the charges – Monday 15 May
2017
The panel raised a concern that the dates set out in Schedule E (April 2006 to October
2007) fell outside the time period identified in the header of the charges against Mr
Harrison. The panel therefore sought clarification from the NMC in respect of charge
4.1, in particular as to the commencement of Mr Harrison’s engagement at Arden Vale
and the subsequent applicability or otherwise of the provisions set out in Schedule E.
Mr Unwin referred the panel to the evidence which confirmed that Mr Harrison was the
appointed Responsible Individual for Arden Vale from 2005. He acknowledged,
however, that the time period identified in the header of the charges was incorrect; he
submitted that it was, most likely, an administrative error. He thus made an application
to amend the header as follows:
That you, whilst employed by Castlebeck Care (Teesdale) Limited as a Regional
Operations Director/ Regional Operations Manager between 2006 and June 2012…
Mr Unwin that the proposed amendment only impacted upon charge 4.1, had no
bearing on the remaining allegations, and that the substance of the remaining
allegations remained unchanged.
Page 63 of 142
The legal assessor referred the panel to Rule 28 of the Rules, which states:
28.—(1) At any stage before making its findings of fact … the Conduct and Competence
Committee, may amend—
(a) the charge set out in the notice of hearing; or
(b) the facts set out in the charge, on which the allegation is based,
Unless, having regard to the merits of the case and the fairness of the proceedings, the
required amendment cannot be made without injustice.
(2) Before making any amendment under paragraph (1), the Committee shall consider
any representations from the parties on this issue.
The legal assessor emphasised the requirement to consider representations from the
parties before making any amendment to a charge. She advised that it was in the
interests of justice and fairness for reasonable attempts to be made to contact Mr
Harrison in order to seek his representations on the application. She advised that the
proposed amendment was substantial in that, without it, there was arguably no case for
Mr Harrison to answer in respect of charge 4.1.
Mr Unwin provided an undertaking for contact to be made with Mr Harrison as advised.
The panel afforded Mr Unwin sufficient time to do so, and decided to reserve its
judgement in respect of this application until such time as Mr Unwin was in a position to
address the panel on this matter.
On Tuesday 16 May 2017, Mr Unwin provided the following update to the panel:
Mr Harrison, in his written representations to the NMC, asserted that he assumed
responsibility for Arden Vale in 2007. The NMC witness relied upon in support of charge
Page 64 of 142
4.1 against Mr Harrison was Witness 23; it was Witness 23’s evidence that Mr Harrison
was the ‘Responsible Individual’ of Arden Vale from its opening in October 2005. In
making that assertion, Witness 23 appeared to rely upon a certificate of registration in
which Mr Harrison was identified as the ‘Responsible Individual’. The ‘Date of
Registration’ was recorded as 27 October 2005. The certificate date, however, was 6
November 2007.
Mr Unwin acknowledged that this document was inconclusive in regard to Mr Harrison’s
position in 2006. He informed the panel that steps were being taken to locate the
original certificate and that, until such time as the position was clarified, contact with Mr
Harrison was being postponed.
On Thursday 18 May 2017, Mr Unwin provided the following update to the panel:
Witness 23 had informed the NMC that there was no record of a certificate of
registration pre-dating 2007. As such, the NMC did not seek to proceed in respect of
paragraphs 1-32 of Schedule E. Mr Unwin told the panel that Mr Harrison would be put
on notice of the application and would be given an opportunity to respond to it. It was
therefore Mr Unwin’s intention to make a formal application to amend the header of the
charges on Friday 19 May, in order to give sufficient time to Mr Harrison to respond,
should he wish to do so.
Determination on application to amend the header of the charges – Friday 19 May
2017
On Friday 19 May 2017, Mr Unwin made a formal application to amend the header of
the charges against Mr Harrison to read as follows:

Page 65 of 142
That you, whilst employed by Castlebeck Care (Teesdale) Limited as a Regional
Operations Director/ Regional Operations Manager between 2007 and June 2012…
Mr Unwin submitted that the proposed amendment was relevant only to charge 4.1. In
light of this application, the NMC sought to withdraw paragraphs 1-32 of Schedule E.
In regard to the notice period afforded to Mr Harrison in respect of this application, Mr
Unwin informed the panel that communication to Mr Harrison about the proposed
amendment was not sent until approximately 16:00 the previous day. As an aside, Mr
Unwin explained that earlier communication had been sent to Mr Harrison, at the
panel’s request, in relation to any further representations he may wish to make in
response to the allegations; no response had been received from Mr Harrison, as at the
time of Mr Unwin’s submission. Mr Unwin further informed the panel that the NMC had
sent communication in the months leading up to this substantive hearing, and that no
response from Mr Harrison had been received. Mr Unwin submitted that other than his
early engagement with the NMC, Mr Harrison appeared to have disengaged from these
proceedings.
Mr Unwin outlined the evidential basis for the application. Whilst Witness 7 was unable
to specify at what stage Mr Harrison took over responsibility of Units in the Midlands
region, she confirmed that Mr Harrison was in post, in a role almost identical to that of
Regional Operations Director, prior to her commencing her employment in 2008. In any
event, Witness 7 confirmed that Registrant A, as Senior Manager, reported to Mr
Harrison. Witness 7 also confirmed that Registrant A was employed as Manager of
Arden Vale between May 2007 and June 2008.
Mr Unwin directed the panel’s attention to the Healthcare Commission inspection report,
following an announced inspection of Arden Vale on 18 October 2007. The report noted
that, since Arden Vale’s registration in 2005, there had been a number of temporary
Managers in post. It went on to state that during the inspection visit, the Healthcare

Page 66 of 142
Commission had registered the current Manager, Registrant A, as a fit person to run the
establishment.
Mr Unwin then directed the panel’s attention to a copy of the notes from the
investigatory meeting held with Mr Harrison on 3 August 2011. In relation to Arden Vale,
Mr Harrison said that he “did not commission Arden or appoint Managers”. He went on
to confirm, however, that he had appointed Registrant A’s predecessor. In that regard,
Mr Unwin submitted that if Registrant A was in post at Arden Vale from May 2007, Mr
Harrison must have been in post prior to that. In any event, Mr Harrison appointed
Registrant A as Manager of Arden Vale.
In those circumstances, Mr Unwin submitted that the evidence of Mr Harrison himself,
during the investigation meeting, supported the inference that he must have been
responsible for Arden Vale at least by the time of the October 2007 inspection.
As to whether the proposed amendment could be made without injustice, Mr Unwin
submitted that the substantial change was to effectively withdraw all paragraphs of
Schedule E that predated 2007. He said that Mr Harrison had been put on notice of the
substance of the charge in question, throughout these proceedings; it was Mr Harrison’s
case that he was responsible for Arden Vale from 2007. Mr Unwin conceded that there
was no evidence to demonstrate that, prior to 2007, Mr Harrison had responsibility for
Arden Vale. Mr Unwin submitted that it was unlikely that Mr Harrison’s response to the
allegations would have been any different, had the application to amend the header of
the charges been made earlier on in these proceedings.
In all of those circumstances, Mr Unwin submitted that the substance of charge 4.1
would not be altered significantly by correcting the dates in the header of the charges so
as to reflect the evidence.

Page 67 of 142
In reaching its decision, the panel had regard to the submissions made by Mr Unwin
and it accepted the advice of the legal assessor, who referred to Rule 28 of the Rules,
which states:
28.—(1) At any stage before making its findings of fact … the Conduct and Competence
Committee, may amend—
(a) the charge set out in the notice of hearing; or
(b) the facts set out in the charge, on which the allegation is based,
Unless, having regard to the merits of the case and the fairness of the proceedings, the
required amendment cannot be made without injustice.
As to the merits of the case, the panel took account of Mr Harrison’s undated written
statement to the NMC, in which he acknowledged that he “was part of the team that
failed to ensure that all of the vulnerable people within Castlebeck were protected from
abuse”. The panel further took note that it was Mr Harrison’s case that he assumed
managerial responsibility for the Midlands region in 2007. The panel had regard to the
documentary evidence referred to by Mr Unwin and was satisfied that the evidential
basis of his application made plain that Mr Harrison was responsible for Arden Vale at
least at the time of the Healthcare Commission inspection in October 2007.
The panel took note of the efforts made by the NMC to engage Mr Harrison in these
proceedings. The panel was informed that there was no working contact number on
record for Mr Harrison. It was further informed that attempts had been made, on
Thursday 18 May 2017 and in the months leading up to the hearing, to contact Mr
Harrison, and that these attempts had been unsuccessful. Whilst Mr Harrison had been
given less than 24 hours’ notice of this application, the panel considered that being
afforded more time was unlikely to result in a response from Mr Harrison, particularly in
light of his apparent disengagement in these proceedings.

Page 68 of 142
In all of the circumstances, the panel was satisfied that the proposed amendment would
not cause Mr Harrison any unfairness or injustice. It therefore agreed to Mr Unwin’s
application. The panel was mindful that the amendment would not bind it in regard to
any decision reached in respect of the allegations.
Mr Harrison’s position – Monday 22 May 2017
Mr Unwin informed the panel that on Friday 19 May 2017, Mr Harrison responded to an
email from his NMC Case Officer, in relation to the NMC’s application to amend the
header of the charges in this case. Mr Harrison stated that he would make himself
available to the panel, should it wish to hear from him. He also stated that he could not
attend the hearing in person, but that he could be contacted by email or telephone. Mr
Harrison, in his email, gave no objection to the NMC’s application to amend the header
of the charges in his case.
Determination on submission of offering no evidence – Monday 22 May 2017
Mr Unwin informed the panel that Mr Harrison was the Regional Operations Manager
with responsibility for the Midlands region from 2007, and was subsequently the
Regional Operations Director, with responsibility for Winterbourne View in 2008. Mr
Unwin told the panel that upon further review of the evidence in this case it appeared
that, prior to and including 2008, Winterbourne View was under the remit of another
Regional Operations Director, Individual GG. According to Registrant A, in her
investigation meeting on 17 August 2011, Mr Harrison resumed responsibility for
Winterbourne View in 2009. This was supported by Witness 7, who confirmed that Mr
Harrison was responsible for Winterbourne View from January 2009.

Page 69 of 142
In light of the above, Mr Unwin submitted that the NMC did not seek to proceed with
paragraphs 1-12 of Schedule A, which had been originally relied upon to support charge
1.1.
The panel was satisfied that there was no case for Mr Harrison to answer in respect of
paragraphs 1-12 of Schedule A in light of the submissions from Mr Unwin.
Mr Harrison’s response to the charges – Wednesday 24 May 2017
Mr Harrison participated in the hearing by telephone on 24 May 2017. He made
admissions to the following charges:
1.1
1.2
1.4
1.6.1
1.8
1.9
1.10
1.11
1.12
2.1
3.1
4.1
4.2
5.1
5.2
6.1
7.1

Page 70 of 142
Mr Harrison also admitted that by virtue of the above charges, his fitness to practise is
impaired by reason of his misconduct.
In accordance with Rule 24(5) of the Rules, the panel found proved the charges
indicated above, by virtue of Mr Harrison’s admissions.
Determination on facts – Monday 5 June 2017
In reaching its determination on facts, the panel had regard to all the evidence adduced,
including the oral evidence and the exhibited documents. It heard submissions from Mr
Unwin and accepted the comprehensive advice of the legal assessor.
The burden of proof rests entirely upon the NMC. Mr Harrison does not have to prove or
disprove anything. The standard of proof is the civil standard, namely the balance of
probabilities. This means that, for a fact to be found proved, the NMC must satisfy the
panel that what is alleged to have happened is more likely than not to have occurred.
The panel heard evidence on behalf of the NMC from the following witnesses who held
the positions (as listed below) at the relevant time:
Witness 1, Activities Coordinator, Wast Hills;
Witness 2, Researcher, BBC;
Witness 3, Charge Nurse, Winterbourne View;
Witness 4, Compliance Inspector, CQC;
Witness 5, Compliance Manager, CQC;
Witness 6, Patient E’s mother;
Witness 7, HR Director, Castlebeck (later Danshell);
Witness 8, Nurse, Arden Vale;

Page 71 of 142
Witness 9, Support Worker, Winterbourne View;
Witness 10, Nurse, Winterbourne View;
Witness 11, Support Worker, Winterbourne View;
Witness 12, Patient D’s mother;
Witness 13, Independent Consultant;
Witness 14, Head of Strategy and Commissioning, SGC;
Witness 15, Senior Practitioner, Safeguarding Team, SGC; and
Witness 16, Chief Operating Officer, Castlebeck.
Witness 1
Witness 1 was an anxious and nervous witness, who was evidently traumatised by the
events at Winterbourne View about which he spoke. His recall, on occasion, was poor;
this could understandably have been due to the passage of time. Although employed by
Castlebeck from September 2009 to June 2010, his specific experience of Winterbourne
View was limited to a period of approximately two months. His evidence was of some
assistance in providing a comparison, particularly of the systems in place and the
provision of care to service users, between his primary place of employment (Wast Hills,
Birmingham) and Winterbourne View.
Witness 1’s evidence was inconsistent and contradictory at times. In his exhibit entitled
‘My Responses To Some Questions Asked By The Media’, Witness 1 stated that “I had
many concerns and expressed them to a few different Managers, I discussed most of
them in person but those that I emailed always went unanswered”. In his oral evidence,
he confirmed that the only Manager at Winterbourne View to whom he had raised his
concerns was Registrant C. He also confirmed that he did not report any concerns, via
email, whilst at Winterbourne View. That being said, his evidence was consistent when
he spoke of his overall relationship with Registrant C, raising concerns with Registrant
C; and how ‘unreceptive’ Registrant C appeared when concerns were raised.

Page 72 of 142
The panel was satisfied that Witness 1 did his best to assist in these proceedings by
giving evidence. The usefulness and reliability of his evidence, however, was limited.
Witness 2
Witness 2 was balanced, fair and professional. He spoke not only of the instances of
abuse he directly observed, as depicted in the BBC Panorama documentary, but also of
the good care that was provided by some staff members to the patients at Winterbourne
View. He also acknowledged that as the Managers at Winterbourne View were not
regularly present on patient floors, they most likely did not or would not necessarily have
had knowledge of the abuse that was occurring.
As to the specific allegations in this case, Witness 2’s evidence was of limited value.
Overall, however, the panel was satisfied that he was a credible, consistent and reliable
witness and that he gave evidence in good faith.
Witness 3
Witness 3 gave evidence in respect of events which led to his whistle-blowing email,
addressed to Registrant C, dated 11 October 2010, as well as in respect of record
keeping, documentation, training and supervision, and incident reporting systems. He
presented as being very experienced in caring for patients with challenging behaviours.
He was balanced and fair, had a good recollection of the matters about which he spoke,
and was candid about what he could not recall. He also made concessions where
appropriate, acknowledging, for example, that he may have misunderstood the purpose
of a meeting that was held a few days after his whistle-blowing email, and whether or
not the copy of the email in Registrant D’s possession at that meeting was in fact his
whistle-blowing email. He was clear in his view as to his expectations, and the
accountabilities, of each registrant in this case.

Page 73 of 142
Witness 3’s prior relationship with Individual K was explored to some extent in cross-
examination, the implication being that when he commenced employment at
Winterbourne View, he had been “on the lookout” for abuse. The panel was not
persuaded by this line of questioning, and was satisfied, on the basis of Witness 3’s
evidence, that he did not seek out employment at Winterbourne View with an ulterior or
sinister motive. Furthermore, there was some suggestion that he, as a Charge Nurse,
ought to have taken action himself to address concerns he had identified. In this regard,
the panel was acutely aware that he worked in Winterbourne View for approximately
three months, during which time he was evidently persistent in his desire to effect
positive changes in Winterbourne View, frequently reporting and escalating his
concerns to management. Witness 3 was clearly traumatised by the abuse that was
uncovered in the BBC Panorama documentary; he was unable to work as a Registered
Nurse for some months after its transmission. He confirmed that he did not personally
witness the severity of the abuse depicted in the footage.
The panel was satisfied that Witness 3 was a credible, consistent and reliable witness
and that he gave evidence in good faith.
Witness 4
Witness 4 provided useful contextual evidence in respect of CQC methodologies and
documentation. Her testimony, insofar as her recollection and the documentation before
her allowed, was fair and balanced. She confirmed that she had undertaken only one
CQC inspection, in December 2009; she was thus unable to speak to wider issues in
respect of other inspections conducted at Winterbourne View. Due to the passage of
time and her limited involvement with Winterbourne View, her overall recall and the
value of her evidence, outside of her written NMC witness statement, were limited. That
being said, the panel was satisfied that she tried her best to assist in these proceedings.
Overall the panel was satisfied that she was a credible, consistent and reliable witness
and that she gave evidence in good faith.

Page 74 of 142
Witness 5
Witness 5 had a good understanding of her role as a witness in these proceedings,
providing factual evidence and not seeking to offer any personal views or opinions
unless specifically sought. She was a highly experienced Registered Nurse with a
background in mental health. She gave useful, contextual evidence in regard to CQC
methodologies in the inspection process (prior and subsequent to the BBC Panorama
documentary), and spoke more specifically about the CQC inspections in May 2011, in
which she took part. She was clear in her view as to the responsibilities and
accountabilities of each registrant in this case. Her testimony, insofar as her recollection
and the documentation before her allowed, was fair and balanced. Whilst her recall
about matters or details not contained in her NMC witness statement was limited, the
panel was assisted by her contemporaneous notes, made at the time of the inspection
in May 2011.
The panel was satisfied that Witness 5 was a credible, consistent and reliable witness
and that she gave evidence in good faith.
Witness 6
Witness 6, Patient E’s mother, had a clear recollection of the conversation she said she
had had with Registrant A after her (Witness 6’s) daughter had re-enacted an incident
when she had been “decked” by Individual U. She also recalled her feelings at the lack
of response she received from the various practitioners, including Registrant A, who
were present at the CPA meeting that took place directly after this conversation.
Witness 6 had had direct professional experience in a care setting and was engaged in
her daughter’s care. She told the panel that, from her point of view, she had had a
professional and positive relationship with Registrant A. Whilst she spoke of her

Page 75 of 142
subsequent lack of trust in Winterbourne View and its staff following transmission of the
BBC Panorama documentary, the panel was satisfied that she bore Registrant A no
malice and had no ulterior motive in giving evidence in these proceedings. In that
regard, the panel was mindful that her evidence to the NMC came about as a result of
her wish to assist her daughter in these proceedings.
The panel was satisfied that Witness 6 was a credible, consistent and reliable witness
and that she gave evidence in good faith.
Witness 7
Witness 7 provided considerable evidence in regard to Castlebeck processes, practices
and systems, and was clear in respect of the primary accountabilities of each registrant
in this case. There were, however, occasions when her testimony was not entirely
objective but rather veered into opinion evidence, speaking about what she would have
expected in the circumstances as opposed to what actually happened. It was also
apparent that she had formed opinions of the standards she had expected of some of
the registrants, whilst not being a clinician herself. There were, furthermore, occasions
when she did not provide direct responses to questions put to her. The panel therefore
accepted her evidence with some reservation.
That being said, the panel was satisfied that Witness 7 did her best to assist in giving
evidence in these proceedings. The panel was further satisfied that she was a
consistent witness and was credible and reliable in respect of matters in which she was
experienced.
Witness 8
Witness 8 was a measured and balanced witness. She had a good recollection of the
matters about which she spoke, and was candid about what she could not recall. The

Page 76 of 142
panel noted that she made a contemporaneous record of instances of restraint, as set
out in her NMC witness statement and in her report to the Manager of Arden Vale,
whose name she was unable to recall. The contemporaneous record was of
considerable assistance to the panel, bearing in mind the passage of time since the
allegations about which she spoke.
Witness 8 spoke of the Manager of Arden Vale (reasonably inferred to be Registrant A)
in positive terms, commenting on the support Registrant A had offered her during their
meeting and Registrant A’s undertaking to address the concerns raised in her (Witness
8’s) report. Witness 8 was candid in her acknowledgement that she did not follow up
with Castlebeck as to whether her concerns were indeed investigated.
It was evident to the panel that the events about which Witness 8 spoke had had an
impact on her. Her employment at Arden Vale was her first professional employment as
a Registered Nurse post qualification. She worked at Arden Vale for approximately
three weeks, during which time she had observed what she considered were excessive
restraints and abuse of patients. She took action in reporting her concerns to Registrant
A in the first instance, in her resignation letter to Castlebeck and again, after
transmission of the BBC Panorama documentary. Her account was consistent
throughout.
The panel was satisfied that Witness 8 was a credible and reliable witness and that she
gave evidence in good faith.
Witness 9
Witness 9 spoke of her experiences whilst working in Winterbourne View as a Support
Worker. Whilst not a qualified professional at the time, the panel took note that she
voiced opinions about the appropriateness or otherwise of matters not entirely within her
remit. She further spoke of her relationship with Registrant A in particularly negative

Page 77 of 142
terms; the panel was mindful that Registrant A was not aware of her evidence in this
regard and was thus not in a position to respond to it. The panel was therefore
somewhat hesitant about Witness 9’s objectivity.
Witness 9 gave evidence in regard to incidents of restraint about which, she said, she
had no particular concerns. For example, she spoke of an occasion when Patient G’s
wrist was broken following a restraint; it was Witness 9’s evidence that she observed
the Nurse involved restrain the patient, that she “[didn’t] believe it was particularly
forceful… we heard this ‘popping’ sound… I can honestly say I don’t think he did it
particularly forcefully”. The panel took further note that Witness 9 was named in a
complaint letter from Patient E, dated 22 July 2010, in which the patient described being
restrained by a number of staff members. The panel was concerned about the extent to
which the witness may have been inculcated into the ‘Castlebeck way’. The panel
therefore attached less weight to her evidence.
Witness 10
Witness 10 was a balanced, measured and compelling witness. She was open and
transparent in respect of her ongoing contact with Registrant D. This contact, she
confirmed, was limited primarily to social media.
Witness 10 provided useful contextual evidence in respect of the working environment,
processes and systems, incidents and incident reporting at Winterbourne View at the
material time. She had a good recollection of the matters about which she spoke, and
was candid about what she could not recall. Of the two patient incidents about which
she spoke, the panel took into account that her evidence was supported by
contemporaneous incident forms. In her oral evidence, she spoke in detail about the
particular incidents, telling the panel that she could recall the events very clearly. It was
apparent to the panel that these incidents, and the impact on the patients at

Page 78 of 142
Winterbourne View when they viewed the BBC Panorama documentary, were clearly
distressing for her.
The panel was satisfied that Witness 10 was a credible, consistent and reliable witness
and that she gave evidence in good faith.
Witness 11
Witness 11 did her best to assist the panel in giving evidence in these proceedings and
was candid about what she could not recall. However, there were a number of
inconsistencies and contradictions between her account as set out in her statement to
the police, her account in her NMC witness statement and her oral evidence; in
particular, with regard to the chronology as to when and to whom she reported the
incidents about which she spoke. In relation to one incident, Witness 11 asserted that
her account in her NMC witness statement, dated 24 November 2013, was more
accurate than her account in her police statement, dated 5 October 2011. In relation to
another incident, she relied on her account in her police statement as being an accurate
version of events, as opposed to her NMC witness statement. It was apparent to the
panel that the witness spoke of what she believed she would have done in the
circumstances, i.e. her view as to the appropriate ‘chain of command’ in regard to
reporting concerns, rather than basing her testimony on her recollection of actual
events.
Moreover, Witness 11 made a number of assumptions with regard to what she
considered to be a lack of action taken by Registrant D in response to concerns raised.
She acknowledged, however, that she made these assumptions as she was not aware
of what action, if any, had in fact been taken. When taken to the relevant documentary
evidence, she conceded that appropriate action had indeed been taken by Registrant D
and that nothing more could have been done by Registrant D.

Page 79 of 142
The inconsistencies and contradictions in Witness 11’s evidence fundamentally led the
panel to question its reliability. The panel therefore attached limited weight to her
testimony.
Witness 12
Witness 12 had a clear recollection of her visits and telephone conversations with her
son, Patient D, during the course of which he would report his concerns about
Winterbourne View. It was, however, apparent to the panel that management at
Winterbourne View did not inform the witness of, or involve her in, matters relating to
her son during his stay in Winterbourne View; for example, she was not privy to his care
records or incident forms, and was not asked to provide written comments or
statements following the disclosures by her son. Her limited involvement in wider
matters was such that her overall evidence was of limited value to the panel in its
consideration of the allegations. That being said, the panel was satisfied that the
witness did her best to assist these proceedings by giving evidence. It was further
satisfied that she gave evidence in good faith.
Witness 13
Witness 13 presented as a professional, measured and fair witness, who was highly
experienced at a senior level. She provided a very useful overview of Castlebeck and its
Units, and her evidence with regard to the accountabilities of members of the
management team was of considerable assistance to the panel. She had a clear
recollection of her observations, as set out in her report following her review of 12
Castlebeck Units (not including Winterbourne View) and was able to elaborate on her
report during the course of her oral evidence.
The panel was satisfied that Witness 13 was a credible, consistent and reliable witness
and that she gave evidence in good faith.

Page 80 of 142
Witness 14
Witness 14 was clear about the limited nature of his role in respect of these
proceedings. He was the Head of Strategy and Commissioning at South
Gloucestershire Council (“SGC”) at the material time; he was not a clinician. His
evidence was confined to a ‘document-scoping’ exercise. That being said, the panel
was satisfied that he did his best to assist in giving evidence in these proceedings. The
panel was further satisfied that he was a consistent witness and was credible and
reliable in respect of matters about which he was an expert.
Witness 15
Witness 15 was defensive in her responses and, when questioned on certain matters,
appeared unwilling to provide her professional judgement. She was not prepared to
comment on documentation she herself collated for the purpose of the NMC’s
investigation, notwithstanding the fact that she was not in post, as Senior Practitioner in
the safeguarding team at SGC, until April 2011 (despite asserting, in her witness
statement, that she had been employed in this role since April 2010). Furthermore,
when asked to provide her professional judgment on the increase in the number of
safeguarding alerts to SGC post transmission of the BBC Panorama documentary, she
appeared unconcerned by this and trivialised, to a degree, the contents of those alerts.
In the panel’s view, Witness 15 did not make a positive attempt to assist in these
proceedings. The panel attached limited weight to her evidence.
Witness 16
Witness 16 was a highly experienced ‘turn-around’ consultant and, as a Registered
Nurse, had a clear view of what constituted good nursing care, particularly from the

Page 81 of 142
point of view of patients. He was a compelling witness, whose evidence corresponded
closely with that of Witness 13. He made plain to the panel that, notwithstanding the
corporate failings in this case and the operational pressures faced by, in particular, Mr
Harrison, Registrant A and Registrant C, his expectations of each registrant in the
circumstances were clear. He acknowledged the wider, systemic failings in regard to
Winterbourne View, but was unwavering in his view of the role of Registered Nurses in
that environment.
The panel was satisfied that Witness 16 was a credible, consistent and reliable witness
and that he gave evidence in good faith.
The panel also heard evidence from Mr Harrison. He was open and transparent in his
responses, conceding that he limited his personal involvement in matters where he
ought not to have. He was candid in acknowledging that he left tasks for others to
complete and would not check up on progress. His accounts throughout were
consistent. The panel was satisfied that he was a credible and reliable witness and that
he gave evidence in good faith.
At the close of his final submissions on facts, Mr Unwin presented general observations
which he invited the panel to take into account. The panel were to bear in mind the
historical nature of these allegations and the effect which that had on witness
recollection and the quality and availability of evidence relating to matters which had
occurred some 7-8 years previously.
Further, there were evidential considerations to be had on account of Winterbourne
View's closure shortly after the Panorama broadcast, and the organisation's entering
into administration. This inevitably had an effect on the availability of documents
both before the panel, and also before the CQC. Quite distinct from those events, both
the CQC and SGC had changed their systems which also affected the availability of
documents. Despite there being a considerable amount of documents placed before

Page 82 of 142
the panel, therefore, those documents were nevertheless unlikely to amount to a
complete picture of what took place and what was available for inspection by the CQC.
Finally, Mr Unwin broadly submitted that the failures which had been alleged and
identified occurred both inside and outside Castlebeck. The Serious Case Review had
identified failings also by the CQC and SGC. Further, on this issue, those failings within
Castlebeck were not all attributable, nor attributed, to one registrant. The Serious Case
Review identified problems occurring at Winterbourne View prior even to Registrant A's
engagement there, and Witnesses 13 and 16 both gave evidence of considerable
failings on the part of the Board at Castlebeck.
The panel considered these observations to have been commendably made by Mr
Unwin in the interests of fairness for all parties.
The panel made the following findings of fact in respect of the charges:
That you, whilst employed by Castlebeck Care (Teesdale) Limited as a Regional
Operations Director/ Regional Operations Manager between 2007 and June 2012:
1 In relation to Winterbourne View:
1.1 Did not ensure that Winterbourne View met any or all of the national minimum
standards for independent healthcare, under the Care Standards Act 2000,
listed in Schedule A
Admitted and found proved.
1.2 Did not ensure that Winterbourne View was compliant with any or all of the
Health and Social Care Act 2008 essential standards listed in Schedule B

Page 83 of 142
Admitted and found proved.
1.3 Did not apply to register with the Care Quality Commission as the accountable
officer at the hospital under Part 2 of The Controlled Drugs (Supervision of
Management and Use) Regulations 2006.
No case to answer.
1.4 Did not ensure that an action plan was submitted to the Healthcare Commission
following an inspection on 24 March 2009
Admitted and found proved.
1.5 Did not ensure that Individual X was registered with the Care Quality
Commission as Manager of Winterbourne View at any time from January 2010
It was Witness 5’s evidence that on 21 January 2011 the CQC issued a certificate of
registration in the name of Registrant A, as the CQC had been told that she was the
Manager of the Hospital. The certificate registered Registrant A to carry on the
regulated activities at the Hospital. At the time of Witness 5’s visit in May 2011, she was
informed by Registrant C that Registrant A did not work at the Hospital and was
managing another Castlebeck unit. Witness 5 said that the CQC had not received any
notification from Castlebeck as regards the new management arrangements at the
Hospital. She said that Registrant C’s application to register was received by the CQC
on 19 April 2011 (it was dated 11 April 2011) and rejected on 21 April 2011, on the
Page 84 of 142
basis that it did not contain all the required documents and an out of date application
form had been used citing earlier legislation.
Witness 7 stated that Registrant A was unable to register with the CQC as Manager of
Chesterholme as she was the Registered Manager of Winterbourne View at the time of
its closure. Individual CC emailed Mr Harrison on 6 May 2011 to establish whether
Registrant A had cancelled her registration with the CQC. Mr Harrison responded on the
same day, stating “Yes they have been informed but only verbally at their last visit to the
unit. I need to send the appropriate written notification to them which I have to admit
had completely slipped my mind”.
Whilst Mr Harrison had suggested, in his oral evidence, that “we had gone through the
registration process with the CQC, completed all the forms and application and
submitted [Registrant C’s] qualification and registration details… we were just
waiting…”, his email to Individual CC indicated otherwise.
Mr Harrison was the Responsible Individual for Winterbourne View at the material time,
and was the Regional Operations Director for nine Castlebeck Units. He had an
obligation to ensure that Winterbourne View fully complied with all appropriate statutory
requirements as regulated by the CQC; this encompassed the requirement to ensure
that the Hospital’s Manager was registered as such with the CQC. Registrant C, for
whom Mr Harrison was responsible, did not apply to register as Manager of
Winterbourne View until April 2011.
On the basis of the evidence before it, the panel was in no doubt that Mr Harrison failed
to discharge his duty as required. Accordingly, the panel found charge 1.5 proved.
1.6 Following a whistle blowing complaint from Individual O on 11 October 2010:

Page 85 of 142
1.6.1 Did not ensure that any or all identified staff were suspended;
1.6.2 Did not ensure that an investigation was promptly conducted;
1.6.3 Did not ensure that a Serious Untoward Incident Form was completed.
Charge 1.6.1 was admitted by Mr Harrison and found proved.
In respect of charges 1.6.2 and 1.6.3, the panel gave careful regard to the following
evidence:
Witness 3 explained that he sent his whistle-blowing email, in which he set out his
concerns in relation to Winterbourne View, to Registrant C on 11 October 2010. A
senior staff meeting was held a few days later, attended by Witness 3, Registrant C,
Registrant D and Individual F. Witness 3 said that Registrant C left the meeting early
and the concerns raised in Witness 3’s email were not discussed.
On 16 October 2010 Witness 3 forwarded a copy of his email to Registrant A,
highlighting that the issues raised in his email had not been addressed. Registrant A
replied to Witness 3, by email on 17 October 2010, stating that Mr Harrison, Regional
Operations Director, was aware of his concerns.
Registrant A responded to Witness 3’s email on the same day. She said that she was
aware of his concerns and was under the impression that Registrant C and Registrant D
had had a meeting with him the week before. She said that she would meet with him on
Monday 18 October when she was due to visit the Hospital. She also confirmed that Mr
Harrison was aware of his concerns and that she would advise Witness 3 as to Mr
Harrison’s input, if Witness 3 wanted him to ‘lead’.
Witness 3 responded to Registrant A on 17 October 2010. He said that he was not
aware that Registrant A was due to meet with him on 18 October; he confirmed that he
was not available to meet that day. He suggested meeting the following week. Witness

Page 86 of 142
3 did not hear anything further. He contacted the CQC on three occasions raising
concerns in relation to care practices at Winterbourne View but received no response.
He subsequently reported his concerns to BBC Panorama.
It was Witness 5’s evidence that the whistle-blowing concerns should have been
followed up with the whistle-blower, reported within the organisation, advice sought, and
promptly reported to the local authority safeguarding team and to the CQC.
The panel had sight of a document exhibited by Witness 7 in which she summarised a
telephone conversation with Mr Harrison on 16 May 2011; according to that summary,
Mr Harrison could not recall the final outcome of his meeting with the safeguarding team
and Witness 3. He went on to say “maybe not done it quite as we should have done”.
According to Witness 7’s note from the investigation meeting held with Mr Harrison on 3
August 2011, Mr Harrison confirmed that Registrant A emailed him a copy of Witness
3’s whistle-blowing email, which Mr Harrison picked up on the following Monday (18
October 2011). Mr Harrison, in his email response to Registrant A, suggested that the
matter be reported to the safeguarding team. Registrant C arranged discussions with
Individual DD in the safeguarding team. Mr Harrison chased Registrant C on 22
October, and was told that the matter had been escalated to Individual DD’s Manager.
Mr Harrison said, at the meeting, that as far as he was concerned, the safeguarding
process was instigated and was ongoing. In January 2011, Mr Harrison and Registrant
C met with the safeguarding team and the CQC to close off the matter. According to the
notes of the meeting, there was no suggestion to do anything else and the only
expectation was for Registrant C to start/complete an internal investigation.
Mr Harrison also confirmed, in the meeting, that he informed Individual CC of the
whistle-blowing complaint, and that it was discussed at Regional Operations meetings.
He was unable to provide an answer when asked why staff members were not
suspended. He said that he made an assumption that staff members would have been
Page 87 of 142
suspended. According to the notes of his disciplinary hearing on 7 March 2012, Mr
Harrison acknowledged that he should have been more involved in following through
with staff suspensions.
It was Witness 7’s view, in her investigation report into Mr Harrison, that there was a
“lack of urgency” on his part, as well as a “failure to grasp the seriousness of the
complaints which had been raised”.
In a letter from the Chief Executive Officer of Castlebeck to the Associate Director of
Strategic Commissioning and Safeguarding (Northumberland Care NHS Trust), dated
13 June 2011, it was reported that the whistle-blowing email was “received in October in
the week [Registrant A] was ceasing any involvement with Winterbourne View and other
services in the Midlands to move to Chesterholme and she was aware that the Hospital
Manager and Regional Operations Director were handling the whistleblower allegations
and had referred these onto adult safeguarding…” In a subsequent letter dated 13 July
2011, the Chief Executive Officer repeated that Registrant A had passed on the
responsibility (in relation to addressing Witness 3’s whistle-blowing email) to Mr
Harrison.
According to a document exhibited by Witness 15 entitled ‘Chronology of Significant
Events’, the requirement for a SUI was not identified until 4 May 2011. When this was
put to Mr Harrison in evidence, he replied “I couldn’t comment. As far as I was aware,
everything had been done… and I was regularly assured by [Registrant C] that this was
the case”.
It was apparent, from Mr Harrison’s oral evidence, that he was of the view that an
investigation was instigated by Registrant C; he said “[Registrant C] had been asked to
look into [Witness 3’s] concerns… HR were aware… and he followed the advice that
had been given”. He acknowledged however, in his oral evidence, that his meeting with
external agencies in relation to the whistle-blowing concerns “took too long”. According
Page 88 of 142
to Mr Harrison, the overall responsibility for taking control of such a situation lay with the
Managing Director (Individual CC) and the HR Director (Witness 7).
Mr Harrison was the Responsible Individual, and Regional Operations Director, for
Winterbourne View at the material time, and Registrant C reported to him. According to
Mr Harrison’s job description he had a “responsibility for the identification of all risks
which have a potential adverse affect on the Company’s ability to maintain quality of
care and the safety of patients… and for the taking of positive action to eliminate or
reduce these… [and] ensure that risk management is a key component of…
management including risk assessment and appropriate action plans”. On the basis of
the evidence before it, the panel reached the conclusion that Mr Harrison failed to
discharge this obligation.
It was evident that no prompt investigation was undertaken following Witness 3’s
whistle-blowing complaint in October 2010. There was nothing before the panel to
suggest that Mr Harrison had taken appropriate and proactive steps to supervise and
monitor Registrant C in addressing the concerns. Rather, he appeared to suggest that
there was little more required of him in the circumstances, having reported the concerns
to Individual CC and Witness 7. He said that it would have been for the appointed HR
representative to have met with Witness 3 and to have kept him updated as to the
progress of any investigation. As far as Mr Harrison was concerned, “I passed it on to
my Managing Director, who was the Responsible Individual”. Mr Harrison agreed to
meet with Witness 3 after he was notified of the whistle-blowing concerns. Mr Harrison
was aware that Registrant A’s responsibility for Winterbourne View had ceased by this
point. He was also of the view that Registrant C, who was directly accountable to Mr
Harrison, was taking some action in addressing Witness 3’s concerns. It was therefore
unclear to the panel as to why he had assumed that he had no further role to play in
these matters. In the panel’s view, Mr Harrison’s oral evidence was indicative of a
disregard for his personal accountability in the circumstances. The panel was in no
doubt that Mr Harrison failed to provide the appropriate level of guidance, direction and

Page 89 of 142
supervision to Registrant C in the circumstances, and failed to ensure that the Whistle-
blowing Policy was being complied with.
For all the reasons set out above, the panel found charge 1.6.2 and 1.6.3 proved.
1.7 Did not ensure that one or more patients who were admitted to the Hospital
were suitable for admission;
It was Witness 13’s evidence that the responsibility for admitting patients at the time
was with the Manager of the service and their Line Manager, the Regional Operations
Director.
According to Witness 13, Mr Harrison admitted during the appeal hearing that service
users had been inappropriately admitted to the services he was responsible for as
Regional Operations Director. Mr Harrison said that he had raised concerns about the
admission of patients with his Line Manager, but he said that he was “under pressure”
from the Board to admit patients for “financial reasons”. Witness 13 said that Mr
Harrison was a very senior Board level employee of Castlebeck and she was concerned
that a person of his seniority had not acted as a whistle-blower, when he had concerns
about the service that would have a significant impact on patient care.
According to the notes of the investigation meeting held with Registrant A on 17 August
2011, Registrant A stated that she would put blocks on admissions, which was backed
by Mr Harrison. She also said that her strongest advice to Registrant C was to be “very
very aware” of admissions and the pressures put on him by the relevant team.
At Mr Harrison’s appeal hearing on 17 May 2012, Mr Harrison said that he had asked
for “no more admission until staff were sorted”. He said that this “often was ok but
sometimes [he was] asked to take admissions”.

Page 90 of 142
In his oral evidence to the panel Mr Harrison suggested that he had “very little input on
who was admitted” to the Hospital, other than being involved in discussions with the
referral team and Registrant C. He said that the assessment procedure involved senior
management who “decided which admission was appropriate”. He said that he assisted
Registrant C, if they felt under pressure from senior management; he said that “we had
weekly conference calls about admissions… [the referral team], [Witness 7], [Individual
CC], the Unit Managers… also, we had been instructed to staff at minimum levels…
there were many discussions about the appropriateness of admission…” He went on to
say that if issues became apparent only after admission, there was not much that could
be done as the patient was already in the Hospital.
Mr Harrison said that there was “immense pressure to fill beds… unless we could give a
very good reason not to admit a [patient]”. He confirmed that he had raised his concerns
about admissions with his Line Manager. He also said that “there were no deliberate
admissions that were not considered appropriate”.
The panel had regard to Mr Harrison’s job description which made plain that he was
required to “work towards ensuring that every appropriate action is taken to ensure
occupancy targets are met and where possible maximum occupancy is obtained”. The
panel heard evidence that Winterbourne View operated as a profit-making company and
that the mechanism by which patients were admitted was financially driven. The panel
accepted that there was considerable pressure placed upon Units to admit patients in
order to secure maximum occupancy. However, Mr Harrison was also responsible “for
the identification of all risks which have a potential adverse affect on the Company’s
ability to maintain quality of care and the safety of patients… and for the taking of
positive action to eliminate or reduce these…” He was aware of the ongoing issues in
relation to staffing at Winterbourne View. He was aware of the patients’ high levels of
needs and challenging behaviour. He was aware of the ongoing concerns in relation to
the adequacy of the training provided to staff to ensure the safe provision of care. He

Page 91 of 142
was also aware that the level of supervision of staff at the Hospital was “not always”
adequate. The panel was in no doubt that he was in a position to take appropriate
action in ensuring that only those patients suitable for admission were admitted; there
was no evidence that he did so.
Accordingly, the panel found charge 1.7 proved.
1.8 Did not ensure that staff at Winterbourne View received sufficient training to
provide appropriate care
Admitted and found proved.
1.9 Did not ensure that all staff at Winterbourne View received adequate
supervision and/or supervision records
Admitted and found proved.
1.10 Did not ensure that there were adequate systems in place for the analysis
and/or review of patient incidents at Winterbourne View
Admitted and found proved.
1.11 Did not ensure that there were adequate systems in place to prevent excessive
use of restraint
Admitted and found proved.

Page 92 of 142
1.12 Did not ensure that patients at Winterbourne View were protected from verbal
and physical abuse by members of staff;
Admitted and found proved.
2 In relation to Rose Villa:
2.1 Did not ensure that Rose Villa was compliant with any or all of the Health and
Social Care Act 2008 essential standards listed in Schedule C
Admitted and found proved.
3 In relation to Croxton Lodge:
3.1 Did not ensure that Croxton Lodge was compliant with any or all of the Health
and Social Care Act 2008 essential standards listed in Schedule D
Admitted and found proved.
4 In relation to Arden Vale:
4.1 Did not ensure that Arden Vale met any or all of the national minimum
standards for independent healthcare, under the Care Standards Act 2000, for
independent healthcare listed in Schedule E

Page 93 of 142
Admitted and found proved.
4.2 Did not ensure that Arden Vale was compliant with any or all of the Health and
Social Care Act 2008 essential standards listed in Schedule F
Admitted and found proved.
5 In relation to Cedar Vale
5.1 Did not ensure that Cedar Vale met any or all of the national minimum
standards for independent healthcare, under the Care Standards Act 2000,
listed in Schedule G
Admitted and found proved.
5.2 Did not ensure that Cedar Vale was compliant with any or all of the Health and
Social Care Act 2008 essential standards listed in Schedule H
Admitted and found proved.
6 In relation to Willow House
6.1 Did not ensure that Willow House was compliant with any or all of the Health
and Social Care Act 2008 essential standards listed in Schedule I
Admitted and found proved.

Page 94 of 142
7 In relation to The East Midlands Centre for Neurobehavioural Rehabilitation
7.1 Did not ensure that The East Midlands Centre for Neurobehavioural
Rehabilitation was compliant with any or all of the Health and Social Care Act
2008 essential standards listed in Schedule J
Admitted and found proved.
Determination on interim order (upon adjourning) – Thursday 8 June 2017
No application was made by the NMC for the imposition of an interim order. Attempts
were made to contact Mr Harrison for his representations. These attempts were
unsuccessful.
In accordance with Article 31(2) of the Nursing and Midwifery Order (2001) and Rule
32(5) of the Rules, the panel considered whether an interim order should be imposed.
Article 31 of the Order outlines the criteria for the imposition of an interim order. The
panel may make an interim order on one or more of three grounds:
Where it is satisfied that it is necessary for the protection of members of the
public;
Where it is satisfied that such an order is otherwise in the public interest;
Where it is satisfied that such an order is in the interests of the registrant.

Page 95 of 142
The panel, having carefully considered the matter and having accepted the advice of
the legal assessor, was not satisfied that any of the three grounds were met. Therefore
no interim order will be placed on Mr Harrison’s registration.

Page 96 of 142
The hearing resumed on 3, 4 and the morning of 5 July 2017 ‘in camera’, and from the
afternoon of 5 July 2017 in public session.
Determination on misconduct and impairment – Wednesday 5 July 2017
Mr Harrison’s evidence
The panel heard evidence from Mr Harrison, by telephone, at this stage of the
proceedings.
Mr Harrison told the panel that he accepted its findings of fact. He said that they had
been “well-established”.
Mr Harrison told the panel that he was “put in charge of a very very large and well-
scattered area to support… it meant an awful lot of time spent moving to and from
different Units”, which meant that he was unable to dedicate sufficient time in each Unit
as he would have liked and which would have “made a difference”. He said “there was
nothing I could do about that, that was how the territory was divided between us
Regional Operations Directors”.
Mr Harrison told the panel that the primary lesson he had learned, as a result of the
failings identified at Winterbourne View, was “to say no to people when they’re putting
on extra pressure to take work on, and explain why I can’t do it… and be able to, and
have the courage to, say no to my employer”. He said that he was not able to offer the
support that was required, as he was “too thinly spread” and, as a result, “ultimately
everyone within the organisation suffer[ed] to a degree”.
Mr Harrison said that he had learned “to be more thorough in checking if things are
done… and not just accepting that they are done… that was the biggest thing for me…
[and] when my superior began to break up the team that was put in place, to be more

Page 97 of 142
robust in my challenges and make sure the support stays where it’s required, and
evidently where it was required”. He went on to say that he had learned “having the
courage to say no when people are asking unreasonable things of you… and
developing arguments for that… [and] when concerns are raised, to act upon them and
follow them through fully”.
Mr Harrison told the panel that he had not worked in a care environment since 2012, as
he was told by the NMC that he was not able to renew his nursing registration until the
conclusion of these proceedings.
In respect of his current employment status, Mr Harrison explained that he was privately
contracted to provide training to assist people in gaining their Level 4 Management
qualification. He said that, in his current role, he managed a team of approximately six
people. He primarily worked in one location, which enabled his team to “bring their
concerns to me and expect me to advise and support them… which I have to do a lot
more robustly… I go through processes with them and… rather than relying on others, I
follow through personally and made sure outcomes are achieved”. He told the panel
that working from one office made it easier to facilitate two-way communication.
As to remorse, Mr Harrison told the panel that “it’s difficult to put into words... it has had
a profound effect on me and my outlook towards things… [as to those most affected by
events at Winterbourne View] the people who suffered the horrible abuse… [and] its
wider than that… there were other members of the team who were put through
unnecessary trauma because of this… if [Winterbourne View] was managed better, it
could have been avoided”.
When asked to comment on the proactive steps he could have taken in the
circumstances, Mr Harrison said that he could have spent time within the Unit and
offered more direct support; that said, he stated that it was “difficult to give the support
that was obviously required… can’t do much remotely… reliance on reports and emails

Page 98 of 142
wasn’t enough. Really, the biggest support would be to ensure that there was sufficient
and experienced support available to a rapidly developing area… and being in a
position to put in a stronger case for that support to my superiors”.
Mr Harrison told the panel that there were instances of Root Cause Analyses “occurring
very robustly… we had investigated some incidents that resulted in dismissals…” In
relation to staff supervision, he said “I knew it wasn’t 100% up to date, but I knew there
had been huge improvements in the regularity of sessions…” In relation to those
charges concerning a failure to meet CQC standards, he said that he was “surprised…
how wide the issues had been… previous CQC reports were fine or only minor issues
identified. So, the change was quite surprising”.
Mr Harrison said that he was aware of one particular patient admission, referred to by
Witness 31 in his oral evidence to the panel on behalf of Registrant D, who was of
particular concern and who, in Witness 31’s view, contributed to an increase in patient
incidents. Mr Harrison said “we tried to ensure that we got the appropriate staffing levels
to manage and support the patients. That didn’t always happen. We took on the
admission expecting what we were told to expect, and it was quite different when the
patient arrived”. He said that issues in relation to patient admissions were reported
monthly in management reports, and discussed in weekly conference calls
When asked if he was aware of an increase in the number of restraints used on patients
at Winterbourne View, Mr Harrison replied, “not as an individual issue… some of the
patients were a lot more demanding [and] the demands on staff were increasing
proportionately”.
Mr Harrison said that he did have concerns about Registrant C’s performance as a
Manager “but those were concerns that could have been sorted with support… like
when my superiors decided to take [Registrant A] out of the area and [Registrant C did
not receive] the support that he needed”.

Page 99 of 142
Mr Harrison said that he accepted that “all the charges are serious, there’s no hiding
from that at all. Serious enough for an investigatory meeting, for this process to be gone
through, and rightly so. I don’t deny that”. He acknowledged that “public trust in the
profession is damaged because of the nature of what had happened… [that’s]
unavoidable”. In regard to public perception of him personally, he replied “loss of trust…
and anger in public opinion about what happened at Winterbourne View”.
Mr Harrison told the panel that he was unsure as to whether he would return to the
nursing profession. He did, however, make efforts to keep his nursing knowledge up to
date since 2012, by reading journals and keeping abreast of nursing news. He said that
he had undertaken relevant training in his current role which were, to a degree,
applicable to the nursing profession, including safeguarding, equality and diversity, first
aid and moving and handling.
In addition to his oral evidence, the panel was also provided with a letter written by Mr
Harrison which had been attached to his ‘Standard Directions Form’ dated October
2014. In that letter, amongst other things, Mr Harrison had written, “I accept fully that it
was my responsibility as part of the overall care team to ensure that he [sic] the people
within our care received the best possible care and I believe that I worked hard as part
of a team to achieve this in very difficult circumstances… I have been a Nurse now for
over 20 years and my record has been exemplary. I have never been subject to any
kind of investigation prior to this one… I asked for my appraisal and supervision records
to support this but they were never sent to me”.
Submissions
The panel then invited submissions on the matters of misconduct and current
impairment.

Page 100 of 142
As to misconduct, Mr Unwin referred the panel to the case of Roylance v General
Medical Council [2000] 1 A.C. 311, in particular to the judgment of Lord Clyde who
described misconduct as “a word of general effect, involving some act or omission
which falls short of what would be proper in the circumstances. The standard of
propriety may often be found by reference to the rules and standards ordinarily required
to be followed by a medical practitioner … [the] misconduct must be serious.”
Mr Unwin submitted that the case of Roylance was of some assistance in relation to
practitioners with management or administrative roles: “[Roylance] was both a
registered medical practitioner and chief executive of a hospital. In each capacity he
had a duty to care for the safety and well-being of the patients. As chief executive that
duty arose out of his holding of that appointment. As a registered medical practitioner he
had the general obligation to care for the sick. That duty did not disappear when he took
on the appointment but continued to co-exist with it.”
Mr Unwin also referred the panel to the case of Calhaem v General Medical Council
[2007] EWHC 2606 (Admin), in which Jackson J derived the following relevant
principles from a review of the authorities:
“(1) Mere negligence does not constitute ‘misconduct’ … Nevertheless, and depending
upon the circumstances, negligent acts or omissions which are particularly serious may
amount to “misconduct”.
(2) A single negligent act or omission is less likely to cross the threshold of ‘misconduct’
than multiple acts or omissions. Nevertheless, and depending upon the circumstances,
a single negligent act or omission, if particularly grave, could be characterised as
‘misconduct’”.
Furthermore, Mr Unwin referred the panel to the case of R (on the application of
Remedy UK Ltd) v General Medical Council [2010] EWHC 1245 (Admin), in which Elias

Page 101 of 142
LJ derived the following principles from Roylance and other authorities: “[Misconduct]
need not arise in the context of a doctor exercising his clinical practice…” but can be in
“the exercise of administrative or managerial functions, where they are part of the day to
day practice of a professional doctor. These functions include the matters identified in
Sadler, such as proper record-keeping, adequate patient communication, proper
courtesy shown to patients and so forth… the obligation to take responsibility for the
care of patients does not cease simply because a doctor is exercising managerial or
administrative functions one step removed from direct patient care. Depending upon the
nature of the duties being exercised, a continuing obligation to focus on patient care
may co-exist with a range of distinct administrative duties, even where other doctors
with a different specialty have primary responsibility for the patients concerned.”
Mr Unwin invited the panel to have regard to the NMC’s publications, ‘The NMC code of
professional conduct: standards for conduct, performance and ethics’ (November 2004)
(“the 2004 Code”) and ‘The code: Standards of conduct, performance and ethics for
nurses and midwives’ (May 2008) (“the 2008 Code”). He submitted that the Codes were
an important reference for assessing whether the facts found proved amounted to a
falling short of the standards expected of a Registered Nurse. He submitted that not
every breach of the relevant Code amounted to misconduct; the breach must be
sufficiently serious. He further submitted that a series of incidents not individually
serious enough to constitute misconduct may be considered cumulatively to be
sufficiently serious.
Mr Unwin submitted that in assessing the seriousness of the failings found proved, the
panel should have regard to its findings about what, if any, steps were taken by each
registrant, as well as its findings about the context of systemic corporate failings, and
what could reasonably be known by the registrants at the time, without the benefit of
hindsight.
Mr Unwin referred the panel to the following provisions of the Codes:

Page 102 of 142
Arden Vale: (the 2004 Code)
Charge 4.1
As a registered nurse … you are personally accountable for your practice. In caring for
patients and clients, you must:
act to identify and minimise risk to patients and clients.
Paragraphs 1.3, 1.4, 4.6, 8.1 and 8.3
Winterbourne View, Rose Villa, Croxton Lodge, Cedar Vale, Willow House and The
East Midlands Centre for Neurobehavioural Rehabilitation: the 2008 Code
Charges 1.1, 1.2, 2.1 and 4.2
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
make the care of people your first concern, treating them as individuals and
respecting their dignity
work with others to protect and promote the health and wellbeing of those in your
care, their families and carers, and the wider community
provide a high standard of practice and care at all times
Paragraphs 4, 12, 15, 16, 22, 30, 31, 33, 34, 35 and 61
Charge 1.4

Page 103 of 142
Mr Unwin submitted that in light of the panel’s finding in respect of the corresponding
charge against Registrant A (charge 2.4), the panel was invited to disregard its finding
in respect of charge 1.4 for the purpose of this stage of the hearing.
Charge 1.5
Paragraphs 30 and 33
Charge 1.6 in its entirety
Paragraphs 22, 32, 54 and 61
Charge 1.7
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
make the care of people your first concern, treating them as individuals and
respecting their dignity
Paragraphs 32, 33 and 34
Charge 1.8 and 1.9
Paragraphs 23, 29 and 31
Charge 1.10
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
provide a high standard of practice and care at all times
Paragraph 22
Page 104 of 142
Charges 1.11 and 1.12
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
make the care of people your first concern, treating them as individuals and
respecting their dignity
work with others to protect and promote the health and wellbeing of those in your
care, their families and carers, and the wider community
Paragraphs 16, 34, 35, 54 and 61
Charges 3.1, 5.1, 5.2, 6.1 and 7.1
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
provide a high standard of practice and care at all times
Paragraphs 22, 30, 33 and 35
As to the matter of impairment, Mr Unwin submitted that this was not limited to the
question of whether a registrant presented a risk to the health, safety and/or welfare of
the public, but also encompassed a careful consideration of the public interest.
Mr Unwin referred the panel to the case of Council for Healthcare Regulatory
Excellence v (1) Nursing and Midwifery Council (2) Grant [2011] EWHC 927 (Admin), in
particular paragraphs 70, 71, 74, 75 and 76 of the judgment. He also referred to the
questions outlined by Dame Janet Smith in her 5th report on Shipman (as endorsed in
the case of Grant):

Page 105 of 142
“Do our findings of fact in respect of the [registrant’s] misconduct […] show that [his]
fitness to practise is impaired in the sense that [he]:
a. has in the past acted and/or is liable in the future to act so as to put a patient or
patients at unwarranted risk of harm; and/or
b. has in the past brought and/or is liable in the future to bring the [nursing]
profession into disrepute; and/or
c. has in the past breached and/or is liable in the future to breach one of the
fundamental tenets of the [nursing] profession; and/or
d. has in the past acted dishonestly and/or is liable to act dishonestly in the future.”
Mr Unwin reminded the panel that Mr Harrison had admitted that his fitness to practise
is impaired by reason of his misconduct. Nevertheless, Mr Unwin acknowledged that
impairment was a matter for the panel’s assessment and judgement.
Mr Unwin submitted that the panel had found, largely on the basis of Mr Harrison’s own
admissions, that Mr Harrison had failed to ensure that several Units within his
responsibility were compliant with essential regulatory standards. Mr Unwin contended
that Mr Harrison’s numerous failings at Winterbourne View, Rose Villa, and Arden Vale
were especially serious, including practices of inappropriate restraint, and at
Winterbourne View, abuse of extremely vulnerable patients. Mr Unwin reminded the
panel of Mr Harrison’s admission that, as Regional Operations Director, he did not
ensure that patients were protected from abuse. In those circumstances, Mr Unwin
submitted that Mr Harrison had acted in a way so as to put patients at unwarranted risk
of harm, brought the profession into disrepute and breached a fundamental tenet of the
nursing profession.
Mr Unwin invited the panel to give careful consideration to Mr Harrison’s evidence
during the course of these proceedings; Mr Harrison told the panel that he was unable
to spend sufficient time at Winterbourne View because of the large number of Units he
Page 106 of 142
was required to cover over a wide geographic area. Mr Unwin referred the panel to the
evidence of Witness 13 and Witness 16, who spoke of the proactive steps they would
have expected Mr Harrison to take in identifying issues, performance managing the Unit
managers and escalating concerns. They also spoke of Mr Harrison’s failure to act
appropriately when serious whistleblowing concerns were brought to his attention.
It was Mr Harrison’s evidence that he had reflected upon the importance of being more
robust in ‘pushing back’ when an employer were to put him in a position where he could
not provide the necessary support to others in the organisation. In light of this evidence,
Mr Unwin submitted that the panel may be concerned about the degree of Mr Harrison’s
insight into his specific failings and the relatively vague and general nature of his
reflection.
Panel’s decision
In reaching its decision, the panel had regard to all the evidence before it, and the
submissions made by Mr Unwin.
The panel accepted the advice of the legal assessor, who referred the panel to the
cases cited by the advocates and, additionally, to the case of Schodlok v General
Medical Council [2015] EWCA Civ 769. In that case, Lord Justice Vos criticised the
panel’s decision to take into account the proven incidents of non-serious misconduct in
determining that the doctor’s fitness to practise was impaired. He said that he was not of
the view that a few allegations of misconduct, which were held individually not to be
serious, could or should be regarded collectively as serious misconduct. However, the
legal assessor commended the remarks of Lord Justice Beatson, who commented that
a cumulative approach to the consideration of misconduct should in principle be open to
the panel, provided that this approach was made clear to the practitioner and that he or
she was aware that this was a possibility. He said that where there were a large number
of findings of non-serious misconduct, particularly where they were of the same or

Page 107 of 142
similar misconduct, it should in principle be open for a fitness to practise panel to find
that, cumulatively, they were to be regarded as serious misconduct capable of impairing
a practitioner’s fitness to practise.
The legal assessor also referred to the case of Johnson and Maggs v NMC [2013]
EWHC 2140 (Admin), which addressed the danger of judging conduct with the benefit of
hindsight.
The panel was advised that, in relation to impairment by reason of misconduct, it must
engage in a two stage process: it must first consider whether, on the facts found proved,
Mr Harrison’s failures and omissions amounted to misconduct; and second, if so,
whether his fitness to practise is currently impaired by reason of that misconduct.
The panel, in reaching its decision, accepted that there was no burden or standard of
proof at this stage and exercised its own professional judgement.
The panel was aware that not every instance of falling short from what would be proper
in the circumstances, and not every breach of the Code, would be sufficiently serious to
be described as misconduct, going to a registrant’s fitness to practise. Accordingly, the
panel had careful regard to the context and circumstances of the matters found proved.
With regard to the prevailing circumstances prominent in this case, the panel
considered the following:
The complex needs, challenging behaviours and vulnerabilities of the patient
group at Winterbourne View.
Mr Harrison joined Castlebeck in 1991, initially as a Staff Nurse. He was
promoted to Senior Staff Nurse, Charge Nurse, Deputy Manager, Manager,
Senior Manager, Area Manager, Regional Operations Manager and Regional
Operations Director. He therefore had significant knowledge and experience of
Castlebeck’s working practices.

Page 108 of 142
Mr Harrison had an overarching responsibility for all patients across all the Units
within his region. He was the designated CQC Responsible Individual of Arden
Vale, Winterbourne View, Croxton Lodge and Cedar Vale and, as a result, had
specific regulatory responsibilities and accountabilities over and above those in
his capacity as Regional Operations Director.
Mr Harrison’s higher degree of accountability and responsibility in light of his
seniority. He was the most senior member of staff with direct responsibility for the
nine Units, with responsibility to supervise, guide, support and manage
operational practices at a senior level, and ensure compliance with regulatory
essential standards.
Mr Harrison had direct access to the Castlebeck Board and had numerous
opportunities to effect positive change, particularly with regard to Winterbourne
View.
Mr Harrison’s direct line management of Registrant C was extremely limited and,
overall, insufficient, particularly in the context of Registrant A’s support being
withdrawn.
Mr Harrison had numerous opportunities to investigate areas of concerns and
apparent discrepancies; for example, there was only one entry (dated 24 March
2010) in the Winterbourne View Complaints record log after 2009. This obvious
anomaly ought to have caused Mr Harrison, at the very least, to question
Registrant C.
In the exercise of his responsibilities, Mr Harrison appeared primarily to rely on
verbal feedback from his staff and placed a significant degree of trust in those
staff members to ‘get on with their job’.
Mr Harrison was in receipt of the monthly management reports completed by Unit
Managers in relation to areas of concerns in the Units including staffing, training,
risk management and supervision. There was limited evidence before the panel
that Mr Harrison formally escalated concerns raised to the Castlebeck Board.
A number of charges concerned documentation which was not available to the
CQC Compliance Inspectors during their visits of Winterbourne View in May

Page 109 of 142
2011. Some relevant documentation was later identified following the closure of
Winterbourne View, as evidenced in the material considered for the purpose of
the Serious Case Review. The documentation before the panel at this
substantive hearing was not likely, therefore, to have formed an accurate,
complete or global picture of Winterbourne View.
Charge 4.1
The Healthcare Commission inspection of Arden Vale took place on 18 October 2007.
Of the national minimum standards inspected, under the Care Standards Act 2000, only
two standards were ‘not met’. Nine standards were ‘almost met’ and five standards were
‘met’.
The panel was mindful of the evidence of Registrant A, Manager of Arden Vale at the
time. Registrant A told the panel that the outcome of the inspection “confirmed” what
she already knew, and that she was not given the opportunity to embed any significant
changes as she was constantly moved from one Unit to the next.
The panel was further mindful that it was not provided with any documentary evidence
in the form of previous Healthcare Commission/CQC reports against which it could
consider a comparison or assess what improvements, if any, had been made in the
Unit.
Having regard to the totality of the findings of the inspection carried out on 18 October
2007, in the context of the prevailing circumstances in Registrant A’s and Mr Harrison’s
case, the panel concluded that Mr Harrison’s failures were not sufficiently serious to
amount to misconduct.
Charges 1.1, 1.2, 2.1 and 4.2
Page 110 of 142
With regard to charge 1.1, the panel took account of the following:
Of the standards inspected, following the Healthcare Commission inspection of
Winterbourne View on 24 March 2009, six standards were ‘not met’ and two standards
were ‘met’.
Of the standards inspected, following the CQC inspection on 15 December 2009,
five standards were ‘almost met’ and 12 standards were ‘met’. There were no standards
inspected which were ‘not met’.
There was, evidently, a pattern of improvement. The panel also considered the
testimonies of both Registrant A and Mr Harrison who spoke of positive CQC
inspections which were not put before the panel. Having regard to the evidence before
it, the panel concluded that Mr Harrison’s failures were not sufficiently serious to amount
to misconduct.
With regard to charge 1.2, the panel took into account the following:
All 10 standards inspected, following the CQC inspection of Winterbourne View in
May/June 2011, were identified as ‘major concerns’.
Mr Harrison was the Responsible Individual for Winterbourne View. In that capacity, he
was responsible for ensuring the quality of the service provided by the Unit. As Regional
Operations Director, he was responsible for ensuring that all Units fully complied with all
appropriate statutory standards and requirements as regulated by the CQC.
Mr Harrison was acutely aware of the support that Registrant C required in the
operational management of the Unit. There was little evidence before the panel of any
steps taken by him to address the specific and identified deficiencies in the service
provided by Winterbourne View. The panel carefully considered the findings of this

Page 111 of 142
inspection against the findings in 2009; the deterioration in the quality of the service
provided was stark. As Regional Operations Director and Responsible Individual, Mr
Harrison was ultimately responsible and accountable for that deterioration.
The panel determined that Mr Harrison’s failures exposed patients to an unwarranted
risk of harm, particularly when considering that the standards inspected in May/June
2011 related to fundamental and essential nursing care, including ‘safeguarding people
who use services from abuse’, ‘care and welfare of people who use services’,
‘management of medicines’ and ‘records’.
With regard to charge 2.1, the panel took account of the following:
Of the standards inspected, following the CQC inspection of Rose Villa in June and July
2011, three standards were identified as ‘major concerns’, two standards as ‘moderate
concerns’ and two standards as ‘minor concerns’.
The panel was mindful that it was not provided with any documentary evidence in the
form of previous Healthcare Commission/CQC reports against which it could consider a
comparison or assess what improvements, if any, had been made in the Unit.
On the basis of the limited evidence before it, the panel was not of the view that it could
safely conclude a finding of misconduct.
With regard to charge 4.2, the panel took account of the following:
Mr Harrison was the Responsible Individual for Arden Vale from 2007. In that capacity,
he was responsible for ensuring the quality of the service provided by the Unit. As
Regional Operations Director, he was responsible for ensuring that all Units fully
complied with all appropriate statutory standards and requirements as regulated by the
CQC.

Page 112 of 142
The panel carefully considered the findings of the inspection in June 2011 against the
findings in October 2007; the deterioration in the quality of the service provided was
stark. There was an evident deterioration in the Unit’s compliance with essential
standards following the inspection in October 2007, to the extent that 11 standards were
identified as ‘major concerns’ and one standard as ‘moderate concerns’. As Regional
Operations Director and Responsible Individual, Mr Harrison was ultimately responsible
and accountable for that deterioration. Of concern to the panel was, according to the
notes of his disciplinary hearing on 7 March 2012, Mr Harrison’s apparent lack of
awareness of any issues in Arden Vale. This was, in the panel’s view, inexcusable and
unjustifiable, given his role and responsibilities at the time.
The panel determined that Mr Harrison’s failures exposed patients to an unwarranted
risk of harm, particularly when considering that the standards inspected in May/June
2011 related to fundamental and essential nursing care, including ‘safeguarding people
who use services from abuse’, ‘care and welfare of people who use services’,
‘management of medicines’ and ‘records’.
The panel determined that Mr Harrison’s failures in respect of charges 1.2 and 4.2 were
sufficiently serious as to amount to misconduct. The panel further determined that his
failures were in breach of the following provisions of the Code:
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
make the care of people your first concern, treating them as individuals and
respecting their dignity
work with others to protect and promote the health and wellbeing of those in your
care, their families and carers, and the wider community

Page 113 of 142
provide a high standard of practice and care at all times
4 You must act as an advocate for those in your care, helping them to access relevant
health and social care, information and support.
12 You must share with people, in a way they can understand, the information they
want or need to know about their health.
15 You must uphold people’s rights to be fully involved in decisions about their care.
16 You must be aware of the legislation regarding mental capacity, ensuring that people
who lack capacity remain at the centre of decision making and are fully safeguarded.
22 You must work with colleagues to […] maintain the safety of those in your care.
30 You must confirm that the outcome of any delegated task meets required standards.
31 You must make sure that everyone you are responsible for is supervised and
supported.
33 You must inform someone in authority if you experience problems that prevent you
working within this code or other nationally agreed standards.
34 You must report your concerns in writing if problems in the environment of care are
putting people at risk.
35 You must deliver care based on the best available evidence or best practice.
61 You must uphold the reputation of your profession at all times.
Page 114 of 142
The panel was not minded to consider that the other instances (charges 1.1 and 2.1)
should be accumulated to find a further allegation of misconduct against Mr Harrison, as
the panel could not safely conclude on the evidence that there was any degree of
misconduct in respect of these charges on the part of Mr Harrison.
Charge 1.4
The panel took into account that the corresponding charge against Registrant A was
found, on the evidence before it, not proved. Notwithstanding Mr Harrison’s admission,
it cannot be said that there was a failure on his part and, therefore, no misconduct
arises.
Charge 1.5
Mr Harrison was the Regional Operations Director and Responsible Individual for
Winterbourne View at the material time. He had an obligation to ensure that
Winterbourne View fully complied with all appropriate statutory requirements as
regulated by the CQC; this encompassed the requirement to ensure that the Hospital’s
Manager was registered as such with the CQC. Registrant C, for whom Mr Harrison had
direct line management responsibility, did not apply to register as Manager of
Winterbourne View until April 2011.
Whilst Registrant A took steps to assist and prompt Registrant C to register with the
CQC as Registered Manager, it was Mr Harrison’s responsibility to ensure that this had
happened. As a result of Registrant C’s failure to register with the CQC, the lines of
management accountability were blurred by the time the BBC Panorama documentary
was aired. This had serious implications for Registrant A, who was still formally
registered with the CQC as Registered Manager.

Page 115 of 142
The panel determined that Mr Harrison’s failure to discharge his obligation as required
was sufficiently serious as to amount to misconduct. The panel further determined that
his failures were in breach of the following provisions of the Code:
30 You must confirm that the outcome of any delegated task meets required standards.
33 You must inform someone in authority if you experience problems that prevent you
working within this code or other nationally agreed standards.
Charge 1.6 in its entirety
Mr Harrison was aware of the whistle-blowing complaint raised by Witness 3. Whilst he
‘suggested’ to Registrant A that the matter be reported to the safeguarding team, and
having chased Registrant C on 22 October, he took few proactive steps to address what
were serious safeguarding allegations. Despite his overarching responsibility for
Winterbourne View, he was unable to explain why staff members were not suspended
or why a SUI was not reported until 4 May 2011, some seven months later. He said that
he made an assumption that staff members would have been suspended. It was
Witness 7’s evidence, the sentiment of which was echoed by the panel, that there was a
lack of urgency on Mr Harrison’s part, and a failure to grasp the seriousness of the
complaints which had been raised.
Whilst he acknowledged that his meeting with external agencies in relation to the
whistle-blowing concerns “took too long”, Mr Harrison sought to place blame on others.
According to Mr Harrison, the overall responsibility for taking control of this situation lay
with the Managing Director (Individual CC) and the HR Director (Witness 7).
Mr Harrison was the Responsible Individual, and Regional Operations Director, for
Winterbourne View at the material time, and Registrant C reported to him. He was
responsible for identifying all risks which had the potential to undermine the quality of

Page 116 of 142
care and the safety of patients and taking action to address and manage those risks. Mr
Harrison failed to discharge this obligation.
Mr Harrison was aware of the need to supervise and monitor Registrant C in the
circumstances. He was aware that Registrant A’s responsibility for Winterbourne View
had ceased by this point. In the panel’s view, Mr Harrison displayed a disregard for his
personal accountability in the circumstances. He failed to provide the appropriate level
of guidance, direction and supervision to Registrant C and failed to ensure that the
Whistle-blowing Policy was being complied with.
The panel was in no doubt, given the substance and severity of the concerns raised by
Witness 3, that Mr Harrison’s failures were significant and placed the patients at
Winterbourne View at serious and unwarranted risk of harm. The panel determined that
Mr Harrison’s failures were sufficiently serious as to amount to misconduct. The panel
further determined that his failures were in breach of the following provisions of the
Code:
22 You must work with colleagues to […] maintain the safety of those in your care.
30 You must confirm that the outcome of any delegated task meets required standards.
31 You must make sure that everyone you are responsible for is supervised and
supported.
32 You must act without delay if you believe that you, a colleague or anyone else may
be putting someone at risk.
34 You must report your concerns in writing if problems in the environment of care are
putting people at risk.

Page 117 of 142
54 You must act immediately to put matters right if someone in your care has suffered
harm for any reason.
61 You must uphold the reputation of your profession at all times.
Charge 1.7
Despite Mr Harrison’s suggestion that he had “very little input on who was admitted” to
the Hospital, the panel was not so persuaded. Whilst the panel recognised and
acknowledged the pressure placed upon Units to admit patients in order to secure
maximum occupancy, Mr Harrison was in a position of considerable seniority and had
direct access to the Castlebeck Board. He was therefore in an influential position to
effect positive change and, ultimately, to ensure the safety of all patients, new and
existing, and staff members at the Hospital. He was aware of the patients’ high levels of
need and challenging behaviours. He was aware of the ongoing concerns in relation to
the adequacy of the training provided to staff to ensure the safe provision of care. He
was aware that the level of supervision of staff at the Hospital was “not always”
adequate. He was also aware of the concerns raised by Individual K and Witness 3, and
the increase in patient incidents and use of restraint following the admission of one
particular patient in December 2010.
It was incumbent upon Mr Harrison to ensure that the Hospital was able to meet the
needs of the patients sought to be admitted. He ought to have analysed the potential
adverse impact of unsuitable admissions on other patients in the Hospital as well on
staffing levels, and on staff members in general. His failure to discharge his
responsibilities in the circumstances would have had a direct impact on the safety of
newly admitted patients, existing patients and staff members, staffing numbers, and the
ability of staff members to provide the level of safe and effective care required.

Page 118 of 142
As a result of his significant failure, Mr Harrison placed patients and staff at serious and
unwarranted risk of harm. The panel determined that his failure was sufficiently serious
as to amount to misconduct. The panel further determined that his failure was in breach
of the following provisions of the Code:
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
make the care of people your first concern, treating them as individuals and
respecting their dignity
30 You must confirm that the outcome of any delegated task meets required standards.
31 You must make sure that everyone you are responsible for is supervised and
supported.
32 You must act without delay if you believe that you, a colleague or anyone else may
be putting someone at risk.
33 You must inform someone in authority if you experience problems that prevent you
working within this code or other nationally agreed standards.
34 You must report your concerns in writing if problems in the environment of care are
putting people at risk.
61 You must uphold the reputation of your profession at all times.
Charges 1.8 and 1.9

Page 119 of 142
Training and supervision of staff are, individually and jointly, fundamental and critical to
the provision of safe, appropriate and effective care.
In light of the complexities and vulnerabilities of the patients at Winterbourne View, it
was crucial that staff members received the training required to provide proper and
appropriate care to patients. It was also crucial that staff members were supervised and
supported in their roles; effective supervision is, undoubtedly, key to the development of
good nursing skills and knowledge, reflective practice, confidence, competence and
morale.
Mr Harrison was the Responsible Individual for Winterbourne View. In that capacity, he
was responsible for ensuring the quality of the service provided by the Unit. As Regional
Operations Director, he was responsible for ensuring that all Units fully complied with all
appropriate statutory standards and requirements as regulated by the CQC. Moreover,
he was part of the corporate group established specifically in relation to training, of
which Witness 7, as HR Director, was also a member.
There was no evidence before the panel that the steps taken by Mr Harrison with regard
to training and supervision were sufficiently vigorous or reasonable. In light of his
responsibilities, and the direct access he had to the Castlebeck Board which placed him
in an advantageous and influential position to effect positive change, the panel found Mr
Harrison’s failures to be significant and had an impact on the overall quality of care
offered to, and received by, the patients at Winterbourne View. Additionally, Mr
Harrison, as the Responsible Individual for Winterbourne View, could and should have
raised any concerns that were not being addressed by the Castlebeck Board with the
CQC. The panel also had in mind Mr Harrison’s own failure to provide adequate
supervision to Registrant C to ensure that he was carrying out his role as Manager of
Winterbourne View to the standard required.

Page 120 of 142
The panel was satisfied that its findings in respect of the corresponding charges faced
by Registrant A can be distinguished by the identified actions taken by her in her
respective role as against Mr Harrison’s inaction/inadequacy of his actions and,
fundamentally, his overarching responsibility as Regional Operations Director and
Responsible Individual.
The panel determined that Mr Harrison’s failures were sufficiently serious as to amount
to misconduct. The panel further determined that his failures were in breach of the
following provisions of the Code:
23 You must facilitate students and others to develop their competence.
29 You must establish that anyone you delegate to is able to carry out your instructions.
31 You must make sure that everyone you are responsible for is supervised and
supported.
Charge 1.10
As an experienced Manager of considerable seniority and authority, and in light of his
overarching responsibilities as Regional Operations Director and Responsible
Individual, Mr Harrison had a corporate responsibility to identify incidents at
Winterbourne View and ensure that such incidents were appropriately and adequately
analysed/reviewed. MDTs were, at the time, the prime mechanism used for reviewing
and analysing patient incidents. There was no evidence before the panel to suggest that
MDTs had been used effectively in this regard.
The panel took account of the evidence of Witness 5, who stated that
accidents/incidents in daily care notes did not correspond with accident/incident forms.
She further stated that forms were not always being completed after a patient restraint.

Page 121 of 142
It was her evidence that the accuracy and completion of such documents were
important in analysing and establishing trends and patterns. She said that “The
provider’s policy should set out the responsibilities for following up incidents, which is
usually a management responsibility. Follow up is necessary to consider trends/themes
and identify the learning and actions to prevent reoccurrence”. In addition, it was
reported in the Serious Case Review that “It is significant that the number of incident
forms do not tally with reference to incidents in the hospital’s nursing and medical
records… There were many incidents noted in the patient chronologies which were
based on the dispersed records of 20 former patients… The extent of such incidents
does not appear to have been shared during review meetings”. The panel was mindful
that Mr Harrison countersigned SUI forms completed by Unit/Deputy Managers and
would therefore have had considerable knowledge of patient incidents.
Mr Harrison’s failure in such a critical area of patient care was, in the panel’s judgement,
sufficiently serious to amount to misconduct. The panel was in no doubt that his failure
was such that it would be regarded as “deplorable” by fellow practitioners. The panel
further determined that his failure was in breach of the following provisions of the Code:
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
work with others to protect and promote the health and wellbeing of those in your
care, their families and carers, and the wider community
provide a high standard of practice and care at all times
22 You must work with colleagues to […] maintain the safety of those in your care.
32 You must act without delay if you believe that you, a colleague or anyone else may
be putting someone at risk.

Page 122 of 142
34 You must report your concerns in writing if problems in the environment of care are
putting people at risk.
Charges 1.11 and 1.12
Mr Harrison had an overarching responsibility to ensure the quality of the service
provided by Winterbourne View and ensure that it complied with all appropriate statutory
standards and requirements as regulated by the CQC. He had overall responsibility for
ensuring the Unit’s compliance with Castlebeck’s Physical Intervention Policy. He ought
to have taken steps to satisfy himself that there were adequate systems in place to
prevent the excessive use of restraint. This included, but was not limited to, his
responsibility to adequately review and scrutinise patient documentation; corporate
monitoring and identification of the number and nature of restraints; reviewing the
increasing level of staff turnover; and discussing all of these areas with Registrant C to
identify how any local issues could be properly addressed.
Mr Harrison’s failures related to fundamental and essential aspects of nursing care that
he was required to provide in a senior managerial capacity, including safeguarding the
health and wellbeing of vulnerable patients. His responsibilities were significant and the
interventions required of him were crucial. It is without doubt that the welfare of such a
vulnerable patient group was paramount. He was well placed to have identified and
acted upon the matters found proved in this case.
Moreover, in the panel’s judgement, Mr Harrison had allowed the culture, subsequently
uncovered by BBC Panorama, to develop and persist in Winterbourne View. He was
aware of concerns surrounding the inappropriate admission of patients with challenging
and complex needs; he was aware of staffing issues including staffing shortages and
insufficient training provided to staff to provide appropriate care to patients; and he was
aware that Registrant C required ongoing support. He was, at the time, a very

Page 123 of 142
experienced senior Manager with direct access to the Castlebeck Board. There was no
doubt that he ought to have taken more robust and proactive steps to address the
above issues, in light of his primary responsibility to protect patients.
The panel concluded that Mr Harrison’s failure in his fundamental duty of care to the
patients was sufficiently serious to amount to misconduct, and was such that it would be
regarded as “deplorable” by fellow practitioners. The panel further determined that his
failures, with regard to both charges 1.11 and 1.12, were in breach of the following
provisions of the Code:
The people in your care must be able to trust you with their health and wellbeing
To justify that trust, you must:
make the care of people your first concern, treating them as individuals and
respecting their dignity
work with others to protect and promote the health and wellbeing of those in your
care, their families and carers, and the wider community
provide a high standard of practice and care at all times
[…] uphold the reputation of your profession.
16 You must be aware of the legislation regarding mental capacity, ensuring that people
who lack capacity remain at the centre of decision making and are fully safeguarded.
26 You must consult and take advice from colleagues when appropriate.
32 You must act without delay if you believe that you, a colleague or anyone else may
be putting someone at risk.

Page 124 of 142
33 You must inform someone in authority if you experience problems that prevent you
working within this code or other nationally agreed standards.
34 You must report your concerns in writing if problems in the environment of care are
putting people at risk.
35 You must deliver care based on the best available evidence or best practice.
54 You must act immediately to put matters right if someone in your care has suffered
harm for any reason.
61 You must uphold the reputation of your profession at all times.
Charges 3.1, 5.1, 5.2, 6.1 and 7.1
With regard to charge 3.1, the panel took account of the following:
Of the standards inspected, following the CQC inspection of Croxton Lodge on 8 March
2011, one standard was identified as ‘moderate concerns’, two standards as ‘minor
concerns’ and 13 were ‘compliant’.
Of the standards inspected, following the CQC inspection on 6 and 11 June 2011, three
standards were identified as ‘major concerns’, one standard as ‘moderate concerns’ and
one standard was ‘compliant’. The panel noted that only five standards were inspected
on this occasion compared to 16 in the inspection just a few months before.
Further, the panel was mindful that the most recent inspection took place soon after the
transmission of the BBC Panorama documentary and this may have had an impact on
the staff and the inspection process. On that basis, the panel determined that the

Page 125 of 142
evidence did not, in all likelihood, represent a sufficiently accurate picture of the Unit in
order to enable the panel to establish the seriousness, or otherwise, of Mr Harrison’s
admitted failure. It was not safe, therefore, to conclude that Mr Harrison had engaged in
misconduct in respect of this charge.
In respect of charges 5.1 and 5.2, the panel took account of the following:
Of the standards inspected, following the Healthcare Commission inspection of Cedar
Vale on 27 May 2008, four standards were ‘almost met’ and four standards were ‘met’.
Of the standards inspected, following the Healthcare Commission inspection on 13
January 2009, 12 standards were ‘not met’, three were ‘almost met’ and 10 were ‘met’.
Of the standards inspected, following the CQC inspection on 1 and 2 June 2009, eight
standards were ‘not met’, four were ‘almost met’ and seven were ‘met’.
Of the standards inspected, following the CQC inspection on 25 January 2010, one
standard was ‘not met’, three were ‘almost met’ and eight were ‘met’.
Of the standards inspected, following the CQC inspection on 7 June 2011, one standard
was identified as ‘major concerns’, four as ‘moderate concerns’ and one as ‘minor
concerns’.
There was, evidently, a pattern of improvement. Having regard to the evidence before it,
the panel concluded that Mr Harrison’s failures were not sufficiently serious to amount
to misconduct.
With regard to charge 6.1, the panel took account of the following:

Page 126 of 142
Of the standards inspected, following the CQC inspection of Willow House on 8 June
2011, one standard was identified as ‘moderate concerns’ and one as ‘minor concerns’.
Notwithstanding Mr Harrison’s admission, the panel was not satisfied that the findings of
the CQC inspection were sufficiently serious to warrant a finding of misconduct.
With regard to charge 7.1, the panel took account of the following:
Of the standards inspected, following the CQC inspection of The East Midlands Centre
for Neurobehavioural Rehabilitation on 23 June 2011, one standard was identified as
‘moderate concerns’ and two as ‘minor concerns’.
Notwithstanding Mr Harrison’s admission, the panel was not satisfied that the findings of
the CQC inspection were sufficiently serious to warrant a finding of misconduct.
In summary, the panel concluded that Mr Harrison’s failures as set out, and found
proved, in charges 1.2, 1.5, 1.6 in its entirety, 1.7, 1.8, 1.9, 1.10, 1.11, 1.12 and 4.2,
amounted to misconduct. The panel was not minded to consider that the other
instances where the panel had found elements of culpability falling short of misconduct
should be accumulated to find a further allegation of misconduct against Mr Harrison.
The panel then went on to consider the question of impairment. In considering Mr
Harrison’s fitness to practise the panel reminded itself of its duty to protect patients and
its wider duty to satisfy the public interest which includes declaring and upholding
proper standards of conduct and behaviour, and the maintenance of public confidence
in the profession and the regulatory process.
“Impairment of fitness to practise” has no statutory definition. However, the NMC has
defined “fitness to practise” as a registrant’s suitability to remain on the register without
restriction.
Page 127 of 142
The panel was assisted by the following observations of Mrs Justice Cox in the case of
Grant:
“In determining whether a practitioner’s fitness to practise is impaired by reason of
misconduct, the relevant panel should generally consider not only whether the
practitioner continues to present a risk to members of the public in his or her current
role, but also whether the need to uphold proper professional standards and public
confidence in the profession would be undermined if a finding of impairment were not
made in the particular circumstances.”
[Paragraph 74]
The panel further took into account the approach formulated by Dame Janet Smith in
her 5th report on Shipman, as outlined above in Mr Unwin’s submissions. In its
assessment of all the evidence, and in light of its determinations thus far, the panel
concluded that limbs a), b) and c) were engaged in this case. There could be no
question that Mr Harrison’s failures exposed patients to serious and unwarranted risk of
harm.
Registered Nurses are required to make the care of patients their first concern, work
with others to protect and promote the health and wellbeing of patients, and provide a
high standard of practice and care at all times; these are fundamental tenets of the
nursing profession. The public needs to have trust and confidence in Registered
Nurses, particularly those in a senior managerial capacity, to provide a high standard of
care to vulnerable patients by ensuring, fundamentally, that appropriate systems are in
place to safeguard the health and wellbeing of those patients. In the panel’s judgement,
as Regional Operations Director and Responsible Individual for Arden Vale and,
primarily, Winterbourne View, Mr Harrison failed to act in such a way as to justify the
trust and confidence which the patients in his care, his colleagues, and members of the

Page 128 of 142
public ought to have been able to place in him. As a result of his failures, Mr Harrison
significantly undermined the reputation of the nursing profession.
The panel therefore determined that Mr Harrison’s fitness to practise was, at the time,
impaired.
In considering whether Mr Harrison’s fitness to practise is currently impaired, the panel
had regard to the issues of future risk and public confidence. The panel has a duty not
only to protect patients, but also to safeguard the public interest. This includes the
declaring and upholding of proper standards of conduct and of behaviour, and the
maintenance of public confidence in the profession and the regulatory process.
With regard to future risk, the panel considered whether Mr Harrison’s misconduct was
easily remediable, whether it had been remedied and whether it was highly unlikely to
be repeated. In considering these questions, the panel had particular regard to the issue
of insight. The panel recognised that the level of insight shown by a practitioner is
central to a proper determination of that practitioner’s fitness to practise.
To effectively remediate past failings, Registered Nurses must demonstrate insight into
their behaviour and undertake sufficient remedial steps to address the concerns in
question.
Mr Harrison told the panel that when he attempted to pay his nursing registration fee in
2012, he was informed by an NMC member of staff that he was not permitted to renew
his nursing registration until the conclusion of these NMC proceedings. As a
consequence, he has not worked as a Registered Nurse since 2012.
In the absence of any information from the NMC to rebut Mr Harrison’s assertion, the
panel was concerned that this apparent misinformation would have had an adverse
impact on Mr Harrison’s ability to undertake full and meaningful remediation.

Page 129 of 142
Nevertheless, Mr Harrison did speak of reading journals to keep his general nursing
knowledge up to date, for which the panel afforded him some credit. However, of
concern to the panel was an apparent absence of sufficient awareness by him of the
considerable deficiencies in his practice as a senior Manager and Registered Nurse in a
care environment, and the crucial need, therefore, to address those deficiencies.
As to the matter of insight, the panel considered the following:
Mr Harrison has, to an extent, engaged in these proceedings and with the NMC. He
made admissions to the majority of the charges against him and admitted that his
current fitness to practise is impaired. He acknowledged the findings made by the panel,
describing them as well-established”. He accepted the seriousness of all the charges
and that “public trust in the profession is damaged because of the nature of what had
happened”.
Mr Harrison recognised some of the appropriate actions that were required of him at the
time, including the need for confident, robust and evidence-based challenge of the
decisions made by the Castlebeck Board; the need to conduct necessary checks to
ensure that delegated tasks were completed appropriately; spending more time in each
of the Units for which he was responsible and accountable; and providing support to his
staff members.
In respect of his current employment, Mr Harrison explained that he was privately
contracted to provide training to assist people in gaining their Level 4 National
Vocational Qualification. He described how his current working environment was a
positive change to that of Castlebeck; he said that working primarily in one location
made it easier for his staff to bring concerns directly to him, and allowed him to respond
“more robustly” and “follow through personally [to make] sure outcomes are achieved”.

Page 130 of 142
That being said, Mr Harrison had not, in the panel’s view, demonstrated sufficient and
meaningful acknowledgement and acceptance of his personal failures, as Regional
Operations Director and Responsible Individual. Nor had he demonstrated sufficient
understanding of the gravity and significance of the impact of his failures on the patients
and their families, junior colleagues for whom he was required to act as a role model,
senior colleagues who were frustrated and let down by his inaction, the profession, and
the wider public interest in terms of public confidence in him as a Registered Nurse and
the nursing profession generally. The panel was not entirely persuaded by his repeated
assertions that he was unable to provide the level of support and attention that was
required in each of the Units due to geographical difficulties; in light of his seniority, and
significant responsibilities and accountabilities, he would have been expected to take
appropriate steps to ensure that he discharged his obligations as required to the best of
his ability and to notify the appropriate individuals if he was unable to carry out these
obligations.
Whilst Mr Harrison told the panel that his remorse was “difficult to put into words”, he
went on to say that the events had had a “profound effect” on him personally, and on his
outlook. He then made reference to “the people who suffered the horrible abuse… and if
[Winterbourne View] was managed better, it could have been avoided”, but went into no
detail about how the patients actually suffered as a result of his own failures and at the
hands of those staff members for whom he, as Regional Operations Director and
Responsible Individual, had overall responsibility. There was insufficient evidence to
suggest that Mr Harrison had fully assessed the incidents in question objectively. There
was, furthermore, insufficient evidence of recognition by him as to what could and
should be done differently, by him, in the future to avoid a recurrence of similar issues.
There was no evidence of any references or testimonials to attest to his competence
and conduct as a Registered Nurse and/or Manager in a care environment.
Page 131 of 142
In the panel’s view, Mr Harrison’s evidence was demonstrative of a lack of sufficient
insight. He has not, in the panel’s judgement, demonstrated the depth of insight and
reflection necessary to embark effectively upon the process of remediation.
In the absence of sufficient evidence of remediation, remorse and insight, the panel was
unable to conclude that Mr Harrison’s misconduct had been remedied. He has provided
limited reassurance that his misconduct will not reoccur in the future. The panel,
therefore, concluded that there remains a real risk of repetition.
The panel had in mind that any approach to the issue of whether fitness to practise
should be regarded as impaired must take into account, not only the need to protect
members of the public, but also the collective need to maintain confidence in the
profession as well as declaring and upholding proper standards of conduct and
behaviour. The panel is well aware that these are particularly important considerations
given that there is no power under the NMC rules to issue a warning if there is a finding
of no impairment (Grant, paragraph 73).
The panel determined that this is a case where the firm declaration of professional
standards so as to promote public confidence in the profession is required. The panel
was of the view that reasonable members of the public in full possession of all the facts
would be appalled by the extent of Mr Harrison’s misconduct in light of the
vulnerabilities and complexities of the patients at Winterbourne View. The panel
determined that such a departure from the standards expected of Mr Harrison must
engage public interest considerations. The panel therefore concluded that a finding of
no impairment would fundamentally undermine proper professional standards and
public confidence in the profession, and significantly damage the regulatory process.
Accordingly, the panel determined that Mr Harrison’s fitness to practise is currently
impaired by reason of his misconduct, on both public protection and public interest
grounds.

Page 132 of 142
Determination on sanction – Thursday 6 July 2017
Following its determination on misconduct and impairment, the panel invited
submissions on the matter of sanction.
Mr Jeffs referred the panel to the NMC’s ‘Indicative sanctions guidance to panels’
(September 2016) (“ISG”). He reminded the panel that the overarching objective of the
NMC is the protection of the public, which involves the pursuit of the following
objectives: to protect, promote and maintain the health, safety and well-being of the
public; to promote and maintain public confidence in the professions; and to promote
and maintain proper professional standards and conduct for members of those
professions. He submitted that these objectives should be at the forefront of the panel’s
mind, particularly in the light of its finding that Mr Harrison continues to pose a risk of
harm to the public.
Mr Jeffs reminded the panel that the purpose of sanction is not to be punitive but to
protect the public interest. He submitted that the public interest may include the safe
return to practise of a Registered Nurse; however this must be balanced against other
public interest considerations.
Mr Jeffs further reminded the panel to consider all sanctions available in ascending
order, and to ensure that the sanction imposed meets the risk of harm identified in this
case.
Mr Jeffs submitted that any sanction imposed must be both appropriate and
proportionate. In that regard, he submitted that any interference with Mr Harrison’s
ability to practise must be no more than necessary to satisfy the public interest, which
includes the protection of the public.
Page 133 of 142
Mr Jeffs commended the prevailing circumstances identified by the panel, in detail, in its
determination on misconduct and current impairment. He acknowledged that the
prevailing circumstances accurately captured the mischief and seriousness of the
conduct found proved; the potential for harm to patients, colleagues and members of
the public; and the potential for harm to the profession. He therefore adopted the factors
identified by the panel as aggravating features in this case. In addition, he submitted
that as a result of Mr Harrison’s failures, Mr Harrison allowed the unacceptable culture
of abuse to develop and persist in Winterbourne View. Mr Jeffs invited the panel to have
regard to the lack of evidence of sufficient remediation and insight, and full
acknowledgement, on Mr Harrison’s part of the extent of his failures. Mr Jeffs reminded
the panel of Mr Harrison’s direct access to the Castlebeck Board and his ability
therefore to influence positive change. Mr Jeffs further reminded the panel of Mr
Harrison’s lack of proactive management.
Mr Jeffs contended that Mr Harrison placed patients at serious and unwarranted risk of
harm; Mr Harrison’s failures arose from basic, fundamental and essential elements of
nursing care. Mr Harrison was obliged to safeguard the very vulnerable patients in
Winterbourne View, who were entitled to receive a high level of care but did not do so.
Mr Jeffs further contended that Mr Harrison’s failures placed members of staff at
unwarranted risk of harm. Moreover, Mr Jeffs submitted that compliance with CQC
standards was “not an optional extra”; these essential standards were an important way
of assessing how Units were operating and to ensure safety and good governance.
As an aggravating feature, Mr Jeffs invited the panel to have in mind the fact that Mr
Harrison has not worked in a registered environment since the events in question. Mr
Jeffs acknowledged the panel’s reference to Mr Harrison being under a
misapprehension that he was not entitled to practise as a Registered Nurse. Mr Jeffs
submitted that whilst there was no evidence to demonstrate precisely the advice or
information given to Mr Harrison on that matter, Mr Harrison was, as a matter of fact,

Page 134 of 142
entitled to practise as a Registered Nurse and a ‘search’ of his PIN would have shown
that fact.
Mr Jeffs submitted that the harm caused to the patients at Winterbourne View were
brought to the fore “in the most public way”, which undoubtedly caused harm to the
reputation of the nursing profession.
As to mitigating features in this case, Mr Jeffs reminded the panel of Mr Harrison’s
engagement in these proceedings, although Mr Jeffs invited the panel to weigh this
against Mr Harrison’s obligation, as a Registered Nurse, to cooperate with regulatory
investigations. Mr Jeffs reminded the panel of Mr Harrison’s admissions to the majority
of the charges against him and to the matter of current fitness to practise. Mr Jeffs
reminded the panel of its finding that Mr Harrison had demonstrated some remorse and
had made attempts to keep his general nursing knowledge up to date. Mr Jeffs also
informed the panel that apart from the matters in this case, there is no evidence of any
previous or subsequent adverse disciplinary or regulatory findings against Mr Harrison.
In reaching its decision, the panel addressed the matter of sanction in the light of Mr
Harrison’s failures, as found proved, and in accordance with its determination on
misconduct and impairment. The panel noted that the question of sanction was a matter
for its own independent judgement.
The panel accepted the advice of the legal assessor, which included advice to disregard
Mr Jeff’s submission that Mr Harrison’s failure to work in a registered environment was
an aggravating feature. Further, the panel took account of the guidance set out in the
ISG. It had regard to the principle of proportionality, weighing Mr Harrison’s interests
against the public interest. The panel bore in mind that the purpose of a sanction was
not to be punitive, although it might have that effect; rather, it was intended to protect
patients and serve the wider public interest. The wider public interest included

Page 135 of 142
promoting and maintaining public confidence in the profession and the NMC as its
regulator, and promoting and maintaining proper standards of conduct and behaviour.
The panel acknowledged that any sanction imposed must be no more than would be
necessary to protect the public and satisfy the public interest.
In keeping with its detailed decision on current impairment, the panel considered that
the following aggravating features applied in this case:
The patients at Winterbourne View were highly vulnerable and were entitled to
expect a Registered Nurse in a senior managerial capacity to protect and
safeguard their health and wellbeing.
Mr Harrison was an experienced Registered Nurse with considerable experience
of Castlebeck and was therefore familiar with its working practices. Whilst he was
the most senior Manager at an operational level, as a Registered Nurse he was
at all times bound to abide by the primary and fundamental principles of good,
safe and effective nursing care. This included his obligation to escalate matters
which place patients at risk of unwarranted harm; in this case, Mr Harrison
should have reported concerns to, at least, the CQC and he failed to do so.
In light of his knowledge and awareness of the significant and persistent
concerns in Winterbourne View including staffing, training, supervision, patient
incidents and patient admissions, Mr Harrison’s material failure to provide
proactive management and support in general, and with particular regard to
Registrant C, undoubtedly contributed to the poor practices, standards of care
and abuse that continued at the Hospital.
Mr Harrison’s lack of awareness of the ongoing status of his Units’ CQC
compliance was inexcusable and unjustifiable.
Mr Harrison has not accepted full accountability and responsibility for his failures.
He sought, at times, to place blame on others and on the company.

Page 136 of 142
The systemic abuse of patients at Winterbourne View, as uncovered publicly by
the BBC Panorama documentary, significantly damaged the reputation of the
nursing profession.
The panel rejected Mr Jeff’s submission that the fact that Mr Harrison has not since
worked in a registered environment should be regarded as an aggravating feature (in
fairness to Mr Jeffs, he accepted, after hearing the advice of the legal assessor, that this
fact should more appropriately have been referred to as a ‘relevant feature’). Mr
Harrison had told the panel that he was informed by an NMC member of staff that he
was not permitted to renew his nursing registration until the conclusion of these
proceedings, and he therefore laboured under the misapprehension that he was not
entitled to practise as a Registered Nurse. No evidence was presented by the NMC to
rebut Mr Harrison’s assertion. If a Registered Nurse is informed, directly or indirectly, by
their regulator that they are not permitted to practise as a Registered Nurse, it is
unreasonable to place the responsibility on the individual to seek information to the
contrary. The panel also acknowledged that Mr Harrison is entitled not to work in a
registered capacity.
As to the mitigating features in this case, the panel considered that the following
applied:
Mr Harrison was not afforded the level of support he ought to have received from
the Castlebeck Board and there was undoubtedly a degree of pressure placed
upon him to prioritise the company’s financial interests.
Apart from the matters in this case, there is no evidence of any previous or
subsequent adverse disciplinary or regulatory findings against Mr Harrison.
Mr Harrison has taken some steps to keep his general nursing knowledge up to
date.
Mr Harrison had engaged, to an extent, in these proceedings.

Page 137 of 142
Mr Harrison had made admissions to the majority of the charges against him,
including the more serious allegations, and admitted that his current fitness to
practise is impaired.
Mr Harrison demonstrated some remorse.
Mr Harrison demonstrated some insight and reflection.
Mr Harrison demonstrated some learning from his experiences at Castlebeck.
Under Article 29 of the Nursing and Midwifery Council Order 2001, the panel, when
considering sanction, can consider the following courses of action in ascending order,
beginning with the least restrictive sanction: take no action, make a caution order for
one to five years, make a conditions of practice order for no more than three years,
make a suspension order for a maximum of one year, or make a striking-off order.
The panel concluded that there were no exceptional circumstances in this case which
would justify taking no action. The panel considered that to take no action would be
manifestly inappropriate given the seriousness and extent of the misconduct found.
Furthermore, the panel considered that taking no action would be wholly insufficient for
the purpose of upholding public confidence in the nursing profession and in the NMC as
its regulator.
The panel then considered whether to make a caution order. The panel bore in mind
that such an order would not restrict Mr Harrison’s ability to practise. As above, the
panel concluded that a caution order would be wholly inappropriate. Such an order
would not properly mark the seriousness of the misconduct found, nor would it be
sufficient to protect the public or satisfy the wider public interest. This is not a case at
the lower end of the spectrum of impaired fitness to practise.
The panel next considered the imposition of a conditions of practice order. The panel
noted that this sanction primarily focuses on remedying identifiable areas of concern
within a registrant’s clinical practice or skills that may require retraining, assessment

Page 138 of 142
and supervision. In addition, it requires the potential and willingness of a registrant to
respond positively to any conditions imposed.
The wide-ranging misconduct established in this case concerned fundamentally Mr
Harrison’s failures in a managerial capacity. Whilst elements of his misconduct may, in
principle, be capable of being addressed by appropriate conditions of practice, there
was evidence before the panel which suggested that his overall misconduct was
compounded by an attitudinal problem. Mr Harrison’s management was passive,
apathetic and, despite his knowledge and awareness of matters that placed patients at
unwarranted risk of harm, lacked the urgency that was required of him.
The panel was mindful of its earlier finding that Mr Harrison had not demonstrated
sufficient insight into his misconduct and had not taken full responsibility for his failures.
The panel took account of the absence of sufficient recognition and acknowledgement
by Mr Harrison of the significant impact of his failings on the patients and their families
and the profession.
In the light of the panel’s finding that there remains a real risk of repetition and,
therefore, a risk of serious harm to patients (for all the reasons set out above), the panel
determined that conditions of practice could not be devised which would satisfactorily
address Mr Harrison’s misconduct. In all the circumstances the panel concluded that,
given the seriousness and extent of his misconduct, a conditions of practice order would
not be sufficient to protect the public, nor would it satisfy the wider public interest. The
panel therefore determined that a conditions of practice order would be an insufficient
sanction in all the circumstances of this case.
The panel next considered imposing a suspension order. A suspension order is
intended to convey a message to the registrant, the profession and the wider public as
to the gravity of the unacceptable and inappropriate behaviour, but which, in the
particular circumstances of a case, falls short of being fundamentally incompatible with
Page 139 of 142
continued registration. A period of suspension can also serve to provide a practitioner
with an opportunity to reflect on their misconduct and to take action to commence or
complete the process of remediation.
The misconduct in this case was not limited to a single incident. It comprised a pattern
and history of failures on Mr Harrison’s part to act in the best interests of the patients in
his care, over a considerable period of time. In respect of each of the matters found to
amount to misconduct, Mr Harrison’s failure was accompanied by an identifiable risk of
serious harm.
In its preceding determination, the panel concluded that Mr Harrison failed to
demonstrate and deliver safe nursing care. He was in a position to influence positive
change for the benefit of the patients and staff for whom he had overall accountability,
and did not do so. As a result, he placed patients at serious and unwarranted risk of
harm and the consequences of his failures were significant, given the particular
vulnerabilities and complexities of the patients for whom he was responsible. By virtue
of his misconduct, Mr Harrison failed in his overriding duty as a Registered Nurse to
safeguard and maintain the health and wellbeing of patients.
The public would be protected temporarily by the imposition of a suspension order. The
panel also took into account Mr Harrison’s extensive and otherwise unblemished
nursing career. However, in the particular circumstances of this case, the panel
concluded that such an order, even for the maximum period of 12 months, would not
satisfy the wider public interest, in declaring and upholding standards of behaviour and
maintaining public confidence in the profession. The panel therefore determined that a
suspension order would not be a sufficient sanction.
Mr Harrison’s misconduct represented a significant and serious departure from the
standards expected of him as a Registered Nurse in a managerial capacity. His
overarching duty was to safeguard the vulnerable patients in his care. In this case, he

Page 140 of 142
failed to discharge that duty. He acted in such a way that could foreseeably have
resulted in harm. Given the particular vulnerability of this patient group, Mr Harrison was
in a crucial position, and was depended upon, to protect the patients in his care. His
failure to act on a significant number of occasions was a breach of the trust incumbent
upon him as a Registered Nurse.
For all those reasons, the panel concluded that Mr Harrison’s misconduct is
fundamentally incompatible with him continuing to be a Registered Nurse.
Mr Harrison’s failures, in the context of his position as Regional Operations Director and
Responsible Individual, fundamentally undermine public trust and confidence in the
nursing profession. He failed to use his privileged position to protect and promote the
health and wellbeing of vulnerable patients. His failures are unequivocally serious.
The panel therefore determined that a striking-off order is the proportionate and
appropriate sanction. A lesser sanction would not be sufficient to satisfy the wider public
interest in maintaining confidence in the profession and its regulator and in declaring
and upholding proper standards of conduct and performance.
The panel was mindful that such an order could have a financial and professional
impact on Mr Harrison. Nevertheless, the panel concluded that his interests were
outweighed by the public interest in this matter.
Accordingly, the panel has determined to direct the Registrar to strike Mr Harrison’s
name from the Register.
Mr Harrison will be advised that his name will be removed from the NMC register. He
may not apply for restoration until five years after the date that this decision takes effect.
Anyone who enquires about his registration will be advised of this.

Page 141 of 142
Determination on interim order – Thursday 6 July 2017
The striking off order will take effect 28 days from the date when notice of it is deemed
to have been served upon Mr Harrison.
The panel considered whether it was appropriate to impose an interim order to cover
the appeal period before the substantive order takes effect, or to cover any time
required for an appeal of the substantive decision in this case to be heard.
Article 31 of the Order outlines the criteria for the imposition of an interim order. The
panel may make an interim order on one or more of three grounds:
Where it is satisfied that it is necessary for the protection of members of the
public;
Where it is satisfied that such an order is otherwise in the public interest;
Where it is satisfied that such an order is in the interests of the registrant.
The panel may make an interim conditions of practice order or an interim suspension
order for a maximum period of 18 months.
Mr Jeffs made an application for the imposition of an interim suspension order for a
period of 18 months on the grounds that it was necessary for public protection and that
it was otherwise in the public interest. He submitted that an interim suspension order
was appropriate and proportionate, in light of the panel’s determinations thus far. He
further submitted that an 18 month interim order was necessary to allow for any appeal
process.
In reaching its decision, the panel had regard to the submissions made by Mr Jeffs and
it accepted the advice of the legal assessor.

Page 142 of 142
For all the reasons set out in the panel’s determination thus far, and in all the
circumstances of this case, the panel decided to impose an interim suspension order on
the grounds that it was necessary for public protection and that it was otherwise in the
public interest. The panel first considered an interim conditions of practice order but
determined that, for the reasons set out in its determination on sanction, such an order
would not be appropriate.
The panel considered that, in the light of the reasons set out above for imposing a
striking off order, members of the public would be put at risk of harm, and confidence in
the NMC’s regulatory process would be damaged if, pending an appeal, there was no
interim order preventing Mr Harrison from working as a Registered Nurse before the
substantive order takes effect.
The panel determined that the order should run for a period of 18 months to allow for
any appeal process. The panel considered this to be an appropriate and proportionate
period.
If at the end of the appeal period of 28 days Mr Harrison has not lodged an appeal, the
interim order will lapse and will be replaced by the substantive order. On the other hand,
if he does lodge an appeal, the interim order will continue to run until the conclusion of
the appeal.
That concludes these proceedings.
Copyright © 2022 FDOKUMEN