
An acquired acyltransferase promotes Klebsiella pneumoniae ...

Guidelines for the treatment of Community-acquired Pneumonia: predictors of adherence
and outcome
Rosario Menéndez1 MD, Antoni Torres2 MD, Rafael Zalacaín3 MD, Javier Aspa4 MD, Juan J
Martín-Villasclaras5 MD, Luis Borderías6 MD, José M Benítez-Moya7 MD, Juan Ruiz-Manzano8
MD, Felipe Rodríguez de Castro9 MD, José Blanquer10 MD, Diego Pérez11 MD, Carmen Puzo12
MD, Fernando Sánchez-Gascón13 MD, José Gallardo14 MD, Carlos Álvarez15 MD, Luis
Molinos16 MD on behalf of the NEUMOFAIL Group
This article has an online data supplement, which
is accessible from this issue's table of content online at
www.atsjournals.org".
From the:
1 Servicio de Neumología, Hospital Universitario La Fe, Valencia, Spain
2 Instituto de Neumología y Alergia, Hospital Clinic (Red Gira FIS-ISCIII-03/063), Barcelona,
Spain
3 Servicio de Neumología, Hospital de Cruces, Bilbao, Spain
4 Servicio de Neumología, Hospital de la Princesa, Madrid, Spain
5 Servicio de Neumología, Hospital Carlos Haya, Malaga, Spain
6 Servicio de Neumología, Hospital San Jorge, Huesca, Spain
7 Servicio de Neumología, Hospital Virgen de la Macarena, Sevilla, Spain
8 Servicio de Neumología, H Germans Trias i Pujol, Badalona, Spain
9 Servicio de Neumología, Hospital Dr Negrín, Las Palmas de Gran Canaria, Spain
10 Cuidados Intensivos, Hospital Clínico, Valencia, Spain
11 Servicio de Neumología; Hospital Clínico, Valencia, Spain
AJRCCM Articles in Press. Published on June 3, 2005 as doi:10.1164/rccm.200411-1444OC
Copyright (C) 2005 by the American Thoracic Society.

12 Servicio de Neumología, Hospital San Pablo, Barcelona, Spain
13 Servicio de Neumología, Hospital General Universitario, Murcia, Spain
14 Servicio de Neumología, Hospital General, Guadalajara, Spain
15 Servicio de Neumología, Hospital 12 de Octubre, Madrid, Spain
16 Servicio de Neumología, Hospital Ntra Sra de Covadonga, Oviedo
Correspondence and reprint requests:
Rosario Menéndez, MD. Servicio de Neumología. Hospital Universitario La Fe,
Avda. de Campanar 21, 46009 Valencia. Spain
Tel: (+34) 96 3862764
Fax: (+34) 96 1973089
e-mail: [email protected]
Alternative for correspondence:
Antoni Torres, MD. Instituto de Neumología y Cirugía Torácica. Hospital Clinic,
Villaroel 180. 08030 Barcelona. Spain
Tel: (+34) 93 2275779
Fax: (+34) 92 2275454
e-mail: [email protected]
This study was supported by a grant from SEPAR (Sociedad Española de Neumología y Cirugía
Torácica) and Pfizer Spain. Data analyses were facilitated by Red-Respira (RTIC C03/11).
Running title: Adherence to guidelines in pneumonia
Descriptor number: 128
Word count (excluding abstract, references): 2588

1
Abstract
Rationale: Some studies highlight the association of better clinical responses with adherence to
guidelines for empirical treatment of community-acquired pneumonia (CAP), but little is known
about factors which influence this adherence.
Objectives: Our objectives were to identify factors influencing adherence to the guidelines for
empirical treatment of CAP, and to evaluate the impact of adherence on outcome.
Methods: We studied 1288 patients with CAP admitted to 13 Spanish hospitals. Collected
variables included the patients clinical and demographic data, initial severity of the disease,
antibiotic treatment, and specialty and training status of the prescribing physician.
Measurements and Main Results: Adherence to guidelines was high (79.7%) with significant
differences between hospitals (range 47-97%) and physicians: pneumologists (81%), pneumology
residents (84%), non pneumology residents (82%), other specialists (67%). The independent
factors related to higher adherence were hospital, physician characteristics and initial high risk
class of Fine, while admission to intensive care unit decreased adherence. Seventy-four patients
died (6.1%) and treatment failure was found in 175 (14.2%). After adjusting for risk class of
Fine, adherence to the guidelines was found protective for mortality (OR 0.55; 95%CI: 0.3-0.9)
and for treatment failure (OR:0.65; 95%CI:0.5-0.9). Treatment prescribed by pneumologists and
residents was associated with lower treatment failure (OR:0.6; 95%CI: 0.4-0.9)
Conclusions: Adherence to guidelines mainly depends on the hospital, and the specialty and
training status of prescribing physicians. Non-adherence was higher in non-pneumology
specialists, and is an independent risk factor for treatment failure and mortality.
(Word count = 239)
Key words: Mortality, antibiotic, compliance, pneumologist, resident

2
Introduction
Community acquired pneumonia (CAP) has an incidence of 3 to 5 cases per 1000 persons, and a
mortality of 5 to 15% in hospitalized patients(1). Initial antibiotic treatment is key for the
resolution of infection and for prognosis, with higher mortality if the treatment is inappropriate.
The difficulty in selecting the appropriate antibiotics arises because CAP can be caused by
multiple organisms, which cannot be identified on clinical and radiographic findings, and the
conventional microbiologic methods have limited sensitivity and specificity(2).
It has been shown that the shorter the time between diagnosis and initiation of treatment, the
better the impact on prognosis(3, 4), and this is more effective than adequacy to results of
microbiologic tests if this delays treatment(5, 6). Thus, usually the antibiotic treatment is chosen
empirically at the time of diagnosis. Evidence based guidelines have been developed by scientific
societies to assist physicians in the selection of antibiotics(7-9) and to reduce variability in
clinical care(10).
Some studies have shown that adherence to guidelines results in reduced need for hospitalization,
shorter stays, and lower mortality. Nevertheless, adherence is very variable among clinicians(11)
and may be due to individual disposition(12, 13). Halm et al identified factors associated with
non-adherence to guidelines for the decision of hospitalizing patients with CAP(14), but there is
little information regarding factors which influence adherence to guidelines for the selection of
treatment of CAP(13).
The differences in adherence to guidelines between specialists in pneumology and other
physicians have not been studied enough, and it is not known if adherence is also influenced by

3
patient characteristics such as comorbid condition or initial severity. This is an important issue
because some processes of care for CAP with an impact on outcome could be improved(15-17),
and the choice of antibiotic treatment is one of the processes associated with differences in the
outcome of hospitalized CAP(18-20). Efforts should be directed to identify factors which
influence the adherence to guidelines in order to prepare strategies to improve it.
The primary objective of this study was to evaluate adherence to the Spanish guidelines for the
empirical antibiotic treatment of CAP, and to identify factors related to compliance with these
guidelines. In the study we analyzed factors associated to the characteristics of the patients, the
initial severity of the infection, and the specialty and training status of the prescribing physician.
Furthermore, we aimed to study the impact of adherence on treatment failure and mortality. A
part of this work has been published as an abstract (21).
4
Patients and Methods. Word count 499
Design and study population
Between October 2000 and April 2001, a multi-center observational prospective study was
carried-out in 15 Spanish hospitals(22). All hospitals belong to the Spanish National Health
System and have a pneumology service. The study cohort comprised non immunosupressed adult
patients hospitalized because of CAP (Additional details provided in the online data supplement).
The attending physician prescribed the initial empirical antibiotic therapy. Compliance with the
latest consensus Spanish guidelines SEQ-SEPAR(23) was evaluated. Data on the prescribing
physician were collected and categorized as: pneumologist (four years trained), other internal
medicine specialist, resident in pneumology (undergoing training), or resident in another
specialty. Initial empirical treatment was considered to adhere to guidelines when antibiotics
were prescribed as follows: In hospitalized CAP: either 3rd generation cephalosporin (cefotaxime
or ceftriaxone) or amoxycillin-clavulanate combined or not with a macrolide, or fluoroquinolone
(3rd or 4th generation) in monotherapy; in patients admitted to the intensive care unit (ICU), 3rd or
4th generation cephalosporin combined with intravenous macrolide or with intravenous
fluoroquinolone (levofloxacin) (see Table E1 in the online data supplement). All other antibiotic
regimens were considered as being non-adherent to guidelines. Outcome variables were treatment
failure(22) and mortality. (Additional details in the online data supplement).
Data collection
Demographic and clinical characteristics and analytical data have been described elsewhere(22).
For the present study data of age, gender, prior antibiotic treatment, adherence to guidelines,
comorbidity, signs of initial severity and PSI or risk class of Fine (24) were analyzed.
Statistical study

5
Univariate analysis. Statistical analyses were performed using the SAS 8.2 software program.
Qualitative variables were compared using the chi-square test. Differences in quantitative
variables were assessed with ANOVA test or with Kruskal-Wallis test when appropriate. Values
of p ≤0.05 were considered significant. Variables dichotomized for univariate analysis were
tachycardia (≥100 bpm), tachypnea (≥30 bpm), hypotension (systolic blood pressure ≤90), and
hypoxemia (Pa O2 ≤60 mmHg).
Multivariate analysis. A logistic regression analysis to predict adherence to guidelines was
performed using as independent variables those found significant in univariate analyses
(unemployed status, previous antibiotic treatment, confusion, hypotension, admission to ICU,
PSI, hospital, and prescribing physician). The PSI was dichotomized as risk class I or >I, based
on the found overall adherence (70.5% for risk class I and 77-82% for the rest). Four dummy
variables for each prescribing physician were introduced into the model so as to analyze the
independent effect of each physician category. Interactions between hospital, physicians,
comorbid conditions and PSI were assessed.
Two logistic regression analyses were performed to assess the impact of adherence and
prescribing physician on mortality and treatment failure. The independent variables were:
adherence, prescribing physician and PSI dichotomized as low (Fine risk classes I-III) and high
(risk classes IV-V).
The logistic regression analyses were performed with a likelihood ratio-based stepwise method.
Variables which reached a p-value ≤0.05 were considered significant and their odds ratios with
95% confidence intervals were calculated. The Hosmer and Lemeshow goodness-of-fit test was
used to evaluate the adequacy of the models(25). The areas under the receiver-operator
characteristic (ROC) curves were also calculated.

6
Results
The original study comprised 1424 patients from 15 Spanish hospitals. Data on the prescribing
physician were available for 1228 patients (additional details provided in the online data
supplement), who were included in the study. Eighty six (7%) were admitted to ICU, 74 died
(6.1%), and 175 had treatment failure (14.2%). The main demographic characteristics, co-
morbidities and PSI scores have been published elsewhere(22).
The initial empirical therapy prescribed on admission was adherent to the SEQ-SEPAR
guidelines in 979 patients (79.7%); of those adherence was 80% in patients hospitalized in ward
(921/1142), and 67.4% in those admitted to ICU (58/86), p<0.05. (Additional details on antibiotic
regimes are provided in the online data supplement). Adherence to guidelines differed between
hospitals with a range of 47-97% (see Table E2 in the on line supplement).
The initial treatment was prescribed as follows: 786 (64%) by residents (239 (19%) by a resident
in pneumology and 547 (45%) by a resident in other specialties), 244 (20%) by a trained
specialist in pneumology, and 198 (16%) by other specialists in internal medicine. In patients
hospitalized in ward, adherence to the guidelines with respect to physician was: pneumologists
187/230 (81%), pneumology residents 196/231 (85%), residents of other specialties 427/524
(82%) and other specialists 111/157 (71%), p<0.05. In patients admitted to ICU, it was as
follows: pneumologists 10/14 (71%), pneumology residents 5/8 (63%), residents of other
specialties 21/23 (91%) and other specialists 22/41 (54%), p <0.05.
Table 1 shows the adherence to guidelines in the whole group stratified according to the
characteristics and co-morbidities of the patients. We did not find significant differences with
regard to age, gender, or tobacco and alcohol intake. Adherence was lower in patients who were
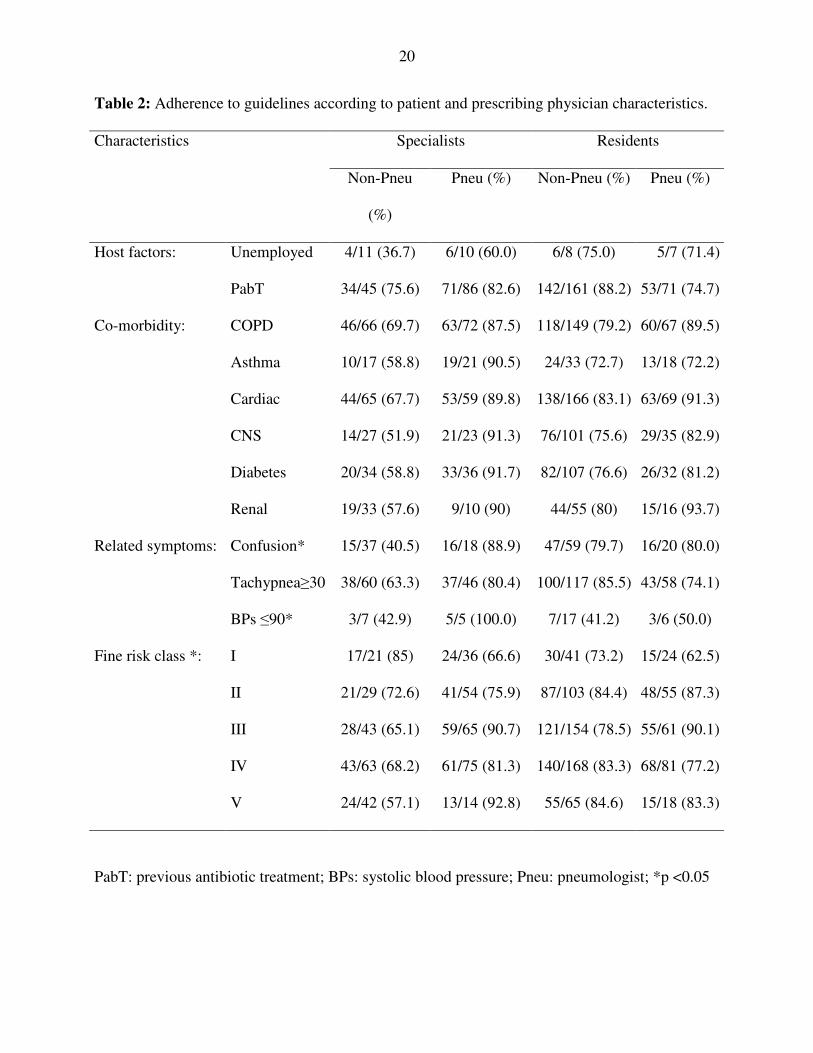
unemployed, with confusion and with hypotension. Table 2 shows the results of adherence
stratified by characteristics of the patients as well as the prescribing physician. The presence of
7
co-morbidity decreased adherence to guidelines when the treatment was prescribed by a non-
pneumology specialist. Adherence with respect to initial severity also showed differences
between prescribing physicians: The pneumology specialists and residents had increased
adherence to the guidelines in patients with severe CAP (risk class V) while, in the non-
pneumology specialists, this was significantly (p<0.05) decreased.
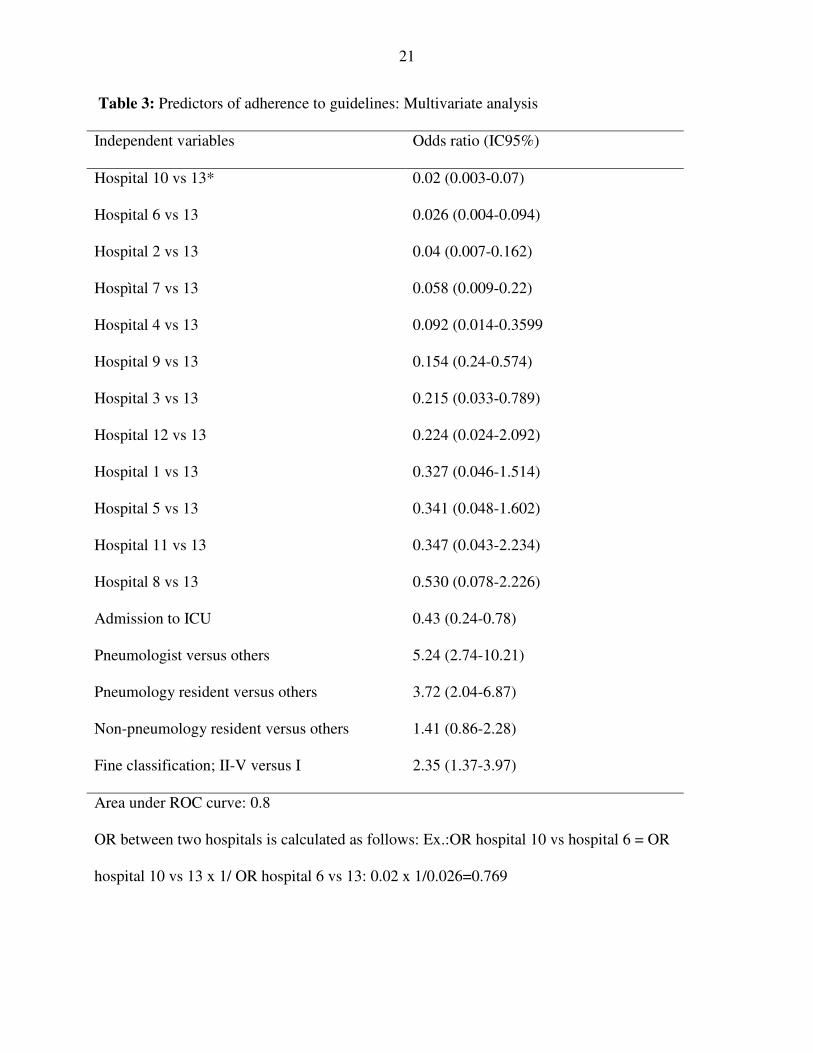
Multivariate adherence predictors. A stepwise regression logistic analysis of 1134 patients was
performed to predict adherence. The independent variables included were unemployed status,
previous antibiotic treatment, confusion, hypotension (systolic blood pressure ≤90), admission to
ICU, risk class of Fine, hospital, and prescribing physician. Interactions between hospital,
physicians, comorbid conditions and initial severity were assessed and not found. The χ2
goodness-of-fit analysis demonstrated the adequacy of the model (p: 0.2). The independent
factors related to higher adherence were hospital, physician characteristics and initial high risk
class of Fine, while admission to intensive care unit decreased adherence (Table 3).
ADHERENCE AND OUTCOME: TREATMENT FAILURE AND MORTALITY
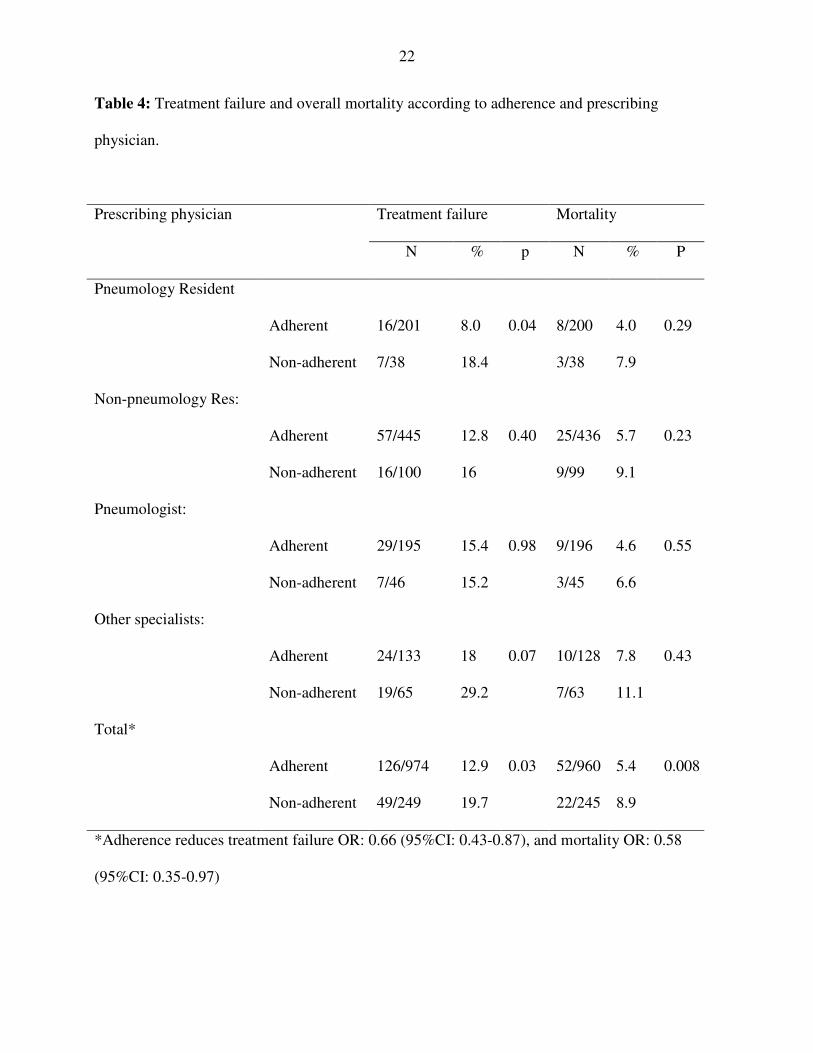
Univariate statistical analyses: Seventy-four patients died (6.1%) and treatment failure was
found in 175 (14.2%). The overall treatment failure (19.7% vs 13%) and mortality (8.9% vs
5.4%) were significantly greater in the group of patients treated with schedules non-adherent to
the guidelines (Table 4). Adherence reduced treatment failure (unadjusted OR: 0.66, 95%CI:
0.43-0.87) and mortality (OR:0.58, 95%CI: 0.35-0.97). For patients admitted to the ward
treatment failure in the adherent group was 10.9 % versus 13.1% in the non adherent group,
(p:0.36) and mortality was 3.9% versus 6.4% respectively (p=0.09). In ICU, patients who
8
received adherent treatment, treatment failure was 44.8% versus 71.4% (p:0.02), and mortality
was 29.3% versus 29.6% respectively (p=0.6). (see Table E3 for patients stratified by ICU and
non-ICU in the online supplement)
Comparing the prescribing physicians, we found that patients treated by non-pneumology
specialists with schemes not adherent to the guidelines showed a greater percentage of treatment
failure and death (albeit the latter not reaching statistical significance).
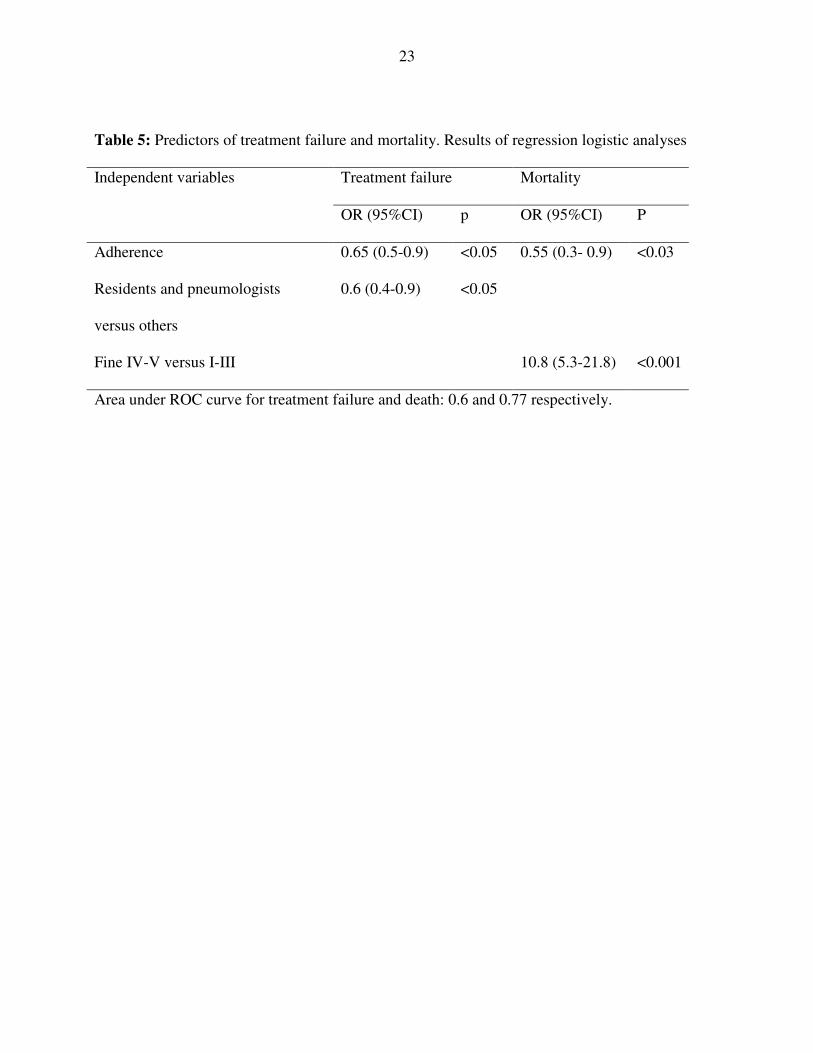
Multivariate analysis: After adjustment for initial severity, adherence to the guidelines (OR:
0.65, 95% CI:0.5-0.9) and treatment prescribed by the pneumologist or the residents were
protective against treatment failure, while only adherence was protective against mortality (OR
0.55; 95%CI: 0.3-0.9) (Table 5). The χ2 goodness-of-fit analysis demonstrated the adequacy of
the model (p: 0.22).
.

9
Discussion
The most relevant findings of our study are: 1) adherence to guidelines greatly differs between
hospitals and is significantly lower in non pneumology specialists, 2) patients with confusion and
hypotension are treated more often with regimens which do not comply with guidelines; 3) non-
pneumology specialists have a lower adherence to the guidelines when treating patients with
severe CAP and greater risk for treatment failure; 4) adherence to the guidelines is an
independent protective factor for treatment failure and death.
In our study, 85% of the patients received the initial treatment from a pneumologist or a resident,
with a high global adherence to guidelines although with great differences among hospitals. We
have confirmed the large variability in compliance with guidelines between hospitals even in the
same country(26). Differences between hospitals prove the heterogeneity in treating CAP and
possibly are due to different reasons, such as local epidemiological peculiarities and, mainly, a
shared collective attitude. In the three hospitals where the adherence of
pneumologists/pneumology residents was the lowest (Hospitals 6, 9 and 12), the global
adherence was also low. This might reflect the effect of non-adherence of pneumologists on the
behavior of others physicians. In general, our findings reveal that trained and trainee
pneumologists showed a high degree and a similar pattern of compliance.
This higher grade of adherence by the pneumologists is, probably, due to the better access these
clinicians have to recommended guidelines, the rapid dissemination of current guidelines, and the
capacity for prompt decision by the specialist. Clinicians in the course of their training are, as
well, very receptive to the information made available by the scientific societies, and sensitive to
the opinions of the experts(14). Clinicians in non-related fields employ treatment schemes that,
often, do not adhere to the specialist guidelines and, as such, our findings sound the alert

10
regarding lack of adherence when the treatment is provided by clinicians who are not specialists
in the patient’s specific condition (27).
In some countries many patients with CAP are treated by general practitioners or other
specialists, so there is a need to disseminate and implement guidelines among those physicians.
Switzer et al (28) found different and low levels of awareness of guidelines between generalists
and even pneumologists. They found that a positive attitude towards guidelines correlated with a
higher awareness and adherence more than specialty itself did. Other reasons for non-adherence
could include the difficulty in the application of the guidelines in some individual patients.
When analyzing patient characteristics associated with adherence to the guidelines, we found a
pattern of behavior, which was similar between the residents and pneumologists, with respect to
patient co-morbidity and signs of severity of CAP. The presence of concomitant diseases almost
doubled the lack of adherence in other specialists, especially in patients with diabetes, or CNS
and renal disorders, without an evident explanation. These data are important since co-morbidity
is frequent among hospitalized CAP patients(29), and is the cause of poor prognosis(30, 31).
Compliance with guidelines was lower in the two extremes of severity of CAP, in the most
severe, that is, those admitted to ICU, and in the least severe cases (risk class I of Fine).
Furthermore, the behavior of physicians was opposite between pneumologists and other
specialists in these circumstances: while in severe CAP (Fine risk class V), adherence was higher
for pneumology specialists and residents and lower for non-pneumology specialists, the opposite
happened in risk class I. This is of considerable notice, because the former are at very high risk of
death, and mortality increases if the prescribed treatment does not adhere to the guidelines. Signs
11
of severity of CAP, such as hypotension and confusion were associated with lower adherence,
specially in non-pneumology specialists. These signs of severity are widely known by
pneumologists, and well documented on the severity scales that are commonly used in the
management of CAP(24, 32). Our results highlight an area warranting improvement in the
management of CAP(33). In countries where patients are treated by non-pneumology specialists,
it would be important to confirm our findings to increase the awareness of signs of severity of
CAP.
The initial antibiotic treatment is among the processes and outcome measures used to asses the
quality of hospital care(34, 35). Several studies have found lower mortality when the antibiotic
treatment is adherent to guidelines(19, 36-38). Our results confirm the independent protective
effect of adherence to guidelines on mortality and treatment failure. In a prior publication we
found that treatment failure was lower when treatment was adherent, and it was independently
associated with fluorquinolone, but the independent effect of the prescribing physician was not
analyzed(22).In addition to adherence, when the treatment was prescribed by the pneumologist or
residents, the treatment failure was lower. Marrie et al(39) found that clinicians who treat a
higher volume of patients with pneumonia achieve better outcomes, which could explain our
findings.
The independent effect of adherence on mortality was demonstrated after adjusting by risk class
of Fine. However, since ours was an observational non-randomized study, possible limitations
are that factors not assessed by the Fine risk class, or confounding variables that were not
measured, could have influenced the outcome. These could include differences in the
characteristics of the hospitals, differences in the management of CAP between hospitals (39), or

12
factors arising during hospitalization. Another limitation is that we don’t have a code for the
actual medical provider and therefore we cannot perform clustered or hierarchical analyses.
In summary, we found that adherence to guidelines for the empirical treatment of CAP differs
considerably between hospitals and prescribing physicians. The pattern of adherence in the
residents was similar to that in pneumologists, in relation to co-morbidity and severity of CAP.
Adherence to guidelines was an independent protective factor for treatment failure and mortality.
Our findings identify factors associated with non-adherence, and highlight inefficiencies and
heterogeneity in clinical practice. Strategies for achieving better adherence need to be
implemented to improve our medical practice.

13
Appendix
Investigators in the NEUMOFAIL research study group:
Rosalía Domenech. Hospital Universitario La Fe, Valencia
Malina Ioanas. Hospital Clinic, Barcelona
Ainhoa Gómez Bonilla. Hospital de Cruces, Bilbao
Olga Rajas. Hospital de la Princesa, Madrid
Marta Arzola. Hospital Carlos Haya, Málaga
Agustín Valido. Hospital Virgen Macarena de Sevilla
Felipe Andreo. Hospital Germans Trias i Pujol, Badalona
Alicia López. Hospital Dr. Negrín, Las Palmas de Gran Canaria
Manuel Brufal. Hospital San Pablo, Barcelona
Damian Malia. Hospital General de Murcia
14
References
1. Kaplan V, Angus DC, Griffin MF, Clermont G, Scott Watson R, Linde-Zwirble WT.
Hospitalized community-acquired pneumonia in the elderly: age- and sex-related patterns of care
and outcome in the United States. Am J Respir Crit Care Med 2002; 165:766-772.
2. San Pedro GS, Campbell GD, Jr. Limitations of diagnostic testing in the initial
management of patients with community-acquired pneumonia. Semin Respir Infect 1997; 12:300-
307.
3. Houck PM, Bratzler DW, Nsa W, Ma A, Bartlett JG. Timing of antibiotic administration
and outcomes for medicare patients hospitalized with community-acquired pneumonia. Arch
Intern Med 2004; 164:637-644.
4. Meehan TP, Fine MJ, Krumholz HM, Scinto JD, Galusha DH, Mockalis JT, Weber GF,
Petrillo MK, Houck PM, Fine JM. Quality of care, process, and outcomes in elderly patients with
pneumonia. Jama 1997; 278:2080-2084.
5. El-Solh AA, Aquilina AT, Dhillon RS, Ramadan F, Nowak P, Davies J. Impact of
invasive strategy on management of antimicrobial treatment failure in institutionalized older
people with severe pneumonia. Am J Respir Crit Care Med 2002; 166:1038-1043.
6. Sanyal S, Smith PR, Saha AC, Gupta S, Berkowitz L, Homel P. Initial microbiologic
studies did not affect outcome in adults hospitalized with community-acquired pneumonia. Am J
Respir Crit Care Med 1999; 160:346-348.
7. Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD, Dean
N, File T, Fine MJ, Gross PA, et al. Guidelines for the management of adults with community-
acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention.
Am J Respir Crit Care Med 2001; 163:1730-1754.

15
8. Bartlett JG, Dowell SF, Mandell LA, File Jr TM, Musher DM, Fine MJ. Practice
guidelines for the management of community-acquired pneumonia in adults. Infectious Diseases
Society of America. Clin Infect Dis 2000; 31:347-382.
9. BTS Guidelines for the Management of Community Acquired Pneumonia in Adults.
Thorax 2001; 56 Suppl 4:IV1-64.
10. Fine JM, Fine MJ, Galusha D, Petrillo M, Meehan TP. Patient and hospital characteristics
associated with recommended processes of care for elderly patients hospitalized with pneumonia:
results from the medicare quality indicator system pneumonia module. Arch Intern Med 2002;
162:827-833.
11. Feagan BG, Marrie TJ, Lau CY, Wheeler SL, Wong CJ, Vandervoort MK. Treatment and
outcomes of community-acquired pneumonia at Canadian hospitals. Cmaj 2000; 162:1415-1420.
12. Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, Rubin HR. Why
don't physicians follow clinical practice guidelines? A framework for improvement. Jama 1999;
282:1458-1465.
13. Marras TK, Chan CK. Use of guidelines in treating community-acquired pneumonia.
Chest 1998; 113:1689-1694.
14. Halm EA, Atlas SJ, Borowsky LH, Benzer TI, Metlay JP, Chang YC, Singer DE.
Understanding physician adherence with a pneumonia practice guideline: effects of patient,
system, and physician factors. Arch Intern Med 2000; 160:98-104.
15. Battleman DS, Callahan M, Thaler HT. Rapid antibiotic delivery and appropriate
antibiotic selection reduce length of hospital stay of patients with community-acquired
pneumonia: link between quality of care and resource utilization. Arch Intern Med 2002;
162:682-688.
16
16. Englert J, Davis KM, Koch KE. Using clinical practice analysis to improve care. Jt Comm
J Qual Improv 2001; 27:291-301.
17. Marrie TJ, Lau CY, Wheeler SL, Wong CJ, Vandervoort MK, Feagan BG. A controlled
trial of a critical pathway for treatment of community-acquired pneumonia. CAPITAL Study
Investigators. Community-Acquired Pneumonia Intervention Trial Assessing Levofloxacin. Jama
2000; 283:749-755.
18. File TM. Community-acquired pneumonia. Lancet 2003; 362:1991-2001.
19. Dean NC, Silver MP, Bateman KA, James B, Hadlock CJ, Hale D. Decreased mortality
after implementation of a treatment guideline for community-acquired pneumonia. Am J Med
2001; 110:451-457.
20. Gleason PP, Meehan TP, Fine JM, Galusha DH, Fine MJ. Associations between initial
antimicrobial therapy and medical outcomes for hospitalized elderly patients with pneumonia.
Arch Intern Med 1999; 159:2562-2572.
21. Menendez R, Torres A, Neumofail Group. Adherence to guidelines for treatment of
community-acquired pneumonia. Related factors. Proc Am Thoracic Soc 2005; 2:A797.
22. Menendez R, Torres A, Zalacain R, Aspa J, Martin Villasclaras JJ, Borderias L, Benitez
Moya JM, Ruiz-Manzano J, Rodriguez de Castro F, Blanquer J, et al. Risk factors of treatment
failure in community acquired pneumonia: implications for disease outcome. Thorax 2004;
59:960-965.
23. Frias J, Gomis M, Prieto J, Mensa J, Bouza E, Garcia-Rodriguez JA, Torres A, Dorca J,
Zalacain R, Garcia de Lomas J. [Initial empirical antibiotic treatment of community-acquired
pneumonia]. Rev Esp Quimioter 1998; 11:255-261.
17
24. Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, Coley CM,
Marrie TJ, Kapoor WN. A prediction rule to identify low-risk patients with community-acquired
pneumonia. N Engl J Med 1997; 336:243-250.
25. Hosmer D, Lemeshow S. Applied logistic regression, John Wiley & Sons, Inc ed, New
York. 1989.
26. Campbell SG. The use of clinical practice guidelines for community-acquired pneumonia
in hospitals in Atlantic Canada. Can Respir J 2004; 11:301-303.
27. Dean NC, Silver MP, Bateman KA. Frequency of subspecialty physician care for elderly
patients with community-acquired pneumonia. Chest 2000; 117:393-397.
28. Switzer GE, Halm EA, Chang CC, Mittman BS, Walsh MB, Fine MJ. Physician
awareness and self-reported use of local and national guidelines for community-acquired
pneumonia. J Gen Intern Med 2003; 18:816-823.
29. Fine MJ, Stone RA, Singer DE, Coley CM, Marrie TJ, Lave JR, Hough LJ, Obrosky DS,
Schulz R, Ricci EM, et al. Processes and outcomes of care for patients with community-acquired
pneumonia: results from the Pneumonia Patient Outcomes Research Team (PORT) cohort study.
Arch Intern Med 1999; 159:970-980.
30. Mortensen EM, Coley CM, Singer DE, Marrie TJ, Obrosky DS, Kapoor WN, Fine MJ.
Causes of death for patients with community-acquired pneumonia: results from the Pneumonia
Patient Outcomes Research Team cohort study. Arch Intern Med 2002; 162:1059-1064.
31. Greenfield S, Aronow HU, Elashoff RM, Watanabe D. Flaws in mortality data. The
hazards of ignoring comorbid disease. Jama 1988; 260:2253-2255.
32. Lim WS, van der Eerden MM, Laing R, Boersma WG, Karalus N, Town GI, Lewis SA,
Macfarlane JT. Defining community acquired pneumonia severity on presentation to hospital: an
international derivation and validation study. Thorax 2003; 58:377-382.
18
33. Meehan TP, Weingarten SR, Holmboe ES, Mathur D, Wang Y, Petrillo MK, Tu GS, Fine
JM. A statewide initiative to improve the care of hospitalized pneumonia patients: The
Connecticut Pneumonia Pathway Project. Am J Med 2001; 111:203-210.
34. Nathwani D, Rubinstein E, Barlow G, Davey P. Do guidelines for community-acquired
pneumonia improve the cost-effectiveness of hospital care? Clin Infect Dis 2001; 32:728-741.
35. Barlow GD, Lamping DL, Davey PG, Nathwani D. Evaluation of outcomes in
community-acquired pneumonia: a guide for patients, physicians, and policy-makers. Lancet
Infect Dis 2003; 3:476-488.
36. Dudas V, Hopefl A, Jacobs R, Guglielmo BJ. Antimicrobial selection for hospitalized
patients with presumed community-acquired pneumonia: a survey of nonteaching US community
hospitals. Ann Pharmacother 2000; 34:446-452.
37. Menendez R, Ferrando D, Valles JM, Vallterra J. Influence of deviation from guidelines
on the outcome of community-acquired pneumonia. Chest 2002; 122:612-617.
38. Mortensen EM, Restrepo M, Anzueto A, Pugh J. Effects of guideline-concordant
antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J
Med 2004; 117:726-731.
39. Marrie TJ, Carriere KC, Jin Y, Johnson DH. Mortality during hospitalisation for
pneumonia in Alberta, Canada, is associated with physician volume. Eur Respir J 2003; 22:148-
155.

19
Table 1: Adherence to guidelines, according to risk factors and co-morbidity.
Risk factor present
Yes No
Adherence/Total (%) Odds ratio p
Host factors: Unemployed 21/36 (58.3) 958/1192 (80.4) 0.3 (0.2-0.7) 0.001
PabT 300/363 (82.6) 677/863 (78.5) 1.3 (1-2) 0.095
Co-morbidity: COPD 287/354 (81.0) 666/846 (78.7) 1.1 (0.8-1.6) 0.402
Asthma 66/89 (74.2) 893/1115 (80.1) 0.7 (0.4-1.1) 0.181
Cardiac 298/359 (83.0) 676/861 (78.5) 1.4 (1-2) 0.07
CNS 140/186 (75.3) 836/1039 (80.5) 0.7 (0.5-1.1) 0.105
Diabetes 161/209 (77.0) 816/1014 (80.5) 0.8 (0.5-1.1) 0.26
Renal 87/114 (76.3) 894/1108 (80.7) 0.7 (0.5-1.4) 0.3
Related symptoms: Confusion 94/134 (70.2) 879/1088 (80.8) 0.6 (0.4-0.8) 0.004
Tachypnea≥30 218/281 (77.6) 761/947 (80.4) 0.8 (0.6-1.1) 0.309
BPs ≤90 18/35 (51.4) 962/1193 (80.6) 0.3 (0.1-0.5) 0.001
PabT: previous antibiotic treatment; CNS: central nervous system; BPs: systolic blood pressure
20
Table 2: Adherence to guidelines according to patient and prescribing physician characteristics.
Specialists ResidentsCharacteristics
Non-Pneu
(%)
Pneu (%) Non-Pneu (%) Pneu (%)
Host factors: Unemployed 4/11 (36.7) 6/10 (60.0) 6/8 (75.0) 5/7 (71.4)
PabT 34/45 (75.6) 71/86 (82.6) 142/161 (88.2) 53/71 (74.7)
Co-morbidity: COPD 46/66 (69.7) 63/72 (87.5) 118/149 (79.2) 60/67 (89.5)
Asthma 10/17 (58.8) 19/21 (90.5) 24/33 (72.7) 13/18 (72.2)
Cardiac 44/65 (67.7) 53/59 (89.8) 138/166 (83.1) 63/69 (91.3)
CNS 14/27 (51.9) 21/23 (91.3) 76/101 (75.6) 29/35 (82.9)
Diabetes 20/34 (58.8) 33/36 (91.7) 82/107 (76.6) 26/32 (81.2)
Renal 19/33 (57.6) 9/10 (90) 44/55 (80) 15/16 (93.7)
Related symptoms: Confusion* 15/37 (40.5) 16/18 (88.9) 47/59 (79.7) 16/20 (80.0)
Tachypnea≥30 38/60 (63.3) 37/46 (80.4) 100/117 (85.5) 43/58 (74.1)
BPs ≤90* 3/7 (42.9) 5/5 (100.0) 7/17 (41.2) 3/6 (50.0)
Fine risk class *: I 17/21 (85) 24/36 (66.6) 30/41 (73.2) 15/24 (62.5)
II 21/29 (72.6) 41/54 (75.9) 87/103 (84.4) 48/55 (87.3)
III 28/43 (65.1) 59/65 (90.7) 121/154 (78.5) 55/61 (90.1)
IV 43/63 (68.2) 61/75 (81.3) 140/168 (83.3) 68/81 (77.2)
V 24/42 (57.1) 13/14 (92.8) 55/65 (84.6) 15/18 (83.3)
PabT: previous antibiotic treatment; BPs: systolic blood pressure; Pneu: pneumologist; *p <0.05
21
Table 3: Predictors of adherence to guidelines: Multivariate analysis
Independent variables Odds ratio (IC95%)
Hospital 10 vs 13*
Hospital 6 vs 13
Hospital 2 vs 13
Hospìtal 7 vs 13
Hospital 4 vs 13
Hospital 9 vs 13
Hospital 3 vs 13
Hospital 12 vs 13
Hospital 1 vs 13
Hospital 5 vs 13
Hospital 11 vs 13
Hospital 8 vs 13
Admission to ICU
Pneumologist versus others
0.02 (0.003-0.07)
0.026 (0.004-0.094)
0.04 (0.007-0.162)
0.058 (0.009-0.22)
0.092 (0.014-0.3599
0.154 (0.24-0.574)
0.215 (0.033-0.789)
0.224 (0.024-2.092)
0.327 (0.046-1.514)
0.341 (0.048-1.602)
0.347 (0.043-2.234)
0.530 (0.078-2.226)
0.43 (0.24-0.78)
5.24 (2.74-10.21)
Pneumology resident versus others 3.72 (2.04-6.87)
Non-pneumology resident versus others 1.41 (0.86-2.28)
Fine classification; II-V versus I 2.35 (1.37-3.97)
Area under ROC curve: 0.8
OR between two hospitals is calculated as follows: Ex.:OR hospital 10 vs hospital 6 = OR
hospital 10 vs 13 x 1/ OR hospital 6 vs 13: 0.02 x 1/0.026=0.769
22
Table 4: Treatment failure and overall mortality according to adherence and prescribing
physician.
Treatment failure MortalityPrescribing physician
N % p N % P
Pneumology Resident
Adherent 16/201 8.0 0.04 8/200 4.0 0.29
Non-adherent 7/38 18.4 3/38 7.9
Non-pneumology Res:
Adherent 57/445 12.8 0.40 25/436 5.7 0.23
Non-adherent 16/100 16 9/99 9.1
Pneumologist:
Adherent 29/195 15.4 0.98 9/196 4.6 0.55
Non-adherent 7/46 15.2 3/45 6.6
Other specialists:
Adherent 24/133 18 0.07 10/128 7.8 0.43
Non-adherent 19/65 29.2 7/63 11.1
Total*
Adherent 126/974 12.9 0.03 52/960 5.4 0.008
Non-adherent 49/249 19.7 22/245 8.9
*Adherence reduces treatment failure OR: 0.66 (95%CI: 0.43-0.87), and mortality OR: 0.58
(95%CI: 0.35-0.97)
23
Table 5: Predictors of treatment failure and mortality. Results of regression logistic analyses
Treatment failure MortalityIndependent variables
OR (95%CI) p OR (95%CI) P
Adherence 0.65 (0.5-0.9) <0.05 0.55 (0.3- 0.9) <0.03
Residents and pneumologists
versus others
0.6 (0.4-0.9) <0.05
Fine IV-V versus I-III 10.8 (5.3-21.8) <0.001
Area under ROC curve for treatment failure and death: 0.6 and 0.77 respectively.
1
ONLINE DATA SUPLEMENT
Guidelines for the Treatment of Community-acquired Pneumonia: Predictors of
Adherence and Outcome
Rosario Menéndez MD, Antoni Torres MD, Rafael Zalacaín MD, Javier Aspa MD, Juan J
Martín-Villasclaras MD, Luis Borderías MD, José M Benítez-Moya MD, Juan Ruiz-Manzano
MD, Felipe Rodríguez de Castro MD, José Blanquer MD, Diego Pérez MD, Carmen Puzo MD,
Fernando Sánchez-Gascón MD, José Gallardo MD, Carlos Álvarez MD, Luis Molinos MD, on
behalf of the NEUMOFAIL Group
2
Patients and methods:
Selection criteria:
The study cohort comprised adult patients (>16 years of age) hospitalized with community-
acquired pneumonia (CAP)(E1). The inclusion criteria were: clinical picture compatible with
CAP, with at least two clinical symptoms and a new radiographic infiltrate. Patients with
previous neoplasm but without immunosuppressive treatment within the preceding 6 months,
and residents in nursing homes were also included. Exclusion criteria were: patients admitted
within the previous15 days, appearance of pneumonia after admission, transplant patients or
those with neoplasm who had recently received immunosuppressive treatment,
leukopenia<1000/mm3 or neutropenia<500/mm3 except if attributable to pneumonia, and HIV-
positive patients with severe immunosuppression (CD4<100). Patients who died within the
first 48 hours after admission were not included, to avoid cases that might reflect the
progression of very severe illness and whose clinical course would remain unchanged despite
antimicrobial therapy.
Data collection.
The data collected for this analysis included data of patients: demographic characteristics,
comorbid condition, signs of severity and chest radiographic findings. Data of the prescribing
physician were classified as: resident of pneumology, resident of other specialty, pneumologist
and non-pneumology specialist. Hospital where patient was admitted was codified with a
number.
The following data of patients were recorded: age, gender, smoking and alcohol habits (>80
gr/day), co-morbid disease (central nervous system (CNS) disorder, cardiac, pulmonary, liver
or renal diseases, diabetes), antimicrobial treatment before admission and employment status.
Initial severity signs collected were: acute confusion, respiratory and heart rate, and systolic

3
and diastolic blood pressure. Hypotension was defined as systolic blood pressure <90 mmHg,
tachypnea as ≥ 30 bpm and tachycardia ≥ 100 bpm.
Comorbid condition was defined as by Arancibia (E2):
CNS disorders: presence of chronic vascular or nonvascular encephalopathy with or
without dementia.
Heart disease: treatment for coronary artery disease, congestive heart failure or the
presence of heart valve disease.
Pulmonary disease: treatment for asthma or chronic obstructive pulmonary disease
(COPD), or the presence of interstitial lung disorders.
Liver disease: underlying viral or toxic liver disease.
Renal disease: underlying renal disease with abnormal serum creatinine not related to the
episode of pneumonia.
Diabetes mellitus: diagnosis of glucose intolerance and treatment with oral antidiabetic
drugs or insulin.
The initial risk class or PSI index(E3) was used to asses the severity of illness at presentation
and was also recorded. The radiographic findings collected were: number of involved lobes
(multilobar was considered as infiltrate of ≥ 2 lobes), and the presence of pleural effusion.
Follow-up protocol:
Treatment failure was classified as early (<72 hours) or late (>72 hours) (E1). Late treatment
failure was defined as persistence/reappearance of fever and symptoms, hemodynamic
instability, the appearance (Pa O2 <60 mm Hg or saturation <90% with a Fi O2 of 0.21) or
impairment of respiratory failure, radiographic progression, or new infectious foci after 72 h of
antimicrobial treatment. Early treatment failure was considered when patient developed clinical
deterioration within 72 hours of treatment, caused by one or more of the following causes:
hemodynamic instability, appearance or impairment of respiratory failure, need of mechanical
4
ventilation, radiographic progression or the appearance of new metastatic infectious foci
(modified from Arancibia et al(E2). Mortality follow-up was assessed until 30 days after
diagnosis of CAP.
Antimicrobial treatment and Adherence
The initial empirical treatment was the antibiotic therapy received during the first 24 hours no
matter if it had been prescribed in the emergency department or in the ward. Treatment was
considered adherent when antimicrobial therapy was compliant with the Spanish guidelines
SEQ-SEPAR(E4), which are depicted in Table E1. Guideline-adherent 3rd or 4th generation
cephalosporin included: cefotaxime, ceftriaxone, cefepime. Guideline-adherent macrolides
included: erythromycin, clarithromycin and azithromycin. Guideline-adherent intravenous
fluoroquinolone was levofloxacin. All other antibiotic regimens were considered non-adherent
to the guidelines, including partially adherent ones, and even if additional antibiotic agents
were added to an adherent one.
Results
The original cohort of patients included 1,424 patients from 15 Spanish hospitals(E1), but it
was not possible to collect data of the prescribing physician in two hospitals. Thus, data were
available for 1228 patients and the other 196 were excluded. To evaluate the consequences of
excluding these 196 patients, a statistical analysis of homogeneity was performed. There were
no significant differences with respect to age (p=0.14), gender (p=0.44), the presence of
comorbidity (p=0.26) and initial severity measured by risk class of Fine (p=0.07).
Adherence to guidelines:
There was a wide difference in adherence to guidelines between hospitals (range: 48.7-
97.2%), and in the percentage of residents and specialist physicians prescribing empirical
treatment (Table E2).

5
The regimens prescribed in intensive care unit (ICU) were compliant with the SEQ-SEPAR
guidelines in 58/86 (67.4%), with the following antibiotic schedules: 3rd generation
cephalosporin + macrolide 49 (57%), 3rd generation cephalosporin plus intravenous
levofloxacin 7 (8.1%); 4th generation cephalosporin + macrolide 2 (2.3%); and other non-
adherent antimicrobial regimens in the other 28 patients.
The regimens used for patients hospitalized in ward were adherent to guidelines in 921/1142
(80.6%), and the prescribed antibiotics were: 3rd generation cephalosporin + macrolide 396
(34.6%), amoxycillin-clavulanate plus macrolide 46 (4%); 3rd generation cephalosporin alone
103 (9%); amoxycillin-clavulanate alone 194 (17%); levofloxacin 182 (16%), while other non-
adherent antimicrobial regimens were used for the other 221 patients.
Multivariate statistical analysis: A stepwise regression logistic analysis was performed using
adherence to guidelines as the dependent variable. Independent variables were those which had
reached statistical significance in the univariate analysis. Those variables were: admission to
the ICU, risk class of Fine, confusion, hypotension, unemployment status, hospital and
prescribing physician. The initial severity, as measured by the Fine risk class, was re-codified
into 2 categories, Fine I versus Fine II-V, since there were significant differences between risk
class I and the rest. Four dummy variables for each prescribing physician -that is
pneumologists versus the other three groups, and the same for the rest- were introduced into
the model so as to analyze the independent effect of each physician category. The 13 hospitals
where prescribing physician was recorded were included in the model as another independent
variable.
The calculated mathematical model had an area under the ROC curve of 0.80, and the analysis
of effects showed that the hospital was the most explanatory variable (Wald chi-square 96.5,
p<0.0001), followed by the prescribing physician (Wald chi-square 31.2, p<0.0001), risk class

6
of Fine (Wald chi-square 12.6, p=0.0004), and admission to ICU (Wald chi-square 5.6,
p=0.01). One hospital was found statistically different with a higher percentage of adherence
while 7 hospitals were found to have significantly lower percentages.
Treatment failure and mortality.
Seventy-four patients died (6.1%) and treatment failure was found in 175 (14.2%). The results
of therapeutic response and mortality in the whole cohort stratified by prescribing physician
and admission to ICU are depicted in Table E3.

7
Table E1: Empirical antibiotic treatments adherent to SEQ-SEPAR guidelines.
- 3rd or 4th generation cephalosporin + iv macrolide CAP in ICU.
- 3rd or 4th generation cephalosporin + iv fluoroquinolone (levofloxacin)
- 3rd generation cephalosporin (cefotaxime or ceftriaxone)
- 3rd generation cephalosporin + macrolide
- amoxycillin-clavulanate
- amoxycillin-clavulanate + macrolide
CAP in ward
- 3rd or 4th generation fluoroquinolone
8
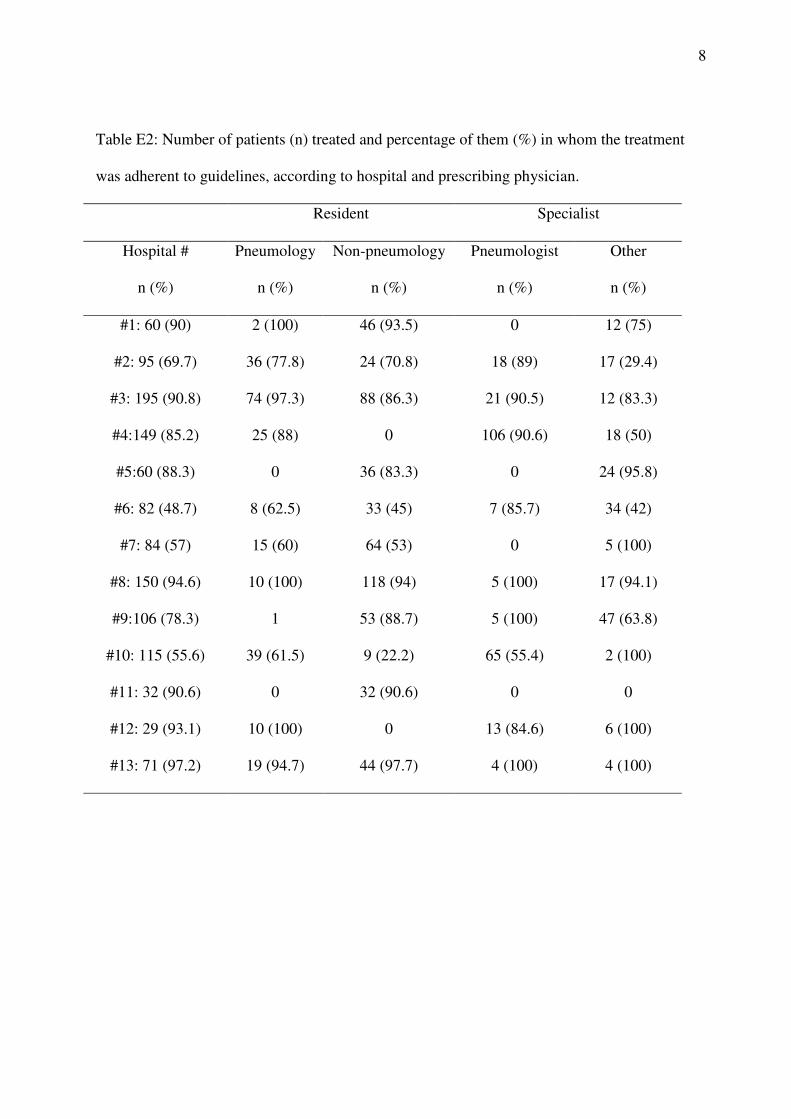
Table E2: Number of patients (n) treated and percentage of them (%) in whom the treatment
was adherent to guidelines, according to hospital and prescribing physician.
Resident Specialist
Hospital #
n (%)
Pneumology
n (%)
Non-pneumology
n (%)
Pneumologist
n (%)
Other
n (%)
#1: 60 (90) 2 (100) 46 (93.5) 0 12 (75)
#2: 95 (69.7) 36 (77.8) 24 (70.8) 18 (89) 17 (29.4)
#3: 195 (90.8) 74 (97.3) 88 (86.3) 21 (90.5) 12 (83.3)
#4:149 (85.2) 25 (88) 0 106 (90.6) 18 (50)
#5:60 (88.3) 0 36 (83.3) 0 24 (95.8)
#6: 82 (48.7) 8 (62.5) 33 (45) 7 (85.7) 34 (42)
#7: 84 (57) 15 (60) 64 (53) 0 5 (100)
#8: 150 (94.6) 10 (100) 118 (94) 5 (100) 17 (94.1)
#9:106 (78.3) 1 53 (88.7) 5 (100) 47 (63.8)
#10: 115 (55.6) 39 (61.5) 9 (22.2) 65 (55.4) 2 (100)
#11: 32 (90.6) 0 32 (90.6) 0 0
#12: 29 (93.1) 10 (100) 0 13 (84.6) 6 (100)
#13: 71 (97.2) 19 (94.7) 44 (97.7) 4 (100) 4 (100)

9
Table E3: Treatment failure and mortality stratified by prescribing physician and admission to
ICU
Treatment failure Mortality
Prescribing physician Cases % Cases %
Pneumology Resident: Non ICU
ICU
19/231
4/8
8.2
50
6/230
5/8
2.6
62.5
Total 23/239 9.6 11/238 4.6
Non-pneumology Res: Non ICU
ICU
61/522
12/23
11.6
52.1
27/512
7/23
5.2
30.4
Total 73/545 13.4 34/535 6.3
Pneumologist: Non ICU
ICU
29/227
7/14
12.7
50
11/223
1/14
4.9
7
Total 37/241 15.3 12/241 4.9
Other specialists: Non ICU
ICU
20/157
23/41
12.7
56.1
5/167
12/41
2.9
29.2
Total 43/198 21.7 17/208 8.1
Total Non ICU
ICU
129/1137
46/86
11.3
53
49/1132
25/86
4.3
29.1
10
REFERENCES
E1. Menendez R, Torres A, Zalacain R, Aspa J, Martin Villasclaras JJ, Borderias L, Benitez
Moya JM, Ruiz-Manzano J, Rodriguez de Castro F, Blanquer J, et al. Risk factors of treatment
failure in community acquired pneumonia: implications for disease outcome. Thorax 2004;
59:960-965.
E2. Arancibia F, Ewig S, Martinez JA, Ruiz M, Bauer T, Marcos MA, Mensa J, Torres A.
Antimicrobial treatment failures in patients with community-acquired pneumonia: causes and
prognostic implications. Am J Respir Crit Care Med 2000; 162:154-160.
E3. Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, Coley CM,
Marrie TJ, Kapoor WN. A prediction rule to identify low-risk patients with community-
acquired pneumonia. N Engl J Med 1997; 336:243-250.
E4. Frias J, Gomis M, Prieto J, Mensa J, Bouza E, Garcia-Rodriguez JA, Torres A, Dorca J,
Zalacain R, Garcia de Lomas J. Initial empirical antibiotic treatment of community-acquired
pneumonia. Rev Esp Quimioter 1998; 11:255-261.
Copyright © 2022 FDOKUMEN




















