General practitioners' judgement of chronic heart failure in the oldest old: Insights from the...
8
General practitioners' judgement of chronic heart failure in the oldest old: Insights from the BELFRAIL study ☆ Miek Smeets a, ⁎, Jan Degryse a,b , Bert Aertgeerts a , Stefan Janssens c , Wim Adriaensen a,b , Catharina Matheï a , Gijs Van Pottelbergh a,d , Pierre Wallemacq e , Jean-Louis Vanoverschelde f , Bert Vaes a,b a Department of Public Health and Primary Care, KU Leuven (KUL), Leuven, Belgium b Institute of Health and Society, Université Catholique de Louvain (UCL), Brussels, Belgium c Department of Cardiovascular Diseases, Universitair Ziekenhuis Gasthuisberg, KU Leuven (KUL), Leuven, Belgium d Department of Health and Technology, Leuven University College, Leuven, Belgium e Laboratory of Analytical Biochemistry, Cliniques Universitaires St Luc, Université Catholique de Louvain (UCL), Brussels, Belgium f Department of Cardiology, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain (UCL), Brussels, Belgium abstract article info Article history: Received 15 April 2015 Accepted 2 May 2015 Available online 5 May 2015 Keywords: Heart failure General practice Diagnosis Mortality Aged, 80 and over Background and objectives: Conflicting evidence exists about the value of general practitioners' (GPs') diagnoses of chronic heart failure (CHF), especially in older persons. Therefore, the relationship between GPs' judgement of CHF and objective cardiac abnormalities and their respective prognostic value for 5-year mortality in patients aged 80 and older was studied. Methods and results: These analyses were embedded within the prospective, population-based BELFRAIL study. At baseline, 525 patients (mean age 85 ± 3.7 years, 37% men) were clinically assessed by their GPs, had NT- proBNP levels determined and received a detailed echocardiography at home. GPs were asked to judge the pres- ence of CHF and to list their arguments in favour or against CHF. Cause-specific mortality was collected until 5.2 ± 0.25 years after baseline. GPs suspected CHF in 154 patients (29%). The prevalence of objective cardiac ab- normalities was 35% (n = 183). GPs' judgement predicted objective cardiac abnormalities inaccurately (sensitiv- ity 45% (95% CI 38–53), specificity 79% (95% CI 75–83)). However, both objective cardiac abnormalities and GPs' diagnoses of CHF were good predictors of 5-year mortality (HR 2.1 (95% CI 1.6–2.7) vs 1.7 (95% CI 1.3–2.3), re- spectively). Furthermore, the presence of objective cardiac abnormalities was not significantly better than GPs' judgement in identifying patients at risk for mortality, although a trend for better cardiovascular mortality risk classification was noted (NRI 10% (95% CI −2 to 21%), P = 0.13). Conclusions: Although GPs' judgement of CHF and objective cardiac abnormalities correlated poorly, the validity of GPs' clinical judgement for mortality risk stratification was demonstrated. © 2015 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Chronic heart failure (CHF) is a prevalent disease that affects older persons in particular [1,2]. In Europe, the first clinical presentation of heart failure usually takes place in the general practice setting [3]. Early diagnosis of heart failure is important to initiate treatment in a timely manner to delay progression to overt heart failure [1]. However, conflicting evidence exists about the value of general prac- titioners' (GPs') diagnoses of CHF [4–6]. Several studies have reported the poor validity of GPs' diagnoses, reporting both under- and over-di- agnoses [4–6]. This finding could be explained by the non-specific nature of heart failure symptoms and signs, especially in older persons [4,6,7] and by the observation that GPs underuse objective cardiac mea- surements such as natriuretic peptides and echocardiography [6,8,9]. Furthermore, GPs' reasoning when considering a diagnosis of CHF is mainly studied by case-vignette studies [10,11]. However, little is known about GPs' reasoning on real patients in daily practice. Gaining insight in how GPs reach a diagnosis of CHF is important, as this can pro- vide points of action to improve the diagnostic process. On the other hand, GPs' diagnoses can successfully identify patients at high risk of death, raising doubt about their poor validity [12]. However, to date, no study has been able to investigate the relationship between GPs' diagnoses and the presence of objective cardiac measure- ments and to compare their long-term predictive capacities. The current study hypothesized that there is a weak correlation between GPs' judge- ment of the presence of CHF in older persons and a standardized defini- tion of cardiac abnormalities but that both approaches are successful in identifying older patients at risk for mortality. International Journal of Cardiology 191 (2015) 120–127 ☆ All the authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. ⁎ Corresponding author at: Kapucijnenvoer 33, Blok J Bus 7001, 3000 Leuven, Belgium. E-mail address: [email protected] (M. Smeets). http://dx.doi.org/10.1016/j.ijcard.2015.05.002 0167-5273/© 2015 Elsevier Ireland Ltd. All rights reserved. Contents lists available at ScienceDirect International Journal of Cardiology journal homepage: www.elsevier.com/locate/ijcard
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of General practitioners' judgement of chronic heart failure in the oldest old: Insights from the...

International Journal of Cardiology 191 (2015) 120–127
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r .com/ locate / i j ca rd
General practitioners' judgement of chronic heart failure in the oldestold: Insights from the BELFRAIL study☆
Miek Smeets a,⁎, Jan Degryse a,b, Bert Aertgeerts a, Stefan Janssens c, Wim Adriaensen a,b, Catharina Matheï a,Gijs Van Pottelbergh a,d, Pierre Wallemacq e, Jean-Louis Vanoverschelde f, Bert Vaes a,b
a Department of Public Health and Primary Care, KU Leuven (KUL), Leuven, Belgiumb Institute of Health and Society, Université Catholique de Louvain (UCL), Brussels, Belgiumc Department of Cardiovascular Diseases, Universitair Ziekenhuis Gasthuisberg, KU Leuven (KUL), Leuven, Belgiumd Department of Health and Technology, Leuven University College, Leuven, Belgiume Laboratory of Analytical Biochemistry, Cliniques Universitaires St Luc, Université Catholique de Louvain (UCL), Brussels, Belgiumf Department of Cardiology, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain (UCL), Brussels, Belgium
☆ All the authors take responsibility for all aspects of tbias of the data presented and their discussed interpretat⁎ Corresponding author at: Kapucijnenvoer 33, Blok J B
E-mail address: [email protected] (M. S
http://dx.doi.org/10.1016/j.ijcard.2015.05.0020167-5273/© 2015 Elsevier Ireland Ltd. All rights reserved
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 15 April 2015Accepted 2 May 2015Available online 5 May 2015Keywords:Heart failureGeneral practiceDiagnosisMortalityAged, 80 and over
Background and objectives: Conflicting evidence exists about the value of general practitioners' (GPs') diagnosesof chronic heart failure (CHF), especially in older persons. Therefore, the relationship between GPs' judgement ofCHF and objective cardiac abnormalities and their respective prognostic value for 5-year mortality in patientsaged 80 and older was studied.Methods and results: These analyses were embedded within the prospective, population-based BELFRAIL study.At baseline, 525 patients (mean age 85 ± 3.7 years, 37% men) were clinically assessed by their GPs, had NT-proBNP levels determined and received a detailed echocardiography at home. GPswere asked to judge the pres-ence of CHF and to list their arguments in favour or against CHF. Cause-specific mortality was collected until5.2 ± 0.25 years after baseline. GPs suspected CHF in 154 patients (29%). The prevalence of objective cardiac ab-normalities was 35% (n=183). GPs' judgement predicted objective cardiac abnormalities inaccurately (sensitiv-
ity 45% (95% CI 38–53), specificity 79% (95% CI 75–83)). However, both objective cardiac abnormalities and GPs'diagnoses of CHF were good predictors of 5-year mortality (HR 2.1 (95% CI 1.6–2.7) vs 1.7 (95% CI 1.3–2.3), re-spectively). Furthermore, the presence of objective cardiac abnormalities was not significantly better than GPs'judgement in identifying patients at risk for mortality, although a trend for better cardiovascular mortality riskclassification was noted (NRI 10% (95% CI −2 to 21%), P = 0.13).Conclusions: Although GPs' judgement of CHF and objective cardiac abnormalities correlated poorly, the validityof GPs' clinical judgement for mortality risk stratification was demonstrated.© 2015 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Chronic heart failure (CHF) is a prevalent disease that affects olderpersons in particular [1,2]. In Europe, the first clinical presentation ofheart failure usually takes place in the general practice setting [3].Early diagnosis of heart failure is important to initiate treatment in atimely manner to delay progression to overt heart failure [1].
However, conflicting evidence exists about the value of general prac-titioners' (GPs') diagnoses of CHF [4–6]. Several studies have reportedthe poor validity of GPs' diagnoses, reporting both under- and over-di-agnoses [4–6]. This finding could be explained by the non-specific
he reliability and freedom fromion.us 7001, 3000 Leuven, Belgium.meets).
.
nature of heart failure symptoms and signs, especially in older persons[4,6,7] and by the observation that GPs underuse objective cardiac mea-surements such as natriuretic peptides and echocardiography [6,8,9].Furthermore, GPs' reasoning when considering a diagnosis of CHF ismainly studied by case-vignette studies [10,11]. However, little isknown about GPs' reasoning on real patients in daily practice. Gaininginsight in howGPs reach a diagnosis of CHF is important, as this can pro-vide points of action to improve the diagnostic process.
On the other hand, GPs' diagnoses can successfully identify patientsat high risk of death, raising doubt about their poor validity [12].However, to date, no study has been able to investigate the relationshipbetween GPs' diagnoses and the presence of objective cardiac measure-ments and to compare their long-termpredictive capacities. The currentstudyhypothesized that there is aweak correlation betweenGPs' judge-ment of the presence of CHF in older persons and a standardized defini-tion of cardiac abnormalities but that both approaches are successful inidentifying older patients at risk for mortality.
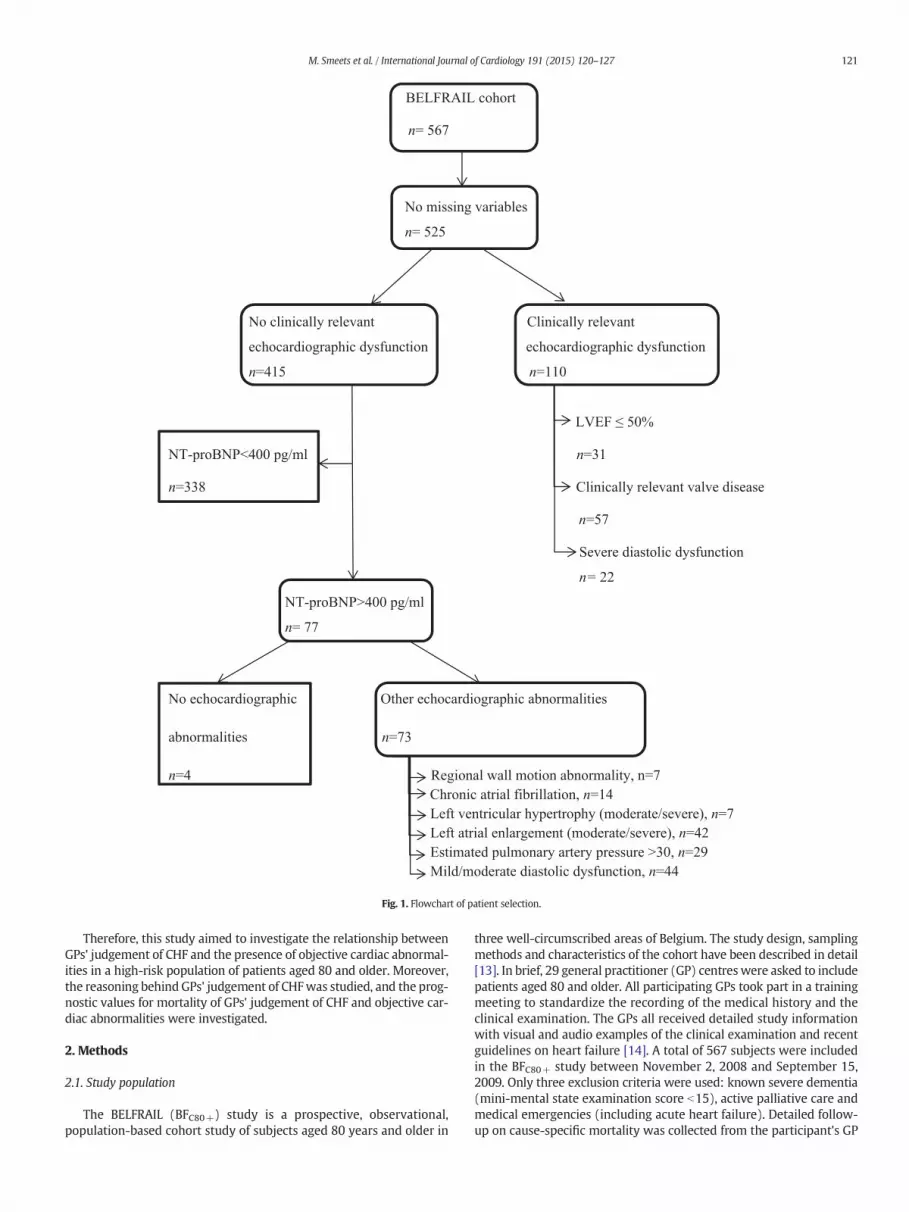
Fig. 1. Flowchart of patient selection.
121M. Smeets et al. / International Journal of Cardiology 191 (2015) 120–127
Therefore, this study aimed to investigate the relationship betweenGPs' judgement of CHF and the presence of objective cardiac abnormal-ities in a high-risk population of patients aged 80 and older. Moreover,the reasoning behind GPs' judgement of CHFwas studied, and the prog-nostic values for mortality of GPs' judgement of CHF and objective car-diac abnormalities were investigated.
2. Methods
2.1. Study population
The BELFRAIL (BFC80+) study is a prospective, observational,population-based cohort study of subjects aged 80 years and older in
three well-circumscribed areas of Belgium. The study design, samplingmethods and characteristics of the cohort have been described in detail[13]. In brief, 29 general practitioner (GP) centreswere asked to includepatients aged 80 and older. All participating GPs took part in a trainingmeeting to standardize the recording of the medical history and theclinical examination. The GPs all received detailed study informationwith visual and audio examples of the clinical examination and recentguidelines on heart failure [14]. A total of 567 subjects were includedin the BFC80+ study between November 2, 2008 and September 15,2009. Only three exclusion criteria were used: known severe dementia(mini-mental state examination score b15), active palliative care andmedical emergencies (including acute heart failure). Detailed follow-up on cause-specific mortality was collected from the participant's GP

122 M. Smeets et al. / International Journal of Cardiology 191 (2015) 120–127
until 5.2 ± 0.25 years after inclusion and baseline evaluation. All of theparticipants in the study provided informed consent, and the Biomedi-cal Ethics Committee of the Medical School of the Université catholiquede Louvain (UCL) of Brussels approved the study. All clinical and labora-tory tests were performed in accordance with the declaration ofHelsinki.
2.2. Standardized clinical assessment
Each GP recorded the medical history and performed a clinical ex-amination of their patients at baseline. The history included questionsabout the presence of dyspnea (according to the dyspnea scale of themedical research council [MRC]) [15], invalidating fatigue, orthopnea,edema of the lower extremities, palpitations and nocturnal cough. Theclinical examination consisted of a blood pressure measurement onboth arms that was repeated after 2 min. Heart rate, heart rhythm (reg-ular or irregular) and breathing rate at rest (cut-off N20 breaths/min)were measured. Heart auscultation was performed to detect S3 and S4heart sounds or a cardiacmurmur, and lung auscultationwasperformedto detect crepitation. The apex beat was palpated and recorded whenabnormal. Jugular venous pressure (JVP) wasmeasured and noted if in-creased, and the presence of hepatojugular reflux (HJR) and edema ofthe lower extremities was checked.
Cardiovascular risk factors were defined as a positive response of theGP with respect to the presence of hypertension, diabetes mellitus orhyperlipidemia. Patient smoking status was recorded, and the bodymass index (BMI) was calculated. Cardiac morbidities were defined asa history of angina pectoris, myocardial infarction, known cardiomyop-athy, a history of decompensated heart failure, chronic atrial fibrillationor known valvular heart disease. GPs reported important cardiac inter-ventions, including percutaneous transluminal coronary angioplasty orstenting; coronary, valve or peripheral vascular surgery; and the place-ment of cardiac devices. Other cardiovascular morbidities were definedas a history of transient ischemic attack, stroke or known peripheral ar-terial disease. Non-cardiovascular co-morbidities were defined as thepresence of depression, COPD, renal insufficiency, anaemia andosteoarthritis.
The Anatomic Therapeutic Chemistry classification system was ap-plied to register medication use [16]. Data on relevant cardiovascularmedications, including cardiac glycosides, diuretics, β-blockers, calciumantagonists, angiotensin-converting enzyme inhibitors and angiotensinII receptor blockers, were used.
A 12-lead electrocardiogram (ECG) was recorded by the clinicalresearch assistant at baseline on a QRS Universal ECG device (QRS diag-nostics, Plymouth, Minnesota, USA, www.qrsdiagnostic.com). A singlecardiologist blinded to all other study results analysed all ECGs accord-ing to theMinnesota Code Classification System for Electrocardiograph-ic Findings [17]. Minnesota Code 8-1-3 was used to define atrialfibrillation on ECG.
2.3. GPs' judgement of the presence of CHF
After the standardized clinical assessment, GPs were asked to recordtheir judgement of the presence of CHF and to estimate their degree ofcertainty (Likert scale: 2–10–25–50–75–90–98% certainty). Further-more, GPs were asked to note, in free text, their arguments in favouror against the presence of CHF. GPs were blinded to the results of allother study visits. An independent researcher (MS) first coded thereported arguments into specific categories similar to the free text(e.g., absence of dyspnea) and afterwards into major categories
Notes to Table 1:°, Chi-square test; &, Mann–WhitneyU-test; ⁎, according to theMRC (Medical Research Council)or irregular heart rhythm in clinical examination; μ, diuretics, ACE-I, angiotensin II RB or digitaSD, standard deviation; JVP, jugular venous pressure; HJR, hepatojugular reflux; BMI, bodymaspulmonary disease; ECG, electrocardiogram; LVH, left ventricular hypertrophy; LBBB, left bund
(absence or presence of symptoms, signs, cardiovascular risk factors,cardiovascular antecedents, antecedent of decompensated heart failure,non-cardiac morbidities).
2.4. Objective cardiac measurements
The serum NT-proBNP levels were measured using a Dade-Dimension® Xpand (Siemens, Deerfield, USA) assay. The coefficient ofvariation ranged from 3.9 to 4.3%.
Echocardiograms were performed at baseline using a commerciallyavailable portable system (CX50, Philips, Andover, Massachusetts, USA)with M-mode, 2-dimensional and pulsed, continuous-wave and colour-flow Doppler capabilities. The echocardiograms were performed at thestudy participant's home by a single cardiologist who was blinded tothe clinical characteristics and laboratory test results. A complete exami-nation, in accordancewith the recommendations of the American Societyof Echocardiography and the European Association of Echocardiography(ASE-EAE), was performed [18]. The method, prevalence of echocardio-graphic abnormalities and quality of the echocardiographic images havebeen previously described in detail [19]. Briefly, left ventricular (LV) sys-tolic functionwas calculatedusing Simpson's biplanemethod [18]. Systol-ic dysfunction was defined as an LV ejection fraction (LVEF) ≤50%. Thefunction of themitral and aortic valves was evaluated using colour Dopp-ler echocardiography after optimizing the gain andNyquist limit. Stenoticand regurgitant valve diseaseswere evaluated according to semiquantita-tive and quantitative methods recommended by the American Society ofEchocardiography [20,21]. Subjectswith prosthetic valveswere evaluatedseparately [20]. Clinically relevant valve diseasewas defined asmitral ste-nosis of any severity, severe aortic stenosis (aortic valve area b1 cm2),moderate or severemitral regurgitation, andmoderate or severe aortic re-gurgitation. The diastolic function was assessed using mitral flow veloci-ties obtained by pulsed Doppler and pulsed tissue Doppler at the levelof the mitral annulus [22]. Additional apical and parasternal views forassessing tissue velocity (colour tissue Doppler) were also recorded. TheASA–EAE guidelines were used to assess the presence of diastolic dys-function [22].
2.5. Reference standard
The reference standard of objective cardiac abnormalities was de-fined as the presence of clinically relevant echocardiographic dysfunc-tion (LVEF ≤ 50, clinically relevant valve disease and severe diastolicdysfunction) or as another functional or structural echocardiographicabnormality in combination with an elevated serum NT-proBNP level(≥400 pg/ml) (Fig. 1) [14,23–25]. Other functional or structural echo-cardiographic abnormalities were defined as regional wall motion ab-normality (RWMA), moderate and severe left atrial enlargement or LVhypertrophy, an estimated pulmonary artery pressure above30 mm Hg, chronic atrial fibrillation or mild/moderate diastolic dys-function [1,18,22]. Second, objective cardiac abnormalities in combina-tion with at least one typical heart failure symptom and sign werestudied as a proxy for symptomatic heart failure.
2.6. Data analysis
Continuous variables were presented as mean± standard deviation(SD) or as medians and inter-quartile ranges (IQR). Categorical datawere presented as frequencies and proportions. Baseline variableswere compared using the Chi-squared test (categorical variables) orMann–Whitney U test (continuous variables). Cohen's kappa coefficient
dyspnea scale; §, breathing frequency N20/min; $, tachycardia (heart rate N100 bpm) and/lis.s index; PTCA, percutaneous transluminal coronary angioplasty; COPD, chronic obstructivele branch block; ACE, angiotensin converting enzyme; RB, receptor blocker.
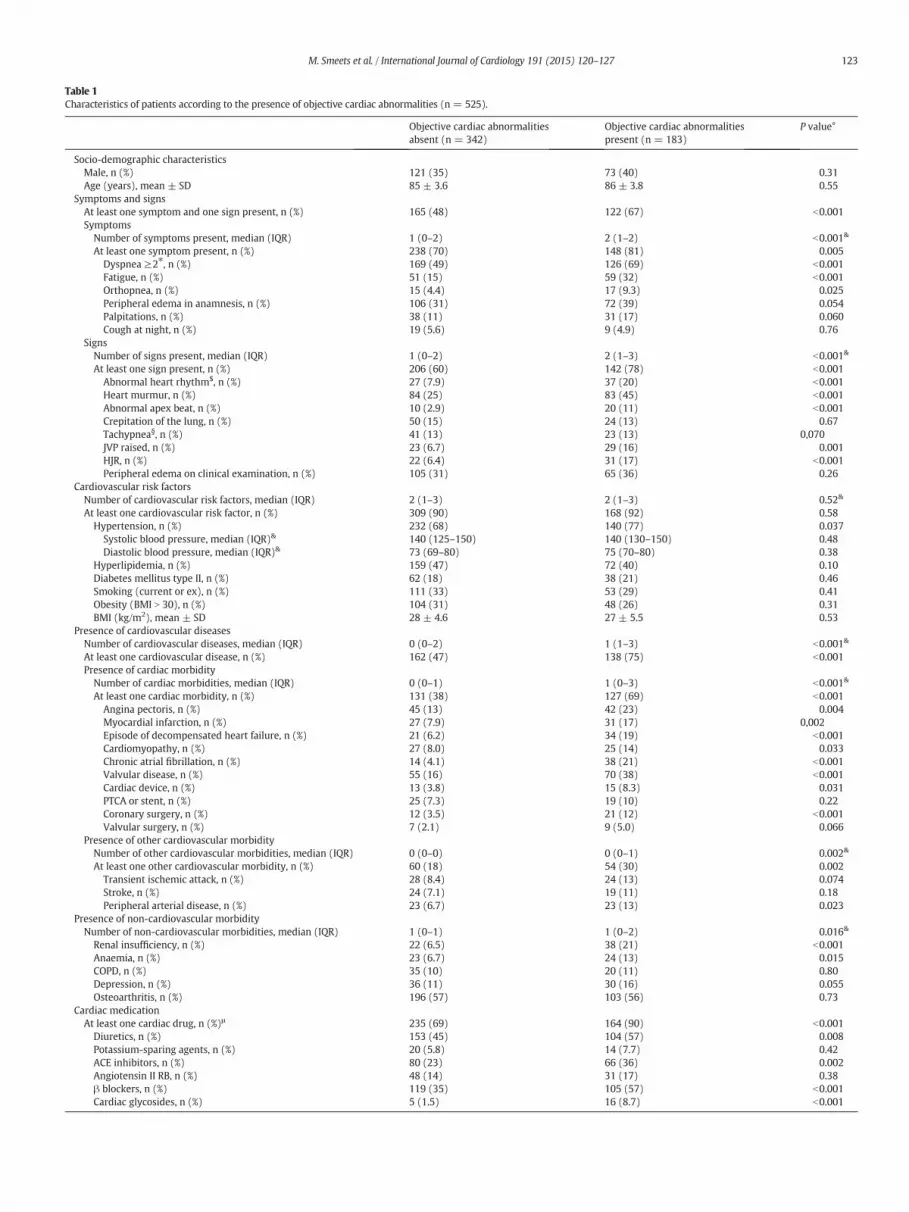
Table 1Characteristics of patients according to the presence of objective cardiac abnormalities (n = 525).
Objective cardiac abnormalitiesabsent (n = 342)
Objective cardiac abnormalitiespresent (n = 183)
P value°
Socio-demographic characteristicsMale, n (%) 121 (35) 73 (40) 0.31Age (years), mean ± SD 85 ± 3.6 86 ± 3.8 0.55
Symptoms and signsAt least one symptom and one sign present, n (%) 165 (48) 122 (67) b0.001SymptomsNumber of symptoms present, median (IQR) 1 (0–2) 2 (1–2) b0.001&
At least one symptom present, n (%) 238 (70) 148 (81) 0.005Dyspnea ≥2⁎, n (%) 169 (49) 126 (69) b0.001Fatigue, n (%) 51 (15) 59 (32) b0.001Orthopnea, n (%) 15 (4.4) 17 (9.3) 0.025Peripheral edema in anamnesis, n (%) 106 (31) 72 (39) 0.054Palpitations, n (%) 38 (11) 31 (17) 0.060Cough at night, n (%) 19 (5.6) 9 (4.9) 0.76
SignsNumber of signs present, median (IQR) 1 (0–2) 2 (1–3) b0.001&
At least one sign present, n (%) 206 (60) 142 (78) b0.001Abnormal heart rhythm$, n (%) 27 (7.9) 37 (20) b0.001Heart murmur, n (%) 84 (25) 83 (45) b0.001Abnormal apex beat, n (%) 10 (2.9) 20 (11) b0.001Crepitation of the lung, n (%) 50 (15) 24 (13) 0.67Tachypnea§, n (%) 41 (13) 23 (13) 0,070JVP raised, n (%) 23 (6.7) 29 (16) 0.001HJR, n (%) 22 (6.4) 31 (17) b0.001Peripheral edema on clinical examination, n (%) 105 (31) 65 (36) 0.26
Cardiovascular risk factorsNumber of cardiovascular risk factors, median (IQR) 2 (1–3) 2 (1–3) 0.52&
At least one cardiovascular risk factor, n (%) 309 (90) 168 (92) 0.58Hypertension, n (%) 232 (68) 140 (77) 0.037
Systolic blood pressure, median (IQR)& 140 (125–150) 140 (130–150) 0.48Diastolic blood pressure, median (IQR)& 73 (69–80) 75 (70–80) 0.38
Hyperlipidemia, n (%) 159 (47) 72 (40) 0.10Diabetes mellitus type II, n (%) 62 (18) 38 (21) 0.46Smoking (current or ex), n (%) 111 (33) 53 (29) 0.41Obesity (BMI N 30), n (%) 104 (31) 48 (26) 0.31BMI (kg/m2), mean ± SD 28 ± 4.6 27 ± 5.5 0.53
Presence of cardiovascular diseasesNumber of cardiovascular diseases, median (IQR) 0 (0–2) 1 (1–3) b0.001&
At least one cardiovascular disease, n (%) 162 (47) 138 (75) b0.001Presence of cardiac morbidityNumber of cardiac morbidities, median (IQR) 0 (0–1) 1 (0–3) b0.001&
At least one cardiac morbidity, n (%) 131 (38) 127 (69) b0.001Angina pectoris, n (%) 45 (13) 42 (23) 0.004Myocardial infarction, n (%) 27 (7.9) 31 (17) 0,002Episode of decompensated heart failure, n (%) 21 (6.2) 34 (19) b0.001Cardiomyopathy, n (%) 27 (8.0) 25 (14) 0.033Chronic atrial fibrillation, n (%) 14 (4.1) 38 (21) b0.001Valvular disease, n (%) 55 (16) 70 (38) b0.001Cardiac device, n (%) 13 (3.8) 15 (8.3) 0.031PTCA or stent, n (%) 25 (7.3) 19 (10) 0.22Coronary surgery, n (%) 12 (3.5) 21 (12) b0.001Valvular surgery, n (%) 7 (2.1) 9 (5.0) 0.066
Presence of other cardiovascular morbidityNumber of other cardiovascular morbidities, median (IQR) 0 (0–0) 0 (0–1) 0.002&
At least one other cardiovascular morbidity, n (%) 60 (18) 54 (30) 0.002Transient ischemic attack, n (%) 28 (8.4) 24 (13) 0.074Stroke, n (%) 24 (7.1) 19 (11) 0.18Peripheral arterial disease, n (%) 23 (6.7) 23 (13) 0.023
Presence of non-cardiovascular morbidityNumber of non-cardiovascular morbidities, median (IQR) 1 (0–1) 1 (0–2) 0.016&
Renal insufficiency, n (%) 22 (6.5) 38 (21) b0.001Anaemia, n (%) 23 (6.7) 24 (13) 0.015COPD, n (%) 35 (10) 20 (11) 0.80Depression, n (%) 36 (11) 30 (16) 0.055Osteoarthritis, n (%) 196 (57) 103 (56) 0.73
Cardiac medicationAt least one cardiac drug, n (%)μ 235 (69) 164 (90) b0.001Diuretics, n (%) 153 (45) 104 (57) 0.008Potassium-sparing agents, n (%) 20 (5.8) 14 (7.7) 0.42ACE inhibitors, n (%) 80 (23) 66 (36) 0.002Angiotensin II RB, n (%) 48 (14) 31 (17) 0.38β blockers, n (%) 119 (35) 105 (57) b0.001Cardiac glycosides, n (%) 5 (1.5) 16 (8.7) b0.001
123M. Smeets et al. / International Journal of Cardiology 191 (2015) 120–127
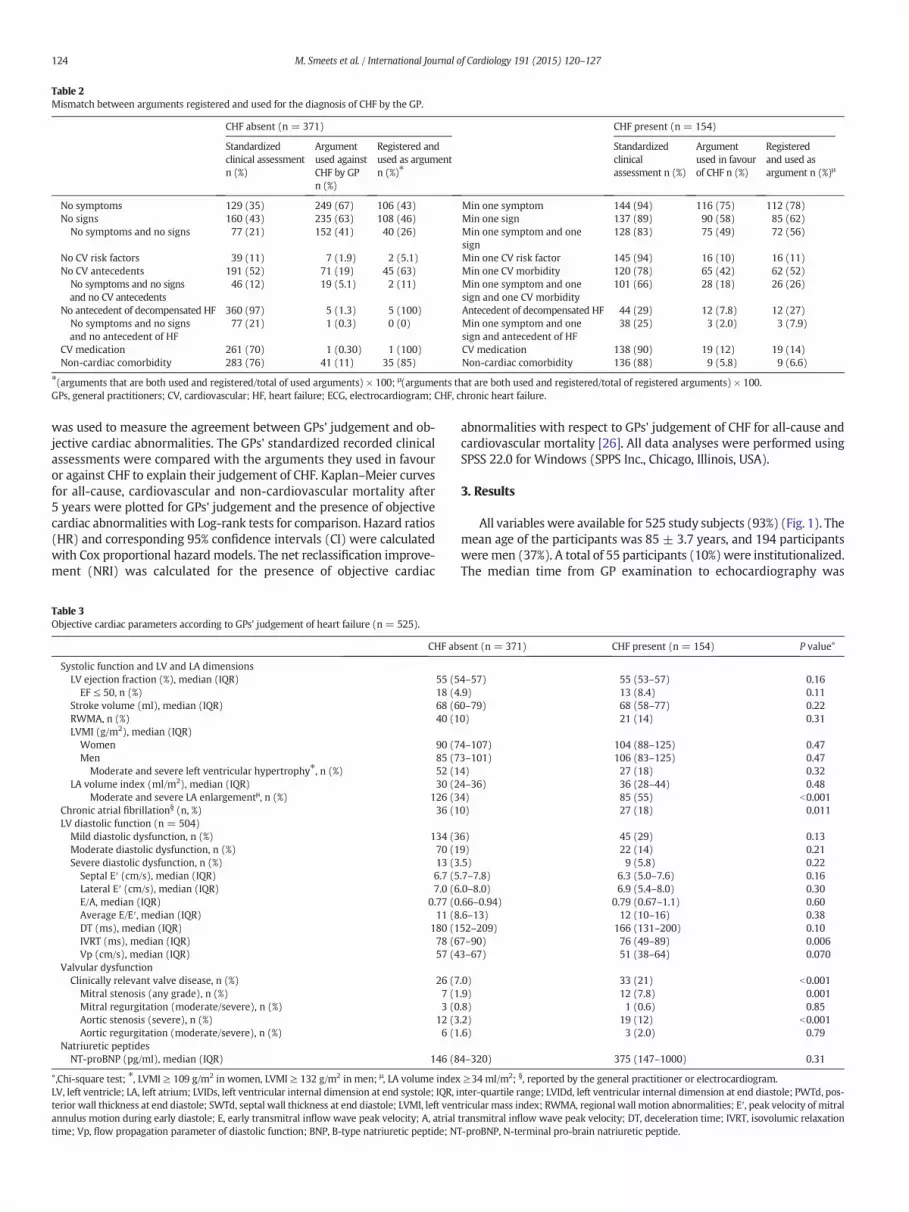
Table 2Mismatch between arguments registered and used for the diagnosis of CHF by the GP.
CHF absent (n = 371) CHF present (n = 154)
Standardizedclinical assessmentn (%)
Argumentused againstCHF by GPn (%)
Registered andused as argumentn (%)⁎
Standardizedclinicalassessment n (%)
Argumentused in favourof CHF n (%)
Registeredand used asargument n (%)μ
No symptoms 129 (35) 249 (67) 106 (43) Min one symptom 144 (94) 116 (75) 112 (78)No signs 160 (43) 235 (63) 108 (46) Min one sign 137 (89) 90 (58) 85 (62)
No symptoms and no signs 77 (21) 152 (41) 40 (26) Min one symptom and onesign
128 (83) 75 (49) 72 (56)
No CV risk factors 39 (11) 7 (1.9) 2 (5.1) Min one CV risk factor 145 (94) 16 (10) 16 (11)No CV antecedents 191 (52) 71 (19) 45 (63) Min one CV morbidity 120 (78) 65 (42) 62 (52)
No symptoms and no signsand no CV antecedents
46 (12) 19 (5.1) 2 (11) Min one symptom and onesign and one CV morbidity
101 (66) 28 (18) 26 (26)
No antecedent of decompensated HF 360 (97) 5 (1.3) 5 (100) Antecedent of decompensated HF 44 (29) 12 (7.8) 12 (27)No symptoms and no signsand no antecedent of HF
77 (21) 1 (0.3) 0 (0) Min one symptom and onesign and antecedent of HF
38 (25) 3 (2.0) 3 (7.9)
CV medication 261 (70) 1 (0.30) 1 (100) CV medication 138 (90) 19 (12) 19 (14)Non-cardiac comorbidity 283 (76) 41 (11) 35 (85) Non-cardiac comorbidity 136 (88) 9 (5.8) 9 (6.6)
⁎(arguments that are both used and registered/total of used arguments) × 100; μ(arguments that are both used and registered/total of registered arguments) × 100.GPs, general practitioners; CV, cardiovascular; HF, heart failure; ECG, electrocardiogram; CHF, chronic heart failure.
124 M. Smeets et al. / International Journal of Cardiology 191 (2015) 120–127
was used to measure the agreement between GPs' judgement and ob-jective cardiac abnormalities. The GPs' standardized recorded clinicalassessments were compared with the arguments they used in favouror against CHF to explain their judgement of CHF. Kaplan–Meier curvesfor all-cause, cardiovascular and non-cardiovascular mortality after5 years were plotted for GPs' judgement and the presence of objectivecardiac abnormalities with Log-rank tests for comparison. Hazard ratios(HR) and corresponding 95% confidence intervals (CI) were calculatedwith Cox proportional hazard models. The net reclassification improve-ment (NRI) was calculated for the presence of objective cardiac
Table 3Objective cardiac parameters according to GPs' judgement of heart failure (n = 525).
CHF ab
Systolic function and LV and LA dimensionsLV ejection fraction (%), median (IQR) 55 (5EF ≤ 50, n (%) 18 (4
Stroke volume (ml), median (IQR) 68 (6RWMA, n (%) 40 (1LVMI (g/m2), median (IQR)Women 90 (7Men 85 (7
Moderate and severe left ventricular hypertrophy⁎, n (%) 52 (1LA volume index (ml/m2), median (IQR) 30 (2
Moderate and severe LA enlargementμ, n (%) 126 (3Chronic atrial fibrillation§ (n, %) 36 (1LV diastolic function (n = 504)
Mild diastolic dysfunction, n (%) 134 (3Moderate diastolic dysfunction, n (%) 70 (1Severe diastolic dysfunction, n (%) 13 (3Septal E′ (cm/s), median (IQR) 6.7 (5Lateral E′ (cm/s), median (IQR) 7.0 (6E/A, median (IQR) 0.77 (0Average E/E′, median (IQR) 11 (8DT (ms), median (IQR) 180 (1IVRT (ms), median (IQR) 78 (6Vp (cm/s), median (IQR) 57 (4
Valvular dysfunctionClinically relevant valve disease, n (%) 26 (7Mitral stenosis (any grade), n (%) 7 (1Mitral regurgitation (moderate/severe), n (%) 3 (0Aortic stenosis (severe), n (%) 12 (3Aortic regurgitation (moderate/severe), n (%) 6 (1
Natriuretic peptidesNT-proBNP (pg/ml), median (IQR) 146 (8
°,Chi-square test; ⁎, LVMI ≥ 109 g/m2 in women, LVMI ≥ 132 g/m2 in men; μ, LA volume indexLV, left ventricle; LA, left atrium; LVIDs, left ventricular internal dimension at end systole; IQR, iterior wall thickness at end diastole; SWTd, septal wall thickness at end diastole; LVMI, left venannulus motion during early diastole; E, early transmitral inflow wave peak velocity; A, atrialtime; Vp, flow propagation parameter of diastolic function; BNP, B-type natriuretic peptide; NT
abnormalities with respect to GPs' judgement of CHF for all-cause andcardiovascular mortality [26]. All data analyses were performed usingSPSS 22.0 for Windows (SPPS Inc., Chicago, Illinois, USA).
3. Results
All variables were available for 525 study subjects (93%) (Fig. 1). Themean age of the participants was 85 ± 3.7 years, and 194 participantsweremen (37%). A total of 55 participants (10%)were institutionalized.The median time from GP examination to echocardiography was
sent (n = 371) CHF present (n = 154) P value°
4–57) 55 (53–57) 0.16.9) 13 (8.4) 0.110–79) 68 (58–77) 0.220) 21 (14) 0.31
4–107) 104 (88–125) 0.473–101) 106 (83–125) 0.474) 27 (18) 0.324–36) 36 (28–44) 0.484) 85 (55) b0.0010) 27 (18) 0.011
6) 45 (29) 0.139) 22 (14) 0.21.5) 9 (5.8) 0.22.7–7.8) 6.3 (5.0–7.6) 0.16.0–8.0) 6.9 (5.4–8.0) 0.30.66–0.94) 0.79 (0.67–1.1) 0.60.6–13) 12 (10–16) 0.3852–209) 166 (131–200) 0.107–90) 76 (49–89) 0.0063–67) 51 (38–64) 0.070
.0) 33 (21) b0.001
.9) 12 (7.8) 0.001
.8) 1 (0.6) 0.85
.2) 19 (12) b0.001
.6) 3 (2.0) 0.79
4–320) 375 (147–1000) 0.31
≥34 ml/m2; §, reported by the general practitioner or electrocardiogram.nter-quartile range; LVIDd, left ventricular internal dimension at end diastole; PWTd, pos-tricular mass index; RWMA, regional wall motion abnormalities; E′, peak velocity of mitraltransmitral inflow wave peak velocity; DT, deceleration time; IVRT, isovolumic relaxation-proBNP, N-terminal pro-brain natriuretic peptide.
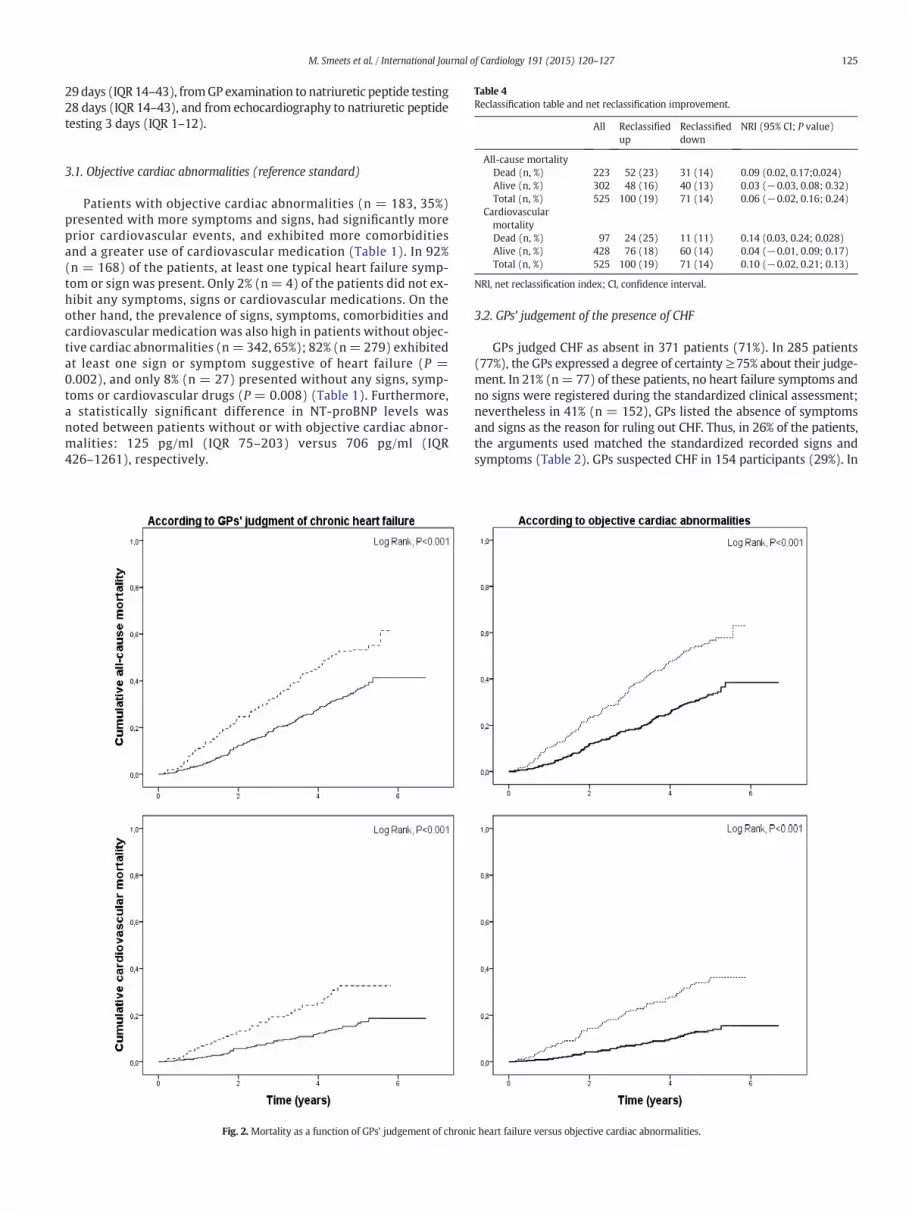
Table 4Reclassification table and net reclassification improvement.
All Reclassified Reclassified NRI (95% CI; P value)
125M. Smeets et al. / International Journal of Cardiology 191 (2015) 120–127
29days (IQR 14–43), fromGP examination to natriuretic peptide testing28 days (IQR 14–43), and from echocardiography to natriuretic peptidetesting 3 days (IQR 1–12).
up down
All-cause mortalityDead (n, %) 223 52 (23) 31 (14) 0.09 (0.02, 0.17;0.024)Alive (n, %) 302 48 (16) 40 (13) 0.03 (−0.03, 0.08; 0.32)Total (n, %) 525 100 (19) 71 (14) 0.06 (−0.02, 0.16; 0.24)
CardiovascularmortalityDead (n, %) 97 24 (25) 11 (11) 0.14 (0.03, 0.24; 0.028)Alive (n, %) 428 76 (18) 60 (14) 0.04 (−0.01, 0.09; 0.17)Total (n, %) 525 100 (19) 71 (14) 0.10 (−0.02, 0.21; 0.13)
NRI, net reclassification index; CI, confidence interval.
3.1. Objective cardiac abnormalities (reference standard)
Patients with objective cardiac abnormalities (n = 183, 35%)presented with more symptoms and signs, had significantly moreprior cardiovascular events, and exhibited more comorbiditiesand a greater use of cardiovascular medication (Table 1). In 92%(n = 168) of the patients, at least one typical heart failure symp-tom or sign was present. Only 2% (n= 4) of the patients did not ex-hibit any symptoms, signs or cardiovascular medications. On theother hand, the prevalence of signs, symptoms, comorbidities andcardiovascular medication was also high in patients without objec-tive cardiac abnormalities (n= 342, 65%); 82% (n= 279) exhibitedat least one sign or symptom suggestive of heart failure (P =0.002), and only 8% (n = 27) presented without any signs, symp-toms or cardiovascular drugs (P = 0.008) (Table 1). Furthermore,a statistically significant difference in NT-proBNP levels wasnoted between patients without or with objective cardiac abnor-malities: 125 pg/ml (IQR 75–203) versus 706 pg/ml (IQR426–1261), respectively.
Fig. 2. Mortality as a function of GPs' judgement of chroni
3.2. GPs' judgement of the presence of CHF
GPs judged CHF as absent in 371 patients (71%). In 285 patients(77%), the GPs expressed a degree of certainty ≥75% about their judge-ment. In 21% (n= 77) of these patients, no heart failure symptoms andno signs were registered during the standardized clinical assessment;nevertheless in 41% (n = 152), GPs listed the absence of symptomsand signs as the reason for ruling out CHF. Thus, in 26% of the patients,the arguments used matched the standardized recorded signs andsymptoms (Table 2). GPs suspected CHF in 154 participants (29%). In
c heart failure versus objective cardiac abnormalities.
126 M. Smeets et al. / International Journal of Cardiology 191 (2015) 120–127
90 patients (58%), the GPs expressed a degree of certainty ≥75% abouttheir judgement. The presence of at least one heart failure sign andsymptom was registered in 83% (n = 128) of these patients duringthe standardized clinical assessment, but these arguments were onlyused in 49% (n = 75) to support the diagnosis of CHF, representing amatch in 56% of these patients. The results of previous technical exam-inations or a previous diagnosis by a cardiologist (before the study base-line) were used as arguments in a minority of cases against CHF(cardiologist, n = 5, 1%; echocardiography, n = 9, 1.7%) or in favourof CHF (cardiologist, n = 4, 0.8%; echocardiography, n = 4, 0.8%).
3.3. Correlation between GPs' judgement of CHF and objective cardiacabnormalities
The presence of objective cardiac abnormalities, the reference stan-dard, matched with GPs' diagnoses of CHF in 54% (n = 83) of patients.This result represented a sensitivity of 45% (95% CI 38–53), a specificityof 79% (95% CI 75–83), a positive predictive value (PPV) of 54% (95% CI46–62) and a negative predictive value (NPV) of 73% (95% CI 68–78) forGPs' judgement. The Cohen's kappa coefficientwas 0.26 (P b 0.001). Theprevalence of objective cardiac abnormalities in combination with atleast one typical heart failure symptom and sign was 23% (n = 122).By comparing this toGPs' judgement of CHF, 397patientswere correctlyclassified, with a sensitivity of 61% (95% CI 51–69), specificity of 80%(95% CI 76–84), a PPV of 48% (95% CI 40–56) and a NPV of 87% (95%CI 83–90). Cohen's kappa coefficient was 0.36 (P b 0.001).
The prevalence of clinically relevant echocardiographic dysfunctionwas 15% (n = 57) in patients without and 34% (n = 53) in patientswith a GP's diagnosis of CHF (P b 0.001) andmainly accounted for a dif-ference in the prevalence of clinically relevant valve disease (7%, n=26vs 21%, n= 33, P b 0.001) (Table 3). Furthermore, the prevalence of leftatrial enlargement was higher in subjects with a diagnosis of CHF(P b 0.001), which is most likely related to the higher prevalence ofchronic atrial fibrillation (P=0.011). No other major differences in ob-jective cardiac measurements were detected between both groups(Table 3).
Patientswithout objective cardiac abnormalities (n=71) butwith aGP's diagnosis of CHF (false positives) were more symptomatic and hadmore cardiac morbidities compared with the correctly classified pa-tients (true negatives) (at least one symptom, n = 64, 90% vs n =179, 66%, P b 0.001; at least one cardiac morbidity, n = 44, 62% vsn=87, 32%, P b 0.001). Similarly, patients with objective cardiac abnor-malities (n=100) butwithout a CHF diagnosis by a GPwere less symp-tomatic and had less cardiac antecedents than their true positiveequivalents (at least one symptom, n = 69, 69% vs n = 80, 96%,P b 0.001; at least one cardiac morbidity, n = 61, 61% vs n = 66, 80%,P = 0.007).
3.4. Prognostic value of GPs' judgement of CHF and objective cardiacabnormalities
In the 5-year follow-up period, 223 patients (43%) died. There wasno loss to follow-up. Non-cardiovascular and cardiovascular deathsaccounted for 56% (n=124) and 43% (n=97) of all deaths, respective-ly (1% unknown cause (n=2)). In total, 55% (n=84) of subjects with aGP's diagnosis and 57% (n = 105) with objective cardiac abnormalitiesdied. Furthermore, 64% (n = 53) of patients with a GP's diagnosis andobjective cardiac abnormalities died. Of patients with objective cardiacabnormalities and at least one symptom and sign, 61% (n = 74) died.
Both GPs' judgement and the presence of objective cardiac abnor-malities, the reference standard, were good predictors of all-cause (HR1.7 (95% CI 1.3–2.3) vs 2.1 (95% CI 1.6–2.7), respectively) and cardiovas-cular mortality (HR 2.2 (95% CI 1.5–3.3) vs 3.0 (95% CI 2.0–4.5), respec-tively) (Fig. 2). Objective cardiac abnormalities were not significantlybetter than GPs' judgement of CHF in identifying patients at risk formortality, although a trend for better cardiovascular mortality risk
classification was observed (NRI 10% (95% CI −2 to 21%), P = 0.13)(Table 4).
4. Discussion
The present study demonstrates that GPs' judgement of CHF in theoldest old ismore thanmerely the sum of symptoms, signs, and risk fac-tors for heart failure. GPs' judgement extends beyond a paper case eval-uation. Despite a weak correlation between GPs' clinical judgement andobjective cardiac abnormalities, both were able to successfully identifypatients at high risk of death. Furthermore, objective cardiac abnormal-ities were not better at identifying high risk subjects, although a trendfor better cardiovascular mortality risk classification with respect toGPs' judgement was noted.
In this population-based cohort study of the oldest old, a 35% preva-lence of objective cardiac abnormalities and a 23% prevalence of objec-tive cardiac abnormalities in combination with at least one heart failuresymptom and signwere found. These findings are consistentwith othercommunity studies that screened older subjects, reporting a prevalenceof 23% of CHF [4,5] to 52% [27] of echocardiographic dysfunction. Thepoor accordance between GPs' diagnoses of CHF and objective cardiacmeasurements has been described previously, with reports of similarNPVs (77% to 81%) and lower PPVs (23% to 41%) than the currentstudy [4,5]. The previously reported mortality rates of patients withCHF vary widely depending on the definition of CHF used, age and set-ting. Only a few recent population-based studies describe long-termmortality rates in the oldest old with CHF [12,28]. The Helsinki Ageingstudy reported a 4-year mortality rate of 46% with an annual deathrate of 15% for CHF patients, consistent with the current findings [28].De Giuli et al. reported very high three-year mortality rates of 70% inmen and 63% in women aged 85 and older with a GP's diagnosis ofCHF. Because of the accordance with hospital mortality rates, the au-thors emphasized the reliability of a GP's diagnosis of CHF [12].
The present study is thefirst comprehensive study describing the re-lationship among GPs' judgement of CHF, objective cardiac measure-ments and mortality in older persons. By choosing GPs' judgementinstead of a once registered diagnosis of CHF, we were able to rule outpoor record keeping as a cause of poor correlation. Furthermore, studiesin the oldest old, especially in the community, are scarce, making ourdata even more valuable. However, a few limitations of the currentstudy should be noted. First, the choice of objective cardiac abnormali-ties as the reference standard, instead of an expert-panel diagnosis ofheart failure, could be seen as a limitation of our study. However, onlysmall differences were found when studying the correlation betweenthe reference standard combined with at least one heart failure symp-tom and sign and the GPs' judgement of CHF. Furthermore, an expertpanel evaluation is often a paper evaluation, which makes it difficultto grasp the full clinical context, especially in a heterogeneous popula-tion of the oldest old. Second, participating GPs evaluated only theirown included patients, possibly inducing heterogeneity in the clinicaljudgement of CHF [10,11]. However, all participating GPs were trainedto standardize the medical history taking and the clinical examinationto limit this risk as much as possible.
Although little overlap was observed between GPs' judgement ofCHF and objective cardiac abnormalities, both approaches were able toidentify high-risk subjects for mortality. Compared with GPs' judge-ment, objective cardiac abnormalities better classified patients whodied within 5 years after baseline, but this effect was counterbalancedby a larger misclassification of subjects who survived after 5 years,resulting in a non-significant NRI. Only a trend for better cardiovascularmortality risk classification was found for objective cardiac abnormali-ties with respect to GPs' judgement. By identifying patients at risk formortality, these analyses demonstrated the validity of GPs' judgement.
Additionally, little overlapwas observed between the symptomsandsigns GPs registered during the standardized clinical assessment andthe actual arguments they used in favour or against CHF. In this
127M. Smeets et al. / International Journal of Cardiology 191 (2015) 120–127
population of the oldest old, the symptoms, signs and risk factors forheart failure were almost equally prevalent in patients with or withoutobjective cardiac abnormalities. Hence, GPs could not base their judge-ment on themere presence or absence of symptoms, signs or risk factorsfor heart failure. However, it remains unclear how the GPs interpretedthe available arguments. It is likely that the holistic approach of the GPfacilitated the ‘reading’ and interpretation of the symptoms, signs andrisk factors within the global performance of these patients. This hy-pothesis will be the subject of future analyses within the BELFRAILcohort.
Moreover, the question arises whether or not the current definitionof CHF should be applied to the very old. The specificity of typical signsand symptoms decreases drastically in the old, and the prevalence ofstructural and functional abnormalities of the heart increases with age[29]. In the light of a shift towards more comprehensive, less disease-oriented care [30] especially in complex geriatric patients with a highburden of multimorbidity and polypharmacy, perhaps the existing con-cept of heart failure in the old should be revisited. CHF could be evaluat-ed using a horizontal approach as themanifestation of clinically relevantcardiac abnormalities, taking full account of the interaction with con-comitant, chronic conditions. Moreover, the clinical impact could beevaluated by objectively measuring the physical performance of the pa-tient in addition to self-reported non-specific symptoms.
Conflict of interest
None.
Acknowledgements
This studywasmade possible by the participating GPs. The BELFRAILstudy (B40320084685) was supported by an unconditional grant fromthe Fondation Louvain.
References
[1] J.J. McMurray, S. Adamopoulos, S.D. Anker, et al., ESC guidelines for the diagnosisand treatment of acute and chronic heart failure 2012: the Task Force for the Diag-nosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Soci-ety of Cardiology. Developed in collaboration with the Heart Failure Association(HFA) of the ESC, Eur. J. Heart Fail. 14 (8) (August 2012) 803–869.
[2] G.S. Bleumink, A.M. Knetsch, M.C. Sturkenboom, et al., Quantifying the heart failureepidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure TheRotterdam Study, Eur. Heart J. 25 (18) (September 2004) 1614–1619.
[3] J.G. Cleland, A. Cohen-Solal, J.C. Aguilar, et al., Management of heart failure in prima-ry care (the IMPROVEMENT of Heart Failure Programme): an international survey,Lancet 360 (9346) (November 23 2002) 1631–1639.
[4] H.C. Hancock, H. Close, J.M.Mason, et al., High prevalence of undetected heart failurein long-term care residents: findings from the Heart Failure in Care Homes(HFinCH) study, Eur. J. Heart Fail. 15 (2) (February 2013) 158–165.
[5] M. Barents, I.C. van der Horst, A.A. Voors, J.L. Hillege, F.A. Muskiet, M.J. de Jongste,Prevalence and misdiagnosis of chronic heart failure in nursing home residents:the role of B-type natriuretic peptides, Neth. Hear. J. 16 (4) (April 2008) 123–128.
[6] C. Fonseca, Diagnosis of heart failure in primary care, Heart Fail. Rev. 11 (2) (June2006) 95–107.
[7] I. Oudejans, A. Mosterd, J.A. Bloemen, et al., Clinical evaluation of geriatric outpa-tients with suspected heart failure: value of symptoms, signs, and additional tests,Eur. J. Heart Fail. 13 (5) (May 2011) 518–527.
[8] H.C. Hancock, H. Close, A. Fuat, J.J. Murphy, A.P. Hungin, J.M. Mason, Barriers to accu-rate diagnosis and effective management of heart failure have not changed in thepast 10 years: a qualitative study and national survey, BMJ Open 4 (3) (2014)e003866.
[9] U. Dahlstrom, J. Hakansson, K. Swedberg, A. Waldenstrom, Adequacy of diagnosisand treatment of chronic heart failure in primary health care in Sweden, Eur. J.Heart Fail. 11 (1) (January 2009) 92–98.
[10] Y. Skaner, L. Backlund, H. Montgomery, J. Bring, L.E. Strender, General practitioners'reasoning when considering the diagnosis heart failure: a think-aloud study, BMCFam. Pract. 6 (1) (January 15 2005) 4.
[11] Y. Skaner, J. Bring, B. Ullman, L.E. Strender, The use of clinical information in diag-nosing chronic heart failure: a comparison between general practitioners, cardiolo-gists, and students, J. Clin. Epidemiol. 53 (11) (November 2000) 1081–1088.
[12] F. De Giuli, K.T. Khaw, M.R. Cowie, G.C. Sutton, R. Ferrari, P.A. Poole-Wilson, Inci-dence and outcome of persons with a clinical diagnosis of heart failure in a generalpractice population of 696,884 in the United Kingdom, Eur. J. Heart Fail. 7 (3)(March 16 2005) 295–302.
[13] B. Vaes, A. Pasquet, P. Wallemacq, et al., The BELFRAIL (BFC80+) study: apopulation-based prospective cohort study of the very elderly in Belgium, BMCGeriatr. 10 (2010) 39.
[14] K. Dickstein, A. Cohen-Solal, G. Filippatos, et al., ESC guidelines for the diagnosis andtreatment of acute and chronic heart failure 2008: the Task Force for the Diagnosisand Treatment of Acute and Chronic Heart Failure 2008 of the European Society ofCardiology. Developed in collaboration with the Heart Failure Association of theESC (HFA) and endorsed by the European Society of Intensive Care Medicine(ESICM), Eur. J. Heart Fail. 10 (10) (October 2008) 933–989.
[15] C.M. Fletcher, The clinical diagnosis of pulmonary emphysema; an experimentalstudy, Proc. R. Soc. Med. 45 (9) (September 1952) 577–584.
[16] M. Pahor, E.A. Chrischilles, J.M. Guralnik, S.L. Brown, R.B. Wallace, P. Carbonin, Drugdata coding and analysis in epidemiologic studies, Eur. J. Epidemiol. 10 (4) (August1994) 405–411.
[17] H. Blackburn, A. Keys, E. Simonson, P. Rautaharju, S. Punsar, The electrocardiogramin population studies. A classification system, Circulation 21 (June 1960)1160–1175.
[18] R.M. Lang, M. Bierig, R.B. Devereux, et al., Recommendations for chamber quantifica-tion, Eur. J. Echocardiogr. 7 (2) (March 1 2006) 79–108.
[19] B. Vaes, N. Rezzoug, A. Pasquet, et al., The prevalence of cardiac dysfunction and thecorrelation with poor functioning among the very elderly, Int. J. Cardiol. 155 (1)(February 23 2012) 134–143.
[20] M.A. Quinones, C.M. Otto, M. Stoddard, A. Waggoner, W.A. Zoghbi, Recommenda-tions for quantification of Doppler echocardiography: a report from the DopplerQuantification Task Force of the Nomenclature and Standards Committee of theAmerican Society of Echocardiography, J. Am. Soc. Echocardiogr. 15 (2) (February2002) 167–184.
[21] W.A. Zoghbi, M. Enriquez-Sarano, E. Foster, et al., Recommendations for evaluationof the severity of native valvular regurgitation with two-dimensional and Dopplerechocardiography, J. Am. Soc. Echocardiogr. 16 (7) (July 2003) 777–802.
[22] S.F. Nagueh, C.P. Appleton, T.C. Gillebert, et al., Recommendations for the evaluationof left ventricular diastolic function by echocardiography, Eur. J. Echocardiogr. 10 (2)(March 2009) 165–193.
[23] P. Van Royen, S. Boulanger, P. Chevalier, et al., Aanbeveling voor goede medischepraktijkvoering: Chronisch hartfalen, Huisarts Nu 40 (2011) 158–186.
[24] B. Vaes, D. Gruson, P.G. Van, et al., The impact of confounders on the test perfor-mance of natriuretic peptides for cardiac dysfunction in subjects aged 80 andolder, Peptides 38 (1) (November 2012) 118–126.
[25] S. Toggweiler, O. Borst, F. Enseleit, et al., NT-proBNP provides incremental prognos-tic information in cardiac outpatients with and without echocardiographic findings,Clin. Cardiol. 34 (3) (March 2011) 183–188.
[26] M.J. Pencina, R.B. D'Agostino Sr., R.B. D'Agostino Jr., R.S. Vasan, Evaluating the addedpredictive ability of a newmarker: from area under the ROC curve to reclassificationand beyond, Stat. Med. 27 (2) (January 30 2008) 157–172.
[27] F. Yousaf, J. Collerton, A. Kingston, et al., Prevalence of left ventricular dysfunction ina UK community sample of very old people: the Newcastle 85+ study, Heart 98(19) (October 2012) 1418–1423.
[28] M. Kupari, M. Lindroos, A.M. Iivanainen, J. Heikkila, R. Tilvis, Congestive heart failurein old age: prevalence, mechanisms and 4-year prognosis in the Helsinki AgeingStudy, J. Intern. Med. 241 (5) (May 1997) 387–394.
[29] M.M. Redfield, S.J. Jacobsen, J.C. Burnett Jr., D.W. Mahoney, K.R. Bailey, R.J.Rodeheffer, Burden of systolic and diastolic ventricular dysfunction in the commu-nity: appreciating the scope of the heart failure epidemic, JAMA 289 (2) (January 82003) 194–202.
[30] M.J. De, R.G. Roberts, M. Demarzo, et al., Tackling NCDs: a different approach is need-ed, Lancet 379 (9829) (May 19 2012) 1860–1861.