
Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders
17
Abstract Gene expression investigations within psychiatry have implicated a number of different genes that are associated with major psychiatric disorders, with the majority of these studies carried out in brains from patients with schizophrenia. In post-mortem brain studies, alterations in the expression of genes involved in oligodendrocyte functioning and myelina- tion, mitochondrial-related functions and energy metab- olism as well as synaptic structure and transmission have been identified. To an extent these alterations reflect changes in mRNAs and proteins previously reported in neuropathological investigations of psychi- atric disorders. The advent of assessing gene expres- sion changes in the blood of patients with psychiatric disorders may allow us to correlate these findings to brain-related changes and hence to potentially identify biomarkers for detection, intervention and treatment. However, while microarray technology has opened the way for high-throughput gene expression analysis, a significant number of methodological and technical questions still exist with their application. It is there- fore necessary that a stringent approach be adopted by researchers when designing gene expression studies and precaution taken as to the final analysis and inter- pretation of the data generated. The aim of this chapter is to provide a balanced view of microarray investiga- tions in the blood and brain in major psychiatric disor- ders by highlighting the benefits and pitfalls of such studies in identifying candidate genes. The relation- ship between these alterations and endophenotypes in identifying such biomarkers will be discussed as well as potential strategies to overcome weaknesses within studies and how to improve future investigations. Keywords Psychiatry • microarray • schizophrenia • gene • endophenotype • expression Abbreviations ACHR: Acetylcholine receptor; AMPA1: 22-aminomethylphenylaceticacid;Apo:Apolipoprotein; ATP1A3: Na + /K + -ATPase alpha 3 subunit I; BDNF: Brain derived neurotrophic factor; BTG1: B-cell translocation gene 1; CAD: Carbamoyl-phosphate synthetase 2, aspartate transcarbamylase and dihydro- orotase; CCK: Cholecystokinin; CD14: Cell differen- tiation 14; CHI3L1: Chitinase 3 like 1; CNP: Cyclic nucleotide phosphodiesterase; dlPFC: Dorsolateral prefrontal cortex; DRD2: Dopamine receptor D2; EBV: Epstein Barr virus; EDGF: Epidermal derived growth factor; ER: Endoplasmic reticulum; FGF: Fibroblast growth factor; GABA: Gamma-amino butyric acid; GAD67: Glutamate decarboxylase-67; GAP-43: Growth associated protein-43; Giα1: G-protein inhibitory alpha1; GluR1–2: Glutamate receptor 1–2; GNA01: Guanine nucleotide binding protein alpha 1; GSK3A: Glycogen synthase kinase 3 alpha; HER3: Heregulin-3; HNRPA3: Heterogeneous nuclear ribonucleoprotein A3; HERC2: Heat domain and rcc1-like domain 2; HLA-DRB1 major: Histocompatibility complex DR beta 1; HML-2: Human macrophage lectin 2; HSPB1: Heat shock protein beta 1; SERPINA3: Alpha-1- antichymotrypsin A3; IFITM1: Interferon induced protein with tetratricopeptide repeats 1; Kir2.3: Potassium channel inward rectifying 2.3; LARS2: Leucyl-tRNA synthetase, mitochondrial; LCM: Laser capture microdissection; MAG: Myelin associated glycoprotein; MAL: Myelin and lymphocyte protein; Chapter 42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders Gursharan Chana, Janet Kwok, Stephen J. Glatt, Ian P. Everall, and Ming T. Tsuang G. Chana, J. Kwok, I. P. Everall, and M. T. Tsuang Department of Psychiatry, University of California, San Diego, La Jolla, CA, 92093-0603 S. J. Glatt Department of Psychiatry and Behavioral Sciences, State University of New York, Syracuse, NY, 13210 M.S. Ritsner (ed.), The Handbook of Neuropsychiatric Biomarkers, Endophenotypes and Genes, 77 © Springer Science + Business Media B.V. 2009
Transcript of Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders
Abstract Gene expression investigations within psychiatry have implicated a number of different genes that are associated with major psychiatric disorders, with the majority of these studies carried out in brains from patients with schizophrenia. In post-mortem brain studies, alterations in the expression of genes involved in oligodendrocyte functioning and myelina-tion, mitochondrial-related functions and energy metab-olism as well as synaptic structure and transmission have been identifi ed. To an extent these alterations refl ect changes in mRNAs and proteins previously reported in neuropathological investigations of psychi-atric disorders. The advent of assessing gene expres-sion changes in the blood of patients with psychiatric disorders may allow us to correlate these fi ndings to brain-related changes and hence to potentially identify biomarkers for detection, intervention and treatment. However, while microarray technology has opened the way for high-throughput gene expression analysis, a signifi cant number of methodological and technical questions still exist with their application. It is there-fore necessary that a stringent approach be adopted by researchers when designing gene expression studies and precaution taken as to the fi nal analysis and inter-pretation of the data generated. The aim of this chapter is to provide a balanced view of microarray investiga-tions in the blood and brain in major psychiatric disor-ders by highlighting the benefi ts and pitfalls of such studies in identifying candidate genes. The relation-ship between these alterations and endophenotypes in
identifying such biomarkers will be discussed as well as potential strategies to overcome weaknesses within studies and how to improve future investigations.
Keywords Psychiatry • microarray • schizophrenia • gene • endophenotype • expression
Abbreviations ACHR: Acetylcholine receptor; AMPA1: 2 2-aminomethyl phenylacetic acid; Apo: Apolipoprotein; ATP1A3: Na + /K + -ATPase alpha 3 subunit I; BDNF: Brain derived neurotrophic factor; BTG1: B-cell translocation gene 1; CAD: Carbamoyl-phosphate synthetase 2, aspartate transcarbamylase and dihydro-orotase; CCK: Cholecystokinin; CD14: Cell differen-tiation 14; CHI3L1: Chitinase 3 like 1; CNP: Cyclic nucleotide phosphodiesterase; dlPFC: Dorsolateral prefrontal cortex; DRD2: Dopamine receptor D2; EBV: Epstein Barr virus; EDGF: Epidermal derived growth factor; ER: Endoplasmic reticulum; FGF: Fibroblast growth factor; GABA: Gamma-amino butyric acid; GAD67: Glutamate decarboxylase-67; GAP-43: Growth associated protein-43; Giα1: G-protein inhibitory alpha1; GluR1–2: Glutamate receptor 1–2; GNA01: Guanine nucleotide binding protein alpha 1; GSK3A: Glycogen synthase kinase 3 alpha; HER3: Heregulin-3; HNRPA3: Heterogeneous nuclear ribonucleoprotein A3; HERC2: Heat domain and rcc1-like domain 2; HLA-DRB1 major: Histocompatibility complex DR beta 1; HML-2: Human macrophage lectin 2; HSPB1: Heat shock protein beta 1; SERPINA3: Alpha-1-antichymotrypsin A3; IFITM1: Interferon induced protein with tetratricopeptide repeats 1; Kir2.3: Potassium channel inward rectifying 2.3; LARS2: Leucyl-tRNA synthetase, mitochondrial; LCM: Laser capture microdissection; MAG: Myelin associated glycoprotein; MAL: Myelin and lymphocyte protein;
Chapter 42Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders
Gursharan Chana, Janet Kwok, Stephen J. Glatt, Ian P. Everall, and Ming T. Tsuang
G. Chana, J. Kwok, I. P. Everall, and M. T. TsuangDepartment of Psychiatry, University of California, San Diego, La Jolla, CA, 92093-0603
S. J. Glatt Department of Psychiatry and Behavioral Sciences, State University of New York, Syracuse, NY, 13210
M.S. Ritsner (ed.), The Handbook of Neuropsychiatric Biomarkers, Endophenotypes and Genes, 77© Springer Science + Business Media B.V. 2009

78 G. Chana et al.
MARCKS: Myristolated alanine-rich C-kinase substrate; TGF-beta 1: Transforming growth factor beta 1; erbB2: Erythroblastic leukemia viral oncogene homolog 2; MOBP: Myelin-oligodendrocyte basic protein; MBP: Myelin basic protein; MOG: Myelin-oligodendrocytic protein; MM: Mismatch; MT2A: Metallothionein 2A; NPY: Neuropeptide Y; Neurod1: Neurogenic differentiation 1; NRG-1: Neuregulin-1; NMDA1: N-methyl, d-aspartate 1; NSF: N-ethylmaleimide sensi-tive fusion protein; PEA-15: Phosphoprotein enriched in astrocytes 15; PDE4D: Phosphodiesterase 4D; PLP: Proteolipid protein; PM: Perfect match; PMI: Post-mortem interval; PMP22: Peripheral myelin protein 22; qRT-PCR: Quantitative real time PCR; RMA: Robust multichip analysis algorithm; SELENBP1: Selenium binding protein-1; SFRS1: Splicing factor, arginine/serine rich 1; SNP: Single nucleotide polymorphism; SPR: Sepiapterin reductase; SOX10: SRY-related homeobox gene 10; SMDF: Sensory and motor neuron derived factor; S100: Calcium binding protein A1; TGF-a: Transforming growth factor-alpha; TRAF4: Tumour necrosis factor receptor associated factor 4; VAMP-1: Vesicle associate membrane protein-1; XBP1: X box binding protein 1
Overview
The use of microarray technology to assess gene expression changes in major psychiatric disorders has increased rapidly over the past 2 decades. This increase has been fuelled primarily by a vast body of neuro-pathological literature failing to demonstrate consis-tent changes in candidate proteins in brains of patients with these disorders. Therefore, the premise behind gene expression investigations has been to identify candidate mRNAs and genes in the brains of patients which can then be validated and related at the protein level to provide us with clues as to the etiology of these disorders. This reversal in the traditional scientifi c pro-cess has allowed us to take a more global view of gene expression changes related to these polygenic psychi-atric disorders. However, while some interesting fi nd-ings have emerged from microarray investigations, they have unfortunately not always been replicated by independent research groups when using different
brain cohorts. This discrepancy in results may be partially attributed to inconsistencies in methodologies and platforms used for analysis; however, it is also largely a consequence of the heterogeneous nature of these disorders as well as general variability in gene expres-sion patterns between individuals that may in part result from lifestyle. Nevertheless, as microarray tech-nology and tools to assess gene expression data become more consistent we are now beginning to build up gene expression profi les for major psychiatric disorders. The construction of such profi les between disorders may eventually help in the separation of their overlap-ping clinical profi les and problems with differential diagnosis faced by clinicians.
One recent area of interest in gene expression studies in psychiatry has been to assess changes in mRNA tran-scripts in the blood of patients. These blood-based gene expression studies are potentially very powerful as they may enable the identifi cation of potential biomarkers which could ultimately be used as diagnostic and prog-nostic indicators. While the discovery of such markers would greatly advance psychiatry, the realization of this may take some time to achieve. This chapter will begin by giving a brief discussion of the study design of microarray investigations prior to covering current gene expression fi ndings in the blood and also in the brain in major psychiatric disorders. The impact of endopheno-types on these gene expression changes will also be discussed together with their potential role in helping to identify biomarkers. Finally, we will look at technical problems associated with gene expression studies and how solving these will help to get us closer to the goal of identifying biomarkers for psychiatric disorders.
Introduction
Historically, diagnoses of psychiatric disorders have always been problematic due to overlapping symptom-atology. This differential diagnosis can be illustrated by the Kraepelinian dichotomy. Kraepelin’s original classifi cation separated schizophrenia and bipolar dis-order into two distinct disease entities. However, with advances in diagnosis and genetic studies it is clear that the profi les of these two disorders demonstrate signifi cant overlap. Such overlap makes the differen-tial diagnoses of these psychiatric disorders diffi cult. An ideal scenario to overcome this diffi culty would be

42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders 79
to have a distinct genetic profi le for each disorder. This would not only clarify and aid diagnoses but would also allow us to screen at-risk individuals for develop-ing these disorders. While this ideal may not be achiev-able in the near future, the use of high-throughput genetic technology such as microarrays are greatly facilitating the building of gene expression profi les and identifi cation of biomarkers.
Locating candidate genes for major psychiatric disorders is an intrinsically diffi cult task; psychiatric disorders are not simple Mendelian traits, and have complex genetic architecture. Endophenotypes are her-itable traits that have specifi c genes associated with them (genes that may or may not already be identifi ed), yet are not directly related to symptoms of the disease or disorder in question and are not typically considered in the diagnosis and screening. These specifi c pheno-types have been suggested to bear a closer relationship to the etiological processes than the actual diagnostic measures,1 indicating that the link between genes and endophenotypes is stronger than that between genes and the phenotype. Recent research into the genetics of schizophrenia now consider endophenotypes to aid our understanding of this polygenic disorder with probable multiple etiologies.2 However, with a lack of consistent changes in genes and their expression levels in schizo-phrenia and major psychiatric disorders they remain as clinically defi ned disorders.
Endophenotypes for major psychiatric disorders include neuroanatomical, neurophysiological, bioche-mical, endocrinological, cognitive and psychological distinctions, and will be discussed in more details in the following sections. Due to these endophenotypes having the potential to alter (or be altered by) gene expression it may be warranted to consider their infl u-ence when designing gene expression studies and also interpreting data gathered from them. In doing so it is feasible that certain knowledge of endophenotypes will help us to better understand and categorize genes into various biological, cellular and molecular pro-cesses related to major psychiatric disorders.
Designing Microarray Investigations
One of the main limitations of designing post-mortem gene expression investigations is the availability of well characterized and matched brain samples from
candidate regions of interest. Once this obstacle has been overcome many steps can be taken when design-ing gene expression studies in order to reduce the rates of false discovery. Attempting to control for potential confounds in blood-based investigations present over-lapping and different sets of external variables that can infl uence gene expression. The most obvious variable that can add power to a gene expression study is the number of patient samples available for investigation. As previously mentioned, however, this is often lim-ited in post-mortem studies by the availability of tis-sue, with competition for samples between researchers. For post-mortem investigations, matching of clinical and demographic variables that are known to affect RNA quality and hence gene expression fi ndings should be attempted. When this is not achievable the variable should be included as a covariate in the fi nal analysis. These variables include factors such as age, gender, agonal period and cause of death, medication histories, history of drug abuse, pH and post-mortem interval (PMI) (for review see Bunney et al.3). Ideal matching of all or even half of these parameters is however, rarely achieved. For blood-based gene expression studies there are even more variables that can signifi cantly affect gene expression. These include, but are not limited to; diet, smoking, time of last meal, time of day, any medications used, and frequency of exercise.4 These variables may also affect post-mortem brain changes but to a lesser extent than blood which is a much more dynamic changing substrate. Some con-trol over these variables for blood based investigations can potentially be achieved by the researcher, i.e. patients could be asked to give a fasting blood sample fi rst thing in the morning before eating. Additional questionnaires pertaining to the patient’s lifestyle can also be administered in order to glean as much infor-mation as possible regarding potential infl uences on gene expression changes. For blood-based gene expres-sion studies it is also worthwhile attempting the recruit-ment of fi rst-degree relatives. This has the potential for differentiating disease-related genes from medication-related genes or genes that change in response to chronic mental illness.
To address the question of endophenotypes in the design of blood-based gene expression investigations, this can theoretically be carried out in two ways. The fi rst method would be to pre-sort patients into different categories based on their clinical or perhaps biological profi le prior to conducting the gene expression analysis

80 G. Chana et al.
or alternatively by carrying out post-hoc analysis of gene expression data by different endophenotypes. Ideally, pre-sorting would be the chosen method as it would set the framework for the microarray investiga-tion. For example, patients could be separated on the basis of structural brain changes observed, such that patients with certain structural brain abnormalities would be grouped and compared to those lacking the abnormality. Separating patients on the basis of their genotype represents another pre-sorting approach. The use of single nucleotide polymorphisms (SNPs) found to confer susceptibility to schizophrenia or other major psychiatric disorders could be utilized. However, with SNP studies in major psychiatric disorders being rela-tively controversial and inconsistent this may not be a reliable way to separate patient groups until putative risk-conferring variants are widely replicated. While a post-hoc analysis of endophenotypes on observed gene expression changes would be easier to carry out, it would be more diffi cult to establish a connection between the already-determined changes in gene expression to the endophenotypes of interest. However, to properly utilize the potential impact of endopheno-types in gene expression investigations, the endophe-notypes must serve to steer the experimentation, so that the alterations in gene expression changes can be attributed to the specifi c intermediary phenotypes. In fact, current research into the genetics of psychiatric disorders tends to lean towards evaluating the predic-tive power of an endophenotype conditioned upon the liability of schizophrenia, rather than looking at the predictive power of an endophenotype given the liabil-ity of schizophrenia (Lenzenweger, http://www.schizo-phreniaforum.org/for/live/transcript.asp?liveID = 46). In this manner, current research does not address the utility of endophenotypes.
In order to pre-sort patients, questionnaires may be administered to group subjects prior to gene expres-sion analysis using microarrays. During screening, the patients could be pre-sorted into different groups according to the specifi c phenotype exhibited, which would allow us to observe the impact of the patients’ specifi c endophenotypes on the changes in the expres-sion of their genes (or vice versa). In this manner, the pathway from genotype to phenotype would be observed. Such endophenotypic parameters could include surveying the patients according to the afore-mentioned distinctions: neuroanatomical, neurophysi-ological, biochemical, endocrinological, cognitive and
psychological. Patients may also be categorized according to their clinical profi les, utilizing their medi-cal records to determine the effect of certain diseases, events or medical conditions on the genetic suscepti-bility for the psychiatric disorder. Examples of the latter are prenatal hypoxia or a low APGAR at birth or a family history of schizophrenia. An important consid-eration in dividing patient groups is the reliability of the data used to separate these endophenotype sub-populations. If consistent and reliable data on specifi c parameters cannot be obtained it maybe more prudent not to make the division.
Choosing a Platform
Selecting a microarray platform for a gene expression study depends largely on the aims of the investigation. For major psychiatric disorders, the majority of investi-gators have tended to employ high-throughput micro-array gene chips that encompass the whole human genome. This approach is warranted due to a lack of information regarding etiological mechanisms for major psychiatric disorders. Nevertheless, a fairly broad choice still exists when selecting a genome-wide chip for screening patient brain or blood samples. While a detailed technical dissection of different microarray platforms is beyond the scope of this review, it is worth-while considering the major strengths and weaknesses of the various arrays. Many of the microarray studies in psychiatry have utilized gene chips produced by Affymetrix (Santa Clara, USA). However, other main competitors for the whole human gene chip market include Codelink, Agilent, Applied Biosystems and Illumina.
The primary reason for this early adoption of Affymetrix gene chips was due to the highly automated process by which they are manufactured. This process comprises the use of highly specifi c photolithographic masks and a solid phase DNA synthesis to construct 25 bases probes on the surface of the chip.5 Other plat-forms such as Agilent, Codelink and Illumina utilize 60–70 bases probe sets which are more sensitive in detecting mRNA signal than the 25mer probe sets used by Affymetrix. However with this increased sensitivity potentially comes an increase in false-positive fi nd-ings. Affymetrix increase their specifi city of detection by including 11 probe sets which are averaged following

42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders 81
analysis of the chip post-hybridization. Also contained on the chip are mismatch (MM) probe sets. These probe sets are identical to the perfect match (PM) probes with the exception of a single base difference located in a central position. The MM probes serve as controls for specifi c hybridization and facilitate back-ground correction due to cross-hybridization signals.5 The newer Affymetrix U133 plus 2.0 platform has been utilized by more recent investigations in psychiatry. This gene chip comprises probes for analysis of over 47,000 transcripts, including the entire human genome and provides a comprehensive way to assess global gene expression changes. This chip has recently been superseded by the Affymetrix Exon arrays that are also capable of assessing gene expression of splice variants by surveying multiple probes for each exon in the genome. This novel technology will help to better understand the contribution of individual variants to overall gene expression and hence better relate to gene function. With the inclusion of alternative splicing events, the number of features per microarray chip has jumped from approx. 470,000 to 2–3 million. This large increase in data necessitate the evolution of pro-grams used to read chip data and also to assess differ-ential gene expression between groups.
However, with the further development of microar-ray technology, Affymetrix’s competitors are also begin-ning to produce highly reproducible arrays for analyzing whole human genome expression. For instance Ilumina’s latest chip sets are also produced in a highly automated way, utilizing a randomly self-assembled silica bead pool with attached oligonucleotide probes that are recorded on specifi c locations on a patterned substrate.6 Due to the small size of the bead used for this procedure, the density of these arrays can be up to 40,000 times greater than that of spotted arrays.7
Another deciding factor for choosing a microarray platform is how well gene expression changes detected on the platform can be validated by quantitative real time PCR (qRT-PCR). This validation of microarray fi ndings using qRT-PCR is of major importance given the enhanced sensitivity of detection by this technique and therefore this process adds confi dence in gene expression changes observed on microarrays.
The fi nal and perhaps most important decision in choosing a microarray platform lies in the ability of the researcher to compare their data on gene expres-sion changes with what has been generated by other research groups. A number of studies to date, looking
at cross-platform comparisons, have unfortunately seen a very low level of correlation in gene expression,8,9 even with mRNA samples derived from relatively homogenous tissue sources, such as transformed cell lines. This has led to the conclusion that gene expres-sion data cannot be combined reliably between plat-forms. Knowledge of this result has often led researchers to choose platforms on the basis of what past investigations have utilized. While the logic behind this choice is concrete, it does to a certain extent preclude an informed decision based on merits of indi-vidual platforms. Furthermore, recent comparisons of cross-platform correlations have yielded more concor-dant data,10–13 suggesting that either the technology, or the scientists’ ability to harness it, is improving.
Post-mortem Brain Gene Expression Investigations
Early post-mortem gene expression studies of the brain in schizophrenia utilized pooled samples of RNA in order to identify gene expression changes between control and patient groups. While these studies were cost-effi cient using a small number of microarray chips, they masked many of the signifi cant gene expression differences that may have existed between groups but which may have been hidden by within-group heterogeneity and/or variability. Therefore, cur-rent post-mortem gene expression investigations tend to use one gene chip per sample when carrying out their analysis. Mirnics et al. (2000), were the fi rst to conduct a high-throughput gene expression study for schizophrenia that compared 250 functional gene groups between matched pairs of patients and controls. While differences in specifi c genes were not consistent between the pairs they did observe down-regulation of functional gene groups. The most convincing of their fi ndings related to a down-regulation of genes encod-ing pre-synaptic proteins.14 Included in this list were the genes for N-ethylmaleimide sensitive factor and synapsin II. These changes were subsequently vali-dated by in situ hybridization. Interestingly, regulator of G protein signaling 4 (RGS4), a gene that has received much attention from family-based genetic association studies in schizophrenia was also shown to be dysregulated. Since this fi rst study by Mirnics many different post-mortem microarray investigations for

82 G. Chana et al.
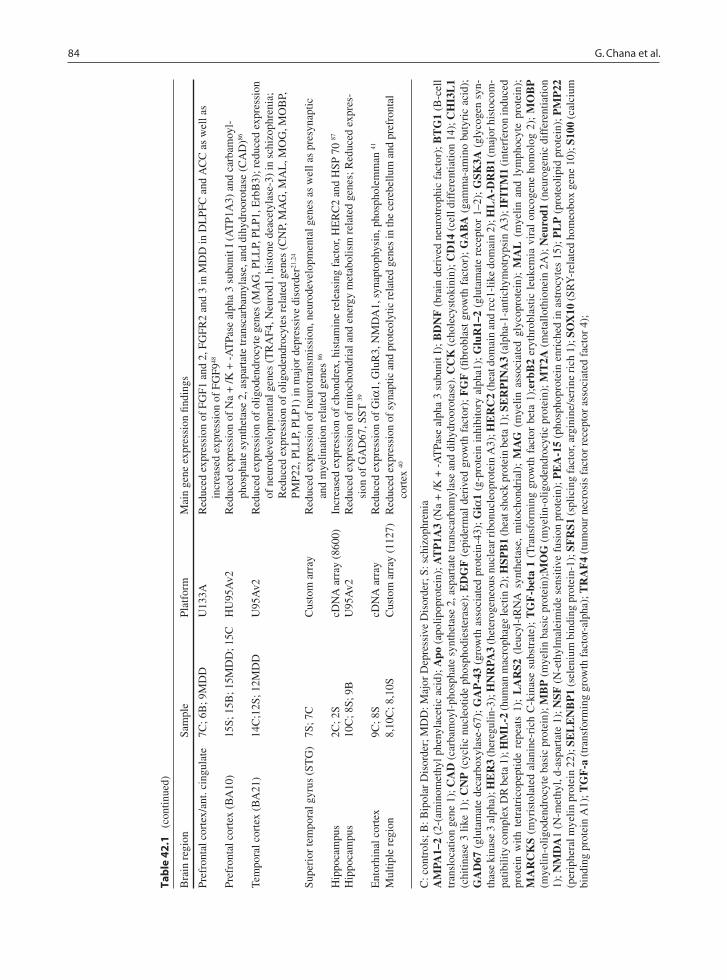
schizophrenia have been carried out in a number of dif-ferent brain regions. The majority of these have focused on schizophrenia and gene expression changes in the dorsolateral prefrontal cortex (dlPFC). The main rea-son for the dlPFC being chosen as a candidate region is due to the relatively consistent cognitive and func-tional defi cits seen in patients with schizophrenia,15–18 functions that are associated with the dlPFC. The study design and main fi ndings of these investigations are summarized in Table 42.1 below.
Looking at the post-mortem microarray studies, one of the most consistent fi ndings has been reductions in genes related to myelin structure and oligodendrocyte functioning in the prefrontal cortex in schizophrenia,19–22 with reductions also being demonstrated in bipolar dis-order and major depressive disorder.20,23,24
While demyelination has not been observed in schizophrenia or bipolar disorder, alterations in oligo-dendrocyte numbers and associated proteins have been demonstrated histopathologically25–28 together with alterations in white matter visualized via diffusion ten-sor imaging.29–31 Given the close relationship between oligodendrocytes and axons, and their role in maintain-ing effi cient neurotransmission, it seems logical that alterations in oligodendrocytes or myelin proteins could cause disruption in normal transmission and hence potentially lead to dysfunctional circuitry in schizophre-nia and other major mental illnesses. Genes related to metabolism and mitochondrial pathways are another ontological group that have been found to be reduced in expression in schizophrenia by a number of different studies20,32–35 and have also been observed in bipolar dis-order.34 Gene expression changes related to mitochon-drial genes that are involved in energy pathways were initially reported by Middleton et al., in 2002 in schizo-phrenia. This investigation demonstrated reductions in transcripts associated with regulation of ornithine, polyamine metabolism, the mitochondrial malate shut-tle system, the tricarboxyclic acid cycle, and amino-acid and ubiquitin metabolism. While the investigations that followed have also shown alterations in mitochondrial and metabolism related genes there has been no overlap in gene lists between studies. Nevertheless, reductions in metabolically related genes, especially in the prefron-tal cortex of schizophrenic subjects fi ts in well with reductions in prefrontal activity shown via functional neuroimaging studies in patients performing working memory tasks.17,36 One potential confounder of the mito-chondrial gene expression fi ndings observed in both
bipolar disorder and schizophrenia maybe agonal-pH state. In a recent study by Vawter and colleagues 28% of genes related to mitochondrial function were found to be differentially expressed between control brains at low and high pH respectively.37
Other relatively consistent changes that have been observed in post-mortem gene expression investigations in schizophrenia and bipolar disorder have been altera-tions in synaptic and synaptic-related genes together with genes encoding neurotransmitters and their associ-ated proteins.14,19,38–41 Of interest, these fi ndings relate to reductions in synaptic proteins such as SNAP-25 and vesicle associate membrane protein-1 (VAMP-1) observed in the PFC of schizophrenics42–44 as well as reductions in GAD-67,45–47 a key enzyme involved in the synthesis of gamma amino butyric acid (GABA). While it is worthwhile relating mRNA changes to these protein alterations reported by post-mortem investigations it should be noted that it has been the inconsistencies in post-mortem neuropathological fi ndings that have led investigators to turn to microarray technology. A point to note here is that microarray investigations have also been relatively inconsistent in their fi ndings, and while these inconsistencies may be related to methodological differences it is likely more associated with the complex nature of the disorders under investigation. These uncer-tainties highlight the strength of microarray analyses in general, which is their ability to generate novel hypo-theses to be tested subsequently, rather than to provide ultimate validation of existing biological theories of a given mental illness.
Post-mortem microarray investigations for major depressive disorder have been less numerous within psychiatry but are beginning to increase in number. One interesting fi nding has been by Evans et al., in 2004 who demonstrated dysregulation of fi broblast growth factor (FGF) genes.48 This study reported reductions in FGF2, a neuroprotective FGF and also increases in FGF9, also known as glial growth factor. Taken together these fi ndings may represent a key neurotrophic system that is dysregulated in major depressive disorder. Directly correlated to this fi nding we also observed reductions in FGF2 and an upregulation of FGF9 in vitro in human fetal brain aggregates exposed to cortisol.49 As hypercortisolemia is a defi ning feature in MDD, our fi ndings may corroborate a role for FGFs in MDD etiology. Replication of post-mortem fi ndings and expansion of in vitro experiments are necessary before a causative role for FGFs in MDD can be achieved.

42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders 83
Tab
le 4
2.1
Po
st-m
orte
m m
icro
arra
y in
vest
igat
ions
in m
ajor
psy
chia
tric
dis
orde
rs
Bra
in r
egio
nSa
mpl
ePl
atfo
rmM
ain
gene
exp
ress
ion
fi ndi
ngs
Pref
ront
al c
orte
x (B
A10
)15
C; 1
5S; 1
5B; 1
5MD
DH
uGen
eFL
(60
00)
Red
uced
neu
rope
ptid
e Y
in s
chiz
ophr
enia
and
bip
olar
dis
orde
r54
Pref
ront
al c
orte
x (B
A10
)15
C; 1
3S; 1
1B; 1
1MD
DU
95A
v2R
educ
ed g
enes
for
rec
epto
rs, c
hann
els
or tr
ansp
orte
rs in
bip
olar
dis
orde
r; I
ncre
ased
gen
es f
or
stre
ss r
espo
nse
prot
eins
or
mol
ecul
ar c
hape
rone
s in
bip
olar
dis
orde
r. R
educ
ed S
OX
10 in
sc
hizo
phre
nia;
incr
ease
d L
AR
S2 in
sch
izop
hren
ia a
nd b
ipol
ar d
isor
der78
,79
Pref
ront
al c
orte
x (B
A9)
6(10
) C
; 6(1
0) S
cDN
A a
rray
(70
00)
Red
uced
pre
syna
ptic
(NSF
, Syn
apsi
n II
); re
duce
d G
AB
A a
nd g
luta
mat
e ne
urot
rans
mis
sion
(G
AD
67, A
MPA
1–2,
Glu
R1–
2)14
Pref
ront
al c
orte
x (B
A9)
11(5
0)C
; 11(
54)S
; 14B
U13
3AR
educ
ed m
yelin
and
olig
oden
droc
ytic
gen
es (
MO
BP,
MO
G, M
AG
, PL
P, M
BP)
in s
chiz
ophr
e-ni
a an
d bi
pola
r di
sord
er; r
educ
ed m
etab
olic
and
incr
ease
d ox
idat
ive
stre
ss g
enes
20,3
2
Pref
ront
al c
orte
x (B
A9/
47)
19C
; 19M
DD
U13
3AN
o de
tect
able
dif
fere
nces
bet
wee
n de
pres
sion
and
sui
cide
and
con
trol
s80
Pref
ront
al c
orte
x (B
A47
)6C
; 6S
cDN
A a
rray
(1,
373)
Red
uced
ast
rocy
tic a
nd o
ligod
endr
ocyt
e ge
nes
(PE
A-1
5, S
100,
MA
L, M
BP,
MO
BP)
; red
uced
gr
owth
/neu
rotr
ophi
c fa
ctor
s (B
DN
F, E
DG
F, T
GF-
a, tr
kB, e
rbB
1)81
Pref
ront
al c
orte
x (B
A46
)12
C; 1
2SH
uGen
eFL
(60
00)
Red
uced
mye
lin r
elat
ed (
MA
G, C
NP,
MA
L, H
ER
3); I
ncre
ased
dev
elop
men
tal (
GA
P-43
, M
AR
CK
S) a
nd in
crea
sed
GA
BA
neu
rotr
ansm
issi
on (
GA
D67
, GA
BA
-A)19
Pref
ront
al c
orte
x (B
A46
)35
C; 3
3S; 3
4BU
133A
Red
uced
mito
chon
dria
l-re
late
d ge
nes
in s
chiz
ophr
enia
and
bip
olar
dis
orde
r; m
edic
atio
n fr
ee
bipo
lar
patie
nts
show
ed in
crea
sed
expr
essi
on34
Pref
ront
al c
orte
x (B
A46
)35
S; 3
3S; 3
4BC
usto
m a
rray
Incr
ease
d ex
pres
sion
of
HM
L-2
in b
ipol
ar d
isor
der
and
schi
zoph
reni
a82
Pref
ront
al c
orte
x10
C; 1
0BcD
NA
arr
ay (
1200
)R
educ
ed T
GF-
beta
1; i
ncre
ased
Cas
pase
8 a
nd e
rbB
283
Pref
ront
al c
orte
x15
C; 1
5S; 1
5B;
15M
DD
Cus
tom
arr
ay (
300)
; In
crea
sed
apoL
1; Q
RT-
PC
R (
incr
ease
d A
poL
2 an
d L
4 in
sch
izop
hren
ia)84
Pref
ront
al c
orte
x27
C; 1
9SU
133A
Incr
ease
d ex
pres
sion
of
SEL
EN
BP1
, BT
G1,
HN
RPA
3 an
d SF
RS1
; red
uced
exp
ress
ion
of
GSK
3A, H
LA
-DR
B163
Pref
ront
al c
orte
x35
B, 3
5CC
usto
m a
rray
(19
K)
Red
uced
mito
chon
dria
l/ele
ctro
n tr
ansp
ort g
enes
(E
TC
com
plex
I, E
TC
Com
plex
IV
, ET
C
Com
plex
V)23
Pref
ront
al c
orte
x14
C; 1
4SC
usto
m a
rray
Incr
ease
d ex
pres
sion
of
gene
s re
late
d to
imm
une
and
chap
eron
e fu
nctio
n (S
ER
PIN
A3,
IFI
TM
1,
IFIT
M2,
IFI
TM
3, C
HI3
L1,
MT
2A, C
D14
, HSP
B1,
HSP
A1B
, HSP
A1A
)85
Pref
ront
al c
orte
x14
C; 1
4SC
usto
m a
rray
Red
uced
exp
ress
ion
of G
AB
A r
elat
ed g
enes
(G
AD
67, G
AB
AT
1, N
PY, S
ST, C
CK
, GA
BA
R
subu
nits
a1,
a2,
b3,
g2,
d)38
(con
tinue
d)
84 G. Chana et al.
Pref
ront
al c
orte
x/an
t. ci
ngul
ate
7C; 6
B; 9
MD
DU
133A
Red
uced
exp
ress
ion
of F
GF1
and
2, F
GFR
2 an
d 3
in M
DD
in D
LPF
C a
nd A
CC
as
wel
l as
incr
ease
d ex
pres
sion
of
FGF9
48
Pref
ront
al c
orte
x (B
A10
)15
S; 1
5B; 1
5MD
D; 1
5CH
U95
Av2
Red
uced
exp
ress
ion
of N
a +
/K +
-A
TPa
se a
lpha
3 s
ubun
it I
(AT
P1A
3) a
nd c
arba
moy
l-ph
osph
ate
synt
heta
se 2
, asp
arta
te tr
ansc
arba
myl
ase,
and
dih
ydro
orot
ase
(CA
D)86
Tem
pora
l cor
tex
(BA
21)
14C
;12S
; 12M
DD
U95
Av2
Red
uced
exp
ress
ion
of o
ligod
endr
ocyt
e ge
nes
(MA
G, P
LL
P, P
LP1
, Erb
B3)
; red
uced
exp
ress
ion
of n
euro
deve
lopm
enta
l gen
es (
TR
AF4
, Neu
rod1
, his
tone
dea
cety
lase
-3)
in s
chiz
ophr
enia
; R
educ
ed e
xpre
ssio
n of
olig
oden
droc
ytes
rel
ated
gen
es (
CN
P, M
AG
, MA
L, M
OG
, MO
BP,
PM
P22,
PL
LP,
PL
P1)
in m
ajor
dep
ress
ive
diso
rder
21,2
4
Supe
rior
tem
pora
l gyr
us (
STG
)7S
; 7C
Cus
tom
arr
ayR
educ
ed e
xpre
ssio
n of
neu
rotr
ansm
issi
on, n
euro
deve
lopm
enta
l gen
es a
s w
ell a
s pr
esyn
aptic
an
d m
yelin
atio
n re
late
d ge
nes
86
Hip
poca
mpu
s2C
; 2S
cDN
A a
rray
(86
00)
Incr
ease
d ex
pres
sion
of
chon
drex
, his
tam
ine
rele
asin
g fa
ctor
, HE
RC
2 an
d H
SP 7
0 87
Hip
poca
mpu
s10
C; 8
S; 9
BU
95A
v2R
educ
ed e
xpre
ssio
n of
mito
chon
dria
l and
ene
rgy
met
abol
ism
rel
ated
gen
es; R
educ
ed e
xpre
s-si
on o
f G
AD
67, S
ST 39
Ent
orhi
nal c
orte
x9C
; 8S
cDN
A a
rray
Red
uced
exp
ress
ion
of G
iα1,
Glu
R3,
NM
DA
1, s
ynap
toph
ysin
, pho
spho
lem
man
41
Mul
tiple
reg
ion
8,10
C; 8
,10S
Cus
tom
arr
ay (
1127
)R
educ
ed e
xpre
ssio
n of
syn
aptic
and
pro
teol
ytic
rel
ated
gen
es in
the
cere
bellu
m a
nd p
refr
onta
l co
rtex
40
C: c
ontr
ols;
B: B
ipol
ar D
isor
der;
MD
D: M
ajor
Dep
ress
ive
Dis
orde
r; S
: sch
izop
hren
iaA
MPA
1–2
(2-(
amin
omet
hyl p
heny
lace
tic a
cid)
; Apo
(ap
olip
opro
tein
); A
TP
1A3
(Na
+ /K
+ -
AT
Pase
alp
ha 3
sub
unit
I); B
DN
F (
brai
n de
rive
d ne
urot
roph
ic f
acto
r); B
TG
1 (B
-cel
l tr
ansl
ocat
ion
gene
1);
CA
D (
carb
amoy
l-ph
osph
ate
synt
heta
se 2
, asp
arta
te tr
ansc
arba
myl
ase
and
dihy
droo
rota
se).
CC
K (
chol
ecys
toki
nin)
; CD
14 (
cell
diff
eren
tiatio
n 14
); C
HI3
L1
(chi
tinas
e 3
like
1);
CN
P (
cycl
ic n
ucle
otid
e ph
osph
odie
ster
ase)
; E
DG
F (
epid
erm
al d
eriv
ed g
row
th f
acto
r);
FG
F (
fi bro
blas
t gr
owth
fac
tor)
; G
AB
A (
gam
ma-
amin
o bu
tyri
c ac
id);
G
AD
67 (
glut
amat
e de
carb
oxyl
ase-
67);
GA
P-4
3 (g
row
th a
ssoc
iate
d pr
otei
n-43
); G
iα1
(g-p
rote
in i
nhib
itory
alp
ha1)
; G
luR
1–2
(glu
tam
ate
rece
ptor
1–2
); G
SK3A
(gl
ycog
en s
yn-
thas
e ki
nase
3 a
lpha
); H
ER
3 (h
ereg
ulin
-3);
HN
RPA
3 (h
eter
ogen
eous
nuc
lear
ribo
nucl
eopr
otei
n A
3); H
ER
C2
(hea
t dom
ain
and
rcc1
-lik
e do
mai
n 2)
; HL
A-D
RB
1 (m
ajor
his
toco
m-
patib
ility
com
plex
DR
bet
a 1)
; HM
L-2
(hum
an m
acro
phag
e le
ctin
2);
HSP
B1
(hea
t sho
ck p
rote
in b
eta
1); S
ER
PIN
A3
(alp
ha-1
-ant
ichy
mot
ryps
in A
3); I
FIT
M1
(int
erfe
ron
indu
ced
prot
ein
with
tet
ratr
icop
eptid
e re
peat
s 1)
; L
AR
S2 (
leuc
yl-t
RN
A s
ynth
etas
e, m
itoch
ondr
ial)
; M
AG
(m
yelin
ass
ocia
ted
glyc
opro
tein
); M
AL
(m
yelin
and
lym
phoc
yte
prot
ein)
; M
AR
CK
S (m
yris
tola
ted
alan
ine-
rich
C-k
inas
e su
bstr
ate)
; T
GF
-bet
a 1
(Tra
nsfo
rmin
g gr
owth
fac
tor
beta
1);
erbB
2 er
ythr
obla
stic
leu
kem
ia v
iral
onc
ogen
e ho
mol
og 2
); M
OB
P
(mye
lin-o
ligod
endr
ocyt
e ba
sic
prot
ein)
; MB
P (
mye
lin b
asic
pro
tein
);M
OG
(m
yelin
-olig
oden
droc
ytic
pro
tein
); M
T2A
(m
etal
loth
ione
in 2
A);
Neu
rod1
(ne
urog
enic
dif
fere
ntia
tion
1); N
MD
A1
(N-m
ethy
l, d-
aspa
rtat
e 1)
; NSF
(N
-eth
ylm
alei
mid
e se
nsiti
ve f
usio
n pr
otei
n); P
EA
-15
(pho
spho
prot
ein
enri
ched
in a
stro
cyte
s 15
); P
LP
(pr
oteo
lipid
pro
tein
); P
MP
22
(per
iphe
ral m
yelin
pro
tein
22)
; SE
LE
NB
P1
(sel
eniu
m b
indi
ng p
rote
in-1
); S
FR
S1 (
splic
ing
fact
or, a
rgin
ine/
seri
ne r
ich
1); S
OX
10 (
SRY
-rel
ated
hom
eobo
x ge
ne 1
0); S
100
(cal
cium
bi
ndin
g pr
otei
n A
1); T
GF
-a (
tran
sfor
min
g gr
owth
fac
tor-
alph
a); T
RA
F4
(tum
our
necr
osis
fac
tor
rece
ptor
ass
ocia
ted
fact
or 4
);
Tab
le 4
2.1
(c
ontin
ued)
Bra
in r
egio
nSa
mpl
ePl
atfo
rmM
ain
gene
exp
ress
ion
fi ndi
ngs

42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders 85
Blood Based Gene Expression Investigations
Due to the use of blood for gene expression analysis being a relatively new concept, the number of blood-based microarray investigations for major psychiatric disorders are not as numerous as those for post-mortem brain. The main fi ndings so far from these investiga-tions are summarized in Table 42.2 above. Half of these studies have focused on assessing gene expres-sion changes in lymphoblastoid cells cultured from patients with schizophrenia and bipolar disorder. The earliest one of these studies was that by Kakiuchi et al in 2003. The authors of this study reported a reduction in expression in XBP1 in a pair of twins discordant for bipolar disorder versus a control twin pair. XBP1 is a pivotal gene in the endoplasmic reticulum (ER) stress response and therefore is of interest in the light of elevation in stress response molecules such as cortisol in patients with bipolar disorder. In addition, they found that a polymorphism substitution at position 116 (C—G) in the promoter region of XBP1 lymphoblasts derived from Japanese bipolar patients conferred a reduced ER stress response that was rescued by treat-ment with the mood stabilizer valproate.50 More recently, they extended their fi nding by demonstrating that lithium treatment also was more effective in
patients with the 116C allele as opposed to patients homozygous for 116G.51 While this fi nding directly relates the codon substitution to a known mood-stabi-lizing agent, validation of this interesting fi nding in a separate larger independent patient cohort is warranted. In the largest microarray study of lymphoblastoid cells so far by Vawter et al., 2004 it was found that the expression of NPY and GNA01 were reduced in schizophrenia as well as an increase in the mitochon-drial-related gene MDH1.52 Changes in NPY have been observed by some post-mortem investigations in schizophrenia and bipolar disorder and are therefore of interest.53–55 It should be noted that even for this study sample numbers were relatively small with only fi ve schizophrenic and nine control subjects. Moreover, studies that utilized lymphoblastoid cell lines utilized Epstein Barr virus (EBV) to transform PBMCs, an effect which in itself could lead to changes in gene expression.
Recently peripheral blood microarray fi ndings have implicated a SMDF, a splice variant of NRG-1 in patients with schizophrenia. This fi nding for NRG1 refl ects previous genetic association studies that have found a susceptibility for schizophrenia to be associ-ated with NRG1 polymorphisms.56,57 More recently, evidence for reduced NRG1 levels in the PFC of brains of patients with schizophrenia and unipolar depression
Table 42.2 Blood-based microarray investigations in major psychiatric disorders
Source Sample Platform Main gene expression fi ndings
Lymphoblastoid cells 1C; 2B U95Av2 Reduced expression of ER stress response gene XBP1 in affected twins50
Lymphoblastoid cells 9C; 5S Custom array (1127) Reduced expression of NPY, GNA01, MDH1 in schizophrenia52
Lymphoblastoid cells 2B cDNA array (2400) Increased expression of alpha1B-AR in bipolar prior to lithium treatment. Chronic lithium treatment reduced alpha1B-AR, ACHR, PDE4D, SPR in lithium responders88
Peripheral blood sample 33S; 5B U133A Increased expression of NRG-1 variant SMDF in patients with schizophrenia89
Peripheral blood sample 10C; 13S Custom array (3200) Increased expression of DRD2 and Kir2.3 in drug naïve schizophrenic subjects90
Peripheral blood sample 24(17) C; Custom array (3200) Increased expression of SELENBP1, GSK3alpha in 30 (30S); schizophrenia; Reduced expression of BTG1, HLADRB1, (7)B HNRPA3, SFRS1 in schizophrenia63,69
Peripheral blood sample 21 C; 21B U133A 2.0 Reduced expression of electron transfer chain genes in bipolar cultured lymphocytes following glucose deprivation versus controls with increased expression67
ACHR (acetylcholine receptor); DRD2 (dopamine receptor D2); ER (endoplasmic reticulum); GNA01 (guanine nucleotide binding protein alpha 1); Kir2.3 (potassium channel inward rectifying 2.3); MDH1 (malate dehydrogenase 1); NPY (neuropeptide Y); NRG-1 (neuregulin-1); PDE4D (phosphodiesterase 4D); SPR (sepiaterin reductase); SMDF (sensory and motor neuron derived factor); XBP1 (X box binding protein 1)

86 G. Chana et al.
has also emerged.58 While some studies have failed to demonstrate association of NRG1 to schizophrenia,59–61 recent meta-analyses have supported a relationship.57,62 In a comparative blood and brain gene expression study we demonstrated that the gene for selenium binding protein-1 (SELENBP1) was upregulated in both compartments in schizophrenia.63 In a follow-up qRT-PCR study looking at a separate brain cohort, our group also observed increased SELENBP1 expression in the dlPFC of patients with schizophrenia. Interes-tingly, the expression of SELENBP1 was signifi cantly correlated with psychosis in a combined sample of schizophrenia and bipolar disorder patients regardless of their diagnosis.64
However, while increased expression in SELENBP1 in the DLPFC in schizophrenia may be present, the functional relevance of this upregulation remains to be elucidated. One potential mechanism may be related to its potential role as a neurogenic factor evi-denced by two investigations demonstrating its ability to promote neurite outgrowth in the rat cerebral cor-tex65 as well as co-localization with actin in growing tips of human neuroblastoma SY5Y cells.66 Given that reductions in synaptic and dendritic arbors have been observed in the brains of patients with schizophrenia, elevated SELENBP1 may play a compensatory role in restoring neuronal connectivity and functioning. Further work to better defi ne this tentative mechanism is being carried out.
Finally, in a recent study by Naydenov et al., reduc-tion in the expression of electron transport chain genes in lymphocytes isolated from patients with bipolar dis-order following glucose deprivation was seen.67 This reduction was in contrast to an upregulation seen in normal controls. This fi nding indicates that patients with bipolar disorder may lack the ability to correct functional defi cits in the blood and hence potentially also within the brain.
Methodological Considerations for Psychiatric Microarray Investigations
An innate diffi culty in conducting microarray investi-gations in the brain is the gene expression diversity that will exist between cell types and various brain regions.68 While many of the studies listed above in Table 42.1 defi ne Brodmann areas for sampling, the
proportion of neurons and glia that make up the fi nal constituent cells for RNA extraction remain largely unknown. This is due to variation in the proportion of gray and white matter sampled. A potential way around this variation is by the use of laser capture microdis-section (LCM) to extract out individual cell types and analyze their gene expression separately. While the collection of targeted cells may appear to be more advantageous compared to homogenizing macroscopic blocks of brain tissue LCM is not without confounders. One of these is that it is very labor-intensive to gener-ate enough cells for RNA extraction and subsequent gene expression analysis. Secondly, dissection of indi-vidual cells from brain tissue inevitably leads to sampling of some of the interstitial neuropil, with the extent of this being variable between cases. Nevertheless, with the development of more automated techniques for LCM and increased precision this method represents a novel approach to assess gene expression changes in specifi c brain cell populations in major psychiatric dis-orders and brain-related disorders. This may also extend to the assessment of sub-populations of neu-rons and glia, i.e. assessment of gene expression changes in interneuronal populations in BA9. Other challenges that face brain microarray studies include (1) variability introduced by genetic diversity, (2) effects of disease treatment on gene expression, (3) differential diagnoses, (4) co-morbidity with other dis-orders, (5) variation in age, PMI, pH, and drug abuse between groups in a cohort, (6) limited sample sizes with a limited number of samples yielding high-quality RNA for investigation, and (7) variability in platform types and methods for hybridization.68
With the exception of PMI all of these factors also affect blood-based gene expression investigations. Further confounding variables for blood based studies, as previously mentioned, include diet, exercise, smok-ing, time of last meal and perhaps most importantly the patients’ immune status. All these factors can affect gene expression in the blood and hence matching and normalization where possible should be attempted when designing such studies. Just as with brain microarray investigations, blood contains several different cell types within its constituents. These cell types fall primarily into three categories; erythrocytes, leukocytes and thrombocytes. With leukocytes com-prising the immune component of blood, focus has been cast on assessing gene expression in this cellular sub-population. However, even within this cell category

42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders 87
several cell types exist; neutrophils, eosinophils, baso-phils, lymphocytes, monocytes and macrophages. As these cell types possess varied roles within the blood, this would be refl ected in their gene expression profi les. Furthermore, based on the immune status of an indi-vidual (i.e. immunosupressed due to infection) different proportions of these cell types may be present. While this signifi cant variability in gene expression paints a rather bleak picture for blood-based microarray inves-tigations to identify biomarkers for disease, specifi c patterns of gene expression have nevertheless been observed in blood samples of patients with schizophre-nia, bipolar disorder and controls.69,70 In an attempt to circumnavigate problems with cell variability in blood samples, some researchers have chosen to transform and culture B-lymphocytes into lymphoblastoid cells lines using Epstein Barr virus prior to microarray anal-ysis (see Table 42.2). While these studies have the advantage of assessing gene expression effects in a relatively homogenous cell population free from the temporal state of individuals, effects of exposure to virus and chromosomal alterations during culture must be considered as a confounder.71
Cross-Platform Comparison and Ontological Analysis
A signifi cant amount of variability lies in gene expression data generated from different microar-ray platforms and in the tools used for analysis. More recent studies have demonstrated better correlation between platforms, however even a 10% divergence will lead to differences in thousands of transcripts between platforms. A contributing element to this plat-form variability lies in the relative sensitivity of the platforms in detecting low abundance transcripts. The sensitivity of platforms in detecting low abundance transcripts is determined to a large extent by the length of oligonucleotide probes present on the array. Probes with a longer length i.e. 60–70 bases are more sensi-tive than probes with a 25-base sequence. One prob-lem with this longer probe length is that it is more prone to cross react with other transcripts and hence its specifi city may be reduced. Due to these relative incon-sistencies it is important that changes in gene expres-sion levels detected via microarrays be validated by qRT-PCR.
Post-hoc analysis of microarray data using onto-logical tools represents another area for potential error in generating false-positive and false-negative results. Firstly, analysis of individual chip image fi les are com-pleted with programs such as robust multichip analysis algorithm (RMA). RMA consists of a three-step pro-cedure involving background adjustment, quantile normalization and fi nally summarizing gene intensi-ties across probes. The next step in the analysis is determining a suitable cut-off for genes differentially regulated. Most researchers will use fold-change rela-tive to controls as their cut-off, however the value cho-sen for this is often arbitrary and tends to vary from study to study based largely on the genes of interest. Given that major psychiatric disorders have complex genetic etiologies this method of fi ltering may lead to increased generation of false-positive and false-nega-tive results. Another way in which researchers select a cut-off may be based on the signifi cance level of the gene differing between control and disease groups. This is typically set to a threshold of p = 0.05. While this method may also be seen as subjective it repre-sents a relatively more unbiased approach to choosing a cut-off, even though the relevance of the integer maybe questionable. While it maybe worthwhile attempting to adjust this scientifi cally dogmatic p-value threshold it is diffi cult to arrive at a good rational for a particular correction approach i.e. if a Bonferroni cor-rection were applied to the data one could argue to divide the p-value by the number of genes being inves-tigated. In the case of whole genome arrays this would eliminate most gene expression changes and would be over-exclusive.
Once gene lists are fi ltered ontological programs such as GoSurfer, GoMiner, OntoExpress, DAVID, Metacore and Ingenuity can be utilized to separate gene lists according to biological, cellular and molecular classification. This ontological profiling shifts the emphasis of microarray fi ndings away from single genes and instead focus is placed on categories where a signifi cant number of genes have been dysregulated. However, variations in databases and methods used for this step also exist and hence potentially introduce another layer of complexity. For example the probabil-ity of gene A being included in process Z depends on how much information the particular company who maintains an ontological program has curated about the function of gene A, furthermore very little infor-mation is know about certain genes so they will never

88 G. Chana et al.
populate a process. Thus molecular processes or networks generated by ontological programs are biased to genes for which there is more published data. Nevertheless, these programs allow us to take a more global view of gene expression changes and to hypoth-esize about certain mechanistic pathways that maybe causatively involved. Standardization of fi ltering and also ontological profi ling will inevitably lead to less variability between research groups and therefore increase the robustness of fi ndings.
Gene Expression and Endophenotypes
Schizophrenia and other major psychiatric disorders have demonstrated defi nite genetic origins, but unlike simpler diseases that follow Mendelian frameworks, their genetic architecture cannot be deconstructed as simply. Microarray investigations provide effective high-throughput gene expression analysis, however, utilizing the potential impact of endophenotypes on gene expression may enhance our ability to tease out disease-related genes and identifying potential bio-markers. Endophenotypes are heritable traits that are exhibited by those with the disorders, but are not directly symptomatic, nor are they normally associated with the disorders in terms of clinical diagnoses. Recent research gives strong evidence that endopheno-types may play a strong role in aiding the screening of patients for psychiatric disorders, especially because they are easier to analyze than the typical phenotypes, and because they may be strongly linked with the etiol-ogy of the psychiatric disorders (Flint & Munafo, 2007), Psychiatric disorders such as schizophrenia have very complex genetic architecture, due to the multiple genetic sources that individually alter suscep-tibility by a small degree while interacting with each other and the environment.72
Examples of endophenotypes and the potential identifi cation of biomarkers can be observed in a number of scientifi c articles. Flint and Munafo (2007) identi-fi ed six different categories of endophenotypes that can correlate with the disorder: anatomical, develop-mental, electrophysiological, metabolic, sensory and psychological/cognitive. Indeed, differences in neuro-anatomical structure have been attributed to schizo-phrenia and bipolar disorder. The genetic risk of schizophrenia was associated with distributed gray
matter volume defi cits in the bilateral fronto-striato-thalamic and left lateral temporal regions, whereas those with bipolar disorder demonstrated a genetic liability linked to gray matter defi cits only in the right anterior cingulate gyrus and ventral striatum.73 Genetic risk for the disorders is thus associated with gray matter structural endophenotypes, and so determination of the genetic basis of this change in gray matter may shed light on the genetic root of schizophrenia.
As already mentioned, endophenotype examination may follow either a post-hoc analysis, once the gene expression changes have been evaluated in patients with major psychiatric disorders, or endophenotypes could also be used to pre-sort patients into different groups. Both methods would ultimately attempt to fur-ther categorize and differentiate psychiatric disorders into their genetic composition in order to improve diagnosis and thus treatment. An interesting approach would be to run all patient samples blind to diagnosis followed by separation of profi les by certain endophe-notypes where data is available. In relation to blood gene expression investigations this could be done by analysis of a number of different physiological and biological factors including assessment of altered sin-gle nucleotide polymorphisms (SNPs). By separating out on the basis of endophenotypes and then compar-ing these profi les to those generated by clinical symp-tomatology common and distinguishing genes of interest between endophenotypes and psychiatric disorders may be found. When correlated with clinical data this may enable the identifi cation of a set or sets of genes that can be used for diagnosis and prognosis; i.e. patient X is a diabetic characterized by a group of dysregulated genes which are in turn related to a more frequent occurrence of psychosis. If such data is made available to a clinician it would allow them to conduct a more individualized diagnosis and treatment plan as well as enabling screening of potentially affected fam-ily members. However, as already mentioned this causative link for major psychiatric disorders is likely to rely on a number of different gene clusters.
Future Directions
Microarray investigations assessing gene expression for major psychiatric disorders in the brain have greatly increased our power to detect candidate genes for these

42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders 89
disorders. Nevertheless, signifi cant problems exist in terms of methodological and technical issues with microarrays. Probably the biggest problem facing microarray studies is the need for standardization. This includes further standardization of diagnosis, collec-tion and processing of samples, platform design and evolution in consistency, laboratory techniques and tools used for analysis. Many problems exist within these individual categories, the details of which have been discussed elsewhere.3,68,71 Problems associated with the differential diagnosis of major psychiatric dis-orders are a consequence of overlapping phenotypes between these disorders. A lack of consistent biomark-ers for major psychiatric disorders makes differential diagnosis for the trained psychiatrist a diffi cult task. The solution to this problem may potentially come at the end of the evolution of microarray investigations in the blood, whereby enough data would have been generated to reliably identify biomarkers and hence aid in differentiating between disorders.
With regard to sample collection in microarray investigations, approaches for the collection of brain material for post-mortem study and RNA extraction are well established. For blood-based investigations a number of different methods exist for the isolation of leukocytes and extraction of RNA. These different methodologies lead to differential sampling of sub-types of cells and hence signifi cant contribution of gene expression differences, an effect mirrored in brain studies where different proportions of neurons and glia may be sampled from cortical and sub-cortical regions. Isolation of specifi c lymphocyte types in blood-based studies may be achievable by the use of techniques such as immunolabelling with beads for specifi c cell-surface markers and in brain investigations via LCM. However, such techniques are relatively ineffi cient in obtaining suffi cient numbers of cells in order to yield enough RNA for microarray investigation. Nonetheless, as these techniques evolve a better isolation of indi-vidual cell populations will be achieved and will lead to a greater sensitivity in detecting gene expression changes in the blood and brain of patients with major psychiatric disorders.
Another confounding variable touched upon earlier is the effects of medications on gene expression changes. These effects occur in both blood and brain and hence require consideration and inclusion of rele-vant controls. In studies generating lymphoblastoid cells from patients, treatment of these cells with atypical
antipsychotics followed by assessment of gene expres-sion effects may help in separating disease-related versus medication-related genes. However, as already mentioned above the process of cell immortalization by infection with EBV may critically alter the cell’s gene expression pattern and therefore cloud results. In vitro and in vivo investigation represent another pos-sible route for investigating medication related effects. Some investigations have already demonstrated these effects by alterations in transcripts in rats and cell lines exposed to typical and atypical antipsychotics.74–77 The most straightforward way to assess medication effects is to study fi rst-episode or unmedicated patients; how-ever these subjects are diffi cult to identify and study.
As already mentioned, genetic studies of major psy-chiatric disorders may indeed be enhanced by using endophenotypes. Since these endophenotypes are con-sidered to be simpler and more prominent, researchers in the fi eld of behavioral science are able to design clearer experiments. By pre-sorting patients according to endophenotype, the scope of the analysis is greatly narrowed; instead studying a large population of schizophrenic patients and performing wide-range microarray investigations, samples of patients can then be studied according to the neuroanatomical, behav-ioral, biochemical etc. correlates. This in turn can be related to clinical phenotype and may be a marker indicative of diagnosis or prognosis.
Conclusion
With the advent of blood-based gene expression inves-tigations in patients with major psychiatric disorders, we may have moved one step closer to identifying potential biomarkers. However, care must be taken in the initial stages of these studies to avoid over-inter-pretation of such generated data and the creation of white elephants that cannot be replicated. By imple-menting careful study design many of these potential confounders can be reduced or accounted for. Further still, separation of specifi c cell populations for study including both blood and brain compartments will allow us to glean more knowledge as to the mechanism of gene dysregulation. The fi eld of microarray plat-form design and development is also very fast-moving. With microarray platforms continuing to evolve the ability to detect splice variants of transcripts is now a

90 G. Chana et al.
reality as well as incorporating single nucleotide polymorphism (SNP) analysis for a more detailed understanding of gene-based expression changes. This then also can be related to other epigenetic mechanisms that have the potential to infl uence gene expression changes and will allow us to not only understand gene expression changes but also what in-built mechanisms may be regulating them. The ability to mine and extract useful data requires standardization in analysis techniques and the free distribution of data to all researchers. An example of this can be seen in the Stanley Foundation’s online genomics database (https://www.stanleygenomics.org/) whereby study results from numerous investigators and platforms have been summarized. Finally, analyzing the tran-scriptome using microarrays must be coupled to other evolving fi elds such as proteomics and metabolomics. Adopting such an approach will greatly facilitate our search for biomarkers in psychiatry as it provides a multi-pronged approach for identifi cation and validation purposes. These techniques will also allow us to look more closely at endophenotypes and their common and specifi c contributions to major psychiatric disorders.
References
1. Flint J, Munafo MR. The endophenotype concept in psychi-atric genetics. Psychological Medicine 2007;37:163–180.
2. Cannon TD, Keller MC. Endophenotypes in the genetic analyses of mental disorders. Annual Review of Clinical Psychology 2006;2:267–290.
3. Bunney WE, Bunney BG, Vawter MP, et al. Microarray technology: a review of new strategies to discover candidate vulnerability genes in psychiatric disorders. The American Journal of Psychiatry 2003;160:657–666.
4. Radich JP, Mao M, Stepaniants S, et al. Individual-specifi c variation of gene expression in peripheral blood leukocytes. Genomics 2004;83:980–988.
5. Hardiman G. Microarray platforms – comparisons and con-trasts. Pharmacogenomics 2004;5:487–502.
6. Fan JB, Chee MS, Gunderson KL. Highly parallel genomic assays. Nature Reviews 2006;7:632–644.
7. Michael KL, Taylor LC, Schultz SL, Walt DR. Randomly ordered addressable high-density optical sensor arrays. Analytical Chemistry 1998;70:1242–1248.
8. Tan PK, Downey TJ, Spitznagel EL, Jr., et al. Evaluation of gene expression measurements from commercial microarray platforms. Nucleic Acids Research 2003;31(19):5676–5684.
9. Hollingshead D, Lewis DA, Mirnics K. Platform infl uence on DNA microarray data in postmortem brain research. Neurobiological Disease 2005;18(3):649–655.
10. Bosotti R, Locatelli G, Healy S, et al. Cross platform microarray analysis for robust identifi cation of differentially expressed genes. BMC Bioinformatics 2007;8 Suppl 1:S5.
11. Wang Y, Barbacioru C, Hyland F, et al. Large scale real-time PCR validation on gene expression measurements from two commercial long-oligonucleotide microarrays. BMC Genomics 2006;7:59.
12. Schlingemann J, Habtemichael N, Ittrich C, et al. Patient-based cross-platform comparison of oligonucleotide microar-ray expression profi les. Laboratory Investigation; A Journal of Technical Methods and Pathology 2005;85:1024–1039.
13. Shippy R, Sendera TJ, Lockner R, et al. Performance evalu-ation of commercial short-oligonucleotide microarrays and the impact of noise in making cross-platform correlations. BMC Genomics 2004;5:61.
14. Mirnics K, Middleton FA, Marquez A, et al. Molecular characterization of schizophrenia viewed by microarray analysis of gene expression in prefrontal cortex. Neuron 2000;28:53–67.
15. Goldman-Rakic PS. Working memory dysfunction in schizophrenia. The Journal of Neuropsychiatry and Clinical Neurosciences 1994;6:348–357.
16. Goldberg TE, Weinberger DR, Berman KFet al. Further evi-dence for dementia of the prefrontal type in schizophrenia? A controlled study of teaching the Wisconsin Card Sorting Test. Archives of General Psychiatry 1987;44:1008–1014.
17. Wible CG, Anderson J, Shenton ME, et al. Prefrontal cortex, negative symptoms, and schizophrenia: an MRI study. Psychiatry Research 2001;108:65–78.
18. Wolf DH, Gur RC, Valdez JN, et al. Alterations of fronto-temporal connectivity during word encoding in schizophre-nia. Psychiatry Research 2007;154:221–232.
19. Hakak Y, Walker JR, Li C, Wong WH, et al. Genome-wide expression analysis reveals dysregulation of myelination-related genes in chronic schizophrenia. Proceedings of the National Academy of Sciences of the United States of America 2001;98:4746–4751.
20. Tkachev D, Mimmack ML, Ryan MM, et al. Oligodendrocyte dysfunction in schizophrenia and bipolar disorder. Lancet 2003;362:798–805.
21. Aston C, Jiang L, Sokolov BP. Microarray analysis of post-mortem temporal cortex from patients with schizophrenia. Journal of Neuroscience Research. 2004;77:858–866.
22. Tkachev D, Mimmack ML, Huffaker SJ, et al.. Further evi-dence for altered myelin biosynthesis and glutamatergic dysfunction in schizophrenia. The International Journal of Neuropsychopharmacology/Offi cial Scientifi c Journal of the Collegium Internationale Neuropsychopharmacologicum (CINP) 2007;10:557–563.
23. Sun X, Wang JF, Tseng M, Young LT. Downregulation in com-ponents of the mitochondrial electron transport chain in the postmortem frontal cortex of subjects with bipolar disorder. Journal of Psychiatry and Neuroscience 2006;31:189–196.
24. Aston C, Jiang L, Sokolov BP. Transcriptional profi ling reveals evidence for signaling and oligodendroglial abnormalities in the temporal cortex from patients with

42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders 91
major depressive disorder. Molecular Psychiatry 2005;10:309–322.
25. Flynn SW, Lang DJ, Mackay AL, et al. Abnormalities of myelination in schizophrenia detected in vivo with MRI, and post-mortem with analysis of oligodendrocyte proteins. Molecular Psychiatry 2003;8:811–820.
26. Uranova N, Orlovskaya D, Vikhreva O, et al. Electron microscopy of oligodendroglia in severe mental illness. Brain Research Bulletin 2001;55:597–610.
27. Uranova NA, Vostrikov VM, Orlovskaya DD, Rachmanova VI. Oligodendroglial density in the prefrontal cortex in schizophrenia and mood disorders: a study from the Stanley Neuropathology Consortium. Schizophrenia Research 2004;67:269–275.
28. Hof PR, Haroutunian V, Copland C, et al. Molecular and cellular evidence for an oligodendrocyte abnor-mality in schizophrenia. Neurochemical Research. 2002;27:1193–1200.
29. Davis KL, Stewart DG, Friedman JI, et al. White matter changes in schizophrenia: evidence for myelin-related dysfunction. Archives of General Psychiatry. 2003;60:443–456.
30. Stewart DG, Davis KL. Possible contributions of myelin and oligodendrocyte dysfunction to schizophrenia. International Review of Neurobiology 2004;59:381–424.
31. Cheung V, Cheung C, McAlonan GM, et al. A diffusion ten-sor imaging study of structural dysconnectivity in never-medicated, fi rst-episode schizophrenia. Psychological Medicine 2008;38:877–885.
32. Prabakaran S, Swatton JE, Ryan MM, et al. Mitochondrial dysfunction in schizophrenia: evidence for compromised brain metabolism and oxidative stress. Molecular Psychiatry 2004;9:684–697, 643.
33. Konradi C. Gene expression microarray studies in polygenic psychiatric disorders: applications and data analysis. Brain Research Brain Research Reviews 2005;50:142–155.
34. Iwamoto K, Bundo M, Kato T. Altered expression of mito-chondria-related genes in postmortem brains of patients with bipolar disorder or schizophrenia, as revealed by large-scale DNA microarray analysis. Human Molecular Genetics 2005;14:241–253.
35. Pongrac J, Middleton FA, Lewis DA, et al. Gene expression profi ling with DNA microarrays: advancing our understand-ing of psychiatric disorders. Neurochemical Research 2002;27:1049–1063.
36. Achim AM, Lepage M. Episodic memory-related activation in schizophrenia: meta-analysis. British Journal of Psychiatry 2005;187:500–509.
37. Vawter MP, Tomita H, Meng F, et al. Mitochondrial-related gene expression changes are sensitive to agonal-pH state: implications for brain disorders. Molecular Psychiatry 2006;11:615, 663–679.
38. Hashimoto T, Arion D, Unger T, et al. Alterations in GABA-related transcriptome in the dorsolateral prefrontal cortex of subjects with schizophrenia. Molecular Psychiatry 2008;13(2):147–161.
39. Konradi C, Eaton M, MacDonald ML, et al. Molecular evi-dence for mitochondrial dysfunction in bipolar disorder. Archives of General Psychiatry 2004;61:300–308.
40. Vawter MP, Barrett T, Cheadle C, et al. Application of cDNA microarrays to examine gene expression differences in schizophrenia. Brain Research Bulletin 2001;55:641–650.
41. Hemby SE, Ginsberg SD, Brunk B, et al. Gene expression profi le for schizophrenia: discrete neuron transcription pat-terns in the entorhinal cortex. Archives of General Psychiatry 2002;59:631–640.
42. Young CE, Arima K, Xie J, et al. SNAP-25 defi cit and hip-pocampal connectivity in schizophrenia. Cerebral Cortex 1998;8:261–268.
43. Honer WG, Falkai P, Chen C, et al. Synaptic and plasticity-associated proteins in anterior frontal cortex in severe men-tal illness. Neuroscience 1999;91:1247–1255.
44. Fatemi SH, Earle JA, Stary JM, et al. Altered levels of the synaptosomal associated protein SNAP-25 in hippocampus of subjects with mood disorders and schizophrenia. Neuroreport 2001;12:3257–3262.
45. Guidotti A, Auta J, Davis JM, et al. Decrease in reelin and glutamic acid decarboxylase67 (GAD67) expression in schizophrenia and bipolar disorder: a postmortem brain study. Archives of General Psychiatry 2000;57:1061–1069.
46. Volk DW, Austin MC, Pierri JN, et al. Decreased glutamic acid decarboxylase67 messenger RNA expression in a sub-set of prefrontal cortical gamma-aminobutyric acid neurons in subjects with schizophrenia. Archives of General Psychiatry 2000;57:237–245.
47. Woo TU, Walsh JP, Benes FM. Density of glutamic acid decarboxylase 67 messenger RNA-containing neurons that express the N-methyl-D-aspartate receptor subunit NR2A in the anterior cingulate cortex in schizophrenia and bipolar disorder. Archives of General Psychiatry 2004;61:649–657.
48. Evans SJ, Choudary PV, Neal CR, et al. Dysregulation of the fi broblast growth factor system in major depression. Proceedings of the National Academy of Sciences of the United States of America 2004;101:15506–15511.
49. Salaria S, Chana G, Caldara F, et al. Microarray analysis of cultured human brain aggregates following cortisol expo-sure: implications for cellular functions relevant to mood disorders. Neurobiology of Disease 2006;23:630–636.
50. Kakiuchi C, Iwamoto K, Ishiwata M, et al. Impaired feed-back regulation of XBP1 as a genetic risk factor for bipolar disorder. Nature Genetics 2003;35:171–175.
51. Kakiuchi C, Ishiwata M, Hayashi A, Kato T. XBP1 induces WFS1 through an endoplasmic reticulum stress response element-like motif in SH-SY5Y cells. Journal of Neurochemistry 2006;97:545–555.
52. Vawter MP, Ferran E, Galke, B, et al. Microarray screening of lymphocyte gene expression differences in a multiplex schizophrenia pedigree. Schizophrenia Research 2004;67:41–52.
53. Frederiksen SO, Ekman R, Gottfries CG, et al. Reduced concentrations of galanin, arginine vasopressin, neuropep-tide Y and peptide YY in the temporal cortex but not in the hypothalamus of brains from schizophrenics. Acta Psychiatrica Scandinavica 1991;83:273–277.
54. Kuromitsu J, Yokoi A, Kawai T, et al. Reduced neuropeptide Y mRNA levels in the frontal cortex of people with schizo-phrenia and bipolar disorder. Brain Research Gene Expression Patterns 2001;1:17–21.
92 G. Chana et al.
55. Iritani S, Kuroki N, Niizato K, Ikeda K. Morphological changes in neuropeptide Y-positive fi ber in the hippocampal formation of schizophrenics. Progress in Neuro-Psychopharmacology & Biological Psychiatry 2000;24:241–249.
56. Thomson PA, Christoforou A, Morris SW, et al. Association of Neuregulin 1 with schizophrenia and bipolar disorder in a second cohort from the Scottish population. Molecular Psychiatry 2007;12:94–104.
57. Li D, Collier DA, He L. Meta-analysis shows strong positive association of the neuregulin 1 (NRG1) gene with schizo-phrenia. Human Molecular Genetics 2006;15:1995–2002.
58. Bertram I, Bernstein HG, Lendeckel U, et al. Immunohistochemical evidence for impaired neuregulin-1 signaling in the prefrontal cortex in schizophrenia and in unipolar depression. Annals of the New York Academy of Sciences 2007;1096:147–156.
59. Rosa A, Gardner M, Cuesta MJ, et al. Family-based associa-tion study of neuregulin-1 gene and psychosis in a Spanish sample. American Journal of Medical Genetics B Neuropsychiatric Genetics 2007.
60. Duan J, Martinez M, Sanders AR, et al. Neuregulin 1 (NRG1) and schizophrenia: analysis of a US family sample and the evidence in the balance. Psychological Medicine 2005;35:1599–1610.
61. Thiselton DL, Webb BT, Neale BM, et al. No evidence for linkage or association of neuregulin-1 (NRG1) with disease in the Irish study of high-density schizophrenia families (ISHDSF). Mol Psychiatry 2004;9:777–783; image 729.
62. Munafo MR, Thiselton DL, Clark TG, Flint J. Association of the NRG1 gene and schizophrenia: a meta-analysis. Molecular Psychiatry 2006;11:539–546.
63. Glatt SJ, Everall IP, Kremen WS, et al. Comparative gene expression analysis of blood and brain provides concurrent validation of SELENBP1 up-regulation in schizophrenia. Proceedings of the National Academy of Sciences of the United States of America 2005;102:15533–15538.
64. Kanazawa T, Chana G, Glatt SJ, et al. The utility of SELENBP1 gene expression as a biomarker for major psy-chotic disorders: replication in schizophrenia and extension to bipolar disorder with psychosis. American Journal of Medical Genetics B Neuropsychiatric Genetics 2008; 147B(6):686–689.
65. Zhao Z, Nair SM, Chou DK, et al. Expression and role of sulfoglucuronyl (HNK-1) carbohydrate and its binding pro-tein SBP-1 in developing rat cerebral cortex. Journal of Neuroscience Research. 2000;62:186–205.
66. Miyaguchi K. Localization of selenium-binding protein at the tips of rapidly extending protrusions. Histochemistry and Cell Biology 2004;121:371–376.
67. Naydenov AV, MacDonald ML, Ongur D, Konradi C. Differences in lymphocyte electron transport gene expres-sion levels between subjects with bipolar disorder and nor-mal controls in response to glucose deprivation stress. Archives of General Psychiatry 2007;64:555–564.
68. Mirnics K, Levitt P, Lewis DA. Critical appraisal of DNA microarrays in psychiatric genomics. Biological Psychiatry 2006;60:163–176.
69. Tsuang MT, Nossova N, Yager T, et al. Assessing the validity of blood-based gene expression profi les for the classifi cation
of schizophrenia and bipolar disorder: a preliminary report. American Journal of Medical Genetics B Neuropsychiatric Genetics 2005;133:1–5.
70. Bowden NA, Weidenhofer J, Scott RJ, et al. Preliminary investigation of gene expression profi les in peripheral blood lymphocytes in schizophrenia. Schizophrenia Research. 2006;82:175–183.
71. Iwamoto K, Kato T. Gene expression profi ling in schizo-phrenia and related mental disorders. Neuroscientist 2006;12:349–361.
72. Riley B, Kendler KS. Molecular genetic studies of schizophrenia. European Journal of Human Genetics 2006;14:669–680.
73. McDonald C, Bullmore ET, Sham PC, et al. Association of genetic risks for schizophrenia and bipolar disorder with specifi c and generic brain structural endophenotypes. Archives of General Psychiatry. 2004;61:974–984.
74. Kontkanen O, Lakso M, Wong G, Castren E. A functional genomic study of the effects of antipsychotic agent chlo-rpromazine in PC12 cells. Clinical Chemistry and Laboratory Medicine 2000;38(9):911–915.
75. Kontkanen O, Lakso M, Wong G, Castren E. Chronic antip-sychotic drug treatment induces long-lasting expression of fos and jun family genes and activator protein 1 complex in the rat prefrontal cortex. Neuropsychopharmacology. 2002;27(2):152–162
76. Chen ML, Chen CH. Microarray analysis of differentially expressed genes in rat frontal cortex under chronic risperidone treatment. Neuropsychopharmacology 2005;30:268–277.
77. Takahashi Y, Kumanishi T, Hayashi S. Using a DNA microarray method to examine gene expression in brain from clozapine-injected mice. Annals of the New York Academy of Sciences 2004;1025:561–569.
78. Iwamoto K, Kakiuchi C, Bundo M, et al. Molecular charac-terization of bipolar disorder by comparing gene expression profi les of postmortem brains of major mental disorders. Molecular Psychiatry 2004;9:406–416.
79. Munakata K, Iwamoto K, Bundo M, Kato T. Mitochondrial DNA 3243A > G mutation and increased expression of LARS2 gene in the brains of patients with bipolar disor-der and schizophrenia. Biological Psychiatry 2005;57:525–532.
80. Sibille E, Arango V, Galfalvy HC, et al. Gene expression profi ling of depression and suicide in human prefrontal cor-tex. Neuropsychopharmacology 2004;29:351–361.
81. Sugai T, Kawamura M, Iritani S, et al. Prefrontal abnormal-ity of schizophrenia revealed by DNA microarray: impact on glial and neurotrophic gene expression. Annals of the New York Academy of Sciences 2004;1025:84–91.
82. Frank O, Giehl M, Zheng C, et al. Human endogenous retro-virus expression profi les in samples from brains of patients with schizophrenia and bipolar disorders. Journal of Virology 2005;79:10890–10901.
83. Bezchlibnyk YB, Wang JF, McQueen GM, Young LT. Gene expression differences in bipolar disorder revealed by cDNA array analysis of post-mortem frontal cortex. Journal of Neurochemistry 2001;79:826–834.
84. Mimmack ML, Ryan M, Baba H, et al. Gene expression analysis in schizophrenia: reproducible up-regulation of several members of the apolipoprotein L family located in a high-susceptibility locus for schizophrenia on chromosome

42 Gene Expression Changes and Potential Impact of Endophenotypes in Major Psychiatric Disorders 93
22. Proceedings of the National Academy of Science U S A. 2002;99(7):4680–4685
85. Arion D, Unger T, Lewis DA, et al. Molecular Evidence for Increased Expression of Genes Related to Immune and Chaperone Function in the Prefrontal Cortex in Schizophrenia. Biological Psychiatry. 2007;62(7):711–721.
86. Bowden NA, Scott RJ, Tooney PA. Altered gene expression in the superior temporal gyrus in schizophrenia. BMC Genomics 2008;9:199.
87. Chung C, Tallerico T, Seeman P. Schizophrenia hippocam-pus has elevated expression of chondrex glycoprotein gene. Synapse 2003;50:29–34.
88. Sun X, Young LT, Wang JF, et al. Identifi cation of lithium-regulated genes in cultured lymphoblasts of lithium respon-sive subjects with bipolar disorder. Neuropsychopharmacology 2004;29:799–804.
89. Petryshen TL, Middleton FA, Kirby A, et al. Support for involvement of neuregulin 1 in schizophrenia pathophysiology. Molecular Psychiatry 2005;10:366–374, 328.
90. Zvara A, Szekeres G, Janka Z, et al. Over-expression of dop-amine D2 receptor and inwardly rectifying potassium channel genes in drug-naive schizophrenic peripheral blood lympho-cytes as potential diagnostic markers. Disease Markers 2005;21:61–69.




















