FINGERNAILS yourselves." the nails upon which Ronchesel ...
16
A DISCOURSE ON NAIL GROWI;TH AND UNUSUAL FINGERNAILS BY 'WILLIAM B. BEANT, M.D. IOWN.A CITY THE TEXT "Divide your attentions equally between books and men. The strength of the student of books is to sit still-two or tlhree hours at a stretch- eating the heart out of a subject with pencil and note-book in hand, de- termined to master the details and intricacies, focusing all your energies on its difficulties. Get accustomed to test all sorts of book problems and state- ments for yourself, and take as little as possible on trust. The Hunterian 'Do not think, but try' attitude of mind is the imiiportant one to cultivate. The question came up one day, when discussing the grooves left on the nails after fever, how long it took for the nail to grow out, from root to edge. A majority of the class had no further interest; a few looked it up in books; two men marked their nails at the root with nitrate of silver, and a few months later had positive knowledge on the subject. They showed the proper spirit. The little points that come up) in your reading try to test for yourselves. " AW ILLIAM OSLER-The Student Life Textbooks only touch upon many interesting diseases of the nails and curious shapes and colors they may acquire. Occupational alterations of the nails upon which Ronchesel of Providence lhas written fascinating papers, are the subject of great neglect. Indeed the Bible mentions finger- nails only once. Information about nail growth is still sketchy but is developing. The large group of clinical conditions in which the nail may be altered sharply and often specifically has not been reviewed systematically. Before I comment about the miscellany of strange nails I lhave selected at random from my notes and slides, I want to tell you of observations miade on the growth of my own left thumbnail. I am now well along in the twenty-first year of the study. Thus it is coming of age.2' 3 I have discussed before this society and elsewhere the importance of the seemiingly trivial and lminute in medicine.4' This series of observations is another aspect of "multum in parvo". The quotation from Osler wlicil is the Imlotto for this essay I had read often, certainly four or five times, before I reactedl and began a venture which has continued far beyond the few months of the students wlhose From The Department of Medicine, College of Medicine, University of Iowa, Iowa City, Iowa. 152
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of FINGERNAILS yourselves." the nails upon which Ronchesel ...
A DISCOURSE ON NAIL GROWI;TH AND UNUSUALFINGERNAILS
BY 'WILLIAM B. BEANT, M.D.
IOWN.A CITY
THE TEXT
"Divide your attentions equally between books and men. The strengthof the student of books is to sit still-two or tlhree hours at a stretch-eating the heart out of a subject with pencil and note-book in hand, de-termined to master the details and intricacies, focusing all your energies onits difficulties. Get accustomed to test all sorts of book problems and state-ments for yourself, and take as little as possible on trust. The Hunterian'Do not think, but try' attitude of mind is the imiiportant one to cultivate.The question came up one day, when discussing the grooves left on thenails after fever, how long it took for the nail to grow out, from root to edge.A majority of the class had no further interest; a few looked it up in books;two men marked their nails at the root with nitrate of silver, and a fewmonths later had positive knowledge on the subject. They showed theproper spirit. The little points that come up) in your reading try to test foryourselves. "
AW ILLIAM OSLER-The Student Life
Textbooks only touch upon many interesting diseases of the nails andcurious shapes and colors they may acquire. Occupational alterations ofthe nails upon which Ronchesel of Providence lhas written fascinatingpapers, are the subject of great neglect. Indeed the Bible mentions finger-nails only once. Information about nail growth is still sketchy but isdeveloping. The large group of clinical conditions in which the nail may bealtered sharply and often specifically has not been reviewed systematically.Before I comment about the miscellany of strange nails I lhave selectedat random from my notes and slides, I want to tell you of observations miadeon the growth of my own left thumbnail. I am now well along in thetwenty-first year of the study. Thus it is coming of age.2' 3 I have discussedbefore this society and elsewhere the importance of the seemiingly trivialand lminute in medicine.4' This series of observations is another aspectof "multum in parvo".The quotation from Osler wlicil is the Imlotto for this essay I had read
often, certainly four or five times, before I reactedl and began a venturewhich has continued far beyond the few months of the students wlhose
From The Department of Medicine, College of Medicine, University of Iowa, IowaCity, Iowa.
152

NAIL GROWTH AND UNUSUAL FINGERNAILS
curiosity led them-i to do their little exercise in observation. The oppor-tunity for making a long-term study was waiting patiently for anyonewith the idea plus persistence. Ten years ago I reported the result of thefirst decade of studies and elsewhere have made a muore detailed analysisof the growth pattern from the records miiade for 20 years.3
Figure 1 illustrates the way I marked the nail and had it photograplhecd.A camera with a fixed focal distance and a little stall into whichl mny
FIG. 1. Photograph of the nail indicating tattoo mark, the transverse line and the.overlying grid used to facilitate measurement.
153

1WILLIAM B. BEAN
thumbnail fits snugly allowed recordings to check the observed progressionof the marked point. A tiny tattoed mark in the skin at the base of thenail and the separation of nail from the distal free edge were the points ofreference. The grid made measuring easy. I use a little file such as isused to score small glass vials before breaking them, to notch the nail.Notes were kept on a card. On the first day of each miiontlh a sharp trans-verse line was filed just where the nail emerged from under the cuticle-This progressed towards the free edge as the nail grew. The distance fromithe place where the nail was scored to the free edge was exactly 1.45 cmii.The distance has not changed during the 20 years of the study. Photo-graphs taken at weekly intervals for the last two years enabled me to makemore detailed observations, but they did not disclose any erratic spurts ordelays not to be found in the month-to-month data.
OBSERVATIONSThe number of days required for each monthly ml-ark to reach the free
edge of the nail is recorded in Figure 2. MIany observers have found sea-sonal variation with a slight acceleration in sutimmer and retardation incold weather. I have never observed any such trend, even though themethod was accurate enough to have discovered it. MIy suspicion is thatspending so much time indoors with central heating and air conditioning,despite walking or bicycling to and from work, getting regular exercise, Ido not have enough exposure to climatic extremes. Anyhow there has beenno seasonal variation in the rate of growth.Near the end of the first ten years of the study I got mumps. During
the ten days I was ill the nail stopped growing completely, as indicatedin the striking delay for the month when I was sick (Fig. 2). This was thefirst time such an observation of the effect of infection with a comparablebefore and after control had ev-er been made. Since the publication of thisobservation in 1953, it has been amply and repeatedly confirmed, especiallyin studies in children where one may anticipate a variety of sharp andgenerally self-limited infections.6The curve of growth was a plateau for the first five years; a somewhat
higher plateau for the next twelve years; and then came a sharp rise in thenumber of days it takes for the nail to grow out, a grim reminder of theaging process. If one forgot the shifting baseline and concentrated on ab-solute rate of growth, he might conclude that the last three years had beenworse than having mumps. Fortunately the process of aging is so gentlethat most of us can conceal it for a time at least from ourselves or bravelytry to brush it aside.
For those who like statistics the figures for the rate of nail growth inmillimeters per day at the age of thirty-two was 0.123. At the age of
15*4

NAIL GROWTH AND UNUSUAL FINGERNAILS15
0 5 110 115 120 125 130 135 140
Cincinnati, 0.1942 -5riganAl/a.
- - - ~~~~~California Desert1943 Fort Knox, Ky.
1944 --- ~ColoradoFort Knox, Ky.Y
1945 ......... .......Pacific.. ~~~~~~Fort Knox, Ky.Y
1946.......1-Man Days per Year
1947 '~~~~~~~~~~~~Cincinnati,0.
1950... ...
1951~ ~ ~ ~ ~ ~ Wiscansin.......1952 lowa City,Ia.~~~~--------
............. W sco si1948 ...Io.a..City,...a.
19549 .....Iowa.City.Ia,wss I~~~~~~~~~~~~~owaCity, la.--Norh-Cao--n
1956IwaCty a
1958 WisowasitynaI.............. /~~~~~owa City, /a.
Iowa City,, Ia.
1954.......... ~$Europe1961
. .......IO Wa City, a
0955..1..1.12.12.13.13..4... ...Total Days -ofotGrowthin
Fi..Tetyy...ud.f...guthO.tehoiona a is inicted,AMotby month the....number....ofdysrqurdfo.hemrkli.dw.tefis.f.ah.otto5reac the.. end.. ofteni.Tedt.ieteaeaefrte1otsadteln
conectng heminicaes he aratin oer he eas o th stdy
I 'a"5

WILLIAM B. BEAN
forty-two 0.110 and then at the age of fifty-two 0.105. I must express mysorrow that there is no climatological effect worth reporting. No changesoccurred during desert exposure or several months of daily exposure of6-8 hours to a temperature of 1100 or more in a laboratory hot room.Those with presbyopia may notice that during the first decade there were
two months where I simply forgot to put the little mark down. I do notknow how long it took my nail to grow in those months. This accounts forthe lacunae in the chart, the missing front teeth. Perhaps a better memoryor force of habit helped me to avoid any such omissions during the seconddecade.Two other personal observations are of note. An occasional injury to the
thumb, instead of producing a blood blister under the nail has produceda splinter hemorrhage. I marked it separately. It moved outward atexactly the same rate as the monthly marks. The other observation isthat on the left side of the thumb nail there is a faint longitudinal streaksomewhat darker than the rest of the nail. Wlhen I trim the nail evenlyand press the two ends of the clipping together, the nails bends in thisspot and breaks easily. This is probably caused by a small area deficientin germinal cells; possibly a result of some forgotten injury.Many observations have been made about nail growth. These may be
summed up briefly by saying that others have described a spurt of adoles-cent nail growth and have verified the slowing of linear growth withaging. There is variation of growth among families and individuals, pre-sumably a genetic difference. Somie families are fast growers, others areslow. Boys and men have a tendency for nails to grow a little faster tllanthose of girls and women. In pregnancy the rate of growth may be in-creased by as much as a third. Likewise in hyperthyroidism there is anincreased rate of growth. Starvation, lactation, and the use of antimitoticdrugs regularly reduce the rate of nail growth.
I believe that the notion of growth after death is an error based on theshrinkage of the skin which sets in with a tendency to pull away from thefree edge of the nail. The cuticle retracts, too. In any event, mitosis ceasesand no new mitoses occur after death.The remaining observations are randomn. N\o effort was made to exhaust
the topic of minor and important variations in nail growth. I mentionclubbing, the most dramatic and commonly observed clinical alteration,well understood clinically but not in terms of pathophysiology, only toeinphasize the point that we still have a lot to learn.
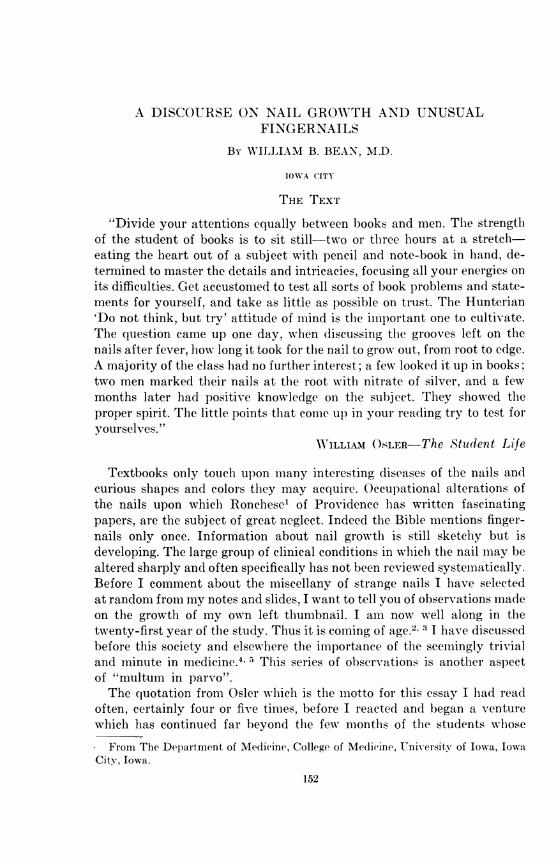
Persons with clubbing have an increased rate of nail growth (Fig. 3).There is a comparable but not always as great an increase in growth whenpalmar erythemia occurs (Fig. 4). Those who have observed the accelera-tion of nail growth during pregnancy have not mentioned an association
156
NAIL GROWTH AND UNUSUAL FINGERNAILS
FIG. 3. Extensive clubbing of the nails in a patient with chronic pulmonary disease.
FIG. 4 a: Palmar erythema of pregnancy indicating the extension of the region ofv-asodilatation to involve the skin around the base of the nail; b: the nails after de-livery.
with palmar erythema which occurs in a fairly high proportion of pregnantwomen. I have observed that in persons with liver disease and palmarerythema the nail grows more rapidly than it does after the palmar ery-thema disappears. When palmar erythema is well advanced there is a
157

WILLIAM B. BEAN
tendency for the accentuated erythema of the palmar portion of the distalphalanx to encompass the skin at the base of the nail. Temperature in suchregions is increased indicating an enhanced blood flow. Presumably thegrowth is a manifestation of forced feeding.
In persons with universal angiomatosis7 the nail tends to be bluishand somewhat pale but squeezing the finger below the base of the nail re-sults in a great suffusion and reddening of the nail itself.White nails or leukonychia totalis have a ground-glass appearance often
with an obscuring of the lunula (Fig. 5). Terry8 called attention to leu-konychia as a stigma of liver disease but his controls were not extensive.I have seen leukonychia totalis in approximately 7% of men and 4% ofwomen without signs of liver disease in the last 650 patients I have seenin consultation. It has been somewhat more common in persons withpalmar erythema. It was not associated with liver disease or pregnancy.It is very important to distinguish the "white nail" from the pallid nailof anemia. In an anemic person if one grips the finger at the distal jointand squeezes, ordinarily the nail as well as the fingertip become red. In aperson with white nails this does not occur because of the thickening ofthe underlying matrix. The venous plexuses which accommodate the blood,upon which the vascular element of skin color depends are too deep to beseen. Instead of total leukonychia some people have a margin of one or twomillimeters at the free end of the nail which has the usual color.Most of us at some time or another have noted in ourselves or in others
the white spots, irregularly arranged, in one or more nails. Rarely theyappear just as the nail emerges but more often are seen further towards
FIG. 5. White nails compared with those of normal pink color.
1.58

NAIL GROWTH AND UNUSUAL FINGERNAILS
the tip. They grow out at the same rate as the nail; tend to become largerin the middle of the nail; and then as the free edge is reached they tend tofade away. A variation of this phenomenon can be produced by the simpleexpedient of injecting a little bubble of air into or Just below the nail.According to Mlitchell and others the cells in the nail bed, though ordi-narily not involved in the continuing proliferation of keratin, may becomeenclosed in the nail plate.9 There is no known connection with minor in-jury. Why some people tend to have a great many such white spots andothers have none at all is a mystery. They can be used as a reasonablyaccurate measuring rod to follow the progress of nail growth.
Last year Dr. James Clifton and I observed two patients who had theextraordinary abnormality depicted in Figure 6. Between a third andalmost a half of the distal portion of the nail they had a red, slightly orangecolor. Most of this color faded out when the free edge of the nail waspressed though the area which had been red was still distinguished by agray color. Botlh patients with this nail lesion had renal disease. One diedof uremia. The other had only moderate renal failure associated withprolonged diabetes. This alteration suggests a change which a formerpresident of this association, Dr. Hal Thomas, reported in the JohnsHopkins Hospital Bulletin.'0 He described a pigmentary change whichgrew out with the nail in a thyrotoxic patient. In our one patient who hasbeen under observation for many months, the pattern has not changed.
FIG 6. Increased vascularity causing a red discoloration of the nail. Most of the redcolor could be caused to fade out by strong pressure.
159

WILLIAM B. BEAN
It seems unlikely that Mueller's suggestion of distal infarction of thenail bed is the explanation for this phenomenon."1
Dr. Plummer at the Mayo Clinic was the first to emphasize the impor-tance of onycholysis in thyrotoxicosis.12 A large part, sometimes morethan half, of the nail loses its intimate connection with the bed. From thetip back to approximately the middle, the nail becomes detached. Thisalteration is slowly corrected by effective treatment of thyrotoxicosis andhas been observed to recur in circumstances where thyroid overactivityrecurs. The cause of onycholysis in patients with disease of the thyroidis not known.
If the condition I call "congenital displastic angiectasis"7 involves a handor a foot in localized gigantism with much overgrowth of the underlyingbone and muscle, a number of grotesque, irregular alterations in the nailmay occur with a tendency to distortion, deformity and increased andirregular growth (Fig. 7).The nails of the hands and the feet in Maffucci's syndrome may be
utterly disorganized13' 14 (Fig. 8).Onychogryposis is the cheerful name given to the long, horn-like nail
which may grow when the nails are not trimmed.'5 It may be seen in someother circumstances also, perhaps associated with fungus disease, rarely
.........
FIG. 7. Deformity of the nails in congenital dysplastic angiomatosis.FIG. 8. Distortion and loss of the nails in Maiffucci's svnadrome.
160

NAIL GROWTH AND UNUSUAL FINGERNAILS
with psoriasis which in itself may produce a variety of pittings, scarringsand discolorations of the nails. Dr. Gray and I had an opportunity toobserve one such patient whose astonishingly curved and elongated toe-nails had grown out and arched back. This young woman, after the deathof her father who had regularly trimmed her nails in the past, refused totrim her own toenails or let anyone else do it.'5 (Fig. 9)The nail in arachnodactyly or Marfan's syndrome may be extraordi-
narily long and gracile though it is not really deformed.16 Its resemblanceto the fingernails depicted in journals given over to milady's latest fashionsis clear and both are reminiscent of the elongated hands and nails so oftenportrayed by El Greco.
In Osler's disease, hereditary hemorrhagic telangiectasia, one may finda linear red streak in the fingernail which, even upon careful inspection,looks exactly like a splinter hemorrhage. It has this easily distinguisheddifference, however. It fades out completely or nearly completely when thenail is pressed upon, whereas the splinter hemorrhage does not fade. InOsler's disease one sees much more extensive and spectacular lesions on thepalmar surface of the fingers, the lips, the tongue, the ears, the mucouslining of the nasal septum and elsewhere.One may find sharp transverse lines and bands (Fig. 10) and longitudi-
nal streaks or ridges after trauma has dislocated and messed up the nail
FIG. 9. Onchogryposis.
161
WILLIAM B. BEAN
root (Fig. 11); or they may be caused by a nevus which tends to be moreeasily seen in adult life.A rather fancy sport is seen in the so-called "tennis racquet thumb" in
which there is a bulbous deformity of the distal phalanx of the thumb, thenail being perhaps two or three times as wide as it is long and the lengthbeing only about half what would be expected in a normal nail. Thisanomaly is ordinarily confined to the thumbs, though I have seen oneperson with several fingers affected too. Whoever named it "tennis racquetthumb" must have been thinking of the blunt weapons used in tennis inthe reign of Henry VIII whom, I amn happy to recall, his contemporaryPollard described as "extremely fond of tennis at which game it is theprettiest tlhing in the world to see him play, his fair skin glowing througha shirt of the finest texture."There is a variety of transverse bands whlichl are imiarks recalling the
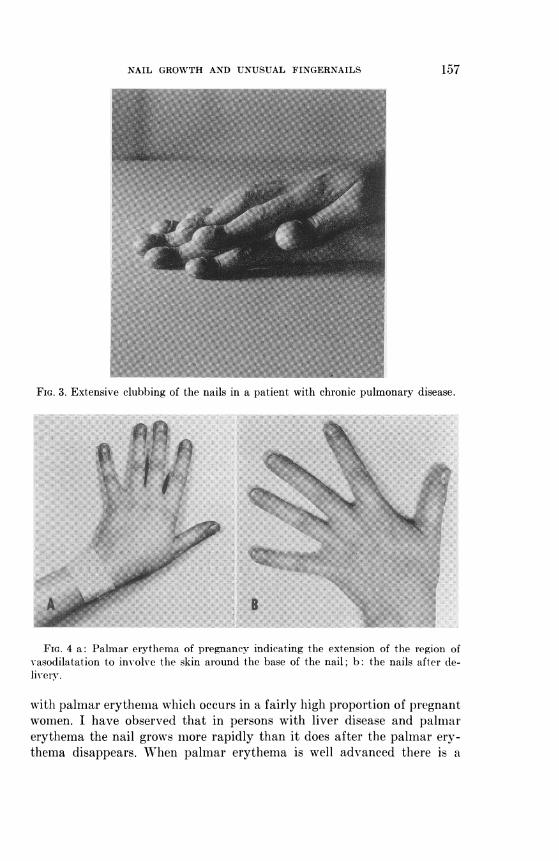
occurrence of some acute crisis, usually of a life-threatening variety. Some-times they follow a severe automiiobile accident, an exsanguinating hemor-rhage, a sharp bout of lobar pneumonia, a myocardial infarct, or a desper-ate operation. One may see a variation on this phenomenon in the nailof a person in whom congenital cyanotic heart disease has been correctedsurgically or in a patient with bacterial endocarditis where the sharp
FIG. 10. Distal half of nail is clubbed. The proximal part is normal and the sharpline marking the alteration is noted in the highlights. Heale(d bacterial endocarditis.
162

NAIL GROWTH AND UNUSUAL FINGERNAILS
break between the outgrowing clubbed nail and the new normiial nail maybe striking (Fig. 10). Transverse lines, the so-called Beau's lines or Mees'lines, have a high specificity when associated with peripheral neuritis. Dr.John Hunt17 recently showed me a patient at the Veterans AdministrationHospital in Iowa City in whom two transverse marks were detected. Hecalled to my attention Wigand's paper on "The Nail Band of Mees inArsenical Polyneuritis."'17 18 The characteristic of this band is that itbegins to emerge six to eight weeks after the poisoning has taken place.If there are two episodes of poisoning there may be two parallel bands,giving a very gaudy effect. This association of bands and peripheral neu-ritis should lead one to look for suicidal, homicidal or accidental arsenicpoisoning. Very rarely thallium may produce somewhat the same effect.In the patient we observed careful investigation disclosed that, owing to ahigh titer of connubial infelicity, this citizen's wife had made an attempt todo him in with arsenic. Having failed the first round, she made anothereffort, so he had two bands across his nail. A further pertinent observationis that growth of the nail has been taking place for approximately twomonths before it first emerges from beneath the cuticle. This correctionin chronometry must be used in estimating the time at which some clinicalcalamity occurred in a person with deep, transverse grooves or breaks inthe nail.
Dr. Lewis January showed me a patient of his whose nails grew out adifferent color after a very serious operation for correction of multiplecongenital cardiac anomalies. The operation itself was not very effectiveand the patient's clinical condition was deteriorating during the period
FIG. 11. A ridge on the nail associated with an anomaly in the groove of the nail.Similar discolored streaks may be caused by a nevus. Sometimes they may be associ-ated with the distortion produced by injury.
163

164 WILLIAM B. BEAN
when the part of his nails which grew out after the operation had a dis-tinctly yellow cast.Among the conditions which the late Dr. Terry observed in his quest for
unusual features about the nails was the red demi-lune or lunula in con-gestive failure. In the ordinary person the half moon has a clear, ground-glass appearance, lighter than the immediately distal portion from whicha darker red halo radiates. In the person with congestive failure who ex-hibits the red half moons, the most intense red color is at the base of thenail as it appears from beneath the cuticle. This fades out so that the sharpedge of the demi-lune remains as a pallid region beyond which the intensityof the redness increases occasionally with a slightly cyanotic tint. I havenot looked for this particular alteration systematically, but I have ob-served that the phenomenon may disappear after the congestive failureis effectively treated and the patient has recovered. It occurs in manypeople with no heart trouble.Bearn and McKusick observed an azure discoloration of the lunula in a
patient with Wilson's disease.20 Though I have looked for this alteration insevaral persons with Wilson's disease I have not found it. My colleague,Dr. Robert Hodges,21 has observed that the fingerprints in persons withWilson's disease, and in some members of their family who have no clinicalstigma of Wilson's disease, are distinguished by a sharp abnormalityin the whole pattern of fingerprints.21
Finally, I call to your attention a monstrous finger, a still unexplainedvariety of localized gigantism.22 Just as the circulation, the temperature,the form and architecture of the underlying bone miiay be perfect butmerely overgrown, so the nail is large but apparently normal. It is wellformed but much bigger than its mate on the opposite hand. I am unawareof any studies that have been done on the rate of growth of nails as theymight be influenced by pachydermatous and proliferative cutaneous as-pects of acromegaly.
THE BENEDICTION
"The oracle of old made it the top of wisdom to know oneself but didnot fix credit to that fragment of self knowledge which enables a man tokeep count of his own pulse."
P. M. LATHAM, fromAphor?isms from Latham-Ed. William B. BeanPrairie PressIowa City, Iowa, 1962
REFERENCES1. RONCHESE, F.: Peculiar Nail Anomalies, A.M.A. Arch. Derm. & Syph. 63: 565-580,
1951.

NAIL GROWTH AND UNUSUAL FINGERNAILS 165
2. BEAN, WILLIAM B.: A Note on Fingernail Growth, J. Invtest. Derm. 20: 27-31, 1953.3. BEAN, WILLIAM B.: 'Nail Growth: A Twenty Year Study, Arch. Ift. Med., in press.4. BEAN, WILLIAm B.: The Medical Utility of the Rare, the Obscure, the Small and
the Trivial, Trans. Amer. Clin. & Climat. Assoc. 72: 38-44, 1961.5. BEAN, WILLIAM B.: The Humanities in Medicine: The Medical and Scientific Sig-
nificance of the Seemingly Small, Trivial and Insignificant, The Groedel Lecture,Am. J. Cardiology 9: 1-11, 1962.
6. SIBINGA, M. S.: Observations on Growth of Fingernails in Health and Disease,Pediatrics 24: 225, 1959.
7. BEAN, W. B.: Vascular Spiders and Related Lesions of the Skin, Charles C Thomas,Springfield, Illinois, 1958.
8. TERRY, R.: White Nails in Hepatic Cirrhosis, T'he Latncet 1: 757-759, 1954.9. MITCHELL, J. C.: A Clinical Study of Leukonychia, Brit. J. Derm. 65: 121-130, 1953.
10. THOMAS, H. M., JR.: Pigment in the Nails During Hyperthyroidism, Bulletin ofthe Johns Hopkins Hospital 52: 315-322, 1933.
11. MULLER, O.: Die Kapillaren der Menschelichen Kbrperoberffische in Gesunden undKranken Tagen, Verlag Ferdinand Enke in Stuttgart, 1922.
12. BOOTHBY, W. M. AND PLUMNIER, W. A.: Diseases of the Thyroid, in Christians Ox-ford Medicine, Chapter XV-A, Oxford University Press, New York.
13. BEAN, WILLIAMi B.: Dyschondroplasia and Hemangiomata (Maffucci's Syndrome),Arch. It. Med. 95: 767-778, 1955.
14. BEAN, WILLIAM B.: Dysehondroplasia and Hemangiomata (Maffucci's Syndrome)II, Arch. Int. Med. 102: 544-549, 1958.
15. GRAY, C. W. AND BEAN, W. B.: A Note on Long Curv-ed Nails, Arch. Derm. 75: 126-128, 1957.
16. BEAN, W. B. AND FLEMIING, J. G.: Arachnodactvlv: Report of a Case ComplicatingPregnancv at Term, Ohio State Mlled. J. 36: 155-160, 1940.
17. HUNT, JOHN: Personal Communication.18. WIGAND, R. D.: The Nail Band of Mees in Arsenical Polyneuritis, M1eanrlchenler
Medizinische WVochenschrift No. 31, Atugust 2, 832-4, 1940.19. TERRY, R.: Red Half-Moons in Cardiac Failure, The Lanicet 2: 842-844, 1954.20. BEARN, A. G. AND McKUSICK, V. A.: Azure Lunulae: An UJnusual Change in the
Fingernails in Two Patients with Hepatolenticular Degeneration (Wilson's Dis-ease), JAMA 166: 903-905, 1958.
21. HODGES, R. E., M.D. AND SInON, J. R., PH.D.: Relationship Between FingerprintPatterns and Wilson's Disease, J. Lab. ct Clin. Mled. 60: 629-640, 1962.
22. BEAN, W. B. AND PETERSON, P. K.: Note on a Monstrouis Finger, Arch. Imit. Med.104: 433-438, 1959.
DISCUSSION
DR. MORTON- HANIBURGER (Cincinnati): I wouild like to ask Dr. Bean a (quiestion withregard to one of his slides. Is the appearance of the douible line in arsenic poisoningsimply an occasional finding or is this a fairly uniform thing?
DR. BEAN: In the first place, I perhaps gave you the wrong impression. This man'swife, I believe, was giving him arsenic in divided doses and I think these two transverselines represent effects of two separate episodes of administration of arsenic, each prob-ably occupying several days-until caution overhauled enthusiasm. As far as I know.,two lines have no significance in terms of indicating arsenic poisoning, indicating onlytwo separate attempts.
DR. STEWART WOLF (Oklahoma City): Doctor Bean, I wonder if you will comment

WILLIAM B. BEAN
with regard to nail growth and hyperthyroidism and also in connection with the bitingof the nails.
DR. BEAN: In hyperthyroidism the nail does grow faster, though the observationsare not very extensive.
Some people with hyperthyroidism bite their nails and biting nails is associated witha faster growth. I have not made any observation myself but persons who bite theirnails have been reported to have a rate of growth between twenty-five and fifty per
cent faster than normal. The nail takes about half of the time to grow out that it doesin the normal person as though the bounty of nature was supplying the extravagantneed.
DR. WORTH DANIELS (Washington, D.C.): With regard to the nails, I would like tosay that I had an interesting experience with an elderly woman who was in failure withauricular fibrillation. I did not suspect hyperthyroidism. However, this lady, whentreated with I-131, made a complete recovery and within a year had a relapse. Further,within three years of her relapse, she had, on her nails, begun to have that dirty littlereversed half moon at the bottom of the nails and so obviously this change in the nailbegins quite rapidly after the beginning of hyperthyroidism.
I would like to ask you one question, Bill. Last summer, one of my grandsons said,"Poppa, why do fingernails grow faster than toenails?" Well, I talked to him aboutthis without too much knowledge. What is your answer to that?
DR. BEAN: I don't know why the toenails grow at all. (Laughter) This is the kind ofquestion that I love to discuss but I have no knowledge. The observation is quite right,that toenails grow only about two-thirds as fast as fingernails. There is some variationin the growth of the different nails in any given individual. Right-handed people havethe nails on the right grow just a little faster than on the left hand; and there are alsoother variations.
I do not have any idea why toenails grow so slowly. I suspect it has to do with eithercirculation or the fact that the ordinary movement and wear and tear of the hand isconsiderably more than the feet. Perhaps this stimulates growth. But I do not know theanswer.
DR. FRANCIS RACKEMANN (Boston): Is there any relation of growth of nails to occu-
pation and in connection with those people whose hands are always warm? I havereference to a dishwasher, who possibly keeps them in warm water as opposed, ofcourse, to the truck driver, whose hands might always be cold?
DR. BEAN: Dr. Rackemann, I don't know whether there is truth in that or not. Isuppose there is.
Dr. Ronchese of Providence has gathered together an extraordinary collectionof occupational works on the nails which identify to those in on the secret what sort oftrade someone is engaged in. For instance, a banjo player has callouses and frayednails where he has been fingering the strings. I don't know whether nails grow fasterin somebody who keeps his hands in warm water or not.
Observations that were made recently by a British naval officer indicated that whilethe crew was in the Mediterranean nails grew at a normal rate. When that same crew
went up to the Arctic for a period of about six or seven weeks, he continued the study.The nail growth of the group slowed down appreciably. When they again came backto the warmer waters growth picked up again. This is the most convincing example ofthe effect of environment.
I suspect that the fact that my own nails do not show seasonal variation is a resultof the fact that I live a sheltered life-central heating in winter and air-conditioning insummer and, therefore, seasons do not mean to me the same thing they might tosomebody living outdoors.
166

NAIL GROWTH AND UNUSUAL FINGERNAILS
DR. THOMAS FINDLEY (Augusta): I believe that Dr. Muercke of Chicago has de-scribed a transv erse white line which he says is characteristic of low albumin content ofthe blood. Will you comment on that?
DR. BEAN: Actually, he has written about the uiniformally white nail rather thanwhite band, and he believes this is connected with hypoalbuminemia. I have made ob-serv-ations which indicate that you certainly need not have anything wrong with serumalbumin to have white nails. I conclude he happened to be looking for it in a group ofpeople who were not very well nourished. I am not sure that there isn't some relation-slip. Perhaps one finds it more often with people with hypoalbuminemia. But I knowthat it may occur without hypoalbuminemia, as a familial or congential affair.
DR. RIc1IARD VILTER (Cincinnati): Apparently the opposite nail formation to club-bing is the spoon that occurs in iron deficiency anemia. This has been very interestingto me. It doesn't occur in this country very often but every once in awhile we dlo seeit. However, once the patient with spoon nail is placed on iron, the nail appears to benormal within ten days to two weeks.
I have explained this to myself and perhaps inadvisedly to others as a replacementof something in the nail bed which shrinks away during the iron deficiency state. Iwould like to have a more erudite explanation from Dr. Bean as to this.
DR. BEAN: I would love to be able to explain it but I can't. I doubt if it is the irondeposit. I do not have the vaguest idea why they should change so rapidly.
DR. WALTER PALMER (Chicago): I have just one final quiestion.Is there any racial (lifference? It seems to me that this is more common in Negroes.
I have reference to the clubbing.DR. BEAN: Well, I really cannot tell you that. Clubbing certainly does occur irrespec-
tive of race and I don't know of any study of incidence in the same kind of disease withreference to race. I am not aware of that although, it may be true.
DR. ROBERT MASON (Baltimore): Perhaps I missed this point, Dr. Bean. Has thedistance between the nail bed and the border changed any in length in this period?This might indicate to you perhaps that the rate of growth may have changed.
DR. BEAN: The length of the nail bed is precisely the same as it was twenty yAearsago. As far as I am personally concerned I hope I have grown in wisdom but I have-riot in length.
167'