Field Actions Science Reports, Special Issue 10
96
Field Actions Science Reports The journal of field actions Special Issue 10 | 2014 Improving Health Among Immigrant Populations Édition électronique URL : http://journals.openedition.org/factsreports/3195 ISSN : 1867-8521 Éditeur Institut Veolia Référence électronique Field Actions Science Reports, Special Issue 10 | 2014, « Improving Health Among Immigrant Populations » [En ligne], mis en ligne le 28 avril 2014, consulté le 20 mars 2020. URL : http:// journals.openedition.org/factsreports/3195 Ce document a été généré automatiquement le 20 mars 2020. Creative Commons Attribution 3.0 License
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Field Actions Science Reports, Special Issue 10
Field Actions Science ReportsThe journal of field actions
Special Issue 10 | 2014Improving Health Among Immigrant Populations
Édition électroniqueURL : http://journals.openedition.org/factsreports/3195ISSN : 1867-8521
ÉditeurInstitut Veolia
Référence électroniqueField Actions Science Reports, Special Issue 10 | 2014, « Improving Health Among ImmigrantPopulations » [En ligne], mis en ligne le 28 avril 2014, consulté le 20 mars 2020. URL : http://journals.openedition.org/factsreports/3195
Ce document a été généré automatiquement le 20 mars 2020.
Creative Commons Attribution 3.0 License

SOMMAIRE
FACTS Special Issue on Migration and HealthIntroductionMarc B. Schenker et Heather E. Riden
Access to Health Care Across Generational Status for Mexican-Origin Immigrants inCaliforniaEva M. Durazo et Steven P. Wallace
Physicians’ knowledge and communication about traditional, complementary andalternative medicine use among Latino patients at Kaiser Permanente, Oakland CAIngrid Bauer et Juan J. Guerra
Does Intergenerational Solidarity Buffer the Negative Effects of Residential Mobility?Evidence for U.S. ChildrenBrian Joseph Gillespie
Demographic and migration-related risk factors for low-level smoking in a farm workingsample of Latinos (the MICASA study)Erik J. Rodriquez, Maria T. Stoecklin-Marois, Tamara E. Hennessy-Burt, Daniel J. Tancredi et Marc B. Schenker
Depression, perceived stress and nervios associated with injury in the MICASA Study, aCalifornia farm worker populationHong Xiao, Maria Stoecklin-Marois, Chin-shang Li, Stephen A. McCurdy et Marc Schenker
Migration & Self-Rated Health: Comparing Occupational Cohorts in California & Spain(MICASA and ITSAL Projects)Emily Sousa, Maria Stoecklin-Marois, Jose Miguel Martinez, Fernando G. Benavides et Marc Schenker
Field Actions Science Reports, Special Issue 10 | 2014
1
FACTS Special Issue on Migrationand HealthIntroduction
Numéro spécial FACTS sur l'immigration et la santé
HECHOS Número especial sobre migración y salud
Marc B. Schenker and Heather E. Riden
1 Migration has, and will continue to be, a natural phenomenon for all living species. In
fact, approximately one seventh of the global population is migrant. The major causes of
global migration are likely to increase in the future – these include environmental
change, political conflict, and demographic and economic disparities. Migration can have
many positive effects, but it also can have negative impacts on the health of the migrant
in the origin, transit and destination locations. As we will see, these negative impacts
include mental health, chronic diseases, and occupational injuries. Despite higher
negative health outcomes compared to native residents, immigrants often have less
access to health care through social systems and their lower income status reduces their
opportunity to purchase services.
2 Study at the intersection of migration and health is highly multidisciplinary, and requires
unique approaches from numerous disciplines and specialties, including epidemiology,
sociology, public health, political science and anthropology. While the multidisciplinary
nature of the field can make it difficult for researchers to ‘talk to each other’ given the
different terminology and methodologies used across disciplines, this feature facilitates
valuable breadth and depth on the subject matter. There is also great opportunity to
better understand and improve the health of immigrant populations through
interdisciplinary collaboration in the study of migration and health. In addition to being a
multidisciplinary field of study, migration and health is topically diverse. Areas of study
span generational migration trends, mental health, human trafficking and refugees,
occupational injury risk, health care access and affordability, and rural to urban
migration – just to name a few. While Latino and Mexican immigrant experiences are
Field Actions Science Reports, Special Issue 10 | 2014
2
largely the focus of this special issue, the topics raised are relevant for immigrants from
other ethnic groups and countries around the world.
3 Topics covered in this special issue include:
1. Health care access across generations among Mexican immigrants;
2. U.S. physician knowledge of culturally specific alternative medicines;
3. Protective factors and residential mobility;
4. Low-level smoking among Latino farmworkers;
5. The association between mental health and occupational injuries in Latino farm workers;
and
6. A comparative investigation of self-reported health status in the U.S. and Spain.
4 Using the lens of the upcoming enactment of the Affordable Care Act (ACA), Eva Durazo
examines the effect of generational status on access to health care among immigrants of
Mexican-origin. She examines access to health care services among first, second, and
third generation Mexican- Americans compared to U.S.-born non-Latino Whites. Durazo
finds generational status to be a significant predictor of health care utilization, with first
and second generation Mexican Americans being significantly less likely than U.S.-born
non-Latino Whites to have health insurance. Third generation Mexican-Americans show
no difference in access to care when compared to U.S.-born non-Latino Whites. She
concludes that the ACA will benefit Mexican-Americans; however, restrictions to
insurance coverage due to immigration status may negatively impact first and second
generation immigrants more significantly. While Durazo focuses on Mexican immigrants,
the ACA is expected to create the opportunity for many immigrants to obtain health
insurance, depending on their immigration status.
5 Many Latinos use some form of traditional, complementary, or alternative medicine
(TCAM) in addition to, or in lieu of, seeking medical care from a physician. Forms of
TCAM include herbal remedies, spiritual practices, massage, and over the counter (OTC)
medication. The use of TCAM is often not reported to physicians. Through questionnaires
completed by physicians in Oakland, California, Ingrid Bauer explores physician
knowledge of Latino beliefs and practices related to TCAM use. Respondents described
their attitude toward TCAM as non-judgmental and many believe they have a good
understanding of Latino health beliefs and folk illnesses. It was more common for
physicians to know and ask about patient use of OTC and prescription medication than
herbal remedies or traditional healers.
6 Looking at migration broadly, as the residential relocation of a family from one locale to
another, Brian Gillespie is interested in whether intergenerational solidarity can help
offset the negative effects of moving on children. The parent-child relationship is found
to significantly buffer the negative educational and behavioral effects of moving on
children. Intergenerational solidarity is a significant predictor of behavior problems after
a residential relocation. While the focus of this study was relocations internal to the U.S.,
the findings suggest the important role of intergenerational solidarity on child academic
and behavioral outcomes for all families. Given the increased pressures and challenges of
transnational migration, parent-child relationships may play an even greater role.
7 Tobacco use is widely accepted as negatively impacting public health and cigarette
smoking is one of the most preventable causes of death in the U.S. Erik Rodriquez
examines low-level smoking (defined as smoking one to five cigarettes per day) among a
cohort of Latino farmworkers in California. Rodriquez finds that among this group,
Field Actions Science Reports, Special Issue 10 | 2014
3
current smokers are more likely to be low-level smokers, rather than smoking 6+
cigarettes per day (CPD). He also notes that while low-level smoking is more common
among Latino immigrants to California, there is some evidence that these smokers may
increase the number of cigarettes they smoke (and the associated health risks) over time.
The differing characteristics of low-level smokers and those who smoke 6+ CPD suggest
targeted smoking cessation interventions may be valuable.
8 Hong Xiao explores the association between mental health and occupational injuries
among Latino agricultural workers. While previous research has documented a link
between depression and agricultural occupational injuries, there has been less focus on
Latino workers – a demographic that makes up a significant portion of this workforce.
Xiao found depression and nervios to be significantly associated with occupational
injuries, while perceived stress and family support were not. This work highlights the
potential role of employers and public health officials to address both mental health
outcomes and occupational injuries hand-in-hand.
9 In a comparative study, Emily Sousa investigates self-reported health in association with
occupational cohorts among Moroccan-born workers in Spain and Mexican-born workers
in the U.S. Despite demographic differences (in age, age at migration, education, and
history of agricultural work), Mexican-women were found to be twice as likely as
Moroccan-born women to report poor health. Similarly, Mexican-born men were more
than three times as likely to report poor health compared to Moroccan-born men. These
findings may be due in part to differences in socio-demographic characteristics,
agricultural work experiences, self-rated health and cultural differences, as well as actual
health differences. Sousa advocates for additional comparative research to explore health
effects across migrant populations.
Summary
10 Immigrants globally have reduced access to health care and social services relative to
native born residents. Public policy and legislation, such as the Affordable Care Act, have
the potential to improve immigrants’ access to care, however the impact will be dictated
in large part by immigration law and eligibility requirements. Those immigrants who are
able to access health care may face barriers due to physicians’ lack of knowledge of
cultural traditions and beliefs. Better education for health providers of immigrants’
beliefs and customs is necessary to facilitate thorough and effective treatment. Mental
health is an emerging area of study relative to migrants and deserves greater attention.
The association between depression and occupational injury, and conversely the
protective impact of intergenerational solidarity and engagement in social groups,
suggest an opportunity to improve health outcomes through mental health interventions.
Given the global nature of migration, with established patterns (such as that between
Latin America and the U.S. or Northern Africa and Europe), comparative studies offer
insight into the shared experiences of migrants as well as the potential to improve
immigrant health via effective strategies employed elsewhere. It is also true that the
central themes of migration and health transcend geography, and much can be learned,
both positive and negative, from examples around the world.
11 Across core areas of education, research, and outreach, the COEMH employs a
multidisciplinary approach to study and understand the complex field of migration and
health. The COEMH’s Research Training Workshop supports and fosters the intellectual
Field Actions Science Reports, Special Issue 10 | 2014
4

growth of future leaders in the field. The papers presented in this special issue exemplify
key areas of inquiry spanning different disciplines and lay the groundwork for future
studies on global trends in migration and health research.
Acknowledgments
12 We wish to acknowledge financial and personnel support from the University of
California Global Health Institute, Center of Expertise on Migration and Health, the
Health Initiative of the Americas and the Migration and Health Research Center that
made possible the Research Training Workshop. We thank faculty members who
participated in the Workshop and provided valuable feedback to student presenters:
Frank Bean, David Lopez Carr, Xochitl Castaneda, Shannon Gleeson, Luis Guarnizo,
Patrick Marius Koga, Alfonso Rodriquez-Lainz, Steve McCurdy, Michael Rodriguez, Marc
Schenker, Steffanie Strathdee, Steve Wallace, and Leslie Wilson. We also thank the
Workshop participants who fostered rich conversations and will lead the research agenda
in migration and health in the future.
ABSTRACTS
Migration is a global phenomenon involving hundreds of millions of people, with major social
and economic impacts on migrants in their countries of origin and destination and on their
communities. In the U.S., California is by far the most affected state by these population
movements. The University of California Global Health Institute (UCGHI), Center of Expertise on
Migration and Health (COEMH) is devoted to systematically studying the health consequences of
global population movements and developing more effective strategies to address them. A key
objective of the Center is to enhance educational opportunities related to migration and health.
To do this, the Center implements graduate education, conducts research on immigrant and
refugee communities, establishes distance education opportunities, and develops transnational
collaborations. These activities provide a rich, real-world environment for training the next
generation of leaders who will respond to emerging health issues related to migration. The
Center’s annual Research Training Workshop is one such activity, resulting in rich discussions,
cross-disciplinary interactions, and invaluable learning opportunities.
This special issue on migration and health stems from the Research Training Workshop held on
June 21-23, 2011, which was organized by COEMH. The workshop brought nineteen graduate
students and postdoctoral fellows together in a multi-disciplinary setting to present their
research and receive constructive feedback from University of California faculty members. Each
paper presented in this special issue represents a unique issue related to migration and health.
L'immigration est un phénomène mondial qui concerne des centaines de millions de personnes,
et qui a des conséquences socio-économiques majeures sur les migrants dans leur pays d'origine
et dans leur pays de destination, et également sur leurs communautés. Aux Etats-Unis, la
Californie est de loin l'état le plus touché par ces mouvements de population. Le COEMH (Center
of Expertise on Migration and Health) de l’UCGHI (University of California Global Health
Institute), est spécialisé dans l'étude systématique des conséquences des mouvements de
Field Actions Science Reports, Special Issue 10 | 2014
5

population sur la santé et dans l'élaboration de stratégies efficaces pour y remédier. L'un des
objectifs clés du Centre est d'accroître les opportunités d'apprentissage liées à l'immigration et à
la santé. Pour cela, le Centre met un œuvre un enseignement supérieur, conduit des recherches
sur les communautés d'immigrants et de réfugiés, crée des opportunités d'enseignement à
distance, et développe des collaborations transnationales. Ces activités constituent un
environnement concret permettant de former la prochaine génération de dirigeants qui devra
faire face aux problèmes de santé émergents liés à l'immigration. Le Research Training Workshop
est l'une des initiatives annuelles du Centre. Il consiste en des débats approfondis, des
interactions pluridisciplinaires et des opportunités d'apprentissage utiles.
Ce numéro spécial consacré à l'immigration et à la santé découle du Research Training Workshop
organisé par le COEMH du 21 au 23 juin 2011. Cet atelier a réuni dix-neuf étudiants diplômés et
post-doctorants dans un contexte pluridisciplinaire qui ont présenté leurs travaux de recherche
et reçu des commentaires constructifs de la part des membres de la faculté de l'Université de
Californie. Chaque article de ce numéro spécial traite d'un sujet spécifique lié à l'immigration et à
la santé.
La migración es un fenómeno de escala mundial que involucra a cientos de millones de personas
y tiene un impacto social y económico tanto en los inmigrantes, como ensus países de origen y
destino, y en las comunidades en las que viven. En los Estados Unidos, el estado más afectado por
estos movimientos de población es California. El Centro de Expertos en Migración y Salud
(COEMH por sus siglas en inglés) del Instituto de Salud Global de la Universidad de California
(UCGHI por sus siglas en inglés) se dedica a realizar estudios sistemáticos sobre las consecuencias
que estos movimientos de población mundial tienen sobre la salud, a fin de crear estrategias
efectivas para abordarlos. Un objetivo clave del Centro es mejorar las oportunidades educativas
relacionadas con la inmigración y la salud. Para ello, el Centro imparte enseñanza universitaria,
realiza estudios sobre las comunidades de inmigrantes y refugiados, crea oportunidades de
educación a distancia y desarrolla colaboraciones transnacionales. Estas actividades
proporcionan un ambiente rico en experiencias reales para formar a la próxima generación de
líderes que darán respuesta a los problemas de salud emergentes relacionados con la migración.
Una de estas oportunidades que el Centro ofrece anualmente es el Taller de Formación e
Investigación que propicia profusos debates, e interacciones interdisciplinarias, además de
valiosas oportunidades de aprendizaje.
Este número especial sobre inmigración y salud nació a partir del Taller de Formación e
Investigación celebrado del 21 al 23 de junio de 2011, organizado por COEMH. El taller reunió a 19
estudiantes de postgrado y becarios posdoctorales en un entorno multidisciplinario dónde
pudieron presentar sus investigaciones y escuchar opiniones constructivas por parte del cuerpo
de docentes de la Universidad de California. Cada trabajo presentado en este número especial
representa un aspecto único relacionado con la migración y la salud.
INDEX
Keywords: Agriculture, Alternative medicine, Farmworker, Health, Immigrant, Latino, Mental
health, Migration, Occupation, Smoking
Field Actions Science Reports, Special Issue 10 | 2014
6
Access to Health Care AcrossGenerational Status for Mexican-Origin Immigrants in CaliforniaAccès aux soins des différentes générations d'immigrants d'origine mexicaine en
Californie
Acceso a cuidados de salud en las distintas generaciones de inmigrantes de
origen mexicano en California
Eva M. Durazo and Steven P. Wallace
Introduction
1 The passage of health care reform in 2010, known as the Patient Protection and
Affordable Care Act (ACA), will potentially extend health insurance coverage to the
majority of the currently uninsured United States (U.S.) population. Latinos, especially
Mexican immigrants, have the highest rates of uninsurance, making the implementation
of the ACA particularly important for this group. Yet many Latinos face a number of
social and economic factors, in addition to health insurance, that shape their ability to
access health services when they need them. California is home to the largest number of
Latinos of Mexican-origin in the country, making it a natural location to investigate the
range of issues they face in access to health care and in assessing the possible
implications of the ACA. Limiting the analysis to one state also avoids the possible
confounding of differences in state health policy with group-specific access issues.
2 A key component of the ACA is to increase insurance coverage through a series of
insurance exchanges and expansion of Medicaid (KFF 2011). In California alone, it is
expected that 1.7 million of the total uninsured will be eligible to participate in the
insurance exchanges and an additional 2.3 million will be newly eligible to receive
Medicaid (Pourat, Kinane and Kominski 2011; Pourat, Martinez and Kominski 2011). Many
Latinos, because of their high rates of uninsurance, stand to benefit from health care
Field Actions Science Reports, Special Issue 10 | 2014
7
reform. In 2007, 30% of Mexican-origin Latinos in California had no health insurance,
compared to 16% of all adults statewide (CHIS 2007). As California begins to prepare for
the implementation of health care reform, there is a need to better understand the health
care access patterns of the Latino population, particularly what factors, in addition to
insurance, affect their access to health care.
3 Immigrants often experience limited access to health care, which is especially true for
Latino immigrants of Mexican-origin (Lara et al. 2005; Morales et al. 2002). Studies find
that access to care increases for Latino immigrants the longer they are in the U.S. (Lara et
al. 2005; Ortega et al. 2007; Wallace et al. 2008). Several reasons may account for the access
barriers Mexican-origin Latinos experience. For example, recent immigrants are more
likely to have jobs that do not provide insurance (Carrasquillo et al. 2000). Latinos, both
immigrant and U.S.-born, have high rates of low socioeconomic status (Lara et al. 2005;
Portes and Rumbaut 2001), which makes it impossible to privately purchase insurance
and can result in other financial barriers, such as not being able to afford high out-of-
pocket costs or losing a day’s wages to take off from work to seek care. Other barriers to
accessing care include a lack of familiarity with the U.S. health care system, limited
English proficiency, or documentation status (Cordasco et al. 2011; Vargas Bustamante et
al. 2010). These obstacles to accessing care can differ in their impact and effect for each
Latino subgroup. Latinos are a heterogeneous group with various demographic
characteristics, such as immigrant status, time in the U.S., nativity, acculturation, and
generational status, that can result in a variety of access patterns and barriers to health
care.
Assimilation Theories and Generational Status
4 Recent research has begun to examine the role of generational status on health and
access (Acevedo-Garcia et al. 2010; Afable-Munsuz et al. 2010; Burgos et al. 2005; Popkin
and Udry 1998; Ta, Holk and Gee 2010). Generational status moves beyond the foreign-
born versus U.S.-born dichotomy found in most research by disaggregating the U.S.-born
into second, third and later generations since immigration. Immigrant health research
typically focuses on the first (immigrant) generation, although there is a growing
attention to the second generation (immigrants’ U.S.-born children) as well. Few studies
examine the third generation, limiting our understanding of the impact of immigrant
integration into mainstream society on health and access. In order to examine
generational status and its association with access to care, this study focuses on Mexican
Americans, which make up 83% of the Latino population in California (U.S. Census 2010)
and have an established history in the United States with several generations in
California (Pew Hispanic 2011).
5 Traditional assimilation theory would posit that by the third generation the economic
and social integration of Mexicans would make them mostly indistinguishable from the
larger non-Latino population (Portes and Rumbaut 2001; Portes and Zhou 1998). However
continued immigration from Mexico, the proximity of Mexico to the U.S., and the
availability of resources and opportunities might create divergent patterns (Portes and
Rumbaut 2001; Portes and Zhou 1998; Telles and Ortiz 2008). Segmented assimilation
theory identifies alternate paths in the assimilation processes of Mexicans and other
racial minority immigrant groups. A first path follows the classical route to assimilation
in which immigrants are integrated into the mainstream and lose their ethnic identity,
Field Actions Science Reports, Special Issue 10 | 2014
8
usually by the third generation; a second path involves upward economic mobility while
also maintaining the group’s ethnic identity (Portes and Zhou 1998). An alternative
course, downward assimilation, leads in the opposite direction in which the immigrant
group retains an ethnic identity and faces barriers that cause socioeconomic stagnation
and limited social mobility, resulting in high rates of poverty (Portes and Zhou 1998).
6 Examining Latinos by generational status allows for a better understanding of the access
of U.S.-born Latinos, as well as the level of integration into U.S. society for immigrants
and the later generations. Generational status may serve as a proxy for the unique racial
and immigrant experiences of Latinos, taking into consideration the larger social context
that can facilitate or impede integration into the mainstream over time. Each generation
may vary on several characteristics, such as in their levels of education, economic status,
racialized experiences, place of residence, current and potential social mobility and social
integration levels, all of which can impact access to health services.
7 We draw on immigrant health research and sociological assimilation theories to better
understand health care access for Mexican-origin individuals by generational status.
Generational status is conceptualized as the number of generations the respondent is
removed from the time of immigration (Rumbaut 2004; Telles and Ortiz 2008). Following
Portes and Rumbaut (2001), this study defines first generation Mexicans as individuals
born in Mexico currently living in the U.S., second generation Mexican Americans as U.S.-
born individuals with at least one foreign-born parent, and third generation Mexican
Americans as U.S.-born individuals with both parents born in the U.S. With cross-
sectional data we are limited to examining generation since immigration as cohorts, as
opposed to generations within families, which would directly link generation from parent
to child to grandchild. This is an important distinction because although with generation
since immigration we examine different generations, those cohorts have similar
historical experiences (Rumbaut 2004; Telles and Ortiz 2008). Since we are not sampling
by families we cannot measure intergenerational change, but instead examine changes by
cohorts.
8 This study has two aims. First, to examine how access to health care services for first,
second, and third generation Mexican Americans compares to that of U.S.-born non-
Latino Whites (hereafter referred to at U.S.-born Whites). Using U.S.-born Whites as a
benchmark, the study observes how access measures differ for each Mexican generation.
Secondly, we identify if there is improvement in access to care with each passing
generation, and if so, if improvements in access of the later Mexican generations leads to
an equalizing of access.
Methods
Data
9 The study uses the 2007 California Health Interview Survey (CHIS) public use file. CHIS is a
random-digit-dial telephone survey of all counties in California conducted every two
years. A small sample of cell phone owners with no landline are also surveyed. A complex
sampling design, which includes geographic-stratification and oversampling, ensures that
small counties and minority populations are represented in the sample (CHIS
Methodology 2009). CHIS data is collected in English, Spanish, and several Asian
languages. The final sample consists of 51,048 adults, of which 825 are cell phone owners
Field Actions Science Reports, Special Issue 10 | 2014
9
without a landline. The 2007 CHIS has a screener completion rate of 35.5%, and 52.8% of
those screened completed a full interview. These rates are comparable to similar
telephone surveys (CHIS Methodology 2009).
Sample
10 Analysis of this study is limited to adults ages 18 and over who identify as Latino of
Mexican origin (n=7,001) and U.S.-born non-Latino Whites (n=30,615). Thus we exclude all
other Latino subgroups, other racial groups and foreign-born non-Latino Whites. U.S.-
born Whites serve as the comparison group since they are the dominant population and
generally experience the least barriers to access and use of care. The U.S.-born White
reference group consists of those born in the U.S., excluding the foreign-born generation,
which may have some barriers to access because of their immigrant status.
Dependent Variables
11 The study focuses on three dependent variables, all of which are yes/no dichotomous
measures. Access to care outcomes include the following: being insured all or part of the
past year, visited the doctor in the past year, and visited the emergency room (ER) in the
past year. These measures have previously been used in the literature to measure access
and use of health care (Ortega et al. 2007; Vargas Bustamante et al. 2009; Weineck et al.
2000). As a measure of access, having insurance is an enabling factor that, when available,
can facilitate the use of health care services (Anderson 1995; Spatz et al. 2010). Seeing a
doctor in the past year measures the ability to access and use health services, and can
increase the likelihood of receiving preventive care as well as the timely treatment of
chronic diseases. Visiting the ER is a measure of access to health services, albeit an
undesired use because of the high costs and usual delay of care related with ER visits.
Alternatively, use of the ER can be an indicator of poor access to primary care resulting
from an inability to navigate the health care system.It can also be an indicator of poorer
health, resulting in increased use of emergency services (Ku and Matani 2001). For this
study, we expect higher levels of access to correspond with having insurance, having had
a doctor visit, and visiting the ER.
Independent Variables
12 The main predictor, generational status, is constructed from a combination of variables
including self-reported race/ethnicity, nativity, and parent nativity. Respondents must
have self-identified as Latino of Mexican-origin or U.S.-born White. Generational status
was then assigned based on the respondents’ and their parents’ place of birth. The
resulting generation variable consists of four categories that distinguish between the
following: U.S.-born Whites (reference); third generation Mexican Americans who are
born in the U.S. and identify as Latino of Mexican origin with both parents born in the
U.S.; second generation Mexican Americans who are born in the U.S. and identify as
Latino of Mexican origin with at least one foreign born parent; and first generation
Mexicans who are born in Mexico and identify as Latino of Mexican origin. There is no
way of distinguishing the third generation from later generations, thus this category
includes third and subsequent generation Mexican Americans. In addition, since coding
Field Actions Science Reports, Special Issue 10 | 2014
10

generational status relies on self-identity, it is likely that some third and higher
generation Mexican American no longer identify as Mexican Americans and are therefore
missing from the analysis.
13 A series of covariates are included in the logistic regression model in order to control for
factors the literature indicates impact access and use of health care services (Anderson
1995; Weinick et al. 2000). These variables include: gender, age, marital status, education
level, income, insurance status, and self-reported health status. Having health insurance
all or part of the past year is used as a covariate for all outcomes, except when insurance
is the dependent variable. Insurance can be a facilitator to health care and those with
insurance will be expected to have better access and increased use of services (Anderson
1995). Socioeconomic status, measured here by education, income level, and insurance
status, is an important factor to consider for Mexican-origin individuals because research
finds differences in socioeconomic status by generational status (Acevedo-Garcia et al.
2010; Telles and Ortiz 2008). The literature identifies additional factors that impact
access, such as language or citizenship status, that are not included in the final model
because of the lack of variation in the second and third generations. While
documentation status may be pertinent to the access of health care for first generation
immigrants, this information is not available when using public use files.
Statistical Analyses
14 Analysis begins with descriptive statistics of all variables. Percentages for the dependent
and independent categorical variables are presented for each Mexican-origin generation
and U.S.-born Whites. Multivariate analysis using binomial logistic regression is
conducted on each of the three access outcome variables in order to determine whether
each Mexican generational status differs from U.S.-born Whites. For each dependent
variable, two models are created. The first model establishes the bivariate association
between generational status and the access outcome variable. The second model includes
the covariates previously listed in order to examine how the generation variable changes
once controlling for demographic and socioeconomic differences in the population.
STATA software version 11.2 was used for all analyses (Stata 2009). The analysis uses the
probability and replicate weights provided by CHIS in order to account for the complex
sampling design in calculating standard errors (CHIS Methodology 2009).
Results
15 Table 1 provides descriptive statistics for the outcome and independent variables for the
total sample and by generational status. About twenty percent of the total sample of
adults has poor access to health care. One in five of the total sample does not have health
insurance, about 18% have not seen a doctor in the past year, and 18% have had an ER
visit in the past year. First generation Mexicans generally have the lowest rates of access,
with increasing rates for subsequent generations. U.S.-born Whites have the highest rate
of access. Access rates for second and third generation Mexican Americans fall in
between, with the third generation reaching similar rates to that of U.S.-born Whites.
Field Actions Science Reports, Special Issue 10 | 2014
11
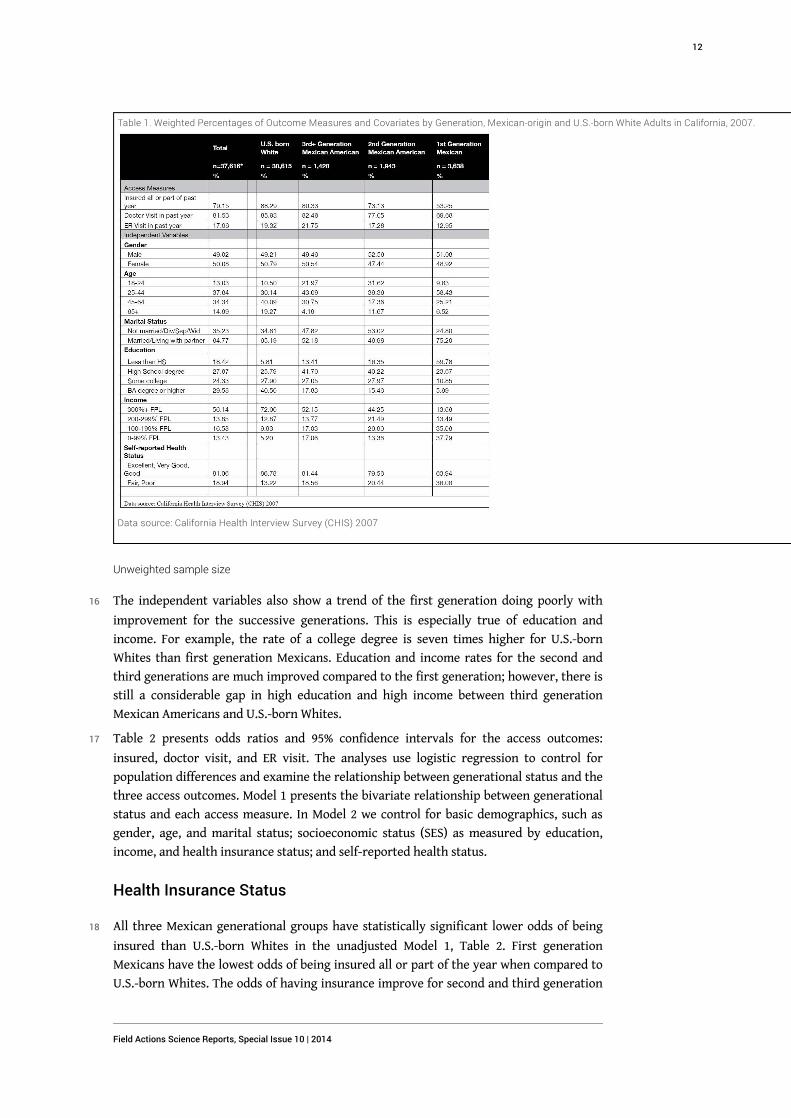
Table 1. Weighted Percentages of Outcome Measures and Covariates by Generation, Mexican-origin and U.S.-born White Adults in California, 2007.
Data source: California Health Interview Survey (CHIS) 2007
Unweighted sample size
16 The independent variables also show a trend of the first generation doing poorly with
improvement for the successive generations. This is especially true of education and
income. For example, the rate of a college degree is seven times higher for U.S.-born
Whites than first generation Mexicans. Education and income rates for the second and
third generations are much improved compared to the first generation; however, there is
still a considerable gap in high education and high income between third generation
Mexican Americans and U.S.-born Whites.
17 Table 2 presents odds ratios and 95% confidence intervals for the access outcomes:
insured, doctor visit, and ER visit. The analyses use logistic regression to control for
population differences and examine the relationship between generational status and the
three access outcomes. Model 1 presents the bivariate relationship between generational
status and each access measure. In Model 2 we control for basic demographics, such as
gender, age, and marital status; socioeconomic status (SES) as measured by education,
income, and health insurance status; and self-reported health status.
Health Insurance Status
18 All three Mexican generational groups have statistically significant lower odds of being
insured than U.S.-born Whites in the unadjusted Model 1, Table 2. First generation
Mexicans have the lowest odds of being insured all or part of the year when compared to
U.S.-born Whites. The odds of having insurance improve for second and third generation
Field Actions Science Reports, Special Issue 10 | 2014
12
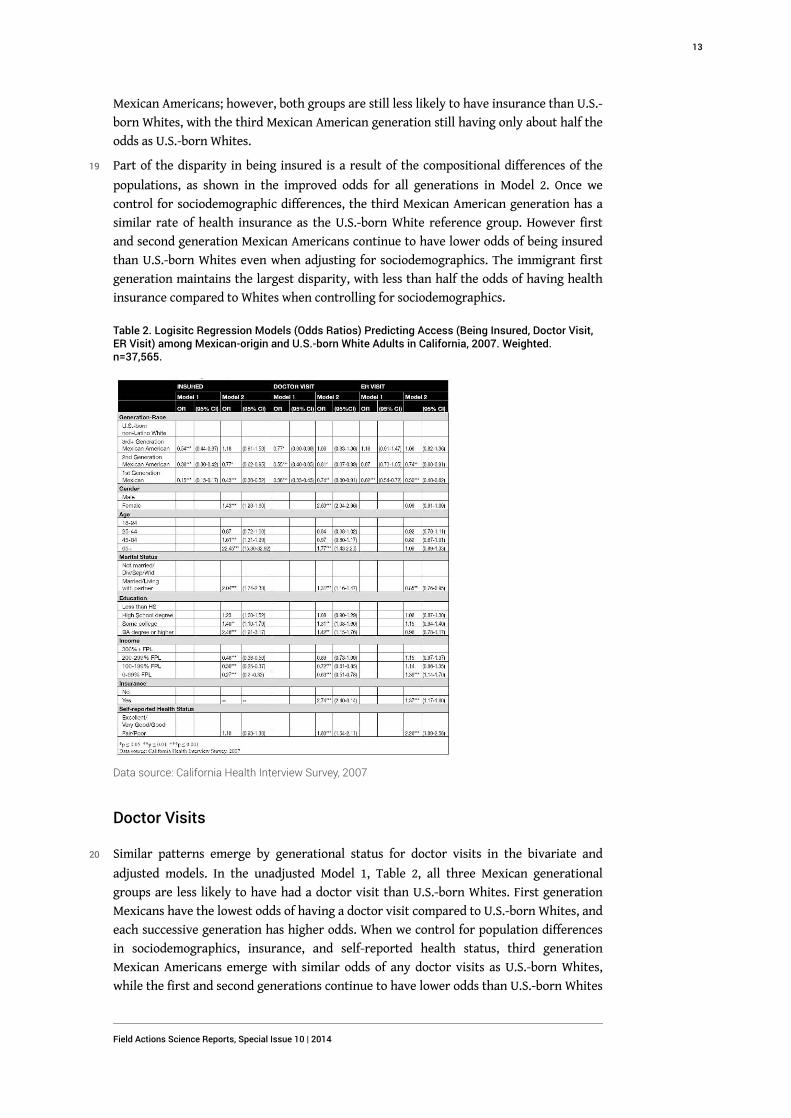
Mexican Americans; however, both groups are still less likely to have insurance than U.S.-
born Whites, with the third Mexican American generation still having only about half the
odds as U.S.-born Whites.
19 Part of the disparity in being insured is a result of the compositional differences of the
populations, as shown in the improved odds for all generations in Model 2. Once we
control for sociodemographic differences, the third Mexican American generation has a
similar rate of health insurance as the U.S.-born White reference group. However first
and second generation Mexican Americans continue to have lower odds of being insured
than U.S.-born Whites even when adjusting for sociodemographics. The immigrant first
generation maintains the largest disparity, with less than half the odds of having health
insurance compared to Whites when controlling for sociodemographics.
Table 2. Logisitc Regression Models (Odds Ratios) Predicting Access (Being Insured, Doctor Visit,ER Visit) among Mexican-origin and U.S.-born White Adults in California, 2007. Weighted.n=37,565.
Data source: California Health Interview Survey, 2007
Doctor Visits
20 Similar patterns emerge by generational status for doctor visits in the bivariate and
adjusted models. In the unadjusted Model 1, Table 2, all three Mexican generational
groups are less likely to have had a doctor visit than U.S.-born Whites. First generation
Mexicans have the lowest odds of having a doctor visit compared to U.S.-born Whites, and
each successive generation has higher odds. When we control for population differences
in sociodemographics, insurance, and self-reported health status, third generation
Mexican Americans emerge with similar odds of any doctor visits as U.S.-born Whites,
while the first and second generations continue to have lower odds than U.S.-born Whites
Field Actions Science Reports, Special Issue 10 | 2014
13
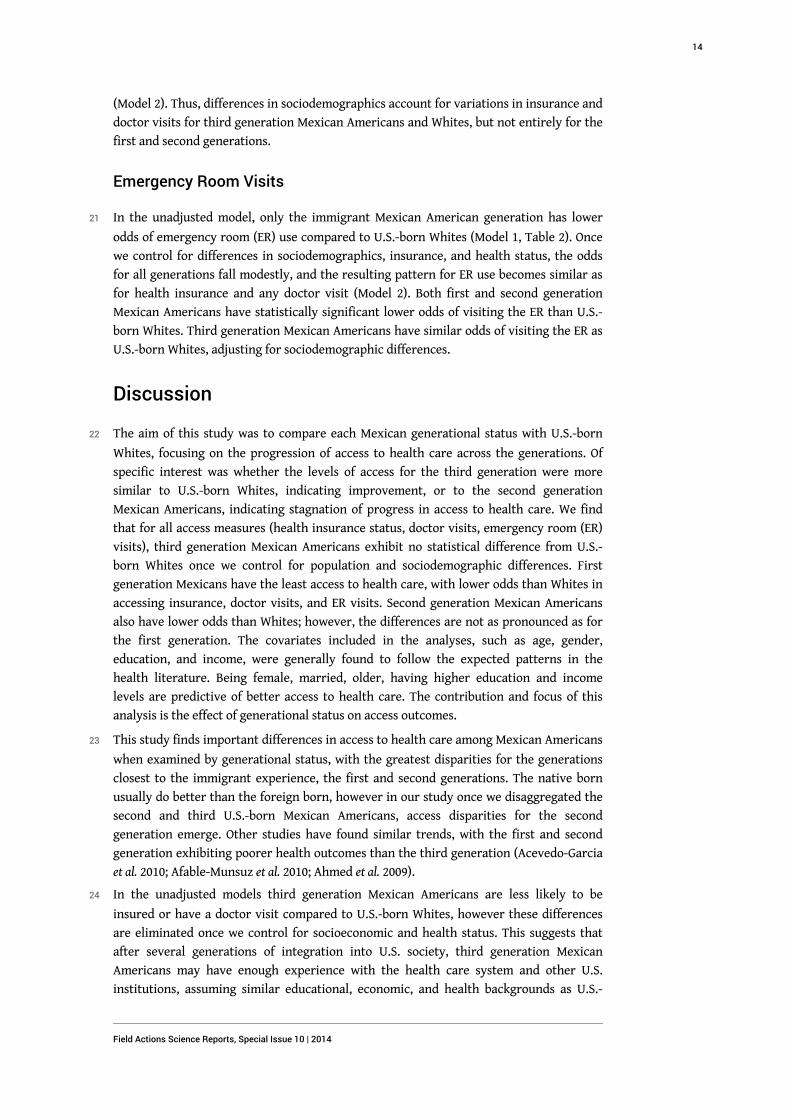
(Model 2). Thus, differences in sociodemographics account for variations in insurance and
doctor visits for third generation Mexican Americans and Whites, but not entirely for the
first and second generations.
Emergency Room Visits
21 In the unadjusted model, only the immigrant Mexican American generation has lower
odds of emergency room (ER) use compared to U.S.-born Whites (Model 1, Table 2). Once
we control for differences in sociodemographics, insurance, and health status, the odds
for all generations fall modestly, and the resulting pattern for ER use becomes similar as
for health insurance and any doctor visit (Model 2). Both first and second generation
Mexican Americans have statistically significant lower odds of visiting the ER than U.S.-
born Whites. Third generation Mexican Americans have similar odds of visiting the ER as
U.S.-born Whites, adjusting for sociodemographic differences.
Discussion
22 The aim of this study was to compare each Mexican generational status with U.S.-born
Whites, focusing on the progression of access to health care across the generations. Of
specific interest was whether the levels of access for the third generation were more
similar to U.S.-born Whites, indicating improvement, or to the second generation
Mexican Americans, indicating stagnation of progress in access to health care. We find
that for all access measures (health insurance status, doctor visits, emergency room (ER)
visits), third generation Mexican Americans exhibit no statistical difference from U.S.-
born Whites once we control for population and sociodemographic differences. First
generation Mexicans have the least access to health care, with lower odds than Whites in
accessing insurance, doctor visits, and ER visits. Second generation Mexican Americans
also have lower odds than Whites; however, the differences are not as pronounced as for
the first generation. The covariates included in the analyses, such as age, gender,
education, and income, were generally found to follow the expected patterns in the
health literature. Being female, married, older, having higher education and income
levels are predictive of better access to health care. The contribution and focus of this
analysis is the effect of generational status on access outcomes.
23 This study finds important differences in access to health care among Mexican Americans
when examined by generational status, with the greatest disparities for the generations
closest to the immigrant experience, the first and second generations. The native born
usually do better than the foreign born, however in our study once we disaggregated the
second and third U.S.-born Mexican Americans, access disparities for the second
generation emerge. Other studies have found similar trends, with the first and second
generation exhibiting poorer health outcomes than the third generation (Acevedo-Garcia
et al. 2010; Afable-Munsuz et al. 2010; Ahmed et al. 2009).
24 In the unadjusted models third generation Mexican Americans are less likely to be
insured or have a doctor visit compared to U.S.-born Whites, however these differences
are eliminated once we control for socioeconomic and health status. This suggests that
after several generations of integration into U.S. society, third generation Mexican
Americans may have enough experience with the health care system and other U.S.
institutions, assuming similar educational, economic, and health backgrounds as U.S.-
Field Actions Science Reports, Special Issue 10 | 2014
14

born Whites. The third generation may have more resources and experiences than the
first or second generations that allow them to better navigate the health care system,
advantages that come from being born in the U.S. and having U.S. born parents. However,
persisting health access barriers between third generation Mexican Americans and U.S.-
born Whites at the bivariate level are in part the result of continued educational and
income disparities between the two groups, such as the poverty rate that is three times
higher for third generation Mexican Americans than for U.S.-born Whites.
25 We also considered differences in age cohorts between Mexican-origin Latinos and U.S.-
born Whites as a possible source of the observed disparities in access to care. Second and
third generation Mexican Americans are younger with a smaller older adult population
compared to U.S.-born Whites, thus we performed a sensitivity analysis restricting the
groups to ages 18-64. Differences in doctor visits observed between second and third
generation Mexican Americans and Whites disappear after restricting the age and
adjusting for sociodemographics. Thus, differences in doctor visits may be driven in part
by the size of the older U.S.-born White population. However, excluding ages 65 and over
from the analysis had little impact on the patterns for insurance status and ER visits,
suggesting that there are differences between U.S.-born Whites and Mexican Americans
by generation not accounted by age variations in the population.
26 While controlling for socioeconomic status and other population variations eliminates
differences in access for third generation Mexican Americans and U.S.-born Whites in our
study, disparities in other related dimensions continue to exist. Research has observed
educational and occupational segregation and discrimination in U.S. institutions against
all Latinos, regardless of immigration status or generation (Portes and Zhou 1993; Telles
and Ortiz 2008; Williams 1999). These observations are supported by legal findings that
legislation at the state level allowing police to inquire about immigration status leads to
racial profiling and discrimination (Bauer 2009; Cervantes et al. 1995; Sabia 2010). A
variety of reasons explain the bivariate disparities in health care access and
socioeconomics between Mexican Americans of all generations and U.S.-born Whites. In
the short term, the ACA’s expansion of health insurance should significantly reduce the
health care access disparities between third generation Mexican Americans and U.S.-born
Whites; in the long-term, it is important to improve educational and occupational equity
to remove the underlying basis for the access disparities for Latinos of all generations.
27 This study finds that those closer to the immigrant experience, first generation
immigrants and the second generation children of immigrants, have worse access to
health care compared to U.S.-born Whites, even after controlling for demographics and
socioeconomic status. Our findings suggest that generational status may be serving as a
proxy for the broader social and structural barriers that Latinos face in accessing health
care. Specifically, first generation Mexicans may face obstacles in accessing health care
due to citizenship and documentation status, language barriers, and limited skills in
navigating the U.S. health care system (Cordasco et al. 2011; Kandula et al. 2007; Vargas
Bustamante et al. 2010). Structural factors, such as where immigrants live and the
availability of quality health services, can also be barriers in accessing health care
(Cordasco et al. 2011; Osypuk et al. 2009). Fear of U.S. institutions, in particular of the
health care system, is another potential obstacle to accessing care for undocumented first
generation Mexican immigrants and all Latinos in general. These fears may have been
heightened as policy discussions for the ACA often coincide with increased anti-
immigrant sentiment (Galarneau 2011). Few studies have examined the actual impact of
Field Actions Science Reports, Special Issue 10 | 2014
15

fear and anti-immigrant policy on health care access, and those that have find less use of
services or are inconclusive (Berk and Schur 2001; Spetz et al. 2000). While the ACA may
provide insurance to many immigrants in California, several other factors will continue
to impact their health care access and use. Undocumented immigrants, the most
vulnerable among Latino immigrants and those least likely to have health insurance
(Vargas Bustamante et al. 2010) will not be able to participate in the ACA, which may
create or further intensify barriers for the undocumented and their families. Our study is
unable to directly account for many of these social and structural factors that affect
health care access for immigrants, nevertheless generational status may serve to broadly
capture the barriers Mexican Americans experience.
28 Second generation Mexican Americans have a demographic and socioeconomic profile
that is similar to that of the third generation, but the second generation follow the access
patterns of the first generation with lower odds of being insured, having a doctor visit, or
having an ER visit compared to U.S.-born Whites. What might explain the differences in
access between second generation Mexican Americans and U.S.-born Whites, considering
that the second generation should not have the citizenship or language barriers that the
first generation might encounter? Although this study accounts for education and income
differences, socioeconomic status may impact the second generation in such a way that
those with low education and low incomes are at a greater disadvantage when accessing
and using health care than those within the second generation with higher incomes and
education. Other studies have found varying socioeconomic gradients between
generations, which may not have been captured in this study (Acevedo-Garcia et al. 2010;
Ahmed et al. 2009).
29 There are additional factors that impact access to health care for the second generation
that we have not been able to address in our study. These factors may include residence
in segregated neighborhoods, experiences with discrimination, or poor quality of care
(Ahmed et al. 2009; Smedley et al. 2003; Viruell-Fuentes 2007). Additionally, considering
segmented assimilation theory the second generation may be experiencing limited social
mobility, which would impact their educational and occupational opportunities. A
segmented labor force may place the second generation at a disadvantage with low-
paying jobs with minimal health benefits or sick leave (Valenzuela Jr. and Gonzalez 2000),
discouraging them from seeking care. Residence in segregated neighborhoods can result
in less availability of services or poorer quality of care for the second generation,
deterring access to services (Acevedo-Garcia et al. 2003). Having an immigrant parent may
impact the social and human capital of the second generation (Portes and Rumbaut 2001),
resulting in limited knowledge or resources in navigating the health care system. Future
studies should consider the social context for the second generation and the experiences
that may be impacting their access to care. Using a life course perspective may be
especially useful for the second generation as barriers experienced in early life as the
children of immigrants, such as limited socioeconomic status or limited family and
neighborhood resources, may last into adulthood and impact access to health care.
Limitations and Strengths
30 The results of this study should be considered within the context of several limitations.
The CHIS is a cross-sectional survey, which limits the establishment of a causal
relationship between generational status and access to health care measures. There may
Field Actions Science Reports, Special Issue 10 | 2014
16
be other variables that we have not considered that confound the possible effect of
generation on access to health care. Additionally, all access measures are self-reported,
leaving the dependent variables prone to historical inaccuracies and response bias. The
findings are specific to California, which has historical and policy differences from other
states that might result in varying access patterns. There may also be third generation
Mexican Americans that no longer identify with being of Mexican or Latino descent,
which would result in excluding the most assimilated from the analysis. However,
excluding the most assimilated from the study strengthens our findings of the third
generation having access patterns similar to U.S.-born Whites, even without those who
are most assimilated.
31 Despite the limitations, this is one of a few studies to examine access to care and the role
of generational status among Mexican Americans, specifically including the third
generation. While generational status is not a new dimension of research in immigrant
health, this study is able to further disaggregate the U.S.-born population by generation.
Additionally, the study is based on the California Mexican-origin population, a state with
one of the largest concentration of Latinos. Results from this study may anticipate the
health trends for Latinos at the national level.
Policy Recommendations and Conclusion
32 This study finds that those closest to the immigrant experience, specifically Mexican
immigrants and U.S.-born Mexican Americans of immigrant parents, have the lowest
rates of health insurance and utilization of health care. There are several policy
recommendations that can be enacted immediately and over the long term to address the
access barriers of these populations. The Affordable Care Act (ACA) presents a unique
opportunity to extend health insurance coverage to an unprecedented number of
individuals. Estimates predict that between 1.8 and 2.7 million individuals will be able to
receive health insurance through the ACA in California; however several groups will still
remain uninsured, for example segments of the Latino population or some Californians
with limited English abilities (Lucia et al. 2012). Specific strategies and policies can be
implemented now in order for the ACA to incorporate the largest amount of eligible
individuals. Based on our findings, third generation Mexican Americans may benefit the
most from health care reform since the elimination of socioeconomic barriers improves
health insurance status and access to care most for this group. First and second
generation Mexican Americans may not fare as well as the third generation and require
additional assistance to improve access.
33 Most significantly, access may be improved through the ACA with focused and increased
outreach to the Mexican American groups with the least access, the first and second
generations. Reaching out to these groups and informing them of ways in which they may
be eligible for the ACA can increase access to health insurance. Outreach will need to be
available in both English and Spanish and dispel any fears for immigrants involved with
the residency process or those belonging to mixed families (Gomez and Artiaga 2011). In
addition to education and outreach for ACA eligibility, issues of navigating the health
care system will also need to be addressed. Mexican immigrants may be unfamiliar with
the health care system in the U.S. and Mexican Americans born to immigrant parents
may lack the knowledge and capital if they were not exposed to the health care system
across their lifespan.
Field Actions Science Reports, Special Issue 10 | 2014
17
34 Outreach and education is critical, but just as important is who is providing the
information. Established ethnic organizations and trusted community programs will be
instrumental in providing ACA outreach for immigrants and second generation Mexican
Americans, as well as with improving navigation of the health care system (Gomez and
Artiaga 2011). Community health workers, or promotoras, have long been used in the
Latino population to improve outreach and program implementation because of the trust
and cultural capacity brought by the community health workers (Elder et al. 2009; Swider
2002). Use of community organizations will be important to increase the number of
applicants to the ACA and to increase the use of appropriate health care utilization by
first and second generation Mexican Americans.
35 Also, as with any recent policy implementation, the application process can be new and
confusing. Streamlining the application process and simplifying the documentation
needed to apply, especially for Medicaid, can facilitate access to health insurance for first
and second Mexican Americans, and all eligible individuals (Gomez and Artiaga 2011).
While community organization can provide assistance and set up processes that work on
the ground, state and federal governments will need to ensure that ACA information is
available and provided in accessible formats for all individuals, including for those with
limited education levels or with limited English language abilities. Additionally, support
for safety net clinics will be critical to provide continued access to low-income and racial/
ethnic minority populations (Andrulis and Siddiqui 2011).
36 In addition to the implementation of the ACA, other policies will be needed over time to
promote equity of access for first and second generation Mexican Americans. For the
generations closest to immigration, additional factors beyond health insurance and
socioeconomic status impact access to health care. Addressing quality of care,
discrimination within the health care system, and educating first and second generation
Mexican Americans of their eligibility to benefits and health programs may improve
health care access in the immediate term. Improving educational and occupational
opportunities for immigrants and their children will be critical to improving health and
access for current and future generations.
Conclusion
37 We find generational status to be a significant predictor to accessing health care services.
Specifically, first and second generation Mexican Americans are less likely to have
insurance, see a doctor, and visit the ER than U.S.-born Whites. Despite the differences in
access by generational status, policies rarely address the unique factors that distinguish
the Latino immigrant and U.S.-born population. This study finds that even when
adjusting for sociodemographics, generational status remained a predictor for health
insurance, limited doctor and ER visits. Further research into the unique experiences of
each generation, especially the second generation, can provide a better understanding as
to why some groups continue to face obstacles in accessing health care. However several
strategies can be implemented to address the access barriers of first and second
generation Mexican Americans, in particular when considering the implementation of
Affordable Care Act.
Field Actions Science Reports, Special Issue 10 | 2014
18
Acknowledgements
38 We thank Vilma Ortiz for her valuable comments to an early version of the paper. Helpful
comments were also provided by Xóchitl Castañeda and Shannon Gleeson.
BIBLIOGRAPHY
Acevedo-Garcia, D., Bates, L. M., Osypuk, T. L., and N. McArdle (2010), “The Effect of Immigrant
Generation and Duration on Self-rated Health Among U.S. Adults 2003-2007”, Social Science &
Medicine, Vol. 71, pp.1161-1172.
Acevedo-Garcia, D., Lochner, K. A., Osypuk, T. L., and S. V. Subramanian (2003), “Future
Directions in Residential Segregation and Health Research: A Multilevel Approach”, American
Journal of Public Health, Vol. 93, No. 2, pp. 215-221.
Afable-Munsuz A., Ponce, N. A., Rodriguez, M., and E. J. Perez-Stable (2010), “Immigrant
Generation and Physical Activity Among Mexican, Chinese & Filipino Adults in the US.” Social
Science & Medicine, Vol. 70, No. 12, pp. 1997-2005.
Ahmed, A. T., Quinn, V. P., Caan, B., Sternfield, B., Haque, R., and S. K. Van Den Eeden (2009),
“Generational Status and Duration of Residence Predict Diabetes Prevalence Among Latinos: the
California Men's Health Study”, BMC Public Health, Vol. 9, 392.
Anderson, R.M. (1995), “Revisiting the Behavioral Model and Access to Medical Care: Does it
Matter?”, Journal of Health Social Behavior, Vol. 36, pp. 1-10.
Andrulis, D. P., and N. J. Siddiqui (2011), “Health Reform Holds Both Risks and Rewards for Safety-
Net Providers and Racially and Ethnically Diverse Patients”, Health Affairs, Vol. 30, No. 10, pp.
1830-1836.
Bauer, M. (2009), “Under Siege: Life for Low-Income Latinos in the South”, The Southern Poverty
Law Center, accessed February 2012 at www.splcenter.org/sites/default/files/downloads/
UnderSiege.pdf.
Berk, M. and C. Schur (2001), “The Effect of Fear on Access to Care Among Undocumented Latino
Immigrants”, Journal of Immigrant Health, Vol. 3, No. 3, pp. 151-156.
Burgos, A. E., Schetzina, K. E., Dixon, L. B., and F. S. Mendoza (2005), “Importance of Generational
Status in Examining Access To and Utilization of Health Care Services by Mexican American
Children”,Pediatrics, Vol. 115, No. 3, pp. e322-30.
California Health Interview Survey (2007), accessed on August 2011 at www.askchis.com.
California Health Interview Survey (2009), “CHIS 2007 Methodology Series: Report 4 – Response
Rate”, Los Angeles, CA: UCLA Center for Health Policy Research, accessed August 2011 at
www.askchis.com/pdf/CHIS2007_method4.pdf.
Field Actions Science Reports, Special Issue 10 | 2014
19
Carrasquillo, O., Carrasquillo, A., and S. Shea (2000), “Health Insurance Coverage of Immigrants
Living in the United States: Differences by Citizenship Status and Country of Origin.” American
Journal of Public Health, Vol. 90, No. 6, pp. 917-923.
Cervantes, N., Khokha, S., and B. Murray (1995), “Hate Unleashed: Los Angeles in the Aftermath of
Proposition 187”, Chicano-Latino Law Review, Vol. 17, No. 1, pp. 1-23, http://heinonline.org/HOL/
Page?collection=journals&handle=hein.journals/chiclat17&type=Image&id=13.
Cordasco, K. M., Ponce, N. A., Gatchell, M. S., Traudt, B., and J. J. Escarce (2011), “English Language
Proficiency and Geographical Proximity to a Safety Net Clinic as a Predictor of Health Care
Access”, Journal of Immigrant and Minority Health, Vol. 13, No. 2, pp. 260-267.
Elder, J. P., Ayala, G. X., Parra-Median, D., and G. A. Talavera (2009), “Health Communication in
the Latino Community: Issues and Approaches”, The Annual Review of Public Health, Vol. 30, pp.
227-251.
Galarneau, C (2011), “Still Missing: Undocumented Immigrants in Health Care Reform”, Journal of
Health Care for the Poor and Underserved, Vol. 22, pp. 422-428.
Gomez, O. C., and Artiaga, S (2011), “Connecting Eligible Immigrant Families to Health Coverage
and Care: Key Lessons from Outreach and Enrollment Workers”, The Kaiser Commission on
Medicaid and the Uninsured, available at www.KFF.org/KCMU, No. 8249.
Kandula, N. R., Lauderdale, D. S., and D. W. Baker (2007), “Differences in Self-Reported Health
Among Asians, Latinos, and Non-Hispanic Whites: The Role of Language and Nativity”, Annals of
Epidemiology, Vol. 17, No. 3, pp. 191-198.
KFF (2011), “Summary of New Health Reform Law”, Focus on Health Care, Kaiser Family Foundation,
accessed August 2011 at www.kff.org/healthreform/upload/8061.pdf.
Ku, L. and S. Matani (2001), “Left Out: Immigrants’ Access To Health Care And Insurance”, Health
Affairs, Vol. 20, No. 1, pp. 247-256.
Lara, M., Gamboa, C., Kahramanian, M. I., Morales, L. S., and D. E. Hayes-Bautista (2005),
“Acculturation and Latino Health in the United States: A Review of the Literature and its
Sociopolitical Context”, Annual Review Public Health, Vol. 26, pp. 367–397.
Lucia, L., Jacobs, K., Dietz, M., Graham-Squire, D., Pourat, N., and D. H. Roby (2012), “After
Millions of Californians Gain Health Coverage under the Affordable Care Act, who will Remain
Uninsured?”, accessed October 2012, http://laborcenter.berkeley.edu/healthcare/
aca_uninsured12.pdf.
Morales, L. S., Lara, M., Kington, R. S., and R. O. Valdez (2002), “Socioeconomic, Cultural, and
Behavioral Factors Affecting Hispanic Health Outcomes”, Journal of Health Care for the Poor and
Underserved, Vol. 13, No. 4, pp. 477-503.
Ortega, A. N., Fang, H., Perez, V. H., Rizzo, J. A., Carter-Pokras, O., Wallace, S. P., and L. Gelberg
(2007), “Health Care Access, Use of Services, and Experiences Among Undocumented Mexicans
and Other Latinos”, Archives of Internal Medicine, Vol. 167, No. 21, pp. 2354-2360.
Osypuk, T. L., Diez Roux, A. V., Hadley, C., and N. R. Kandula (2009), “Are Immigrant Enclaves
Healthy Places to Live? The Multi-Ethnic Study of Atherosclerosis”, Social Science & Medicine,
Vol.69, pp. 110-120.
Pew Hispanic Center (2011), “The Mexican-American Boom: Births Overtake Immigration”,
accessed August 2011, http://pewhispanic.org/files/reports/144.pdf.
Field Actions Science Reports, Special Issue 10 | 2014
20
Popkin, B. M. and J. R. Udry (1998), “Adolescent Obesity Increases Significantly in Second and
Third Generation U.S. Immigrants: the National Longitudinal Study of Adolescent Health”,The
Journal of Nutrition, Vol. 128, No. 4, pp. 701-706.
Portes, A. and R. Rumbaut (2001), Legacies: The Story of the Immigrant Second Generation,University
of California.
Portes, A. and M. Zhou (1993), “The New Second Generation: Segmented Assimilation and Its
Variants.” Annals of the American Academy of Political and Social Science, Vol.530, pp. 74-96.
Pourat ,N., Kinane, C. M., and G. F. Kominski (2011), “Who Can Participate in the California Health
Benefit Exchange? A Profile of Subsidy-Eligible Uninsured and Individually Insured”, Los Angeles,
CA: UCLA Center for Health Policy Research, accessed August 2011 at www.healthpolicy.ucla.edu/
pubs/files/benefitexchange-may2011.pdf.
Pourat, N., Martinez, A. E., and G. F. Kominski (2011), “Californians Newly Eligible for Medi-Cal
under Health Care Reform”, Los Angeles, CA: UCLA Center for Health Policy Research, accessed
August 2011 at www.healthpolicy.ucla.edu/pubs/files/medicalpb-may2011.pdf.
Rumbaut, R. G. (2004), “Ages, Life Stages, and Generational Cohorts: Decomposing the Immigrant
First and Second Generations in the United States”, International Migration Review, Vol. 38, No. 3,
pp. 1160-1205.
Sabia, D. (2010), “The Anti-Immigrant Fervor in Georgia: Return of the Nativist or Just Politics as
Usual?”, Politics & Policy, Vol. 38, No.1, pp. 53-80.
Smedley, B. D., Stitch, A. Y., and A. R. Nelson (2003), Unequal Treatment: Confronting Racial and
Ethnic Disparities in Health Care, The National Academies Press, Washington DC.
Spatz, E. S., Ross, J. S., Desai, M. M., Canavan, M. E., and H. M. Krumholz (2010), “Beyond
Insurance Coverage: Usual Source of Care in the Treatment of Hypertension and
Hypercholesterolemia. Data from the 2003-2006 National Health and Nutrition Examination
Survey”, American Heart Journal, Vol. 160, No.1, pp. 115-121.
Spetz, J., Baker, L., Phibbs, C., Pedersen, R., and S. Tafoya (2000), “The Effect of Passing an ‘Anti-
immigrant’ Ballot Proposition on the Use of Prenatal Care by Foreign-Born Mothers in
California”, Journal of Immigrant Health, Vol. 2, No. 4, pp. 203-212.
Stata, (2009). College Station, Texas. Stata Corporation.
Swider, S. M. (2002), “Outcome Effectiveness of Community Health Workers: An Integrative
Literature Review”, Public Health Nursing, Vol. 19, No. 1, pp. 11-20.
Ta, V. M., Holck, P., and G. C. Gee (2010), “Generational Status and Family Cohesion Effects on the
Receipt of Mental Health Services Among Asian Americans: Findings from the National Latino
and Asian American Study”, American Journal of Public Health, Vol. 100, No. 1, pp.115-121.
Telles, E. E. and V. Ortiz (2008), Generations of Exclusion: Mexican Americans, Assimilation, and Race,
Russell Sage Foundation.
Valenzuela Jr, A. and E. Gonzalez (2000), “Latino Earnings Inequality: Immigrant and Native-born
Differences”, Prismatic Metropolis: Inequality in Los Angeles, Russell Sage Foundation, pp. 249-278.
Vargas Bustamante, A., Fang, H., Rizzo, J. A., and A. N. Ortega (2009), “Understanding Observed
and Unobserved Health Care Access and Utilization Disparities Among U.S. Latino Adults”,
Medical Care Research and Review, Vol. 66, pp. 561-577.
Field Actions Science Reports, Special Issue 10 | 2014
21

Vargas Bustamante, A., Fang, H., Garza, J., Carter-Pokras, O., Wallace, S. P., and J. A. Rizzo (2010),
“Variations in Healthcare Access and Utilization Among Mexican Immigrants: The Role of
Documentation Status”, Journal of Immigrant and Minority Health, Vol. 66, pp. 561-577.
Viruell-Fuentes E. A. (2007), “Beyond Acculturation: Immigration, Discrimination, and Health
Research Among Mexicans in the United States”, Social Science & Medicine, Vol. 65, pp. 1524-1535.
Wallace, S. P., Gutierrez, V. F., and X. Castaneda (2008), “Access to Preventive Services for Adults
of Mexican Origin”, Journal of Immigrant and Minority Health, Vol. 10, pp. 363–371.
Weineck, R. M., Zuvekas, S. H., and J. W. Cohen (2000), “Racial and Ethnic Differences in Access To
and Use of Health Care Services, 1977 to 1996”, Medical Care Research and Review, Vol. 57, Suppl. 1,
pp. 36-54
Williams, D. R. (1999), “Race, Socioeconomic Status, and Health: The Added Effects of Racism and
Discrimination”, Annals New York Academy of Sciences, Vol. 896, pp. 173-188.
U.S. Census (2010), American Community Survey, 2007. In, Steven Ruggles, J. Trent Alexander,
Katie Genadek, Ronald Goeken, Matthew B. Schroeder, and Matthew Sobek. Integrated Public Use
Microdata Series: Version 5.0 [Machine-readable database]. Minneapolis: University of
Minnesota, 2010, accessed August 2011 at http://usa.ipums.org/usa/sda/
ABSTRACTS
The Patient Protection and Affordable Care Act (ACA) of 2010 expands health insurance coverage
to a substantial number of persons without health insurance. In California, Latinos, especially
Mexican immigrants, have one of the highest rates of uninsurance, making the ACA particularly
important for that group. Using the 2007 California Health Interview Survey, this study examines
how the generation in the U.S. of individuals of Mexican-origin is associated with their access to
health insurance, doctor visits, and emergency room visits in California compared to that of U.S.-
born non-Latino Whites. Results indicate that third generation Mexican Americans have similar
levels of being insured, having a doctor visit, and having an ER visit compared to Whites,
controlling for demographic, socioeconomic, and health status. First generation (immigrant)
Mexicans have the least access to health care services with lower odds than Whites of accessing
care across all measures. Second generation Mexican Americans also have lower odds than
Whites, however, the differences are not as pronounced as for the first generation. This study
finds that there are important differences in access to health care among Mexican Americans by
generational status, with the greatest disparities for the generations closest to the immigrant
experience. Implementation of the ACA will benefit Mexican Americans across generational
statuses, but gaps will likely remain for first and second generation Mexican Americans.
Le Patient Protection and Affordable Care Act (ACA), voté en 2010, étend la couverture
d'assurance-maladie à un grand nombre de personnes qui en étaient jusqu’à présent dénués.
Cette loi est particulièrement importante pour les Latinos de Californie, et en particulier pour les
immigrés mexicains, le groupe ethnique qui présente l'un des taux de non-assurance les plus
élevés. En se basant sur l'enquête 2007 California Health Interview Survey, cette étude examine le
lien entre la génération des individus d'origine mexicaine vivant aux Etats-Unis et leur accès à
l'assurance-maladie, aux médecins et aux urgences en Californie comparé aux Blancs non latinos
nés aux Etats-Unis. Les résultats indiquent que les Américains d’origine mexicaine de troisième
génération ont des taux similaires de non-assurance, de visites chez le médecin et de visites aux
urgences à ceux des Blancs, pour des statuts démographique, socioéconomique, et de santé
comparables. Les Mexicains de première génération (immigrants) sont ceux qui ont le moins
Field Actions Science Reports, Special Issue 10 | 2014
22

accès aux services de santé avec moins de chances que les Blancs d'accéder aux soins pour tous
les groupes de mesures. Les Américains d’origine mexicaine de deuxième génération ont
également moins accès aux soins que les Blancs mais les différences sont moins prononcées que
pour la première génération. Cette étude montre qu'il existe des différences notables au niveau
de l'accès aux soins entre les Américains d’origine mexicaine en fonction du degré de génération,
les disparités les plus importantes concernant les générations les plus proches de la date
d'arrivée dans le pays. L'application de l'ACA va bénéficier aux Américains d’origine mexicaine
des différentes générations mais des écarts vont probablement perdurer pour les première et
deuxième générations.
La Ley de Protección al Paciente y Cuidado Asequible (ACA por sus siglas en inglés) de 2010
amplía la cobertura del seguro de salud a un importante número de personas que carece de dicho
seguro. En California, los latinos, especialmente los inmigrantes mexicanos, registran una de las
tasas más altas de no-asegurados, lo que convierte a ACA en una ley especialmente importante
para ellos. Usando la Encuesta de Salud de California de 2007, este estudio examina como la
generación a la que pertenecen los individuos de origen mexicano en California afecta su acceso a
seguro médico, a consultas médicas y a consultas en la sala de emergencias en comparación con
los blancos no-latinos nacidos en Estados Unidos. Controlando demografía, nivel socioeconómico
y estado de salud, los resultados indican que la tercera generación de estadounidenses de origen
mexicano tienen un nivel similar de cobertura, consultas médicas y atención en salas de
emergencias comparados con los blancos. La primera generación de mexicanos (inmigrantes)
registra el menor acceso a los servicios de cuidados de salud y menor probabilidad que los
blancos de acceder a cuidados en todas las categorías. La segunda generación de estadounidenses
de origen mexicano también tienemenos probabilidades que los blancos, aunque las diferencias
no son tan pronunciadas como en la primera generación. Este estudio concluye que existen
importantes diferencias en el acceso al cuidado de salud entre los estadounidenses de origen
mexicano dependiendo de la generación a la que pertenecen, con las diferencias más grandes en
la generación más cercana a la experiencia migratoria.. La implementación de ACA beneficiará a
las distintas generaciones de estadounidenses de origen mexicano, aunque probablemente sigan
existiendo deficiencias para la primera y segunda generación.
INDEX
Mots-clés: ACA, Accès aux soins des Latinos, Accès aux soins en Californie, Statut générationnel
Palabras claves: ACA – (siglas en inglés de Affordable Care Act), Acceso a cuidado de salud en
California, Acceso a salud de los latinos, Estado generacional
Keywords: ACA, California health care access, Generational status, Latino health access
AUTHORS
EVA M. DURAZO
M.P.H., UCLA Fielding School of Public Health, Department of Community Health Sciences, P.O.
Box 951772, Los Angeles, CA 90095-1772, [email protected]
STEVEN P. WALLACE
Ph.D., UCLA Fielding School of Public Health, Department of Community Health Sciences and
Center for Health Policy Research
Field Actions Science Reports, Special Issue 10 | 2014
23
Physicians’ knowledge andcommunication about traditional,complementary and alternativemedicine use among Latino patientsat Kaiser Permanente, Oakland CAConnaissances et attitudes des médecins vis-à-vis du recours à la médecine
traditionnelle, à la médecine complémentaire et à la médecine alternative des
patients latinos du Kaiser Permanente, d'Oakland en Californie
El conocimientos y comunicación sobre el uso de medicina tradicional,
complementaria y alternativa entre doctores y los pacientes latinos del centro
Kaiser Permanente, Oakland (California)
Ingrid Bauer and Juan J. Guerra
Introduction
1 California has the largest Latino population in the nation, with over 14 million Latinos
representing 38% of the state’s total population1. Latinos have lower overall mortality and
infant mortality than non-Hispanic white and black Americans, a phenomenon known as
the “Latino health paradox” 2-4. At the same time, Latinos suffer disproportionately high
rates of diabetes, HIV/AIDS, tuberculosis, certain cancers, depression, and death from
homicide or incarceration.
2 Many social factors contribute to Latino health disparities, including income, lack of
access to health care, insurance status, immigration status, language barriers, working
conditions, environmental contamination, neighborhood safety, and unhealthy lifestyles4,6. Cultural barriers between patients and health care providers, as well as individual-
Field Actions Science Reports, Special Issue 10 | 2014
24
and institutional-level discrimination, also contribute to poor health among Latinos and
other ethnic minorities 7.
3 Cultural competence, cultural humility, and patient-centered communication have all
been promoted as strategies for reducing health inequities 8-12. Since the federal Office of
Minority Health released its standards for Culturally and Linguistically Appropriate
Services (CLAS) in 2000, many health care systems have complied with language services
standards. However, cross-cultural communication skills and knowledge about the
particular health beliefs and practices of Latinos remain an area of weakness in health
care research and practice 13.
4 For many Latinos, their health beliefs and practices do not fit within the framework of
Western biomedicine, which has been cited as a barrier to care 4,14. Although rates of use
vary by region and national origin, at least 25% of Latinos use some form of traditional,
complementary or alternative medicine (TCAM) 15,16. Some studies show that up to three
quarters of Mexican-Americans use TCAM 17.
5 A common theme throughout Latino cultures is a holistic perspective on health, where
spirituality, physical and mental/emotional health are equally important and intertwined18-21. Illness may result from natural causes or may be related to emotional, spiritual, or
supernatural causes. Folk illnesses, also known as “culture-bound syndromes,” are
collections of symptoms not recognized by conventional medicine but with popularly
understood mechanisms of causation and often treated using TCAM. Commonly cited folk
illnesses include ataque de nervios (nervous attack), susto (fright), mal de ojo (evil eye),
empacho (blocked bowel in children), caída de mollera (fallen fontanel), and caida de matríz
(fallen uterus) 11,22.
6 Herbal remedies, folk chiropractors (sobadores), massage, spiritual practices, and
relaxation techniques are some of the most frequently reported forms of TCAM among
Latinos 16. Over-the-counter (OTC) and non-prescribed prescription drugs (purchased
across the border or under-the-table in the U.S.) also form part of the
“ethnopharmacology” of Latinos 23. Despite much curiosity about folk healers, such as
curanderos, most studies indicate that no more than 4% of Latinos have visited such a
healer within the past year 17,19,24,25, although other studies report rates as high as 13%21,26.
7 Self-care through diet and lifestyle, as well as herbal home remedies, appear to be the
most important features of Latino health maintenance and are the first steps many
Latinos take before consulting a medical professional 22,27,28. In fact, some argue that the
preference for self-care and natural remedies leads Latinos to seek conventional medical
treatment as a last resort 21.
8 Of particular concern to physicians and public health officials is the underreporting of
TCAM by Latino patients. Studies have shown that up to 80% of Latino patients do not
report TCAM use to their physician 29. Poor communication not only increases the risk of
herb-drug interactions or missing potentially serious health problems, but also points to
a profound breakdown in the patient-provider relationship. Improving clinicians’
communication skills and knowledge of patients’ health beliefs and practices can enhance
doctor-patient relationships and improve health outcomes 11,30.
9 Lacking among research on Latino health beliefs, practices, and outcomes is an
investigation of what health care providers who serve Latinos know about their patients’
health beliefs and practices and how they communicate with their patients about TCAM.
Field Actions Science Reports, Special Issue 10 | 2014
25

This study exploresthe cultural knowledge and communication skills of physicians
regarding Latino health beliefs and TCAM practices at a bilingual clinic in Oakland,
California. Later stages of the research will examine the health beliefs and practices of
Latino patients served by the same clinic. Research questions include: (1) How do
physicians rate their understanding of Latino patients’ health beliefs and use of TCAM
and pharmaceuticals? (2) Which TCAM therapies do they consider most effective or most
problematic? and (3) How do physicians communicate with Latino patients about TCAM
and health beliefs?
Methods
10 This is an exploratory mixed methods study at Salud en Español (SE), a bilingual module
at Kaiser Permanente in Oakland, California, founded in September 2009. SE serves a
diverse Latino patient population from across Alameda County, providing medical
services in family and internal medicine, obstetrics and gynecology, and pediatrics. The
study involves questionnaires conducted with 10 SE physicians and a telephone survey of
65 adult Latina patients. Results from provider questionnaires conducted May through
July 2011 are presented here. The results from patient surveys will be presented
separately. The study was approved by the Kaiser Permanente Institutional Review Board
and the UC Berkeley Committee on the Protection of Human Subjects.
Questionnaire instrument
11 All physicians at SE were invited to participate in a 20-minute questionnaire administered
in person by the graduate student researcher. The questionnaire included questions
pertaining to (1) personal background and use of TCAM; (2) knowledge about Latino
patients’ TCAM use; and (3) communication with patients about TCAM. Both open-ended
and scaled questions were included; notes were taken to record responses to open-ended
questions, as audio recording was not permitted.
Analysis
12 Physician questionnaires were analyzed using qualitative techniques. Scaled questions
were analyzed to generate frequencies that described the characteristics, knowledge and
skills of the group of interviewees. Open-ended questions were coded and sorted into
themes, and lists of herbs, supplements, OTC, and prescription medications were sorted
and compared.
Results
Demographics
13 Participants included 10 physicians (3 men and 7 women), including 6 internal medicine
doctors, 3 family practice physicians, and one pediatrician. Their ages ranged from 32 to
57 years old, and their length in practice ranged from 5 to 31 years since beginning their
medical residency training. All of the physicians self-identified as Hispanic or Latino/a.
Nine physicians felt most comfortable with English but also spoke Spanish fluently; one
Field Actions Science Reports, Special Issue 10 | 2014
26
felt equally comfortable speaking both languages. Eight were born in the US; one was
born in Mexico and another in Trinidad and Tobago.
14 The participants had diverse experiences with using TCAM in their personal health
maintenance. Three physicians had no experience using any TCAM therapy. The other
seven physicians had some experience with some kind of TCAM, including herbal
medicine, yoga, meditation, tai chi, acupuncture, and other TCAM practices (massage,
acupressure osteopathy, reiki, craniosacral therapy). None had ever visited a curandero or
other traditional/folk Latino healer.
15 Physicians had varying levels of cultural competency training. Six of the 10 participants
mentioned receiving information about cultural health beliefs and practices during an
orientation when they began working at Kaiser Permanente, while three reported having
participated in cultural competency programs elsewhere. One physician leads such
trainings at Kaiser Permanente and other settings. Five physicians underwent
“extensive” cultural competency training during their medical residency training or
fellowships at academic institutions.
Cultural Knowledge
16 The majority of physicians felt that they had some knowledge and understanding
regarding their Latino patients’ health belief system (Table 1). One participant did not
respond to this set of questions because she did not feel that she could generalize about
all of her Latino patients due to the diversity of their cultural backgrounds and
socioeconomic status.
17 The physicians had a wide distribution of knowledge and understanding about folk
illnesses. Physicians expressed a greater understanding of ataque de nervios (nervous
attack), mal de ojo (evil eye), susto (fright), and caída de matriz (fallen uterus). They
reported less understanding of empacho (blocked stomach) and caida de mollera (fallen
fontanel). Another commonly encountered syndrome mentioned by three physicians was
the description of low back pain as dolor de riñones (kidney pain) in the absence of urinary
tract symptoms. Two others cited the widespread belief that exposure to cold air causes
illness.
18 Similarly, physicians varied in their level of knowledge and understanding about Latino
patients’ use of traditional, alternative and complementary therapies. Nine out of ten
reported having some knowledge of herbal remedies commonly used by their Latino
patients, while they had more knowledge about their patient’s use of OTC medications
and non-prescribed prescription drugs.
19 Four participants discussed how socioeconomic status, educational attainment, and level
of acculturation, as well as patients’ experiences with health care in their country of
origin, affect Latino patients’ health beliefs and practices. Among less acculturated
immigrants, said one doctor, “they first try herbal remedies, then they get antibiotics
from a friend, then they call me.” More traditional/less acculturated immigrants “are
more deferential; they will nod and say ‘yes’, but they don’t necessarily trust me.” The
physicians agreed that Kaiser Permanente members were more likely to believe in and
use Western medicine than traditional systems, possibly due to education, income,
acculturation, and their membership in a managed care plan. “Most of these folk illnesses
don’t come up in my patients, except some older or recent migrants,” said one physician.
Field Actions Science Reports, Special Issue 10 | 2014
27
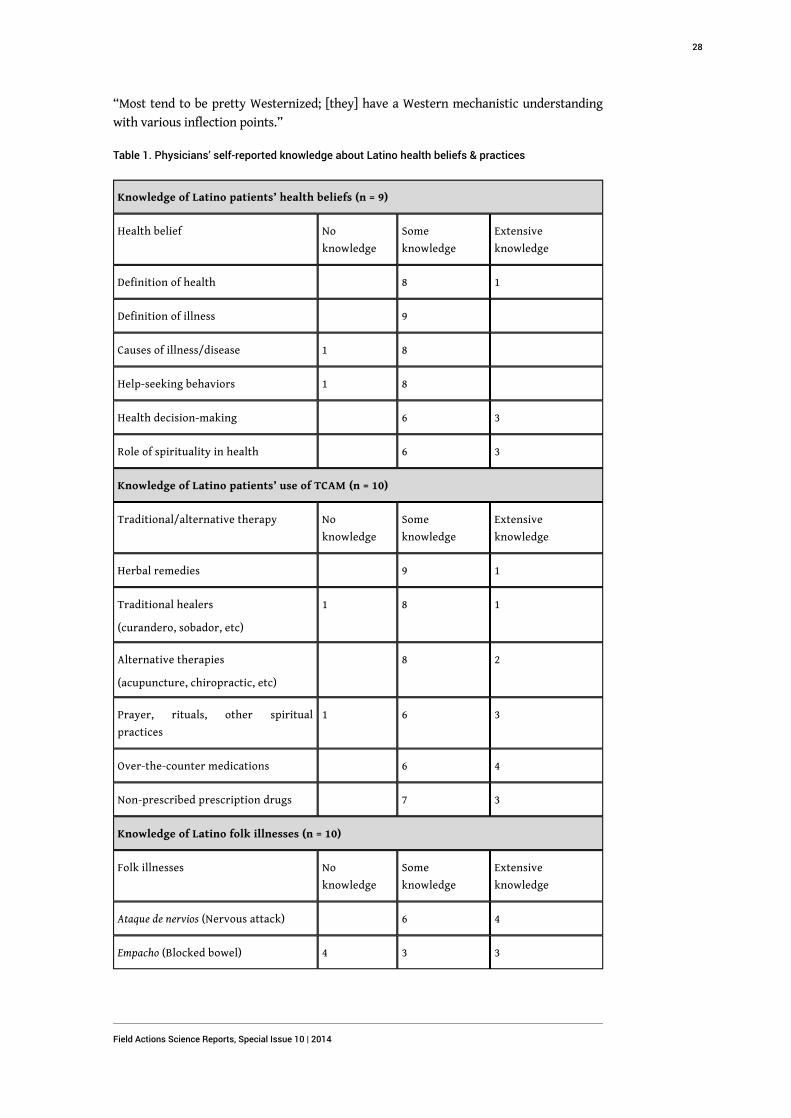
“Most tend to be pretty Westernized; [they] have a Western mechanistic understanding
with various inflection points.”
Table 1. Physicians’ self-reported knowledge about Latino health beliefs & practices
Knowledge of Latino patients’ health beliefs (n = 9)
Health belief No
knowledge
Some
knowledge
Extensive
knowledge
Definition of health 8 1
Definition of illness 9
Causes of illness/disease 1 8
Help-seeking behaviors 1 8
Health decision-making 6 3
Role of spirituality in health 6 3
Knowledge of Latino patients’ use of TCAM (n = 10)
Traditional/alternative therapy No
knowledge
Some
knowledge
Extensive
knowledge
Herbal remedies 9 1
Traditional healers
(curandero, sobador, etc)
1 8 1
Alternative therapies
(acupuncture, chiropractic, etc)
8 2
Prayer, rituals, other spiritual
practices
1 6 3
Over-the-counter medications 6 4
Non-prescribed prescription drugs 7 3
Knowledge of Latino folk illnesses (n = 10)
Folk illnesses No
knowledge
Some
knowledge
Extensive
knowledge
Ataque de nervios (Nervous attack) 6 4
Empacho (Blocked bowel) 4 3 3
Field Actions Science Reports, Special Issue 10 | 2014
28
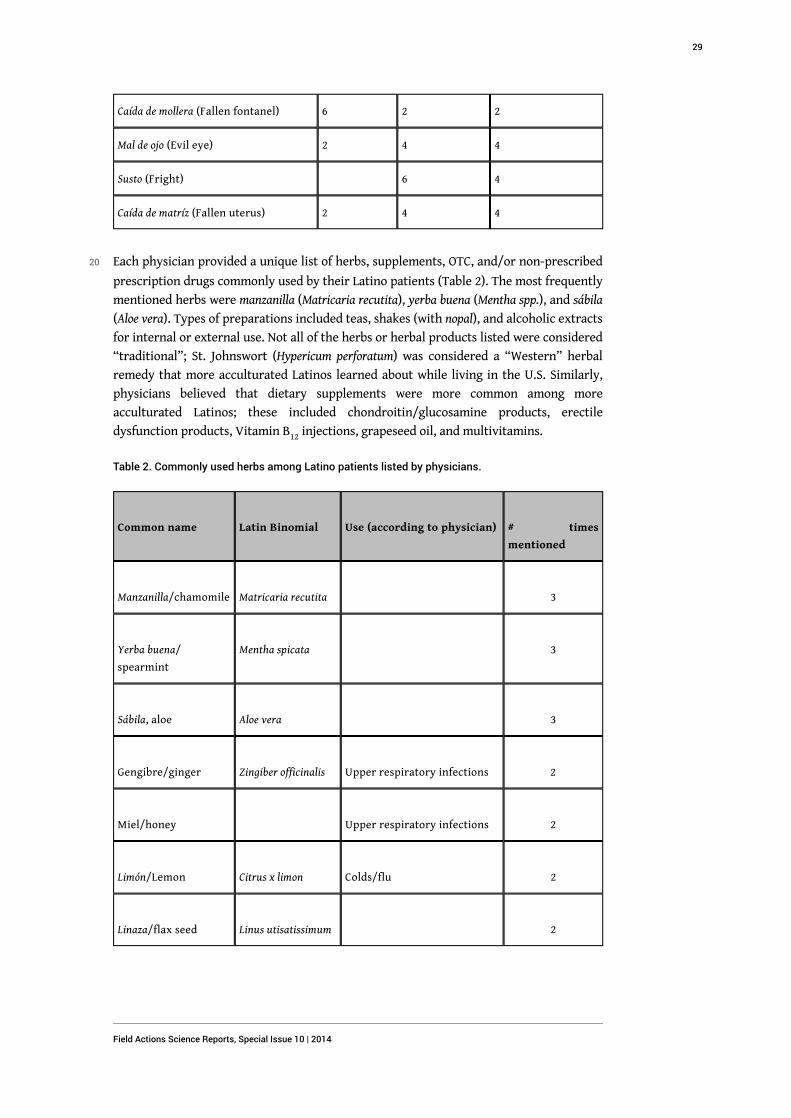
Caída de mollera (Fallen fontanel) 6 2 2
Mal de ojo (Evil eye) 2 4 4
Susto (Fright) 6 4
Caída de matríz (Fallen uterus) 2 4 4
20 Each physician provided a unique list of herbs, supplements, OTC, and/or non-prescribed
prescription drugs commonly used by their Latino patients (Table 2). The most frequently
mentioned herbs were manzanilla (Matricaria recutita), yerba buena (Mentha spp.), and sábila
(Aloe vera). Types of preparations included teas, shakes (with nopal), and alcoholic extracts
for internal or external use. Not all of the herbs or herbal products listed were considered
“traditional”; St. Johnswort (Hypericum perforatum) was considered a “Western” herbal
remedy that more acculturated Latinos learned about while living in the U.S. Similarly,
physicians believed that dietary supplements were more common among more
acculturated Latinos; these included chondroitin/glucosamine products, erectile
dysfunction products, Vitamin B12 injections, grapeseed oil, and multivitamins.
Table 2. Commonly used herbs among Latino patients listed by physicians.
Common name Latin Binomial Use (according to physician) # times
mentioned
Manzanilla/chamomile Matricaria recutita
3
Yerba buena/
spearmint
Mentha spicata
3
Sábila, aloe Aloe vera
3
Gengibre/ginger Zingiber officinalis Upper respiratory infections 2
Miel/honey
Upper respiratory infections 2
Limón/Lemon Citrus x limon Colds/flu 2
Linaza/flax seed Linus utisatissimum
2
Field Actions Science Reports, Special Issue 10 | 2014
29
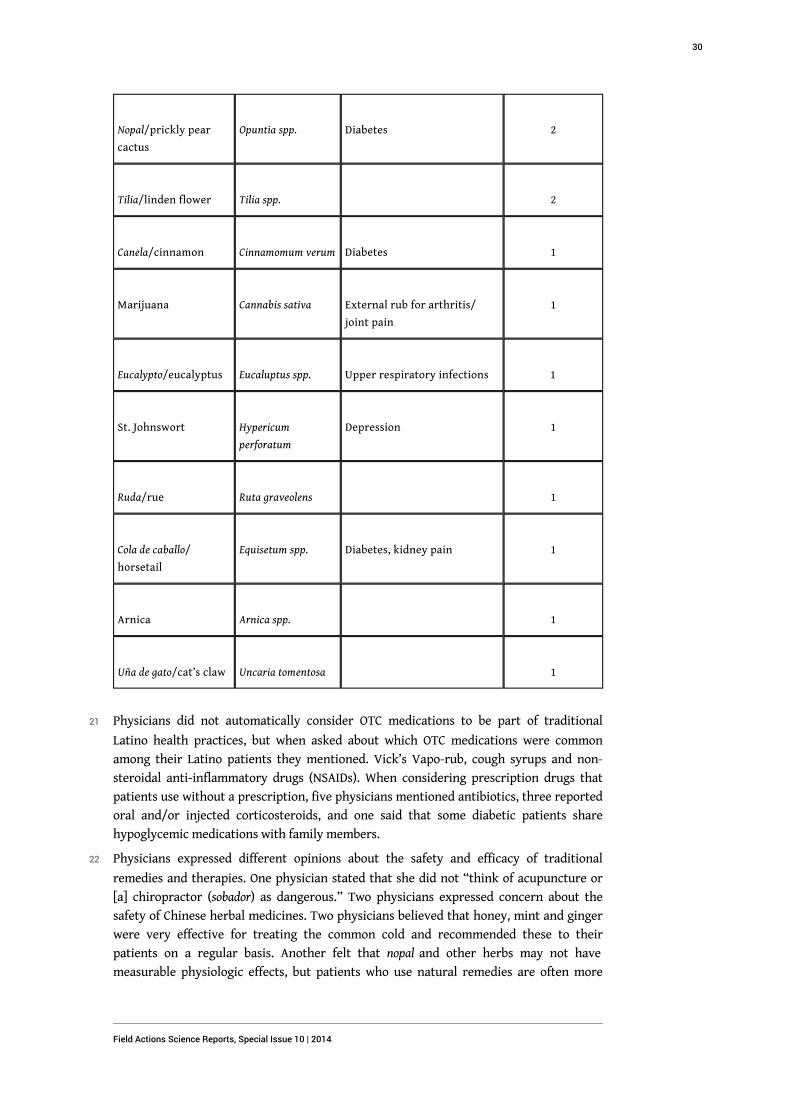
Nopal/prickly pear
cactus
Opuntia spp. Diabetes 2
Tilia/linden flower Tilia spp.
2
Canela/cinnamon Cinnamomum verum Diabetes 1
Marijuana Cannabis sativa External rub for arthritis/
joint pain
1
Eucalypto/eucalyptus Eucaluptus spp. Upper respiratory infections 1
St. Johnswort Hypericum
perforatum
Depression 1
Ruda/rue Ruta graveolens
1
Cola de caballo/
horsetail
Equisetum spp. Diabetes, kidney pain 1
Arnica Arnica spp.
1
Uña de gato/cat’s claw Uncaria tomentosa
1
21 Physicians did not automatically consider OTC medications to be part of traditional
Latino health practices, but when asked about which OTC medications were common
among their Latino patients they mentioned. Vick’s Vapo-rub, cough syrups and non-
steroidal anti-inflammatory drugs (NSAIDs). When considering prescription drugs that
patients use without a prescription, five physicians mentioned antibiotics, three reported
oral and/or injected corticosteroids, and one said that some diabetic patients share
hypoglycemic medications with family members.
22 Physicians expressed different opinions about the safety and efficacy of traditional
remedies and therapies. One physician stated that she did not “think of acupuncture or
[a] chiropractor (sobador) as dangerous.” Two physicians expressed concern about the
safety of Chinese herbal medicines. Two physicians believed that honey, mint and ginger
were very effective for treating the common cold and recommended these to their
patients on a regular basis. Another felt that nopal and other herbs may not have
measurable physiologic effects, but patients who use natural remedies are often more
Field Actions Science Reports, Special Issue 10 | 2014
30
willing to make significant changes to their diet and lifestyle, which makes a difference
for patients with chronic diseases, such as diabetes. On the other hand, another physician
had experience with diabetic patients who used sweetened fruit smoothies containing
nopal, resulting in elevated blood glucose from the extra sugar, the opposite of the
intended therapeutic effect.
23 Physicians were more concerned with the misuse or mislabeling of pharmaceuticals. Six
of the participants considered the use of non-prescribed antibiotics to be a major problem
among Latinos (especially for viral infections), due to increased bacterial resistance and
the danger of home-administered injections. Four of the ten physicians mentioned
corticosteroids as a problem, either as injections for pain or allergies, or as an unlisted
ingredient in “natural” pain relief formulas obtained in Mexico. These products, said two
physicians, may also contain unlabeled NSAIDs, which posed a risk of gastric, hepatic or
renal damage. One also considered weight-loss products being sold in Latino communities
to be dangerous.
24 Six physicians could not think of any significant herb-drug interactions that they knew of
or had encountered in clinical practice. One mentioned the potential for reactions
between warfarin and ginkgo or between chondroitin-glucosamine and cholesterol
medications. Another physician mentioned St. Johnswort as posing a risk, as well as herbs
that interact with statin drugs. Two felt that the lack of regulation of herbal products and
supplements made it difficult to assess their safety or the risk of herb-drug interactions.
Attitudes and Communication Skills
25 All of the physicians described their way of communicating with their Latino patients
about their health beliefs and practices as open-minded and/or nonjudgmental. They
agreed that asking point-blank “what they think is going on” and “what they’re doing for
the problem,” including “anything natural,” was the best way to elicit information about
the patient’s explanatory model and use of TCAM. They reported that patients are usually
quite forthcoming with this information. “That’s where the ‘mal de ojo’ comes up. It’s not
usually their chief complaint, but it comes out when I ask them what’s going on.”
26 Three physicians emphasized the importance of understanding how patients understand
their illness, in part because the patient population is very diverse and health literacy
varies from person to person. One physician stated the following:
I always ask patients about how they understand their illness. Then we can tailor or
customize how much time I have to spend on health education. Because of time
issues, ‘tell me what you know about hypertension or diabetes’ is a good starting
point, to determine how much do they need to know.
27 Besides tailoring health education during initial patient visits, asking how the patient
understands his or her illness at follow-up visits was seen as important “because things
can get lost in translation and over time people develop their own understanding of their
own health.” One physician felt that asking about the patient’s perspective was most
important for psychosocial issues, where the problem was less clear-cut than physical
complaints.
28 Responding to patients’ information about TCAM in a nonjudgmental way was seen as the
best way to build trust with patients and keep the lines of communication open. A
participant reported:
Field Actions Science Reports, Special Issue 10 | 2014
31
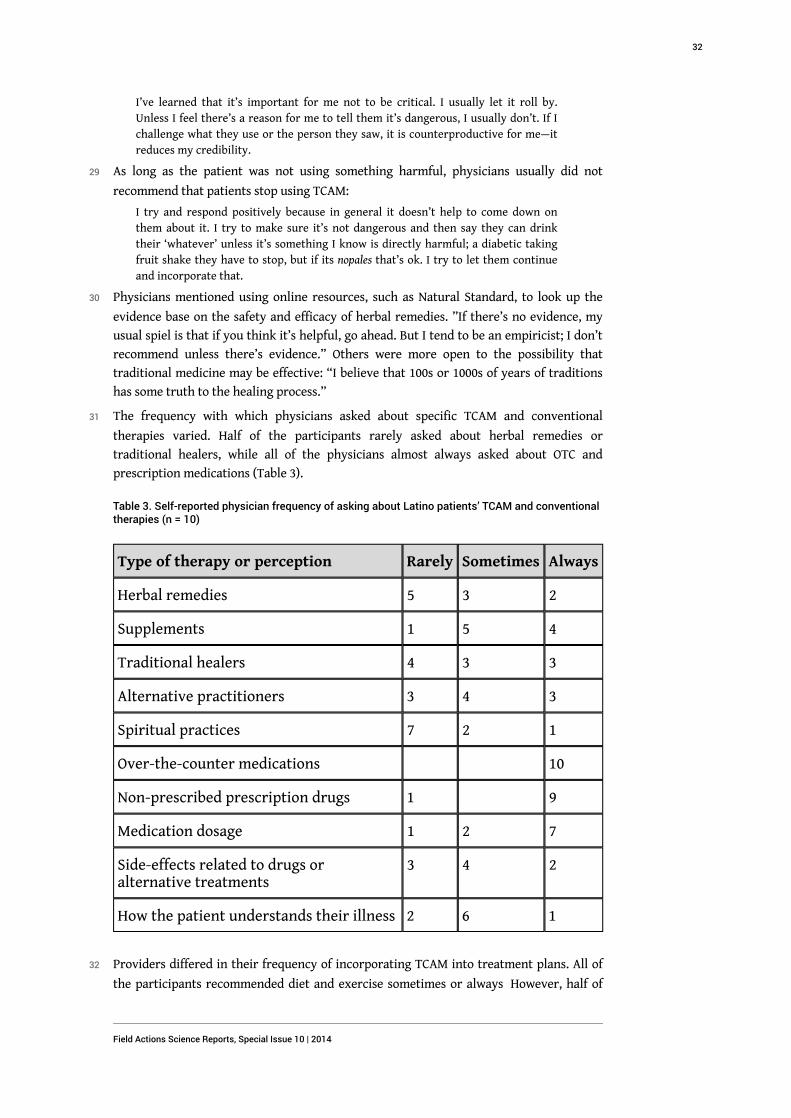
I’ve learned that it’s important for me not to be critical. I usually let it roll by.
Unless I feel there’s a reason for me to tell them it’s dangerous, I usually don’t. If I
challenge what they use or the person they saw, it is counterproductive for me—it
reduces my credibility.
29 As long as the patient was not using something harmful, physicians usually did not
recommend that patients stop using TCAM:
I try and respond positively because in general it doesn’t help to come down on
them about it. I try to make sure it’s not dangerous and then say they can drink
their ‘whatever’ unless it’s something I know is directly harmful; a diabetic taking
fruit shake they have to stop, but if its nopales that’s ok. I try to let them continue
and incorporate that.
30 Physicians mentioned using online resources, such as Natural Standard, to look up the
evidence base on the safety and efficacy of herbal remedies. ”If there’s no evidence, my
usual spiel is that if you think it’s helpful, go ahead. But I tend to be an empiricist; I don’t
recommend unless there’s evidence.” Others were more open to the possibility that
traditional medicine may be effective: “I believe that 100s or 1000s of years of traditions
has some truth to the healing process.”
31 The frequency with which physicians asked about specific TCAM and conventional
therapies varied. Half of the participants rarely asked about herbal remedies or
traditional healers, while all of the physicians almost always asked about OTC and
prescription medications (Table 3).
Table 3. Self-reported physician frequency of asking about Latino patients’ TCAM and conventionaltherapies (n = 10)
Type of therapy or perception Rarely Sometimes Always
Herbal remedies 5 3 2
Supplements 1 5 4
Traditional healers 4 3 3
Alternative practitioners 3 4 3
Spiritual practices 7 2 1
Over-the-counter medications 10
Non-prescribed prescription drugs 1 9
Medication dosage 1 2 7
Side-effects related to drugs oralternative treatments
3 4 2
How the patient understands their illness 2 6 1
32 Providers differed in their frequency of incorporating TCAM into treatment plans. All of
the participants recommended diet and exercise sometimes or always However, half of
Field Actions Science Reports, Special Issue 10 | 2014
32
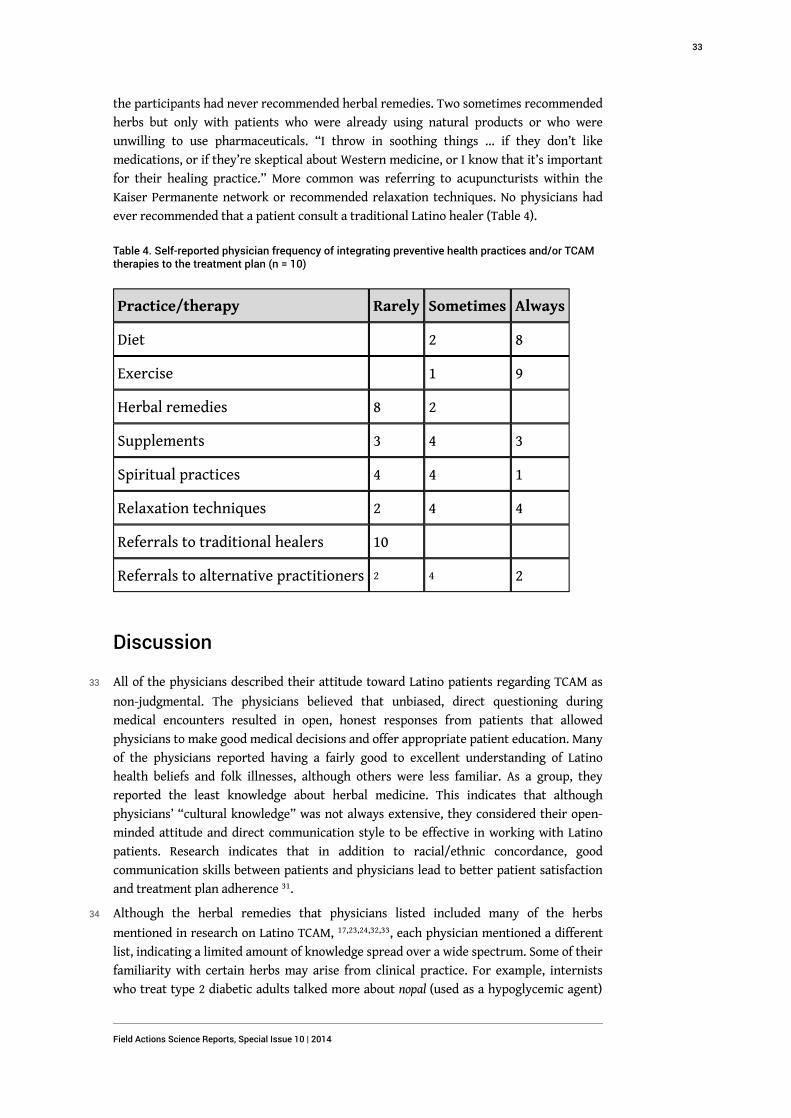
the participants had never recommended herbal remedies. Two sometimes recommended
herbs but only with patients who were already using natural products or who were
unwilling to use pharmaceuticals. “I throw in soothing things … if they don’t like
medications, or if they’re skeptical about Western medicine, or I know that it’s important
for their healing practice.” More common was referring to acupuncturists within the
Kaiser Permanente network or recommended relaxation techniques. No physicians had
ever recommended that a patient consult a traditional Latino healer (Table 4).
Table 4. Self-reported physician frequency of integrating preventive health practices and/or TCAMtherapies to the treatment plan (n = 10)
Practice/therapy Rarely Sometimes Always
Diet 2 8
Exercise 1 9
Herbal remedies 8 2
Supplements 3 4 3
Spiritual practices 4 4 1
Relaxation techniques 2 4 4
Referrals to traditional healers 10
Referrals to alternative practitioners 2 4 2
Discussion
33 All of the physicians described their attitude toward Latino patients regarding TCAM as
non-judgmental. The physicians believed that unbiased, direct questioning during
medical encounters resulted in open, honest responses from patients that allowed
physicians to make good medical decisions and offer appropriate patient education. Many
of the physicians reported having a fairly good to excellent understanding of Latino
health beliefs and folk illnesses, although others were less familiar. As a group, they
reported the least knowledge about herbal medicine. This indicates that although
physicians’ “cultural knowledge” was not always extensive, they considered their open-
minded attitude and direct communication style to be effective in working with Latino
patients. Research indicates that in addition to racial/ethnic concordance, good
communication skills between patients and physicians lead to better patient satisfaction
and treatment plan adherence 31.
34 Although the herbal remedies that physicians listed included many of the herbs
mentioned in research on Latino TCAM, 17,23,24,32,33, each physician mentioned a different
list, indicating a limited amount of knowledge spread over a wide spectrum. Some of their
familiarity with certain herbs may arise from clinical practice. For example, internists
who treat type 2 diabetic adults talked more about nopal (used as a hypoglycemic agent)
Field Actions Science Reports, Special Issue 10 | 2014
33
than other physicians. The pediatrician and family medicine doctors were more familiar
with folk illnesses that affect children, such as empacho and caída de mollera. A lack of
formal training or evidence-base for herbal remedies or supplements prevented some
physicians from recommending them to patients.
35 Physicians may have reported asking more about OTC and prescription medications and
having a better understanding of how Latino patients used these products because they
are more familiar with pharmaceuticals than with herbal medications. Similarly, while
physicians did not volunteer much knowledge about herb-drug interactions or dangerous
herbal remedies, they were worried about the misuse of antibiotics, corticosteroids,
NSAIDs, and weight-loss drugs. This concern may stem not only from the potency and
potential danger of these medications over herbs, but also from more physician
knowledge about these drugs.
36 While all of the physician participants identified somehow as Latino or Hispanic, they
have experienced multiple processes of acculturation that may have limited their
understanding and use of Latino health beliefs and practices. They all grew up and
attended medical school in the U.S., and for all but two, English was their first language.
37 Medical education in the US inculcates physicians with a scientific culture that
emphasizes objectivity and excludes many TCAM modalities 34. Although they had all
participated in some type of cultural competency training, none of the physicians had
extensive education in herbal medicine or other TCAM modalities. Increasing physician
knowledge about the safety, efficacy, and potential interactions of herbs may raise their
rate of asking about these remedies 35.
38 Physicians’ concerns with their Latino patients’ use of non-prescribed medications
highlight the importance of including these therapies in studies of Latino TCAM use.
Ethnopharmacology encompasses more than herbal remedies and traditional healing
practices by including studies of why and how people use and understand the mechanism
of modern pharmaceuticals 23. Socioeconomic barriers to health care, as well as cultural
beliefs about efficacy, and greater comfort using familiar medications from one’s native
country, are all factors that contribute to the self-prescription of antibiotics and other
drugs 36. In regards to antibiotics, besides their inefficacy against viral infections,
infectious disease specialists and public health officials are concerned with the rise in
antibiotic resistance resulting from inappropriate antibiotic use and point to the need for
culturally-appropriate interventions that target consumers as well as vendors of these
antibiotics 37. The literature does not include a discussion of problems with Latinos’
misuse of corticosteroids or NSAIDS for pain management, but physicians’ concerns point
to a need to research this issue.
39 The physicians’ open, nonjudgmental approach may help patients feel more comfortable
volunteering information about TCAM. While a physician’s attitude is important for
increasing patient comfort, studies indicate that physicians may also need to ask more
explicitly about TCAM and other health issues in order to elicit information 30,38. Some
physicians mentioned that unlike community-based clinics serving mostly recent, low-
income immigrants, Kaiser Permanente Latino members are more educated and
acculturated, and thus less likely to use TCAM. However, providers’ assumptions that
their patients do not use much TCAM may prevent them from asking regularly 30. Patient
data gathered in the second stage of this study will demonstrate if providers’ assumption
that Latino Kaiser Permanente members use less TCAM than lower-income Latino
patients matches patients’ actual rates of use.
Field Actions Science Reports, Special Issue 10 | 2014
34
Limitations
40 This research was limited by the questionnaire format; more open-ended questions and
audio recording of responses may have helped to capture physicians’ knowledge and
attitudes. The questions asked physicians to generalize about all Latinos, which did not
effectively capture the diversity of the patients they serve. Furthermore, the data is based
on self-reporting, rather than observations of physician behavior in clinical encounters,
so it is difficult to know if what providers say they do actually happens in clinical
practice.
41 Because these physicians all identify as Latino/a and work with a primarily Latino patient
population within a bilingual module, their cultural knowledge, communication skills,
and attitudes toward TCAM may not be representative of other groups of physicians
within Kaiser Permanente. As employees of a managed care organization, they may have
different clinical guidelines or time constraints than physicians working in other medical
contexts.
Conclusions
42 This study demonstrated that in regards to Latino patients’ health beliefs and TCAM,
physicians at Kaiser Permanente’s Salud en Español module consider their
communication style to be direct and their attitude open-minded. Their level of
knowledge about specific health beliefs and TCAM modalities varies from very low to
quite extensive, with the least amount of knowledge falling in the realm of herbal
remedies. The physicians’ primary safety concerns are not about herbs or traditional
healers, but about the misuse of non-prescribed prescription drugs, such as
corticosteroids and antibiotics. Rather than understanding and communicating more
about TCAM, physicians felt that developing skills to quickly assess the educational level
and health literacy of their patients would improve patient-provider communication and
lead to better health outcomes.
Acknowledgements
43 The authors would like to acknowledge the UC Global Health Institute (UCGHI) for
providing partial funding for the presentation and review of this work.
BIBLIOGRAPHY
(1) Ennis SR, Rios-Vargas M, Albert NG (2011), “The Hispanic Population: 2010”, US Census Bureau
http://www.census.gov/prod/cen2010/briefs/c2010br-04.pdf
Field Actions Science Reports, Special Issue 10 | 2014
35

(2) Hummer RA, Powers DA, Pullman SG, Gossman GL, Frisbie WP (2007), “Paradox Found (Again):
Infant Mortality Among the Mexican-Origin Population in the United States”, Demograph,y Vol.
44, No. 3, pp. 441-457.
(3) Lara M, Gamboa C, Kahramanian MI, Morales LS, Hayes Bautista DE (2005), “Acculturation and
Latino health in the United States: A review of the literature and its sociopolitical context”,
Annual Review of Public Health, Vol. 26, pp. 367-397.
(4) Morales L, Lara M, Kington R, Valdez R, Escarce J (2002), “Socioeconomic, cultural and
behavioral factors affecting Hispanic health outcomes”, J Health Care Poor Underserved, Vol. 14, No.
4, pp. 477-503.
(5) Network for a Healthy California--Latino Campaign (2010), “Latino Health Statistics. 2009”,
www.cdph.ca.gov/programs/cpns/Documents/Network-FV-LC-
LatinoHealthStatistics2009.pdf.
(6) Betancourt JR, Carrillo JE, Green AR, Maina A (2004), “Barriers to health promotion and
disease prevention in the Latino population”, Clin.Cornerstone, Vol. 6, No. 3, pp. 16-29.
(7) Smedley BD, Stith AY, Nelson AR (eds.) (2003), Unequal treatment: confronting racial and ethnic
disparities in healthcare, Washington, DC: National Academies Press.
(8) Cross TL et al (1989), Towards a culturally competent system of care: a monograph on effective
services for minority children who are severely emotionally disturbed, Washington, DC: Georgetown
University Child Development Center, CASSP Technical Assistance Center.
(9) Betancourt JR, Green AR, Carrillo JE, II OA (2003), “Defining Cultural Competence: A Practical
Framework for Addressing Racial/Ethnic Disparities in Health and Health Care”, Public Health
Reports, Vol. 118, No. 4, pp. 293-302.
(10) Tervalon M, Murray-Garcia J (1998), “Cultural humility versus cultural competence: A critical
distinction in defining physician training outcomes in multicultural education”, Journal of Health
Care to the Poor and Underserved, Vol. 9, No. 2, pp. 117-125.
(11) Flores G (2000), “Culture and the patient-physician relationship: Achieving cultural
competency in health care”, Journal of Pediatrics, Vol. 136, No. 1, pp. 14-23.
(12) Teal CR, Street RL (2009), “Critical elements of culturally competent communication in the
medical encounter: A review and model”, Social Science and Medicine, Vol. 68, No. 3, pp. 533-543.
(13) Brach C, Fraser I (2000), “Can Cultural Competency Reduce Racial And Ethnic Health
Disparities? A Review And Conceptual Model”, Medical Care Research and Review, Vol. 57,
Supplement 1, pp. 181-217.
(14) Parangimalil G (2001), “Latino health in the new millenium: the need for a culture-centered
approach”, Sociological Spectrum Vol. 21, pp. 423-429.
(15) Ortiz BI, Shields KM, Clauson KA, Clay PG (2007), “Complementary and Alternative Medicine
Use Among Hispanics in the United States”, Annals of Pharmacotherapy, Vol. 41, No. 6, pp.
994-1004.
(16) Graham R, Ahn A, Davis R, O'Connor B, Eisenberg D, Phillips R (2005), “Use of complementary
and alternative medical therapies among racial and ethnic minority adults: results from the 2002
National Health Interview Survey”, Journal of the National Medical Association, Vol. 97, No. 4, pp.
535-545.
Field Actions Science Reports, Special Issue 10 | 2014
36
(17) Rivera JO, Ortiz M, Lawson ME, Verma KM (2002), “Evaluation of the use of complementary
and alternative medicine in the largest United States-Mexico border city”, Pharmacotherapy, Vol.
22, pp. 256-264.
(18) Kiesser M, Mcfadden J, Belliard JC (2006), “An interdisciplinary view of medical pluralism
among Mexican-Americans”, Journal of Interprofessional Care, Vol. 20, No. 3, pp. 223-234.
(19) Murguía A, Peterson RA, Cecilia Zea M (2003), “Use and Implications of Ethnomedical Health
Care Approaches among Central American Immigrants”, Health and Social Work, Vol. 28, No. 1, pp.
43-51.
(20) Ness R, Wintrob R (1981), “Folk healing: a description and synthesis”, American Journal of
Psychiatry, Vol. 138, No. 11, pp. 1477-1481.
(21) Lopez R (2005), “Use of alternative folk medicine by Mexican American women”, Journal of
Immigrant Health, Vol. 7, No. 1, pp. 23-31.
(22) Sanchez MS (2007), “Mexican American Women's Pathways to Health”, Family & Community
Health, Vol. 30, Supplement 1, pp. S43-S52.
(23) Waldstein A (2006), “Mexican migrant ethnopharmacology: Pharmacopoeia, classification of
medicines and explanations of efficacy”, Journal of Ethnopharmacology, Vol. 108, No. 2, pp. 299-310.
(24) Zeilmann CA, Dole EJ, Skipper BJ, McCabe M, Dog TL, Rhyne RL (2003), “Use of herbal
medicine by elderly Hispanic and non-Hispanic white patients”, Pharmacotherapy, Vol. 23, pp.
526-532.
(25) Higginbotham JC, Trevino FM, Ray LA (1990), “Utilization of curanderos by Mexican
Americans: prevalence and predictors. Findings from HHANES 1982-84”, American Journal of Public
Health, Vol. 80 (Suppl), pp. 32-35.
(26) Keegan L (1996), “Use of Alternative Therapies among Mexican Americans in the Texas Rio
Grande Valley”, Journal of Holistic Nursing, Vol. 14, No. 4, pp. 277-294.
(27) Mendelson C (2003), “Creating Healthy Environments: Household-Based Health Behaviors of
Contemporary Mexican American Women”, Journal of Community Health Nursing, Vol. 20, No. 3, pp.
147-159.
(28) Zapata J, Shippee-Rice R (1999), “The Use of Folk Healing and Healers by Six Latinos Living in
New England: A Preliminary Study”, Journal of Transcultural Nursing, Vol. 10, No. 2, pp. 136-142.
(29) Mikhail N, Wali S, Ziment I (2004), “Use of Alternative Medicine among Hispanics”, Journal of
Alternative and Complementary Medicine, Vol. 10, No. 5, pp. 851-859.
(30) Shelley BM, Sussman AL, Williams RL, Segal AR, Crabtree BF (2009), “'They Don't Ask Me So I
Don't Tell Them': Patient-Clinician Communication About Traditional, Complementary, and
Alternative Medicine”, Annals of Family Medicine, Vol. 7, No. 2, pp. 139-147.
(31) Street RL Jr, O'Malley KJ, Cooper LA, Haidet P (2008), “Understanding concordance in
patient-physician relationships: personal and ethnic dimensions of shared identity”, Annals of
Family Medicine Vol. 6, No. 3, pp. 198-205.
(32) Kay M, Yoder M (1987), “Hot and cold in women's ethnotherapeutics: The American-Mexican
west”, Social Science and Medicine, Vol. 25, No. 4, pp. 347-355.
(33) Risser AL, Mazur LJ (1995), “Use of Folk Remedies in a Hispanic Population”, Archives of
Pediatric and Adolescent Medicine, Vol. 149, No. 9, pp. 978-981.
(34) Taylor JS (2003), “Confronting ‘culture’ in medicine's ‘culture of no culture’", Academic
Medicine, Vol. 78, No. 6, pp. 555-559.
Field Actions Science Reports, Special Issue 10 | 2014
37

(35) Gaylord SA, Mann JD (2007), “Rationales for CAM Education in Health Professions Training
Programs”, Academic Medicine ,Vol. 82, No. 10, pp. 927-933.
(36) Coffman MJ, Shobe MA, O'Connell B (2008), “Self-Prescription Practices in Recent Latino
Immigrants”, Public Health Nursing, Vol. 25, No. 3, pp. 203-211.
(37) Céspedes A, Larson E (2006), “Knowledge, attitudes, and practices regarding antibiotic use
among Latinos in the United States: Review and recommendations”, American Journal of Infection
Control, Vol. 34, No. 8, pp. 495-502.
(38) Julliard K, Vivar J, Delgado C, Cruz E, Kabak J, Sabers H (2008), “What Latina patients don't
tell their doctors: a qualitative study”, Annals of Family Medicine, Vol. 6, No. 6, pp. 543-549.
ABSTRACTS
Understanding Latinos’ health beliefs and traditional, complementary and alternative medicine
(TCAM) practices, and improving cross-cultural communication skills may improve quality of
care and reduce health disparities. Although studies have examined the health beliefs and
practices of Latino patients, few have examined the knowledge, attitudes, and communication
skills of health care providers in regards to Latino TCAM use. This paper discusses the results
from 10 physician questionnaires, which form part of a larger mixed-methods study of patients
and physicians at a bilingual clinic at Kaiser Permanente in Oakland, California. Physicians had a
range of knowledge regarding health beliefs and practices common among Latinos, but all
reported an open and non-judgmental attitude during patient interactions and were permissive
of TCAM therapies they considered safe. Physicians believed that TCAM use decreased with
acculturation and varied by ethnicity, education and income. Physicians were more concerned
with the misuse of prescription drugs among Latino patients than the potential for herbal
toxicity or herb-drug interactions. The results indicate a need to include questions about
pharmaceuticals in future research on Latino health practices, and also point to the need for
research on how education, income and acculturation affect health beliefs and TCAM practices
within different Latino subgroups.
La compréhension des croyances des Latinos en matière de santé et de leur recours aux
médecines traditionnelle, complémentaire et alternative, et l'amélioration des compétences en
matière de communication interculturelle peut faire progresser la qualité des soins et réduire les
disparités dans le domaine de la santé. Plusieurs études se sont penchées sur les croyances et les
pratiques des Latinos en matière de santé mais peu se sont intéressées aux connaissances, aux
attitudes et aux aptitudes en communication des professionnels de santé à l'égard des médecines
TCA utilisées par les Latinos. Cette étude discute des résultats de 10 questionnaires complétés par
des médecins, qui font partie d'une étude à méthodologie mixte à grande échelle portant sur des
patients et des médecins d’une clinique bilingue du Kaiser Permanente à Oakland en Californie.
Les médecins ont montré qu’ils avaient un large éventail de connaissances concernant les
croyances et les pratiques liées à la santé répandues dans la communauté latino, et tous ont
rapporté une attitude ouverte et sans jugement pendant les entretiens avec les patients et se sont
montrés tolérants vis-à-vis des traitements traditionnels, complémentaires et alternatifs qu'ils
considéraient comme sans danger. Les résultats montrent que les médecins estiment que le
recours aux médecines TCA diminue avec l'acculturation et varie en fonction de l'ethnicité, de
l'éducation et du revenu. Les médecins sont davantage préoccupés par le mauvais usage que font
les patients latinos des médicaments prescrits que par le risque de toxicité des plantes ou des
interactions plantes-médicaments. Les résultats indiquent le besoin d'inclure des questions sur
les produits pharmaceutiques dans les futurs travaux de recherche sur les pratiques de santé des
Field Actions Science Reports, Special Issue 10 | 2014
38

Latinos, et pointent sur la nécessité d'étudier la manière dont l'éducation, le revenu et
l'acculturation affectent les croyances en matière de santé et le recours aux médecines TCA dans
les différents sous-groupes de Latinos.
Entender las creencias respecto a la salud, y las prácticas de medicina tradicional,
complementaria y alternativa entre los latinos, así como mejorar las habilidades de
comunicación interculturales, podrían mejorar la calidad de la atención y reducir las
desigualdades de salud. Aunque se han realizado estudios que han examinado las creencias y
prácticas relacionadas a la salud de los pacientes latinos, pocos se han centrado en el
conocimiento, las actitudes y las habilidades de los profesionales de la salud para comunicarse
respecto al uso de la medicina tradicional, complementaria y alternativa entre los latinos. Este
trabajo analiza los resultados de 10 cuestionarios médicos que forman parte de un estudio más
amplio (que utiliza distintos métodos) de pacientes y profesionales médicos en una clínica
bilingüe de Kaiser Permanente en Oakland (California). Los médicos contaban con conocimientos
sobre las creencias y prácticas de salud habituales entre los latinos, aunque todos ellos
manifestaban mantener una actitud abierta sin prejuicios durante las interacciones con los
pacientes y eran permisivos con las terapias de medicina tradicional, complementaria y
alternativa que consideraban seguras. Los profesionales médicos consideraban que dichas
prácticas disminuían con la asimilación cultural y variaban según la etnia, el nivel educativo y el
nivel de ingresos. A los facultativos les preocupaba más la mala utilización de las recetas de
medicamentos entre los pacientes latinos que la posible toxicidad de las hierbas o la interacción
entre medicamentos y hierbas. Los resultados indican que es necesario incluir preguntas sobre
productos farmacéuticos en futuros estudios sobre prácticas de salud entre los latinos, así como
resaltar la necesidad de investigar cómo la educación, el nivel de ingresos y la asimilación
cultural afectan a las creencias de salud y las prácticas de medicina tradicional, complementaria
y alternativa en los distintos subgrupos latinos.
INDEX
Mots-clés: Attitudes des médecins, Communication interculturelle, Compétences culturelles,
Disparités en matière de santé, Femmes latinos, Médecine complémentaire et alternative,
Médecine traditionnelle
Keywords: Complementary and alternative medicine, Cross-cultural communication, Cultural
competence, Health disparities, Latinas, Physician attitudes, Traditional medicine
Palabras claves: Actitudes de los médicos, Competencia cultural, Comunicación intercultural,
Disparidades de salud latinas, Medicina complementaria y alternativa, Medicina tradicional
AUTHORS
INGRID BAUER
BS, University of California, San Francisco, School of Medicine, 5441 Broadway, Oakland, CA
94618, [email protected]
JUAN J. GUERRA
MD, Kaiser Permanente Medical Center, Oakland, California
Field Actions Science Reports, Special Issue 10 | 2014
39
Does Intergenerational SolidarityBuffer the Negative Effects ofResidential Mobility?Evidence for U.S. Children
La solidarité intergénérationnelle atténue-t-elle les effets négatifs de de la
mobilité résidentielle ?Étude sur des enfants américains
¿La solidaridad intergeneracional neutraliza los efectos negativos de los cambios
de residencia?Pruebas sobre niños estadounidenses
Brian Joseph Gillespie
Introduction
1 The recent economic downturn has destabilized housing for low and middle-class
populations with the harmful effects of tighter housing budgets, refinancing, foreclosure,
etc. In addition to this, evictions and relocations are occurring with greater frequency
and forcing individuals to move. According to the Current Population Survey, about 37.1
million Americans (12.5% of the population) moved between 2008 and 2009 (U.S. Census
Bureau 2010). Among these movers, 67.3% relocated within the same county, 17.2%
moved to another county and 12.6% relocated across state lines.1 The relatively high
percentage of Americans (and particularly families with children) that relocates annually
continues to raise concerns for researchers and practitioners (Jelleyman and Spencer
2008; Ersing, Sutphen, and Loeffler 2009).
2 Especially in trying economic times, it is important to better understand the effects of
residential mobility on individuals and families. For the most part, research has shown
negative outcomes for residentially mobile children, yet to date, few studies have
advanced to help understand what factors might serve to cushion the negative effects
Field Actions Science Reports, Special Issue 10 | 2014
40

associated with residential mobility. For instance, to what extent can intergenerational
solidarity (i.e., parent-child closeness) offset the negative effects of moving for children?
3 Intergenerational solidarity has long been a major focus in the study of the family. The
parent-adolescent relationship, specifically closeness between parent and child, occupies
a central place in most conceptions of the socialization process. This is because the family
is one of, if not the primary, focus of emotional energy during adolescence. The main
focus of this paper is whether or not intergenerational solidarity helps to offset the
negative effects of moving on children.
Prior Research and Theory
Residential Mobility and Child Outcomes
4 Research widely focuses on two specific outcomes of mobility on children: academic
achievement and behavior problems. Scholars have consistently found that compared
with non-mobile children, mobile children experience significantly more behavior
problems, (Simpson and Fowler 1994; Haynie, South, and Bose 2006; Gillespie 2013),
poorer health outcomes (Gillespie and Bostean, 2013), as well as negative academic
outcomes, such as dropping out (Coleman 1988; Haveman, Wolfe, and Spaulding 1991;
South, Haynie, and Bose 2005), decreased academic performance (Ingersoll, Scamman,
and Eckerling 1989; Tucker, Marx, and Long 1998), and grade retention (Simpson and
Fowler 1994).
5 One possible reason given for the differences in outcomes between mobile and non-
mobile children is the loss of social capital experienced by both the child and the parents
in the move (Coleman 1988; Stack 1994; Pribesh and Downey 1999; Pettit and McLanahan
2003). Household characteristics that predict selection into migration can complicate the
picture, as moves can be instigated by family disruptions, such as divorce, that negatively
affect child outcomes (Astone and McLanahan 1994; Tucker, Marx, and Long 1998;
Norford and Medway 2002). At the same time, long-distance moves are more common for
families with higher levels of education and household income (Tucker, Marx, and Long
1998; Fischer 2002), which are positively related to child outcomes (Davis-Kean 2005).
6 Outside of individual and household predictors, such as marital disruption (Madigan and
Hogan 1991), the major debates on residential mobility and child outcomes have centered
largely on community and family support.
Community and Family Protective Factors
7 The most well-known way of measuring community and family protective factors is
through the transmission and maintenance of social capital, a concept that has been
popularized by James Coleman. Over the past two decades, Coleman’s (1988) work on
social capital has inspired scholars to view where a person lives as promoting the
formation and maintenance of social ties that are paramount in forming a child’s ability
to excel in educational settings. Coleman’s key point is that interactions between
individuals and institutions (i.e., parents, teachers, schools, and community) are
resources that provide children with assets that increase their abilities, achievement-
levels, and general welfare. These social and community ties are broken when a family
relocates, resulting in a loss of social capital. Negative effects may be even worse when
Field Actions Science Reports, Special Issue 10 | 2014
41
families relocate repeatedly: e.g., “…for families that have moved often, the social
relations that constitute social capital are broken at each move” (Coleman 1988: 113).
8 Coleman argues that the concentration of social interactions among parents, between
parent and child, and between parents and community institutions (e.g., school) close
intergenerational relations and, in turn, create pathways to the attainment of social
capital. He charges that moving erodes family and community ties to social capital and
that this has important and negative effects on child outcomes. However, it has not been
considered whether or not the parent-child bond (arguably the social capital dimension
least affected by a move) can serve to buffer the negative effects of broken social and
community-level ties after relocation.
Intergenerational Solidarity
9 Research on the effects of the parent-child relationship on child outcomes has, for the
most part, shown that high quality intergenerational relationships are beneficial for
children. For instance, Aseltine, Gore, and Colten (1998) found a significant relationship
between parent-child closeness and decreased depression and externalizing behavior
problems in children. Others (Conger, Ge, Elder, Lorenz, and Simons 1994) found that
positive parent-child relationships buffer the negative emotional and behavioral effects
of divorce on children. In a longitudinal study, Hair, Moore, Garrett, Ling, and Cleveland
(2008) found that adolescent intergenerational cohesion was associated with greater
young adult mental well-being. However, little is known about whether parent-child
closure can offset the negative effects of moving associated with loss of community-level
social capital.
10 Few people question the value of a strong parent-child relationship. Close
intergenerational bonding during adolescence has been linked to a number of positive
outcomes, such as fewer behavior problems (Aseltine, Gore, and Colten 1998; Hair, Moore,
Garrett, Ling, and Cleveland 2008) and higher educational attainment (Bronte-Tinkew,
Scott, and Lilia 2010). Again, it should stand that the parent-child relationship (ostensibly
the dimension of social capital left most intact after a move) will help to buffer the
negative effects of moving on children over and above parent-community and child-
community social capital.
11 The act of moving is a decision made almost completely by parents, albeit sometimes with
children’s interests a major concern. Further, the decision to move (and where to move)
is made almost completely by parents, and this decision is expected to have consequences
on children’s behavior and achievement. However, in the same respect, a strong parent-
child relationship might buffer the negative effects of community-based social capital
loss for parents and children alike.
Research Question and Hypothesis
12 Following from the research discussed in the previous section, the main research
question being considered is: does intergenerational solidarity moderate the relationship
between residential mobility and child academic and behavioral outcomes? It is expected
that since the parent-child relationship remains relatively intact it will offset the loss of
community-based social capital and negative behavioral and achievement effects after a
Field Actions Science Reports, Special Issue 10 | 2014
42
move. This research question linking mobility and child outcomes is tested with measures
for an extensive set of child and family characteristics and community-based social
capital.
Data and Methods
National Longitudinal Survey of Youth (NLSY) Information and
Sampling
13 The National Longitudinal Survey of Youth (NLSY79) is a longitudinal study of a
representative sample of 12,696 American men and women aged 14 to 21 in 1979. The
children of the female NLSY79 respondents are also surveyed biennially starting in 1986
and these NLSY79 Child and Young Adult data files can be linked with the original NLSY79
to assess intergenerational phenomena and outcomes. The present study utilizes data
only from the 2000, 2002, 2004, and 2006 survey waves because respondents’ residential
mobility was not assessed in the NLSY until 2000.The age ranges for children during the
2000 wave of interviews is from 5.83 – 15.17, and the ages of the mothers in the study
ranged from 36-40 at the time of the 2000 interview.
14 Multiple children are surveyed in each household, giving the NLSY a useful hierarchical
design. High response rates (between 85 – 90%) also contribute to the validity of the
analysis. This rate has been maintained because data are primarily collected in the
respondent’s home through face-to-face interviews. This study utilizes the records of
3,168 adolescent respondents.
Variables and Measures
Child Outcomes
15 Academic achievement was measured using the NLSY79 Child and Youth respondent’s 2000,
2002, 2004, and 2006 Peabody Individual Achievement Test (PIAT) scores. The PIAT is a
widely used measure of academic achievement for children. Since 1986, the children in
this study have been assessed biennially between ages five and 15. Each assessment
begins with five age-appropriate questions and progresses to more advanced concepts.
The reading recognition test measures word recognition and pronunciation ability, and
the math test measures basic math skills and concepts.
16 The behavioral problems measure was measured using Peterson and Zill’s (1986) Behavior
Problems Index (BPI). This index consists of 28 questions, drawn primarily from the
widely used Child Behavior Checklist (Achenbach and Edelbrock 1981) along with other
widely used child behavior scales. The respondent’s mother indicates whether a
statement about the child’s behavior is “often true,” “sometimes true,” or “never true.”
17 Because the purpose of this analysis is to assess the effects of moving and several other
theoretical predictor variables on changes in educational achievement and behavior
problems, it is important to use longitudinal data which includes measures of the
predictors and outcomes in a person-year format. This allows for consideration of social
capital for each survey wave in the analysis. Adequately controlling for past behaviors
before a move occurs is crucial; otherwise, associating changes in child outcomes after
moving cannot be done confidently. The sample consists of children who completed the
Field Actions Science Reports, Special Issue 10 | 2014
43
PIAT and BPI for the 1998 (baseline), 2000, 2002, 2004, and 2006 survey rounds. The PIAT is
administered starting at age five, and the behavior problems assessment begins at age
four; neither examination is recorded after age 15.
Control Variables
Individual and Household Characteristics
18 Individual and household characteristics include time variant variables, such as annual
household income, age, and whether or not a family change (e.g., marital disruption)
occurred between any of the survey waves. Dummy variables for marital status marked
whether or not a respondent’s parent was married, never married, divorced, remarried,
separated, or widowed across each survey wave. Time-invariant variables include the
child’s sex, birth order, mother’s age at child’s birth, mother’s highest year of education
completed (measured once in 2000), family structure (father in household or not), and the
number of children in the respondent’s household. Children were assigned to racial
groups based on the primary racial identification of their mothers as Black, Hispanic, or
Non-Black/Non-Hispanic. All other variables in the analysis vary across survey waves.
Social Capital
19 Interaction between parents and community institutions was measured using two variables:
how often a child’s parent volunteers at the child’s school reported as never or almost
never (0), once or twice a term (1), once a month (2), once or twice a month (3),or once a
week or more (4) (Morgan and Sørensen 1999), and, following Coleman (1988), a
dichotomous variable marking whether or not a child attends Catholic school.2
20 Interaction between child and community institutions was measured by whether or not the
child participates in extracurricular activities (White and Gager 2007); how often he/she
attends religious services as coded as about once a week (1), about once a month (2), a few
times a year (3), or never (4) (Parcel and Dufur 2001); and how often the child feels lonely
or wishes he or she has more friends as measured as being never or hardly ever (1),
sometimes (2), or often (3).
Key Independent Variables
21 The potentially disruptive act of residential mobility is captured by a variable marking
whether a respondent did not move (0), moved locally (1), or moved across city, county,
or state boundaries.
22 Intergenerational solidarity was measured by the level of closeness the respondent reported
feeling to his/her mother, reported as being not very close (1), fairly close (2), quite close
(3), or extremely close (4).
Analytic Strategy
23 Linear Mixed Modeling (LMM) was used to examine the moderation effects of
intergenerational solidarity on the relationship between moving and child academic and
behavioral outcomes. Models were run separately for each of these two child outcomes.
Field Actions Science Reports, Special Issue 10 | 2014
44

24 This study applied an upward two-step preliminary modeling procedure employed by
Singer and Willett (2003): (a) an unconditional means model, and (b) and unconditional
growth model.3 First, the unconditional means model is the preliminary verification for
whether LMM is appropriate for this analysis by partitioning the total variation in the
outcome variable (BPI or PIAT). The intra-class correlation coefficient (ICC) measures the
proportion of variance in the outcome variable that is due to between-children
differences rather than differences within children over time.
25 LMM is a flexible and powerful method for the analysis of longitudinal data. In LMM,
independent observations are not assumed, meaning that between-subject and within-
subject effects are both considered. This modeling structure is also flexible in its use of
missing information. Other models use listwise deletion of cases if a complete trajectory
is not available for an individual. LMM, on the other hand, accounts for all respondents in
the data set and is, therefore, arguably a better model for unbalanced panel data sets like
the NLSY where not every respondent is observed in every year. Lastly, LMM allows for
the analysis of hierarchically organized data. In this study, four models (A through D)
were tested on three levels using an LMM structure. The first of these three levels
consisted of households, the second was the individual child nested in each household
and the last level, time, was measured by interview round and nested within each child.
26 The Hausman specification test validated these models (results not shown). LMM assumes
that the dependent variable be conditionally normal. Shapiro-Wilkins, and Skewness/
Kurtosis testing (not shown), indicate that both dependent variables were distributed
reasonably normally. Stata estimated the fixed and random effects as well as the
reliability and correlation coefficients. Variance inflation factors were checked in order
to assess for severe multicollinearity in the model (average VIF: 1.24).Analysis of the
correlation matrix (not shown) indicates that none of the observed relationships between
the independent variables in the models were very strong.
Results
Sample Characteristics in 2000 (Valid N=3,168)
27 The average household income for families in the sample from the 2000 wave was
approximately $55,000 per year. The majority of the children in the sample (52%) were
boys, only a slightly larger percent than the entire NLSY population sample (51%). The
mean age of children in the sample at the time of the 2000 wave was 10.8 (SD= 2.45). Half
of the sample mothers identified as Non-Black, Non-Hispanic (50.44), 28.6% identified as
Black, and 20.9% identified as Hispanic.
28 About three-fourths of the sample (75.82%) did not move while 15.27% moved locally and
8.91% moved across city, county, or state lines. The sample statistics on mobility are
reasonably consistent with recent reported rates of residential mobility in the United
States (U.S. Census Bureau, 2010).
Field Actions Science Reports, Special Issue 10 | 2014
45
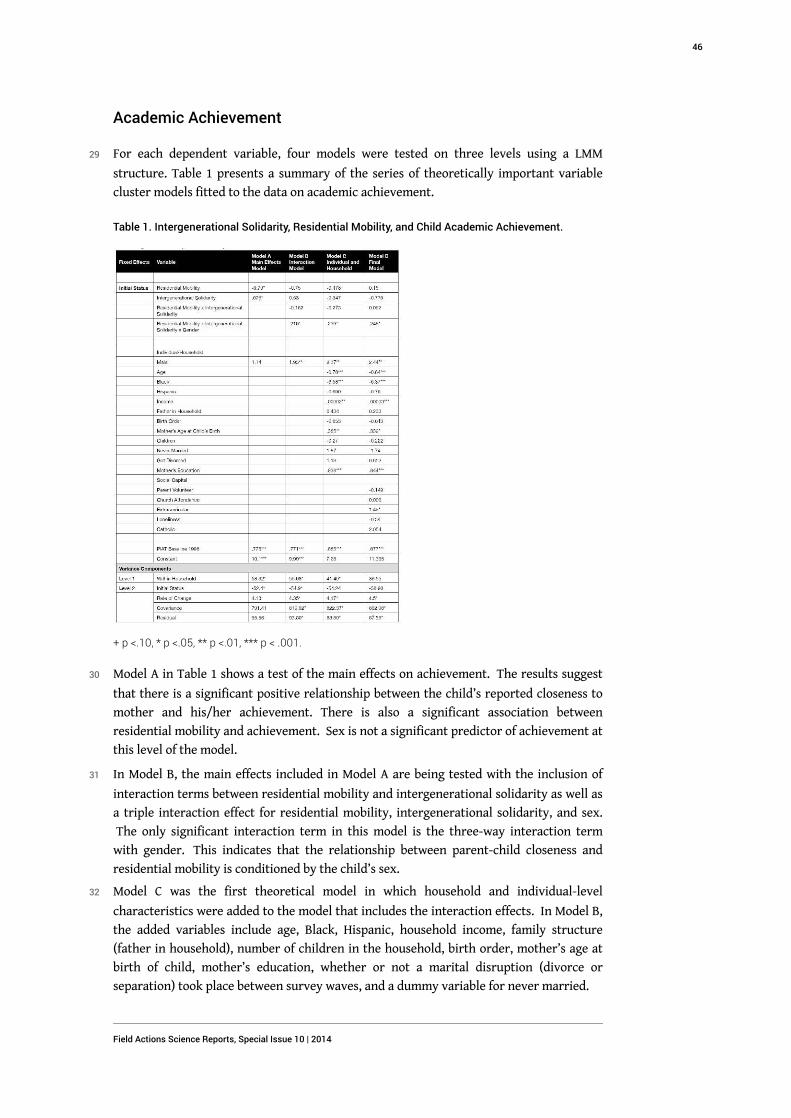
Academic Achievement
29 For each dependent variable, four models were tested on three levels using a LMM
structure. Table 1 presents a summary of the series of theoretically important variable
cluster models fitted to the data on academic achievement.
Table 1. Intergenerational Solidarity, Residential Mobility, and Child Academic Achievement.
+ p <.10, * p <.05, ** p <.01, *** p < .001.
30 Model A in Table 1 shows a test of the main effects on achievement. The results suggest
that there is a significant positive relationship between the child’s reported closeness to
mother and his/her achievement. There is also a significant association between
residential mobility and achievement. Sex is not a significant predictor of achievement at
this level of the model.
31 In Model B, the main effects included in Model A are being tested with the inclusion of
interaction terms between residential mobility and intergenerational solidarity as well as
a triple interaction effect for residential mobility, intergenerational solidarity, and sex.
The only significant interaction term in this model is the three-way interaction term
with gender. This indicates that the relationship between parent-child closeness and
residential mobility is conditioned by the child’s sex.
32 Model C was the first theoretical model in which household and individual-level
characteristics were added to the model that includes the interaction effects. In Model B,
the added variables include age, Black, Hispanic, household income, family structure
(father in household), number of children in the household, birth order, mother’s age at
birth of child, mother’s education, whether or not a marital disruption (divorce or
separation) took place between survey waves, and a dummy variable for never married.
Field Actions Science Reports, Special Issue 10 | 2014
46
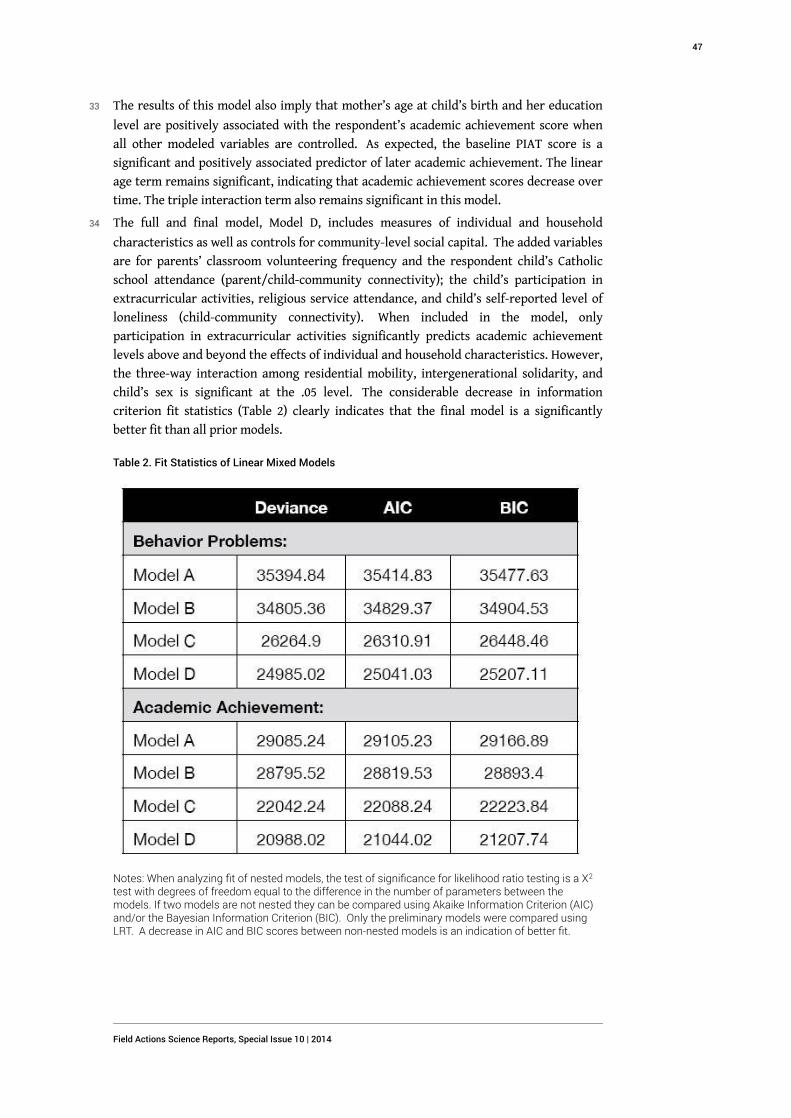
33 The results of this model also imply that mother’s age at child’s birth and her education
level are positively associated with the respondent’s academic achievement score when
all other modeled variables are controlled. As expected, the baseline PIAT score is a
significant and positively associated predictor of later academic achievement. The linear
age term remains significant, indicating that academic achievement scores decrease over
time. The triple interaction term also remains significant in this model.
34 The full and final model, Model D, includes measures of individual and household
characteristics as well as controls for community-level social capital. The added variables
are for parents’ classroom volunteering frequency and the respondent child’s Catholic
school attendance (parent/child-community connectivity); the child’s participation in
extracurricular activities, religious service attendance, and child’s self-reported level of
loneliness (child-community connectivity). When included in the model, only
participation in extracurricular activities significantly predicts academic achievement
levels above and beyond the effects of individual and household characteristics. However,
the three-way interaction among residential mobility, intergenerational solidarity, and
child’s sex is significant at the .05 level. The considerable decrease in information
criterion fit statistics (Table 2) clearly indicates that the final model is a significantly
better fit than all prior models.
Table 2. Fit Statistics of Linear Mixed Models
Notes: When analyzing fit of nested models, the test of significance for likelihood ratio testing is a X2
test with degrees of freedom equal to the difference in the number of parameters between themodels. If two models are not nested they can be compared using Akaike Information Criterion (AIC)and/or the Bayesian Information Criterion (BIC). Only the preliminary models were compared usingLRT. A decrease in AIC and BIC scores between non-nested models is an indication of better fit.
Field Actions Science Reports, Special Issue 10 | 2014
47
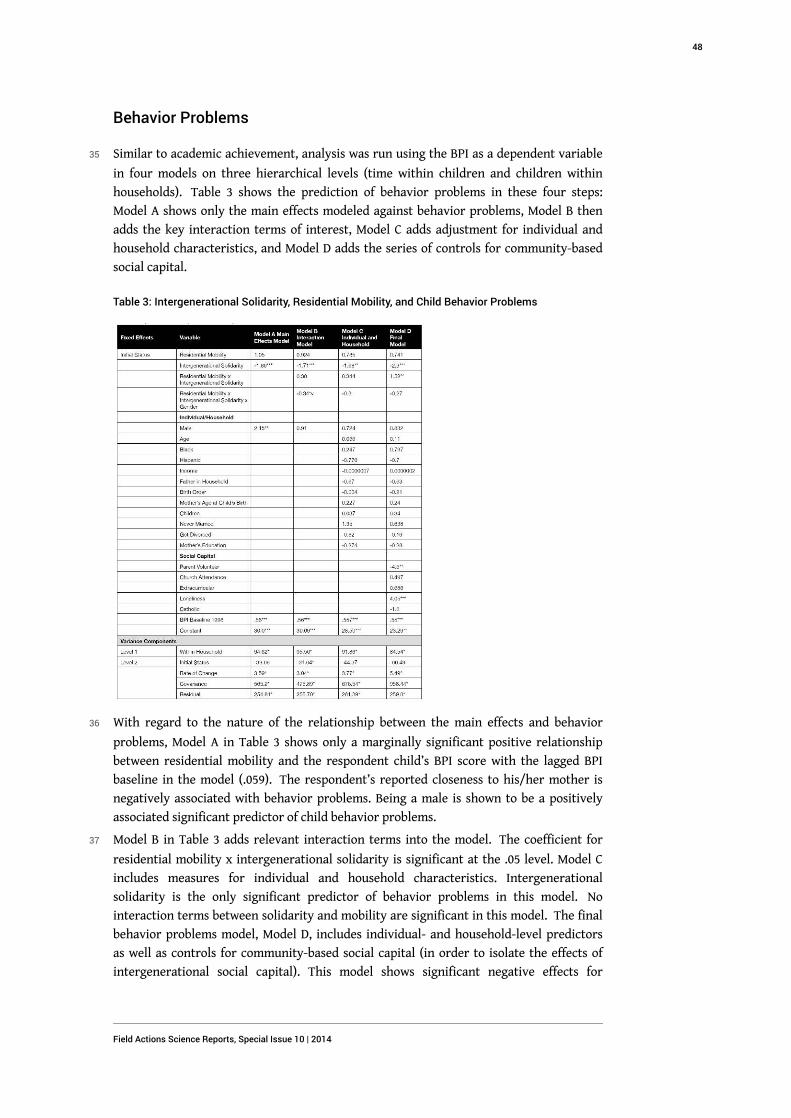
Behavior Problems
35 Similar to academic achievement, analysis was run using the BPI as a dependent variable
in four models on three hierarchical levels (time within children and children within
households). Table 3 shows the prediction of behavior problems in these four steps:
Model A shows only the main effects modeled against behavior problems, Model B then
adds the key interaction terms of interest, Model C adds adjustment for individual and
household characteristics, and Model D adds the series of controls for community-based
social capital.
Table 3: Intergenerational Solidarity, Residential Mobility, and Child Behavior Problems
36 With regard to the nature of the relationship between the main effects and behavior
problems, Model A in Table 3 shows only a marginally significant positive relationship
between residential mobility and the respondent child’s BPI score with the lagged BPI
baseline in the model (.059). The respondent’s reported closeness to his/her mother is
negatively associated with behavior problems. Being a male is shown to be a positively
associated significant predictor of child behavior problems.
37 Model B in Table 3 adds relevant interaction terms into the model. The coefficient for
residential mobility x intergenerational solidarity is significant at the .05 level. Model C
includes measures for individual and household characteristics. Intergenerational
solidarity is the only significant predictor of behavior problems in this model. No
interaction terms between solidarity and mobility are significant in this model. The final
behavior problems model, Model D, includes individual- and household-level predictors
as well as controls for community-based social capital (in order to isolate the effects of
intergenerational social capital). This model shows significant negative effects for
Field Actions Science Reports, Special Issue 10 | 2014
48
intergenerational solidarity and also the interaction between intergenerational solidarity
and residential mobility on behavior problems. Therefore, closeness to mother is a
significant predictor of behavior problems and these effects increase after a residential
move takes place (locally or across distance).
38 Residual plotting for both behavior problems and academic achievement models revealed
constant variance and indicated that neither model’s residual errors deviate from a
normal distribution. Additional diagnostics plotting the best linear unbiased predicted
values (BLUPs) for random effects did not provide evidence of extremely unusual random
child or household effects in either model.
Discussion
39 The current study tested the moderation of intergenerational solidarity on the
relationship between residential mobility and adolescent outcomes. It was hypothesized
that intergenerational solidarity and residential mobility would interact to significantly
affect adolescent behavior and achievement above and beyond other theoretically
important variables (including measures for other dimensions of social capital).
40 To test these hypotheses with the greatest rigor, a longitudinal analysis was conducted
that involved four conditional growth models incorporating clustered theoretically
important variables (i.e., individual/household characteristics and community-based
social capital). In light of mixed research on the relationship between social capital and
residential mobility effects for children, it was important to analyze how the parent-child
relationship might cushion the effects of mobility and attendant loss community-based
social capital.
41 It was expected that the parent-child relationship would significantly buffer the negative
academic and behavioral effects of moving on children. This is because the
intergenerational form of social capital is arguably the one dimension of capital to remain
relatively intact once a move takes place. This hypothesis is supported by this research.
42 The effect in Model D, Table 3, shows a significant positive association between behavior
problems and an interaction between residential mobility and intergenerational
solidarity. Controlling for all other theoretically important variables, intergenerational
solidarity is a significant predictor of behavior problems, and this is especially so after a
residential relocation takes place. For academic achievement, this association holds but
only when conditioned by gender.
43 These analyses are subject to several caveats. Measuring child outcomes across only four
waves of this longitudinal survey does not allow for analysis of behavior and achievement
to the extent that the relationship between residential mobility and academic
achievement and/or behavior problems takes longer than two, four, or six years to
develop.Reverse causation may also be present in the models above. For instance,
problem behavior may cause children to have distant relationships with their parents.
Also, because only the children of NLSY female respondents are surveyed, father-child
and father-community interaction (other than what is reported by the mother) cannot be
assessed as a component of intergenerational solidarity or community-based social
capital. The information available for a child’s mother is not necessarily available for the
child’s father. Moreover, because of the NLSY design, children raised in single-father
homes are not included in the sample. With the rise of joint custody arrangements, this is
Field Actions Science Reports, Special Issue 10 | 2014
49

an important limitation to this study, if only because this study’s main focus is on the
parent-child relationship.
Conclusion
44 The effect of moving on child outcomes was successfully modeled with a hierarchical
design to compensate for time as it is nested within children and children nested within
households. Intergenerational solidarity significantly interacts with residential mobility
to predict adolescent behavior and achievement outcomes. As such, intergenerational
solidarity is one dimension of social capital that needs purposeful consideration in
residential mobility research because it appreciably offsets negative child academic and
behavioral outcomes.
45 The findings of the current study are important in a number of ways. First, the data show
that intergenerational solidarity does significantly offset the negative behavioral and
achievement effects of residential mobility, even when controlling for the effects of
individual/household-level variables and community-level social capital. Second, the
research indicates that in a study of child outcomes, generally, there are different
significant predictors and interactions for behavior problems than there are for academic
achievement in adolescence even though prior researchers had posited similarly negative
effects of moving on a range of child outcomes (Coleman 1988; Hendershott 1989; Hagan,
MacMillan, and Wheaton 1996; Norford and Medway 2002).
46 Moving is difficult—it is arguably one of life’s most stressful commonly occurring events.
Residentially mobile children, especially those who move frequently, are at a risk for a
host of negative behavioral and academic outcomes. However, these potentially harmful
effects may be forestalled by social services and policy commitment to help mobile
children and families adjust to their new schools and communities. These approaches to
intervention are based on a multidisciplinary effort that would include social workers,
educators, school administrators, and the community at large.
47 In other words, community leaders and other practitioners ought to be mindful of these
effects and help to improve parent-community and child-community social capital,
especially among mobile and hypermobile families. For instance, community health
practitioners might facilitate community-based functions that provide opportunities for
recent “transplants” to network—this would be especially beneficial for high-mobility
communities.
48 At the same time, community and school involvement for residentially mobile families
relies, at least in part, on whether or not the school community reaches out to involve
them and help them adjust. Thus, school-based services focused on residentially mobile
individuals and families would help encourage parental involvement in school activities
and functions. People will never stop moving—but helping integrate mobile families into
their destination communities is a good start at alleviating the negative social,
behavioral, and academic effects of residential mobility on children.
Field Actions Science Reports, Special Issue 10 | 2014
50
Acknowledgments
49 The author would like to thank the Center of Expertise on Migration and Health, Michael
Rodriguez, and David Lopez-Carr for their advice and comments on earlier drafts of this
manuscript.
BIBLIOGRAPHY
Achenbach, T. M. and C. S. Edelbrock (1981), “Behavioral Problems and Competencies Reported
by Parents of Normal and Disturbed Children Aged Four through Sixteen”, Monographof the Society
for Research in Child Development, Vol. 46, No. 1, pp. 1-82.
Aseltine, R. H. Jr., S. Gore, and M.E. Colten (1998), "The Co-Occurrence of Depression and
Substance Abuse in Late Adolescence", Development and Psychopathology, Vol. 10, pp. 549-70.
Astone, N.M. and S. McLanahan (1994), “Family Structure, Residential Mobility, and School
Dropout: A Research Note”, Demography, Vol. 31, No. 4, pp. 575-84.
Bronte-Tinkew, J., M.E. Scott, and E. Lilia (2010), "Single Custodial Fathers' Involvement and
Parenting: Implications for Outcomes in Emerging Adulthood", Journal of Marriage and Family, Vol.
72, pp. 1107-27.
Coleman, J.S. (1988), “Social Capital in the Creation of Human Capital”, American Journal of
Sociology, Vol. 94 (Supplement: Organizations and Institutions: Sociological and Economic
Approaches to the Analysis of Social Structure), pp. 95-120.
Conger, R.D., X. Ge, G.H. Elder, Jr., F.O. Lorenz, and R.L. Simons (1994), "Economic Stress, Coercive
Family Process, and Developmental Problems of Adolescents", Child Development, Vol. 65, pp.
541-61.
Davis-Kean, P.E. (2005), “The Influence of Parent Education and Family Income on Child
Achievement: The Indirect Role of Parental Expectations and the Home Environment”, Journal of
Family Psychology, Vol. 19, No. 2, pp. 294-304.
Ersing, R. L., R.L. Sutphen, and D.N. Loeffler (2009), “Exploring the Impact and Implications of
Residential Mobility: From the Neighborhood to the School”, Advances in Social Work, Vol. 10, No.
1, pp. 1-18.
Fischer, C.S. (2002), “Ever-more Rooted Americans”, City and Community, Vol. 1, No. 2, pp. 177-98.
Gillespie, B.J. (2013), "Adolescent Behavior and Achievement, Social Capital, and the Timing of
Geographic Mobility", Advances in Life Course Research, Vol. 18, No. 3, pp. 223-233.
Gillespie, B.J., and G. Bostean (2013), "Socioeconomic Status, Residential Mobility, and Health", In
K. Fitzpatrick (Ed.), Poverty in America: A Crisis among America’s Most Vulnerable, Vol. II, pp.
33-57. Santa Barbara: Praeger.
Field Actions Science Reports, Special Issue 10 | 2014
51
Hagan, J., R. MacMillan, and B. Wheaton (1996), “New Kid in Town: Social Capital and the Life
Course Effects of Family Migration on Children”, American Sociological Review, Vol. 61, No. 3,
pp.368-85.
Hair, E.C., K.A. Moore, S.B. Garrett, T. Ling, and K. Cleveland (2008), "The Continued Importance
of Quality Parent-Adolescent Relationships during Late Adolescence", Journal of Research on
Adolescence, Vol. 18, pp. 187-200.
Haveman, R., B. Wolfe, and J. Spaulding (1991), “Childhood Events and Circumstances Influencing
High School Completion”, Demography, Vol. 28, No. 1, pp. 133-57.
Haynie, D.L., S.J. South, and S. Bose (2006), “The Company You Keep: Adolescent Mobility and
Peer Behavior”, Sociological Inquiry, Vol. 76, No. 3, pp. 397-426.
Hendershott, A.B. (1989), “Residential Mobility, Social Support and Adolescent Self-Concept”,
Adolescence, Vol. 24, No. 93, pp. 217-32.
Ingersoll, G.M., J.P. Scamman, and W.D. Eckerling (1989), “Geographic Mobility and Student
Achievement in an Urban Setting”, Educational Evaluation and Policy Analysis, Vol. 11, No. 2, pp.
143-49.
Jelleyman, T. and N. Spencer (2008), “Residential Mobility in Childhood and Health Outcomes: A
Systematic Review”, Journal of Epidemiology and Community Health, Vol. 62, pp. 584-92.
Madigan, T.J. and D.P. Hogan (1991), “Kin Access and Residential Mobility among Young
Mothers”, Social Science Quarterly, Vol. 72, No. 3, pp. 615-22.
Morgan, S.L., and A.B. Sørensen (1999), "Parental Networks, Social Closure, and Mathematics
Learning: A Test of Coleman's Social Capital Explanation of School Effects", American Sociological
Review, Vol. 64, No. 5, pp. 661-681.
Norford, B.C. and F.J. Medway (2002), “Adolescents’ Mobility Histories and Present Social
Adjustment”, Psychology in the Schools, Vol.39, No. 1, pp. 51-62.
Parcel, T.L. and M.J. Dufur (2001), "Capital at Home and at School: Effects on Child Social
Adjustment", Journal of Marriage and the Family, Vol. 63, No. 1, pp. 32-47.
Peterson, J.L. and N. Zill (1986), “Marital Disruption, Parent-Child Relationships, and Behavior
Problems in Children”, Journal of Marriage and the Family, Vol. 48, No. 2, pp. 295-307.
Pettit, B. and S. McLanahan (2003), “Residential Mobility and Children’s Social Capital: Evidence
from an Experiment”, Social Science Quarterly, Vol. 84, No. 3, pp. 632-49.
Pribesh, S. and D.B. Downey (1999), “Why are Residential and School Moves Associated with Poor
School Performance?”, Demography, Vol. 36, No. 4, pp. 521–34.
Simpson, G.A. and M.G. Fowler (1994), “Geographic Mobility and Children's Emotional/Behavioral
Adjustment and School Functioning”, Pediatrics, Vol. 93, No. 2, pp. 303-9.
Singer, J.D. and J.B. Willett (2003), Applied Longitudinal Data Analysis: Modeling Change and Event
Occurrence, Oxford University Press, New York, NY.
South, S.J., D.L. Haynie, and S. Bose (2005), “Student Mobility and School Dropout”, Social Science
Research, Vol. 36, pp. 68-94.
Stack, S. (1994), “The Effect of Geographic Mobility on Premarital Sex”, Journal of Marriage and the
Family, Vol. 56, No. 1, pp. 204-8.
Tucker, C.J., J. Marx, and L. Long (1998), “’Moving on’: Residential Mobility and Children's School
Lives”, Sociology of Education, Vol. 71, No. 2, pp. 111-29.
Field Actions Science Reports, Special Issue 10 | 2014
52

U.S. Bureau of the Census (2010), Geographic Mobility: March 2008 to March 2009. Current Population
Reports, Washington DC: U.S. Government Printing Office.
White, A.M. and C.T. Gager (2007), "Idle Hands and Empty Pockets? Youth Involvement in
Extracurricular Activities, Social Capital, and Economic Status", Youth & Society, Vol. 39, No. 1,
pp.75-111.
NOTES
1. A large portion of the mobility rate in America can be accounted for by a subpopulation of
hypermobile households (Clark and Davies-Withers 2007). Therefore, these CPS figures might
underestimate rates of residential mobility because these figures do not reflect multiple moves
made by those who moved more than once within a year.
2. Coleman argues that Catholic school is indicative of social ties in the larger community that
are based on members’ religious affiliation.
3. The preliminary models confirmed significance for each dependent variable and are not
presented in the tables.
ABSTRACTS
This longitudinal study examines the moderation effects of parent-child closeness on residential
mobility and two important adolescent outcomes. Children’s behavior problems and academic
achievement test scores were compared across four survey waves of the National Longitudinal
Survey of Youth (2000, 2002, 2004, and 2006) and matched to data from their mothers' reports
from the National Longitudinal Survey of Youth 1979. The results suggest that controlling for
other dimensions of social capital (i.e., child-community and parent-community), the negative
behavioral effects of moving are buffered by the reported level of emotional closeness to one’s
parent. That is, the closer a child reports being to his/her parent, the fewer behavior problems
this child will experience following relocation. Furthermore, the negative academic effects of
moving are moderated by intergenerational solidarity and conditioned by sex. This indicates
that the reported level of parent-child closeness (vis-à-vis residential mobility) is significantly
altered by sex for achievement outcomes.
Cette étude longitudinale examine les effets de modération de la proximité parent-enfant sur la
mobilité résidentielle et deux résultats importants liés aux adolescents. Les problèmes
comportementaux des enfants et leurs performances scolaires ont été comparés d'après les
résultats de quatre vagues d'enquête du National Longitudinal Survey of Youth (2000, 2002, 2004,
et 2006), et appariés aux résultats d’une enquête conduite auprès de leurs mères, le National
Longitudinal Survey of Youth 1979. Selon les résultats, et en tenant compte des autres
dimensions du capital social (à savoir communauté des enfants et communauté des parents), les
effets comportementaux négatifs de la mobilité sont atténués par le degré rapporté de proximité
affective avec un parent. En effet, plus un enfant se dit proche de son père/sa mère, moins il aura
de problèmes comportementaux après un déménagement. De plus, les effets négatifs de la
mobilité sur les résultats scolaires sont pondérés par la solidarité intergénérationnelle et
Field Actions Science Reports, Special Issue 10 | 2014
53

conditionnés par le sexe. Cela indique que le degré de proximité parent-enfant rapporté (vis-à-
vis de la mobilité résidentielle) est considérablement influencé par le sexe en ce qui concerne les
résultats scolaires.
El presente estudio longitudinal examina los efectos de moderación que la cercanía entre padres
e hijos tiene sobre el cambio de residencia y dos importantes resultados entre los adolescentes.
Se han comparado los problemas de comportamiento y las calificaciones académicas de los niños
en cuatro fases del Estudio Longitudinal Nacional de Juventud (2000, 2002, 2004 y 2006) y se han
contrastado los datos con la información que facilitaron las madres en dicho estudio en 1979. Los
resultados sugieren que, si se controlan otras dimensiones del capital social (es decir, comunidad
infantil y comunidad de padres), los efectos negativos sobre el comportamiento que tiene el
mudarse se ven contrarrestados por el nivel de cercanía emocional con los progenitores. De tal
modo, cuanto más cercano admite un niño estar de sus padres, menores serán sus problemas de
comportamiento tras la reubicación. Así mismo, los efectos académicos negativos que conllevan
los traslados se ven aminorados por la solidaridad intergeneracional y además están
condicionados por el sexo. En este aspecto, el nivel de cercanía que se afirma tener entre padres e
hijos (con respecto al cambio de residencia) varía significativamente según el sexo en cuanto a
resultados académicos.
INDEX
Palabras claves: Adolescencia, Cambio de residencia, Capital social, Problemas de
comportamiento, Resultados académicos, Solidaridad intergeneracional
Mots-clés: Adolescence, Capital social, Mobilité résidentielle, Problèmes comportementaux,
Résultats scolaires, Solidarité intergénérationnelle
Keywords: Academic Achievement, Adolescence, Behavior Problems, Intergenerational
Solidarity, Residential Mobility, Social Capital
AUTHOR
BRIAN JOSEPH GILLESPIE
Ph.D., Assistant Professor, Department of Sociology, Sonoma State University, 1801 E. Cotati
Avenue, Rohnert Park, CA 94928, e-mail: [email protected]
Field Actions Science Reports, Special Issue 10 | 2014
54
Demographic and migration-relatedrisk factors for low-level smoking ina farm working sample of Latinos(the MICASA study)Facteurs de risque démographiques et liés à l'immigration d'un échantillon
d’ouvriers agricoles latinos (étude MICASA)
Factores de riesgo relacionados a demográfia y migración en un grupo muestra
de trabajadores agrícolas latinos que fumaban poco (el estudio MICASA)
Erik J. Rodriquez, Maria T. Stoecklin-Marois, Tamara E. Hennessy-Burt,Daniel J. Tancredi and Marc B. Schenker
Background
1 The most preventable cause of death in the U.S. is cigarette smoking (Mokdad, Marks, et
al., 2004, Mokdad, Marks, et al., 2005). In national and regional surveys Latinos have been
found to smoke at a lower rate than non-Latino Whites and non-Latino Blacks. The
national estimate of smoking prevalence among adult Latinos is 14.5% compared to 22.1%
of non-Latino Whites and 21.3% of non-Latino Blacks (Centers for Disease Control and
Prevention, 2010). Rates of smoking among Latinos have been found to differ by sex,
ethnicity, and acculturation level. Nineteen percent of Latino men smoke compared to
only 9.8% of Latino women (Centers for Disease Control and Prevention, 2010). Among
Latino ethnic groups, rates of smoking are highest among Puerto Ricans and lowest
among Central Americans (Perez-Stable, Ramirez, et al., 2001). Among Latino women,
higher levels of acculturation are associated with increased smoking (Markides, Coreil
and Ray, 1987, Marin, Perez-Stable and Marin, 1989, Haynes, Harvey, et al., 1990, Coreil,
Ray and Markides, 1991, Samet, Howard, et al., 1992, Palinkas, Pierce, et al., 1993, Cantero,
Richardson, et al., 1999, Coonrod, Balcazar, et al., 1999, Sundquist and Winkleby, 1999,
Field Actions Science Reports, Special Issue 10 | 2014
55
Acevedo, 2000). However, associations between acculturation and smoking among men is
less consistently reported (Bethel and Schenker, 2005).
2 More recently, studies have examined the phenomenon of low-level smoking, defined as
smoking one to five cigarettes per day (CPD) on average. A daily smoker is someone who
reports smoking every day while a non-daily smoker reports smoking only some days.
Among adult smokers in the U.S., Latinos are much more likely than non-Latinos to be
low-level daily smokers (Trinidad, Perez-Stable, et al., 2009). In California, 70% of Latino
smokers are either low-level or non-daily smokers (Zhu, Pulvers, et al., 2007). Further, the
number of cigarettes smoked per day is lower for Latinos. Nationally, Latino smokers on
average smoke 6.7 CPD compared to 14.9 CPD for non-Latino White smokers and 9.3 CPD
for non-Latino Black smokers (Substance Abuse and Mental Health Services
Administration, 2006). Smoking among Latino farm worker populations has been found to
be predominantly low-level smoking (Gamsky, Schenker, et al., 1992, Garcia, Matheny
Dresser and Zerr, 1996).
3 Research on the prevalence of low-level smoking in the U.S. is limited. Even less data exist
on the characteristics, risk factors, and public health significance of low-level smoking
(Reitzel, Costello, et al., 2009). The purpose of this study was to characterize low-level
smokers and identify demographic, migration-related, and psychosocial risk factors for
low-level smoking in a population of Latino farm workers in California.
Methods
Study Design and Recruitment
4 The Mexican Immigration to California: Agricultural Safety and Acculturation (MICASA)
study is a prospective cohort study conducted among Latino hired farm worker families
(Stoecklin-Marois, Hennessy-Burt and Schenker, 2011). Sampling consisted of households
residing in the town of Mendota, located in the San Joaquin Valley of California. Mendota
was chosen for its large proportion of agricultural workers and Latino immigrants (U.S.
Census Bureau). A two-stage stratified area probability sampling design was used. In the
first step census blocks were randomly selected from a list of all census blocks in Mendota
and enumerators walked door-to-door to map out all dwellings in 62 selected census
blocks. In the second step enumerators acquired demographic information about adult
individuals residing in each dwelling including age, sex, years lived in Mendota, and
involvement in agricultural work. Households that contained at least one hired farm
worker were randomly ordered and contacted sequentially for recruitment. Further
details regarding the sampling design methods and recruitment of participants have been
described previously (Stoecklin-Marois, Hennessy-Burt and Schenker, 2011).
Informed Consent
5 Prior to obtaining written informed consent, a verbal and written description of the study
objectives and procedures were provided to each participant. The study description and
written informed consent were provided in Spanish, the primary language of
participants. All study procedures were approved by the University of California, Davis
Institutional Review Board.
Field Actions Science Reports, Special Issue 10 | 2014
56
Participant Eligibility
6 Men and women were eligible to participate in the study if they were 18 to 55 years of
age, self-identified as Mexican or Central American, resided in Mendota at the time of the
baseline interview, and worked or had a household member who worked in agriculture
for at least 45 days in the last year. Eligibility for the present analysis included
completion of both the baseline and follow-up interviews.
Rates of Participation
7 From these households, 803 participants completed the baseline interview and 620 (77.2%
) subsequently completed the follow-up interview. For individuals who were not
recruited, reported reasons for not participating included distrust, no time or interest,
and unwillingness to disclose personal information.
Data Collection and Questionnaire Instruments
8 The recruitment and baseline interviews of participants were conducted between January
2006 and April 2007. Participant follow-up interviews were conducted between November
2008 and February 2010. Both the baseline and follow-up questionnaires were
interviewer-administered in Spanish and most interviews were conducted in the
participant’s home. Both the baseline and follow-up interviews assessed demographic
characteristics, work history, smoking and psychosocial factors. Migration-related factors
were assessed only at the baseline interview and frequent mental distress was assessed
for the first time at the follow-up interview.
Demographic Characteristics and Migration-Related Factors
9 Demographic characteristics assessed included participant sex, date of birth, marital
status, educational attainment, annual household income, and number of years worked in
agriculture. Migration-related factors included country of birth, age at immigration to
the U.S., number of years lived in the U.S., and acculturation level. In order to better
capture the multi-dimensionality of an individual’s level of acculturation, the revised
version of the Acculturation Rating Scale for Mexican Americans (ARSMA-II) was used
(Cuellar, Arnold and Maldonado, 1995). Two acculturation level categories were
established: low and medium or high (medium/high).
Smoking-Related Outcomes and Low-Level Smoking
10 Questions from the ATS-DLD-78-A were used to assess cigarette smoking (American
Thoracic Society). Participants who reported ever smoking at least 100 cigarettes (5
packs) in the follow-up interview were classified as smokers. Those who reported
smoking a cigarette within the past 30 days of the follow-up interview were identified as
current smokers. Current smokers were then classified as either low-level smokers,
defined as individuals smoking one to five CPD on average since they began smoking, or
individuals smoking 6+ CPD on average according to the follow-up interview. Both
smoking groups included daily and non-daily smokers. Individuals who met the criterion
Field Actions Science Reports, Special Issue 10 | 2014
57
for smoking but had not smoked a cigarette within the past 30 days were categorized as
former smokers.
11 Three participants were excluded from the analysis because their smoking status at the
follow-up interview could not be determined. These three participants reported current
smoking at the baseline interview but never smoking at the follow-up interview. Three
additional participants were missing data for the age that they last smoked cigarettes.
These data were imputed by subtracting the number of years since each participant quit
smoking cigarettes from that participant’s age at the follow-up interview.
Psychosocial and Quality of Life Factors
12 Among the psychosocial factors assessed in the baseline interview were depressive
symptoms, perceived stress, family support, and nervios. Depressive symptoms were
assessed using a validated screening instrument developed from questions on the Center
for Epidemiologic Studies Depression Scale (CES-D) and the Diagnostic Interview Schedule
(DIS) from the National Institutes of Mental Health (Burnam, Wells, et al., 1988). Items
were coded according to the method by Burnam and colleagues later creating a
probability of depressive symptoms. The Perceived Stress Scale questions were rated on a
Likert scale and included the following: “how often have you dealt successfully with daily
problems and hassles?”, “how often have you coped well with important changes that
were taking place in your life?”, “how often have you felt confident about your being able
to handle your personal problems?”, “how often have you been able to control your anger
in your life?”, “how often have you felt that you were on top of things?”, and “how often
did you feel that things were going well?” (Cohen, Kamarck and Mermelstein, 1983).
13 The assessment of family support was based upon seven items from the Provisions of
Social Relations Scale and consisted of the following statements: “no matter what
happens, I know that my family will always be there for me should I need them”, “I’m not
sure if I can completely rely on my family”, “my family lets me know they think I’m a
worthwhile person”, “people in my family have confidence in me”, “people in my family
provide me with help in finding solutions to my problems”, “I know my family will always
stand by me”, and “I know I can count on my family for financial assistance should I need
it” (Turner, Frankel and Levin, 1983). Cronbach’s alpha coefficients for perceived stress
and family support were 0.80 and 0.88, respectively. Scores for both perceived stress and
family support were created by summing responses for each item; with higher scores
indicating higher levels of stress and family support. These scores were then
dichotomized by using the mean and/or median as a cut-off point. Scores above this
established cut-off point were designated as having a “high” level of perceived stress or
family support.
14 A culturally-specific condition known as nervios was assessed. Nervios has been
previously described as a generalized condition of distress that can be expressed with
somatic and psychological symptoms (Salgado de Snyder, Diaz-Perez and Ojeda, 2000).
Participants were classified as having nervios based upon an affirmative response to the
question “sometimes in your life, have you ever suffered from nervios?”. Fair or poor
(fair/poor) self-rated health and frequent mental distress were assessed using the
Healthy Days Core Module of the Health-Related Quality of Life instrument from the
Centers for Disease Control and Prevention (CDC HRQOL – 4) (Centers for Disease Control
and Prevention).
Field Actions Science Reports, Special Issue 10 | 2014
58

Statistical methods
15 Univariate analyses were performed on all variables by calculating means, medians, and
standard deviations for continuous variables and frequencies and proportions for
nominal and ordinal variables. Bivariate analyses examined smoking outcome variables
by each predictor of interest. One-way analysis of variance F-tests and chi-square tests for
association were used to assess statistical significance by smoking group for continuous
and categorical study variables, respectively. Multinomial logistic regression was used to
model low-level smoking and smoking 6+ CPD, separately, against the reference category
of never and former smoking combined (never/former smoking). Survey data analysis
procedures for logistic regression analyses were used to adjust confidence intervals and
hypotheses tests for the probability sampling design. All analyses were performed using
Statistical Analysis Software, Version 9.2 (SAS Institute Inc., Cary, North Carolina).
Results
16 Since patterns of smoking differ between men and women, analyses of demographic
characteristics were stratified by sex. Mean age of participants at the follow-up interview
was 40.8 years, but men tended to be older than women (p<0.01) (Table 1). The cohort
was roughly balanced by sex with 45% men and 55% women. Although 95% of the cohort
was married or living with someone at the follow-up interview, a significantly larger
proportion of women reported being single, divorced, separated, or widowed (p<0.01).
Women were more educated than men; 39% of women versus 29% of men had completed
a higher than primary school education (p=0.03). Average annual incomes were low in the
population with over three fourths of participants reporting household incomes <$30,000.
17 One hundred percent of men versus 83% of women ever worked in agriculture (p<0.0001;
data not shown). Additionally, men had significantly more work experience in agriculture
than women with men reporting an average of 17.7 years compared to 10.5 years for
women (p<0.0001).
18 Sixty-eight percent of participants were born in Mexico and 29% of participants were
born in either El Salvador or another Central American country. Overall, the average
number of years lived in the U.S. was 15.6 and men had a longer residency than women
(18.4 vs. 13.5 years, p<0.0001). Men immigrated to the U.S. 2.5 years earlier, on average,
than women. Despite men immigrating earlier and living in the U.S. longer, men and
women did not differ significantly by acculturation level. The vast majority of both sexes
were classified with a low level of acculturation.
Field Actions Science Reports, Special Issue 10 | 2014
59
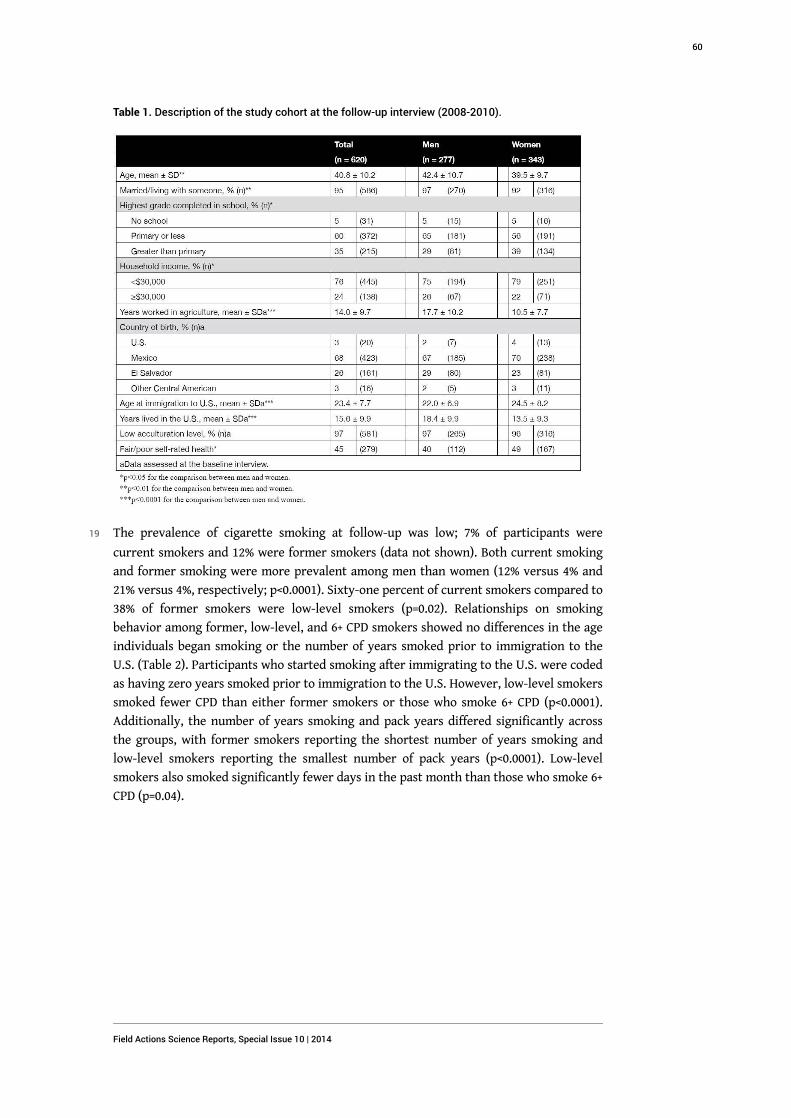
Table 1. Description of the study cohort at the follow-up interview (2008-2010).
19 The prevalence of cigarette smoking at follow-up was low; 7% of participants were
current smokers and 12% were former smokers (data not shown). Both current smoking
and former smoking were more prevalent among men than women (12% versus 4% and
21% versus 4%, respectively; p<0.0001). Sixty-one percent of current smokers compared to
38% of former smokers were low-level smokers (p=0.02). Relationships on smoking
behavior among former, low-level, and 6+ CPD smokers showed no differences in the age
individuals began smoking or the number of years smoked prior to immigration to the
U.S. (Table 2). Participants who started smoking after immigrating to the U.S. were coded
as having zero years smoked prior to immigration to the U.S. However, low-level smokers
smoked fewer CPD than either former smokers or those who smoke 6+ CPD (p<0.0001).
Additionally, the number of years smoking and pack years differed significantly across
the groups, with former smokers reporting the shortest number of years smoking and
low-level smokers reporting the smallest number of pack years (p<0.0001). Low-level
smokers also smoked significantly fewer days in the past month than those who smoke 6+
CPD (p=0.04).
Field Actions Science Reports, Special Issue 10 | 2014
60
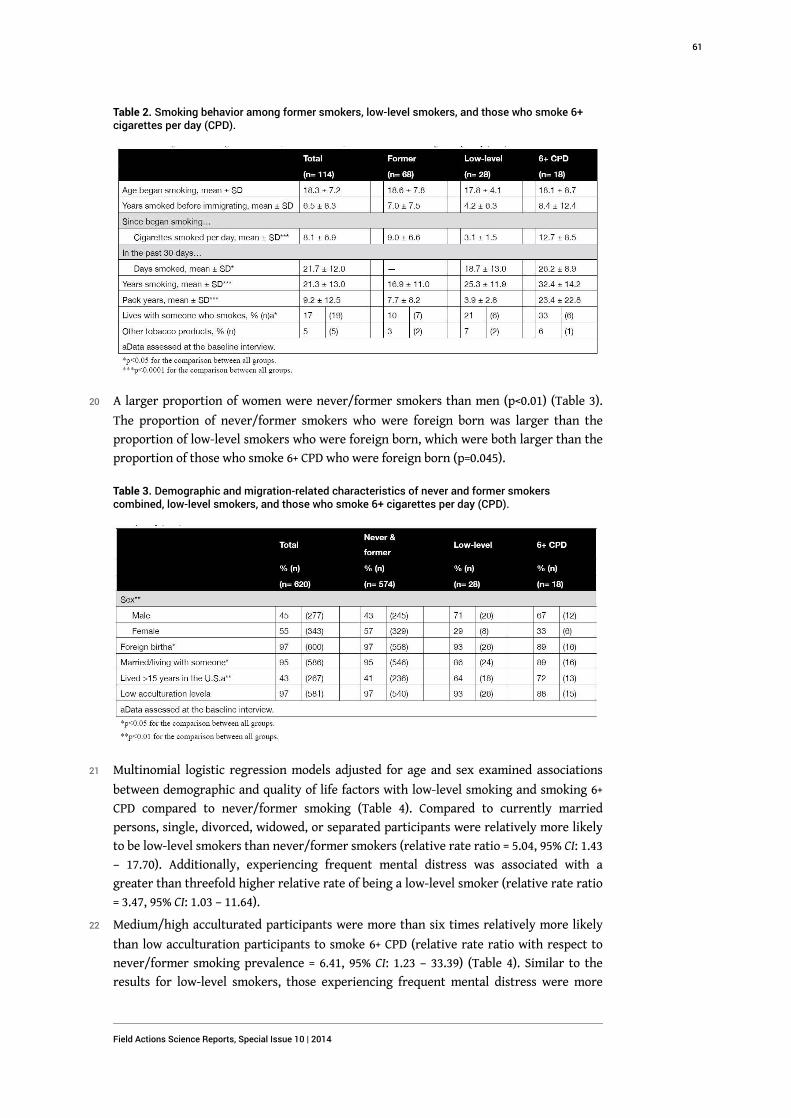
Table 2. Smoking behavior among former smokers, low-level smokers, and those who smoke 6+cigarettes per day (CPD).
20 A larger proportion of women were never/former smokers than men (p<0.01) (Table 3).
The proportion of never/former smokers who were foreign born was larger than the
proportion of low-level smokers who were foreign born, which were both larger than the
proportion of those who smoke 6+ CPD who were foreign born (p=0.045).
Table 3. Demographic and migration-related characteristics of never and former smokerscombined, low-level smokers, and those who smoke 6+ cigarettes per day (CPD).
21 Multinomial logistic regression models adjusted for age and sex examined associations
between demographic and quality of life factors with low-level smoking and smoking 6+
CPD compared to never/former smoking (Table 4). Compared to currently married
persons, single, divorced, widowed, or separated participants were relatively more likely
to be low-level smokers than never/former smokers (relative rate ratio = 5.04, 95% CI: 1.43
– 17.70). Additionally, experiencing frequent mental distress was associated with a
greater than threefold higher relative rate of being a low-level smoker (relative rate ratio
= 3.47, 95% CI: 1.03 – 11.64).
22 Medium/high acculturated participants were more than six times relatively more likely
than low acculturation participants to smoke 6+ CPD (relative rate ratio with respect to
never/former smoking prevalence = 6.41, 95% CI: 1.23 – 33.39) (Table 4). Similar to the
results for low-level smokers, those experiencing frequent mental distress were more
Field Actions Science Reports, Special Issue 10 | 2014
61
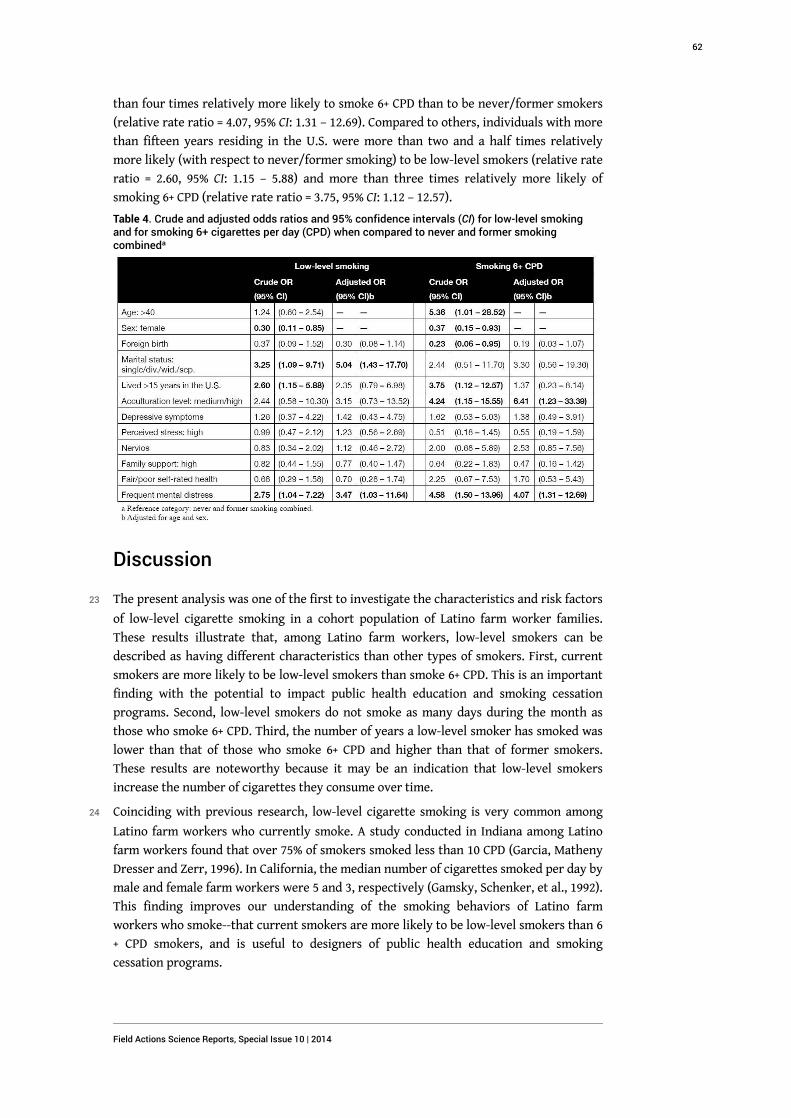
than four times relatively more likely to smoke 6+ CPD than to be never/former smokers
(relative rate ratio = 4.07, 95% CI: 1.31 – 12.69). Compared to others, individuals with more
than fifteen years residing in the U.S. were more than two and a half times relatively
more likely (with respect to never/former smoking) to be low-level smokers (relative rate
ratio = 2.60, 95% CI: 1.15 – 5.88) and more than three times relatively more likely of
smoking 6+ CPD (relative rate ratio = 3.75, 95% CI: 1.12 – 12.57).
Table 4. Crude and adjusted odds ratios and 95% confidence intervals (CI) for low-level smokingand for smoking 6+ cigarettes per day (CPD) when compared to never and former smokingcombineda
Discussion
23 The present analysis was one of the first to investigate the characteristics and risk factors
of low-level cigarette smoking in a cohort population of Latino farm worker families.
These results illustrate that, among Latino farm workers, low-level smokers can be
described as having different characteristics than other types of smokers. First, current
smokers are more likely to be low-level smokers than smoke 6+ CPD. This is an important
finding with the potential to impact public health education and smoking cessation
programs. Second, low-level smokers do not smoke as many days during the month as
those who smoke 6+ CPD. Third, the number of years a low-level smoker has smoked was
lower than that of those who smoke 6+ CPD and higher than that of former smokers.
These results are noteworthy because it may be an indication that low-level smokers
increase the number of cigarettes they consume over time.
24 Coinciding with previous research, low-level cigarette smoking is very common among
Latino farm workers who currently smoke. A study conducted in Indiana among Latino
farm workers found that over 75% of smokers smoked less than 10 CPD (Garcia, Matheny
Dresser and Zerr, 1996). In California, the median number of cigarettes smoked per day by
male and female farm workers were 5 and 3, respectively (Gamsky, Schenker, et al., 1992).
This finding improves our understanding of the smoking behaviors of Latino farm
workers who smoke--that current smokers are more likely to be low-level smokers than 6
+ CPD smokers, and is useful to designers of public health education and smoking
cessation programs.
Field Actions Science Reports, Special Issue 10 | 2014
62
25 Statewide, representative data in California has shown that the prevalence of daily low-
level smoking among Latinos in the general population is between 16% and 22% (Zhu,
Pulvers, et al., 2007). However, among non-daily Latino smokers the prevalence of low-
level smoking is between 80% and 85%. In the present analysis, we could not clearly
identify daily and non-daily smokers because smokers were not asked whether they
smoke “every day” or “some days”. However, the prevalence of smoking 30 days in the
past month among low-level smokers was 54% and among those who smoke 6+ CPD was
83% (p=0.04). This would indicate that low-level smokers in the present analysis are non-
daily smokers. Not only is the prevalence of low-level smoking high among Latinos, but
Latinos have been found to have increased odds of low-level smoking compared to Blacks
or Asian/Pacific Islanders. Using nationally representative data, from the Tobacco Use
Supplement of the Current Population Survey, Trinidad and colleagues estimated that
Latinos have 4.6 higher odds of being low-level daily smokers compared to Non-Latino
Whites (Trinidad, Perez-Stable, et al., 2009).
26 The characteristics and risk factors of low-level smoking in the Latino population have
not been well established in the literature. One study examining low-level smoking
attempted to understand the associations of demographic characteristics, tobacco
dependence, withdrawal, and cessation with low-level smoking among Latinos from a
randomized clinical control trial (Reitzel, Costello, et al., 2009). Research into the
characteristics and risk factors of low-level smoking among other ethnic groups is limited
to a few studies that examined associations with smoking ≤10 CPD. Among African
Americans, smoking ≤10 CPD in young adulthood has been linked to factors in late
adolescence such as perceived discrimination, peer smoking, and youth maladaptive
characteristics as well as less parental educational attainment and parental smoking
(Fagan, Brook, et al., 2009). Among Asian Americans, being a woman, highly educated, not
Korean (compared to Chinese), and being a bilingual speaker with high English
proficiency compared to being an English-only speaker were factors associated with
smoking ≤9 CPD (Tong, Nguyen, et al., 2009).
27 In the present analysis, being single, divorced, widowed, or separated was found to be
strongly associated with being a low-level smoker. Research has found that low-level
smokers are more likely not to be married (Hyland, Rezaishiraz, et al., 2005). Additionally,
frequent mental distress was associated with a more than threefold higher relative rate of
low-level smoking (with respect to never/former smoking). Reasons why marital status
and mental distress are associated with low-level smoking have not been well
investigated. Being married or living with someone may be protective of social pressures
to smoke from other family members, friends, and coworkers (Coreil, Ray and Markides,
1991).
28 A population-based study using data from the California Tobacco Survey by Zhu and
colleagues found that only 36% of low-level smokers at baseline remained low-level
smokers 20 months later compared to 82% of 6+ CPD daily smokers. Additionally, they
observed that 21% of low-level smokers at baseline increased their cigarette consumption
to that of 6+ CPD daily smokers 20 months later (Zhu, Sun, et al., 2003). These findings
give some context to the results observed in the present analysis regarding the number of
years smoking and smoking group. Low-level smokers were found to smoke for fewer
years than those who smoke 6+ CPD. This may be because low-level smokers are more
likely to change their cigarette consumption over time.
Field Actions Science Reports, Special Issue 10 | 2014
63

29 Conclusions drawn from the present analysis should be interpreted with caution due to
the small numbers of smokers in each group. Other limitations due to the sample size of
current smokers include the inability to identify characteristics and establish risk factors
by sex, Latino ethnicity, or daily/non-daily status. However, strengths of the present
study include its use of data from a representative, random sample of farm worker
families in California, its effort to describe and characterize low-level smokers using
demographic, migration-related, and psychosocial approaches, and its contribution to the
understanding of the high prevalence of low-level smoking among Latinos. These findings
warrant consideration of smoking behaviors, demographic characteristics, and quality of
life factors when targeting current smokers for smoking education and cessation
programs; particularly among Latinos and underserved populations such as farm
workers. Among the recommendations for future research are to investigate the self-
perceptions of low-level smokers as being smokers or non-smokers and to examine the
characteristics and risk factors of daily and non-daily low-level smoking separately.
Acknowledgements
30 The authors of the present analysis give much gratitude and appreciation to the MICASA
study participants and local field staff, with special thanks to Gloria Andrade, Alex
Cervantes, Ana Cervantes, and Giselle Garcia. Funding for the MICASA study was provided
by the National Institute for Occupational Safety and Health (2U500H007550 and
RO1OH009293) and The California Endowment. The authors would also like to
acknowledge the UC Global Health Institute (UCGHI) for providing partial funding for the
presentation and review of this work.
BIBLIOGRAPHY
Acevedo, M. C. (2000), "The Role of Acculturation in Explaining Ethnic Differences in the Prenatal
Health-Risk Behaviors, Mental Health, and Parenting Beliefs of Mexican American and European
American at-Risk Women", Child Abuse Negl, Vol.24, No.1, pp. 111-127.
American Thoracic Society "Ats-Dld-78-A", www.cdc.gov/niosh/atswww.txt.
Bethel, J. W. and M. B. Schenker (2005), "Acculturation and Smoking Patterns among Hispanics: A
Review", Am J Prev Med, Vol.29, No.2, pp. 143-148.
Burnam, M. A., K. B. Wells, B. Leake and J. Landsverk (1988), "Development of a Brief Screening
Instrument for Detecting Depressive Disorders", Med Care, Vol.26, No.8, pp. 775-789.
Cantero, P. J., J. L. Richardson, L. Baezconde-Garbanati and G. Marks (1999), "The Association
between Acculturation and Health Practices among Middle-Aged and Elderly Latinas", Ethn Dis,
Vol.9, No.2, pp. 166-180.
Centers for Disease Control and Prevention "Health-Related Quality of Life (Hrqol)",
www.cdc.gov/hrqol/index.htm.
Field Actions Science Reports, Special Issue 10 | 2014
64
Centers for Disease Control and Prevention (2010), "Vital Signs: Current Cigarette Smoking
among Adults Ages ≥ 18 Years - United States, 2009", Morbidity and Mortality Weekly Report,
Vol.59, No.35, pp. 1135-1140.
Cohen, S., T. Kamarck and R. Mermelstein (1983), "A Global Measure of Perceived Stress", J Health
Soc Behav, Vol.24, No.4, pp. 385-396.
Coonrod, D. V., H. Balcazar, J. Brady, S. Garcia, et al. (1999), "Smoking, Acculturation and Family
Cohesion in Mexican-American Women", Ethn Dis, Vol.9, No.3, pp. 434-440.
Coreil, J., L. A. Ray and K. S. Markides (1991), "Predictors of Smoking among Mexican-Americans:
Findings from the Hispanic Hanes", Prev Med, Vol.20, No.4, pp. 508-517.
Cuellar, I., B. Arnold and R. Maldonado (1995), "Acculturation Rating Scale for Mexican
Americans-Ii: A Revision of the Original Arsma Scale", Hispanic Journal of Behavioral Sciences,
Vol.17, No.3, pp. 275-304.
Fagan, P., J. S. Brook, E. Rubenstone, C. Zhang, et al. (2009), "Longitudinal Precursors of Young
Adult Light Smoking among African Americans and Puerto Ricans", Nicotine Tob Res, Vol.11,
No.2, pp. 139-147.
Gamsky, T. E., M. B. Schenker, S. A. McCurdy and S. J. Samuels (1992), "Smoking, Respiratory
Symptoms, and Pulmonary Function among a Population of Hispanic Farmworkers", Chest,
Vol.101, No.5, pp. 1361-1368.
Garcia, J. G., K. S. Matheny Dresser and A. D. Zerr (1996), "Respiratory Health of Hispanic Migrant
Farm Workers in Indiana", Am J Ind Med, Vol.29, No.1, pp. 23-32.
Haynes, S. G., C. Harvey, H. Montes, H. Nickens, et al. (1990), "Patterns of Cigarette Smoking
among Hispanics in the United States: Results from Hhanes 1982-84", Am J Public Health, Vol.80
Suppl, pp. 47-53.
Hyland, A., H. Rezaishiraz, J. Bauer, G. A. Giovino, et al. (2005), "Characteristics of Low-Level
Smokers", Nicotine Tob Res, Vol.7, No.3, pp. 461-468.
Marin, G., E. J. Perez-Stable and B. V. Marin (1989), "Cigarette Smoking among San Francisco
Hispanics: The Role of Acculturation and Gender", Am J Public Health, Vol.79, No.2, pp. 196-198.
Markides, K. S., J. Coreil and L. A. Ray (1987), "Smoking among Mexican Americans: A Three-
Generation Study", Am J Public Health, Vol.77, No.6, pp. 708-711.
Mokdad, A. H., J. S. Marks, D. F. Stroup and J. L. Gerberding (2004), "Actual Causes of Death in the
United States, 2000", JAMA, Vol.291, No.10, pp. 1238-1245.
Mokdad, A. H., J. S. Marks, D. F. Stroup and J. L. Gerberding (2005), "Correction: Actual Causes of
Death in the United States, 2000", JAMA, Vol.293, No.3, pp. 293-294.
Palinkas, L. A., J. Pierce, B. P. Rosbrook, S. Pickwell, et al. (1993), "Cigarette Smoking Behavior and
Beliefs of Hispanics in California", Am J Prev Med, Vol.9, No.6, pp. 331-337.
Perez-Stable, E. J., A. Ramirez, R. Villareal, G. A. Talavera, et al. (2001), "Cigarette Smoking
Behavior among Us Latino Men and Women from Different Countries of Origin", Am J Public
Health, Vol.91, No.9, pp. 1424-1430.
Reitzel, L. R., T. J. Costello, C. A. Mazas, J. I. Vidrine, et al. (2009), "Low-Level Smoking among
Spanish-Speaking Latino Smokers: Relationships with Demographics, Tobacco Dependence,
Withdrawal, and Cessation", Nicotine Tob Res, Vol.11, No.2, pp. 178-184.
Field Actions Science Reports, Special Issue 10 | 2014
65

Salgado de Snyder, V. N., M. J. Diaz-Perez and V. D. Ojeda (2000), "The Prevalence of Nervios and
Associated Symptomatology among Inhabitants of Mexican Rural Communities", Cult Med
Psychiatry, Vol.24, No.4, pp. 453-470.
Samet, J. M., C. A. Howard, D. B. Coultas and B. J. Skipper (1992), "Acculturation, Education, and
Income as Determinants of Cigarette Smoking in New Mexico Hispanics", Cancer Epidemiol
Biomarkers Prev, Vol.1, No.3, pp. 235-240.
Stoecklin-Marois, M. T., T. E. Hennessy-Burt and M. B. Schenker (2011), "Engaging a Hard-to-
Reach Population in Research: Sampling and Recruitment of Hired Farm Workers in the Micasa
Study", J Agric Safety Health, Vol.In press, pp.
Substance Abuse and Mental Health Services Administration (2006), "Past Month Cigarette Use
among Racial and Ethnic Groups", The NSDUH Report, No.30, pp.
Sundquist, J. and M. A. Winkleby (1999), "Cardiovascular Risk Factors in Mexican American
Adults: A Transcultural Analysis of Nhanes Iii, 1988-1994", Am J Public Health, Vol.89, No.5, pp.
723-730.
Tong, E. K., T. Nguyen, E. Vittinghoff and E. J. Perez-Stable (2009), "Light and Intermittent
Smoking among California's Asian Americans", Nicotine Tob Res, Vol.11, No.2, pp. 197-202.
Trinidad, D. R., E. J. Perez-Stable, S. L. Emery, M. M. White, et al. (2009), "Intermittent and Light
Daily Smoking across Racial/Ethnic Groups in the United States", Nicotine Tob Res, Vol.11, No.2,
pp. 203-210.
Turner, R. J., B. G. Frankel and D. M. Levin (1983), "Social Support: Conceptualization,
Measurement, and Implications for Mental Health", Research in Community and Mental Health,
JAI Press, Greenwich, CT, pp. 67-111.
U.S. Census Bureau "American Fact Finder", http://factfinder2.census.gov/.
Zhu, S. H., K. Pulvers, Y. Zhuang and L. Baezconde-Garbanati (2007), "Most Latino Smokers in
California Are Low-Frequency Smokers", Addiction, Vol.102 Suppl 2, pp. 104-111.
Zhu, S. H., J. Sun, S. Hawkins, J. Pierce, et al. (2003), "A Population Study of Low-Rate Smokers:
Quitting History and Instability over Time", Health Psychol, Vol.22, No.3, pp. 245-252.
ABSTRACTS
Cigarette smoking is the most preventable cause of death in the U.S. Research regarding the
phenomenon of low-level smoking, defined as smoking one to five cigarettes per day (CPD) on
average, is increasing as its high prevalence is better recognized. The Mexican Immigration to
California: Agricultural Safety and Acculturation (MICASA) study is a prospective cohort study of
Latino hired farm worker families that assesses respiratory health, including patterns and
behaviors of cigarette smoking. The purpose of the present analysis was to establish
demographic, migration-related, and psychosocial characteristics and risk factors for low-level
smoking. Seven percent of participants were current smokers, 61% of them being low-level
smokers. Low-level smokers did not smoke as many days during the past month as those who
smoke 6+ CPD (p=0.04). Low-level smokers were more likely than never and former smokers
combined not to be married and to experience frequent mental distress. Those who smoke 6+
CPD were also more likely than never and former smokers combined to experience frequent
mental distress and to be more acculturated. Low-level smokers have characteristics and risk
factors that set them apart from other types of smokers. This increased understanding of low-
Field Actions Science Reports, Special Issue 10 | 2014
66

level smokers can enhance public health education and smoking cessation programs targeted at
Latinos.
Le tabagisme est la principale cause de décès évitable aux Etats-Unis. La recherche sur le
tabagisme faible, défini comme la consommation d'une à cinq cigarettes par jour (CPJ) en
moyenne, se développe car la forte prévalence de ce type de tabagisme est de mieux en mieux
reconnue. L'étude MICASA (The Mexican Immigration to California : Agricultural Safety and
Acculturation) est une étude de cohorte prospective portant sur des familles d'ouvriers agricoles
latinos salariés qui évalue la santé respiratoire, y compris les modes et comportements face au
tabagisme. La présente analyse a pour but de déterminer les caractéristiques démographiques,
psychosociales et liées à l'immigration et les facteurs de risque pour le tabagisme faible. Sept
pour cent des participants étaient des fumeurs et 61 % d'entre eux étaient des petits fumeurs. Au
cours du mois précédent, les petits fumeurs n'avaient pas fumé autant de jours que ceux qui
avaient fumé 6+ CPJ (p=0,04). Les petits fumeurs étaient plus susceptibles d'être célibataires et de
connaître des épisodes fréquents de détresse mentale que les personnes n'ayant jamais fumé et
les anciens fumeurs. Ceux qui fumaient 6+ CPJ étaient également plus susceptibles de connaître
des épisodes fréquents de détresse mentale et d'être plus acculturés que les personnes n'ayant
jamais fumé et que les anciens fumeurs. Les petits fumeurs ont des caractéristiques et des
facteurs de risque qui les mettent à part des autres types de fumeurs. Cette meilleure
compréhension des petits fumeurs peut améliorer l'éducation en matière de santé publique et les
programmes de lutte contre le tabagisme destinés aux Latinos.
En los Estados Unidos fumar cigarrillos es la causa de muerte que más puede prevenirse. Las
investigaciones de fumadores con bajos niveles de consumo, definido como el consumo de uno a
cinco cigarrillos por día en promedio (CDP por sus siglas en inglés), están aumentando en cuanto
su alta prevalencia se conoce mejor. El estudio Migración Mexicana a California: Seguridad en la
Agricultura y Aculturación (MICASA por sus siglas en inglés) evaluó la salud pulmonar de una
cohorte de trabajadores del campo y sus familias, incluyendo sus patrones de conducta en
relación a fumar cigarrillos. El propósito del presente análisis fue establecer las características
demográficas y psicológicas, así como las relacionadas a la migración y los factores de riesgo de
los fumadores con bajos niveles de consumo de cigarrillos. Siete por ciento de los participantes
eran fumadores, de ellos 61% lo hacían en un bajo nivel. Los fumadores con bajos niveles de
consumo no fumaron tantos días durante el mes anterior como aquellos que fumaban 6+ (p=0.04).
Los fumadores con bajos niveles tenían más probabilidades de no estar casados y experimentaban
angustia mental con más frecuencia. Aquellos que fumaban 6+ CDP tenían mayor probabilidad
que los que no fumaban nunca y de los que dejaron de fumar combinados a experimentar
angustia mental y estaban más aculturados. Los fumadores con bajos niveles tenían
características y factores de riesgo que los diferenciaba de los otros tipos de fumadores. Este
mejor entendimiento de los fumadores con bajos niveles de consumo puede mejorar la educación
pública y los programas para dejar de fumar que se enfocan en los latinos.
INDEX
Mots-clés: Acculturation, Agriculture, Epidémiologie, Hispaniques/Latinos, Psychosocial,
Tabagisme
Palabras claves: Aculturación, Agricultura, Consumo de tabaco, Epidemiología, Hispanos/
latinos, Psicosocial
Keywords: Acculturation, Agriculture, Epidemiology, Hispanics/Latinos, Psychosocial, Smoking
Field Actions Science Reports, Special Issue 10 | 2014
67
AUTHORS
ERIK J. RODRIQUEZ
Ph.D., M.P.H., University of California, Western Center for Agricultural, Health and Safety Center
for Tobacco Control Research and Education, 530 Parnassus Ave, Ste 366, Box 1390 - San
Francisco, CA 94143-1390, [email protected]
MARIA T. STOECKLIN-MAROIS
Ph.D., M.P.H., University of California, Davis Department of Public Health Sciences, Western
Center for Agricultural Health and Safety
TAMARA E. HENNESSY-BURT
M.S., University of California, Davis Department of Public Health Sciences, Western Center for
Agricultural Health and Safety
DANIEL J. TANCREDI
Ph.D., UC Davis School of Medicine Department of Pediatrics, Western Center for Agricultural
Health and Safety
MARC B. SCHENKER
M.D., M.P.H., University of California, Davis Department of Public Health Sciences, Western
Center for Agricultural Health and Safety
Field Actions Science Reports, Special Issue 10 | 2014
68
Depression, perceived stress andnervios associated with injury in theMICASA Study, a California farmworker populationDépression, stress ressenti et état de nervosité associés à des blessures dans
l'étude MICASA portant sur une population d'ouvriers agricoles en Californie
Depresión, percepcion de estrés y nervios asociados con lesiones según el estudio
MICASA realizado entre la población agrícola de California
Hong Xiao, Maria Stoecklin-Marois, Chin-shang Li, Stephen A. McCurdyand Marc Schenker
Introduction
1 Farming is an arduous occupation (Schenker 1996; Schenker 2010) and produces a high
number of related injuries. Agriculture ranks among the three occupational groups with
the highest occupational fatality rate (Schenker 2010). The occupational fatality rate in
agriculture remained high (22/100,000 workers) during the 1990s (Rautiainen and
Reynolds 2002). The United States Department of Agriculture (USDA) reported a fatality
rate of 28/100,000 workers in 2002. In California, there are more than 20,000 disabling
non-fatal injuries each year among agricultural workers, and it is estimated that the
actual number may be even higher (Villarejo and Baron 1999). National data suggest that
livestock, machinery, and falls are the most important sources for farm worker injury
(Meyers 1998). Strains and sprains are the most common injuries among migrant farm
workers in California (McCurdy, Samuels et al. 2003).
2 California’s agriculture industry generates products worth over $36 billion/year, and
relies primarily on hired farm labor in all aspects of production (CDFA 2008). Hired farm
workers are often immigrants with little or no safety training who face language and
Field Actions Science Reports, Special Issue 10 | 2014
69

cultural barriers and may experience additional challenges because of their
undocumented status (Schenker 2010). These characteristics place farm workers at high
risk of injury (Schenker 2010; Villarejo, McCurdy et al. 2010).
3 Psychological hazards have been associated with agricultural work, (Gregoire 2002)
including depression (Sanne, Mykletun et al. 2004), stress (Simkin, Hawton et al. 1998),
and low level of social support (Linn and Husaini 1987). The 12 month prevalence of mood
disorder was 9.5% in US adult population according to Kessler and colleagues’ report
(Kessler, Chiu et al. 2005). Only half of them received minimally adequate treatment
(Wang, Lane et al. 2005). Women are 50 % more likely to experience a mood disorder than
men during their lifetime. Latinos are more likely to experience a mood disorder than
non-Latinos during their lifetime (Kessler, Berglund et al. 2005). Linn and Husaini
reported a 20% prevalence of depression among Tennessee farm residents (Linn and
Husaini 1987). Eight percent of Ohio cash grain farmers screened positive for depressive
symptoms (Elliott, Heaney et al. 1995), and a 9.3% prevalence of depressive symptoms was
reported in Colorado farmers (Stallones, Lefft et al. 1995). Depression has been associated
with occupational injuries in agriculture (Park, Sprince et al. 2001; Tiesman, Peek-Asa et
al. 2006). However, there have been only few studies on mental health outcomes and
injury among Latino farm workers (Alderete, Vega et al. 2000).
4 Compared to non-Hispanic whites and other ethnic groups, a higher prevalence of
depressive symptoms was also observed among a Latino adolescent population, especially
among those living in rural areas and those with low socio-economic status (Mikolajczyk,
Bredehorst et al. 2007). Nervios is a culturally-interpreted syndrome which is expressed
with a variety of somatic symptoms, such as headaches, fatigue, diarrhea, or dizziness;
and psychological symptoms such as feeling sad, irritable, angry, or absent-minded
(Salgado de Snyder, Diaz-Perez et al. 2000). Nervios represents the physical and emotional
pain that may arise from family poverty, legal status, gender roles, rural background and
social isolation and other stresses, and is expressed in anger and powerlessness (Salgado
de Snyder, Diaz-Perez et al. 2000). Nervios has been significantly associated with stress
and depressive symptoms in Latinos (Weller, Baer et al. 2008).
5 The National Institute for Occupational Safety and Health (NIOSH) has identified stress as
a serious occupational health problem in agriculture (Carruth and Logan 2002). More
than 50% of female farmers have reported symptoms of stress (Berkowitz and Perkins
1985). Social support had ameliorating effects on life stress and was more protective of
psychological health among men, compared to women (Falcon, Todorova et al. 2009).
Despite the importance of psychosocial factors, there are few studies examining these in
the context of agricultural injury. The purpose of this study was to assess psychosocial
factors, including depression, nervios, social support and perceived stress, and their
relationship with injury among a population-based sample of Latino hired farm workers
in California.
Methods
Sample description and eligibility
6 The Mexican Immigration to California: Agricultural Safety and Acculturation (MICASA)
study is a population-based cohort study of occupational exposures and health in farm
workers. Data for this analysis were derived from the MICASA baseline interview
Field Actions Science Reports, Special Issue 10 | 2014
70
undertaken in 2006-2007. Eligible participants included men and women, 18-55 years old,
who identified themselves as Mexican, Central American, Hispanic or Latino, with at least
one member of the household engaged in farm work for at least 45 days in the last year
and residing in Mendota, CA at the time of the interview.
Sample and recruitment
7 A stratified area probability design was used with census block as the primary sampling
unit. A two-stage enumeration was employed to obtain information on age, gender,
nationality, farm work, and years living in Mendota for each adult member of the
household. Further details of the procedure are documented elsewhere (Stoecklin-Marois,
T.E.Hennessy-Burt et al. 2011). A random list of eligible, enumerated households was
created, and households were approached and asked to participate in the study. There
were a total of 467 households, comprising 843 adults who were recruited and completed
a baseline interview. Of these, 759 individuals answered “yes” to the question “have you
ever worked in agriculture?” and are included in this analysis.
Data collection
8 All data collection was done by a local field team in Mendota. The interviewer-
administered questionnaire assessed demographic characteristics, smoking status,
acculturation, nutrition, occupational and environmental risk factors, psychosocial
factors such as depression, perceived stress, and nervios, as well as a variety of health
outcomes including injuries. Baseline interviews were conducted with participants
between January 2006 and April 2007. Written consent in Spanish was obtained from each
participant, and trained interviewers conducted all interviews in Spanish. Participants
received $15 gift cards for completing the interview. All study procedures were approved
by the University of California, Davis Institutional Review Board.
Outcome measurement
9 A qualifying injury was defined as bodily damage within the 12 months prior to interview
due to exposure to energy and requiring the need for medical care, loss of consciousness,
at least one-half day of lost work time, or restriction from normal activities. All qualifying
injuries, whether occupationally related or not, were included in the analysis.
Exposure measurement
10 The primary exposure measurements were self-reported assessments of depression,
perceived stress, family support, and nervios. Depression was assessed with an eight-item
screener for depressive disorders developed by Burnam and colleagues, based upon the
Center for Epidemiologic Studies Depression Scale (CES-D) (Burnam, Wells et al. 1988).
These elements are scored and calculate the probability of being depressed using a
regression algorithm. A value of 0.06 was used as the cut-point for possible depression,
according to suggested criteria by Burnam et al.
11 Perceived stress was measured with a six items drawn from the 14-item Perceived Stress
Scale (Cohen, Kamarck et al. 1983). Items assessed included: 1) “how often have you dealt
Field Actions Science Reports, Special Issue 10 | 2014
71
successfully with daily problems and hassles?”; 2) “how often have you coped well with
important changes that were taking place in your life?” 3) “how often have you felt
confident about your being able to handle your personal problems?”; 4) “how often have
you been able to control your anger in your life?”; 5) “how often have you felt that you
were on top of things?” and 6) “how often did you feel that things were going well?”
Responses were assessed on a four-point Likert scale ranging from “never” to “all the
time.” Scores for perceived stress were obtained by summing all items and was included
as a continuous variable in logistic regression models. The internal reliability coefficient,
Cronbach’s alpha for the six items on the Perceived Stress scale was 0.80.
12 Family support was assessed with seven items drawn from the Family Dimension of the
Provision of Social Relations (PSR) Scale (Turner, Grindstaff et al. 1990). Participants rated
each statement on a Likert scale response ranging from strongly disagree to strongly
agree. Items included statements such as: “No matter what happens, I know my family
will always be there for me should I need them,” and, “I am not sure if I can completely
rely on my family.” Responses were summed to create a continuous index for inclusion in
logistic regression models. The internal reliability coefficient, Cronbach’s alpha for the
seven items on the Family Support scale, was 0.88.
13 Nervios was assessed by an affirmative response to the question, “Sometimes in your life
have you suffered from nervios?” (Salgado de Snyder, Diaz-Perez et al. 2000). Symptoms
of nervios assessed were having an idea stuck in your mind, feeling distracted or absent-
minded, feeling sad, down or depressed, and feeling irritable or angry. Participants were
also asked how much their nervios interfered with activities and what they believed
caused their nervios.
Statistical analysis
14 Initial descriptive statistic analyses were conducted for injury and the psychosocial
exposure measures and important covariates. Logistic regression was subsequently
employed to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for assessing
the association between psychosocial exposure variables and injury, with adjustment for
relevant potential confounders, including age, gender, current smoking, and years of
working in agriculture. Although gender and current smoking were not confounders in
this analysis, they were retained in the models because other studies have reported
associations with injury (Ratzlaff, Gillies et al. 2007). “Years of working in agriculture”
was correlated with age and was not a cofounder and thus was not included in models for
analyses. Final models were adjusted for age, gender and current smoking. All analyses
were conducted using SAS 9.1.3 (Cary, North Carolina, USA).
Results
Demographic characteristics
15 Overall, 759 participants, 339 (44.7%) women and 420 (55.3%) men, were included in the
present analysis. Ninety-four percent of participants were married or living with
someone. More than half worked in agriculture 11+ years, and 64% earned less than
$20,000/year. Nearly two-thirds of the subjects were born in Mexico and 27.6% were born
Field Actions Science Reports, Special Issue 10 | 2014
72
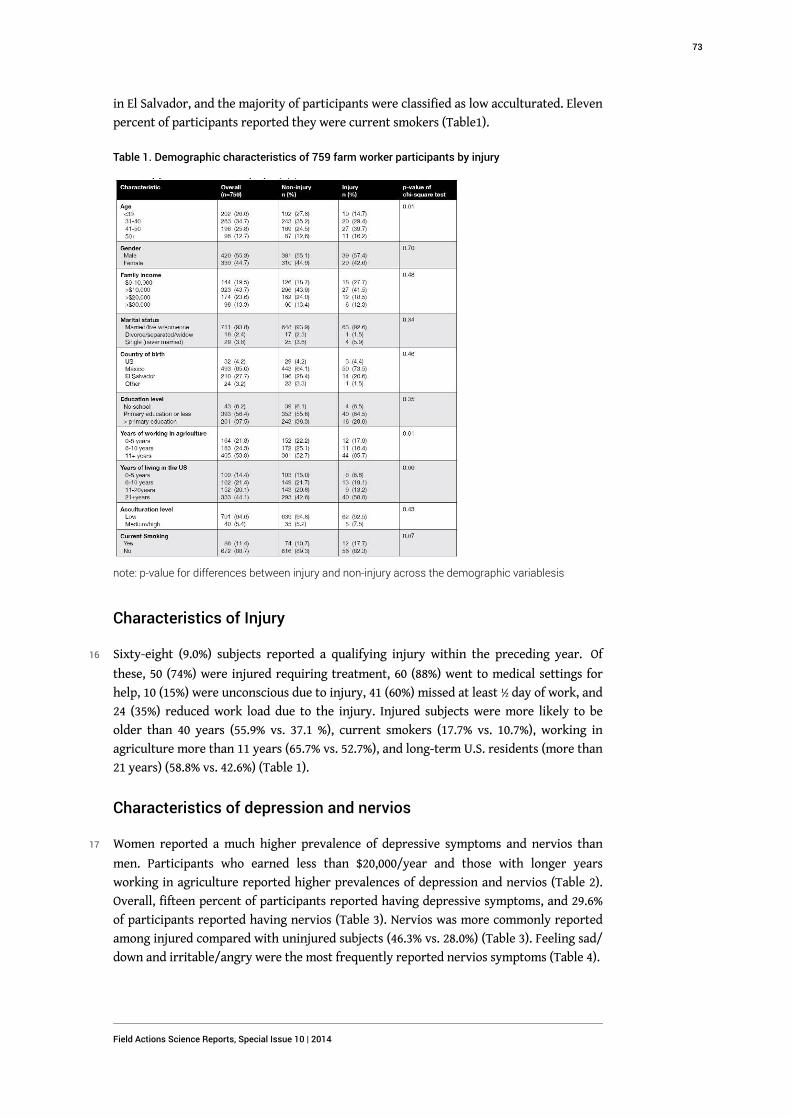
in El Salvador, and the majority of participants were classified as low acculturated. Eleven
percent of participants reported they were current smokers (Table1).
Table 1. Demographic characteristics of 759 farm worker participants by injury
note: p-value for differences between injury and non-injury across the demographic variablesis
Characteristics of Injury
16 Sixty-eight (9.0%) subjects reported a qualifying injury within the preceding year. Of
these, 50 (74%) were injured requiring treatment, 60 (88%) went to medical settings for
help, 10 (15%) were unconscious due to injury, 41 (60%) missed at least ½ day of work, and
24 (35%) reduced work load due to the injury. Injured subjects were more likely to be
older than 40 years (55.9% vs. 37.1 %), current smokers (17.7% vs. 10.7%), working in
agriculture more than 11 years (65.7% vs. 52.7%), and long-term U.S. residents (more than
21 years) (58.8% vs. 42.6%) (Table 1).
Characteristics of depression and nervios
17 Women reported a much higher prevalence of depressive symptoms and nervios than
men. Participants who earned less than $20,000/year and those with longer years
working in agriculture reported higher prevalences of depression and nervios (Table 2).
Overall, fifteen percent of participants reported having depressive symptoms, and 29.6%
of participants reported having nervios (Table 3). Nervios was more commonly reported
among injured compared with uninjured subjects (46.3% vs. 28.0%) (Table 3). Feeling sad/
down and irritable/angry were the most frequently reported nervios symptoms (Table 4).
Field Actions Science Reports, Special Issue 10 | 2014
73
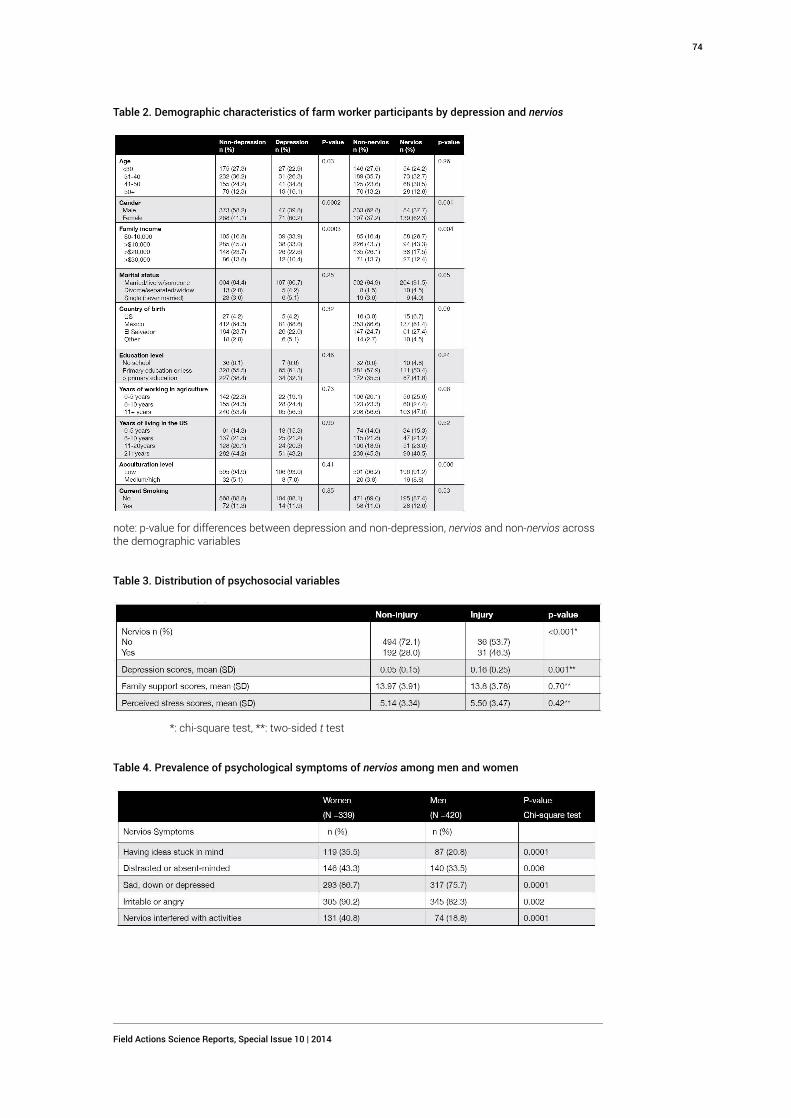
Table 2. Demographic characteristics of farm worker participants by depression and nervios
note: p-value for differences between depression and non-depression, nervios and non-nervios acrossthe demographic variables
Table 3. Distribution of psychosocial variables
*: chi-square test, **: two-sided t test
Table 4. Prevalence of psychological symptoms of nervios among men and women
Field Actions Science Reports, Special Issue 10 | 2014
74
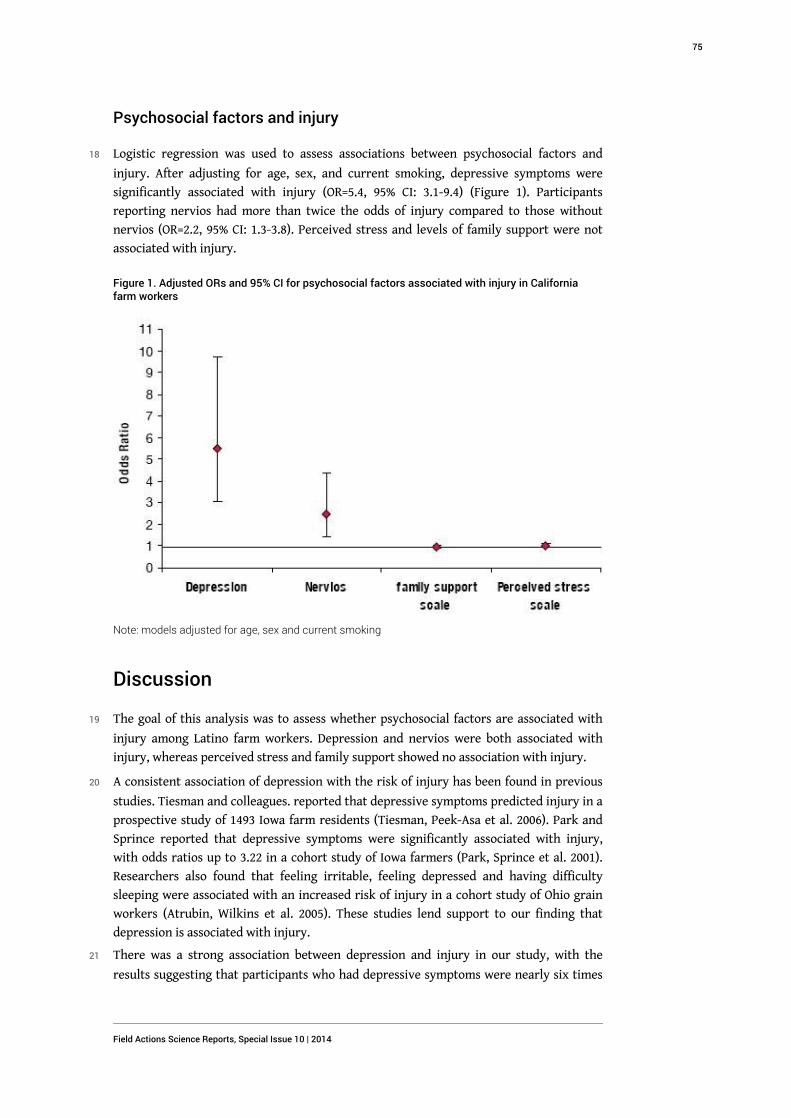
Psychosocial factors and injury
18 Logistic regression was used to assess associations between psychosocial factors and
injury. After adjusting for age, sex, and current smoking, depressive symptoms were
significantly associated with injury (OR=5.4, 95% CI: 3.1-9.4) (Figure 1). Participants
reporting nervios had more than twice the odds of injury compared to those without
nervios (OR=2.2, 95% CI: 1.3-3.8). Perceived stress and levels of family support were not
associated with injury.
Figure 1. Adjusted ORs and 95% CI for psychosocial factors associated with injury in Californiafarm workers
Note: models adjusted for age, sex and current smoking
Discussion
19 The goal of this analysis was to assess whether psychosocial factors are associated with
injury among Latino farm workers. Depression and nervios were both associated with
injury, whereas perceived stress and family support showed no association with injury.
20 A consistent association of depression with the risk of injury has been found in previous
studies. Tiesman and colleagues. reported that depressive symptoms predicted injury in a
prospective study of 1493 Iowa farm residents (Tiesman, Peek-Asa et al. 2006). Park and
Sprince reported that depressive symptoms were significantly associated with injury,
with odds ratios up to 3.22 in a cohort study of Iowa farmers (Park, Sprince et al. 2001).
Researchers also found that feeling irritable, feeling depressed and having difficulty
sleeping were associated with an increased risk of injury in a cohort study of Ohio grain
workers (Atrubin, Wilkins et al. 2005). These studies lend support to our finding that
depression is associated with injury.
21 There was a strong association between depression and injury in our study, with the
results suggesting that participants who had depressive symptoms were nearly six times
Field Actions Science Reports, Special Issue 10 | 2014
75
more likely to have been injured at work than those without depressive symptoms. One
possible mechanism is that depression reduces concern about personal protection leading
to injury (Beseler and Stallones 2010). It is also possible that psychological stress impedes
a worker’s perception, assessment, judgment, and ability to respond to short-term
demands on attention and readiness (acute stress reaction) (Schaubroeck and Ganster
1993), degrading safety performance and ultimately leading to injury (Kidd, Scharf et al.
1996).
22 In the Ontario Farm Family Health Study (Simpson, Sebastian et al. 2004), financial
concerns were a prominent source of stress. Financial problems were significantly
associated with depression in Colorado farm workers (Beseler and Stallones 2010), a
population in which depression was associated with injury. In our study, income was also
associated with depression, and injury was more frequent among participants earning
less than $10,000/year. As two-thirds of participants earned $20,000 or less annually in
our study, financial concerns are likely to be important for this population. For example,
financially stressed workers paid piece-rate may work at a rapid and unsafe pace to
maximize income, increasing the risk of injury (McCurdy, Samuels et al. 2003).
23 In the Mexican American Prevalence and Services Survey (MAPSS), Mexican immigrants
had a lower rate of psychiatric symptoms and disorders than did US-born Mexican
Americans migrant farm workers in Fresno County, California (Alderete, Vega et al. 2000).
However, a cross-national study found that migrants were at higher risk than non-
migrants for psychiatric symptoms (Breslau, Borges et al. 2011). The prevalence of
psychiatric symptoms might be more strongly associated with the age at migration rather
than the duration of living in the U.S. based on the finding that Mexican-origin Latinos
who spent their childhood in the U.S. had worse mental health status than those who did
not migrate (Breslau, Borges et al. 2011). In our study, increased age was significantly
associated with depression. No association was observed between depression and
acculturation or years of living in the U.S.
24 Hispanic immigrants are less likely to use mental health services compared to non-
Hispanics, but they do use general practitioners over specialists for mental health care
(Vega, Kolody et al. 1999). They prefer counseling or counseling plus medication over
antidepressant medication alone (Dwight-Johnson, Lagomasino et al. 2010). It has been
suggested that individual education, transportation assistance, family involvement,
providing Spanish-speaking staff, and offering different services in a single community
primary care location could improve attendance and keep them in treatment (Santiago-
Rivera, Kanter et al. 2010) so as to better control depressive symptoms and decrease the
risk of injury.
25 Nervios was strongly associated with injury in our study. Chen et al. reported that many
personality traits are associated with increasing risks of unintentional injuries. One
possible mechanism may be poor judgment and impulsivity leading to injuries (Chen,
Sinclair et al. 2008). We are not aware of any literature reporting nervios associated with
injury among farm workers.
26 In an Ontario farm family health cross-sectional study, a significant association was
observed between perceived stress and farm injury among operators working on farms
(Simpson, Sebastian et al. 2004). However, in our study we did not observe an association
between perceived stress and injury. This may relate to social and cultural differences
between the predominantly White Ontario population and our Hispanic population,
potentially affecting both risk for injury and reporting.
Field Actions Science Reports, Special Issue 10 | 2014
76
27 Social support is viewed as a protective factor according to the stress buffering model of
social support (Cohen and Wills 1985). However, we did not find a significant association
between family support and injury. Social support may not play a key role in preventing
injury although it may indirectly be associated with injury by mediating stress. Since our
population included primarily married subjects, we may also have not included subjects
with the least social support (e.g. single males) and our findings may not be generalizable
to that population.
28 There were some limitations in this study: First, temporality of the association is
uncertain in cross-sectional studies because of potential reciprocal relationship between
depression or nervios and injury. Nervios was assessed at any time in the person’s life.
Therefore, it is not certain if the injury preceded or followed the nervios condition.
Secondly, study data were based on self-report, which is subject to recall bias. Finally, this
study focused on Latino farm workers in California, and results might not be
generalizable to other industries and ethnic groups.
29 On the other hand, there were strengths of this study in the use of a representative
population-based sample of a hard to reach demographic group, large sample size, and
strict data quality control and data management. Although study data are based on self-
report, we used standardized questions from the National Health and Nutrition
Examination Survey. Interviews were conducted in Spanish by trained personnel,
minimizing interview biases. Strict data quality control and management was performed
to minimize information bias and ensured the validity and precision of the study.
Conclusions
30 Psychosocial variables were strongly associated with injury in this sample of California
Hispanic farm workers. These findings may be useful for guiding prevention and
management of injury. For example, persons with psychiatric symptoms, especially
depression and nervios, represent a high-risk group for injury and may benefit from
recognizing this and more intensive educational and other measures for prevention. Also,
persons suffering agricultural injury should be evaluated and monitored for psychiatric
symptoms that may have preceded their injury or resulted from it. Further research is
needed to confirm the temporality of the association between psychosocial variables and
injury and to evaluate the effectiveness of prevention and treatment measures.
Acknowledgments
31 This study is supported by National Institute for Occupational Safety and Health
(Research agreements: 2U50OH007550 and 1R01OH009293). The authors appreciate the
advice and support from Dr. Robert Harrison at the University of California, San
Francisco, Hennessy-Burt T.E. (data management), and MICASA field team. Statistical and
database architect support was derived through Grant Number UL1 RR024146 from the
National Center for Research Resources (NCRR), a component of the National Institutes of
Health (NIH) and NIH Roadmap for Medical Research, and its contents are solely the
responsibility of the authors and do not necessarily represent the official view of NCRR or
NIH. The authors also acknowledge the UC Global Health Institute (UCGHI) for providing
partial funding for the presentation and review of this work.
Field Actions Science Reports, Special Issue 10 | 2014
77

BIBLIOGRAPHY
Alderete, E., W. A. Vega, et al. (2000). "Lifetime prevalence of and risk factors for psychiatric
disorders among Mexican migrant farmworkers in California." Am J Public Health 90(4): 608-614.
Atrubin, D., J. R. Wilkins, 3rd, et al. (2005). "Self-reported symptoms of neurotoxicity and
agricultural injuries among Ohio cash-grain farmers." Am J Ind Med 47(6): 538-549.
Berkowitz, A. D. and H. W. Perkins (1985). "Correlates of psychosomatic stress symptoms among
farm women: a research note on farm and family functioning." J Human Stress 11(2): 76-81.
Beseler, C. L. and L. Stallones (2010). "Safety knowledge, safety behaviors, depression, and
injuries in Colorado farm residents." Am J Ind Med 53(1): 47-54.
Breslau, J., G. Borges, et al. (2011). "Migration from Mexico to the United States and subsequent
risk for depressive and anxiety disorders: a cross-national study." Arch Gen Psychiatry 68(4):
428-433.
Burnam, M. A., K. B. Wells, et al. (1988). "Development of a brief screening instrument for
detecting depressive disorders." Med Care 26(8): 775-789.
Carruth, A. K. and C. A. Logan (2002). "Depressive symptoms in farm women: effects of health
status and farming lifestyle characteristics, behaviors, and beliefs." J Community Health 27(3):
213-228.
CDFA (2008). IT Governance Project & Portfolio Management. C.D.O.F.A. Agriculture.
Chen, G., S. Sinclair, et al. (2008). "Personality disorders and nonfatal unintentional injuries
among US adults." Inj Prev 14(3): 180-184.
Cohen, S., T. Kamarck, et al. (1983). "A global measure of perceived stress." J Health Soc Behav 24
(4): 385-396.
Cohen, S. and T. A. Wills (1985). "Stress, social support, and the buffering hypothesis." Psychol
Bull 98(2): 310-357.
Dwight-Johnson, M., I. T. Lagomasino, et al. (2010). "Effectiveness of collaborative care in
addressing depression treatment preferences among low-income Latinos." Psychiatr Serv 61(11):
1112-1118.
Elliott, M., C. A. Heaney, et al. (1995). "Depression and perceived stress among cash grain farmers
in Ohio." Journal of Agricultural Safety and Health 1(3): 177-184.
Falcon, L. M., I. Todorova, et al. (2009). "Social support, life events, and psychological distress
among the Puerto Rican population in the Boston area of the United States." Aging Ment Health
13(6): 863-873.
Gregoire, A. (2002). "The mental health of farmers." Occup Med (Lond) 52(8): 471-476.
Kessler, R. C., P. Berglund, et al. (2005). "Lifetime prevalence and age-of-onset distributions of
DSM-IV disorders in the National Comorbidity Survey Replication." Arch Gen Psychiatry 62(6):
593-602.
Field Actions Science Reports, Special Issue 10 | 2014
78
Kessler, R. C., W. T. Chiu, et al. (2005). "Prevalence, severity, and comorbidity of 12-month DSM-
IV disorders in the National Comorbidity Survey Replication." Arch Gen Psychiatry 62(6):
617-627.
Kidd, P., T. Scharf, et al. (1996). "Linking stress and injury in the farming environment: a
secondary analysis of qualitative data." Health Educ Q 23(2): 224-237.
Linn, J. G. and B. A. Husaini (1987). "Determinants of psychological depression and coping
behaviors of Tennessee farm residents." Journal of Community Psychology 15(4): 503-513.
McCurdy, S. A., S. J. Samuels, et al. (2003). "Agricultural injury in California migrant Hispanic
farm workers." Am J Ind Med 44(3): 225-235.
Meyers, J. (1998). Injuries among farm workers in the United States-1995. P. H. S. United States
Department of Health and human Services, CDC, NIOSH Cincinnati OH.
Mikolajczyk, R. T., M. Bredehorst, et al. (2007). "Correlates of depressive symptoms among Latino
and Non-Latino White adolescents: findings from the 2003 California Health Interview Survey."
BMC Public Health 7: 21.
Park, H., N. L. Sprince, et al. (2001). "Risk factors for work-related injury among male farmers in
Iowa: a prospective cohort study." J Occup Environ Med 43(6): 542-547.
Ratzlaff, C. R., J. H. Gillies, et al. (2007). "Work-related repetitive strain injury and leisure-time
physical activity." Arthritis Rheum 57(3): 495-500.
Rautiainen, R. H. and S. J. Reynolds (2002). "Mortality and morbidity in agriculture in the United
States." J Agric Saf Health 8(3): 259-276.
Salgado de Snyder, V. N., M. J. Diaz-Perez, et al. (2000). "The prevalence of nervios and associated
symptomatology among inhabitants of Mexican rural communities." Cult Med Psychiatry 24(4):
453-470.
Sanne, B., A. Mykletun, et al. (2004). "Farmers are at risk for anxiety and depression: the
Hordaland Health Study." Occup Med (Lond) 54(2): 92-100.
Santiago-Rivera, A. L., J. W. Kanter, et al. (2010). "Latino Immigrants with Depression: An Initial
Examination of Treatment Issues at a Community Clinic." J Immigr Minor Health.
Schaubroeck, J. and D. C. Ganster (1993). "Chronic demands and responsivity to challenge." J Appl
Psychol 78(1): 73-85.
Schenker, M. B. (1996). "Preventive medicine and health promotion are overdue in the
agricultural workplace." J Public Health Policy 17(3): 275-305.
Schenker, M. B. (2010). "A global perspective of migration and occupational health." Am J Ind
Med 53(4): 329-337.
Simkin, S., K. Hawton, et al. (1998). "Stress in farmers: a survey of farmers in England and Wales."
Occup Environ Med 55(11): 729-734.
Simpson, K., R. Sebastian, et al. (2004). "Stress on the farm and its association with injury." J Agric
Saf Health 10(3): 141-153.
Stallones, L., M. Lefft, et al. (1995). "Depressive symptoms among Colorado farmers." J. Agric.
Safety and Health 1(1): 37-43.
Stoecklin-Marois, T.E.Hennessy-Burt, et al. (2011). Engaging a hard-to reach population in
research: Sampling and recruitment of hired farm workers in the MICASA study. Davis, UC
DAVIS.
Field Actions Science Reports, Special Issue 10 | 2014
79

Tiesman, H. M., C. Peek-Asa, et al. (2006). "Depressive symptoms as a risk factor for unintentional
injury: a cohort study in a rural county." Inj Prev 12(3): 172-177.
Turner, R. J., C. F. Grindstaff, et al. (1990). "Social support and outcome in teenage pregnancy." J
Health Soc Behav 31(1): 43-57.
Vega, W. A., B. Kolody, et al. (1999). "Gaps in service utilization by Mexican Americans with
mental health problems." Am J Psychiatry 156(6): 928-934.
Villarejo, D. and S. L. Baron (1999). "The occupational health status of hired farm workers."
Occup Med 14(3): 613-635.
Villarejo, D., S. A. McCurdy, et al. (2010). "The health of California's immigrant hired
farmworkers." Am J Ind Med 53(4): 387-397.
Wang, P. S., M. Lane, et al. (2005). "Twelve-month use of mental health services in the United
States: results from the National Comorbidity Survey Replication." Arch Gen Psychiatry 62(6):
629-640.
Weller, S. C., R. D. Baer, et al. (2008). "Susto and nervios: expressions for stress and depression."
Cult Med Psychiatry 32(3): 406-420.
ABSTRACTS
Introduction: While many studies report on the risks of agricultural injury, few have examined
psychosocial factors associated with injury, especially among Latino farm workers. We examined
psychological factors, including depression, perceived stress, social support and nervios that may
be associated with an increased risk of injury. Methods: MICASA is a population-based study of
occupational exposures and health in farm workers. An interviewer-administered questionnaire
collected data on 759 Latinos, 18-55 years old, engaged in farm work and residing in Mendota, CA.
The questionnaire assessed self-reported psychosocial factors and injury risk. A qualifying injury
was defined as one with the need for medical care, going to a medical setting, loss of
consciousness, >½ day lost work time or restricted from normal activities. Results: Mean age was
37.9 years. 65.0% of participants were born in Mexico and 27.7% were born in El Salvador. The
past-year cumulative incidence of injury was 9.0%. A higher cumulative incidence of past-year
injury was observed among participants older than 40 years (55.9% vs. 37.1 %), current smokers
(17.7% vs. 10.7%), working in agriculture more than 11 years (65.7% vs. 52.7%), and long-term U.S.
residents (more than 21 years) (58.8% vs. 42.6%). After adjusting for age, sex, and current
smoking, depression (OR=5.4, 95% CI: 3.1-9.4) and nervios (OR=2.2, 95% CI: 1.3-3.8) were
significantly associated with injury. Conclusions: The findings may be useful for guiding
prevention and management of injury. Further cohort research to confirm the temporality of the
association between psychosocial variables and injury is needed.
Introduction : De nombreuses études ont examiné les risques de blessures en milieu agricole mais
peu se sont intéressées aux facteurs psychosociaux associés à ces blessures, en particulier parmi
les ouvriers agricoles latinos. Nous avons étudié les facteurs psychologiques, notamment la
dépression, le stress ressenti, le soutien social et l'état de nervosité qui peuvent être liés à un
risque accru de blessures. Méthodes : L'étude MICASA est une étude de population qui porte sur
les expositions professionnelles et la santé des ouvriers agricoles. Un questionnaire rempli par un
enquêteur a permis de recueillir des données sur 759 Latinos, de 18 à 55 ans, ouvriers agricoles et
résidant à Mendota, en Californie. Ce questionnaire a évalué les facteurs psychosociaux auto-
déclarés et le risque de blessure. Une blessure admissible a été définie comme une blessure
Field Actions Science Reports, Special Issue 10 | 2014
80

impliquant des soins médicaux, une visite dans un établissement médical, une perte de
connaissance, >½ journée d'arrêt de travail ou d'activités limitées. Résultats : L'âge moyen était
de 37,9 ans. 65,0 % des participants étaient nés au Mexique et 27,7 % au Salvador. L'incidence
cumulée de blessures l'année précédente était de 9,0 %. Une plus grande incidence cumulée de
blessures l'année précédente a été observée parmi les participants âgés de plus de 40 ans (55,9 %
vs. 37,1 %), les fumeurs (17,7 % vs. 10,7 %), ceux travaillant dans l'agriculture depuis plus de 11
ans (65,7 % vs. 52,7 %), et les résidents américains de longue durée (plus de 21 ans) (58,8 % vs. 42,6
%). Après ajustement en fonction du sexe et du tabagisme, la dépression (OR=5,4, IC à 95 % :
3,1-9,4) et l'état de nervosité (OR=2,2, IC à 95 % : 1,3-3,8) ont été associés de manière significative
à des blessures. Conclusions : Les résultats peuvent être utiles pour orienter la prévention et la
prise en charge des blessures. D'autres études de cohortes sont nécessaires pour confirmer la
temporalité de l'association entre les variables psychosociales et les blessures.
Introducción: Aunque se han realizado numerosos estudios sobre los riesgos de lesiones en la
agricultura, pocos son los que han examinado los factores psicosociales asociados a dichas
lesiones, especialmente entre los trabajadores agrícolas latinos. Hemos estudiado los factores
psicosociales, tales como la depresión, el estrés percibido, el apoyo social y los nervios, que
pueden asociarse a un mayor riesgo de lesiones. Métodos: MICASA es un estudio de población
sobre exposiciones y salud occupacionales en trabajadores agrícolas. Un cuestionario realizado
por entrevistador recogió datos de 759 latinos, de entre 18 y 55 años de edad, que realizaban
labores agrícolas y con residencia en Mendota (California). El cuestionario evaluaba los factores
sociales y el riesgo de lesiones declarados por los encuestados. Las lesiones por las que calificaban
para el estudio eran aquellas que requerían asistencia médica o la visita a un centro médico, que
implicaban pérdida de conciencia o pérdida de más de medio día de trabajo o que restringían la
realización de actividades normales. Resultados: La edad media era de 37.9 años. El 65,0% de los
participantes eran originarios de México y el 27.7% de El Salvador. La incidencia acumulada de
lesiones del año pasado fue del 9.0%. Se observó una mayor incidencia acumulada de lesiones el
año pasado entre participantes de más de 40 años (55.9% contra 37.1 %), fumadores activos (17.7%
contra 10.7%), que llevan trabajando en la agricultura más de 11 años (65.7% contra 52.7%) y los
residentes en Estados Unidos por un largo plazo (más de 21 años) (58.8% contra 42.6%). Tras
ajustar los resultados por edad, sexo, condición de fumador, la depresión (OR=5,4; 95% IC: 3,1-9,4)
y los nervios (OR=2,2, 95% IC: 1.3-3.8) se asociaron de forma importante a las lesiones.
Conclusiones: Las conclusiones extraídas pueden ser de utilidad para guiar la prevención y
manejo de lesiones. Es necesario realizar otros estudios de cohortes para confirmar la
temporalidad de la asociación entre las variables psicosociales y las lesiones.
INDEX
Mots-clés: Agriculture, Blessure, Dépression, Etat de nervosité, Stress ressenti
Palabras claves: Agricultura, Depresión, Estrés percibido, Lesiones, Nervios
Keywords: Agriculture, Depression, Farmworker, Hispanic, Injury, Latino, Nervios, Perceived
Stress, Stress
AUTHORS
HONG XIAO
MD, PHD MPH, University of California, Davis, Department of Public Health Sciences - One Shields
Ave., University of California, Davis; Davis, CA 95616-8638, [email protected]
Field Actions Science Reports, Special Issue 10 | 2014
81

MARIA STOECKLIN-MAROIS
PhD, MPH, University of California, Davis, Department of Public Health Sciences - One Shields
Ave., University of California, Davis; Davis, CA 95616-8638
CHIN-SHANG LI
PhD, University of California, Davis, Department of Public Health Sciences - One Shields Ave.,
University of California, Davis; Davis, CA 95616-8638
STEPHEN A. MCCURDY
MD, MPH, University of California, Davis, Department of Public Health Sciences - One Shields
Ave., University of California, Davis; Davis, CA 95616-8638
MARC SCHENKER
MD, MPH, University of California, Davis, Department of Public Health Sciences - One Shields
Ave., University of California, Davis; Davis, CA 95616-8638
Field Actions Science Reports, Special Issue 10 | 2014
82
Migration & Self-Rated Health:Comparing Occupational Cohorts inCalifornia & Spain (MICASA andITSAL Projects)Immigration et Santé auto-évaluée : Comparaison de cohortes professionnelles
en Californie et en Espagne (Etudes MICASA et ITSAL)
Migración y autoevaluación del estado de salud: comparación de cohortes
ocupacionales en California y España (proyectos MICASA e ITSAL)
Emily Sousa, Maria Stoecklin-Marois, Jose Miguel Martinez, Fernando G.Benavides and Marc Schenker
Introduction
1 Global migration is a growing phenomenon. In 2010, 214 million people were reported to
be living outside their countries of birth [1]. As an incorporated group, these
international migrants would comprise the 5th largest country in the world [2].
Motivations for leaving one’s country of origin are complex, as are the resulting health
implications. The sheer number of international migrants makes the potential burden of
related public health issues important to consider.
2 Immigration may impact infectious disease, chronic disease, and health care access, as
well as occupational injury and illness. Health implications of migration are commonly
studied from the perspective of receiving nations, with protective outcomes among
newly-arrived foreign-born individuals, followed by declining health with time in the
host country [3-5]. The initial health advantages of immigration are often attributed to
protective cultural factors and selective migration (the healthy immigrant effect) [5, 6]. A
person’s age at the time of migration is also of issue, with the health of those who migrate
as pre-adolescents or adolescents differentiated from that of those who migrate at later
Field Actions Science Reports, Special Issue 10 | 2014
83
stages of development, and more closely resembling the health of native-born individuals
in the host country [4]. Given migration’s magnitude and complicated relationship with
health, research in this area is critical.
3 Migration is often attributed to an imbalance of resources, from land and natural
resources to job opportunities, underemployment and economic strength. This article
utilizes the United Nations definition of migrant workers as people who are paid for
services in states in which they are not nationals [7]. Such migrant workers are abundant,
sending roughly $414 billion in remittances in 2009, $307 billion of which went to
developing countries [8]. This population is especially relevant in a public health context
because of the potential impact of occupational exposures. Differences in work exposures
may exist between host and sending societies, and between foreign-born and native-born
workers within host countries. The volume and diversity of experiences of migrant
workers make public health research in these populations both interesting and
important.
4 Self-rated health is a measure of general health that has been associated with mortality in
various studies across cultures and populations [9-12]. Participants rank their health on a
Likert scale, and responses are dichotomized into good and poor health. The measure is
subjective, and is generally associated with sex and age. Existing literature has found
females and older individuals tend to report higher proportions of poor health than their
male and younger counterparts, respectively [9]. The measure is also valuable because of
its quick and cost-effective collection, making it assessable in a variety of research
settings.
5 Comparative studies of migratory trends provide an opportunity to determine if the
impacts of migration have commonalities across migrant streams, and if so, which factors
are specific to individual country relationships, host and sending societies, and which
factors are observed in multiple settings. Previous studies have looked at the specific
comparison between North Africa-Europe migration and Mexico-USA migration, as well
as migration experiences in host countries across Europe [13, 14]. Guendelman et al.
found similar trends in birth outcomes in North Africa-Europe migration and Mexico-USA
migration. Bollini et al. reported an association between immigrant integration policy
and birth outcomes across Europe. These studies take immigration to be an exposure in
and of itself, and add to existing immigration research by comparing outcomes across
situations. This type of work remains uncommon and is an area of powerful potential in
the field.
6 Spain is of particular interest in migration studies due to the rich migrant history and
transformation in the past decade from a country of net emigration to one of net
immigration [15, 16]. California is also a prime location for immigration research as the
state’s southern border makes up part of the most crossed international border in the
world [17], and one out of every four Californians are foreign-born [18]. In the interest of
parallelism and building on comparative migration research, this analysis compares
Moroccan-born workers in Spain and Mexican-born workers in California.
7 Occupational health is often explored epidemiologically through occupational cohorts,
defined as samples of workers from the same field and/or professional organizations with
similar exposures. Ultimately, experts in the field have noted that, “the choice of
occupational cohort will be influenced by research objectives, and inevitably will be
determined by the availability of data necessary for cohort enumeration, exposure
assessment, and health outcome evaluation” [19]. Migration-related variables are not
Field Actions Science Reports, Special Issue 10 | 2014
84
universally collected in occupational datasets, so the design and analyses conducted in
this study have been guided by the use of available, comparable data to optimize progress
in an emerging field.
8 The goal of this study is to assess self-rated health in occupational cohorts of Moroccan-
born workers in the Immigration, Work and Health (ITSAL) study and Mexican-born
workers in the Mexican Immigration to California: Agricultural Safety and Acculturation
(MICASA) study. Hypotheses tested examine the variability of poor self-rated health by
gender, age, age at migration, and occupation to allow for optimally unbiased comparison
of health status across migratory trends, with the aim of identifying appropriate next
steps in research and optimal public health planning.
Methods
9 This study presents a comparison of two independently collected samples of foreign-born
workers – one of Mexican-born workers in Mendota, California, USA, and the other of
Moroccan-born workers in four cities across Spain (Barcelona, Huelva, Madrid and
Valencia).
Data Collection
10 The MICASA project studies a longitudinal occupational cohort of farm workers in
Mendota, California. Exposures of interest include acculturation, smoking, and other
occupational and environmental health issues potentially relevant to the health of this
population.
11 Stratified area probability sampling was used with census block as the primary sampling
unit [20-22]. A household enumeration procedure identified all dwellings in randomly
selected census blocks and individuals residing in these dwellings. Further details of the
methodology is submitted elsewhere for publication [23]. Eligible individuals were 18-55
years old, residing in Mendota at the time of baseline interviews (2006-2007), living in a
household with at least one person who worked in agriculture a minimum of 45 days in
the previous year, who self-identified as Mexican or Central American, and consented to
participate in the study. Interviews were conducted with a 70% household response rate.
12 Research objectives and methods were explained to potential participants in Spanish.
Individuals choosing to participate in the study provided written consent in Spanish. The
study was approved by the University of California, Davis, Institutional Review Board.
Data presented here were collected as part of the second wave of the study between 2008
and 2010. The survey tool used for the follow-up interview included standardized,
validated scales, focusing on sociodemographics, residential conditions and exposures,
smoking, occupational history and exposures, and a variety of specific and holistic health
measures. At follow-up, 640 individuals were interviewed, of which 424 (66%) were
Mexican-born.
13 The ITSAL project studies immigration, work and health in Spain. Data presented here are
from a cross-sectional sample taken 2008-2009 (wave 1) that utilized a 74-item
questionnaire to assess sociodemographics, the migration process, occupational and
economic variables, employment conditions, working conditions, occupational risk
Field Actions Science Reports, Special Issue 10 | 2014
85

prevention activities, participation in trade unions, physical and mental health, and
overall evaluation of individuals’ experiences working in Spain.
14 Quota sampling was used to construct a sample of 2,434 foreign-born workers, with
quotas set by nationality, gender, and area of residence in Spain [20-22]. Moroccan-born
individuals (n=625) living in Barcelona, Huelva, Madrid or Valencia (four Spanish cities
with high proportions of foreign-born residents) were interviewed. Inclusion criteria
consisted of living in Spain for at least one year and working in Spain for at least three
months (professional athletes, artists, graduate students and business executives were
excluded), not being a Spanish citizen or married to a native Spaniard, and adequate
Spanish language abilities for interview participation. Interviews were conducted with a
55.8% response rate [24]. All selected individuals within the inclusion criteria were
invited to participate in the study and given an informational letter explaining their
rights and guaranteeing individual confidentiality. Participation was voluntary, with
consent implied by completion of the survey [25].
Measures
15 The following variable definitions were used for both samples: sex, age (categorical – 18
to 30, 31 to 40, 41+ years old), age at migration (categorical – under 13, 13 to 17, 18+ years
old), education (at most primary, secondary, post secondary), and work experience in
agriculture (yes, no).
16 Self-rated health was used as an outcome in both samples. Participants in both studies
were asked to rate their health. Responses were dichotomized into good health or poor
health, as is standard in research with this outcome [6, 9].
17 In the MICASA study, the question read, “Would you say that in general your health is…”
with the following possible responses: excellent, very good, good, fair, and poor.
Excellent, very good, and good were combined to represent good health, and fair and
poor categories were grouped to represent poor health. In the ITSAL study, the question
read, “How would you rate your health right now?” with the following possible responses:
very good, good, fair, poor, and very poor. Very good and good categories were joined to
represent good health, and the fair, poor and very poor were merged to represent poor
health.
Analysis
18 Comparisons were made between the samples overall and with respect to self-rated
health. Variables of interest included sex, age, age at migration, education, and work
experience in agriculture. Chi-square tests were done to assess significant differences.
Log-binomial models [26-29] were constructed to obtain prevalence ratios and respective
95% confidence intervals for poor self-rated health, stratified by sex and adjusted for age.
All analyses were completed with SAS version 9.2 (SAS Institute Inc., Cary, NC, USA).
Results
19 The two samples differ significantly by sex, age, education and experience working in
agriculture (Table 1). The Mexican-born sample was gender balanced, while males
Field Actions Science Reports, Special Issue 10 | 2014
86

comprised 84% of the Moroccan-born sample. Individuals in the Mexican-born sample
were significantly older (41 vs. 31 years old), less educated, and more likely to have
worked in agriculture than their Moroccan-born counterparts (p<0.001). We observed
these same differences among males and females independently. Additionally, among
men, a larger proportion of Mexican-born individuals immigrated before age 18.
Table 1. Sociodemographic profile of Mexican-born and Moroccan-born samples, overall and bygender.
20 Differences also existed between the samples according to self-rated health (Table 2).
Overall, 42% of Mexican-born participants reported poor health compared to 14% of
Moroccan-born participants. This was seen in every stratum by age, age at migration,
education, and agricultural work overall, and remained significant when stratified by
gender, with the exception of age at migration and education in females.
Field Actions Science Reports, Special Issue 10 | 2014
87
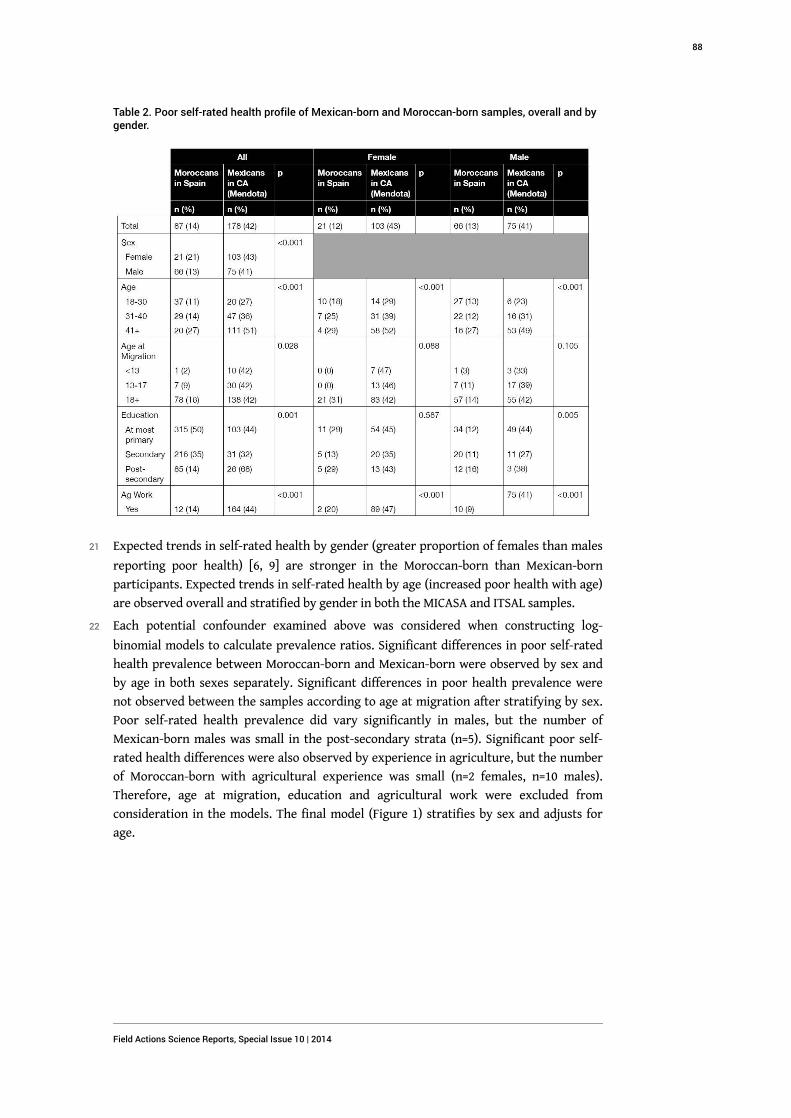
Table 2. Poor self-rated health profile of Mexican-born and Moroccan-born samples, overall and bygender.
21 Expected trends in self-rated health by gender (greater proportion of females than males
reporting poor health) [6, 9] are stronger in the Moroccan-born than Mexican-born
participants. Expected trends in self-rated health by age (increased poor health with age)
are observed overall and stratified by gender in both the MICASA and ITSAL samples.
22 Each potential confounder examined above was considered when constructing log-
binomial models to calculate prevalence ratios. Significant differences in poor self-rated
health prevalence between Moroccan-born and Mexican-born were observed by sex and
by age in both sexes separately. Significant differences in poor health prevalence were
not observed between the samples according to age at migration after stratifying by sex.
Poor self-rated health prevalence did vary significantly in males, but the number of
Mexican-born males was small in the post-secondary strata (n=5). Significant poor self-
rated health differences were also observed by experience in agriculture, but the number
of Moroccan-born with agricultural experience was small (n=2 females, n=10 males).
Therefore, age at migration, education and agricultural work were excluded from
consideration in the models. The final model (Figure 1) stratifies by sex and adjusts for
age.
Field Actions Science Reports, Special Issue 10 | 2014
88
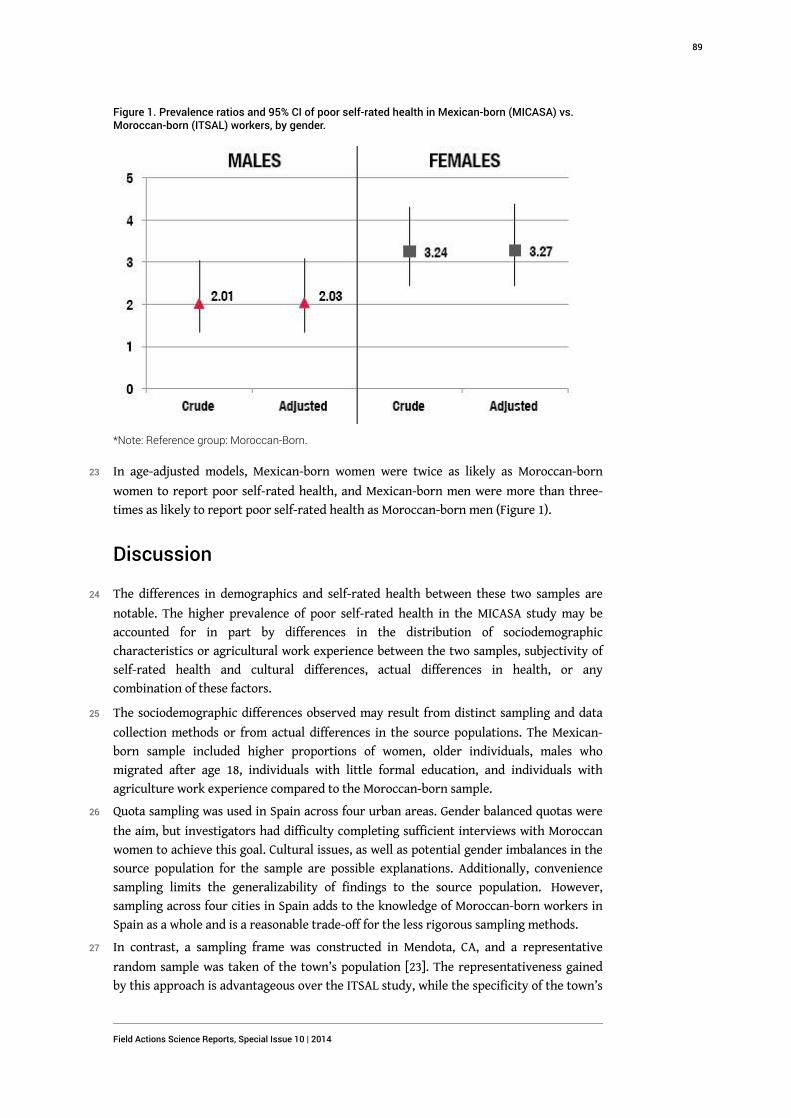
Figure 1. Prevalence ratios and 95% CI of poor self-rated health in Mexican-born (MICASA) vs.Moroccan-born (ITSAL) workers, by gender.
*Note: Reference group: Moroccan-Born.
23 In age-adjusted models, Mexican-born women were twice as likely as Moroccan-born
women to report poor self-rated health, and Mexican-born men were more than three-
times as likely to report poor self-rated health as Moroccan-born men (Figure 1).
Discussion
24 The differences in demographics and self-rated health between these two samples are
notable. The higher prevalence of poor self-rated health in the MICASA study may be
accounted for in part by differences in the distribution of sociodemographic
characteristics or agricultural work experience between the two samples, subjectivity of
self-rated health and cultural differences, actual differences in health, or any
combination of these factors.
25 The sociodemographic differences observed may result from distinct sampling and data
collection methods or from actual differences in the source populations. The Mexican-
born sample included higher proportions of women, older individuals, males who
migrated after age 18, individuals with little formal education, and individuals with
agriculture work experience compared to the Moroccan-born sample.
26 Quota sampling was used in Spain across four urban areas. Gender balanced quotas were
the aim, but investigators had difficulty completing sufficient interviews with Moroccan
women to achieve this goal. Cultural issues, as well as potential gender imbalances in the
source population for the sample are possible explanations. Additionally, convenience
sampling limits the generalizability of findings to the source population. However,
sampling across four cities in Spain adds to the knowledge of Moroccan-born workers in
Spain as a whole and is a reasonable trade-off for the less rigorous sampling methods.
27 In contrast, a sampling frame was constructed in Mendota, CA, and a representative
random sample was taken of the town’s population [23]. The representativeness gained
by this approach is advantageous over the ITSAL study, while the specificity of the town’s
Field Actions Science Reports, Special Issue 10 | 2014
89

population limits the generalizability of the results to farm workers living in Mendota or
potentially in other comparable California Central Valley farming communities.
28 Selection bias may have been introduced by language restrictions established as
eligibility criteria in the ITSAL project. It is possible that Moroccan-born workers who
speak Spanish were not representative of the general population of Moroccan-born
workers in Spain.
29 Regardless of the sources of the demographic differences, poor self-rated health is
generally understood to be more prevalent in females than males, with age, and lower
levels of education [9]. However, even when prevalence ratios were calculated and
stratified by gender and adjusted for age, Mexican-born individuals in the MICASA sample
reported poorer general health than Moroccan-born individuals in the ITSAL sample. The
lower education level among Mexican-born participants would be expected to increase
the prevalence of poor self-rated health, so this may account for some of the discrepancy
in the ratios. While models were adjusted for age, ratios adjusted for other possible
confounders could not be calculated due to model convergence concerns.
30 The differences in the prevalence of poor self-rated health between the MICASA and
ITSAL samples may have resulted from the subjectivity of the measure. Latino
populations are understood to somatize emotional issues into physical health concerns,
and such cultural impacts on the concept of health may play a role in the differences seen
between these two samples [30-32]. Research has shown a positive relationship between
poor self-rated health and mortality among US Latinos as a whole, as well as those living
in the US for at least 10 years [33]. At baseline interview in the MICASA study (two to four
years before the data analyzed here were collected), study participants had lived in the
US 15.5 years on average. Thus, it is plausible here that such an association may hold.
31 Self-rated health has been used as an overall health assessment. This construct has been
associated with morbidity and mortality and validated across cultures and communities
[9, 10, 34-36]. However, self-rated health’s associations remain to be researched with
more specific health measures. In addition, self-rated health’s inherent subjectivity
cannot be discounted when considering potential explanations.
32 True differences in health status between the samples may also explain differences
observed in poor self-rated health prevalence in this study. Self-rated health, while
subjective, is a valid health measure with implications for mortality, if not also for
decreased health-related quality of life. The public health implications of such a
difference in health status across populations could be substantial and are important for
policy planning as well as future research.
33 Comparative research would do well to continue exploring health effects across
migrations, distinguishing commonalities as well as factors unique to individual
situations. Such an understanding will be valuable to immigration health research, as
well as public health planning, to ensure optimal health outcomes in our increasingly
mobile world.
Acknowledgments
34 Funding for the MICASA study was provided by the National Institute for Occupational
Safety and Health (2U500H007550 and RO1OH009293) and The California Endowment.
Funding for the ITSAL project was provided by the Fondo de Investigación Sanitaria,
Field Actions Science Reports, Special Issue 10 | 2014
90
Instituto de Salud Carlos III in 2005 (PI050497, PI052202, PI052334), 2006 (PI061701), and
2007 (PI0790470).
35 The authors would like to thank staff at the Western Center for Agriculture & Health and
the Center for Occupational Health Research (CiSal), especially Tamara Hennesy-Burt.
The authors would also like to acknowledge the UC Global Health Institute (UCGHI) for
providing partial funding for the presentation and review of this work. We would also like
to acknowledge the contribution of the MICASA field team, with special thanks to Gloria
Andrade, Alex Cervantes, Ana Cervantes, and Giselle Garcia. Most of all, we thank the
participants for sharing their experiences and making this study possible.
BIBLIOGRAPHY
1. United Nations (2008), "United Nations' Trends in Total Migrant Stock: The 2008 Revision",
http://esa.un.org/migration
2. United Nations (2008), "United Nations' World Population Prospects: The 2008 Revision,
Highlights", http://esa.un.org/unpd/wpp2008/pdf/WPP2008_Highlights.pdf.
3. Abraido-Lanza, A.F., M.T. Chao, and K.R. Florez (2005), "Do healthy behaviors decline with
greater acculturation? Implications for the Latino mortality paradox", Soc Sci Med, Vol. 61, No.
6, pp. 1243-55.
4. Breslau, J., et al. (2009), "Immigration to the USA and risk for mood and anxiety disorders:
variation by origin and age at immigration", Psychol Med, Vol. 39, No. 7, pp. 1117-27.
5. Gushulak, B.D. and D.W. MacPherson (2006), "The basic principles of migration health:
population mobility and gaps in disease prevalence," Emerg Themes Epidemiol, Vol. 3, p. 3.
6. Newbold, K.B. (2005), "Self-rated health within the Canadian immigrant population: risk and
the healthy immigrant effect", Soc Sci Med, Vol. 60, No. 6, pp. 1359-70.
7. United Nations (2003), United Nations Convention on the Protection of the Rights of All
Migrant Workers and Members of Their Families.
8. World Bank (2011), "World Bank's Migration and Remittances Factbook 2011", http://
go.worldbank.org/QGUCPJTOR0.
9. Idler, E.L. and Y. Benyamini (1997), "Self-rated health and mortality: a review of twenty-seven
community studies", J Health Soc Behav, Vol. 38, No. 1, pp. 21-37.
10. Jiang, Y. and J.E. Hesser (2009), "Using item response theory to analyze the relationship
between health-related quality of life and health risk factors", Prev Chronic Dis, Vol. 6, No. 1, p.
A30.
11. Cook, C., R. Pietrobon, and E. Hegedus (2007), "Osteoarthritis and the impact on quality of life
health indicators", Rheumatol Int, Vol. 27, No. 4, pp. 315-21.
12. Cook, E.L. and J.S. Harman (2008), "A comparison of health-related quality of life for
individuals with mental health disorders and common chronic medical conditions", Public
Health Rep, Vol. 123, No. 1, pp. 45-51.
Field Actions Science Reports, Special Issue 10 | 2014
91
13. Bollini, P., et al. (2009), "Pregnancy outcome of migrant women and integration policy: a
systematic review of the international literature", Soc Sci Med, Vol. 68, No. 3, pp. 452-61.
14. Guendelman, S., et al. (1999), "Birth outcomes of immigrant women in the United States,
France, and Belgium", Matern Child Health J, Vol. 3, No. 4, pp. 177-87.
15. Agudelo-Suarez, A., et al. (2009), "Discrimination, work and health in immigrant populations
in Spain", Soc Sci Med, Vol. 68, No. 10, pp. 1866-74.
16. Ahonen, E.Q., et al. (2009), "A qualitative study about immigrant workers' perceptions of their
working conditions in Spain", J Epidemiol Community Health, Vol. 63, No. 11, pp. 936-42.
17. Glenday, C., (2009) Guinness World Records, Random House Digital.
18. PPIC (2011), "Just the Facts: Immigrants in Calfornia", http://www.ppic.org/content/pubs/
jtf/JTF_ImmigrantsJTF.pdf
19. Checkoway, H. and E. Eisen (1998), "Developments in Occupational Cohort Studies", Epidemiol
Rev, Vol. 20, No. 1, pp. 100-111
20. Faugier, J. and M. Sargeant (1997), "Sampling hard to reach populations", J Adv Nurs, Vol. 26,
No. 4, pp. 790-7.
21. Muhib, F.B., et al. (2001), "A venue-based method for sampling hard-to-reach populations",
Public Health Rep, Vol. 116, Suppl 1, pp. 216-22.
22. Spring, M., et al. (2003), "Sampling in difficult to access refugee and immigrant communities",
J Nerv Ment Dis, Vol. 191, No. 12, pp. 813-9.
23. Stoecklin-Marois MT, H.-B.T., Schenker MB. (Submitted 2011), "Engaging a hard-to reach
population in research: Sampling and recruitment of hired farm workers in the MICASA study".
24. Delclos, C.E., et al. (2011), "From questionnaire to database: field work experience in the
'Immigration, work and health survey' (ITSAL Project)", Gac Sanit.
25. Sousa, E., et al. (2010), "Immigration, work and health in Spain: the influence of legal status
and employment contract on reported health indicators", Int J Public Health, Vol. 55, No. 5, pp.
443-51.
26. Greenland, S. (2004), "Model-based estimation of relative risks and other epidemiologic
measures in studies of common outcomes and in case-control studies", Am J Epidemiol, Vol. 160,
No. 4, pp. 301-5.
27. Savu, A., Q. Liu, and Y. Yasui (2010), "Estimation of relative risk and prevalence ratio", Stat
Med, Vol. 29, No. 22, pp. 2269-81.
28. Skov, T., et al. (1998), "Prevalence proportion ratios: estimation and hypothesis testing", Int J
Epidemiol, Vol. 27, No. 1, pp. 91-5.
29. Spiegelman, D. and E. Hertzmark (2005), "Easy SAS calculations for risk or prevalence ratios
and differences", Am J Epidemiol, Vol. 162, No. 3, pp. 199-200.
30. Angel, R. and P.J. Guarnaccia (1989), "Mind, body, and culture: somatization among
Hispanics", Soc Sci Med, Vol. 28, No. 12, pp. 1229-38.
31. Finch, B.K., B. Kolody, and W.A. Vega (2000), "Perceived discrimination and depression among
Mexican-origin adults in California", J Health Soc Behav, Vol. 41, No. 3, pp. 295-313.
32. Vega, W.A. and H. Amaro (1994), "Latino outlook: good health, uncertain prognosis", Annu
Rev Public Health, Vol. 15, pp. 39-67.
Field Actions Science Reports, Special Issue 10 | 2014
92

33. Finch, B.K., et al. (2002), "Validity of self-rated health among Latino(a)s", Am J Epidemiol, Vol.
155, No. 8, pp. 755-9.
34. Chandola, T. and C. Jenkinson (2000), "Validating self-rated health in different ethnic groups",
Ethn Health, Vol. 5, No. 2, pp. 151-9.
35. Cavlak, U., et al. (2009), "A new tool measuring health-related quality of life (HRQOL): the
effects of musculoskeletal pain in a group of older Turkish people", Arch Gerontol Geriatr, Vol.
49, No. 2, pp. 298-303.
36. Jiang, Y. and J.E. Hesser (2006), "Associations between health-related quality of life and
demographics and health risks. Results from Rhode Island's 2002 behavioral risk factor survey",
Health Qual Life Outcomes, Vol. 4, p. 14.
ABSTRACTS
International migration is a growing global phenomenon. The magnitude of the global
population living outside their countries of origin substantiates the value of considering
potential public health issues and their population-wide burden. As migration has yet to be
generally accepted as an exposure in and of itself, and encompasses a wide range of experiences
and health effects, a measure of overall health is well suited for this research. This study
compares self-rated health between two independently collected occupational cohorts as part of
the ITSAL study in Spain and the MICASA study in Mendota, California, USA. We observed
greater gender balance in the MICASA sample than the ITSAL sample, where there was a
substantial male majority. Mexican-born workers in the MICASA sample tended to be older, less
educated, and more likely to work in agriculture than their Moroccan-born counterparts in the
ITSAL study. We also observed a higher prevalence of poor self-rated health in the MICASA
sample compared to the ITSAL sample. Differences may be due to sampling and data collection
issues, cultural issues and the subjectivity of self-rated health as an outcome, as well as actual
health differences. Further research is needed to determine common and distinct migration-
related public health issues.
L'immigration internationale est un phénomène mondial en plein essor. Le pourcentage élevé de
personnes dans le monde vivant dans un pays autre que son pays d'origine justifie l'intérêt de
prendre en compte les problèmes de santé publique potentiels et le fardeau que cela implique à
l'échelle de la population. Alors que l'immigration n'est pas encore généralement reconnue
comme une exposition en soi, et englobe un large éventail d'expériences et d'effets sur la santé,
une évaluation de la santé globale est tout à fait appropriée pour cette étude. Cette étude
compare la santé auto-évaluée de deux cohortes professionnelles, les donnés ayant été recueillies
indépendamment dans le cadre de l'étude ITSAL en Espagne et de l'étude MICASA à Mendota, en
Californie. Nous avons observé un plus grand équilibre entre les sexes dans l'échantillon MICASA
que dans l'échantillon ITSAL, dans lequel il y avait une majorité considérable d'hommes. Les
ouvriers de l'échantillon MICASA nés au Mexique avaient tendance à être plus âgés, à avoir un
niveau d'instruction moindre, et à être plus susceptibles de travailler dans l'agriculture que leurs
homologues nés au Maroc de l'étude ITSAL. Nous avons également observé une plus forte
prévalence de mauvaise santé auto-évaluée dans l'échantillon MICASA que dans l'échantillon
ITSAL. Les différences peuvent être dues aux méthodes d'échantillonnage et de recueil des
données, à des aspects culturels et à la subjectivité des résultats de la santé auto-déclarée, ainsi
qu'à de réelles différences en matière de santé. D'autres études sont nécessaires pour déterminer
les problèmes de santé publique liées à l'immigration communs et distincts.
Field Actions Science Reports, Special Issue 10 | 2014
93

La migración internacional es un fenómeno creciente a nivel mundial. La magnitud de la
población mundial que vive fuera de su país de origen justifica el valor del estudio de los
problemas potenciales para la salud pública y la carga que supone para la población en general.
Debido a que todavía no se ha aceptado de forma generalizada que la migración supone una
exposición por sí misma y al hecho de que abarca una amplia gama de experiencias y efectos para
la salud, una medición de la salud en general parece apropiada para este estudio. En este trabajo
se compara la autoevaluación de la salud entre dos cohortes ocupacionales analizadas
independientemente como parte del estudio ITSAL en España y el estudio MICASA en Mendota
(California, Estados Unidos.). Hemos observado un mayor equilibrio entre sexos en la muestra de
MICASA que en la de ITSAL, donde había una importante mayoría masculina. Los trabajadores de
origen mexicano de la muestra de MICASA tendían a ser mayores, con menor nivel educativo y
con mayor probabilidad de trabajar en la agricultura que los colegas de origen marroquí del
estudio ITSAL. Asimismo, hemos observado una mayor prevalencia de salud deficiente en la
muestra de MICASA en comparación con la muestra de ITSAL. Las diferencias pueden deberse a
problemas de muestreo y de recopilación de datos, a aspectos culturales y a la subjetividad de los
resultados de la autoevaluación de la salud, así como a verdaderas diferencias de salud.
Asimismo, es necesario realizar otros estudios para determinar qué aspectos de salud pública
relacionados con la migración se comparten y cuáles son diferentes.
INDEX
Keywords: Epidemiology, Immigrant Workers, Occupational Health, Self-Reported Health, Spain,
United States
Palabras claves: Autoevaluación de salud, Epidemiología, España, Estados Unidos, Salud
ocupacional, Trabajadores inmigrantes
Mots-clés: Epidemiologie, Espagne, Etats-Unis, Santé au travail, Santé auto-déclarée,
Travailleurs immigrés
AUTHORS
EMILY SOUSA
MPH, University of California, Davis, Department of Public Health Sciences, Western Center for
Agricultural Health and Safety, 1 Shields Ave., Davis, CA 95616, [email protected]
MARIA STOECKLIN-MAROIS
MPH, PhD, University of California, Davis, Department of Public Health Sciences, Western Center
for Agricultural Health and Safety, 1 Shields Ave., Davis, CA 95616
JOSE MIGUEL MARTINEZ
PhD, Universitat Pompeu Fabra, Center for Investigation of Occupational Health
FERNANDO G. BENAVIDES
MD, PhD, Universitat Pompeu Fabra, Center for Investigation of Occupational Health
Field Actions Science Reports, Special Issue 10 | 2014
94
MARC SCHENKER
MD, MPH, University of California, Davis, Department of Public Health Sciences, Western Center
for Agricultural Health and Safety, 1 Shields Ave., Davis, CA 95616
Field Actions Science Reports, Special Issue 10 | 2014
95