
Stories to Tell to Children: Fifty-One Stories With Some Suggestions ...
Failure of Computerized Treatment Suggestions to Improve Health Outcomes of Outpatients
with Uncomplicated Hypertension: Results of a Randomized Controlled Trial
Michael D. Murray, Pharm.D., M.P.H., Lisa E. Harris, M.D., J. Marc Overhage, M.D., Ph.D., Xiao-Hua Zhou, Ph.D., George J. Eckert, M.A.S., Faye E. Smith, M.A., Nancy Nienaber Buchanan, M.A.,
Fredric D. Wolinsky, Ph.D., Clement J. McDonald, M.D., and William M. Tierney, M.D.
Study Objective. To assess the effects of evidence-based treatmentsuggestions for hypertension made to physicians and pharmacists using acomprehensive electronic medical record system.
Design. Randomized controlled trial with a 2 x 2 factorial design of physicianand pharmacist interventions, which resulted in four groups of patients:physician intervention only, pharmacist intervention only, intervention byphysician and pharmacist, and intervention by neither physician norpharmacist (control).
Setting. Academic primary care internal medicine practice.Subjects. Seven hundred twelve patients with uncomplicated hypertension.Measurements and Main Results. Suggestions were displayed to physicians
on computer workstations used to write outpatient orders and topharmacists when filling prescriptions. The primary end point was generichealth-related quality of life. Secondary end points were symptom profileand side effects from antihypertensive drugs, number of emergencydepartment visits and hospitalizations, blood pressure measurements,patient satisfaction with physicians and pharmacists, drug therapycompliance, and health care charges. In the control group, implementationof care changes in accordance with treatment suggestions was observed in26% of patients. In the intervention groups, compliance with suggestionswas poor, with treatment suggestions implemented in 25% of patients forwhom suggestions were displayed only to pharmacists, 29% of those forwhom suggestions were displayed only to physicians, and 35% of the groupfor whom both physicians and pharmacists received suggestions (p=0.13).Intergroup differences were neither statistically significant nor clinicallyrelevant for generic health-related quality of life, symptom and side-effectprofiles, number of emergency department visits and hospitalizations,blood pressure measurements, charges, or drug therapy compliance.
Conclusion. Computer-based intervention using a sophisticated electronicphysician order-entry system failed to improve compliance with treatmentsuggestions or outcomes of patients with uncomplicated hypertension.
Key Words: computers, practice guidelines, hypertension, randomizedcontrolled trials.
(Pharmacotherapy 2004;24(3):324–337)

COMPUTERIZED HYPERTENSION TREATMENT SUGGESTIONS Murray et al
Hypertension is a prevalent cause of cardio-vascular morbidity, mortality, and rising healthcare costs. In the United States, it affects 50–62million people and its prevalence may be rising.1,
2 Between 1991 and 1999 patient self-report datafrom the Centers for Disease Control andPrevention showed a 2% increase in theprevalence of hypertension.3 The disease is animportant antecedent of enormously expensive,major cardiovascular complications. Indeed, anestimate of health care expenditures owing tohypertension and its complications for 1998 was$108 billion.4 To reduce the prevalence ofhypertension, improve its treatment, and preventits complications, the Joint National Committee(JNC) on Prevention, Detection, Evaluation, andTreatment of High Blood Pressure providedevidence-based guidelines.5–7 Their purpose is toreduce the overall burden of suffering and costsof the disease by preventing it, by encouraging itsearly detection, and, when diagnosed, bypromoting lifestyle modifications, effectivepharmacotherapy, and therapy compliance.However, despite the availability of such expertguidelines and a variety of effective drugs andlifestyle modifications, hypertension remainsdifficult to control: only one fourth of treatedpatients have adequately controlled bloodpressure.1
Although there are a variety of barriers tophysician adherence to guidelines,8 a majorproblem is that guidelines are numerous andcomplicated, thereby decreasing prospects ofrecall by physicians while caring for patients inbusy practices.9–11 Furthermore, becauseguidelines exist for many chronic diseases,physicians are often not aware of them12 or havedifficulty retrieving relevant information for eachdisorder when necessary. Finally, simplyproviding clinicians with more documents
containing guidelines is overwhelming13 and doesnot improve compliance,14–20 and the guidelinesquickly become outdated.21–23 Because patientswith complex treatment regimens refill drugprescriptions on a regular basis between clinicvisits, pharmacists with good lines of communi-cation to caring physicians may be able to notifyphysicians about patients whose regimens do notconform to guidelines or who are not takingdrugs according to instructions.
The increasing use of computers in health careoffers the hope of better organization and readyaccess to updated information to improve thequality of patient care,24 including practiceguidelines.25–27 Access to guidelines by computercan be as simple as making relevant text available.At the other end of the spectrum, displayingpatient- and problem-specific messages at thepoint of care would seem to have advantages;however, it requires a comprehensive, integratedelectronic information system. Having such asystem with comprehensive, computer-basedphysician order-entry and pharmacy management,we conducted a randomized controlled trial ofguideline-based hypertension managementsuggestions to primary care physicians writingorders and pharmacists dispensing drugs topatients in a large internal medicine practice.
Methods
Setting
After approval by the institutional reviewboard, this study was conducted at a large, inner-city, academic, internal medicine practiceaffiliated with the Indiana University School ofMedicine. The primary venues for this studywere the general medicine practice and theWishard Memorial Hospital outpatient pharmacy,which, at the time of the study, were located onefloor apart in the Regenstrief Health Center. Bothmedicine practice and outpatient pharmacy usethe electronic Regenstrief medical records system(RMRS)28 to deliver everyday care and have doneso for more than 25 years. This is not a purelyinvestigational system.
At the time of this study, the medicine practiceincluded more than 150 faculty general internistsand internal medicine residents who providedprimary care to approximately 13,000 adultsduring more than 50,000 visits annually in fouridentical, adjacent practices that each hadseparate physician, nursing, and clerical staffs.Each practice met during 8 half-day sessions/week,with each session attended by 2–3 faculty and
325
From the Department of Medicine, Indiana UniversitySchool of Medicine (Drs. Murray, Harris, Overhage,McDonald, and Tierney, and Mr. Eckert), RegenstriefInstitute (Drs. Murray, Harris, Overhage, McDonald, andTierney, and Ms. Smith and Ms. Buchanan), Department ofPharmacy Practice, Purdue University School of Pharmacy(Dr. Murray), and Roudebush VA Medical Center (Dr.Tierney), Indianapolis, Indiana; the Department ofBiostatistics, HSR&D Center of Excellence, VA Puget SoundHealth Care System, University of Washington, Tacoma,Washington (Dr. Zhou); and St. Louis University School ofPublic Health, St. Louis, Missouri (Dr. Wolinsky).
Supported by a grant (R01 HS07763) from the Agency forHealthcare Research and Quality, Rockville, Maryland.
Address reprint requests to Michael D. Murray, Pharm.D.,M.P.H., Regenstrief Institute, Regenstrief Health Center,Sixth Floor, 1050 Wishard Boulevard, Indianapolis, IN46202-2872; e-mail: [email protected].

PHARMACOTHERAPY Volume 24, Number 3, 2004
3–5 residents. Faculty physicians practiced 1–5sessions/week, fellows practiced 1–2 sessions,and residents 1 session/week.
At the beginning of each academic year, newphysicians were randomly assigned to assume theprimary care practices and patient panels ofdeparting physicians.29 Residents were primarycare providers, although they briefly presentedpatients to a faculty physician. New patientswere assigned to the next available primary carephysician and to a specific practice session. Suchassignments were permanent unless a changewas requested by the patient, which was rare(< 2% of patients). Repeated studies foundpatient characteristics and physician practicepatterns to be similar among the four practicesand their half-day sessions.30, 31
Subjects
Eligibility for this study required that patientshave evidence in their electronic medical recordsof hypertension as an active outpatient diagnosisor, in the absence of such a diagnosis, all of thefollowing: at least two systolic blood pressuremeasurements of 140 mm Hg or greater, at leasttwo diastolic blood pressure measurements of 90mm Hg or greater, and a prescription for at leastone antihypertensive agent. Qualifying anti-hypertensive agents were angiotensin-convertingenzyme (ACE) inhibitors, b-blockers, calciumchannel blockers, oral clonidine and topicalpatch, diuretics, and other less commonlyprescribed drugs such as methyldopa andreserpine. Because our intent was to focus onpatients with uncomplicated hypertension (andhence without other major indications forantihypertensive therapy, such as b-blockersamong patients with ischemic heart disease),patients were excluded from participation if theyhad evidence (diagnoses or test results)indicating the presence of a cardiovascularcomplication such as coronary artery disease,myocardial infarction, stroke, heart failure, orrenal insufficiency.
Study Design
This was a randomized controlled trial using a2 x 2 factorial design involving physician andpharmacist interventions. To avoid contaminationof physicians practicing in the same session, werandomly assigned half of the 32 practicesessions to receive the physician intervention(described below). We first randomized tointervention or control status the practice
sessions attended by faculty physicians withmore than 1 session/week. We then randomizedall remaining practice sessions to intervention orcontrol status. By doing so, each practice sessionhad an equal number of intervention and controlsessions, and all physicians in sessions had thesame study status.
We also randomly assigned pharmacists tointervention and control status, separatelyrandomizing 11 with full-time and 9 with part-time positions. Half of patients receiving care inphysician-intervention sessions and halfreceiving care in physician-control sessions werethen randomly assigned to receive all prescrip-tions from intervention pharmacists (describedbelow) whenever they filled any prescription forany condition in the Wishard outpatientpharmacy. Remaining patients were required tohave all prescriptions filled by control pharmacists.This randomization of practice sessions,pharmacists, and patients resulted in four groupsof patients: physician intervention only,pharmacist intervention only, intervention byphysician and pharmacist, and intervention byneither physician nor pharmacist (control).
A full-time research assistant recruitedparticipants between January 1, 1994, and May 1,1996, by approaching potentially eligible patientsin the medicine practice waiting room duringregularly scheduled appointments. Potentialparticipants who were able to communicate(could hear and speak English and understandinstructions), had access to a working telephone,and were willing to provide written informedconsent were enrolled. Full enrollmentinterviews were performed within the month bytelephone. Participating physicians andpharmacists were unaware of the studyhypothesis and outcomes being measured.
Treatment Guidelines and Suggestions
We used evidence-based guidelines publishedby the JNC on Prevention, Detection, Evaluation,and Treatment of High Blood Pressure.5, 6 Thestudy proposal had been written during the fifthcommittee session (JNC V) and implementedduring the sixth (JNC VI); treatment suggestionswere consistent with both sets of guidelines.Recognizing that effective guidelines must beboth evidence based and translated into localaccepted standards of practice,32, 33 we presentedhypertension treatment considerations orsuggestions of the JNC expert panel to a localpanel of expert general internists and cardiologists,
326

COMPUTERIZED HYPERTENSION TREATMENT SUGGESTIONS Murray et al
each of whom read and graded each suggestion asacceptable as written, acceptable after makingminor modifications, or unacceptable withoutmajor modifications. The panel adjudicated eachsuggestion considered unacceptable by any panelmember. After approval by the expert panel, weused a locally developed computer decisionsupport system to encode approved suggestionsinto computer workstations that generalmedicine practice physicians used to write allinpatient and outpatient orders.28, 34, 35
Data necessary to generate care suggestionswere derived from the RMRS.28 Treatmentsuggestions fell into five major categories:
• Reducing systolic blood pressure to below140 mm Hg and diastolic blood pressure tobelow 90 mm Hg by increasing dosages ofantihypertensive drugs or by encouragingpatient adherence to the antihypertensiveregimen where indicated
• Promoting therapy with thiazides or b-blockers as first-line agents as indicated inJNC reports
• Providing warnings about common sideeffects of antihypertensive drugs
• Encouraging treatment of uncontrolledcomorbid conditions (e.g., diabetes, hyper-cholesterolemia) or preferential use of someantihypertensive drugs with specific comor-bidities (e.g., ACE inhibitors for patients withdiabetes)
• Encouraging regular exercise, smokingcessation, and weight reduction, with drugtherapy compliance and patient educationstressed for all intervention patients
The goal of this study was to determine thedirect effects of computerized treatmentguidelines for hypertension rather than theirindirect effects as an educational tool. Theapproved treatment suggestions were availableonline to all intervention and control physiciansand pharmacists. Before beginning the study, wealso provided each primary care physician with aprinted, referenced summary of the locallyapproved guidelines for managing hypertension,presented as accepted standards of care for theadult medicine practice. Pharmacists had accessto these same materials on their computer work-stations. Names of consensus panel memberswere included, together with a summary of thedevelopment process. Two physician investigators(WMT, JMO) presented medicine grand roundson the role of evidence-based practice guidelinesin primary care and the role of computer decision
support systems in quality improvement.11 Asummary of the JNC VI guidelines was includedin this presentation. A pharmacist investigator(MDM) presented a similar program tooutpatient pharmacists. In addition, one of theinvestigators met with each interventionphysician and pharmacist (individually or insmall groups) to present the rationale for thestudy and instruct them in guidelines andcomputer-based presentation of care suggestions.
Physician Intervention Protocol
For each outpatient visit, the physicianreceived the patient’s paper chart and a patient-specific encounter form that included thepatient’s active outpatient problem list, activedrugs, and computer-based reminders forpreventive care and monitoring for adverse drugreactions. This form was printed the night beforeeach scheduled visit. After examining a patient,the physician used an order-writing workstation28,
34, 35 to write orders for drugs, tests, nursingactivities, and consultations. If they chose to,physicians could print patient education materials,type visit notes, and record other information.Using data from patients’ electronic medicalrecords and data entered by physicians after thevisit, the workstation identified care suggestionsfor the treatment of hypertension for whichpatients (regardless of study group) were eligible.
The computer-based ordering system generatedthese care suggestions36 for both intervention andcontrol groups; however, the suggestions weredisplayed by the computer to physicians and/orpharmacists for patients randomized to theappropriate intervention groups. This allowed usto assess the numbers and types of interventionsthat the control group was eligible to receive aswell as those in the three intervention groups.For patients in the physician intervention group,all care suggestions based solely on earlier RMRSdata were generated at the time that theencounter form was printed and were displayedat the end of the drug list. All hypertension caresuggestions for intervention patients weredisplayed as “suggested orders” on physicians’workstations when they wrote orders afterpatient visits (Figure 1). This computer screendisplayed the actual suggested order, possibleactions for each order (order or omit), and a briefexplanation of the rationale for the order.Physicians could list full guidelines and literaturecitations associated with the specific suggestionsby using the workstation’s “help” key.
327

PHARMACOTHERAPY Volume 24, Number 3, 2004
During the study, an enrolled patient couldvisit the medicine practice for unscheduled carewhen his or her physician was not available.When this occurred, the system delivered caresuggestions only when both the patient and thepatient’s primary care physician had beenrandomized to the physician intervention group.In all other situations, the system withheld caresuggestions. Also, throughout the study, long-standing computer-generated reminders11, 29 fornonstudy conditions were presented whenindicated to all physicians.
Pharmacist Intervention Protocol
When any patient brought a new or refillprescription (written in any affiliated clinic,physician’s office, or Wishard Hospital emergencydepartment) to the Wishard outpatient pharmacy,a pharmacy technician entered the data into theRMRS pharmacy module.37, 38 This was requiredfor all prescriptions because it was the only wayto generate and complete a financial transactionfor prescriptions in the outpatient pharmacy.After entering prescription data, a high-speedprinter created a label to affix to the patient’sdrug container. The technician who filled theprescription notified the pharmacist for allintervention patients. The labeled drug productwas checked by a pharmacist who dispensed the
agent to the patient and provided counseling.For this study we created the pharmacist
intervention recording system (PIRS). Thissoftware program was used by all Wishardpharmacists to document all pharmaceutical careinterventions provided to any outpatient.39 Forpatients enrolled in this study only (regardless ofstudy group), care suggestions generated by theRMRS or the outpatient workstations (inresponse to data entered by the physician, e.g.,new antihypertensive prescriptions) were storedin the PIRS. For patients randomized to receivecare from an intervention pharmacist who hadsuch care suggestions, the high-speed printerprinted a note together with drug containerlabels directing the pharmacist to the PIRS todisplay care suggestions that were identical tothose viewed by intervention physicians. Anintervention patient’s prescription could be filledonly by an intervention pharmacist unless nointervention pharmacists were available. (Weworked with the pharmacy department to makesure that both intervention and control pharmacistswere present on most shifts in the outpatientpharmacy.)
On receiving suggestions, the pharmacist hadthree options: fill the prescription(s) as written,discuss the intervention suggestion(s) with thepatient and encourage subsequent discussions
328
Figure 1. Example of an order-entry screen used by study physicians. Treatment with an angiotensin-converting enzyme(ACE) inhibitor is recommended for a patient with diabetes and renal insufficiency.

COMPUTERIZED HYPERTENSION TREATMENT SUGGESTIONS Murray et al
with his or her primary care physician, or contactthe ordering physician by telephone or by page.During the first few months of the study, somepharmacists stated that discussing some issueswith patients was ineffective and they frequentlywere reluctant to contact busy physicians. Wetherefore added a fourth option: the pharmacistcould e-mail a brief message to the physician onthe workstation network. The next time thatphysician logged onto the workstation, thepharmacist’s message was displayed and thephysician could access the patient’s electronicmedical record, use the workstation to write anorder or a memorandum to consider thesuggestion during the next visit, or do nothing.Of importance, the pharmacist interventiondisplayed information to an interventionpharmacist whenever an intervention patientcame to the Wishard outpatient pharmacy to fillany prescription, written from any outpatientencounter site, any time of the day or night.
Data Collection
We considered a patient to be eligible for anevidence-based suggestion if a care suggestionwas generated for a scheduled visit betweenenrollment and closeout dates. Regardless of thenumber of times the patient visited the practiceor the outpatient pharmacy during the study,each care suggestion was counted only once. Wedefined guideline adherence as the patient’sreceipt of the suggested drug, dosage adjustmentor test at any time between the date thesuggestion was first generated and 30 days afterthe patient’s study closeout date. We created aguideline adherence score for each patient bysumming all care suggestions complied withdivided by the number suggested. Not includedin our calculation of adherence score wascounseling about smoking cessation, exercise, orweight loss, which we could not measureaccurately.
The primary outcome variable was generichealth-related quality of life. Secondary patientoutcomes were symptom and side-effect profiles,number of emergency department visits orhospitalizations for all causes in general andheart disease specifically (ischemic heart disease,heart failure), blood pressure measurements,drug therapy compliance, direct health carecharges, and patient satisfaction with physicianand pharmacist. After enrollment, a researchassistant called each patient at home andadministered a baseline survey that included the
Short Form (SF)-36,40 a generic indicator ofhealth-related quality of life that was validatedlocally,41, 42 and the hypertension-specific Bulpittquestionnaire.43 The SF-36 produces measures ofhealth status across eight physical and mentaldimensions, and the Bulpitt questionnairemeasures symptoms and antihypertensive drugside effects across physical and psychologicaldomains. Drug therapy compliance was assessedwith specific instruments44, 45 and by calculatingthe medication possession ratio,46 also locallyvalidated,47 which uses archived computerprescription refill information.
At the beginning of the twelfth month afterenrollment, telephone interviewers made severalattempts, as necessary, to obtain a closeoutinterview. If unsuccessful by the end of thetwelfth month, research assistants attempted toadminister the interview during patients’scheduled visits to the practice. After 15 monthsafter enrollment, no further attempts were made.To avoid bias, all research assistants andinterviewers interviewed patients in all studygroups and were blinded to group assignmentduring both enrollment and closeout interviews.From patients’ RMRS records, we extractedevidence of all-cause and heart disease–specificemergency department visits and hospitalizationsand death dates. We used a validated list of heartdisease–specific diagnoses indicating ischemia orheart failure.48 Data were extracted from theRMRS to assess physician and pharmacistcompliance with care suggestions.
To assess the validity of care suggestionsrelative to information in the chart, oneinvestigator (JMO) reviewed paper and electronicrecords of a 10% random sample (72) of enrolledpatients. Four paper charts could not be located.For each suggestion, all paper and electronicnotes and patient data for all practice encountersduring the study were searched for evidence thatthe care suggestion was invalid or that thephysician disagreed with it. We found no casesin which treatment suggestions were faulty andphysician agreement with suggestions wascomplete.
Statistical Analyses
The unit of analysis for all outcomes was thepatient. We controlled for correlation of responsesamong patients of individual physicians byemploying random effects generalized linearmodels and generalized estimating equations49 toaccount for correlations of results among patients
329
PHARMACOTHERAPY Volume 24, Number 3, 2004
treated by individual physicians who were targetsof the intervention. The other target was thepharmacist. However, there was no one-to-oneassignment of individual pharmacists toindividual patients, and as such no correctionwas possible for the effect of individual pharmacists.
Before the study began, we performed poweranalyses that indicated that we needed 500evaluable patients to have 80% power to detect 1standard error of measurement change insubscale scores of the SF-36 question-naire. Thestandard error of measurement is a measure of
330
2063 potentially eligible patientsmade a scheduled visit
1332 contacted by aresearch assistant
830 were eligible and signedinformed consent
731 missed by research assistants
206 were ineligible:114 had no telephone 21 were non-communicative 15 were nursing home residents 13 were prisoners 43 for some other reason
65 refused to participate
1036 agreed to be interviewed forstudy eligibility
53 could not be reached byphone for baseline interview
777 were contacted by telephonefor baseline interview
171 control(no intervention)
180 pharmacistintervention
181 physicianintervention
180 bothinterventions
47 with no visits orcare suggestions
44 with no close-outinterview
49 with no visits orcare suggestions
64 with no close-outinterview
48 with no visits orcare suggestions
57 with no close-outinterview
38 with no visits orcare suggestions
64 with no close-outinterview
Analyzed:171 utilization114 rule compliance127 survey results
Analyzed:180 utilization117 rule compliance116 survey results
Analyzed:181 utilization123 rule compliance124 survey results
Analyzed:180 utilization125 rule compliance116 survey results
296 refused to participate
712 were randomized
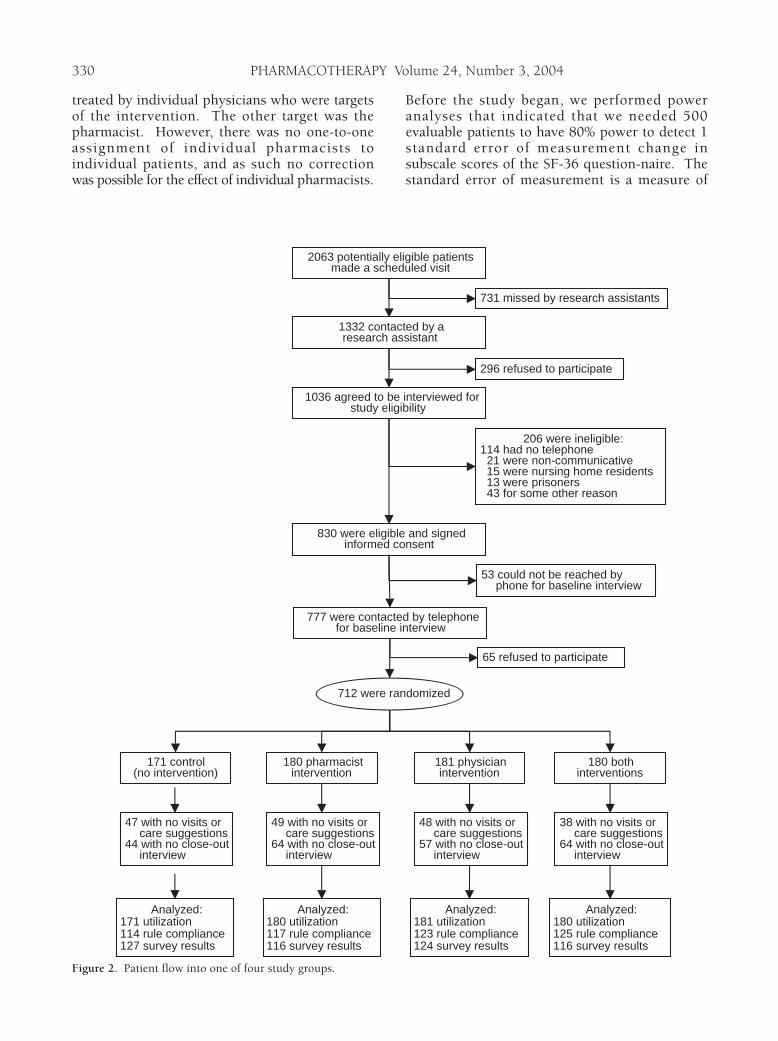
Figure 2. Patient flow into one of four study groups.
COMPUTERIZED HYPERTENSION TREATMENT SUGGESTIONS Murray et al
statistically significant changes in quality-of-lifescores that takes into account the distribution ofresponses among subjects and the reliability(Cronbach’s coefficient a) of scale scores.50, 51 Weanticipated attrition of 25% of subjects duringthe study, so we sought to enroll 700 patientswith hypertension as defined above.
We used analysis of variance to comparepatients’ guideline adherence rates among thefour study groups and the Student t tests toassess separate effects of physician and phar-macist interventions. We compared numbers ofprimary care visits during subjects’ time in thestudy and adverse events such as hospitalizationsamong study groups using Poisson regression.We created overall and subscale scores for the SF-36,40 Bulpitt,43 and physician satisfactioninstruments52 as described. We then usedanalysis of covariance to compare these scoresamong groups, using baseline scores andindicators for ceiling and floor effects ascovariates. We classified patients as improved orworse on quality-of-life measures if their scoreschanged by more than 1 standard error ofmeasurement,50, 51 which we compared amongstudy groups using logistic regression. Chargesand the medication possession ratio wereanalyzed using Wald-type tests for log-normaldata possibly with zeros.53 Comparisons for drugcompliance measures were made using logisticregression44 and analysis of covariance modelswith baseline scores and indicators for ceilingand floor effects as covariates.45
Results
Patient flow during the study is shown inFigure 2. A total of 712 patients were enrolled.Our randomization of the medicine practice
sessions resulted in 171 patients in the controlgroup, 180 whose pharmacist received theintervention, 181 whose physician received theintervention, and 180 for whom both pharmacistand physician received the intervention. Thenumbers of patients available for analysis werecomparable across these four groups.
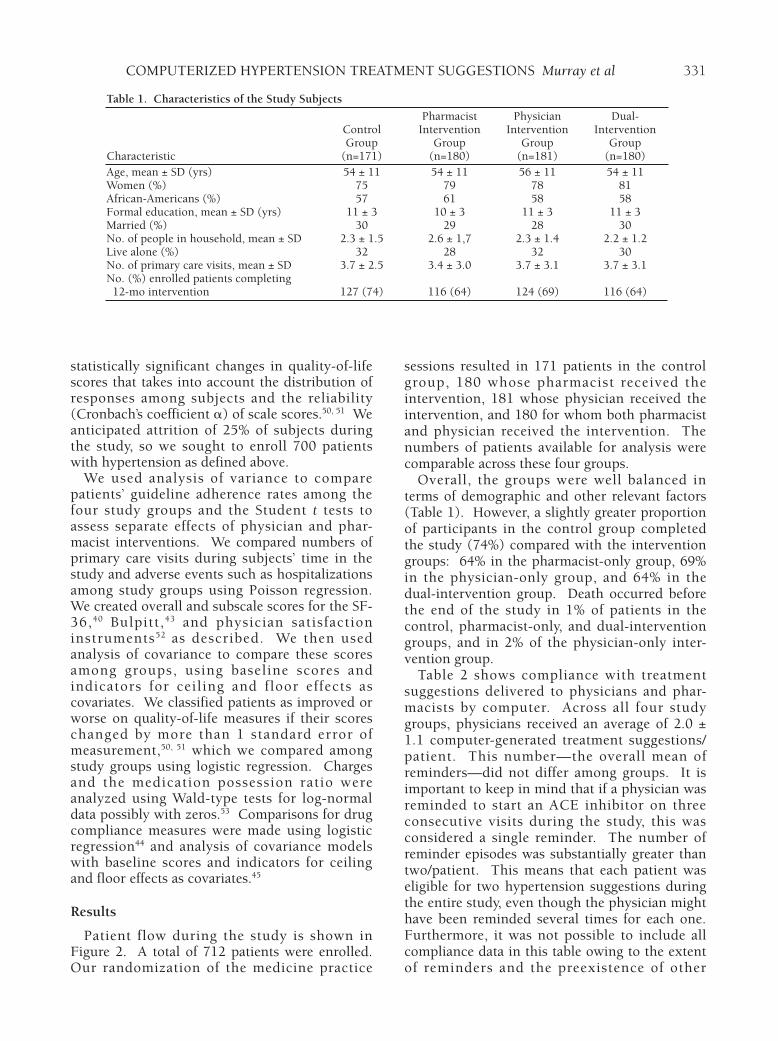
Overall, the groups were well balanced interms of demographic and other relevant factors(Table 1). However, a slightly greater proportionof participants in the control group completedthe study (74%) compared with the interventiongroups: 64% in the pharmacist-only group, 69%in the physician-only group, and 64% in thedual-intervention group. Death occurred beforethe end of the study in 1% of patients in thecontrol, pharmacist-only, and dual-interventiongroups, and in 2% of the physician-only inter-vention group.
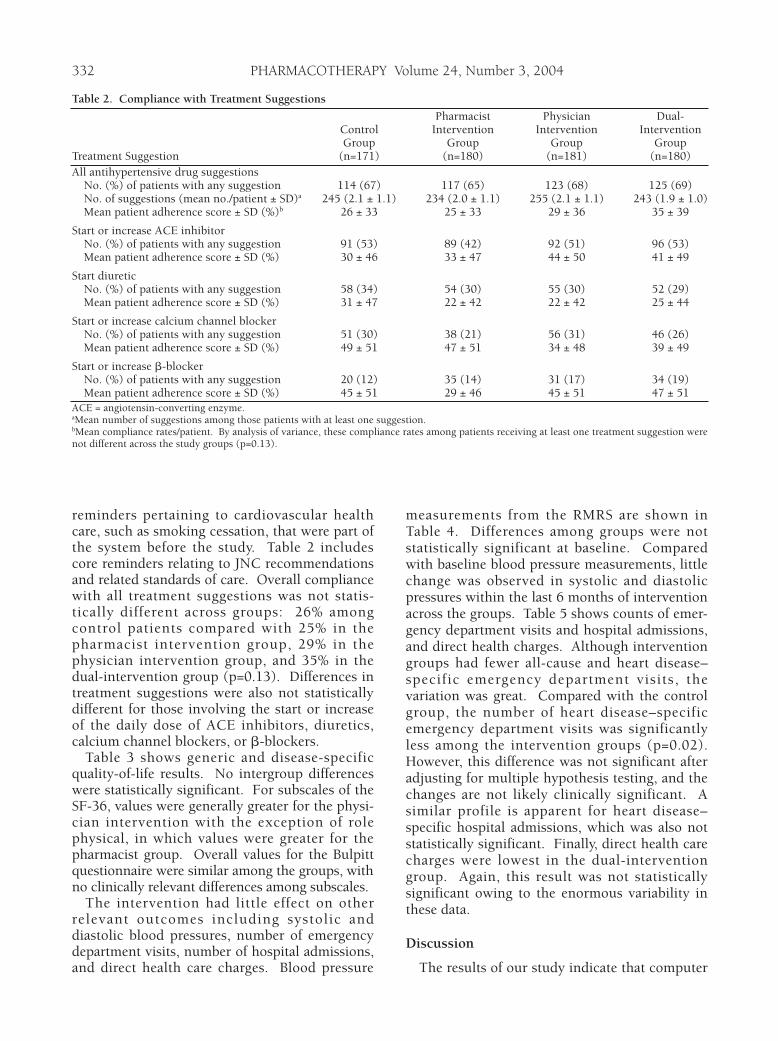
Table 2 shows compliance with treatmentsuggestions delivered to physicians and phar-macists by computer. Across all four studygroups, physicians received an average of 2.0 ±1.1 computer-generated treatment suggestions/patient. This number—the overall mean ofreminders—did not differ among groups. It isimportant to keep in mind that if a physician wasreminded to start an ACE inhibitor on threeconsecutive visits during the study, this wasconsidered a single reminder. The number ofreminder episodes was substantially greater thantwo/patient. This means that each patient waseligible for two hypertension suggestions duringthe entire study, even though the physician mighthave been reminded several times for each one.Furthermore, it was not possible to include allcompliance data in this table owing to the extentof reminders and the preexistence of other
331
Table 1. Characteristics of the Study Subjects
Pharmacist Physician Dual-Control Intervention Intervention InterventionGroup Group Group Group
Characteristic (n=171) (n=180) (n=181) (n=180)Age, mean ± SD (yrs) 54 ± 11 54 ± 11 56 ± 11 54 ± 11Women (%) 75 79 78 81African-Americans (%) 57 61 58 58Formal education, mean ± SD (yrs) 11 ± 3 10 ± 3 11 ± 3 11 ± 3Married (%) 30 29 28 30No. of people in household, mean ± SD 2.3 ± 1.5 2.6 ± 1,7 2.3 ± 1.4 2.2 ± 1.2Live alone (%) 32 28 32 30No. of primary care visits, mean ± SD 3.7 ± 2.5 3.4 ± 3.0 3.7 ± 3.1 3.7 ± 3.1No. (%) enrolled patients completing12-mo intervention 127 (74) 116 (64) 124 (69) 116 (64)
PHARMACOTHERAPY Volume 24, Number 3, 2004
reminders pertaining to cardiovascular healthcare, such as smoking cessation, that were part ofthe system before the study. Table 2 includescore reminders relating to JNC recommendationsand related standards of care. Overall compliancewith all treatment suggestions was not statis-tically different across groups: 26% amongcontrol patients compared with 25% in thepharmacist intervention group, 29% in thephysician intervention group, and 35% in thedual-intervention group (p=0.13). Differences intreatment suggestions were also not statisticallydifferent for those involving the start or increaseof the daily dose of ACE inhibitors, diuretics,calcium channel blockers, or b-blockers.
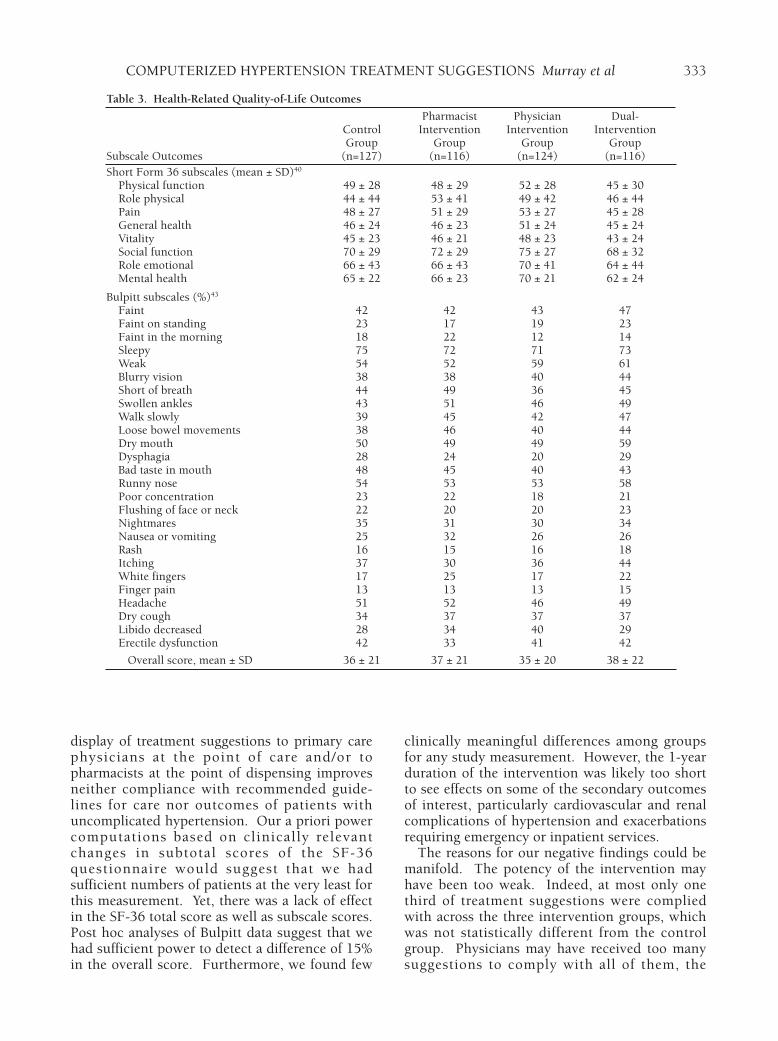
Table 3 shows generic and disease-specificquality-of-life results. No intergroup differenceswere statistically significant. For subscales of theSF-36, values were generally greater for the physi-cian intervention with the exception of rolephysical, in which values were greater for thepharmacist group. Overall values for the Bulpittquestionnaire were similar among the groups, withno clinically relevant differences among subscales.
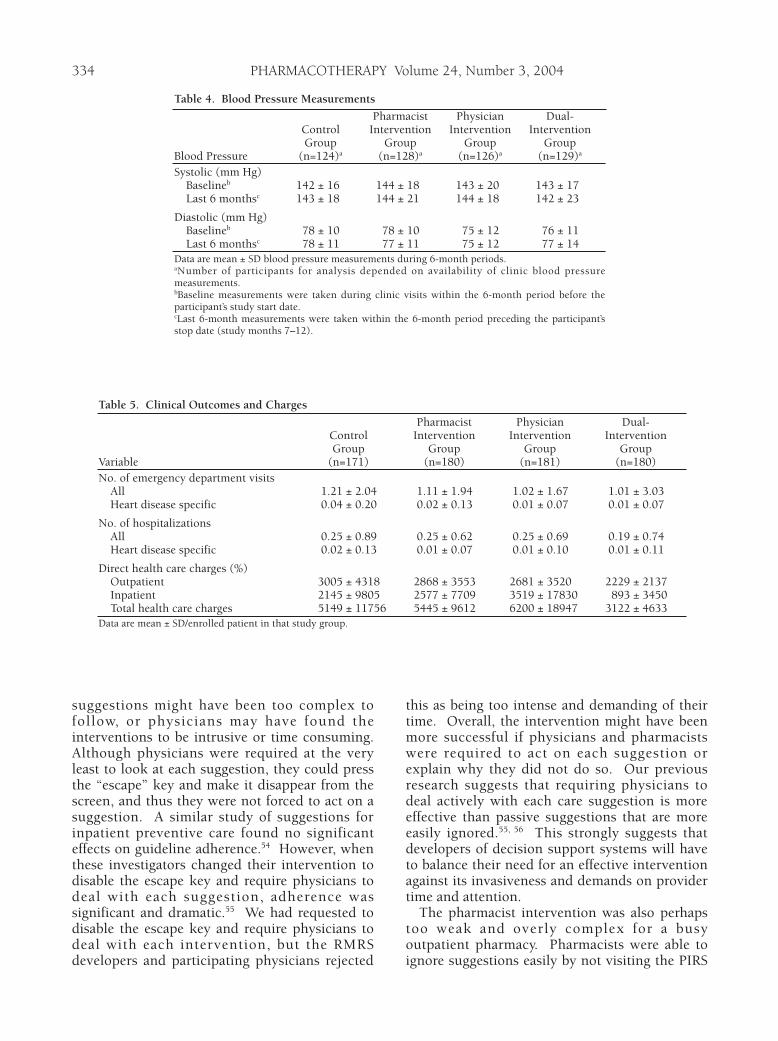
The intervention had little effect on otherrelevant outcomes including systolic anddiastolic blood pressures, number of emergencydepartment visits, number of hospital admissions,and direct health care charges. Blood pressure
measurements from the RMRS are shown inTable 4. Differences among groups were notstatistically significant at baseline. Comparedwith baseline blood pressure measurements, littlechange was observed in systolic and diastolicpressures within the last 6 months of interventionacross the groups. Table 5 shows counts of emer-gency department visits and hospital admissions,and direct health charges. Although interventiongroups had fewer all-cause and heart disease–specific emergency department visits, thevariation was great. Compared with the controlgroup, the number of heart disease–specificemergency department visits was significantlyless among the intervention groups (p=0.02).However, this difference was not significant afteradjusting for multiple hypothesis testing, and thechanges are not likely clinically significant. Asimilar profile is apparent for heart disease–specific hospital admissions, which was also notstatistically significant. Finally, direct health carecharges were lowest in the dual-interventiongroup. Again, this result was not statisticallysignificant owing to the enormous variability inthese data.
Discussion
The results of our study indicate that computer
332
Table 2. Compliance with Treatment Suggestions
Pharmacist Physician Dual-Control Intervention Intervention InterventionGroup Group Group Group
Treatment Suggestion (n=171) (n=180) (n=181) (n=180)All antihypertensive drug suggestions
No. (%) of patients with any suggestion 114 (67) 117 (65) 123 (68) 125 (69)No. of suggestions (mean no./patient ± SD)a 245 (2.1 ± 1.1) 234 (2.0 ± 1.1) 255 (2.1 ± 1.1) 243 (1.9 ± 1.0)Mean patient adherence score ± SD (%)b 26 ± 33 25 ± 33 29 ± 36 35 ± 39
Start or increase ACE inhibitorNo. (%) of patients with any suggestion 91 (53) 89 (42) 92 (51) 96 (53)Mean patient adherence score ± SD (%) 30 ± 46 33 ± 47 44 ± 50 41 ± 49
Start diureticNo. (%) of patients with any suggestion 58 (34) 54 (30) 55 (30) 52 (29)Mean patient adherence score ± SD (%) 31 ± 47 22 ± 42 22 ± 42 25 ± 44
Start or increase calcium channel blockerNo. (%) of patients with any suggestion 51 (30) 38 (21) 56 (31) 46 (26)Mean patient adherence score ± SD (%) 49 ± 51 47 ± 51 34 ± 48 39 ± 49
Start or increase b-blockerNo. (%) of patients with any suggestion 20 (12) 35 (14) 31 (17) 34 (19)Mean patient adherence score ± SD (%) 45 ± 51 29 ± 46 45 ± 51 47 ± 51
ACE = angiotensin-converting enzyme.aMean number of suggestions among those patients with at least one suggestion.bMean compliance rates/patient. By analysis of variance, these compliance rates among patients receiving at least one treatment suggestion werenot different across the study groups (p=0.13).
COMPUTERIZED HYPERTENSION TREATMENT SUGGESTIONS Murray et al
display of treatment suggestions to primary carephysicians at the point of care and/or topharmacists at the point of dispensing improvesneither compliance with recommended guide-lines for care nor outcomes of patients withuncomplicated hypertension. Our a priori powercomputations based on clinically relevantchanges in subtotal scores of the SF-36questionnaire would suggest that we hadsufficient numbers of patients at the very least forthis measurement. Yet, there was a lack of effectin the SF-36 total score as well as subscale scores.Post hoc analyses of Bulpitt data suggest that wehad sufficient power to detect a difference of 15%in the overall score. Furthermore, we found few
clinically meaningful differences among groupsfor any study measurement. However, the 1-yearduration of the intervention was likely too shortto see effects on some of the secondary outcomesof interest, particularly cardiovascular and renalcomplications of hypertension and exacerbationsrequiring emergency or inpatient services.
The reasons for our negative findings could bemanifold. The potency of the intervention mayhave been too weak. Indeed, at most only onethird of treatment suggestions were compliedwith across the three intervention groups, whichwas not statistically different from the controlgroup. Physicians may have received too manysuggestions to comply with all of them, the
333
Table 3. Health-Related Quality-of-Life Outcomes
Pharmacist Physician Dual-Control Intervention Intervention InterventionGroup Group Group Group
Subscale Outcomes (n=127) (n=116) (n=124) (n=116)Short Form 36 subscales (mean ± SD)40
Physical function 49 ± 28 48 ± 29 52 ± 28 45 ± 30Role physical 44 ± 44 53 ± 41 49 ± 42 46 ± 44Pain 48 ± 27 51 ± 29 53 ± 27 45 ± 28General health 46 ± 24 46 ± 23 51 ± 24 45 ± 24Vitality 45 ± 23 46 ± 21 48 ± 23 43 ± 24Social function 70 ± 29 72 ± 29 75 ± 27 68 ± 32Role emotional 66 ± 43 66 ± 43 70 ± 41 64 ± 44Mental health 65 ± 22 66 ± 23 70 ± 21 62 ± 24
Bulpitt subscales (%)43
Faint 42 42 43 47Faint on standing 23 17 19 23Faint in the morning 18 22 12 14Sleepy 75 72 71 73Weak 54 52 59 61Blurry vision 38 38 40 44Short of breath 44 49 36 45Swollen ankles 43 51 46 49Walk slowly 39 45 42 47Loose bowel movements 38 46 40 44Dry mouth 50 49 49 59Dysphagia 28 24 20 29Bad taste in mouth 48 45 40 43Runny nose 54 53 53 58Poor concentration 23 22 18 21Flushing of face or neck 22 20 20 23Nightmares 35 31 30 34Nausea or vomiting 25 32 26 26Rash 16 15 16 18Itching 37 30 36 44White fingers 17 25 17 22Finger pain 13 13 13 15Headache 51 52 46 49Dry cough 34 37 37 37Libido decreased 28 34 40 29Erectile dysfunction 42 33 41 42
Overall score, mean ± SD 36 ± 21 37 ± 21 35 ± 20 38 ± 22
PHARMACOTHERAPY Volume 24, Number 3, 2004
suggestions might have been too complex tofollow, or physicians may have found theinterventions to be intrusive or time consuming.Although physicians were required at the veryleast to look at each suggestion, they could pressthe “escape” key and make it disappear from thescreen, and thus they were not forced to act on asuggestion. A similar study of suggestions forinpatient preventive care found no significanteffects on guideline adherence.54 However, whenthese investigators changed their intervention todisable the escape key and require physicians todeal with each suggestion, adherence wassignificant and dramatic.55 We had requested todisable the escape key and require physicians todeal with each intervention, but the RMRSdevelopers and participating physicians rejected
this as being too intense and demanding of theirtime. Overall, the intervention might have beenmore successful if physicians and pharmacistswere required to act on each suggestion orexplain why they did not do so. Our previousresearch suggests that requiring physicians todeal actively with each care suggestion is moreeffective than passive suggestions that are moreeasily ignored.55, 56 This strongly suggests thatdevelopers of decision support systems will haveto balance their need for an effective interventionagainst its invasiveness and demands on providertime and attention.
The pharmacist intervention was also perhapstoo weak and overly complex for a busyoutpatient pharmacy. Pharmacists were able toignore suggestions easily by not visiting the PIRS
334
Table 4. Blood Pressure Measurements
Pharmacist Physician Dual-Control Intervention Intervention InterventionGroup Group Group Group
Blood Pressure (n=124)a (n=128)a (n=126)a (n=129)a
Systolic (mm Hg)Baselineb 142 ± 16 144 ± 18 143 ± 20 143 ± 17Last 6 monthsc 143 ± 18 144 ± 21 144 ± 18 142 ± 23
Diastolic (mm Hg)Baselineb 78 ± 10 78 ± 10 75 ± 12 76 ± 11Last 6 monthsc 78 ± 11 77 ± 11 75 ± 12 77 ± 14
Data are mean ± SD blood pressure measurements during 6-month periods.aNumber of participants for analysis depended on availability of clinic blood pressuremeasurements.bBaseline measurements were taken during clinic visits within the 6-month period before theparticipant’s study start date.cLast 6-month measurements were taken within the 6-month period preceding the participant’sstop date (study months 7–12).
Table 5. Clinical Outcomes and Charges
Pharmacist Physician Dual-Control Intervention Intervention InterventionGroup Group Group Group
Variable (n=171) (n=180) (n=181) (n=180)No. of emergency department visits
All 1.21 ± 2.04 1.11 ± 1.94 1.02 ± 1.67 1.01 ± 3.03Heart disease specific 0.04 ± 0.20 0.02 ± 0.13 0.01 ± 0.07 0.01 ± 0.07
No. of hospitalizationsAll 0.25 ± 0.89 0.25 ± 0.62 0.25 ± 0.69 0.19 ± 0.74Heart disease specific 0.02 ± 0.13 0.01 ± 0.07 0.01 ± 0.10 0.01 ± 0.11
Direct health care charges (%)Outpatient 3005 ± 4318 2868 ± 3553 2681 ± 3520 2229 ± 2137Inpatient 2145 ± 9805 2577 ± 7709 3519 ± 17830 893 ± 3450Total health care charges 5149 ± 11756 5445 ± 9612 6200 ± 18947 3122 ± 4633
Data are mean ± SD/enrolled patient in that study group.

COMPUTERIZED HYPERTENSION TREATMENT SUGGESTIONS Murray et al
on the study workstation. It is important to notethat the pharmacist intervention differedconsiderably from the physician intervention.Unlike the intervention for physicians whoreceived suggestions as they wrote orders forpatients they had just seen, the pharmacistintervention most often required a technicianwho was monitoring the printer to notify thepharmacist that a message had been received onthe printer, and the pharmacist then had to moveto a separate workstation for the suggestion.Furthermore, in contrast to physicians, phar-macists could not legally write treatment orders.On the positive side, pharmacists had a chance toview treatment suggestions whenever patientscame to the pharmacy, not just when they werevisiting their primary care physicians or whenthey were having antihypertensive drugsprescribed or filled. This would explain theresults of our earlier reports of pharmacist workpatterns that intervention pharmacists had highnumbers of interactions with patients andphysicians.37 However, despite increased patientand physician encounters, there were nomeasurable effects on adherence to hypertensiontreatment guidelines and patient-centeredoutcomes.
At the end of the study we asked physiciansand pharmacists for their thoughts about theintervention. Physicians generally thought thatguidelines were a good educational tool, aconvenient source of information, and intendedto improve the quality of care. But manybelieved that guidelines were “cookbook”medicine and too rigid to apply to individualpatients. They thought that the guidelineshampered their autonomy and were simplyintended to decrease health care costs.Pharmacists, although interested, were hamperedby constraints on dispensing time, their need tobe notified about an intervention by a technician,and a somewhat cumbersome PIRS data-entryform for logging interventions.
Although these results are discouraging, we donot believe that they suggest abandoningcomputerized treatment suggestions for thiscondition. Rather, we believe that the resultshave several lessons that would be instructive toothers. First, careful attention must be given tothe presentation or display of treatmentsuggestions and the ease with which physicianscan act on them or even ignore them. Second,besides making suggestions easy to implement,incentives may help increase compliance.Positive incentives to clinicians or teams of
practitioners may be worthwhile; however, theyshould come only after attempts to improveawareness of the objectives and content ofguidelines.12, 57 Objectives implicit in implementingpractice guidelines are to improve the quality andeffectiveness of care and reduce variations in theaccess and delivery of that care at predictablecosts.58, 59
Conclusion
Improvements in the quality and effectivenessof care or the associated effect on healthoutcomes cannot be achieved without betteradherence to treatment guidelines by clinicianswho are provided with timely, patient-specificsuggestions. Providing treatment suggestions toclinicians while caring for patients using asophisticated electronic medical record systemdoes not improve compliance with acceptedpractice guidelines or outcomes of patients withuncomplicated hypertension.
Acknowledgment
We thank Beverly Clark for her secretarial supporton this manuscript.
References1. Muntner P, He J, Roccella EJ, Whelton PK. The impact of JNC-
VI guidelines on treatment recommendations in the USpopulation. Hypertension 2002;39:897–902.
2. American Heart Association. 2002 heart and stroke statisticalupdate. Dallas, TX: American Heart Association, 2001.
3. Centers for Disease Control and Prevention. State-specifictrends in self-reported blood pressure screening and high bloodpressure—United States, 1991 to 1999. MMWR Morb MortalWkly Rep 2002;51:456–60.
4. Hodgson T, Cai L. Medical care expenditures for hypertension,its complications and its comorbidities. Med Care2001;39:599–615.
5. JNC V Coordinating Committee. The fifth report of the JointNational Committee on Prevention, Detection, Evaluation, andTreatment of High Blood Pressure (JNC V). Arch Intern Med1993;153:154–83.
6. JNC VI Coordinating Committee. The sixth report of the JointNational Committee on Prevention, Detection, Evaluation, andTreatment of High Blood Pressure (JNC VI). Arch Intern Med1997;157:2413–46.
7. JNC VII Coordinating Committee. The seventh report of theJoint National Committee on Prevention, Detection,Evaluation, and Treatment of High Blood Pressure. JAMA2003;289:2560–72.
8. Cabana MD, Rand C, Powell WW, Abboud P, Rubin HR. Whydon’t physicians follow clinical practice guidelines. JAMA1999;282:1458–65.
9. Hagemeister J, Schneider CA, Sven B, et al. Hypertensionguidelines and their limitations—the impact of physicians’compliance as evaluated by guideline awareness. J Hypertens2001;19:2079–86.
10. McDonald CJ. Medical heuristics: the silent adjudicators ofclinical practice. Ann Intern Med 1996;124:56–62.
11. Tierney WM. Improving clinical decisions and outcomes withinformation: a review. J Med Inform 2001;62:1–9.
335
PHARMACOTHERAPY Volume 24, Number 3, 2004
12. Hyman DJ, Pavl ik VN . Se l f -reported hypertensiontreatment practices among primary care physicians: bloodpressure threshold, drug choices and the role of guidelinesand evidence-based medicine. Arch Intern Med 2000;160:2281–6.
13. Conti CR. Guidelines, guidelines, and more guidelines. ClinCardiol 2002;25:1–2.
14. Siegel D, Lopez J. Trends in antihypertensive drug use in theUnited States: do the JNC V recommendations affectprescribing? JAMA 1997;278:1745–8.
15. Mehta SS, Wilcox CS, Schulman KA . Treatment ofhypertension in patients with comorbidities: results from thestudy of hypertensive prescribing practices (SHyPP). Am JHypertens 1999;12:333–40.
16. Swales JD. Current clinical practice in hypertension: TheEISBERG (evaluation and interventions for systolic bloodpressure elevation—regional and global) project. Am Heart J1999;138:S231–7.
17. Chalmers J. Implementation of guidelines for management ofhypertension. Clin Exp Hypertens 1999;21:647–57.
18. Gupta L, Ward JE, Hayward RSA. Clinical practice guidelinesin general practice: a national survey of recall, attitudes andimpact. Med J Am 1997;166:69–72.
19. Troein M, Gardell B, Selander S, Rastam L. Guidelines andreported practice for the treatment of hypertension andhypercholesterolemia. J Intern Med 1997;242:173–8.
20. Lomas J, Anderson GM, Domnick-Pierre K, et al. Do practiceguidelines guide practice? The effect of a consensus statementon the practice of physicians. N Engl J Med 1989;321:1306–11.
21. Shekelle PG, Ortiz ERS, Morton SC, Eccles MP, GrimshawJM, Woolf SH. Validity of the Agency for Healthcare Researchand Quality clinical practice guidelines: how quickly doguidelines become outdated? JAMA 2001;286:1461–7.
22. Goldstein MK, Hoffman BB, Coleman RW, et al. Implementingclinical practice guidelines while taking account of changingevidence: ATHENA DSS, an easily modifiable decision-supportsystem for managing hypertension in primary care. Proc AmMed Inform Assoc Annu Symp 2000:300–4.
23. Eccles MP, Rousseau N, Freemantle N. Updating evidence-based clinical guidelines. J Health Serv Res Pol2002;7:98–1003.
24. McDonald CJ, Tierney WM. Computer-stored medical records.Their future role in medical practice. JAMA 1988;259:3433–40.
25. Caironi PVC, Portoni L, Combi C, Pinciroli F, Ceri S.HyperCare: a prototype of an active database for compliancewith essential hypertension therapy guidelines. Proc Am MedInform Assoc Annu Symp 1997:288–92.
26. Tierney W, Overhage J, Takesue B, et al. Computerizingguidelines to improve care and patient outcomes: the exampleof heart failure. JAMA 1995;2:316–22.
27. Morris AH. Developing and implementing computerizedprotocols for standardization of clinical decisions. Ann InternMed 2000;132:373–83.
28. McDonald CJ, Overhage JM, Tierney WM, et al . TheRegenstrief medical record system: a quarter centuryexperience. Int J Med Inform 1999;54:225–53.
29. Tierney WM, Miller ME, Hui SL, McDonald CJ. Practicerandomization and clinical research. The Indiana experience.Med Care 1991;29:JS57–64.
30. McDonald CJ, Hui SL, Smith DM, et al. Reminders tophysicians from an introspective computer medical record. Atwo-year randomized trial. Ann Intern Med 1984;100:130–8.
31. Tierney WM, Miller ME, McDonald CJ. The effect on testordering of informing physicians of the charges for outpatientdiagnostic tests. N Engl J Med 1990;322:1499–525.
32. Tierney WM, Overhage JM, McDonald CJ. Computerizingguidelines: factors for success. Proc Am Med Inform AssocAnnu Symp 1996:459–62.
33. Woolf S. Practice guidelines: a new reality in medicine. ArchIntern Med 1990;150:1811–18.
34. McDonald CJ, Tierney WM . The medical gopher—amicrocomputer system to help find, organize and decide aboutpatient data. West J Med 1986;145:823–9.
35. Tierney WM, Miller ME, Overhage JM, McDonald CJ.Physician inpatient order writing on microcomputerworkstations. Effects on resource utilization. JAMA1993;269:379–83.
36. Overhage JM, Mamlin B, Warvel J, Warvel J, Tierney W,McDonald CJ. A tool for provider interaction during patientcare: G-CARE. J Am Med Inform Assoc 1995;2(suppl):178–82.
37. Murray MD, Loos B, Tu W, et al. Work patterns of ambulatorycare pharmacists with access to electronic guideline-basedtreatment suggestions. Am J Health-Syst Pharm 1999;56:225–32.
38. Murray MD, Loos B, Tu W, et al. Effects of computer-basedprescribing on pharmacist work patterns. J Am Med InformAssoc 1998;5:546–53.
39. Overhage J, Lukes A. Practical, reliable, comprehensivemethod for characterizing pharmacists’ clinical activities. Am JHealth-Syst Pharm 1999;56:2444–50.
40. McHorney C, Ware J Jr. Construction and validation of analternate form general mental health scale for the medicaloutcomes study short-form 36-item health survey. Med Care1995;33:15–28.
41. Wolinsky F, Stump T. A measurement model of the medicaloutcomes study 36-item short-form health survey in a clinicalsample of disadvantaged, older, black, and white men andwomen. Med Care 1996;34:537–48.
42. Dexter P, Stump T, Tierney W, Wolinsky F. The psychometricproperties of the SF-36 health survey among older adults in theclinical setting. J Clin Geropsychol 1996;2:225–37.
43. Bulpitt C, Fletcher A. The measurement of quality of life inhypertensive patients: a practical approach. Br J Clin Pharmacol1990;30:353–64.
44. Inui T, Carter W, Pecoraro R. Screening for noncomplianceamong patients with hypertension: is self-report the bestavailable measure? Med Care 1981;19:1061–4.
45. Morisky D, Green L, Levine D. Concurrent and predictivevalidity of a self-reported measure of medication adherence.Med Care 1986;24:67–74.
46. Steiner J, Koepsell T, Fihn S, Inui T. A general method ofcompliance assessment using centralized pharmacy records.Description and validation. Med Care 1988;26:814–23.
47. Murray M, Harris L, Overhage J, Zhou X, Smith F, Tierney W.Association between medication possession ratio and reportedcompliance [abstr]. J Gen Intern Med 1997;12:77.
48. Murray MD, Deer MM, Ferguson JA, et al. Open-labelrandomized trial of torsemide compared with furosemidetherapy for patients with heart failure. Am J Med 2001;111:513–20.
49. Liang KY, Zeger SL . Longitudinal data analysis usinggeneralized estimating equations. Biometrika 1988;73:13–22.
50. Dudek F. The continuing misinterpretation of the standarderror of measurement. Psychol Bull 1979;86:335–7.
51. Wyrwich KW, Tierney WM, Wolinsky FD. Further evidencesupporting a SEM-based criterion for identifying meaningfulintra-individual changes in health-related quality of life. J ClinEpidemiol 1999;52:861–73.
52. Stump T, Dexter P, Tierney W, Wolinsky F. Measuring patientsatisfaction with physicians among older and diseased adults inthe outpatient setting: a comparison of three instruments. MedCare 1995;33:958–72.
53. Zhou X, Tu W. Comparisons of several independent populationmeans when their samples contain non-zero log-normal andpossibly zero observations. Biometrics 1999;55:645–51.
54. Overhage JM, Tierney WM, McDonald CJ . Computerreminders to implement preventive care guidelines forhospitalized patients. Arch Intern Med 1996;156:1551–6.
55. Dexter PR, Perkins S, Overhage JM, Maharry K, Kohler RB,McDonald CJ. A computerized reminder system to increase theuse of preventive care for hospitalized patients. N Engl J Med2001;345:965–70.
56. Litzelman DK, Dittus RS, Miller ME, Tierney WM. Requiringphysicians to respond to computerized reminders improvestheir compliance with preventive care protocols. J Gen InternMed 1993;8:311–17.
336
COMPUTERIZED HYPERTENSION TREATMENT SUGGESTIONS Murray et al
57. Litzelman DK, Tierney WM. Physicians’ reasons for failing tocomply with computerized preventive care guidelines. J GenIntern Med 1996;11:497–9.
58. McGuire L. A long run for a short jump: understanding clinical
guidelines. Ann Intern Med 1989;113:705–8.59. Audet A, Greenfield S, Field M. Medical practice guidelines:
current activities and future directions. Ann Intern Med1990;113:709–14.
337
Copyright © 2022 FDOKUMEN




















