
Factors associated with self-reported use of dental health services among older Greek and Italian...
8
DENTAL HEALTH SERVICES Factors associated with self-reported use of dental health services among older Greek and Italian immigrants Rodrigo Mariiio, CD, PhD"; Clive Wright, MD'; Margot Schofield, PhD3; Hanny Calache BDSc, MDSc'; Victor Minichiello, PhD' 'School of Dental Science, University of Melbourne, Victoria, 3000, Australia; 'Ministry of Health, Wellington, New Zealand; 'School of Health, University of New England, Armidale, New South Wales, Australia; 'Dean, Faculty of Education Health and Professional Studies, University of New England, Armidale, New South Wales, Australia. 'Corresponding author: [email protected] Spec Care Dentist 25(1): 29-36. 2005 Introduction The increase in life expectancy, the combined effect of advances in medicine, and other social and economic factors have improved tooth retention among older adults, creat- ing a greater need for this population to seek regular dental health care. The nature of oral health care needs, thus, has changed dramatically. Oral health is critical to people's physical, emotional and social functioning, quality of life and well being. In addition, oral health problems are related to local and systemic morbidity; for example, loss of chewing efficiency may lead to poor nutritional health due to a preference for softer foods that are typically high in carbohydrates and low in fiber and Regular dental visits not only provide opportunities for early diagnosis and treat- ment of oral diseases and conditions, but also allow for health promotion, oral hygiene education and maintenance of a good oral health status.' However, older adults have been described as the least likely group to seek dental care.4 Factors associated with the use of dental health services by older adults include: age, gender, level of education, social support and connectedness, income, general and dental health status, oral health knowledge and attitudes, perceived oral health needs, oral pain or discomfort, physical disabilities and chronic condition^.^ I3 Underutilization of dental health services appears to be common in immi- grant group^,'^^'^ with the most common- ly cited barriers being the cost of dental care, lack of minority oral health profes- sionals, patients' lack of awareness of services and facilities, and difficulties communi~ating.'~~'~~'~ Over the past two decades the pro- portion of Australians using dental health services has increased substantial- ly from 48.8% in 1985 to 59.5% in 1999.",19 However, the Australian data do not offer a clear picture on the oral health status or use of dental health serv- ices by culturally and linguistically diverse (CALD) populations, particularly those aged 65 and older. Further, the characteristics of these groups are so diverse that assumptions coming from mainstream studies, despite the possible inclusion of immigrant participants, may not be applicable to or reliable for immi- grants. Since planning of dental health serv- ices is dependent on the quality of cur- rent local data,zo we considered this study both timely and important to undertake, with the aim of learning more about the use of dental health services by specific CALD groups in Melbourne, Australia. To reduce the heterogeneity created by grouping together all CALD denomi- nations, this study specifically included Spec Care Dentist 25(1) 2005 29
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Factors associated with self-reported use of dental health services among older Greek and Italian...

D E N T A L H E A L T H S E R V I C E S
Factors associated with self-reported use of dental health services among older Greek and Italian immigrants Rodrigo Mariiio, CD, PhD"; Clive Wright, MD'; Margot Schofield, PhD3; Hanny Calache BDSc, MDSc'; Victor Minichiello, PhD'
'School of Dental Science, University of Melbourne, Victoria, 3000, Australia; 'Ministry of Health, Wellington, New Zealand; 'School of Health, University of New England, Armidale, New South Wales, Australia; 'Dean, Faculty of Education Health and Professional Studies, University of New England, Armidale, New South Wales, Australia. 'Corresponding author: [email protected]
Spec Care Dentist 25(1): 29-36. 2005
I n t r o d u c t i o n The increase in life expectancy, the combined effect of advances in medicine, and other social and economic factors have improved tooth retention among older adults, creat- ing a greater need for this population to seek regular dental health care. The nature of oral health care needs, thus, has changed dramatically. Oral health is critical to people's physical, emotional and social functioning, quality of life and well being. In addition, oral health problems are related to local and systemic morbidity; for example, loss of chewing efficiency may lead to poor nutritional health due to a preference for softer foods that are typically high in carbohydrates and low in fiber and
Regular dental visits not only provide opportunities for early diagnosis and treat- ment of oral diseases and conditions, but also allow for health promotion, oral hygiene education and maintenance of a good oral health status.' However, older adults have been described as the least likely group to seek dental care.4 Factors associated with the use of dental health services by older adults include: age, gender, level of education, social support and connectedness, income, general and dental health status, oral health knowledge and attitudes, perceived oral health needs, oral pain or discomfort, physical disabilities and chronic condition^.^ I 3
Underutilization of dental health services appears to be common in immi- grant group^,'^^'^ with the most common- ly cited barriers being the cost of dental care, lack of minority oral health profes- sionals, patients' lack of awareness of services and facilities, and difficulties c o m m u n i ~ a t i n g . ' ~ ~ ' ~ ~ ' ~
Over the past two decades the pro- portion of Australians using dental health services has increased substantial- ly from 48.8% in 1985 to 59.5% in 1999.",19 However, the Australian data do not offer a clear picture on the oral health status or use of dental health serv- ices by culturally and linguistically diverse (CALD) populations, particularly
those aged 65 and older. Further, the characteristics of these groups are so diverse that assumptions coming from mainstream studies, despite the possible inclusion of immigrant participants, may not be applicable to or reliable for immi- grants.
Since planning of dental health serv- ices is dependent on the quality of cur- rent local data,zo we considered this study both timely and important to undertake, with the aim of learning more about the use of dental health services by specific CALD groups in Melbourne, Australia.
To reduce the heterogeneity created by grouping together all CALD denomi- nations, this study specifically included
Spec Care Dent is t 25(1) 2005 29
D E N T A L H E A L T H S E R V I C E S
Greek and Italian older adults. Greek and Italian immigration to Australia grew rapidly in the 1950s and early 1960s, with the Australian state of Victoria as the most common destination. In 1996, 49% of all Greeks living in Australia were in Victoria. That year, close to 42% of all Italians living in Australia also lived in Victoria, making them the largest CALD group in that state.*’
The implications of oral health in the quality of life of older adults and in the aging process itself emphasize the impor- tance of investigating the use of dental services by these groups to better under- stand the socio-cultural context through which oral health decisions are made.” We launched this study of older adults from Greek or Italian backgrounds, liv- ing in Melbourne, to estimate their use of dental health care services, identify self-reported barriers to dental health services utilization and examine factors associated with the older adults’ use of dental services.
Methods The targeted sainple comprised men and women aged 55 years or older from Greek and Italian backgrounds, who were members of ethnic clubs for older adults in Melbourne, Australia. Lists of Greek (n = 59) and Italian (n = 90) clubs were obtained from the Greek and Italian welfare associations in the Australian state of Victoria (Australian- Greek Welfare Society and Commitato di Assistenza Italiana, respectively). Information from these organizations indicates that these clubs for older adults provide a venue for meetings and social activities for about 16,000 Greeks and about 26,000 Italians. However, lists of individual club participants were not available for either immigrant group. This fact, as well as limitations in time and resources, led us to use a non-ran- dom, convenience sample of volunteers for the study
P rocedure Trained hi-cultural and fully bilingual Greek-English or Italian-English research
30 Spec Care Dent is t 25(1) 2005
assistants contacted each club coordina- tor and arranged a meeting to discuss the project. The club coordinators were asked for permission to address the club membership to recruit volunteers for this study Once individual written consent was obtained, volunteers were asked to undergo a structured interview and a clinical examination. Participants were not paid for their participation in this study. Data collection extended from October 2000 to mid-June 2001.
The interview consisted of 107 ques- tions that covered a variety of topics including: socio-demographic and immi- gration characteristics; use of oral health care services; perception of oral health status and oral health needs; and oral hygiene habits. The instrument also included questions about attitudes to oral health and knowledge of causes and risk factors for dental caries, periodontal disease and oral cancer. To collect infor- mation on quality of life, interviewers used a number of previously validated scales: Short-Form 12 (SF-12),23 Australian Nutritional Screen Initiative (ANSI)z4 and the short version of the Oral Health Impact Profile (OHIP-14).25 Questions were developed in English and translated into the target languages (Greek and Italian) following Brislin’s me thodology.’6
at the clubs’ facilities using overhead light, dental mirrors and Community Periodontal Index Clinical data were recorded following criteria and rec- ommendations from well-established methods for oral health data collec- t i~n.*~,’* Radiographic examinations were not performed, and teeth were not dried before scoring.
Dental examinations were conducted
Measu res Selected socio-demographic, psychoso- cia1 and clinical variables were used to identify factors that could influence the use of dental health services for older Greeks and Italians.
Socio-demographic. In addition to age and gender, data were collected for the following socio-demographic vari- ables: living arrangement, occupation
before retirement, educational level and possession of a State or Commonwealth Health Concession Card.
“Living arrangement” was classified into four groups: living alone; living with spouse; living with spouse and daugh- terkon; and other living arrangements. “Occupation before retirement” was clas- sified into three groups, based on the Australian Industrial Classification2’: managers, professionals, para-profession- als, trades clerks and personal services; laborers and related workers, which included those job categories that were poorly defined; and not in paid jobs. “Educational level” was classified into three categories: no formal education or incomplete primary education; complete primary education or incomplete second- ary education; and complete secondary or tertiary education. Participants also were asked whether they had a health care card (coded as “yes” or “no”).
Self-assessments of health. Participants were asked to describe their oral health status in comparison to other people of their same age. Response options included: “much better,” “bet- ter,” “about the same,” “worse” and “much worse.” A lack of responses in the extreme categories at both ends of the range led us to collapse the scale into the adjacent moderate categories.
To measure physical and mental health status, we used the SF-12. The SF- 12 covers many aspects of health and has been validated for use with adults of all ages.233o Physical and Mental Health Component Summary Scores were calcu- lated for each ~a r t i c ipan t .~~
Oral health knowledge and atti- tudes. The oral health knowledge index consisted of the sum of correct responses to 38 questions about symptoms and causes of dental caries, periodontal dis- ease and oral cancer. Oral health atti- tudes were measured by seven items con- cerned with the inevitability of oral dis- ease in older adults, desirability of keep- ing natural teeth and the efficacy of pre- ventive behaviors, such as self-examina- tion and dental visits. Higher scores rep- resent more positive attitudes.
Perceived need for dental health care. From a list of seven options, partic-
Factors associated w i th dental services use b y older immigrants

D E N T A L H E A L T H S E R V I C E S
ipants were asked to indicate the type of dental treatment they thought they might need. Treatment options included: tooth extraction, relief of dental pain, dental crown or fillings, dentures, soft tissue consultation, gum treatment and other treatments. A Dental Health Treatment Needs Index was created by adding posi- tive responses.
Clinical data. During the dental examination, we recorded: decayed sur- faces (DS), filled surfaces (FS) and num- ber of teeth present. Number of teeth was divided into four groups: no teeth, 1 to 10 teeth, 11 to 20 teeth and more than 20 teeth.
ent variable, “use of dental services,” was investigated by asking participants to indicate the time interval since the last dental visit, with response options based on the National Dental Telephone Interview SurveyLy: 12 months or less, 12 months to 2 years, 2 to 5 years, and more than 5 years. For the multivariate analysis, dental attendance was dichotomised as a dependent variable according to whether or not a participant had visited the dentis! within the last 12 months.
Self-perceived barrier to care. We assessed self-perceived barriers to dental health care service by asking whether any of the following responses prevented the respondent from seeking dental care: cost, availability of dentists, time waiting for appointments, rude behavior from dentist; rude behavior from non-dentists; location of services; waiting time in the dental office, fear of dental treatments, physical disability, general health prob- lems, and communication or language problems. Respondents were asked to indicate “yes” or “no” for each response option.
We then added the number of “yes” responses to establish a Barriers to Dental Health Care Index.
the University of New England (Armidale, NSW) and Dental Health Services Victoria (DHSV) Ethics and Research Committees.
Use of dental services. The depend-
Ethics approvals were obtained from
Analys is The analysis provides basic descrip-
tive information on selected socio-demo- graphic, psychosocial, dental status and use of dental health service variables. Univariate associations between use of dental health services and a number of demographic, oral health knowledge and attitudes, and dental health variables were computed as unadjusted odds ratios and 95% confidence intervals, using logistic regression. Data manipulation and analyses were done using SPSS (SPSS 10.0”, SPSS Inc., Chicago).
To test if any combination of socio- demographic, psychosocial or clinical variables, provided a multivariate expla- nation of the use of dental health care services, a decision tree analysis was per- formed for each migrant group using the KnowledgeSEEKERa software program (ANGOSS Software Corp.; Toronto, Canada).3z This corresponds to a multi- variate stepwise decision making proce- dure, which selects the independent vari- able that best separates groups according to frequency or scores of the dependent variables. The procedure also allows the identification of combinations of risks and non-linear relations between the pre- dictors and the outcome ~ a r i a b l e . ~ ~ . ~ ’ Several alternative models were tested and the one that explained a larger pro- portion of the variance was kept as the final.
will not be attempted here, however, to better interpret the results it must be noted that KnowledgeSEEKERB splits data sets into new, homogeneous subsets of data (nodes).33 At each node, all pre- dictor variables are considered to further split the node. The node of best partition is based on the selection of that variable which produces the highest level of sig- nificance. This process continues until no more significant splits can be found.33 To determine if the relationship between the outcome variable and the independ- ent variable was significant, the signifi- cance level was set at 0.20, for the explo- ration level, resulting in a “bushy” deci- sion tree. In the next step, to avoid asso- ciation patterns that may be found by chance, the resulting tree was pruned
A detailed explanation of this method
back until the significance level of the lowest branch was lower than 0.01.’4
Resul t s We recruited participants from 16 clubs for older Greek adults and 22 clubs for older Italian immigrants. A total of 751 older adults volunteered to participate; however, 14 participants were younger than the defined age criteria, and incom- plete information was recorded for three adults on the dental visits. Of the remaining 734 respondents, 374 were from Greek background and 360 from Italian background, with about 63% of each group being female.
Greek and Italian participants dif- fered on a number of socio-demographic characteristics. For example, among Greek participants the mean age was 66.90 years (k 6.6 y), while the mean age for Italian participants was 69.95 years (k 6.4 y) (p < 0.001). Greekpar- ticipants were less likely to have no for- mal education or incomplete primary education compared with Italians (37.2% and 56.2%, respectively), and more likely to have completed primary education (47.4%) compared with Italian partici- pants (27.9%). The remaining 15.4% of Greeks and 15.9% of Italians had higher levels of education. Differences by level of education reached statistical signifi- cance at the 0.001 level of significance.
Greek participants were less likely than Italians to live alone (10.7% vs. 20.2%, respectively) and more likely to live with their children (13.1% vs. 5.5%, respectively) or in other living arrange- ments (22.0% vs. 15.8%, respectively) (p < 0,001). The remaining 54.2% of Greeks and 58.5% of Italians lived with their spouses. A health care card was held by 96% in both groups.
Perceived b a r r i e r s to use o f d e n t a l s e r v i c e s Most participants (44.3%) reported two barriers to dental health services; 10.5% and 9.5% reported one and three barri- ers, respectively; and the remainder, 10.3%, reported between four and eleven
Marii io et a/. Spec Care Dentist 25jl) 2005 31
D E N T A L H E A L T H S E R V I C E S
Used dental service I n I in last &tnonths
barriers. In addition, 186 participants (25.4%) reported no barriers to care. Overall, the three most frequent barriers to care cited by participants were the length of waiting lists (62.6%); the wait- ing time in the dental office (51.9%); and the cost of services (23.9%).
For Greek participants, length of the waiting list was the most frequently men- tioned barrier (87.0%), followed by wait- ing time in the dental clinic (85.3%). For this group, no other barrier to accessing dental health services was reported by more than 6.0% of the participants. For Italian participants, cost of services was the most frequently cited barrier (45.4%), followed by length of waiting list (38.3%), and language and communication barriers (21.1%). In addition, waiting time in the dental office and availability of services influenced 18.5% and 16.9%, respectively, among Italian immigrants. Among Italians, no other category was reported by more than 12% of the sample.
Odds ratio (95% CI) I I Used dental service
Odds Ratio 1 n I in last :;o)months (95% CI)
Time since last dental visit Overall 42.6% of participants (40.4% Greek and 45.0% of Italians) reported having been to the dentist in the previ- ous 12 months. Ninety-eight partici- pants (13.2%) reported that their last visit to the dentist had been more than 12 months and less than two years ago. An additional 21.5% had not been to the dentist within the last five years, and 22.7% (n = 166) had not been for more than five years. Ethnic groups did not differ by time since last visit.
Living alone
Living with spouse
Factors associated with the use of dental health services
40 40.0 0.98 (0.49 - 1.95) 73 47.9 1.16 (0.68 - 1.98) 202 40.6 1 .oo 208 44.2 1 .oo
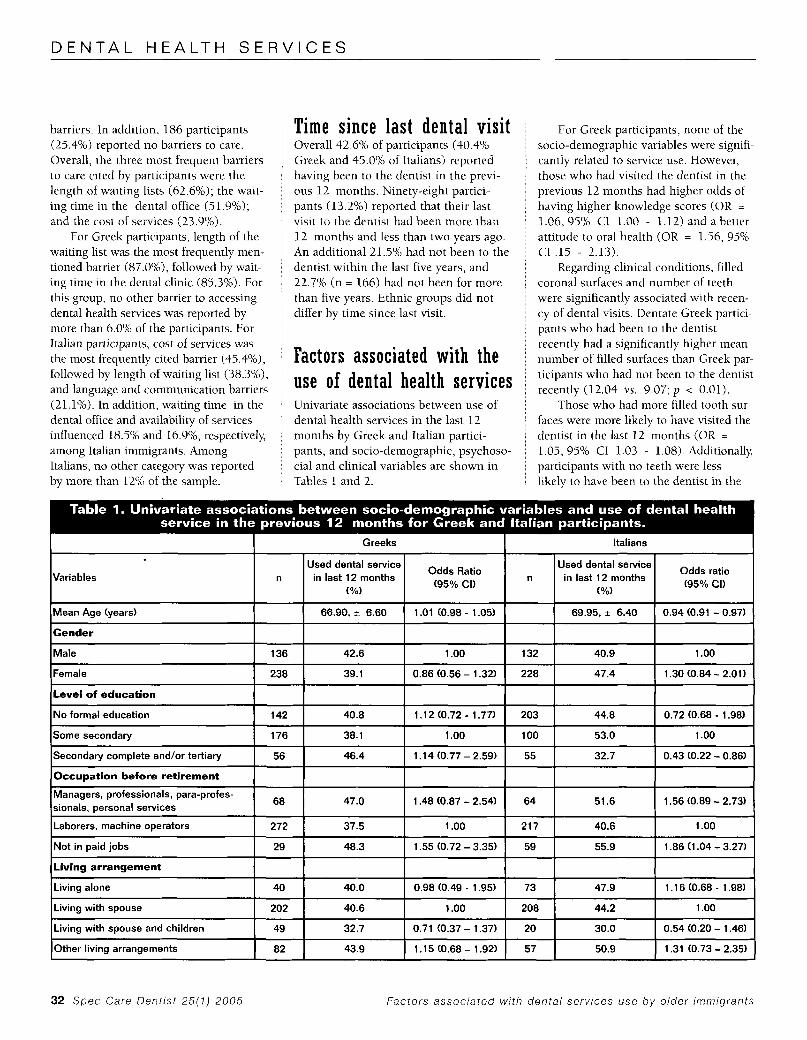
Univariate associations between use of dental health services in the last 12 months by Greek and Italian partici- pants, and socio-demographic, psychoso- cia1 and clinical variables are shown in Tables 1 and 2.
For Greek participants, none of the socio-demographic variables were signifi- cantly related to service use. However, those who had visited the dentist in the previous 12 months had higher odds of having higher knowledge scores (OR =
1.06, 95% CI 1.00 - 1.12) and a better attitude to oral health (OR = 1.56, 95% CI .15 - 2.13).
Regarding clinical conditions, filled coronal surfaces and number of teeth were significantly associated with recen- cy of dental visits. Dentate Greek partici- pants who had been to the dentist recently had a significantly higher mean number of filled surfaces than Greek par- ticipants who had not been to the dentist recently (12.04 vs. 9.07; p < 0.01).
Those who had more filled tooth sur- faces were more likely to have visited the dentist in the last 12 months (OR =
1.05, 95% CI 1.03 - 1.08). Additional13 participants with no teeth were less likely to have been to the dentist in the
I I Greeks I Italians I
Variables
I I I I I I
Occupation before retirement I I I I 68 I 47.0 1 1.48 (0.87 -2.54) I 64 I 51.6 1 1.56 (0.89 - 2.73) Managers, professionals, para-profes- I sionals, personal services
ILaborers, machine operators I 272 I 37.5 I 1 .oo I 217 I 40.6 I 1.00 I lNot in paid jobs I 29 I 48.3 I 1.55 (0.72 - 3.35) I 59 I 55.9 I 1.86 (1.04 - 3.27) I (Living arrangement I I I I I I I
ILiving with spouse and children I 49 I 32.7 I 0.71 (0.37 - 1.37) I 20 I 30.0 I 0.54 (0.20 - 1.46) I lother living arrangements I 82 I 43.9 I1.15(0.68-1.92) I 57 I 50.9 I 1.31 (0.73 - 2.35) I
32 Spec Care Dent ist 25(7) 2005 Factors associated wi th dental services use by older immigrants
D E N T A L H E A L T H S E R V I C E S
67.23 (6.75)
67.23 (6.75)
previous 12 months than those with teeth (OR = 0.14; 95% CI 0.06 - 0.32).
For Italian participants, each added year of age decreased the likelihood of having had a dental visit (OR = 0.94, 95% CI 0.91 - 0.97), and those with at least some secondary education were less likely to have visited the dentist in the previous 12 months compared to those who had less education (OR = 0.43, 95% CI 0.22 - 0.86).
Oral health knowledge was significant- ly and positively associated with recency of dental visits among Italians (OR = 1.05, 95% CI 1.00 - 1.09). Among the clinical variables, dentate Italians who had been to the dentist had a significantly higher num- ber of filled surfaces than those who had not visited the dentist in the last 12 months (13.04 vs. 8.12; OR = 1.06, 95% CI 1.03 - 1.08). Edentulous Italians were less likely to have been to the dentist in the previous 12 months (OR = 0.28,95% C = 0.14 - 0.55) than those with teeth.
1.05 (1.03 - 1.08)
0.94 (0.80 - 1.1 1)
Mu l t iva r i a t e a n a l y s i s The combination of five socio-demographic
No teeth
1-1 0 teeth
1 1-20 teeth
More than 20 teeth
m Vlslt = 40 4%
59 13.6 0.14 (0.06 - 0.32) 59 22.0 0.28 (0.1 4 - 0.55)
42 37.2 0.55 (0.27 - 1.1 0) 45 44.4 0.78 (0.40 - 1.53)
123 41.5 0.65 (0.40 - 1.061 107 51.4 1.03 (0.62 - 1.70)
142 52.1 1 .oo 50.7
I a 1.001 I
20 teeth br more - Less tA20 teeth
I V K . 0 1 1 7 PK.001 1 I . I Dentate Edentate
Visit = 40.9%
I Y lsit = ++ 9 x N= 38
I- P = O ~ 1 Score
Vlsit = 41 5% Vlslt = 63 3%
<01 I h g m t h spduse ody and other
lN
I
t- PJOOl I may not add up to agree mth the trunkdue to rmssmgvalues
Knowledge Score
N= 32
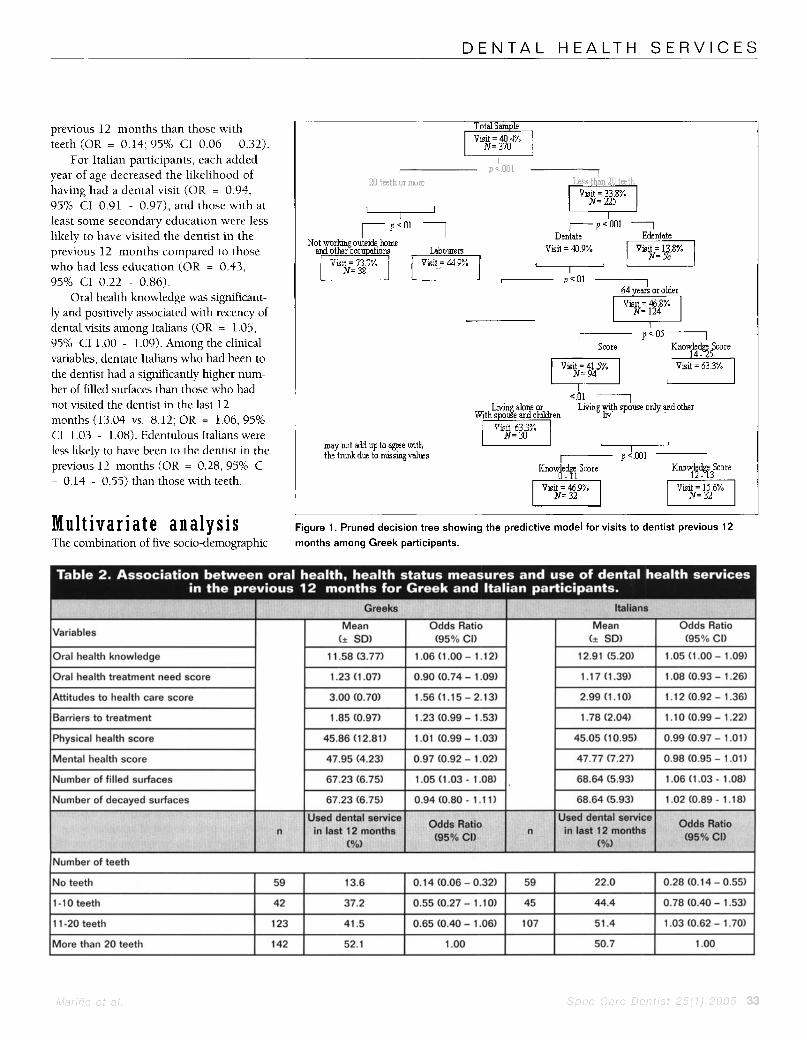
- Figure 1. Pruned decision tree showing the predictive model for visits to dentist previous 12 months among Greek participants.
Ivariabies i Oral health knowledge
Barriers to treatment I
(+ SD) (95% CI)
11.58 (3.77) 1.06 (1 .OO - 1.12) I 12.91 (5.20) I 1.05 (1.00 - 1.09) I
I 3.00(0.70) I1.56(1.15-2.13) I I 1.85 (0.97) I 1.23 (0.99 - 1.53) 1 1.78(2.04) I l.lO(O.99-1.22) I
Number of filled surfaces I INurnber of decayed surfaces I
I 68.64 (5.93) I 1.06 (1.03 - 1.08) I I 68.64 (5.93) I 1.02 (0.89 - 1.18) I
D E N T A L H E A L T H S E R V I C E S
I P S . 0 5 1 Not w o r h g Labourers qld outslde home other occuxLatlom
N= 360
KEY [- P C 0 2 1 p = Probabhty N = Nunbermgroup Bmners to care Bamers to care NOTE Sample sue III eachbranch
the t d due to rmssmgvalues may not add up to a p e wth $q Vlslt 51 0% -1 Vlslt = 75 5%
Dentate
N= 292
I I
~ n o w ~ t & Score 0.9 I Visit = 29.4%
N=51 I
Edentate pG&q
K ~ ~ W M & Score 10 - 25 -1
N= 98 N= 77
variables (age, gender, education level, occupation before retirement and living arrangement), seven psychosocial vari- ables (oral health knowledge, self per- ceived oral health needs, attitudes to dental care, perceived barriers to dental care, self-assessed oral health status, and Physical and Mental Health Component Summary Scores) and three clinical vari- ables (number of filled tooth surfaces, number of decayed tooth surfaces, and number of teeth) explained 17% and 13% of the variance in use of dental health services among Greek and Italian participants, respectively.
Among dentate Greek participants (see Figure I), in addition to number of teeth, age, occupation before retirement, and oral health knowledge, living arrangements emerged as a significant additional predictor of dental health service utilization. A larger proportion of those who lived alone or with their spouse and children had visited the den- tist in the previous 12 months, com- pared to those who lived with their
34 Spec Care Dent ist 25(1) 2005
spouse only or children only or had other living arrangements. In fact, among the latter group, those who had interme- diate oral health knowledge were among those with the lowest proportion of visits to the dentist in the previous 12 months (15.6%). Another group with few dental visits were those who were edentulous (13.8%). Those who had the highest pro- portion of visits to the dentist were those with more than 20 teeth who reported not working outside home or working before retirement in occupations other than laborers (73.7%).
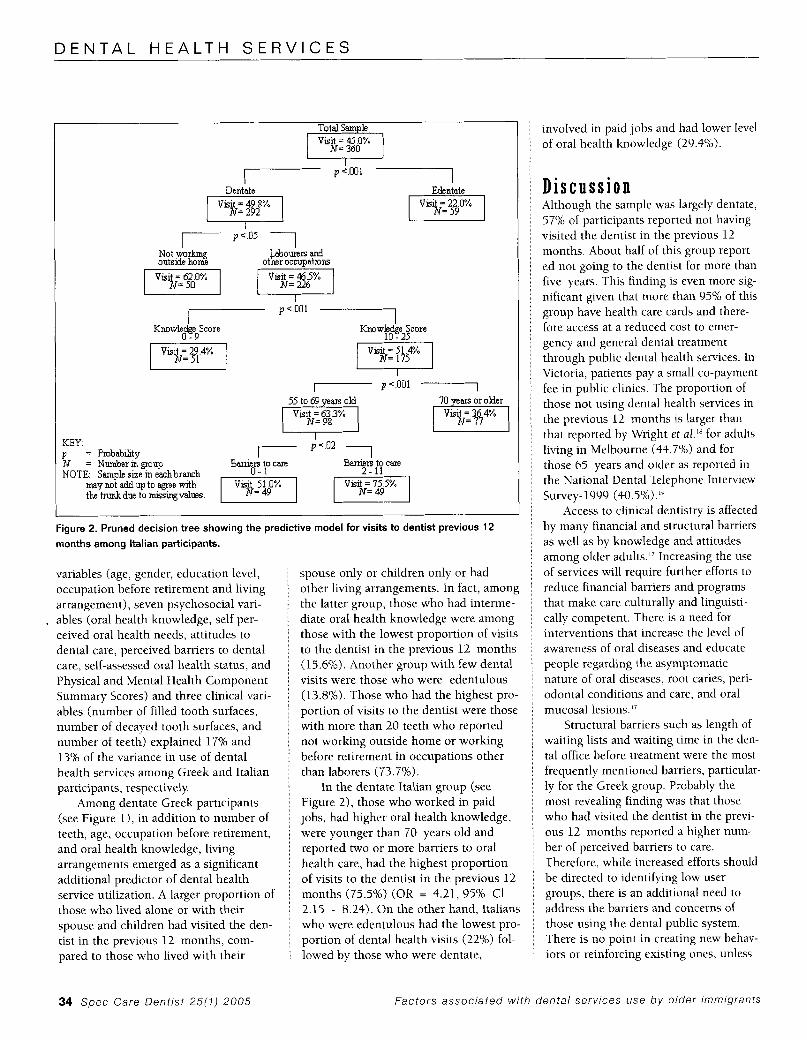
In the dentate Italian group (see Figure 2), those who worked in paid jobs, had higher oral health knowledge, were younger than 70 years old and reported two or more barriers to oral health care, had the highest proportion of visits to the dentist in the previous 12 months (75.5%) (OR = 4.21, 95% C1 2.15 - 8.24). On the other hand, Italians who were edentulous had the lowest pro- portion of dental health visits (22%) fol- lowed by those who were dentate,
involved in paid jobs and had lower level of oral health knowledge (29.4%).
Discuss ion Although the sample was largely dentate, 57% of participants reported not having visited the dentist in the previous 12 months. About half of this group report- ed not going to the dentist for more than five years. This finding is even more sig- nificant given that more than 95% of this group have health care cards and there- fore access at a reduced cost to emer- gency and general dental treatment through public dental health services. In Victoria, patients pay a small co-payment fee in public clinics. The proportion of those not using dental health services in the previous 12 months is larger than that reported by Wright et al.'" for adults living in Melbourne (44.7%) and for those 65 years and older as reported in the National Dental Telephone Interview Survey- 1999 (40.5%) .Iy
Access to clinical dentistry is affected by many financial and structural barriers as well as by knowledge and attitudes among older adults." Increasing the use of services will require further efforts to reduce financial barriers and programs that make care culturally and linguisti- cally competent. There is a need for interventions that increase the level of awareness of oral diseases and educate people regarding the asymptomatic nature of oral diseases, root caries, peri- odontal conditions and care, and oral mucosal lesions."
Structural barriers such as length of waiting lists and waiting time in the den- tal office before treatment were the most frequently mentioned barriers, particular- ly for the Greek group. Probably the most revealing finding was that those who had visited the dentist in the previ- ous 12 months reported a higher num- ber of perceived barriers to care. Therefore, while increased efforts should be directed to identifying low user groups, there is an additional need to address the barriers and concerns of those using the dental public system. There is no point in creating new behav- iors or reinforcing existing ones, unless
Factors associated w i th dental services use b y older immigrants

D E N T A L H E A L T H S E R V I C E S
services exist to support these messages, and the target population has the oppor- tunity to use dental health services.
Data provided here did not support some of the commonly assumed barriers to accessing dental health care services. For example, distance and physical health status, were not among the most commonly mentioned barriers to use of health services." However, this sample must be considered to represent healthy, reasonably well and autonomous older adults, or adults who are handicapped only to a level that does not affect dependency. Therefore, physical health might not be a main barrier. Importantly, language and communication were sig- nificant barriers only for Italian partici- pants. Although the final multivariate model contained significant explanatory variables of dental health service use, mediated in a manner consistent with the literature on use of dental health services by older adults, a number of commonly described predictors were not present. A possible explanation for this lack of effect of commonly described pre- dictors, might be that conclusions derived from mainstream studies might not be fully applicable to CALD popula- tions. Alternatively, traditional predictors must be questioned since older adults these days have more natural teeth than in the past and therefore, different oral health needs and demands for services.
Reports show that dentate adults tend to use dental health care services more frequently than those who are edentulous.'y However, it also has been demonstrated that the use of dental health services tends to decrease after retirement.'53h A parallel decline in dental health status in older adult populations also has been reported.'" This has impor- tant program and policy implications. For example, an intensification of out- reach programs for populations around retirement age, aimed at identifying and treating oral diseases and conditions might be more appropriate and success- ful for this age group. That is, programs should target these adults before they stop seeking routine dental health care, before dental health care is not seen as a high health priority, or before they
become medically impaired. This should be viewed, not only as a cost-effective, but also as an appropriate and socially just intervention.
The information provided has to be considered within the limitations of the study design. The most obvious limita- tion is the potential for recall bias in ask- ing older people to report retrospectively on dental visits. In addition, the sample consisted of volunteers recruited from older persons clubs in Melbourne, this self-selection may limit the representa- tiveness of the findings. Participants may not be considered representative of the Greek or Italian older adult population attending clubs. Another limitation was the lack of distinction between dental visits. A basic variation, particularly rele- vant to public dental services, exists between a visit for emergency and gener- al dental care, for example. However, the purpose of this study was to gain an ini- tial understanding of the use of dental health services and identifying factors associated with their use among older adults in immigrant populations.
model has been developed, rather, that a step has been made toward providing a basis for future research models. The explanatory power of the final models was not large (between 13% and 17% of the variance). Present results suggest that variables not considered in this analysis might add explanatory power to the models. These might include other his- torical considerations, both dental and personal, and provider-related variables such as age, gender or ethnic back- ground."
representative sample of older immi- grants, the importance of these variables in explaining the use of dental health care services. Future research should explore the reasons for discrepancies with the literature on predictors of the use of dental health care services and make a distinction between dental visits. Further exploration of the oral health behaviors of specific groups of older immigrants, learning how to reach these groups and overcoming barriers to care are important goals in dentistry. With
It is not claimed here that a definitive
Future studies should confirm, in a
this information, health providers can most appropriately target programs and policies to reduce inequalities in access to preventive services and treatment for all Australians.
A c k n o w l e d g m e n t The authors would like to acknowledge the support received from the Commitato di Assistenza Italiana (CO.AS.IT.) and the Australian-Greek Welfare Society, the participants and the participating clubs. In particular, we would like to acknowledge the staff of the project for assisting with data collec- tion.
R e f e r e n c e s 1. Shay K, Ship JA. The importance of oral
Health in the older patient. J Am Geriatr Soc 43:1414-22, 1995.
2. Gordon SR, Kelley SL, Sybyl JR, Mill M, Kramer A, Jahnigen DW. Relationship in very elderly veterans of nutritional status, self-perceived chewing ability, dental status, and social isolation. J Am Gerialr Soc 33:334-9, 1985.
3. Dolan TA, Peek CP, Stuck AS, Beck JC. Functional health and dental service use among older adults. J Gerontol 53(A):M413- M48, 1998.
4. Gift HC, Newman JF! How older adults use oral health care services: results of a National Health Interview Survey. J Am Dent Assoc 124:89-93, 1993.
5. Murtomaa H, Laine P, Masalin K. Dental health practices among Finnish adults. Community Dent Health 1:131-40, 1984.
6. Schou L. Oral health, oral health care and oral health promotions among older adults: social and behavioral dimensions. In: Cohen L, Gift H. eds. Disease Prevention and Oral Health Promotion. Copenhagen: Munskgaard; pp. 215-70, 1995.
7. Clarke M, Clarke SJ, Jagger C. Social interven- tion and the elderly: a randomized con- trolled trial. A m J Epidemiol 136:1571-3, 1992.
8. Barnard PD. National Oral Health Survey, Australia 1987-1988. Department Health, Housing, Local Government and Community Services. Canberra: Australian Government Publishing Services, 1993.
Marifio et a / . Spec Care Dent ist 25(1) 2005 35
D E N T A L H E A L T H S E R V I C E S
9. Tennstedt SL, Branbilla DL, fetter AM, McGuire HM. Understanding dental service use by older adults: sociobehavioral factors vs need. J Public Health Dent 54:211-9, 1994.
10. Jones JA, Fedele DJ, Bolden AJ, Bloom B. Gains in dental care not shared by minority elders. J Public Health Dent 54:39-46, 1994.
11. Petersen PE, Holst D. Utilization of dental health services. In: Cohen L, Gift H, eds. Disease Prevention and Oral Health Promotion. Copenhagen: Munskgaard; pp 230-8, 1995.
12. Schou L, Eadie D. Qualitative study of oral health norms and behaviour among elderly people in Scotland. Community Dent Health 8:53-8, 1991.
13. Davidson PL, Andersen RM. Determinants of dental care utilization for diverse ethnic and age groups. Adv Dent Res 11:254-62, 1997.
14. Young RF, Bukoff A, Waller JB Jr, Blount SB. Health status, health problems and practices among refugees from the Middle East, Eastern Europe and Southeast Asia. Int Migr Rev 21:760-82, 1987.
refugees in Sweden. Swed DentJ 94 Supp1:l- 40, 1993.
15. Zimmerman M. Oral health in groups of
16. Williams SA, Godson JH, Ahmed 1A. Dentists’ perceptions of difficulties encoun- tered in providing dental care for British Asians. Community Dent Health 12:30-4, 1995.
17. Marino RJ, Minichiello VM, Wright FAC, Schofield MJ. Oral health beliefs and prac- tices among Greek and Italian older Australians: a focus group approach. Australasj Ageing 21:193-8, 2002.
36 Spec Care Dent ist 25(1) 2005
18. Wright FAC, Gebart-Eaglemont JE, Olsen CB, Hammond RH, Jago JD. A longitudinal socio-dental study of adult oral health in Melbourne, 1985-1990. Melbourne, Victoria, AUS: The University of Melbourne. Community Dental Health Monograph Series No. 8, 1991.
19. Australian Institute of Health and Welfare. Oral health and access to dental care. Adelaide: AIHW Dental Statistics and Research Unit. 2001.
20. Bourgeois D, Nihtila A, Mersel A. Prevalence of caries and edentulousness among 65-74 year olds in Europe. Bull WHO 76:413-7, 1998.
21. Department of Immigration and Multicultural Affairs (Australia). 2002 Available from: URL: http://www.immi .gov.au/statistics/infosum- mary/ summaqchtm. Accessed February 11, 2002.
22. Andersen RM, Davidson PL. Ethnicity, aging and oral health outcomes: a conceptual framework. Adv Dent Res 11:203-9, 1997.
23. Ware J Jr, Kosinski M, Keller SD. A 12-item short form survey: construction of scales and preliminary test of reliability and validi- ty Med Care 34:220-33, 1996.
tiative. AustralasianJ Ageing 15:14-6, 1996.
short-form oral health impact profile. Community Dent Oral Epidemiol 25:284-90, 1997.
24. Lipski PS. Australian nutrition screening ini-
25. Slade GD. Derivation and validation of a
26. Brislin RW. Back-translation for cross-cultur- a1 research.J Cross Cult Psychol 1:185-216, 1970.
27. World Health Organization. Oral health sur- veys: basic methods. 4th. ed. Geneva: WHO, 1997.
28. National Center for Health Slatistics. NHANES I11 Oral Health Examination. Training Manual. Rockville, MD; NCHS, 1987.
29. Australian Bureau Statistics. Australian Standard Industrial Classification. Canberra: Australian Government Publishing Services, 1985.
30. Schofield MJ, Mishra G. Validity of the SF-12
4
compared with the SF-36 Health Survey in pilot studies of the Australian Longitudinal Study on Women’s Health. J Health Psychol 3:259-71, 1998.
31. Ware J , Kosinski M, Keller 5. SF-12: how to score the SF-12 Physical and Mental Health Summary Scales. Boston, MA: The Health Institute, New England Medical Center, 1995.
32. FirstMARK Technologies. KnowledgeSEEKER user’s guide. Ottawa; Ontario, 1990.
33. Biggs D, DeVille 8, Suen E. A method of choosing muhiway partitions for classifica- tion and decision trees. J Appl Stat 1991;18:49-62.
34. McKenzie DP, Patrick DMc, Wallace CS, Le HL, Copolov DL, Bruce SS. Constructing a minimal diagnostic decision tree. Methods InJ Med 1993;32: 16 1-6.
35. Tryon, AE Organization and methods of delivering geriatric oral health care. In: Chauncey H, Epstein S, Rose CL, Hefferren JJ, eds. Clinical Geriatric Dentistry Chicago, IL: American Dental Association; 1985. pp. 205-15.
36. U.S. Department of Health and Human Services. Oral health of United States adults. Bethesda, MD: National Institute of Dental Research. NIH Pub No. 87-2868, 1987.
Factors associated w i th dental servlces use b y older immigrants




















