
Diminution of eIF4E activity suppresses parkin mutant phenotypes
Upload
independentCategory
view
0download
0
www.elsevier.com/locate/humpath
Human Pathology (2009) 40, 1224–1233
Original contribution
Expression and prognostic significance of metalloproteasesand their inhibitors in luminal A and basal-like phenotypesof breast carcinoma☆
Luis O. González MDa,b,c, María D. Corte PhDa,b, Sara Junquera MDa,Raquel González-Fernández PhDd, José M. del Casar PhDa,b,e, Carmen García MDa,Alejandro Andicoechea PhDa,b,e, Julio Vázquez PhDa,b,Román Pérez-Fernández PhDd, Francisco J. Vizoso PhDa,b,e,⁎
aUnidad de Investigación, Hospital de Jove, 33290 Gijón, SpainbInstituto Universitario de Oncología del Principado de Asturias, 33006 Oviedo, SpaincServicio de Anatomía Patológica, Hospital de Jove, 33290 Gijón, SpaindDepartamento de Fisiología, Facultad de Medicina, 15782 Universidad de Santiago de Compostela, SpaineServicio de Cirugía General, Hospital de Jove, 33290 Gijón, Spain
Received 2 September 2008; revised 1 December 2008; accepted 3 December 2008
0d
Keywords:Breast cancer;Matrix metalloproteases;Metastasis;Tissue inhibitors of matrixmetalloproteases
Summary To analyze the expression and prognostic value of matrix metalloproteases and their tissueinhibitors in luminal A and basal-like breast carcinomas, an immunohistochemical study was performedon cancer specimens from 93 randomly selected patients with invasive primary ductal tumors of thebreast (46 with and 47 without distant metastasis) and with luminal A (n = 48) (ER+, HER2−) or basal-like (HER2−, ER−, PgR−) (n = 45) lesions. Luminal B cases were too few to analyze. Specimens werealso studied using tissue microarrays and specific antibodies against matrix metalloproteases 1, 2, 7, 9,11, 13, and 14 and tissue inhibitors 1, 2, and 3. There were no significant differences in matrixmetalloprotease or tissue inhibitor expression in the 2 phenotypes of tumors. In basal-like carcinomas,high scores for matrix metalloproteases 9 and 11 were significantly associated with a high distantmetastasis rate. Likewise, data showed associations between matrix metalloprotease/tissue inhibitorexpression by either stromal fibroblasts or mononuclear inflammatory cells and distant relapse-freesurvival in both tumor phenotypes. In addition, in infiltrating luminal A and basal-like tumors, weidentified a prometastatic phenotype of mononuclear inflammatory cells, showing a high matrixmetalloprotease/tissue inhibitor molecular profile. Expression of matrix metalloproteases and tissueinhibitors is related to the characteristics of breast tumor cells. As prognostic factors in breastcarcinomas of both luminal A and basal-like phenotypes, our results point to the importance of theexpression of matrix metalloproteases and tissue inhibitors by the stromal cells.© 2009 Elsevier Inc. All rights reserved.
☆ This work was supported by a grant from FIS-PI040137 Fondo de invesrsión Sanitaria del Instituto Carlos III (FIS-Spain) and Obra Social Cajastur.⁎ Corresponding author. Hospital de Jove, Servicio de Cirugía General, 33290 Gijón, Spain.
046-8177/$ – see front matter © 2009 Elsevier Inc. All rights reserved.oi:10.1016/j.humpath.2008.12.022

1225Expression and prognostic significance of metalloproteases
1. Introduction
Breast cancer is the quintessential sickness affectingwomen in industrialized countries (22% of all cancers). Themortality rate has been stable for several years, in spite of theincreasing incidence of the disease. Nowadays, breast canceris the second leading cause of cancer death. Clinicians arefaced with the challenge of accurate diagnosis. Althoughclinical signs of disseminated disease occur in fewer than10% of women at the time of diagnosis, in about half ofapparently localized tumors, the disease relapses in the formof metastases within 5 years after surgery.
It is difficult to predict the occurrence of distantmetastases because breast cancer is a heterogeneous diseaseencompassing complex pathologic entities. Even in patientswith apparently similar clinical profiles, there is a range ofclinical behaviors that influence the accuracy of prediction ofdistant metastases. This is why data such as nodal status,tumor size, grade, patient age, and tumor hormone receptorstatus as prognostic variables seem insufficient. Newprognostic factors are indispensable to improve the classicrisk classification.
Recent DNA microarray profiling of frozen breast cancersamples has identified distinct subtypes associated with anarray of clinical outcomes [1-3]. Using an intrinsic set of 534genes, Sorlie et al [2] analyzed the expression profiles of 115independent tumor samples, categorizing them into 4 groups:luminal (estrogen receptor positive [ER+]), HER2 over-expressing, normal breast like, and basal like. Basal like istriple-negative breast cancer characterized by absence of ER,progesterone receptors (PgR), and HER2 [2]. The molecularsubtype and prognostic expression profile of a primary breasttumor were shown to be maintained throughout its metastaticprocess [4]. Several other studies have shown the potentialclinical value of this classification. For instance, the basal-like subtype comprises about 19% of the tumors. They havea poor prognosis, as assessed by relapse-free survival [2,5,6].Additional opportunities to identify or validate molecularsignatures are provided by molecular profiling using alimited number of protein biomarkers. Thus, basal epithelialcells can be stained with antibodies to keratins 5/6, whereasluminal epithelial cells can be stained with antibodies againstkeratins 8/18 [7-9]. The prevalence of basal-like breastcancers and their poor prognosis have been validated byrecent immunohistochemical studies on formalin-fixedparaffin-embedded archival tumors [7,8,10,11]. The rolesof molecules in tumor, the metastasis development, and thephenotypes of breast carcinomas are yet to come to theforefront of cancer research; we also need to expand matrixmetalloprotease (MMP) research.
The human MMP family currently consists of 28members of homologous zinc-dependent endopeptidases.These can either be divided into 8 structural classes orgrouped depending on their substrate specificity and primarystructure. Finally, MMPs can be clustered into subgroups ofcollagenases (MMP-1, 8, and 13), gelatinases (MMP-2 and
9), stromelysins (MMP-3, 10, 11), membrane-associatedMMPs (MMP-14, 15, 16, 17, 23, 24, and 25), and othernovel MMPs [12,13].
MMPs are synthesized as inactive zymogens, which areactivated by other MMPs or by serine proteases in apredominant and pericellular manner. Their activity isspecifically inhibited by metalloprotease tissue inhibitors(TIMPs) or by nonspecific protease inhibitors (eg, α2-macroglobulin). Inhibitors 1, 2, 3, and 4 are the 4 TIMPsknown to exist. The balance between MMPs and theirinhibitors is essentially altered in those physiologic condi-tions where rapid remodeling of extracellular matrixhappens. Cancer is a result of pathologic cellular growth.Interestingly, MMPs are expressed by different tissues atvarious stages of their development and are conspicuouslyabsent in normal cells of adult organisms [14]. Growthfactors and cytokines secreted by either tumor or stromalcells [15] regulate the expression of MMPs in neoplastictissues in a paracrine manner. That MMPs promotemetastases exclusively by modulating the remodeling ofextracellular matrix is a dogma easily challenged by therobust data available. Researchers also have been able toidentify MMPs' ability to impact tumor cell behavior in vivothrough their ability to cleave growth factors, cell surfacereceptors, cell adhesion molecules, and chemokines/cyto-kines [16-18]. Furthermore, MMPs may produce a moreaggressive phenotype via generation of apoptosis-resistantcells by cleaving proapoptotic factors [19]. MMPs may alsoregulate angiogenesis in cancer in 2 contrary directions:positively, through their ability to mobilize proangiogenicfactors [20], and negatively, by generating angiogenesisinhibitors, such as angiostatin and endostatin, which are thencleaved from large protein precursors [18]. Consequently,several MMPs, in particular, the gelatinases MMP-2 [19-24]and MMP-9 [23,25], have been studied as prognostic factorsin breast cancer and are associated with a poor outcome invarious subsets of patients. Likewise, several other MMPs,such as MMP-7 [26], MMP-11 [24,26], MT1-MMP (MMP-14) [25], and MMP-13 [27], may be overexpressed or relatedto clinical outcome in breast cancer. On the other hand, it isnow assumed that TIMPs are multifactorial proteins involvedin the induction of proliferation as well as in the inhibition ofapoptosis [28,29]. Thus, some TIMPs, such as TIMP-1[30,31] or TIMP-2 [25,32], may be overexpressed or relatedto clinical outcomes in breast cancer.
These researchers feel these findings are relevant to theattempt to characterize cancer cell behavior. One aim ofour present study was to analyze the possible relationsbetween the expression of MMPs and TIMPs of clinicalinterest in breast cancer and the 2 most frequent cancersubtypes according to the new molecular taxonomy:luminal A and basal-like phenotypes. Considering theheterogeneous nature of these tumor subtypes, we alsoinvestigated the prognostic value of MMP/TIMP expres-sion in reference to the occurrence of distant metastasis inboth subgroups of tumors.

1226 L. O. González et al.
2. Materials and methods
2.1. Patient selection, patient characteristics, andtissue specimen handling
We selected women with the following inclusion criteria:invasive ductal carcinoma, with at least 10 histopathologi-cally assessed axillary lymph nodes and a minimum of 5years of follow-up in those women without recurrence. Theexclusion criteria were the following: metastatic disease atpresentation, history of any type of malignant tumor, bilateralbreast cancer at presentation, receipt of any type ofneoadjuvant therapy, development of locoregional recur-rence during the follow-up period, development of a secondprimary cancer, and absence of sufficient tissue in theparaffin blocks for manufacturing the tissue microarrays(TMAs). From a total of 1053 patients fulfilling these criteriaand treated between 1990 and 2001, we randomly selected asample of 111 patients. We divided these patients in to 4groups of similar size and stratified them with regard to nodalstatus and development of metastatic disease, which was thekey variable of the study. This classification had for an endensuring the statistical power of the survival analysis, as wellas the inclusion of a significant number of events in both thenode-positive and node-negative subgroups (half of caseswith distant metastasis during the follow-up period in each ofthese subgroups). From this overall group, we selected 93patients with luminal A or basal-like tumors in accordancewith the criteria set out below, which were the most frequentphenotypes in our population.
Women were treated according to the guidelines used inour institution. The study adhered to national regulations andwas approved by our institution's ethics and investigationcommittee. The end point was distant metastatic relapse. Themedian follow-up period was 84 months in patients withoutmetastasis and 66 months in patients with metastasis.
2.2. TMAs and immunohistochemistry studies
Routinely fixed (overnight in 10% buffered formalin)paraffin-embedded tumor samples stored in our pathologylaboratory files were used. Histopathologically representa-tive tumor areas were defined on hematoxylin and eosin–stained sections and marked on the slide. Tumor tissue arrayblocks were obtained by punching a tissue cylinder (core)with a diameter of 1.5 mm through a histologicallyrepresentative area of each donor tumor block, which wasthen inserted into an empty recipient tissue array paraffinblock using a manual tissue arrayer (Becker Instruments, SunPrairie, WI) as described elsewhere [33]. Collection of tissuecores was carried out under highly controlled conditions.Areas of nonnecrotic cancerous tissue were selected by 2experienced pathologists (L. O. González and A. M.Merino). Two cores were used for each case. From the 111tumor samples available, 3 tissue array blocks were prepared,
each containing 37 samples, as well as internal controls,including 4 normal breast tissue samples from 2 healthywomen who underwent reductive mammary surgery.
Serial 5-μm sections were consecutively cut with amicrotome (Leica Microsystems GmbH, Wetzlar, Germany)and transferred to adhesive-coated slides. One section fromeach tissue block was stained with hematoxylin and eosin,and these slides were reviewed to confirm that the samplewas representative of the original tumor. Immunohistochem-istry staining was done on these sections using a TechMateTM50 autostainer (DAKO, Glostrup, Denmark). Antibodiesfor MMPs and TIMPs were obtained from Neomarker (LabVision Corporation, Fremont, CA). The dilution for eachantibody was established on the basis of negative andpositive controls (1/50 for MMP-2, 7, and 14 and TIMP-2; 1/100 for MMP-9 and 13 and TIMP-1 and 3; 1/200 for MMP-1and 11). We used mouse anti-ER clone 1D5, anti-PR clonePgR 636 (ready for use), rabbit polyclonal anti-HER2/neuoncoprotein at a dilution of 1/250, anti-p53 clone DO-7 at adilution of 1/75, Ki-67 clone MIB-1 at a dilution of 1/50,anti-EGFR clone 2-18c9 (ready for use) (DakoCytomation,Glostrup, Denmark), and anti-cytokeratin 5 (anti-CK5) cloneXM26 (Lab Vision) ready for use.
Tissue sections were deparaffinized in xylene and thenrehydrated in graded concentrations of ethyl alcohol (100%,96%, 80%, 70%, and then water). To enhance antigenretrieval for some antibodies, we microwave treated TMAsections (H2800 Microwave Processor; EBSciences, EastGranby, CT) in citrate buffer (Target Retrieval Solution,DAKO) at 99°C for 16 minutes. Endogenous peroxidaseactivity was blocked by incubating the slides in peroxidase-blocking solution (DAKO) for 5 minutes. The EnVisionDetection Kit (DAKO) was used as the staining detectionsystem. Sections were counterstained with hematoxylin,dehydrated with ethanol, and permanently coverslipped.
2.3. TMA analysis
For each antibody preparation, the location of immunor-eactivity, percentage of stained cells, and staining intensitywere determined. All the cases were semiquantified for eachprotein-stained area. An image analysis system with theOlympus BX51 microscope and analySIS software (SoftImaging System, Münster, Germany) was used as follows:tumor sections were stained with antibodies according to themethod explained above and counterstained with hematox-ylin. There are different optical thresholds for both stains.Each core was scanned with a power objective (originalmagnification ×400) in 2 fields per core. Fields were selectedby searching for the stained areas. The computer programselects and traces a line around antibody-stained areas(higher optical threshold, red spots), with the remainingnonstained areas (hematoxylin-stained tissue with loweroptical threshold) standing out as a blue background. Anyfield has an area ratio of stained (red) and nonstained (blue)

Table 1 Significant associations between tumor characteristicsand breast cancer subtypes in 93 patients
Patient and tumorcharacteristics
Luminal A Basal like P
n (%) n (%)
Total 48 (43.2) 45 (40.5)Cytokeratin 5 .001Negative 37 (80.4) 25 (56.8)Positive 9 (19.6) 19 (43.2)p53 .009Negative 46 (95.8) 35 (77.8)Positive 2 (4.2) 10 (22.2)EGFR .0001Negative 43 (89.6) 14 (31.1)Positive 5 (14.4) 20 (44.5)
1227Expression and prognostic significance of metalloproteases
areas. A final area ratio was obtained by averaging 2 fields.To evaluate immunostaining intensity, we used a numericscore ranging from 0 to 3: 0, no staining; 1, weak staining; 2,moderate staining; and 3, intense staining. Using an Excelspreadsheet, the mean score was obtained by multiplying theintensity score (I) by the percentage of stained cells (PC), andthe results were added (total score, I × PC). This overallscore was then averaged with the number of cores for eachpatient. If there was no tumor in a particular core, no scorewas given.
Furthermore, whole-tissue sections from tumor blocksfrom a subset of 10 cases were compared with thecorresponding TMA discs regarding expression of eachMMP and TIMP. Those cases were selected randomly, andthe clinicopathologic data were similar to those from thewhole series. Each whole-tissue section was scanned with alens (original magnification ×400) in 10 fields selected bysearching for the protein-stained areas, as described above.
Staining for ERs and PgRs was scored according to themethod described by Allred et al [34] and HER2 stainingaccording to the criteria used for the Herceptest. Controlsincluded breast cancer tissue with known immunoreactivityfor each antibody. Negative controls had the primaryantibody replaced by antibody diluent (DAKO).
Ki-67 and p53 were scored according to percentage ofstained cells. A case was considered positive if at least 15%or 25% of cells were stained, respectively. Staining of EGFRwas defined as any staining of tumor cell membranes abovebackground level, whether complete or incompletecircumferentially.
2.4. Definition of breast cancer subtypes
We established the following subtypes: luminal A (ER+,HER2−), luminal B (ER+, HER2+), HER2+ (HER2+, ER−,PgR−), and basal like (ER−, PgR−, HER2−) [8,10,11].
2.5. Western blot analysis
Western blotting of MMP-11, 13, and 14 and TIMP-2 from6 luminal A breast carcinomas or human placenta (used as apositive control for MMPs) was performed as previouslydescribed [36]. Briefly, 80 μg of cytosol extract was subjectedto 12% SDS-PAGE electrophoresis, transferred to a nitrocellu-lose membrane, and blocked. Blots were then immunolabeledovernight at 4°C with a monoclonal anti-MMP-11 (1:200,LabVision, Fremont, CA, USA), anti-MMP-13 (1:200;Calbiochem, Barcelona, Spain), anti-MMP-14 antiserum,anti-TIMP-2 antiserum (1:200, LabVision), or an anti-β-actinmonoclonal antibody (1:2500; Sigma-Aldrich, St Louis, MO)to confirm that equivalent amounts of total protein had beenadded to each well. After several washes, membranes wereincubated with goat anti-mouse IgG (1:2500, for MMP-11 and-13) or 1:5000 anti-rabbit IgG (for MMP-14 and TIPM-2)peroxidase-conjugated second antibody using the ECL™
Western blotting analysis system (Amersham Biosciences,Pittsburg, PA, USA). Finally, the immunoreactive bands weredetected by autoradiography.
2.6. Statistical analysis
Patients were subdivided into groups on the basis of thedefinition of breast cancer subtypes. Immunostaining scoresfor each protein were expressed as median (range).Comparison of immunostaining values between groupswas made with the Mann-Whitney or Kruskal-Wallis test.Differences in percentages were calculated with the χ2 test.To calculate metastasis-free survival analysis, we used theCox univariate method. To examine interactions of differentprognostic factors in a multivariate analysis, we used theCox regression model. In the multivariate analysis, weincluded only parameters that achieved statistical signifi-cance for relapse-free survival or overall survival in the log-rank test. Statistical tests were 2 sided at P b .05. Expressionprofiles were analyzed by the unsupervised hierarchicalclustering method, which organizes protein bases on treestructure similarity. Data were reformatted as follows: −3designated negative staining, 3 was positive staining, andmissing data were left blank. The score values werereformatted (positive-negative) choosing the median as thecutoff value. We used the Cluster 3.0 program (averagelinkage, Pearson correlation). Results were displayed withTreeview [35]. The SPSS 11.5 program (SPSS Inc,Chicago, IL) was used for all calculations.
3. Results
A total of 48 tumors (43.2%) were of luminal type A, 8(7.2%) of luminal type B, 45 (40.5%) basal like, and theremaining 10 (9.1%) HER2+ type. For the present study, weselected only the 2 most frequent types: luminal type A andbasal like. Our results did not show significant differencesbetween these types with regard to patient age, menopausal

1228 L. O. González et al.
status, tumor size, stage, nodal status, histologic grade, or Ki-67 expression (data not shown). However, we foundsignificantly more common expression of CK5 (P = .01),p53 (P = .009) and EGFR (P = .0001) in tumors with thebasal-like phenotype (Table 1).
Fig. 1 Representative examples of TMAs for the different MMPs andimmunohistochemical staining of CK5 in tumoral cells (A) and immunohiluminal A carcinoma: immunohistochemical staining of ER in tumoralfibroblastic cells (D), original magnification ×400.
More than 1800 determinations in cancer specimens from93 patients were evaluated on TMAs. Minimal internalvariance of score data in duplicate tissue cores from the samepatients was detected, showing a high agreement for eachprotein (r N 0.95 and P b .0001). We had previously
TIMPs (original magnification ×200). Example of basal-like tumor:stochemical staining of MMP-9 in fibroblastic cells (B). Example ofcell (C) and negative immunohistochemical staining of MMP-9 in

1229Expression and prognostic significance of metalloproteases
described a validation study for MMPs and TIMPs ininvasive breast carcinomas [26].
Fig. 1 shows examples of TMAs with immunostaining foreach protein evaluated. There was wide variability in theimmunostaining scores. In the overall population of tumors,the median score was 139 (range, 20-285) for MMP-1, 0 (0-246) for MMP-2, 127 (0-270) for MMP-7, 72 (0-273) forMMP-9, 160 (0-270) for MMP-11, 63 (0-192) for MMP-13,84 (0-261) for MMP-14, 146 (0-270) for TIMP-1, 121 (0-240) for TIMP-2, and 121 (0-272.4) for TIMP-3. However,there were no significant differences in scores for the MMPsor TIMPs in the 2 tumor phenotypes. We also investigatedthe tumors with regard to the cellular type expressing eachfactor (data not shown). We found no significant differencesin protein expression by the 2 tumor phenotypes.
We also investigated the possible prognostic value of theexpression of MMPs and TIMPs in luminal A as well as inbasal-like tumors. Our reason for doing so is that luminal Aand basal-like tumors are the most numerous types in ourpopulation. A poor prognosis in basal-like carcinomas(Table 2) was significantly associated with high scores forMMP-9 and 11. We further analyzed the possible associa-tions between the expression of MMPs or TIMPs by eachcellular type and prognosis, but for neither MMPs nor TIMPsexpression by cancerous cells were there significant
Table 2 Cox univariate (HR) and multivariate (RR) analysis of relatioluminal A and basal-like tumors
Luminal A
No. ofpatients
Eventfrequency
HR (95% CI) RR (95%
MMP-9Score b median vsN median
24/24 7/15 2.6 (1-6.3) 2.6 (1-6.
Fibroblasts (−) vs (+) 44/4 18/4 3.1 (1-9.2) 3.1 (1-9.MIC (−) vs (+) 45/3 19/3 3.8 (1-13.6) 3.8 (1-13MMP-11Score b median vsN median
21/27 7/15 1.9 (0.8-4.8) -
Fibroblasts (−) vs (+) 19/29 4/18 4.9 (1.6-14.9) -MIC (−) vs (+) 33/15 8/14 5.9 (2.4-14.4) 5.9 (2.4-MMP-13Fibroblasts (−) vs (+) 26/22 8/14 2.7 (1.1-6.4) 2.7 (1.1-MIC (−) vs (+) 31/17 10/12 3 (1.2-7) 3 (1.2-7)MMP-14MIC (−) vs (+) 22/26 5/17 4 (1.4-11.1) 7.6 (2.4-TIMP-2Score b median vsN median
22/26 6/16 2.6 (1-6.7) 2.6 (1-6.
Fibroblasts (-) vs (+) 26/19 7/15 4.8 (1.9-11.9) 4.8 (1.9-MIC (−) vs (+) 32/16 8/14 5.8 (2.4-14) 5.8 (2.4-Clustering (MIC)Group 1 vs Group 2 16/32 15/7 7.9 (3.1-19.7) 7.9 (3.1-
CI indicates confidence interval; HR, hazard ratio; RR, relative risk; MIC, mini⁎ P b .05.⁎⁎ P b .001.
associations with the occurrence of metastasis. However,our results did show associations between MMP/TIMPexpression by either fibroblasts or mononuclear inflamma-tory cells and distant relapse-free survival. These facts pointto the importance of stromal cells as prognostic indicators inboth luminal A and basal-like tumors. Thus, in luminal Atumors, expression of MMP-9 and 13 and TIMP-2 byintratumoral fibroblasts was significantly associated with ashorter relapse-free survival time, whereas the expression ofMMP-9, 11, 13, and 14 and TIMP-2 by mononuclearinflammatory cells was significantly associated with shorterrelapse-free survival (Table 2). With regard to the groups oftumors of the basal-like phenotype, the expression of MMP-9 and 11 and TIMP-2 by intratumoral fibroblasts wassignificantly associated with a shorter relapse-free survival,and the expression of MMP-9, 11, and 13 and TIMP-2 bymononuclear inflammatory cells was associated with shorterrelapse-free survival (Table 2). Multivariate analysis accord-ing to the Cox model demonstrated that the expression ofseveral MMPs/TIMPs was significantly and independentlyassociated with relapse-free survival (Table 2). However, ourresults showed no significant associations among MMP-1, 2,and 7; TIMP-1 and 3; and relapse-free survival. Significantassociations failed to appear in luminal A type as well as inbasal-like tumors (data not shown).
n between MMP and TIMP expression and relapse-free survival in
Basal like
CI) No. ofpatients
Eventfrequency
HR (95% CI) RR (95% CI)
3) ⁎ 22/22 9/16 2.3 (1-5.4) 2.4 (1-5.5) ⁎
2) ⁎ 35/10 16/10 3.9 (1.7-8.8) 2.4 (1-5.8) ⁎
.6) ⁎ 40/5 21/5 4.1 (1.4-11.7) 5.6 (1.9-16.3) ⁎
22/23 9/17 2.5 (1.1-5.6) 2.3 (1-5.3) ⁎
11/34 2/24 7.3 (1.7-31.7) 4.7 (1-21.7) ⁎
14.4) ⁎⁎ 32/13 13/13 4.1 (1.8-9.2) 3.2 (1.4-7.5) ⁎
6.4) ⁎ 18/27 7/19 2.2 (0.9-5.3) -⁎ 33/12 16/10 1.9 (0.8-4.4) 3.1 (1.1-8.9) ⁎
24) ⁎⁎ 22/23 7/19 5.3 (2-13.8) -
7) ⁎ 22/23 9/17 2.1 (0.9-4.8) -
11.9) ⁎ 27/18 9/17 7.5 (3.2-17.6) 6.7 (2.8-16.3) ⁎⁎
14) ⁎⁎ 26/19 13/13 1.3 (0.6-2.8) 2.6 (1.1-6.1) ⁎
19.7) ⁎⁎ 36/9 17/9 2.6 (1.1-5.9) ⁎ 3.6 (1.5-8.5) ⁎
mum inhibitory concentration.

Fig. 2 Hierarchical clustering analysis of global MMPs/TIMPs expressions in the different cell types of breast cancer as measured by immunohistochemistry on TMA in luminal A andbasal-like tumors. Graphical representation of hierarchical clustering results for score values, taken the median value as cutoff point, in luminal A (A) and basal-like (B) tumors and formononuclear inflammatory cells in luminal A (C) and basal-like tumors (D). Rows, tumoral samples; columns, MMPs/TIMPs. Protein expressions are depicted according to a color scale: red,positive staining; green, negative staining; gray, missing data. Two major clusters of tumors (1 and 2) are shown in each case.
1230L.
O.González
etal.
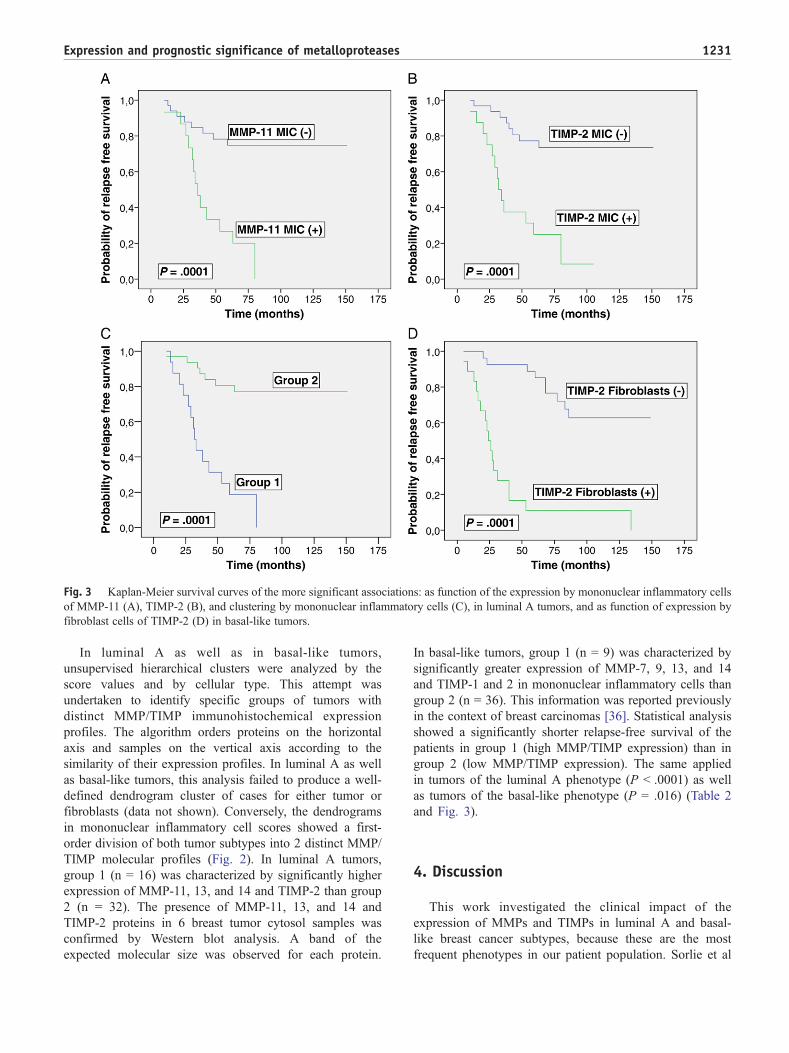
Fig. 3 Kaplan-Meier survival curves of the more significant associations: as function of the expression by mononuclear inflammatory cellsof MMP-11 (A), TIMP-2 (B), and clustering by mononuclear inflammatory cells (C), in luminal A tumors, and as function of expression byfibroblast cells of TIMP-2 (D) in basal-like tumors.
1231Expression and prognostic significance of metalloproteases
In luminal A as well as in basal-like tumors,unsupervised hierarchical clusters were analyzed by thescore values and by cellular type. This attempt wasundertaken to identify specific groups of tumors withdistinct MMP/TIMP immunohistochemical expressionprofiles. The algorithm orders proteins on the horizontalaxis and samples on the vertical axis according to thesimilarity of their expression profiles. In luminal A as wellas basal-like tumors, this analysis failed to produce a well-defined dendrogram cluster of cases for either tumor orfibroblasts (data not shown). Conversely, the dendrogramsin mononuclear inflammatory cell scores showed a first-order division of both tumor subtypes into 2 distinct MMP/TIMP molecular profiles (Fig. 2). In luminal A tumors,group 1 (n = 16) was characterized by significantly higherexpression of MMP-11, 13, and 14 and TIMP-2 than group2 (n = 32). The presence of MMP-11, 13, and 14 andTIMP-2 proteins in 6 breast tumor cytosol samples wasconfirmed by Western blot analysis. A band of theexpected molecular size was observed for each protein.
In basal-like tumors, group 1 (n = 9) was characterized bysignificantly greater expression of MMP-7, 9, 13, and 14and TIMP-1 and 2 in mononuclear inflammatory cells thangroup 2 (n = 36). This information was reported previouslyin the context of breast carcinomas [36]. Statistical analysisshowed a significantly shorter relapse-free survival of thepatients in group 1 (high MMP/TIMP expression) than ingroup 2 (low MMP/TIMP expression). The same appliedin tumors of the luminal A phenotype (P b .0001) as wellas tumors of the basal-like phenotype (P = .016) (Table 2and Fig. 3).
4. Discussion
This work investigated the clinical impact of theexpression of MMPs and TIMPs in luminal A and basal-like breast cancer subtypes, because these are the mostfrequent phenotypes in our patient population. Sorlie et al

1232 L. O. González et al.
[37] suggested that when it comes to the treatment ofdifferent breast tumors, one shoe does not fit all. In fact, thecontrary is the case. Because tumor subtypes represent apanoply of disease entities, a variety of therapeutic strategieswould be beneficial.
A case in point is the luminal subtype. Its genes areregulated by estrogen, and it is characterized by highexpression of ER. This tumor shows a high response rate tohormone therapy. However, therapies targeting the ER or theHER2 oncogene would not be effective against basal-likebreast cancers, as indeed has been reported, because thissubtype typically fails to express either of these proteins. Inaddition, although studies conducted by van de Rijn et al [7],Nielsen et al [8], and Callagy et al [10] have established thatluminal tumors (ER+) are associated with a better survivalrate, the presence of basal-like tumors has been associatedwith higher mortality rates [11]. However, we found nosignificant association between the phenotypic subtypes ofbreast tumors and the expression of MMPs by tumor cells.The MMPs are key elements in tumor invasion andmetastasis through their role in degradation of the stromalconnective tissue and basement membrane components,which are, particularly because some components, especiallythe interstitial collagens, are resistant to proteolytic attack,degraded only by MMPs.
The heterogeneous nature of particular tumor subtypes iswell established. For instance, patients with aggressivesubgroups of tumors, such as hormone-negative lesions,stand as excellent candidates to profit from aggressivetherapy [38]. If we refine treatment accuracy whenidentifying additional prognostic factors from breast carci-noma subtypes, we would increase the survival rate.Instances are found, for example, in results demonstratingthat high scores of MMP-9 and 11 are significantlyassociated with a poor prognosis in basal-like carcinomas.Likewise, MMP-9 (gelatinase B) is related to tumor invasionand metastasis via its capacity to degrade the type IVcollagen found in basement membranes [39] and induceangiogenesis [17]. Our results reproduce findings by Li et al[40] and Vizoso et al [26] documenting that high MMP-9expression correlates significantly with tumor aggressive-ness and poor prognosis. Similarly, results in studiesundertaken by Chenard et al [41], Ahmad et al [42], andVizoso et al [26] parallel our findings that high levels ofMMP-11 (stromelysin-3) are associated with tumor progres-sion and poor prognosis.
In addition, we have provided further evidence thatsubgroups differing in prognosis demonstrate expression ofMMPs or TIMPs by either stromal fibroblasts or mono-nuclear inflammatory cells. The same finding applies toluminal A and basal-like tumors. This is robust evidence thatbiologic aspects from cells of the tumor stroma influence theprognosis of both luminal A and basal-like tumors. Thesefindings point again to the prognostic role of the stromal cellsand match previous results demonstrating that molecularexpressions are an independent factor in predicting the
occurrence of distant metastasis in invasive breast cancer[26,36]. In addition, in the present study, we further analyzedthe possible existence of different patterns of MMP andTIMP expression in luminal A as well as basal-like tumors.In luminal A tumors, we found that 33.3% (group 1) showeda phenotype of inflammatory mononuclear cells overexpres-sing MMP-9, 11, 13, and 14 and TIMP-2 that wassignificantly associated with shorter relapse-free survival.Likewise, a significant association with shorter relapse-freesurvival was seen in the 20% of basal-like tumors (group 1)having a phenotype of inflammatory mononuclear cellsoverexpressing MMP-9, 11, and 13 and TIMP-2. Althoughthis latter subgroup of basal-like tumors comprises a smallpercentage of the cases, it is noteworthy that the over-expression of MMP/TIMP in mononuclear inflammatorycells has already been reported by us. We mentioned it whenconferring about invasive ductal carcinomas for the subset oftumors showing prometastatic mononuclear inflammatorycells defined by a high MMP/TIMP profile [36]. Thus, ourdata are in accordance with the increasing evidence thattumor behaviors such as angiogenesis, growth, and invasion[43-45] are promoted by leukocyte infiltration, which canstimulate proliferation and invasiveness of cancer cells byinflammation with secretion of cytokines, growth factors,chemokines, and proteases.
In summary, our research data point to the expressions ofMMPs and TIMPs in breast tumors being connected to thesignature of the tumor cells. The importance of theexpression of these factors by the stromal cells as prognosticfactors in breast carcinomas of both luminal A and basal-likephenotypes is underlined by our results. Further studies ofmore cases are necessary to assess whether MMPs andTIMPs are found in less common breast tumors such asluminal B and HER2+ phenotypes.
Acknowledgment
We thank to Dr Antonio Merino for collaboration inhistopathologic evaluation of tumors and Diana González forassistance in editing the manuscript.
References
[1] Sorlie T, Perou CM, Tibshirani R, et al. Gene expression patterns ofbreast carcinomas distinguish tumor subclasses with clinical implica-tions. Proc Natl Acad Sci U S A 2001;98:10869-74.
[2] Sorlie T, Tibshirani R, Parker J, et al. Repeated observation of breasttumor subtypes in independent gene expression data sets. Proc NatlAcad Sci U S A 2003;100:8418-23.
[3] Bertucci F, Viens P, Hingamp P, Nasser V, Houlgatte R, Birnbaum D.Breast cancer revisited using DNA array-based gene expressionprofiling. Int J Cancer 2003;103:565-71.
[4] Weigelt B, Hu Z, He X, et al. Molecular portraits and 70-geneprognosis signature are preserved throughout the metastatic process ofbreast cancer. Cancer Res 2005;65:9155-8.

1233Expression and prognostic significance of metalloproteases
[5] van 't Veer LJ, Dai H, van de Vijver MJ, et al. Gene expressionprofiling predicts clinical outcome of breast cancer. Nature 2002;415:530-6.
[6] Sotiriou C, Neo SY, McShane LM, et al. Breast cancer classificationand prognosis based on gene expression profiles from a population-based study. Proc Natl Acad Sci U S A 2003;100:10393-8.
[7] van de Rijn M, Perou CM, Tibshirani R, et al. Expression ofcytokeratins 17 and 5 identifies a group of breast carcinomas with poorclinical outcome. Am J Pathol 2002;161:1991-6.
[8] Nielsen TO, Hsu FD, Jensen K, et al. Immunohistochemical andclinical characterization of the basal-like subtype of invasive breastcarcinoma. Clin Cancer Res 2004;10:5367-74.
[9] Matos I, Dufloth R, Alvarenga M, Zeferino LC, Schmitt F. p63,cytokeratin 5, and P-cadherin: three molecular markers to distinguishbasal phenotype in breast carcinomas. Virchows Arch 2005;447:688-94.
[10] Callagy G, Cattaneo E, Daigo Y, et al. Molecular classification ofbreast carcinomas using tissue microarrays. Diagn Mol Pathol 2003;12:27-34.
[11] Jacquemier J, Ginestier C, Rougemont J, et al. Protein expressionprofiling identifies subclasses of breast cancer and predicts prognosis.Cancer Res 2005;65:767-79.
[12] Overall CM, Lopez-Otin C. Strategies for MMP inhibition in cancer:innovations for the post-trial era. Nat Rev Cancer 2002;2:657-72.
[13] Demers M, Couillard J, Belanger S, St-Pierre Y. New roles for matrixmetalloproteinases in metastasis. Crit Rev Immunol 2005;25:493-523.
[14] Stamenkovic I. Matrix metalloproteinases in tumor invasion andmetastasis. Semin Cancer Biol 2000;10:415-33.
[15] Meller D, Li DQ, Tseng SC. Regulation of collagenase, stromelysin,and gelatinase B in human conjunctival and conjunctivochalasisfibroblasts by interleukin-1beta and tumor necrosis factor-alpha. InvestOphthalmol Vis Sci 2000;41:2922-9.
[16] Sternlicht MD, Werb Z. How matrix metalloproteinases regulate cellbehavior. Annu Rev Cell Dev Biol 2001;17:463-516.
[17] Egeblad M, Werb Z. New functions for the matrix metalloproteinasesin cancer progression. Nat Rev Cancer 2002;2:161-74.
[18] Rifkin DB, Mazzieri R, Munger JS, Noguera I, Sung J. Proteolyticcontrol of growth factor availability. Apmis 1999;107:80-5.
[19] Fingleton B, Vargo-Gogola T, Crawford HC, Matrisian LM. Matrilysin[MMP-7] expression selects for cells with reduced sensitivity toapoptosis. Neoplasia 2001;3:459-68.
[20] Stetler-Stevenson WG. Matrix metalloproteinases in angiogenesis: amoving target for therapeutic intervention. J Clin Invest 1999;103:1237-41.
[21] Cornelius LA, Nehring LC, Harding E, et al. Matrix metalloprotei-nases generate angiostatin: effects on neovascularization. J Immunol1998;161:6845-52.
[22] Ferreras M, Felbor U, Lenhard T, Olsen BR, Delaisse J. Generationand degradation of human endostatin proteins by various proteinases.FEBS Lett 2000;486:247-51.
[23] Jones JL, Glynn P, Walker RA. Expression of MMP-2 and MMP-9,their inhibitors, and the activator MT1-MMP in primary breastcarcinomas. J Pathol 1999;189:161-8.
[24] Duffy MJ, Maguire TM, Hill A, McDermott E, O'Higgins N.Metalloproteinases: role in breast carcinogenesis, invasion andmetastasis. Breast Cancer Res 2000;2:252-7.
[25] Talvensaari-Mattila A, Paakko P, Turpeenniemi-Hujanen T. Matrixmetalloproteinase-2 (MMP-2) is associated with survival in breastcarcinoma. Br J Cancer 2003;89:1270-5.
[26] Vizoso FJ, Gonzalez LO, Corte MD, et al. Study of matrixmetalloproteinases and their inhibitors in breast cancer. Br J Cancer2007;96:903-11.
[27] Nielsen BS, Rank F, Lopez JM, et al. Collagenase-3 expression inbreast myofibroblasts as a molecular marker of transition of ductalcarcinoma in situ lesions to invasive ductal carcinomas. Cancer Res2001;61:7091-100.
[28] Chantrain CF, Shimada H, Jodele S, et al. Stromal matrixmetalloproteinase-9 regulates the vascular architecture in neuroblas-toma by promoting pericyte recruitment. Cancer Res 2004;64:1675-86.
[29] Wurtz SO, Schrohl AS, Sorensen NM, et al. Tissue inhibitor ofmetalloproteinases-1 in breast cancer. Endocr Relat Cancer 2005;12:215-27.
[30] Jiang Y, Goldberg ID, Shi YE. Complex roles of tissue inhibitors ofmetalloproteinases in cancer. Oncogene 2002;21:2245-52.
[31] Baker AH, George SJ, Zaltsman AB, Murphy G, Newby AC.Inhibition of invasion and induction of apoptotic cell death of cancercell lines by overexpression of TIMP-3. Br J Cancer 1999;79:1347-55.
[32] Ree AH, Florenes VA, Berg JP, Maelandsmo GM, Nesland JM,Fodstad O. High levels of messenger RNAs for tissue inhibitors ofmetalloproteinases (TIMP-1 and TIMP-2) in primary breast carcino-mas are associated with development of distant metastases. ClinCancer Res 1997;3:1623-8.
[33] Parker RL, Huntsman DG, Lesack DW, et al. Assessment ofinterlaboratory variation in the immunohistochemical determinationof estrogen receptor status using a breast cancer tissue microarray. AmJ Clin Pathol 2002;117:723-8.
[34] Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic andpredictive factors in breast cancer by immunohistochemical analysis.Mod Pathol 1998;11:155-68.
[35] Eisen MB, Spellman PT, Brown PO, Botstein D. Cluster analysis anddisplay of genome-wide expression patterns. Proc Natl Acad Sci U S A1998;95:14863-8.
[36] Gonzalez LO, Pidal I, Junquera S, et al. Overexpression of matrixmetalloproteinases and their inhibitors in mononuclear inflammatorycells in breast cancer correlates with metastasis-relapse. Br J Cancer2007;97:957-63.
[37] Sorlie T, Wang Y, Xiao C, et al. Distinct molecular mechanismsunderlying clinically relevant subtypes of breast cancer: geneexpression analyses across three different platforms. BMC Genomics2006;7:127.
[38] Rakha EA, El-Sayed ME, Green AR, Lee AH, Robertson JF, Ellis IO.Prognostic markers in triple-negative breast cancer. Cancer 2007;109:25-32.
[39] Jones JL, Walker RA. Control of matrix metalloproteinase activity incancer. J Pathol 1997;183:377-9.
[40] Li HC, Cao DC, Liu Y, et al. Prognostic value of matrixmetalloproteinases (MMP-2 and MMP-9) in patients with lymphnode–negative breast carcinoma. Breast Cancer Res Treat 2004;88:75-85.
[41] Chenard MP, O'Siorain L, Shering S, et al. High levels of stromelysin-3 correlate with poor prognosis in patients with breast carcinoma. Int JCancer 1996;69:448-51.
[42] Ahmad A, Hanby A, Dublin E, et al. Stromelysin 3: an independentprognostic factor for relapse-free survival in node-positive breastcancer and demonstration of novel breast carcinoma cell expression.Am J Pathol 1998;152:721-8.
[43] Coussens LM, Werb Z. Inflammation and cancer. Nature 2002;420:860-7.
[44] Daniel D, Chiu C, Giraudo E, et al. CD4+ T cell–mediated antigen-specific immunotherapy in a mouse model of cervical cancer. CancerRes 2005;65:2018-25.
[45] Adams TE, Alpert S, Hanahan D. Non-tolerance and autoantibodies toa transgenic self antigen expressed in pancreatic beta cells. Nature1987;325:223-8.
Copyright © 2022 FDOKUMEN




















