Childbirth Series Section Four: Understanding Cesarean Birth ...
Upload
itguardianghCategory
view
4download
0
Evoking the Guardian Angel: Childbirth Care in a
Palestinian HospitalSahar Hassan-Bitar, Laura Wick
Institute of Community and Public Health, Birzeit University, Ramallah, West Bank,Occupied Palestinian Territory. E-mail: [email protected]
Abstract: The purpose of this study was to assess the quality of maternity care in a large,public, Palestinian referral hospital, as a first step in developing interventions to improve safety andquality of maternity care. Provider interviews, observation and interviews with women were usedto understand the barriers to improved care and prepare providers to be receptive to change. Someof the inappropriate practices identified were forbidding female labour companions, routine useof oxytocin to accelerate labour, restriction of mobility during labour and frequent vaginalexaminations. Magnesium sulfate was not used for pre-eclampsia or eclampsia, and post-partumhaemorrhage was a frequent occurrence. Severe understaffing of midwives, insufficient supervisionand lack of skills led to inadequate care. Use of evidence-based practices which promotenormal labour is critical in settings where resources are scarce and women have large families. Thereport of this assessment and dissemination meetings with providers, hospital managers,policymakers and donors were a reality check for all involved, and an intervention plan toimprove quality of care was approved. In spite of the ongoing climate of crisis and whatever elsemay be going on, women continue to give birth and to want kindness and good care forthemselves and their newborns. This is perhaps where the opportunity for change should begin.A2007 Reproductive Health Matters. All rights reserved.
Keywords: childbirth, post-partum period, emergency obstetric care, quality of care, humanresources, provider-patient relations, Occupied Palestinian Territory
ALTHOUGH childbirth in some developingcountries has shifted from the home to thehospital, the institutionalisation of birth
has not always been accompanied by improvedpractices or outcomes.1 The components of effec-tive childbirth care based on scientific evidencehave been well documented and disseminated,2,3
yet there seems to be a lag in the adoption ofbest practice both in developed and developingcountries. Situating birth in its local environmentcontributes to understanding the complexity anddiversity of childbirth care provision and whathas shaped it.4 A local needs assessment helpsto understand what factors shape maternitycare in a particular setting and what strategiesmight be most effective in adopting evidence-based best practices.
The purpose of this study was to assess thequality of maternity care in a large Palestinianreferral hospital, as a first step in developinginterventions to improve childbirth care formothers and newborns. However, in order tounderstand the barriers to quality care, it is nec-essary to situate the birthing environmentwithin the larger social, economic, and politicalcontext. The ongoing Israeli occupation ofPalestine has contributed to a situation offragmented, under-resourced and unregulatedhealth services. The separation wall and over500 checkpoints5 in the Occupied PalestinianTerritory limit access to maternity care andimpede the effective organisation of and accessto health care. Rising poverty, encompassingover 60% of the population,6 is an additional
A 2007 Reproductive Health Matters.All rights reserved.
Reproductive Health Matters 2007;15(30):103–1130968-8080/06 $ – see front matterPII: S0968-8080 (07 )30321-2www.rhm-elsevier.com www.rhmjournal.org.uk
103

S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
barrier to accessing services in the private andnon-governmental sector.
Most births (97%) take place in hospitals orclinics.7 Since the Palestinian Ministry of Healthtook over responsibility from the Israeli Ministryof Defense for the health sector in 1994, it hasencouraged all women to give birth in hospi-tals, phasing out community midwives anddayas (traditional birth attendants).8 The 17public hospitals in the West Bank and Gazahave become the place of birth for 56% of the103,870 annual births,9 primarily for the poor.However, the increasingly overcrowded andunder-staffed maternity wards of public hospi-tals have compounded the risks for birthingwomen of unpredictable lack of access to mater-nity facilities and sub-optimal perinatal care.Whereas previously high-risk cases and com-plications from the West Bank were referred tothe major Palestinian referral hospital in Jeru-salem, with the restricted access to Jerusalemsince 2000, most are now treated in the localpublic hospitals.
Due toahigh total fertility rateof 4.6,7maternaland child health services comprise a large andcritical portion of health service utilisation.Although antenatal care coverage is high(97%),7 the overall quality is poor.10 Intrapartumcare in West Bank maternity facilities is fre-quently not based on scientific evidence,11 in spiteof the dissemination of national standards andguidelines. Few health care providers and wardmanagers were trained in how to instruct theirstaff in the use of these guidelines where manysystemic and institutional obstacles impedeimplementation. The population-based caesar-ean delivery rate has doubled in the past decadefrom6% in1996 to 12.8% in2004,7 and the publichospitals’ caesarean rate reached 15.7% in 2004.9
Women leave the hospital within 24 hours aftera vaginal birth and three days after a caesareansection, and only one-third consult a maternalhealth provider during the six-week period there-after.7 Almost all Palestinian women breastfeedtheir babies (96%), althoughexclusivebreastfeed-ing is not always practised, but a large majority(66%) continue to breastfeed at 9–12 months.7
Our study setting was a general referral publichospital located in the middle governorate of theWest Bank with 155 beds (including 36 mater-nity beds), treating about 20,000 in-patient and70,000 emergency cases each year. It was one of
104
the hospitals that had recently been made amajor referral hospital to replace the one inJerusalem. We chose this hospital because ofits high delivery rate, serving primarily poorwomen in the area, unlike most maternity hos-pitals in the non-governmental and privatesector. Approximately 4,000 births took placethere annually, which was free of charge forthose holding the public insurance instituted bythe Ministry of Health for the poor during thesecond uprising in September 2000. Its proxim-ity enabled the researcher to spend an extensiveperiod of observation in the wards to betterunderstand the childbirth environment. Sinceaffecting change at the policy level is difficultin a weak and unregulated system, this assess-ment aimed to improve childbirth care throughmid-level modifications targeting hospital-basedmidwives, the primary caregivers during normalbirth, as the key agents of change.
MethodologyThe objectives of this study were to assess thequality of maternity care in a large referral hos-pital, to identify the gaps and barriers to betterpractice, to provide baseline data for upgradingservice provision, and to prepare a receptive con-text for change for the interventions to follow.International and local research was reviewed.Practices were assessed according to the latestscientific research on evidence-based obstet-rics.2,3 Two frameworks for the evaluation ofquality of care guided the development ofthe instruments, which were adapted to localconditions: the WHO Safe Motherhood NeedsAssessment Tools12 and the framework for qual-ity of maternity services developed by Hultonet al.13 The overall approach was influenced bythe literature on the adoption of innovations inhealth care as a complex and adaptive process,which needs to take into account local struc-tures, processes and patterns and which requiresflexibility, creativity and interaction for trans-lating research into practice.14
In the hospital, quantitative and qualitativemethods were used to assess technical and sup-portive care during delivery and the immediatepost-partum period. Field observations, recordreviews, case notes, exit interviews with womenand in-depth interviews with providers and wardmanagers were collected between April 2005

S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
and March 2006. The principal investigator (firstauthor) is a Palestinian midwife with experiencein running a busymaternityward. She carried outmost of the fieldwork, which aimed to eliminateone aspect of observer bias, as the staff becameaccustomed to her presence in the ward andwere not intimidated (as might be the case ifthe observer were of a different nationality orprofession), which was also conducive to thesmall budget allocated for this study. Beforebeginning the study, written and oral permissionwere obtained from the General Director of Hos-pitals at the Ministry of Health, the hospitaldirector and the head obstetrician and midwife.
Observations were undertaken for 14 days(120 hours) during different days of the weekand times of day (in the three shifts) in order todocument actual practices and better under-stand childbirth management issues and inter-personal relations. Observations were the bestway to understand the complexity of the birthingenvironment and create relationships of trustwith the providers. In addition to direct obser-vation in the wards, with prepared checklists asa guide, informal group discussions and one-to-one discussions with key informants (pro-viders, managers and hospital administrators,women, clerks and cleaners) added to the richnessand diversity of the information collected.
A total of 64 women and 12 newborns wereobserved using checklists, except for post-partumcare and emergency events, where detailed noteswere taken. Thirty-nine women were observedbetween the beginning of labour and the imme-diate post-partum period, 23 women duringthe post-partum period, two emergency cases,and 12 newborns (Table 1).
Ward registers and medical records werereviewed to collect data on ward statistics, actualpractices and accuracy of record-keeping. Elevenmedical records (nine normal births and two emer-gency events) were audited in detail using struc-tured checklists.
Semi-structured interviews were conductedwith all women who gave birth in the hospital(both normal and caesarean birth) during a two-week period by the researcher and one field-worker (a midwifery teacher from outside thehospital trained for this purpose). After beinginformed of the purpose of the interview (the needto understand women’s views and how theywere treated) and the identity of the interviewer
(not a member of the hospital staff) and beingassured of confidentiality, all of the women choseto participate. Due to the lack of a private place inthe hospital to carry out interviews, 159 womenwere interviewed (either the day following birthor three days later for caesarean operations) indi-vidually by their beds, ensuring privacy as muchas possible by closing the door, making sure thatno providers were in the room at the time, andsitting close to the woman. The 15–30 minuteinterviews were in Arabic and focused on thechoice of place of birth, the current birth expe-rience, woman–provider interactions, and post-partum care. The cases were cross-checked withthe birth register to make sure that no womenhad been overlooked.
Thirty-one in-depth interviews were carriedout by the first author with all but one of thematernity care providers working in the hospi-tal (9 midwives, 14 nurses and 8 physicians)using a semi-structured questionnaire with pri-marily open-ended questions. Each interviewlasted 45–60 minutes, focusing on a descriptionof their work and responsibilities, includingchildbirth practices and care, perceived barriersto quality care, training needs and suggestedstrategies for improvement.
SPSS Version 12 was used to analyse the quan-titative data (closed-ended questions) from theinterviews with women and providers. Observa-tion checklists and record reviews were manuallyanalysed by counting frequencies of variouscomponents of care.
105
S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
Themes were initially identified through thewomen and providers interview guidelines. Theresearcher transcribed the content of the open-ended questions and categorised it accord-ing to the identified themes. Other concerns thatemerged during the interviews were also includedas themes. The content was analysed within thecontext of the overall birthing environment andthe main findings of the study. Field observationnotes were handwritten in the field and thentyped and analysed the following day. In addi-tion, the researcher had many informal discus-sions with the women, health providers, wardsecretary and cleaners to clarify observations.Triangulation was utilised to verify the validity ofqualitative findings from different sources. Forexample, case observations were compared withrelevant records and with the informal discussionswith women and providers. The data were furthervalidated through discussions with providersduring preliminary dissemination meetings.
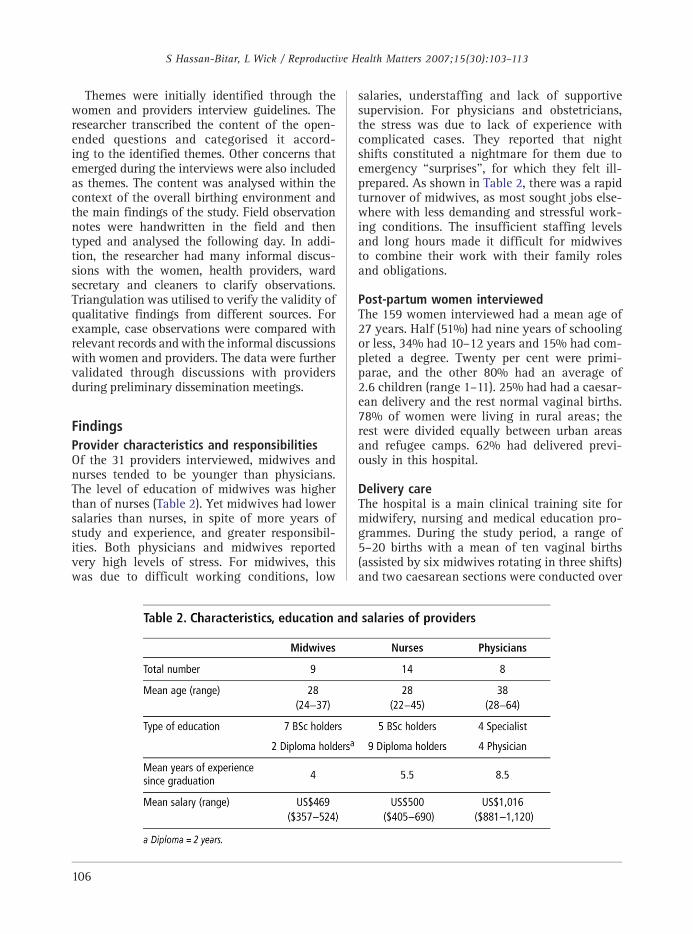
FindingsProvider characteristics and responsibilitiesOf the 31 providers interviewed, midwives andnurses tended to be younger than physicians.The level of education of midwives was higherthan of nurses (Table 2). Yet midwives had lowersalaries than nurses, in spite of more years ofstudy and experience, and greater responsibil-ities. Both physicians and midwives reportedvery high levels of stress. For midwives, thiswas due to difficult working conditions, low
106
salaries, understaffing and lack of supportivesupervision. For physicians and obstetricians,the stress was due to lack of experience withcomplicated cases. They reported that nightshifts constituted a nightmare for them due toemergency ‘‘surprises’’, for which they felt ill-prepared. As shown in Table 2, there was a rapidturnover of midwives, as most sought jobs else-where with less demanding and stressful work-ing conditions. The insufficient staffing levelsand long hours made it difficult for midwivesto combine their work with their family rolesand obligations.
Post-partum women interviewedThe 159 women interviewed had a mean age of27 years. Half (51%) had nine years of schoolingor less, 34% had 10–12 years and 15% had com-pleted a degree. Twenty per cent were primi-parae, and the other 80% had an average of2.6 children (range 1–11). 25% had had a caesar-ean delivery and the rest normal vaginal births.78% of women were living in rural areas; therest were divided equally between urban areasand refugee camps. 62% had delivered previ-ously in this hospital.
Delivery careThe hospital is a main clinical training site formidwifery, nursing and medical education pro-grammes. During the study period, a range of5–20 births with a mean of ten vaginal births(assisted by six midwives rotating in three shifts)and two caesarean sections were conducted over

S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
a 24-hour period. One physician staffed thelabour ward on each shift and one obstetricianwas on call; all of them were men. Midwivesprovided all the care for 91%of the vaginal births.Physicians were expected to prescribe medica-tion, suture episiotomies and assist high-riskand caesarean deliveries. Epidurals for pain reliefwere not available and meperidine was usedinfrequently. Nurses provided post-partum carefor women and newborns after normal andcaesarean birth. Rooming-in and early initiationof breastfeeding had been adopted as hospitalpolicy and routine supplemental liquids or for-mula were not used. The increasing caesareansection ratewas due to the absence of an effective,early referral system for high risk cases to thehospital, unnecessary routine interventionsduring labour, the inadequate competence ofphysicians in making clinical judgements due tooutdated knowledge, obstetricians who werestressed because of working in more than oneinstitution and the declining health of pregnantPalestinian women.
Intra-partum careThere was severe understaffing ofmidwives, giventheir responsibilities and workload. Observationand women’s reports revealed that the motherfrequently went through labour alone, with littlecaregiver support. At birth only one midwife waspresent. This resulted in unsafe birthing practices,involving either insufficient monitoring of thenewborn or inappropriate care of the motherduring the critical third stage of labour.
Infection control was insufficient and sup-plies frequently not available; women often gavebirth without sheets on the beds, only plasticcovers. Furthermore, observations and providers’and women’s reports revealed the use of inap-propriate practices (Table 3) such as restrictingmobility and not allowing eating and drinkingduring labour, routine intravenous infusions withoxytocin during labour, no use of partograms, nofamily support person permitted, infrequent useof non-pharmacological methods of pain relief,no use of active management of the third stageof labour and routine episiotomy for first-timemothers. Women were observed asking for theirnewborns soon after birth to initiate breastfeed-ing, but the midwife had no time to assist them.
This pattern of care was consistent with pro-viders’ reports. Frequent vaginal examinations
were carried out, but not always documented inthe records. Providers reported using oxytocinroutinely to accelerate labour and midwivesadmitted administering it in the intravenousbags without using dropper machines to regu-late dosage, due to lack of equipment, and fre-quently neglecting to put on a label.
When therewasmore thanonebirth at the sametime, newborns were placed together under theonly warmer in the delivery room, and sometimesno identification bracelets were put on the babies.One full-term newborn, left unattended, fell outof the warmer and had to be taken to intensivecare. Another, born at 39 weeks, Apgar 8/9, andweighing 2kg had breathing difficulties. He waskept in the busy labour and delivery room forobservation for more than five hours, and diedunattended. Cases 1 and 2 that follow are repre-sentative of many of the cases we observed.
Case 1At 9:30am, a 27-year-old woman, para 3, fullterm, was admitted to the hospital complain-ing of labour pains. A fetal heart monitor wasplaced for about ten minutes. Her case wasstraightforward without any significant historyof complications in previous pregnancies. Aspart of the admission procedure, the physicianconducted a vaginal exam and documented6 cm dilation. The midwife repeated the vaginal
107

S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
exam, and the labouring woman was guidedto the delivery room where she was placed inthe lithotomy position on a delivery bed. Anintravenous cannula was inserted and an infu-sion fluid was initiated. Two units of oxytocinwere added to the infusion bag. However, nolabel was placed on the bag to show the addi-tional medication. The bladder was emptied usinga catheter. The woman was ready to deliver within15 minutes. Although the main door of the roomwas partially closed, the woman without anysheet was exposed continually to the many staffand patients. The woman was assisted by themidwife in giving birth at 9:45am. Immediatelyafter birth, the midwife placed a towel from themother’s belongings on her abdomen for thebaby and asked her to hold the baby while shecut the umbilical cord. The baby was then takento the resuscitator in the next room, which wascold and not prepared for use. The baby wascleaned, suctioned and kept on a table near thewarmer, not under it, as another premature babywas occupying the resuscitator. After checkingthe woman’s uterus, the midwife returned to thenewborn, placed the cord clamp, weighed anddressed him. Then, without washing her hands,she continued to care for the other, prematurebaby. She returned to the mother for the deliveryof the placenta, cleaned her and administeredsyntrometrine intra-muscular injection while theintravenous drip was still running. Blood pressureand fundal height were measured only once. Therecords were filled in by the other midwife on duty.
Case 2A pre-term newborn, weighing 1800 gm wasbrought in to the labour and delivery ward by aphysician from the operating theatre, after a
108
caesarean section. Both midwives were busy andunavailable when the physician called for them,and no one answered him. He put the babyunder the warmer and went to leave by theexternal, main door. I (first author) was observ-ing in the main corridor and just could notremain silent. I asked him: ‘‘How come you leftthis newborn on the table without even check-ing if the warmer was on, or whether there was amidwife to provide care?’’ Without asking who Iwas, the physician went back and checked thewarmer, which was cold. He turned it on, driedthe newborn and gave her oxygen until one ofthe midwives took over about 20 minutes later.This reminded me of the comment of one of thephysicians who used to work at this hospital:
‘‘Those newborns certainly must have a guardianangel as it’s only God who takes care of them.’’
Post-partum careMany women did not receive adequate post-partum care. According to women’s reports,only 10% were asked about bleeding aftervaginal birth, and only 13% had their lochia(discharge from the uterus during the puerpe-rium) checked. These findings were consistentwith nurses’ reports. More than half of post-partum women did not have their blood pressuretaken, regardless of mode of delivery. Althoughhalf the nurses reported checking episiotomies,it was noted through observations that this wasnot done. Post-partum haemorrhage remained afrequent emergency, according to women andproviders and the review of emergency cases.Magnesium sulfate, the drug of choice, was notused when pre-eclampsia or eclampsia occurred.Table 4 details the obstetric complications in

S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
women that were observed by the first author orwhat was ‘‘voluntarily reported’’ by midwivesduring the period of field work. We heard stafftalking among themselves about other cases, butthe records were incomplete and did not allowus to track them, and we decided not ask fordetails, as doing so might have been perceivedas threatening.
The nurses’ knowledge of maternity care wasvery limited. None of the nurses reported pro-viding any care or monitoring of newborns.Observation and women’s interviews indicatedthat women breastfed their babies in the post-partum period, but without any assistance fromnurses or any health education.
Provider–patient relationsAlthough most women (87% with normaldelivery and 90% with caesarean section)reported that their birth attendants were ‘‘nice’’to them, only about half of them felt that thehealth care providers were friendly or polite.While 36% of women who considered their birthattendant to be ‘‘nice’’ reported that she was kind,patient, respectful and acceptable, 20% said shewas nice only because she did not shout at them.Sometimes women were shouted at, sometimesconsidered ignorant and difficult to deal with,sometimes neglected and frequently not assisted,informed or consulted.
‘‘Thank God, they did not shout at me’’(Primigravida, 17 years old, 7 years education)
‘‘The midwife frowned at me, was hot-temperedand shouted at me.’’ (Para 5, 25 years old, 8 yearsof education)
When women were asked if they were encour-aged to ask questions, only 12% with a normaldelivery and 18% with caesareans replied posi-tively. Only 54% of the women said the midwifeor nurse came quickly when they called forassistance. Nurses reported finding it difficult todeal with some of the women and their familieswho had a low level of education. Some womenperceived that they were not all treated equallyand that certain individuals with connectionsgot special care. The women’s reports were con-sistent with the researcher’s observations andinformal discussions with providers.
‘‘The hospital is not clean at all. I am sleeping ona dirty sheet that has a bad smell. There are no
curtains for privacy so that my husband can stayhere without invading other women’s privacy. Asyou can see, I have no pillow and I am sleepingon my hand bag instead.’’ (Para 2, 24 years old,8 years education)
‘‘There are no sheets as you can see. I felt coldand asked the nurse to bring me a blanket; shedid not and replied: ‘So what if you feel cold?’ Icovered myself with my jelbab (long dress). I didnot see any food here!’’ (Primigravida, 22 yearsold, third year university student)
Reasons for suboptimal careSuboptimal care occurred because of a shortageof staff, as shown in the two cases above inwhich one midwife had to assist both in thebirth and care of the newborn. Secondly, therewas a lack of basic supplies and equipment dueto an insufficient budget and/or dependence oninternational funds for items such as identifica-tion bands, linens, gauze and newborn warmers.Thirdly, there was poor management and organi-sation of care as shown in Case 2. Despite thepresence of a specialised neonatal unit, new-borns after caesarean sections were transferredto the busy understaffed labour and deliveryward to be observed and cared for. Fourthly,there was insufficient supervision, as the seniormidwife divided the workload with the othermidwife on duty, which left no time for super-vision. Fifthly, as shown in the findings, therewas outdated knowledge, particularly regardingmanagement of the third stage of labour. Finally,staff felt powerless to effect change. For example,midwives reported that supervision was unsup-portive and they felt powerless being at the bottomof the health system hierarchy, coping withunresponsive authorities.
Forbidding women to have female compan-ions during labour and birth was a decisiontaken at the Ministerial policy level, but mid-wives and physicians agreed with this regulationas they considered family members an obstacleto efficient care. The issue of provider controlof the labour process and environment wasfrequently reported by providers as the mainreason for such inappropriate practices as limit-ing mobility during labour, restricting womento the lithotomy position to give birth, and theroutine use of oxytocin to speed up labour andto free up beds for the next women coming in.
109

S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
Changing providers’ attitudes from controllingto assisting birthing women would thereforeappear to be crucial.
DiscussionIn this hospital the quality of basic childbirthcare was inadequate and not consistent withbest practice. While the results cannot be gen-eralised to other maternity hospitals, communi-cation with health providers and experience inthe field indicate that many of the obstacles inother large institutions in the Occupied Pales-tinian Territory are similar. The results supportfindings from previous studies documentingthe gap between evidence-based practices androutine care in Palestine11, the Arab world15 andother regions of the world as well.16,17 However,this study was able to validate providers’reported practices through observation and exitinterviews with women, to understand furtherthe process of care. The research process stim-ulated health care providers to think, interact andinitiate small changes in their own practice duringthe fieldwork. Moreover, it explored women’sviews in a context where women were rarely con-sulted or included in medical decision-making.
The fact that the first author was a local mid-wife enabled her to build confidence amongthe midwives. While having one researcherdoing all of the fieldwork might be considereda limitation, due to individual bias, it facilitatedestablishing contact and gaining insight intoproblem-solving in this neglected area of hos-pital services. Building trust, motivation and self-esteem in the maternity team helped to empowerthem to initiate change. The process of assess-ment was a way of preparing the ground to bereceptive to change and to motivate the mid-wives to problem-solve. Field observation oftenposes the moral dilemma of observing harmfulpractices without intervening; instead, there isfrequently a time lag between research findingsand their translation into practice. We consid-ered it ethically and strategically unjustifiableto observe evident malpractice without givingstaff immediate feedback, as occurred in Case 2above. Sometimes asking the right question wasenough to initiate a process of change. Simplechanges that evolved during the fieldworkwere the utilisation of identification bands forthe newborns and the acquisition of a second
110
warmer for newborns in the delivery ward. Morecomplex innovations, such as the use of thepartogram, will require more staff and furtheron-the-job training and supervision.
Improving the safety of childbirth, motivat-ing providers, reducing rapid staff turnoverand meeting women’s needs involve systemicchanges, including sufficient staff and ensur-ing enough midwives so that two are presentat every birth – one for the mother and the otherfor the newborn.18 The shortage of midwivesis mainly due to systemic problems in humanresource management, including in determiningthe required numbers of midwives for facilitiesand utilising the most appropriate types of pro-viders. The lack of sufficient staff and suppliesfor the maternity services has been exacerbatedby the recent international financial boycott ofthe elected Palestinian government; providers(particularly midwives) have had to ensure child-birth services for poor women under difficultcircumstances and without receiving their sala-ries for more than ten months. Investing inmidwives as providers of perinatal care duringpregnancy, childbirth and the post-partumperiod has been shown to be effective and sus-tainable and to result in a lower caesarean sec-tion rate.19 This would permit physicians, whoexpressed the need for more support and super-vision, to focus on improving their skills.
Poverty and difficult access to maternity carefacilities have increased the stress and severityof cases that providers have to deal with. Forexample, sometimes due to difficult access forwomen, physicians will induce or acceleratelabour upon their admission to the labour ward.Having recently been made a referral hospital,this hospital needs to train and retain its existingphysicians and attract new physicians who arehighly skilled to cope with the heavy burden ofhigh-risk cases, severe complications and surgi-cal deliveries. This requires political commitmentand awareness among decision-makers, and thetranslation of commitment into budgetary allo-cations and reform of the health system.20 In thePalestinian case, effective internal reform mustalso be accompanied by the end of occupationas a prerequisite to respect for the basic humanright of access to health care.
Caregiver and female relative support to pro-mote normal labour and birth is essential, par-ticularly in a culture that values family support.21

APA
LESTINIANMED
ICALRELIEFSO
CIETY
Palestinian mother’s voices, West Bank, OccupiedPalestinian Territories
S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
Alternative methods of pain relief22,23 have beenshown to be appreciated by women and toreduce interventions, and are particularly impor-tant in a context where epidurals are not avail-able. Oxytocin was used routinely to speed uplabour, in spite of the risks involved with itsuse in a situation where labour was not closelymonitored.24 The benefit of accelerating labouris in itself questionable, particularly where thenormal duration of labour in a study in anotherPalestinian hospital was shown to be relativelyshort.25 A rising trend in the caesarean sectionrate (particularly the primary rate) is a real con-cern for Palestinian women’s health, given thetendency to have large families.
Post-partum care for mothers and newbornswas extremely inadequate. Globally, more thanone half of all newborn deaths occur in the first24 hours after birth and integrated maternal andnewborn care is lifesaving.26 Although exclusivebreastfeeding for 4–6 months remains a chal-lenge, the high initiation of breastfeeding in thehospital was most likely due to the culture ofbreastfeeding rather than specific hospital prac-tices, as women received little support.
Like women all over the world, the Palestinianwomen interviewed wanted to be treated withrespect, sensitivity and equality.27 They werevery enthusiastic about being interviewed andhaving the opportunity to express their opinions.As one woman said, she hoped that when shecame back for her next birth, conditions wouldbe better as she had no other place to give birth.Women were not always treated with empathy andrespect, as the midwives themselves admitted.While such behaviour can be understood in rela-tion to shortage of staff, low status, poor salariesand the inherent stress of obstetrics, the diffi-cult relationship between women and hospitalmidwives and nurses is a multifaceted and uni-versal problem. Poor working conditions are onecause, but lack of communication, a judgmentalattitude and disregard for patients’ knowledgeand concerns are all too frequent componentsof the provider–patient relationship, leading todissatisfaction and lack of uptake of services.28
Such attitudes need to be continually addressedwith regard to the organisation of services, theaccountability of providers and institutions, mid-wifery role models, and an emphasis not only ontechnical competence in maternity care, but alsoon interpersonal relations.
The publication of a detailed report of thisassessment, along with several disseminationmeetings with providers, ward and hospitalmanagers, decision-makers at higher levels anddonors succeeded in attracting attention to thepoor conditions of normal childbirth and emer-gency obstetric care in the public sector. Theassessment helped to raise awareness amongmanagers and decision-makers of the need toallocate more financial support to this neglectedarea of women’s health care. Moreover, theintervention plan to improve the quality of careduring childbirth in this hospital as a pilot projectwas approved and will hopefully be extended toother public hospitals in the future. Carrying outthis assessment in an ongoing climate of crisiswas a reality check for all involved, demonstrat-ing that in spite of whatever may be goingon in the wider world, women continue to givebirth and to want kindness and good care for
111

S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
themselves and their newborns. And this is perhapswhere the opportunity for change needs to begin.
AcknowledgementsWe would like to thank the Theodor-SpringmannFoundation for funding this study, Dr Rita
112
References1. Miller S, Cordero M, Coleman A,
et al. Quality of care ininstitutionalized deliveries: theparadox of the DominicanRepublic. International Journalof Gynecology and Obstetrics2003;82:89–103.
2. Cochrane Database of SystematicReviews Library. At bwww3.interscience.wiley.com/cgi-bin/mrwhome/106568753/HOMEN.Accessed 17 March 2007.
3. World Health Organization.WHO Reproductive HealthLibrary. Geneva7 WHO, 2006.
4. Wrede S, Benoit C, Bourgeault I,et al. Decentred comparativeresearch: context sensitiveanalysis of maternal health care.Social Science and Medicine2006;63:2986–97.
5. UN News Service. Israeliobstacles to free movement inPalestinian territories mount.At: bwww.un.org/apps/news/printnewsAr.asp?nid=20234N.Accessed 19 March 2007.
6. Palestinian Central Bureau ofStatistics. Impact of the IsraeliMeasures on the EconomicConditions of PalestinianHouseholds. Ramallah7PCBS, 2006.
7. Palestinian Central Bureau ofStatistics. Demographic andHealth Survey 2004. FinalReport. Ramallah7 PCBS, 2006.
8. Giacaman R, Wick L,Abdul-Rahim H, et al. Thepolitics of childbirth in thecontext of conflict: policies orde facto practices? Health Policy2005;72:129–39.
9. Ministry of Health. HealthStatus in Palestine: AnnualReport 2004. Gaza7 MOH, 2005.
10. Maram Project.Assessment: Suand Child HealtServices in thethe Gaza Strip 2Maram Project,
11. Wick L, Mikkiet al. ChildbirthInternational JoGynecology and2005;89:174–78
12. World Health OMotherhood NeTools. Geneva7At: bwww.who.reproductive-hesmna_index.en.17 March 2007
13. Hulton L, MatthA Framework fof Quality of CaServices. SouthUniversity ofSouthampton, 2
14. Plsek P. CompleAdoption of InnHealth Care. WaNational InstituCare ManagemeFoundation, 20
15. Choices and ChChanging ChildNetwork. Routinfacility-based mevidence from tBJOG: InternatiObstetrics and G2005;112:1270–
16. Turan JM, Buluet al. Challengeadoption of evimaternity careScience and Me2006;62(9):2196
17. Garner P, MeremVolmink J, et a
Giacaman and Dr Rana Khatib for their con-tinuous support and Sheila Narrainen for herassistance in editing earlier drafts of this paper.We are grateful to all the women, midwives andother providers who shared their experienceswith us.
Baselinervey of Womenh and HealthWest Bank and003. Ramallah72004.N, Giacaman R,in Palestine.urnal ofObstetrics
.rganization. Safeeds AssessmentWHO, 1996.int/alth/MNBH/htmlN. Accessed.ews Z, Stones R.or Evaluationre in Maternityampton7
000.xity and theovation inshington DC7te for Healthnt03.allenges inbirth Researches inaternity care:he Arab world.onal Journal ofynaecology76.t A, Nalbant H,s for thedence-basedin Turkey. Socialdicine–204.ikwu M,
l. Putting
evidence into practice: howmiddle and low incomecountries ‘‘get it together’’. BMJ2004;329(7473):1036–39.
18. WHO/UNFPA/UNICEF/WorldBank. Pregnancy, Childbirth,Postpartum and Newborn Care:A Guide for Essential Practice.Geneva7 WHO, 2003.
19. Rosenblatt R, Dobie SA,Schneeweisser R, et al.Interspecialty differencesin the obstetric care oflow-risk women. AmericanJournal of Public Health1997;87:344–51.
20. World Health Organization.Quality of Care. A Process forMaking Strategic Choices inHealth Systems. Geneva7WHO, 2006.
21. Mosallem M, Rizq D, Thomas L,et al. Women’s attitudes towardspsychosocial support in labourin United Arab Emirates.Archives of Gynaecology andObstetrics 2004;269:181–87.
22. Declercq E, Sakala C, Corry M,et al. Listening to Mothers:Report of the First NationalUS Survey of Women’sChildbearing Experiences.NY7 Harris Interactive forthe Maternity CenterAssociation, 2002.
23. Abushaikha L. Methods ofcoping with labor pain used byJordanian women. Journal ofTranscultural Nursing2007;18:35–40.
24. Dujardin B, Boutsen M, DeSchampheleire I, et al. Oxytocicsin developing countries.International Journal ofGynecology and Obstetrics1995;50:243–51.

113
ResumeCette etude souhaitait evaluer la qualite dessoins obstetricaux dans un grand hopital publicpalestinien, pour preparer des interventionsdestinees a ameliorer la securite et la qualitedes soins obstetricaux. Des entretiens avec lepersonnel de sante, l’observation et des entretiensavec des femmes ont permis de cerner lesobstacles a l’amelioration des soins et de preparerles prestataires a etre receptifs au changement.L’interdiction des accompagnantes pendantl’accouchement, l’utilisation generalisee d’ocytocinepour accelerer le travail, la restriction de lamobilite de la parturiente et la frequence desexamens vaginaux figuraient au nombre despratiques impropres. Le sulfate de magnesiumn’etait pas utilise pour la pre-eclampsie ni pourl’eclampsie, et les hemorragies du post-partumetaient frequentes. Une grave penurie desages-femmes, la supervision insuffisante et lemanque de competences conduisaient a dessoins inadaptes. L’utilisation de pratiques abase factuelle qui encouragent le travailnormal est essentielle dans les milieux pauvresen ressources et ou les femmes ont de nombreuxenfants. Le rapport de cette evaluation et lesreunions avec les prestataires de soins, lesadministrateurs hospitaliers, les decideurs etles donateurs ont montre la realite a toutesles parties prenantes, et un plan d’interventionpour ameliorer la qualite des soins a eteapprouve. En depit du climat actuel de crise,et quels que soient les evenements qui lesentourent, les femmes continuent d’accoucheret de vouloir des soins de qualite, a l’ecoute desmeres et des nouveau-nes. C’est peut-etre laque doit commencer le changement.
ResumenEl proposito de este estudio fue evaluar la calidadde la atencion de maternidad en un importantehospital publico de referencia palestino, como elprimer paso para formular intervenciones a finde mejorar la seguridad y calidad de la atencionde maternidad. Se realizaron entrevistas conlos prestadores de servicios, observaciones yentrevistas con las mujeres para entender lasbarreras a una mejor atencion y preparar a losprestadores de servicios para estar abiertosal cambio. Algunas de las practicas indebidasencontradas fueron laprohibiciondeacompanantesdurante el parto, el uso rutinario de oxitocinapara acelerar el parto, la restriccion de movilidaddurante el parto y examenes vaginales frecuentes.No se utilizo el sulfato de magnesio parapreeclampsia o eclampsia, y la hemorragiaposparto fue una complicacion frecuente. La granescasez de parteras, supervision insuficiente yfalta de habilidades propiciaron una prestacionde atencion inadecuada. El uso de practicasbasadas en evidencia que promuevan el partonormal es fundamental en lugares donde escaseanlos recursos y las mujeres tienen familiasgrandes. El informe de esta evaluacion y lasreuniones de difusion con prestadores de servicios,administradores de hospitales, formuladores depolıticas y donantes fueron una revision de larealidad para todas las partes implicadas, y seaprobo el plan de intervencion para mejorar lacalidad de la atencion. Pese al clima continuode crisis y los demas factores implıcitos, lasmujeres continuan dando a luz y desean recibiruna atencion amable y de calidad para ellas y susrecien nacidos. He aquı donde debe comenzar laoportunidad para realizar cambios.
25. Mikki N, Wick L, Abu-Asab N,et al. Trial of amniotomy in aPalestinian hospital. Journal ofObstetrics and Gynecology2007;27(4):368–73.
26. Sines E, Syed U, Wall S, et al.Postnatal Care: A CriticalOpportunity to Save Mothers
and Newborns. Washington7Population ReferenceBureau, 2007.
27. Yelland J, Small R, Lumley J,et al. Support, sensitivity,satisfaction: Filipino, Turkishand Vietnamese women’sexperiences of postnatal
hospital stay. Midwifery1998;14(3):144–54.
28. Jewkes R, Abrahams N, Mvo Z.Why do nurses abuse patients?Reflections from South Africanobstetric services. SocialScience and Medicine 1998;47(11):1781–95.
S Hassan-Bitar, L Wick / Reproductive Health Matters 2007;15(30):103–113
Copyright © 2022 FDOKUMEN