European Initial Hands-On Experience with HEMOPATCH, a Novel Sealing Hemostatic Patch: Application...
7
European Initial Hands-On Experience with HEMOPATCH, a Novel Sealing Hemostatic Patch: Application in General, Gastrointestinal, Biliopancreatic, Cardiac, and Urologic Surgery ABE FINGERHUT, MD, DSC (HON), FACS, FRCPS (G), FRCS (ED) PROFESSOR SECTION FOR SURGICAL RESEARCH,DEPARTMENT OF SURGERY MEDICAL UNIVERSITY OF GRAZ GRAZ,AUSTRIA - 29 - Surgical Overview SURGICAL TECHNOLOGY INTERNATIONAL XXV SELMAN URANUES, MD, FACS PROFESSOR AND HEAD SECTION FOR SURGICAL RESEARCH CLINICAL DIVISION OF GENERAL SURGERY, DEPARTMENT OF SURGERY MEDICAL UNIVERSITY OF GRAZ GRAZ,AUSTRIA GIUSEPPE MARIA ETTORRE, MD PROFESSOR DEPARTMENT OF HPB SURGERY AND LIVER TRANSPLANTATION SAN CAMILLO HOSPITAL ROME,ITALY EMANUELE FELLI, MD SURGEON DEPARTMENT OF HPB SURGERY AND LIVER TRANSPLANTATION SAN CAMILLO HOSPITAL ROME,ITALY MARCO COLASANTI, MD SURGEON DEPARTMENT OF HPB SURGERY AND LIVER TRANSPLANTATION SAN CAMILLO HOSPITAL ROME,ITALY GREGORIO SCERRINO, MD, PHD SURGEON UNIT OF GENERAL AND EMERGENCY SURGERY, DEPARTMENT OF GENERAL,EMERGENCY AND TRANSPLANT SURGERY UNIVERSITY OF PALERMO,SCHOOL OF MEDICINE PALERMO,ITALY GIUSEPINA IRENE MELFA, MD SURGEON UNIT OF GENERAL AND EMERGENCY SURGERY, DEPARTMENT OF GENERAL, EMERGENCY AND TRANSPLANT SURGERY UNIVERSITY OF PALERMO,SCHOOL OF MEDICINE PALERMO,ITALY CRISTINA RASPANTI, MD SURGEON UNIT OF GENERAL AND EMERGENCY SURGERY, DEPARTMENT OF GENERAL,EMERGENCY AND TRANSPLANT SURGERY UNIVERSITY OF PALERMO,SCHOOL OF MEDICINE PALERMO,ITALY GASPARE GULOTTA, MD PROFESSOR,CHIEF OF DEPARTMENT. UNIT OF GENERAL AND EMERGENCY SURGERY, DEPARTMENT OF GENERAL, EMERGENCY AND TRANSPLANT SURGERY UNIVERSITY OF PALERMO, SCHOOL OF MEDICINE PALERMO,ITALY ALEXANDER MEYER,DR.MED HEAD OF DEPARTMENT DEPARTMENT OF VISCERAL AND VASCULAR SURGERY JOHANNITER HOSPITAL RHEINHAUSEN DUISBURG,GERMANY MARTIN OBERHOFFER, MD CONSULTANT DEPARTMENT OF CARDIAC SURGERY ASKLEPIOS HOSPITAL ST.GEORG HAMBURG,GERMANY MICHAEL SCHMOECKEL, MD, PHD PROFESSOR HEAD OF DEPARTMENT DEPARTMENT OF CARDIAC SURGERY ASKLEPIOS HOSPITAL ST.GEORG HAMBURG,GERMANY LUCA PAOLO WELTERT, MD SURGEON DEPARTMENT OF CARDIAC SURGERY EUROPEAN HOSPITAL ROME,ITALY GRAZIANO VIGNOLINI, MD SURGEON DEPARTMENT OF UROLOGY CAREGGI HOSPITAL,UNIVERSITY OF FLORENCE FLORENCE,ITALY MATTEO SALVI, MD SURGEON DEPARTMENT OF UROLOGY CAREGGI HOSPITAL,UNIVERSITY OF FLORENCE FLORENCE,ITALY LORENZO MASIERI, MD SURGEON DEPARTMENT OF UROLOGY CAREGGI HOSPITAL,UNIVERSITY OF FLORENCE FLORENCE,ITALY GUIDO VITTORI, MD SURGEON DEPARTMENT OF UROLOGY CAREGGI HOSPITAL,UNIVERSITY OF FLORENCE FLORENCE,ITALY GIAMPAOLO SIENA, MD SURGEON DEPARTMENT OF UROLOGY CAREGGI HOSPITAL,UNIVERSITY OF FLORENCE FLORENCE,ITALY ANDREA MINERVINI, MD SURGEON DEPARTMENT OF UROLOGY CAREGGI HOSPITAL,UNIVERSITY OF FLORENCE FLORENCE,ITALY SERGIO SERNI, MD SURGEON DEPARTMENT OF UROLOGY CAREGGI HOSPITAL,UNIVERSITY OF FLORENCE FLORENCE,ITALY MARCO CARINI, MD SURGEON DEPARTMENT OF UROLOGY CAREGGI HOSPITAL,UNIVERSITY OF FLORENCE FLORENCE,ITALY
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of European Initial Hands-On Experience with HEMOPATCH, a Novel Sealing Hemostatic Patch: Application...

European Initial Hands-On Experience withHEMOPATCH, a Novel Sealing Hemostatic Patch:
Application in General, Gastrointestinal,Biliopancreatic, Cardiac, and Urologic Surgery
ABE FINGERHUT, MD, DSC (HON), FACS, FRCPS (G), FRCS (ED)PROFESSOR
SECTION FOR SURGICAL RESEARCH, DEPARTMENT OF SURGERYMEDICAL UNIVERSITY OF GRAZ
GRAZ, AUSTRIA
- 29 -
#590 Fingerhut FINAL
Surgical OverviewSURGICAL TECHNOLOGY INTERNATIONAL XXV
SELMAN URANUES, MD, FACSPROFESSOR AND HEAD SECTION FOR SURGICAL
RESEARCHCLINICAL DIVISION OF GENERAL SURGERY,
DEPARTMENT OF SURGERYMEDICAL UNIVERSITY OF GRAZ
GRAZ, AUSTRIA
GIUSEPPE MARIA ETTORRE, MDPROFESSOR
DEPARTMENT OF HPB SURGERY AND LIVERTRANSPLANTATION
SAN CAMILLO HOSPITALROME, ITALY
EMANUELE FELLI, MDSURGEON
DEPARTMENT OF HPB SURGERY AND LIVERTRANSPLANTATION
SAN CAMILLO HOSPITALROME, ITALY
MARCO COLASANTI, MDSURGEON
DEPARTMENT OF HPB SURGERY AND LIVERTRANSPLANTATION
SAN CAMILLO HOSPITALROME, ITALY
GREGORIO SCERRINO, MD, PHDSURGEON
UNIT OF GENERAL AND EMERGENCY SURGERY,DEPARTMENT OF GENERAL, EMERGENCY AND
TRANSPLANT SURGERYUNIVERSITY OF PALERMO, SCHOOL OF
MEDICINEPALERMO, ITALY
GIUSEPINA IRENEMELFA, MDSURGEON
UNIT OF GENERAL AND EMERGENCY SURGERY,DEPARTMENT OF GENERAL,
EMERGENCY AND TRANSPLANT SURGERYUNIVERSITY OF PALERMO, SCHOOL OF
MEDICINEPALERMO, ITALY
CRISTINA RASPANTI, MDSURGEON
UNIT OF GENERAL AND EMERGENCY SURGERY,DEPARTMENT OF GENERAL, EMERGENCY AND
TRANSPLANT SURGERYUNIVERSITY OF PALERMO, SCHOOL OF
MEDICINEPALERMO, ITALY
GASPARE GULOTTA, MDPROFESSOR, CHIEF OF DEPARTMENT.
UNIT OF GENERAL ANDEMERGENCY SURGERY,
DEPARTMENT OF GENERAL,EMERGENCY AND TRANSPLANT SURGERY
UNIVERSITY OF PALERMO,SCHOOL OFMEDICINE
PALERMO, ITALY
ALEXANDERMEYER, DR.MEDHEAD OF DEPARTMENT
DEPARTMENT OF VISCERAL AND VASCULARSURGERY
JOHANNITER HOSPITAL RHEINHAUSENDUISBURG, GERMANY
MARTIN OBERHOFFER, MDCONSULTANT
DEPARTMENT OF CARDIAC SURGERYASKLEPIOS HOSPITAL ST. GEORG
HAMBURG, GERMANY
MICHAEL SCHMOECKEL, MD, PHDPROFESSOR
HEAD OF DEPARTMENTDEPARTMENT OF CARDIAC SURGERYASKLEPIOS HOSPITAL ST. GEORG
HAMBURG, GERMANY
LUCA PAOLOWELTERT, MDSURGEON
DEPARTMENT OF CARDIAC SURGERYEUROPEAN HOSPITAL
ROME, ITALY
GRAZIANO VIGNOLINI, MDSURGEON
DEPARTMENT OF UROLOGYCAREGGI HOSPITAL, UNIVERSITY OF FLORENCE
FLORENCE, ITALY
MATTEO SALVI, MDSURGEON
DEPARTMENT OF UROLOGYCAREGGI HOSPITAL, UNIVERSITY OF FLORENCE
FLORENCE, ITALY
LORENZOMASIERI, MDSURGEON
DEPARTMENT OF UROLOGYCAREGGI HOSPITAL, UNIVERSITY OF FLORENCE
FLORENCE, ITALY
GUIDO VITTORI, MDSURGEON
DEPARTMENT OF UROLOGYCAREGGI HOSPITAL, UNIVERSITY OF FLORENCE
FLORENCE, ITALY
GIAMPAOLO SIENA, MDSURGEON
DEPARTMENT OF UROLOGYCAREGGI HOSPITAL, UNIVERSITY OF FLORENCE
FLORENCE, ITALY
ANDREAMINERVINI, MDSURGEON
DEPARTMENT OF UROLOGYCAREGGI HOSPITAL, UNIVERSITY OF FLORENCE
FLORENCE, ITALY
SERGIO SERNI, MDSURGEON
DEPARTMENT OF UROLOGYCAREGGI HOSPITAL, UNIVERSITY OF FLORENCE
FLORENCE, ITALY
MARCO CARINI, MDSURGEON
DEPARTMENT OF UROLOGYCAREGGI HOSPITAL, UNIVERSITY OF FLORENCE
FLORENCE, ITALY

- 30 -
#590 Fingerhut FINAL
European initial hands-on experience with HEMOPATCH, a novel sealing hemostatic patch: Application in general, gastrointestinal, biliopancreatic, car-diac and urologic surgeryFINGERHUT/URANUES/ETTORRE/FELLI/COLASANTI/SCERRINO/MELFA/RASPANTI/GULOTTA/MEYER/OBERHOFFER /SCHMOECKEL/WELTERT/VIGNOLINI/SALVI/MASIERI/VITTORI/SIENA/MINERVINI/SERNI/CARINI
INTRODUCTION
TTopical hemostatic agents that can seal tissues and assist in the coagulation cascade of patients undergo-
ing surgery have been readily available for several decades. Using either synthetic or animal/plant-
derived materials, these agents represent a powerful tool to reduce postoperative bleeding
complications in cases where mechanical or energy-driven hemostasis is not possible or insufficient.
Recently, a novel sealing hemostatic patch, HEMOPATCH (Baxter International, Deerfield, IL), was
developed. The device is a thin and flexible patch consisting of a specifically-formulated porous collagen
matrix, coated on one side with a thin protein-binding layer. This gives the patch a dual mechanism of action,
in which the two components interact to achieve hemostasis by sealing off the bleeding surface and initiating
the body’s own clotting mechanisms.
Here we present a series of case reports that outline the quick, effective hemostatic sealing of HEMOPATCH
in a variety of clinical applications, including solid organ, gastrointestinal, biliopancreatic, endocrine,
cardiovascular, and urologic surgeries.
Essentially a feasibility study, these reports demonstrate how HEMOPATCH can be applied to seal almost any
bleeding surface encountered during a range of procedures. Our results show that the device is eminently
capable in both via laparotomy and laparoscopic approaches, and in patients with impaired coagulation or
highly variable anatomies.
In conclusion, our cases document the ease-of-use, application, and immediate hemostatic effect of the patch
across a broad range of surgical settings and paves the way for future randomized clinical trials with more
extensive follow-up.
ABSTRACT
The use of topical agents to seal tis-sues or intervene in the coagulation cas-cade of patients undergoing surgery havebeen used widely in Europe since the1970s.1 The active agents are either syn-thetic or derived from animals or plants.Synthetic agents are better for sealingbut do not intervene in the coagulationcascade.2,3 In contrast, collagen-basedsealants are pro-coagulants, triggeringor accelerating the cascade, but are notsuited for tissue fixation.4 The use oftopical agents to promote these twoactions has given rise to a large numberof experimental and clinical publica-tions. However, the results in these pub-lications have been somewhat
contradictory.5-8Nevertheless, hemostatic agents are
useful agents for reducing postoperativebleeding complications, particularly inspecific areas such as sutures lines,whether anastomotic or not, and theyare especially helpful when these sitesare difficult to access.3 The majority ofrecent evaluations of such agents havefocused on the effect of these agents onthe requirement for blood transfusion.9A novel sealing hemostatic patch,
HEMOPATCH, recently became avail-able. This hemostatic adjunct is a soft,thin, and flexible patch consisting of aporous collagen matrix, which facilitatesclotting, coated on one side with a thinprotein-binding layer known as pen-taerythritol polyethylene glycol ethertetra-succinimidyl glutarate (NHS-
PEG). This coating allows rapid adhe-sion (within two minutes) to lesions viaelectrophilic crosslinking. The patchconsequently has a dual-method mecha-nism of action, in which the two compo-nents interact to achieve hemostasis bysealing off the bleeding surface and initi-ating the body’s own clotting mecha-nisms (Fig. 1). The patch, which issuitable for surgery via laparotomy or aminimal access route, is resorbed intothe body within six to eight weeks.Significant preclinical testing has been
conducted to confirm the hemostaticperformance, biocompatibility and safetyprofile of the patch.4,10,11 Furthermore,feasibility and reliability of applicationwas demonstrated in a preliminary studyof seven patients with confirmed renalmasses undergoing zero-ischemia laparo-

- 31 -
scopic partial nephrectomy.12 In allpatients, the patch was applied to thetumor resection site after suturing of therenal parenchyma, perfecting hemostasisand fixation within two to three minutes.For the current case series, we gath-
ered a series of 17 individual proceduralreports in which the sealing hemostaticpatch was used as an adjunctive hemosta-tic procedure. The cases cover severalsurgical specialties (in some circum-stances, more than one per case), fallingbroadly into the following categories:
�Solid organ: One partial splenic resec-tion, two sectionectomies, one resec-tion for metastases, one for liverabrasion, and one liver trauma
�Gastrointestinal: Two cases of colonicand rectal anastomoses
�Bilio-pancreatic: Two cholecystec-tomies—one for acute cholecysti-tis—and four pancreatic resections,including two Whipple proceduresand two distal pancreatectomies
�Endocrine: One total thyroidectomy�Cardiovascular: Bleeding from onebypass suture line and tissues after dis-section of epicardial fat, one from anaortocoronary bypass at the anasto-mosis of the saphenous vein to theright coronary artery, and one distalsuture-line of an aortic prosthesiscombined with an aortic valve andascending aorta replacement (Wheatprocedure)
�Urological: one partial nephrectomy,one robotic-assisted kidney tumorresection, and one robotic-assistednerve-sparing prostatectomy
Among these, there were severallaparoscopic applications, including twocholecystectomies, a distal pancreatecto-my, a partial splenectomy, a partialnephrectomy, a nerve-sparing prostatec-tomy, and a kidney tumor enucleation(the last two of these also being robotic-assisted procedures).
Selected Case Details
Liver resectionA 63-year-old obese (body mass
index [BMI]=31), hypertensive manwith hepatitis B virus-related liver cir-rhosis (Child-Pugh class A) presentedwith a 5 cm hepatocellular carcinoma.An open 6–7-segment sectionectomywas performed. The liver parenchymal
#590 Fingerhut FINAL
Surgical OverviewSURGICAL TECHNOLOGY INTERNATIONAL XXV
Figure 1. Mechanism of action of the sealing hemostatic patch.
SELECTED CASE DETAILS

- 32 -
division border was sealed off withHEMOPATCH after elective, tradition-al, but incomplete, hemostasis and bil-iostasis (Fig. 2). As shown in the figure,the sealing hemostatic patch achievedgood adherence to the heavily electro-coagulated liver surface. Importantly,the patch stopped the residual oozingfrom the electrocoagulated area. Totalblood loss was 200 cc without any needfor transfusion. Similarly, in another case example of
segment 6–7 sectionectomy, performedon a 31-year-old female with a 7 cmadenoma, HEMOPATCH was used tocomplete hemostasis of the liver surfacewith satisfactory outcome.
Bilio-pancreatic surgeryIn one case, a 54-year-old man with
diabetes and chronic pancreatitis under-went a Whipple procedure.HEMOPATCH was used to preventbleeding following difficult and intra-adventitial dissection of the major ves-sels (portal vein, superior mesentericartery, and vein). As such, no postoper-ative complications were observed.Use of HEMOPATCH in distal pan-
createctomy involved two patients. Thefirst, who underwent laparoscopy, was a49-year-old female with a pancreatictumor, and the second was a 60-year-old woman with pancreatic tail metasta-sis originating from kidney carcinoma.
HEMOPATCH was applied to the prox-imal stump (Fig. 3), and no postopera-tive bleeding or pancreatic fistula wereobserved in either case.
GallbladderTwo patients (one taking antiplatelet
treatment) undergoing laparoscopiccholecystectomy for acute cholecystitishad diffuse bleeding from the liver bedat the end of the procedure.HEMOPATCH was easily inser tedthrough one of the 10 mm trocars,deployed, and applied to the liver bedcorrectly without difficulty. Bothpatients had an uneventful post-opera-tive recovery.
#590 Fingerhut FINAL
European Initial Hands-On Experience with HEMOPATCH, a Novel Sealing Hemostatic Patch: Application in General, Gastrointestinal, Biliopancreatic,Cardiac, and Urologic SurgeryFINGERHUT/URANUES/ETTORRE/FELLI/COLASANTI/SCERRINO/MELFA/RASPANTI/GULOTTA/MEYER/OBERHOFFER /SCHMOECKEL/WELTERT/VIGNOLINI/SALVI/MASIERI/VITTORI/SIENA/MINERVINI/SERNI/CARINI
Figure 2. Placement (left) and subsequent sealing and hemostasis (right) of theliver surface using HEMOPATCH.
Figure 3. Application of HEMOPATCH (outlined) to the transection line on thepancreatic stump.
Figure 4a. Active bleeding following laparoscopic stapled transection of thelower splenic pole.
Figure 4b. HEMOPATCH hemostatic patches were used to seal the wound andprevent further bleeding.
- 33 -
Spleen A 64-year-old woman presented with
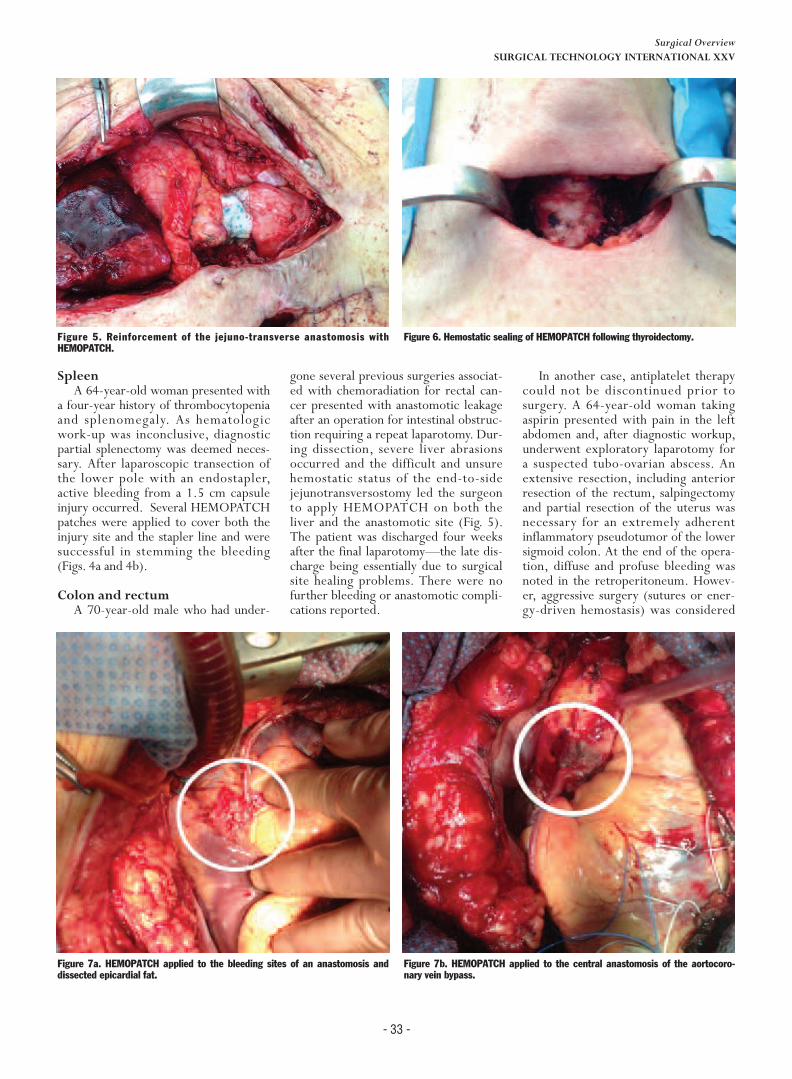
a four-year history of thrombocytopeniaand splenomegaly. As hematologicwork-up was inconclusive, diagnosticpartial splenectomy was deemed neces-sary. After laparoscopic transection ofthe lower pole with an endostapler,active bleeding from a 1.5 cm capsuleinjury occurred. Several HEMOPATCHpatches were applied to cover both theinjury site and the stapler line and weresuccessful in stemming the bleeding(Figs. 4a and 4b).
Colon and rectumA 70-year-old male who had under-
gone several previous surgeries associat-ed with chemoradiation for rectal can-cer presented with anastomotic leakageafter an operation for intestinal obstruc-tion requiring a repeat laparotomy. Dur-ing dissection, severe liver abrasionsoccurred and the difficult and unsurehemostatic status of the end-to-sidejejunotransversostomy led the surgeonto apply HEMOPATCH on both theliver and the anastomotic site (Fig. 5).The patient was discharged four weeksafter the final laparotomy—the late dis-charge being essentially due to surgicalsite healing problems. There were nofurther bleeding or anastomotic compli-cations reported.
In another case, antiplatelet therapycould not be discontinued prior tosurgery. A 64-year-old woman takingaspirin presented with pain in the leftabdomen and, after diagnostic workup,underwent exploratory laparotomy fora suspected tubo-ovarian abscess. Anextensive resection, including anteriorresection of the rectum, salpingectomyand partial resection of the uterus wasnecessary for an extremely adherentinflammatory pseudotumor of the lowersigmoid colon. At the end of the opera-tion, diffuse and profuse bleeding wasnoted in the retroperitoneum. Howev-er, aggressive surgery (sutures or ener-gy-driven hemostasis) was considered
#590 Fingerhut FINAL
Surgical OverviewSURGICAL TECHNOLOGY INTERNATIONAL XXV
Figure 5. Reinforcement of the jejuno-transverse anastomosis withHEMOPATCH.
Figure 6. Hemostatic sealing of HEMOPATCH following thyroidectomy.
Figure 7a. HEMOPATCH applied to the bleeding sites of an anastomosis anddissected epicardial fat.
Figure 7b. HEMOPATCH applied to the central anastomosis of the aortocoro-nary vein bypass.

- 34 -
potentially dangerous for the ureter. AHEMOPATCH was applied to thebleeding area and successfully stoppedthe bleeding without endangering theureter.
Thyroid A 71-year-old man presented with
progressive enlargement of the infrahy-oid neck, which had been developingover the past 10 years. Workup docu-mented two nodules, one hypoechoic,the other semi-liquid. Preoperativefine-needle aspiration led to suspicionof follicular carcinoma. A total bilateral
extracapsular thyroidectomy was there-fore performed through a typicalKocher incision. At the end of theoperation, diffuse bleeding was notedaround the left recurrent laryngealnerve. To avoid damaging the nerve with
energy-driven hemostasis or suture, aHEMOPATCH was inserted along thenerve in the bleeding area, and alsocontralaterally as a preventive measure.After confirmation of effective hemo-stasis (Fig. 6), sustained even after theValsalva maneuver, the incision wasclosed without drainage. The patient
was discharged on the second post-operative day, without any untowardevent or concern as to compressivehematoma or nerve palsy. One monthlater, neither hypocalcemia nor aero-digestive symptoms were observed.
ProstateA 65-year-old male underwent
robot-assisted radical nerve sparingprostatectomy for biopsy-confirmedadenocarcinoma. To control mild post-operative oozing in the operative field,HEMOPATCH was easily inser tedthrough a 10 mm trocar, deployed,placed, and applied without any intra-operative incident along the vascularand neural bundles. One month post-operatively, the patient had normalbladder and erectile function.
CardiacSeveral cases of postoperative
bleeding related to cardiovascularsurgery are included. The first twofocus on coronary artery bypass grafts(CABG) and involved epicardial bleedsarising from the bypass suture line andtissues after dissection of epicardial fat(Fig. 7a), and bleeding from the CABGanastomosis—saphenous vein to theright of the coronary artery (Fig. 7b).In the aorta, the sealing hemostatic
patch was used to reinforce the suture-line to prevent suture-line bleedingfrom a distal aortic prosthesis. Ourcase involved combined aortic valveand ascending aor ta replacement,known as the Wheat procedure(Fig. 8).Another case is particularly illustra-
tive. This 65-year-old, otherwise
#590 Fingerhut FINAL
European Initial Hands-On Experience with HEMOPATCH, a Novel Sealing Hemostatic Patch: Application in General, Gastrointestinal, Biliopancreatic,Cardiac, and Urologic SurgeryFINGERHUT/URANUES/ETTORRE/FELLI/COLASANTI/SCERRINO/MELFA/RASPANTI/GULOTTA/MEYER/OBERHOFFER /SCHMOECKEL/WELTERT/VIGNOLINI/SALVI/MASIERI/VITTORI/SIENA/MINERVINI/SERNI/CARINI
Figure 8. HEMOPATCH placed on the distal suture line after combined replace-ment of the ascending aorta and aortic valve.
Figure 9. Application of band-shaped HEMOPATCH hemostatic patch on graft-to-aorta suture line.
Figure 10. HEMOPATCH placed at the site of the ventricular pacing wires.

healthy, man was admitted to hospitalfor symptomatic aortic valve stenosisand underwent aortic valve replace-ment by implantation of a 23 mm sizeTrifecta™ valve (St. Jude Medical, SaintPaul, Minnesota). At the end of theoperation, diffuse bleeding at the levelof the aortic sutures—persisting afterthe administration of protamine sul-phate and infusion of tranexamicacid—led the surgeon to applyHEMOPATCH, which successfullystopped the bleeding without recourseto surgery. The physical characteristicsof the patch allowed for easy cuttingand shaping to match the geometry ofthe bleeding area (Fig. 9). Postopera-tively, a total of 260 ml was collectedin 24 hours and blood parameters weresatisfactory. No blood transfusion wasnecessary during hospitalization.Finally, HEMOPATCH was used to
prevent bleeding from a ventricularpacing wire in a redo case. By the endof the off-pump CABG procedures, thesternal wires were in place and aHEMOPATCH was easily placed at thesite of the ventricular pacing wires(Fig. 10), an otherwise difficult area toaccess for traditional hemostatic proce-dures.
Discussion
This case series demonstrates theease and rapidity with which the seal-ing hemostatic patch can be applied toalmost any type of bleeding surface,and how equally easy it is to apply vialaparotomy or laparoscopy. These find-ings complement those of the threeexperimental comparative studies onthe patch,4,10,11 as well as the recentlypublished preliminary clinical investi-gation.12Through these procedures, we were
able to show that the patch was effec-tive in several different scenarios.Moreover, the surgeon was able to useit preventively, such as for incompleteor unsatisfactory mechanical or ener-gy-dr iven hemostasis, or in areas
where mechanical or energy-drivenhemostasis would have been dangerousor difficult, essentially due to issues ofaccess. There are a number of limitations to
the current series. These include thelack of controls, the highly selectivenature of the inclusion process, theincomplete medium and long-term fol-low-up for some patients, and theselective use of the patch based on theindividual surgeon’s preferences. Con-sequently, the external validity of thissummary is limited, and generaliza-tions for clinical practice cannot yet bemade.Nonetheless, the findings underline
the facil ity of application and theimmediate hemostatic effect of thepatch. In laparoscopic surgery, it is easyto inser t through a 10 mm trocar,without deformation, flaking or losingany of its active components.12 Thepatch does not require any particularpreparation before application. Thanksto its rapid and firm tissue adherence,inadvertent dislodging is avoidable, andhemostasis can be obtained on verticalstructures, without dropping off due togravity and, finally, its flexibility allowsfirm application to a variety of round-ed or uneven (spleen, kidney, colonic,liver, and vascular) surfaces.
Conclusion
In conclusion, the sealing hemostaticpatch, as shown in these cases, is apromising, valuable addition to therange of available topical hemostaticagents, and is recommended for furtherinvestigation.
Acknowledgement
Editorial support for this manuscriptwas provided by Medicalwriters.com(Zurich, Switzerland). Editorial sup-port was funded by Baxter HealthcareSA.
Conflict of Interest
Professor Fingerhut has receivedpayments from Baxter Healthcare SAfor consulting services. Dr Oberhofferis a speaker for Baxter Healthcare, St.Jude Medical, and Smith & Nephew.
References
1. Martinowitz U, Saltz R. Fibrin sealant. CurrOpin Hematol 1996;3(5):395–402.2. Wallace DG, Cruise GM, Rhee WM, et al.A tissue sealant based on reactive multifunc-tional polyethylene glycol. J Biomed MaterRes B Appl Biomater 2001;58(5):545–55.3. Lodi D, Iannitti T, Palmieri B. Managementof haemostasis in surgery: sealant and glueapplications. Blood Coagul Fibrinolysis2012;23(6):465–72.4. Lewis KM, Spazierer D, Slezak P, et al.Swelling, sealing, and hemostatic ability of anovel biomaterial: A polyethylene glycol-coat-ed collagen pad. J Biomater Appl. 2014;29(5):780–8.5. Orci LA, Oldani G, Berney T, et al. Sys-tematic review and meta-analysis of fibrinsealants for patients undergoing pancreaticresection. HPB 2014;16(1):3–11.6. Fingerhut A, Veyrie N, Ata T, et al. Use ofsealants in pancreatic surgery: critical appraisalof the literature. Digestive Surgery2009;26(1):7–14.7. Aubourg R, Putzolu J, Bouche S, et al. Sur-gical hemostatic agents: assessment of drugsand medical devices. J Visc Surg 2011;148(6):e405–8.8. Uraneus S, Fingerhut A. Splenic Injuries. In:Oestern H, Trentz O, Uranues S, editors.European Manual of Medicine: Head, Tho-racic, Abdominal, and Vascular Injuries.Berlin: Springer; 2011. p. 285–96.9. Carless PA, Anthony DM, Henry DA. Sys-tematic review of the use of fibrin sealant tominimize perioperative allogeneic blood trans-fusion. Br J Surg 2002;89(6):695–703.10.Lewis KM, McKee J, Schiviz A, et al. Ran-domized, controlled comparison of advancedhemostatic pads in hepatic surgical models.ISRN Surg 2014;2014:930803.11.Lewis KM, Schiviz A, Hedrich HC, et al.Hemostatic efficacy of a novel, PEG-coatedcollagen pad in clinically relevant animal mod-els. Int J Surg 2014;12(9):940–4.12.Imkamp F, Tolkach Y, Wolters M, et al.Initial experiences with the HEMOPATCH asa hemostatic agent in zero-ischemia partialnephrectomy. World J Urol 2014.
- 35 -
#590 Fingerhut FINAL
Surgical OverviewSURGICAL TECHNOLOGY INTERNATIONAL XXV
REFERENCES
STI
CONCLUSION
DISCUSSION
ACKNOWLEDGEMENTS
AUTHORS’ DISCLOSURES