Estimating the health benefits and costs associated with ezetimibe coadministered with statin...
16
Clinical Therapeutics/Volume 30, Number 8, 2008 Estimating the Health Benefits and Costs Associated with Ezetimibe Coadministered with Statin Therapy Compared with Higher Dose Statin Monotherapy in Patients with Established Cardiovascular Disease: Results of a Markov Model for UK Costs Using Data Registries Roberta Ara, MScl; Abdullah Pandor, MScl; Indra Tumur, MScl; Suzy Paisley, MA1; Alejandra Duenas, PhD1; Robert Williams, BScl; Anna Wilkinson, MA1; Paul Durrington, MD2; and Jim Chilcott, MSc 1 1Health Economics and Decision Science, School of Health and Related Research, University of Sheffield, Sheffield, United Kingdom; and 2Cardiovascular Research Group, Core Technology Facility, Manchester, United Kingdom ABSTRACT Background: Ezetimibe has been reported to im- prove lipid control in patients with established cardio- vascular disease (CVD). Objective: The aim of this study was to estimate the potential long-term impact on health status of pre- scribing ezetimibe in combination with statin therapy in patients with established CVD and evaluate its cost- effectiveness in a health economic model. Methods: A Markov model was used to compare ezetimibe and statin combination therapy with statin monotherapy. A published relationship linking chang- es in low-density lipoprotein cholesterol and cardio- vascular events was used to estimate the cardiovascu- lar events avoided through lipid-lowering therapies. The model was populated using results of extensive literature searches and a meta-analysis of clinical evi- dence. An adjustment was applied to model second- line lipid-lowering benefits. Conservative assumptions were used to extend the patient pathway beyond the clinical evidence. The analysis took the perspective of the UK Department of Health; therefore, only direct costs were included. Costs were calculated as year- 2006 British pounds. Results: For a cohort of 1000 hypothetical male patients aged 55 years, ezetimibe coadministered with current statin therapy was estimated to prevent a mean of 43 nonfatal myocardial infarctions, 7 nonfatal strokes, and 26 cardiovascular deaths over a lifetime, com- pared with doubling the current statin dose. The events avoided would provide a mean of 134 additional quality-adjusted life-years (QALYs). With a mean in- cremental cost of £3,693,000, the lifetime discounted cost per QALY gained would be £27,475 (95% CI, £27,331-£27,620) and would rise to £32,000 for men aged 75 years. Conclusions: The results suggest that, in some in- stances, ezetimibe coadministration may be cost-effective compared with statin monotherapy, but there are sev- eral limitations with this model. The economic effects of ezetimibe must be revisited when long-term effec- tiveness and safety data become available. (Clin Ther. 2008;30:1508-1523) © 2008 Excerpta Medica Inc. Key words: cost, cost-effectiveness, ezetimibe, statin, cardiovascular disease. INTRODUCTION Serum cholesterol makes an important contribution to the development of atherosclerosis and is an impor- tant determinant of cardiovascular risk. It has been estimated that high cholesterol (hypercholesterolemia) causes 18% of global cerebrovascular disease and 56% of global ischemic heart disease. 1 The British Heart Foundation s and the National Heart Forum 3 suggest that about 46% of premature coronary deaths among those aged <75 years in the United Kingdom Accepted fiorpubfication June 26, 2008. doi:l 0.1016/j.clinthera.2008.08.002 0149-2918/$32.00 © 2008 Excerpta Medica Inc. All rights reserved. 1508 Volume 30 Number8
Transcript of Estimating the health benefits and costs associated with ezetimibe coadministered with statin...

Clinical Therapeutics/Volume 30, Number 8, 2008
Estimating the Health Benefits and Costs Associated with Ezetimibe Coadministered with Statin Therapy Compared with Higher Dose Statin Monotherapy in Patients with Established Cardiovascular Disease: Results of a Markov Model for UK Costs Using Data Registries
Roberta Ara , MSc l ; Abdullah Pandor, MScl; Indra Tumur, MScl ; S u z y Paisley, MA1;
Alejandra Duenas, PhD1; Robert Williams, BScl; Anna Wilkinson, MA1; Paul Durrington, MD2; and Jim Chilcott, MSc 1
1Health Economics and Decision Science, School of Health and Related Research, University of Sheffield, Sheffield, United Kingdom; and 2Cardiovascular Research Group, Core Technology Facility, Manchester, United Kingdom
ABSTRACT Background: Ezetimibe has been reported to im-
prove lipid control in patients with established cardio- vascular disease (CVD).
Objective: The aim of this study was to estimate the potential long-term impact on health status of pre- scribing ezetimibe in combination with statin therapy in patients with established CVD and evaluate its cost- effectiveness in a health economic model.
Methods: A Markov model was used to compare ezetimibe and statin combination therapy with statin monotherapy. A published relationship linking chang- es in low-density lipoprotein cholesterol and cardio- vascular events was used to estimate the cardiovascu- lar events avoided through lipid-lowering therapies. The model was populated using results of extensive literature searches and a meta-analysis of clinical evi- dence. An adjustment was applied to model second- line lipid-lowering benefits. Conservative assumptions were used to extend the patient pathway beyond the clinical evidence. The analysis took the perspective of the UK Department of Health; therefore, only direct costs were included. Costs were calculated as year- 2006 British pounds.
Results: For a cohort of 1000 hypothetical male patients aged 55 years, ezetimibe coadministered with current statin therapy was estimated to prevent a mean of 43 nonfatal myocardial infarctions, 7 nonfatal strokes, and 26 cardiovascular deaths over a lifetime, com- pared with doubling the current statin dose. The events avoided would provide a mean of 134 additional
quality-adjusted life-years (QALYs). With a mean in- cremental cost of £3,693,000, the lifetime discounted cost per QALY gained would be £27,475 (95% CI, £27,331-£27,620) and would rise to £32,000 for men aged 75 years.
Conclusions: The results suggest that, in some in- stances, ezetimibe coadministration may be cost-effective compared with statin monotherapy, but there are sev- eral limitations with this model. The economic effects of ezetimibe must be revisited when long-term effec- tiveness and safety data become available. (Clin Ther. 2008;30:1508-1523) © 2008 Excerpta Medica Inc.
Key words: cost, cost-effectiveness, ezetimibe, statin, cardiovascular disease.
INTRODUCTION Serum cholesterol makes an important contribution to the development of atherosclerosis and is an impor- tant determinant of cardiovascular risk. It has been estimated that high cholesterol (hypercholesterolemia) causes 18% of global cerebrovascular disease and 56% of global ischemic heart disease. 1 The British Heart Foundation s and the National Heart Forum 3 suggest that about 46% of premature coronary deaths among those aged <75 years in the United Kingdom
Accepted fior pubfication June 26, 2008. doi:l 0.1016/j.clinthera.2008.08.002 0149-2918/$32.00
© 2008 Excerpta Medica Inc. All rights reserved.
1508 Volume 30 Number 8

R. Ara et al.
are attributable to raised serum cholesterol. The UK population also has one of the highest mean serum cholesterol levels in the world, with -70% of the population with levels >5.0 mmol/L. 4
Hypercholesterolemia is the largest modifiable risk factor for coronary heart disease (CHD). e,3 Lifestyle factors, including diet, obesity, smoking, and lack of physical activity, are important in the prevention of CHD, but in many cases, pharmaceutical lipid- regulating interventions are also required. Statins in- hibit the hepatic synthesis of cholesterol and are the recommended first-line pharmaceutical approach.5 Com- bination treatment may be an option for patients whose cholesterol levels are not adequately reduced with the maximum tolerated or highest licensed statin dose.
Ezetimibe is a comparatively new cholesterol- lowering drug that inhibits the intestinal absorption of dietary and biliary cholesterol and of plant sterols. Although the evidence base is limited, some short- term clinical data suggest that the combination of ezetimibe and statin therapy may provide an addi- tional low-density lipoprotein cholesterol (LDL-C) reduction compared with statin monotherapy. Long- term clinical data demonstrating a reduction in car- diovascular risk corresponding to the observed ezetimibe-induced cholesterol reduction are awaited. However, based on the evidence currently available, ezetimibe coadministered with a statin is approved for use in the European Union as an adjunct therapy to diet for primary hypercholesterolemia in patients whose cholesterol levels are not sufficiently controlled with a statin alone. 6
In 2003, when ezetimibe became available in Eng- land and Wales, 3854 patients received prescrip- tions for the drug. 7 In 2004, the number had risen to 24,651 patients; an additional 32,309 patients re- ceived ezetimibe in 2005, representing a year-over- year growth rate of 55%. 8,9 The 740,000 prescriptions dispensed in 2005 represented a cost of approximately £26 million 8,9 to the National Health Service in Eng- land and Wales. Based on the limited number of eco- nomic evaluations of ezetimibe, the cost-effectiveness of this treatment in the United Kingdom is open to question. This paper describes an economic evaluation commissioned by the National Institute for Clinical Excellence (NICE) to inform the recent appraisal of ezetimibe for the treatment of primary hypercholester- olemia in the United Kingdom. 1° The aim of this study was to estimate the potential long-term impact on
health status of prescribing ezetimibe in combination with statin therapy in patients with established cardio- vascular disease (CVD) and evaluate its cost-effectiveness in a health economic model.
M ETHODS Overview
We adapted an existing CVD model reported in 20075 to estimate the potential costs and health out- comes associated with ezetimibe coadministered with statin therapy compared with statin monotherapy in patients whose cholesterol levels are not appropriately controlled with a statin alone. The model (constructed in Microsoft Excel 2003) synthesizes the best available evidence on the costs and consequences resulting from the use of ezetimibe combination therapy. The result of a meta-analysis of clinical evidence 1° was used to populate the model, supported by published evidence from extensive literature searches. An adjustment was applied to model second-line lipid-lowering benefits in patients who do not experience adequate lipid control on maximum tolerated statin doses. The relative risks of events were estimated using a published relationship linking changes in LDL-C and CVD events.ll Transi- tions to subsequent events were derived from UK reg- istries; health-state costs and quality-of-life data were obtained from published literature. The uncertainty in input parameters was characterized by probability distributions, and Monte Carlo simulations were used to replicate this uncertainty in the results. Conservative assumptions were employed to extend the patient pathway beyond the clinical evidence. A more detailed description is provided in the following section.
Comparison of Treatment Regimens UK guidelines for statin treatment recommend ini-
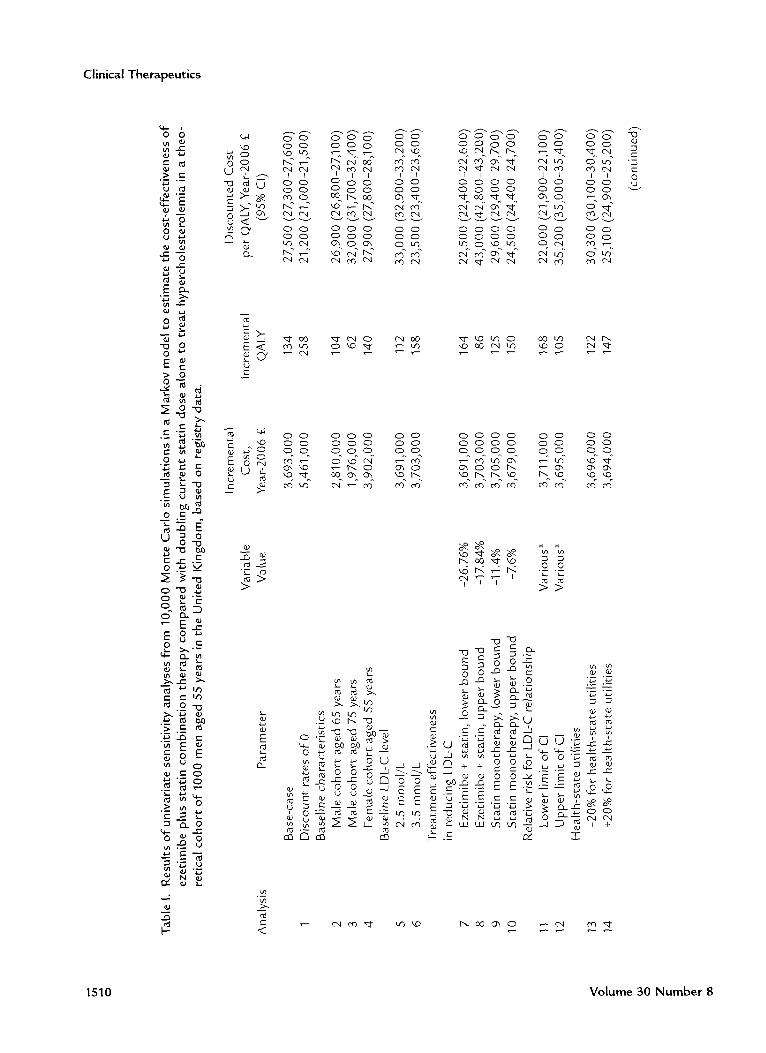
tial therapy with a drug that has a low acquisition cost (taking into account required daily dose and product price per dose). 5 Prescribing data suggest this recommendation is generally followed, with almost 50% of patient-days of statin treatment in England being provided with generic simvastatin, le If ezeti- mibe is to be added to the maximum tolerated statin dose, there are several possible treatment regimens. We report in detail the costs and benefits associated with ezetimibe coadministered with currently pre- scribed statin versus currently prescribed statin titrated by 1 dose increment. Results for several other treat- ment comparisons are summarized in Table I.
August 2008 1509
Clinical Therapeut ics
q _
0 8 ¢,1 ,~ "-- ~1 > ~-
E c,-
"13 0 0
> 0
m
NN~ " ~ I:m
~ e- ._~ 0 . N
o " ~ ~ o 2 " r -
" - E ~
,z ~7.,
e- e- ~
-~ ~- ~
N u o
> m 0
"4-- ~"
°-g8 ~ E - ~
-.2" ~J
O 0 0 0 0 O 0 ~ o ~ ~ % ~ .
O 0 O 0 O 0
~-~ ~ ~ . ~ o o o o o o o
$ °
I I I I I I 0 0 0 0 O 0 0 0 0 0 O 0
4~
E < 2 ( : 7 c -
- '~ ~4
k,O c- ~ o o 0 c-4
L3
O 0 0 0 0 O 0 O 0 0 0 0 O 0 O 0 0 0 0 O 0
0 0 0 0 O 0 O 0 0 0 0 0 O 0 O 0 % ~ o o o o o
~ 0 0 ~ ~ ~
02
c o ~
>
~ ~ . 2 . 2
E
co
~ co
. _ kO ~-, "~D ~ 3 >t. >,t.
~j
" 4 4 ~ - ~ ~ ~ 0 0 ,, ~: ~
~ ~ - ~ a E ~ . _ ~ , ~ ~ . . . . . . . . ~ , ~ _ ~ _
~ S ~ ~ ~ - ~ ~ ~ ~ co.~ ~_~
co c- <
0 0 " ~
o.4 "~
c~ o4 c - f f 0
cO c',l
~'3 £',1
co co
r-" c-"
~o~
o o ~,+
m
1510 V o l u m e 30 N u m b e r 8

R. Ara et al.
~q
kO ~ o 0 0
U
• 2 0 ' n ~.
G . _
O
o4 I
O O
0 0 o4
o4
0 Oh
c'~ I
0 0 ',,0
cO t 'C o4
0 0 0 0 0 0 0 0 0 0 c~ u') u') ',,0 CO CO u') o ~" ~
I I I I I I ~ - CY~ ~ ' 3 ~
I I I
o ~ ~ ~ ~ ~ ~ o o o
o o o o o o o o o o o o o o o o o o o o c-,i c~ c~ u,.) ',,o ',,o ~ co c~
E < LJ r-"
o") o") o") o") o") o") o") o") o") o") o") o")
- '~ ~q
t -
E ~ o , ~ u ,'
cg _= >~
0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
',,0 I '~ I '~ I '~ u') CO c~ CO
- i e-
. m
e- O
m
#
m
>
E
<
O
T
O
u'3 ~
b0 b0 b0 b0 b0 b0 b0 b0 b0 E E E E E E E E E E
0 0 0 0 ~ 0 ~ 04 0 0 0 0 0
C C C
i ",u ~.__E ",~ ~ ' , u "- "- "- ~.__E "-
• - ",~ b 0 " , ~ . - ~ . - b0 m m
E ~ -~ ~ & , ~ '~ ~ '~ ~ - ' : "~ . . . . . . • ~ + ~ + ~ + ~ + ~ + ~ + ~ + ~ + ~ + ~ + ~
• ,~ ~ ",~ ",~ ~ ",~ ~ ",~ ",~ ~ ",~ ~ ",~ ~ ",~ ~ ~ ~ ~ ~ ~ ~ ~ ~ LJJ LJJ LJJ LJJ LJJ LJJ LJJ LJJ LJJ LJJ
#
m
0
c 4~ 2 o = o > C~- ~_ o o
m 73
-U U
, . ' S u
f~ . _ j m
m c g
73 ~_
cg
" 12 < ~ ( 7 *
August 2008 1511

Clinical Therapeutics
Disease Treatment Pathway Markov models are useful for conditions that
involve events that can occur more than once, proba- bilities that change according to the time since a pre- vious event, and risks that continue or increase over time. 13 Because CVD satisfies these requisites, a
Markov model was chosen to represent the patients' clinical pathway; Figure 1 illustrates the health states included. These health states are representative of the main cardiovascular events and were governed by the evidence available to populate effectiveness and transitions.
Commencing in one of the postevent health states, an annual cycle was used for the probability of mov- ing to a subsequent event. In accordance with recom- mendations for conditions associated with fatal events, a lifetime horizon was used to capture the potential long-term consequences of the disease. 14
Age- and sex-specific prevalence data published by the British Heart Foundation were used to distribute patients to initial health states. 15 First- and subsequent- year transitions to CVD events were also age related (Table II). For patients with a history of a CHD event, the probability of subsequent nonfatal myocardial in- farctions (MIs), nonfatal strokes, and cardiovascular deaths were derived from patients in the Nottingham Heart Attack Register. 16 For patients with a history of a stroke, probabilities of subsequent events were derived from patients in the South London Stroke Register. 17
The transitions from transient ischemic attack and sta- ble angina were taken from the existing CVD model. 5
Ezetimibe Effectiveness Data We undertook a systematic review of the evidence
relating to the effectiveness of ezetimibe (coadminis- tered with a statin) compared with statin monothera-
After stable angina
After unstable angina
New
unstable angina
After M I
~ Z ~ After TIA
~ Z ~ After stroke
New ~ Death nonfatal MI (3 health states)
New nonfatal stroke
Figure 1. Health states modeled in 10,000 Monte Carlo simulations in a Markov model to estimate the cost- effectiveness of ezetimibe plus statin combination therapy compared with doubling current statin close alone to treat hypercholesterolemia in a theoretical cohort of 1000 men aged SS years in the United Kingdom, based on registry data. In each cycle, all individuals were at risk of entering the absorbing health state, death, which included health states: Fatal coronary heart disease, Fatal stroke, or death through other causes. Transitions from new-event health states used First-year event rates, whereas transitions from postevent health states used subsequent-year event rates. MI = myo- cardial infarction; TIA = transient ischemic attack.
1512 Volume 30 Number 8

R. Ara et al.
Table II. Examples of annual transitions in a Markov model to estimate the cost-effectiveness of ezetimibe plus statin combination therapy compared with doubling current statin dose alone to treat hyper- cholesterolemia in a theoretical cohort of 1000 men in the United Kingdom, based on registry data.
Cardiovascular Nonfatal M I Nonfatal Stroke Death
Event Age 55 Age 75 Age 55
Stable angina, % 1.45 2.10 0.40
Unstable angina, % Year 1 5.00 4.70 0.30 Year _>2 3.27 10.60 0.09
MI, % Year 1 11.70 8.90 0.30 Year _>2 1.95 2.20 0.10
TIA, % 0.60 0.60 1.20 Year 1 0.60 0.60 4.60 Year _>2 0.56 0.55 1.82
Age 75 Age 55 Age 75 Source
0.90 0.59 1.51 Ward et al s
1.30 6.10 1.66 Gray and Hampton 16 0.43 1.02 1.43 Gray and H a m p t o n 16
1.30 3.13 4.25 Gray and Hampton 16 0.54 1.00 1.73 Gray and Hampton 16
4.20 1.27 3.48 Ward et al s 4.80 2.04 3.86 Wolfe et a117 2.45 0.90 1.94 Wolfe et a117
MI = myocardial infarction; TIA = transient ischemic attack.
py in individuals with hypercholesterolemia. All ran- domized controlled trials (RCTs) of fixed-dose treat- ment regimens with a minimum treatment duration of 12 weeks in individuals aged >18 years with heterozy- gous familial and nonfamilial hypercholesterolemia were included. Meta-analyses were carried out using fixed- and random-effects models using Cochrane Collabo- ration Review Manager 4.2.3 software. Heterogeneity between trial results was explored through consider- ation of the study populations, methods and interven- tions, by examination of the results and, in statistical terms, by Z 2 test for homogeneity and the 12 measure. Further details are available from Ara et al. 1°
Basel ine LDL-C M e a s u r e m e n t s The baseline LDL-C measurement for patients en-
tering the model was assumed to be 3.0 mmol/L. These data were derived from the end-of-treatment measurements observed in the statin monotherapy groups of the studies included in the clinical meta- analysis (see Results).18--~3
Linking the Changes in LDL-C to Cardiovascular Events
A literature search was conducted to identify the most robust methodology to link the changes in sur-
rogate measures to clinical events. 10 A mixture of hard quantitative and soft operational research techniques (strategic choice approach, cognitive maps) were used to review the evidence.i° The results of a meta-analysis conducted by the Cholesterol Treatment Trialists' (CTF) Collaborators was identified as the most appropriate methodology. 11 Using data collected from 90,056 pa- tients enrolled in 14 RCTs of statins, the authors re- ported that a 1-mmol/L reduction in LDL-C was as- sociated with a 23 % reduction in the 5-year incidence of a major coronary event (nonfatal MI or CHD death), and a 21% reduction in major coronary events, coro- nary revascularization, and stroke (Table III). 24 The CIs were used to define normal distributions to describe the uncertainty around the relative risk parameters, and uniform distributions were used for the effective- ness data to account for the greater uncertainty in the data (ie, the data were not obtained from individuals who were not adequately controlled by statin mono- therapy, only very short-term data were available, and an adjustment was required for the effect of second- line treatment).
Costs Our analysis took the perspective of the UK De-
partment of Health; therefore, nonvascular-related health
August 2008 1513

Clinical Therapeutics
Table III. Effectiveness and relative risks in a Markov model to estimate the cost-effectiveness of ezetimibe plus statin combination therapy compared with doubling current statin dose alone to treat hyper- cholesterolemia in a theoretical cohort of 1000 men aged 55 years in the United Kingdom, based on registry data.
Variable
Change in LDL-C, % Due to second-line ezetimibe + st:at:in therapy
Due to second-line titrated statin monotherapy
Relative risk per 1-mmol/L reduction in LDL-C
Nonfatal MI Angina ~ CHD death Nonfatal stroke TIAI
Mean (95% CI) Distribution Source
-22.3 (-26.76 to -17.84)
-9.5 (-11.4 to -7.6)
Uniform Meta-analysis, adjusted for second line
Uniform Knopp, 24 adjusted for second line
0.74 (0.70 to 0.79) Normal 0.74 (0.70 to 0.79) Normal 0.81 (0.75 to 0.87) Normal 0.83 (0.78 to 0.88) Normal 0.83 (0.78 to 0.88) Normal
Baigent el: a111 Baigent el: a111 Baigent el: a111 Baigent el: a111 Baigent et a111
LDbC = low-density lipoprotein cholesterol; MI = myocardial infarction; CHD = coronary heart disease; TIA = transient ischemic attack. *As nonfatal MI. tAs nonfatal stroke.
care costs and indirect costs were not included. 14 Costs for ezetimibe and statins were taken from the British National Formulary (Table IV). e5 The
weighted cost of statin treatment was calculated using the prescribing rates of statins in England for 20058 and the statins costs from the British National Formu- lary in 2006. e5 For instance, if atorvastatin 10 mg represented 19.7% of the total statins prescribed in 2005 and its annual cost in 2006 was £234, then the contribution of atorvastatin 10 mg to the total cost of statin treatment (Table IV) would be approximately £46. It was also assumed that individuals receiving the highest dose of any statin (6.3% of all prescriptions) 1° would remain on that dose. UK-based health-state costs (Table IV) were identified through literature searches, e6-28 Based on data available from short-term studies, minor adverse events were rare for patients receiving ezetimibe treatment, with no serious adverse events having been reported. Therefore, the costs of managing adverse events were not modeled.
Quality of Life In keeping with the NICE reference case, the health
states (Table IV) were populated using the EuroQoL-5D
preference-based utility data.14 Age-dependent utility 36 was adjusted multiplicatively using empiric estimates derived from a systematic literature search for each health state, l° Where possible, data collected on indi- viduals in the United Kingdom were used. No data were found that represented the impact of additional events; therefore, based on clinical opinion, it was as- sumed that second and third events would incur an additional 10% and 15% reduction in utility, respec- tively.10 Based on the current safety profile, no disutili- ty was applied for ezetimibe treatment.
Model Analysis We modeled the costs and benefits for a cohort of
1000 hypothetical male patients aged 55 years with a history of CVD and a baseline LDL-C of 3.0 mmol/L. In line with published guidelines, we discounted the costs and benefits at 3.5% per annum, and a half- cycle correction was applied to both costs and bene- fits. 14 A lifetime horizon was used to capture the full
benefits associated with preventing fatal events. 14 Sen- sitivity analyses were performed because there is al- ways uncertainty in decision analysis. We used 2 meth- ods to characterize this uncertainty: 1-way sensitivity
1514 Volume 30 Number 8

R. A r a e t al .
7n
m ~
E c 0 " - -
u ~ E -'I
~ g o >- oq t r )
~" t r )
. o t~ e- c-
O 0 0
._c o
t~ q - o
"~ 0 T~_-c
0 0
..I3 "7 -~: -~ "n "n
N ~- n o
o ~"
e- e-
> t~
'd E
~5 o
u ~ 0
¢-
,.~ t7 q)
E _ c
0
0 ~" E o ~i
o ~ - ~ ~" 0 ~- ~ T n ~
c ' ~
.E -~ ,- 0
b~
,~ E
¢- ¢-
0 0
,o o ~ o ~ o ~ o ~ b , ° b , ° r-" r-" r-" r-"
.'L- . - - .'L- . - - .'L- . - - .'L- ~ 0 ~q
2 ,_ ~_ n ~_ n ~_ n ~_ n -~-~ - = ~ =.__. =.__. =.__. = . _ _ . z ~ : ' ~
~ E ° ~- ° i ° ~- ° i • s o
. ~ - r ~ G.._ ~ G.._ ~
U c~ c~ c~ c~ U
c~
¢-
0 u
Ix , ,~- Ix , 0 ~ kO
b ( 0 u'~
7 3 7 3 7 3 7 3 ~
7 3 bO bO E E E E
E o o o4 ,~- .~ .~ O o 4 ~ ,-" ,-" ~
. _ q~ q~ 0
~ E ~ ~ ~ ~ ~ ~ - n o ' , ~ > > > > ~ ~ o ~ E E o o .~ .~
q)
¢- ¢- ¢- ¢- ¢-
u
•o• ~- ~( ~- ~ ~ ~ ~ ~ ~__ -~
"7- ~- n c~ c~ c~ c~ c~ c~ ~ - n 7
E . . c
"7 "7 c~ "7 - ~
¢- ¢- ¢- ¢-
# # o ~ z
~ . ~ . ~ . ~ . CO
C'4 C'4 C'4 C'4 C'4 I I I I "
C O C O ~ . n c o ~
v
v v v v
S S S S ~ o C'4 C'4 C'4 C'4 C'4
c~ ¢-
¢- ¢-
~>t>t ~>t>t >t>t~ ¢-
7 3
"7 ¢-
¢-
O o v
A u g u s t 2 0 0 8 1 5 1 5

Clinical T h e r a p e u t i c s
q~
P 0
~ q
~ E E E ~
o
o rg
> ~ ~ ,~ r - .
- p P P
a 3 0 0 0 0 0 0
g g g
N ' - E E E
..~ v v v
t - O
",D
. m
D D D D
E ~ ~ E E ~ E O 0 . . . . . . O 0 O 0 O 0 0
z u # # # ~ u u z z u u z
i i i ,~- u ' ) c ~ C',I c ~ c ~ O C',I ',,0 u ' ) 00 O
O ,-" C'-,I 0 h ',,0 ~ O O O k 0 0
D ~ , ~ - r-. ~ ,.o ~ coo- , n~0O r - . 0 o D ~ '~ ~..~__... ~ ~ ~ ~ r - . : ,5 , : :5 ~ , : :5 o o ~n
bO bO b O ~ r - r - r - o ' )
o ,~ ,~ ,~ ,~._J ,~._j
O O O 0 h I .~
c ~ bO .=-^
> ,~ b~ b~_~ b~ b~ -~ ° ~ b~ b~ b~ b~ b~ b~_~ b~ q,) . - - _ _
g E <>~>~ ,o >~ >~ ~ f~ ~-~ >~ >~ < >~ >~_ >~ >~ ,o>~
-~ % -~ %
LJ-I ~ LJ-I ~
rg rg
- ' " - ' " ~ ~ ._.5 ._.5 >~ >~ < < v v
EE 0 0
E .,u .,u O '7 '7
z E E
~ - 5 r~ . -
z-~
o,I 0 ~
o d ~ ',,0 0 . -
O ~ ~ ~*q ~*q ._~ u") ' ' d ~ ~ ~7
. _ ~ -
~ e , .o~
.__ ~ _
~ . - ~_~
A~ 'u E:-u~ ~ ~
~ < < ~ ,
O u
.2
_c
c
E
i " -
" 5 c~
O E c~ c~
E E :_z _~
c~ v
",~ . O
~. -~ i_~ _c c N ~ 0
._oc ~
i ~ ° m . , ~
0 c
E .E .2 3 o ~.~
4 - - - - -
1 5 1 6 V o l u m e 3 0 N u m b e r 8

R. Ara et al.
analyses and Monte Carlo simulations. One-way sen- sitivity analysis is a procedure in which the central es- timates for key parameters in the model are varied one at a time. New results were generated from the model using the adjusted values and recorded. This process was repeated for all key parameters in the model. One- way sensitivity analyses could inform readers as to which variables drive the results generated by the model, but do not provide information about the over- all uncertainty associated with the model. In addition to varying the baseline characteristics of the cohort (age, sex, LDL-C), the 95% CIs were used to represent the effectiveness of the treatments and the relationship between changes in LDL-C and relative risks of events. Health-state utility values were varied by _+20% and health-state costs were varied by _+50%.
Monte Carlo simulations were used to create a probabilistic sensitivity analysis, which is a method of varying all variables simultaneously to assess the over- all uncertainty in the model. 37 The individual simula- tions (10,000) were generated using random num- bers (0-1) to sample from the distributions. New results were generated by the model, and each of the 10,000 results were stored. The recorded results were then used to illustrate the overall variability in the model using a threshold of £30,000 per quality- adjusted life-year (QALY). 14 The 95% CIs of the mean were estimated using jackknife techniques whereby the variance was estimated by sampling the residuals in the 10,000 samples. Table HI describes the input parameters and probability distributions used in the model.
Incremental Cost-Effectiveness Ratio The primary outcome was the incremental cost-
effectiveness ratio (ICER). The ICER demonstrated the additional cost per QALY gained from Treatment A compared with Treatment B38:
ICER = (Cost Treatment A - Cost Treatment B)
(Utility Treatment A - Utility Treatment B)
RESULTS Clinical Effectiveness
Because there are currently no clinical outcome tri- als, LDL-C surrogate end points were used to repre- sent effectiveness of treatment. Six RCTs (n = 3610) of short duration (all 12 weeks) and varying methodo- logical quality were included. 18-23 Of these, 4 corn-
pared ezetimibe coadministered with simvastatin ver- sus simvastatin alone, 1 compared ezetimibe coad- ministered with atorvastatin versus atorvastatin alone, and i compared ezetimibe coadministered with prava- statin versus pravastatin alone.
Our meta-analysis showed that ezetimibe/statin coadministration was associated with a statistically significant mean reduction in LDL-C (from baseline to end point)of-13.94% (95% CI,-14.90% to-12.98%; P < 0.001) compared with statin alone (Table HI). Al- though there was low heterogeneity (Z 2 = 5.31; P = 0.38, I 2 = 5.8 %), the statistical test was not significant. It was assumed that statin titration of i dose provided an additional 6% reduction in LDL-C. 16
Effectiveness Rates for Second-Line Treatments The evidence used in the meta-analysis was drawn
from studies that included a washout period before commencing study treatments. Because the model ex- amined the benefits associated with add-on treatment for patients who had not achieved an adequate re- sponse to statin monotherapy, the effectiveness of second-line treatments was estimated as follows.
Using data from the studies included in the meta- analysis, the baseline LDL-C measurement was 4.65 retool/L, the mean LDL-C after statin mono- therapy was 2.92 retool/L, and the mean LDL-C after combination therapy was 2.27 mmol/L. The percent- age reductions from baseline to end of treatment were 36.5% and 51.2%, respectively. Using the observed end-of-treatment LDL-C measurement (2.92 retool/L) from statin monotherapy to represent the effectiveness of first-line treatment, and the observed end-of-treatment LDL-C measurement from the ezetimibe and combi- nation therapy, the incremental percentage reduction attributable to second-line treatment was estimated to be 22.3% ([2.92 - 2.27]/2.92).
Assuming that titrating to the next highest dose of statin provided an additional incremental 6% reduc- tion in LDL-C, the total benefit from baseline due to titrated statin treatment would be 42.5% (36.5% + 6.0%). Using the RCT baseline mean LDL-C measure- ment (4.65 retool/L), the absolute LDL-C level after titrating statin therapy would be 2.65 mmol/L (4.65 x [1 - 42.5%]). Therefore, the incremental percentage reduction due to second-line statin therapy would be -9.5% ([2.92 - 2.65]/2.92). The values shown do not match exactly because of rounding in the values used in the calculations.
August 2008 1517

Clinical Therapeutics
Applying the BenetTts of Treatments to Obtain Relative Risks
The absolute reduction in LDL-C was calculated by multiplying the baseline LDL-C by the adjusted per- centage reduction in LDL-C due to second-line treat- ment. The relative risk per event type was then calcu- lated by multiplying the absolute reduction in LDL-C by the relative risk per mmol/L reduction in LDL-C reported by the CTT Collaborators.11
Cost - Ef fec t iveness Probabilistic Cost-Effectiveness Results
The individual results of the probabilistic analyses are shown in Figure 2. Because each symbol in the figure represents an estimate of the ICER when sam- piing from each of the parameter distributions, the ellipses represent the uncertainty in the mean ICER. Using the costs and benefits accrued over a 5-year pe- riod, all points lie well above the £30,000 per QALY
threshold, and the ellipse is small, representing the comparative certainty at this stage. Extrapolating to examine the costs and benefits accrued over longer time periods, the size of the ellipses increases, reflect- ing greater uncertainty in the effectiveness of treat- ment beyond the short term. Using a lifetime horizon, with a mean of £27,500 per QALY gained, 63% of the symbols lie below the £30,000 per QALY thresh- old (Figure 3).
The mean results for 10,000 simulations using a cohort of 1000 male patients aged 55 years are sum- marized in Table V. Ezetimibe coadministered with current statin therapy was estimated to prevent a mean of 43 nonfatal MIs, 7 nonfatal strokes, and 26 cardio- vascular deaths over a lifetime, compared with titrat- ing the current statin treatment by 1 dose. The events avoided would provide a mean of 134 additional QALYs. With a mean incremental cost of £3,693,000, the lifetime discounted cost per QALY gained would
• 5 Years • 10 Years • 20 Years X LiFetime
5 0 0 0 -
4000-
o 3000- o
"-" 2 0 0 0 -
O
1000-
0 0
£30 ,000 per QALYga ined
X x Xx
I I I I I 0.05 0.10 0.15 0.20 0.25
QALY Gained
Figure 2. Cost-effectiveness plane using different time horizons in 10,000 Monte Carlo simulations in a Markov model to estimate the cost-effectiveness ofezet imibe plus statin combination therapy com- pared with doubling current statin close alone to treat hypercholesterolemia in a theoretical cohort of 1000 men aged 55 years in the United Kingdom, based on registry data. Baseline low-density lipoprotein cholesterol was assumed to be 3.0 mmol/L. QALY = quality-adjusted life-year.
1518 Volume 30 Number 8

1.00 -
0.80 -
~>" 0.60- ..O
..O O
0.40-
0.20 -
I 0 60,000
I I 20,000 40,000
Cost per QALYThreshold (£)
R. Ara et al.
Figure 3. Cost-effectiveness acceptability curve horizon in 10,000 Monte Carlo simulations in a Markov model to estimate the cost-effectiveness ofezetimibe plus statin combination therapy compared with dou- bling current statin dose alone to treat hypercholesterolemia in a theoretical cohort of 1000 men aged 55 years in the United Kingdom, based on registry data. Baseline low-density lipoprotein cho- lesterol was assumed to be 3.0 mmol/k. QAkY = quality-adjusted life-year.
be £27,475 (95% CI, £27,331-£27,620). 39 As would be expected, the cost-effectiveness of ezetimibe im- proved over time in the model (Table V).
Univariate Sensitivity Analyses When exploring the impact of varying individual
parameter values, the results for the univariate sensi- tivity analyses (Table I) showed that the ICER for men aged 65 years (analysis 2) was comparable (mean, £26,900) to that for men aged 55 years. The ICER increased to £32,000 per QALY for cohorts aged 75 years (analysis 3), reflecting the limited time during which cost offsets and benefits due to events avoided were accumulated. When varying the baseline LDL-C level modeled (analyses 5 and 6), the ICERs ranged from £23,500 to £33,000 per QALY. Changes to the rates applied to represent the effectiveness from second-line treatment (analyses 7-10) had the largest impact on the model, with ICERs ranging from £22,500 to £43,000 per QALY. Variations in the health-state costs had a negligible impact on the ICER. This was not surprising, given that the cost offsets due to events avoided (£69,000) was small when compared with the
cumulative lifetime difference in the treatment regi- mens (£3,765,000). Adjustments to the utility values associated with health states (analyses 13-14) pro- duced ICERs ranging from £25,100 to £30,300 per QALY.
When comparing ezetimibe coadministered with sim- vastatin 40 mg/d with atorvastatin 40 mg/d, the life- time ICER decreased to approximately £3100 per QALY. Conversely, when comparing ezetimibe plus atorvastatin 40 mg/d with rosuvastatin 40 mg/d, the lifetime ICER increased to approximately £33,500 per QALY.
D I S C U S S I O N
Using a threshold of £20,000 per QALY, our results suggest that ezetimibe plus current statin versus current statin titrated by 1 dose is not a cost-effective alterna- tive in the UK health system, independent of the age at which treatment is started. Although the central esti- mates suggest that this treatment regimen could be considered cost-effective with a threshold of £30,000 per QALY, many of the results from the univariate sen- sitivity analyses were higher than this threshold. When comparing ezetimibe plus generic simvastatin with
August 2 0 0 8 1519

Clinical Therapeutics
Table V. Base-case costs and benefits accrued over different time horizons in 10,000 Monte Carlo simulations in a Markov model to estimate the cost-effectiveness of ezetimibe plus statin combination therapy compared with doubling current statin dose alone to treat hypercholesterolemia in a theoretical cohort of 1000 men aged 55 years in the United Kingdom, based on registry data.
Time Horizon
Variable 5 Years 10 Years 20 Years Lifetime
Total discounted life-years Ezetimibe plus statin Statin monotherapy Incremental difference
Total discounted QALYs Ezetimibe plus statin Statin monotherapy Incremental difference
Total discounted costs, year-2006 £
Ezetimibe plus statin Statin monotherapy Incremental difference
Discounted cost per QALY, mean (95% CI), year-2006 £
4458 7779 11,663 13,260 4453 7757 11,583 13,106
5 22 80 154
2980 5127 7505 8386 2975 5103 7424 8252
5 24 81 134
5,074,000 9,087,000 14,201,000 16,560,000 3,896,000 7 ,027,000 11,050,000 12,867,000 1,178,000 2,060,000 3,151,000 3,693,000
214,725 85,767 39,109 27,475 (213,490-215,956) (85,285-86,247) (38,897-39,321) (27,331-27,620)
QALY = quality-adJusted life-year.
branded atorvastatin, the ICERs were well below the £20,000 per QALY threshold. Conversely, comparing ezetimibe plus branded atorvastatin with branded rosu- vastatin, the ICERs increased well beyond £30,000 per QALY. The results generated by the model were based on the limited clinical evidence currently available and driven by the difference in the costs associated with the regimens being compared. There are several limitations to the evidence base, which are discussed here.
Despite the incomplete clinical evidence, ezetimibe is being prescribed, and the prescribing rates in Eng- land and Wales are increasing rapidly, with a growth rate of 55% between 2004 and 2005. s The introduc- tion of ezetimibe to the lipid-lowering market has placed a substantial additional burden on limited health care budgets. In 2005, -740,000 prescriptions of ezetimibe were dispensed in England and Wales, costing approximately £24 million in England s and £2 million in Wales. 9 It had been estimated that the
total annual cost associated with ezetimibe for England and Wales would be as high as £37 million in 2006.1°
Because of the comparatively recent launch of ezetimibe, economic evaluations of the treatment have been sparse. Several studies were identified that present- ed country-specific results based on adaptations of a core model. 4° To compare the results, the currencies were converted to British pounds using the gross do- mestic product purchasing power parities, 41 and re- suits were adjusted to year-2006 values using the pay and prices annual percentage increase (1.9 % ). le Com- parison with our results was difficult because of the differences in baseline characteristics and treatment regimens evaluated, which included titrations to cho- lesterol goals. The results for Europe (Germany, Spain, or Norway) ranged from £7565 to £49,867 per life- year gained when examining the cost-effectiveness of ezetimibe coadministered with statin versus statin mono- therapy in cohorts with either existing CHD or diabe-
1520 Volume 30 Number 8

R. Ara et al.
tes. 4° The primary analysis in the Canadian study fo- cused on patients aged 65 years who were classified as having very high risk of a CHD event and compared adding ezetimibe to atorvastatin therapy versus ator- vastatin titration. 4~ The results ranged from £26,221 to £45,867 per QALY. The model in these evaluations used the cardiovascular risk algorithm derived from the US Framingham Heart Study to estimate the re- duction in risk due to treatment. 43
There is now substantial and robust evidence of a direct relationship between reductions in LDL-C and cardiovascular risk. 11,40 In the absence of long-term clinical outcome studies, if the cost-effectiveness of ezetimibe is to be compared with other lipid-modifying therapies, the relationship between changes in LDL-C and cardiovascular risk is the most appropriate meth- od available to analysts. However, we caution that the validity of the link modeled between ezetimibe- induced changes in LDL-C and cardiovascular events is pivotal to the accuracy of the results generated us- ing this methodology. In particular, based on the CTT Collaborators' results, we assumed that the relation- ship between changes in LDL-C and relative risk of future clinical events is linear regardless of age, sex, history of CVD, or baseline LDL-C.
A major limitation in the evidence base used for the effectiveness of ezetimibe was that the individuals en- rolled in the studies were given a washout period be- fore treatment and were not individuals who could not achieve adequate lipid control on the maximum tolerated statin treatment. In addition, a great deal of uncertainty exists regarding individual treatment ef- fects 42 and baseline prognostic factors such as heart failure. 43 The experience with cerivastatin has also shown that additional evidence is required before lipid-modifying treatments are routinely prescribed. Furthermore, although clinical researchers have re- ported that ezetimibe therapy reduces LDL-C levels, the possibility that it does not share the same benefits as statin treatments was recently raised by the results of the Ezetimibe and Simvastatin in Hypercholesterol- emia Enhances Atherosclerosis Regression study. 44
Further Research Data from clinical studies reporting cardiovascular
and mortality data associated with ezetimibe treat- ment are required to verify the potential clinical bene- fits and the safety profile of this treatment. In particu- lar, data demonstrating any differential effects when
combining ezetimibe with different types and doses of statins would be very useful for future analysts to es- timate the cost-effectiveness of alternative treatment regimens. In addition, evidence from studies enrolling individuals who are unable to control lipids on statin monotherapy, and from patients using several comedi- cations, such as those with diabetes, would be useful additions to the evidence base.
C O N C L U S I O N S The current evaluation was undertaken to inform policy decision makers in the United Kingdom and provides the best economic information possible given the limitations of the evidence available. The results suggest that, in some instances, ezetimibe coadminis- tration may be cost-effective compared with statin monotherapy. However, there are concerns about the evidence base and there are several limitations to the evidence used in this economic model. When evidence of ezetimibe-induced benefits, in terms of clinical end points, becomes available, the methods and data used should be updated and new results generated.
ACKNOWLEDGMENTS The UK National Coordinating Centre for Health Technology Assessment (NCCHTA) funded this study on behalf of NICE. The opinions and views expressed are those of the authors and are not necessarily those of NICE or the NCCHTA.
Paul Durrington was an International Advisory Board member to Merck & Co., Merck/Sharp & Dohme, and Schering-Plough until the beginning of 2006 and received remuneration for his advice. He resigned his advisory roles to these and other compa- nies when he joined the advisory group to the Com- mission on Human Medicines in 2006.
The authors wish to thank Rachel German for assis- tance in the use of the innovative problem-structuring techniques used in the cost-effectiveness review, and Andrea Shippam for her administrative assistance with research and manuscript preparation.
REFERENCES
1. World Health Organization. The World Health Report 2002--Reducing Risks: Promoting Healthy Life. Geneva, Swit- zerland: World Health Organization; 2002.
2. British Heart Foundation. Reducing your blood choles- terol. Health Information Series No. 3. London, UK: British Heart Foundation; 2004.
August 2008 1521

Clinical Therapeutics
3. McPherson K, Britton A, Causer L. CHD: Estimating the Impact of Changes in Risk Factors. London, UK: Nation- al Heart Forum; 2002.
4. Primatesta P, Poulter NR. Levels of dyslipidaemia and improvement in its management in England: Results from the Health Survey for England 2003. Clin Endocrinol (Oxf). 2006;64: 292-298.
5. Ward S, Lloyd Jones M, Pandor A, et al. A systematic review and eco- nomic evaluation of statins for the prevention of coronary events. Health
Technol Assess. 2007;11:1-160. 6. Committee for Medical Products
for Human Use. Note for Guidance on Clinical Investigation of Medical Products in the Treatment of Lipid Disorders. London, UK: European Medicines Agency; 2004. http://emea.europa. eu /pdf s /h u m a n / e w p / 3 0 2 0 0 3 e n . pdf. Accessed July 21, 2008.
7. Health Care Statistics. Prescription cost analysis, England 2003. Lon- don, UK: Department of Health; 2003. http://www.d h.gov, u k/e n/
Pu blicationsandstatistics/Statistics/ StatisticalWorkAreas/Statistical health
care/DH_4086603. Accessed Octo- ber 9, 2006.
8. National Health Services Health and Social Care Information Cen- tre. Health care statistics. Prescrip- tion cost analysis, 2005. http://www.
ic. n hs.u k/pu bs/prescostanalysis2005. Accessed October 9, 2006.
9. Welsh Assembly Government. Pre- scriptions dispensed in the commu- ni W in Wales, 2000 to 2005 and prescription cost analysis (PCA) data. h t t p : / / n ew.wales.gov, u k / top ics / statistics~headlines~health-2007~ h e a l t h - 2 0 0 6 / h d w 2 0 0 6 0 5 1 8 / ?lang=en. Accessed October 9, 2006.
0. Ara R, Tumur I, Pandor A, et al. Ezetimibe for the treatment of hypercholesterolaemia: A systemat- ic review and economic evaluation. Health Technol Assess. 2008;12:1-232.
1. Baigent C, Keech A, Kearney PM, et al, for the Cholesterol Treatment Trialists' (C1~) Collaborators. EF-
ficacy and safety of cholesterol- lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials ofstat ins [published correction ap- pears in Lancet. 2005;366:1358]. Lancet. 2005;366:1 267-1278.
12. Curtis L, Netten A. Unit costs of health and social care 2006. http:// www. p s s r u . a c , u k /u c /u c 2 0 0 6 contents.htm. Accessed July 3, 2006.
13. Sonnenberg FA, Beck JR. Markov models in medical decision making: A practical guide. Med Decis Making. 1993;13:322-338.
14. National Institute for Clinical Excel- lence (NICE). Guide to the methods of Technology Appraisal (reference NO515). http://www, nice.org, u k/
n iceM edia/pd f/TAP_M ethods, pd f. Accessed September 7, 2006.
15. British Heart Foundation statistics database. BHF 2004. http://www.
h eartst ats. org/ atozp age. asp ?id = 2478. Accessed September 10, 2007.
16. Gray D, HamptonJR. Twenty years' experience of myocardial infarction: The value of a heart attack register. BrJ Clin Pract. 1993;47:292-295.
17. Wolfe CD, Rudd AG, Howard R, et al. Incidence and case fatality rates of stroke subtypes in a multiethnic population:The South London Stroke Register. J Neural Neurosurg Psychiatry.
2002;72:211-216. 18. Bays HE, Ose L, Fraser N, et al, for
the Ezetimibe Study Group. A mul- ticenter, randomized, double-blind, placebo-controlled, factorial design study to evaluate the lipid-altering efficacy and safe W profile of the ezetimibe/simvastatin tablet com- pared with ezetimibe and simva- statin monotherapy in patients with primary hypercholesterolemia. Clin Ther. 2004;26:1 758-1773.
19. Davidson MH, McGarryT, Bettis R, et al. Ezetimibe coadministered with
simvastatin in patients with primary hypercholesterolemia.J Am Coil Car- dial. 2002;40:2125-2134.
20. Goldberg AC, Sapre A, Liu J, et al, for the Ezetimibe Study Group. El-
ficacy and safety of ezetimibe co- administered with simvastatin in patients with primary hypercholes- terolemia: A randomized, double- blind, placebo-controlled trial. Mayo Clin Proc. 2004;79:620-629.
21. Rodney RA, Sugimoto D, Wagman B, et al. Efficacy and safety of co- administration of ezetimibe and simvastatin in African-American pa- tients with primary hypercholestero- lemia. J Nail Med Assoc. 2006;98: 772-778.
22. Ballantyne CM, Houri J, Notarbar- tolo A, et al, for the Ezetimibe Study Group. Effect ofezetimibe coadmin- istered with atorvastatin in 628 pa- tients with primary hypercholester- olemia: A prospective, randomized, double-blind trial. Circulation. 2003; 107:2409-2415.
23. Melani L, Mills R, Hassman D, et al, for the Ezetimibe Study Group. Ef- ficacy and safe W ofezetimibe coad- ministered with pravastatin in pa- tients with primary hypercholester- olemia: A prospective, randomized, double-blind trial. Eur Heart J. 2003;24:717-728.
24. Knopp RH. Drug treatment of lipid disorders. N EnglJ Med. 1999;341 : 498-511.
25. Joint Formulary Committee British Na- tional Formulary. 52nd ed. London, UK: British Medical Association and Royal Pharmaceutical Society of Great Britain; 2006. www.bnf.org.
Accessed October 9, 2006. 26. Palmer S, Sculpher M, Philips Z, et
al. A Cost-Effectiveness Model Compar- ing Alternative Management Strategies for the Use of Glycoprotein lib~Ilia An- tagonists in Non-ST-Elevation Acute Corona~Syndrome. London, UK: Na- tional Institute for Clinical Excel- lence; 2002.
27. Clarke P, Gray A, Legood R, et al. The impact of diabetes-related com- plications on healthcare costs: Re- suits from the United Kingdom Pro- spective Diabetes Study (UKPDS Study No. 65). DiabetMed. 2003;20: 442-450.
1522 Volume 30 Number 8

R. Ara et al.
28. Youman P, Wilson K, HarrafF, Kal- ra L. The economic burden ofstroke
in the United Kingdom. Pharmaco-
Economics. 2003;21(Suppl 1):43-50. 29. Lenzen M, Scholte op Reimer W,
Norekvfil TM, et al. Pharmacologi-
cal treatment and perceived health status during 1-year follow up in patients diagnosed with coronary artery disease, but ineligible for revascularization. Results from the
Euro Heart Survey on Coronary Revascularization. Eur J Cardiovasc
Nuts. 2006;5:115-121. 30. BARI Investigators. Protocol for the
bypass angioplasty revasculariza- tion investigation. Circulation. 1991; 84(Suppl 6):V1-V27.
31. KimJ, Henderson RA, PocockSJ, et al, for the RITA-3 Trial Investiga- tors. Health-related quality of life after interventional or conservative strategy in patients with unstable angina or non-ST-segment eleva- tion myocardial infarction: One- year results of the third Random- ized Intervention Trial of unstable Angina (RITA-3). J Am Coil Cardiol.
2005;45:221-228. 32. Goodacre S, Nicholl J, Dixon S, et
al. Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care. BMJ. 2004;328:254.
33. van Exel N J, Scholte op Reimer WJ, Koopmanschap MA. Assessment of post-stroke quality of life in cost- effectiveness studies: The usefulness of the Barthel Index and the Euro- Qol-5 D. QualLife Res. 2004;13:427- 433.
34. Leeds L, Meara J, Hobson P. The impact ofdischarge to a care home
on longer term stroke outcomes. Clin Rehabil. 2004;18:924-928.
35. Pickard AS, Johnson JA, Feeny DH. Responsiveness of generic health- related quality of life measures in
stroke. Qua/Life Res. 2005;14:207- 219.
36. Kind P, Dolan P, Gudex C, Williams A. Variations in population health status: Results from a United King-
dom national questionnaire survey. BMJ. 1998;316:736-741.
37. Briggs AH. Handling uncertainty in cost-effectiveness models. Pharmaco- Economics. 2000;I 7:479-500.
38. Drummond MF, Sculpher MJ, Tor- rance GW, et al, eds. Methods for the
Economic Evaluation of Health Care Pro-
grammes. 3rd ed. Oxford, UK: Ox- ford University Press; 2005.
39. Law AM. Simulation Modeling ~9" Analy-
sis. 4th ed. New York, NY: McGraw- Hill; 2006.
40. Cook JR, Yin D, Alemao E, et al. Cost-effectiveness ofezetimibe coati-
ministration in statin-treated pa- tients not at cholesterol goal: Ap- plication to Germany, Spain and Norway. PharmacoEconomics. 2004;22
(Suppl 3):49-61.
41. Organisation for Economic Co- operation and Development Pur- chasing Power Parities. http://www.
oecd.org/department/. Accessed
July 3, 2006. 42. Kohli M, Attard C, Lain A, et al.
Cost effectiveness of adding ezeti- mibe to atorvastatin therapy in pa- tients not at cholesterol treatment goal in Canada. PharmacoEconomics.
2006;24:815-830. 43. Anderson KM, Wilson PW, Odell
PM, Kannel WB. An updated coro- nary risk profile. A statement for health professionals. Circulation. 1991 ;
83:356-362. 44. Kastelein JJ, Akdim F, Stroes ES, et
al. Simvastatin with or without ezeti- mibe in Familial hypercholesterolemia. N EngUMed. 2008;358:1431-1443.
Address cor respondence to: Rober t a Ara , MSc, Hea l th Economics and
Decis ion Science, School of Hea l th and Related Research, Univers i ty of
Sheffield, Regent Cour t , 30 Regent Street, Sheffield $1 4DA, Uni ted
Kingdom. E-marl: r .m.ara@sheff ield.ac.uk
August 2008 1S23