Enhancing palliative care delivery in a regional community in Australia
10
370 Australian Health Review August 2006 Vol 30 No 3 Improving the Processes of Care Abstract Although access to palliative care is a fundamen- tal right for people in Australia and is endorsed by government policy, there is often limited access to specialist palliative care services in regional, rural and remote areas. This article appraises the evi- dence pertaining to palliative care service delivery to inform a sustainable model of palliative care that meets the needs of a regional population on the mid-north coast of New South Wales. Expert consultation and an eclectic literature review were undertaken to develop a model of palliative care service delivery appropriate to the needs of the target population and resources of the local community. On the basis of this review, a local palliative care system that is based on a population-based approach to service planning and delivery, with formalised integrated network agreements and role delineation between special- ist and generalist providers, has the greatest potential to meet the palliative care needs of this Aust Health Rev 2006: 30(3): 370–379 regional coastal community. ACCESS TO PALLIATIVE CARE is a fundamental right for people in Australia and is endorsed by government policy. 1,2 Access, a key component of all palliative care service delivery models, implies fairness not determined by geographical loca- tion. 1-5 Despite this ideal, the increasing demand for palliative care in regional, rural and remote areas, combined with the limited number of palliative care specialists, presents considerable challenges for health service planners. 6,7 This discussion document reviews the evidence pertaining to model-of-care development, the policy environment and existing rural palliative care models in operation in rural Australia. This review was conducted to inform the development Jane L Phillips, RN, BA(Science-Nursing), Rural Palliative Care Project Co-ordinator Mid North Coast (NSW) Division General Practice, Coffs Harbour, NSW. Patricia M Davidson, RN, BA, MedEd, PhD, Associate Professor of Nursing; and Western Sydney Area Health Service Debra Jackson, RN, PhD, Professor of Nursing John Daly, RN, BA, BHSc, MEd(Hons), PhD, FINE, FCN(NSW), FRCNA, Professor of Nursing, and Foundation Head, School of Nursing, Family and Community Health University of Western Sydney, Sydney, NSW. Linda Kristjanson, RN, BN, MN, PhD, Pro Vice Chancellor Research and Development Curtin University of Technology, Perth, WA. Margaret L Bennett, RN, BN, General Manager, Coffs Harbour Health Campus North Coast Area Health Service, NSW, Coffs Harbour, NSW. Correspondence: Ms Jane L Phillips, PO Box 920, Coffs Harbour, NSW 2450. [email protected] Enhancing palliative care delivery in a regional community in Australia Jane L Phillips, Patricia M Davidson, Debra Jackson, Linda Kristjanson, Margaret L Bennett and John Daly What is known about the topic? The provision of palliative care in rural and remote areas presents significant service delivery challenges, but it is not known how best to address these challenges. What does this paper add? This paper explores issues related to palliative care service delivery in a rapidly expanding regional coastal community. The paper outlines a population- based planning strategy to enhance capacity. What are the implications for practitioners? The authors propose the development of a palliative care service that builds upon the existing specialist service with greater involvement of generalist providers and ensures service development and delivery is explicitly linked to consumer needs.
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Enhancing palliative care delivery in a regional community in Australia

Improving the Processes of Care
Enhancing palliative care delivery in a regional community in Australia
Jane L Phillips, Patricia M Davidson, Debra Jackson, Linda Kristjanson, Margaret L Bennett and John Daly
370
Jane L Phillips, RN, BA(Science-Nursing), Rural Palliative Care Project Co-ordinator Mid North Coast (NSW) Division General Practice, Coffs Harbour, NSW.
Patricia M Davidson, RN, BA, MedEd, PhD, Associate Professor of Nursing; and Western Sydney Area Health Service Debra Jackson, RN, PhD, Professor of Nursing John Daly, RN, BA, BHSc, MEd(Hons), PhD, FINE, FCN(NSW), FRCNA, Professor of Nursing, and Foundation Head, School of Nursing, Family and Community Health University of Western Sydney, Sydney, NSW.
Linda Kristjanson, RN, BN, MN, PhD, Pro Vice Chancellor Research and Development Curtin University of Technology, Perth, WA.
Margaret L Bennett, RN, BN, General Manager, Coffs Harbour Health Campus North Coast Area Health Service, NSW, Coffs Harbour, NSW.
Correspondence: Ms Jane L Phillips, PO Box 920, Coffs Harbour, NSW 2450. [email protected]
Aust Health Rev ISSN: 0156-5788 1August 2006 30 3 370-379©Aust Health Rev 2006 www.aushealthre-view.com.auImproving the Processes of Care
tal right for people in Australia and is endorsed bygovernment policy, there is often limited access tospecialist palliative care services in regional, ruraland remote areas. This article appraises the evi-dence pertaining to palliative care service deliveryto inform a sustainable model of palliative carethat meets the needs of a regional population onthe mid-north coast of New South Wales.
AbstractAlthough access to palliative care is a fundamen-
Expert consultation and an eclectic literaturereview were undertaken to develop a model ofpalliative care service delivery appropriate to theneeds of the target population and resources ofthe local community. On the basis of this review, alocal palliative care system that is based on apopulation-based approach to service planningand delivery, with formalised integrated networkagreements and role delineation between special-ist and generalist providers, has the greatestpotential to meet the palliative care needs of this
Aust Health Rev 2006: 30(3): 370–379
regional coastal community.
ACCESS TO PALLIATIVE CARE is a fundamentalright for people in Australia and is endorsed bygovernment policy.1,2 Access, a key component ofall palliative care service delivery models, impliesfairness not determined by geographical loca-tion.1-5 Despite this ideal, the increasing demandfor palliative care in regional, rural and remoteareas, combined with the limited number ofpalliative care specialists, presents considerablechallenges for health service planners.6,7
This discussion document reviews the evidencepertaining to model-of-care development, thepolicy environment and existing rural palliativecare models in operation in rural Australia. Thisreview was conducted to inform the development
What is known about the topic?The provision of palliative care in rural and remote areas presents significant service delivery challenges, but it is not known how best to address these challenges.What does this paper add?This paper explores issues related to palliative care service delivery in a rapidly expanding regional coastal community. The paper outlines a population-based planning strategy to enhance capacity.What are the implications for practitioners?The authors propose the development of a palliative care service that builds upon the existing specialist service with greater involvement of generalist providers and ensures service development and delivery is explicitly linked to consumer needs.
Australian Health Review August 2006 Vol 30 No 3

Improving the Processes of Care
of a sustainable model of palliative care deliveryfor the mid-north coast of New South Wales.
Mid-north coast New South WalesThe mid-north coast consists of the Coffs Har-bour, Bellingen and Nambucca local governmentareas (LGA) which now reside within the centralnetwork of the recently created North Coast AreaHealth Service. Although the reorganisation of thearea health service boundaries in NSW occurredsubsequent to the completion of this need assess-ment, this does not alter the significance of thesefindings.8
This area has a population of 97 774 people,with the largest concentrated population residingin the Coffs Harbour LGA and the remainingpopulation in smaller coastal townships, whichare popular holiday destinations, or in inlandfarming communities.9 Over the past 20 years thearea has had the highest population growth inNSW with an annual rate of 2.3%, primarily dueto the internal migration of people over 65 yearsof age.10-11 Many of these people have left behindtheir family, support and kinship networks withthe expectation that services to which they areaccustomed will be readily available in their newregional community.12 A significant number ofresidents are of lower socio-economic status andare welfare recipients.9,13-14 There is a poor trans-port infrastructure in the area and limited accessto community-based aged care-related serv-ices.13,15 A workforce shortage of general practi-tioners, specialists and nurses has been noted.9,15
Significantly, the area has a large Indigenouspopulation, representing about 3.2% of the localpopulation, compared with 1.9% for NSW. Anadditional feature of this area is also the presenceof a well established Punjabi community.16
The Coffs Harbour palliative care service com-menced operation in 198413 and is essentially aseven day per week community-based specialistpalliative care nursing service that provides directcare with minimal community nursing input. Theservice has a designated part-time counsellor;trained volunteers; a visiting palliative care physi-cian service; access to hospital-based allied health
staff; a large loan equipment pool; and a bereave-ment support program. It has strong links withlocally based oncology, renal, neurology and car-diology services and clinical experts. There is asatellite palliative care service that operates inde-pendently from Macksville Health Campus andservices the Nambucca LGA.
Key challenges to palliative care service delivery on the mid-north coastAn extensive review of local epidemiological dataand reports10,15,17 has identified the followingfactors as challenging local palliative care delivery.
Population ageingIt is anticipated that the popularity of the mid-north coast as a preferred retirement destinationfor baby boomers will continue, with 35% of thearea’s population growth expected to be in theover 65 age group by 2031,10 with anticipationthat this area will have the highest proportion ofover-65-year-olds in NSW. Of significance, mid-way through this period the number of deaths isexpected to exceed the number of births.10
As increased age is associated with the onset ofchronic and potentially life-limiting illnesses, formany retirees their new lifestyle is accompaniedby disability. As many people have minimal or nolocal family support and lack the funds to pur-chase additional private health care services15
they are dependent upon community-based serv-ices which are already under significant pressure.
Increased demand for servicesThis unprecedented migration of people over 65years has significant implications for aged andpalliative care services. Although the number ofspecialist palliative care workers has increasedfrom 1.5 full-time equivalents in 1984 to thecurrent level of 6.5 full-time equivalents, theservice now covers a significantly larger geo-graphic area of three LGAs. During the sameperiod, the number of patients referred to thecommunity-based service has increased from 50referrals per year in 1984 to 240 referrals in 2003,
Australian Health Review August 2006 Vol 30 No 3 371

Improving the Processes of Care
with about 40% of these palliative care patientsnow electing to be cared for at home. It isestimated that on any given day, over 110 pallia-tive care patients are registered with the localpalliative care services. Given this continuedgrowth, the specialist palliative care team isunable to meet this level of need within thecurrent model of care.
It is now widely accepted that palliative carehas a role to play at various stages of a person’sdisease, and this is reflected in most contemp-orary definitions.1,2,5 Symptom control has beenidentified as the primary reason for admission topalliative care services in Australia, followed byterminal care.18 Although adults with cancermake up 85%–90% of the palliative care patientprofile in Australia, people with non-malignantprogressive disorders also require access to palli-ative care.1,2,19 Advances in therapeuticapproaches mean that the palliative phase ofboth malignant and non-malignant diseases isoften longer, and determining the terminalphase for some life-limiting diseases is oftendifficult to predict due to the absence of reliableprognostic indicators.20 As a consequence ofthese prolonged illness trajectories community-based services are frequently required to providecare for extended periods of time.21,22
Absence of palliative care bedsAs there are no designated beds on the mid-northcoast, palliative care patients requiring inpatientcare are admitted to one of five local hospitals. Arecent planning framework has estimated that 6.7designated palliative care beds are required forthis population.5
Increased demand from residential aged care facilitiesThe high service demands on the palliative careservice mean that there have been very limitedopportunities to provide input, education andconsultancy to the 12 local residential aged carefacilities, which are collectively providing care to397 high- and 470 low-level care residents.Locally, the majority of high-level care beds areoccupied by the chronically unwell and frail
aged and in many respects function as hos-pices.23 Yet, until recently, the palliative careneeds of these facilities have largely been invisi-ble,18,24,25 with only a little over half (54.55%) ofpalliative care providers in Australia havingengaged in educational initiatives with this sec-tor.18 This is despite the reality that aged careproviders care for a significant number of peopleat the end of life, with local data revealing that80% of all resident deaths were managed onsite.26
Workforce-related issuesDespite the NSW mid-north coast being anidyllic rural location, it has become increas-ingly difficult to attract skilled medical andnursing workforce to the area. The local Divi-sion of General Practice conservatively esti-mates that the area is 12 GPs short of therecommended number, and workload issuesmake it difficult for many GPs to respond in atimely manner to patients in need.27 There islimited coordination of GP input and participa-tion in the management of patients receivingpalliative care, regardless of care setting. Timeconstraints and the lack of financial reward arethe reasons often quoted by local GPs for notconducting home visits, including regular visitsto residential aged care facilities.23
Facilitators to service deliveryIn spite of the challenges listed above, severallocal factors exist to drive the improvement ofpalliative care service delivery.
Health facilities and servicesThere are four public hospitals with at least onefacility in each LGA and an 80 bed privatehospital located in Coffs Harbour. The area’smajor referral hospital is also located in CoffsHarbour and provides a broad range of support-ing specialties consistent with a Level 5 BaseHospital in NSW. A purpose built Cancer CareCentre with a radiotherapy unit and one linearaccelerator has recently been commissioned.There has been a significant expansion in the
372 Australian Health Review August 2006 Vol 30 No 3
Improving the Processes of Care
number of aged care beds with the numbers forthe area now within established planning ratios tomeet anticipated local need.15,28
Information systems and data collectionThroughout Australia there is disparity in pallia-tive care data collection, with services using avariety of definitions and collecting different dataitems. As a consequence there is an inadequatedescription of service provision and consumerneeds.18 The Australian National Sub-Acute andNon-Acute Casemix Classification Study identi-fied a five-phase classification system for pallia-tive care that is independent of the setting and issensitive to changes in the goal of care.2,3,29 Thisdata collection system has recently been imple-mented locally, which will make it easier toaccurately determine and map local palliative careservice need.
Community participationThe local palliative care service benefits fromsignificant local community support, which hasensured the acquisition of a large loan equipmentpool through donated funds. The palliative carevolunteers consist of interested local communitymembers, and there is a voluntary organisationthat assists patients requiring out-of-area medicaltreatment and provides accommodation and sup-port for families at Coffs Harbour Hospital. Abranch of the National Association of Loss andGrief has recently been established and there hasbeen support of an aged care academic positionby a local credit union.
Expansion of locally available education servicesA tertiary education facility has been establishedat Coffs Harbour with the first intake of localbachelor of nursing students commencing in2004. The College of Technical and FurtherEducation (TAFE) conducts enrolled nursing andcare assistants courses, including a designatedpalliative care course. A medical student programwith an onsite campus located at the Base Hospi-tal has recently been established. It is anticipatedthat these locally based initiatives will improve
workforce shortages in the area and adequatelyequip health care providers to work withinregional communities.30
Rural palliative care programThe Mid North Coast Division of General Practiceis one of eight rural divisions in Australia that hasbeen funded as part of the National Rural PalliativeCare Program from 2004 to 2006. This programaims to strengthen local partnerships to improvethe coordination and delivery of local palliativecare services.31 The local project has adopted acollaborative approach to engage local health careorganisations and providers in the delivery ofpalliative care across the care continuum.
MethodsCINAHL, PubMed and MEDLINE electronicdatabases were searched using keywords of“models*”, “rural*”, “palliative care models” and“service delivery models” to identify relevantliterature published in the English language toinform this review. Reference lists of retrievedarticles were searched for additional literature.Relevant journals held locally were handsearched for pertinent articles, and the Internetwas searched using the Google search engine forrelated organisations or electronic documentsusing the keywords listed previously. Relevantpalliative care policy was identified from asearch of Commonwealth, state and Area HealthService and Palliative Care Australia websites.The eclectic and heterogeneous material for thisreview precluded the use of a systematic reviewmethodology.
Findings
Positive policy environmentA number of significant policy frameworksshape the delivery of palliative care serviceswithin Australia. The National Palliative CareStrategy provides a guide for the developmentand implementation of palliative care policies,strategies and services to improve the quality,
Australian Health Review August 2006 Vol 30 No 3 373

Improving the Processes of Care
range and coverage of palliative care.1 A total of$201.2 million has been allocated to palliativecare throughout the 5 years of the AustralianHealth Care Agreement (2003–2008), with oneof the priorities being to increase the range andreach of palliative care services.1 This policy isresponsive to perceived deficits and inequity ofaccess. As part of this commitment the Austral-ian Government has endorsed policy guidelinesaimed at enhancing the delivery of a palliativeapproach to care for older people in residentialaged care facilities.24
The NSW Palliative Care Framework identifieskey elements to promote access, continuity ofcare and standard levels of care, regardless of theservice location.2The majority of funding forpalliative care is derived from the state govern-ment in accordance with the resource distribu-tion formula, and it is the responsibility of eacharea health service to determine how palliativecare is provided locally. In 2001, all area healthservices were requested to prepare an AreaPalliative Care Services Plan in accordance withaccepted palliative care frameworks and stand-ards,2,18 but little is known about whether theseplans have been actioned.
Since 2003, Palliative Care Australia hasreleased three significant policy documentswhich collectively provide guidance for thedevelopment of palliative care services at anational, state, regional and local level. A guide topalliative care service development: a populationbased approach provides a framework to ensurethe equitable access to palliative care for allAustralians which is based on the efficient,effective and ethical use of resources.32 Palliativecare service provision in Australia — a planningguide5 provides a formula for determining thehuman resources needed for the provision ofspecialist palliative care services in Australia.The Standards for providing quality palliative carefor all Australians is an integral tool for theplanning and delivery of a coordinated networkapproach to palliative care provided by bothprimary and specialist service providers.4 Col-lectively these platform policy documents pro-vide a clear framework and guidance for the
development of palliative care services through-out Australia.
Health care organisationIn Australia, palliative care services haveemerged largely as a result of funding initiativessince the 1980s with services operating in out-patient, inpatient and community-based set-tings, with a combination of public and privateproviders utilising both specialist and generalistmodels of care.1-3,13,29,33 Some of these servicesappear to have grown historically, and notalways in response to local population needs.32
To date, minimal systematic investigation hasbeen undertaken on palliative care deliverymodels.2
A recent review of palliative care servicesplans in NSW identified diversity among deliv-ery models, characteristics, target groups, rela-tionships with other services, available resourcesand organisational structures.18 This study wasunable to identify “models of excellence” inprescribed settings and circumstances because ofa lack of a uniform approach to the definitionand collection of both quantitative and qualita-tive data by palliative care services.18 Similardifficulties were encountered by researchers in asystematic review of the literature examiningorganisation of palliative care for rural popula-tions. These authors identified 26 studies suit-able for inclusion in the review, but the diversityand lack of research methods in the reportsmade it difficult to analyse the models.34
The majority of service delivery models inAustralia are specialist services delivering pallia-tive care to a small subset of the population.32
Given that not all people living with a life-limiting illness need, or desire, the same leveland access to specialist palliative care services,access to these scarce specialist services shouldbe based on the level of need.32 A recent reviewof palliative care service delivery in Tasmaniadetermined that formalised clinical partnershipsand role delineation between specialist and gen-eralist services was required for effective andsustainable palliative care delivery.35 This modelexpands upon a population-based approach by
374 Australian Health Review August 2006 Vol 30 No 3
Improving the Processes of Care
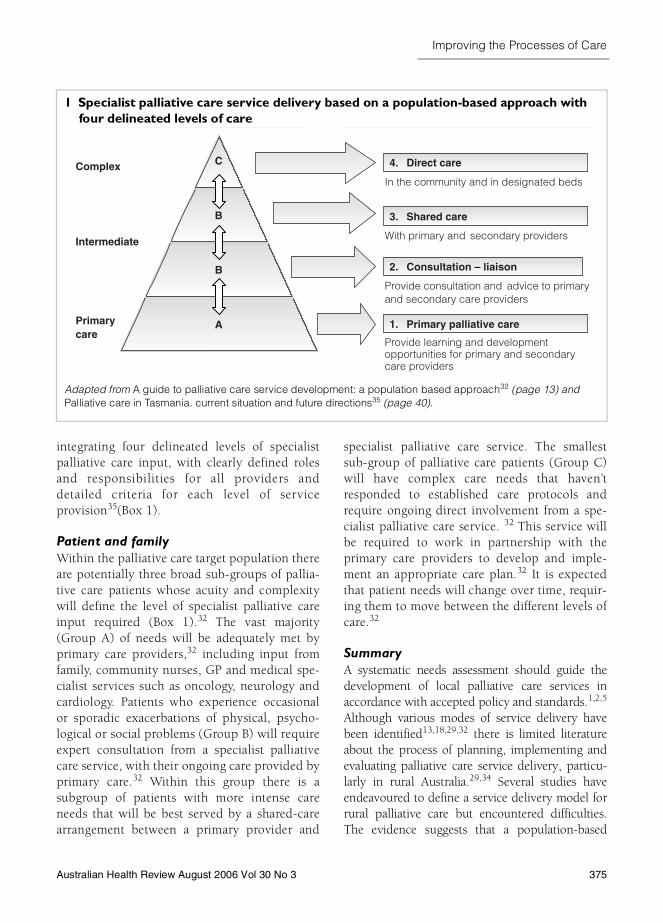
integrating four delineated levels of specialistpalliative care input, with clearly defined rolesand responsibilities for all providers anddetailed criteria for each level of serviceprovision35(Box 1).
Patient and familyWithin the palliative care target population thereare potentially three broad sub-groups of pallia-tive care patients whose acuity and complexitywill define the level of specialist palliative careinput required (Box 1).32 The vast majority(Group A) of needs will be adequately met byprimary care providers,32 including input fromfamily, community nurses, GP and medical spe-cialist services such as oncology, neurology andcardiology. Patients who experience occasionalor sporadic exacerbations of physical, psycho-logical or social problems (Group B) will requireexpert consultation from a specialist palliativecare service, with their ongoing care provided byprimary care.32 Within this group there is asubgroup of patients with more intense careneeds that will be best served by a shared-carearrangement between a primary provider and
specialist palliative care service. The smallestsub-group of palliative care patients (Group C)will have complex care needs that haven’tresponded to established care protocols andrequire ongoing direct involvement from a spe-cialist palliative care service. 32 This service willbe required to work in partnership with theprimary care providers to develop and imple-ment an appropriate care plan.32 It is expectedthat patient needs will change over time, requir-ing them to move between the different levels ofcare.32
SummaryA systematic needs assessment should guide thedevelopment of local palliative care services inaccordance with accepted policy and standards.1,2,5
Although various modes of service delivery havebeen identified13,18,29,32 there is limited literatureabout the process of planning, implementing andevaluating palliative care service delivery, particu-larly in rural Australia.29,34 Several studies haveendeavoured to define a service delivery model forrural palliative care but encountered difficulties.The evidence suggests that a population-based
1 Specialist palliative care service delivery based on a population-based approach with four delineated levels of care
Adapted from A guide to palliative care service development: a population based approach32 (page 13) and Palliative care in Tasmania. current situation and future directions35 (page 40).
C
B
B
APrimarycare
Complex 4. Direct care
3. Shared care
2. Consultation – liaison
1. Primary palliative care
Intermediate
In the community and in designated beds
With primary and secondary providers
Provide consultation and advice to primary and secondary care providers
Provide learning and development opportunities for primary and secondary care providers
Australian Health Review August 2006 Vol 30 No 3 375
Improving the Processes of Care
approach to palliative care service development isthe most appropriate framework for the delivery ofeffective and efficient palliative care.32
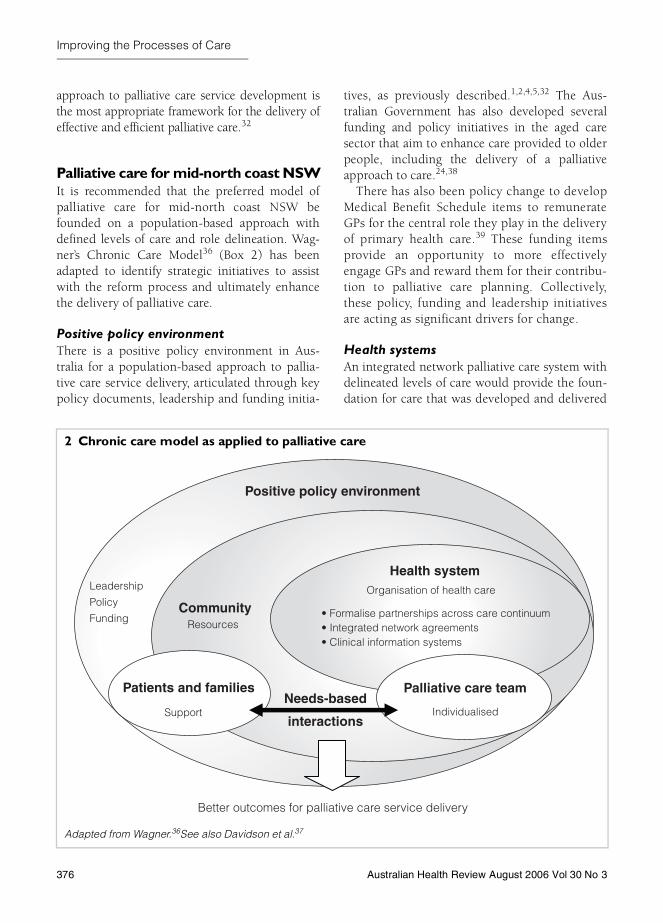
Palliative care for mid-north coast NSWIt is recommended that the preferred model ofpalliative care for mid-north coast NSW befounded on a population-based approach withdefined levels of care and role delineation. Wag-ner’s Chronic Care Model36 (Box 2) has beenadapted to identify strategic initiatives to assistwith the reform process and ultimately enhancethe delivery of palliative care.
Positive policy environmentThere is a positive policy environment in Aus-tralia for a population-based approach to pallia-tive care service delivery, articulated through keypolicy documents, leadership and funding initia-
tives, as previously described.1,2,4,5,32 The Aus-tralian Government has also developed severalfunding and policy initiatives in the aged caresector that aim to enhance care provided to olderpeople, including the delivery of a palliativeapproach to care.24,38
There has also been policy change to developMedical Benefit Schedule items to remunerateGPs for the central role they play in the deliveryof primary health care.39 These funding itemsprovide an opportunity to more effectivelyengage GPs and reward them for their contribu-tion to palliative care planning. Collectively,these policy, funding and leadership initiativesare acting as significant drivers for change.
Health systemsAn integrated network palliative care system withdelineated levels of care would provide the foun-dation for care that was developed and delivered
2 Chronic care model as applied to palliative care
Adapted from Wagner.36See also Davidson et al.37
Organisation of health care
• Formalise partnerships across care continuum• Integrated network agreements• Clinical information systems
Resources
IndividualisedSupport
Leadership
Policy
Funding
Better outcomes for palliative care service delivery
Positive policy environment
Health system
Needs-based
interactions
Palliative care teamPatients and families
Community
376 Australian Health Review August 2006 Vol 30 No 3

Improving the Processes of Care
in accordance with local need and capacity.32,35 Inthis model, the specialist palliative care teamstructure would be retained, but these workerswould deliver care according to the patient’s levelof need and perform the roles outlined in Box 1.The expertise of the specialist palliative careservice will be used more effectively to: developand implement learning and development oppor-tunities for generalist providers; provide a consul-tancy and liaison service; contribute to the sharedcare of patients with more intense needs; andprovide direct care to patients who have the mostcomplex palliative care needs in the communityand acute care setting.32,35
Community health staff, GPs, residential agedcare providers, private nursing services, acutecare providers in both the public and privatesetting, and specialist medical and nursing staffwill need to be actively engaged as partners in thedelivery of palliative care in the network. Thisrequires all health care providers’ roles andresponsibilities to be clearly defined, with policiesand procedures which clearly outline the accessand referral criteria.35 Formalised role delineationpartnership agreements between specialist andgeneralist providers will promote coordination oflimited resources.32 Integration of resources willhelp to overcome the diseconomies of scale whichmight otherwise make discrete services unstaina-ble and improve local palliative care service deliv-ery.35,40
The formalisation of partnerships across thenetwork provides a platform to explore creativealternatives for better continuity and coordinationof local palliative delivery, including initiativessuch as: co-funding of service delivery; utilisingcommon palliative care clinical indicators andassessment and management tools; standardiseddata collection, developing a common language;and the use of end-of-life care pathways by gener-alist health care providers in all care settings.
Yet, creating the proposed integrated networkpalliative care system is not without significantchallenges. It requires a clear commitment by allinvolved to actively work towards reorientating arange of services to ensure that the degree ofproviders’ involvement in palliative care delivery is
determined by the patient’s intensity of need (Box 1).In this model, generalist providers, particularlycommunity nurses, are required to play a greaterrole in the delivery of primary palliative care. Ascommunity nurses currently have limited involve-ment in the provision of palliative care in this localarea, this group of providers will require supportand guidance through the proposed change. Giventhe potential impact the reorientation of care deliv-ery will have on community nurses’ workloads,additional resources need to be allocated.
Capacity building of local services is a keyelement of establishing an integrated network pal-liative care system. There will be a need for skillenhancement and diversification, extended rolesand new scopes of practice for many health careprofessionals, particularly those working in acutecare services, community nursing and residentialaged care,3,24 potentially resulting in the creationof palliative care as a sub-specialty within theseareas.41 The development of a palliative care “linknurse” role within local acute care services andresidential aged care facilities, supported and men-tored by the specialist palliative care team, is astrategy to ensure access to a resources nurse.42,43
Communication strategies for timely sharing ofaccurate clinical information among relevanthealth care providers at different locations is criti-cal.32 The use of patient-held records would enablerelevant health care information to be sharedbetween the patient and providers. There is scopeto explore communication strategies regarding careplanning, including the use of technology such asvideoconferencing, personal digital assistants, pal-liative care-specific data software44 and web-basedclinical information systems.
Palliative care teamIn the proposed model, an individualised pallia-tive care team, which in some cases may be“virtual”, will be created to meet the needs of eachpatient and their family. This team can operate inthe acute care, community and residential agedcare settings and seek the input of the specialistpalliative care team as required. Generalist pro-viders, input into multidisciplinary palliative careplanning forums will assist in building relation-
Australian Health Review August 2006 Vol 30 No 3 377

Improving the Processes of Care
ships across local health care systems, reinforcethe importance of a team approach and enableknowledge sharing that is immediately relevant.45
While enhanced primary care (EPC) items reim-burse general practitioners for their contributionto the care planning process.39
Community resourcesThe target population for palliative care servicedelivery will be people with a life-limiting illnessand caregivers residing in the mid-north coast.Access to the specialist palliative care team will bebased on their intensity of need. 32 Given the levelof community support that currently exists forthe local palliative care service it is important thatthe proposed model be disseminated to the com-munity and processes put in place to enableresources to be shared throughout the local palli-ative care system.
Conclusions and implications for clinical service deliveryThe adoption of a population approach to plan-ning palliative care service delivery on the mid-north coast of NSW is required to ensure moreeffective utilisation of scare resources. An inte-grated palliative care network with delineatedlevels of care would provide the foundation for alocal palliative care system to develop and deliverpalliative care based on local need and capacity.Establishment of palliative care partnerships, for-malising network agreements, role delineationbetween providers and referral and entry criteriaare required, along with appropriate resourcesallocation. A systematic evaluation is needed andmay assist in developing a model of care that isable to be used in other regions.
AcknowledgementsThis paper resulted from the preliminary work under-taken as part of developing the Mid North CoastDivision of General Practice’s 3-year (2003–2006) RuralPalliative Care Project. The research team would like toacknowledge the contribution and support of the MidNorth Coast Division of General Practice and the Pallia-tive Care Team, as well as funding from the Common-
wealth Department of Health and Ageing, NationalRural Palliative Care Program.
Competing interestsThe authors declare that they have no competing interests.
References1 Commonwealth Department of Health and Aged Care.
National Palliative Care Strategy. Canberra: 2000.2 NSW Health. NSW Palliative Care Framework: a guide for
the provision of palliative care in NSW. Sydney: NSWHealth Department, 2001.
3 Perkins D, Owen A. Indicators of fairness and sustainabil-ity in palliative care. 2001. Proceedings of Health Out-comes 2001 — The Odyssey Advances: 7th Annualnational health outcomes conference. Canberra; 2001June 27–28.
4 Palliative Care Australia. Standards for providing qualitypalliative care for all Australians. Canberra: PC Australia,2005.
5 Palliative Care Australia. Palliative care service provision inAustralia: a planning guide. Canberra: PC Australia 2003.
6 Department of Primary Industries and Energy and Depart-ment of Human Services and Health. Rural, remote andmetropolitan area classification. Canberra: Common-wealth of Australia, 1994: 28.
7 White K, Wall D, Kristjanson L. Out of sight out of mind:reframing remoteness in providing palliative care in remoteAustralia. Collegian 2004; 11(3): 29-33.
8 NSW Health Department. Planning better health — minis-ter announces reform of NSW health system. [Mediarelease]. 27 July 2004. Available at: <http://www.heal th.nsw.gov.au/news/2004/index.html#>(accessed Jun 2006).
9 Public Health Information Development Unit. Populationhealth profile of the Mid North Coast Division of GeneralPractice. Population Profile Series No. 22. Adelaide: Com-monwealth of Australia, 2005.
10 Department of Infrastructure Planning and NaturalResources. New South Wales state and regional popula-tion projections. Sydney: Transport and Population DataCentre, 2004.
11 Salt B. The big shift: the Bernard Salt report. Melbourne:Hardie Grant Books, 2001.
12 MacDermott K, Clout J. Fight is on to control the patch.Australian Financial Review 2004 27 Mar: 7.
13 Sach J. Palliative care in rural Australia. Canberra: NationalPalliative Care Program, Commonwealth Department ofHealth and Family Services, 1996.
14 St Lawrence and associates Consulting Services. CoffsHarbour economic profile. Coffs Harbour: NSW Depart-ment of State and Regional Development and Coffs Har-bour City Council, 2003. Available at <http://www.coffsharbour.nsw.gov.au/resources/documents/
378 Australian Health Review August 2006 Vol 30 No 3
Improving the Processes of Care
Coffs_Harbour_Economic_Profile_20032.pdf> (accessedJun 2006).
15 Curran J. Progress on a joint aged services and researchcollaboration at Coffs Harbour [Unpublished report].Southern Cross University and University of New SouthWales, 2004: 23.
16 Bhatti R, Dusenbury V. A Punjabi Sikh community inAustralia: from Indian sojourners to Australian citizens.Woolgoolga: Woolgoolga Neighbourhood Centre Inc,2000.
17 Mid North Coast Area Health Service. Area Palliative CareServices Plan, July 2001–June 2004 [Unpublished]. PortMacquarie: Mid North Coast Area Health Service, 2001.
18 Little Company of Mary Health Care. National PalliativeCare Plan Initiative: final report. 2003.
19 Franks PJ, Salisbury C, Bosanquet N, et al. The level ofneed for palliative care: a systematic review of the litera-ture. Palliat Med 2000; 14: 93-104.
20 Christakis NA, Lamont A. Extent and determinants of errorin doctors’ prognoses in terminally ill patients: prospectivecohort study. BMJ 2000; 320: 469-73.
21 Brookes K, Davidson P, Daly J, Hancock K. Communityhealth nursing in Australia: a critical literature review andimplications for professional development. ContempNurse 2004; 16: 195-207.
22 Davidson PM, Paull G, Introna K, et al. Integrated, collabo-rative palliative care in heart failure: the St George HeartFailure Service experience 1999-2002. J Cardiovasc Nurs2004; 19: 68-75.
23 Phillips J, Davidson PM, Kristjanson L, et al. Residentialaged care: the last frontier for palliative care. J Adv Nurs2006 (in press).
24 Australian Government Department of Health and Ageing.Guidelines for a palliative approach in residential agedCare. Canberra: Department of Health and Ageing, 2004.
25 Grbich C, Maddocks I, Parker D. Palliative care in agedcare facilities for residents with non-cancer diagnosis.Adelaide: Department of Palliative and Supportive Serv-ices, School of Medicine, Flinders University, 2003.
26 Phillips J. Number of deaths in residential aged carefacilities in Coffs Harbour and Bellingen local governmentareas [unpublished data]. Coffs Harbour: Mid North CoastDivision of General Practice, 2004.
27 Spence P. Shortage of general practitioners in Coffs Har-bour and Bellingen local government areas [unpublishedreport]. Coffs Harbour: Mid North Coast Division of Gen-eral Practice, 2004.
28 Commonwealth Department of Health and Ageing. Theresidential care manual. Canberra: DHA, 2002.
29 Cromwell D, Senior K, Owen A, et al. Can the NationalPalliative Care Strategy be translated into a model of carethat works for rural Australia? An answer from the GriffithArea Palliative Care Service (GAPS) experience. Centre forHealth Service Development, University of Wollongong,2003. Available at: <http://ro.uow.edu.au/chsd/>(accessed Jun 2006).
30 Hegney D, McCarthy A, Rogers-Clark C, Gorman D.Retaining rural and remote area nurses. The Queensland,Australia experience. J Nurs Adm 2002; 32: 128-35.
31 Australian Divisions of General Practice. Rural PalliativeCare Program [websi te ]. Ava i lable a t :<http:www.adgp.com.au/site/index.cfm?display=683>(accessed Jun 2006).
32 Palliative Care Australia. A guide to palliative care servicedevelopment: a population based approach. Canberra:PC Australia, 2005.
33 Palliative Care Association of New South Wales. Review ofNSW Health palliative care service plans [unpublishedreport]. Sydney: PCA NSW, 2003.
34 Evans R, Stone D, Elwyn G. Organizing palliative care forrural populations: a systematic review of the evidence.Fam Pract 2003; 20(3): 304-10.
35 Eagar K, Gordon R, Quinsey K, Fildes D. Palliative care inTasmania: current situation and future directions. Wollon-gong: Centre for Health Services Development, Universityof Wollongong, 2004. Available at: <http://ro.uow.edu.au/chsd/13/> (accessed Jun 2006).
36 Wagner EH. Chronic disease management: what will ittake to improve care for chronic illness? Eff Clin Pract1998; 1: 2-4.
37 Davidson PM, Halcomb EJ, Hickman L, et al. Beyond therhetoric: what do we mean by a model of care? Aust J AdvNurs 2006; 23: 47-55.
38 Australian Government Department of Health and Ageing.Aged care general practitioners panels initiative guide-lines Canberra: Australian Government Department ofHealth and Ageing, 2004.
39 Australian Government Department of Health and Ageing.Medicare Benefits Schedule book. Canberra: AustralianGovernment Department of Health and Ageing, 2004.
40 Bidwell S. Successful models of rural health servicedelivery and community involvement in rural health:international literature review. Christchurch: Centre forRural Health, Department of Public Health and Gen-eral Practice, Christchurch School of Medicine andHealth Sciences, University of Otago: 2001. Availableat: <http://www.moh.govt.nz/moh.nsf/238fd5fb4fd051844c256669006aed57/55b8e684cb76f9c7cc256d9f000ace50?OpenDocument> (accessed Jun 2006).
41 Wilkes L, Beale B. Palliative care at home: stress fornurses in urban and rural New South Wales, Australia.Int J Nurs Pract 2001; 7: 306-13.
42 Maddocks I, Parker D, McLeod A, Jenkins P. Palliativecare nurse practitioners in aged care facilities. Adelaide,South Australian Department of Human Services, 1999.
43 Froggatt K, Hoult L. Developing palliative care practice innursing and residential care homes: the role of the clinicalnurse specialist. J Clin Nurs 2002; 11: 802-8.
44 Unique Database Solutions. Palliative Care Clinical Infor-mation System – PalCIS. 2006. Available at: <http://www.palcis.com/vmc_whatis.asp>. (accessed Feb 2006).
45 Dudgeon D, Knott C, Viola R, et al. Managing continuitythrough collaborative care plans: a study of palliative carepatients. Ontario: Canadian Health Services ResearchFoundation, 2004. Available at: <http://www.chsrf.ca/final_research/index_e.php> (accessed Jun 2006).
(Received 17 May 2005, accepted 27 Apr 2006)
Australian Health Review August 2006 Vol 30 No 3 379




















