ELDERLY.pdf - edtna/erca homepage
140
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of ELDERLY.pdf - edtna/erca homepage


Caring for the Elderly Renal PatientA Guide to Clinical Practice
All rights are reserved by the author and publisher, including the rights of reprinting, reproduction in any form and translation. No part of this book may be reproduced, stored in a retrieval system or transmitted, in any form or by means, electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the publisher.
First edition: September 2011
European Dialysis and Transplant Nurses Association/ European Renal Care Association (EDTNA/ERCA)Pilatusstrasse 35, Postfach 3052, 6002 Luzern, Switzerlandwww.edtnaerca.org
ISBN: 978-84-615-1653-7
D.L.: M-29870-2011
Layout, Binding and Printing: Imprenta Tomás HermanosRío Manzanares, 42-44 · E28970 Humanes de MadridMadrid - Spainwww.tomashermanos.com

5
Acknowledgements
6
Caring for the Elderly Renal Patient
Acknowledgements
Last year the EDTNA/ERCA in partnership with 13 Nephrology National Associations conducted a cross-sectional study to describe the attitudes of a sample of renal nurses toward older people and examine the relationship between their personal characteristics and their attitudes. Participants completed the Kogan’s Attitude Towards Old People Scale (KOAP) and a brief questionnaire about demographic, social and educational details. Results of this project will be presented at the 40th EDTNA/ERCA Conference in Ljubljana – Slovenia. They will help to provide specifi c information to renal nurses, in order to provide the best care to the elderly population assisted in renal fi eld. This is a vital concern for an excellent nursing practice.Caring for the Elderly Renal Patient – A Guide to Clinical Practice handbook was produced with the aim to be used as a tool to help renal care professionals in the caring for the elderly patients. As EDTNA/ERCA Publications Coordinator and on behalf EDTNA/ERCA Executive Committee I am pleased to Acknowledge a number of colleagues. First of all, thanks to all the Authors of each chapter because they made possible this book. Second, a special note of acknowledgement to Karen Pugh-Clarke for the considerable amount of work assumed in order to complete this book. She has had also the support of Hildur Einarsdóttir who also deserves our appreciation. Last but not least, thanks to Alessandra Zampieron and Maria Saraiva from EDTNA/ERCA Executive Committee for their great support in the consolidation of this publication.Maria Cruz CasalEDTNA/ERCA Publications Coordinator
7
Acknowledgements
EditorsKaren Pugh-Clarke, RGN, BSc (Hons), MSc, PhD (c). Lead Nurse for Anaemia Management, Chronic Kidney Disease (CKD) Team, University Hospital of North Staffordshire (UHNS) NHS Trust, Stoke-on-Trent, England, UK
Hildur Einarsdóttir, BSc, MSc in nursing, RN, Certifi ed CNS in Chronic Illness, CNS in Nephrology, Landspitali University Hospital, Reykjavík, Iceland
Reviewer and CoordinatorMaria Cruz Casal, RN, Nephrology Unit, 12 Octubre Universitary Hospital, Madrid, Spain

9
Table of Contents

10
Caring for the Elderly Renal Patient
Preface .............................................................................................................. 15
Alessandra Zampieron, RN, BSN, MSN,Coordinator of Studies at School of Nursing, Padua University Hospital, Italy
1. The Aging Process .............................................................................. 19
Nele van Den Noortgate, Geriatric specialist, Department of Geriatric Medicine, Gent, Belgium
2. Theories of Aging & Physiological Changes ......... 31
Karen Pugh-Clarke, RGN, BSc (Hons), MSc, PhD (c). Lead Nurse for Anaemia Management, Chronic Kidney Disease (CKD) Team, University Hospital of North Staffordshire (UHNS) NHS Trust, Stoke-on-Trent, England, UK
3. Meeting the elderly patient in the Renal Clinic: A partnership in care with the multidisciplinary team ....................................................................................................................... 43
Idalina Delfi na Gomes, PhD in Nursing Sciences, lecturer at Lisbon’s College of Nursing and member of UI&DE (Nursing Research and Development Unit), Master on Communication in Health, Lisbon, Portugal

11
Table of Contents
4. Providing Information and Education to the Elderly Renal patient ............................................................................................... 67
Hildur Einarsdóttir, BSc, MSc in nursing, RN, Certifi ed CNS in Chronic Illness, CNS in Nephrology, Landspitali University Hospital, Reykjavík, Iceland
5. The Elderly Patient on Peritoneal Dialysis ............... 79
Aase Riemann, PN, Bc, EDTNA/ERCA Peritoneal Dialysis Consultant, The Netherlands
6. The Elderly Patient on Haemodialysis .......................... 97
Karen Pugh-Clarke, RGN, BSc (Hons), MSc, PhD (c). Lead
Nurse for Anaemia Management, Chronic Kidney Disease (CKD)
Team, University Hospital of North Staffordshire (UHNS) NHS Trust,
Stoke-on-Trent, England, UK
June Turner, RN, Deputy Sister, CKD Team, UHNS NHS Trust, Stoke- on-Trent, England, UK
Hildur Einarsdóttir, BSc, MSc in nursing, RN, Certifi ed CNS in Chronic Illness, CNS in Nephrology, Landspitali University Hospital, Reykjavík, Iceland
7. Legal and Ethical Concerns for the Elderly Renal Patient ............................................................................................ 107
Mumtaz Goolam, MSc (c) Clinical Research, PG Dip (Health
Studies), PG Dip (Advanced Nursing Science), BA (Cur), RN, Dip.
Nurs. & Midwifery, Renal Nurs Cert., UK

12
Caring for the Elderly Renal Patient
8. Nutritional Requirements in Elderly Renal Patients ......................................................................................... 115
Kalliopi-Anna Poulia, MMedSci. Assoc. Nut.r, Clinical Dietitian-Nutritionist, General Hospital of Athens, “Laiko”, Greece
9. Psychosocial Aspects of Caring for the Elderly Renal Patient ........................................................................ 129
Karen Pugh-Clarke, RGN, BSc (Hons), MSc, PhD (c). Lead Nurse for Anaemia Management, Chronic Kidney Disease (CKD) Team, University Hospital of North Staffordshire (UHNS) NHS Trust, Stoke-on-Trent, England, UK

13
Table of Contents


15
Preface
16
Caring for the Elderly Renal Patient
The proportion of older people has increased worldwide and so have the health problems related with ageing, such as renal diseases that often need long-term care. This enhances the need for skilled and experienced healthcare providers, in many health care settings, who can address and meet the needs of older people. Nurses therefore have a pivotal role as care providers for older people and are uniquely positioned to infl uence the quality of their care1.
However, previous studies have indicated that healthcare providers do not enjoy taking care of the elderly due to ignorance and poor attitude2. Care for these patients — who occupy acute-care beds, chronic units, homes for the aged, nursing homes, rehabilitation facilities, other continuing care institutions, or homecare programs — is viewed as low-status by registered nurses, unchallenging, and not what they were trained or hired to provide3. Courtney (2000), in a literature review about this topic4, described that attitudes towards older patients signifi cantly infl uence nurses’ practice, because they reported holding negative attitudes towards older patients held positive attitudes towards restraint use and stereotyped older patients rather than regarding them as individuals. They also did not perceive older patients as being capable of making their own decisions or carrying out important functions.
Due to all these motivations EDTNA/ERCA decided to produce this book. This product would be a support for renal nurses who have the responsibility of taking care of older people. We are sure that the contributions offered by multidisciplinary authors, related to the different aspects of renal geriatric care will help nurses to increase their knowledge about geriatric care. This information can offer an excellent foundation for good nursing practice to better serve the needs of older people.Alessandra Zampieron
17
Preface
ReferencesStevens J, & Herbert M. Ageism and nursing practice in Australia. 1. Royal College of Nursing, Australia’s Discussion Document, No. 3, 1997.
Palmore EB. Ageism: negative and positive (2nd ed). New York: 2. Springer Publishing Company, 1999.
Kuhn JK.. A Nationwide Survey of Student Nurses’ Attitudes Toward 3. Aging and their Intent to Work with Elderly Clients after Graduation. PhD dissertation, Temple University. 1990.
Courtney M, Tong S, Walsh A. Acute-care nurses’ attitudes towards 4. older patients: A literature review. Intern. J. Nurs. Pract. 2000; 6:62-9.


The Aging Process
19

Caring for the Elderly Renal Patient
20
Introduction
Aging is the result of spontaneous and irreversible changes in the body, starting after the end of the phase of development and leading to progressive functional decline ending in the failure of the organism and death. Aging may be defi ned in both biological and sociological terms. Biological defi nitions of aging are derived from processes that are largely beyond human control e.g. declining physical functioning (in the developed world the elderly population is generally defi ned as person’s ≥ 80 years of age). Whereas, sociological defi nitions of aging are based on chronological age driven by age of retirement (≥ 65 years of age in developed countries).
Demographic changes
The concept of the aging society is based on the biological defi nition of the aging process1.With reference to Europe, the greatest (relative) growth in the next forty years will be seen in the proportion of the old old (≥80 years of age) and not in the young old (65-79 years of age). The group of people 100 years and older will increase even more rapidly from 388,960 people in the world in 2011 to 1,619,586 in 2030 (a fi ve-fold increase
Learning outcomes
• To know the biological and sociological defi nitions of aging
• To understand the aging process• To understand the different types of aging: normal,
accelerated or successful
The Aging Process
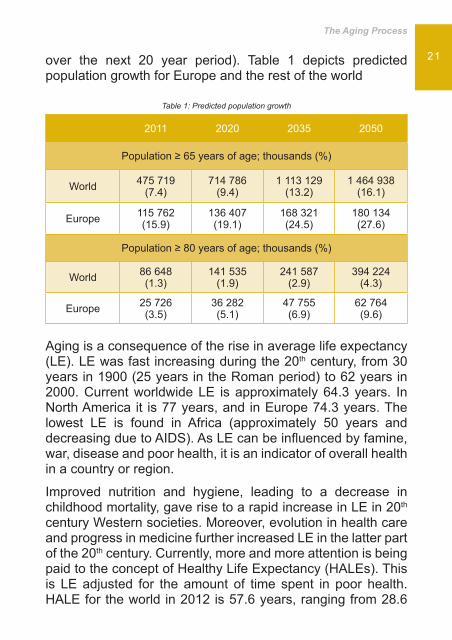
21over the next 20 year period). Table 1 depicts predicted population growth for Europe and the rest of the world
Table 1: Predicted population growth
2011 2020 2035 2050
Population ≥ 65 years of age; thousands (%)
World 475 719 (7.4)
714 786 (9.4)
1 113 129 (13.2)
1 464 938 (16.1)
Europe 115 762 (15.9)
136 407 (19.1)
168 321 (24.5)
180 134 (27.6)
Population ≥ 80 years of age; thousands (%)
World 86 648 (1.3)
141 535 (1.9)
241 587 (2.9)
394 224 (4.3)
Europe 25 726 (3.5)
36 282 (5.1)
47 755 (6.9)
62 764 (9.6)
Aging is a consequence of the rise in average life expectancy (LE). LE was fast increasing during the 20th century, from 30 years in 1900 (25 years in the Roman period) to 62 years in 2000. Current worldwide LE is approximately 64.3 years. In North America it is 77 years, and in Europe 74.3 years. The lowest LE is found in Africa (approximately 50 years and decreasing due to AIDS). As LE can be infl uenced by famine, war, disease and poor health, it is an indicator of overall health in a country or region.
Improved nutrition and hygiene, leading to a decrease in childhood mortality, gave rise to a rapid increase in LE in 20th century Western societies. Moreover, evolution in health care and progress in medicine further increased LE in the latter part of the 20th century. Currently, more and more attention is being paid to the concept of Healthy Life Expectancy (HALEs). This is LE adjusted for the amount of time spent in poor health. HALE for the world in 2012 is 57.6 years, ranging from 28.6

Caring for the Elderly Renal Patient
22 years in countries with low LE to 75 years in countries with high LE.
Heterogeneity in the aging processThe complexity of the aging process gives rise not only to differences between countries, but also to between sexes and even between individuals. The measured sex differences in LE, approximately 62.7 and 66 years for males and females respectively, are not fully understood. They could be biological or life style related e.g. women are less likely to be murdered, drink alcohol excessively, smoke, or drive at excess speed.
Three key determinants (Figure 1) explain the variability in the human aging process. These encompass endogenous processes (genetically determined and cellular senescence due to damage), exogenous processes (environmental and life style factors), and age related diseases (which are infl uenced by the same factors). The interplay between these factors determines whether an individual will have a normal, accelerated, or successful aging process.
Figure 1: Determinants of the human aging process
ENDOGENOUS
AGE RELATED DISEASES
AGING PROCESS
EXOGENOUSGenetically determined• Aging on molecular, cellular, • and organ level
Life style• Environmental factors•

The Aging Process
23Insight into aging is also infl uenced by the methodology used to study the aging process. Consequently, results from cross-sectional studies may differ from those obtained from longitudinal studies. This is evidenced by the results of the following two studies which examine the impact of aging on kidney function. A cross-sectional study of 548 healthy volunteers demonstrated a progressive linear decline in creatinine clearance of 0.9 ml/min/1.73m²/year over the age of 40 years2. However, a longitudinal study of 254 normal subjects, whilst generally confi rming these fi ndings, found that 36% of subjects did not show an absolute decrease in creatinine clearance3. The latter study suggests that age-related loss of glomerular fi ltration rate (GFR) is not a universal phenomenon, and that dietary, metabolic, hormonal, and haemodynamic factors may play a major role in modulating the age-related decrease in renal function.
The interplay between diseases and aging Normal aging is characterised by loss of reserve capacity in the way people are able to cope with secondary aging factors (e.g. stress, trauma, exposure to toxins, and disease) without loss of functional capacity. Diseases can exacerbate the aging process in either a chronic or acute manner.
Chronic diseases such as heart failure (HF), ischemic heart disease, chronic kidney disease (CKD), diabetes mellitus, osteoarthritis, osteoporosis, and chronic bronchitis, occur more frequently in old age, and may cause accelerated loss of function or death (accelerated or pathological aging is possible but not necessary in the presence of chronic diseases).
Alternatively, acute illness such as hip fracture, infl uenza, and exacerbation of chronic HF, may cause an acute and substantial loss of functional capacity. The recovery of this acute loss of function is infl uenced by many factors, some of which are preventable and treatable if recognized at an early

Caring for the Elderly Renal Patient
24 stage. Therefore, early recognition of individuals at risk for developing adverse events after an acute loss of function is fundamental to the care of the elderly.
Aging is clearly more than an accumulation of diseases. More-over, it is a complex interaction of physiological, psychological, sociocultural, and spiritual changes that make older individuals able or unable to cope with internal and external stressors. Ag-ing is a gradual decline infl uenced by many factors, culminat-ing in an inability to cope with imposed stresses. When frailty occurs, the elderly are at high risk for developing geriatric syn-dromes such as sleep disorders, problems with eating or feed-ing, incontinence, confusion, falls, and tissue breakdown.
The concept of frailty
Frailty is defi ned as a physiological syndrome characterized by decreased reserve capacity and resistance to stressors, resulting from cumulative decline across multiple physiologi-cal systems and causing vulnerability to adverse outcomes.4 In the recent years the concept of frailty, as defi ned by Fried et al., has been modifi ed to encompass, not only physiologi-cal systems, but also a decline in psychological, social, and economic status4,5.
Frailty is present in about 3 to 7 % of persons aged 65-75 years. It rises with increasing age, and is evident in>25% of people aged ≥ 90 years6. The prevalence of frailty is also rising in pa-tients with underlying chronic diseases such as CKD. Shlipak et al. found that individuals with CKD have a two- (male) to three-fold (female) risk of developing frailty compared to age- and comorbidity-matched individuals without CKD.7 The signs and symptoms associated with the frailty syndrome are out-lined in Table 2.
The Aging Process
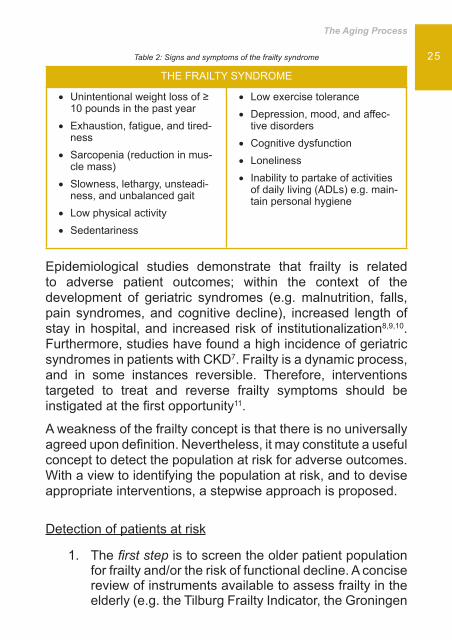
25Table 2: Signs and symptoms of the frailty syndrome
THE FRAILTY SYNDROME
Unintentional weight loss of ≥ • 10 pounds in the past yearExhaustion, fatigue, and tired-• nessSarcopenia (reduction in mus-• cle mass)Slowness, lethargy, unsteadi-• ness, and unbalanced gaitLow physical activity•
Sedentariness•
Low exercise tolerance•
Depression, mood, and affec-• tive disordersCognitive dysfunction•
Loneliness•
Inability to partake of activities • of daily living (ADLs) e.g. main-tain personal hygiene
Epidemiological studies demonstrate that frailty is related to adverse patient outcomes; within the context of the development of geriatric syndromes (e.g. malnutrition, falls, pain syndromes, and cognitive decline), increased length of stay in hospital, and increased risk of institutionalization8,9,10.Furthermore, studies have found a high incidence of geriatric syndromes in patients with CKD7. Frailty is a dynamic process, and in some instances reversible. Therefore, interventions targeted to treat and reverse frailty symptoms should be instigated at the fi rst opportunity11.
A weakness of the frailty concept is that there is no universally agreed upon defi nition. Nevertheless, it may constitute a useful concept to detect the population at risk for adverse outcomes. With a view to identifying the population at risk, and to devise appropriate interventions, a stepwise approach is proposed.
Detection of patients at risk
The 1. fi rst step is to screen the older patient population for frailty and/or the risk of functional decline. A concise review of instruments available to assess frailty in the elderly (e.g. the Tilburg Frailty Indicator, the Groningen
Caring for the Elderly Renal Patient
26 Frailty Indicator, and the Edmonton Frail Scale), including their strengths and weaknesses, is provided by Gill et al12.The 2. second step is to assess the different domains that could be responsible for changes in functionality and pathological ageing. To facilitate this evaluation, geriatricians use a system termed comprehensive geriatric assessment (CGA). CGA assesses for defi cits in different domains of functioning, such as ADLs, cognition, nutrition, continence, and mobility and gait.
Interventions to promote healthy agingActive healthy ageing
Promoting healthy and/or active aging is a key policy objective for most Western societies and globally13. Each older person should be stimulated to active and healthy aging. This concept which is much broader than a concept of physical or mental health should be stimulated and regarded to reduce the risk of chronic diseases and functional decline during the aging process. It makes also the health care provider aware that patients can be in a good physical health but that there may be other factors which infl uence their well-being and quality of life. Ignoring these aspects, will put older patient populations and that it is not by resolving some of chronic health problems, these problems will disappear. Often there are interrelated but there is certainly not always a simple causal relation. Active ageing should prevent for accelerated aging, loss of function and early development of frailty.
Prevention of frailty
The prevention of frailty starts by eliminating events that can diminish physiological reserve capacity (as deterioration of chronic diseases and optimal treatment of underlying diseases) is very important and should be stressed. Moreover patients at risk for developing frailty should be screened

The Aging Process
27regularly and treatable domains (like pain, visual and hearing problems, nutrition, mobility and gait) should be addressed (fi gure 1, situation 1). Due to the complexity and interaction of risk factors, multiple target interventions should be foreseen. Multidisciplinary teamwork is necessary to avoid complications.
Acute events as diseases or accidents like falls can induce a steep decline in physiological capacity as well in the normal aging as in the frail elderly. By an adequate intervention, normal aging people as well as frail elderly, recover from the insult and should be able to function at the previous level; in case of severe damage, like stay in ICU for organ failure, the chance to full recovery become smaller and people can end up in situation of frailty or in the worst case of functional disability. Geriatric rehabilitation can end up in full recovery under the condition that the approach in the acute phase is already oriented to early rehabilitation: mobilization of the limbs to prevent atrophy of the muscles, respiratory exercises, nutritional support, cognitive stimulation, observation of bowel and bladder function, prevention of heart failure, pneumonia and deep venous thrombosis. In short, complications of bed rest and immobility should be addressed from the fi rst minute of hospitalization. That this approach has benefi t on the functional outcome of the elderly at discharge and three month later has been proven in recent meta-analysis comparing the approach on acute geriatric wards with conventional hospital care.14
Caring for the Elderly Renal Patient
28 Referenceswww.who.int/entity/healthinfo1.
Rowe JW, Andres R, Tobin J, Norris AH, Shock NW. The effect of age 2. on creatinine clearance in men: A cross-sectional and longitudinal study. J Gerontol. 1976; 31: 155-163.
Lindeman RD, Tobin J, Shock NW. Longitudinal studies on the rate 3. of decline in renal function with age. J Am Geriatr Soc. 1985; 33: 278-285.
Linda P. Fried, Luigi Ferrucci, Jonathan Darer, Jeff D. Williamson, and 4. Gerard Anderson. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved.
Targeting and Care. 5. J Gerontol Med Soc 2004; 59: M255-M263.
Gobbens RJ, Luijkx KG, Wijnen-Sponselee MT, Schols JM. Towards 6. an integral conceptual model of frailty. J Nutr Health Aging. 2010; 14:175-81.
Shlipak MG, Stehman-Breen C, Fried LF, Song X, Siscovick D, Fried 7. LP, Psaty BM, Newman AB. The presence of frailty in elderly persons with chronic renal insuffi ciency. Am J Kidney Dis. 2004; 43:861-7.
Nancy G. Kutner. Promoting functioning and well-being in older 8. CKD patients: review of recent evidence. Int Urol Nephrol 2008; 40:1151-1158.
Winograd CH, Gerety MB, Chung M, Goldstein MK, Dominguez F Jr, 9. Vallone R. Screening for frailty: criteria and predictors of outcomes. J Am Geriatr Soc 1991; 39:778-84.
Rockwood K, Stadnyk K, MacKnight C, McDowell I, Hébert R, Hogan 10. DB. A brief clinical instrument to classify frailty in elderly people. Lancet 1999; 353:205-6.
Brown CJ, Friedkin RJ, Inouye SK. Prevalence and outcomes of 11. low mobility in hospitalized older patients. J Am Geriatr Soc 2004; 52:1263-70.
Gill TM, Gahbauer EA, Allore HG, et al. Transitions between frailty 12. states among community-living older persons. Arch Intern Med 2006; 166: 418–423.
Victor CR. Aging, Health and Care. 13. The Policy Press, Bristol, United Kingdom 2010.
Baztán JJ, Suárez-García FM, López-Arrieta J, Rodríguez-Mañas 14. L, Rodríguez-Artalejo F. Effectiveness of acute geriatric units on functional decline, living at home, and case fatality among older
The Aging Process
29patients admitted to hospital for acute medical disorders: meta-analysis. BMJ 2009; 22;338:b50. doi: 10.1136/bmj.b50. Review.


Theories of Aging and Physiological Changes
31
Caring for the Elderly Renal Patient
32
Introduction
Aging or senescence may be defi ned as... ‘the accumulation of cellular damage over time that leads to a generalised decline in function and an increased probability of death’1. It is a complex multifactorial process, with much inter-individual variation in the manner and timing of its presentation (seen as differences in ‘biological’ and ‘chronological’ age)1.
Aging is a universal phenomenon in that similar physiological changes occur in all individuals with the passage of time. The focus of this chapter is to examine the physiological changes caused by aging. Prior to addressing the impact of aging on physiological systems, contemporary theories of aging will fi rst be explored.
Theories of aging
Many theories of aging have been proposed. The following text outlines some of the more popular in recent years.
Learning outcomesOn reading this chapter the reader should be able to:
• Outline the current theories of aging• Comprehend how the aging process impacts on
physiological systems• Acknowledge how comprehensive assessment of age
associated physiological changes may individualise and enhance the care of elderly renal patients

Theories of Aging and Physiological Changes
33
The ‘Hayfl ick Limit’• In the 1960s, the biologist Leonard Hayfl ick discovered that cells in culture can divide only about 50 times before they stop. This was termed the ‘Hayfl ick Limit’, and was thought to play a role in the aging process. However, there is little evidence of this occurrence in older adults. Moreover, it does not explain the aging of non-dividing cells e.g. neurons1.
The telomere theory• Telomeres are non-functional areas at the end of each chromosome. Telomerase is an enzyme required to replicate these areas, but many cells do not express it. This leads to a progressive shortening of the telomeres with cell divisions2. Although it has been suggested that this may play a role in the aging process, it would not explain senescence in non-dividing cells1.
The genetic theory• The genetic theory of aging proposes that lifespan is largely determined by the genes we inherit. According to this theory, our potential age is primarily determined at the moment of conception3. There is some evidence to support this. Individuals with parents who have lived long lives are more likely to live long themselves (though this could be partially explained by learned behaviours e.g. food preferences). Furthermore, monozygotic twins (who have the exact same genes) have closer life spans than siblings4. However, overall, genes are thought to account for only around 25% of variance between individuals, probably due to a complex accumulative effect of interaction of several genes rather than a single allelle1.

Caring for the Elderly Renal Patient
34
The hormonal theory• Aging is characterised by a decline in the production of several hormones e.g. testosterone, oestrogen, and growth hormone. This has led to the identifi cation of hormone supplementation as a potential means by which to delay or reverse aging1. Nevertheless, empirical studies have demonstrated that testosterone supplementation in older men5, oestrogen replacement in women6, and growth hormone supplementation7 do not confer signifi cant physiological benefi ts. Moreover, aging is likely to be a much more complex process than could be reversed by such simple interventions1.
To summarise, there is no defi nitive theory of aging. What is evident is that aging is a multifactorial phenomenon; the consequence of numerous degenerative processes.
The impact of aging on physiological systems
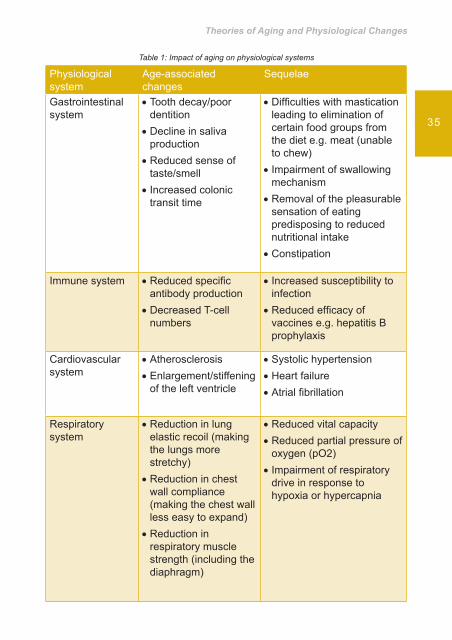
Homeostasis may be defi ned as ... ‘the tendency towards a relatively stable equilibrium between interdependent elements, especially as maintained by physiological processes’8. Namely, it encompasses a collection of physiological processes that maintain a constant body temperature, pH level, blood pressure, and intracellular ion concentrations1. As an individual ages, the body becomes less effi cient at maintaining this constant internal environment. Consequently, minor external stressors may precipitate imbalance. For example, aging is associated with an impaired ability to maintain a constant body temperature. A reduced ability to vasoconstrict or vasodilate peripheral vessels may lead to hypo- or hyperthermia, respectively1. Table 1 depicts the physiological changes brought about by the aging process.
Theories of Aging and Physiological Changes
35
Table 1: Impact of aging on physiological systems
Physiological system
Age-associated changes
Sequelae
Gastrointestinal system
Tooth decay/poor • dentitionDecline in saliva • productionReduced sense of • taste/smell Increased colonic • transit time
Diffi culties with mastication • leading to elimination of certain food groups from the diet e.g. meat (unable to chew)Impairment of swallowing • mechanismRemoval of the pleasurable • sensation of eating predisposing to reduced nutritional intakeConstipation•
Immune system Reduced specifi c • antibody productionDecreased T-cell • numbers
Increased susceptibility to • infectionReduced effi cacy of • vaccines e.g. hepatitis B prophylaxis
Cardiovascular system
Atherosclerosis•
Enlargement/stiffening • of the left ventricle
Systolic hypertension•
Heart failure•
Atrial fi brillation•
Respiratory system
Reduction in lung • elastic recoil (making the lungs more stretchy)Reduction in chest • wall compliance (making the chest wall less easy to expand)Reduction in • respiratory muscle strength (including the diaphragm)
Reduced vital capacity•
Reduced partial pressure of • oxygen (pO2)Impairment of respiratory • drive in response to hypoxia or hypercapnia

Caring for the Elderly Renal Patient
36
Physiological system
Age-associated changes
Sequelae
Nervous system Cognitive changes: •
Reduced new - memory learningReduced new - problem solvingReduced - psychomotor speed
Pathological changes: •
Cerebral atrophy- Cerebral white - matter lesions (leukoaraiosis)
Reduced verbal fl uency•
Diminished ability • to perform complex visuospatial tasks e.g. ascertain the distance between two objectsDementia•
Seizures•
Stroke•
Increased risk of falls •
Endocrine system Loss of the circadian • rhythm of antidiuretic hormone secretionReduced secretion of:•
Aldosterone- Renin- Angiotensin-
Increased atrial • natriuretic peptide levels
Increased nocturnal urine • productionNocturia which may • be associated with an increased incidence of sleep disordersUrinary incontinence•
Musculoskeletal system
Sarcopenia (the age-• related loss of muscle mass, strength, and function)Decreased bone • mineral density
Loss of muscle strength • and enduranceLoss of bone strength•
Increased fall risk•
Increased fracture risk•
Reduction in ability to • perform activities of daily living (ADLs)

Theories of Aging and Physiological Changes
37
Sensory system Visual changes •
Presbyopia - (reduced lens elasticity)Macular - degenerationCataract formation-
Auditory changes •
Presbycusis - (progressive, bilaterally symmetrical perceptive hearing loss)Tinnitus-
Olfactory changes •
Decreased number - of functioning smell receptors
Tongue atrophy •
Diminished - sensitivity to taste
Reduced quality of life • (QOL)Decreased ability to • maintain independenceWeakening sense of • balanceDizziness•
Increased smell threshold • i.e. it requires a more intense smell for it to be identifi ed and differentiated from other smellsReduced appetite•
Suboptimal nutritional • statusWeight loss•
Renal system Decline in renal mass • (primarily from the cortex)Focal • glomerulosclerosis predisposing to loss of nephronsDecline in renal • perfusion
Progressive decline in • glomerular fi ltration rate (GFR)Diminished capacity to • maintain:
Water balance - Acid-base balance-
Increased risk of • nephrotoxicity from drugs or radiocontrast agents
Caring for the Elderly Renal Patient
38
Physiological system
Age-associated changes
Sequelae
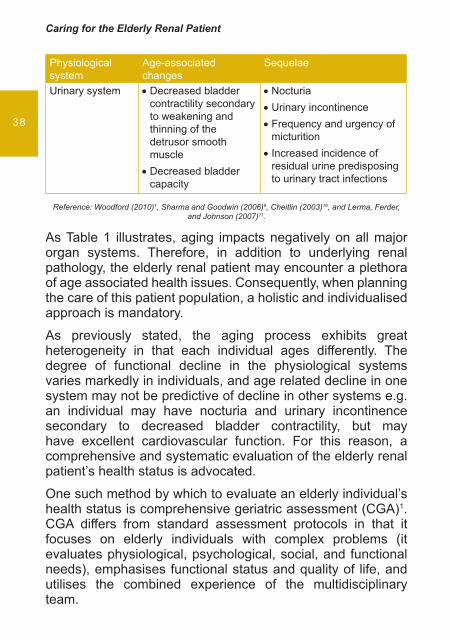
Urinary system Decreased bladder • contractility secondary to weakening and thinning of the detrusor smooth muscleDecreased bladder • capacity
Nocturia•
Urinary incontinence•
Frequency and urgency of • micturitionIncreased incidence of • residual urine predisposing to urinary tract infections
Reference: Woodford (2010)1, Sharma and Goodwin (2006)9, Cheitlin (2003)10, and Lerma, Ferder, and Johnson (2007)11.
As Table 1 illustrates, aging impacts negatively on all major organ systems. Therefore, in addition to underlying renal pathology, the elderly renal patient may encounter a plethora of age associated health issues. Consequently, when planning the care of this patient population, a holistic and individualised approach is mandatory.
As previously stated, the aging process exhibits great heterogeneity in that each individual ages differently. The degree of functional decline in the physiological systems varies markedly in individuals, and age related decline in one system may not be predictive of decline in other systems e.g. an individual may have nocturia and urinary incontinence secondary to decreased bladder contractility, but may have excellent cardiovascular function. For this reason, a comprehensive and systematic evaluation of the elderly renal patient’s health status is advocated.
One such method by which to evaluate an elderly individual’s health status is comprehensive geriatric assessment (CGA)1. CGA differs from standard assessment protocols in that it focuses on elderly individuals with complex problems (it evaluates physiological, psychological, social, and functional needs), emphasises functional status and quality of life, and utilises the combined experience of the multidisciplinary team.
Theories of Aging and Physiological Changes
39
Age related changes in laboratory variables
With reference to Table 1, aging is associated with a progressive decline in GFR. Typically, GFR declines by 1mL/minute/1.73m2 per year over the age of 40 years and the rate of decline in GFR accelerates after the age of 65 years 12. The prevalence of both microalbuminuria (urinary albumin levels of 30-300mg per day) and albuminuria also increases progressively after the age of 40 years11. The increased prevalence is most marked in diabetic and hypertensive subjects but is also observed in patients lacking these risk factors13.
Aging is also associated with changes in laboratory variables related to the diagnosis of anaemia and iron defi ciency. Haemoglobin declines and anaemia prevalence steadily increases with advancing age14. Serum iron, vitamin B12, and folate levels (all aetiological factors in the development of anaemia) may all be suboptimal as a consequence of nutritional inadequacies15. These factors, combined with low levels of endogenous erythropoietin, predispose the elderly renal patient to anaemia. Anaemia is an independent risk factor for hospitalisation and mortality in the elderly16. Therefore, strategies to correct anaemia, in the context of erythropoiesis stimulating agents (ESAs) and iron and vitamin supplementation are fundamental components in the care of this patient population.
Summary
This chapter has explored the physiological consequences of aging. In addition to the sequelae associated with the primary renal disease, the elderly renal patient may encounter a multitude of health related issues. What is evident is that aging is heterogeneous. Thus, a patient focused approach to assessment and subsequent development of care strategies is a priority care objective.

Caring for the Elderly Renal Patient
40
ReferencesWoodford H. 1. Essential Geriatrics. 2nd ed. Radcliffe Publishing Ltd. 2010: 3-19.
Aubert G and Lansdorp PM. Telomeres and aging. 2. Physiological Review. 2008; 88(2): 557-579.
Weinert BT and Timiras PS. Invited review: theories of aging. 3. Journal of Applied Physiology. 2003; 95(4): 1706-1716.
Kirkwood TBL. Evolution of aging. 4. Mechanisms of Aging and Development. 2002; 123(7): 737-745.
Nair KS, Rizza RA, O’Brien P, Dhatariya K, Short KR, Nehra A, Vittone 5. JL, Klee GG, Basu A, Basu R, Cobelli C, Toffolo G, Dalla Man C, Tindall DJ, Melton LJ 3rd, Smith GE, Khosla S, and Jensen MD. DHEA in elderly women and DHEA or testosterone in elderly men. New England Journal of Medicine. 2006; 355(16): 1647-1659.
Hendri6. x SL, Cochrane BB, Nygaard IE, Handa VL, Barnabei VM, Iglesia C, Aragaki A, Naughton MJ, Wallace RB, and McNeeley SG. Effects of estrogen with and without progestin on urinary incontinence. The Journal of the American Medical Association. 2005; 293(8): 935-948.
Liu H, Bravata DM, Olkin I, Nayak S, Roberts B, Garber AM, and 7. Hoffman A. Systematic review: the safety and effi cacy of growth hormone in the healthy elderly. Annals of Internal Medicine. 2007; 146(2): 104-115.
Oxford Dictionary of English.8. 2005. 2nd ed (revised). Oxford University Press.
Sharma G and Goodwin J. Effect of aging on respiratory system 9. physiology and immunology. Clinical Interventions in Aging. 2006; 1(3): 253-260.
Cheitlin MD. Cardiovascular physiology – changes with aging. 10. The American Journal of Geriatric Cardiology. 2003; 12(1): 9-13.
Lerma EV, Ferder L, and Johnson RJ. Geriatric nephrology. In: 11. Feehally J, Floege J, and Johnson RJ. Comprehensive Clinical Nephrology. 3rd ed. Mosby, 2007: 745-753.
Lamb E and Delaney M. 12. Kidney Disease and Laboratory Medicine. ACB Venture Publications. 2009: 22-23.
Jones CA, Francis ME, Eberhardt MS, Chavers B, Coresh J, Engelgau 13. M, Kusek JW, Byrd-Holt D, Narayan KM, Herman WH, Jones CP, Salive M, and Agoda LY. Microalbuminuria in the US population: Third National Health and Nutrition Examination Survey. American Journal of Kidney Diseases. 2002; 39: 445-449.

Theories of Aging and Physiological Changes
41
Artz AS. Anemia and the frail elderly. 14. Seminars in Hematology. 2008; 45(4): 261-266.
Lash AA and Coyer SM. Anaemia in older adults. 15. MEDSURG Nursing. 2008; 17(5): 298-304.
Patel KV and Guralnik JM. Prognostic implications of anaemia in older 16. adults. Haematologica. 2009; 94(1): 1-2.

Meeting the Elderly Patient in the Renal Clinic: A partnership in Care with the Multidisciplinary Team
43

Caring for the Elderly Renal Patient
44
Many factors have been of importance in the development of the concept of partnership and on the citizen’s awareness. In large scale, the movement in favour for the patient’s participation emerges as result of several groups of consumers, ever more informed, claiming for an ever growing humane assistance in the health service, with access to information and the participation on the decision making.
In the recent past, patients were seen as passive care recipients, needing to approach health professionals, the holders of knowledge, for their diseases to be diagnosed and treated. Under such a care model, paternalism was confi gured as a classic model of the relationship between health professionals and the patient, therefore allowing a narrow margin for autonomy and individual freedom1.
We must also contemplate contemporary society, where the emphasis on pragmatism, materialism, utilitarianism, beauty and productivity may contribute towards the values of caring. The contemporary world, over the last few decades, through science, technology, and the pursuit of happiness by production and consumption, has relegated humanist values to a secondary level. Nowadays, one observes the emergence
Learning outcomes
• To review the problems associated with chronic disease within the context of the elderly renal patient
• To be aware about the role of the elderly person in the disease management process
• To refl ect upon the partnership process as a promoter of care for the Elderly with Renal Disease

Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
45
of values indicating their retrieval, such as greater ecological consciousness, greater respect for human rights, and fi ghting against all sorts of discrimination.
Other social questions, such as the increase of consumer rights, the movements composed of associated groups of patients, the elevated costs on Health Care and the increasing awareness of the health care professionals’ fallibility, have driven citizens to get more involved in a more active fashion on the health care services that concern them.
It is from this context of philosophical, social and political new/inversion tendency, that healthcare professionals try to distance themselves, a methodology based on an essentially pragmatic philosophy; one that bases its action on a technical-professional model, valuing overall the biophysiological knowledge and technique, operating in obscure detachment from what is of more importance for the individual, eminent dignity and respectability.
Also worth mentioning is the demographical structure of the world society and the tendency for the global ageing of the population, as well as the development of health policies and strategies that are not alien to the necessities of an ever older population. At an international level, some events and health policies of extreme importance in this process are worth considering, such as the Declaration of Alma-Ata 1978, World Health Organisation (WHO),19981 and the Ottawa Charter for Health Promotion WHO19861, holding as their uttermost intention the promotion of health for all and the participation of the community and the citizens in the promotion of health. It is under this philosophical, social and political framework that the concept of partnership within the health sector becomes increasingly important. Of the defi nitions identifi ed, many extracted from management and training contexts, one can fi nd a common notion: respect for the individuality and subjectivity of the patient as a person, presupposing a combined action between carer and patient on the decision
Caring for the Elderly Renal Patient
46
making process1,2,3,4,5,6,7,8. Other authors identify the client’s empowerment as one of the most important consequences of partnership; the client being described as having the improved ability of being able to decide for oneself10,11,12. Other authors13,14,15 state that empowerment should be seen as a priority for the senior citizens, justifying this with the notion that, along with longevity, there is usually a process that can lead to the loss of one’s power, autonomy and individual independence.
Hoping for a better quality of life (QOL) to evolve along the life span, implying a quest for well-being and QOL, and for a health policy where costs, ethics and the right to live and the right to die with dignity can be appreciated as a whole. This vision drives to acceptance of the non-healing, culminating in a shift of the traditional relationship with the patient. It is then necessary to negotiate with the patient regarding their treatment concerns, including the decisions to make regarding QOL, and the responsibilities that other family members may take concerning the care for the patient, therefore setting up the patient/family link as a care partnership.
The problems associated with chronic disease within the context of the elderly renal patient The present reality of socio-economic and technological alterations and the clinical capacity to control diseases has substantially changed the indices of mortality and morbidity, not only increasing life expectancy, but consequently also increasing the number of people suffering from a chronic disease. A chronic disease is defi ned as a situation that produces signs and symptoms in a person for a variable period of time, displays a prolonged evolution and can only be resolved partially16. Thus, a chronic disease, namely renal disease, can be associated with successive loss of independence and control, moments of anxiety, sadness and low mood. Learning how to deal with a chronic disease depends on the individual
Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
47
characteristics, the way it is accepted by the person and the life projects one may have.
The way in which a chronic disease is experienced by the patient and their family is infl uenced by several factors, namely, the type and stage of the disease, the family structure, the role of the patient in the family and their professional status, their current life stage, and personal and familiar development level, among others17.) Knowing the diagnosis of a chronic disease, such as renal disease, often represents a great shock to the person and is a stress factor. Stress is usually indicated as a process where environmental and cognitive events are combined with behavioural, physiological and psychological consequences18. For the person to manage this situation it is necessary to look for coping mechanisms, defi ned as constant behavioural and cognitive efforts in order to manage specifi c demands, internal and/or external, that are assessed as exceeding the resources of the individual18 Coping is seen as a stabilising factor that facilitates the individual adjustment or adaptation when one faces stressful events, or moments of events. Stress is seen as a process which implicates the management of situations, depending on continuous assessments and reassessments in a dynamical process set between the individual and the environment, and not a rigid way of being19. The consequence of such a defi nition is represented by the utmost importance health professionals assume whilst promoters of the QOL to the individual suffering from the chronic disease, for the reason that, as previously stated, there are huge adaptive differences imposed on the person by the characteristic stressors of the chronic disease.
Thus, when a chronic disease emerges, a group of alterations also arise; alterations dependent on the current life stage of the individual at the initial moment of sickness, conditioning the type of adaptation necessary to embark in a family, social and professional context. The whole process is dynamic and demands the constant follow-up of the patient, in order to

Caring for the Elderly Renal Patient
48
enable that all the team elements care for the patient in an individual manner.
Particularly with regard to kidney disease, health professionals need to adopt different roles to help promote the capabilities elderly people make use of when coping with the disease itself. A situation justifi ed by the impact that chronic illness and prolonged treatment has on the elderly population with great disturbance on their welfare; the evolution and sophistication of therapeutic procedures and the need to help customers in a complex process of adaptation to the illness and to a treatment with repercussions throughout life.
Despite several sources referencing signifi cant evolutions over the past 40 years on the treatment of chronic disease, as well as on the improvement and maintenance of the quality of those suffering from altered renal discharge, many problems remain unsolved affecting the lives of patients and their families.
The relationship between the patient, health professionals and the patient’s family or next of kin are the basis for strategic development that can allow one to live through a chronic disease and achieve the best QOL possible. The Health professionals encounter these clients, the majority of them being elderly adults, throughout the diverse context of their professional practice, and function as the primary carer between the different health subsystems, supporting the client who performs home-based renal replacement therapies.
The primary focus of care, within the context of this patient group, is to support the decision making processes and to establish a partnership with the elderly person in their care.
It is therefore necessary to face the elderly patient considering everything they have seen in the past, i.e. with his Lived Self and his Experienced Self, for individuality is not an abstract notion, rather an acquired construction throughout life. Due to their uncertainty and duration, chronic diseases cannot be cured, and instead have to be managed. Chronic diseases,
Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
49
namely renal disease, represent a complex situation implying coping efforts from the patient. These, as stated by Livenh20, are related not only to the psychosocial adaptation to the chronic disease and incapacity, but also as mediating variables between the incapacity related to the disease, personality attributes, environmental conditions and social-demographical factors.
This approach is only possible in a model where the person is seen as a whole; for example, in a model which links the behaviour and lifestyles of individuals, and recognises the importance of socio-economic, political, cultural and environmental aspects that determine people’s lifestyles and the equilibrium of health in the community. Here, the patient is seen as an active partner in care and the goals set for their recovery are established together with the health professional with no paternalist attitudes. For example, an elderly person suffering from a renal disease participates in the process of prevention or cure of the disease, being responsible for their actions and choices.
Health professionals have to make available to each elderly person their knowledge and accompany them throughout the experience in a process that must be monitored by the patient themselves, seeing them as responsible for their own life project. Therefore, it is necessary that the elderly person is vested with empowerment so that they can resort to decision-making over matters that concern them, such as those related to their lifestyles and their health. These relationships require consent and respect for each other, so that the elderly patient is given the right to participate in their care.
The elderly person as partner in the disease management process Promoting the patient’s autonomy implies the sharing of decision making and the analysis of the decisions together,
Caring for the Elderly Renal Patient
50
giving the patient the right and the power to choose, without the temptation of prescriptive righteous intentions. It is therefore essential to increase the citizens’ participation and active exercise of the right and duty of citizenship which promotes an increase of power and control, allowing empowerment to emerge.
Within a chronic disease context, such as renal disease the management of symptoms depends largely on following a regimen as indicated by health professionals, the fact remains that it is vital that the person in question adheres to the same regimen. Appeals for greater participation of the patient are based on the assumption that patients want and enjoy taking a more active role in their treatment.
When one participates, one more readily agrees to take the necessary steps to improve their health. Adhering is considered important in renal disease because following the recommendations of health professionals is of vital importance for the recovery of the patient. Studies conducted by Kimball21
have shown that better results were obtained when there was an attitude of partnership, which meant that patients accepted their disease and participated in treatment and rehabilitation.
Gomes1 conducted a study that sought to understand the concept of partnership in the process of nursing care for elderly patients and concluded that most patients do not want to continue to take a passive role, but wish, instead, to be active participants in their care. This study also demonstrated that the ideas that nurses hold regarding the elderly person can either facilitate or hinder the process of partnership.
Negative representations held by professionals about the elderly lead to an underestimation in the abilities of the latter, and the lack of a partnership being formed, due to the fact that this view sees the elderly as a sick person, an older person, with a reduction of their physical and mental faculties, further leading to dehumanising them and not respecting their

Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
51
privacy. The professionals who consider elderly people as people with life experience, full of wisdom, with a story to tell, and who have the perception of how important it is to respect the privacy and modesty of the elderly, give them the respect they deserve for being old enough to be their grandparents, and take into account the knowledge they possess, as well as the personal characteristics of the elderly, as being unique and unrepeatable1.
This is something that the entire health care team should be aware of in their dealings with patients, since a partnership cannot exist without a special relationship, which allows focus on the needs of the elderly patient, so that they may voice, speak up and establish a negotiated relationship; demystifying the silent contradictory perception that is characterised by the fact that the elderly often do not speak their minds fearing that no one will attribute importance to what they say due to their age. A partnership thus implies the existence of a situation of communication in opposition to indifference i.e. involves a form of care that must be necessarily reciprocal.
Attention must then be given to the diffi culty that an elderly person may have when trying to participate when lacking ability or the necessary experience. Thus, studies suggested by Gomes (2003) showed that the elderly patients, in most cases, adhere to an active participation in the decision-making process, but the most critically ill patients would prefer a less active role. In this regard, Biley22 conducted a qualitative study which also concluded that patients participate in decision making depending on their health.
Patients’ involvement cannot be generalised, hence the efforts of nurses, in caring for sick people in an individualised manner, are of utmost importance. All healthcare professionals must share the meaning of the actual experience of each person so that care can be truly person-centred i.e. in which they are seen as a partner. It is important that we rethink our practices for the elderly sick people suffering from renal disease so that
Caring for the Elderly Renal Patient
52
the patient becomes the centre of care within a multidisciplinary health team. It is diffi cult to develop organisational models of care when not all team members have the same vision of care. Health professionals need to develop skills for them to be partners, and be better prepared for new challenges and roles advocated by the recognition of the individuality of the person, by current policies of citizenship in health.
In the fi rst conference debating "Institutions and Partnerships" held in France, Zay and Gonnin-Bolo23 provided a minimum defi nition of partnership, that of a compromise negotiated in a joint action. The emphasis on negotiation assumes that in the partnership there is no uniformity or consensus, but a heterogeneity which recognizes the possibility of confl ict, and which requires the construction of a compromise.
The partnership means that the patient actively participates in the process, and can give opinions and offer solutions which harmonise with their lifestyle. Instead of thinking for the patient, health professionals should promote the person to process this refl ection and decision making autonomy. It is understood, therefore, that both the health care team and the patient are in possession of knowledge. Instead of thinking for the patient, the professionals promote the empowerment of the patient, allowing for the refl ection and decision-making needed to make them a partner. The partnership involves undertaking a process that establishes with the person being cared for, and depending on the situation and the patient’s family, a care program that means to identify along with the patient the goals set to achieve by that patient. This entails a negotiation process in which a person's autonomy must be respected above all things.
The partnership process as a promoter of care for elderly people with renal diseaseGomes24 investigated the nature of the care partnership between nurses and elderly patients, and concluded that the
Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
53
process of partnership has, as a key condition, the need to see the elderly person as a being the focus of care. This condition leads to paying attention to the potential development for the care of the SELF, which involves looking at the elderly patient as more than just a being with needs. Another essential issue that emerged was to have the time and space to build a quality relationship that allows the establishment of trust, that meets the elderly patient and helps create an atmosphere for the establishment of commitments.
The structure on which the partnership process underlies, the conditions described above, has the potential to vary or change the type of action or interaction. Thus, when an elderly patient has autonomy, the strategy for building the partnership process in nursing care results in the construction of a joint action, which aims to enable people to take control of the care of the SELF. When an elderly patient is dependent and has no autonomy, the strategy includes the construction of an action in which the nurse provides care for the Other, assuming attitudes the nurses would expect others to have for themselves, or training the family or next-of-kin to do so. These strategies have resulted in securing or assuming the care for the SELF, which contributes to a more centred care in the elderly, enabling him to have more control over his life plan and health or to continue his path in life.
Understanding the meaning of the concept of partnership in the design in which it was developed - as a care for the SELF and as a care for the Other - may, in epistemological terms, be constructive for the practice of care in situations where people are vulnerable or dependent, as in situations of elderly patients with renal disease. Since it allows one to proceed on seeing the person as a being of action in which it has power, due to their uniqueness as a person, it is valued regardless of their circumstance, promoting their autonomy.
The clarifi cation and the interrelationships of the concepts explained which characterise the partnership qualify the

Caring for the Elderly Renal Patient
54
development of the partnership between nurses and elderly patients in the care relationship. However, the adoption of the multidisciplinary team model leads to improved quality of care and the growth of well-being of the patients. This improvement in quality of care may prevent many admissions into both hospitals and nursing homes, with potential economic impact and obvious health gains. This possibility implies a different organisation of care.
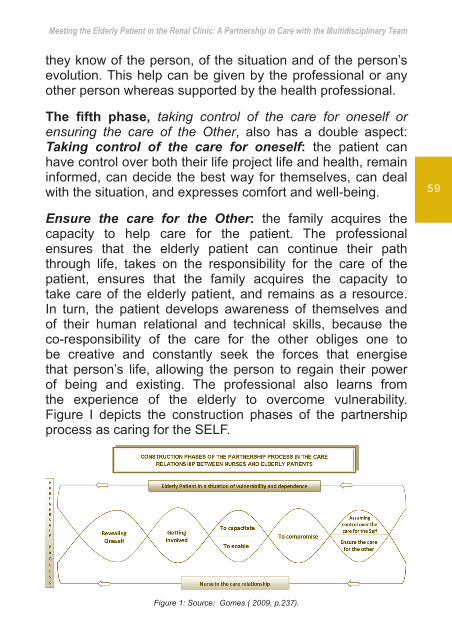
We must, therefore, systemise the construction phases of the partnership process that can help structure a practice of care based on the construction of an action in partnership with the elderly patient with renal disease. This promotes the care of the SELF and helps focus care on the person’s uniqueness.Thus, the construction of the partnership process has been characterised and divided into fi ve stages:
Reveal oneself• Getting involved• Train or enable• Engage• Take control of the SELF or ensure the care of the • Other
Although these categories are listed individually they are interrelated to form a continuum.
The fi rst phase, to reveal oneself, is characterised by making others aware of the person (the patient and the health professional) as a being of projects and care. The professional demand is to know the potential development of a patient in order to help promote their life, health strategy and the achieving of the SELF, whatever their circumstances might be. It has an attitude that mobilises their communication skills to make themselves known and to know the other person; promotes affection by showing affection, sympathy; promotes active listening; shows availability; asks before acting; shows

Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
55
respect for the person; demonstrates ability to understand the person and the ability to assess the situation along with the patient.
The professional, in relation to the patient, must endeavour to know their identity (what is the person, who is the person), what their values are, the culture and context of social inter-relationship, and show respect for the person as a being of rights. They must seek to understand the disease event and the meaning it has in the trajectory of that person’s life, and identify in them the knowledge and personal resources of the patient, in order to deal with the situation. In addition, the professional should give attention to the meaning of people’s lives and their needs, propose solutions to problems that arise, and avoids complications, whilst always seeking to promote refl exivity and personal autonomy at the level of action and decision, taking into account their values and desires.
Sometimes, it may also happen that the elderly person may fi nd himself in a phase of upheaval or denial with regard to the situation of illness or the context in which it is inserted. Given that, the professional should show an attitude of active listening and give time to the elderly patient, respecting their pace.
The second phase, getting involved, is characterised by the creation of a reciprocal space, designed by the establishment of time and space to develop a quality relationship that allows the person to meet and develop a relationship of trust that goes beyond revealing his or herself. At this stage of involvement, the professional tries to identify what is most unique in the elderly client, so that later the acquired data can be put into action and applied to the relationship.
Health professionals should be aware of the importance of time when dealing with elderly patients, so they have to try and seek to structure time slots in the relationship so that they are ready to listen, making themselves available and solicit,
Caring for the Elderly Renal Patient
56
show concern, a person-centred attitude, and respect for the identity of elderly patient and the confi dentiality of such space. The health practitioner endeavours to become familiar with the life context of the patient.
When approaching the patient, the health professional should use an affective attitude, explaining the terms of the relationship and saying what is expected of each one. They should: seek to use strategies for transparency and truth and share information with the patient; show availability - sit, listen to, and fi nd the needs and meet the life project, as well as the health project of the patient – be able to change the planning according to the priorities, concerns and needs of the patient.
The elderly patient, due to the proximity, affection, concern, technical and relational competence that the nurse demonstrates, will be involved in sharing with them, through verbal or body language, look and posture, the surrounding environment and the meaning of their experience. By communicating their concerns the patient allows the practitioner to see the problems and can then, to accept some help, complementing each other in the aid towards what their diffi culties actually are.
The concern and involvement with the elderly patient will help to probe their needs and potentials i.e. to identify whether, and where, there is a lack of knowledge, and the functional limitations resulting from the disease regarding day to day activities. Recognising situations helps people to fi nd their motivations, what gives meaning to their lives, and to jointly identify opportunities and resources for the care of the SELF. These actions aim to fi nd a way to assist in the conduct of the elder based on the knowledge and resources of both partners.
The third phase is two directional: to capacitate or to enable. Capacitating is to build a joint action in developing skills to act and decide. It takes into account the patient’s sharing of their experience of being in a critical condition, the knowledge

Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
57
of both the patient and practitioner to the defi nition of objectives given, the range of dependence and independence of the elder person, as well as the people around the elder in life, maintaining daily living and operational activities, and remediation (symptom control, treatment). In this sense the health professional has to develop an informed process, remaining enlightened, refl ective and negotiable i.e. sharing responsibility and power in mobilizing the uniqueness of the patient in order to help turn potential into actual capacity, so that the patient can assume control over the care process of the SELF.
During the interaction the elderly patient and health professional must articulate their actions, taking into account the uncertainty and unpredictability of the interaction, so that there can be an adjustment in the construction of the action. According to the interactionist’s point of view, people interact with each other through mutual interpretation of actions and meanings that each brings to the interaction, and therefore, not reacting to the actions of others. Therefore, professionals should share the responsibility and power to promote affection and humour when addressing the patient; interacting, listening, asking questions, to jointly continue to identify and validate the need and potential of people, valuing the knowledge that the person holds of the situation, given their priorities. Promoting independence, comfort and help in the choice of the patient and family, facilitating access to resources (community resources), should help the caregiving relatives to build capacity in order to care for the sick person.
Enabling the Care of the Other is an action experience where health professionals and the elderly patients accomplish the state of “being with”, sharing the meanings of the experience, with the professional assuming responsibility of the care that the Other should have with themself if they had the capacity for autonomy. As such, the practitioner uses their knowledge already gathered about the person and their life experience,
Caring for the Elderly Renal Patient
58
via body language decoding or information obtained through the family, and assuming the responsibility of caring that the Other should hold for themselves, that the patient must have, or helping to enable the family to care for the elderly. In this sense, the professional promotes care, acting according to the principles and values of the therapeutic effi cacy and knowledge detained about the person, which holds the identity of the person (who is the person, whose person is it) and what gives meaning to their life.
To enable means being careful and making use of the same care that the patient would have for themselves, if such was possible, in order to anticipate complications, allowing the person comfort, well-being and to continue their path in life, preserving their identity within a social context. The concept hereby described meets the concept of enabling reported by Swanson25 which holds that a care provider that gives possibility is one that uses their expertise for another’s well-being, helping to ease the passage through life transitions and unfamiliar events. On the other hand, the professional shares, the meaning of the experience with the Other, helping clarify their own sense of life, self-care and focusing care on the other.
The fourth phase, committing, is refl ected in a development of joint efforts in seeking to achieve the set objectives to assume or ensure control or progression of the life project and health of the elderly patient, based on the meanings of their experience in the context of their human responses against a critical event and on what gives meaning to their life. Thus, the professional helps to support the commitment that one makes based on what makes sense for the person. Actions carried out aim towards a gradual transition, from a potential capacity into a real capacity, or promote health and help the elderly patient to continue on their life trajectory. Committing with the professional care of the elderly, forces the health professional to be creative and look for what makes sense in relation to what
Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
59
they know of the person, of the situation and of the person’s evolution. This help can be given by the professional or any other person whereas supported by the health professional.
The fi fth phase, taking control of the care for oneself or ensuring the care of the Other, also has a double aspect:Taking control of the care for oneself: the patient can have control over both their life project life and health, remain informed, can decide the best way for themselves, can deal with the situation, and expresses comfort and well-being.
Ensure the care for the Other: the family acquires the capacity to help care for the patient. The professional ensures that the elderly patient can continue their path through life, takes on the responsibility for the care of the patient, ensures that the family acquires the capacity to take care of the elderly patient, and remains as a resource.In turn, the patient develops awareness of themselves and of their human relational and technical skills, because the co-responsibility of the care for the other obliges one to be creative and constantly seek the forces that energise that person’s life, allowing the person to regain their power of being and existing. The professional also learns from the experience of the elderly to overcome vulnerability.Figure I depicts the construction phases of the partnership process as caring for the SELF.
Figure 1: Source: Gomes ( 2009, p.237).
Caring for the Elderly Renal Patient
60
The fi gure I illustrates the stages of the partnership process. These is not always linear because agreements may not be always accomplished, and confl icts and failures may arise during the negotiation process. However, the partnership allows for carrying out the commitments because there is a better understanding of the meanings of the experience of each of the intervenient in the process.
The partnership process is presented as an intervention, based on the construction of an action that aims to promote the care for the SELF.
This process, constituting fi ve stages, promotes the sharing of power in the relation of care towards building the partnership process; promotes and develops the autonomy of the elderly; helps harness the power of existing and to promote comfort and well-being; facilitates integration of the elderly patient in the context of the social inter-relationship, and promotes care more driven to the uniqueness of the elderly person. This enables the elderly patient to have control over their life, ensuring that they can move forward. This is a fundamental principle in the context of which we are focused, the management of chronic disease of the elderly suffering from a renal disease.
The partnership is therefore understood as a social, global, multidimensional, and multicultural process allowing individuals to be a “person” in the extent that they become protagonists of their own existence. Thus, their existence becomes an individual project opened to the community, but in a free form. To deprive people from taking part in the aspects that relate to their very existence is to deprive them of their own life, to deny them their inalienable right to independence and dignity.
CONCLUSIONAs we have been referring throughout the text, chronic diseases due to their characteristics of uncertainty and duration have to be managed rather than cured. Thus a new approach becomes
Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
61
necessary for the health professionals when providing care to chronic patients with renal illness, promoting the management of the disease, where the sick person is the nucleus of that care, rather than focusing only on the healing process.
Today, we cannot provide care in the health area without an extended study about the meanings of people i.e. their values, beliefs and the fundamentals that support their behaviour. Nursing care is based on inter-personal relationships with humans. So accepting the patient as a partner means losing the pretentious attitude of the health professional as one who considers that they know about what is best for the patient. The participation of patients in the decisions will lead to the adoption of negotiating strategies arising from the relations of power present in the complexity of those relationships and the contexts in which they develop the partnership1.
The difference between points of view when one defi nes a certain situation can lead to a negotiation between the parties and make them undertake an effort to reach an acceptable solution between them.
The interrelationship of problematic chronic disease management and the necessity for observing the patient is due to the demands of the contemporary reality in a system ever increasingly constructivist and less positivist. A new health perspective arises that proposes methodologies more consentaneous with the complexity of human experience, in which the health professional must respect and promote the autonomy and individuality of the patient.
In conclusion, only the active participation of the person, associated to the exercise and the duty of citizenship, will promote an increase of power and control empowerment that enables the emergence of a partnership within the process of health care that will help the elderly with renal chronic disease to manage and to adapt to their disease.
Caring for the Elderly Renal Patient
62
Key Points
• A new approach is necessary for the health profession-als when providing care to chronic patients with renal illness, promoting the management of the disease, where the sick person is the core of that care, rather than focusing only on the healing process.
• The participation of patients in the decisions will lead to the adoption of negotiating strategies arising from the relations of power present in the complexity of those relationships and the contexts in which they develop the partnership.
• It is necessary to intervene in partnership with the elderly patient suffering from renal disease concerning treatment, measures to be taken related QOL quality of life and possibilities available both for patients and relatives under the partnership concept.
• The strategies comprise the sharing of meanings including the experience in the construction of a joined action both when the elderly patient has autonomy, or the construction of an action ensured by the nurse when that one does not have autonomy. The consequences of these actions and interactions are the ability to assume or to ensure the care for oneself.
• The development of the partnership process is characterized by fi ve stages: to reveal oneself; involve oneself; to capacitate or to enable; to commit; to take control of himself/herself or to ensure the care of the Other.

Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
63
• Partnership, as the construction of a joint action which promotes the care of Oneself, respects the person’s singularity.
• The construction of an action which has the aim of ensuring to care for the Other, enables the person to assume the control of his/her project of life and health, or to prosecute his/her own trajectory of life, whatever their circumstances are.
Caring for the Elderly Renal Patient
64
References
Gomes, I.D. (2007): Parceria e cuidados de enfermagem: uma 1. questão de cidadania. Coimbra: FORMASAU, Formação e Saúde Lda.
World Health Organization (1998). Health Promotion and Community 2. Action for Health in Developing Countries. Report of a WHO Study Group. Geneva: World Health Organization.
World Health Organization (1986). The Ottawa Charter for 3. Health Promotion. First International Conference on Health Promotion, Ottawa, 21 November. Acedido a 20 de Maio, 2009, em http://www.who.int/healthpromotion/conferences/en
Casey, A. (1988). A partnership with family. Senior Nurse, 8(4), 8-9.4.
Christensen, J. (1993). Nursing partnership. A model for nursing 5. pratice. London: Churchil Livingstone.
ZAY, Danielle (2000): Ensino de Enfermagem: Processos e Percursos 6. de Formação-Balanço de um Projecto, Lisboa in Ministério da Saúde, Departamento dos Recursos Humanos da Saúde.
Hesbeen, Walter (1997): Prendre soin à l’hôpital: inscrire le soin 7. infi rmier dans une perspective soignante, Paris: Intereditions/Masson.
Honoré, B. (1999). Le partenariat dans L’évolution des estrutures de 8. santé. Perspective Soignante, 3, 21-38.
Merini, C. (1999). Le Partenariat en formation espace d`Interculturalit. 9. Vie colloque National. De L`Aipelf/Afi rse, Université Paris XI.
Gallant, M.H., Beaulieu, M.C. & Carnevale, F.A. (2002). Partnership: 10. an analysis of the concept within the nurse-client relationship. Journal of Advanced nursing, 40(2), 149-157.
Hook, M.L. (2006). Partnering with patients - a concept ready for 11. action. Journal of Advanced Nursing, 56(2), 133-143.
Bidmead, C. & Cowley, S. (2005a). A concept analysis of partnership 12. with clients, Community practitioner, 78(6), 203-208.
Thurzs, D. (1993). The case of empowerment. in: the possibilities of 13. empowerment. Journal of the International Federation on Ageing, XX(1), 1-2.
Myers, J. (1993). Personal Empowerment. in: the possibilities of 14. empowerment. Journal of the International Federation on Ageing, 20(1), 3-8.

Meeting the Elderly Patient in the Renal Clinic: A Partnership in Care with the Multidisciplinary Team
65
Cusack, S. & Thompson, W. (1999). Leadership for older adults: aging 15. with purpose and passion. Philadelphia: Brunner/Mazel.
Bolander, Veralyn; Barnes, (1998) Sorensen & Luckman: Enfermagem 16. Fundamental – abordagem psicofi siológica. Lisboa, Lusodidac ta.
Lubkin, Ilene (1995): Chronic illness: impact and interventions. 3rd 17. Edition. London: Jones and Bartlett Publishers.
Lazarus, R.S.& Folkman, S. (1984): Stress, appraisal, and coping, 18. New York, Springer Publishing Company.
Ribeiro, J.L.P. ; Santos, C. (2001): Estudo conservador de adaptação 19. da Ways of Coping Questionnaire a uma amostra e contexto portugueses, Análise Psicológica, 4 (XIX):, pp. 491-502.
Livneh, H. (1999) Psychosocial adaptation to heart diseases: The role 20. of coping strategies. Journal of Reabilitation, 65(3), 24-32.
Kimbal, C.P. (1969): Psychological responses the experience of open 21. heart surgery: I. American Journal of Psychiatry, 126, 3: 348-359.
BILEY, F.C., (1992): Some determinants that patient participation in 22. decision-making about nurse cares, Journal of Advent Nursing, 17, pp. 412-421.
Zay, Danielle & GONNIN-BOLO, A. (1995): Etablissements et 23. partenariats. Stratégies pour des projets communs, Actes du colloque. 14,15, 16, Paris.
GOMES, I. D. (2009): Cuidado de Si a Natureza da Parceria entre 24. o enfermeiro e o doente idoso no domicílio. Lisboa: Instituto de Ciências da Saúde de Lisboa da Universidade Católica Portuguesa. Tese de doutoramento.
Swanson, K. (1991). Empirical Development of Middle Range Theory 25. of Caring, Nursing Research, 40(3), 161-166.

Providing Information and Education to the Elderly Renal Patient
67

Caring for the Elderly Renal Patient
68
Introduction
The mean age of the chronic kidney disease (CKD) population is steadily increasing. This is primarily a function of increased longevity in Western societies and the impact of the aging process on the kidneys1. Although age is no longer a barrier to referral to the renal care team, the education of the elderly requires specifi c considerations. In accordance with Falvo (2011)2, the aims of informing and educating the elderly renal patient are to promote optimal functioning within the limitations of the illness, maintain good health, and facilitate independence. Many health professionals assume that older people can not learn and therefore there is no need to educate them. Research has shown that they can learn but not as fast or in the same way as the younger3,4. There are changes brought on by aging that can affect learning. The age related changes affect the sensory, cardiovascular, respiratory, and musculoskeletal systems, and the socioeconomic status of the elderly3,4. The sensory changes affect all fi ve senses, visual,
Learning outcomes
• Describe the changes brought on by aging that affect the learning process
• List the reasons why educating the elderly may differ from other age groups
• Identify the communication strategies that enhance learning for older individuals
• Discuss the health promotion issues that are important in the care of the elderly renal patient
Providing Information and Education to the Elderly Renal Patient
69
hearing, taste, smell and touch. The visual changes affect colour and depth perception, peripheral vision and increased sensitivity to glare. Hearing high frequency sounds becomes more diffi cult with age. The older patient can often not tolerate long education session due to age related musculoskeletal problems. When planning education to the older renal patient those age related changes should be considered3,4.
Communication issues with the older renal patient
Communication strategies with the older renal patient are essentially the same as with other patients, and include listen-ing, clarifying, giving information, seeking validation of under-standing, using open-ended questions, and maintaining the focus of the communication. It is a two-way process between the patient and the health care professional. Communication is an ongoing, changing and repeating process which includes both verbal and non-verbal signals. Non-verbal communica-tion is estimated to comprise approximately 80% of the com-munication process, and encompasses body language, such as position, eye contact, tone of voice, facial expression and touch. For verbal communication with the older renal patient the following guidelines are recommended:,4,5,6,7
Face the individual• Do not shout or raise the voice• Minimize background sound as it can make hearing • more diffi cult Communicate at eye level e.g. if the patient is sitting • or lying, sit down Touch the individual if appropriate to do so• Use written material to supplement verbal communica-• tionKeep teaching sessions short •

Caring for the Elderly Renal Patient
70
Present material at a comfortable pace controlled by • the patient Ensure that the environment is quiet and conducive to • learning
Establishing a good relationship with the older individual is important to facilitate learning. How the communication is initiated can have signifi cant infl uence on and set the tone for the duration of the interaction. It is important to make the fi rst interaction as positive as possible, and to establish a good rapport. Research had shown that the ability to establish a trusting and empathetic relationship with patients is important in communication effectiveness7. Therefore, acceptance, understanding, trust, and empathy are fundamental to a positive learning relationship.
EDUCATING THE OLDER RENAL PATIENT
Needs assessment
Prior to commencing a programme of education, the educator should assess the older renal patient’s needs and learning style. The needs assessment should include physical and psychosocial needs, education level, reading level, motivation to learn, readiness to learn, present knowledge, and barriers to learning. Problems that affect learning, such as hearing and visual impairment, should be included in the assessment. The presence of diseases that affect cognitive function and the musculoskeletal system should also be assessed.
The patient’s learning style should be formally evaluated, and the preferred method of learning determined. Moreover, if the education is provided in a way that the patient is accustomed to, the recommendations of the education session are more likely to be followed,8,9,10. Several instruments are available to assess learning style. These include Roger Sperry right-brain/left-brain and whole brain thinking and Kolb’s experiential
Providing Information and Education to the Elderly Renal Patient
71
learning model11. The easiest instrument to use is to ask the patient who s/he learns best. The education should then be planed in the preferred way.
Goal of teaching
Following assessment the patient and the educator should set their collaborative goals for learning. These goals are based on the knowledge and skills that the educator perceives as fundamental to the achievement of learning objectives. Goals need to be established in collaboration so the patient and the educator share common goals during the educational session. Once the goals have been set, the educator can plan and structure the education programme with the goals in mind. The goals may additionally assist the educator to arrange the order in which the education is presented3,9.
The individual’s level of education
Nurse educators often rely heavily on printed educational material. As research demonstrates that the reading level of educational material is often beyond the capability of the intended audience3,8, when planning education with the older renal patient careful assessment of the reading level is required. The older today grew up before or during the war and often have much less formal education than is now common. Their reading skills are often limited due to lack of practice and they often are functionally illiterate.
With a view to facilitating understanding on behalf of the elderly renal patient, the following points should be considered8:
Create a positive relationship with the patient and • signifi cant others Negotiate collaborative goals for the education • programme
Caring for the Elderly Renal Patient
72
Use the smallest amount of information needed to • reach the set goals
Divide the education session into small steps •
Ensure that the information is as clear and specifi c as • possible
Avoid medical jargon •
Encourage the patient to repeat the information in their • own words and to demonstrate learned procedures
Ask open ended questions instead of close ended • questions
Encourage and praise the patient in order to keep • motivation high
Repeat the content of the session using different • wording to help the patient to remember
Help the patient to arrange the regime into his/her • daily schedule to make it easier to adapt to and use reminder to learn new habits
Mode of teaching
Education sessions may be group or individual. Whilst providing education in the group environment may be cost effective, it is not always the best method for the elderly renal patient3. Not all patients feel comfortable in the group setting, and would prefer to be taught on an individual basis. Although it seems ideal to educate patients on haemodialysis during treatment time, there are reasons not to do so. Research indicates that patients’ experience a variety of physiological and psychological symptoms during dialysis therapy. These symptoms have negative impact on the patient’s ability to learn. Therefore, education during dialysis sessions should be avoided3,8.
Providing Information and Education to the Elderly Renal Patient
73
Enhancing learning With increasing age, the amount of time that the patient requires to learn new facts and skills increases. The elderly have decreased energy levels, and thus it is important to identify at what time of the day the patient learns most effectively. To enhance learning, the education session should take place in:
A comfortable environment that facilities learning e.g. • in a quiet room that has appropriate lighting A logical sequence beginning with the most important • point fi rstShort sessions with frequent breaks•
Studies suggest that when multiple teaching approaches are used, learning is enhanced8. Therefore, it is pertinent to use a combination of teaching methods, such as verbal education supplemented with written and visual material. Of note, it is important to consider the individual’s preferred learning style, and to use this whenever possible and/or appropriate. Learning will only take place if the older values the information given to him as important. Be specifi c in the education about what the older needs to know, what to do, who and when. The more specifi c the educator is in the education the more likely the older is to follow the recommendation3,8,9.
Learning can be impeded by barriers in the educator and the older. Negative attitudes regardless of their origin can have effect on the teaching and the possibilities that the older fallows the recommendation. Positive attitude can on the other hand facilitate learning1.
Self care and health promotion The goal of management of chronic diseases such as CKD is to achieve the best level of functioning and the lowest level of symptoms at the same time. This goal is hard to reach unless
Caring for the Elderly Renal Patient
74
the patient is active participant in self-management of his/her illness and treatment. Self-management has been described as the process people use to manage their condition, maintain or create meaningful life-roles and deal with the emotional consequences of having chronic illness. This includes having the knowledge and skills to care for themselves, monitor and manage symptoms and identifying problems. The older renal patient can be assisted in self-management through education12, 13.
Component of education to the older renal patient should be health promotion. Health promotion is the process of assisting people to change health habits in order to improve health. For the older renal patient this includes helping him/her to maintain or reach their optimum level of functioning and quality of life. Included in the promotion are also issues such as smoking cessation, drinking alcohol in moderate amounts, eating healthy but in congruity with what the CKD allows and safety at home and while driving2.
Providing Information and Education to the Elderly Renal Patient
75
Key Points
• Older persons can learn but changes related to aging can affect learning. Those changes affect the sensory, cardiovascular, respiratory, and musculoskeletal sys-tems, and the socioeconomic status of the older.
• Same strategies apply to communication with the older person as younger person.
• Assessment of the older person needs, learning style and educational level should be done before starting the education.
• The educator can use many teaching aid to enhance learning in the older. Barriers to learning should be in his/her mind in the education.
Caring for the Elderly Renal Patient
76
References Zhou XJ, Rakheja D, Yu X, Saxena R, Vaziri ND, and Silva FG. The 1. aging kidney. Kidney International 2008; 74(6): 710-720.
Falvo DR. Patient teaching and patient adherence issues for older 2. adults. In: Falvo DR. Effective patient education. A guide to increased adherence. 4th ed. Sudbury: Jones and Bartlett Publishers, 2011; p. 297-325.
Best J. Effective teaching for the elderly: Back to basis. 3. Orthopaedic Nursing 2001; 20(3): 46-52.
Mathers T. The older adult with chronic kidney disease. In: Molzahn A, 4. Butera E, editors. Contemporary nephrology nursing: Principles and practice. 2nd ed. Pitman: American Nephrology Nursing Association, 2006; p. 503-26.
Ebersole P, Hess P. Communicating with elders. In: Ebersole P, Hess 5. P. Geriatric nursing & healthy aging. St. Louis: Mosby Inc., 2001; p. 28-42.
Tabloski PA. Gerontological nursing issues. In: Tabloski PA. 6. Gerontological nursing. Upper Sadler River: Pearson Education Inc., 2006; p. 27-53.
Falvo DR. Communicating effectively on patient teaching: Enhancing 7. patient adherance. In: Falvo DR. Effective patient education. A guide to increased adherence. 4th ed. Sudbury: Jones and Bartlett Publishers, 2011; p. 193-220.
McCormick J. Relating to teaching and learning. In: Molzahn A, Butera 8. E, editors. Contemporary nephrology nursing: Principles and practice. 2nd ed. Pitman: American Nephrology Nursing Association, 2006; p. 885-902.
Falvo DR. Communicating effectively in patient teaching: Enhancing 9. patient adherence. In: Falvo DR. Effective patient education. A guide to increased adherence. 4th ed. Sudbury: Jones and Bartlett Publishers, 2011; p. 193-220.
Cox S, Thomas N, Liossatou A. Giving choice through timely 10. education: How to set up and implement education programmes for CKD. In: Jenkins K, Mahon A. Chronic kidney disease. A guide to clinical practice. Luzern: European Dialysis and Transplant Nurses Association/European Renal Care Association, 2008; p. 19-41.
Kitchie S. Determinants of learning. In Bastable SB. 11. Nurse as educator. Principles of teaching and learning for nursing practice. 3rd ed. Sudbury: Jones and Bartlett Publishers, 2008; p. 93-145.
Providing Information and Education to the Elderly Renal Patient
77
Molzahn AE. Quality of life and chronic kidney disease: Living long 12. and living well. In: Molzahn A, Butera E, editors. Contemporary nephrology nursing: Principles and practice. 2nd ed. Pitman: American Nephrology Nursing Association, 2006; p. 343-358.
Richard CJ. Self-care management in adults undergoing hemodialysis. 13. Nephrology Nursing Journal. 2006; 33(4): 387-94.


The Elderly Patient on Peritoneal Dialysis
79

Caring for the Elderly Renal Patient
80
IntroductionThe invention of the Tenckhoff catheter for peritoneal dialysis in 1968 made it possible to perform intermittent peritoneal dialysis (PD) in patients with chronic renal failure.
Typically 3 short exchanges are manually performed during daytime, followed by one during the night. With this technique the relatively low effi ciency of the peritoneum as a dialysis membrane is compensated by the continuous character of the treatment: 24 hours a day, 7 days a week.
Due to its simplicity CAPD is a home treatment that can be done by patients themselves after a training period of 1 to 2 weeks. Automated peritoneal dialysis (APD) was developed in the nineties. A cycler regulates the short nightly exchanges. This is followed by a long exchange during daytime. Similarly to CAPD, APD is performed daily.
Elderly dialysis patients: haemodialysis (HD) vs peritoneal dialysis (PD)Many recent studies have shown that the survival of new PD patients is better than that of new haemodialysis patients for the fi rst few years of treatment1. Other studies have shown an
Learning outcomes
• Advantages of PD treatment in the elderly renal patient• The importance of an accurate PD training according
elderly patient needs
The Elderly Patient on Peritoneal Dialysis
81
inferior survival rate for PD-patients compared to HD patients, especially for elderly and diabetic patients2 In the prospective study comparing outcomes of older (> 70 years) people on PD and HD, the North Thames Dialysis Study3 there was no signifi cant difference in survival or quality of life between PD and HD patients. The BOLDE-study from 2010 shows that in two closely matched demographic groups of older dialysis patients on HD and PD, health-related quality of life was similar, if not better, in those on PD. The study strongly supports offering PD to all suitable older patients4.
Choice of dialysis modality.
The choice of dialysis modality has a major impact on many aspects of an individual’s life. Therefore lifestyle, social environment and personality, as well as medical factors, need to be considered in the decision-making process. The determinants for quality of care, as rated by the older person, are the values of being independent and being in control of one’s own life. In light of this, PD should be ideally suited to the elderly4 . The European Renal Best Practice (ERBP) Advisory Board stated in 2010 that there is insuffi cient evidence to support a general preference of HD or PD for medical reasons.
In several studies the authors warn for a vicious cycle concerning the possibilities to choose and start on PD: nephrologists may feel inadequately prepared to provide suffi cient care for elderly PD patients, thus further reducing use of PD and training opportunities for this group of patients. Low rates of PD utilization could refl ect a breakdown in the process of care4 .The perception that older patients are more likely to have barriers to PD related to physical problems, social circumstances and cognitive dysfunction, can result in the healthcare team believing that PD at home is not feasible for this patient group4 .

Caring for the Elderly Renal Patient
82
The initial modality choice should therefore be made primarily by the well-informed patient5 and following the preference of the patient.
The decision-making process of the elderly.
Predialysis consultations in order to make a good choice of dialysis could be in the outpatient clinic or unit but visits at home in the daily surroundings of the elderly may feel more comfortable for him becausethere is no need for transportation to the hospital. Family has a very important role in the choice of modality, but there are no doubts that it is the elderly decision at the end.
The elderly has to choose a modality which fi ts best to his way of living. A simple tool of three questions, developed in Sweden (2008), can be used to summarize the wishes of the elderly6.
Advantages and contraindications of PD for the elderly.PD offers the elderly a good cardiovascular stability. The longer preservation of residual renal function also contributes to the maintenance ofvolaemia. This is very important as the elderly are particularly sensitive to disturbances in fl uid balance7
As for all PD-treatments the intensity of the PD-treatment has to fi t with the personal needs and characteristics of the individual patient regarding diet, metabolic problems, peritoneal transport, doses of dialysis fl uid and the haemodynamic situation of the patient8.
The medical advantages of PD in the elderly can be summarized as follows:
Better maintenance of residual renal function• Better control of extra-cellular volume• Slow and continuous extraction of solutes and water•
The Elderly Patient on Peritoneal Dialysis
83
Better removal of middle molecules• Reduced cardiovascular instability and risk of • arrhythmiasNo need of vascular access (diffi cult to achieve in older • diabetic patients with atherosclerotic vessels Reduced risk of transmission of viral diseases• Improvement of anaemia and no loss of iron• 7
Social-economic advantages of PD can be mentioned:
A more liberal diet and water intake• A home therapy with reduced needs for transportation • No waiting time • Avoidance of disequilibrium syndrome •
Reduced costs• 7
Contraindications to PD
The ERBP work group advices not to consider older age, physical or mental inability to perform PD and poor adherence/compliance to therapy as a contraindication to PD. Performing PD requires a minimum of physical skills and mental capacity. It is clear that some physical problems, such as visual impairment and tremor or deformities of the hands, may interfere with PD handling, but in the opinion of the ERBP expert group these problems do not, a priori, preclude the application of PD as a therapy5.
Absolute contraindications are:
Reduced peritoneal surface due to adhesions• Chronic ostomies•
Active intestinal infl ammation•
Caring for the Elderly Renal Patient
84
The following medical contraindications could be seen as rather relative:
Hernia which can be repaired• Fresh aortic prosthesis• Severe peripheral vascular disease• Extensive diverticulitis• Low back pain•
And morbid obesity• 7
psychosocial problems where solutions have to be considered before starting with PD are:
Dementia• Inability to perform self-dialysis• Homelessness• Blindness•
CAPD or APD?
There is as such no reason to prefer CAPD or APD, as long as the dwell time of the patient is matched to his/her peritoneal transport type. Medical outcomes on both modalities have been found to be equal. Following the advice of the ERBP group the choice for CAPD or APD should be guided by the patient’s preference5.
The choice for CAPD or APD is fully depending on the individual situation of the elderly, his physical, psychological state and the amount of support from relatives.
The possibilities to receive support by district nurses in his area are also important.

The Elderly Patient on Peritoneal Dialysis
85
Steps for PD treatmentThe PD treatment starts with the implementation of the PD catheter. For this, the patient has to be admitted for about 2 or 3 days depending on the implantation technique.
Before the implantation several points have to be considered:
Location of the exit-site. • Patients in their seventies and eighties are usually concerned about their body image and sexuality9. Nevertheless the type of the catheter and the location of the exit-site should be discussed with the patient and also it should clearly be marked on the skin for the surgeon. Because of the danger of too much pressure, the exit site has to be placed under or over the belt. The patient must be able to inspect and cleanse the exit-site himself to prevent infection. The selection of the position has preferably to be done in the sitting position and can be diffi cult because of skin wrinkles. Choice of catheter and problems that might infl uence the operation procedure have to be identifi ed before the implantation. The pre- and post-insertion care follows mostly the normal guidelines. (For more detailed see: Handbook Peritoneal Dialysis, a Guide to Clinical Practice, 2009).
It is important to remember that many elderly patients are prescribed anti-aggregant drugs, the most common aspirin. These drugs should be stopped 3-7 days before the catheter implantation to prevent bleeding and development of haematomas at the site of catheter insertion
Home visits.• Specifi c issues of the housing situation of the elderly person have to be considered such as enough space for storing of materials and the distance between the

Caring for the Elderly Renal Patient
86
storing and the place where the PD treatment will take place. A home visit, by nurse, social worker or both before starting with PD gives optimal possibilities to discuss these issues with the patient and relatives. These visits can also be used to become better acquainted with each other. Feelings and fears concerning the treatment can be recognized and discussed. Information can be given about the implantation of the catheter and the following training.
Patient visit to the Unit• Some renal Units organize a patient visit to the Unit to inform the patient and family about procedures, provide some specifi c guidelines and to introduce the renal team. For elderly patients this is extremely useful.
Discharge from the hospital• Discharge of the hospital after the catheter implantation is a “critical moment” for the elderly and his family. The PD-team support is therefore needed.
Training of the elderly to perform PD treatment
Except in cases where the elderly patient is unable to perform PD exchanges by himself he will be trained by the PD-unit staff. This has to be discussed very carefully with the elderly and his family.
Apart from “normal” problems of ESRD-patients such as physical unwellness because of uraemic problems, such as nausea, vomiting, sleep disturbances and confusions, teaching elderly patients may be diffi cult because of diminished cognitive ability.
The Elderly Patient on Peritoneal Dialysis
87
Visual impairment
It is very important to identify: if the patient has the appropriate glasses, or whether he/she is affl icted with cataract or glaucoma which has to be solved/treated. The patient can also have a light sensitivity and problems with depth or colour perceptions.
For the training it is important to provide a well-lighted environment, to be close enough to the patient to allow reading and gestures to be noted and to choose large type and bold print in reading materials.
Hearing
A hearing evaluation with a whisper test in a quiet room may be a cost-effective way of detecting a hearing impairment. Ensure before the training that the patient has a good working hearing aid if needed. The trainer should speak slowly and distinctly allowing the patient to watch the lips of the trainer.
Cognitive status
Cognitive status should be assessed in all elderly ESRD patients. It is important to differentiate between delirium and dementia especially when delirium may need a medical emergency. A delirium can be predisposed by the following factors: drugs, infection, metabolic, endocrine and nutritional causes, cardiovascular and respirator disorders and psychiatric conditions such as depression, anxiety and dementia. A lot of tests can be used to assess the mental state of the elderly. One of the most well-known is the Mini-mental state examination (MMSE).
Do not forget the following when training a patient on PD treatment:
Caring for the Elderly Renal Patient
88
Hearingensure presence and good working order of hearing device if • neededspeak slowly and distinctly, do not shout • use synonyms•
Visionconsider light sensitivity and problems with depth or colour • perceptionsprovide a well-lit environment• be close enough to allow lip reading and gestures to be noted• reading material for teaching: large type and bold print•
Temperature controlelderly chill easily• use a room that is easy to keep warm•
Slow information processingbe patient, repeat information and do not go too fast• present information using different formats• provide review questions•
Mental disordersshort teaching periods (> 30 minutes)•
Stress, arthritis and decreased muscle strengthchoose an easy PD-system or use facilitatory devices•
Talk according patient educationuse simple terms, not medical jargon7 • some elderly people can use internet and different computer • programstraining sessions should be no longer than 20 minutes11
The training may be successful from ‘an intellectual point of view’7 but the performance of exchanges may still be impossible because of trembling or lack of muscular strength. Devices can be offered but is essential to accurately identify patient

The Elderly Patient on Peritoneal Dialysis
89
limitations before leaving it at home with the responsibility to perform by him/her the PD treatment.
Support from family members
Contacts between the family of the elderly and the training-nurses are extremely important before starting. It is necessary to know precisely how much help the family can give and if they want to. Some people are very independent and even if they appear frail or unwell, may want to undertake the training on their own without the support of family members. Other people are reluctant self-carers who appreciate family support10.
It is advisable to invite family to participate in the training even if the patient has the intention to perform the PD technique by himself.
Issues such as where to do the exchanges or place the APD machine, cleaning/sterile procedures, the need to wash hands and tips about storing must be widely discussed with the patient and his family.
More detailed description of PD training programs can be found in The EDTNA/ERCA handbook: Peritoneal Dialysis - A Guide to Clinical Practice, 2009.
Daily care
PD treatment for the fi rst time at home after training is very stressful and should be supervised by the nurse who has done the training.
Next to an optimal training, a successful PD at home will depend on other things such as
The motivation and acceptation of the patient and his • family to do the treatment at home and to deal with all the changes in his life caused by the illness

Caring for the Elderly Renal Patient
90
The possibilities of the patient to get help when needed • from family or community such as the district nurse
It is important to evaluate at regular intervals the storing of all materials and the ability to do the exchanges according to infection control rules. Depending on whether the patient is doing CAPD or APD, the following activities have to be done daily:
Measure of blood pressure and weight1. Choose the right concentration of fl uids2. Carry out all procedures for exchanges: machine, 3. fl uids, catheter care
Daily care of the exit- site4.
Regular evaluations of how the elderly is coping with these activities are important. In case of problems the district-nurse can take over some of the activities or just support the elderly by a daily visit.
Evaluations and retraining
Evaluation of the training and the knowledge of the patient and his family, and the daily application of this in the treatment is important and have to be monitored carefully. Different methods can be used. For elderly the best methods are house visits. The frequency will be depending on the situation of the patient and/or according Unit of reference protocols. Questions can be asked about the technique of the exchanges (connections and cleanliness) and hand washing. Fluid management, peritonitis, exit-site care and quality of daily life have also to be discussed. The ISPD-guidelines advises to do a retraining after special cases such as peritonitis or an exit site-infection12.

The Elderly Patient on Peritoneal Dialysis
91
Visits at the outpatient clinic
Most PD-patients will visit the Unit every 6 to 8 weeks, depending on the individual situation of the patient. For the renal team it is very important to continually consider if the visits of the elderly are necessary. House visits done by the specialist and more use of telecare such as Skype and the use of electronic information systems should be developed and used in the future to prevent traveling and waiting time in the hospitals13.
Admission to hospital
Hospital admissions are an extremely stressful situation for the elderly. Recent research found that 35 % of the frail elderly are in worse condition after discharge than before admittance14. Regular house visits and careful follow-up evaluation should be done after discharge, followed by a retraining, if necessary.
Assisted PD: Care done by the district nurse
Due to the growing number of frail elderly and the positive advantages of PD for the elderly, different centers in Europe have collaborate with district nurses. Assisted PD is implemented in most countries in Western Europe such as the Scandinavian countries, France, UK and the Netherlands. The cost is covered by their national healthcare system. The frequency of the visits depends on the task the district nurse has to perform. The qualifi cation of the visiting person can be different depending on the tasks to perform15.Family assistance is associated with lower peritonitis risks compared with nurses assistance, but not if PD nurses do regular visits16 Assisted PD allows disabled patients to receive dialysis care in the comfort and dignity of their own home and is a promising alternative to in center HD17.
Caring for the Elderly Renal Patient
92
The literature gives different recommendations to improve assisted PD18. Optimal training programs and e-learning programs for the district nurses, delivered by the PD centers are nowadays of great importance. There is still some reluctance to start assisted PD when reimbursement of care is unclear. Research so far shows less costs than hospital haemodialysis, particularly when cost of transport is included19.
Nursing homes have to be moved into accepting care of the elderly with PD. This is by far not the case in many countries. Reasons for this are among others: perceiving that the patient has too many medical problems, lack of reimbursement for the additional time needed to support CAPD-exchanges and nursing shortages.
Summary Working with elderly on PD is a challenge for the renal team. Dependency of help in ADL, physical and learning disabilities etc. can often lead to ethical considerations. Issues about quality of life have to be discussed in the renal team but especially with the older patient and his family. To listen respectfully to what the patient wants is the most important task for the professionals who want to optimize the care for these elderly patients.
The Elderly Patient on Peritoneal Dialysis
93
ReferencesKrediet, R. Peritoneal dialysis: past, present and future. 1. Peritoneal Dialysis, a guide to Clinical Practice, 2009; 16-23.
Collins, AJ et al. Comparison and survival of homedialysis and 2. peritoneal dialysis in the elderly. Seminars in Dialysis, 2002, 15: 98-102.
Lamping DL et al. Clinical outcomes, quality of life, and costs in 3. the North Thames Dialysis Study of elderly people on dialysis: a prospective cohort study. Lancet, 2000; 356: 1543-1550.
Brown E, Johansson L, et al. Broadening Options for Long-term 4. Dialysis in the Elderly (BOLDE): differences in quality of life on peritoneal dialysis compared to haemodialysis for older patients, Nephrology Dialysis Transplantation 2010; 25; 11: 3755-3763.
Covic, A et al. Educating endstage renal disease patients on 5. dialysis modality selection: a clinical advice from the European Renal Best Practice (ERBP) Advisory Board, Nephrology Dialysis Transplantation Plus Advance Access, 2010.
Care for home, decisionsguide, 6. Baxter Sweden, 2008.
Dratwa M, van der Poel M Peritoneal Dialysis in older People, 7. Management Possibilities for the renal team, Baxter Europe, Renal division 2003.
Guidelines Dialysis, the Netherlands, 8. DiaVisie, visitationcommision dialysis departments NfN/V&VN dialysis & Nephrology, 2010.
Gonsalves-Ebrahim L et al. Continuous ambulatory peritoneal dialysis: 9. psychological factors, Psychosomatics 1982; 23 (9): 944-949.
Thomas, N Education and Training in 10. Peritoneal Dialysis, a Guide to Clinical Practice, EDTNA/ERCA 2009; 55-69.
Hall, G et al. New directions in peritoneal dialysis training, 11. Nephrology Nursing Journal, 2004; 31(2): 149-154: 159-163.
Bernardini, J et al. ISPD Guidelines/Recommandations, 12. Peritoneal Dialysis International, 2006; 26 (6): 625-632.
Tinker, A The care of older people-what role for technology? 13. Journal of Clinical Nursing, 2010; 19: abstract: suppl.1.
Smilde, D et al. Care for older in the hospital, 14. Journal of Clinical Nursing, 2010; 19: abstract: suppl. 1.
Castrale, C et al.Peritoneal dialysis in elderly patients: report from the 15. French Peritoneal Dialysis Registry (RDPLF), Nephrology Dialysis Transplantation, 2010; 25 : 255-262.
Caring for the Elderly Renal Patient
94
Verger, C et al. Infl uence of autonomy and type of home assistance on 16. the prevention of peritonitis in assisted automated peritoneal dialysis patients: An analysis of data from the French language Peritoneal Dialysis Registry, Nephrology Dialysis Transplantation, 2007; 22: 1218-1223.
Oliver, MJ et al. Homecare assistance and the utilization of peritoneal 17. dialysis, Kidney International, 2007; 71: 673-678.
Holck, K How can you support the assisted PD-patient’s Self-care 18. Capacity Peritoneal Dialysis, a Guide to Clinical Practice EDTNA/ERCA 2009, 177-185.
Povlsen, J Peritoneal Dialysis for the Elderly, 19. Peritoneal Dialysis, a guide to Clinical Practice 2009, 163-177.

The Elderly Patient on Peritoneal Dialysis
95

The Elderly Patient on Haemodialysis
97
Caring for the Elderly Renal Patient
98
IntroductionHospital based haemodialysis (HD) is the predominant treatment choice for elderly patients entering renal replacement therapy programmes. The reasons for the selection of HD over home based therapies, such as assisted peritoneal dialysis, in this patient population are multifactorial, and include medical and social factors, physician bias, late referral, and education not tailored to the needs of older individuals1. HD in the elderly poses a unique challenge to the multidisciplinary renal care team, in terms of optimising vascular access (VA) and dialysis adequacy, maintaining nutritional status, and preserving quality of life (QOL). The focus of this chapter is to explore HD within the context of the elderly patient. The signifi cance of establishing viable VA will be emphasised, and the role of the renal nurse, in enhancing the patient experience, will be highlighted.
Specifi c characteristics of the elderly HD populationWhen compared to the younger HD population, elderly patients have a signifi cantly higher number of comorbidities. Specifi c
Learning outcomesOn reading this chapter the reader should be able to:
• List the factors which may compromise the creation of successful vascular access in the elderly
• Discuss the role of the nurse in maintaining vascular access patency
• Outline the key components of renal conservative care
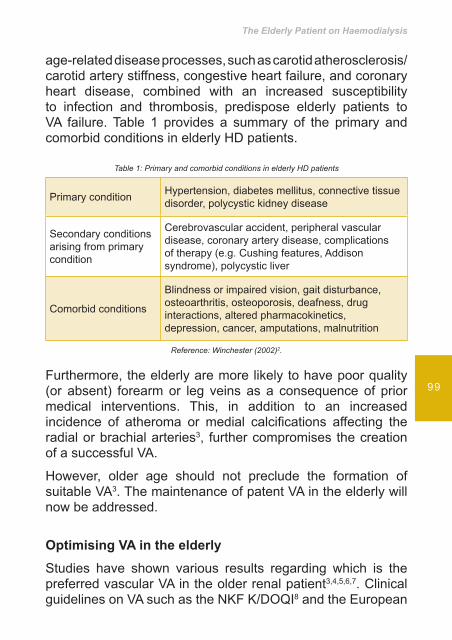
The Elderly Patient on Haemodialysis
99
age-related disease processes, such as carotid atherosclerosis/carotid artery stiffness, congestive heart failure, and coronary heart disease, combined with an increased susceptibility to infection and thrombosis, predispose elderly patients to VA failure. Table 1 provides a summary of the primary and comorbid conditions in elderly HD patients.
Table 1: Primary and comorbid conditions in elderly HD patients
Primary condition Hypertension, diabetes mellitus, connective tissue disorder, polycystic kidney disease
Secondary conditions arising from primary condition
Cerebrovascular accident, peripheral vascular disease, coronary artery disease, complications of therapy (e.g. Cushing features, Addison syndrome), polycystic liver
Comorbid conditions
Blindness or impaired vision, gait disturbance, osteoarthritis, osteoporosis, deafness, drug interactions, altered pharmacokinetics, depression, cancer, amputations, malnutrition
Reference: Winchester (2002)2.
Furthermore, the elderly are more likely to have poor quality (or absent) forearm or leg veins as a consequence of prior medical interventions. This, in addition to an increased incidence of atheroma or medial calcifi cations affecting the radial or brachial arteries3, further compromises the creation of a successful VA.
However, older age should not preclude the formation of suitable VA3. The maintenance of patent VA in the elderly will now be addressed.
Optimising VA in the elderly
Studies have shown various results regarding which is the preferred vascular VA in the older renal patient3,4,5,6,7. Clinical guidelines on VA such as the NKF K/DOQI8 and the European
Caring for the Elderly Renal Patient
100
Best Practice Guidelines (EBPG)9 do not especially discuss VA in the elderly or divide their recommendation into age groups. Both guidelines recommend the arteriovenous fi stula (AVF) as the fi rst choice of VA, then the arteriovenous graft (AVG) and catheter should be the last resource of VA and used only when other options are not available.
Several authors3,5,7,10 advocate the timely placement of VA. Before insertion, a thorough history and physical assessment of the older person should be performed. Included in the history should be events such as former placement of central venous catheters, the presence of a cardiac pacemaker, axillary lymph node dissections and other interventions in the vascular system of the shoulder area. The selection of the VA type inserted should be based on the history, physical assessment and clinical guidelines. The threshold for upper arm AVF should be lower than for younger individuals. The VA should be inserted timely so it has adequate time for maturation, as studies have shown that the elderly have a longer AVF maturation time than younger patients3. Strict control of cardiovascular risk factors, and suitable treatment of cardiovascular disease, is recommended as they are thought to have benefi cial effects on AVF maturation and survival3.
Complications in the VA of the elderly, such as thrombosis, stenosis, infections, and aneurysm are no different than for other age groups11,12. They are related to the type of VA and the anatomic location of the access. The same complication preventions should be used with older patients on HD as for other patients.
As for all age groups, the VA should be assessed regularly after insertion and before all cannulations8,9,12,13. The assessment should consist of inspection, palpation and auscultation. In order to prolong the life of the VA, an appropriate cannulation technique should be utilised. The literature indicates that the rope ladder is the most suitable technique for AVG, and either the rope ladder or button hole technique for AVF12,13.
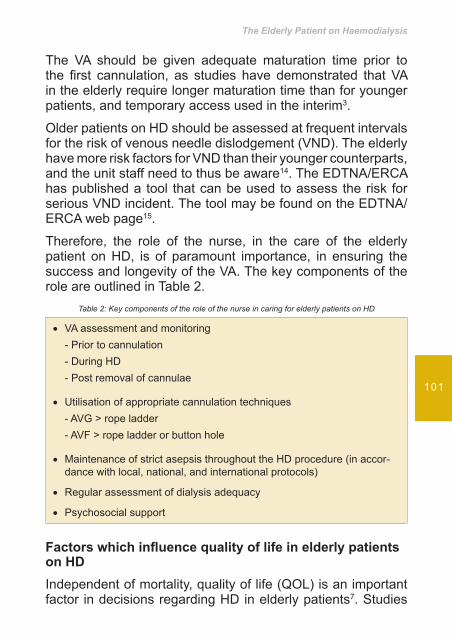
The Elderly Patient on Haemodialysis
101
The VA should be given adequate maturation time prior to the fi rst cannulation, as studies have demonstrated that VA in the elderly require longer maturation time than for younger patients, and temporary access used in the interim3.
Older patients on HD should be assessed at frequent intervals for the risk of venous needle dislodgement (VND). The elderly have more risk factors for VND than their younger counterparts, and the unit staff need to thus be aware14. The EDTNA/ERCA has published a tool that can be used to assess the risk for serious VND incident. The tool may be found on the EDTNA/ERCA web page15.
Therefore, the role of the nurse, in the care of the elderly patient on HD, is of paramount importance, in ensuring the success and longevity of the VA. The key components of the role are outlined in Table 2.
Table 2: Key components of the role of the nurse in caring for elderly patients on HD
VA assessment and monitoring•
- Prior to cannulation- During HD- Post removal of cannulae
Utilisation of appropriate cannulation techniques•
- AVG > rope ladder- AVF > rope ladder or button hole
Maintenance of strict asepsis throughout the HD procedure (in accor-• dance with local, national, and international protocols)
Regular assessment of dialysis adequacy•
Psychosocial support•
Factors which infl uence quality of life in elderly patients on HDIndependent of mortality, quality of life (QOL) is an important factor in decisions regarding HD in elderly patients7. Studies
Caring for the Elderly Renal Patient
102
suggest that most elderly patients would elect dialysis if offered but that relief of symptoms was a major goal rather than survival alone16. Moreover, patients on HD rate their QOL as poorer than age-matched controls17. Factors which may negatively impact on the QOL of elderly patients on HD encompass:
Intradialytic hypotension• Exhaustion• The time consuming nature of travelling to and from • the HD unitFunctional impairment• Failure of VA• Infection e.g. AVF cannulation site, bacteraemia• Frequent hospitalisation•
Withdrawal of the elderly patient from HDOccasionally, HD in elderly patients is initiated with the understanding that it is a time limited trial. Even if this is not the case, elderly HD patients are in general quite ill, and consideration should be given to the possibility of a short lifespan7. Approximately 30% of patients aged ≥ 75 years withdraw from their dialysis at the end of life7. Subsequently, the focus of care becomes symptom control and psychosocial support of the patient and family. With a view to providing holistic care within this context, the role of the Renal Conservative Care Nurse Specialist was created.
Role of the Renal Conservative Care Nurse SpecialistFor some patients, making the decision to withdraw from dialysis may be extremely diffi cult, not only for themselves, but also for their family, friends, and carers. The Renal Conservative Care Nurse Specialist can offer help and support to the patient, family, and the HD team during the decision
The Elderly Patient on Haemodialysis
103
making process when a patient wish to stop dialysis, as this can be a highly emotive subject and a sensitive and diffi cult time for all concerned.
The demands and constraints of HD can take its toll on patients, especially the frail elderly with signifi cant comorbidities. For this population of patients, receiving hospital based HD can be time consuming, and the round journey thrice weekly can be exhausting. Poor tolerance of the HD sessions may contribute to failure to thrive; and frequent hospitalisations, as a result of fl uid overload, poor nutritional status, infections, or problematic vascular access predisposes to overall poor QOL.
When the decision to withdraw from dialysis has been made, consideration needs to be given to what the patient wishes to happen during the last few weeks of life. This may include matters relating to their personal life, funeral wishes, place of death, and dialysis arrangements. A date may be set to stop HD, and it may be helpful to reduce the frequency and duration of the sessions, tailoring the treatment to the individual needs of the patient especially if fl uid removal is required on a need to need basis.
Murtagh et el (2007)18 summarise that in patients with CKD stage 5 aged ≥ 75 years, who receive specialist nephrological care early, and who follow a planned management pathway, the survival advantage of dialysis is substantially reduced by comorbidity and ischaemic heart disease in particular. Therefore it may be prudent to consider conservative care.
Summary This chapter has examined the elderly patient experience in HD. Although the elderly may present with complex medical issues, HD for older individuals should not be viewed as different from the young. This chapter has also highlighted the unique role of the renal nurse, in both optimising VA and supporting the patient who opts for conservative care.

Caring for the Elderly Renal Patient
104
References
Brown EA. Peritoneal dialysis for older people: overcoming the 1. barriers. Kidney International. 2008; 73: S68-71.
Winchester JF. Special clinical problems in geriatric patients. 2. Seminars in Dialysis. 2002; 15(2): 116-120.
Bessias N, Paraskevas KI, Tziviskou E, and Andrikopoulos A. Vascular 3. access in elderly patients with end-stage renal disease. International Urology and Nephrology. 2008; 40: 1133-1142.
Ekbal NJ, Swift PA, Chalisey A, Steele M, Makanjuola D, Chemla 4. E. Hemodialysis access-related survival and morbidity in an elderly population on South West Thames, UK. Hemodialysis International. 2008; (12): S15-S19.
Ismail N, Hakim RM, Oreopoulos DG, Patrikarea A. Renal replacement 5. therapies in the elderly: Part 1. Hemodialysis and chronic peritoneal dialysis. American Journal of Kidney Diseases. 1993; 22(6): 759-782.
Richardson AI, Leake A, Schmieder GC, et al. Should fi stulas really 6. be fi st in the elderly patient? The Journal of Vascular Access. 2009; 10: 199-202.
Wright S, Danziger J. Vascular access for hemodialysis in the elderly. 7. Geriatric Nephrology Curriculum [homepage on the Internet]. c2009 [cited 2011 July 14] Available from: http://www.asn-online.org/education_and_meetings/geriatrics/
NKF K/DOQI. 8. Clinical practice guidelines and clinical practice recommendations. 2006; updates: vascular access [homepage on the Internet]. c2006 [cited 2008 Dec 18] Available from: http://www.kidney.org/professionals/kdoqi/guideline_upHD_PD_VA/index.htm
Tordoir J, Canaud B, Haage P, et al. EBPG on vascular access. 9. Nephrology Dialysis Transplantation. 2007; 22(suppl. 2): ii88-ii117.
Latos DL. Hemodialysis in the elderly: vascular access and initiation 10. of renal replacement therapy. Seminars in Dialysis. 2002; 13(2): 91-93.
Elseviers MM, Van Waeleghem JP. Complications of vascular access: 11. results of a European multi centre study of the EDTNA/ERCA research board. EDTNA/ERCA Journal. 2003: XXIX: 163-167.
McCann M, Einarsdottir H, Van Waeleghem JP, Murphy F, Sedgwick 12. J. Vascular access management II: AVF/AVG cannulation techniques and complications. Journal of Renal Care. 2009; 35(2), 90-98.

The Elderly Patient on Haemodialysis
105
Ball K. Improving arteriovenous fi stula cannulation skills. 13. Nephrology Nursing Journal. 2005; 32(6), 611-617.
Van Waeleghem JP, Chammey M, Lindley E, Pancírová J. Venous 14. needle dislodgement: How to minimise the risk. Journal of Renal Care. 2008; 34(4), 16.
http://www.edtnaerca.org15. /
Ahmed S, Addicott C, Qureshi M, Pendleton N, Clague JE, and Horan 16. MA. Opinions of elderly people on treatment for end-stage renal disease. Gerontology. 1999; 45: 156-159.
Evans RW, Manninen DL, Garrison LP Jr, Hart LG, Blagg CR, Gutman 17. RA, Hull AR, and Lowrie EG. The quality of life of patients with end-stage renal disease. New England Journal of Medicine. 1985; 312: 553-559.
Murtagh FE, Marsh JE, Donohoe P, Ekbal NJ, Sheerin NS, and Harris 18. FE. Dialysis or not? A comparative survival study of patients over 75 years with chronic kidney disease stage 5. Nephrology Dialysis Transplantation. 2007; 22: 1955-1962.

Legal and Ethical Challenges of Caring for the Elderly Renal Patient
107

Caring for the Elderly Renal Patient
108
Caring for elderly renal patients poses a multitude of ethical and legal challenges for healthcare professionals. Key challenges of caring for elderly renal patients include renal replacement therapy decisions, dialysis withdrawal, end of life care and renal transplantation. Withdrawal from dialysis has historically posed the most prominent dilemma.
Empirical evidence1,2,3,is accumulating to illustrate that the incidence of elderly patients receiving life sustaining renal support via an extra corporeal blood circuit (haemodialysis) is escalating. The wisdom of this practice is debatable when poor quality of life (QOL) is often the outcome, and this has resulted in a dichotomy of opinions. The legal and ethical implications of withdrawing life-sustaining haemodialysis, however, appear to be formidable.
The QOL of elderly renal patients receiving haemodialysis is pitiable. This is partly due to their poor tolerance of haemodialysis and their existing co-morbidities4.
Lelie et.al (1999) argue that there are specifi c moral problems attached to life-prolonging medical technologies, for instance the range of questions about stopping treatment when the burden seems to outweigh the benefi ts4. The same authors raise the question of whether the explicit wishes of patients
Learning outcomes
• Identify the ethical issues relating to the care of elderly renal patients
• Understand the legal implications of treatment withdrawal

Legal and Ethical Challenges of Caring for the Elderly Renal Patient
109
and relatives to continue dialysis should be followed under all circumstances.
Ethical concerns regarding patient autonomy, surrogate choice in decision making and benefi cence are evident. Keen (2000)5 describes autonomy as the freedom to determine one’s own actions and behaviour. Parker (1999)6 elaborates that autonomy gives every competent adult the right to decide what may or may not be done to him, and emphasises that any treatment or investigation carried out without consent may amount to an assault or battery. Tobe & Senn (1996)7 suggest that competent patients do wish to discuss life-sustaining treatments, and health care workers should meet this wish in a timely and comprehensive manner, discussing benefi ts and limitations of therapy.
Recent studies8 recommend that dialysis decisions should be made through the process of shared decision-making. Cohen et al. (2000)9 echoes Levine’s work by writing that bioethical approval of decisions to discontinue dialysis is based on the principle of respect for patient autonomy and the belief shared by patients, families and physicians that the promise of a good death is preferable to prolonged and onerous suffering.
Nephrology nurses have a fundamental role as patient advocates. Hewit (2002)10 identifi es that patient advocacy is one of the roles that separates nursing from medical ethics. Moral and ethical reasoning, autonomy and patient empowerment have become inextricably linked with the triad of nurse, patient and advocacy11. However, it must be questioned if nurses possess the authority to challenge either the medical profession or the bureaucratic health care system. Hewitt (2002)10 argue that doctors have felt threatened by nurse advocacy and its encroachment on their traditional role as information givers. Salvage (1985)12 has written of the medical hostility attracted by nurse advocacy. Hewitt (2002)10 describes Beardshaw’s (1981) evidence to demonstrate that as a result of this hostility, nurses have been fearful to speak out for patients, even when

Caring for the Elderly Renal Patient
110
patients were suffering. The Nursing and Midwifery Council (NMC) of the United Kingdom (2008)20 mandates that nurses should act as patient advocates. This statement has been the subject of considerable debate, as the profi ciency of nurses acting as advocates given their minimum knowledge of ethics and the law has been challenged14,19 Changes in legislation are essential to support nurses in the advocacy role.
Fry (1994)15 defi nes benefi cence as the ‘obligation to do good and avoid doing harm’. Acting on this principle means restoring health and alleviating suffering. It is noted in the literature5 that good can be interpreted subjectively, therefore decisions regarding dialysis discontinuation maybe related to subjective judgements. It is increasingly expected that health professionals will inform their clinical decisions with appropriate evidence from research16 .
Surrogate decision-making is occasionally, the only realistic option available. Cohen et al. (2000)9 highlight the fact that dying requires an appreciation of the limited time remaining to patients and families and an extraordinary sensitivity to privacy issues. Patients should explicitly state their preference for end of life care in a written advance directive. Recent studies17,18 provide evidence to support this viewpoint. Rashid (2000)17 defi nes advance directives as living wills or the durable power of attorney for health care that allows individuals to infl uence medical decisions about their care should they lose mental capacity due to acute or chronic illness. Keen (2000)5 has identifi ed that honest and consistent communication and the development of a trusting relationship with staff are signifi cant factors in relation to the ability of the family to act as surrogate decision makers.
In the context of nursing the elderly renal patient this discourse of critical refl ection has illustrated various professional issues. These include the need for interprofessional collaboration, the bureaucratic focus on physiological outcomes and the lack of nurse education in ethico-legal issues. Keen (2000)5 proposes

Legal and Ethical Challenges of Caring for the Elderly Renal Patient
111
that ethico-legal decision-making should be emphasized in the basic education of nurses, thus allowing them to optimally fulfi l their pivotal role of patient advocate. Nurses should also be involved in policy decisions that affect their everyday practice, so that they can become autonomous practitioners, implementing health care policies with an informed perspective, culminating in positive patient outcomes.
The focus has for too long being on physiological outcome measurements, the work should be broadened to encompass standards such as QOL indicators. Nephrology nurses are eminently situated, academically prepared, and professionally qualifi ed to positively affect patient outcomes. This chapter clearly highlights the challenges that paternalism and ethics pose to the present day nephrology nurse, caring for the elderly renal patient20.
Caring for the Elderly Renal Patient
112
References
Mallick, N.P. & Marasi, A.E. 1999. Dialysis in the Elderly, to treat or not 1. to treat? Nephrology Dialysis Transplantation 14(1):37-39.
Schaefer,K.& Rohrich,B. 1999 The dilemma of renal replacement 2. therapy in patients over 80 years of age: Dialysis should not be withheld. Nephrology Dialysis Transplantation 14(1):35-36.
Latos, D.1996. Chronic Dialysis in patients over age 65. 3. Journal of the American Society of Nephrology 7(5): 637-646.
Vecchio, L.D. & Locatelli, F. 2009. Ethical issues in the elderly with 4. renal disease. Clinics in Geriatric Medicine 25(3):543-553.
Lelie, A., Dekkers, W.J.M., Van Hamersvelt, H.W., Huysmans,F.T.M. 5. & Have, A.M.J. 1999. Discontinuing Dialysis: Patient’s wishes and professional judgement. Nephrology Dialysis Transplantation 14(1): 318-321.
Keen, A., 2000. Critical Incident: efl ection on the process of terminal 6. weaning. British Journal of Nursing 9(16): 1059-1062.
Parker, S.1999. Nurses have an important role in consent issues. 7. British Journal of Nursing 8(16): 1048.
Tobe, S.W. & Senn, J.S. 1996. Foregoing renal dialysis: A case study 8. and review of Ethical issues. American Journal of Kidney Diseases 28(1): 147-153.
Levine, D.Z. 2001. Shared decision-making in dialysis: The new RPA/9. ASN Guideline on appropriate initiation and withdrawal of treatment. American Journal of Kidney Diseases 37(5): 1081-1091.
Cohen, L.M., Germain, M., Poppel, D.M., Woods, A. & Kjellstrand, 10. C.M. 2000. Dialysis discontinuation and palliative care. American Journal of Kidney diseases 36(1): 140-144.
Hewitt, J. 2002. A critical review of the arguments debating the role of 11. the nurse advocate. Journal of Advanced Nursing 37(5): 439-445.
Holden, R.J. 1991. Responsibility and Autonomous Nursing Practice. 12. Journal of Advanced Nursing16, 398-403.
Salvage, J.,1985. The Politics of Nursing. LONDON: HEINEMANN.13.
Harris, S. 1996. Issues concerning Patient Advocacy: Personal 14. experiences. Nurs. Critical Care 1(6): 292-295.
Fry S.T. 1994. Ethics in Nursing Practice: A Guide to Ethical Decision 15. Making. Geneva: International Council of Nurses.
Legal and Ethical Challenges of Caring for the Elderly Renal Patient
113
Thompson, C., McCaughan, D., Cullum, M., Sheldon, T. A., Mulhall, 16. A. & Thompson, D.R. 2001. Research information in Nurses Clinical Decision-Making: What is useful? Journal of Advanced Nursing 36(3): 376-388.
Rashid, C. 2000. Philosophical Implications of the use of advance 17. statements (LIVING WILLS). Nursing Standard 14(25): 37-40.
Loftin, L.P. & Beumer, C. 1998 . Collaborative End-of-Life decision 18. making in End Stage renal Disease. ANNA Journal 25(6): 615-617, 597.
Norrie, P. 1997. Ethical Decision Making i Intensive Care: Are Nurses 19. suitable Patient Advocates? Intens Critical Care Nurs. 14, 167-169.
NMC. 2008. 20. Code of Professional Conduct. LONDON: NMC.

Nutritional Requirements in Elderly Renal Patients
115
Caring for the Elderly Renal Patient
116
Introduction As life expectancy increases, the population aged over 65 constantly increases. In 2010-2050 the population over 65 years old is expected to double its percentage (from 7.2% to 16.2%) in world population and to rise from 15.2% to 26.1% in the developed countries1. Despite the great heterogeneity among the elderly, the majority of the older adults suffer from disabilities and chronic diseases that alter their nutritional needs and affect greatly their nutritional status. In Chronic Kidney Disease (CKD) nutritional intervention is of great importance. Specifi c recommendations for the elderly do not exist today and most of the dietary restrictions and advice are based on the recommendations given in younger adults..
Malnutrition in the elderly with CKD Mild to moderate malnutrition affects almost one-third of the dialysis patients, while 6-8% have severe malnutrition, which is associated with increased morbidity and mortality rates2. Moderate to severe malnutritioncan be foundin 10-30%
Learning outcomes
• To gain knowledge and understanding of the importance of maintaining a good nutritional status in elderly with CKD
• To understand the role of dietary interventions in fl uid and electrolyte balance
• To understand the importance of nutritional interventions in optimizing biochemical parameters and reducing long term complications associated with CKD
Nutritional Requirements in Elderly Renal Patients
117
of the patients, however, is an independent risk factor for death among the elderly. Many of these patients also suffer from cardiovascular diseases and other co morbidities, which, independent of any underlying uremia and/or dialysis, impacts negatively both on their quality of life and clinical status. Moreover, their condition is often further exacerbated by dialysis itself, with its acute (e.g., hypotension and sensorial alterations) and chronic complications, including an exacerbation of malnutrition and systemic vascular disease3.
Malnutrition in the elderly is a multifactorial problem, consisting of physiological, social and economic parameters, often referred as the “nine d’s”, namely:
poor dentition - dysgeusia - dysphagia - diarrhea - depression disease- dementia - dysfunction and drugs4, factors which often coexist, resulting in compromised nutritional intake and subsequent poor nutritional status. Malnutrition can occur secondary not only to insuffi cient and/or unbalanced nutritional intake or uraemia, but it may also depend on the patient’s level of tolerance to dialysis and on the dialysis modality. Despite the improvements made to dialysis techniques, the nutritional condition of elderly patients on dialysis for chronic renal failure remains a cause for concern2.
Aims of nutritional therapy To promote a balanced and healthy dietary plan, • covering the special needs of the elderly patients, without a negative effect on the quality of life of the patientTo preserve good nutritional status and prevent • malnutrition and sarcopenia (erosion of skeletal muscle and weakening of the body)To control biochemical parameters related to CKD and • retain them within acceptable rangeTo optimize fl uid control•
Caring for the Elderly Renal Patient
118
Energy intake
Suffi cient energy intake is vital in older renal patients in order to prevent malnutrition, to maintain Body Mass Index within the normal range and to achieve a nitrogen balance. According to the recent recommendations the provision of 35 Kcal/kg can cover the needs of the majority of pre – and dialysis renal patients. In patients over 60 years old it is recommended that lower energy intake, i.e. 30 Kcal/kg/ day could suffi ciently cover their needs, due to the reduced energy expenditure of the above mentioned population, especially when they lead a sedentary way of life5 .
Elderly patients are more susceptible to under nutrition comparing to younger adults due to physiological, psychological and socioeconomic reasons. Anorexia is more common in older patients, which is closely related to age associated alterations in taste and smell, loss of dentition, depression and cognitive decline due to ageing6. In End Stage Renal Disease (ESRD) anorexia and malnutrition affect over 50% of the patients over the age 65 years, and are probably even more frequent in diabetics7For the prevention of energy – protein malnutrition in clinically stable chronic haemodialysis patients, energy intake should be 30-40 Kcal/day, adjusted for age, gender, and physical activity levels8.
For patients undergoing peritoneal dialysis, calories absorbed from the dialysate should be included in the assessment of the nutritional needs of the patients. Sixty to seventy % of the dextrose of the dialysate is absorbed during its stay in the peritoneal cavity9 . Despite the caloric intake by the dextrose in the dialysate, malnutrition is common in PD patients, due to the feeling of fullness that the dialysate causes to the patient, the loss of appetite and/or the increased energy needs in case of a peritonitis. Therefore, the energy intake for elderly PD patients should be 30 Kcal/kg/day, included the calories for the dialysate5 .
Nutritional Requirements in Elderly Renal Patients
119
Protein intake Close control of protein intake is vital for patients with CKD stages 4 – 5. According to a secondary analysis of the Modifi cation of Diet in Renal Disease study, a favourable effect of the tight control of blood pressure and modifi cation of protein intake (i.e. 0.6 g/kg/day) in pre-dialysis patients with Glomerular Filtration Rate (GFR)< 25 ml/min was revealed10. A recent Cochrane review supported the benefi t of the reduction in protein intake in reserving renal function and delaying the progression of renal disease. Nevertheless, the evidence about the exact level of protein intake reduction remains inconclusive11,12.
According to the NKF/ KDOQI protein intake recommendations it should be limited to 0.6 g/kg/day for patients with GFR<30 ml/min, while in EDTNA/ERCA guidelines protein intake for CKD patients can range from 0.6 – 1.0 g/kg/day. Emphasis on the biological value of the proteins should be given, as more than 50% of the protein intake should be of high biological value,i.e. protein from meat, poultry, dairy products and soya5,13. Protein intake should be higher that 1.0g/kg/day in patients with overt malnutrition and/or older than 80 years. In these patients the risk of malnutrition is probably higher than any benefi t from the protein restriction1 .
In patients on dialysis recommendations are similar to the ones for younger patients. Protein intake is more liberal due to the protein losses during the dialysis. These losses can be as high as 10-12 g/session of haemodialysis14 and should be replaced for the achievement of a positive nitrogen balance in these patients. Therefore, dietary intake in stable haemodialysis patients should be between 1.0 and 1.2 g/kg/day, with emphasis on proteins of high biological value5.
In patients undergoing peritoneal dialysis (PD) protein loses in the dialysate can vary greatly, ranging from 4-12 g/day. In cases of peritonitis these losses can be raised further, by
Caring for the Elderly Renal Patient
120
even 70%, resulting in a negative nitrogen balance. Therefore, protein intake of 1.0g/kg/day is considered be the minimum for stable, non-catabolic patients. Higher levels of protein intake are recommended for patients with peritonitis or catabolic stress, when it is suggested an intake of 1.5 g/kg/day15.
Phosphate and CalciumHyperphosphatemia is a common problem for patients with late stages of CKD. Phosphorus retention is directly connected to the development of secondary hyperparathyroidism16. Serum phosphate should be kept within the range of 2.7- 4.6 mg/dl (0.87 – 1.49 mmol/L) in patients with CKD stage 3 and 4. Dietary phosphorus intake should be limited in case of abnormal laboratory values of serum phosphate. In patients with early stages of CKD, who follow a low protein diet, the restriction in phosphorus is easy to be achieved, since they are advised to limit their intake of the main dietary sources of this mineral (i.e. dairy products, meat and animal protein)5.
Disturbed balance of phosphorus and calcium can increase the soft tissue and vascular calcifi cation, leading to higher cardiovascular disease prevalence and mortality in patients with stage 3 to 5 CKD17. Therefore, the balance between phosphate and calcium is crucial. More specifi cally, the calcium phosphate product (corrected calcium x phosphate) should be maintained < 55 mg2/dl2 in these patients5
For patients in dialysis the restriction of dietary phosphate is more complex, and they should get advices from a renal dietitian, in order to limit their phosphate without limiting their protein intake. According to the NKF/ KDOQI and the European guidelines, phosphate intake should be limited to 800 – 1000 mg/ day. High protein foods, with lower phosphate content should be recommended, in combination with non –dietary strategies, i.e. phosphate binders. Calcium intake should not exceed 2000 mg, including calcium obtained from
Nutritional Requirements in Elderly Renal Patients
121
calcium-based phosphate binders, for the management of renal bone disease and metabolism5,13
Potassium
Hyperkalaemia is common in patients with stage 4 to 5 CKD, raising their risk of sudden cardiac death. Renal insuffi ciency, constipation, metabolic acidosis, lean body mass catabolism and insuffi cient dialysis are some of the causes of hyperkalaemia in these patients18. Moreover, medical therapies such as angiotensin – converting enzyme inhibitors, angiotensine receptive blockers, beta-blockers, potassium sparing diuretics, non steroidal anti-infl ammatory drugs, corticosteroids and cyclosporine use can contribute to hyperkalaemia19.
Serum potassium should be monitored and potassium intake restrictions should be followed in case of abnormal laboratory values5. In patients with stage 5 renal disease, potassium intake should be limited from 2,000 to 3,000 mg/day (8-17 mg/kg/day). In haemodialysis patients with pre-dialysis serum potassium > 6 mmol/l, a daily intake of potassium of 1950 – 2730 mg (50-70 mmol) or 1 mmol/kg IBW is recommended5,8.
Since normal bowel function can also contribute to normal serum potassium values, elderly patients often suffer for hyperkalaemia due to constipation. Constipation is a common problem in older age and since large intestine increases stool potassium content in order to compensate the renal insuffi ciency, high blood potassium levels are rather common. Therefore, the prevention of constipation can help in achieving normal serum potassium levels19. And since restriction in potassium intake include restriction in whole grain foods, fruits and vegetables, dietary fi ber supplements may be a solution to the prevention of constipation.

Caring for the Elderly Renal Patient
122
Sodium and Fluids
Sodium restriction is essential in elderly patients with CKD. Having in mind that older people often suffer from heart failure apart from CKD, sodium intake should be rather limited in daily basis1. In CKD, as urine output decreases, sodium fi ltration decreases as well. In stage 4 and 5 CKD patients’ sodium intake should be limited to 2000 – 2300 mg/day (80 – 100 mmol/l)5,8. Sodium restriction can also contribute to better fl uid intake control through lowering thirst sensation20.
Fluid intake should be restricted only if edemas or fl uid retention is experienced. In patients undergoing haemodialysis, hypertension is strongly connected to insuffi cient fl uid intake between haemodialysis sessions. Fluid control should be monitored by the interdialytic weight gain, which should be approximately less than 1 kg per day, or 4 – 4.5% of dry body weight (edema free body weight) to avoid fl uid overload. To achieve that, fl uid intake should be matched to the volume removed during the treatment and should be limited to 1000 ml plus the remnant urine output/ day5,8. In older adults the reduction of the sensation of thirst may facilitate the restriction in fl uids. Lower fl uids intake though may increase the risk of constipation and subsequent hyperkalaemia.
In PD patients the fl uid equilibrium is controlled by ultrafi ltrate (i.e. the fl uids removed by the dialysate) and dietary fl uid restriction is easier to be achieved. Ultrafi ltrate production can be infl uenced by the concentration of the dialysate and fl uid retention can be prevented by the use of dialysate with higher dextrose concentration. It should be stressed though that the use of hypertonic solutions raises the risk of obesity, hypertriglyceridemia, and peritoneal membrane distraction. For this reason, better fl uid control is essential. In PD patients fl uids should be limited to 800 ml plus ultrafi ltration plus urine output20

Nutritional Requirements in Elderly Renal Patients
123
Vitamins and minerals Vitamin and mineral requirements is still a controversial issue in CKD patients. Renal patients may be in danger of vitamin defi ciencies due to compromised dietary intake and/ or appetite, dietary restrictions leading to insuffi cient intake of nutrients, the process of dialysis which raises water soluble vitamin losses and other pathological problems that could raise the patients’ needs19. (Table 1)
Table 1: Recommended dietary intake and supplements of vitamins in adult haemodialysis patients8
Vitamins Daily Recomendation
Thiamine (B1) 1.1 – 1.2 mg supplement
Ribofl avin (B2) 1.1 – 1.3 mg supplement
Pyridoxine (B6) 10 mg supplement
Ascorbic Acid (C) 75 – 90 mg supplement
Folic Acid 1 mg supplement
Cobalamine (B12) 2.4 mg supplement
Niacine (B3) 14-16 mg supplement
Biotine (B8) 30 μg supplement
Pantothenic Acid (B5) 5 mg supplement
Retinol (A) 700 – 900 μg intake – no supplement
A-tocopherol (E) 400 – 800 IU supplement
Vitamin K 90 – 120μg intake – no supplement
ConclusionThe necessary dietary restrictions for CKD patients may be valuable even for older patients. Nevertheless, when dealing with elderly renal patients we should always bear in mind that in the long run efforts to improve health status via severe dietary restrictions may result in defi ciencies and higher risk

Caring for the Elderly Renal Patient
124
of malnutrition and frailty in older age. Restrictive diets, even if they have proven benefi ts for CKD patients (i.e. protein and sodium restrictive diets) should be handled with care in older individuals, in order to assure the promotion of an optimum nutritional status and a good quality of life.
Nutritional Requirements in Elderly Renal Patients
125
References Darmon, P., et al., Restrictive diets in the elderly: never say never 1. again? Clin Nutr, 2010 29(2): p. 170-4.
Lacquaniti, A., et al., Malnutrition in the elderly patient on dialysis. 2. Ren Fail, 2009. 31(3): p. 239-45.
Jahromi, S.R., et al., Malnutrition predicting factors in hemodialysis 3. patients. Saudi J Kidney Dis Transpl, 2010. 21(5): p. 846-51.
Robbins, L.J., Evaluation of weight loss in the elderly. 4. Geriatrics, 1989 44(4): p. 31-34.
NKF-KDOQI, Clinical practice guidelines for nutrition in CRF. 5. American Journal of Kidney Diseases, 2000. 35(6): p. S9, S56-63.
Hays, N.P. and S.B. Roberts, The anorexia of aging in humans. 6. Physiol. Behav., 2006. 88(3): p. 257-66.
Cano, N.J., et al., Malnutrition in hemodialysis diabetic patients: 7. evaluation and prognostic infl uence. Kidney Int, 2002. 62(2): p. 593-601.
Fouque, D., et al., EBPG guideline on nutrition. 8. Nephrology Dialysis Transplantation, 2007. 22(Suppl 2): p. ii45-87.
Heimbürger, O., et al., A quantitative description of solute and fl uid 9. transport during peritoneal dialysis. Kidney International 1992. 41: p. 1320-1332.
Levey, A.S., et al., Effects of dietary protein restriction on the 10. progression of advanced renal disease in the Modifi cation of Diet in Renal Disease Study. American Journal of Kidney Diseases,1996. 27(5): p. 652-63.
Fouque, D., M. Laville, and J.P. Boissel, Low protein diets for chronic 11. kidney disease in non diabetic adults. Cochrane Database Syst. Rev, 2006. 19(2): p. CD001892.
Levey, A.S., et al., Effect of dietary protein restriction on the progression 12. of kidney disease: long-term follow-up of the Modifi cation of Diet in Renal Disease (MDRD) Study. American Journal of Kidney Diseases, 2006. 48(6): p. 879-88.
Dietitians Special Interest Group, 13. European Guidelines for the Nutritional Care of Adult Renal Patients.2002, European Dialysis and Transplantation Nurses Association / European Renal Care Association.
Ikizler, T.A., et al., Amino acid and albumin losses during hemodialysis. 14. Kidney International, 1994. 43(3): p. 830-7.
Caring for the Elderly Renal Patient
126
Bergström, J., et al., Protein and Energy Intake, Nitrogen Balance 15. and Nitrogen Losses in Patients Treated with Continuous Ambulatory Peritoneal Dialysis. Kidney International, 1993. 44: p. 1048-1057.
Slatopolsky, E., The role of calcium, phosphorus and vitamin D 16. metabolism in the development of secondary hyperparathyroidism. Nephrology Dialysis Transplantation, 1998. 13(suppl 3 ): p. 3-8.
Block, G.A., et al., Association of serumphosphorus and calcium x 17. phosphate product with mortality risk in chronic hemodialysis patients: a national study. American Journal of Kidney Diseases,1998. 27: p. 394-401.
Bansal, V., Potassium metabolism in renal failure: non-dietary rationale 18. for hyperkalaemia. .Journal of Renal Nutrition,1992. 2(suppl. 1): p. 8-12.
Beto, J.A. and V.K. Bansal, Medical Nutrition Therapy in chronic 19. renal failure: integrating clinical practice guidelines. Journal of the American Dietetic Association, 2004. 104(404-409).
Mailloux, L.U. and A.S. Levey, Hypertension in patients with chronic 20. renal disease. American Journal of Kidney Diseases 1998. 32(Supp. 3 ): p. S120-S141.

Nutritional Requirements in Elderly Renal Patients
127

Psychosocial Aspects of Caring for the Elderly Renal Patient
129

Caring for the Elderly Renal Patient
130
IntroductionEarlier chapters of this handbook have focused on the physiological aspects of caring for the elderly renal patient, in terms of renal replacement therapies (peritoneal dialysis and haemodialysis) and the maintenance of adequate nutritional status. Whilst this is important, of equal importance is the psychosocial care of this patient population. Elderly renal patients, in addition to the illness burden imposed by underlying renal dysfunction, encounter a multitude of psychological and sociological issues which impact on well being and quality of life (QOL). The focus of this chapter is to explore the psychosocial component of elderly renal patient care. The opening section of this chapter will seek to defi ne the psychosocial context of older age and renal disease. Psychosocial factors specifi c to this patient population will be identifi ed, prior to outlining the fundamental constituents of care.
The psychosocial contextThe term psychosocial may be defi ned as ... ‘relating to the interrelation of social factors and individual thoughts and behaviour’1. Hence, the psychosocial context encompasses both a psychological and social component, and describes
Learning outcomesOn reading this chapter the reader should be able to:
• List the psychosocial implications of older age• Describe the psychosocial stressors inherent to renal
disease• Acknowledge the uniqueness of the individual when
planning psychosocial interventions
Psychosocial Aspects of Caring for the Elderly Renal Patient
131
the individual’s psychological development in, and interaction with, their social environment. Of primary importance within this defi nition is the individual’s interface with their social world. This incorporates not only family members, but also the wider community.
The psychosocial implications of older ageAging is accompanied by numerous physiological (see Chapter 2), psychological, and sociological changes. As individual’s age, serious and chronic health issues may arise, comprising physiological and psychosocial well being2. Health issues may impinge upon the QOL experienced by the older individual, and there is an increased risk of becoming functionally dependent and losing one’s automony2.
For the older adult, maintaining independence and autonomy are of utmost importance3. Moreover, in Western culture, independence is considered a core indicator of successful aging4. Ill health presents psychosocial consequences for individuals of all ages, of which the notion of stigma or spoilt identity is of considerable signifi cance5. Those with chronic illnesses (e.g. chronic kidney disease, diabetes mellitus, cardiovascular disease, rheumatoid arthritis, and Alzheimer’s disease), which are extremely prevalent in the elderly, come to acquire a highly stigmatised status. This is a consequence, through the extensive duration of their illness, of their inability to demonstrate the social attributes of independence, autonomy, and self-determination5. Such groups are thus negatively evaluated and disempowered via notions of social stigma and stereotyping5.
Loss of independence and autonomy, and the social roles that may accompany this (e.g. being the primary caregiver for a spouse and an active member of the local community), may precipitate feelings inadequacy and worthlessness and impact negatively on psychological well being.

Caring for the Elderly Renal Patient
132
Psychological health is an important component of the experience in later life, and signifi cantly infl uences the QOL of individuals. Whilst this statement is not unique to the elderly – it probably holds true for the rest of the population – older age and life do pose specifi c challenges in terms of illness and disability and stressful life events such as bereavement or the admission of family and friends into long term care5. Table 1 depicts the psychosocial implications of older age.
Table 1: Psychosocial implications of older age
Psychological implications Social implicationsGrief over losses e.g.•
Independence- Loved ones (bereavement)- Health (through chronic illness) -
Depression•
Embarrassment and shame at • conditions and status e.g.
Incontinence- Dependence- llness perceived as a weakness-
Anxiety disorders e.g.•
Panic disorder- Post traumatic stress disorder - (following a signifi cant life event e.g. life threatening illness)Specifi c phobias- Obsessive-compulsive disorder- Social phobia (or social anxiety - disorder)Generalised anxiety disorder-
Fear of death and dying•
Perceived vulnerability•
Loneliness as a consequence of • social isolation
Loss of social roles e.g. • caregiver to family members such as spouse, children, and grandchildrenSocial isolation e.g. unable to get • out and about as a consequence of ill health and disabilityPoverty due to an absence of paid • employmentLoss of social support through • the death of family members and friendsInability to partake of social • activitiesSocial exclusion •
Reference: Victor (2010)5 and Low, Smith, Burns, and Jones (2008)6.
Psychosocial Aspects of Caring for the Elderly Renal Patient
133
The psychosocial implications of renal diseaseAn individual’s adaptation to the changes occurring during aging is often compromised by the presence of chronic disease. This is particularly true among patients with chronic kidney disease (CKD)2. The physiological, psychological, and sociological stresses associated with CKD are immense, and the illness burden of CKD on patients is said to surpass that of other chronic diseases7.
The steady decline in kidney function typically results in CKD stage 5 (kidney failure), necessitating the instigation of renal dialysis in order to sustain life. The regimen of dialysis is at the least distressing, and imposes a series of limitations that impact on all aspects of the individual’s life2, 8.
Furthermore, CKD rarely exists as a single disease entity. For the majority of patients, CKD co-exists with several other co-morbidities, such as diabetes mellitus and hypertension2. Consequently, co-morbidities may further compromise a patients’ well being, within the context of increasing the risk of hospitalisation and intensifying patient perception of ill health2. Therefore, the elderly renal patient encounters a multitude of physiological and psychosocial stressors, as a function of older age in combination with chronic illness and various co-morbidities. Table 2 summarises the psychosocial implications of renal disease.
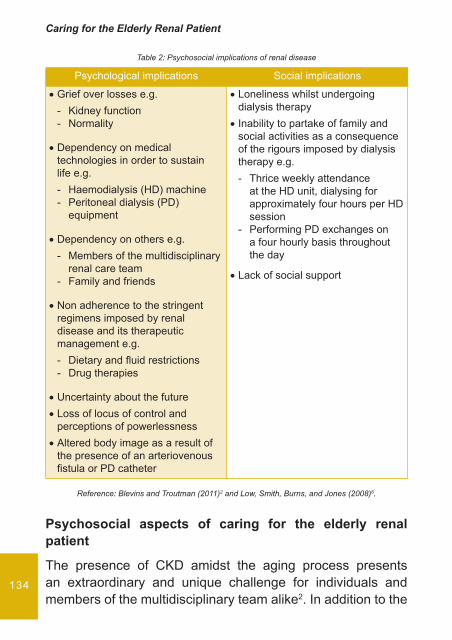
Caring for the Elderly Renal Patient
134
Table 2: Psychosocial implications of renal disease
Psychological implications Social implications
Grief over losses e.g.•
Kidney function- Normality-
Dependency on medical • technologies in order to sustain life e.g.
Haemodialysis (HD) machine- Peritoneal dialysis (PD) - equipment
Dependency on others e.g.•
Members of the multidisciplinary - renal care teamFamily and friends-
Non adherence to the stringent • regimens imposed by renal disease and its therapeutic management e.g.
Dietary and fl uid restrictions- Drug therapies-
Uncertainty about the future•
Loss of locus of control and • perceptions of powerlessnessAltered body image as a result of • the presence of an arteriovenous fi stula or PD catheter
Loneliness whilst undergoing • dialysis therapyInability to partake of family and • social activities as a consequence of the rigours imposed by dialysis therapy e.g.
Thrice weekly attendance - at the HD unit, dialysing for approximately four hours per HD sessionPerforming PD exchanges on - a four hourly basis throughout the day
Lack of social support•
Reference: Blevins and Troutman (2011)2 and Low, Smith, Burns, and Jones (2008)6.
Psychosocial aspects of caring for the elderly renal patient
The presence of CKD amidst the aging process presents an extraordinary and unique challenge for individuals and members of the multidisciplinary team alike2. In addition to the
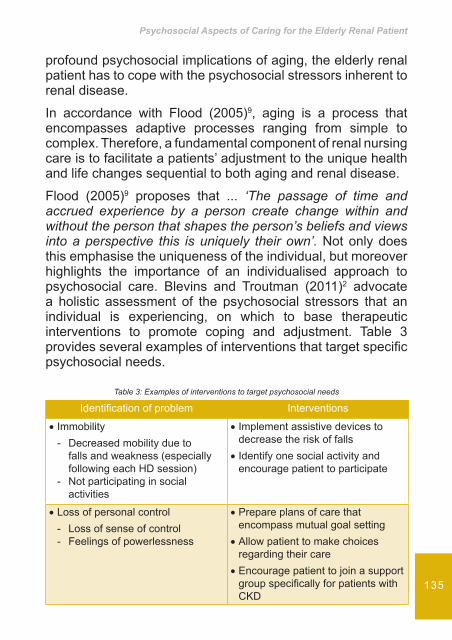
Psychosocial Aspects of Caring for the Elderly Renal Patient
135
profound psychosocial implications of aging, the elderly renal patient has to cope with the psychosocial stressors inherent to renal disease.
In accordance with Flood (2005)9, aging is a process that encompasses adaptive processes ranging from simple to complex. Therefore, a fundamental component of renal nursing care is to facilitate a patients’ adjustment to the unique health and life changes sequential to both aging and renal disease.
Flood (2005)9 proposes that ... ‘The passage of time and accrued experience by a person create change within and without the person that shapes the person’s beliefs and views into a perspective this is uniquely their own’. Not only does this emphasise the uniqueness of the individual, but moreover highlights the importance of an individualised approach to psychosocial care. Blevins and Troutman (2011)2 advocate a holistic assessment of the psychosocial stressors that an individual is experiencing, on which to base therapeutic interventions to promote coping and adjustment. Table 3 provides several examples of interventions that target specifi c psychosocial needs.
Table 3: Examples of interventions to target psychosocial needs
Identifi cation of problem Interventions
Immobility•
Decreased mobility due to - falls and weakness (especially following each HD session)Not participating in social - activities
Implement assistive devices to • decrease the risk of fallsIdentify one social activity and • encourage patient to participate
Loss of personal control•
Loss of sense of control- Feelings of powerlessness-
Prepare plans of care that • encompass mutual goal settingAllow patient to make choices • regarding their careEncourage patient to join a support • group specifi cally for patients with CKD
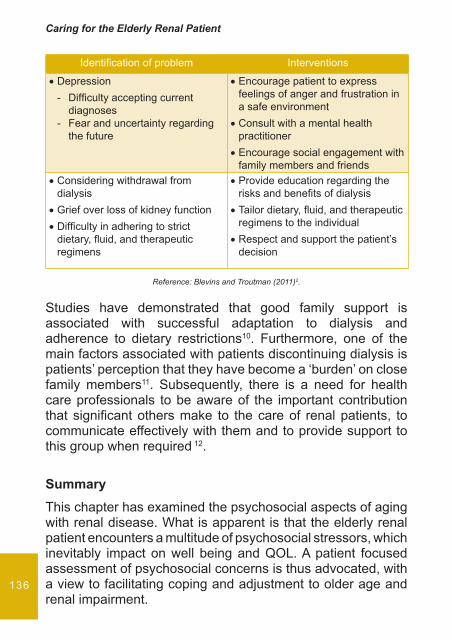
Caring for the Elderly Renal Patient
136
Identifi cation of problem Interventions
Depression•
Diffi culty accepting current - diagnosesFear and uncertainty regarding - the future
Encourage patient to express • feelings of anger and frustration in a safe environmentConsult with a mental health • practitionerEncourage social engagement with • family members and friends
Considering withdrawal from • dialysisGrief over loss of kidney function•
Diffi culty in adhering to strict • dietary, fl uid, and therapeutic regimens
Provide education regarding the • risks and benefi ts of dialysisTailor dietary, fl uid, and therapeutic • regimens to the individualRespect and support the patient’s • decision
Reference: Blevins and Troutman (2011)2.
Studies have demonstrated that good family support is associated with successful adaptation to dialysis and adherence to dietary restrictions10. Furthermore, one of the main factors associated with patients discontinuing dialysis is patients’ perception that they have become a ‘burden’ on close family members11. Subsequently, there is a need for health care professionals to be aware of the important contribution that signifi cant others make to the care of renal patients, to communicate effectively with them and to provide support to this group when required 12.
SummaryThis chapter has examined the psychosocial aspects of aging with renal disease. What is apparent is that the elderly renal patient encounters a multitude of psychosocial stressors, which inevitably impact on well being and QOL. A patient focused assessment of psychosocial concerns is thus advocated, with a view to facilitating coping and adjustment to older age and renal impairment.

Psychosocial Aspects of Caring for the Elderly Renal Patient
137
ReferencesOxford Dictionary of English.1. 2005. 2nd ed (revised). Oxford University Press.
Blevins C and Troutman MF. Successful aging theory and the 2. patient with chronic renal disease: application in the clinical setting. Nephrology Nursing Journal. 2011; 38(3): 255-260, 270.
Perrig-Cheiello P, Perrig W, Ucbelbacher A, and Stahelin H. Impact of 3. physical and psychological resources on functional autonomy in old age. Psychological Health and Medicine. 2006; 11(4): 470-484.
Ford A, Haug M, Strange K, Gaines A, Noelker L, and Jones P. 4. Sustained personal autonomy: a measure of successful aging. Journal of Aging and Health. 2000; 12(4): 470-489.
Victor CR. 5. Aging, Health and Care. The Policy Press. 2010: 7-36.
Low J, Smith G, Burns A, and Jones L. The impact of end-stage kidney 6. disease (ESKD) on close persons: a literature review. Nephrology Dialysis Transplantation. 2008; 2: 67-79.
Stewart M. Nursing review: sexual dysfunction in the patient on 7. hemodialysis. Nephrology Nursing Journal. 2006; 33(6): 631-641.
Campos G. The experience of persons with chronic renal disease in 8. hemodialysis: meanings attributed for the patients. Online Brazilian Journal of Nursing. 2007; 6(3): 16.
Flood M. A mid-range theory of successful aging. 9. The Journal of Theory Construction and Testing. 2005; 9(2): 35-39.
Kimmel PL. Psychosocial factors in adult end-stage renal disease 10. patients treated with hemodialysis: correlates and outcomes. American Journal of Kidney Diseases. 2000; 35(Suppl 1): S132-S140.
Ashby M, Hoog C, Kellehear A, Kerr P, Brooks D, Nicholls K, and 11. Forrest M. Renal dialysis abatement: lessons from a social study. Palliative Medicine. 2005; 19: 389-396.
Robert Wood Johnson Foundation. ESRD workgroup fi nal report 12. summary on end-of-life care: recommendations to the fi eld. Nephrology Nursing Journal. 2003; 30: 59-63.