
Effectiveness of the social-emotional prevention program as a function of children's baseline risk...
32
This article was downloaded by: [BCU Cluj-Napoca], [Catrinel Alice Ştefan] On: 25 February 2014, At: 01:26 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK European Early Childhood Education Research Journal Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/recr20 Effectiveness of the social-emotional prevention program as a function of children's baseline risk status Catrinel A. Ştefan a & Mircea Miclea a a Department of Psychology, Babeş-Bolyai University, Cluj-Napoca, Romania Published online: 20 Feb 2014. To cite this article: Catrinel A. Ştefan & Mircea Miclea (2014) Effectiveness of the social-emotional prevention program as a function of children's baseline risk status, European Early Childhood Education Research Journal, 22:1, 14-44, DOI: 10.1080/1350293X.2013.865359 To link to this article: http://dx.doi.org/10.1080/1350293X.2013.865359 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms- and-conditions
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Effectiveness of the social-emotional prevention program as a function of children's baseline risk...

This article was downloaded by: [BCU Cluj-Napoca], [Catrinel Alice Ştefan]On: 25 February 2014, At: 01:26Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
European Early Childhood EducationResearch JournalPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/recr20
Effectiveness of the social-emotionalprevention program as a function ofchildren's baseline risk statusCatrinel A. Ştefana & Mircea Micleaa
a Department of Psychology, Babeş-Bolyai University, Cluj-Napoca,RomaniaPublished online: 20 Feb 2014.
To cite this article: Catrinel A. Ştefan & Mircea Miclea (2014) Effectiveness of the social-emotionalprevention program as a function of children's baseline risk status, European Early ChildhoodEducation Research Journal, 22:1, 14-44, DOI: 10.1080/1350293X.2013.865359
To link to this article: http://dx.doi.org/10.1080/1350293X.2013.865359
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

Effectiveness of the social-emotional prevention program as afunction of children’s baseline risk status
Catrinel A. Stefan* and Mircea Miclea
Department of Psychology, Babes-Bolyai University, Cluj-Napoca, Romania
ABSTRACT: We report here findings from a community-based multifacetedprevention program which was implemented concomitantly as a universal andindicated intervention. Screening of social competence development was used toselect preschool children targeted by the indicated intervention (high risk), andby the universal intervention (moderate and low risk). The intervention’seffectiveness on children’s behaviors at home increased as a function of higherbaseline risk status and higher parental attendance rates. The results also suggestthat short, four session parent training is sustainable, generating attendance ratesup to 60%. The intervention’s effectiveness on parent behaviors was onlypartially sustained by significant within intervention group trends. The resultsindicate that the use of parent training in community-based interventions sustainskills transfer from the classroom to parent–child interactions. Furthermore, themost consistent effects were found for moderate risk children, suggesting thatuniversal interventions might be efficient for this marginally at risk category.
RESUME: Dans cette étude nous rapportons les résultats d’un structurecommunautaire de prévention à plusieurs aspects, qui a été mise en oeuvresimultanément en tant qu’intervention universelle et indiquée. Le niveau dedéveloppement des compétences sociales a été utilisé comme critère de sélectiondes enfants ciblés par l’intervention indiquée (risque élevé) mais aussi parl’intervention universelle (risque modéré et faible). L’efficience de l’interventionsur les comportements des enfants à la maison a augmenté comme une fonctiond’un plus haut risque de base et d’un niveau plus élevé de présence parentale.Les résultats suggèrent également qu’un court stage de quatre sessions pour lesparents génère un taux de présence allant jusqu’à 60%. L’efficience del’intervention concernant les comportements des parents n’a été quepartiellement soutenue à l’intérieur du groupe. Les résultats indiquent le fait quel’utilisation des stages parentaux dans le contexte des interventions dans lacommunauté soutient le transfert de compétences de la classe aux interactionsparent-enfant. En outre, les effets les plus importants de l’intervention ont étéidentifiés à l’intérieur du groupe à risque modéré, ce qui suggère le fait que lesinterventions universelles pourraient être efficaces pour cette catégorie de risquemarginal.
ZUSAMMENFASSUNG: Wir berichten hier über die Ergebnisse einesgemeindebasierten vielfältigen Präventionsprogrammes, das als Kombination vonallgemeiner Prävention (für alle Kinder) und spezifischer Prävention (für Kinderaus Risikofamilien) konzipiert wurden. Auf der Grundlage eines Screeningssozialer Kompetenzen wurden die beteiligten Kinder in drei Gruppen aufgeteilt(hohes, moderates und geringes Risiko). Das Interventionsprogramm umfasste
© 2014 EECERA
*Corresponding author. Email: [email protected]
European Early Childhood Education Research Journal, 2014Vol. 22, No. 1, 14–44, http://dx.doi.org/10.1080/1350293X.2013.865359
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
ein Curriculum zum sozialen Lernen in der Kindergruppe, Training der Lehrkräfteund Elterntraining. Die Ergebnisse belegen positive Auswirkungen sowohl auf dasVerhalten der Kinder zuhause als auch auf die Beteiligung von Eltern an denMaßnahmen. Sie belegen, dass ein kurzes Elterntraining mit vier Sitzungen dieBeteiligung von Eltern nachhaltig auf bis zu 60% erhöhen kann. Allerdingsließen sich nicht in allen Bereichen Effekte des Trainings belegen. Elterntrainingfördert die Übertragung von erlernten Kompetenzen von derKindertageseinrichtung auf Eltern-Kind-Interaktionen. Die deutlichsten Effektewurden jedoch für Kinder mit mittlerem Risiko gefunden; dies weist darauf hin,dass allgemeine Präventionsansätze besonders für Kinder wirksam sind, die nichtzu Risikogruppen im engeren Sinne gehören.
RESUMEN: En el presente estudio informamos sobre los resultados de un(a)programa de prevención comunitaria con múltiples facetas, que fue puesto enpráctica concomitante como una intervención universal y una intervenciónindicada. El examen del desarrollo de las competencias sociales ha sido (estado)usado para seleccionar a los niños preescolar para (a) los que fue orientada laintervención indicada (riesgo elevado) y la intervención universal (riesgomoderado y bajo). La efectividad de la intervención acerca de loscomportamientos de los niños en casa aumenta (toma aumento) como función depertenencia a la categoría de mayor riesgo y mayor índice de presencia paternal.Los resultados también sugieren, que una formación (trainera) paternal corta decuatro sesiones es sostenible y produce un índice de presencia hasta 60%. Laefectividad de la intervención acerca de los comportamientos paternales fuesostenida solamente en parte por tendencias significativas(ntes) dentro de losgrupos de intervención. Los resultados indican que el uso de una formación(trainera) paternal en el contexto de una intervención comunitaria sostiene latransferencia de la habilidad de la clase a las interacciones entre padres y niños(interactuación). Además, los efectos más consistentes fueron encontrados paralos niños de riesgo moderado, sugieriendo que las intervenciones universalespodrían ser eficientes para esta categoría de riesgo marginal.
Keywords: prevention; preschool; social-emotional competencies; parenting;universal and indicated prevention
A large body of empirical evidence suggests that adequate development of social andemotional competencies in preschool children favor long term adaptive outcomes. Lit-erature in the field of developmental psychology emphasizes that social and emotionalcompetencies are protective factors against mental health problems (Caldarella andMerrell 1997; Engels et al. 2001), as well as key prerequisites for school adjustment(Linares et al. 2005; Trentacosta et al. 2006). Moreover, social and emotional compe-tencies have been shown to be relatively stable over time from preschool to adolescence(Abe and Izard 1999; Eisenberg et al. 1999). Maladaptive behaviors such as non-compliance, poor emotion regulation skills and aggression resulting from deficientdevelopment of children’s competencies during preschool place them at risk forconduct disorders (Hastings et al. 2000; Cole, Teti, and Zahn-Waxler 2003).
Efforts to prevent these negative outcomes have been taken by developing a numberof prevention programs for preschoolers, especially in the US and Australia. However,meta-analyses from the field of early education show that the criteria of evidence-basedinterventions are met by only a few prevention programs worldwide (Webster-Strattonand Taylor 2001; Stefan and Miclea 2010). There is obviously a gap between knowl-edge about children’s normative and atypical development and applied research on
European Early Childhood Education Research Journal 15
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

prevention/intervention, and this calls for more efforts to design and implement earlyeducation programs for preschoolers. The main rationale of such an undertaking isthat once behavior problems escalate past the preschool years, negative interactionpatterns become more stable, and rehabilitating children with diagnosed conductdisorders is much more difficult and can result in higher costs (Cunningham,Bremner, and Boyle 1995).
Social-Emotional Prevention Program (SEP) was developed as a multifaceted(child-, teacher-, parent-focused) intervention. SEP draws its objectives and contentsfrom already existing evidence-based interventions, but also takes into account thespecific intervention needs of Romanian preschoolers, teachers and parents.The need for a community-based intervention is mostly related to recent changes inthe Romanian educational system. One important educational outcome defined in theLaw of Education, namely school readiness, is conceptualized as a combination ofsocial, emotional, cognitive and autonomy competencies developed in preschool inorder to ensure children’s ability to adapt to school requirements in the 1st grade andbeyond. Although this perspective was translated in guidelines for activities aimed atdeveloping children’s social and emotional competencies, there is still a need for amore comprehensive and systematic approach. The main rationale of our interventionwas to deliver an intensive, short-format program with the explicit objective of includ-ing all children from the classroom. Therefore, we opted for an intervention framework,which would allow us to work with both high and low risk children. An approach com-bining the delivery of universal (for all children) and indicated (for high risk children)prevention programs was initiated by the Fast Track research group (Conduct ProblemsPrevention Research Group [CPPRG] 1999a, 1999b). SEP was built drawing from thishybrid framework, and its components were adapted according to the rationaledescribed below.
The first component of this intervention program was the classroom curriculum,which was developed according to the latest trends emphasizing emotion awarenessand emotion regulation as key for appropriate social interactions (Lemerise andArsenio 2000; Izard 2001). From this perspective, our intervention highly resemblesthe Fast Track program, and the classroom curriculum from The Incredible Yearsprogram (Webster-Stratton 2000). The main characteristic of these programs is thatthey target both emotional (i.e., emotion understanding, emotion regulation) andsocial competencies (i.e., problem-solving, peer skills), and the contents of ourprogram reflect this separate conceptualization. However, compared to the original fra-mework we excluded small group social skills training for high risk children. Someresearchers advocate the use of small group training for high risk children in order todevelop their social skills, but there is an increasing amount of empirical evidencesuggesting that in fact high risk children do not benefit from such strategies(Lochman and Wells 2002; van Lier, Vuijk, and Crijnen 2005), which are in fact coun-terproductive and reinforce existing negative behaviors. Consequently, both the univer-sal and indicated prevention level consisted of similar intervention strategies.
The second intervention strategy from the Fast Track program was the teacher train-ing. The need for training in behavior management strategies is explained by the factthat most teachers deal with children’s inappropriate behaviors using punishment(Lewis and Sugai 1999), and are less oriented towards establishing a consistent andresponsive environment, which rewards positive behaviors (Bear et al. 2000). In fact,teachers’ use of positive discipline strategies (e.g., rule setting, establishing logical con-sequences for misbehavior, timeout) is consistent with lower levels of high risk
16 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

children’s misconduct (Filcheck et al. 2004). Besides targeting high risk children’saggressive and non-compliant behaviors as indicated by the Fast Track program,research on successful implementation of community-based prevention programssuggests that they are dependant on the amount of support and skill-building strategiesthat teachers offer children in daily interactions in the classroom. Lewis and Sugai(1999) argued that a deflection from negative developmental trajectories cannot beachieved only through classroommanagement strategies, but also by preparing teachersto provide children with meaningful learning opportunities in ecological settings thatallow skill internalization and generalization. Findings from efficacy studies lend indir-ect support to this perspective, because implementing classroommanagement strategiesis necessary, but not sufficient for obtaining significant intervention effects. Forexample, Paths to Alternative Thinking Strategies (PATHS) Curriculum included con-sultations in the teacher training, which were found to foster positive effects and facili-tate high quality implementation of activities designed to develop children’s social andemotional competencies (Kam, Greenberg, and Walls 2003; Domitrovich, Cortes, andGreenberg 2007). Consequently, our teacher training component was aimed at acquir-ing classroom management skills and coaching skills for supporting children in acquir-ing age-appropriate social and emotional competencies.
The third component of the Fast Track program was the parent training. Parent-focused interventions were initially developed for supporting parents of childrenwith clinically-relevant symptoms to deal with their children’s misbehaviors, and topromote less use of harsh and inconsistent parenting strategies, which were shown tobe associated with higher levels of non-compliance and aggression in children(Chang et al. 2003; Dennis 2006). Although data reflecting intervention effectivenesson parenting strategies are somewhat conflicting (Webster-Stratton and Hammond1997), several arguments can be cited for promoting parenting programs as part of com-munity-based interventions. First, universal prevention programs which are largelyaimed towards developing children’s social and emotional competencies, failed toexert significant changes in children’s externalizing problems in the classroom or athome (Domitrovich et al. 2007). Second, additional research on mechanisms respon-sible for changes in children’s behaviors, have suggested that programs which pairchild-focused activities with teacher training exert positive effects in terms of lowerlevels of externalizing problems especially for high risk children (Raver et al. 2009;Webster-Stratton 1998; Webster-Stratton, Reid, and Hammond 2001). In spite ofthese findings, when these children were evaluated by their parents, they did notreport any changes in their misbehaviors at home. This problem raised questionswhether prevention programs mainly aimed at skill-building in the classroom are infact less likely to be efficient in addressing children’s misbehaviors at home, sincemost studies suggest that skill transfer and generalization from classroom to parent–child interactions are either low or take longer time to be achieved, if parents are notinvolved in the intervention (Webster-Stratton et al. 2001).
In the Fast Track program, parent training was delivered as an exclusive interven-tion strategy for parents of high risk children. Dadds and Roth (2008) have raised somequestions regarding such an approach, which might be responsible for high rates ofdropout among parents, who are likely to reject intervention programs that singlethem out. We opted for an intervention strategy, which would allow all parents, irre-spective of their child’s risk status to participate in the parent training. In order toachieve this, we were inspired by the ‘minimally sufficient’ intervention frameworkdefined by the developers of the Triple P – Positive Parenting Program (Turner and
European Early Childhood Education Research Journal 17
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

Sanders 2006; Zubrick et al. 2005). From this perspective parents of high risk childrenare in need of more refined intervention strategies, emphasizing skill development,while parents of low risk children should be exposed to information providing strat-egies. More precisely, our intervention was similar at the content level for parents ofat risk and low risk children, but assumed that different intervention mechanismssupport skill transfer and generalization for these two categories of children: infor-mation providing strategies for parents of low risk children, and skill developmentfor parents of high risk children.
Another concern we attempted to address was related to the training’s sustainability(Dadds and Roth 2008). Long intervention formats encompassing 14–28 training ses-sions are appropriate for children who already exhibit behavior problems, but in orderto ensure parent attendance at the population level a brief consultation format is needed.For this reason, we opted for a short four session training program, thus maximizing theintake of relevant information that would maintain parents’ interest in attending thetraining sessions. As suggested by Kazdin and Wassell (1999), parental engagementin the intervention is largely related to perceived relevance of intervention for their chil-dren and themselves. Since it is known that usually there is a self-selective process, inwhich parents who perceive their children as more difficult are more interested inattending (Prinz and Sanders 2007) and parents of low risk children are more likelyto drop out (Andrews and Erskine 2001), we provided parents with the possibility torequest short individual sessions, as well as participating in the group training. Weexpected that such a flexible format would prompt parents of at risk children to seekfurther support and assistance, but also maintain low risk parents’ interest inparticipating.
Methods for establishing risk status
Beside program components and intervention strategy, it is important to note themethod employed for efficacy testing in the Fast Track program (CPPRG 1999a,1999b). As already stated, this hybrid framework involved separate testing of interven-tion efficacy for the receivers of the universal intervention and indicated intervention,respectively. The most common strategy for identifying high risk children involveddetermining risk status based on either below cut-off scores on measures of externaliz-ing problems (Webster-Stratton, Reid, and Stoolmiller 2008), or pre-existing risk suchas low family income or high rates of juvenile delinquency in a given community(CPPRG 1999a, 1999b; Raver et al. 2009). In a meta-analytic review, Durlak andWells (1998) argued that a screening procedure for deficient social skills might beoptimal for identifying high risk children targeted by indicated interventions and itshould precede assessment of externalizing problems. More precisely, screeningwould result in identifying two groups: high risk children, who receive scores in thelowest 10 percentile, and low risk children. However, we sustain a further divisionof the low risk group into a moderate risk category, comprising marginally at risk chil-dren, and low risk category. This rationale is sustained by prevalence reports indicatingthat up to one third of all preschool children exhibit signs of behavioral and emotionalproblems, which may result in adverse long-term outcomes (Prinz and Sanders 2007).Our interest in the intervention dynamics for the moderate risk group was to identify towhat extent this marginally at risk group can account for the universal intervention’sefficacy, since their potential for competence development should be the highestamong children targeted by the universal intervention.
18 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

A second issue concerning risk assessment is the source of the data used for estab-lishing risk status. Assessments for risk status for preschoolers are most often con-ducted using teacher and parent reports of children’s behaviors. Decisions regardingearly intervention result from aggregating teacher’s and parent’s evaluations, but innon-clinical samples this procedure is not applied. The reason for employing separateassessments for the same child, is accounted for by data from meta-analytical studiesobtained by Achenbach, Dumenci, and Rescorla (2002), indicating that teacher andparent ratings in non-clinical samples of preschool-aged children show low correlationcoefficients (r = .35). These results suggest that in fact young children tend to be moresensitive to the context of interaction, and that their behaviors show some importantvariations depending on the quality of adult–child interaction, which needs to beacknowledged in evaluating an intervention’s outcomes.
The present study
Our intervention program was designed as a multifaceted community-based interven-tion comprising of child-, teacher- and parent-centered activities. The aim of thisstudy was to assess the intervention’s effectiveness on children’s behaviors at home,as well as and parent practices, since a detailed account of changes in classroom beha-viors was provided elsewhere (Stefan and Miclea 2012). More precisely, we were inter-ested in evaluating children’s social-emotional competencies and behavior problems, aswell as parental stress and discipline strategies as a result of implementing our preven-tion program. Also, in keeping with the Fast Track framework (CPPRG 1999a, 1999b),we were interested in determining the intervention’s effects differentially for the indi-cated (high risk children), and the universal (moderate and low risk children) interven-tion levels.
Method
Participants
Children
The initial sample consisted of 204 children (121 intervention and 83 control) frompreschools in the urban area of Cluj-Napoca (Romania), for which we obtained par-ental consent to participate in this study (the initial number of parents approachedfor the study was 275). The final sample included 89 children (42 boys and 47girls) in the intervention group and 69 children (29 boys and 40 girls), with meanages of 50.7 months (SD = 0.50), and 48.6 months (SD = 0.53), respectively.Thirty-two intervention participants (24%) and 14 (16%) from the comparisongroup did not complete one or both post-intervention assessments. Dropout ratesbetween 15% and 30% indicate a normal attrition rate for this type of study. Riskstatus and demographic characteristics for dropout and non-dropout participantsare presented in Table 1.
Children were included in one of the three risk categories based on parent ratingsof social and emotional competence development. Social competence screeningresulted in the following distribution: 16 high risk, 30 moderate risk, and 43 lowrisk children in the intervention group, as well as 12 high risk, 24 moderate risk,and 33 low risk children in the comparison group. Screening measures were com-pleted by mothers: 93.1% from the intervention group, and 85.5% from the
European Early Childhood Education Research Journal 19
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

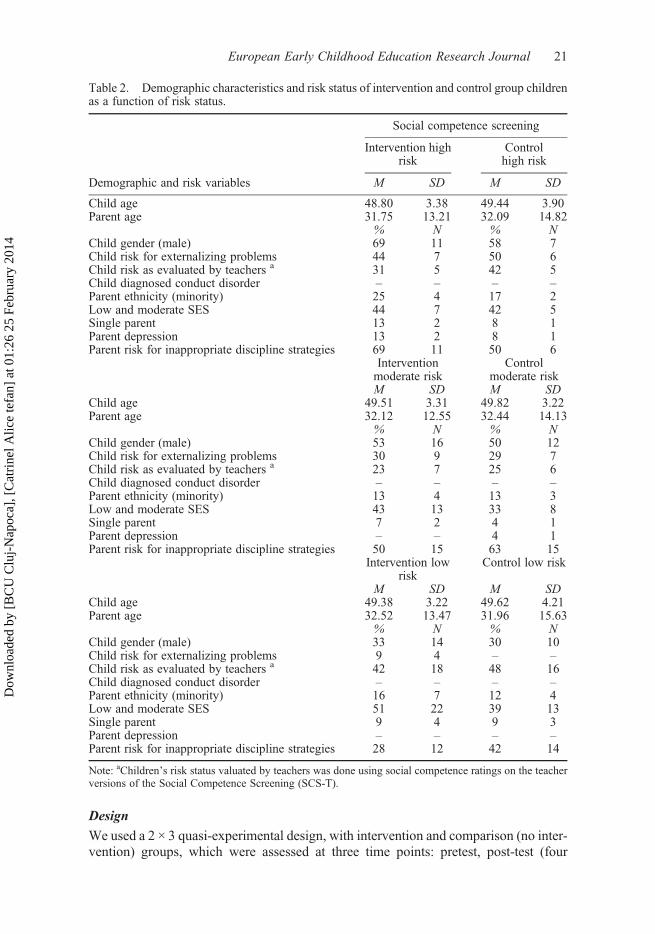
comparison group, respectively. For each risk group from the intervention and com-parison group, we established the presence of additional risk factors described inTable 2.
Teachers
There was a total of n = 28 teachers included in this study, half of which attended theteacher training, and consequently were responsible for implementing the activitiesfrom the classroom curriculum. The mean age of the teachers in the interventiongroup was M = 41.29 (SD = 11.83), while for those of the control group was M =40.71 (SD = 11.32). All teachers included in this study had at least two years experiencein working with preschool children, were university graduates, and participated in atleast one postgraduate training in classroom management techniques, which are man-datory for teachers as part of their ongoing professional training.
Parents
The final sample included 87 parents from the intervention group and 69 from thecontrol group, with mean ages of 32.2 (SD = 6.56) and 34.1 (SD = 7.21). Additionaldemographic and risk status characteristics of the parent sample are provided inTable 2.
Table 1. Risk status and demographic factors for dropout and non-dropout participants fromthe intervention and control groups.
Final sample (N = 158) Dropout (N = 46)
Intervention(%)
Control(%)
Intervention(%)
Control(%)
ECS-Pa 17.9 17.4 6.3 21.4SCS-Pa 17.9 15.9 9.4 7.1SSRS Behavior Problemsb 21.3 20.3 21.9 21.4PPI harsh, inconsistent parenting,
and PSI-SF parent stressc44.8 50.7 56.3 42.9
Low and middle SESd 43.8 46.3 34.4 35.7Minority statuse 12.4 8.7 9.4 7.1Single parent 13.5 14.5 12.5 14.3Mother depression 2.2 2.9 – –Child diagnosed mental health
problems– – – –
Note: ECS-P = Emotion Competence Screening-Parent; SCS-P = Social Competence Screening-Parent;SSRS = Social Skills Rating System; PPI = Parent Practices Interview; PSI-SF = Parent Stress Index-ShortForm.aCutoff scores based on Romanian norms for ECS-P and SCS-P.bCutoff score for SSRS Behavior Problems scale determined on the basis of results obtained by the split-halfmethod.cRisk determined by below cutoff scores on at least one of the following scales: Harsh Discipline,Inconsistent Discipline from PPI, and Parenting Stress from PSI-SF, using the split-half method.dSES categories were established based on mothers’ level of education: low SES included parents with atmost 8 classes completed, while middle SES was associated with a minimum of high school diploma.eMinorities included Hungarian, German, or Gipsy children.
20 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
Design
We used a 2 × 3 quasi-experimental design, with intervention and comparison (no inter-vention) groups, which were assessed at three time points: pretest, post-test (four
Table 2. Demographic characteristics and risk status of intervention and control group childrenas a function of risk status.
Social competence screening
Intervention highrisk
Controlhigh risk
Demographic and risk variables M SD M SD
Child age 48.80 3.38 49.44 3.90Parent age 31.75 13.21 32.09 14.82
% N % NChild gender (male) 69 11 58 7Child risk for externalizing problems 44 7 50 6Child risk as evaluated by teachers a 31 5 42 5Child diagnosed conduct disorder – – – –Parent ethnicity (minority) 25 4 17 2Low and moderate SES 44 7 42 5Single parent 13 2 8 1Parent depression 13 2 8 1Parent risk for inappropriate discipline strategies 69 11 50 6
Interventionmoderate risk
Controlmoderate risk
M SD M SDChild age 49.51 3.31 49.82 3.22Parent age 32.12 12.55 32.44 14.13
% N % NChild gender (male) 53 16 50 12Child risk for externalizing problems 30 9 29 7Child risk as evaluated by teachers a 23 7 25 6Child diagnosed conduct disorder – – – –Parent ethnicity (minority) 13 4 13 3Low and moderate SES 43 13 33 8Single parent 7 2 4 1Parent depression – – 4 1Parent risk for inappropriate discipline strategies 50 15 63 15
Intervention lowrisk
Control low risk
M SD M SDChild age 49.38 3.22 49.62 4.21Parent age 32.52 13.47 31.96 15.63
% N % NChild gender (male) 33 14 30 10Child risk for externalizing problems 9 4 – –Child risk as evaluated by teachers a 42 18 48 16Child diagnosed conduct disorder – – – –Parent ethnicity (minority) 16 7 12 4Low and moderate SES 51 22 39 13Single parent 9 4 9 3Parent depression – – – –Parent risk for inappropriate discipline strategies 28 12 42 14
Note: aChildren’s risk status valuated by teachers was done using social competence ratings on the teacherversions of the Social Competence Screening (SCS-T).
European Early Childhood Education Research Journal 21
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

months after pretest), and at three-months follow-up. A hallmark of clinical controlledtrials is randomization which takes place at the individual level, but in our study randomassignment to one of the intervention or control conditions was done at the classroomlevel making this a partially-randomized controlled trial. We also opted for using an‘intent to treat’ approach in the data analyses, which means that all available datawere included regardless of whether the children and their parents participated or notto at least 75% of the intervention activities.
Procedures
Preschool headmasters were approached at their monthly meeting to join this project bypresenting the rationale and purpose of the prevention program. Five sites from theurban area of Cluj-Napoca entered the pilot program. From each location we selectedat least two matched classrooms (age, location, size, ethnic composition), and half ofthe 14 classrooms were randomly assigned (via a lottery) to either the intervention orto the comparison condition. All selected locations provided similar conditions forenrolled children in terms of the number of hours children spent in the classrooms(eight h/day), classroom size (20–25 children), curriculum requirements, and numberof assigned teachers (two/classroom).
Parents from the intervention classrooms were asked to attend a meeting with theprogram developer. The main aim of this session was to introduce parents to thecontent of the intervention, and was meant to provide a positive framing. Because par-ental perceptions are highly important and guide decisions about involvement, weemphasized the skill-building approach of the intervention, and the fact that such aprogram supports children’s social and academic adjustment, as well as parents’ability to provide care and age-appropriate learning opportunities for their children.Parents were asked to provide written consent for their children’s participation to theintervention and received a set of questionnaires to be filled out within a week. All chil-dren for which parents returned questionnaires and provided consent underwent otherpretest evaluations involving teacher rated questionnaires and direct assessmentsthrough experimental tasks.
During the initial screening and evaluation procedures, which took place in January2009, we began implementing the first two modules of the teacher training. For the nextfour months, teachers were responsible for implementing the five modules of the class-room curriculum, which were preceded by consultations. Consultations with theprogram developer were intended to ensure that teachers were familiar with the activi-ties and that they were prepared to provide children with supportive strategies for com-petence development. Four parent group training session also took place betweenFebruary and May 2009, and individual training sessions were also held at parents’request. Post-test evaluations were completed in June 2009, and follow-up data werecollected in the beginning of the next school year, in October 2009.
Children, teachers, and parents from the control group had no contact with the inter-vention program, and only participated in pretest, post-test, and follow-up assessments.
Intervention
In the next sections, we provide a short description of the classroom curriculum, teacherand parent trainings.
22 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
Classroom curriculum
The classroom curriculum included 37 teacher implemented activities, aimed at devel-oping children’s emotional competencies (emotion recognition and emotion regu-lation), and social competencies (compliance to rules, problem-solving, and prosocialbehaviors such as turn-taking, toy sharing, and cooperation during group play activi-ties). The first module included activities for rule compliance (e.g., listening toothers, asking permission before speaking, gathering toys, etc.). Teachers encouragedrule compliance using antecedent-focused strategies (e.g., visual cues, reminders), aswell as consequence-focused strategies (e.g., praise, logical consequences). Thismodule was followed by training in emotion recognition and involved a variety ofgames designed to practice knowledge about emotions such as happiness, sadness,fear, and anger. Lessons consisted of mime games and drawing activities, whichemphasized knowledge about specific facial cues, while stories and card sortinggames, offered children the opportunity to practice emotion vocabulary. Another cat-egory of activities dealt with children’s ability to establish links between events andparticular emotions. Children’s knowledge about emotions was also developed inorder to prepare them for learning appropriate ways of regulating anger-elicitingsituations. In the third module, children were taught the ‘turtle technique’ (Robin,Schneider, and Dolnick 1976), which was found effective in dealing with angeroutbursts in both normative and clinically referred samples. This technique enhanceschildren’s ability to deal with anger arousal by: (1) retreating into the turtle shell toavoid amplifying the negative emotion (anger); (2) taking three deep breaths asmeans of tension reduction, probably by decreasing sympathetic activation of the per-ipheral nervous system, and reorienting attention by focusing on breathing rather thanthe negative emotion; and (3) thinking about an appropriate solution to the problem, inorder to negotiate conflict resolution. The forth classroom module was designed toteach children to identify problems and find appropriate solutions. Teachers usedpuppet play scenarios depicting possible conflicts with other children (e.g., refusingto share a toy, being excluded from group play, being hit), or with adults (e.g., refusingto do something that the teacher/parent asked, lying, not following rules, having to waitfor something they want). Puppet play was followed by teachers asking children toeither evaluate the solutions provided by the characters in the story/vignette, or tofind solutions themselves. In both types of activities, children were required to roleplay appropriate solutions and teachers modeled prosocial behaviors (e.g., waiting,turn-taking, asking for help, offering to help). The final intervention module mainlycapitalizes on prosocial behaviors taught in the previous section, and was intended toteach how such behaviors help establish and maintain friendships. These behaviorswere taught by teachers who coached children during group play activities, whichcould only be completed by working and communicating with the other childrenfrom the group.
Teacher training
Teacher training was delivered in group workshops scheduled to take place over eightsessions. The first module covered classroom management strategies which werediscussed in terms of preventive strategies such as rules, the use of high probabilitycommands, and routines, as well as using praise and rewards to effectively motivatepositive behaviors. The next part of the training highlighted the importance of positivediscipline strategies. The training was meant to emphasize that negative behaviors can
European Early Childhood Education Research Journal 23
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

be dealt with in a non-aggressive and constructive manner. Three intervention methods(i.e., ignoring, logical consequences and time-out) were discussed and provided guide-lines for using them for dealing with different types of negative behaviors. The secondmodule introduced training teachers in effective communication strategies and buildinga positive teacher–parent partnership. This included teaching them to deal with com-munication blockers such as criticizing or promptly offering solutions, but alsoencouraging them to allow parents to get involved in children’s activities in the class-room by organizing joint activities (e.g., field trips, parties, contests, etc.). The finalmodule included five consultation sessions, which preceded each classroom interven-tion module. The sessions were organized around three discussion topics: developmen-tal milestones for social and emotional competence development, methods for coachingsocial and emotional competencies, and the content of the classroom curriculum. Thisapproach was intended to ensure that teachers became familiar with the activities, andthat they were able to implement them accurately.
Parent training
The parent training included two strategies: group training sessions and individualtraining sessions, which were held at parents’ request.
Group training included four sessions lasting between 90 to 120 minutes each, andcovered developmental milestones for social and emotional competencies, coachingstrategies for assisting children’s competence development, and discipline strategies.The first module involved familiarizing parents with developmental milestones inchildren’s compliance. This adjustment in parental expectations regarding childrenwas followed by teaching parents strategies to decrease non-compliance such as estab-lishing rules, formulating action oriented commands, and developing daily routines.The next module introduces parents to strategies for developing children’s emotionknowledge and emotion regulation. Specific activities were suggested for developingchildren’s emotion vocabulary (e.g., stories, discussing emotions), and parents wereencouraged to provide a safe environment for emotion expression, which wouldpromote children’s learning about appropriate ways to deal with negative emotions.Parents were also suggested strategies needed for supporting children’s anger manage-ment: a description of the rationale and steps involved in the ‘turtle technique’, tipsabout how to reorient attention or to help children discover appropriate solutions toanger-eliciting situations. The behavior management component of the module wasfocused on how parents can effectively use praise, activities and symbolic reinforce-ments as strategies for increasing children’s positive behaviors. The third modulewas intended to further approach coaching strategies by teaching parents to problem-solve with their children, and problem-solving strategies were suggested in order toprevent aggressive behaviors (e.g., waiting, turn-taking, offering help). Moreover,the trainer emphasized the fact that decelerating negative behaviors is not achievedby excessive punishment. During this session, the trainer discussed the negative conse-quences that harsh and/or inconsistent discipline strategies have on children’s behavior,and suggested alternative discipline strategies such as ignoring, logical consequences,and time-out. The fourth parent session aimed at introducing parents to the notion ofspending ‘quality time’ with their child. The trainer suggested specific parent–child activities and provided examples of how parents can get involved in children’splay in order to coach their social behaviors (e.g., toy sharing, turn-taking, orcooperation).
24 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

The individual training component included short 20–30 minutes sessions and theywere only held at parents’ request. These sessions were largely based on behavior analy-sis methods and were aimed at: identifying the behavior problem, providing parents witha conceptualization of the problem in terms of activating events-behavior-consequences,and establishing an intervention plan. Follow-up sessions were provided for evaluatingprogress, and if necessary additional steps and suggestions were made.
Training delivery and attendance
The first two modules of the teacher training were implemented one week before thestart of the classroom curriculum. Each of the five classroom modules was precededby consultations, which were intended on one hand to familiarize teachers with theobjectives and contents of the activities, and on the other hand to ensure consistencyin implementing the activities, as two teachers were assigned to each classroom.This meant that one teacher implemented the activities during one week, while theother teacher implemented them during the consecutive week.
Fidelity checklists were used not only to ensure similar program delivery amongdifferent teachers, but to also guide and remind them about strategies used in orderto consolidate knowledge acquired by children in previous modules. During eachweek, the trainer conducted one classroom observation for each intervention site inorder to determine whether the projected activity was implemented, and whether itwas done according to previously discussed activity objectives and description. Ana-lyzing the data from the fidelity checklists in all intervention sites the percent ofimplemented activities was above 90%. Teachers were also asked to indicate childattendance for each of the 37 activities from the emotional and social development cur-riculum, which showed that only eight out of 89 (9%) had attended less than 75% of thetotal number of activities.
Regarding parental involvement with the group training sessions, the records indi-cated that 10 (11.5%) parents did not participate in any training session, 30 (34.5%)attended 1–2 sessions, while 47 (54.0%) took part in 3–4 sessions. From the totalnumber of parents who participated in at least one training session (69 parents), 58were mothers, eight fathers, and in three cases both mother and father attended.Also, 13 (14.6%) parents requested individual training sessions, eight attended twoindividual sessions of approximately 40–60 minutes, while the remaining five wereprovided with additional training throughout three individual sessions lastingbetween 60 and 90 minutes.
Measures
The dependant variables employed for testing the effectiveness of this multi-focusedprevention program were related to children’s behaviors at home: social and emotionalcompetencies, behavior problems, expressive emotion recognition, and positive/negative problem-solving strategies, as well as parent behaviors: harsh parenting,inconsistent parenting, positive parenting, appropriate discipline, and parental stress.
Parent assessment of social and emotional competencies
The Social Competence Screening for Preschoolers – Parent Form (SCS-P; Micleaet al. 2010) consists of 12 items assessing compliance to rules, interpersonal skills,
European Early Childhood Education Research Journal 25
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

and prosocial behavior (e.g., ‘The child easily accepts changes in game rules’; ‘Thechild shares his/her toys without being told’). The Emotion Competence Screeningfor Preschoolers – Parent Form (ECS-P; Miclea et al. 2010) contains 14 items asses-sing aspects related to emotion understanding, emotion expression, and emotion regu-lation (e.g.,‘The child recognizes that others feel happy, angry, sad, or afraid’; ‘Thechild shows patience until receiving attention or a reward’). The answers on both instru-ments were coded on a 5-point Likert scale, where 1 = almost never and 5 = almostalways. The SCS-P showed high internal consistency, α Cronbach ranging from .85to .88, while Cronbach’s α = .72–.79, indicated good internal consistency for theECS-P. Other reliability and validity data, as well as sensitivity and specificityindices were provided in detail elsewhere (Stefan et al. 2009).
Children’s social skills were also assessed by their parents using the Social Compe-tence scale from the Social Skills Rating System – Preschool (Parent Form) (SSRS;Gresham and Elliott 1990). This scale comprises four 10-item subscales: Cooperation(e.g., ‘Helps you with household tasks without being asked’), Assertion (e.g., ‘Receivescriticism well’), Responsibility (e.g., ‘Asks permission before using another familymember’s property’), and Self-control (e.g., ‘Controls temper in conflict situationswith you’). Each item was rated on a 3-point Likert scale, measuring the frequencyof a specific behavior, where 0 = never and 2 = very often. Internal consistency coeffi-cients for the Social Competence scale were high and ranged from .85 to .88.
Parent assessment of behavior problems
The Behavior Problem summary scale from the SSRS (Gresham and Elliott 1990) wasused to evaluate parental perceptions of children’s maladaptive behaviors. This scalecomprised 10 items (e.g., ‘Argues with others’; ‘Disturbs ongoing activities’). Theanswers were rated on a 3-point Likert scale, where 0 = never and 2 = very often.Internal consistency coefficients for the summary scales varied between α = .73–.77,indicating good reliability. Since the norms for behavior problems were obtained onUS samples, we derived cut-off points for our sample, which were computed usingthe split-half method (median -1SD). We obtained separate cut-offs for boys andgirls, since independent samples t test revealed significant differences, with boysbeing rated significantly higher on behavior problem scales than girls (p < .01).
Direct assessment of children’s emotion recognition and social problem-solving
We assessed children’s emotion recognition using a modified version of the AffectiveKnowledge Test (AKT; Denham 1986), replacing the original ‘puppet task’ involvingsmiley-type facial features, with an ecological set of stimuli consisting of human facesselected from the NimStim Face Stimulus data base (Tottenham et al. 2002). Similarlywith the AKT, we used this task in order to evaluate expressive emotion recognition,more precisely children’s ability to name the following emotions: happiness, anger,sadness, and fear. The children in this study were presented with a computerizedversion of the task. For the Expressive task each child viewed four 14x14 cm cardswith male or female faces and was asked ‘How does he/she feel’. The order of presen-tation was counterbalanced across participants. Each child could earn 2 points for cor-rectly identifying the emotion, 1 point for naming an emotion with a similar emotionalvalence as the target, and 0 points for incorrectly naming the emotion. The task wasrecorded by a Sony DCR-SR3 camera and two blind coders rated separately the
26 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

children’s performance. Two-way random intraclass correlation coefficients (ICCs) forthe expressive task ranged from .92 to .96 for happiness, .91 to 0.93 for anger, .87 to .91for sadness, and .84 to .86 for fear.
In order to assess children’s problem-solving skills we used a modified version ofthe Social Problem Solving Test (SPST-R; Webster-Stratton 1990). The initial task con-sisted of 13 vignettes describing conflict situations. For the purposes of this study weselected five situations which were previously used in prevention studies: adult disap-proval (#1), rejection from a friend (#2), toy access (#3), unjust treatment from anotherchild (#4), and making a mistake (#5). Each child was presented the vignettes togetherwith a picture depicting the situation in order to facilitate their answers. After each vign-ette, the child was asked to say ‘What would he/she do’. The answers were codedaccording to two categories: positive (P) and negative (N) problem-solving strategies.Positive strategies included apologizing, finding another toy or friend to play with,asking for help from an adult, etc.; in the negative category we included aggressivebehaviors such as hitting, name calling, destroying a toy, non-compliance and lying.For each type of category the children could receive a score from 0 to 5 points. Thetask was recorded by a Sony DCR-SR3 camera. Two-way random ICCs ranged from.88 to .91 for positive problem-solving strategies.
Parent self-reports
We used a modified version of the original LIFT Parenting Practices Interview (PPI;Webster-Stratton et al. 2001) to evaluate parental discipline strategies. This measureincluded five of the seven initial scales: Harsh Discipline, Inconsistent Discipline,Appropriate Discipline, Positive Parenting, and Monitoring. We ran a confirmatoryfactor analysis using a principal component analysis (PCA) to establish factor loadings.The model confirmed the proposed factor structure. Items loading below .30 on a par-ticular factor were dropped. The resulting scales were Harsh Discipline comprising 12items (e.g., ‘Raise your voice [scold or yell]’; ‘Slap or hit your child’), Inconsistent Dis-cipline nine items (e.g., ‘Threaten to punish him/her [but not really punish him/her]’;‘Ignore misbehavior’), Appropriate Discipline 11 items (e.g., ‘ Give him/her a brieftimeout away from family’; ‘Take away privileges [like TV, playing with friends]’),Positive Parenting 10 items (e.g., ‘I believe in using rewards to teach my child howto behave’; ‘Giving children a reward for good behavior is bribery’), and Monitoringseven items (e.g., ‘Giving children lots of free, unsupervised time helps them learnto be more responsible’; ‘Children who are not supervised by an adult are morelikely to develop behavior problems’). Each item was coded on a 7-point Likertscale, where 1 = strongly disagree and 7 = strongly agree. Cronbach’s αs rangedbetween .68 and .82, except for the Monitoring scale for which we obtained α = .39.As a result, this scale was dropped from our analysis due to its low internal consistency.Cut-off points for the Harsh and Inconsistent Discipline scales were computed using thesplit-half method.
Parent stress ratings were obtained form a self-report questionnaire, the ParentStress Index-Short Form (PSI-SF, Abidin 1995). This measure contains three basicscales comprised of 12 items each: Parental Distress (e.g., ‘Since having a child Ifell that I am almost never able to do things that I like to do’), Childrearing Stress(e.g., ‘My child seems to cry or fuss more often than most children’), and DifficultChild (e.g., ‘My child turned out to be more of a problem than I had expected’). ATotal Stress score is derived by summing the results from the basic scale, and this
European Early Childhood Education Research Journal 27
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

was the measure used in this study. Each item was scored on a 5-point Likert scale,where 1 = strongly disagree and 5 = strongly agree. The internal consistency washigh, with αs ranging from .86 to .91. The cut-off score for at risk parents was obtainedusing the split-half method.
Results
Attrition and group equivalence
The analyses comparing children who remained in the project at follow-up, with thosewho completed pretest assessments showed no significant differences in the number ofdropouts from the intervention and comparison group (Table 1). Differences betweendropouts and non-dropouts on risk and demographic variables were examined usingt and chi-square tests separately for the intervention and comparison groups, and no sig-nificant differences (ps > .05) were found. Analysis comparing the intervention andcomparison group participants who remained in the study at follow-up yielded no sig-nificant differences on any demographic or risk factor variables (ps > .05). Furthertesting for group equivalence on demographic and risk factor variables was conductedwithin each risk category, but revealed that intervention and comparison groups did notdiffer significantly (ps > .05) (Table 2).
Baseline equivalence
For all variables we ran independent samples t tests on pretest scores to determine base-line equivalence. Our data indicated that there were significant pretest differences (ps< .05) for two constructs measuring child behaviors: expressive emotion recognition inthe high risk social competence group, and ECS-P in the low risk emotion competencegroup. Where parental behaviors were concerned pretest significant differences (ps< .05) were found for the appropriate discipline measure from the high risk emotionalcompetence group. For these measures, ANCOVAs covarying pretest on post-test andfollow-up data, were used in order to establish the intervention’s effectiveness.
Statistical analysis
Data analysis was done using a mixed ANOVA with a between-subject variable (inter-vention vs comparison group) and a within-subject variable (pretest, post-test, andfollow-up). We report here the group by time interaction effect as an indicator of a sig-nificant trend within one or both groups. When the interaction effect was significant, weconducted paired samples t tests within each group separately, and significance levelwas adjusted using a Bonferroni correction for multiple comparisons. If the analysisindicated the presence of a significant within group effect, we proceeded to run inde-pendent samples t tests on post-test and follow-up scores, in order to draw conclusionson group differences. Besides statistical significance, we also established effect sizesusing Cohen’s d computed as the mean group difference divided by the pooled standarddeviations. Results are reported in three sections for each of the risk groups establishedusing the social competence screening instrument for children’s behaviors at home andparenting practices.
28 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

Results for the high risk group
Child outcomes
The results for the high risk group showed the presence of significant interactioneffects for both the screening measure and the SSRS Social Competence scale (ps< .05) (Table 3). Subsequent independent sample t tests showed that interventiongroup children improved significantly on social skill ratings compared to their compari-son group counterparts on the SCS-P, t(26) = 2.21, p < .05, as well as SSRS t(26) =2.01, p < .05. Follow-up group differences were still in favor of the interventiongroup on both measures, t(26) = 2.26, p < .05, and t(26) = 2.10, p < .05, respectively,which indicated the maintenance of the intervention’s effects. For the externalizing pro-blems we found a significant interaction effect, F(1, 26) = 8.56, p < .01. However, atpost-test there was only a marginally significant difference in favor of the interventiongroup (p < .10). When the difference was computed for children whose parent’sattended the intervention, the intervention group scored significantly lower on thismeasure than comparison group children, t(18) =−2.04, p < .05.
Although immediately post-test this difference was only marginally significant,based on follow-up results we found significantly less aggressive and non-compliantbehaviors for intervention group children compared to control group children, t(26)=−2.41, p < .05, and also for intervention children whose parents participated to theintervention, t(18) =−2.06, p < .05.
Mixed ANOVAs for children’s declarative knowledge indicated the presence ofsignificant interaction effects (ps < .05) for expressive emotion recognition and positiveproblem-solving strategies, but not for negative problem-solving strategies. Groupdifference for the expressive emotion recognition task was established usingANCOVA, which indicated that intervention group children outperformed controlgroup children, t(26) = 2.14, p < .05. The group difference at follow-up was t(26) =3.70, p < .01, suggesting that the intervention’s effect was maintained. Data on positiveproblem-solving strategies showed that at post-test intervention group children pro-vided significantly more prosocial answers to potential anger-eliciting situations com-pared to control group children, t(26) = 2.01, p < .05. Follow-up analysis indicated thatthe intervention’s effects were maintained, t(26) = 2.18, p < .05.
Parent outcomes
Mixed ANOVAs yielded significant (ps < .05) interaction effects for inconsistent dis-cipline, appropriate discipline and positive parenting strategies (Table 4). Followingpaired t tests on pre- to post-test data showed that the difference was significant forintervention group parents (ps < .05), while control group parents did not improve.However, there were no significant differences (ps > .05) between the interventionand comparison groups immediately post-test or at follow-up on any of the threemeasures of parental behaviors. The outcomes for harsh discipline and parent stressshowed no significant (ps > .05) interaction effects.
Results for the moderate risk group
Child outcomes
Parent ratings on the SCS-P yielded a significant time by group interaction effect, F(1,52) = 5.64, p < .05 (Table 5). Independent samples t test on post-test scores confirmedthat the intervention group had significantly improved their social skills compared to
European Early Childhood Education Research Journal 29
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
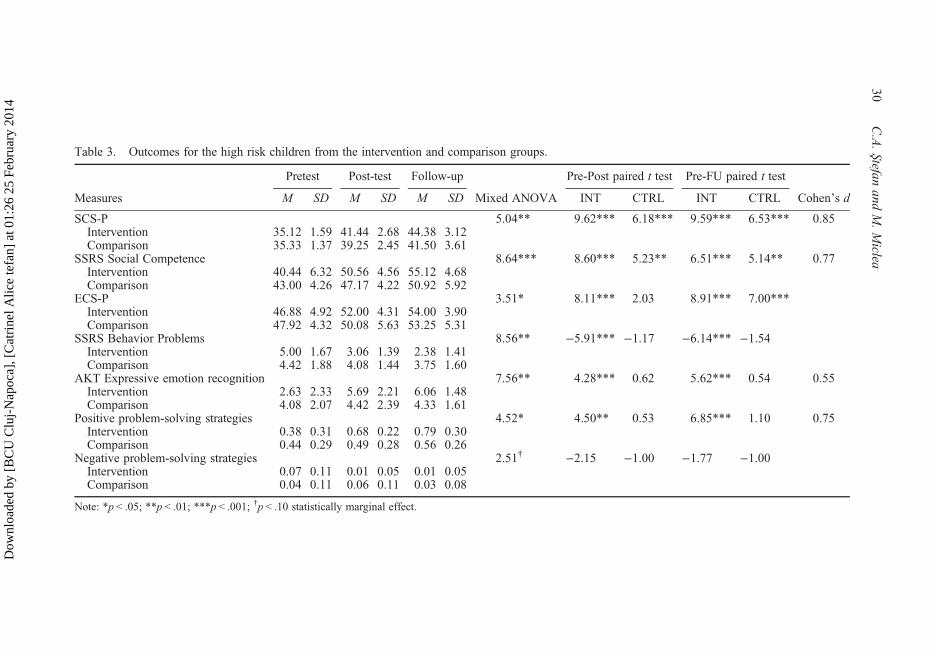
Table 3. Outcomes for the high risk children from the intervention and comparison groups.
Pretest Post-test Follow-up Pre-Post paired t test Pre-FU paired t test
Measures M SD M SD M SD Mixed ANOVA INT CTRL INT CTRL Cohen’s d
SCS-P 5.04** 9.62*** 6.18*** 9.59*** 6.53*** 0.85Intervention 35.12 1.59 41.44 2.68 44.38 3.12Comparison 35.33 1.37 39.25 2.45 41.50 3.61
SSRS Social Competence 8.64*** 8.60*** 5.23** 6.51*** 5.14** 0.77Intervention 40.44 6.32 50.56 4.56 55.12 4.68Comparison 43.00 4.26 47.17 4.22 50.92 5.92
ECS-P 3.51* 8.11*** 2.03 8.91*** 7.00***Intervention 46.88 4.92 52.00 4.31 54.00 3.90Comparison 47.92 4.32 50.08 5.63 53.25 5.31
SSRS Behavior Problems 8.56** −5.91*** −1.17 −6.14*** −1.54Intervention 5.00 1.67 3.06 1.39 2.38 1.41Comparison 4.42 1.88 4.08 1.44 3.75 1.60
AKT Expressive emotion recognition 7.56** 4.28*** 0.62 5.62*** 0.54 0.55Intervention 2.63 2.33 5.69 2.21 6.06 1.48Comparison 4.08 2.07 4.42 2.39 4.33 1.61
Positive problem-solving strategies 4.52* 4.50** 0.53 6.85*** 1.10 0.75Intervention 0.38 0.31 0.68 0.22 0.79 0.30Comparison 0.44 0.29 0.49 0.28 0.56 0.26
Negative problem-solving strategies 2.51† −2.15 −1.00 −1.77 −1.00Intervention 0.07 0.11 0.01 0.05 0.01 0.05Comparison 0.04 0.11 0.06 0.11 0.03 0.08
Note: *p < .05; **p < .01; ***p < .001; †p < .10 statistically marginal effect.
30C.A.Stefan
andM.Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

Table 4. Outcomes for parents of high risk children from the intervention and comparison groups.
Pretest Post-test Follow-upPre-Post paired t
test Pre-FU paired t test
Measures M SD M SD M SD Mixed ANOVA INT CTRL INT CTRL Cohen’s d
Harsh Discipline 1.57 −1.52 0.49 −1.98 −0.12Intervention 2.68 0.50 2.54 0.46 2.50 0.40Comparison 2.59 0.70 2.64 0.72 2.58 0.67
Inconsistent Discipline 5.97** −3.07* 0.82 −3.35* 0.70Intervention 3.10 0.73 2.76 0.57 2.77 0.58Comparison 3.06 0.88 3.14 0.99 3.15 0.85
Appropriate discipline 6.91** 4.77** 0.86 5.55*** 0.92Intervention 4.24 0.75 4.76 0.73 4.78 0.70Comparison 4.61 0.80 4.68 0.76 4.72 0.76
Positive parenting 3.19* 3.06* 0.49 2.95* 0.41Intervention 5.70 0.63 6.04 0.60 6.03 0.57Comparison 5.65 0.54 5.69 0.43 5.69 0.42
Parent stress 1.38 −1.31 −0.30 −2.54† −0.51Intervention 74.13 14.44 69.93 14.06 66.25 13.69Comparison 75.50 9.44 74.67 11.12 74.00 11.29
Note: *p < .05; **p < .01; ***p < .001; †p < .10 statistically marginal effect.
European
Early
Childhood
Education
Research
Journal31D
ownl
oade
d by
[B
CU
Clu
j-N
apoc
a], [
Cat
rine
l Alic
e te
fan]
at 0
1:26
25
Febr
uary
201
4
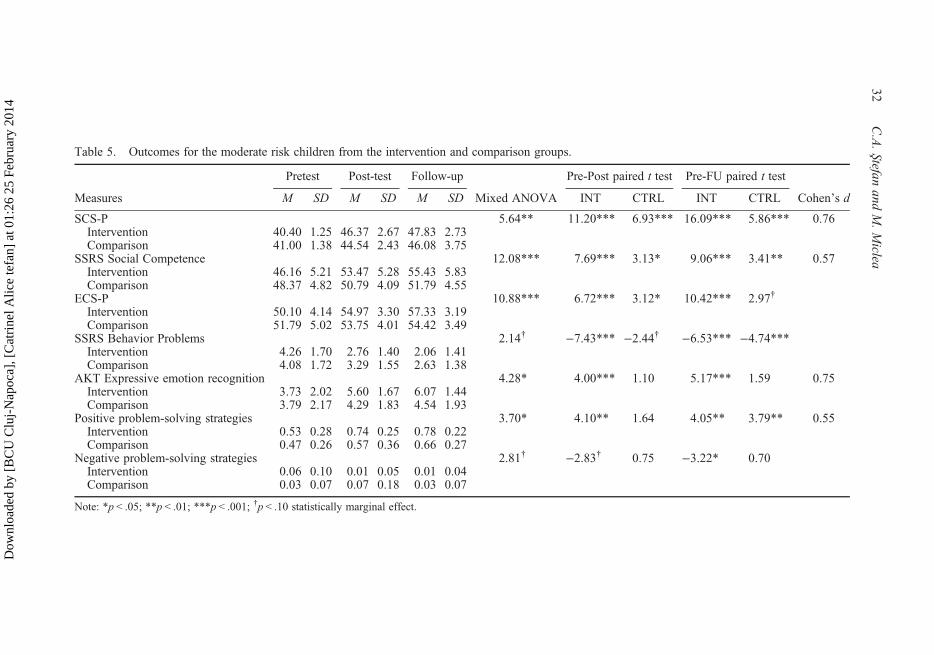
Table 5. Outcomes for the moderate risk children from the intervention and comparison groups.
Pretest Post-test Follow-up Pre-Post paired t test Pre-FU paired t test
Measures M SD M SD M SD Mixed ANOVA INT CTRL INT CTRL Cohen’s d
SCS-P 5.64** 11.20*** 6.93*** 16.09*** 5.86*** 0.76Intervention 40.40 1.25 46.37 2.67 47.83 2.73Comparison 41.00 1.38 44.54 2.43 46.08 3.75
SSRS Social Competence 12.08*** 7.69*** 3.13* 9.06*** 3.41** 0.57Intervention 46.16 5.21 53.47 5.28 55.43 5.83Comparison 48.37 4.82 50.79 4.09 51.79 4.55
ECS-P 10.88*** 6.72*** 3.12* 10.42*** 2.97†
Intervention 50.10 4.14 54.97 3.30 57.33 3.19Comparison 51.79 5.02 53.75 4.01 54.42 3.49
SSRS Behavior Problems 2.14† −7.43*** −2.44† −6.53*** −4.74***Intervention 4.26 1.70 2.76 1.40 2.06 1.41Comparison 4.08 1.72 3.29 1.55 2.63 1.38
AKT Expressive emotion recognition 4.28* 4.00*** 1.10 5.17*** 1.59 0.75Intervention 3.73 2.02 5.60 1.67 6.07 1.44Comparison 3.79 2.17 4.29 1.83 4.54 1.93
Positive problem-solving strategies 3.70* 4.10** 1.64 4.05** 3.79** 0.55Intervention 0.53 0.28 0.74 0.25 0.78 0.22Comparison 0.47 0.26 0.57 0.36 0.66 0.27
Negative problem-solving strategies 2.81† −2.83† 0.75 −3.22* 0.70Intervention 0.06 0.10 0.01 0.05 0.01 0.04Comparison 0.03 0.07 0.07 0.18 0.03 0.07
Note: *p < .05; **p < .01; ***p < .001; †p < .10 statistically marginal effect.
32C.A.Stefan
andM.Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
the control group, t(52) = 2.60, p < .05. Moreover, parent ratings on this measure ofsocial competence was still significantly higher for intervention group children atfollow-up, t(52) = 2.07, p < .05, indicating that the intervention’s effects were main-tained. Similar results were found for the other measure of social skills, post-testscores showed that intervention group children were rated significantly higher onsocial competence than comparison group children, t(52) = 2.04, p < .05, and sub-sequent analysis on follow-up data confirmed the maintenance of the intervention’seffects, t(52) = 2.51, p < .05. However, mixed ANOVA indicated no significant (p> .05) interaction effect for children’s behavior problems.
For children’s performance on the experimental tasks, we found significant inter-action effects (ps < .05) for expressive emotion recognition and positive problem-solving. Group comparisons indicated that intervention group children named correctlysignificantly more emotions than comparison group children, t(52) = 2.74, p < .01, andused significantly more positive problem-solving strategies than comparison groupchildren, t(52) = 2.04, p < .05. At follow-up, the intervention’s effects for emotion rec-ognition were maintained, t(52) = 3.33, p < .01, while group differences were only mar-ginally significant (p < .10) in favor of intervention group children for positiveproblem-solving.
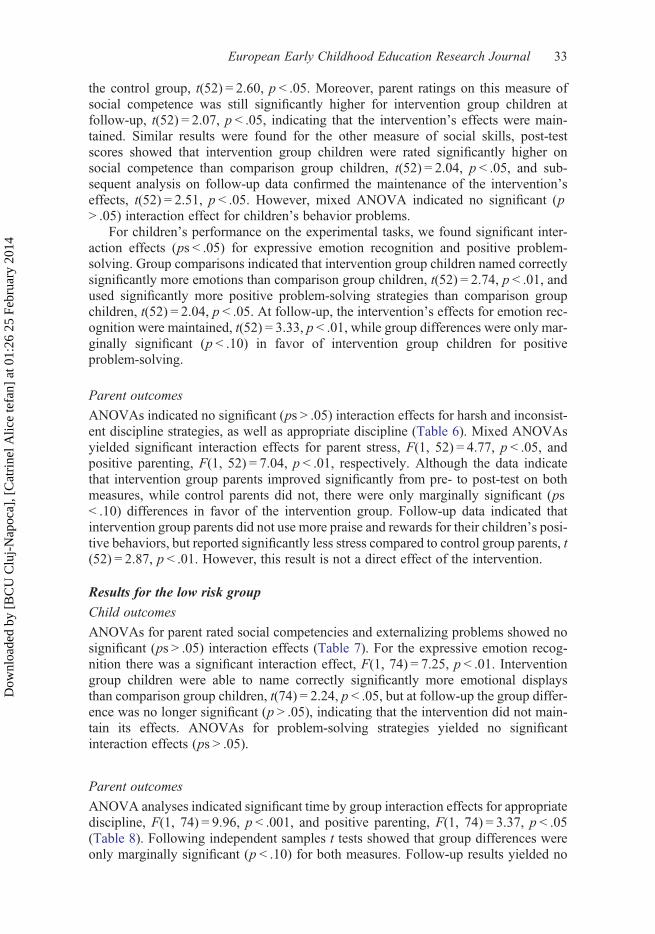
Parent outcomes
ANOVAs indicated no significant (ps > .05) interaction effects for harsh and inconsist-ent discipline strategies, as well as appropriate discipline (Table 6). Mixed ANOVAsyielded significant interaction effects for parent stress, F(1, 52) = 4.77, p < .05, andpositive parenting, F(1, 52) = 7.04, p < .01, respectively. Although the data indicatethat intervention group parents improved significantly from pre- to post-test on bothmeasures, while control parents did not, there were only marginally significant (ps< .10) differences in favor of the intervention group. Follow-up data indicated thatintervention group parents did not use more praise and rewards for their children’s posi-tive behaviors, but reported significantly less stress compared to control group parents, t(52) = 2.87, p < .01. However, this result is not a direct effect of the intervention.
Results for the low risk group
Child outcomes
ANOVAs for parent rated social competencies and externalizing problems showed nosignificant (ps > .05) interaction effects (Table 7). For the expressive emotion recog-nition there was a significant interaction effect, F(1, 74) = 7.25, p < .01. Interventiongroup children were able to name correctly significantly more emotional displaysthan comparison group children, t(74) = 2.24, p < .05, but at follow-up the group differ-ence was no longer significant (p > .05), indicating that the intervention did not main-tain its effects. ANOVAs for problem-solving strategies yielded no significantinteraction effects (ps > .05).
Parent outcomes
ANOVA analyses indicated significant time by group interaction effects for appropriatediscipline, F(1, 74) = 9.96, p < .001, and positive parenting, F(1, 74) = 3.37, p < .05(Table 8). Following independent samples t tests showed that group differences wereonly marginally significant (p < .10) for both measures. Follow-up results yielded no
European Early Childhood Education Research Journal 33
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
Table 6. Outcomes for parents of moderate risk children from the intervention and comparison groups.
Pretest Post-test Follow-upPre-Post paired t
test Pre-FU paired t test
Measures M SD M SD M SD Mixed ANOVA INT CTRL INT CTRL Cohen’s d
Harsh Discipline 1.74 −1.09 −0.60 −2.42† −0.29Intervention 2.35 0.61 2.26 0.49 2.14 0.45Comparison 2.64 0.91 2.62 0.90 2.64 0.90
Inconsistent Discipline 2.53† −2.95† 0.61 −2.69† −1.19Intervention 2.87 0.84 2.64 0.83 2.57 0.72Comparison 2.89 0.83 2.93 0.83 2.80 0.82
Appropriate discipline 0.08 2.31† 1.84 2.21† 2.56†
Intervention 4.49 0.73 4.68 0.60 4.73 0.43Comparison 4.29 0.65 4.43 0.68 4.50 0.57
Positive parenting 7.04** 4.03** −0.34 5.63*** −0.21Intervention 5.50 0.65 5.77 0.53 5.86 0.52Comparison 5.52 0.64 5.47 0.66 5.50 0.61
Parent stress 4.77** −3.56** −0.05 −3.83** 1.65Intervention 67.97 18.14 62.00 14.80 60.33 13.35Comparison 70.83 18.62 70.71 19.95 71.46 15.09
Note: *p < .05; **p < .01; ***p < .001; †p < .10 statistically marginal effect.
34C.A.Stefan
andM.Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

Table 7. Outcomes for the low risk children from the intervention and comparison groups.
Pretest Post-test Follow-upPre-Post paired t
test Pre-FU paired t test
Measures M SD M SD M SD Mixed ANOVA INT CTRL INT CTRL Cohen’s d
SCS-P 1.71 3.79** 0.97 3.70** 2.27†
Intervention 48.44 4.08 50.58 3.94 50.86 3.96Comparison 49.39 4.27 49.19 3.58 51.21 2.90
SSRS Social Competence 0.51 2.81† 0.96 3.48** 2.36†
Intervention 55.70 6.63 58.56 6.78 60.19 7.71Comparison 57.42 7.35 58.70 8.45 60.61 7.70
ECS-P 4.14** 3.80** 1.29 7.09*** 2.20Intervention 54.95 5.00 57.09 4.19 59.28 4.84Comparison 56.03 5.62 56.91 4.53 57.70 4.68
SSRS Behavior Problems 1.54 −3.21** −0.82 −3.63** −1.44Intervention 2.26 1.76 1.58 1.40 1.40 1.15Comparison 1.85 1.33 1.64 1.43 1.48 1.18
AKT Expressive emotion recognition 7.25** 6.82*** 2.07 7.82*** 3.26** 0.51Intervention 3.44 1.99 5.84 1.48 6.14 1.44Comparison 4.27 2.07 4.97 1.90 5.64 1.64
Positive problem-solving strategies 1.87 6.13*** 1.83 6.60*** 2.89†
Intervention 0.53 0.26 0.76 0.27 0.78 0.26Comparison 0.55 0.29 0.66 0.24 0.71 0.25
Negative problem-solving strategies 0.72 −0.50 −0.80 1.00 −0.50Intervention 0.01 0.05 0.01 0.04 0.01 0.03Comparison 0.03 0.07 0.05 0.11 0.02 0.07
Note: *p < .05; **p < .01; ***p < .001; †p < .10 statistically marginal effect.
European
Early
Childhood
Education
Research
Journal35D
ownl
oade
d by
[B
CU
Clu
j-N
apoc
a], [
Cat
rine
l Alic
e te
fan]
at 0
1:26
25
Febr
uary
201
4

Table 8. Outcomes for parents of low risk children from the intervention and comparison groups.
Pretest Post-test Follow-upPre-Post paired t
test Pre-FU paired t test
Measures M SD M SD M SD Mixed ANOVA INT CTRL INT CTRL Cohen’s d
Harsh Discipline 1.74 −1.09 −0.60 −2.42† −0.29Intervention 2.46 0.65 2.40 0.56 2.29 0.59Comparison 2.46 0.65 2.62 0.90 2.64 0.90
Inconsistent Discipline 1.80 −2.11 0.62 −1.80 −0.67Intervention 2.67 0.94 2.54 0.75 2.54 0.67Comparison 2.81 0.87 2.86 0.79 2.80 0.82
Appropriate discipline 9.96*** 4.13*** 0.71 5.54*** 0.34Intervention 4.56 0.82 4.87 0.76 4.95 0.70Comparison 4.83 0.89 4.76 0.89 4.80 0.84
Positive parenting 3.37* 3.29*** 0.78 4.21*** 1.29Intervention 5.66 0.55 5.84 0.42 5.87 0.41Comparison 5.55 0.68 5.61 0.59 5.65 0.59
Parent stress 1.37 −1.16 −1.01 −1.75 0.22Intervention 61.19 13.69 59.67 10.32 58.47 10.31Comparison 58.45 11.79 56.67 12.06 59.03 14.02
Note: *p < .05; **p < .01; ***p < .001; †p < .10 statistically marginal effect.
36C.A.Stefan
andM.Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

significant (p > .05) group difference for appropriate discipline, but intervention groupparents reported significantly more positive parenting strategies than control groupparents, t(74) = 2.01, p < .05. For all other parent outcomes we found no significant(ps > .05) time by group interaction effects.
Discussion
Our objective was to deliver a multifocussed intervention program as both a universaland indicated prevention program for three- to four-year-old children. The results dis-cussed here concern the changes in children’s behaviors at home, and the changes inparent behaviors. The analyzed data rely on parental evaluations of children’s beha-viors, as well as objective measures of emotion recognition and social problem-solving, as well as parental self-ratings of discipline strategies and stress levels. Thedata are discussed for two intervention levels: the indicated intervention (high riskgroup) and the universal intervention (moderate and low risk groups).
Our findings for the high risk group are sustained by previous research on high riskchildren showing that parents perceive improvements in their children’s acquired socialcompetencies as a result of participation to selective (CPPRG 1999a) or indicated pre-vention programs (Webster-Stratton et al. 2008). However, we only found improve-ments on the criterion measure, but not regarding parental ratings of children’semotional competence development, for which we only found a within group trend.Prevention of aggressive and non-compliant behaviors was one of the main aims ofour intervention program. Parents reported reductions in high risk children’s externaliz-ing behaviors, but a significant effect was in fact obtained only for those children,whose parents attended at least 75% of the intervention sessions. These resultsmimic those from prevention programs targeting at risk children, which suggestthat significant group differences are not detectable in community samples (Webster-Stratton 1998; Webster-Stratton et al. 2001). As a result, only when children whoseparents attended the parent training are compared to the comparison group, significantintervention effects emerge.
Data from high risk group indicated that intervention children performed signifi-cantly better on objective tasks of emotion naming and positive problem-solving strat-egies. Although previous research has employed such measurements for testing theefficacy of community-based interventions for low social-economic status (SES)children (Webster-Stratton et al. 2008), these results are the first to provide insightinto children’s declarative knowledge in the context of an indicated intervention.However, no such effects were found for negative problem-solving strategies (aggres-sion, non-compliance, and isolation/avoidance). This might be a consequence of thefact that participants in this study were not children with early-onset conduct disordersfor whom effects on negative problem-solving strategies were previously reported(Webster-Stratton and Hammond 1997; Webster-Stratton and Reid 2003).
Where parent behaviors are concerned, we need to acknowledge the fact that theintervention showed no consistent group effects on measures of discipline strategiesand stress, but rather significant within intervention group trends. Contrary to ourexpectations, we did not find any changes in relation to harsh parenting, which is con-sidered the most robust predictor of children’s behavior problems (Snyder et al. 2005;Bradley and Corwyn 2007). Harsh parenting is highly associated with maternaldepression (Chronis et al. 2007), low SES parents (Curtner-Smith et al. 2006), aswell as clinical intensity child behavior problems (Gutermuth Anthony et al. 2005).
European Early Childhood Education Research Journal 37
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

It is obvious that our sample included only small percentages of parents and childrencorresponding to these risk profiles, and therefore, the lack of significant changesmight be a result of the fact that actually most parents who scored below the cut-offpoint for harsh parenting, do not exhibit the increased levels of punitive strategieswhich are found in high risk parent samples. A similar explanation could be appliedto the lack of effects on parental stress, which is more consistently associated withincreased use of harsh parenting strategies (Gutermuth Anthony et al. 2005). Significanttrends for inconsistent parenting strategies have been found for the high risk socialcompetence group and mirror to some extent results obtained by the Fast Trackgroup, indicating that parents of at risk children tend to be more consistent in theirdisciplining styles after participating to group training sessions (CPPRG 1999a).Previously reported improvements for appropriate parenting and increased use ofpraise have been associated with intervention outcomes for parents of clinicallyreferred children (Webster-Stratton and Hammond 1997) or parents from disadvan-taged socio-economic backgrounds (Webster-Stratton et al. 2001).
In this next section, we will provide a discussion for the universal intervention levelwhich targeted moderate and low risk children. Our data from the moderate risk groupare in consensus with previous results reported by Domitrovich et al. (2007) from a uni-versal intervention, suggesting that parents observed improved social skills at homeafter their children participated to a classroom based intervention. An interestingpattern of results emerged for the moderate risk group which showed consistentimprovements in terms of better developed social and emotional competencies,whereas the high risk group only improved in terms of social competencies. Thesedata suggest that in fact parents observe the most consistent gains in terms of social-emotional development for moderate risk children rather than high risk children, butthis effect is no longer observable for low risk children, for whom the universal inter-vention did not exert significant improvements on parent rated competencies. Interven-tion children from the moderate risk group showed a significant post-test trend forexpressive emotion recognition and significant gains in the use of positive problem-solving strategies. These data are the first objective evaluations reported for low riskchildren in a community-based intervention, the only other data come from either chil-dren with diagnosed conduct problems (Webster-Stratton and Hammond 1997), orthose from low-income families (Webster-Stratton et al. 2008). However, the lack ofsignificant group effects for the low risk group is not surprising in the context of sig-nificant gains in performance on these tasks made by comparison group children andsupports the fact that parents of low risk children did not rate their children significantlybetter on measures of social and emotional development.
Based on findings reported in the literature we did not expect to find any significantintervention effects on harsh and/or inconsistent parenting strategies, as well as parentstress at the universal intervention level. Our expectations were largely supported by theoutcome measures for parental self-reports suggesting no intervention effects on thesemeasures for moderate and low risk groups, except for significant trends for positiveparenting strategies. Although other indicated interventions reported that parents ofhigh risk children are more likely to benefit in terms of developing protective strategiessuch as the use of appropriate discipline strategies and praise (Brotman et al. 2005), thiseffect should be interpreted cautiously and future studies will need to confirm whether itis a replicable or a singular effect.
In summary, the data from this study offer empirical support to our assumption thata multifaceted prevention program can be delivered and evaluated at the same time as a
38 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
universal and indicated prevention program. One of our main concerns was to provideparents with a sustainable intervention program, which would allow us to deliver in ashort amount of time relevant information for all parents, independent of their chil-dren’s risk status. As suggested by Kazdin and Wassell (2000) parents are morelikely to attend such interventions, if they believe that it is suitable for their needs.Attendance rates of 30% confirmed our expectations that low risk parents are themost likely to drop out, while moderate and high risk parents’ attendance rates of55–60% suggest that those who perceive their children as more ‘difficult’ are moreinclined to participate (Prinz and Sanders 2007). Moreover, almost all parents whorequested the added individual training sessions evaluated their children’s skill devel-opment in the high risk range, and also reported high levels of behavior problems. Also,there seems to be a relationship between parent participation to the training sessions andthe intervention’s effectiveness on children’s behaviors at home, as effect sizesdecreased as a function of children’s lower risk status and lower parent attendance rates.
While we expected to find that the moderate risk group was the primary beneficiaryof the universal intervention based on our data for children’s classroom behaviors(Stefan and Miclea 2012) a rather unexpected finding was that better developedsocial-emotional competencies, as well as better performance on the objective taskswere found for moderate risk children and not low risk children. This effect can beexplained by assuming that similar attendance rates for moderate risk and high riskparents would have an influence on parents’ perceptions of children’s gains. Therefore,progress for moderate risk children could be more easily detectable by parents, becausethe levels of behavior problems in this group are lower (30%) than in the high riskgroup (40–50%).
The parent training did not exert significant differences between group effects onparental behaviors, but rather within group trends. The data on parent behaviorssupport three assertions. First, the significant trends obtained for positive parentingstrategies for parents of all risk categories suggests that in some instances commu-nity-based interventions actually work in terms of boosting protective factors such asappropriate discipline and positive parenting, rather than decreasing harsh and/or incon-sistent parenting strategies (Brotman et al. 2005). Second, consistent improvements inpositive parenting strategies is a reflection of the fact that parents of children with lesssevere aggressive and non-compliant behaviors are more interested in developing andencouraging appropriate behaviors. And third, effects on parental inconsistency forhigh risk parents could be explained by the fact that in normative samples parentstend to be more inconsistent in their disciplining strategies in relation to boys comparedto girls (Kim et al. 2005).
This study was also among the few that used screening for social competence devel-opment as a strategy for detecting risk categories, and it suggests that this can be auseful alternative to the more widely used assessment of externalizing problems.This conclusion is supported by three aspects. First, our data on Romanian childrenare consistent with researches indicating that higher rates of externalizing symptomsare more common among boys than girls (Chaplin, Cole, and Zahn-Waxler 2005).Indeed, 60 to 70% of the high risk children were boys, who scored in the lowest 10percentiles on both the SCS-T and SSRS. Second, children rated as high risk onmeasures of social-emotional development received similar high risk ratings onmeasures of externalizing problems in 40–50% of cases from their parents, while inour previous study based on teacher rated competencies, overlapping below cut-offscores were reported for 60–75% of children (Stefan and Miclea 2012). This might
European Early Childhood Education Research Journal 39
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

indicate that at least for screening purposes, the assessment of skill development couldbe particularly useful, because parents tend to rate their children lower on externalizingproblems than teachers (De Los Reyes and Kazdin 2005). And third, although we didnot use a measure of externalizing problems in order to obtain risk status, our results arehighly similar to those of Achenbach et al. (2002), who found that teacher and parentratings of externalizing behaviors show low correlation coefficients. Overlappingteacher and parent ratings of risk based on social and emotional competence screeningoccurred in this study in 30–35% of the cases, suggesting that these informants holddifferent perspectives on children’s adaptive and maladaptive behaviors.
Limitations and future directions
One mechanism responsible for changes in high risk children are behavior managementtechniques. However, as most prevention programs have indicated besides these tech-niques, parents should be able to develop their children’s competencies as means of pre-venting escalation of aggressive and non-compliant behaviors (Sanders and Morawska,2005). However, it is difficult to be precise about which intervention componentresulted in the observed effects on children’s and parents’ behaviors. Future studieswill need to address the differential impact of the information-based and behavior man-agement approaches. Furthermore, it is not clear whether the effects on children’s beha-viors at home are a result of the parent training, the classroom curriculum, the teachertraining, or interactions between these intervention strategies. In order to draw suchconclusions, it would be interesting for future studies to compare the effects of theclassroom curriculum, the parent training, and the combined effect of the two on chil-dren’s social-emotional competencies and behavior problems (Webster-Stratton et al.2001).
The results of this study relied on questionnaire ratings and experimental tasksrather than objective measure of changes in children’s negative behaviors. Anotherlimitation of this study might be the fact that parent ratings are not supported by obser-vational measures evaluating changes in children’s misbehaviors at home. However,since this was a community-based intervention such strategies might prove too invasivefor parents, mainly due to the fact that observational methods are more frequentlyemployed in studies on clinically referred children (Webster-Stratton and Hammond1997; Webster-Stratton and Reid 2003).
The intervention’s impact on parental behaviors lends indirect support to the asser-tion that although community-based interventions are less likely to produce significanteffects on parental behaviors, since the levels of risk in these samples is relatively low.However, we feel that an important limitation of our study is related to the fact that mostof the participating parents came from high and middle SES backgrounds, and thus, thepossibility to generalize these findings to parents that would most probably exhibitmore risk factors is very low. A selective prevention approach targeting economicallydisadvantaged children and their parents, or an early intervention program wouldprovide a more accurate evaluation of the program’s efficiency regarding parentalbehaviors.
Another limit is related to the fact that most parents included in this training weremothers, and both child and parental behavior evaluations came from one parent. Moreresearchers have called for including fathers in these trainings, because of the increasedrole they tend to have gained in children’s education, and because of the fact that theyare mostly unprepared for such tasks, lacking experience and necessary skills for
40 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014

effective childrearing practices (Pollack 1995). As other researchers have suggested,the presence of fathers is necessary for obtaining a more comprehensive perspectiveon the intervention’s effects, although such effects were shown to be more difficultto achieve (Morawska and Sanders 2006; Helfenbaum-Kun and Ortiz 2007).However, one possible future direction would be including fathers in the intervention,and evaluating the outcomes from both parents’ perspective. It would also be helpful forfuture studies to assess the moderating effect that quality time has on parental percep-tions of changes in the use of effective discipline strategies. Studies have indicated thatparental involvement in terms of play time, special parent–child activities, and emotion-al availability have a positive impact on children’s development (Snyder 2007), andmight actually operate as mediators of positive discipline strategies.
Conclusions
SEP constitutes the first attempt to provide preschool children, teachers and parentsfrom Romania with a comprehensive approach to developing social and emotionalcompetencies and preventing behavior problems. This community-based programrelied on a dual approach, combining the delivery of an indicated and a universal inter-vention. The data reported here show that providing parents with the possibility toattend the training irrespective of their children’s risk status generated high attendancerates. These translated into consistent intervention effects on both high and moderaterisk children. While we expected to find effects at the indicated intervention level,the results for the universal intervention provide a more complex perspective on theprogram’s effectiveness. It seems that parents of moderate risk children make up thelargest percent of attending parents from the non-risk group. In turn, moderate risk chil-dren show the most consistent improvement, suggesting that universal interventionsmight benefit these marginally at risk children. Further research is however neededfor a better understanding of the intervention mechanisms which facilitate positive out-comes for different risk categories targeted in community-based settings.
ReferencesAbe, J. A., and C. E. Izard. 1999. “A Longitudinal Study of Emotion Expression and Personality
Relations in Early Development.” Personality Processes and Individual Differences 77:566–577.
Abidin, R. R. 1995. Parenting Stress Index: Professional Manual. 3rd ed. Florida: Odessa, FL.Achenbach, T. M., L. Dumenci, and L. A. Rescorla. 2002. “Ten-Year Comparisons of Problems
and Competencies for National Samples of Youth: Self, Parent, and Teacher Reports.”Journal of Emotional and Behavioral Disorders 10: 194–203.
Andrews, G., and A. Erskine. 2001. “Within Our Reach: The Economics of Prevention.”Current Opinion in Psychiatry 14: 103–105.
Bear, G. G., C. Webster-Stratton, M. J. Furlong, and S. Rhee. 2000. “Preventing Aggression andViolence.” In Preventing School Problems-Promoting School Success, edited by K. M.Minke and G. G. Bear, 1–69. MD: NASP.
Bradley, R. H., and R. F. Corwyn. 2007. “Externalizing Problems in the Fifth Grade: Relationswith Productive Activity, Maternal Sensitivity, and Harsh Parenting from Infancy ThroughMiddle Childhood.” Developmental Psychology 43: 1390–1401. doi: 10.1037/0012-1649,43.6.1390.
Brotman, L. M., K. K. Gouley, D. Chesir-Teran, T. Dennis, R. G. Klein, and P. Shrout. 2005.“Prevention for Preschoolers at High Risk for Conduct Problems: Immediate Outcomes onParenting Practices and Child Social Competence.” Journal of Clinical Child andAdolescent Psychology 34: 724–734.
European Early Childhood Education Research Journal 41
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
Caldarella, P., and K. W. Merrell. 1997. “Common Dimensions of Social Skills of Children andAdolescents: A Taxonomy of Positive Behaviors.” School Psychology Review 26: 264–278.
Chang, L., D. Schwartz, K.A. Dodge, and C. McBride-Chang. 2003. “Harsh Parenting inRelation to Child Emotion Regulation and Aggression.” Journal of Family Psychology17: 598–606. doi: 10.1037/0893-3200.17.4.598.
Chaplin, T. M., P. M. Cole, and C. Zahn-Waxler. 2005. “Parental Socialization of EmotionExpression: Gender Differences and Relations to Child Adjustment.” Emotion 5: 80–88.doi: 10.1037/1528-3542.5.1.80.
Chronis, A. M., B. B. Lahey, W. E. Pelham, Jr., S. H. Hall Williams, B. L. Baumann, H. Kipp,… P. J. Rathouy. 2007. “Maternal Depression and Early Positive Parenting Predict FutureConduct Problems in Young Children with Attention-Deficit/Hyperactivity Disorder.”Developmental Psychology 43: 70–82. doi: 10.1037/0012-1649.43.1.70.
Cole, P. M., D. O. Teti, and C. Zahn-Waxler. 2003. “Mutual Emotion Regulation and theStability of Conduct Problems between Preschool and Early School Age.” Developmentand Psychopathology 15: 1–18. doi: 10.1017/S0954579403000014.
Conduct Problems Prevention Research Group. 1999a. “Initial Impact of the Fast TrackPrevention Trial for Conduct Problems: I. The High Risk Sample.” Journal of Consultingand Clinical Psychology 67: 631–647. doi: 10.1037/0022-006X.67.5.631.
Conduct Problems Prevention Research Group. 1999b. “Initial Impact of the Fast TrackPrevention Trial for Conduct Problems: II. Classroom Effects.” Journal of Consultingand Clinical Psychology 67: 648–657. doi: 10.1037/0022-006X.67.5.648.
Cunningham, C. E., R. Bremner, and M. Boyle. 1995. “Large Group Community-BasedParenting Programs for Families of Preschoolers at Risk for Disruptive BehaviorDisorders: Utilization, Cost Effectiveness, and Outcome.” Journal of Child Psychologyand Psychiatry 36: 1141–1159.
Curtner-Smith, M. E., A. M. Culp, R. Culp, C. Scheib, K. Owen, A. Tilley,… , P. W. Coleman.2006. “Mothers’ Parenting and Young Economically Disadvantaged Children’s Relationaland Overt Bullying.” Journal of Child and Family Studies 15: 181–193.
Dadds, M. R., and J. H. Roth. 2008. “Prevention of Anxiety Disorders: Results of a UniversalTrial with Young Children.” Journal of Child and Family Studies 17: 320–335. doi: 10.1007/s10826-007-9144-3.
De Los Reyes, A., and A. E. Kazdin. 2005. “Informant Discrepancies in the Assessment ofChildhood Psychopathology: A Critical Review, Theoretical Framework, andRecommendations for Further Study.” Psychological Bulletin 131: 483–509. doi: 10.1037/0033-2909.131.4.483.
Denham, S. A. 1986. “Social Cognition, Social Behavior, and Emotion in Preschoolers:Contextual Validation.” Child Development 57: 194–201.
Dennis, T. 2006. “Emotional Self-Regulation in Preschoolers: The Interplay of Child ApproachReactivity, Parenting, and Control Capacities.” Developmental Psychology 42: 84–97. doi:10.1037/0012-1649.42.1.84.
Domitrovich, C. E., R. C. Cortes, and M. T. Greenberg. 2007. “Improving Young Children’sSocial and Emotional Competence: A Radomized Trial of the Preschool ‘PATHS’ curricu-lum.” The Journal of Primary Prevention 28: 67–91. doi: 10.1007/s10935-007-0081-0.
Durlak, J. A., and A. M. Wells. 1998. “Evaluation of Indicated Preventive Intervention (second-ary prevention) Mental Health Programs for Children and Adolescents.” American Journalof Community Psychology 26: 775–802.
Eisenberg, N., I. K. Guthrie, B. C. Murphy, S. A. Shepard, A. Cumberland, and G. Carlo. 1999.“Consistency and Development of Prosocial Dispositions: A Longitudinal Study.” ChildDevelopment 70: 1360–1372.
Engels, C. M. E., C. Finkenauer, W. Meeus, and M. Dekovic. 2001. “Parental Attachment andAdolescents’s Emotional Adjustment: Associations with Social Skills and RelationalCompetence.” Journal of Counseling Psychology 48: 428–439.
Filcheck, H. A., C. B. McNeil, L. A. Greco, and R. S. Bernard. 2004. “Using a Whole-ClassToken Economy and Coaching of Teacher Skills in a Preschool Classroom to ManageDisruptive Behavior.” Psychology in the Schools 4: 351–361. doi: 10.1002/pits.10168.
Gresham, F. M., and S. N. Elliott. 1990. Social Skills Rating System. Circle Pines, MN:American Guidance Service.
42 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
Gutermuth Anthony, L., B. J. Anthony, D. N. Glanville, D. Q. Naiman, C. Waandres, and S.Shaffer. 2005. “The Relationship between Parenting Stress, Parenting Behavior andPreschoolers’s Social Competence and Behavior Problems in the Classroom.” Infant andChild Development 14: 133–154. doi: 10.1002/icd.385.
Hastings, P. D., C. Zahn-Waxler, J. Robinson, B. Usher, and D. Bridges. 2000. “TheDevelopment of Concern for Others in Children with Behavior Problems.”Developmental Psychology 36: 531–546. doi: 10.1037//0012-1649.36.5.531.
Helfenbaum-Kun, E. D., and C. Ortiz. 2007. “Parent-Training Groups for Fathers of HeadStart Children: A Pilot Study of their Feasibility and Impact on Child Behavior and Intra-Familial Relationships.” Child and Family Behavior Therapy 29: 47–64. doi: 10.1300/J019v29n02_04.
Izard, C. E. 2001. “Emotional Intelligence or Adaptive Emotions?” Emotion 1: 249–257.Kam, C.-M., T. M. Greenberg, and T. C. Walls. 2003. “Examining the Role of Implementation
Quality in School-Based Prevention Using the PATHS Curriculum.” Prevention Science 4:55–63. doi: 10.1023/A:1021786811186.
Kazdin, A. E., and G. Wassell. 1999. “Barriers to Treatment Participation and TherapeuticChange Among Children Referred for Conduct Disorder.” Journal of Clinical ChildPsychology 28: 160–172.
Kazdin, A. E., and G. Wassell. 2000. “Therapeutic Changes in Children, Parents, and FamiliesResulting from Treatment of Children with Conduct Problems.” Journal of AmericanAcademy of Child and Adolescent Psychiatry 39: 414–420.
Kim, H-J., D. H. Arnold, P. H. Fisher, and A. Zeljo. 2005. “Parenting and Preschoolers’Symptoms as a Function of Child Gender and SES.” Child and Family Behavior Therapy27: 23–41. doi: 10.1300/J019v27n02_03.
Lemerise, A. E., and R. C. Arsenio. 2000. “An Integrated Model of Emotion Processes andCognition in Social Information Processing.” Child Development 71: 107–118. doi: 10.1111/1467-8624.00124.
Lewis, T. J., and G. Sugai. 1999. “Effective Behavior Support: A System Approach to ProactiveSchoolwide Management.” Focus on Exceptional Children 31: 1–24.
van Lier, P. A. C., P. Vuijk, and A. A. M. Crijnen. 2005. “Understanding Mechanisms ofChange and Development of Antisocial Behavior: The Impact of a UniversalIntervention.” Journal of Abnormal Child Psychology 33: 521–535. doi: 10.1007/s10802-005-6735-7.
Linares, L. O., N. Rosbruch, B. M. Stern, E. M. Edwards, G. Walker, B. H. Abikoff, and J. M. I.Alvir. 2005. “Developing Cognitive-Social-Emotional Competencies to Enhance AcademicLearning.” Psychology in the Schools 42: 405–418. doi: 10.1002/pits.20066.
Lochman, J. E., and C. K. Wells. 2002. “The Coping Power Program at the Middle-SchoolTransition: Universal and Indicated Prevention Effects.” Psychology of AddictiveBehaviors 16: S40–S54. doi: 10.1037//0893-164X.16.4S.S40.
Miclea, M., A. Balaj, M. Porumb, D. Porumb, and S. Porumb. 2010. PEDa: The DevelopmentalAssessment Platform for 3-6/7 year Old Children. Cluj-Napoca: ASCR Publishing.
Morawska, A., and M. R. Sanders. 2006. “A Review of Engagement and Strategies to PromoteEngagement with Parenting Interventions.” Journal of Children’s Services 1: 29–40. doi:10.1108/1746660200600004.
Pollack, W. S. 1995. “A Delicate Balance: Fatherhood and Psychological Transformation-aPsychotherapeutic Perspective.” In Becoming a Father, edited by J. L. Shapiro, M. H.Diamond, and M. Greenberg, 316–331. New York, NY: Springer Publishing Company.
Prinz, R. J., and M. R. Sanders. 2007. “Adopting a Population-Level Approach to Parenting andFamily Support Interventions.” Clinical Psychology Review 27: 739–749. doi: 10.1016/j.cpr.2007.01.005.
Psychological Assessment Resources, Inc.Raver, C. C., S. M. Jones, C. Li-Grining, F. Zhai, W. M. Metzger, and B. Solomon. 2009.
“Targeting Children’s Behavior Problems in Preschool Classrooms: A Cluster-Randomized Controlled Trial.” Journal of Consulting and Clinical Psychology 77: 302–316. doi: 10.1037/a0015302.
Robin, A., M. Schneider, and M. Dolnick. 1976. “The Turtle Technique: An Extended CaseStudy of Self-Control in the Classroom.” Psychology in the Schools 13: 449–453.
European Early Childhood Education Research Journal 43
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014
Sanders, M. R., and A. Morawska. 2005. “Can Changing Parental Knowledge, DysfunctionalExpectations and Attributions, and Emotion Regulation Improve Outcomes for Children?”In Encyclopedia on Early Childhood Development, edited by R. E. Tremblay, R. G., Barr,and R. De. V. Peters, 1–8. Montreal, Quebec: Centre of Excellence for Early ChildhoodDevelopment. Accessed March 13, 2012. www.excellence-earlychildhood.ca.
Snyder, K. A. 2007. “A Vocabulary of Motives: Understanding how Parents Define QualityTime.” Journal of Marriage and Family 69: 320–340.
Snyder, J., A. Cramer, J. Afrank, and R. G. Patterson. 2005. “The Contributions of IneffectiveDiscipline and Parental Hostile Attributions of Child Misbehavior to the Development ofConduct Problems at Home and School.” Developmental Psychology 41: 30–41. doi: 10.1037/0012-1649.41.1.30.
Stefan, C. A., A. Balaj, M. Porumb, M. Albu, and M. Miclea. 2009. “Preschool Screening forSocial and Emotional Competencies – Development and Psychometric Properties.”Cognition, Brain, Behavior. An Interdisciplinary Journal 13: 121–146.
Stefan, C. A., and M. Miclea. 2010. “Prevention Programs Targeting Emotional and SocialDevelopment in Preschoolers: Current Status and Future Directions.” Early ChildDevelopment and Care 180: 1103–1128.
Stefan, C. A., and M. Miclea. 2012. “Classroom Effects of a Hybrid Universal and IndicatedPrevention Program for Preschool Children: A Comparative Analysis Based on Socialand Emotional Competence Screening.” Early Education and Development 23: 393–426.doi: 10.1080/10409289.2011.554756.
Tottenham, N., A. Borscheid, K. Ellertsen, J. D. Marcus, and A. C. Nelson. 2002.“Categorization of Facial Expressions in Children and Adults: Establishing a LargerStimulus Set. Poster Presented at the Cognitive Neuroscience Society annual meeting,San Francisco.
Trentacosta, C. J., C. E. Izard, A. J. Mostow, and S. E. Fine. 2006. “Children’s EmotionalCompetence and Attentional Competence in Early Elementary School.” SchoolPsychology Quarterly 21: 148–170. doi: 10.1521/scpq.2006.21.2.148.
Turner, K. M. T., and R. M. Sanders. 2006. “Dissemination of Evidence-Based Parenting andFamily Support Strategies: Learning from the Triple P – Positive Parenting Program SystemApproach.” Aggression and Violent Behavior 11: 176–193. doi: 10.1016/j.avb.2005.07.005.
Webster-Stratton, C. 1990. “Long-Term Follow-Up of Families with Young Conduct-ProblemChildren: From Preschool to Grade School.” Journal of Clinical Child Psychology 19:1344–1349.
Webster-Stratton, C. 1998. “Preventing Conduct Problems in Head Start Children: StrengtheningParent Competencies.” Journal of Consulting and Clinical Psychology 66: 715–730.
Webster-Stratton, C. 2000. “The Incredible Years Training Series.” Juvenile Justice Bulletin.Washington, DC: Office of Juvenile Justice and Delinquency Prevention.
Webster-Stratton, C., and M. Hammond. 1997. “Treating Children with Early-Onset ConductProblems: A Comparison of Child and Parent Training Interventions.” Journal ofConsulting and Clinical Psychology 65: 93–109. doi: 10.1037/0022-006X.65.1.93.
Webster-Stratton, C., and J. M. Reid. 2003. “Treating Conduct Problems and StrengtheningSocial and Emotional Competence in Young Children: The Dina Dinosaur Program.”Journal of Emotional and Behavioral Disorders 2: 130–143.
Webster-Stratton, C., M. J. Reid, and M. Hammond. 2001. “Preventing Conduct Problems,Promoting Social Competence: A Parent-Teacher Training Partnership in Head Start.”Journal of Clinical Child Psychology 30: 283–302.
Webster-Stratton, C., M. J. Reid, and M. Stoolmiller. 2008. “Preventing Conduct Problems andImproving School Readiness: Evaluation of the Incredible Years Teacher and ChildTraining Programs in High-Risk Schools.” The Journal of Child Psychology andPsychiatry 49: 471–488. doi: 10.1111/j.1469-7610.2007.01861.x.
Webster-Stratton, C., and T. Taylor. 2001. “Nipping Early Risk Factors in the Bud: PreventingSubstance Abuse, Delinquency, and Violence in Adolescence Through InterventionsTargeted at Young Children (0–8 years).” Prevention Science 2: 165–192.
Zubrick, S. R., A. K. Ward, S. R. Silburn, D. Lawrence, A. A. Williams, E. Blair, D. Robertson,and R. M. Sanders. 2005. “Prevention of Child Behavior Problems through UniversalImplementation of a Group Behavioral Family Intervention.” Prevention Science 6:176–193. doi: 10.1007/s11121-005-0013-2.
44 C.A. Stefan and M. Miclea
Dow
nloa
ded
by [
BC
U C
luj-
Nap
oca]
, [C
atri
nel A
lice
tefa
n] a
t 01:
26 2
5 Fe
brua
ry 2
014




















