Effectiveness of Empowerment-Based Self-Management Interventions on Patients with Chronic Metabolic...
15
Evidence Review Effectiveness of Empowerment-Based Self-Management Interventions on Patients with Chronic Metabolic Diseases: A Systematic Review and Meta-Analysis Chia-Chi Kuo, RN, MSN • Chiu-Chu Lin, RN, PhD • Fu-Mian Tsai, RN, MSN Keywords chronic metabolic disease, empowerment, literature review, metabolic syndrome, self-management, systematic review and meta-analysis ABSTRACT Background: Management of chronic metabolic diseases has recently become an important global health issue. Extensive research on empowerment-based self-management interventions (EBSMIs) for patients with chronic metabolic diseases has been conducted, but no systematic review has evaluated their effects. Aim: To evaluate the effects of EBSMIs on patients with chronic metabolic diseases. Methods: A systematic review and meta-analysis was conducted. Five electronic databases (Airiti Library, CINAHL, Cochrane Library, PubMed/ MEDLINE, and Index of Taiwan Periodical Literature System) were searched from the earliest year available to October 2012. Controlled trials about the effectiveness of interventions on patients with chronic metabolic diseases were included. Each study was appraised by three reviewers and assigned a level of evidence based on the modified Jadad scale. Extracted data were entered and analyzed using Review Manager 5.2. Findings: Nineteen studies were reviewed. Most studies showed that EBSMIs improved patients’ hemoglobin A1c test (HbA1c) (p < .00001), waist circumference (p = .02), and empowerment level (p = .004). Four studies compared the effect on body weight and body mass index, but the overall effect was not significant (p = .33 and .73, respectively). Five studies compared the effect on self-efficacy, four of which indicated significant increase. However, the overall effect on self-efficacy was not compared because studies used different scales. Linking Evidence to Action: EBSMIs improved HbA1c test results, waist circumference, self- efficacy, and empowerment level in patients with chronic metabolic diseases. When implementing the EBSMIs, healthcare institutions need to provide training programs related to empowerment from which health professionals can acquire competence in patient empowerment. Moreover, healthcare leaders should assess and overcome barriers (e.g., time, manpower, cost, etc.) to implementing EBSMIs in clinical settings. INTRODUCTION People with metabolic syndrome must adjust their lifestyle to prevent disease progression and promote well-being (Ford, 2005). Metabolic syndrome is defined as the multiplex risk factors aggregation, such as abdominal obesity, dyslipidemia, raised blood pressure (BP), insulin resistance, or glucose intol- erance (Grundy, Brewer, Cleeman, Smith, & Lenfant, 2004a). These risk factors lead to multiple chronic diseases such as cardiovascular disease, diabetes, and chronic kidney disease (Raimundo & Lopes, 2011). Thus, people with metabolic syn- drome need to change their lifestyles. Effective strategies of lifestyle change include regular physical activity, weight reduc- tion and maintenance, and continuous dietary modification (Grundy, Hansen, Smith, Cleeman, & Kahn, 2004b). One tra- ditional education program is a health professional-centered care model, which focuses on patients’ compliance (Anderson & Funnell, 2000). Under this compliance model, it is difficult for health professionals to help patients change their behaviors and maintain a healthy lifestyle day-to-day because patients lack the awareness, autonomy, and self-efficacy to manage their dis- ease (Anderson & Funnell, 2000; Funnell, Tang, & Anderson, 2007; Grundy et al., 2004b). On the other hand, the care model of empowerment is a patient-centered approach (Funnell et al., 2007). In the empowerment model, healthcare professionals work together with patients to assist the patients to be self- aware of their concerns or needs, find their barriers to lifestyle change, learn the knowledge and skills needed to manage their disease, and utilize resources to solve the problems they Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 301 C 2014 Sigma Theta Tau International
Transcript of Effectiveness of Empowerment-Based Self-Management Interventions on Patients with Chronic Metabolic...

Evidence Review
Effectiveness of Empowerment-BasedSelf-Management Interventions on Patientswith Chronic Metabolic Diseases: ASystematic Review and Meta-AnalysisChia-Chi Kuo, RN, MSN • Chiu-Chu Lin, RN, PhD • Fu-Mian Tsai, RN, MSN
Keywords
chronic metabolicdisease,
empowerment,literature review,
metabolicsyndrome,
self-management,systematic reviewand meta-analysis
ABSTRACTBackground: Management of chronic metabolic diseases has recently become an importantglobal health issue. Extensive research on empowerment-based self-management interventions(EBSMIs) for patients with chronic metabolic diseases has been conducted, but no systematicreview has evaluated their effects.
Aim: To evaluate the effects of EBSMIs on patients with chronic metabolic diseases.
Methods: A systematic review and meta-analysis was conducted. Five electronic databases (AiritiLibrary, CINAHL, Cochrane Library, PubMed/ MEDLINE, and Index of Taiwan Periodical LiteratureSystem) were searched from the earliest year available to October 2012. Controlled trials aboutthe effectiveness of interventions on patients with chronic metabolic diseases were included.Each study was appraised by three reviewers and assigned a level of evidence based on themodified Jadad scale. Extracted data were entered and analyzed using Review Manager 5.2.
Findings: Nineteen studies were reviewed. Most studies showed that EBSMIs improved patients’hemoglobin A1c test (HbA1c) (p < .00001), waist circumference (p = .02), and empowermentlevel (p = .004). Four studies compared the effect on body weight and body mass index, butthe overall effect was not significant (p = .33 and .73, respectively). Five studies compared theeffect on self-efficacy, four of which indicated significant increase. However, the overall effect onself-efficacy was not compared because studies used different scales.
Linking Evidence to Action: EBSMIs improved HbA1c test results, waist circumference, self-efficacy, and empowerment level in patients with chronic metabolic diseases. When implementingthe EBSMIs, healthcare institutions need to provide training programs related to empowermentfrom which health professionals can acquire competence in patient empowerment. Moreover,healthcare leaders should assess and overcome barriers (e.g., time, manpower, cost, etc.) toimplementing EBSMIs in clinical settings.
INTRODUCTIONPeople with metabolic syndrome must adjust their lifestyleto prevent disease progression and promote well-being (Ford,2005). Metabolic syndrome is defined as the multiplex riskfactors aggregation, such as abdominal obesity, dyslipidemia,raised blood pressure (BP), insulin resistance, or glucose intol-erance (Grundy, Brewer, Cleeman, Smith, & Lenfant, 2004a).These risk factors lead to multiple chronic diseases such ascardiovascular disease, diabetes, and chronic kidney disease(Raimundo & Lopes, 2011). Thus, people with metabolic syn-drome need to change their lifestyles. Effective strategies oflifestyle change include regular physical activity, weight reduc-tion and maintenance, and continuous dietary modification(Grundy, Hansen, Smith, Cleeman, & Kahn, 2004b). One tra-
ditional education program is a health professional-centeredcare model, which focuses on patients’ compliance (Anderson& Funnell, 2000). Under this compliance model, it is difficultfor health professionals to help patients change their behaviorsand maintain a healthy lifestyle day-to-day because patients lackthe awareness, autonomy, and self-efficacy to manage their dis-ease (Anderson & Funnell, 2000; Funnell, Tang, & Anderson,2007; Grundy et al., 2004b). On the other hand, the care modelof empowerment is a patient-centered approach (Funnell et al.,2007). In the empowerment model, healthcare professionalswork together with patients to assist the patients to be self-aware of their concerns or needs, find their barriers to lifestylechange, learn the knowledge and skills needed to managetheir disease, and utilize resources to solve the problems they
Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 301C© 2014 Sigma Theta Tau International

Empowerment-Based Self-Management Interventions
PubMed/ MEDLINE (1950–2012): n = 13
Cochrane Library (1998–2012): n = 31
CINAHL (1995– 2012): n = 33
Airiti Library (1990–2012): n = 5 (Chinese articles)
ITPLS (1970–2012): n = 2 (Chinese articles)
Reasons for exclusion after screening abstract or full text: Not clinical controlled trial: n = 36 Not chronic disease: n = 1 Not adult subjects: n = 3 No description of results: n = 5 Scale development: n = 1
Reasons for exclusion after screening abstract or full text: Not clinical controlled trial: n = 4
Papers included in analysis: n = 19
Search strategy: “empowerment” AND (“self-management” OR “self-care”) AND (“metabolic syndrome” OR “diabetes” OR “hypertension” OR “hyperlipidemia” OR “obesity”): n = 86
Related articles: n = 2
Duplicate papers excluded after screening titles: n = 15
Duplicate papers excluded after screening titles: n = 2
Figure 1. Flowchart of literature search process and results.
encounter (Anderson & Funnell, 2005). In other words, theempowerment care model could facilitate patients’ auton-omy and abilities to self-manage their disease and furtherachieve their desired goals (Anderson et al., 2009; Anderson &Funnell, 2010; Aujoulat, d’Hoore, & Deccache, 2007).
Empowerment-based self-management interventions (EB-SMIs) have been used widely for patients with chronic condi-tions such as diabetes (Anderson et al., 2009; Cooper, Booth,& Gill, 2009; Deakin, Cade, Williams, & Greenwood, 2006;Naik, Teal, Rodriguez, & Haidet, 2011) and hypertension (Figaret al., 2006), as well as for weight management (Mayer-Daviset al., 2001, 2004). These protocols share a patient-centeredapproach and partnership, self-awareness and self-motivation,self-care or self-management, problem solving, and reflectionconcepts (Anderson et al., 2005; Figar et al., 2006; Naik et al.,2011; Sigurdardottir, Benediktsson, & Jonsdottir, 2009). How-ever, the overall effects of different protocols on patients withchronic diseases remain unclear. Thus, the aim of this studywas to explore the research effects of EBSMIs for patients withchronic metabolic diseases using systematic literature reviewand meta-analysis.
METHODSSelection CriteriaTypes of studies. Studies of individual randomized controlledtrials (RCTs), controlled trials, and quasi-experimental designwere included.
Types of participants. Patients with chronic metabolic dis-eases such as metabolic syndrome, diabetes, hypertension, hy-
perlipidemia, or obesity were included. Nonadult subjects (<18years) were excluded.
Types of interventions. This review considered any empow-erment and self-management concept interventions.
Types of outcome measures. Effects of EBSMIs on knowl-edge, behavioral, physiological, or psychological outcomes onpatients with chronic metabolic diseases were included.
Search MethodsTo obtain more comprehensive literature, we searched studiespublished in Chinese and English from five databases (Air-iti Library, CINAHL, Cochrane Library, PubMed/MEDLINE,and the Index of the Taiwan Periodical Literature System)from the earliest available date to October 2012. The searchterms used were “empowerment” AND (“self-management”OR “self-care”) AND (“metabolic syndrome” OR “diabetes” OR“hypertension” OR “hyperlipidemia” OR “obesity”). Related ar-ticles identified in the database searches were also reviewedto identify additional pertinent studies. Individual controlledclinical trials that examined EBSMIs for adults with chronicmetabolic diseases were included in the analysis. Duplicatepublications, qualitative studies, and review articles were ex-cluded. Figure 1 illustrates the search and selection processused in this study.
Search OutcomeA total of 86 Chinese- and English-language publications wereidentified in the initial search. Primary appraisal of titles,abstracts, or full texts was used to screen the articles. After
302 Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315.C© 2014 Sigma Theta Tau International

Evidence Reviewscreening, 19 studies fit the inclusion criteria (Figure 1). Thefull texts of these articles were obtained for analysis.
Quality AppraisalThree reviewers used the modified Jadad scale, which hasshown excellent validity and reliability (intraclass correlationcoefficient = .90), to appraise the quality of each clinical trial(Oremus et al., 2001). The scale has eight items: random-ization, appropriateness of randomization, blinding, appropri-ateness of blinding, withdrawals-dropouts, inclusion-exclusioncriteria, adverse effects, and statistical analysis. Each item isscored as 0 or 1; total scores range from 0 to 8, with higherscores indicating higher quality of the study.
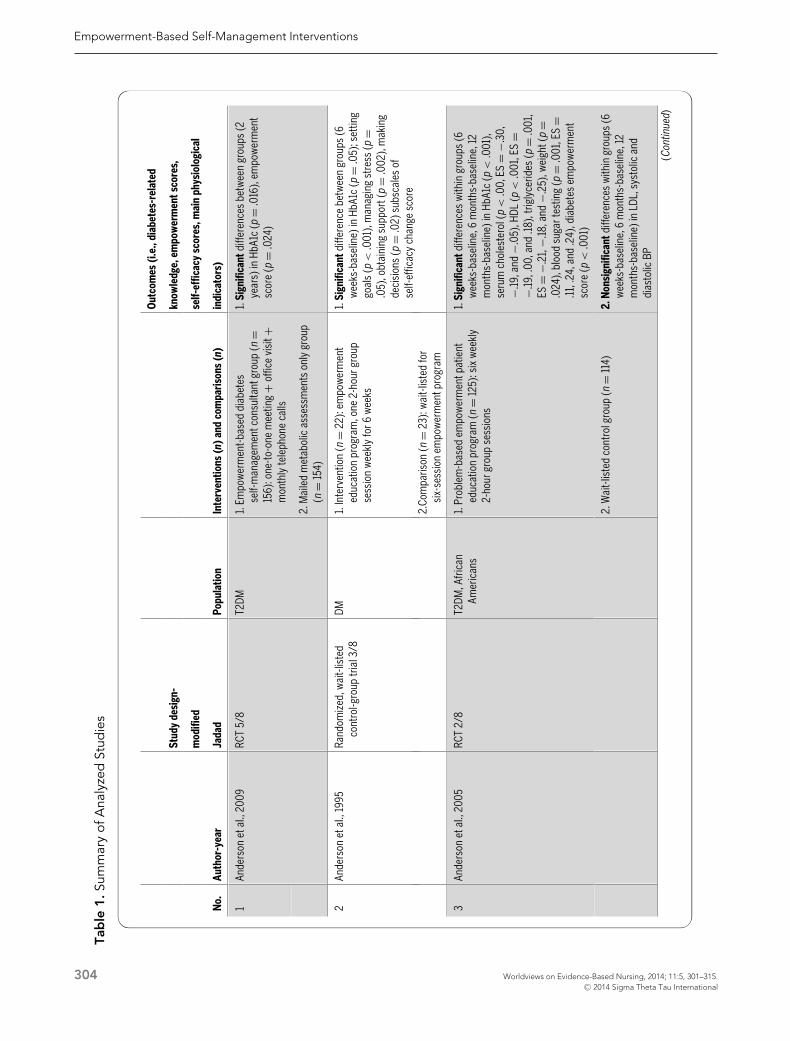
Data Abstraction and SynthesisThe study population and design, method-timing-duration ofintervention and comparisons, main results, and quality of eachstudy were abstracted and assessed (Table 1). Meta-analysis wasused to pool the data (e.g., mean, standard deviation, effect size,etc.) from studies to determine the overall effect. Data were an-alyzed using Review Manager 5.2 software (The Cochrane Col-laboration, Copenhagen, Denmark). Considering the varyingintervention protocols and disease types of study participants,we used a random effects model to estimate the overall effectconservatively. To help readers evaluate the strength level ofan intervention, we calculated the effect size of interventionoutcomes (e.g., knowledge score, self-efficacy, cholesterol, etc.)that cannot be pooled to compare using Review Manager 5.2(Table 1).
RESULTSStudy Participants and Study DesignsPatients in the 19 intervention studies had diabetes (n = 18;94.74%; Anderson et al., 1995, 2005, 2009; Cooper et al.,2009; Deakin et al., 2006; Forlani, Zannoni, Tarrini, Mel-chionda, & Marchesini, 2006; Kuo, Tsay, & Yang, 2002; Mc-Carrier et al., 2009; Mayer-Davis et al., 2001, 2004; Naik et al.,2011; Pena-Purcell, Boggess, & Jimenez, 2011; Piatt et al., 2006;Ruggiero et al., 2010; Sigurdardottir et al., 2009; Simmons,Gamble, Foote, Cole, & Coster, 2004; Spencer et al., 2011; Utzet al., 2008), hypertension (Figar et al., 2006), or diabetes com-bined with a weight problem (Mayer-Davis et al., 2001, 2004).Thus, most EBSMIs have been applied in diabetes research.The designs of the 19 studies were 13 RCTs, three randomizedpilot studies (McCarrier et al., 2009; Mayer-Davis et al., 2001;Ruggiero et al., 2010), one controlled trial (Forlani et al., 2006),and two quasi-experimental studies (Pena-Purcell et al., 2011;Utz et al., 2008).
Study QualityOf the 19 published studies describing EBSMIs for patientswith chronic metabolic diseases, 6 (31.58%) were determinedto be of good quality (modified Jadad scale score �5; Table 1).
Major Elements of EBSMIsMost of the studies in our review lacked descriptions of inter-vention mechanisms and operational definitions; moreover,most intervention protocols were not described clearly. How-ever, we try to extract the major elements of EBSMIs to helpreaders to apply the abstract concept of empowerment to clin-ical practice. These major elements include: building partner-ship, identifying one’s problems or concerns, self-awareness,self-motivation, goal setting and action planning, utilization ofresources, communication with healthcare professionals, over-coming obstacles, problem solving, and reflection or review ofchanges (Anderson et al., 1995, 2005, 2009; Cooper et al.,2009; Deakin et al., 2006; Figar et al., 2006; Forlani et al.,2006; Kuo et al., 2002; McCarrier et al., 2009; Mayer-Daviset al., 2001, 2004; Naik et al., 2011; Pena-Purcell et al., 2011;Piatt et al., 2006; Ruggiero et al., 2010; Sigurdardottir et al.,2009; Simmons et al., 2004; Spencer et al., 2011; Utz et al.,2008).
Intervention EffectsThe 19 intervention studies used a variety of outcome indi-cators (Table 1), but all of these EBSMIs, which emphasizedintegrated strategies and long-term follow-up, had positivepatient outcomes. The effects of knowledge-based, behav-ioral, physiological, and psychological indicators are presentedbelow.
Knowledge-based indicators. Three studies (Deakin et al.,2006; Naik et al., 2011; Sigurdardottir et al., 2009) indicatedthat interventions significantly improved patients’ diabetes-related knowledge, whereas two studies (Piatt et al., 2006;Simmons et al., 2004) found no significant change in suchknowledge. Fourteen studies (73.68%) did not measure pa-tients’ knowledge of their disease.
Behavioral indicators. Some studies indicated that interven-tions significantly improved patients’ self-care activities (Kuoet al., 2002; Pena-Purcell et al., 2011), BP control (Figar et al.,2006), or self-monitoring (Cooper et al., 2009; Mayer-Daviset al., 2004). One study (Utz et al., 2008) reported a trendtoward improved self-care activities. Other studies showed nosignificant improvement in patients’ self-care activities, e.g.,diet, exercise, foot care, insulin use (Anderson et al., 2005;Cooper et al., 2009; Sigurdardottir et al., 2009; Simmonset al., 2004), and self-monitoring (Sigurdardottir et al., 2009;Simmons et al., 2004).
Physiological indicators. Most studies indicated that in-terventions resulted in significant improvement in one ormore physiological indicators, including glycated hemoglobin(HbA1c) level (Anderson et al., 1995, 2005, 2009; Cooper et al.,2009; Deakin et al., 2006; Kuo et al., 2002; Mayer-Daviset al., 2004; Piatt et al., 2006; Simmons et al., 2004; Spenceret al., 2011; n = 10; 52.63%), fasting blood glucose (Ander-son et al., 2005; Mayer-Davis et al., 2001), frequency of hy-perglycemia (Deakin et al., 2006), cholesterol and triglyceride
Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 303C© 2014 Sigma Theta Tau International
Empowerment-Based Self-Management Interventions
Tab
le1.S
umm
ary
ofA
naly
zed
Stud
ies
Outcomes(i.e.,diabetes-related
Studydesign-
knowledge,empowermentscores,
modified
self-efficacyscores,mainphysiological
No.
Author-year
Jadad
Population
Interventions(n)andcomparisons(n)
indicators)
1Andersonetal.,2009
RCT5/8
T2DM
1.Empowerment-baseddiabetes
self-managementconsultantgroup(n
=156):one-to-onemeeting
+officevisit+
monthlytelephonecalls
1.Significantdifferencesbetweengroups(2
years)inHbA1c(p
=.016),empowerment
score( p
=.024)
2.Mailedmetabolicassessmentsonlygroup
(n=154)
2Andersonetal.,1995
Randomized,wait-listed
control-grouptrial3/8
DM1.Intervention(n
=22):empowerment
educationprogram,one2-hourgroup
sessionweeklyfor6weeks
1.Significantdifferencebetweengroups(6
weeks-baseline)inHbA1c( p
=.05);setting
goals(p
<.001),managingstress(p
=.05),obtainingsupport(p
=.002),making
decisions( p
=.02)subscalesof
self-efficacychangescore
2.Comparison(n
=23):wait-listedfor
six-sessionempowermentprogram
3Andersonetal.,2005
RCT2/8
T2DM,African
Americans
1.Problem-basedempowermentpatient
educationprogram(n
=125):sixweekly
2-hourgroupsessions
1.Significantdifferenceswithingroups(6
weeks-baseline,6months-baseline,12
months-baseline)inHbA1c( p
<.001),
serumcholesterol(p
<.00,ES
=−.30,
−.19,and
−.05),HDL(p
<.001,ES
=−.19,.00,and.18),triglycerides( p
=.001,
ES=
−.21,−.18,and
−.25),weight(p
=.024),bloodsugartesting(p
=.001,ES
=.11,.24,and.24),diabetesempowerment
score( p
<.001)
2.Wait-listedcontrolgroup(n
=114)
2.Nonsignificantdifferenceswithingroups(6
weeks-baseline,6months-baseline,12
months-baseline)inLDL,systolicand
diastolicBP
(Continued)
304 Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315.C© 2014 Sigma Theta Tau International

Evidence ReviewTa
ble
1.C
ontin
ued
Outcomes(i.e.,diabetes-related
Studydesign-
knowledge,empowermentscores,
modified
self-efficacyscores,mainphysiological
No.
Author-year
Jadad
Population
Interventions(n)andcomparisons(n)
indicators)
4Cooperetal.,2009
RCT4/8
T2DM
1.Educationgroup(n
=30):LookAfter
Yourselfprogram,2-hourgroupsessions
weeklyfor8weeks
1.Significantdifferencesbetweengroups(6
months-baseline)inHbA1c(p
=.005)
2.Controlgroup(n
=36)
2.Nonsignificantdifferencesbetweengroups
(6months-baseline,12months-baseline)in
BMI
5Deakinetal.,2006
Double-blindRCT7/8
T2DM
1.Interventiongroup(n
=150):X-PERT
program,sixweekly2-hoursessions
1.Significantdifferencesbetweengroups
(baseline,4months,and14months)in
HbA1c( p
<.001),bodyweight(p
<.001),
BMI(p
<.001),waistcircumference
(p<.001),diabetesknowledgescore(p
<
.001,ES
=.15,.91,and.52),totaldiabetes
empowermentscore( p
=.04)
2.Controlgroup(n
=141)
6Figaretal.,2006
RCT6.5/8
HTN,>65-year-old1.Patientempowerment-basedmodel(PEM)
group(n
=30):interventionfrequency-
durationnotdescribed
1.Significantdifferencebetweengroups(3
months)innight-timesystolicBP(p
=.02,
ES=
−.65)
2.Compliance-basedmodel(CM)group(n
=30)
2.Nonsignificantdifferencesbetweengroups
(3months)indaytimeandofficeBP
7Forlanietal.,2006
Controlledtrial2/8
T1DM,�65-year-old1.Empowerment-basedinterventiongroup(n
=54):eightfortnightly2-hoursessions,
8–10patientspergroup
1.Significantdifferencesbetweengroups(12
months-baseline)ingeneralhealth(p
=.043,intervention-controlwithingroupsES
=.33/−.05)
2.Controlgroup(n
=36)
8Kuoetal.,2002
RCT3/8
T2DM,>18-year-old,
Taiwanese
1.Interventiongroup(n
=34):empowerment
trainingprogram,2hour/weekfor8weeks1.Significantdifferencesbetweengroups
(baseline,8weeks,3months)in
empowerment(p
=.766,<.001,and
<.001),self-efficacy( p
=.460,.029,and
<.001,ES
=−.18,.55,and1.10)
2.Controlgroup(n
=33)
2.Significantdifferencesbetweengroups
(ANCOVA)inHbA1c( p
=.033)
(Continued)
Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 305C© 2014 Sigma Theta Tau International

Empowerment-Based Self-Management Interventions
Tab
le1.C
ontin
ued
Outcomes(i.e.,diabetes-related
Studydesign-
knowledge,empowermentscores,
modified
self-efficacyscores,mainphysiological
No.
Author-year
Jadad
Population
Interventions(n)andcomparisons(n)
indicators)
9Mayer-Davisetal.,2001
Randomizedpilotstudy4/8T2DM&BMI�25
kg/m2 ,
�50-year-old
1.Lifestyleplusempowermentevaluation
interventiongroup(n
=23):8-weekweight
managementinterventionwithweekly
groupactivitysessions,formalevaluation
by“toolbox”
1.Significantdifferenceswithingroups(8
weeks-baseline)inmeanweight(p
<.01),
BMI(p
<.01),fastingbloodglucose
( p<.01,ES
=−.52)
2.Lifestyleinterventiongroup(n
=23):
8-weekweightmanagementintervention,
informalevaluation
10Mayer-Davisetal.,2004
RCT4/8
DM&BMI�25
kg/m2 ,
�45-year-old
1.Intensivelifestylegroup(n
=49):weekly
corecurriculum(1-hoursessions)forfirst4
months(intensive),fortnightlyfor2months
(transition),monthlyfor6months
(maintenance)
1.Significantdifferencesamonggroups(6
months-baseline)inBMI(p
<.001),HbA1c
(p<.0001)
2.Reimbursablelifestylegroup(n
=47):
condensedversionofintensivelifestyle
intervention;three1-hourgroupsessions,
oneindividualsession
2.Nonsignificantdifferencesamonggroups(6
months-baseline)intotalcholesterol,LDL,
HDL,triglycerides,systolic,anddiastolicBP
3.Usualcaregroup(n
=56)
11McCarrieretal.,2009
Randomizedpilotstudy6.5/8T1DM&HbA1c
�7.0%,
21–49-year-old
1.Interventiongroup(n
=41):usualcare
+nursepractitioner-aidedweb-basedcase
managementprogram;1-hourconsultation,
one-to-oneinstructionwithwebmodule
(fivewebsites),weeklye-mailcontactwith
casemanagertodiscussindividualgoals
andrecords
1.Significantdifferencebetweengroups(12
months-baseline)indiabetes-related
self-efficacy( p
=.044,intervention-control
withingroupsES
=.23/
−.26)
2.Controlgroup(n
=36)
2.Nonsignificantdifferencebetweengroups
(12months-baseline)inaverageHbA1c
( p=.16)
(Continued)
306 Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315.C© 2014 Sigma Theta Tau International

Evidence ReviewTa
ble
1.C
ontin
ued
Outcomes(i.e.,diabetes-related
Studydesign-
knowledge,empowermentscores,
modified
self-efficacyscores,mainphysiological
No.
Author-year
Jadad
Population
Interventions(n)andcomparisons(n)
indicators)
12Naiketal.,2011
RCT3/8
T2DM&HbA1c
�7.5%,50–90-
year-old
1.Interventiongroup(n
=44):empowerment
interventionarm(conceptualmetaphor,
team-basedlearningmethods),1-hour
groupsession(8–10patientspergroup),
10-minuteone-on-oneconsultation
1.Significantdifferencesbetweengroups(3
months)inunderstandingofdiabetesABCs
( p<.0001,betweengroupsES
=4.04)
2.Comparisongroup(n
=41)
13Pena-Purcelletal.,2011
Quasi-experimentalpilot
study3/8
T2DM,>40-year-old,
Hispanic-Latino
1.Interventiongroup(n
=71):fiveweekly
1.5–2-hourlessons,groupclasses
1.Significantdifferencesbetweengroups(5
weeks-baseline)inself-efficacy( p
<.001)
2.Controlgroup(n
=64)
2.Nonsignificantdifferencebetweengroups
(3months)inaverageHbA1c(p
=.077)
14Piattetal.,2006
RCT3/8
DM1.Chroniccaremodel(CCM)group(n
=27):
oneproblem-basedlearningsession,6
monthsofindividualconsultationon
“diabetesdays”
1.Significantdifferencesamonggroups(12
months-baseline)inHbA1c(p
=.01),HDL
(p=.05)
2.Providereducationonlygroup(n
=32):one
problem-basedlearningsession,
consultationavailable
2.Nonsignificantdifferencesamonggroups
(12months-baseline)insystolicand
diastolicBP,diabetesknowledge,and
empowermentscore
3.Usualcaregroup(n
=46)
15Ruggieroetal.,2010
Randomizedpilotstudy4/8T2DM&HbAlc
�7%,
�50-year-old
1.Medicalassistantcoaching(MAC)group(n
=25):diabeteseducationhandbook
+diabetesself-careandbehavioralcoaching
for6months(onebriefsession
+twoclinic
visits
+fourmonthlytelephonecalls)
1.Significantlyincreased(6months-baseline)
diabetesempowermentscoreinMACgroup
versusnochangeinTAUgroup( p
<.01)
2.Treatmentasusual(TAU)group(n
=25):
diabeteseducationhandbook
+treatment
asusual
2.Nonsignificantdifferenceamonggroups(6
months-baseline)inHbA1c(p
>.05)
3.Nocontactcontrol(NCC)group(n
=50)
(Continued)
Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 307C© 2014 Sigma Theta Tau International

Empowerment-Based Self-Management Interventions
Tab
le1.C
ontin
ued
Outcomes(i.e.,diabetes-related
Studydesign-
knowledge,empowermentscores,
modified
self-efficacyscores,mainphysiological
No.
Author-year
Jadad
Population
Interventions(n)andcomparisons(n)
indicators)
16Sigurdardottiretal.,2009
RCT6.5/8
T2DM&HbAlc
�7.5%,
�65-year-old
1.Interventiongroup(n
=28):oneindividual
1–2-hoursession
+weekly15–20-minute
telephonecallsfor5weeks
1.Significantdifferencesbetweengroups
(baseline,3months,and6months)in
diabetesknowledgescore( p
=.001,
betweengroupsES
=.40,1.25,and1.57)
2.Controlgroup(n
=25)
2.Nonsignificantdifferencesbetweengroups
(baseline,3months,and6months)in
HbA1c,weight,BMI,waistcircumference,
diabetesempowermentscore
17Simmonsetal.,2004
RCT7/8
T1DM&T2DM,HbAlc
�8.5%,18–
65-year-old
1.Passportgroup(n
=193):receivedDiabetes
Passportwith11sections
1.Significantdifferencesbetweengroups(12
months-baseline)inHbA1c(p
=.017),BMI
( p=.028)
2.Controlgroup(n
=150)
2.Nonsignificantdifferencesbetweengroups
(12months-baseline)insystolicand
diastolicBP,totalcholesterolknowledge
score
18Spenceretal.,2011
RCT4.5/8
T2DM,�18-year-old,
AfricanandLatino
Americans
1.Interventiongroup(n
=72):Eleven2-hour
groupsessions,two1-hourhomevisits
(individualsessions)permonth,fortnightly
telephonecalls;6-monthinterventionperiod
1.Significantdifferencebetweengroups(6
months-baseline)inHbA1c(meanchange
=−.8,95%CI
=−1.2to
−.4,p
<.01);
significantimprovementinLDL(mean
change
=−10,95%CI
=−17to
−2, p
<
.05)ininterventiongroup
2.Controlgroup(n
=92)
2.Nonsignificantdifferencesbetweengroups
(6months-baseline)insystolicanddiastolic
BP,andBMI
19Utzetal.,2008
Quasi-experimental,
randomlyassigned5/8
T2DM,�18-year-old,
AfricanAmericans1.GroupDSME(Diabetesself-management
education)(n
=7):eightweekly2-hour
educationalsessions
1.Trendsofimproved(3months-baseline)in
HbA1c,andself-efficacy(GroupDSME/
IndividualDSMEwithingroupES
=.89/
−.20)
2.IndividualDSME(n
=8):threeeducation
sessionsinweeks1,4,8
Note.RCT,randomizedcontrolledtrial;T2,type2;DM,diabetesmellitus;HTN,hypertension;T1,type1;BMI,bodymassindex;HbAlc,glycatedhemoglobinlevel;HDL,high-densitylipoprotein;LDL,low-density
lipoprotein;BP,bloodpressure;ES,effectsize
=Cohen’sd
=M1(treatmentmeanorposttestmean)–M2(controlmeanorpretestmean)/pooled(SD 1
+SD 2÷2).
308 Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315.C© 2014 Sigma Theta Tau International

Evidence Review
Study or subgroup
1.1.1 HbA1c~6 weeks
Anderson et al. 1995
Anderson et al. 2005Subtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.40, df = 1 (P = 0.53); I² = 0%
Test for overall effect: Z = 0.66 (P = 0.51)
1.1.2 HbA1c~3 months
Kuo et al. 2002Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 1.03 (P = 0.30)
1.1.3 HbA1c~6 months
Ruggiero et al. 2010
Sigurdardottir et al.2009
Spencer et al. 2011Subtotal (95% CI)
Heterogeneity: Tau² = 0.14; Chi² = 5.18, df = 2 (P = 0.08); I² = 61%
Test for overall effect: Z = 1.72 (P = 0.09)
1.1.4 HbA1c~12 months
Cooper et al. 2009
McCarrier et al. 2009
Simmons et al. 2004Subtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.09, df = 2 (P = 0.96); I² = 0%
Test for overall effect: Z = 2.87 (P = 0.004)
1.1.5 HbA1c~14 months
Deakin et al. 2006Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 4.00 (P < 0.0001)
1.1.6 HbA1c~24 months
Anderson et al. 2009Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 2.03 (P = 0.04)
Total (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 9.09, df = 10 (P = 0.52); I² = 0%
Test for overall effect: Z = 6.37 (P < 0.00001)
Test for subgroup differences: Chi² = 3.13, df = 5 (P = 0.68), I² = 0%
Mean
-0.73
-0.4
-0.65
-0.17
-0.08
-0.8
0
-0.37
-0.3
-0.6
0.05
SD
2.95
2.02
1.78
1.67
1.41
1.05
2.51
1.26
1.5
1.37
1.87
Total
22
117139
3434
25
28
58111
30
41
193264
150150
122122
820
Mean
-0.04
-0.28
-0.2
0.37
-0.12
0
0.3
0.11
0.1
0.1
0.53
SD
2.77
2.15
1.79
1.55
0.85
1.1
2.2
1.4
1.6
1.6
1.86
Total
23
108131
3333
50
25
69144
36
36
150222
141141
126126
797
Weight
0.8%
7.9%8.8%
3.2%3.2%
3.9%
6.2%
16.9%26.9%
1.8%
6.6%
21.5%29.9%
20.1%20.1%
11.0%11.0%
100.0%
IV, Random, 95% CI
-0.69 [-2.36, 0.98]
-0.12 [-0.67, 0.43]-0.17 [-0.69, 0.34]
-0.45 [-1.30, 0.40]-0.45 [-1.30, 0.40]
-0.54 [-1.32, 0.24]
0.04 [-0.58, 0.66]
-0.80 [-1.17, -0.43]-0.47 [-1.00, 0.07]
-0.30 [-1.45, 0.85]
-0.48 [-1.08, 0.12]
-0.40 [-0.73, -0.07]-0.41 [-0.69, -0.13]
-0.70 [-1.04, -0.36]-0.70 [-1.04, -0.36]
-0.48 [-0.94, -0.02]-0.48 [-0.94, -0.02]
-0.50 [-0.65, -0.35]
Experimental Control Mean difference Mean difference
IV, Random, 95% CI
-2 -1 0 1 2Favours [experimental] Favours [control]
Figure 2. Forest plot of HbA1c.
levels (Anderson et al., 2005), high-density (Anderson et al.,2005; Piatt et al., 2006) and low-density lipoprotein (Spenceret al., 2011), weight (Anderson et al., 2005; Deakin et al.,2006; Mayer-Davis et al., 2001, 2004), waist circumference(Deakin et al., 2006), body mass index (BMI; Deakin et al.,2006; Mayer-Davis et al., 2001, 2004; Simmons et al., 2004),night-time systolic BP and other symptoms (Figar et al., 2006).
Three studies (McCarrier et al., 2009; Ruggiero et al., 2010;Utz et al., 2008) reported an insignificant trend toward im-provement in HbA1c levels. Other studies found no significantchange in HbA1c level (McCarrier et al., 2009; Pena-Purcellet al., 2011; Ruggiero et al., 2010; Sigurdardottir et al., 2009; n= 4; 21.05%), weight and waist circumference (Sigurdardottiret al., 2009), BMI (Cooper et al., 2009; Sigurdardottir et al.,
Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 309C© 2014 Sigma Theta Tau International

Empowerment-Based Self-Management Interventions
Study or subgroup
2.1.1 Waist circumference ~6 months
Sigurdardottir et al.2009Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 1.49 (P = 0.14)
2.1.2 Waist circumference~14 months
Deakin et al. 2006Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 1.85 (P = 0.06)
Total (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.29, df = 1 (P = 0.59); I² = 0%
Test for overall effect: Z = 2.31 (P = 0.02)
Test for subgroup differences: Chi² = 0.29, df = 1 (P = 0.59), I² = 0%
Mean
-5.1
-3
SD
11.66
11.25
Total
2828
150150
178
Mean
-0.4
-0.2
SD
11.3
14.25
Total
2525
141141
166
Weight
18.6%18.6%
81.4%81.4%
100.0%
IV, Random, 95% CI
-4.70 [-10.89, 1.49]-4.70 [-10.89, 1.49]
-2.80 [-5.76, 0.16]-2.80 [-5.76, 0.16]
-3.15 [-5.83, -0.48]
Experimental Control Mean difference Mean difference
IV, Random, 95% CI
-10 -5 0 5 10Favours [experimental] Favours [control]
Figure 3. Forest plot of waist circumference.
2009; Spencer et al., 2011), systolic and diastolic BP (Andersonet al., 2005; Mayer-Davis et al., 2004; Piatt et al., 2006; Sim-mons et al., 2004; Spencer et al., 2011), daytime BP (Figar et al.,2006), cholesterol (Mayer-Davis et al., 2004; Simmons et al.,2004), triglycerides and high-density lipoprotein (Mayer-Daviset al., 2004), or low-density lipoprotein (Anderson et al., 2005;Mayer-Davis et al., 2004). Most studies reported no significantreduction in BP, body weight, BMI, or blood lipid measure-ments, possibly because most interventions (n = 18; 94.74%)were based on diabetes care and these effects were not readilyvisible.
Of the 19 studies included, 11 presented the mean and stan-dard deviation of HbA1c, body weight, waist circumference,or BMI. These original data were inputted to Review Manager5.2. The random effects model of meta-analysis was used toanalyze the overall effect. The pooled mean difference (pooledeffect size) for HbA1c, and waist circumference between postand pretest of two groups were −.50%, and −3.15 cm (pooledsample size = 1617 and 344; 95% CI = −.65 to −.35 and −5.83to −.48, respectively); and the overall effect of experimentalgroups had more significant improvement than that of controlgroups (Z = 6.37, p < .00001; Z = 2.31, p = .02, respectively,Figures 2 and 3). The pooled mean difference (pooled effectsize) for body weight and BMI was −1.34 kg and −.14 kg/m2
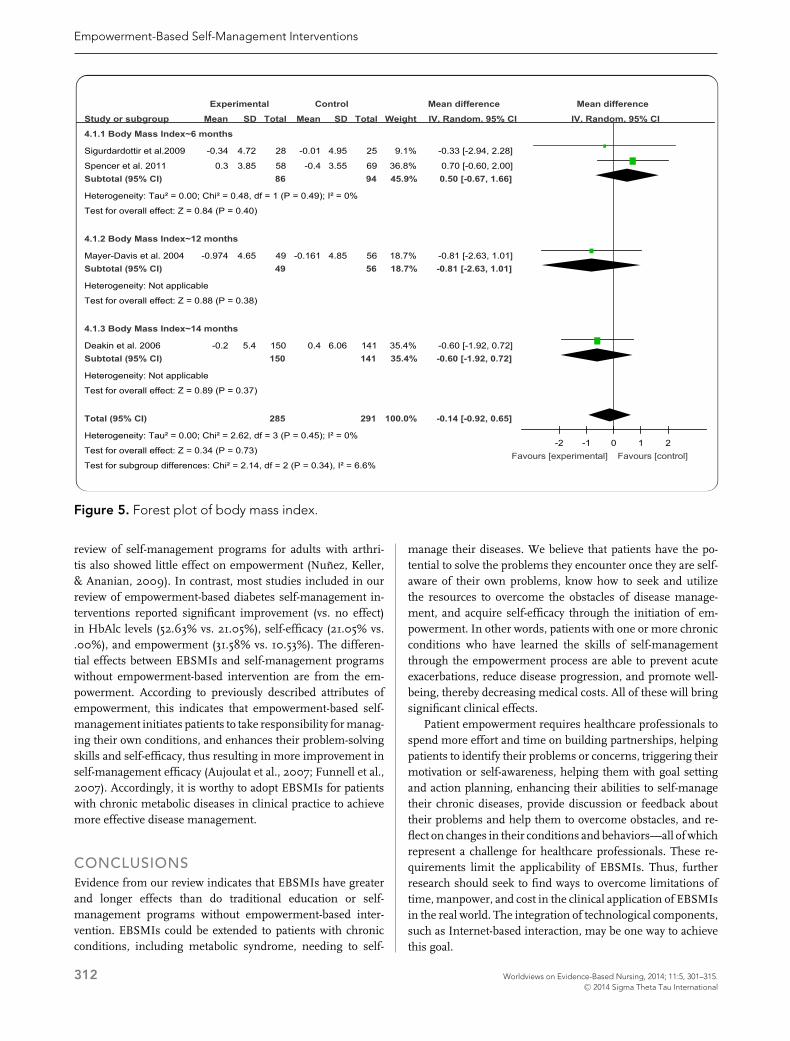
(pooled sample size = 661 and 576, 95% CI = −4.04 to 1.36and −.92 to .65, respectively), and the overall effect had no sta-tistically significant difference between two groups (Z = .97, p= .33 and Z = .34, p = .73, respectively, Figures 4 and 5).
Psychological indicators. Some studies indicated that inter-ventions significantly increased patients’ self-efficacy (Ander-son et al., 1995; Kuo et al., 2002; McCarrier et al., 2009; Pena-
Purcell et al., 2011; n = 4; 21.05%) and empowerment level(Anderson et al., 2005, 2009; Deakin et al., 2006; Kuo et al.,2002; Piatt et al., 2006; Ruggiero et al., 2010; n = 6; 31.58%).One study (Utz et al., 2008) showed a trend toward increasedself-efficacy, and two (Piatt et al., 2006; Sigurdardottir et al.,2009) showed no significant improvement in empowerment.Some studies reported significant improvement in patients’comprehension of diabetes (Anderson et al., 2005, 2009), ef-fectiveness of treatment (Cooper et al., 2009), satisfaction withdiabetes care (Anderson et al., 2009; Deakin et al., 2006), at-titudes toward diseases (Anderson et al., 1995, 2005; Cooperet al., 2009), anxiety, depression, general health, and generalwell-being (Forlani et al., 2006), and quality of life (Andersonet al., 2009; Forlani et al., 2006). Only one study (Andersonet al., 1995) showed no significant improvement in patientsatisfaction. Most studies did not report the effects of interven-tions on self-efficacy (n = 14; 73.69%) and empowerment (n =11; 57.89%).
Five studies presented the mean and standard deviation ofdiabetes empowerment scores. The pooled mean difference(pooled effect size) was .23 (pooled sample size = 719, 95%CI = .07 to .39), and the overall effect of experimental groupshad more significant increase than that of control groups (Z =2.84, p = .004, Figure 6).
DISCUSSIONThe findings of this systematic review indicate that EBSMIs im-proved HbA1c test results, waist circumference, self-efficacy,and empowerment level in patients with chronic metabolicdiseases. Because no published review has examined em-powerment and self-management together, we systematically
310 Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315.C© 2014 Sigma Theta Tau International

Evidence Review
Study or subgroup
3.1.1 Body Weight~6 weeks
Anderson et al. 2005Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.27 (P = 0.79)
3.1.2 Body Weight~6 months
Sigurdardottir et al.2009Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.12 (P = 0.91)
3.1.3 Body Weight~12 months
Mayer-Davis et al. 2004Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
3.1.4 Body Weight~14 months
Deakin et al. 2006Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.82 (P = 0.41)
Total (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.12, df = 3 (P = 0.99); I² = 0%
Test for overall effect: Z = 0.97 (P = 0.33)
Test for subgroup differences: Chi² = 0.12, df = 3 (P = 0.99), I² = 0%
Mean
-0.68
-0.6
-2.2
-0.5
SD
19.93
15.85
16.81
14.65
Total
111111
2828
4949
150150
338
Mean
0.09
-0.1
-0.3
1.1
SD
21.25
15.6
18.35
18.21
Total
101101
2525
5656
141141
323
Weight
23.6%23.6%
10.1%10.1%
16.1%16.1%
50.2%50.2%
100.0%
IV, Random, 95% CI
-0.77 [-6.33, 4.79]-0.77 [-6.33, 4.79]
-0.50 [-8.98, 7.98]-0.50 [-8.98, 7.98]
-1.90 [-8.63, 4.83]-1.90 [-8.63, 4.83]
-1.60 [-5.41, 2.21]-1.60 [-5.41, 2.21]
-1.34 [-4.04, 1.36]
Experimental Control Mean difference Mean difference
IV, Random, 95% CI
-10 -5 0 5 10Favours [experimental] Favours [control]
Figure 4. Forest plot of body weight.
reviewed the studies on EBSMIs and also compared their dif-ference with studies focused only on self-management. Theimplications of our findings and risk of bias are also discussedbelow.
Study Quality and Risk of BiasThe quality of the 19 trials varied widely. Most of the studieshad moderate to high quality (4 to 7 scores), which could haveintroduced biases that can lead to over- and underestimatesof intervention effectiveness (Cook, Mulrow, & Haynes, 1997).Thirteen studies did not have adequate description of powercalculation for the sample (Anderson et al., 1995, 2005, 2009;Forlani et al., 2006; Kuo et al., 2002; Mayer-Davis et al., 2001;Naik et al., 2011; Pena-Purcell et al., 2011; Piatt et al., 2006; Rug-giero et al., 2010; Simmons et al., 2004; Spencer et al., 2011;Utz et al., 2008), which could have type 1 error. According to theCochrane Collaboration’s “Risk of bias” tool, 11 studies (Ander-son et al., 1995, 2005, Cooper et al., 2009; Forlani et al., 2006;Kuo et al., 2002; Mayer-Davis et al., 2001, 2004; Naik et al.,
2011; Pena-Purcell et al., 2011; Ruggiero et al., 2010; Spenceret al., 2011) did not have adequate procedure for random se-quence or allocation concealment, which could induce poten-tial selection bias. Eighteen studies (except Kuo et al., 2002) didnot follow intention-to-treatment analysis, which could induceattrition bias. In addition, we only reviewed published articlesin English and Chinese, which could lead to reporting bias andlanguage bias.
Intervention EffectsSelf-management education has become an integral part ofprimary care for patients with chronic diseases (Bodenheimer,Lorig, Holman, & Grumbach, 2002). Systematic reviewsof studies focused only on self-management programs forpatients with chronic diseases showed no significant differ-ence in glycemic control in patients with diabetes (66.67%), nodifference in action plans in patients with asthma (52.17%; Bo-denheimer et al., 2002), and weak evidence of improved HbA1clevels in patients with diabetes (Coster & Norman, 2009). A
Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 311C© 2014 Sigma Theta Tau International
Empowerment-Based Self-Management Interventions
Study or subgroup
4.1.1 Body Mass Index~6 months
Sigurdardottir et al.2009
Spencer et al. 2011Subtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.48, df = 1 (P = 0.49); I² = 0%
Test for overall effect: Z = 0.84 (P = 0.40)
4.1.2 Body Mass Index~12 months
Mayer-Davis et al. 2004Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
4.1.3 Body Mass Index~14 months
Deakin et al. 2006Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.89 (P = 0.37)
Total (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 2.62, df = 3 (P = 0.45); I² = 0%
Test for overall effect: Z = 0.34 (P = 0.73)
Test for subgroup differences: Chi² = 2.14, df = 2 (P = 0.34), I² = 6.6%
Mean
-0.34
0.3
-0.974
-0.2
SD
4.72
3.85
4.65
5.4
Total
28
5886
4949
150150
285
Mean
-0.01
-0.4
-0.161
0.4
SD
4.95
3.55
4.85
6.06
Total
25
6994
5656
141141
291
Weight
9.1%
36.8%45.9%
18.7%18.7%
35.4%35.4%
100.0%
IV, Random, 95% CI
-0.33 [-2.94, 2.28]
0.70 [-0.60, 2.00]0.50 [-0.67, 1.66]
-0.81 [-2.63, 1.01]-0.81 [-2.63, 1.01]
-0.60 [-1.92, 0.72]-0.60 [-1.92, 0.72]
-0.14 [-0.92, 0.65]
Experimental Control Mean difference Mean difference
IV, Random, 95% CI
-2 -1 0 1 2Favours [experimental] Favours [control]
Figure 5. Forest plot of body mass index.
review of self-management programs for adults with arthri-tis also showed little effect on empowerment (Nunez, Keller,& Ananian, 2009). In contrast, most studies included in ourreview of empowerment-based diabetes self-management in-terventions reported significant improvement (vs. no effect)in HbAlc levels (52.63% vs. 21.05%), self-efficacy (21.05% vs..00%), and empowerment (31.58% vs. 10.53%). The differen-tial effects between EBSMIs and self-management programswithout empowerment-based intervention are from the em-powerment. According to previously described attributes ofempowerment, this indicates that empowerment-based self-management initiates patients to take responsibility for manag-ing their own conditions, and enhances their problem-solvingskills and self-efficacy, thus resulting in more improvement inself-management efficacy (Aujoulat et al., 2007; Funnell et al.,2007). Accordingly, it is worthy to adopt EBSMIs for patientswith chronic metabolic diseases in clinical practice to achievemore effective disease management.
CONCLUSIONSEvidence from our review indicates that EBSMIs have greaterand longer effects than do traditional education or self-management programs without empowerment-based inter-vention. EBSMIs could be extended to patients with chronicconditions, including metabolic syndrome, needing to self-
manage their diseases. We believe that patients have the po-tential to solve the problems they encounter once they are self-aware of their own problems, know how to seek and utilizethe resources to overcome the obstacles of disease manage-ment, and acquire self-efficacy through the initiation of em-powerment. In other words, patients with one or more chronicconditions who have learned the skills of self-managementthrough the empowerment process are able to prevent acuteexacerbations, reduce disease progression, and promote well-being, thereby decreasing medical costs. All of these will bringsignificant clinical effects.
Patient empowerment requires healthcare professionals tospend more effort and time on building partnerships, helpingpatients to identify their problems or concerns, triggering theirmotivation or self-awareness, helping them with goal settingand action planning, enhancing their abilities to self-managetheir chronic diseases, provide discussion or feedback abouttheir problems and help them to overcome obstacles, and re-flect on changes in their conditions and behaviors—all of whichrepresent a challenge for healthcare professionals. These re-quirements limit the applicability of EBSMIs. Thus, furtherresearch should seek to find ways to overcome limitations oftime, manpower, and cost in the clinical application of EBSMIsin the real world. The integration of technological components,such as Internet-based interaction, may be one way to achievethis goal.
312 Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315.C© 2014 Sigma Theta Tau International

Evidence Review
Study or subgroup
5.1.1 Diabetes Empowerment Scores~6 weeks
Anderson et al. 2005Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.59 (P = 0.55)
5.1.2 Diabetes Empowerment Scores~6 months
Ruggiero et al. 2010
Sigurdardottir et al.2009Subtotal (95% CI)
Heterogeneity: Tau² = 0.07; Chi² = 3.51, df = 1 (P = 0.06); I² = 72%
Test for overall effect: Z = 1.81 (P = 0.07)
5.1.3 Diabetes Empowerment Scores~14 months
Deakin et al. 2006Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 1.13 (P = 0.26)
5.1.4 Diabetes Empowerment Scores~24 months
Anderson et al. 2009Subtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 2.51 (P = 0.01)
Total (95% CI)
Heterogeneity: Tau² = 0.01; Chi² = 7.42, df = 4 (P = 0.12); I² = 46%
Test for overall effect: Z = 2.84 (P = 0.004)
Test for subgroup differences: Chi² = 2.83, df = 3 (P = 0.42), I² = 0%
Mean
0.25
0.61
0.2
0.6
0.28
SD
0.65
0.61
0.61
1.25
0.77
Total
106106
21
2849
100100
119119
374
Mean
0.19
-0.04
0
0.4
0.04
SD
0.73
0.62
0.4
1.2
0.72
Total
8686
19
2544
9191
124124
345
Weight
26.5%26.5%
12.5%
19.1%31.6%
14.2%14.2%
27.6%27.6%
100.0%
IV, Random, 95% CI
0.06 [-0.14, 0.26]0.06 [-0.14, 0.26]
0.65 [0.27, 1.03]
0.20 [-0.08, 0.48]0.40 [-0.03, 0.84]
0.20 [-0.15, 0.55]0.20 [-0.15, 0.55]
0.24 [0.05, 0.43]0.24 [0.05, 0.43]
0.23 [0.07, 0.39]
Experimental Control Mean difference Mean difference
IV, Random, 95% CI
-1 -0.5 0 0.5 1Favours [control] Favours [experimental]
Figure 6. Forest plot of empowerment scores.
In addition, the abstract nature of the concept of empower-ment limits its application. Future qualitative and quantitativeresearch should be conducted to facilitate discussion of themechanism of empowerment and facilitate its application. Re-searchers also need to clearly state operational definitions usedin study protocols to facilitate their clinical application.
This review focused on studies on adult participants receiv-ing the intervention, so the results may not be generalizedto other age population. Accordingly, we suggest the reviewscan be extended to evaluate the effects of EBSMIs on youngor old population groups. Our review also revealed that fewstudies have explored the effectiveness of EBSMIs in chronicmetabolic diseases such as hypertension and obesity; thus, wesuggest the implementation and evaluation of such interven-tions could be extensively conducted for patients with diversechronic conditions.
Findings from our systematic review indicate that interven-tions based on empowerment could help patients self-managetheir chronic conditions and achieve a balanced life. There-
fore, healthcare professionals should integrate empowermentstrategies to help patients self-manage their chronic conditions.WVN
LINKING EVIDENCE TO ACTIONEmpowerment-based self-management interventions
(EBSMIs) include a patient-centered care model emphasiz-ing a collaborative approach to supporting patients’ auton-omy and facilitating patients’ self-directed behavior change.Through EBSMIs, patients improve their ability to iden-tify their own problems related to living with a chroniccondition, to self-regulate behaviors, to seek and utilize re-sources to deal with their problems, and to evaluate theeffectiveness of their actions. Briefly, EBSMIs can enhancepatients’ abilities to control their disease as well as resolvedisease-life conflicts, thereby assisting patients to achievea balanced life. Healthcare professionals should keep the
Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 313C© 2014 Sigma Theta Tau International

Empowerment-Based Self-Management Interventions
following principles in mind to implement EBSMIs in theclinical setting.
� EBSMIs should be based on the philosophy ofpatient-centered approach.
� Healthcare professionals should maintain a part-nership with their patients while implementingEBSMIs.
� The EBSMIs should cover the following cru-cial elements: building partnership, identifyingone’s problems or concerns, self-awareness, self-motivation, goal setting and action planning, uti-lization of resources, communication with health-care professionals, overcoming obstacles, problemsolving, and reflection or review of changes.
� Healthcare leaders should assess and overcomebarriers (e.g., time, manpower, cost, etc.) whenthey want to carry out the EBSMIs in clinical set-tings.
� Healthcare institutions should provide trainingprograms related to empowerment to assist health-care professionals in acquiring competence in pa-tient empowerment.
Author information
Chia-Chi Kuo, Advanced Practice Nurse, Emergency Depart-ment, Chi-Mei Medical Center, and doctoral candidate, Schoolof Nursing, Kaohsiung Medical University, and Assistant Pro-fessor, Department of Nursing, Chang Jung Christian Uni-versity, Tainan, Taiwan; Chiu-Chu Lin, Professor, College ofNursing, Kaohsiung Medical University, Kaohsiung, Taiwan;Fu-Mian Tsai, Lecturer, Department of Nursing, Chung HwaUniversity of Medical Technology & doctoral candidate, Schoolof Nursing, Kaohsiung Medical University, Kaohsiung, Taiwan
Address correspondence to Dr. Chiu-Chu Lin, School of Nurs-ing, Kaohsiung Medical University, No. 100, Shi-Chuan 1stRd., San Ming District, Kaohsiung 80708, Taiwan, ROC; [email protected]
This research received no specific grant from any fundingagency in the public, commercial, or not-for-profit sectors.
Accepted 29 June 2014Copyright C© 2014, Sigma Theta Tau International
ReferencesAnderson, R., & Funnell, M. (2000). Compliance and adherence
are dysfunctional concepts in diabetes care. Diabetes Educator,26(4), 597–604. doi: 10.1177/014572170002600405
Anderson, R. M., & Funnell, M. M. (2005). Patient empower-ment: Reflections on the challenge of fostering the adoption
of a new paradigm. Patient Education Counseling, 57(2), 153–157.doi: 10.1016/j.pec.2004.05.008
Anderson, R. M., & Funnell, M. M. (2010). Patient empowerment:Myths and misconceptions. Patient Education and Counseling,79(3), 277–282. doi: 10.1016/j.pec.2009.07.025
Anderson, R. M., Funnell, M. M., Aikens, J. E., Krein, S. L., Fitzger-ald, J. T., Nwankwo, R., . . . Tang, T. S. (2009). Evaluating theefficacy of an empowerment-based self-management consultantintervention: Results of a two-year randomized controlled trial.Therapy Patient Education, 1(1), 3–11. doi: 10.1051/tpe/2009002
Anderson, R. M., Funnell, M. M., Butler, P. M., Arnold, M. S.,Fitzgerald, J. T., & Feste, C. C. (1995). Patient empowerment.Results of a randomized controlled trial. Diabetes Care, 18(7),943–949. doi: 10.2337/diacare.18.7.943
Anderson, R. M., Funnell, M. M., Nwankwo, R., Gillard, M. L.,Oh, M., & Fitzgerald, J. T. (2005). Evaluating a problem-basedempowerment program for African Americans with diabetes:Results of a randomized controlled trial. Ethnicity & Disease, 15(4),671–678. doi: 10.1051/tpe/2009002
Aujoulat, I., d’Hoore, W., & Deccache, A. (2007). Patientempowerment in theory and practice: Polysemy or ca-cophony? Patient Education and Counseling, 66, 13–20. doi:10.1016/j.pec.2006.09.008
Bodenheimer, T., Lorig, K., Holman, H., & Grumbach, K. (2002).Patient self-management of chronic disease in primary care. TheJournal of the American Medical Association, 288(19), 2469–2475.doi: 10.1001/jama.288.19.2469
Cook, D. J., Mulrow, C. D., & Haynes, R. B. (1997). Systematic re-views: Synthesis of best evidence for clinical decisions. Academiaand Clinic Annals, 126(5), 376–380.
Cooper, H., Booth, K., & Gill, G. (2009). A trial of empowerment-based education in type 2 diabetes—Global rather thanglycaemic benefits. Insulin, 4(1), 61–67. doi: 10.1016/S1557-0843(09)80006-7
Coster, S., & Norman, I. (2009). Cochrane reviews of educationaland self-management interventions to guide nursing practice:A review. International Journal of Nursing Studies, 46, 508–528.doi: 10.1016/j.ijnurstu.2008.09.009
Deakin, T. A., Cade, J. E., Williams, R., & Greenwood, D. C. (2006).Structured patient education: The diabetes X-PERT Programmemakes a difference. Diabetes Medication, 23(9), 944–954. doi:10.1111/j.1464-5491.2006.01906.x
Figar, S., Galarza, C., Petrlik, E., Hornstein, L., Loria, G. R., Wais-man, G., . . . de Quiros, F. G. (2006). Effect of education onblood pressure control in elderly persons: A randomized con-trolled trial. American Journal of Hypertension, 19(7), 737–743.doi: 10.1016/j.amjhyper.2005.10.005
Ford, E. (2005). Risks for all-cause mortality, cardiovascular dis-ease, and diabetes associated with the metabolic syndrome:A summary of the evidence. Diabetes Care, 28(7), 1769–1778.
Forlani, G., Zannoni, C., Tarrini, G., Melchionda, N., & March-esini, G. (2006). An empowerment-based educational programimproves psychological well-being and health-related quality oflife in Type 1 diabetes. Journal Endocrinological Investigation,29(5), 405–412.
Funnell, M., Tang, T., & Anderson, R. (2007). FromDSME to DSMS: developing empowerment-based diabetesself-management support. Diabetes Spectrum, 20(4), 221–226.
314 Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315.C© 2014 Sigma Theta Tau International

Evidence ReviewGrundy, S. M., Brewer, H. B., Cleeman, J. I., Smith, S.
C., & Lenfant, C. (2004a). Definition of metabolic syn-drome: Report of the National Heart, Lung, and Blood In-stitute/American Heart Association conference on scientificissues related to definition. Circulation, 109(3), 433–438. doi:10.1161/01.CIR.0000111245.75752.C6
Grundy, S. M., Hansen, B., Smith, S. C., Cleeman, J. I., & Kahn,R. A. (2004b). Clinical management of metabolic syndrome:Report of the American Heart Association/National Heart, Lung,and Blood Institute/American Diabetes Association Conferenceon scientific issues related to management. Circulation, 109(4),551–556.
Kuo, P. L., Tsay, S. L., & Yang, C. (2002). The effectiveness ofempowerment training on the HbA1c, self-efficacy and self-careamong diabetes patients. Formosan Journal of Medicine, 6(6),848–857.
McCarrier, K. P., Ralston, J. D., Hirsch, I. B., Lewis, G., Mar-tin, D. P., Zimmerman, F. J., & Goldberg, H. I. (2009). Web-based collaborative care for type 1 diabetes: A pilot random-ized trial. Diabetes Technology & Therapeutics, 11(4), 211–217. doi:10.1089/dia.2008.0063
Mayer-Davis, E. J., D’Antonio, A., Martin, M., Wandersman, A.,Parra-Medina, D., & Schulz, R. (2001). Pilot study of strategiesfor effective weight management in type 2 diabetes: Poundsoff with empowerment. Family & Community Health, 24(2), 27–35.
Mayer-Davis, E. J., D’Antonio, A. M., Smith, S. M., Kirkner,G., Levin, M. S., Parra-Medina, D., & Schultz, R. (2004).Pounds off with empowerment (POWER): A clinical trial ofweight management strategies for black and white adults withdiabetes who live in medically underserved rural communi-ties. American Journal of Public Health, 94(10), 1736–1742. doi:10.2105/AJPH.94.10.1736
Naik, A. D., Teal, C. R., Rodriguez, E., & Haidet, P. (2011). Knowingthe ABCs: A comparative effectiveness study of two methods ofdiabetes education. Patient Education and Counseling, 82(1) 1–7.doi: 10.1016/j.pec.2011.01.010
Nunez, D. E., Keller, C., & Ananian, C. D. (2009). A review ofthe efficacy of the self-management model on health outcomesin community-residing older adults with arthritis. Worldviewson Evidence Based Nursing, 6(3), 130–148. doi: 10.1111/j.1741-6787.2009.00157.x
Oremus, M., Wolfson, C., Perrault, A., Demers, L., Momoli, F.,& Moride, Y. (2001). Interrater reliability of the modified Jadadquality scale for systematic reviews of Alzheimer’s disease drug
trials. Dementia and Geriatric Cognitive Disorders, 12(3), 232–236.doi: 10.1159/000051263
Pena-Purcell, N. C., Boggess, M. M., & Jimenez, N. (2011). Anempowerment-based diabetes self-management education pro-gram for Hispanic/Latinos: A quasi-experimental pilot study. Di-abetes Educator, 37(6), 770–779. doi: 10.1177/0145721711423319
Piatt, G. A., Orchard, T. J., Emerson, S., Simmons, D., Songer, T. J.,Brooks, M. M., . . . Zgibor, J. C. (2006). Translating the chroniccare model into the community: Results from a randomizedcontrolled trial of a multifaceted diabetes care intervention. Di-abetes Care, 29(4), 811–817. doi: 10.2337/diacare.29.04.06.dc05-1785
Raimundo, M., & Lopes, J. (2011). Metabolic syndrome, chronickidney disease, and cardiovascular disease: A dynamic and life-threatening triad. Cardiology Research & Practice, 2011, Article ID747861, 1–16. doi: 10.4061/2011/747861
Ruggiero, L., Moadsiri, A., Butler, P., Oros, S., Berbaum, M.,Whitman, S., & Cintron, D. (2010). Supporting diabetesself-care in underserved populations: A randomized pilot studyusing medical assistant coaches. Diabetes Educator, 36(1), 127–131. doi: 10.1177/0145721709355487
Sigurdardottir, A., Benediktsson, R., & Jonsdottir, H. (2009). In-struments to tailor care of people with type 2 diabetes. Jour-nal of Advanced Nursing, 65(10), 2118–2130. doi: 10.1111/j.1365-2648.2009.05040.x
Simmons, D., Gamble, G. D., Foote, S., Cole, D. R., & Coster, G.(2004). The New Zealand diabetes passport study: A randomizedcontrolled trial of the impact of a diabetes passport on risk factorsfor diabetes-related complications. Diabetic Medicine: A Journal ofthe British Diabetic Association, 21(3), 214–217. doi: 10.1111/j.1464-5491.2004.01047.x
Spencer, M. S., Rosland, A., Kieffer, E. C., Sinco, B. R., Valerio, M.,Palmisano, G., . . . Heisler, M. (2011). Effectiveness of a com-munity health worker intervention among African Americanand Latino adults with type 2 diabetes: A randomized controlledtrial. American Journal of Public Health, 101(12), 2253–2260. doi:10.2105/AJPH.2010.300106
Utz, S.W., Williams, I. C., Jones, R., Hinton, I., Alexander, G., Yan,G., . . . Oliver, M. N. (2008). Culturally tailored intervention forrural African Americans with type 2 diabetes. Diabetes Education,34(5), 854–865. doi: 10.1177/0145721708323642
doi 10.1111/wvn.12066WVN 2014;11:301–315
Worldviews on Evidence-Based Nursing, 2014; 11:5, 301–315. 315C© 2014 Sigma Theta Tau International