
Effect of tegaserod in chronic constipation: A randomized, double-blind, controlled trial
12
Effect of Tegaserod in Chronic Constipation: A Randomized, Double-Blind, Controlled Trial JOHN F. JOHANSON, ARNOLD WALD, GERVAIS TOUGAS, WILLIAM D. CHEY, JAMES S. NOVICK, ANTHONY J. LEMBO, FIONA FORDHAM, MARY GUELLA, and BRIGITTE NAULT VOL. 2, NO. 9 September 2004
Transcript of Effect of tegaserod in chronic constipation: A randomized, double-blind, controlled trial

Effect of Tegaserod in Chronic
Constipation: A Randomized,
Double-Blind, Controlled Trial
JOHN F. JOHANSON, ARNOLD WALD, GERVAIS TOUGAS,
WILLIAM D. CHEY, JAMES S. NOVICK, ANTHONY J. LEMBO,
FIONA FORDHAM, MARY GUELLA, and BRIGITTE NAULT
VOL. 2, NO. 9 September 2004

Effect of Tegaserod in Chronic Constipation: A Randomized,Double-Blind, Controlled Trial
JOHN F. JOHANSON,* ARNOLD WALD,‡ GERVAIS TOUGAS,§,� WILLIAM D. CHEY,¶
JAMES S. NOVICK,# ANTHONY J. LEMBO,** FIONA FORDHAM,� MARY GUELLA,‡‡ andBRIGITTE NAULT�
*University of Illinois College of Medicine, Rockford, Illinois; ‡Division of Gastroenterology, Hepatology & Nutrition, University of PittsburghMedical Center, Pittsburgh, Pennsylvania; §Division of Gastroenterology, McMaster University, Intestinal Disease Research Programme,Hamilton, Ontario, Canada; ¶University of Michigan Health System, Ann Arbor, Michigan; #Charm City Research, Towson, Maryland;**Department of Gastroenterology, Beth Israel Deaconess Hospital, Boston, Massachusetts; �Novartis Pharma AG, Basel, Switzerland; and‡‡Novartis Pharmaceuticals Corporation, East Hanover, New Jersey
Background & Aims: Chronic constipation is a commongastrointestinal disorder. The aim of this study was toevaluate the efficacy, safety, and tolerability of tegas-erod, a serotonin subtype 4 receptor partial agonist inpatients with chronic constipation. Methods: This was arandomized, double-blind, placebo-controlled study. Af-ter a 2-week baseline, patients received tegaserod 2 mgtwice daily (n � 450), tegaserod 6 mg twice daily (n �451), or placebo (n � 447) for 12 weeks, followed by a4-week withdrawal period. Responders were those pa-tients having been treated for at least 7 days with anincrease of >1 complete spontaneous bowel move-ment/week vs. baseline during weeks 1–4 (primary vari-able) and weeks 1–12 (secondary variable). Other sec-ondary variables included patient assessment ofconstipation symptoms (number of bowel movements,stool form, abdominal bloating/distention, straining,and abdominal pain/discomfort), and global assess-ment of constipation and bowel habits. Results: Re-sponder rates for complete spontaneous bowel move-ment during weeks 1–4 were significantly greater(P < 0.0001) in the tegaserod 2 mg twice daily (41.4%)and 6 mg twice daily groups (43.2%) vs. placebo(25.1%). This effect was maintained over 12 weeks.Statistically significant improvements over placebo wereobserved across the majority of secondary variables forboth tegaserod doses. No rebound effect was observedafter treatment withdrawal. Tegaserod was well toler-ated; headache and nasopharyngitis, the most frequentadverse events, were more common in the placebogroup than in either tegaserod group. Conclusions: Over12 weeks, tegaserod treatment produced significant im-provements in chronic constipation symptoms and wasalso safe and well tolerated.
Constipation is a common problem. Population-basedstudies indicate that approximately 10%–20% of
otherwise healthy people report 1 or more symptoms ofchronic constipation,1 with some reports in the U.S.suggesting a prevalence rate exceeding 30%.2 Defini-
tions of this disorder vary markedly, likely explainingthe wide variation in prevalence, but generally includeinfrequent passage of stools associated with persistentsymptoms of straining, hard or lumpy stools, and afeeling of incomplete evacuation.3
Constipation is associated with substantial direct andindirect health care costs. In the U.S., the disorder promptsan estimated 2.5 million physician visits per year, with100,000 referrals to gastroenterologists.4 It has been esti-mated that the majority of these visits (85%) result in aprescription for a laxative. Indeed, the annual expenditurefor laxatives in the U.S. is estimated at $800million.4 Thesefigures probably underestimate the true treatment costsassociated with chronic constipation, because individualstypically attempt to treat this persistent condition them-selves before seeking medical attention.
Traditional treatments such as laxatives and dietarymodifications have been primarily directed towards in-creasing gastrointestinal (GI) motility and stool fre-quency. Although such treatment approaches lead toimprovement in stool frequency, they can be associatedwith side effects, including abdominal distention anddiscomfort.5–7 Available data regarding the efficacy oflaxatives and fiber in treating constipation are limited,with many randomized trials using short treatment du-rations.8 There is an unmet medical need for a well-tolerated and effective therapy for patients with chronicconstipation that not only increases bowel frequency butalso relieves the multiple symptoms associated with thedisorder, such as straining, bloating, hard stools, feelings
Abbreviations used in this paper: AEs, adverse events; BM, bowelmovement; CSBM, complete spontaneous bowel movement; ECG,electrocardiogram; GI, gastrointestinal; 5-HT4, serotonin subtype 4receptor; IBS-C, IBS with constipation; ITT, intent-to-treat; SAEs, seriousadverse events; SBM, spontaneous bowel movement.
© 2004 by the American Gastroenterological Association1542-3565/04/$30.00
PII: 10.1053/S1542-3565(04)00356-8
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:796–805

of incomplete evacuation, and abdominal pain/discom-fort.
Tegaserod is a selective agonist at the serotonin sub-type 4 (5-HT4) receptor and has been shown to augmentthe peristaltic reflex, enhance intestinal secretion, andreduce visceral hypersensitivity.9–13 Tegaserod interactswith enteric 5-HT4 receptors, resulting in amplificationof peristaltic and secretory reflexes in response to endog-enous mucosal stimulation.14 Previous studies with te-gaserod have shown enhanced promotile activity in ani-mals,15 healthy volunteers,16–17 and patients sufferingfrom irritable bowel syndrome with constipation (IBS-C).18 Given the known pharmacodynamic actions oftegaserod, and its documented efficacy profile inIBS-C,19–22 the aim of the current study was to assess theefficacy, safety, and tolerability of tegaserod in patientswith chronic constipation.
Materials and MethodsStudy Design
This was a randomized, double-blind, placebo-con-trolled study involving patients with chronic constipationrecruited from 105 centers in North and South America (Ar-gentina, Brazil, Canada, Chile, Colombia, United States, andVenezuela). The study comprised a 2-week baseline periodfollowed by a 12-week treatment period. Patients who com-pleted the treatment period or discontinued from the studyprematurely were encouraged to enter a 4-week withdrawalperiod, during which no medication was taken. During thetreatment phase, patients were randomized to receive eithertablets containing tegaserod 2 mg, tegaserod 6 mg, or placebo,twice daily, within 30 minutes of morning and evening meals.A double-dummy packaging technique was used to mask theslightly different sizes of the 2 and 6 mg tablets. Afterinitiation of therapy, each patient was seen by a study inves-tigator at weeks 4, 8, 12, and 16 to collect and verify diary dataand to assess safety and tolerability.
Randomization was performed using a validated computer-ized system that automated the random assignment of treat-ment groups. All personnel involved remained blinded tostudy medications until the time of unblinding. Drug codeswere broken and data were made available for analysis after thestudy was complete, the data file verified, and protocol viola-tions determined. The study was performed in accordance withthe Declaration of Helsinki and the US 21 Code of FederalRegulations regarding informed patient consent and institu-tional review board approval.
Study Population
Eligible patients were men or women �18 years of agewith a history of constipation of �6 months. Constipation wasdefined as an average of �3 complete spontaneous bowelmovements (CSBM)/week, associated with at least 1 of thefollowing symptoms on �25% of occasions: straining, incom-
plete evacuation, and hard and/or very hard stools. A bowelmovement (BM) was considered to be complete if it wasassociated with a feeling of complete evacuation and sponta-neous if the patient had not used a laxative or undergone anenema within the preceding 24 hours.
Before entering the study, patients answered a questionnairerelated to their constipation symptoms during the preceding 6months. The questions specifically inquired about the durationof constipation, the patient’s main symptoms associated withconstipation, the patient’s use of laxatives and other medica-tions for constipation, the number of spontaneous bowel move-ments (SBM)/week, and the percentage of SBM with hard/veryhard stools, incomplete evacuation, or straining.
Investigators were asked to record relevant medical condi-tions affecting each patient. Patients whose constipation andsymptoms were associated with a known disease of the colon,and those with documented pelvic floor dysfunction, metabolicor neurologic disturbances, or any other disease that couldinterfere with study completion, were excluded from enteringthe study. Individuals who were not constipated during thebaseline period, as well as those experiencing loose or waterystools for �3 days during baseline, those who were not com-pliant with completion of their diary assessments during base-line, and those taking prohibited medication (i.e., drugs af-fecting GI motility) for �2 days during baseline were alsoexcluded from the study.
The use of medications affecting GI motility was not al-lowed during the study; such medications were discontinuedbefore baseline. Patients were instructed to use bisacodyl as arescue medication only if they had not experienced a bowelmovement in the previous 96 hours. Nonpharmacologic ther-apies affecting the GI system (e.g., acupuncture, colonic irri-gation) were not allowed during the study, and patients wereinstructed not to change their lifestyle, diet, or fiber intake.
Efficacy and Safety/TolerabilityAssessments
Throughout the study (including the baseline andwithdrawal periods), patients recorded their symptoms in apaper diary. On a daily basis, they recorded the time of BM (ifany) and associated characteristics (sensation of incompleteevacuation [yes/no], straining, and stool form). Straining wasevaluated using a 3-point scale (no straining/acceptable strain-ing/too much straining). Stool form was assessed using the7-point Bristol Stool Form scale, ranging from 1 (separate hardstools, like nuts) to 7 (watery, unformed stools).23 In addition,patients recorded on a daily basis the intake of other medica-tion and, in the case of laxatives, the time of intake.
On a weekly basis, patients assessed their satisfaction withbowel habits using a 5-point ordinal scale (0 � a great dealsatisfied, 1 � a good deal satisfied, 2 � moderately satisfied,3 � hardly satisfied, 4 � not at all satisfied) and the bother-someness of constipation, abdominal distention/bloating, andabdominal pain/discomfort (each measured using a 5-pointordinal scale in which 0 � not at all bothersome, 1 � hardlybothersome, 2 � moderately bothersome, 3 � a good dealbothersome, 4 � a very great deal bothersome).
September 2004 TEGASEROD IN CHRONIC CONSTIPATION 797

To assess the effect of treatment on quality of life and healthstatus, patients also completed quality of life questionnaires atbaseline, week 4, and week 12. The results of these assessmentswill be presented in a subsequent publication.
All adverse events (AEs) and serious AEs (SAEs), eitherreported by the patient or discovered by the physician follow-ing questioning or by physical examination, were recorded anddescribed by duration, severity, and relationship to studytreatment. Safety evaluations included standard laboratorytests (hematology, biochemistry, and urinalysis), measurementof vital signs, physical examinations, and central evaluation ofelectrocardiogram (ECG) parameters.
Statistical Analysis
The primary efficacy variable was the responder rate forCSBM during the first 4 weeks (weeks 1–4) of double-blindtreatment. Responders were those with a mean increase of �1CSBM/week compared with baseline, provided that they hadcompleted at least 7 days of treatment. Prospectively plannedsecondary efficacy variables included the responder rate forCSBM during the whole 12 weeks of active treatment (weeks1–12), and at each weekly time point in the study; the changefrom baseline in mean number of CSBM, SBM, and BM overweeks 1–4, weeks 1–12, and at each weekly time point;weekly evaluations of individual constipation symptoms; daysof laxative intake; and median time to first CSBM and SBM. Inaddition, the percentages of patients with �3 CSBM/weekduring weeks 1–4 and weeks 1–12, and �7 days of treatmentwere determined for each treatment group. The percentageimprovement from baseline in mean number of CSBM, SBM,and BM per week was calculated in a post-hoc analysis.
Sample size calculations were performed using the nQueryAdvisor software (Statistical Solutions, Saugus, MA), based onthe primary efficacy variable. Assuming a response rate of 30%in the placebo group and 42% in at least 1 of the tegaserodgroups, it was calculated that 395 patients per treatment armwould be sufficient to achieve 90% power in detecting atreatment difference based on a 2-sided �2 test without con-tinuity correction at a significance level of 0.025 (0.025 wasused to maintain the overall significance level at 5% whenusing the Hochberg correction for multiple testing).
Efficacy analyses were performed using the intent-to-treat(ITT) population, defined as all randomized patients, irrespec-tive of whether or not they actually took study medication.Safety/tolerability analyses were conducted using data onlyfrom randomized patients who received �1 dose of studymedication (safety population).
The CSBM responder rates (those with an increase of �1CSBM/week compared with baseline) and the percentage ofpatients with �3 CSBM/week during weeks 1–4 and weeks1–12 were analyzed using logistic regression models adjustingfor center, gender, and baseline number of CSBM/week. Be-cause each dose of tegaserod was compared with placebo sep-arately in these analyses, the Hochberg adjustment for multi-ple comparisons was used to assess the statistical significance ofthese multiple tests, although the P values presented here arethe nominal (unadjusted) P values. Analyses of time to CSBM
and SBM were performed using survival analysis methods,censoring patients at the end of treatment. Estimates for thesevariables derive from Kaplan–Meier survival curves, and Pvalues derive from log-rank tests. Analyses of the other sec-ondary efficacy variables were performed weekly and overweeks 1–4 and weeks 1–12 using van Elteren tests, stratifiedby center. In these cases, values for each patient over the periodof interest were summarized by the mean over the period,normalized to a 7-day period.
Results
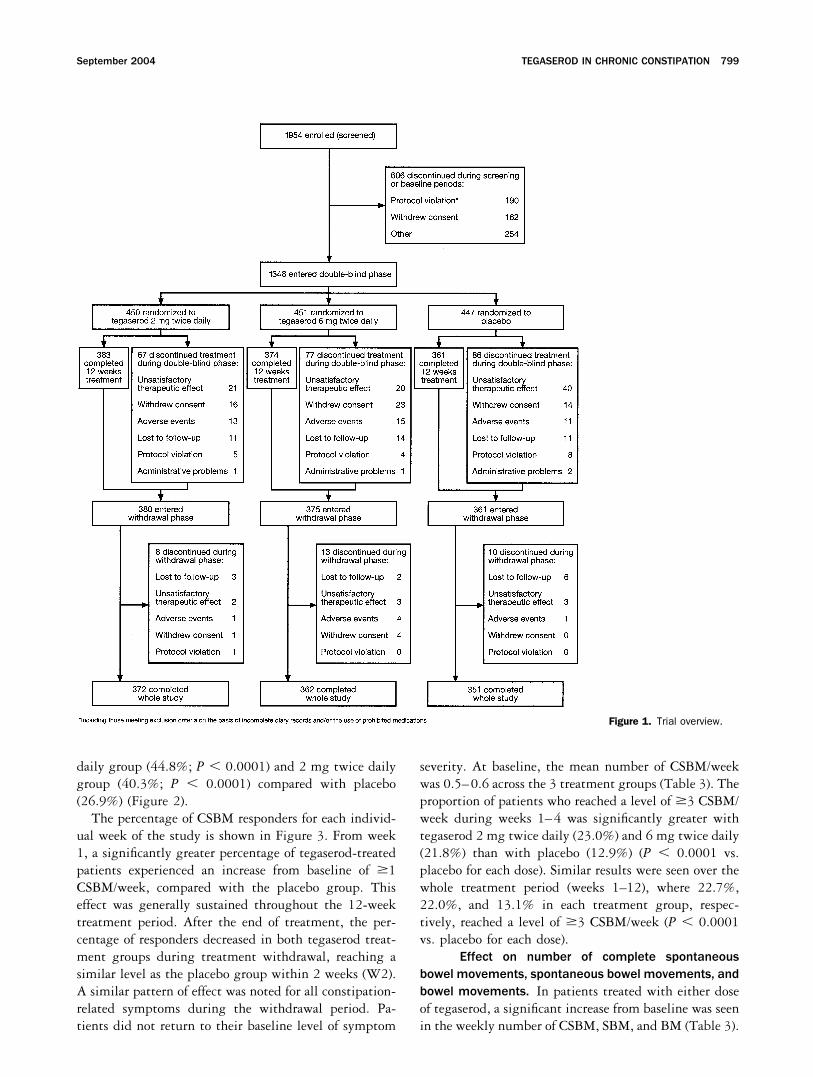
A total of 1954 patients were screened, and ofthese, 1348 were randomized to receive treatment withtegaserod 2 mg twice daily (n � 450), tegaserod 6 mgtwice daily (n � 451), or placebo (n � 447) (Figure 1).Overall, 82.9% completed the double-blind treatmentphase and 97.2% completed the withdrawal period.
Patient Demographics and History ofConstipation Symptoms
Patient demographics were similar across the 3treatment groups (Table 1). The majority of patientswere women and Caucasian, with a mean age of approx-imately 47 years. Patients were chronically constipated,as the mean duration of constipation before study entrywas approximately 19 years (Table 2). Symptoms ofconstipation and the use of laxatives (based on the 6months before study entry) were also comparable amongthe treatment groups. Abdominal bloating/distentionand infrequent defecation were the main complaints. Aprevious medical history of IBS was reported in 4.2% ofrandomized patients.
Effect of Tegaserod on Frequency of BowelMovements
Tegaserod treatment resulted in a marked effecton the frequency of BM, as assessed by a number ofefficacy parameters.
Complete spontaneous bowel movement re-sponder rate. The percentage of patients who experi-enced an increase from baseline of �1 CSBM/week dur-ing the first 4 weeks of treatment (primary efficacyvariable) was significantly higher in both tegaserodgroups compared with placebo (P � 0.0001 for bothdoses; Figure 2). In the tegaserod 6 mg twice dailygroup, 43.2% were responders, compared with 41.4%and 25.1% in the tegaserod 2 mg twice daily and placebogroups, respectively. This effect was maintained over theentire treatment period (i.e., during weeks 1–12) with asignificantly higher responder rate in the tegaserod 6 mgtwice
798 JOHANSON ET AL. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 2, No. 9
daily group (44.8%; P � 0.0001) and 2 mg twice dailygroup (40.3%; P � 0.0001) compared with placebo(26.9%) (Figure 2).
The percentage of CSBM responders for each individ-ual week of the study is shown in Figure 3. From week1, a significantly greater percentage of tegaserod-treatedpatients experienced an increase from baseline of �1CSBM/week, compared with the placebo group. Thiseffect was generally sustained throughout the 12-weektreatment period. After the end of treatment, the per-centage of responders decreased in both tegaserod treat-ment groups during treatment withdrawal, reaching asimilar level as the placebo group within 2 weeks (W2).A similar pattern of effect was noted for all constipation-related symptoms during the withdrawal period. Pa-tients did not return to their baseline level of symptom
severity. At baseline, the mean number of CSBM/weekwas 0.5–0.6 across the 3 treatment groups (Table 3). Theproportion of patients who reached a level of �3 CSBM/week during weeks 1–4 was significantly greater withtegaserod 2 mg twice daily (23.0%) and 6 mg twice daily(21.8%) than with placebo (12.9%) (P � 0.0001 vs.placebo for each dose). Similar results were seen over thewhole treatment period (weeks 1–12), where 22.7%,22.0%, and 13.1% in each treatment group, respec-tively, reached a level of �3 CSBM/week (P � 0.0001vs. placebo for each dose).
Effect on number of complete spontaneousbowel movements, spontaneous bowel movements, andbowel movements. In patients treated with either doseof tegaserod, a significant increase from baseline was seenin the weekly number of CSBM, SBM, and BM (Table 3).
Figure 1. Trial overview.
September 2004 TEGASEROD IN CHRONIC CONSTIPATION 799
Onset of action. The median time to first CSBM(� 95% confidence intervals) was significantly shorter inpatients treated with tegaserod 6 mg twice daily (73 � 45hours; P � 0.0001) and 2 mg twice daily (117 � 66 hours;P � 0.01) than in the placebo group (229 � 123 hours).
Patients receiving tegaserod also experienced their firstSBM significantly faster than patients receiving placebo(Figure 4). As with CSBM, the 95% confidence intervalwidths were much smaller in the tegaserod groups (ap-proximately 3.5 hours in both tegaserod groups) than inthe placebo group (approximately 15 hours).
Effect of Tegaserod on Other Aspects ofBowel Function
Tegaserod not only significantly improved thefrequency of BM, but also the quality of BM, as assessedby secondary efficacy variables. Significant differences infavor of both doses of tegaserod were seen across themajority of these variables during the study (Table 4). Ingeneral, changes from baseline were slightly greater withthe 6 mg twice daily dose compared with the 2 mg twicedaily dose.
Laxative Use
At baseline, the use of rescue laxatives (meannumber of days/week) was comparable across the 2 mgtwice daily group (0.6 days/week), 6 mg twice dailygroup (0.6 days/week), and the placebo group (0.6 days/week). During the double-blind treatment period, use oflaxatives decreased compared with baseline (to 0.3 days/week, 0.4 days/week, and 0.4 days/week, respectively).Although a greater reduction in laxative use was seen inthe tegaserod 2 mg twice daily group, the difference wasnot significantly different from placebo.
Safety and Tolerability
Overall, 62.0% of patients in the safety popula-tion reported �1 AE during the 12-week treatmentperiod (61.2%, 62.2%, and 62.6% in the tegaserod 2 mgtwice daily group, 6 mg twice daily group, and placebogroup, respectively). The most frequently reported AEsin the tegaserod 2 and 6 mg twice daily groups wereheadache (9.2% and 9.8%, respectively) and nasophar-yngitis (7.6% and 8.4%, respectively), both of whichoccurred more frequently with placebo (12.8% and
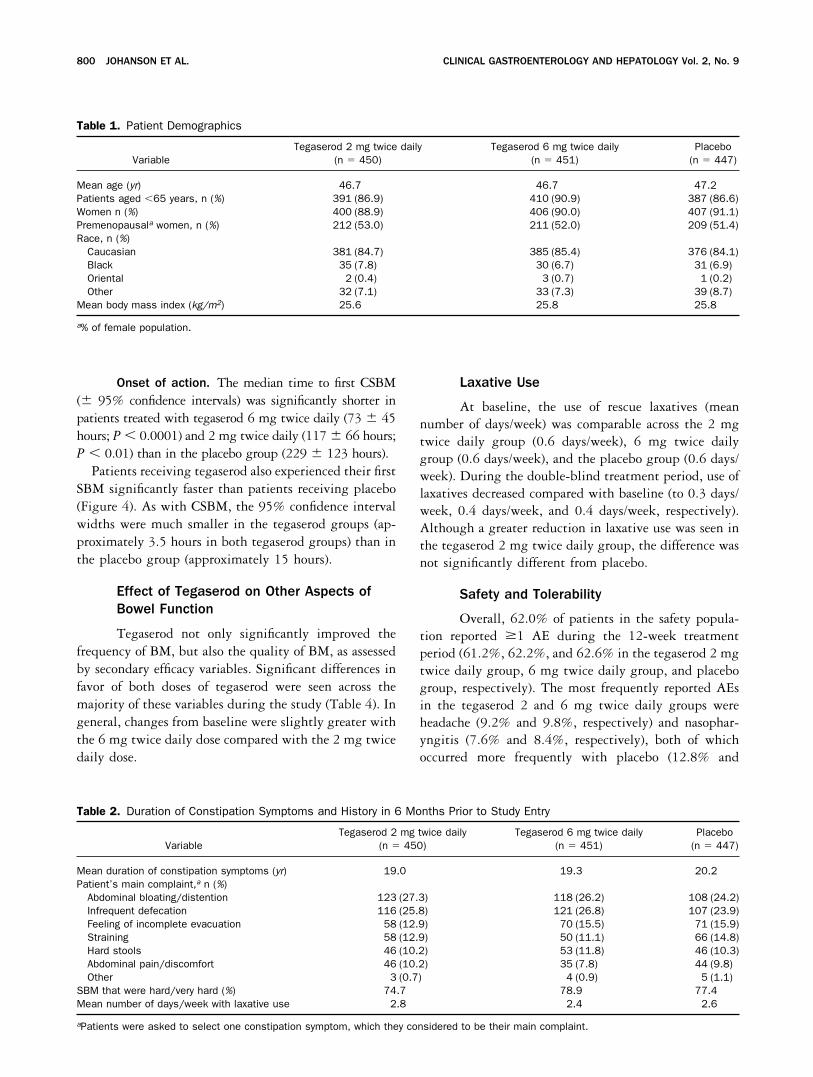
Table 1. Patient Demographics
VariableTegaserod 2 mg twice daily
(n � 450)Tegaserod 6 mg twice daily
(n � 451)Placebo(n � 447)
Mean age (yr) 46.7 46.7 47.2Patients aged �65 years, n (%) 391 (86.9) 410 (90.9) 387 (86.6)Women n (%) 400 (88.9) 406 (90.0) 407 (91.1)Premenopausala women, n (%) 212 (53.0) 211 (52.0) 209 (51.4)Race, n (%)Caucasian 381 (84.7) 385 (85.4) 376 (84.1)Black 35 (7.8) 30 (6.7) 31 (6.9)Oriental 2 (0.4) 3 (0.7) 1 (0.2)Other 32 (7.1) 33 (7.3) 39 (8.7)
Mean body mass index (kg/m2) 25.6 25.8 25.8
a% of female population.
Table 2. Duration of Constipation Symptoms and History in 6 Months Prior to Study Entry
VariableTegaserod 2 mg twice daily
(n � 450)Tegaserod 6 mg twice daily
(n � 451)Placebo(n � 447)
Mean duration of constipation symptoms (yr) 19.0 19.3 20.2Patient’s main complaint,a n (%)Abdominal bloating/distention 123 (27.3) 118 (26.2) 108 (24.2)Infrequent defecation 116 (25.8) 121 (26.8) 107 (23.9)Feeling of incomplete evacuation 58 (12.9) 70 (15.5) 71 (15.9)Straining 58 (12.9) 50 (11.1) 66 (14.8)Hard stools 46 (10.2) 53 (11.8) 46 (10.3)Abdominal pain/discomfort 46 (10.2) 35 (7.8) 44 (9.8)Other 3 (0.7) 4 (0.9) 5 (1.1)
SBM that were hard/very hard (%) 74.7 78.9 77.4Mean number of days/week with laxative use 2.8 2.4 2.6
aPatients were asked to select one constipation symptom, which they considered to be their main complaint.
800 JOHANSON ET AL. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 2, No. 9

10.8%, respectively). Diarrhea was more common integaserod 2 and 6 mg twice daily groups (4.5% and7.3%, respectively) than in the placebo group (3.8%). Ingeneral, episodes of diarrhea were of mild to moderateseverity, occurred early (median of 5.5 days after the startof tegaserod 6 mg twice daily treatment), did not requiretreatment with antidiarrheal drugs, and in the majorityof cases (86.1% in the 6 mg twice daily group), occurredonly once during the study. The median duration ofdiarrhea in all treatment groups was 2.0 days. Tegaserodtreatment did not result in any cases of electrolyte im-balance.
The percentage of patients who discontinued treat-ment due to AEs was similar across all 3 treatmentgroups (3.1%, 3.8%, and 2.5% for tegaserod 2 mg twicedaily, 6 mg twice daily, and placebo, respectively). In-dividual AEs leading to discontinuation were also similaracross treatment groups with the exception of diarrhea(0.4%, 0.9%, and 0% for tegaserod 2 mg twice daily, 6mg twice daily, and placebo, respectively) and abdominalpain (1.1%, 0%, and 0%, respectively). SAEs were re-ported for 13 patients (1.0% overall; 4 patients in each ofthe tegaserod groups and 5 in the placebo group) duringthe double-blind phase, none of which were deemed bythe investigators as being related to study treatment.There were no clinically relevant changes observed in anyof the treatment groups for hematology, biochemistry,urinalysis, vital signs, or ECG parameters. No deathsoccurred during the study.
AEs reported during the withdrawal period were sim-ilar among the 3 groups (15.8%, 20.8%, and 20.2% ofpatients in the tegaserod 2 mg twice daily, 6 mg twicedaily, and placebo groups, respectively), with no evi-dence of a rebound effect. Seven patients (0.6% overall)experienced SAEs during the withdrawal period, none ofwhich were suspected by the investigators to be relatedto study treatment.
DiscussionThe results of this large multinational, random-
ized, double-blind, placebo-controlled study show thattegaserod, a selective, partial agonist at the 5-HT4 re-ceptor, is an effective and well-tolerated treatment forpatients with chronic constipation. This prospectivestudy demonstrates an effective treatment for chronicconstipation over 12 weeks.
Although chronic constipation is associated with awide spectrum of persistent symptoms, infrequent BMare generally viewed as a defining and clinically sig-nificant symptom.3,7 This study evaluated the effectsof tegaserod treatment on the frequency of BM byassessing the weekly number of CSBM, SBM, and BM.The primary efficacy variable (percentage of patientsreporting an increase of �1 CSBM/week over baselineduring the first 4 weeks of treatment) is a reliable andobjective measure of bowel frequency that has beenused in investigational studies of prucalopride inchronic constipation.24 The definition of CSBM usedin this study combines a subjective measure of BMassociated with a sense of complete evacuation with anobjective measure of the number of BM, thereby iden-tifying BM that relieve symptoms caused by chronicconstipation.25 By excluding BM that were producedby the patient taking laxatives or undergoing enemas,the primary endpoint accurately reflected the effect oftegaserod on bowel frequency and facilitated the anal-ysis of multiple constipation symptoms in a singlemeasure.
Results for the primary efficacy variable significantlyfavored both doses of tegaserod over placebo, and thiseffect was sustained over the entire study duration. Te-gaserod demonstrated a rapid and predictable effect onbowel function, with patients experiencing their firstCSBM and SBM significantly faster than placebo pa-
Figure 2. Complete spontaneous bowel movement responder ratesduring weeks 1–4 (primary efficacy variable) and weeks 1–12.
Figure 3. Weekly responder rate throughout the study.
September 2004 TEGASEROD IN CHRONIC CONSTIPATION 801

tients. The widths of 95% confidence intervals for me-dian time to first CSBM were narrower in the tegaserodgroups, particularly 6 mg twice daily, than in the pla-cebo group, suggesting that the occurrence of first CSBMwas also less variable. A similar trend was seen for timeto first SBM.
For patients with chronic constipation, who on aver-age experience only 0.5 CSBM/week, an increase of �1CSBM from baseline represents a clinically significantimprovement.26,27 However, it may be argued that pa-tients having �3 CSBMs/week are still constipated andresponse should therefore be defined as an increase to �3CSBM/week. Even when this more stringent definitionwas examined, tegaserod remained significantly superior(P � 0.0001) to placebo during the first 4 weeks oftreatment and over the entire study duration.
A large proportion of patients with chronic constipa-tion also complain of symptoms such as bloating, strain-ing, and abdominal pain/discomfort, and report passinghard stools. Indeed, in this study abdominal bloating/distention was the main complaint reported by patientsin the 6 months before study entry. Statistically signif-icant improvements (P � 0.05) were seen for both dosesof tegaserod over placebo across the majority of symp-toms assessed, supporting the results of the primaryefficacy variable.
As expected from the findings of previous clinicalstudies in patients with IBS-C,19–22 tegaserod also
showed a beneficial effect on abdominal bloating/disten-tion and abdominal pain/discomfort. Only 125 patients(9.3%) reported abdominal pain as their main symptomcomplaint during the 6 months before study entry. Be-cause abdominal pain is a feature of IBS, this small groupof patients may include those with IBS as well as thosereporting some form of abdominal pain at baseline.20 Avery small proportion of enrolled patients were alsoknown to have a prior or current history of formallydiagnosed IBS (56/1348, 4.2%). If all patients selectingabdominal pain as their main complaint at baseline hadundiagnosed IBS, the overall number of patients withIBS would, at most, still be a minority (181 patients, or13.4% of the population at baseline, assuming no overlapof patients).
Stool form and straining were improved, as were sat-isfaction with bowel habits and overall bothersomeness ofconstipation. Furthermore, the proportion of patientsreporting a sense of complete evacuation with a BM wassignificantly higher in the tegaserod groups comparedwith placebo.
A 4-week withdrawal period, during which patientsdid not take any study medication, assessed whethercessation of tegaserod treatment would cause a reboundeffect (i.e., symptoms becoming worse or more severethan when the patient entered the study). Consistentwith the findings from a similarly designed study inpatients with IBS-C,21 symptoms did not return to theirbaseline level of severity during treatment withdrawaland were comparable in severity to those seen in theplacebo group within 2 weeks.
The ability of tegaserod to improve the multiplesymptoms of chronic constipation was expected, based onthe pharmacodynamic profile of this agent, the findingsof early mechanistic studies,9–11 and the results of severalstudies in patients with IBS-C.19–22 These effects in-clude augmentation of peristaltic motor activitythroughout the GI tract and increased intestinal secre-tion,11,16–18 both of which are important targets in theeffective management of chronic constipation.
Traditionally, laxatives have been the primary ap-proach to the treatment of chronic constipation, despiteFigure 4. Time to first spontaneous bowel movement.
Table 3. Effect of Tegaserod on Bowel Frequency From Baseline to Weeks 1–12
Variable Mean (� SD)
Tegaserod 2 mg twice daily(n � 437)
Tegaserod 6 mg twice daily(n � 440)
Placebo(n � 431)
Baseline Weeks 1–12 Baseline Weeks 1–12 Baseline Weeks 1–12
Number of CSBM/week 0.5 (� 0.8) 1.9a (� 2.3) 0.6 (� 0.8) 1.9a (� 2.1) 0.6 (� 0.9) 1.3 (� 1.7)Number of SBM/week 3.6 (� 3.3) 5.5a (� 4.0) 3.5 (� 3.4) 5.4a (� 3.8) 3.7 (� 3.3) 4.6 (� 3.2)Number of BM/week 4.6 (� 3.2) 6.2a (� 3.7) 4.7 (� 3.2) 6.1a (� 3.5) 4.7 (� 3.1) 5.4 (� 3.0)
NOTE. Patients with data available at baseline and at least 1 of the 12 weeks during the treatment period.aChange from baseline statistically significant vs. placebo (P � 0.0001).
802 JOHANSON ET AL. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 2, No. 9

the fact that a meta-analysis has shown they do notdemonstrate efficacy beyond 4 weeks.28 It is thereforeimportant to recognize that treatment with tegaserodresulted in sustained improvement across all the keysymptoms of constipation over the entire 12-week treat-ment period.
In addition to being effective in relieving the multiplesymptoms of chronic constipation, tegaserod was safe andwell tolerated. The most frequently reported AEs wereheadache and nasopharyngitis, both of which occurredmore frequently with placebo than tegaserod. Diarrheaoccurred more frequently with tegaserod than with pla-cebo, likely representing an enhanced physiologic re-sponse to treatment. In general, however, diarrhea wasmild, transient (typically occurring a few days after ini-tiation of treatment and resolving after approximately 2days), and self-limited. Only 0.4% and 0.9% of patientstreated with tegaserod 2 mg twice daily and 6 mg twicedaily, respectively, were discontinued from the studybecause of diarrhea. Treatment with tegaserod did notresult in electrolyte imbalance, an abnormality whichmay be associated with the frequent use of osmoticlaxatives.6
In conclusion, this prospective study shows that tega-serod provides rapid, predictable, and consistent relief ofthe persistent symptoms of chronic constipation, includ-ing BM, straining, incomplete evacuation, hard/lumpystools, abdominal bloating/distention, and abdominalpain/discomfort. Significant benefits over placebo weredemonstrated during the first week of treatment andwere generally maintained throughout the 12-weektreatment period. Tegaserod was also safe and well tol-erated in this population.
References1. Talley NJ, Jones M, Nuyts G, Dubois D. Risk factors for chronic
constipation based on a general practice sample. Am J Gastro-enterol 2003;98:1107–1111.
2. Talley NJ, Weaver AL, Zinsmeister AR, Melton III LJ. Functionalconstipation and outlet delay: a population-based study. Gastro-enterology 1993;105:781–790.
3. Thompson WG, Longstreth GF, Drossman DA, Heaton KW, IrvineEJ, Müller-Lissner SA. Functional bowel disorders and functionalabdominal pain. Gut 1999;45(suppl II):43–47.
4. Faigel DO. A clinical approach to constipation. Clin Cornerstone2002;4:11–21.
5. Heaton KW, Cripps HA. Straining at stool and laxative taking in anEnglish population. Dig Dis Sci 1993;38:1004–1008.
6. Gattuso JM, Kamm MA. Adverse effects of drugs used in
Table 4. Effect of Tegaserod on Secondary Efficacy Variables (Weeks 1–12)
Variable Mean (� SD)
Tegaserod 2 mg twice daily Tegaserod 6 mg twice daily Placebo
Baseline Weeks 1–12 Baseline Weeks 1–12 Baseline Weeks 1–12
Daily straining score ofSBMa
1.3 (� 0.5) 0.9i (� 0.4) 1.3 (� 0.5) 0.9i (� 0.4) 1.2 (� 0.5) 1.1 (� 0.4)
Number of days/weekwith too muchstrainingb
1.3 (� 1.2) 0.9 (� 1.0) 1.3 (� 1.2) 0.8 (� 0.9) 1.3 (� 1.3) 1.1 (� 1.1)
Percentage of SBMwith a sensation ofcompleteevacuationc
17.6 (� 24.3) 34.6i (� 29.0) 18.1 (� 23.8) 35.7i (� 27.3) 18.1 (� 23.6) 28.5 (� 27.0)
Stool form score ofSBMd
2.9 (� 1.2) 3.5i (�1.1) 2.9 (� 1.2) 3.7i (� 1.0) 2.8 (� 1.2) 3.2 (� 1.1)
Satisfaction with bowelhabit scoree
3.1 (� 0.8) 2.3i (� 0.9) 3.1 (� 0.8) 2.3i (� 0.9) 3.0 (� 0.9) 2.6 (� 0.9)
Bothersomeness ofconstipation scoref
2.7 (� 0.8) 2.1i (� 0.9) 2.8 (� 0.9) 2.1i (� 0.9) 2.7 (� 0.9) 2.3 (� 0.9)
Bothersomeness ofabdominal bloating/distention scoreg
2.7 (� 0.9) 2.0i (� 0.9) 2.7 (� 1.0) 2.1 (� 0.9) 2.7 (� 1.0) 2.3 (� 0.9)
Bothersomeness ofabdominal pain/discomfort scoreh
2.3 (� 1.0) 1.8i (� 0.9) 2.2 (� 1.1) 1.8i (� 0.9) 2.3 (� 1.1) 2.0 (� 0.9)
NOTE. Patients with data available at baseline and for at least 1 week during the treatment period.an � 401, 378, 390 for tegaserod 2 mg twice daily, 6 mg twice daily, and placebo, respectively.bn � 437, 440, 431 for tegaserod 2 mg twice daily, 6 mg twice daily, and placebo, respectively.cn � 402, 378, 390 for tegaserod 2 mg twice daily, 6 mg twice daily, and placebo, respectively.dn � 400, 378, 390 for tegaserod 2 mg twice daily, 6 mg twice daily, and placebo, respectively.en � 423, 424, 418 for tegaserod 2 mg twice daily, 6 mg twice daily, and placebo, respectively.fn � 422, 424, 416 for tegaserod 2 mg twice daily, 6 mg twice daily, and placebo, respectively.gn � 422, 424, 416 for tegaserod 2 mg twice daily, 6 mg twice daily, and placebo, respectively.hn � 422, 423, 416 for tegaserod 2 mg twice daily, 6 mg twice daily, and placebo, respectively.iChange from baseline statistically significant vs. placebo (P � 0.05).
September 2004 TEGASEROD IN CHRONIC CONSTIPATION 803

the management of constipation and diarrhoea. Drug Saf1994;10:47–65.
7. Lembo A, Camilleri M. Chronic constipation. N Engl J Med2003;349:1360–1368.
8. Tramonte SM, Brand MB, Mulrow CD, Amato MG, O’Keefe ME,Ramirez G. The treatment of chronic constipation in adults. Asystematic review. J Gen Intern Med 1997;12:15–24.
9. Grider JR, Foxx-Orenstein AE, Jin JG. 5-Hydroxytryptamine(4) re-ceptor agonists initiate the peristaltic reflex in human, rat, andguinea pig intestine. Gastroenterology 1998;115:370–380.
10. Jin JG, Foxx-Orenstein AE, Grider JR. Propulsion in guinea pigcolon induced by 5-hydroxytryptamine (HT) via 5-HT4 and5-HT3 receptors. J Pharmacol Exp Ther 1999;288:93–97.
11. Stoner MC, Arcuni JC, John JL, Kellum M. A selective 5-HT4receptor agonist induces cAMP-mediated Cl� efflux from ratcolonocytes (abstr). Gastroenterology 1999;116:G287.
12. Schikowski A, Thewissen M, Mathis C, Ross H-G, Enck P. Sero-tonin type-4 receptors modulate the sensitivity of intramuralmechanoreceptive afferents of the cat rectum. Neurogastroen-terol Motil 2002;14:221–227.
13. Coffin B, Farmachidi JP, Rueegg P, Bastie A, Bouhassira D.Tegaserod, a 5-HT4 receptor partial agonist, decreases sensitiv-ity to rectal distension in healthy subjects. Aliment PharmacolTher 2003;17:577–585.
14. Gershon MD. Serotonin and its implication for the managementof irritable bowel syndrome. Rev Gastroenterol Disord 2003;3(suppl 2):S25–S34.
15. Nguyen A, Camilleri M, Kost LJ, Metzger A, Sarr MG, Hanson RB,Fett SL, Zinsmeister AR. SDZ HTF 919 stimulates canine co-lonic motility and transit in vivo. J Pharmacol Exp Ther1997;280:1270–1276.
16. Degen L, Matzinger D, Merz M, Appel-Dingemanse S, OsborneS, Luchinger S, Bertold R, Maecke H, Beglinger C. Tegaserod,a 5-HT4 receptor partial agonist, accelerates gastric emptyingand gastrointestinal transit in healthy male subjects. AlimentPharmacol Ther 2001;15:1745–1751.
17. Appel-Dingemanse S. Clinical pharmacokinetics of tegaserod,a serotonin 5-HT(4) receptor partial agonist with promotileactivity. Clin Pharmacokinet 2002;41:1021–1042.
18. Prather CM, Camilleri M, Zinsmeister AR, McKinzie S, ThomfordeG. Tegaserod accelerates orocecal transit in patients with con-stipation-predominant irritable bowel syndrome. Gastroenterol-ogy 2000;118:463–468.
19. Lefkowitz M, Shi Y, Schmitt C, Krumholz S, Tanghe J. The 5-HT4partial agonist, tegaserod, improves abdominal discomfort/painand normalizes altered bowel function in irritable bowel syn-drome. Am J Gastroenterol 1999;94:266.
20. Müller-Lissner SA, Fumagalli I, Bardhan KD, Pace F, Pecher E,Nault B, Rueegg P. Tegaserod, a 5-HT(4) receptor partial agonist,relieves symptoms in irritable bowel syndrome patients with ab-dominal pain, bloating and constipation. Aliment Pharmacol Ther2001;15:1655–1666.
21. Novick J, Miner P, Krause R, Glebas K, Bliesath H, Ligozio G,Rüegg P, Lefkowitz M. A randomized, double-blind, placebo-con-trolled trial of tegaserod in female patients suffering from irritablebowel syndrome with constipation. Aliment Pharmacol Ther2002;16:1877–1888.
22. Kellow J, Lee OY, Chang FY, Thongsawat S, Mazlam MZ, Yuen H,Gwee K, Bak YT, Jones J, Wagner A. An Asia-Pacific, double blind,placebo controlled, randomised study to evaluate the efficacy,safety, and tolerability of tegaserod in patients with irritablebowel syndrome. Gut 2003;52:671–676.
23. Lewis SJ, Heaton KW. Stool form scale as a useful guide tointestinal transit time. Scand J Gastroenterol 1997;32:920–924.
24. Sloots CE, Poen AC, Kerstens R, Stevens M, De Pauw M, VanOene JC, Meuwissen SG, Felt-Bersma RJ. Effects of prucaloprideon colonic transit, anorectal function and bowel habits in
patients with chronic constipation. Aliment Pharmacol Ther2002;16:759–767.
25. Stewart WF, Liberman JN, Sandler RS, Woods MS, Stemhagen A,Chee E, Lipton RB, Farup CE. Epidemiology of constipation(EPOC) study in the United States: relation of clinical subtypes tosociodemographic features. Am J Gastroenterol 1999;94:3530–3540.
26. Sandler RS, Drossman DA. Bowel habits in young adults notseeking health care. Dig Dis Sci 1987;32:841–845.
27. Pare P, Ferrazzi S, Thompson WG, Irvine EJ, Rance L. An epide-miological survey of constipation in Canada: definitions, rates,demographics, and predictors of health care seeking. Am J Gas-troenterol 2001;96:3130–3137.
28. Jones MP, Talley NJ, Nuyts G, Dubois D. Lack of objective evi-dence of efficacy of laxatives in chronic constipation. Dig Dis Sci2002;47:2222–2230.
Address requests for reprints to: Brigitte Nault, Clinical ResearchManager, Novartis Pharma AG, Basel, Switzerland CH-4002. e-mail:[email protected]; fax: (41) 61-324-9249.This research was funded by Novartis Pharma AG.John F. Johanson has been a paid consultant for Novartis Pharma,
Sucampo Pharmaceuticals, and GlaxoSmithKline. He is also a mem-ber of the Speakers Bureau for Novartis Pharma.Arnold Wald has received research support, is a member of the
Speakers Bureau, and has been a paid consultant to Novartis Pharma,GlaxoSmithKline, Solvay, Johnson and Johnson, and Boehringer In-gelheim.Gervais Tougas has received research support, has been a member
of the Speakers Bureau, and has been a paid consultant for AstraZen-eca, Novartis Pharma, Janssen-Ortho, Johnson and Johnson, Solvay,Takeda, Merck, SK Pharmaceuticals, and Dynogen Pharmaceuticals.Dr. Tougas is now an employee of Novartis Pharma.William Chey has been a paid consultant for Novartis Pharma,
GlaxoSmithKline, Solvay, and Janssen. He has received research sup-port from Vela and Janssen, and honoraria from Novartis Pharma andGlaxoSmithKline. He is a member of the Speakers Bureau for NovartisPharma.James Novick has been a paid consultant for Novartis Pharma, and
he is a member of the Speakers Bureau for Novartis Pharma.Anthony Lembo has been a paid consultant for Novartis Pharma and
GlaxoSmithKline, and he is a member of the Speakers Bureau forNovartis Pharma.Fiona Fordham, Mary Guella, and Brigitte Nault are employees of
Novartis Pharma.The authors thank the following investigators for their involvement
in conducting this study: Argentina: Alfredo Curras, Policlínica Ban-caria, Buenos Aires; Juan A. De Paula, Hospital Italiano, Buenos Aires;Jose Carlos German, Fundación Rusculleda, Cordoba; Guido Iantorno,Hospital Udaondo, Buenos Aires; Rodolfo Pedrana, Hospital de Clíni-cas, Buenos Aires. Brazil: Eduardo A. Andre, Hosp. Servidor PúblicoEstadual de São Paulo, São Paulo; Ricardo Aires Correa, HospitalUniversitário Walter Cantidio, Fortaleza; Carlos F. Francisconi, Hospitaldas Clínicas da Universidade Federal do Rio Grande do Sul, PortoAlegre; Jose Alves Freitas, Faculdade de Medicina de Catanduva,Hospital Emílio Carlos, Catanduva; Helio Moreira Jr., Hospital Univer-sitário, Goiânia. Canada: Jack Amar, St-Paul’s Hospital, Vancouver;Jeffrey Axler, Toronto Digestive Disease Associates, Downsview;Charles Bernstein, Health Science Centre, Winnipeg; Michel Boivin,Hôpital Saint-Luc du CHUM, Montréal; Ronald Ford Bursey, HealthScience Centre, St-Johns; Naoki Chiba, Surrey GI Research, Guelph;Lawrence Cohen, North Toronto GI Associates, Toronto; Richard Fe-dorak, GILDR Group, Edmonton; Robert Hilsden, Health Sciences Cen-tre, University of Calgary, Calgary; Pierre Pare, Hopital St-Sacrement,Quebec; Gervais Tougas, McMaster University Medical Centre, Hamil-ton; Geoffrey Turnbull, Queen Elizabeth II HSC, Halifax; Stephen Van-ner, Hotel Dieu Hospital, Kingston; Alain Watier, Centre de Recherche
804 JOHANSON ET AL. CLINICAL GASTROENTEROLOGY AND HEPATOLOGY Vol. 2, No. 9

Clinique, Sherbrooke; Eddie Wasser, Sound Medical Research, To-ronto; Lawrence Worobetz, Royal University Hospital, Saskatoon.Chile: Carlos Briceno, Hospital Regional de Concepcion, Concepcion;Edmundo Hofmann, Clinical Alemana de Temuco, Temuco. Columbia:Pablo Archila, Fundacion Clinica Shaio — Unidad de Gastroenterologia,Bogota D.C.; Mario Rey, Centro Gastroenterologico de la 93, BogotaD.C.; Jose Velez, Centro de Profesionales, Bogota D.C. United States:J. Tyler Baber, Physicians Group Research Clinic, Little Rock; JayBeckwith, Medical Center Professional Bldg, Fort Worth; William R.Berry, Longmont Medical Research, Longmont; Charles A. Birbara,Clinical Pharmacology Study Group, Worchester; Kristine Bordenave,ABQ Medical, Albuquerque; Terry D. Box, Intermountain West Gastro-enterology, Salt Lake City; Donald Brandon, California Research Foun-dation, San Diego; Patricia Buchanan, River Road Medical Group,Eugene; William D. Chey, University of Michigan, Ann Arbor; Gregory V.Collins, Charlotte Clinical Research, Charlotte; Michael P. DeMicco,Advanced Clinical Research Institute, Anaheim; Benjamin J. Dolin,nTouch Research, Peoria; Douglas Drossman, University of North Caro-lina Center for Functional GI and Motility Disorders, Chapel Hill; Kul-winder S. Dua, Denver Health and Hospital, Denver; Steven L. Duckor,AGMG Clinical Research, Orange; David Ferrera, Sacramento ResearchMedical Group, Sacramento; James I. Fidelholtz, Hilltop PhysiciansInc., Cincinnati; Michael Goldstein, Long Island Gastrointestinal Re-search Group, Great Neck; Daniel E. Gremillion, Nashville ClinicalResearch, Nashville; John F. Johanson, Rockford GastroenterologyAssociates, Rockford; John Jolley, San Rafael; Mario Kamionkowski,Gastroenterology Associates of Cleveland, Inc., Lyndhurst; SeymourKatz, Long Island Clinical Research Associates, Great Neck; Barry P.Kaufman, Atlantic Gastroenterology, Egg Harbor; Terry D. Klein, Heart-land Research Associates, Wichita; George Koval, West Hills Gastro-enterology Associate, PC, Portland; Steven Krumholz, Waterside Clin-ical Research, West Palm Beach; Christopher Lahr, CarolinaConstipation Center, Charleston; Mark Lamet, Center for Gastrointes-tinal Disorders, Hollywood; James LaSalle, Medical Arts ResearchCollaborative, Excelsior Springs; Paul J. Lebovitz, Allegheny UniversityHospital, Pittsburgh; Anthony Lembo, Beth Israel Deaconess MedicalCenter, Boston; John E. Lowe, Utah Digestive Health Institute, S. Og-den; Barry Lubin, Hampton Roads Center for Clinical Research, Nor-
folk; Douglas W. Mapel, Lovelace Scientific Resources, Inc., Albuquer-que; Barry Migicovsky, BMMD Research, Inc., Pembroke Pines; PhilipMiner, Oklahoma Foundation for Digestive Research, Oklahoma City;David Morris, Healthcare Research Consultants, Tulsa; Morry Mosko-vitz, Valley Gastroenterology Associates, Beaver Falls; Susan G.Moster, Gastroenterology Associates of North Texas Research, FortWorth; Paul Norwood, Valley Research, Fresno; James S. Novick,Charm City Research, Towson; J. Mark Provenza, Louisiana ResearchCenter, Shreveport; U. Prakesh Rau, Healthsouth Clin Research atBraintree Rehabilitation Hosp, Braintree; Ernie Riffer, Central PhoenixMedical Clinic, L.L.C., Phoenix; Dennis Ruff, Healthcare Discoveries,P.A., San Antonio; Jon R. Schmidt, Radiant Research, Lakewood; LeahM. Schmidt, Advance Clinical Therapeutics, Tucson; Colleen Schmitt,Southeastern Clinical Research, Chattanooga; Howard L. Schwartz,Miami Research Associates, Miami; Jerrold Schwartz, Northwest Gas-troenterologists, S.C., Arlington Heights; Michael Schwartz, Jupiter Re-search Associates, Jupiter; Ronald Schwarz, Multispeciality ResearchAssociates of North Carolina, Raleigh; Bavikatte Shivakumar, Gastro-intestinal Clinics of the Quad Cities, Davenport; Bruce H. Short, Pinna-cle Medical Research, Overland Park; Ann Silverman, William Beau-mont Hospital, Royal Oak; William B. Smith, New Orleans Center ForClinical Research, New Orleans; Edy Soffer, Cleveland Clinic Founda-tion, Cleveland; Malcolm Sperling, Edinger Medical Group Clinical Re-search Center, Fountain Valley; Eugene J. Spiotta, Southern MedicalResearch, Memphis; Jan H. Tanghe, Ridgeview Research, Chaska;Timothy Trainor, North Shore Research, East Slidell; Arnold Wald,University of Pittsburgh Medical Center, Pittsburgh; Mark Walton, Ex-press Care Clinical Research, Colorado Springs; David J. Wenzel, Bos-ton Clinical Research Center, Wellesley Hills; Robert J. Williams, Geor-gia Clinical Professionals Group, Augusta; Troy Williams, PivotalResearch Center, Peoria; John T. Witte, Idaho Gastroenterology, Boise;Robert A. Wohlman, Northwest Gastroenterology Assoc., Bellevue;Lawrence D. Wruble, Memphis Gastroenterology Group, Memphis;Alvin Zfass, VCU Health System, Richmond. Venezuela: Maribel Liz-arzabal, Hospital Universitario de Maracaibo, Maracaibo-Zulia; RamonPinero, Hospital Vargas de Caracas, San Jose-Caracas; Jose MiguelVelasquez, Hospital General ‘Dr. Domingo Luciani’, Caracas.
September 2004 TEGASEROD IN CHRONIC CONSTIPATION 805

ZEL-RP-0437-B




















