
Effect of contralateral finger touch on grip force control in individuals with multiple sclerosis
6
Effect of contralateral finger touch on grip force control in individuals with multiple sclerosis Veena Iyengar a , Marcio J. Santos a , Michael Ko b , Alexander S. Aruin a, * a Department of Physical Therapy (MC 898), University of Illinois at Chicago, 1919 W Taylor Street, Chicago, IL 60612, USA b Department of Neurology, Loyola University, 2160 South First Avenue, Maywood, IL 60153, USA article info Article history: Accepted 15 December 2008 Available online 24 February 2009 Keywords: Grip force control Finger touch Multiple sclerosis (MS) abstract Objective: It was recently shown that the magnitude of grip force utilized to lift and transport a hand- held object decreased if a light touch from the contralateral finger is provided [Aruin AS. Support-specific modulation of grip force in individuals with hemiparesis. Arch Phys Med Rehabil 2005;86:768–75]. The rationale of the study is to find out whether or not the individuals with multiple sclerosis (MS) have the same behavior as control subjects. Methods: Eight patients with MS and eight control subjects performed the task of lifting and transporting an instrumented object with provision of light touch of the contralateral index finger to the wrist of the target arm and without it. The tasks of placing the object on a shelf and a simulation of a drinking maneu- ver were studied. Peak grip force, force ratio, latency, and time lag were recorded and analyzed. Results: The mean peak grip force decreased in conditions with application of light finger touch in patients and control subjects while performing both the experimental tasks. The force ratio also improved with application of light finger touch. Conclusions: Individuals with MS apply smaller grip force if they utilize a finger touch. Significance: Findings provide better understanding of how patients with MS control grip force and suggest that a light touch approach could be considered as a valuable modality in the rehabilitation of these patients. Ó 2008 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. 1. Introduction A prerequisite for the elaborate use of the human hand during manipulation of objects is the ability to produce, maintain and reg- ulate grip force (GF). Successful object manipulations are based on the application of forces that are large enough to prevent slips but are not excessive preventing fatigue and damage of the lifted object. Thus, appropriate regulation of grip force is essential to per- form various activities of daily living such as drinking, eating, but- toning a shirt, etc. In addition, proper modulation of grip force is crucial for the performance of a number of work-related activities (Holewski et al., 1988; Bell-Krotoski, 1991; Gilles and Wing, 2003; Nowak and Hermsdorfer, 2004). The capability to scale grip forces in order to lift an object depends on many factors such as age, gender, handedness, age and disease (Johansson et al., 1992; Cole and Rotella, 2002; Gilles and Wing, 2003; Nowak et al., 2004b). Thus, elderly persons apply larger grip forces to manipulate an object as compared to younger individuals (Thornbury and Mistretta, 1981; Cole et al., 1998, 1999; Cole and Rotella, 2001, 2002; Gilles and Wing, 2003). Also, individuals with stroke, cerebellar disorders, cerebral palsy and impaired tactile sensibility commonly produce inefficiently ele- vated grip forces while performing simple daily tasks (Gordon and Duff, 1999; Lowe and Freivalds, 1999; Hermsdorfer et al., 2003; Nowak et al., 2003a). Studies have shown that a light finger touch (< 0:1 N) on a sta- tionary object in the environment provides sensory information that reduces postural sway in standing individuals (Jeka and Lack- ner, 1994; Jeka, 1997; Lackner et al., 1999, 2001). It was also dem- onstrated in experiments involving lifting of an object with two hands that when a second hand provides support to the object, the grip force needed to lift the object is reduced (Scholz and Latash, 1998). Moreover, recent studies revealed that a light touch of the contralateral finger provided to the wrist of the target arm is associated with decreasing grip force while performing lifting tasks in individuals with hemiparesis (Aruin, 2005) and healthy individ- uals (Iyengar et al., 2007). Multiple sclerosis (MS) is an inflammatory demyelinating dis- ease of the central nervous system (CNS) that is characterized by the loss of myelin in the brain and spinal cord. Individuals with MS usually present with impairments in visual, somatosensorial, and motor systems leading to tremors, balance disturbances, and fatigue. Also, the hand coordination and motor function are largely 1388-2457/$36.00 Ó 2008 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.clinph.2008.12.029 * Corresponding author. Tel.: +1 312 355 0904; fax: +1 312 996 4583. E-mail address: [email protected] (A.S. Aruin). Clinical Neurophysiology 120 (2009) 626–631 Contents lists available at ScienceDirect Clinical Neurophysiology journal homepage: www.elsevier.com/locate/clinph
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Effect of contralateral finger touch on grip force control in individuals with multiple sclerosis

Clinical Neurophysiology 120 (2009) 626–631
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier .com/locate /c l inph
Effect of contralateral finger touch on grip force control in individualswith multiple sclerosis
Veena Iyengar a, Marcio J. Santos a, Michael Ko b, Alexander S. Aruin a,*
a Department of Physical Therapy (MC 898), University of Illinois at Chicago, 1919 W Taylor Street, Chicago, IL 60612, USAb Department of Neurology, Loyola University, 2160 South First Avenue, Maywood, IL 60153, USA
a r t i c l e i n f o
Article history:Accepted 15 December 2008Available online 24 February 2009
Keywords:Grip force controlFinger touchMultiple sclerosis (MS)
1388-2457/$36.00 � 2008 International Federation odoi:10.1016/j.clinph.2008.12.029
* Corresponding author. Tel.: +1 312 355 0904; faxE-mail address: [email protected] (A.S. Aruin).
a b s t r a c t
Objective: It was recently shown that the magnitude of grip force utilized to lift and transport a hand-held object decreased if a light touch from the contralateral finger is provided [Aruin AS. Support-specificmodulation of grip force in individuals with hemiparesis. Arch Phys Med Rehabil 2005;86:768–75]. Therationale of the study is to find out whether or not the individuals with multiple sclerosis (MS) have thesame behavior as control subjects.Methods: Eight patients with MS and eight control subjects performed the task of lifting and transportingan instrumented object with provision of light touch of the contralateral index finger to the wrist of thetarget arm and without it. The tasks of placing the object on a shelf and a simulation of a drinking maneu-ver were studied. Peak grip force, force ratio, latency, and time lag were recorded and analyzed.Results: The mean peak grip force decreased in conditions with application of light finger touch inpatients and control subjects while performing both the experimental tasks. The force ratio alsoimproved with application of light finger touch.Conclusions: Individuals with MS apply smaller grip force if they utilize a finger touch.Significance: Findings provide better understanding of how patients with MS control grip force and suggestthat a light touch approach could be considered as a valuable modality in the rehabilitation of these patients.� 2008 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved.
1. Introduction
A prerequisite for the elaborate use of the human hand duringmanipulation of objects is the ability to produce, maintain and reg-ulate grip force (GF). Successful object manipulations are based onthe application of forces that are large enough to prevent slips butare not excessive preventing fatigue and damage of the liftedobject. Thus, appropriate regulation of grip force is essential to per-form various activities of daily living such as drinking, eating, but-toning a shirt, etc. In addition, proper modulation of grip force iscrucial for the performance of a number of work-related activities(Holewski et al., 1988; Bell-Krotoski, 1991; Gilles and Wing, 2003;Nowak and Hermsdorfer, 2004).
The capability to scale grip forces in order to lift an objectdepends on many factors such as age, gender, handedness, ageand disease (Johansson et al., 1992; Cole and Rotella, 2002; Gillesand Wing, 2003; Nowak et al., 2004b). Thus, elderly persons applylarger grip forces to manipulate an object as compared to youngerindividuals (Thornbury and Mistretta, 1981; Cole et al., 1998,1999; Cole and Rotella, 2001, 2002; Gilles and Wing, 2003). Also,
f Clinical Neurophysiology. Publish
: +1 312 996 4583.
individuals with stroke, cerebellar disorders, cerebral palsy andimpaired tactile sensibility commonly produce inefficiently ele-vated grip forces while performing simple daily tasks (Gordonand Duff, 1999; Lowe and Freivalds, 1999; Hermsdorfer et al.,2003; Nowak et al., 2003a).
Studies have shown that a light finger touch (< 0:1 N) on a sta-tionary object in the environment provides sensory informationthat reduces postural sway in standing individuals (Jeka and Lack-ner, 1994; Jeka, 1997; Lackner et al., 1999, 2001). It was also dem-onstrated in experiments involving lifting of an object with twohands that when a second hand provides support to the object,the grip force needed to lift the object is reduced (Scholz andLatash, 1998). Moreover, recent studies revealed that a light touchof the contralateral finger provided to the wrist of the target arm isassociated with decreasing grip force while performing lifting tasksin individuals with hemiparesis (Aruin, 2005) and healthy individ-uals (Iyengar et al., 2007).
Multiple sclerosis (MS) is an inflammatory demyelinating dis-ease of the central nervous system (CNS) that is characterized bythe loss of myelin in the brain and spinal cord. Individuals withMS usually present with impairments in visual, somatosensorial,and motor systems leading to tremors, balance disturbances, andfatigue. Also, the hand coordination and motor function are largely
ed by Elsevier Ireland Ltd. All rights reserved.
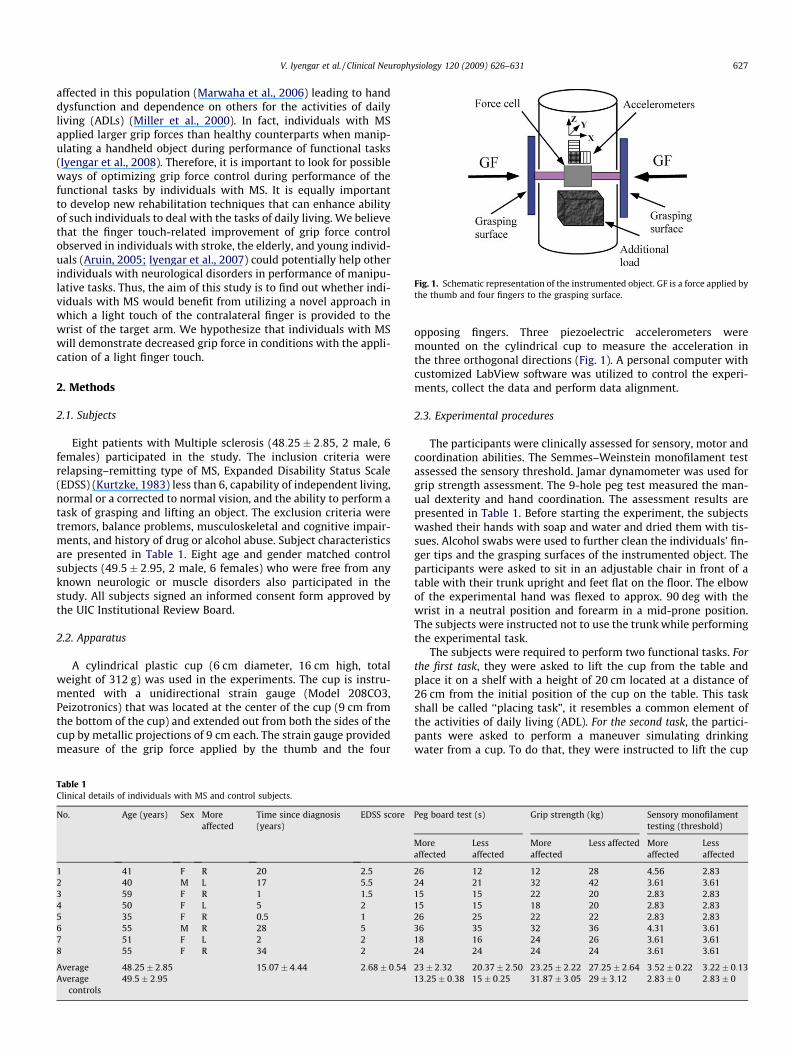
Fig. 1. Schematic representation of the instrumented object. GF is a force applied bythe thumb and four fingers to the grasping surface.
V. Iyengar et al. / Clinical Neurophysiology 120 (2009) 626–631 627
affected in this population (Marwaha et al., 2006) leading to handdysfunction and dependence on others for the activities of dailyliving (ADLs) (Miller et al., 2000). In fact, individuals with MSapplied larger grip forces than healthy counterparts when manip-ulating a handheld object during performance of functional tasks(Iyengar et al., 2008). Therefore, it is important to look for possibleways of optimizing grip force control during performance of thefunctional tasks by individuals with MS. It is equally importantto develop new rehabilitation techniques that can enhance abilityof such individuals to deal with the tasks of daily living. We believethat the finger touch-related improvement of grip force controlobserved in individuals with stroke, the elderly, and young individ-uals (Aruin, 2005; Iyengar et al., 2007) could potentially help otherindividuals with neurological disorders in performance of manipu-lative tasks. Thus, the aim of this study is to find out whether indi-viduals with MS would benefit from utilizing a novel approach inwhich a light touch of the contralateral finger is provided to thewrist of the target arm. We hypothesize that individuals with MSwill demonstrate decreased grip force in conditions with the appli-cation of a light finger touch.
2. Methods
2.1. Subjects
Eight patients with Multiple sclerosis (48:25� 2:85, 2 male, 6females) participated in the study. The inclusion criteria wererelapsing–remitting type of MS, Expanded Disability Status Scale(EDSS) (Kurtzke, 1983) less than 6, capability of independent living,normal or a corrected to normal vision, and the ability to perform atask of grasping and lifting an object. The exclusion criteria weretremors, balance problems, musculoskeletal and cognitive impair-ments, and history of drug or alcohol abuse. Subject characteristicsare presented in Table 1. Eight age and gender matched controlsubjects (49:5� 2:95, 2 male, 6 females) who were free from anyknown neurologic or muscle disorders also participated in thestudy. All subjects signed an informed consent form approved bythe UIC Institutional Review Board.
2.2. Apparatus
A cylindrical plastic cup (6 cm diameter, 16 cm high, totalweight of 312 g) was used in the experiments. The cup is instru-mented with a unidirectional strain gauge (Model 208CO3,Peizotronics) that was located at the center of the cup (9 cm fromthe bottom of the cup) and extended out from both the sides of thecup by metallic projections of 9 cm each. The strain gauge providedmeasure of the grip force applied by the thumb and the four
Table 1Clinical details of individuals with MS and control subjects.
No. Age (years) Sex Moreaffected
Time since diagnosis(years)
EDSS score
1 41 F R 20 2.52 40 M L 17 5.53 59 F R 1 1.54 50 F L 5 25 35 F R 0.5 16 55 M R 28 57 51 F L 2 28 55 F R 34 2
Average 48:25� 2:85 15:07� 4:44 2:68� 0:54Average
controls49:5� 2:95
opposing fingers. Three piezoelectric accelerometers weremounted on the cylindrical cup to measure the acceleration inthe three orthogonal directions (Fig. 1). A personal computer withcustomized LabView software was utilized to control the experi-ments, collect the data and perform data alignment.
2.3. Experimental procedures
The participants were clinically assessed for sensory, motor andcoordination abilities. The Semmes–Weinstein monofilament testassessed the sensory threshold. Jamar dynamometer was used forgrip strength assessment. The 9-hole peg test measured the man-ual dexterity and hand coordination. The assessment results arepresented in Table 1. Before starting the experiment, the subjectswashed their hands with soap and water and dried them with tis-sues. Alcohol swabs were used to further clean the individuals’ fin-ger tips and the grasping surfaces of the instrumented object. Theparticipants were asked to sit in an adjustable chair in front of atable with their trunk upright and feet flat on the floor. The elbowof the experimental hand was flexed to approx. 90 deg with thewrist in a neutral position and forearm in a mid-prone position.The subjects were instructed not to use the trunk while performingthe experimental task.
The subjects were required to perform two functional tasks. Forthe first task, they were asked to lift the cup from the table andplace it on a shelf with a height of 20 cm located at a distance of26 cm from the initial position of the cup on the table. This taskshall be called ‘‘placing task”, it resembles a common element ofthe activities of daily living (ADL). For the second task, the partici-pants were asked to perform a maneuver simulating drinkingwater from a cup. To do that, they were instructed to lift the cup
Peg board test (s) Grip strength (kg) Sensory monofilamenttesting (threshold)
Moreaffected
Lessaffected
Moreaffected
Less affected Moreaffected
Lessaffected
26 12 12 28 4.56 2.8324 21 32 42 3.61 3.6115 15 22 20 2.83 2.8315 15 18 20 2.83 2.8326 25 22 22 2.83 2.8336 35 32 36 4.31 3.6118 16 24 26 3.61 3.6124 24 24 24 3.61 3.61
23� 2:32 20:37� 2:50 23:25� 2:22 27:25� 2:64 3:52� 0:22 3:22� 0:1313:25� 0:38 15� 0:25 31:87� 3:05 29� 3:12 2:83� 0 2:83� 0

628 V. Iyengar et al. / Clinical Neurophysiology 120 (2009) 626–631
and move it close to the mouth, hold it in that position for a coupleof seconds and then bring it back to the starting position. A strawwas used to make it easy for the subjects to perform the task with-out tilting the cup. This task would be referred as the ‘‘drinkingtask.”
In both tasks the subjects were instructed to lift the object usingthe opposition of the thumb and four fingers in a self-paced man-ner after hearing an auditory signal and to maintain similar speedof movement throughout all the series. They were instructed tokeep the cup vertical at all times during the task and the experi-menter paid a special attention to the object position. These twotasks were performed with and without the provision of a lightcontralateral finger touch. In the touch conditions the participantswere instructed to touch the wrist of the experimental hand whileperforming the experimental tasks. They were also instructed notto apply force to the wrist but slightly touch it with the tip ofthe index finger. The subjects were asked to apply the light touchbefore grasping the object and maintain it throughout the move-ment and through that particular series (5 trials). The order of ser-ies (tasks and conditions) was randomized for each subject. Theintervals between the trials were 8 s; the intervals between con-secutive series were about 1 min so that fatigue was never an issue.The subjects performed 2–3 practice trials in each series prior tothe start of data collection and were instructed to complete thetasks within each experimental series as similar as possible.
Both hands were assessed for the patients with MS and healthysubjects. The upper extremities of the healthy subjects were clas-sified as dominant and non-dominant based on self report. Thehands of the patients with MS were classified into more affectedand less affected based on diagnosis and self report and were alsoconfirmed by the outcome of the peg board, sensory and gripstrength tests.
2.4. Data processing
The signals from the force sensor and three accelerometerswere sampled at 100 Hz with a 16-bit resolution using LabViewsoftware and stored for off-line processing on a computer. The dataprocessing included viewing each trial on a monitor screen andaligning them using the first deflection of the vertical accelerome-ter signal from its baseline, which reflected the moment of lift offof the object. Then, the mean of five trials for each condition wascalculated and analyzed in a MATLAB program. The following out-come measures were obtained. Peak grip force (PGF), the maxi-mum grip force applied by the thumb and four fingers on thecup during the task performance (N); peak of grip force difference(PGFd) that is the difference between the grip force in no touchcondition and in condition with the finger touch provided (N);the vertical acceleration was used to calculate the moment of liftoff of the object as the first detectable abrupt change in the accel-eration; maximal load force (LFmax), calculated as the product ofthe mass of the object (m) and the vector sum of the horizontal(Y), lateral (X) and vertical (Z) acceleration (A) taking into accountgravity (g) (N) (Nowak et al., 2004a); force ratio (PGF=LFmaxÞ, calcu-lated using two steps: first the time course of the force ratio wasobtained, then the PGF=LFmax peak value was extracted from thetime course during the acceleration phase. This force ratio givesan estimate of the efficiency of the grip force (Nowak, 2004); thelatency of grip force, measured as the time difference betweenthe initiation of grip force application and the time of object liftoff; and the time lag, calculated as the time difference betweenthe time of peak grip force (TPGFÞ, and time of peak of load force(TLFmaxÞ (ms). Finally, the velocity of the movement was calculatedby integrating the vectorial sum of acceleration signal usingMatLab software.
Descriptive statistics were obtained for all relevant subjectcharacteristics such as age, gender, EDSS score, time in secondsfor the 9-hole peg board test, strength measurement using Jamardynamometer and sensitivity using Semmes–Weinstein monofila-ment test. Repeated measures ANOVAs with two factors (conditionand side) were performed for each group and task separately foreach of five dependent variables (velocity, PGF, force ratio, timelag, and latency). The interactions between the side and conditionswere also computed. In addition, two-way ANOVAs (group andside) were performed to compare the PGF difference between thetouch and no touch conditions and between groups for each task(placing and drinking). A post-hoc analysis was used to detectthe differences within factors for both repeated measures ANOVAsand two-way ANOVAs. Statistical significance was set at p < 0:05.
3. Results
3.1. Movement velocity
Individuals with MS performed the placing task with averagevelocity of 52:57� 4:14 m=s and 57:97� 4:04 m=s while liftingthe object with the more and less affected hands, respectively.When a contralateral finger touch was available, the average veloc-ity was 52:98� 3:93 m=s for more affected and 54:57� 4:89 m=sfor less affected hands, respectively. Control subjects demonstratedaverage velocity of movement of 57:29� 3:60 m=s and56:75� 2:48 m=s in no touch conditions while using their domi-nant hand and non-dominant hand. When they utilized a contra-lateral finger touch, velocity of the task was 57:53� 3:96 for thedominant and 54:33� 2:47 m=s for the non-dominant hands,respectively. The difference between the velocity of the task per-formed with and without a finger touch in patients and in controlsubjects was not statistically significant (F1;7 ¼ 0:59, p = 0.808).Both groups of subjects performed the drinking task with a slowervelocity as compared to the placing task. Thus, the average velocityof movement for patients with MS was 31:06� 3:53 m=s and30:67� 3:35 m=s for the more and less affected hands, respec-tively; with provision of a contralateral finger touch the averagevelocity of the movement was 31:00� 3:69 m=s and30:07� 2:96 m=s, for the more and less affected hands, respec-tively. Control subjects performed the task with average velocityof 33:40� 4:57 m=s using their dominant hand and30:88� 4:15 m=s with their non-dominant hand. When a contra-lateral finger touch was available, they performed the task withthe average velocity of 34:96� 4:76 m=s using their dominantand 30:46� 3:85 m=s while using their non-dominant hands,respectively. The effects of a group, sides, and a finger touch onaverage velocity of the task were not statistically significant(F1;7 ¼ 0:29, p = 0.95).
3.2. Grip force
The mean peak grip force applied to the cup by the patientswith MS during the no touch condition in the placing task was17:54� 1:58 N and 16:31� 3:44 N for the more and less affectedhands, respectively. When a contralateral finger touch was avail-able, grip force was reduced by 23:47� 6:0% reaching13:64� 1:58 N in the more affected hand and was reduced by20:66� 3:52% reaching 13:88� 3:40 N in the less affected hand(Fig. 2). Repeated measures ANOVA revealed significant differencewithin the group due to the touch condition (F1;7 ¼ 57:82,p < 0:01). A post-hoc analysis uncovered statistical significancebetween the condition of touch and no touch in both the moreaffected (p = 0.003) and less affected hands (p = 0.03). The gripforce applied by the control subjects’ dominant and non-dominant
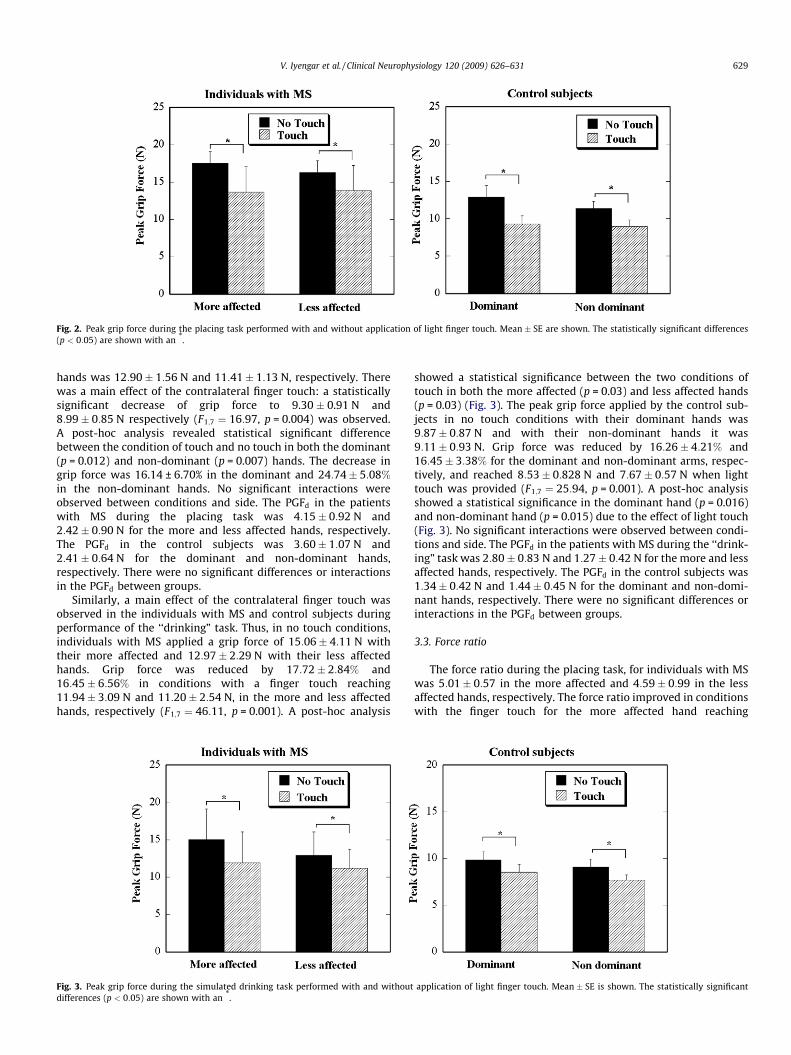
Fig. 2. Peak grip force during the placing task performed with and without application of light finger touch. Mean � SE are shown. The statistically significant differences(p < 0:05) are shown with an *.
V. Iyengar et al. / Clinical Neurophysiology 120 (2009) 626–631 629
hands was 12:90� 1:56 N and 11:41� 1:13 N, respectively. Therewas a main effect of the contralateral finger touch: a statisticallysignificant decrease of grip force to 9.30 � 0.91 N and8:99� 0:85 N respectively (F1;7 ¼ 16:97, p = 0.004) was observed.A post-hoc analysis revealed statistical significant differencebetween the condition of touch and no touch in both the dominant(p = 0.012) and non-dominant (p = 0.007) hands. The decrease ingrip force was 16.14 ± 6.70% in the dominant and 24:74� 5:08%
in the non-dominant hands. No significant interactions wereobserved between conditions and side. The PGFd in the patientswith MS during the placing task was 4:15� 0:92 N and2:42� 0:90 N for the more and less affected hands, respectively.The PGFd in the control subjects was 3:60� 1:07 N and2:41� 0:64 N for the dominant and non-dominant hands,respectively. There were no significant differences or interactionsin the PGFd between groups.
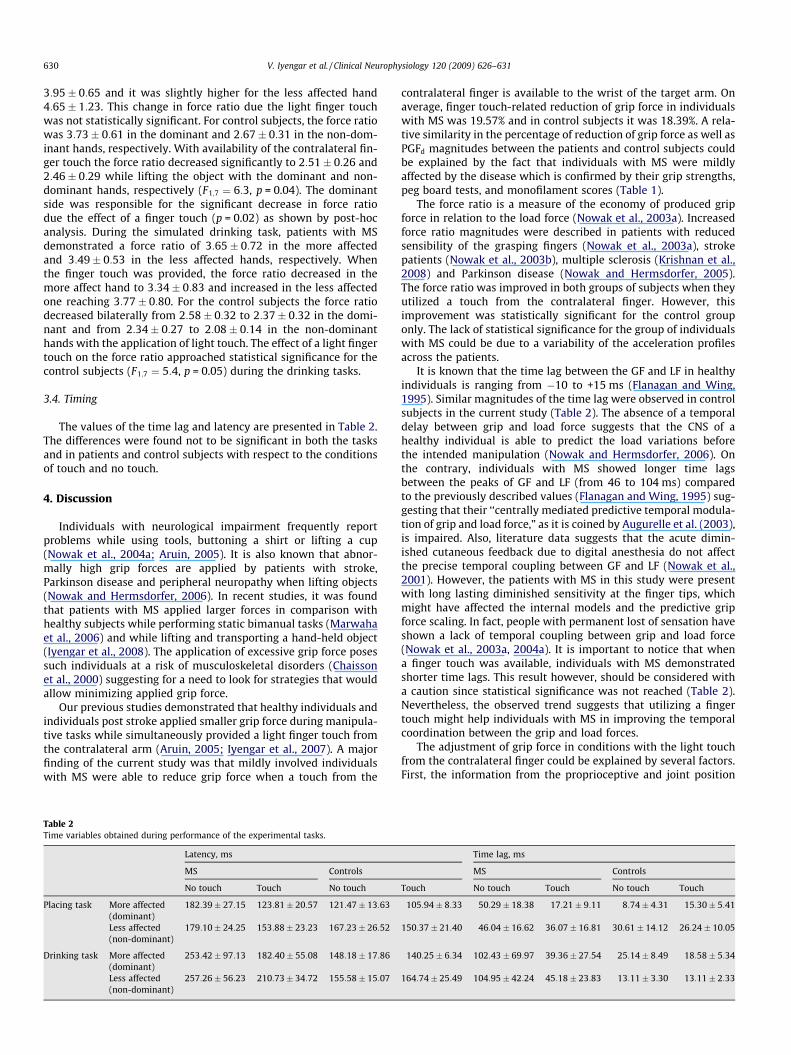
Similarly, a main effect of the contralateral finger touch wasobserved in the individuals with MS and control subjects duringperformance of the ‘‘drinking” task. Thus, in no touch conditions,individuals with MS applied a grip force of 15:06� 4:11 N withtheir more affected and 12:97� 2:29 N with their less affectedhands. Grip force was reduced by 17:72� 2:84% and16:45� 6:56% in conditions with a finger touch reaching11:94� 3:09 N and 11:20� 2:54 N, in the more and less affectedhands, respectively (F1;7 ¼ 46:11, p = 0.001). A post-hoc analysis
Fig. 3. Peak grip force during the simulated drinking task performed with and withoutdifferences (p < 0:05) are shown with an *.
showed a statistical significance between the two conditions oftouch in both the more affected (p = 0.03) and less affected hands(p = 0.03) (Fig. 3). The peak grip force applied by the control sub-jects in no touch conditions with their dominant hands was9:87� 0:87 N and with their non-dominant hands it was9:11� 0:93 N. Grip force was reduced by 16:26� 4:21% and16:45� 3:38% for the dominant and non-dominant arms, respec-tively, and reached 8:53� 0:828 N and 7:67� 0:57 N when lighttouch was provided (F1;7 ¼ 25:94, p = 0.001). A post-hoc analysisshowed a statistical significance in the dominant hand (p = 0.016)and non-dominant hand (p = 0.015) due to the effect of light touch(Fig. 3). No significant interactions were observed between condi-tions and side. The PGFd in the patients with MS during the ‘‘drink-ing” task was 2:80� 0:83 N and 1:27� 0:42 N for the more and lessaffected hands, respectively. The PGFd in the control subjects was1:34� 0:42 N and 1:44� 0:45 N for the dominant and non-domi-nant hands, respectively. There were no significant differences orinteractions in the PGFd between groups.
3.3. Force ratio
The force ratio during the placing task, for individuals with MSwas 5:01� 0:57 in the more affected and 4:59� 0:99 in the lessaffected hands, respectively. The force ratio improved in conditionswith the finger touch for the more affected hand reaching
application of light finger touch. Mean � SE is shown. The statistically significant
630 V. Iyengar et al. / Clinical Neurophysiology 120 (2009) 626–631
3:95� 0:65 and it was slightly higher for the less affected hand4:65� 1:23. This change in force ratio due the light finger touchwas not statistically significant. For control subjects, the force ratiowas 3:73� 0:61 in the dominant and 2:67� 0:31 in the non-dom-inant hands, respectively. With availability of the contralateral fin-ger touch the force ratio decreased significantly to 2:51� 0:26 and2:46� 0:29 while lifting the object with the dominant and non-dominant hands, respectively (F1;7 ¼ 6:3, p = 0.04). The dominantside was responsible for the significant decrease in force ratiodue the effect of a finger touch (p = 0.02) as shown by post-hocanalysis. During the simulated drinking task, patients with MSdemonstrated a force ratio of 3:65� 0:72 in the more affectedand 3:49� 0:53 in the less affected hands, respectively. Whenthe finger touch was provided, the force ratio decreased in themore affect hand to 3:34� 0:83 and increased in the less affectedone reaching 3:77� 0:80. For the control subjects the force ratiodecreased bilaterally from 2:58� 0:32 to 2:37� 0:32 in the domi-nant and from 2:34� 0:27 to 2:08� 0:14 in the non-dominanthands with the application of light touch. The effect of a light fingertouch on the force ratio approached statistical significance for thecontrol subjects (F1;7 ¼ 5:4, p = 0.05) during the drinking tasks.
3.4. Timing
The values of the time lag and latency are presented in Table 2.The differences were found not to be significant in both the tasksand in patients and control subjects with respect to the conditionsof touch and no touch.
4. Discussion
Individuals with neurological impairment frequently reportproblems while using tools, buttoning a shirt or lifting a cup(Nowak et al., 2004a; Aruin, 2005). It is also known that abnor-mally high grip forces are applied by patients with stroke,Parkinson disease and peripheral neuropathy when lifting objects(Nowak and Hermsdorfer, 2006). In recent studies, it was foundthat patients with MS applied larger forces in comparison withhealthy subjects while performing static bimanual tasks (Marwahaet al., 2006) and while lifting and transporting a hand-held object(Iyengar et al., 2008). The application of excessive grip force posessuch individuals at a risk of musculoskeletal disorders (Chaissonet al., 2000) suggesting for a need to look for strategies that wouldallow minimizing applied grip force.
Our previous studies demonstrated that healthy individuals andindividuals post stroke applied smaller grip force during manipula-tive tasks while simultaneously provided a light finger touch fromthe contralateral arm (Aruin, 2005; Iyengar et al., 2007). A majorfinding of the current study was that mildly involved individualswith MS were able to reduce grip force when a touch from the
Table 2Time variables obtained during performance of the experimental tasks.
Latency, ms
MS Controls
No touch Touch No touch
Placing task More affected(dominant)
182:39� 27:15 123:81� 20:57 121:47� 13:63
Less affected(non-dominant)
179:10� 24:25 153:88� 23:23 167:23� 26:52
Drinking task More affected(dominant)
253:42� 97:13 182:40� 55:08 148:18� 17:86
Less affected(non-dominant)
257:26� 56:23 210:73� 34:72 155:58� 15:07
contralateral finger is available to the wrist of the target arm. Onaverage, finger touch-related reduction of grip force in individualswith MS was 19.57% and in control subjects it was 18.39%. A rela-tive similarity in the percentage of reduction of grip force as well asPGFd magnitudes between the patients and control subjects couldbe explained by the fact that individuals with MS were mildlyaffected by the disease which is confirmed by their grip strengths,peg board tests, and monofilament scores (Table 1).
The force ratio is a measure of the economy of produced gripforce in relation to the load force (Nowak et al., 2003a). Increasedforce ratio magnitudes were described in patients with reducedsensibility of the grasping fingers (Nowak et al., 2003a), strokepatients (Nowak et al., 2003b), multiple sclerosis (Krishnan et al.,2008) and Parkinson disease (Nowak and Hermsdorfer, 2005).The force ratio was improved in both groups of subjects when theyutilized a touch from the contralateral finger. However, thisimprovement was statistically significant for the control grouponly. The lack of statistical significance for the group of individualswith MS could be due to a variability of the acceleration profilesacross the patients.
It is known that the time lag between the GF and LF in healthyindividuals is ranging from �10 to +15 ms (Flanagan and Wing,1995). Similar magnitudes of the time lag were observed in controlsubjects in the current study (Table 2). The absence of a temporaldelay between grip and load force suggests that the CNS of ahealthy individual is able to predict the load variations beforethe intended manipulation (Nowak and Hermsdorfer, 2006). Onthe contrary, individuals with MS showed longer time lagsbetween the peaks of GF and LF (from 46 to 104 ms) comparedto the previously described values (Flanagan and Wing, 1995) sug-gesting that their ‘‘centrally mediated predictive temporal modula-tion of grip and load force,” as it is coined by Augurelle et al. (2003),is impaired. Also, literature data suggests that the acute dimin-ished cutaneous feedback due to digital anesthesia do not affectthe precise temporal coupling between GF and LF (Nowak et al.,2001). However, the patients with MS in this study were presentwith long lasting diminished sensitivity at the finger tips, whichmight have affected the internal models and the predictive gripforce scaling. In fact, people with permanent lost of sensation haveshown a lack of temporal coupling between grip and load force(Nowak et al., 2003a, 2004a). It is important to notice that whena finger touch was available, individuals with MS demonstratedshorter time lags. This result however, should be considered witha caution since statistical significance was not reached (Table 2).Nevertheless, the observed trend suggests that utilizing a fingertouch might help individuals with MS in improving the temporalcoordination between the grip and load forces.
The adjustment of grip force in conditions with the light touchfrom the contralateral finger could be explained by several factors.First, the information from the proprioceptive and joint position
Time lag, ms
MS Controls
Touch No touch Touch No touch Touch
105:94� 8:33 50:29� 18:38 17:21� 9:11 8:74� 4:31 15:30� 5:41
150:37� 21:40 46:04� 16:62 36:07� 16:81 30:61� 14:12 26:24� 10:05
140:25� 6:34 102:43� 69:97 39:36� 27:54 25:14� 8:49 18:58� 5:34
164:74� 25:49 104:95� 42:24 45:18� 23:83 13:11� 3:30 13:11� 2:33

V. Iyengar et al. / Clinical Neurophysiology 120 (2009) 626–631 631
sense receptors of the contralateral arm might be utilized togetherwith information obtained from the arm that is performing the lift-ing task. This could enhance the sensorial input allowing bettermodulation of grip force (Nowak et al., 2001; Iyengar et al.,2007). Second, it has been shown that light finger touch providesspatial cues, which, similarly to vision, could enhance the controlof position of the body segments in space (Jeka and Lackner,1994; Lackner et al., 1999, 2001; Iyengar et al., 2007). Third, thiscould be the effect of perception that one hand is supporting theother (even if there is no physical support provided), thus helpingin the reduction of grip force. While the results supporting thissuggestion are not available at the moment, a testimony of oneof the patients participating in this study, who perceived it mucheasier to accomplish the experimental task with the applicationof a light touch compared to no touch conditions, could be consid-ered as an indication that this is a possible scenario.
There are three issues that we would like to address. First,relates to the experimental protocol that might have involvedsome changes of the vertical orientation of the object during thetask performance. It was shown in the literature that changes inthe orientation of the object or resultant torque could be associatedwith changes in the grip force applied to the instrumented object(Gao et al., 2005). While the subjects were instructed to keep theinstrumented object vertically at all times, it is possible that theorientation changed in some trials. As such this could be consid-ered as a limitation of the study. Second, it is apparent that theexact mechanism of the finger touch-related grip force reductionis still a matter of debates. While the outcome of the current studydemonstrated the ability of individuals with MS studied here tominimize grip force when a contralateral finger touch is provided,it does not provide additional explanations about the mechanismof such a reduction. As such, additional studies focused on betterunderstanding of the mechanism of grip force reduction areneeded. Third, it is known that MS patients tend to apply largergrip forces than healthy individuals. As such, application of forcethat is greater than required potentially predisposes them to mus-culoskeletal trauma like repeated use injuries and cumulative trau-ma disorders. The utilization of a light finger touch helped in thereduction of grip forces applied and economized the grip force pro-duction in individuals with MS. It is possible that such a decreasein the grip force production can lead to delay in the onset of fatigue(which is one of their major complaints in this population) andmight decrease the susceptibility to other musculoskeletal injuries.
5. Conclusion
The results of the present study suggest that the patients withMS studied here might benefit from the application of light fingertouch from the contralateral hand during performance of simpletasks of daily living such as placing a book on a shelf or feedingor drinking from a glass. Moreover, the outcome of the study canbe used to develop a new rehabilitation approach which wouldhelp patients in economizing their grip force, thus, enabling themto perform more activities independently.
Acknowledgement
This study was supported by a grant from the National MultipleSclerosis Society.
References
Aruin AS. Support-specific modulation of grip force in individuals with hemiparesis.Arch Phys Med Rehabil 2005;86:768–75.
Augurelle AS, Smith AM, Lejeune T, Thonnard JL. Importance of cutaneous feedbackin maintaining a secure grip during manipulation of hand-held objects. JNeurophysiol 2003;89:665–71.
Bell-Krotoski J. Advances in sensibility evaluation. Hand Clin 1991;7:527–46.Chaisson CE, Zhang Y, Sharma L, Felson DT. Higher grip strength increases the risk of
incident radiographic osteoarthritis in proximal hand joints. OsteoarthritisCartilage 2000;8(Suppl. A):S29–32.
Cole KJ, Rotella DL. Old age affects fingertip forces when restraining anunpredictably loaded object. Exp Brain Res 2001;136:535–42.
Cole KJ, Rotella DL. Old age impairs the use of arbitrary visual cues for predictivecontrol of fingertip forces during grasp. Exp Brain Res 2002;143:35–41.
Cole KJ, Rotella DL, Harper JG. Tactile impairments cannot explain the effect of ageon a grasp and lift task. Exp Brain Res 1998;121:263–9.
Cole KJ, Rotella DL, Harper JG. Mechanisms for age-related changes of fingertip forcesduring precision gripping and lifting in adults. J Neurosci 1999;19:3238–47.
Flanagan JR, Wing AM. The stability of precision grip forces during cyclic armmovements with a hand-held load. Exp Brain Res 1995;105:455–64.
Gao F, Latash ML, Zatsiorsky VM. Internal forces during object manipulation. ExpBrain Res 2005;165:69–83.
Gilles MA, Wing AM. Age-related changes in grip force and dynamics of handmovement. J Mot Behav 2003;35:79–85.
Gordon AM, Duff SV. Fingertip forces during object manipulation in children withhemiplegic cerebral palsy. I: Anticipatory scaling. Dev Med Child Neurol1999;41:166–75.
Hermsdorfer J, Hagl E, Nowak DA, Marquardt C. Grip force control during objectmanipulation in cerebral stroke. Clin Neurophysiol 2003;114:915–29.
Holewski JJ, Stess RM, Graf PM, Grunfeld C. Aesthesiometry: quantification ofcutaneous pressure sensation in diabetic peripheral neuropathy. J Rehabil ResDev 1988;25:1–10.
Iyengar V, Santos MJ, Aruin AS. Does the location of the touch from the contralateralfinger application affect grip force control while lifting an object? Neurosci Lett2007;425:151–5.
Iyengar V, Santos MJ, Aruin AS. Grip force control in patients with multiplesclerosis: effect of contralateral finger touch. In: UIC student research forum,UIC forum, 2008. p. 35.
Jeka JJ. Light touch contact as a balance aid. Phys Ther 1997;77:476–87.Jeka JJ, Lackner JR. Fingertip contact influences human postural control. Exp Brain
Res 1994;100:495–502.Johansson RS, Riso R, Hager C, Backstrom L. Somatosensory control of precision grip
during unpredictable pulling loads. I: Changes in load force amplitude. ExpBrain Res 1992;89:181–91.
Krishnan V, de Freitas PB, Jaric S. Impaired object manipulation in mildly involvedindividuals with multiple sclerosis. Motor Control 2008;12:3–20.
Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expandeddisability status scale (EDSS). Neurology 1983;33:1444–52.
Lackner JR, DiZio P, Jeka J, Horak F, Krebs D, Rabin E. Precision contact of thefingertip reduces postural sway of individuals with bilateral vestibular loss. ExpBrain Res 1999;126:459–66.
Lackner JR, Rabin E, DiZio P. Stabilization of posture by precision touch of the indexfinger with rigid and flexible filaments. Exp Brain Res 2001;139:454–64.
Lowe BD, Freivalds A. Effect of carpal tunnel syndrome on grip force coordination onhand tools. Ergonomics 1999;42:550–64.
Marwaha R, Hall SJ, Knight CA, Jaric S. Load and grip force coordination in static bimanualmanipulation tasks in multiple sclerosis. Motor Control 2006;10:160–77.
Miller DM, Rudick RA, Cutter G, Baier M, Fischer JS. Clinical significance of themultiple sclerosis functional composite: relationship to patient-reportedquality of life. Arch Neurol 2000;57:1319–24.
Nowak DA. Different modes of grip force control: voluntary and externally guidedarm movements with a hand-held load. Clin Neurophysiol 2004;115:839–48.
Nowak DA, Glasauer S, Hermsdorfer J. Grip force efficiency in long-term deprivationof somatosensory feedback. Neuroreport 2003a;14:1803–7.
Nowak DA, Glasauer S, Hermsdorfer J. How predictive is grip force control in thecomplete absence of somatosensory feedback. Brain 2004a;127:182–92.
Nowak DA, Hermsdorfer J. Analysis of grip force during object manipulation.Method for the objective measurement of physiological normal and impairedhand function. Nervenarzt 2004;75:725–33.
Nowak DA, Hermsdorfer J. Grip force behavior during object manipulation inneurological disorders: toward an objective evaluation of manual performancedeficits. Mov Disord 2005;20:11–25.
Nowak DA, Hermsdorfer J. Objective evaluation of manual performance deficits inneurological movement disorders. Brain Res Rev 2006;51:108–24.
Nowak DA, Hermsdorfer J, Glasauer S, Philipp J, Meyer L, Mai N. The effects of digitalanaesthesia on predictive grip force adjustments during vertical movements ofa grasped object. Eur J Neurosci 2001;14:756–62.
Nowak DA, Hermsdorfer J, Topka H. Deficits of predictive grip force control duringobject manipulation in acute stroke. J Neurol 2003b;250:850–60.
Nowak DA, Rothwell J, Topka H, Robertson MM, Orth M. Grip force behavior inGilles de la Tourette syndrome. Mov Disord 2004b;20:217–23.
Scholz J, Latash M. A study of bimanual synergy associated with holding anobjectPlease provide the volume number for the reference ‘Scholz and Latash(1998)’.. Hum Mov Sci 1998:753–79.
Thornbury JM, Mistretta CM. Tactile sensitivity as a function of age. J Gerontol1981;36:34–9.




















