E:\review\or-2018\or may.pmd - E-Magazine....::... - Odisha Gov
Upload
khangminh22Category
view
0download
0
1
ENVIRONMENTAL AND OCCUPATIONAL HEALTH MONTHLY E-MAGAZINE
VOLUME 3 ISSUE - 9
October 2020
UNIQUE FORUM FOR INDUSTRIAL PHYSICIANS AND SAFETY PERSONNELS
e-MagazineOCCUCLAVE
• Walking Out of the Doors of Death Story of COVID Survival• "Second Wave" of COVID-19 Pandemic• Role of Occupational Health Professionals in Health Promotion• International Lead Poisoning Prevention Week 2020

2
IN THIS ISSUE
07
03Editor's Desk
About AEOHD
EVENT HIGHLIGHTS
Hall of Fame AEOHD Digiconnect Academic Platform
ARTICLES
International Lead Poisoning Prevention Week 2020
Role of Occupational Health Professionals in Promotion of Health Education & Training For Prevention of Occupational Health Problems in Industry
"Second Wave" of COVID-19 Pandemic
COVID-19 Pandemic: Occupational Health Practitioner’s Perception
Walking Out of the Doors of Death Story of COVID Survival
QUIZOCCUCLAVE e-Quiz
Quiz Answers
UPCOMING WORLD HEALTH DAYSBreast Cancer Awareness
World Sight Day
World Arthritis Day
World Osteoporosis Day
22
42
34
42 43 43
05
13
18 23 27 35
Secretariat
Association of Environmental and Occupational Health Delhi #2057, Tower 3B, Landcraft Golf Links, NH- 24 Near Columbia Asia Hospital, Ghaziabad - 201002 (U.P)
Email: [email protected]; [email protected]
Disclaimer : This e-Magazine is in continuation of Volume-I & II of our OCCUCLAVE e-Magazine, 24 monthly issues of which were successfully published by the
Association of Environmental & Occupational Health, Delhi.The information on this e-Magazine is for information purposes only. The opinion expressed in each article is the opinion of its author and does not necessarily reflect the opinion of e-Magazine. Therefore, e-Magazine carries no responsibility
for the opinion expressed thereon. Any form of reproduction of any content on this e-Magazine without the written permission of the publisher is strictly prohibited. All Rights Reserved © OCCUCLAVE e-Magazine / Managed By: ENOCH Trust.

3
Editor’s DeskInvest in Mental HealthHi All, Mental health is one of the most neglected areas of public health. Close to 1 billion people are living with a mental disorder, 3 million people die every year from the harmful use of alcohol and one person dies every 40 seconds by suicide. This year, millions of people around the world have been affected by the COVID-19 pandemic, which is having a further impact on people’s mental health.Worldwide October is observed as a focus month for mental health. On 10th October, we are observing the World Mental health Day .The goal for this year is – “Increased investment in Mental health”WHO, together with partner organizations, united for Global Mental Health and the World Federation for Mental Health, is calling for a massive scale-up in investment in mental health? To encourage public action around the world, a World Mental Health Day campaign, Move for mental health: let’s invest is been initiated.
Let’s all ensure to do our bit & encourage the following - • During COVID times , encourage employees to speak up , be open & share their
thoughts• Let’s build capacity among managers to handle any concerns sensitively & respectively• Initiate suitable adjustments and accommodations to build a more agile workplace.Let’s try to make our workplaces healthy and stigma free from mental health issues.Regards,Dr Ashish Vijay Jain
References:https://www.who.int/campaigns/world-mental-health-day/world-mental-health-day-2020
4
Dr. S. P. Chaudhry Dr. Shashi Bhushan Dr. Shriniket Mishra
Dr. Angela Sharma Dr. Pawan K. Gupta
Rakesh Veer Garg Sandeep Kumar
Dr. Kamla FartyalDr. Rajiv Kumar JainDr. Sandeep SharmaDr. Gajendra Kumar
Editorial Advisory Board
Editorial Board

5
Association of Environmental and Occupational Health Delhi (AEOHD) is the association of Industrial physicians from PSU’s, Indian Railways, ESIC, Government organizations and other Corporate Industrial physicians working with an aim to study Occupational Health issues of Industrial Workers, it’s prevention and management.
AEOHD is also the Delhi State Branch of the Indian Association of Occupational Health (IAOH) which is the all India parent body.
Internationally IAOH is affliated to The International Commision on Occupational Health (ICOH) & is committed to enable Occupational Health professionals to make global work places healthy, safe and green.
ICOH is recognised by the United Nations as a non-governmental organisation (NGO) and has close working relationships with ILO, WHO, UNEP and ISSA.
Association of Environmental and Occupational Health Delhi
(Delhi State Branch of IAOH)
About

6
Dear Friends,
We know that there is a Tsunami of webinars & information around the globe. In this scenario we need to have sequential decision making with a Dexterous Approach to learn from these events & come back & discuss on your own DigiConnect Platform. This is just like coming home, discussing & filtering the useful information which is of some practical importance to all of us. So stay tuned for every Saturday Prime Time at 6:30 PM to share & learn from each other.
You all can come forward & share your views & Best Practices of your Organizations which shall empower every one of us to fight the Pandemic & hear the pearls of Guidance from our Seniors in IAOH Leaders Please do register for your own Program.
You are cordially invited every Saturday prime time at 6.30 pm to join us on this platform, interact & share their valuable inputs. Learned speakers from different industries & specialties have shared their views in last Issues of this webinar Series-1. Those who have missed it can revisit them on our AEOHD DigiConnect You Tube Channel.
We are quite confident that anything is possible when you have the right people to associate & support us. These are times when we have to take care of each other, our families and our society more than ever.
COVID Pandemic is a challenge but we all industrial physicians have proved that we are good in crisis times, learning from each other & helping society to protect both the lives & livelihood. We have adopted to the new ways of working & wish to invite you all. Please Stay Tuned every Saturday to share & learn from each other, on our AEOHD DigiConnect Academic Platform. This shall help to create a positive atmosphere in these gloomy times.
Environmental & Occupational Health DigiConnect Webinar Academic Platform
(Tune in Every Saturday Prime Time 6.30PM IST India)
Dr Sandeep SharmaProgram Moderator

7
Hall of Fame Environmental & Occupational Health
DigiConnect Webinar Academic Platform
Eminent Speakers Series - 1 • Issue - 1 on 26th April, 2020
Topic: "COVID-19 - The GSK Experience"
Dr. Ashish Vijay Jain
Series - 1 • Issue - 2 on 29th April, 2020
Topic : “In the Face of a Pandemic: Ensuring Safety and Health at Work”
Dr. Rajiv Kumar Jain
Series - 1 • Issue - 3 on 4th May, 2020
Topic : "COVID-19 Testing Methodologies & Path to Vaccine Development and
Evaluation of Therapies" Dr. Puneet Chandna
Series - 1 • Issue - 4 on 9th May, 2020
Topic : "Indian Response v/s Global Response to Mitigate the COVID-19
Situation" Dr. T. Rajgopal
Series - 1 • Issue - 5 on16th May, 2020
Topic : "Minding Your Minds During & After Lock down Due to COVID-19
Pandemic" Dr. S Sivaramakrishnan (Dr Siva)
Series - 1 • Issue - 6 on 23rd May, 2020
Topic : "COVID-19 Pandemic: A Bane or a Boon for Occupational Health Physicians"
Dr. Shrinivas Shanbhag
Series - 1 • Issue - 7 on 30th May, 2020
Topic: “Nintedanib in Idiopathic Pulmo-nary Fibrosis and Extension of Benefit in
SSC-ILD” Dr. Manav Manchanda
Series - 1 • Issue - 8 on 30th May, 2020
Topic : "Pandemics - Then and Now"
Dr. Shyam Pingle
Series - 1 • Issue - 9 on 6th June, 2020
Topic: “Return to Work with COVID 19 – Issues and Strategies for Prevention at
Industrial Workplaces” Dr. Shriniket Mishra
Series - 1 • Issue - 9 on 6th June, 2020
Topic : “Diagnosis and Management of cITP"
Dr. Nitin Sood
Series - 1 • Issue - 9 on 6th June, 2020
Topic: “Road Ahead for Imatinib Treated Patients"
Dr. Amit Bhargava
Series - 1 • Issue - 10 on 13th June, 2020
Topic : “Non Diabetic Renal Disease in Diabetics"
Dr. Jitendra Kumar
Series - 1 • Issue - 10 on 13th June, 2020
Topic: “Work from Home - A NEW NORMAL - Health Perspective"
Dr. Ramanjeet Singh Awal
Series - 1 • Issue - 11 on 20th June, 2020
Topic : “Lysosomal Storage Disorders - Diagnosis & Management"
Dr. Ratna Puri
Series - 1 • Issue - 12 on 21th June, 2020
Topic: "Quick Tips for Work from Home Ergonomics”
Dr. Reena Valecha
Series - 1 • Issue - 14 on 27th June, 2020
Topic : “Cytokine Storm- An Evil: Role of CytoSorb in Critically ill COVID Patients"
Dr. Neera Gupta
Dr S Sivaramakrishnan (Dr Siva)
Medical graduate from the University of Mumbai with post-
graduation in Occupational Health and Hospital Administration. Retired as the Vice President, Medical & Occupational Health at
Siemens Ltd. Heading the Occupational Health Services in India for all Siemens entity for 20 years.
Worked as Medical Officer, Tata Power for 12 years. Working as :-
1. Medical Consultant – Siemens Enterprise Communications Pvt Ltd.
2. Medical Advisor – SAP India 3. Life Style Management Consultant – PD Hinduja National
Hospital, Mahim, Mumbai 4. Life Style Management Consultant – Jupiter Hospital, Thane 5. Managing Director, Lifestyle Enhancing Solutions (INDIA)
Pvt. Ltd.
Awards:
Awarded the OHSF IAOH Oration by the Indian Association of Occupational Health at the 61st National Conference held in February 2011 at Vadodara.
Awarded Fellowship by the Indian Association of Occupational Health at the 60th National Conference on Occupational Health held in February 2010
Awarded the Life Time achievement Award for the contributions in the field of Occupational Health in India by the IAOH, Jamnagar Branch
L & T Oration, Golden Jubilee Commemoration Award Oration, ADM Memorial Oration, Dr KM Bhansali Memorial Oration, Britannia Award & Resource Person Award.
Professional achievements
Worked as Occupational Health Physician for 32 years Past President of Indian Association of Occupational Health, during the Golden Jubilee year. Past General Secretary IAOH. Past President IAOH, Mumbai Branch Presently the National Secretary (INDIA) for International Commission on Occupational Health
(ICOH). Trustee Member of the Worksafe India Fund. Ex Member of CII National Committee on Health and Population. Ex Co-Chairman of the Committee on Environmental Safety & Health of Bombay Chamber of
Commerce and Industries (BCCI). Ex. Visiting faculty IIM, Bangalore Conducting regular Life-Style Management workshop Authored and co-authored many papers on Occupational Health at the National and International
Conferences Visiting faculty at TISS Chairman Advisory Board, Occupational Health, Lokmanya Hospital, Pune. Member of the advisory Board of IJOEM (Indian Journal of Occupational and Environmental
Medicine). Published a chapter on Life Style Management in the book Occupational and Environmental Health
– A Practical Manual Participated in the Global Health Clinic: Healthcare Management for Physician Executives at
Harvard Medical School, Boston, USA in 2007

8
Series - 1 • Issue - 15 on 4th July, 2020
Topic: “Management of Hip Fractures in Corona Times in Elderly"
Dr. Yuvraj Kumar
Series - 1 • Issue - 14 on 27th June, 2020
Topic :“COVID-19 Precautionary & Preventive Measures followed in Our Site/
Organisation" Dr. Nidhi Dhawan Chopra
Series - 1 • Issue - 17on 25th July, 2020Topic: “Myeloproliferative Neoplasms
(MPNs): Thinking Beyond Hydroxyurea (HU)"
Dr. Rahul Bhargava
Series - 1 • Issue - 16 on18th July, 2020
Topic : “Therapeutic Inertia & Insulin Initation in T2DM Patients"
Dr. Praveen R
Series - 1 • Issue - 18 on 01st August, 2020
Topic: “Crisis Standard of Care in COVID 19 – It's Application in EMS,
Emergency Department and ICU" Dr. (Prof.) Tamorish Kole
Series - 1 • Issue - 17 on 25th July, 2020
Topic: “Bone Marrow Transplantation(BMT) in Myeloproliferative Neoplasms
(MPNs) - When it Required" Dr. Meet Kumar
Series - 1 • Issue - 19 on 7th August, 2020
Topic: “Tomotherapy the New Kid on the Block for Radiation Oncology"
Dr. G.K. Jadhav
Series - 1 • Issue - 19 on 7th August, 2020
Topic : “Interesting Cases in Oncology During COVID 19”
Dr. Manish K. Singhal
Series - 1 • Issue - 21 on 15th August, 2020
Topic: “Independence Day Musings: Looking Back, Looking Forward”
Dr. Rajiv Kumar Jain
Series - 1 • Issue - 20 on 8th August, 2020
“AEOHD Discussion with Dr. Anshuman Kumar, COVID 19 Challenges,
Solutions & Opportunities"Dr. Anshuman Kumar
Series - 1 • Issue - 23 on 29th August, 2020
Topic: “Challenges and Strategies for Improving Healthcare Outcomes of Head
and Neck Cancer in India” Dr. Tejas Pandya
Series - 1 • Issue - 22 on 22nd August, 2020
Topic: “Artificial Intelligence: What is it and How is it Changing the Practice of
Medicine?” Dr. Vidur Mahajan
Series - 1 • Issue - 25 on 29th Sep., 2020 Topic: Lung Cancer Outcomes -
Diagnosis to Current Management - With Interesting Cases“Optimal Management of
EGFRm NSCLC Patients” Dr. Manish K. Singhal
Series - 1 • Issue - 24 on 05th September, 2020
TTopic: “Improving Outcomes in Locally Advanced Head and Neck Cancer:
Current Landscape” Dr. Vikas Talreja
Series - 1 • Issue - 27 on 26th September, 2020
Topic : “Idiopathic Pulmonary Fibrosis (IPF) & Systemic Scelorosis Associated -
Interstitial Lung Disease (SSc-ILD)” Dr. Vaibhav Chachra
Series - 1 • Issue - 26 on19th September, 2020
Topic: “Diagnosis & Management of Severe Aplastic Anemia”
Dr. Rayaz Ahmed

9
Series - 1 • Issue - 24 on 05th September, 2020
These kinds of webinars require a meticulous, very careful, precious and well-organized planning.
COVID 19 EPID updates facts, figures, statistics and “hot spots of India as well as global” has really made it a huge success.
Dr Vikas Talreja presentation reflects most popular and latest developments in triple modality of treatment in oncology.
Series - 1 • Issue - 25 on 29th September, 2020
Dr Rajiv Jain is enthusiastic, passionate and very much concerned about the grim situation prevailing in INDIA.
Dr Manish has explained targeted, individualized chemotherapy while proactively managing its side effects.
Thank you, Dr Sandeep, without you it wouldn’t have been possible to update our knowledge especially during COVID and lock down situation.
Series - 1 • Issue - 26 on 19th September, 2020
COVID EPID updates presentation of COVID SARS 2 is superb & informative.
Dr Rayaz Ahmed very nicely explained the causes of aplastic anemia & beautifully explained definitive diagnosis strategy & latest management protocols in the management of Aplastic anemia.
Series - 1 • Issue - 27 on 26th September, 2020
COVID EPID updates is highly educative and helpful to Occupational and Public Health Physicians.
Dr Vaibhav’s presentation & explanations on this great topic of “Idiopathic Pulmonary Fibrosis” were quite fruitful. Take home messages were early screening, monitoring, periodic assessment, diagnosis & early treatment as per the US or UK evidence-based guidelines.
Dr. M. Thyaga Raju Muniswamappa
TestimonialsEnvironmental & Occupational Health
DigiConnect Webinar Series
10
Event Highlights
September 2020 Event Highlights
During the celebration 61st IndianOil Day, Mr SM Vaidya, Chairman IndianOil along with the Board of Directors, felicitated Dr Sandeep Sharma for his contribution & dedicated efforts during COVID 19 Pandemic to ensure that the IOCians across the Nation are
Safe & Healthy
Chairman IndianOil felicitating Dr Sandeep Sharma

11
COVID-19 EPID UPDATESFrom
ENVIRONMENTAL & OCCUPATIONAL HEALTH
DIGICONNECT SERIESDR RAJIV KUMAR JAIN
MBBS; DCH; MD; DNB (HEALTH ADMIN.INC HOSPTAL ADMIN) MNAMS; FIPHA; FAEOHD
DIPLOMA IN CHINESE LANGUAGE

12
13
due to long-term health effects, with the highest burden in developing regions. Even though there is wide recognition of the harmful effects of lead and many countries have taken action, exposure to lead, particularly in childhood, remains of key concern to health care providers and public health officials worldwide. An important source of lead exposure, particularly in children, is paint containing high levels of lead. These paints are still widely available and used in many countries for decorative purposes, although good alternatives without added lead are available. Policy BackgroundRecognizing the continuing need for action to stop exposure to lead from paint, the second session of the International Conference on Chemicals Management in 2009 nominated lead in paint as an emerging policy issue for voluntary cooperative action for risk reduction by countries under the Strategic Approach to International Chemicals Management (SAICM) policy framework. This led to the establishment of the Global Alliance to Eliminate Lead Paint (the Lead Paint Alliance) in 2011, under the joint leadership of the United Nations Environment Programme (UNEP) and the World Health Organization (WHO). The primary goal of the Alliance is to promote
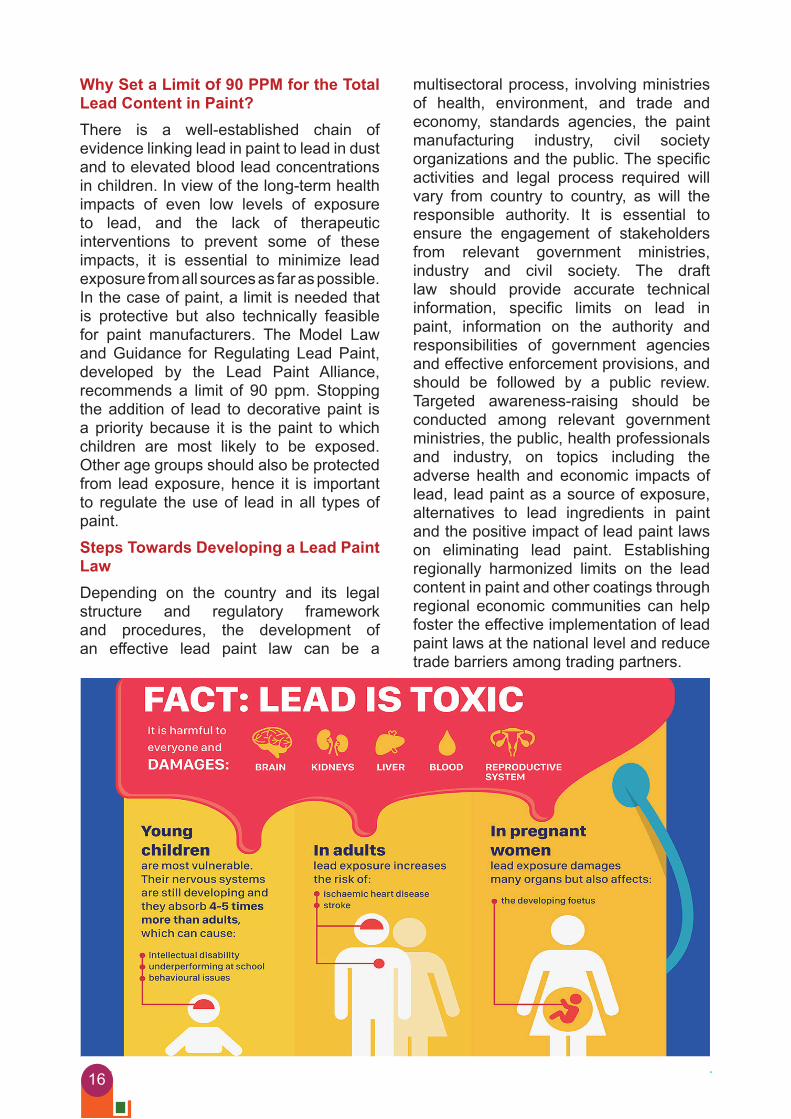
Accelerate The Global Phase Out Of Lead Paint The eighth International Lead Poisoning Prevention Week (ILPPW) takes place on 25–31 October 2020. This week of action is an initiative of the Global Alliance to Eliminate Lead Paint (the Lead Paint Alliance), which is jointly led by the UN Environment Programme and WHO. The manufacture and sale of lead paint is still permitted in over 60% of countries, presenting a continuing and future source of lead exposure for children and workers. The focus of this year’s week of action is on the need to accelerate progress towards the global phase out of lead paint through regulatory and legal measures. The IssueLead is a well-recognized toxicant that has wide-ranging health impacts, in particular affecting the neurological, cardiovascular, gastrointestinal and haematological systems. Young children are particularly vulnerable because they have higher exposures than adults and because lead affects the developing brain, potentially resulting in reduced intellectual ability. The Institute for Health Metrics and Evaluation1 estimated that in 2017 lead exposure accounted for 1.06 million deaths and 24.4 million years lost to disability and death
International Lead Poisoning Prevention Week 2020
DR RAJIV KUMAR JAIN
MBBS; DCH; MD; DNB; MNAMS; FIPHA; FAEOHD; Diploma in Chinese Language.Member, Management Committee, Scientific Committee on Epidemiology in Occupational Health, International Commission on Occupational Health (ICOH)Vice President, Association of Environmental and Occupational Health, Delhi (AEOHD)
ARTICLE

14
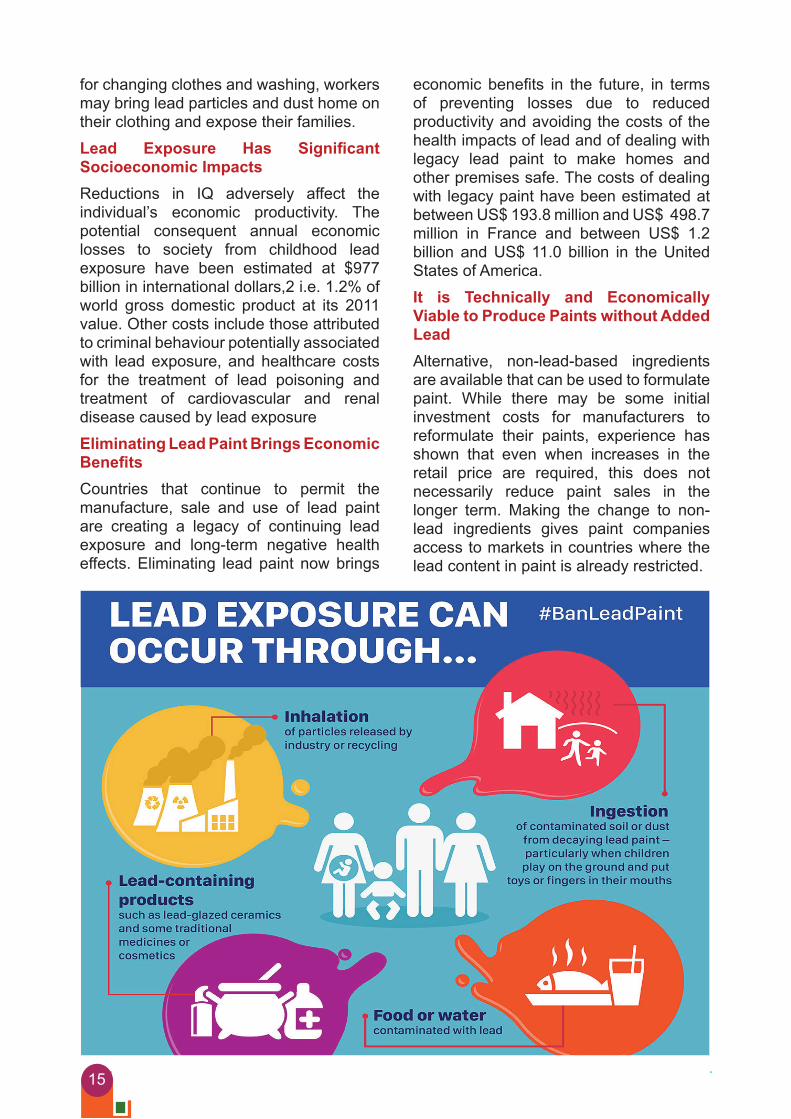
Lead Exposure Causes Wide-Ranging Health Effects and Environmental Impacts The toxicity of lead has been known for centuries; however, it is only in recent decades that the impact of chronic low-level lead exposure on multiple body systems has been understood. Studies to date have been unable to identify any level of exposure that has no harmful effects in children or adults. Young children are especially vulnerable to lead toxicity, and even low levels of exposure can result in reduced intelligence quotient (IQ), reduced attention span, increased antisocial behaviour and reduced educational attainment. Exposure in adults is associated with increased risk of cardiovascular disease, including hypertension and coronary heart disease. As a consequence of these health impacts, the burden of disease from lead exposure is high: the Institute for Health Metrics and Evaluation (IHME) estimated that, in 2017, lead exposure accounted for 1.06 million deaths and the loss of 24.4 million years of healthy life (disability-adjusted life years (DALYs)) worldwide. Lead is, furthermore, a well-documented ecotoxicant, posing threats to both aquatic and terrestrial ecosystems.Mechanisms Of Exposure to Lead From Paint Lead compounds can be added to paint as pigments, driers and to provide corrosion resistance, resulting in a high lead content, which may be in the order of thousands of parts per million (ppm). While the paint remains intact, the lead content is not a hazard; however, as the paint ages, it starts to crumble and flake, releasing lead into household dust. Young children are vulnerable to lead exposure from contaminated dust and flaking paint. They spend a lot of time on the ground and ingest lead-contaminated dust through normal hand-to-mouth behaviour. These exposures can result in elevated blood lead concentrations and lead poisoning. Workers can be exposed to lead during paint manufacture, application and removal. If facilities are not available at the workplace
the global phase-out of lead paint through the establishment of appropriate legally binding measures to stop the manufacture, import, export, distribution, sale and use of lead paints in every country. This goal has received further support in the WHO Road map to enhance health sector engagement in the Strategic Approach to International Chemicals Management towards the 2020 goal and beyond (decision WHA70(23)), which includes national action to phase out the use of lead paint. The elimination of lead paint will contribute to the achievement of the following Sustainable Development Goal targets.• 3.9: By 2030 substantially reduce the
number of deaths and illnesses from hazardous chemicals and air, water, and soil pollution and contamination.
• 12.4: By 2020, achieve the environmentally sound management of chemicals and all wastes throughout their life cycle, in accordance with agreed international frameworks, and significantly reduce their release to air, water and soil in order to minimize their adverse impacts on human health and the environment.
The CampaignInternational lead poisoning prevention week (ILPPW) is an initiative of the Lead Paint Alliance. The aim of the week of action is to• Raise awareness about health effects
of lead exposure;• Highlight the efforts of countries and
partners to prevent led exposure, particularly in children; and
• Urge further action to eliminate lead paint through regulatory action at country level.
Governments, civil society organizations, health partners and others are encouraged to organize campaigns during ILPPW. A range of materials to support campaign activities have been developed by the Lead Paint Alliance and are made available by WHO. We invite campaign organizers to register their events on our webpage so that others can see what events are happening in their area.
15
economic benefits in the future, in terms of preventing losses due to reduced productivity and avoiding the costs of the health impacts of lead and of dealing with legacy lead paint to make homes and other premises safe. The costs of dealing with legacy paint have been estimated at between US$ 193.8 million and US$ 498.7 million in France and between US$ 1.2 billion and US$ 11.0 billion in the United States of America.It is Technically and Economically Viable to Produce Paints without Added Lead Alternative, non-lead-based ingredients are available that can be used to formulate paint. While there may be some initial investment costs for manufacturers to reformulate their paints, experience has shown that even when increases in the retail price are required, this does not necessarily reduce paint sales in the longer term. Making the change to non-lead ingredients gives paint companies access to markets in countries where the lead content in paint is already restricted.
for changing clothes and washing, workers may bring lead particles and dust home on their clothing and expose their families.Lead Exposure Has Significant Socioeconomic Impacts Reductions in IQ adversely affect the individual’s economic productivity. The potential consequent annual economic losses to society from childhood lead exposure have been estimated at $977 billion in international dollars,2 i.e. 1.2% of world gross domestic product at its 2011 value. Other costs include those attributed to criminal behaviour potentially associated with lead exposure, and healthcare costs for the treatment of lead poisoning and treatment of cardiovascular and renal disease caused by lead exposureEliminating Lead Paint Brings Economic Benefits Countries that continue to permit the manufacture, sale and use of lead paint are creating a legacy of continuing lead exposure and long-term negative health effects. Eliminating lead paint now brings
16
multisectoral process, involving ministries of health, environment, and trade and economy, standards agencies, the paint manufacturing industry, civil society organizations and the public. The specific activities and legal process required will vary from country to country, as will the responsible authority. It is essential to ensure the engagement of stakeholders from relevant government ministries, industry and civil society. The draft law should provide accurate technical information, specific limits on lead in paint, information on the authority and responsibilities of government agencies and effective enforcement provisions, and should be followed by a public review. Targeted awareness-raising should be conducted among relevant government ministries, the public, health professionals and industry, on topics including the adverse health and economic impacts of lead, lead paint as a source of exposure, alternatives to lead ingredients in paint and the positive impact of lead paint laws on eliminating lead paint. Establishing regionally harmonized limits on the lead content in paint and other coatings through regional economic communities can help foster the effective implementation of lead paint laws at the national level and reduce trade barriers among trading partners.
Why Set a Limit Of 90 PPM for the Total Lead Content in Paint? There is a well-established chain of evidence linking lead in paint to lead in dust and to elevated blood lead concentrations in children. In view of the long-term health impacts of even low levels of exposure to lead, and the lack of therapeutic interventions to prevent some of these impacts, it is essential to minimize lead exposure from all sources as far as possible. In the case of paint, a limit is needed that is protective but also technically feasible for paint manufacturers. The Model Law and Guidance for Regulating Lead Paint, developed by the Lead Paint Alliance, recommends a limit of 90 ppm. Stopping the addition of lead to decorative paint is a priority because it is the paint to which children are most likely to be exposed. Other age groups should also be protected from lead exposure, hence it is important to regulate the use of lead in all types of paint.Steps Towards Developing a Lead Paint Law Depending on the country and its legal structure and regulatory framework and procedures, the development of an effective lead paint law can be a

17
Conclusions WHO has identified lead as one of the 10 chemicals of major public health concern globally. While young children are the ones most vulnerable to the toxic effects of lead, in fact all age groups can be adversely affected by exposure to lead. The health consequences of lead exposure can also result in significant negative economic and social impacts at the population level.Lead paint is an important, but preventable, source of exposure to lead. Already, 72 WHO Member States (73 United Nations Member States) have shown that it is possible to restrict the use of lead in paint, and many paint companies have already reformulated or committed to reformulating their paints. Eliminating lead paint globally is therefore entirely possible and will yield both individual and societal benefits for years to come. For governments, regulating lead paint is an important primary prevention measure to tackle a priority chemical of public health concern. This action contributes to mainstreaming primary prevention in the sound management of chemicals. It also creates an opportunity for the health and environment sectors to work together to protect public health and preserve the integrity of ecosystems. Such joint activity supports the implementation of the WHO Chemicals Roadmap and the Strategic Approach to International Chemicals Management.
References• Alexander FW (1974). The uptake of lead by children in
differing environments. Environ Health Perspect. 7:155–9. doi:10.1289/ehp.747155.
• American Academy of Pediatrics Committee on Environmental Hazards (1972). Lead content of paint applied to surfaces accessible to young children. Pediatrics. 49(6):918–21.
• American Academy of Pediatrics Council on Environmental Health (2016). Prevention of childhood lead toxicity. Pediatrics. 138(1):e20161493. doi:10.1542/peds.2016 1493.
• da Rocha Silva JP, Salles FJ, Leroux IN, da Silva Ferreira APS, da Silva AS, Assunção NA et al. (2018). High blood lead levels are associated with lead concentrations in households and day care centers attended by Brazilian preschool children. Environ Pollut. 239:681–8. doi:10.1016/j. envpol.2018.04.080.
• GBD 2017 Risk Factor Collaborators (2018). Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 392:1923–94 (https://doi.org/10.1016/S0140– 6736(18)32225–6).
• Goldman RH, Weissman L (2019). A diagnosis to chew on. N Engl J Med. 381:466–73. doi:10.1056/ NEJMcps1900774.
• Health Canada (2019). Fifth report on human biomonitoring of environmental chemicals in Canada. Ottawa: Health Canada (https:// www.canada.ca/en/health-canada/services/ environmental-workplace-health/reports-publications/environmental-contaminants/fifth-report-humanbiomonitoring.html).
• Keller B, Faciano A, Tsega A, Ehrlich J (2017). Epidemiologic characteristics of children with blood lead levels ≥45 μg/dL. J Pediatr. 180:229–34 (https:// doi.org/10.1542/gr.37–1-8).
• Lanphear BP, Rauch S, Auinger P, Allen RW, Hornung RW (2018). Low-level lead exposure and mortality in US adults: a population-based cohort study. Lancet Public Health. 3(4):e177–e184 (https://www. thelancet.com/journals/lanpub/ article/PIIS2468– 2667(18)30025–2/fulltext).
• NCPC Serbia (2019). Lead paint reformulation technical guidelines. In: Demonstration pilots with paint manufacturers in small and medium sized enterprises (SMEs) executed in eight countries [Project Output 1.1][website]. National Cleaner Production Centre of Serbia (http://www.saicm.org/ Implementation/GEFProject/LeadinPaintComponent/Output11/tabid/7974/language/en-US/Default.aspx).
• NYU Lagone Health (2020). Economic costs of childhood lead exposure in low- & middle-income countries. In: NYU Lagone Health [website]. New York: New York University Lagone Health (https://med. nyu.edu/departments-institutes/pediatrics/divisions/ environmental-pediatrics/research/policy-initiatives/ economic-costs-childhood-lead-exposure-low-middleincome-countries).
• Ongking J (2018). We can’t be green until lead is out of the scene. Polymers Paint Colour Journal: Going Green, October 2018 (https://issuu.com/dmgeventscg/ docs/ppcj_oct_18/24).
• SCS Global Services (2019). Sycwin Coating & Wires receives Lead Safe Paint® certification for all paint brands. In: SCS Global Services. Emeryville (CA): SCS Global Services (https://www. scsglobalservices.com/news/sycwin-coating-wiresreceives-lead-safe-paint-certification-for-all-paintbrands).
• Ziegler EE, Edwards BB, Jensen RL, Mahaffey KR, Fomon SJ (1978). Absorption and retention of lead by infants. Pediatric Res. 12(1):29–34. doi:10.1203/00006450–197801000–00008.
18
It has been further documented by various research workers that migrant worker- a common feature in developing countries like India — who have neither vocational training nor previous industrial experience are predisposed to high risks of accidents and occupational diseases.To protect the health of workers, ILO vide its recommendation 1959 (No.112) has suggested for establishment of Occupational Health Service with training and education of employees as one of the essential constituents besides others. In our country we are also propagating the idea of Occupational Health Service and working at the same time to implement the recommendation.The modern trends in Occupational Health and Safety in the developed countries are also three dimensional:
1. By research, education and effective training of the working people
2. By establishing occupational health services.
3. By effective legislative measures
Occupational Health aims at the promotion and maintenance of Highest degree of physical, mental and social well-being of workers in all occupations. It is a known fact that "No occupation is without any occupational disorder and further there is no occupational disorder which is not preventable." Therefore, the preventive program must play a vital role in the industrial growth of a country.In industrial situations all over the world — occupational disorders due to ill-effects of various physical, chemical and biological agents are causing great concern. In India also the occupational health status of man at work is getting due importance. The adverse health effects of various agents are found to be more amongst the workers exposed to specific pollutants. Physical agents like noise, heat had also contributed significantly in causing ill-health to the man at work.Accident investigations have also revealed that unsafe acts are leading to a greater number of accidents than the unsafe conditions.
Dr. Sandeep Sharma
Secretary, AEOHD Ex-Joint Secretary IAOH India
Organizing Secretary OCCUCON 2017National Representative of MEDICHEM in India
& Deputy General Manager Corporate HSE IndianOil Corporation Limited
Role of Occupational Health Professionalsin Promotion of Health Education & Training
For Prevention of Occupational Health Problems in Industry
ARTICLE
19
Therefore, the training must play a vital role in the prevention program of Occupational Health problems of industrial workers of the World in general and of India in particular.Role of Factory Medical OfficerThe Factory Medical Officer will have to play a very important and key role of a catalyst and a change agent. He must convey the intention of Management to all concerned that "Around here, we support positive health practices". He must see that Health Education and training for preventing occupational diseases becomes on integral part of the company's Education and Training policy. Towards this end he must take the following steps1. Determining Needs:
Administer a questionnaire based on the findings of Occupational Health studies for identification of training needs. This will help in designing need-based training packages for different level of personnel in an organization
2. Involve People:Training employees to function as a health promotion leadership committee member is an effective way to prepare an organization’s action team to make a functional contribution to the occupational health promotion effort. This committee should consist of employees from all levels of the organization and should represent as many departments as possible. Leadership committee members can serve as advocates for this occupational health promotion process, problem solvers for issues that arise and an effective communication vehicle for propagating program events.
3. Heighten Interest and Awareness:Occupational Health Promotion is a communications intensive effort, Newsletters, bulletin boards, posters, etc. can all be used to promote and market the process. The factory medical officer plays a vital role in the communication process by writing
supportive statements and messages in company publications. This send a powerful message to all employees that occupational health promotion is a mainstream business function.
4. Secure Leadership Commitment: It is critical for managers to know why Occupational Health promotion is a compelling priority business need and how they can get involved. One way to do this is to involve the whole management team in your health education and training effort.
5. Introduce Employees:Getting employees started as a group is essential for the success of the program. Employees usually have a limited vision of what is possible in their working lives. Orientation to Occupational Health promotion efforts of the factory broaden employees’ image of the situation in which he is supposed to work and the associated health hazards. This motivates them to get involved in the occupational health promotion effort of the factory. These sessions are an excellent opportunity for employees to hear firsthand from management about the organization’s commitment to occupational health promotion.
6. Create a vision of Health enhancing Lifestyle Possibilities:Providing health enhancement interventions communicates to employees that the organization is interested in their personal development as well as their prevention from health risks. These programs include titles such as Interpersonal Communication, Self Esteem, Creative Thinking, Job Satisfaction, Managing Change and deal less with avoiding illness and more with maximizing personal potential.
7. Equip People with Skills for on-Going Support:Recharging enthusiasm and support are always an issue with Occupational

20
Health promotion programs. Employees need to have opportunities to learn more about Occupational Health promotion topics and provide support to the efforts of the company. This can be accomplished through regular scheduled support group meetings organized by the Factory Medical Officers. Continual reinforcement by managers of the importance of occupational health during work group meetings keeps the message alive that the organization is committed to employee’s well-being.
8. Create a Healthy Organization: Clearly, this is the biggest challenge, but the most important step Managers need to look for ways to create occupational health enhancing norms and to eliminate those norms which blocks the efforts. Above all, managers need to maintain their commitment to productivity through health promotion and to stay involved themselves.
Role of an Occupational Health NurseOccupational and environmental health nursing is the specialty practice that focuses on promoting and restoring health, preventing illness and injury, and protecting workers and community groups from environmental hazards. Occupational and Environmental Health Nurses have a combined knowledge of health and business that they blend with healthcare expertise to balance the requirement for a safe and healthful work environment with a “healthy” bottom line.They can provide worker education and administrative controls for safe work supplies like masks, gloves, cleanser, and disinfectants; handwashing and workstation cleaning protocols; elevator use; cafes and food courts; public transportation; supplier deliveries and practices; and safe interaction with customers and clients. OH Nurses can identify signs and symptoms of traumatic stress, and provide coping skills and emotional resilience that will keep employees happy, healthy, and on the job.
Through their recognized value as business partners, OH Nurses implement Occupational Health service programs and provide budgetary input.They develop policies and procedures that align with company visions and missions, and supervise, direct, and mentor co-workers in the effort to impact corporate improvement and workers’ health and safety, thus contributing positively to the financial bottom line.Role of an Industrial Hygienist Industrial hygienists use environmental monitoring and analytical methods to detect the extent of worker exposure and employ engineering, work practice controls, and other methods to control potential health hazards at the workplace, as Industrial hygiene is the science of anticipating, recognizing, evaluating, and controlling workplace conditions that may cause workers' injury or illness. Industrial Hygienist is responsible for selecting and using instrumentation to monitor workplace during the identification and control phases of industrial hygiene projects, recommend relevant control techniques & maintain the control measure.To Summarize:The following three paragraphs summarize the principles of ethics on which is based the international code of ethics for Occupational Health professionals prepared by the International Commission on Occupational Health- ICOH 1. Occupational practice must be
performed according to the highest professional standards and ethical principles. Occupational Health professionals must solve the health and social wellbeing of the workers individually and collectively they also contribute to environmental and community health.
2. Occupational Health professionals are experts who must enjoy full professional independence in the execution of their functions. They must acquire and maintain the competence necessary
21
for their duties and require conditions which allow them to carry out their task according to good practice and professional ethics.
3. The obligations of Occupational Health professionals include protecting the life and the health of worker respecting human dignity and promoting the highest ethical principles in Occupational Health policies and programs. Integrity in professional conduct, impartiality and protection of the confidentiality after health data and of the privacy of workers are part of these obligations.
As for the international code of ethics for Occupational Health professionals, the physician should:1. Accord the highest priority to the Health
and Safety of individuals in both the workplace and the environment.
2. Practice on a scientific basis with integrity and strive to acquire and maintain adequate knowledge and expertise upon which to render professional service.
3. Relate honestly and ethically in all professional relationships
4. Strive to expand and disseminate medical knowledge and participate in ethical research efforts as appropriate
5. Keep confidential all individual medical information, releasing such information only when required by law or overriding public health considerations, or to other physicians according to accepted medical practice, or to others at the request of the individual
6. Recognize that employers may be entitled to counsel about an individual's medical work fitness but not to diagnosis or specific details except in compliance with laws and regulations
7. Communicate to individuals and/or groups any significant observations and recommendations concerning their health or safety, and
8. Recognize those medical impairments in ourselves and others including chemical dependency and abusive personal practices which interfere with one's ability to follow the above principles, and take appropriate measures
Disclaimer: The information shared, is solely intended, for the benefit of young industrial physicians & is contributed from the archives of what we have learnt from the views, thoughts, and opinions expressed by our great teachers.
Any updates in the present context may please be verified
22
1. Which of the following is a Good Cholesterol:
(a) LDL (b) VLDL (c) HDL (d) None of the above
2. What is the most common cause of back Pain:
(a) A Slipped Disc (b) A Trapped Nerve (c) An Injury to a Muscle (d) Usually There no Obvious Physical
Cause
3. An Allergen is a substance that can trigger:
(a) Loose motion (b) Alopecia (c) Allergic reaction (d) Bleeding from Gums
4. Relative humidity (RH) must be maintained below in occupied indoor areas:
(a) <50% (b) <40% (c) <75% (d) <60%
5. NIHL is normally described as being:
(a) Permanent (b) Painless (c) Progressive(d) All of the above
6. Best method to control bleeding is:(a) Direct pressure (b) Pressure point (c) Elevation (d) None
7. An ideal Body Mass Index score is… (a) 25-30(b) 30-35(c) 20-25 (d) 15-20
8. Which factor does not affect blood pressure?
(a) Being overweight(b) Sweating heavily(c) Smoking(d) Physical inactivity 9. You may need a tetanus shot if...(a) You step on a rusty nail (b) You are bitten by a dog(c) You scratch yourself with a rose bush
thorn while gardening(d) All of the above
10. Time required to develop Noise Induced Hearing Loss is
(a) 6-10 months (b) 1-2 months (c) 6-12 Years (d) 1-2 Years
A Unique New Initiative of OCCUCLAVE Editorial Team : OCCUCLAVE e-Quiz
Instructions for the e-Quiz : Please read the questions carefully & note down the correct answers on a seperate piece of paper.
e-QuizOCCUCLAVE
COVID-19Quiz
Note : The correct answers of this e-Quiz are available on page no. 34 of the OCCUCLAVE e-Magazine
23
"Second Wave" of COVID-19 Pandemic
DR AJAY SATI
Consultant Physician Occupational Health and Wellness
Zen MultiSpecialty HospitalChembur, Mumbai
ARTICLE
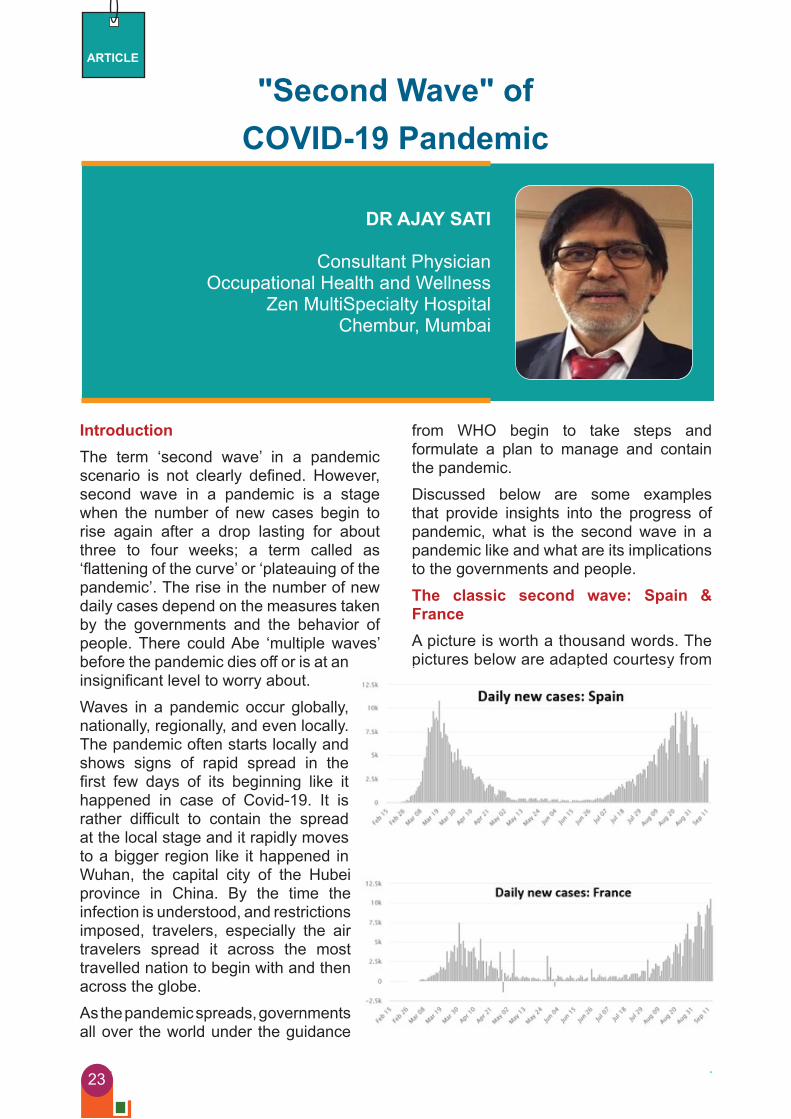
IntroductionThe term ‘second wave’ in a pandemic scenario is not clearly defined. However, second wave in a pandemic is a stage when the number of new cases begin to rise again after a drop lasting for about three to four weeks; a term called as ‘flattening of the curve’ or ‘plateauing of the pandemic’. The rise in the number of new daily cases depend on the measures taken by the governments and the behavior of people. There could Abe ‘multiple waves’ before the pandemic dies off or is at an insignificant level to worry about.Waves in a pandemic occur globally, nationally, regionally, and even locally. The pandemic often starts locally and shows signs of rapid spread in the first few days of its beginning like it happened in case of Covid-19. It is rather difficult to contain the spread at the local stage and it rapidly moves to a bigger region like it happened in Wuhan, the capital city of the Hubei province in China. By the time the infection is understood, and restrictions imposed, travelers, especially the air travelers spread it across the most travelled nation to begin with and then across the globe. As the pandemic spreads, governments all over the world under the guidance
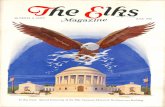
from WHO begin to take steps and formulate a plan to manage and contain the pandemic.Discussed below are some examples that provide insights into the progress of pandemic, what is the second wave in a pandemic like and what are its implications to the governments and people.The classic second wave: Spain & FranceA picture is worth a thousand words. The pictures below are adapted courtesy from

24
worldometers.info and they depict the ‘second wave’ happening in Spain and France. In between the two waves was a period when the number of cases plateaued followed by hitting a new low that prompted governments to open up the economy. As the economic activity gains momentum number of cases rise. Frequent increase in the number of daily cases occurs which is then followed by a slow constant increase in the number of daily cases. As long as the number of cases and deaths are manageable by the available healthcare infrastructure governments do not impose lockdown restrictions again.Experiences during the first wave make people more careful and less fearful during the second wave. Economic activity that continues during the second wave also indicates that the healthcare capacity is not overstretched. Lockdown is reimposed in varying degrees if cases rise beyond the capacity of healthcare infrastructure. Both people and governments begin to realize that the pandemic is here to stay and that livelihood is as important as life.The take-off second wave: UK & Italy U.K and Italy are on the verge of having the second wave as there is a constant
daily upswing happening in the number of daily cases as noted in the illustration alongside. If restrictions are not imposed immediately the second wave will occur soon. As I start to write this on 15th September 2020, the British Prime Minister Boris Johnson has imposed some restrictions in the UK as the number of new daily cases rise to 3000 – it has lowered the limit on the number of people allowed to
meet from 30 to 6. There could be more restrictions coming. As compared to the UK, Italy doesn’t yet have the constant increase in the number of daily cases as evident in the illustration alongside. Once a constant increase is noted the government steps in to impose appropriate restrictions. The timing of restrictions is important; too early will derail the economic gains and a delay will impact both the economic gains as well as healthcare capacity.The impending second wave: Germany The illustration alongside for Germany is indicative that the country is getting ready for the ‘second wave’ unless timely tough measures are put in place. The number of new daily cases have not reached the levels that were seen at the start or the first wave. Frequent increase in the number of daily cases with fall in between
after the plateau are indications of an impending second wave. The moment there are constant daily upswings the scene is set for the second wave and the government acts to impose restrictions before the healthcare capacity gets overstretched. It is important that imposition of restrictions is well-timed as discussed earlier as it has impact
on economic gains as well as healthcare capacity.

25
The complex second wave: USAThe pattern seen for USA in the picture is indicative of the various ways this virus behaves depending on the environment provided. The first wave in US was smaller compared to the second wave. The first wave although had a peak did not have a fall and merged into a heightened plateau of around 20,000 daily cases lasting 4 weeks from 10th May to 10th June 2020 and without a further substantial decrease in the number of daily cases the second wave took off. The second wave was bigger than the first wave and had a peak and a fall that is continuing. It will take a couple of weeks more before a flattening of the curve occurs, if at all, as a third wave could quickly kick off just as the second wave occurred quickly after the first wave.
The complex behavior of the second wave is in accordance with the behavior of the government and the public alike. If the lockdown restrictions were to continue during the first wave until a drop in number of daily cases it is possible that the plateau though prolonged would have further flattened to reduce the number. In the absence of continuing lockdown restrictions and perhaps the disobedience on part of a section of population the second wave came on rather quickly and the daily cases began to rise, more than in the first wave and persisted for about 10 weeks from 25th June to 10th September. There is a drop in the number of daily cases occurring now that could increase again after a plateau if restrictions fail or are not imposed and that could mean a quick ‘third wave’.
The incomplete first wave: IndiaIndia appears to be a case where even the first wave is not yet peaked, is still continuing and is incomplete. That clearly means that the first wave is not yet over as can be seen in the illustration alongside. The second wave if at all it occurs is far away. Typically, a pandemic peaks followed by a gradual fall in the number of cases and a subsequent flattening of the curve or a plateau for 3 to 4 weeks after which due to reopening of economic activity there are frequent increase in the number of daily cases which lead to the second wave. In a country of the size of India there was enormous impact of lockdown and restarting of economic activity was necessary despite rising number of daily cases; the compulsion was not political
but a humanitarian one to prevent excessive unrest and unemployment and its repercussions that includes a fall in GDP. The big fat first wave seen in India is for two reasons – the spread to rural areas and its 1.4 billion population. Appropriate steps have been taken by the government whenever the number of daily cases exceed the healthcare capacity to
handle it.More than 4000 friends, well-wishers,
Local ‘second wave’ in an incomplete national ‘first wave’: Mumbai / DelhiThe cities of Delhi and Mumbai are examples, wherein a second wave has set in while India is still to complete the classic first wave. There are many such examples all over India and across the globe. This happens when the local government initially controls the spread effectively
26
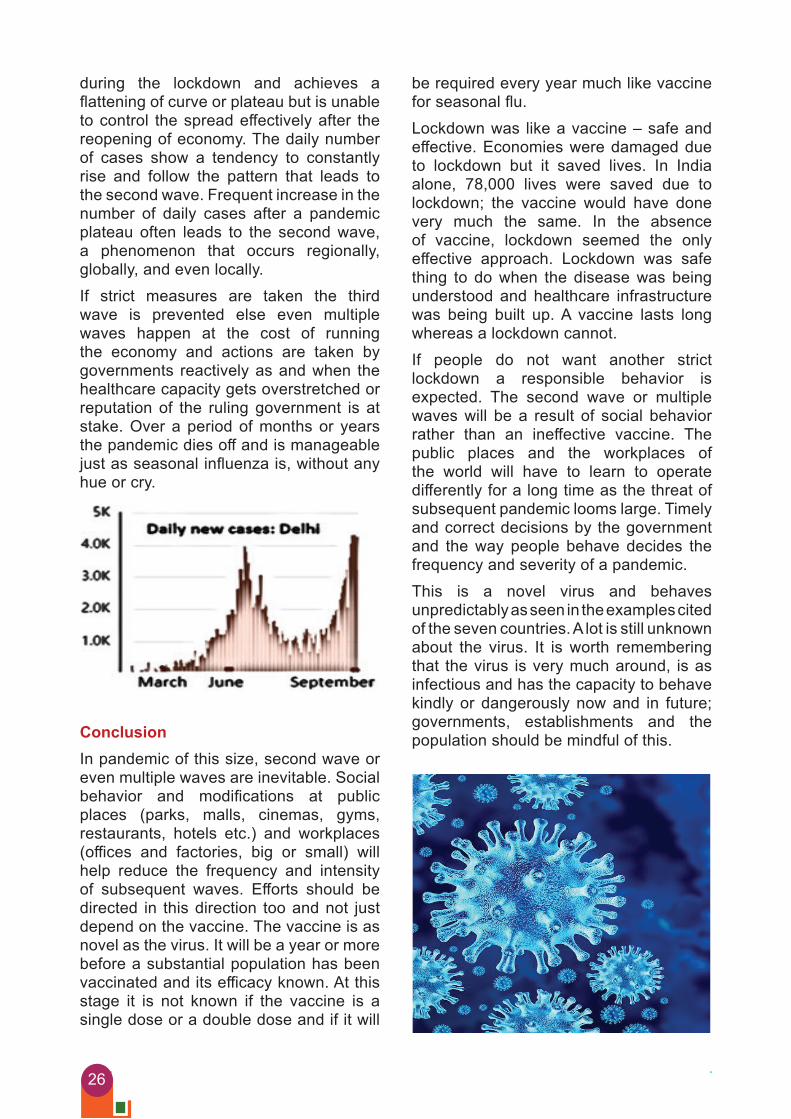
during the lockdown and achieves a flattening of curve or plateau but is unable to control the spread effectively after the reopening of economy. The daily number of cases show a tendency to constantly rise and follow the pattern that leads to the second wave. Frequent increase in the number of daily cases after a pandemic plateau often leads to the second wave, a phenomenon that occurs regionally, globally, and even locally. If strict measures are taken the third wave is prevented else even multiple waves happen at the cost of running the economy and actions are taken by governments reactively as and when the healthcare capacity gets overstretched or reputation of the ruling government is at stake. Over a period of months or years the pandemic dies off and is manageable just as seasonal influenza is, without any hue or cry.
Conclusion In pandemic of this size, second wave or even multiple waves are inevitable. Social behavior and modifications at public places (parks, malls, cinemas, gyms, restaurants, hotels etc.) and workplaces (offices and factories, big or small) will help reduce the frequency and intensity of subsequent waves. Efforts should be directed in this direction too and not just depend on the vaccine. The vaccine is as novel as the virus. It will be a year or more before a substantial population has been vaccinated and its efficacy known. At this stage it is not known if the vaccine is a single dose or a double dose and if it will
be required every year much like vaccine for seasonal flu. Lockdown was like a vaccine – safe and effective. Economies were damaged due to lockdown but it saved lives. In India alone, 78,000 lives were saved due to lockdown; the vaccine would have done very much the same. In the absence of vaccine, lockdown seemed the only effective approach. Lockdown was safe thing to do when the disease was being understood and healthcare infrastructure was being built up. A vaccine lasts long whereas a lockdown cannot. If people do not want another strict lockdown a responsible behavior is expected. The second wave or multiple waves will be a result of social behavior rather than an ineffective vaccine. The public places and the workplaces of the world will have to learn to operate differently for a long time as the threat of subsequent pandemic looms large. Timely and correct decisions by the government and the way people behave decides the frequency and severity of a pandemic.This is a novel virus and behaves unpredictably as seen in the examples cited of the seven countries. A lot is still unknown about the virus. It is worth remembering that the virus is very much around, is as infectious and has the capacity to behave kindly or dangerously now and in future; governments, establishments and the population should be mindful of this.

27
COVID-19 Pandemic: Occupational Health Practitioner’s Perception
Dr. J. Vijay Rao
Chief Medical SuperintendentNuclear Fuel Complex
ECILHyderabad
ARTICLE
of SARS-CoV-2 Infection and the high mortality rate, development of a vaccine is an urgent task. Vaccination will restrict the spread of COVID-19 and reduce mortality. Intensive research and development of vaccines is currently underway in China, Russia, India, the USA, & other countries.’ According to WHO, on Aug 13, 2020, 29 candidate COVID-19 vaccines based on different platforms (vectored, DNA, mRNA, inactivated etc.) were being tested in clinical trials.Prevention of SARS-CoV2 infection might be achieved by targeting the spike protein (glycoprotein S), which interacts with the ACE2 receptor and enables entry of SARS-CoV-2 into the cell. Blocking this interaction decreases viral internalisation and replication. Most vaccines that are currently in development target glycoprotein S as the main antigen. The structure and function of the SARC-CoV-2 Glycoprotein is similar to that of other highly pathogenic beta corona viruses, such as Middle East respiratory syndrome COVID (MERS-CoV) and severe acute respiratory syndrome corona virus (SARS-CoV). ’Glycoprotein S consists of two subunits S1 contains a receptor-binding domain (RBD), which interacts with the ACE2 receptor on the cell surface S2 mediates the fusion of viral and cell membranes via formation of a six-helix bundle fusion core. To protect against SARS-CoV2 infection, it is important to
Adapting to the changed conditions while accepting new challenges has always been integral part of a learning curve. COVID-19 pandemic has yet again proved that we, industrial physicians are equipped to handle any crisis, learning from each other and being a part of technological revolution it has brought about. This demanding situation on both body and mind has resulted in stress of a different kind, often expressed as anxiety, anger, short temperedness etc. though this cannot be avoided, it can for sure be directed and managed. Covid-19 was first reported in Wuhan, China, during the end of Dec. 2019. The disease is an acute respiratory illness ranging in severity from mild to severe, with death in some cases: many infected people are asymptomatic. Since the end of Jan. 2020, cases of COVID-19 have been reported in more than 200 countries around the globe. On March 11, 2020, WHO described the spread of COVID-19 as a pandemic.The causative agent of COVID-19 is the beta corona virus severe acute respiratory syndrome corona virus 2. (SARS-CoV2) SARS-CoV2 can be transmitted in many ways, with the main route of via contact with infected people (eg. by secretions, particularly droplet). As of Sep. 19, 2020, there have been more than 21 million laboratory confirmed cases of SARS-CoV2 infection, and more than 7,50,000 deaths. Because of the rapid global spread

28
form neutralizing anti bodies targeting S1 RBD, S1 N- terminal domain, or the S2 region: these antibodies block binding of the RBD to the ACE 2 receptor and prevent S2 mediated membrane fusion or entry into the host cell, thus inhibiting viral infection. Developing a vaccine (particularly during a pandemic) it is important to consider a productive response must develop in a short time (eg. up to 1 month). Moreover, previous work on vaccines for MERS - CoV and SARS-CoV showed that both humoral and cellular (cytotoxic) immune responses are important to induce a protective immune response. To achieve these goals, one of the most attractive options is for vaccines to be based on recombinant viral vectors, which can induce humoral and cellular immune responses and form protective immunity after one or two doses. Recombinant adenovirus vectors have been used for a long time, with safety confirmed in many clinical studies of various preventive and therapeutic drugs. Moreover, the long – term effects of vectors based on adenoviruses have been investigated, by contrast with newer methods that remain to be studied long term. For formation of a robust long lasting immune response a pre-boost vaccination is advisable which is widely used with registered vaccines for diseases including hepatitis B” and Ebola virus disease. When using vector based vaccines immune responses are formed not only to the target antigen but also to the vector component. As a result, the best vaccination scheme is heterologous vaccination, when different viral vectors are used to over come any negative effects of immune response to vector components. Such an approach was successfully used with an Ebola virus disease vaccine developed in Russia and licensed in 2015. A novel, heterologous adenoviral vector based vaccine was designed against SARS-CoV-2 suitable for prime boost vaccinations. This vaccine was with two recombinant adenovirus vectors and was developed as two formulations (frozen [Gam-COVID-Vac] and lyophilised [Gam-COVID-Vac-lyo]). It was aimed to assess safety and immunogenicity of both vaccine formulations and to compare
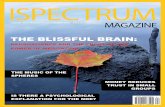
the humoral immune response with that recorded in people who have recovered from COVID-19. A key role for all clinicians advising about return to work is to acquire some understanding of the task requirements of their patient’s work and to assess and advise about the patient’s functional capability both in the short term and in the context of their prognosis. In the current COVID-19 pandemic, clinicians in many settings may be asked to provide guidance on return to work for individuals. This will be particularly important during the phased relaxation of the current lockdown measures. Many of the millions of workers returning to work will have underlying health conditions and they, and possibly their employers, will be seeking advice from their General Practitioners, hospital specialists, nurse practitioners, allied health professionals and others, as well as occupational health (OH) specialists. In doing so, these clinicians will need to take into account the COVID-19 infection risk arising from underlying health conditions (i.e medical/clinical vulnerability) as well as the individual’s workplace, work activities and work environment.illustrates the key areas for consideration in providing such guidance. A brief summary guide and resource list are provided in Section 2. This section provides more detailed guidance in navigating each step of the process and working through the risk assessment and risk judgement processes. Specific tools and illustrative examples are provided for this purpose. Medical vulnerability risk will require clinical assessment of the clinical history and risk factors. Workplace infection transmission risk assessment remains the duty of the employer and guidance and references to assist with this are provided. The employer has significant responsibilities for ensuring an adequate risk assessment is carried out and that all reasonable control measures are implemented and maintained. Many workers may also be able to access advice from their employer’s occupational health (OH) service. Discussion of risks and recommendations with individual employees is important for a successful return to work.

29
Work place transmission risk assessment and controlAll employers will require to undertake a risk assessment of their workplace and work activities and to implement control measures to reduce COVID-19 related risks for transmission of infection, in accordance with the 5 steps approach adopted by the Health & Safety Executive (HSE) for all risk assessments.The lowest risk position is likely to be working from home however, there are many occupations whereby this is not reasonably practicable.COVID-19 transmission arises mainly from:
• Contact with contaminated surfaces• Droplet spread - e.g. coughs and
sneezesAerosol spread can occur mainly in healthcare settings and aerosol generating procedures (AGPs) would be regarded as high risk.Identify risks of COVID-19 transmissionFigure 2. Outlines some main considerations for employers. An awareness of these work-based COVID-19 transmission risk factors will also assist clinicians in discussing return to work risks with their patients. This list is not exhaustive and there may be other risk factors specific for particular workplaces.
Figure 1. COVID-19 Return To Work (RTW) advice considerations
workplaceriskassessment
Medical / clinical vulnerability risk asessment
Overall OH risk assessment
Health promotion
DEICE - Discussion ofemployee's ideas,
concerns & expections
RTW advice

30
Figure 2. General considerations for assessing COVID-19 workplace exposure and transmission risk
Work tasks
• Patient/Service user
• Public facing
• Close contact necessary?
Work place travel
• To and from work
• In the course of work
• Public transport
• Private vehicles
Work place hygiene
• Increased cleaning schedule
• High touch surfaces
Work location• Clinical setting• Customer/Client homes• Retail/Hospitality• Office/Contact centre• Factory
Work movement• Entering and leaving
work• Changing areas• Toilets• Lunch/Breakout areas
Personal hygiene
• Ability to wash hands• Sanitizer• Catch it, Kill it, Bin it
Work Organisation• Ability to maintain social
distancing at work > 2m• Number of different
people sharing a workplace
Personal protective equipment (PPE)• Aavailability• Need• How it is used
Avoidance of symptomatic people
• Particular concern for health / social care providers
Once risk factors for transmission of COVID-19 infection have been considered and practicable control measures have been applied, an overall workplace risk judgement should be made. It is the risk of transmission of COVID-19 through work activities that needs to be assessed. Figure 3 below outlines a simple table of risk factors that can be used to summarise the residual risk of COVID-19 transmission through work activities. It describes some of the main situations related to work whereby the risk of exposure to infection can occur.
The overall workplace risk judgment would be the highest risk level reached (i.e. colored risk category) for any specific risk factor, after control measures are implemented. Low risk is likely to mean working from home or isolated, non-shared office working.The overall workplace COVID-19 transmission risk together with the medical vulnerability risk will be necessary in order to make an overall OH risk assessment and provide return to work advice to individual workers tailored to their specific work environment/activities.

31
Figure 3. Risk factors that can be used to evaluate the residual risk of COVID-19 transmission through work activities
Based on risk after control measures are implemented**Framework for workplace COVID-19 risk
Risk Factors
Patient care/Individuals cared for in the community/Public facing
Risk ID
1
Low** Standard Medium High
Travel to and from work
Workplace entry and exit
4
5
Ability to maintain social distancing at work >2m
Number of different people sharing the workplace
2
3
Workplace environment cleanliness control
Ability to avoid symptomatic people
8
9
Availability and use of PPE
Ability to maintain hand hygiene
6
7
(*) A low risk environment is likely to be home working or isolated, non-shared office working(**) The overall workplace risk judgement would be the highest risk level reached (i.e. coloured risk category) for any specific risk factor, after control measures are implemented.A workplace risk assessment is required to ensure that all reasonable steps are taken by employers to reduce the risk of COVID-19 transmission in the course of work. The lowest risk position is likely to be working from home however, there are many occupations whereby this is not feasible or practicable.
In order to provide individual advice to workers/patients, an assessment of the overall workplace risk of COVID-19 transmission is needed.The risk factors in the tables below outline some of the main situations related to work whereby the risk of exposure to infection can occur.See the examples below to illustrate this. The overall workplace risk judgement would be the highest risk level reached (i.e. coloured risk category) for any specific risk factor, after control measures are implemented.
32
Risk Factors
Patient care/Individuals cared for in the community/Public facing
Risk ID
1
Low** Standard Medium High
Travel to and from work
Workplace entry and exit
4
5
Ability to maintain social distancing at work >2m
Number of different people sharing the workplace
2
3
Workplace environment cleanliness control
Ability to avoid symptomatic people
8
9
Availability and use of PPE
Ability to maintain hand hygiene
6
7
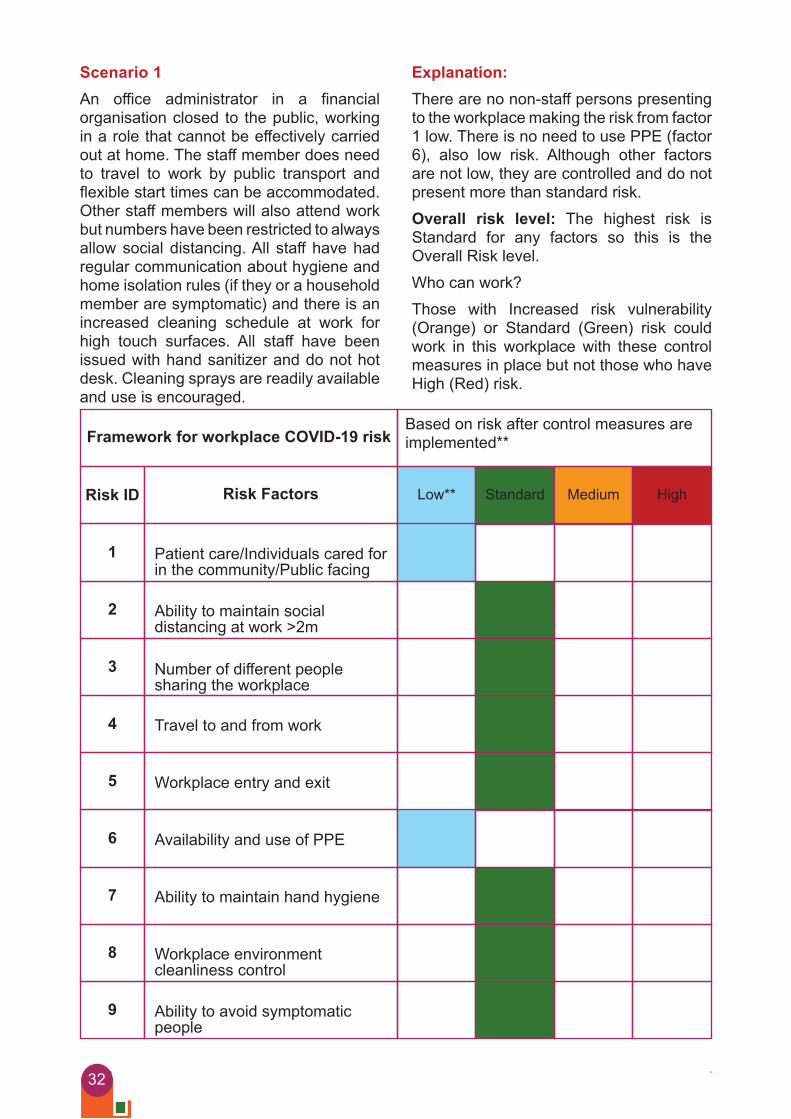
Scenario 1An office administrator in a financial organisation closed to the public, working in a role that cannot be effectively carried out at home. The staff member does need to travel to work by public transport and flexible start times can be accommodated. Other staff members will also attend work but numbers have been restricted to always allow social distancing. All staff have had regular communication about hygiene and home isolation rules (if they or a household member are symptomatic) and there is an increased cleaning schedule at work for high touch surfaces. All staff have been issued with hand sanitizer and do not hot desk. Cleaning sprays are readily available and use is encouraged.
Explanation:There are no non-staff persons presenting to the workplace making the risk from factor 1 low. There is no need to use PPE (factor 6), also low risk. Although other factors are not low, they are controlled and do not present more than standard risk.Overall risk level: The highest risk is Standard for any factors so this is the Overall Risk level.Who can work?Those with Increased risk vulnerability (Orange) or Standard (Green) risk could work in this workplace with these control measures in place but not those who have High (Red) risk.
Based on risk after control measures are implemented**Framework for workplace COVID-19 risk

33
Scenario 2A role involves providing social care to a service user with Cerebral Palsy in the service user’s own home. There is a close staff team of five support workers, and they are limited to reduce infection risk. The service user requires physical assistance for toileting, washing and dressing. Members of the service user’s family are not visiting at present due to the social distancing rules. All staff know how to recognise symptoms of potential COVID-19 in themselves and family members and know not to present to work in these situations. PPE is available but is used for the direct provision of personal care within two metres.The staff team also check the temperature of the service user and note the absence of symptoms of COVID-19 at each staff changeover. The support workers all drive private vehicles to the service user’s home.Explanation:There is service user facing work (the main focus of the work for prolonged periods) which would present a medium risk. It is not possible to maintain social distancing for some periods of the shift although there are mechanisms in place to screen for symptoms in the service user. Being in close contact at times creates an increased risk, which is reduced with PPE worn. The close staff team leads to a low level of workplace sharing and cleanliness can be maintained on shift. If the service user became symptomatic for potential COVID-19, then the risk would elevate to high risk.Overall Risk Level:Because of the low number of staff and a single service user who is monitored for potential COVID-19 symptoms, whilst they are asymptomatic, the overall risk would be Medium, as this is the highest risk level presented by the risk factors.Who can work?Workers with Increased (Orange) or
Standard (Green) risk can work here but not those who have High (Red) risk. If COVID - 19 symptoms present in the service user, only Standard vulnerability support workers can work here.Important information for treating PhysiciansA BRIEF UNDERSTANDING OF CYTOKINE STORM Cytokine storm has no definition. Broadly speaking, it denotes a hyperactive immune response characterized by the release of interferons, interleukins, tumor-necrosis factors, chemokines, and several other mediators. These mediators are part of a well-conserved innate immune response necessary for efficient clearance of infectious agents. Cytokine storm implies that the levels of released cytokines are injurious to host cells. For example, a recent post-mortem report of patients with COVID-19 ARDS identified severe vascular injury, including alveolar microthrombi that were 9 times more prevalent than found in post-mortem studies of patients with influenza ARDSHow re-infections are determinedWhat is COVID-19 re-infection?When patient test positive for SARS-CoV2 less than 3 months after onset of symptoms, the test could represent a new infection.Recovered patients can still have non –infectious virus fragments in their bodies that show up as positive results in RTpcr tests.If a positive test occurs more than 3 months after a person’s symptom onset, there is a possibility of re-infection.How to establish re-infection?Determining re-infection is a challenge.Scientists have to use genetic sequencing and match entire or pieces of the viral genetic material gathered from the first and the second swab samples of the patient.There are subtle differences in the genetic
34
material of different strains of SARS-CoV2.If differences show up during sequencing, it clearly a case of re-infection.Post COVID-19 ImpactPositive tests long after recoveryPCR - Picks up SARS-CoV2 RNA fragments of viruses – no threat.Serious Lingering EffectsHeart: Estimated 20% of COVID-19 Patients suffer Myocarditis; no age group is spared. ArrythmiasNeuropsychological: Estimation 33% COVID fog - depression, cognitive impairment, PTSD. Psychosis.Neurological: Numbness of limbs, myasthenia gravis 3 cases, demyelination, stroke, anosmia-all induced by COVID-19 induced inflammation & toxemia.Diabetes: Sudden onset diabetes or worsening of existing DM. Beta cell destruction.Renal Injury: Chronic renal failure for a subset of recovered patients.General: Long – Haulers 20% fatigue, mal regulation of BP, HR and body temp-dysautonomia?
Conclusion Globally all efforts are being made to prevent the spread of COVID-19 virus. However, until we get complete control over the situation, it is important that we make some changes to our lifestyle. Going
beyond the use of masks, maintaining physical distancing, and use of sanitizers, it is now necessary to adopt some changes in our personal, familial and public lives.Today, work related stress is the most difficult or stressful than anything else one could ever imagine. Excessively high work loads coupled with unrealistic deadline are making people stressed and reeling under tremendous pressure. Creating a work life balance demands both equal attention and adequate energy. With the alarming rate and escalating effects of COVID-19 (Corona virus) pandemic, the vibes around the world have turned negative. In such situations, stress and panic is normal among people from all walks of life. Hence, one needs to control the mind and send positive energy. The main idea behind is that our mind should not be dependant on what is happening outside but should deal with what is happening inside. If a person can control his mind, he can fight and win any battle. Exercise, meditation and relaxation techniques, etc will help persons to control mind and body also.References: -1. SOM-COVID-19 return to work guide for
health professionals advising patients and employers.
2. On line publication on 4th September, 2020 The Lancet - Safety and immunogenicity of an rAd26 and rAd5 vector – based heterologus prime boost COVID-19 vaccine in 2 Formulations: Two open, non-randomised phase ½ studies from Russia.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31866-3.
Answ
ers
1. C
2. D
3. C
4. D
5. D
OCCUCLAVE e-Quiz6. A
7. C
8. B
9. B
10. D

35
Dear Friends I have gone through a serous journey of corona virus infection past two weeks, the experience is worth sharing, I am enclosing various factors how they influence one’s recovery and damage.ExposureDay -1- on 29 Aug 2020, I met 15 patients (supposedly not affected by Corona) for their serious painful conditions. One of them accidentally removed his mask and spoke on my face, but I didn’t suspect anything.cough and difficulty breathing should seek medical attention. Initial SymptomsDay-2- on 30 Aug, Sunday I felt feverish, nose block, mild cough and joint pains. I felt suspicious and started of with conservative medication Dolo 650, anti-histamine like Montek LC, steam inhalation and garglingDay-3- on 31 Aug, my wife and son also had minimal symptoms, my cough has increased and felt breathless in the night. I was sure that we were hit by Covid-19 and decided to isolate ourselves in three different rooms. Became Corona PositiveDay-4- on 01 Sept, we went to laboratory and tested for SARS-cov2 and to my surprise,
I was declared positive; son was also declared positive and wife was negative. I was skeptical about the RT-PCR, the current gold standard test can give false results in 30% of people. This created a trouble to keep her in quarantine from both of us in the same house. We managed to give her food in her room, she did have some diarrhea. Son was largely asymptomatic with a bit loss of taste and smell. Medication started: Doxycycline 100mg twice a day in addition to normal ones to all of us. Status Me - Corona Positive - SymptomaticWife - Corona Negative-Mildly SymptomaticSon - Corona Positive - Asymptomatic Worst Times During Night My symptoms began vigorously, cough became severe in the night, I was sleeping in the drawing room, breathing became difficult with worsening cough. I walked out of the door and did some Taichi breathing, but in vain. Took steam inhalation several times. Choking sensation continued. Day -5- on 02 Sept, discussed with some colleagues, and the was hell of a confusion, there is no single proper methodology of medication, took a decision on my own and started off
Walking Out of the Doors of Death Story of COVID Survival
Prof Dr S Bakhtiar Choudhary
MD (Switzerland) D.Litt. (Sri Lanka)
Ph.D. (USA)
ARTICLE
36
• Favipiravir (Fabi flu) to reduce the viral infection and load
• Prednisolone 20 mg twice a day to reduce the reaction of the body against the virus
• Vit D3 60000 IU one dose daily• Other vitamins (I was sure that
Ivermectin and HCQS were of no use)
Fever was on between 100-102 FH; Night was terrific with chocking and breathing difficulty and dam medical brain reminding all the complications of Covid. But on the other side, years of martial arts training, control over breathing and not having any disease such as diabetes, hypertension and hypothyroidism (Co-morbidities) were the blessing in disguise. Somehow managed that nightDay -6- on 03 Sept, the day of nightmare, day time was better, as the night approached, cough became so terrible, with each bought of cough, bladder and bowl were embarrassingly leaking. Took Oxygen saturation, it was ranging between 85-92%, that means significant less supply of oxygen to my lungs and brain. Whole night I was getting up coughing, doing inhalation, gargling and of course doing some mental training. I had decided, whatever the situation may be, I am not going to go to hospital and die in ICU. I was able to sleep only on my back for few min every hour. I didn’t wake my family members, I had to climb 20 steps to go to toilet with SOB (Shortness of Breath) grade III, barely was able breath. I remember our commando course saying, when going gets tougher, the tough get going My experience of motivating thousands of players, patients and students did come handy in driving myself. Fear in the mind pushed me in too many negative thoughts, i.e. I didn’t write my will? Who will repay the loans, who will publish my research works and bla bla… Day-7- on 04 Sept, Good news was I got up with no fever (probably anti-viral did work). I called my friend John from Tenet to test my blood values to check
for complications if any. As expected, D Dimor, IL 6, CBP, HRCRP, Ferritin were all in abnormal ranges indicating that I might go in to vascular complications. I didn’t start any aspirin or HCQS. I knew, as the inflammation comes down things would improve. Nights were still terrible.Day-8-10- From Sept 05 - 07, day time I was better with no taste and smell, but by night things were same. I called for Oxygen generator to improve my night difficulties; this machine was invaluable in improving my O2 saturation. Night struggle continued with lot of secretions, irritating cough and the miserable nights. We improved our cooking daily mutton, chicken, eggs, orange juice. Recovery BeganDay-11-15- From Sept 08 - 12, Oxygen discontinued, Saturation improved, cough persisted, Shortness of breath persists. Secretions are still there, sleep slightly improved. Steroid tapering began, stopped antibiotic, breathing exercises and nutritious food are helping me to get back to action.Day-16- Sept 13 on wards, Things have improved, little cough, weakness and found it difficult to talk more than few minutes. WE are going test on 15 September; post Covid complications are well known and we need to exercise our minds unravelling those unknown dangers.Day-18- Sept 15 Our RT-PCR tested negative, all my IL6, D Dimor, Ferritin, HsCRP came down to normal levels. Chest HRCT scans have findings of CO-RADS. 3/4 for both of us and my son got chest clear. Now we need to fight with post Covid complications if any. Lessons Learnt Why so many doctors who are dying daily during frontline job? Are there any risk factors apart from direct dose of virus infection?Yes, the doctors, medical staff who died due to Covid were largely affected by their pre-existing diseases like diabetes, Hypertension and obesityPoor
37
Micronutrient status is equally responsible; our dedicated medical fraternity must take care of themselves with regard to timing and composition of nutritionBody weight management is of paramount importance in maintaining intrinsic immunity, Physical exercise, sleep and rest are three important cardinals of immunity to maintain, biorhythm of Human body which in turn solidifies the immune system, Doctors cannot afford to die because of ignorance and inability to protect themselves. They are needed because, the more power the more responsibility…Vit D deficiency pandemic opened doors To Covid pandemic?Yes, people with low Vit D status (almost 95% of the world population) are highly susceptible to viral infections including covid-19, but you may then ask me why did I get it? The answer is very clear, when I got directly exposed to a Covid person who spoke on my face without mask, probably the dose of infection could not be prevented. Because my good Vit D status, probably saved me from hospitalization and allowed faster recovery. One must have an appropriate vitamin status of the body to prevent cytokine storms in the body and complications.Can we boost our immunity all of a sudden?Absolutely baseless, suddenly eating zinc, vitamins (Few can help), drinking kada, and ayurvedic Kashaya cannot raise your immunity overnight. Immunity is not a ready-made item which can be boosted on the spot.To your surprise, my wife had a severe gastritis after drinking AYUSH promoted kada made of Tulasi and what not. Please improve your basic food habits, abstain from alcohol and smoking and sleep tight to boost your immunity.How much you have earned??? all that mattersHaving affected by covid-19, made me
realize to think ‘how much I have earned’? More than 4000 friends, well-wishers, patients and some unknown people had extended their heartfelt wishes for our recovery, people have called restlessly to know about the progress, many had sent delicious cooked food and there was no shortage of medicine supply. People, relatives from my village and patients from far off villages performed prayers for our recovery. Constant blessings from old parents and families were the best vaccines one can afford. Living in Giving, the philosophy of life… Today I walked out of the doors of Death not because of anti-viral drug but I believe it’s because of so many factors. I had seen war, met major accidents, had narrow escapes during Motorcycle rally’s and worst of situations in my 60 years of life. I have saved more than 6000 people from surgery and saved more than 120 people from Covid itself; I had planted more than a lakh of trees to mother earth in my life.When it comes to taking back, it took so much of efforts to hold on to one small life for 5 days of of life and death during Corona Invasion. I have realized that I have yet another chance to give and give to believe in my philosophy of “Living in Giving”People, relatives from my village and patients from far off villages performed prayers for our recovery. Constant blessings from old parents and families were the best vaccines one can afford. Living with CoronaWe are going to live with corona for couple of years without any doubt. We may achieve herd immunity as the more numbers get infected, sacrifices of people at risk is going to be inevitable. Vaccine? I am not sure it’s going to work or cause more danger? we don’t know. Life should go on with suitable guidelines and law-abiding attitude (Not spreading virus to others). Let’s respect humans, nature and mother earth.

C O N F E R E N C E
A S I A • EUROPEN O RT H A M E R I C A
E M P O W E R I N G W O R K P L A C E M E N T A L H E A L T H
23–25 November 2020 | ONLINE
DELEGATE BROCHUREEUROPE, ASIA AND NORTH AMERICA
T H I S C A N H A P P E N E V E N T S . C O M
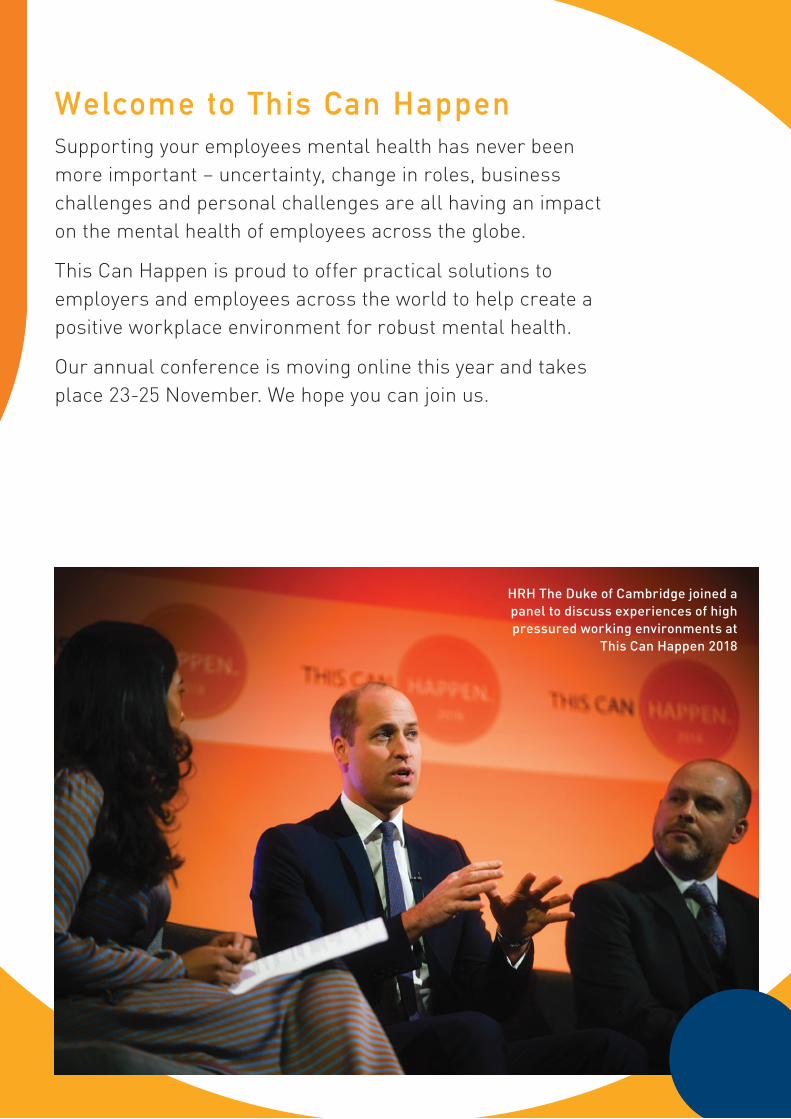
39
2
Welcome to This Can HappenSupporting your employees mental health has never been more important – uncertainty, change in roles, business challenges and personal challenges are all having an impact on the mental health of employees across the globe.
This Can Happen is proud to offer practical solutions to employers and employees across the world to help create a positive workplace environment for robust mental health.
Our annual conference is moving online this year and takes place 23-25 November. We hope you can join us.
HRH The Duke of Cambridge joined a panel to discuss experiences of high pressured working environments at
This Can Happen 2018

40
3
Conference main stage
Live speaker Q&A
Resource centre
Exhibition
Networking hub
Live video chat
Scheduled video
meetings
Personalised agenda
Resources bag
Reasons to attend this November:
Unlimited access to a three-day virtual conference
All presentations available on demand for one month after event
30+ sessions available – create your own Agenda across three days
Interactive Exhibition Hall featuring leading suppliers
Network with 3,000+ international delegates – share ideas and find solutions

41
8
Book now to join us: th iscanhappenevents .com
T H I S C A N H A P P E N 2 0 2 0 – O N L I N E E V E N T T I C K E T S
£ + V A T $
Group of 5 tickets 1,250.00 1,625.00
Group of 10 tickets 2,495.00 3,250.00
Group of 50 tickets 9,950.00 12,950.00
TCH Friends Package (inc. 30 online tickets) 4,950.00 6,350.00
TCH Friends PLUS Package (inc. 60 online tickets) 9,950.00 12,950.00
Melanie Brown sharing her experience with domestic abuse
For further details please email:in fo@tchevents .com
42
Upcoming World Health DaysBreast Cancer Awareness
October 01
Breast cancer occurs when some breast cells begin to grow abnormally. Breast cancer is the most common cancer in women, it does occur in men as well. Since 2006, October is International Breast Cancer Awareness Month
World Sight DayOctober 10
Eyes play an important role in movement and enjoyment of life. Therefore, it is impor-tant to maintain the eye health well; as it has the only job of capturing light, then all different parts of the eye system work together and connect with neurons that transmit and translate messages directly to the brain as visual images. The World Sight Day is globally observed on the second Thursday of October each year
43
World Arthritis DayOctober 12
Arthritis means inflammation or swelling of one or more joints. It describes more than 100 conditions that affect the joints, tissues around the joint, and other connective tis-sues. Specific symptoms vary depending on the type of arthritis, but usually include joint pain and stiffness. Treatment varies according to the severity and type of the con-dition. World Arthritis Day is celebrated every year on 12th October.
World Osteoporosis DayOctober 20
World Osteoporosis Day (WOD), marked on October 20 each year, is designated by WHO to raising global awareness of the prevention, diagnosis and treatment of osteo-porosis, especially after the age of 50. Osteoporosis constitutes a heavy burden on individuals in the future, if not detected and treated early. Although there are very ef-fective treatments, osteoporosis is often not diagnosed early, therefore, we must seek timely assessment and treatment to reduce the human, social, and economic burden.
44
A Unique Virtual Platform for Learning & Sharing for Industrial Physicians,
Occupational Health Physicians, Public Health Specialist & Other Related
Stakeholders.
Environmental & Occupational Health DigiConnect Webinar Academic Platform
(Tune in Every Saturday Prime Time 6.30PM IST India)
Copyright © 2022 FDOKUMEN