
Dopamine transporter levels in cocaine dependent subjects
7
Available online at www.sciencedirect.com Drug and Alcohol Dependence 98 (2008) 70–76 Dopamine transporter levels in cocaine dependent subjects Paul Crits-Christoph a,∗ , Andrew Newberg b , Nancy Wintering b , Karl Ploessl b , Mary Beth Connolly Gibbons a , Sarah Ring-Kurtz a , Robert Gallop c , Julie Present a a Department of Psychiatry, University of Pennsylvania, 3535 Market Street, Suite 650, Philadelphia, PA 19104, USA b Division of Nuclear Medicine, Department of Radiology, University of Pennsylvania, 110 Donner Building, Hospital of the University of Pennsylvania, 3400 Spruce Street, Philadelphia, PA 19104, USA c Department of Statistics and Applied Mathematics, West Chester University, 323B Anderson Hall, West Chester, PA 19383, USA Received 12 October 2007; received in revised form 19 March 2008; accepted 21 April 2008 Available online 20 June 2008 Abstract Cocaine use is a significant problem in the US and it is well established that cocaine binds to the dopamine transporter (DAT) in the brain. This study was designed to determine if the DAT levels measured by 99m Tc TRODAT SPECT (single photon emission computed tomography) brain scans are altered in cocaine dependent subjects and to explore clinical correlates of such alterations. SPECT brain scans were acquired on 21 cocaine dependent subjects and 21 healthy matched controls. There were significantly higher DAT levels in cocaine dependent subjects compared to controls for the anterior putamen (p = 0.003; Cohen’s d effect size = 0.98), posterior putamen (p < 0.001; effect size = 1.32), and caudate (p = 0.003; effect size = 0.97). DAT levels in these regions were 10%, 17%, and 8% higher in the cocaine dependent subjects compared to controls. DAT levels were unrelated to craving, severity of cocaine use, or duration of cocaine use, but DAT levels in the caudate and anterior putamen were significantly (p < 0.05) negatively correlated with days since last use of cocaine. © 2008 Elsevier Ireland Ltd. All rights reserved. Keywords: Dopamine transporter; Cocaine dependence; SPECT 1. Introduction Cocaine binds to the dopamine transporter (DAT) in the brain (Ritz et al., 1987), thereby blocking uptake resulting in increases in synaptic dopamine in the striatum and the nucleus accum- bens (Di Chiara and Imperato, 1988; Egilmez et al., 1995). The magnitude of the blockage of the DAT in humans correlates with the degree of self-reported “high” from cocaine (Volkow et al., 1997). Aspects of the mechanism of cocaine binding to the dopamine transporter have been studied at the cellular level (Chen and Reith, 2000). Studies have revealed that cocaine induces increases in the plasma membrane DAT immunoreac- tivity (Little et al., 2002) and results in the movement of DAT to the cell surface (Daws et al., 2002). In vitro autoradiographic studies of cocaine binding in brain sections from nonhuman primates have found the highest density ∗ Corresponding author at: Department of Psychiatry, University of Pennsyl- vania, 3535 Market Street, Suite 650, Philadelphia, PA 19104, USA. Tel.: +1 215 662 7993; fax: +1 215 349 5171. E-mail address: [email protected] (P. Crits-Christoph). of binding sites for cocaine in the basal ganglia, the brain region with the highest density of dopamine terminals (Madras and Kaufman, 1994). In humans, autoradiographic studies of post- mortem striatal specimens from cocaine users have revealed significant increases in DAT binding sites (Little et al., 1993), and specific increases in the density of high affinity sites on the DAT (Staley et al., 1994), compared with control subjects. Additionally, in nonhuman primates, exposure to cocaine over an 18-month period, compared to animals not exposed to cocaine, has been found to lead to a higher density of DAT binding sites, specifically in the ventral striatum where the shell of the nucleus accumbens is found (Letchworth et al., 2001). Though most studies support the claim that cocaine use causes an increase in DAT levels, there are some investigations yielding different findings in animals including lower uptake in the nucleus accum- bens, or no changes in the striatum, when measured 24 h after the last of 3 daily administrations of cocaine in rats (Izenwasser and Cox, 1990). Similarly, normal levels of DAT have been reported in the autopsied brains of chronic cocaine users (Wilson et al., 1996). It has been speculated that differences across studies in brain regions examined, time elapsed since last cocaine use, and 0376-8716/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.drugalcdep.2008.04.014
Transcript of Dopamine transporter levels in cocaine dependent subjects

A
Tbccew(©
K
1
(ibmwetlitt
s
vT
0d
Available online at www.sciencedirect.com
Drug and Alcohol Dependence 98 (2008) 70–76
Dopamine transporter levels in cocaine dependent subjects
Paul Crits-Christoph a,∗, Andrew Newberg b, Nancy Wintering b, Karl Ploessl b,Mary Beth Connolly Gibbons a, Sarah Ring-Kurtz a, Robert Gallop c, Julie Present a
a Department of Psychiatry, University of Pennsylvania, 3535 Market Street, Suite 650, Philadelphia, PA 19104, USAb Division of Nuclear Medicine, Department of Radiology, University of Pennsylvania, 110 Donner Building,
Hospital of the University of Pennsylvania, 3400 Spruce Street, Philadelphia, PA 19104, USAc Department of Statistics and Applied Mathematics, West Chester University, 323B Anderson Hall, West Chester, PA 19383, USA
Received 12 October 2007; received in revised form 19 March 2008; accepted 21 April 2008Available online 20 June 2008
bstract
Cocaine use is a significant problem in the US and it is well established that cocaine binds to the dopamine transporter (DAT) in the brain.his study was designed to determine if the DAT levels measured by 99mTc TRODAT SPECT (single photon emission computed tomography)rain scans are altered in cocaine dependent subjects and to explore clinical correlates of such alterations. SPECT brain scans were acquired on 21ocaine dependent subjects and 21 healthy matched controls. There were significantly higher DAT levels in cocaine dependent subjects compared toontrols for the anterior putamen (p = 0.003; Cohen’s d effect size = 0.98), posterior putamen (p < 0.001; effect size = 1.32), and caudate (p = 0.003;
ffect size = 0.97). DAT levels in these regions were 10%, 17%, and 8% higher in the cocaine dependent subjects compared to controls. DAT levelsere unrelated to craving, severity of cocaine use, or duration of cocaine use, but DAT levels in the caudate and anterior putamen were significantlyp < 0.05) negatively correlated with days since last use of cocaine.2008 Elsevier Ireland Ltd. All rights reserved.
owKmsatA1hsas
eywords: Dopamine transporter; Cocaine dependence; SPECT
. Introduction
Cocaine binds to the dopamine transporter (DAT) in the brainRitz et al., 1987), thereby blocking uptake resulting in increasesn synaptic dopamine in the striatum and the nucleus accum-ens (Di Chiara and Imperato, 1988; Egilmez et al., 1995). Theagnitude of the blockage of the DAT in humans correlatesith the degree of self-reported “high” from cocaine (Volkow
t al., 1997). Aspects of the mechanism of cocaine bindingo the dopamine transporter have been studied at the cellularevel (Chen and Reith, 2000). Studies have revealed that cocainenduces increases in the plasma membrane DAT immunoreac-ivity (Little et al., 2002) and results in the movement of DAT to
he cell surface (Daws et al., 2002).In vitro autoradiographic studies of cocaine binding in brainections from nonhuman primates have found the highest density
∗ Corresponding author at: Department of Psychiatry, University of Pennsyl-ania, 3535 Market Street, Suite 650, Philadelphia, PA 19104, USA.el.: +1 215 662 7993; fax: +1 215 349 5171.
E-mail address: [email protected] (P. Crits-Christoph).
ifiblCi1b
376-8716/$ – see front matter © 2008 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.drugalcdep.2008.04.014
f binding sites for cocaine in the basal ganglia, the brain regionith the highest density of dopamine terminals (Madras andaufman, 1994). In humans, autoradiographic studies of post-ortem striatal specimens from cocaine users have revealed
ignificant increases in DAT binding sites (Little et al., 1993),nd specific increases in the density of high affinity sites onhe DAT (Staley et al., 1994), compared with control subjects.dditionally, in nonhuman primates, exposure to cocaine over an8-month period, compared to animals not exposed to cocaine,as been found to lead to a higher density of DAT binding sites,pecifically in the ventral striatum where the shell of the nucleusccumbens is found (Letchworth et al., 2001). Though mosttudies support the claim that cocaine use causes an increasen DAT levels, there are some investigations yielding differentndings in animals including lower uptake in the nucleus accum-ens, or no changes in the striatum, when measured 24 h after theast of 3 daily administrations of cocaine in rats (Izenwasser and
ox, 1990). Similarly, normal levels of DAT have been reportedn the autopsied brains of chronic cocaine users (Wilson et al.,996). It has been speculated that differences across studies inrain regions examined, time elapsed since last cocaine use, and

Alco
ti
tbciduc1icptdoltbaitibse
uia(c9
tfc
2
2
ttnsBb
2
dCwdocs
CCdythroawenuAozb
2
gwbai
tc7b
1fo8jw
Tt0o1
TPoebwriiSsarnci
o
P. Crits-Christoph et al. / Drug and
ype of radioligand used for quantifying DAT may explain thenconsistency of the findings (Volkow et al., 1996).
The long-term behavioral effects of cocaine may be relatedo alterations in dopamine transmission that follow from DATlockade. As a consequence of high levels of synaptic dopamine,hronic cocaine use is associated with reduction in availabil-ty of dopamine D2 receptors that persists 3–4 months afteretoxification (Volkow et al., 1993). Imaging studies have doc-mented higher DAT levels for recently (about 4 days) abstinentocaine-using subjects compared to control (Malison et al.,998; Jacobsen et al., 2000). No studies, however, have exam-ned DAT levels as a function of clinical characteristics ofocaine use among active cocaine dependent subjects. Based onrimate data on duration and dosage of cocaine exposure in rela-ion to DAT (Letchworth et al., 2001), it would be expected thaturation of cocaine use and severity of cocaine usage (amountf use in past month) might be associated with higher DATevels. Because withdrawal symptoms appear related to a deple-ion in dopamine (Dackis and Gold, 1985), abstinence woulde expected to be associated with a recovery of DAT levels,lthough the time period for recovery to relatively normal levelss uncertain. Craving is another clinical characteristic of sus-ained cocaine use that might be associated with alterationsn DAT. Studies have found that increased mu-opioid receptorinding, another neurotransmitter system that affects dopamineystems in the brain, is positively corrected with craving (Zubietat al., 1996; Gorelick et al., 2005).
In this study, 99mTc TRODAT-1 was used to image DAT levelssing single photon emission computed tomography (SPECT)n 21 cocaine dependent patients who were recently abstainingnd 21 healthy controls. The following hypotheses were tested:a) there is significantly greater 99mTc TRODAT-1 uptake forocaine patients compared to controls, and (b) the pattern of9mTc TRODAT-1 uptake will co-vary with clinical characteris-ics of cocaine use: negatively for time since last use, positivelyor amount of cocaine being used, positively for duration ofocaine addiction, and positively for craving.
. Methods
.1. Subjects
Cocaine dependent subjects were currently seeking outpatient counseling forheir cocaine use. The control sample contained 21 age-matched healthy volun-eers. All healthy volunteers included in the study had no significant medical,eurological or psychiatric diseases. All subjects gave written informed con-ent and all procedures for this study were approved by the Institutional Reviewoard and Radiation Safety Committee of the University of Pennsylvania andy the Food and Drug Administration.
.2. Clinical assessments
For the treatment-seeking subjects, a DSM-IV diagnosis of cocaine depen-ence was made by a trained doctoral level psychologist using the Structuredlinical Interview for DSM-IV (First et al., 1994). Cocaine dependent subjects
ere excluded if they met diagnostic criteria for current opioid dependence,ementia, other irreversible organic brain syndrome, or if there was evidencef current psychotic symptoms or a medical illness that can create markedhange in mental state. Clinical characteristics of cocaine use were also mea-ured at this initial assessment. Craving was assessed with a three-item Cocainecs(wt
hol Dependence 98 (2008) 70–76 71
raving Scale (Weiss et al., 1997, 2003). The three questions on the Cocaineraving Scale were “please rate how strong your desire was to use cocaineuring the last 24 h,” “please imagine yourself in the environment in whichou previously used drugs and/or alcohol. . .if you were in this environmentoday, what is the likelihood that you would use cocaine?” and “please rateow strong your urges are for cocaine when something in the environmenteminds you of it.” Response options ranged from 0 for “no desire/likelihoodf use” to 9 for “strong desire/likelihood of use.” The composite score wassum of these three items, ranging from 0 to 27. Severity of cocaine useas measured using an item from the Addiction Severity Index (McLellan
t al., 1992) administered by trained interviewers. The item asked about theumber of days of cocaine use during the past month. Duration of cocainese (in years) was obtained by self-report as part of a cocaine history form.n observed urine sample was also obtained at this assessment visit. Ann-site analysis system was used to screen the urines for illicit opioids, ben-yolecognine (a cocaine metabolite), amphetamines, methamphetamines, andenzodiazepines.
.3. Imaging
After completing diagnostic and other assessments for the treatment pro-ram, cocaine dependent patients were scheduled to receive the SPECT scan,hich was generally completed within two weeks of the diagnostic visit butefore treatment began. When patients arrived for the SPECT scan, they weresked to report the day of their last use. Patients were excluded from the studyf they reported use of cocaine within the past 24 h.
At the start of the scan, individuals were placed at rest on the imaging table inhe supine position. An intravenous catheter was placed in an antecubital vein andapped with a well containing normal saline. Subjects were then injected with40 MBq (20 mCi) of 99mTc TRODAT-1. Vital signs and EKGs were recordedefore and after the injection.
Patients were scanned 3–4 h following the administration of 99mTc TRODAT-. All images were acquired on a triple headed gamma camera equipped withan beam collimators (Picker Prism 3000XP, Cleveland, OH). The camera res-lution is 6.7 mm with a spatial resolution for reconstructed SPECT scans of–10 mm. The acquisition parameters included a continuous mode with 40 pro-ection angles over a 120◦ arc to obtain data in a 128 × 128 matrix with a pixelidth of 2.11 mm and a slice thickness of 3.56 mm.
All images were processed and reconstructed using the same procedure.ransverse reconstruction backprojection was applied to the raw data. A But-
erworth, low pass filter was then applied with an order of 4 and a cutoff of.351 cm−1. Photon attenuation correction was performed using Chang’s firstrder correction method using an attenuation coefficient of 0.11 cm−1 (Chang,978).
The frames that were acquired from 3 to 4 h after the injection of 99mTcRODAT-1 were summed and imported into an image analysis package calledETVIEW. Image analysis was performed blinded to the clinical diagnosisf each patient. A standardized template containing six regions of inter-st (ROIs) was transposed manually onto subregions of the right and leftasal ganglia (caudate, anterior putamen and posterior putamen). The regionsere different shapes to accommodate the different structures (some more
ound and some more oblong) and ranged from 7 to 14 pixels (correspond-ng to an area of 3–62 mm2). This standardized template had been validatedn previous studies (Amsterdam and Newberg, 2007; Newberg et al., 2007;wanson et al., 2005). Basal ganglia ROIs were placed on 3 consecutivelices so that the ROIs were within each structure both on each slice andcross the slices (i.e., in the x, y, and z dimensions). In this manner, theyepresent a “punch biopsy” of each of the structures. In addition, begin-ing 5 slices above the basal ganglia, an elliptical ROI was placed on twoonsecutive slices of the supratentorial uptake representing non-specific bind-ng.
An example scan of a cocaine dependent subject showing the placementf the basal ganglia ROIs is given in Fig. 1. Distribution volume ratios were
alculated for these ROIs based upon a reference region consisting of theupratentorial structures above the basal ganglia and the following equation:ROI-Reference Region)/Reference Region. Right and left values for each areaere averaged to yield final scores for the caudate, anterior putamen, and pos-erior putamen.

72 P. Crits-Christoph et al. / Drug and Alcohol Dependence 98 (2008) 70–76
Fig. 1. TRODAT SPECT scan of a cocaine subject showing placement of therad
or9
T(brhlrta0bptvw
3
WSahldAac
Table 1Demographic and clinical characteristics of cocaine dependent and controlsubjects
Characteristic Cocaine dependentsubjects (N = 21)
Controlsubjects(N = 21)
Age, mean (S.D.) 42.8 (6.2) 40.3 (7.0)Sex, n (%) male 16 (76.2) 14 (66.7)
Race, n (%)Caucasian 1 (4.8) 11 (52.4)African-American 18 (85.7) 8 (38.1)Hispanic 2 (9.5) 0Native American/Alaskan 0 2 (9.5)
Smoke cigarettes, n (%) 19 (90.5) 2 (9.5%)Days used alcohol (past 30), mean(S.D.)
7.4 (7.3) NA
Days used cocaine (past 30), mean(S.D.)
12.1 (7.5) 0
Days since last use of cocaine, mean(S.D.)
7.5 (9.7) 0
Years of cocaine use, mean (S.D.) 11.7 (5.6) 0
Days used other psychotropic druguse in past 30 days, mean (S.D.)
Heroin 0 0Methamphetamine 0 0Marijuana 1.7 (3.0) 0
N
ospu(Wnur
8WscAan
(ardpgp
egions of interest over the caudate, anterior and posterior putamen. The ROIsre smaller than the actual structures so they represent a “punch biopsy” ofopamine transporter binding.
Full kinetic modeling of the uptake of 99mTc TRODAT-1 in the striatumf cocaine dependent subjects has not been performed. However, the aboveatio method using a reference region has been employed in other studies using9mTc TRODAT-1 and was expected to be adequate for the following reasons.he peak uptake of 99mTc TRODAT-1 is typically in the range of 30–40 min
Kushner et al., 1999). Moreover, studies of 99mTc TRODAT-1 uptake in bothaboons (Acton et al., 1999) and humans (Acton et al., 2000) have examined theelationship between data from the reference region (ratio) method employedere and full kinetic analysis based on rapid arterial blood sampling (using non-inear regression analysis and graphical analysis measures of distribution volumeatios). In the range of 3–4 h post-injection, the correlations between data fromhe simpler reference region method and data from full kinetic analysis werebove 0.80 in humans; at 4–5 h post-injection, these correlations were above.90 (Acton et al., 2000). The timing of the scans in our study was typicallyetween 3 and 4.5 h post-injection, substantially beyond the expected point ofeak uptake in non-cocaine users. In addition, in the Acton et al. (2000) study,here was a nonsignificant relationship between peak equilibrium time and higheralues of distribution volume ratios, suggesting that longer time to peak uptakeas not strongly affected by DAT levels.
. Results
For the cocaine dependent patients, 1 identified himself ashite, 18 as African American, and 2 as Other (Table 1).
eventy-six percent (n = 16) of the sample were men. The aver-ge age of patients was 42.8 (S.D. = 6.2) years. More thanalf (12 patients; 57%) were employed and 16 patients (76%)ived alone. Most (67%) used crack cocaine, and the average
ays of use in the month prior to treatment was 12.1 days.t the time of the scans, patients had last used cocaine onverage 7.5 days (S.D. = 9.7; range = 2–39) previously. No dis-repancies were found between the urine screen for cocaine
cf1c
A = not assessed.
btained at the intake assessment and the self-report of daysince last use obtained at the SPECT scan visit (i.e., for allatients who reported last use at a time point earlier than therine screen, the urine result was negative for cocaine). Most90.5%) of the cocaine dependent patients smoked cigarettes.
hile alcohol was not the primary drug of abuse, the averageumber of days in the past 30 drinking alcohol was 7.4. Nose of heroin or methamphetamines in the past 30 days waseported.
The control sample was also mostly male (14/21; 67%), withpatients identifying themselves as African American, 11 ashite, and 2 Other (Table 1). The average age of the control
ample was 40.3 (S.D. = 7.0) years. None of the subjects in theontrol sample had used illicit drugs during the past month.
minority (9.5%) were smokers; none were abusing alcohol,lthough the numbers of days of alcohol use in the past 30 wasot assessed.
Multivariate analysis of variance testing for between-groupcontrol vs. cocaine dependent patients) mean differences acrossll three regions (anterior putamen, posterior putamen, caudate)evealed that 99mTc TRODAT-1 uptake in cocaine depen-ent subjects was higher than controls (F = 6.14, D.F. = 3.38,= 0.0016). Univariate t-tests were significant for between-roup differences for the anterior putamen (t = 3.18; D.F. = 40;= 0.003), posterior putamen (t = 4.27; D.F. = 40; p < 0.001), andaudate (t = 3.14; D.F. = 40; p = 0.003). Effect sizes were large
or these between-group differences (Table 2). DAT levels were0%, 17%, and 8% higher in the cocaine dependent subjectsompared to controls for the anterior putamen, posterior puta-
P. Crits-Christoph et al. / Drug and Alcohol Dependence 98 (2008) 70–76 73
Table 2Mean DAT binding scores for cocaine dependent subjects and normal controls
DAT binding: brain region Cocaine dependent subjects N = 21 Normal controls N = 21 Effect size
Mean (S.D.) Mean (S.D.) Cohen’s d p-Value
CAP
md
ctiraiuts
4
dbgcpp
aiilf
tpotaaSnua
mttDapcwa
wca
F(
audate 3.17 (0.25)nterior putamen 2.95 (0.28)osterior putamen 2.50 (0.28)
en, and caudate, respectively. Examples of scans for a cocaineependent subject and a control subject are shown in Fig. 2.
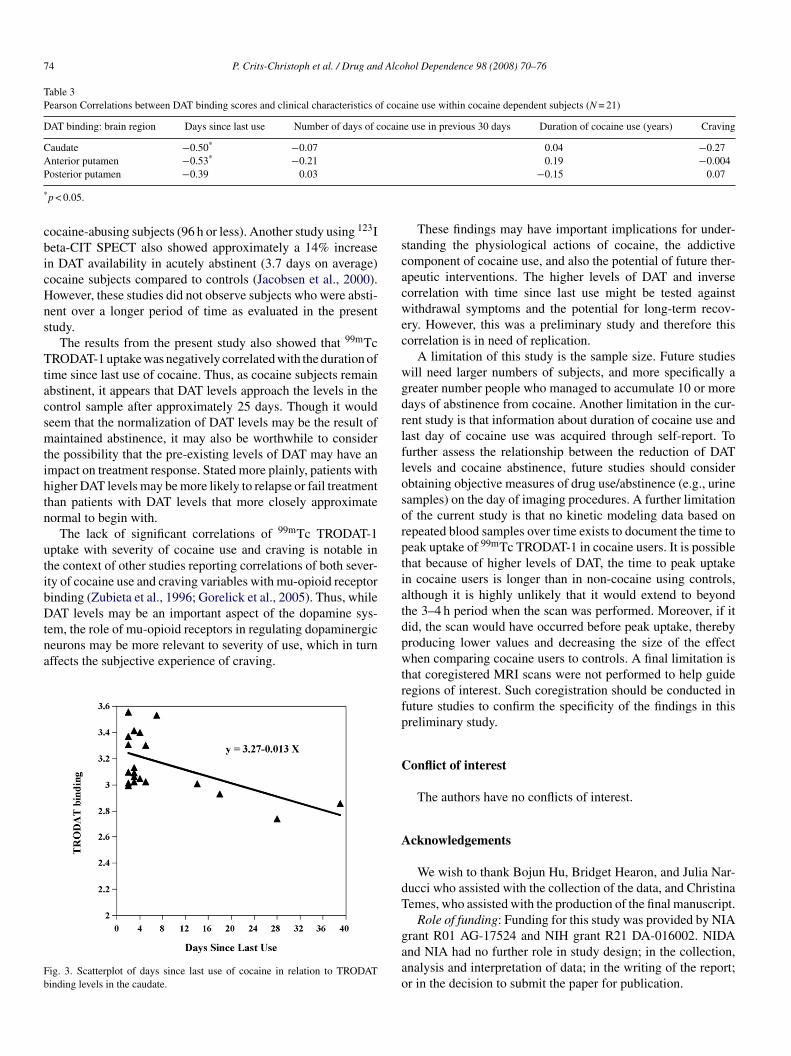
Pearson correlation between 99mTc TRODAT-1 uptake andlinical characteristics of cocaine use revealed a significant rela-ion between days since last use and 99mTc TRODAT-1 updaten the caudate and anterior putamen (Table 3). No significantelationships were observed between 99mTc TRODAT-1 updatend duration of cocaine usage, amount of cocaine use, or crav-ng. Using a regression equation predicting 99mTc TRODAT-1ptake in the caudate from days since last use, it was estimatedhat DAT levels would return to normal levels (mean of controlample) by 25.4 days (Fig. 3).
. Discussion
The results support the first hypothesis, that there are groupifferences in 99mTc TRODAT-1 uptake and hence DAT levelsetween cocaine patients and controls. All three specific subre-ions of the basal ganglia (anterior putamen, posterior putamen,audate) were significantly different in cocaine patients com-ared to controls, although the effects were strongest for theutamen regions.
It is possible that confounds between the cocaine dependentnd control samples may explain the between-group differences
n DAT levels. For example, the groups differed in rates of smok-ng. Smoking, however, has been associated with decreased DATevels (Krause et al., 2002; Newberg et al., 2007), and thus thisactor would have hindered between-group differences givencSSn
ig. 2. TRODAT SPECT scan of a control subject (A) and a cocaine subject (B) showarrow).
2.94 (0.23) 0.97 0.0032.68 (0.26) 0.98 0.0032.14 (0.25) 1.32 <0.001
he higher percentage of smokers among the cocaine dependentatients relative to the controls. The groups also likely differedn alcohol use, although the exact amount of alcohol use inhe control sample was not assessed (but there were no alcoholbusers). Animal and human studies of DAT in relationship tolcohol have yielded mixed results (Carroll et al., 2006; Ho andegre, 2001; Tupala et al., 2001; Budygin et al., 2001), thus it isot clear how alcohol use may have affected the results. Othernmeasured confounds, such as past psychiatric disorders, maylso be relevant to the findings.
These findings are generally consistent with previous ani-al studies which have evaluated changes in the DAT related
o cocaine administration and withdrawal. One study showedhat rats receiving cocaine for 3 days showed an increase in theAT half life which lasted approximately 7 days (Kimmel etl., 2001). A review of a number of other animal studies sup-orts the notion that in the short-term withdrawal period fromocaine, there may be an increase of DAT levels in the striatumhich may return to normal or even decrease over time (Kuhar
nd Pilotte, 1996; Sharpe et al., 1991).The current 99mTc TRODAT-1 findings are also consistent
ith several human studies that have evaluated the DAT inocaine patients. Studies of post-mortem brains demonstratedn overall increase of DAT in the striatum of cocaine abusers
ompared to controls (Little et al., 1999; Mash et al., 2002;taley et al., 1994). Malison et al. (1998) used 123I beta-CITPECT and found that striatal dopamine transporters were sig-ificantly increased (approximately 20%) in acutely abstinenting increased TRODAT binding in the anterior putamen of the cocaine subject
74 P. Crits-Christoph et al. / Drug and Alcohol Dependence 98 (2008) 70–76
Table 3Pearson Correlations between DAT binding scores and clinical characteristics of cocaine use within cocaine dependent subjects (N = 21)
DAT binding: brain region Days since last use Number of days of cocaine use in previous 30 days Duration of cocaine use (years) Craving
Caudate −0.50* −0.07 0.04 −0.27Anterior putamen −0.53* −0.21 0.19 −0.004P
*
cbicHns
Ttacsmtihtn
utibDtna
Fb
scacwec
wgdrlflosorptiat
osterior putamen −0.39 0.03
p < 0.05.
ocaine-abusing subjects (96 h or less). Another study using 123Ieta-CIT SPECT also showed approximately a 14% increasen DAT availability in acutely abstinent (3.7 days on average)ocaine subjects compared to controls (Jacobsen et al., 2000).owever, these studies did not observe subjects who were absti-ent over a longer period of time as evaluated in the presenttudy.
The results from the present study also showed that 99mTcRODAT-1 uptake was negatively correlated with the duration of
ime since last use of cocaine. Thus, as cocaine subjects remainbstinent, it appears that DAT levels approach the levels in theontrol sample after approximately 25 days. Though it wouldeem that the normalization of DAT levels may be the result ofaintained abstinence, it may also be worthwhile to consider
he possibility that the pre-existing levels of DAT may have anmpact on treatment response. Stated more plainly, patients withigher DAT levels may be more likely to relapse or fail treatmenthan patients with DAT levels that more closely approximateormal to begin with.
The lack of significant correlations of 99mTc TRODAT-1ptake with severity of cocaine use and craving is notable inhe context of other studies reporting correlations of both sever-ty of cocaine use and craving variables with mu-opioid receptorinding (Zubieta et al., 1996; Gorelick et al., 2005). Thus, whileAT levels may be an important aspect of the dopamine sys-
em, the role of mu-opioid receptors in regulating dopaminergiceurons may be more relevant to severity of use, which in turnffects the subjective experience of craving.
ig. 3. Scatterplot of days since last use of cocaine in relation to TRODATinding levels in the caudate.
dpwtrfp
C
A
dT
gaao
−0.15 0.07
These findings may have important implications for under-tanding the physiological actions of cocaine, the addictiveomponent of cocaine use, and also the potential of future ther-peutic interventions. The higher levels of DAT and inverseorrelation with time since last use might be tested againstithdrawal symptoms and the potential for long-term recov-
ry. However, this was a preliminary study and therefore thisorrelation is in need of replication.
A limitation of this study is the sample size. Future studiesill need larger numbers of subjects, and more specifically areater number people who managed to accumulate 10 or moreays of abstinence from cocaine. Another limitation in the cur-ent study is that information about duration of cocaine use andast day of cocaine use was acquired through self-report. Tourther assess the relationship between the reduction of DATevels and cocaine abstinence, future studies should considerbtaining objective measures of drug use/abstinence (e.g., urineamples) on the day of imaging procedures. A further limitationf the current study is that no kinetic modeling data based onepeated blood samples over time exists to document the time toeak uptake of 99mTc TRODAT-1 in cocaine users. It is possiblehat because of higher levels of DAT, the time to peak uptaken cocaine users is longer than in non-cocaine using controls,lthough it is highly unlikely that it would extend to beyondhe 3–4 h period when the scan was performed. Moreover, if itid, the scan would have occurred before peak uptake, therebyroducing lower values and decreasing the size of the effecthen comparing cocaine users to controls. A final limitation is
hat coregistered MRI scans were not performed to help guideegions of interest. Such coregistration should be conducted inuture studies to confirm the specificity of the findings in thisreliminary study.
onflict of interest
The authors have no conflicts of interest.
cknowledgements
We wish to thank Bojun Hu, Bridget Hearon, and Julia Nar-ucci who assisted with the collection of the data, and Christinaemes, who assisted with the production of the final manuscript.
Role of funding: Funding for this study was provided by NIA
rant R01 AG-17524 and NIH grant R21 DA-016002. NIDAnd NIA had no further role in study design; in the collection,nalysis and interpretation of data; in the writing of the report;r in the decision to submit the paper for publication.
Alco
dmrtPot
R
A
A
A
B
C
C
C
D
D
D
E
F
G
H
I
J
K
K
K
K
L
L
L
L
M
M
M
M
N
R
S
S
S
T
V
P. Crits-Christoph et al. / Drug and
Contributors: Paul Crits-Christoph and Andrew Newbergesigned the study and wrote the protocol. Sarah Ring-Kurtzanaged the literature searches and summaries of previous
elated work. Julie Present helped with the editing and format-ing of the text. Robert Gallop undertook the statistical analysis.aul Crits-Christoph and Andrew Newberg wrote the first draftf the manuscript. All authors contributed to and have approvedhe final manuscript.
eferences
cton, P.D., Kushner, S.A., Kung, M.P., Mozley, P.D., Plossl, K., Kung,H.F., 1999. Simplified reference region model for the kinetic analysis of[99mTc]TRODAT-1 binding to dopamine transporters in nonhuman primatesusing single-photon emission tomography. Eur. J. Nucl. Med. 26, 518–526.
cton, P.D., Meyer, P.T., Mozley, P.D., Plossl, K., Kung, H.F., 2000. Simplifiedquantification of dopamine transporters in humans using [99mTc]TRODAT-1 and single photon emission tomography. Eur. J. Nucl. Med. 27,1714–1718.
msterdam, J.D., Newberg, A.B., 2007. A preliminary study of dopaminetransporter binding in bipolar and unipolar depressed patients and healthycontrols. Neuropsychobiology 55, 167–170.
udygin, E.A., Phillips, P.E., Wightman, R.M., Jones, S.R., 2001. Terminaleffects of ethanol on dopamine dynamics in rat nucleus accumbens: an invitro voltammetric study. Synapse 42, 77–79.
arroll, M.R., Rodd, Z.A., Murphy, J.M., Simon, J.R., 2006. Chronic ethanolconsumption increases dopamine uptake in the nucleus accumbens of highalcohol drinking rats. Alcohol 40, 103–109.
hang, L.T., 1978. A method for attenuation correction in radionuclide com-puted tomography. IEEE Trans. Nucl. Sci. 25, 638–643.
hen, N., Reith, M.E., 2000. Structure and function of the dopamine transporter.Eur. J. Pharmacol. 405, 329–339.
ackis, C.A., Gold, M.S., 1985. New concepts in cocaine addic-tion: the dopamine depletion hypothesis. Neurosci. Biobeh. Rev. 9,469–477.
aws, L.C., Callaghan, P.D., Moron, J.A., Kahlig, K.M., Shippenberg, T.S.,Javitch, J.A., Galli, A., 2002. Cocaine increases dopamine uptake and cellsurface expression of dopamine transporters. Biochem. Bioph. Res. Co. 290,1545–1550.
i Chiara, G., Imperato, A., 1988. Drugs abused by humans preferentiallyincrease synaptic dopamine concentrations in the mesolimbic system offreely moving rats. Proc. Nat. Acad. Sci. U.S.A. 85, 5274–5278.
gilmez, Y., Jung, M.E., Lane, J.D., Emmett-Oglesby, M.W., 1995. Dopaminerelease during cocaine self-administration in rats: effect of SCH23390. BrainRes. 701, 142–150.
irst, M.B., Spitzer, R.L., Gibbon, M., Williams, B.W., 1994. Structured Clin-ical Interview for Axis I DSM-IV Disorders––Patient Edition. AmericanPsychiatric Press, Washington D.C.
orelick, D.A., Kim, Y.K., Bencherif, B., Boyd, S.J., Nelson, R., Copersino,M., Endres, C.J., Dannals, R.F., Frost, J.J., 2005. Imaging brain mu-opioidreceptors in abstinent cocaine users: time course and relation to cocainecraving. Bio. Psychiatry 57, 1573–1582.
o, M., Segre, M., 2001. Individual and combined effects of ethanol and cocaineon the human dopamine transporter in neuronal cell lines. Neurosci. Lett.299, 229–233.
zenwasser, S., Cox, B.M., 1990. Daily cocaine treatment produces a persistentreduction in [3H]dopamine uptake in vitro in rate nucleus accumbens butnot in striatum. Brain Res. 531, 338–341.
acobsen, L.K., Staley, J.K., Malison, R.T., Zoghbi, S.S., Seibyl, J.P., Kosten,T.R., Innis, R.B., 2000. Elevated central serotonin transporter binding avail-
ability in acutely abstinent cocaine-dependent patients. Am. J. Psychiatry157, 1134–1140.immel, H.L., Carroll, F.I., Kuhar, M.J., 2001. RTI-76, an irreversible inhibitorof dopamine transporter binding, increases locomotor activity in the rat athigh doses. Brain Res. 897, 157–163.
V
hol Dependence 98 (2008) 70–76 75
rause, K.H., Dresel, S.H., Krause, J., Kung, H.F., Tatsch, K., Ackenheil, M.,2002. Stimulant-like action of nicotine on striatal dopamine transporterin the brain of adults with attention deficit hyperactivity disorder. Int. J.Neuropsychopharmacol. 5, 111–113.
uhar, M.J., Pilotte, N.S., 1996. Neurochemical changes in cocaine withdrawal.Trends Pharmacol. Sci. 17, 260–264.
ushner, S.A., McElgin, W.T., Kung, M.P., Mozley, P.D., Plossl, K., Meegalla,S.K., Mu, M., Dresel, S., Vessotskie, J.M., Lexow, N., Kung, H.F., 1999.Kinetic modeling of [99mTc]TRODAT-1: a dopamine transporter imagingagent. J. Nuclear. Med. 40, 150–158.
etchworth, S.R., Nader, M.A., Smith, H.R., Friedman, D.P., Porrino, L.J., 2001.Progression of changes in dopamine transporter binding site density as aresult of cocaine self-administration in rhesus monkeys. J. Neurosci. 21,2799–2807.
ittle, K.Y., Elmer, L.W., Zhong, H., Zhang, L., 2002. Cocaine induction ofdopamine transporter trafficking to the plasma membrane. Mol. Pharmacol.61, 436–445.
ittle, K.Y., Kirkman, J.A., Carroll, F.I., Clark, T.C., Duncan, G.E., 1993.Cocaine use increases [3H]WIN 35428 binding sites in human striatum.Brain Res. 628, 17–25.
ittle, K.Y., Zhang, L., Desmond, T., Frey, K.A., Dalack, G.W., Cassin, B.J.,1999. Striatal dopaminergic abnormalities in human cocaine users. Am. J.Psychiatry 156, 238–245.
adras, B.K., Kaufman, M.J., 1994. Cocaine accumulates in dopamine-richregions of primate brain after i.v. administration: comparison with mazindoldistribution. Synapse 18, 261–275.
ash, D.C., Pablo, J., Ouyang, Q., Hearn, W.L., Izenwasser, S., 2002. Dopaminetransport function is elevated in cocaine users. J. Neurochem. 81, 292–300.
alison, R.T., Best, S.E., van Dyck, C.H., McCance, E.F., Wallace, E.A., Laru-elle, M., Baldwin, R.M., Seibyl, J.P., Price, L.H., Kosten, T.R., Innis, R.B.,1998. Elevated striatal dopamine transporters during acute cocaine absti-nence as measured by [123I] beta-CIT SPECT. Am. J. Psychiatry 155,832–834.
cLellan, A.T., Kushner, H., Metzger, D., Peters, R., Smith, I., Grissom, Pet-tinati, H., Argeriou, M., 1992. The fifth edition of the Addiction SeverityIndex. J. Subst. Abuse 9, 199–213.
ewberg, A., Lerman, C., Wintering, N., Ploessl, K., Mozley, P.D., 2007.Dopamine transporter binding in smokers and nonsmokers. Clin. Nucl. Med.32, 452–455.
itz, M.C., Lamb, R.J., Goldberg, S.R., Kuhar, M.J., 1987. Cocaine receptors ondopamine transporters are related to self-administration of cocaine. Science237, 1219–1223.
harpe, L.G., Pilotte, N.S., Mitchell, W.M., De Souza, E.B., 1991. Withdrawalof repeated cocaine decreases autoradiographic [3H]mazindol-labelling ofdopamine transporter in rat nucleus accumbens. Eur. J. Pharmacol. 203,141–144.
taley, J.K., Hearn, W.L., Ruttenber, A.J., Wetli, C.V., Mash, D.C., 1994.High affinity cocaine recognition sites on the dopamine transporter areelevated in fatal cocaine overdose victims. J. Pharmacol. Exp. Ther. 271,1678–1685.
wanson, R.L., Newberg, A.B., Acton, P.D., Siderowf, A., Wintering, N., Alavi,A., Mozley, P.D., Plossl, K., Udeshi, M., Hurtig, H., 2005. Differences in[99mTc]TRODAT-1 SPECT binding to dopamine transporters in patientswith multiple system atrophy and Parkinson’s disease. Eur. J. Nucl. Med.Mol. Imaging 32, 302–307.
upala, E., Kuikka, J.T., Hall, H., Bergstrom, K., Sarkioja, T., Rasanen, P.,Mantere, T., Hiltunen, J., Vepsalainen, J., Tiihonen, J., 2001. Measurementof the striatal dopamine transporter density and heterogeneity in type 1 alco-holics using human whole hemisphere autoradiography. Neuroimage 14,87–94.
olkow, N.D., Fowler, J.S., Wang, G.J., Hitzemann, R., Logan, J., Schlyer, D.J.,Dewey, S.L., Wolf, A.P., 1993. Decreased dopamine D2 receptor availabilityis associated with reduced frontal metabolism in cocaine abusers. Synapse
14, 169–177.olkow, N.D., Wang, G.J., Fischman, M.W., Foltin, R.W., Fowler, J.S., Abumrad,N.N., Vitkun, S., Logan, J., Gatley, S.J., Pappas, N., Hitzemann, R., Shea,C.E., 1997. Relationship between subjective effects of cocaine and dopaminetransporter occupancy. Nature 386, 827–830.

7 Alco
V
W
W
W
6 P. Crits-Christoph et al. / Drug and
olkow, N.D., Wang, G.J., Fowler, J.S., Logan, J., Hitzemann, R., Gatley,S.J., MacGregor, R.R., Wolf, A.P., 1996. Cocaine uptake is decreased inthe brain of detoxified cocaine abusers. Neuropsychopharmacology 14,159–168.
eiss, R.D., Griffin, M.L., Hufford, C., Muenz, L.R., Najavits, L.M., Jans-
son, S.B., Kogan, J., Thompson, H.J., 1997. Early prediction of initiation ofabstinence from cocaine: use of a craving questionnaire. Am. J. Addict. 6,224–231.eiss, R.D., Griffin, M.L., Mazurick, C., Berkman, B., Gastfriend, D.R., Frank,A., Barber, J.P., Blaine, J., Salloum, I., Moras, K., 2003. The relationship
Z
hol Dependence 98 (2008) 70–76
between cocaine craving, psychosocial treatment, and subsequent cocaineuse. Am. J. Psychiatry 160, 1320–1325.
ilson, J.M., Levey, A.I., Bergeron, C., Kalasinsky, K., Ang, L., Peretti, F.,Adams, V.I., Smialek, J., Anderson, W.R., Shannak, K., Deck, J., Niznik,H.B., Kish, S.J., 1996. Striatal dopamine, dopamine transporter, and vesic-
ular monoamine transporter in chronic cocaine users. Ann. Neurol. 40,428–439.ubieta, J.K., Gorelick, D.A., Stauffer, R., Ravert, H.T., Dannals, R.F., Frost,J.J., 1996. Increased mu opioid receptor binding detected by PET in cocaine-dependent men is associated with cocaine craving. Nat. Med. 2, 1225–1229.



![Non-amine dopamine transporter probe [3H]tropoxene distributes to dopamine-rich regions of monkey brain](https://static.fdokumen.com/doc/165x107/63224d2f050768990e0fcb6c/non-amine-dopamine-transporter-probe-3htropoxene-distributes-to-dopamine-rich.jpg)
















