
Does Off-Pump Coronary Surgery Reduce Postoperative Acute Renal Failure? The Importance of...
9
DOI: 10.1016/j.athoracsur.2007.05.054 2007;84:1496-1502 Ann Thorac Surg Bivona, Paolo Bosco, Sabina Gallina and Antonio M. Calafiore Michele Di Mauro, Massimo Gagliardi, Angela L. Iacò, Marco Contini, Antonio The Importance of Preoperative Renal Function Does Off-Pump Coronary Surgery Reduce Postoperative Acute Renal Failure? http://ats.ctsnetjournals.org/cgi/content/full/84/5/1496 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2007 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 3, 2013 ats.ctsnetjournals.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Does Off-Pump Coronary Surgery Reduce Postoperative Acute Renal Failure? The Importance of...

DOI: 10.1016/j.athoracsur.2007.05.054 2007;84:1496-1502 Ann Thorac Surg
Bivona, Paolo Bosco, Sabina Gallina and Antonio M. Calafiore Michele Di Mauro, Massimo Gagliardi, Angela L. Iacò, Marco Contini, Antonio
The Importance of Preoperative Renal FunctionDoes Off-Pump Coronary Surgery Reduce Postoperative Acute Renal Failure?
http://ats.ctsnetjournals.org/cgi/content/full/84/5/1496located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2007 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 3, 2013 ats.ctsnetjournals.orgDownloaded from

DPoMMaD
cip
pmcds2mgfa
npra
AcweDr
vsm[opgfat
A
AUI
©P
CA
RD
IOV
ASC
ULA
R
oes Off-Pump Coronary Surgery Reduceostoperative Acute Renal Failure? The Importancef Preoperative Renal Functionichele Di Mauro, MD, Massimo Gagliardi, MD, Angela L. Iacò, MD,arco Contini, MD, Antonio Bivona, MD, Paolo Bosco, MD, Sabina Gallina, MD,
nd Antonio M. Calafiore, MD
epartment of Cardiac Surgery, University of Catania, Catania, Italy, and Department of Cardiology, University of Chieti, ItalyivtruItg0e
roWcotp
Background. Off-pump was compared with on-pumporonary artery bypass graft surgery to evaluate thempact of cardiopulmonary bypass on the incidence ofostoperative acute renal failure (ARF).Methods. From November 1994 to December 2001, 2,943
atients having multivessel surgical disease underwentyocardial revascularization. Ninety patients were ex-
luded because of incompleteness of data, intraoperativeeath, or preoperative chronic dialysis. The analysis wasplit: one analysis included 1,724 (862 each group) of,618 patients with normal preoperative creatinine (<1.5g/dL), and the second analysis included 160 (80 each
roup) of 215 patients with preoperative abnormal renalunction; in both analyses matched groups were selectedpplying propensity score.Results. In the group with normal preoperative creati-
ine, the incidence of 30-day ARF was 5.4% (2.9% off-ump versus 7.9% on-pump; p < 0.001). Stepwise logisticegression confirmed that cardiopulmonary bypass was
n independent variable for increased postoperative ARFdfd
irlfCvnntiTo
M
PFw
niversity of Catania, Ferarrotto Hospital, Via Citelli, Catania, 95124,taly; e-mail: [email protected].
2007 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
ncidence (odds ratio, 3.3), as well as age and reduced leftentricular ejection fraction. Receiver operating charac-eristic curves showed that cardiopulmonary bypass du-ation was a predictor of higher ARF incidence (areander the curve, 0.79) with a cutoff value of 66 minutes.n the patients with abnormal renal function preopera-ively, the incidence of ARF was similar between theroups (16.3% on-pump versus 12.5% off-pump; p �.499). Acute renal failure had an important impact onarly (odds ratio, 3.6) and late mortality (hazard ratio, 4.1).Conclusions. Off-pump surgery plays an important
enoprotective role and provides better early and lateutcome in patients with normal preoperative creatinine.hen the preoperative creatinine is abnormal, the surgi-
al strategy does not seem to have any influence. Theccurrence of ARF significantly impairs early and long-erm mortality, and the surgical strategy does not im-rove outcomes.
(Ann Thorac Surg 2007;84:1496–503)
© 2007 by The Society of Thoracic Surgeonscute renal failure (ARF) is a very common compli-cation after cardiac surgery (8% to 30%) [1–4]. In
ase of coronary artery bypass graft surgery, its incidenceas estimated between 1.4% and 19.5% [2, 4–10]. Postop-
rative ARF increases early mortality (7% to 38%) [1–4, 7].ialysis is required in 1% to 5% of cases, with a mortality
ate of roughly 60% [11].The above-mentioned data justify the efforts in pre-
enting perioperative and postoperative renal failure. Asome therapeutic strategies, like dopamine infusion,annitol, and furosemide, showed controversial results
11–13], several studies focused on the pathogenetic basisf postoperative renal dysfunction. Cardiopulmonary by-ass (CPB) was demonstrated to be the main cause oflomerular and tubular dysfunction or damage [14]. Inact, the markers of glomerular function (creatinine clear-nce) and damage (microalbuminuria) as well as ofubular function (fractional excretion of sodium) and
ccepted for publication May 18, 2007.
ddress correspondence to Dr Calafiore, Division of Cardiac Surgery,
amage (urinary N-acetyl-�-glucosaminidase) wereound to be significantly higher in on-pump patients,uring and after CPB [14, 15].Causes of the detrimental effects of CPB on kidney are
nflammatory response, nonpulsatile flow, hemodilution,enal hypoperfusion, low output syndrome, atheroembo-ism, increased levels of circulating catecholamines, andree hemoglobin [2, 12, 16–19]. However, the impact ofPB on postoperative renal complications is still contro-ersial, whether preoperative renal function is normal orot [5–10, 20, 21]. These conflicting results and the limitedumber of large comparative studies on this particular
opic caused us to analyze retrospectively our experiencen patients with normal and abnormal renal function [3].he impact of postoperative renal function impairmentn early and late outcome was also investigated.
aterial and Methods
opulationrom November 1994 to December 2001, 2,943 patients
ith multivessel coronary disease underwent isolated0003-4975/07/$32.00doi:10.1016/j.athoracsur.2007.05.054
by on June 3, 2013 als.org

mcidiiptcf2(da
coa
A
wm(sc
A
smpgc
PAvcipboe
SO
nsawbcO
tIe(cwrC
CAutAceaa(asda
FA3icwff
SDctwWFa
Tt
C
A
FE
CUDPCEL23ARE
A
1497Ann Thorac Surg DI MAURO ET AL2007;84:1496–503 OFF-PUMP SURGERY AND RENAL FAILURE
CA
RD
IOV
ASC
ULA
R
yocardial revascularization. Ninety of them were ex-luded because of incompleteness of data (n � 59),ntraoperative death (n � 11), or preoperative chronicialysis (n � 20). Globally, 2,833 patients were included
n the study. Creatinine values, the most diffuse, even ifmperfect, marker of renal function, were recorded in allatients in this study. The entire group was then split in
wo subgroups and analyzed separately. Analysis A in-luded 2,618 patients with normal preoperative renalunction (creatinine �1.5 mg/dL). Analysis B included15 patients with abnormal preoperative renal functioncreatinine �1.5 mg/dL). This cutoff value was selected asiscriminatory of altered preoperative renal functionccording to the literature [3] and to our laboratory.These patients were included in other previous publi-
ations of ours. Use of our database was authorized byur institutional review board on October 2004. Theuthorization waived patient consent.
NALYSIS A. From the entire group of 2,618 patients 1,724ere selected by means of propensity score and sampleatching to obtain two groups of 862 patients each
on-pump and off-pump coronary artery bypass grafturgery), with similar preoperative and perioperativeharacteristics.
NALYSIS B. From the entire group of 215 patients 160 wereelected by means of propensity score and sampleatching to obtain two groups of 80 patients each (on-
ump and off-pump coronary artery bypass graft sur-ery), with similar preoperative and perioperativeharacteristics.
atient Selectionllocation to off-pump surgery was on the basis of theessel size (�1.2 mm) and the absence of diffuse coronaryalcifications. In the presence of mechanical or electricnstability, the patient was selected preferably for on-ump surgery. The final decision was dependent on theasis and the expertise of the surgeon responsible for theperation. Patients converted to on-pump were consid-red in the off-pump group (intention to treat).
urgical TechniqueN-PUMP. Cardiopulmonary bypass was instituted by can-ulation of the ascending aorta and right atrium. Atandard circuit with a hollow-fiber membrane oxygen-tor and a roller pump was used. The body temperatureas kept at 37°C. Myocardial protection was achievedy means of intermittent antegrade warm bloodardioplegia.FF-PUMP. The technique of exposure and stabilization of
he target coronary vessel has already been reported [22].n the most recent years, an apical suction was used toxpose in particular the lateral and the inferior wallXpose, Guidant Corporation, Cupertino, CA). When theoronary artery was exposed, stabilization was achievedith a pressure (Acces Ultima System, Guidant Corpo-
ation) or suction (Axius Vacuum 2 System, Guidant
orporation) stabilizer.pt
ats.ctsnetjournDownloaded from
linical Data Collection, Monitoring, and Definitionset of perioperative data was collected for all patients
ndergoing myocardial revascularization at our institu-ion. The following variables were recorded and defined.cute renal failure was defined as postoperative blood
reatinine equal or higher than 2.0 mg/dL if the preop-rative value was normal (�1.5 mg/dL), or increment oft least 1 mg/dL if preoperative renal function wasltered. Mortality included death from any cause duringearly mortality) or after (late mortality) the first 30 daysfter surgery. Postoperative creatinine value was mea-ured every postoperative day for each patient untilischarge; the peak value was considered for thenalysis.
ollow-Upll the patients were followed up in our outpatient clinic
, 6, and 12 months after surgery and thereafter at yearlyntervals. The more recent information was obtained byalling the patient or the referring cardiologist. Follow-upas 100% complete and ended on June 30, 2006. Mean
ollow-up of survivors was 7.5 � 1.9 years. Two hundredorty-three patients were still alive 10 years after surgery.
tatistical Analysisata are reported as mean � standard deviation for
ontinuous variables, or otherwise as a percentage. Sta-istical analysis comparing two groups was performedith the Mann-Whitney U test. In case of paired data, theilcoxon signed rank test was applied. Pearson �2 or
isher’s exact test was used to compare categorical vari-bles. Stepwise logistic regression was used to realize a
able 1. Analysis A: Preoperative Characteristics Accordingo Surgical Strategy
haracteristicOff-Pump(n � 862)
On-Pump(n � 862) p Value
ge (y) 63.9 � 9.5 64.2 � 9.1 0.494�75 y 103 (11.9%) 112 (13.0%) 0.512
emale sex 142 (16.5%) 154 (17.9%) 0.443F 0.589 � 0.130 0.581 � 0.131 0.265�0.85 43 (5.0%) 40 (4.6%) 0.736
reatinine (mg/dL) 1.02 � 0.21 1.02 � 0.21 1.000rgency 179 (20.8%) 183 (21.3%) 0.813iabetes 203 (23.5%) 203 (23.5%) 1.000revious AMI 401 (46.5%) 400 (46.4%) 0.961OPD 51 (5.9%) 53 (6.1%) 0.840CV 211 (24.5%) 213 (24.7%) 0.911M disease 134 (15.5%) 132 (15.3%) 0.911-vessel disease 309 (35.8%) 267 (31.0%) 0.123-vessel disease 553 (64.2%) 595 (69.0%) 0.123nastomoses/patients 2.6 � 0.7 2.6 � 0.7 0.717edo 9 (1.0%) 6 (0.7%) 0.437uroSCORE 4.7% 4.6% 0.813
MI � acute myocardial infarction; COPD � chronic obstructive
ulmonary disease; ECV � extracardiac vasculopathy; EF � ejec-ion fraction; LM � left main coronary artery.
by on June 3, 2013 als.org
n[aTL�po
iamrCiolroprfriaCw
R
APi
5(nmcpro0s1
hpleTrh4pnAc
ip(uisuf
F
Tt
C
a
FE
CUDPCEL23ARE
Apt
1498 DI MAURO ET AL Ann Thorac SurgOFF-PUMP SURGERY AND RENAL FAILURE 2007;84:1496–503
CA
RD
IOV
ASC
ULA
R
onparsimonious model to calculate the propensity score22] (the probability of being selected for on-pump given
set of preoperative risk factors already reported [23]).he model fit was evaluated using the Hosmer andemeshow test (analysis A: �2 � 3.22; p � 0.92; analysis B:2 � 3.96; p � 0.86). Then, a sample matching waserformed: each off-pump patient was matched with then-pump patient having the closest propensity score.Stepwise logistic regression was used to verify the
mpact of CPB on higher incidence of postoperative ARFnd early mortality as well as the impact of ARF on earlyortality; The results of stepwise logistic regression were
eported as odds ratio (OR), 95% confidence limits (95%L), and probability value. Receiver operating character-
stic curve was used to identify the cutoff predictive valuef CPB duration; area under the curve, 95% confidence
imits, probability value, sensitivity and specificity wereeported [24]. Actuarial survival was obtained by meansf Kaplan-Meier method; Ten-year survival was re-orted. Statistical differences were investigated with log-ank test. Time-to-event (mortality) analysis was per-ormed by a multivariate Cox proportional-hazardegression. The results of Cox analysis were reported asnstantaneous relative risk ratio (hazard ratio), 95% CL,nd probability value. The SPSS software (SPSS, Inc,hicago, IL) was used. Probability values less than 0.05ere considered significant.
esults
nalysis Areoperative and perioperative characteristics were sim-
able 2. Analysis B: Preoperative Characteristics Accordingo Surgical Strategy
haracteristicOff-Pump(n � 80)
On-Pump(n � 80) p Value
ge (y) 69.4 � 8.2 68.9 � 8.2 0.900�75 y 26 (31.0%) 31 (23.7%) 0.237
emale sex 9 (11.3%) 12 (15.0%) 0.482F 0.540 � 0.138 0.528 � 0.139 0.221�0.35 6 (7.5%) 7 (8.8%) 0.722
reatinine (mg/dL) 2.40 � 1.60 2.39 � 1.88 0.821rgency 20 (25.0%) 24 (30.0%) 0.479iabetes 18 (22.5%) 20 (25.0%) 0.710revious AMI 40 (50.0%) 38 (47.5%) 0.752OPD 8 (10.0%) 7 (8.8%) 0.786CV 23 (28.8%) 24 (30.0%) 0.862M disease 15 (18.8%) 15 (18.8%) 1.000-vessel disease 26 (32.5%) 29 (36.3%) 0.618-vessel disease 54 (67.5%) 51 (63.8%) 0.618nastomoses/patients 2.7 � 0.8 2.7 � 0.9 0.846edo 1 (1.3%) 2 (2.5%) 1.000uroSCORE 9.8% 10.6% 0.625
MI � acute myocardial infarction; COPD � chronic obstructiveulmonary disease; ECV � extracardiac vasculopathy; EF � ejec-
ion fraction; LM � left main coronary artery.
lar in both groups (Table 1). The incidence of ARF was r
ats.ctsnetjournDownloaded from
.4% (93 cases), significantly higher in on-pump patients7.9% versus 2.9%; p � 0.001). Mean preoperative creati-ine value was identical for each group (1.02 � 0.21g/dL). In the postoperative period the peak value of
reatinine was 1.26 � 0.64 mg/dL (p � 0.001 versusreoperative value); in the off-pump group creatinineose to 1.19 � 0.5 mg/dL (p � 0.001), whereas in then-pump group it increased to 1.33 � 0.72 mg/dL (p �.001). Hence, the percentage increment of creatinine wasignificantly higher in the on-pump group (30.4% versus6.6%; p � 0.001).
The incidence of ARF was higher in off-pump patientsaving lateral wall revascularization (3.6% versus 0.7%;� 0.011; OR, 5.4; 95% CL, 1.3 to 9.5; p � 0.024), whereas
ateral wall revascularization did not produce any differ-nce in on-pump patients (7.9% versus 7.8%; p � 0.976).he ARF rate for off-pump patients having lateral wallevascularization was lower than that for the groupaving on-pump surgery (3.6% versus 7.9%; p � 0.001). In92 (57.0%) off-pump patients, side clamping was used toerform proximal anastomoses. This grade of aortic ma-ipulation did not produce any significant increment ofRF rate (2.2% no aortic manipulation versus 3.0% side
lamping; p � 0.424).Patients with ARF showed a postoperative peak creat-
nine value of 2.72 � 1.81 mg/dL, significantly higher thanatients with normal postoperative renal function
1.17�0.26 mg/dL; p � 0.001). Dopamine infusion wassed in 91 of 93 patients (97.8%) with postoperative ARF;
n the remaining 2 patients, diuretic therapy and fluidupply were able to treat the ARF. Hemofiltration wassed in 3 patients (3.2%). Complete recovery of renal
unction (creatinine �1.5 mg/dL) was achieved in 29 of 88
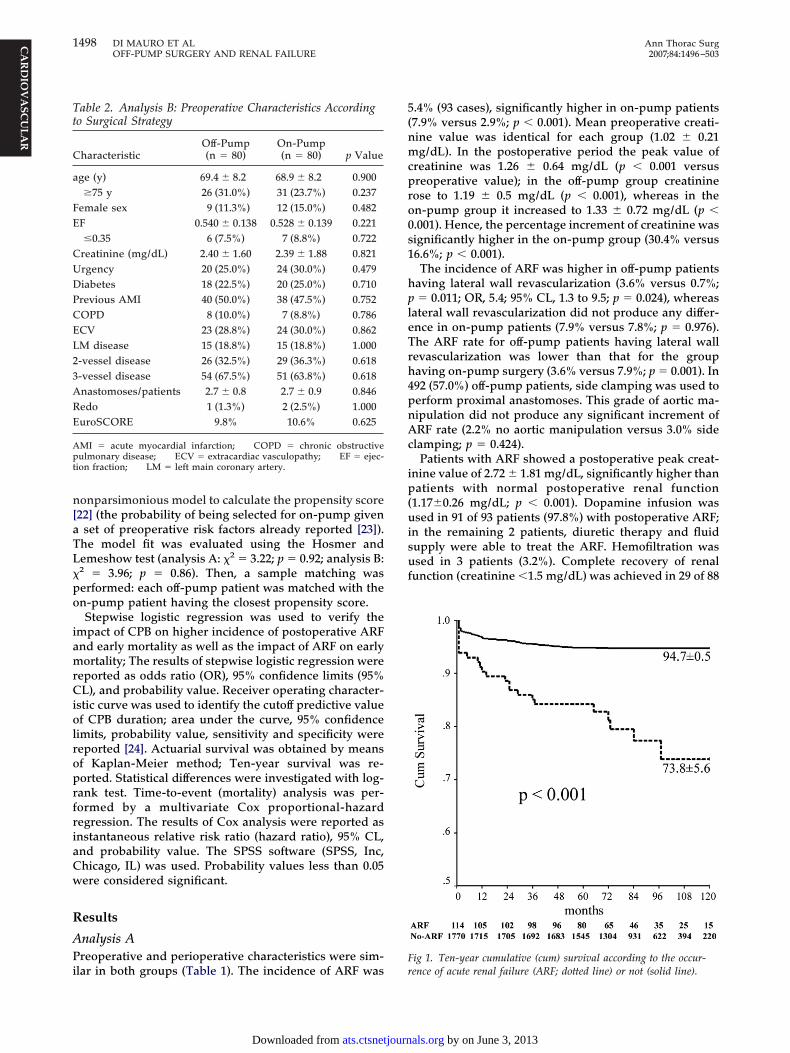
ig 1. Ten-year cumulative (cum) survival according to the occur-
ence of acute renal failure (ARF; dotted line) or not (solid line).by on June 3, 2013 als.org

sspw
iiaeCit0mt5
APi1tpsp(gwmc2p
t0Pph1orsuemd(m
EOT60(ochtw
pept
T
OAA
A ratio.
T
O
A
A
A
1499Ann Thorac Surg DI MAURO ET AL2007;84:1496–503 OFF-PUMP SURGERY AND RENAL FAILURE
CA
RD
IOV
ASC
ULA
R
urvivors (33.0%); 1 patient (1.1%) did not recover andtarted the dialysis on the nephrology ward. Twenty-nineatients (33.0%) were discharged to the cardiology wardith creatinine equal to or greater than 2.0 mg/dL.Stepwise logistic regression confirmed that CPB was an
ndependent variable for increased postoperative ARFncidence (OR, 3.3; 95% CL, 1.9 to 5.1; p � 0.001) as well asge (OR, 1.02; 95% CL, 1.004 to 1.05; p � 0.0299) andjection fraction equal or lower than 0.35 (OR, 2.6; 95%L, 1.5 to 6.1; p � 0.0081). Receiver operating character-
stic curves showed that CPB duration played an impor-ant predictive role (area under the curve, 0.79; 95% CL,.72 to 0.85; p � 0.001) and identified a cutoff value of 66inutes, above which the risk of developing postopera-
ive ARF was higher (sensitivity and specificity, 70%; OR,.3; 95% CL, 3.6 to 8.0; p � 0.001).
nalysis Breoperative and perioperative characteristics were sim-
lar in both groups (Table 2). The incidence of ARF was3.8% (23 patients), without significant differences be-ween groups (16.3% on-pump versus 12.5% off-pump;
� 0.499). Mean preoperative creatinine value wasimilar for each group (Table 2). In the postoperativeeriod the peak value of creatinine was 2.87 � 1.96 mg/dL
p � 0.001 versus preoperative value); in the off-pumproup creatinine rose to 2.84 � 1.65 mg/dL (p � 0.001),hereas in the on-pump group it increased to 2.86 � 2.22g/dL (p � 0.001). The percentage of increment of
reatinine was similar in both groups (22.4% versus1.5%; p � 0.873). The incidence of ARF was similar inatients having or not having lateral wall revasculariza-
able 3. Impact of Postoperative Acute Renal Failure on 10-Y
10-Year Mortality
ARF
Patients Deaths, n (%) Pa
verall 114 23 (20.2) 1nalysis A 91 15 (16.5) 1nalysis B 23 8 (34.8)
RF � acute renal failure; CL � confidence limits; HR � hazard
able 4. Ten-Year Outcome for On-Pump Versus Off-Pump in
10-Year Mortality
On-Pump
Patients Deaths, n (%) Pa
verall 942 66 (7.0)ARF 81 17 (21.0)No ARF 861 49 (5.7)nalysis A 862 57 (6.6)ARF 68 13 (19.1)No ARF 794 44 (5.5)nalysis B 80 9 (11.3)ARF 13 4 (30.8)No ARF 67 5 (7.5)
RF � acute renal failure; CL � confidence limits; HR � hazard ratio.
ats.ctsnetjournDownloaded from
ion either in case of off-pump (11.7% versus 15.0%; p �.705) or on-pump surgery (19.7% versus 0%; p � 0.112).atients with postoperative ARF showed a postoperativeeak creatinine value of 4.30 � 2.04 mg/dL, significantlyigher than patients who did not experience ARF (2.60 �.83 mg/dL; p � 0.001). Dopamine infusion was used in 14f 23 patients (60.9%) with postoperative ARF; in theemaining 9 patients (39.1%), diuretic therapy and fluidupply were enough to treat the ARF. Hemofiltration wassed in 1 patient (4.3%). Among the 22 patients whoxperienced ARF and survived the first postoperativeonth, 1 patient (4.3%) did not recover and started the
ialysis on the nephrology ward. Twenty-one patients95.5%) were discharged to the cardiology ward with a
ean creatinine value of 3.38 � 1.09 mg/dL.
arly Outcomeverall early mortality was 1.7% (32 of 1,884 patients).he impact of ARF on early mortality was relevant (n �; 5.3% ARF group versus n � 26; 1.5% no-ARF group; p �.011). Off-pump surgery did not reduce early mortalityn � 11; 1.2% off-pump group versus n � 21; 2.1%n-pump group; p � 0.074). Stepwise logistic regressiononfirmed that ARF was an independent variable forigher 30-day mortality in the overall analyzed popula-
ion (OR, 3.6; 95% CL, 1.5 to 9.1; p � 0.004). No patientho underwent postoperative dialysis died.In analysis A, early mortality was 1.6% (28 of 1,724
atients), again significantly higher in patients experi-ncing ARF (5.5% ARF group versus 1.4% no-ARF group;� 0.003). Off-pump surgery provided lower early mor-
ality (0.9% off-pump versus 2.3% on-pump; p � 0.022).
ortality
No ARF Cox Analysis
s Deaths, n (%) HR 95% CL p Value
94 (5.3) 4.1 2.6–6.4 �0.00178 (4.8) 3.7 2.1–6.5 �0.00116 (11.7) 3.0 1.3–7.0 0.011
h Strata
Off-Pump Cox Analysis
s Deaths, n (%) HR 95% CL p Value
50 (5.3) 1.3 0.91–1.9 0.1416 (18.2) 1.1 0.4–2.7 0.879
44 (4.8) 1.2 0.8–1.8 0.43236 (4.2) 1.6 1.1–2.4 0.0282 (8.7) 2.0 0.5–9.0 0.356
34 (4.1) 1.4 0.9–2.1 0.16414 (17.5) 0.6 0.3–1.4 0.2364 (40.0) 0.7 0.2–2.7 0.546
10 (14.3) 0.5 0.2–1.5 0.210
ear M
tient
,770,633137
Eac
tient
94233
90986223
839801070
by on June 3, 2013 als.org

M(9m
psAgo1
as
LTi(BaFi02p
oip
ltfoe
C
Ir(pT1otAcwfi
Cgono(t
Fppo
Fpn
1500 DI MAURO ET AL Ann Thorac SurgOFF-PUMP SURGERY AND RENAL FAILURE 2007;84:1496–503
CA
RD
IOV
ASC
ULA
R
ultivariate analysis confirmed that postoperative ARFOR, 3.4; 95% CL, 1.2 to 9.2; p � 0.017) and CPB (OR, 2.3;5% CL, 1.05 to 5.3; p � 0.041) were risk factors for earlyortality.In analysis B, 4 patients (2.5%) died within the first
ostoperative month; in this analysis, there were notatistical differences between patients with or withoutRF (n � 1; 4.3% ARF group versus n � 2; 2.2% no-ARFroup; p � 0.466) and in those undergoing on-pump orff-pump surgery (n � 3; 3.7% off-pump group versus n �; 1.3% on-pump group; p � 0.620).
Concerning 1,907 patients surviving the first postoper-tive month, ARF prolonged the postoperative hospitaltay from 4.6 � 2.9 to 6.7 � 5.3 days (p � 0.001).
ate Outcomeen-year survival was 93.6% � 0.6%, significantly higher
n patients with preoperative normal creatinine value94.5% � 0.6%, analysis A versus 83.2% � 3.7%, analysis; p � 0.001) and in patients who experienced postoper-tive ARF (73.8% � 5.6% versus 94.7% � 0.5%; p � 0.001;ig 1); a worse survival for the ARF group was found both
n analysis A (80.5% � 4.8% versus 95.3% � 0.5%, p �.001) and in analysis B (54.8% � 13.7% versus 89.1% �.7%; p � 0.005). Cox analysis confirmed the impact ofostoperative ARF on late outcome (Table 3).Table 4 summarizes 10-year outcome in on-pump and
ff-pump groups according to occurrence of ARF or not,n each strata (overall, analysis A, and analysis B). On-
ig 2. Ten-year cumulative (cum) survival for on-pump and off-ump surgery according to the type of analysis: analysis A, off-ump (solid line); analysis A, on-pump (dashed line); analysis B,ff-pump (dotted line); analysis B, on-pump (dash-dot line).
ump surgery resulted in being a risk factor for worse A
ats.ctsnetjournDownloaded from
ate outcome in analysis A (hazard ratio, 1.6; 95% CL, 1.1o 2.4; p � 0.028). Figures 2 and 3 show 10-year survivalor on-pump and off-pump surgery according to the typef analysis (A or B) and the occurrence or not of postop-rative ARF.
omment
n patients with normal preoperative renal function, theate of ARF was significantly higher in on-pump patients7.9% versus 2.9%; p � 0.001), as was the postoperativeeak value of creatinine and the increment of creatinine.hese findings are consistent with the literature (1.4% to0%) [5, 7, 9]. Stepwise logistic regression confirmed thatn-pump patients with normal preoperative renal func-ion have a threefold increment of the risk to developRF. The same result was obtained by Stallwood and
olleagues [7], who analyzed a cohort of 2,199 patientsith preoperative creatinine values less than 200 �mol/L,nding that CPB was a risk factor for ARF.Another important result from our analysis is that a
PB longer than roughly 1 hour (66 minutes) raised withood accuracy (70%) the risk of ARF (OR, 5.3). Althoughthers stated that prolonged CPB may produce ARF [1],one of them reported any cutoff value. However,ff-pump likely plays the main renoprotective roleARF: 2.9% for off-pump versus 5.0% for CPB shorterhan 66 minutes; p � 0.033; OR, 2.7; p � 0.029).
ig 3. Ten-year cumulative (cum) survival for on-pump and off-ump surgery according to occurrence of acute renal failure (ARF) orot: no-ARF, off-pump (solid line); no-ARF, on-pump (dashed line);
RF, off-pump (dotted line); ARF, on-pump (dash-dot line).by on June 3, 2013 als.org

Atd
c[ootop
sopwrpf
botfeLsat
oprpgrvlistIsp
libc
opiata(rep
casK
mirefBsP1asea
inmbbnpsmrlsois
abcbcdd
R
1501Ann Thorac Surg DI MAURO ET AL2007;84:1496–503 OFF-PUMP SURGERY AND RENAL FAILURE
CA
RD
IOV
ASC
ULA
R
dditionally, advanced age and very low ejection frac-ion were found to impair renal function, as alreadyemonstrated [1, 5, 7, 9].Again, in analysis B, the incidence of ARF (13.0%) was
onsistent with that reported by others (5.9% to 19.5%)5, 6, 8]. In this case, attempts to find any impact of CPBn ARF failed. Both groups showed the same incrementf creatinine value in the postoperative period. Althoughhe small sample size could reduce the statistical powerf analysis B, the same results were achieved in anotherropensity-based analysis comparing larger cohorts [8].To better understand the results of our study, we
hould answer the following questions. Why does evenff-pump surgery impair renal function? Why does CPBrovide a significant higher incidence of ARF in patientsith normal preoperative renal function? Why does the
enoprotective role of off-pump surgery seem to disap-ear in patients with preoperative abnormal renal
unction?The inflammatory response does not differ greatly
etween on-pump and off-pump groups [25, 26]. Inff-pump patients with good preoperative renal reserve,he inflammatory response may cause a mild renal dys-unction, resulting more in a slight increment of postop-rative creatinine than in a clinical picture of ARF.ikewise, preoperative dysfunctioning kidneys are moreusceptible, and the inflammatory response may causen important renal dysfunction or damage, even similaro that produced by CPB.
Transient circulatory failure and global hypoperfusion,ccurring in case of exposure of the lateral vessels, couldrovide another possible explanation for postoperativeenal impairment in off-pump surgery [21]. In our series,atients with preoperative normal renal function under-oing off-pump surgery showed a significantly higherate of ARF in case of lateral wall revascularization (3.6%ersus 0.7%). In patients with normal renal function,ateral wall revascularization may be performed on beat-ng heart, being very careful to avoid transient hypoten-ion, but when it occurs, the likelihood of ARF is lowerhan with on-pump surgery (3.6% versus 7.9%; p � 0.001).n case of preoperative abnormal renal function, tran-ient circulatory failure does not seem to have anyarticular relevance.Finally, atheroembolism as a result of aortic manipu-
ation is addressed as another possible cause of renalmpairment [27]. This can occur even in off-pump surgeryecause of side clamping. However, in our series sidelamping did not influence the rate of ARF.
These speculations help us not only to depict the rolef off-pump surgery in case of either normal or alteredreoperative renal function, but also to explain the major
mpact of CPB on postoperative renal impairment. Actu-lly, although off-pump surgery produces an inflamma-ory response similar to CPB, the latter is responsible for
more rapid (C5a and C5b-9) and more profoundC5b-9) expression of complement activation, which areesponsible for tubular epithelial cell lesion by an isch-mia–reperfusion mechanism [18]. Moreover, the non-
ulsatile flow of CPB is strongly correlated with in-ats.ctsnetjournDownloaded from
reased likelihood of renal dysfunction, especially ifssociated with hypotension [9]. Recently, the relation-hip between hemodilution and ARF was confirmed byarkouti and associates [19].Postoperative ARF was demonstrated to increase earlyortality (7% to 38%) [1–4, 7]. The occurrence of ARF
mpacted negatively on early mortality (OR, 3.7). Thisesult was mainly related to patients with normal preop-rative renal function; in fact, ARF was found to be a riskactor for early mortality in analysis A but not in analysis. Furthermore, ARF prolonged postoperative hospitaltay from 4.6 � 2.9 days to 6.7 � 5.3 days (p � 0.001).ostoperative ARF caused a significant impairment of0-year survival (hazard ratio, 4.1), confirmed in bothnalysis A (3.7) and analysis B (3.0). Moreover, off-pumpurgery can provide an important protective role on botharly and late outcome of patients with normal preoper-tive renal function.In conclusion, avoiding CPB can be the most important
tem to prevent as much as possible ARF in patients withormal preoperative creatinine. In patients with abnor-al preoperative creatinine, off-pump coronary artery
ypass graft surgery does not seem to add any benefit,ut further analysis on a larger cohort of patients isecessary to better clarify its role in this subset ofatients. When CPB has to be necessarily used, wehould remember that the longer the CPB duration, theore important the renal damage is, with a cutoff point of
oughly 1 hour. In case of off-pump lateral wall revascu-arization, it is very important to keep arterial pressuretable to prevent even transient renal hypoperfusion. Theccurrence of postoperative renal failure has a great
mpact on early and late mortality, and the surgicaltrategy cannot improve them.
The main limitation is the retrospective nature of thenalysis. Moreover, the results found in analysis B shoulde confirmed in a larger cohort of patients. The use ofreatininemia as a marker of renal function is not perfect,ut it is by far the most widely used in the centers ofardiac surgery, as creatinine clearance is difficult toetermine and it is often based on formulas rather thanirect observation.
eferences
1. Corwin HL, Sprague SM, DeLaria GA, Norusis MJ. Acuterenal failure associated with cardiac operations: a case-control study. J Thorac Cardiovasc Surg 1989;98:1107–12.
2. Andersson LG, Ekroth R, Bratteby LE, Hallhagen S, WesslenO. Acute renal failure after coronary surgery: a study ofincidence and risk factors in 2009 consecutive patients.Thorac Cardiovasc Surg 1993;41:237–41.
3. Chertow GM, Lazarus JM, Christiansen CL, Cook EF, Ham-mermeister KE, Grover F, Daley J. Preoperative renal riskstratification. Circulation 1997;95:878–84.
4. Mangano CM, Diamondstone LS, Ramsay JG, Aggarwal A,Herskowitz A, Mangano DT. Renal dysfunction after myo-cardial revascularization: risk factors, adverse outcomes, andhospital resource utilization—the Multicenter Study of Peri-operative Ischemia Research Group. Ann Intern Med 1998;128:194–203.
5. Gamoso MG, Phillips-Bute B, Landolfo KP, Newman MF,Stafford-Smith M. Off-pump versus on-pump coronary ar-
by on June 3, 2013 als.org

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
I
Depppirygssos3c�b
n
1502 DI MAURO ET AL Ann Thorac SurgOFF-PUMP SURGERY AND RENAL FAILURE 2007;84:1496–503
©P
CA
RD
IOV
ASC
ULA
R
tery bypass surgery and postoperative renal dysfunction.Anesth Analg 2000;91:1080–4.
6. Ascione R, Nason G, Al-Ruzzeh S, Ko C, Ciulli F, AngeliniGD. Coronary revascularization with or without cardiopul-monary bypass in patients with preoperative nondialysis-dependent renal insufficiency. Ann Thorac Surg 2001;72:2020–5.
7. Stallwood MI, Grayson AD, Mills K, Scawn ND. Acute renalfailure in coronary artery bypass surgery: independenteffect of cardiopulmonary bypass. Ann Thorac Surg 2004;77:968 –72.
8. Chukwuemeka A, Weisel A, Maganti M, et al. Renal dys-function in high-risk patients after on-pump and off-pumpcoronary artery bypass surgery: a propensity score analysis.Ann Thorac Surg 2005;80:2148–53.
9. Weerasinghe A, Athanasiou T, Al-Ruzzeh S, et al. Functionalrenal outcome in on-pump and off-pump coronary revascu-larization: a propensity-based analysis. Ann Thorac Surg2005;79:1577–83.
0. Schwann N, Horrow J, Strong M, Chamchad D, Guerraty A,Wechsler A. Does off-pump coronary artery bypass reducethe incidence of clinically evident renal dysfunction aftermultivessel myocardial revascularisation? Anesth Analg2004;99:959–64.
1. Zanardo G, Michielon P, Paccagnella A, et al. Acute renalfailure in the patient undergoing cardiac operation. Preva-lence, mortality rate, and main risk factors. J Thorac Cardio-vasc Surg 1994;107:1489–95.
2. Hickey PR, Buckley MJ, Philbin DM. Pulsatile and nonpul-satile cardiopulmonary bypass: review of a counterproduc-tive controversy. Ann Thorac Surg 1983;36:720–37.
3. Regragui IA, Izzat MB, Birdi I, Lapsley M, Bryan AJ, AngeliniGD. Cardiopulmonary bypass perfusion temperature doesnot influence perioperative renal function. Ann Thorac Surg1995;60:160–4.
4. Ascione R, Lloyd CT, Underwood MJ, Gomes WJ, AngeliniGD. On-pump versus off-pump coronary revascularization:evaluation of renal function. Ann Thorac Surg 1999;68:493–8.
5. Loef BG, Epema AH, Navis G, Ebels T, van Oeveren W,Henning RH. Off-pump coronary revascularization attenu-ates transient renal damage compared with on-pump coro-nary revascularization. Chest 2002;121:1190–4.
6. Ramsay JG. The respiratory, renal, and hepatic systems:
effect of cardiac surgery and cardiopulmonary bypass. In:al function prior to surgery (analysis A), patients under-
grsMfimpferoysv0
cpd
2007 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
Mora CT, ed. Cardiopulmonary bypass. New York: Springer-Verlag, 1995:147–68.
7. Suen WS, Mok CK, Chiu SW, et al. Risk factors for devel-opment of acute renal failure (ARF) requiring dialysis inpatients undergoing cardiac surgery. Angiology 1998;49:789–800.
8. Zhou W, Farrar CA, Abe K, et al. Predominant role for C5b-9in renal ischemia/reperfusion injury. J Clin Invest 2000;105:1363–71.
9. Karkouti K, Beattie WS, Wijeysundera DN, et al. Hemodilu-tion during cardiopulmonary bypass is an independent riskfactor for acute renal failure in adult cardiac surgery. J Tho-rac Cardiovasc Surg 2005;129:391–400.
0. Schwann NM, Horrow JC, Strong MD 3rd, Chamchad D,Guerraty A, Wechsler AS. Does off-pump coronary arterybypass reduce the incidence of clinically evident renal dys-function after multivessel myocardial revascularization?Anesth Analg 2004;99:959–64.
1. Tang AT, Knott J, Nanson J, Hsu J, Haw MP, Ohri SK. Aprospective randomised study to evaluate the renoprotectiveaction of beating heart coronary surgery in low risk patients.Eur J Cardiothoracic Surg 2002;22:118–23.
2. Blackstone EH. Comparing orange and apples. J ThoracCardiovasc Surg 2002;123:8–15.
3. Calafiore AM, Di Mauro M, Canosa C, Di Giammarco G,Iaco AL, Contini M. Myocardial revascularization with andwithout cardiopulmonary bypass: advantages, disadvan-tages and similarities. Eur J Cardiothorac Surg 2003;24:953– 60.
4. Jones MC, Athanasiou T. Summary receiver operating char-acteristic curve analysis techniques in the evaluation ofdiagnostic tests. Ann Thorac Surg 2005;79:16–20.
5. Biglioli P, Cannata A, Alamanni F, et al. Biological effects ofoff-pump versus on-pump coronary artery surgery: focus oninflammation, haemostasis and oxidative stress. Eur J Car-diothorac Surg 2003;24:260–9.
6. Wehlin L, Vedin J, Vaage J, Lundahl J. Activation of comple-ment and leukocyte receptors during on- and off pumpcoronary artery bypass surgery. Eur J Cardiothorac Surg2004;25:35–42.
7. Doty JR, Wilentz RE, Salazar JD, Hruban RH, Cameron DE.Atheroembolism in cardiac surgery. Ann Thorac Surg
2003;75:1221–6.NVITED COMMENTARY
i Mauro and colleagues [1] investigated the renoprotectiveffect of off-pump coronary artery bypass surgery com-ared with on-pump surgery using cardiopulmonary by-ass. The authors stratified the analysis into two groups: (A)atients with normal baseline renal function (serum creat-
nine � 1.5 mg/dL) and (B) patients with abnormal baselineenal function (serum creatinine � 1.5 mg/dL). Their anal-sis addressed the following question: Does off-pump sur-ery have a renoprotective effect compared with on-pumpurgery with cardiopulmonary bypass support? Propensitycore matching was used to balance patients undergoingn-pump and off-pump surgery in both of the analyticaltrata. The outcomes of the analyses were survival and0-day acute renal failure, defined as a postoperative serumreatinine of �2.0 (mg/dL) if the baseline creatinine was1.5 mg/dL or a 1.0 mg/dL increase in creatinine if theaseline creatinine was �1.5 mg/dL.Among propensity-matched patients with normal re-
oing off-pump surgery were less likely to have acuteenal failure develop (2.9%) than patients undergoingurgery with cardiopulmonary bypass support (7.9%).
ultivariable stepwise logistic regression analysis con-rmed that cardiopulmonary bypass with more than 66inutes of pump time was a significant independent
redictor of acute renal failure as well as low ejectionraction � 35%. However, among patients with pre-xisting abnormal renal function (analysis B), the occur-ence of acute renal failure at 30 days was similar forff-pump (12.5%) and on-pump (16.3%) patients. Ten-ear survival analysis demonstrated a similar findinghowing off-pump surgery with significantly higher sur-ival in comparison with on-pump for analysis A (p value.026), but not with analysis B (p value 0.230).The authors extended their primary hypothesis to
ompare the survivorship of patients undergoing on-ump versus off-pump surgery but stratified by the
evelopment of postoperative acute renal failure. The0003-4975/07/$32.00doi:10.1016/j.athoracsur.2007.06.059
by on June 3, 2013 als.org

DOI: 10.1016/j.athoracsur.2007.05.054 2007;84:1496-1502 Ann Thorac Surg
Bivona, Paolo Bosco, Sabina Gallina and Antonio M. Calafiore Michele Di Mauro, Massimo Gagliardi, Angela L. Iacò, Marco Contini, Antonio
The Importance of Preoperative Renal FunctionDoes Off-Pump Coronary Surgery Reduce Postoperative Acute Renal Failure?
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/84/5/1496including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/84/5/1496#BIBL
This article cites 26 articles, 21 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/84/5/1496#otherarticleThis article has been cited by 19 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/coronary_disease Coronary disease
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 3, 2013 ats.ctsnetjournals.orgDownloaded from




















