
Death caused by cardioinhibitory reflex cardiac arrest—A systematic review of cases
7
Death caused by cardioinhibitory reflex cardiac arrest—A systematic review of cases Bettina Schrag *, Paul Vaucher, Marc D. Bollmann, Patrice Mangin University Centre of Legal Medicine, Lausanne-Geneva, Rue Michel-Servet 1, 1211 Gene `ve 4, Switzerland 1. Introduction Parry in 1799, Waller in 1862, and Landois in 1865 were among the first authors to report that a compression of the side of the neck could lead to circulatory collapse [1]; however, they gave no pathophysiological explanation for the phenomenon. In 1868, Czermak [2] wrote that it was the result of direct excitation of the vagal nerve. Hering [3] in 1924 performed animal experiments and observed that compression of the neck influenced heart rate. He explained this observation by a mechanical stimulation of the carotid sinus, thus describing the arterial baroreflex. Franke [4] delineated in his papers different types of responses of the syndrome of the carotid sinus with important interindividual variations. The regulatory effect of carotid sinus stimulation is often used in cardiology for diagnosis [5] and therapy [6]. The evaluation of the dangers of neck compression without restriction of the arterial flow remains unresolved in forensic medical practice. It is generally accepted [7] that a blow or a short compression of the side of the neck stimulating the carotid sinus can lead to circulatory collapse resulting from activation of an arterial baroreflex controlling the heart rate. This cardioinhibitory reflex cardiac arrest (CiRCA) has, however, not been observed in animal experimental settings [8]. In legal medicine, there is therefore a need to study the circumstances of death when CiRCA has been mentioned to understand the possible underlying mechanisms that could explain why and when such stimulation leads to death. We performed a systematic review to identify published cases in which CiRCA was evoked as a possible mechanism of death. This observational study aimed to describe conditions in which CiRCA was thought to be possible and to review authors’ conclusions in the light of current knowledge. 2. Materials and methods 2.1. Search strategy Our search strategy included both published cases in biomedical journals and those published in textbooks. To retrieve cases from published articles, we used no restrictions for time or language. Many articles were expected to be indexed before the 1970s without an abstract. Our search strategy therefore had to include as many terms as possible that might be included in titles. To achieve an optimal balance between sensitivity and specificity, we used as many terms as feasible to restrict our search to articles that referred to death caused by a reflex following trauma to the neck (Box 1). Titles and abstracts, when available, were extracted from Medline, Embase (1974–current), and ISI Web of Knowledge on June 25, 2009. Duplicates were automatically discarded by the reference managing software (Endnote 2.0) at importation, and those that the software did not identify were manually discarded. Forensic Science International 207 (2011) 77–83 ARTICLE INFO Article history: Received 26 July 2010 Received in revised form 30 August 2010 Accepted 9 September 2010 Available online 20 October 2010 Keywords: Neck trauma Death Sudden Baroreflex Carotid ABSTRACT Forensic pathologists often refer to the cardioinhibitory reflex cardiac arrest (CiRCA) following short neck trauma as a mechanism of death. We sought via a systematic review of the literature to identify circumstances under which carotid bifurcation stimulation could lead to death. Two independent reviewers selected case studies or reports from Medline, ISI Web of Knowledge, and Embase. Circomstances and contributory factors were extracted for each case. From the available data, authors independently assessed whether CiRCA was highly probable (no alternative explanation possible), probable (alternative explanation possible), or unlikely (alternative explanation highly probable). A narrative approach was used to define circumstances in which CiRCA remained possible. From the 48 published cases evoking CiRCA as a possible cause of death between 1881 and 2009, 28 were most likely to result of other mechanism of death (i.e., cerebral hypoxia due to carotid compression, mechanical asphyxia, myocardial infarction). CiRCA remained possible for 20 cases (including five based on anecdotal evidence only) with only one case with no alternative explanation other than CiRCA. Our findings support the presumption that reflex cardiac arrhythmia due to carotid bifurcation stimulation cannot provoke death alone. Actual state of knowledge suggests CiRCA might be contributory to death in the presence of drug abuse and/or cardiac pathology, often associated with physical and/or mental excitation. ß 2010 Elsevier Ireland Ltd. All rights reserved. * Corresponding author. Tel.: +41 22 379 55 84; fax: +41 22 372 96 53. E-mail address: [email protected] (B. Schrag). Contents lists available at ScienceDirect Forensic Science International journal homepage: www.elsevier.com/locate/forsciint 0379-0738/$ – see front matter ß 2010 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.forsciint.2010.09.010
Transcript of Death caused by cardioinhibitory reflex cardiac arrest—A systematic review of cases

Death caused by cardioinhibitory reflex cardiac arrest—A systematicreview of cases
Bettina Schrag *, Paul Vaucher, Marc D. Bollmann, Patrice Mangin
University Centre of Legal Medicine, Lausanne-Geneva, Rue Michel-Servet 1, 1211 Geneve 4, Switzerland
1. Introduction
Parry in 1799, Waller in 1862, and Landois in 1865 were amongthe first authors to report that a compression of the side of the neckcould lead to circulatory collapse [1]; however, they gave nopathophysiological explanation for the phenomenon. In 1868,Czermak [2] wrote that it was the result of direct excitation of thevagal nerve. Hering [3] in 1924 performed animal experiments andobserved that compression of the neck influenced heart rate. Heexplained this observation by a mechanical stimulation of thecarotid sinus, thus describing the arterial baroreflex. Franke [4]delineated in his papers different types of responses of thesyndrome of the carotid sinus with important interindividualvariations. The regulatory effect of carotid sinus stimulation isoften used in cardiology for diagnosis [5] and therapy [6].
The evaluation of the dangers of neck compression withoutrestriction of the arterial flow remains unresolved in forensicmedical practice. It is generally accepted [7] that a blow or a shortcompression of the side of the neck stimulating the carotid sinus canlead to circulatory collapse resulting from activation of an arterial
baroreflex controlling the heart rate. This cardioinhibitory reflexcardiac arrest (CiRCA) has, however, not been observed in animalexperimental settings [8]. In legal medicine, there is therefore a needto study the circumstances of death when CiRCA has beenmentioned to understand the possible underlying mechanisms thatcould explain why and when such stimulation leads to death.
We performed a systematic review to identify published casesin which CiRCA was evoked as a possible mechanism of death. Thisobservational study aimed to describe conditions in which CiRCAwas thought to be possible and to review authors’ conclusions inthe light of current knowledge.
2. Materials and methods
2.1. Search strategy
Our search strategy included both published cases in biomedical journals andthose published in textbooks. To retrieve cases from published articles, we used norestrictions for time or language. Many articles were expected to be indexed beforethe 1970s without an abstract. Our search strategy therefore had to include as manyterms as possible that might be included in titles. To achieve an optimal balancebetween sensitivity and specificity, we used as many terms as feasible to restrict oursearch to articles that referred to death caused by a reflex following trauma to theneck (Box 1). Titles and abstracts, when available, were extracted from Medline,Embase (1974–current), and ISI Web of Knowledge on June 25, 2009. Duplicateswere automatically discarded by the reference managing software (Endnote 2.0) atimportation, and those that the software did not identify were manually discarded.
Forensic Science International 207 (2011) 77–83
A R T I C L E I N F O
Article history:Received 26 July 2010Received in revised form 30 August 2010Accepted 9 September 2010Available online 20 October 2010
Keywords:Neck traumaDeathSuddenBaroreflexCarotid
A B S T R A C T
Forensic pathologists often refer to the cardioinhibitory reflex cardiac arrest (CiRCA) following shortneck trauma as a mechanism of death. We sought via a systematic review of the literature to identifycircumstances under which carotid bifurcation stimulation could lead to death. Two independentreviewers selected case studies or reports from Medline, ISI Web of Knowledge, and Embase.Circomstances and contributory factors were extracted for each case. From the available data, authorsindependently assessed whether CiRCA was highly probable (no alternative explanation possible),probable (alternative explanation possible), or unlikely (alternative explanation highly probable). Anarrative approach was used to define circumstances in which CiRCA remained possible. From the 48published cases evoking CiRCA as a possible cause of death between 1881 and 2009, 28 were most likelyto result of other mechanism of death (i.e., cerebral hypoxia due to carotid compression, mechanicalasphyxia, myocardial infarction). CiRCA remained possible for 20 cases (including five based onanecdotal evidence only) with only one case with no alternative explanation other than CiRCA. Ourfindings support the presumption that reflex cardiac arrhythmia due to carotid bifurcation stimulationcannot provoke death alone. Actual state of knowledge suggests CiRCA might be contributory to death inthe presence of drug abuse and/or cardiac pathology, often associated with physical and/or mentalexcitation.
! 2010 Elsevier Ireland Ltd. All rights reserved.
* Corresponding author. Tel.: +41 22 379 55 84; fax: +41 22 372 96 53.E-mail address: [email protected] (B. Schrag).
Contents lists available at ScienceDirect
Forensic Science International
journal homepage: www.elsev ier .com/ locate / forsc i in t
0379-0738/$ – see front matter ! 2010 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.forsciint.2010.09.010
To identify cases from textbooks, we manually searched references from articlesand from identified textbooks. When possible, original reports of cases wereexplored. We then tracked cases back to their earliest published report. A librarianobtained copies of historical medical textbooks for us to use for reading andretrieving cases.
Finally, to identify cases eventually reported in the grey literature, we consultedexperts for information about any known case that our search strategy did notidentify. We used no language restriction and employed interpreters if texts werenot written in English, French, German, or Italian.
2.2. Article selection
One author excluded all articles that did not in any way concern the neck or acompressive mechanism. Two reviewers then independently selected articles basedon titles and abstracts. Articles were discarded if they did not concern humans andmechanical stimulation of the carotid sinus, if individuals survived, if death wasclearly reported from a cause other than CiRCA, or if initial cardiac arrest was notsudden. From this first selection, the reviewers collected and read the full articles.
We then used the following criteria to select articles: They had to include at leastone case in which a victim died, the death had to be related to a sudden necktrauma, and authors had to have mentioned CiRCA as a plausible cause of death. Ifreviewers had discordant views on these criteria, the study was retained for thenext step, which involved achieving consensus after discussion with all currentauthors once both reviewers individually extracted the data.
2.3. Textbooks and non-indexed articles
References from each retained article were screened to detect cases fromtextbooks and non-indexed articles. The institution librarian retrieved the sources,which the authors then reviewed. In turn, references from textbooks and non-indexarticles were manually searched to find original descriptions of cited cases.
2.4. Data extraction
Whenthe information was available, two reviewers extracted the following for eachidentified case and entered it into an Excel sheet: gender, age, profession, history ofcardiovascular disease,historyofsubstanceabuse,suddenneck trauma,circumstancesof trauma, sequence of events, presence of witnesses, duration of trauma, local necklesions, other lesions or signs, cardiac and cerebral status, toxicological findings, andgenetic investigations. In addition, when possible, original authors were contacted forfurther details when published descriptions of cases were unclear.
2.5. Synthesis
Three experienced experts in forensic medicine reviewed each case indepen-dently. They were asked to report their interpretation of possible likely mechanismof death related to the described neck trauma. Furthermore, for each case they hadto report whether they thought CiRCA was highly probable (no alternativeexplanation possible), probable (alternative explanation possible), or unlikely(alternative explanation highly probable). Mechanism of death was defined as thesuccession of events that best explains the link between the initial cause (usuallyneck trauma) and death [9]. Cases for which the three reviewers did not all agreewere discussed until a consensus was reached.
Description of victims’ age, gender, and presence of local injury of the carotidbifurcation were recapitulated in another table. Contributory factors (history ofcardiovascular disease, alcohol, drugs, acquired and congenital electrical cardiacabnormalities, excited delirium) were also reported when available. The restrictednumber of cases made it impossible to synthesize results using a meta-analysis.Alternatively, a narrative approach to interpret conditions that could favor CiRCAwas used instead.
Box 1. Search strategy
#1 Death
death OR deaths OR die OR died OR decline OR declines OR declined ORmortal OR mortality OR life threatening OR life endangerment OR deceaseOR deceased OR perish OR perished OR arrest OR heart failure OR cardiacfailure OR myocardial failure
#2 Reflex
sudden OR abrupt OR immediate OR short OR brief OR unexpected ORunexplained OR reflex OR reflexes OR baroreflex OR baroreflexes ORcirculatory collapse OR Hering OR vasovagal OR vagal OR cardioinhibitory
#3 Trauma
violence OR violent OR trauma OR traumatic OR injury OR injured OR lesionOR strangulation OR strangulations OR compression OR pressure ORstimulation OR stimulations OR excitation OR choke OR choking
#4 Localization
neck OR throat OR gullet OR carotid OR carotids OR baroreceptor ORbaroreceptors
#1 AND #2 AND #3 AND #4
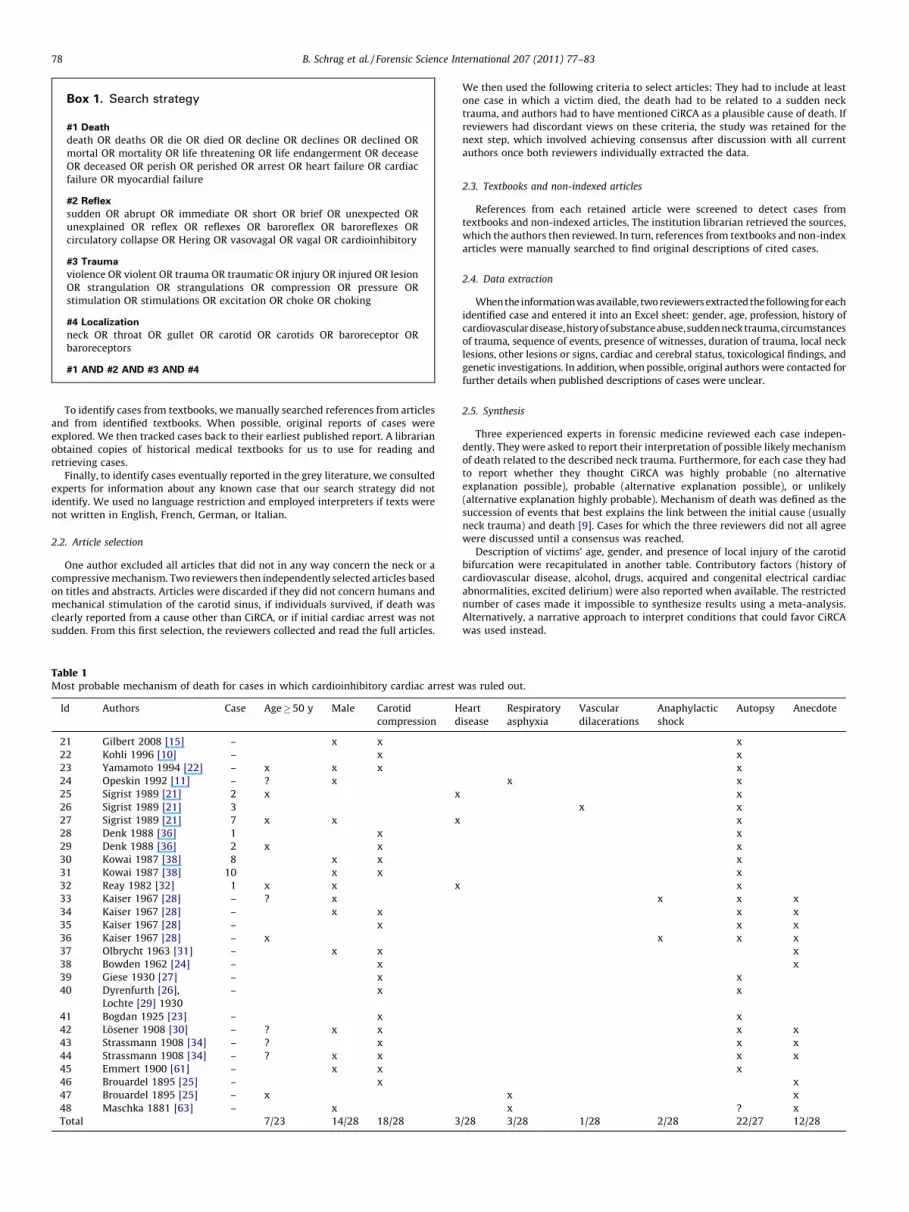
Table 1Most probable mechanism of death for cases in which cardioinhibitory cardiac arrest was ruled out.
Id Authors Case Age!50 y Male Carotidcompression
Heartdisease
Respiratoryasphyxia
Vasculardilacerations
Anaphylacticshock
Autopsy Anecdote
21 Gilbert 2008 [15] – x x x22 Kohli 1996 [10] – x x23 Yamamoto 1994 [22] – x x x x24 Opeskin 1992 [11] – ? x x x25 Sigrist 1989 [21] 2 x x x26 Sigrist 1989 [21] 3 x x27 Sigrist 1989 [21] 7 x x x x28 Denk 1988 [36] 1 x x29 Denk 1988 [36] 2 x x x30 Kowai 1987 [38] 8 x x x31 Kowai 1987 [38] 10 x x x32 Reay 1982 [32] 1 x x x x33 Kaiser 1967 [28] – ? x x x x34 Kaiser 1967 [28] – x x x x35 Kaiser 1967 [28] – x x x36 Kaiser 1967 [28] – x x x x37 Olbrycht 1963 [31] – x x x38 Bowden 1962 [24] – x x39 Giese 1930 [27] – x x40 Dyrenfurth [26],
Lochte [29] 1930– x x
41 Bogdan 1925 [23] – x x42 Losener 1908 [30] – ? x x x x43 Strassmann 1908 [34] – ? x x x44 Strassmann 1908 [34] – ? x x x x45 Emmert 1900 [61] – x x x46 Brouardel 1895 [25] – x x47 Brouardel 1895 [25] – x x x48 Maschka 1881 [63] – x x ? xTotal 7/23 14/28 18/28 3/28 3/28 1/28 2/28 22/27 12/28
B. Schrag et al. / Forensic Science International 207 (2011) 77–8378
3. Results
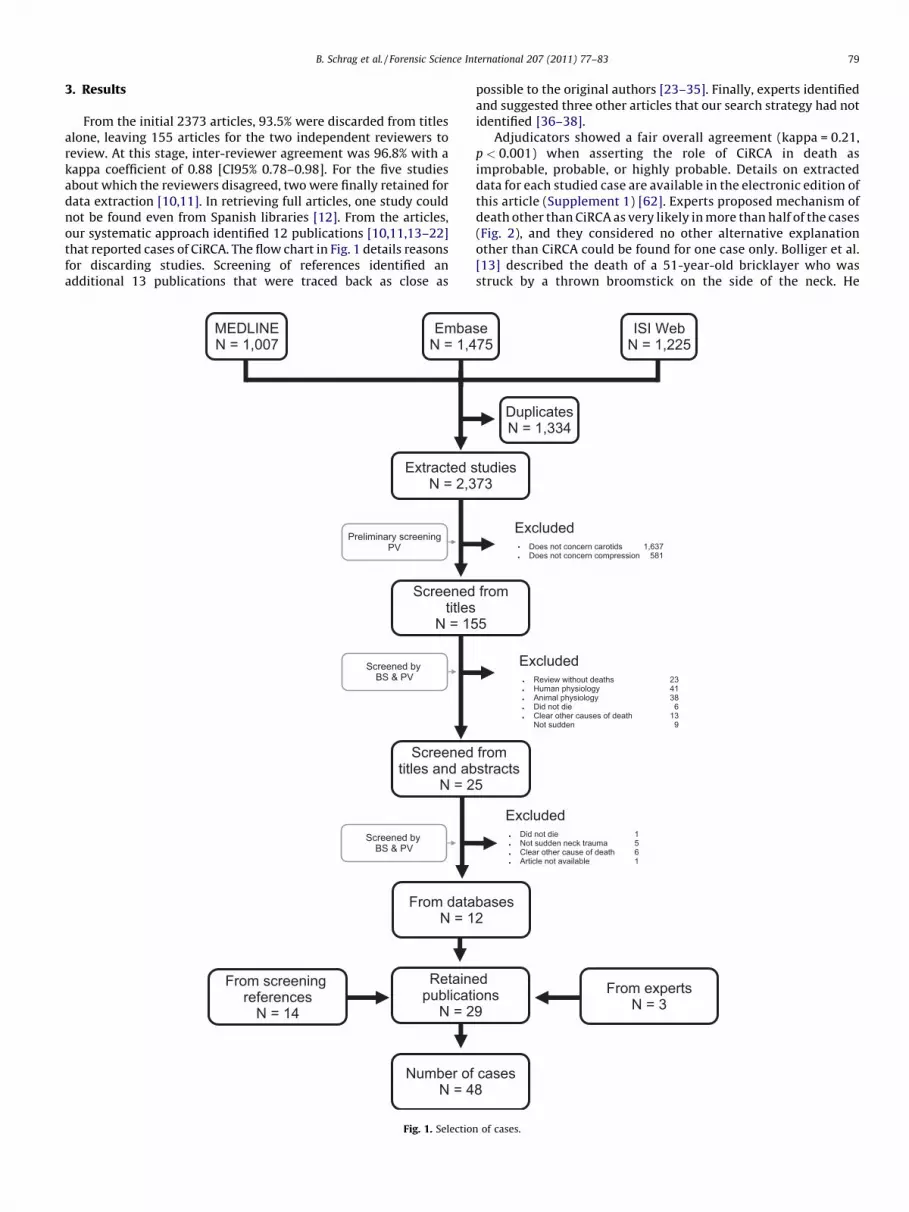
From the initial 2373 articles, 93.5% were discarded from titlesalone, leaving 155 articles for the two independent reviewers toreview. At this stage, inter-reviewer agreement was 96.8% with akappa coefficient of 0.88 [CI95% 0.78–0.98]. For the five studiesabout which the reviewers disagreed, two were finally retained fordata extraction [10,11]. In retrieving full articles, one study couldnot be found even from Spanish libraries [12]. From the articles,our systematic approach identified 12 publications [10,11,13–22]that reported cases of CiRCA. The flow chart in Fig. 1 details reasonsfor discarding studies. Screening of references identified anadditional 13 publications that were traced back as close as
possible to the original authors [23–35]. Finally, experts identifiedand suggested three other articles that our search strategy had notidentified [36–38].
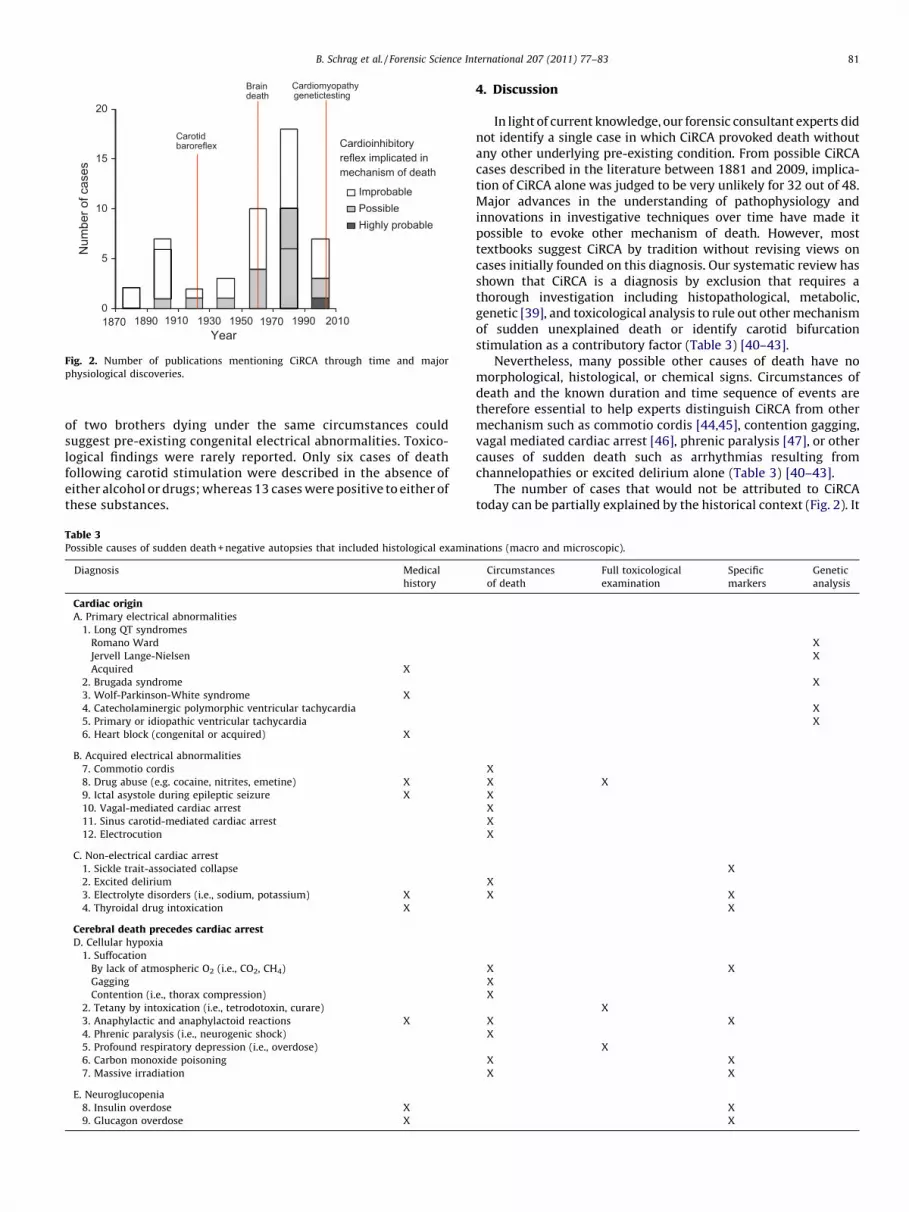
Adjudicators showed a fair overall agreement (kappa = 0.21,p < 0.001) when asserting the role of CiRCA in death asimprobable, probable, or highly probable. Details on extracteddata for each studied case are available in the electronic edition ofthis article (Supplement 1) [62]. Experts proposed mechanism ofdeath other than CiRCA as very likely in more than half of the cases(Fig. 2), and they considered no other alternative explanationother than CiRCA could be found for one case only. Bolliger et al.[13] described the death of a 51-year-old bricklayer who wasstruck by a thrown broomstick on the side of the neck. He
[()TD$FIG]
MEDLINEN = 1,007
EmbaseN = 1,475
ISI WebN = 1,225
Extracted studiesN = 2,373
Screened fromtitles
N = 155
ExcludedDoes not concern carotids 1,637Does not concern compression 581
DuplicatesN = 1,334
Preliminary screeningPV
Screened by BS & PV
Screened from titles and abstracts
N = 25
From screening references
N = 14
ExcludedReview without deaths 23Human physiology 41Animal physiology 38Did not die 6Clear other causes of death 13Not sudden 9
From databasesN = 12
ExcludedDid not die 1Not sudden neck trauma 5 Clear other cause of death 6Article not available 1
From expertsN = 3
Retained publications
N = 29
Screened by BS & PV
Number of casesN = 48
Fig. 1. Selection of cases.
B. Schrag et al. / Forensic Science International 207 (2011) 77–83 79
collapsed immediately, and bradycardic electromechanical dis-sociation was measured 10 min after trauma. Other than locallesions of the carotid bifurcation, no other signs could explain thedeath. However, even in this case, the original authors reportedthat the victim had cardiovascular disease. Including this case,CiRCA could not be excluded for 20 reported deaths. During the1970s and 1980s, many cases of death associated with exciteddelirium or overdose were observed during interventionsinvolving police force. CiRCA was then mentioned as a possiblecontributory factor of death. These deaths were retained as
possibly related to CiRCA. For the 28 remaining cases, expertsconsidered other mechanism of death as much more likely.Cerebral hypoxia resulting from prolonged carotid compressionwas the most likely reported mechanism, one that seemed to havebeen neglected especially for cases reported before the 1950s(Table 1). Anaphylactic shock, myocardial infarction, and drown-ing were also probable causes of death among the selected cases.Contributory factors are given in Table 2. Genetic analysis forcardiac congenital electrical abnormalities was never assessed inany of the reported cases. Olbrycht’s [31] strange anecdotal story
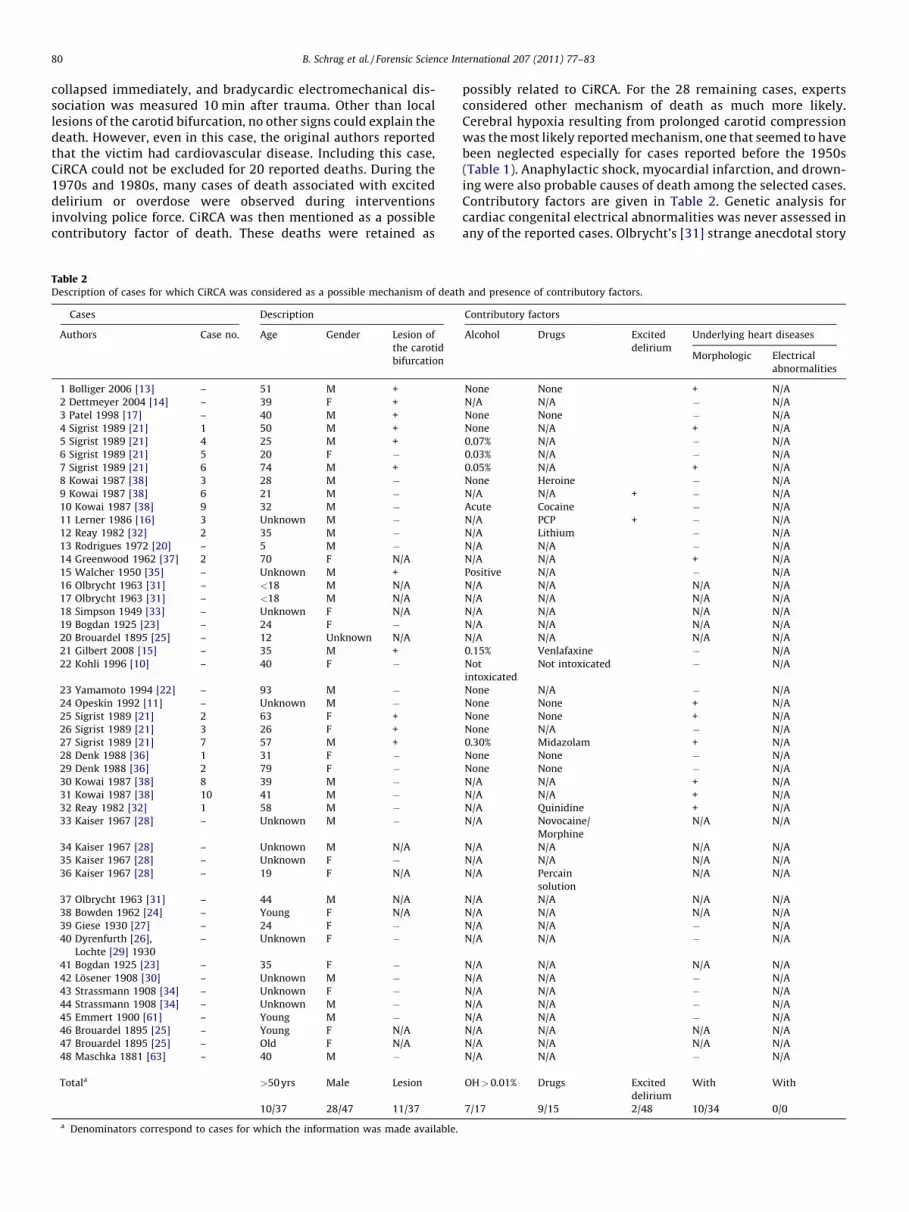
Table 2Description of cases for which CiRCA was considered as a possible mechanism of death and presence of contributory factors.
Cases Description Contributory factors
Authors Case no. Age Gender Lesion ofthe carotidbifurcation
Alcohol Drugs Exciteddelirium
Underlying heart diseases
Morphologic Electricalabnormalities
1 Bolliger 2006 [13] – 51 M + None None + N/A2 Dettmeyer 2004 [14] – 39 F + N/A N/A " N/A3 Patel 1998 [17] – 40 M + None None " N/A4 Sigrist 1989 [21] 1 50 M + None N/A + N/A5 Sigrist 1989 [21] 4 25 M + 0.07% N/A " N/A6 Sigrist 1989 [21] 5 20 F " 0.03% N/A " N/A7 Sigrist 1989 [21] 6 74 M + 0.05% N/A + N/A8 Kowai 1987 [38] 3 28 M " None Heroine " N/A9 Kowai 1987 [38] 6 21 M " N/A N/A + " N/A10 Kowai 1987 [38] 9 32 M " Acute Cocaine " N/A11 Lerner 1986 [16] 3 Unknown M " N/A PCP + " N/A12 Reay 1982 [32] 2 35 M " N/A Lithium " N/A13 Rodrigues 1972 [20] – 5 M " N/A N/A " N/A14 Greenwood 1962 [37] 2 70 F N/A N/A N/A + N/A15 Walcher 1950 [35] – Unknown M + Positive N/A " N/A16 Olbrycht 1963 [31] – <18 M N/A N/A N/A N/A N/A17 Olbrycht 1963 [31] – <18 M N/A N/A N/A N/A N/A18 Simpson 1949 [33] – Unknown F N/A N/A N/A N/A N/A19 Bogdan 1925 [23] – 24 F " N/A N/A N/A N/A20 Brouardel 1895 [25] – 12 Unknown N/A N/A N/A N/A N/A21 Gilbert 2008 [15] – 35 M + 0.15% Venlafaxine " N/A22 Kohli 1996 [10] – 40 F " Not
intoxicatedNot intoxicated " N/A
23 Yamamoto 1994 [22] – 93 M " None N/A " N/A24 Opeskin 1992 [11] – Unknown M " None None + N/A25 Sigrist 1989 [21] 2 63 F + None None + N/A26 Sigrist 1989 [21] 3 26 F + None N/A " N/A27 Sigrist 1989 [21] 7 57 M + 0.30% Midazolam + N/A28 Denk 1988 [36] 1 31 F " None None " N/A29 Denk 1988 [36] 2 79 F " None None " N/A30 Kowai 1987 [38] 8 39 M " N/A N/A + N/A31 Kowai 1987 [38] 10 41 M " N/A N/A + N/A32 Reay 1982 [32] 1 58 M " N/A Quinidine + N/A33 Kaiser 1967 [28] – Unknown M " N/A Novocaine/
MorphineN/A N/A
34 Kaiser 1967 [28] – Unknown M N/A N/A N/A N/A N/A35 Kaiser 1967 [28] – Unknown F " N/A N/A N/A N/A36 Kaiser 1967 [28] – 19 F N/A N/A Percain
solutionN/A N/A
37 Olbrycht 1963 [31] – 44 M N/A N/A N/A N/A N/A38 Bowden 1962 [24] – Young F N/A N/A N/A N/A N/A39 Giese 1930 [27] – 24 F " N/A N/A " N/A40 Dyrenfurth [26],
Lochte [29] 1930– Unknown F " N/A N/A " N/A
41 Bogdan 1925 [23] – 35 F " N/A N/A N/A N/A42 Losener 1908 [30] – Unknown M " N/A N/A " N/A43 Strassmann 1908 [34] – Unknown F " N/A N/A " N/A44 Strassmann 1908 [34] – Unknown M " N/A N/A " N/A45 Emmert 1900 [61] – Young M " N/A N/A " N/A46 Brouardel 1895 [25] – Young F N/A N/A N/A N/A N/A47 Brouardel 1895 [25] – Old F N/A N/A N/A N/A N/A48 Maschka 1881 [63] – 40 M " N/A N/A " N/A
Totala >50 yrs Male Lesion OH>0.01% Drugs Exciteddelirium
With With
10/37 28/47 11/37 7/17 9/15 2/48 10/34 0/0
a Denominators correspond to cases for which the information was made available.
B. Schrag et al. / Forensic Science International 207 (2011) 77–8380
of two brothers dying under the same circumstances couldsuggest pre-existing congenital electrical abnormalities. Toxico-logical findings were rarely reported. Only six cases of deathfollowing carotid stimulation were described in the absence ofeither alcohol or drugs; whereas 13 cases were positive to either ofthese substances.
4. Discussion
In light of current knowledge, our forensic consultant experts didnot identify a single case in which CiRCA provoked death withoutany other underlying pre-existing condition. From possible CiRCAcases described in the literature between 1881 and 2009, implica-tion of CiRCA alone was judged to be very unlikely for 32 out of 48.Major advances in the understanding of pathophysiology andinnovations in investigative techniques over time have made itpossible to evoke other mechanism of death. However, mosttextbooks suggest CiRCA by tradition without revising views oncases initially founded on this diagnosis. Our systematic review hasshown that CiRCA is a diagnosis by exclusion that requires athorough investigation including histopathological, metabolic,genetic [39], and toxicological analysis to rule out other mechanismof sudden unexplained death or identify carotid bifurcationstimulation as a contributory factor (Table 3) [40–43].
Nevertheless, many possible other causes of death have nomorphological, histological, or chemical signs. Circumstances ofdeath and the known duration and time sequence of events aretherefore essential to help experts distinguish CiRCA from othermechanism such as commotio cordis [44,45], contention gagging,vagal mediated cardiac arrest [46], phrenic paralysis [47], or othercauses of sudden death such as arrhythmias resulting fromchannelopathies or excited delirium alone (Table 3) [40–43].
The number of cases that would not be attributed to CiRCAtoday can be partially explained by the historical context (Fig. 2). It
Table 3Possible causes of sudden death + negative autopsies that included histological examinations (macro and microscopic).
Diagnosis Medicalhistory
Circumstancesof death
Full toxicologicalexamination
Specificmarkers
Geneticanalysis
Cardiac originA. Primary electrical abnormalities
1. Long QT syndromesRomano Ward XJervell Lange-Nielsen XAcquired X
2. Brugada syndrome X3. Wolf-Parkinson-White syndrome X4. Catecholaminergic polymorphic ventricular tachycardia X5. Primary or idiopathic ventricular tachycardia X6. Heart block (congenital or acquired) X
B. Acquired electrical abnormalities7. Commotio cordis X8. Drug abuse (e.g. cocaine, nitrites, emetine) X X X9. Ictal asystole during epileptic seizure X X10. Vagal-mediated cardiac arrest X11. Sinus carotid-mediated cardiac arrest X12. Electrocution X
C. Non-electrical cardiac arrest1. Sickle trait-associated collapse X2. Excited delirium X3. Electrolyte disorders (i.e., sodium, potassium) X X X4. Thyroidal drug intoxication X X
Cerebral death precedes cardiac arrestD. Cellular hypoxia
1. SuffocationBy lack of atmospheric O2 (i.e., CO2, CH4) X XGagging XContention (i.e., thorax compression) X
2. Tetany by intoxication (i.e., tetrodotoxin, curare) X3. Anaphylactic and anaphylactoid reactions X X X4. Phrenic paralysis (i.e., neurogenic shock) X5. Profound respiratory depression (i.e., overdose) X6. Carbon monoxide poisoning X X7. Massive irradiation X X
E. Neuroglucopenia8. Insulin overdose X X9. Glucagon overdose X X
[()TD$FIG]
20
Braindeath
Cardiomyopathygenetictesting
15
Carotidbaroreflex Cardioinhibitory
reflex implicated in
Improbable
mechanism of death
10 Possible
Highly probable
Num
ber
of c
ases
5
01870 1890 1910 19501930 1970 20101990
Year
Fig. 2. Number of publications mentioning CiRCA through time and majorphysiological discoveries.
B. Schrag et al. / Forensic Science International 207 (2011) 77–83 81

was only in 1924 that Hering [3] described the mechanical carotidbifurcation baroreflex in animal experimentation. At this time,brain cell death was believed to be related to hemorrhage and notto hypoxia [48]. In 1938, anesthetists noted that nitrous oxidecould cause death by cerebral hypoxia [49]. In 1950, brain deathwas defined and soon became the official definition of the death ofan individual [50]. When citing CiRCA, textbooks refer to old casesthat usually happened before knowledge of the possible mecha-nism of sudden cardiac deaths was available. CiRCA as a possiblemechanism of death may therefore often have been used byforensic experts without precautions as a default diagnosis [7].
Carotid stimulation incontestably can induce bradycardia andeventually syncope in a minority of individuals [51–55]. Followingprolonged repeated stimulations, experimental studies havereported cases of short, self-limited asystolic cardiac arrest of 2–9 s [56,57] and severe ventricular fibrillation without bradycardia[58]. Rossen et al. [59] did not, however, observe any cardiac arrestin more than 100 healthy strangled subjects, although when theneck compression was maintained for over 30 s, he did notebradycardia. Similar observations have been reported in the‘‘deadly broomstick’’ case in which an injury of the carotidbifurcation was observed [13]. Apparently, potentially fatal cardiacevents following carotid sinus stimulation could be more related toexisting underlying conditions than to the stimulation itself.Observations have shown that responses to sinus carotidstimulation have important interindividual variations and thatthere is no evidence suggesting that carotid stimulation alone canprovoke death. The mechanism of death following combined effectof excitation, drugs and carotid bifurcation stimulation remaindiscussable. Increased need in oxygen could diminish the lapse oftime before brain cell death occurs. Furthermore, cardiacarrhythmia induced by carotid stimulation could diminish bloodcirculation and favor cerebral hypoxia. On the other hand,substances such as cocaine are known to induce cardiac electricalabnormalities which could favor cardiac arrest. Sound scientificexperimental data are lacking to know which of these twomechanisms take place [60].
The only studies that support a link between CiRCA and deathare observational and remain insufficient to infer a causal link. Thisstudy has important limitations. Interpretations are highlydependent of reported information from publications which areless complete than true observations at the time of autopsies.Furthermore, publications most often do not report presence orabsence of contributory factors. Finally, the small number ofreported cases from the literature makes it difficult to generalizeour findings to all possible cases. The scarcity of deaths followingcarotid stimulations suggests that if such a causal link were toexist, particular pre-existing acquired or primary underlyingelectrical, biochemical, molecular, or morphological cardiacabnormalities are also required.
5. Conclusions
In forensic practice, authors usually report CiRCA as a probablemechanism of death when no other explanation can be found or isknown at the time of autopsy. With major advances in forensicmedicine throughout the last century, it has become difficult toexclude other possible mechanism of death for most reported casesof CiRCA. Our findings suggest that, reflex cardiac arrhythmia dueto carotid bifurcation stimulation cannot provoke death withoutthe presence of contributory factors. Actual state of knowledgesuggests CiRCA might be contributory to death in the presence ofdrug abuse and/or cardiac pathology, often associated withphysical and/or mental excitation. Circumstances of death, knownduration and time sequence of events, medical history, macro-scopic and microscopic autopsy findings, and metabolic, genetic,
and toxicological analyses are therefore essential to document andsupport CiRCA death.
Conflict of interest and ethical standards
This study was entirely financed by the University Center ofLegal Medicine, Lausanne, Geneva. Authors are all employees ofthis institution and are affiliated to the Geneva University Hospital,the University of Geneva or the University Hospital of Vaud. Theauthors declare that they have no conflict of interest. This studycomplies with the current Swiss laws and regulations for medicalresearch.
Acknowledgments
We thank Anne Monbaron for her thorough investigations infinding original old textbooks and articles all over Europe and TonyFracasso for his constructive critical appraisal of our firstmanuscript. We also thank San Francisco Edit for reviewing ourEnglish and improving this article.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in
the online version, at doi:10.1016/j.forsciint.2010.09.010.
References
[1] T. Lewis, Vasovagal syncope and the carotid sinus mechanism, BMJ 1 (1932) 873–876.
[2] J.N. Czermak, Untersuchungen uber die Wirkung starker Vagus-Reizung auf denHerzschlag, Pflug. Arch. Eur. J. Physiol. 1 (1) (1868) 644–650.
[3] H.E. Hering, Die Sinusreflexe vom Sinus caroticus werden durch einen Nerven(Sinnesnerv) vermittelt, der ein Ast des Nervus glossopharyngeus ist, Munch.Med. Wschr. 71 (1924) 1265–1266.
[4] H. Franke, Herzrhythmusstorungen beim hyperaktiven Carotissinus-Reflex, In-ternist (Berl.) 9 (July (7)) (1968) 289–296.
[5] P. Schweitzer, L.E. Teichholz, Carotid sinus massage. Its diagnostic and therapeuticvalue in arrhythmias, Am. J. Med. 78 (4) (1985) 645–654.
[6] D.S. Hess, T. Hanlon, M. Scheinman, R. Budge, J. Desai, Termination of ventriculartachycardia by carotid sinus massage, Circulation 65 (3) (1982) 627–633.
[7] B. Schrag, P. Mangin, P. Vaucher, M.D. Bollmann, Death caused by cardioinhibitoryreflex; what experts believe, Am. J. Forensic Med. Pathol., 31, in press.
[8] A. Sawaguchi, T. Funao, Experimental studies on the cause of death from thecompression of neck (Japanese), J. Tokyo Women’s Med. Coll. 45 (8) (1975) 675–686.
[9] J.V. DiMaio, D. DiMaio, Forensic Pathology, 2nd ed., CRC Press, Washington, DC,2001.
[10] A. Kohli, S.K. Verma, B.B.L. Agarwal, Accidental strangulation in a rickshaw,Forensic Sci. Int. 78 (1) (1996) 7–11.
[11] K. Opeskin, K.A.P. Lee, Death by greyhound, Forensic Sci. Int. 56 (1) (1992) 51–57.
[12] H.A. Abrines, Inhibitory mechanism in death by strangulation, Diabetic Med. 28(October (74)) (1956) 2265, passim.
[13] S. Bolliger, T. Plattner, U. Zollinger, The deadly broomstick: an unusual missileinjury to the neck, Am. J. Forensic Med. Pathol. 27 (4) (2006) 304–306.
[14] R. Dettmeyer, H. Grass, C. Diefenbach, B. Madea, Lethal carotid sinus syndrome.Unusual complication after puncture of the carotid artery during positioning of aSheldon catheter, Rechtsmedizin 14 (2) (2004) 117–121.
[15] J.D. Gilbert, L. Jensen, R.W. Byard, Further observations on the speed of death inhanging, J. Forensic Sci. 53 (5) (2008) 1204–1205.
[16] S.E. Lerner, R.S. Burns, Legal issues associated with PCP abuse—the role of theforensic expert, NIDA Res. Monogr. 64 (1986) 229–236.
[17] F. Patel, Vasovagal death from screwdriver stabbing of the neck, J. Clin. ForensicMed. 5 (4) (1998) 205–206.
[18] A. Perez, Sudden death caused by neck compression, Diabetic Med. 27 (September(66)) (1955) 2145–2146.
[19] M.S. Pollanen, D.A. Chiasson, J.T. Cairns, J.G. Young, Unexpected death related torestraint for excited delirium: a retrospective study of deaths in police custodyand in the community, Can. Med. Assoc. J. 158 (12) (1998) 1603–1607.
[20] A.C. Rodrigues, M. De Almeida, Sudden death by reflex vagal inhibition, Rev.Paulista Med. 81 (2) (1973) 85–88.
[21] T. Sigrist, K. Meier, U. Zollinger, Traumatic carotid sinus reflex death, Beitr.Gerichtlichen Med. 47 (1989) 257–266.
[22] K. Yamamoto, T. Hayase, H. Matsumoto, K. Ojima, Y. Yamamoto, A grooveobserved in the face of an old man who probably died from acute asphyxia,Jpn. J. Legal Med. 48 (2) (1994) 92–95.
B. Schrag et al. / Forensic Science International 207 (2011) 77–8382

[23] G. Bogdan, Trois cas de mort par inhibition, Ann. Med. Legale Criminol. Police Sci.5 (1925) 322–327.
[24] K.M. Bowden, The larynx, J. Forensic Med. 9 (1962) 10–16.[25] Brouardel p. La mort et la mort subite, Librairie J.-B. Bailliere et Fils ed., Paris, 1895.[26] Dyrenfurth, Steinbiss, Betrachtungen zum Fall ‘‘von Dielingen’’, Aertzliche Sach-
verstandigen-Zeitung 21 (1930) 321–323.[27] Giese, Bemerkungen zur der Mitteilung von Prof. Lochte: ‘‘Uber einen Fall von Tod
durch Erdgosseln und uber die Bedeutung des Sinus caroticus (Hering)’’ in dies.Zeitschrift 15. Bd., 5. Heft. Dtsch. Z. Ges. Gerichtl. Med. 15 (1930) 572–574.
[28] J. Kaiser, Anatomisch-physiologische Grundlagen und gerichtlich-medizinischeKasuistik des sogenannten Reflextodes bei mechanischen Reizen an Hals undweiblichem Genitale, Institut fur gerichtliche Medizin, Universitat Marburg,Marburg, 1967.
[29] H. Lochte, Uber einen Fall von Tod durch Erdrosseln und uber die Bedeutung desSinus caroticus (Hering), Dtsch. Z. Ges. Gerichtl. Med. 15 (1930) 419–432.
[30] Losener, Ueber den Tod durch Erwurgen von gerichtsarztlichen Standpunkt,Vjschr Gerichtl. Med. 36 (1908) 10–80.
[31] J.S. Olbrycht, Beitrage zur Lehre uber den Tod durch Erhangen, Dtsch. Z. Ges.Gerichtl. Med. 54 (1963) 407–423.
[32] D.T. Reay, J.W. Eisele, Death from law enforcement neck holds, Am. J. ForensicMed. Pathol. 3 (3) (1982) 253–258.
[33] K. Simpson, Deaths from vagal inhibition, Lancet 1 (April (6553)) (1949) 558–560.[34] F. Strassmann, Tod durch Erwurgen oder gewaltsames Anfassen des Halses?
Vjschr. Gerichtl. Med. 36 (1908) 282–294.[35] K. Walcher, Leitfaden der gerichtlichen Medizin fur Arzte und
Medizinstudierende, Urban & Schwarzenberg, Munchen/Berlin, 1950.[36] W. Denk, J. Missliwetz, Mechanism of action of forearm strangulation technics, Z.
Rechtsmed. 100 (2–3) (1988) 165–176.[37] R.J. Greenwood, D.A. Dupler, Death following carotid sinus pressure, JAMA 181
(August) (1962) 605–609.[38] E.K. Koiwai, Deaths allegedly caused by the use of ‘‘choke holds’’ (shime-waza), J.
Forensic Sci. 32 (2) (1987) 419–432.[39] Clinical indications for genetic testing in familial sudden cardiac death syn-
dromes: an HRUK position statement, Heart 94(April (4)) (2008) 502–507.[40] S. Berger, J.D. Kugler, J.A. Thomas, D.Z. Friedberg, Sudden cardiac death in children
and adolescents: introduction and overview, Pediatr. Clin. North Am. 51 (5)(2004) 1201–1209.
[41] M. Borjesson, A. Pelliccia, Incidence and aetiology of sudden cardiac death inyoung athletes: an international perspective, Br. J. Sports Med. 43 (9) (2009) 644–648.
[42] Z. Lim, K. Gibbs, J.E. Potts, S. Sanatani, A review of sudden unexpected death in theyoung in British Columbia, Can. J. Cardiol. 26 (January (1)) (2010) 22–26.
[43] S.S. Chugh, K. Reinier, C. Teodorescu, A. Evanado, E. Kehr, M. Al Samara, et al.,Epidemiology of sudden cardiac death: clinical and research implications, Prog.Cardiovasc. Dis. 51 (3) (2008) 213–228.
[44] B.J. Maron, N.A. Estes 3rd., Commotio cordis, N. Engl. J. Med. 362 (March (10))(2010) 917–927.
[45] B.J. Maron, T.E. Gohman, S.B. Kyle, N.A. Estes 3rd, M.S. Link, Clinical profile andspectrum of commotio cordis, JAMA 287 (March (9)) (2002) 1142–1146.
[46] B. Takase, R. Kato, K. Arakawa, F. Ohsuzu, M. Ishihara, Vagal nerve-mediatedvasospasm-induced lethal ventricular fibrillation, J. Electrocardiol. 39 (2) (2006)183–187.
[47] S.J. Davies, ‘‘C3, 4, 5 Keeps the Diaphragm Alive.’’ Is phrenic nerve palsy part of thepathophysiological mechanism in strangulation and hanging? Should diaphragmparalysis be excluded in survived cases?: a review of the literature, Am. J. ForensicMed. Pathol. 31(March (1)) (2010) 100–102.
[48] A.N. Clarkson, B.A. Sutherland, I. Appleton, The biology and pathology of hypoxia-ischemia: an update, Arch. Immunol. Ther. Exp. (Warsz.) 53 (3) (2005) 213–225.
[49] J.D. O’Brien, A.T. Steegmann, Severe degeneration of the brain following nitrousoxide-oxygen anesthesia, Ann. Surg. 107 (4) (1938) 486–491.
[50] P. Mollaret, M. Goulon, Le coma depasse (memoire prelimenaire), Rev. Neurol.(Paris) 101 (1959) 3–15.
[51] E. Gadermann, N. Heinz, J. Saegler, The syncope of the carotid sinus syndrome andits treatment, Internist 14 (10) (1973) 502–510.
[52] M.L. Smith, K.A. Ellenbogen, D.L. Eckberg, Sympathoinhibition and hypotension incarotid sinus hypersensitivity, Clin. Auton. Res. 2 (6) (1992) 389–392.
[53] A.L. Baskerville, D.L. Eckberg, M.A. Thompson, Arterial pressure and pulse intervalresponses to repetitive carotid baroreceptor stimuli in man, J. Physiol. 297 (1979)61–71.
[54] D.L. Eckberg, Adaptation of the human carotid baroreceptor-cardiac reflex, J.Physiol. 269 (3) (1977) 579–589.
[55] V.F. Nager, Die kardioinhibitorischen Carotissinusdruck-Effekte im Ekg. bei Herz-und Kreislaufgesunden, Helvetical Med. Acta 28 (1961) 42–62.
[56] E. Gadermann, N. Heinz, J. Saegler, Die Synkopen des Carotissinus-Syndroms undihre Behandlung, Internist (Berl.) 14 (10) (1973) 502–510.
[57] G.H. Heidorn, A.P. McNamara, Effect of carotid sinus stimulation on the electro-cardiograms of clinically normal individuals, Circulation 14 (6) (1956) 1104–1113.
[58] M.V. Cohen, Ventricular fibrillation precipitated by carotid sinus pressure: casereport and review of the literature, Am. Heart J. 84 (5) (1972) 681–686.
[59] R. Rossen, H. Kabat, J.P. Anderson, Acute arrest of cerebral circulation in man,Arch. Neurol. Psychiatry 50 (1943) 510–528.
[60] W.J. Kleemann, R. Urban, U. Graf, H.D. Troger, Kann ein Griff an den Hals zumreflektorischen Herztod fuhren? in: B. Brinkmann, K. Puschel (Eds.), Ersticken,Springer-Verlag, Berlin, 1990, pp. 14–20.
[61] C. Emmert, Lehrbuch der gerichtlichen Medizin, Georg Thieme, Leipzig, 1900.[62] A. Schmidtmann, Handbuch der gerichtlen Medizin. 9. Auflage des Casper-
Limanschen Handbuches, Berlin, August Hirschwald, 1905.[63] J. Maschka, Handbuch der Gerichtlichen Medicin, Tubingen, H. Laupp’schen
Buchhandlung, 1881.
B. Schrag et al. / Forensic Science International 207 (2011) 77–83 83




















