DATA REVOLUTION - International Pharmaceutical ...
27
THE OFFICIAL JOURNAL OF INTERNATIONAL PHARMACY JOURNAL VOL.33, NO.2 - JULY 2015 CROWD POWER being used in research DATA REVOLUTION Lab Boxes BRINGING LEARNING TO LIFE NEW SERVICES for MS and other complex patients
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of DATA REVOLUTION - International Pharmaceutical ...
T H E O F F I C I A L J O U R N A L O F
INTERNATIONAL PHARMACY JOURNAL
VOL.33, NO.2 - JULY 2015
CROWD POWERbeing used in research
DATA REVOLUTION
Lab Boxes
BRINGING LEARNING TO LIFE
NEW SERVICES for MS and other complex patients

2 3INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
INTERNATIONAL PHARMACY JOURNAL
The International Pharmacy Journal is the official journal of the International
Pharmaceutical Federation (FIP) and began in 1912 as the Bulletin de la Fédération
Internationale Pharmaceutique. Subscription is a benefit to all members— individual
or otherwise — of FIP, with readership spanning 95 countries. The IPJ is published
electronically, three times a year. ISSN 2213-7890
SCOPE
The IPJ keeps its readership in touch with pharmacy around the world. The aim is to
communicate developments and work in pharmaceutical science, practice and
education & workforce in order to contribute to the mission of FIP: to improve global
health by advancing pharmacy practice and science to enable better discovery,
development, access to and safe use of appropriate, cost-effective, quality medicines
worldwide.
The IPJ reports on pharmacy matters affecting the global community or specific regions
or countries, offering in-depth coverage, summaries and unique content. The IPJ strives
to inform and inspire. It updates readers on FIP’s position and work on important
pharmacy issues as well as on relevant activities of FIP member organisations.
EDITORIAL POLICY
All articles published reflect the views of the authors and are not necessarily those of
FIP or the journal editors. The use of specific names of companies or products does
not imply endorsement or recommendation by FIP or the journal editors. Although all
reasonable efforts have been made to verify information, the publisher accepts no
responsibility for omissions or inaccuracies. In no event shall FIP be liable for any
damages arising as a result of interpretation and use of published information.
COPYRIGHT & PERMISSIONS
Copyright ©2015 by the International Pharmaceutical Federation, The Hague, the
Netherlands. All reproduction rights, including photocopying reserved. FIP members
may download or print one hard copy of the IPJ for personal non-commercial use or
study only. Permission to copy articles must be obtained from the Editorial Office.
EDITORS
Lowell Anderson, Lin-Nam Wang
EDITORIAL ADVISORY PANEL
Luc Besançon (Netherlands), Shazia Qasim Jamshed (Malaysia), Charles Alan Lyles
(USA), José Manuel Martinez Sesmero (Spain), Oliver van der Spek (Netherlands)
EDITORIAL OFFICE
Andries Bickerweg 5, 2517 JP The Hague, The Netherlands
T +31 70 302 1987
F +31 70 302 1999
www.fip.org
ART DIRECTION/LAYOUT
NoSuchCompany, Rotterdam, The Netherlands
GUIDANCE FOR CONTRIBUTORS & ADVERTISEMENTS
Contact the Editorial Office.
News round-up 4Around the globe 10 Getting practical: the FIP project giving students much
needed lab experience 17Interview Marie Lindquist: Taking to song about
medicines safety 19Master your pharmacy information 24
Science
Crowd power being applied to research 26
Expert tips on communicating your research 30
Practice
New pharmacy services and better care for patients
with multiple sclerosis 32Pharmacy-generated record, public health resource 36How real-world data are improving access to medicines 38
Education & workforce
What might be the quickest path to equip hospital pharmacists
for the information age? 40What workforce data tell us 43
View from the USA Big data and the pharmacist —
caution advised 44View from the UK Community pharmacies deserve
a renaissance 46Panama Where pharmacy is on the rise 48Nine things About Middle East respiratory syndrome 51
In this issue
Did you know that when you opened this digital issue of the IPJ, your (anonymous) “click” was counted? We can track in which countries this issue was read, which articles and for how long. We use these data to make reader-driven improvements to the journal. All this is feasible because of technology.
Technological advancements have changed the ways in
which data are generated, gathered and analysed. They have
widened the range of data that is created. They have made it
so that data now exist in mammoth volumes and are
produced faster than ever before. They have made it possible
to trawl through existing data and conduct complex analysis
of new data, or of aggregates of old and new. This is the data
revolution: the world of crowd-sourced data, real-world and
real-time data, big data and data mining.
Around this time last year, the United Nations put together a
data revolution advisory group to inform the post-2015
Millennium Development Goals debate. The group’s work
culminated in a report, “A World that Counts”, which contains
examples of how the data revolution is already improving
general quality of life. One healthcare-related example is the
Mtrac programme in Uganda, which uses text message (SMS)
surveys completed by health workers to signal outbreaks of
malaria and let officials know how much medicine is
available. Since its start, the number of facilities out of stock
of artemisinin-based therapies has fallen dramatically from
80 to 15%. We commend this report to you as a
comprehensive overview. In particular, the advisory group
warns that major gaps are appearing between “data haves”
and “data have-nots”.
This issue of the IPJ, however, focuses on some of the
concepts of data revolution as they relate to pharmacy.
The UN group highlighted a need for standards, and a feature
(p12) reports on initiatives to ensure the integrity of health
The new medicines classed as
“ESSENTIAL”
7
Make PHARMACY count in the data revolution
data. Another article describes how scientific data are being
generated by crowd-sourcing in order to do things like
predict how cancer patients will respond to treatment (p26).
And we take a look at how data gathering is being used for
new pharmacy services (p32).
Of course, when pharmacists think of data, patient safety
will be high on the list. We took the opportunity to ask the
director of the Uppsala Monitoring Centre, which carries out
the WHO International Drug Monitoring Programme, about
the current extent of data mining in pharmacovigilance, the
difficulties and potentials. In the interview, you can also read
her view on Twitter as a way of monitoring adverse effects
and find out what she had to say about research on
thalidomide (p19).
At the very foundation of what we all do are data. These
numbers turn into information when given meaning and, at
the top of this pyramid (once the information is applied) is
knowledge. In other words, data and information are
fundamental to evidence-based practice.
To take full advantage of the data revolution, we need to be
aware of the changes taking place, to have an understanding
of the technology and to recognise and manage the potential
dangers.
Pharmacy counts. We hope this issue of the IPJ will prompt you to think about
how and why it counts.
news round-up
qualityaccountability
health
4 5INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
UNESCO RENEWS UNIQUE AGREEMENT TO DEVELOP PHARMACY EDUCATION WITH FIP
Development of pharmacy education around the world through a unique collaboration between
the International Pharmaceutical Federation (FIP), University College London School of Pharmacy
and the United Nations Educational, Scientific and Cultural Organization (UNESCO) is to continue
for a further four years.
The collaboration is a UNESCO-sponsored initiative known as the Global Pharmacy Education Development Network (GPhEd).
Launched in 2010, this was the first initiative for health professionals under UNESCO’s University Twinning and Networking
Programme (UNITWIN). This global network has brought together pharmacy schools and stakeholders from across the globe with
aims of synchronising powerful development in pharmacy and pharmaceutical sciences education, improving communication for
scientific innovation and healthcare outcomes and, ultimately, enabling attainment of Millennium Development Goals.
UNESCO has renewed the agreement with FIP “in light of the very good results achieved”. Major achievements of the network so
far have included the development a Global Pharmacy Workforce Observatory (which collates pharmacy workforce data with the
long-term aim of improving access to medicines and care; see p43) and the
creation of a Centre of Excellence across Africa (which currently works to
enhance professional education in pharmacy schools in Uganda, Ghana,
Nigeria, Zambia, Namibia and Malawi).
“Being reaccredited for a further four years shows that the network has
credibility and value for UNESCO and the wider development community, and
that our project goals continue to be relevant and successful,” said Jennifer
Marriot, director of the FIP UNESCO-UNITWIN collaboration.
“The renewal will support further work to enhance education, development
and workforce planning at global level, including a new venture with Monash
University, Australia, to develop a ‘global community of practice for pharmacy
educators’,” said GPhEd coordinator Ian Bates.
“Such projects make the future very exciting for our global network. Using the
UNITWIN banner we are able to provide better linkages with countries and
promote the whole initiative better at global level,” Professor Bates added.
FIP ANNUAL REPORT 2014 PUBLISHED“Together we are stronger” is the title of FIP’s annual report for 2014, published in May.
It reflects the fact that the number of FIP’s national member organisations grew to a
record number — 132 — last year. The report, which is now available online, shares
highlights from 2014 as well as giving an overview of the main issues FIP is currently
working on, such as green pharmacy and mental health.
“Outcomes of pharmacists working together, such as bringing about new laws,
clearly demonstrate strength in numbers. It could also be said that uniting over such
issues inspires pride in our profession,” says FIP President Carmen Peña in the report.
Stakeholders around the world have been brought
together for education
A roadmap for health measurement and accountability was
endorsed by global health leaders from governments,
academia, research institutions and civil society last month.
The endorsements were given at the “Measurement and
accountability for results in health” summit in Washington,
USA, organised by the World Health Organization, the World
Bank Group and the US Agency for International Development.
Explaining the importance of the summit, Ties Boerma,
director of the Department of Health Statistics and
Information Systems at the WHO, said: “Low-quality data are
being used to inform decisions on allocation of limited health
resources — undermining the quality of those decisions. There
is a lack of a coordinated global approach between countries
and development partners on what information countries
should collect to measure progress in health.”
Dr Boerma pointed out that health is a central component in
the new set of sustainable development goals (which will be
finalised later this year) and that every country needs robust
and reliable health information systems: “They need to be
able to generate their own data to monitor health
programmes and report on progress.”
Furthermore, he said that international partners and donors,
as well as domestic ministries of finance, are demanding
stronger evidence that investments in health are producing
results. However, “virtually all of the 80 low- and lower-middle-
income countries have major gaps in skills, tools and
resources to build quality health information systems.”
For several years, leaders from United Nations agencies and
global health partnerships have been “making increasingly
loud calls for more and better health data” and the summit
heralded a new approach to this, he said.
The health measurement and accountability roadmap
outlines investments and concrete actions and targets that
countries can adopt. Participants at the summit also agreed a
five-point call to action, including the more effective use of
data, openly sharing and standardising data, and promoting
accountability.
Work on establishing a global collaborative for measurement
and accountability is continuing, Dr Boerma added.
100 CORE HEALTH INDICATORS PUBLISHED
A global reference list of 100 core health
indicators was launched by the World
Health Organization last month.
Developed by a multi-agency working
group chaired by the WHO’s Director-
General over the past two years, the list
is intended to provide concise
information on health situations and
trends at national and global level. It is
hoped that this will serve as a global
standard, reducing the excessive and
duplicative reporting requirements that
currently burden countries, improving
harmonisation, and enhancing
efficiency and availability of data.
The list is divided into four main areas:
health status, risk factors, service
coverage and health systems. “It covers
the full spectrum of health priorities,
including maternal and child health,
infectious diseases and emerging
priorities such as non-communicable
diseases and universal health
coverage,” said Ties Boerma, director of
the WHO’s Department of Health
Statistics and Information Systems.
“All indicators were selected because
they are scientifically robust and have
a track record of being used for
measurement in countries. The list will
be a living document to be updated
periodically as new priorities emerge
and interventions change,” Dr Boerma
added.
The health measurement and accountability roadmap outlines concrete
actions and targets that countries can adopt
Indicators
selected for
scientific
robustness
HEALTH LEADERS COMMIT TO IMPROVING QUALITY AND SHARING DATA

news round-up
7VOL 33, NO.2 - JULY 2015
Five new direct-acting oral antivirals for hepatitis C, including
sofosbuvir and daclatasvir, are now listed, even though their
high prices mean they remain unaffordable for low-income
countries despite some efforts to reduce prices.
The WHO said that new breakthroughs made in cancer
treatment in recent years prompted it to revise the full cancer
segment of the Essential Medicines List: 52 products were
reviewed and 30 treatments confirmed, 16 being new
medicines. “Some of these medicines produce relevant
survival benefits for cancers with high incidence, such as
trastuzumab for breast cancer,” explained Kees De Joncheere,
WHO director of essential medicines. “Other treatment
regimens for rare cancers such as leukemia and lymphoma,
which can cure up to 90% of patients, were added to set a
global standard,” Dr De Joncheere said.
In addition, after about 45 years of scarce innovation for TB
medicines, five new products have now been included in the
list. Four of these, including bedaquiline and delamanid,
target multi-drug-resistant TB.
“When new effective medicines emerge to safely treat serious
and widespread diseases, it is vital to ensure that everyone
who needs them can obtain them,” said WHO director-
general, Margaret Chan. “Placing them on the WHO Essential
Medicines List is a first step in that direction.”
The WHO Expert Committee on the Selection and Use of
Essential Medicines has also recommended supporting
off-label uses in cases where there is clear evidence of major
health benefits but no licensed indication, such as for many
medicines for children.
Increasingly, governments and institutions around the world
are using the WHO list to guide the development of their own
essential medicines lists, because they know that every
medicine listed has been vetted for efficacy, safety and
quality, and that there has been a comparative cost-
effectiveness evaluation with other alternatives in the same
class of medicines, the WHO says.
In brief
ALERT ON FAKE MENINGITIS VACCINES ISSUED
As reports of 5,855 suspected cases of meningococcal
meningitis, including 406 deaths, come from Niger, the
WHO has issued an alert over fake meningitis vaccines.
It calls for increased vigilance with Mencevax ACW
(50 doses per vial), which may bear a genuine batch
number but false manufacturing and expiry dates.
Details.
RECORD HAUL OF ILLEGAL MEDICINES
Potentially dangerous medicines to the value of
US$81m were seized during the week of Operation
Pangea in June, according to Interpol. This year’s
Pangea VIII was the largest ever internet-focused
operation and saw 20.7 million illicit and counterfeit
medicines seized — more than twice the amount
confiscated during the 2013 operation. A total of 115
countries took part in Pangea VIII, resulting in 156
arrests worldwide, the suspension of 550 online
advertisements for illicit pharmaceuticals and 2,414
websites being taken offline. More.
NEW COUNTERFEIT MEDICINES HANDBOOK AVAILABLE
A handbook for healthcare professionals entitled “All
you need to know about spurious medicines” has been
developed by the World Health Professions Alliance,
under the lead of FIP, and in cooperation with the
Indian Pharmaceutical Association. It contains tips on
preventing and detecting counterfeit medicines as
well as advice on how to change behaviours.
GROUND-BREAKING MEDICINES CLASSED AS ESSENTIAL
New treatments for hepatitis C, a variety of cancers and multi-drug resistant tuberculosis appear in the latest Model List of Essential Medicines, published by the World Health Organization in May.
Sofosbuvir has
been placed on
the essential
medicines list
despite its
high price
© Serge001 |
Dreamstime.com
“PHARMACIST: YOUR PARTNER IN HEALTH”

news round-up
8 9INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
EXPLORE POOLED PROCUREMENT OF VACCINES, WHA SAYS
A resolution to improve access to sustainable supplies of
affordable vaccines — a key issue for low- and middle-income
countries — was an outcome of this year’s World Health
Assembly (WHA). The resolution urged member states to
increase transparency around vaccine pricing and explore
pooling the procurement of vaccines. It requested the WHO
Secretariat to report on barriers that may undermine robust
competition and barriers to enabling price reductions for new
vaccines. The resolution also recommended scaling up
advocacy efforts to improve understanding of the value of
vaccines and to allay fears leading to vaccine hesitancy.
Speaking at the WHA, FIP pointed out that the joint WHO-FIP
guidelines on good pharmacy practice emphasise that
pharmacists should be used to their full potential in
education to address vaccination hesitancy and resistance.
Full FIP statement on the Global Vaccines Action Plan.
DECADES OF PROGRESS IN TB WILL BE UNDONE UNLESS AMR IS ADDRESSED The billions of dollars invested in the Global Fund to Fight
AIDS, TB and Malaria by national governments will be under
threat unless urgent action is taken to address antimicrobial
resistance (AMR), Joanne Carter, vice-chair of the Stop TB
Partnership Coordinating Board said at the United Nations
in New York last month. Referring to a review on AMR
commissioned by the UK Prime Minister and published in May
(“Securing new drugs for future generations: the pipeline of
antibiotics”), Dr Carter said its findings “brought to light the
potentially massive scale and devastating impact of drug-
resistant TB and other AMR infections in both human and
economic terms. Decades of progress will be undone . . .
unless we address this challenge now.”
In April, a World Health Organization report revealed that only
a quarter of countries that responded to a survey on response
to AMR have national plans to preserve antimicrobial
medicines. The survey was part of a country situation analysis
(from 2013 to 2014) to determine the extent to which effective
practices and structures to address AMR have been put in place
and where gaps remain. The full report, “Worldwide country
situation analysis: Response to antimicrobial resistance”, is
available online.
GROWING FOCUS ON NEED TO IMPROVE HUMAN RESOURCES FOR HEALTH Calls to strengthen the health workforce
are growing, according to the Global
Health Workforce Alliance. At the World
Health Assembly (WHA) it was revealed
that a review of the WHA resolutions
made between 2000 and 2014 found that
many of the 374 resolutions on technical
themes generated by World Health
Organization member states contained
calls for the development of human
resources for health policy, data/
information and education/training of
individual health personnel for skills
enhancement.
Several of the agenda items tabled for
discussion at this year’s assembly,
including those on antimicrobial
resistance, Ebola, epilepsy, malaria,
nutrition, polio, public health, surgical
care and anaesthesia, and emergencies,
preparedness and surveillance, also had
health workforce implications. The WHO
Global Strategy on Human Resources for
Health is tabled for discussion by the next
WHA in May 2016.
FIP AT THE 2015 WORLD HEALTH ASSEMBLYINDICATION DETAILS WOULD HELP FIGHT AMR Putting indications on prescriptions would enable pharmacists to support
the responsible prescribing of antibiotics, said FIP during the World Health
Assembly discussion of antimicrobial resistance. The federation also
highlighted that diagnostic tools could easily be integrated into pharmacy
practice, citing as an example the UK National Chlamydia Screening
Programme, which helps to reach the at-risk population via point-of-care
testing in pharmacies. Similar models can be used for other infections,
such as syphilis, FIP said. Full statement.
PHARMACISTS SHOULD BE PARTNERS IN MENTAL HEALTH It is becoming more widely recognised that mental healthcare requires a
comprehensive approach with common services and resource
mobilisation, according to a statement submitted by FIP at the World
Health Assembly. The assembly was given two pharmacy examples of
moves in this direction, in the form of recent policies from Australia
(“A framework for pharmacists as partners in mental health care”) and
the USA (through the development of a pharmacy speciality of
psychopharmacology and behavioural health matters). Full statement.
INPUT ON PLAN TO COMBAT COUNTERFEITSRegulation of those who deal with raw materials in addition to active
pharmaceutical ingredient manufacturers is recommended, FIP said on
behalf of the World Health Professions Alliance during the World Health
Assembly. This is because we now have a highly fragmented supply chain
where overseeing reliable and complete traceability of the real sources of
raw materials is problematic. Full statement.
FIRST WHPA COLLABORATIVE PRACTICE AWARD WON BY ANTI-TOBACCO GROUPAn international award for bringing together several health
professions in a major collaborative project was won by the
Thai Health Professional Alliance Against Tobacco (THPAAT) in
May. The alliance, set up 10 years ago to increase the
awareness of tobacco hazards and to improve the health of
the people of Thailand, was presented with the award by the
World Health Professions Alliance at a ceremony in Geneva,
Switzerland. Accepting the award, THPAAT president Somsri
Pausawasdi said: “It was clear that the best way to
accomplish our goals was to create a collaborative
interprofessional team and so the medical association
collaborated with the Thai Health Foundation and recruited
four more organisations, including the pharmacy council, the
nurses’ association, the dental association and the public
health association, to join the team.”
FIP is a founding member of the WHPA.
NEW REPORT SHOWS 400 MILLION HAVE NO ACCESS TO ESSENTIAL HEALTH SERVICESFour hundred million people do not have access to
essential health services and 6% of people in low- and
middle-income countries are tipped into or pushed further
into extreme poverty because of health spending,
according to a report released by the World Health
Organization and the World Bank Group last month.
The report “Tracking universal health coverage” is the first
of its kind to measure health service coverage and financial
protection to assess countries’ progress towards universal
health coverage. It looked at global access to essential
health services, including family planning, antenatal care,
skilled birth attendance, child immunisation, antiretroviral
therapy, tuberculosis treatment, and access to clean water
and sanitation, in 2013.
“This report is a wake-up call: It shows that we’re a long
way from achieving universal health coverage. We must
expand access to health and protect the poorest from
health expenses that are causing them severe financial
hardship,” said Tim Evans, senior director of health,
nutrition and population at the World Bank.
The WHO and the World Bank recommend that countries
pursuing universal health coverage should aim to achieve a
minimum of 80% population coverage of essential health
services, and that everyone everywhere should be
protected from catastrophic and impoverishing health
payments. “Health policies and programmes should focus
on providing quality health services for the poorest people,
women and children, people living in rural areas and those
from minority groups,” said Marie-Paule Kieny, WHO
assistant director-general, health systems and innovation.
The report is the first in a series that the WHO and the
World Bank Group will produce on tracking progress
towards universal health coverage across countries.
The World Health Assembly took place in Geneva,
Switzerland, from 18 to 26 May 2015
Essential health services
include family planning,
child immunisation,
antiretroviral therapy and
tuberculosis treatment
© L
ore
nz
Tim
m |
Dre
am
stim
e.c
om

around the globe
11VOL 33, NO.2 - JULY 2015INTERNATIONAL PHARMACY JOURNAL10
Community pharmacists in England are to get access to Summary Care
Records (SCRs; national electronic patient records) under new plans.
Around 96% of people have an SCR, which contains up-to-date clinical
information sourced from general practitioners. Following pilots across
140 sites, it was found that in 92% of cases where the SCR was accessed
by a pharmacist, patients did not need to be sent elsewhere in the
National Health Service, and in 18% of cases the risk of medication
errors was avoided. The UK Government plans to invest £7.5m in the
training and tools that community pharmacists will need to use SCRs.
FRANCE
PHARMACISTS RAISE ALARM THAT “PURPLE DRANK” HAS BECOME POPULAR WITH TEENS
A dangerous cocktail containing pharmacy medicines and
known as “purple drank” is becoming increasingly popular
with French teenagers, pharmacists in France report.
The practice of mixing cough linctus (usually containing codeine
and promethazine) with soft drinks is believed to originate from US
hip hop culture and has featured in a number of rap songs.
AUSTRALIA
GOVERNMENT STICKS BY RECOMMENDATION ON BIOLOGICAL SWITCHING
Following continued debate, the Australian Government has made a statement in support of the recent recommendation by the
Pharmaceutical Benefits Advisory Committee (PBAC) that doctors and pharmacists be able to substitute originator biologicals
with biosimilars. The Alliance for Safe Biologic Medicines, which represents originator companies, said that Australia “would
break with widely held international standards by becoming the first and only nation to allow pharmacy-level substitution of
biologic[al] medicines without physician involvement”. The PBAC maintains that if it recommends a biosimilar is substitutable
patients can be given the choice of taking the original biologic or the substitute biosimilar, just as they have a choice with
generic versions of synthetic molecule drugs.
ITALY
MEDICINES THEFT IS THE NEW PHARMACEUTICAL CRIME WAVE
An investigation of thefts of high-cost medicines from Italian hospitals has led to the
discovery of a vast transnational crime network. Medicines theft is emerging as the
new frontier of pharmaceutical crime, say the authors of a Transcrime report.
They found that, in Italy between 2006 and 2013, one in 10 hospitals reported thefts
of pharmaceuticals, suffering an average loss of €330,000 each time. The police
investigation revealed a complex mechanism of false invoicing that allowed stolen
medicines to re-enter the European market, with Eastern Europe and Greece appearing
to be popular destinations.
GLOBAL
ANOTHER GOOD REASON TO PROMOTE MEASLES VACCINATION
Vaccination against measles protects against other infectious and
potentially fatal diseases such as pneumonia and meningitis, scientists
say. The measles virus kills white blood cells that have a memory of past
infections, resulting in “immune amnesia”. It was previously thought that
this amnesia (ie, loss of immunity) was short but statistical analysis now
shows that it lasts, on average, 27 months. More.
SOUTH AFRICA
HOSPITALS EXPERIENCING SHORTAGES OF BASIC MEDICINES
Hospitals in KwaZulu-Natal province are running out of a wide range of medicines, including paracetamol. A health department
spokesman said that shortages are affecting both private and public sectors but the impact is being felt more in the public
sector because of the volumes involved. Manufacturer difficulties obtaining active pharmaceutical ingredients, quality
problems, and procurement and distribution issues have been blamed.
GERMANY
HEALTHCARE PROFESSIONS JOIN FORCES AGAINST INCLUSION OF HEALTH SECTOR IN TTIP
Five major healthcare professional
organisations in Germany, including
pharmacists, have jointly called for the
health sector to be excluded from the
Transatlantic Trade and Investment
Partnership (TTIP), the free trade
agreement being developed by the EU and
the USA. The organisations see a risk that
a market-oriented healthcare sector will
jeopardise the social principle that
characterises EU systems. In their joint
declaration, they say that health services
should not be equated with other
market-oriented services. Free trade
agreements explained.
SPAIN
PHARMACISTS DOUBLE ADHERENCE AND REDUCE MEDICINES PROBLEMS
Pharmacists’ interventions increased
adherence to treatment from 35% to 75.7%,
and reduced drug-related problems by
33.4%, according to the first results of the
ADHIERETE Programme. Findings also
indicated that participating in the
programme increased patient-perceived
quality of life by an average of 5.5 points.
The study was conducted at 51 pharmacies
with 114 elderly, non-adherent patients with
chronic conditions and multiple medicines.
GHANA
PHARMACISTS TO SIT ON COUNCIL OF NEW HEALTH FACILITIES REGULATOR
The Pharmaceutical Society of Ghana is to sit on the 10-member
council of Ghana’s newly established Health Facility Regulatory
Agency (HEFRA). The agency has been set up by the country’s Ministry
of Health to regulate public and private healthcare facilities.
Regulatory activities will focus on consumer protection in terms of
availability of human resources for health service delivery, availability
of appropriate health products, including pharmaceuticals, as well as
minimum standards for health facilities and services.
FINLAND
PHARMACY ADVICE SAVES €1BN A YEAR
Pharmacy advice significantly reduces the load on primary healthcare (GP and
emergency visits) and saves nearly €1bn each year, according to a
PricewaterhouseCoopers report commissioned by the Association of Finnish
Pharmacies. Most of the savings are generated by self-care management services in
minor ailments and advice on the responsible use of non-prescription medicines.
Pharmacy advice is also estimated to reduce visits to GPs by up to six million each year.
ENGLAND
COMMUNITY PHARMACISTS GET ACCESS TO PATIENT MEDICAL RECORDS
USA
NEW LAW ALLOWS PHARMACISTS TO ADMINISTER FLU VACCINE TO CHILDREN
Children as young as nine years of age can now
be immunised against influenza by their
community pharmacist under a new law in the
US state of Pennsylvania. The law aims to
boost vaccination rates and reduce influenza
cases by increasing access and convenience.
The Pennsylvania Department of State
estimates there are 8,816 licensed pharmacists
with the authority to administer the vaccines
with parental consent.
SWEDEN
PARACETAMOL BANNED FROM SUPERMARKETS
Sale of paracetamol tablets from
Swedish supermarkets is to cease
from 1 November, the country’s
medical products agency has
announced. The restriction of
paracetamol tablet sales to
pharmacies follows research
showing a 40% increase in
paracetamol-related poisoning,
since paracetamol tablets went
on general sale.
12 13INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
WHAT IS BIG DATA?The McKinsey Global Institute defines big data as
“datasets whose size is beyond the ability of typical
database software tools to capture, store, manage and
analyse.” What differentiates big data from previous
data is its three Vs: volume, variety and velocity.
The NIH is at the forefront of moves among policymakers and
research organisations to create an ethical and operational
framework for the collection, organisation, storage, and
analysis of big data. It is embarking on research projects that
bring together some of the major challenges posed. Last month,
the NIH revealed details of a research scheme on HIV prevention
which would explore “the potential for big data approaches and
methodology to address key questions” relating to gaps in HIV
knowledge. The scheme will involve investigation of social and
behavioural characteristics of population groups and networks,
gender and ethnic disparities in disease acquisition,
evolutionary relationships among groups of molecular
organisms, and ethical, legal and policy issues.
The research would be looking out for “unexpected
correlations through analysis of diverse data”. With the help
of big data approaches, these data may “reveal events that
are rare, unseen in traditional datasets and are transient”,
the NIH said in its announcement of the project. The
organisation wants to use big data science “technologies,
computing, informatics and analytics to address gaps in our
understanding of HIV transmission risks, social networks and
the HIV treatment continuum, including co-morbidities such
as cancer”, it says.
Thorny issue of privacyAlong with other leading research organisations, the NIH
has also been trying to tackle the thorny issue of privacy
with regard to personal data in big data research projects.
This means ensuring compliance with ethical norms and
legal rules at national and international levels. It also
involves taking a stance on the issue of whether complete
anonymity can be assured even after all evidence of personal
identity has been stripped out of data sources, as laid down
by legislation like the US Health Insurance Portability and
Accountability Act (HIPAA).
It has become clear that the process of de-identification can
be reversed so that anonymised data can be re-identified as
a result of advances in analytics and computer software.
Using only a computer, an internet connection and publicly
accessible online resources, researchers at the Whitehead
Institute for Biomedical Research, based at the
Massachusetts Institute of Technology (MIT), were able to
identify individuals who had anonymously submitted
personal genetic material in genomics studies. >>
By 2020 the amount of data being held globally is forecast to
be 44 times larger than it was in 2009. Big data (see Box) has
been predicted to radically raise efficiencies and quality of
healthcare, transform outcomes and improve research and
development of new drugs — all at a much lower cost. It is
also predicted to greatly accelerate the use of personalised
medicines.
It may eventually achieve some or all of these things. But it
will probably take longer than previously expected. “There
has been a lot of hype about it,” Martin Kohn, chief medical
scientist at Sentrian, Aliso Viejo, California, a pioneer in
remote monitoring of patients with chronic disease, said at a
conference on big data in London, UK, last month. “It’s not
the solution to all healthcare’s problems. On the other hand
it will certainly help to find answers.”
Today’s new technologies have resulted in a massive increase
in data being stored — data that are easily accessible and
that can be quickly distributed around the world. There are
already opportunities for health information exchanges
between different data points in the delivery of care,
according to IMS Health, the pharmaceuticals and healthcare
information services company. Among the new data sources
in medicine are electronic medical records (EMRs), insights
from social media, a wealth of real-world information on
treatment practices, patient compliance and health
outcomes, and data on what works and does not work with
individuals, the company says.
“Enormous amounts of data are now stored in data warehouses, data lakes and the cloud in a mix that has varied levels of quality.”
With biomedical data, the range of sources becomes more
varied, but this can make data collection and analysis more
difficult. The National Institutes of Health (NIH), part of the
US Department of Health and Human Sciences and the US
Government’s medical research agency, describes
biomedical big data sources as including “diverse, complex,
disorganised, massive and multimodal data being generated
by researchers, hospitals, and mobile devices around the
world”. More specifically, those data include “imaging,
phenotypic, molecular, exposure, health, behavioural and
many other types of data”, the NIH says. These data could be
used to discover new drugs or to determine the genetic and
environmental causes of human disease. Yet many barriers
need to be overcome before these objectives can be
achieved. These include, according to the NIH, “the unwieldly
amount of information, lack of organisation and access to
data and insufficient training in data science methods
[all of which] make it difficult for big data’s full powers to
be harnessed”.
BIG DATA: How far are we from the revolution in healthcare?
Big data has been widely touted to have the powers not only to revolutionise healthcare but science itself. Sean Milmo reports on the reality and recent developments.

BIGDATA
14 15INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
Since then the NIH has joined with the Broad Institute of MIT
and Harvard University and 140 other medical, research and
campaign organisations around the world to set up the Global
Alliance for Genomics and Health to enable the international
sharing of genomic and clinical data. It has already drawn up a
regulatory framework and technical guidelines.
The framework, which the alliance wants to become a global
standard, is guided by the United Nations 1948 Universal
Declaration of Human Rights, in particular the rights to
privacy and to “share in scientific advancement and its
benefits”. It applies to “the use of data that have been
consented to by donors (or their legal representatives) and/
or approved for use by competent bodies or institutions in
compliance with national and international laws, general
ethical principles, and best practice standards”, according to
the framework.
What about quality assurance?Together with privacy matters, another important issue with
big data is its quality. According to the Global Alliance, data
of acceptable quality would be “accurate, verifiable,
unbiased, proportionate and current so as to enhance
interoperability and replicability.”
Enormous amounts of data are now stored in data
warehouses, data lakes and the cloud in a mix that has varied
levels of quality. “A large proportion of these data can be
flawed and it could take a long time to sort out what data are
flawed,” Dr Kohn said. For example, a lot of data from
laboratory studies will have been subject to the strict rules
of Good Laboratory Practice (GLP), a standard which was first
drawn up in the 1970s with its worldwide expansion since
becoming the responsibility of the Paris-based Organisation
for Economic Co-operation and Development. But there is
also much data from research laboratories, mainly in
universities and other academic institutions, which cannot
gain GLP status due to lack of equipment and manpower.
Academics have been in lengthy disputes with regulatory
authorities over the acceptability of the conclusions of their
non-GLP studies in areas like risks to human health and the
environment from certain industrial chemicals. This battle is
likely to intensify in the era of big data.
The different ways in which and the different purposes for
which data is collected may also pose problems. A working
group set up by the US National Heart, Lung and Blood
Institute to examine big data opportunities pointed out in a
report last year the challenges of dealing with data from
EMRs because they are designed for medical care rather than
clinical research. EMR data not only differ in quality from
data, for example, from carefully organised comparative
cohort studies, but they can be inconsistent because of the
contrasting ways in which EMR systems are organised and
physicians collect information. Mobile health devices, such
In a draft policy on sharing of genomic data issued last year
NIH stipulated that it expects researchers to obtain personal
consent for the use of data from de-identified clinical
specimens and cell lines. “Given growing concerns about
re-identification, it is no longer ethically tenable simply to
re-identify clinical specimens or derived cell lines to generate
data for research use without an individual’s consent,” the
NIH explained. Generally, individuals do not legally own the
data in their patient record or other data sources. But
acknowledgement that patients should give their consent to
the use of their genomic and other clinical data would seem
to override that.
“It has become clear that the process of de-identification can be reversed so that anonymised data can be re-identified as a result of advances in analytics and computer software.”
The NIH envisages that strict privacy rules will ultimately
benefit research rather than hinder it. “Obtaining consent for
broad future research uses will facilitate access to greater
volumes of data and ultimately will reduce the costs and
burdens associated with sharing research data,” it said.
In a White Paper issued two years ago, the NIH complained
that not only are the research and medical communities not
organised to seize the extraordinary opportunities of big
data but they are not on a path to do so. “If we remain on the
current path, the likely outcome will be a hodgepodge of
balkanised systems [inhibiting] learning and improving
healthcare.”
Mobile health devices are becoming another
large-scale source of data of variable quality
as watches that measure blood pressure, heart rates and
other health indicators, are becoming another large-scale
source of data of variable quality.
Initiatives are gradually being taken to standardise the
quality of data in major data sources, particularly in the way
they are collected and recorded. The European Medicines
Agency (EMA) has been issuing detailed guidelines to
pharmaceutical companies on the operation of an up-to-date
database on details of all authorised medicines on the
European market. The EMA wants to ensure that all the data
are entered in an accurate and standardised manner. The US
Government has introduced a scheme for giving incentives to
healthcare providers to make “meaningful use” of EMRs by
raising the quality of the data in the records so that they can
be shared and do more to improve outcomes for patients.
With regard to wearable medical devices, the Institute of
Electrical and Electronics Engineers (IEEE) has drawn up a
standard for blood pressure meters which do not depend on
the traditional blood pressure cuffs.
“With the availability of a standardised way to evaluate and
calibrate devices, the hope is that more manufacturers will
be encouraged to develop wearable, cuffless blood-pressure
monitors and more healthcare practitioners will be
encouraged to use them,” said Carole Carey, chair of IEEE’s
standards committee.
With more data sources becoming standardised, the quality
of the analysis of the information itself will become less of an
issue on the grounds that, generally, the results of analytics
are only as robust as the data. With big data the analytics are
centred on mathematical models and the algorithms into
which they are integrated to provide a set of step-by-step
operations for processing the data. In the financial world
faulty, hastily constructed algorithms are considered by
economists to be responsible for the 2008 crisis and the 2010
Flash Crash in which the US stock market plunged into the
steepest daily decline in its history. In healthcare and related
sectors, algorithms are worked out much more carefully with
some taking years to put together.
“With more data sources becoming standardised, the quality of the analysis of the information itself will become less of an issue.”
Once personalised medicine becomes a widespread
phenomenon the mass of algorithms for processing healthcare
data will have to be uniformly consistent and reliable. This will
raise the question of whether the main conventional method
of testing the quality, safety and efficacy of new drugs will
continue to be the randomised clinical trial based on a
comparison of evidence from a group of patients and a control
group. “With personalised medicines, a big weakness with
randomised clinical trials is that they cover groups of patients
not individuals,” said Dr Kohn.
It is likely that with the testing of drugs, randomised clinical
trials will continue to be applied to assess quality, safety and
efficacy — but with the help of big data. Mathematicians are
already claiming that they can draw up models that can
safely — at least theoretically — amalgamate data from
good laboratory practice and good clinical practice studies
with data from less closely controlled sources.
For that to become a reality, acceptable ways will have to be
established for verifying the qualities of a vast array of
different data sources, which would be a lengthy process.
16 17INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
GETTING PRACTICAL: the FIP project giving students
much needed lab experience
Chemistry is the backbone of pharmacy. It touches everything
from drug synthesis to identifying counterfeits. So most
people would agree that laboratory practice is an essential
component of pharmacy learning and few would imagine a
pharmacy school where the teaching is all theory and no
practice. But this was the case at the University of Malawi
Pharmacy Department until last year. A lack of simple
laboratory equipment meant that the students at the country’s
first ever pharmacy school were unable to gain necessary
hands-on laboratory experience. Under the auspices of the FIP
UNESCO-UNITWIN programme, however, a solution has been
provided: the Lab Box.
The Lab Box is simply a box containing enough basic
equipment to allow a student to conduct simple experiments
throughout the pharmacy curriculum. Jennifer Marriott,
director of the FIP UNESCO-UNITWIN programme explained
the concept: “Malawi needs pharmacists. In 2012 it had just 73
pharmacists and 174 pharmacy technicians for a population of
around 16 million. There has been progress in that the first
school of pharmacy opened in 2006 but a lack of resources has
hampered learning and the acquisition of skills. The need for
laboratory equipment was identified in 2014 during general
FIP UNESCO-UNITWIN discussions in Lusaka, and during a later
visit to Malawi, and we developed the Lab Box concept.”
Costs and other logistics had to be worked out: what exactly
should go into each box to improve educational outcomes in
an affordable way; who would be a suitable supplier; what
would be the best way to get them to their destination; and
where would the money come from?
The project brought together the University of Malawi
Pharmacy Department, FIP’s Academic Pharmacy Section and
the FIP UNESCO-UNITWIN collaboration. After much
deliberation, a list of contents — 24 different types of item
— was developed, a supplier was found and air freight was
selected. As for costs (each Lab Box cost US$99 plus US$44.66
for transport), these were met by the Academic Pharmacy
Section from project funds and a private donation.
In September 2014, 50 lab boxes were carefully packed into a
pallet and dispatched, arriving in Malawi just over three
weeks later. But this was not straightforward since, in many
developing countries, airfreighted foreign shipments are not
delivered to the recipient’s door, Lutz Heide, a visiting
professor at the university, told IPJ. Nor do airport or customs
offices automatically inform recipients of the arrival of
shipments. “One lesson was that the recipient needs to be
proactive and expedite customs clearance. This is important
since goods that remain too long in a port are at risk of
damage or pilferage,” he said.
News of a project that promises to make an impact on the future healthcare workforce in developing countries came out of Malawi last month. Lin-Nam Wang reports.
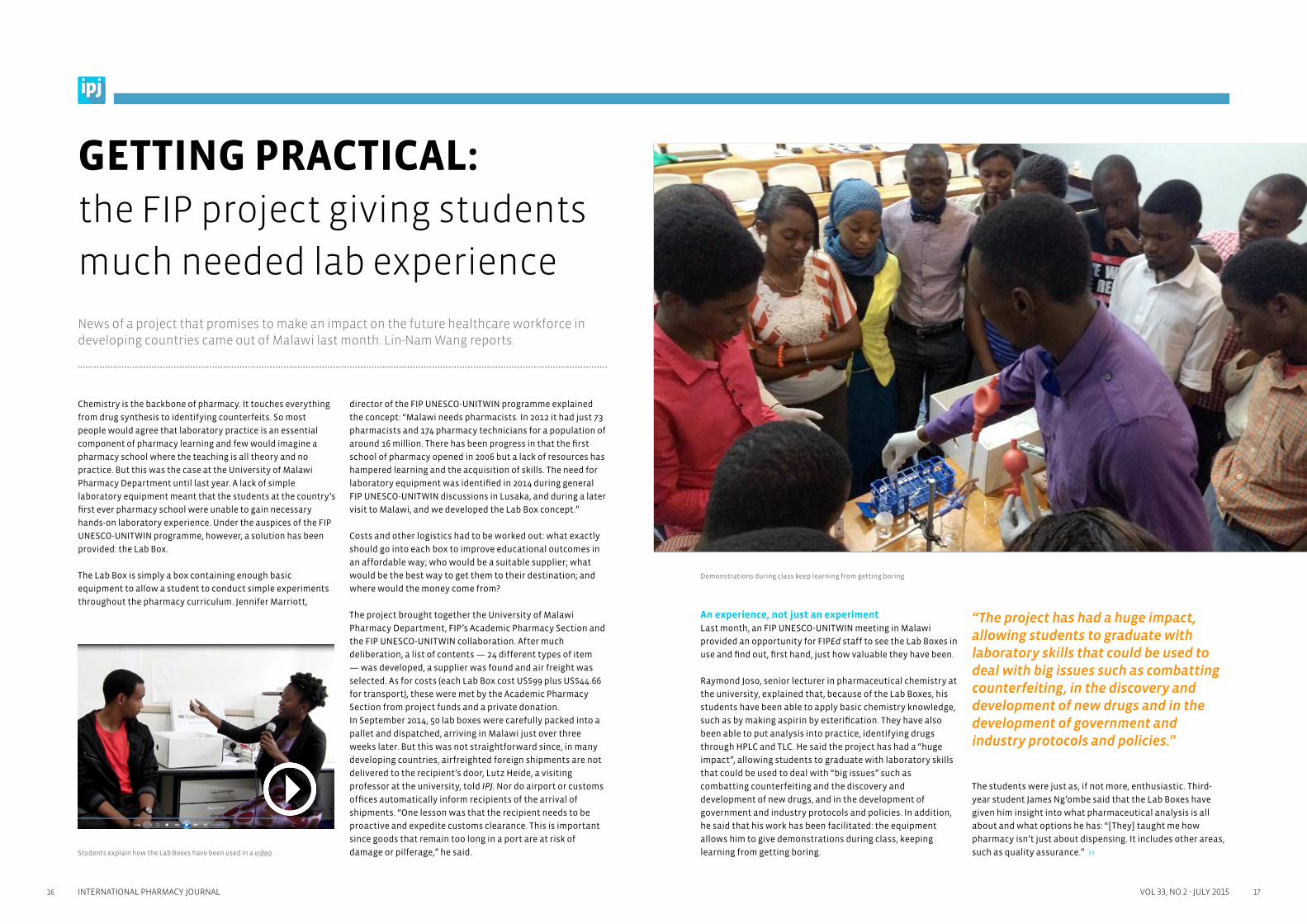
An experience, not just an experimentLast month, an FIP UNESCO-UNITWIN meeting in Malawi
provided an opportunity for FIPEd staff to see the Lab Boxes in
use and find out, first hand, just how valuable they have been.
Raymond Joso, senior lecturer in pharmaceutical chemistry at
the university, explained that, because of the Lab Boxes, his
students have been able to apply basic chemistry knowledge,
such as by making aspirin by esterification. They have also
been able to put analysis into practice, identifying drugs
through HPLC and TLC. He said the project has had a “huge
impact”, allowing students to graduate with laboratory skills
that could be used to deal with “big issues” such as
combatting counterfeiting and the discovery and
development of new drugs, and in the development of
government and industry protocols and policies. In addition,
he said that his work has been facilitated: the equipment
allows him to give demonstrations during class, keeping
learning from getting boring.
“The project has had a huge impact, allowing students to graduate with laboratory skills that could be used to deal with big issues such as combatting counterfeiting, in the discovery and development of new drugs and in the development of government and industry protocols and policies.”
The students were just as, if not more, enthusiastic. Third-
year student James Ng’ombe said that the Lab Boxes have
given him insight into what pharmaceutical analysis is all
about and what options he has: “[They] taught me how
pharmacy isn’t just about dispensing. It includes other areas,
such as quality assurance.” >>
Demonstrations during class keep learning from getting boring
Students explain how the Lab Boxes have been used in a video

interview
19VOL 33, NO.2 - JULY 201518 INTERNATIONAL PHARMACY JOURNAL
Next in line “Liberia and Sierra Leone have already contacted us with
requests for Lab Boxes,” Professor Marriott said. Not only
does Sierra Leone have a fragile healthcare system, figures
from the Pharmacy Board of Sierra Leone indicate that the
country had only 124 registered pharmacists for six million
people in 2014.
“Ultimately our work is all about helping to ensure sufficient
coverage of pharmacists around the world and there was no
better place to start than in Africa, where pharmacists are so
desperately needed. This is part of the general mission of FIP,”
she explained. The Lab Boxes are to enable laboratory classes
to support classroom teaching. Before they can be dispatched,
however, we need to ensure that they can be properly used.
This means knowing that a suitable laboratory is available,
laboratory manuals are in place, and that someone will be
responsible for their care and storage, she added.
“Feedback from students and staff of the University of
Malawi has been documented in a video that’s now available
online. I invite people to watch it so they can see for
themselves the big impact that these simple boxes have had,”
Professor Marriott said.
“[The Lab Boxes] are helpful because I’m a visual learner.
[They] helped me to understand the things I’ve been learning
in class,” he added.
Another student, Twambilire Mhango, said that the Lab Boxes
have made learning “more than an experiment”. Rather, they
have provided an experience.
Nettie Dzabala, head of the Pharmacy Department said: “[The
Lab Boxes have] motivated students. We see they are more
confident in chemistry. It is a dream come true for us. . . . I’m
very pleased about this development because we do need
pharmacists who are able and competent.”
A complete evaluation of the project is now planned. The Lab
Box contents will be reviewed but the students have already
made suggestions, such as for a mortar and pestle — “the
emblem of pharmacy” — and Petri dishes — “to protect any
drugs made from contamination” — to be included. Dr Joso
suggested that that the inclusion of retort stands and
burettes would allow students to conduct titrations. He also
said that the Lab Boxes could easily be tailored to enable
advanced chemistry practicals. A survey will be used to
measure relevance, improved learning outcomes and
satisfaction. And there are problems to be solved since the
supply of reagents is a continuing problem. But, perhaps most
importantly, replicability will be looked into.
The Uppsala Monitoring Centre (UMC) has provided scientific
leadership and operational support to the World Health
Organization’s International Drug Monitoring Programme
(WHO PIDM) since 1978. How would you describe the
programme?
The WHO PIDM brings almost 150 countries together in an
effort to improve patient safety. This global
pharmacovigilance network was started with the aim to
ensure that early signs of previously unknown medicine-
related safety problems would be identified and information
about them shared and acted on. Each country contributes
data from their post-marketing safety surveillance systems
to the WHO global database of suspected adverse drug
reactions, Vigibase, which is hosted by UMC. The aim of our
work is to enable patients and health professionals to make
wise decisions in their use of medicines.
What activities does the UMC carry out?
For almost 40 years we’ve supported existing national
pharmacovigilance centres and the establishment of
new national centres by our continued development
of core activities, such as data analysis. We also have a
responsibility to the pharmaceutical industry, academia
and professional organisations and networks, public
health programmes, and to a growing number of patient/
consumer organisations, all relying on the continued supply,
maintenance and development of our products and services.
We have pharmacists in every part of UMC, contributing
their specialist skills to research, data entry, database
management and production of output, data content
management, methodology and clinical research, technical
and scientific support, education, training and advocacy, and
sales and customer support. >>
“In all parts of the world, patient-reported harm or concerns about safety of medicines will increase exponentially as part of the big data and social media revolution.”
MARIE LINDQUIST: Taking to song about
medicines safety
Data are the bricks that build pharma-
covigilance but it’s knowing what to do with
the information that makes the difference.
IPJ talked challenges in pharmacovigilance,
roles for pharmacists and thalidomide with
Marie Lindquist, director of the Uppsala
Monitoring Centre in Sweden.

interview
20 21INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
Deciding if the risks of a medicine outweigh its benefits will
never be black and white. It’s about dealing with uncertainty,
trying to find the best balance between warning too early,
which could cause unnecessary panic and the withdrawal of
useful medicines; and too late, causing patient harm that
could have been avoided. Signal detection is not made more
difficult with the growing amount of data; in order to do our
job properly, we need more data, not less — the challenges
are to get good quality, relevant data, with as little delay as
possible, in a format that can be accessed and analysed
combining efficient IT technology, artificial and human
intelligence and experience.
Signal detection and analysis is a stepwise process. Once the
first suspicion of a possible drug-related problem has been
raised, we use different methods and data sources to build
knowledge gradually. It is important to keep in mind that a
signal is tentative and we, at the early stage, will not have
enough information to establish beyond doubt a causal
relationship between a medicine and a reported adverse effect.
A causal relationship of an adverse effect by a drug is always
a degree of probability. There are always other possible
causes that need to be considered in a single case or a study;
the competing probabilities need to be evaluated and made
transparent. Assessing the likelihood of causality is a
particular challenge if the suspected adverse reaction is a
common medical problem — a few case reports could be
nothing more than a chance finding.
There seems to be a trend in organisations applying data
mining to health. What’s the current extent of use of data
mining in pharmacovigilance, the difficulties and potentials?
I’m proud to say that we in the UMC pioneered the use of
data mining techniques to screen large healthcare data sets.
We started in the 90s developing our signal detection
process for the case reports in VigiBase to combine a first
screening using data mining and disproportionality analysis
with a subsequent manual clinical assessment of potential
signals, and then went on to apply the same technique to
find signals in electronic healthcare records. Nowadays most
major regulators and pharmaceutical companies use similar
techniques to ours to find new signals in their case report
databases. There are different formulas in use, but they are
all based on the same principle: looking at reporting
frequencies relative to a background of other reports to
identify associations that stand out. Using data mining to
recognise patterns is a way to help determine at-risk groups.
But automated screening is not going to do the trick on its
own — it can only generate potential signals — and has to be
combined with manual assessment and clinical judgement.
The main advantage is that by using computer technology to
do what it does well — sifting through huge amounts of data
— we can focus human effort to areas where it is best suited.
This issue of the IPJ focuses on data in health. How would you
sum up the use of data to create new knowledge and
evidence in pharmacovigilance?
The role of pharmacovigilance is to gather the best available
evidence on how medicines work in real life, in the most
cost-efficient and timely fashion. We need to systematically
collect data on possible adverse effects of medicines; and
then organise it and provide information in a way that is
valuable and relevant to improved patient safety.
After these first steps the information must be analysed,
interpreted and communicated; this is what builds the
knowledge base which will support good decision-making in
therapy. Data are the basis for all pharmacovigilance, but I
think the emphasis must move much more towards what we
make of the data, and how we ensure that it is transformed
to useful clinical information. A big challenge is that we have
to constantly re-examine our conclusions based on evolving
knowledge.
The WHO PIDM covers 95% of the world’s population.
What sorts of tools are used?
We obviously need to be effective both in our use of
technology and in the way we communicate to our audiences.
I think there has been too much emphasis on the former in
pharmacovigilance. IT tools are only the medium, not an end.
We have to focus more on how to reach the people we need
to reach, in a way that suits their needs, not ours.
“Today, open access to data is an important feature of the modern society where people expect to be included in decisions regarding their health.”
VigiBase holds information about 11 million individuals who
have been adversely affected by their use of medicines. It’s
our duty to make sure that this information is available so
that it can be used to prevent harm to future patients. For
many years we’ve developed search tools that we’ve made
available to all countries in the PIDM. But this is not enough.
Today, open access to data is an important feature of modern
society where people expect to be included in decisions
regarding their health. That’s why we’ve developed an
easy-to-use interface that can be accessed from a computer
or smartphone: VigiAccess.org allows anyone in the world
access to summarised information from VigiBase.
With the rapidly growing amount of data, is signal detection
getting more difficult?
Last year US researchers looked at Twitter as a way of
monitoring adverse effects. Could this or other social media
really be a viable pharmacovigilance approach?
I wouldn’t call social media a pharmacovigilance approach,
but it’s an untapped, and potentially useful source of data
and we should definitely embrace it. It will provide us with
better insight into problems with medicines, as perceived
by patients.
Until recently, much of our information of possible adverse
drug reactions (ADRs) has come from health professionals.
I’m excited about a new public-private partnership project
including UMC, WEB-RADR, investigating how we can make
the best use of mobile technology and patient-reported data
in social media.
The WHO PIDM was set up after the thalidomide disaster.
This old drug is now being used for new indications, such as
leprosy and multiple myeloma. What research and
monitoring is the UMC doing on this?
Thalidomide has shown to be useful for these new
indications, but we are concerned about reported harm to
fetuses, either during a clinically indicated use or by
accidental or off-label use. It could be that, in spite of strict
regulatory measures, the current controls are not
comprehensive enough to cover the vulnerabilities within
the entire supply and use chain. More research needs to be
done to fully understand the mechanism of thalidomide
embryopathy, and we need diagnostic criteria to establish
cases of fetal malformations with a reasonable level of
certainty. To address these issues a consensus meeting was
organised in 2014 by the UK Thalidomide Trust, and hosted by
WHO in Geneva. Several areas for research were outlined and
we are now developing methods for diagnosing
embryopathies, which could be extended to monitor the
effects of other medicines used during pregnancy.
Turning to new drugs, do biosimilars and biotech products
present any added challenges for pharmacovigilance?
Yes. Similar is not identical. Even slight differences between
molecules as a result of changed production processes may
be important both from the safety and effectiveness
perspective. Immunogenicity is a particular risk area for
biologicals, with the possibility of new reactions and
syndromes occurring.
Biologicals are often used for orphan diseases, and here we have
the problem of doing studies in small populations; we can’t
assemble enough controls to know if the treatment is effective,
and it will take a long time to establish the safety profile. >>
MARIE LINDQUIST QUICK FIREPharmacist Marie Lindquist became director of the
Uppsala Monitoring Centre in 2009. During her long
tenure at the centre Dr Lindquist has worked in data
management, research and IT development.
Significant milestones
Being part of the team that developed the first
routine signal detection process in
pharmacovigilance using data mining technology;
deciding I had the broad interests, skills and
determination needed to take on the challenge to
lead this unique organisation into the future.
Inspiration Being with thoughtful people who have
courage, integrity and a sense of humour, and who,
like me, want to do something important and useful
for this world.
Perfect weekend Lazy mornings with several cups of
tea, time to relax, think, go for walks or work in the
garden, and lively discussions and good food with
people that are close to me.
Visiting Uppsala? Don’t miss The Gustavianum
museum with its anatomical theatre and fika at Cafe
Guntherska by the River Fyris.
Swedish fika: coffee with something sweet and delicious

interview
22 23INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
Active risk planning and management is, therefore, critical when
these products are released for real-life clinical use.
We need to get much better at communicating and training
health professionals and patients to report more details for
these products. It’s not good enough to have ADR reporting
on the substance level — in the absence of an agreed precise
nomenclature allowing for a distinction between different
products, as a minimum requirement, the brand name must
be used.
Recent legislation requires the pharmaceutical industry to
develop risk management plans for new medicines. What’s
your opinion on this new application of post-marketing
pharmacovigilance?
Any serious pharmaceutical company and regulator will
always have done risk management as part of their safety
work; whether they called it “risk management” 20 years ago
is another question. I think it’s good that there’s now
legislative support for rigorous risk management practices
— but there’s a risk that the requirements related to the
production of the plans themselves become so detailed and
extensive that more effort is spent producing risk
management plans than doing the work. Risk management
planning per se is not changing our relations with industry.
“We now have a situation where medicines with limited safety profiles are made available to large populations in a short time, in places with little or no pharmacovigilance capacity.”
But the accelerated market entry of new medicines in low-
and middle-income countries will affect us directly, in that
we now have a situation where medicines with limited safety
profiles are made available to large populations in a short
time, in places with little or no pharmacovigilance capacity.
We will need real-life risk management in real time.
In its quest to increase reporting of side effects, the UMC
recently branched into the music world with its “Take & Tell”
song (see Box). But the lyrics only direct people to “Let your
doctor know”. What about pharmacists?
There’s a very simple reason for only including doctor in the
“Take & Tell” song: have you ever tried rhyming health
professional? Phar-ma-co-vigi-lance was bad enough, but we
felt it had to be included. On a more serious note, of course I
think that pharmacists have an important role in pharma-
covigilance — after all I’m a pharmacist myself! “Take & Tell”
is just a fun way of getting through the media noise of today
to be able to spread the serious and important message that
everyone can contribute to safer use of medicines.
“Pharmacists with their pharmacological and kinetic expertise have a unique contribution to make as part of the healthcare delivery team.”
Pharmacists with their pharmacological and kinetic expertise
have a unique contribution to make as part of the healthcare
delivery team. Also, pharmacists contribute to rational use of
medicines by keeping an eye on the risk of interactions and
suboptimal combination of drugs. As a pharmacist you’re
trained to be meticulous, and attention to detail is critical to
ensure that good quality data are collected and recorded
when an ADR, or any other problem in relation to medicines, is
suspected. When assessing new signals of possible ADRs,
pharmacists’ knowledge in pharmaceutics and pharmacology
is very important. So I’m not surprised that many national
pharmacovigilance centres are run by pharmacists.
What new types and applications of data do you predict in
the field of pharmacovigilance?
In all parts of the world, patient-reported harm or concerns
about safety of medicines will increase exponentially as part
CAMPAIGN
UMC’s Take & Tell campaign launched last month urges
people to be more active in pharmacovigilance.
A website explains side effects and what action to take,
an introduction to the WHO global database of suspected
adverse drug reactions, an application to allow people to
keep track of side effects and a campaign song.
of the data and social media revolution. The challenge for
pharmacovigilance here is to make use of diverse and
unstructured data in a way that helps other patients.
In low- and middle-income countries there will be much more
data coming from product-based surveillance projects done
as part of major roll-outs of donated medicines. In many of
these countries the resources and ability to do post-
marketing surveillance throughout the life cycle of all drugs
will likely continue to be limited. But things are changing,
and much needed efforts are now put into strengthening
overall regulatory systems and the harmonisation of
pharmacovigilance practices and processes across regions.
Perhaps most important is that there’s a new generation of
people now who are more than ready and able to apply agile
processes and the latest mobile technology which will
accelerate development.
The original aim of pharmacovigilance was to find new
suspected ADRs, mainly to new drugs. Only a broader look at
all the factors leading to adverse patient outcomes on
medication will reduce the burden of drug-induced morbidity
and mortality; including harm caused by sub-standard and
adulterated drugs, medication error and antibiotic
resistance. These are global problems, but posing particular
challenges in countries with limited regulatory and patient
safety systems.
“It does not make sense that hard pressed health professionals in poor countries should be asked to fill in many forms for the same patient, who happens to have several diseases, treated with medicines through different public health programmes.”
I’m pushing the principle that data collection should follow
the patient, not the drug. It does not make sense that
hard-pressed health professionals in poor countries should
be asked to fill in many forms for the same patient, who
happens to have several diseases, treated with medicines
through different public health programmes.
Safety assessment of new medicines in low- and middle-
income countries rely on the implementation of sustainable
pharmacovigilance processes and life-cycle management of
patient safety data; and robust and good quality data
collection and analytical tools. UMC will contribute actively
to these developments.
ABOUT THE UPPSALA MONITORING CENTRE
Uppsala Monitoring Centre (UMC) advances the
science of pharmacovigilance and inspires patient
safety initiatives all over the world. As an
independent, non-profit foundation, it engages
stakeholders who share its vision and collaborates to
build a global patient safety culture. As a leader in the
research and development of new scientific methods,
it explores the benefits and risks of medicines to help
minimise harm to patients, and offers products and
services used by health authorities and life-science
companies worldwide. For almost 40 years, it has
provided scientific leadership and operational
support to the WHO Programme for International
Drug Monitoring, expanding the global
pharmacovigilance network to reach more than 95%
of the world’s population.

25VOL 33, NO.2 - JULY 201524 INTERNATIONAL PHARMACY JOURNAL
Not-to-miss congress sessions
D5: INFORMATION MASTERY (Thursday 1 October; 09:00–12:00)
• Information mastery overview — Vimal Kishore (Xavier University of Louisiana, USA)
• Preparing a database to provide on-the-minute updated information about medicines/health products —
Sandra Lino (Associação Nacional das Farmácias, Portugal)
• Hands on demonstration of the use of high quality information mastery resources —
Timothy Chen (University of Sydney, Australia)
D6: EVIDENCE-BASED PRACTICE SKILLS (Thursday 1 October; 14:30–17:30)
• Barriers to EBP — Greg Duncan (Monash University, Australia)
• Techniques for empowering the pharmacist: skills to practise EBP — Safeera Hussainy (Monash University, Australia)
• Educational strategies to overcome barriers to EBP: model for an environment with limited resources —
P.T. Thomas (Taylor’s University, Malaysia)
B4: HOW TO USE SURVEYS TO GENERATE LOCALLY RELEVANT EVIDENCE THROUGH PRACTICE(Friday 2 October; 09:00–12:00)
• Survey research design: why survey designs matter — Parisa Aslani (University of Sydney, Australia)
• Survey studies: advantages and limitations — Carl Schneider (University of Sydney, Australia)
• Steps in survey research: developing and validating the survey instrument —
Anandi Law (Western University of Health Sciences, USA)
• Interactive workshop
Full congress programme.
Master your pharmacy information
The increasing use of medicines and expanding professional
roles mean pharmacists need to work smarter. Rapid changes,
such as mutations and resistance in infectious diseases and
emerging epidemics, make it imperative that they keep up
to date.
It is one thing to desire to use evidence-based practice (EBP),
but another to be able to use it routinely and effectively in
view of competing priorities in real practice environments,
says Vimal Kishore, professor of pharmacy at Xavier
University of Louisiana, USA.
So, how can EBP be ensured when pharmacists’ daily tasks
are growing? One solution is to become more efficient, and
one of the best ways to do this in time-constrained
environments is to exercise information mastery, he says.
Professor Kishore, an expert in research methods and
literature evaluation, explains that information mastery is
a tool: “an approach to quickly find pre-appraised and
summarised science-driven, relevant and high-quality
evidence”. And he believes that “its use applies to all
pharmacists, irrespective of their role”.
Professor Kishore will be giving an overview of this important
skill at this year’s FIP congress in Düsseldorf. In particular,
he will be explaining how information mastery (which is
time-efficient) differs from critical appraisal (which is time-
intensive). His presentation is part of two sessions (D5 and D6;
see Box) dedicated to using databases and ensuring EBP.
Session D5 will focus on information mastery and is not only
aimed at practitioners. One of the objectives of the session is
that participants learn how to incorporate this important
skill into curricula. “The teachings of EBP differ widely not
only across global regions but even within countries.
Information mastery as a formal required course is missing in
the majority of the pharmacy education system. It is
important to ensure that pharmacy students are exposed to
information mastery early on in their studies and throughout
their education,” Professor Kishore says.
Dealing with barriersSession D6 will help participants with further areas of EBP.
According to Professor Kishore, in order to adopt EBP
successfully, pharmacists have to be aware of the barriers and,
more importantly, how to overcome them. “Differences in
cultural, social, and religious attitudes towards modern
medicine serve as a major barrier to EBP around the world and
within regions of a given country. For example, herbal medicine
is revered in China, Ayurveda in India and homoeopathy in
other parts of the world, including Germany, although
acceptable evidence is not always available,” he says.
These sessions will also be relevant to pharmacists in
electronic-resource-poor practice environments. Professor
Kishore explains that information can be broken into three
categories: (1) electronic resources requiring paid
subscription; (2) credible electronic resources available
without subscription; and (3) non-electronic resources
generally produced as annual/semiannual reports available
free or at minimal cost. The plan is to make available a list of
such non-electronic resources based on various pharmacy
relevant classifications during sessions D5 and D6, he says.
With a wealth of rapidly evolving information at your fingertips, but little time to find — let alone analyse — what is most relevant to you, what can be done? Adian Magomedov reports.
Vimal Kishore
Contributing to the evidenceBesides being able to use information efficiently, pharmacists
themselves can generate valuable new evidence, Professor
Kishore says. For example, they can collect locally relevant
data by conducting survey studies through their own
pharmacies. But, he warns, “high quality surveys are not as
easy to design or conduct as people might think. A substantial
proportion of published pharmacy survey studies fail to meet
highest quality standards, primarily in robustness of design.”
To this end, he is chairing a session at the congress (B4) that
will concentrate on how to use surveys to generate locally
relevant evidence through practice, which will include an
interactive workshop.
The barriers to EBP and generating locally relevant
information are well known. The real question is what to do
about them. At these three congress sessions, you will be able
to find out.
“Information mastery as a formal required course is missing in the majority of the pharmacy education system.”
26 27INTERNATIONAL PHARMACY JOURNAL
science
VOL 33, NO.2 - JULY 2015
How crowd power is being applied to researchCrowd-based mentality has slowly been pervading our daily activities. Need a ride? Crowd-source it through Uber or numerous others. How about a place to stay? Find one through AirBnB. With the rise of on-demand access and technology, it may come as no surprise that science and research are also turning to crowd-sourcing. Timothy Dy Aungst finds about a landscape of citizen scientists, gamers and e-patients.
Crowd-sourcing data simply means collecting data from a
large group of people rather than from a more traditional
source. In health research, this could mean collecting data
from an online patient community rather than through a
clinical trial. The benefits of crowd-sourcing data include cost
reductions, overcoming logistical barriers and access to larger
datasets. The growing popularity of crowd-sourcing is due, in
part, to rapid advancements in technology, including
smartphones and their applications (apps), the internet and
social media.
Many organisations are looking for ways to integrate these
new technologies with medicine. For example, the charity
Cancer Research UK has recruited “citizen scientists” to help
with its projects, speeding up the identification of biomarkers
and the analysis of tumour samples. It has created a platform
— Cell Slider — to teach the public what to look for in images
of breast tumour samples, and to allow them to contribute to
image processing. Researchers can then look at what trends
are being spotted by these citizen scientists. One way in
which such information might be used is to predict how
patients will respond to treatment.
“With [our] first crowd-sourced citizen scientist project,
Cell Slider, it took just three months to score pathology
images which had taken researchers 18 months [previously],”
Hannah Keartland, Cancer Research UK’s citizen science
programme manager, told the IPJ. “Our absolute priority is
making sure that Cancer Research UK’s citizen science
products are genuinely useful to researchers. To do this, we
need to invest a lot of time in rigorous scientific validation.
We also recognise that this is crucial to convincing
researchers that they can trust our crowd-sourcing products,”
Ms Keartland added.
Gaming accelerating health researchCancer Research UK then expanded to other projects using
gaming to engage people and reward those who invest their
time. For instance, its “Genes in Space” game requires players
to pilot a spaceship collecting a fictional “element alpha”. But
they have to find the best space route and that means plotting
a course through real DNA microarray data and finding the
highly irregular bands medical researchers look for. By
crowd-sourcing players around the world through a game
available on smartphones, researchers have a large number of
people helping to peruse medical data faster than they could
alone. In another game, “Reverse the Odds”, players can help to
identify bladder cancer biomarkers though solving a puzzle.
Again, players spend time identifying patterns in real samples.
“Our two innovative mobile games have also attracted a lot of
attention globally which has helped raise awareness of Cancer
Research UK and of our citizen science activity. Over 50% of the
people playing our games are outside the UK,” Ms Keartland
said. Moreover, she said that “gamification” of research has
enabled the charity to tap into totally new audiences — people
who would not normally support it. However, she added: “This
is not without its challenges. We need to make sure that the
game-play element incentivises players to carry out accurate
analysis as that is what is most important to us.” She also
recognises that games have a limited shelf-life, and that
learning to increase the sustainability of these research games
is key to continual research benefits.
Making use of online patient communities Beyond citizen science, several companies are using data
collected from e-patients (patients who are equipped, enabled,
empowered and engaged in their health and healthcare
decisions, especially through use of technology) and online
patient groups, through mobile apps and social media to
evaluate diseases and determine what treatments work. For
example, CureTogether is crowd-sourcing quantitative data
and patient responses to different treatments. It recently
announced the first results from its ongoing “study” of
arthritis treatments, evaluating the top 10 overall treatments
according to patients. It is also running similar “studies” on
treatments for Crohn’s disease, anxiety, bipolar disorder and
acid reflux. Scientists and health professionals at universities
and medical research companies across the USA are now
tapping into this patient-driven research initiative as a means
of evaluating ongoing or possible new treatments.
“Patients are equally likely to report issues with their medicines online as they are to share a picture of their latest meal.”
Walgreens, one of the largest retail pharmacy chains in the
USA, is also getting in on the action. It has partnered with
PatientsLikeMe to provide an online portal through which
patients who get prescriptions from Walgreens can access
collated data and compare their treatments with those of
other patients; what degree of success patients have
experienced and how long the medicine took to work.
Crowd-sourcing patient experiences with medical treatments
is quickly turning into a new realm of data acquisition
previously unattainable outside of clinical trials. Data
collected from patients’ experiences and their health journeys
may be especially useful for rare diseases where finding large
patient groups can be difficult.
Social media for pharmacovigilanceThrough Walgreens’s portal, patients can also find out about
the side effects experienced by others, illustrating how
platforms that serve as online communities could also be
used for pharmacovigilance. Patients’ experience data are
also actively being mined by government agencies as a new
source of information about adverse drug reactions. The US
Food and Drug Administration (FDA) traditionally relied on its
Adverse Event Reporting System (FAERS) and its MedWatch
programme for healthcare providers to identify and report
medical device and drug adverse events. But although this
system is recognised and used nationally, it can be
cumbersome and does not capture all data in the populace.
Taking that into consideration, attention turned to social
media as a potential resource to mine: researchers have
identified that patients are equally likely to report issues with
their medicines online as they are to share a picture of their
latest meal. In their Drug Safety paper “Digital drug safety
surveillance: Monitoring pharmaceutical products in Twitter”
(2014;37: 343–350), Freifeld et al evaluated over seven months,
Twitter posts that were related to 23 medical products.
They identified and analysed 4,401 Tweets related to adverse
events. Patients’ experiences with treatments on social media
may be an untapped resource that can be looked at as a future
means of pharmacovigilance and may offer an improvement
over current resources.
PatientsLikeMe recently announced a partnership with the
FDA to evaluate potential adverse events through its platform.
This may offer an advantage over Twitter (where only 140
characters can be communicated) in determining significance.
It remains to be seen whether such sources of data will be
beneficial to federal agencies and pharmaceutical industries.
Mobile data gathering to make predictionsThe widespread uptake of smartphones by a sizable portion
of the populace and the increased ability of these devices
to collect data from the environment (eg, accelerometer,
global positioning system [GPS], camera, microphone) poses
a new means of crowd-sourcing data. Take, for instance, the
HealthyDay app, which informs patients in real-time about
their risks for allergies, cold and influenza based on local data
(via built-in GPS). Other users in the same location manually
Quantitative data and
patient responses to
different treatments can
be crowd-sourced
28 INTERNATIONAL PHARMACY JOURNAL
science
medical research. Through collecting all kinds of data,
smartphones could also potentially reduce clinic visits and
other logistical barriers that researchers face.
Ethical conundrums and what the future may bringAlthough there are many examples of how crowd-sourcing is
disrupting the sphere of medical research, patient
engagement and healthcare advancement overall, there are
several limitations. Foremost is the ethical concern
regarding patient safety and confidentiality. Researchers
seeking to engage society as a means of crowd-sourced data
must ensure patients’ information is properly collected,
stored and protected from misuse. Other issues facing
researchers concern the accuracy and robustness of
crowd-sourced data that could either supplement or replace
traditional research methods. The medical community may
see itself having to adjust to new research parameters and
coming up with new methods to meet the potential data
overload that research may soon encounter.
Researchers and medical practitioners are now able to reach
and engage with a larger audience, enabling crowd-sourced
data collection to be a turning point in medical research.
Although these changes may prove beneficial, there are still
many unanswered questions. These include which
technology works, whether tapping into social media is a
worthwhile endeavor, and whether online patient groups will
really be a boon to expanding data sources. Rapid changes in
technology could also pose their own barriers, leaving
researchers and the field of medicine always trying to catch
up with the next big thing, never affirming the benefits or
harm of currently widespread accepted technological
advances. Other issues include competition by start-up
companies, pharmaceutical companies and even technology
powerhouses that have previously stayed away from
healthcare, all looking to delve into the realm of crowd-
sourced medical research to make the next big discovery or
possibly devise a means of monetising this potentially
limitless data source. Crowd-sourcing is here to stay. We will
be talking about it more in the next few years and it will most
definitely be a game changer in the way patients are treated.
or automatically feed in data when using the app to report
symptoms or vital statistics (eg, temperature). Other data such
as pollen count are also pulled and added to the information.
HealthyDay users can then compare themselves with other
members in their community and see if there has been any
increase in illnesses in their area. Health professionals
can also use these sorts of app to identify possible health
concerns arising in their area. However, the data gathering
is not without problems. Google Flu, for example, which has
tracked the spread of the influenza across parts of the world
based on browser search patterns, has been criticised for
failing to predict pandemics such as swine flu.
Crowd-sourcing data to plot out health patterns is in its
infancy but the reality is that with the growth and
capabilities of information analytics and mobile devices
real-time data could soon play a significant role in disease
control and patient care. This, in part, is highlighted by the
expansive role that Apple has entrusted in its smartphones
and its recently released ResearchKit platform, which will
allow medical researchers to crowd-source data from
iPhones. Users can choose to join clinical studies sponsored
by large academic institutions on a range of conditions such
as Parkinson’s disease and cardiac disease. This demonstrates
a paradigm shift in medical research. Pharmaceutical
companies are also taking an interest in exploiting
smartphones to broaden their patient engagement and
ABOUT THE AUTHORTimothy Dy Aungst is assistant professor at MCPHS
University, USA. He has provided consultancy services
to Iodine, Inc. He was previously an editor for
iMedicalApps, where he reviewed mobile medical
applications.
FUNDING THE NEXT MEDICAL BREAKTHROUGH
Crowd-sourced funding of medical research is here. Using
websites like KickStarter and Indiegogo, small companies
and individuals have seen success in their raising of funds
for their different products or business ventures.
Researchers have similarly turned an eye towards
crowd-funding as an alternative to traditional grants and
funding initiatives that have become much scarcer and
more competitive. Several online crowd-funding ventures
have come into being aimed at the scientific researching
community. Examples include Experiment, Walacea and
Consano. Here, scientists and researchers can pitch their
proposed research projects and receive funding from the
public, who can then see the research outcomes and the
results of their investments revealed in real-time. While
crowd-funding may be a potential option for researchers to
get help with their projects, currently there are limited
data to support the widespread use of these services or to
evaluate the overall impact of crowd-funded goals in the
wide scheme of medical research.
Systems approaches for better medicines and health
Join leading pharmaceutical scientists from around the world to discuss cutting-
edge research and up-and- coming developments at the Pharmaceutical Sciences
World Congress 2017 in Stockholm, Sweden.
THE SYSTEMS THERAPEUTICS APPROACH
Systems biology has emerged as a novel
scientifi c discipline, which focuses on the
analysis of biological networks as the basis
for the functioning of biological systems.
Systems analysis will revolutionise medicines
and health research.
This will impact on both the pharmaceutical
sciences and pharmacy practice, says
congress chairman Professor Meindert
Danhof.
In research, systems biology offers a novel
approach to:
i) Identifying pathways of disease;
ii) Discovering drug targets; and
iii) Discovering biomarkers (for monitoring
of the treatment response).
In practice, this will lead to the intro duction
of “systems therapeutics” interventions
which are:
i) Personalised (both with respect to the
selection of drug(s) and dosing regimens);
ii) Disease modifying (with emphasis on pre-
emptive and preventive treatments); and
iii) Complex (such as multi-target drugs,
rational drug-drug combinations,
drug-device combinations).
Pharmaceutical Sciences World Congress 2017Stockholm, Sweden21-24 May 2017
WHO NEEDS TO KNOW ABOUT IT?
The introduction of systems therapeutics will impact on the entire
chain, from drug discovery and design through to development,
regulation and use. This calls for a multi disciplinary approach with
contributions from the entire spectrum of subdisciplines in the
pharmaceutical sciences and pharmacy practice. We must join forces.
www.fi p.org/pswc2017
#FIPCongress
0091_PSWC2017_advert_v4.indd 1 31-03-15 11:34
www.fip.org/pswc2017
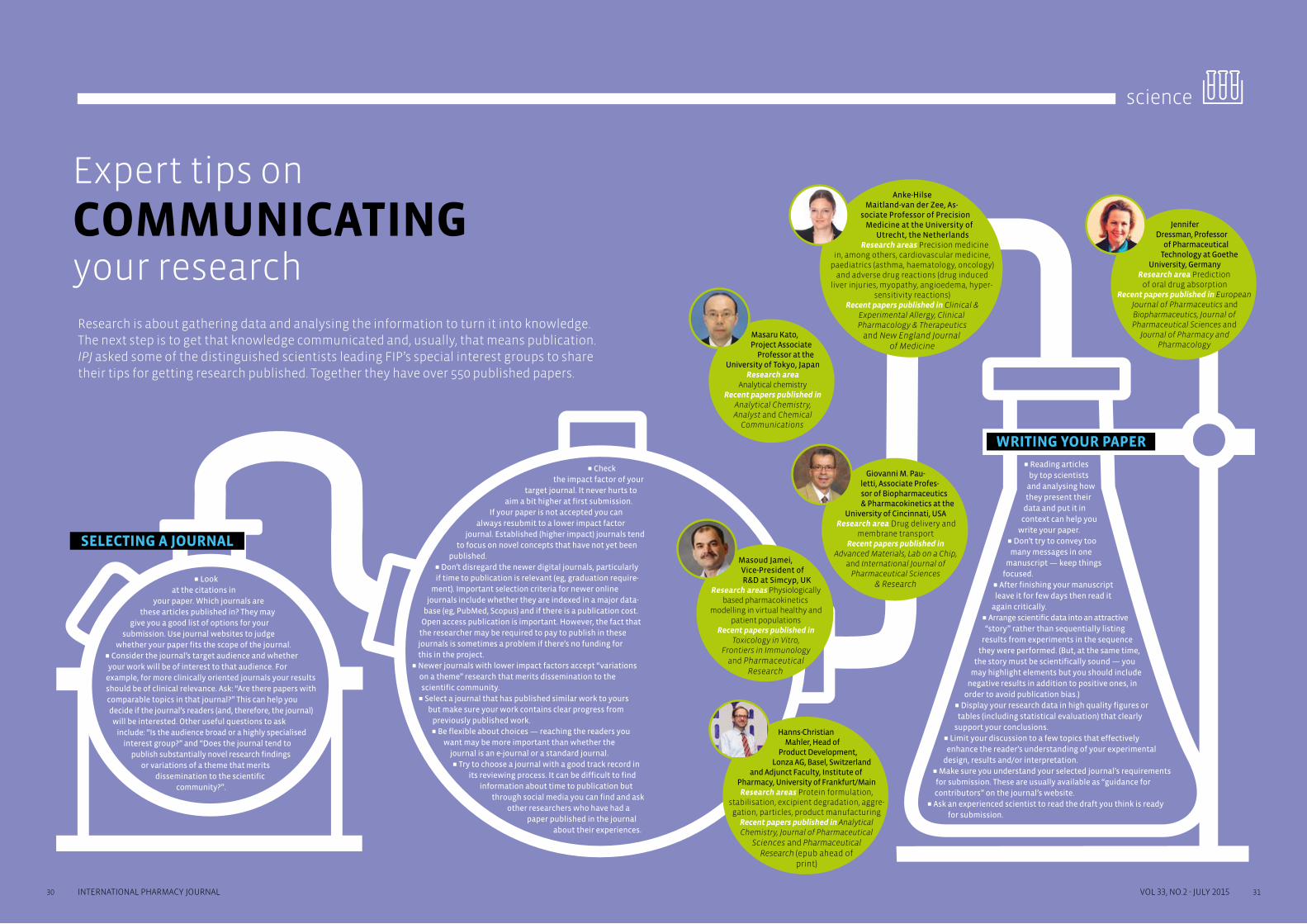
30 31INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
science
Expert tips on
COMMUNICATING your research
Research is about gathering data and analysing the information to turn it into knowledge. The next step is to get that knowledge communicated and, usually, that means publication. IPJ asked some of the distinguished scientists leading FIP’s special interest groups to share their tips for getting research published. Together they have over 550 published papers.
SELECTING A JOURNAL
WRITING YOUR PAPER
N Reading articles by top scientists
and analysing how they present their
data and put it in context can help you
write your paper.N Don’t try to convey too many messages in one
manuscript — keep things focused.
N After finishing your manuscript leave it for few days then read it
again critically.N Arrange scientific data into an attractive “story” rather than sequentially listing
results from experiments in the sequence they were performed. (But, at the same time,
the story must be scientifically sound — you may highlight elements but you should include
negative results in addition to positive ones, in order to avoid publication bias.)
N Display your research data in high quality figures or tables (including statistical evaluation) that clearly
support your conclusions.N Limit your discussion to a few topics that effectively enhance the reader’s understanding of your experimental
design, results and/or interpretation.N Make sure you understand your selected journal’s requirements for submission. These are usually available as “guidance for contributors” on the journal’s website.
N Ask an experienced scientist to read the draft you think is ready for submission.
N Look at the citations in
your paper. Which journals are these articles published in? They may
give you a good list of options for your submission. Use journal websites to judge
whether your paper fits the scope of the journal. N Consider the journal’s target audience and whether your work will be of interest to that audience. For
example, for more clinically oriented journals your results should be of clinical relevance. Ask: “Are there papers with comparable topics in that journal?” This can help you decide if the journal’s readers (and, therefore, the journal) will be interested. Other useful questions to ask
include: “Is the audience broad or a highly specialised interest group?” and “Does the journal tend to
publish substantially novel research findings or variations of a theme that merits
dissemination to the scientific community?”.
N Check the impact factor of your
target journal. It never hurts to aim a bit higher at first submission.
If your paper is not accepted you can always resubmit to a lower impact factor
journal. Established (higher impact) journals tend to focus on novel concepts that have not yet been
published.N Don’t disregard the newer digital journals, particularly if time to publication is relevant (eg, graduation require-
ment). Important selection criteria for newer online journals include whether they are indexed in a major data-
base (eg, PubMed, Scopus) and if there is a publication cost. Open access publication is important. However, the fact that
the researcher may be required to pay to publish in these journals is sometimes a problem if there’s no funding for this in the project.
N Newer journals with lower impact factors accept “variations on a theme” research that merits dissemination to the scientific community.
N Select a journal that has published similar work to yours but make sure your work contains clear progress from
previously published work.N Be flexible about choices — reaching the readers you
want may be more important than whether the journal is an e-journal or a standard journal. N Try to choose a journal with a good track record in
its reviewing process. It can be difficult to find information about time to publication but
through social media you can find and ask other researchers who have had a
paper published in the journal about their experiences.
Anke-Hilse Maitland-van der Zee, As-
sociate Professor of Precision Medicine at the University of
Utrecht, the NetherlandsResearch areas Precision medicine
in, among others, cardiovascular medicine, paediatrics (asthma, haematology, oncology)
and adverse drug reactions (drug induced liver injuries, myopathy, angioedema, hyper-
sensitivity reactions)Recent papers published in Clinical &
Experimental Allergy, Clinical Pharmacology & Therapeutics
and New England Journal of Medicine
Hanns-Christian Mahler, Head of
Product Development, Lonza AG, Basel, Switzerland
and Adjunct Faculty, Institute of Pharmacy, University of Frankfurt/MainResearch areas Protein formulation,
stabilisation, excipient degradation, aggre-gation, particles, product manufacturing
Recent papers published in Analytical Chemistry, Journal of Pharmaceutical
Sciences and Pharmaceutical Research (epub ahead of
print)
Jennifer Dressman, Professor
of Pharmaceutical Technology at Goethe
University, GermanyResearch area Prediction
of oral drug absorptionRecent papers published in European
Journal of Pharmaceutics and Biopharmaceutics, Journal of Pharmaceutical Sciences and
Journal of Pharmacy and Pharmacology
Giovanni M. Pau-letti, Associate Profes-sor of Biopharmaceutics & Pharmacokinetics at the
University of Cincinnati, USAResearch area Drug delivery and
membrane transportRecent papers published in
Advanced Materials, Lab on a Chip, and International Journal of
Pharmaceutical Sciences & Research
Masoud Jamei, Vice-President of R&D at Simcyp, UK
Research areas Physiologically based pharmacokinetics
modelling in virtual healthy and patient populations
Recent papers published in Toxicology in Vitro,
Frontiers in Immunology and Pharmaceutical
Research
Masaru Kato, Project Associate
Professor at the University of Tokyo, Japan
Research area Analytical chemistry
Recent papers published in Analytical Chemistry, Analyst and Chemical
Communications

32 33INTERNATIONAL PHARMACY JOURNAL VOL 33, NO.2 - JULY 2015
patient has reported as outcomes and barriers, pill box
opening and side effects. The web platform even has an
algorithm developed to detect macular oedema — if the
pharmacist selects certain combinations of side effects,
potential macular oedema is flagged. The platform also
allows free text entries. “But it’s not just about the data. It’s
about creating relationships,” Professor Bugnon stressed.
Furthermore, although one role of data is the feedback, a
second is to prove performance of the service: “Twenty years
ago we were paid only a margin on drugs, 10 years ago a fee
for service was paid. Now it’s about the effectiveness of the
service. If you want to prove this, you need the data.”
Outcomes and satisfaction“We have a high level of satisfaction. The neurologist is
happy with the work we are doing and to have contact with
the patient once or twice a year because she knows we are
following a process,” Professor Bugnon said.
He has presented preliminary data on the outcomes of this
project (see Box) but explained that his team were obliged to
allow a minimum follow-up time. In October they will have two
years’ worth of data from his first patient, and more analysis is
planned. Nevertheless, when it is estimated that 50% of
patients don’t take their medicines as prescribed,1 a pharmacy
service that produces 97–99% adherence is impressive. >>
practice
Complex treatments and complex patients are the markets of
the future. Prime examples where this applies are oncology
and HIV. Another such market is multiple sclerosis (MS), says
Olivier Bugnon, professor of clinical pharmacy practice at
Policlinique Médicale Universitaire, Lausanne, Switzerland.
In 2013, his community pharmacy, which is located in a
primary care centre, began a risk management service for
patients prescribed fingolimod, based on gathering data
from patient interviews and electronic pill boxes.
“In many instances the complex patient market does not
come to the community pharmacist. My idea was to prepare
pharmacists of the future for complex drugs. I believed we
could add more information on the use of drugs in routine
care. For example, effectiveness, side effects and barriers for
drug intake can be recorded,” Professor Bugnon said.
How it worksThe first dose of fingolimod must be taken in the neurologist’s
clinic, with close initial monitoring for at least six hours
(particularly to follow potential cardiovascular side effects),
and further monitoring after that. “The first two weeks is
really important because you have to be 100% adherent or
you have to start again,” Professor Bugnon explained.
Once the doctor and patient have taken the decision to begin
treatment, the pharmacist becomes involved, and explains
the pharmacy risk management programme to the patient
during the initial six-hour monitoring in hospital. The patient
is given a choice to receive care under the programme or to
follow the usual course of care (ie, no special service). Under
the programme, fingolimod is dispensed into an electronic
pill box that detects opening — an indication of adherence
— and at each refill, data are retrieved from the box, which
FIGURES AND FINDINGS
From October 2013 to October 2014, 72 patients
starting fingolimod were approached for inclusion in
the programme. Of these 61% (44) accepted, of which
32 patients were served by the Policlinique Médicale
Universitaire (PMU) pharmacy and 12 by other
accredited community pharmacies.
Of the PMU patients, 25% (8) left the programme (two
due to relocations, one due to a change in prescription,
one due to a loyalty conflict with his usual pharmacist
and four for other reasons).
Mean follow-up was 180 days per patient. Average
adherence according to pill count was 99%. Average
adherence according to electronic pill box data was 97%.
Motivational interviews revealed that facilitators and
barriers to adherence were related to treatment
factors (eg, medication schedule, association with a
ritual), psycho-cognitive factors (eg, anxiety, existence
of treatment goals) and socio-economic factors (eg,
education, social support).
New pharmacy services and better care for patients with
MULTIPLE SCLEROSIS
the patient brings back to the pharmacy. On refill,
motivational interviews are conducted by the pharmacist,
who has been trained to provide the service. “We help
patients to find their own [adherence] solutions by
suggesting different strategies,” Professor Bugnon said.
Data are entered into a web platform and the pharmacist
submits a report of what was discussed to the doctor. “So we
have a complete collaboration system. The future of the
healthcare system has to be integrated,” he added. There are
criteria in place for referral back to the physician.
The web platform was developed by Professor Bugnon’s
team. It integrates the elements of the risk management plan
and guides the pharmacist’s consultation with the patient.
So, for example, the platform ensures that at three months
the patient is asked specifically about any skin complaints.
“The web platform ensures that the service is standardised
and that the pharmacist follows a process. Just as you buy
quality-assured aspirin in different pharmacies, so should
pharmacy services [in different pharmacies] be
standardised,” he told IPJ.
“It’s about the effectiveness of the service. If you want to prove this, you need the data.”
The data Patients using the service authorise the pharmacist and
doctor to share their data and use it for research. Data
collected include the severity of the MS, patient
expectations, the questions the patient has asked, what the
Collecting and sharing adherence and side-effect data from patients with multiple sclerosis is key to a new risk management service in Swiss pharmacies. Lin-Nam Wang reports.

34 INTERNATIONAL PHARMACY JOURNAL
practice
Finding remuneration“The fingolimod project development was funded by an
unrestricted grant from Novartis, but there has been interest
from other drug companies, especially because neurologists
are asking them to pay for the service. This is testament that
doctors recognise the benefits of the service,” Professor
Bugnon said.
A Novartis spokesman told the IPJ: “[We] considered the
integrated care programme for MS patients who were
starting treatment with an oral disease-modifying therapy
for the first time to be a very valuable project. In addition to
supporting patients with their new treatment, this project
assessed patient reported outcomes and treatment
adherence over time. In the past few years, several scientific
publications highlighted that drug adherence, especially for
oral formulations, is a critical success factor for the [efficacy]
of a drug, as medicines are only fully effective if they are
taken on a regular basis.”
The Swiss already have a pharmacy service for adherence that
is paid for through the health insurance system but Professor
Bugnon thinks a new source of funding could be found for
similar services and that this source should be the
pharmaceutical industry.
“Industry should pay because they now have to prove to
medicines authorities that the drug is effective and efficient,
beyond the clinical trial evidence required for licensing.
Moreover, the usual pharmacovigilance is for severe side
effects but we have no idea about minor side effects. We have
no idea about effectiveness. Without this you don’t know
anything about the real effectiveness of the drug and the
safety. The service could also be used to provide data to prove
the value of a medicine,” he said.
The programme highlights patients’ needs and brings new
data about safety and use of fingolimod in real life. “In real
life, we need to keep in mind three Es: efficacy, efficiency and
effectiveness. I have the feeling that community pharmacy is
the right place to prove this as a partner of industry,”
Professor Bugnon added.
Future directions“In Switzerland, the competition for fingolimod provision was
a mail order company. Pharmacy should want to keep
complex patients. This sort of programme is a good strategy,”
Professor Bugnon told IPJ.
Fingolimod must be taken once daily but there are other
medicines for which patients could benefit from similar
services: dimethyl fumarate is one since it has twice daily
dosing in MS. Professor Bugnon’s team has also tested
programmes for oncology and immunoglobulin self-infusion.
“I believed we could add more information on the use of drugs in routine care. For example, effectiveness, side effects and barriers for drug intake can be recorded.”
In addition, new regulations mean that the pharmaceutical
industry is responsible for following medicines post-launch
but this is difficult for it to do in primary care beyond the
number of boxes provided. Pharmacy adherence services
could offer a solution, Professor Bugnon believes. “If you
speak about adherence you have to collect a lot of data and
such a service could easily be adapted to provide post-
marketing surveillance,” he said.
He is now looking to talk to the pharmaceutical industry
about further funding but is wary that it can be sensitive over
the issue of side effects. There needs to be internal
commitment to side-effect notification within the company,
he said.
“A year ago I had no MS patients. Today I have 39 in my pharmacy.”
Professor Bugnon is a strong activist in finding new models of
care and remuneration for community pharmacy, and it
seems he is well on his way to achieving his goals: “A year ago I
had no MS patients. Today I have 39 in my pharmacy.”
REFERENCE
1. Brown MT, Bussell JK. Medication adherence: WHO cares?
Mayo Clin Proc 2011;86(4):304–14.
Olivier Bugnon
75thFIP WORLD
CONGRESS
The 2015 FIP congress is organised
mrahpopxE htiw noitarob alloc ni
lacituecamrahp tsegral eht si hcihw
trade fair in Europe.
A.
SENICIDEM
Just what are the scope and limitations of
scientifi c evidence? From complementary
medicines and cancer immunotherapy to
novel biopharmaceutics tools and effects
of drugs on driving – discover what is
known and what it really means._
B. PRACTICE THROUGH SCIENCE AND
ECITCARP HGUORHT ECNEICS
How do advances in science affect the
advice you give? And how can information
from practice make the knowledge we have
more powerful? It’s not only up to scientists
to gather the evidence! Among the topics in
this congress stream are how food impacts
on drug effi cacy and the use of surveys to
generate locally relevant evidence._
C.
WITH THE HUMAN TOUCH
?yldneirf -tneitap eb tnempoleved gurd naC
Can care in a world of innovation and
dna emoC ?dertnec-tneitap eb ssergorp
fi nd out fi rst hand from colleagues who are
making innovations in science and practice._
D. GNIVEIHCA ROF PAG EHT GNISOLC
PROFESSIONAL EXCELLENCE
What needs to be done to ensure
advanced practice and professional
ecrofkrow cigetarts tuoba raeH ?ecnellecxe
ycamrahp ni noitasilaiceps ,tnempoleved
senicidem hcihw ni syaw tnereffid eht dna
eht dnuora deveihca gnieb si noitasimitpo
globe. Excellence is achievable!_
E. TARGETING YOUR INTEREST
Are environmental issues your passion?
Are you concerned about violence in the
workplace or how to cope in a disaster?
Or do you want to be a great leader? This
fi nal congress stream covers all these areas
and more!_
For more information please visit:
www.fi p.org/dusseldorf2015
Better practice – science based, nevird ecnedive
scimedaca dna srehcraeser ,srenoititcarp setivni ,ynamreG ,frodlessüD ni ssergnoc PIF 5102 ehT
ycamrahp elbissop tseb eht sdrawot gnikrow fo eussi eht otni evled ot dlrow eht revo lla morf
.nevird ecnedive eb ot sah dna secneics lacituecamrahp no desab eb dluohs hcihw ,ecitcarp
th FIP World Congress of Pharmacy secneicS lacituecamrahP dna
Düsseldorf, Germany29 September - 3 October 2015
DUS_advert_IPJ_A4_v2.indd 1 23-10-14 13:37
36) DUS_advert_IPJ_A4_def.pdf 1 16-07-15 14:27

36 37INTERNATIONAL PHARMACY JOURNAL
practice
VOL 33, NO.2 - JULY 2015
Pharmacy-generated record,
public health resource In 2007, a shared electronic patient medicines record was established by law in France, the French Chamber of Pharmacists being in charge of its implementation. Isabelle Adenot and Olivier Porte give an update of how the system has expanded, and Jean-Charles Rochard gives an insight into demographic data gathered by the French Chamber.
The French pharmaceutical record (Dossier Pharmaceutique;
DP) is a shared electronic patient record aimed at securing the
safety of drug dispensing, by reducing drug interactions and
stopping medicines that are no longer required. A further aim is
to improve the coordination, continuity and thus quality of care.
The DP lists all the medicines dispensed to the patient in any
French community pharmacy in the preceding four months
(period extended to 21 years for vaccines and three years for
biological medicines). Prescription and over-the-counter
medicines are included. Since launch, the use of the DP has
security and confidentiality requirements. Being able to
monitor the dispensing of a particular medicine over the
territory in real time is an asset for those carrying out
epidemiological studies. French health authorities (eg, the
Medicines Agency, the Health Ministry and the Institute for
DEMOGRAPICS DATA TO PREPARE FOR THE FUTUREIn France, all practising pharmacists must be registered with the French Chamber of Pharmacists (74,492 pharmacists in
January 2015, including pharmacists working in clinical biology laboratories, industry and wholesalers). The register
allows us to have an exact picture of the demographic situation of the profession/workforce and of the range of
pharmacy establishments. This is a valuable tool for decision-makers when they discuss pharmacy issues. For 20 years,
we have published our data (available at www.ordre.pharmacien.fr) annually. To answer specific requests, we are also
able to cross-reference our data with other data, regarding doctors for instance.
As in previous years, our data show that community pharmacies are evenly spread over the French territory, including
rural areas. There are 22,510 community pharmacies in France (one per 2,936 inhabitants), one third of which are located
in towns with fewer than 5,000 inhabitants. We also notice that community pharmacists are increasingly joining forces
with each other to form partnerships for owning community pharmacies. — Jean-Charles Rochard
been gradually extended to hospitals, and new services are
being developed to allow the dissemination of health alerts,
batch recalls and drug shortage notifications. We are also
currently developing a new service using the DP infrastructure
for medicines verification.
By law, the French Chamber of Pharmacists (Ordre Nationale
des Pharmaciens), was charged with the responsibility of
developing the DP system. For community pharmacies,
implementation started in 2007 and 99.2% of French
community pharmacies are now involved. Some 38.1 million
patient records have been created, making the DP the second
largest patient record system in Europe after the summary
care record system in England (50 million patients; [see pXX
for news]). In terms of activity, the DP in community
pharmacies is the most widely used health record in Europe
with more than one million pieces of information shared
among French pharmacists every day (a total of 330 million
pieces of information in 2014).
On top of that, 195 hospitals are now involved. Hospital
pharmacists have been able to access the DP since October
2012. More recently, since spring 2013, a trial has been
ongoing to extend DP access to hospital physicians working
in emergency, anaesthetic and geriatric departments.
The first assessments have shown a major benefit regarding
medicines reconciliation (when a patient enters a hospital,
the DP allows the identification of 90% of the medicines the
patient is currenlty taking). A consequence is a reduction in
the number of patients requiring readmission to hospital on
account of drug problems.
Today, four billion dispensed medicines are recorded in our
statistical database. Data protection laws require all data to
be anonymised. And because of that the DP system has strict
Public Health Surveillance) have commissioned more than 20
such studies dealing with one particular medicinal product,
a group of medicines or a whole therapeutic class.
The DP: A hub now providing a full range of services
PUBLIC HEALTH BODIES
DP SERVICES
HEALTHCARE PROFESSIONALS
• Pharma companies • Wholesalers • Pharmacists
Public health nationwide statistics
Pharmacist software access
LE DOSSIER PHARMACEUTIQUE
Web access Healthcare alerts
Batch recalls, supply
shortage notification
• Community pharmacists • Hospital pharmacists • Hospital physicians
Access restricted (to dedicated team of the French Chamber of
Pharmacists)
DP FAST PASS
FAST : Fast Access Service to TreatmentsPASS : Portal for Alarms & Sanitary Security
THE DP: A hub now providing a full range of services
Since 2013, a trial has been ongoing to extend DP to emergency, anaesthetic and
geriatric hospital departments

38 39INTERNATIONAL PHARMACY JOURNAL
practice
VOL 33, NO.2 - JULY 2015
How REAL-WORLD DATA are improving access to medicines
Although randomised clinical trials (RCTs) are considered the
gold standard method for establishing efficacy, in general,
these use a standardised therapy in a selected group of
patients and are typically restricted to evaluating specific
discrete interventions one at a time. As such, RCTs fail to assess
complex interactions within a study arm, fail to establish
continuous relationship and fail to elucidate if the benefits/
harms of a treatment are drug-specific or mechanistic.
Traditional RCTs focus more on evaluating the efficacy of
simple therapies and less on the delivery of care, and it is said
that RCTs have internal validity but not external validity. For
assessing effectiveness of combinations and for evaluating
all these issues in RCTs, many study arms would be required.
For example, it would take 32 different study arms to examine
all the possible combinations of just five treatments, making
the costs of conducting RCTs that evaluate all these issues
prohibitive. This is where real-world data (RWD) have a role
to play.
The International Society for Pharmacoeconomics and
Outcome Research has defined RWD as everything that goes
beyond what is normally collected in the phase III clinical
trials programme in terms of efficacy. It is also conveniently
labelled as anything that is not interventional. Many
healthcare decision-makers are developing policies that
integrate evidence from different sources. Importantly, it is
being accepted that other sources of data can contribute to
the evidence base (eg, demonstrating how a drug works in
populations not studied in the trial, or relative to another
drug not included in the study).
In real-world studies, the actual care that patients receive in
clinics is recorded. Rather than having strict inclusion and
exclusion criteria, all patients — including those with
co-morbidities — have to be treated. Such studies generate
long-term efficacy and safety data along with economic
assessment under pragmatic conditions.
Data sources for RWD can be supplements to traditional
registration RCTs; large, simple trials known as pragmatic
clinical trials; registries; administrative data; health surveys;
and electronic health record and medical chart reviews.
Although some governments are making efforts to permit
patients and researchers greater access to data, most of the
health-related data are aggregated and curated by private
companies. In most cases, charging for access to such data is
integral to their business plans. In many cases, the data have
been transformed in some fashion by the company collecting
the data, and therefore considered as intellectual property.
Access may also be restricted to government-sponsored
datasets.
Improving access to medicineThe past few years have seen RWD being used to improve
access to medicines. For example, in July 2011, the
Pharmaceutical Benefits Advisory Committee in Australia
(PBAC) evaluated Yervoy (ipilimumab) for the treatment of
patients with stage III or IV malignant melanoma. The
submission presented a single phase III, randomised double-
blind trial. In the first two submissions, the PBAC did not
recommend the drug, noting that, although it demonstrated
In a paper published in Breathe recently (2015;11:26-38) a group of academics presented the importance of real-world research in respiratory medicine, such as exploring the links between asthma and obesity. But real-world data are also improving access to medicines. José Manuel Martínez Sesmero explains.
improved efficacy, it had an inferior safety profile and there
was considerable uncertainty regarding the eligible patient
population and costs associated with the treatment. On the
third submission in November 2012, the manufacturer
presented four new pieces of evidence related to the
durability of Yervoy’s effect and three new pieces of
information related to recent, real-world, post-registration
data. These new data demonstrated that the drug increased
survival (compared with gp100 peptide) and that there was
evidence of a plateau in effect. There was also evidence that
the effect was durable. Citing this new evidence (and a
decrease in price), the PBAC recommended the product.
Another example, from Scotland, is where RWD helped
demonstrate improvement in quality of life (QoL) with Zaltrap
(aflibercept). In June 2013, the Scottish Medicines Consortium
(SMC) reviewed Zaltrap in combination with FOLFIRI
chemotherapy for the treatment of adults with metastatic
colorectal cancer. The SMC evaluated one randomised,
placebo-controlled phase III study and, despite
demonstrating significantly longer overall survival, Zaltrap
was not recommended because of the lack of a sufficiently
robust economic analysis. In a February 2014 resubmission,
the licence holder included two open-label studies assessing
safety and quality of life. This RWE was used to revise the
utility values within the economic model. The SMC
recommended Zaltrap because the new data demonstrated a
substantial improvement in QoL. In addition, the licence
holder also presented a patient access scheme, which
improved the cost-effectiveness evaluation of Zaltrap.
A further example comes from France, where RWD helped
confirm the effectiveness of a drug for a rare inherited
disorder, Pompe disease. In 2006, Haute Autorité Santé (HAS)
reviewed Myozyme (alglucosidase alfa) for the treatment of
late-onset Pompe disease. The HAS evaluated interim analysis
from a non-comparative trial and observational data from an
expanded access programme. The HAS did not recommend
Myozyme because the efficacy/safety ratio was not well
established. In 2010, the HAS recommended the drug based
on newly submitted data: a larger randomised control trial, an
observational study of 44 patients, and data from the French
Pompe Disease registry. Data from the observational studies
confirmed that the drug improved the six-minute walk test
and seated vital capacity.
Important role, despite the issuesThere are a number of issues with collection of RWD, for
example: lack of good quality and sufficiently representative
databases in many countries; incomplete databases; the
presence of many asymptomatic cases (an issue with
retrospective observation of data); and more chances of bias
and confounding in prospective real-world studies (as it is
without randomisation). Yet RWD has an important role to
play in the evaluation of epidemiology and burden of disease,
treatment patterns, compliance, persistence, and health
outcomes of different treatments.
Health research, including health outcomes and comparative
effectiveness research, is on the cusp of a golden era of access
to digitised RWD that promises to transform the way in which
we understand and practise medicine and pharmacy. Part of
this transformation will be driven by the quantity of RWD that
will be generated as well as the broader interest in big data
(see pp 12). The era of digitised RWD and big data holds great
promise for the transformation of healthcare. Yet this promise
can only be fully realised if access to data is broadened, if
connectivity between datasets is improved, if the methods for
analysing large datasets are advanced, communication of
evidence is encouraged and put in the right context, and if
there are clear standards for how privacy can be maintained
that also recognise that no solution is entirely secure.
© D
eca
de3
d |
Dre
am
stim
e.c
om
Colorectal cancer has been treated with medicine made accessible because of
real-world data

40 41INTERNATIONAL PHARMACY JOURNAL
education & workforce
VOL 33, NO.2 - JULY 2015
“Looking ahead to the next 50 years, it is not a stretch to imagine that the ability to manipulate and extract information from data will be as important as the ability to write.”
The information age is finally dawning for a hold-out sector in
the global economy: healthcare. This will likely produce
dramatic changes to the landscape of patient care, bringing
both opportunities and challenges to patients, providers and
payers. Looking ahead to the next 50 years, it is not a stretch
to imagine that the ability to manipulate and extract
information from data will be as important as the ability to
write. Leaders in the profession of pharmacy should realise
that this paradigm shift suggests that we should adopt new
skills and transform our practices accordingly. We need to
prioritise data manipulation and analysis skills in both the
pedagogical and practice settings.
Practice transformationAccomplishing this practice transformation will be more
difficult than agreeing with it in concept. The challenges are
many, starting with the fact that analytic skills are generally
lacking in pharmacy curricula both in the USA and
elsewhere.1–3 Accordingly, pharmacists around the world have
consistently voiced an appreciation of the value of analytic
endeavours, but at the same time feel ill-prepared to practise
them.4–7 These realities present significant obstacles toward
accomplishing the laudable goal recently upheld by the
editor-in-chief of the American Journal of Health-System
Pharmacy: to develop pharmacy residents as practice-based
researchers. Here, a classic “chicken or egg” paradox presents
itself. How are mentors and trainers to teach trainees these
analytic skills when the mentors and trainers feel inadequate
regarding these very skills?
One rather obvious answer to this dilemma is to increase
exposure to these topics within the pharmacy school
curricula.8 This could be accomplished through didactic
courses dedicated to health information technology, research
design, statistics and the like. It could be supplemented by
providing opportunities for students to gain practical
experience, either by conducting their own project work or by
assisting their school’s faculty. In any case, to prepare
pharmacists to succeed in the healthcare information age,
these efforts should include a sharp focus on manipulation
and analysis of large data sets. As our clinical information
systems evolve to provide access to richer, more complicated
data sets, the importance of mastering data manipulation
skills will increase. These skills have been somewhat
overlooked in favour of research design, analysis,
interpretation and communication.9 While these latter skills
What might be the quickest path to equip HOSPITAL PHARMACISTS for the information age?
Kenneth Shermock shares two US models that are helping pharmacists develop as practice-based researchers, able to manage data.
are undoubtedly essential, analysis and subsequent steps in
the research process presume that data have been properly
cleaned, manipulated and assembled into an analytic data set.
Viable strategiesEven in the best case scenario, where increased emphasis in
college of pharmacy curricula on research design, data
management and analysis happens quickly, there will still be
a substantial lag before these skills make it to the front lines
in the form of newly graduated pharmacists. Are there viable
strategies that pharmacy leaders can take to hasten the
arrival of these skills in their departments? There are two
successful examples that share a common element: they
involve hiring a formally trained pharmacist into a
department of pharmacy to lead the department’s efforts in
this regard. >>
1. TOPICS IN KAISER PERMANENTE
COLORADO’S PHARMACY INVESTIGATOR
TRAINING PROGRAMME
1 Introduction to the research process
2 Study objectives and design
3 Biostatistics, Health Insurance Portability and
Accountability Act and other regulatory issues
4 Data collection
5 Interpreting and presenting research findings
6 Manuscript preparation
2. TOPICS IN THE JOHNS HOPKINS
STATA TRAINING SESSIONS
Session 1 Introduction to Stata and basic data
management
Session 2 Intermediate data management
Session 3 Working with dates and string variables
Session 4 Analysis of categorical dependent variables
Session 5 Simple logistic regression
Session 6 Multivariable logistic regression
Session 7 Analysis of continuous dependent
variables, two groups
Session 8 Analysis of continuous dependent
variables, three or more groups
Session 9 Simple and multivariable linear regression
Session 10 Graphics

42 43INTERNATIONAL PHARMACY JOURNAL
education & workforce
VOL 33, NO.2 - JULY 2015
of pharmacists per 10,000 population over the period 2006–12
apart from South East Asia, which has seen a decline in
density, he explained.
The methodology used for the 2015 report is to identify
countries where data are available across at least two out of
three time points (2006, 2009 and 2012) and, for countries
where there is a gap in one data point, to undertake a
literature search to capture the missing data. The data will
then be plotted over the three time points so that trends can
be identified and discussed.
“This new report, however, will not only gather data but will also focus on identifying trends.”
As countries’ populations and economies change over the
years, will the pharmacy workforce density mirror the
changes? Will pharmacy be ready to meet the health demands
of the populations it serves? The data we collect will provide
the knowledge to answer such questions. However, “it is not
simply a matter of considering a head count of pharmacists
per country over time. Changing epidemiology and disease
burden at country level as well as population increases need
to be considered, and an assessment made as to whether the
development of pharmacy human resources has adapted and
made an impact over time,” Mr John said.
It is essential to monitor the global pharmacist workforce
trends at regular intervals so that decisions can be made as to
how countries can deploy their workforce. There is also an
increasing international transfer of healthcare professionals.
The WHO is rightly pushing for health equity as a global human
right and having access to a pharmacist is key to that because
medicines are one of the most important health interventions.
For almost a decade, the FIP Education Initiative has been gathering data about the pharmacy workforce from around the world. Its latest report is due to be published in October. Andreia Bruno explains the importance of these data and what they reveal
Many countries aspire to universal health coverage. To
achieve that, they need a health workforce — including
pharmacists — that can meet the health demand of the
population it serves. It is important, therefore, to monitor
trends in the workforce to see whether countries are
successfully approaching their health coverage goals.
In 2006, 2009 and 2012, FIP conducted pharmacy workforce
surveys, and analysed, monitored and reported on the status
of the pharmacy workforce at country level. The reach of the
surveys has grown each time, with 34 countries responding to
the 2006 survey, 56 in 2009 and 90 countries and territories in
2012, representing 2.5 million pharmacists and nearly one and
a half million technicians and support workers.
“The range of countries identified as having data for each of
the time points covered all the World Health Organization
regions, with Europe having the most countries with data
available and South East Asia the least,” said Christopher
John, the Global Workforce Observatory lead.
A key message from all three Global Pharmacy Workforce
Reports so far is that pharmacy workforce density varies
considerably between countries and WHO regions but
generally correlates with population numbers and country
level economic development indicators. “Those countries and
territories with lower economic indicators tended to have
relatively fewer pharmacists and pharmacy technicians,”
Mr John said.
Identifying important trendsThe fourth Global Pharmacy Workforce Report is in
preparation, with publication expected in October 2015. This
new report, however, will not only gather data but will also
focus on identifying trends, since there are now enough data
compiled over a long-enough period to begin to do this,
Mr John said. For example, after the 2012 report, we could see
that all WHO regions experienced an increase in the density
What WORKFORCE DATA tell us
At the first example, Kaiser Permanente Colorado, a clinical
pharmacy research team (CPRT) was assembled within the
department of pharmacy, led by a PhD-trained pharmacist
and including four staff members and two post-doctoral
fellows.10 The CPRT was established in 2004 to formally drive
the departmental research agenda, including resident trainee
research. Their approach involves review of potential resident
project ideas, using standardised criteria and oversight of the
project process. The CPRT also conducts a series of six classes
for their residents, offered at strategic times throughout the
residency year (see Box 1, p41). The percentage of resident
projects published in a peer-reviewed journal increased after
the CPRT was established from 47% to 86% (P=0.001). While
data management does not appear to be a primary focus,
their programme has achieved impressive results in terms of
publication rate.
“How are mentors and trainers to teach trainees these analytic skills when the mentors and trainers feel inadequate regarding these very skills?”
A second organisation, The Johns Hopkins Hospital, supports
the Center for Medication Quality and Outcomes (CMQO) within
their pharmacy department that is also led by a PhD-trained
pharmacist. The CMQO has three main missions: (1) to support
the department’s research enterprise, (2) to conduct quality
improvement and business intelligence assessments, and (3) to
manage the data infrastructure required to accomplish the first
two missions. Similar to Kaiser’s CPRT, the CMQO has a highly
structured process for reviewing and conducting residents’
projects. Additionally, the CMQO has developed a series of 10
classes to train clinical specialists and residents how to
manage and analyse data using Stata statistical software (see
Box 2). These 10 classes are offered multiple times during the
year. As clinical specialists become more proficient, they are
added to the roster of instructors in this curriculum. Using
these data management and analysis skills, the department has
published over 30 peer-reviewed publications in each of the
past four years. Moreover, these efforts have been used to
effect change within the organisation and have sent a strong
message that the department of pharmacy considers evidence-
based quality improvement as one of its core functions. To
support mission number 3, we are recruiting a data architect,
who will specialise in pulling data from disparate sources to
assemble data sets that will be used both for “one-off” research
purposes as well as for continuous quality improvement and
business intelligence.
Things in commonIt is notable that these two successful ventures have some
things in common and some differences. They share
dedicated personnel who are formally trained and are
responsible for promoting the research enterprise in their
departments. They also provide training programmes to
assist members of their departments to conduct practice-
based research. Interestingly, both the targets of and the
content in the training programmes differ. One is offered to
residents and focuses holistically on the research process,
but appears to de-emphasise data management. The other is
offered to both clinical pharmacy specialists and trainees,
but focuses on data management and analysis using
sophisticated software at the expense of other topics
relevant to conducting successful research. It is likely that a
hybrid model that trains clinical pharmacy specialists and
combines the two curricula might be the quickest path to
preparing our front-line pharmacists to take full advantage of
the increased access to data we are just beginning to see.
REFERENCES
1. Awaisu A, Alsalimy N. Pharmacists’ involvement in and
attitudes toward pharmacy practice research: a
systematic review of the literature. Res Social Adm Pharm
2015:1–24.
2. Fuji KT, Galt KA. Research skills training for the doctor of
pharmacy in US schools of pharmacy: a descriptive study.
Int J Clin Pharm 2009;17:115–21.
3. Phillips JA, Gabay MP, Ficzere C et al. Curriculum and
instructional methods for drug information, literature
evaluation, and biostatistics: survey of US pharmacy
schools. Ann Pharmacother 2012;46:793–801.
4. Awaisu A, Bakdach D, Elajez RH et al. Hospital
pharmacists’ self-evaluation of their competence and
confidence in conducting pharmacy practice research.
Saudi Pharm J 2014:1–9.
5. Elkassem W, Pallivalapila A, Hail MA et al. Advancing
pharmacy practice research agenda: views and
experiences of pharmacists in Qatar. Int J Clin Pharm
2013;35:692–6.
6. Kanjanarach T, Numchaitosapol S, Jaisa-ard R. Thai
pharmacists’ attitudes and experiences of research. Res
Social Adm Pharm 2012;8:58–9.
7. Perreault MM, Thiboutot Z, Burry LD et al. Canadian
survey of critical care pharmacists’ views and
involvement in clinical research. Ann Pharmacother
2012;46:1167–73.
8. Brazeau GA, Meyer SM, Belsey M et al. Preparing pharmacy
graduates for traditional and emerging career
opportunities. Am J Pharm Educ 2009;73:1–11.
9. Lee MW, Clay PG, Kennedy WK et al. The essential research
curriculum for doctor of pharmacy degree programs.
Pharmacotherapy 2010;30:966.
10. Olson KL, Irwin AN, Billups SJ et al. Impact of a clinical
pharmacy research team on pharmacy resident research.
Am J Health-Syst Pharm 2015;72:309–16.
opinion
44 INTERNATIONAL PHARMACY JOURNAL 45VOL 33, NO.2 - JULY 201544 INTERNATIONAL PHARMACY JOURNAL
Big data seems to be ubiquitous. Everywhere you look, there it is.
Big data is primarily a dynamic repository of clinical, social
and other personal information that can be used to have a
powerful and precise impact on targeted individuals, who
could be consumers of healthcare or other goods and services.
In 2011, US healthcare data alone reached 150 exabytes.
Those data include not only health records, and direct from
machine data, but also spoken words.1 Driven by current
policies, healthcare data are digitised and hold an
unprecedented potential to improve the quality of healthcare
delivery and reduce costs. Big data promises to support
healthcare functions such as clinical decision-making,
disease surveillance, and population health management.
There are reports of data-driven innovations that combine
Stories of the use of prescribing data to tailor advertising of medicines and the re-identification of anonymised data are coming out of the USA, which is among the front-runners in the big data revolution. Pharmacists know the ethical issues attached to handling patient data, but in the data revolution perhaps they need to think again.
By Fadia T. Shaya, Professor in Pharma-ceutical Health Services Research, and Priyanka Gaitonde, Research Associate, both at the University of Maryland School of Pharmacy, USA
BIG DATA and the pharmacist: caution advised
community settings. Pharmacists’ mastery in analytics of
medical data can foster partnerships with the physicians
where they would own the medication safety domain and help
physicians overcome barriers to medication safety, such as
time limitations and alert fatigue.7
In spite of its advantages, big data presents many opportunities
for inadvertent malpractice. Pharmacists need to rigorously
train and retrain periodically on patient confidentiality and
related legal requirements. They also need to remember that
data are only as good as the method used to collect them.
Considering that the field around big data is still evolving,
collection and reporting methods have not been yet
standardised. Therefore, despite what may be indicated
electronically, the pharmacist-patient-physician interaction in
a most HIPAA-compliant environment remains rudimentary,
and cannot be substituted by, but only be aided by big data.
REFERENCES
1. Institute of Health Technology Transformation.
Transforming health care through big data - Strategies for
leveraging big data in the health care industry. Updated
2013. Accessed July, 2015.
http://c4fd63cb482ce6861463-bc6183f1c18e748a49b87a259
11a0555.r93.cf2.rackcdn.com/iHT2_BigData_2013.pdf
2. Krisberg K. Big data key to improve healthcare. Updated
2014. Accessed July, 2015.
https://www.aamc.org/newsroom/reporter/
january2014/366338/big-data.html
3. Nikfarjam A, Sarker A, O’Connor K, et al. Pharmacovigilance
from social media: Mining adverse drug reaction mentions
using sequence labeling with word embedding cluster
features. Journal of the American Medical Information
Association. 2015;22(3):671–81. doi: 10.1093/jamia/ocu041
[doi].
4. Raghupathi W, Raghupathi V. Big data analytics in
healthcare: Promise and potential. Health Information
Science and Systems. 2014;2:3. eCollection 2014. doi:
10.1186/2047-2501-2-3 [doi].
5. National Institutes of Health (NIH). Data management
infrastructure for a national precision medicine cohort.
Updated 2015. Accessed July 2015.
http://www.nih.gov/precisionmedicine/workshop-
20150528-backgrounder.pdf
6. Robertson J, Pettypiece S. They know you buy Viagra and
they want to sell you more. Bloomberg. Updated 2014.
Accessed July, 2015.
http://www.bloomberg.com/news/articles/2014-12-10/
they-know-you-buy-viagra-and-they-want-to-sell-you-more
7. Wild D. Combing through big data yields big benefits.
Pharmacy Practice News. 2013. Accessed July, 2015.
electronic health records (EHRs) and geospatial software to
map geographical spikes in diseases such as influenza, or use
algorithms to help identify patients at risk for undiagnosed
conditions, provide data to physicians in real time and
provide precision in target care.2, 3
“Patients may be under a false sense of security.”
Many payers are deploying mobile apps to help patients
manage their care and coverage. Through analytics, payers can
monitor adherence to drug and treatment regimens and detect
trends that lead to individual and population wellness
benefits.4 The vision of precision medicine is to take the
revolution of big data further by building an evidence base
large enough to support pattern detection and correlations
among different types of data, including molecular level
genetic information to patients’ healthcare use, and make
treatment options patient-specific.5 The key to this vision is a
large national cohort of willing patients who would disclose
sensitive personal data thus making its security a high priority.
Potential vulnerabilitiesUS legislation (eg, the Health Insurance Portability and
Accountability Act; HIPAA) and healthcare providers’ (including
pharmacists) code of ethics cover the issue of patient
confidentiality, but it is not clear how much security belies
patients’ personal and medical data. Patients may be under a
false sense of security. Indeed, even with a process known as
“matchback”, which enables the tracking of patients’ drug use
and preferences via their prescription records, without their
names being exchanged, there is the potential for security
breaches. That fact exposes a potential vulnerability in the
system that claims privacy and security about the pharmacy
data.6 In the USA, the Health Information Technology for
Economic and Clinical Health (HITECH) Act has empowered
patients to view, download, and transmit their own health
records. But it has also made them targets of direct and
personalised advertising by pharmaceutical companies.
Marketing departments view this as a lucrative avenue to
promote products to patients, side-lining physicians,
pharmacists and insurers who previously stood between the
drug makers and consumers.
“In spite of its advantages, big data presents many opportunities for inadvertent malpractice.”
Use of big data in pharmacies happens at different levels.
One level is catering to the demands of the retail business
and analysing data to help provide a convenient shopping
experience while the other level is using the data to improve
and monitor medication adherence. However, pharmacists
have full access to sensitive personal medical information
conveyed to them by prescription records, by the patient
during counselling or via medical records if the pharmacy
partners with a healthcare organisation. Big data will thus help
pharmacists to better track patient behaviour, decisions and
rationale and provide patient-centric care efficiently. With
additional training, pharmacists can master the challenge of
data mining for insights from a healthcare data ecosystem that
includes prescription data, unstructured physician notes,
medical images, genomic data, and data from consumer’s
buying behaviour. This would put pharmacists on the forefront
of patient care, but at the same time provide a myriad of
opportunities to inadvertently violate confidentiality in

opinion
46 INTERNATIONAL PHARMACY JOURNAL 47VOL 33, NO.2 - JULY 201546 INTERNATIONAL PHARMACY JOURNAL
Thanks to worldwide action to make real the concept of
pharmaceutical care, today pharmacists in most countries are
looking forward to an expansion of their professional roles.
In many healthcare systems, there is a growing realisation
that pharmacists have much to offer and moves are being
made to put into place the leadership, the retraining and the
resources required to help them fulfil their potential, for the
benefit of patients.
In the drive to “reprofessionalise” pharmacists, there has
been less action on creating an equally promising future for
the community-based pharmacy. According to the thinkers
behind the concept of pharmaceutical care, the pharmacist
of the future will be less involved in dispensing, so little
Technology-enabled patients need technology-enabled health hubs. Could this be the future role of community pharmacies?
By Darrin Baines, Professor in Health Economics, Coventry University, UK
Community pharmacies deserve a renaissance
we can now scan our own groceries. In relation to pharmacy,
this direction suggests that community pharmacy shelves
should be cleared of commercial goods, turning the premises
into a hub for technology-enabled patients. I suggest the
following five steps for creating an innovative model of a
technology-enabled pharmacy:
1. Refit the “front of house” as a technology-hub that allows
patients to connect with the pharmacy, local doctors, the
healthcare system, pharmaceutical companies, charities,
other patients and the like
2. Exploit the time that patients wait for their prescriptions
by connecting them to a technology-enabled task, such as
reporting on their medicines use, watching an interactive
educational programme, completing a questionnaire, or
being an expert-patient in a study
3. Network the pharmacy hub into the wider healthcare
community, including providers, patient groups and
private companies — and by doing so become the port of
first call for patients — and coordinate their care through
the pharmacy’s technology enabled network
4. Retrain pharmacists in healthcare technology not just
medicines optimisation
5. Educate and enable the public to become technology-
enabled pharmacy users
The notion of a technology-enabled pharmacy must prove
itself in practice. However, the argument is clear: although
individual pharmacists are focusing on new roles for the craft
of pharmacy, there is now an urgent need to match this focus
with a technology-enabled new lease of life — a renaissance
— for the community pharmacy.
REFERENCES
1. Baines D. Dispensing: it’s time to let go. Pharmaceutical
Journal 2015;294:113–14.
2. Baines D. Pharmacists as dispensers and formation of the
PPA. Prescriber 2014;25:33–4.
3. Baines D. Has pharmacy run out of time? Pharmaceutical
Journal 2008;281:21.
attention need be placed on rejuvenating community
pharmacy premises because their importance will diminish
as the profession focuses on patients and not dispensing.
They believe the future of profession lies with the pharmacist
not the pharmacy.1
The demand for new roles for pharmacists against a
background of relative disinterest in pharmacies as
professional spaces is ironic: without local pharmacies, the
profession of pharmacy might not have thrived over the past
200-plus years. If the pharmacy had not been such an
important part of the landscape in our cities and towns,
dispensing might have been performed in-house by doctors
or vast publicly funded dispensaries might have become
popular. In other words, there is a strong argument that
suggests pharmacists only exist as a profession because of
their pharmacies.2 Therefore, today’s pharmacists walk away
from their professional “homes” at their professional peril.
From the perspective of pharmacists who have spent many
years dispensing medicines, the idea that there is a
professional life beyond the pharmacy is appealing. However,
the concept that the profession can en masse exist outside its
historical place of work is an unproven ideal. Given current
demand, a proportion of the profession could work with
patients on a regular basis, reviewing their medicines. But,
there is a limit to the number of pharmacists that are needed
to work as “knowledge managers” outside their traditional
homes. Moreover, if money is released from dispensing to
fund medicines optimisation and other activities for patients,
healthcare commissioners may decide that doctors or nurses
should be employed (instead of pharmacists) to do this work.
Could it be easier to train a doctor or nurse in pharmacology
and related skills than to train pharmacists in diagnosis,
medicines and all the other things they need to know to work
with patients safely and effectively?
Technology is everythingIn any profession, the exploration of new roles must always
be welcome. However, I suggest that an equal effort should be
put into finding new roles for pharmacies. Throughout
history, pharmacies have evolved in response to customer
demands and changes in technology, from new drugs to the
introduction of computers. The pharmacy profession should
now ask how pharmacies should evolve. Just because the
outside of a pharmacy remains the same, it does not mean
that the inside must do so. Instead of walking away from the
community pharmacy, there should be immediate action on
how best to transform its space into a technology hub ready
for the future. I will not expand fully on the technological
future of pharmacy here, as I have considered that subject
elsewhere,3 but the following trends are clear:
• Consumers will become more technology-enabled
• Healthcare will be built around the technology-enabled
patient
• Medicines will move away from compounded powders
into technology-assisted interventions (for example,
the future patient will used mobile technology to assist
in coordinating, receiving and reporting on their
prescribed care)
As patients will need somewhere to go if their technology
needs updating, reprogramming or fixing, perhaps the
pharmacy should become the healthcare technology shop of
the future. Think of banking and the grocery industry.
Big banking and supermarket chains are reducing workforces
in their local outlets and using technology instead. We can
now do our own banking, without a member of counter staff;
Darrin Baines
“Without local pharmacies the profession of pharmacy might not have thrived over the past 200-plus years.”

profile
48 INTERNATIONAL PHARMACY JOURNAL 49VOL 33, NO.2 - JULY 201548 INTERNATIONAL PHARMACY JOURNAL
Another challenge the country has had to face was a serious
counterfeiting situation in 2006 in which several people died.
The incident had a marked effect on general awareness of the
problems caused by counterfeit medicines and in the
development of policies and more stringent professional
practices to ensure the integrity and safety of drugs. Dr
Quintero said that the episode had forced the Panamanian
health authorities to instigate greater controls on the entry of
raw materials and medicines into the country. A national
pharmacovigilance centre has also been created.
Medicines shortages and new medicinesThe pharmaceutical industry in Panama manufactures about
10% of the drugs that reach the domestic market. Among the
drugs that the country exports are antibiotics, generally
presented as powders for reconstitution. Dr Quintero added
that in the Colón Free Trade Zone (a large entity near the
Atlantic entrance to the Panama Canal dedicated to re-
exporting a wide variety of merchandise to Latin America and
the Caribbean) there is a facility for the secondary packaging
of products so that they comply with the requirements of
other markets in South America. Panama is suffering from
drug shortages. There are several reasons for this, Dr Quintero
said. The high degree of regulation in the country means that
some manufacturers prefer not to register their products.
Tests to confirm medicines’ identity and concentration are
Pro mundi beneficio: for the benefit of the world. Panama’s motto seems particularly apt currently because the country’s benefit to the world will increase next year when the project to double the capacity of its famous canal will be completed. With the country set to leap on to the world stage and its national pharmacy organisation celebrating 10 years of FIP membership, Graeme Smith finds out from the President of the Colegio Nacional de Farmacéuticos de Panama how Panamanian pharmacy is living up to its country’s motto.
PANAMAWhere pharmacy is on the rise
Pharmacists in Panama are perceived as “consultants of the
community, counsellors of the people, the professional who
has more time than a doctor to give you healthcare or
recommend a good therapy”, said Nereida Quintero, President
of the Colegio Nacional de Farmacéuticos de Panama.
However, Dr Quintero also acknowledged the reality of a
World Health Organization report which pointed out that
indigenous and rural populations have limited access to
health services.
“Panama has adopted international standards proposed by the WHO and FIP for good pharmacy practice.”
The country’s capital, Panama City, is home to almost half of
the country's population of 3.6 million people and Dr Quintero
said that the health profile of Panamanian people is
characterised by the effects of demographic and
epidemiological polarisation. Communicable diseases remain
prevalent, especially among rural and poor people, and
pharmacists have to be familiar with tropical diseases typical
of the region, such as Chagas disease.
But such diseases coexist with the increasingly visible
chronic-degenerative conditions seen in ageing urban
populations. Dr Quintero added that a trend towards
urbanisation is seeing an emergence of problems such as
obesity, alcoholism and drug abuse, and “high incidences of
non-communicable diseases have forced the pharmaceutical
profession towards training in complex therapeutic regimens.”
In addition, her country’s pharmacists, as major participants
in the healthcare team, need to be aware of processes
surrounding how the country deals with natural disasters,
such as earthquakes, landslides and floods (and the
associated water-borne diseases). According to the World
Bank, Panama ranks 14th among countries most exposed to
multiple hazards based on land area.
The WHO has also said that Panama’s health code, which
dates from 1947, needs to be reformed. Dr Quintero agreed.
But she said it was important not to undermine what had
already been achieved. In particular, she said, the drugs
market was extremely important and there were forces that
wanted to ignore the many established controls in that
market. “We must always remember that medicines are a
social good and that the practice of pharmacy has always
been and will always be aimed at protecting public health.”
Panama has a fast growing economy and its greater exposure
to the world on account of the canal expansion project means
that “we have to strengthen health and put greater emphasis
on drug controls and the practice of the profession,” she said.
expensive. And drugs in Panama are generally more expensive
than in the rest of the region. Added to this is a shortage of
the raw materials required to produce drugs.
(For the benefit of countries, like Panama, that have
experienced medicines shortages, FIP has produced a report of
its International Summit on Medicines Shortages, held in
Toronto, Canada, in June 2013. Available in English and Spanish,
the document contains suggested solutions and recommen-
dations that may help alleviate the associated problems.)
“Scientists are investigating some types of fungi found in the fur of the three-toed sloth as a source of new anti-cancer, anti-parasitic and anti-bacterial compounds.”
Yet Panama may also be the source of new medicines. Some
40% of the country is covered by jungle that contains some
flora and fauna species found nowhere else in the world, and
teams of scientists are now investigating some types of fungi
found in the fur of the three-toed sloth (Bradypus variegatus)
as a source of new anti-cancer, anti-parasitic and anti-
bacterial compounds. >>
Ima
ge
: © Y
an
ik C
ha
uvi
n |
Dre
am
stim
e.c
om
profile
51VOL 33, NO.2 - JULY 201550 INTERNATIONAL PHARMACY JOURNAL
Researcher Sarah Higginbotham and colleagues from the
Smithsonian Tropical Research Institute based in Panama
have described how they used a culture-based approach to
examine fungal communities associated with the coarse,
outer hair of this sloth (PLoS One 2014; 9[1]: e84549). They
isolated fungi with bioactivity against: Trypanosoma cruzi,
the causal agent of Chagas disease; Plasmodium falciparum,
the causal agent of malaria; the human breast cancer cell line
MCF-7; and a range of Gram-negative and Gram-positive
human pathogenic bacteria. Could Panama find itself a cradle
of new drug discovery? Watch this space!
A decade of FIP membershipThe Colegio Nacional de Farmacéuticos de Panama was
created in 1963 to regulate the functioning of pharmaceutical
establishments. Now celebrating 10 years of FIP membership,
the Colegio has over 2,600 pharmacists registered with it,
of whom around 60% are active. It promotes scientific
advancement, cooperates with universities in the training of
pharmacists, sees that those exercising the pharmaceutical
profession do so within the law, promotes and defends the
honour of the profession, and upholds ethical standards.
The IPJ asked Dr Quintero why it was important for the
Colegio to be a member of FIP. “It is important because you
have more access to better information strategies for
national pharmaceutical services,” she said.
Panama has adopted international standards proposed by
the WHO and FIP for good pharmacy practice, and is working
towards improving pharmaceutical care with respect to
access to medicines, the quality of medicines and the
responsible use of drugs.
“FIP membership: More access to better information strategies for national pharmaceutical services.”
Another outcome of the Colegio’s FIP membership is that its
country’s universities that teach pharmacy have begun to
mark World Pharmacists Day with special training sessions
and radio broadcasts, among other activities. (This year’s
World Pharmacists Day, on 25 September, will have the theme
“Pharmacist: your partner in health”).
Pharmacy in Panama is “on the rise” with much domestic and
foreign investment in it, Dr Quintero said. “Belonging to an
international organisation that brings together all the
thinking from the pharmaceutical world provides a window
of opportunity for Panamanian pharmacists to participate in
the updating, promotion and enhancement of the profession
through their awareness of global pharmaceutical activities.”
ABOUT MIDDLE EAST RESPIRATORY SYNDROME
Nine things...
As the IPJ went to press, 26 countries had reported cases of Middle East respiratory syndrome
(MERS). In the current outbreak Korea had 181 confirmed cases with 33 deaths. A suspected
MERS sufferer in Thailand had been declared disease-free and a case had been confirmed in
China. Here are nine things you should know about MERS.
PHARMACY AND HEALTH IN PANAMA
Panama’s oldest pharmacy school, at University of Panama
School of Pharmacy, was founded in 1920 and has produced
more than 2,000 graduates.
Currently around 916 pharmacists work for the state; the
remainder work on boards, non-governmental organisations
or for private companies.
Since January 2001, a qualified pharmacist must be present in
any pharmaceutical establishment.
Medical doctors may not own a pharmacy in Panama but
pharmacies may be owned by anyone else as long as a
registered pharmacist is employed.
The health of most of the Panamanian population is covered
by the public sector through the Ministry of Health and
funded through a system of social security. Those who can
afford to pay use services provided by the private sector.
“Pharmacists in Panama are perceived as consultants of the community, counsellors of the people.”
She concluded: “Panama has become a centre of world trade
and has good things and new technologies. We also have new
threats and we must learn to anticipate advances in our field
to ensure the health of our nationals and visitors. . . . We learn
from the experiences of other countries and we can share our
knowledge and experience and so contribute to the world.”
ACKNOWLEDGEMENT
With thanks to Gonçalo Sousa Pinto and Margareth Charry for
translations.
Nereida Quintero
1.Middle East respiratory syndrome (MERS) is a viral
respiratory illness caused by a novel coronavirus that
was first reported in Saudi Arabia in 2012. The source is
unknown, but it is thought the disease may have
arisen through human contact with camels.
5.Since 2013, cases of MERS have
arisen across the world. Most cases
outside the Arabian peninsula have
been associated with contact with
infected individuals who have
travelled from that area. Countries
affected outside Arabia include
China, France, Germany, Thailand,
the UK and the USA. A cluster of
cases in South Korea, where the
original case does not appear to
have had any contact with camels
or the Arabian peninsula, has been
concerning.
6.A World Health Organization
Emergency Committee met in June to
discuss the situation in Korea.
It concluded that the country’s lack of
awareness about MERS and suboptimal
infection prevention and control
measures in its hospital had
contributed to the outbreak. The
committee has issued advice to
affected countries.
7.There is no vaccine against
MERS, although the possibility of
developing one is being explored.
Advice on prevention is the same as
for other respiratory diseases and
includes rigorous hand-washing, use
and disposal of tissues, avoiding
personal contact with sick people,
and cleaning and disinfection of
surfaces and objects like door
handles, for instance.
2.Symptoms are similar to those of other respiratory illnesses and
include cough, shortness of breath and fever. Gastrointestinal
symptoms have also been reported. More severe complications can
develop, such as pneumonia and kidney failure. However some
infected people have displayed no symptoms at all.
8.Currently there is no
recommendation that anyone
need change their travel plans on
account of MERS.
9.The WHO recently issued a statement
on best practices for naming new
human infectious diseases (such as
MERS). It recommends against using
geographical locations in names
because this is unscientific and has the
potential seriously to affect people’s
lives and livelihoods.
4.Presence of the disease is confirmed by
laboratory testing. High quality supportive
care is the keystone of patient management.
Convalescent plasma, interferon and lopinavir
may be considered for specific treatment
(Public Health England). The WHO has interim
guidance on the clinical management of severe
acute respiratory infections when novel
coronavirus is suspected.
3.MERS kills three to four out of every 10
people infected. However most of those who
die usually have underlying medical
conditions, such as diabetes or cancer.
Healthcare workers in contact with MERS
patients are particularly at risk of infection.
For others, the risk is generally low since there
is no indication of sustained transmission
from person to person in the community.