Precision medicine/personalized medicine: a critical analysis ...

CPAHG
C
Ea
Es
C
I
Ppdb
F(HoIAkA
PN
wa
A©
Review and Special Articles
urbing Problem Drinking withersonalized-Feedback InterventionsMeta-Analysis
eleen Riper, PhD, MSc, Annemieke van Straten, PhD, Max Keuken, BSc, Filip Smit, PhD,erard Schippers, PhD, Pim Cuijpers, PhD
ontext: The effectiveness of personalized-feedback interventions to reduce problem drinking hasbeen evaluated in several RCTs and systematic reviews. A meta-analysis was performed toexamine the overall effectiveness of brief, single-session personalized-feedback interven-tions without therapeutic guidance.
videncecquisition:
The selection and analyses of studies were conducted in 2008. Fourteen RCTs ofsingle-session personalized-feedback interventions without therapeutic guidance wereidentified, and their combined effectiveness on the reduction of problematic alcoholconsumption was evaluated in a meta-analysis. Alcohol consumption was the primaryoutcome measure.
videnceynthesis:
The pooled standardized-effect size (14 studies, 15 comparisons) for reduced alcoholconsumption at post-intervention was d�0.22 (95% CI�0.16, 0.29; the number needed totreat�8.06; areas under the curve�0.562). No heterogeneity existed among the studies(Q�10.962; p�0.69; I2�0).
onclusions: The use of single-session personalized-feedback interventions without therapeuticguidance appears to be a viable and probably cost-effective option for reducingproblem drinking in student and general populations. The Internet offers ampleopportunities to deliver personalized-feedback interventions on a broad scale, andproblem drinkers are known to be amenable to Internet-based interventions. Moreresearch is needed on the long-term effectiveness of personalized-feedback interven-tions for problem drinking, on its potential as a first step in a stepped-care approach,and on its effectiveness with other groups (such as youth obliged to use judicial serviceprograms because of violations of minimum-age drinking laws) and in other settings(such as primary care).(Am J Prev Med 2009;36(3):247–255) © 2009 American Journal of Preventive Medicine
lsnmavo
bgsosofsbc
ntroduction
roblem drinking is a major public health issue,particularly due to its high prevalence in adult1,2
and student populations.3,4 It is these groups ofroblem drinkers—and not those with severe alcoholependence, as is often thought—who account for theulk of the alcohol-related harm in the general popu-
rom the Innovation Centre of Mental Health and TechnologyRiper, Smit), Trimbos Institute (Netherlands Institute of Mentalealth and Addiction), Utrecht; the Department of Clinical Psychol-
gy and Institute for Research in Extramural Medicine (EMGO)nstitute (Riper, van Straten, Smit, Cuijpers), Vrije Universiteit;msterdam Medical Centre (Schippers), Cognitive Science (Keu-en), Institute for Interdisciplinary Studies, University of Amsterdam,msterdam, The NetherlandsAddress correspondence and reprint requests to: Heleen Riper,
hD, MSc, Trimbos Institute, P.O. Box 725, 3500 AS Utrecht, Theetherlands. E-mail: [email protected] full text of this article is available via AJPM Online at
cww.ajpm-online.net; 1 unit of Category-1 CME credit is also avail-ble, with details on the website.
m J Prev Med 2009;36(3)2009 American Journal of Preventive Medicine • Published by
ation.5,6 Problem drinking causes a formidable array oferious health problems7 and a heavy social and eco-omic burden.8,9 Besides short-term and long-termorbidity1,2 and mortality,10 the consequences include
cute unintended injuries, sexual and physical assault,iolence-related trauma, vandalism, and poor academicr work performance.11,12
Early identification and brief interventions haveeen increasingly advocated as cost-effective strate-ies to curb problem drinking.8,13–15 Evidence istrongest for brief interventions in primary and sec-ndary care,6,16 –18 but effectiveness has also beenhown in settings such as the general population19 –21
r student communities.22–25 Less encouraging is theact that the implementation of brief interventions istill hampered by constraints such as a limited num-er of professionals who administer them, the diffi-ulty of contacting problem drinkers, and the high
osts of implementation and delivery.21,26,27 As a2470749-3797/09/$–see front matterElsevier Inc. doi:10.1016/j.amepre.2008.10.016

can
fpaowtppbsd(tmsmntotOctmv
befainaigppmwpoacatpgsvmfiia
pwi
E
I
Ts
1
2
3
4
S
Ff
F
2
onsequence, as many as 80% of problem drinkersre not yet receiving help.28 –30 Innovative ways areeeded for reaching out to them.Brief personalized feedback (i.e., personalized-
eedback interventions) could be one such strategy,31
roviding personal feedback regarding an individual’slcohol-consumption patterns. This feedback may consistf different components, such as an overview of meaneekly alcohol consumption; blood alcohol concentra-
ion levels (BAC); associated health and social risks ofroblem drinking; or self-help guidelines to changeroblematic alcohol consumption. Normative feed-ack is another important component of many per-onalized-feedback interventions. It enables problemrinkers to compare their own alcohol consumptionin terms of frequency, quantity, or other measures)o the level of their own cohort—such as the average
an or woman in the general population or theirtudent peer group32–34—as well as to the recom-ended guidelines for sensible drinking. The ratio-ale of normative feedback is that such comparisons
rigger an awareness in problem drinkers of theirwn drinking patterns and the risks they are taking,hus motivating them to reduce their alcohol use.33
ne underlying explanation for such behavioralhange is that many problem drinkers overestimatehe alcohol consumption of others while underesti-
ating their own.35–37 Personalized-feedback inter-entions may consist only of normative feedback.38
Personalized feedback began as a component of evidence-ased, face-to-face individual or group motivational-nhancement interventions.17,39 Today, personalized-eedback interventions are being successfully provided asutonomous, face-to-face self-help interventions in bothndividual and group formats. Technologic advances alsoow enable the delivery of automated mail, computer,nd Internet-based personalized feedback. This includesndividual single-session interventions without therapeuticuidance, provided in various settings and to variousopulations.22,24,31,40 The systematic review by White25 onersonalized feedback for college students has shown thatail- or web-based personalized-feedback interventionsithout professional guidance were as effective in studentopulations as brief face-to-face interventions. Studies38,41
n needs assessment in problem-drinking populationslso suggest that personalized feedback is a highly practi-al method for the target groups concerned. Bothdults and students often prefer to use self-help interven-ions without therapeutic involvement to address theirroblem drinking instead of more-intensive individual orroup treatments.41,42 Given these promising results withingle-session, stand-alone, personalized-feedback inter-entions, it was decided to assess their effectiveness in aeta-analysis. To the best of our knowledge, this is therst meta-analysis to focus on brief personalized-feedback
nterventions without professional guidance for young
nd adult problem drinkers. The expectation was that o48 American Journal of Preventive Medicine, Volume 36, Num
ersonalized-feedback interventions for problem drinkersould be more effective than non-intervention in reduc-
ng problem drinking.
vidence Acquisition
dentification and Selection of Studies
he relevant studies were identified in 2008, using severalystematic search strategies:
. Systematic searches were carried out in the followingbibliographical databases: MEDLINE; PsycINFO (1985 topresent); Science Citation Index Expanded; Social Sci-ences Citation Index; Arts & Humanities Citation Index®
(1988 to present); CINAHL®; EMBASE; the CochraneDrug and Alcohol Group Specialised Register; the Co-chrane Effective Practice and Organisation of Care Group;the Alcohol and Alcohol Problems Science Database; andETOH (etoh.niaaa.nih.gov; 1972 to 2003). Text and keywords indicative of personalized-feedback interventions forproblem drinking (personalized feedback, personalized normativefeedback, self-help, brief intervention, brief psychotherapy, bibliother-apy) were combined with terms referring to the content ofthe problem (problem drinking, binge drinking, hazardous drink-ing, alcohol abuse, alcoholism—both MeSH terms and free textwords); the setting (primary care, general population, community,Internet, adults, students, mail, web-based); and the studydesign (RCTs). These search strategies were combinedwith the optimal search strategy for RCTs designed by theUnited Kingdom’s Cochrane Centre.43
. References were examined relating to earlier meta-analysesand systematic reviews on brief interventions, self-help inter-ventions, and personalized-feedback interventions forproblem drinking.6,16,18–21,31,44–53
. Unpublished literature was searched by scanning Disserta-tion Abstracts and Digital Dissertations.
. Reference lists of retrieved papers were screened, andpapers that possibly met inclusion criteria were retrievedand studied (Figure 1). No language restrictions wereapplied.
election of Primary Studies
or inclusion in the meta-analysis, studies on personalizedeedback for problem drinkers were selected that (1) applied
igure 1. Flow chart of study selection resulting in inclusion
f 14 studies (15 comparisons)ber 3 www.ajpm-online.net

awwba((vpp
uiatreAasCba
M
AosoabTacobf
M
Etaie�a
eaegoctt
rshsd
soTdawrifirumeips
nNtsoo�
dv(tossIiimeaf
eppffaAo
ED
TsfBlma
M
randomized–controlled design (including control groupsith assessment only and no treatment, with wait-listing, andith a semi-placebo in the form of an alcohol-informationrochure); (2) reported data that were usable for meta-nalytic procedures; (3) assessed alcohol-drinking behaviore.g., frequency or quantity) as a primary outcome measure;4) applied individually focused personalized-feedback inter-entions; and (5) delivered the interventions without thera-eutic support, with a maximum duration of 15 minutes perarticipant (Table 138,54–64).The assessment of studies for inclusion in the review was
ndertaken by two independent raters. Preselection from thenitial search was based on information derived from titles,bstracts, and key words; if they yielded insufficient informa-ion to assess the inclusion criteria, then the full paper wasetrieved. All papers excluded at this stage were re-checked tonsure that all potentially relevant papers had been retrieved.ll retrieved papers were assessed for inclusion using thebove criteria (Table 138,54–64); any disagreement was re-olved by discussion and consensus. Using SPSS version 15,ohen’s � was used to assess the agreement on inclusionetween the two raters (��0.72, which reflects a substantialgreement).
ethodologic Quality Assessment of Primary Studies
t least 25 scales are available to assess the validity and qualityf RCTs.43 As there is no evidence that the more elaboratecales give more reliable assessments of validity than simplernes, an approach was used like the one suggested by Higginsnd Green43 and like the ones applied in several reviews ofrief interventions for problem drinking in primary care.6,12
his resulted in four basic criteria for assessing the validitynd quality of the studies analyzed: (1) allocation toondition by an independent third party, (2) the adequacyf random-allocation concealment to respondents, (3) thelinding of assessors of outcomes, and (4) attrition inollow-up data.
eta-Analysis
ffect sizes (d) were calculated by subtracting (at post-test)he average score of the control condition (Mc) from theverage score of the experimental condition (Me) and divid-ng the result by the average of the standard deviations of thexperimental and control conditions (SDec). An effect size of0.15 can be regarded as small, 0.45 as moderate, and �0.90
s large.65
Effect-size calculations were restricted to instruments thatxplicitly measured alcohol consumption (Table 138,54–64). Ifstudy used more than one alcohol measure, the mean of theffect sizes was calculated, giving each study (or contrastroup) a single effect size. In one study38 where more thanne experimental condition was compared to a controlondition, the number of participants in the control condi-ion was divided evenly over the experimental conditions sohat each participant was used only once in the meta-analysis.
The pooled mean effect sizes were calculated using bothandom- and fixed-effects models. A fixed-effects model as-umes that all studies in the meta-analysis are considered toave been conducted under similar conditions with similarubjects. The only difference among studies is their power to
etect the outcome of interest. In a random-effects model, parch 2009
tudies are regarded as having been drawn from a populationf studies. Effect sizes may vary due to error across studies.his allows for more uncertainty in the meta-analytical data,oes not make the (possibly too restrictive) assumption thatll studies are exact replications, and generally producesider CIs around the pooled estimates. By implication, theandom-effects model is more conservative in flagging signif-cant results. In the absence of heterogeneity (see below), thexed- and the random-effects models produce the sameesults. In that case, the more simple fixed-effects model issually preferred. As the analyzed studies used differenteasures (both continuous and dichotomous) to indicate
ffectiveness, some ORs had to be converted into effect sizesn terms of Cohen’s d. This was done using the formularovided by the Comprehensive Meta-Analysis program ver-ion 2.2.021.
Next, the mean effect sizes were converted into the numbereeded to treat (NNT) and area under the curve (AUC).66 TheNT estimates how many people must receive the intervention
o achieve a good clinical outcome in one person; hence, amaller NNT is better than a large one. The AUC is a measuref an intervention’s effectiveness; a score �0.50 indicates that itsutcome is superior to that in the control condition, and a score0.50 indicates that it is inferior.This analysis also tested whether genuine differences un-
erlay the results of the studies (heterogeneity) or whetherariations in findings were attributable to chance alonehomogeneity).67 The Q statistic was calculated as an indica-or of homogeneity. A significant Q rejects the null hypothesisf homogeneity and shows that the variability among effectizes is greater than what would likely have resulted fromampling error alone in the primary studies. Additionally, the2 statistic, an indicator of heterogeneity, was calculated; 0%ndicates no observed heterogeneity, and larger values showncreasing heterogeneity, with 25% regarded as low, 50% as
oderate, and 75% as high.67 As heterogeneity was non-xistent in all analyses and the differences between the fixed-nd random-effects results were negligible, only the resultsrom the fixed-effects model are reported here.
Meta-regression analyses were performed to assess whetherffect sizes decayed over time and whether multicomponentersonalized feedback differed in impact in comparison toersonalized normative feedback alone. To assess and adjustor any publication bias, a fail-safe analysis was conducted, aunnel plot was constructed, and Duval and Tweedie’s trim-nd-fill analysis was performed. The Comprehensive Meta-nalysis program version 2.2.021 was used for all suchperations.
vidence Synthesisescription of the Primary Analyzed Studies
he combined literature search generated 406 ab-tracts and yielded 14 studies (Boon B, Instituteor Addiction Research, unpublished findings, 2006;oon B, Institute for Addiction Research, unpub-
ished findings, 2008)38,54 – 64 (15 comparisons) thatet the inclusion criteria (Table 138,54 – 64). The
nalysis involved a total of 3682 participants (1904 in
ersonalized-feedback conditions and 1778 in con-Am J Prev Med 2009;36(3) 249
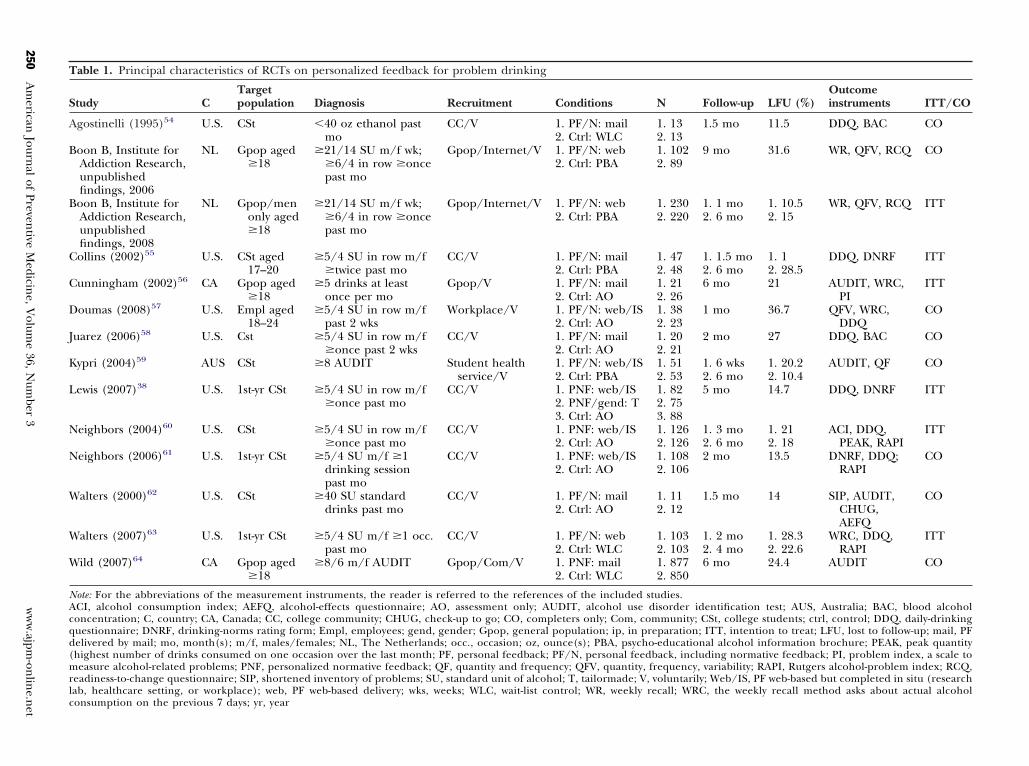
Table 1. Principal characteristics of RCTs on personalized feedback for problem drinking
Study CTargetpopulation Diagnosis Recruitment Conditions N Follow-up LFU (%)
Outcomeinstruments ITT/CO
Agostinelli (1995)54 U.S. CSt �40 oz ethanol pastmo
CC/V 1. PF/N: mail2. Ctrl: WLC
1. 132. 13
1.5 mo 11.5 DDQ, BAC CO
Boon B, Institute forAddiction Research,unpublishedfindings, 2006
NL Gpop aged�18
�21/14 SU m/f wk;�6/4 in row �oncepast mo
Gpop/Internet/V 1. PF/N: web2. Ctrl: PBA
1. 1022. 89
9 mo 31.6 WR, QFV, RCQ CO
Boon B, Institute forAddiction Research,unpublishedfindings, 2008
NL Gpop/menonly aged�18
�21/14 SU m/f wk;�6/4 in row �oncepast mo
Gpop/Internet/V 1. PF/N: web2. Ctrl: PBA
1. 2302. 220
1. 1 mo2. 6 mo
1. 10.52. 15
WR, QFV, RCQ ITT
Collins (2002)55 U.S. CSt aged17–20
�5/4 SU in row m/f�twice past mo
CC/V 1. PF/N: mail2. Ctrl: PBA
1. 472. 48
1. 1.5 mo2. 6 mo
1. 12. 28.5
DDQ, DNRF ITT
Cunningham (2002)56 CA Gpop aged�18
�5 drinks at leastonce per mo
Gpop/V 1. PF/N: mail2. Ctrl: AO
1. 212. 26
6 mo 21 AUDIT, WRC,PI
ITT
Doumas (2008)57 U.S. Empl aged18–24
�5/4 SU in row m/fpast 2 wks
Workplace/V 1. PF/N: web/IS2. Ctrl: AO
1. 382. 23
1 mo 36.7 QFV, WRC,DDQ
CO
Juarez (2006)58 U.S. Cst �5/4 SU in row m/f�once past 2 wks
CC/V 1. PF/N: mail2. Ctrl: AO
1. 202. 21
2 mo 27 DDQ, BAC CO
Kypri (2004)59 AUS CSt �8 AUDIT Student healthservice/V
1. PF/N: web/IS2. Ctrl: PBA
1. 512. 53
1. 6 wks2. 6 mo
1. 20.22. 10.4
AUDIT, QF CO
Lewis (2007)38 U.S. 1st-yr CSt �5/4 SU in row m/f�once past mo
CC/V 1. PNF: web/IS2. PNF/gend: T3. Ctrl: AO
1. 822. 753. 88
5 mo 14.7 DDQ, DNRF ITT
Neighbors (2004)60 U.S. CSt �5/4 SU in row m/f�once past mo
CC/V 1. PNF: web/IS2. Ctrl: AO
1. 1262. 126
1. 3 mo2. 6 mo
1. 212. 18
ACI, DDQ,PEAK, RAPI
ITT
Neighbors (2006)61 U.S. 1st-yr CSt �5/4 SU m/f �1drinking sessionpast mo
CC/V 1. PNF: web/IS2. Ctrl: AO
1. 1082. 106
2 mo 13.5 DNRF, DDQ;RAPI
CO
Walters (2000)62 U.S. CSt �40 SU standarddrinks past mo
CC/V 1. PF/N: mail2. Ctrl: AO
1. 112. 12
1.5 mo 14 SIP, AUDIT,CHUG,AEFQ
CO
Walters (2007)63 U.S. 1st-yr CSt �5/4 SU m/f �1 occ.past mo
CC/V 1. PF/N: web2. Ctrl: WLC
1. 1032. 103
1. 2 mo2. 4 mo
1. 28.32. 22.6
WRC, DDQ,RAPI
ITT
Wild (2007)64 CA Gpop aged�18
�8/6 m/f AUDIT Gpop/Com/V 1. PNF: mail2. Ctrl: WLC
1. 8772. 850
6 mo 24.4 AUDIT CO
Note: For the abbreviations of the measurement instruments, the reader is referred to the references of the included studies.ACI, alcohol consumption index; AEFQ, alcohol-effects questionnaire; AO, assessment only; AUDIT, alcohol use disorder identification test; AUS, Australia; BAC, blood alcoholconcentration; C, country; CA, Canada; CC, college community; CHUG, check-up to go; CO, completers only; Com, community; CSt, college students; ctrl, control; DDQ, daily-drinkingquestionnaire; DNRF, drinking-norms rating form; Empl, employees; gend, gender; Gpop, general population; ip, in preparation; ITT, intention to treat; LFU, lost to follow-up; mail, PFdelivered by mail; mo, month(s); m/f, males/females; NL, The Netherlands; occ., occasion; oz, ounce(s); PBA, psycho-educational alcohol information brochure; PEAK, peak quantity(highest number of drinks consumed on one occasion over the last month; PF, personal feedback; PF/N, personal feedback, including normative feedback; PI, problem index, a scale tomeasure alcohol-related problems; PNF, personalized normative feedback; QF, quantity and frequency; QFV, quantity, frequency, variability; RAPI, Rutgers alcohol-problem index; RCQ,readiness-to-change questionnaire; SIP, shortened inventory of problems; SU, standard unit of alcohol; T, tailormade; V, voluntarily; Web/IS, PF web-based but completed in situ (researchlab, healthcare setting, or workplace); web, PF web-based delivery; wks, weeks; WLC, wait-list control; WR, weekly recall; WRC, the weekly recall method asks about actual alcoholconsumption on the previous 7 days; yr, year
250A
merican
Journal
ofPreven
tiveM
edicine,
Volum
e36,
Num
ber3
ww
w.ajpm
-onlin
e.net
tf
fopFuRtetoABfie(wdI2ltpdBiultiam
TstI2fieB2alae
csORirsf
EC
FuRpommhI
Fa
b
M
rol conditions). The number of participants rangedrom 11 to 877 per condition per comparison.
All38,54–58,60–64 but one study59 used nonclinical samplesrom settings either in the community, in higher education,r at work. Nine studies38,54,55,58–63 recruited their partici-ants, aged 17–24 years, from higher-education institutions.our studies (Boon B, Institute for Addiction Research,npublished findings, 2006; Boon B, Institute for Addictionesearch, unpublished findings, 2008)56,64 recruited from
he general adult population, and one study57 targetedmployees in a work setting. Six studies54–56,58,62,64 deliveredhe personalized-feedback interventions by mail, and thether eight did so via the Internet (Boon B, Institute forddiction Research, unpublished findings, 2006;oon B, Institute for Addiction Research, unpublishedndings, 2008).38,57,59–61,63 Five studies38,57,59–61 deliv-red the personalized-feedback interventions in situi.e., a research laboratory, health service clinic, or atork). Six54–56,58,62,64 of the remaining nine studieselivered the intervention by mail; three (Boon B,nstitute for Addiction Research, unpublished findings,006; Boon B, Institute for Addiction Research, unpub-ished findings, 2008)63 enabled participants to accesshe intervention via the Internet at their venue ofreference. Eight studies38,55–58,60,61,63 used bingerinking as the primary inclusion criterion; two (Boon, Institute for Addiction Research, unpublished find-
ngs, 2006; Boon B, Institute for Addiction Research,npublished findings, 2008) used drinking in excess of a
ow-risk drinking guideline (including binge drinking;wo59,64 used the AUDIT68 screening test (with a score of �8ndicating problem drinking); and two studies used themount of alcohol intake (�40 oz. ethanol in the pastonth54 and �40 standard drinks in the past month62).
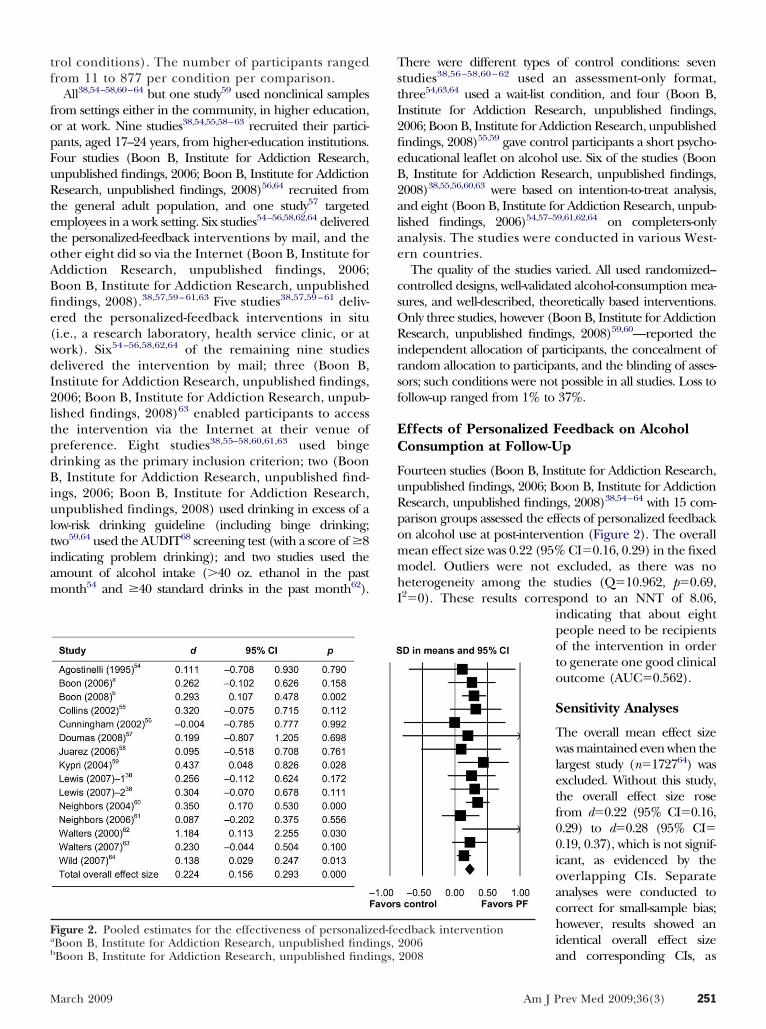
igure 2. Pooled estimates for the effectiveness of personalizBoon B, Institute for Addiction Research, unpublished findi
Boon B, Institute for Addiction Research, unpublished findings,arch 2009
here were different types of control conditions: seventudies38,56 –58,60 – 62 used an assessment-only format,hree54,63,64 used a wait-list condition, and four (Boon B,nstitute for Addiction Research, unpublished findings,006; Boon B, Institute for Addiction Research, unpublishedndings, 2008)55,59 gave control participants a short psycho-ducational leaflet on alcohol use. Six of the studies (Boon, Institute for Addiction Research, unpublished findings,008)38,55,56,60,63 were based on intention-to-treat analysis,nd eight (Boon B, Institute for Addiction Research, unpub-ished findings, 2006)54,57–59,61,62,64 on completers-onlynalysis. The studies were conducted in various West-rn countries.The quality of the studies varied. All used randomized–
ontrolled designs, well-validated alcohol-consumption mea-ures, and well-described, theoretically based interventions.nly three studies, however (Boon B, Institute for Addictionesearch, unpublished findings, 2008)59,60—reported the
ndependent allocation of participants, the concealment ofandom allocation to participants, and the blinding of asses-ors; such conditions were not possible in all studies. Loss toollow-up ranged from 1% to 37%.
ffects of Personalized Feedback on Alcoholonsumption at Follow-Up
ourteen studies (Boon B, Institute for Addiction Research,npublished findings, 2006; Boon B, Institute for Addictionesearch, unpublished findings, 2008)38,54–64 with 15 com-arison groups assessed the effects of personalized feedbackn alcohol use at post-intervention (Figure 2). The overallean effect size was 0.22 (95% CI�0.16, 0.29) in the fixedodel. Outliers were not excluded, as there was no
eterogeneity among the studies (Q�10.962, p�0.69,2�0). These results correspond to an NNT of 8.06,
indicating that about eightpeople need to be recipientsof the intervention in orderto generate one good clinicaloutcome (AUC�0.562).
Sensitivity Analyses
The overall mean effect sizewas maintained even when thelargest study (n�172764) wasexcluded. Without this study,the overall effect size rosefrom d�0.22 (95% CI�0.16,0.29) to d�0.28 (95% CI�0.19, 0.37), which is not signif-icant, as evidenced by theoverlapping CIs. Separateanalyses were conducted tocorrect for small-sample bias;however, results showed anidentical overall effect size
edback intervention2006
ed-fengs,
and corresponding CIs, as2008
Am J Prev Med 2009;36(3) 251

rmsfCdiptp
dCnybwt
DM
Taaadaenatdpppb
tvsapfpbtfm
igicin
dtWctWedtmtfipn
L
SibosmdiAabitq
C
PmfiatpetivadmcIfcusac
2
eported for the pooled standardized difference ineans. Meta-regression analyses did not establish
ignificant differences in the effects of personalized-eedback interventions over time (�� – 0.006, 95%I� – 0.014, 0.0015, p�0.12), nor could a significantifference be established for personalized-feedback
nterventions inclusive of normative feedback andersonalized-feedback interventions based solely on
his normative feedback (��0.09, CI� – 0.05, 0.24,�0.22).Duval and Tweedie’s trim-and-fill analysis did not
etect any publication bias (observed d�0.22, 95%I�0.16, 0.29; adjusted d�0.22, 95% CI�0.15, 0.29);either did the funnel plot analysis. The fail-safe anal-sis indicated that 122 studies with null effects have toe added to the database before the pooled effect sizeould be no longer significant (p�0.05). In view of
hese results, we believe that our results are robust.69,70
iscussionain Findings
his meta-analysis shows that single-session, individu-lly personalized feedback without professional guid-nce can be an effective intervention for reducing riskylcohol consumption in young and adult problemrinkers. Adverse consequences in terms of increasedlcohol use among participants resulting from theirxposure to personalized-feedback interventions wereot identified.12 These results may indicate that person-lized feedback is an effective intervention for differentarget groups across different settings, using a variety ofelivery modes. Despite the modest effect sizes overall,ersonalized feedback could have a major health im-act at the population level, in view of the highercentage of problem drinkers who potentially couldenefit.49
The effect sizes reported here are comparable tohose from several other meta-analyses of brief inter-entions to curb problem drinking. Those were in themall-to-moderate range, both for college students22
nd the adult population in both nonclinical andrimary care samples.6,17,19,20,71 The NNT of 8.06
ound in this meta-analysis for the overall effect ofersonalized feedback seems appreciable, given therief and unguided nature of the intervention. It is inhe range of those NNTs (i.e., from 772 to 823) reportedor brief, face-to-face alcohol-reduction advice in pri-
ary care.The meta-analysis by Carey et al.22 indicated that
ndividual brief interventions are more effective thanroup interventions for college drinkers (with d rang-ng from 0.11 to 0.41 on several alcohol-related out-ome measures). This study also showed that briefnterventions based on motivational interviewing and
ormative feedback are more effective than those that t52 American Journal of Preventive Medicine, Volume 36, Num
o not include these features. In a review dedicatedo personalized-feedback interventions for students,
hite25 found more favorable results for written andomputer-based personalized-feedback interventionshan for face-to-face individual or group interventions;
alters and Neighbors31 found similar results. Theffectiveness of personalized feedback may thereforeepend not on personal contact but on the content ofhe feedback, such as normative feedback and the
ode of mail and web-based delivery.24,25 For example,his meta-analysis showed that personalized normativeeedback was as effective as multi-component personal-zed feedback. Further research into the effective com-onents is, however, required to evaluate the robust-ess of this observation.
imitations
everal limitations need to be taken into account whennterpreting the results of this study. First, this meta-analysis isased on 14 primary studies; the findings can be generalizednly to the groups studied,73 who were at-risk drinkers intudent and general populations. Second, some studies hadethodologic drawbacks such as small samples54,55,62 or
ropout rates above 30% (Table 138,54–64). Third, all stud-es relied on self-reported alcohol-consumption measures.lthough there is some concern about the reliabilitynd validity of such measures,38,74 they are currently theest option available.12,75 Indeed, their validity actually
mproves in interventions delivered online, which facili-ate self-disclosure in comparison to pen-and-paperuestionnaires.38,42,76
onclusion
ersonalized feedback without therapeutic guidanceay be cost effective in view of the minimal time and
nancial investments needed to make it widely avail-ble. It is expected that this potential cost effectiveness,he attractiveness of personalized feedback for partici-ants,77 and the diffusion potential could be greatlyxpanded by delivering it over the Internet. Many ofhe traditional impediments to implementing briefnterventions could be overcome thereby.27,57 The ad-antages of web-based delivery include the widespreadvailability of personalized feedback to underserved orifficult-to-reach groups such as college students, fe-ale problem drinkers,22,40 and those in geographi-
ally dispersed areas,27,42 many of whom now haventernet access.78 Brief web-based personalized-eedback interventions appear to be more readily ac-epted by both young and mature risky drinkers, as thenobtrusive nature of the intervention allays fears oftigmatization and violation of privacy.79,80 The constantvailability of these web-based interventions makes it moreonvenient to take part.40 Information and Communica-
ion Technologies (ICT) also now facilitates personal-ber 3 www.ajpm-online.net

nhIggiyoagtsa
ccptIwimirrplmtritvtrmp
pieycstpieisdbfRssi
vit
smgf(ciawbss
Wp
e
t
R
1
1
1
1
1
M
eeds assessments, including those necessary for publicealth interventions.81 A further advantage is that thenternet—in particular, the advent of Web 2.0 technolo-ies82—facilitates the gathering of knowledge about tar-eted groups as well as their active participation in thenterventions. The use of ICT devices in group settings iset another promising avenue, as shown by the recent RCTf LaBrie et al.83 among college students. This study evalu-ted the effectiveness of a professionally guided, interactive,roup-specific, personalized, normative-feedback interven-ion by means of personal digital handhelds. Results demon-trated the effectiveness of this intervention on reducinglcohol consumption at 2-month follow-up.
All such features of web-based personalized feedbackould increase the effectiveness of intervening, andould make it possible—as Neighbors et al.61 haveointed out—to reach out with preventive interven-ions to people in different settings and on a large scale.n a public health approach to problem drinking, itould therefore seem beneficial to integrate personal-
zed feedback into the first stage of a stepped-careodel for problem drinking. A stepped-care approach
s based on the rationale that problem drinkers firsteceive a brief, low-threshold intervention that has aeasonable chance of success. For those for whomersonalized feedback, for example, does not work, the
evel of treatment can be stepped up in terms ofore-intensive interventions with increasing levels of
herapeutic involvement and related cost. It therefore isecommended that personalized feedback be furthernvestigated. However, many of the expected advan-ages still lack an empirical basis, while potential disad-antages have not yet been fully investigated. Alterna-ive strategies to reach out to high-risk drinkers are alsoequired, because with effect sizes in the small-to-edium range, not all high-risk drinkers benefit from
ersonalized feedback.In addition, research into the cost effectiveness of
ersonalized-feedback interventions is required. Whilet is expected that personalized feedback can be deliv-red at low cost, the empirical evidence for this is notet available. Cost-effectiveness studies should also in-lude evaluations of effective recruitment strategies foringle-session personalized-feedback interventions, ashe latter could involve higher costs than the actualersonalized-feedback intervention itself. Future stud-
es should focus on factors that influence the long-termffectiveness of personalized feedback, as well as exam-ning the groups (e.g., youth obliged to use judicialervice programs because of violations of minimum-agerinking laws and adults obliged to use these programsecause of convictions for alcohol-impaired driving)or which it might have greater or lesser effectiveness.esearch should also explore its applicability to other
ettings, such as primary care. As is the case in collegeettings, a whole range of barriers exist to implement-
ng interventions in primary care. These involve moti-arch 2009
ating and training general practitioners to use thentervention, a lack of pragmatic screening interven-ions,26,27,44,45 and the costs of implementation.21,84
Future research should investigate the role thatingle-session personalized feedback could play in pri-ary care with and without the involvement of the
eneral practitioner. As the effects of personalizedeedback appear comparable to those of more intensiveand hence costly and intrusive) brief interventions, itould be of interest to a range of stakeholders, includ-ng university officials, public health planners, insur-nce companies, and employers. In addition, it isorthwhile to further investigate the potential applica-ility of a single session for altering lifestyle behaviorsuch as overeating or common mental health disordersuch as depression.
e thank Karin Mutsaers; this study would not have beenossible without her contribution.We are grateful to Michael Dallas for English-language
dits.No financial disclosures were reported by the authors of
his paper.
eferences1. Murray CJ, Lopez AD. The global burden of disease: a comprehensive
assessment of mortality and disability from diseases, injuries, and riskfactors in 1990 and projected to 2020. Cambridge MA: Harvard School ofPublic Health, 1996.
2. WHO. WHO expert committee on problems related to alcohol consump-tion. Second report. World Health Organ Tech Rep Ser 2007;1–7.
3. Knight JR, Wechsler H, Kuo M, Seibring M, Weitzman ER, Schuckit MA.Alcohol abuse and dependence among U.S. college students. J StudAlcohol 2002;63:263–70.
4. Wechsler H, Lee JE, Kuo M, Seibring M, Nelson TF, Lee H. Trends incollege binge drinking during a period of increased prevention efforts.Findings from 4 Harvard School of Public Health college alcohol studysurveys: 1993–2001. J Am Coll Health 2002;50:203–17.
5. Heather N, Kaner E. Brief interventions against excessive alcohol consump-tion. In: Warell DA, Cox TM, Firth JD, et al, eds. Oxford textbook ofmedicine. Oxford: Oxford University Press, 2003.
6. Kaner EF, Beyer F, Dickinson HO, et al. Effectiveness of brief alcoholinterventions in primary care populations. Cochrane Database Syst Rev2007;CD004148.
7. White HR, Jackson KM. Social and psychological influences on emergingadult drinking. Alcohol Res Health 2004;28:182–90.
8. Anderson P, Baumberg B. Alcohol in Europe. A public health perspective.London: Institute of Alcohol Studies, 2006.
9. Smit F, Cuijpers P, Oostenbrink J, Batelaan N, de Graaf R, Beekman A.Costs of nine common mental disorders: implications for curative andpreventive psychiatry. J Ment Health Policy Econ 2006;9:193–200.
0. Holman CD, English DR, Milne E, Winter MG. Meta-analysis of alcohol andall-cause mortality: a validation of NHMRC recommendations. Med J Aust1996;164:141–5.
1. Hingson R, Heeren T, Winter M, Wechsler H. Magnitude of alcohol-relatedmortality and morbidity among U.S. college students ages 18–24: changesfrom 1998 to 2001. Annu Rev Public Health 2005;26:259–79.
2. Whitlock EP, Polen MR, Green CA, Orleans T, Klein J. Behavioralcounseling interventions in primary care to reduce risky/harmful alcoholuse by adults: a summary of the evidence for the U.S. Preventive ServicesTask Force. Ann Intern Med 2004;140:557–68.
3. Freemantle N, Gill P, Godfrey C, et al. Brief interventions and alcohol use.Qual Health Care 1993;2:267–73.
4. IOM. Broadening the base of treatment of alcohol problems: report of a
study by a committee of the Institute of Medicine. Washington DC:National Academy Press, 1990.Am J Prev Med 2009;36(3) 253
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
2
5. USDHHS. The Surgeon General’s call to action to prevent and reduceunderage drinking. Washington DC: Office of the Surgeon General, 2007.
6. Ballesteros J, Duffy JC, Querejeta I, Arino J, Gonzalez-Pinto A. Efficacy ofbrief interventions for hazardous drinkers in primary care: systematicreview and meta-analyses. Alcohol Clin Exp Res 2004;28:608–18.
7. Burke BL, Arkowitz H, Menchola M. The efficacy of motivational interview-ing: a meta-analysis of controlled clinical trials. J Consult Clin Psychol2003;71:843–61.
8. Cuijpers P, Riper H, Lemmers L. The effects on mortality of brief interventionsfor problem drinking: a meta-analysis. Addiction 2004;99:839–45.
9. Apodaca TR, Miller WR. A meta-analysis of the effectiveness of bibliother-apy for alcohol problems. J Clin Psychol 2003;59:289–304.
0. Moyer A, Finney JW, Swearingen CE, Vergun P. Brief interventions for alcoholproblems: a meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction 2002;97:279–92.
1. Raistrick D, Heather N, Godfrey C. Review of the effectiveness of treatmentfor alcohol problems. London: National Treatment Agency for SubstanceMisuse, 2006.
2. Carey KB, Scott-Sheldon LA, Carey MP, DeMartini KS. Individual-levelinterventions to reduce college student drinking: a meta-analytic review.Addict Behav 2007;32:2469–94.
3. Ehrlich PF, Haque A, Swisher-McClure S, Helmkamp J. Screening and briefintervention for alcohol problems in a university student health clinic. J AmColl Health 2006;54:279–87.
4. Larimer ME, Cronce JM. Identification, prevention, and treatment revis-ited: individual-focused college drinking prevention strategies 1999–2006.Addict Behav 2007;32:2439–68.
5. White HR. Reduction of alcohol-related harm on U.S. college campuses: theuse of personal feedback interventions. Int J Drug Policy 2006;17:310–9.
6. Kaner EF, Lock CA, McAvoy BR, Heather N, Gilvarry E. A RCT of threetraining and support strategies to encourage implementation of screeningand brief alcohol intervention by general practitioners. Br J Gen Pract1999;49:699–703.
7. Moyer A, Finney JW. Brief interventions for alcohol problems: factors thatfacilitate implementation. Alcohol Res Health 2005;28:44–50.
8. Anderson P. The risk of alcohol [dissertation]. Nijmegen, The Nether-lands: Radboud University, 2003.
9. Andrews G, Issakidis C, Sanderson K, Corry J, Lapsley H. Utilising surveydata to inform public policy: comparison of the cost-effectiveness oftreatment of ten mental disorders. Br J Psychiatry 2004;184:526–33.
0. Cunningham JA, Breslin FC. Only one in three people with alcohol abuseor dependence ever seek treatment. Addict Behav 2004;29:221–3.
1. Walters ST, Neighbors C. Feedback interventions for college alcoholmisuse: what, why and for whom? Addict Behav 2005;30:1168–82.
2. Chan KK, Neighbors C, Gilson M, Larimer ME, Alan MG. Epidemiologicaltrends in drinking by age and gender: providing normative feedback toadults. Addict Behav 2007;32:967–76.
3. Larimer ME, Turner AP, Anderson BK, et al. Evaluating a brief alcoholintervention with fraternities. J Stud Alcohol 2001;62:370–80.
4. Marlatt GA, Baer JS, Kivlahan DR, et al. Screening and brief interventionfor high-risk college student drinkers: results from a 2-year follow-upassessment. J Consult Clin Psychol 1998;66:604–15.
5. Borsari B, Carey KB. Descriptive and injunctive norms in college drinking:a meta-analytic integration. J Stud Alcohol 2003;64:331–41.
6. Borsari B, Carey KB. Peer influences on college drinking: a review of theresearch. J Subst Abuse 2001;13:391–424.
7. Miller WR, Toscova RT, Miller JH, Sanchez V. A theory-based motivationalapproach for reducing alcohol/drug problems in college. Health EducBehav 2000;27:744–59.
8. Lewis MA, Neighbors C, Oster-Aaland L, Kirkeby BS, Larimer ME. Indi-cated prevention for incoming freshmen: personalized normative feedbackand high-risk drinking. Addict Behav 2007;32:2495–508.
9. Miller WR, Rollnick S. Motivational interviewing: preparing people forchange. New York: Guilford Press, 2002.
0. Cunningham JA, Humphreys K, Koski-Jannes A, Cordingley J. Internet andpaper self-help materials for problem drinking: is there an additive effect?Addict Behav 2005;30:1517–23.
1. Cunningham JA, Wild TC, Bondy SJ, Lin E. Impact of normative feedbackon problem drinkers: a small-area population study. J Stud Alcohol2001;62:228–33.
2. Chiauzzi E, Green TC, Lord S, Thum C, Goldstein M. My student body: ahigh-risk drinking prevention web site for college students. J Am CollHealth 2005;53:263–74.
3. Cochrane Collaboration. Cochrane handbook for systematic reviews of
interventions. Oxford: Cochrane Collaboration, 2008.54 American Journal of Preventive Medicine, Volume 36, Num
4. Beich A, Thorsen T, Rollnick S. Screening in brief intervention trialstargeting excessive drinkers in general practice: systematic review andmeta-analysis. BMJ 2003;327:536–42.
5. Bertholet N, Daeppen JB, Wietlisbach V, Fleming M, Burnand B. Reduc-tion of alcohol consumption by brief alcohol intervention in primary care:systematic review and meta-analysis. Arch Intern Med 2005;165:986–95.
6. Bien TH, Miller WR, Tonigan JS. Brief interventions for alcohol problems:a review. Addiction 1993;88:315–35.
7. Emmen MJ, Schippers GM, Bleijenberg G, Wollersheim H. Effectiveness ofopportunistic brief interventions for problem drinking in a general hospi-tal setting: systematic review. BMJ 2004;328:318.
8. Gould RA, Clum GA. A meta-analysis of self-help treatment approaches.Clin Psychol Rev 1993;13:169–86.
9. Kahan M, Wilson L, Becker L. Effectiveness of physician-based interven-tions with problem drinkers: a review. CMAJ 1995;152:851–9.
0. Mains JA, Scogin FR. The effectiveness of self-administered treatments: apractice-friendly review of the research. J Clin Psychol 2003;59:237–46.
1. Miller WR, Wilbourne PL. Mesa Grande: a methodological analysis of clinicaltrials of treatments for alcohol use disorders. Addiction 2002;97:265–77.
2. Poikolainen K. Effectiveness of brief interventions to reduce alcohol intake inprimary health care populations: a meta-analysis. Prev Med 1999;28:503–9.
3. Wilk AI, Jensen NM, Havighurst TC. Meta-analysis of randomized controltrials addressing brief interventions in heavy alcohol drinkers. J Gen InternMed 1997;12:274–83.
4. Agostinelli G, Brown JM, Miller WR. Effects of normative feedback onconsumption among heavy drinking college students. J Drug Educ1995;25:31–40.
5. Collins SE, Carey KB, Sliwinski MJ. Mailed personalized normative feed-back as a brief intervention for at-risk college drinkers. J Stud Alcohol2002;63:559–67.
6. Cunningham JA, Koski-Jannes A, Wild TC, Cordingley J. Treating alcoholproblems with self-help materials: a population study. J Stud Alcohol2002;63:649–54.
7. Doumas DM, Hannah E. Preventing high-risk drinking in youth in theworkplace: a web-based normative feedback program. J Subst Abuse Treat2008;34:263–71.
8. Juarez P, Walters ST, Daugherty M, Radi C. A randomized trial ofmotivational interviewing and feedback with heavy drinking college stu-dents. J Drug Educ 2006;36:233–46.
9. Kypri K, Saunders JB, Williams SM, et al. Web-based screening and briefintervention for hazardous drinking: a double-blind randomized con-trolled trial. Addiction 2004;99:1410–7.
2. Neighbors C, Larimer ME, Lewis MA. Targeting misperceptions of descrip-tive drinking norms: efficacy of a computer-delivered personalized norma-tive feedback intervention. J Consult Clin Psychol 2004;72:434–47.
1. Neighbors C, Lewis MA, Bergstrom RL, Larimer ME. Being controlled bynormative influences: self-determination as a moderator of a normativefeedback alcohol intervention. Health Psychol 2006;25:571–9.
2. Walters ST, Bennett ME, Miller JH. Reducing alcohol use in collegestudents: a controlled trial of two brief interventions. J Drug Educ2000;30:361–72.
3. Walters ST, Vader AM, Harris TR. A controlled trial of web-based feedbackfor heavy drinking college students. Prev Sci 2007;8:83–8.
4. Wild TC, Cunningham JA, Roberts AB. Controlled study of brief person-alized assessment-feedback for drinkers interested in self-help. Addiction2007;102:241–50.
5. Lipsey MW, Wilson DB. Practical meta-analysis. Thousand Oaks CA: SagePublications, 2001.
6. Kraemer HC, Morgan GA, Leech NL, Gliner JA, Vaske JJ, Harmon RJ.Measures of clinical significance. J Am Acad Child Adolesc Psychiatry2003;42:1524–9.
7. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistencyin meta-analyses. BMJ 2003;327:557–60.
8. Saunders JB, Aasland OG, Babor TF, Defuentes-Merillas L, Grant M.Development of the alcohol use disorders identification test (AUDIT):WHO collaborative project on early detection of persons with harmfulalcohol consumption—II. Addiction 1993;88:791–804.
9. Hedges LV, Waddington T. From evidence to knowledge to policy:research synthesis for policy formation. Rev Educ Res 1993;63:345–52.
0. Wilson DB. Meta-analyses in alcohol and other drug abuse treatmentresearch. Addiction 2000;95(3S):419–38.
1. Vasilaki EI, Hosier SG, Cox WM. The efficacy of motivational interviewingas a brief intervention for excessive drinking: a meta-analytic review.
Alcohol 2006;41:328–35.ber 3 www.ajpm-online.net

7
7
7
7
7
7
7
7
8
8
8
8
M
2. National Health Committee. Guidelines for recognising, assessing andtreating alcohol and cannabis abuse in primary care. Wellington, NewZealand: National Health Committee, 1999.
3. Heather N. Interpreting the evidence on brief interventions for excessivedrinkers: the need for caution. Alcohol 1995;30:287–96.
4. Hustad JT, Carey KB. Using calculations to estimate blood alcohol concen-trations for naturally occurring drinking episodes: a validity study. J StudAlcohol 2005;66:130–8.
5. Laforge RG, Borsari B, Baer JS. The utility of collateral informant assess-ment in college alcohol research: results from a longitudinal preventiontrial. J Stud Alcohol 2005;66:479–87.
6. Kypri K, Gallagher SJ, Cashell-Smith ML. An Internet-based surveymethod for college student drinking research. Drug Alcohol Depend2004;76:45–53.
7. Kypri K, Saunders JB, Gallagher SJ. Acceptability of various brief interven-
tion approach2003;38:626–arch 2009
8. Internet World Stats. World Internet users and population stats. 2008.www.internetworldstats.com./stats.htm.
9. Curry SJ. eHealth research and healthcare delivery beyond interventioneffectiveness. Am J Prev Med 2007;32:S127–S130.
0. Simon-Arndt CM, Hurtado SL, Patriarca-Troyk LA. Acceptance of web-based personalized feedback: user ratings of an alcohol misuse preventionprogram targeting U.S. Marines. Health Commun 2006;20:13–22.
1. Copeland J, Martin G. Web-based interventions for substance use disorders:a qualitative review. J Subst Abuse Treat 2004;26:109–16.
2. Musser J, O’Reilly T, the O’Reilly Radar Team. Web 2.0 principles and bestpractices: an O’Reilly radar report. 2006. radar.oreilly.com/research/web2-report.html.
3. LaBrie JW, Hummer JF, Neighbors C, Pedersen ER. Live interactivegroup-specific normative feedback reduces misperceptions and drinking incollege students: a randomized cluster trial. Psychol Addict Behav
14.
es for hazardous drinking among university students. Alcohol8.2008;22:141–8.84. Boyd GM, Faden V. Overview. J Stud Alcohol 2002;14:6–
Did you know?You can personalize the American Journal of Preventive Medicine website to meet your
individual needs.Visit www.ajpm-online.net today to see what else is new online!
Am J Prev Med 2009;36(3) 255
Copyright © 2022 FDOKUMEN