
Cultural concepts of tuberculosis and gender among the general population without tuberculosis in...
11
Cultural concepts of tuberculosis and gender among the general population without tuberculosis in rural Maharashtra, India Sachin R. Atre 1 , Abhay M. Kudale 1 , Sudhakar N. Morankar 1 , Sheela G. Rangan 1 and Mitchell G. Weiss 2 1 The Foundation for Research in Community Health, Pune, India 2 Swiss Tropical Institute, Basel, Switzerland Summary Gender-specific patterns of experience, meaning, and behaviour for tuberculosis (TB) require consideration to guide control programmes. To clarify concepts of gender, culture, and TB in a rural endemic population of Maharashtra, India, this study of 80 men and 80 women employed qualitative and quantitative methods of cultural epidemiology, using a locally adapted semi-structured Explanatory Model Interview Catalogue (EMIC) interviews are instruments for cultural epidemiological study of the distribution of illness-related experiences, meanings, and behaviours. This interview queried respondents without active disease about vignettes depicting a man and woman with typical features of TB. Emotional and social symptoms were frequently reported for both vignettes, but more often considered most distressing for the female vignette; specified problems included arranging marriages, social isolation, and inability to care for children and family. Job loss and reduced income were regarded most troubling for the male vignette. Men and women typically identified sexual experience as the cause of TB for opposite-sex vignettes. With wider access to information about TB, male respondents more frequently recommended allopathic doctors and specialty services. Discussion considers the practical significance of gender-specific cultural concepts of TB. keywords gender, tuberculosis, cultural epidemiology, stigma, help seeking, vulnerability Introduction Mycobacterium tuberculosis has infected one-third of the world’s population and imposes a global burden of an estimated 8 million new cases and 1.8 million deaths yearly (WHO 2002). The morbidity and mortality caused by tuberculosis (TB) currently place it among the highest priorities for disease control. India ranks first among high- burden countries for TB (Floyd et al. 2002), and every year 2.2 million people are added to the existing 15 million cases as 450 000 die (Misra el al. 2003). Although effective treatment for curing TB has been available for several decades, the control of TB in developing countries has been particularly complex. This is because, apart from structural problems, TB control efforts have been affected by socio- cultural barriers and ‘gender’, which influence TB at every stage from symptom awareness to outcome of the disease (Uplekar et al. 2001). Being sensitive areas to study, document and quantify, relevant socio-cultural aspects of control remain neglected by both policy makers and programme implementers. Gender perspective Many aspects of health policy and programming generally and specific features of TB control require careful attention to the role of gender (Vlassoff & Moreno 2002). The framework outlined by Uplekar et al. (2001) indicates the various ways in which gender may be relevant to strategies for control, suggesting a number of questions that require study. A gender perspective may help to clarify observed differences in rates of TB between men and women, accounting for social contexts of exposure and differential vulnerability to infection. Attention to gender should also help to explain known sex differences in the accessibility and utilization of health care resources, and to show how social meanings influence social responses and the stigma targeting people with TB. Social discrimination on the basis of TB disease status may result from various factors, such as perceived dangerousness and contagiousness, or adverse judgments that attribute the condition to immoral behaviour and blame the victim for acquiring the disease. Social determinants of support and rejection influence the ways that people in the general population without TB interact with people who are symptomatic from the disease (Vlassoff et al. 2000). Epidemiological evidence indicates that TB everywhere, including low- and middle-income countries, is more prevalent among men than women. This fact may be explained by gender differences in the social pattern of interactions, as men have more chance of social mixing Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004 1228 ª 2004 Blackwell Publishing Ltd
Transcript of Cultural concepts of tuberculosis and gender among the general population without tuberculosis in...
Cultural concepts of tuberculosis and gender among the general
population without tuberculosis in rural Maharashtra, India
Sachin R. Atre1, Abhay M. Kudale1, Sudhakar N. Morankar1, Sheela G. Rangan1 and Mitchell G. Weiss2
1 The Foundation for Research in Community Health, Pune, India2 Swiss Tropical Institute, Basel, Switzerland
Summary Gender-specific patterns of experience,meaning, andbehaviour for tuberculosis (TB) require consideration
to guide control programmes. To clarify concepts of gender, culture, and TB in a rural endemic population
ofMaharashtra, India, this study of 80men and 80women employed qualitative and quantitativemethods
of cultural epidemiology, using a locally adapted semi-structured ExplanatoryModel InterviewCatalogue
(EMIC) interviews are instruments for cultural epidemiological study of the distribution of illness-related
experiences, meanings, and behaviours. This interview queried respondents without active disease about
vignettes depicting a man and woman with typical features of TB. Emotional and social symptoms were
frequently reported for both vignettes, but more often considered most distressing for the female vignette;
specified problems included arranging marriages, social isolation, and inability to care for children and
family. Job loss and reduced income were regarded most troubling for the male vignette. Men and women
typically identified sexual experience as the cause of TB for opposite-sex vignettes. With wider access to
information about TB, male respondents more frequently recommended allopathic doctors and specialty
services. Discussion considers the practical significance of gender-specific cultural concepts of TB.
keywords gender, tuberculosis, cultural epidemiology, stigma, help seeking, vulnerability
Introduction
Mycobacterium tuberculosis has infected one-third of the
world’s population and imposes a global burden of an
estimated 8 million new cases and 1.8 million deaths
yearly (WHO 2002). The morbidity and mortality caused
by tuberculosis (TB) currently place it among the highest
priorities for disease control. India ranks first among high-
burden countries for TB (Floyd et al. 2002), and every year
2.2 million people are added to the existing 15 million
cases as 450 000 die (Misra el al. 2003). Although effective
treatment for curing TB has been available for several
decades, the control of TB in developing countries has been
particularly complex. This is because, apart from structural
problems, TB control efforts have been affected by socio-
cultural barriers and ‘gender’, which influence TB at every
stage from symptom awareness to outcome of the disease
(Uplekar et al. 2001). Being sensitive areas to study,
document and quantify, relevant socio-cultural aspects of
control remain neglected by both policy makers and
programme implementers.
Gender perspective
Many aspects of health policy and programming generally
and specific features of TB control require careful attention
to the role of gender (Vlassoff & Moreno 2002). The
framework outlined by Uplekar et al. (2001) indicates the
various ways in which gender may be relevant to strategies
for control, suggesting a number of questions that require
study.
A gender perspective may help to clarify observed
differences in rates of TB between men and women,
accounting for social contexts of exposure and differential
vulnerability to infection. Attention to gender should also
help to explain known sex differences in the accessibility
and utilization of health care resources, and to show how
social meanings influence social responses and the stigma
targeting people with TB. Social discrimination on the
basis of TB disease status may result from various factors,
such as perceived dangerousness and contagiousness, or
adverse judgments that attribute the condition to immoral
behaviour and blame the victim for acquiring the disease.
Social determinants of support and rejection influence the
ways that people in the general population without TB
interact with people who are symptomatic from the disease
(Vlassoff et al. 2000).
Epidemiological evidence indicates that TB everywhere,
including low- and middle-income countries, is more
prevalent among men than women. This fact may be
explained by gender differences in the social pattern of
interactions, as men have more chance of social mixing
Tropical Medicine and International Health
volume 9 no 11 pp 1228–1238 november 2004
1228 ª 2004 Blackwell Publishing Ltd

with people outside the home, including people with TB,
whereas women are more likely to spend most of their time
in the community around their homes (Liefooghe 1998).
Several studies have examined the influence of gender on
help-seeking behaviour for TB and indicate the need for a
better understanding of the role of behavioural factors in TB
control (Rangan&Uplekar 1998; Hudelson 1999).Women
appear more likely to neglect their illness until they become
too sick either to lead their normal lives or even to seek
medical help (Finch et al. 1991; WHO 1991). Review of
Liefooghe et al. (1997) shows that women face more
barriers to reach needed treatment for TB than men, which
can be attributed to cultural ideas about women’s more
restricted role in the home and community; this makes them
less likely to seek help outside. A study by Needham et al.
(2001) among pulmonary TB patients in Lusaka, Zambia,
reported greater lag time (including patient and provider
delay) fromsymptomonset to diagnosis forwomen.Delayed
help seeking (HS) arising from gender disparities in access
and perceived needs and entitlements to care may also play a
significant role in Maharashtra and other parts of India.
Stigma may delay HS and lead patients to drop out of
treatment. Because of their social vulnerability, women
may be especially susceptible to the impact of stigma.
Research in Kerala, India, suggests that stigma may
adversely influence participation in the DOTS pro-
grammes, resulting in poorer treatment outcomes, and this
effect of stigma may be more pronounced among women
(Balasubramanian et al. 2000).
Cultural epidemiology of tuberculosis
As a framework for studying the social determinants of
health problems, cultural epidemiology arose from efforts
to apply an integrated formulation of anthropological and
epidemiological principles to health research (Weiss 2001).
Cultural epidemiology is concerned not only with rates of
disorders but also the distribution of categories of illness-
related experience, meaning, and behaviour. Findings from
anthropological research identify the locally relevant
aspects of illness that influence risk and response, sug-
gesting a causal web of interactions linking culture, gender
and illness; cultural epidemiological study further examines
the findings of ethnographic study to clarify their distri-
bution of categories and their impact on TB control (Weiss
2001). Such socio-cultural health studies are concerned
with patterns of personal distress (PD), social stigma,
perceived causes (PC) and HS for TB. To study the patterns
of TB-related experience, meaning, and behaviour in the
general population, male and female vignettes depicting
typical features of TB have been used as the focus of
interview questions.
This report presents findings from socio-cultural study of
TB as it is explained in the general population. It was
conducted in villages of rural Pune District, Maharashtra,
India. The objective of this study was to specify the
distribution of TB-related illness experiences, meanings
and behaviours, examining categories of PD, PC, and HS
with reference to narrative contexts of respondents’
accounts, as reported by the general population of people
without TB. It also aimed to identify gender differences
among men and women interviewed with questions about
a vignette describing someone of the same sex as the
respondent and someone of the opposite sex.
Methodology
Setting and sample selection
Pune district is located in the western part of Maharashtra
State in India. The District TB Centre (DTC) is located in
Pune City and serves a population of about 3.6 million
people in rural areas and 2.7 million in urban areas. The
Revised National Tuberculosis Control Programme
(RNTCP), which follows the policy guidelines of the
WHO’s DOTS strategy, was implemented in the district in
October 1998. Although the annual case detection rate
remained 187 per 100 000 for India in the year 1999
(WHO 2001a), rates in rural areas were lower (nearly 70
per 100 000) (DTC 1999). The study took place at a time
when a major shift in the programme (from the former
National TB Programme to the RNTCP) was underway.
Rural areas were selected for the present study of gender
and TB, attentive to differential barriers to health services,
educational status of women, and access to household
resources. In rural areas of the district, farming is a
predominant occupation, followed by unskilled agri-
cultural labour. Women are housewives and also involved
in farm work on either family-owned or other’s land. To
earn a livelihood, a significant proportion of the male
population is moving in and out of crowded slum areas in
big cities such as Pune and Mumbai, which also presents a
threat of transmitting infectious diseases.
A total of 20 villages, where patients have been
registered and treated in the National TB Programme were
selected randomly for the study from six tehsil (subdistrict/
administrative units) of Pune District within a radius of
60 km from Pune city. To elicit community perceptions of
TB and people who have it, 160 respondents (80 men and
80 women) who personally and whose immediate family
members did not currently have active TB were studied
with EMIC interviews. A sample was drawn from these
villages using a multistage sampling procedure. The sex
and age distribution of the sample is specified in Table 1.
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
ª 2004 Blackwell Publishing Ltd 1229

EMIC interview for community study
EMIC interviews are instruments for assessing represen-
tations of illness or specified health problems from the
perspective of affected persons, their families, or (as in
this study) their community. These interviews were
developed and locally adapted in pilot testing, and the
research interviews were completed between November
1998 and June 1999. Female researchers interviewed
women respondents and male researchers interviewed
men. A systematic ‘spontaneous and probe’ methods
for eliciting responses to open-ended and prompted
queries was adapted. Response categories of PD, PC, and
HS that were coded from the narrative content of
answers to open-ended questions were designated spon-
taneous. Responses that were coded based on acknow-
ledgement or rejection of categories specified in the
question were designated probed. The EMIC interviews
studied patterns of distress, which referred not only to
the disease-specific symptoms, but also to the broader
range of effects of TB. Stigma, constituting an aspect of
the adverse social impact of the disease, was studied.
Perceived causes were elicited to examine respondents’
ideas about the meaning of TB. Recommendations for
HS, sources of information about TB, and personal
interactions with people with TB were studied to provide
a descriptive cultural epidemiological account suitable for
gender comparison.
The structure of the EMIC interview used in this study
is outlined in Appendix 1. The male and female
vignettes, depicting classical symptoms of TB in a local
cultural context, which were the reference for the EMIC
questions, are presented in Appendix 2. The interview
schedule was pretested in eight villages, and the initial
phase of pretesting provided an opportunity to train
interviewers. Subsequent pretesting with these trained
interviewers evaluated questions under field conditions.
Interview data consisting of codes that were marked on
the interview sheet and qualitative narrative accounts, were
maintained separately. An interviewer and a data recorder
participated in each interview, and the coding was
discussed for a consensus rating.
Analysis
Bivariate analysis using Epi Info, version 6 compared
responses concerning male and female vignettes for
categories of distress, stigma, PC, and other variables
elaborated in the EMIC interviews. Spontaneous and
probed responses, wherever applicable, were tabulated in
frequency tables. The Cochran-Armitage trend test was
used to test the significance of associations for cross-
tabulated data, acknowledging the greater prominence of
spontaneous, compared with probed responses. The
chi-square test was used for a single level of reporting
(e.g. most important perceived cause).
Qualitative gender differences were examined using the
MAXqda software program to compare coded text seg-
ments from the interview responses for male and female
vignettes and for men and women respondents. Coded text
segments, based on topics of the cultural epidemiological
framework studied with the EMIC interviews, were
retrieved from selected respondents to facilitate qualitative
comparison of narrative accounts, examining topics in
context.
Results
Sample characteristics
Among the 160 respondents, 62% were below 45 years
of age, with a mean age of 39.7 years (39.4 years for
women and 39.9 years for men). Most (88%) respond-
ents were married, and one-third (33%) of the respond-
ents were illiterate. Most (78%) women respondents
were engaged in household work, and many of these
were also engaged in unpaid labour on their family-
owned land. Most of the male respondents were involved
in farming, and others worked as unskilled labourers and
in small-scale merchandising.
Recognition of tuberculosis
The majority (62%) of respondents identified the health
problem depicted in the vignette as TB. Asthma, cough,
AIDS, and pneumonia were the other conditions reported
by the remaining respondents. Less than one in five (17%)
respondents could not specify any name for the health
problem depicted in the vignette, and there were no
differences in the responses of men and women
respondents.
Table 1 Sample distribution
Agegroup
(years)
Male vignette Female vignette
Menrespondents
(N ¼ 40)
Womenrespondents
(N ¼ 40)
Menrespondents
(N ¼ 40)
Womenrespondents
(N ¼ 40)
20–29 10 10 10 10
30–39 10 10 10 10
40–49 10 10 10 1050–59 10 10 10 10
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
1230 ª 2004 Blackwell Publishing Ltd
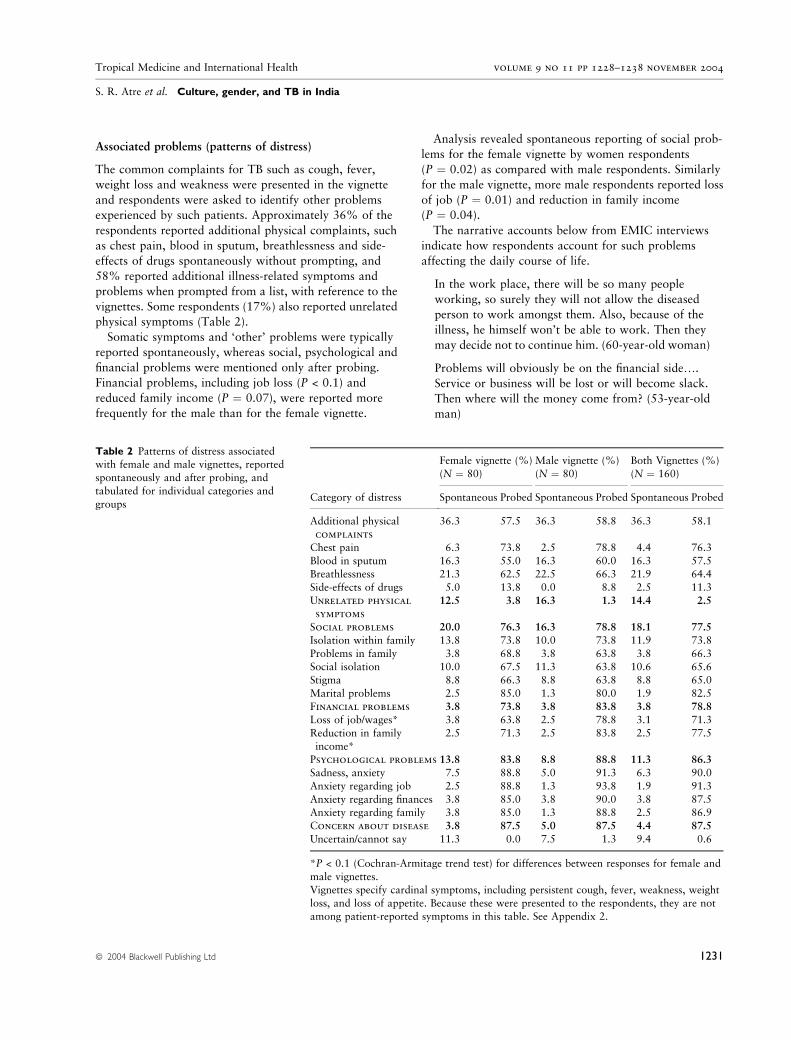
Associated problems (patterns of distress)
The common complaints for TB such as cough, fever,
weight loss and weakness were presented in the vignette
and respondents were asked to identify other problems
experienced by such patients. Approximately 36% of the
respondents reported additional physical complaints, such
as chest pain, blood in sputum, breathlessness and side-
effects of drugs spontaneously without prompting, and
58% reported additional illness-related symptoms and
problems when prompted from a list, with reference to the
vignettes. Some respondents (17%) also reported unrelated
physical symptoms (Table 2).
Somatic symptoms and ‘other’ problems were typically
reported spontaneously, whereas social, psychological and
financial problems were mentioned only after probing.
Financial problems, including job loss (P < 0.1) and
reduced family income (P ¼ 0.07), were reported more
frequently for the male than for the female vignette.
Analysis revealed spontaneous reporting of social prob-
lems for the female vignette by women respondents
(P ¼ 0.02) as compared with male respondents. Similarly
for the male vignette, more male respondents reported loss
of job (P ¼ 0.01) and reduction in family income
(P ¼ 0.04).
The narrative accounts below from EMIC interviews
indicate how respondents account for such problems
affecting the daily course of life.
In the work place, there will be so many people
working, so surely they will not allow the diseased
person to work amongst them. Also, because of the
illness, he himself won’t be able to work. Then they
may decide not to continue him. (60-year-old woman)
Problems will obviously be on the financial side….
Service or business will be lost or will become slack.
Then where will the money come from? (53-year-old
man)
Table 2 Patterns of distress associatedwith female and male vignettes, reported
spontaneously and after probing, and
tabulated for individual categories and
groupsCategory of distress
Female vignette (%)
(N ¼ 80)
Male vignette (%)
(N ¼ 80)
Both Vignettes (%)
(N ¼ 160)
Spontaneous Probed Spontaneous Probed Spontaneous Probed
Additional physical
complaints
36.3 57.5 36.3 58.8 36.3 58.1
Chest pain 6.3 73.8 2.5 78.8 4.4 76.3
Blood in sputum 16.3 55.0 16.3 60.0 16.3 57.5Breathlessness 21.3 62.5 22.5 66.3 21.9 64.4
Side-effects of drugs 5.0 13.8 0.0 8.8 2.5 11.3
Unrelated physical
symptoms
12.5 3.8 16.3 1.3 14.4 2.5
Social problems 20.0 76.3 16.3 78.8 18.1 77.5
Isolation within family 13.8 73.8 10.0 73.8 11.9 73.8
Problems in family 3.8 68.8 3.8 63.8 3.8 66.3Social isolation 10.0 67.5 11.3 63.8 10.6 65.6
Stigma 8.8 66.3 8.8 63.8 8.8 65.0
Marital problems 2.5 85.0 1.3 80.0 1.9 82.5
Financial problems 3.8 73.8 3.8 83.8 3.8 78.8
Loss of job/wages* 3.8 63.8 2.5 78.8 3.1 71.3
Reduction in family
income*
2.5 71.3 2.5 83.8 2.5 77.5
Psychological problems 13.8 83.8 8.8 88.8 11.3 86.3
Sadness, anxiety 7.5 88.8 5.0 91.3 6.3 90.0
Anxiety regarding job 2.5 88.8 1.3 93.8 1.9 91.3
Anxiety regarding finances 3.8 85.0 3.8 90.0 3.8 87.5Anxiety regarding family 3.8 85.0 1.3 88.8 2.5 86.9
Concern about disease 3.8 87.5 5.0 87.5 4.4 87.5
Uncertain/cannot say 11.3 0.0 7.5 1.3 9.4 0.6
*P < 0.1 (Cochran-Armitage trend test) for differences between responses for female and
male vignettes.Vignettes specify cardinal symptoms, including persistent cough, fever, weakness, weight
loss, and loss of appetite. Because these were presented to the respondents, they are not
among patient-reported symptoms in this table. See Appendix 2.
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
ª 2004 Blackwell Publishing Ltd 1231

What will happen to the family and her children?
What will happen to her life? Since she will be unable
to work outside, she has to work in the home. She
may start feeling that if I was in good health, I would
have earned money for the family and me. (53-year-
old woman)
Stigma: indicators of stigma
Nine interview questions were formulated as indicators of
stigma. Most respondents (85%) acknowledged dimin-
ished self-esteem as a feature of the illness depicted in
the vignettes, explaining that such people think less of
themselves and that they hide their disease from others
(Table 3). A 38-year-old man explained why disclosing TB
was a greater problem for women:
A woman will hide the disease more than a man
because she will have a fear of social isolation and less
respect from others.
About half (48%) of the respondents said that people are
likely to treat such a person with TB in ways that would be
embarrassing. About 60% of respondents anticipated
support from a spouse for both vignettes. The narrative
accounts of social responses indicated that a woman was
obliged to support her husband with such a disease, but a
man did not have the same obligation to support his wife.
In fact, many considered the man free to leave her, or he
could send her to her parent’s home. Some women, like the
middle-aged respondent quoted below, resented that:
Men don’t have any problem, but a woman has to
handle everything. Even if her husband is ill, she has
to look after him and treat him well because her
husband is the only support for lifetime and to take
care of husband is her duty. But she can’t expect this
kind of help from her husband if she falls ill. Such is
the fate of women.
Problems in an ongoing marriage were reported more for
the female vignette (P ¼ 0.09). In addition, qualitative
accounts emphasized the impact of the illness on the ability
of a woman to marry. People did not want their sons to
marry a girl who has had TB because of fear of the disease
getting passed on to her children. It is widely accepted that
when a girl develops TB after her marriage, she is often sent
back to her natal house, and the man will then marry
another girl. Women were not more concerned, however,
about problems arranging a marriage, and it appeared that
among respondents, more men identified this as a potential
problem (P ¼ 0.1).
Perceived causes
Respondents identified various categories of PC, which
were grouped under nine broad headings, and these
findings are summarized in Table 4. Most respondents
identified categories under the headings ingestion (89%)
and health-injury-illness (97%) as common causes for TB
for both vignettes.
Addictions (smoking, alcohol, and drugs) as a cause of
TB, were specified significantly more often for the male
vignette. However, significantly more male respondents
also mentioned the same causes for the illness in the
female vignette (P < 0.0001) also. Prior health care
problems or injuries, environmental factors and sexual
experiences were commonly reported as the most
important cause of TB. In response to the interviews
based on the female vignette, significantly more women
than men reported health-illness-injury (30% vs. 7.5%)
and psychological factors (17.5% vs. 0%) as the most
important perceived cause. Although women specified a
psychological cause more frequently for the female
vignette, no men identified a psychological cause as most
important for either of the vignettes.
More male respondents mentioned ‘contact’ as a cause in
case of female vignette than women (P ¼ 0.004). Men
more frequently identified sexual experience as the most
important perceived cause for the female vignettes than
women respondents (P ¼ 0.05), and both men and women
more frequently identified sexual experience as a cause in
the opposite sex. For some respondents sexual relations in
the absence of disease were sufficient to transmit TB, but
Table 3 Indicators of stigma for female and male vignettes
Stigma variables
Female vignette
(N ¼ 80) (%)
Male vignette
(N ¼ 80) (%)
Yes Possibly Yes Possibly
Hide disease 75.0 6.3 81.3 7.5Think less of self 85.0 2.5 85.0 3.8
Community thinks less
of patient
68.8 5.0 67.5 12.5
Community thinks lessof family
42.5 8.8 35.0 12.5
Hurting behaviour 32.5 21.3 28.8 15.0
Problems in arranging
marriage
15.0 27.5 12.5 36.3
Spouse support 57.5 37.5 58.8 28.8
Problems in current
marriage
10.0 16.3 21.3 17.5
Problems in family
to marry
23.8 27.5 28.8 22.5
There were no statistically significant differences between
responses for female and male vignettes.
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
1232 ª 2004 Blackwell Publishing Ltd

Table 4 Perceived causes associated with
female and male vignettes, reported
spontaneously and after probing, andtabulated for individual categories and
groupsPerceived causes
Female vignette (%)(N ¼ 80)
Male vignette (%)(N ¼ 80)
Both vignettes (%)(N ¼ 160)
Spontaneous Probed Spontaneous Probed Spontaneous Probed
Uncertain/cannot say 21.3 00.0 20.0 0.0 20.6 0.0
Ingestion 27.5 56.3 33.8 60.0 30.6 58.1
Food 12.5 18.8 13.8 23.8 13.1 21.3
Water 3.8 22.5 10.0 21.3 6.9 21.9
Contaminated food/water
6.3 47.5 8.8 33.8 7.5 40.6
Contaminated food
vector
2.5 48.8 2.5 45.0 2.5 46.9
Alcohol* 3.8 27.5 18.8 62.5 11.3 45.0
Smoking* 2.5 27.5 13.8 67.5 8.1 47.5
Tobacco/misheri 8.8 51.3 11.3 58.8 10.0 55.0
Abused drugs* 2.5 35.0 8.8 66.3 5.6 50.6
Health-illness-injury 33.8 62.3 26.3 71.3 30.0 66.9
Prescribed medicines 2.5 10.0 3.8 7.5 3.1 8.8
Injury/accident 0.0 18.8 1.3 16.3 0.6 17.5Insect bite 0.0 22.5 1.3 21.3 0.6 21.9
Physical exertion 1.3 30.0 1.3 31.3 1.3 30.6
Blood problems 0.0 72.5 3.8 82.5 1.9 77.5
Prior illness 18.8 47.5 16.3 60.0 17.5 53.8Pregnancy/child birth 1.3 35.0 0.0 21.3 0.6 28.1
Congenital 3.8 36.3 0.0 38.8 1.9 37.5
Weakness 15.0 57.5 11.3 58.8 13.1 58.1
Heredity 12.5 40.0 2.5 57.5 7.5 48.8
Psychological 12.5 40.0 2.5 57.5 7.5 48.8
Mental stress 3.8 35.0 2.5 30.0 3.1 32.5
Mind worry 8.8 41.3 7.5 37.5 8.1 39.4
Environmental 26.3 70.0 28.8 70.0 27.5 70.0
Sanitation 7.5 63.8 5.0 71.3 6.3 67.5
Air pollution 2.5 52.5 2.5 60.0 2.5 56.3Personal hygiene 3.8 70.0 3.8 75.0 3.8 72.5
Germ/infection 8.8 80.0 11.3 67.5 10.0 73.8
Contamination/contact 6.3 65.0 6.3 63.8 6.3 64.4
Proximity to patient 8.8 72.5 12.5 70.0 10.6 71.3Air borne 2.5 65.0 5.0 62.5 3.8 63.8
Traditional/cultural 6.3 50.0 6.3 47.5 6.3 48.8
Pollution 0.0 33.8 0.0 30.0 0.0 31.9Ayurvedic concept 0.0 27.5 0.0 27.5 0.0 27.5
Heat/cold in the body 5.0 25.0 2.5 28.8 3.8 26.9
Climate 1.3 16.3 3.8 15.0 2.5 15.6
Sexual experience 16.3 56.3 15.0 45.0 15.6 50.6
Supernatural-karma-
traditional
11.3 32.5 6.3 42.5 8.8 37.5
Karma 8.8 30.0 5.0 35.0 6.9 32.5
Fate/god/stars 10.0 31.3 5.0 40.0 7.5 35.6
Supernatural 1.3 13.8 0.0 26.3 0.6 20.0
Evil eye 0.0 5.0 0.0 10.0 0.0 7.5
*P < 0.01 (Cochran-Armitage trend test) for differences between responses for maleand female vignettes.
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
ª 2004 Blackwell Publishing Ltd 1233

for others, sex was a risk to the other party only if one had
the disease:
If both are clear then there will not be any problem,
but if one is suffering from the illness then the other
gets affected. (58-year-old woman)
Some of the categories were specified only after probing;
for example, respondents tended not to identify heredity as
a cause unless asked directly. More male respondents
mentioned heredity as a cause of TB for the female vignette
(P ¼ 0.1) and vice versa (P ¼ 0.09). Some respondents
explained that a pregnant woman with a cough might pass
the disease to the foetus:
If a mother has it, then it will pass on to the next
generation. Once it is in the family, it will continue.
(28-year-old woman)
During pregnancy, if there is cough and that remains
for a long time, then it will result in this illness. (40-
year-old woman)
The following account indicates how germs are under-
stood in the community to cause TB, and how they
produce symptoms:
If there are more holes in the lungs, then it will cause
tuberculosis. The person will get cough. Germs will be
there and they will cause swelling. (50-year-old man)
Although there was no difference in reports for male and
female vignettes, more women respondents identified
supernatural and karma-related causes of TB for the male
vignette (P ¼ 0.001).
Outcome of illness
Respondents were asked about the outcome of the disease
generally, and specifically with and without treatment.
Most respondents expressed confidence in the ability of the
available treatment to cure the disease, stating they
definitely thought it could be cured (60%) or indicating
that possibility even if they were not certain of it (29%).
Cure was not just a matter of taking medicines, however,
and many respondents noted that a wholesome diet was an
essential component of effective treatment (Table 5):
After taking an X-ray or consulting the doctor, we can
say that (she has TB). If she starts eating food, one may
expect 50–75% improvement. (28-year-old woman)
By taking regular medicines in consultation with the
doctor, a patient can definitely be cured. His body
and health will improve, paleness will reduce and
freshness will appear again. He can then go and mix
with the people in the community. (A male
respondent)
Men were more optimistic in their expectations of a cure
for the condition for both male and female vignettes. For
the male vignette, 75% of men were more definite about
prospects for cure and 20% indicated the possibility,
compared with 40% of women who were definite about
prospects for cure and 50% who indicated the possibility
(P < 0.01). Men were also more confident about cure for
the female vignette, 75% responding definitely curable and
17% possibly, compared with 50% of women who were
definite and 30% who indicated the possibility of cure
(P < 0.05):
There will be an improvement in the condition, and
we understand that from reduced cough and less
breathlessness. The disease will be cured in some
cases, but it may not be cured in others. (A female
respondent)
Among the indications of cure, respondents specified
relief from somatic symptoms, restoration of appetite, and
the return of a healthy look on the face. Some respondents
emphasized more technical clinical indicators, such as an
improvement in the condition on X-ray; some also referred
to the authority of the doctor, specifying a doctor’s
certification as an indication of cure. A middle-aged
woman said:
After taking an X-ray, the doctor has to tell us. How
can we tell from the face only? If the condition is
really bad, then one can recognize it from the face.
Otherwise only a photo (X-ray) can show the scar on
the rib.
Table 5 Most important perceived cause associated with
female and male vignettes
Perceived cause
Female vignette (%)
(N ¼ 80)
Male vignette (%)
(N ¼ 80)
Women Men Both Women Men Both
Ingestion 7.5 12.0 9.8 7.5 20.0 13.8
Health/injury/illness 30.0 7.5 18.8* 22.5 10.0 16.3
Heredity 5.0 7.5 6.3 2.5 0.0 1.3Psychological 17.5 0.0 8.8* 5.0 0.0 2.5
Environmental 7.5 20.0 13.8 15.0 25.0 20.0
Traditional/cultural 5.0 2.5 3.8 0.0 2.5 1.3
Sexual experience 7.5 35.0 21.3* 10.0 25.0 17.5Karma/traditional 5.0 5.0 5.0 07.5 7.5 7.5
Uncertain 12.5 10.0 11.3 30.0 5.0 17.5*
*P < 0.01 (chi-square test) for differences between women and
male respondents.
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
1234 ª 2004 Blackwell Publishing Ltd

When they spoke about the medical authority of cure,
respondents typically referred to the X-ray, rather than
sputum examination, which has become the official diag-
nostic method of the RNTCP.
Recommended help seeking
When asked to recommend sources of help for the people
depicted in the vignettes, two-thirds of the respondents
recommended government sources and one-third recom-
mended private doctors for both male and female vignettes.
Compared with women, men clearly preferred the higher
levels of health services, such as rural hospital, TB hospital,
District TB Centre, and government hospital (Table 6). The
reasons for recommending private practitioners were their
easy accessibility and confidence in their effectiveness,
often discussed in their narrative account with reference to
prior positive experience. The lower cost of government
services, however, made them attractive. Seeking help from
a health care provider was not necessarily sufficient in
itself, and for some respondents a broader cultural context
of religious support was important: ‘First we must look to
god, and then we will ask to go to the clinic’, a woman
explained.
Younger people rejected old ideas that discriminated
against women, including assumptions that they should
return to their parents’ house, or that it was unnecessary to
spend money on treatment for a woman. Although such
respondents personally rejected such views, they acknow-
ledged that these were common ideas and values in the
community.
Sources of information
Respondents were asked how people came to know about
the health problems we were asking about. Significantly
more men (74%) than women (15%) identified the mass
media (mainly television and radio) as sources of infor-
mation about TB (P < 0.05). A common reason by which
respondents accounted for this gender difference were that
women’s work leaves little time and less opportunity for
access to mass media. Women were also generally
considered more likely to be illiterate and less mobile.
More men (31%) also identified health services as a source
of information than women (14%), and from interactions
with others in the community (Table 7). A middle-aged
male respondent reported:
I have seen and heard the advertisements (about TB)
on TV and radio. I have also read about this in
government hospitals.
Women were thought more likely to learn about the
disease from their personal and local experience and
interactions with affected family members, neighbours, or
others in the community:
I have seen people who have died because of TB.
(33-year-old woman)
When I was staying in Pune, one of the boys from our
relative’s family was having it. My father also had TB
earlier. I came to know about the disease from going
to the hospital to visit them. (A female respondent)
Table 6 Help seeking reported for female and male vignettes
Help seeking
Female vignette
(N ¼ 80) (%)
Male vignette
(N ¼ 80) (%)
Women Men Both Women Men Both
Home remedies 35.0 32.5 33.8 37.5 12.5 25.0
Self-medication 30.0 30.0 30.0 45.0 27.5 36.3Pharmacist 32.5 30.0 31.3 45.0 30.0 37.5
Health worker 67.5 77.5 72.5 70.0 75.0 72.5
Primary health
centre/subcentre
57.5 35.0 46.3 47.5 35.0 41.3
Rural hospital 40.0 80.0 60.0** 40.0 77.5 58.8**
Government hospital 15.0 72.5 43.8** 30.0 65.0 47.5**
DTC 55.0 77.5 66.3* 52.5 72.5 62.5*
TB hospital 30.0 72.5 51.3** 42.5 65.0 53.8*Public sector 2.5 0.0 1.3 0.0 0.0 0.0
Private doctor-
specialist
0.0 0.0 0.0 0.0 2.5 1.3
Private sector-no
qualification
17.5 32.5 25.0 30.0 30.0 30.0
Private hospital-
nursing home
10.0 20.0 15.0 10.0 15.0 12.5
Traditional healer 37.5 30.0 33.8 37.5 22.5 30.0
Faith healer 25.0 22.5 23.8 30.0 25.0 27.5
*P < 0.05 and **P < 0.01 (chi-square test) for differences
between men and women respondents.
Table 7 Sources of information about TB
Sources
Women (%)
(N ¼ 80)
Men (%)
(N ¼ 80)
Both (%)
(N ¼ 160)
Mass media 15.1 73.9 44.4**
Formal education 2.5 7.5 5.0
Reading material 3.8 11.3 7.5People around 37.5 60.1 48.8**
TB patients 23.8 20.0 21.9
Experience 36.3 13.8 25.0
Health personnel 13.8 31.3 22.5*
*P < 0.05 and **P < 0.01 (chi-square test) for differencesbetween men and women respondents.
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
ª 2004 Blackwell Publishing Ltd 1235

Discussion
This study of the cultural epidemiology of TB-related
illness experience, meaning, and behaviour highlights
cultural and gender-specific features of TB in the general
population of endemic village communities of Pune
District in western Maharashtra. People were well aware
of the condition; they could identify it from the symptoms
depicted in our research vignettes, and they regarded TB
as a serious health problem. Physical suffering was the
hallmark of the disease. Social and emotional problems,
however, were also commonly reported as important
features of the overall illness experience, but mostly in
response to probe questions about this aspect of the
illness, rather than reported in spontaneous answers to
open-ended queries. Social and emotional suffering also
conformed to gender roles and associations – financial
problems for men, and emotional and social problems
for women were mentioned. The findings indicate a
substantial gender-specific hidden burden of social and
psychological suffering, which is a feature of TB, as
it is with other chronic stigmatized conditions, that
may often be ignored in clinical consultations (WHO
2001b).
Complementing our assessment of illness experience, the
meaning and PC of the disease also identified gender-
specific findings consistent with other studies. Women
respondents attributed the disease depicted in the female
vignette to psychological problems, but none of the male
respondents reported psychological causes for either of the
vignettes.
Men more frequently attributed TB to sexual experien-
ces and socially unacceptable behaviour, particularly for
the female vignette. This association between TB and
sexual behaviour has been identified in other studies and in
other settings. Nichter (1994) reported excessive and
inappropriate sex as a perceived cause of TB in the
Philippines; Uplekar and Rangan (1996) found that soci-
ally unacceptable behaviour, like sex with prostitutes and
menstruating women, was associated with the onset of TB
in western India. Such ideas provide a basis for community
ideas for stigmatizing women, justifying a man’s right to
desert his wife and remarry because according to this view,
she is not merely a passive victim but also blameworthy.
The cross-gender mistrust of sexual promiscuity, although
directed more by men against women, was also directed by
women against men, providing a rationale for women to
chastise the sexual promiscuity of their men, for when it is
identified as a cause. Such findings indicate the moral basis
of risk and vulnerability to the disease, which justifies and
supports community responses to TB, both support and
stigmatization.
Some PC persist as a tacit undercurrent in the meaning of
TB, acknowledged only after probing. Heredity reflects a
particular aspect of contagiousness and contamination, not
just from person to person, as indicated by reports of
spread by contact, but also across generations from parent
to child. Such concerns naturally affect marriage prospects,
and they are especially troubling in a culture where families
are responsible for arranging their children’s marriage.
Typically we expect this worry about prospects for
arranging a marriage to be more of a concern for women.
Although qualitative accounts reflected this, we did not
observe more frequent reports of it in the female vignette,
as expected.
Concerning the dissemination of information about TB
in the community, and especially with reference to public
health priorities for early HS, findings showed that men
were better served by formal media. More limited access
to public health educational communications about TB
may contribute to women’s shame and self-blame in poor
settings, and also to patient delays in HS. More women
had fewer definite ideas about the cause of TB for men,
and they more frequently referred to karma, which
typically is used as a cultural metaphor for fate, literally,
the effect of deeds in a previous life, when other causes
cannot be specified. Such findings suggest the need for
innovative approaches to disseminate public health infor-
mation about TB to women, perhaps using women’s
groups or activities of the primary health care system
more effectively.
With regard to advice about HS, male respondents more
frequently than women recommended higher levels of
health care services. Both the financial dependence of
women on male decision-makers in the household for
access to outside health care, and lack of information
about the need for treatment in response to symptoms of
TB may have contributed to lower rates of women
recommending appropriate levels of health seeking for
symptoms of recognized TB. A less optimistic response of
women concerning the effectiveness of treatment and
prospects for cure may also reflect limited access to
education and broader gender-based disadvantage, inclu-
ding limited expectations of social supports for women,
and perhaps personal experience in the community
suggesting poorer outcomes for women who present late
for treatment.
Studies suggest, however, that in the face of limited
access, women who do eventually come for treatment may
have better rates of treatment adherence and outcome
(Johansson et al. 1999). Smith (1994) explains that such
findings may reflect the persistence of those particular
women who manage to overcome the barriers of limited
access to health care. Insofar as our findings indicate
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
1236 ª 2004 Blackwell Publishing Ltd

greater socio-economic barriers faced by women and the
greater social and emotional burden of TB borne by them,
they are consistent with Smith’s argument. The more
specific questions about gender differences in rates of TB,
access to treatment, diagnosis, treatment adherence, and
outcome, however, constitute a broader agenda for gender
studies of TB well beyond the scope of this report.
This cultural epidemiological study has demonstrated
gender-specific features of the community-perceived bur-
den of TB affecting men and women and reported by them.
The perceptions of people without TB in the village
communities of our study reflect a mixture of optimism
regarding the availability of treatment for TB and scepti-
cism about the possibility of prevailing over a disease that
not only burdens affected individuals, but also their
families and even the next generation. Although we found
evidence that some respondents rejected the stigma and
social discrimination traditionally associated with TB (e.g.
sending married women back to their natal homes), the
range of community responses also highlights the persisting
vulnerability of women and the hidden emotional and
social burden of TB.
Our findings indicate views of the general population
suggesting limited community support for women with TB,
their limited access to treatment, and more limited access
to information about TB from informed sources. These are
crucial considerations for TB control, and our findings
should also be complemented with studies of people with
TB and health care providers who treat them in these
communities. Efforts to enhance the gender sensitivity of
health services and to promote community awareness of
TB will nevertheless benefit from attention to the findings
presented here.
Acknowledgements
Financial support of the Swiss Agency for Development
and Cooperation is gratefully acknowledged. We also
thank the following persons for their assistance and
contributions to the research: Dr N.H. Antia, Director,
FRCH, for encouragement throughout; Ms Deepali
Deshmukh, Dr Nishi Suryawanshi and Mr Omprakash
Patil for inputs in the design and initial field research
activities; Dr N.F. Mistry for support in developing the
manuscript; Prof. R.K. Mutatkar, Honorary Professor,
Health Sciences, University of Pune and Dr M.W.
Uplekar, Medical Officer, WHO Stop TB Programme,
for inputs in developing the study and consultation
throughout; and Dr A.K. Chakraborty, Epidemiology
Analyst, Bangalore, and other members of the research
advisory committee organized by FRCH for their review
and consultation. We appreciate the cooperation of the
State and District TB Officers and Health staff, Patients
and Community respondents.
References
Balasubramanium VN, Oommen K & Samuel R (2000) DOT or
not? Direct observation of anti-tuberculosis treatment and pa-
tient outcomes, Kerala State, India. The International Journal of
Tuberculosis and Lung Disease 4 (Suppl. 5), 409–413.
DTC (1999) Quarterly Reports. District Tuberculosis Centre,
Pune, India.
Finch PJ, Millard FJ & Maxwell JD (1991) Risk of tuberculosis in
immigrant Asians: culturally acquired immunodeficiency?
Thorax 46 (Suppl. 1), 1–5.
Floyd K, Blanc L & Raviglione M (2002) Resources required for
global tuberculosis control. Science 295, 2040–2041.
Hudelson P (1999) Gender issues in the detection and treatment of
tuberculosis. In: Tuberculosis: an Interdisciplinary Perspective
(eds JD Porter & JM Grange) Imperial College Press, London,
339–355.
Misra R, Chatterjee R & Rao S (2003) India Health Report.
Oxford University Press, New Delhi, India.
Johansson E, Long N, Divan V & Winkvist A (1999) Attitudes to
compliance with tuberculosis treatment among men and women
in Vietnam. The International Journal of Tuberculosis and Lung
Disease 3 (Suppl. 10), 862–868.
Liefooghe R (1998) Gender differences in beliefs and attitudes
towards tuberculosis and their impact on tuberculosis control:
what do we know? In: Gender and Tuberculosis (eds VK Diwan,
A Thorson & A Winkvist) An International Research
Workshop, Nordic School of Public Health, Goteborg,
Sweden, 89–105.
Liefooghe R, Baliddawa JB, Kipruto EM, Vermeire C &
De Munynck AO (1997) From their own perspective: a Kenyan
community’s perception of tuberculosis. Tropical Medicine
and International Health 2, 809–821.
Needham DM, Foster SD, Tomlinson G & Godfrey-Faussett P
(2001) Socio-economic, gender and health services factors
affecting diagnostic delays for tuberculosis patients in urban
Zambia.Tropical Medicine and International Health6, 256–259.
Nichter M (1994) Illness semantics and international health: the
weak lungs/tuberculosis complex in the Philippines. Social
Science and Medicine 38, 649–663.
Rangan S & Uplekar MW (1998) Gender perspectives of access to
health and tuberculosis care. In: Gender and Tuberculosis (eds
VK Diwan, A Thorson & A Winkvist) An International
Research Workshop, Nordic School of Public Health, Goteborg,
Sweden, 107–125.
Smith I (1994) Women and tuberculosis: gender issues and
tuberculosis control in Nepal. MA Dissertation, Nuffield Insti-
tute of Health, University of Leeds.
Uplekar MW & Rangan S (1996) Tackling TB: the Search for
Solutions. The Foundation for Research in Community Health,
Bombay, India.
Uplekar MW, Rangan S, Weiss MG, Ogden J, Borgdorff MW &
Hudelson P (2001) Attention to gender issues in tuberculosis
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
ª 2004 Blackwell Publishing Ltd 1237
control. The International Journal of Tuberculosis and Lung
Disease 5 (Suppl. 3), 220–224.
Vlassoff C & Moreno CG (2002) Placing gender at the center of
health programming: challenges and limitations. Social Science
and Medicine 54, 1713–1723.
Vlassoff C, Weiss MG, Ovuga E et al. (2000) Gender and the
stigma of onchocercal skin disease in Africa. Social Science and
Medicine 50, 1353–1368.
Weiss M (2001) Cultural epidemiology: an introduction and
overview. Anthropology and Medicine 8 (Suppl. 1), 5–29.
WHO (1991) Maternal Mortality: a Global Fact Book. WHO,
Geneva.
WHO (2001a) Global DOTS Expansion Plan: Progress in TB
Control in High-Burden Countries. (WHO/CDS/STB/2001.11)
WHO, Geneva.
WHO (2001b) The ‘undefined and hidden’ burden of mental
health problems. http://www.who.int/mediacentre/factsheets/
fs218/en, (accessed on 20 September 2004).
WHO (2002) Global Tuberculosis Control. (WHO/CDS/TB/
2002.295) WHO, Geneva.
Authors
Sachin R. Atre, Abhay M. Kudale, Sudhakar N. Morankar and Sheela G. Rangan, The Foundation for Research in Community Health,
85, 3 & 4 Trimiti B, Anand Park, Aundh, Pune 411007, India. Tel.: +91 020 25887020; Fax: +91 20 25881308;
E-mail: [email protected]
Mitchell G. Weiss, Swiss Tropical Institute, Department of Public Health and Epidemiology, Socinstrasse 57, CH-4002 Basel,
Switzerland. Tel.: +41 61 284 8284; Fax: +41 62 271 7951; E-mail: [email protected] (corresponding author)
Appendix 1
Structure of the EMIC Interview for respondents without
TB in the general population of rural Pune District.
1. Socio-cultural characteristics
• Demographic data, including age, sex, occupation,
education, religion, and marital status.
• Socio-economic information about household, including
livelihood activities and income. Open-ended questions
(yielding ‘spontaneous’ responses) and focused queries
(yielding ‘probed’ responses) about particular categories,
and narrative accounts with reference to the condition
depicted in a vignette inquire about the following topics.
2. Identification of condition and help seeking
• Recommendations for help seeking
• Anticipated treatment from various types of providers
• Anticipated outcome with and without treatment
3. Patterns of distress
• Somatic symptoms
• Illness-related family issues and social problems
• Financial problems
• Psychological problems
• Most troubling among the above
• Indicators of stigma
4. Perceived causes
• Ingestion
• Health-illness-injury
• Heredity
• Environmental
• Traditional-cultural
• Sexual
• Karma-supernatural
• Most important among the above
5. Sources of information about TB
Appendix 2
Vignettes depicting TB, which served as reference for
queries of the EMIC interview.
Male vignette
A male ‘Raghu’ is 23 years old. He has been suffering from
cough and fever since 2 months. He keeps bringing out
sputum while coughing. He does not have any appetite and
has lost a lot of weight. He feels so weak that he is not able
to continue any more with his daily work on farms.
Female vignette
A female ‘Manju’ is 18 years old. She has been suffering
from cough and fever since 2 months. She keeps bringing
out sputum while coughing. She does not have any appetite
and has lost a lot of weight. She feels so weak that she is
not able to continue any more with her daily work at
home.
Tropical Medicine and International Health volume 9 no 11 pp 1228–1238 november 2004
S. R. Atre et al. Culture, gender, and TB in India
1238 ª 2004 Blackwell Publishing Ltd




















