Global Travel Restrictions during COVID-19 Outbreak - The ...
Upload
independentCategory
view
1download
0
JOBNAME: No Job Name PAGE: 1 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: B490C734/v2503/blackwell/journals/pme_v11_i11/pme_988
Correlates of Perceived Pain-RelatedRestrictions among Women with Fibromyalgiapme_988 1..10
Peter Przekop, DO, PhD,†,‡,††,* Mark G. Haviland,PhD,* Kelly R. Morton, PhD,§,¶ Keiji Oda, MPH,**and Gary E. Fraser, MD, PhD**,††
*Department of Psychiatry, Loma Linda UniversitySchool of Medicine and Loma Linda, California, USA;
†Departments of Pediatrics and Neurology, LomaLinda University School of Medicine, Loma Linda,California, USA;
‡Betty Ford Center, Rancho Mirage, California, USA;
§Department of Family Medicine, Loma LindaUniversity School of Medicine, Loma Linda, California,USA;
¶Department of Psychology, Loma Linda UniversitySchool of Science and Technology, Loma Linda,California, USA;
**Department of Epidemiology and Biostatistics, LomaLinda University School of Public Health, Loma Linda,California, USA;
††Department of Internal Medicine, Loma LindaUniversity School of Medicine, Loma Linda, California,USA
Reprint requests to: P. Przekop, DO, PhD, Departmentof Psychiatry, Loma Linda University School ofMedicine, Loma Linda, CA, 92350, USA. Tel:909-558-9502; Fax: 909-558-9595; E-mail:[email protected].
Abstract
Objective. To identify correlates of perceived pain-related restrictions in a community sample ofwomen with fibromyalgia.
Methods. The fibromyalgia group was composed ofwhite women with a self-reported, physician-givenfibromyalgia diagnosis (N = 238) from the Biopsy-chosocial Religion and Health Study (BRHS). BRHSrespondents had participated in the larger AdventistHealth Study-2. To identify associations with pain-related restrictions, we used hierarchical linear
regression. The outcome measure was subjects’pain-related restrictions (one SF-12 version 2-item).Predictors included age, education, body massindex (BMI), sleep apnea, and fibromyalgia treat-ment in the last year, as well as standardized mea-sures for trauma, major life stress, depression, andhostility. To better interpret the findings, pain-related restrictions also were predicted in womenwith osteoarthritis and no fibromyalgia.
Results. Women with fibromyalgia reporting themore severe pain-related restrictions were thosewho had experienced trauma accompanied byphysical pain, were older, less educated, moredepressed, more hostile, had high BMI scores, andhad been treated for fibromyalgia in the last12 months (adjusted R2 = 0.308). Predictors inwomen with osteoarthritis were age, BMI, treatmentin the last 12 months, experience of a major lifestressor, and greater depression symptom severity(adjusted R2 = 0.171).
Conclusions. In both groups, age, BMI, treatment inthe last 12 months, and depression predicted pain-related restrictions. Experience of a traumatic eventwith physical pain was the strongest predictor in thefibromyalgia group. These findings may be useful inconstructing novel treatments and prevention strat-egies for pain-related morbidity in fibromyalgiapatients.
Key Words. Fibromyalgia; Osteoarthritis; Pain;Central Nervous System; Trauma; Stress
Introduction
Fibromyalgia and Chronic Pain
Pain that persists for more than 3 months is consideredchronic [1]. Perhaps the most perplexing, controversial,disabling, and difficult-to-treat of all chronic pain condi-tions is fibromyalgia. Fibromyalgia patients account formore medical cost, medication use, physician visits, anddisability compared with other chronic pain patients [2,3];therefore, identifying correlates of pain-related functionalstatus may improve care in this patient group.
Fibromyalgia Pain
Patients with fibromyalgia report constant, widespread,amplified body pain (hyperalgesia) and pain to superficialand deep palpation that is out of proportion to the intensity
Pain Medicine 2010; 11: **–**Wiley Periodicals, Inc.
1
123
4
56789
1011121314151617181920212223242526272829303132333435363738
39
40414243444546474849505152
535455565758596061626364656667686970717273747576777879808182838485
86
878889909192939495969798
99
100101102103104

JOBNAME: No Job Name PAGE: 2 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: 892734FB/v2503/blackwell/journals/pme_v11_i11/pme_988
of applied pressure (allodynia). Recent evidence suggeststhat fibromyalgia pain may be modulated at the level of thecentral nervous system (CNS) [4,5]. Functional imagingstudies have shown alterations in brain networks in bothfibromyalgia and other chronic pain patients [6,7]. Despitethese similarities, fibromyalgia patients report more pain-related problems relative to other pain patients with com-parable pain ratings [8,9]. This may be due, in part, todifferences in genetic predisposition, life experiences,coping strategies, cognitive styles, and co-morbidities[10,11].
Correlates of Fibromyalgia, Pain, andPain-Related Restrictions
Previous work suggests that traumatic events can influ-ence the onset and progression of various diseases suchas depression, anxiety disorders, and chronic pain (includ-ing fibromyalgia), and often there are associated CNSchanges [7,12–16]. Many factors have been associatedwith pain and restrictions in fibromyalgia patients includingtraumatic events. In a recent study, fibromyalgia preva-lence was associated with having experienced bothsexual and physical assault/abuse [17]. What remainsunclear, however, is whether negative life events (i.e., trau-matic and major life stress experiences) can predict theextent of perceived pain-related restrictions in fibromyalgiapatients.
In fibromyalgia patients, depression increases somaticcomplaints and functional disability [18], and can predictthe extent of pain and functional restrictions [19]. Copingstyles such as catastrophizing, the inability to identifyemotions, and hostility (which entails isolation and mistrustof others) can lead to increased pain and disability infibromyalgia patients [20,21].
Age, education, weight, and sleep disorders also caninfluence pain-related restrictions. Fibromyalgia patientswho are younger and better educated maintain higherfunctional status [22]. Moreover, fibromyalgia patients whoare overweight report increased disability, decreasedquality of life, and lower pain thresholds [23]. The relation-ship between sleep problems and musculoskeletal pain isnot completely understood, but nonrestorative sleep isassociated with increased pain sensitivity [24].
Research Aim
The present study was designed to identify factors asso-ciated with perceived pain-related restrictions in a national(United States), community sample of women with fibro-myalgia. Our primary aim was to determine whethervarious factors—shown to be related to pain severity andfunctional restrictions in previous studies—would be posi-tively related/make independent contributions to painrestriction prediction in fibromyalgia. In designing thisstudy, we sought to both identify and confirm potentiallytreatable factors—not yet evaluated together in a singlestudy—in this difficult-to-treat patient population. To better
interpret the results, we predicted pain-related restrictionsin another pain group, women with osteoarthritis (andwithout fibromyalgia).
Method
Data Source
Data were from the Biopsychosocial Religion and HealthStudy (BRHS [25]). BRHS investigators randomly sampled20,000 of the 96,000 respondents to the Adventist HealthStudy (AHS-2 [26]); of the 20,000 receiving a mailed ques-tionnaire, 10,988 provided usable BRHS surveys. TheAHS-2 is a cohort study investigating the interrelationshipsamong cancer, diet, and lifestyle among Seventh-DayAdventists, whereas the BRHS is a study of the interrela-tionships among traumatic and major life stressors, reli-gion, and health/mental health. Seventh-Day Adventistsendorse many healthy lifestyle commitments, which areanchored in their faith; for example, only 1% smoke, 7%consume alcohol, and fewer than half eat meat.
Subjects
Fibromyalgia subjects in the present study were the 238White women answering “yes” to a yes–no question, “Hasa physician ever diagnosed you with fibromyalgia,” andproviding responses to both the gender and race/ethnicityquestions. The number of respondents answering “no” tothe fibromyalgia question and answering the gender andrace/ethnicity questions was 3,624. The numbers of menand Black women meeting these criteria were too smalland precluded meaningful analyses.
Measures
Dependent Variable
Pain ratings were based on subjects’ answers to theSF-12 version 2 [27] item, “During the past 4 weeks, howmuch did pain interfere with your normal work (includingboth work outside the home and housework)?” Ratingswere on a 5-point scale, ranging from 1 (not at all) to 5(extremely). This criterion represents a snapshot, that is,how the women perceived the extent to which pain hadinterfered with their lives in the month preceding thesurvey.
Independent Variables
Age (in years) is a continuous variable. Education is athree-level categorical variable, high school or less, somecollege, and college graduate or higher. Body mass index(BMI, weight scaled by height) is a self-reported continu-ous variable. Labels have been given to three scoreranges (obesity � 30, overweight = 25–29.9, andnormal = 18.5–24.9) [28]. Our sleep disorder measure(sleep apnea) was coded yes = 1 and no = 0, based onsubjects’ answers to the question, “Has a physician ever
2
Przekop et al.
123456789
1011
12
13141516171819202122232425262728293031323334353637383940414243444546
47
48495051525354555657585960
616263
64
6566676869707172737475767778798081
82
8384858687888990919293
94
9596979899
100101102103104105106107
108
109110111112113114115116117118119

JOBNAME: No Job Name PAGE: 3 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: 9CA23DE0/v2503/blackwell/journals/pme_v11_i11/pme_988
diagnosed you with sleep apnea?” Fibromyalgia status(treated the last 12 months) was coded yes = 1 andno = 0.
Trauma and major life stress items were from a modifiedversion of the Trauma Assessment in Adults and Ryff andcolleagues’ child abuse scales [29–31]. In this section ofthe questionnaire, subjects were asked about “differenttypes of stressful or difficult life events” (both in child andadulthood, with no event timeline). We classified the itemsas either a traumatic experience or a major life stressor.The traumatic experiences are those that likely involvedactual or threatened death (actual death of anotherperson) or serious injury (or threat to one’s physical integ-rity), and elicited intense reactions, such as fear, helpless-ness, or horror [32–34]. We then grouped the items bytrauma type: 1) life-threatening accident (one question,“Have you ever been in a really bad accident—car, atwork, or somewhere else—and thought you might bekilled or injured?), 2) emotional abuse/neglect (two ques-tions about mother or father insulting, swearing at, orignoring between ages 5 and 15 years), 3) physicalassault/abuse (two assault questions, actual and threat-ened in subject’s lifetime; four abuse questions betweenage 5 and 15 years, mother or father pushing, slapping,throwing objects, kicking, biting, striking with an object),and 4) sexual assault/abuse (three questions, actual andthreatened in one’s lifetime).
The major life stressors are serious illness (e.g., cancer,leukemia, AIDS, and multiple sclerosis), abortion (self/intimate partner), miscarriage (self/intimate partner),divorce/separation, homelessness, and death of a child.For each of these trauma/stressor variables, subjectswere given a score of 0 in the category if their answers toall of the questions in that category were no/never (andgiven a score of 1, if otherwise).
With one exception, traumatic experience and major lifestressor classification/scoring is consistent with Havilandet al. [17]. They grouped bad accident with war, naturaldisaster, and witnessing someone being killed. Only “badaccident” was related to the pain criterion in the presentstudy, so it was isolated as a single trauma variable.
For depression severity, we used the 11-item version of theCenter for Epidemiological Studies-Depression Scale(CES-D) (each item rated on a three-point scale, rangingfrom 0 or rarely/none to 2 or much/most of the time), whichwe converted to full 20-item CES-D equivalent scores [35].CES-D equivalent scores of �16 are considered high; andthis cut-point often is used to screen for clinical depression.For hostility, we used a modified version of the 9-itemCook–Medley hostility scale [36]. Items were rated on a 1–4scale (originally a true-false format): 1 = definitely false,2 = tends to be false, 3 = tends to be true, and 4 = defi-nitely true. Total scores are expressed as average itemscores. Missing item values for these two scales werereplaced with the average of available items if subjects hadanswered at least eight of the depression and seven of thehostility items.
Data Analyses
To evaluate the bivariate relationships between indepen-dent variables and the dependent variable (pain ratings),we used correlation (age, BMI, depression, and hostility),one-way analysis of variance (education), and t-tests forindependent samples (sleep apnea, fibromyalgia status,traumatic experiences, and major life stressors).
To evaluate multivariate relationships, we used hierarchicallinear regression (presented are standardized betas,P-values, and adjusted R2s for each stage). Entered at thefirst stage was a set of personal/health variables (age,education, BMI, sleep apnea, and fibromyalgia status). Atstage two, the traumatic/major life stress set was entered,and at stage three, the psychological set (depression andhostility). For all tests of statistical significance, alpha wasset at 0.05.
Based on the results of the multivariate analysis, wecreated two “extreme” subgroups and compared theiraverage pain ratings; in one group were those womenpossessing all of the associated factors, and, in the othergroup, those possessing none.
Finally, we ran a parallel analysis (hierarchical regression)with the women in the larger sample answering “yes” tothe osteoarthritis question (“Has a physician ever diag-nosed you with osteoarthritis?”), “no” to the fibromyalgiaquestion, and with complete information on all of theindependent variables. The independent variables werethe same as those in the fibromyalgia analysis, with oneexception: fibromyalgia status was replaced with osteoar-thritis status (again, treated in the last 12 months).
Results
Descriptive statistics for the 238 women with fibromyal-gia are shown in Tables 1 and 2. Subjects’ average agewas 62.6 years (SD = 10.8), and approximately three-quarters had either attended or graduated from college.Traumatic experiences and major life stressors werestrikingly common. Moreover, subjects’ average depres-
Table 1 Women with a physician-givenfibromyalgia diagnosis: descriptive statistics(continuous variables) and their relationships topain ratings
N Range Mean SDCorrelationwith pain
Age 233 38–88 62.6 10.8 0.12BMI 236 16.8–75.9 29.2 8.0 0.24Depression 237 0.7–48.6 15.7 10.4 0.35Hostility 234 1–3.3 2.1 0.49 0.18
P < 0.05 shown in boldface type.BMI = body mass index.
3
Fibromyalgia Pain Predictors
123456789
10111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061
6263646566676869707172737475767778798081828384858687888990919293949596979899
100101102103104
105
106107108109110111112113114115116117118119120121122123

JOBNAME: No Job Name PAGE: 4 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: 940C49B3/v2503/blackwell/journals/pme_v11_i11/pme_988
sion scores (15.7) were just under an establishedscreening criterion for clinical depression (�16), and theiraverage BMIs (29.2) were just under the obesity criterion(�30) (39.1% met the screening criterion for clinicaldepression and 27.3% for obesity). Slightly less than afifth (18.1%) reported sleep apnea, and 45% reportedhaving been treated for fibromyalgia in the last12 months.
Subjects’ perceived pain ratings are shown in Figure 1. Inresponse to the question, “During the past 4 weeks, howmuch did pain interfere with your normal work (includingboth work outside the home and housework)?” slightlyless than half responded quite a bit (n = 75, 31.8%) orextremely (n = 38, 16.1%), and, a fifth, moderately (n = 50,21.2%). The mean score (�SD) was 3.21 � 1.26 on the5-point scale.
The bivariate relationships between predictor variablesand the pain criterion are shown in Tables 1 and 2. Greaterpain interference was associated with lower education,higher BMI, sleep apnea, treated for fibromyalgia in the
Table 2 Women with a physician-given fibromyalgia diagnosis: descriptive statistics (categoricalvariables) and their relationships to pain ratings
n %
Pain ratings
PMean SD
Education† 0.002High school or less 69 29.1 3.5 1.2Some college 105 44.3 3.3 1.3College graduate or higher 63 26.6 2.7 1.2
Sleep apneaYes 43 18.1 3.8 1.1 0.000No 190 79.8 3.1 1.3
Fibromyalgia Tx last 12 months‡ 0.000Yes 98 45.0 3.6 1.2No 120 55.0 2.8 1.2
Bad accident‡ 0.014Yes 102 42.9 3.4 1.2No 136 57.1 3.0 1.3
Emotional abuse/neglect‡ 0.217Yes 104 45.2 3.3 1.2No 126 54.8 3.1 1.3
Physical assault/abuse‡ 0.001Yes 123 53.7 3.5 1.1No 106 46.3 2.9 1.3
Sexual assault/abuse‡ 0.067Yes 109 46.6 3.4 1.2No 125 53.4 3.1 1.3
Major life stressor‡ 0.072Yes 168 71.2 3.3 1.2No 68 28.8 3.0 1.3
† One-way analysis of variance.‡ t-Test for independent samples.P < 0.05 shown in boldface type.
Figure 1 Pain responses of women with aphysician-given fibromyalgia diagnosis (n = 236).
4
Przekop et al.
123456789
10111213141516171819202122232425262728293031323334353637
38
39404142434445464748495051525354555657585960
616263
JOBNAME: No Job Name PAGE: 5 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: A36B6851/v2503/blackwell/journals/pme_v11_i11/pme_988
last 12 months, having been in a bad accident, the expe-rience of physical assault/abuse, and higher depressionand hostility scores.
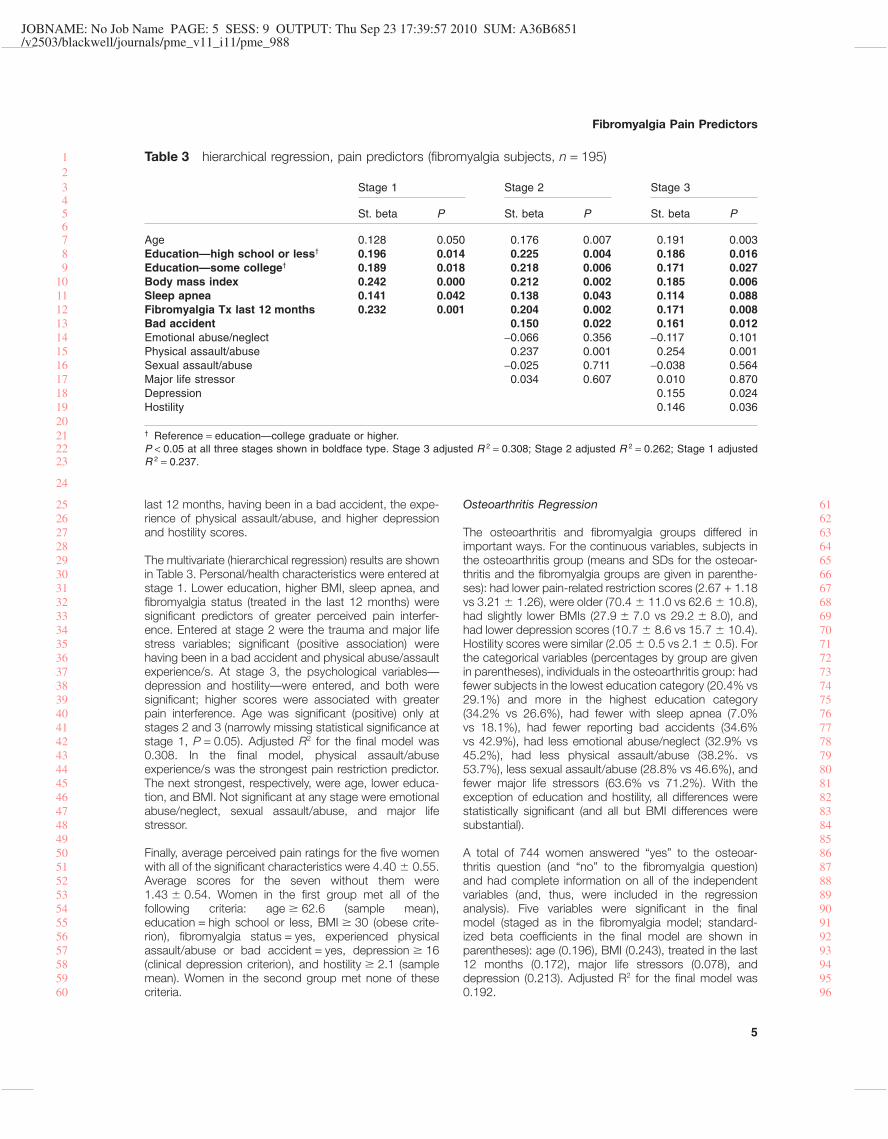
The multivariate (hierarchical regression) results are shownin Table 3. Personal/health characteristics were entered atstage 1. Lower education, higher BMI, sleep apnea, andfibromyalgia status (treated in the last 12 months) weresignificant predictors of greater perceived pain interfer-ence. Entered at stage 2 were the trauma and major lifestress variables; significant (positive association) werehaving been in a bad accident and physical abuse/assaultexperience/s. At stage 3, the psychological variables—depression and hostility—were entered, and both weresignificant; higher scores were associated with greaterpain interference. Age was significant (positive) only atstages 2 and 3 (narrowly missing statistical significance atstage 1, P = 0.05). Adjusted R2 for the final model was0.308. In the final model, physical assault/abuseexperience/s was the strongest pain restriction predictor.The next strongest, respectively, were age, lower educa-tion, and BMI. Not significant at any stage were emotionalabuse/neglect, sexual assault/abuse, and major lifestressor.
Finally, average perceived pain ratings for the five womenwith all of the significant characteristics were 4.40 � 0.55.Average scores for the seven without them were1.43 � 0.54. Women in the first group met all of thefollowing criteria: age � 62.6 (sample mean),education = high school or less, BMI � 30 (obese crite-rion), fibromyalgia status = yes, experienced physicalassault/abuse or bad accident = yes, depression � 16(clinical depression criterion), and hostility � 2.1 (samplemean). Women in the second group met none of thesecriteria.
Osteoarthritis Regression
The osteoarthritis and fibromyalgia groups differed inimportant ways. For the continuous variables, subjects inthe osteoarthritis group (means and SDs for the osteoar-thritis and the fibromyalgia groups are given in parenthe-ses): had lower pain-related restriction scores (2.67 + 1.18vs 3.21 � 1.26), were older (70.4 � 11.0 vs 62.6 � 10.8),had slightly lower BMIs (27.9 � 7.0 vs 29.2 � 8.0), andhad lower depression scores (10.7 � 8.6 vs 15.7 � 10.4).Hostility scores were similar (2.05 � 0.5 vs 2.1 � 0.5). Forthe categorical variables (percentages by group are givenin parentheses), individuals in the osteoarthritis group: hadfewer subjects in the lowest education category (20.4% vs29.1%) and more in the highest education category(34.2% vs 26.6%), had fewer with sleep apnea (7.0%vs 18.1%), had fewer reporting bad accidents (34.6%vs 42.9%), had less emotional abuse/neglect (32.9% vs45.2%), had less physical assault/abuse (38.2%. vs53.7%), less sexual assault/abuse (28.8% vs 46.6%), andfewer major life stressors (63.6% vs 71.2%). With theexception of education and hostility, all differences werestatistically significant (and all but BMI differences weresubstantial).
A total of 744 women answered “yes” to the osteoar-thritis question (and “no” to the fibromyalgia question)and had complete information on all of the independentvariables (and, thus, were included in the regressionanalysis). Five variables were significant in the finalmodel (staged as in the fibromyalgia model; standard-ized beta coefficients in the final model are shown inparentheses): age (0.196), BMI (0.243), treated in the last12 months (0.172), major life stressors (0.078), anddepression (0.213). Adjusted R2 for the final model was0.192.
Table 3 hierarchical regression, pain predictors (fibromyalgia subjects, n = 195)
Stage 1 Stage 2 Stage 3
St. beta P St. beta P St. beta P
Age 0.128 0.050 0.176 0.007 0.191 0.003Education—high school or less† 0.196 0.014 0.225 0.004 0.186 0.016Education—some college† 0.189 0.018 0.218 0.006 0.171 0.027Body mass index 0.242 0.000 0.212 0.002 0.185 0.006Sleep apnea 0.141 0.042 0.138 0.043 0.114 0.088Fibromyalgia Tx last 12 months 0.232 0.001 0.204 0.002 0.171 0.008Bad accident 0.150 0.022 0.161 0.012Emotional abuse/neglect -0.066 0.356 -0.117 0.101Physical assault/abuse 0.237 0.001 0.254 0.001Sexual assault/abuse -0.025 0.711 -0.038 0.564Major life stressor 0.034 0.607 0.010 0.870Depression 0.155 0.024Hostility 0.146 0.036
† Reference = education—college graduate or higher.P < 0.05 at all three stages shown in boldface type. Stage 3 adjusted R 2 = 0.308; Stage 2 adjusted R 2 = 0.262; Stage 1 adjustedR 2 = 0.237.
5
Fibromyalgia Pain Predictors
123456789
1011121314151617181920212223
24
252627282930313233343536373839404142434445464748495051525354555657585960
616263646566676869707172737475767778798081828384858687888990919293949596

JOBNAME: No Job Name PAGE: 6 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: 95830E5F/v2503/blackwell/journals/pme_v11_i11/pme_988
Discussion
The primary purpose of the present study was to identifyfactors—including traumatic life events—that were asso-ciated with the extent of perceived pain-related restrictionsin women self-reporting a physician-given fibromyalgiadiagnosis. In the final regression model, older age, lowereducation, higher BMI, treatment for fibromyalgia in thelast 12 months, experiencing a bad accident or physicalassault/abuse, and higher depression, and hostilityscores, all were associated with greater pain-relatedrestrictions in the fibromyalgia group. In the osteoarthritisgroup, only older age, higher BMI, treatment for osteoar-thritis in the last 12 months, major life stressors, anddepression were predictors of pain-related restrictions.
In contrast to the fibromyalgia group, traumatic events(having been in a bad accident or experiencing physicalassault/abuse), hostility, and education were not associ-ated with pain-related restrictions in the osteoarthritisgroup. Particularly noteworthy is that traumatic experi-ences accompanied by physical pain (bad accident orphysical abuse/assault) were the strongest predictors ofpain-related restrictions in our cohort of women with fibro-myalgia (and not in women with osteoarthritis). On theother hand, having experienced at least one major lifestressor (e.g., serious illness, abortion, miscarriage,divorce/separation, homelessness, or death of a child)predicted pain restrictions for women with osteoarthritisbut not for women with fibromyalgia. Future research maybe designed to elucidate the process by which thesecontrasting stressors lead to pain-related restrictions inthe two disease groups.
Life Experience and Pain-Related Restriction
In the fibromyalgia group, the strongest predictor of pain-related interference was the traumatic life experience ofphysical assault/abuse. In previous studies, traumatic lifeexperiences have been shown to influence subsequentbehavior, health trajectories, as well as CNS andhypothalamic-pituitary-adrenal (HPA) axis function andstructure [37]. In our fibromyalgia subjects, 72.5% hadexperienced physical trauma (physical assault/abuse or abad accident) and concomitant acute pain. This supportsthe possibility that traumatic events predisposed somewomen to later develop fibromyalgia, hypersensitivity topain [17,38], and mood disorders.
Traumatic events can influence brain function [39]; when atraumatic event occurs, brain neural networks assess theevent for controllability. Events perceived to be uncontrol-lable affect the degree of stress mediator release andsubsequent neuroplastic changes that, in turn, alter neu-ronal function and presumably lessen one’s ability tohandle further stress [40]. Although unproven, it is pos-sible that similar changes may be relevant to participantsin the present study.
There is growing evidence that adverse life experiencescan lead to alterations in HPA axis function, which in turn
can affect normal brain function, especially frontal lobe/executive function, and have lasting effects [41]. Thisoccurs, in part, from altered levels of biogenic amines [41].Similar alterations in neurotransmitter levels and synapticfunction have been reported in fibromyalgia patients[42–44], and have been hypothesized to contribute tocognitive alterations, such as catastrophizing, depression,hostility, “fibro fog” (cognitive impairment), and the inabilityto modulate pain and pain’s effects. In the present study,greater perceived pain-related restrictions in the fibromy-algia group were associated with having experienced“physical” traumatic events (i.e., physical assault/abuseand bad accident). Future studies should uncover whether1) these events can lead to changes in CNS function infibromyalgia patients and 2) the influence of the timecourse of such events.
Other Correlates of Pain-Related Restriction
Depression was associated with worse pain-relatedrestrictions in both the fibromyalgia and the osteoarthritisgroups, despite depression scores being considerablylower on average in the osteoarthritis group. Among thefibromyalgia cohort, 39.1% had CES-D equivalentscores � 16 (typically used as a screen for clinical depres-sion), and the group’s mean depression scores fell justshort of this criterion. In previous studies, fibromyalgiapatients have reported poorer quality of life, lower func-tional status, and more psychiatric symptoms thanpatients with other pain conditions [9,45–47]. In fact,some suggest that depression exerts a greater effect onfibromyalgia patients than on patients with other pain syn-dromes [9]. Moreover, fibromyalgia patients with concomi-tant mood disorders report more intense somaticcomplaints, pain levels, and functional restrictions thanpatients with other pain syndromes [18,19]. Our data,however, show that depressive symptoms—regardless ofseverity—predict pain-related restrictions in both individu-als with fibromyalgia and osteoarthritis, although the fibro-myalgia group reported both worse depression and higherpain-related restrictions.
Hostility also predicted pain-related restrictions in thefibromyalgia cohort. Hostility often has been defined asgeneral cynicism, interpersonal mistrust, and lack of socialsupport [48]. Hostility relates to a cognitive style that ismaladaptive and has been associated with the progres-sion of various diseases, including cardiovascular disease[49]. A recent large community-based study reported thathostility was significantly associated with depression [50].The mechanism by which hostility relates to pain-relatedrestrictions in the fibromyalgia group is unknown but mayrelate to a cognitive style [51] that may lead to perceivedpain-related restrictions.
In both groups, older age and higher BMI were associatedwith an increase in pain-related restrictions, and, in thefibromyalgia group, low education was a significant pre-dictor. Advancing age has been associated with a declinein functional ability in fibromyalgia patients, with an esti-mated 4% decline in functional capacity for each year of
6
Przekop et al.
123456789
10111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061
6263646566676869707172737475767778798081828384858687888990919293949596979899
100101102103104105106107108109110111112113114115116117118119120121122

JOBNAME: No Job Name PAGE: 7 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: B076DFCB/v2503/blackwell/journals/pme_v11_i11/pme_988
advancing age [22]. In agreement with our findings, pre-vious studies have shown that low education levels gen-erally are associated with poor health outcomes [52], andincreased depression rates [53]. Obesity has been shownto have a negative effect on the musculoskeletal system[54]. In our fibromyalgia sample, 27.3% of the subjectsmet the National Heart, Lung, and Blood Institute criteriafor obesity [28]. Obesity in fibromyalgia patients leads togreater disability, poorer quality of life, and reduced painthresholds [23]. It is likely that increased age and beingoverweight/obese increase stress to a system that alreadyis unable to handle the ever present burden of pain.
Thus, older age, high BMI, having treatment within the last12 months, and depression emerge as common factorsthat predict perceived pain-related restrictions in womenwith fibromyalgia and osteoarthritis, whereas traumaticexperiences, hostility, and low education are specific tofibromyalgia.
Study Strengths
The present sample was a relatively large, communitygroup. In many fibromyalgia studies, researchers havestudied smaller groups in clinical (treatment) settings. Anadditional strength is that the BRHS survey containeddetailed lifetime trauma/stressor questions, thus, allowingus to clarify the relationship between specific traumas andstressors, as well as other correlates that lead to per-ceived pain-related restrictions in women with fibromyalgiaand osteoarthritis. Our sample size and comprehensivequestionnaire afforded us the ability to evaluate a largenumber of variables in a single study. Moreover, our rela-tively large cohort of women with osteoarthritis allowed forsimilar meaningful comparisons to be made in this group.
Study Limits
First, our fibromyalgia criterion was based on yes–noanswers to a single question, “Has a physician ever diag-nosed you with fibromyalgia?” Although clearly an imper-fect criterion, Haviland et al. [17] have provided somesupport for its validity: 1) their reported rates were reason-able given sample age and composition, and the rate forwomen was higher than that of men, and 2) individualsreporting a fibromyalgia diagnosis had more pain, lessenergy, worse sleep, higher depressive symptom scores,and diagnoses of depression and irritable bowel syn-drome (life-to-date). Second, although our pain criterion isinterpretable, it does not necessarily represent painintensity/severity or disability. Third, our trauma/stressdata are uncorroborated, self-reported, “point events,”and we had no measures/indices of chronic stress/present anxiety, which both have long been associatedwith chronic pain. Fourth, this is a unique sample,although how this may limit generalizability is not obvious.Fifth, only 50% of those sent questionnaires responded(although the response rate for white women—the groupfrom which the present samples were drawn—was 62%),and finally, this is a cross-sectional, not longitudinal, studyand a secondary data analysis.
Conclusion
We have identified a number of associations with per-ceived pain-related restrictions in women with fibromyalgiaand contrasted these with pain predictors for women withosteoarthritis. The factors that provide the most strikingcontrast is traumatic events accompanied by physicalpain, which predicted greater perceived pain-related inter-ference in the fibromyalgia group only. Thus, individualswith fibromyalgia who have experienced traumatic lifeevents may be predisposed to greater pain-related restric-tions than those who have not experienced trauma [55].The fibromyalgia subgroup with the most extreme painrestrictions in the present study may have been geneticallypredisposed to cope poorly with past and present stres-sors. Future studies could be designed to explore theintriguing relationships between genetic predisposition,traumatic life events, and present pain-related restrictions.Successful treatment likely will occur only after the devel-opment of treatment paradigms that consider the fullspectrum of the fibromyalgia disease phenotype we havereported. Strategies that consider, for example, corticalalterations and past and present cognitive, physical, andemotional elements of disease, have been successful intreating chronic pain patients [56]. Our results underscorethe importance of investigating traumatic experienceswhen approaching fibromyalgia patients or those suscep-tible for the development of the disease. In the ideal sce-nario, traumatic events would be prevented, but whenpresent, they should be addressed in the predisease orearly disease stage. Finally, the reported data may helpresearchers design novel studies that explore genetic andepigenetic factors underlying the development of riskfactors for perceived pain-related restrictions in fibromyal-gia patients.
Acknowledgments
Funding for this study was from the National Institute onAging (Biopsychosocial Religion and Health Study,5R01AG026348-05) and from the National Cancer Insti-tute for the parent study (Adventist Health Study 2, 5R01CA094594).
References1 Merskey H, Bogduk N. Classification of Chronic Pain.
Seattle, WA: IASP Press; 1994.
2 White LA, Birnbaum AG, Kaltenboeck A, et al.Employees with fibromyalgia: Medical comorbidity,healthcare costs, and work loss. J Occup Environ Med2008;50:13–24.
3 Silverman S, Dukes EM, Johnston SS, et al. The eco-nomic burden of fibromyalgia: Comparative analysiswith rheumatoid arthritis. Curr Med Res Opin 2009;25:829–40.
4 Shweinhardt P, Sauro KM, Bushnell MC. Fibromyalgia:A disorder of the brain? Neuroscientist 2008;14:415–21.
7
Fibromyalgia Pain Predictors
123456789
10111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061
6263646566676869707172737475767778798081828384858687888990919293949596979899
100101102103104105106107108109110111112113114115116117118119120121122
JOBNAME: No Job Name PAGE: 8 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: 73698B6B/v2503/blackwell/journals/pme_v11_i11/pme_988
5 Williams DA, Clauw DJ. Understanding fibromyalgia:Lessons from the broader pain research community. JPain 2009;10:777–91.
6 Apkarian AV, Bushnell MC, Treede R-D, Zubieta J-K.Human brain mechanisms of pain perception andregulation in health and disease. Eur J Pain 2005;9:463–84.
7 Tracey I. Imaging pain. Br J Anaesth 2008;101:32–9.
8 DeWalt DA, Reed GW, Pincus T. Further clues torecognition of patients with fibromyalgia from a simple2-page multidimensional health assessment question-naire (MDHAQ). Clinical Experiments Rheumatology2004;22:453–61.
9 Gormsen L, Rosenberg R, Bach FW, Jensen TS.Depression, anxiety, health related quality of life andpain in patients with chronic fibromyalgia and neuro-pathic pain. Eur J Pain 2010;14:127, e1–8.
10 Turk DC, Flor H. Primary fibromyalgia is greater thantender points: Towards a multiaxial taxonomy. J Rheu-matol 1989;16:80–6.
11 Thieme K, Turk DC, Flor H. Comorbid depression andanxiety in fibromyalgia syndrome: Relationship tosomatic and psychosocial variables. Psychosom Med2004;66:827–44.
12 Heim C, Nemeroff CB. The role of childhood trauma inthe neurobiology of mood and anxiety disorders: Pre-clinical and clinical studies. Biol Psychiatry2001;49:1023–39.
13 Caspi A, McClay J, Moffitt TE, et al. Role of genotypein the cycle of violence in maltreated children. Science2002;297:851–4.
14 Leonardo ED, Hen R. Anxiety as a developmentaldisorder. Neuropsychopharmacology 2008;33:134–40.
15 Pittenger C, Duman RS. Stress, depression, and neu-roplasticity: A convergent mechanism. Neuropsy-chopharmacology 2008;33:88–109.
16 Paras ML, Hassan-Murad M, Chen P, et al. Sexualabuse and lifetime diagnosis of somatic disorders: Asystematic review and meta-analysis. JAMA2009;302:550–61.
17 Haviland MG, Morton KR, Oda K, Fraser GE. Trau-matic experiences, major life stressors, and self-reporting a physician-given fibromyalgia diagnosis.Psychiatry Res 2010;177:335–41.
18 White KP, Nielson WR, Harth M, Ostbye T, SpeechleyM. Chronic widespread musculo-skeletal pain with
and without fibromyalgia: Psychological distress in arepresentative community adult sample. J Rheumatol2002;29:588–94.
19 Forseth KO, Husby G, Gran JT, Forre O. Prognosticfactors for the development of fibromyalgia in womenwith self-reported musculoskeletal pain. A prospectivestudy. J Rheumatol 1999;26:2458–67.
20 Geisser ME, Casey KL, Brucksch CB, et al. Percep-tion of noxious and innocuous heat stimulation amonghealthy women and women with fibromyalgia: Asso-ciation with mood, somatic focus, and catastrophiz-ing. Pain 2003;102:243–50.
21 Sayar K, Gulec H, Topbas M. Alexithymia and angerin patients with fibromyalgia. Clin Rheumatol 2004;23:441–8.
22 Rutledge DN, Jones K, Jones CJ. Predicting highphysical functioning in people with fibromyalgia. JNurs Scholarsh 2007;39:319–24.
23 Neumann L, Lerner E, Glazer Y, et al. A cross-sectional study of the relationship between body massindex and clinical characteristics, tenderness mea-sures, quality of life, and physical functioning in fibro-myalgia patients. Clin Rheumatol 2008;12:1543–7.
24 Moldofsky H. Rheumatic manifestations of sleep dis-orders. Curr Opin Rheumatol 2010;22:59–63.
25 Lee JW, Morton KR, Walters J, et al. Cohort profile:The Biopsychosocial Religion and Health Study(BRHS). Int J Epidemiol 2009;38:1470–8.
26 Butler TL, Fraser GE, Beeson WL, et al. Cohort profile:The Adventist Health Study-2 (AHS-2). Int J Epidemiol2008;37:260–5.
27 Ware JE Jr, Kosinski M, Dewey JE. How to ScoreVersion 2 of the SF-12® Health Survey. Lincoln, RI:QualityMetric, Inc.; 2002.
28 National Heart, Lung, and Blood Institute. 2009. Cal-culate your body mass index. Available at: http://www.nhlbisupport.com/bmi/ (accessed August 2010).
29 Cusack KJ, Frueh BC, Brady KT. Trauma historyscreening in a community mental health center. Psy-chiatr Serv 2004;55:157–62.
30 Ryff CD, Singer BH, Palmersheim KA. Social inequali-ties in health and well-being: The role of relational andreligious protective factors. In: Brim OG, Ryff CD,Kessler RC, eds. How Healthy Are We?: A NationalStudy of Well-Being at Midlife. Chicago: University ofChicago Press; 2004:90–123.
31 McHugo GJ, Caspi Y, Kammerer N, et al. The assess-ment of trauma history in women with co-occurring
8
Przekop et al.
11
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
616263646566676869707172737475767778798081828384858687888990919293949596979899
100101102103104105106107108109110111112113114115116117118119120121

JOBNAME: No Job Name PAGE: 9 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: 6EAA4C2F/v2503/blackwell/journals/pme_v11_i11/pme_988
substance abuse and mental disorders and a historyof interpersonal violence. J Behav Health Serv Res2005;32:113–27.
32 Lazarus RS, Folkman S. Stress, Appraisal, andCoping. New York: Springer; 1984.
33 Shalev AY. Stress versus traumatic stress: From acutehomeostatic reactions to chronic psychopathology. In:van der Kolk BA, McFarlane AC, Weisaeth L, eds.Traumatic Stress: The Effects of Overwhelming Expe-rience on Mind, Body, and Society. New York: Guil-ford; 1996:77–101.
34 American Psychiatric Association. DSM-IV-TR. Wash-ington, DC: American Psychiatric Association; 2000.
35 Kohout FJ, Berkman LF, Evans DA, Cornoni-HuntleyJ. Two shorter forms of the CES-D Depression Symp-toms Index. J Aging Health 1993;5:179–93.
36 Strong DR, Kahler CW, Greene RL, Schinka J. Isolat-ing a primary dimension within the Cook–Medley Hos-tility Scale: A Rasch analysis. Pers Indiv Differ2005;39:21–33.
37 Hyman S. How adversity gets under the skin. NatNeurosci 2009;12:241–3.
38 Raphael K, Marbach J, Klausner J. Myofascial facepain. Clinical characteristics of those with regional vswidespread pain. J Am Dent Assoc 2000;131:161–71.
39 Lupien SJ, McEwen BS, Gunnar MR, Heim C. Effectsof stress throughout the lifespan on the brain, behav-ior, and cognition. Nat Rev Neurosci 2009;10:434–45.
40 Maier SF, Watkins LR. Stressor controllability andlearned helplessness: The roles of the dorsal raphenucleus, serotonin, and corticotrophin-releasingfactor. Neurosci Biobehav Rev 2005;29:829–41.
41 Arnsten AF. Stress signaling pathways that impair pre-frontal cortex structure and function. Nat Rev Neurosci2009;10:410–22.
42 Russell IJ, Vaeroy H, Javors M, Nyberg F. Cerebrospi-nal fluid biogenic amines metabolites in fibromyalgia/fibrositis syndrome and rheumatoid arthritis. ArthritisRheum 1992;35:550–6.
43 Larson AA, Giovengo SL, Russell IJ, Michalek JE.Changes in the concentrations of amino acids in thecerebrospinal fluid that correlate with pain in patientswith fibromyalgia: Implications for nitric oxide path-ways. Pain 2000;87:201–11.
44 Wood PB, Glabus MF, Simpson R, Patterson JC.Changes in gray matter in fibromyalgia: Correlationwith dopamine metabolism. J Pain 2009;10:609–18.
45 Picavet HS, Hoeymans N. Health related quality of lifein multiple musculoskeletal diseases: SF-36 andEQ-5D in the DMC3 study. Ann Rheum Dis2004;63:723–9.
46 Hoffman DL, Dukes EM. The health status burden ofpeople with fibromyalgia: A review of studies thatassessed health status with the SF-36 or the SF-12.Int J Clin Pract 2008;62:115–26.
47 Verbunt JA, Pernot DH, Smeets RJ. Disability andquality of life in patients with fibromyalgia. HealthQuality Life Outcomes 2008;6:8. doi:10.1186/1477-7525-6-8. Available at: http://www.hqlo.com/content/6/1/8 (accessed August 2010).
48 Hardy JD, Smith TW. Cynical hostility and vulnerabilityto disease: Social support, life stress, and physiologi-cal response to conflict. Health Psychol 1988;7:447–59.
49 Suls J, Bunde J. Anger, anxiety, and depression as riskfactors for cardiovascular disease: The problems andimplications of overlapped affective dispositions.Psychol Bull 2005;131:260–300.
50 Nabi H, Sing-Manoux A, Ferrie JE, et al. Hostility anddepressive mood: Results form the Whitehall II Pro-spective Cohort Study. Psychol Med 2010;40:405–13.
51 Sullivan MJ, Rodgers WM, Kirsch I. Catastrophizing,depression, and expectancies for pain and emotionaldistress. Pain 2001;91:147–54.
52 Pignone M, DeWalt DA, Sheridan S, Berkman N, LohrKN. Interventions to improve health outcome forpatients with low literacy: A systematic review. J GenIntern Med 2005;20:185–92.
53 Lopez-Leon S, Choy WC, Aulchenko YS, et al.Genetic factors influence the clustering of depressionamong individuals with lower socioeconomic status.Plos One 2009;4:e5069.
54 Anandacoomarasamy A, Fransen M, March L. Obesityand the musculoskeletal system. Curr Opin Rheuma-tol 2009;21:71–7.
55 Goldenberg DM. The interface of pain and mood dis-turbances in the rheumatic diseases. Semin ArthritisRheum [Epub ahead of print] 2009;••:••–••. doi:10.1016/j.semarthrit.2008.11.005.
56 Przekop P, Przekop A, Haviland MG, Riggs ML. Neu-rocognitive enhancement for the treatment of chronicpain. J Bodywork Mov Ther [Epub ahead of print]2009;••:••–••. doi: 10.1016/j.jbmt.2009.10.003.
9
Fibromyalgia Pain Predictors
22
33
123456789
10111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455565758596061
6263646566676869707172737475767778798081828384858687888990919293949596979899
100101102103104105106107108109110111112113114115116117118119

JOBNAME: No Job Name PAGE: 10 SESS: 9 OUTPUT: Thu Sep 23 17:39:57 2010 SUM: 236712A0/v2503/blackwell/journals/pme_v11_i11/pme_988
Toppan Best-set Premedia LimitedJournal Code: PME Proofreader: EmilyArticle No: 988 Delivery date: 23 September 2010Page Extent: 9 CopyEditor: Tet
AUTHOR QUERY FORM
Dear Author,During the preparation of your manuscript for publication, the questions listed below have arisen. Please
attend to these matters and return this form with your proof.Many thanks for your assistance.
QueryReferences
Query Remark
q1 AUTHOR: Please check these website addresses in the Reference List andconfirm that they are correct.
q2 AUTHOR: Please provide the volume number and page range for Reference55.
q3 AUTHOR: Please provide the volume number and page range for Reference56.
Copyright © 2022 FDOKUMEN