Refracture And Mortality Following Hospitalization For Severe ...

http://mdm.sagepub.com
Medical Decision Making
DOI: 10.1177/0272989X06290494 2006; 26; 313 Med Decis Making
Peter H. Ditto, Jill A. Jacobson, William D. Smucker, Joseph H. Danks and Angela Fagerlin Life-Sustaining Treatment Preferences
Context Changes Choices: A Prospective Study of the Effects of Hospitalization on
http://mdm.sagepub.com/cgi/content/abstract/26/4/313 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
On behalf of:
Society for Medical Decision Making
can be found at:Medical Decision Making Additional services and information for
http://mdm.sagepub.com/cgi/alerts Email Alerts:
http://mdm.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://mdm.sagepub.com/cgi/content/refs/26/4/313 Citations
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

UTILITIES AND PREFERENCES
MEDICAL DECISION MAKING/JUL–AUG 2006 313
Objective. Policy and law encouraging individuals to docu-ment their wishes for life-sustaining medical treatment inadvance of serious illness assumes that these wishes are unaf-fected by changes in health condition. To test this assumption,the authors examine the life-sustaining treatment prefer-ences of a sample of elderly adults prior to, soon after, andseveral months after a hospitalization experience. Subjectsand Methods. As part of the Advance Directives, ValuesAssessment, and Communication Enhancement (ADVANCE)project, 401 individuals older than age 65 participated in 3annual interviews. A subsample of 88 individuals who werehospitalized for greater than 48 hours during the course of thestudy participated in an additional “recovery” interview con-ducted soon after their release from the hospital (M = 14 dayspostdischarge). At each interview, subjects indicated theirdesire to receive 4 life-sustaining medical treatments in 4 seri-ous illness scenarios. Results. Treatment preferences showed
a significant “hospitalization dip,” with subjects reporting lessdesire to receive life-sustaining treatment at the recovery inter-view than they did at the annual interview conducted prior tohospitalization, but with desire returning to near prehospital-ization levels at the annual interview conducted severalmonths after hospitalization. This dip was more pronouncedin preferences for cardiopulmonary resuscitation and artifi-cial nutrition and hydration than in preferences for less inva-sive treatments. Conclusions. Preferences for life-sustainingtreatment are dependent on the context in which they aremade, and thus individuals may express different treatmentpreferences when they are healthy than when they are ill.These results challenge a key psychological assumptionunderlying the use of instructional advance directives inend-of-life decision making. Key words: end-of-life decisionmaking; advance directives; life-sustaining treatment prefer-ences. (Med Decis Making 2006;26:313–322)
Context Changes Choices: A ProspectiveStudy of the Effects of Hospitalization on
Life-Sustaining Treatment Preferences
Peter H. Ditto, PhD, Jill A. Jacobson, PhD, William D. Smucker, MD,Joseph H. Danks, PhD, Angela Fagerlin, PhD
An important shift has occurred in Americanmedicine over the past 2 decades toward
acknowledging the fundamental right of seriously illindividuals to make their own choices about the useof life-sustaining medical treatment.1 Assertion of thisright in actual end-of-life situations, however, is com-plicated by the fact that at the time decisions must be
made about whether to use or forgo such treatment,many patients are already so sick that they have lostthe capacity to make these choices for themselves.2
Instructional advance directives (e.g., living wills)are widely endorsed as the solution to this problem.3–6
On the surface, the solution seems elegant in its sim-plicity. If wishes for the use of life-sustaining treat-ment are recorded prior to incapacitating illness, thenpatients’ ability to influence the medical care theyreceive can be maintained even after they have lostthe ability to decide for themselves.
Policy and law encouraging the use of instructionaladvance directives, however, rests on a number ofpsychological assumptions of questionable validity.7,8
Most fundamentally, reliance on treatment prefer-ences generated in advance of serious illness assumesthat healthy individuals can anticipate their reactionsto future disease states and predict their preferences
Received 24 February 2005 from the Department of Psychology andSocial Behavior, University of California, Irvine (PHD); Department ofPsychology, Queen’s University (JAJ); Department of Family Practice,Summa Health System (WDS); Center for Advanced Study of Language,University of Maryland (JHD); and VA Center for Practice Managementand Outcomes Research, University of Michigan (AF). Financial supportfor these studies was provided by grants from the Agency for HealthcareResearch and Quality (HS08180), the Applied Psychology Center atKent State University, and the Summa Health System Foundation.Dr. Fagerlin is supported by an MREP early career award from the US
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

314 • MEDICAL DECISION MAKING/JUL–AUG 2006
for various life-sustaining treatments. If healthy indi-viduals cannot predict accurately their reactions toserious illness—for example, because life-sustainingtreatment decisions are affected by changes in anindividual’s physical or psychological condition—then treatment decisions made in advance of seriousillness should not be taken as authentic representa-tions of the decisions an incapacitated individualwould make if he or she were currently able.
In fact, the assumption that healthy individualscan predict accurately their reactions to futureillness is challenged by growing bodies of researchin both the psychological and medical literatures.Research on “affective forecasting,” for example, hasshown that individuals make systematic errorswhen trying to predict their emotional reactions andbehavioral choices in future situations.9,10 Similarly,a number of studies have found healthy people toassign different utilities to disease states and treat-ments than do individuals with direct personalexperience with the disease or treatment.11–15
The best of these studies use prospective designs inwhich assigned utilities from the same individuals arecollected both prior to and after experiencing theevent of interest.12,13,16 In a well-known study byChristensen-Szalanski,12 for instance, preferences forthe use of anesthesia during labor were solicitedseveral times before, during, and after childbirth.One month before labor and in early labor, womenexpressed a clear preference to avoid anesthesia. Aslabor progressed and the women experienced signifi-cant discomfort, however, preferences shifted stronglytoward choosing anesthesia. Importantly, when thesame women were interviewed again 1 month afterdelivery, they had returned to their prechildbirth pref-erence for avoiding anesthesia.
If life-sustaining treatment choices show a similarcontext dependency, the underlying premise ofinstructional advance directives is challenged. Of
course, the ideal prospective study in which prefer-ences stated by a healthy individual are compared tothose of that same individual when incapacitated isimpossible. A more feasible alternative is to examinelife-sustaining treatment preferences stated beforeand after treatment for a condition that requires hos-pitalization but is not so serious as to result in inca-pacitation or the use of life-sustaining therapy. Thefrequency of hospitalization in older adults makes it amenable to prospective examination. Moreover,although in most cases it will be only a relativelyweak approximation of the impact caused by life-threatening illness requiring decisions about the useof life-sustaining treatment, any hospitalizationexperience is likely to result in some importantdegree of discomfort, dependency, and distress. Iflife-sustaining treatment preferences change afterexperience with non-life-threatening hospitaliza-tion, this result would certainly cast doubt on thestability of such preferences in the face of more seri-ous illness.
This study uses a prospective design, modeledafter Christensen-Szalanski,12 to examine elderlyadults’ desire for the use of life-sustaining medicaltreatment prior to, soon after, and several months aftera hospitalization experience. Most previous studieshave found that individuals having direct experiencewith health states and treatments assign higher utili-ties to them (i.e., perceive them more positively) thando individuals without such experience.11,13–15 Arecent study of current and former colostomy patientshas also found that individuals for whom a medicalcondition has been resolved assign lower utilities tothe condition than do individuals currently experi-encing the condition.17 In contrast, the Christensen-Szalanski study12 found that women seemed toperceive labor more negatively (i.e., as more painful)while they were experiencing it than they did beforeor well after the experience. Similarly, past researchhas found increases in depression (one likely result ofhospitalization) to be associated with both increased18
and decreased19 desire for life-sustaining treatment.Thus, although prior studies offer conflicting guid-ance regarding the specific effects hospitalizationmight have on life-sustaining treatment preferences,they converge on the prediction that any preferencechange resulting from hospitalization is itself likely tobe temporary and will change again as any physicaldiscomfort and/or emotional distress caused by hos-pitalization dissipates over the course of recovery.Thus, our general prediction was that life-sustainingtreatment preferences would be context dependent,and they would vary significantly depending on
DITTO AND OTHERS
Department of Veterans Affairs (MRP 04-222). The funding agreementensured the authors’ independence in designing the study, interpretingthe data, writing, and publishing the report. The authors acknowledgethe assistance of Helen Anderson, N. Sharleen Boley, Miriam Curran,Mary J. Kennard, Pat Leonard, and Isabel Ricker in data collection andJanet Long in coordinating data collection. We also gratefully acknowl-edge the contributions of Kristen Coppola, Renate Houts, and JamilaBookwala. Revision accepted for publication 4 January 2006.
Address correspondence to Peter H. Ditto, PhD, Department ofPsychology & Social Behavior, 3340 Social Ecology II, University ofCalifornia, Irvine, Irvine, CA 92697-7085; e-mail: [email protected].
DOI: 10.1177/0272989X06290494
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

whether they were elicited prior to, soon after, or sev-eral months after hospitalization.
METHOD
Overview
This investigation used data collected as part ofthe Advance Directives, Values Assessment, andCommunication Enhancement (ADVANCE) pro-ject.20,21 The ADVANCE project was a 3-phase longi-tudinal study intended to test several assumptionsunderlying the use of instructional advance directives.The first phase of data collection (time 1) involved arandomized controlled trial assessing the effectivenessof different types of advance directive interventionsfor improving the agreement between elderly outpa-tients’ and their surrogates’ life-sustaining treatmentchoices.20 Phase 2 focused on the longitudinal sta-bility of patients’ preferences measured 1 (time 2)and 2 (time 3) years after the initial phase 1 inter-view.21 Phase 3, the focus of the present investiga-tion, used a prospective design involving a subset ofpatients who happened to be hospitalized duringtheir participation in the project.
Subjects and Data Collection
ADVANCE subjects were recruited from lists ofoutpatients aged 65 and older obtained from 6 pri-mary care practices affiliated with Summa HealthSystems in Akron, Ohio.20 Potential subjects werecontacted by letter and later by telephone to deter-mine their eligibility and willingness to participatein a 2-year longitudinal study investigating the life-sustaining treatment preferences of older adults.Initial interview data were collected from 401subjects at time 1, and 332 (83%) of these subjectsremained in the study through time 3.
On a weekly basis, hospital admissions personnelnotified ADVANCE project staff whenever one of oursubjects was hospitalized for more than 48 hours ateither of Summa Health System’s 2 hospitals. Duringthe 2 years of the study, 103 subjects (26% of the totalsample) met this hospitalization criterion at least once.Slightly more subjects were hospitalized betweentimes 1 and 2 (58%) than between times 2 and 3.
Hospitalized subjects were contacted to completean additional interview that was scheduled to takeplace as soon as possible after the subject had beenreleased from the hospital. We will refer to this as therecovery interview because it was designed to reflectsubject preferences in the midst of their recovery from
the hospitalization experience. For all analyses,subjects’ prehospitalization interview data came fromtheir most recent annual interview prior to the hospi-talization that prompted their recovery interview(either time 1 or time 2), and their posthospitalizationinterview data came from their next annual interview(either time 2 or time 3). The amount of time that hadtranspired since the annual interview immediatelyprior to the subjects’ hospitalization did not affect thescheduling of their recovery interview. However, aminimum delay of 3 months between their recoveryinterview and their next annual interview was insti-tuted to allow subjects time to recover sufficientlyfrom their illness episode.
Of the 103 eligible subjects, 4 were unable to com-plete the recovery interview (e.g., 1 died within 2 weeks of being discharged, 1 was in a coma), 2 wereunreachable, and 9 refused to participate. The hos-pitalized subjects who did and did not complete arecovery interview did not differ significantly interms of their age, gender, education, or their base-line physical or mental health scores. Ultimately,interview data were collected successfully from 88subjects (85% of the hospitalized sample) during orimmediately after their first hospitalization (M = 14days following discharge).a
Life-Support Preferences Questionnaire
At each annual interview, subjects completed theLife-Support Preferences Questionnaire (LSPQ20)assessing desire to receive medical treatment in 9 dif-ferent medical scenarios. To minimize respondentburden during the recovery interview, a shortenedversion was used that focused on only 4 of the 9health scenarios: Alzheimer’s disease, terminal can-cer with pain, coma with no chance of recovery, andstroke with a slight chance of recovery. Subjects imag-ined themselves in each medical condition and indi-cated if they would want to receive each of 4 medicaltreatments that varied in invasiveness: 1) cardiopul-monary resuscitation (CPR) for cardiac arrest, 2) arti-ficial nutrition and hydration (ANH) for inability toeat or drink, 3) gall bladder surgery (GBS) for a life-threatening gall bladder infection, and 4) antibioticsfor life-threatening pneumonia. Ratings were made ona 5-point scale ranging from 1 = definitely do not wanttreatment to 5 = definitely want treatment.
CONTEXT CHANGES CHOICES
UTILITIES AND PREFERENCES 315
a. Of the 88 subjects, 16 people (18%) were rehospitalized during thecourse of the study, and only 2 of these subjects refused to complete an inter-view after their second hospitalization. To avoid statistical dependency causedby using data from the same 14 people more than once, all the analyses wereconducted using only the data from the subjects’ first hospitalization.
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

316 • MEDICAL DECISION MAKING/JUL–AUG 2006
Secondary Measures
To glean additional information about what mightaccount for any preference changes caused byhospitalization, a number of measures were includedthat could be used in moderator analyses. At all ofthe interviews, the short form of the Center forEpidemiologic Studies–Depression Scale (CES-D22)served as a measure of depressive symptomatology.Two items were used to assess the subjects’ generalhealth (5-point scale from excellent to poor) and phys-ical pain (5-point scale from none to severe) at therecovery interview, and these same questions also werecompleted at the annual interviews as part of theMedical Outcomes Study Short Form (SF-3623).Finally, 3 questions asked at the recovery interviewassessed subjects’ perceptions of the seriousness of theillness for which they required hospitalization (“Howwould you rate the seriousness of your current ill-ness?” “How likely do you think it is that you willreturn to your normal day-to-day functioning afterthis illness?” “How soon do you think you will returnto your normal day-to-day functioning after this ill-ness?”. For each question, the same basic 5-point scaleswere used, ranging from extremely (serious/likely/soon) to not at all (serious/likely/soon).
Analysis
An overall treatment preference index was createdby averaging subjects’ responses to the 16 individualpreference judgments (preferences for each of 4 life-sustaining treatments in each of 4 illness scenarios).In addition, separate indices were created for each ofthe 4 treatments by averaging preferences for eachtreatment across the 4 scenarios.b Changes in life-sustaining treatment preferences over time were ana-lyzed with repeated-measures analyses of variance(ANOVAs) with interview (prehospitalization, recov-ery, posthospitalization) as the within-subjects factor.These ANOVAs were followed up with contrastanalyses to clarify whether the pattern of any signifi-cant changes in preferences across interviews tendedto be linear (consistent increases or decreases in pref-erences over time) or quadratic (e.g., a spike or dip inpreferences at the recovery interview) in form.
To examine possible moderators of preferencechange, a series of general linear model analyses wasconducted, with interview as the within-subjects
factor and 1 of the following variables used as a con-tinuous between-subjects factor: perceived serious-ness of illness ratings, length of hospitalization, anddifference scores representing changes in depressivesymptomatology, general health, and bodily pain fromprehospitalization to recovery.
Finally, an additional set of analyses was conductedto assess the clinical relevance of preference changeacross interviews. First, the 5-point preference scaleswere dichotomized into “want treatment” (“definitelywant,” “probably want,” or “unsure”) and “don’t wanttreatment” (“probably do not want” and “definitely donot want”) categories,20,21,24–26 and the proportion ofwant and don’t-want treatment responses remainingstable across the 3 interviews was calculated. It is pos-sible, however, that a substantial portion of the insta-bility captured by these dichotomized data representsvery minor changes in preferences (e.g., from probablywant to unsure). To account for this possibility, weexamined the mean magnitude of utility loss acrossinterviews. We assumed that our response scale was alinear measure of utility and that no change in decision(e.g., from probably to definitely want/do not want orvice versa) represented zero loss. Once a change indecision occurred, however (even from probablywant/do not want to unsure), each scale point changewas counted as 1 unit of utility loss. We calculated themean magnitude of utility loss (overall and for eachlife-sustaining treatment) using prehospitalizationpreferences to predict recovery interview preferences.For purposes of comparison, we also calculated simi-lar utility loss measures for an actuarial decision strat-egy of using the most common preference in oursample (in every case, this was to not want treatment)to predict recovery preferences.27,28 The utility lossassociated with the preference-based and actuarialstrategies was compared with dependent t tests.
RESULTS
Sample Characteristics
Characteristics of the sample are shown in Table 1.Subjects were mostly European Americans (94%)who, at time 1, ranged in age from 65 to 94 years (M= 73.6). The sample contained roughly equalnumbers of females (52%) and males, and a slightmajority were high school graduates (M = 12.4 yearsof school). At the time of the hospital interview, 59%of subjects reported having an advance directive(either a living will or a durable power of attorneyfor health care).
DITTO AND OTHERS
b. Similar results were obtained when preferences were averaged foreach scenario across the 4 treatments.
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

On average, subjects were hospitalized for 1 week(M = 7.2 days, SD = 14.3). In general, subjects rated theirillness as “somewhat” to “pretty serious” (M = 3.6) butbelieved that they were “pretty likely” to return to nor-mal (M = 4.3) and to do so “pretty soon” (M = 3.7). The2 most common reasons for hospitalization were ortho-pedic surgery (24%) and cardiovascular disease (19%).Only 2 of the 4 hypothetical illness conditions coveredin the LSPQ were among the reasons for hospitalizationin this sample: 10% had cancer and 4% had a stroke.
Subjects’ self-reported mental and physical health wascompared across interviews using repeated-measures
ANOVAs and linear and quadratic contrast analyses.Subjects’ self-reported general health changed signifi-cantly over time, F(2, 158) = 3.06, P = 0.05, and onlythe quadratic contrast was significant, F(1, 79) = 6.29,P = 0.01. As expected, subjects reported poorer generalhealth at the time of the recovery interview comparedto their annual interviews (see Table 1). Subjects alsoexperienced marginal changes in depressive symp-toms, F(2, 152) = 2.78, P < 0.07, with subjects tendingto report more depressive symptoms during the recov-ery interview than at either annual interview. However,neither the quadratic nor the linear contrast analysiswas significant. Subjects’ ratings of bodily pain did notdiffer significantly over time.
Change in Treatment Preferencesacross Interviews
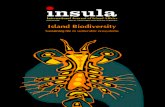
Repeated-measures ANOVAs comparing meandesire for treatment across the 3 interviews showedsignificant differences for the total LSPQ score,F(2, 154) = 3.79, P < 0.05, and the CPR and ANHsubindices, Fs = 4.57, Ps < 0.02. In all 3 cases, the qua-dratic contrasts were significant, Fs = 4.28, Ps < 0.03.As shown in Figure 1, subjects’ preferences for receiv-ing CPR and ANH showed a “hospitalization dip” atthe recovery interview. That is, subjects expressedless interest in receiving each treatment immediatelyafter hospitalization than they did either prior to
CONTEXT CHANGES CHOICES
UTILITIES AND PREFERENCES 317
Table 1 Sample Characteristics
Variable Patients (N == 88)
Mean age (SD) 73.6 (5.6)Gender, no. (%) female 46 (52)Race, no. (%) European
American 83 (94)Mean years of 12.4 (2.6)
education (SD)No. (%) with AD/living will 15 (17)No. (%) with DPAHC 1(1)No. (%) with both 36 (40)Reason for hospitalization, no. (%)
Orthopedic 21 (24)Cardiovascular 17 (19)Cancer 9 (10)Digestive 9 (10)Pneumonia 8 (9)Infection 8 (9)Fainted 7 (8)Stroke 4 (4)Miscellaneous 5 (5)
Mean seriousness 3.6 (1.1)of illness (SD)
Mean likelihood of 4.3 (0.9)returning to normal (SD)
Mean speed of returning 3.7 (0.9)to normal (SD)
Prehospitalization Recovery Posthospitalization
Mean 6.0 (5.2) 7.4 (5.4) 6.6 (5.0)CES-D (SD)
Mean 3.2 (0.9) 2.9 (0.9) 3.1 (0.9)generalhealth(SD)
Mean 3.3 (1.4) 3.6 (1.3) 3.5 (1.2)bodilypain(SD)
Note: AD = advance directive; CES-D = Center for EpidemiologicalStudies–Depression Scale-10; DPAH = durable power of attorney forhealth care.
1.0
2.0
3.0
4.0
5.0
Pre-Hospital Recovery Post-Hospital
CPR ANH GBS Antibiotics
Figure 1 Mean treatment preferences at the prehospitalization,recovery, and posthospitalization interviews. CPR, cardiopul-monary resuscitation; ANH, artificial nutrition and hydration;GBS, gall bladder surgery.
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

318 • MEDICAL DECISION MAKING/JUL–AUG 2006
hospitalization or in the months after hospitalization.The same pattern of means was seen on the totalLSPQ score (prehospital M = 2.21, recovery M = 1.98,posthospital M = 2.09). Preferences for GBS andantibiotics showed no significant differences acrossinterviews.
The analyses examining potential moderators ofpreference change showed no evidence that changesin desire for life-sustaining treatment across the inter-views was affected by subjects’ perceptions of theseriousness of their illness, the length of their hospi-tal stay, or the magnitude of changes in their depres-sive symptomatology, perceived general health, orbodily pain from prehospitalization to recovery.c
Stability of Want and Don’t-WantResponses across Interviews
Table 2 presents the percentage of want and don’t-want responses changing and remaining stablebetween the prehospitalization and recovery inter-views. As can be seen in that table, want treatmentresponses were considerably less stable than don’t-want treatment responses when responses were aggre-gated across all LSPQ items as well as for the CPR,ANH, and GBS items aggregated separately. Across allLSPQ responses, for example, 87% of responses indi-cating refusal of treatment prior to hospitalizationremained stable at the recovery interview. In contrast,43% of cases in which participants wanted to receivetreatment prior to hospitalization changed to don’t-want treatment responses at the recovery interview(stability = 57%). Only antibiotic preferences did notshow a similar pattern.
Because of our particular interest in the fate ofresponses changing from wanting treatment at the pre-hospitalization interview to refusing treatment at therecovery interview, Table 3 compares the recovery-to-post-hospitalization stability of these judgments tothat of responses showing a consistent refusal of treat-ment in the first 2 interviews. Again consideringresponses aggregated across all LSPQ items, 90% ofpreferences showing a consistent pattern of treatmentrefusal from prehospitalization to recovery alsoremained stable from recovery to posthospitalization.In contrast, fully 50% of the responses showing achange from want to don’t-want treatment from pre-hospitalization to recovery shifted back to want treat-ment at the posthospitalization interview.
Utility Loss
In general, utility loss was modest (typically lessthan 1 unit) for both the preference-based and actuar-ial strategies across all treatments. Most important,however, the utility loss associated with usingsubjects’ prehospitalization preferences to predict theirrecovery preferences was generally very similar to theloss associated with the very simple actuarial strategyof predicting recovery preferences from the sample’smodal response. For example, the preference-basedapproach was actually a slightly (though not signifi-cantly) less accurate strategy (i.e., it produced moremean utility loss) than the actuarial approach for CPR(.55 v. .45) and ANH preferences (.42 v. .35) and for theindex averaging across all 16 treatment preferences
DITTO AND OTHERS
Table 2 Stability of Want and Don’t-WantTreatment Responses between the
Prehospitalization and Recovery Interviews
Recovery
Treatment Prehospital Don’t Want Want % Stable
CPR Don’t want 225 18 93Want 56 44 44
ANH Don’t want 250 19 93Want 41 33 45
GBS Don’t want 180 39 82Want 51 74 59
Antibiotics Don’t want 147 48 75Want 44 107 71
Total LSPQ Don’t want 802 124 87Want 192 258 57
Note: Units are responses rather than participants. ANH, artificialnutrition and hydration; CPR, cardiopulmonary resuscitation; GBS, gallbladder surgery; LSPQ, Life-Sustaining Treatment PreferencesQuestionnaire.
c. Two dichotomous variables, timing of subjects’ hospitalization(between the time 1 and 2 annual interviews or between the time 2 and 3annual interviews) and whether or not the subject had an advance directive(either instructional or proxy), were also examined as potential moderators ofpreference change across the interviews. Significant Advance Directive ×Interview interactions were found for the total Life-Support PreferencesQuestionnaire (LSPQ) index, F(2, 152) = 3.65, P < 0.001, and for the car-diopulmonary resuscitation (CPR), artificial nutrition and hydration (ANH),and antibiotics subindices, Fs = 3.11, Ps < 0.05. The pattern of these interac-tions, however, is difficult to interpret. For CPR and ANH preferences, bothadvance directive groups showed a tendency to want less treatment at therecovery interview compared to the annual interviews, quadratic contrastFs = 3.55, Ps < 0.07. The interaction for these preferences seems to be a func-tion of a tendency for subjects with an advance directive to show a smallerdecrease in desire for treatment from the prehospitalization to the recoveryinterview, but a larger increase in desire for treatment from the recovery to theposthospitalization interview, than did individuals without an advance directive.The interaction pattern for antibiotic preferences was different. Subjects with anadvance directive showed a significant linear decrease in desire for antibioticsover time, F(1, 76) = 6.52, P < 0.01, whereas subjects without an advance directive showed a nonsignficant trend (P < 0.15) in the other direction.
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

(.67 v. .57). Only in the case of antibiotic preferenceswas the preference-based approach statistically supe-rior to the actuarial one (.66 v. 1.07), t(85) = 3.64, P < 0.001.
DISCUSSION
This study used a prospective design to examinethe life-sustaining treatment preferences of 88 olderadults before hospitalization, during their recovery fromthe hospitalization, and several months after recovery.We found that treatment preferences elicited duringrecovery from an important, but not life-threatening, ill-ness were different from those stated both prior to andmonths after hospitalization.
Specifically, subjects reported less desire for life-sustaining medical treatment during the recoveryinterview than they did during the annual interviewconducted prior to their hospitalization. If we were toconsider just these 2 data points, one plausible expla-nation would be that direct experience with the dis-comforts of hospitalization caused an enduring changein our subjects’ attitudes about the value of extendinglife via aggressive medical treatment. Following thelessons of Christensen-Szalanski’s12 study of anesthesiapreferences, however, we continued to track our subjects’treatment preferences in the months after their hospi-talization. This follow-up measurement highlighted thetemporary nature of preference changes observed in theimmediate context of a medical event. Instead of hospi-talization causing an enduring decline in subjects’desire for life-sustaining treatment, patients’ change inpreferences was shown to be fleeting, as preferencesreturned to near prehospitalization levels at the next
regular annual interview (conducted at least 3 monthsafter hospitalization). This pattern of contextual changeis very similar to that found by both Christensen-Szalanski12 and in a recent study comparing percep-tions of current and former colostomy patients.17
Although a significant hospitalization dip wasfound on the overall index combining all 16 prefer-ence judgments, the effect was most pronounced inpreferences for the most invasive treatments of CPRand ANH. These treatments are the focus of many end-of-life decisions, and at an intuitive level, they mightseem to be the treatments about which people shouldhave the most clear-cut and stable opinions. Thus, animportant contribution of the current study is to doc-ument that preferences for these prototypical exam-ples of life-sustaining treatment may be particularlydependent on the context in which they are elicited.
Further insight into the specific pattern of contex-tual change observed in the current study is revealedby examining the proportion of want and don’t-wanttreatment responses changing across the interviews.Consistent with the hospitalization dip pattern foundin the primary analyses, instability in treatment pref-erences across interviews occurred primarily for indi-viduals who initially indicated their desire to receivetreatment at the prehospitalization interview. TakingCPR decisions as an example, whereas treatmentrefusal decisions remained highly stable across all 3interviews, 56% of all decisions to receive CPR at theprehospitalization interview changed to decisions torefuse treatment at the recovery interview, and 56% ofthose initially unstable decisions changed back towanting CPR by the time of the posthospitalizationinterview several months later. These findings suggest
CONTEXT CHANGES CHOICES
UTILITIES AND PREFERENCES 319
Table 3 Stability of Don’t-Want Treatment Responses between Recovery and PosthospitalizationInterviews by Prehospitalization Treatment Preferences
Posthospital
Treatment Prehospital to Recovery Don’t Want Want % Stable
CPR Don’t want → don’t want 189 24 89Want → don’t want 24 30 44
ANH Don’t want → don’t want 222 14 94Want → don’t want 24 15 62
GBS Don’t want → don’t want 143 25 85Want → don’t want 20 28 42
Antibiotics Don’t want → don’t want 125 12 91Want → don’t want 23 19 55
Total LSPQ Don’t want → don’t want 679 75 90Want → don’t want 91 92 50
Note: Units are responses rather than participants. ANH, artificial nutrition and hydration; CPR, cardiopulmonary resuscitation; GBS, gall bladdersurgery; LSPQ, Life-Sustaining Treatment Preferences Questionnaire.
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

320 • MEDICAL DECISION MAKING/JUL–AUG 2006
that physicians and family makers should be sensitiveto the possibility that decisions to receive life-sustainingtreatment stated by healthy individuals may be partic-ularly susceptible to contextual change and, more gen-erally, that even the seemingly modest changes inpreferences observed in analyses of the undi-chotomized scale responses can have clinically rele-vant implications. When faced with essentially a50-50 chance that decisions expressed at any giventime will change with changes in an individual’shealth condition, the task of divining a patient’s “true”end-of-life wishes becomes difficult. The utility lossanalyses confirm that, in the current study, usingpatients’ prehospitalization desire for life-sustainingtreatment to predict their desire for the same treat-ments in the immediate aftermath of hospitalizationwas a no more accurate strategy than simply predict-ing recovery interview preferences from the mostcommon preference stated by the sample.
Strengths, Limitations, and Future Directions
An important strength of this study was its prospec-tive design. We elicited elderly subjects’ preferencesfor life-sustaining treatment in future hypotheticalhealth states prior to an unplanned hospitalization,which then allowed us to compare these decisions tothose made in the recovery period. Moreover, by col-lecting these prospective data in the context of a 2-yearlongitudinal study, we were able to interview patientsagain months after their hospitalization—data thatyielded valuable information about the context depen-dency of patients’ treatment preferences.
One limitation of the study design was the lack ofa no-hospitalization control group that was inter-viewed near the same time as our hospitalized sam-ple. Although this would have been an ideal methodof confirming the causal role of the hospitalizationexperience in our findings, the U-shaped pattern ofpreference change observed in the current study isnot easily explained by the simple passage of time.
Another key limitation of the study is that we exam-ined a small, relatively healthy sample of individuals,most of whom did not experience life-threatening ill-ness. Smaller than ideal samples are a common afflic-tion of prospective studies. Prospective studies also, bydefinition, examine only a select and potentiallyunique subgroup of the larger study sample. The cur-rent study was generally quite successful, however, inthat we were able to use more than 20% of the totalADVANCE sample due to the substantial rate of hospi-talization in older adults. Moreover, a compelling argu-ment can be made that finding significant preference
change after relatively minor hospitalization experi-ences does not bode well for the stability of treatmentpreferences in the face of more serious illness or injury.
Still, it would be valuable for future research toreplicate the current findings in a sample of individu-als confronted with more serious illness for 2 generalreasons. First, studying individuals experiencing andthen recovering from serious illness would help to betteraddress questions about the psychological mecha-nisms underlying contextual changes in treatmentpreferences. In addition to documenting preferencechanges associated with hospitalization, a second goalof the current study was to begin to specify why suchpreference changes might occur. We collected dataabout subjects’ physical and psychological states thatmight be expected to change with hospitalization andthus might account for changes in life-sustaining treat-ment choices. The reported moderator analyses wereintended to address such issues in that if, for example,the dip in desire for treatment was most pronouncedfor those individuals showing the largest increasesin depressive symptoms from prehospitalization torecovery, then a key role for depression in preferencechange would be suggested. None of the health statefactors we examined, however, were significant mod-erators of preference change. One likely contributor tothe inconclusiveness of these analyses was that thehealth state factors themselves showed relatively littlechange across interviews. In a sample of individualsfacing hospitalization for more serious health condi-tions, more dramatic changes in health state would be expected, and these changes would greatly facili-tate identification of moderating (or even mediating)variables.
The first reason for examining treatment preferencechange in individuals facing serious illness, therefore,is because the magnitude of effects may be greaterthan in individuals facing less serious health threats.The second reason is that the pattern of effects maydiffer as well. In the current study, hospitalizationwas associated with a decreased desire for life-sus-taining medical treatment. Consider, however, thecommon intuitive example of the individual whosteadfastly asserts his or her wish to forgo heroic med-ical treatment while healthy but becomes moreaggressive about life-prolonging treatment once facedwith the genuine possibility of death. A more theoret-ically sophisticated version of this pattern is consis-tent with research showing an impact bias in affectiveforecasting.10 That is, a number of studies have shownthat individuals tend to overestimate both the magni-tude and duration of their affective reactions to futurelife events.14,16,29,30 This impact bias would predict that
DITTO AND OTHERS
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

healthy individuals should tend to underestimatetheir interest in receiving life-sustaining treatment interminal illness situations (believing that they wouldrespond more poorly to the illness than they would inactuality). No data currently exist to confirm whetherthis pattern of preference change, or the one found inthe current study, best characterizes how preferencesfor life-sustaining treatment made by healthy individ-uals might change in response to a real end-of-lifescenario. As noted earlier, an ideal test examiningwhether life-sustaining treatment preferences remainstable into periods of incapacitating illness (the timewhen treatment instructions in advance directiveswould be consulted) is not possible. Still, the moreclosely researchers can approximate this ideal bystudying samples of individuals experiencing andthen recovering from serious illness, the more valid(and specific) are the conclusions that can be drawn.The growing body of theoretical work regardingpeople’s ability to predict their future feelings andchoices10,14,31,32 can be drawn upon to refine predic-tions of how hypothetical and “real” health decisionsmight be expected to diverge for different medicalconditions and in varying decision contexts.
Conclusions
The current study is the latest addition to expand-ing bodies of research questioning 1) the stability oflife-sustaining treatment preferences over time andacross changes in an individual’s health condi-tion18,19,21,26,33 and 2) the general ability of individualsto predict accurately their future feelings and behav-ioral choices.9–16 As a whole, this work presents aformidable empirical challenge to the almost univer-sal advocacy of instructional advance directivesfound in modern American medicine. If treatmentpreferences made by healthy individuals cannot betaken as accurate representations of the treatmentchoices those individuals would make in actual end-of-life scenarios, then the value of documenting life-sustaining treatment preferences in instructionaladvance directives is suspect.
At first blush, this statement might be taken asan endorsement of the idea that the treatment prefer-ences of seriously ill individuals should be givenpriority over preferences expressed by healthy indi-viduals imagining (presumably in good faith and withdue consideration) their future illness. To the con-trary, however, the assumption that choices made inthe throes of serious illness are somehow “better”(i.e., more authentic) than decisions made by healthyindividuals in the calm detachment of hypothetical
consideration can be questioned from many angles.1,34–36
In many judgment situations, this valuation would bereversed, and emotional detachment would be seen aspreferable to emotional involvement as a context foroptimal decision making.
As empiricists, the goal of psychologists and decisionscientists is to pursue a more sophisticated understand-ing of how preferences for life-sustaining treatment areaffected by changes in an individual’s physical andemotional state and to document the conditions underwhich treatment preferences stated by healthy and illpeople are likely to differ. This empirical understand-ing can only be translated into clear policy guidance,however, if it then serves as input into an equallysophisticated ethical analysis regarding how to assignvalue to decisions made within the different contextsprovided by health and illness.
REFERENCES
1. Dresser R. Precommitment: A misguided strategy for securingdeath with dignity. Texas Law Rev. 2003;81:1823–47.2. Bradley E, Walker L, Blecher BB, Wettle T. Assessing capacity
to participate in discussions of advance directives in nursinghomes: findings from a study of the Patient Self DeterminationAct. J Am Ger Soc. 1997;45:79–83.3. American Association of Retired Persons. Tomorrow’s
Choices: Preparing Now for Future Legal, Financial, and HealthCare Decisions. Washington, DC: American Association of RetiredPersons; 1988.4. American Geriatrics Society Public Policy Committee. AGS
Position Statement: Medical Treatment Decisions ConcerningElderly Persons. New York: American Geriatrics Society; 1991.5. Orentlicher D. Advance medical directives. JAMA. 1990;263:
2365–7.6. 101st Congress—Second Session. Patient Self-Determination
Act. 1990; Public Laws 101-508 to 101-548.7. Ditto PH. Self-determination, substituted judgment, and the psy-
chology of end-of-life medical decision making. In: Werth J, BlevinsD, eds. Psychosocial Issues Near the End of Life: A Resource forProfessional Care Providers. Washington, DC: APA Press; 2006.8. Fagerlin A, Schneider, CE. Enough: the failure of the living
will. Hastings Center Report. 2004;34:30–42.9. Loewenstein G, Schkade D. Wouldn’t it be nice? Predicting
future feelings. In: Diener E, Schwarz N, Kahneman D, eds. HedonicPsychology: Scientific Approaches to Enjoyment, Suffering andWell-Being. New York: Russell Sage Foundation; 1999.10. Wilson TD, Gilbert DT. Affective forecasting. In: Zanna M, ed.Advances in Experimental Social Psychology (Vol. 35). New York:Elsevier; 2003.11. Boyd NF, Sutherland, HJ, Heasman KZ, Tritchler DL,Cummings BJ. Whose utilities for decision analysis? Med DecisMaking. 1990;10:58–67.12. Christensen-Szalanski JJ. Discount functions and the measure-ment of patients’ values: women’s decisions during childbirth.Med Decis Making. 1984;4:47–58.
CONTEXT CHANGES CHOICES
UTILITIES AND PREFERENCES 321
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from

322 • MEDICAL DECISION MAKING/JUL–AUG 2006
13. Jansen SJT, Stiggelbout, AM, Wakker PP, et al. Unstable pref-erences: a shift in valuation or an effect of the elicitation proce-dure? Med Decis Making. 2000;20:62–71.
14. Riis J, Loewenstein G, Baron J, et al. Ignorance of hedonicadaptation to hemodialysis: a study using ecological momentaryassessment. J Exp Psych Gen. 2005;134:3–9.
15. Sackett DL, Torrance GW. The utility of different health statesas perceived by the general public. J Chronic Dis. 1978;31:697–704.
16. Schkade DA, Kahneman D. Does living in California makepeople happy? A focusing illusion in judgments of life satisfac-tion. Psychol Sci. 1998;9:340–6.
17. Smith DM, Sherriff RL, Damschroder L, et al. Misrememberingcolostomies? Former patients give lower utility ratings than do cur-rent patients. Health Psychol. In press.
18. Danis M, Garrett J, Harris R, Patrick DL. Stability of choicesabout life-sustaining treatments. Ann Intern Med. 1994;120:567–73.
19. Rosenfeld KE, Wenger NS, Phillips RS, et al. Factors associatedwith change in resuscitation preference of seriously ill patients. TheSUPPORT investigators. Study to Understand Prognoses andPreferences for Outcomes and Risks of Treatments. Arch Intern Med.1996;156:1558–64.
20. Ditto PH, Danks JH, Smucker WD, et al. Advance directives asacts of communication: a randomized controlled trial. Arch InternMed. 2001;161:421–30.
21. Ditto PH, Smucker WD, Danks JH, et al. Stability of olderadults’ preferences for life-sustaining medical treatment. HealthPsychol. 2003;22:605–15.
22. Andresen EM, Carter WB, Malmgren JA, Patrick DL. Screeningfor depression in well older adults: evaluation of a short form ofthe CES-D. Am J Prev Med. 1994;10:77–84.
23. Ware JE, Sherbourne CD. The MOS 36-item Short-Form HealthSurvey (SF-36). Med Care. 1992;30:473–83.
24. Seckler AB, Meier DE, Mulvihill M, et al. Substituted judgment:how accurate are proxy predictions? Ann Intern Med. 1991;115:92–8.25. Uhlmann RF, Pearlman RA, Cain KC. Physicians’ and spouses’predictions of elderly patients’ resuscitation preferences. J Gerontol.1988;43:M115–21.26. Emanuel LL, Emanuel EJ, Stoeckle JD, Hummel LR, Barry MJ.Advance directives: stability of patients’ treatment choices. ArchIntern Med. 1994;154:209–17.27. Houts R, Smucker WD, Jacobson JA, et al. Predicting elderlyoutpatients’ life-sustaining treatment preference over time: themajority rules. Med Decis Making. 2002;22:39–52.28. Smucker WD, Houts R, Danks JH, et al. Modal preferences pre-dict elderly patients’ life-sustaining treatment preferences as wellas chosen surrogates. Med Decis Making. 2000;20:271–80.29. Gilbert DT, Pinel EC, Wilson TD, Blumberg SJ, Wheatley TP.Immune neglect: a source of durability bias in affective forecasting.J Pers Soc Psychol. 1998;75:617–38.30. Wilson TD, Wheatley TP, Meyers JM, Gilbert DT, Axsom D.Focalism: a source of durability bias in affective forecasting. J PersSoc Psychol. 2000;78:821–36.31. Trope Y, Liberman, N. Temporal construal. Psychol Rev.2003;110:401–21.32. VanBoven L, Loewenstein G. Social projection of transient vis-ceral feelings. Person Soc Psychol Bull. 2003;29:1159–68.33. Carmel S, Mutran E. Stability of elderly persons’ expressedpreferences regarding the use of life-sustaining treatments. SocSci Med. 1999;49:303–11.34. Elster J. Ulysses and the Sirens. Cambridge, UK: CambridgeUniversity Press; 1979.35. Emanuel L. Appropriate and inappropriate use of advancedirectives. Journal Clin Ethics. 1994;5:357–9.36. Ditto PH, Hawkins NA, Pizarro DA. Imagining the end of life.Motivation & Emotion. In press.
DITTO AND OTHERS
at UNIV OF MARYLAND on April 8, 2009 http://mdm.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN