Investigating Word of Mouth as Advertising Tool for Mobile ...
Upload
independentCategory
view
1download
0
Resuscitation (2006) xxx, xxx—xxx
TRAINING AND EDUCATIONAL PAPER
Comparison of mouth-to-mouth, mouth-to-maskand mouth-to-face-shield ventilation bylay persons�
Peter Paala,∗, Markus Falkb, Gunther Sumannc, Florian Demetzd,Werner Beikirchere, Elisabeth Grubere,John Ellertonf, Hermann Bruggerg
a Department of Anaesthesiology and Intensive Care Medicine, Mountain Rescue Service provided by the
South Tyrolean Alpine Association, International Commission for Mountain Emergency Medicine ICARMEDCOM, Innsbruck Medical University, Anichstrasse 35, A-6020 Innsbruck, Austriab Inova Q Inc., St. Lorenznerstrasse 34, I-39031 Bruneck, Italyc Department of Anaesthesiology and Critical Care Medicine, Division for General and Surgical IntensiveCare Medicine, International Commission for Mountain Emergency Medicine ICAR MEDCOM, InnsbruckUniversity, Anichstrasse 35, A-6020 Innsbruck, Austriad Clinic for Anaesthesiology, International Commission for Mountain Emergency Medicine ICAR MEDCOM,LMU University Munich, Grosshadern, 81377 Munich, Germanye Department of Anaesthesiology, General Hospital of Bruneck, Spitalstrasse 11, I-39031 Bruneck, Italyf Mountain Rescue Council England and Wales, International Commission for Mountain EmergencyMedicine ICAR MEDCOM, Pinfold, Nicholson Lane, Penrith, Cumbria CA11 7UL, Englandg Mountain Rescue Service provided by the South Tyrolean Alpine Association, President of theInternational Commission for Mountain Emergency Medicine (ICAR MEDCOM) Europastrasse 17, I-39031Bruneck, ItalyReceived 12 November 2004; received in revised form 17 February 2005; accepted 14 March 2005
KEYWORDSFace-shield;Mouth-to-mouthventilation;Mouth-to-mouthresuscitation;Pocket-mask;
SummaryObjective and methods: A prospective randomised study on 70 volunteers withoutprevious first aid education (42 males, 28 females, mean age 17) was performedto compare mouth-to-mouth ventilation (MMV, n = 24) versus mouth-to-pocket-maskventilation (MPV, n = 25) and mouth-to-face-shield ventilation (MFV, n = 21), and toevaluate if an instruction period of 10 min would be sufficient to teach lay per-sons artificial ventilation. Every volunteer performed three ventilation series usinga bench model of an unprotected airway.
� A Spanish translated version of the summary of this article appears as Appendix in the online version atdoi:10.1016/j.resuscitation.2005.03.024.
∗ Corresponding author. Tel.: +43 512 504 80448.E-mail address: [email protected] (P. Paal).
0300-9572/$ — see front matter © 2005 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.resuscitation.2005.03.024
RESUS-2893; No. of Pages 7

2 P. Paal et al.
Stomach inflation;Training;Ventilation
Results: MMV and MPV show higher mean tidal volume (TV) than MFV (values ofseries 3: 976 ± 454 and 868 ± 459 versus 604 ± 328 ml, P = 0.002 and P = 0.025, respec-tively). We found a higher inter-individual variation in TV than in previous studies(P = 0.031). The recommended TV of 700—1000 ml was reached in only 23%, mostfrequently with MPV (MMV 16.7%, MPV 32%, MFV 19%) but the difference was notsignificant (P = 0.391). However, we found a significantly higher percentage with aTV below 700 ml with MFV (MMV 33.3%, MPV 36%, MFV 66.7% P = 0.047) and a signifi-cantly higher percentage of TV exceeding 1000 ml with MMV (MMV 50%, MPV 32%, MFV14.3%) (P = 0.039). ‘‘Stomach’’ inflation was highest with MMV (79.2%) followed by MPV(52%) and MFV (42.9%) (P = 0.034). We found further differences between the sexes;males produced a higher TV (P = 0.003) and a higher percentage of stomach inflation(P = 0.029).Conclusion: MPV showed the best ventilation quality. It resulted in a more adequateTV than MMV and MFV and lower stomach inflation than MMV. Only a relatively lowpercentage of ventilations were within the recommended range for TV and this may berelated to the short training duration. We found different performances between thesexes, a high inter-individual variation and mainly a low ventilation quality. There-fore, further studies have to focus more on teaching duration, sex differences andventilation quality.© 2005 Elsevier Ireland Ltd. All rights reserved.
Introduction
Mouth-to-mouth-ventilation (MMV) is the standardtechnique for ventilation in Basic Life Support.
efficacy of face shields has not been documented
needed to train lay persons sufficiently in these ven-tilation techniques.
Our study aimed to compare MMV with MPV andMFV, and to assess if a short period of instruction of
and spirometry. All subjects were healthy and clas-swf
iiibib
conclusively’’, and suggested that ‘‘healthcare pro-fessionals and rescuers with a duty to respondshould use face shields only as a substitute formouth-to-mouth breathing and should use mouth-to-mask or bag-mask devices at the first opportu-nity’’.15
So far no prospective study has been carried outon the efficiency of MMV in comparison with mouth-to-mask and MFV, provided by lay persons. More-over, no data has been published yet, on the time
ified as ASA I.16 Expiratory vital capacity VCexas 4705 ± 625 ml for males and 3564 ± 458 ml for
emales.After the medical check each participant was
nstructed alone in the ILCOR 200015 guidelinesn one of two rooms by a teacher in a standard-sed way, using the same instruction flow charts inoth rooms. Teachers were physicians experiencedn CPR and a total of three teachers alternatedetween the rooms every half an hour. The venti-
MMV has been proven to be an efficient ven-tilation method.1—3 Nevertheless some authorshave noted a lack of willingness to ventilatea patient by the mouth-to-mouth technique inwitnessed respiratory arrest,4 because of con-cern about a potential infection.5—7 Due to thesepotential risks, rescuers prefer to use a bar-rier device during ventilation in CPR.3,4,8 Saferventilation techniques for lay rescuer ventila-tion have been developed to overcome the prob-lems inherent to MMV. Mouth-to-mask and mouth-to-face-shield ventilation techniques (MFV) havebeen introduced to encourage lay rescuers to per-form artificial ventilation; their effectiveness wasstudied thoroughly.1,2,8—14 Several mouth-to-mask-ventilation devices met the criteria for adequateventilation.1,10,11 On the other hand mouth-to-faceshield devices failed to demonstrate the capacityto provide sufficient tidal volume (TV).9 There-fore, the ILCOR 2000 guidelines stated that ‘‘the
10 min would be sufficient to teach lay rescuers thenecessary skills for proper ventilation.
Methods
The study was undertaken in a high school inBruneck, Italy, at 840 m above sea level. Sev-enty unpaid, voluntary students (28 females, 42males) participated having given informed, writ-ten consent. Mean age was 17.3 ± 0.7 years (range16—20). Mean height was 178.4 ± 6.1 cm for malesand 167.2 ± 6.3 cm for females. No differences insex or age distribution was observed between thethree ventilation groups (P = 0.57 Chi-Square Test).No volunteer had attended any first aid instructionbefore.
Before the tests every participant underwent ahealth check consisting of a questionnaire, physi-cal examination, weight and height measurement,
Comparison of mouth-to-mouth, mouth-to-mask and mouth-to-face-shield 3
lation technique was explained and then demon-strated by the instructor, and finally the candi-date performed ventilation under guidance of theinstructor. The theoretical and practical teach-ing was performed on a Laerdal Little AnneTM
and lasted for 10 min. The teacher did not influ-ence the outcome (P = 0.295, ANOVA). Accordingto the ILCOR 2000 guidelines sufficient ventila-tion is regarded as evident chest excursion. Ran-domisation was accomplished by distributing thealphabetically arranged candidates alternatively tothe two teaching rooms. In each room a venti-lation technique was assigned using a randomi-sation table balanced for sex: MMV (n = 24), MPV(Laerdal Pocket MaskTM) (n = 25), MFV (Laerdal FaceShield) (n = 21). The number of persons in the MFVgroup was limited to 21 due to the number of faceshields.
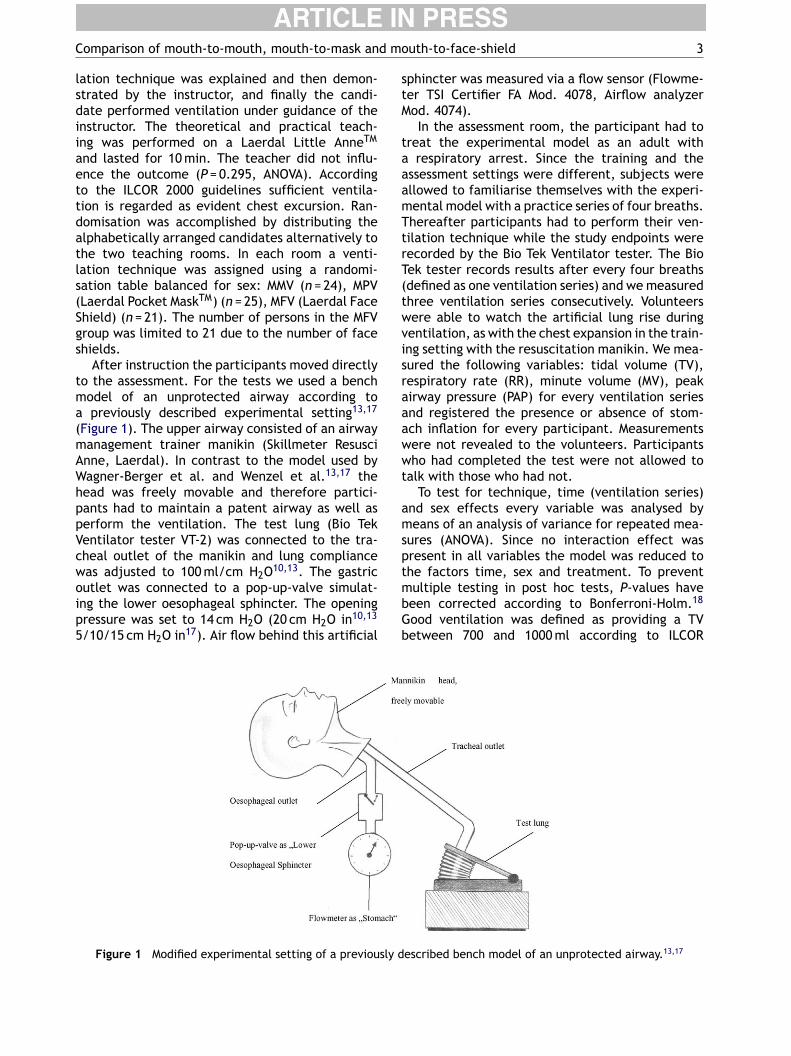
After instruction the participants moved directlyto the assessment. For the tests we used a benchmodel of an unprotected airway according toa previously described experimental setting13,17
(Figure 1). The upper airway consisted of an airwaymanagement trainer manikin (Skillmeter ResusciAnne, Laerdal). In contrast to the model used byW 13,17
hppVcwoip5
sphincter was measured via a flow sensor (Flowme-ter TSI Certifier FA Mod. 4078, Airflow analyzerMod. 4074).
In the assessment room, the participant had totreat the experimental model as an adult witha respiratory arrest. Since the training and theassessment settings were different, subjects wereallowed to familiarise themselves with the experi-mental model with a practice series of four breaths.Thereafter participants had to perform their ven-tilation technique while the study endpoints wererecorded by the Bio Tek Ventilator tester. The BioTek tester records results after every four breaths(defined as one ventilation series) and we measuredthree ventilation series consecutively. Volunteerswere able to watch the artificial lung rise duringventilation, as with the chest expansion in the train-ing setting with the resuscitation manikin. We mea-sured the following variables: tidal volume (TV),respiratory rate (RR), minute volume (MV), peakairway pressure (PAP) for every ventilation seriesand registered the presence or absence of stom-ach inflation for every participant. Measurementswere not revealed to the volunteers. Participantswho had completed the test were not allowed tot
amsptmbGb
sly d
agner-Berger et al. and Wenzel et al. theead was freely movable and therefore partici-ants had to maintain a patent airway as well aserform the ventilation. The test lung (Bio Tekentilator tester VT-2) was connected to the tra-heal outlet of the manikin and lung complianceas adjusted to 100 ml/cm H2O10,13. The gastricutlet was connected to a pop-up-valve simulat-ng the lower oesophageal sphincter. The openingressure was set to 14 cm H2O (20 cm H2O in10,13
/10/15 cm H2O in17). Air flow behind this artificial
Figure 1 Modified experimental setting of a previou
alk with those who had not.To test for technique, time (ventilation series)
nd sex effects every variable was analysed byeans of an analysis of variance for repeated mea-
ures (ANOVA). Since no interaction effect wasresent in all variables the model was reduced tohe factors time, sex and treatment. To preventultiple testing in post hoc tests, P-values haveeen corrected according to Bonferroni-Holm.18
ood ventilation was defined as providing a TVetween 700 and 1000 ml according to ILCOR
escribed bench model of an unprotected airway.13,17
4 P. Paal et al.
standards15 and stomach inflation was counted aspresent/absent. Data was analysed first by meansof a logistic regression to test for sex and techniqueeffects. Since no interaction was present betweensex and technique we compared data by means ofthe Chi-Square test. Correlation was assessed bymeans of the Partial Correlation Coefficient con-trolling for sex. To evaluate our observed vari-ance in TV we calculated pooled standard devia-tions (square root of the weighted mean variances)from our and published data and compared themby means of the F-Test. A P-value less than 0.05was considered significant and SPSS 7.5 (SPSS Inc.,Chicago, Illinois) software was used for statisticalanalysis. Data are reported as mean and standarddeviation or frequencies as appropriate.
Results
The results of the three test series with MMV,MPV and MFV regarding TV, MV, PAP, ventila-tion quality and stomach inflation are given inTable 1. For TV we found overall significant dif-
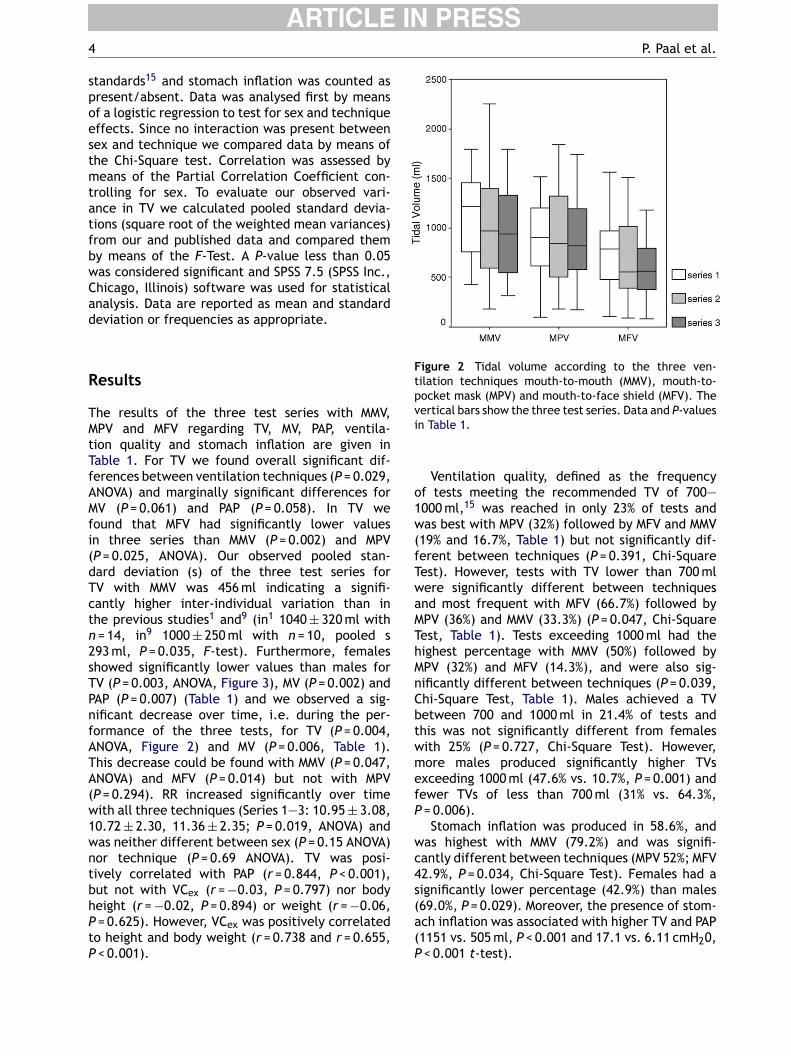
Figure 2 Tidal volume according to the three ven-tilation techniques mouth-to-mouth (MMV), mouth-to-pocket mask (MPV) and mouth-to-face shield (MFV). Thevertical bars show the three test series. Data and P-valuesin Table 1.
Ventilation quality, defined as the frequencyof tests meeting the recommended TV of 700—1000 ml,15 was reached in only 23% of tests andwas best with MPV (32%) followed by MFV and MMV(19% and 16.7%, Table 1) but not significantly dif-ferent between techniques (P = 0.391, Chi-SquareTest). However, tests with TV lower than 700 mlwere significantly different between techniquesand most frequent with MFV (66.7%) followed byMPV (36%) and MMV (33.3%) (P = 0.047, Chi-SquareTest, Table 1). Tests exceeding 1000 ml had thehighest percentage with MMV (50%) followed byMPV (32%) and MFV (14.3%), and were also sig-nificantly different between techniques (P = 0.039,Chi-Square Test, Table 1). Males achieved a TVbetween 700 and 1000 ml in 21.4% of tests andthis was not significantly different from femaleswith 25% (P = 0.727, Chi-Square Test). However,more males produced significantly higher TVsexceeding 1000 ml (47.6% vs. 10.7%, P = 0.001) andfewer TVs of less than 700 ml (31% vs. 64.3%,P = 0.006).
Stomach inflation was produced in 58.6%, andwas highest with MMV (79.2%) and was signifi-cantly different between techniques (MPV 52%; MFV4s(a(P
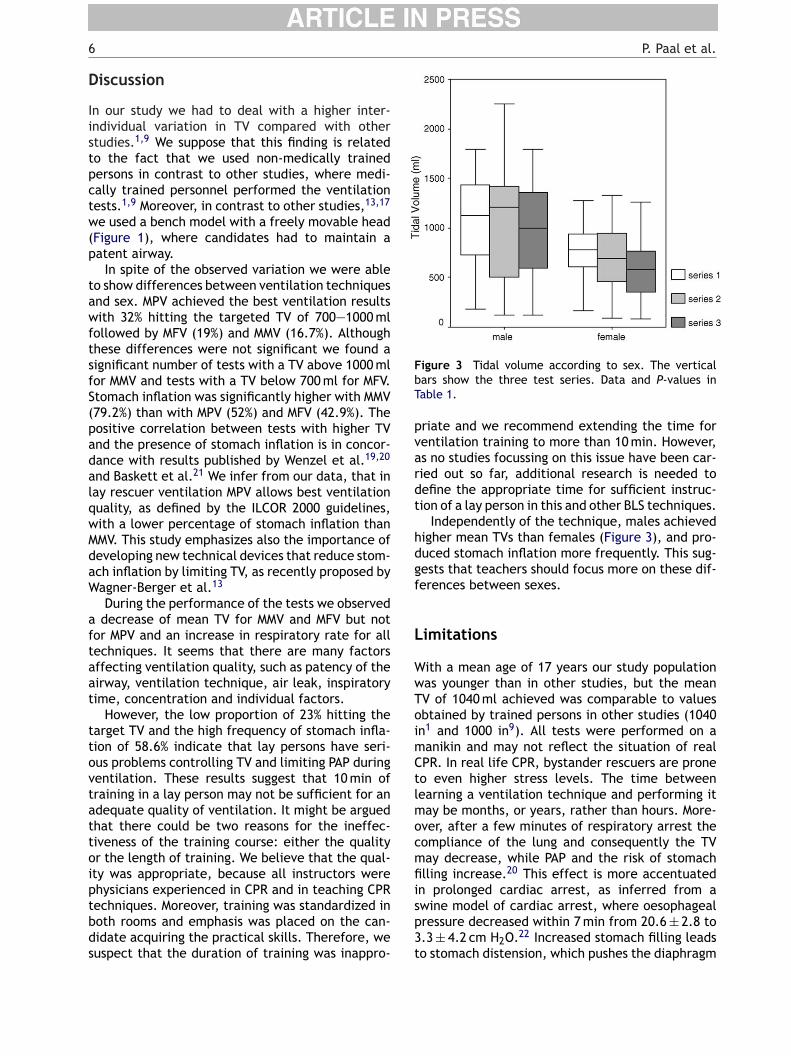
ferences between ventilation techniques (P = 0.029,ANOVA) and marginally significant differences forMV (P = 0.061) and PAP (P = 0.058). In TV wefound that MFV had significantly lower valuesin three series than MMV (P = 0.002) and MPV(P = 0.025, ANOVA). Our observed pooled stan-dard deviation (s) of the three test series forTV with MMV was 456 ml indicating a signifi-cantly higher inter-individual variation than inthe previous studies1 and9 (in1 1040 ± 320 ml withn = 14, in9 1000 ± 250 ml with n = 10, pooled s293 ml, P = 0.035, F-test). Furthermore, femalesshowed significantly lower values than males forTV (P = 0.003, ANOVA, Figure 3), MV (P = 0.002) andPAP (P = 0.007) (Table 1) and we observed a sig-nificant decrease over time, i.e. during the per-formance of the three tests, for TV (P = 0.004,ANOVA, Figure 2) and MV (P = 0.006, Table 1).This decrease could be found with MMV (P = 0.047,ANOVA) and MFV (P = 0.014) but not with MPV(P = 0.294). RR increased significantly over timewith all three techniques (Series 1—3: 10.95 ± 3.08,10.72 ± 2.30, 11.36 ± 2.35; P = 0.019, ANOVA) andwas neither different between sex (P = 0.15 ANOVA)nor technique (P = 0.69 ANOVA). TV was posi-tively correlated with PAP (r = 0.844, P < 0.001),but not with VCex (r = −0.03, P = 0.797) nor bodyheight (r = −0.02, P = 0.894) or weight (r = −0.06,P = 0.625). However, VCex was positively correlatedto height and body weight (r = 0.738 and r = 0.655,P < 0.001).
2.9%, P = 0.034, Chi-Square Test). Females had aignificantly lower percentage (42.9%) than males69.0%, P = 0.029). Moreover, the presence of stom-ch inflation was associated with higher TV and PAP1151 vs. 505 ml, P < 0.001 and 17.1 vs. 6.11 cmH20,< 0.001 t-test).
Comparison of mouth-to-mouth, mouth-to-mask and mouth-to-face-shield 5
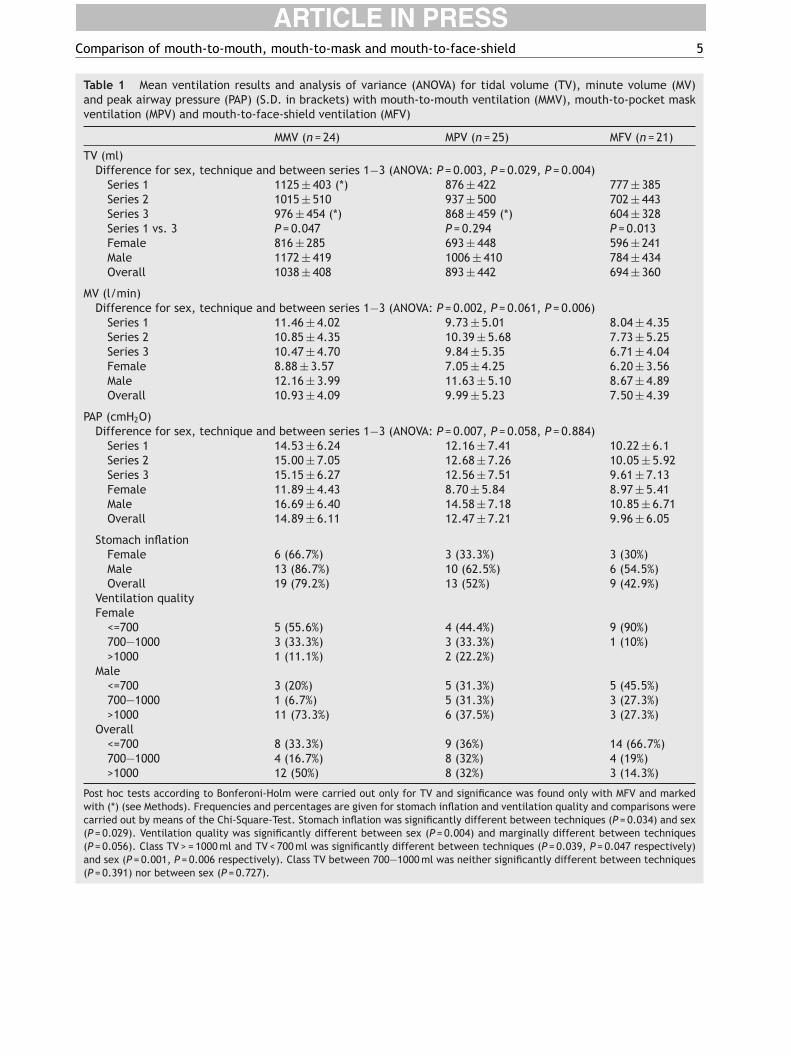
Table 1 Mean ventilation results and analysis of variance (ANOVA) for tidal volume (TV), minute volume (MV)and peak airway pressure (PAP) (S.D. in brackets) with mouth-to-mouth ventilation (MMV), mouth-to-pocket maskventilation (MPV) and mouth-to-face-shield ventilation (MFV)
MMV (n = 24) MPV (n = 25) MFV (n = 21)
TV (ml)Difference for sex, technique and between series 1−3 (ANOVA: P = 0.003, P = 0.029, P = 0.004)
Series 1 1125 ± 403 (*) 876 ± 422 777 ± 385Series 2 1015 ± 510 937 ± 500 702 ± 443Series 3 976 ± 454 (*) 868 ± 459 (*) 604 ± 328Series 1 vs. 3 P = 0.047 P = 0.294 P = 0.013Female 816 ± 285 693 ± 448 596 ± 241Male 1172 ± 419 1006 ± 410 784 ± 434Overall 1038 ± 408 893 ± 442 694 ± 360
MV (l/min)Difference for sex, technique and between series 1−3 (ANOVA: P = 0.002, P = 0.061, P = 0.006)
Series 1 11.46 ± 4.02 9.73 ± 5.01 8.04 ± 4.35Series 2 10.85 ± 4.35 10.39 ± 5.68 7.73 ± 5.25Series 3 10.47 ± 4.70 9.84 ± 5.35 6.71 ± 4.04Female 8.88 ± 3.57 7.05 ± 4.25 6.20 ± 3.56Male 12.16 ± 3.99 11.63 ± 5.10 8.67 ± 4.89Overall 10.93 ± 4.09 9.99 ± 5.23 7.50 ± 4.39
PAP (cmH2O)Difference for sex, technique and between series 1−3 (ANOVA: P = 0.007, P = 0.058, P = 0.884)
Series 1 14.53 ± 6.24 12.16 ± 7.41 10.22 ± 6.1Series 2 15.00 ± 7.05 12.68 ± 7.26 10.05 ± 5.92Series 3 15.15 ± 6.27 12.56 ± 7.51 9.61 ± 7.13Female 11.89 ± 4.43 8.70 ± 5.84 8.97 ± 5.41Male 16.69 ± 6.40 14.58 ± 7.18 10.85 ± 6.71Overall 14.89 ± 6.11 12.47 ± 7.21 9.96 ± 6.05
Stomach inflationFemale 6 (66.7%) 3 (33.3%) 3 (30%)Male 13 (86.7%) 10 (62.5%) 6 (54.5%)Overall 19 (79.2%) 13 (52%) 9 (42.9%)
Ventilation qualityFemale
<=700 5 (55.6%) 4 (44.4%) 9 (90%)700—1000 3 (33.3%) 3 (33.3%) 1 (10%)>1000 1 (11.1%) 2 (22.2%)
Male<=700 3 (20%) 5 (31.3%) 5 (45.5%)700—1000 1 (6.7%) 5 (31.3%) 3 (27.3%)>1000 11 (73.3%) 6 (37.5%) 3 (27.3%)
Overall<=700 8 (33.3%) 9 (36%) 14 (66.7%)700—1000 4 (16.7%) 8 (32%) 4 (19%)>1000 12 (50%) 8 (32%) 3 (14.3%)
Post hoc tests according to Bonferoni-Holm were carried out only for TV and significance was found only with MFV and markedwith (*) (see Methods). Frequencies and percentages are given for stomach inflation and ventilation quality and comparisons werecarried out by means of the Chi-Square-Test. Stomach inflation was significantly different between techniques (P = 0.034) and sex(P = 0.029). Ventilation quality was significantly different between sex (P = 0.004) and marginally different between techniques(P = 0.056). Class TV > = 1000 ml and TV < 700 ml was significantly different between techniques (P = 0.039, P = 0.047 respectively)and sex (P = 0.001, P = 0.006 respectively). Class TV between 700—1000 ml was neither significantly different between techniques(P = 0.391) nor between sex (P = 0.727).
6 P. Paal et al.
Discussion
In our study we had to deal with a higher inter-individual variation in TV compared with otherstudies.1,9 We suppose that this finding is relatedto the fact that we used non-medically trainedpersons in contrast to other studies, where medi-cally trained personnel performed the ventilationtests.1,9 Moreover, in contrast to other studies,13,17
we used a bench model with a freely movable head(Figure 1), where candidates had to maintain apatent airway.
In spite of the observed variation we were ableto show differences between ventilation techniquesand sex. MPV achieved the best ventilation resultswith 32% hitting the targeted TV of 700—1000 mlfollowed by MFV (19%) and MMV (16.7%). Althoughthese differences were not significant we found asignificant number of tests with a TV above 1000 mlfor MMV and tests with a TV below 700 ml for MFV.Stomach inflation was significantly higher with MMV(79.2%) than with MPV (52%) and MFV (42.9%). Thepositive correlation between tests with higher TVand the presence of stomach inflation is in concor-dance with results published by Wenzel et al.19,20
21
Figure 3 Tidal volume according to sex. The verticalbars show the three test series. Data and P-values inTable 1.
priate and we recommend extending the time forventilation training to more than 10 min. However,as no studies focussing on this issue have been car-ried out so far, additional research is needed todefine the appropriate time for sufficient instruc-tion of a lay person in this and other BLS techniques.
Independently of the technique, males achievedhigher mean TVs than females (Figure 3), and pro-duced stomach inflation more frequently. This sug-gests that teachers should focus more on these dif-ferences between sexes.
Limitations
With a mean age of 17 years our study populationwas younger than in other studies, but the meanTV of 1040 ml achieved was comparable to valuesobtained by trained persons in other studies (1040in1 and 1000 in9). All tests were performed on amanikin and may not reflect the situation of realCPR. In real life CPR, bystander rescuers are proneto even higher stress levels. The time betweenlearning a ventilation technique and performing itmay be months, or years, rather than hours. More-ocmfiisp3t
and Baskett et al. We infer from our data, that inlay rescuer ventilation MPV allows best ventilationquality, as defined by the ILCOR 2000 guidelines,with a lower percentage of stomach inflation thanMMV. This study emphasizes also the importance ofdeveloping new technical devices that reduce stom-ach inflation by limiting TV, as recently proposed byWagner-Berger et al.13
During the performance of the tests we observeda decrease of mean TV for MMV and MFV but notfor MPV and an increase in respiratory rate for alltechniques. It seems that there are many factorsaffecting ventilation quality, such as patency of theairway, ventilation technique, air leak, inspiratorytime, concentration and individual factors.
However, the low proportion of 23% hitting thetarget TV and the high frequency of stomach infla-tion of 58.6% indicate that lay persons have seri-ous problems controlling TV and limiting PAP duringventilation. These results suggest that 10 min oftraining in a lay person may not be sufficient for anadequate quality of ventilation. It might be arguedthat there could be two reasons for the ineffec-tiveness of the training course: either the qualityor the length of training. We believe that the qual-ity was appropriate, because all instructors werephysicians experienced in CPR and in teaching CPRtechniques. Moreover, training was standardized inboth rooms and emphasis was placed on the can-didate acquiring the practical skills. Therefore, wesuspect that the duration of training was inappro-
ver, after a few minutes of respiratory arrest theompliance of the lung and consequently the TVay decrease, while PAP and the risk of stomachlling increase.20 This effect is more accentuated
n prolonged cardiac arrest, as inferred from awine model of cardiac arrest, where oesophagealressure decreased within 7 min from 20.6 ± 2.8 to.3 ± 4.2 cm H2O.22 Increased stomach filling leadso stomach distension, which pushes the diaphragm
Comparison of mouth-to-mouth, mouth-to-mask and mouth-to-face-shield 7
more cranially thus worsening the compliance ofthe respiratory system.20,23 CPR is a complex tech-nique and it may be speculative to transfer resultsfrom an experimental setting to CPR in real circum-stances.
Conclusions
We infer from our data that MPV leads to bestventilation quality in bystander CPR. MPV resultsin a more appropriate TV than MMV and MFV andlower stomach inflation than MMV. The efficiencyof ventilation with MFV was not adequate in accor-dance to previous publications.9 MPV seems to havesubstantial advantages over MMV: MPV reduces therisk of infection and should lower the barrier fora bystander to perform CPR. Additionally, PAP ismoderate, resulting in less stomach inflation thanwith MMV. Handling is simple and mask displace-ment unlikely once in place. An additional oxy-gen source can be applied on some masks increas-ing the inspiratory oxygen fraction;11,24 this shouldimprove outcome further.25
A
ToattBrR
R
tion courses and mouth-to-mouth resuscitation. Semin Der-matol 1995;14:205—11.
7. Friedland GH, Saltzman BR, Rogers MF, Kahl PA, LesserML, Mayers MM, et al. Lack of transmission of HTLV-III/LAVinfection to household contacts of patients with AIDS orAIDS- related complex with oral candidiasis. N Engl J Med1986;314:344—9.
8. Safar P. Pocket mask for emergency artificial ventilation andoxygen inhalation. Crit Care Med 1974;2:273—6.
9. Simmons M, Deao D, Moon L, Peters K, Cavanaugh S. Benchevaluation: three face-shield CPR barrier devices. RespirCare 1995;40(6):618—23.
10. Johannigman JA, Branson RD, Davis K, Hurst JM. Techniquesof emergency ventilation: a model to evaluate tidal vol-ume, airway pressure and gastric insufflation. J Trauma1991;31:93—8.
11. Thomas AN, Hyatt J, Chen JL, Barker SJ. The Laerdal pocketmask: effects of increasing supplementary oxygen flow.Anaesthesia 1992;47:967—71.
12. Breakell A, Townsend-Rose C. An improved pocket rescuemask incorporating a novel breathing indicator. Resuscitation2001;50:185—7.
13. Wagner-Berger HG, Wenzel V, Stallinger A, Voelckel WG,Rheinberger K, Stadlbauer KH, et al. Decreasing peak flowrate with a new bag-valve mask device: effects on respira-tory mechanics, and gas distribution in a bench model of anunprotected airway. Resuscitation 2003;57:193—9.
14. Fuerst RS, Banner MJ, Melker RJ. Gastric inflation in theunintubated patient: a comparison of common ventilatingdevices. Ann Emerg Med 1992;21:636.
1
1
1
1
1
2
2
2
2
2
2
cknowledgements
he authors thank Alfred Niederhofer MPhil, headf the high school Realgymnasium in Bruneck, andll students who participated. We are also indebtedo Michael de Zordo and the members of the Moun-ain Rescue Service, provided by the Alpine Club ofruneck, for technical and logistic support. Mate-ial was provided by the South Tyrolean Mountainescue Service.
eferences
1. Hess D, Ness C, Oppel A, Rhoads K. Evaluation of mouth-to-mask ventilation devices. Respir Care 1989;34:191—5.
2. Hess D, Baran C. Ventilatory volumes using mouth-to-mouth, mouth-to-mask, and bag-valve-mask-techniques. AmJ Emerg Med 1985;3:292—6.
3. Wenzel V, Lindner KH, Prengel AW. Ventilation dur-ing cardiopulmonary resuscitation (CPR). A literaturestudy and analysis of ventilation strategies. Anaesthesist1997;46:133—41.
4. Melanson SW, O’Gara K. EMS provider reluctance to per-form mouth-to-mouth resuscitation. Prehosp Emerg Care2000;4:48—52.
5. Figura N. Mouth-to-mouth-ventilation and Helicobacterpylori infection. Lancet 1996;347:1342.
6. Sun D, Bennett RB, Archibald DW. Risk of acquiring AIDSfrom salivary exchange through cardiopulmonary resuscita-
5. Anonymous Part 3: Adult basic life support. Resuscitation2000;36:42—6.
6. American Society of Anesthesiologists Inc. New classificationof physical status. Anesthesiology 1963;24:111.
7. Wenzel V, Idris A, Banner MJ, Kubilis PS, Williams Jr JL.Influence of tidal volume on the distribution of gas betweenthe lungs and stomach in the nonintubated patient receivingpositive-pressure ventilation. Crit Care Med 1998;26:364—8.
8. Holm S. A simple sequentially rejective multiple test proce-dure. Scand J Stat 1979;6:65—70.
9. Wenzel V, Keller C, Idris AH, Dorges V, Lindner KH, Brima-combe JR. Effects of smaller tidal volumes during basic lifesupport ventilation in patients with respiratory arrest: goodventilation, less risk? Resuscitation 1999;43:25—9.
0. Wenzel V, Idris AH, Banner MJ, Kubilis PS, Band R, WilliamsJr JL, et al. Respiratory system compliance decreases aftercardiopulmonary resuscitation and stomach inflation: impactof large and small tidal volumes on calculated peak airwaypressure. Resuscitation 1998;38:113—8.
1. Baskett P, Nolan J, Parr M. Tidal volumes which are per-ceived to be adequate for resuscitation. Resuscitation1996;31:231—4.
2. Bowmann FP, Menegazzi JJ, Check BD, Duckett TM. Loweresophageal sphincter pressure during prolonged cardiacarrest and resuscitation. Ann Emerg Med 1995;26:216—9.
3. Berg MD, Idris Ah, Berg RA. Severe ventilatory compromisedue to gastric distension during cardiopulmonary resuscita-tion. Resuscitation 1998;36:71—3.
4. Wenzel V, Idris AH, Banner MJ, Fuerst RS, Tucker KJ. Thecomposition of gas given by mouth-to-mouth ventilation dur-ing CPR. Chest 1994;104:1806—10.
5. Idris AH, Volker W, Becker LB, Banner MJ, Orban DJ. Doeshypoxia or hypercarbia independently affect resuscitationfrom cardiac arrest? Chest 1995;108:522—8.
Copyright © 2022 FDOKUMEN