
Communication about standard treatment options and clinical trials: can we teach doctors new skills...
10
Communication about standard treatment options and clinical trials: can we teach doctors new skills to improve patient outcomes? † Jürg Bernhard 1,2 *, Phyllis Butow 3,4 , Julie Aldridge 5 , Ilona Juraskova 3 , Karin Ribi 1 and Richard Brown 6 1 IBCSG Coordinating Center, Efngerstrasse 40, 3008 Bern, Switzerland 2 Department of Medical Oncology, Inselspital, Bern University Hospital, 3010 Bern, Switzerland 3 Centre for Medical Psychology and Evidence-based Decision-making (CeMPED), School of Psychology, The University of Sydney, Camperdown, NSW 2006, Australia 4 Psycho-oncology Co-operative Research Group (PoCoG), The University of Sydney, NSW 2006, Australia 5 IBCSG Statistical Center, Dana-Farber Cancer Institute, Department of Biostatistics and Computational Biology, 450 Brookline Avenue, LW2, Boston, MA 02115, USA 6 Department of Social and Behavioral Health, Virginia Commonwealth University School of Medicine, 1112 East Clay Street, Richmond, VA 23298, USA *Correspondence to: IBCSG Coordinating Center, Efnger- strasse 40, 3008 Bern, Swit- zerland. Email: juerg.bernhard@ ibcsg.org † This trial was orally presented at the International Psycho- Oncology Society (IPOS) Conference, 21–25 June 2009, Vienna. Received: 9 September 2010 Revised: 7 June 2011 Accepted: 8 June 2011 Abstract Background: The International Breast Cancer Study Group conducted a phase III trial in Australian/New Zealand (ANZ) and Swiss/German/Austrian (SGA) centres on training doctors in clear and ethical information delivery about treatment options and strategies to encourage shared decision making. Methods: Medical, surgical, gynaecological and radiation oncologists, and their patients for whom adjuvant breast cancer therapy was indicated, were eligible. Doctors were randomised to participate in a workshop with standardised teaching material and role playing. Patients were recruited in the experimental and control groups before and after the workshop. Results: In ANZ centres, 21 eligible doctors recruited a total of 304 assessable patients. In SGA centres, 41 doctors recruited 390 patients. The training was well accepted. There was no overall effect on patient decisional conict (primary endpoint) 2 weeks after the consultation. Overall, patients were satised with their treatment decision, their consultation and their doc- tors’ consultation skills. Considerable variation was observed in patient outcomes between SGA and ANZ centres; the effect sizes of the intervention were marginal (<0.2). Conclusions: Shared decision making remains a challenge. A sustained training effect may require more intensive training tailored to the local setting. Cross-cultural differences need attention in conducting trials on communication interventions. Copyright © 2011 John Wiley & Sons, Ltd. Keywords: communication skills training; shared decision making; cross-cultural differences; breast cancer; oncology Introduction During the past decade, there has been a growing ex- pectation that patients should participate in decisions about their medical care and give informed consent not only to clinical trials but also to standard treat- ments. As communities in Western societies have be- come better informed about health care issues, patient expectations and medical ethics have moved from a paternalistic model to one promoting partnership and patient autonomy (e.g., Declaration of Helsinki [1]). Oncologists have advocated involving patients in decision making, particularly when the potential gains of treatment must be weighed up against the adverse effects [2–4]. Many patients with cancer today want to participate in decisions about their care [5,6]. Actively participating or knowing one has choice in treatment decision making is benecial to patients [7–9]. Not all patients, however, prefer decisional control, particularly if faced with distressing and unfamiliar situations [10]. Prescribing increased involvement for all patients could be as paternalistic as encourag- ing none. This concern has led to the paradigm of shared decision making (SDM) in which doctors tailor involvement to a patient’s desired level of con- trol rather than aiming for overall patient participa- tion [11,12]. Decision-making preferences of patients with can- cer are not always met [13–16], and often on- cologists do not elicit these [17,18]. Oncologists’ Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology Psycho-Oncology (2011) Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/pon.2044
Transcript of Communication about standard treatment options and clinical trials: can we teach doctors new skills...

Communication about standard treatment options andclinical trials: can we teach doctors new skills to improvepatient outcomes?†
Jürg Bernhard1,2*, Phyllis Butow3,4, Julie Aldridge5, Ilona Juraskova3, Karin Ribi1 and Richard Brown61IBCSG Coordinating Center, Ef!ngerstrasse 40, 3008 Bern, Switzerland2Department of Medical Oncology, Inselspital, Bern University Hospital, 3010 Bern, Switzerland3Centre for Medical Psychology and Evidence-based Decision-making (CeMPED), School of Psychology, The University of Sydney, Camperdown,NSW 2006, Australia4Psycho-oncology Co-operative Research Group (PoCoG), The University of Sydney, NSW 2006, Australia5IBCSG Statistical Center, Dana-Farber Cancer Institute, Department of Biostatistics and Computational Biology, 450 Brookline Avenue, LW2,Boston, MA 02115, USA6Department of Social and Behavioral Health, Virginia Commonwealth University School of Medicine, 1112 East Clay Street, Richmond, VA 23298,USA
*Correspondence to: IBCSGCoordinating Center, Ef!nger-strasse 40, 3008 Bern, Swit-zerland. Email: [email protected]
†This trial was orally presentedat the International Psycho-Oncology Society (IPOS)Conference, 21–25 June 2009,Vienna.
Received: 9 September 2010Revised: 7 June 2011Accepted: 8 June 2011
AbstractBackground: The International Breast Cancer Study Group conducted a phase III trial inAustralian/New Zealand (ANZ) and Swiss/German/Austrian (SGA) centres on training doctorsin clear and ethical information delivery about treatment options and strategies to encourageshared decision making.
Methods: Medical, surgical, gynaecological and radiation oncologists, and their patients forwhom adjuvant breast cancer therapy was indicated, were eligible. Doctors were randomisedto participate in a workshop with standardised teaching material and role playing. Patientswere recruited in the experimental and control groups before and after the workshop.
Results: In ANZ centres, 21 eligible doctors recruited a total of 304 assessable patients. InSGA centres, 41 doctors recruited 390 patients. The training was well accepted. There was nooverall effect on patient decisional con!ict (primary endpoint) 2weeks after the consultation.Overall, patients were satis"ed with their treatment decision, their consultation and their doc-tors’ consultation skills. Considerable variation was observed in patient outcomes betweenSGA and ANZ centres; the effect sizes of the intervention were marginal (<0.2).
Conclusions: Shared decision making remains a challenge. A sustained training effect mayrequire more intensive training tailored to the local setting. Cross-cultural differences needattention in conducting trials on communication interventions.Copyright © 2011 John Wiley & Sons, Ltd.
Keywords: communication skills training; shared decision making; cross-cultural differences;breast cancer; oncology
Introduction
During the past decade, there has been a growing ex-pectation that patients should participate in decisionsabout their medical care and give informed consentnot only to clinical trials but also to standard treat-ments. As communities in Western societies have be-come better informed about health care issues, patientexpectations and medical ethics have moved from apaternalistic model to one promoting partnershipand patient autonomy (e.g., Declaration of Helsinki[1]).Oncologists have advocated involving patients in
decision making, particularly when the potentialgains of treatment must be weighed up against theadverse effects [2–4]. Many patients with cancer
today want to participate in decisions about theircare [5,6]. Actively participating or knowing onehas choice in treatment decision making is bene!cialto patients [7–9].Not all patients, however, prefer decisional control,
particularly if faced with distressing and unfamiliarsituations [10]. Prescribing increased involvementfor all patients could be as paternalistic as encourag-ing none. This concern has led to the paradigmof shared decision making (SDM) in which doctorstailor involvement to a patient’s desired level of con-trol rather than aiming for overall patient participa-tion [11,12].Decision-making preferences of patients with can-
cer are not always met [13–16], and often on-cologists do not elicit these [17,18]. Oncologists’
Copyright © 2011 John Wiley & Sons, Ltd.
Psycho-OncologyPsycho-Oncology (2011)Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/pon.2044

perceptions may be inconsistent with patients’ statedpreferences, for example, in elderly patients [19].These dif!culties are heightened when discussing aclinical trial [20–23].These issues suggest that targeted training in SDM
is warranted. Communication training in decisionmaking regarding standard care has been shown tobe effective in a randomised controlled trial in thefamily practice setting [24]. We are not aware ofsimilar studies in the oncology setting. Studies in de-cision making regarding cancer clinical trials arelimited by pre-post designs [17,25]. Jenkins et al.showed improved con!dence and competence inclinicians and nurses after training in communicationabout randomised clinical trials of cancer therapy[25]. In a pilot study by Brown et al. oncologistsvaried considerably in their SDM behaviours [23].This group conducted a phase II trial that developedand evaluated a model to promote SDM during in-formed consent discussions. Oncologists used somebehaviours of SDM (e.g., less coercion) more fre-quently after this training. Patients in the post-training cohort showed more positive attitudes toclinical trials [17].We expanded this curriculum for SDM for both
clinical trials and standard options [17], testing thisintervention in an international randomised con-trolled trial. Doctors were trained in clear and ethicalinformation delivery of standard treatment optionsand clinical trials and of strategies to encourageSDM with patients with early breast cancer. Wehypothesised a bene!cial impact on decisional con-"ict in patients of trained doctors.The relevance of decisional con"ict to prefer-
ence-sensitive decisions in early breast cancer iswell documented [26–28]. The potential bene!ts ofadjuvant chemotherapy for postmenopausal patientsin terms of prolongation of disease-free and overallsurvival must be balanced against the toxicity oftreatment [29]. In younger premenopausal patients,age-adjusted risk pro!les are complicated, consider-ing the trade-offs between delayed endocrine symp-toms but higher risk of permanent menopause withchemotherapy and the immediate but reversible en-docrine symptoms with goserelin [30]. Such cost–bene!t ratios may be dif!cult for patients to assess,causing decisional con"ict.This report focuses on patient outcomes from our
trial and discusses methodological issues relevantto trials on SDM interventions. Doctor outcomeswill be presented elsewhere.
Doctors, patients and methods
The International Breast Cancer Study Group(IBCSG) conducted Trial 33–03 in centres inAustralia and New Zealand (referred to as ANZ)and Switzerland, Germany and Austria (referred toas SGA), with the doctor as the unit of block rando-misation after strati!cation for centre. The ethics
committees of all participating centres (Appendix)approved the protocol.Medical, surgical, radiation and gynaecological
oncologists, working in major cancer centres orclinics (including private oncologists) and involvedin the treatment of patients with early breast cancer,and their patients for whom adjuvant therapy forbreast cancer was indicated, were eligible. The fol-lowing patient criteria were additionally required:lower age limit of 18 years, adequate knowledge oflocal language (English or German) and being men-tally and physically capable of participating. Doctorparticipation was independent of previous or con-current participation in other types of communica-tion training; previous communication training wasdocumented.
Procedures and measures
Centres with high patient accrual to adjuvant breastcancer trials were invited to join this trial. Local trialcoordination was supported and monitored by a cen-tral coordinator for ANZ and SGA, respectively. Af-ter giving informed consent, doctors at participatingcentres were enrolled concurrently. Following base-line assessment and before the scheduled trainingworkshop, they were randomly assigned to the ex-perimental (training workshop) or control (no train-ing workshop) group. Doctors in the control groupwere offered the training after completing trialfollow-up.Patients of enrolled doctors were recruited before
their doctors were randomised (pre-randomisationcohort) and after the workshop, if assigned (post-randomisation cohort). Local staff identi!ed eligi-ble patients within a "exible time window of about12months in each randomisation cohort. For eachdoctor, 5–10 patients were to be enrolled in thepre-randomisation and 8 or more in the post-randomisation cohort.Trial outcomes were selected on the basis of stud-
ies that evaluated decision aids designed to facilitateSDM [31]. Within 2weeks of their initial consulta-tion discussing treatment options, patients gaveinformed consent and completed a baseline question-naire gathering demographics; preferences for infor-mation (degree of detail required on a Likert scalefrom ‘prefer few details’ to ‘prefer as many detailsas possible’ and type of information required ‘onlyinformation needed to care for myself properly’,‘only good news’ or ‘all possible news both goodand bad’ [32]) and involvement in decision making(single choice among !ve speci!c statements froma doctor-focused decision to a patient-focused deci-sion [32]); quality of life indicators [33] comprisingphysical well-being, mood, coping effort [34],thought of actually having treatment [35], treatmentburden [36] and burden of self-determined problem;and state anxiety by Spielberger [37]. Research
J. Bernhard et al.
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon

nurses or data managers assisted patients in the com-pletion of the questionnaire if necessary.At two additional time points, 2 weeks and
4months after the initial consultation, patients weremailed a questionnaire with pre-paid, addressed re-turn envelope. In addition to the baseline measures,the 2-week questionnaire assessed satisfaction with:decision (total score, six items [38]), consultation(total score, 25 items, adapted from [39,40])and doctor communication in discussing standardtreatment options (total score, 12 items [17]) andclinical trials(total score, four items [17]); patient’sknowledge of diagnosis and treatment options(multiple choice items among speci!c statements,study-developed measure); amount of information re-ceived, involvement preference and actual involve-ment (all adapted from the corresponding baselinemeasures); and decisional con"ict by O’Connor [41]as primary endpoint (total score, 12 items). The4-month questionnaire re-assessed satisfaction withdecision, quality of life and state anxiety. If the coor-dinator did not receive a questionnaire in due time,she or he contacted the patient.Prior to randomisation and 4months after rando-
misation, doctors completed the Maslach BurnoutInventory as used by Ramirez [42] (three subscales:depersonalization (!ve items), emotional exhaustion(nine items), and personal accomplishment (eightitems)), and study developed measures of satisfac-tion with their communication and the training. Inthe study by Ramirez, burnout was more prevalentamong consultants who felt insuf!ciently trained incommunication and management skills [42]. We ex-plored the potential in"uence of doctor stress andburnout on the difference in decisional con"ict be-tween randomisation groups, because this may havebeen a potential confounder of doctors’ ability tobene!t from training.All the patient measures were in English for ANZ
and in German for SGA centres. Only the anxietyand quality of life measures were available in multi-ple languages. For the others, German versions wereadapted from the English version according to stan-dardised procedures. Reliability (internal consis-tency) was con!rmed in the German version ofthese scales (scores ranging from 0.71 to 0.95).
The training
The training consisted of a 7-h interactive face-to-face workshop with one to two follow-up tele-phone calls over 2months. The elements of thistraining were evidence-based [17], incorporatingpresentation of principles [43], a video modellingideal behaviour and role-play practice. The trainingfocused on four key concepts: ensure a shared deci-sion-making framework; structure information intoa sequence or order; ensure the inclusion of different,speci!c types of information in a clear manner; and
consider the disclosure of speci!c controversial in-formation and avoid coercive communication [43].The workshops were held at the participating cen-
tres and conducted in the local language by one totwo clinical psychologists with experience in inter-actional skills training. The teaching materials werein English (i.e., strategies document and teachingvideo). Before the workshop, participants wereexpected to have read the strategies document. Foreach participant, two audio-taped consultations weretranscribed and analysed by the research team usingthe Decision Analysis System for Oncology [44,45].Con!dential written feedback concerning these tapeswas provided at the end of the workshop. One monthlater, the trainer called the doctors to reinforce andextend learning.
Statistical analysis
The target accrual was 44 doctors (22 per rando-mised group) to detect a 0.25-point difference indecisional con"ict between the two groups with90% power, a = 0.05 and 10 patients per doctor(pre-randomisation and post-randomisation cohorts).On the basis of a prospectively de!ned interim anal-ysis (2006) of 19 ANZ doctors (average of eightpatients each), which yielded an intra-class correla-tion of 0.05 and S2 (variance within doctors plus var-iance among doctors) of 0.34, 19 SGA doctors (eightpatients each) were required to detect a 0.25-pointdifference in decisional con"ict with 90% power.Language cohorts were de!ned by location: ANZ
(English) and SGA (German). All analyses were un-dertaken, and results are presented separately by lan-guage due to potential cultural differences.The primary outcome measure was patient deci-
sional con"ict. The secondary patient outcomes de-scribed previously (e.g., satisfaction with decision)were explored.The difference in decisional con"ict between the
randomised groups (Trainingpost!Trainingpre)!(Controlpost!Controlpre) 2weeks after the consulta-tion was estimated by a mixed effects model, withdata at the patient level and doctor as a random effect.A two-sided p-value of 0.05 was considered signi!-cant. Doctor and patient characteristics between ran-domisation groups were considered in the models,but the individual factors that showed a statisticallysigni!cant treatment difference did not contributeto the decisional con"ict scores and had no substan-tial impact on the estimates of the training effect;thus, the !nal models did not adjust for these factors.Estimated mean differences, standard errors and95% CIs based on the mixed models for decisionalcon"ict were reported according to data collectionpoint (pre-randomisation or post-randomisation)and randomisation group. Effect size (ES) was calcu-lated as the estimate divided by the product of thestandard error and the square root of the degrees offreedom. In an exploratory analysis, mixed models
Discussing standard treatment and trials
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon
for decisional con"ict accounted for the three doctorstress and burnout subscales, respectively, as mea-sured 2weeks post-randomisation. The secondarypatient endpoints were similarly analysed by mixedeffects models, with multiple assessments over time.The mean scores by randomisation group at eachdata collection point are plotted. Adjustments werenot made for multiple testing. The analyses usedSAS 9.2 (SAS Institute, Cary, NC, USA).
Results
Sample description and patient characteristics
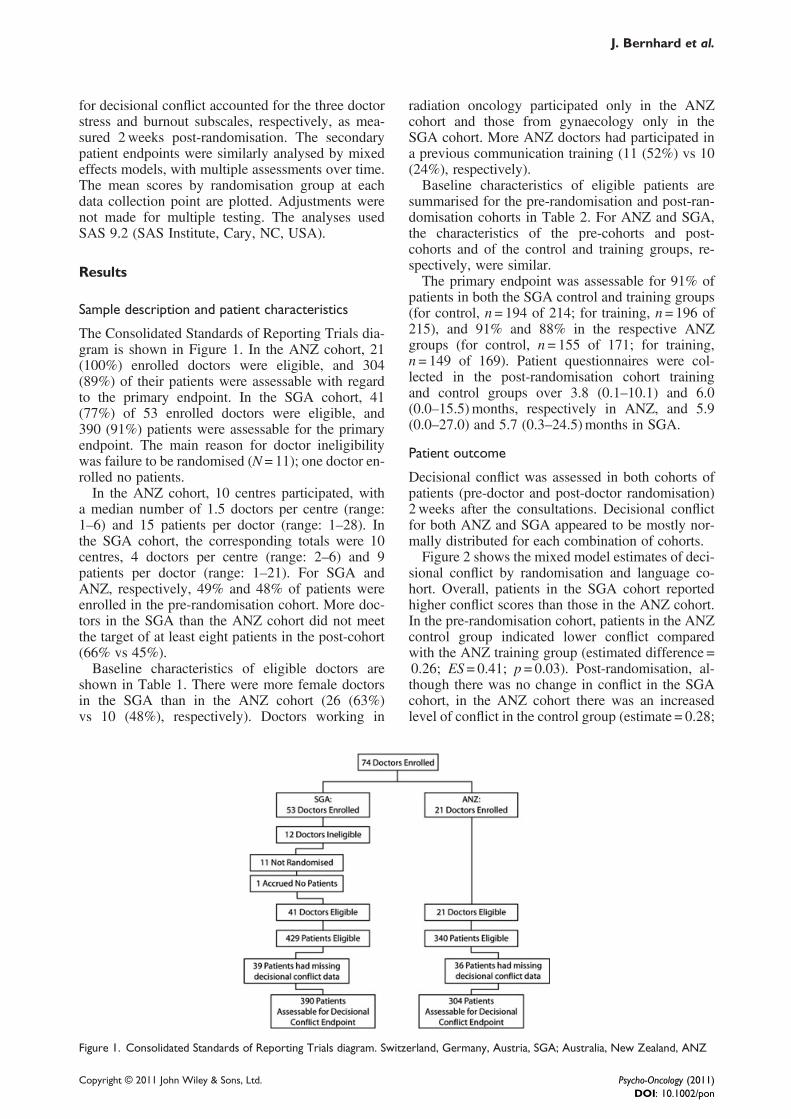
The Consolidated Standards of Reporting Trials dia-gram is shown in Figure 1. In the ANZ cohort, 21(100%) enrolled doctors were eligible, and 304(89%) of their patients were assessable with regardto the primary endpoint. In the SGA cohort, 41(77%) of 53 enrolled doctors were eligible, and390 (91%) patients were assessable for the primaryendpoint. The main reason for doctor ineligibilitywas failure to be randomised (N = 11); one doctor en-rolled no patients.In the ANZ cohort, 10 centres participated, with
a median number of 1.5 doctors per centre (range:1–6) and 15 patients per doctor (range: 1–28). Inthe SGA cohort, the corresponding totals were 10centres, 4 doctors per centre (range: 2–6) and 9patients per doctor (range: 1–21). For SGA andANZ, respectively, 49% and 48% of patients wereenrolled in the pre-randomisation cohort. More doc-tors in the SGA than the ANZ cohort did not meetthe target of at least eight patients in the post-cohort(66% vs 45%).Baseline characteristics of eligible doctors are
shown in Table 1. There were more female doctorsin the SGA than in the ANZ cohort (26 (63%)vs 10 (48%), respectively). Doctors working in
radiation oncology participated only in the ANZcohort and those from gynaecology only in theSGA cohort. More ANZ doctors had participated ina previous communication training (11 (52%) vs 10(24%), respectively).Baseline characteristics of eligible patients are
summarised for the pre-randomisation and post-ran-domisation cohorts in Table 2. For ANZ and SGA,the characteristics of the pre-cohorts and post-cohorts and of the control and training groups, re-spectively, were similar.The primary endpoint was assessable for 91% of
patients in both the SGA control and training groups(for control, n= 194 of 214; for training, n= 196 of215), and 91% and 88% in the respective ANZgroups (for control, n= 155 of 171; for training,n= 149 of 169). Patient questionnaires were col-lected in the post-randomisation cohort trainingand control groups over 3.8 (0.1–10.1) and 6.0(0.0–15.5)months, respectively in ANZ, and 5.9(0.0–27.0) and 5.7 (0.3–24.5)months in SGA.
Patient outcome
Decisional con"ict was assessed in both cohorts ofpatients (pre-doctor and post-doctor randomisation)2weeks after the consultations. Decisional con"ictfor both ANZ and SGA appeared to be mostly nor-mally distributed for each combination of cohorts.Figure 2 shows the mixed model estimates of deci-
sional con"ict by randomisation and language co-hort. Overall, patients in the SGA cohort reportedhigher con"ict scores than those in the ANZ cohort.In the pre-randomisation cohort, patients in the ANZcontrol group indicated lower con"ict comparedwith the ANZ training group (estimated difference =0.26; ES= 0.41; p= 0.03). Post-randomisation, al-though there was no change in con"ict in the SGAcohort, in the ANZ cohort there was an increasedlevel of con"ict in the control group (estimate = 0.28;
Figure 1. Consolidated Standards of Reporting Trials diagram. Switzerland, Germany, Austria, SGA; Australia, New Zealand, ANZ
J. Bernhard et al.
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon

ES = 0.17: p = 0.003). This change exceeded the im-provement in the training group (estimate =!0.14;ES = 0.09; p= 0.13). In summary, the training appearedto have no overall effect on decisional con"ict in eitherlanguage cohort.Because the patients in the pre-randomisation con-
trol group in the ANZ cohort displayed a low deci-sional con"ict that seemed to have in"uenced the
overall outcome, we further investigated their charac-teristics and compared them with those of all otherpatients. Compared with the other pre-randomisationcohort, patients from the ANZ control group wereyounger (median age: 48 vs 57.5 years) and morelikely to be node positive (48% vs 37%).Overall, patients were satis!ed with their treat-
ment decision (Figure 3a). Although there were
Table 1. Baseline characteristics of eligible doctors by language cohort (SGA, ANZ) and randomisation group (control, training)
Switzerland/Germany/Austria (SGA) Australia/New Zealand (ANZ)
Control Training Control Training
N % N % N % N %
n 20 100 21 100 11 100 10 100Gender
Male 7 35 8 38 6 55 5 50Female 13 65 13 62 5 45 5 50
SpecialtyMedical oncology 6 30 5 24 6 55 6 60Radiology — — — — 3 27 3 30Surgeon 2 10 2 10 2 18 1 10Gynaecologist 12 60 14 67 — — — —
InstitutionPublic 20 100 20 95 7 64 7 70Private — — 1 5 — — — —Both — — — — 4 36 3 30
Previous training in communication skills 6 30 4 19 5 45 6 60Med (Range) Med (Range) Med (Range) Med (Range)
Age in years 33 (27, 44) 34 (24, 48) 47 (33, 58) 44 (38, 62)Previous years of practice 6 (1, 18) 6 (1, 24) 16 (2, 35) 20.5 (8, 37)Average number of patients per doctor recruited to trials over 6monthsa 15 (5, 200) 15 (3, 55) 15 (5, 50) 8 (3, 20)
Med, median.aRefers to any trial.
Table 2. Baseline characteristics of eligible patients by language cohort (SGA, ANZ) and randomisation group (control, training)(includes both pre-doctor and post-doctor randomization cohorts)a
Switzerland/Germany/Austria (SGA) Australia/New Zealand (ANZ)
Control Training Control Training
N % N % N % N %
n 214 100 215 100 171 100 169 100Nodal status
Missing 3 1 8 4 2 1 7 4Negative 138 64 129 60 100 58 96 57Positive 73 34 78 36 69 40 66 39
Grade of tumour1 2 1 10 5 8 5 9 52 31 14 27 13 30 18 38 223 100 47 84 39 79 46 63 37Missing 81 38 94 44 54 32 59 35
Hormone receptor statusMissing 10 5 12 6 20 12 25 15Negative 39 18 39 18 36 21 41 24Positive 165 77 164 76 115 67 103 61Training in medical !eld 27 13 39 18 41 24 33 20
Med (Range) Med (Range) Med (Range) Med (Range)Age (years) 58 (24, 85) 58 (31, 88) 50.5 (27, 81) 53 (30, 83)Tumour size (cm) 2 (0.2, 8) 2 (0, 12) 1.9 (0.1, 25) 2 (0.3, 40)
Med, median.aTwenty-eight patients with missing data on decisional con!ict are included.
Discussing standard treatment and trials
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon

some tendencies in the expected direction, there wasno overall effect by the training in the secondary pa-tient outcomes in either language cohort. The ESswere consistently marginal (ES< 0.2). For example,patients in both the SGA and ANZ cohorts reportedmore involvement in decision making in the traininggroup after the workshop as compared with the con-trol group (Figure 3b), but this was not statisticallysigni!cant (p = 0.08 for SGA and p = 0.24 forANZ). There was higher satisfaction with doctor’sconsultation skills for patients in ANZ than forpatients in SGA, and all cohorts showed improvedsatisfaction with doctor’s consultation skills exceptfor the ANZ control group (Figure 3c), althoughnot statistically signi!cant (p= 0.08 for SGA andp= 0.26 for ANZ). Anxiety slightly decreased overtime for all cohorts. Patients in the SGA (Figure 4a)and ANZ (Figure 4b) cohorts reported comparableanxiety levels at each time point. The quality of lifeindicators showed similar !ndings (data not shown).When doctors’ stress and burnout factors were
accounted for in the mixed effects models for deci-sional con"ict, the ESs became slightly larger inthe SGA cohort but remained low. There was no in-"uence by these factors on the ESs in the ANZ co-hort (data not shown).
Discussion
We studied the effectiveness of our communicationskills training cross-culturally within an experimen-tal design. To increase homogeneity, we tailoredour intervention to consultations in which adjuvanttreatment options for early breast cancer were dis-cussed, with or without a clinical trial. There wasconsiderable variation in patient outcomes betweenthe SGA and ANZ cohorts and no substantial train-ing effect. Overall, patients were satis!ed with theirtreatment decision, their consultation and their doc-tors’ consultation skills.
Most previous communication trainings have fo-cused on general interaction skills or the deliveryof bad news [46]. Such interventions have a bene!-cial effect mainly on doctor outcomes, for example,increased empathic responses [47]. Training inSDM has been studied less frequently [17,25] andits effect on patient outcomes has been studied infew controlled designs [48,49].There is some suggestion of a dose–response ef-
fect based on trials of general communication skills[47], although the minimal training duration for asustainable effect is unclear. The only trial with anenduring effect over 12months was based on a 3-day workshop [50,51]. In our trial, doctors enrolledpatients over the course of approximately 1 year inboth the pre-randomisation and post-randomisationcohorts. Such a window was necessary to study theeffect of the training on a suf!cient number ofpatients in real consultations. Our 1-day workshopmay not have been suf!ciently intensive for such awide interval of outcome evaluation. Enrollingactors portraying a patient in a shorter time frame be-fore and after the training may be more sensitive tocommunication changes [25], at least in the shortterm. However, this approach loses the ecologicalvalidity of showing a real bene!t to real patientsfrom doctor communication skills training.Logistically, the trial was very demanding. Job ro-
tation and maternity leaves of fellows had a negativeimpact on patient accrual particularly in the SGApost-randomisation cohort, resulting in fewerpatients per doctor than projected. Whether the doc-tors selectively enrolled their patients is not known.Although the pre-randomisation and post-randomi-sation cohorts were similar, individual patient differ-ences may still have clouded the intervention effects.Although we might have reduced this effect with anadditional random assignment of the patients, thiswas not feasible. Most centres were not able to com-ply with the original requirement to enrol patients inconsecutive order and document reasons for non-
Figure 2. Decisional con!ict (primary endpoint) based on estimates from the mixed model by randomisation group and language co-hort. Treatment comparisons are made in terms of differences in the patients of each randomised doctor, pre-randomisation andpost- randomisation, adjusting for language Switzerland, Germany, Austria/Australia, New Zealand (SGA/ANZ). Overall, scores of!2 of decisional con!ict are considered as ‘no dif"culty in decision making’
J. Bernhard et al.
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon

participation. Our mixed effects model accounted forpotential clustering effects to the extent possible.We chose centres that already had a high accrual
to clinical trials. These centres were experienced inclinical research, had designated staff for local coor-dination and data management and generally had ahigher accrual overall and thus may have contributedto a faster recruitment to studies such as ours. Com-munication skills of these providers may alreadyhave been at an advanced level. In particular, somedoctors had previously participated in other typesof communication training. We did not exclude thesedoctors because we explicitly focused our interven-tion on SDM. Whether this lowered the impact ofthe training on the observed outcomes is not known.
It is also possible that these more experienced doc-tors were more motivated for this training. Finally,the lower con"ict scores in the ANZ cohort may re-late to the widespread availability of nurses forbreast cancer in ANZ sites who provide signi!cantinformation to patients.It was dif!cult for doctors to organise time for
telephone coaching after the workshop. Compliancewith these calls was not satisfactory. We did not for-mally document how the doctors used their trainedskills. As an alternative, we suggest an individualfollow-up based on the facilitator’s participation ina doctor’s real consultation with feedback providedafter the consultation. This procedure would poten-tially be more meaningful to the doctor and thus a
Figure 3. Patients’ satisfaction with decision (a), patient preferences for involvement in decision making (b) and satisfaction with doc-tor consultation skills (c) based on mean scores by randomisation group and language cohort. Switzerland, Germany, Austria, SGA;Australia, New Zealand, ANZ
Discussing standard treatment and trials
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon

promising approach to reinforce and extend learning.As a consequence, the impact of the training wouldlikely be enhanced and more likely to impact patientoutcomes. Practicing discussion of speci!c trials cur-rently recruiting at the local centre may improveskills implementation.Whether patients might be more responsive to
SDM interventions than doctors is an intriguingquestion. It is not the patient’s responsibility to ad-just his or her communication skills when confrontedwith cancer. However, to enhance their participationin decision making as they move through the cancertrajectory, short interventions incorporating decisioncoaching may be useful [52].In summary, training our doctors in SDM with a
1-day workshop and support materials did not ap-pear to bene!t their patients in a measurable way.Elwyn et al. have summarised the main conditionsfor SDM to become part of mainstream clinical prac-tice: ready access to evidence-based informationabout treatment options; guidance on how to weighup the pros and cons of different options; and a sup-portive clinical culture that facilitates patient engage-ment [53]. Our intervention targeted the secondcondition. We propose the development of a moreintensive module, more speci!cally adapted to localneeds and with individual follow-up based on real-time supervision of the doctors’ communication withtheir patients. Both between and within the ANZ andSGA cohorts, we were faced with different clinical
cultures regarding the facilitation of patient engage-ment. Cross-cultural differences and local settingsneed more systematic attention in conducting trialson communication interventions.
AcknowledgmentsThis trial was a collaborative effort between the Centre for Med-ical Psychology and Evidence-based Decision-making, Schoolof Psychology, University of Sydney, and the InternationalBreast Cancer Study Group (IBCSG). It needed considerablelogistic efforts.
We would like to thank the doctors who participated in thetrial, the patients who took the time to complete the question-naires, the data managers and local coordinators in the participat-ing centres and Peter Zoller, Cornelia Zuberbühler, MonikaDzidowska, Gwynneth Wong, Gina Bark and Anna-Lena Lopezfor central trial coordination.
We would like to thank the National Breast Cancer Foundationof Australia, Oncosuisse/Swiss Cancer League (OCS–01165-09-2001/KLS–01648-02-2005), Deutsche Krebshilfe (106668), andIBCSG for funding this trial. The IBCSG Statistical Center (J.A.)is partially funded through a grant from the US National CancerInstitute (CA-75362).Con!ict of interest: There are no !nancial disclosures from anyauthors.
Appendix of participating centres, doctorsand local coordinators
AustraliaSt Vincent’s Hospital, Melbourne: R. Snyder, W.Burns, A. Dowling and Nadia Ranieri
Figure 4. Patient state anxiety in the Switzerland, Germany, Austria (a) and the Australia, New Zealand (b) cohort over time based onmean scores by randomisation group
J. Bernhard et al.
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon
Maroondah Hospital, Maroondah: J. Chirgwin andSuzanne GiddingsRoyal Prince Alfred Hospital, Sydney: S. Pendlebury, J.Beith, A. Hamilton and Gina BarkSir Charles Gairdner Hospital, Perth: C. Saunders, L.Jackson, N. Spry, F. Cameron, M. Taylor, R. Chee,Anna Davies and Philippa KellyFlinders Medical Center, Adelaide: B. Koczwara andAlison RichardsWestmead Hospital, Sydney: V. Ahern, P. Harnettand Mary CooperNepean Cancer Care Center, Penrith: N. Wilckenand Penny Murie
New ZealandAuckland Hospital, Auckland: P. Thompson, V.Harvey and Joline OngWaikato Hospital, Hamilton: I. Campbell and JenniScarletDunedin Hospital, Dunedin: D. Perez and AlisonWylie
SwitzerlandKantonsspital St. Gallen: B. Thürlimann, A. Casty,M. Hoe"iger and A. MüllerInselspital Bern: S. Aebi,M. Rabaglio and C. Baumann
GermanyUniversitätsklinik Frankfurt: M. Liszka, S. Loibl, K.Schmidt, V. Gies and H. TrümperFrauenklinik Technische Universität München:K. Miska, U. Euler, D. Paepke, K. Gauger and A.BaumgärtnerUniversitätsfrauenklinik Kiel: C. Crohns, I. Mein-hold-Heerlein, A. Ulrich, S. Grebe, J. Haller, A.Lüesse and J. DürkopKrankenhaus München Schwabing: Andrea Schulte,Alexandra von Holle and Sabine SchmidUniversitätsklinikum Jena: O. Camara, J. Hermann, A.Egbe, A. Kavallaris, H. Winzer, B. Härtwig andS. Krauspe
AustriaWilhelminenspital Wien: H. Lass, T. Scholl, M.Brunbauer and M. Riegler-KeilAllgemeines Krankenhaus Wien: C. Singer, Y.Yücel, D. Gschwantler-Kaulich, A. Fink-Retter, D.Bikas and M. TeaLandeskrankenhaus Feldkirch: M. Knauer, R.Köberle-Wührer and P. Elke
References
1. World Medical Association (WMA), Declaration ofHelsinki. Ethical Principles for Medical Research InvolvingHuman Subjects. 2008: Seoul.
2. Simes RJ et al. Randomised comparison of procedures forobtaining informed consent in clinical trials of treatmentfor cancer. Br Med J (Clin Res Ed) 1986;293(6554):1065–1068.
3. Goodwin PJ. Reversible ovarian ablation or chemotherapy:are we ready for quality of life to guide adjuvant treatment
decisions in breast cancer? J Clin Oncol 2003; 21(24):4474–4475.
4. Whelan T et al. Mastectomy or lumpectomy? Helpingwomen make informed choices. J Clin Oncol 1999;17(6):1727–1735.
5. Ravdin PM, Siminoff IA, Harvey JA. Survey of breastcancer patients concerning their knowledge and expec-tations of adjuvant therapy. J Clin Oncol 1998;16(2):515–521.
6. Parker PA et al. Breaking bad news about cancer: patients’preferences for communication. J Clin Oncol 2001;19(7):2049–2056.
7. Street RLJ, B Voigt. Patient participation in deciding breastcancer treatment and subsequent quality of life. Med DecisMaking 1997;17(3): p. 298–306.
8. Fallow!eld LJ et al. Psychological outcomes of differenttreatment policies in women with early breast cancer outsidea clinical trial. Br Med J 1990;301(6752):575–580.
9. Coulter A. Do patients want a choice and does it work? BMJ2010; 341: c4989.
10. Butow PN et al. The dynamics of change: cancer patients’preferences for information, involvement and support. AnnOncol 1997;8(9):857–863.
11. Fallow!eld L. Offering choice of surgical treatment towomen with breast cancer. Patient Educ Couns 1997;30(3):209–214.
12. Guadagnoli E, P Ward. Patient participation in decision-making. Soc Sci Med 1998;47(3): 329–339.
13. Ford S, Scho!eld T and Hope T. Are patients’ decision-making preferences being met? Health Expect 2003;6(1):72–80.
14. Bilodeau BA and Degner LF. Information needs, sources ofinformation, and decisional roles in women with breast can-cer. Oncol Nursing Forum 1996;23(4):691–696.
15. Gattellari M, Butow PN, Tattersall MH. Sharing decisions incancer care. Soc Sci Med 2001;52(12): 1865–1878.
16. Sutherland HJ et al. Cancer patients: their desire for infor-mation and participation in treatment decisions. J RoyalSoc Med 1989;82(May):260–263.
17. Brown RF et al. Seeking informed consent to cancer clinicaltrials; evaluating the ef!cacy of doctor communication skillstraining. Psycho-Oncology 2007;16(6): 507–516.
18. Degner LF et al. Information needs and decisional prefer-ences in women with breast cancer. JAMA 1997;277(18):1485–1492.
19. Elkin EB et al. Desire for information and involvementin treatment decisions: elderly cancer patients’ prefer-ences and their physicians’ perceptions. J Clin Oncol2007;25(33):5275–5280.
20. Benson AB 3rd et al. Oncologists’ reluctance to accruepatients onto clinical trials: an Illinois Cancer Center study.J Clin Oncol 1991;9(11):2067–2075.
21. Olver IN et al. The adequacy of consent forms for informingpatients entering oncological clinical trials. Ann Oncol1995;6(9):867–870.
22. Fleissig A, Jenkins V, Fallow!eld L. Results of an interven-tion study to improve communication about randomisedclinical trials of cancer therapy. Eur J Cancer 2001;37(3):322–331.
23. Brown RF et al. Seeking informed consent to cancer clinicaltrials: describing current practice. Soc Sci Med 2004;58(12):2445–2457.
24. Elwyn G et al. Achieving involvement: process outcomesfrom a cluster randomized trial of shared decisionmaking skill development and use of risk communica-tion aids in general practice. Fam Pract 2004;21(4):337–346.
25. Jenkins V et al. Discussing randomised clinical trials of can-cer therapy: evaluation of a Cancer Research UK trainingprogramme. BMJ 2005;330(7488):400.
26. Waljee JF, Rogers MA, Alderman AK. Decision aids andbreast cancer: do they in"uence choice for surgery and
Discussing standard treatment and trials
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon

knowledge of treatment options? J Clin Oncol 2007;25(9):1067–1073.
27. Rini C et al. Cognitive and emotional factors predictingdecisional con"ict among high-risk breast cancer survi-vors who receive uninformative BRCA1/2 results. HealthPsychol 2009;28(5): 569–578.
28. Juraskova I, et al. Improving informed consent: pilot of a de-cision aid for women invited to participate in a breast cancerprevention trial (IBIS-II DCIS). Health Expect 2008;11(3):252–262.
29. Goldhirsch A et al. Costs and bene!ts of adjuvant therapy inbreast cancer: a quality-adjusted survival analysis. J ClinOncol 1989;7(1):36–44.
30. Bernhard J et al. Adjuvant chemotherapy followed by goser-elin compared with either modality alone: the impact onamenorrhea, hot "ashes, and quality of life in premeno-pausal patients—the International Breast Cancer StudyGroup Trial VIII. J Clin Oncol;2007. 25(3):p.263–270.
31. O’Connor AM et al. Decision aids for people facing healthtreatment or screening decisions. Cochrane Database SystRev 2003(2):CD001431.
32. Cassileth BR et al. Information and participation prefer-ences among cancer patients. Ann Intern Med 1980;92(6):832–836.
33. Bernhard J et al. Quality of life assessment in patients re-ceiving adjuvant therapy for breast cancer: the IBCSG ap-proach. The International Breast Cancer Study Group. AnnOncol 1997;8(9):825–835.
34. Hurny C et al. The Perceived Adjustment to Chronic IllnessScale (PACIS): a global indicator of coping for operablebreast cancer patients in clinical trials. Swiss Group forClinical Cancer Research (SAKK) and the InternationalBreast Cancer Study Group (IBCSG). Support Care Cancer1993;1(4):200–208.
35. Coates A, Glasziou P, McNeil D. On the receiving end--III.Measurement of quality of life during cancer chemotherapy.Ann Oncol 1990;1(3):213–217.
36. Bernhard J et al. Patients’ estimation of overall treatmentburden: why not ask the obvious? J Clin Oncol 2002;20(1):65–72.
37. Spielberger CD. Manual for the State-Trait Anxiety Inven-tory STAI (Form Y). 1983, Consulting Psychologists Press:Palo Alto, CA.
38. Holmes-Rovner M et al. Patient satisfaction with health caredecisions: the satisfaction with decision scale. Med DecisMaking 1996;16(1):58–64.
39. Roter D. Patient participation in the patient-provider interac-tion: the effects of patient question asking on the quality of
interaction, satisfaction and compliance. Health EducMonogr 1977;5:281–315.
40. Korsch BM, Gozzi EK, Francis V. Gaps in doctor-patientcommunication. 1. Doctor-patient interaction and patientsatisfaction. Pediatrics 1968;42:855–871.
41. O’Connor AM. Validation of a decisional con"ict scale.Med Decis Making 1995;15:25–30.
42. Ramirez AJ et al. Mental health of hospital consultants: theeffects of stress and satisfaction at work. Lancet 1996;347(9003):724–728.
43. Brown RF et al. Developing ethical strategies to assistoncologists in seeking informed consent to cancer clinicaltrials. Soc Sci Med 2004;58(2):379–390.
44. Brown RF et al. Sharing decisions in breast cancer care: de-velopment of the Decision Analysis System for Oncology(DAS-O) to identify shared decision making during treat-ment consultations. Heal Expect 2010;14:29–37.
45. Butow P et al. Shared decision making coding systems: howdo they compare in the oncology context? Patient EducCouns 2010;78(2):261–268.
46. Stiefel F et al. Communication skills training in oncology: aposition paper based on a consensus meeting among Euro-pean experts in 2009. Ann Oncol 2010;21(2):204–207.
47. Barth J, Lannen P. Ef!cacy of communication skills trainingcourses in oncology: a systematic review and meta-analysis.Ann Oncol 2011;22(5):1030–1040.
48. Edwards A et al. Patient-based outcome results from a clus-ter randomized trial of shared decision making skill devel-opment and use of risk communication aids in generalpractice. Fam Pract 2004;21(4):347–354.
49. Watson E et al. Informed decision making and prostatespeci!c antigen (PSA) testing for prostate cancer: a ran-domised controlled trial exploring the impact of a briefpatient decision aid on men’s knowledge, attitudes andintention to be tested. Patient Educ Couns 2006;63(3):367–379.
50. Fallow!eld L et al. Ef!cacy of a Cancer Research UKcommunication skills training model for oncologists:a randomised controlled trial. Lancet 2002;359(9307):650–656.
51. Fallow!eld L et al. Enduring impact of communicationskills training: results of a 12-month follow-up. Br J Cancer2003;89(8):1445–1449.
52. Kennedy AD et al. Effects of decision aids for menorrhagiaon treatment choices, health outcomes, and costs: a random-ized controlled trial. BMJ 2002;288(21):2701–2708.
53. Elwyn G et al. Implementing shared decision making in theNHS. BMJ 2010; 341:c5146.
J. Bernhard et al.
Copyright © 2011 John Wiley & Sons, Ltd. Psycho-Oncology (2011)DOI: 10.1002/pon




















