common spinal problems -...
116
COMMON SPINAL PROBLEMS (โรคของกระดูกสันหลังที่พบบอย) ผศ.นพ.ตอพงษ บุญมาประเสริฐ หนวยโรคกระดูกสันหลัง ภาควิชาออรโทปดิกส คณะแพทยศาสตร มหาวิทยาลัยเชียงใหม
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of common spinal problems -...

COMMON SPINAL PROBLEMS
(โรคของกระดูกสันหลังที่พบบอย)
ผศ.นพ.ตอพงษ บุญมาประเสริฐหนวยโรคกระดูกสันหลัง ภาควิชาออรโทปดิกส
คณะแพทยศาสตร มหาวิทยาลัยเชียงใหม

หัวขอการบรรยาย
ทบทวนกายวิภาคศาสตร และการทํางานของกระดูกสันหลัง
อาการวิทยาและแนวทางการวินิจฉัยอาการของโรคปวดหลัง-ปวดคอ
การอานภาพรังสีวิทยาที่ใชในการตรวจวินิจฉัยโรคปวดหลัง-ปวดคอ
โรคที่ทําใหเกิดอาการปวดหลัง และอาการปวดคอ ที่พบบอย
Acute Back Strain
Herniated Nucleus Pulposus (HNP)
Degenerative Lumbar Spinal Canal Stenosis (SCS)
Spondylolysis & Spondyloisthesis
Cervical Spondylosis – Radiculopathy - Myelopathy
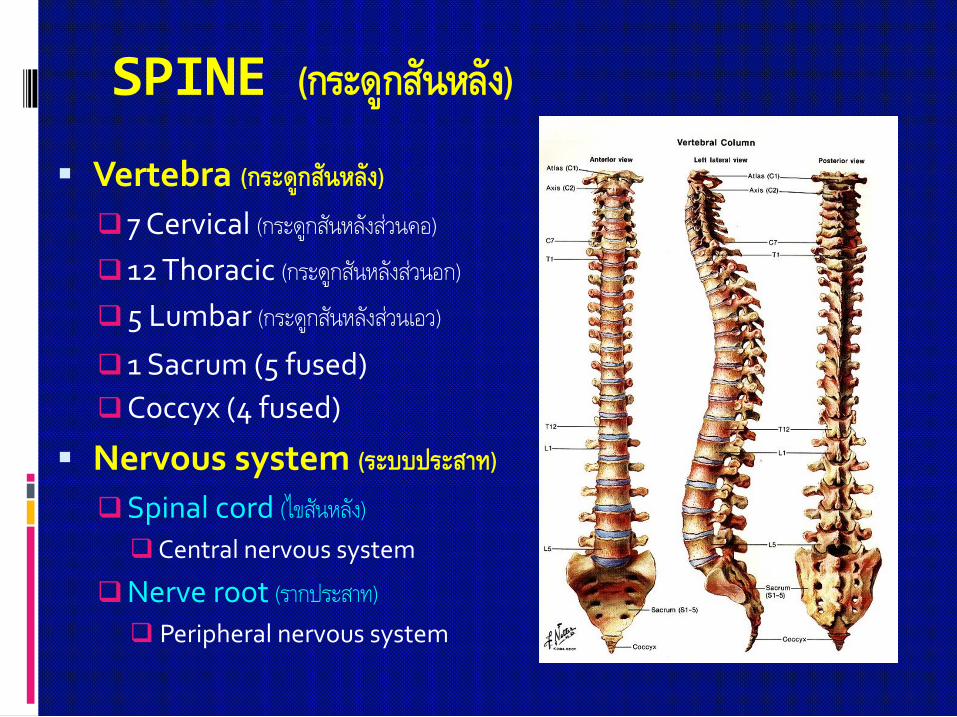
SPINE (กระดูกสันหลัง)
Vertebra (กระดูกสันหลัง)
7 Cervical (กระดูกสันหลังสวนคอ)
12 Thoracic (กระดูกสันหลังสวนอก)
5 Lumbar (กระดูกสันหลังสวนเอว)
1 Sacrum (5 fused)
Coccyx (4 fused)
Nervous system (ระบบประสาท)
Spinal cord (ไขสันหลัง)
Central nervous system
Nerve root (รากประสาท)
Peripheral nervous system

หนาที่ของกระดูกสันหลัง
ปองกันอันตรายแกระบบประสาท*** (ไขสันหลังและเสนประสาท)
โครงสรางแกนกลาง
การเคลื่อนไหว
สรางเม็ดเลือด
เปนที่เกาะของกลามเนื้อและเสนเอ็น
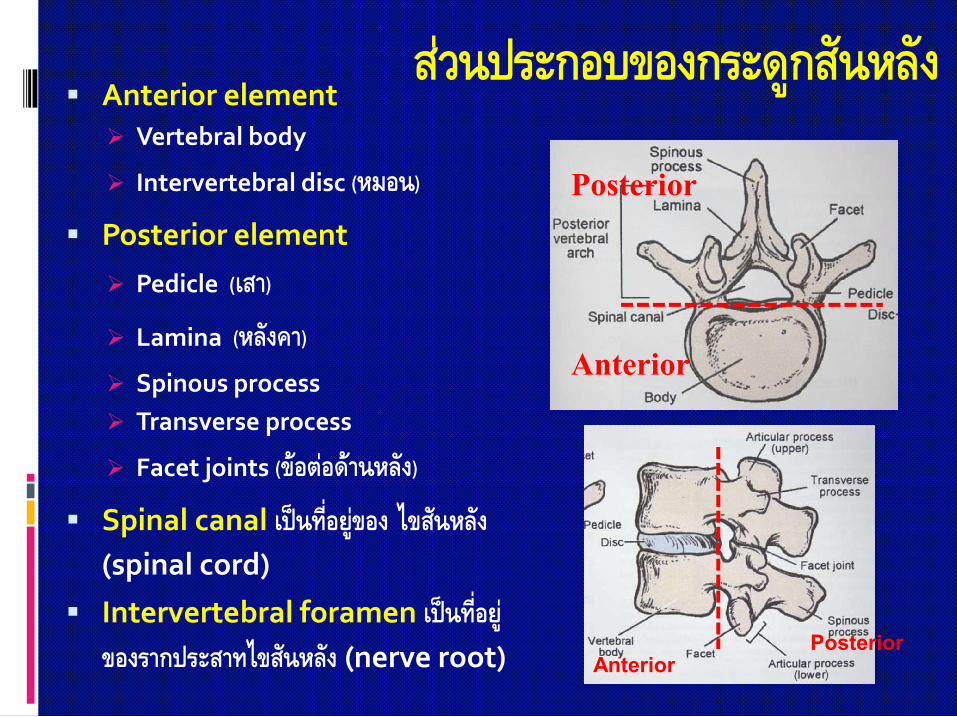
สวนประกอบของกระดูกสันหลัง Anterior element
Vertebral body
Intervertebral disc (หมอน)
Posterior element
Pedicle (เสา)
Lamina (หลังคา) Spinous process
Transverse process
Facet joints (ขอตอดานหลัง)
Spinal canal เปนที่อยูของ ไขสันหลัง (spinal cord)
Intervertebral foramen เปนที่อยูของรากประสาทไขสันหลัง (nerve root)
Anterior
Posterior
AnteriorPosterior
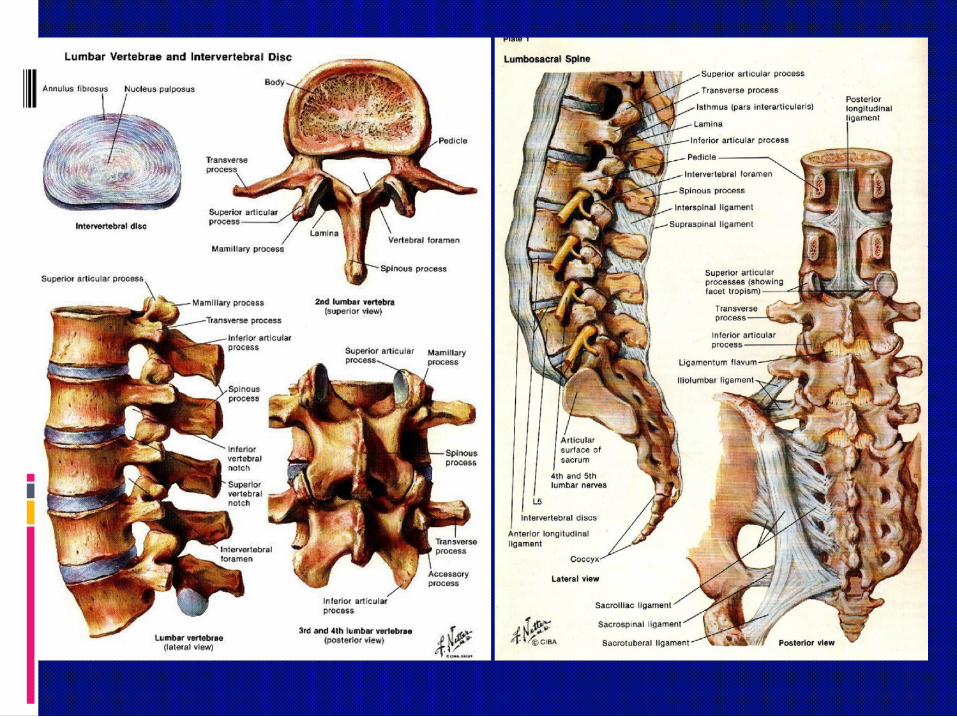
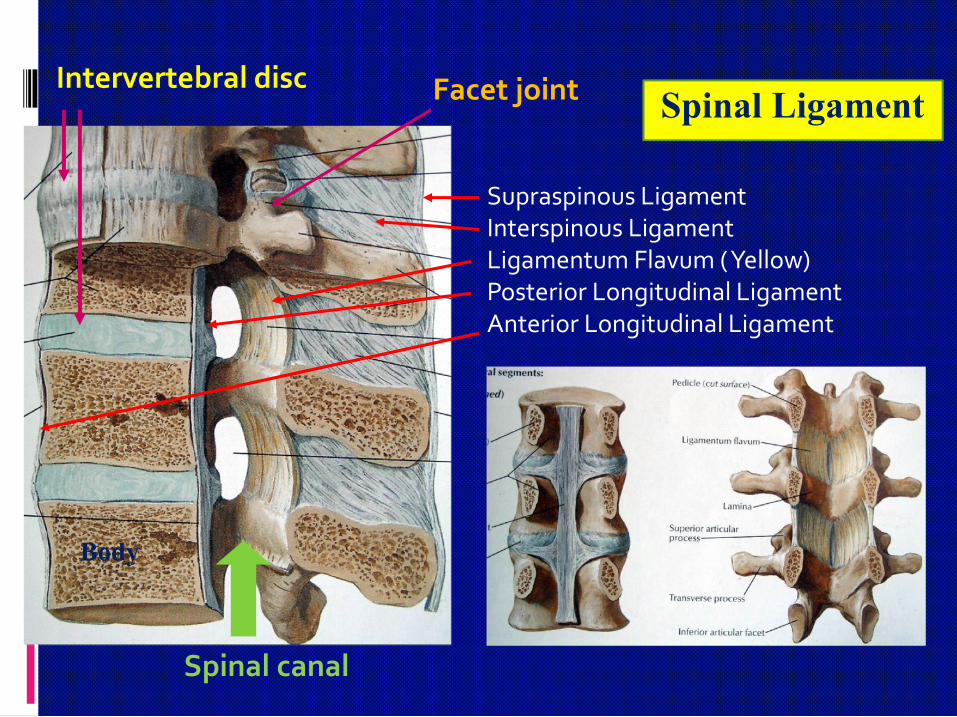
Intervertebral disc
Spinal canal
Body
Facet joint
Supraspinous LigamentInterspinous LigamentLigamentum Flavum ( Yellow)Posterior Longitudinal LigamentAnterior Longitudinal Ligament
Spinal Ligament


Vertebraand
Spinal Cord
Spinal cord & surroundings
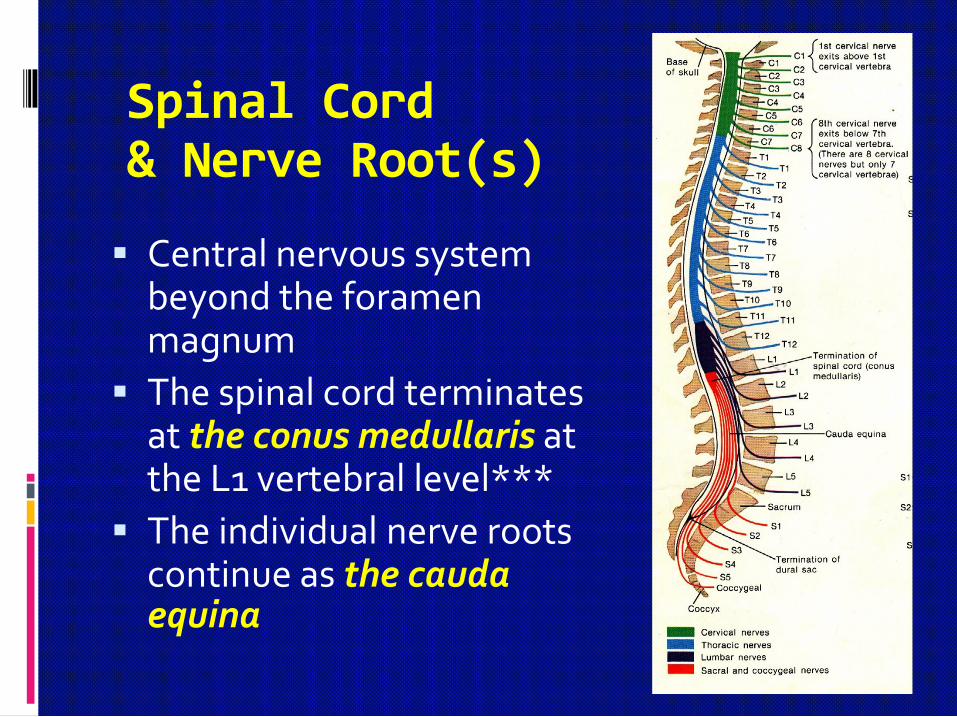
Spinal Cord& Nerve Root(s)
Central nervous system beyond the foramen magnum
The spinal cord terminates at the conus medullaris at the L1 vertebral level***
The individual nerve roots continue as the caudaequina

Facet joints
Intervertebraldisc
Joints of the Lumbar Spine Functional Spinal Unit= 2 vertebrae +1 disc + 2 facet joints
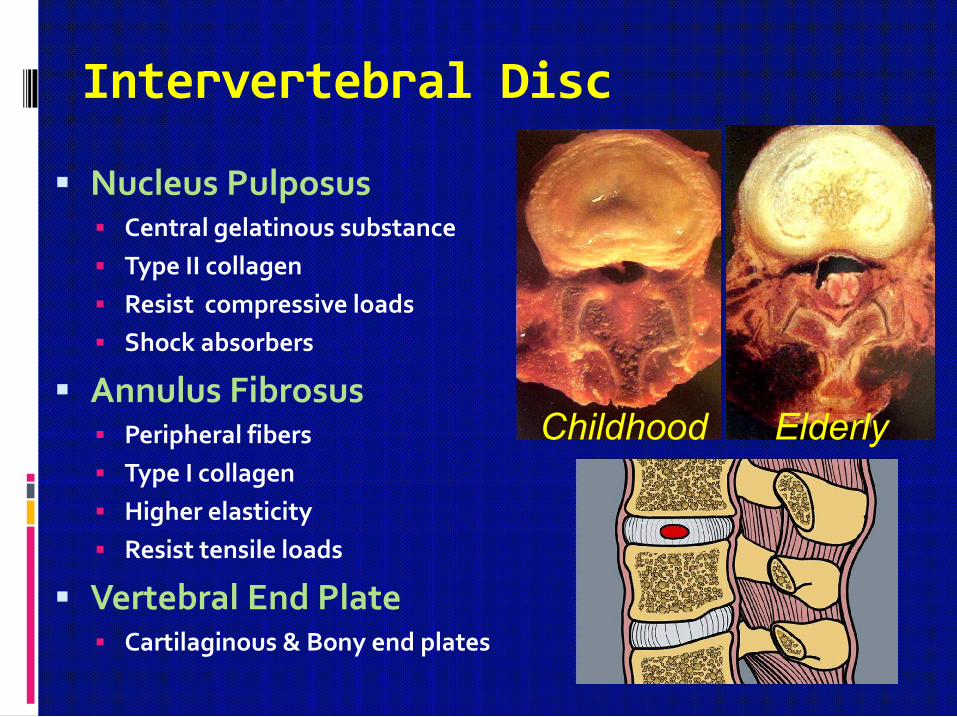
Intervertebral Disc
Nucleus Pulposus Central gelatinous substance
Type II collagen
Resist compressive loads
Shock absorbers
Annulus Fibrosus Peripheral fibers
Type I collagen
Higher elasticity
Resist tensile loads
Vertebral End Plate Cartilaginous & Bony end plates
Childhood Elderly

คํานิยามและคําศัพทเกี่ยวกับโรคกระดูกสันหลัง
Spondylo- : spine (กระดูกสันหลัง)
Spondylosis : degenerative (โรคกระดูกสันหลังเสื่อม)
Cervical spondylosis
Lumbar spondylosis
Spondylitis : infection, inflammation (อักเสบ)
Bacterial, TB, epidural abscess (อักเสบติดเชื้อ)
AS : ankylosing spondylitis (อักเสบไมติดเชื้อ)
Spondylolisthesis (ขอตอปลองกระดูกสันหลังเลื่อน)
Scoliosis (โรคกระดูกสันหลังคด)

Case LBP
ผูปวยหญิงไทยคู อายุ 46 ป
อาชีพ เกษตรกร
ภูมิลําเนา อ.หางดง จ.เชียงใหม
Chief complaint
ปวดหลังราวลงขาซาย 1 ปกอนมารพ.
เริ่มจากการซักประวัติผูปวยกอน
History taking
Age
Younger patients: strain, trauma
Older patients: tumor, infection, degenerative
Onset
Gradual, slow – degenerative mechanical pain
Sudden and severe – osteoporotic compression fracture
Characterization of symptoms
Mechanical pain – muscle strain, myofascial pain
Localized pain – trauma, tumor, infection
Radicular pain – HNP, stenosis of the foramen

Location Leg pain aggravated by walking and standing but
relieved by sitting suggests spinal stenosis
Anterior thigh pain suggests upper lumbar radiculopathy or hip disease
Posterior thigh pain suggests lower lumbar radiculopathy or sciatica
Effect of positional change Unrelieved with position change – cancer, infection
Relieved when supine, increased when position is changed – mechanical
Aggravated by flexion – HNP
Aggravated by extension – SCS, facet syndrome
History taking

History taking
Mechanism of injury/ onset of symptoms
Relieving/aggravating symptoms
Systemic symptoms
Bowel or bladder symptoms –
cauda equina compression syndrome
Areas of numbness
Leg pain (sciatica ± neurogenic claudication)
Underlying diseases Previous treatment

Physical examination
Inspection
Integument
Posture
Gait

Physical examination

Adolescent
Idiopathic scoliosis Neuromusclar scoliosisNeurofibromatosisMeningocele

CONGENITAL KYPHOSIS
Failure of formation
Failure of segmentation
ACQUIRED KYPHOSIS
InfectionOsteoporosisTumorTrauma
Kyphosis
Physical examination
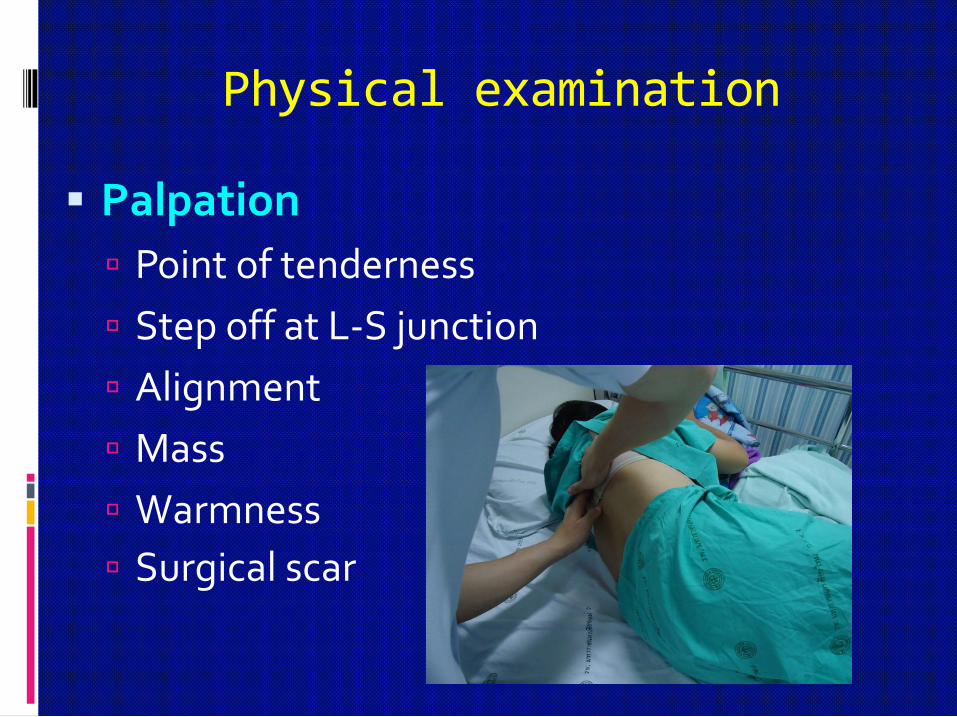
Palpation
Point of tenderness
Step off at L-S junction
Alignment
Mass
Warmness
Surgical scar

NORMAL BACK MOTION
กมตัว (A) 40˚-60˚
แอนหลัง (B) 20˚-35˚
เอียงตัวไปดานขาง (C) 15˚-20˚
บิดเอี้ยวลําตัว (D,E) 3˚-18˚
23
(A) (B)
(C) (D) (E)
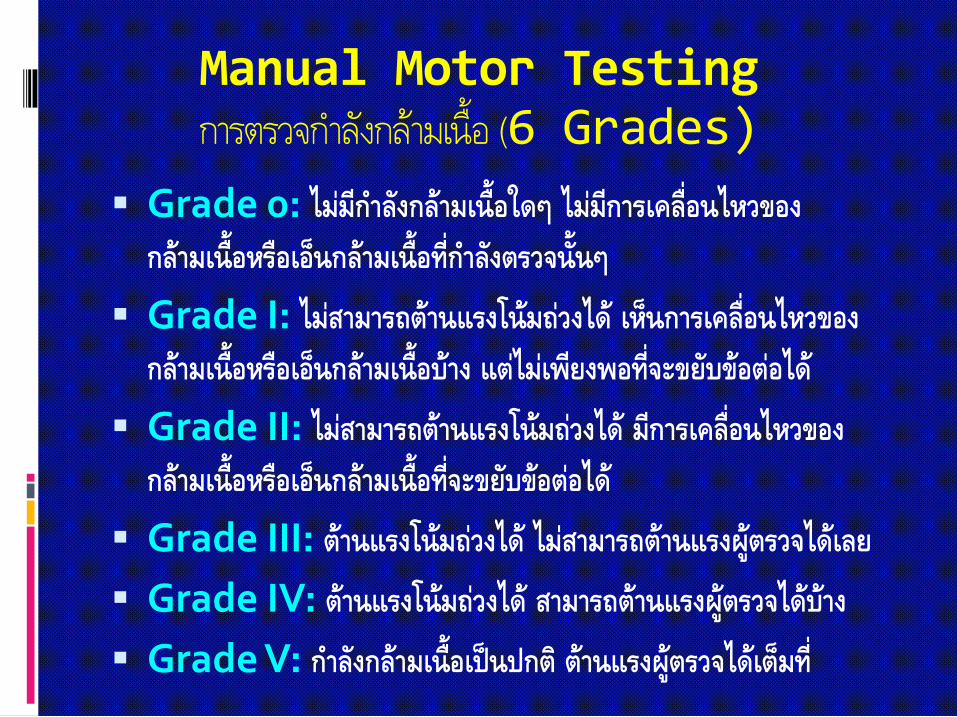
Manual Motor Testingการตรวจกําลังกลามเนื้อ (6 Grades)
Grade 0: ไมมีกําลังกลามเนื้อใดๆ ไมมีการเคลื่อนไหวของกลามเนื้อหรือเอ็นกลามเนื้อที่กําลังตรวจนั้นๆ
Grade I: ไมสามารถตานแรงโนมถวงได เห็นการเคลื่อนไหวของกลามเนื้อหรือเอ็นกลามเนื้อบาง แตไมเพียงพอที่จะขยับขอตอได
Grade II: ไมสามารถตานแรงโนมถวงได มีการเคลื่อนไหวของกลามเนื้อหรือเอ็นกลามเนื้อที่จะขยับขอตอได
Grade III: ตานแรงโนมถวงได ไมสามารถตานแรงผูตรวจไดเลย
Grade IV: ตานแรงโนมถวงได สามารถตานแรงผูตรวจไดบาง
Grade V: กําลังกลามเนื้อเปนปกติ ตานแรงผูตรวจไดเต็มท่ี

Neurologic Examination
Motor Iliopsoas – hip flexion (L1-L2)
Quadriceps – knee extension, hip adduction (L3-4)
Tibialis anterior – ankle dorsiflexion/ inversion (L4)
Extensor hallucis longus – great toe extension(L5)
Gluteus medius – hip abduction (L5)
Peroneus longus and brevis –ankle eversion(S1)
Flexor hallucis longus – great toe flexion (S1)
Bowel/bladder sphincter (S2-5)
Sensation
Sensory dermatomal area
Reflexes
L4 (knee jerk)
S1 (ankle jerk)
S2-4 (rectal exam; bulbocavernosus reflex)

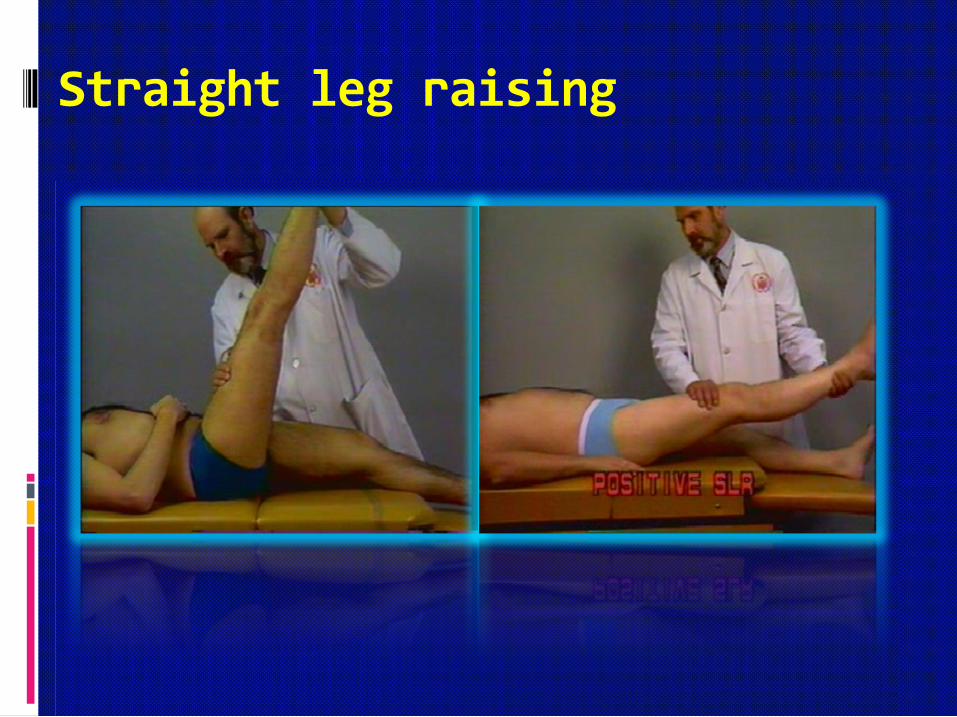
Straight leg raising

Symptomatology of Back Pain
Low back pain
Spondylogenic
Neurogenic
Viscerogenic
Vasculogenic
Psychogenic
Sciatica
Pain along the sciatic nerve distribution
Claudication Neurogenic vs Vascular claudication
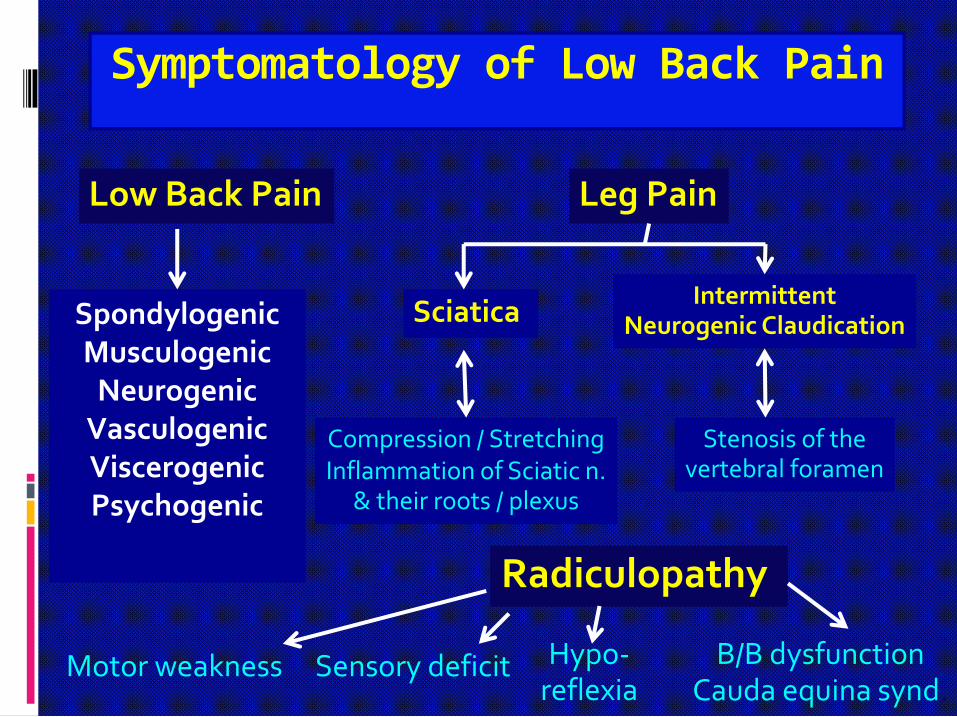
Symptomatology of Low Back Pain
Low Back Pain Leg Pain
Sciatica Intermittent
Neurogenic Claudication
Compression / StretchingInflammation of Sciatic n.
& their roots / plexus
Stenosis of thevertebral foramen
SpondylogenicMusculogenic
NeurogenicVasculogenicViscerogenicPsychogenic
Radiculopathy
Motor weakness Sensory deficit Hypo-reflexia
B/B dysfunctionCauda equina synd.

Leg Pain-Sciatica
Pain along sciatic nerve distribution
พยาธิสภาพใดก็ตามที่กด ทับ ดึง รั้ง เสนประสาท sciatic และ แขนงของมัน

Leg Pain- Intermittent Neurogenic Claudication
พยาธิสภาพที่ทําใหโพรงกระดูกสันหลังตีบแคบลง ทําใหการไหลเวียนน้ําไขสันหลัง (CSF) ไมสะดวก เกิดการคั่งของเสียและการอักเสบตอรากประสาท

Vascular vs Neurogenic
intermittent claudication (1)
Test Vascular NeurogenicPain Crampy, tight Sharp, ache, numbness
Walking Distal Proximal pain, calf pain
Proximal Distal pain, thigh pain
Uphill walking Symptoms develop sooner
Symptoms develop later
Rest Relief with standing still Relief with sitting, bending
Bicycle test Symptoms develop No symptoms develop
Lying flat Relief May exacerbate
Walking distance
Constant Variable

Vascular vs Neurogenicintermittent claudication (2)
Test Vascular Neurogenic Pulses Diminished Normal
Bruits Likely Not likely
Skin Shiny, no hair Normal
Atrophy Rare Occasional
Weakness Rare Occasional
Back pain Uncommon Common
Spine ROM Normal Often decreased

Nerve root
RadiculopathyMotor disturbanceSensory disturbanceHyporeflexia
Lower motor neuron
Spinal cord
Myelopathy• Sensory disturbance
• Motor disturbance
• Bowel and bladder dysfunction
• Hyperreflexia
• Spasticity
• Abnormal reflexes : Clonus,Babinski, Hoffmann,Lhermitte,Inverted radial reflex
Upper motor neuron

Plain X-rays LS-spine of Lumbar Degenerative Diseases
L1
L2
L3
L4
L5
Pedicle Pedicle
Facet jointsFacet joints
Intervertebral disc
Vertebral body
Spinous process
Spinousprocess
Transverseprocess
SI joint
Intervertebralforamen
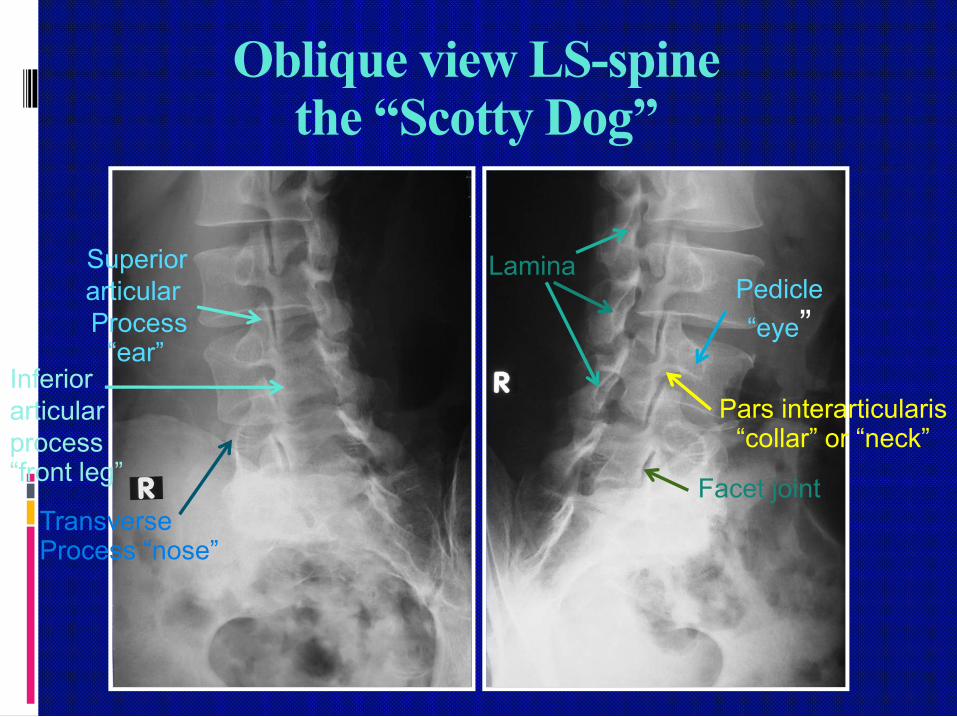
Oblique view LS-spinethe “Scotty Dog”
SuperiorarticularProcess
“ear”
Pedicle
“eye”
Inferior articularprocess“front leg”
Pars interarticularis“collar” or “neck”
TransverseProcess “nose”
Facet joint
Lamina

Lumbar Myelography
Injection of the contrast media into subarachnoid spacePerform radiographic exam., Adv.: evaluate dynamic motion
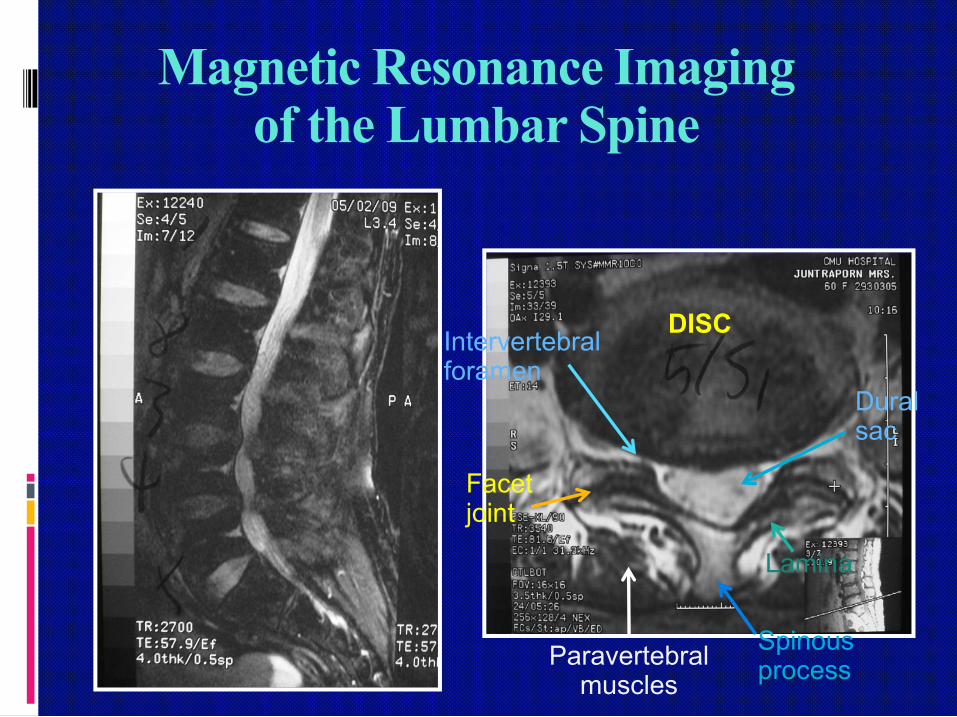
Magnetic Resonance Imagingof the Lumbar Spine
DISC
Lamina
Paravertebralmuscles
Spinousprocess
Facetjoint
Duralsac
Intervertebralforamen

สาเหตุของอาการ “ปวดเอว”
กลามเนื้อหลังอักเสบ เฉียบพลันและเรื้อรัง
หมอนรองกระดูกสันหลังกดทับรากประสาท
ขอตอกระดูกสันหลังเสื่อม
ชองกระดูกสันหลังตีบแคบ
ขอตอกระดูกสันหลังเสื่อม ความไมมั่นคงของกระดูก สันหลัง

• Most common back problem
• Partial injury of muscle, fascia, • tendon, annulus fibrosus• Long-standing poor posture• Non radiated back pain • No neurological involvement
Neck strainMid-back strainLow back strain
:
Diagnosis • History …. Pain relate to traumatic event
• Clinical findings :- localized pain and tenderness- pain on back / neck movement- decrease range of motion- back muscle spasm- deformity…. Scoliosis, Kyphosis
• Laboratory finding …. normal• X- rays findings …..normal

Back Strain
Chronic, acute-on-chronic inflammation of the back muscles
Repetitive use, Malposture
No precise lesion demonstrable
Predisposing factors
Overweight
Muscle flabbiness
Debilitating illness
Poor posture
Heavy lifting
Back Strain
TreatmentTreatment
Conservative treatment :• Limit activity• Supports• Physical therapy• Drugs … Analgesic, NSAIDs
• ExerciseMuscle relaxants
LBP - is a self-limiting,
benign disorder in the
vast majority of adults

Herniated Nucleus Pulposus(HNP)
Displacement of the central area of the disc (nucleus) resulting in impingement on the lumbo-sacral nerve root
Common cause of LBP & leg pain (sciatica, claudication)
Common at L4-5, L5-S1
Posterolateral direction
Predisposing factors
Age degeneration
Injury

HNP

Male > Female
Age 30-50 year
Job requiring heavy lift, Lift on twisted
Low income
Cigarette smoking
Acute subacute onset
Back pain and/or sciatica

Lumbar Disc Herniation
Low back pain : acute onset related to an innoceousmovement
Sciatica : aggravated bysitting and relievedby lying down or standing
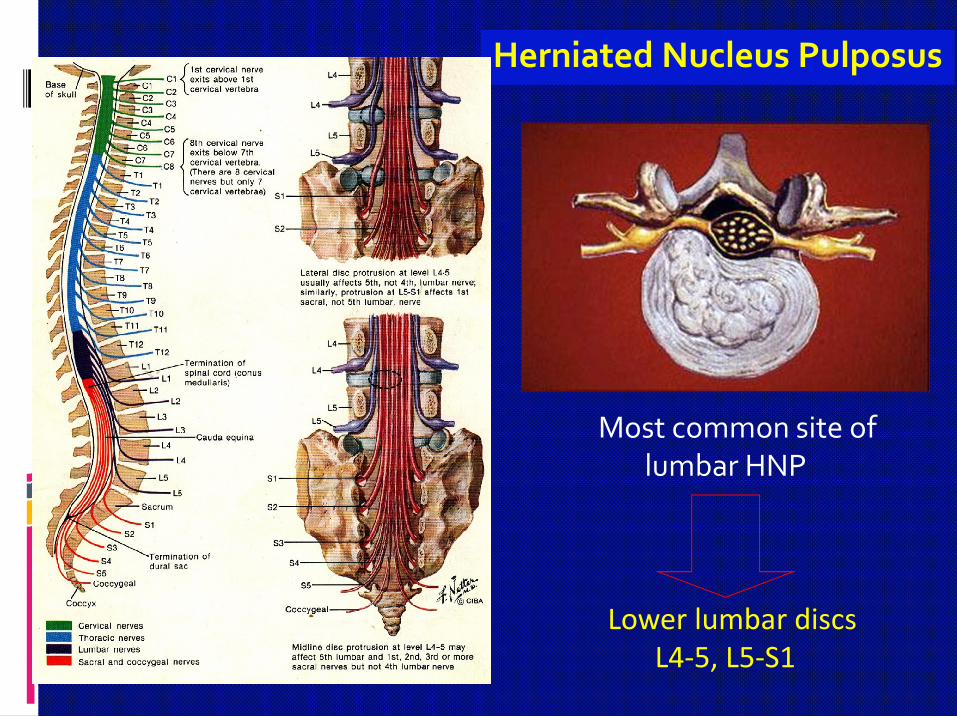
Most common site of lumbar HNP
Lower lumbar discsL4-5, L5-S1
Herniated Nucleus Pulposus

Neurological Examination

Herniated Nucleus Pulposus(HNP)
Lumbar HNP- very common
Location: low back to lower leg
Quality: sharp, shooting, burning paresthesia in lower leg
S/S: positive straight leg-raising test, weakness, hyporeflexia
Imaging: plain film, myelogram, CT, MRI (most sensitive)
90% treated by conservative Rx
Only 5-10% required surgery

Herniated Nucleus Pulposus(HNP)
Treatment
Conservative treatment
Rest, Restriction of motion
NSAIDs & analgesics
Physical therapy
Aerobic conditioning
Lumbar epidural steroid injection
Surgical discectomy

Non - operative treatment (90%)• Patient education• Rest • Medication : analgesics, anti-inflammatory drugs steroid,muscle relaxants,
anti-depressants, anti-convulsants• Physical therapy : lumbar traction ,
diathermyexercise, supports
• Modification of activities , Support• Occupational therapy• Psychotherapy • Spinal injection
Treatment of Disc Herniation

Treatment of Lumbar Disc Herniation
Operative Treatment
Indications - loss of bowel and bladder function(Cauda equina syndrome)
- progressive neurological deficit- failure conservative treatment- excruciating pain
Procedures: Discectomy - Anterior / PosteriorNucleolysisSpinal Fusion Disc Prosthesis Replacement
Posterior Lumbar Disc Herniation“disc excision”
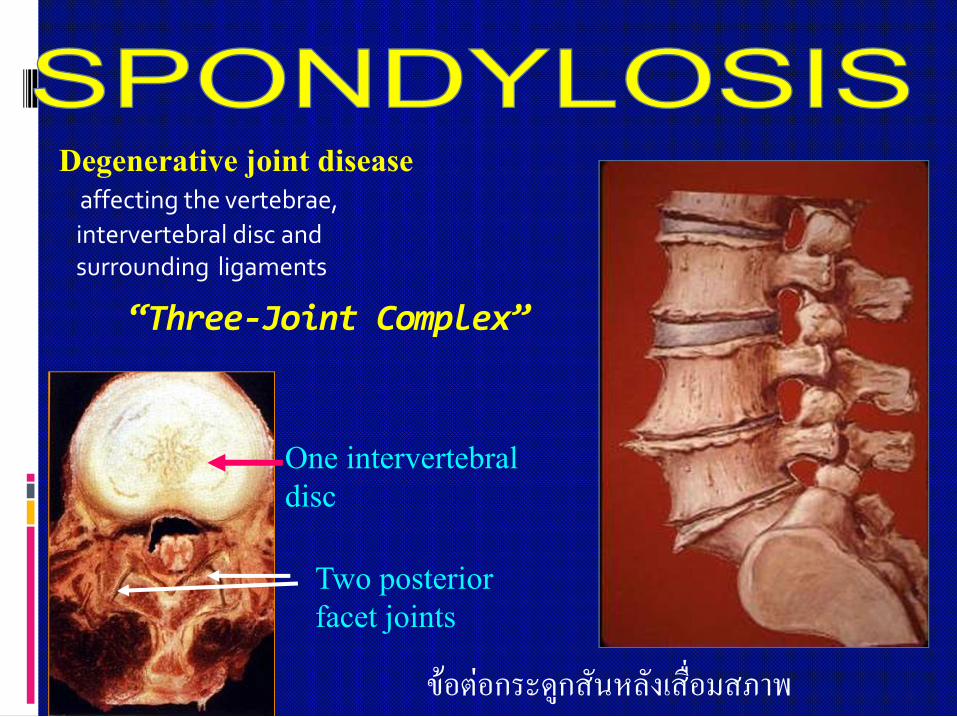
Degenerative joint disease affecting the vertebrae,
intervertebral disc and surrounding ligaments
“Three-Joint Complex”
One intervertebral disc
Two posterior facet joints
ขอตอกระดูกสันหลังเสื่อมสภาพ
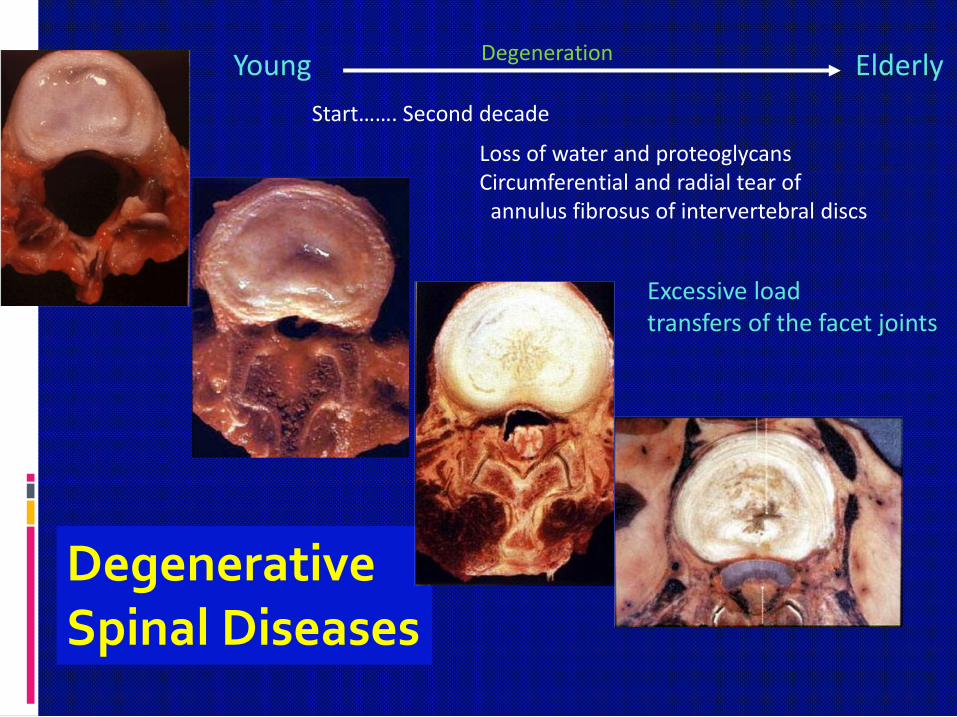
DegenerativeSpinal Diseases
Young Elderly
Start……. Second decade
Loss of water and proteoglycansCircumferential and radial tear of
annulus fibrosus of intervertebral discs
Excessive loadtransfers of the facet joints
Degeneration

Intervertebral disc
Decrease disc volumeDecrease disc height
( space )Laxity of annular ligamentSubluxation of discOsteophyte formation
Facet joints
Degeneration of articular cartilageSynovitisDecrease joint spaceLaxity of joint capsuleSubluxation of jointOsteophyte formationFacet joint hypertrophyLUMBAR
SPONDYLOSIS
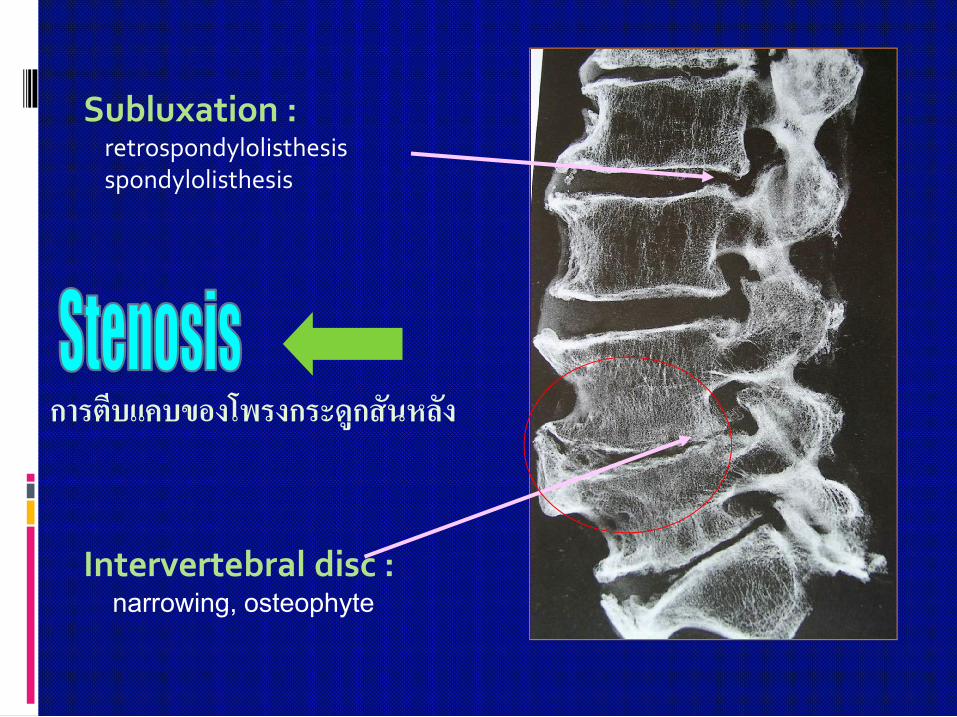
Subluxation :retrospondylolisthesisspondylolisthesis
Intervertebral disc :narrowing, osteophyte
การตีบแคบของโพรงกระดูกสันหลัง

Degenerative arthritis :osteophyte, laxity
Facet joint hypertrophyFacet joint subluxation
Decrease spinal canal volume

Spinal canal stenosisSpinal canal stenosis
Spondylotic changes leading to spinal deformity and spinal instability

Degenerative Lumbar Diseases
Wear-tear process
Degenerative Disc Disease + Osteoarthritis of the facet joints
Low back pain
Leg pain: sciatica + neurogenic claudication
90% conservative treatment

Investigations-Imaging
Plain radiographs- AP, lateral, oblique
Flexion-extension lateral view
Myelography
CT myelography
MRI
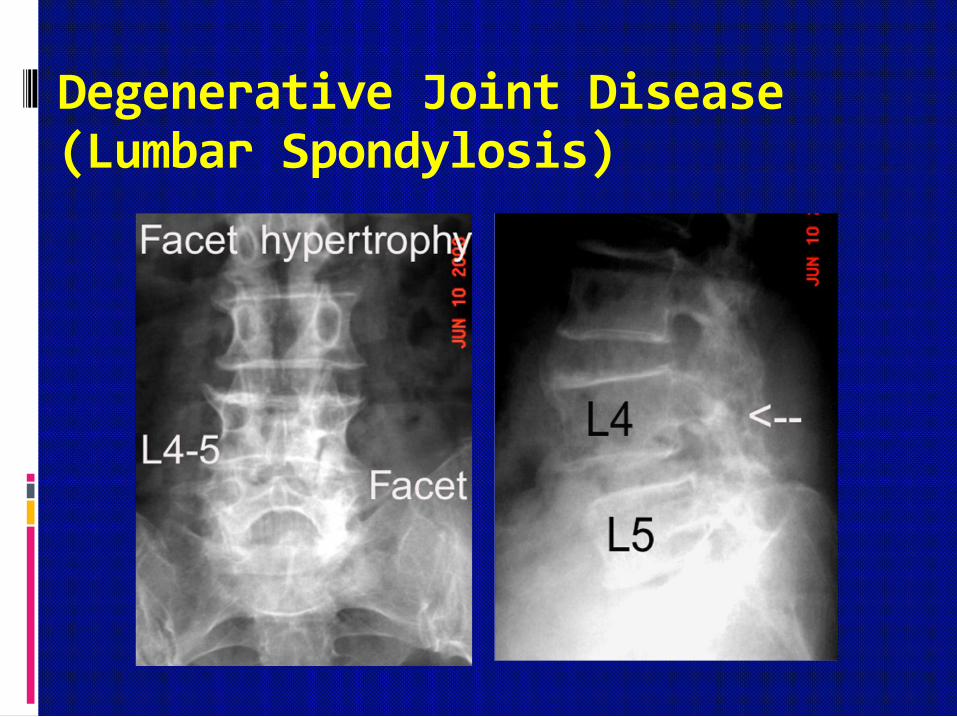
Degenerative Joint Disease(Lumbar Spondylosis)
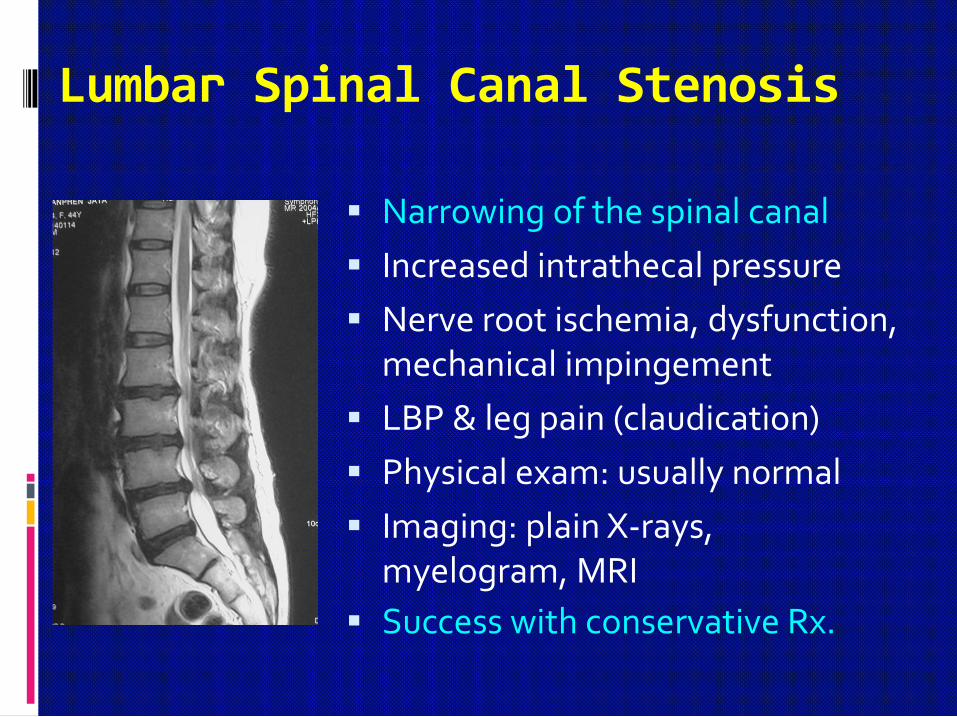
Lumbar Spinal Canal Stenosis
Narrowing of the spinal canal
Increased intrathecal pressure
Nerve root ischemia, dysfunction, mechanical impingement
LBP & leg pain (claudication)
Physical exam: usually normal
Imaging: plain X-rays, myelogram, MRI
Success with conservative Rx.

Defect of pars interarticularis of the vertebra
Forward displacement (olisthesis) of one vertebra over another

Symptoms and signs of spondylolysis
Low back pain or aching radiating into the buttock and thigh
Limitation of back movement
No neurological deficit

SPONDYLOLYSISSPONDYLOLYSIS
Plain X-rays
position – Oblique view“Scotty Dog pattern”
Pars interarticularisPars interarticularis

Spondylolysis(defect of pars interarticularis)
Lateral view Oblique view

Lumbar Spondylolisthesis
Isthmic spondylolisthesisL5-S1 (common)
Degenerative spondylolisthesisL4-5 (common)
Pars defect Facet arthrosis+
Disc degeneration

Symptoms and signs of Spondylolisthesis
Low back pain radiating into the buttock and thigh
Sciatica
Intermittent claudication
Limitation of back movement
Visible and palpable step off
Hamstring tightness
Paravertebral muscle spasm
Hyperlordosis
Abnormal gait
Neurological deficit (motor, sensory, reflex changes)

Treatment of Spondylolisthesis
Non-operative treatment
Restriction of activityLumbosacral corset/brace
Medications
Exercise
Physical therapy
Operative indicationsContinued back and sciatic painProgressive slippingProgressive neurological deficit
Operative procedurePosterolateral spinal fusion
with/without decompressionPosterior spinal instrumentation and
fusion with or without decompression
Anterior spinal fusion
Management of Low Back Pain
“Primary care interventions”
Patient education (brief education, back school)
Medications
Common analgesics, Muscle relaxants, Opioid analgesics
Physical modalities
Superficial heat/cold, Electrotherapy, Traction therapy
Manual therapy
Spinal manipulation therapy, Massage
Other interventions
Acupuncture
Management of Low Back Pain
“Secondary / Tertiary care interventions”
Medications
Adjunctive analgesics (antidepressants, anticonvulsants)
Injections
Epidural steroid injections
Facet injections
Soft tissue injections (trigger point, local anesthetic)
Other approaches & Alternative medicines
Surgery
Decompression & Fusion surgery

การรักษาโดยวิธีไมผาตัด
การปฏิบัติตนที่ถูกตอง
การพักการใชงาน
การรักษาโดยการใชยา
การทํากายภาพบําบัด
การใชเครื่องพยุงกระดูกสันหลัง
การฝงเข็ม การจัดกระดูก

Education
Activity modification
• Posture
• Lifestyle
Physical activity
Smoking cessation
Weight reduction
Back school

LEVEL 1 TREATMENT
“Active Observation”
Activities as tolerated
NSAIDs ***
Analgesics
Muscle relaxants
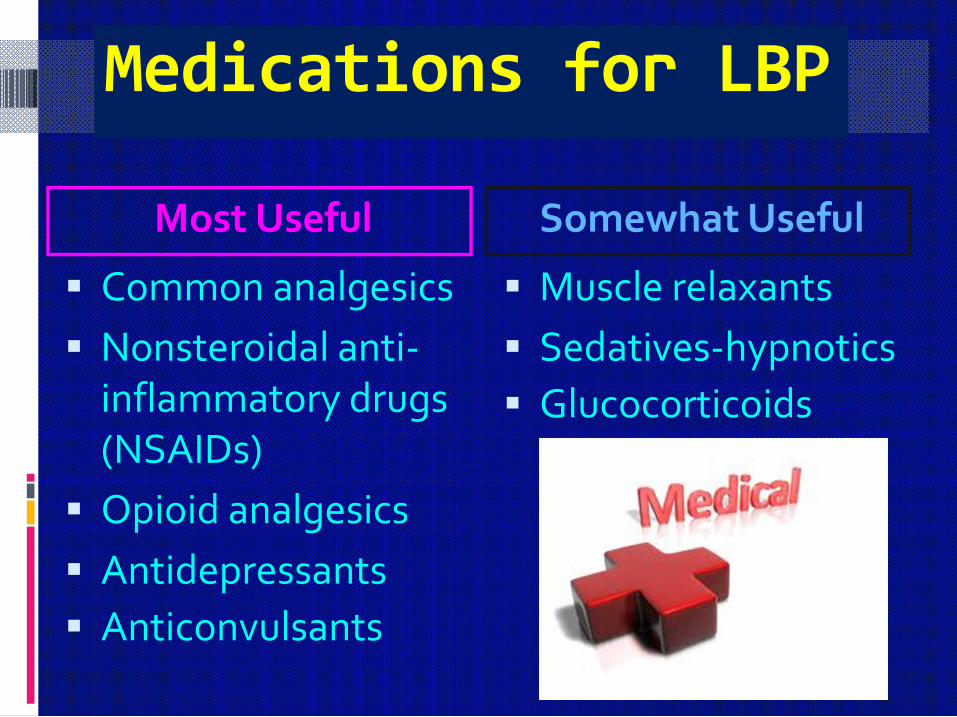
Medications for LBP
Most Useful
Common analgesics
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Opioid analgesics
Antidepressants
Anticonvulsants
Somewhat Useful
Muscle relaxants
Sedatives-hypnotics
Glucocorticoids

LEVEL 2 TREATMENT
Physical Therapy
Active
Passive

Conservative Treatment
Lumbar support Assistive device

Lumbar Traction

Lumbar Stabilization Exercise

Lumbar Strengthening Exercise

LEVEL 3 TREATMENT
Injection Therapy
Epidural steroids
Nerve blocks
Trigger point injections
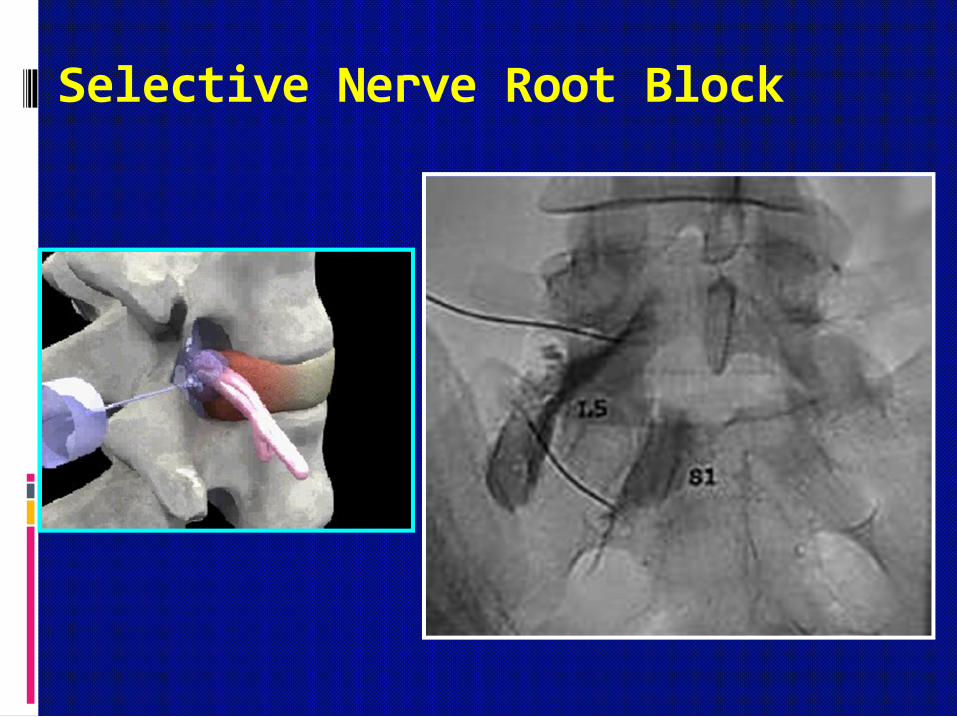
Selective Nerve Root Block

LEVEL 4 TREATMENT
Anesthesiologists
Physical therapists
Occupational therapists
Psychologists
Neurologists
Etc.
Multidisciplinary Pain Management

การรักษาโดยวิธีผาตัด
(SURGICAL TREATMENT) การผาตัดระบายความดันในชอง
กระดูกสันหลัง
การผาตัดเชื่อมขอตอกระดูกสันหลัง
I. ไมใชโลหะดามกระดูกสันหลัง
II. ใชโลหะดามกระดูกสันหลัง การผาตัดแกไขความผิดรูป
การผาตัดขอหมอนรองกระดูกสันหลังเทียม
การผาตัดแบบเนื้อเย่ือบาดเจ็บนอย
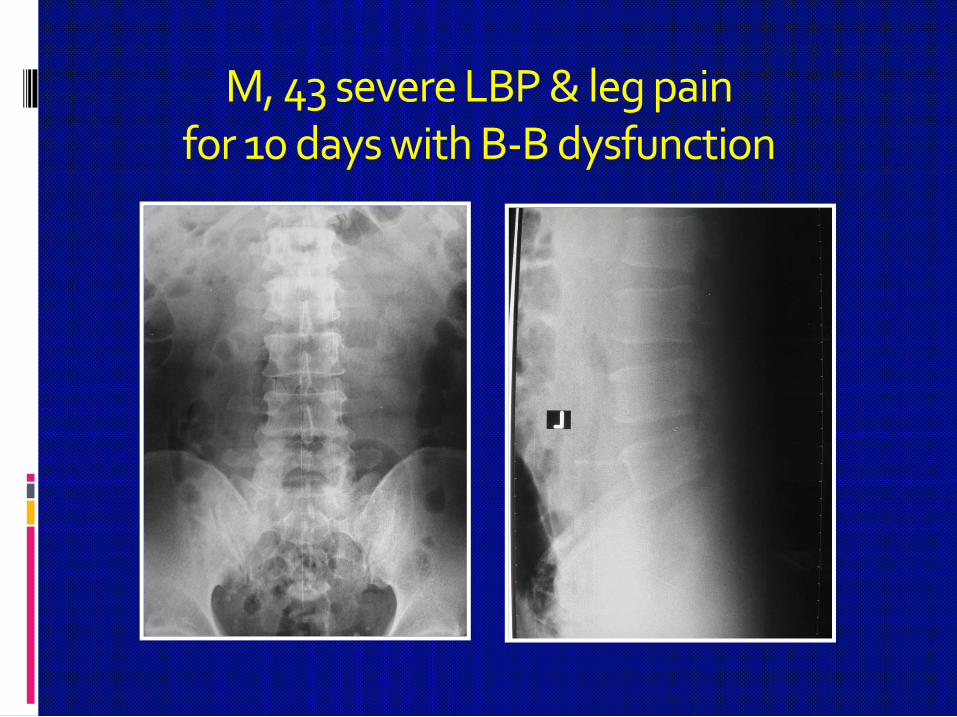
M, 43 severe LBP & leg pain for 10 days with B-B dysfunction

M, 43 severe LBP & leg pain for 10 days with B-B dysfunction

MRI LS-spine

Large HNP L4-5 Disc Sequestration
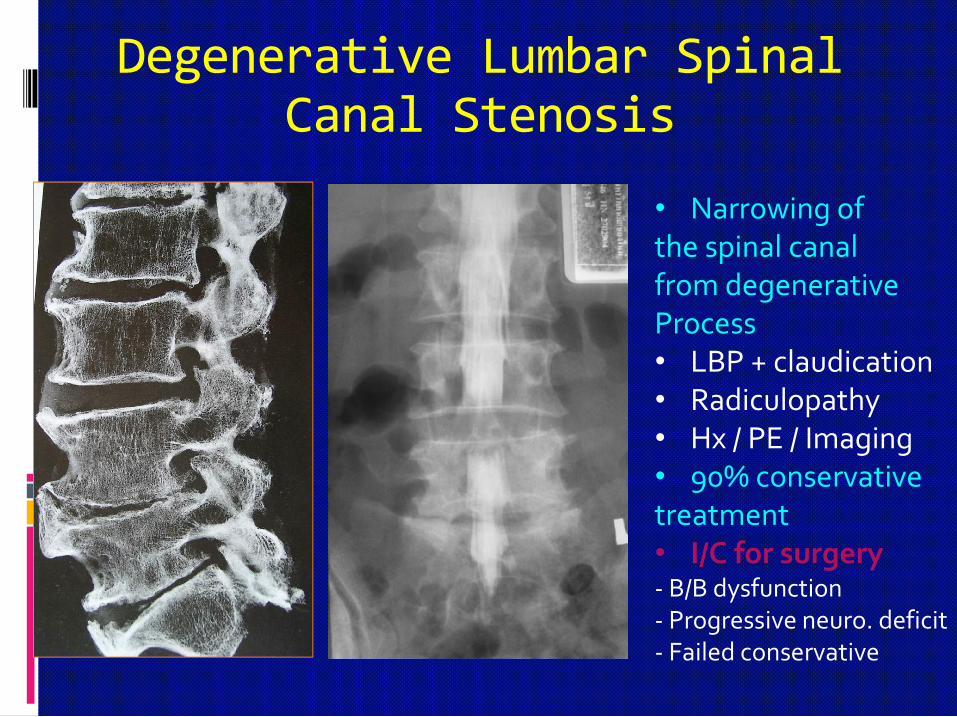
Degenerative Lumbar Spinal Canal Stenosis
• Narrowing ofthe spinal canalfrom degenerative Process• LBP + claudication• Radiculopathy • Hx / PE / Imaging• 90% conservativetreatment• I/C for surgery- B/B dysfunction- Progressive neuro. deficit- Failed conservative
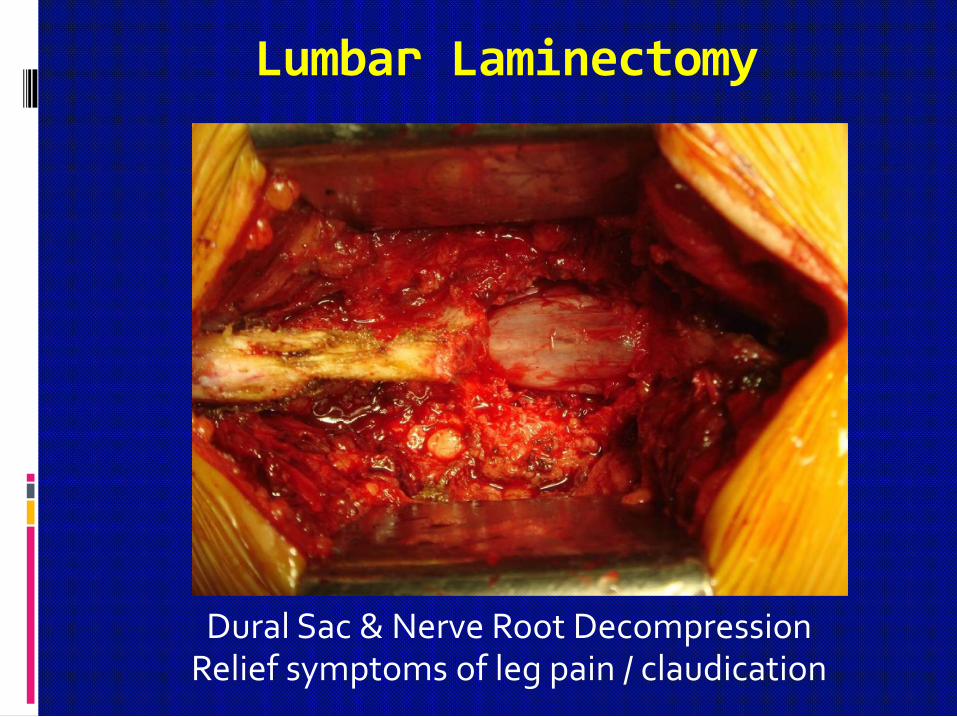
Lumbar Laminectomy
Dural Sac & Nerve Root DecompressionRelief symptoms of leg pain / claudication

Treatment of Spondylolisthesis
Non-operative treatment
Restriction of activityLumbosacral corset/brace
Medications
Exercise
Physical therapy
Operative indicationsContinued back and sciatic pain
Progressive slippingProgressive neurological deficit
Operative proceduresPosterolateral spinal fusion with/without decompressionPosterior spinal instrumentation and fusion with or without decompressionAnterior spinal fusion

Faculty of Medicine
Chiang MaiUniversity

Cervical Vertebra (C1-C7)
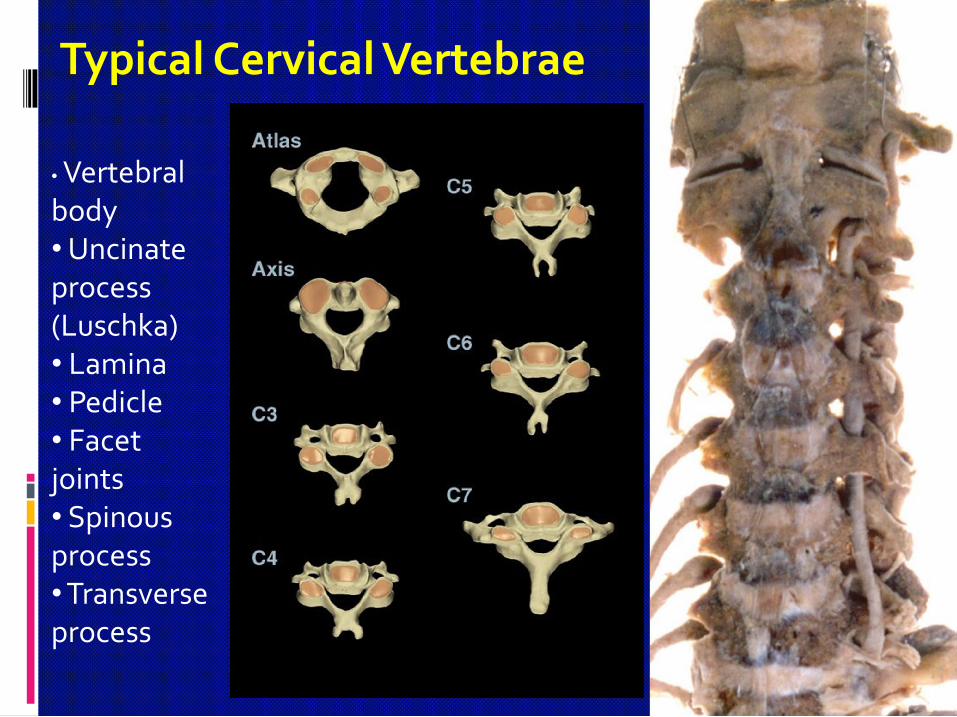
• Vertebralbody• Uncinateprocess(Luschka)• Lamina• Pedicle• Facet joints• Spinousprocess• Transverseprocess
Typical Cervical Vertebrae
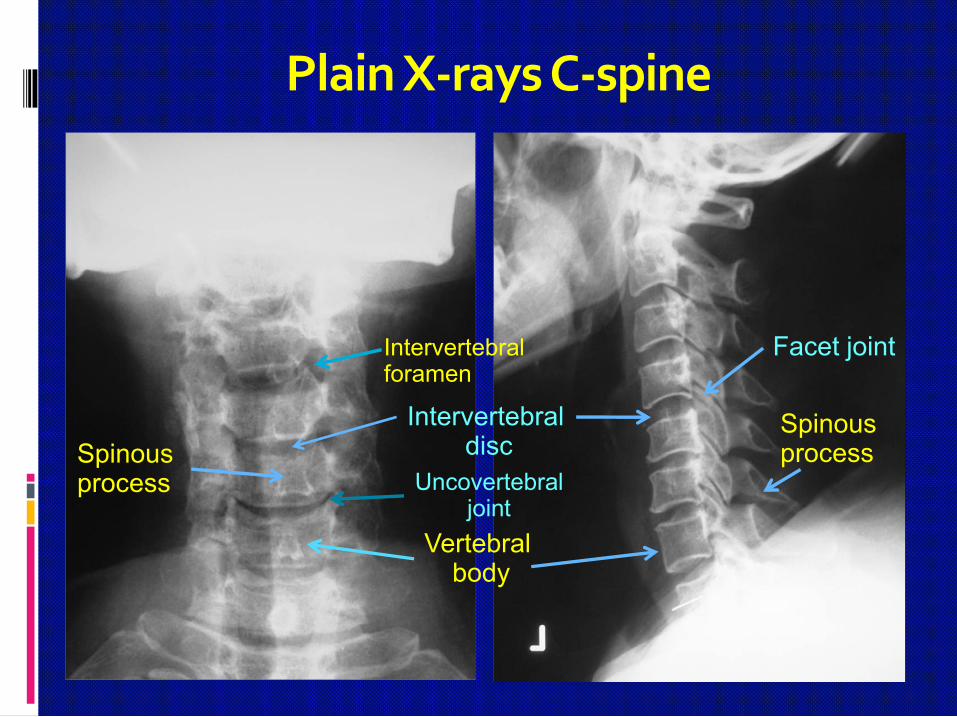
Plain X-rays C-spine
Intervertebral disc
Vertebral body
Uncovertebraljoint
Intervertebralforamen
Spinous process
Spinous process
Facet joint
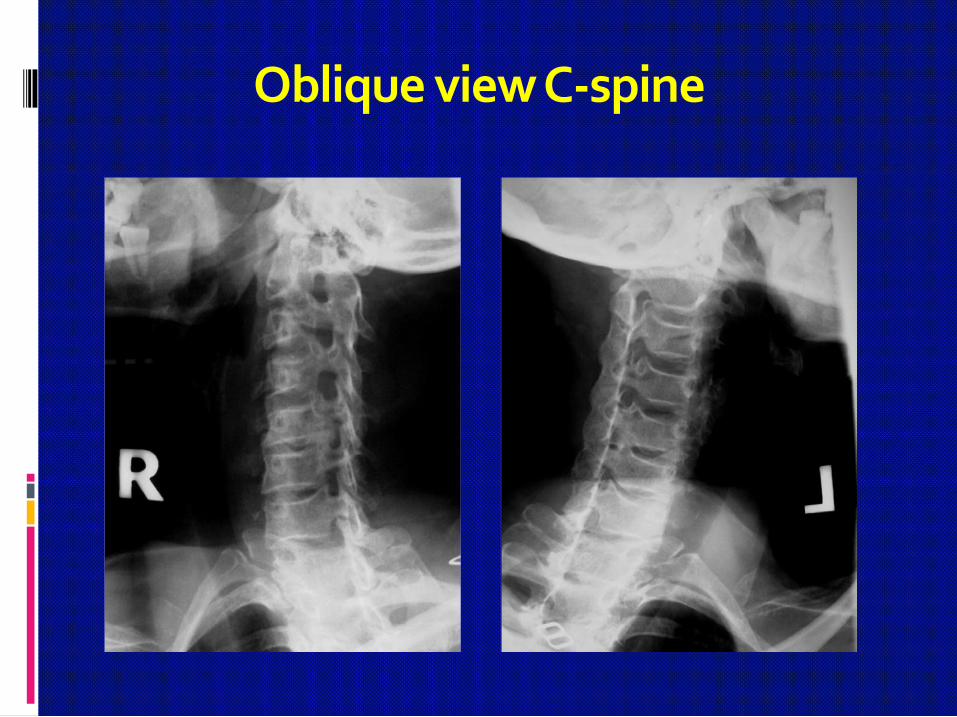
Oblique view C-spine

Magnetic Resonance Imagingof the Cervical Spine
Common Cervical Spine Disorders
Degenerative diseases*** Acute cervical strain Cervical spondylosis Cervical radiculopathy Cervical spondylotic myelopathy (CSM) Cervical disc herniation
Infectious diseases Bacterial vs TB
Tumors Metastasis
Inflammatory diseases Rheumatoid arthritis
Miscellaneous Ossification of the ligament: OPLL, OYL
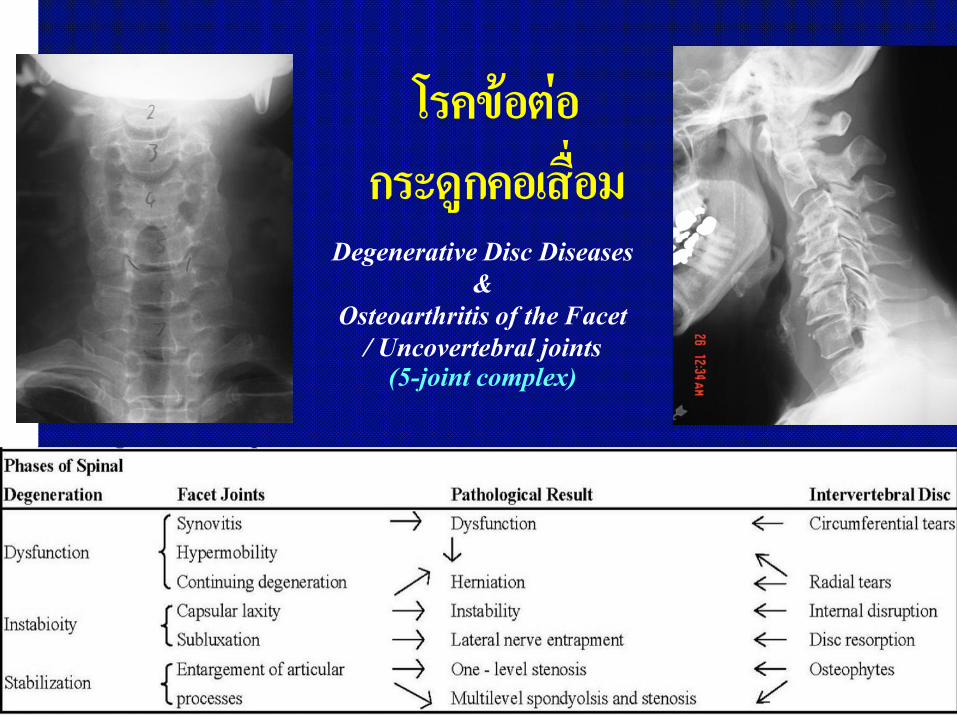
โรคขอตอกระดูกคอเสื่อม
Degenerative Disc Diseases&
Osteoarthritis of the Facet / Uncovertebral joints
(5-joint complex)

โรคขอตอกระดูกคอเสื่อม
Disc degeneration
Facet joint arthropathy
Osteophyte formation
Uncovertebral joint hypertrophy
Hypertrophy of the ligamentum flavum
Loss of lordosis
Segmental instability
AXIAL NECK PAIN …RADICULOPATHY …MYELOPATHY ………

Degenerative Cervical Diseases
Wear-tear process
Symptomatology
Axial neck pain
Radiculopathy
Myelopathy
Hx / PE / Imaging
Mostly conservative Rx
Activity modification
Medication
Physical therapy
Surgery: C-myelopathy
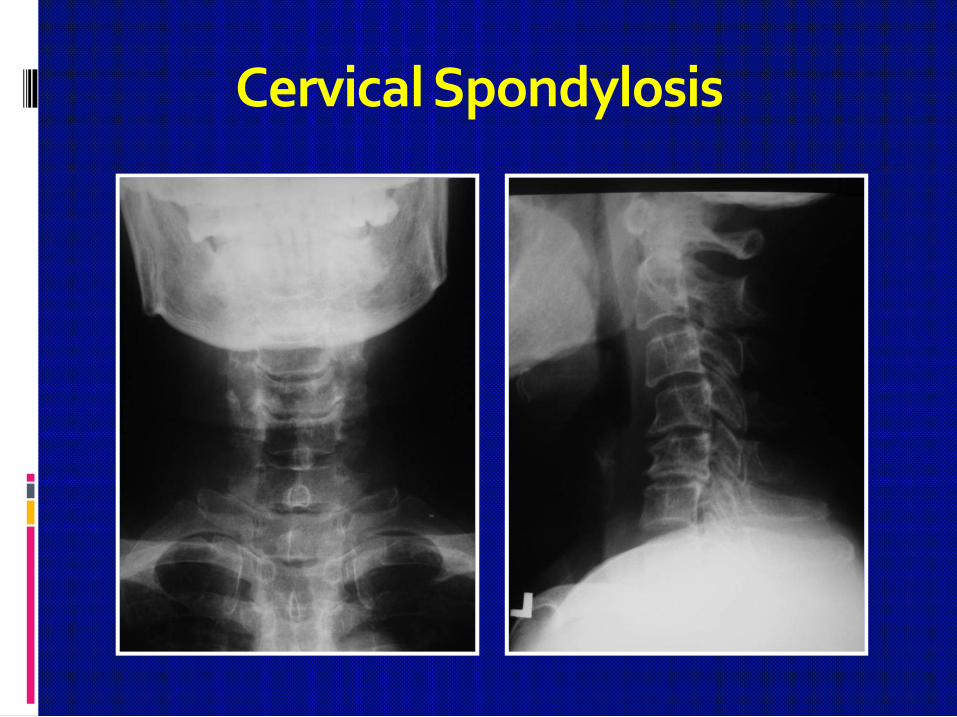
Cervical Spondylosis


Cervical Disc Herniation
Cervical Radiculopathy
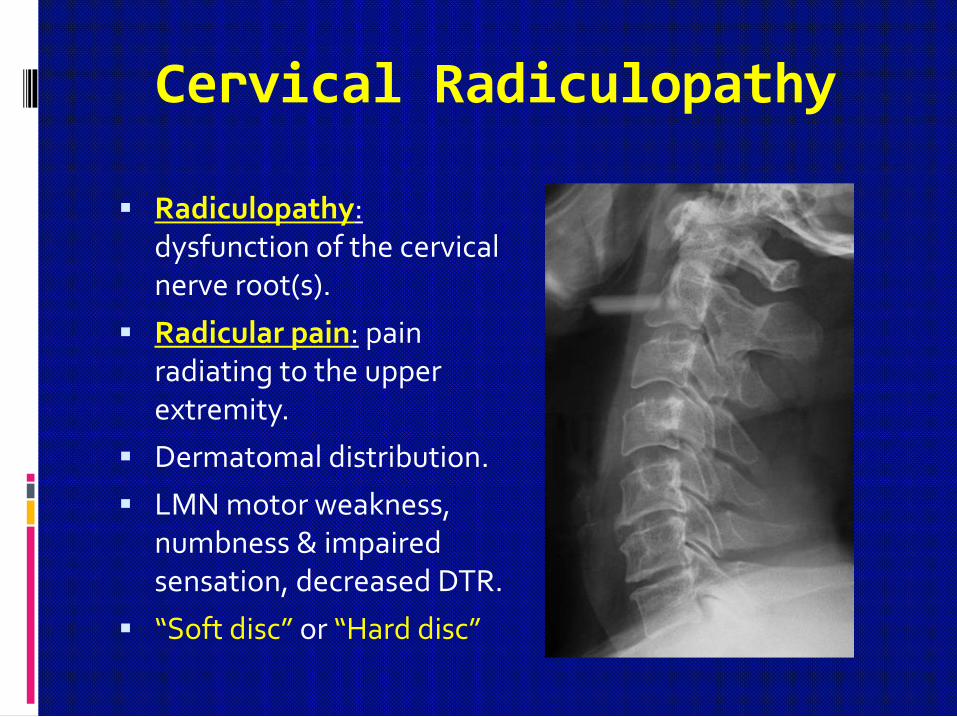
Radiculopathy:dysfunction of the cervical nerve root(s).
Radicular pain: pain radiating to the upper extremity.
Dermatomal distribution.
LMN motor weakness, numbness & impaired sensation, decreased DTR.
“Soft disc” or “Hard disc”

Cervical Spondylotic Radiculopathy

Cervical Spondylotic Myelopathy (CSM)spinal cord dysfunction secondary to extrinsic compression of the cord or its vascular supply,
or both, that caused by degenerative diseases of the spine
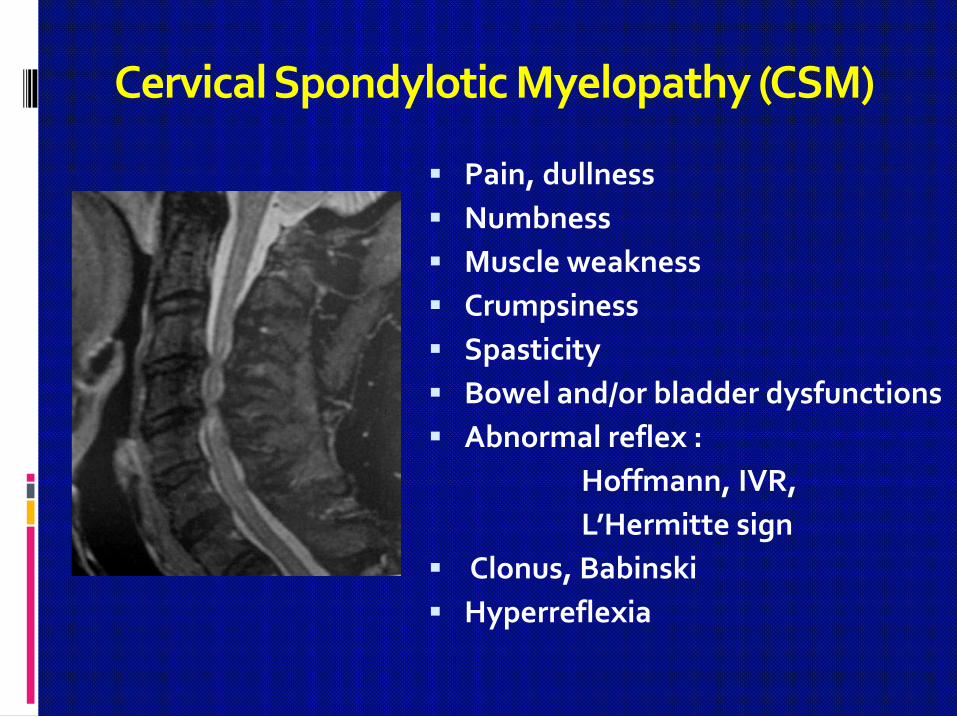
Cervical Spondylotic Myelopathy (CSM)
Pain, dullness
Numbness
Muscle weakness
Crumpsiness
Spasticity
Bowel and/or bladder dysfunctions
Abnormal reflex :
Hoffmann, IVR,
L’Hermitte sign
Clonus, Babinski
Hyperreflexia

Intrinsic Hand Muscle Weakness
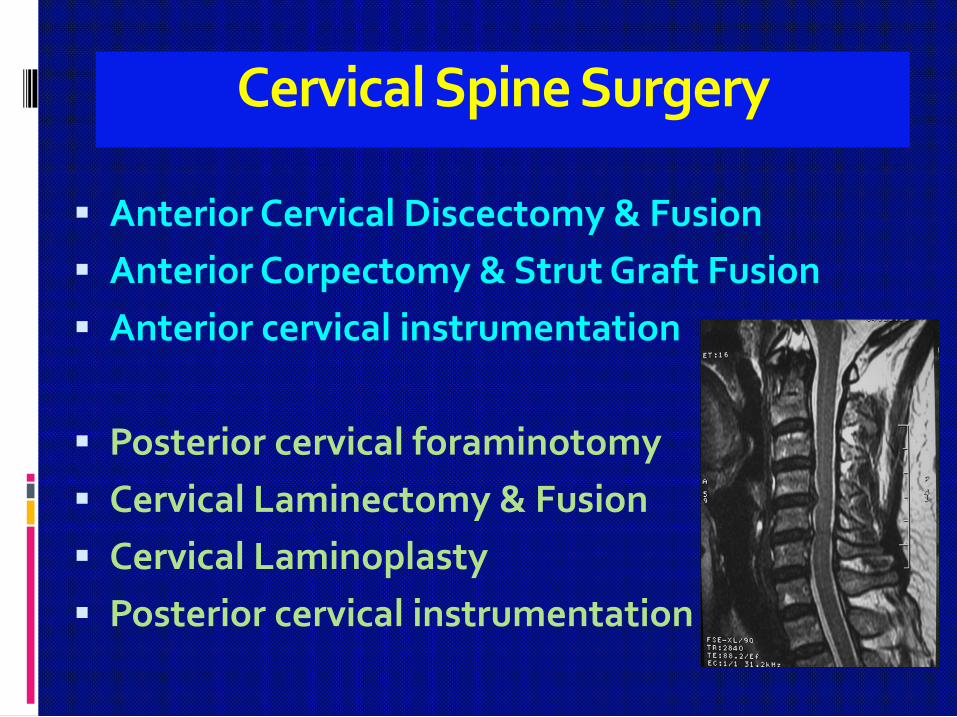
Cervical Spine Surgery
Anterior Cervical Discectomy & Fusion
Anterior Corpectomy & Strut Graft Fusion
Anterior cervical instrumentation
Posterior cervical foraminotomy
Cervical Laminectomy & Fusion
Cervical Laminoplasty
Posterior cervical instrumentation
Anterior Cervical Discectomy (Decompression)
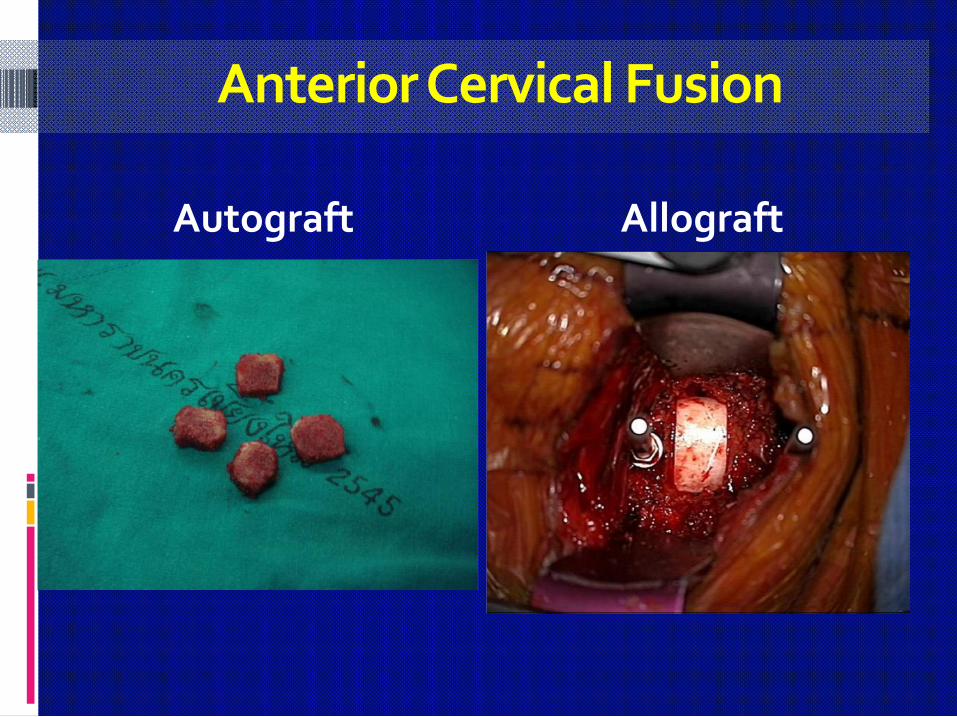
Anterior Cervical Fusion
Autograft Allograft
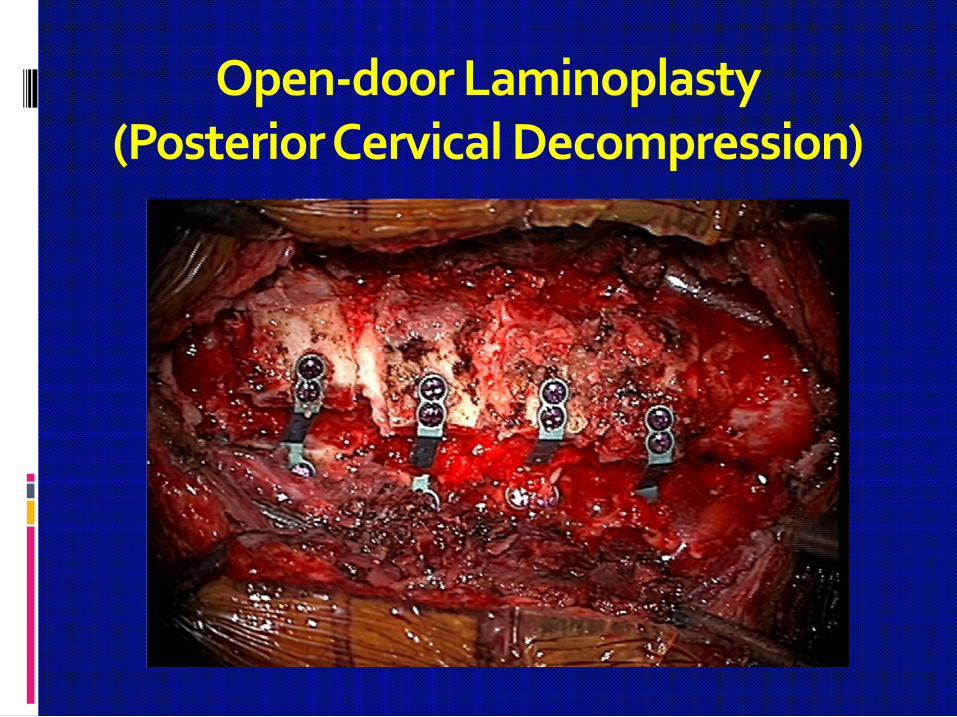
Open-door Laminoplasty(Posterior Cervical Decompression)

THANK YOUFOR YOUR KIND ATTENTION
T. Bunmaprasert, MD.