
National Education, Pulp Fiction and the Contradictions of Colonialism

Available online at www.sciencedirect.com
4 (2009) 253–265
History of the Family 1Colonialism and the health transition: Aboriginal Australians andpoor whites compared, Victoria, 1850–1985
Janet McCalman a,⁎, Len Smith b, Ian Anderson a, Ruth Morley c, Gita Mishra d
a Centre for Health & Society, University of Melbourne, Victoria, 3010, Australiab Australian Demographic & Social Research Institute, Australian National University, Canberra, ACT, 0200, Australia
c University of Melbourne Department of Paediatrics and Murdoch Children's Research Institute, Royal Children's Hospital,Melbourne, 3052, Australia
d MRC Unit for Lifelong Health and Ageing, Department of Epidemiology & Public Health, University College, London, WC1B 5JU, UK
Abstract
This paper presents the results of the first two longitudinal historical cradle-to-grave datasets constructed in Australia: theAboriginal population of the state of Victoria, reconstituted backwards using genealogical research and vital registrations, 1835–1930; and an impoverished European population born at the Melbourne Lying-In Hospital, 1857–1900 and traced until 1985. Itinvestigates the hypothesis that the health transition in indigenous people was different from that of the dominant non-indigenouspopulation. Both of these studied sub-populations were highly stressed, resulting in high infant mortality and persistent tuberculosismortality. The Aboriginal population suffered the additional burdens of racism and social exclusion, even though after the passageof the 1886 ‘Half-Castes Act’, the majority of Aboriginal Victorians were legally ‘white’. The impact of that legislation and thesystematic exclusion of Aboriginal Victorians from federal entitlements in the twentieth century sent the Aboriginal healthtransition into reverse. The contrasting fates of poor whites and ‘unofficial blacks’ during the health transition demonstrate thehealth burdens of inequality and racial discrimination, and reveal that ‘the gap’ in life expectancy between Indigenous and non-Indigenous Australians is a historical product of long-term government policy and exclusion from citizenship and its entitlements.© 2009 Elsevier Inc. All rights reserved.
1. Introduction
Our challenge for the future is to embrace a newpartnership between Indigenous and non-IndigenousAustralians. The core of this partnership for the futureis closing the gap between Indigenous and non-Indigenous Australians on life expectancy, educationalachievement and employment opportunities. This new
⁎ Corresponding author. Tel.: +61 3 8344 9107.E-mail address: [email protected] (J. McCalman).
1081-602X/$ - see front matter © 2009 Elsevier Inc. All rights reserved.doi:10.1016/j.hisfam.2009.04.005
partnership on closing the gap will set concrete targetsfor the future: within a decade to halve the wideninggap in literacy, numeracy and employment outcomesand opportunities for Indigenous children, within adecade to halve the appalling gap in infant mortalityrates between Indigenous and non-Indigenous childrenand, within a generation, to close the equally appalling17-year life gap between Indigenous and non-Indigenous when it comes to overall life expectancy.
— Prime Minister Kevin Rudd, Apology toAustralia's Indigenous Peoples, 13 February 2008

254 J. McCalman et al. / History of the Family 14 (2009) 253–265
The new Australian federal government is nowcommitted to ‘closing the gap’ between Indigenousand non-Indigenous life expectancy, but the demogra-phy of that gap—its dimensions, structure and history—is poorly understood (AHRC, 2008). Vital registrationsfall within state jurisdictions and imperfectly identifypeople as indigenous or non-indigenous. Not only isthere the immediate challenge of quickly amassingadequate data to monitor the ‘gap’, there is also a limitedunderstanding of how the gap evolved: did Indigenousand non-Indigenous Australians experience differenthealth transitions? Has the gap narrowed or widenedover time and has that varied across regions andjurisdictions? How does it compare with the epidemio-logical history of disadvantaged non-Indigenous Aus-tralians? Population health, like an individual's lifecourse and biography, is a historical phenomenon,where the past casts a long shadow across generations.This paper investigates the hypothesis, first proposed byKunitz, that Indigenous Australians experienced aprofoundly different mortality transition from that ofnon-indigenous Australians (Kunitz, 1994, p. 82–120).This hypothesis will be tested by a comparative analysisbetween the all-age survival of five decadal birth cohortsof Aboriginal Victorians and impoverished whites, bornbetween 1851 and 1900.
Data exist for only about 65%of the current Indigenouspopulation, and from that data, estimates of the extent ofthe gap vary. None the less, in a rich, developed nation thatenjoys sixth place on theWorldDevelopment Index of lifeexpectancy, Australian Indigenous people's statisticsmatch those of India and Pakistan or the most deprivedcommunities in Glasgow (Anderson, Crengle, LeialohaKamaka, & Chen, 2006).
The lack of data, both current and historical, is mostacute in Victoria where its distinctive history of nativeadministration rendered most of the Indigenous popula-tion statistically ‘invisible’ for almost a century.Estimates of ‘the gap’ in Victoria range from 15 to20 years in life expectancy at birth between Indigenousand non-indigenous Victorian males. This lack of strongdata was the first purpose for the exercise of populationreconstitution backwards via genealogies.
In 1770, when Captain Cook sighted and mapped theeastern coast of Australia for the British, there wereprobably around 60,000 Aboriginal people living in whatis now Victoria. Along the Murray River, they lived insuch densities that their health indicatorsmatched those ofNeolithic farmers. On the comparatively rich volcanicsoils of the Western District, they had constructedcomplex eel farms and stone houses. Each languagegroup was mapped on an ecological niche; and each
culture was the result of a precise reciprocity betweenhuman life and the natural world that had been built overthousands of years (Lourandos, 1997; Smith et al., 2008,pp. 533–51; Webb, 1995).
In a fateful historical co-incidence, at the time that theFirst Fleet was landing at Sydney Cove in January 1788,smallpox was moving slowly down the continent fromthe north coast people who had contact with Macassantrepang fishermen. It reached Port Jackson in late 1788.Some time later, it found its way down to the densepopulations along the Murray and then into central andwestern Victoria. Australia, with its lack of herd animalsand scattered human populations, had no exposure tozoonoses and their variants (Campbell, 2002). It is nowbelieved that this first impact of smallpox on animmunologically naïve population cut the VictorianAboriginal population by half. A second smallpoxepidemic swept through eastern Australia in the late1820s and early 1830s, just before permanent whitesettlement began in Port Phillip, and again cut thepopulation of Aboriginal Victorians by half. WhenEuropean settlement began in 1835, it was believed thatthe Aboriginal population of Victoria was just 15,000.Within a decade there were 5000, and in place of theonce 60,000 Aborigines of Victoria, there were six and ahalf million sheep (Broome, 2005).
Victoriawas settled byEuropeans in themid 1830s andremained a pastoral outpost until the discovery of gold in1851. Suddenly the small settlementwas over-run by half-a-million fortune seekers. Nearly all paid their own way;the vast majority were literate and skilled; half of themstayed to settle permanently. Victoria thereby enjoyed adistinctive start as a settler colony with a high proportionof modern, educated people committed to building asociety that was better than the one they had left behind.Among themwere many professional men—Scottish andIrish doctors, men of science, Anglo-Irish lawyers—andgifted individuals forced to emigrate because of tubercu-losis. Among the skilled workingmen were disillusionedradicals who now found a blank slate onwhich to inscribethe Chartist principles of manhood suffrage, the secretballot, payment of members of parliament and fairelections (Serle, 1977).
The advance of the squatters and their millions ofsheep from the mid-1830s had been disastrous forAboriginal people, who lost access to water and huntinglands. If they took sheep instead of kangaroos, if theydisputed rights to water, if they fought back, if theyresisted the rape or abduction of women, they werekilled. The moving frontier was led by ruthlessentrepreneurs whose flocks were guarded by formerconvicts, often maddened by loneliness and rum in the

255J. McCalman et al. / History of the Family 14 (2009) 253–265
bush (Critchett, 1990). Everywhere in the nineteenthcentury, the moving frontier took its greatest toll onAboriginal women of reproductive age who becameinfertile, died prematurely or simply ‘disappeared’.From 1834 to 1851, the numbers fell from 15,000 toan official count of under 3000 people.
At the same time, the colonial administrations wereofficially committed to a ‘civilising mission’ to the peoplewhose land and lives were being stolen. Mindful of thedisaster in Van Diemen's Land, and influenced by theunusual proportion of enlightened, modern men amongthe gold rush generation, the Colony of Victoria was to leadthe way in the administration of ‘native affairs’. It was earlyto establish a protectorate (1838), and the first to set up aboard of protection (1861), official stations and missions,and a structure of surveillance that later became the modelfor other colonies and states. The expectation was thatAboriginal society would melt away in the face of a‘superior culture’, and that the financial charge on the statefor the care of the remnants of Aboriginal Victoria woulddecline in concert with the ‘dying of the race’. However, assoon as Aboriginal family groups were collected togetherunder the Board's protection and kept in permanentlocations, sexual relationships between Aboriginalwomen and white men continued to produce part-Aboriginal children who remained with their mothers onthe reserves, adding to the population and the fiscal burden.To resolve the financial dilemma and accelerate assimila-tion, the 1886 Half-Castes Act forced all Aboriginal peopleofmixed-ancestry to leave the reserves, live apart from their‘full-blood’ relatives and make their own way in whitesociety as ‘legalwhites’. Lacking skills, family support, andnever recognised by white society as ‘white’, these‘fractional Aborigines’ were caught in a twilight zonebetween two systems of entitlements: a psychologicallyand economically corrosive limbo that endured until the1960s: too ‘white’ to be ‘black’ and too ‘black’ to beallowed to be ‘white’ (Broome, 2005; Smith et al., 2008).
With Federation in 1901, the Commonwealth Govern-ment over the next 60 years introduced entitlements inpensions, child endowment, returned soldiers' repatria-tion benefits, and family support. All these entitlementseither covertly or overtly excluded those Aboriginalpeoplewhowere defined as ‘really black’ under the states'and territories' jurisdictions, and too often did not extendthese entitlements to ‘unofficial part-Aborigines’, expli-citly denying their applications for pensions, land and therights of citizenship on the grounds that they were ‘notwhite enough’(Commonwealth of Australia, 2006). Thiscan be understood as a ‘racialised rationing’ of publicresources, that was integrated within the structure of thedeveloping social welfare state and the fiscal arrange-
ments of Federation. Likewise, it was mixed-ancestrychildren who were the target of ‘child removal’, to cuttheir connections with mothers and family who were‘really black’. And in Victoria, at least, marriage waspoliced lest the ‘colour be strengthened’ by ‘marryingback’ (Australian Human Rights Commission, 1997).
The irony of the Victorian history of native admin-istration, is that it now appears that the present-day,resurgent Aboriginal population of almost 30,000people at the last census, is essentially descended fromthat half of the total population that was taken on to thereserves in the 1870s, while those who remained outsidethe Board's control were too isolated and weakened tobe able to regroup and rebuild. Today, the Indigenouspopulation of Victoria is entirely of part-Aboriginaldescent. The destruction of Aboriginal Victoria between1835 and 1885 must rate as one of the most rapid andcatastrophic colonial dispossessions of the nineteenthcentury (Smith et al., 2008). See Fig. 1.
But not all the European settlers were to be winners,and our study compares the survival and familyformation of Aboriginal people under colonial controlwith that of poor whites who were also excluded andvulnerable. The poor whites included some of thearound 20,000 former convicts who found their way toVictoria, despite the passing of a law in 1852 to preventany Van Diemen's Lander with a convict record fromentering the colony(Shaw, 1996). We still do not knowhow many former convicts successfully re-inventedthemselves, reared enduring families and becamefounding fathers and mothers of the Australian people.Many were too damaged and sick to be able to cope withfreedom. Perhaps only a third of the 75,000 men andwomen transported to Van Diemen's Land were to go onto becoming Founders as well as Survivors in themaking of modern Australia. That is the purpose ofanother project now under way.
Many former convicts who arrived in Victoria beforethe gold rush came as bonded servants of squatters andsettlers; assisted immigrants often found themselvesquickly employed, and single women were, almost asquickly, married. But the gold rush was an entirelydifferent challenge. Nearly all the gold seekers paid theirway or had deserted ships that brought settlers to theports. Many were single, male adventurers followingopportunity around the globe and many of those left forother gold fields when the alluvial gold ran out. Marriedcouples could find survival difficult as men left womenand children unsupported in Melbourne, or took themfrom mining camp to mining camp. Infant mortality wasappalling as women struggled to start motherhoodwithout the support of their own mothers and extended

Fig. 1. Victorian Aboriginal population 1780–2001.
256 J. McCalman et al. / History of the Family 14 (2009) 253–265
family, in a hot climate, in shantytowns withoutsanitation and reliable water, and in a continent offlies (McCalman, 2005). Social and family networkswere essential to survival, and those who arrived with anetwork or who were skilled at forming new ones,thrived. Around a third of the 208,000 people who diedaged 12 years or older between 1836 and 1888 inVictoria, according to the Pioneers' Index of Births,Marriages and Deaths, departed this life without awitness who knew their father's name. (Mothers'identities were a little more likely to be remembered,at least by given name.) Thus they could be said to havedied ‘without friends’, amongst strangers who did notknow their personal history or who had never cared toremember (McCalman, 2009).
Gold mining and pioneering took a toll on bodies andminds: broken and amputated limbs, injured spines,shattered hopes, all of which aggravated disconnected-ness. Alcohol was a ready escape from both physicaland mental pain. Cheap, adulterated, high-proof spiritswere the preferred beverages until the 1880s (Smith,2006, pp. 137–158). It is probable that more men died inmining accidents than made fortunes, hence it wascommon for women with children to find themselveswidowed, deserted or dependent on an incapacitatedbreadwinner. Marriage rates were high in this frontiersociety with its surplus of young males, but women stillfound themselves pregnant, unmarried and unprotected.The plight of single, deserted or widowed womenneeding support and care in childbirth was sufficiently
acute by 1856, for a charitable lying-in hospital to befounded, and it survives today as the Royal Women'sHospital. Its lying-in and infirmary wards took in thehomeless, single and near destitute and it is from thebabies born of these women that we have reconstituted asample population of severely disadvantaged Eur-opeans: the Lying-In Hospital Birth Cohort, 1857–1985 (hereafter the LIH Birth Cohort) (McCalman,1999).
Similarly, we have reconstituted the VictorianAboriginal population from 1855 to the present day,using genealogy to identify the very large number ofKoori people who were not counted by the adminis-trative system as ‘official Aborigines’ but who were inevery way discriminated against in daily life as ‘tooblack’ to be white. This dataset is the Koori HealthResearch Database (hereafter the KHRD).
2. Materials and methods
The births, deaths and marriages of both reconstitutedpopulations were extracted from the same dataset: theVital Registrations of Victoria, which are searchable asindexes on CD ROM and publicly available to variouscut-off years: 1907 (previously 1920) for births, 1920 formarriages and 1985 for deaths. Vital registration began inVictoria in 1853, under the direction of William HenryArcher, a disciple of Dr William Farr, chief statistician ofthe General Register Office of England and Wales(Hopper, 1986). Archer's disciplined superintendence of

Fig. 2. Infant mortality (percent) by birth weight, according tosocioeconomic status at birth.
257J. McCalman et al. / History of the Family 14 (2009) 253–265
a team of trained assistant registrars operating all over thecolony, ensured early compliance which captured thebirths, deaths and marriages of both Europeans andAboriginal people in contact with white society or whosedeaths came to public notice. No attempt was made toconceal the complicity of leading citizens in the fatheringof part-Aboriginal children, and the names of leadingpastoralists are to be found on many birth certificatesalong with the Aboriginal mothers. People who wished toevade the notice of the authorities—concealing births andinfant deaths—were gradually brought under statesurveillance by the 1880s. Causes of death were definedaccording to Farr's nosologies and a well-organisedcolonial medical profession ensured that those nosologieswere used.
The most remarkable characteristic of Archer's vitalregistration regime was the attention given to recordingfamily history on the certificates from informationprovided by named witnesses to the death. Providedwitnesses were cognisant of the deceased's lineage, thedeceased's certificate recorded both parents' names,mother's maiden name, parents' occupations and placesof birth; the deceased's place of birth, occupation, usualplace of residence and place of death, dates and places ofmarriage, spouses' names and condition (divorced,deceased) and all children, both living and dead, withnames and ages. The witness to the death must alsoprovide name and address. This level of detail makesVictoria's vital registrations among the best in the world(Larson, 1994). Silences and mistakes in this personalrecord can often be read as indications of disconnected-ness from kin and community.
Inquests were traced for both populations. Child(industrial school) and family welfare (Charity Organi-zation Society) case records, criminal records and warservice records were also used for both datasets. Thesource materials for the LIH Birth Cohort were theLabour Ward registers and allied medical records fromthe Royal Women's Hospital, 1857–1900. Thesecomprised admissions of women (around half ofwhom were unmarried) who had been assessed by acommittee as lacking adequate support for a home birth,or who were admitted as destitute emergency cases.
Immigration and convict transportation records andlocal government rate books were used. The KHRDgenealogies were recorded in a commercial genealogicalsoftware product and exported to a customised databaseprepared by the eScholarship Research Centre (eSRC) atthe University of Melbourne. Additional historicalrecords were the colonial censuses and the abundantrecords of the Victorian Aboriginal Protection Board inits various incarnations. Trained historians conducted all
the nominal record linkage and identities were con-firmed only after triangulation of vital records, otherfamily connections and geographical locations.
The two populations were divided into decadal birthcohorts that were matched against events, policyinterventions and socio-economic change with specialreference to Victoria.
Survival analysis was then performed for bothpopulations, divided into historical cohorts and infantmortality and tuberculosis mortality were analysed. Fulldescriptions of the compilation and characteristics of theLIH Birth Cohort and of the KHRD have been publishedelsewhere (McCalman, Morley, & Mishra, 2008; Smithet al., 2008).
3. Ethics
The records used are all publicly available apart fromthe Citizens' Welfare Service case records, which wereaccessed only with the permission and control of thecustodian, the Bouverie Centre. The Aboriginal gene-alogy remains in the custody ofMuseumVictoria and canbe viewed according to protocols developed by theMuseum.All individuals are de-identified before analysis.
4. Results
4.1. The LIH Birth Cohort 1857–1985
From 16,278 registered live births between 1857 and1990, death certificates were traced for 8590 or 53%. Ofthese, 1283 (15%) died in the first 28 days; 3019 (35%)died age 1–12 months; 1350 (16% died 1–40 years) and2938 (34%) died aged 40 or more years. Half of thefound cohort (4302/8590) died in infancy (before age1 year). The biological and social characteristics of the47% of babies not traced to a death certificate mostresembled those who died in infancy, and the infantmortality of those traced was imputed to be likely to

Fig. 3. Infant mortality (percent) by cohort, according to socio-economic status at birth.
258 J. McCalman et al. / History of the Family 14 (2009) 253–265
have applied to the full cohort. The gravest risk to anewborn's future was having an unmarried or poorlysupported mother and that risk was embodied in a clearsocial gradient in normal birth weights. Birth weightwas also a determinant of survival, see Fig. 2.
When the LIH cohort was divided into decadalcohorts, infant mortality by socio-economic statuschanged over time, and in unison, suggesting that thefactors that effected the change affected all mothers andbabies. Infant deaths in these four cohorts were: 784/1487(1857–1870), 1147/1971 (1871–1880), 1286/1286/2106 (1881–1890), 1079/3020 (1891–1900)(McCalman et al., 2008), see Fig. 3.
This is shown by the manner in which infantmortality fell in the LIH cohort, independently of thetrend for Melbourne as a whole. The critical interven-tions were 1) the introduction of antiseptic midwifery
Fig. 4. Infant mortality in LIH Birth Cohort, c
(1887) in the hospital that reduced neonatal mortality forall SES groups born in the hospital; and 2) the coercivecontrol of private nurses in the campaign to suppress‘baby farming’ with the Infant Life Protection Act(effective from 1893). This was a targeted medical andpolicy intervention, foreshadowing the successfulcampaigns to reduce infant mortality in poor countriessince the 1940s. (Chicago is a useful internationalcomparator, being another New World ‘instant city’ ofimmigrants with carefully studied infant and childmortality (Preston & Haines, 1991). See Fig. 4.
The all-age survival curves for the four decadal LIHbirth cohorts revealed the fall in infant mortality in the1890–1900 cohort to have been the only significantchange in survival and that no cohort displayed anychange in life-expectancy after the age of 15 years forthe entire period. See Fig. 5.
4.2. The KHRD 1855–1930 Cohort
The KHRD reconstitution has added a new popula-tion of previously ‘invisible Aborigines’ to the enumera-tions of Aboriginal people by the Aboriginal ProtectionBoard and the Victorian Censuses that were conductedby the police. The results were surprising in tworespects: first those who remained outside the Board'scontrol from the 1870s, but who were known to theauthorities and recorded by the police, were pushed bythe moving frontier to the dry north west of the colonywhere they appear to have disappeared. Second, thecurrent Koori community of Victoria (around 30,000people at the last census) appears to be almost entirelydescended from those taken under the Board's ‘protec-tion’ on to the reserves in the 1870s. See Fig. 6.
ompared with Melbourne and Chicago.

Table 1KHRD decadal cohorts.
KHRD decadal cohorts Births with recorded deaths Total births
1841–1850 151 1651851–1860 143 1911861–1870 136 2251871–1880 200 3551881–1890 233 4211891–1900 210 4461901–1910 260 5281911–1920 219 5791921–1930 211 5361931–1940 182 5971941–1950 112 606After 1950 94 319Fig. 5. LIH Births: survival by cohort.
259J. McCalman et al. / History of the Family 14 (2009) 253–265
The KHRD contains the recorded deaths of 2633individuals of all ages. Not all have birth records and thetracing of deaths is progressively censored for thoseborn after 1895 because of the restriction on publicaccess to death certificates from the Victorian Registrar.Similarly, births and marriages could be searched onlyas far as 1920. The KHRD includes many deathcertificates for people who were born before coloniza-tion and before registration, thus it contains the recordsof ‘solitaries’ who were found, even though theirgenealogy is not known. The underlying softwareenables individuals to be viewed in their family contextand individually.
Survival analysis was performed only on those forwhom we had both birth and death certificates. SeeTable 1.
Aboriginal infant mortality appears less severe thanin the LIH Birth Cohort, but premature death in adult lifemore common. It is likely that infant mortality was
Fig. 6. Evidence from KHRD of Aboriginal Victorians' movements
under-recorded until the Aboriginal population wascollected on to the reserves in the 1870s and closelymonitored by the bureaucracy. On the other hand,deceased adults were better recorded both inside andoutside the reserves, simply through normal policesurveillance of the community. See Fig. 7.
4.3. Comparing Aborigines and ‘poor whites’
The most significant difference between the Abor-igines and ‘poor whites’ is the direct impact ofgovernment policy on the mortality of Aboriginalpeople, in particular once so many were consigned to‘invisibility’ by the 1886 Half-Castes Act. Figs. 9–11demonstrate the effect of the 1886 Half–Castes Act andthe 1890s depression on mortality at progressive agecohorts for Aborigines compared to the smoother,unchanging survival curves for the poor whites afterthe age of 15 years. The chronology of the 1886 Act and
into and out of the census and Protection Board populations.
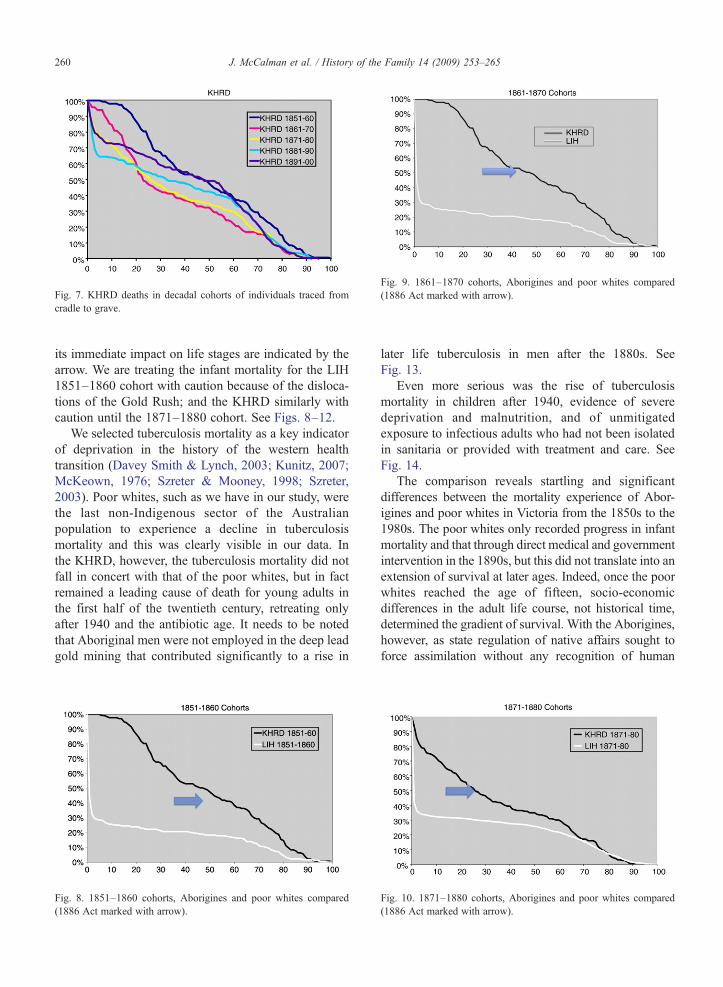
Fig. 7. KHRD deaths in decadal cohorts of individuals traced fromcradle to grave.
Fig. 9. 1861–1870 cohorts, Aborigines and poor whites compared(1886 Act marked with arrow).
260 J. McCalman et al. / History of the Family 14 (2009) 253–265
its immediate impact on life stages are indicated by thearrow. We are treating the infant mortality for the LIH1851–1860 cohort with caution because of the disloca-tions of the Gold Rush; and the KHRD similarly withcaution until the 1871–1880 cohort. See Figs. 8–12.
We selected tuberculosis mortality as a key indicatorof deprivation in the history of the western healthtransition (Davey Smith & Lynch, 2003; Kunitz, 2007;McKeown, 1976; Szreter & Mooney, 1998; Szreter,2003). Poor whites, such as we have in our study, werethe last non-Indigenous sector of the Australianpopulation to experience a decline in tuberculosismortality and this was clearly visible in our data. Inthe KHRD, however, the tuberculosis mortality did notfall in concert with that of the poor whites, but in factremained a leading cause of death for young adults inthe first half of the twentieth century, retreating onlyafter 1940 and the antibiotic age. It needs to be notedthat Aboriginal men were not employed in the deep leadgold mining that contributed significantly to a rise in
Fig. 8. 1851–1860 cohorts, Aborigines and poor whites compared(1886 Act marked with arrow).
later life tuberculosis in men after the 1880s. SeeFig. 13.
Even more serious was the rise of tuberculosismortality in children after 1940, evidence of severedeprivation and malnutrition, and of unmitigatedexposure to infectious adults who had not been isolatedin sanitaria or provided with treatment and care. SeeFig. 14.
The comparison reveals startling and significantdifferences between the mortality experience of Abor-igines and poor whites in Victoria from the 1850s to the1980s. The poor whites only recorded progress in infantmortality and that through direct medical and governmentintervention in the 1890s, but this did not translate into anextension of survival at later ages. Indeed, once the poorwhites reached the age of fifteen, socio-economicdifferences in the adult life course, not historical time,determined the gradient of survival. With the Aborigines,however, as state regulation of native affairs sought toforce assimilation without any recognition of human
Fig. 10. 1871–1880 cohorts, Aborigines and poor whites compared(1886 Act marked with arrow).

Fig. 11. 1881–1890 cohorts, Aborigines and poor whites compared(1886 Act marked with arrow).
Fig. 13. Tuberculosis deaths: Aborigines and Poor Whites compared.
261J. McCalman et al. / History of the Family 14 (2009) 253–265
rights, land rights, economic needs, welfare and theburdens and barriers of racial prejudice, people underwenta health transition in reverse, where tuberculosis and earlyadult death increased along with exclusion and denial ofentitlements.
5. Discussion
These longitudinal datasets reveal the differingdemographic regimes of two impoverished andexcluded sub-populations in an otherwise prosperousand healthy colonial society. They also display theimpact of racial marginalization on the Aboriginalpeople over time in comparison to the impact of povertyand social exclusion across the population. However,the trajectories of the health transition were significantlydifferent, and that difference provides some insight intothe structure of the ‘gap’ between Indigenous and non-indigenous health and survival that persists today. Thegenesis of this research project was Kunitz's hypothesisthat the health transition in Aboriginal Australians wasdistinctive and that models derived from British
Fig. 12. 1891–1900 cohorts, Aborigines and poor whites compared(1886 Act marked with arrow).
experience were not relevant (Kunitz, 1994). What wehave found is that this health transition was more thandifferently timed; it went into reverse.
Kermack et al were the first to observe that the healthtransition in nineteenth century Britain advanced in birthcohorts and was driven by improvements in child healthand welfare that began in the late 1860s. As eachsuccessive generation was better nourished and nurturedand the infectious environment was progressivelymitigated, healthier childhoods resulted in longer-livingadults. The exception to this was infant mortality, until
Fig. 14. KHRD: proportion of respiratory deaths by age group and era.

262 J. McCalman et al. / History of the Family 14 (2009) 253–265
Kermack et al. perceived that it fell a generation after theimprovement in child health, and that healthier motherswere necessary to better infant survival (Kermack,McKendrick, & McKinlay, 1934; Davey Smith & Kuh,2001). In the historical debate over the mechanisms thatbrought about this improvement in child health, the roleof community-level reform of household behaviour,street sanitation and food safety, led by local govern-ment medical officers has become apparent (Hardy,1993). Access to medical advice, in particular with babyfeeding and the care and isolation of sick children, couldmake all the difference in survival for even the poorestfamilies. It was precisely this type of intervention ininner Melbourne for nurses and mothers who were inwalking distance of the Children's Hospital in Carlton,combined with the coercive supervision of privatenurses, that accelerated the learning of safer artificialfeeding amongst the impoverished babies in the Lying-In Hospital cohorts (McCalman et al., 2008).
Australian historical studies of all-cause and cause-specific mortality have used this British model as itlargely fits the all-Australia data, with Australia showinga small advantage in survival until the British caught upafter World War II (Taylor, Lewis, & Powles, 1998a,b).However, as Kunitz advises, macro population studiesconceal as much as they reveal, losing the fine-graineddetail on those sectors of the population where change isoccurring in that they can become buried in geographi-cal regions that are very similar. Indeed, recent work onhealth transitions has called for attention to be paid tothe specifics of a society's history, social composition,cultural values and institutions (Caldwell, 1992; Kunitz,2007).
Cohort analysis makes it possible to tie subtlechanges in health and mortality to external socio-economic conditions over time. A new colonial societysuch as Victoria, swept by rapid population growth,ecological disruption and fatal social dislocation forboth Indigenous people and vulnerable newcomers,provided an unstable environment for the young. Thetiming of these crises was different from that in England,with the crisis of urbanization and industrialization notcoming until the 1870s and 1880s. While the skilled andthe able did well in the boom of the 1880s, the unskilledremained trapped in the informal economy. The 1890sthen brought a severe economic depression that provedto be the beginning of a stagnant economy until 1938(Forster, 1988). This schema of the diachronic progressof each cohort is mapped against the gradual introduc-tion of supportive entitlements by the colonial govern-ment until 1900 and by the Commonwealth governmentafter 1901. The Aboriginal story sits below the schema
because Aboriginal people in Victoria lived in a parallelsub-society where these entitlements were denied themuntil the 1960s, either ‘legally’ because they wereconsidered ‘too black’ and still ‘came under the Act’ or‘illegally’ because they were discriminated against. SeeFig. 15.
The survival curves of the poor whites reveal that theonly significant improvements in life expectancy werederived from the fall in infant mortality in the 1890s as theresult of direct biomedical and welfare intervention.Otherwise, even though causes of death changed in thetwentieth century, adult survival did not change sig-nificantly apart from a small improvement in women'smean age of death for those who began child bearing after1900 as their fertility declined (McCalman et al., 2008).End of life socio-economic status—the outcome of theadult life course—were the determinants of life span forthose poor whites who lived beyond the age of 15 years.And the widest divide in life span was between those whoremained in the inner city, trapped in the informaleconomy, and those who found regular employment.While biomedical advance made no impact on survival ata population level other than in infant feeding and care inthe 1890s, social entitlements that provided land andhousing, either as war service homes or welfare housingafter the 1950s, had an effect on the living conditions andthe welfare of the children of these ‘poor whites’ overtime. This upward mobility after 1945 was apparent fromthe place of death when cohort members died in the careof their children. On the other hand, their own life-courseswere lived under the long shadowof a pre-1914 childhood(McCalman et al., 2008).
The Aboriginal birth cohorts reveal the particularprivations inflicted on infants, children and adults by thedislocations of colonization. Aboriginal infant mortalitywas less extreme than with the babies of unsupported,destitute white women, probably simply because ofbreast-feeding; but exposure to their sick mothers'respiratory diseases was fatal. The separation of familiesby the 1886 Half-Castes Act, and the terrible struggle tosurvive as young adults during the unemployment of the1890s depression, shortened the lives of those born ofeach successive cohort as it passed through thathistorical crisis. Sick, distressed parents, exclusion,poor nutrition in pregnancy and childhood, continuingintimate contact with people with active tuberculosis, allserved to ‘widen the gap’ over time between indigenousand non-indigenous life expectancy from the 1870s forkey vulnerable age-groups.
Most startling was the rise in childhood tuberculosismortality, indicative of continuing exposure by under-nourished and neglected children. We can see this as

Fig. 15. History, entitlements and exclusion.
263J. McCalman et al. / History of the Family 14 (2009) 253–265
evidence of real decline in community cohesion, socialcapital and material security during the twentiethcentury, just as the non-indigenous poor began tobenefit from the increase in state and federal welfarebenefits. In modern health transition terms, the biome-dical interventions such as hospitalization and isolationthat could make a difference in containing tuberculosiswere rarely available to Aboriginal Victorians. Goodprimary medical care was difficult to access for thevarious Aboriginal communities living in fear of thestate authorities who might remove their children. InMooroopna, Jackson's Track, the forest near Framling-ham, people were living rough, isolated lives withouttransport, running water and sanitation. The ‘gap’ wasthus created by a ‘gap’ in entitlements that encapsulatedthe racial discrimination that excluded AboriginalVictorians not just from citizenship, but also frommodernity and its benefits. As Anderson and Whytehave argued elsewhere, ‘Federation’ was ‘bad’ forAboriginal health (Anderson & Whyte, 2006).
The KHRD cohort provides a window into how ‘thegap’ was historically structured: that exclusion from
entitlements and discrimination prevented AustralianAboriginal people, in Victoria at least, from ‘catchingup’ to even the most impoverished whites. Their lifeexpectancy was worse than that of the most disadvan-taged, socially excludedwhites living off casual work andwelfare in the inner city. The continuing death toll fromtuberculosis, while it retreated amongst whites, testified toa ‘widening of the gap’ as the rest of Australian societybecame healthier and wealthier and the relative andabsolute exclusion of Aboriginal people became worse.
The final word should be from the record of the past.In July 1939, the Victorian Charity Organization Societywas asked to investigate the case of Lily Barlow. Mr.Burdeu of the Aborigines' Uplift Society had written onher behalf to the Archbishop of Melbourne, recom-mending her as ‘a dear Christian woman’. He went on:
Miss LB has been a domestic for years, quite capableand clean. Of late, due to infirmity of years she has hada light position looking after an aged person, but nowshe must relinquish work altogether at the age of 62.She is thoroughly civilized and no different from

264 J. McCalman et al. / History of the Family 14 (2009) 253–265
another woman only for the colour of her skin. She is 3/4 black, I should say, perhaps scarcely that. She wassent by the Board of Protection of Aborigines to thepension office with a view to getting an old agepension as she would have received had she even been50 per cent white. She was refused on the grounds thatthe blood predominance was aboriginal. She camesobbing to me and I assured her that I would take upher case for we have a half promise that there will be analteration to the law to enable approved aborigines toobtain the rights of whites. Meanwhile I told her Iwould try to get her State assistance which she isentitled to if she resumes an Aboriginal status inFramlingham aboriginal station, or as a native put it tome last night, ‘if she returns to the ashes of thecampfire’ (Citizens' Welfare Service, 1939).
This is the lived history of ‘the gap’.
Acknowledgement
This research is funded by the Australian ResearchCouncil.
References
Anderson, I., Crengle, S., Leialoha Kamaka, M., & Chen, T. (2006).Indigenous health in Australia, New Zealand, and the Pacific.Lancet, 367, 1775−1785.
Anderson, I., &Whyte, D. (2006). Australian Federalism andAboriginalHealth. Australian Aboriginal Studies, 2, 5−16.
Australian Human Rights Commission (AHRC 1997). Bringing themhome: The 'Stolen Children' report, http://www.hreoc.gov.au/social_justice/bth_report/index.html
Australian Human Rights Commission (AHRC August 2006). Astatistical overview of Aboriginal and Torres Strait islander peoplesin Australia, http://www.hreoc.gov.au/Social_Justice/statistics/index.html
Australian Human Rights Commission (AHRC 2008). Close the Gap:Indigenous Health Equality Summit, Statement of Intent, Canberra,March 20, 2008, http://www.hreoc.gov.au/Social_Justice/health/statement_intent.html
Broome, R. (2005). Aboriginal Victorians: A History since 1800.Sydney: Allen & Unwin.
Caldwell, J. C. (1992). Old and new factors in health transitions. HealthTransition Review, 2.
Campbell, J. (2002). Invisible Invaders: Smallpox and other diseases inAboriginal Australia, 1780–1880. Melbourne: Melbourne Univer-sity Press.
Citizens' Welfare Service (1939, 7 December). Case Records of theCharity Organization Society, Case 59327. University of MelbourneArchives.
Critchett, J. (1990). A Distant Field of Murder.Melbourne: MelbourneUniversity Press.
Davey Smith, G., & Kuh, D. (2001). Commentary: William OgilvyKermack and the childhood origins of adult health and disease.International Journal of Epidemiology, 30, 696−703.
Davey Smith, G., & Lynch, J. (2003). Commentary: Social capital,social epidemiology and disease aetiology. International Journalof Epidemiology, 33, 691−700.
Forster, C. (1988). Unemployment and the Australian economicrecovery of the 1930s. In R. Gregory & N.G. Butlin (Eds.), Re-covery from the depression: Australia and the world economy inthe 1930s. Cambridge: Cambridge University Press.
Hardy, A. (1993). The epidemic streets: infectious disease and the riseof preventive medicine, 1850–1900. Oxford: Oxford UniversityPress.
Hopper, J. (1986). The contribution of WH Archer to Vital Statistics inthe Colony of Victoria. Australian Journal of Statistics, 28,124−137.
Kermack, W. O., McKendrick, A. G., & McKinlay, P. L. (1934). Death-rates in Great Britain and Sweden and some general regularities andtheir significance. Lancet, 223, 698−703.
Kunitz, S. J. (1994). Disease and Social Diversity. New York: OxfordUniversity Press.
Kunitz, S. J. (2007). The Health of Populations. New York: OxfordUniversity Press.
Larson, A. (1994). Growing Up in Melbourne: Family life in the latenineteenth century, Canberra, Demography Program. AustralianNational University.
Lourandos, H. (1997). Continent of Hunter–Gatherers: new perspec-tives in Australian pre-history. Cambridge: Cambridge UniversityPress.
McCalman, J. (1999). Sex and Suffering: women's health and awomen's hospital. Baltimore: Johns Hopkins University Press.
McCalman, J. (2005). All just melted with heat”: Mothers, babies and‘hot winds’ in colonial Melbourne. In T. Sherratt, Tom Griffiths, &Libby Robin (Eds.), A change in the weather: Climate and culturein Australia. Canberra: National Museum of Australia Press.
McCalman, J. (2009). “To die without friends: Solitaries, drifters andfailures in a New World society” in Graeme Davison, Pat Jalland,& Wifrid Prest (Eds.), Body and Mind in British and AustralianHistory: Essays in honour of FB Smith. Melbourne UniversityPublishing.
McCalman, J., & Morley, R. (2008). Inequalities of gender and health11857–1985: A long-run perspective from theMelbourne Lying-InHospital Birth Cohort. Australian Journal of Social Issues, 43,29−44.
McCalman, J., Morley, R., & Mishra, G. (2008). A health transition:Birth weights, households and survival in an Australian working-class population sample born 1857–1900. Social Science &Medicine, 66, 1070−1083.
McKeown, T. (1976). The Modern Rise of Population. London:Edward Arnold.
Preston, S. H., & Haines (1991). Michael R, The Fatal Years; ChildMortality in Late Nineteenth Century America. Princeton NewJersey: Princeton University Press.
Serle, G. (1977). The Golden Age: a history of the colony of Victoria1851–1861. Melbourne: Melbourne University Press.
Shaw, A. G. L. (1996). A History of the Port Phillip District.Melbourne: Melbourne University Press.
Smith, F. B. (2006). Curing alcoholism in Australia, 1880s–1920s.Journal of Australian Colonial History, 8, 137−158.
Smith, L., McCalman, J., Anderson, I., Smith, S., Evans, J., McCarthy, G.,et al. (2008). Fractional Identities: the political arithmetic of AboriginalVictorians. Journal of Interdisciplinary History, 38, 533−551.

265J. McCalman et al. / History of the Family 14 (2009) 253–265
Szreter, S. (2003). Author response: Debating mortality trends in 19thcentury Britain. International Journal of Epidemiology, 33,705−709.
Szreter, S., & Mooney, G. (1998). Urbanization, mortality, and thestandard of living debate: new estimates of the expectation of life atbirth in nineteenth-century British cities. Economic HistoryReview, 51, 84−112.
Taylor, R., Lewis, M., & Powles, J. (1998). The Australian mortalitydecline: all-cause mortality 1788–1990. Australian and NewZealand Journal of Public Health, 22, 27−36.
Taylor, R., Lewis, M., & Powles, J. (1998). The Australian mortalitydecline: cause specific mortality 1907–1990. Australian and NewZealand Journal of Public Health, 22, 37−44.
Webb, S. (1995).Palaeopathology of Aboriginal Australians: health anddisease across a hunter–gatherer continent. Cambridge: CambridgeUniversity Press.
Copyright © 2022 FDOKUMEN














![[Olufemi Taiwo] How Colonialism Preempted Modernit(Book Fi org)](https://static.fdokumen.com/doc/165x107/6313f17dc32ab5e46f0ca687/olufemi-taiwo-how-colonialism-preempted-modernitbook-fi-org.jpg)




