
Cognitive‐Behavioral Psychotherapy for Children and Adolescents With Posttraumatic Stress Disorder...
12
S P ,E C I A L ART ICLE Cognitive-Behavioral Psychotherapy for Children and Adolescents with OCD: A Review and Recommendations for Treatment JOHN S. MARCH, M.D., M.P.H. ABSTRACT Objective: To critically review the published literature on cognitive-behavioral psychotherapy for obsessive-compulsive disorder (OGD) in children and adolescents. Method: The psychiatric and psychological literature was systematically searched for "studies" applying cognitive-behavioral principles to children and adolescents with OGD. Results: Thirty- two investigations, most of them single case reports, were identified. Despite manifold differences in terminology and theoretical framework, all but one showed some benefit for cognitive-behavioral interventions. Graded exposure and response prevention form the core of treatment; anxiety management training and OGD-specific family interventions may play an adjunctive role. Poor compliance, inadequately documented and inconsistently applied treatment, and lack of exportability were recurrent problems. Conclusions: Abundant clinical and emerging empirical evidence suggest that cognitive-behavioral psychotherapy, alone or in combination with pharmacotherapy, is an effective treatment for OGD in children and adolescents. Future research in this area will need to focus on comparisons of cognitive- behavioral psychotherapy to other treatments, on component analyses, and on the application of exportable protocol- driven treatments to divergent patient populations. J. Am. Acad. Child Ado/esc. Psychiatry, 1995, 34, 1:7-18. Key Words: obsessive-compulsive disorder, behavior therapy, cognitive therapy, follow-up studies, treatment, children and adoiescents. Obsessive-compulsive disorder (OCD) is more com- mon than once thought, affecting approximately 0.5% to 1.0% of children and adolescents at any given time (Flament et al., 1988). Since one third to one half of adults develop the disorder during childhood or adolescence (Rasmussen and Eisen, J990), childhood- onset OCD also is an important predictor of adult morbidity. Cognitive-behavioral psychotherapy (CBT) has been shown to be an effective treatment for OCD in adults (Baer, 1992; Marks et al., 1988), where it is often combined with pharmacotherapy (Greist, 1992). Accepted january 26, 1994. Dr. March is with the Program in Child and AdolescentAnxiety Disorders, Division of Child Psychiatry, Department of Psychiatry, Duke University Medical Center, and the Department ofPsychology: Social and Health Sciences, at Duke University. This work was supported in part by a NIMH Scientist Development Award for Clinicians (I K20 MH00981-01) to Dr. March. Correspondence to Dr. March, Department ofPsychiatry, DUMC Box 3527, Durham, NC 21110. InterNet: [email protected]. 0890-8567/95/3401-0007$03.00/0©1995 by the American Academy of Child and Adolescent Psychiatry. J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 34:1, JANUA'!ty 1995 Although empirical support remains weak, CBT also may be the psychotherapeutic treatment of choice for children and adolescents with OCD (Rapoport et al., 1992). Nonetheless, clinicians routinely complain that patients will not comply with behavioral treatments and parents routinely complain that clinicians are poorly trained in the application of CBT to child patients with OCD. This article reviews the current status of CBT for children and adolescents with OCD, addressing empiri- cal documentation, acceptability of treatment, and ex- portability, among other issues, and concludes by making specific recommendations regarding cognitive- behavioral interventions for young persons with OCD. COGNITIVE-BEHAVIORAL PSYCHOTHERAPY FOR OCD IN ADULTS As illustrated by recent lay publications (Baer, 1991; Foa and Wilson, 1991), CBT has become the psycho- therapeutic treatment of choice for adults with OCD. Treatment generally involves a three-stage approach 7
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Cognitive‐Behavioral Psychotherapy for Children and Adolescents With Posttraumatic Stress Disorder...
S P,E C I A L ART I C L E
Cognitive-Behavioral Psychotherapy for Childrenand Adolescents with OCD: A Review and
Recommendations for Treatment
JOHN S. MARCH, M.D., M.P.H.
ABSTRACT
Objective: To critically review the published literature on cognitive-behavioral psychotherapy for obsessive-compulsive
disorder (OGD) in children and adolescents. Method: The psychiatric and psychological literature was systematically
searched for "studies" applying cognitive-behavioral principles to children and adolescents with OGD. Results: Thirty
two investigations, most of them single case reports, were identified. Despite manifold differences in terminology and
theoretical framework, all but one showed some benefit for cognitive-behavioral interventions. Graded exposure and
response prevention form the core of treatment; anxiety management training and OGD-specific family interventions
may play an adjunctive role. Poor compliance, inadequately documented and inconsistently applied treatment, and
lack of exportability were recurrent problems. Conclusions: Abundant clinical and emerging empirical evidence suggest
that cognitive-behavioral psychotherapy, alone or in combination with pharmacotherapy, is an effective treatment
for OGD in children and adolescents. Future research in this area will need to focus on comparisons of cognitive
behavioral psychotherapy to other treatments, on component analyses, and on the application of exportable protocol
driven treatments to divergent patient populations. J. Am. Acad. Child Ado/esc. Psychiatry, 1995, 34, 1:7-18. Key
Words: obsessive-compulsive disorder, behavior therapy, cognitive therapy, follow-up studies, treatment, children
and adoiescents.
Obsessive-compulsive disorder (OCD) is more common than once thought, affecting approximately 0.5%to 1.0% of children and adolescents at any given time(Flament et al., 1988). Since one third to one halfof adults develop the disorder during childhood oradolescence (Rasmussen and Eisen, J990), childhoodonset OCD also is an important predictor of adultmorbidity. Cognitive-behavioral psychotherapy (CBT)has been shown to be an effective treatment for OCDin adults (Baer, 1992; Marks et al., 1988), where it isoften combined with pharmacotherapy (Greist, 1992).
Accepted january 26, 1994.Dr. March is with the Program in Child and AdolescentAnxiety Disorders,
Division of Child Psychiatry, Department of Psychiatry, Duke University
Medical Center, and the Department ofPsychology: Socialand Health Sciences,at Duke University.
This work was supported in part by a NIMH Scientist Development Awardfor Clinicians (I K20 MH00981-01) to Dr. March.
Correspondence to Dr. March, Department ofPsychiatry, DUMC Box 3527,
Durham, NC 21110. InterNet: [email protected]/95/3401-0007$03.00/0© 1995 by the American Academy
of Child and Adolescent Psychiatry.
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 34:1, JANUA'!ty 1995
Although empirical support remains weak, CBT alsomay be the psychotherapeutic treatment of choice forchildren and adolescents with OCD (Rapoport et al.,1992). Nonetheless, clinicians routinely complain thatpatients will not comply with behavioral treatments andparents routinely complain that clinicians are poorlytrained in the application of CBT to child patientswith OCD.
This article reviews the current status of CBT forchildren and adolescents with OCD, addressing empirical documentation, acceptability of treatment, and exportability, among other issues, and concludes bymaking specific recommendations regarding cognitivebehavioral interventions for young persons with OCD.
COGNITIVE-BEHAVIORAL PSYCHOTHERAPY
FOR OCD IN ADULTS
As illustrated by recent lay publications (Baer, 1991;Foa and Wilson, 1991), CBT has become the psychotherapeutic treatment of choice for adults with OCD.Treatment generally involves a three-stage approach
7

MARCH
co nsis ting of informatio n gathering, therapist-assistedexposure and response prevention (E/RP), and homework assignme nts. The seco nd element, therapi stassisted exposure, often can be eliminated in favorof patient-di rect ed homework. Compo nent ana lysessugges t that expos ure is th e active ingre dient of treatment (Em melkam p et al., 1989). Relaxa tio n has beenshown to be an inert compo nent of behavioral treatment for O CD, and sometimes it is used as an activeplaceb o (Marks, 1987). Simi larly, cog ni tive interventions probably are less importan t than E/RP in reducing
OCD sympto ms (Emmelkamp and Beens, 1991). Bothgraded exposure and flooding procedures have shownem pirical and clinical support (M arks, 1987). Predictors of a successful response to behavior therapyinclude th e presence of overt rituals, the desire to
elimi na te sympto ms, ability to mon ito r and reportsym ptoms, absence of complicati ng comorbid co nditions, an d willingness to coo perate with treatmen t (Foaand Emrnelkamp, 1983). Behavior therapy is oftensuccessfully combined with ph arm acotherap y wi th aserotonin reuptake inhibito r (G reist, 1992 ). Furthermo re, since antiexposure instructio ns (in wh ich patientsare enco urage d not to resist th eir obsessions and ritu als)atte n uate th e effectiveness of drug trea tme nt (M arkset al., 1988), the combina tion of d rug and behavioraltherapies may be the treatment of choice for O CD inpa tients req uiring medication (Greist, 1992) .
COGNITIVE-BEHAVIORAL PSYCHOTHERAPY FOR
OCD IN YOUNG PERSONS
Method
Us ing MEDLINE, PsychLit, the Obsessive-Compulsive In formation Center at the Dean Foundation inM ad ison , W isconsin, and an informal survey of professional colleagues, the psychiatric and psych ologicalliteratu re was systema tically searched for published andunpubl ished reports that explici tly or im plici tly appliedcog ni t ive-behavio ral prin ciples and th erap ies to O CDin chi ldre n and adolescents. Reference lists of selectedarticles were scanned for mor e recent or omitt ed papers.Excluded from consideration were arti cles conce rni ngthe so-called O C spectr um disorders (such as tr ichotillomania), "com pulsive" behaviors manifesting as imp ulse disorders (such as stealing), or repetitive beha viors(such as com pulsively flipping light swi tches) in mentally reta rded chi ldren.
8
Types of Investigations
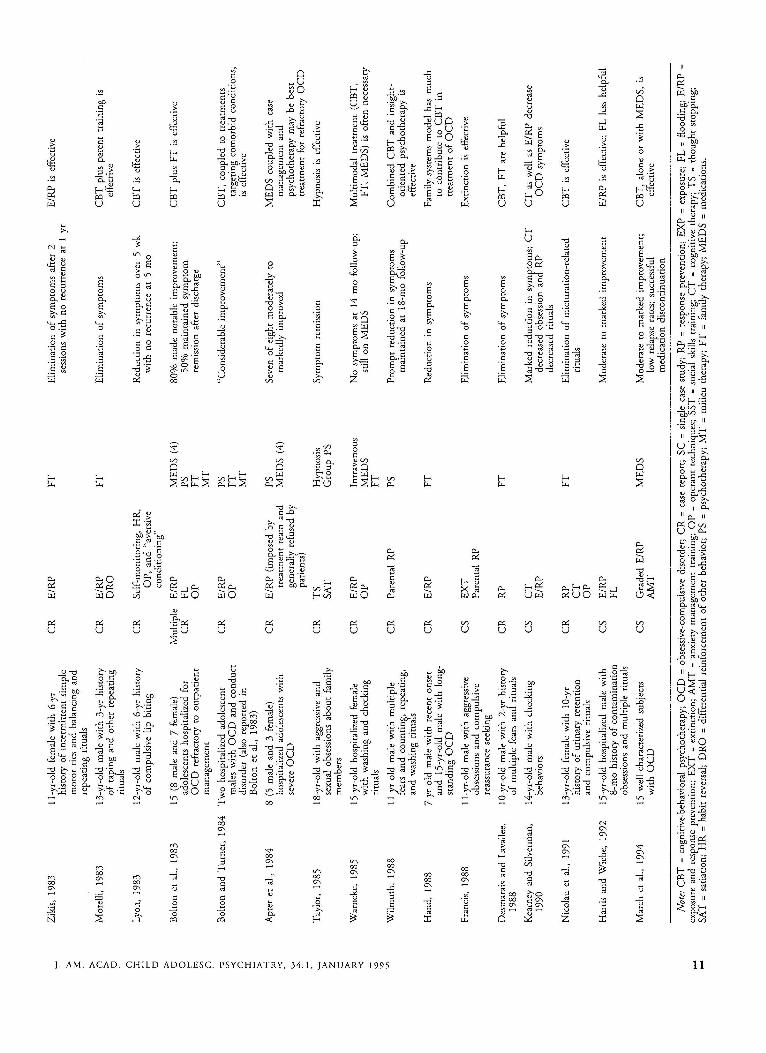
T hirty-two art icles describ ing th e no npharmacological treatment of OCD in one or more ch ild andado lescent subjects were identified (Table 1). T h isrepresents a substantial inc rease from th e 13 art iclesidentified by Wolf an d Rapop ort in their 1988 reviewof th is to pic (Wolff and Rapoport , 1988) and reflectsthe na ture of the literat ure searc h rather than a profusion of recent reports. Twenty-five of the 32 investigations are case reports, as defin ed by insubstantialdescriptions of assessment, treatmen t, and outcomewith little or no accompan ying qu antitative data. O nepresents an case series of systematically assessed childrenand ado lescents treated with a newly developed, protocol-driven treatment (March et al., 1994). The remaining investigati on s are single case studies, definedas any report that provides a quanti tative baselineassessme nt plus either assessme nt across multiple sym pto m domains (mult iple baseline design) or treatments(such as an ABAB design). No published investiga tio ns
used contrasting group designs compari ng treatments orcomponents of treat ments, and th ere were no systematicreplicat ion studies.
Assessment Issues
Diagnosis and Symptom Profile. Accura te assessme ntis essential to the skillful application and evalua tionof behavioral t reat m ents (Thyer, 19 91 ) , but was no t
a strength of the cited investigatio ns taken as a who le.O nly 2 of 32 articles used struc tu red interviews toidentify subjects as hav ing OCD (Francis, 1988; Kearney and Silverman, 1990). Severa l others used scalarmeasures, such as the M audsley O bsessional Inventory(Stern berge r and Burns, 1990) and Leyton Obsession alInventory (Berg et al., 1988), that assess OCD butare not truly diagnostic. One used the Yale-BrownObsessive Com pulsive Scale (March et al., 1994), whichis currently considered the inst rument of choice forrating O CD sympto ms (Goodma n et al., 1989). Mostinvestigat ions relied instead on rathe r haph azard clinicaldesc ript ions to cha racterize sym ptomatology in individual subjec ts. Similarly, just th ree of th e reviewed investigations assessed comorbidity using either categorical orscalar meas ures (Fra ncis, 1988; Kearney and Silverman,1990; March et al., 1994), altho ugh severa l mentionedtic d isorders or dep ression as factors complicating treatment. Since corn orbidir y may pred ict the nature and
J. AM. ACAD. C H IL D ADOL ESC. PSY CH IATRY, 34 : 1 , JANUARY 19 9 5

outcome of treatment (Dar and Greist, 1992), failureto systematically assess comorbid conditions is a critical deficiency.
Demographics and Severity. Both males and femalesare represented in the treated population as are youngerchildren to older adolescents (age range 6 to 18 years).Other demographic variables, such as ethniciry or socioeconomic status, were generally not well documented.Nine of the 32 investigations focused on hospitalizedchildren or adolescents, most of whom were hospitalized for long periods. All were hospitalized with severeOCD as the primary indication. However, other thancomments about "severe" OCD, no study of hospitalized children and only one outpatient study (Marchet al., 1994) provided quantitative measures of symptom severity, although Bolton et al. (1983) linkedseverity to time occupied by OCD in a global fashion.This is a notable deficiency, since children and adolescents with OCD vary widely with respect to the impactof the disorder on level of functioning. Moreover,severely ill patients who improve markedly with treatment may nonetheless fail to normalize so that globalimprovement and clinical status must be judgedindependently.
Outcome Measures. Most of the cited investigationsrelied on unsubstantiated parent reports to documentwhat happened during treatment. Six of 32 investigations, all single case studies, systematically monitoredthe process and outcome of treatment using measuresthat sampled specific symptom domains, such as washing versus avoidance; functional domains, such as homeor school; or symptomatic distress during exposure,such as subjective units of discomfort. A few of thehospital-based investigations used symptom counts byhospital staff (see, for example, Bolton et aI., 1983).Two others used self-report checklists, such as thefrequency of hand washing, rather than direct observational measures (Ong and Leng, 1979; Stanley, 1980).Since reliable and valid assessment of outcome acrosstime is a key feature ofwell-designed treatment outcomestudies, the lack of adequate assessments alone relegatesa great deal of the work in this area to hypothesisgeneration.
Treatments
Careful specification of treatments is a prerequisiteto the empirical evaluation of treatment efficacy. Levelof detail and conceptual clarity varied widely between
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 34:1, JANUARY 1995
COGNITIVE-BEHAVIORAL TREATMENT OF OCD
investigations; however, cited investigations were approached using consistent behavioral terminology. Forexample, when O'Connor (1983) encouraged his patient's parents not to attend to reassurance seeking,this intervention was termed extinction, even thoughO'Connor conceptualized it in the language of systemicfamily therapy. Of the 32 investigations, only one(March et aI., 1994) used a treatment protocol documented in manual form. Most of the cited investigations, including the single case studies, used multiplebehavioral treatments, mixing and matching behavioraltherapies with nonbehavioral interventions, such asfamily therapy or supportive psychotherapy, dependingon the needs of the particular child.
For heuristic purposes, treatment approaches havebeen divided into exposure-based treatments, anxietymanagement training, operant treatments, and nonbehavioral psychotherapies.
Exposure-Based Treatments
Exposure. As applied to OCD, the exposure principledepends on the fact that anxiety usually attenuatesafter sufficient duration of contact with the fearedstimulus (Dar and Greist, 1992). Thus a child withcontamination fears must come into and remain incontact with "contaminated" objects until his or heranxiety decreases substantially. Repeated exposure isassociated with lessened anxiety across exposure trialsuntil the child no longer fears contact with a particularphobic stimulus. Exposure can be implemented in agradual (sometimes termed graded) fashion or throughflooding, with exposure targets under either therapistor patient control. In graded exposure, the child rankshis or her OCD symptoms from the easiest to hardestto resist, in the process generating a stimulus hierarchythat serves as the focus for organizing E/RP. In contrastto graded exposure, which begins at the easy end ofthe stimulus hierarchy, flooding involves prolongedexposure to the most anxiety-provoking stimuli on thehierarchy in order to shorten treatment and maximizebenefit (Dar and Greist, 1992).
Counting satiation (described below) as exposure,slightly more than one half of the cited investigations(17 of 32) included a formal exposure procedure,although all relied on naturalistic in vivo exposure.Most applied exposure in a graded fashion, with targetschosen or suggested by the therapist rather than bythe patient. While two investigations used flooding to
9
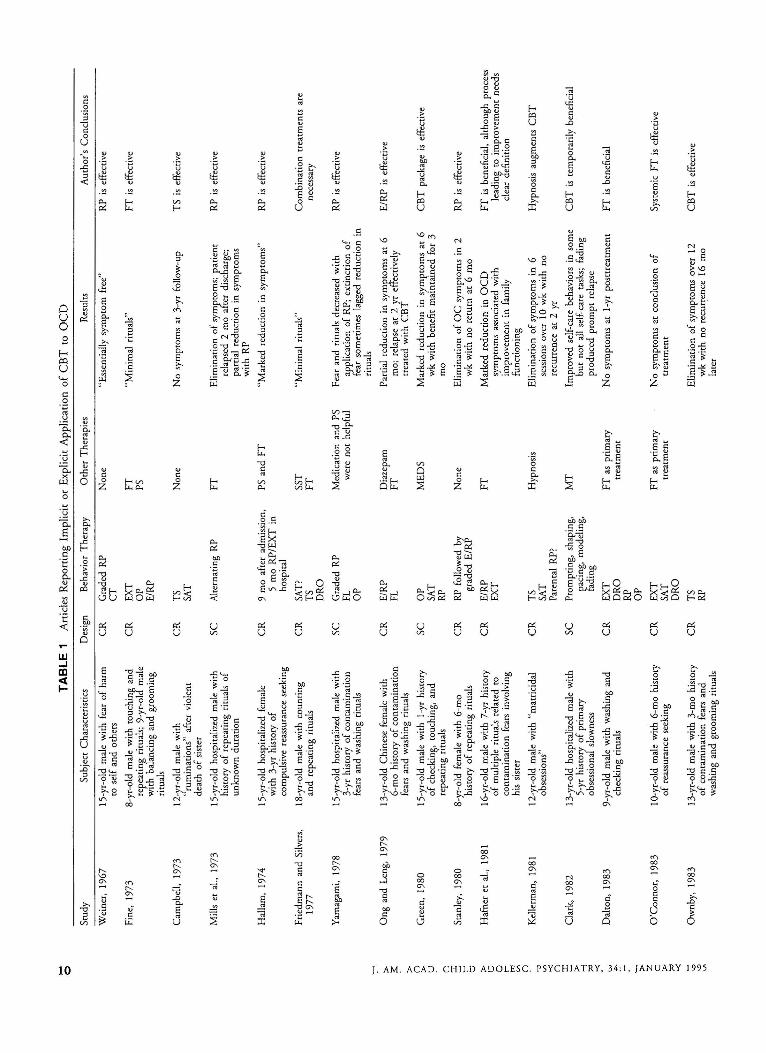
.... TABLE 1 Articles Reporting Implicit o r Expl icit App lica tio n of CBT to OCD0
Study Subject Characteristics Design Behavior T herapy Other Th erapies Results Author's Conclusions
Weiner, 1967 l S-yr-old male with fear of harm CR Graded RP None "Essentially symptom free.. RP is effectiveto self and oth ers CT
Fine, 1973 8-yr-old male with touchinJ and CR EXT FT "Minimal rituals" FT is effectiverepeating rituals; 9-yr-ol male OP PSwith balancing and grooming E/RPrituals
Campbell, 1973 12-yr-old male with CR TS None No symptoms at 3-yr follow-up TS is effective, ruminations" after violent SATdeath of sister
Mills et al., 1973 l S-yr-old hospitalized male with SC Alternating RP FT Elimination of symtc toms; patient RP is effectivehistory of repeating rituals of relapsed 2 mo a er discharge;unknown dur ation part ial reduction in symproms
with RP
Hallam, 1974 IS-yr-old hospitalized female CR 9 mo after admission, PS and FT "Marked reduction in symptoms.. RP is effectivewith 3-yr history of S mo RP/EXT incompulsive reassurance seeking hospital
Friedmann and Silvers, 18-yr-old male with counting CR SAT? SST "M inimal rituals" Combination treatments are1977 and repeating rituals TS FT necessary
ORO
Yamagami, 1978 l S-yr-old hospitalized male with SC Graded RP Medication and PS Fear and rituals decreased with RP is effective3-yr history of contamination FL were not helpful application of RP; extinction offears and washing rituals OP fear sometimes lagged reduction in
rituals~
>- Ong and Leng, 1979 13-yr-old Chinese female with CR ElRP Diazepam Partial reduction in symJ.toms at 6 E/RP is effective3:: 6-mo history of contamination FL FT mo; relapse at 2 yr e ecrively
>- fears and washing rituals treated with CBT()
Green, 1980 I S-yr-old male with l -yr history SC OP MEDS Marked reduct ion in symproms at 6 CBT package is effective>-tJ of checking, touching, and SAT wk with benefit maint ained for 3() repeating rituals RP mo::r: Stanley, 1980 8-yr-old female with 6-mo CR RP followed by None Elimination of OC symptoms in 2 RP is effectiver- history of repeating rituals graded E/ RP wk with no return at 6 motJ
>- Hafner et al., 1981 l S-yr-old male with 7-yr history CR E/RP FT Marked reduction in OCD FT is beneficial, although processtJ of multiple rituals related to EXT symptoms associated with leadinJ, to improvement needs0r- contamination fears involving improvement in family clear efinition
'" his sister functioningV>()
Kellerman, 1981 12-yr-old male with "matricidal CR IS Hypnosis Elimination of symptoms in 6 Hypnosis augments CBT..,obsessions" SAT sessions over 10 wk with noV>
-< Parent al RP? recurrence at 2 yr()
::r: Clark, 1982 13-yr-old hospitalized male with SC Promp ting. shaping, MT Improved self-care behaviors in some CBT is temporarily beneficial:;-l S-yr history of primary pacing, modeling. but not all self-care tasks; fading
'" obsessional slowness fading produced prompt relapse.:-<
Dalton, 1983 9-yr-old male with washing and CR EXT FT as primary No symptoms at l- yr posttr eatment FT is beneficial\.»"'- checking rituals ORO treatment
RP
'> OPZ O'Connor, 1983 l O-yr-old male with 6-mo history CR EXT FT as primary No symptoms at conclusion of Systemic FT is effectivec>- of reassurance seeking SAT treatment treatment
'" ORO-<- Ownby, 1983 13-yr-old male with 3-mo history CR IS Elimination of symptoms over 12 CBT is effective<c<c of contamination fears and RP wk with no recurrence 16 moV>
washing and grooming rituals later
Zik
is,
1983
11-y
r-ol
dfe
mal
ew
ith6-
yrC
RE
/RP
FT
Eli
min
atio
nof
sym
ptom
saf
ter
2E
/RP
isef
fecr
ive
>-hi
stor
yof
inte
rmit
tent
sim
ple
sess
ions
wir
hno
recu
rren
cear
1yr
$:m
otor
tics
and
bala
ncin
gan
d
>-re
peat
ing
ritu
als
oM
orel
li,19
8313
-yr-
old
mal
ew
ith3-
yrhi
stor
yC
RE
/RP
FT
Eli
min
atio
nof
sym
ptom
sC
BT
plus
pare
nttr
aini
ngis
>-of
tapi
ngan
dot
her
repe
atin
gO
RO
effe
ctiv
eo
ritu
als
o ::r:L
yon,
1983
12-y
r-ol
dm
ale
with
6-yr
hist
ory
CR
Sel
f-m
onit
orin
g,H
R,
Red
uctio
nin
sym
ptom
sov
er5
wk
CB
Tis
effe
ctiv
er-
ofco
mpu
lsiv
elip
bitin
gO
P,an
d"a
vers
ive
with
nore
curr
ence
at5
mo
tJco
ndit
ioni
ng>- tJ
Bol
ton
etaI
.,19
8315
(8m
ale
and
7fe
mal
e)M
ulti
ple
E/R
PM
ED
S(4
)80
%m
ade
nota
ble
impr
ovem
ent;
CB
Tpl
usFT
isef
fect
ive
0ad
oles
cent
sho
spita
lized
for
CR
FLPS
50%
mai
ntai
ned
sym
ptom
r- ~O
CD
refr
acto
ryto
outp
atie
ntO
PF
Tre
mis
sion
afte
rdi
scha
rge
om
anag
emen
tM
T
'"B
olto
nan
dT
urne
r,19
84T
wo
hosp
italiz
edad
oles
cent
CR
E/R
PPS
"Con
side
rabl
eim
prov
emen
t"C
BT
,co
uple
dto
trea
tmen
tsV
> -<m
ales
with
OC
Dan
dco
nduc
tO
PF
Tta
rget
ing
com
orbi
dco
ndit
ions
,o
diso
rder
(als
ore
pone
din
MT
isef
fect
ive
::r: :;B
olto
net
aI.,
1983
)-i
Apt
eret
aI.,
1984
8(5
mal
ean
d3
fem
ale)
CR
E/R
P(i
mpo
sed
byPS
Seve
nof
eigh
tm
oder
atel
yto
ME
DS
coup
led
with
case
'" :<ho
spita
lized
adol
esce
nts
with
trea
tmen
tte
aman
dM
ED
S(4
)m
arke
dly
impr
oved
man
agem
ent
and
'"se
vere
OC
Dge
nera
llyre
fuse
dby
psyc
hoth
erap
ym
aybe
best
"'pa
tient
s)tr
eatm
ent
for
refr
acto
ryO
CD
~T
aylo
r,19
8518
-yr-
old
with
aggr
essi
vean
dC
RT
SH
ypno
sis
Sym
ptom
rem
issi
onH
ypno
sis
isef
fect
ive
>-se
xual
obse
ssio
nsab
out
fam
ilySA
TG
roup
PSZ C
mem
bers
>-W
arne
ke,
1985
15-y
r-ol
dho
spita
lized
fem
ale
CR
E/R
PN
osy
mpt
oms
at14
mo
follo
w-u
p;M
ulri
mod
altr
eatm
ent
(CB
T,
'"In
trav
enou
s-<
with
was
hing
and
chec
king
OP
ME
DS
still
onM
ED
SFT
,M
ED
S)is
ofte
nne
cess
ary
-ri
tual
sF
T<
o -o v.W
ilm
uth,
1988
lI-y
r-ol
dm
ale
with
mul
tipl
eC
RPa
rent
alR
PPS
Pro
mpt
redu
ctio
nin
sym~toms
Com
bine
dC
BT
and
insi
ght-
fear
san
dco
unti
ng,
repe
atin
g,m
aint
aine
dat
18-m
ool
low
-up
orie
nted
psyc
hoth
erap
yis
and
was
hing
ritu
als
effe
ctiv
e
Han
d,19
887-
yr-o
ldm
ale
with
rece
nton
set
CR
E/R
PF
TR
educ
tion
insy
mpt
oms
Fam
ily-s
yste
ms
mod
elha
sm
uch
and
15-y
r-ol
dm
ale
with
long
-to
cont
ribu
teto
CB
Tin
stan
ding
OC
Dtr
eatm
ent
ofO
CD
Fran
cis,
1988
lI-y
r-ol
dm
ale
with
aggr
essi
veC
SE
XT
Eli
min
atio
nof
sym
ptom
sE
xtin
ctio
nis
effe
ctiv
eob
sess
ions
and
com
puls
ive
Pare
ntal
RP
reas
sura
nce
seek
ing
Des
mar
ais
and
Lav
alle
e,l O
vyr-
old
mal
ew
ith2-
yrhi
stor
yC
RR
PF
TE
lim
inat
ion
ofsy
mpt
oms
CB
T,
FTar
ehe
lpfu
l19
88of
mul
tiple
fear
san
dri
tual
s
Kea
rney
and
Silv
erm
an,
14-y
r-ol
dm
ale
with
chec
king
CS
CT
Mar
ked
redu
ctio
nin
sym
ltom
s;C
TC
Tas
wel
las
E/R
Pde
crea
se19
90be
havi
ors
E/R
Pde
crea
sed
obse
ssio
nan
RP
OC
Dsy
mpt
oms
decr
ease
dri
tual
s
Nic
olau
eraI
.,19
9113
-yr-
old
fem
ale
with
lO-y
rC
RR
PF
TE
lim
inat
ion
ofm
ictu
rari
on-r
elar
edC
BT
isef
fect
ive
hist
ory
ofur
inar
yre
tent
ion
CT
ritu
als
and
com
puls
ive
ritu
als
OP
Har
ris
and
Wie
be,
1992
lS-y
r-ol
dho
spita
lized
mal
ew
ithC
SE
/RP
Mod
erat
eto
mar
ked
impr
ovem
ent
E/R
Pis
effe
ctiv
e;FL
less
help
ful
8-m
ohi
stor
yof
cont
amin
atio
nFL
obse
ssio
nsan
dm
ultip
leri
tual
s
Mar
chet
aI.,
1994
15w
ell-
char
acte
rize
dsu
bjec
tsC
SG
rade
dE
/RP
ME
DS
Mod
erat
eto
mar
ked
impr
ovem
ent;
CB
T,
alon
eor
with
ME
DS
,is
with
OC
DA
MT
low
rela
pse
rate
s;su
cces
sful
effe
ctiv
em
edic
atio
ndi
scon
tinu
atio
n
Not
e:C
BT
=co
gniti
ve-b
ehav
iora
lps
ycho
ther
apy;
OC
D=
obse
ssiv
e-co
mpu
lsiv
edi
sord
er;
CR
=ca
sere
port
;SC
=si
ngle
case
stud
y;R
P=
resp
onse
prev
enti
on;
EX
P=
expo
sure
;FL
=fl
oodi
ng;
E/R
P=
-ex
posu
rean
dre
spon
sepr
even
tion;
EX
T=
extin
ctio
n;A
MT
=an
xiet
ym
anag
emen
ttr
aini
ng;
OP
=op
eran
tte
chni
ques
;SS
T=
soci
alsk
ills
trai
ning
;C
T=
cogn
itive
ther
apy;
TS
=th
ough
tst
oppi
ng;
-SA
T=
satia
tion;
HR
=ha
bit
reve
rsal
;O
RO
=di
ffer
entia
lre
info
rcem
ent
ofot
her
beha
vior
;PS
=ps
ycho
ther
apy;
MT
=m
ilieu
ther
apy;
FT=
fam
ilyth
erap
y;M
ED
S=
med
icar
ions
.

MARCH
treat adolescents with OCD (Bolton and Turner, 1984;Harris and Wiebe, 1992), young persons with OCDunderstandably abhor "therapeutic" surprises (Lenane,1989), and the intensity of miscalculated exposure isalmost alwayssurprising and aversive. Stated differently,a therapist's idea about what constitutes an appropriateE/RP target may not match the child's with respectto motivation to resist OCD or ability to tolerateanxiety. Thus what appears to be graded exposure tothe therapist may turn out to be flooding for the child.Failure in an exposure task generally reinforces anxiety,and not infrequently disrupts the therapeutic relationship. For this reason, Harris and Weibe (1992) recommended that young persons with OCD receive gradedE/RP, with targets for both under control of the patient.They did not, however, specify how the therapist canhelp patients choose appropriate E/RP targets. Werecently proposed using cartographic and story metaphors to negotiate just such a mechanism (j.S. Marchand K. Mulle, "How J Ran OCD Off My Land''®:A Cognitive-Behavioral Program [or the Treatment ofObsessive-Compulsive Disorder in Children and Adolescents, unpublished) and demonstrated the effectivenessof this approach in a series of 15 patients (Marchet al., 1994).
Response Prevention. The response prevention principle states that adequate exposure depends on blockingrituals or avoidance behaviors (Dar and Greist, 1992).Thus a child with contamination fears must not onlytouch "contaminated" objects but must refrain fromritualized washing until his or her anxiety attenuates.Since many phobic stimuli occur naturally throughoutthe day, response prevention targets can be selectedindependently of contrived exposure targets under theassumption that the child cannot avoid exposure. Forexample, a boy with doorway balancing rituals willinvariably need to go through doors. Not avoidingdoors, or refraining from executing balancing ritualsas he proceeds through them, is an example of anoncontrived response prevention strategy. Twenty-sixof the 32 investigations successfully used responseprevention (see Mills et al., 1973, for example). Ofthose that did not, some involved an OCD subtype,such as obsessional slowness, for which response prevention is not indicated or is difficult to implement. Mostinvestigations failed to explicitly separate exposure fromresponse prevention; many failed to distinguish response prevention selected voluntarily by the child
12
from that enforced by parents or hospital staff. Bothcan be effective, but the level of short-term distressand oppositional behavior associated with the latterstrategy is virtually always higher. In addition, it isoften difficult to train parents to interrupt or preventrituals, and constant supervision, necessary to preventsurreptitious washing, for example, is difficult to implement outside hospital settings.
Extinction. Technically, response prevention is anextinction procedure, since blocking rituals or avoidance behaviors removes the negative reinforcementeffect of the rituals or avoidance. However, adoptingthe convention that exists in the literature, extinctionis defined here as the elimination of OCD-relatedbehaviors through removal of parental positive reinforcement. For example, parents may reduce OC symptoms by systematically ignoring compulsive reassuranceseeking (Hallam, 1974). Extinction often producesrapid effects and is readily monitored. On the otherhand, extinction (especially ignoring) is difficult toimplement when the child's behavior is bizarre or whenthe behaviors are frequent. Like response prevention,extinction can be effected with (or more commonlywithout) the child's consent. For example, Francis usedextinction to successfully treat an l l-year-old boy withaggressive obsessions and compulsive reassurance seeking (Francis, 1988). As with E/RP, we found thatplacing extinction targets under the child's controlled to increased compliance and improved outcomes(March et al., 1994).
Anxiety Management Strategies
Packaged anxiety management trammg (AMT) isan effective treatment for children with generalizedanxiety (Kendall, 1991), but has not yet been testedempirically in children and adolescents with OCD. Inadults, AMT is ineffective for OCD and has been usedas an active placebo (Marks, 1987). However, childrenwith OCD often have other anxiety disorders (Flamentet al., 1988), and AMT could benefit patients bytargeting comorbid conditions that might interfere withOCD treatment. Moreover, studies in adults haveshown that the level of anxiety during exposure isless important than exposure duration and consequentattenuation of anxiety (Marks, 1987). Thus AMT alsomay facilitate exposure through reducing the amplitudeof exposure-related anxiety (March et al., 1994).
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 34:1, JANUARY 1995

Relaxation and Breathing Training. Progressive mu scle relaxation and diaphragmatic breathing train inghave been successfully applied to child ren and ado lescents with separation anxiety and overanxious disord ers(Kendall, 1991 ; T hyer , 199 1). Several of 32 investigations mentioned relaxat ion , but only one specificallyimpl emented progressive muscl e relaxation or breathingtra ining (March et al., 1994) , and the role of thesestrategies in trea ting childre n and ado lescents withOCD remains un certa in.
Cognitive Therapies. Cognitive the rap ies for O CDinclude techniqu es based both in exposure, such assatiation, and in anxiety management, such as thoughtsto pping or cognitive restr uctu ring (N eziroglu andN eum an, 1990). Satiation is a form of massed pract icein which patient s repeat the ir obsessions vocally orin writing to induce exposure. Before impl ementingsatia tion, it is impor tant to distinguish obsessions fromment al ritu als that are appropriate targets for responseprevention. Satiation typically has been applied to
patients with primary obsessional O C D, and 6 ofthe 32 investiga tions successfully applied satiation to"obsessional" patients . Adjunctive hypn osis provedhelp ful in implementing satiation in a boy with aggressive obsessions (T aylor, 1985 ). In cont rast to satiationprocedures, which exaggerate obsessions, two investigations formally used thought stopping- a techniquedesigned to interrupt rather than to challenge obsessions-to treat obsessional adolescents (Ca m pbell,1973; Kellerma n, 198 1). As part of a multico mponentapproach to OCD treatm ent, thought stopping mayenable E/RP in some patients (Ma rch et aI., 1994). Incogn itive restructuring, the therap ist helps the pat ientdirectly challenge the reality of obsessions and thenecessity of compulsions (Emmelkamp and Beens,1991 ). Kearney and Silverma n used expos ure andrational em ot ive therapy to treat rituals and obsessions,respectively, in a single-subject, alternating-weeks design. Exposure primarily reduced rituals; rat ional emotive therapy reduced obsessions (Kearney andSilverman, 1990 ). In our preliminary case series, cognitive restruc turing in the form of " bossing back O CD"seemed to benefi t patients primarily by facilitati ngcompliance with E/RP (March et al., 1994). Thusit remains unclear whether cogn itive therapy simpl yenco urages exposure or provides dir ect antio bsession al effeers.
J. A M . ACAD . C H I l. D AD O l. ESc:. PSYCHI AT RY, 34 : 1, JANUARY 19 9 5
C OGN IT IV E-BE H AV I O RA L T REAT M EN T OF Oe D
Habit Reversal. N egative affects, such as anxiety,guilt, or disgust , predict com pulsions, such as washin gin response to conta mination fears, that respond nicelyto E/RP. No t all OC symptoms involve negative affects,however. Some O CD pat ients, particularly those onthe boun dary with the tic disorders, exhibit "sensoryincompleteness"-the feeling that an act ion has to becompleted "enough" or "just so"-often accompaniedby stereorypic repeating rituals (Rasmussen and Eisen ,1992). For those pat ient s in who m O CD resembl es acomplex tic-like repeating ritual, habi t reversal procedures, such as those descr ibed for trichot illom an ia orT ou rette's syndrome (Baer, 1992; Vitulano et al.,1992), can sometimes be help ful alone or in combination with response prevent ion. In habit reversal, patientsand their fami lies are taught thought stopping, visualization , relaxation, competing motoric responses, andrelapse prevention stra tegies. Although habit reversalis in wide use in subspecialty clinic anxiety programs,habit reversal procedures have received little empiricalattent ion in children or adolescents with OCD. Cli nica lexper ience suggests that habit reversal like E/ RP is lesspromising for tic disorders, which may be driven in partby abnormal processing of sensori motor infor mation(Kane, 1994; Leckma n er al., 1993) , than for symptomconstellations, such as trichotillomania (Swedo, 1993),that more closely resemble OCD.
Operant and Related Procedures
Operant Techniques. O perant proced ures are in theory defined by their effects. In clinical practice, however ,operant techniques reduce to the appli cation of rewardsand punishm ents plus negative reinforcement. Sincethere is no em pirical or clin ical sup port for the prop osition that positive reinforcement affects OCD symptomsdirectly, many investigations used positive reinforce ment on an adju nctive basis to encourage exposure.For example, we rou tinely use pr izes for compl etingexposure tasks and reward ceremonies for masteringimp ortant steps along the way to eliminatin g OCD(March et al., 1994). Taking the opposite tack, severalinvest igat ions attem pted to impleme nt punishme nt(imposition of an aversive event) or response -cost (removal of a positive event ) procedures. Altho ugh onereport "showed" a reduction in OCD symptoms usingresponse-cost in the form of reducing privileges (Apteret al., 1984; see Lyon, 1983, for a similar example),methodological problems, the absence of replication,
13

MARCH
and abundant clinical evidence that punishment increases resistance to treatment preclude endorsementof aversive techniques for children and adolescents withOCD. Finally, none of the cited investigations usednegative reinforcement procedures, defined here as theremoval of an aversive event in order to increase adesired behavior. However, OCD is itself a negativereinforcer, so that a reduction in presumably aversiveOCD symptoms through spontaneous or planned exposure should produce an increase in adaptive E/RP.Consistent with this idea, Flament et al. noted thatchildren from the NIMH cohort who did well seemedto have spontaneously discovered saying "no" to OCD(Flament et al., 1990). As part of negotiating gradedexposure, we explicitly use the negative reinforcementvalue of OCD to encourage compliance with treatment(March et al., 1994).
Modeling and Shaping. Modeling, defined as demonstrating more appropriate or adaptive behaviors, isfrequently used during therapist-assisted exposure.Modeling can be overt (the child understands that thetherapist is providing a demonstration) or covert (thetherapist informally models a behavior). Closely relatedto modeling, shaping consists of positively reinforcingsuccessive approximations to a target behavior. Forexample, an AIDS-phobic child might be reinforcedfor coming closer and closer to an HIV-positive personbefore finally shaking hands (shaping/exposure), anaction that the child has seen the therapist take withoutharm on previous occasions (modeling). With childpatients, modeling helps reduce anticipatory anxietyas well as providing an opportunity for cognitive strategizing in the form of constructive self-talk (Thyer,1991). Obsessional slowness may represent a specificindication for modeling and shaping procedures sinceexposure has proven less useful than shaping proceduresin this population (Ratnasuriya et al., 1991). Clinically,children with primary obsessional slowness generallyrespond poorly to both behavioral and pharmacologicalinterventions, often relapsing when therapist-assistedshaping, limit setting, and temporal speeding procedures are withdrawn (Wolff and Rapoport, 1988). Andalthough Clark successfully used shaping proceduresto treat a 13-year-old boy with obsessional slowness(Clark, 1982), most clinicians and researchers agreethat this subtype is ripe for cognitive-behavioral innovation in both adults and youth (March et al., 1990a).
14
Diffirential Reinforcement of Other Behaviors andOvercorrection. Differential reinforcement of other behaviors (ORO) depends on extinction (systematicallyignoring problem behaviors) while simultaneously reinforcing more adaptive behaviors. Overcorrection involves substitution via massed practice of a moreadaptive for a less adaptive behavior in the same domainof functioning. In OCD, for example, a parent mightignore reassurance seeking around contaminationthemes (extinction) while paying more attention toschoolwork (ORO) and emphasizing a greater frequency of chores involving appropriate cleaning (overcorrection). Both ORO and overcorrection implicitlyfoster response prevention. Of the cited investigations,the family therapy-oriented investigations in particularfavored ORO or overcorrection, although none described the interventions in behavioral terminology,and no study empirically validated either procedure.
Nonbehavioral Psychotherapeutic Techniques
A variety of psychotherapeutic techniques, not systematically applied or conceptually linked, have beenbrought to bear on children and adolescents withOCD. Examples include individual and group psychotherapies, hypnosis, and family therapy. Some, such asO'Connor's (1983) family treatment of OCD, containunacknowledged behavioral components. Others explicitly combine treatment approaches. For example,Kellerman used hypnosis to implement thought stopping and E/RP to treat matricidal obsessions in a 12year-old boy (Kellerman, 1981); we routinely use storymetaphors (White and Epston, 1990), like giving OCDa "nasty nickname" against which the child can dobattle, to support cognitive-behavioral interventions(March etal., 1994).
Individual and Group Psychotherapy. As it has inadults (Esman, 1989), psychodynamic psychotherapyhas proven disappointing as a treatment for OCD inchildren and adolescents (Hollingsworth et al., 1980).Nevertheless, many investigations included supportiveor psychodynamic psychotherapy as part of the treatment package. Often these interventions seemed aimedat increasing compliance with E/RP or at comorbidconditions, particularly personality dysfunction. Forexample, Apter et al. (1984) reported that their hospitalized adolescent patients refused behavior therapy, butgot better with supportive psychotherapy and ward
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 34:1, JANUARY 1995

milieu therapy, suggesting that these additional measures permitted implicit if not explicit application ofexposure-based treatments. Clinically, long-standingOCD often damages self-esteem and interferes withpeer relationships. Thus insight-oriented psychotherapymay become more important as the effects of OCDrecede with successful treatment. Social skills trainingalso may playa role in selected patients with OCD,especially those with comorbid nonverbal learning disabilities that interfere with the pragmatics of socialemotional communication (March et aI., 1990b;Voeller, 1990).
Family Therapy. While OCD is substantially heritable (Lenane et aI., 1990; Riddle er aI., 1990), familydysfunction is neither sufficient nor necessary clinicallyfor the genesis of OCD (Lenane, 1989). Nevertheless,families affect and are affected by the disorder. Typicalconcerns include parental or sibling involvement inrituals, difficulty dealing with sexual or aggressive obsessions, and differences ofopinion about how to deal withOCD symptoms. As in schizophrenia, high "expressedemotion" in families may exacerbate OCD in affectedfamily members (Hibbs et aI., 1991). Moreover, OCDfrequently unsettles social and community interactions,including those with health care professionals who mayor may not understand the disorder (Hand, 1988).Thirteen of the 32 investigations cited here includedexplicit family interventions as part of treatment forOCD. While these interventions frequently focusedon implementing extinction or response preventionprocedures, several adopted systemic family therapyapproaches where OCD represented a metaphor forfamily dysfunction (Dalton, 1983; O'Connor, 1983).These investigations tended to encourage E/RP as a"paradoxical intervention," making it impossible todetermine how or whether the family interventionadded to conventional if implicit cognitive-behavioralapproaches. Until future research establishes a preferredcontext, CBT for OCD can be administered in anindividual or family setting, depending on the needsof the child. For most patients, the combination ofindividual sessions plus focused family work will provebest (March et al., 1994). Family therapy or maritalcounseling should be recommended as part of thechild 's treatment for OCD only if family dysfunctionor marital discord represents a constraint to the application of treatments directed specifically at OCD.
J . AM . ACAD . CHILD ADOLESC . PSYCHIATRY, 34:1, JANUARY 1995
COGNITIVE-BEHAVIORAL TREATMENT OF OCD
CONCLUSION
Abundant clinical and emerging empirical evidencesuggests that CBT, alone or in combination withpharmacotherapy, is an effective treatment for OCDin children and adolescents. Unlike other psychotherapeutic techniques that have been applied to OCD,CBT presents a logically consistent and compellingrelationship between the disorder, the treatment, andthe specified outcome. Moreover , the empirical literature shows no support for the now discredited mythsofsymptom substitution, danger of interrupting rituals,uniformity of learned symptoms, and incompatibilitywith pharmacotherapy (Baer, 1992). And as Baer alsopoints out, CBT neither ignores thoughts nor discountsmeaning (Baer, 1992), although OCD symptomsthemselves perhaps are best seen as CNS hiccups devoidof intrinsic meaning. Finally, CBT is not simplistic.Helping patients make rapid and difficult behaviorchange over short time intervals takes considerable skillcoupled to highly focused treatment.
Ideally, young persons with OCD should first receiveCBT, and if not rapidly responsive, or if experiencingmarked depression, a selectiveserotonin reuptake inhibitor . However, some physicians and their patients willprefer to begin with CBT in hopes of avoiding theneed for medication and the side effects that mayaccompany pharmacotherapy. Others will choose medication first, trying to avoid the time, effort, expense,and anxiety associated with cognitive-behavioral interventions. Still others will prefer to combine the twoapproaches.
Clinically, pharmacotherapy and CBT work welltogether, and many children with OCD likely requireor would benefit from pharmacotherapy (Rapoportet al., 1992). In our CBT caseseries, where the majorityof subjects also were treated with medication (Marchet aI., 1994), the average magnitude of improvementwas larger and relapse rates were lower than usuallyseen with medication alone (DeVeaugh et aI., 1992;Leonard et aI., 1989). Thus concurrent CBT, includingbooster treatments during medication discontinuation,may improve both short- and long-term outcome inmedication-responsive patients, including those forwhom ongoing pharmacotherapy proves necessary (Leonard et aI., 1993).
It should be emphasized, however, that empiricaldocumentation regarding the efficacy of CBT in child
15

MARCH
subjects with OCD remains weak, especially whencontrasted with the robust empirical evidence favoringpharmacotherapy (Rapoport et al., 1992). For themost part, currently published investigations fail to (1)adequately define and assess inclusion/exclusion criteria,OCD symptoms, functional impairment, and com orbid conditions; (2) apply reliable and valid measures oftreatment outcome that cross symptom and functionaldomains; (3) assess subjects pretreatment, posttreatment, and at follow-up; (4) use distinct levels of assessment, including, for example, neuroimaging,psychophysiology, behavior, and family methodologies;and (5) implement contrasting group designs, usingrandomized assignment or carefully specified singlesubject designs. Moreover, only recently has the application ofCBT to OCD in young persons been adequatelydocumented in a treatment manual (March et al.,1994); thus replication studies and the exportation ofsuccessful techniques to clinical settings have beenimpeded.
Given these caveats, the following treatment recommendations regarding implementation of CBT foryoung persons with OCD currently seem reasonable(March and Mulle, in press; March et al., 1994; Wolffand Rapoport, 1988):
• It is generally preferable to describe OCD in amedical context, that is as a neurobehavioral disordet,
and not as a bad habit.• Giving OeD a "nasty nickname" against which the
child can do battle helps keeps the focus on OCDas the identified problem.
• In most subtypes of OCD, graded E/RP is thefoundation of treatment.
• With the admonition that the child must makeprogress, the choice of E/RP targets IS best left tothe child.
• Implementing AMT as a "tool kit" to use duringE/RP improves compliance with E/RP.
• While the focus of treatment must be on the child'sstruggle with OCD, involving family members inthe treatment process frequently is essential to a
satisfactory outcome.• Many, if not most, patients will require or would
benefit from concurrent pharmacotherapy with aserotonin reuptake inhibitor.
Future research in this area will need to focus onthe following areas. First, controlled trials comparing
16
medications, behavior therapy, and combination treatment to controls are necessary to determine whethermedications and behavior therapy are synergistic oradditive in their effects on symptom reduction. Second,follow-up studies will be necessary to evaluate the longterm benefit of CBT, including examining whetherbooster CBT reduces relapse rates in patients discontinuing medications. Third, dismantling strategies arenecessary to examine the relative contributions of
specific treatment components to symptom reductionand treatment acceptability. A comparison of E/RP,anxiety management, and combination treatment is a
logical starting point. Fourth, CBT can be administeredas an individual- or family-based treatment, and comparison of these two approaches will be necessary todetermine which is more effective in which children.Fifth, OCD subtypes, such as obsessional slowness,
primary obsessional OCD, and tic-like OCD, bedevilthe field and are ripe for behavioral innovation. Sixth,other putative predictors of treatment resistance, suchas nonverbal learning disabilities (March et al., 1990b)or family dysfunction (Hand, 1988), need to be examined vis-a-vis their interactions with behavioral treatments. Finally, the application of protocol-driventreatments to different patient populations should increase generalizibility of results as well as provide arationale for exporting research-based treatments intoclinical settings to the benefit of children and adolescents with OeD.
REFERENCES
Apter A, Bernhout E, Tyano S (1984), Severe obsessive compulsive disorderin adolescence: a report of eighr cases. J Adolesc 7:349-358
Baer L (1991), Getting Control. Boston: Little, Brown, and CompanyBaer L (1992), Behavior therapy for obsessive-compulsive disorder and
trichorillomania. Implications for To urcrrc syndrome. Ad" Neurol58:333-340
Berg CZ, Whiraker A, Davies M, Flamcnr MF, Rapoport JL (1988), Thesurvey form of the Leyton Obsessional Inventory-Child Version: normsfrom an epidemiological study, J Am Acad Child Adolesc Psychiatry27:759-763
Bolton D, Collins S, Steinberg D (1983), The treatment of obsessivecompulsive disorder in adolescence: a report of fifteen cases. 131' JPsychiatry 142:456-464
Bolron D, Turner D (1984), Obsessive-compulsive neurosis with conductdisorder in adolescence: a report of rwo cases. J Child Psychol Psychiatry 25:133-Ll9
Campbell L (1973), A variation of thought stopping in a twelve-year-oldboy: a case report. J Behau Ther Exp Psychiatry 4:69-70
Clark D (1982), Primary obsessional slowness: a nursing treatment programme with a Ll yeat old male adolescent. 13ehav Res Ther20:289-292
Dalton P (1983), Family treatment of an obsessive-compulsive child: acase report. Fran Process 22:99-108
J. AM. ACAD. CHILD ADOLESC. PSYCHIATRY, 34:1, JANUARY 1995
Dar R, Grcist J (1992), Behavior therapy for obsessive-compulsive disorder.Psychiatr Gin North Alii 15:885-894
Desmarais P, Lavallee Y (1988), Severe obsessive-compulsive syndrome ina 10 year old: a .3 year follow-up. Can J Psychiall] 33:405-408
DeVeaugh CJ, Moroz C, Biederman Jet nl. (1992), Clomipramine hydrochloride in childhood and adolescent obsessive-compulsive disorder: amulticenter rrial. ] Alii Acad Child Adolesc Psychiall] 31 :45-49
Emmelkamp PM, Beens H (1991), Cognitive therapy with obsessivecompulsive disorder: a comparative evaluation. Behn u Res Ther29:293-300
Emmelkamp P, van Linden S, van den Hcuvcll R, Uphan M, SandermanR (1989), Home-based treatment of obsessive-compulsive patients:inrcrscssion interval and therapist involvement'. BehnoResTher27:89-93
Esman A (1989), Psychoanalysis in general psychiatry: obsessive-compulsivedisorder as a paradigm. ] Alii Psycboanal Assoc 37:319-3.'36
Fine S (1973), Family therapy and a behavioral approach to childhoodobsessive-compulsive neurosis. Arch Gen Psychiatry 28:695-697
Flamenr MF, Koby E, Rapoport JL et al, (1990), Childhood obsessivecompulsive disorder: a prospective follow-up study. ] Child Psycho!p,ychiatl] 31 :.%3-380
Flamcnr MF, Whitaker A, Rapoport JL ct al. (1988), Obsessive compulsivedisorder in adolescence: an epidemiological study. ] Alii Acad ChildAdolcsc Psychir/ll] 27:764-71
Foa E, Emmelkamp I' (1983), Failures ill Behauior Therapy. New York:Wiley and Sons
Foa E, Wilson R (1991), Stop Obsessing! New York: BantamFrancis G (1988), Childhood obsessive-compulsive disorder: extinction of
compulsive reassurance seeking. ] Anxiety Disord 2:361-368Friedmann C, Silvers F (1977), A multimodality approach to inpatient
treatment ofobsessive-compulsive disorder. Am] Psychotbcr 31:456-465Goodman WK, Price LH, Rasmussen SA et al. (1989), The Yale-Brown
Obsessive Compulsive Scale. 11. Validity. Arch Gen Psychiatry46:1012-1016
Green D (1980), A behavioral approach to the treatment of obsessionalrituals: an adolescent case study. ] Adolesc 3:297-306
Greist JH (1992), An inregrated approach ro treatment of obsessive compulsive disorder. ] Gin Psychirltl] 53(suppl):38-41
Hafner R, Gilchrist 1', Bowling J, Kalucy R (1981), The rrcarrucnr ofobsessional neurosis in a family setting. Awt N Z] Psychiatry 15: 145-151
Hallam R (1974), Extinction of ruminations: a case study. Hehr/ll Ther5:565-568
Hand 1 (1988), Obsessive-compulsive paricnrs and their families. In:Handbook of Brbauioral Family Thempy, Halloon M, cd. New York:Guilford Press, PI' 231-256
Harris C, Wiebe [) (1992), An analysis of response prevention and Hoodingprocedures in the treatment of adolescent obsessive compulsive disorder.] Bcliau Tbcr !:xp Psychirltl] 2.'3: 107-115
Hibbs ED, Hamburger SD, Lcnanc M ct al, (199l), Determinants ofexpressed emotion in f'"11ilies of disturbed and normal children.] ChildPsycho! Psychirltl] 32:757-770
Hollingsworth C, Tangnay 1', Crossman I. (1980), Long-term outcome ofobsessive compulsive disorder in childhood. JAm Acad Child PsycbiaII] 19:134-144
Kane M (1994), Case srudy: premonitory urges as "atrcntional tics" inTourcrrc's syndrome. ] Am Acad Child Adolesc Psychiatry 33:805-808
Kearney CA, Silverman WK (1990), Treatment of an adolescent withobsessive-compulsive disorder by alternating response prevention andcognitive therapy: an empirical analysis. ] Behn» 71?Cr Exp Psychiatl]21:.3')17
Kellerman J (1981), Hypnosis as an adjunct to thought stopping andcovert rcinforccrncnr in the treatment of homicidal obsession in atwelve-year-old boy. Int ] Gin J;:yp Hyp» 29:129-135
Kendall I' (1991), Child and Adolescent Therapy. New York: Guilford PressI.eckman J, Walker D, Cohen D (1993), Premonitory urges in Tourcttc's
syndrome. Am] Psychiatry 150:98-102Lcnane M (1989), Families in obsessive-compulsive disorder. In: Obsessive
CompulsiveDisorderin Children find Adolescents, Rapoport J, cd. Washington, DC: American Psychiatric Press
J. AM. ACAD, C1I1I.D ADOLESC. PSYCHIATRY, 34:1, JANUARY 1995
COGNITIVE-BEHAVIORAL TREATMENT OJ' OCD
Lcnanc MC, Swedo SE, Leonard H, Pauls DL, Sccery W, Rapoport JL(I990), Psychiatric disorders in first degree relatives of children andadolescents with obsessive compulsive disorder.] Am Acad Child AdolescPsychiatl] 29:407-412
Leonard HI., Swede SE, I.cnanc MC ct al. (1993), A 2- to 7-year followup study of 54 obsessive-compulsive children and adolescents. ArchGen Psychiatry 50:429-439
Leonard HI., Swedo SE, Rapoport JL ct al, (1989), Treatment of obsessivecompulsive disorder with clomipramine and desipramine in childrenand adolescents. A double-blind crossover comparison, Arch Gen Psycbintl] 46:1088-1092
Lyon L (1983), A behavioral treatment of compulsive lip-biting. ] Beha»E~p p,ychiatry 14:275-276
March J, Jobnston H, Greist J (1990a), The future of research in obsessivecompulsive disorder. In: Obsessive-Compulsive Disorder, [cnikc M, BacrI., Minichcllo W, cds, Littleton, MA: PSG
March J, Johnston H, Jefferson J, Grcisr J, Kobak K, Mazza J (1990b),Do subtle neurological imparimcnrs predict treatment resistance inchildren and adolescents with obsessive-compulsive disorder? .I ChildAdolesc Psycbopbarmacol 1:133-140
March J, Mullc K (in press), Cognitive-behavioral psychotherapy forobsessive-compulsive disorder. In: Psychosocial Treatments jiJr Child and
Adolescent Disorders, Hibbs E, Jensen P, cds, Washington, DC: AmericanPsychological Press
March JS, Mulle K, Herbel B (1994), Behavioral psychotherapy for childrenand adolescents with obsessive-compulsive disorder: an open trial of anew protocol-driven treatment package. ] Am Acrid Child AdolescPsychiatry 33:333-341
Marks I (I987), Fears, Phobias, and Rituals. New York: Oxford University Press
Marks 1M, Lelliott P, Basoglu M cr al. (I 988), Clomipramine, self-exposureand therapist-aided exposllte for obsessive-compulsive rituals. HI']Psychiatl] 152:522-534
Mills H, Agras S, Barlow D, Mills J (I 973), Compulsive rituals treatedby response prevention. Arch Gen Psychiatry 28:524-529
Morelli G (1983), Adolescent compulsion: a case study involving cognitivebehavioral treatment. Psycho! Rep 53:519-522
Neziroglu 1', Neuman J (1990), Three treatment approaches lor obsessions.] Cogn Psychother4:377-392
Nicolau R, Toro J, Perez PC (I991), Behavioral treatment of a case ofpsychogenic urinary retention. ] Behau Ther Exp Psychiatry 22:63-68
O'Connor J (I983), Why can't I get hives: brief strategic therapy with anobsessional child. Fam Process 22:201-209
Ong S, Leng Y (I 979), The treatment of an obsessive-compulsive girl in thecontext of Malaysian Chinese culture. AlistN;(] Psychiatry 13:255-259
Ownby R (I983), A cognitive behavioral intervention for compulsivehandwashing with a thirteen year-old-boy. Psycho!Sch 20:219-222
Rapoport JL, Swedo SE, Leonard HI. (1992), Childhood obsessive compulsive disorder. ] Clin Psychiatry 53(suppl):6-11
Rasmussen SA, Eisen JL (I 990), Epidemiology of obsessive compulsivedisorder.] Clin Psychiatry 51 (suppl):.'3-1 0, discussion 14
Rasmussen SA, Eisen JL (1992), The epidemiology and differential diagnosisof obsessive compulsive disorder. ] Gin Psychiatry 53(suppl):4-1 ()
Rarnasuriya RH, Marks 1M, Forshaw DM, Hymas NF (1991), Obsessiveslowness revisited. Br ] Psychiatry 159:273-274
Riddle MA, Scahill I., King R ct al. (I990), Obsessive compulsive disorderin children and adolescents: phenomenology and family history. ] AmAcad Child Adolesc Psychirltl] 29:766-772
Sl<.lnlcy L (1980), Trcnuucut or ri t ual ist ic behavior in all cigllt-ycar-old
girl by response prevention. ] Child Psycho! Psychiatl), 21 :85-90Sternberger LG, Burns GL (1990), Maudsley Obsessional-Compulsive
Inventory: obsessions and compulsions in a nonclinical sample. BehnuRes Ther 28:337-340
Swedo S (1993), Trichotillomania. Psychiatr Ann 23:402-407Taylor R (I985), Imagery for the treatment of obsessional behavior: a case
study. Am] Clin Hypn 27: 175-179Thycr BA (1991), Diagnosis and treatment of child and adolescent anxiety
disorders. Behnu Modl]' 15:.'3 10-325
17

MARCH
Virulano LA, King RA, Scahi ll L, Cohen DJ (1992), Behavioral treatmentof children and adolescents with trichotillomania. j Am Acad ChildAdolesc Psychiatry 31: 139-146
Voeller K (1990), Right hemisphere deficit syndrome in children: a neur ological perspect ive. Int j Pediatr 5:163- 170
Warncke L (1985), Intr avenous chlorimipramine in the treatment ofobsessional disorder in adolescence: a case report . j Clin Psychiatry46:100 -103
Weiner I (1967), Behavior therapy in obsessive-compulsive neurosis: treatment of an adolescent boy. Psycbother TheOlY Res Pract 4:27-29
White M , Epsron D (1990 ), Narrative Means to Therapeutic Ends. N ewYork: WW Norton
Willmuth ME (1988) , Cognitive-behavioral and insight-oriented psychotherapy of an eleven-year-old boy with obsessive-com pulsive disorder.Am j Psycbother 42:472-478
Wolff R, Rapop ort J (1988) , Behavioral treatment of childhood obsessivecompulsive disord er. Behav Modif 12:252-266
Yamagami T (197 8), Changes of behavior, fear and thought in the treatme ntby response prevention. Folia Psychiatry Neurol[pn 32:77-83
Z ilcis P (198 3), T reatment of an l l -year-old obsessive-compulsive ritua lizerand tiquer girl with in vivo exposure and response prevention. BehavPsychother I 1:75-81
Call for Submissions
The new Clinical Perspectives Section of the Journal reflects an attempt to acknowledge formally the value of clinical observations, perspectives, wisdom, guidelines, and pearls.Submissions should be short (750 to 1,500 words), concise, clear, pithy, and focused.Clinical Perspectives reflects the Journal's continuing attempt to provide the latest information for clinical practice in addition to building a knowledge base for the field grounded onformal research. We encourage questions, comments, and submissions sent to MichaelJellinek, M. D., Assistant Editor, Clin ical Perspectives, Massachusetts General Hosp ital, 15Parkman Street-ACC 725, Boston, MA 02 114.
18 J . AM, AC AD , C H I LD AD O LESC. PSY C H IATRY, 34 : 1, JANU ARY 1995




















