Cognitive Behavior Therapy in First-Episode Psychosis With a Focus on Depression, Anxiety, and...
12
Cognitive Behavior Therapy in First-Episode Psychosis With a Focus on Depression, Anxiety, and Self-Esteem Nasrettin Sönmez, Oslo University Hospital and University of Oslo Roger Hagen, Norwegian University of Science and Technology, Trondheim Ole A. Andreassen and Kristin Lie Romm, Oslo University Hospital, Institute of Clinical Medicine, University of Oslo Marit Grande and Lene Hunnicke Jensen, Oslo University Hospital Anthony P. Morrison, Prestwich Hospital, Manchester Ingrid Melle and Jan I. Røssberg, Oslo University Hospital and University of Oslo Although several reviews show that cognitive behavioral therapy (CBT) is an effective treatment for patients with chronic psychosis, the effects of CBT on patients with a first-episode psychosis are less clear. Patients undergoing a first-episode psychosis are unique in that not only are they struggling with the symptoms of the disease, but also the realization of the diagnosis. Understanding how the disease will impact their lives with respect to changes in social goals, roles, and status can also lead to depression, anxiety and low self-esteem. The main aim of the present study is to describe two clinical cases in order to demonstrate the application of CBT in first-episode psychosis patients in an early stage of their psychosis. The two cases are individuals who were in an ongoing CBT trial for first-episode psychosis patients with symptoms of social anxiety, depression, and low self-esteem. Individual case formulations based on these symptoms were developed. Psychoeducation, normalizing, evaluation of negative automatic thoughts and dysfunctional schematic beliefs, and focusing on the negative consequences of safety behavior were the main treatment targets in attempting to improve the patients’ symptoms and functioning. Both patients showed improvement in depressive symptoms, self-esteem, and general functioning. The cases described suggest that treatment designed to target depression, anxiety, and self-esteem in patients with first-episode psychosis could have potential beneficial effects; specific studies of this approach are recommended. A CCORDING to current treatment guidelines (National Institute for Health and Clinical Excellence, 2009), it is of importance to establish comprehensive treatment programs combining pharmacological and psychosocial interventions for patients with first-episode psychosis. Such programs have demonstrated improvement in prognosis and promoted recovery and social/occupational function- ing (Craig et al., 2004; Garety et al., 2006; Hegelstad et al., 2012; Jeppesen et al., 2005; McGorry, Killackey, & Yung, 2008; Thorup et al., 2005). Cognitive behavioral therapy (CBT) for psychosis has received increased interest over the last decade. Several reviews show that CBT is an effective treatment for patients with chronic psychosis with regard to improvement of hallucinations, delusions, negative symptoms, recovery, depressive symptoms, social anxiety, insight, and number of relapses (Bustillo, Lauriello, Horan, & Keith, 2001; Gould, Mueser, Bolton, Mays, & Goff, 2001; Haddock, Morrison, Hopkins, Lewis, & Tarrier, 1998; Rector & Beck, 2001; Tarrier, 2005; Tarrier & Wykes, 2004; Turkington, Dudley, Warman, & Beck, 2004; Wykes, Steel, Everitt, & Tarrier, 2008; Zimmermann, Favrod, Trieu, & Pomini, 2005). Several national guidelines also recommend CBT as a routine treatment for patients with a psychotic disorder (Lehman et al., 2004). However, most of the existing CBT studies have been performed on samples of patients with a long-established diagnosis of schizophrenia/psychotic disorder. Relatively few studies have been performed among patients in the early stages of a first-episode psychosis. This is significant as the needs and goals of a patient with a first-episode psychosis may be quite different from a patient with a long history of psychosis and involvement with mental health services. First-episode psychosis patients, besides experienc- ing hallucinations and delusions, often also suffer from "emotional dysfunction." Emotional dysfunction has been described in the literature as symptoms of depression, Keywords: cognitive behavioral therapy; first-episode psychosis; depression; anxiety; low self-esteem 1077-7229/13/xxx-xxx$1.00/0 © 2013 Association for Behavioral and Cognitive Therapies. Published by Elsevier Ltd. All rights reserved. CBPRA-00471; No of Pages 12: 4C Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in First-Episode Psychosis With a Focus on Depression, Anxiety, and Self- Esteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.1016/j.cbpra.2013.06.001 Cognitive and Behavioral Practice xx (2013) xxx-xxx www.elsevier.com/locate/cabp
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Cognitive Behavior Therapy in First-Episode Psychosis With a Focus on Depression, Anxiety, and...

CBPRA-00471; No of Pages 12: 4C
Cognitive and Behavioral Practice xx (2013) xxx-xxxwww.elsevier.com/locate/cabp
Cognitive Behavior Therapy in First-Episode Psychosis With a Focus onDepression, Anxiety, and Self-Esteem
Nasrettin Sönmez, Oslo University Hospital and University of OsloRoger Hagen, Norwegian University of Science and Technology, Trondheim
Ole A. Andreassen and Kristin Lie Romm, Oslo University Hospital, Institute of Clinical Medicine, University of OsloMarit Grande and Lene Hunnicke Jensen, Oslo University Hospital
Anthony P. Morrison, Prestwich Hospital, ManchesterIngrid Melle and Jan I. Røssberg, Oslo University Hospital and University of Oslo
Keywdepr
1077© 20Publ
PleEst
Although several reviews show that cognitive behavioral therapy (CBT) is an effective treatment for patients with chronic psychosis, theeffects of CBT on patients with a first-episode psychosis are less clear. Patients undergoing a first-episode psychosis are unique in thatnot only are they struggling with the symptoms of the disease, but also the realization of the diagnosis. Understanding how the diseasewill impact their lives with respect to changes in social goals, roles, and status can also lead to depression, anxiety and low self-esteem.The main aim of the present study is to describe two clinical cases in order to demonstrate the application of CBT in first-episodepsychosis patients in an early stage of their psychosis. The two cases are individuals who were in an ongoing CBT trial for first-episodepsychosis patients with symptoms of social anxiety, depression, and low self-esteem. Individual case formulations based on thesesymptoms were developed. Psychoeducation, normalizing, evaluation of negative automatic thoughts and dysfunctional schematicbeliefs, and focusing on the negative consequences of safety behavior were the main treatment targets in attempting to improve thepatients’ symptoms and functioning. Both patients showed improvement in depressive symptoms, self-esteem, and general functioning.The cases described suggest that treatment designed to target depression, anxiety, and self-esteem in patients with first-episode psychosiscould have potential beneficial effects; specific studies of this approach are recommended.
A CCORDING to current treatment guidelines (NationalInstitute for Health and Clinical Excellence, 2009),
it is of importance to establish comprehensive treatmentprograms combining pharmacological and psychosocialinterventions for patients with first-episode psychosis. Suchprograms have demonstrated improvement in prognosisand promoted recovery and social/occupational function-ing (Craig et al., 2004; Garety et al., 2006; Hegelstad et al.,2012; Jeppesen et al., 2005; McGorry, Killackey, & Yung,2008; Thorup et al., 2005).
Cognitive behavioral therapy (CBT) for psychosis hasreceived increased interest over the last decade. Severalreviews show that CBT is an effective treatment for patientswith chronic psychosis with regard to improvement ofhallucinations, delusions, negative symptoms, recovery,
ords: cognitive behavioral therapy; first-episode psychosis;ession; anxiety; low self-esteem
-7229/13/xxx-xxx$1.00/013 Association for Behavioral and Cognitive Therapies.ished by Elsevier Ltd. All rights reserved.
ase cite this article as: Sönmez et al., Cognitive Behavior Therapy in Fireem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
depressive symptoms, social anxiety, insight, and numberof relapses (Bustillo, Lauriello, Horan, & Keith, 2001;Gould, Mueser, Bolton, Mays, & Goff, 2001; Haddock,Morrison, Hopkins, Lewis, & Tarrier, 1998; Rector & Beck,2001; Tarrier, 2005; Tarrier & Wykes, 2004; Turkington,Dudley, Warman, & Beck, 2004; Wykes, Steel, Everitt, &Tarrier, 2008; Zimmermann, Favrod, Trieu, & Pomini,2005). Several national guidelines also recommend CBT asa routine treatment for patients with a psychotic disorder(Lehman et al., 2004).
However, most of the existing CBT studies have beenperformed on samples of patients with a long-establisheddiagnosis of schizophrenia/psychotic disorder. Relativelyfew studies have been performed among patients in theearly stages of a first-episode psychosis. This is significantas the needs and goals of a patient with a first-episodepsychosis may be quite different from a patient with a longhistory of psychosis and involvement with mental healthservices. First-episode psychosis patients, besides experienc-ing hallucinations and delusions, often also suffer from"emotional dysfunction." Emotional dysfunction has beendescribed in the literature as symptoms of depression,
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

2 Sönmez et al.
anxiety, and reduced self-esteem. The emotional sequelaeassociated with receiving a chronic mental illness diagnosishas also been underexamined in the literature for thosewho are newly diagnosed and experiencing a first episodeof psychosis. The importance of emotional dysfunction infirst-episode psychosis is reflected by the fact that studiesshow the highest prevalence rate of suicide and suicidalbehavior the first year after the start of treatment (Barrettet al., 2010; Melle et al., 2006; Verdoux et al., 2001). Sim-ilarly, people experiencing a first-episode psychosis arelikely to experience significant levels of internalized stigma(Brohan, Gauci, Sartorius, & Thornicroft, 2011) and dif-ficulty adjusting to the labels or diagnoses that are givento them. Such emotional processes may be an importanttarget for treatment intervention in first episode psychosis(Birchwood, 2003; Birchwood and Trower, 2006; Morrison,2009a).
In line with this, Haddock and Lewis (2005) describethe importance of developing treatments that are specificto the different phases of psychotic illness. Specific treat-ment is especially important in first-episode psychosisas symptoms can change rapidly at this stage, and alsobecause this early stage of the disorder can result in majorchanges in the patient’s life. Rather than applying treat-ment that is standard across all stages of psychotic illness,treatment programs for first-episode psychosis patientsneed to be individually tailored to meet the specific needsof each patient.
To our knowledge, eight randomized clinical trials(RCT) have examined the effect of CBT on patients with afirst-episode psychosis (Edwards et al., 2006; Fowler et al.,2009; Haddock et al., 1999; Jackson et al., 2008; Jolley et al.,2003; Lewis et al., 2002; Power et al., 2003; Tarrier et al.,2004). In four of these studies, the main aim was to reducepositive psychotic symptoms (Haddock et al., 1999; Jolley etal., 2003; Lewis et al., 2002; Tarrier et al., 2004), while theother four studies aimed specifically to reduce suicidality,cannabis use, posttraumatic symptoms and improve socialrecovery among first-episode psychosis patients, respective-ly (Edwards et al., 2006; Fowler et al., 2009; Jackson et al.,2008; Power et al., 2003). There is a tendency that studiestargeting specific symptoms show better outcome resultsthan studies targeting general psychotic symptoms. Fowlerand colleagues reported important benefits among patientswith nonaffective psychosis who had social recoveryproblems, while Jackson et al. proved that CBT is aneffective method in helping people adopt to the traumaticaspects of a first-episode psychosis. Power and colleaguesshowed that CBT is effective in the management of suicideideation. In a review focusing on CBT and first-episodepsychosis, Morrison concludes that there is only modestsupport for the evidence of the effectiveness of CBT forpatients with first-episode psychosis and that the evaluatedstudies have flaws both in study design and with regard to
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
the extent that the treatment approach and intended goalsare relevant to the concerns of patients with first-episodepsychosis (Morrison, 2009b). Furthermore, studies exam-ining the effect of CBT for patients with a first-episodepsychosis should target specific difficulties for this group ofpatients, such as depression, anxiety, low self-esteem, PTSD,and a reduction of distress and problematic behaviorassociated with positive psychotic symptoms.
Few of the aforementioned first-episode psychosisstudies have specifically targeted problems related to emo-tional dysfunction. There has been an increased interest inthe role of emotions or emotional dysfunction in psychosisduring the last decade. The term “emotional dysfunction”is used interchangeably with symptoms of mood and anx-iety disorders, including PTSD, negative schematic beliefs,and reduced self-esteem. According to Birchwood (2003),Birchwood and Trower (2006), and Morrison (2009a),CBT for patients with a first-episode psychosis should aimat developing a case formulation based on the patient’semotional dysfunction, as these problems are common inpatients with first-episode psychosis and are related to thedevelopment, and the maintenance, of positive (e.g., hallu-cinations and delusions) and negative (e.g., flat affect andapathy) symptoms.
Depression in schizophrenia has a prevalence ratevarying between 7% and 75% and is associated with pooroutcome, frequent relapse, rehospitalization, and in-creased suicidality (Caldwell & Gottesman, 1990; Heilaet al., 1997; Herz & Lamberti, 1995; Romm et al., 2010;Roy, Thompson, & Kennedy, 1983). The rate of socialanxiety disorder in the first year following a first episode ofpsychosis has been reported to be between 43% and 50%(Cosoff & Hafner, 1998; Pallanti, Quercioli, & Hollander,2004; Romm et al., 2012). Low self-esteem in individualswith psychotic disorder is also common andmay be relatedto poor clinical outcomes (Barrowclough et al., 2003;Bowins & Shugar, 1998; Romm et al., 2011). Self-esteem is acomplex concept comprising appraisal of self-worth basedon personal achievements and the anticipated evaluationof others. In psychotic disorders low self-esteem has beenimplicated both in the development of delusions and themaintenance of psychotic symptoms (Bentall, Corcoran,Howard, Blackwood, & Kinderman, 2001; Garety, Kuipers,Fowler, Freeman, & Bebbington, 2001). Smith et al. (2006)found that low mood, low self-esteem, and negative sche-matic beliefs can contribute to the development of symp-toms of psychosis.
Thus, there is a strong case to be made for provision ofCBT for patients with first-episode psychosis that focuseson emotional dysfunction in addition to positive symp-toms (Birchwood & Trower, 2006). We aim to demon-strate that CBT focusing on different aspects of emotionaldysfunction can be a helpful intervention for patients withfirst-episode psychosis. Two case studies are included.
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

3CBT for First-Episode Psychosis
MethodParticipants
The two cases presented in this paper are part of astructured pilot program of CBT for emotional dysfunction(e.g., depressive symptoms, social anxiety, and self-esteem)in patients with first-episode psychosis at our universityclinic.
Materials and ProcedureThe patients were offered 26 sessions of therapy during
a 6-month period and the same therapist treated bothcases. The study was approved by the regional researchethics committee. Clinical assessment was carried out bytrained psychiatrists and clinical psychologists. Diagnosiswas based on the Structured Clinical Interview for DSM-IVAxis I disorders (SCID-I) (2004). Symptom level was mea-sured with the Structural Clinical Interview of the Positiveand Negative Symptom Scale (SCI-PANSS; Kay, Fiszbein,& Opler, 1987), and the Global Assessment of Function-ing Scale (GAF; Jones, Thornicroft, Coffey, & Dunn,1995) split version (Pedersen, Hagtvet, & Karterud, 2007).Severity of depressive symptoms was assessed using theCalgary Depression Scale for Schizophrenia (CDSS;Addington, Addington, & Schissel, 1990). The CDSS wasspecifically developed to assess depression in schizophre-nia and prevent overlap with negative and extrapyramidalsymptoms. Self-esteem was measured using the RosenbergSelf-Esteem Scale (RSES; Rosenberg, 1989). This is a10-item self-administered questionnaire answered on a4-point Likert scale, ranging from strongly disagree tostrongly agree. A higher score indicates better self-esteem.Two different raters assessed the patients on clinical mea-sures at baseline and at the end of therapy.
In order to protect patient anonymity, a number ofessential details have been altered in these two case studies.All case reports were anonymized. Written informed con-sent was given by the two patients described.
Case I: Self-Esteem and DepressionBackground
Jonathan is a 27-year-old man with a family history ofschizophrenia (mother). He had few friends duringchildhood and was bullied at school. The other childrenmade jokes about him, but they did not physically abusehim. His psychotic symptoms started when he was 25 yearsold. The duration of untreated psychosis was 2 years.He started to hear voices that said negative things abouthim. The voices were unfamiliar to him. After approxi-mately 2 months of hearing voices, he began to experi-ence thoughts of being controlled by the devil. He wasadmitted to hospital and received antipsychotic medication(Aripiprazol). While an in-patient he received a diagnosisof paranoid schizophrenia. Aripiprazol was effective inreducing his psychotic symptoms, and Jonathan was con-
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
siderednonpsychotic after amonth at the hospital.He livedwith his mother during therapy. He was referred to CBTdue to low self-esteem and several depressive episodes thatoccurred before, during, and after the psychotic episode.
EngagementIn the first session the therapist informed Jonathan
about the basic principles of CBT and explained howpsychotic symptoms often develop based on the stress-vulnerability model (Zubin & Spring, 1977). The impor-tance of active participation and collaboration was em-phasized early in the therapy by explaining the importanceof homework and developing a problem list and goals forthe forthcoming sessions. A particular effort was made toclarify Jonathan's own expectations of the therapy.
Problem List and GoalsThe next step in the treatment process was to make a
problem list. As homework, Jonathan made a list of whathe thought were the most important aspects of his illnessto work with, both during and between therapy sessions.With the help of the therapist, the following list wascreated: low self-esteem, depression/suicidality, and lackof motivation. Jonathan related his lack of self-esteemto his avoidant behavior in social settings. As Jonathanplanned to start studying at the university 2 months afterthe start of therapy, he and the therapist agreed to focuson how he could manage to follow the schedule at theuniversity.
Case FormulationThe case formulation developed by Morrison (2001) is
displayed in Figure 1. This case formulation is appli-cable for use by both patients with a first-episode psychosisand therapists. In order to develop a case formulation,Jonathan and the therapist explored a specific stressfulsituation during the previous week. The formulationaimed to clarify how his thoughts and feelings might beaffected by his assumptions about himself, others, andthe world. The role of his early experiences and earlierlife events in shaping such assumptions was also investi-gated and included in the case formulation. A friend’squestion about what Jonathan thought about psychologyserved as a concrete situation for an ABC formulation.This question generated a thought that others could readsigns from Jonathan’s face, and therefore could see thathe went to a psychologist for treatment. These thoughtstriggered a schematic belief that he is boring, different,and ugly, and as a consequence of having these thoughtshe became anxious, sad, and paranoid. His reaction tothis line of thinking was to withdraw from social situationsin order to avoid these unpleasant thoughts and feelings.The case formulation is displayed in Figure 2.
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

What happened? (Event/intrusion)
How I make sense of it
Beliefs about yourself and others
Life experiences
What do you do How does itwhen this happens? make you feel?
Figure 1. Case formulation as described by Morrison (2001). From “The Interpretation of Intrusions in Psychosis: An Integrative CognitiveApproach to Hallucinations and Delusions,” by A. P. Morrison, 2001, Behavioral and Cognitive Psychotherapy, 29, p. 261. Adapted withpermission of the author.
A friend asks,“What do you think about psychology?”
Do I have a sign on me that says goes to a psychologist?
I am boring, different and ugly
Mother with schizophrenia, bullied at school
Don’t socialize Sad, paranoid anxious
Be quiet
Figure 2. A Case Formulation for Jonathan
4 Sönmez et al.
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in First-Episode Psychosis With a Focus on Depression, Anxiety, and Self-Esteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.1016/j.cbpra.2013.06.001

5CBT for First-Episode Psychosis
Course of TreatmentA situation similar to that described above occurred
at a school party where a schoolmate asked him, “Iseverything ok?” Drawing on the ABC formulation: (A) heinterpreted this remark as indicating that his schoolmatecould see that something was wrong with him and that hewas unwell and different from his schoolmates; (B) hestarted feeling angry, frustrated, and forced into a corner;(C) the next step in therapy was to help Jonathan comeup with alternative explanations for his negative thoughts(Table 1).
After creating an ABC formulation, the therapist usedSocratic questioning to see if there were other ways tointerpret and understand the situation. To what extentJonathan believed in the different interpretations was ratedon a scale from 0 (not at all) to 100 (totally right). AfterSocratic questioning, his interpretations (Is it somethingwrong with me? What is wrong with me? Do they think that I amnot well? Am I different?), at first rated at 70, were reduced toa rating of 20. As a result of Socratic questioning and ananalysis of the situation, Jonathan came up with new andmore realistic interpretations: It is kind of my friend to ask andShe demonstrates that she cares. He then rated his confidencein these new interpretations of the situations as 80. Thesealternative interpretations made Jonathan happier andmore relaxed. The CBT strategies described above wereused repeatedly in therapy and Jonathan gradually beganto apply them as part of his homework. As a conse-quence of this he gained more self-confidence and feltless depressed.
Lack of motivation was another item on Jonathan’sproblem list. He felt that he lacked motivation to dothings that he felt everyone else could do, such as visitingfriends or going shopping. In order to get an overviewof his daily activities, Jonathan was asked to write down allhis activities the following week and rate how enjoyablethe experiences were with a score from 0 to 100. Theassessment of Jonathan’s homework in the next sessiondemonstrated that Jonathan in fact was quite active. Inparticular, he spent time with friends nearly every day, anactivity that he rated high on the satisfaction scale. Afterreviewing this homework exercise he stated, “I can nowsee that I am actually much more active in participatingin different activities than I thought I was.”
The last phase of therapy focused predominantly onJonathan’s schematic beliefs. His basic assumptions were
Table 1An ABCDE Formulation
A B
A schoolmateasks at a party“Is everything ok?”
Is something wrong with me? What is itabout me that shows that everything is not ok?They think that I am unwell. Am I different?
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
that he was ugly and that no one possibly could like him.Together with the therapist, Jonathan evaluated the evi-dence for and against this belief. According to Jonathan,the evidence supporting this assumption was: “I have nosense of humor,” “I speak little and I do not come up withanything smart to say,” “I lack spontaneity and socialintelligence.” The following line of Socratic questioningwas used to challenge these assumptions: “What is theadvantage of thinking like this?” “How many people havesaid that this is the way you are?” “Will you ever get theright answer concerning these questions and, if so, willyou ever trust the answers?” According to Jonathan, aclose friend described him as interesting, kind, empa-thetic, polite, open, and positive. Many other friends andfamily members had also described him in such a way.No one had described him as boring and ugly. He thenrealized that there were no advantages to thinking insuch a way. He also realized that there was no evidencesupporting such negative assumptions about himself. Asa consequence of this new way of thinking, Jonathanbelieved less in his negative description of himself and hisself-esteem increased.He started to realize that his appraisalof himself did not correspond with other people’s views ofhim. This made it easier for him to speak with other peopleand talk in class at the university.
These interventions are illustrated in the transcriptfrom a session in the middle of the therapy (Session 16):
THERAPIST (T): You have very often stated that youhave no sense of humor, lack spontaneity and socialintelligence, and that you are boring and ugly. Howmany people have actually said that directly to you?
JONATHAN (J): Hmmm … I am not sure. I don’t thinkanyone actually has said it to me directly… No,nobody has. . . . It is just the way it is.
T: But how would one of your friends or yourmother describe you?
J: I am not sure… I think my mother would describeme as interesting, polite, open and positive…
T: And your closest friends?
J: Pretty much the same way, I think.
C D E
Angry, frustrated,forced into acorner.
So nice that she is asking.She demonstrates that shecares.
Happy,important,well.
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

6 Sönmez et al.
PE
T: So how come you don’t believe them?
J: It’s just a fact … something I feel strongly inside….I feel that I am boring and lack social intelligence.I have nothing to speak with other people about.Nobody can possibly like me. I am boring and ugly.
T: Yes, but nobody has, in your entire life, describedyou like that. Nobody has ever directly said to youthat you are boring and ugly. Do you rememberthat we talked about different core beliefs thatpeople have and how these beliefs are ideas wehave about ourselves? They are not necessarily trueor false but we are certainly affected by them….
J: Yes … I remember.
T: Fine. What about if I said that you have no reasonto believe that you are boring, ugly, lack spontaneity,and actually most people, including myself, see youas a positive and interesting person. What would youthink about that?
J: That wouldn’t change my opinion about myself.You are paid to say things that cheer me up. . . .
T: What if we went out of the office and I asked mycolleagues?
J: They wouldn’t know. They know nothing aboutme.
T: But if they did?
J: They would probably say the same things as you.They are probably all paid to cheer people up.
T: If we ask 100 people about how you are, and alldescribed you the way your mother and friends did,would you believe them or would you still think sonegatively about yourself?
J: I am not sure. Probably . . . People always say nicethings to each other. They want to be polite anddon’t say negative things about each other.
T: Okay. So in fact this is a question that has nocorrect answer… It is impossible to find out whetherit is true or false?
J: Yes, I think so.
T: How come? And how do you think we shoulddeal with that? What if you, say about ten years from
lease cite this article as: Sönmez et al., Cognitive Behavior Therapy in Firsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
now, got an answer you really trusted…? The “true”answer… and that answer was in fact more in linewith how your mother and friends describe you.What about the fact that you are going to havethese negative assumptions about yourself in tenyears and then you discover that you really havebeen thinking wrongly about yourself for no reasonat all?
J: I see your point, but what if, in fact, I am right—that I really am boring and ugly with no socialcompetence?
T: Yeah … What about that? The worst scenariowould be that you would have been satisfied withyourself in all the ten years. I think that would makeyou more satisfied and less depressed. If it shouldbe correct, ten years from now, that you are a badand socially incompetent person, then you at leastprobably would have energy to handle and dealwith it.
J: There is actually no way I can get the correctanswer to this question. You are probably right . . .
The last four sessions in therapy focused on relapseprevention. Jonathan was afraid of a relapse and aresultant hospitalization. The final sessions thereforefocused on early warning signals for a psychotic relapse,and also the fact that an increase in symptoms over a shortperiod did not necessarily mean that he would need to beadmitted to hospital.
ResultsCase I: Self-Esteem and Depression
At the end of treatment (24 sessions), Jonathanshowed a major improvement in both his symptoms andfunctioning. This is illustrated by the split version of theGAF scores used in the present study. At the start oftreatment, the GAF symptom score was rated as 47, whichincreased to 72 by the end of therapy. The GAF function-ing score increased from 46 to 70. This constitutes a 25%improvement in functioning and symptoms.
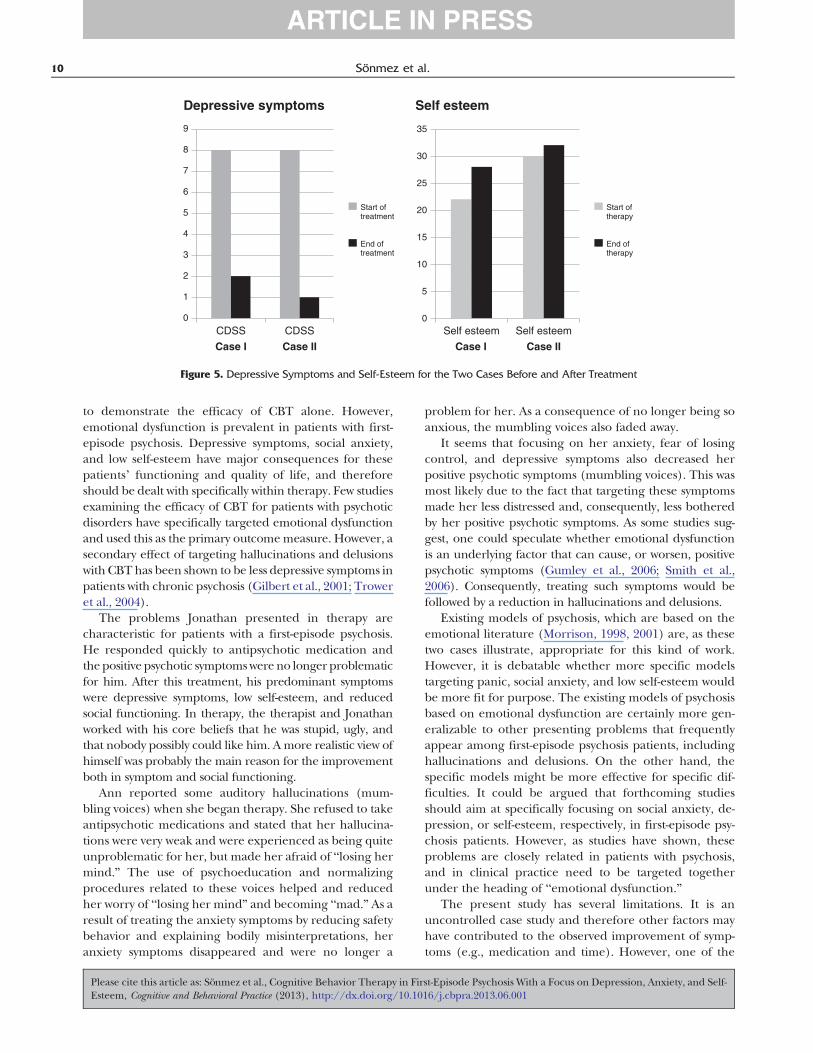
During therapy Jonathan’s depressive symptoms im-proved gradually; his suicidal thoughts disappeared, hebecame more optimistic about the future, had more pos-itive thoughts about himself, was less disappointed abouthimself, and began to enjoy the company of other people.This considerable improvement in depressive symptomsis illustrated by a decrease from 8 to 2 in the total CDSSscore. Consequently, according to the usual cutoff scoreof the CDSS (CDSS ≥ 6), he was no longer depressed atthe end of therapy. Self-esteem, as measured by the RSES,improved from 22 to 28 during the intervention. This
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

7CBT for First-Episode Psychosis
constitutes a 20% increase. Jonathan described a consid-erable change in his view of himself. At the end of thetherapy he was more satisfied with himself and thoughtthat he had a lot of good qualities. He no longer feltashamed of himself or that everyone else was better thanhim. Perhaps most importantly, he was no longer afraidof appearing stupid in the presence of other people.Jonathan said that during therapy he had learned togenerate more realistic assumptions about himself. Hewas more relaxed in challenging situations and hadlearned strategies of dealing with different problemsin life. The main outcome measures are illustrated inFigures 4 and 5.
The PANSS scores further illustrate the improvementin his symptomatology. The total PANSS scores decreasedfrom 48 to 32. Jonathan was scored with a low total PANSSscore at the beginning of therapy and, although therewas a decrease in total PANSS score, it was not significant(20% decrease). Concerning the specific PANSS subscales,the PANSS positive symptoms subscale scores decreasedfrom 11 to 8 during treatment, and the PANSS negativesubscale scores decreased from 11 to 7. The generalpsychopathology score on the PANSS decreased from 26to 17. However, Jonathan’s main problem was not thepositive psychotic symptoms. Like many other patients witha first-episode psychosis, he rapidly recovered from positivepsychotic symptoms after receiving antipsychotic medica-tions, but still struggled with depressive symptoms and lowself-esteem.
Case II: Anxiety and DepressionBackground
Ann is a 23-year-old woman. She has a brother withschizophrenia. Ann received a diagnosis of unspecifiedpsychosis. She worked as a teacher in primary school. Herpsychotic symptoms consisted of auditory hallucinationsand somatic delusions. She heard what she describedas “mumbling” and “annoying” voices. She could notdescribe what the voices said and they did not seem tocome from a specific person. Furthermore, when shelooked at herself in the mirror she saw her body changing.She was afraid that she was losing control of her mind andthat she was going mad. She refused to use antipsychoticmedication.
EngagementEngagement with therapy was an important target of
the first sessions. Ann had the understanding of herpsychosis that “something wrong was going on in hermind.” Psychoeducation about the different forms ofpsychotic symptoms was given. In the first phase of therapyan emphasis was put on normalization. Information aboutthe fact that both hallucinations and delusional ideas arefrequently experienced by healthy, normal people madeher less anxious about her symptoms. Education about
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
situations that often initiate positive psychotic symptoms,such as drug abuse, grief, traumatic events and fever,madeher even more relaxed concerning her own experiences.This normalization process was probably of major im-portance in enabling Ann to engage in therapy.
The normalizing process is illustrated in the transcriptfrom the second session:
THERAPIST (T): You said the first time we met that youwere afraid of going mad and the reason was thefact that you heard voices that no one else did.What kind of voices/sounds were they?
ANN (A): It was just some mumbling. They were notreally voices . . . although it sounded like a screamor something. I was terrified….
T: Okay, and you started to fear that you were goingmad and that you were unable to be with yourfriends, go to work and concentrate. You panickedand you said that you were more depressed whenyou thought that you were going mad and unableto function?
A: Yes. I was terrified. Especially the first time I ex-perienced this. Now, I am actually more depressedthan anxious.
T: Do you have any idea about how common it is tohear voices? Do you know, or have you heard about,other people who sometimes have heard voices orsounds?
A: No. I have not heard about other people ex-periencing things like this. Except that I know thatthe people who hear voices are totally crazy. Theyare often admitted to hospitals and are not able tofunction at all. No work and no family or children.
T: That’s actually not the entire truth. . . . Actually,many people experience hearing voices or soundsand they are not at all “totally crazy.” A lot of famouspeople have actually heard voices. You have prob-ably heard about Gandhi and Anthony Hopkins?
A: Yes. Of course I have heard about them. Did theyreally hear voices?
T: Yes, they did, and if you ask people on the streetmany would say that they sometimes have heardsounds or voices that people standing close to themcould not hear. It is actually very common. It isespecially common after grief and sorrow and afterusing drugs.
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

8 Sönmez et al.
A: That’s interesting. I now remember that one ofmyfriends from high school had a grandmother whoheard voices after her husband died. She becamebetter after a while, I think. . . .
T: Yes, she probably did. It is actually quite commonin different stressful situations to hear voices. Likeyou… As you told me in the last session, you havegone through some quite stressful periods lately. . . .
Problem List and GoalsFor homework after the third session, Ann had to write
down what kind of problems she wanted to work within therapy in order of importance. She considered theanxiety she experienced in certain situations as beingthe most problematic issue. Second on her list were herdepressive symptoms, and third were intrusive thoughts(e.g., “What if I harm the children at school?”).
Case FormulationA specific situation that Ann had recently experienced
as disturbing was chosen for the construction of the caseformulation. The situation (A) involved Ann sitting athome by herself listening to music. She suddenly had athought that she was losing her mind and would becomemad. She assumed that the world was crazy and that shewas evil. These thoughts were followed by an assumptionthat something was wrong with her (B). She became veryanxious, and handled her fear with the use of safety
Alone at home, liste
I am losing my mI am going ma
The world is crazThere is something
Brother with sch
Sit calmly
Breathe deeply
Figure 3. A Case Form
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
behaviors such as sitting quietly and breathing deeply (C).The case formulation is illustrated in Figure 3.
Course of TreatmentClark’s (1986) model of panic disorder was used to
formulate the fear/anxiousness Ann was experiencing indifferent situations. For example, listening to music trig-gered feelings of panic, fear, anxiety, and nervousness.The thoughts she had were that “something dangerousis happening to me and I am going mad.” The bodilyreaction she experienced when having these thoughts wasa feeling of being unwell, restless, and overwhelmed. Anntried to cope with these situations by talking to herselfand instructing herself to “breathe calmly” and “think aboutsomething else,” but these instructions were not helpful incoping with the emotional consequences of the situation.The therapist drew the panic circle on the white-boardand explained it in detail to Ann, including examples ofsafety behavior and an explanation of how such behaviorsincrease anxiety.
One of the safety behaviors Ann used when she ex-perienced anxiety was that she stayed at home, whichmade it impossible for her to work. The therapist en-couraged Ann to start working again. After a closer lookat the case formulation she understood that her safetybehaviors made her situation worse. After 2 weeks in ther-apy she returned to work and the symptoms of nervousnessand anxiety became less troublesome, although she occa-sionally still had the thought, “What if I am going mad?”
ning to music
ind.d
y. I am evil.wrong with me.
izophrenia
Anxious, fear
ulation for Ann
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

0
10
20
30
40
50
60
70
80
GAF Symptoms GAF Function GAF Symptoms GAF function
Start of therapy End of therapy
Case I Case II
Figure 4.GAF Symptoms and Function Before and After Treatmentfor the Two Cases
9CBT for First-Episode Psychosis
Psychoeducation and Socratic questioning made thisthought less stressful for her. The therapist asked suchquestions as, “What do youmeanby ‘goingmad’?” and “Arethese thoughts really dangerous?” Focusing on her fearhelped Ann to reduce the fear and anxiety that had beenvery stressful for her. However, the fear was to some extentreplaced by depression. In order to address this issue intherapy, the content of Ann’s depressive thoughts wasidentified. She stated that she felt alone, different, notinterested in other people, not able to be herself, havingdiffering values than others, and feeling something heavyin herself which she described as a “big lump.” As aconsequence of experiencing these negative thoughts, thefocus on the following sessions was on Ann’s depression.However, she said that there were some advantages tohaving these depressive thoughts, and that she was notquite sure if she wanted to get rid of them. She thoughtthat she would become less reflective, less empathetic,and stupid, but also happier and more sociable if she wereto stop having these depressive thoughts. As a homeworkexercise she was asked to write down pros and cons forher assumptions, and to what extent she wanted to workwith this in the therapy. She concluded that she wantedto address this problem in therapy, and the forthcomingsessions were mainly focused on the pros and cons forhaving depressive symptoms. According to Ann, the useof Socratic questioning helped her to see that there wasno reason to believe that getting rid of her depressionwould make her less reflective, less empathetic, and less“intellectually deep.” The final sessions focused on relapseprevention and means of preventing the use of safetybehaviors as a strategy for getting rid of unwanted thoughtsand feelings.
Ann reported feeling better at the end of therapy(21 sessions) with regard to symptoms and functioning.She was working regularly as an assistant in a primaryschool and planned to start studying at the university thefollowing semester.
Ann was mostly troubled with anxiety and depression,while at the start of therapy she had a relatively normallevel of functioning and self-esteem. Her improvement isillustrated in her GAF symptom scores, which increasedfrom 57 to 70 (13 %), and her GAF function score, whichincreased from 68 to 73 during treatment (5%). Ann’sanxiety and fear of losing control resolved quickly afterpsychoeducation and normalizing procedures of hersymptoms. Furthermore, she improved by focusing on thenegative consequences of her safety behavior (breathingdeeply, sitting quietly, and not going to work). Of primaryimportance concerning her improvement was the fact thatshe went back to work only 2 weeks after starting treatment.
Annwas considerably depressed at the start of treatment.She had no suicidal thoughts but was pessimistic about thefuture, felt that shewas a failure andwas disappointed about
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
herself. She had also lost her interest in other people andeasily became tired. These depressive symptoms disap-peared during treatment, which is illustrated by the CDSSscore. Ann scored considerably lower on the CDSS, with adecrease from 8 at the start of treatment to 1 at the end oftreatment. Her self-esteem was quite high at the start oftreatment with a score of 30 on the RSES, which increasedto 32 by the end of treatment. Themain outcomemeasuresare illustrated in Figures 4 and 5.
The PANSS positive symptoms subscale score decreasedfrom 13 to 11, and the negative subscale decreased from9 to 7 from the start to the end of treatment. Althoughshe receive no antipsychotic medication, the generalpsychopathology subscale reduced from 25 to 18. As withJonathan, the focus in therapy was not aimed at reducingpositive psychotic symptoms.
Discussion
Treatment programs for first-episode psychosis patientsneed to be individually tailored in order tomeet the uniqueand specific needs of each patient. This individualizationshould be a general rule for every therapy, but is especiallycrucial for first-episode psychosis patients because thispatient group has a wide variation in symptoms, problems,and goals. As illustrated in the two cases described in thepresent paper, Jonathan struggled mostly with depressivesymptoms, low self-esteem, lack of motivation, and reducedsocial functioning, andAnnmostly with anxiety, depression,intrusive thoughts, and auditory hallucinations (mumblingvoices). Consequently, the CBT interventions in the twocases were quite different.
The effectiveness of CBT in the treatment of differentpsychiatric disorders, including chronic psychosis andschizophrenia, has been demonstrated (Turkington et al.,2004; Wykes et al., 2008; Zimmermann et al., 2005). As thetreatment of first-episode psychosis patients is usuallyfocused on hallucinations and delusions, which respondquickly to antipsychotic medication, it has been difficult
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001
Depressive symptoms
0
1
2
3
4
5
6
7
8
9
CDSS CDSS
Start of treatment
End of treatment
Self esteem
0
5
10
15
20
25
30
35
Self esteem Self esteem
Start of therapy
End of therapy
Case I Case II Case IICase I
Figure 5. Depressive Symptoms and Self-Esteem for the Two Cases Before and After Treatment
10 Sönmez et al.
to demonstrate the efficacy of CBT alone. However,emotional dysfunction is prevalent in patients with first-episode psychosis. Depressive symptoms, social anxiety,and low self-esteem have major consequences for thesepatients’ functioning and quality of life, and thereforeshould be dealt with specifically within therapy. Few studiesexamining the efficacy of CBT for patients with psychoticdisorders have specifically targeted emotional dysfunctionand used this as the primary outcomemeasure. However, asecondary effect of targeting hallucinations and delusionswith CBThas been shown to be less depressive symptoms inpatients with chronic psychosis (Gilbert et al., 2001; Troweret al., 2004).
The problems Jonathan presented in therapy arecharacteristic for patients with a first-episode psychosis.He responded quickly to antipsychotic medication andthe positive psychotic symptomswere no longer problematicfor him. After this treatment, his predominant symptomswere depressive symptoms, low self-esteem, and reducedsocial functioning. In therapy, the therapist and Jonathanworked with his core beliefs that he was stupid, ugly, andthat nobody possibly could like him. Amore realistic view ofhimself was probably the main reason for the improvementboth in symptom and social functioning.
Ann reported some auditory hallucinations (mum-bling voices) when she began therapy. She refused to takeantipsychotic medications and stated that her hallucina-tions were very weak and were experienced as being quiteunproblematic for her, but made her afraid of “losing hermind.” The use of psychoeducation and normalizingprocedures related to these voices helped and reducedher worry of “losing her mind” and becoming “mad.” As aresult of treating the anxiety symptoms by reducing safetybehavior and explaining bodily misinterpretations, heranxiety symptoms disappeared and were no longer a
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
problem for her. As a consequence of no longer being soanxious, the mumbling voices also faded away.
It seems that focusing on her anxiety, fear of losingcontrol, and depressive symptoms also decreased herpositive psychotic symptoms (mumbling voices). This wasmost likely due to the fact that targeting these symptomsmade her less distressed and, consequently, less botheredby her positive psychotic symptoms. As some studies sug-gest, one could speculate whether emotional dysfunctionis an underlying factor that can cause, or worsen, positivepsychotic symptoms (Gumley et al., 2006; Smith et al.,2006). Consequently, treating such symptoms would befollowed by a reduction in hallucinations and delusions.
Existing models of psychosis, which are based on theemotional literature (Morrison, 1998, 2001) are, as thesetwo cases illustrate, appropriate for this kind of work.However, it is debatable whether more specific modelstargeting panic, social anxiety, and low self-esteem wouldbe more fit for purpose. The existing models of psychosisbased on emotional dysfunction are certainly more gen-eralizable to other presenting problems that frequentlyappear among first-episode psychosis patients, includinghallucinations and delusions. On the other hand, thespecific models might be more effective for specific dif-ficulties. It could be argued that forthcoming studiesshould aim at specifically focusing on social anxiety, de-pression, or self-esteem, respectively, in first-episode psy-chosis patients. However, as studies have shown, theseproblems are closely related in patients with psychosis,and in clinical practice need to be targeted togetherunder the heading of “emotional dysfunction.”
The present study has several limitations. It is anuncontrolled case study and therefore other factors mayhave contributed to the observed improvement of symp-toms (e.g., medication and time). However, one of the
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

11CBT for First-Episode Psychosis
patients refused medication and still improved. A ran-domized controlled trial examining the effect of CBTin emotional dysfunction among first-episode psychosispatients is needed and is under way.
We propose that individually tailored CBT, focusingon depression, anxiety, and low self-esteem, would be ef-fective in the treatment of first-episodepsychosis patients, ashas been suggested previously (Birchwood & Trower, 2006;Morrison, 2009a, 2009b). The two cases presented in thisstudy demonstrate that CBT is applicable and acceptableto first-episode psychosis patients and that individuallyadjusted case formulations are essential for planning anddesigning therapy. This necessitates a continuous updatingof case formulation and the patient’s problem list in orderto satisfy the patient’s specific needs in different phases ofthe therapy.
References
Addington, D., Addington, J., & Schissel, B. (1990). A depression ratingscale for schizophrenics. Schizophrenia Research, 3, 247–251.
Barrett, E. A., Sundet, K., Faerden, A., Nesvag, R., Agartz, I., Fosse,R., … Melle, I. (2010). Suicidality before and in the early phases offirst episode psychosis. Schizophrenia Research, 119, 11–17.
Barrowclough, C., Tarrier, N., Humphreys, L., Ward, J., Gregg, L., &Andrews, B. (2003). Self-esteem in schizophrenia: relationshipsbetween self-evaluation, family attitudes, and symptomatology. Journalof Abnormal Psychology, 112, 92–99.
Bentall, R. P., Corcoran, R., Howard, R., Blackwood, N., & Kinderman, P.(2001). Persecutory delusions: A review and theoretical integration.Clinical Psychology Review, 21, 1143–1192.
Birchwood, M. (2003). Pathways to emotional dysfunction in first-episode psychosis. British Journal of Psychiatry, 182, 373–375.
Birchwood, M., & Trower, P. (2006). The future of cognitive-behaviouraltherapy for psychosis: Not a quasi-neuroleptic. British Journal ofPsychiatry, 188, 107–108.
Bowins, B., & Shugar, G. (1998). Delusions and self-esteem. CanadianJournal of Psychiatry, 43, 154–158.
Brohan, E., Gauci, D., Sartorius, N., &Thornicroft, G. (2011). Self-stigma,empowerment and perceived discrimination among people withbipolar disorder or depression in 13 European countries: TheGAMIAN-Europe study. Journal of Affective Disorders, 129, 56–63.
Bustillo, J., Lauriello, J., Horan, W., & Keith, S. (2001). Thepsychosocial treatment of schizophrenia: An update. AmericanJournal of Psychiatry, 158, 163–175.
Caldwell, C. B., & Gottesman, I. I. (1990). Schizophrenics kill themselvestoo: A review of risk factors for suicide. Schizophrenia Bulletin, 16,571–589.
Clark, D. M. (1986). A cognitive approach to panic. Behaviour Researchand Therapy, 24, 461–470.
Cosoff, S. J., & Hafner, R. J. (1998). The prevalence of comorbid anxietyin schizophrenia, schizoaffective disorder and bipolar disorder.Australian and New Zealand Journal of Psychiatry, 32, 67–72.
Craig, T. K., Garety, P. A., Power, P., Rahaman, N., Colbert, S.,Fornells-Ambrojo, M., & Dunn, G. (2004). The Lambeth EarlyOnset (LEO) Team: Randomised controlled trial of the effective-ness of specialised care for early psychosis. BMC Psychiatry, 6, 329.
Edwards, J., Elkins, K., Hinton, M., Harrigan, S. M., Donovan, K.,Athanasopoulos, O., &McGorry, P. (2006). Randomized controlledtrial of a cannabis-focused intervention for young people with first-episode psychosis. Acta Psychiatrica Scandinavica, 114, 109–117.
Fowler, D., Hodgekins, J., Painter, M., Reilly, T., Crane, C., Macmillan,I., et al. (2009). Cognitive behaviour therapy for improving socialrecovery in psychosis: A report from the ISREP MRC TrialPlatform Study (Improving Social Recovery in Early Psychosis).Psychological Medicine, 39, 1627–1636.
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
Garety, P. A., Craig, T. K., Dunn, G., Fornells-Ambrojo, M., Colbert, S.,Rahaman, N., … Power, P. (2006). Specialised care for earlypsychosis: Symptoms, social functioning and patient satisfaction—randomised controlled trial. British Journal of Psychiatry, 188, 37–45.
Garety, P. A., Kuipers, E., Fowler, D., Freeman, D., & Bebbington, P. E.(2001). A cognitive model of the positive symptoms of psychosis.Psychological Medicine, 31, 189–195.
Gilbert, P., Birchwood, M., Gilbert, J., Trower, P., Hay, J., Murray, B., …Miles, J. (2001). An exploration of evolved mental mechanisms fordominant and subordinate behaviour in relation to auditoryhallucinations in schizophrenia and critical thoughts in depres-sion. Psychological Medicine, 31(6), 1117–1127.
Gould, R. A., Mueser, K. T., Bolton, E., Mays, V., & Goff, D. (2001).Cognitive therapy for psychosis in schizophrenia: An effect sizeanalysis. Schizophrenia Research, 48, 335–342.
Gumley, A. F., Karatzias, A. F., Power, K. F., Reilly, J. F., McNay,L. F., & O'Grady, M. (2006). Early intervention for relapse inschizophrenia: Impact of cognitive behavioural therapy on negativebeliefs about psychosis and self-esteem. British Journal of ClinicalPsychology, 45, 247–260.
Haddock, G., & Lewis, S. (2005). Psychological interventions in earlypsychosis. Schizophrenia Bulletin, 31, 697–704.
Haddock, G.,Morrison, A. P., Hopkins, R., Lewis, S., & Tarrier, N. (1998).Individual cognitive-behavioural interventions in early psychosis.British Journal of Psychiatry Suppl, 172, 101–106.
Haddock, G., Tarrier, N., Morrison, A. P., Hopkins, R., Drake, R., &Lewis, S. (1999). A pilot study evaluating the effectiveness ofindividual inpatient cognitive-behavioural therapy in early psycho-sis. Social Psychiatry and Psychiatric Epidemiology, 34, 254–258.
Hegelstad, W. T., Larsen, T. K., Auestad, B., Evensen, J., Haahr, U., Joa,I., …McGlashan, T. (2012). Long-term follow-up of the TIPS earlydetection in psychosis study: Effects on 10-year outcome. AmericanJournal of Psychiatry, 4, 374–380.
Heila, H., Isometsa, E. T., Henriksson, M. M., Heikkinen, M. E.,Marttunen, M. J., & Lonnqvist, J. K. (1997). Suicide andschizophrenia: A nationwide psychological autopsy study on age-and sex-specific clinical characteristics of 92 suicide victims withschizophrenia. American Journal of Psychiatry, 154, 1235–1242.
Herz, M. I., & Lamberti, J. S. (1995). Prodromal symptoms and relapseprevention in schizophrenia. Schizophrenia Bulletin, 21, 541–551.
Jackson, H. J., McGorry, P. D., Killackey, E., Bendall, S., Allott, K.,Dudgeon, P., … Harrigan, S. (2008). Acute-phase and 1-yearfollow-up results of a randomized controlled trial of CBT versusBefriending for first-episode psychosis: The ACE project. Psycho-logical Medicine, 38, 725–735.
Jeppesen, P., Petersen, L., Thorup, A., Abel, M. B., Oehlenschlaeger,J., Christensen, T. O., … Nordentoft, M. (2005). Integratedtreatment of first-episode psychosis: effect of treatment onfamily burden: OPUS trial. British Journal of Psychiatry, Suppl 48,85–90.
Jolley, S., Garety, P., Craig, T., Dunn, G., White, J., & Aitken, M. (2003).Cognitive therapy in early psychosis: A pilot randomized controlledtrial. Behavioural and Cognitive Psychotherapy, 31, 473–478.
Jones, S. H., Thornicroft, G., Coffey, M., & Dunn, G. (1995). A briefmental health outcome scale-reliability and validity of the GlobalAssessment of Functioning (GAF). British Journal of Psychiatry, 166,654–659.
Kay, S. R., Fiszbein, A., & Opler, L. A. (1987). The positive and negativesyndrome scale (PANSS) for schizophrenia. Schizophrenia Bulletin,13, 261–276.
Lehman, A. F., Kreyenbuhl, J., Buchanan, R. W., Dickerson, F. B.,Dixon, L. B., Goldberg, R., … Steinwachs, D. (2004). TheSchizophrenia Patient Outcomes Research Team (PORT): up-dated treatment recommendations 2003. Schizophrenia Bulletin, 30,193–217.
Lewis, S., Tarrier, N., Haddock, G., Bentall, R., Kinderman, P.,Kingdon, D., … Dunn, G. (2002). Randomised controlled trial ofcognitive-behavioural therapy in early schizophrenia: acute-phaseoutcomes. British Journal of Psychiatry, Suppl 43, s91–s97.
McGorry, P. D., Killackey, E., & Yung, A. (2008). Early interventionin psychosis: Concepts, evidence and future directions. WorldPsychiatry, 7, 148–156.
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001

12 Sönmez et al.
Melle, I., Johannesen, J. O., Friis, S., Hahr, U., Joa, I., Larsen, T. K., …McGlashan, T. (2006). Early detection of the first episode ofschizophrenia and suicidal behavior. British Journal of Psychiatry,163(5), 800–804.
Morrison, A. P. (1998). A cognitive analysis of the maintenance ofauditory hallucinations: Are voices to schizophrenia what bodilysensations are to panic? Behavioural and Cognitive Psychotherapy, 26,289–302.
Morrison, A. P. (2001). The interpretation of intrusions in psychosis:An integrative cognitive approach to hallucinations and delusions.Behavioural and Cognitive Psychotherapy, 29, 257–276.
Morrison, A. P. (2009a). A cognitive behavioural perspective on therelationship between childhood trauma andpsychosis. Epidemiologia ePsichiatria Sociale, 18, 294–298.
Morrison, A. P. (2009b). Cognitive behaviour therapy for first episodepsychosis: Good for nothing or fit for purpose? Psychosis, 1(2),103–112.
National Institute forHealth andClinical Excellence. (2009). Schizophrenia.Core interventions in the treatment and management of schizophrenia inprimary and secondary care (update). National Clinical Practice GuidelineNumber 82. London: Author.
Pallanti, S., Quercioli, L., & Hollander, E. (2004). Social anxiety inoutpatients with schizophrenia: A relevant cause of disability.American Journal of Psychiatry, 161, 53–58.
Pedersen, G., Hagtvet, K. A., & Karterud, S. (2007). Generalizabilitystudies of the Global Assessment of Functioning-Split version.Comprehensive Psychiatry, 48, 88–94.
Power, P. J., Bell, R. J., Mills, R., Herrman-Doig, T., Davern, M., Henry,L., … McGorry, P. D. (2003). Suicide prevention in first episodepsychosis: The development of a randomised controlled trial ofcognitive therapy for acutely suicidal patients with early psychosis.Australian and New Zealand Journal of Psychiatry, 37, 414–420.
Rector, N. A., & Beck, A. T. (2001). Cognitive behavioral therapy forschizophrenia: An empirical review. Journal of Nervous and MentalDisease, 189, 278–287.
Romm, K. L., Melle, I., Thoresen, C., Andreassen, O. A., & Rossberg,J. I. (2012). Severe social anxiety in early psychosis is associatedwith poor premorbid functioning, depression, and reduced qualityof life. Comprehensive Psychiatry, 53(5), 434–440.
Romm, K. L., Rossberg, J. I., Berg, A. O., Barrett, E. A., Faerden, A.,Agartz, I., et al. (2010). Depression and depressive symptoms infirst episode psychosis. Journal of Nervous and Mental Disease, 198,67–71.
Romm, K. L., Rossberg, J. I., Hansen, C. F., Haug, E., Andreassen, O. A.,& Melle, I. (2011). Self-esteem is associated with premorbidadjustment and positive psychotic symptoms in early psychosis.BMC Psychiatry, 11(36), 2–8.
Rosenberg, M. (1989). Society and the adolescent self-image. (Rev. ed.).Middletown, CT: Wesleyan University Press.
Roy, A., Thompson, R., & Kennedy, S. (1983). Depression in chronicschizophrenia. British Journal of Psychiatry, 142, 465–470.
Smith, B., Fowler, D. G., Freeman, D., Bebbington, P., Bashforth, H.,Garety, P., … Kuipers, E. (2006). Emotion and psychosis: Links
Please cite this article as: Sönmez et al., Cognitive Behavior Therapy in FirEsteem, Cognitive and Behavioral Practice (2013), http://dx.doi.org/10.10
between depression, self-esteem, negative schematic beliefs anddelusions and hallucinations. Schizophrenia Research, 86, 181–188.
Tarrier, N. (2005). Cognitive behaviour therapy for schizophrenia: Areview of development, evidence and implementation. Psychotherapyand Psychosomatics, 74, 136–144.
Tarrier, N., Lewis, S., Haddock, G., Bentall, R., Drake, R., Kinderman,P., … Dunn, G. (2004). Cognitive-behavioural therapy in first-episode and early schizophrenia: 18-month follow-up of a rando-mised controlled trial. British Journal of Psychiatry, 184, 231–239.
Tarrier, N., & Wykes, T. (2004). Is there evidence that cognitivebehaviour therapy is an effective treatment for schizophrenia?A cautious or cautionary tale? Behaviour Research and Therapy, 42,1377–1401.
Thorup, A. F., Petersen, L. F., Jeppesen, P. F., Ohlenschlaeger, J. F.,Christensen, T. F., Krarup, G. F., et al. (2005). Integrated treatmentameliorates negative symptoms in first episode psychosis—Resultsfrom the Danish OPUS trial. Schizophrenia Research, 79(1), 95–105.
Trower, P., Birchwood, M., Meaden, A., Byrne, S., Nelson, A., & Ross, K.(2004). Cognitive therapy for command hallucinations: Rando-mised controlled trial. British Journal of Psychiatry, 184, 312–320.
Turkington, D., Dudley, R., Warman, D. M., & Beck, A. T. (2004).Cognitive-behavioral therapy for schizophrenia: A review. Journalof Psychiatric Practice, 10, 5–16.
Verdoux, H., Liraud, F., Gonzales, B., Assens, F., Abalan, F., & van Os, J.(2001). Predictors and outcome characteristics associated withsuicidal behaviour in early psychosis: A two-year follow-up of firstadmitted subjects. Acta Psychiatrica Scandinavica, 103(5),347–354.
Wykes, T., Steel, C., Everitt, B., & Tarrier, N. (2008). Cognitive behaviortherapy for schizophrenia: Effect sizes, clinical models, andmethodological rigor. Schizophrenia Bulletin, 34, 523–537.
Zimmermann, G., Favrod, J., Trieu, V. H., & Pomini, V. (2005). Theeffect of cognitive behavioral treatment on the positive symptomsof schizophrenia spectrum disorders: A meta-analysis. SchizophreniaResearch, 77, 1–9.
Zubin, J., & Spring, B. (1977). Vulnerability: A new view of schizophrenia.Journal of Abnormal Psychology, 86, 103–126.
This study was supported by ExtraStiftelsen Helse og Rehabilitering.The founding source had no further role in the study design, thecollection, analysis and interpretation of data, the writing of the reportor the decision to submit the paper for publication. The authorsdeclare that there are no conflicts of interest.
Address correspondence to Nasrettin Sönmez, Oslo UniversityHospital (TIPS Sor Ost) Centre of Competence for Early Interventionin Psychosis, Fritdjof Nansens vei 12, 0369 Oslo, Norway; e-mail:[email protected].
Received: April 24, 2012Accepted: June 5, 2013Available online xxxx
st-Episode Psychosis With a Focus on Depression, Anxiety, and Self-16/j.cbpra.2013.06.001