Researchers and Clinicians: A Growing Divide or Narrowing Gap

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
Top Lang DisordersVol. 27, No. 1, pp. 37–49Copyright c© 2007 Wolters Kluwer Health | Lippincott Williams & Wilkins
Clinicians as CommunicationPartnersDeveloping a Mediated DiscourseElicitation Protocol
Julie A. Hengst, PhD; Melissa C. Duff, PhD
This article presents the development and piloting of a mediated discourse elicitation protocol.Grounded in situated theories of communication and informed by mediated discourse analysis,this protocol selectively samples familiar discourse types in a manner designed to preserve inter-actional aspects of communication. Critically, the mediated discourse elicitation protocol concep-tualizes the entire session (not just targeted tasks) and both client and clinician talk (not just clientmonologues) as clinical/research data. Using situated discourse analysis techniques, we presenttwo pilot sessions. Surprisingly, in the first session the clinician had difficulty shifting from a clini-cal stance (e.g., offering prompts, directing talk) to a reciprocal conversational stance during targetcommunicative activities (e.g., being an audience to client narratives). Thus, we revised the pro-tocol to better specify the clinician’s dynamic role and conducted a second pilot session withstrikingly different results. Broadly, these findings reveal that complex interactional discourse canbe elicited in clinical settings and that mediated discourse analysis provides rich theoretical andmethodological resources to empower clinicians in examining, accounting for, and flexibly shift-ing their discourse roles in order to better achieve clinical goals. Key words: adult neurogenics,clinical discourse, discourse analysis, discourse elicitation tasks, mediated activity
THE role of the speech–language patholo-gist (SLP) in discourse elicitation proce-
dures is broadly grounded in issues of clini-cal discourse. Researchers (e.g., Leahy, 2004)have identified ways that prevailing clinicaldiscourse practices limit opportunities for,and patterns of, participation for cliniciansand clients alike. In traditional clinical con-texts, the clinician assumes the role of ex-pert or person-in-charge, whereas clients areoffered the role of novice or person-seeking-help. As an expert-in-charge, clinicians as-sume the rights and responsibilities for initi-
From the Department of Speech and Hearing Science,University of Illinois at Urbana-Champaign(Dr Hengst); and the Department of Neurology,Division of Cognitive Neuroscience, University ofIowa College of Medicine, Iowa City (Dr Duff).
Corresponding author: Julie A. Hengst, PhD, Depart-ment of Speech and Hearing Science, University of Illi-nois, 901 S Sixth St, Champaign, IL 61820 (e-mail:[email protected]).
ating, managing, and evaluating the contentand form of client talk. To control the dis-course, clinicians use imperatives, interview-style questions, task prompts, and initiation–response–evaluation routines (Leahy, 2004;Simmons-Mackie & Damico, 1999), which arealso a hallmark of instructional discourse inschools (see Mehan, 1979).
In her study of SLP feedback during ses-sions with aphasic clients, Simmons-Mackie,Damico, and Damico (1999) found thatnegative evaluations were frequently indirect(e.g., asking for a repetition rather thanexplicitly critiquing a response) and thatfeedback was often vague, with its successdependent on the client interpreting it withina clinician–client framework (e.g., cliniciansilence after client utterance indicates inad-equate response and need for client to tryagain). In a study of group sessions withbrain-injured adults, Kovarsky, Kimbarow,and Kastner (1999) reported that SLPs fo-cused attention on clients’ cognitive-linguistic
37

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
38 TOPICS IN LANGUAGE DISORDERS/JANUARY–MARCH 2007
abilities by offering frequent evaluations ofthe form of client productions while minimiz-ing response to content, and by keeping activ-ities focused on therapeutic topics and goals.This growing body of research on clinical dis-course practices of SLPs points to ways thatthese practices in effect suppress the compe-tencies of the client and limit the role of theclinician.
Holland (1998), in a response to Kagen’s(1998) article on supported conversation, ar-gued that clinical training approaches mayactually make it harder for SLPs to carryon meaningful conversations with aphasicadults. Kagen documented that laypeoplewere able to successfully adopt supportedconversation techniques to improve their in-teractions with aphasic adults, whereas SLPsfound such strategies difficult to implement.Holland suggested that the SLPs’ poor perfor-mance could (in part) be accounted for bythe way the field of speech–language pathol-ogy pulls clinicians away from the businessof being effective communicators in conver-sational interactions. Theoretical and method-ological traditions define conversational inter-actions as nontherapeutic, focusing insteadon isolated linguistic units produced by indi-vidual speakers. Thus, clinicians are trained tofocus attention on client talk by adopting animpersonal, distanced stance. Indeed, accord-ing to Holland, the common sentiment amongclinicians seems to be that although conversa-tion with clients may be important for build-ing rapport, it is not an integral part of thera-peutic procedures.
The two main approaches to obtainingdiscourse samples from individuals with neu-rogenic cognitive-linguistic communicationdisorders focus on attenuating the presence ofthe clinician. Traditional linguistic approachesto discourse elicitation (see Cherney,Shadden, & Coelho, 1998) focus on discourseas a multisentence linguistic unit producedby individual speakers. Discourse level tasksare designed to focus on a client’s abilityto organize and produce different typesof discourse (e.g., narrative, descriptive,procedural) under controlled task conditions.
During elicitation, the clinician presents theclient with appropriate prompts (e.g., “tellme everything you see happening in thispicture”) and limits her own contributionsto follow-up prompts (e.g., “Is that all yousee?”).
As an alternative to eliciting controlledclient monologues, researchers and clini-cians interested in interactional dimensionsof discourse (see Damico, Oelschlaeger, &Simmons-Mackie, 1999; Lesser & Perkins,1999) have drawn on conversational analysis(CA) to argue for the importance of record-ing conversations that occur in the course ofeveryday activities to meet the routine needsof the participants. CA approaches argue thatto capture more “natural”samples for analysis,ideally the clinician should not participate inthe conversations. The clinician’s role is lim-ited to identifying communication partnersand situations appropriate for analysis, facili-tating recording, and analyzing the samples.While traditional linguistic approaches seekthe controlled conditions of a clinical settingto isolate client competence, the CA-based ap-proach rejects clinical spaces as artificial. TheCA approach seeks the authenticity of every-day, nonclinical settings in order to capturethe communicative work of coparticipants inan interaction. Yet, each approach in its ownway sees clinician talk as a source of interfer-ence and positions the clinician as an outsiderto, rather than a direct participant in, the dis-course being sampled.
The alternative we take here is mediateddiscourse analysis (Norris & Jones, 2005;Scollon, 2001; Wertsch, 1998). It concep-tualizes discourse within a broader unit ofanalysis—mediated action. It insists on care-ful attention to concrete, situated action andthe cultural resources (whether languages ortools, other people, or long-established andtaught routines) that mediate action. It fo-cuses clinicians’ attention on (1) all partic-ipants (not just speakers) as active collabo-rators in an interaction; (2) all communica-tive resources (not just language) as the rel-evant mediational tools; and (3) goal-directedactivity (not accurate production of discourse

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
Clinicians as Communication Partners 39
forms) as the motives for communicative in-teractions. Mediated discourse analysis as-sumes that we must consider chains of activitythat are longer than the immediate sequencesof a given interaction, including histories ofinteractions between particular people, or inspecific situations, social identities, genres,and so on. Taking a mediated approach to dis-course elicitation shifts attention away fromwho is in charge (e.g., clinician or client) orwhere the interactions take place (e.g., clinic,home). It focuses instead on what activitiesparticipants are engaged in and how media-tional means (e.g., social/communicative his-tories and resources) are being deployed inand around these activities. This perspectiveallows professionals to imagine and begin todescribe alternative clinical stances, includingthat of the clinician as a communication part-ner in the discourse being sampled.
Several years ago we began a line of re-search exploring the interrelationship of lan-guage and memory by studying the discoursepractices of adults with anterograde amne-sia. We were particularly interested in howprofound, isolated memory deficits might im-pact the interactional elements of discourse.Our access to these participants, set by theterms of a broader study, was limited to ses-sions in a clinical-research setting. Therefore,we wanted to structure a protocol that wouldallow us to systematically collect meaning-ful, interactional data in a clinical context. Inthis institutional setting, which by conventionforegrounded clinician-controlled discourse,the challenge we faced was to implementan elicitation protocol that fostered a moresymmetrical communicative relationship be-tween the clinician and the client.
Drawing on theories of communication asmediated action, we designed a mediated dis-course elicitation protocol and piloted it witha woman with amnesia. Reviewing that ses-sion, we concluded that our protocol had un-derspecified key interactional elements of thetarget discourse and that routine clinician dis-course practices were surprisingly resistant tochange.
In this article, we narrate how our initialprotocol was designed theoretically, how the
pilot revealed problems implementing it, howwe revised the protocol to better specify dis-cursive reception roles of the clinician in thetarget activities, and how striking changes inthe discourse were observed during the sec-ond piloting.
DEVELOPING A MEDIATED DISCOURSE
ELICITATION PROTOCOL
The mediated discourse elicitation proto-col was designed to selectively target a rangeof familiar discourse types relevant to explor-ing the interrelationships of language use andmemory impairments, yet to do so in a man-ner sensitive to its interactional complexities.Critically, the mediated discourse elicitationprotocol conceptualized the whole session(as opposed to only the targeted tasks) asthe elicitation protocol. It focused on spe-cific, or targeted, discourse types as conversa-tionally shaped (as opposed to isolated clientmonologues). Research on discourse abilitiesof adult neurogenic populations focuses onfour discourse types (narrative, descriptive,procedural, and conversational) and has sug-gested that cognitive and linguistic demandsvary considerably with discourse type, thenature of discourse tasks, and familiarity ofprompts (see Cherney et al., 1998). Thus, theprotocol targeted multiple samples of thesefour discourse types.
Conversational discourse was elicitedfirst, in part because it was the most open-ended of the discourse types and also to helpestablish the conversational frame critical forthe remainder of the protocol. The goal wasto obtain a 10-min conversation between theclient and clinician covering multiple topicsof mutual interest (e.g., sharing experiences,discussing current events). The protocol didnot specify a set of topics, or interview-stylequestions. Instead, the clinician was to drawon her own repertoire of appropriate topicsfor a casual conversation between acquain-tances, as well as to follow up on topicsoffered by the client.
Narrative discourse was targeted sec-ond using three story-generating prompts(frightening experience, historical event,

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
40 TOPICS IN LANGUAGE DISORDERS/JANUARY–MARCH 2007
personal/family story) designed to elicitpersonal narratives in a conversationalframework. We chose story generationbecause it was assumed to be more demand-ing than tasks in which clients describestory sequences using picture promptsor retell stories from verbal models. Wefocused on personal narratives becausethey were a well-documented commu-nicative practice in everyday talk acrosssocial and professional settings (e.g.,Ochs & Capps, 2001), and thus wouldbe more consistent with everyday discoursepractices.
Descriptive discourse was targeted third us-ing three visual prompts, two that were se-lected for their clinical relevance (cookie thiefdrawing, Norman Rockwell painting) and oneof a salient event (World Trade Center attack).
Procedural discourse was targeted fourthwith three prompts based on daily activi-ties (making a sandwich, grocery shopping,changing a tire). In order to frame the clientas an expert on the requested topic, the clin-ician personalized the prompts (e.g., tell mehow to make your favorite sandwich) and dis-played interest in the client’s expertise (e.g.,taking notes).
Finally, by conceiving of the entire sessionas the protocol, we treated discourse ob-tained throughout the session (between aswell as during target tasks) as data, allowingfor systematic analysis of interactional dis-course elements (e.g., client following/takingconversational lead) and creating opportuni-ties for unplanned target discourse samples(e.g., conversational stories).
Defining discourse as mediated actionmade it critical to specify the clinician’s role inits production. In our initial protocol, we iden-tified two interactional frames—a clinician-directed frame and a reciprocal frame—andcalled for the clinician to shift her com-municative stance, or footing (see Goffman,1981), between these two frames at appro-priate times throughout the session. Duringthe clinician-directed frame, which was usedfor pretask and posttask interactions, the clin-ician was the expert-in-charge managing clini-cal business, providing task instructions and
prompts, and moving the session forward.During the reciprocal frame, which was usedduring targeted discourse tasks and to cre-ate opportunities for spontaneous conversa-tion between tasks, the clinician adopted thestance of communication partner by provid-ing appropriate interactional responses (e.g.,being a good audience for storytelling). Thereciprocal frame called for the clinician to fo-cus on the content of the client’s utterances;to be an active interactional partner (e.g., pro-vide meaningful verbal/nonverbal backchan-nel supports); and to avoid passing judgmenton the quantity, quality, or form of clienttalk. Written out, the mediated discourseelicitation protocol listed the three promptsfor each of the four target discourse typeswith notations reminding the clinician to shifther stance between the two interactionalframes.
PARTICIPANTS
Melissa Duff (second author) served as theclinician-researcher in charge of data collec-tion. At the time, she was a doctoral stu-dent and a licensed SLP with 5 years of ex-perience working in medical settings. Melissawas comfortable working with adults with ac-quired brain injuries and had extensive experi-ence with various formal and informal assess-ment techniques. In addition, she had beenworking for 2 years in the Amnesia ResearchLab, serving as clinical coordinator, handlingscheduling and neuropsychological testing foramnesic participants.
We selected “Susan” (a pseudonym) to pi-lot the mediated discourse elicitation proto-col. Susan was a 54-year-old wife, mother, andretired hairdresser with a 4-year history ofprofound amnesia due to bilateral hippocam-pal damage from an anoxic episode. Formaltesting documented her language and intel-lectual abilities to be within normal limits,while scores on memory tasks indicated thather memory was severely impaired. Susan wasfriendly and outgoing, and had been a regu-lar participant in the Amnesia Research Lab. Itwas, in fact, Susan’s easy conversational man-ner, comfort in this setting, and history with

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
Clinicians as Communication Partners 41
Melissa that made her perfect for piloting theprotocol.
Piloting the protocol---The first session
The first pilot session took place duringone of Susan’s regular visits to the lab. Melissascheduled it for the first hour of Susan’s 4-hrtesting schedule in an attempt to limit the in-fluence of the controlled clinician–client rolesthat were typical of the standardized paper-and-pencil testing and computer experimentsconducted in the lab. On this day, Susan wasin good spirits. As was typical, Melissa rein-troduced herself (Susan does not explicitly re-member Melissa from session to session) andreviewed the day’s schedule with Susan.
If viewed as a traditional discourse elici-tation task focusing on client performancein isolation from the broader communica-tive context, the results of this first ses-sion would have certainly been successful—Melissa moved the session through all targettasks, Susan responded to all prompts, andthe 19-min session yielded clean data withroughly equal amounts of time devoted toeach of the four discourse types. However,as an initial attempt to implement the medi-ated discourse elicitation protocol, the ses-sion was disappointing. Melissa reported thatthroughout the session she was conflicted asto what she, as the clinician, was allowedto say. Consequently, she felt she had reliedon the clinician-directed frame and had notadopted the role of communication partnerfor the target discourse. She felt that her at-tempts at small talk were too scripted (e.g.,she limited herself to predetermined topics)and could not recall following up on topics in-troduced by Susan. In effect, her interactionswith Susan felt stiff and Susan’s discourse onthe target tasks seemed flat and disengaged—a pattern not representative of interactionsMelissa had witnessed with Susan on other oc-casions, even earlier that day.
Reviewing the tape, we identified severalways that Melissa had maintained an authori-tative (though friendly) clinical stance duringthe session. Melissa minimized her own con-tributions while maximizing opportunities for
Susan to make comments, express opinions,and tell stories. Melissa directed Susan to talk,introducing topics and tasks almost exclu-sively with imperatives (e.g., “tell me aboutyour wedding day”)or questions (“Do you gar-den or anything?”).Even during the target con-versation, Melissa maintained control of thediscourse by providing topics for Susan to talkabout, while offering few opinions, stories, orcomments of her own. In fact, Melissa intro-duced all 10 of the topics and did so by askingSusan questions (“Wow, so what do you thinkof the weather we’ve been having?”).
Throughout the session, Melissa’s feedback,particularly at the end of tasks, was usuallybrief and carried a general evaluation ofSusan’s production or compliance (e.g.,“okay”; “that was a fine story”). Very littleinteraction occurred between target tasks,and Susan made almost no offers of topicsoutside of the ones introduced by Melissa.
In addition, there was evidence that Su-san aligned to the role of client or researchsubject—she demonstrated little conversa-tional initiative, generally waiting to be di-rected to talk and limiting herself to topics in-troduced by Melissa. She also focused on theadequacy of her responses, commenting onher memory deficits (“I don’t remember anyof that”),and seeking reassurance that she wasperforming the tasks adequately (“Did I messthat one up?”).Melissa interpreted these com-ments to indicate that Susan, in the absence ofother explanations, was construing the targetdiscourse tasks as activities designed to assessher memory impairment.
The impact of Melissa’s clinical stanceon the discourse samples obtained can beseen nicely in the narrative discourse. Thenarrative discourse task, including all threeprompts, was 46 turns long. Melissa’s instruc-tions to Susan were minimal (“Now I’m go-ing to have you just . . .tell me some stories”)and did little to motivate the task, to indicatehow the task was related to research or clin-ical goals, or to clarify what aspects of sto-rytelling (e.g., accuracy, performance) wereimportant here. The excerpt presented inExample 1 begins four turns into the narrative

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
42 TOPICS IN LANGUAGE DISORDERS/JANUARY–MARCH 2007
discourse tasks, immediately after Melissa hasgiven the first story prompt—“Can you tell methe most frightening experience. . .that you’vehad in your life?”
Example 1: Excerpt from response to fright-ening story prompt in session one. (see Ap-pendix for Transcription Key):
4 S: hm. . . . . . . . . .10. . . . . . . . . . the only thingthat comes to mind is going on this sillyroller coaster and [shakes head “no”] and Icouldn’t hardly get out [laughs]
5 M: Well tell me about that.
6 S: It was just so scary that..2.. myknees just buckled when I tried toget out of it in the car [laughs] when itwas over with,..2.. that’s about it, I neverhad any major . . . .4. . . . burglars or robbersor anything like that. [shakes head “no”]
7 M: Well tell me more about this rollercoaster.
8 S: Just . . . ..5. . . .. I’m sacred of heights. . . 3. . . and (uh) . . . 3. . . that was probably mybig thing, going through loops and every-thing, it was a great huge big roller coaster,the scariest thing ever happen in my life isthis..2..this problem [laughs & nods head“yes”]
9 M: What problem is that?
10 S: No memory [shakes head “no”]
11 M: No memory.
12 S: No memory, . . . 3. . . yeah, . . . 3. . . like. . . being stranded somewhere and..2.. nothaving a clue how to get home or..2.. re-membering telephone [shakes head “no”]numbers or, . . .you know . . . . . . 6. . . . . .
13 M: So these things have happened . . . toyou or you’re afraid they’re going to.
14 S: No::::, I’m- I’ve- [nods head “yes”then shakes head “no”] my family’s beenwonderful.
15 M: Mhm
16 S: They . . . don’t want me out their sight[laughs and shakes head “no”]. They havejust absolutely been wonderful, . . . but I’malways scared that it’s going to happen youknow? Ronald caught me one time, . . . I juststood where I was supposed to stay and wait
for him you know and he was late, and whenhe came up I had a little tear in my eye and hefelt so bad [laughs] yeah, but I know if I juststood there he would be there you know?
In the turns that follow, Susan rules out po-tentially frightening experiences such as bur-glaries or robberies (turn 6) and offers de-scriptions of two possible stories that couldbe considered frightening. The first story(turns 4–8) is about how she was scared dur-ing a roller coaster ride, and the second story(turns 8–16) was about fears related to heramnesia and one particular time when shewas left waiting. Melissa did not follow up onthe details of these narratives or respond totheir emotional tones. That is, she did not dis-play the kind of active listenership expectedfrom a conversational partner truly interestedin the story being told. Instead, Melissa main-tained a clinical stance (turns 5, 7, 9, 11,13), instructing Susan to say more and clari-fying story topics. For her part, Susan neverbroke into a full-bodied performance of ei-ther story by setting the scene, narrating a de-tailed sequence of events, or using engagingstorytelling elements (e.g., changing speakingprosody, including gestures, using reportedspeech).
REFINING THE MEDIATED DISCOURSE
SAMPLING PROTOCOL---TARGETING
MULTIPLE FRAMES
Because we had expected that our proto-col would be relatively easy to administer, wewere both quite surprised by this initial out-come. Melissa was an experienced clinicianhighly familiar with this population and was askilled communicator. In addition, Susan, de-spite her amnesia, was outgoing and capableof participating in conversations, and she andMelissa had engaged in many conversationsprior to this session. So, what went wrong?Why was it so difficult for both Melissa andSusan to draw on and display their conversa-tional skills within this clinical context?
As a communication partner outside ofthe clinical context, Melissa would have felt

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
Clinicians as Communication Partners 43
free to share her own stories, offer her ownopinions, and generally comment on and re-spond to what Susan had said. However, inthe clinical context, where the focus wason getting a sample of Susan’s discourse,Melissa’s history with controlled clinical tasksand well-established clinical discourse prac-tices worked to limit her participation, as shekept her opinions to herself and her speak-ing turns brief. Consequently, Susan took upa stance consistent with the traditional clientrole in a typical clinical setting. Collabora-tively their patterns of interaction through-out the session worked against their function-ing as more reciprocal communication part-ners. Clearly, the interactional components ofour original protocol, which primarily statedwhen the clinician should shift her stancebetween the reciprocal and clinician-directedframes, were insufficient to guide moment-by-moment clinical decisions.
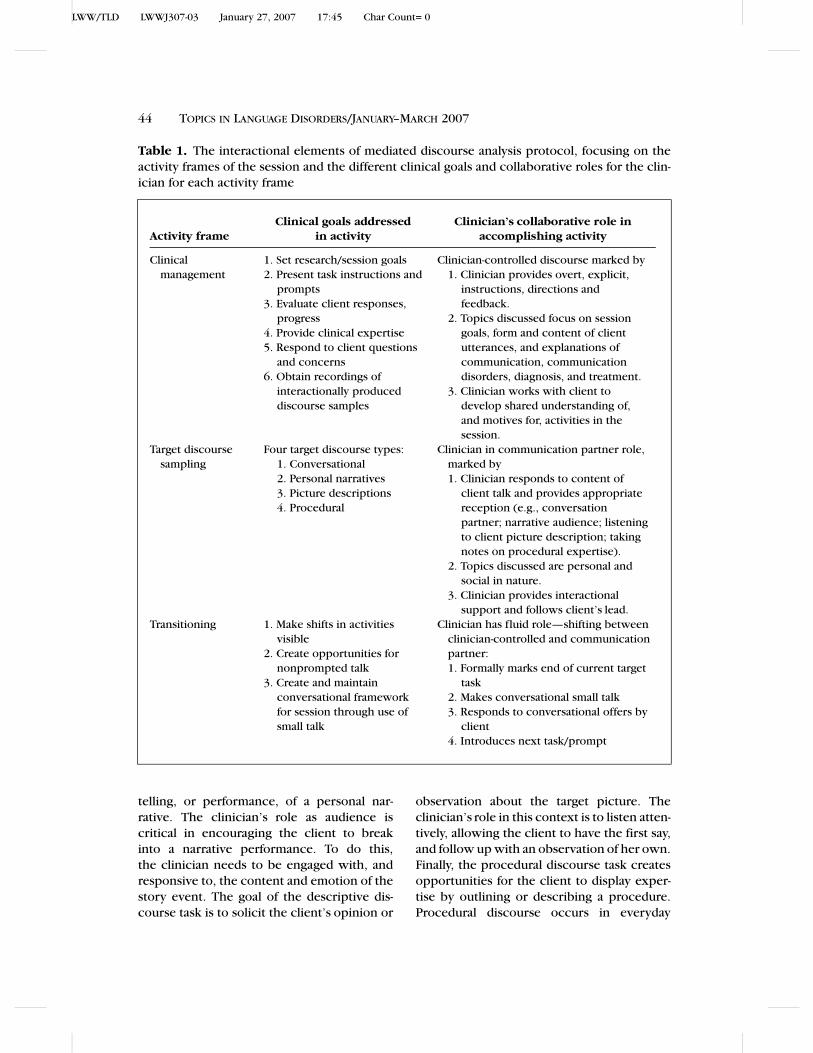
To better specify the clinician’s dynamicrole in the elicitation process, we revised theprotocol to focus on goal-directed activitiesinstead of the two interactional frames. Ouraim was to allow the clinician to make inter-actional choices at any point throughout thesession by asking herself: What is the currentactivity? What clinical goals does this activ-ity address? How should I collaborate withthe client to accomplish this activity? Table 1lists the three goal-directed activities (clinicalmanagement, target discourse sampling, andtransitioning) and the clinical goals and col-laborative role of the clinician during each ofthese three activities.
The first activity is clinical management.This acknowledges that the clinician carries aprofessional responsibility to display and useher position of authority in ways that serveclinical, institutional, and research goals. Inthis position, the clinician is expected to takecharge of the overall session and provideexpert judgments. However, unlike the oftenassumed, vague, and indirect ways of display-ing clinical control and expertise that havebeen documented in traditional clinical prac-tices (see literature review), the mediateddiscourse elicitation protocol calls for overt
and direct clinical discourse practices. Inthis way, the clinician is expected to clearlydisplay, through verbal and nonverbal means,when she is exercising her control of the ses-sion and fulfilling her role of communicationexpert. Specifically, this includes explicitlystating, establishing, and negotiating clinicalgoals; clearly explaining, motivating, present-ing, and managing materials for target tasks;openly taking responsibility for institutionalmanagement issues; and providing direct andspecific evaluations of client’s performanceas needed.
The purpose of adopting overt clinical dis-course practices here is twofold. First, logis-tically, a clear display of a managerial stanceallows both parties to more easily differenti-ate clinical management activities from othersession activities (see below). Second, instru-mentally, an overt and direct explanation ofclinical (or research) goals provides an oppor-tunity to motivate the tasks. During our evalu-ation of the first protocol session, it appearedthat Susan misinterpreted the discourse tasksas memory assessments, and thus workedto shape her narratives as memory displays(e.g., recalling story details) instead of as con-versational stories. Overt discussion of clin-ical goals should keep the client from hav-ing to guess about task motivations and fa-cilitate client and clinician collaboration. Fi-nally, such an explicit focus reflects the em-phasis in theories of mediated action on thecentrality of motives and goals to all situatedactivity.
The second activity, target discourse sam-pling, focuses on obtaining conversationallyproduced discourse samples. In this activity,the clinician adopts an important supportingrole within the target discourse by serving asan appropriate communicative partner. Thegoal of the conversational task is to obtain a10-min reciprocal conversational exchange.By focusing on swapping stories and opinions,as is typical of causal conversation, the clini-cian’s role includes making conversational of-fers and responding conversationally to offersmade by the client. The goal of the narrativediscourse task is to obtain a conversational
LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
44 TOPICS IN LANGUAGE DISORDERS/JANUARY–MARCH 2007
Table 1. The interactional elements of mediated discourse analysis protocol, focusing on theactivity frames of the session and the different clinical goals and collaborative roles for the clin-ician for each activity frame
Clinical goals addressed Clinician’s collaborative role in
Activity frame in activity accomplishing activity
Clinical
management
1. Set research/session goals
2. Present task instructions and
prompts
3. Evaluate client responses,
progress
4. Provide clinical expertise
5. Respond to client questions
and concerns
6. Obtain recordings of
interactionally produced
discourse samples
Clinician-controlled discourse marked by
1. Clinician provides overt, explicit,
instructions, directions and
feedback.
2. Topics discussed focus on session
goals, form and content of client
utterances, and explanations of
communication, communication
disorders, diagnosis, and treatment.
3. Clinician works with client to
develop shared understanding of,
and motives for, activities in the
session.
Target discourse
sampling
Four target discourse types:
1. Conversational
2. Personal narratives
3. Picture descriptions
4. Procedural
Clinician in communication partner role,
marked by
1. Clinician responds to content of
client talk and provides appropriate
reception (e.g., conversation
partner; narrative audience; listening
to client picture description; taking
notes on procedural expertise).
2. Topics discussed are personal and
social in nature.
3. Clinician provides interactional
support and follows client’s lead.
Transitioning 1. Make shifts in activities
visible
2. Create opportunities for
nonprompted talk
3. Create and maintain
conversational framework
for session through use of
small talk
Clinician has fluid role—shifting between
clinician-controlled and communication
partner:
1. Formally marks end of current target
task
2. Makes conversational small talk
3. Responds to conversational offers by
client
4. Introduces next task/prompt
telling, or performance, of a personal nar-rative. The clinician’s role as audience iscritical in encouraging the client to breakinto a narrative performance. To do this,the clinician needs to be engaged with, andresponsive to, the content and emotion of thestory event. The goal of the descriptive dis-course task is to solicit the client’s opinion or
observation about the target picture. Theclinician’s role in this context is to listen atten-tively, allowing the client to have the first say,and follow up with an observation of her own.Finally, the procedural discourse task createsopportunities for the client to display exper-tise by outlining or describing a procedure.Procedural discourse occurs in everyday

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
Clinicians as Communication Partners 45
conversational settings, such as getting arecipe from a friend or explaining how to usea new piece of equipment. Speakers oftenrecite the procedure in a manner that allowsthe listener to accomplish, or write, the steps,and listeners often seek confirmation of theprocedure by restating the steps. Thus, theclinician’s collaborative role in the protocolincludes writing down the procedures pre-sented by the client and reading them backto the client for confirmation.
The third activity, transitioning, highlightsthe importance of attending to the workof, and opportunities for, shifting activitiesthroughout the session. During transitioning,the clinician overtly marks the shift in activi-ties both verbally (e.g., “okay, now we needto move on to the next task”) and nonver-bally (e.g., picking up a clipboard, chang-ing posture). Opportunities for unplanned in-teractions are created by initiating conversa-tional small talk and following the client’s con-versational leads. Transitioning is not limitedto the moments between targeted tasks, butmay be initiated by the client (or clinician)at any time during the session. For example,in the first session when Susan commentedon her poor memory or the adequacy of herresponses to task prompts (“I don’t know ifI’m doing this right”),Melissa could have iden-tified such utterances as transitioning activ-ity by ratifying the shift to clinical manage-ment and overtly restating the goals of thetask (e.g., “Remember this is not a memorytest”).
Piloting the protocol---The second
session
Working with an amnesic client providedan opportunity to conduct the second pilotsession with minimal concern for how learn-ing might impact the results. The second ses-sion occurred approximately 10 months afterthe initial one. As in the first session, Susanwas in good spirits and Melissa (re)introducedherself and reviewed the schedule, which be-gan with the revised protocol. The pilot ses-sion that followed, however, was quite differ-ent from the first one.
During the second session, which lasted45 min, Susan and Melissa produced morethan double the turns and words than theydid the first session, and talk time (esti-mated by total number of words produced)was more evenly distributed between them.Indeed, during the first session, in whichMelissa worked to limit her talk time, Susanproduced twice as many words as Melissa(1432 and 730, respectively). In the secondsession, however, Melissa actually producedmore words (3315) than did Susan (2602).Melissa’s increased talk time included morediscussion of research and task goals as wellas more side conversations during which bothMelissa and Susan made comments and of-fered stories.
Compared to the first session, Melissa feltthat their interactions throughout this sec-ond session had “loosened up.” The sessionflowed easily from task-to-task and topic-to-topic. At various times both Melissa and Su-san took the conversational lead. As the con-versational partner in the target discourse,Melissa confidently took on diverse interac-tional roles. Overall, Melissa reported thattheir interactions during this second sessionwere more consistent with Susan’s conver-sational engagement outside of the clinicroom.
In reviewing the videotape, there was clearevidence that Melissa shifted her stance to ac-complish target activities. As the clinician incharge, Melissa took on a directive and openstance, clarifying what she was, and was not,looking for (e.g., “There are no wrong an-swers here, all I am interested in . . . is tosee how you communicate”).Melissa returnedto this overt directive stance at the begin-ning and end of each target task, resumingher role as session manager, moving them for-ward through the protocol, and clarifying thegoals of the various tasks. The length and con-tent of Melissa’s turns varied across activities.Within the conversational task, Melissa usedher own comments, opinions, and stories toshape the discourse into a back-and-forth, orswapping, pattern. She introduced topics bysharing her own experiences (e.g., “My dad

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
46 TOPICS IN LANGUAGE DISORDERS/JANUARY–MARCH 2007
uhm.1. he had a truck, he didn’t have to go. . . you know cross-country, he pretty muchstayed in the Midwest”),by reintroducing pasttopics (e.g., “one of these past times whenyou were in you told me that you used to workin a . . . salon”),and by following up on emerg-ing topics. Susan’s talk was also more varied.She responded to topics Melissa raised, initi-ated topics of her own, and made fewer com-ments about her memory impairment or theaccuracy of her responses. On the few occa-sions when Susan did mention her memorydeficit, Melissa shifted to a clinical frame toovertly restate the research goals.
The difference in these two sessions is dis-played nicely in the narrative samples. Thistime Susan and Melissa devoted more thanfour times as many turns (199 turns) to thenarrative discourse tasks than in the first ses-sion (46 turns). In addition, Melissa clarifiedthe task goals by telling Susan that she wantedto hear her tell stories, not test her mem-ory. She focused Susan’s attention on whatit meant to be a good storyteller by ask-ing her who the good storytellers were inher family. Example 2 begins with Susan’sturn right after Melissa had given the fright-ening story prompt: “the first story I wantyou to tell me is about your most frighteningexperience.”
Example 2: Response to frightening storyprompt in session two (see Transcription Keyin Appendix 1).
14 S: Frightening experience . . . 3 . . . fright-ening experience . . . 3. . . have I had one
of those. . . .4. . . . okay..2..it was no- not too
frightening, but uhm, I was working at the
beauty shop..2..
15 M: Mhm
16 S: a:::nd everybody had gone to leave and
there was about nine of us . . . that worked in
there
17 M: Mhm
18 S: and everybody had gone and I was
there with keys to close up and I was work-
ing on my last customer
19 M: Uhm
20 S: and it was like . . . nine o‘c lock atnight, . . . a::nd there was a door at bothends . . . [gestures as if pointing at doors] ofthe shop, that went straight through [moveshands side to side] the shop again, a::ndwhen I look up . . . and there was a manstanding there and the door was locked youand it was like..2.. “Can I help you?” youknow
21M: Oh my gosh!
22 S: It was like “Ohhh! Gosh what is this!”. . . and we had already had the cash dooropen a::nd . . . [moves hand as if openingdrawer] yeah
23 M: Mhm
24 S: everything opened and you could seethere was no money
25 M: Right
26 S: You could see that from the outsideeven but uh..2.. he’s standing there and he’she’s really nervous you could tell he wasshaking and and I was . . . a little alarmed andmy customer was very alarmed you knowand . . .
27 M: Oh well, at least there was someoneelse there.
28 S: Yeah [nods head “yes”]
29 M: For a minute I was thinking it was justyou.
30 S: Yeah, but she was like a hundred yearsold so [laughs::::::::::]
31 M: [laughs] So she was useless to you?
32 S: Yes, mh [nods head “yes”] and fi-nally I ge- I- you know . . . “Can I help you?”. . .Uhm, . . . very nervously he says “Yeah Ineed uh change for the vending machine.”I said “Okay [nods head “yes”] I can do thatyou know” I said “that’s all I got is change.”
33 M: Mhm
34 S: I said “I don’t have any bills you know.”So I- I gave it to him and..2.. and I let himout cause I had to unlock the door youknow and uh . . . 3. . . my customer immedi-ately got up and called her husband and toldhim what happened you know . . . he camestraight down . . .with his handgun [laughs]
35 M: Oh wow!

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
Clinicians as Communication Partners 47
Throughout the 37 turns of this story-telling, Melissa displayed her engagement inSusan’s emerging conversational narrative.While Susan settled on a frightening storyto tell, presented a description of the scene,and set up the story events to follow (turns14, 16, 18), Melissa provided backchannel re-sponses to signal her involvement in the un-folding narrative (turns 15, 17, 19). In turn 20,Susan presented the initial frightening event(“a man standing there”), and dramatized thetelling with use of gestures (pointing to imag-inary doors, moving hands side to side) anddirect reported speech (“‘Can I help you?”’).In turn 21, Melissa’s response (“Oh my gosh!”)marked her continued affective involvementin the story. Susan highlighted Melissa’s re-sponse by recasting it as her own responsewithin the story to the stranger’s sudden ap-pearance: “Ohhh! Gosh what is this!” For theremainder of the storytelling, Melissa contin-ued to respond to the narrative by reflectingstory emotions and clarifying story details. Atthe end, she not only agreed that it was ascary story but even offered a more dramaticsetting for the tale (“I picture it being a darknight”).Throughout the telling, Susan capital-ized on Melissa’s affective audience displaysof involvement to construct a successful, dra-matic narrative.
CONCLUSIONS---THEORETICAL AND
CLINICAL IMPLICATIONS
We have presented this account of our de-velopment of a mediated discourse analysisprotocol because we found the process ofworking through it quite striking. It was strik-ing to both of us that the initial protocol—although theoretically grounded, explicitlytalked through and written up, implementedby an experienced clinician-researcher, andpiloted with a client who had good commu-nication skills—had failed to achieve its goals.It was striking, too, that the revised protocol,grounded in an analysis of what went wrongand why, took such a different approach fromthe first. Finally, it was striking how quantita-tively and qualitatively different the discourse
produced in the second session was from thatof the first session. In short, we found thatthis process of protocol development and pi-loting clarified for us both the challenges andthe means of enacting a mediated discourseapproach in a clinical setting.
When discussing these findings with oth-ers, we are often met with the response thatsome clinicians are simply better communica-tors than others. The implication seems to bethat effective communication in clinical set-tings is a mystery, perhaps a natural gift forsome, but in any case beyond serious analysisor instruction. For a field constituted on thepremise of clinical intervention to improvelinguistic and communicative abilities, such aview is decidedly odd.
We suspect, in addition to prevailing clin-ical training practices suggested by Holland(1998), that it is precisely the asymmetricalpower relations, the ideology of authority (seeKovarsky et al., 1999), that has kept cliniciandiscourse outside the circle of analysis and in-tervention. Even conversational analysts, whohave detailed and critiqued the effects ofthe traditional forms in clinical settings, seemto have accepted their manifestations as in-evitable (hence the need to collect samplesoutside of any clinical influence). As we pre-sented here, although we found the combinedweight of dominant theories of language as in-dividual competence, of ideologies of profes-sional expertise and authority, and of historiesof socialization into clinical practices to bestronger than anticipated, we also found themamenable to our interventions. In short, in themicrocosm of this story, we see dynamics andforces we believe to be widely present in ourfield.
Broadly, these results reveal that SLPs’ ex-pertise in communicative analysis can effec-tively be applied to reshaping clinical prac-tices. Discourse elicitation procedures shouldaim to sample monitor, and sustain specifictypes of interaction and goal-directed dis-course. Such procedures call on cliniciansto reject the conventional wisdom that sam-pling procedures should be simplified andclinician “interference” should be minimized.

LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
48 TOPICS IN LANGUAGE DISORDERS/JANUARY–MARCH 2007
Clinicians cannot rely on the assumption ei-ther that a task prompt will simply producethe desired discourse type or that collectingdiscourse samples at home or in communitysettings will guarantee a more meaningful orcollaborative interaction. This analysis (alongwith our experience using the revised proto-col in more than 40 sessions) makes it clearthat complex interactional discourse can beelicited between clinicians and clients in clini-cal settings. Finally, this experience reinforcesour perception that theories of mediated ac-tion and mediated discourse analysis offer rich
resources for reconceptualizing communica-tion as situated, sociocultural practice. Thisreconceptualization focuses on how activitiesare shifted, sustained, and juggled; on howcommunication is collaboratively supportednot only by co-present participants but alsoby histories of use; and on how personaland social motives and goals infuse and ani-mate communicative activity. This new focusstrikes us as productive grounds for empower-ing clinicians to reimagine their roles in clin-ical contexts and to flexibly wield their dis-course to achieve clinical goals.
REFERENCES
Cherney, L. R., Shadden, B. B., & Coelho, C. A. (Eds.).
(1998). Analyzing discourse in communicatively im-paired adults. Gaithersburg, MD: Aspen.
Damico, J. S., Oelschlaeger, M., & Simmons-Mackie, N.
(1999). Qualitative methods in aphasia research: Con-
versational analysis. Aphasiology, 13(9–11), 667–679.
Goffman, E. (1981). Forms of talk. Philadelphia: Univer-
sity of Pennsylvania Press.
Holland, A. L. (1998). Why can’t clinicians talk to aphasic
adults? Aphasiology, 12, 844–847.
Kagen, A. (1998). Supported conversation for adults with
aphasia: Methods and resources for training conversa-
tional partners. Aphasiology, 12, 816–830.
Kovarsky, D., Kimbarow, M., & Kastner. (1999). The con-
struction of incompetence during group treatment
with traumatically brain injured adults. In D. Ko-
varsky, J. F. Duchan, & M. Maxwell (Eds.), Construct-ing (in)competence: Disabling evaluations in clini-cal and social interaction (pp. 291–311). Mahwah,
NJ: Erlbaum.
Leahy, M. M. (2004). Therapy talk: Analyzing therapeutic
discourse. Language, Speech, and Hearing Servicesin Schools, 35(1), 70–81.
Lesser, R., & Perkins, L. (1999). Cognitive neuropsychol-
ogy and conversation analysis in aphasia: An intro-ductory casebook. London: Whurr Publishers.
Mehan, H. (1979). Learning lessons. Cambridge, MA: Har-
vard University Press.
Norris, S., & Jones, R. H. (Eds.). (2005). Discourse in ac-tion: Introducing mediated discourse analysis. Lon-
don, UK: Routledge.
Ochs, E., & Capps, L. (2001). Living narrative: Creatinglives in everyday storytelling. Cambrige, MA: Harvard
University Press.
Scollon, R. (2001). Mediated discourse [The nexus ofpractice]. London, UK: Routledge.
Simmons-Mackie, N., & Damico, J. (1999). Social role ne-
gotiation in aphasia therapy: Competence, incompe-
tence, and conflict. In D. Kovarsky, J. F. Duchan, & M.
Maxwell (Eds.), Constructing (in)competence: Dis-abling evaluations in clinical and social interaction(pp. 313–342). Mahwah, NJ: Erlbaum.
Simmons-Mackie, N., Damico, J. S., & Damico, H. L.
(1999). A qualitative study of feedback in aphasia treat-
ment. American Journal of Speech-Language Pathol-ogy, 8(3), 218–230.
Wertsch, J. V. (1998). Mind as action. New York, NY: Ox-
ford University Press.
LWW/TLD LWWJ307-03 January 27, 2007 17:45 Char Count= 0
Clinicians as Communication Partners 49
Appendix
Transcription Key
Symbol Meaning
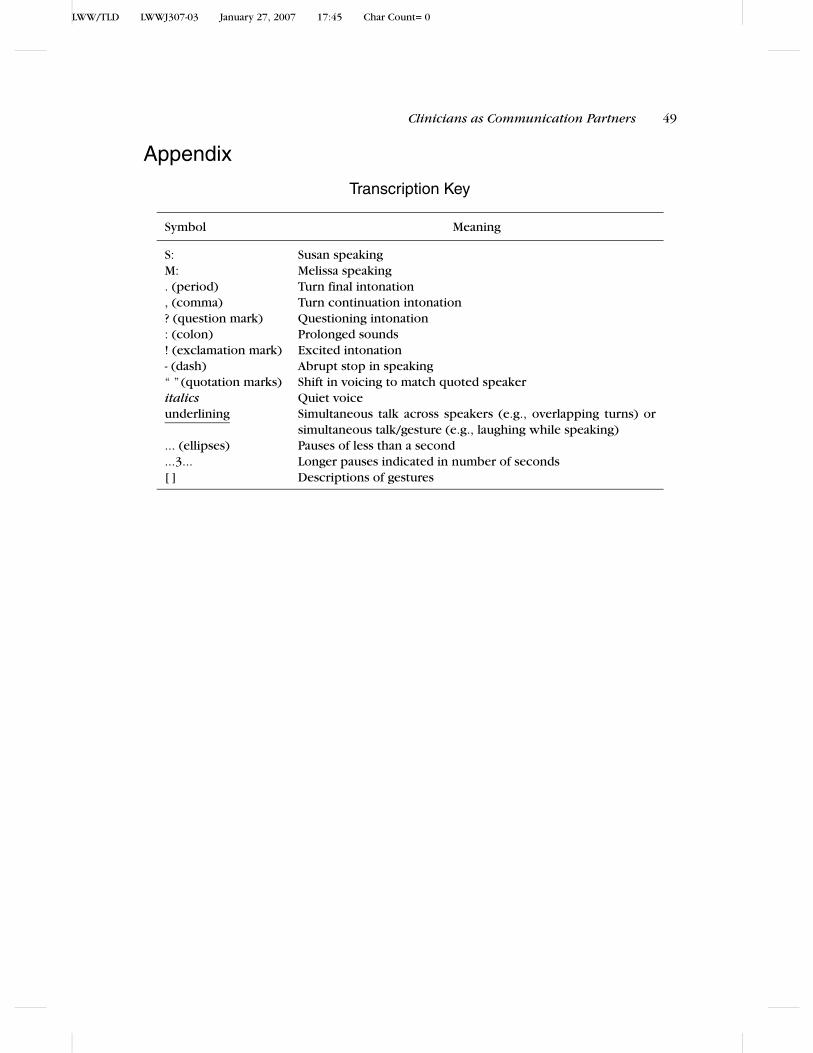
S: Susan speakingM: Melissa speaking. (period) Turn final intonation, (comma) Turn continuation intonation? (question mark) Questioning intonation: (colon) Prolonged sounds! (exclamation mark) Excited intonation- (dash) Abrupt stop in speaking“ ” (quotation marks) Shift in voicing to match quoted speakeritalics Quiet voiceunderlining Simultaneous talk across speakers (e.g., overlapping turns) or
simultaneous talk/gesture (e.g., laughing while speaking)... (ellipses) Pauses of less than a second...3... Longer pauses indicated in number of seconds[ ] Descriptions of gestures
Copyright © 2022 FDOKUMEN