Clinical significance of worsening portal hypertension during long-term medical treatment in...
9
Clinical significance of worsening portal hypertension during long-term medical treatment in patients with cirrhosis who had been classified as early good-responders on haemodynamic criteria Carlo Merkel 1, * , Massimo Bolognesi 1 , Annalisa Berzigotti 2 , Piero Amodio 1 , Lucia Cavasin 1 , Ilaria Maria Casarotto 1 , Marco Zoli 2 , Angelo Gatta 1 1 Department of Clinical and Experimental Medicine, University of Padua, Italy; 2 Department of Internal Medicine, Ageing and Nephrology, University of Bologna, Italy Background & Aims: It is established that cirrhotic patients who respond to beta-blockers by lowering their hepatic venous pres- sure gradient (HVPG) to 612 mmHg or by P20% of the baseline values are protected from bleeding. However, it is not known whether the effect remains unchanged over the treatment period. Methods: A group of 24 patients with cirrhosis and oesophageal varices, treated with beta-blockers ± nitrates, good-responders on haemodynamic criteria, were followed for up to 76 months with sequential HVPG measurements. Another group of 16 patients was used for validation. Results: HVPG worsened in 10 of the 24 patients during follow- up. Changes in HVPG correlated to concomitant changes in liver function parameters. Variceal bleeding occurred in four of the 10 patients whose HVPG had worsened (bleed; 3–21 months after the measured increase in HVPG) and in none of those with stable HVPG (p = 0.02). Patients with increased HVPG also had shorter survival (p = 0.05). Worsening of HVPG was an indepen- dent predictor of death, additive to Child-Pugh or MELD scores, in a time-dependent Cox’s regression analysis. This relationship was confirmed in the validation group. Conclusions: Worsening HVPG during follow-up in patients who had initially been good-responders to medical treatment is related to worsening in hepatic function. The maintenance of a good haemodynamic response to medical treatment of portal hypertension is an excellent predictor of outcome in these patients. Ó 2009 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. Introduction Beta-blockers reduce the likelihood of a first variceal bleed in patients with cirrhosis and oesophageal varices ‘at risk’ [1] and they represent the currently recommended first line treatment for the primary prophylaxis in these patients [2,3]. The associa- tion of beta-blockers and long-acting nitrates is useful in prevent- ing variceal re-bleeding [2], while the available evidence for its use in primary prophylaxis is conflicting [4–6]. The response to 1–3 months of treatment with beta-blockers allows discrimination of patients who will be protected from bleeding in the long term [7–9] from those who will not. Indeed, it has been observed that patients whose hepatic venous pres- sure gradient (HVPG) decreases to 12 mmHg or less, or who exhibit a decrease in HVPG P 20% of the baseline values, are protected from bleeding (good-responders), while nearly all bleeds occur in those patients who do not meet these haemody- namic criteria. It is generally assumed that medical prophylaxis of variceal bleeding should be kept indefinitely, despite no clear evidence that treatment discontinuation is actually dangerous. The only clues that this might be the case are the following: (i) withdrawal of treatment was followed by the restoration of baseline risk of bleeding [10] in one clinical trial; (ii) amongst patients on long- term treatment classified as good-responders at 3 months, vari- ceal bleeding during further follow-up only occurred in those who were withdrawn from treatment for any reason in one study [8]. It has also been suggested that long-term treatment with beta-blockers may lead to tachyphylaxis, i.e. a decrease in phar- macological activity due to a re-adjustment of the vascular homeostatic mechanisms which had been perturbed by treat- ment [11]. A detailed analysis of these complex relationships is difficult because the long-term effect of treatment is interconnected with the natural history of the disease, which is characterized by a more or less progressive worsening in hepatic function and portal hypertension. Thus it is hard to discriminate between the loss of pharmacological activity and the spontaneous progression of the underlying disease. To date, the clinical significance of the time-course of the response to treatment of portal hypertension, as assessed by Journal of Hepatology 2010 vol. 52 j 45–53 Keywords: Hepatic venous pressure gradient; Beta-blockers; Nitrates; Indocya- nine green; Child-Pugh score; MELD score; Variceal bleeding. Received 12 January 2009; received in revised form 23 July 2009; accepted 30 July 2009; available online 23 October 2009 * Corresponding author. Address: Dipartimento di Medicina Clinica e Sperimen- tale, Università di Padova, via Giustiniani, 2, 35126 Padova, Italy. Tel.: +39 049 821 2282; fax: +39 049 875 4179. E-mail address: [email protected] (C. Merkel). Abbreviations: HVPG, Hepatic venous pressure gradient; ICG-IHC, Indocyanine g- reen intrinsic hepatic clearance; CP, Child-Pugh; MELD, Model for end-stage liver disease. Research Article
Transcript of Clinical significance of worsening portal hypertension during long-term medical treatment in...

Research Article
Clinical significance of worsening portal hypertension duringlong-term medical treatment in patients with cirrhosis who had
been classified as early good-responders on haemodynamic criteria
Carlo Merkel1,*, Massimo Bolognesi1, Annalisa Berzigotti2, Piero Amodio1, Lucia Cavasin1,Ilaria Maria Casarotto1, Marco Zoli2, Angelo Gatta1
1Department of Clinical and Experimental Medicine, University of Padua, Italy; 2Department of Internal Medicine, Ageing and Nephrology,University of Bologna, Italy
Background & Aims: It is established that cirrhotic patients who Introduction
respond to beta-blockers by lowering their hepatic venous pres-sure gradient (HVPG) to 612 mmHg or by P20% of the baselinevalues are protected from bleeding. However, it is not knownwhether the effect remains unchanged over the treatment period.Methods: A group of 24 patients with cirrhosis and oesophagealvarices, treated with beta-blockers ± nitrates, good-responderson haemodynamic criteria, were followed for up to 76 monthswith sequential HVPG measurements. Another group of 16patients was used for validation.Results: HVPG worsened in 10 of the 24 patients during follow-up. Changes in HVPG correlated to concomitant changes in liverfunction parameters. Variceal bleeding occurred in four of the10 patients whose HVPG had worsened (bleed; 3–21 monthsafter the measured increase in HVPG) and in none of those withstable HVPG (p = 0.02). Patients with increased HVPG also hadshorter survival (p = 0.05). Worsening of HVPG was an indepen-dent predictor of death, additive to Child-Pugh or MELD scores,in a time-dependent Cox’s regression analysis. This relationshipwas confirmed in the validation group.Conclusions: Worsening HVPG during follow-up in patients whohad initially been good-responders to medical treatment isrelated to worsening in hepatic function. The maintenance of agood haemodynamic response to medical treatment of portalhypertension is an excellent predictor of outcome in thesepatients.� 2009 European Association for the Study of the Liver. Publishedby Elsevier B.V. All rights reserved.Journal of Hepatology 20
Keywords: Hepatic venous pressure gradient; Beta-blockers; Nitrates; Indocya-nine green; Child-Pugh score; MELD score; Variceal bleeding.Received 12 January 2009; received in revised form 23 July 2009; accepted 30 July2009; available online 23 October 2009*Corresponding author. Address: Dipartimento di Medicina Clinica e Sperimen-tale, Università di Padova, via Giustiniani, 2, 35126 Padova, Italy. Tel.: +39 049821 2282; fax: +39 049 875 4179.E-mail address: [email protected] (C. Merkel).Abbreviations: HVPG, Hepatic venous pressure gradient; ICG-IHC, Indocyanine g-reen intrinsic hepatic clearance; CP, Child-Pugh; MELD, Model for end-stage liverdisease.
Beta-blockers reduce the likelihood of a first variceal bleed inpatients with cirrhosis and oesophageal varices ‘at risk’ [1] andthey represent the currently recommended first line treatmentfor the primary prophylaxis in these patients [2,3]. The associa-tion of beta-blockers and long-acting nitrates is useful in prevent-ing variceal re-bleeding [2], while the available evidence for itsuse in primary prophylaxis is conflicting [4–6].
The response to 1–3 months of treatment with beta-blockersallows discrimination of patients who will be protected frombleeding in the long term [7–9] from those who will not. Indeed,it has been observed that patients whose hepatic venous pres-sure gradient (HVPG) decreases to 12 mmHg or less, or whoexhibit a decrease in HVPG P 20% of the baseline values, areprotected from bleeding (good-responders), while nearly allbleeds occur in those patients who do not meet these haemody-namic criteria.
It is generally assumed that medical prophylaxis of varicealbleeding should be kept indefinitely, despite no clear evidencethat treatment discontinuation is actually dangerous. The onlyclues that this might be the case are the following: (i) withdrawalof treatment was followed by the restoration of baseline risk ofbleeding [10] in one clinical trial; (ii) amongst patients on long-term treatment classified as good-responders at 3 months, vari-ceal bleeding during further follow-up only occurred in thosewho were withdrawn from treatment for any reason in one study[8]. It has also been suggested that long-term treatment withbeta-blockers may lead to tachyphylaxis, i.e. a decrease in phar-macological activity due to a re-adjustment of the vascularhomeostatic mechanisms which had been perturbed by treat-ment [11].
A detailed analysis of these complex relationships is difficultbecause the long-term effect of treatment is interconnected withthe natural history of the disease, which is characterized by amore or less progressive worsening in hepatic function and portalhypertension. Thus it is hard to discriminate between the loss ofpharmacological activity and the spontaneous progression of theunderlying disease.
To date, the clinical significance of the time-course of theresponse to treatment of portal hypertension, as assessed by
10 vol. 52 j 45–53

Research Article
sequential HVPG measurements, in patients with cirrhosis under-going prophylaxis of variceal bleeding has not been studied sys-tematically. The aim of the present study was to assess whetherworsening portal hypertension: (i) occurs during long-term fol-low-up; (ii) is associated to progression of hepatic dysfunction,and (iii) has predictive value for bleeding and/or survival in acohort of patients with cirrhosis and oesophageal varices at riskof bleeding, under medical treatment for primary prophylaxis,classified as good-responders on haemodynamic criteria.Patients and methods
Patients
In and outpatients with cirrhosis under the care of the Department of Clinical andExperimental Medicine of the University of Padua between June 2001 and July2004, were prospectively evaluated for inclusion into this study if they fulfilledthe following criteria: [1] clinical or histological diagnosis of cirrhosis, [2] age18–70 years, [3] presence of oesophageal varices classified as F2 or F3 accordingto Beppu’s classification [12,4] informed consent to participate in the study, [5] no
Fig. 1. Cohort selection profile: the gray
46 Journal of Hepatology 20
history of previous variceal bleeding, previous treatment for portal hypertension,Child-Pugh (CP) score [13] > 11, contraindications to beta-blockers or long-actingnitrates, portal vein thrombosis, neoplastic disease at any site.
Based onto these criteria, 42 patients were considered. They underwent aclinical and laboratory assessment and hepatic vein catheterization for the mea-surement of HVPG. Subsequently, all patients received oral nadolol starting at thedose of 40 mg/day in a single daily administration, according to the resting heartrate, with a target of a 25% decrease or a heart rate of 50 bpm. Five patients hadside-effects leading to treatment withdrawal and were removed from the studypopulation. The remaining 37 patients were re-evaluated after 1 month of treat-ment; 13 patients met the criteria for good-response and were therefore includedin the study. The remaining 24 patients received also isosorbide mononitrate at20–40 mg/day and were re-evaluated by hepatic vein catheterization after 2–3 months of treatment. A further 11 patients who met criteria for good-responseunder combined treatment were included in the study. The 13 patients who didnot respond to combined therapy (4 with alcoholic, 8 with virus-related and onewith cryptogenic cirrhosis) were offered endoscopic band ligation, which wasaccepted by eight. Five of these eight patients, who were kept on drug treatmentuntil endoscopic eradication of varices, were also monitored with sequentialHVPG measurements and are included as a separate group for comparative pur-poses. The overall selection procedure is depicted in Fig. 1. The protocol con-formed to the Helsinki declaration (1975), Edinburgh review (2000), and wasapproved by the Ethics Committee of the Medical Faculty of the University of Pad-ua. Written informed consent was obtained from each patient.
area marks the selected patients.
10 vol. 52 j 45–53
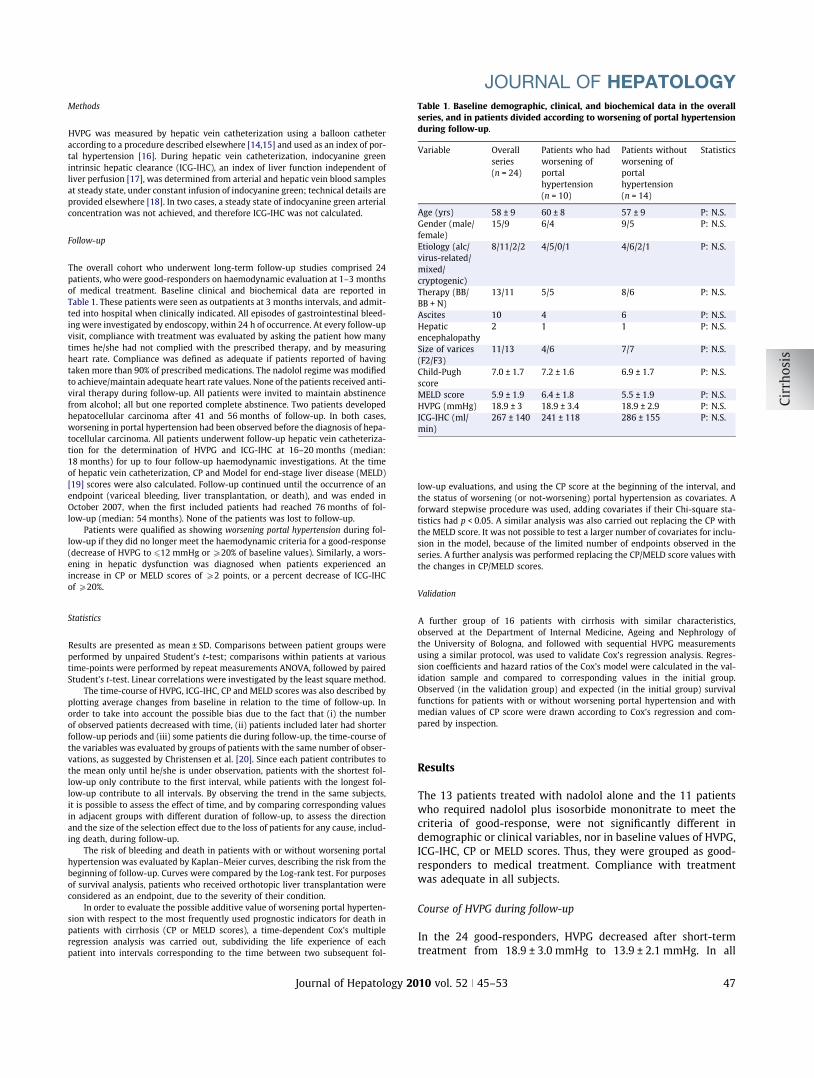
Table 1. Baseline demographic, clinical, and biochemical data in the overallseries, and in patients divided according to worsening of portal hypertensionduring follow-up.
JOURNAL OF HEPATOLOGY
MethodsHVPG was measured by hepatic vein catheterization using a balloon catheteraccording to a procedure described elsewhere [14,15] and used as an index of por-tal hypertension [16]. During hepatic vein catheterization, indocyanine greenintrinsic hepatic clearance (ICG-IHC), an index of liver function independent ofliver perfusion [17], was determined from arterial and hepatic vein blood samplesat steady state, under constant infusion of indocyanine green; technical details areprovided elsewhere [18]. In two cases, a steady state of indocyanine green arterialconcentration was not achieved, and therefore ICG-IHC was not calculated.
Follow-up
The overall cohort who underwent long-term follow-up studies comprised 24patients, who were good-responders on haemodynamic evaluation at 1–3 monthsof medical treatment. Baseline clinical and biochemical data are reported inTable 1. These patients were seen as outpatients at 3 months intervals, and admit-ted into hospital when clinically indicated. All episodes of gastrointestinal bleed-ing were investigated by endoscopy, within 24 h of occurrence. At every follow-upvisit, compliance with treatment was evaluated by asking the patient how manytimes he/she had not complied with the prescribed therapy, and by measuringheart rate. Compliance was defined as adequate if patients reported of havingtaken more than 90% of prescribed medications. The nadolol regime was modifiedto achieve/maintain adequate heart rate values. None of the patients received anti-viral therapy during follow-up. All patients were invited to maintain abstinencefrom alcohol; all but one reported complete abstinence. Two patients developedhepatocellular carcinoma after 41 and 56 months of follow-up. In both cases,worsening in portal hypertension had been observed before the diagnosis of hepa-tocellular carcinoma. All patients underwent follow-up hepatic vein catheteriza-tion for the determination of HVPG and ICG-IHC at 16–20 months (median:18 months) for up to four follow-up haemodynamic investigations. At the timeof hepatic vein catheterization, CP and Model for end-stage liver disease (MELD)[19] scores were also calculated. Follow-up continued until the occurrence of anendpoint (variceal bleeding, liver transplantation, or death), and was ended inOctober 2007, when the first included patients had reached 76 months of fol-low-up (median: 54 months). None of the patients was lost to follow-up.
Patients were qualified as showing worsening portal hypertension during fol-low-up if they did no longer meet the haemodynamic criteria for a good-response(decrease of HVPG to 612 mmHg or P20% of baseline values). Similarly, a wors-ening in hepatic dysfunction was diagnosed when patients experienced anincrease in CP or MELD scores of P2 points, or a percent decrease of ICG-IHCof P20%.
Statistics
Results are presented as mean ± SD. Comparisons between patient groups wereperformed by unpaired Student’s t-test; comparisons within patients at varioustime-points were performed by repeat measurements ANOVA, followed by pairedStudent’s t-test. Linear correlations were investigated by the least square method.
The time-course of HVPG, ICG-IHC, CP and MELD scores was also described byplotting average changes from baseline in relation to the time of follow-up. Inorder to take into account the possible bias due to the fact that (i) the numberof observed patients decreased with time, (ii) patients included later had shorterfollow-up periods and (iii) some patients die during follow-up, the time-course ofthe variables was evaluated by groups of patients with the same number of obser-vations, as suggested by Christensen et al. [20]. Since each patient contributes tothe mean only until he/she is under observation, patients with the shortest fol-low-up only contribute to the first interval, while patients with the longest fol-low-up contribute to all intervals. By observing the trend in the same subjects,it is possible to assess the effect of time, and by comparing corresponding valuesin adjacent groups with different duration of follow-up, to assess the directionand the size of the selection effect due to the loss of patients for any cause, includ-ing death, during follow-up.
The risk of bleeding and death in patients with or without worsening portalhypertension was evaluated by Kaplan–Meier curves, describing the risk from thebeginning of follow-up. Curves were compared by the Log-rank test. For purposesof survival analysis, patients who received orthotopic liver transplantation wereconsidered as an endpoint, due to the severity of their condition.
In order to evaluate the possible additive value of worsening portal hyperten-sion with respect to the most frequently used prognostic indicators for death inpatients with cirrhosis (CP or MELD scores), a time-dependent Cox’s multipleregression analysis was carried out, subdividing the life experience of eachpatient into intervals corresponding to the time between two subsequent fol-
Journal of Hepatology 20
low-up evaluations, and using the CP score at the beginning of the interval, andthe status of worsening (or not-worsening) portal hypertension as covariates. Aforward stepwise procedure was used, adding covariates if their Chi-square sta-tistics had p < 0.05. A similar analysis was also carried out replacing the CP withthe MELD score. It was not possible to test a larger number of covariates for inclu-sion in the model, because of the limited number of endpoints observed in theseries. A further analysis was performed replacing the CP/MELD score values withthe changes in CP/MELD scores.
Validation
A further group of 16 patients with cirrhosis with similar characteristics,observed at the Department of Internal Medicine, Ageing and Nephrology ofthe University of Bologna, and followed with sequential HVPG measurementsusing a similar protocol, was used to validate Cox’s regression analysis. Regres-sion coefficients and hazard ratios of the Cox’s model were calculated in the val-idation sample and compared to corresponding values in the initial group.Observed (in the validation group) and expected (in the initial group) survivalfunctions for patients with or without worsening portal hypertension and withmedian values of CP score were drawn according to Cox’s regression and com-pared by inspection.
Results
The 13 patients treated with nadolol alone and the 11 patientswho required nadolol plus isosorbide mononitrate to meet thecriteria of good-response, were not significantly different indemographic or clinical variables, nor in baseline values of HVPG,ICG-IHC, CP or MELD scores. Thus, they were grouped as good-responders to medical treatment. Compliance with treatmentwas adequate in all subjects.
Course of HVPG during follow-up
In the 24 good-responders, HVPG decreased after short-termtreatment from 18.9 ± 3.0 mmHg to 13.9 ± 2.1 mmHg. In all
10 vol. 52 j 45–53 47
-20%
-25%
-30%
-35%
-40%at definition ofgood response
18 months 36 months 54 months 72 months
perc
ent c
hang
e in
HVP
G
80%
60%
40%
20%
0%at definition ofgood response
18 months 36 months 54 months 72 months
perc
ent c
hang
e in
ICG
-IHC
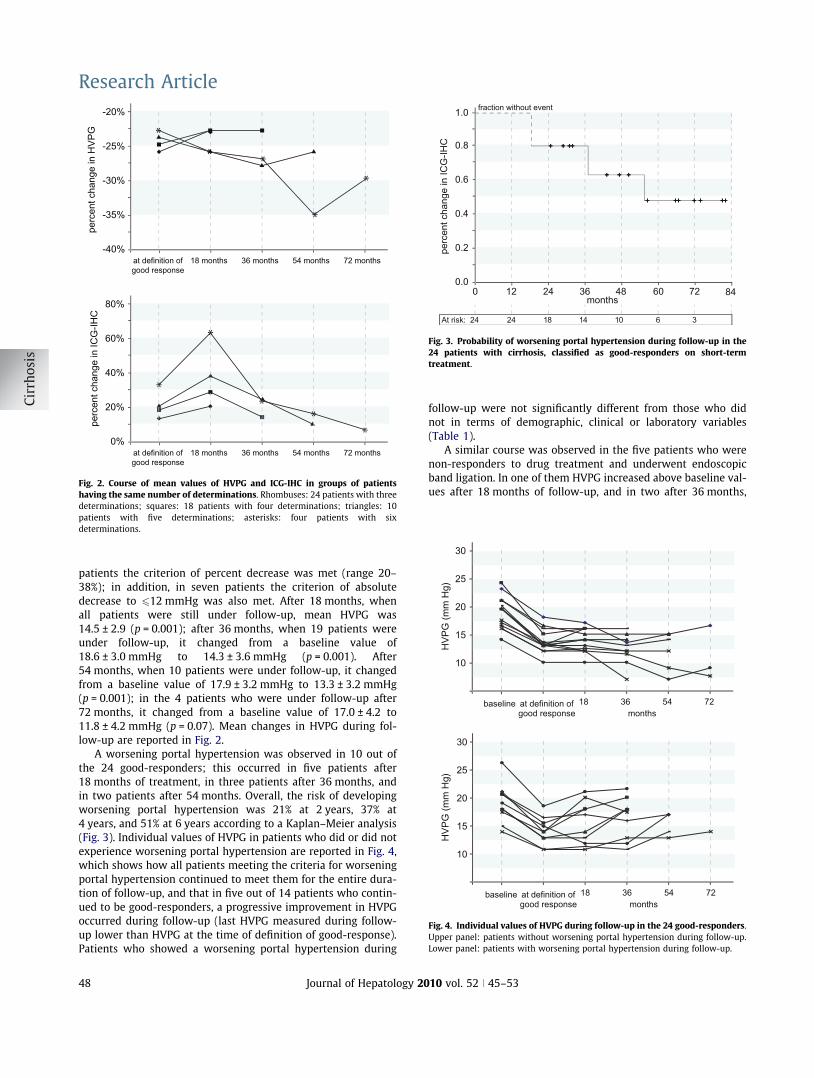
Fig. 2. Course of mean values of HVPG and ICG-IHC in groups of patientshaving the same number of determinations. Rhombuses: 24 patients with threedeterminations; squares: 18 patients with four determinations; triangles: 10patients with five determinations; asterisks: four patients with sixdeterminations.
0.8
0.6
0.4
0.2
0.0120 24 36 48 60
At risk:
fraction without event
perc
ent c
hang
e in
ICG
-IHC
1.0
72 84
2424 18 14 10 6 3
months
Fig. 3. Probability of worsening portal hypertension during follow-up in the24 patients with cirrhosis, classified as good-responders on short-termtreatment.
25
20
15
30
10
at definition ofgood response
baseline
HVP
G (m
m H
g)
months36 54 7218
25
20
15
30
10
at definition ofgood response
baseline
HVP
G (m
m H
g)
months36 54 7218
Fig. 4. Individual values of HVPG during follow-up in the 24 good-responders.Upper panel: patients without worsening portal hypertension during follow-up.Lower panel: patients with worsening portal hypertension during follow-up.
Research Article
patients the criterion of percent decrease was met (range 20–38%); in addition, in seven patients the criterion of absolutedecrease to 612 mmHg was also met. After 18 months, whenall patients were still under follow-up, mean HVPG was14.5 ± 2.9 (p = 0.001); after 36 months, when 19 patients wereunder follow-up, it changed from a baseline value of18.6 ± 3.0 mmHg to 14.3 ± 3.6 mmHg (p = 0.001). After54 months, when 10 patients were under follow-up, it changedfrom a baseline value of 17.9 ± 3.2 mmHg to 13.3 ± 3.2 mmHg(p = 0.001); in the 4 patients who were under follow-up after72 months, it changed from a baseline value of 17.0 ± 4.2 to11.8 ± 4.2 mmHg (p = 0.07). Mean changes in HVPG during fol-low-up are reported in Fig. 2.
A worsening portal hypertension was observed in 10 out ofthe 24 good-responders; this occurred in five patients after18 months of treatment, in three patients after 36 months, andin two patients after 54 months. Overall, the risk of developingworsening portal hypertension was 21% at 2 years, 37% at4 years, and 51% at 6 years according to a Kaplan–Meier analysis(Fig. 3). Individual values of HVPG in patients who did or did notexperience worsening portal hypertension are reported in Fig. 4,which shows how all patients meeting the criteria for worseningportal hypertension continued to meet them for the entire dura-tion of follow-up, and that in five out of 14 patients who contin-ued to be good-responders, a progressive improvement in HVPGoccurred during follow-up (last HVPG measured during follow-up lower than HVPG at the time of definition of good-response).Patients who showed a worsening portal hypertension during
48 Journal of Hepatology 20
follow-up were not significantly different from those who didnot in terms of demographic, clinical or laboratory variables(Table 1).
A similar course was observed in the five patients who werenon-responders to drug treatment and underwent endoscopicband ligation. In one of them HVPG increased above baseline val-ues after 18 months of follow-up, and in two after 36 months,
10 vol. 52 j 45–53

400
300
200
at definition ofgood response
baseline
ICG
-IHC
(ml/m
in)
months18
350
250
150
25
20
15
30
10
at definition ofpoor response
baseline
HVP
G (m
m H
g)
months
36 54 72
36 54 7218
Fig. 5. Individual values of HVPG and ICG-IHC in the five poor-responders todrug treatment, who were treated with endoscopic band ligation andunderwent sequential HVPG measurements.
0
-0.5
-1
0.5
-1.5
at definition ofpoor response
Cha
nge
in C
P sc
ore
months36 54 7218
1
1
0.5
0
1.5
-0.5
at definition ofpoor response
Cha
nge
in M
ELD
sco
re
months36 54 7218
2
*
**
*
*
**
*
*
*
Fig. 6. Course of mean values of Child-Pugh and MELD scores in groups ofpatients having the same number of determinations. Rhombuses: 24 patientswith three determinations; squares: 18 patients with four determinations;triangles: 10 patients with five determinations; asterisks: four patients with sixdeterminations.
JOURNAL OF HEPATOLOGY
while in the other two it was unchanged or slightly decreasedthroughout the observation period (Fig. 5).
Course of ICG-IHC
In the 24 good-responders, baseline ICG-IHC averaged267 ± 140 mL/min, and did not change significantly in the shortterm (292 ± 140 mL/min; p = 0.31) or after 18 months of follow-up (324 ± 187 mL/min; p = 0.07). No significant changes frombaseline values were observed in the 18 patients who were mon-itored at 36 months of treatment (from 243 ± 110 to263 ± 102 mL/min; p = 0.33), or in the 10 patients who weremonitored at 54 months of treatment (from 256 ± 89 to257 ± 104 mL/min; p = 0.98). Mean changes in ICG-IHC duringfollow-up are reported in Fig. 2.
A decrease in ICG-IHC greater than 20% from baseline wasobserved during follow-up in seven patients: in one at short term,in 3 after 18 month, in 2 after 36 months and in one after54 months. Values of ICG-IHC during follow-up were inverselycorrelated to Child-Pugh score (rs = �0.25; p = 0.05), confirmingthe value of ICG-IHC as an index of hepatic function.
In the five patients who were non-responders to drug treat-ment and underwent endoscopic band ligation a similar coursewas observed. Only one patient showed a decrease in ICG-IHCof more than 20% (Fig. 5); the same individual exhibited a con-comitant increase in HVPG.
Course of CP score
In the 24 good-responders, baseline CP score averaged 7.0 ± 1.7,and did not change in the short term (6.3 ± 0.9; p = 0.18) or after
Journal of Hepatology 20
18 months of treatment (6.7 ± 1.5; p = 0.20). In the 19 patientsmonitored at 36 months, CP score was not significantly differentfrom baseline (from 7.2 ± 1.8 to 7.1 ± 1.7; p = 0.87). In contrast, inthe 10 patients monitored at 54 months, a significant increase inCP score was observed (from 6.3 ± 1.0 to 7.0 ± 1.3; p = 0.05). Inthe four subjects monitored at 72 months of treatment, CP scorewas not different from baseline (from 6.2 ± 0.5 to 6.0 ± 1.4;p = 0.79). Mean changes in CP score during follow-up are shownin Fig. 6. An increase in CP score of P2 points was observed inseven patients, in 2 after 18 months of follow-up, in 2 after36 months, and in 3 after 54 months.
Course of MELD score
In the 24 good-responders, baseline MELD score averaged5.9 ± 1.9, and did not change in the short term (5.6 ± 1.5;p = 0.14) or after 18 months of treatment (5.7 ± 1.9; p = 0.55). Inthe 19 patients monitored at 36 months, MELD score was mar-ginally increased from baseline (from 5.8 ± 1.9 to 6.4 ± 1.7;p = 0.06) and in the 10 patients monitored at 54 months of fol-low-up, a significant increase in MELD score was observed (from4.9 ± 1.1 to 6.2 ± 1.7; p = 0.01). In the four subjects monitored at72 months of treatment, MELD score was not different from base-line (from 4.8 ± 1.0 to 5.3 ± 1.8; p = 0.40). Mean changes in MELDscore during follow-up are reported in Fig. 6. An increase in MELDscore of P2 points was observed in four patients, in 1 after18 months of follow-up, in 2 after 36 months, and in 1 after54 months.
10 vol. 52 j 45–53 49

0.8
0.6
0.4
0.2
0.0120 24 36 48 60
At risk:
fract
ion
with
out e
vent
1.0
6
Bleeding
Death or OLT
10 4 1 1610 5 1 1
months
Fig. 7. Risk of variceal bleeding or death from a diagnosis of worsening portalhypertension.
0.8
0.6
0.4
0.2
0.0120
At risk:
cum
ulat
ive
surv
ival
1.0
72 84
14141010
24 36 48 60
14 10 8 6 310 9 5 4 2
months
Log-rank test: 3.80, p = 0.02
with worsening in portal hypetension
without worsening in portal hypetensionB
0.8
0.6
0.4
0.2
0.0120 24 36 48 60
At risk:
fract
ion
with
out b
leed
ing
1.0
72 84
14141010
14 10 8 6 310 9 5 4 2
months
Log-rank test: 5.14, p = 0.02
with worsening in portal hypetension
without worsening in portal hypetensionA
Fig. 8. (Panel A) Kaplan–Meier plot of the risk of variceal bleeding from thebeginning of the observation in patients who developed (solid line) or did notdevelop (dotted line) worsening portal hypertension during follow-up. (Panel B)Kaplan–Meier plot of survival or OLT from the beginning of follow-up in patientswho developed (solid line) or did not develop (dotted line) worsening portalhypertension during follow-up.
Research Article
Relationships between worsening portal hypertension andaggravation in liver dysfunction
At the time of detection of worsening portal hypertension, the 10relevant patients showed a significantly larger increase in CPscore than that observed at the same time of follow-up in the14 patients who did not show worsening portal hypertension(0.7 ± 0.04 vs. �0.3 ± 0.03; p = 0.04). A significant inverse correla-tion was also found between percent changes in HVPG and inICG-IHC observed at the same time (r = �0.27; p = 0.029), and adirect one between percent changes in HVPG and changes in CPscore (rs = 0.25; p = 0.048).
Clinical events during follow-up
During follow-up, four patients had variceal bleeding, two under-went hepatic transplantation and 11 died of liver-related causes.Ten patients met the criteria for worsening portal hypertensionduring follow-up (i.e. loss of the haemodynamic criteria forgood-response to medical treatment (Fig. 3)). Amongst them, fourhad a variceal bleeding during follow-up, with an interval of 3–21 months from the diagnosis of worsening portal hypertension(Fig. 7). None of the patients maintaining the haemodynamic cri-teria for good-response had variceal bleeding during follow-up(Fisher’s exact test p = 0.02). According to a Kaplan–Meier analy-sis, the risk of bleeding in patients with worsening portal hyper-tension was significantly higher than that of patients withoutworsening portal hypertension (30% vs. 0% at 42 months) (Log-rank test: p = 0.02) (Fig. 8A).
Table 2. Statistical parameters of the time-dependent Cox’s regression models predi
*Hazard ratio calculated for an increase in one point of CP or MELD score.
50 Journal of Hepatology 20
The 10 patients who experienced worsening portal hyperten-sion had a higher risk of death compared to those without wors-ening portal hypertension. Indeed, nine out of 10 patients whohad worsening portal hypertension died or underwent hepatictransplantation during follow-up, versus four out of 14 of thosewho did not have worsening portal hypertension (Fisher’s exacttest: p = 0.01). Kaplan–Meier analysis showed a lower probabilityof survival in patients with worsening portal hypertension, com-
cting death in the 24 patients with cirrhosis.
10 vol. 52 j 45–53

JOURNAL OF HEPATOLOGY
pared to those without worsening portal hypertension (10% vs.37% at 72 months, Log-rank test: p = 0.05) (Fig. 8B). A furtherKaplan–Meier analysis, performed considering the two patientswho underwent liver transplantation as ‘censored’, producedvery similar results (Log-rank test: p = 0.01). The median survivalafter the diagnosis of worsening portal hypertension was18 months (range 5–51 months) (Fig. 7).The time-depended Cox’s multiple regression analysis showedthat both the CP score at each time-point and the condition ofworsening (or not-worsening) portal hypertension were indepen-dent predictors of death or transplantation, and that worseningportal hypertension was more strongly associated with mortalitythan the CP score (Table 2). Very similar results were obtainedwhen the CP score was replaced by the MELD score (Table 2).Models testing the addition of changes in CP or MELD scores toworsening portal hypertension as predictor covariates did notresult in significantly improved regression fits (p = 0.32 andp = 0.35, respectively).
Validation
In the 16 patients of the validation group worsening portalhypertension occurred in nine patients. Three bleedings occurredafter 24, 25 and 36 months, respectively. In all of them worseningportal hypertension had been observed prior to bleeding. The riskof bleeding was higher in patients who had worsening portalhypertension (3 out of 9) than in those who kept a good-response(0 out of 7); Chi-square = 2.8; p = 0.09). Two patients died ofliver-related causes after 30 and 34 months, respectively. Threewere transplanted after 23, 24 and 46 months, respectively. Therisk of death or transplant was 44% (4 out of 9) in those whoexperienced worsening portal hypertension versus 14% (1 outof 7) in those who did not. This difference did not reach statisticalsignificance (chi-square = 1.66; p = 0.19) due to the small numberof events.
The time-dependent Cox’s regression analysis confirmedworsening portal hypertension and CP score as predictors ofdeath or transplantation, with very similar statistical parameters.Regression coefficients were 1.93 and 0.44, respectively, similarto 2.16 and 0.44, as observed in the initial population; conse-
0.8
0.6
0.4
0.2
0.030 6 9 12 15
cum
ulat
ive
surv
ival
1.0
18months
Fig. 9. Validation of the Cox’s model. Survival function for the time betweentwo subsequent determinations for patients with (narrow lines) or without (boldlines) worsening portal hypertension observed in the validation group (solidlines) and expected according to the initial group (dashed lines).
Journal of Hepatology 20
quently hazard ratios were 6.8 and 1.55, respectively, similar invalue to 7.1 and 1.55, as observed in the initial population. Hence,observed (in the validation group) and expected (in the initialgroup) survival functions for patients with or without worseningportal hypertension were very similar (Fig. 9).
Discussion
Prophylaxis of variceal bleeding with beta-blockers is the pre-ferred treatment option for patients with varices at risk of bleed-ing, since it decreases the underlying risk of bleedingapproximately by half (from 30% to 14% at 2 years [1]). Patientswho are good-responders to a short-term course of drug treat-ment are generally protected, and their risk of bleeding is approx-imately 4–5% at two years [1]. In the present series of patientstreated with beta-blockers or beta-blockers plus nitrates, classi-fied as good-responders on haemodynamic criteria, the overallrisk of bleeding was low (0% at 2 years, 12% at 4 years and 17%at 6 years), and comparable to that expected according to theavailable literature [1].
However, all available evidence on the clinical value of fulfill-ing haemodynamic criteria of good-response is based on theassessment of the effect of a 1–3 month course of treatment[7–9], and very limited information is available on the long-termcourse of HVPG in patients undergoing prophylaxis of varicealbleeding. The only published report is related to a group ofpatients under pharmacological treatment for prevention of re-bleeding, comprising good- and poor-responders at short term,who were re-evaluated after 12–18 months of treatment [21].In that study, worsening portal hypertension was seldomobserved, and was mainly linked to discontinuation of treatmentor alcohol intake, but no information was available on HVPG inthe following years of follow-up. Keeping a good-response wasa significant predictor of a favourable outcome, and the authorsinterpreted the less favourable CP scores in patients with wors-ened portal pressure as a consequence of the lack of effect oftreatment, although the opposite could not be completely ruledout.
Although it has been observed in many trials that most bleed-ings occur in the first year of treatment, and the risk shows a ten-dency to decrease thereafter, there is a general consensus thattreatment should be continued indefinitely [10]. The long-termhaemodynamic effect of treatment, beyond the first year of treat-ment, has never been investigated prospectively. It is conceivablethat, in a long-term study like the present one, portal hyperten-sion may increase progressively despite treatment, eitherbecause of pharmacological tachyphylaxis, or because of the pro-gression of the disease itself. Uncertainties on this subject are fur-ther increased by some methodological problems frequentlyencountered in the published studies, such as selection bias dueto survival, and regression towards the mean. The first bias isrelated to the fact that only patients who improve or remain sta-ble can be monitored long term, while patients who worsen anddie are absent from the long-term data. This implies that long-term observations contain a biased number of patients with afavourable prognosis. The second mechanism is related to the factthat patients are entered into a study when they have particularlyabnormal values of a variable, and this variable will show a spon-taneous tendency to improve when patients are reviewed duringfollow-up. The combination of these mechanisms is probably at
10 vol. 52 j 45–53 51

Research Article
the basis of: (i) the observation [22] that a small subset ofuntreated patients with portal hypertension can show long-termimprovement in portal pressure; (ii) the frequent finding of a longterminal tail without events in the Kaplan–Meier plots of clinicaltrials of treatment of portal hypertension; (iii) the good long-term course of HVPG seen in the subgroup of our patients whowere followed up for 72 months in the present study.Since it has been shown that treatment with beta-blockers orbeta-blockers plus nitrates [23,24] does not impair liver func-tion, changes in ICG-IHC or in CP or MELD scores should be con-sidered an expression of the evolution of the underlying liverdisease. Indeed, the plots of mean changes of subjects withthe same number of follow-up measurements (Figs. 2 and 6)suggest that at the beginning there is a regression towards themean effect, followed by a slowly progressive impairment inliver function.
In the present series a worsening portal hypertension wasseen in 40% of patients, after a follow-up time ranging from 18to 54 months. This worsening would have been unpredictableon the basis of the clinical, biochemical or haemodynamic dataavailable at the beginning of follow-up. Nevertheless, the correla-tions observed between an increase in HVPG and a decrease inICG-IHC or aggravation of the CP score, together with the signif-icantly larger increase in CP score in patients who had concomi-tant worsening portal pressure, suggest that the aggravation ofliver disease led to worsening portal hypertension and increasedHVPG despite the ongoing medical treatment. In other words,worsening in portal hypertension in these patients should notbe interpreted as a clue that the efficacy of medical treatmenthas been lost, but as a condition in which medical treatment con-tains an increase in HVPG which would be much more obvious inits absence. Definite proof that this is the case could only beobtained by determining HVPG after withdrawal of treatment,but it would be unethical because of the risks of bleeding dueto rebound phenomena. The observation that a similar courseof aggravation in HVPG was also seen in the small group ofpoor-responders who received endoscopic band ligation (Fig. 5)lends further support to this interpretation.
This study is the first to report on the clinical events followingworsening portal hypertension during medical treatment for theprophylaxis of variceal bleeding. A limited number of varicealbleeds occurred during follow-up in those patients who wereearly good-responders according to haemodynamic criteria.However, all these bleeds occurred after over two years of treat-ment, and only amongst those patients who had worsening portalhypertension, and after a diagnosis of worsening in HVPG, indi-cating that worsening portal hypertension is a specific, althoughnot a sensitive, indicator of the risk of bleeding. The same coursewas seen in the validation group collected in a different tertiaryreferral centre. Bleeding occurred after a variable interval (3–21 months) after a diagnosis of aggravation of portal hyperten-sion, suggesting that worsening portal hypertension is a contrib-uting but not exclusive factor leading to hemorrhage. Overall, theoutcome of the patients who bled was poor, since median sur-vival was 24 months from the observation of worsening in portalhypertension.
The present data do not provide an answer to whetherpatients showing a worsening in portal hypertension should bemaintained on medical treatment or switched to endoscopictreatment, because the risk of bleeding of band-ligated patientswith this specific history is unknown. If we assume that this risk
52 Journal of Hepatology 20
may be similar to that of early non-responders to drug treatment,in whom band ligation was recently reported to be very effective[25], our data may support the decision to switch such patients toband ligation.
Considering that our data suggest that worsening portalhypertension is a clue to progression of the underlying liver dis-ease, it is not surprising that worsening portal hypertension wasalso associated with shorter survival. We could not identify obvi-ous causes of worsening HVPG in our patients, besides the spon-taneous aggravation of their liver disease. Indeed, compliancewas adequate throughout the follow-up: liver cancer, whichdeveloped in two patients, was always observed after worseningin HVPG, and none of the patients received antiviral treatment.The predictive value of worsening portal hypertension was inde-pendent of that of the CP/MELD score, and more directly linked tosurvival than these scores. This suggests that aggravation in por-tal hypertension occurs earlier than that of conventional bio-chemical or clinical data, and identifies patients who are proneto disease progression. The predictive value of worsening portalhypertension was confirmed in the validation group observedin Bologna.
The main findings of this study represent an expansion of aprevious observation that baseline HVPG is an important predic-tor of the clinical events occurring in the course of the disease,including ascites, encephalopathy, and hepato-renal syndrome[26], and that keeping a good hemodynamic response to medicaltreatment at one year has a favourable effect on the clinicalevents in the prevention of re-bleeding [21]. These events arethe consequence of the progression of fibrosis and derangementof hepatic microvasculature and HVPG seems to be the bestand most direct available surrogate marker of such changes [27].
These data, although validated in a small independent sample,need to be confirmed in larger series, with less strict criteria ofinclusion, and in other clinical settings. If confirmed, this wouldsupport the clinical importance of demonstrating the mainte-nance of the haemodynamic response to medical treatment, aspatients whose HVPG remains low are very well protected frombleeding in the long term and their liver disease is unlikely toprogress. Obviously, such potential benefits should be weighedagainst the costs and the discomforts of repeated HVPG measure-ment, which are not trivial.
In conclusion, in patients with cirrhosis under medical pro-phylaxis of variceal bleeding, who are early good-responders onhaemodynamic criteria, few variceal bleedings occur duringlong-term follow-up. In addition, these bleeds are confined topatients who show a worsening portal hypertension as expressedby the loss of haemodynamic criteria of good-response. Thisworsening is related to the aggravation of liver disease and isan important predictor of risk of death, independently of CP orMELD scores.
Acknowledgement
C.M., M.B., P.A., L.C., I.C., and A.G. declared that they do not have arelationship with the manufacturers of the drugs involved eitherin the past or present and did not receive funding from the man-ufacturers to carry out their research. They received support fromthe Italian Ministry of Education, University and Research (Rome,Italy) for this study. The other authors who have taken part in thisstudy declared that they do not have anything to disclose regard-ing funding or conflict of interest with respect to this manuscript.
10 vol. 52 j 45–53

JOURNAL OF HEPATOLOGY
The study was supported by a grant from the Italian Ministry ofEducation, University, and Research (Rome, Italy).References
[1] D’Amico G, Pagliaro L, Bosch J. The treatment of portal hypertension: a meta-analytic review. Hepatology 2005;41:386–400.
[2] Garcia Tsao G, Sanyal AJ, Grace ND, Carey WPractice Guideline Committee ofAASLDPractice Parameters Committee AGA. Prevention and management ofgastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology2007;46:922–938.
[3] Garcia-Tsao G, Bosch J, Groszmann RJ. Portal hypertension and varicealbleeding. Unresolved issues. Hepatology 2008;47:1764–1772.
[4] Merkel C, Marin R, Enzo E, Donada G, Cavallarin G, Torboli P, et al.Randomised trial of nadolol alone or with isosorbide mononitrate forprimary prophylaxis of variceal bleeding in cirrhosis. Lancet1996;348:1677–1681.
[5] Garcia-Pagan JC, Morillas R, Banares R, Albillos A, Villanueva C, Vila C, et al.Propranolol plus placebo versus propranolol plus isosorbide-5-mononitratein the prevention of a first variceal bleeding: a double-blind RCT. Hepatology2003;37:1260–1266.
[6] D’Amico G, Pasta L, Politi F, Vizzini G, Traina M, Caltagirone M, et al.Isosorbide mononitrate with nadolol compared to nadolol alone forprevention of the first bleeding in cirrhosis. A double-blind placebo-controlled randomized trial. Gastroenterol Int 2002;15:40–50.
[7] Groszmann R, Bosch J, Grace ND, Conn HO, Garcia-Tsao G, Navasa M, et al.Hemodynamic events in a prospective randomised trial of propranololversus placebo in the prevention of a first variceal hemorrhage. Gastroen-terology 1990;99:1401–1407.
[8] Merkel C, Bolognesi M, Sacerdoti D, Bombonato G, Bellini B, Bighin R, et al.The hemodynamic response to medical treatment of portal hypertension as apredictor of clinical effectiveness in the primary prophylaxis of varicealbleeding in cirrhosis. Hepatology 2000;32:930–934.
[9] Turnes JC, Garcia-Pagan J, Abraldes M, Hernandez-Guerra A, Dell’Era A, Bosch J.Pharmacological reduction of portal pressure and long-term risk of firstvariceal bleeding in patients with cirrhosis. Am J Gastroenterol 2006;101:1–7.
[10] Abraczinkas DR, Ookubo R, Grace ND, Groszmann RJ, Bosch J, Garcia-Tsao G,et al. Propranolol for prevention of first variceal hemorrhage: a lifetimecommitment? Hepatology 2001;34:1096–1102.
[11] Elkayam U. Tolerance to organic nitrates: evidence, mechanism, clinicalrelevance, and strategies for prevention. Ann Intern Med 1991;114:667–677.
[12] Beppu K, Inokuchi K, Koyanagi N, Nakayama S, Sakata H, Kitano S, et al.Prediction of variceal hemorrhage by esophageal endoscopy. GastrointestEndosc 1981;27:213–218.
Journal of Hepatology 20
[13] Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transectionof the esophagus for bleeding oesophageal varices. Br J Surg 1973;60:646–664.
[14] Merkel C, Bolognesi M, Bellon S, Zuin R, Noventa F, Finucci G, et al.Prognostic usefulness of hepatic vein catheterization in patients withcirrhosis and esophageal varices. Gastroenterology 1992;102:973–979.
[15] Groszmann RJ, Wongcharatrawee S. The hepatic venous pressure gradient:anything worth doing should be done right. Hepatology 2004;39:280–282.
[16] Armonis A, Patch D. Burroughs AK Hepatic venous pressure gradient: an oldtest as a new prognostic marker in cirrhosis? Hepatology 1997;25:245–248.
[17] Bass L, Keiding S, Winkler K, Tygstrup N. Enzymatic elimination ofsubstances flowing through the intact liver. J Theor Biol 1976;61:393–409.
[18] Merkel C, Bolognesi M, Finucci GF, Angeli P, Caregaro L, Rondana M, et al.Indocyanine green intrinsic hepatic clearance as a prognostic index ofsurvival in patients with cirrhosis. J Hepatol 1989;9:16–22.
[19] Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Themeau TM, Kosberg CL,et al. A model to predict survival in patients with end-stage liver disease.Hepatology 2001;33:464–470.
[20] Christensen E, Schlichting P, Fauerholdt L, Juhl E, Poulsen H, Tygstrup N.Changes in laboratory variables with time in cirrhosis: prognostic andtherapeutic significance. Hepatology 1985;5:843–853.
[21] Villanueva C, Lopez-Balaguer JM, Aracil C, Kolle L, Gonzales B, Minana J, et al.Maintenance of hemodynamic response to treatment for portal hyperten-sion and influence on complications of cirrhosis. J Hepatol2004;40:757–765.
[22] Vorobioff J, Groszmann RJ, Picabea E, Gamen M, Villavicencio R, Bordato J,et al. Prognostic value of hepatic venous pressure gradient measurement inalcoholic cirrhosis: a 10 year prospective study. Gastroenterology1996;111:701–709.
[23] Merkel C, Gatta A, Sacerdoti D, Bolognesi M, Rondana M, Caregaro L, et al.Long-term effect of nadolol on quantitative liver function tests in patientswith cirrhosis. Eur J Clin Pharmacol 1988;34:501–504.
[24] Merkel C, Sacerdoti D, Bolognesi M, Buonamico P, Sticca A, Amodio P, et al.Effect of chronic treatment with nadolol plus isosorbide mononitrate onliver blood flow and liver metabolic activity in cirrhosis. Eur J GastroenterolHepatol 1999;11:1221–1225.
[25] Dell’Era A, Cubero Sotela J, Fabris FM, Petazzi G, Reati R, et al. Primaryprophylaxis of variceal bleeding in cirrhotic patients: a cohort study. DigLiver Dis 2008;40:936–943.
[26] Ripoll C, Groszmann R, Garcia-Tsao G, Grace N, Burroughs AK, Planas R, et al.Hepatic venous pressure gradient predicts clinical decompensation inpatients with compensated cirrhosis. Gastroenterology 2007;133:481–488.
[27] Gluud C, Brok J, Gong Y, Koretz RL. Hepatology may have problems withputative surrogate outcome measures. J Hepatol 2007;46:734–742.
10 vol. 52 j 45–53 53