CLINICAL PLACEMENT ONBOARDING MANUAL
90
1 Dr. Billie Madler, DNP, APRN, FNP, FAANP Chair, Graduate Nursing 701.355.8266 [email protected] Dr. Jenna Herman, DNP, APRN, FNP-C FNP Program Coordinator 701.355.8116 [email protected] Jody Martin Clinical Placement Liaison Graduate Nursing 701.355.8127 [email protected] Dr. Annie Gerhardt, DNP, APRN, FNP-C FNP Clinical Competence Coordinator 701.319.1101 [email protected] CLINICAL PLACEMENT ONBOARDING MANUAL Family Nurse Practitioner Program University of Mary 7500 University Drive Bismarck, ND 58504
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of CLINICAL PLACEMENT ONBOARDING MANUAL

1
Dr. Billie Madler, DNP, APRN, FNP, FAANP Chair, Graduate Nursing 701.355.8266 [email protected]
Dr. Jenna Herman, DNP, APRN, FNP-C FNP Program Coordinator 701.355.8116 [email protected]
Jody Martin Clinical Placement Liaison Graduate Nursing 701.355.8127 [email protected]
Dr. Annie Gerhardt, DNP, APRN, FNP-C FNP Clinical Competence Coordinator 701.319.1101 [email protected]
CLINICAL PLACEMENT
ONBOARDING MANUAL
Family Nurse Practitioner Program
University of Mary
7500 University Drive
Bismarck, ND 58504

2
Table of Contents
Introduction/Purpose of Clinical Experiences ............................................................................................ 3 Overview of Clinical Courses ....................................................................................................................... 3 Types of Clinical Facilities............................................................................................................................ 3 Preceptor Qualifications ............................................................................................................................. 4 Clinical Placement Process .......................................................................................................................... 4
Clinical Placement Overview ........................................................................................................... 4 Clinical Process Steps ...................................................................................................................... 5 Preparing for Clinical Placement ..................................................................................................... 7 Common Additional Expectations of Clinical Facilities ................................................................... 9 Clearance to Begin Clinical Experience ........................................................................................... 9
Miscellaneous Clinical Concerns ............................................................................................................... 10 Student Liability Insurance............................................................................................................ 10 Clinical Travel Requirements ........................................................................................................ 10 Clinical Attendance ....................................................................................................................... 10 Working during Clinical Courses ................................................................................................... 11 On-call Hours................................................................................................................................. 11 Surgical Hours ............................................................................................................................... 11
Characteristics of the Clinically Engaged Student .................................................................................... 11 Other Student Clinical Responsibilities ..................................................................................................... 14 Professional Behavior ............................................................................................................................... 16 Establishing Baseline Student Clinical Competence ................................................................................. 16 Overview of Student Clinical Evaluation Methods ................................................................................... 16
Clinical Placement Meetings ......................................................................................................... 17 NP Skills Checklist .......................................................................................................................... 17 Student Clinical Objectives/Evaluation ......................................................................................... 17 Clinical Conference Group Meetings ............................................................................................ 17 Clinical Site Visit ............................................................................................................................ 17 Typhon Entries .............................................................................................................................. 18 Dictations ...................................................................................................................................... 18 Preceptor Typhon Evaluations ...................................................................................................... 18 Hotseat Competency Testing ........................................................................................................ 19
Appendices A. Graduate Nursing Student Health Requirements ................................................................... 20 B. NP Skills Checklist …………………………………………………………………………………………………………….. 22 C. Clinical Placement Information Form ..................................................................................... 26 D. Student Clinical Contract with Objectives/Evaluation Examples ........................................... 29 E. 3 Minute Clinical Presentation ................................................................................................ 36 F. Typhon Guidelines/Examples ................................................................................................. 42 G. Dictation Requirements .......................................................................................................... 46 H. Clinical Site Visit Tool .............................................................................................................. 56 I. Selecting the Appropriate E/M Coding ................................................................................... 62 J. Hotseat Pearls ......................................................................................................................... 64 K. Preceptor Thank You Letter with Preceptor Benefits ............................................................. 76

3
Introduction
Clinical rotations are an important component of the academic experience in the BSN to DNP program and are
critical to the formation of competent Family Nurse Practitioner (FNP) graduates. This manual intends to serve
as a roadmap for common questions surrounding clinical requirements, placements, and expectations.
Purpose of Clinical Experiences
Planned clinical experiences, guided by qualified and competent preceptors are essential for student growth
and development in clinical and professional skills necessary for preparedness to function as a competent
nurse practitioner upon graduation. Under careful supervision of clinical preceptors, students apply classroom
principles to real life experiences in healthcare settings.
The clinical experience sets the stage for students to begin their professional networking. It is a time when students are marketing themselves and the University of Mary. They are on stage and not only are they being assessed by preceptors but also by nurses, clinic staff on their performance with histories, physicals, diagnosis and management. Students are being assessed on their professionalism, communication style, personality, interpersonal relationship skills, teamwork mentality, etc. And equally important, students are representing the University of Mary FNP program and their interactions are a direct reflection of our program. How students market themselves can affect the program either positively or negatively for generations to come.
Overview of Clinical Courses
FNP students will complete a minimum of 1180 clinical hours during their course of study. Of these, a
minimum of 900 will be in direct patient care. This manual discusses important information related to the
direct patient care clinical experiences required of FNP students.
In the final clinical course NUR 960, the required number of clinical hours is 400. Student must engage care of
the primary care population for a minimum of 150 hours during this course and may not have more than 3
unique clinical placements.
The first year of the program provides challenging coursework foundational to the preparation of students for
direct patient care experiences. Direct patient care experiences will commence fall semester of year 2 in the
FNP program of study. Table 1 outlines the direct patient care clinical courses and their position in the
program of study.
Table 1
FNP Direct Patient Care Clinical Courses
Course Number Course Name Number of Required Hours Semester/Year
NUR 759 Primary Care Clinical 200 Fall of Year 2 NUR 859 Women and Children Clinical 150 Summer of Year 2 or Fall of Year 3 NUR 869 Special Populations Clinical 150 Summer of Year 2 or Fall of Year 3 NUR 960 Seminar and Practicum 400 Spring of Year 3
Types of Clinical Facilities
Direct patient care experiences occur in a wide range of clinical settings. The type of setting will be dependent
on the clinical course and faculty’s suggestions based on previous clinical experience exposure and
performance. The care delivered at the setting must match the objectives of the course. Table 2 offers
examples of clinical settings based on clinical course.
Table 2

4
Examples of Clinical Settings by Course
Course Number Course Name Example of Clinic Setting NUR 759 Primary Care Clinical Primary Care/Family Practice Clinic, Federally Qualified
Health Center, Long Term Care Facility NUR 859 Women and Children Clinical OB/GYN Clinic, Pediatric Clinic, Family Practice Clinic NUR 869 Special Populations Clinical Orthopedics, Cardiology, Pulmonology, Pain Management,
Dermatology, Rheumatology, Neurology, Oncology, Nephrology, Urgent Care, Hospitalist, Emergency, etc
NUR 960 Seminar and Practicum Primary Care/Family Practice Clinic, Federally Qualified Health Center, Mental Health, Diabetes Management, Long
Term Care Facility OB/GYN Clinic, Pediatric Clinic, Family Practice Clinic
Orthopedics, Cardiology, Pulmonology, Pain Management, Dermatology, Rheumatology, Neurology, Oncology,
Nephrology, Urgent Care, Hospitalist, Emergency, etc
Preceptor Qualifications
To assure students can fulfill clinical obligations of each course, it is important for the University of Mary FNP
faculty to carefully screen and, to the best of their ability, select preceptors who are motivated to teach, are
willing to devote time to student’s learning, and are ready to allow students hands on experiences in practice
and clinical documentation. A minimum of 200 hours with a nurse practitioner, over the course of the program
of study, is a University of Mary program requirement.
Preceptor qualifications are verified by several means including a review of the preceptor credentials,
curriculum vitas, and from previous evaluations of that preceptor. Other means include web inquiries for
biographies commonly found on clinical agency pages and contacts to medical staff service or credentialing
offices for verification of preceptor qualifications.
Basic preceptor qualifications required include the following:
• Nurse Practitioner, Certified Nurse Midwife, Physician (MD), Osteopathic Physician (DO), Physician
Assistant (PA).
• Current licensure in state of proposed clinical preceptorship (except providers practicing in US
government settings).
• Preceptor’s practice is in an area related to content of clinical course.
• A minimum of one year of work experience.
Clinical Placement Process The clinical placement process is a collaborative effort between FNP Faculty, Graduate Nursing Clinical
Placement Liaison, the student, the healthcare organization, and the preceptor. In accordance with the
Commission on Collegiate Nursing Education, the program maintains overall responsibility for determining and
securing placement of students in clinical experiences.
Designated FNP faculty are responsible for approving a potential preceptor and clinical setting prior to the
pursuit of a clinical placement. Faculty consider the credentials of potential preceptors, the appropriateness
of the clinical site regarding the clinical course, and the population served in relationship to the intended
objectives of the experience. Upon approval from faculty, the Graduate Clinical Placement Liaison makes an
initial communication to request a clinical rotation with the preceptor, communicates if the placement was
5
secured or not, and executes necessary paperwork for secured placements between students, faculty, clinical
organization, and preceptor.
What you can expect
Faculty work to place students with preceptors who work in settings near the student’s home, however, that is
not always possible or appropriate to the objectives of the placement. See Clinical Travel Requirements
section for additional information.
In many cases, the clinical placement process can take months to accomplish. Therefore, it is important to
plan and begin placement work early. Ongoing, timely communication between FNP Faculty, Graduate
Nursing Clinical Placement Liaison, and the student is important to facilitate the process.
Life happens. Sometimes secured placements fall through at the last minute. Sometimes finalized placements
do not occur in a timely manner (this may be due to a variety of causes including preceptors or clinical sites
are not responsive, delay in signed agreements, legal review of affiliation agreements are not approved,
additional backgrounds studies are needed and cause delays, etc.). As professionals, faculty, students, and
staff must be prepared to adapt and rise to the occasion.
Faculty, staff will use Monday.com, a cloud-based project management application, to organize the work
associated with each student’s placement and to facilitate communication between and among faculty, staff,
and students.
Steps in the Clinical Placement Process
Coordinating a clinical placement can be challenging, however the rewards of a quality clinical experience are
invaluable to the future success of graduates. A well-defined clinical placement process is in the Graduate
Nursing Student Handbook. Listed below are the key activities associated with the clinical placement process.
Please note:
1. Students are not allowed to inquire with prospective preceptors until granted permission by the
Graduate Nursing Clinical Placement Liaison.
2. Care is taken to place the students with a preceptor and a location that will best equip them to
achieve required clinical competencies associated with that course. While a goal is to place the
student in a location in or near their home community, or somewhere the student has friends or
family, occasions do arise that the student will be required to travel for their clinical experience. All
students can expect that they will be required to travel for clinical experiences during their program
of study.
3. State regulations may prevent the University of Mary from placing students in some states. In
circumstances the student is contemplating moving to a different state, it is advisable for that
student to communicate early with the FNP Program Coordinator.
Clinical Placement Process:
1. During December of Year 1, the student will receive an invite to Monday.com, CastleBranch Registration, and instructions for completing renewal Background Check Requirements.
2. Student completes and submits an online Clinical Placement Information Form (Appendix C) and NP Skills Checklist (Appendix B) to Monday.com.

6
3. Student completes CastleBranch and Background Check Requirements and continues updates through out the ENTIRE FNP Program.
4. Student schedules a Clinical Placement Planning Meeting January of First Year. A sign up will be sent to students University of Mary email by the FNP Clinical Competency Coordinator.
5. Student meets with FNP Clinical Faculty and Graduate Nursing Clinical Placement Liaison to review Clinical Placement Information Form, NP Skills Checklist to discuss and plans are made for clinical practice sites/preceptors during the Clinical Placement Planning Meeting.
6. Faculty approves proposed clinical placement plan, preceptor, and setting. 7. Graduate Nursing Clinical Placement Liaison:
a. Verifies if student requirements are in place (i.e., immunizations, required certifications, criminal background check). If not in place, no further work on placement continues.
b. Makes contacts to student placement coordinators at potential preceptors’ affiliated practice settings.
c. Documents notes related to dates/types of communications, response to communications, etc. d. Determines if interagency contracts are in place for potential setting. If interagency
agreements are not in place, sends University of Mary Memorandum of Understanding for signatures or forwards clinical site’s affiliation agreement to University of Mary’s Legal Counsel for review and approval. Once draft is approved, sends on to collect signatures.
e. Communicates accepted or declined placements to faculty and student. f. Moves to alternative placement options when necessary (i.e. declined placement, untimely
communication from potential preceptor or organization, etc.). g. Inquires about site-specific paperwork (HIPAA, confidentiality forms, verification of background
checks and immunization requirements). Sends paperwork to student, collects and submits to clinical site. (Some sites use online attestation, and others require UMary to “sign off” on forms or rosters (Excel spreadsheets) and submits back to clinical site.
h. Inquires about computer access, badging, parking, etc. as needed and/or passes on information to the student.
i. Asks for scheduling instructions and contact information, as needed. j. Adds clinical site and preceptor into Typhon.
8. Once a preceptor has accepted a student, two documents must be in place: a. Affiliation Agreement/Memorandum of Understanding (MOU) (agreement between the
University of Mary and the organization where the clinical experience will occur).
b. Letter of Agreement (an agreement between the preceptor and the FNP program). The letter of
agreement contains the following information:
• Student name
• Student responsibilities
• University name
• Course number
• Clinical site/organization name and address
• Timeframe, number of hours requesting, and specialty area
• Preceptor’s name and address
• Preceptor responsibilities
• Clinical faculty name and contact information
• Clinical faculty responsibilities
• FNP Clinical Competence Coordinator name and contact information

7
• FNP Clinical Competence Coordinator responsibilities
5. Graduate Nursing Clinical Placement Liaison creates and sends the letter of agreement to the approved
preceptor. The letter of agreement must be signed and returned by the preceptor, FNP Competence
Coordinator, clinical faculty, and FNP student before initiating the clinical experience.
6. In addition to the letter of agreement, the Graduate Nursing Clinical Placement Liaison sends a copy of
the University sponsored liability insurance coverage on students is sent to the facility.
7. Graduate Nursing Clinical Placement Liaison gathers any additional required pre-courses, scheduling
information, contact information, etc. and provides a Clinical Approval Letter to the student upon
verified completion and signing of the Memorandum of Agreement and Clinical Letter of Agreement.
This step may take 2 - 3 weeks. The student cannot begin scheduling or start clinicals until this letter
has been received and any additional facility requested requirements (such as EPIC training) are
completed by the student.
8. Graduate Nursing Clinical Placement Liaison, in collaboration with students, ensures the preceptor and
clinical site information is up to date in the clinical tracking system (Typhon®).
9. Student establishes their clinical schedule in collaboration with their preceptor within two weeks of
receiving clinical placement confirmation. Clinical faculty will establish the timeframe within each
semester for clinical placement completion to ensure necessary course material has been covered
prior to the rotation. This timeframe, along with the means by which the preceptor would like to be
contacted for scheduling, will be communicated to the student via the Graduate Nursing Clinical
Placement Liaison.
10. Students enter their clinical schedule into the clinical tracking system (Typhon®), as well as log each
patient encounter and track daily time logs. The FNP Clinical Competence Coordinator and assigned
clinical faculty from each respective course will monitor both the online clinical schedule and Typhon®
patient encounter entries.
11. FNP Clinical Competence Coordinator will communicate with preceptors at the beginning of the
semester. This communication is meant to strengthen the connection between the preceptor and
clinical faculty. The message will include the preceptor manual, reiterate student expectations and
extend contact information for the preceptor to reach faculty.
12. Student facilitates the scheduling of a clinical site visit near the midpoint of the student’s experience
with clinical faculty and the preceptor. The purpose of the site visit will be to evaluate the student’s
experience, the student’s performance and clinical site effectiveness. This clinical site visit may occur
by one of several mechanisms (i.e., in person, over the phone, or technologically facilitated). It is the
student’s responsibility to schedule the site visit.
13. Student notifies the FNP Clinical Competence Coordinator once they have completed all clinical
experiences.
14. FNP Clinical Competence Coordinator will send the preceptor a student evaluation. Students must also
complete an evaluation of the clinical site. Students are strongly encouraged to save a copy of the
evaluation in their e-Portfolio.
15. FNP Clinical Competence Coordinator will send the preceptor a thank you note and a letter
documenting the hours of service provided on behalf of the FNP Program, student, and faculty.
16. Student sends a thank you card to their preceptors for their time and commitment.
8
Preparation for Clinical Placement
In order to begin the clinical placement process, students are required to submit several documents noting
they are a healthy and safe student that meets the requirements of the assigned clinical sites. The student will
be asked to submit documents or certificates of course completion to a variety of databases including
CastleBranch (https://www.castlebranch.com/sign-in), Typhon
(https://www3.typhongroup.net/np/data/login.asp?facility=), and/or other facility databases such as
MyClinicalExchange, or site specific healthcare websites for onboarding students.
It is imperative to be responsive to any requests for additional documentation within a TIMELY manner. If
students fail to keep their requirements or submit documents timely, the University of Mary will not be able to
proceed with clinical placement. At minimum clinical placement takes two months, though for many clinical
sites, especially any military, Indian Health Service, or Government Facility, it may take six to twelve months to
complete the clinical placement process. It is essential for the student to read, understand, and follow any
requests from your Graduate Nursing Clinical Placement Liaison, FNP Clinical Competence Coordinator, or the
specific clinical placement facilities so contracts and plans can be made well in advance to solidify an
experience that will be of benefit to the student as they progress through the program.
For the Graduate Nursing Clinical Liaison to begin work on student placements, it is necessary for all immunizations and the criminal background checks to be up to date and to remain up to date throughout the entirety of the clinical experience.
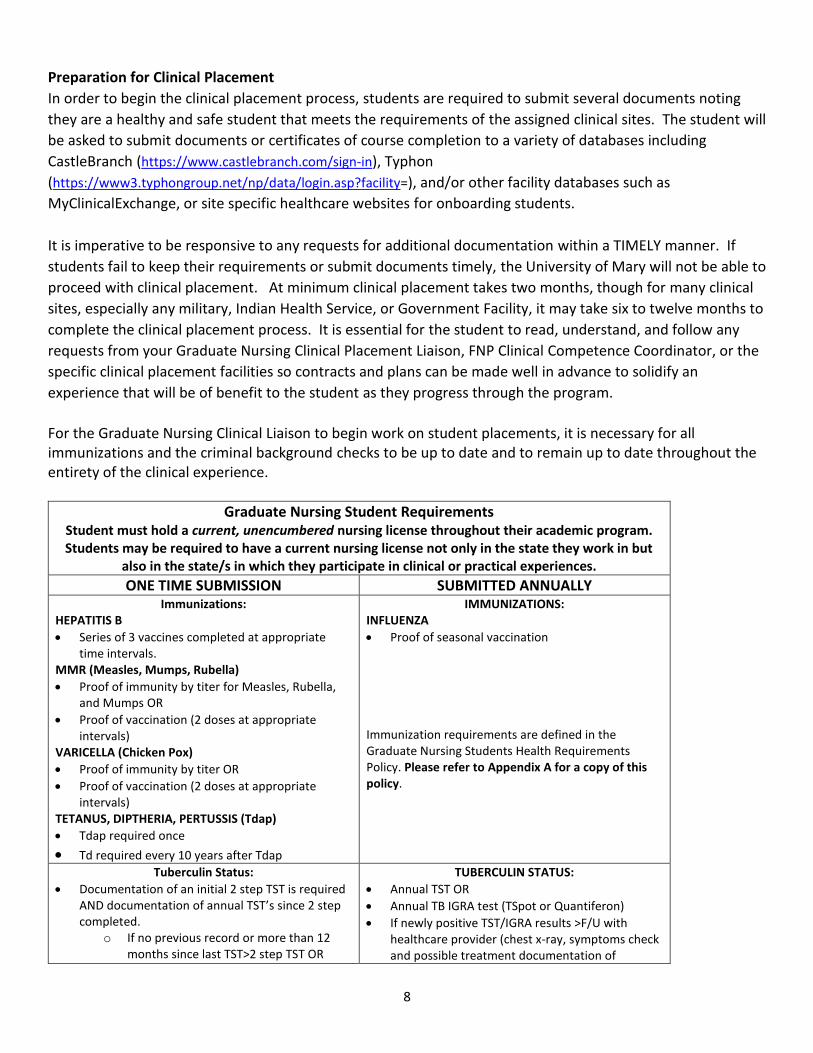
Graduate Nursing Student Requirements Student must hold a current, unencumbered nursing license throughout their academic program. Students may be required to have a current nursing license not only in the state they work in but
also in the state/s in which they participate in clinical or practical experiences. ONE TIME SUBMISSION SUBMITTED ANNUALLY
Immunizations: HEPATITIS B
• Series of 3 vaccines completed at appropriate time intervals.
MMR (Measles, Mumps, Rubella)
• Proof of immunity by titer for Measles, Rubella, and Mumps OR
• Proof of vaccination (2 doses at appropriate intervals)
VARICELLA (Chicken Pox)
• Proof of immunity by titer OR
• Proof of vaccination (2 doses at appropriate intervals)
TETANUS, DIPTHERIA, PERTUSSIS (Tdap)
• Tdap required once
• Td required every 10 years after Tdap
IMMUNIZATIONS: INFLUENZA
• Proof of seasonal vaccination
Immunization requirements are defined in the Graduate Nursing Students Health Requirements Policy. Please refer to Appendix A for a copy of this policy.
Tuberculin Status:
• Documentation of an initial 2 step TST is required AND documentation of annual TST’s since 2 step completed.
o If no previous record or more than 12 months since last TST>2 step TST OR
TUBERCULIN STATUS:
• Annual TST OR
• Annual TB IGRA test (TSpot or Quantiferon)
• If newly positive TST/IGRA results >F/U with healthcare provider (chest x-ray, symptoms check and possible treatment documentation of

9
o Negative TB IGRA test (Tspot or Quantiferon) within 12 months OR
o If negative TST within 12 months > one step TST
• If newly positive TST or TB IGRA > F/U by health care provider (chest x-ray, symptoms check and possible treatment documentation of absence of active M. TB disease) and need to complete health questionnaire
• If history of positive TST>provide documentation of TST reading, provide proof of chest x-ray documenting absence of M.TB, medical treatment and negative symptoms check OR
o If history of BCG vaccine >TST Skin Testing as above or TB IGRA (TSpot or Quantiferon). If negative >OK; if positive > follow-up as above.
absence of active M. TB disease) and may need to complete health questionnaire.
• Previously documented + TST results and prior negative chest x-ray results: submit annual symptom check completed within one year from healthcare provider.
BACKGROUND CHECK Annual background re-check.
TRAININGS/CERTIFICATIONS: Students are responsible to locate, register and fund all required certification courses. The student is also
responsible to upload a copy into their Medical Document Manager on CastleBranch.
• American Heart Association (AHA) BLS Healthcare Provider Card
• Prior to NUR836 o Pediatric Advanced Life Support (PALS) o Advanced Cardiac Life Support (ACLS) o Trauma Nursing Core Certification (TNCC)
BACKGROUND CHECK A National Criminal background check upon admission to program and updated annually. Please refer to your Graduate Nursing Student Handbook for more specific information/requirements.
SIGNED RELEASE OF INFORMATION
• Kept on file with program COMPLETED MEDIA RELEASE
• Kept on file with program CV/RESUME/BIOSKETCH
• CV/Resume/BioSketch/Professional Headshot Picture will be uploaded upon admission. Student will be responsible for updating CV/BioSketch annually to include contact information.
ADDITIONAL SITE SPECIFIC REQUIREMENTS THAT MAY APPLY
On request from an affiliated organization for which the student is engaged in a learning experience, the
Graduate Nursing Program will share student immunization information. At times, affiliated
organizations may have additional health requirements. In these situations, the student will be
held responsible for compliance with these requirements. Please see additional note below.
Additional requirements may include the following:
• Drug screen (Please see “Policy on Drug Testing” in Graduate Nursing Student Handbook
• Personal Health Insurance
• Vehicle Insurance (for access to VA and Military Clinical Sites)
• Hepatitis A Vaccine
• Proof of US Citizenship
• Color Blind Test
• HIPAA and/or OSHA Training
• Department of Human Services Background Study
• EPIC or other computerized documentation training
Common Additional Expectations of Clinical Facilities
Most clinical facilities employ staff in clinical education departments that assume the role of working with
Universities to coordinate the placements of students. Many have their own algorithm for determining how
individuals are prioritized for placements (employee or not, program, etc.). Nearly all restrict programs or
students from asking preceptors directly regarding their willingness to be a preceptor.
Agencies have their own timelines that they follow which sometimes does not line up well with the timeline needs of the program. This challenge can complicate the seamless placement of students.
Immunizations, background checks, sometimes drug testing, completion of the facilities unique onboarding
process (which requires separate paperwork and training usually on Electronic Health Records take time.

10
Unfortunately, these hours don’t count toward the clinical requirement – and students must accommodate
the meetings times the clinical agency offers to them for this training.
Clearance to Begin Clinical Experience
1. All clinical and FNP placements must be secured and approved by University of Mary Faculty.
2. Students are NOT to attempt to request, contact, or schedule their own clinical experiences unless
given explicit direction to do so by the Graduate Nursing Clinical Placement Liaison or FNP Clinical
Competence Coordinator.
3. Once the Graduate Nursing Clinical Placement Liaison has verified completion and signing of the
Memorandum of Agreement and Clinical Letter of Agreement, the Graduate Nursing Clinical Placement
Liaison will gather any additional required pre-courses, scheduling information, contact information,
etc. and provide a Clinical Approval Letter to the student. This step may take 2 - 3 weeks. The student
cannot begin scheduling or start clinicals until this letter has been received and any additional facility
requested requirements (such as EPIC training) are completed by the student.
Miscellaneous Clinical Concerns
Student Liability Insurance
A group policy of liability insurance is provided by the University of Mary. As a practice discipline, nursing deals
with the public and may be subject to litigation. Therefore, liability insurance is mandatory for all nurse
graduate students. A separate fee will appear on the student financial billing statement annually. Liability
insurance provides coverage only during approved clinical rotations and time frames. This is not a health
insurance policy. Students must maintain their own health insurance.
Clinical Travel Requirements The University of Mary will place students in clinical experiences that are expected to provide students with the best tools and experiences necessary to meet program objectives, support future clinical practice, and obtain the most independent opportunities to practice as a student. Depending on where a student is located, there may not be access to necessary preceptors who can assist with providing adequate clinical exposure to meet program requirements. Travel will be required. Some clinical sites do provide housing; however, it is not the standard. Students are responsible for their own transportation and lodging expenses incurred for any experiences related to their academic program of study. Students are not allowed to transport clients, due to liability concerns.
Clinical Attendance Clinical attendance is mandatory. Students are required to enter their clinical schedule into the Typhon Clinical
Tracking Software. Students are required to be at their clinical site during their scheduled clinical hours. The Typhon Calendar will be used as needed to verify student compliance with clinical hours and planning clinical site visits. No missed hours of clinical will count towards a student’s total number of required hours. Students must complete the required number of clinical hours per semester to successfully progress in their program of study. If an extenuating circumstance creates an unforeseen absence such as illness, family emergency, or inclement weather, the student must contact both their preceptor and clinical faculty as soon as possible. It is the student’s responsibility to assess the safety of travel conditions if travel to clinical is required. Any time lost must be made up during the same semester. In extenuating circumstances, arrangements are to be made with course faculty and the FNP Program Coordinator to find an alternative clinical site.

11
Failure to Adhere to Attendance Requirements Consequences of a single unexcused absence for a scheduled synchronous class meeting may result in any of the following: * Dismissal from the course * 5% reduction in overall course grade * A zero for the related assignment Absence from scheduled clinical experiences and/or class without prior approval will be recorded as an unexcused absence. Two unexcused absences will place student on probation. Notification of this status will be given in writing. Further unexcused absences may result in termination from the program. Working during Clinical Courses Some students will ask to complete clinical placement where they work. Students may complete clinical hours where they work, however, students MAY NOT conduct hours within the same department where the student is normally in an administrative or leadership position and or other relationship that may results in a conflict of interest. For example, student is working part-time as a clinical manager in an urgent care clinic, then returns to complete clinicals under a provider and with clinical staff the student is responsible for “managing” during regular working hours. This situation results in a potential conflict of interest.
Most students will work a part-time or PRN status while in the FNP program. The first year is more feasible, however, once clinical courses start, most students find it very difficult to keep up with all the rigors and requirements of a doctoral nursing practice program. Placements will not be based on specific student scheduling needs. Work will not be an accepted excuse for missing clinical or mandatory student meetings/presentations/institute. If students choose to continue working, it is crucial that an employer be flexible with the student’s work schedule, as most offices operate on a Monday to Friday, 8 am to 5 pm schedule, which will conflict with scheduled clinical and class periods. Overall, the University of Mary Graduate Nursing Program highly recommends that students do not work, or work only a minimal number of hours, during clinical course semesters.
On-Call Hours
A preceptor may be on call for a 24-hour period or longer, but the maximum number of hours a student may
count towards their clinical in a 24-hour period is 16 hours. Furthermore, students may only log the hours
they are actively engaged in patient care. On-call hours may not be logged.
Surgical Hours
If the facility and preceptor are willing, students can follow and assist in surgery. Students may use a portion of the clinical hours spent in the Operating Room (OR) for credit during the clinical experience depending on the length of the clinical experience. Students will need to communicate with Clinical Faculty prior to entering the OR regarding how many hours may be applied for clinical credit. Students would still include these patient exposures in the Typhon Clinical Tracking System. Characteristics of the Clinically Engaged Student
Be open and willing to extract as much experience and knowledge from each one of your clinical preceptors and clinical sites. Always be asking the question, how can I apply this experience to my FNP objectives and future clinical practice? Each student depending on their location may have different and varied sites, but all students can expect their clinical experiences to meet program objectives.

12
Here are some comments to contemplate as you embark on the clinical experience:
• Always keep in mind the two primary goals of clinical training: To learn to care for patients in an
independent role and to help develop professional identity as a nurse practitioner.
o It is easy to be distracted by worries about how well you are doing and what your teachers and
preceptors think about your performance. However, maintaining a clear focus on these two
goals above will help you maintain perspective during challenging times of your clinical
experience.
o Consider each placement as an “audition” for future placements. The reputation you develop
while in your clinical rotations can open doors for future rotations, and even future
employment. Alternatively, a negative experience with a student can impact a sites’ willingness
to place future students.
o Formally thank each preceptor and staff who assisted you at the end of each clinical rotation
with at least a thank you note.
• Be prepared for clinical rotations.
o Prepare both academically and mentally for your rotations. From an educational perspective,
look ahead to each rotation. Have the appropriate resources available before you start the
rotation. Ask questions of previous students.
o You will find that each preceptor has their own way of doing things and their own personality.
Although this may feel a bit strange when you experience it (you will certainly find some
rotations more comfortable than others) and take some getting used to, don’t be surprised, and
try to take advantage of seeing how different preceptors view the world of clinical practice.
• Work-life Balance
o Work-life balance can be a major struggle. Consider cooking for the week on your day off and
stock up on healthy snacks and easy to prepare foods. Recharge on your days off by doing
something that gives you joy or peace of mind. For some it’s exercise, for others it could be
watching television, brunch with friends, or writing in a journal.
• Don’t underestimate your abilities.
o The clinical experience is intended to help you apply the basic science knowledge you have
acquired over the last semesters to real patients. This is an extremely difficult, frustrating, and
often painful experience. At times you will feel as though you don’t know anything, and it is not
uncommon for students to say that the more they experience, the more they realize how little
they actually know. But don’t forget that you DO know a lot, and that over time things will
become easier! Remember that those who are supervising and teaching you were at one point
in the exact same position as you will be, and possibly not that long ago. Students also make
major contributions to patient care and patient care teams, so always remember that your
presence and engagement are valued.
o During your rotation make your presence meaningful every day. If you are reliable and
enthusiastic, you will be entrusted with a range of tasks, from minor to major. Most preceptors
care less about your ability to ask every content question and more about your dedication to
patient care and desire to improve your knowledge and skills during the rotation.
o Keep track of to-do items for patients cared for during the day. If everything has been
completed, volunteer to help with other patients by offering to run samples to the lab, call a

13
pharmacy to confirm a patient’s medication list, or find a clinically relevant article and
summarize for the next day. Your effort to go above and beyond will be noted.
• Don’t overestimate your abilities.
o It is also important that you understand your own strengths and limitations to optimize your
clinical learning. Many students feel as though they always need to have the correct answer or
never need to ask for help in order to be successful. This approach can be a great hindrance
when learning clinical practice. It is perfectly acceptable to indicate what you know and don’t
know. You preceptors understand that you are early in training and that different students
progress at different rates when transitioning from the classroom to the clinics. Do prepare to
the best of your abilities. It’s ok to tell people what you need help with in order to fill in your
knowledge and skill gaps.
• Take advantage of this incredibly unique period in your professional training.
o This will be the only time you will be able to become intensively involved with the different
disciplines. So, despite the expected stress and anxiety that you will undoubtedly experience,
when able find times to relax and enjoy the process.
• Contact your preceptor within a week of gaining approval to schedule or reach out to your preceptor.
o Ask about where to meet or how best to contact them on your first day so you know what to do
when you arrive. Some work in areas that have employee-only access or are at a different
location depending on the day of the week, so you need to have a plan for how you’ll connect
before you get there.
o Ask about particular resources you should bring.
o Ask up front how your preceptor prefers to field questions.
▪ For many practices, asking questions as you go is routine. However, some practices are
fast paced and more conducive to fielding groups of questions every few hours or at the
end of the day.
▪ You want to ask as many questions as you can while on a rotation. Preceptors are gold
mines for clinical pearls, career advice, and patient care strategies, and you don’t want
to miss out on their insight.
▪ However, it is best to limit questions while in the presence of the patients.
▪ It is best to just ask your preceptor when it is best to ask questions.
o Ask about presentation preference.
▪ You’ll surely be practicing your patient presentation skill before your first rotations.
However, what a preceptor wants from a presentation will vary based on the specialty
and patient status.
▪ If someone is an established patient coming in for a specific complaint, a problem-
focused presentation is appropriate. For a brand-new patient, you’ll want to cover a full
history and highlight any items relevant to their presenting complaint. But, without
asking, it’s hard to know what your preceptor prefers.
▪ Usually what is most important to the preceptor is that students can determine what is
RELEVANT to a patient. They do not have time to sit through an entire medical history
on someone they have known for three years and are coming in for a check-up.
▪ Preceptors want to see that students can triage the information they gain from a history
and physical and tell the preceptor the essentials for a patient with a certain diagnosis
or under a particular treatment.

14
▪ Please see Three Minute Clinical Presentation Tips in the appendix for further
recommendations.
o Come ready for the environment.
▪ If you are entering a pediatric rotation, have quick access and be well versed in the
treatment of otitis media, pharyngitis, and upper respiratory guidelines. Same if moving
into a women’s health rotation – you should have ready access to ACOG pap guidelines
and prenatal care recommendations.
▪ Always dress professionally but understanding the environment you will be in will help
you to adapt accordingly. For example, high heels may not be the most functional
shoes. Please review at length the Graduate Nursing Student Handbook requirements
on “Dress Code for Clinical Rotations”.
▪ Pack a lunch and a few extra snacks. You never know what a new rotation may hold in
terms of available food or lunch hours. Until you get a lay of the land, bring food with
you.
▪ Even if there are places to eat nearby, some practices are too busy to break for lunch.
Going on a new rotation is like starting a new job every 5 – 6 weeks and can be mentally
exhausting. Do not assume you can make it throughout without some calories.
o Honor your role with patients.
▪ One of the most difficult things as a student is not answering a question.
▪ It is in our nature to be helpful. We want to fill in the blanks for patients when they
have questions, or sometimes provide a positive spin on something that we probably
shouldn’t.
▪ You might be 80% sure of something, but if you are not solid on an answer or feel like
you are providing false hope, leave the question for your preceptor.
▪ Clinical rotations are an excellent way to observe how providers handle difficult patient
questions. You don’t have to worry about doing this yet, so maintain your role as a
student and just learn how you MIGHT handle difficult issues in the future.
▪ Don’t start guessing or talking over your preceptor on diagnosis or treatments. This may
cause undo anxiety for the patient and more time than needed by the preceptor to
address un-needed concerns. Work with your preceptor on how and when to best
discuss student findings and recommendations (either with or without the patient
present).
o Show up early; stay to the end.
▪ Preceptors understand you have a lot to do in school, but arriving at least 10 minutes
early and staying until the work is done (without constant checking of your phone) will
go a long way!
▪ You may not be interested in a particular field of study, but there’s always something to
learn. Preceptors are always volunteers, so even if you think you would never want to
work in their specialty, respect that they are using their time to help you.
▪ Every preceptor is a potential reference and a connection for job hunting in the future.
Even if you are bored, or would rather be somewhere else, it’s in your best interest to
stay engaged. Don’t get caught with your cell phone causing distractions. Shut it off. Or
if needed for entering patient encounters, be certain the provider and staff are aware of

15
how you are using your phone. Many will unfortunately assume other non-student
engaged activities.
Other Student Clinical Responsibilities When registered in DNP Clinical Courses, the NP student is responsible for:
• Following all Graduate Nursing Student Handbook requirements.
• Following the administrative policies, regulations, standards, practices (such as universal precautions) and procedures of the contracted (affiliated) clinical facilities.
• Safeguarding the confidentiality of client information.
• Providing their own transportation to and from the clinical facilities. If a clinical preceptor travels to an outreach site, the student may ride with the clinical preceptor or with facility transportation at their own risk. The University of Mary and Clinical Facility are not responsible should an unforeseen accident occur.
• Reporting to the preceptor on time and as scheduled. On time should be 15 minutes prior to the start of the clinical experience.
• Providing appropriate and timely notification to Clinical Faculty when conflicts or concerns arise in the clinical setting. This may be a patient, clinical site, preceptor, or variety of other concerns that may interfere with the student’s clinical experience.
• Conforming to the standards of professional practice established by the preceptor, affiliated clinical facilities, and any applicable regulating body while participating in the preceptor experience. Understand and practice within the scope of advanced practice nursing as regulated by the Nurse Practice Act in the state where clinical experiences will be completed
• Coming prepared to the clinical site with a stethoscope, lab coat, name tag, be ready with EMR access before arriving at clinical.
• Wearing a University of Mary identification badge while in the clinical practice area and/or student identification badge per the facilities requirements.
• Checking e-mail DAILY. Students registered in NP courses may have short turn-around times for returning needed documents, therefore it is imperative to be checking e-mail accounts frequently.
• Keeping course faculty fully appraised of your ability to complete the clinical hours in the expected time frame as clinical contracts do include specific dates. If it becomes apparent to the student or the approved preceptor that the student or preceptor will not be able to meet his/her agreed upon obligations, it is the student’s responsibility to inform the course faculty of the situation to promptly. This allows time to locate an alternative preceptor under whom the expectations can be met or make other arrangements to drop the class or take an incomplete until the course clinical requirements can be completed.
• Keeping the FNP clinical faculty, FNP Program Coordinator, and or FNP Clinical Competence Coordinator appraised of any personal crisis that arises that may prevent completion of any courses while attending the University of Mary. All faculty and administrators are well aware that certain situations may arise while students are enrolled in graduate studies and will make every effort to help the student decide what can and should be done about your educational responsibilities at the time of crisis. The key to any sound decision or alternative plan requires that you make the University of Mary aware of your situation. Decisions about tuition refund, dropping a course or courses, taking a leave of absence, obtaining assistance from Student Services can be done in a satisfactory manner when you notify and discuss the situation immediately.
• Facilitating a clinical site visit between FNP Clinical Faculty and Preceptor.
• Seeing a minimum of one to two patients per hour on most days depending on the complexity of the patient.
16
• Maintaining an accurate and timely electronic clinical log of patient encounters and clinical hours on a weekly basis in the Typhon Clinical Tracking System. Students may be asked to hold on clinical attendance until caught up with clinical work. Typhon Entries must be made for each patient with whom the student has involvement. Entries allow faculty to assess the experience and eventually the competence of the student. Please see Appendix F: Typhon Guidelines/Examples for more detailed information.
• Updating NP Clinical Skills Checklist at the end of each clinical course.
• Completing the following evaluations in the Typhon Clinical Tracking System: Student Evaluation of Preceptor(s) and Student Evaluation of Clinical Site(s).
• Notifying the FNP Clinical Competence Coordinator upon completion of all clinical hours for the course. This allows the FNP Clinical Competence Coordinator to send out the Preceptor and Student Evaluation Forms and a Thank You Letter/Verification of Hours to the Preceptor.
Professional Behavior The highest standard of professional behavior, ethics, and integrity are expected of each University of Mary student. Nurse practitioners have a responsibility for the welfare, well-being, and betterment of their patients, along with a responsibility to maintain their own professional and personal well-being in and out of the clinical setting. Each University of Mary student is expected to treat all fellow course mates, faculty, University of Mary personnel, preceptors, clinical facility staff, and patients with courtesy and respect and with regard for their dignity.
If a student has been found to have fallen short of these expectations (this may include but are not limited to statements of concern for lack of engagement in the clinical experience or professional behavior either verbally or by written evaluation, community complaints of student representation of the University of Mary, alcohol or drug related offenses, disruptive behavior, concerns of any form of harassment), the University of Mary will follow set protocols as found in the Graduate Nursing Student Handbook. The safeguarding of patient care and safety is paramount, and the University of Mary will enforce disciplinary measures to include dismissal from the program whenever necessary and/or if continued behaviors are not resolved.
Please review Graduate Nursing Student Handbook under Principles of Professionalism, Academic and Professional Behavioral Standards Review, Graduate Nursing Academic Progression Committee, and Graduate Nursing Satisfactory Progression.
Establishing Baseline Student Clinical Competence
The NP skills checklist is a document utilized to track the clinical skills development of NP students as they
progress through the program. The tracking system is started and maintained by each individual student for
several reasons. Documentation of skills allows preceptors to assess the level of the student’s experience so
that each preceptor can provide a variety of clinical experiences. This snapshot of a student’s abilities and
experiences can help to ensure a continuing progression throughout their program of study. Also, as a new
graduate, the student will be able to inform potential employers what kind of experience he or she can bring
to the table on day one of employment.
Overview of Student Clinical Evaluation Methods Course, student, preceptor, and faculty evaluations are an expected part of any clinical experience. These evaluations are important not only because they are required by regional and national accreditation bodies, but also because the evaluations provide information that leads to future improvement of student, program, and the University of Mary. Grading in the clinical courses at a minimum includes consideration of your self-evaluation of clinical objectives, growth of NP Skills, clinical site visits (may be via phone, in-person, other

17
technology-assisted means), clinical logs (through Typhon Clinical Tracking Software), quality of written assignments including dictations, preceptor’s appraisal of your skills, your contributions to group discussions, and your performance in Hotseat Competencies.
On at least three occasions during the FNP program, students will have a formative assessment meeting with the FNP Clinical Competence Coordinator to discuss their current FNP Skills, clinical performance, Hotseat Competencies, and overall clinical competence to update the student, plan further clinical experiences, and/or decide on continued progression through the FNP program. As faculty, we are excited to have this time to work with you one on one as you grow in your professional development!
Clinical Placement Planning Meetings Clinical Placement Planning meetings occur a minimum of three times over the course of the student’s program of study. Members of this meeting include a faculty representative, the Graduate Nursing Clinical Placement Liaison, and the individual student. Meeting occurrences follow the general schedule below:
• Meeting 1: January of Year 1
• Meeting 2: September or October of Year 2
• Meeting 3: February or March of Year 2
The purpose of these meetings is to discuss the clinical placement process, develop a clinical placement plan, onboard students to clinical expectations, and determine current stage of clinical competence against expected stage of clinical competence. Students will schedule Clinical Placement Planning meetings through an electronic signup sent to their University of Mary webmail accounts. If the clinical placement plan as minimal changes from the first meeting, Meetings 2 and 3 may be very brief communication completed via phone, email, or face to face during institute sessions. At least two weeks prior to the first meeting, students must: 1) complete/update/submit a Clinical Placement Information Form, 2) submit a completed NP Skills Check List, and 3) ensure immunization, certification, and background check requirements are up to date in CastleBranch. NP Skills Checklist While clinical skills may be just one of many abilities needed in today’s healthcare world, they are still extremely important. The NP Skills Checklist is used to help track your progression and exposure to various clinical skills throughout the program. The progression can be shared with FNP Clinical Faculty, your preceptors, and future employers to demonstrate the skills you may need, but more importantly, the skills you have already mastered. Student Clinical Objectives/Evaluation The student will write individualized clinical objectives to be reviewed and approved by their assigned FNP Clinical Faculty PRIOR to starting the clinical experience. The student is to return a preceptor signed copy of the student’s clinical objectives to clinical faculty preferably within 7 days of starting the clinical experience. At the end of the experience, complete a self-evaluation of your progress related to your specific clinical objectives. This document will serve as an example of your clinical growth throughout each experience. Clinical Conference Group Meetings Learning in the FNP Program takes many different forms including lecture, lab, and clinical. Your clinical faculty will be monitoring Typhon and clinical dictations. However, direct communication with your clinical faculty is an important factor in the faculty person’s overall assessment of your clinical competence progression.

18
Over the course of the clinical courses there will be at least two meetings to convene with your clinical faculty
and small group of peers. These meetings will be placed on the course calendar and will take place via virtual
technology. The student is responsible for communicating with their clinical faculty when they believe they
have completed their clinical experience. Students will be assigned to reflect on several areas from their
clinical experience. Topics that are to be covered will be made available in the course announcements before
the first assigned meeting. Students are expected to be full participants.
Clinical Site Visit
Clinical site visits augment the evaluation process and take place at approximately the midpoint of the
student’s clinical hours. The site visits may occur in person, by phone, or virtual technology. During the clinic
site visit the FNP Clinical Competence Coordinator will make inquiries related to specific characteristics of the
clinical experience and the student’s performance. This visit is further enhanced through direct or technology
assisted observation of the student in direct patient care encounters.
Typhon Entries
Typhon is a patient tracking system used to document patient encounters throughout clinical experiences. It will be used to track clinical competencies. It can be accessed at https://www.typhongroup.net/np/data/login.asp?facility. University of Mary’s facility number is 7201. Each student will be provided a user name and password. An orientation is provided prior to the first major clinical experience course. There are student tutorials available for review once a student is logged in. The following are guidelines to follow when using the system.
• Clinical schedules must be entered by the student into Typhon as soon as they are established AND NO LESS THAN ONE WEEK PRIOR TO START OF CLINICALS. Students may not start clinicals until their schedule is entered into the Typhon system and their Clinical Objectives have been submitted in Canvas for Faculty Approval.
• It is required that all patient encounters be entered. Remember, you are building your database of experiences. You want Typhon to showcase the variety of conditions, diagnostics, pharmacological plans, and procedures that you have had exposure and experience with. The quality of what you put in impacts the quality of the product you will have at the end. It should be your goal to maximize this tool’s potential as a professional marketing portfolio for you in the future.
Clinical logs must be completed on a WEEKLY basis, however it is highly recommended that students enter
encounters daily. All entries of patient encounters from the previous week must be entered in Typhon by
Monday of each week! Should students become more than 1 week behind on Typhon entries, they will not
be allowed to continue with the clinical experience until caught up.
Dictations
The purpose for evaluation of dictations/documentations is to appraise your critical thinking skills as well as
your proficiency regarding assessment, diagnosis/impression, and development of a plan of care. In addition,
assessments of clinical documentation assists with quantification of a student’s ability to formulate an
accurate, clear, well organized record that reflects and facilitates sound clinical thinking. If at all able, do take
the opportunity to document for your preceptors. However, ALL dictations submitted for grading must be self-
typed and submitted in a word document. No COPIED or facility-based dictations are allowed. Be sure your
dictations are complete but scrubbed of any patient identifying information (birthdate, medical record
numbers, names, etc.). This assignment is a learning tool. Specific rubric criteria for each clinical course will be
provided. Although various clinical sites may use a different format and or electronic templates, the student

19
must follow University prescribed dictations. For example, some clinical sites will note “All systems negative”
or Cardiovascular Assessment is negative. This will not suffice for program requirements because FNP Clinical
Faculty are assessing your ability to include pertinent information, exclude unneeded elements, complete and
document appropriate physical exams using medical terminology. Therefore, students will be required to
write out full review of systems and exam findings.
Preceptor Typhon Evaluations At the end of the clinical experience an electronic evaluation is completed by each preceptor using the Clinical Evaluation form located in NPST/Typhon. This evaluation is essential for educational and evaluation processes. Preceptors are encouraged to discuss the evaluation with the student prior to its completion. Preceptors are expected to intervene directly and immediately should the student provide unsafe or inappropriate care in the clinical facility. Students are encouraged to save their Typhon evaluations after each clinical rotation because it demonstrates your competence and can be helpful for future employment. It offers a skills report of your clinical. Hotseat Competency Testing
Student clinical competence is further evaluated by faculty during practical testing that occurs on campus at
the conclusion of each clinical course. Using a simulated scenario, the student is evaluated on their history,
physical exam, clinical decision making, diagnosis, management, and patient education competence. This
competency testing is coined “hot seat” because they are evaluated in real time by at least two faculty while
also being observed by their peers. This is a Pass/Fail requirement for continued progression in the FNP
Program. If a student fails the Hotseat Competency, several other factors are taken into consideration. Based
on an overall assessment of the student’s performance in the clinical setting and FNP course work, students
may be required to repeat the course, repeat another Hotseat Competency, complete additional clinical
hours, or work one on one with faculty followed by another Hotseat Competency. The final recommendation
will be made based on feedback from at least two clinical faculty. Please see Appendix J for further
information.

20
Appendix A
Graduate Nursing Student Health Requirements
GRADUATE NURSING STUDENT HEALTH REQUIREMENTS
It is the responsibility of the graduate nursing student to comply with the following requirements and provide documentation of all required immunizations to the Graduate Nursing Program at least one full semester prior to any course with a clinical experience (this includes non-direct patient care experiences). Immunization records must be provided on letterhead or other form clearly labeled with the name of the provider or agency who administered the immunizations. Positive titers are acceptable evidence of immunity status. Healthcare agencies that the student participates in clinical experiences have similar requirements. Failure to meet these expectations will prevent the student from entering a clinical experience. Instructions:
1. All items listed, with the exception of Hepatitis B, are MANDATORY FOR ALL STUDENTS. Only persons born before January 1, 1957 are exempt from having to submit this information.
2. Persons born before January 1, 1957 must submit a copy of a valid driver’s license, passport, or birth certificate to establish proof of age.
3. Please label all pages of immunization records with appropriate identification including your current name if it is different from what is on the record.
Immunizations Required Influenza Vaccine
Submit proof of influenza vaccine within the last year Tetanus-diphtheria (Td or Tdap) Submit proof of a tetanus booster which is less than 10 years old Rubeola (provide ONE of the following) Submit dates of immunization with live virus vaccine (if born after 1968 proof of TWO doses required) Submit blood titer results proving immunity Mumps (provide ONE of the following) Submit date of immunization with live virus vaccine Submit blood titer results proving immunity Rubella (provide ONE of the following) Submit dates of immunization with live virus vaccine Submit blood titer results proving immunity Varicella (provide ONE of the following) Submit dates of immunization Submit blood titer results proving immunity Tuberculin skin test (TB or PPD)
Submit documentation of one of the following: 1. initial two step TB test and annual PPD within the last 12 months 2. results from T-SPOT.TB within the last 12 months 3. results QuantiFERON (QFT) within the last 12 months 4. results of either an initial T-SPOT.TB or QuantiFERON (QFT) and PPD within the last 12 months
Students with a positive past TB skin test must complete the annual TB questionnaire initially and annually, while enrolled. While enrolled, annual PPDs, T-SPOT.TB, or QuantiFERON results are required.
Hepatitis B Although not required, Hepatitis B vaccination series is highly recommended. If completed submit dates of immunization or submit serology proving immunity. Students who chose not to receive the vaccine must sign a form indicating they are familiar with the risks and
decline the vaccine.

21

22
Appendix B
NP Skills Checklist
The student should update and share the Family Nurse Practitioner Student Skill Set with their assigned preceptor at the beginning
of each clinical experience. This document is meant to help preceptors understand the student’s degree of experience with skills
identified in the document below.
Student Name: Date: Phone: Email:
Current Term of Study:
Course Title:
Total Hours Required for this Clinical Placement: Total Hours Required for the Clinical Course this Semester: Total Clinical Hours Completed Prior to beginning this experience: Total Clinic Hours Required for Program:
Current Certifications:
BLS
PALS
ACLS
ATLS
Other _______
Computer Skills:
Epic
McKesson
Cerner
Meditech
Dragon Dictation
EClinical Works
Word
Excel
Other___________
Brief Background of Nursing Experiences/Specialty Areas:
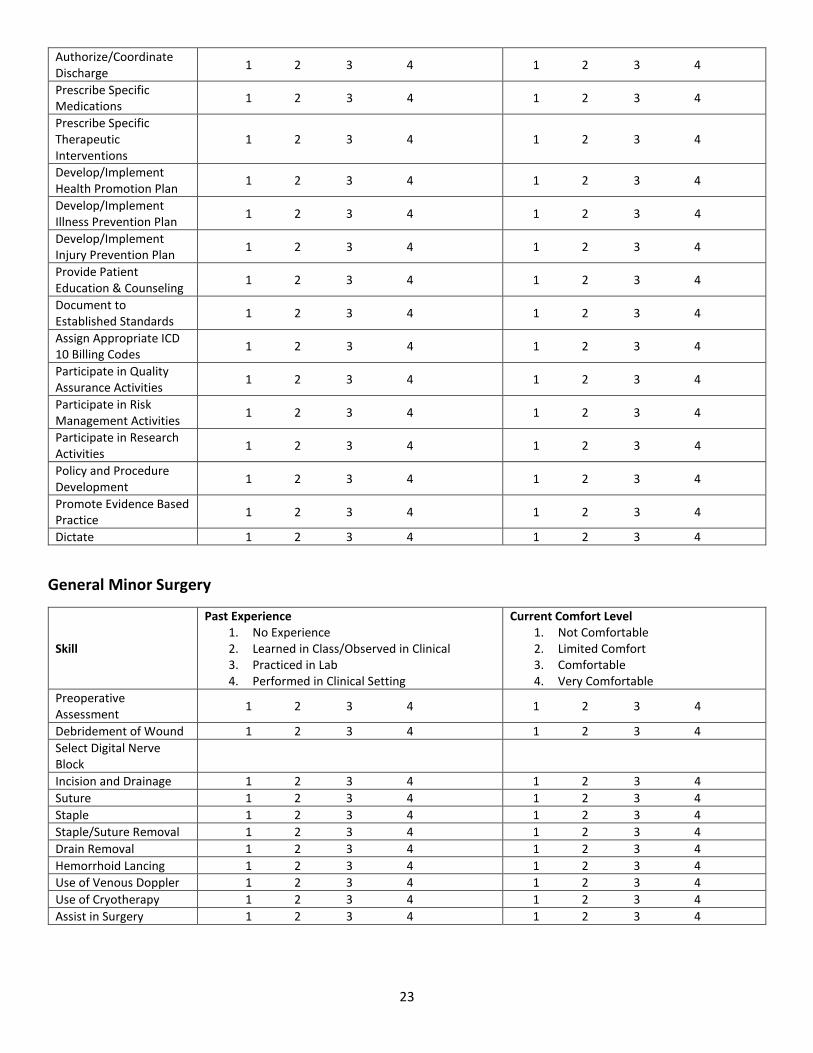
The responses below represent a self-reflection of degree of past experience and current comfort level for each skill:
General Nurse Practitioner Skills
Skill
Past Experience 1. No Experience 2. Learned in Class/Observed in Clinical 3. Practiced in Lab 4. Performed in Clinical Setting
Current Comfort Level 1. Not Comfortable 2. Limited Comfort 3. Comfortable 4. Very Comfortable
Obtain Complete Health History
1 2 3 4 1 2 3 4
Perform Complete Physical Exam
1 2 3 4 1 2 3 4
Order/Perform Diagnostic Tests
1 2 3 4 1 2 3 4
Interpret Clinical Findings
1 2 3 4 1 2 3 4
Develop Differential Diagnoses
1 2 3 4 1 2 3 4
Develop Health Care Problems List
1 2 3 4 1 2 3 4
Develop/Implement Plan for Patient
1 2 3 4 1 2 3 4
Arrange Referrals/Consults
1 2 3 4 1 2 3 4
Authorize/Coordinate Admission
1 2 3 4 1 2 3 4
23
Authorize/Coordinate Discharge
1 2 3 4 1 2 3 4
Prescribe Specific Medications
1 2 3 4 1 2 3 4
Prescribe Specific Therapeutic Interventions
1 2 3 4 1 2 3 4
Develop/Implement Health Promotion Plan
1 2 3 4 1 2 3 4
Develop/Implement Illness Prevention Plan
1 2 3 4 1 2 3 4
Develop/Implement Injury Prevention Plan
1 2 3 4 1 2 3 4
Provide Patient Education & Counseling
1 2 3 4 1 2 3 4
Document to Established Standards
1 2 3 4 1 2 3 4
Assign Appropriate ICD 10 Billing Codes
1 2 3 4 1 2 3 4
Participate in Quality Assurance Activities
1 2 3 4 1 2 3 4
Participate in Risk Management Activities
1 2 3 4 1 2 3 4
Participate in Research Activities
1 2 3 4 1 2 3 4
Policy and Procedure Development
1 2 3 4 1 2 3 4
Promote Evidence Based Practice
1 2 3 4 1 2 3 4
Dictate 1 2 3 4 1 2 3 4
General Minor Surgery
Skill
Past Experience 1. No Experience 2. Learned in Class/Observed in Clinical 3. Practiced in Lab 4. Performed in Clinical Setting
Current Comfort Level 1. Not Comfortable 2. Limited Comfort 3. Comfortable 4. Very Comfortable
Preoperative Assessment
1 2 3 4 1 2 3 4
Debridement of Wound 1 2 3 4 1 2 3 4
Select Digital Nerve Block
Incision and Drainage 1 2 3 4 1 2 3 4
Suture 1 2 3 4 1 2 3 4
Staple 1 2 3 4 1 2 3 4
Staple/Suture Removal 1 2 3 4 1 2 3 4
Drain Removal 1 2 3 4 1 2 3 4
Hemorrhoid Lancing 1 2 3 4 1 2 3 4
Use of Venous Doppler 1 2 3 4 1 2 3 4
Use of Cryotherapy 1 2 3 4 1 2 3 4
Assist in Surgery 1 2 3 4 1 2 3 4

24
Orthopedic
Skill
Past Experience 1. No Experience 2. Learned in Class/Observed in Clinical 3. Practiced in Lab 4. Performed in Clinical Setting
Current Comfort Level 1. Not Comfortable 2. Limited Comfort 3. Comfortable 4. Very Comfortable
Remove External Fixators with Pin
1 2 3 4 1 2 3 4
Instruct Crutch Walking 1 2 3 4 1 2 3 4
Cast 1 2 3 4 1 2 3 4
Splint 1 2 3 4 1 2 3 4
Arthrocentesis 1 2 3 4 1 2 3 4
Interpret Basic Orthopedic X-rays
Spine
Upper Extremity
Pelvis
Lower Extremity
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4
1 2 3 4 1 2 3 4 1 2 3 4 1 2 3 4
Cardiac/Pulmonology
Skill
Past Experience 1. No Experience 2. Learned in Class/Observed in Clinical 3. Practiced in Lab 4. Performed in Clinical Setting
Current Comfort Level 1. Not Comfortable 2. Limited Comfort 3. Comfortable 4. Very Comfortable
Distinguish Type of Pacemaker
1 2 3 4 1 2 3 4
Perform/Interpret 12-lead EKG
1 2 3 4 1 2 3 4
Instruct Use of Incentive Spirometer
1 2 3 4 1 2 3 4
Interpret Pulmonary Function Testing
1 2 3 4 1 2 3 4
Interpret Chest X-ray 1 2 3 4 1 2 3 4
Interpret ABG’s 1 2 3 4 1 2 3 4
Educate Use: MDI; Aerochamber; Peak Flow Meter
1 2 3 4 1 2 3 4
Gynecology/Urology
Skill
Past Experience 1. No Experience 2. Learned in Class/Observed in Clinical 3. Practiced in Lab 4. Performed in Clinical Setting
Current Comfort Level 1. Not Comfortable 2. Limited Comfort 3. Comfortable 4. Very Comfortable
Obtain Fetal Heart Tones
1 2 3 4 1 2 3 4
Obtain Pap Smear 1 2 3 4 1 2 3 4
Interpret Wet Prep Microscopy
1 2 3 4 1 2 3 4

25
Obtain Vaginal Cultures 1 2 3 4 1 2 3 4
Obtain Group B Strep Culture
1 2 3 4 1 2 3 4
Obtain Post Void Residual
1 2 3 4 1 2 3 4
Dermatology
Skill
Past Experience 1. No Experience 2. Learned in Class/Observed in Clinical 3. Practiced in Lab 4. Performed in Clinical Setting
Current Comfort Level 1. Not Comfortable 2. Limited Comfort 3. Comfortable 4. Very Comfortable
Shave Biopsy 1 2 3 4 1 2 3 4
Punch Biopsy 1 2 3 4 1 2 3 4
Excision Biopsy 1 2 3 4 1 2 3 4
Wart Cryotherapy 1 2 3 4 1 2 3 4
Miscellaneous
Skill
Past Experience 1. No Experience 2. Learned in Class/Observed in Clinical 3. Practiced in Lab 4. Performed in Clinical Setting
Current Comfort Level 1. Not Comfortable 2. Limited Comfort 3. Comfortable 4. Very Comfortable
Eye Fluorescein Stain 1 2 3 4 1 2 3 4
Corneal Abrasion ID 1 2 3 4 1 2 3 4
Removal of Foreign Body:
Eye
Nose
Ear
1 2 3 4 1 2 3 4 1 2 3 4
1 2 3 4 1 2 3 4 1 2 3 4
Ingrown Toe Nail Removal
1 2 3 4 1 2 3 4
Audiometry Interpretation
1 2 3 4 1 2 3 4
Other_____________ 1 2 3 4 1 2 3 4

26
Appendix C
Clinical Placement Information Form
Graduate Nursing: Clinical Placement Information
First Name Last Name Previous/Maiden Name
Current Street Address
Address Line 2
City State/Province/Region
Postal/Zip Code Country
Phone Number for Facilitating Clinical Placement
( )
Any possible city or state movements during the program?
NO
YES
Please Describe
Current Employer
Current Employer Street Address
Address Line 2
City State/Province/Region

27
Postal/Zip Code Country
Hometown City Hometown State
I have family or friends that I can stay within the following cities:
Potential Preceptors and Clinical Sites (List any and all possibilities including specialties):
Previous Place of Employment
Last Date Employed at Previous Employment Site
Address Line 2
City State/Province/Region

28
Postal/Zip Code Country
I have work experience or professional interests in the following areas:
Med-Surg
Family Medicine
Internal Medicine
Orthopedics
Mental Health
OB/GYN
Pediatrics
ICU
Emergency Medicine
Urgent Care
Hospital Medicine
Rural Health
Pain Management & Rehabilitation
Oncology
Surgery
Cardiovascular
Any additional notes or comments that may help facilitate scheduling clinical experiences:

29
Appendix D
Student Clinical Practice Contract/Objective and Evaluation Example Clinical Practice Contract
Pass/Fail
Directions:
Complete the following Clinical Practice Contract for all four semesters of 759, 859, 869, and 960. This document will need to be updated each semester.
Clinical Contract Purpose:
The clinical contract represents the student's personal objectives for clinical learning and should be a reflection the overall program/course objectives. Prior to
beginning the clinical experience, the student will author clinical activities and a clinical objectives evaluation plan. At the conclusion of the clinical experience,
the student will complete this document with an evaluation of their achievement of the identified clinical objectives.
The Clinical Practice Contract (minus the clinical evaluation) should be completed prior to the beginning of your clinical experience and must be approved by
your designated clinical faculty for that course.
Process:
This contract should be completed prior to the beginning of your clinical experience and approved by designated faculty. After forming a professional draft of
this contract, consult with designated faculty to identify if there are needed edits or opportunities for improvement. Make those changes as appropriate, sign
the document, have your preceptor sign the document, and then turn it into the drop box by the due date indicated on the course calendar. The instructor will
have final approval authority for your contract.
Clinical Learning Objectives:
Define your overall focuses for the course.
Clinical Activities to Achieve Objectives:
Description of your plan to meet the objectives. How will the objectives be carried out and with whom? Try to make them measurable so evaluation can be
objective.
Clinical Evaluation Plan:
Description of your plan for evaluation of your progress in meeting your objectives/clinical activities.
Clinical Evaluation Summary:
Broad statement of how your activities for the semester were met.

30
EXAMPLE - Clinical Practice Contract
POINTERS: Clinical Learning Objective 1 should flow with the Clinical Activities 1, Clinical Evaluation Plan 1, and Clinical Evaluation Summary 1. Note how the
Clinical Activities and Clinical Evaluation Plan provide MEASUREABLE and REALISTIC tasks and outcomes. This will significantly improve your ability to fully
evaluate the meets or does not meet for each of your objectives. This document needs to be approved by both your clinical faculty and preceptor. This
should serve as a talking tool with your preceptor in regards to how you learn best. Be sure to ask for feedback and modify based on your preceptors
willingness to follow through with your plan or if they have recommended changes based on how the preceptor prefers to assist with advancing your skills.
The Clinical Activities and Evaluation Plan may also need modification depending on what is realistic with that specific clinical environment.
Name: Course Number: Credits/Hours: Semester/Year:
NUR 759 Program Year 2/Primary Care Clinical
Clinical Learning Objectives: (Address the
following elements)
ASSESSMENT
- History-Subjective Data
1. Increase my competency in collecting
thorough histories based upon patient
complaint.
- Physical – Objective Data
2. Increase my competency in performing
a comprehensive physical examination
using accurate, evidence-based
techniques.
- Health Promotion & Risks
3. Identify health and psychosocial risks
when implementing treatment plan.
- Differential Diagnosis
4. Gain experience in creating a list of differential diagnoses as indicated by the patient’s presenting problem.
MANAGEMENT
- Clinical Reasoning
5. Demonstrate skill in interpreting
pertinent biopsychosocial evidence
derived from individual and family
assessments including health histories,
Clinical Activities
(How, with whom):
1. Collect at least 1-3 histories per
clinical day under the direction of
my preceptor.
2. Perform at least one focused
and at least one comprehensive
physical examinations per clinical
day as indicated by the patient
complaint under the supervision
of my preceptor.
3. Identify at least one health
promotion/preventive activity per
patient (immunizations, tobacco,
exercise, preventive screening,
etc).
4. Generate at least four
differential diagnoses per
presenting problem for the
patients I see on clinical days.
5. Analyze the information
received from each physical
examination, health history, and
laboratory/diagnostic studies for
at least 2 patients per clinical day
of active participation, suggesting
Clinical Evaluation Plan:
1. Request feedback from my
preceptor regarding my
competence on history taking after
every two clinical days of active
participation.
2. Request feedback from my
preceptor regarding my
competence on performing
comprehensive physical
examinations after every two
clinical days of active participation.
3. Review with preceptor personal
understanding of recommended
health promotion/preventive
activities for at least 2 patients
each clinical day.
4. Verify my list of differential
diagnosis with my preceptor on at
least 1 – 2 patients per clinical day.
5. Verify correct interpretation of
patient case, diagnostics, and
management plan with preceptor
on at least 3 patients a day.
Clinical Evaluation Summary
(Complete at end of
semester):
1. My preceptor was not
present for the majority of
histories that I collected, but
simply heard my reports. He
denied any area for
improvement.
2. While I performed various
comprehensive examinations,
my preceptor was not present
to observe my technique and
critique my skills. However, he
reported that my assessments
were accurate, and assisted
me with techniques when I
was uncertain.
3. My preceptor stated that
there was no specific area in
which I need improvement—I
just need experience.
Preceptor noted I was
appropriately applying the US
Preventive Service Guidelines
for patients reviewed.

31
physical examinations, laboratory and
diagnostic sources, and current literature.
- Diagnostic Strategies & Interpretation
6. Order and interpret appropriate
diagnostic tests for patients based on
history and physical findings.
- Patient Care Management
7. Demonstrate competence in developing
appropriate treatment plans in order to
provide patient-centered, evidence-based
care.
- Documentation & Presentation
8. Present assessment data, both orally
and written, in an organized manner.
-Patient & Family Relationships
9. Establish a relationship with the
patient/family characterized by mutual
respect, empathy, and cultural
considerations.
- Evaluation
10. Participate in review of patient
outcomes and follow through.
- Patient Education
11. Provide anticipatory guidance that is age, developmentally, and culturally appropriate to assist the client in assuming responsibilities for self-care and health-promotion such as healthy nutritional and physical activity practices.
LEADERSHIP & PROFESSIONAL ROLE
- Accountability & Professionalism
12. Demonstrate accountability for own
learning and professional behaviors
(punctuality, confidentiality, respect, and
communication).
proposed diagnoses based on
these findings.
6. Order at least two diagnostic
tests per day if indicated by a
patient’s examination findings and
personally review the laboratory,
ECG, and imaging results of each
patient I work with, consulting my
resources, such as Epocrates,
Nursing Central, Squire’s
Radiology, and UpToDate, as
needed to increase my
understanding.
7. Formulate management plans
based on current evidence,
utilizing resources such as
UpToDate, Epocrates, etc., for at
least two patients per clinical day
of active participation.
8. Orally inform my preceptor
regarding the history, physical,
and examination findings of each
patient I see independently.
Complete at least five dictations
on patients throughout the clinical
experience.
9. Collaborate with patient/family
in decision making for patient
centered care.
10. Consider possible impact of
life transitions and health status
on patient outcomes for each
patient.
11. Provide anticipatory guidance
regarding nutrition, physical
activity, and developmental
6. Verify appropriateness of
recommended diagnostic tests for
each patient with preceptor.
7. Suggest appropriate
pharmacologic and non-
pharmacologic interventions for at
least two patients per clinical day.
Verify appropriate dosing and
indications with preceptor.
8. Request feedback from
preceptor regarding my
performance in providing both oral
and written assessments every two
clinical days of active participation
and for each dictation completed.
9. By the end of the rotation
request feedback from preceptor
regarding my interactions with
patients and family members.
10. Discuss with preceptor possible
impact of life transitions and health
status on patient outcomes for at
least 2 patients per clinical day.
11. By the end of the rotation,
request feedback from preceptor
regarding ability to provide
appropriate patient education and
discharge planning
recommendations.
12. By the end of the rotation,
request feedback from preceptor
and other clinical staff regarding
professional behavior and
encourage preceptor and other
staff to correct me early if any
4. Many of the patients I saw
presented for established
conditions, decreasing the
need for developing
differential diagnoses. Thus, I
developed little practice in
this regard. However, there
were several occasions where
I suggested possible diagnoses
for my preceptor to verify.
Will need to continue working
on this skill.
5.6. &7. The management plans for my patients were developed primarily by my preceptors. However, I would question them at times, or suggest other strategies. For instance, if a diabetic patient presented with multiple cardiac risk factors, I would suggest that we have the patient begin taking low-dose aspirin. Thus, my skills have grown in this area, but I have much room for improvement. 8. My preceptor reported that
my oral presentations and
charting was “fine,” but
encouraged me to become
more concise in my notes. By
the end of the experience, I
did all the charting for the HPI,
ROS, and physical
examinations for the patients I
saw. I feel that I have fully met

32
- Role & Healthcare Systems
13. Identify roles of interprofessional
healthcare members in delivery of
specialty services to provide a continuum
of patient care.
expectations for each patient seen
in clinic.
12. Arrive prepared and in
appropriate clinical dress at least
15 minutes prior to start of clinical
day.
13. Consider roles of
interprofessional healthcare
members in delivery of specialty
services for each patient as
indicated throughout the clinical
experience.
concerns noted throughout the
experience.
13. Discuss with preceptor roles of
interprofessional healthcare
members in delivery of specialty
services for at least one patient per
clinical day.
this objective but will continue
to advance with experience.
9. Received positive
compliments from patients,
“She did a good job.”
Preceptor noted patients were
comfortable with me and I
was able to develop a quick
rapport with patients and
family members.
10. Able to discuss potential
impact of planned treatment
protocol for each patient
throughout the clinical
experience with the preceptor
and or clinic nurse.
11. Always asked by preceptor
when each patient needed to
return for follow-up or next
evaluation. By the end of the
rotation, preceptor did not
have to correct my
recommendations.
12. Positive feedback
received from clinic staff and
preceptor. Noted I was a “joy
to work with” and appreciated
for “working so hard, coming
early, and staying to the end.”
13. Able to spend time with
radiologist, physical therapist,
and occupational therapist for
about 1 hour each during
clinical experience. Preceptor
feels it is imperative to
provide patient care as a team

33
and know/understand the
various roles. Whenever a
patient required additional
team care, discussed purposes
and to request specific actions
or consult required. Also
advised to review
expectations with the patient
so that they are prepared as
well.
NUR 859 Program Year 2/Women and Children Clinical
Clinical Learning Objectives:
(Address the following elements)
ASSESSMENT
- History-Subjective Data
- Physical – Objective Data
- Health Promotion & Risks
- Differential Diagnosis
MANAGEMENT
- Clinical Reasoning
- Diagnostic Strategies & Interpretation
- Patient Care Management
- Documentation & Presentation
-Patient & Family Relationships
- Evaluation
- Patient Education
LEADERSHIP & PROFESSIONAL ROLE
- Accountability & Professionalism
- Role & Healthcare Systems
Clinical Activities
(How, with whom):
Clinical Evaluation Plan: Clinical Evaluation Summary
(Complete at end of
semester):
NUR 869 Program Year 2/Special Populations Clinical

34
Clinical Learning Objectives:
(Address the following elements)
ASSESSMENT
- History-Subjective Data
- Physical – Objective Data
- Health Promotion & Risks
- Differential Diagnosis
MANAGEMENT
- Clinical Reasoning
- Diagnostic Strategies & Interpretation
- Patient Care Management
- Documentation & Presentation
-Patient & Family Relationships
- Evaluation
- Patient Education
LEADERSHIP & PROFESSIONAL ROLE
- Accountability & Professionalism
- Role & Healthcare Systems
Clinical Activities
(How, with whom):
Clinical Evaluation Plan: Clinical Evaluation Summary
(Complete at end of
semester):
NUR 960 Program Year 3/Seminar and Practicum
Clinical Learning Objectives:
(Address the following elements)
ASSESSMENT
- History-Subjective Data
- Physical – Objective Data
- Health Promotion & Risks
- Differential Diagnosis
MANAGEMENT
- Clinical Reasoning
- Diagnostic Strategies & Interpretation
- Patient Care Management
- Documentation & Presentation
-Patient & Family Relationships
- Evaluation
- Patient Education
LEADERSHIP & PROFESSIONAL ROLE
Clinical Activities
(How, with whom):
Clinical Evaluation Plan: Clinical Evaluation Summary
(Complete at end of
semester):

35
- Accountability & Professionalism
- Role & Healthcare Systems
I agree to accept the responsibility of fulfilling this agreement.
Student Signature: __________________________ Date: _______________________________
*******************************************************************************************************
I agree to accept the responsibility of serving as the preceptor. I have reviewed Clinical Scholarship Practice Contract developed by this student and am in
agreement with the objectives sought. I have verified that an institutional contract is concurrent for this experience.
Preceptor Name (typed): ______________________________________________________________________
Preceptor Signature: ___________________________________________________ Date: __________________________

36
Appendix E 3 Minute Clinical Case Presentation
The ability to deliver short and succinct oral case presentations is a core skill for any provider. Effective oral case presentations help facilitate the transfer of information among providers and are essential to delivering quality patient care. Oral case presentations are also a key component of how students are assessed during their clinical experiences. Displays how much the student knows and or doesn’t know for future learning.
At its core, an oral case presentation functions as an argument. It is the job of the presenter to share the pertinent facts of a patient’s case with other members of the medical care team and establish a clear diagnosis and treatment plan. Thus, the presenter should strive to include details to support the proposed diagnosis and argue against alternative diagnoses, and exclude extraneous information. While this task may seem daunting at first, with practice, it will become easier. That said, if you are unsure if a particular detail is important to your patient’s case, it is probably best to be safe and include it.
During your clinical experiences, you and in particular your preceptor, do not have the time for lengthy presentations of every detail. The following framework below can be applied to patients in most settings with slight modifications.
STYLE As the presenter, strive to deliver an interesting presentation that keeps your preceptor or other team members engaged:
• Be Confident o Speak clearly at the loudest volume appropriate to protect patient privacy, vary your tone to
emphasize the most important details, and maintain eye contact.
• Minimize Fidgeting o Stand up straight and avoid unnecessary, distracting movements.
• Use Your Notes; But Avoid Just Reading o Glance at your notes, but there is no better way to lose your preceptor’s attention than to simply
read your notes to them.
• Be Honest o Given the importance of presentations in guiding medical care, never report false information to
the team. If you are unsure about a particular detail, it is fine to say so. DON’T GUESS!!
LENGTH The length of your presentation will depend on a variety of factors, including the complexity of your patient, your audience, and the specialty covering. For an outpatient family practice clinic, you should strive for 2 – 5 minutes. Ideal length should be 3 minutes. STRUCTURE Expectations may vary among preceptors for patient presentations, so either before your first patient or after your first time delivery, check in with the preceptor to identify how they would prefer you best present a patient. Once you have presented, check in to identify any recommendations for change.
PRESENTING THE PATIENT
1. Opener a. Every oral presentation should begin with a brief one-liner that contains the patient’s name, age,
relevant past medical history, and chief complaint. Remember the chief complaint is the reason that the patient sought medical care in his or her words. Example: “Ms. Green is a 78 year old

37
female with a past history of COPD who presents to the clinic after noting increased productive cough and shortness of breath at home.”
b. If the patient is a female presenting for a GYN complaint, the opening should include gravida para status. Example: “Ms. Joe is a 44 year old G4P4 previously healthy female patient presenting with heavy vaginal bleeding for the last 3 weeks.”
c. For a young child consider the following: “Emma is a developmentally normal 15 month-old female without previous congenital or chronic disease presenting with nasal drainage and cough for 10 days, now with fever of 102.” Or: “Tigen is a 10 month old male patient with down’s syndrome presenting with a 5 day history of nasal and eye drainage.”
d. Introductory sentence: Mr./Mrs./Ms.____ was in his/her usual state of ____ (e.g., excellent health/poor health) until ____(e.g., three days prior to admission) when he/she developed the ___ (acute/gradual) onset of _____. The introductory sentence may include details of past medical history if the patient’s illness directly relates to an ongoing chronic disease.
e. Don’t mention that an event occurred “on Saturday”, rather refer to the time relative to the day of presentation, e.g. 3 days ago...
f. Other Good Examples: “Mr. Smith is a 55 year-old man with a long history of diabetes mellitus, cirrhosis, and chronic obstructive lung disease, who presents with a chief complaint of fever and productive cough…”; “Mrs. Jones is a 39 year-old woman who was electively admitted for evaluation of exertional dyspnea. Her active problems include rheumatoid arthritis and hypertension. She was in her normal state of health until…”
g. Comparison of Bad/Good Examples: BAD: “…his problem list includes coronary artery disease – myocardial infarction x 2, the last in 1996, multiple negative rule-outs since, ejection fraction equaled 35% in 1994; diabetes mellitus x 10 years, insulin requiring for five years, complicated by retinopathy; chronic obstructive lung disease – with a FEV1* of 1.2 liters and steroid dependence…” GOOD: …his active problems include coronary artery disease, diabetes mellitus, and chronic obstructive lung disease…. In the Bad Example the listener will forget the chief complaint by the time you reach the history of present illness. The Good Example is concise and does not interrupt the listener’s train of thought between the chief complaint and the history of present illness; relevant information about each of these problems should be introduced when appropriate in the “HPI” or “other medical problems.”
2. History of Present Illness a. Following the opener, elaborate on why the patient sought care. Describe the events that preceded
the patient’s presentation in chronological order. OPQRST or OLDCARTS are very helpful here. b. OPQRST
i. Onset of patient’s symptoms; ii. Palliative or Provoking factors that make symptoms better or worse;
iii. Quality of symptoms (how the patient describes the symptoms); iv. Region of the body where the patient is experiencing concern and if the symptoms is pain,
whether the pain Radiates to another location or is well localized; v. Severity of the symptoms and any other associated Symptoms;
vi. Time course of the symptoms (how they have changed over time and whether the patient has experienced them before.
c. OLDCARTS i. Onset
ii. Location/radiation iii. Duration iv. Character v. Aggravating Factors

38
vi. Relieving Factors vii. Timing
viii. Severity d. Include any other details that may support your final diagnosis or rule out alternative diagnosis. For
example, if concerned about a pulmonary embolism and patient had a recent long-distance flight, then that would be worth mentioning.
e. Good Examples: “Mr. Smith has a long history of chronic obstructive lung disease characterized by two block dyspnea on exertion, FEV1 of 1.0 liter, and home oxygen therapy. He was in this usual state of health until three days ago when he developed the gradual worsening of his shortness of breath, associated with a cough productive of yellow sputum and a fever of 102”. “Mr. White has a long history of coronary artery disease characterized by three myocardial infarctions, the most recent in 1995, ventricular tachycardia treated with amiodarone, and congestive heart failure. He was in his usual state of health, with angina occurring once per week, until last night, while watching a football game, he developed the acute onset of severe substernal chest heaviness…”
f. Bad Example: A poorly characterized and too brief history of present illness: “Elderly man presents for evaluation of chest pain. He was well until three weeks ago when he began to feel chest heaviness whenever he exerted himself. He saw his local doctor who prescribed antacids with little benefit. The pain woke him last night so he came back to the clinic today for evaluation. His other problems include…….” A more complete example: “72 year old previously healthy male presents for evaluation of chest pain. He was in his usual state of excellent health until three weeks ago when he started developing the gradual onset of intermittent chest pain, characterized as poorly localized deep substernal heaviness which radiated to his left shoulder, lasting about five minutes per episode, occurring several times a day, aggravated by exertion and relieved by rest. Associated with the pain were shortness of breath and nausea. One week ago he was seen by a local doctor who, without other testing, diagnosed gastritis and prescribed antacids without benefit. The chest pain was stable until two hours ago, when he awoke with a more severe version of the same pain that lasted until he presented here to the clinic. Currently at rest he has no pain. There is no history of cough, heartburn, weight loss, or fever, chills or sweats. The patient’s risk factors for coronary artery disease include a positive family history and a cholesterol of 310 in 1998. He has no history of high blood pressure or diabetes and has never smoked cigarettes.”
3. Review of Systems a. The review of systems is sometimes included in the history of present illness, but may also be
separated. Given the potential breadth of the review of systems (meaning a comprehensive list of questions that may be asked), when presenting, ONLY report information that is relevant to your patient’s condition. Most commonly the information provided in the HPI is all that is needed for your initial 3 minute presentation.
4. Past Medical History a. This should include any additional medical history that was not highlighted in the opener, but
pertinent to the chief complaint to include other chronic medical problems; recent or past surgeries; past or recent hospitalizations, ER visits, or clinic visits; current medications or recently discontinued medications; and allergies. If no pertinent past medical history information is pertinent, it is acceptable to note: “No significant past medical or surgical history”. Or past medical and surgical history is non-contributory.”
b. Example: “…his other medical problems include insulin-requiring diabetes for 12 years, complicated by retinopathy, polyneuropathy, and nephropathy. His recent creatinine was 1.7…”

39
5. Family History
a. Relevant family history should include any relevant conditions that run in the patient’s family, with an emphasis on first-degree relatives.
6. Social History a. Pertinent information may include living situation, occupation, alcohol and tobacco use, other
substance use. b. You may also need to include relevant details about the patient’s education level, travel history,
history of animal and occupational exposures, and religious beliefs. For example, it would be worth mentioning that your anemic patient is a Jehovah’s Witness to guide medical decisions regarding blood transfusions.
c. It is often the social history that explains why the patient has fallen ill now, as opposed to some other time or not at all: patients may have chaotic lives and little social support so don’t have the help they need to follow therapeutic recommendations, few financial resources and can’t afford their meds, depression and feelings of hopelessness about their conditions, etc. These factors, if not addressed, will tend to lead to rehospitalizations. If appropriate, include information about the patient’s personal wishes for health such as advance directives (their living will and durable power of attorney) including discussion concerning these issues.
7. Physical Exam a. Start with vital sign’s including Temperature, Heart Rate, Blood Pressure, Respiratory Rate, and
Oxygen Saturation. Include postural changes when relevant. b. Include pertinent findings of your physical exam, including general impression of the patient
(including whether they appear “sick” or not). Depending on the “system” affected, you will want to include specific areas again based on the chief complaint. For example, for chief complaint of cough – will need to include a minimum of HEENT, Respiratory, Cardiovascular, Abdomen, and Extremities.
c. General description – be colorful, allow the listener to visualize the patient. “The patient was short of breath” is inferior to “the patient was sitting on the edge of the bed, leaning forward and gasping for breath.”
d. Mention only the relevant positive findings and relevant negative findings. e. Use concise but complete descriptions of positive findings. Resist the urge to report an exam as
being “normal”. Instead, report your findings in medical terminology. For example, if a patient presents with chief complaint of “abdominal pain” and the exam is currently normal, should report “the patient’s abdomen is soft, non-tender, and nondistended, with normoactive bowel sounds. No guarding or rebound tenderness is present. No CVA tenderness.”
8. Any known lab findings past or recent pertinent to the current problem a. If any previous labs, imaging, or other diagnostics were obtained pertinent to your diagnosis (such
as with a recent ER visit or hospitalization), these could be included here. You do not have to report the results of every test that was ordered.
9. Assessment a. This is the most important part of your presentation and gives you the opportunity to show your
preceptor how much you really know. b. Provide 3 – 5 of the most possible differential diagnosis, but then note your most likely diagnosis
and what further diagnostics one should consider to validating this diagnosis.

40
c. Explain why you think each diagnosis is or is not the final diagnosis. Be sure to rule out potentially life-threatening conditions (unless you think your patient has one). For the COPD patient previously noted above you may need to note why you don’t believe the symptoms are due to congestive heart failure or a pulmonary emboli.
d. Consider the following format: “…the patient’s major presenting problem is ____ (best positive statement you can make; say “chest pain” and avoid statements like “rule-out myocardial infarction”). The differential diagnosis includes ____, ______, and _____. The diagnosis of _____appears to be the most likely of these because ______.
e. Example: “...the patient’s main problem is chest pain, which could be due to a myocardial infarction, a dissecting aortic aneurysm, pericarditis, and a variety of other diagnoses such as pneumonia, pulmonary embolus, or esophageal disease. MI seems most likely, because his description of chest pain is classic for angina and because his ECG reveals a new injury current in the inferior leads.”
f. While your assessment can be similar to your opener, is should not be identical: “Ms. Joe is a 78 year old female with past history of COPD presenting with SOB and cough in the setting of a URI who is now stable on 2 liters of supplemental oxygen delivered via nasal cannula. Symptoms thought to be secondary to an acute exacerbation of COPD.” “There is no previous history of CAD, denies chest pain, fever. No evidence of fluid overload. Negative for PE risk factors including recent travel, previous DVT/PE, estrogen exposure, recent surgery, or known clotting disorder for the patient or in immediate family members. Grandchildren have been staying with patient and have been ill with URI symptoms.”
g. If the diagnosis is apparent just based on history and exam, then include the supporting diagnostic criteria. For example: “Most likely diagnosis is a bacterial sinus infection based on 14 day history of mucopurulent nasal drainage, nausea, bilateral maxillary sinus tenderness, cough, that is not relieved with 5 days of continued antihistamine and decongestants.”
10. Recommended Plan of Action. a. Include additional studies for supporting or ruling out diagnosis. If known diagnosis, include your
treatment plan, education, and follow-up recommendations. Example for sinusitis patient: “Patient has NKDA, no recent exposure to antibiotics, non-smoker. Would advise treatment of Amoxicillin 875 mg po BID for 7 days. Should start to note improvement in 2 – 3 days. Recheck in 10 – 14 days if symptoms have not completely cleared. Return sooner if signs of allergic reaction, fever, no improvement in 2 -3 days, or other new or worsening symptoms. Home adjunct treatments would include adequate fluids, sleeping upright, steamy showers or facial steam baths, nasal saline spray/washes.”
11. Common Mistakes in Oral Presentation a. Slow labored rhythm - a wandering, disorganized and desultory presentation is the most
common problem encountered in early students. The ability to convert a written history and physical examination into a compressed presentation requires careful thought and practice. Ask your preceptor how long a presentation they would like. You should maintain eye contact with your listener during the presentation, which means that you should refer to notes and not read your write-up. In order to keep it under 5 minutes, you will need to PRACTICE with role play cases. This is helpful to do with a classmate who can give you feedback and then let you try again. It is also worth video-taping or at least recording yourself and listening to the play-back – then you can give yourself feedback.
b. History of present illness too brief - 90% of correct diagnoses come from the history alone; do not sabotage your listener’s understanding of the case by omitting important information. The HPI portion of the oral presentation, as a general rule, should take 1/3 to 1/2 of the

41
presentation time. Common pitfalls include incomplete characterization of the major symptoms, omitting pertinent negatives or positive ROS questions, and omitting specific information about past history that relates to the present problem.
c. Failure to use parallel reference points - in both write-ups and oral presentation, relate time in “hours/days/weeks prior to admission”. Avoid “at 2:00 in the morning of last Wednesday” or “on May 25th; instead, say “three hours prior to admission”, or “at 2:00 am, three days prior to admission”.
d. Editorializing in the middle of the presentation - avoid comments like “do you even want to hear this?…” or “cardiac examination revealed a systolic murmur….well, I thought heard it, but the resident didn’t…so maybe it isn’t there….I don’t really know….”
e. Use of negative statements instead of positive statements. Positive statements add color and accuracy to your presentation. “Chest Xray shows normal heart size” is better than “chest X-ray shows no cardiomegaly”. “In summary, this patient’s problem is acute dyspnea” is better than “the patient’s problem is rule-out pneumonia”.
f. Repetition- vary your sentence structure. An overly repetitious presentation is monotonous for the listener. “On pulmonary exam, the lungs were normal…on cardiac exam, the heart sounds were…, on lymph node exam, there were no cervical nodes…etc” is difficult to listen to and unnecessary – your listener knows that S1 and S2 are part of the cardiac exam! Use brief descriptive sentences: “an S3 gallop was heard at the left lower sternal border.”
g. Disorganization - this problem is a result of lack of rehearsal. Stopping at the end of the HPI to say “Oh, I can’t believe I forgot to tell you this” will kill a presentation. Or “…in summary, this patient…wait, I forgot to tell you the most important thing…” You need to be aware that this can happens even with careful preparation. The best advice when you forget something crucial to your presentation, is to work it in as soon as possible and don’t make a big deal about it.
h. Physical findings presented without proper terminology - for example, “lymph node exam shows some small cervical nodes” is not as descriptive as “…there were three soft tender mobile nodes in the left anterior cervical chain which measure 1 x 1 x 2 cm each…” Commitment to accuracy will improve your physical examination skills.
i. Diagnoses used instead of descriptions in the physical examination - diagnoses belong in the assessment, descriptions in the physical examination. For example, avoid “exam showed the murmur of mitral regurgitation” …instead say “a 2/6 holosystolic murmur was heard at the apex when radiated to the axilla”. Avoid “skin exam showed psoriatic lesions on the elbows…”: instead, say “there were several 2 cm. diameter round plaques with silver scale distributed on the extensor surface of the elbows…”
Remember to practice! Remain professional and formal, using the same format each time and you will become proficient in this essential skill!

42
Appendix F
Typhon Guidelines
Typhon is a patient tracking system used to document patient encounters throughout clinical experiences. It will be used to track clinical competencies. It can be accessed at https://www.typhongroup.net/np/data/login.asp?facility. University of Mary’s facility number is 7201. Each student will be provided a user name and password. An orientation is provided prior to the first major clinical experience course. There are student tutorials available for review once a student is logged in. The following are guidelines to follow when using the system.
• Clinical schedules must be entered by the student into Typhon as soon as they are established AND NO LESS THAN ONE WEEK PRIOR TO START OF CLINICALS. Students may not start clinicals until their schedule is entered into the Typhon system and their Clinical Objectives have been submitted in Canvas for Faculty Approval.
• It is required that all patient encounters be entered. Remember, you are building your database of experiences. You want for it to showcase the variety of conditions, diagnostics, pharmacological plans, and procedures that you have had exposure and experience with. The quality of what you put in impacts the quality of the product you will have at the end. It should be your goal to maximize this tool’s potential as a professional marketing portfolio for you in the future.
• Clinical logs must be completed on a WEEKLY basis, however it is highly recommended that students enter encounters daily. All entries of patient encounters from the previous week must be entered in Typhon by Monday of each week! Should students become more than 1 week behind on Typhon entries, they will not be allowed to continue with the clinical experience until caught up. The Typhon system has a "lock" that only allows students to provide entries for a set number of days. If you are locked out from entering clinical data, the student will need to contact their clinical faculty for permission to enter their data and reschedule clinicals until they are caught up with previous encounters. The student will also need to contact their clinical preceptor with an update and reason for being unable to proceed with the clinical experience until further notice. This has become a facility requirement in many professional practices - when providers are more than a week behind on dictations, they are not allowed to see patients and required to take a personal day off to "catch up" on required documentation. Once the student is caught up, they will need to re-notify their faculty members and clinical preceptor to resume the clinical experience.
• Student must enter clinical hours in the time log.
Typhon Patient Encounter Entry Requirements
• Document your family practice, orthopedics, and mental health rotation patients.
• All required fields must be completed
• Pharmacologic management must be entered
• Skills observed, assisted with or completed independently must be recorded on the skills checklist within typhon
• CPT codes are required for procedures (splinting, I&D, laceration repair…) as well as diagnostics that were ordered (labs, x-rays, EKGs, CTs, ultrasounds…).
• An E/M code is required to be entered for each patient encounter.
• ICD-10 codes are required for all patient encounters. This is the diagnosis code. There may be more than one.
• The notes section can be used to enter brief details of the encounter for purposes of recall and to help the faculty person reviewing the encounter understand the context of the visit and management plan.

43
• All Typhon entries must be approved by the student’s clinical faculty. Those left unapproved will need to be addressed by the students.
Typhon Entries Rubric
Criteria Criterion Fully Met Criterion Partially Met Criterion Not Met
Timeliness Typhon entries for each week are submitted in full by Monday for the clinical encounters the student has participated in during the previous week. 5.0 pts
Less than all Typhon entries are submitted by Monday for patient encounters from the preceding week. 3.0 pts
No patient encounters are entered. 0.0 pts
Entry Flow Each entry has sufficient information to demonstrate congruency between the chief complaint, diagnostics, diagnosis, and management plan. Students are encouraged to include 1-2 sentence to enter brief details of the encounter for purposes of demonstrating critical thinking or relationship of encounter details to management plan.
5.0 pts
Most entries have sufficient information to demonstrate congruency between the chief complaint, diagnostics, diagnosis, and management plan. Students are encouraged to include 1-2 sentence to enter brief details of the encounter for purposes of demonstrating critical thinking or relationship of encounter details to management plan.
3.0 pts
Entries include minimal information. 0.0 pts
Pharmacologic management
Pharmacologic actions from patient encounters are included in each entry as appropriate.
3.0 pts
Pharmacologic actions are missing on many encounters that would have drug management.
0.0 pts
Skills Each encounter that a skills was performed is noted in the skills list as either observed, assisted or completed independently.
2.0 pts
Skills are not entered in Typhon.
0.0 pts
Coding ICD-10, CPT, and E/M codes are entered for each patient encounter.
5.0 pts
Coding not done 0.0pts

44
Examples of Primary Care Typhon Entries

45
Examples of Women’s Health Typhon Entries
Examples of ER/Urgent Care Typhon Entries

46
Appendix G Dictation Requirements
Dictation Expectations
The purpose for evaluation of dictations/documentations is to appraise your critical thinking skills as well as
your proficiency in regard to assessment, diagnosis/impression, and development of a plan of care. In
addition, assessments of clinical documentation assists with quantification of a student’s ability to formulate
an accurate, clear, well organized record that reflects and facilitates sound clinical thinking.
If you are not allowed to dictate, dictations must be self-typed and submitted. Dictations should reflect the
criteria below and will be evaluated using the evaluation tool provided. For some courses, students may have
to self-correct dictations and details will be outlined in individual clinical course syllabi. The required number
of dictations required is outlined in course syllabi.
Documentation criteria
o Documentation is clear and well organized.
o Appropriate medical terminology and anatomical descriptions are utilized.
o No redundancy (repetitious words, phrases, and other distracting information are omitted).
o Format follows a standard. Narratives such as the HPI and Exam have a logical flow.
o HPI is fully developed and includes location, duration, timing, character, severity, provocative/palliative
factors and/or other features appropriate for the reason for presentation.
o Physical exam includes vital signs, height and weight for all children and for others as appropriate, and any
relevant developmental data.
o Appropriate diagnostic tests are performed/ordered.
o Assessment and diagnosis reflect the patient’s symptoms and diagnostic tests
o Clinical decision making is documented regarding diagnostics, differential diagnosis, treatment plan and
follow-up.
o Management plan is appropriate for the diagnosis and accurately addresses the problem identified.
o Management plan is economically sound.
o Management plan includes plans for evaluation/follow-up care (as appropriate).
o Management plan is individualized to the patient’s age and development, culture, religion, family,
environment, education, and/or any other unique concerns uncovered in assessment.
o Level of visit and documentation consistent with E/M guidelines key components
Number of Dictations
o The student must satisfactorily complete 8 Dictations/Documentations
o 3 of the dictations need to be comprehensive H&Ps
o 5 focused H&Ps
o All dictations must represent a different presenting complaint or age category for the comprehensive
exam
o Demonstrate a variety of common health problems
o All dictation must be self-corrected. For example when you receive your dictation back, review the
protocol material for any missing questions, system examinations, management….etc. Make these
corrections on the typed form.

47
o The dictation grading rubric will be used for evaluation of submitted dictations
o You must demonstrate competency on your focused exam documentations. You will be allowed only TWO
different repeats of your documentation if you receive an initial fail.
o The following web sites may be of some help as you begin to provide E/M guideline based documentation
(refer to resources supplied in NUR 567)

48
Comprehensive History and Physical Examination Rubric
Other Considerations when documentation is for a female patient.
HPI – First sentence should include age, parity, LMP and present problem (details about cc and other relevant information).
Menstrual History Menarche, duration, flow and cycle length of menses, IMB (intermenstrual bleeding), or contact bleeding, dysmenorrheal, PMS, climacteric
Gynecologic History Breast history – history of breast disease, breast feeding, the use of SBE (Self Breast Exam), last mammogram (if applicable); previous gyn surgery (can include surgical history),
history of infertility, history of DES (diethylstilbestrol) use by patients mother, last pap smear - history of abnormal pap.
Contraceptive/ Sexual Current method/patients satisfaction with current method
History Past Methods, current sexual activity, number of partners, new partner in the last 3 months, condom use, history of sexual abuse.
PMH Include infectious diseases (gonorrhea, chlamydia, syphilis, herpes, genital warts, trichomonas, HIV, TB, rheumatic fever, hepatitis)
Social History Marital status, employment, age and health of children, social supports
ROS Concentrate of GY/GI; pertinent negatives may include, abnormal discharge, abnormal bleeding, dyspareunia, abdominal/pelvic pain, dysuria, hesitancy, urgency, incontinence, change in bowel habits, rectal
bleeding. For post/perimenopausal woman – hot flashes/night sweats, vaginal dryness, abnormal bleeding, irritability, depression, mood changes.
PE: At a minimum: Vital Signs, Thyroid, Breasts, Lungs, Heart, Abdomen, Extremities, Pelvic Exam, External genitalia, vagina, cervix, uterus abdomen, recto-vaginal
Other Considerations when documentation is for a pediatric patient.
A number of factors distinguish the pediatric from the adult history and physical exam. Depending on the age of the patient, the primary historian may be the patient and/or another person, usually the parent.
Developmental factors are commonly considered. The differential diagnosis of a condition may vary depending on the age of the patient. Health care maintenance (e.g., immunizations and safety issues) and social
issues play a major role in emergent and routine care. Therefore, key items must be considered for inclusion within the documentation note including: informant, prenatal history, birth and neonatal history, feeding
history, immunization history, developmental/behavioral history, HEADDSS for the adolescents. For the physical exam: be sure to include head circumference, growth curves, etc. for appropriate age levels along with
appropriate developmental assessment.
Comprehensive Examination Rubric
Criterion Criterion
Fully Met
Criterion
Partially Met
Criterion
Inadequately
Met
Criterion Not
Met
Chief Complaint:
Patient initials, age, and CC present. No identifying data 5pts 3pts 2pts 0pts
History of Present Illness: 15pts 10pts 6pts 0pts

49
Thoroughly documents all pertinent history components for type of note; includes critical as well as supportive information. HPI is fully developed
and includes location, duration, timing, character, severity provocative/palliative factors, pertinent positives and pertinent negatives when
appropriate.
Past medical, family, and social history:
Thoroughly documents all history components for PMH, FH, SH are included. Allergies, prescribed and over the counter medicines currently
being used are noted. Evidence of extensive chart review. Includes vocational history when appropriate, current living situation,
tobacco/alcohol/drug history, & medical history of first degree relatives.
10pts 8pts 6pts 0pts
Review of Systems:
Complete review of systems is included. 10pts 8pts 6pts 0pts
General Survey/Vital Signs:
General survey includes complete set of vital signs, height and weight, BMI, and other relevant data. 5pts 3pts 2pts 0pts
Physical Examination:
All systems assessed. Appropriate descriptors are used to articulate the physical findings. 15pts 10pts 6pts 0pts
Labs/Diagnostics:
Pertinent lab and diagnostic findings are included with provider interpretation of any abnormal labs. Includes all pertinent labs, or references what
should have been obtained
10pts 8pts 6pts 0pts
Management Plan:
States/identifies all appropriate final diagnosis/problem list. Each problem is addressed, either separately or as a constellation of problems, and a
differential diagnosis is provided for each problem or problem constellation. Use of tests is discussed for each major problem. A complete,
reasonable plan for each problem is suggested. Shares constructs that led to decisions and diagnostic decision making related to management
plan, disposition, consult, and/or follow up recommendations. Includes appropriate patient education/anticipatory guidance, health promotion,
pharmacological and non-pharmacological measures, consult/referral, and follow-up recommendations. Demonstrates practice recommendations
based on evidenced based practice.
15pts 10pts 6pts 0pts
Evaluation and Management Coding:
Evaluation and management coding is stratified into the appropriate level of complexity based on the nature and number of clinical problems,
amount and complexity of the data reviewed during the encounter, and/or the risk of morbidity and mortality to the patient. When appropriate,
accurate procedure codes included with supporting documentation within the dictation
5pts 3pts 2pts 0pts
Organization and Grammar:
Documentation is clear and well organized without spelling errors. Correct medical terminology is used. Redundant words, phrases, and other
distracting information are omitted. Record has a logical flow.
10pts 8pts 6pts 0pts

50
Focused or Episodic History and Physical Examination Rubric
Other Considerations: Female GYN/OB Examination
HPI – First sentence should include age, parity, LMP and present problem (details about cc and other relevant information).
Menstrual History Menarche, duration, flow and cycle length of menses, IMB (intermenstrual bleeding), or contact bleeding, dysmenorrheal, PMS, climacteric
Gynecologic History Breast history – history of breast disease, breast feeding, the use of SBE (Self Breast Exam), last mammogram (if applicable); previous gyn surgery (can include surgical history),
history of infertility, history of DES (diethylstilbestrol) use by patients mother, last pap smear - history of abnormal pap.
Contraceptive/ Sexual Current method/patients satisfaction with current method
History Past Methods, current sexual activity, number of partners, new partner in the last 3 months, condom use, history of sexual abuse.
PMH Include infectious diseases (gonorrhea, chlamydia, syphilis, herpes, genital warts, trichomonas, HIV, TB, rheumatic fever, hepatitis)
Social History Marital status, employment, age and health of children, social supports
ROS Concentrate on GYN/GU/GI; pertinent negatives may include, abnormal discharge, abnormal bleeding, dyspareunia, abdominal/pelvic pain, dysuria, hesitancy, urgency, incontinence, change in bowel habits, rectal
bleeding. For post/perimenopausal woman – hot flashes/night sweats, vaginal dryness, abnormal bleeding, irritability, depression, mood changes.
PE: At a minimum: Vital Signs, Thyroid, Breasts, Lungs, Heart, Abdomen, Extremities, Pelvic Exam, External genitalia, vagina, cervix, uterus abdomen, recto-vaginal
Other Considerations: Pediatric Examination
A number of factors distinguish the pediatric from the adult history and physical exam. Depending on the age of the patient, the primary historian may be the patient and/or another person, usually the parent.
Developmental factors are commonly considered. The differential diagnosis of a condition may vary depending on the age of the patient. Health care maintenance (e.g., immunizations and safety issues) and social
issues play a major role in emergent and routine care. Therefore, key items must be considered for inclusion within the documentation note including: informant, prenatal history, birth and neonatal history, feeding
history, immunization history, developmental/behavioral history, HEADDSS for the adolescents. For the physical exam: be sure to include head circumference, growth curves, etc. for appropriate age levels along with
appropriate developmental assessment.
Focused Problem Rubric
Criterion Criterion
Fully Met
Criterion
Partially Met
Criterion
Inadequately
Met
Criterion Not
Met
Chief Complaint:
Targeted CC present without the inclusion of extraneous information. Patient initials and age present without identifying data. 5pts 3pts 2pts 0pts
History of Present Illness:
HPI is targeted toward the reason for presentation without the inclusion of extraneous information. HPI is fully developed and includes location,
duration, timing, character, severity provocative/palliative factors, pertinent positives and pertinent negatives.
15pts 10pts 6pts 0pts

51
Focused Problem Rubric
Past medical, family, and social history:
Elements of the PMH that expand on the CC and HPI are included, yet irrelevant information is excluded. Elements of the FH and SH that
expand on the CC and HPI are included, yet irrelevant information is excluded.
10pts 8pts 6pts 0pts
Review of Systems:
Elements of the ROS that expand on the CC and HPI are included, yet irrelevant information is excluded 10pts 8pts 6pts 0pts
General Survey/Vital Signs:
General survey includes vital signs, height and weight, BMI, and other relevant data related to CC. 5pts 3pts 2pts 0pts
Physical Examination:
All systems assessed focus on the CC. Appropriate descriptors are used to articulate the physical findings. 15pts 10pts 6pts 0pts
Labs/Diagnostics:
Pertinent lab and diagnostic findings are included along with appropriate comments regarding abnormal labs and inclusion of pertinent positives. 10pts 8pts 6pts 0pts
Management Plan:
States/identifies appropriate final diagnosis. Shares constructs that led to decisions and diagnostic decision making related to management plan,
disposition, consult, and/or follow up recommendations. Includes appropriate patient education/anticipatory guidance, health promotion,
pharmacological and non-pharmacological measures, consult/referral, and follow-up recommendations. Demonstrates practice recommendations
based on evidenced based practice.
15pts 10pts 6pts 0pts
Evaluation and Management Coding:
Evaluation and management coding is stratified into the appropriate level of complexity based on the nature and number of clinical problems,
amount and complexity of the data reviewed during the encounter, and/or the risk of morbidity and mortality to the patient. When appropriate,
accurate procedure codes included with supporting documentation within the dictation.
5pts 3pts 2pts 0pts
Organization and Grammar:
Documentation is clear and well organized without spelling errors. Correct medical terminology is used. Redundant words, phrases, and other
distracting information are omitted. Record has a logical flow.
10pts 8pts 6pts 0pts

52
DICTATION EXAMPLE USED WITH PERMISSION
Date of Service: 06/29/18 Initials: R. W. MRN: XXXXXXX General Patient Information: Age: 29 years Sex: Female Race: Caucasian Primary historian: Patient, Patient’s mother Chief complaint: Nausea, dizzy, overheated History of Present Illness: R.W. is an otherwise healthy 29-year-old female who presents to the emergency room by private vehicle with complaints of nausea, fatigue, and feeling overheated. Reports that she was out in the boat for about two hours this afternoon in 90-degree weather. States she began feeling ill and fatigued while on the boat, and lay down for a rest once returning home. She woke up feeling nauseated, which was unrelieved with ODT Zofran and lying in an air-conditioned environment. She has had at least one episode of emesis. Reports associated dizziness, lightheadedness, malaise, weakness, headache, muscle/abdominal cramping, and heart palpitations. She states she drank one bottle of water today. Denies any previous history of heat exhaustion or heat stroke, but states she is “sensitive” to the sun and does not feel well when in a warm environment for prolonged periods. Denies feeling ill prior to this experience. Past Medical History
- Cervical Cancer (2016) - Renal calculi
Surgical History
- Septoplasty (2018) - Adenoidectomy (2018)
Family History
- Noncontributory. Social History R. W. lives with her family. States that she is not worried about recurrent heat symptoms and has no sun exposure at her work. She is on vacation for a week, and has been spending time on the water for the past few days. Reports that she does not drink much water normally. Medications
- Albuterol 8 gm IH as directed PRN - Spironolactone 25 mg PO bedtime - Norethindrone-Ethinyl Estrad 1 each PO daily - Fluoxetine HCl 20 mg PO daily - Metformin 1,000 mg PO daily - Bupropion HCl 150 mg PO daily
Allergies
- Penicillins – Nausea and vomiting Review of Systems:

53
General: Denies fever or chills. Reports malaise and fatigue. Head: Reports headaches and a history of migraines. No trauma. Eyes: Denies visual changes, visual loss, blurring, or double vision. Gastrointestinal: Reports nausea, vomiting, and abdominal pain. Denies appetite changes or diarrhea. Respiratory: Denies shortness of breath. Cardiac/Peripheral vascular: Reports a brief period of palpitations which have since resolved. No chest pain or peripheral edema. Musculoskeletal: Reports muscle weakness and generalized muscle cramping. Genitourinary: No dysuria, hematuria, or other urinary symptoms. Integumentary: Reports rash over arms and upper chest. Neurologic: Denies seizures or changes in level of consciousness. Physical examination: Vital Signs: Heart rate 88, Temperature 36.8 C tympanic, Respiratory rate 17, Oxygen saturations 97% on room air, BP 154/97, Height 1.57 m, Weight 85.275 kg, BMI 34.4 kg/m2
General appearance: This is a pleasant female in no acute distress who appears her stated age. She appears pale and fatigued, but is conversant and answers questions appropriately. Eyes: Sclera nonicteric. Pupils are equal, round, and 2mm in size. EOMs intact, with horizontal nystagmus noted. Pharynx: Mucous membranes moist. Cardiac/Peripheral vascular: Heart rate is tachycardic with regular rhythm. No murmurs, gallops, clicks, or splitting. No peripheral edema. Gastrointestinal: Abdomen rounded, with no evident pulsations. Bowel sounds active x4 quadrants. Abdomen soft to palpation and tender in the upper quadrants. No guarding or rigidity. Respiratory: Respirations easy, even, and unlabored. No cyanosis. Lung sounds clear to auscultation, equal bilaterally, and free of adventitious sounds. No cough noted. Integumentary: Scattered maculopapular rash noted over upper chest and arms bilaterally. No evidence of sweating or diaphoresis. Musculoskeletal: No tremors. Demonstrates no functional deficits. Strength equal in upper extremities. Gait unobserved. Neurologic: The patient is alert and oriented x4. Speech is clear. No confusion noted. Cranial nerves II-XII grossly intact. Labs/Diagnostics
1. CBC with differential - WBC 9.9 - RBC 4.18 - HGB 13.1 - HCT 39.8 - MCV 95 - MCH 31 - MCHC 33 - Plt Count 380 - Neutrophils 70 - Lymphocytes 21 - Monocytes 7 - Eosinophils 1 - Basophils 0 2. BMP - Sodium 140 - Potassium 4.2 - Chloride 106 - Carbon Dioxide 27 - Anion Gap 7.5

54
- BUN 10 - Creatinine 1.0 - Est Cr Clr Drug Dosing 65.65 - Estimated GFR (MDRD) >60 - Glucose 93 - Calcium 9.5 3. Magnesium 2.0 4. Urinalysis - Urine Color Yellow - Urine Appearance Cloudy - Urine pH 5.0 - Ur Specific Gravity 1.025 - Urine Protein Negative - Urine Glucose Normal - Urine Ketones Negative - Urine Occult Blood Large - Urine Nitrite Negative - Urine Bilirubin Small - Urine Urobilinogen Normal - Ur Leukocyte Esterase Negative - Urine RBC 10-20 – Reports she is spotting with her period. - Urine WBC 0-5 - Ur Epithelial Cells Moderate - Amorphous Sediment Few - Urine Bacteria Few - Urine Mucus Few
Assessment
1. Heat exhaustion, unspecified – ICD 10 T67.5 Differential Diagnoses Differential diagnoses for heat exhaustion are as follows:
1. Migraine headache – The patient’s nausea, vomiting, and frontal headache suggest possible migraine headache, which is congruent with the patient’s history. However, she states that this does not feel like a typical migraine for her, and its association with other symptoms of heat exhaustion support that as the primary diagnosis.
2. Heat stroke – The patient’s history of feeling overheated, along with her numerous somatic complaints and lack of hydration make this a possibility. However, her lack of neurological symptoms, such as seizures and decreased level of consciousness, reduce this possibility. Additionally, her normal temperature on exam supports heat exhaustion as the primary diagnosis.
Plan 1. Heat exhaustion – The patient’s sudden onset of symptoms after spending time in the heat supports this
diagnosis. Her laboratory studies were unremarkable. - The patient refused IV hydration and anti-nausea medications here. She was given 1 dose of ODT Zofran and
reported that her symptoms resolved following this medication (with the exception of a mild frontal headache). - Zofran script provided for ongoing nausea. - Pt should drink a minimum of 8-10 glasses of water daily and increase water intake when in the heat. - Avoid strenuous activities in hot weather. Wear cool, breathable clothing to reduce excess heat exposure. - Take cool showers or baths as needed to reduce the symptoms of heat rash. - Discussed the need to be cautious with heat exposure in the future, as the patient will likely be prone to
recurrences. - Seek immediate care if experiencing seizures, difficulty breathing, ongoing nausea and vomiting, or any other
concerning symptoms.

55
Total Time Spent: 25 minutes Signed: Jenise Ropp, RN, FNP-s E/M CPT Codes: #1 - 85025 - BLOOD COUNT; COMPLETE CBC, AUTOMATED (HGB, HCT, RBC, WBC, & PLATELET) & AUTOMATED DIFFERENTIAL WBC #2 - 81015 - URINALYSIS; MICROSCOPIC ONLY #3 - 80048 - BASIC METABOLIC PANEL (CALCIUM, TOTAL) #4 - 83735 - MAGNESIUM #5 - 99281 - EMERGENCY DEPT VISIT, 3 KEY COMPONENTS: PROB FOCUS HX; PROB FOCUS EXAM; STRTFWD MED DECISION
1. History a. HPI – Extended b. ROS – Extended c. PFSH – Pertinent d. History – Detailed
2. Exam – Detailed 3. MDM
a. Number of Diagnoses – 1 (Self-limited or minor) b. Complexity of data reviewed: 1 (review or order clinical lab tests) c. Risk: Minimal (One self-limited or minor problem)
4. Overall MDM – Straightforward Complexity

56
Appendix H
Clinical Site Visit Tool
Clinical Site Visit Guide
"Mid-Term FACULTY Evaluation of CLINICAL SITE, PRECEPTOR, and STUDENT"
OVERALL SUMMARY:
The degree to which the FACULTY determines the CLINICAL EXPERIENCE to:
1. Facilitate the students’ ability to engage in learning activities that contribute to the growth and development related to course, clinical, and/or personal
objectives established for the precepted experience.
Strongly Agree Agree Disagree Strongly Disagree
2. Promote student integration of new knowledge and attainment of program outcomes.
Strongly Agree Agree Disagree Strongly Disagree
3. Foster interprofessional collaborative practices.
Strongly Agree Agree Disagree Strongly Disagree

57
4. Meet the identified academic and/or experiential qualifications required of a preceptor.
Strongly Agree Agree Disagree Strongly Disagree
6
Name of Preceptor and Phone Number
Enter a response
7
Site Name and Address
Enter a response
5 What type of clinical site visit was performed?
Onsite Visit, Primary preceptor and student present
Onsite Visit, Secondary preceptor and student present
Phone Visit with Preceptor
Additional Comments:

58
8
Primary Practice Type
9
QUESTIONS FOR PRECEPTOR and/or STUDENT:
Has the student reviewed their clinical objectives with you?
What is the average number of patients per clinical day the student is exposed to?
What types of patients are being seen/evaluated by the student?
Can you describe a typical day with the student?
Enter a response
10
QUESTION FOR PRECEPTOR - Interviewing and History Taking
What PROMOTES or NEGATES YOUR CONFIDENCE for the student to have independence with seeing and then presenting a case to you?
Explain your assessment of the student's approach to establishing rapport, identifying a chief complaint and collecting a history.
Adult Health (Ages 19 - 99+)
Family Practice (All ages)
Pediatrics (Ages 18 and below)
Women's Health
OB
ER
Hospitalist
Specialist
OTHER - Note in text box below.
Additional Comments:

59
Enter a response
11
QUESTION FOR PRECEPTOR - Physical Exam
What parts of the physical exam do you feel the student needs more experience in or can you given me an example of an occasion the student did
remarkably well during their physical exam?
Can you please comment on degree of competence the student has displayed with any psychomotor skills (i.e. procedures/specialty exams) you’ve
observed during the student’s rotation?
Enter a response
12
QUESTION FOR PRECEPTOR - Documentation
How would you rate the student’s use of medical terminology and encounter documentation?
If not able to document, can the student scribe for you?
Enter a response
13
QUESTION FOR PRECEPTOR - Critical Thinking/Application of Knowledge - Management Planning
Are there examples of the student’s performance in critical thinking, appropriate decision making, and diagnostic test interpretation that you can share with
me?
Can you describe an example of how the student has or has not grown in ability to formulate a management plan, engage in consultation/referral, and
provide patient education?
Enter a response

60
14
QUESTION FOR PRECEPTOR - Professionalism
Can you share examples that indicate the student’s degree of professionalism throughout the rotation (for example, mannerisms, attire, timeliness,
communication with patients/staff)?
Enter a response
15
QUESTION FOR PRECEPTOR - Opportunities/Strengths
During the time you had with our student can you provide areas of opportunities for improvement that I could share with the student?
Can you share strengths regarding the student exhibited during their rotation?
Enter a response
16
QUESTION FOR PRECEPTOR - University Relationship
Is there anything the University of Mary can improve on for facilitating/improving the university/student/preceptor relationship and interactions?
Enter a response

61
Questions for Faculty Observation of Clinical Site
YES NO NA
17
Preceptor makes time for student to review chart and plan care
with preceptor before patient encounter, as appropriate for
student’s developmental level.
Additional Comments
18
Preceptor makes time for student to review visit and plan of care
after encounter.
Additional Comments
19
Preceptor provides opportunities for student to learn how to
consult appropriately.
Additional Comments
62
20
Expectations for student performance are consistent with
accepted professional competencies for safe beginning-level
practitioner.
Additional Comments
21
Preceptor requires problem-focused documentation of patient
care that is accurate and complete.
Additional Comments
YES NO NA
22
Preceptor provides opportunities for students to learn
prescribing, triage, evaluation, development of interprofessional
relationships, and follow-up of laboratory results.
Additional Comments

63
23
A preceptor reviews and signs all student documentation of care.
Additional Comments
24
The preceptor demonstrates a philosophy that fosters holistic
care as demonstrated by the practice philosophy statement,
charting, or observed patient care.
Additional Comments
25
The practice site can be accessed safely by the student.
Additional Comments
26
The site has adequate space for students to work, study, and
rest (e.g., dictation, access computer desk space).

64
Additional Comments
YES NO NA
27
Clinic staff welcomes student/faculty. Pleasant and friendly
environment.
YES NO NA
Additional Comments
28
FACULTY observation of STUDENT with CLINICAL PATIENT:
Please provide a brief description of the patient case encounter observed.
29
EVALUATION OF STUDENT WITH CLINICAL PATIENT
RATING SCALE
1 - NOVICE

65
Knows the general rules to help perform tasks; relies on guidelines/standards on which to base treatment/management, rather than on previous past
experience. Student: Requires guidance to determine which guidelines/standards to choose; beginning to develop differentials, recognize some normal
versus abnormal conditions.
2 - ADVANCED BEGINNER
Has had some prior experience with which to frame judgments and formulate management plans; requires supportive cues but less so than beginner
stage. Student: Increasingly independent in their ability to develop a differential list and use guidelines/standards to formulate a management plan;
increasingly recognizes normal versus abnormal conditions.
3 - COMPETENT
More past experiences upon which to base their clinical reasoning and judgement; developing the ability to prioritize care and formulate management
plans; gaining efficiency in clinical practice. Student: Increasingly independent in their ability to develop a differential list and use guidelines/standards to
formulate a management plan; increasingly recognizes normal versus abnormal conditions (in specific populations); starting to recognize the need for
consultation and referral.
4 - PROFICIENT
Able to anticipate patient course from previous experience; ability to prioritize care and formulate management plans based on previous experience;
efficient clinical practice; developing intuition. Student: Independent in their ability to develop a differential list and use guidelines/standards to formulate
a management plan; recognizes normal versus abnormal conditions in most populations; recognizes the need for consultation and referral.
5 - EXPERT
Confident; solid knowledge base on which to formulate judgements and develop management plans; intuitive ability to quickly read patient situations.
Student: exceptional in their ability to perform independently; intuitive grasp of patient situations; recognizes the need for consultation and referral.
NOVICE
ADVANCED
BEGINNER COMPETENT PROFICIENT EXPERT

66
HISTORY
COLLECTION:
Employs skillful
interviewing
techniques to
identify
pertinent
positive and
pertinent
negative
historical data
in the adult
patient
population.
Gathers
relevant
historical
health data for
patients of all
ages.
Additional Comments
HISTORY
COLLECTION:
Distinguishes
between
relevant and
irrelevant
subjective data.
67
NOVICE
ADVANCED
BEGINNER COMPETENT PROFICIENT EXPERT
Additional Comments
PHYSICAL
EXAMINATION:
Performs an
indicated
timely and
organized
physical exam
to differentiate
normal from
abnormal to
identify
obvious and
subtle findings.
Differentiate
normal from
abnormal
findings,
and/or change
across the
lifespan.
Additional Comments

68
PHYSICAL
EXAMINATION:
Identifies
obvious and
subtle findings
of significance.
Additional Comments
PHYSICAL
EXAMINATION:
Modifies the
physical exam
with regard to
the chief
complaint and
history of
present illness.
Additional Comments
NOVICE ADVANCED
BEGINNER
COMPETENT PROFICIENT EXPERT

69
DIAGNOSIS:
Formulates
appropriate
differential
diagnoses based
on client data.
Additional Comments
NOVICE
ADVANCED
BEGINNER COMPETENT PROFICIENT EXPERT
DIAGNOSIS:
Selects
appropriate
diagnostic
modalities
necessary for
evaluation of
client
condition.
Additional Comments

70
DIAGNOSIS:
Selects and
conduct
appropriate
screening
procedures as
deemed
appropriate.
Additional Comments
MANAGEMENT:
Initiates nursing
and medical
interventions to
promote
health, treat
health
alterations, and
to prevent
illness using
evidencebased
resources.
Additional Comments

71
MANAGEMENT:
Recognizes
indications for
pharmaceutical
management.
Additional Comments
NOVICE ADVANCED
BEGINNER
COMPETENT PROFICIENT EXPERT
MANAGEMENT:
Calculates and
prescribes
appropriate
medication
doses based on
client
characteristics
(age, weight,
etc.)
NOVICE
ADVANCED
BEGINNER COMPETENT PROFICIENT EXPERT
Additional Comments

72
MANAGEMENT:
Performs procedures
as indicated.
Additional Comments
TEACHING:
Assesses client
readiness to learn.
Additional Comments
TEACHING: Informs
clients at an
educational level
best suited for their
optimal
understanding.
Additional Comments
TEACHING: Aware of
a variety of
resources for

73
counseling and
referral.
Additional Comments
NOVICE ADVANCED
BEGINNER
COMPETENT PROFICIENT EXPERT
COMMUNICATION:
Gives a brief,
succinct case
presentation with
appropriate
terminology in an
organized manner.
Additional Comments
NOVICE
ADVANCED
BEGINNER COMPETENT PROFICIENT EXPERT

74
COMMUNICATION:
Accurately
documents history
and physical in the
client’s medical
record succinctly
and systematically.
Additional Comments
COMMUNICATION:
Informs the client
of their health
status including
diagnosis,
management,
therapeutics,
consultations, and
referrals.
Additional Comments

75
LEADERSHIP and
ROLE
INTEGRATION: The
student is
punctual, has a
professional
appearance in all
clinical
experiences,
displays initiative,
and possesses
interpersonal skills
that promote
effective
interactions with
healthcare team
members and
patients
Additional Comments
30
Please provide any additional comments or concerns for the clinical site visit.
Enter a response

76
Appendix I Choosing the Correct Outpatient E/M Coding

77

78
Appendix J Hotseat Competency Pearls
Student clinical competence is further evaluated by faculty during practical testing that occurs on campus at
the conclusion of each clinical course. Using a simulated scenario the student is evaluated on their history,
physical exam, clinical decision making, diagnosis, management, and patient education competence. This
competency testing is coined “hot seat” because they are evaluated in real time by faculty while also being
observed by their peers.
This is a PASS/FAIL requirement. If a student fails the Hotseat Competency, several other factors are taken into
consideration. Based on an overall assessment of the student’s performance in the clinical setting and FNP course work,
students may be required to repeat the course, repeat another Hotseat Competency, complete additional clinical hours,
or work one on one with faculty followed by another Hotseat Competency. The final recommendation will be made
based on feedback from at least two clinical faculty.
• Each student will be assigned a case pertinent to the clinical course most recently completed. Primary Care Clinical Experience will include cases that commonly present to an outpatient family practice clinic. Acute and Emergent Cases will be presented to students after completing their Acute and Emergent Clinical.
• One instructor will be the patient and another instructor will be the Examiner. Both will assist in evaluating student competence.
• The expectation is for the student to present to the patient just like you would in that clinical setting.
• The student will conduct a focused history and physical exam just as you would in that clinical setting. If it is a complaint that requires a more comprehensive evaluation such as a preventive exam, you will modify your questions and exam to meet that criteria.
• Each student will only have 15 - 20 minutes for your history and exam.
• Please bring any assessment tools (stethoscope, etc) or references (procedure books, EKG manual, ACLS or TNCC algorithms, etc) that you want readily available.
• Dress professionally.
• When conducting the exam, the student is to assume their findings are normal unless the instructor states something is abnormal - for example: as you are listening to the heart - (the instructor might state "you hear a grade 3/6 systolic murmur") - if nothing is said - assume it is a normal exam. If you are assessing a sprained ankle - ("you see moderate swelling with bruising to the heel area, but no deformity, no bony tenderness, pain moderate over anterior talofibular ligament" - this is what you will note in your exam findings. If you are concerned the "Examiner" will not realize what you are assessing - tell your patient - "I'm listening to your heart now". "I'm checking your abdomen for any tenderness or abnormalities." etc...
• During the exam portion be sure you are conducting your exam appropriately. For example, listening to the correct locations over the carotid and instructing the patient to hold their breath for a few seconds. Listening to the correct locations of the heart. If you are observed listening to just two areas of the back and two areas on the front chest – this is an obvious fail.
• If you have an orthopedic complaint - you are expected to complete a true hands on focused musculoskeletal exam.
• The only exception would be to verbalize breast, rectal, and GU exams.
• After completing the exam - you will need to direct any planning and recommendations to the "patient" in regard to your findings along with any recommendations or plans for further evaluation, including labs and diagnostics. If no further testing, you will make an excuse to step away from the patient to order your diagnostics or review studies completed and put together a discharge plan. We

79
are also assessing your ability to communicate fully with the patient, conduct appropriate exams, and transition from history/exam/and discharge. You can complete your history along with your examination.
• After you "step away" from the patient, the Examiner will hand you your requested test results (the tests you told the patient you would be ordering), give you a verbal report, or show you x-rays if available through the computer for review. If a procedure is required such as suturing, you will be provided the materials to perform.
• You can then do a brief check in with their peers - "did I miss anything?" "my initial plan is this... am I on target?". This step gives you a "safety net" and "consult" - which I would hope and assume you will probably do to start out in your new career; and gives the other students a chance to be involved in multiple cases. Listening students – HELP your colleagues!!! Like in the real world we tend to be so caught up with our own patients – we don’t always “listen” and or provide the best direction. Thus – it is an art to know when your consultants are truly hearing you and which ones provide the best recommendations.
• For a couple of the cases - an outside consult may be needed - then the Examining Instructor would be the consultant. Otherwise - you will have little interaction with the Examiner. If you need to call a specialist, DO!!
• The testing student will then finish reviewing diagnostics and writing out a final discharge plan, prescriptions, admit or transfer orders, etc. while another student will begin - then swap again to close off with your patient.
• Like an actual patient you will need to decide to treat and discharge home, or if needed admit, or transfer your patients. If admitting or transferring, you will need to note type of acuity, transfer needs, and provide a report to your accepting provider. Be prepared with what you need to communicate for the safety of your patient.
• The student will complete a documentation note following the Hotseat. Documentation templates will be available for the student to use. However, if you have a template you prefer to use or feel more comfortable writing out on your own – that is acceptable as well. Be sure to accurately document any procedures performed.
• As a reminder - only document what you completed or observed and remain focused to your specific case. If you are asked to complete a "physical" - obviously you will gather more material. If it is a focused complaint - will want to focus on items specific for your case. At the end of the Hotseat Experience, all documentation will be collected and used for assessing competency.
• Some cases are quite short - others a little longer depending on the clinical setting.
• There are some cases that have x-rays, EKG’s, available in the Canvas Hot Seat Sandbox; and some cases that have pictures or videos.
• There will be a brief closing debriefing, then can still complete/finish your "dictation" or documentation template while the other students are completing their hot seats. We will collect the dictations at the end of the experience. A final debriefing will be completed via GOTOMEETING within the month following Hotseat examinations.
• An example of a Hotseat Case and Evaluation Form is provided for your review.
• You got this!! Do your best to have fun and show your stuff!
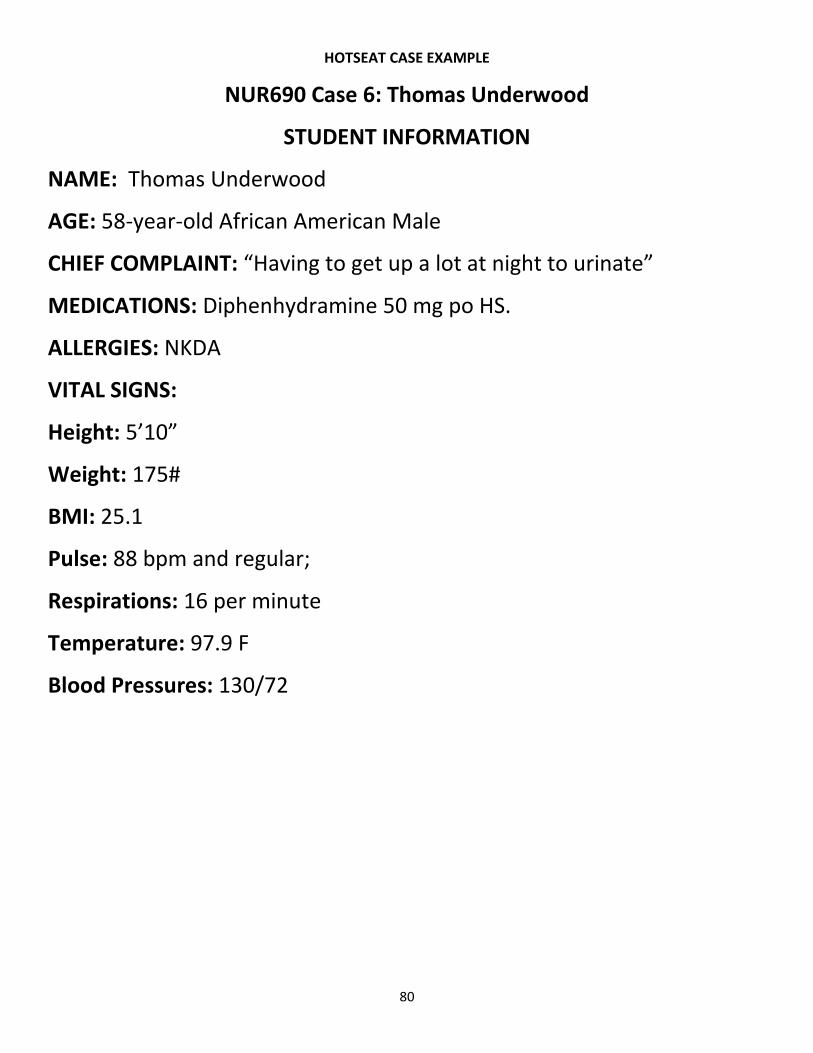
80
HOTSEAT CASE EXAMPLE
NUR690 Case 6: Thomas Underwood
STUDENT INFORMATION
NAME: Thomas Underwood
AGE: 58-year-old African American Male
CHIEF COMPLAINT: “Having to get up a lot at night to urinate”
MEDICATIONS: Diphenhydramine 50 mg po HS.
ALLERGIES: NKDA
VITAL SIGNS:
Height: 5’10”
Weight: 175#
BMI: 25.1
Pulse: 88 bpm and regular;
Respirations: 16 per minute
Temperature: 97.9 F
Blood Pressures: 130/72

81
Thomas Underwood
Presenting Complaint: “Having to get up a lot at night to urinate” Final Diagnosis: Benign Prostatic Hypertrophy, Symptoms worsened by antihistamine use Patient Demographics: Age: 58 years old Gender: Male; African American
Case Objectives:
• Obtain a through history and physical examination based on the
presenting complaint.
• Develop a comprehensive list of differential diagnosis.
• Identify appropriate diagnostic studies, consultations, if indicated, to
further clarify definitive diagnosis.
• Note final diagnosis.
• Provide patient education plan with necessary written instructions,
transfer, referral, or admission.
• Complete a written documentation note.
Case Setting: Clinic

82
Chief Complaint: “Having to get up a lot at night to urinate.”
History of Present Illness: Mr. Underwood is a 58-year-old African American male who
presents with the chief complaint of “having to get up a lot at night to urinate.” The nocturia
began approximately 2 years ago and consisted of having to get up once at night to urinate;
however, for the past month this has increased to three to four times per night. It interferes
with the quality and quantity of his sleep, leaving him drowsy at work the following day. In
addition, he is experiencing urinary urgency, urgency frequency, sensation of incomplete
bladder emptying after voiding, difficulty starting stream, straining to continue stream, weaker
force and diameter of the stream, and postvoid dribbling. He has not noticed an abnormal or
unusual odor to his urine. He is not having any abdominal pain, back pain, flank pain, fever,
nausea, vomiting, urinary incontinence, urethral discharge, bowel changes, leg weakness, or
paresthesias affecting the trunk or lower extremities.
Past Medical History: Mild Seasonal Allergic Rhinitis – Currently Controlled with
diphenhydramine started 1 month ago. No previous hospitalizations. Has NOT had age
appropriate immunizations or screening evaluations.
Past Surgical History: None
Past Family History: Unremarkable – negative for prostate or bladder cancer.
MEDICATIONS: Diphenhydramine 50 mg PO HS for the last month. No
other OTC, Herbal, or Vitamins.
ALLERGIES: NKDA
SOCIAL HISTORY: Smoker 1 ppd for last 40 years. Drinks alcohol on occasion (two drinks every
2 to 3 months). Married. Children are grown and out of the house. Business manager for a
construction company.
Last Visit to Health Care Provider: Over 8 years ago.
REVIEW OF SYSTEMS:
General: Denies recent anorexia, weight loss, night sweats, true fatigue.
Genitourinary: Denies gross hematuria. Denies erectile dysfunction.
Sleep History: Normally goes to bed at 10 pm and watches television until midnight. Does not
consume beverages during this time period. Does admit in last month has increased
caffeinated beverage intake to 5 to 10 drinks during work hours to “stay awake and alert.”

83
All other ROS negative.
PHYSICAL EXAM:
Vital Signs: Height: 5’10” Weight: 175# BMI: 25.1 Pulse: 88 bpm and regular; Respirations: 16 per minute
Temperature: 97.9 F Blood Pressures: 130/72
General: Alert and oriented. No acute distress. Appears well.
CVS: Regular rate and rhythm, without murmurs, gallops, or rubs. Apical impulse is nondisplaced and without
any thrills.
Respiratory: Lung fields are clear and equal bilaterally.
Abdomen: Active bowel sounds in all four quadrants. Soft, non-tender. No masses or organomegaly. Rectal
examination is normal except for a slightly enlarged, smooth prostate with a shallow medial furrow. Normal in
consistency and does not reveal any masses or indentations.
Genitourinary: Both testicles are descended and without masses; scrotal sacs are nontender and without
abnormal masses; midline urethra; and status postcircumcision. No lesions, lymphadenopathy, or hernias are
identified.
Skin: Warm and dry without rash. No new lesions. No edema to lower extremities
DIAGNOSTIC TESTING:
Post Void Residual Urine (PVR): 155 mL (normal: <100-200)
PSA: 4.5 ng/ml (normal: <4)
UA: Unremarkable
Serum Creatinine: 0.8 mg/dl (normal male: 0.6 – 1.2)
FINAL DIAGNOSIS:
1. Benign Prostatic Hypertrophy – Symptoms worsened by antihistamine usage (In view of negative
findings with additional history questions, physical exam, and diagnostic results, most likely diagnosis.
PLAN:
1. Medications:
• Stop diphenhydramine and try topical cromolyn sodium for allergic rhinitis. Symptoms of BPH can be
worsened by patients taking antihistamines. Other medications that exacerbate BPH symptoms include
anticholinergics, decongestants, tranquilizers, and alpha-adrenergic agonists.
• Start Tamsulosin 0.4 mg 30 minutes before bed: can increase to 0.8 mg if patient tolerates and
continues to be symptomatic. Tamsulosin, as well as any other alpha-blocker, is an appropriate first-
line agent to treat BPH. If maximum dosage does not produce the desired results (or is not tolerated by
the patient), then the addition of a 5alpha-reductase inhibitor, which is generally considered a second-
line agent, should be considered. However, it would not be totally incorrect to begin a patient with
severe symptoms on both. If this combination fails, a urology consult is indicated for additional

84
evaluation, confirmation of diagnosis, the addition of an anticholinergic agent, and/or surgical
intervention.
2. Decrease if possible eliminate caffeine, and avoid fluids 4 to 6 hours before bedtime. Caffeine can increase
urinary frequency because it is both a bladder irritant and a diuretic. This urinary frequency can occur both
during the day and at night; hence, eliminating caffeine from his diet is likely to reduce the frequency of
nocturia. Eliminating fluids (especially caffeine and alcohol) 4 to 6 hours before bedtime will make less urine
during the night and hopefully reduce frequency of nocturia.
3. Schedule for a Prostatic Ultrasound. The PSA level is slightly elevated; however, considering current symptoms and
DRE findings, it is most likely caused by BPH. However, because the PSA is slightly elevated, it could represent an early
prostate carcinoma in addition to the BPH. Risk factors for prostate cancer include tobacco use, African American
descent, age, and current symptoms of change.
7. Final recommendations pending ultrasound. Consider Urology consult if Ultrasound is of concern and or no
improvement in symptoms in 4 – 6 weeks. Return to clinic in 4 weeks for recheck of symptoms. Sooner if new
or worsening concerns.

85
NUR690 Case 6: Thomas Underwood
HOT SEAT Competency Rubric
Evaluation Criteria Rating Scale Comments
Communication 1. Establishes rapport 1 2 3 4 5 NA 2. Interviews patient with confidence 1 2 3 4 5 NA 3. Identifies patient’s chief complaint and patient concerns
• Determines what the client thinks may be diagnosis or cause of problem
1 2 3 4 5 NA
4. Preserves alertness to patient clues 1 2 3 4 5 NA 5. Maintains control in difficult patient encounters
1 2 3 4 5 NA
6. Shows use of pre-encounter dates from patient or nurse’s comments/notes
1 2 3 4 5 NA
Knowledge 1. Conducts history in a manner that assists provider to narrow differential
• Timing/onset/duration/frequency
• Location/radiation
• Character or quality
• Quantity/severity
• Associating factors
• Aggravating factors
• Alleviating factors
• Past medical history
• Family medical history
• Personal and social history
• Current medications
• Allergies
• Review of systems
1 2 3 4 5 NA
• Onset of nocturia 2 years ago – with once a night.
• Much worse the last month – coincided with start of nightly diphenhydramine, now 3 – 4 times a noc.
• Interferes with quality and quantity of sleep. Drowsy at work.
• Experiencing urinary urgency, urgency frequency, sensation of incomplete bladder emptying after voiding, difficulty starting stream, starting to continue stream, weaker force and diameter of stream, and post void residual.
• Denies unusual or abnormal urine odor.
• Denies abdominal pain, back pain, flank pain, fever, nausea, vomiting, urinary incontinence, urethral discharge, bowel changes, leg weakness, or paresthesias affecting the trunk or lower extremities.
• Family history negative for bladder, prostate, or other cancers.
ESSENTIAL:
• Elicit recent history of anorexia, weight loss, night sweats, or true fatigue. Constitutional symptoms could indicate the presence of an associated malignancy including prostate or bladder cancer.
• Any gross hematuria? Can be associated with nephrolithiasis, bladder cancer, or urinary tract infection. Regardless of symptoms, patients with painless hematuria in conjunction with risk factors for bladder cancer are considered to have bladder cancer until proven otherwise. Bladder cancer risk factors include male gender, Caucasian race, advancing age, cigarette smoking, aniline dye (found in fabric dye, hair coloring, and wood stains) exposure, some medications (phenacetin and chloranaphazine), and previous radiation therapy especially an external beam.
• Does he have any problems with erectile dysfunction? Because his symptoms could be caused by prostatic tissue hypertrophy and the currently accepted theory is that prostate gland enlargement, which is associated with the normal aging process, results from decreasing testosterone levels (which also occur with the normal aging process), it is important to determine whether the patient is experiencing symptoms suggestive of a decreased testosterone state. One of the primary symptoms caused by hypotestosteronism is ED.
• How much caffeine does he consume in the average day? Caffeine is considered to be a bladder irritant and diuretic. Excessive caffeine intake can increase urinary output and frequency of voiding, including at night.
Non-Essential

86
• Smoker 40 pack year • What is his bedtime routine? Routine night routines usually will not have an effect on voiding unless involves fluid intake. Bedtime routines do have an effect on overall sleep efficiency.
2. Shows evidence of critical thinking
• Summarizes history findings 1 2 3 4 5 NA
3. Conducts physical exam appropriate to patient complaint
• Chooses systems appropriate to presenting complaint and history findings
• Conducts an organized sequence of exam to minimize position changes yet promotes examiner efficiency
• Communicates to the client the exam technique instructions and findings
• Order of exam techniques (inspection, auscultation, percussion, palpation)
• Performs techniques correctly
1 2 3 4 5 NA ESSENTIAL
• Abdominal Examination. Identify if presence or absence of distended bladder, irregularities to shape of bladder or renal mass. Provides useful information in formulating his list of differential diagnosis and evaluated complications for those conditions.
• Rectal and prostate examination. DRE permits abnormalities in size, consistency, contour, and tenderness of prostate gland to be identified. Important to remember, when prostate gland is responsible for patient’s symptoms, its oval size does NOT correlate well with the severity of these symptoms. Specific attention should be made to tone of anal sphincter. Generally accepted that strength of the anal sphincter tone correlates with strength of urinary bladder sphincter tone.
• Genital examination. Assess for abnormalities that lend support for or against conditions on list of potential diagnosis along with information regarding coexisting conditions (phimosis, hypospadias, epididymitis, or urethritis) that might contribute to nocturia.
NONESSENTIAL
• Skin Examination. There are very few urogenital skin concerns that can cause specifically nocturia. Dysuria if noted could be related to a skin secondary infection or other cause.
• Heart and Lung Examination. Ideally, a heart and lung examination should be performed on all patients regardless of the reason for the clinical encounter; however, in the “real world” time constraints in the clinical setting, we want to focus on the areas that with provide the best “bang for the buck”. Therefore the only essential H and P points need to provide the most useful clinical information for guiding diagnostic studies and formulate correct diagnosis and treatment plans.
4. Demonstrates ability to summarize history and physical findings in a manner to provide a list of differential diagnosis and possible primary diagnosis (es)
1 2 3 4 5 NA Differential Diagnosis: BPH, Prostate CA, Caffeine Overuse, Medication Adverse Symptom, Bladder Cancer, Colon Cancer, Phimosis, epididymitis, urethritis, urethral tumor, DM, Diabetes insipidus, heart failure, cystitis, pyelonephritis, glomerulonephritis, renal cancer, staghorn calculus, renal trauma, lower UTI, nephrolithiasis.
5. Critically considers diagnostic work up pertinent or necessary to patient problem
1 2 3 4 5 NA Essential
• UA. Evaluate for systemic diseases (DM, diabetes insipidus, heart failure); infectious process of urinary tract (cystitis, pyelonephritis, glomerulonephritis); renal abnormality (renal carcinoma, stone)

87
• PSA. Most experts agree that if the PSA score is below 4.0, the likelihood of prostate CA is very small. However, if greater than 10, likelihood is much higher. No consensus on levels from 4 to 10. Risk factors for prostate cancer include advancing age, positive family history, African American, smoking, unhealthy diet (including red meat, high fat), and low fiber (vegetables).
• Serum Creatinine. Generally proportional to renal function. All older men with urinary symptoms should have a creat to ensure kidney function is not compromised or contributing to their condition.
Nonessential
• PVR – Marked BPH can cause obstructive uropathy. Depending on clinical guideline – AUA SI score noting moderate to severe BPH symptoms should be screened. Other experts note not needed if H and P are consistent with diagnosis of BPH and without evidence of obstructive uropathy.
• Prostatic US Today – Not indicated based on benign exam findings. However, if abnormal PSA, then further consideration advised prior to Urology Consult.
6. Interprets diagnostic data accurately 1 2 3 4 5 NA 7. Considers cultural variations that will impact patient management
1 2 3 4 5 NA
Resource Utilization 1. Employs current and dated references 1 2 3 4 5 NA 2. Exhibits proficient use of web-based references
1 2 3 4 5 NA
3. Demonstrates use of evidence-based medicine
1 2 3 4 5 NA
Patient Management Plan 1. Provides most probably diagnosis(es) for patient encounter
1 2 3 4 5 NA Essential BPH, increased symptoms due to antihistamine use.
2. Articulates effective patient education concerning management plan, follow-up, and preventive care as appropriate
1 2 3 4 5 NA Essential
• Stop Antihistamine. Consider nasal atrovent or nasal steroid instead.
• Start Tamsulosin 0.4 mg 30 minutes before bed, can increase 0.8 mg if patient tolerates and continues to be symptomatic.
• Scheduled for Prostatic US – if abnormal, or not improvement with medication, refer to urology.
• Risks and benefits of medication.
• Follow-up recommendations
3. Chooses appropriate pharmacologic and/or non-pharmacologic interventions
1 2 3 4 5 NA
4. Demonstrates consideration of use of collaborative patient management
1 2 3 4 5 NA
5. Includes patient education at disposition as well as at teachable moments in patient encounter
1 2 3 4 5 NA
6. Arranges referral or consultation in effective manner
1 2 3 4 5 NA

88
Final Summary Final Evaluation 1 2 3 4 5 PASS FAIL
Final Comments
Adapted from: Scott, P.M. (2012). Cases in Clinical Medicine. Sudbury, MA: Jones and Bartlett Learning, LLC.
Tool Definitions
1 - Novice: Knows the general rules to help perform tasks; relies on guidelines/standards on which to base
treatment/management, rather than on previous past experience. Student: Requires guidance to determine which
guidelines/standards to choose; beginning to develop differentials, recognize some normal versus abnormal conditions.
2 - Advanced beginner: Has had some prior experience with which to frame judgements and formulate management
plans; requires supportive cues but less so than beginner stage. Student: Increasingly independent in their ability to
develop a differential list and use guidelines/standards to formulate a management plan; increasingly recognizes normal
versus abnormal conditions.
3 - Competent: More past experiences upon which to base their clinical reasoning and judgement; developing the ability
to prioritize care and formulate management plans; gaining efficiency in clinical practice. Student: Increasingly
independent in their ability to develop a differential list and use guidelines/standards to formulate a management plan;
increasingly recognizes normal versus abnormal conditions (in specific populations); starting to recognize the need for
consultation and referral.
4 - Proficient: Able to anticipate patient course from previous experience; ability to prioritize care and formulate
management plans based on previous experience; efficient clinical practice; developing intuition. Student: Independent

89
in their ability to develop a differential list and use guidelines/standards to formulate a management plan; recognizes
normal versus abnormal conditions in most populations; recognizes the need for consultation and referral.
5 - Expert: Confident; solid knowledge base on which to formulate judgements and develop management plans; intuitive
ability to quickly read patient situations. Student: exceptional in their ability to perform independently; intuitive grasp of
patient situations; recognizes the need for consultation and referral.
References
Burns, C., Beauchesne, M., Ryan-Krause, P., & Sawin, K. (2006). Mastering the preceptor role: Challenges of clinical teaching. Journal
of Pediatric Health Care, 20(3), 172-183.Latham, C. L. & Fahey, L. J. (2006). Novice to expert advanced practice nurse role
transition: Guided student self-reflection. Journal of Nursing Education, 45(1), 46-48.
Copeland, H. L., & Hewson, M. G. (2000). Developing and testing and instrument to measure the effectiveness of clinical teaching in
an academic medical center. Academic Medicine, 75(2), 161-166.
Latham, C. L. & Fahey, L. J. (2006). Novice to expert advanced practice nurse role transition: Guided student self-reflection. Journal
of Nursing Education, 45(1), 46-48.
Scott, P.M. (2012). Cases in Clinical Medicine. Sudbury, MA: Jones and Bartlett Learning, LLC.

90
Appendix K Preceptor Thank You Letter
Noted below is a copy of the Preceptor Thank You Letter that is sent out to each University of Mary Preceptor on University of Mary Letter Head. Preceptors also have the option of becoming a Clinical Practice Professor. Students are encouraged to communicate these benefits with their preceptor and consider this opportunity after they graduate and are eligible to also become a University of Mary Preceptor.
Dear Preceptor,
Thank you for your contribution to the clinical and professional development of Student during the
summer semester of XXXX school year for xx clinical hours. The University of Mary appreciates how you
honor the professional duty of mentoring the next generation of healthcare providers. We have high standards for
our students and realize that in order for them to reach their full potential they need the challenge and guidance of
professionals such as you.
Please keep a copy of this letter for your records. It serves as documentation of
the number of hours worked with a student. These hours may contribute to your
recertification application to some national certification bodies (i.e. AANP and
ANCC).
Please know your service is appreciated by not only Student, but also by the entire University of Mary Family Nurse
Practitioner Program faculty. The time and energy you expend as a preceptor is significant and we want to
recognize your efforts. For your contributions, the University of Mary bestows upon you the title of University of
Mary Clinical Practice Professor and encourages you to use this title as part of your professional documentation.
A definition of the Clinical Practice Professor role at the University of Mary can be found at this link.
I am excited to share with you that Clinical Practice Professors are provided eligibility for University of Mary
tuition benefits, access to the Welder Library, and opportunities for free continuing education. Information related
to each of these benefits are provided in the links below:
• University of Mary Tuition Benefit – Preceptors are eligible for 100% discount on 8 semester hour credits/year for undergraduate degree credits and 50% graduate degree credits (classroom setting) and 50% tuition benefit for online undergraduate and graduate degree programs. Preceptors who would like to take advantage of this option are encourage to contact Dr. Billie Madler, Chair of Graduate Nursing Education at 701-355-8266 or by email at [email protected].
• Welder Library
• Continuing Education Opportunities
We do require having on file a resume or curriculum vitae (CV) for all Clinical Practice Professors. If you have
not previously provided a copy, forward your resume or CV to me at [email protected].
Please know we will always welcome your ideas. If you have any recommendations for our program or comments
regarding your time with our student, please feel free to contact me. Also, if you should need any additional
documentation of your hours spent with our students, I can be reached at 701-319-1101 or by email at
[email protected]. I look forward to continuing our partnership in this exciting and rewarding venture.
With many thanks,
Annie M. Gerhardt, DNP, APRN, FNP-C FNP Clinical Competence Coordinator, Associate Professor
Doctorate of Nursing Practice, Family Nurse Practitioner Program