Cholecystitis. - Karachi Kings (KK) Nursing College
21
Advanced Concept of Nursing- II UNIT- V Advance Nursing Management In The Name of God (A PROJECT OF NEW LIFE HEALTH CARE SOCIETY ,KARACHI) Advance Nursing Management of GIT diseases. Cholecystitis. Shahzad Bashir RN, BScN, DCHN,MScN (Std.DUHS) Instructor New Life College of Nursing Updated on June 08, 2016
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Cholecystitis. - Karachi Kings (KK) Nursing College
Advanced Concept of Nursing- IIUNIT- V
Advance Nursing Managementof GIT diseases.
Cholecystitis.
In The Name of God
(A PROJECT OF NEW LIFE HEALTH CARE SOCIETY, KARACHI)
UNIT- VAdvance Nursing Management
of GIT diseases.
Cholecystitis.Shahzad Bashir
RN, BScN, DCHN,MScN (Std.DUHS)Instructor
New Life College of NursingUpdated on June 08, 2016

Objectives:By the end of this presentation, the students willbe able to:
Define cholecyctitis. Discuss the pathophysiology of cholecystitis. List the types of cholecystitis. Identify the clinical features of cholecystitis. Elaborate the investigations of cholecystitis. Explain the medical and nursing management
of cholecyctitis. Cite nursing diagnosis of cholecyctitis.
Define cholecyctitis. Discuss the pathophysiology of cholecystitis. List the types of cholecystitis. Identify the clinical features of cholecystitis. Elaborate the investigations of cholecystitis. Explain the medical and nursing management
of cholecyctitis. Cite nursing diagnosis of cholecyctitis.
8/22/2016 2


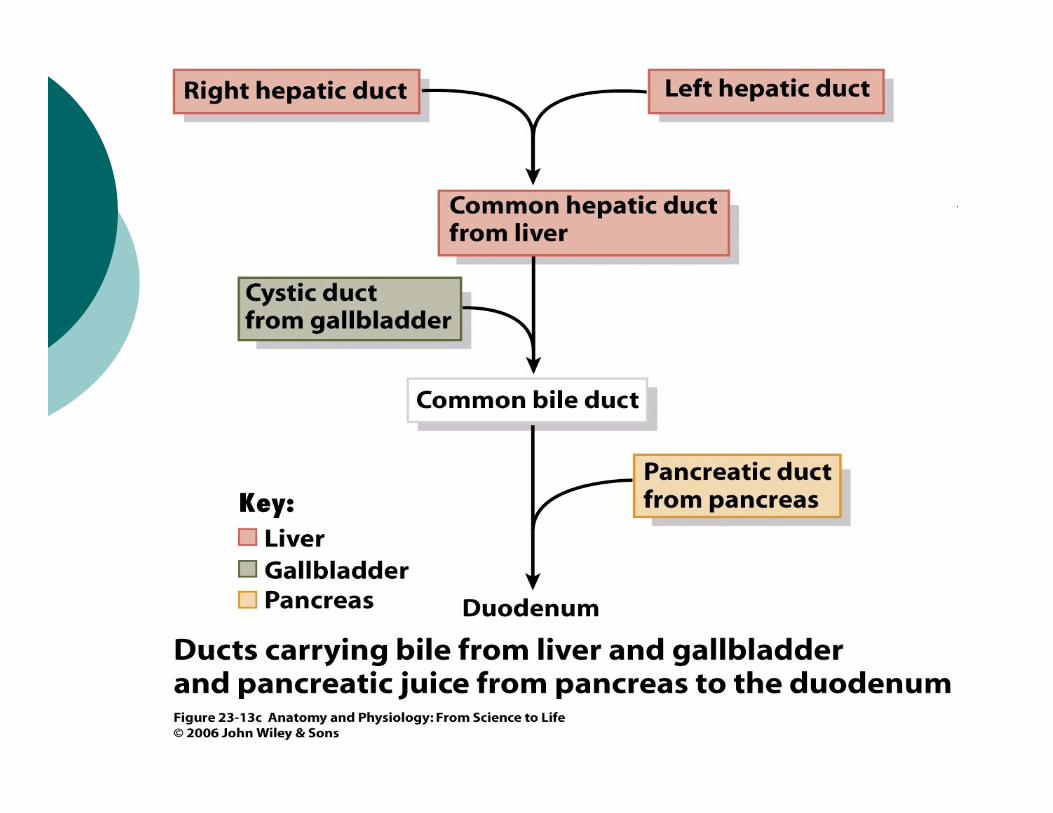
Gallbladder When food enters the duodenum, the gallbladder contracts and the sphicter
of Oddi relaxes (valve in the common bile duct), allowing bile to enter theintestine.
Cholecystitis - inflammation of gallbladder usually develops in assoc. withgallstones. But can occur from bacterial invasion or biliary spasm. Jaundice,bile obstruction not common. Blockage of bile flow from GB
Gallbladder becomes fibrotic and contracted, which result in decreasedmotility and deficient absorption.
3x4” pear shaped hollow organ underside of liver
Cholilithiasis- over time the concentration of bile in the gallbladder mayresult in insoluble stones, especially if bile contains high amounts ofcholesterol.
When food enters the duodenum, the gallbladder contracts and the sphicterof Oddi relaxes (valve in the common bile duct), allowing bile to enter theintestine.
Cholecystitis - inflammation of gallbladder usually develops in assoc. withgallstones. But can occur from bacterial invasion or biliary spasm. Jaundice,bile obstruction not common. Blockage of bile flow from GB
Gallbladder becomes fibrotic and contracted, which result in decreasedmotility and deficient absorption.
3x4” pear shaped hollow organ underside of liver
Cholilithiasis- over time the concentration of bile in the gallbladder mayresult in insoluble stones, especially if bile contains high amounts ofcholesterol.
6
Conti….
Cholesterol stones form and block drainage of bilefrom gallbladder, which causes spasm, GBbecomes inflamed, edematous and distended. Thiscongestion leads to changes in GB circulationwhich eventually causes necrosis. Bacterialgrowth also develops.
Cholesterol stones form and block drainage of bilefrom gallbladder, which causes spasm, GBbecomes inflamed, edematous and distended. Thiscongestion leads to changes in GB circulationwhich eventually causes necrosis. Bacterialgrowth also develops.
7
Gallbladder
Function- storage depot for bile Cholecystitis- inflammation of the
gallbladder wall, acute infection Cholelithiasis - presence of gallstones
Function- storage depot for bile Cholecystitis- inflammation of the
gallbladder wall, acute infection Cholelithiasis - presence of gallstones
Cholecystitis
Inflammation of gallbladder is called ascholecystitis.
Two types of cholecystitis.
Acute cholecystitis Chronic cholecyctitis
Inflammation of gallbladder is called ascholecystitis.
Two types of cholecystitis.
Acute cholecystitis Chronic cholecyctitis
8/22/2016 9

Acute cholecystitis
Acute cholecystitis is acute inflammation of gallbladder.
It is precipitated 90% of time by gallstones obstructionof neck or cystic duct.
Acalculous cholecystitis describes acute gallbladderinflammation in the absence of obstruction bygallstones.
For example: Surgical procedure, sever trauma, severeburns etc.
Acute cholecystitis is acute inflammation of gallbladder.
It is precipitated 90% of time by gallstones obstructionof neck or cystic duct.
Acalculous cholecystitis describes acute gallbladderinflammation in the absence of obstruction bygallstones.
For example: Surgical procedure, sever trauma, severeburns etc.
8/22/2016 10
Clinical features
Right upper quadrant pain Pain radiates to right scapula and right shoulder Fever Anorexia Tachycardia Diaphoresis Nausea & vomiting Jaundice
Right upper quadrant pain Pain radiates to right scapula and right shoulder Fever Anorexia Tachycardia Diaphoresis Nausea & vomiting Jaundice
8/22/2016 11
Pathophysiology (Calculus Cholecystitis) A gallbladder stone obstructs bile outflow.
Bile remaining in the gallbladder initiates a chemicalreaction.
It causes autolysis and edema
The blood vessels in the gallbladder are compressed,compromising its vascular supply.
Gangrene of gallbladder with perforation may result.
Bacteria play a minor role in acute Cholecystitis .i.e.Enterococci, Staphylococci , E. coli
A gallbladder stone obstructs bile outflow.
Bile remaining in the gallbladder initiates a chemicalreaction.
It causes autolysis and edema
The blood vessels in the gallbladder are compressed,compromising its vascular supply.
Gangrene of gallbladder with perforation may result.
Bacteria play a minor role in acute Cholecystitis .i.e.Enterococci, Staphylococci , E. coli
8/22/2016

Pathophysiology (Acalculus Cholecystitis) Acalculous Cholecystitis describes acute
gallbladder inflammation in the absence ofobstruction by gallstones.
Acalculous Cholecystitis occurs after majorsurgical procedures, severe trauma, or burns
It results from alterations in fluids andelectrolytes and in regional blood flow in thevisceral circulation.
Acalculous Cholecystitis describes acutegallbladder inflammation in the absence ofobstruction by gallstones.
Acalculous Cholecystitis occurs after majorsurgical procedures, severe trauma, or burns
It results from alterations in fluids andelectrolytes and in regional blood flow in thevisceral circulation.
8/22/2016
Cholecystitis: Pathophysiology The most common cause is cholelithiasis; obstructing the cystic and
or common bile ducts.
Can be acute or chronic
Bile is used for digestion of fats. It’s produced in the liver and storedin the gallbladder. When the concentration of bilirubin in the bloodincreases to greater than 2mg/dl, jaundice occurs.
Acute- gallstones partially/completely obstruct CBD
Chronic Cholecystitis- results from inefficient emptying of bile bygallbladder and gallbladder muscle wall disease persists.
Chronic- may be caused by or lead to formation of gallstones(cholelithiasis)
The most common cause is cholelithiasis; obstructing the cystic andor common bile ducts.
Can be acute or chronic
Bile is used for digestion of fats. It’s produced in the liver and storedin the gallbladder. When the concentration of bilirubin in the bloodincreases to greater than 2mg/dl, jaundice occurs.
Acute- gallstones partially/completely obstruct CBD
Chronic Cholecystitis- results from inefficient emptying of bile bygallbladder and gallbladder muscle wall disease persists.
Chronic- may be caused by or lead to formation of gallstones(cholelithiasis)

Investigations
Ultrasonography The use of ultrasound is based on reflected
sound waves.
Ultrasonography can detect calculi in thegallbladder or a dilated common bile duct.
To detect gallstones with 95% accuracy.
Ultrasonography The use of ultrasound is based on reflected
sound waves.
Ultrasonography can detect calculi in thegallbladder or a dilated common bile duct.
To detect gallstones with 95% accuracy.
8/22/2016 15
Cholescintigraphy
Cholescintigraphy is used successfully in thediagnosis of acute cholecystitis
A radioactive agent (Technitum 99-M) isadministered intravenously
It is taken up by the hepatocytes and excretedrapidly through the biliary tract
The biliary tract is then scanned, and images ofthe gallbladder and biliary tract are obtained
Cholescintigraphy is used successfully in thediagnosis of acute cholecystitis
A radioactive agent (Technitum 99-M) isadministered intravenously
It is taken up by the hepatocytes and excretedrapidly through the biliary tract
The biliary tract is then scanned, and images ofthe gallbladder and biliary tract are obtained
8/22/2016 16
Nursing Diagnosis
Altered nutrition: less than body requirementrelated to inadequate bile secretion
Deficient knowledge related to dietarymodifications, medications, self care activities
Acute pain related to inflammation of gallbladder Impaired skin integrity related to vomiting Risk for infection Knowledge deficit
Altered nutrition: less than body requirementrelated to inadequate bile secretion
Deficient knowledge related to dietarymodifications, medications, self care activities
Acute pain related to inflammation of gallbladder Impaired skin integrity related to vomiting Risk for infection Knowledge deficit
8/22/2016 17
Nursing InterventionsS/P CholecystectomyLap vs. Open CholecystecomyLOCVital signsPulmonary Hygiene (cough deep breath, ambulate, turnand position incentive spirometer)Splinting to reduce painPain managementMonitor wound incision /S/S of infectionMonitor T-tube drainage (initially bloody, then green-brown bile)T-tube initially may drain >400ml/day then shouldgradually decrease
Lap vs. Open CholecystecomyLOCVital signsPulmonary Hygiene (cough deep breath, ambulate, turnand position incentive spirometer)Splinting to reduce painPain managementMonitor wound incision /S/S of infectionMonitor T-tube drainage (initially bloody, then green-brown bile)T-tube initially may drain >400ml/day then shouldgradually decrease
Care of the T-tube
Report sudden increases in drainage or amountsexceeding 1000ml/day
Keep drainage bag below level of GB Inspect surrounding skin Maintain flow by gravity Never irrigate, clamp or aspirate without order Clamp 1 to 2 hours AC and PC Monitor and document the client’s response to food
Report sudden increases in drainage or amountsexceeding 1000ml/day
Keep drainage bag below level of GB Inspect surrounding skin Maintain flow by gravity Never irrigate, clamp or aspirate without order Clamp 1 to 2 hours AC and PC Monitor and document the client’s response to food
Nursing Interventions:Patient Education
Dietary counseling: Low fat diet Weight reduction Fat-soluble vitamins and bile salts to enhance
absorptions and aid digestion Avoid gas-forming foods Smaller more frequent meals Activity precautions 4-6 weeks Care of T-tube
Dietary counseling: Low fat diet Weight reduction Fat-soluble vitamins and bile salts to enhance
absorptions and aid digestion Avoid gas-forming foods Smaller more frequent meals Activity precautions 4-6 weeks Care of T-tube
References Brunner, L. S., Suddarth, D. S., & Smeltzer, S. C.
(2008). Brunner & Suddarth's textbook of medical-surgical nursing (12th ed.). Philadelphia: LippincottWilliams & Wilkins.
Porth, MC. (6th ED). Pathophysiology. (2002).Philadelphia. USA. Lippincott Willams& Willkins,
A Wolters Kluwer Company
McPhee, J. S., & Papadakis, A. M. (2011). CurrentMedical Diagnosis and Treatment.(50th ED). Chicago. USA: Mc Graw Hill
Brunner, L. S., Suddarth, D. S., & Smeltzer, S. C.(2008). Brunner & Suddarth's textbook of medical-surgical nursing (12th ed.). Philadelphia: LippincottWilliams & Wilkins.
Porth, MC. (6th ED). Pathophysiology. (2002).Philadelphia. USA. Lippincott Willams& Willkins,
A Wolters Kluwer Company
McPhee, J. S., & Papadakis, A. M. (2011). CurrentMedical Diagnosis and Treatment.(50th ED). Chicago. USA: Mc Graw Hill
![gkbZZZZ Ldwy ijh{kk] fnlEcj & 2017 Ldwy ijh{kk] fnlEcj ... - mpsos](https://static.fdokumen.com/doc/165x107/63261e906d480576770ca006/gkbzzzz-ldwy-ijhkk-fnlecj-2017-ldwy-ijhkk-fnlecj-mpsos.jpg)






![Kings Mountain Telephone Directory [1959] - DigitalNC](https://static.fdokumen.com/doc/165x107/63204c5aeb38487f6b0f9149/kings-mountain-telephone-directory-1959-digitalnc.jpg)