Blogging pragmatics and pedagogy: An adventure in faculty development

Sociology of Health & Illness Vol. 21 No.2 1999 ISSN 0141–9889, pp. 163–186
Children as informal interpreters in GP consultations: pragmatics and ideology
Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
Department of Sociology, University of Surrey
Abstract This paper explores the views of General Practitioners (GPs)about the appropriateness of children undertaking a task ofinterpretation between the GP and an adult patient in primaryheath care consultations. We argue that the operational con-straints that GPs face because of the limited availability ofprofessional interpreters or bi-lingual Health Advocates createsituations where children are accepted in this role by GPs, subjectto specific limitations and contingencies. The contingent natureof perceptions of children’s acceptability as informal interpretersis shown to be related primarily to the nature of the medicalconsultation in terms of whether it is likely to be straightforward,complex or sensitive. At the same time GPs express an ideologi-cal opposition to the appropriateness of this task for childrengenerally. This ideological opposition is explicitly linked by GPsto broader constructions of a ‘proper’ childhood, characterisedas a time of innocence and freedom from worry.
Keywords: children, general practitioners, competence, health advocates,interpreters
Introduction
One major aim of a consultation between a general practitioner (GP) andtheir patient is to share ideas about the ‘diagnostic’ significance of apatient’s trouble, the doctor’s treatment action or preventative advice, andthe consequences of illness and its treatment’ (Tuckett et al. 1985: 204).Effective communication between the GP and patient, then, becomes anessential component of the consultation process.
The achievement of effective communication is fraught with difficulties,and depends in part on the content of the interaction between patient and© Blackwell Publishers Ltd/Editorial Board 1999. Published by Blackwell Publishers, 108 Cowley Road,Oxford OX4 1JF, UK and 350 Main Street, Malden MA 02148, USA.

doctor. Ritchey et al. (1995) found that what they termed ‘accuracy’ of com-munication was strongly influenced by the type of information that wasbeing sought or could be sought by the doctor. They identified four types ofcommunication, and found that the degree of accuracy for each type ofcommunication varied considerably. For example, in examining patients’and doctors’ understandings of what had been communicated in a just-con-cluded consultation, the highest degree of shared perception between doctorand patient (reported independently of each other) was about informationelicited or conveyed in relation to the task of diagnosis—‘technical task’communications. In contrast, there was greatest divergence around percep-tions of what information had been conveyed or elicited in relation to thehealth lifestyle of the patient, and their psychosocial circumstances. There was a tendency by both the doctors and the patients to rely on stereotypicalassumptions in these two domains and to avoid direct communicationabout them.
In addition, major difficulties can arise when the GP and patient do notshare a common language. It has been well documented that the most effec-tive consultations are those occurring between GPs and patients who notonly speak the same language but are also from the same cultural back-ground (Waitzkin 1991: 24). However, as Shackman (1984: 56) and othershave found, even where there is a concordance of language and culture,problems of communication can still arise, with detrimental outcomes forboth patient and GP. It follows, then, that where GP and patient differ inboth first language and cultural background such communication problemswill be exacerbated. Indeed, Hornberger et al. (1996: 846) suggest thatwhere there is a lack of concordance there is the potential risk that patientswill have their access to good quality health compromised.
One response to language barriers between doctors and patients has beenthe employment by service providers of interpreters, bi-lingual Linkworkersor Health Advocates (Smaje 1995: 126). Each of these three professionalroles offers a distinctive approach to assisting patients with communication.Professional interpreters undertake interpretation between languages, oper-ating primarily at a technical linguistic level. The bi-lingual Linkworkers’role goes further, encompassing interpretation, explanations about how thehealth system works, and encouragement of uptake of services available.These workers generally aim to act as a link between women and health careprofessionals (Hicks and Hayes 1991). The bi-lingual Health Advocateapproach is more proactive on behalf of the patient in that they also offercultural information to professionals, challenge discrimination, andempower the patient to make informed decisions (Baylov 1996). In short,Linkworkers primarily represent the views of health professionals topatients, whereas Health Advocates represent the views of patients to healthprofessionals (Smaje 1995).
Despite the initiative to provide Linkworker and bi-lingual HealthAdvocates, which started in the UK in the 1980s, provision has never been
164 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999
at a level sufficient to cover all medical consultations where assistance withcommunication might be needed. This has resulted in other strategies beingadopted by individual GP practices, often on an ad hoc basis, includingemployment of quasi-professionals such as bi-lingual receptionists who canbe called on to interpret if a Health Advocate is not available, and the useof bi-lingual friends or relatives of the patient, often described as ‘informalinterpreters’ (Schott and Henley 1996: 100). Informal interpreters can becharacterised as being brought into the consultation by the patient, havingsome skills (although they may be quite limited) in translating between tworelevant languages, but not having any informal or professional training inthe task of interpretation. The extent to which the use of informal inter-preters is accepted suggests an attention to linguistic difficulties in commu-nication and a setting aside of those issues to which Linkworker andHealth Advocates can attend. The use of children as informal interpreterstakes this linguistic focus, and the exclusion of other aspects ofdoctor–patient communication, even further. The use of informal inter-preters is generally treated by health professionals as of only limitedacceptability. Shackman (1984: 13), for example, argues that the use ofinformal interpreters is suitable only as a short-term measure for emer-gency GP consultations.1
What little research there has been into the use of informal interpretersfor medical consultations has not shown it to be a particularly satisfactoryarrangement. Ebden et al. (1988: 347) examined encounters between hospi-tal out-patients staff and non-English speaking patients where relatives ofthe patient acted as informal interpreters. They found that, even with whatthey regarded as the two best interpreters, at least a quarter of all questionsasked were mistranslated or not translated at all. Mistranslation tended tooccur for anatomical and technical words because of cultural differences inthe ways that body parts were named. Questions or terms that were nottranslated at all, tended to reflect bodily taboos.
Research by The Health Education Authority (1994) into the ‘Health andLifestyles’ of Black and minority ethnic groups in England, and their reviewof the literature in this area, confirmed the difficulties that can arise withinformal interpreters. For example the HEA study reported that:
Patients who use informal interpreters report difficulties. These includeinhibitions in talking about women’s health issues via the husband or sonor daughter, as well as problems with inaccuracy and interpretation(HEA 1994: 66).
Ebden et al. (1988) also drew attention to the problem of embarrassmentwhere children were in the role of informal interpreter:
Children found it embarrassing to translate questions about menstruationor bowel movements to their parents (Ebden et al. 1988: 347).
Children as informal interpreters in GP consultations 165
© Blackwell Publishers Ltd/Editorial Board 1999

In general, professional opinion is opposed to the use of children as infor-mal interpreters. Rack (1982) has made the most emphatic statement aboutthis in terms of the universal unsuitability of children for the task of inter-preting in health encounters:
Under no circumstances should children be asked to interpret medicaldetails for their parents. It appears to us to be unethical, unprofessional,uncivilised and totally unacceptable (Rack 1982: 199–200).
This view is supported by others such as Schott and Henley (1996: 101), andShackman (1984: 13). However, Rack does not elaborate on this injunctionagainst the use of children, based through it is on an appeal to a number ofmoral grounds rather than any systematic empirical analysis of children inthe role of informal interpreter. In making statements like these Rack, andothers, do not consider whether children2 are always unsuitable for thistask, whether the patients who rely on their children to interpret for themare in favour of this or are reluctantly acquiescent to the practice in the faceof no apparent alternative, or whether health professionals with experienceof encounters where children act as interpreters support or oppose this ingeneral. Indeed, little empirical evidence is available on the extent to whichchildren do fulfill the role of informal interpreters, nor on the views andexperiences of those involved in such situations.
Drawing on in-depth interviews with GPs working in a London healthauthority with a large number of minority ethnic communities, this papermakes a contribution to empirical evidence in this area by exploring theviews of one set of health professionals—GPs—who have experience ofmedical consultations where children are enlisted as informal interpretersbetween a parent who is a patient, and the GP.
The research project
This paper reports on part of a larger Department of Health funded projectto examine barriers that face children from minority ethnic groups whenaccessing primary care services (Cohen et al. forthcoming). The project con-sisted of two stages: interviews with GPs, and focus groups with parentsfrom a variety of minority ethnic backgrounds. Here, we report on theanalysis of the GP interviews.
Thirty-eight in-depth tape recorded interviews were carried out by thefirst author between March and July 1997 with GPs working in the City andEast London Health Authority Area (known locally as ELCHA). This innerLondon health authority has a diversity of minority ethnic communities. Ofthe three boroughs covered by ELCHA the resident minority ethnic popula-tion (as defined by the Census 1991) made up 34 per cent of the populationin Hackney, 42 per cent in Newham and 35 per cent in Tower Hamlets(OPCS 1993: 398).
166 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999
Sampling strategyA purposive sample of GPs was identified using Patton’s (1987) criterion ofmaximum variation sampling. Patton’s sampling scheme creates a respon-dent selection framework based on one or two themes that the researcheridentifies as critical to the research question. Respondents are then selectedto represent the range of variation around those themes. In this research,the two themes chosen as most relevant were: languages (first and second)spoken by the GPs, and the advertised availability of bi-lingual HealthAdvocates at the GP practice. The ELCHA directory of GPs (ELCHA,1997) provided an appropriate sampling frame as well as providing informa-tion on languages spoken by the GPs. Sampling and selection was alsostructured to reflect location of GP practice (across the three LondonBoroughs covered by ELCHA), and practice size.
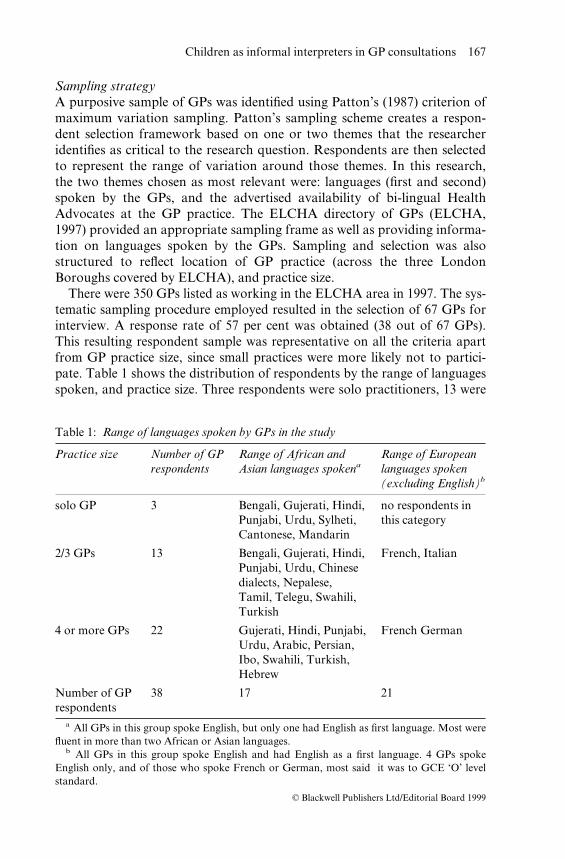
There were 350 GPs listed as working in the ELCHA area in 1997. The sys-tematic sampling procedure employed resulted in the selection of 67 GPs forinterview. A response rate of 57 per cent was obtained (38 out of 67 GPs).This resulting respondent sample was representative on all the criteria apartfrom GP practice size, since small practices were more likely not to partici-pate. Table 1 shows the distribution of respondents by the range of languagesspoken, and practice size. Three respondents were solo practitioners, 13 were
Children as informal interpreters in GP consultations 167
© Blackwell Publishers Ltd/Editorial Board 1999
Table 1: Range of languages spoken by GPs in the study
Practice size Number of GP Range of African and Range of Europeanrespondents Asian languages spokena languages spoken
(excluding English)b
solo GP 3 Bengali, Gujerati, Hindi, no respondents inPunjabi, Urdu, Sylheti, this categoryCantonese, Mandarin
2/3 GPs 13 Bengali, Gujerati, Hindi, French, ItalianPunjabi, Urdu, Chinesedialects, Nepalese, Tamil, Telegu, Swahili,Turkish
4 or more GPs 22 Gujerati, Hindi, Punjabi, French GermanUrdu, Arabic, Persian,Ibo, Swahili, Turkish,Hebrew
Number of GP 38 17 21respondents
a All GPs in this group spoke English, but only one had English as first language. Most werefluent in more than two African or Asian languages.
b All GPs in this group spoke English and had English as a first language. 4 GPs spokeEnglish only, and of those who spoke French or German, most said it was to GCE ‘O’ levelstandard.

in partnerships of two or three GPs, and 22 were in partnerships of 4 or more.The main reason given for non response was ‘too busy’. Of the 38 respon-dents, 17 spoke Asian or African languages.
The approach taken in the interview was that of a purposeful conversa-tion (Burgess 1984: 102), with the researcher using a topic guide. As Mason(1996) notes qualitative interviews are epistemologically appropriate whereemphasis is placed on the construction of social explanations. The use of in-depth interviews allowed the GP respondents to identify the issues they feltwere important or meaningful in relation to their experiences of using chil-dren as informal interpreters. In addition, this interview format also allowedthe interviewer to probe the respondents’ accounts more extensively than isusually afforded by other methods such as semi-structured interviews.
Extent of GP experience of children as informal interpretersGPs in the study varied greatly as to whether or not they had recent experi-ence of consultations where children had acted as informal interpreters. GPsfrom the same minority ethnic community as their patients, or who couldspeak one or more of the language spoken by their patients, were the leastlikely to have had recent experience of children acting as interpreters, aswould be expected. However, the majority of GPs (24 out of 38) had hadrecent consultations with adult patients where a child had undertaken therole of informal interpreter. The frequency of this occurrence rangedbetween one and fifteen consultations a week, with two to three consulta-tions a week being the more common.
In one instance a GP reported having a child of five act as an informalinterpreter but on average the youngest reported age was between six andeight years old. Minor children of all ages were equally likely to act as infor-mal interpreters, as were both girls and boys.
Enlisting children as informal interpreters: general contexts
It was clear from the interview data that the use of children as informalinterpreters was an option reserved by both parents and GPs for situationswhere professional bi-lingual Health Advocates or quasi-professional inter-preters (such as bi-lingual receptionists) were not available. The availabilityof bi-lingual Health Advocates reflected levels of regular demand for theirservices. Where there was little demand for such advocates they were nor-mally booked in advance to come to the surgery by the patient or the prac-tice on an ‘as required’ basis. One GP who worked in a practice wheredemand for Health Advocates was ‘sporadic’, found this arrangement farfrom satisfactory:
I think the advocates are in very short supply. The problem is, theconsultations we have with people who require advocates are sufficiently
168 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999

sporadic. It is very difficult to have an advocate when you want one, thatis the problem. It is just not practical to arrange for an advocate to bearound at a specific time during the week when a patient who can’t speakEnglish is going to have their peptic ulcer or their back sprain or what-ever it is, just organisational difficulties (50).
Where demand was high, Health Advocates attended certain weekly surgeries or clinics on a regular basis. Paradoxically, this arrangement wasthe case for the majority of GPs interviewed who had recent experience ofchildren acting as informal interpreters. This paradox arose becausealthough regular, Health Advocate cover was provided on average for onlytwo surgeries and one clinic session each week. Only three GPs had regulardaily coverage but this tended to be for morning surgeries only. For patientsto make use of the health advocacy service, therefore, their appointmenthad to coincide with a session covered by the Health Advocate. This couldbe planned for advance bookings but was governed by chance for emer-gency appointments. One GP commented:
We do however have a lot of situations where people, because it is veryhard to plan to get sick and need to see the Doctor then, they can’t get tophone the interpreters the following day and book an appointment forthe following week. We do often find we are seeing people in sort of acutesituations where young children are interpreters (38).
A small number of practices coped with the lack of Health Advocates byrelying upon bi-lingual receptionists who could function as quasi-profes-sional interpreters. They were employed directly by the practice itself andwere usually called upon to interpret for patients when there were no HealthAdvocates on duty. This arrangement was considered unsatisfactory by theGPs, first, because the receptionists were taken away from their usual recep-tion duties, and secondly, because they did not have any formal training forthis role. In addition this arrangement depended on whether they were onduty at the time of the consultation.
Only five GPs reported accessing Language Line, a national telephoneinterpreting service launched in 1990 (Halahmy 1990: 94). Communicationbetween GP and patient is assisted via a three way telephone conversationwith the interpreter. GPs were generally positive about this service, becauseit did not depend on being booked in advance, nor were there any restric-tions on the languages that were being offered. However, not all GPs wereaware of this service and many who were, said that the cost was too high forregular use and was reserved only for exceptional emergencies. One practicemade unlimited use of the service for historical reasons, resulting in a lowincidence in that practice of children being used as informal interpreters,despite the high percentage of registered patients requiring assistance withcommunication.
Children as informal interpreters in GP consultations 169
© Blackwell Publishers Ltd/Editorial Board 1999

It is clear that GPs do not generally follow the advice of Rack and othersnever to use children as informal interpreters. The quite frequent use of chil-dren for this task by the majority of GPs in the study reflects the need forassistance with communication during medical consultations and a lack ofalternative formal options. At the same time GPs experienced a tensionbetween a general reluctance to have children taking on the task of inter-pretation on the one hand, and a professional responsibility to proceed witha consultation once a patient is in the surgery on the other. This responsibil-ity was given a high priority, reflecting as it does, the organisation of accessto GP services and the GPs’ own professional goals.
. . . only yesterday I had a . . . family, children are going to school, bigchildren, and they know English and they come and act as interpreters.Not very satisfactory situation but at least the main problem can beidentified (22).
Priority was also placed on the importance of determining the seriousness ofpatients’ illnesses, and the possible consequences of failing to do this.
The unsatisfactory nature of these arrangements from the GP perspectiveis generally evident, however. One GP, when asked how he dealt with con-sultations where interpreting was needed but a Health Advocate was notavailable, described managing:
. . . as best as one can. At the time you try and deal with what needsdealing with there and then and beyond that one would try and arrangefor them to come back at a time with an advocate or interpreter (50).
Others said that using children as informal interpreters was ‘not a situationwe would choose to be in’ (05), and ‘something we discourage’ (43). In prac-tice, though, the immediate need to proceed with the consultation tended tooverride reluctance to place children in the role of interpreter, although notin all the cases as we show later.
Only two GPs suggested that parents may actively prefer their children tointerpret on their behalf, rather than have a Health Advocate. This prefer-ence was attributed to parents feeling that confidentiality was more likely tobe maintained by their child than by a Health Advocate who may be wellknown in the community in which the parent lived. This was seen to be thecase particularly for intimate personal health issues, such as reproductiveproblems, and socially sensitive problems such as domestic violence. One ofthese GPs commented:
I think if there was a problem with domestic violence or something theywere reporting, they wouldn’t want someone outside of the home to know. . . they wouldn’t want that kind of thing to get out and women will putup with a lot just to keep, obviously they have got their pride and they
170 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999

wouldn’t want people to know that they were being knocked about, orthat somebody had a drink problem for instance, so it’s only the familythat’s to know, so they would probably be reluctant to use an advocate in that situation (54).
Another felt that:
. . . lots of them come with their mothers and I think they feel that theywould rather, especially if it was gynaecological, they would prefer to doit through the daughter (20).
The actual enrolment of children into the task of interpreting in a medicalconsultation was usually initiated by the adult patient bringing along a childto act as interpreter:
. . . they bring the children along specifically (50).
The grandmother comes or the mother comes and she brings the childwith her. She knows she will have some communication problem and thatactually the child is brought in specifically for the purpose mostly,sometimes opportunistically the child happens to be here and the motherspeaks a bit of English and then the child will help with one or two wordshere and there . . . But usually more often the situation arises that thepatient has brought this child with them (52).
However, analysis of the GPs’ accounts of using children as informalinterpreters suggests that, where a Health Advocate or other interpreter isnot available, the GP each time makes a decision whether or not to acceptthe child for the role of informal interpreter. This decision is influenced to alarge extent by two main factors, assessed by the GP at the start of the con-sultation or early in the proceedings: the complexity of the process of diag-nosis, and the ‘sensitivity’ of the problem the patient has presented with orthe ‘sensitivity’ of the diagnosis process.
Accepting children as informal interpreters: the impact of complexity in theconsultation
The process of children acting as informal interpreters begins, then, with thepresentation of them for that role by the adult patient in the absence ofalternative arrangements. Subsequent to this, the GPs indicated that theyassessed the level of complexity and sensitivity involved in examining thepatient and reaching a diagnosis, and, on the basis of this assessment,accepted the child as an informal interpreter or postponed the consultationuntil an adult interpreter (informal or otherwise) would be available.
Children as informal interpreters in GP consultations 171
© Blackwell Publishers Ltd/Editorial Board 1999

Consultations described as ‘straightforward’ were seen unproblematicallyas suitable situations for children to undertake translation of questions andanswers between the patient and doctor:
. . . I think if it’s a pretty straightforward situation then carry on . . . (03).
The GPs characterised straightforward consultations as situations wherepatients presented minor ailments such as coughs, colds and sore throats oreasily diagnosable conditions. In these consultations GPs felt they were ableto make a clear diagnosis and advise on a treatment plan without muchintrusion into the patient’s life history or bodily boundary. These straight-forward encounters were seen as acceptable for the presence and use of chil-dren to interpret between the GP and patient:
. . . there are occasionally straightforward situations like somebody hascome in with a cough and, or a sore throat, that kind of situation is quiteeasy, it’s not very personal and it’s okay, it’s been possible to use a childin that way, or it’s been relatively okay . . . (05).
The acceptability of straightforward consultations did not depend solely onthe site or simplicity of the presenting symptoms, although these were criti-cal. The high incidence of the types of illnesses in this category—coughs,colds, sore throats—in itself presented a resource that the GP drew upon.This resource was constructed upon an assumption that children interpret-ing on behalf of the adult patients with these symptoms were likely them-selves to have experienced these types of illnesses and so be familiar with theconcepts used to describe them. Furthermore, diagnosis of these symptomscould be achieved using the simple language that GPs felt children couldeasily understand:
. . . we put it in a very simple English you know in such a way that they(minor children) could understand what we really want, we don’t use anytechnical words or complicated things you know, we put it in a very simpleway and then they ask their parents and they will tell us back . . . (22).
So, typically a straightforward consultation was characterised by diagnosisbeing achievable through the use of simple questions and answers, and chil-dren being perceived as generally competent to translate these (GP respon-dents generally indicated that children over the age of 5 years were usuallycapable of this level of translation in their experience). Additionally, thelikelihood that the child had themselves experienced the same sort of signsand symptoms and so would be able to understand the concepts employedby the doctor was an important factor in judging children to be competentenough to be translators in the consultation. Crucially, straightforward con-sultations involved illnesses or conditions which related to non-taboo parts
172 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999

of the body or bodily functions. In cases where these three factors were pre-sent GPs felt that the risk of making a misdiagnosis or the consequences ofmisdiagnosis were low.
By contrast, consultations that the GPs categorised as ‘complex’ werethose where the process of diagnosis was more complicated, and so the riskof misdiagnosing the condition was high, or the potential consequences ofmisdiagnosis were serious. In these situations proceeding with the consulta-tion using a child as interpreter was not generally seen as appropriate,although the GPs indicated that they might attempt to proceed if it seemedthat the child could cope with translating complex concepts and questions.This pragmatism was prompted by concerns on the GPs’ part that it couldbe essential that some information about the presenting problem wasgained, in case immediate action was needed.
GPs indicated that the difficulty with these consultations related in thefirst instance to concerns that the child might have a limited, or even a com-plete lack of, understanding of the particular concepts being used in theprocess of diagnosing the problem. This could be true of quite simpleaspects of the diagnosis process such as identifying the relevant affectedparts of the body verbally through naming them. For example, one GPdescribed a consultation in which a teenage son who was interpreting for hismother, kept mentioning the word ‘stomach’ as the area of the bodyaffected by ill-health, yet his mother kept pointing to her throat:
. . . he was saying that her stomach was a problem, but she kept onreferring to here (points to throat), I said do you mean the stomach or doyou mean the throat, he’d actually just got the words wrong, he’d thoughtthat stomach had meant throat . . . (27).
In this case, the GP drew on the mother’s behaviour to conclude that therewas a translation problem. The possibility of mistranslation between lan-guages increases the complexity of the diagnosis process and subsequent risks.
A second source of difficulty that GPs identified was the problem ofestablishing equivalent concepts between languages. As one GP suggested,this task was difficult enough even for a Health Advocate:
Apparently there is no Bengali or Sylheti word for stress or depressed orthese things, so anyway all that side is very difficult to access even with aHealth Advocate (59).
Not all difficulties in communication were linked to linguistic translation.What could be termed ‘cultural performances’ of illnesses were seen aspotentially problematic. The way in which patients expressed their symp-toms was seen by many GPs to be connected to the cultural backgroundand level of education of the patient. Knowledge of the different ways thatpatients expressed symptoms was seen as an essential component of making
Children as informal interpreters in GP consultations 173
© Blackwell Publishers Ltd/Editorial Board 1999

a correct diagnosis where there were cultural or language differencesbetween patient and doctor. One GP, fluent in the language of the minorityethnic group patients referred to in this extract, illustrated this:
. . . they describe to you what they feel . . . if they are having a gastriculcer, they will first come to see you complaining of a headache. How areyou supposed to know it’s a tummy ache . . . the indigestion is actuallybeing transmitted to the head, the pain moves about, but they are feelingit more psychologically, they are getting stressed out by the pain andhence they are getting the headaches. They complain more about theheadaches than they are about their tummy and hence, it’s complicated.They get worked up over an illness, which then ends up giving themanother illness, and they’ll describe that illness. It will be the leg ache, thesleepless night, it won’t be the tummy ache . . . I’ve learnt, that if theycomplain of headaches, its almost always certainly something else, then Ihave to examine them top to bottom because I know it’s something else.Often you find it’s epigastric pain and you press their tummy, that’stender, you give them the tablets, that clears, the headache clears, and thesleepless nights clear, to a GP listening to them, headaches, sleeplessnights, they think stress, I’ll give them sleeping tablets, but they havemissed the cause (28).
This perception of problems with cultural performance formed one of thebases of concern over the ability of children to interpret not just languagebut also culturally-specific presentations of the felt effects of illness and dis-ease. The implication is that children lack the knowledge and skills requiredfor linguistic and/or cultural mediation in this type of consultation and socannot be accepted into the role of interpreter. In circumstances where GPswere faced with managing a consultation about what they suspected was apsychosomatic or somatised illness, parents would be asked (via the child)to re-book the appointment for a time when a Health Advocate was avail-able. However, as can be seen, even with adults acting as interpreters, thesituation may continue to be less than straightforward.
Facilitating interpretation in consultationsThe very need to facilitate the task of interpretation could in itself transforma straightforward consultation into a complex one. The GPs described vari-ous ways in which they worked with the child undertaking the interpretingto achieve communication:
. . . I have to make sure that my English language is at a level that theycan understand . . . (55).
and in turn the child also seemed to work actively to facilitate translatingresponses from the adult patient to the GP:
174 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999

. . . you can give a big sentence or paragraph talking and then they willtranslate the gist of it . . . (57).
If it became clear to the GP that the child was having difficulties under-standing the concepts being used or translating a word between two lan-guages, non-verbal strategies were often successfully employed to clarifywith the child or parent what was being said. One GP gave the example of asituation where the child was having difficulty translating the concept oftemperature. The GP used non-verbal behaviour to communicate directlywith the parent, in the hope that the parent would be able to understandwhat was being asked and therefore help their child to communicate theiranswer to the GP:
Sometimes it creates confusion because the child cannot understand intheir own language how to relay the message to their parent. So I have touse sign language as well. Body language as well and explain and themother understands and replies back to the daughter . . . Say for exampletemperature, I put my hand on my head, I start shivering then I shakemyself, imitate and show to the mother exactly what I mean . . . (35).
Whilst it would seem that GPs had some success in clarifying what wasbeing said through the use of non-verbal strategies and entering into a dis-cussion with the child about the concepts being used, these strategies werereported as only useful in establishing which part of the body was affectedby the ill health and which symptoms were being experienced. Such strate-gies could not be used when the GP wanted to discuss their diagnosis ortreatment plan.
So the appropriateness of proceeding with a complex consultation using achild as an interpreter was subject to doubt because of the intricacy of theprocess of gathering information for diagnosis, the potential difficulty oftranslating culture-specific concepts between languages. Moreover, therewas the question of the imperviousness of some types of communication,such as those relating to explanations of treatment and intervention, tofacilitation through non-verbal means. Facilitated communication was further inhibited by the child being unlikely to have experienced any of thesigns or symptoms themselves and so removing the resource of understand-ing which could be drawn upon by the GP, the child or the patient instraightforward consultations.
However, in complex consultations the GPs were usually at least comfort-able with trying to establish via the child the symptoms and location in thebody of the illness. This was not the case for another category of consulta-tions described as ‘sensitive’.
Children as informal interpreters in GP consultations 175
© Blackwell Publishers Ltd/Editorial Board 1999

Rejecting children as informal interpreters: the impact of ‘sensitive’ consultations
All but two GPs with experience of children acting as informal interpretersmade it clear that it was unsatisfactory for children to be involved in consul-tations that related to reproductive health or personal emotional difficulties,such as marital problems. These were the types of consultations that theGPs categorised as ‘sensitive’. One GP summarised this feeling:
. . . it is problematic when I find out that the son or daughter is there andI have to ask the questions about the family planning and the cervicalsmear and their sexual history and personal questions which I feel myselfthat it is not an ideal situation where it should be conveyed through a sonor daughter. I normally tell the children look I need to ask certainpersonal questions, could you please bring an interpreter for the nextappointment . . . where they (parents) can bring somebody who speaksEnglish and come and tell me more about their personal history . . . (35).
The majority of GPs chose to do as the above GP had done, and not askthe parent any personal questions, even though such questions were essen-tial to arriving at the correct diagnosis for abdominal pain. This reluctancewas in complete contrast to complex consultations, where GPs appeared tohave less inhibition asking questions relating to other body areas, such asthe stomach or leg and where they would work to clarify misunderstoodconcepts with the child. The following dialogue between researcher and GPtypifies these issues:
GP: . . . if their [the patient’s] main concern is that they have tummy acheor that when they have their monthly period it is painful, it’s timethat the discussion stops there because the other leading questionsare too delicate for the youngster to relate to the mother . . . thequestions I need to ask are such that I’ll delve into areas that are toosensitive for the child really.
R: In what way are they too sensitive for the child?GP: I mean if you ask the child do you have pain during intercourse, do
you have vaginal discharge, I wouldn’t ask that sort of question.R: Is it not really something that children should know about?GP: I wouldn’t ask youngsters of eight to ask their mother, that sort of
thing, it does not do well for the child asking the mother do youhave pain during intercourse or vaginal discharge it doesn’t makesense to the child, because the child will ask me what, obviously itsgoing to ask ‘what’, ‘what’, ‘what do you mean?’
R: So then you have to start explaining.GP: Yes, it limits my consultation, it limits the questions I will ask, I will
176 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999

only ask questions that deal with the rest of the body, but if I needto ask more sensitive questions I will ask the child, ‘tell your motherto come with an adult’ (53).
Only a minority of GPs continued with sensitive consultations using achild as an interpreter and this was with reservations about the appropriate-ness of doing so. As the following GP’s account indicates, the decision toproceed could be made on the basis of whether the child was perceived to be‘worldly wise’:
. . . And it’s quite difficult to judge whether you should do it at all [theconsultation] if it’s a sexual or gynaecological, one tends to try and judgeit by the child’s reaction, they are very often worldly wise . . . (01).
On the whole, teenage daughters were considered ‘worldly wise’ enoughto interpret in sensitive consultations. GPs based their assessment of thechild on the assumption that because teenage girls had periods, they wouldat least be able to understand the concepts being used in the consultation. Incommon with straightforward consultations, shared physiological or patho-logical experiences were treated as creating a resource that could be drawnupon during the consultation to facilitate communication. As one GPdescribed when asked for reasons why teenage girls could assist with sensi-tive consultations:
One is, as I said, that somebody below 12, it is difficult to understand forexample if their mother is talking about periods, under 12 it is difficult.By 12 most of the girls have had periods so they will know what we aretalking about. That’s one. Secondly you start looking on them as a bit ofa semi-adult by that time so that is the only reason (33).
Conversely absence of shared physiological experiences between the adultand the child was problematic:
. . . the child is dealing with concepts that they have no understanding orexperience with . . . for example, how can a seven-year-old ask in theirlanguage whether the mother is having period problems or ask if theydon’t know what a period is . . . (50).
Thus, where the child’s own likely body or health related experiences aredeemed available as a resource that can be drawn on in sensitive consulta-tions, GPs considered it less inappropriate to use a child as an informalinterpreter for personal or intimate problems.
It became clear that the acceptability to the GP of the child as an inter-preter in a sensitive consultation was strongly influenced by the child’s gen-der and age together. For example, the two GPs who said it was acceptable
Children as informal interpreters in GP consultations 177
© Blackwell Publishers Ltd/Editorial Board 1999

for children to act as informal interpreters if the family preferred it for con-fidential reasons were referring to teenage daughters in the examples theygave. In contrast, GPs were categorical that they never asked teenage sonsto interpret in sensitive consultations. Apart from the obvious reason thatthey had no personal experience of menstruation, and thus there was nopossibility of a constructed bodily resource, the anticipation of feelings of‘embarrassment’ that would be experienced by both mother and son waskey. The consequence of this was that discussion of reproductive healthbetween mother and son was viewed as taboo:
You can’t expect a 13-year-old boy, you can’t really ask through himabout his mother’s periods. There are some subjects that I feel are taboo.You can’t ask things like that it is just too embarrassing, not for me butfor them, the parent and child (67).
The taboos associated with certain topics were central to the classificationof some consultations as sensitive and hence as generally inappropriate con-texts for children to undertake interpreting. However, the operation of thetaboos was clearly contingent on the gender and likely physiological experi-ences of the child who might be used to interpret between the doctor andadult patient.
So, in sensitive consultations, the appropriateness of proceeding withusing the child as an interpreter was governed not by issues about errors indiagnosis arising out of miscommunication, but rather by the status of thebody part or function that was implicated in the problem the patient waspresenting. The competence of the child to translate particular concepts wasassessed in relation to the likelihood of that child having experienced anaspect (not necessarily pathological) of the illness or condition the adultpatient was experiencing. However, even more critical was the gender of thechild, with girls being seen as potentially acceptable in relation to questionsabout taboo topics, or taboo parts or functions of the body for their moth-ers, whilst boys never were. Finally, sensitive consultations need not neces-sarily be complex and could be amenable to simple questions and answers,but this did not override the constraining effect of taboo.
Children as informal interpreters: contingent competence and ideologicalunease
For the GPs in this study, the appropriateness of proceeding with a consul-tation where a child had been brought along by the adult patient to act asan interpreter is a highly contingent decision. The GP is faced on the onehand with the professional imperative of achieving ‘a consultation’ at thepoint at which the patient presents themselves as in need of medical help.On the other hand, the suitability of a child for the role of informal inter-
178 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999
preter is generally considered to be low. Most GPs took pragmatic decisionsbased on their assessment of the likely nature of the consultation—straight-forward, complex or sensitive—and the perception of the child’s compe-tence to act as a communication mediator. The nature of this competencevaried depending on the nature of the consultation, the child’s own bi-lingual competence and the extent to which communication could be sup-plemented by non-verbal means, as well as the likelihood that the child hadexperience of similar problems or experiences relevant to the problem forwhich the adult patient was seeking medical help. In certain circumstancesthe gender of the child was also highly relevant.
Nonetheless, the pragmatic need to proceed with the consultation if pos-sible stood in tension with a general ideological reluctance to use children asinterpreters. This raises the question, though, of the basis of the ideologicalunease about the use of children as interpreters. In part, reluctance to usechildren was attributed by GPs to whether they were sufficiently competentto translate between GP and patient. However, despite the GPs havingexperience of children being able to take on the role of interpreter success-fully, only two GPs were generally positive about children occupying thisrole. For the majority of the respondents there remained fundamental con-cerns about the effects on children:
I don’t feel that it’s right really, they are having to grow up before theirtime in many ways. I think it puts a burden on them and it’s quiteinappropriate really, but it’s clearly better than nothing . . . (27).
When GPs spoke about the general inappropriateness of using children asinterpreters this was usually on the basis of much wider issues relating to theemotional impact on children of being party to their parent’s illness, theimpact on the normal dynamics of the parent–child relationship in that itcould become ‘reversed’, and the inappropriateness of certain knowledgeabout adult life being shared with children. The following comments illus-trate these themes:
. . . it’s not right, it’s not fair really that the children should be doing that.It also puts a huge responsibility on children makes them feel presumably,makes them feel very responsible for their parent’s ill health, makes them,puts them in a role of parenting when they should, they should be the onewho is parented (44).
I think it is a responsibility for the child that is, there is a terrible feelingof how it would grow up and take too much responsibility too soonwhich is sad for them. I also think it is sad for parents to be dependent ontheir children in that way. Very disempowering for them as parents and ashuman beings to sort of have to depend on their kids to do that. I think itmust be difficult for both parties (45).
Children as informal interpreters in GP consultations 179
© Blackwell Publishers Ltd/Editorial Board 1999

Children shouldn’t worry about their parents being ill, should they? (43).
These comments embody appeals to an ideology of childhood and par-ent–child relations which essentially constructs childhood as a time of inno-cence, a time of development where the child grows up but not too fast. Thischildhood innocence is partly based on maintaining an absence of know-ledge about certain aspects of the world, those aspects which are categorisedas ‘intimate’ or ‘personal’. On the whole it would seem that in medicalencounters these are matters related to gynaecological problems or issues:
. . . they may be discussing things that are more intimate than they shouldbe talking about (47).
Many GPs indicated broad concerns about the ‘emotional’ impact onchildren of taking on the interpreter role and through that gaining know-ledge about their parent’s health status and embodied sexual activities.Concern was expressed that children could become emotionally over-whelmed by coming into contact with aspects of adult life normally hiddenfrom them. The perception was that the effects of children coming into con-tact with such issues through their role in the medical consultation were‘unhealthy’ for the parent–child relationship. Adults normatively haveexclusive knowledge about specific aspects of their own lives—in particularin arenas relating to bodily functions, health and illness, mental health, sex-ual activity and sexuality. However, children gain access to these boundedknowledges when undertaking the interpreting role by virtue of having tocommunicate such knowledge between adult patient and doctor. Thisthreatens the innocence of childhood and children then ‘grow up tooquickly’, and disrupts a parent–child relationship based on an uneven distri-bution of knowledge (see Harre 1986 on this latter point).
In contrast, the two GPs who were positive about children acting as infor-mal interpreters for their parents, and who cited families that preferred touse teenage daughters to interpret in sensitive consultations, felt that suchchildren’s self-esteem benefited from being given responsibility for their par-ent’s health problems. The benefit of this was seen as giving children anopportunity to acquire and test out rational thought skills, which in turn,would help them to access health care more effectively for themselves in thefuture. This was contrasted with children who did not have this experience:
Because they are given the responsibility of speaking on behalf of themum, that gives them more confidence than some of the English children.So when they aren’t well, they understand what’s required of them in aconsultation and they can be more assertive because that’s what they areused to. In that sense they are then clearer sometimes about what theywant, than say a white child who is not used to that. Well, I think chil-dren respond to having a bit of responsibility, some children enjoy that,
180 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999

having responsibility, I would say on the whole they can give a betteraccount than the child who is always spoken for, you know, when peoplespeak on their behalf (54).
Overall, though, most of the GPs interviewed expressed reservationsabout the use of children for interpreting on behalf of an adult patient onthe basis of what might be termed ideological inappropriateness. Their con-tinuing sense of unease with children occupying this role related partly toviews about the effect it could have on the parent–child relationship if thechild gained knowledge about the parent’s health, body and activitiesbeyond what is considered the normal bounds (vague as they are), and if thechild takes on a burden of worry from that. A further source of uneaseseemed to be the taboos relating to sexual knowledge and the exposure ofchildren to sexually connoted knowledge in the course of translatingbetween adult patient and doctor during the medical consultation. Thisunease would seem to argue for childhood being preserved as a time ofinnocence, and for GPs to have a role as moral guardians within this, pro-tecting both child and adult patient from infringements of this innocenceand the inappropriate sharing of knowledge or worry.
Discussion and conclusions
The position that Rack (1982) asserts, that children should not be used asinterpreters in medical consultations under any circumstances, discussed atthe beginning of the paper, does not hold in practice for the GPs involved inthis study. In the absence of ready access to bi-lingual Health Advocates,professional interpreting services such as Language Line, or quasi-professional interpreters, GPs are willing to accept for this task the childthat the adult patient has brought with them, in the context of a profes-sional imperative to achieve a consultation once the patient has entered thedoctor’s surgery. This acceptance of the child as interpreter, however, is notautomatic. The acceptance or rejection of having a child as the informalinterpreter is contingent on both the perceived linguistic ability of the child,and the initial evaluation of the nature of the consultation as appropriate ornot for the child’s participation. Straightforward consultations, i.e. thoseinvolving easily-diagnosed and common conditions, are not seen as posingproblems, provided the child can assist with communication in terms ofinterpretation and translation of words and concepts. Even where thechild’s linguistic and conceptual ability does not match the translation task,the GP will work to facilitate communication across the two languages byemploying simplified English to be translated and non-verbal communica-tion of concepts that seem not to have been understood.
The more problematic situations from the GP’s point of view are thoseconsultations where the process of diagnosis is more complex, the concepts
Children as informal interpreters in GP consultations 181
© Blackwell Publishers Ltd/Editorial Board 1999

involved are unfamiliar or outside the experience of the child, or the natureof the presenting problem and/or the process of differential diagnosisinvolves topics that are sensitive or personal. In these situations the GPsindicated that they preferred not to use the child but would rather delay theconsultation until a time when a bi-lingual Health Advocate could be presentor an adult informal interpreter would be available. Complex consultationswere seen as problematic because of doubts on the GPs’ part that the con-ceptual and linguistic skills needed would be within the capability of thechild undertaking the interpretation, whereas sensitive consultations weremainly seen as problematic because of the knowledge the child mightacquire, or be exposed to, in the course of translating questions and answers.
One context for the reluctance of GPs to use children as informal inter-preters in sensitive consultations is the reported difficulty that doctors havewith communication about certain types of information. It has been claimedthat in the face of medical uncertainty (Yoels and Clair 1994, Mizrahi 1984)or avoidance of embarrassing or ambiguous encounters (Ritchey et al. 1995)doctors prefer to focus on the task of diagnosis, with communication pri-marily directed towards obtaining information relevant to that task. In thechild-interpreted consultations considered in this paper, sensitive consulta-tions may present particular problems for a doctor’s preferred focus on thediagnostic task, since the ease of doing this is undermined by the lack of ashared language, and by the taboos attendant on certain types of knowledgethat might be elicited or presented in the course of diagnosis where childrenare involved in the process of communication. Thus, the use of a child as aninformal interpreter in a sensitive consultation is problematic in a multipli-city of ways. In the GP accounts these knowledge taboos were related primarily to normative constructions of childhood as a time of innocence.Such innocence was seen to be threatened by the knowledge that childrenmight gain about taboo matters and about the adult patient during thecourse of translating questions and answers.
Straightforward consultations did not pose a threat to knowledge taboos,nor to the doctor’s ability to focus on diagnostic information. However, ifthe doctor’s focus on eliciting and exchanging diagnostic information wascompromised, such as when the child lacked sufficient linguistic or concep-tual skills to effect doctor–patient communication without much help, astraightforward consultation could transform into a complex one. Thisunderlines the high priority placed on what Ritchey et al. (1995) term ‘tech-nical task’ communication, with ‘psychosocial’ and ‘lifestyle’ communica-tion problems not even entering the frame in the GP accounts.
However, concern about using children as informal interpreters seems to gofurther than anxieties about the effectiveness of this, or the impact on the com-munication preferences of the doctor. Despite GPs being clear about the con-tingent acceptability of using children as informal interpreters their accountsseemed to suggest an underlying persistent ideological unease with using chil-dren at all, regardless of the child’s ability to take on the role of informal inter-
182 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999

preter, and this universal unease related to concerns that children could beharmed in unspecified ways through participating in the interpreter role.3
The identification by GPs of specific circumstances in which it would beinappropriate for children to undertake the role of informal interpreterrested on a defence of childhood as a time of innocence. The more gener-alised ideological unease expressed by the GPs reflects the coupling of child-hood as a time of innocence with it being framed as a time of development,a preparatory phase for adulthood (Jenks 1982, Alanen 1990). The childwho comes to know things before their time through being party to adultsinteracting with each other, as in the case of being the informal interpreterin a medical encounter, is in double jeopardy. Not only may their innocencebe dispersed but this precocious knowledge may then have a damagingeffect on their development into stable, adjusted adults. The unease aboutchildren acting as informal interpreters is principally focused not on the effi-cacy of the medical encounter but rather on the impact on the child as adeveloping subject. The restriction of children in particular arenas wherethey might encounter adults interacting with each other is often justified interms of risks to their mental health and psychological development(Qvortrup 1994). Children are constructed as needing protection from thecorrupting influence of the adult world.
A further source of ideological unease is the perception that through theprocess of children undertaking the tasks of translating for the adult patientand the GP, the normal moral order of the family is disturbed, partlybecause the child may learn things about the parent in the course of inter-preting for them and the GP, and partly because children do not usuallyspeak on behalf of adults. The social order of the family is characterised byan uneven distribution of power between adults and children in favour ofthe adults, the assumption of authority by the adults over the child, and theuneven distribution of knowledge in the family as both a process and out-come of the social order (Oldman 1994). Children gaining knowledge abouttheir parents’ health, bodies or private activities threatens the normative dis-tribution of knowledge in the family. Hutchby and Moran-Ellis (1998) sug-gest that parents take as one of their main tasks the establishment ofboundaries around the forms of knowledge to which children can haveaccess, and it would seem from this study that this responsibility for regula-tion of knowledge is also undertaken by other adults in defence of a particu-lar construction of childhood and moral family order. In the case ofchildren interpreting in medical consultations the GPs’ accounts indicatedthat they assumed a responsibility for the policing of the moral order of thefamily primarily through attempts to regulate the knowledge children mightbe exposed to in the course of the consultation, or through reconstructingthe knowledge as appropriate for display in the medical domain. This recon-struction of knowledge was possible where the child could be identified ashaving experienced the same or relevant physiological or pathophysiologicalevents as the adult patient. Responsibility for regulation is assumed by the
Children as informal interpreters in GP consultations 183
© Blackwell Publishers Ltd/Editorial Board 1999

GP despite the adult patient having chosen to bring the child along as aninterpreter in the first place.
In all types of consultation where children take on the role of informalinterpreter, they become positioned as an intermediary between the GP andthe adult patient. Children speaking on behalf of adult others disrupts socialrelations. Indeed, children speaking on behalf of themselves is still treated asproblematic in many arenas. For example, it is only relatively recently thatchildren have been seen as potentially competent respondents in research(Alderson 1995, Butler and Shaw 1996), and where children do have warrantto speak it is often in contexts where that warrant depends on their presenceor voice being mediated by adults (Lee 1998, De Montigny 1998). Therefore,children speaking on behalf of an adult, especially on behalf of a parent, isperceived by the GPs as presenting a potential threat to the normative distri-bution of power and authority in the family. Children are usually present inmedical encounters either as the object of the encounter when their parentsspeak on their behalf and act as intermediaries between the child and themedic, or as uninvolved adjuncts to the adult when the adult is the object ofthe encounter. This reflects a normative relationship between adults and chil-dren which can be characterised as one of protection and exclusion (Bardy1994). GPs felt unable to manage the disruption to the parent–child relation-ship in the way they managed disruption to the distribution of knowledgebetween parents and children, since the very acceptance of children into therole of informal interpreters, driven though it was by the absence of alterna-tive sources of interpretation, meant that the child was speaking on behalf ofthe parent however straightforward and non-taboo the problem was. Thisinability to directly manage the perceived reversal of an aspect of thechild–parent relationship in this respect makes, we suggest, a major contri-bution to the persistent ideological unease apparent in the GP accounts, anunease which was independent of the nature of the consultation.
The pragmatic demands of achieving a consultation are thus in tensionwith perceived threats both to the moral order of the family and to the ideo-logy of childhood as a time of innocence. Management of this tension, weargue, is achieved through the contingent construction both of the compe-tence of the child to act as an informal interpreter, and the appropriatenessof the child taking on that role. But, even where children display compe-tence in successfully undertaking the role of informal interpreter, theyremain enmeshed in the ideology of childhood and the process of familiali-sation. To that extent, whilst Rack’s emphatic injunction against the use ofchildren as interpreters is not followed in practice, it still represents a strongideological position.
Address for correspondence: Jo Moran-Ellis, Department of Sociology,University of Surrey, Guildford, Surrey, GU2 5XH.e-mail: Suzanne Cohen: [email protected]; Jo Moran-Ellis: [email protected]; Chris Smaje: [email protected].
184 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999

Acknowledgements
We are grateful to the NHS South Thames (Mother and Child Heath programme)which funded the project on which this paper is based. We would like to thankProfessor Sara Arber for her role in guiding the project, and Dr. Geoff Cooper forhis helpful comments on an earlier draft of this paper. The paper represents theviews of the authors and not the NHS executive.
Notes
1 ‘Emergency consultations’ is used to indicate those GP consultations where thepatient insists on seeing the GP at short notice, usually on the day they ask for anappointment or as a home visit.
2 In this paper, and in the research reported, the term children is used for childrenand young people up to the age of 18 years.
3 It is not possible to ascertain from these interviews with GPs whether the non-English speaking parents share this unease or act within the same ideologicalframework as regards the appropriateness of their children taking on an inter-preting role However, our early analysis of the focus group interviews with par-ents does suggest a shared concern and similar constructions of a ‘proper’childhood as the GPs (Cohen et al. forthcoming).
References
Alanen, L. (1990) Rethinking childhood socialization, the family and childhood,Sociological Studies of Child Development, 3, 13–28.
Alderson, P. (1995) Listening to Children. London: Barnardo’s.Bardy, M. (1994) The Manuscript of the 100 years project. In Qvortrup, J., Bardy,
M., Sgritta, G. and Wintersberger, H. (eds) (1994) Childhood Matters. Aldershot:Avebury.
Baylov, A. (1996) Defining Advocacy. Paper presented at Supporting the Community:a Transnational Seminar on Access and Advocacy, Hopscotch Asian Woman’sCentre (26 December 1996).
Burgess, R.G. (1984) In the Field: an Introduction to Field Research. London: Allenand Unwin.
Butler, I. and Shaw, I. (1996) A Case of Neglect? Children’s Experiences and theSociology of Childhood. Aldershot: Avebury.
Cohen, S., Arber, S. and Smaje, C. (forthcoming) Barriers to the Effective Use ofPrimary Health Care Services by Children from Minority Ethnic Groups in EastLondon. Unpublished Report to South Thames NHS Executive.
De Montigny, G. (1998) In the company of strangers: being a child in care. InHutchby, I. and Moran-Ellis, J. (eds) Children and Social Competence: Arenas ofAction. London: Falmer.
Ebden, P., Bhatt, A., Carey, O.J. and Harrison, B. (1988) The bi-lingual consulta-tion. The Lancet, 8581 i, 347.
Children as informal interpreters in GP consultations 185
© Blackwell Publishers Ltd/Editorial Board 1999

ELCHA (1997) Health Directory for City and Hackney, Tower Hamlets andNewham. East London and the City Health Authority.
Halahmy, R. (1990) Communication on call, Social Work Today, 26 July 1990, 24–5.Harre, R. (1986) The step to social constructionism. In Richards, M. and Light, P.
(eds) Children of Social Worlds. Oxford: Blackwell and Polity.Health Education Authority (1994) Health and Lifestyles: Black and Minority Ethnic
Groups in England. London: Health Education Authority.Hicks, C. and Hayes, L. (1991) Linkworkers in antenatal care: facilitators of equal
opportunities in health provision or salves for management conscience?, HealthServices Management Research 4, 2, 89–93.
Hornberger, J.C., Gibson, C.D., Wood, W., Dequeldre, C., Corso, I., Palla, B. andBloch, D.A. (1996) Eliminating language barriers for non-English speakingpatients, Medical Care, 34, 8, 845–56.
Hutchby, I. and Moran-Ellis, J. (1998) Children and Social Competence: Arenas ofAction. London: Falmer Press.
Jenks, C. (1982) Sociology of Childhood: Essential Readings. London: Batsford.Lee, N. (1998) Towards an immature sociology, Sociological Review, 46, 3, 458–82.Mason, J. (1996) Qualitative Researching. London: Sage.Mizrahi, T. (1984) Coping with patients: subcultural adjustments to the conditions
of work among internists-in-training, Social Problems, 32, 156–65.Oldman, D. (1994) Adult–child relations as class relations. In Qvortrup, J., Bardy,
M., Sgritta, G. and Wintersberger, H. (eds) Childhood Matters. Aldershot:Avebury.
OPCS (1993) Morbidity Statistics from General Practice—4th National Study1991/92. London: HMSO.
Patton, M.Q. (1987) How to Use Qualitative Methods in Evaluation. Newbury ParkCalif.: Sage.
Qvortrup, J. (1994) Childhood matters: an introduction. In Qvortrup, J., Bardy, M.,Sgritta, G. and Wintersberger, H. (eds) Childhood Matters. Aldershot: Avebury.
Rack, P. (1982) Race, Culture and Mental Disorder. London: Tavistock.Ritchey, F.J., Yoels, W.C., Clair, J.M. and Allman, R.M. (1995) Competing medical
and social ideologies and communication accuracy in medical encounters,Research in the Sociology of Health Care, 12, 189–211.
Schott, J. and Henley, A. (1996) Culture, Religion and Childbearing in a MultiracialSociety: Handbook for Health Professionals. Oxford: Butterworth Heinemann.
Shackman, J. (1984) The Right to be Understood: a Handbook on Working with,Employing and Training Community Interpreters. London; HEC: NationalExtension College.
Smaje, C. (1995) Health Race and Ethnicity: Making Sense of the Evidence. London:Kings Fund Institute.
Tuckett, D., Boulton, M., Olson, C. and Williams, A. (1985) Meetings BetweenExperts: An Approach to Sharing Ideas in Medical Consultations. London andNew York: Tavistock Publications.
Waitzkin, H. (1991) The Politics of Medical Encounters. New Haven: YaleUniversity Press.
Yoels, W.C. and Clair, J.M. (1994) Never enough time: how medical residents man-age a scarce resource, Journal of Contemporary Ethnography, 23, 185–213.
186 Suzanne Cohen, Jo Moran-Ellis and Chris Smaje
© Blackwell Publishers Ltd/Editorial Board 1999
Copyright © 2022 FDOKUMEN