Chamoli 2018.pdf - Institute of Economic Growth
79
MONITO NATIONAL RURAL HEA MINIST P IN UNI NATIO A REPORT ON ORING OF IMPORTANT COMPONENTS OF ALTH MISSION PROGRAMME IMPLEMENTATI IN CHAMOLI, UTTARAKHAND SUBMITTED TO TRY OF HEALTH AND FAMILY WELFARE GOVERNMENT OF INDIA DR. SURESH SHARMA MS. VARSHA SHUKLA POPULATION RESEARCH CENTRE, NSTITUTE OF ECONOMIC GROWTH IVERSITY ENCLAVE, DELHI 110007 DECEMBER, 2018 ONAL HEALTH MISSION ION PLAN
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Chamoli 2018.pdf - Institute of Economic Growth
MONITORING
NATIONAL RURAL HEALTH
MINISTRY OF
P
INSTITUTE OF
UNIVERSITY
NATIONAL HEALTH MISSION
A REPORT ON
ONITORING OF IMPORTANT COMPONENTS OF
EALTH MISSION PROGRAMME IMPLEMENTATION
IN CHAMOLI, UTTARAKHAND
SUBMITTED TO
INISTRY OF HEALTH AND FAMILY WELFARE
GOVERNMENT OF INDIA
DR. SURESH SHARMA
MS. VARSHA SHUKLA
POPULATION RESEARCH CENTRE,
NSTITUTE OF ECONOMIC GROWTH
NIVERSITY ENCLAVE, DELHI 110007
DECEMBER, 2018
NATIONAL HEALTH MISSION
MPLEMENTATION PLAN
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
2222
Contents
Executive Summary ...................................................................................................................................... 8
Strengths ................................................................................................................................................... 8
Weakness .................................................................................................................................................. 9
1. Introduction ............................................................................................................................................. 11
1.1 Background ....................................................................................................................................... 11
1.2 Objective ........................................................................................................................................... 11
1.3 Methodology ..................................................................................................................................... 12
1.4 Socio Economic and Demographic Profile ....................................................................................... 13
1.5 Key Health Indicators ....................................................................................................................... 15
2. Health Infrastructure ............................................................................................................................... 16
3. Human Resource and Training Status ..................................................................................................... 18
3.1 Human Resource Availability ........................................................................................................... 18
3.2 Training Status .................................................................................................................................. 19
4. Maternal Health ...................................................................................................................................... 19
4.1 Delivery Services .............................................................................................................................. 19
4.2 Maternal Scheme .............................................................................................................................. 22
4.2.1 JSY ............................................................................................................................................. 22
4.2.2 JSSK ........................................................................................................................................... 22
4.3 Maternal Death .................................................................................................................................. 23
5. Child Health ............................................................................................................................................ 24
5.1 Immunisation .................................................................................................................................... 24
5.2 Neonatal Health ................................................................................................................................ 26
5.2.1 Infrastructure and Services ......................................................................................................... 26
5.3 Rastriya Bal Surakha Karyakaram .................................................................................................... 27
6. Family Planning ...................................................................................................................................... 28
7. Rashtriya Kishor Swasthya Karyakram .................................................................................................. 29
8. Aurvedic Yoga Unanisiddh And Homopathy (AYUSH) ........................................................................ 29
9. Quality in Health Services ...................................................................................................................... 29
9.1 Biomedical Waste & Infection Control ............................................................................................ 30
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
3333
9.2 Information, Education and Management ......................................................................................... 30
10. Community Process .............................................................................................................................. 31
11. Disease Control Programme ................................................................................................................. 31
11.1 Communicable Disease ................................................................................................................... 31
11.2 Non Communicable Disease ........................................................................................................... 32
12. HMIS .................................................................................................................................................... 33
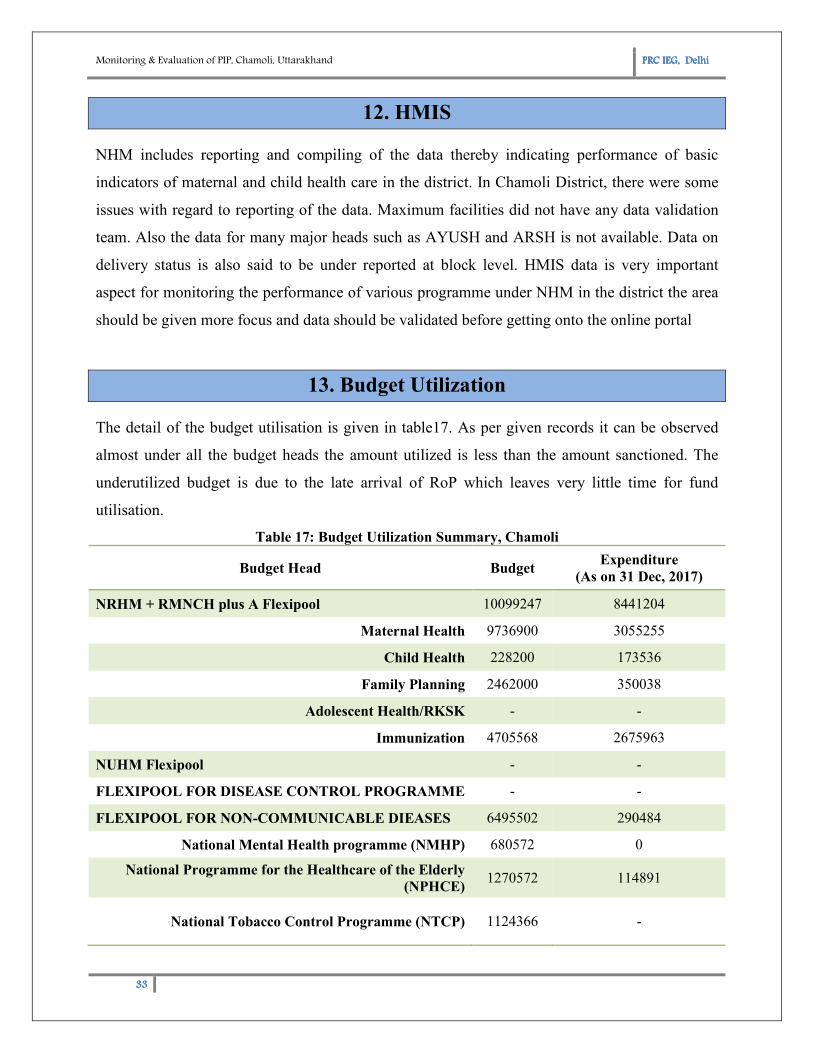
13. Budget Utilization ................................................................................................................................. 33
15. Facility Wise Observation ..................................................................................................................... 34
15.1 Distict Hospital Gopeshwar, Chamoli ............................................................................................ 34
15.2 Community Health Center, Karanprayag, Chamoli ........................................................................ 36
15.3 Primary Health Centre, Chamoli ..................................................................................................... 39
15.4 Sub-Centre, Nandprayag ................................................................................................................. 40
15.5 Sub-Centre, Simli ............................................................................................................................ 41
16. Conclusion and Recommendations ................................................................................................... 42
Appendix ..................................................................................................................................................... 44
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
4444
Table 1: List of Visited Healthcare Facilities in Chamoli District, Uttarakhand, 2018 .............................. 12
Table 2: Key Socio-Economic and Demographic Indicators: All India, Uttarkhand & Chamoli District .. 14
Table 3: Key Health Indicators, Chamoli, Uttarakhand .............................................................................. 15
Table 4: Health Infrastructures, Chamoli, Uttarakhand .............................................................................. 17
Table 5: Transport Facility, Chamoli, Uttarakhand .................................................................................... 17
Table 6: Human Resource under NHM: Chamoli, Uttarakhand ................................................................. 18
Table 7: JSY Payment Status, Chamoli ...................................................................................................... 22
Table 8: JSSK beneficiaries, Chamoli ........................................................................................................ 23
Table 9: Maternal Death Status, Chamoli ................................................................................................... 23
Table 10: Details of Infrastructure and Services under Neonatal Health .................................................... 26
Table 11: Neonates Health Status ............................................................................................................... 26
Table 12: RBSK progress report, Chamoli ................................................................................................. 27
Table 13: Family planning achievement in the district ............................................................................... 28
Table 14: Quality in health care services- BMW and Infection control ..................................................... 30
Table 15: Status of ASHA, Chamoli ........................................................................................................... 31
Table 16: Disease control programme progress District (Communicable Diseases) .................................. 32
Table 17: Budget Utilization Summary, Chamoli ...................................................................................... 33
Table 18: Service delivery in last two years, District Hospital ................................................................... 35
Table 19: Service delivery status for last two years, CHC, Karanprayag ................................................... 37
Table 20: Service delivery status for last two years, PHC, Chamoli .......................................................... 39
Table 21: Service delivery status for last two years, Sub-centre Nandprayag ............................................ 41
Table 22: Service delivery status for last years, Sub-centre Simli .............................................................. 42
List of TablesList of TablesList of TablesList of Tables
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
5555
Figure 1: Map of District Chamoli, Uttarakhand ........................................................................................ 13
Figure 2: Institutional Deliveries and home deliveries, Chamoli, Uttarakhand .......................................... 16
Figure 3: ANC1 registration vs. ANC3 Coverage, Chamoli ...................................................................... 20
Figure 4: HomeDeliveries: SBA Assisted vs Non SBA Assisted ............................................................... 21
Figure 5: Home Deliveries vs Institutional Deliveries ................................................................................ 21
Figure 6: Immunisation Status, Chamoli .................................................................................................... 25
Figure 7: District Hospital, Chamoli ........................................................................................................... 34
Figure 8: CHC Karanprayag, Chamoli ....................................................................................................... 36
Figure 9: Unhygienic toilets, CHC, Karanprayag ....................................................................................... 38
Figure 10: PHC, Chamoli ........................................................................................................................... 39
Figure 11: Sub Centre, Nandprayag ............................................................................................................ 40
Figure 12: Sub Centre, Simli ...................................................................................................................... 41
List of List of List of List of FiguresFiguresFiguresFigures
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
6666
This is to express our deepest gratitude to all those who have extended their timely support and
helping in hand in completing this report.
We would like to express our special thanks of gratitude to Smt. Rajnesh Jain, Deputy General
(Stats) and Smt. Navanita Gogoi, Director (Stats) Ministry of Health and Family Welfare,
Government of India for assigning the work of monitoring of the important components of NHM
Programme Implementation Plan to Population Research Centre, Institute of Economic Growth,
Delhi.
We are very grateful to Dr. Rashmi Purohoti, for devoting her valuable time and giving us some
valuable inputs for our monitoring and evaluation purpose. We are also thankful to Mr. Vinod
Bahuguna for coordinating the facility visit. Further we would also Mr. Deepak Khanduri,
District Programme Manager for his coordination and support.
The monitoring and evaluation relies heavily on the cooperation and support from the health
facility, we thank the health facility staff for their active involvement, cooperation and
enthusiasm during the monitoring visits in the districts. We are very grateful to the health facility
staff particularly MOIC’s, ANMs and BPM for sharing with us valuable information.
Last but not the least special, I would like to thank to Mr. Rahul Kumarand Ms. Sangam Singh
for their invaluable support and coordination throughout the visit.
December, 2018 Dr. Suresh Sharma
Ms. Varsha Shukla
Population Research Centre
Institute of Economic Growth, Delhi
AcknowledgementAcknowledgementAcknowledgementAcknowledgement
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
7777
List of AbbreviationsList of AbbreviationsList of AbbreviationsList of Abbreviations
ANC Ante Natal Care MCTS Mother and Child Tracking System
ANM Auxiliary Nurse Midwife MDR Maternal Death Review
AYUSHAyurveda, Yoga & Naturopathy, Unani,
Siddha and HomoeopathyMMU Mobile Medical Unit
BEMOC Basic Emergency Obstetric Care MoHFW Ministry of Health and Family Welfare
BMW Biomedical waste MOIC Medical Officer In- Charge
BSU Blood Storage Unit NBCC New Born Care Corner
CDMO Chief District Medical Officer NBSU New Born Stabilization Unit
CHC Community Health Centre NSSK Navjat Shishu Suraksha Karyakram
DH District Hospital NSV No Scalpel Vasectomy
DMPA Depot Medroxyprogesterone Acetate OCP Oral Contraceptive Pill
DPM District Programme Manager OPD Out Patient Department
ECG Electrocardiography OPV Oral Polio Vaccines
EMOC Emergency Obstetric Care PIP Programme Implementation Plan
FRU First Referral Unit PNC Post Natal Care
HMIS Health Management Information System PPP Public Private Partnership
IEC Information, Education and
CommunicationPRC Population Research Centre
IMEPInfection Management and Environment
PlanRBSK Rashtriya Bal Suraksha Karyakram
IPD In Patient Department RCH Reproductive Child Health
IUCD Intra Uterine Contraceptive Device RKS Rogi Kalyan Samiti
IYCF Infant and Young Child Feeding RPR Rapid Plasma Reagin
JSSK Janani Shishu Suraksha Karyakram SBA Skilled Birth Attendant
JSY Janani Suraksha Yojana SKS Swasthya Kalyan Samiti
LHV Lady Health Visitor SN Staff Nurse
LSAS Life Saving Anaesthetic Skill SNCU Special New Born Care Unit
LT Laboratory Technician TFR Total Fertility Rate
M&E Monitoring and Evaluation TT Tetanus Toxoid
VHND Village Health and Nutrition Day
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
8888
Executive Summary
It is the monitoring and evaluation of PIP of NHM. A collaborative team of Population Research
Centre, Delhihad visited the selected district to interview and monitor the health functionaries in
the district hospital, CHCs, PHCs and sub centres to assess the availability of funds and
infrastructure and evaluate the performance of the district on various indicators. The report is
prepared by PRC Delhi based on the framed scheduled prepared for collection of data from the
district and observation made during the visit.
The major strength and weaknesses in the functioning of NHM activities in the district are as
follows:
Strengths
� Major Key economic indicators have shown appreciable improvement in the district.
Institutional deliveries have increased significantly whereas IMR and MMR witnessed a
downward trend.
� Two days in the week have been dedicated for immunization in the district.Proper
immunization cards are maintained in DH, PHCs and CHCs. ANMs are actively involved
in the process of immunization. Immunisation room in all the facilities are well
maintained.
� The installation of the biometric system for recording attendance of employees and also
cameras are serving a role in keeping the rules and policies of centres intact.
� ILR (Ice Lined Refrigerator) and deep freezer have been established at the sub centres as
well. And the staffs have received training regarding the operation of the same. Visited
Sub centres were also receiving Annual Maintenance Grant in the district.
� Physical Infrastructure of all the facilities visited was very well maintained. Waiting area
in the all facilities was well constructed.
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
9999
� RBSK was functioning well in the district; team member was working diligently to
provide services to the school going children.
Weakness
� Funds usually arrive late in the district, which leaves only 3-4 months for the fund
utilisation. Also, the roadmap is helpful for realigning the financial processes, however,
till last year the district never received the road map for fund utilisation.
� Information, Education and Management (IEC) materials are very essential for
generating awareness among the patient. IEC is displayed well throughout the facilities;
However, no IEC was displayed in Hindi which essential for all the facilities as they
majorly deal with rural, illiterate population.
� Approachability of most of the sub-centres was impassable. Out of 113 sub centres
approximately 20 were accredited and only one sub-centre Nandprayag, was conducting
deliveries in the district. Owing to the topology of the district, the service delivery at the
rest of the sub centre level is restricted to immunization, VHNDs, and suchlike.
� ASHA’s were working efficiently in the district. ASHA’s in the district were
multitasking, giving training, conducting survey under AYUSHMAN Bharat, however no
extra incentive or payment was given to them for rendering these extra services. Also,
HBNC Kit and Sari received by ASHA’s were reported to be meagre quality.
� Zero availability of Nischay kit in the district since last one year.
� Since 2013, no training has been conducted for RBSK in the district.
� HMIS (Health Management Information System) and RCH (Reproductive and Child
Health) portal data entry operator post is vacant since last one and half year.
� Severe shortage of ANM (Auxiliary Nurse Midwife) was reported in the district. In
several blocks two sub centres were being managed by one ANM, hence the currently
working ANM are becoming overburdened with work.
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
10101010
� Mobile Medical Units (MMUs) under NHM is a key strategy to facilitate access to public
health care particularly to people living in remote, difficult, under-served and unreached
areas. However, no MMU or Arogya Ratham was functional throughout the district.
� No provision of waste collection in the district. Due to geographical constraints bidding
rates are extremely high for BMW pickup.
� Non-availability of Vitamin and IFA tablets since last two years was reported in the
district.
� ARSH clinic is not established throughout the district.
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
11111111
1. Introduction
1.1 Background
National Health Mission (NHM) was launched on April, 2005 with mission to outreach the
under-served population of the country and provide them with essential healthcare services.
Since then it has become integral part in providing quality health care services especially to the
vulnerable group. Given its achievement in providing affordable, equitable and quality
healthcare services in March 2018 it has been further extended to continue till March 2020.
National Health Mission encloses two sub-missions, National Urban Health mission and
National Rural health Mission.
Over the years the funds allotted to the National Health Mission have increased considerably
with the vision to cater the increasing needs of the population for health care services. Hence
quality assessment of the programme implementation is extremely important as it will help in
further planning and resource allocation. Therefore, the Ministry of Health and Family Welfare
(MoHFW) has entrusted Population Research Centre (PRC) for quality monitoring of key
components of NRHM Programme Implementation Plan (PIP).While engaging with the task,
PRCs would identify critical concerns in implementation of NRHM activities and also evolve
suitable quality parameters to monitor the various components. As a part of qualitative reports,
the PRCs are required to observe and comment on status of the following key areas mentioned in
the Records of Proceedings (ROPs):
� Mandatory disclosure on the State NRHM website
� Components under key conditionality and new innovation
� Strategic areas identified in the roadmap for priority action
� Key strengths and weaknesses in the implementation of the program
1.2 Objective
Monitoring covers quality service delivery at all levels, physical infrastructure, financial
expenditure report, and strengths of the health institution. The main objective of whole
monitoring and evaluation are stated below:
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
12121212
1. To get clear picture of the district current health situation, status of programme
implementation; addressing the loopholes and registering its achievements.
2. Understanding the community level participation, gaps in different community level
processes and help take appropriate community level actions to bridge up the gap.
3. Suggesting them to get equipped with tools and skills required for better service delivery.
And get them exposed to various replicable public health facilities, models, and
programmes.
4. Understanding the effectiveness of the programme at the grass root level, sharing the
observations at various facility levels and suggesting them to come up with new
innovations to address emerging health issues and better implementation of existing
programmes.
1.3 Methodology
Ministry of Health and Family Welfare has assigned the task of monitoring the health status of
Chamoli, Uttarakhand to PRC Delhi. The report is based on secondary data, collected from the
CMO office and other health facilities visited. PRC, Delhi visited the district office to interact
with CMO, Dy. CMO, DPM and other officers of the district.Health profile of the district was
discussed intensively and higher authorities were questioned on broad areas under NHM such as
maternal health, child health, family planning, human resource, infrastructure etc.
The report is based on both qualitative and quantitative survey. Before visiting the field, a
structured questionnaire (Appendix) prepared on various important aspects of NHM activities,
has been send to the respective facilities Nodal officers. Further on the visit the questionnaire is
cross checked and discussed in detail. After a valuable discussion with the ACMO few selected
facilities were visited for monitoring purpose. The healthcare facilities visited are listed below:
Table 1: List of Visited Healthcare Facilities in Chamoli District, Uttarakhand, 2018
Facility Type Name of the facility
District Hospital District Hospital, Chamoli
Community Health Centre CHC Karnprayag
Primary Health Centre PHC Chamoli
Sub-Centre 1.SC Nandprayag
2.SC Simli
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand
13131313
Apart from discussion with various health officials the team also interviewed various
beneficiaries to obtain their perspective on the various NHM schemes. The report has attempted
to support the health functionaries in identifying their key strengths and
Appreciating the facilities for their efforts and achievements, encou
effectively on the gaps identified during the survey and take appropriate actions within their
respective capacities
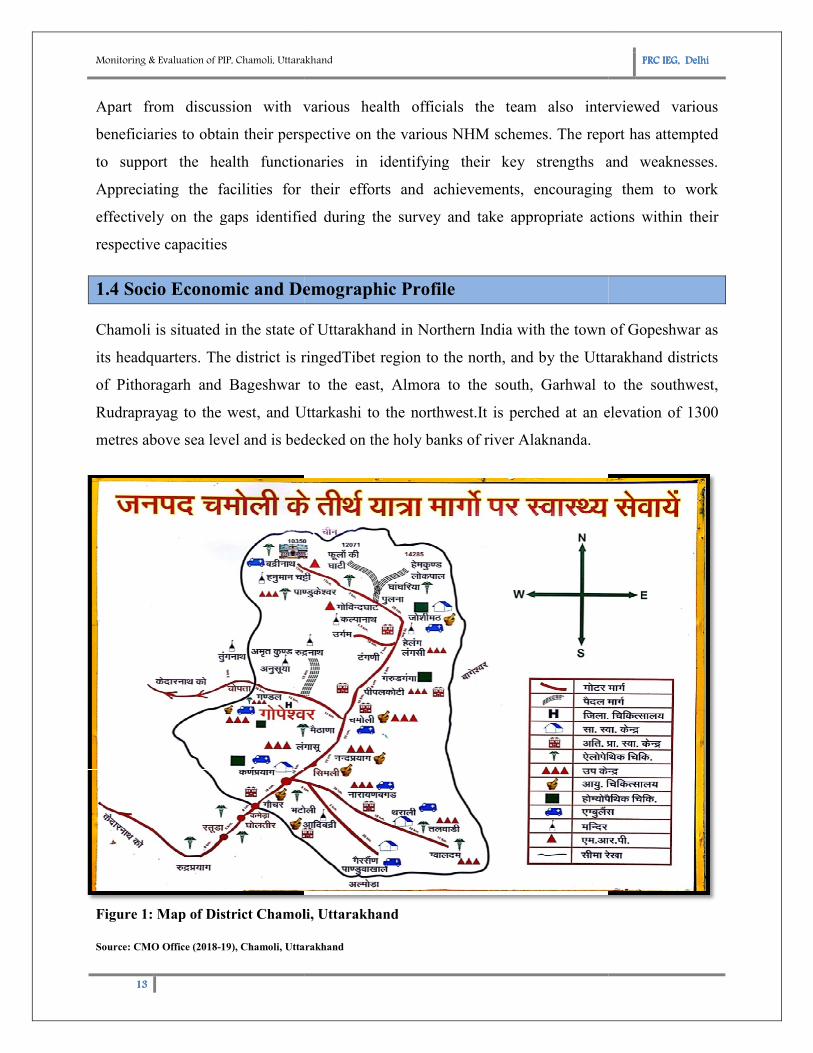
1.4 Socio Economic and Demographic Pro
Chamoli is situated in the state of Uttarakhand in Northern India with the town of
its headquarters. The district is ringed
of Pithoragarh and Bageshwar to the east, Almora to the
Rudraprayag to the west, and Uttarkashi to the northwest.
metres above sea level and is bedecked on the holy banks of river Alaknanda.
Figure 1: Map of District Chamoli, Uttarakhand
Source: CMO Office (2018-19), Chamoli, Uttarakhand
Chamoli, Uttarakhand
Apart from discussion with various health officials the team also interviewed various
perspective on the various NHM schemes. The report has attempted
to support the health functionaries in identifying their key strengths and
Appreciating the facilities for their efforts and achievements, encouraging them to work
effectively on the gaps identified during the survey and take appropriate actions within their
1.4 Socio Economic and Demographic Profile
is situated in the state of Uttarakhand in Northern India with the town of
ringedTibet region to the north, and by the Uttarakhand districts
of Pithoragarh and Bageshwar to the east, Almora to the south, Garhwal to the southwest,
Rudraprayag to the west, and Uttarkashi to the northwest.It is perched at an elevation of 1300
metres above sea level and is bedecked on the holy banks of river Alaknanda.
t Chamoli, Uttarakhand
, Chamoli, Uttarakhand
PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
Apart from discussion with various health officials the team also interviewed various
perspective on the various NHM schemes. The report has attempted
to support the health functionaries in identifying their key strengths and weaknesses.
raging them to work
effectively on the gaps identified during the survey and take appropriate actions within their
is situated in the state of Uttarakhand in Northern India with the town of Gopeshwar as
Tibet region to the north, and by the Uttarakhand districts
south, Garhwal to the southwest,
It is perched at an elevation of 1300
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
14141414
Chamoli hosts a variety of destinations of pilgrim and tourists' interest places such as Badrinath,
Hemkund Sahib, Valley of Flowers and Auli. Chamoli also happened to be a birthplace of
"Chipko movement". Chamoli proved itself "the most spectacular in its natural assets; be it
scenery, valley aspects, water-edges, floristic varieties, dramatic landform or the climatic
cardinalities. Chamoli district occupies an area of approximately 8030 square kilometers.
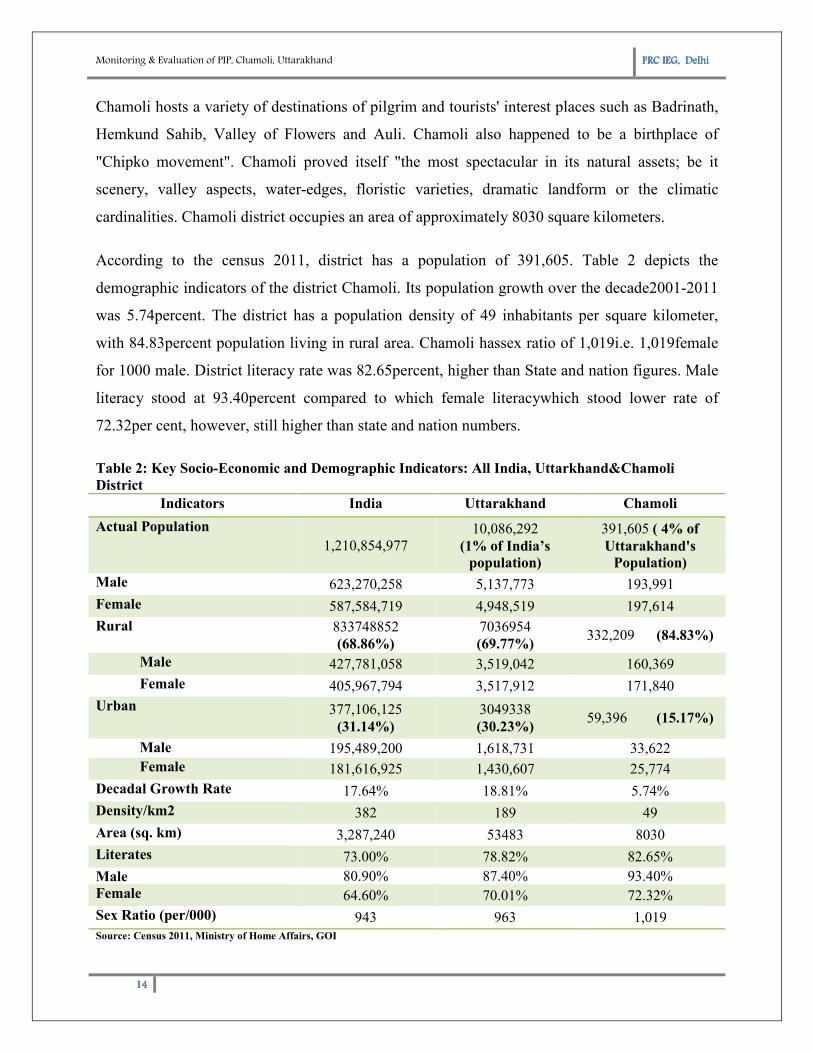
According to the census 2011, district has a population of 391,605. Table 2 depicts the
demographic indicators of the district Chamoli. Its population growth over the decade2001-2011
was 5.74percent. The district has a population density of 49 inhabitants per square kilometer,
with 84.83percent population living in rural area. Chamoli hassex ratio of 1,019i.e. 1,019female
for 1000 male. District literacy rate was 82.65percent, higher than State and nation figures. Male
literacy stood at 93.40percent compared to which female literacywhich stood lower rate of
72.32per cent, however, still higher than state and nation numbers.
Table 2: Key Socio-Economic and Demographic Indicators: All India, Uttarkhand&Chamoli
District
Indicators India Uttarakhand Chamoli
Actual Population
1,210,854,977
10,086,292
(1% of India’s
population)
391,605 ( 4% of
Uttarakhand's
Population)
Male 623,270,258 5,137,773 193,991
Female 587,584,719 4,948,519 197,614
Rural 833748852
(68.86%)
7036954
(69.77%) 332,209 (84.83%)
Male 427,781,058 3,519,042 160,369
Female 405,967,794 3,517,912 171,840
Urban 377,106,125
(31.14%)
3049338
(30.23%) 59,396 (15.17%)
Male 195,489,200 1,618,731 33,622
Female 181,616,925 1,430,607 25,774
Decadal Growth Rate 17.64% 18.81% 5.74%
Density/km2 382 189 49
Area (sq. km) 3,287,240 53483 8030
Literates 73.00% 78.82% 82.65%
Male 80.90% 87.40% 93.40%
Female 64.60% 70.01% 72.32%
Sex Ratio (per/000) 943 963 1,019
Source: Census 2011, Ministry of Home Affairs, GOI
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
15151515
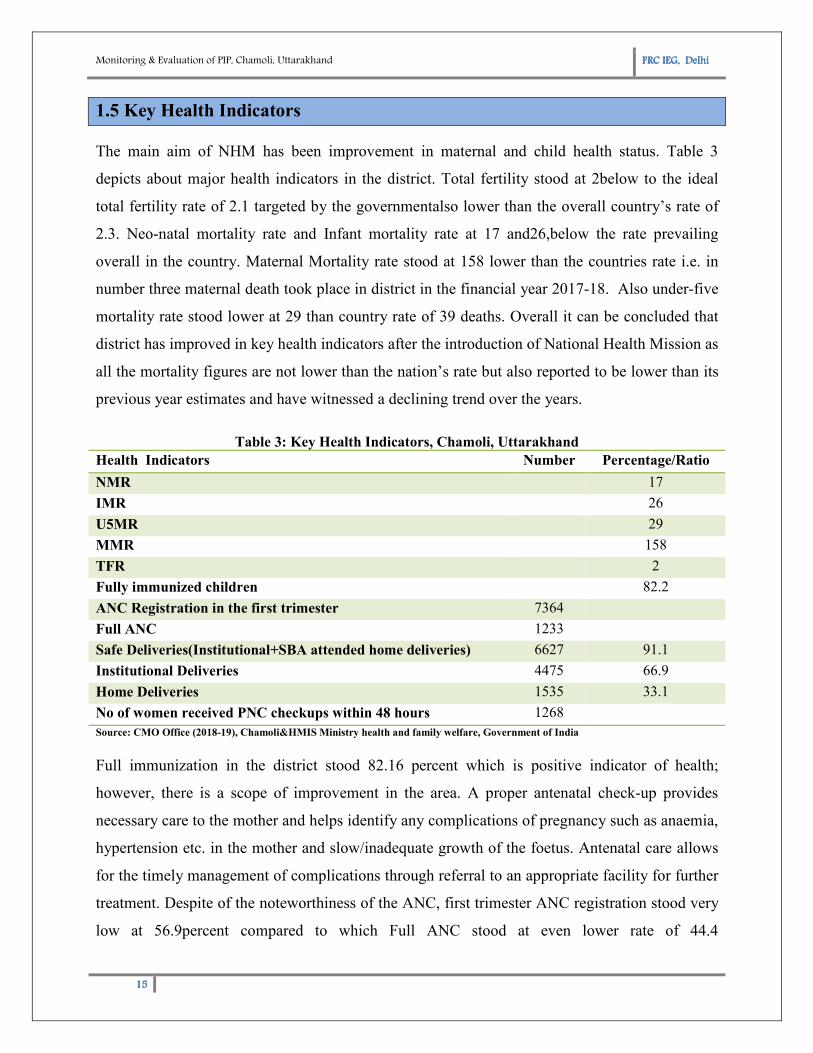
1.5 Key Health Indicators
The main aim of NHM has been improvement in maternal and child health status. Table 3
depicts about major health indicators in the district. Total fertility stood at 2below to the ideal
total fertility rate of 2.1 targeted by the governmentalso lower than the overall country’s rate of
2.3. Neo-natal mortality rate and Infant mortality rate at 17 and26,below the rate prevailing
overall in the country. Maternal Mortality rate stood at 158 lower than the countries rate i.e. in
number three maternal death took place in district in the financial year 2017-18. Also under-five
mortality rate stood lower at 29 than country rate of 39 deaths. Overall it can be concluded that
district has improved in key health indicators after the introduction of National Health Mission as
all the mortality figures are not lower than the nation’s rate but also reported to be lower than its
previous year estimates and have witnessed a declining trend over the years.
Table 3: Key Health Indicators, Chamoli, Uttarakhand
Health Indicators Number Percentage/Ratio
NMR 17
IMR 26
U5MR 29
MMR 158
TFR 2
Fully immunized children 82.2
ANC Registration in the first trimester 7364
Full ANC 1233
Safe Deliveries(Institutional+SBA attended home deliveries) 6627 91.1
Institutional Deliveries 4475 66.9
Home Deliveries 1535 33.1
No of women received PNC checkups within 48 hours 1268
Source: CMO Office (2018-19), Chamoli&HMIS Ministry health and family welfare, Government of India
Full immunization in the district stood 82.16 percent which is positive indicator of health;
however, there is a scope of improvement in the area. A proper antenatal check-up provides
necessary care to the mother and helps identify any complications of pregnancy such as anaemia,
hypertension etc. in the mother and slow/inadequate growth of the foetus. Antenatal care allows
for the timely management of complications through referral to an appropriate facility for further
treatment. Despite of the noteworthiness of the ANC, first trimester ANC registration stood very
low at 56.9percent compared to which Full ANC stood at even lower rate of 44.4
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand
16161616
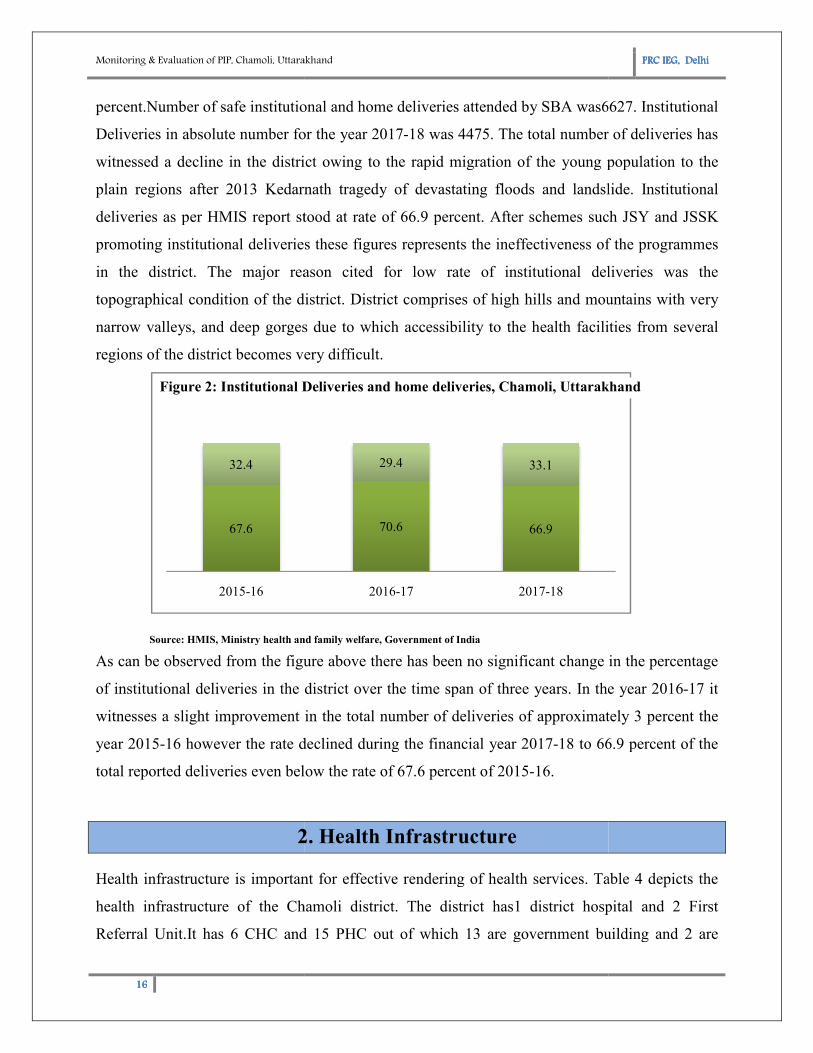
percent.Number of safe institutional and
Deliveries in absolute number for the year 2017
witnessed a decline in the district owing to the rapid migration of the young population to the
plain regions after 2013 Kedarnath tragedy of devastating floods and landslide. Institutional
deliveries as per HMIS report stood at ra
promoting institutional deliveries these
in the district. The major reason cited for low rate of institutional deliveries was the
topographical condition of the district. D
narrow valleys, and deep gorges
regions of the district becomes very difficult.
Source: HMIS, Ministry health and family welfare, Government of India
As can be observed from the figure above there has been no significant change in the
of institutional deliveries in the district over the time span of three years. In the year 2016
witnesses a slight improvement in the total number of deliveries of approximately 3 percent the
year 2015-16 however the rate declined during t
total reported deliveries even below the rate of 67.6 percent of 2015
2. Health Infrastructure
Health infrastructure is important for effective rendering of health services.
health infrastructure of the Chamoli
Referral Unit.It has 6 CHC and
67.6
32.4
2015-16
Institutional DeliveriesFigure 2: Institutional Deliveries and home deliveries, Chamoli, Uttarakhand
Chamoli, Uttarakhand
institutional and home deliveries attended by SBA was6627.
Deliveries in absolute number for the year 2017-18 was 4475. The total number of deliveries has
witnessed a decline in the district owing to the rapid migration of the young population to the
plain regions after 2013 Kedarnath tragedy of devastating floods and landslide. Institutional
deliveries as per HMIS report stood at rate of 66.9 percent. After schemes such JSY and JSSK
ng institutional deliveries these figures represents the ineffectiveness of the programmes
in the district. The major reason cited for low rate of institutional deliveries was the
dition of the district. District comprises of high hills and moun
deep gorges due to which accessibility to the health facilities from several
regions of the district becomes very difficult.
Ministry health and family welfare, Government of India
As can be observed from the figure above there has been no significant change in the
of institutional deliveries in the district over the time span of three years. In the year 2016
witnesses a slight improvement in the total number of deliveries of approximately 3 percent the
16 however the rate declined during the financial year 2017-18 to 66.9 percent of the
total reported deliveries even below the rate of 67.6 percent of 2015-16.
2. Health Infrastructure
Health infrastructure is important for effective rendering of health services. Table
Chamoli district. The district has1 district hospital and
CHC and 15 PHC out of which 13 are government building and
70.6 66.9
29.4 33.1
2016-17 2017-18
Institutional Deliveries Home Deliveries: Institutional Deliveries and home deliveries, Chamoli, Uttarakhand
PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
6627. Institutional
number of deliveries has
witnessed a decline in the district owing to the rapid migration of the young population to the
plain regions after 2013 Kedarnath tragedy of devastating floods and landslide. Institutional
te of 66.9 percent. After schemes such JSY and JSSK
figures represents the ineffectiveness of the programmes
in the district. The major reason cited for low rate of institutional deliveries was the
istrict comprises of high hills and mountains with very
due to which accessibility to the health facilities from several
As can be observed from the figure above there has been no significant change in the percentage
of institutional deliveries in the district over the time span of three years. In the year 2016-17 it
witnesses a slight improvement in the total number of deliveries of approximately 3 percent the
18 to 66.9 percent of the
Table 4 depicts the
district hospital and 2 First
are government building and 2 are
: Institutional Deliveries and home deliveries, Chamoli, Uttarakhand
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
17171717
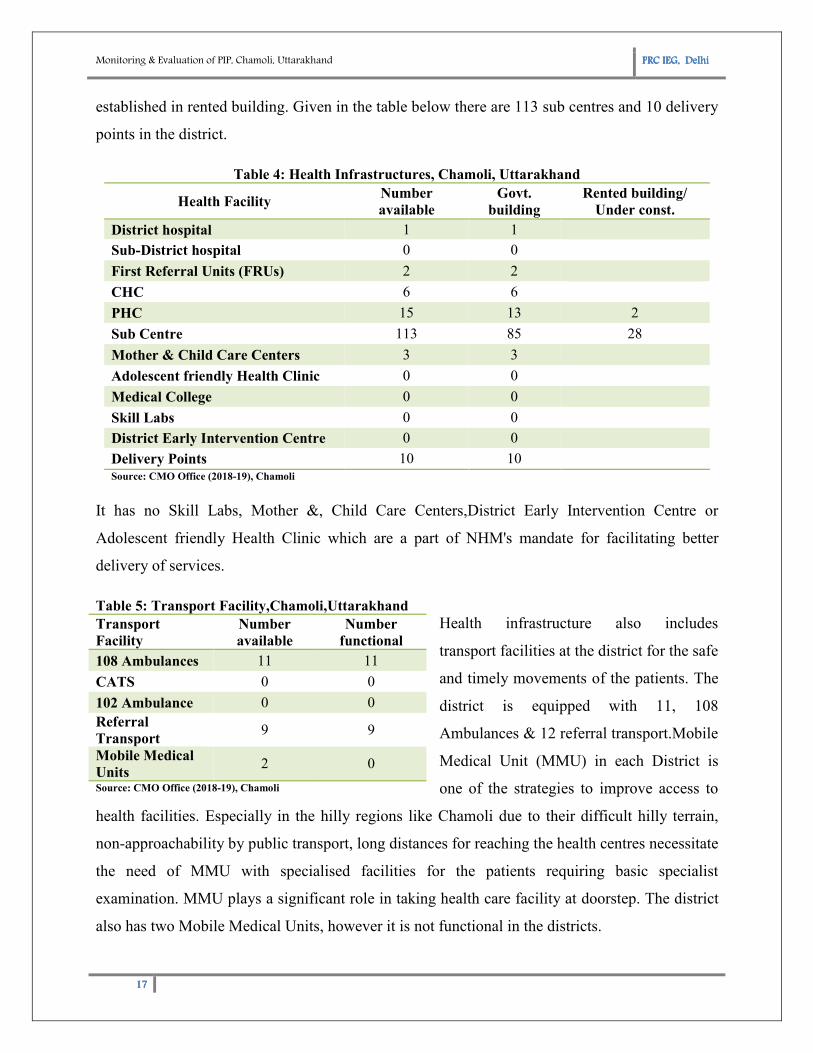
established in rented building. Given in the table below there are 113 sub centres and 10 delivery
points in the district.
Table 4: Health Infrastructures, Chamoli, Uttarakhand
Health Facility Number
available
Govt.
building
Rented building/
Under const.
District hospital 1 1
Sub-District hospital 0 0
First Referral Units (FRUs) 2 2
CHC 6 6
PHC 15 13 2
Sub Centre 113 85 28
Mother & Child Care Centers 3 3
Adolescent friendly Health Clinic 0 0
Medical College 0 0
Skill Labs 0 0
District Early Intervention Centre 0 0
Delivery Points 10 10
Source: CMO Office (2018-19), Chamoli
It has no Skill Labs, Mother &, Child Care Centers,District Early Intervention Centre or
Adolescent friendly Health Clinic which are a part of NHM's mandate for facilitating better
delivery of services.
Table 5: Transport Facility,Chamoli,Uttarakhand
Health infrastructure also includes
transport facilities at the district for the safe
and timely movements of the patients. The
district is equipped with 11, 108
Ambulances & 12 referral transport.Mobile
Medical Unit (MMU) in each District is
one of the strategies to improve access to
health facilities. Especially in the hilly regions like Chamoli due to their difficult hilly terrain,
non-approachability by public transport, long distances for reaching the health centres necessitate
the need of MMU with specialised facilities for the patients requiring basic specialist
examination. MMU plays a significant role in taking health care facility at doorstep. The district
also has two Mobile Medical Units, however it is not functional in the districts.
Transport
Facility
Number
available
Number
functional
108 Ambulances 11 11
CATS 0 0
102 Ambulance 0 0
Referral
Transport 9 9
Mobile Medical
Units 2 0
Source: CMO Office (2018-19), Chamoli
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
18181818
3. Human Resource and Training Status
3.1 Human Resource Availability
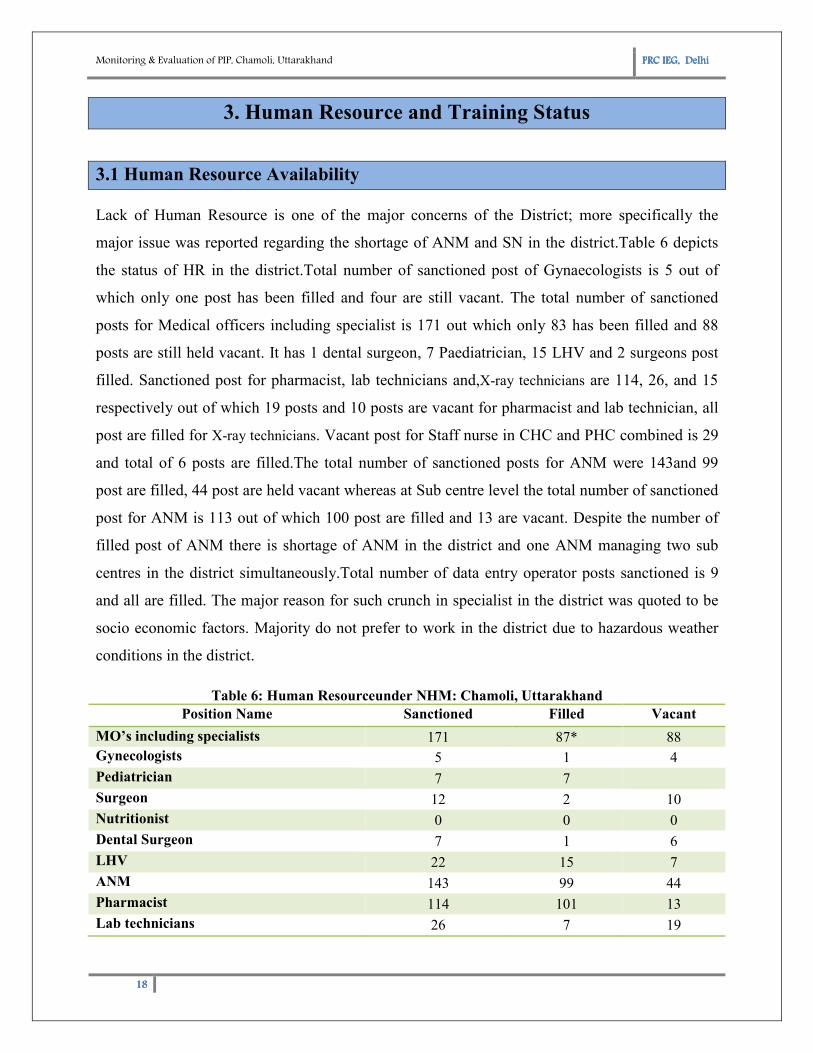
Lack of Human Resource is one of the major concerns of the District; more specifically the
major issue was reported regarding the shortage of ANM and SN in the district.Table 6 depicts
the status of HR in the district.Total number of sanctioned post of Gynaecologists is 5 out of
which only one post has been filled and four are still vacant. The total number of sanctioned
posts for Medical officers including specialist is 171 out which only 83 has been filled and 88
posts are still held vacant. It has 1 dental surgeon, 7 Paediatrician, 15 LHV and 2 surgeons post
filled. Sanctioned post for pharmacist, lab technicians and,X-ray technicians are 114, 26, and 15
respectively out of which 19 posts and 10 posts are vacant for pharmacist and lab technician, all
post are filled for X-ray technicians. Vacant post for Staff nurse in CHC and PHC combined is 29
and total of 6 posts are filled.The total number of sanctioned posts for ANM were 143and 99
post are filled, 44 post are held vacant whereas at Sub centre level the total number of sanctioned
post for ANM is 113 out of which 100 post are filled and 13 are vacant. Despite the number of
filled post of ANM there is shortage of ANM in the district and one ANM managing two sub
centres in the district simultaneously.Total number of data entry operator posts sanctioned is 9
and all are filled. The major reason for such crunch in specialist in the district was quoted to be
socio economic factors. Majority do not prefer to work in the district due to hazardous weather
conditions in the district.
Table 6: Human Resourceunder NHM: Chamoli, Uttarakhand
Position Name Sanctioned Filled Vacant
MO’s including specialists 171 87* 88
Gynecologists 5 1 4
Pediatrician 7 7
Surgeon 12 2 10
Nutritionist 0 0 0
Dental Surgeon 7 1 6
LHV 22 15 7
ANM 143 99 44
Pharmacist 114 101 13
Lab technicians 26 7 19
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
19191919
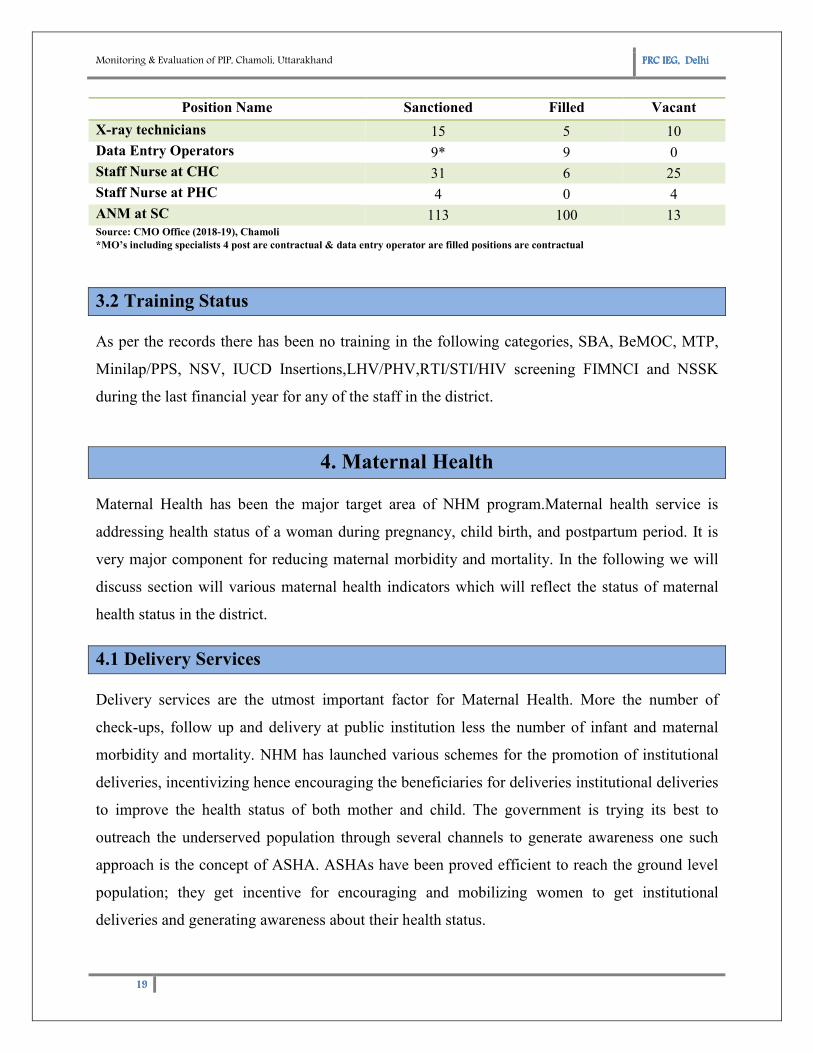
Position Name Sanctioned Filled Vacant
X-ray technicians 15 5 10
Data Entry Operators 9* 9 0
Staff Nurse at CHC 31 6 25
Staff Nurse at PHC 4 0 4
ANM at SC 113 100 13 Source: CMO Office (2018-19), Chamoli
*MO’s including specialists 4 post are contractual & data entry operator are filled positions are contractual
3.2 Training Status
As per the records there has been no training in the following categories, SBA, BeMOC, MTP,
Minilap/PPS, NSV, IUCD Insertions,LHV/PHV,RTI/STI/HIV screening FIMNCI and NSSK
during the last financial year for any of the staff in the district.
4. Maternal Health
Maternal Health has been the major target area of NHM program.Maternal health service is
addressing health status of a woman during pregnancy, child birth, and postpartum period. It is
very major component for reducing maternal morbidity and mortality. In the following we will
discuss section will various maternal health indicators which will reflect the status of maternal
health status in the district.
4.1 Delivery Services
Delivery services are the utmost important factor for Maternal Health. More the number of
check-ups, follow up and delivery at public institution less the number of infant and maternal
morbidity and mortality. NHM has launched various schemes for the promotion of institutional
deliveries, incentivizing hence encouraging the beneficiaries for deliveries institutional deliveries
to improve the health status of both mother and child. The government is trying its best to
outreach the underserved population through several channels to generate awareness one such
approach is the concept of ASHA. ASHAs have been proved efficient to reach the ground level
population; they get incentive for encouraging and mobilizing women to get institutional
deliveries and generating awareness about their health status.
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand
20202020
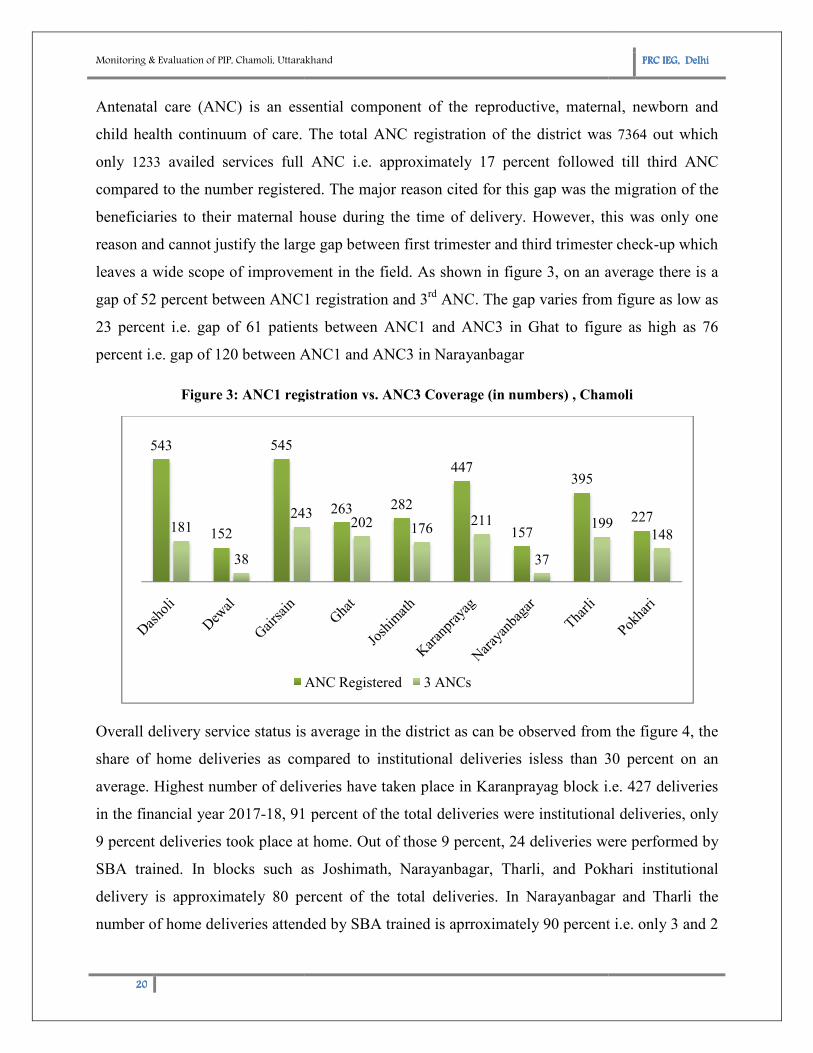
Antenatal care (ANC) is an essential component of the reproductive, maternal, newborn and
child health continuum of care.
only 1233 availed services full
compared to the number registered. The major reason cited for this gap was the migration of the
beneficiaries to their maternal house during the time of delivery. However
reason and cannot justify the large gap between
leaves a wide scope of improvement in the field.
gap of 52 percent between ANC1 registration and 3
23 percent i.e. gap of 61 patients
percent i.e. gap of 120 between ANC1 and ANC3 in
Figure 3: ANC1 registration vs
Overall delivery service status is
share of home deliveries as compared to institutional deliveries
average. Highest number of deliveries have taken place in Karanprayag block i.e. 427 deliver
in the financial year 2017-18, 91 percent of the total deliveries were institutional deliveries, only
9 percent deliveries took place at home. Out of those 9 percent, 24 deliveries were performed by
SBA trained. In blocks such as
delivery is approximately 80 percent of the total deliveries. In Narayanbagar and Tharli the
number of home deliveries attended by SBA trained is aprroximately 90 percent i.e. only 3 and 2
543
152
545
181
38
243
Chamoli, Uttarakhand
ntenatal care (ANC) is an essential component of the reproductive, maternal, newborn and
child health continuum of care. The total ANC registration of the district was
ANC i.e. approximately 17 percent followed till
compared to the number registered. The major reason cited for this gap was the migration of the
beneficiaries to their maternal house during the time of delivery. However, this was only one
reason and cannot justify the large gap between first trimester and third trimester check
scope of improvement in the field. As shown in figure 3, on an a
cent between ANC1 registration and 3rd
ANC. The gap varies from figure as low as
61 patients between ANC1 and ANC3 in Ghat to figure as high as
between ANC1 and ANC3 in Narayanbagar
: ANC1 registration vs. ANC3 Coverage (in numbers) , Chamoli
is average in the district as can be observed from the figure
share of home deliveries as compared to institutional deliveries isless than 30
average. Highest number of deliveries have taken place in Karanprayag block i.e. 427 deliver
18, 91 percent of the total deliveries were institutional deliveries, only
9 percent deliveries took place at home. Out of those 9 percent, 24 deliveries were performed by
n blocks such as Joshimath, Narayanbagar, Tharli, and Pokhari
delivery is approximately 80 percent of the total deliveries. In Narayanbagar and Tharli the
number of home deliveries attended by SBA trained is aprroximately 90 percent i.e. only 3 and 2
263 282
447
157
395
243202 176
211
37
199
ANC Registered 3 ANCs
PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
ntenatal care (ANC) is an essential component of the reproductive, maternal, newborn and
The total ANC registration of the district was 7364 out which
followed till third ANC
compared to the number registered. The major reason cited for this gap was the migration of the
this was only one
third trimester check-up which
on an average there is a
ANC. The gap varies from figure as low as
to figure as high as 76
Chamoli
in the district as can be observed from the figure 4, the
isless than 30 percent on an
average. Highest number of deliveries have taken place in Karanprayag block i.e. 427 deliveries
18, 91 percent of the total deliveries were institutional deliveries, only
9 percent deliveries took place at home. Out of those 9 percent, 24 deliveries were performed by
Pokhari institutional
delivery is approximately 80 percent of the total deliveries. In Narayanbagar and Tharli the
number of home deliveries attended by SBA trained is aprroximately 90 percent i.e. only 3 and 2
227199148

Monitoring & Evaluation of PIP, Chamoli, Uttarakhand
21212121
deliveries are attended by non- SBA trained in Narayanbangar and Tharli, respectively. In blocks
such as Dasholi and Ghat the number of home
deliveries is as high as 162 and 105, respectively. But for block Ghat all the home deliveries are
attended by SBA trained which i
As evident from the figure the performance of the district in
given the geographical constraints
non SBA trained home deliveries is greater than the SBA trained, in all the other blocks share of
SBA trained home deliveries is hig
of the district is satisfactory given its topological
improvement which can be achieved by
increasing the number ANM and SN required for the catering the outreach population.
162
64
110
105
32
37
21
46
20
117
390
234
Dasholi
Dewal
Gairsain
Ghat
Joshimath
Karanprayag
Narayanbagar
Tharli
Pokhari
Home Deliveries Institutional Deliveries
Figure 5: Home Deliveries vs Institutional
Deliveries
Chamoli, Uttarakhand
SBA trained in Narayanbangar and Tharli, respectively. In blocks
such as Dasholi and Ghat the number of home
deliveries is as high as 162 and 105, respectively. But for block Ghat all the home deliveries are
attended by SBA trained which is appreciable.
As evident from the figure the performance of the district in delivery services
constraints of the district. Except for the block Dewal where the share of
non SBA trained home deliveries is greater than the SBA trained, in all the other blocks share of
is higher than the share of non SBA trained. Overall performance
of the district is satisfactory given its topological constraints however there
can be achieved by increasing the efficiency of transport facility and also
ng the number ANM and SN required for the catering the outreach population.
274
145
206
222
117
390
72
234
64
Institutional Deliveries
127
16
89
105
16
24
18
18
28
Dasholi
Dewal
Gairsain
Ghat
Joshimath
Karanprayag
Narayanbagar
Tharli
Pokhari
SBA assisted Non
: Home Deliveries vs Institutional Figure 4: HomeDeliveries: SBA Assisted vs
Non SBA Assisted
PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
SBA trained in Narayanbangar and Tharli, respectively. In blocks
deliveries is as high as 162 and 105, respectively. But for block Ghat all the home deliveries are
services is satisfactory
of the district. Except for the block Dewal where the share of
non SBA trained home deliveries is greater than the SBA trained, in all the other blocks share of
her than the share of non SBA trained. Overall performance
however there is a scope of
increasing the efficiency of transport facility and also
ng the number ANM and SN required for the catering the outreach population.
127
105
18
18
35
48
21
0
16
13
3
2
18
Non-SBA
: HomeDeliveries: SBA Assisted vs
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
22222222
4.2 Maternal Scheme
The sharp decline in percentage of home deliveries and rising proportion of institutional
deliveries is due to success of the schemes Janani Suraksha Yojna (JSY) and Janani Shishu
Suraksha Karyakaram launched by the Government of India.
4.2.1 JSY
Janani Suraksha Yojana is an initiative for safe motherhood under NRHM. It aims at reducing
maternal and neo mortality rate, promoting institutional deliveries among poor pregnant women
by incentivizing them through cash benefits for getting institutional deliveries. The initiative is
working well in the district and also the level of awareness among the beneficiaries is
satisfactory in the district.
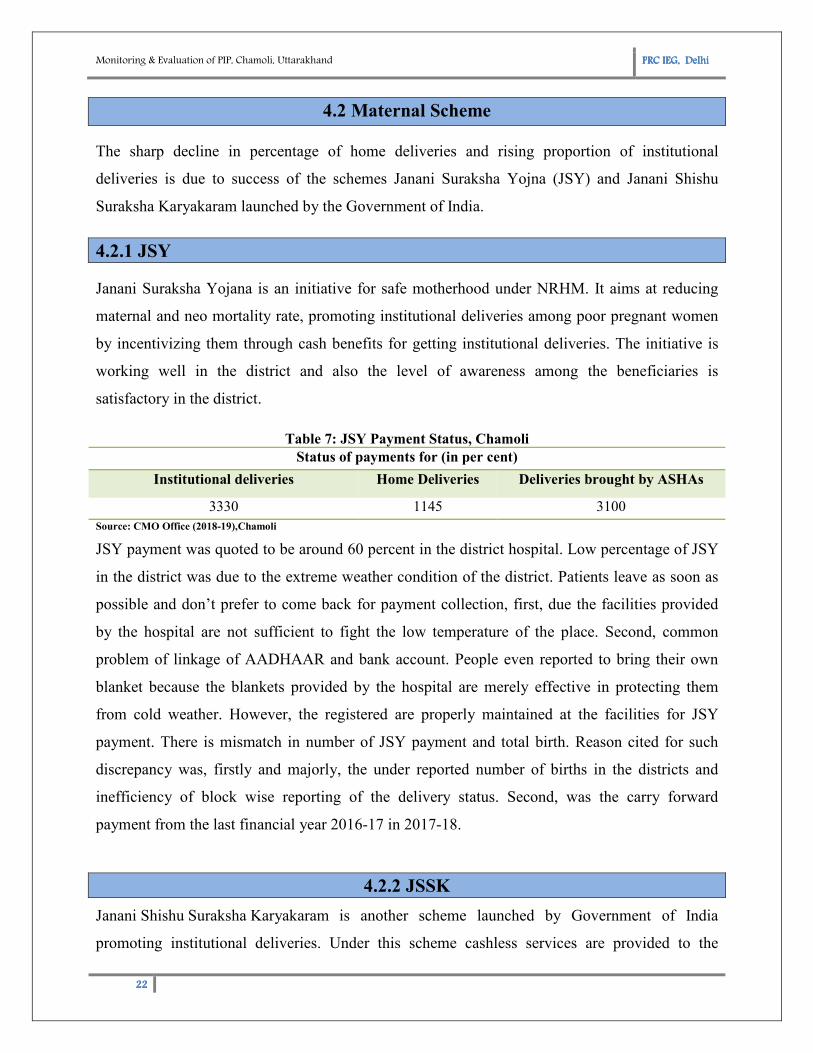
Table 7: JSY Payment Status, Chamoli
Status of payments for (in per cent)
Institutional deliveries Home Deliveries Deliveries brought by ASHAs
3330 1145 3100
Source: CMO Office (2018-19),Chamoli
JSY payment was quoted to be around 60 percent in the district hospital. Low percentage of JSY
in the district was due to the extreme weather condition of the district. Patients leave as soon as
possible and don’t prefer to come back for payment collection, first, due the facilities provided
by the hospital are not sufficient to fight the low temperature of the place. Second, common
problem of linkage of AADHAAR and bank account. People even reported to bring their own
blanket because the blankets provided by the hospital are merely effective in protecting them
from cold weather. However, the registered are properly maintained at the facilities for JSY
payment. There is mismatch in number of JSY payment and total birth. Reason cited for such
discrepancy was, firstly and majorly, the under reported number of births in the districts and
inefficiency of block wise reporting of the delivery status. Second, was the carry forward
payment from the last financial year 2016-17 in 2017-18.
4.2.2 JSSK
Janani Shishu Suraksha Karyakaram is another scheme launched by Government of India
promoting institutional deliveries. Under this scheme cashless services are provided to the
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
23232323
pregnant woman and new born in form of free drug, free food, free diagnostics, and free
transport or any other cost which might be incurred during the process of delivery till 30 days
after birth.
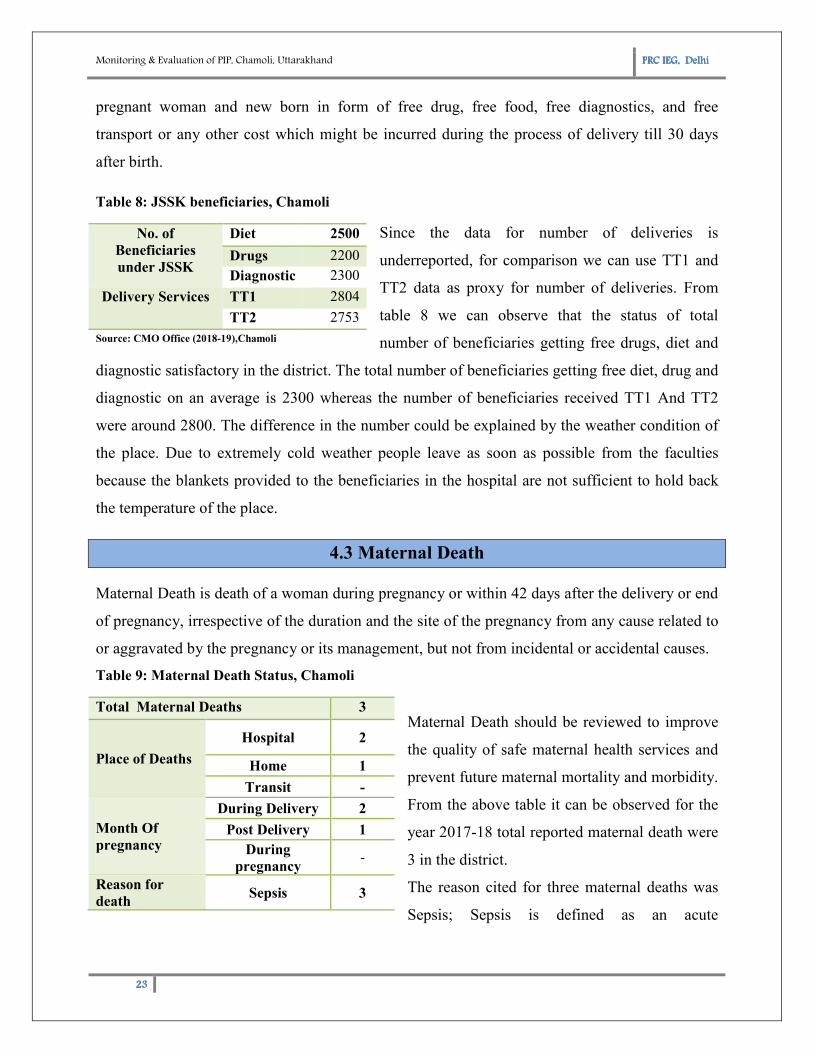
Table 8: JSSK beneficiaries, Chamoli
Since the data for number of deliveries is
underreported, for comparison we can use TT1 and
TT2 data as proxy for number of deliveries. From
table 8 we can observe that the status of total
number of beneficiaries getting free drugs, diet and
diagnostic satisfactory in the district. The total number of beneficiaries getting free diet, drug and
diagnostic on an average is 2300 whereas the number of beneficiaries received TT1 And TT2
were around 2800. The difference in the number could be explained by the weather condition of
the place. Due to extremely cold weather people leave as soon as possible from the faculties
because the blankets provided to the beneficiaries in the hospital are not sufficient to hold back
the temperature of the place.
4.3 Maternal Death
Maternal Death is death of a woman during pregnancy or within 42 days after the delivery or end
of pregnancy, irrespective of the duration and the site of the pregnancy from any cause related to
or aggravated by the pregnancy or its management, but not from incidental or accidental causes.
Table 9: Maternal Death Status, Chamoli
Maternal Death should be reviewed to improve
the quality of safe maternal health services and
prevent future maternal mortality and morbidity.
From the above table it can be observed for the
year 2017-18 total reported maternal death were
3 in the district.
The reason cited for three maternal deaths was
Sepsis; Sepsis is defined as an acute
No. of
Beneficiaries
under JSSK
Diet 2500
Drugs 2200
Diagnostic 2300
Delivery Services TT1 2804
TT2 2753
Source: CMO Office (2018-19),Chamoli
Total Maternal Deaths 3
Place of Deaths
Hospital 2
Home 1
Transit -
Month Of
pregnancy
During Delivery 2
Post Delivery 1
During
pregnancy -
Reason for
death Sepsis 3
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
24242424
inflammatory response syndrome secondary to an infectious focus. Out of the three deaths two
took place at Hospital and during delivery while one at the home and post-delivery.
5. Child Health
The Child Health programme under NRHM stresses upon improving child health and nutrition
status and address the factors contributing to neonatal, infant and under-five mortality and
morbidity. The programme focus on following areas;
1. Immunisation
• Intensification of Routine Immunisation
• Eliminating Measles and Japanese Encephalitis related deaths
• Polio Eradication
2. Neonatal Health
• Essential new born care (at every ‘delivery’ point at time of birth)
• Facility based sick newborn care (at FRUs & District Hospitals)
• Home Based Newborn Care and Home Based Young Care (HBYC) Programme
3. Nutrition
• Promotion of optimal Infant and Young Child Feeding Practices under Mother’s
Absolute Affection (MAA) Programme
• Micronutrient supplementation (Vitamin A, Iron Folic Acid)
• Management of children with severe acute malnutrition
• National De-worming Day
4. Management of Common Child hood illnesses
• Management of Childhood Diarrhoeal Diseases & Acute Respiratory Infections
5.1 Immunisation
Immunization Programme is one of the key interventions for protection of children from life
threatening conditions, which are preventable. It is one of the largest immunization programme
in the world and a major public health intervention in the country. Immunization activities have
been an important component under National Rural Health Mission (NRHM) since 2005.
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand
25252525
Mission Indradhanush
To strengthen and re-energize the programme and achieve full immunization coverage for all
children and pregnant women at a
Indradhanush” in December 2014.
death rate but targets to reduce diseases and death due to vaccine preventable diseases. It aims to
increase full immunization coverage in India to
The four phases of Mission Indradhanush have reached to more than 2.53 crore children and 68
lakh pregnant women with life-saving vaccines.
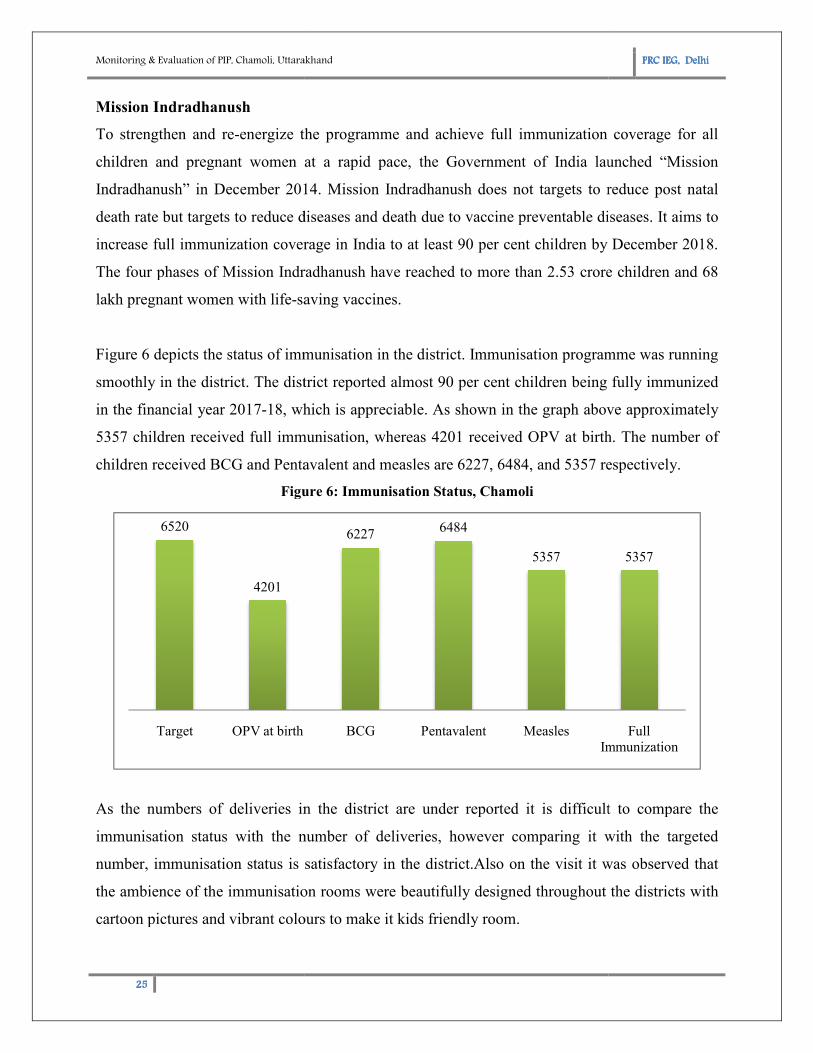
Figure 6 depicts the status of immunisation in the district. Immunisation programme was running
smoothly in the district. The district reported almost
in the financial year 2017-18, which is appreciable.
5357 children received full immunisation
children received BCG and Pentavalent and measles are 6227, 6484, and 5357 respectively.
Figure
As the numbers of deliveries in the district are under reported it is difficult to compare the
immunisation status with the number of deliveries, however comparing it with the targeted
number, immunisation status is satisf
the ambience of the immunisation rooms were beautifully designed throughout the districts with
cartoon pictures and vibrant colours to make it kids friendly room.
6520
4201
Target OPV at birth
Chamoli, Uttarakhand
energize the programme and achieve full immunization coverage for all
children and pregnant women at a rapid pace, the Government of India launched “Mission
Indradhanush” in December 2014. Mission Indradhanush does not targets to reduce post natal
death rate but targets to reduce diseases and death due to vaccine preventable diseases. It aims to
ull immunization coverage in India to at least 90 per cent children by December 2018.
The four phases of Mission Indradhanush have reached to more than 2.53 crore children and 68
saving vaccines.
Figure 6 depicts the status of immunisation in the district. Immunisation programme was running
The district reported almost 90 per cent children being fully immunized
, which is appreciable. As shown in the graph above approximately
children received full immunisation, whereas 4201 received OPV at birth. The number of
children received BCG and Pentavalent and measles are 6227, 6484, and 5357 respectively.
Figure 6: Immunisation Status, Chamoli
As the numbers of deliveries in the district are under reported it is difficult to compare the
immunisation status with the number of deliveries, however comparing it with the targeted
number, immunisation status is satisfactory in the district.Also on the visit it was observed that
the ambience of the immunisation rooms were beautifully designed throughout the districts with
cartoon pictures and vibrant colours to make it kids friendly room.
62276484
5357
BCG Pentavalent Measles
Immunization
PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
energize the programme and achieve full immunization coverage for all
rapid pace, the Government of India launched “Mission
Mission Indradhanush does not targets to reduce post natal
death rate but targets to reduce diseases and death due to vaccine preventable diseases. It aims to
children by December 2018.
The four phases of Mission Indradhanush have reached to more than 2.53 crore children and 68
Figure 6 depicts the status of immunisation in the district. Immunisation programme was running
per cent children being fully immunized
in the graph above approximately
01 received OPV at birth. The number of
children received BCG and Pentavalent and measles are 6227, 6484, and 5357 respectively.
As the numbers of deliveries in the district are under reported it is difficult to compare the
immunisation status with the number of deliveries, however comparing it with the targeted
actory in the district.Also on the visit it was observed that
the ambience of the immunisation rooms were beautifully designed throughout the districts with
5357
Full
Immunization
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
26262626
5.2 Neonatal Health
Neonatal health refers to the critical care that a newborn requires especially for first 28 days after
birth. Following section shed light on the indicators that will explain about status of neonatal
health in the district.
5.2.1 Infrastructure and Services
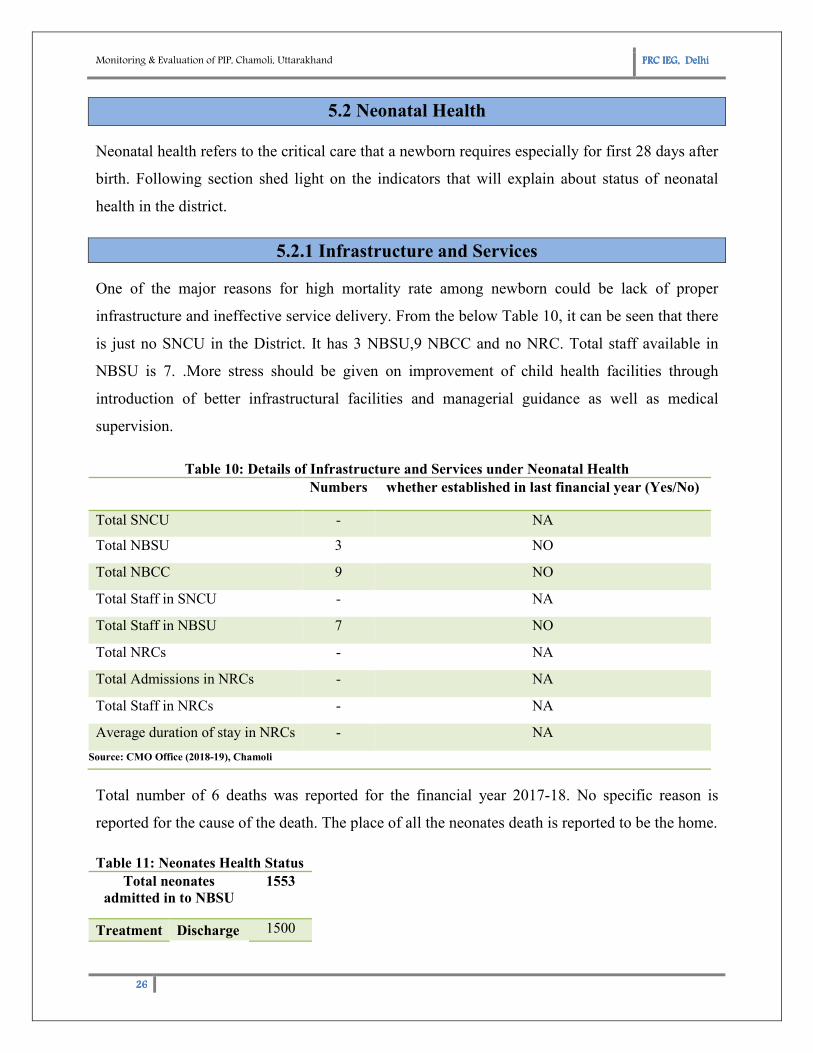
One of the major reasons for high mortality rate among newborn could be lack of proper
infrastructure and ineffective service delivery. From the below Table 10, it can be seen that there
is just no SNCU in the District. It has 3 NBSU,9 NBCC and no NRC. Total staff available in
NBSU is 7. .More stress should be given on improvement of child health facilities through
introduction of better infrastructural facilities and managerial guidance as well as medical
supervision.
Table 10: Details of Infrastructure and Services under Neonatal Health
Numbers whether established in last financial year (Yes/No)
Total SNCU - NA
Total NBSU 3 NO
Total NBCC 9 NO
Total Staff in SNCU - NA
Total Staff in NBSU 7 NO
Total NRCs - NA
Total Admissions in NRCs - NA
Total Staff in NRCs - NA
Average duration of stay in NRCs - NA
Source: CMO Office (2018-19), Chamoli
Total number of 6 deaths was reported for the financial year 2017-18. No specific reason is
reported for the cause of the death. The place of all the neonates death is reported to be the home.
Table 11: Neonates Health Status
Total neonates
admitted in to NBSU
1553
Treatment Discharge 1500
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
27272727
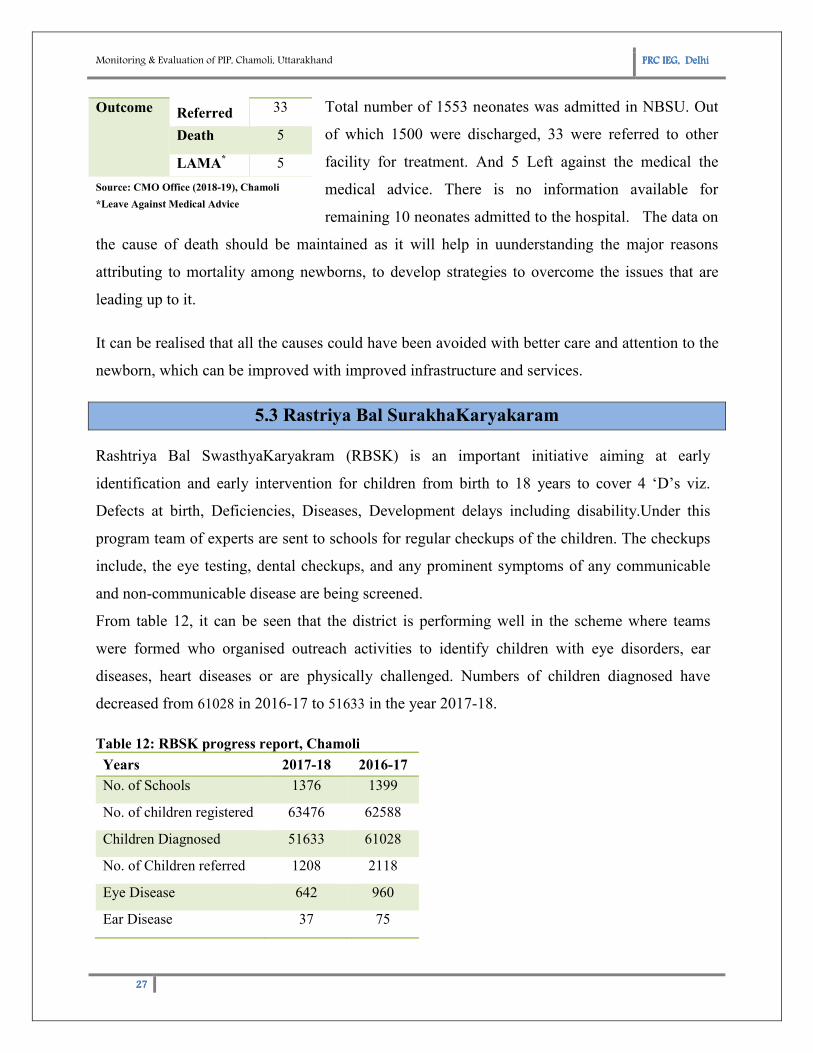
Total number of 1553 neonates was admitted in NBSU. Out
of which 1500 were discharged, 33 were referred to other
facility for treatment. And 5 Left against the medical the
medical advice. There is no information available for
remaining 10 neonates admitted to the hospital. The data on
the cause of death should be maintained as it will help in uunderstanding the major reasons
attributing to mortality among newborns, to develop strategies to overcome the issues that are
leading up to it.
It can be realised that all the causes could have been avoided with better care and attention to the
newborn, which can be improved with improved infrastructure and services.
5.3 Rastriya Bal SurakhaKaryakaram
Rashtriya Bal SwasthyaKaryakram (RBSK) is an important initiative aiming at early
identification and early intervention for children from birth to 18 years to cover 4 ‘D’s viz.
Defects at birth, Deficiencies, Diseases, Development delays including disability.Under this
program team of experts are sent to schools for regular checkups of the children. The checkups
include, the eye testing, dental checkups, and any prominent symptoms of any communicable
and non-communicable disease are being screened.
From table 12, it can be seen that the district is performing well in the scheme where teams
were formed who organised outreach activities to identify children with eye disorders, ear
diseases, heart diseases or are physically challenged. Numbers of children diagnosed have
decreased from 61028 in 2016-17 to 51633 in the year 2017-18.
Table 12: RBSK progress report, Chamoli
Outcome Referred 33
Death 5
LAMA* 5
Source: CMO Office (2018-19), Chamoli
*Leave Against Medical Advice
Years 2017-18 2016-17
No. of Schools 1376 1399
No. of children registered 63476 62588
Children Diagnosed 51633 61028
No. of Children referred 1208 2118
Eye Disease 642 960
Ear Disease 37 75
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
28282828
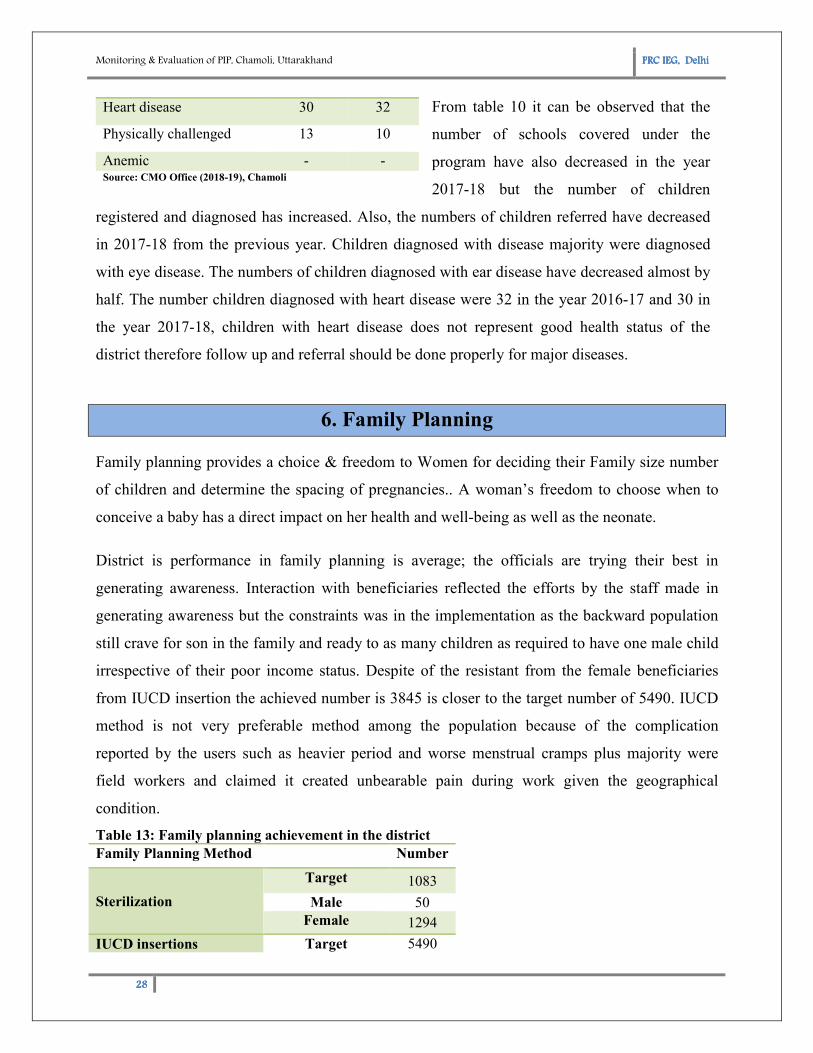
From table 10 it can be observed that the
number of schools covered under the
program have also decreased in the year
2017-18 but the number of children
registered and diagnosed has increased. Also, the numbers of children referred have decreased
in 2017-18 from the previous year. Children diagnosed with disease majority were diagnosed
with eye disease. The numbers of children diagnosed with ear disease have decreased almost by
half. The number children diagnosed with heart disease were 32 in the year 2016-17 and 30 in
the year 2017-18, children with heart disease does not represent good health status of the
district therefore follow up and referral should be done properly for major diseases.
6. Family Planning
Family planning provides a choice & freedom to Women for deciding their Family size number
of children and determine the spacing of pregnancies.. A woman’s freedom to choose when to
conceive a baby has a direct impact on her health and well-being as well as the neonate.
District is performance in family planning is average; the officials are trying their best in
generating awareness. Interaction with beneficiaries reflected the efforts by the staff made in
generating awareness but the constraints was in the implementation as the backward population
still crave for son in the family and ready to as many children as required to have one male child
irrespective of their poor income status. Despite of the resistant from the female beneficiaries
from IUCD insertion the achieved number is 3845 is closer to the target number of 5490. IUCD
method is not very preferable method among the population because of the complication
reported by the users such as heavier period and worse menstrual cramps plus majority were
field workers and claimed it created unbearable pain during work given the geographical
condition.
Table 13: Family planning achievement in the district
Heart disease 30 32
Physically challenged 13 10
Anemic - - Source: CMO Office (2018-19), Chamoli
Family Planning Method Number
Sterilization
Target 1083
Male 50 Female 1294
IUCD insertions Target 5490
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
29292929
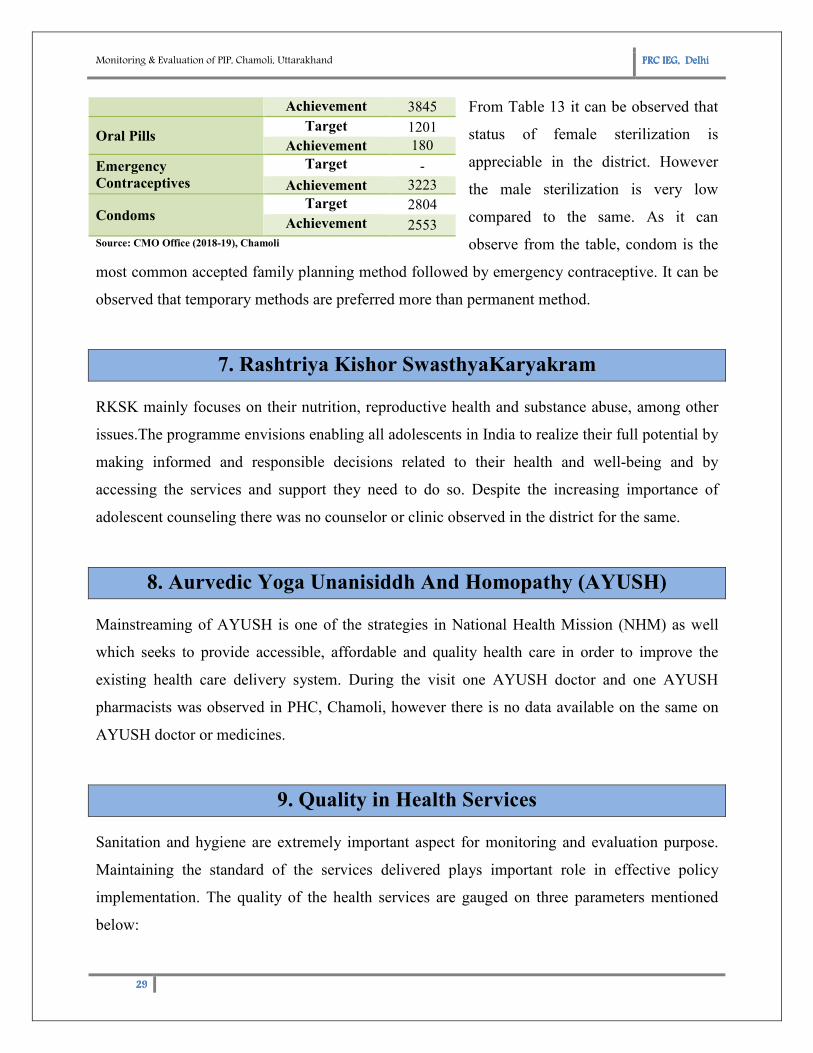
From Table 13 it can be observed that
status of female sterilization is
appreciable in the district. However
the male sterilization is very low
compared to the same. As it can
observe from the table, condom is the
most common accepted family planning method followed by emergency contraceptive. It can be
observed that temporary methods are preferred more than permanent method.
7. Rashtriya Kishor SwasthyaKaryakram
RKSK mainly focuses on their nutrition, reproductive health and substance abuse, among other
issues.The programme envisions enabling all adolescents in India to realize their full potential by
making informed and responsible decisions related to their health and well-being and by
accessing the services and support they need to do so. Despite the increasing importance of
adolescent counseling there was no counselor or clinic observed in the district for the same.
8. Aurvedic Yoga Unanisiddh And Homopathy (AYUSH)
Mainstreaming of AYUSH is one of the strategies in National Health Mission (NHM) as well
which seeks to provide accessible, affordable and quality health care in order to improve the
existing health care delivery system. During the visit one AYUSH doctor and one AYUSH
pharmacists was observed in PHC, Chamoli, however there is no data available on the same on
AYUSH doctor or medicines.
9. Quality in Health Services
Sanitation and hygiene are extremely important aspect for monitoring and evaluation purpose.
Maintaining the standard of the services delivered plays important role in effective policy
implementation. The quality of the health services are gauged on three parameters mentioned
below:
Achievement 3845
Oral Pills Target 1201
Achievement 180
Emergency
Contraceptives
Target -
Achievement 3223
Condoms Target 2804
Achievement 2553 Source: CMO Office (2018-19), Chamoli
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
30303030
1. Biomedical Waste & Infection Control
2. Information, Education And Management
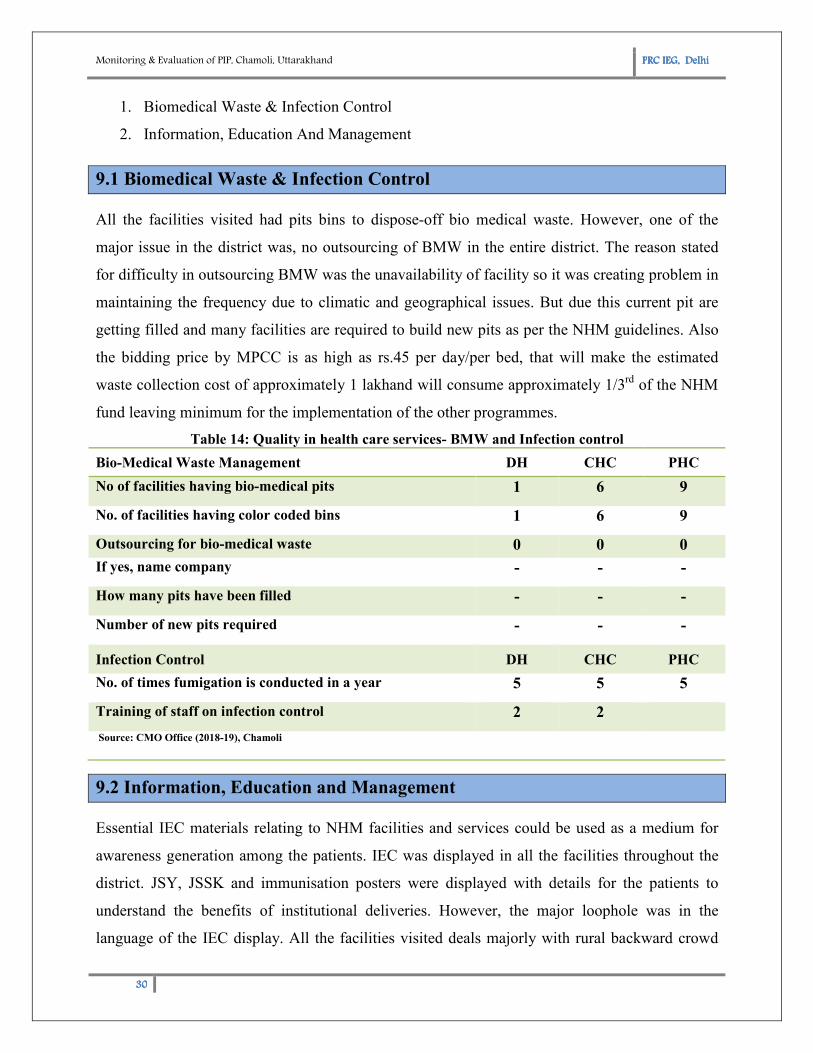
9.1 Biomedical Waste & Infection Control
All the facilities visited had pits bins to dispose-off bio medical waste. However, one of the
major issue in the district was, no outsourcing of BMW in the entire district. The reason stated
for difficulty in outsourcing BMW was the unavailability of facility so it was creating problem in
maintaining the frequency due to climatic and geographical issues. But due this current pit are
getting filled and many facilities are required to build new pits as per the NHM guidelines. Also
the bidding price by MPCC is as high as rs.45 per day/per bed, that will make the estimated
waste collection cost of approximately 1 lakhand will consume approximately 1/3rd
of the NHM
fund leaving minimum for the implementation of the other programmes.
Table 14: Quality in health care services- BMW and Infection control
Bio-Medical Waste Management DH CHC PHC
No of facilities having bio-medical pits 1 6 9
No. of facilities having color coded bins 1 6 9
Outsourcing for bio-medical waste 0 0 0
If yes, name company - - -
How many pits have been filled - - -
Number of new pits required - - -
Infection Control DH CHC PHC
No. of times fumigation is conducted in a year 5 5 5
Training of staff on infection control 2 2
Source: CMO Office (2018-19), Chamoli
9.2 Information, Education and Management
Essential IEC materials relating to NHM facilities and services could be used as a medium for
awareness generation among the patients. IEC was displayed in all the facilities throughout the
district. JSY, JSSK and immunisation posters were displayed with details for the patients to
understand the benefits of institutional deliveries. However, the major loophole was in the
language of the IEC display. All the facilities visited deals majorly with rural backward crowd
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
31313131
which is not very literate, hence IEC display in English will of no use in such areas. Therefore
the IEC display should be in Hindi for the general public to understand.
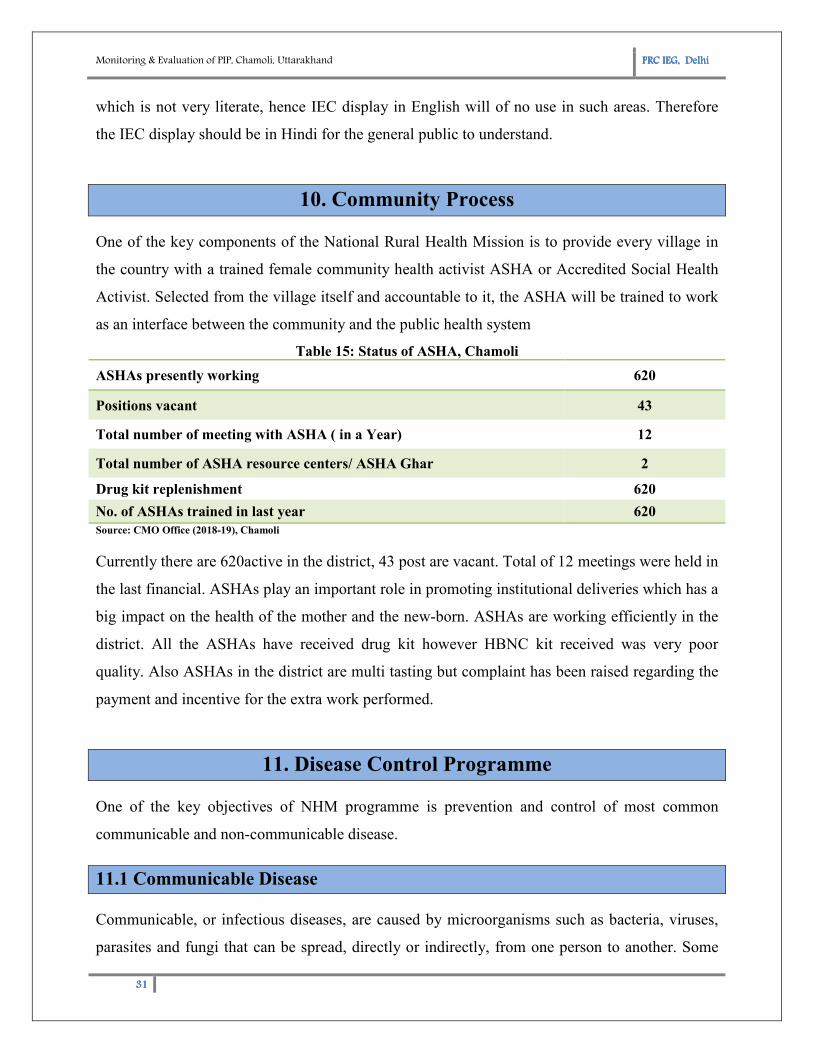
10. Community Process
One of the key components of the National Rural Health Mission is to provide every village in
the country with a trained female community health activist ASHA or Accredited Social Health
Activist. Selected from the village itself and accountable to it, the ASHA will be trained to work
as an interface between the community and the public health system
Table 15: Status of ASHA, Chamoli
ASHAs presently working 620
Positions vacant 43
Total number of meeting with ASHA ( in a Year) 12
Total number of ASHA resource centers/ ASHA Ghar 2
Drug kit replenishment 620
No. of ASHAs trained in last year 620
Source: CMO Office (2018-19), Chamoli
Currently there are 620active in the district, 43 post are vacant. Total of 12 meetings were held in
the last financial. ASHAs play an important role in promoting institutional deliveries which has a
big impact on the health of the mother and the new-born. ASHAs are working efficiently in the
district. All the ASHAs have received drug kit however HBNC kit received was very poor
quality. Also ASHAs in the district are multi tasting but complaint has been raised regarding the
payment and incentive for the extra work performed.
11. Disease Control Programme
One of the key objectives of NHM programme is prevention and control of most common
communicable and non-communicable disease.
11.1 Communicable Disease
Communicable, or infectious diseases, are caused by microorganisms such as bacteria, viruses,
parasites and fungi that can be spread, directly or indirectly, from one person to another. Some
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
32323232
are transmitted through bites from insects while others are caused by ingesting contaminated
food or water. Most common forms of spread include fecal-oral, food, sexual intercourse, insect
bites, contact with contaminated fomites, droplets, or skin contact. Some examples of the
communicable disease include HIV, hepatitis A, B and C, measles, salmonella, measles and
blood-borne illnesses.
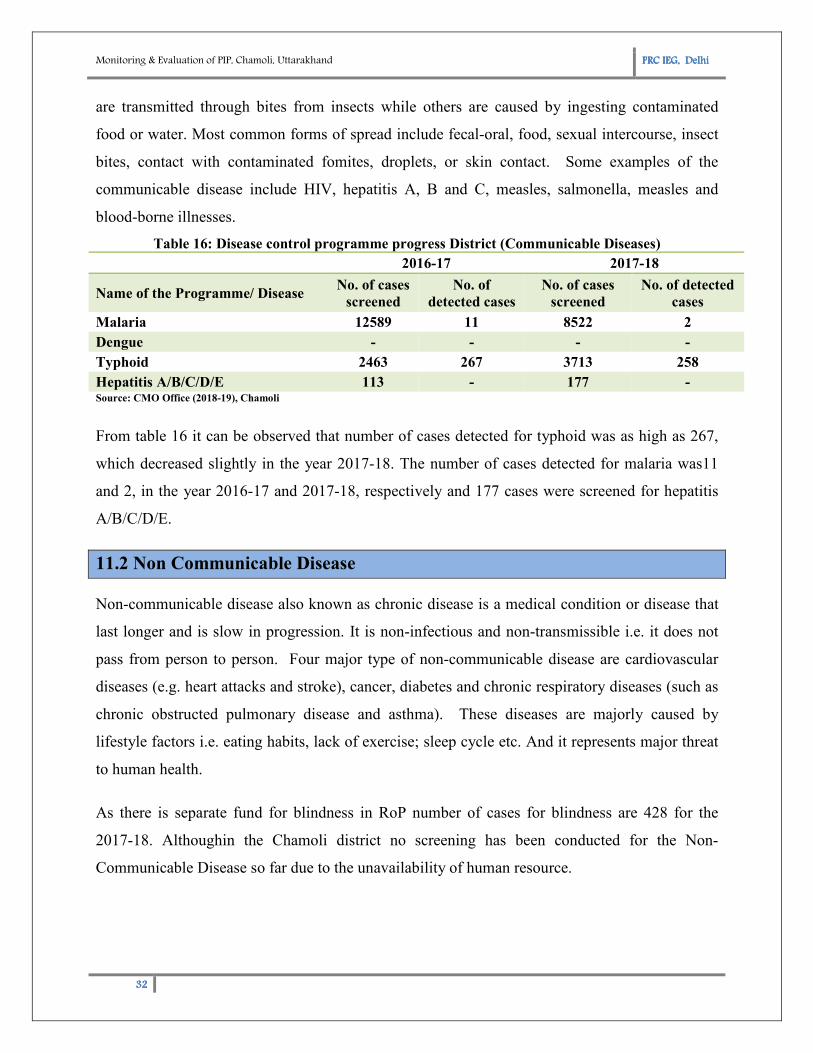
Table 16: Disease control programme progress District (Communicable Diseases)
2016-17 2017-18
Name of the Programme/ Disease No. of cases
screened
No. of
detected cases
No. of cases
screened
No. of detected
cases
Malaria 12589 11 8522 2
Dengue - - - -
Typhoid 2463 267 3713 258
Hepatitis A/B/C/D/E 113 - 177 - Source: CMO Office (2018-19), Chamoli
From table 16 it can be observed that number of cases detected for typhoid was as high as 267,
which decreased slightly in the year 2017-18. The number of cases detected for malaria was11
and 2, in the year 2016-17 and 2017-18, respectively and 177 cases were screened for hepatitis
A/B/C/D/E.
11.2 Non Communicable Disease
Non-communicable disease also known as chronic disease is a medical condition or disease that
last longer and is slow in progression. It is non-infectious and non-transmissible i.e. it does not
pass from person to person. Four major type of non-communicable disease are cardiovascular
diseases (e.g. heart attacks and stroke), cancer, diabetes and chronic respiratory diseases (such as
chronic obstructed pulmonary disease and asthma). These diseases are majorly caused by
lifestyle factors i.e. eating habits, lack of exercise; sleep cycle etc. And it represents major threat
to human health.
As there is separate fund for blindness in RoP number of cases for blindness are 428 for the
2017-18. Althoughin the Chamoli district no screening has been conducted for the Non-
Communicable Disease so far due to the unavailability of human resource.
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
33333333
12. HMIS
NHM includes reporting and compiling of the data thereby indicating performance of basic
indicators of maternal and child health care in the district. In Chamoli District, there were some
issues with regard to reporting of the data. Maximum facilities did not have any data validation
team. Also the data for many major heads such as AYUSH and ARSH is not available. Data on
delivery status is also said to be under reported at block level. HMIS data is very important
aspect for monitoring the performance of various programme under NHM in the district the area
should be given more focus and data should be validated before getting onto the online portal
13. Budget Utilization
The detail of the budget utilisation is given in table17. As per given records it can be observed
almost under all the budget heads the amount utilized is less than the amount sanctioned. The
underutilized budget is due to the late arrival of RoP which leaves very little time for fund
utilisation.
Table 17: Budget Utilization Summary, Chamoli
Budget Head Budget Expenditure
(As on 31 Dec, 2017)
NRHM + RMNCH plus A Flexipool 10099247 8441204
Maternal Health 9736900 3055255
Child Health 228200 173536
Family Planning 2462000 350038
Adolescent Health/RKSK - -
Immunization 4705568 2675963
NUHM Flexipool - -
FLEXIPOOL FOR DISEASE CONTROL PROGRAMME - -
FLEXIPOOL FOR NON-COMMUNICABLE DIEASES 6495502 290484
National Mental Health programme (NMHP) 680572 0
National Programme for the Healthcare of the Elderly
(NPHCE) 1270572 114891
National Tobacco Control Programme (NTCP) 1124366 -
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
34343434
Budget Head Budget Expenditure
(As on 31 Dec, 2017)
National Programme for Prevention and Control of
Cancer, Diabetes, Cardiovascular Diseases and Stroke
(NPCDCS)
2179770 -
INFRASTRUCTURE MAINTENANCE 3439245 -
Source: CMO Office (2018-19), Chamoli
15. Facility Wise Observation
15.1 Distict Hospital Gopeshwar, Chamoli
District HospitalGopeshwar is located in Near Head Post Office, Gopeshwar-Chamoli Road,
Chamoli. The hospital was 100 bedded. It is located in block Dasholi and has a catchment
population of 19000.Below mentioned are some major points observed in the facility visited:
� District hospital fares extremely well on all
assessments with respect to the infrastructure availability and maintenance.The area was
optimally utilised and waiting area was well constructed and maintained. It also received
kaya-kalp award for the year 2016-17.
� Hospital has functional labour room, NBCC, and cleans wards.
� Waste is segregated in colour coded bins. And pits are established for BMW.
� Functional laundry/ washing services, dietary
services, and drug storage facilities are
available.
� The DH has all equipment available including
BP Instrument, Stethoscope, Sterilised delivery
sets, neonatal, paediatric and Adult
Resuscitation kit, weighing machine (adult and
child), Needle Cutter, Radiant Warmer, Suction
apparatus, Facility for Oxygen Administration,
Foetal Doppler/CTG, Mobile light, Delivery
Figure 7: District Hospital, Chamoli
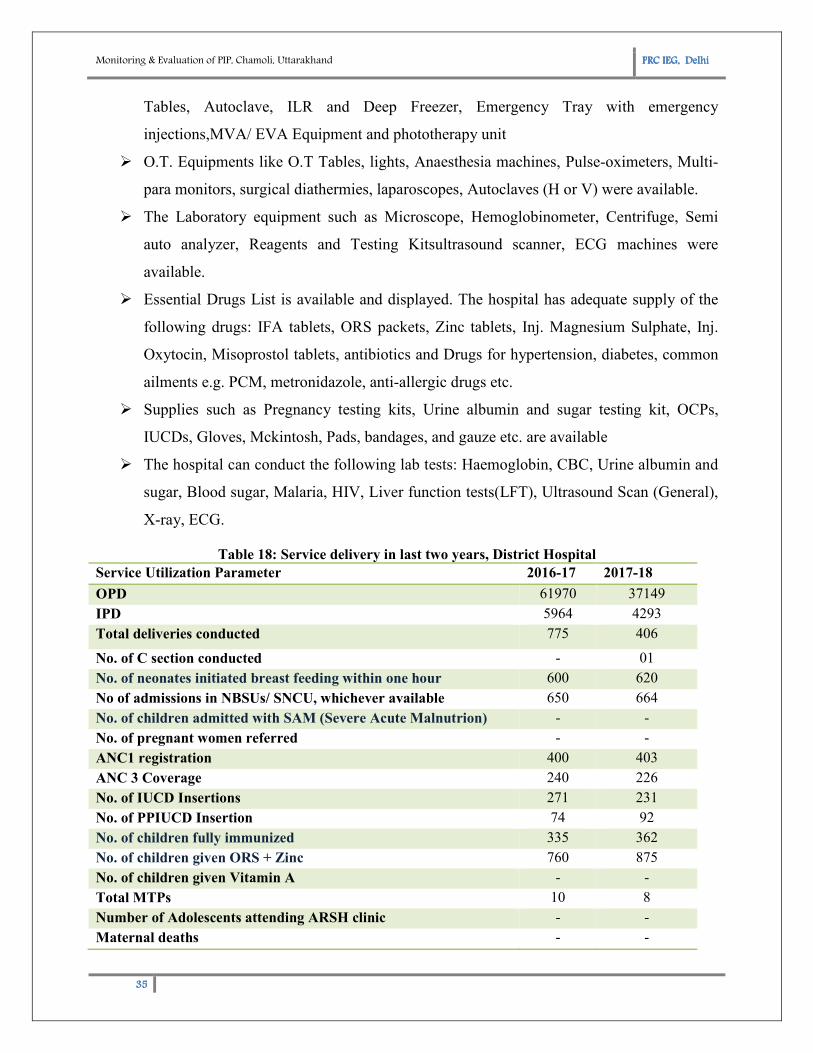
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
35353535
Tables, Autoclave, ILR and Deep Freezer, Emergency Tray with emergency
injections,MVA/ EVA Equipment and phototherapy unit
� O.T. Equipments like O.T Tables, lights, Anaesthesia machines, Pulse-oximeters, Multi-
para monitors, surgical diathermies, laparoscopes, Autoclaves (H or V) were available.
� The Laboratory equipment such as Microscope, Hemoglobinometer, Centrifuge, Semi
auto analyzer, Reagents and Testing Kitsultrasound scanner, ECG machines were
available.
� Essential Drugs List is available and displayed. The hospital has adequate supply of the
following drugs: IFA tablets, ORS packets, Zinc tablets, Inj. Magnesium Sulphate, Inj.
Oxytocin, Misoprostol tablets, antibiotics and Drugs for hypertension, diabetes, common
ailments e.g. PCM, metronidazole, anti-allergic drugs etc.
� Supplies such as Pregnancy testing kits, Urine albumin and sugar testing kit, OCPs,
IUCDs, Gloves, Mckintosh, Pads, bandages, and gauze etc. are available
� The hospital can conduct the following lab tests: Haemoglobin, CBC, Urine albumin and
sugar, Blood sugar, Malaria, HIV, Liver function tests(LFT), Ultrasound Scan (General),
X-ray, ECG.
Table 18: Service delivery in last two years, District Hospital
Service Utilization Parameter 2016-17 2017-18
OPD 61970 37149
IPD 5964 4293
Total deliveries conducted 775 406
No. of C section conducted - 01
No. of neonates initiated breast feeding within one hour 600 620
No of admissions in NBSUs/ SNCU, whichever available 650 664
No. of children admitted with SAM (Severe Acute Malnutrion) - -
No. of pregnant women referred - -
ANC1 registration 400 403
ANC 3 Coverage 240 226
No. of IUCD Insertions 271 231
No. of PPIUCD Insertion 74 92
No. of children fully immunized 335 362
No. of children given ORS + Zinc 760 875
No. of children given Vitamin A - -
Total MTPs 10 8
Number of Adolescents attending ARSH clinic - -
Maternal deaths - -
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
36363636
Service Utilization Parameter 2016-17 2017-18
Still births - 02
Neonatal deaths 6 5
Infant deaths 5 -
Source: DH Gopeshwar, (2018-19),Chamoli
� From the table above it can be served that the number of OPD and IPD decreased in the
year 2017-18 compared to the last financial year.
� The total number of deliveries conducted also decreased by 50 percent. The major reason
for decrease in OPD, IPD and number of deliveries is the migration of the population to
the plains.
� ANC1 registration increased meagrelyfrom 400 in 2016-2017 to 403 in 2017-18
whereasANC 3 coverage decreased in the year 2017-18 to 226 from 240 in the year
2016-17.
� No. Of IUCD insertion alsodecreased from271 in the year 2-16-17 tp 231 in the year
2017-18. No. of PPIUCD have shown a slight growth by 18 in the year 2017-18.
ANTARA was launched in the district and has reached its second dose.
� No maternal deathwas reported in 2016-17 or 2017-18.No still birth was reported in the
year 2016-17 however 2 still birthwere reported in the last financial year and 5 neonates
death.
� Total number of fully immunised children has increased from 335 in 2016-17 to 362 in
2017-18.Also the number of children given ORS + Zinc increased.
� JSY payments were reported to be approximately 60%. PFMS staff inefficiency was
stated to be one of the reason for low rate of settlement of JSY payments
� All data bases are regularly updated. Records are maintained for OPD, IPD, ANC, PNC,
Line listing of severely anaemic pregnant women, Labour room, OT, Immunisation,
Referral Register (In and Out), MDR, Drug Stocks and Payment under JSY
� Information about various schemes was displayed well in the hospital.
15.2 Community Health Center,Karanprayag, Chamoli
Community Health Centre Karanprayaghas the catchment population of 51119. The facility
covered 205 villages. The facility was 40 bedded. The average OPD was 100 per day.
Figure 8: CHC Karanprayag, Chamoli
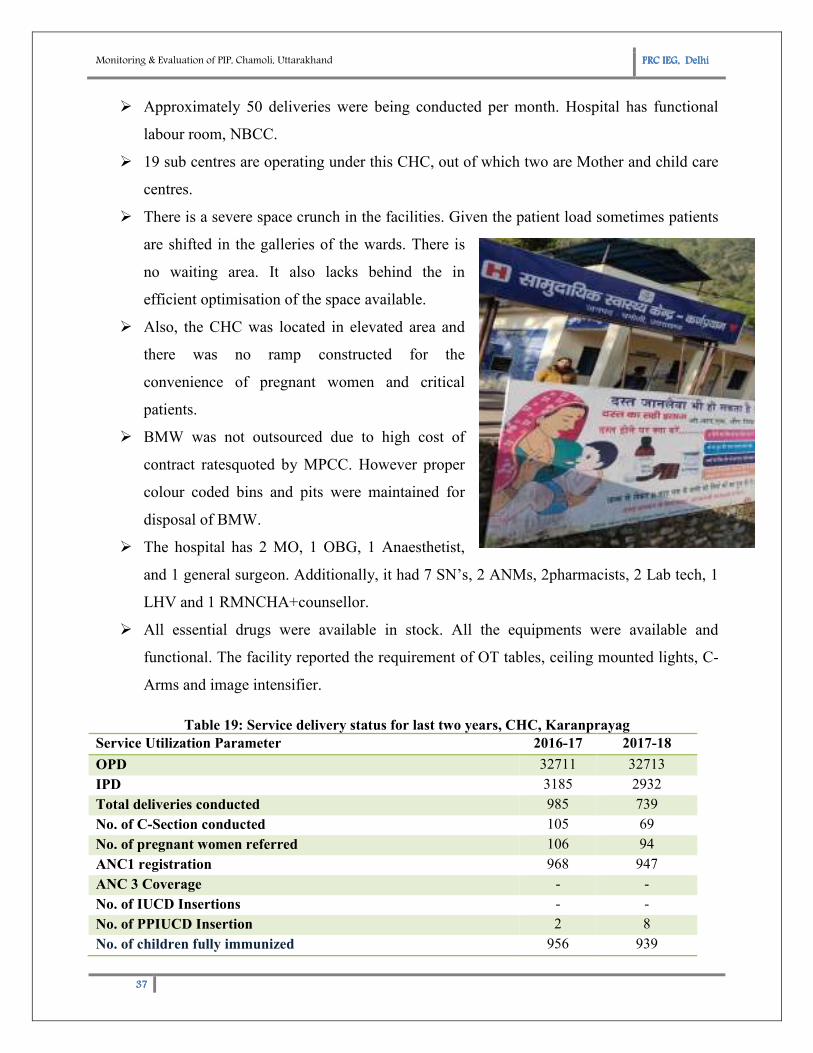
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
37373737
� Approximately 50 deliveries were being conducted per month. Hospital has functional
labour room, NBCC.
� 19 sub centres are operating under this CHC, out of which two are Mother and child care
centres.
� There is a severe space crunch in the facilities. Given the patient load sometimes patients
are shifted in the galleries of the wards. There is
no waiting area. It also lacks behind the in
efficient optimisation of the space available.
� Also, the CHC was located in elevated area and
there was no ramp constructed for the
convenience of pregnant women and critical
patients.
� BMW was not outsourced due to high cost of
contract ratesquoted by MPCC. However proper
colour coded bins and pits were maintained for
disposal of BMW.
� The hospital has 2 MO, 1 OBG, 1 Anaesthetist,
and 1 general surgeon. Additionally, it had 7 SN’s, 2 ANMs, 2pharmacists, 2 Lab tech, 1
LHV and 1 RMNCHA+counsellor.
� All essential drugs were available in stock. All the equipments were available and
functional. The facility reported the requirement of OT tables, ceiling mounted lights, C-
Arms and image intensifier.
Table 19: Service delivery status for last two years, CHC, Karanprayag
Service Utilization Parameter 2016-17 2017-18
OPD 32711 32713
IPD 3185 2932
Total deliveries conducted 985 739
No. of C-Section conducted 105 69
No. of pregnant women referred 106 94
ANC1 registration 968 947
ANC 3 Coverage - -
No. of IUCD Insertions - -
No. of PPIUCD Insertion 2 8
No. of children fully immunized 956 939
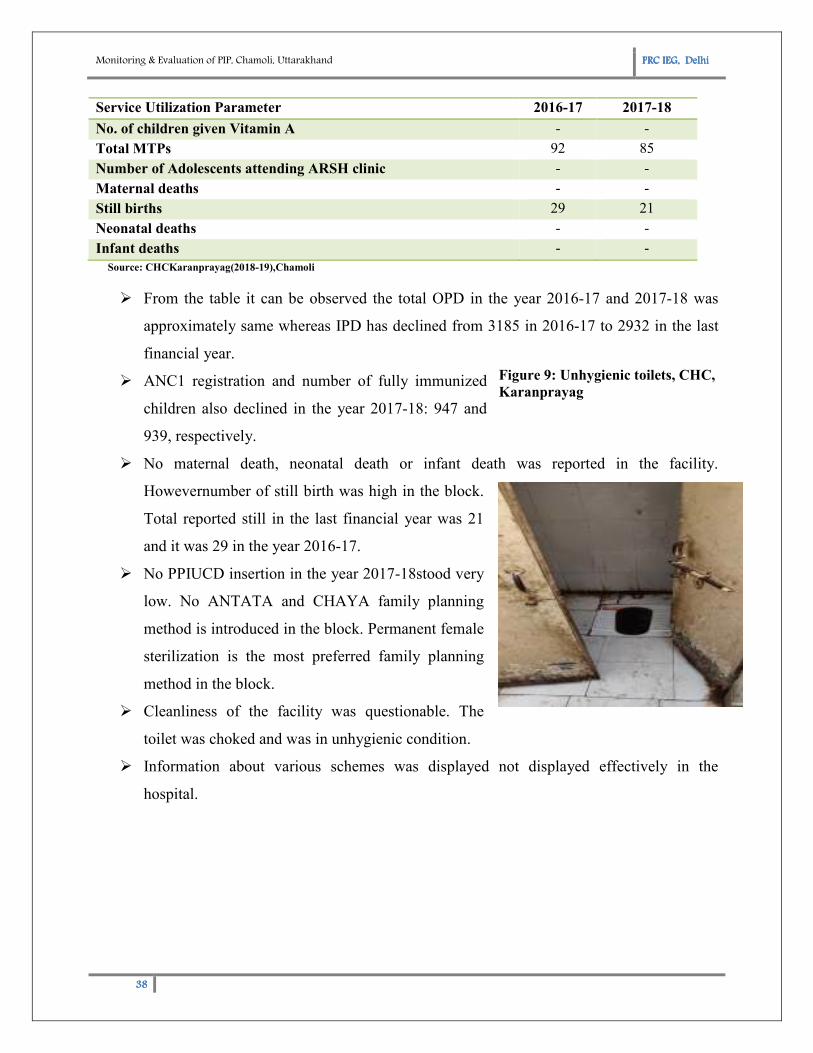
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
38383838
Service Utilization Parameter 2016-17 2017-18
No. of children given Vitamin A - -
Total MTPs 92 85
Number of Adolescents attending ARSH clinic - -
Maternal deaths - -
Still births 29 21
Neonatal deaths - -
Infant deaths - -
Source: CHCKaranprayag(2018-19),Chamoli
� From the table it can be observed the total OPD in the year 2016-17 and 2017-18 was
approximately same whereas IPD has declined from 3185 in 2016-17 to 2932 in the last
financial year.
� ANC1 registration and number of fully immunized
children also declined in the year 2017-18: 947 and
939, respectively.
� No maternal death, neonatal death or infant death was reported in the facility.
Howevernumber of still birth was high in the block.
Total reported still in the last financial year was 21
and it was 29 in the year 2016-17.
� No PPIUCD insertion in the year 2017-18stood very
low. No ANTATA and CHAYA family planning
method is introduced in the block. Permanent female
sterilization is the most preferred family planning
method in the block.
� Cleanliness of the facility was questionable. The
toilet was choked and was in unhygienic condition.
� Information about various schemes was displayed not displayed effectively in the
hospital.
Figure 9: Unhygienic toilets, CHC,
Karanprayag
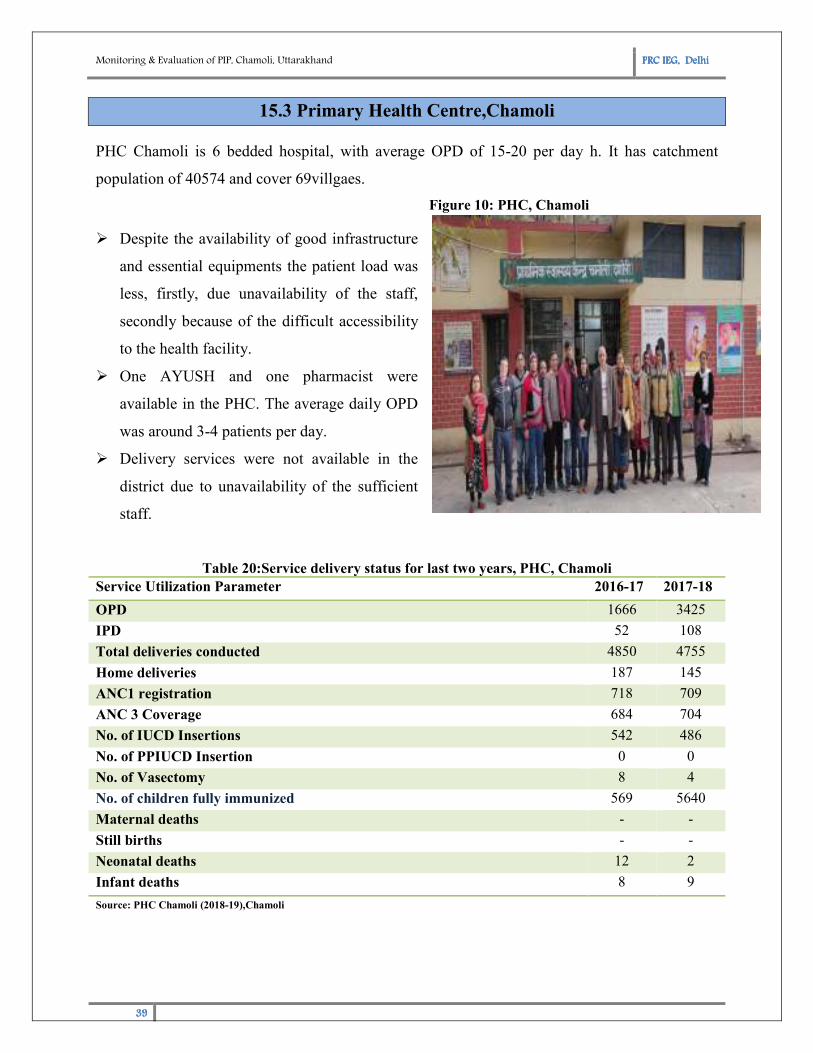
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
39393939
15.3 Primary Health Centre,Chamoli
PHC Chamoli is 6 bedded hospital, with average OPD of 15-20 per day h. It has catchment
population of 40574 and cover 69villgaes.
� Despite the availability of good infrastructure
and essential equipments the patient load was
less, firstly, due unavailability of the staff,
secondly because of the difficult accessibility
to the health facility.
� One AYUSH and one pharmacist were
available in the PHC. The average daily OPD
was around 3-4 patients per day.
� Delivery services were not available in the
district due to unavailability of the sufficient
staff.
Table 20:Service delivery status for last two years, PHC, Chamoli
Service Utilization Parameter 2016-17 2017-18
OPD 1666 3425
IPD 52 108
Total deliveries conducted 4850 4755
Home deliveries 187 145
ANC1 registration 718 709
ANC 3 Coverage 684 704
No. of IUCD Insertions 542 486
No. of PPIUCD Insertion 0 0
No. of Vasectomy 8 4
No. of children fully immunized 569 5640
Maternal deaths - -
Still births - -
Neonatal deaths 12 2
Infant deaths 8 9
Source: PHC Chamoli (2018-19),Chamoli
Figure 10: PHC, Chamoli
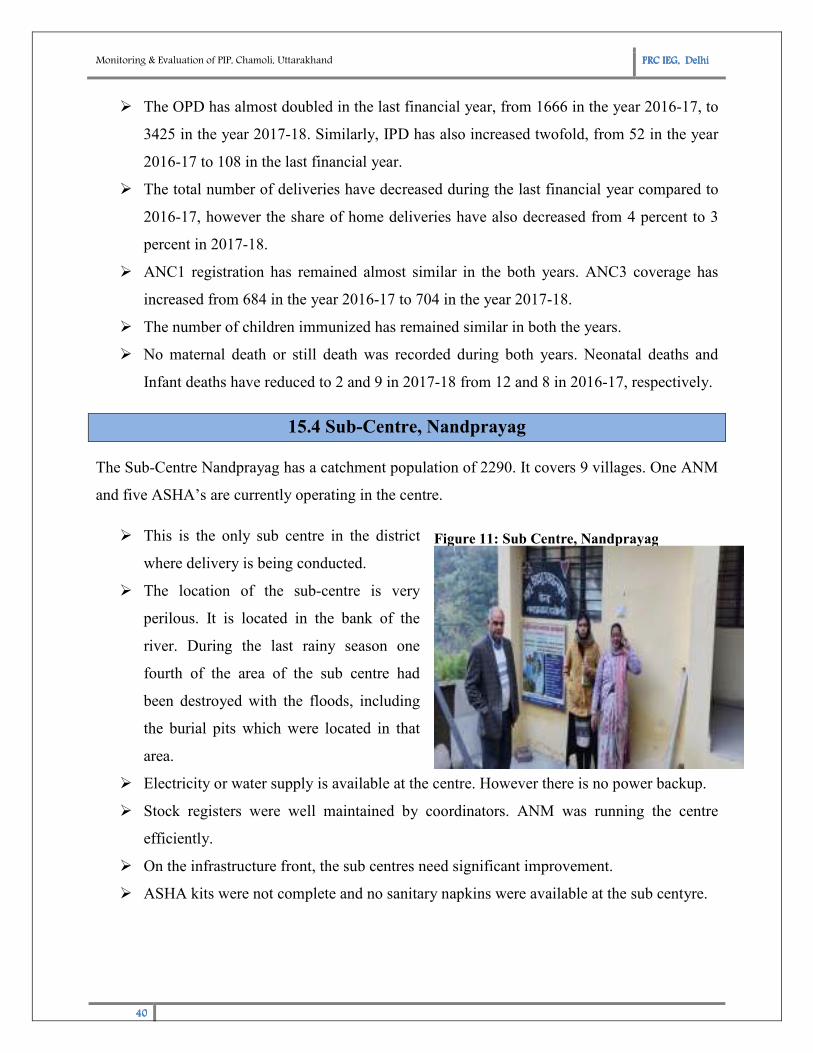
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
40404040
� The OPD has almost doubled in the last financial year, from 1666 in the year 2016-17, to
3425 in the year 2017-18. Similarly, IPD has also increased twofold, from 52 in the year
2016-17 to 108 in the last financial year.
� The total number of deliveries have decreased during the last financial year compared to
2016-17, however the share of home deliveries have also decreased from 4 percent to 3
percent in 2017-18.
� ANC1 registration has remained almost similar in the both years. ANC3 coverage has
increased from 684 in the year 2016-17 to 704 in the year 2017-18.
� The number of children immunized has remained similar in both the years.
� No maternal death or still death was recorded during both years. Neonatal deaths and
Infant deaths have reduced to 2 and 9 in 2017-18 from 12 and 8 in 2016-17, respectively.
15.4 Sub-Centre, Nandprayag
The Sub-Centre Nandprayag has a catchment population of 2290. It covers 9 villages. One ANM
and five ASHA’s are currently operating in the centre.
� This is the only sub centre in the district
where delivery is being conducted.
� The location of the sub-centre is very
perilous. It is located in the bank of the
river. During the last rainy season one
fourth of the area of the sub centre had
been destroyed with the floods, including
the burial pits which were located in that
area.
� Electricity or water supply is available at the centre. However there is no power backup.
� Stock registers were well maintained by coordinators. ANM was running the centre
efficiently.
� On the infrastructure front, the sub centres need significant improvement.
� ASHA kits were not complete and no sanitary napkins were available at the sub centyre.
Figure 11: Sub Centre, Nandprayag
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
41414141
Table 21: Service delivery status for last two years, Sub-centreNandprayag
Service Utilization Parameter 2016-17 2017-18
Number of estimated pregnancies 41 40
No. of pregnant women given IFA 35 58
Number of deliveries conducted at SC 12 5
Number of deliveries conducted at home 0 0
ANC1 registration 35 58
ANC3 coverage 27 32
No. of IUCD insertions 32 41
No. of children fully immunized 48 53
No. of children given Vitamin A
No. of children given IFA Syrup 25
No. of still birth recorded
Neonatal deaths recorded 1
Number of VHNDs attended 17 17
Number of VHNSC meeting attended Source: Sub-Centre, Nandprayag, Chamoli
� The number of deliveries conducted during the last financial year have decreased to 5
from 12 in the year 2016-17
� The number of ANC registration has increased 35 to 58 in the year 2017-18. Similarly
ANC3 coverage has also increased to 32 from 27 in the last the financial year.
� No neonatal death or still birth was recorded during the last financial year.
� Number of VHND meeting attended remained same for both the years.
15.5 Sub-Centre, Simli
Sub-centreBughani has a catchment population of 2495. It covers 10 villages. It has One ANM
and Five ASHAs operating the facility.
� No delivery was being conducted at the centre. The
service delivery at the sub centre level is restricted to
immunization, VHNDs, and suchlike
� The facility was not easily accessible. The road to the
facility is extremely dangerous especially for the
pregnant women.
� Immunisation camp and VHND is held every week of
the month, on Wednesday and Saturday, respectively
Figure 12: Sub Centre, Simli
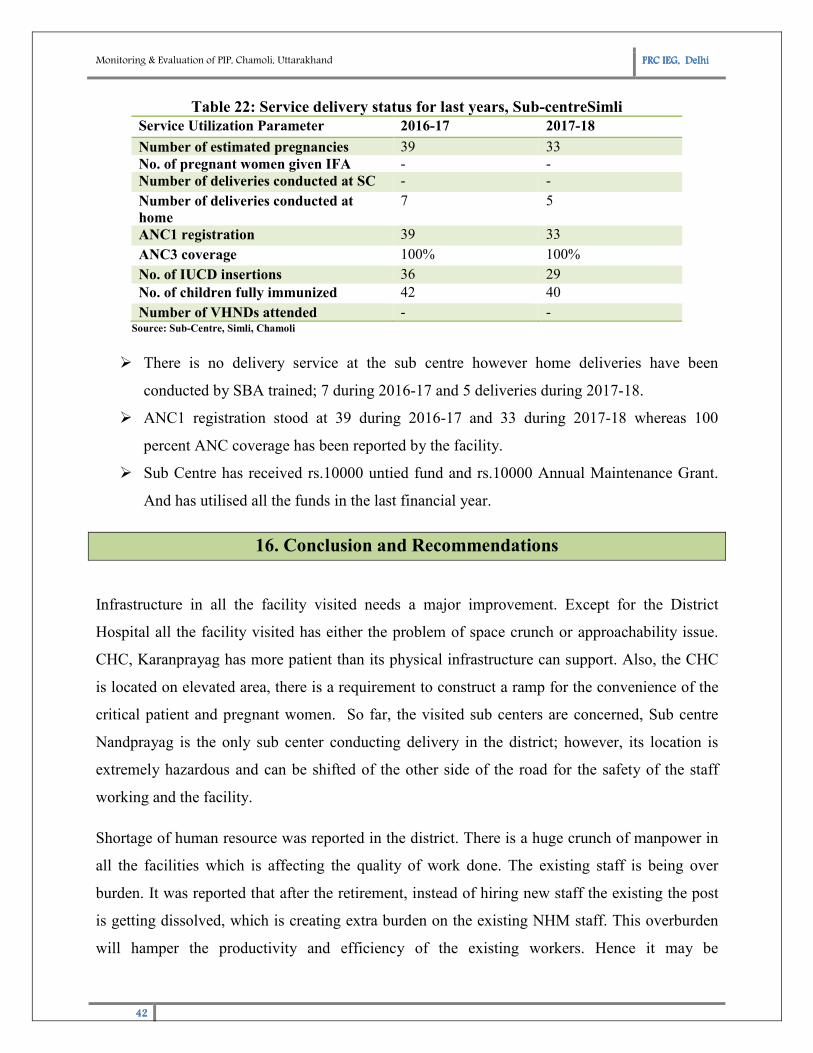
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
42424242
Table 22: Service delivery status for last years, Sub-centreSimli
Service Utilization Parameter 2016-17 2017-18
Number of estimated pregnancies 39 33
No. of pregnant women given IFA - -
Number of deliveries conducted at SC - -
Number of deliveries conducted at
home
7 5
ANC1 registration 39 33
ANC3 coverage 100% 100%
No. of IUCD insertions 36 29
No. of children fully immunized 42 40
Number of VHNDs attended - - Source: Sub-Centre, Simli, Chamoli
� There is no delivery service at the sub centre however home deliveries have been
conducted by SBA trained; 7 during 2016-17 and 5 deliveries during 2017-18.
� ANC1 registration stood at 39 during 2016-17 and 33 during 2017-18 whereas 100
percent ANC coverage has been reported by the facility.
� Sub Centre has received rs.10000 untied fund and rs.10000 Annual Maintenance Grant.
And has utilised all the funds in the last financial year.
16. Conclusion and Recommendations
Infrastructure in all the facility visited needs a major improvement. Except for the District
Hospital all the facility visited has either the problem of space crunch or approachability issue.
CHC, Karanprayag has more patient than its physical infrastructure can support. Also, the CHC
is located on elevated area, there is a requirement to construct a ramp for the convenience of the
critical patient and pregnant women. So far, the visited sub centers are concerned, Sub centre
Nandprayag is the only sub center conducting delivery in the district; however, its location is
extremely hazardous and can be shifted of the other side of the road for the safety of the staff
working and the facility.
Shortage of human resource was reported in the district. There is a huge crunch of manpower in
all the facilities which is affecting the quality of work done. The existing staff is being over
burden. It was reported that after the retirement, instead of hiring new staff the existing the post
is getting dissolved, which is creating extra burden on the existing NHM staff. This overburden
will hamper the productivity and efficiency of the existing workers. Hence it may be
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
43434343
recommended that the post should not be dissolved and new recruits should be hired to manage
the work load efficiently. Also, the shortage of ANM and staff nurse was reported in the district.
It was highlighted that one ANM is handling two sub centers simultaneously in the district. PHC,
Chamoli reported shortage of SN due to which they are unable to handle much patient
load.Therefore, the sanctioned post of the ANM and staff nurse may be increased in the district.
ANM’s in the district are working efficiently and effectively. Given the geographical condition
of the district they have been travelling distance to reach the remote areas which are not
accessible to DH, CHC and PHC. Moreover, they are giving additional training, conducting
survey under AYUSHMAN Bharat, however no extra incentive or payment was given to them
for rendering these extra services. Empowering ASHA via incentives is extremely important to
improve access to health facilities because they play a significant role in taking health care
facility at doorstep.
Biomedical Waste Collection pricing should be regulated. Currently there is no mechanism of
waste collection in the entire district, and pits are getting full. MPCC biding rates are so high that
it will consume one-fourth of the NHM funds, leaving very little for rest of the
programmes/schemes. Also due to topographical reason very few firms are operating in the near
area and also their rates are very high. Therefore, the pricing should be regulated so that
hospitals, especially district hospital may have the facility of waste collection.
Data reporting of the district is poor. Block-wise delivery status is under-reported, also no
information is available on AYUSH doctor and ARSH. Data validation team should be formed at
all the centres because data feeding without validation gives absurd figures on the portal. Wrong
figures on the portal can degrade the district performance and ranking therefore data validation
before data feeding is extremely important.
As per the records there was no training was held for the year 2017-18. Training programme
should be organised so that more staff can be trained which will result in improved efficiency
and productivity of the staff.
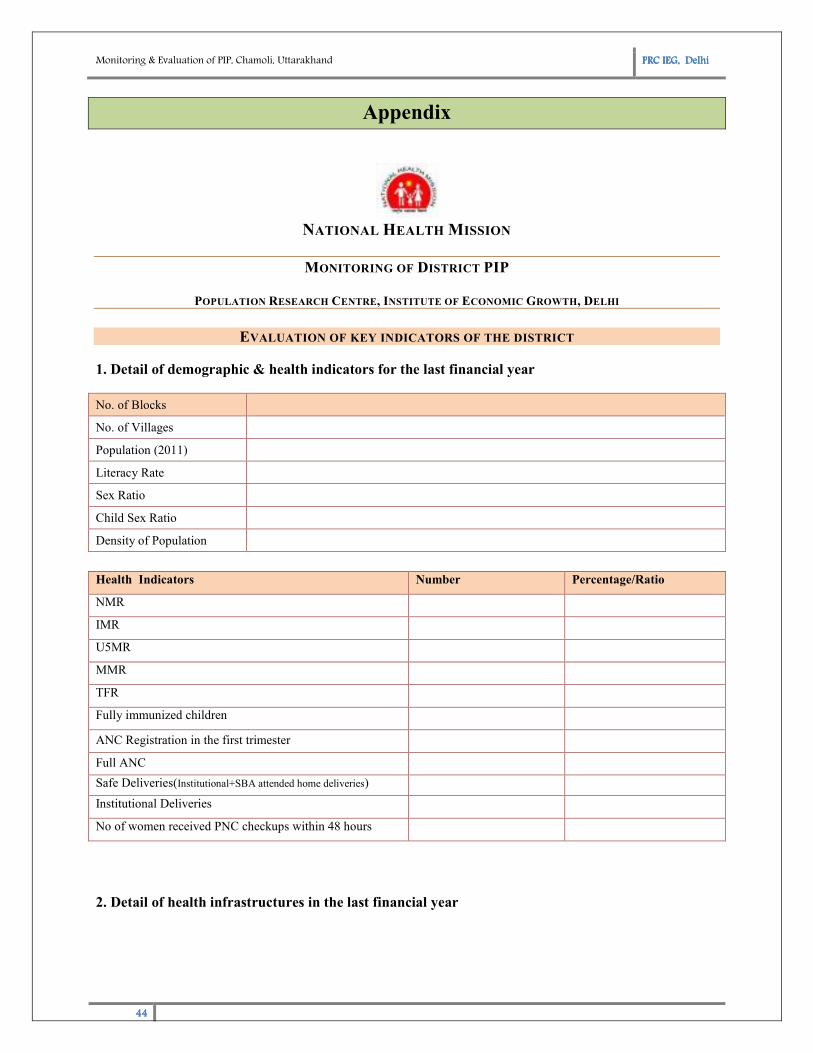
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
44444444
Appendix
NATIONAL HEALTH MISSION
MONITORING OF DISTRICT PIP
POPULATION RESEARCH CENTRE, INSTITUTE OF ECONOMIC GROWTH, DELHI
EVALUATION OF KEY INDICATORS OF THE DISTRICT
1. Detail of demographic & health indicators for the last financial year
No. of Blocks
No. of Villages
Population (2011)
Literacy Rate
Sex Ratio
Child Sex Ratio
Density of Population
Health Indicators Number Percentage/Ratio
NMR
IMR
U5MR
MMR
TFR
Fully immunized children
ANC Registration in the first trimester
Full ANC
Safe Deliveries(Institutional+SBA attended home deliveries)
Institutional Deliveries
No of women received PNC checkups within 48 hours
2. Detail of health infrastructures in the last financial year
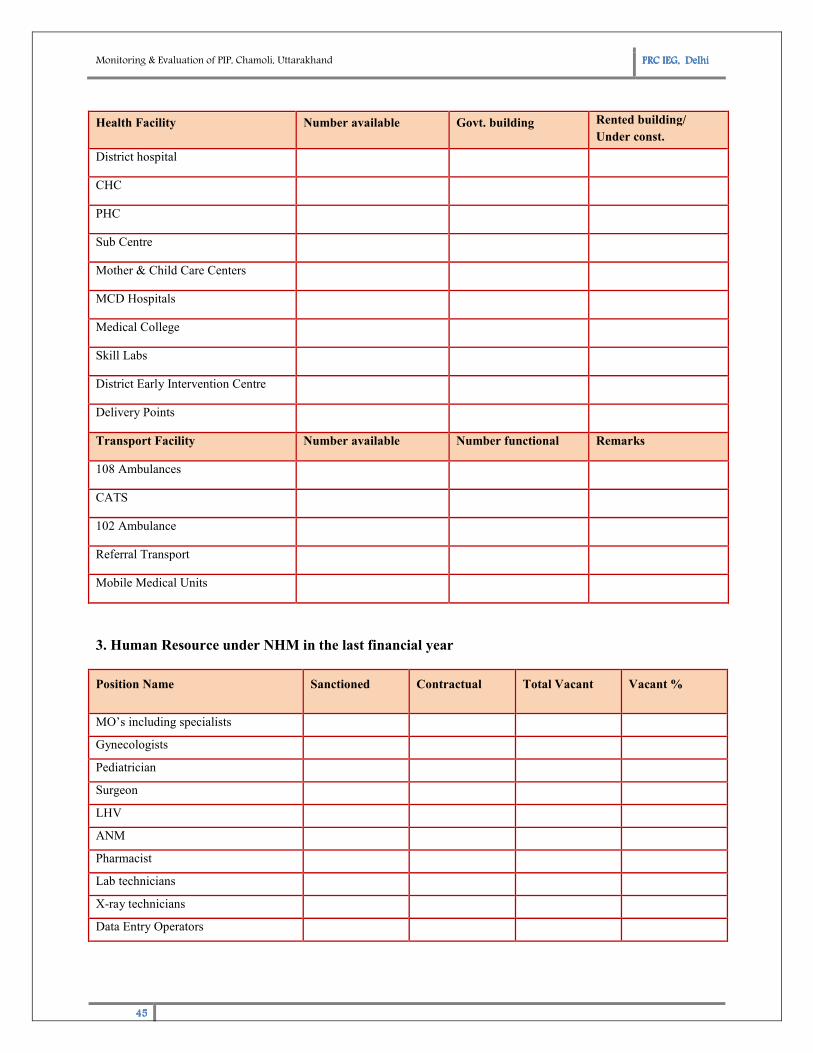
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
45454545
3. Human Resource under NHM in the last financial year
Position Name Sanctioned Contractual Total Vacant Vacant %
MO’s including specialists
Gynecologists
Pediatrician
Surgeon
LHV
ANM
Pharmacist
Lab technicians
X-ray technicians
Data Entry Operators
Health Facility Number available Govt. building Rented building/
Under const.
District hospital
CHC
PHC
Sub Centre
Mother & Child Care Centers
MCD Hospitals
Medical College
Skill Labs
District Early Intervention Centre
Delivery Points
Transport Facility Number available Number functional Remarks
108 Ambulances
CATS
102 Ambulance
Referral Transport
Mobile Medical Units
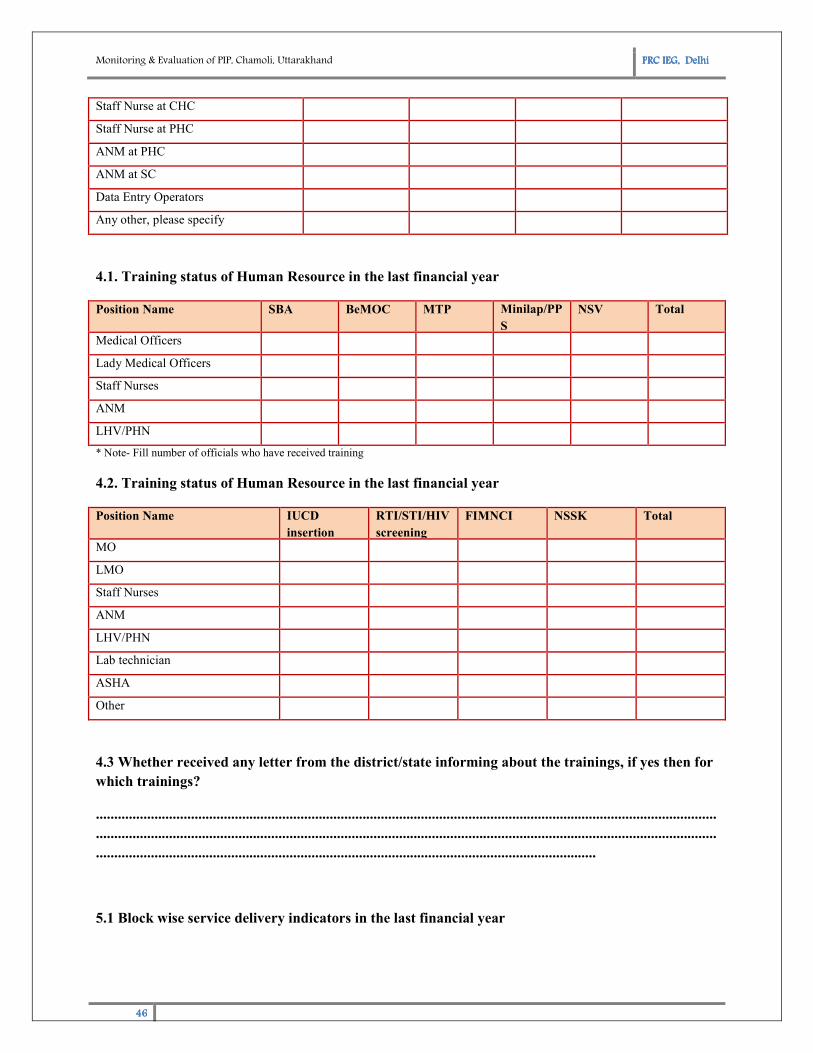
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
46464646
Staff Nurse at CHC
Staff Nurse at PHC
ANM at PHC
ANM at SC
Data Entry Operators
Any other, please specify
4.1. Training status of Human Resource in the last financial year
Position Name SBA BeMOC MTP Minilap/PP
S
NSV Total
Medical Officers
Lady Medical Officers
Staff Nurses
ANM
LHV/PHN
* Note- Fill number of officials who have received training
4.2. Training status of Human Resource in the last financial year
Position Name IUCD
insertion
RTI/STI/HIV
screening
FIMNCI NSSK Total
MO
LMO
Staff Nurses
ANM
LHV/PHN
Lab technician
ASHA
Other
4.3 Whether received any letter from the district/state informing about the trainings, if yes then for
which trainings?
..........................................................................................................................................................................
..........................................................................................................................................................................
.........................................................................................................................................
5.1 Block wise service delivery indicators in the last financial year
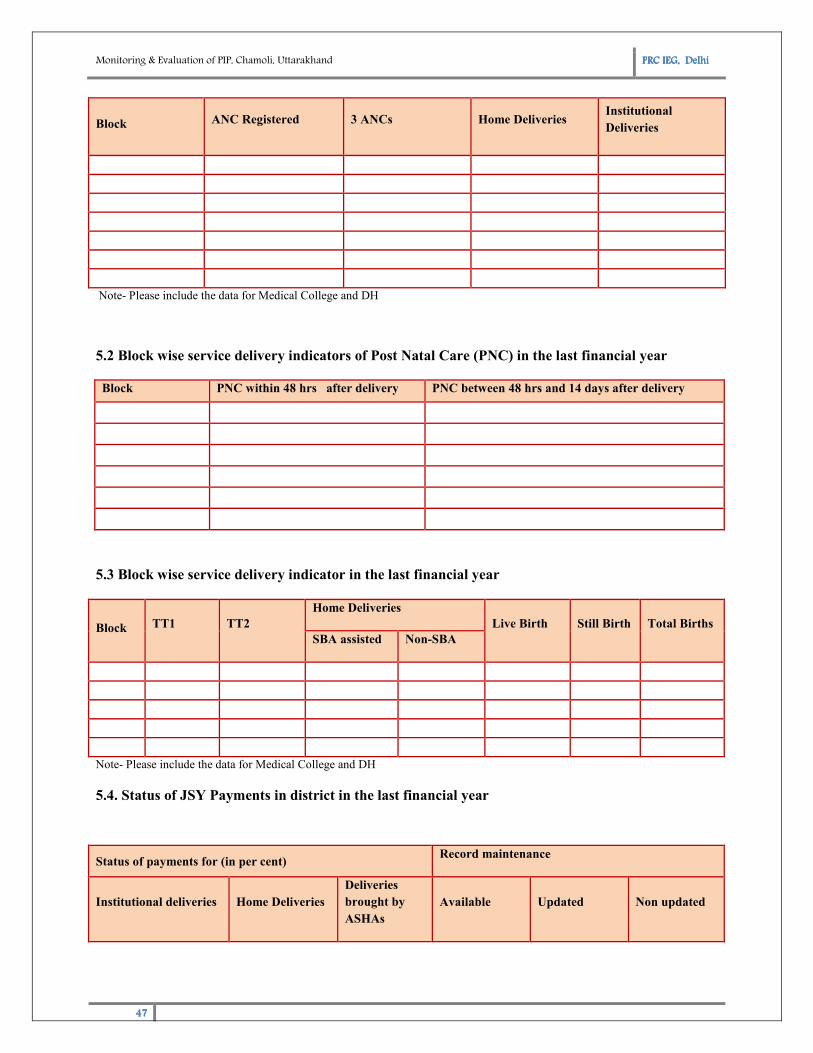
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
47474747
Block ANC Registered 3 ANCs Home Deliveries Institutional
Deliveries
Note- Please include the data for Medical College and DH
5.2 Block wise service delivery indicators of Post Natal Care (PNC) in the last financial year
Block PNC within 48 hrs after delivery PNC between 48 hrs and 14 days after delivery
5.3 Block wise service delivery indicator in the last financial year
Note- Please include the data for Medical College and DH
5.4. Status of JSY Payments in district in the last financial year
Block TT1 TT2
Home Deliveries
Live Birth Still Birth Total Births
SBA assisted Non-SBA
Status of payments for (in per cent) Record maintenance
Institutional deliveries Home Deliveries
Deliveries
brought by
ASHAs
Available Updated Non updated
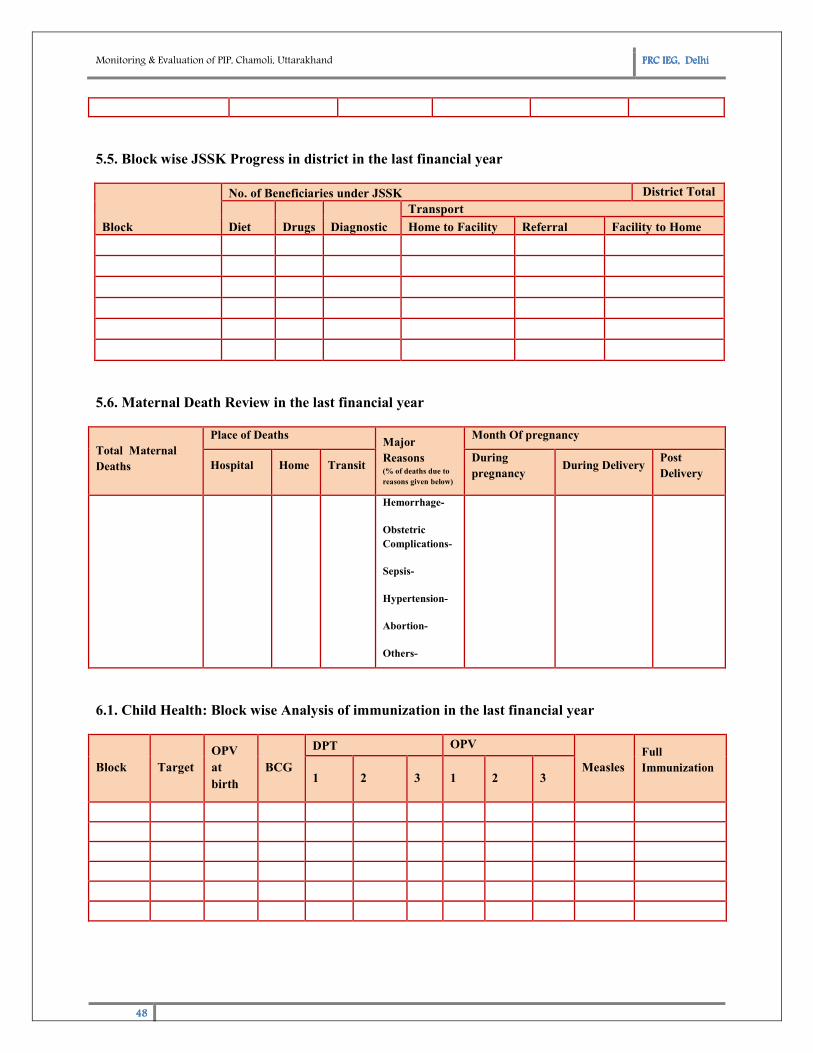
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
48484848
5.5. Block wise JSSK Progress in district in the last financial year
Block
No. of Beneficiaries under JSSK District Total
=
Diet Drugs Diagnostic
Transport
Home to Facility Referral Facility to Home
5.6. Maternal Death Review in the last financial year
Total Maternal
Deaths
Place of Deaths Major
Reasons (% of deaths due to
reasons given below)
Month Of pregnancy
Hospital Home Transit During
pregnancy During Delivery
Post
Delivery
Hemorrhage-
Obstetric
Complications-
Sepsis-
Hypertension-
Abortion-
Others-
6.1. Child Health: Block wise Analysis of immunization in the last financial year
Block Target
OPV
at
birth
BCG
DPT OPV
Measles
Full
Immunization
1 2 3 1 2 3
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
49494949
6.2. Child Health: Detail of infrastructure & Services under Neonatal Health, in the last financial
year
Numbers whether established in last financial year (Yes/No)
Total SNCU
Total NBSU
Total NBCC
Total Staff in SNCU
Total Staff in NBSU
Total NRCs
Total Admissions in NRCs
Total Staff in NRCs
Average duration of stay in NRCs
6.4. Neonatal Health: (SNCU, NRCS & CDR) in the last financial year
Total Death
Place of Death Major Reasons for
death
(% of deaths due to reasons given
below) Hospital Home Transit
Prematurity-
Birth Asphyxia-
Diarrhea-
Sepsis-
Pneumonia-
Others-
6.5. Rashtriya Bal Suraksha Karyakram (RBSK), Progress Report in the last two financial years
Years No. of
Schools No. of children
registered
Children
Diagnosed
No. of
Children
referred
Eye
Disease
Ear
Disease
Heart
disease
Physically
challenged Anemic
2017-18
2016-17
7. Family Planning Achievement in District in the last financial year
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
50505050
Block
Sterilization IUCD insertions Oral Pills Emergency
Contraceptives Condoms
T M F T A T A T A T A
T-Target, A-Achievement, M-Male, F-Female
8. ARSH/RKSK Progress in District in the last financial year
Block
No. of
Counseling
session held
conducted
No. of Adolescents
who attended the
Counseling sessions
No of Anemic Adolescents IFA tablets
given
No. of
RTI/STI cases Severe
Anemia
Any
Anemic
9. Quality in health care services
Bio-Medical Waste Management DH CHC PHC
No of facilities having bio-medical pits
No. of facilities having color coded bins
Outsourcing for bio-medical waste
If yes, name company
How many pits have been filled
Number of new pits required
Infection Control
No. of times fumigation is conducted in a year
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
51515151
Training of staff on infection control
10. Community process in District in the last financial year
Last status of ASHAs (Total number of ASHAs)
ASHAs presently working
Positions vacant
Total number of meeting with ASHA ( in a Year)
Total number of ASHA resource centers/ ASHA Ghar
Drug kit replenishment
No. of ASHAs trained in last year
Name of trainings received
1)
2)
3)
11.2 Disease control programme progress District (Non-Communicable Diseases)
Name of the
Programme/ Disease
2015-16 2016-17 2017-18
No. of cases
screened
No. of
detected
cases
No. of cases
screened
No. of detected
cases
No. of cases
screened
No. of detected
cases
Diabetes
Hypertension
Osteoporosis
Heart Disease
Others, if any
12. AYUSH progress District in the last financial year
Block No. of facilities with AYUSH No. of AYUSH Doctors No. of patients received treatment
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
52525252
health centers
13. Budget Utilisation Parameters:
Sl. no Scheme/Programme
Funds
Sanctioned Utilized
13.1 RCH Flexible Pool
13.2 NHM Flexible Pool
13.3 Immunization cost
13.4 NIDDCP
13.5 NUHM
13.6 Communicable disease Control Programmes
13.7 Non Communicable disease Control Programmes
13.8 Infrastructure Maintenance
14. HMIS/MCTS progress District in the last financial year
HMIS/MCTS Remarks
Is HMIS implemented at all the facilities Yes No
Is MCTS implemented at all the facilities Yes No
Is HMIS data analyzed and discussed with concerned staff at state and
district levels for necessary corrective action to be taken in future? Yes No
Do programme managers at all levels use HMIS data for monthly
reviews? Yes No
Is MCTS made fully operational for regular and effective monitoring
of service delivery including tracking and monitoring of severely
anemic women, low birth weight babies and sick neonates
Yes No
Is the service delivery data uploaded regularly Yes No
Is the MCTS call centre set up at the District level to check the
veracity of data and service delivery? Yes No
Is HMIS data analyzed and discussed with concerned staff at state Yes No
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
53535353
and district levels for necessary corrective action to be taken in future?
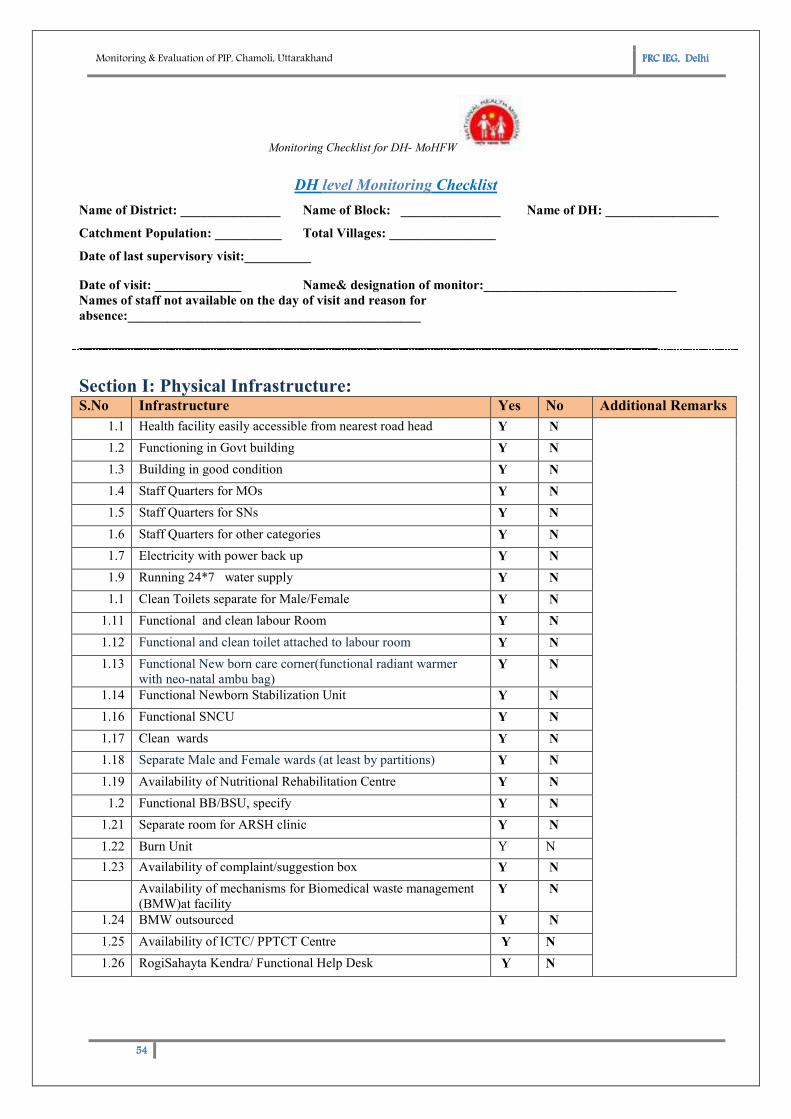
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
54545454
Monitoring Checklist for DH- MoHFW
DH level Monitoring Checklist
Name of District: _______________ Name of Block: _______________ Name of DH: _________________
Catchment Population: __________ Total Villages: ________________
Date of last supervisory visit:__________
Date of visit: _____________ Name& designation of monitor:_____________________________
Names of staff not available on the day of visit and reason for
absence:____________________________________________
_______________________________________________________________________________________
Section I: Physical Infrastructure: S.No Infrastructure Yes No Additional Remarks
1.1 Health facility easily accessible from nearest road head Y N
1.2 Functioning in Govt building Y N
1.3 Building in good condition Y N
1.4 Staff Quarters for MOs Y N
1.5 Staff Quarters for SNs Y N
1.6 Staff Quarters for other categories Y N
1.7 Electricity with power back up Y N
1.9 Running 24*7 water supply Y N
1.1 Clean Toilets separate for Male/Female Y N
1.11 Functional and clean labour Room Y N
1.12 Functional and clean toilet attached to labour room Y N
1.13 Functional New born care corner(functional radiant warmer
with neo-natal ambu bag) Y N
1.14 Functional Newborn Stabilization Unit Y N
1.16 Functional SNCU Y N
1.17 Clean wards Y N
1.18 Separate Male and Female wards (at least by partitions) Y N
1.19 Availability of Nutritional Rehabilitation Centre Y N
1.2 Functional BB/BSU, specify Y N
1.21 Separate room for ARSH clinic Y N
1.22 Burn Unit Y N
1.23 Availability of complaint/suggestion box Y N
Availability of mechanisms for Biomedical waste management
(BMW)at facility Y N
1.24 BMW outsourced Y N
1.25 Availability of ICTC/ PPTCT Centre Y N
1.26 RogiSahayta Kendra/ Functional Help Desk Y N
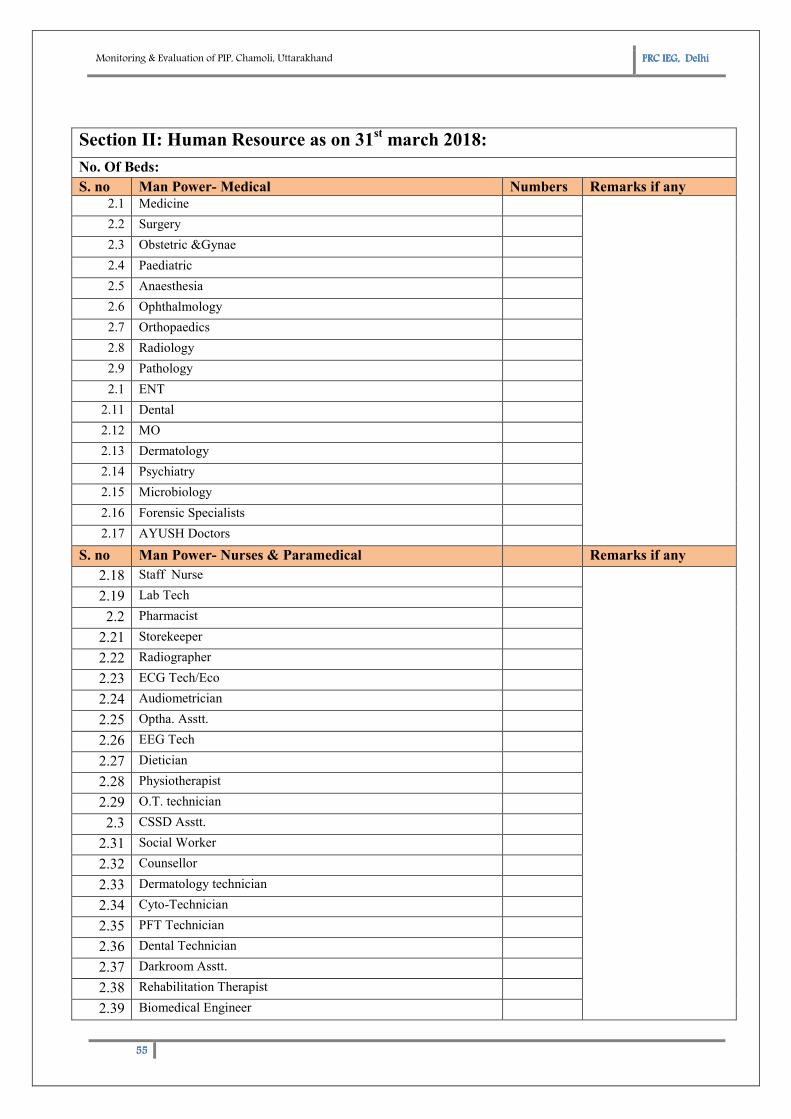
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
55555555
Section II: Human Resource as on 31st march 2018:
No. Of Beds:
S. no Man Power- Medical Numbers Remarks if any 2.1 Medicine
2.2 Surgery
2.3 Obstetric &Gynae
2.4 Paediatric
2.5 Anaesthesia
2.6 Ophthalmology
2.7 Orthopaedics
2.8 Radiology
2.9 Pathology
2.1 ENT
2.11 Dental
2.12 MO
2.13 Dermatology
2.14 Psychiatry
2.15 Microbiology
2.16 Forensic Specialists
2.17 AYUSH Doctors
S. no Man Power- Nurses & Paramedical Remarks if any
2.18 Staff Nurse
2.19 Lab Tech
2.2 Pharmacist
2.21 Storekeeper
2.22 Radiographer
2.23 ECG Tech/Eco
2.24 Audiometrician
2.25 Optha. Asstt.
2.26 EEG Tech
2.27 Dietician
2.28 Physiotherapist
2.29 O.T. technician
2.3 CSSD Asstt.
2.31 Social Worker
2.32 Counsellor
2.33 Dermatology technician
2.34 Cyto-Technician
2.35 PFT Technician
2.36 Dental Technician
2.37 Darkroom Asstt.
2.38 Rehabilitation Therapist
2.39 Biomedical Engineer
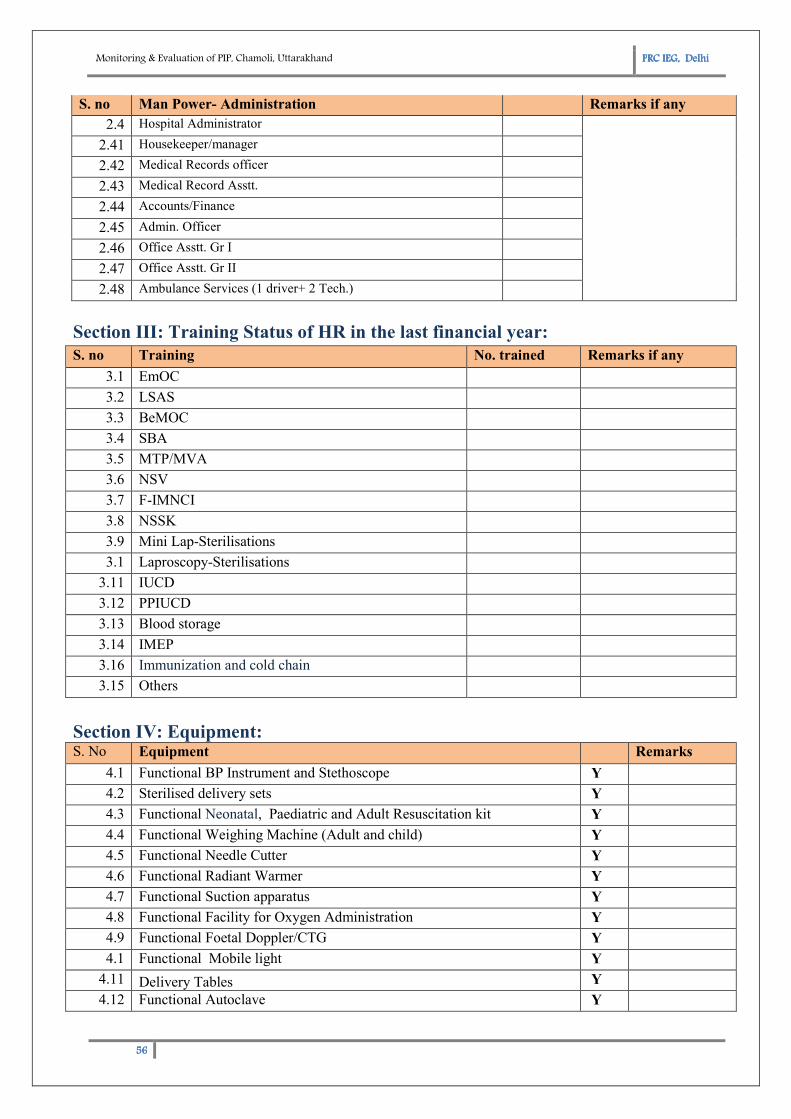
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
56565656
S. no Man Power- Administration Remarks if any
2.4 Hospital Administrator
2.41 Housekeeper/manager
2.42 Medical Records officer
2.43 Medical Record Asstt.
2.44 Accounts/Finance
2.45 Admin. Officer
2.46 Office Asstt. Gr I
2.47 Office Asstt. Gr II
2.48 Ambulance Services (1 driver+ 2 Tech.)
Section III: Training Status of HR in the last financial year:
S. no Training No. trained Remarks if any
3.1 EmOC
3.2 LSAS
3.3 BeMOC
3.4 SBA
3.5 MTP/MVA
3.6 NSV
3.7 F-IMNCI
3.8 NSSK
3.9 Mini Lap-Sterilisations
3.1 Laproscopy-Sterilisations
3.11 IUCD
3.12 PPIUCD
3.13 Blood storage
3.14 IMEP
3.16 Immunization and cold chain
3.15 Others
Section IV: Equipment: S. No Equipment Remarks
4.1 Functional BP Instrument and Stethoscope Y
4.2 Sterilised delivery sets Y
4.3 Functional Neonatal, Paediatric and Adult Resuscitation kit Y
4.4 Functional Weighing Machine (Adult and child) Y
4.5 Functional Needle Cutter Y
4.6 Functional Radiant Warmer Y
4.7 Functional Suction apparatus Y
4.8 Functional Facility for Oxygen Administration Y
4.9 Functional Foetal Doppler/CTG Y
4.1 Functional Mobile light Y
4.11 Delivery Tables Y
4.12 Functional Autoclave Y
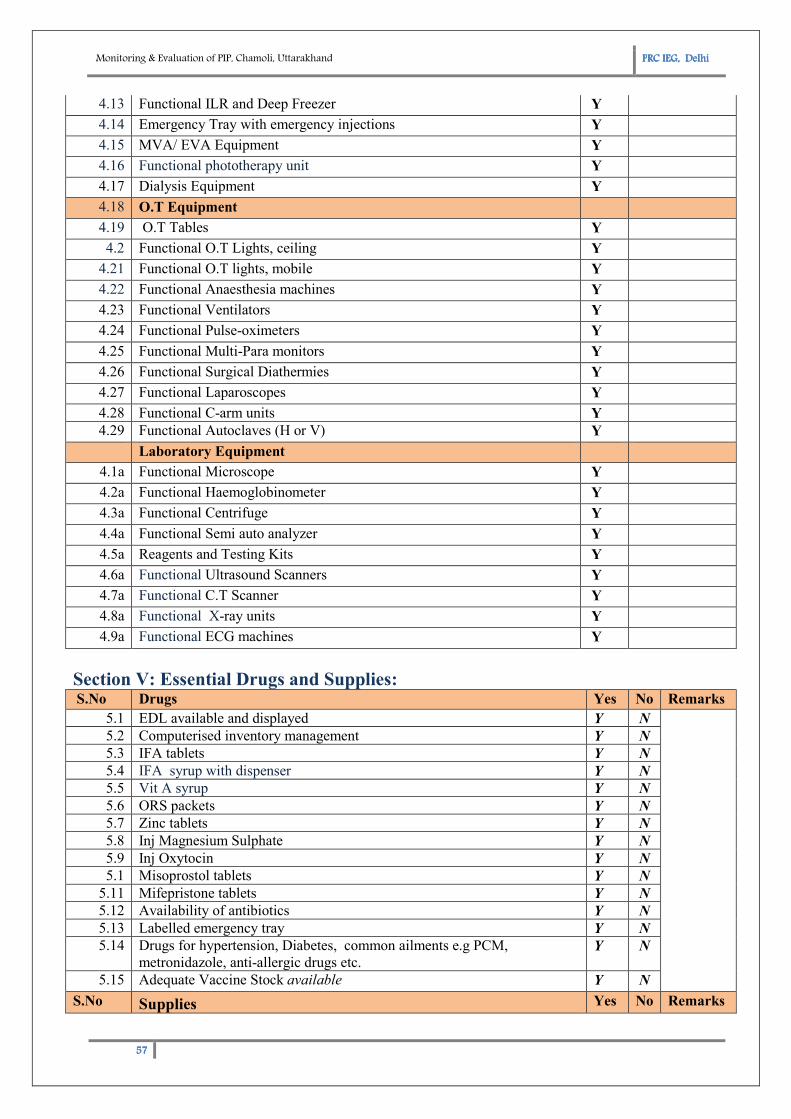
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
57575757
4.13 Functional ILR and Deep Freezer Y
4.14 Emergency Tray with emergency injections Y
4.15 MVA/ EVA Equipment Y
4.16 Functional phototherapy unit Y
4.17 Dialysis Equipment Y
4.18 O.T Equipment
4.19 O.T Tables Y
4.2 Functional O.T Lights, ceiling Y
4.21 Functional O.T lights, mobile Y
4.22 Functional Anaesthesia machines Y
4.23 Functional Ventilators Y
4.24 Functional Pulse-oximeters Y
4.25 Functional Multi-Para monitors Y
4.26 Functional Surgical Diathermies Y
4.27 Functional Laparoscopes Y
4.28 Functional C-arm units Y
4.29 Functional Autoclaves (H or V) Y
Laboratory Equipment
4.1a Functional Microscope Y
4.2a Functional Haemoglobinometer Y
4.3a Functional Centrifuge Y
4.4a Functional Semi auto analyzer Y
4.5a Reagents and Testing Kits Y
4.6a Functional Ultrasound Scanners Y
4.7a Functional C.T Scanner Y
4.8a Functional X-ray units Y
4.9a Functional ECG machines Y
Section V: Essential Drugs and Supplies: S.No Drugs Yes No Remarks
5.1 EDL available and displayed Y N
5.2 Computerised inventory management Y N
5.3 IFA tablets Y N
5.4 IFA syrup with dispenser Y N
5.5 Vit A syrup Y N
5.6 ORS packets Y N
5.7 Zinc tablets Y N
5.8 Inj Magnesium Sulphate Y N
5.9 Inj Oxytocin Y N
5.1 Misoprostol tablets Y N
5.11 Mifepristone tablets Y N
5.12 Availability of antibiotics Y N
5.13 Labelled emergency tray Y N
5.14 Drugs for hypertension, Diabetes, common ailments e.g PCM,
metronidazole, anti-allergic drugs etc. Y N
5.15 Adequate Vaccine Stock available Y N
S.No Supplies Yes No Remarks
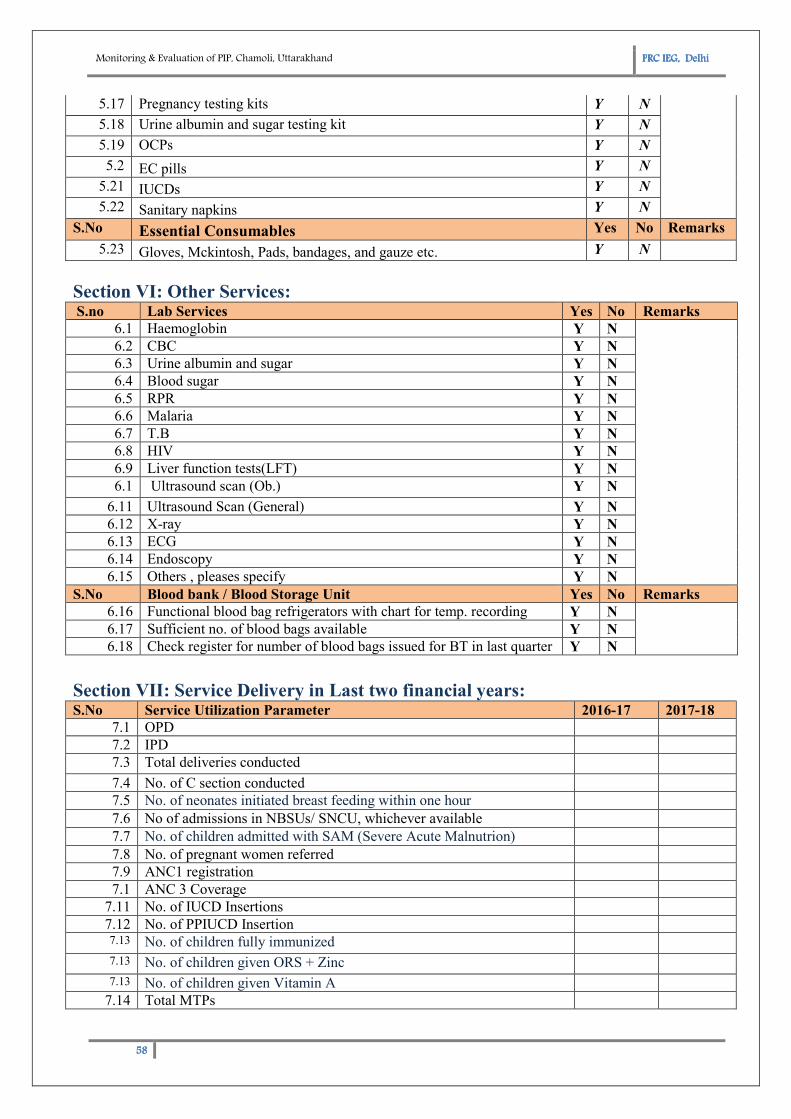
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
58585858
5.17 Pregnancy testing kits Y N
5.18 Urine albumin and sugar testing kit Y N
5.19 OCPs Y N
5.2 EC pills Y N
5.21 IUCDs Y N
5.22 Sanitary napkins Y N
S.No Essential Consumables Yes No Remarks
5.23 Gloves, Mckintosh, Pads, bandages, and gauze etc. Y N
Section VI: Other Services: S.no Lab Services Yes No Remarks
6.1 Haemoglobin Y N
6.2 CBC Y N
6.3 Urine albumin and sugar Y N
6.4 Blood sugar Y N
6.5 RPR Y N
6.6 Malaria Y N
6.7 T.B Y N
6.8 HIV Y N
6.9 Liver function tests(LFT) Y N
6.1 Ultrasound scan (Ob.) Y N
6.11 Ultrasound Scan (General) Y N
6.12 X-ray Y N
6.13 ECG Y N
6.14 Endoscopy Y N
6.15 Others , pleases specify Y N
S.No Blood bank / Blood Storage Unit Yes No Remarks
6.16 Functional blood bag refrigerators with chart for temp. recording Y N
6.17 Sufficient no. of blood bags available Y N
6.18 Check register for number of blood bags issued for BT in last quarter Y N
Section VII: Service Delivery in Last two financial years: S.No Service Utilization Parameter 2016-17 2017-18
7.1 OPD
7.2 IPD
7.3 Total deliveries conducted
7.4 No. of C section conducted
7.5 No. of neonates initiated breast feeding within one hour
7.6 No of admissions in NBSUs/ SNCU, whichever available
7.7 No. of children admitted with SAM (Severe Acute Malnutrion)
7.8 No. of pregnant women referred
7.9 ANC1 registration
7.1 ANC 3 Coverage
7.11 No. of IUCD Insertions
7.12 No. of PPIUCD Insertion 7.13 No. of children fully immunized
7.13 No. of children given ORS + Zinc
7.13 No. of children given Vitamin A
7.14 Total MTPs
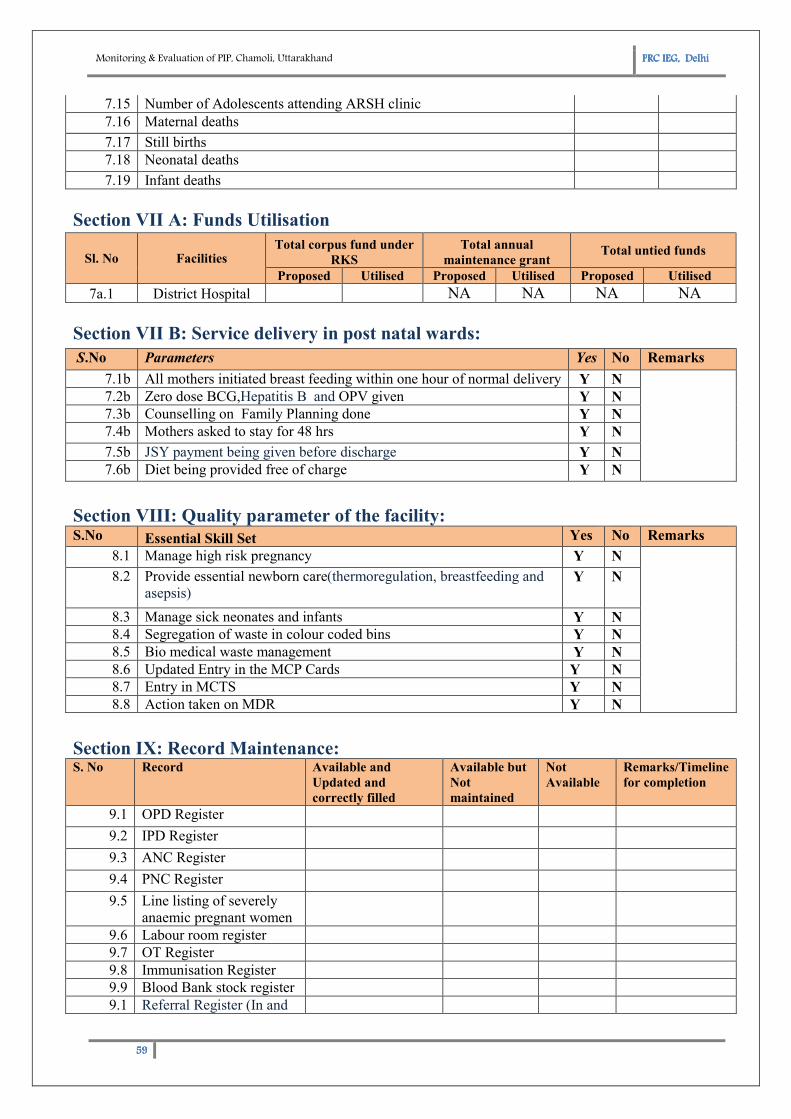
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
59595959
7.15 Number of Adolescents attending ARSH clinic
7.16 Maternal deaths
7.17 Still births
7.18 Neonatal deaths
7.19 Infant deaths
Section VII A: Funds Utilisation
Sl. No Facilities Total corpus fund under
RKS
Total annual
maintenance grant Total untied funds
Proposed Utilised Proposed Utilised Proposed Utilised
7a.1 District Hospital NA NA NA NA
Section VII B: Service delivery in post natal wards:
S.No Parameters Yes No Remarks
7.1b All mothers initiated breast feeding within one hour of normal delivery Y N
7.2b Zero dose BCG,Hepatitis B and OPV given Y N
7.3b Counselling on Family Planning done Y N
7.4b Mothers asked to stay for 48 hrs Y N
7.5b JSY payment being given before discharge Y N
7.6b Diet being provided free of charge Y N
Section VIII: Quality parameter of the facility: S.No Essential Skill Set Yes No Remarks
8.1 Manage high risk pregnancy Y N
8.2 Provide essential newborn care(thermoregulation, breastfeeding and
asepsis) Y N
8.3 Manage sick neonates and infants Y N
8.4 Segregation of waste in colour coded bins Y N
8.5 Bio medical waste management Y N
8.6 Updated Entry in the MCP Cards Y N
8.7 Entry in MCTS Y N
8.8 Action taken on MDR Y N
Section IX: Record Maintenance: S. No Record Available and
Updated and
correctly filled
Available but
Not
maintained
Not
Available
Remarks/Timeline
for completion
9.1 OPD Register
9.2 IPD Register
9.3 ANC Register
9.4 PNC Register
9.5 Line listing of severely
anaemic pregnant women
9.6 Labour room register
9.7 OT Register
9.8 Immunisation Register
9.9 Blood Bank stock register
9.1 Referral Register (In and
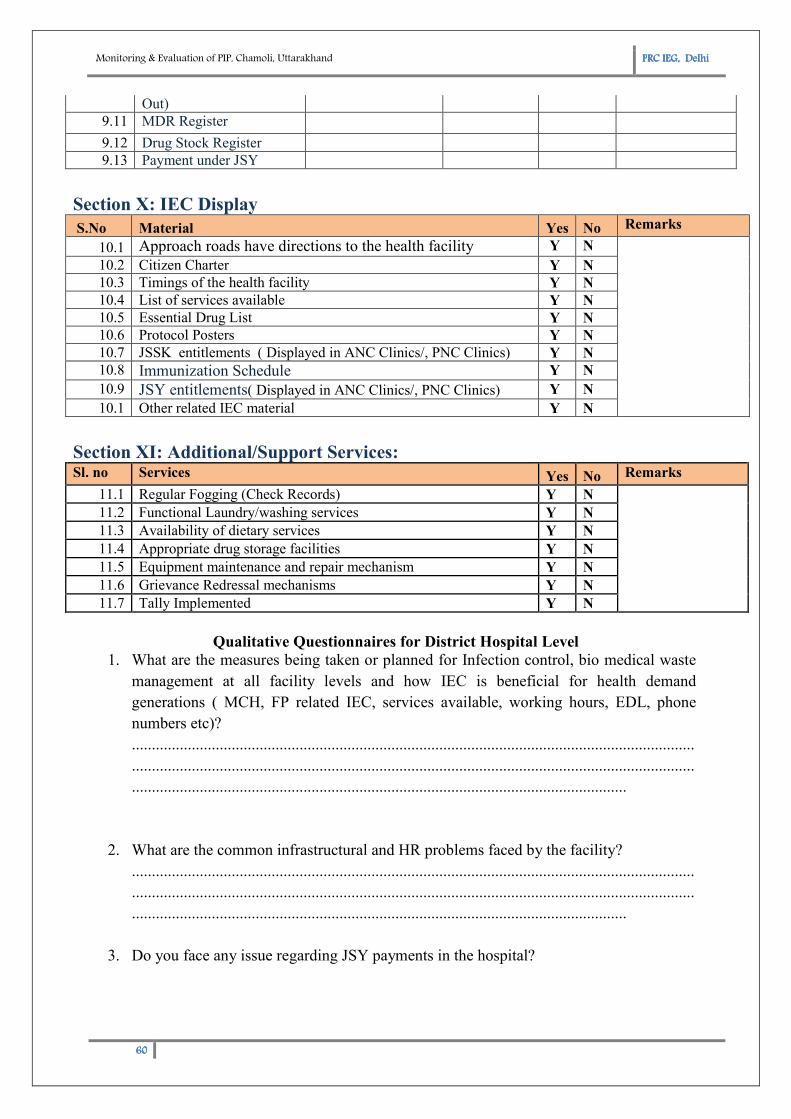
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
60606060
Out)
9.11 MDR Register
9.12 Drug Stock Register
9.13 Payment under JSY
Section X: IEC Display
S.No Material Yes No Remarks
10.1 Approach roads have directions to the health facility Y N
10.2 Citizen Charter Y N
10.3 Timings of the health facility Y N
10.4 List of services available Y N
10.5 Essential Drug List Y N
10.6 Protocol Posters Y N
10.7 JSSK entitlements ( Displayed in ANC Clinics/, PNC Clinics) Y N
10.8 Immunization Schedule Y N
10.9 JSY entitlements( Displayed in ANC Clinics/, PNC Clinics) Y N
10.1 Other related IEC material Y N
Section XI: Additional/Support Services: Sl. no Services Yes No Remarks
11.1 Regular Fogging (Check Records) Y N
11.2 Functional Laundry/washing services Y N
11.3 Availability of dietary services Y N
11.4 Appropriate drug storage facilities Y N
11.5 Equipment maintenance and repair mechanism Y N
11.6 Grievance Redressal mechanisms Y N
11.7 Tally Implemented Y N
Qualitative Questionnaires for District Hospital Level
1. What are the measures being taken or planned for Infection control, bio medical waste
management at all facility levels and how IEC is beneficial for health demand
generations ( MCH, FP related IEC, services available, working hours, EDL, phone
numbers etc)?
.............................................................................................................................................
.............................................................................................................................................
............................................................................................................................
2. What are the common infrastructural and HR problems faced by the facility?
.............................................................................................................................................
.............................................................................................................................................
............................................................................................................................
3. Do you face any issue regarding JSY payments in the hospital?
Monitoring & Evaluation of PIP, Chamoli, Uttarakhand PPPPRC IEG, RC IEG, RC IEG, RC IEG, DelhiDelhiDelhiDelhi
61616161
.............................................................................................................................................
.............................................................................................................................................
............................................................................................................................
4. What is the average delivery load in your facility? Are there any higher referral centres
where patients are being referred?
.............................................................................................................................................
.............................................................................................................................................
............................................................................................................................
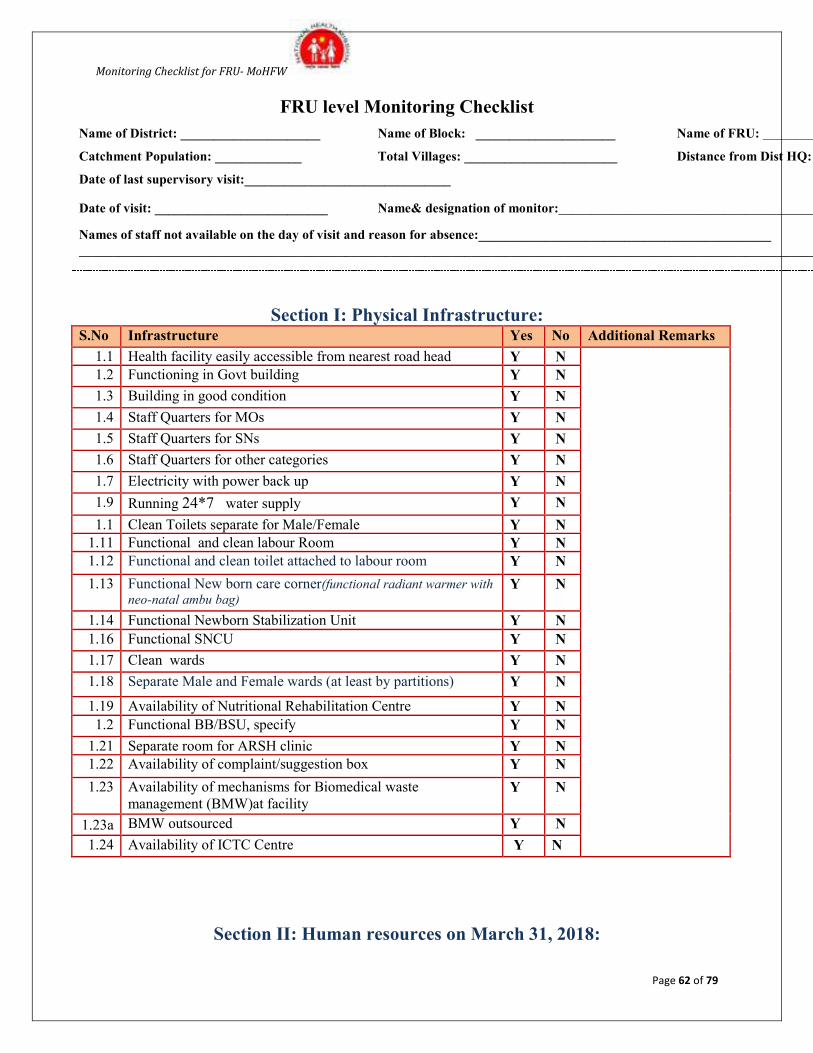
Monitoring Checklist for FRU- MoHFW
Page 62 of 79
FRU level Monitoring Checklist
Name of District: _____________________ Name of Block: _____________________ Name of FRU: ______________________
Catchment Population: _____________ Total Villages: _______________________ Distance from Dist HQ: __________
Date of last supervisory visit:_______________________________
Date of visit: __________________________ Name& designation of monitor:_____________________________________________
Names of staff not available on the day of visit and reason for absence:____________________________________________
_____________________________________________________________________________________________________________________________
Section I: Physical Infrastructure: S.No Infrastructure Yes No Additional Remarks
1.1 Health facility easily accessible from nearest road head Y N
1.2 Functioning in Govt building Y N
1.3 Building in good condition Y N
1.4 Staff Quarters for MOs Y N
1.5 Staff Quarters for SNs Y N
1.6 Staff Quarters for other categories Y N
1.7 Electricity with power back up Y N
1.9 Running 24*7 water supply Y N
1.1 Clean Toilets separate for Male/Female Y N
1.11 Functional and clean labour Room Y N
1.12 Functional and clean toilet attached to labour room Y N
1.13 Functional New born care corner(functional radiant warmer with
neo-natal ambu bag) Y N
1.14 Functional Newborn Stabilization Unit Y N
1.16 Functional SNCU Y N
1.17 Clean wards Y N
1.18 Separate Male and Female wards (at least by partitions) Y N
1.19 Availability of Nutritional Rehabilitation Centre Y N
1.2 Functional BB/BSU, specify Y N
1.21 Separate room for ARSH clinic Y N
1.22 Availability of complaint/suggestion box Y N
1.23 Availability of mechanisms for Biomedical waste
management (BMW)at facility Y N
1.23a BMW outsourced Y N
1.24 Availability of ICTC Centre Y N
Section II: Human resources on March 31, 2018:
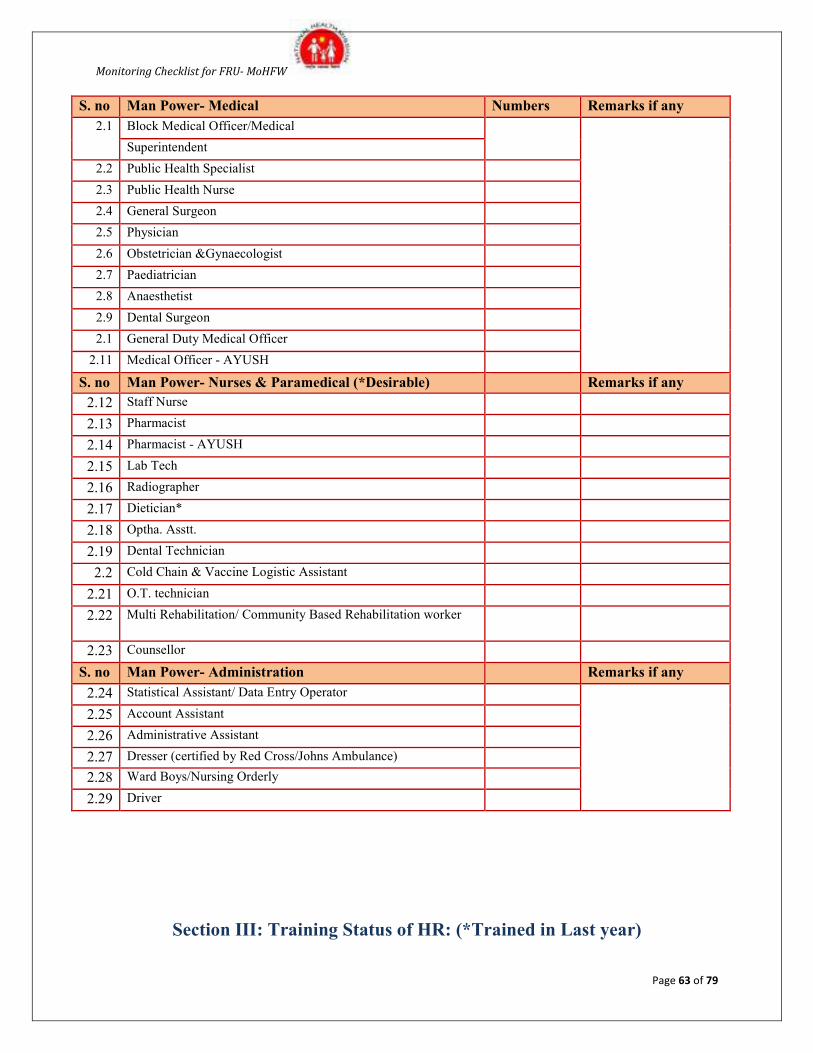
Monitoring Checklist for FRU- MoHFW
Page 63 of 79
S. no Man Power- Medical Numbers Remarks if any
2.1 Block Medical Officer/Medical
Superintendent
2.2 Public Health Specialist
2.3 Public Health Nurse
2.4 General Surgeon
2.5 Physician
2.6 Obstetrician &Gynaecologist
2.7 Paediatrician
2.8 Anaesthetist
2.9 Dental Surgeon
2.1 General Duty Medical Officer
2.11 Medical Officer - AYUSH
S. no Man Power- Nurses & Paramedical (*Desirable) Remarks if any
2.12 Staff Nurse
2.13 Pharmacist
2.14 Pharmacist - AYUSH
2.15 Lab Tech
2.16 Radiographer
2.17 Dietician*
2.18 Optha. Asstt.
2.19 Dental Technician
2.2 Cold Chain & Vaccine Logistic Assistant
2.21 O.T. technician
2.22 Multi Rehabilitation/ Community Based Rehabilitation worker
2.23 Counsellor
S. no Man Power- Administration Remarks if any
2.24 Statistical Assistant/ Data Entry Operator
2.25 Account Assistant
2.26 Administrative Assistant
2.27 Dresser (certified by Red Cross/Johns Ambulance)
2.28 Ward Boys/Nursing Orderly
2.29 Driver
Section III: Training Status of HR: (*Trained in Last year)
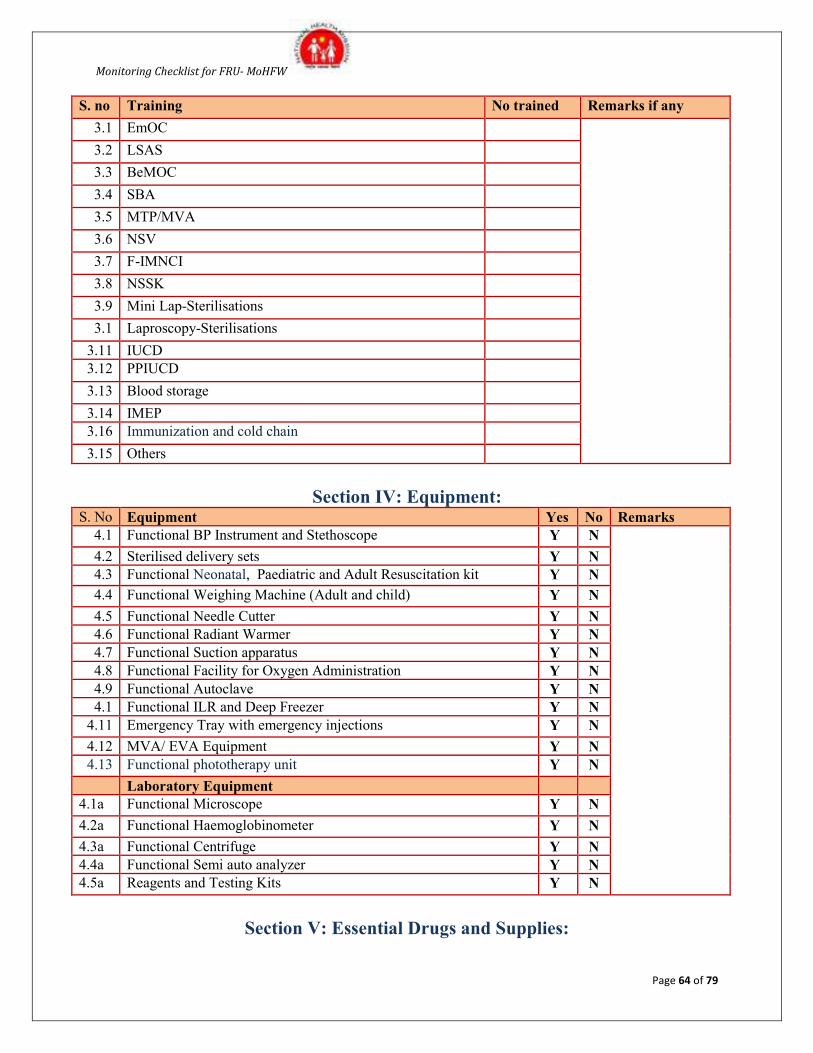
Monitoring Checklist for FRU- MoHFW
Page 64 of 79
S. no Training No trained Remarks if any
3.1 EmOC
3.2 LSAS
3.3 BeMOC
3.4 SBA
3.5 MTP/MVA
3.6 NSV
3.7 F-IMNCI
3.8 NSSK
3.9 Mini Lap-Sterilisations
3.1 Laproscopy-Sterilisations
3.11 IUCD
3.12 PPIUCD
3.13 Blood storage
3.14 IMEP
3.16 Immunization and cold chain
3.15 Others
Section IV: Equipment: S. No Equipment Yes No Remarks
4.1 Functional BP Instrument and Stethoscope Y N
4.2 Sterilised delivery sets Y N
4.3 Functional Neonatal, Paediatric and Adult Resuscitation kit Y N
4.4 Functional Weighing Machine (Adult and child) Y N
4.5 Functional Needle Cutter Y N
4.6 Functional Radiant Warmer Y N
4.7 Functional Suction apparatus Y N
4.8 Functional Facility for Oxygen Administration Y N
4.9 Functional Autoclave Y N
4.1 Functional ILR and Deep Freezer Y N
4.11 Emergency Tray with emergency injections Y N
4.12 MVA/ EVA Equipment Y N
4.13 Functional phototherapy unit Y N
Laboratory Equipment
4.1a Functional Microscope Y N
4.2a Functional Haemoglobinometer Y N
4.3a Functional Centrifuge Y N
4.4a Functional Semi auto analyzer Y N
4.5a Reagents and Testing Kits Y N
Section V: Essential Drugs and Supplies:
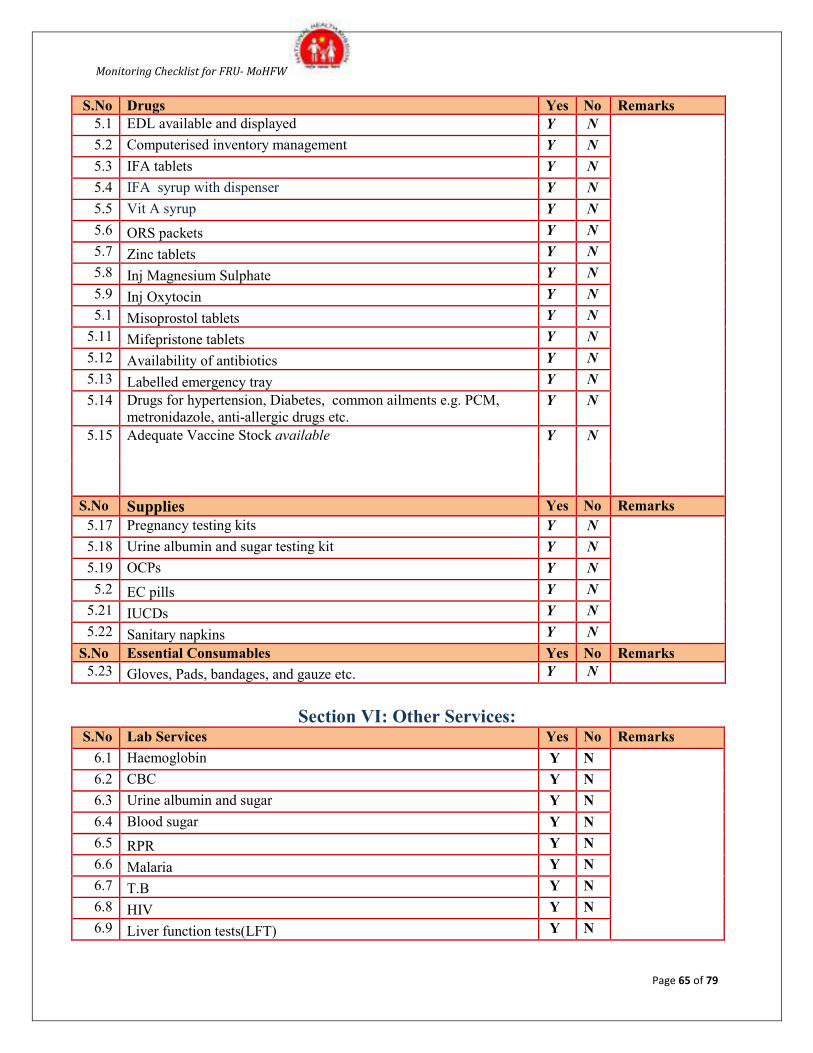
Monitoring Checklist for FRU- MoHFW
Page 65 of 79
S.No Drugs Yes No Remarks
5.1 EDL available and displayed Y N
5.2 Computerised inventory management Y N
5.3 IFA tablets Y N
5.4 IFA syrup with dispenser Y N
5.5 Vit A syrup Y N
5.6 ORS packets Y N
5.7 Zinc tablets Y N
5.8 Inj Magnesium Sulphate Y N
5.9 Inj Oxytocin Y N
5.1 Misoprostol tablets Y N
5.11 Mifepristone tablets Y N
5.12 Availability of antibiotics Y N
5.13 Labelled emergency tray Y N
5.14 Drugs for hypertension, Diabetes, common ailments e.g. PCM,
metronidazole, anti-allergic drugs etc. Y N
5.15 Adequate Vaccine Stock available Y N
S.No Supplies Yes No Remarks
5.17 Pregnancy testing kits Y N
5.18 Urine albumin and sugar testing kit Y N
5.19 OCPs Y N
5.2 EC pills Y N
5.21 IUCDs Y N
5.22 Sanitary napkins Y N
S.No Essential Consumables Yes No Remarks
5.23 Gloves, Pads, bandages, and gauze etc. Y N
Section VI: Other Services: S.No Lab Services Yes No Remarks
6.1 Haemoglobin Y N
6.2 CBC Y N
6.3 Urine albumin and sugar Y N
6.4 Blood sugar Y N
6.5 RPR Y N
6.6 Malaria Y N
6.7 T.B Y N
6.8 HIV Y N
6.9 Liver function tests(LFT) Y N
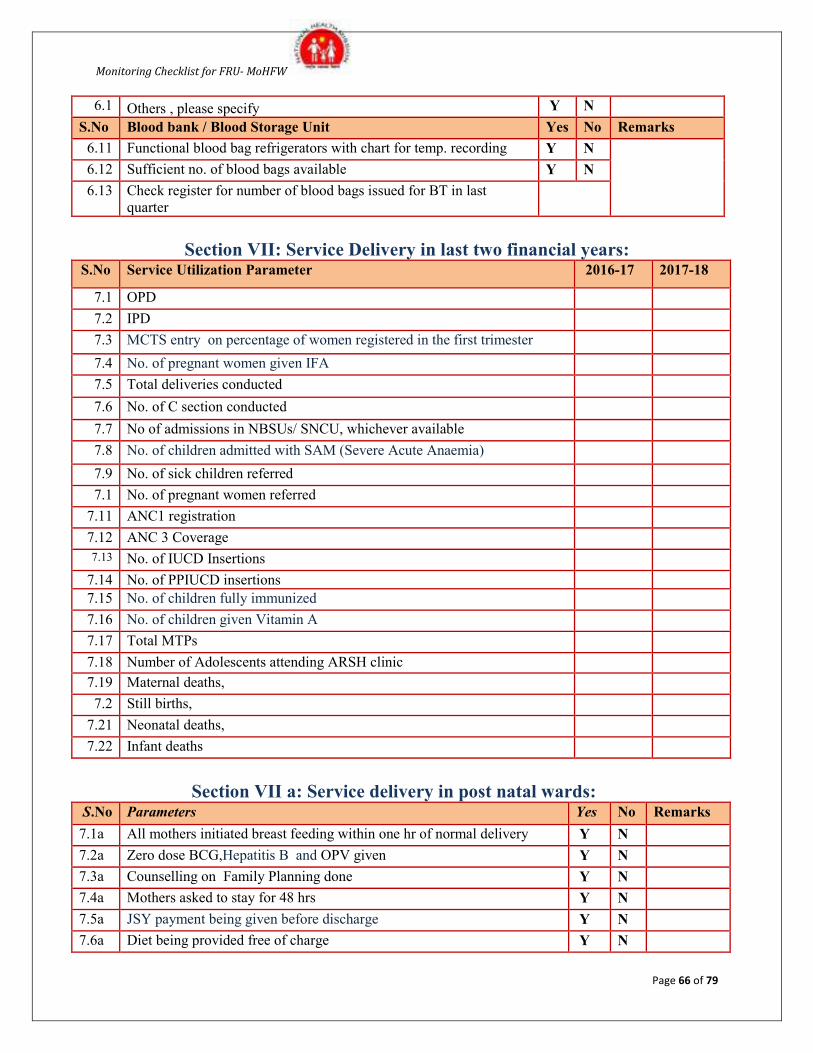
Monitoring Checklist for FRU- MoHFW
Page 66 of 79
6.1 Others , please specify Y N
S.No Blood bank / Blood Storage Unit Yes No Remarks
6.11 Functional blood bag refrigerators with chart for temp. recording Y N
6.12 Sufficient no. of blood bags available Y N
6.13 Check register for number of blood bags issued for BT in last
quarter
Section VII: Service Delivery in last two financial years: S.No Service Utilization Parameter 2016-17 2017-18
7.1 OPD
7.2 IPD
7.3 MCTS entry on percentage of women registered in the first trimester
7.4 No. of pregnant women given IFA
7.5 Total deliveries conducted
7.6 No. of C section conducted
7.7 No of admissions in NBSUs/ SNCU, whichever available
7.8 No. of children admitted with SAM (Severe Acute Anaemia)
7.9 No. of sick children referred
7.1 No. of pregnant women referred
7.11 ANC1 registration
7.12 ANC 3 Coverage
7.13 No. of IUCD Insertions
7.14 No. of PPIUCD insertions
7.15 No. of children fully immunized
7.16 No. of children given Vitamin A
7.17 Total MTPs
7.18 Number of Adolescents attending ARSH clinic
7.19 Maternal deaths,
7.2 Still births,
7.21 Neonatal deaths,
7.22 Infant deaths
Section VII a: Service delivery in post natal wards: S.No Parameters Yes No Remarks
7.1a All mothers initiated breast feeding within one hr of normal delivery Y N
7.2a Zero dose BCG,Hepatitis B and OPV given Y N
7.3a Counselling on Family Planning done Y N
7.4a Mothers asked to stay for 48 hrs Y N
7.5a JSY payment being given before discharge Y N
7.6a Diet being provided free of charge Y N
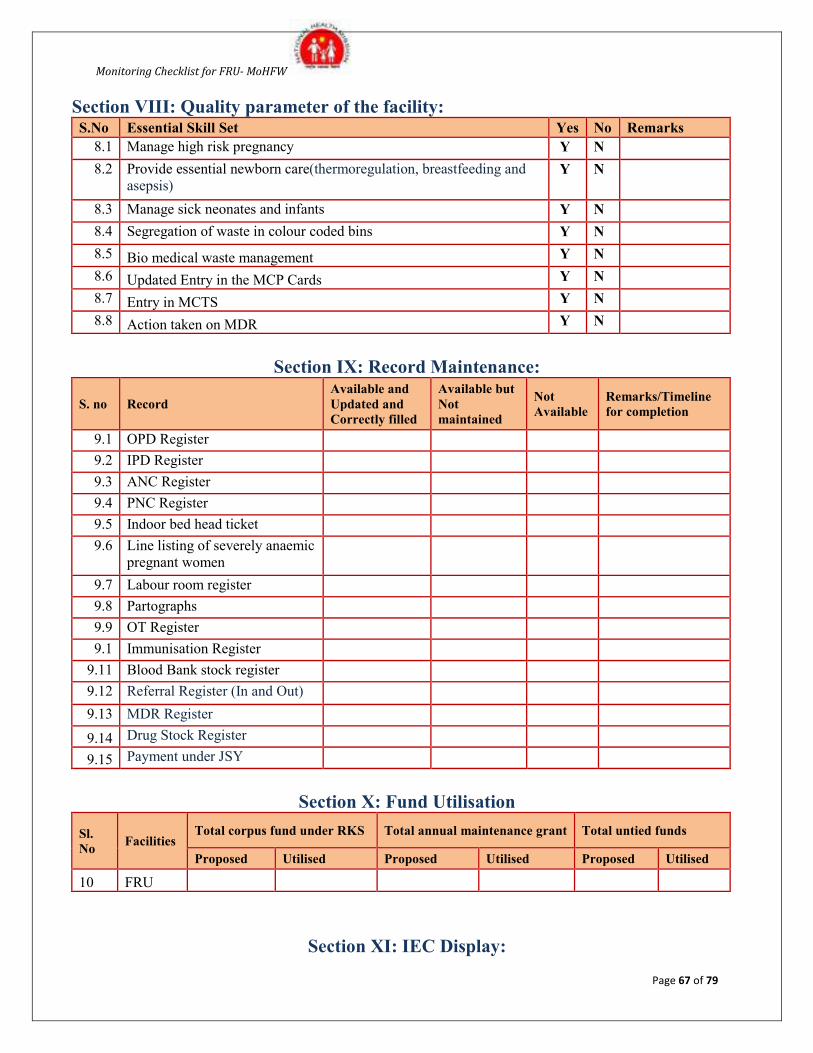
Monitoring Checklist for FRU- MoHFW
Page 67 of 79
Section VIII: Quality parameter of the facility: S.No Essential Skill Set Yes No Remarks
8.1 Manage high risk pregnancy Y N
8.2 Provide essential newborn care(thermoregulation, breastfeeding and
asepsis) Y N
8.3 Manage sick neonates and infants Y N
8.4 Segregation of waste in colour coded bins Y N
8.5 Bio medical waste management Y N
8.6 Updated Entry in the MCP Cards Y N
8.7 Entry in MCTS Y N
8.8 Action taken on MDR Y N
Section IX: Record Maintenance:
S. no Record
Available and
Updated and
Correctly filled
Available but
Not
maintained
Not
Available
Remarks/Timeline
for completion
9.1 OPD Register
9.2 IPD Register
9.3 ANC Register
9.4 PNC Register
9.5 Indoor bed head ticket
9.6 Line listing of severely anaemic
pregnant women
9.7 Labour room register
9.8 Partographs
9.9 OT Register
9.1 Immunisation Register
9.11 Blood Bank stock register
9.12 Referral Register (In and Out)
9.13 MDR Register
9.14 Drug Stock Register
9.15 Payment under JSY
Section X: Fund Utilisation
Sl.
No Facilities
Total corpus fund under RKS Total annual maintenance grant Total untied funds
Proposed Utilised Proposed Utilised Proposed Utilised
10 FRU
Section XI: IEC Display:
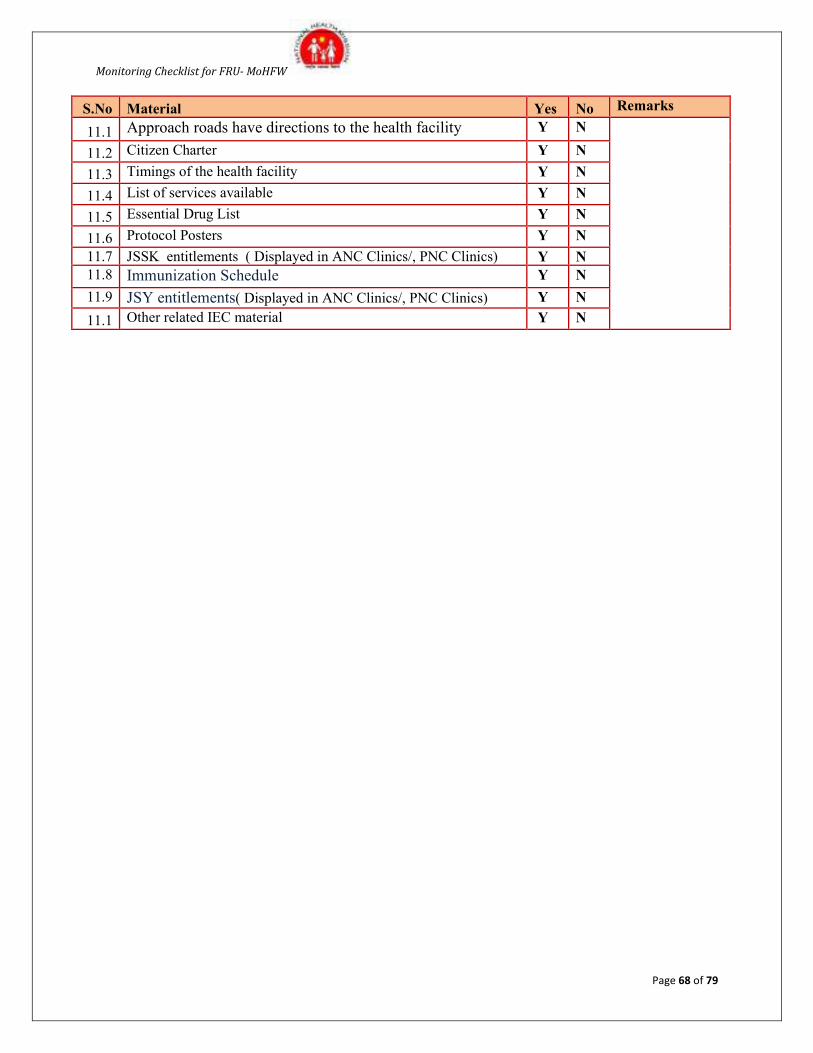
Monitoring Checklist for FRU- MoHFW
Page 68 of 79
S.No Material Yes No Remarks
11.1 Approach roads have directions to the health facility Y N
11.2 Citizen Charter Y N
11.3 Timings of the health facility Y N
11.4 List of services available Y N
11.5 Essential Drug List Y N
11.6 Protocol Posters Y N
11.7 JSSK entitlements ( Displayed in ANC Clinics/, PNC Clinics) Y N
11.8 Immunization Schedule Y N
11.9 JSY entitlements( Displayed in ANC Clinics/, PNC Clinics) Y N
11.1 Other related IEC material Y N
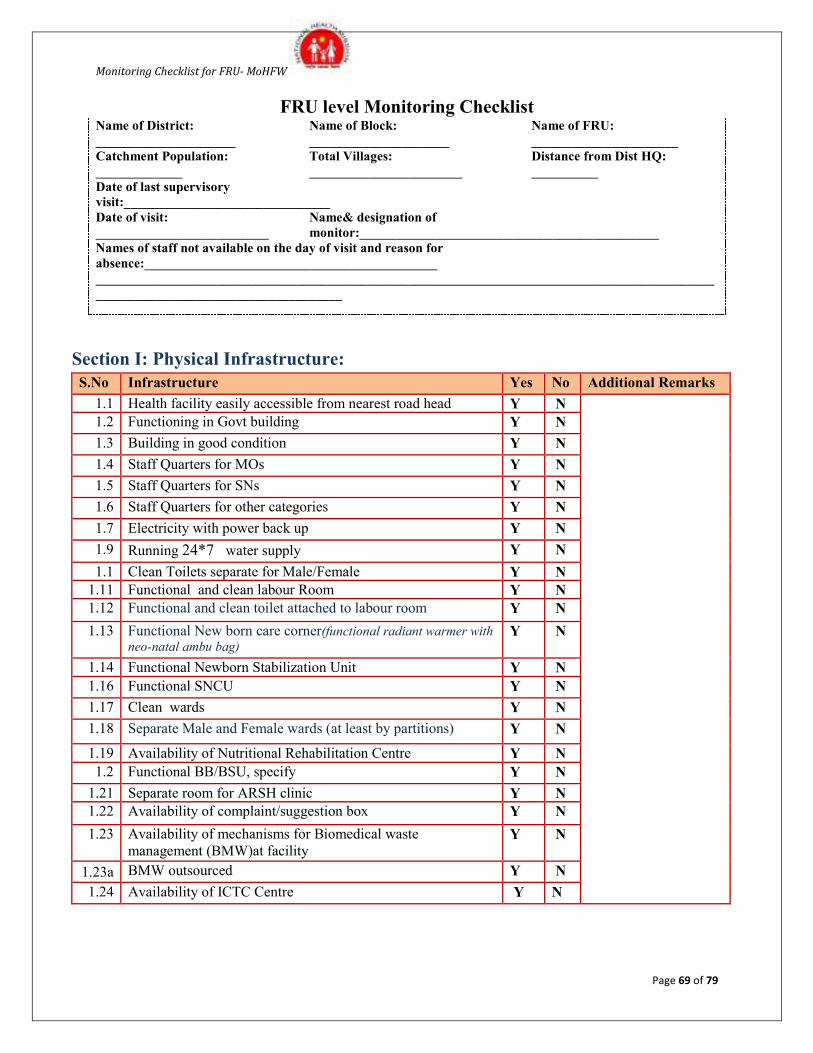
Monitoring Checklist for FRU- MoHFW
Page 69 of 79
FRU level Monitoring Checklist Name of District:
_____________________
Name of Block:
_____________________ Name of FRU:
______________________
Catchment Population:
_____________
Total Villages:
_______________________ Distance from Dist HQ:
__________
Date of last supervisory
visit:_______________________________ Date of visit:
__________________________
Name& designation of
monitor:_____________________________________________
Names of staff not available on the day of visit and reason for
absence:____________________________________________
_____________________________________________________________________________________________
_____________________________________
Section I: Physical Infrastructure:
S.No Infrastructure Yes No Additional Remarks
1.1 Health facility easily accessible from nearest road head Y N
1.2 Functioning in Govt building Y N
1.3 Building in good condition Y N
1.4 Staff Quarters for MOs Y N
1.5 Staff Quarters for SNs Y N
1.6 Staff Quarters for other categories Y N
1.7 Electricity with power back up Y N
1.9 Running 24*7 water supply Y N
1.1 Clean Toilets separate for Male/Female Y N
1.11 Functional and clean labour Room Y N
1.12 Functional and clean toilet attached to labour room Y N
1.13 Functional New born care corner(functional radiant warmer with
neo-natal ambu bag) Y N
1.14 Functional Newborn Stabilization Unit Y N
1.16 Functional SNCU Y N
1.17 Clean wards Y N
1.18 Separate Male and Female wards (at least by partitions) Y N
1.19 Availability of Nutritional Rehabilitation Centre Y N
1.2 Functional BB/BSU, specify Y N
1.21 Separate room for ARSH clinic Y N
1.22 Availability of complaint/suggestion box Y N
1.23 Availability of mechanisms for Biomedical waste
management (BMW)at facility Y N
1.23a BMW outsourced Y N
1.24 Availability of ICTC Centre Y N
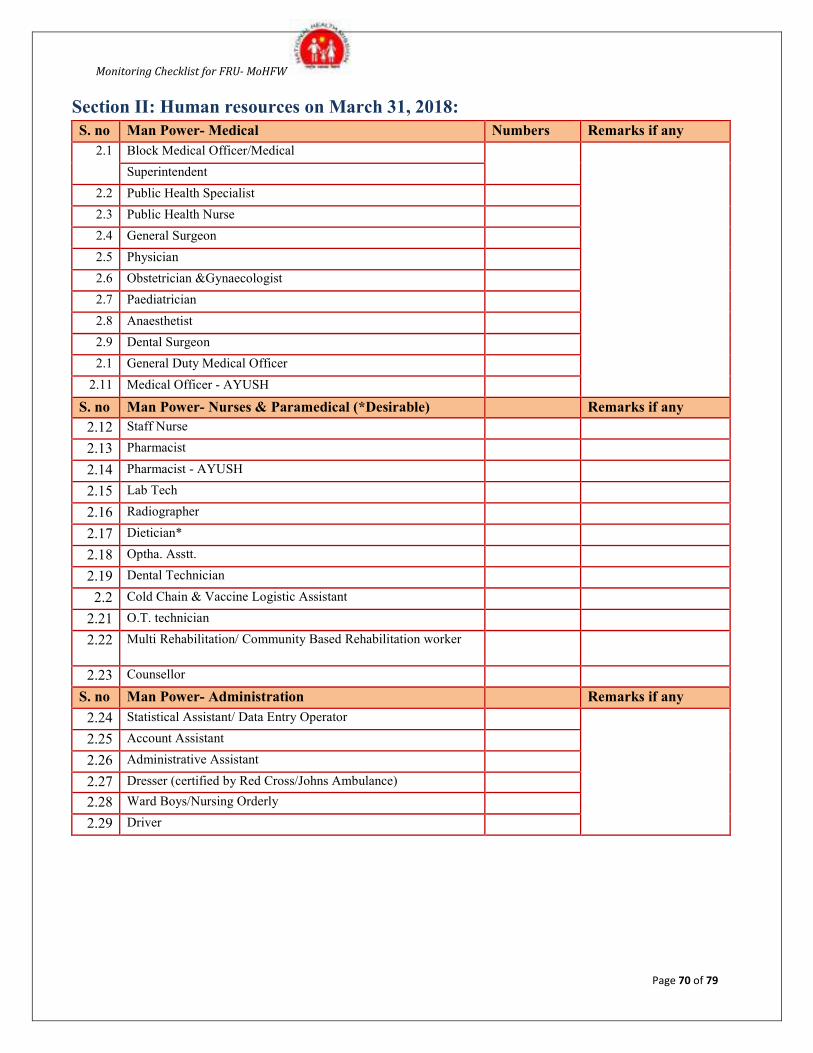
Monitoring Checklist for FRU- MoHFW
Page 70 of 79
Section II: Human resources on March 31, 2018:
S. no Man Power- Medical Numbers Remarks if any
2.1 Block Medical Officer/Medical
Superintendent
2.2 Public Health Specialist
2.3 Public Health Nurse
2.4 General Surgeon
2.5 Physician
2.6 Obstetrician &Gynaecologist
2.7 Paediatrician
2.8 Anaesthetist
2.9 Dental Surgeon
2.1 General Duty Medical Officer
2.11 Medical Officer - AYUSH
S. no Man Power- Nurses & Paramedical (*Desirable) Remarks if any
2.12 Staff Nurse
2.13 Pharmacist
2.14 Pharmacist - AYUSH
2.15 Lab Tech
2.16 Radiographer
2.17 Dietician*
2.18 Optha. Asstt.
2.19 Dental Technician
2.2 Cold Chain & Vaccine Logistic Assistant
2.21 O.T. technician
2.22 Multi Rehabilitation/ Community Based Rehabilitation worker
2.23 Counsellor
S. no Man Power- Administration Remarks if any
2.24 Statistical Assistant/ Data Entry Operator
2.25 Account Assistant
2.26 Administrative Assistant
2.27 Dresser (certified by Red Cross/Johns Ambulance)
2.28 Ward Boys/Nursing Orderly
2.29 Driver
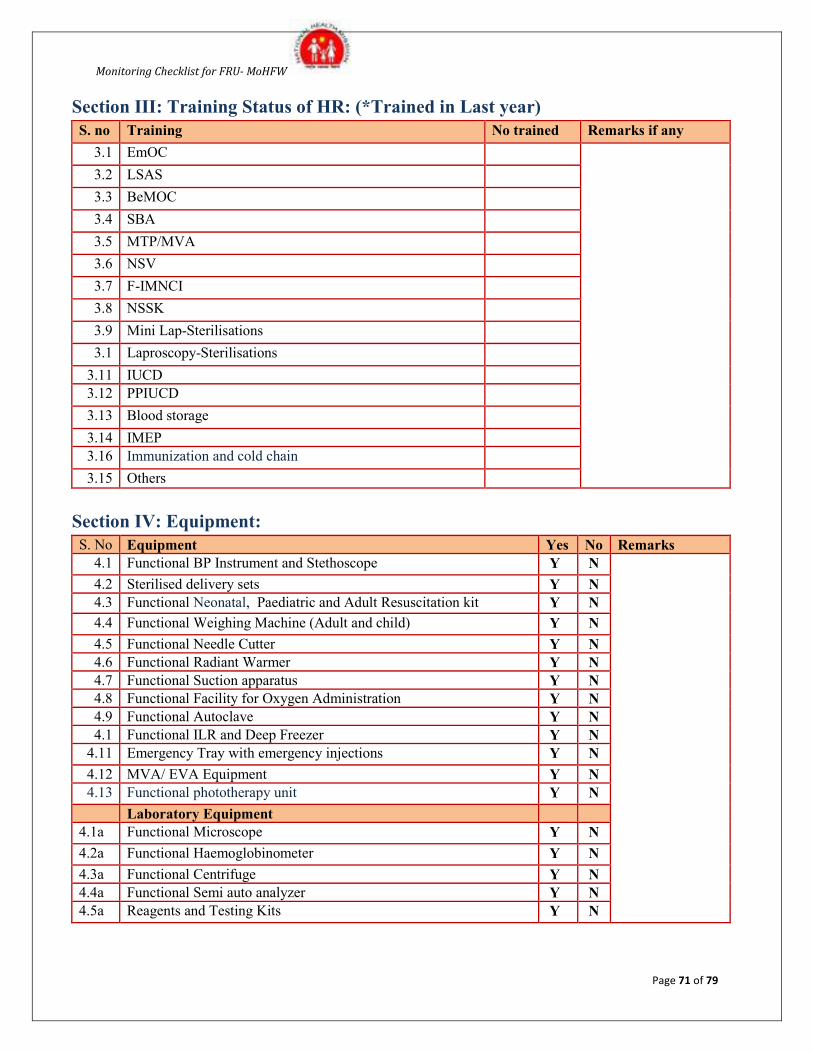
Monitoring Checklist for FRU- MoHFW
Page 71 of 79
Section III: Training Status of HR: (*Trained in Last year)
S. no Training No trained Remarks if any
3.1 EmOC
3.2 LSAS
3.3 BeMOC
3.4 SBA
3.5 MTP/MVA
3.6 NSV
3.7 F-IMNCI
3.8 NSSK
3.9 Mini Lap-Sterilisations
3.1 Laproscopy-Sterilisations
3.11 IUCD
3.12 PPIUCD
3.13 Blood storage
3.14 IMEP
3.16 Immunization and cold chain
3.15 Others
Section IV: Equipment:
S. No Equipment Yes No Remarks
4.1 Functional BP Instrument and Stethoscope Y N
4.2 Sterilised delivery sets Y N
4.3 Functional Neonatal, Paediatric and Adult Resuscitation kit Y N
4.4 Functional Weighing Machine (Adult and child) Y N
4.5 Functional Needle Cutter Y N
4.6 Functional Radiant Warmer Y N
4.7 Functional Suction apparatus Y N
4.8 Functional Facility for Oxygen Administration Y N
4.9 Functional Autoclave Y N
4.1 Functional ILR and Deep Freezer Y N
4.11 Emergency Tray with emergency injections Y N
4.12 MVA/ EVA Equipment Y N
4.13 Functional phototherapy unit Y N
Laboratory Equipment
4.1a Functional Microscope Y N
4.2a Functional Haemoglobinometer Y N
4.3a Functional Centrifuge Y N
4.4a Functional Semi auto analyzer Y N
4.5a Reagents and Testing Kits Y N
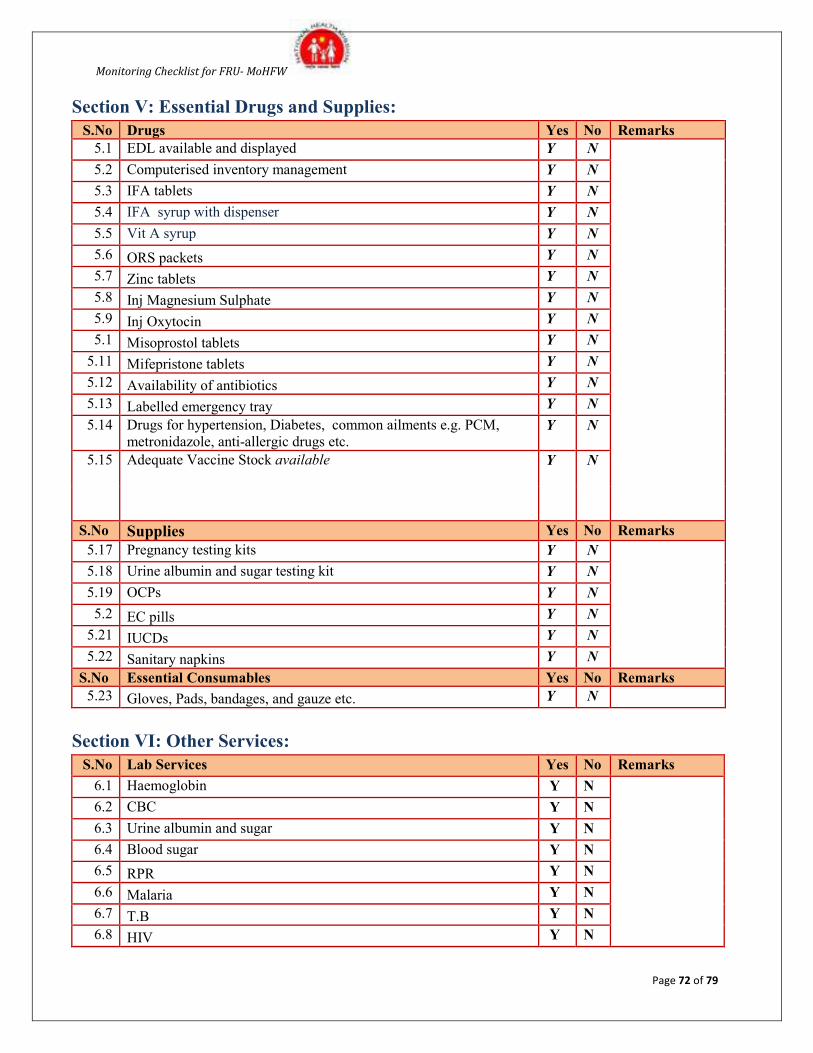
Monitoring Checklist for FRU- MoHFW
Page 72 of 79
Section V: Essential Drugs and Supplies:
S.No Drugs Yes No Remarks
5.1 EDL available and displayed Y N
5.2 Computerised inventory management Y N
5.3 IFA tablets Y N
5.4 IFA syrup with dispenser Y N
5.5 Vit A syrup Y N
5.6 ORS packets Y N
5.7 Zinc tablets Y N
5.8 Inj Magnesium Sulphate Y N
5.9 Inj Oxytocin Y N
5.1 Misoprostol tablets Y N
5.11 Mifepristone tablets Y N
5.12 Availability of antibiotics Y N
5.13 Labelled emergency tray Y N
5.14 Drugs for hypertension, Diabetes, common ailments e.g. PCM,
metronidazole, anti-allergic drugs etc. Y N
5.15 Adequate Vaccine Stock available Y N
S.No Supplies Yes No Remarks
5.17 Pregnancy testing kits Y N
5.18 Urine albumin and sugar testing kit Y N
5.19 OCPs Y N
5.2 EC pills Y N
5.21 IUCDs Y N
5.22 Sanitary napkins Y N
S.No Essential Consumables Yes No Remarks
5.23 Gloves, Pads, bandages, and gauze etc. Y N
Section VI: Other Services:
S.No Lab Services Yes No Remarks
6.1 Haemoglobin Y N
6.2 CBC Y N
6.3 Urine albumin and sugar Y N
6.4 Blood sugar Y N
6.5 RPR Y N
6.6 Malaria Y N
6.7 T.B Y N
6.8 HIV Y N
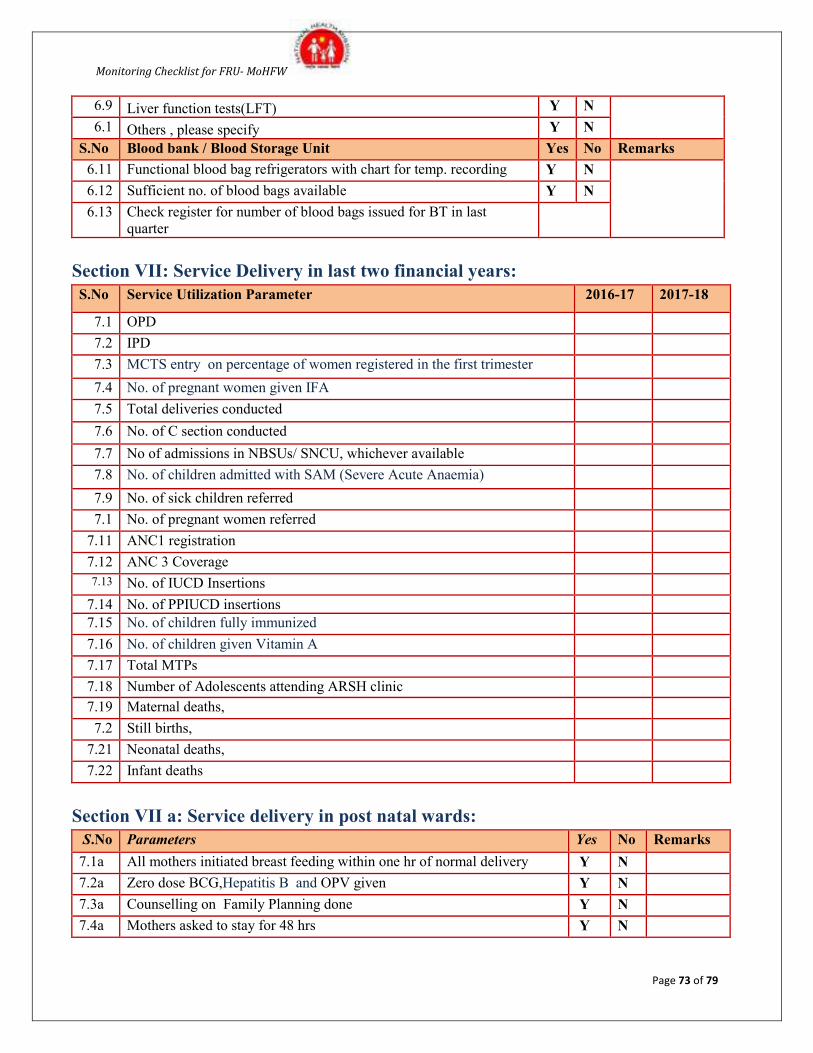
Monitoring Checklist for FRU- MoHFW
Page 73 of 79
6.9 Liver function tests(LFT) Y N
6.1 Others , please specify Y N
S.No Blood bank / Blood Storage Unit Yes No Remarks
6.11 Functional blood bag refrigerators with chart for temp. recording Y N
6.12 Sufficient no. of blood bags available Y N
6.13 Check register for number of blood bags issued for BT in last
quarter
Section VII: Service Delivery in last two financial years:
S.No Service Utilization Parameter 2016-17 2017-18
7.1 OPD
7.2 IPD
7.3 MCTS entry on percentage of women registered in the first trimester
7.4 No. of pregnant women given IFA
7.5 Total deliveries conducted
7.6 No. of C section conducted
7.7 No of admissions in NBSUs/ SNCU, whichever available
7.8 No. of children admitted with SAM (Severe Acute Anaemia)
7.9 No. of sick children referred
7.1 No. of pregnant women referred
7.11 ANC1 registration
7.12 ANC 3 Coverage
7.13 No. of IUCD Insertions
7.14 No. of PPIUCD insertions
7.15 No. of children fully immunized
7.16 No. of children given Vitamin A
7.17 Total MTPs
7.18 Number of Adolescents attending ARSH clinic
7.19 Maternal deaths,
7.2 Still births,
7.21 Neonatal deaths,
7.22 Infant deaths
Section VII a: Service delivery in post natal wards:
S.No Parameters Yes No Remarks
7.1a All mothers initiated breast feeding within one hr of normal delivery Y N
7.2a Zero dose BCG,Hepatitis B and OPV given Y N
7.3a Counselling on Family Planning done Y N
7.4a Mothers asked to stay for 48 hrs Y N
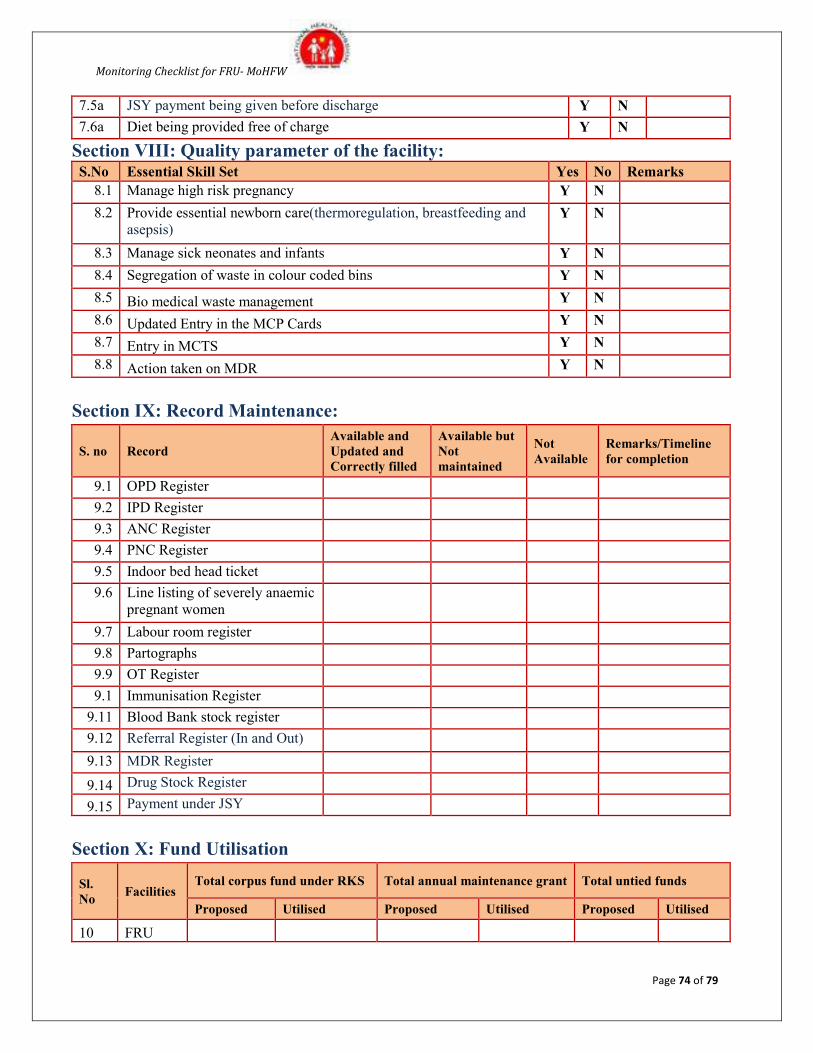
Monitoring Checklist for FRU- MoHFW
Page 74 of 79
7.5a JSY payment being given before discharge Y N
7.6a Diet being provided free of charge Y N
Section VIII: Quality parameter of the facility: S.No Essential Skill Set Yes No Remarks
8.1 Manage high risk pregnancy Y N
8.2 Provide essential newborn care(thermoregulation, breastfeeding and
asepsis) Y N
8.3 Manage sick neonates and infants Y N
8.4 Segregation of waste in colour coded bins Y N
8.5 Bio medical waste management Y N
8.6 Updated Entry in the MCP Cards Y N
8.7 Entry in MCTS Y N
8.8 Action taken on MDR Y N
Section IX: Record Maintenance:
S. no Record
Available and
Updated and
Correctly filled
Available but
Not
maintained
Not
Available
Remarks/Timeline
for completion
9.1 OPD Register
9.2 IPD Register
9.3 ANC Register
9.4 PNC Register
9.5 Indoor bed head ticket
9.6 Line listing of severely anaemic
pregnant women
9.7 Labour room register
9.8 Partographs
9.9 OT Register
9.1 Immunisation Register
9.11 Blood Bank stock register
9.12 Referral Register (In and Out)
9.13 MDR Register
9.14 Drug Stock Register
9.15 Payment under JSY
Section X: Fund Utilisation
Sl.
No Facilities
Total corpus fund under RKS Total annual maintenance grant Total untied funds
Proposed Utilised Proposed Utilised Proposed Utilised
10 FRU
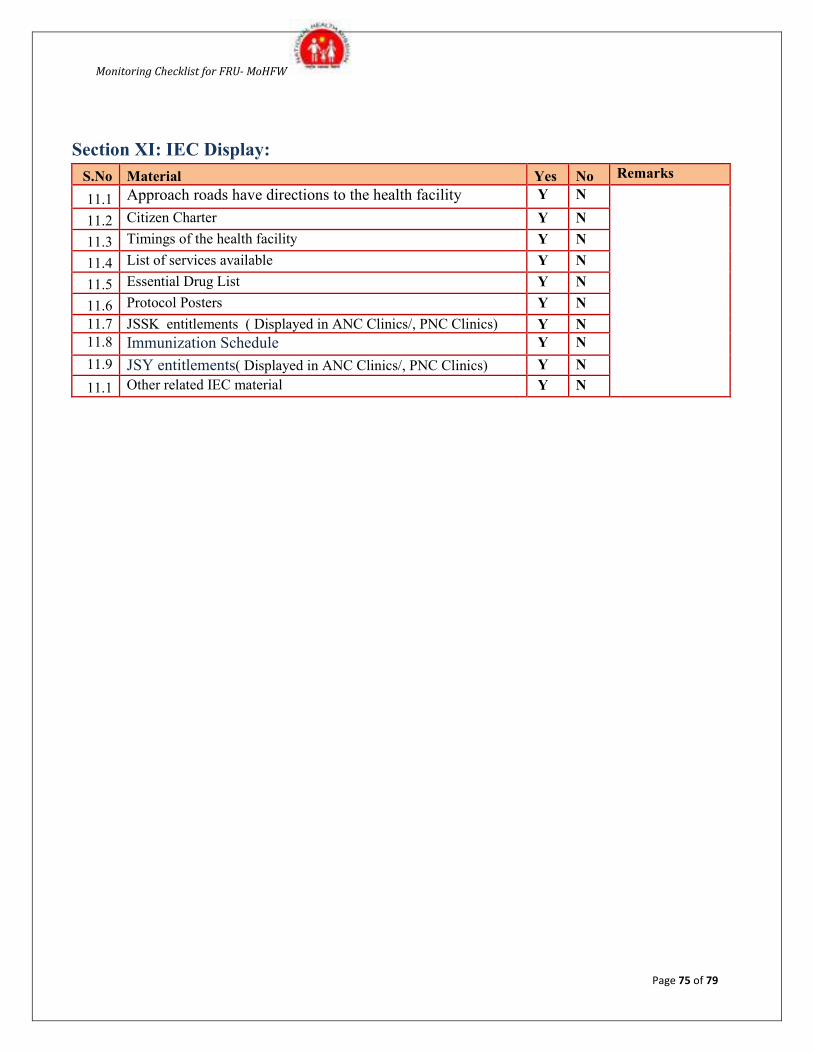
Monitoring Checklist for FRU- MoHFW
Page 75 of 79
Section XI: IEC Display:
S.No Material Yes No Remarks
11.1 Approach roads have directions to the health facility Y N
11.2 Citizen Charter Y N
11.3 Timings of the health facility Y N
11.4 List of services available Y N
11.5 Essential Drug List Y N
11.6 Protocol Posters Y N
11.7 JSSK entitlements ( Displayed in ANC Clinics/, PNC Clinics) Y N
11.8 Immunization Schedule Y N
11.9 JSY entitlements( Displayed in ANC Clinics/, PNC Clinics) Y N
11.1 Other related IEC material Y N
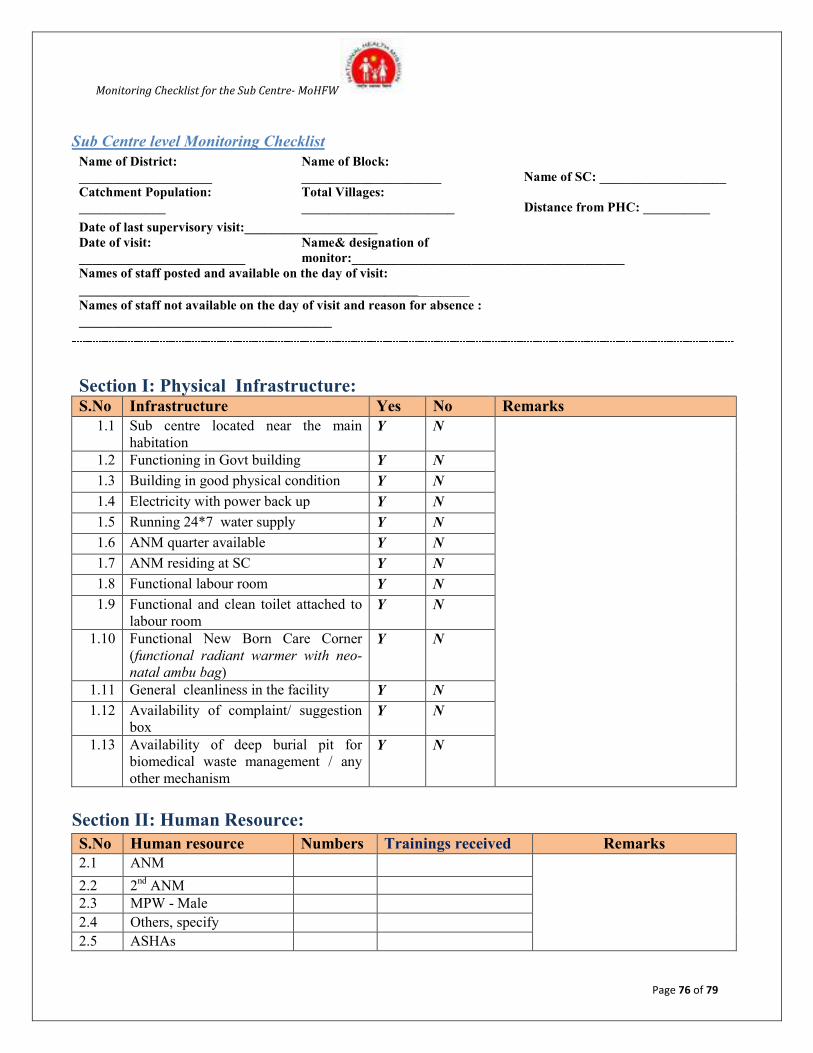
Monitoring Checklist for the Sub Centre- MoHFW
Page 76 of 79
Sub Centre level Monitoring Checklist
Name of District:
____________________
Name of Block:
_____________________ Name of SC: ___________________
Catchment Population:
_____________
Total Villages:
_______________________ Distance from PHC: __________
Date of last supervisory visit:____________________ Date of visit:
_________________________
Name& designation of
monitor:_________________________________________
Names of staff posted and available on the day of visit:
__________________________________________________________
Names of staff not available on the day of visit and reason for absence :
______________________________________
Section I: Physical Infrastructure: S.No Infrastructure Yes No Remarks
1.1 Sub centre located near the main
habitation Y N
1.2 Functioning in Govt building Y N
1.3 Building in good physical condition Y N
1.4 Electricity with power back up Y N
1.5 Running 24*7 water supply Y N
1.6 ANM quarter available Y N
1.7 ANM residing at SC Y N
1.8 Functional labour room Y N
1.9 Functional and clean toilet attached to
labour room Y N
1.10 Functional New Born Care Corner
(functional radiant warmer with neo-
natal ambu bag)
Y N
1.11 General cleanliness in the facility Y N
1.12 Availability of complaint/ suggestion
box Y N
1.13 Availability of deep burial pit for
biomedical waste management / any
other mechanism
Y N
Section II: Human Resource:
S.No Human resource Numbers Trainings received Remarks
2.1 ANM
2.2 2nd
ANM
2.3 MPW - Male
2.4 Others, specify
2.5 ASHAs
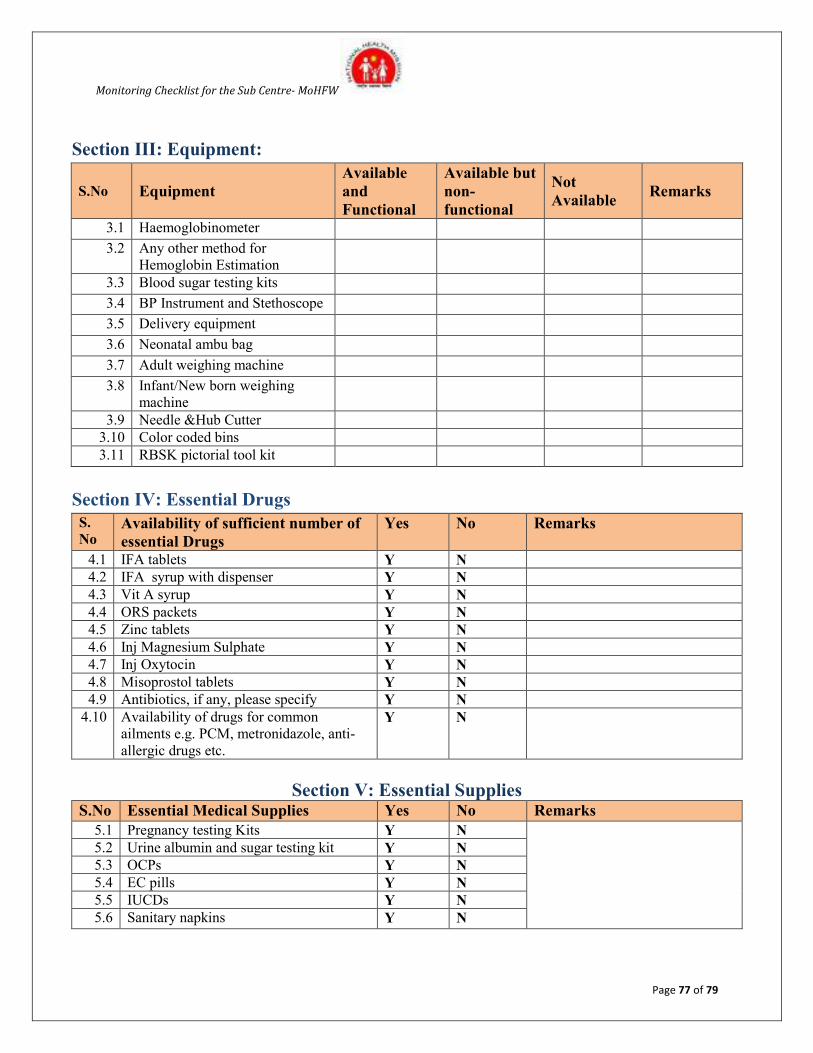
Monitoring Checklist for the Sub Centre- MoHFW
Page 77 of 79
Section III: Equipment:
S.No Equipment
Available
and
Functional
Available but
non-
functional
Not
Available Remarks
3.1 Haemoglobinometer
3.2 Any other method for
Hemoglobin Estimation
3.3 Blood sugar testing kits
3.4 BP Instrument and Stethoscope
3.5 Delivery equipment
3.6 Neonatal ambu bag
3.7 Adult weighing machine
3.8 Infant/New born weighing
machine
3.9 Needle &Hub Cutter
3.10 Color coded bins
3.11 RBSK pictorial tool kit
Section IV: Essential Drugs
S.
No Availability of sufficient number of
essential Drugs
Yes No Remarks
4.1 IFA tablets Y N
4.2 IFA syrup with dispenser Y N
4.3 Vit A syrup Y N
4.4 ORS packets Y N
4.5 Zinc tablets Y N
4.6 Inj Magnesium Sulphate Y N
4.7 Inj Oxytocin Y N
4.8 Misoprostol tablets Y N
4.9 Antibiotics, if any, please specify Y N
4.10 Availability of drugs for common
ailments e.g. PCM, metronidazole, anti-
allergic drugs etc.
Y N
Section V: Essential Supplies S.No Essential Medical Supplies Yes No Remarks
5.1 Pregnancy testing Kits Y N
5.2 Urine albumin and sugar testing kit Y N
5.3 OCPs Y N
5.4 EC pills Y N
5.5 IUCDs Y N
5.6 Sanitary napkins Y N
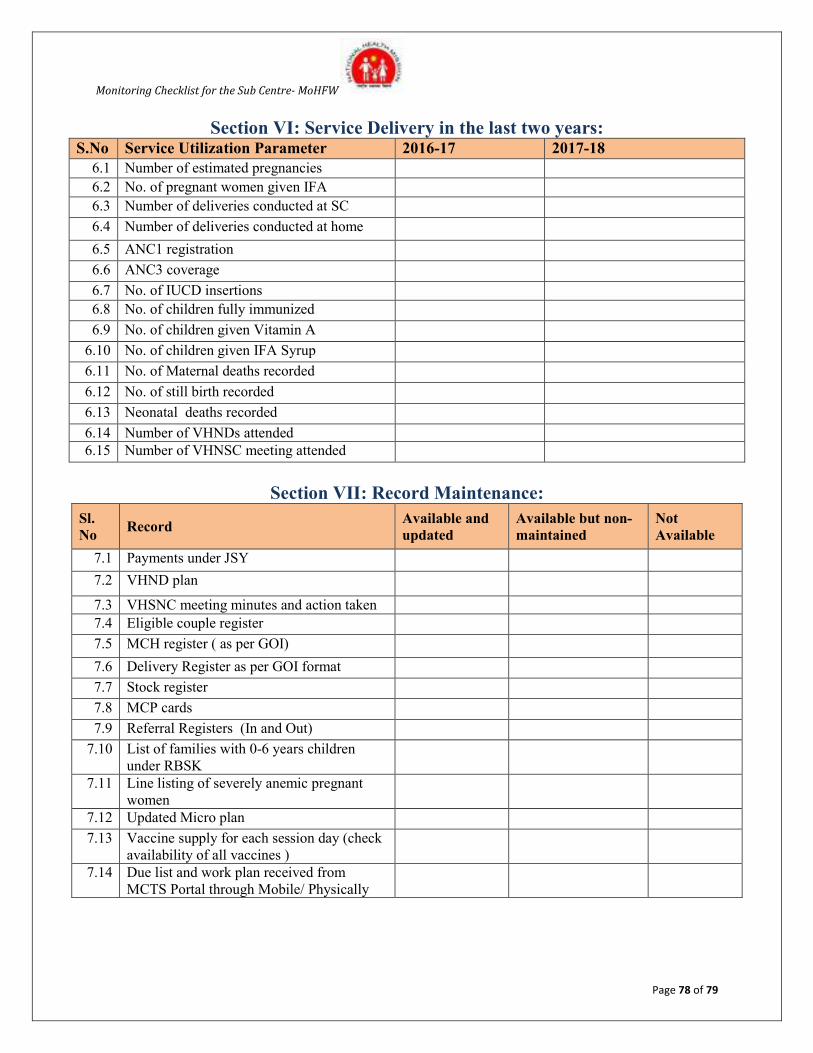
Monitoring Checklist for the Sub Centre- MoHFW
Page 78 of 79
Section VI: Service Delivery in the last two years: S.No Service Utilization Parameter 2016-17 2017-18
6.1 Number of estimated pregnancies 6.2 No. of pregnant women given IFA
6.3 Number of deliveries conducted at SC
6.4 Number of deliveries conducted at home
6.5 ANC1 registration
6.6 ANC3 coverage
6.7 No. of IUCD insertions
6.8 No. of children fully immunized
6.9 No. of children given Vitamin A
6.10 No. of children given IFA Syrup
6.11 No. of Maternal deaths recorded
6.12 No. of still birth recorded
6.13 Neonatal deaths recorded
6.14 Number of VHNDs attended
6.15 Number of VHNSC meeting attended
Section VII: Record Maintenance:
Sl.
No Record
Available and
updated
Available but non-
maintained
Not
Available
7.1 Payments under JSY
7.2 VHND plan
7.3 VHSNC meeting minutes and action taken
7.4 Eligible couple register
7.5 MCH register ( as per GOI)
7.6 Delivery Register as per GOI format
7.7 Stock register
7.8 MCP cards
7.9 Referral Registers (In and Out)
7.10 List of families with 0-6 years children
under RBSK
7.11 Line listing of severely anemic pregnant
women
7.12 Updated Micro plan
7.13 Vaccine supply for each session day (check
availability of all vaccines )
7.14 Due list and work plan received from
MCTS Portal through Mobile/ Physically
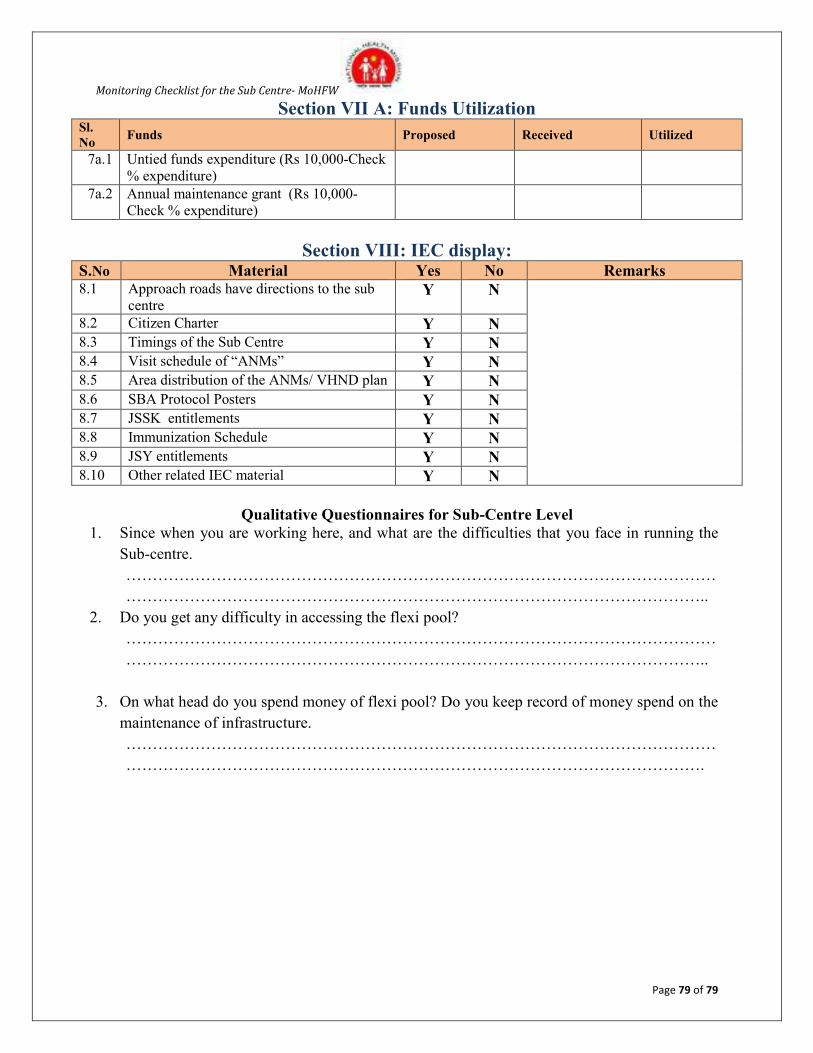
Monitoring Checklist for the Sub Centre- MoHFW
Page 79 of 79
Section VII A: Funds Utilization Sl.
No Funds Proposed Received Utilized
7a.1 Untied funds expenditure (Rs 10,000-Check
% expenditure)
7a.2 Annual maintenance grant (Rs 10,000-
Check % expenditure)
Section VIII: IEC display: S.No Material Yes No Remarks 8.1 Approach roads have directions to the sub
centre Y N
8.2 Citizen Charter Y N 8.3 Timings of the Sub Centre Y N 8.4 Visit schedule of “ANMs” Y N 8.5 Area distribution of the ANMs/ VHND plan Y N 8.6 SBA Protocol Posters Y N 8.7 JSSK entitlements Y N 8.8 Immunization Schedule Y N 8.9 JSY entitlements Y N 8.10 Other related IEC material Y N
Qualitative Questionnaires for Sub-Centre Level
1. Since when you are working here, and what are the difficulties that you face in running the
Sub-centre.
…………………………………………………………………………………………………
………………………………………………………………………………………………..
2. Do you get any difficulty in accessing the flexi pool?
…………………………………………………………………………………………………
………………………………………………………………………………………………..
3. On what head do you spend money of flexi pool? Do you keep record of money spend on the
maintenance of infrastructure.
…………………………………………………………………………………………………
……………………………………………………………………………………………….