Can Spirituality be Taught to Health Care Professionals
13
1 23 Journal of Religion and Health ISSN 0022-4197 Volume 51 Number 3 J Relig Health (2012) 51:879-889 DOI 10.1007/s10943-010-9399-7 Can Spirituality be Taught to Health Care Professionals? Pamela Meredith, Judith Murray, Trish Wilson, Geoff Mitchell & Richard Hutch
Transcript of Can Spirituality be Taught to Health Care Professionals
1 23
Journal of Religion and Health ISSN 0022-4197Volume 51Number 3 J Relig Health (2012) 51:879-889DOI 10.1007/s10943-010-9399-7
Can Spirituality be Taught to Health CareProfessionals?
Pamela Meredith, Judith Murray, TrishWilson, Geoff Mitchell & Richard Hutch
1 23
Your article is protected by copyright and
all rights are held exclusively by Springer
Science+Business Media, LLC. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.

ORI GIN AL PA PER
Can Spirituality be Taught to Health Care Professionals?
Pamela Meredith • Judith Murray • Trish Wilson •
Geoff Mitchell • Richard Hutch
Published online: 1 October 2010� Springer Science+Business Media, LLC 2010
Abstract Although people with life-limiting conditions report a desire to have spiritual
concerns addressed, there is evidence that these issues are often avoided by health care
professionals in palliative care. This study reports on the longitudinal outcomes of four
workshops purpose-designed to improve the spiritual knowledge and confidence of 120
palliative care staff in Australia. Findings revealed significant increases in Spirituality,
Spiritual Care, Personalised Care, and Confidence in this field immediately following the
workshops. Improvements in Spiritual Care and Confidence were maintained 3 month
later, with Confidence continuing to grow. These findings suggest that attendance at
a custom-designed workshop can significantly improve knowledge and confidence to
provide spiritual care.
Keywords Spirituality � Health care professionals � Palliative care
Introduction
Spirituality is a delicate and complex topic that is receiving increasing attention in aca-
demic and medical circles (Sulmasy 2002), with evidence of the importance of spirituality
P. Meredith (&)School of Health and Rehabilitation Sciences, The University of Queensland,St Lucia, QLD 4072, Australiae-mail: [email protected]
J. MurraySchool of Psychology, The University of Queensland, St Lucia, QLD, Australia
T. WilsonMater Health Services, South Brisbane, QLD, Australia
G. MitchellSchool of Medicine, The University of Queensland, Ipswich, QLD, Australia
R. HutchSchool of Religion, The University of Queensland, St Lucia, QLD, Australia
123
J Relig Health (2012) 51:879–889DOI 10.1007/s10943-010-9399-7
Author's personal copy
to both physical and emotional health (Larson and Larson 2003). Within a holistic
approach to health, there is recognition of the need to address existential or spiritual issues
(Sulmasy 2002), and this particularly exists in the field of palliative care (Murphy et al.
2000; Mytko and Knight 1999). Further, the need for spiritual concerns to be taken up by
all disciplines, rather than just those of a religious orientation, has been recognised
(Hermann 2001; Rumbold 2003). Nevertheless, there is also evidence that these issues are
often not broached or addressed by practitioners working with those facing serious health
challenges, even though patients report a desire to address them (Farber et al. 2004; Hart
et al. 2003).
Reasons for failure of health care professionals to address these issues include a lack of
knowledge of the issues, a lack of confidence in broaching spiritual topics, and a lack of
shared language of spirituality outside the confines of traditional religious terminologies
(Kellehear 2000). Illustrating the challenge of providing this care, and indicative of the need
for training, a survey of Australian nurses revealed that, although 97% of registered nurses
believe that they should address patient’s spiritual needs, only 66% felt able to do so
(Barletta and Thompson 2001). Some of the reasons identified within the literature for such
discrepancies include the nurses’ perceived inability to communicate on spiritual matters
(Greasley et al. 2001), pluralism resulting in nurses encountering a wide variety of ideol-
ogies, philosophies and creeds (Laukhuf and Werner 1998), and deficits in nursing edu-
cation in relation to spiritual care (Catanzaro and McMullen 2001). Similar difficulties have
been expressed in other professions: ‘‘Spirituality is not well understood by occupational
therapists and neither do we seem to educate ourselves about it.’’ (Wilding 2002, p. 47).
These difficulties are exacerbated by the multidisciplinary nature of palliative care and
lack of easily defined competencies in spiritual care across disciplines (Gordon and
Mitchell 2004). In addition, issues arise in the perception of spiritual needs as of lesser
priority, the extent of contrasting belief systems, limited staff resources, and training that
fails to enhance knowledge, insight, and confidence (Culliford 2002). However, there is
some evidence that training in spiritual care that focuses on spirituality as a broad concept,
as opposed to religious interpretations, can improve staff attitudes to patients and families,
reduce stress, and build the confidence of staff (Abrams et al. 2005; Wasner et al. 2005), as
well as enhance multidisciplinary collaboration in palliative care (Oppenheimer et al.
2004).
A Training Option
In response to a perceived need, a multidisciplinary team of health and religious profes-
sionals at the University of Queensland, Australia, in consultation with people with life-
limiting illness, their family members, and those employed in the clinical field, developed a
set of training resources. These resources were designed to increase the knowledge and
confidence of staff in the field of palliative care in terms of overcoming hesitancy and/or
difficulty in knowing how to address issues of existential and spiritual care with patients.
The nature of the resources was to ensure the accessibility of the information by health care
practitioners regardless of geographic location or religious affiliation. The resources were
designed to appeal equally to health professionals and pastoral care givers with religious
and non-religious orientations. They were designed to be used as either a self-paced
independent learning package or a workshop that could be delivered by a member of any
profession. The Spirituality in Palliative Care training resource is available, free of charge,
from Palliative Care Australia on their national website at: www.pallcare.org.au. Having
undertaken this developmental task, the next aim was to evaluate the training resources.
880 J Relig Health (2012) 51:879–889
123
Author's personal copy

Study Expectations
In this paper, the outcomes of four pilot workshops using the Spirituality in Palliative Care
package are described. It was anticipated that participation in the workshops would result
in significant gains in measures of spiritual care, spirituality, and confidence to provide
spiritual care in palliative care. Furthermore, it was expected that these gains would be
maintained up to 3 months after workshop attendance. Religiosity, workplace concerns,
stress, anxiety, and depression, although not expected to change in response to the
workshop, were also measured as control variables. In anticipation of these objectives
being met, it is suggested that this training package will prove to be a valuable educational
tool for health care professionals.
Methods
Participants
Participants were a self-selected sample of employees and volunteers in the field of pal-
liative care. Approximately 120 people attended one of four workshops. Pre-workshop
questionnaires were collected for 113 (94.2%) of these (23 ? 26 ? 28 ? 36 at each of the
four workshops, respectively). At the post-workshop stage, 109 questionnaires (96.5%)
were returned, and 69 of the 113 participants (61.1%) completed follow-up questionnaires.
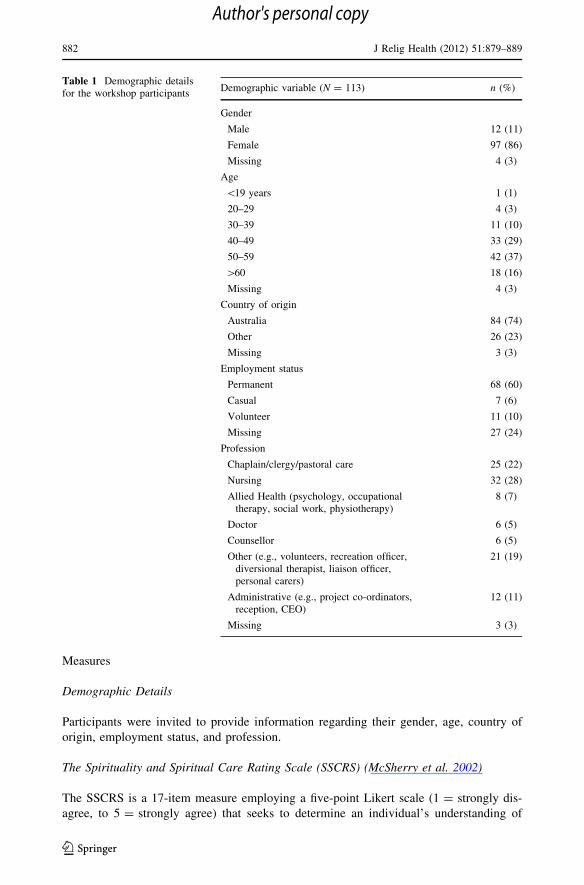
As can be seen from Table 1, participants were predominantly Australian women, older
than 40 years of age, who were employed permanently in the field of palliative care. A
wide range of professions was represented.
Procedure
Following the development of the workshop content by the authors, promotions for the
Queensland pilots were undertaken in three locations: one provincial town (Cairns), one
rural town (Roma), and one metropolitan town (Brisbane). Due to the high numbers of
registrants, two workshops were provided in Brisbane. Promotional material was distrib-
uted through hospital, hospice and palliative care facilities, church groups, and aged care
facilities in the various locations. Participants enrolling in the workshops were sent the pre-
workshop questionnaire as part of their confirmation of registration package. The majority
of participants completed these measures before attendance on the day of the workshop.
Those who forgot to complete their questionnaire prior to the workshop, or who neglected
to bring it with them on the day, were provided with an additional questionnaire to
complete prior to the commencement of the workshop. Workshops were delivered jointly
by a psychologist and a nurse counsellor on the program development team. Participants
completed the post-workshop questionnaire prior to leaving the workshop venue on that
day. Three months following the workshop, participants were sent the follow-up ques-
tionnaire by mail and asked to return the completed questionnaire in a postage-paid
envelope. Ethical clearance for this project was obtained from The University of
Queensland’s Behavioral and Social Science Ethical Review Committee. Confidentiality of
participants was maintained through the use of a confidentiality code—a unique six letter
code generated by the participants from personal information known only to them. This
code was required in order to link pre-, post- and follow-up questionnaires.
J Relig Health (2012) 51:879–889 881
123
Author's personal copy
Measures
Demographic Details
Participants were invited to provide information regarding their gender, age, country of
origin, employment status, and profession.
The Spirituality and Spiritual Care Rating Scale (SSCRS) (McSherry et al. 2002)
The SSCRS is a 17-item measure employing a five-point Likert scale (1 = strongly dis-
agree, to 5 = strongly agree) that seeks to determine an individual’s understanding of
Table 1 Demographic detailsfor the workshop participants
Demographic variable (N = 113) n (%)
Gender
Male 12 (11)
Female 97 (86)
Missing 4 (3)
Age
\19 years 1 (1)
20–29 4 (3)
30–39 11 (10)
40–49 33 (29)
50–59 42 (37)
[60 18 (16)
Missing 4 (3)
Country of origin
Australia 84 (74)
Other 26 (23)
Missing 3 (3)
Employment status
Permanent 68 (60)
Casual 7 (6)
Volunteer 11 (10)
Missing 27 (24)
Profession
Chaplain/clergy/pastoral care 25 (22)
Nursing 32 (28)
Allied Health (psychology, occupationaltherapy, social work, physiotherapy)
8 (7)
Doctor 6 (5)
Counsellor 6 (5)
Other (e.g., volunteers, recreation officer,diversional therapist, liaison officer,personal carers)
21 (19)
Administrative (e.g., project co-ordinators,reception, CEO)
12 (11)
Missing 3 (3)
882 J Relig Health (2012) 51:879–889
123
Author's personal copy

spiritual care. It produces four subscales: (1) ‘‘Spirituality’’, (2) ‘‘Spiritual Care’’, (3)
‘‘Religiosity’’, and (4) ‘‘Personalised Care’’. The Spirituality subscale reflects participants’
beliefs about what constitutes personal spirituality. An example is: ‘‘I believe spirituality is
about finding meaning in the good and bad events of life’’. The Spiritual Care subscale taps
into the beliefs of participants with respect to who is responsible for providing spiritual
care and how spiritual care can be offered e.g., ‘‘I believe we can provide spiritual care by
showing kindness, concern and cheerfulness when giving care’’. Religiosity reflects beliefs
concerning the centrality of religious beliefs to spiritual care, as in the following example:
‘‘I believe spirituality involves only going to Church/Place of Worship’’. Finally, Per-
sonalised Care reflects staff beliefs concerning the interactional nature of spiritual care,
such as: ‘‘I believe spirituality involves personal friendships, relationships’’.
Perception of Workplace Change Schedule (POWCS)(Nolan et al. 1998; Schofield et al. 2005)
The POWCS is a 16-item measure employing a 5-point Likert scale (1 = decreased a lot,
to 5 = increased a lot) that seeks to measure the perceptions of staff with respect to their
workplace. It provides three subscales that measure: (1) perceived ‘‘Strengths’’ of the
workplace (e.g., ‘‘My feelings of being a valued employee have…’’), (2) ‘‘Concerns’’ held
about the workplace (e.g., ‘‘The levels of stress I feel have…’’), and (3) ‘‘Pressures’’ in
terms of workplace demands (e.g., ‘‘My workload has…’’). This measure was included at
only the pre-workshop and follow-up phases to determine if there had been any perceived
changes in the workplace that could account for any changes in outcome measures.
Knowledge and Confidence Scale (KCS) (Murray and Chan, manuscript in preparation)
This is a 15-item measure employing a seven-point Likert scale (1 = very strongly dis-
agree, to 7 = very strongly agree) that was developed by one of the researchers in previous
research looking at provision of care in bereavement and other adverse life events. It
provides two subscales: (1) participant ‘‘Confidence’’ in their ability to provide spiritual
support and (2) participant ‘‘Compassion’’, reflecting the willingness on the part of staff to
view providing support as their role or responsibility. A sample confidence item is: ‘‘I have
skills that I can use to help a person facing death’’, while a sample compassion item is:
‘‘People facing death need to talk about their situation.’’ Because the Cronbach’s alpha for
the Compassion subscale fell below 0.7 at all three data collection stages, the Compassion
scale was not utilised in this study.
Depression Anxiety Stress Scale-21 (DASS-21) (Lovibond and Lovibond 1995;Clara et al. 2001)
The DASS is a 21-item scale that comprises three scales: (1) ‘‘Stress’’, (2) ‘‘Depression’’,
and (3) ‘‘Anxiety’’, each with seven items. Questions are scored on a four-point scale
(0 = did not apply to me at all, to 3 = applied to me very much or most of the time) based
on the previous week. Adequate reliability, convergent and discriminant validity have been
reported, internal consistency, temporal stability, and convergent and discriminant validity
are excellent, and a consistent factor structure has been found (Brown et al. 1997; Clara
et al. 2001; Crawford and Henry 2003; Lovibond and Lovibond 1993). Sample items
include: ‘‘I found it hard to wind down’’ (stress), ‘‘I experienced trembling’’ (anxiety), and
J Relig Health (2012) 51:879–889 883
123
Author's personal copy
‘‘I couldn’t seem to experience any positive feeling at all’’ (depression). The scale was
employed only at pre-workshop and follow-up phases of the project.
Statistical Analyses
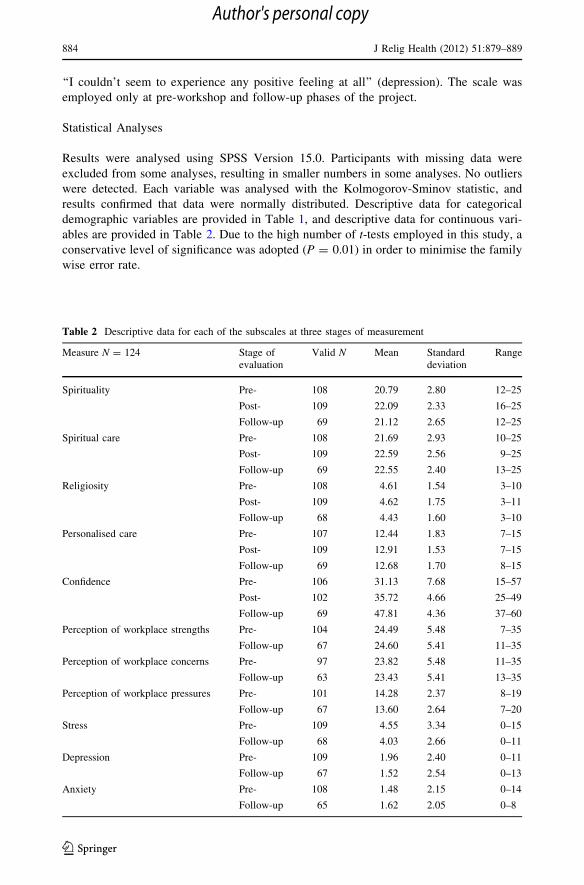
Results were analysed using SPSS Version 15.0. Participants with missing data were
excluded from some analyses, resulting in smaller numbers in some analyses. No outliers
were detected. Each variable was analysed with the Kolmogorov-Sminov statistic, and
results confirmed that data were normally distributed. Descriptive data for categorical
demographic variables are provided in Table 1, and descriptive data for continuous vari-
ables are provided in Table 2. Due to the high number of t-tests employed in this study, a
conservative level of significance was adopted (P = 0.01) in order to minimise the family
wise error rate.
Table 2 Descriptive data for each of the subscales at three stages of measurement
Measure N = 124 Stage ofevaluation
Valid N Mean Standarddeviation
Range
Spirituality Pre- 108 20.79 2.80 12–25
Post- 109 22.09 2.33 16–25
Follow-up 69 21.12 2.65 12–25
Spiritual care Pre- 108 21.69 2.93 10–25
Post- 109 22.59 2.56 9–25
Follow-up 69 22.55 2.40 13–25
Religiosity Pre- 108 4.61 1.54 3–10
Post- 109 4.62 1.75 3–11
Follow-up 68 4.43 1.60 3–10
Personalised care Pre- 107 12.44 1.83 7–15
Post- 109 12.91 1.53 7–15
Follow-up 69 12.68 1.70 8–15
Confidence Pre- 106 31.13 7.68 15–57
Post- 102 35.72 4.66 25–49
Follow-up 69 47.81 4.36 37–60
Perception of workplace strengths Pre- 104 24.49 5.48 7–35
Follow-up 67 24.60 5.41 11–35
Perception of workplace concerns Pre- 97 23.82 5.48 11–35
Follow-up 63 23.43 5.41 13–35
Perception of workplace pressures Pre- 101 14.28 2.37 8–19
Follow-up 67 13.60 2.64 7–20
Stress Pre- 109 4.55 3.34 0–15
Follow-up 68 4.03 2.66 0–11
Depression Pre- 109 1.96 2.40 0–11
Follow-up 67 1.52 2.54 0–13
Anxiety Pre- 108 1.48 2.15 0–14
Follow-up 65 1.62 2.05 0–8
884 J Relig Health (2012) 51:879–889
123
Author's personal copy
Results
Comparisons Between Pre-Workshop, Post-Workshop, and Follow-Up Measures
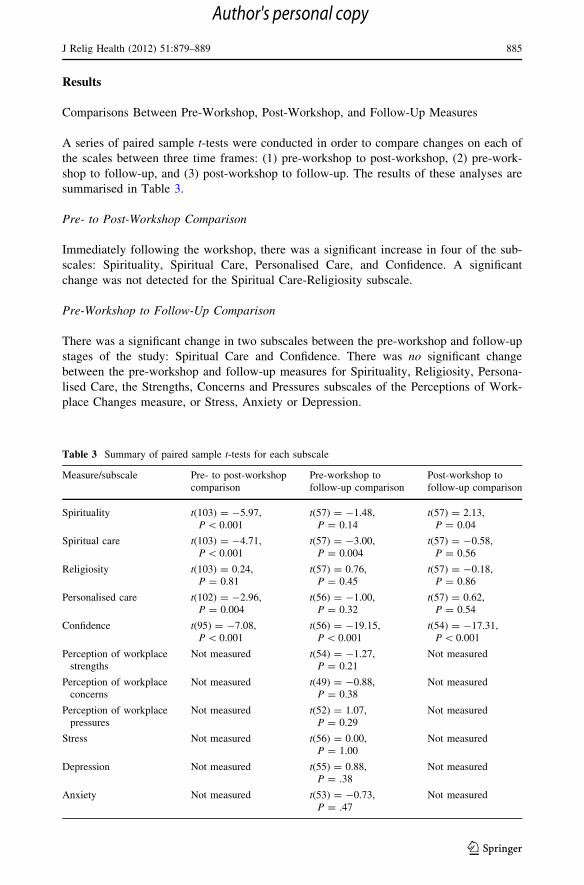
A series of paired sample t-tests were conducted in order to compare changes on each of
the scales between three time frames: (1) pre-workshop to post-workshop, (2) pre-work-
shop to follow-up, and (3) post-workshop to follow-up. The results of these analyses are
summarised in Table 3.
Pre- to Post-Workshop Comparison
Immediately following the workshop, there was a significant increase in four of the sub-
scales: Spirituality, Spiritual Care, Personalised Care, and Confidence. A significant
change was not detected for the Spiritual Care-Religiosity subscale.
Pre-Workshop to Follow-Up Comparison
There was a significant change in two subscales between the pre-workshop and follow-up
stages of the study: Spiritual Care and Confidence. There was no significant change
between the pre-workshop and follow-up measures for Spirituality, Religiosity, Persona-
lised Care, the Strengths, Concerns and Pressures subscales of the Perceptions of Work-
place Changes measure, or Stress, Anxiety or Depression.
Table 3 Summary of paired sample t-tests for each subscale
Measure/subscale Pre- to post-workshopcomparison
Pre-workshop tofollow-up comparison
Post-workshop tofollow-up comparison
Spirituality t(103) = -5.97,P \ 0.001
t(57) = -1.48,P = 0.14
t(57) = 2.13,P = 0.04
Spiritual care t(103) = -4.71,P \ 0.001
t(57) = -3.00,P = 0.004
t(57) = -0.58,P = 0.56
Religiosity t(103) = 0.24,P = 0.81
t(57) = 0.76,P = 0.45
t(57) = -0.18,P = 0.86
Personalised care t(102) = -2.96,P = 0.004
t(56) = -1.00,P = 0.32
t(57) = 0.62,P = 0.54
Confidence t(95) = -7.08,P \ 0.001
t(56) = -19.15,P \ 0.001
t(54) = -17.31,P \ 0.001
Perception of workplacestrengths
Not measured t(54) = -1.27,P = 0.21
Not measured
Perception of workplaceconcerns
Not measured t(49) = -0.88,P = 0.38
Not measured
Perception of workplacepressures
Not measured t(52) = 1.07,P = 0.29
Not measured
Stress Not measured t(56) = 0.00,P = 1.00
Not measured
Depression Not measured t(55) = 0.88,P = .38
Not measured
Anxiety Not measured t(53) = -0.73,P = .47
Not measured
J Relig Health (2012) 51:879–889 885
123
Author's personal copy

Post-Workshop to Follow-Up Comparison
The only significant change between post-workshop and follow-up was an increase in
Confidence scores. There was no significant change in the other four subscales: Spiritual
Care, Spirituality, Religiosity, and Personalised Care subscales of the SSCRS.
Discussion
As identified in the literature, there is a need for health care professionals to increase their
knowledge and confidence in addressing spiritual issues as part of our health care services.
The overall aim of the Spiritual Care in Palliative Care Project was to develop a training
program that would improve the confidence and ability of staff to provide spiritual care in a
palliative care setting. The results of this study suggest that the workshops were successful
in achieving this aim. Immediately following the workshop, participants significantly
increased their Spiritual Care (Spirituality, Spiritual Care, and Personalised Care) and
Confidence in this field. The improvement in the Spiritual care subscale was maintained at
3 months, while the Confidence subscale continued to improve beyond the post-workshop
scores. Thus, over a 3-month period, the workshops contributed to ongoing improvements
in the confidence of staff in providing spiritual care. As anticipated, there was no change in
participants’ level of religiosity: the workshop clearly distinguished between spirituality
and religiosity, and appeared to have no impact on religiosity.
At the same time as participants reported improvements in staff confidence to provide
spiritual support, there were no perceived alterations to workplace demands or to staff levels
of personal stress, anxiety or depression. That is, improvements in spiritual care and con-
fidence cannot be attributed to decreases in workplace concerns or pressures, increases in
workplace strengths, or to positive changes in staff mood or stress levels. Thus, it appears that
identified changes are related more to the self-perceived ability of individual staff members
to provide spiritual care in their everyday encounters with patients and their families.
In addition, workshop participants showed significant improvements in personal spiritu-
ality at the post-workshop phase, as indicated by the Spirituality subscale of the Spirituality
and Spiritual Care Rating Scale (SSCRS). This aspect of personal spirituality enhancement
appears to have had its own effects on the individual, separate from mental health, which, as
previously noted, did not differ significantly over time. That both Spiritual Care and personal
Spirituality improved is consistent with Toomey’s (1999, p. 198) notion that: ‘‘…by seeing
our own spirituality we become better equipped to recognise spiritual things in others’’.
The initial improvements in personal Spirituality and Personalised Care present
immediately post-workshop decreased 3 months post-workshop to be non-significant,
however. While the opportunity for staff in this field to gather together, reflect on clinical
practice, and discuss spiritual matters may nurture one’s spirituality and refuel one’s
capacity to provide personalised care, it appears that this effect does not last. Thus, hosting
gatherings such as these workshops intermittently for staff in palliative care may confer a
significant benefit. Notably, while scores in these personal aspects of spirituality returned
to pre-workshop levels, improvements in spiritual care and confidence in providing support
were maintained at the follow-up stage and, as noted earlier, confidence continued to
improve. This is apparently not the result of the participant’s innate spirituality.
It is possible only to speculate upon the mechanisms behind the apparent success of
these workshops. The positive outcomes could potentially be attributed to a combination or
interaction of a range of factors, including: (a) the nature of the presenters of the
886 J Relig Health (2012) 51:879–889
123
Author's personal copy
workshops, (b) the content and format of the program itself, and/or (c) the emotional and
intellectual benefits of a group of like-minded people gathering collectively. The program
team was comprised of professionals with a range of relevant backgrounds (medical,
nursing, psychology, religion, occupational therapy) and clinical experience. Hence,
potentially ethereal topics were able to be clearly presented in language relevant to
everyday clinicians and situations. For example, core concepts were couched in terms of
‘‘love and fear’’ for clarity and acceptability by all participants, regardless of religious
affiliation. Further, processes guiding workshop development included an extensive liter-
ature review (including recommendations for teaching health professionals), consultation
with an expert reference group drawn from a range of professions, and wide consultation
with key stakeholders. This ensured that the workshops were both comprehensive and
relevant, while also informing a range of design decisions. For example, the teaching and
learning concept of ‘‘different ways of knowing’’ was adopted by using a diversity of
learning resources (poems, music, quotes, movie clips, interviews with people experi-
encing life-limiting illnesses and their families, a reflection journal, and photo montages).
In this way, the team demonstrated that spirituality is more than a cognitive experience—
the workshops engaged sensory, emotional and experiential aspects of the participant in
addition to the cognitive element. Finally, although the workshops were designed to be
delivered by any health professional, training at all four of the evaluated workshops was
provided by people on the project team. While each of these aspects may have contributed
to the observed success, only further tailored research considering the many potential
influencing factors (workshop development, content, personnel, method of delivery, group
processes, and dynamics) could shed further light on this question.
There are a number of considerations that indicate a need for caution in interpreting the
results. Firstly, a self-selection bias may have been introduced in several ways. The par-
ticipants attending each workshop were voluntary registrants, suggesting that those
interested in and open to exploring spiritual elements presented in the workshops may have
been more likely to attend. In addition, although the sample of individuals attending the
workshops was over 120, the rate of questionnaire return at the 3-month follow-up stage
was only 61% of the initial sample. Secondly, the sessions were conducted in English, as
were the evaluations. People whose primary language is not English and who may have a
non-European cultural background may be under-represented, and the study is not appli-
cable to non-European cultures. Thirdly, although workshops were delivered in a range of
settings throughout Queensland, results may not be generalisable to staff and volunteers in
other states of Australia, or in other countries. Finally, there was no control group, so the
observed changes cannot be categorically attributed to the intervention itself. Further
research would help to address these issues.
Although it is a strength of this study that longitudinal measures were obtained, time
constraints on the project made only a 3-month follow-up possible. This may have been
insufficient to determine long-term changes to care offered by staff or any subsequent
changes to the workplace as the result of staff changes. It would be advantageous to review
outcomes about 1 year after the workshop to determine longevity of change.
The measurements in this project relied on the self-report of participants. While this
may have been appropriate given the goal of improving participants’ spiritual care and
confidence, it may have also been valuable to consider more behavioral measures of the
impact of the workshops. For example, the absence of objective measures of actual change
in staff behaviors and care (as determined by colleagues or patients and their families, for
example) meant that reports of change were restricted to subjective perceptions on the part
of staff.
J Relig Health (2012) 51:879–889 887
123
Author's personal copy

Future Directions
There is still much research to be done in relation to this training package. Replications of
this training and outcome study using various samples and altering outcome measures will
strengthen confidence in these findings. While there is now evidence that the workshop,
delivered by the experts who were part of the program development team, has an apparent
beneficial outcome for participants, it remains to be seen whether the content of the
workshop will be similarly helpful for those who elect to take a self-directed study
approach to the online package. Finally, there is a need to measure outcomes for partic-
ipants of workshops delivered by trainers not previously involved in the development of
the package.
Conclusion
As noted by Toomey (1999), the growth of one’s own spirituality involves a complex
journey, yet embarking on this journey equips us to recognise the spiritual lives of those
with whom we work. The aim of the Spiritual Care in Palliative Care Project was to
develop and evaluate a set of staff training resources aimed at encouraging a multidisci-
plinary approach to spirituality and health in palliative care. In order to achieve this aim,
the workshops were focused on improving the awareness, confidence, and ability of the
multidisciplinary group of staff and volunteers to provide spiritual care in palliative care
settings. The evidence reported in this paper suggests that this aim has been met, and that
spirituality can indeed be taught to health care professionals.
Acknowledgments The authors would like to acknowledge the financial support of The AustralianDepartment of Health and Ageing Local Palliative Care Grants—Pastoral Care Counselling and SupportSub-Program. We would also like to express our appreciation to the participants of the workshops whocompleted several questionnaires and to the people with terminal illnesses, their families, and palliative careworkers, who agreed to be interviewed and videoed for the purpose of developing this training package.
References
Abrams, D., Albury, S., Crandell, L., Doka, K., & Harris, R. (2005). The Florida Clergy End-of-LifeEducation Enhancement Project: A description and evaluation. American Journal of Hospice andPalliative Medicine, 22(3), 181–187.
Barletta, J., & Thomsen, M. (2001). Pastoral carers in the hospital context. Australian Journal of PrimaryHealth – Interchange, 7(2), 43–49.
Brown, T. A., Chorpita, B. E., Korotitsch, W., & Barlow, D. H. (1997). Psychometric properties of theDepression Anxiety Stress Scales (DASS) in clinical samples. Behaviour Research and Therapy, 35(1),79–89.
Catanzaro, A. M., & McMullen, K. A. (2001). Increasing nursing student’s spiritual sensitivity. NurseEducator, 26(5), 221–226.
Clara, I. P., Cox, B. J., & Enns, M. W. (2001). Confirmatory factor analysis of the Depression-Anxiety-Stress Scales in depressed and anxious patients. Journal of Psychopathology and Behavioral Assess-ment, 23(1), 61–67.
Crawford, J. R., & Henry, J. D. (2003). The Depression Anxiety Stress Scale (DASS): normative data andlatent structure in a large non-clinical sample. British Journal of Clinical Psychology, 42(2), 111–131.
Culliford, L. (2002). Spirituality and clinical care. British Medical Journal, 325, 1434–1435.Farber, N. J., Urban, S. Y., Collier, V. U., Metzger, M., Weiner, J., & Boyer, E. G. (2004). Frequency and
perceived competence in providing palliative care to terminally ill patients: A survey of primary carephysicians. Journal of Pain and Symptom Management, 28(4), 364–370.
888 J Relig Health (2012) 51:879–889
123
Author's personal copy
Gordon, T., & Mitchell, D. (2004). A competency model for the assessment and delivery of spiritual care.Palliative Medicine, 18(7), 646–651.
Greasley, P., Chiu, L. F., & Gartland, M. (2001). The concept of spiritual care in mental health nursing.Journal of Advanced Nursing, 33(5), 629–637.
Hart, A. R., Kohlwes, R. J., Devo, R., et al. (2003). Hospice patients’ attitudes regarding spiritual discus-sions with their doctors. American Journal of Hospice and Palliative Care, 20, 135–139.
Hermann, C. P. (2001). Spiritual needs of dying patients: A qualitative study. Oncology Nursing Forum,28(1), 67–72.
Kellehear, A. (2000). Spirituality and palliative care: A model of needs. Palliative Medicine, 14, 149–155.Larson, D. B., & Larson, S. S. (2003). Spirituality’s potential relevance to physical and emotional health: A
brief review of quantitative research. Journal of Psychology and Theology, 31(1), 37–51.Laukhuf, G., & Werner, H. (1998). Spirituality: The missing link. Journal of Neuroscience Nursing, 30(1),
60–67.Lovibond, P. F., & Lovibond, S. H. (1993). Manual for the Depression Anxiety Stress Scales (DASS).
Psychology Foundation Monograph. (Available from The Psychology Foundation, Room 1005Mathews Building, University of New South Wales, 2052, Australia).
Lovibond, P. F., & Lovibond, S. H. (1995). The structure of negative emotional states: Comparison of theDepression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav-ioral Research Therapy, 33(3), 335–353.
McSherry, W., Draper, P., & Kendrick, D. (2002). The construct validity of a rating scale designed to assessspirituality and spiritual care. International Journal of Nursing Studies, 39, 723–734.
Murphy, P. L., Albert, S. M., Weber, C. M., Del Bene, M. L., & Rowland, L. P. (2000). Impact of spiritualityand religiousness on outcomes in patients. Neurology, 55(10), 1581–1584.
Murray, J., & Chan, N. (in preparation). Justification and initial development of a scale to measure perceivedconfidence and attitudes to the provision of support to those facing adverse life events.
Mytko, J. J., & Knight, S. J. (1999). Body, mind, and spirit: Towards the integration of religiosity andspirituality in cancer quality of life research. Psycho-Oncology, 8, 439–450.
Nolan, M., Grant, G., Brown, J., & Nolan, J. (1998). Assessing nurses’ work environment: Old dilemmas,new solutions. Clinical Effectiveness in Nursing, 2, 145–156.
Oppenheimer, J. E., Flannelly, K. J., & Weaver, A. J. (2004). A comparative analysis of the psychologicalliterature on collaboration between clergy and mental-health professionals – perspectives from andreligious journals: 1970–1999. Pastoral Psychology, 53(2), 153–162.
Rumbold, B. (2003). Caring for the spirit: Lesson from working with the dying. Medical Journal ofAustralia, 179, s11–s13.
Schofield, I., Tolson, D., Arthur, D., Davies, S., & Nolan, M. (2005). An exploration of the caring attributesand perceptions of work place change among gerontological nursing staff in England, Scotland andChina (Hong Kong). International Journal of Nursing Studies, 42, 197–209.
Sulmasy, D. P. (2002). A biopsychosocial-spiritual model for the care of patients at the end of life.Gerontologist, 42(Special Issue 3), 24–33.
Toomey, M. A. (1999). The art of observation: Reflecting on a spiritual moment. Canadian Journal ofOccupational Therapy, 66(4), 197–199.
Wasner, M., Longaker, C., Fegg, M., Martin, J., & Borasio, G. D. (2005). Effects of spiritual care trainingfor palliative professionals. Palliative Medicine, 19(2), 99–104.
Wilding, C. (2002). Where angels fear to tread: Is spirituality relevant to occupational therapy practice?Australian Occupational Therapy Journal, 49, 44–47.
J Relig Health (2012) 51:879–889 889
123
Author's personal copy