
C Afferent Axons/Fibers
340
C C Afferent Axons/Fibers Synonyms C Fibers Definition One kind of fiber in the peripheral nerve; unmyelinated thin fibers. These high-threshold sensory afferents con- duct very slowly (less than 2 m/s), and are thought to be responsible for the sensation of deep, burning pain that follows ’first pain’ after injury. Although C fibers ma- ture earlier than low-threshold Aβ fibers, anatomically and neurochemically, other aspects of their function are delayed, for example, the phenomenon of neurogenic edema, and the development of functional central con- nections within the spinal cord. A Fibers (A-Fibers) Alpha(α) 2-Adrenergic Agonists in Pain Treatment Infant Pain Mechanisms Insular Cortex, Neurophysiology and Functional Imaging of Nociceptive Processing Magnetoencephalography in Assessment of Pain in Humans Morphology, Intraspinal Organization ofVisceral Af- ferents Nociceptor, Categorization Nociceptors in the Orofacial Region (Temporo- mandibular Joint and Masseter Muscle) Nociceptor(s) Opiates During Development Spinothalamic Tract Neurons, in Deep Dorsal Horn Thalamus, Dynamics of Nociception Vagal Input and Descending Modulation C and A Fibers Definition Nociceptive input is conveyed from the peripheral terminals to the spinal cord, predominantly by two classes of primary afferent fibers. Of these, the slowly- conducting, thinly-myelinated Aδ-fibers mediate ther- mal and mechanical nociception, whereas the unmyeli- nated, polymodal C-fibers are activated by a variety of high-intensity mechanical, chemical, hot and cold stimuli. In addition, low threshold fibers (Aβ) that nor- mally only transfer innocuous sensations like touch, can contribute to neuropathic pain following nerve damage. Opioids in the Periphery and Analgesia Cachexia Definition General ill health and malnutrition that presents as mus- cle wasting, dehydration and reduced behavioral activ- ities in untreated diabetic animals. Neuropathic Pain Model, Diabetic Neuropathy Model CACNA1A Definition CACNA1A is a gene encoding the α1A subunit of a voltage sensitive calcium channel abundantly expressed in neuronal tissue. It is activated by high voltage and gives rise to P/Q-type calcium currents. Mutations in the human gene are related to diseases like spinocere- bellar ataxia type 6, familial hemiplegic migraine and episodic ataxia type 2. In mice, mutations in the or- thologous gene are responsible for the “leaner” and “tottering” phenotypes. Calcitonin Gene-Related Peptide and Migraine Headaches Calbindin Definition Vitamin D-dependent calcium-binding protein that is present in specific sensory neuronal cell types. Spinothalamic Terminations, Core and Matrix Thalamus, Receptive Fields, Projected Fields, Human
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of C Afferent Axons/Fibers

C
C Afferent Axons/Fibers
Synonyms
C Fibers
Definition
One kind of fiber in the peripheral nerve; unmyelinatedthin fibers. These high-threshold sensory afferents con-duct very slowly (less than 2 m/s), and are thought to beresponsible for the sensation of deep, burning pain thatfollows ’first pain’ after injury. Although C fibers ma-ture earlier than low-threshold Aβ fibers, anatomicallyand neurochemically, other aspects of their function aredelayed, for example, the phenomenon of neurogenicedema, and the development of functional central con-nections within the spinal cord.� A Fibers (A-Fibers)� Alpha(α) 2-Adrenergic Agonists in Pain Treatment� Infant Pain Mechanisms� Insular Cortex, Neurophysiology and Functional
Imaging of Nociceptive Processing� Magnetoencephalography in Assessment of Pain in
Humans� Morphology, Intraspinal Organization ofVisceral Af-
ferents� Nociceptor, Categorization� Nociceptors in the Orofacial Region (Temporo-
mandibular Joint and Masseter Muscle)� Nociceptor(s)� Opiates During Development� Spinothalamic Tract Neurons, in Deep Dorsal Horn� Thalamus, Dynamics of Nociception� Vagal Input and Descending Modulation
C and A Fibers
Definition
Nociceptive input is conveyed from the peripheralterminals to the spinal cord, predominantly by twoclasses of primary afferent fibers. Of these, the slowly-conducting, thinly-myelinated Aδ-fibers mediate ther-mal and mechanical nociception, whereas the unmyeli-
nated, polymodal C-fibers are activated by a varietyof high-intensity mechanical, chemical, hot and coldstimuli. In addition, low threshold fibers (Aβ) that nor-mally only transfer innocuous sensations like touch, cancontribute to neuropathic pain following nerve damage.� Opioids in the Periphery and Analgesia
Cachexia
Definition
General ill health and malnutrition that presents as mus-cle wasting, dehydration and reduced behavioral activ-ities in untreated diabetic animals.� NeuropathicPainModel,DiabeticNeuropathyModel
CACNA1A
Definition
CACNA1A is a gene encoding the α1A subunit of avoltage sensitive calcium channel abundantly expressedin neuronal tissue. It is activated by high voltage andgives rise to P/Q-type calcium currents. Mutations inthe human gene are related to diseases like spinocere-bellar ataxia type 6, familial hemiplegic migraine andepisodic ataxia type 2. In mice, mutations in the or-thologous gene are responsible for the “leaner” and“tottering” phenotypes.� Calcitonin Gene-Related Peptide and Migraine
Headaches
Calbindin
Definition
Vitamin D-dependent calcium-binding protein that ispresent in specific sensory neuronal cell types.� Spinothalamic Terminations, Core and Matrix� Thalamus,ReceptiveFields,ProjectedFields,Human

188 Calbindin D–28k
Calbindin D–28k
Definition
A member of the EF-hand family calcium binding pro-teins, which buffer intracellular calcium concentrationand mediate a variety of cellular functions. CalbindinD–28k has six EF-hand domains, but only four of thembind to calcium. Calbindin D–28k has been used asa marker of nerve cells in neuroanatomical studies,since it selectively distributes in subpopulations ofcentral nervous system neurons in specific regions.In the monkey thalamus, calbindin D–28k antibodiesselectively label the matrix domain of the medial ven-troposterior nucleus of the thalamus, which is relatedto trigeminothalamic projection from the caudal spinaltrigeminal nucleus subnucleus caudalis.� Trigeminothalamic Tract Projections
Calbindin-Immunoreceptive Matrix Cells
Definition
Sensory neurons that stain positively for the presence ofvitamin D-dependent calcium-binding protein.� Thalamic Nuclei Involved in Pain, Human and Mon-
key
Calcitonin Gene-Related Peptide
Synonyms
CGRP
Definition
CGRP is a 37-amino acid peptide that is produced bytissue-specific processing of the calcitonin gene. Itbelongs to the Calcitonin/CGRP family which includesother peptides like calcitonin, amylin, adrenomedullinand intermedin. CGRP is comprised of at least twoforms: αCGRP and βCGRP. Whereas αCGRP is foundin DRG neurons of all sizes, βCGRP is localized tosmall- and medium-sized neurons. CGRP functionsprimarily as a neuromodulator and signals via a het-erodimeric receptor complex consisting of a G-proteincoupled receptor (calcitonin-like receptor) and a recep-tor activity modifying protein (RAMP1) and stimulatescAMP formation intracellularly. Release of CGRP fromthe peripheral terminals of DRG neurons contributes toneurogenic inflammation. During this process, CGRPis the most potent vasodilator in the microcirculationidentified so far and acts by relaxing small arteriesand arterioles. Furthermore, CGRP acts together withsubstance P to potentiate plasma extravasation where
proteins from the blood stream pass into the surround-ing tissue. Release of CGRP from the central terminalsof DRG neurons modulates spinal cord neurons, in partby enhancing the actions of substance P. It also plays arole in pain processing.� Alternative Medicine in Neuropathic Pain� Calcitonin Gene-Related Peptide and Migraine
Headaches� Clinical Migraine without Aura� Immunocytochemistry of Nociceptors� Migraine, Pathophysiology� Neuropeptide Release in the Skin� Nociceptor, Categorization� Nociceptors in the Orofacial Region (Meningeal/
Cerebrovascular)� Opioids in the Periphery and Analgesia� Opioid Modulation of Nociceptive Afferents In Vivo� Spinal Cord Nociception, Neurotrophins� Thalamus, Visceral Representation
Calcitonin Gene-Related Peptide andMigraine Headaches
KIRSTEN ARNDT, STEFAN JUST, HENRI DOODS
CNS Pharmacology, Pain Research, BoehringerIngelheim Pharma GmbH & Co. KG, Biberach/Riss,[email protected]
Synonym
CGRP
Definition� Migraine isacomplex,multi-symptom diseaseaffect-ing 10–16% of the western population. It has a higherprevalence in women than in men. Migraine character-istics are its episodic appearance and symptoms suchas unilateral headache, phono- and/or photo-phobia,facial mechanical allodynia and nausea and vomit-ing (Headache Classification Subcommittee of theInternational Headache Society 2004). Preceding theheadache, 20–30% of the patients experience focal neu-rological symptoms termed aura. Based on the presenceor absence of an aura, migraines are classified as either“classical” migraine (migraine with aura), or “com-mon” migraine (migraine without aura). Generally, amigraine attack can be subdivided into different phasesthat include the premonitory phase, headache and thepostdrome. The prevalence of the different symptomsvaries over the phases with e.g. being tired and wearyas approximately equally prominent in all phases and“stiff neck” being most prevalent in the headache andpostdrome phases. Typically, a migraine attack lastsfrom 4 to 72 hours.

C
Calcitonin Gene-Related Peptide and Migraine Headaches 189
� Calcitonin gene-related peptide (CGRP) is a neu-ropeptide and important vasodilator. It is releasedduring migraine attacks. Blockade of CGRP receptorsin humans alleviates migraine pain.
Characteristics
Underlying Causes of a Migraine Attack
Despite many approaches to understand the initiationof migraine attacks, “the migraine trigger” or the phys-iological starting point has not yet been identified. Todate it is also not possible to come up with a primary un-derlying cause for migraines and probably there is morethan one. Several genetic factors have been discussedas rendering a person more susceptible to developingmigraines, as well as disturbances of central neuronalfunction or cranial changes in vasodynamics. Many ofthese hypotheses evolved from studies of one subtypeof migraine patients, the ones experiencing classicalmigraines. Potential genetic defects which might causeclassical migraines include e.g. missense mutations inthe � CACNA1A gene encoding the α1 subunit of thevoltage dependent P/Q type calcium channel, whichaccounts for 50% of an autosomal disease called famil-ial hemiplegic migraine (FHM1). Missense mutationsin the ATP1A2 gene, which encodes the α2 isoformof the enzyme Na, K-ATPase, have been shown to beresponsible for additional cases of FHM.Besides the genetic factors, local disturbances of centralneuronal function, i.e. the cortical spreading depression(CSD) of Leão or activity changes in brainstem/ mid-brain neuronal systems have been hypothesized to bea main cause underlying migraine attacks. In the fore-brain, CSD is a wave of excitation that propagates acrossthe cortex, followed by a wave of suppression. Recentevidence suggests that CSD is the physiological phe-nomenon causing the aura phenomenon of classical mi-graines (Hadjikhani et al. 2001). Whether CSDs also oc-cur in common migraines is not yet known. Neuronaldysfunctionofbrainstem/midbrainneuronalsystemsin-volved in pain inhibition/facilitation has also been sug-gested (Knight and Goadsby 2001; May 2003). HumanfMRI studies during migraine attacks indicate changedneuronal activity in certain brainstem and midbrain ar-eas (Weiller et al. 1995). The anatomical location sug-gests that the function of these regions is associated withadjusting nociceptive information entering the brain byeither inhibiting or facilitating the responses of neuronsand sensory terminals in the brainstem trigeminal nu-cleus caudalis (TNC). Furthermore, extensive changesin vasodynamics have long been implicated in the patho-genesis of migraines, e.g. alterations in intracranial ves-sel diameters followed by reactive changes in extracra-nial vessel diameters were already investigated in 1938by Graham and Wolff. Also, the first specific treatmentemployed, the ergotamines, work as vasoconstrictors.More recent support for the importance of vasodilata-
tion is coming from observations employing transcra-nial laserDopplermeasurements,whichsuggest thatmi-graine attacks are associated with intracranial large ar-terial dilatation on the headache side.Together the possible causes described above providelinks to the observed migraine symptomatology and po-tential underlying mechanisms. They deliver the biolog-ical “hardware” which contributes to migraine patho-genesis. The focus is on the cranial vasculature and thetrigeminal sensory system controlling the vasculatureand transmitting information to brainstem and midbrainnuclei,which in turn monitor and adjust the incoming in-formation. During a migraine attack, adjustments madeby these systems might be reflected by certain symp-toms. As an example, the symptom unilateral throbbingpain at the temples seems to be caused by mechanismslike sensitization of sensory afferents in the periphery.In addition, facial mechanical allodynia might be initi-ated by neuronal sensitization processesadvancing fromsensory to central neurons (Burstein et al. 2000). Under-standing migraine symptoms and the potential mecha-nisms driving an attack is an important basis for under-standing the disease and getting a handle on the essentialmolecular drivers that direct the biological systems to-wards a migraine attack.
The Neuropeptide CGRP, an Important Molecular Player in Mi-graine Attacks
Several molecules have been identified that triggerheadache responses fulfilling the criteria of migraineattacks. Among them are NO released from glyceryltrinitrate (GTN), histamine, prostaglandin E1 andCGRP. These molecules have in common that they in-duce vasodilatation and affect sensory neuron function.The 37 amino acid neuropeptide CGRP has been shownto be one of the most potent vasodilators in human andanimal tissues and is widely distributed throughout thebody. Two isoforms, α and β CGRP are known, whichoriginate from different genes. The isoforms differ byonly 1 and 3 amino acids in rats and humans, respec-tively. The peptides are expressed by primary afferentneurons, which mostly fire in the C- and Aδ fiber range,as well as by motor neurons, the autonomous nervoussystem and central neurons. The CGRP receptor medi-ating CGRP function consists of three components, a Gprotein coupled seven transmembrane receptor elementknown as calcitonin-like receptor (CLR) a receptorassociated membrane protein 1 (RAMP1) and a proteintermed receptor component protein (RCP) (Poyneret al. 2002). While CLR and RAMP1 are membraneconstituents, RCP is a cytoplasmic protein shown tobe crucial for the efficient intracellular coupling of theG protein and adenylate cyclase and thus for the pro-duction of cAMP. Constituents of the CGRP receptorhave been shown to be expressed by peripheral andcentral neurons as well as by smooth muscle cells inthe vascular system.

190 Calcitonin Gene-Related Peptide and Migraine Headaches
Ample evidence that CGRP could play an importantrole in migraine pathophysiology comes from variousstudies investigating the transmitter content of externaljugular vein blood during migraine attacks (Goadsbyand Edvinsson 1994, Sarchielli et al. 2000). These stud-ies demonstrate that levels of CGRP normally found tobe in the lower pM range and below are approximately2-fold increased during acute migraine attacks. Also,increasing the plasma levels by ashort infusion ofCGRPtriggers immediate headaches fellowed by a delayedsevere headache in migraineurs. The symptoms of thedelayed headache are indistinguishable from that of amigraine. Furthermore, current gold standard migrainetreatment with sumatriptan, a 5HT1B/1D agonist, re-duces blood levels of CGRP in humans and in animalexperiments. A relationship between pain intensity andplasma CGRP levels has been suggested. Finally, moredirect evidence for the contribution of CGRP to mi-graine pain was introduced by a recent phase II clinicaltrial. Olesen et al. (2004) investigated the effectivenessof the small molecule CGRP antagonist BIBN4096in reducing migraine pain. In this multicenter, doubleblind, randomized clinical trial, a dose dependent relieffrom migraine pain was observed after BIBN4096 in-travenous administration. The 2.5 mg dose representedthe dose group with the highest patient number. It dis-played a response rate of approximately 66% over 27%for placebo (Fig. 1). A general pain relieving effect wasalready observed 30 min after application of BIBN4096.Significant efficacy over placebo was also observed inother migraine specific secondary endpoints, includingthe pain-free rate, the 24 hr recurrence rate and typicalmigraine associated symptoms like nausea and phono-and/or photo-phobia. The drug was well tolerated andno serious adverse events were observed.In summary, evidence like increased CGRP levels dur-ing an attack, the induction of migraine attacks by in-fusion of CGRP, CGRP levels showing a relationship to
Calcitonin Gene-Related Peptide and Migraine Headaches,Figure 1 Two hr headache response after intravenous administration ofseveral doses BIBN4096 in the phase II clinical trial.
pain intensity and high CGRP levels detected early in anattack, as well as current and future treatment affectingCGRP function, point to a significant contribution of theneuropeptide to the pathogenesis of migraines. CGRPmightbenotonly amarkerbutalso an importantdriverofprocessesunderlyingmigrainesymptomatology.Never-theless, to date its mechanism of action in the migrainesetting is still not fully understood.
Potential Function of CGRP in Migraine
Some insights into the potential function of CGRPcome from animal studies investigating the activity ofthe highly selective and competitive CGRP antago-nist BIBN4096 in the vascular and neuronal system.BIBN4096 has a high affinity for the human CGRP re-ceptor (14.4 pM) and potently reverses CGRP-inducedvasodilatation in various rat and guinea pig vasculartissues as well as human cerebral arteries (Doods 2001).Furthermore, in an in vivo model where an increase infacial blood flow is induced by unilateral electricalstimulation of the trigeminal ganglion, BIBN4096 dosedependently reduces the evoked blood flow with anID50 of 0.003 mg/kg in marmoset monkeys. Recentdetailed investigations into the mechanism of action ofthe antagonist in humans showed that in healthy volun-teers BIBN4096 prevented CGRP-induced extracranialdilatation and concomitantly reduced CGRP-inducedheadaches (Petersen et al. 2005). Together these datasupport thesignificanceofCGRP-inducedvasodynamicchanges in migraine headaches.CGRP and its receptor system are not only expressed bythe vasculature but also by trigeminal and second orderneurons in the brainstem TNC. It therefore might well bethat during migraine attacks increased CGRP levels in-fluence trigeminal neuronal information processing be-sides affecting vasodynamics. Unfortunately, the role ofCGRP is not very well explored in the trigeminal sys-tem. This is especially true for the primary afferent. Inthe central portion, direct application of αCGRP into theTNC increased the firing rate of the neurons. In this set-ting, intravenous administration of theCGRP antagonistBIBN4096 dose dependently inhibited increased activ-ity of TNC neurons. Because the selective CGRP antag-onist BIBN4096 is able to reduce central neuronal activ-ity, the data suggest that CGRP participates in increasingthe activity of and/or sensitizing second orderneurons inthe TNC under these experimental conditions. WhetherCGRP sensitizes central second order neurons directlyor increases thefiring rateof trigeminalneurons that thendrive central sensitization or both has still to be demon-strated.In summary, these experimental animal studies sug-gest that CGRP can affect nociceptive processing inthe trigeminal system. Increased CGRP levels beingpresent during migraine attacks could imply a role ofCGRP in sensitization of primary and/or central neurons

C
Calcium Channels in the Spinal Processing of Nociceptive Input 191
Calcitonin Gene-Related Peptide and Migraine Headaches, Figure 2 Possible points of action of CGRP in migraine pathogenesis.
besides inducing vasodynamic changes in the cranialvasculature (Fig. 2).Although migraine pathogenesis still offers vaguenesswith respect to the trigger(s) and numerous hypotheseson causes and the biological processes behind the symp-toms, the testing of new molecular principles like that oftheCGRPantagonistBIBN4096 opensnewpaths for theunderstanding of underlying mechanisms and the iden-tification of important contributors to this complex dis-ease.
References1. Burstein R, Yarnitsky D, Goor-Aryeh I et al. (2000) An asso-
ciation between migraine and cutaneous allodynia. Ann Neu-rol 47:614–624
2. Doods H (2001) Development of CGRP antagonists for the treat-ment of migraine. Curr Opin Investig Drugs 9:1261–1268
3. Goadsby PJ, Edvinsson L (1994) Neuropeptides in migraine andcluster headache. Cephalalgia 14:320–327
4. Graham JR, Wolff HG (1938) Mechanism of migraine headacheand action of ergotamine tartrate. Arch Neurol Psychia-try 39:737–763
5. Hadjikhani N, Sanchez Del Rio M, Wu O et al. (2001) Mech-anisms of migraine aura revealed by functional MRI in humanvisual cortex. Proc Natl Acad Sci USA 98:4687–4692
6. Headache Classification Subcommittee of the InternationalHeadache Society (2004) The international classification ofHeadache disorders. Cephalalgia 24:9–160
7. Knight YE, Goadsby PJ (2001) The periaqueductal grey mattermodulates trigeminovascular input: a role in migraine? Neuro-science 106:793–800
8. May A (2003) Headache: lessons learned from functional imag-ing. Br Med Bull 65:223–234
9. Olesen J, Diener HC, Husstedt IW et al. (2004) BIBN 4096 BSClinical Proof of Concept Study Group. Calcitonin gene-relatedpeptide receptor antagonist BIBN 4096 BS for the acute treatmentof migraine. N Engl J Med 350:1104–1110
10. Petersen KA, Lassen LH, Birk S et al. (2005) BIBN4096BS an-tagonizes human alpha-calcitonin gene related peptide-induced
headache and extracerebral artery dilatation. J Clin PharmacolTher 77:202–213
11. Poyner DR, Sexton PM, Marshall I et al. (2002) InternationalUnion of Pharmacology. XXXII. The mammalian calcitoningene-related peptides, adrenomedullin, amylin, and calcitoninreceptors. Pharmacol Rev 54:233–246
12. Sarchielli P, Alberti A, Codini M et al. (2000) Nitric oxidemetabolites, prostaglandins and trigeminal vasoactive peptidesin internal jugular vein blood during spontaneous migraineattacks. Cephalalgia 20:907–918
13. Weiller C, May A, Limmroth V et al. (1995) Brain stem activationin spontaneous human migraine attacks. Nat Med 1:658–660
Calcium Channel Blockers
Definition
A class of drugs with the capacity to prevent calciumions from passing through biologic membranes. Theseagentsareused to treathypertension,anginapectorisandcardiac arrhythmias; examples include nifedipine, dilti-azem, verapamil, amlodipene.� Headache Attributed to a Substance or its Withdrawal
Calcium Channels in the SpinalProcessing of Nociceptive Input
HORACIO VANEGAS
Instituto Venezolano de Investigaciones Cientificas(IVIC), Caracas, Venezuela and Institute forPhysiology, Friedrich Schiller University, Jena,[email protected]

192 Calcium Channels in the Spinal Processing of Nociceptive Input
Synonyms
Voltage-Dependent Calcium Channels; VDCCs; volt-age-sensitive calcium channels; VSCCs, high-thresholdcalcium channels; High-Threshold VDCCs; High-Voltage Calcium Channels; HVCCs; Low-ThresholdCalcium Channels; Low-Threshold VDCCs; Low-Voltage Calcium Channels; LVCCs; hyperalgesia;allodynia; spinal dorsal horn; spinal nociceptive trans-mission
Definition
Calcium channels that open upon depolarization(voltage-dependent calcium channels, VDCCs) en-able calcium ions to enter neurons. VDCCs are therebyinvolved in synaptic transmission, changes inmembraneexcitability, intracellular regulation of second and thirdmessengers and expression of genes. Spinal VDCCsthat are opened by relatively largedepolarizations (high-threshold VDCCs) or by small depolarizations (low-threshold VDCCs) are involved in normal nociceptionas well as in the hyperalgesia and allodynia that resultfrom inflammatory and mechanical lesions ofperipheraltissues or from lesions of primary afferents fibers.
Characteristics
Voltage-Dependent Calcium Channels
VDCCs are classified according to their electrophysi-ological properties and their sensitivity to specific an-tagonists (Miljanich and Ramachandran 1995). L-, N-,P/Q- and R-type are high-threshold whereas T-type arelow-threshold VDCCs. Most of what is known regard-ing the role of spinal VDCCs in pain (see Vanegas andSchaible 2000 for a comprehensive review)derives fromstudies based on the use of specific channel antagonistsor blockers (Table 1). By definition, there are no specificblockers for R-type VDCCs; their role in pain mecha-nisms is thereforeunclear. Oneand thesameneuronmayexpress several types of VDCC. An antagonist to onlyone channel type therefore blocks only a fraction of the
Calcium Channels in the Spinal Processing of Nociceptive Input,Table 1 Some antagonists to voltage-dependent calcium channels
channeltype
antagonist
L Benzothiazepines: diltiazemDihydropyridines: nicardipine, nifedipine, nimodipine,nitrendipinePhenylalkylamines: verapamil
N ω -Conopeptides:natural : ω-conotoxin-GVIA, ω-conotoxin-CIVD (AM336)synthetic: SNX-111 (equivalent to ω-conotoxin-MVIIA),SNX-124 (equivalent to ω-conotoxin-GVIA), SNX-159,SNX-239
P/Q ω- Agapeptide: ω-agatoxin-IVA
T ethosuximide
VDCCs present in a neuron or a neuronal ensemble suchas the spinal cord, but the effect of one antagonist maybe additive to the effect of antagonists to other channeltypes.
Animal Models for the Study of VDCCs in Nociception
On the one hand there are the models for “acute” noci-ception, in which brief and intense stimuli are appliedto normal tissues (see Vanegas and Schaible 2000).These stimuli include noxious heat or noxious pressureas applied to skin or joints, application or injectionof algogenic substances such as capsaicin, mustardoil, formalin or acetic acid, and noxious distension ofhollow viscera. Upon stimulus application, withdrawalreflexes and other protective behaviors can be measuredor the response of dorsal spinal nociceptive neurons canbe recorded prior to and during the action of specificVDCC antagonists. Also spinal neuronal responses toelectrical stimulation of nociceptive primary afferentfibers may serve as a measure of nociception.On the other hand, animal models of persistent damageinclude inflammation of skin or joints, surgical wounds,long-lasting hyperexcitability induced by applicationor injection of capsaicin, mustard oil or formalin, lig-ation of peripheral nerves, and diabetic neuropathy(see Vanegas and Schaible 2000). These manipulationsinduce peripheral and central sensitization and theexperimental animals thus respond in an exaggeratedmanner to the “acute” stimuli mentioned above. This isakin to � hyperalgesia and � allodynia, and the effectof specific VDCC antagonists on these exaggeratedresponses can be investigated.It is now possible to generate mice that lack one of themolecular subunits of specific calcium channels and tostudy their nociceptive responses both under normal andunder sensitized conditions. The VDCC defect in theseanimals, however, is not restricted to the spinal cord.
Role of Spinal VDCCs in Nociception
Normal Nociception
In awake and in anesthetized rats, L- and N-type antag-onists may or may not depress responses to mechanicalinnocuous or noxious, thermal noxious and visceralnoxious stimuli, or responses to electrical stimulationof nociceptive afferents (e.g. Malmberg and Yaksh1994; Neugebauer et al. 1996). Blockade of spinalP/Q-type channels causes a slight increase in neu-ronal responses, thus suggesting that they normallyparticipate in predominantly inhibitory mechanisms(Matthews and Dickenson 2001a; Nebe et al. 1999).Finally, blockade of spinal T-type channels causes aninhibition of spinal neuronal responses to electricalstimulation of nociceptive afferents as well as to low-and high-intensity mechanical and thermal stimuli(Matthews and Dickenson 2001b).Mice with a genetically induced lack of N-type VD-CCs may or may not show decreased responses to

C
Calcium Channels in the Spinal Processing of Nociceptive Input 193
“acute” thermal and/or mechanical noxious stimuli(Hatakeyama et al. 2001; Kim et al. 2001; Murakamiet al. 2002; Saegusa et al. 2001). Mice that lack the α1Esubunit (which may be part of the R- or the T-type chan-nel) have normal responses to thermal and mechanicalnoxious stimuli (Saegusa et al. 2000).
Sensitized Nociception
In animal models that utilize nociceptive stimulationby means of capsaicin or mustard oil (see Vanegasand Schaible 2000), blockade of spinal N-type chan-nels always prevents the subsequent exaggeration ofresponses (primary and secondary hyperalgesia and al-lodynia) to “acute” test stimuli. Also, blockade of spinalL- or P/Q-type channels generally prevents secondaryhyperalgesia and allodynia.As regards responses to test stimuli during inflammationor inflammation-like processes such as surgical wounds,blockade of N-type channels in animals has never failedto prevent or attenuate primary hyperalgesia, secondaryhyperalgesia and allodynia or the late, “inflamma-tory” response to formalin injection (see Vanegas andSchaible 2000). The most effective doses of N-typeantagonists, however, cause motor disturbances after30–60 min. In human patients, one intrathecally admin-istered N-type channel blocker alleviated postsurgicalpain but produced severe adverse effects (Atanassoffet al. 2000). On the other hand, blockade of spinal L-type channels has generally prevented the late phase ofthe formalin response and has attenuated primary andsecondary mechanical hyperalgesia and allodynia (butnot thermal hyperalgesia) due to knee inflammation.Finally, blockade of spinal P/Q-type channels beforeand during induction of inflammation prevents the ex-aggeration of responses to stimulation of the inflamedknee or the uninflamed ankle. However, blockade ofP/Q-type channels when central sensitization is alreadyestablished attenuates only responses to stimulationof the sensitized nociceptors in the knee (primary hy-peralgesia and allodynia) but has no influence uponresponses to stimulation of normal nociceptors in theuninflamed ankle (Nebe et al. 1997). The effect of agiven compound on the prevention of a painful condi-tion may therefore be different from its effect on thealleviation of the already established condition.Mice with a genetically induced lack of either N-typeVDCCs or the α1E subunit of VDCCs show an at-tenuation of the late phase of the formalin response(Hatakeyama et al. 2001; Kim et al. 2001; Saegusa etal. 2000; Saegusa et al. 2001). The writhing responseto intraperitoneal acetic acid, a model of visceral noci-ception, may (Kim et al. 2001) or may not (Saegusa etal. 2000; Saegusa et al. 2001) be attenuated.In animals with peripheral nerve damage, spinal appli-cation of antagonists to either L- or P/Q-type VDCCsdoes not alter the hyperalgesia and allodynia, nor theincreased spinal neuronal responses to noxious heat,
pressure or electrical stimulation of nociceptive affer-ents (Matthews and Dickenson 2001a; see Vanegasand Schaible 2000). In contrast, spinal application ofN-type channel antagonists has proven effective againstneuropathic nociceptive behavior in animals (see Vane-gas and Schaible 2000) and against the increased spinalneuronal responses to noxious heat, pressure or elec-trical stimulation of nociceptive afferents induced bynerve damage (Matthews and Dickenson 2001a). Also,mice with a genetically induced lack of N-type VDCCsfail to develop neuropathic behavioral responses afterperipheral nerve damage (Saegusa et al. 2001). Intrathe-cal administration of one N-type antagonist alleviatedneuropathic pain and allodynia in human patients, al-though with considerable adverse effects (Brose et al.1997; Penn and Paice 2000). Finally, the inhibition by aT-type VDCC antagonist of spinal neuronal responsesto noxious heat, pressure or electrical stimulation of no-ciceptive afferents remains unaltered after developmentof neuropathy (Matthews and Dickenson 2001b).
In Summary
PharmacologicalorgeneticreductionofVDCCfunctionmay or may not have an effect upon normal nocicep-tive mechanisms. In situations where inflammation orinflammation-like processes have induced an enhance-ment of spinal nociceptive phenomena (central sensiti-zation), the participation of VDCCs in the spinal pro-cessing of nociceptive input becomes more obvious andreduction ofL-,P/Q-,T-and,particularly,N-typeVDCCfunctionattenuates theexaggerationofresponses tonox-ious and innocuous stimulation. N-type VDCC antago-nists also attenuate the spontaneous pain, the hyperalge-sia and the allodynia that result from damage to primaryafferents, yet with considerable adverse effects.
Potential Therapeutic Use of VDCC Antagonists
Any hope of using VDCC antagonists for alleviating hy-peralgesia and allodynia in a clinical setting must reckonwith several drawbacks. All studies with spinal VDCCantagonists have used the intrathecal route of adminis-tration, which is problematic, especially for compoundsof low water solubility. On the other hand, systemicallyadministered VDCC antagonists may have undesirableeffects on a variety of organs. Sufficiently beneficial ef-fects with VDCC antagonists are attained mostly withdoses that already cause unwanted effects. At the sametime, VDCC antagonists have some positive attributes.They may block the synaptic release of several media-tors involved in nociceptive transmission, hyperalgesiaand allodynia. This would be an advantage over the useof individual antagonists to, e.g. glutamate, � substanceP, neurokinin A and � CGRP. In contrast with opioids,which may also decrease synaptic release,VDCC antag-onistsdonotseemtogiverise to tolerance. Insomecases,normal somethesia and motricity have been spared bydoses that are effective against hyperalgesia and allody-

194 Calcium Spike Bursts
nia. Specific antagonists to various VDCC types can becombined in submaximal doses to achieve a summatedeffect. Finally, VDCC antagonists may synergize with,e.g. opiates and local anesthetics.
References1. Atanassoff PG, Hartmannsgruber MW, Thrasher J et al. (2000)
Ziconotide, a new N-type calcium channel blocker, administeredintrathecally for acute postoperative pain. Reg Anesth Pain Med25:274–278
2. Brose WG, Gutlove DP, Luther RR et al. (1997) Use of intrathe-cal SNX-111, a novel, N-type, voltage-sensitive, calcium channelblocker, in the management of intractable brachial plexus avul-sion pain. Clin J Pain 13:256–259
3. Hatakeyama S, Wakamori M, Ino M et al. (2001) Differentialnociceptive responses in mice lacking the α1B subunit of N-typeCa2+ channels. NeuroReport 12:2423–2427
4. Kim C, Jun K, Lee T et al. (2001) Altered nociceptive responsesin mice deficient in the α1B subunit of the voltage-dependentcalcium channel. Mol Cell Neurosci 18:235–245
5. Malmberg AB, Yaksh TL (1994) Voltage-sensitive calcium chan-nels in spinal nociceptive processing: blockade of N- and P-type channels inhibits formalin-induced nociception. J Neurosci14:4882–4890
6. Matthews EA, Dickenson AH (2001a) Effects of spinally de-livered N- and P-type voltage-dependent calcium channel an-tagonists on dorsal horn neuronal responses in a rat model ofneuropathy. Pain 92:235–246
7. Matthews EA, Dickenson AH (2001b) Effects of ethosuximide, a
T-type Ca2+ channel blocker, on dorsal horn neuronal responsesin rats. Eur J Pharmacol 415:141–149
8. Miljanich GP, Ramachandran J (1995) Antagonists of neuronalcalcium channels: structure, function, and therapeutic implica-tions. Annu Rev Pharmacol Toxicol 35:707–734
9. Murakami M, Fleischmann B, De Felipe C et al. (2002) Painperception in mice lacking the β3 subunit of voltage-activatedcalcium channels. J Biol Chem 277:40342–40351
10. Nebe J, Vanegas H, Neugebauer V et al. (1997) ω-Agatoxin IVA,a P-type calcium channel antagonist, reduces nociceptive pro-cessing in spinal cord neurons with input from the inflamed butnot from the normal knee joint -An electrophysiological studyin the rat in vivo. Eur J Neurosci 9:2193–2201
11. Nebe J, Ebersberger A, Vanegas H et al. (1999) Effect of ω-agatoxin IVA, a P-type calcium channel antagonist, on the de-velopment of spinal neuronal hyperexcitability caused by kneeinflammation in rats. J Neurophysiol 81:2620–2626
12. Neugebauer V, Vanegas H, Nebe J et al. (1996) Effects of N-and L-type calcium channel antagonists on the responses of no-ciceptive spinal cord neurons to mechanical stimulation of thenormal and inflamed knee joint J Neurophysiol 76:3740–3749
13. Penn RD, Paice JA (2000) Adverse effects associated with theintrathecal administration of ziconotide. Pain 85:291–296
14. Saegusa H, Kurihara T, Zong S et al. (2000) Altered pain re-sponses in mice lacking the α1E subunit of the voltage-dependentCa2+ channel. Proc Natl Acad Sci USA 97:6132–6137
15. Saegusa H, Kurihara T, Zong S et al. (2001) Suppression of in-flammatory and neuropathic pain symptoms in mice lacking theN-type Ca2+ channel. EMBO J 20:2349–2356
16. Vanegas H, Schaible H-G (2000) Effects of antagonists to high-threshold calcium channels upon spinal mechanisms of pain, hy-peralgesia and allodynia. Pain 85:9–18
Calcium Spike Bursts
� Burst Activity in Thalamus and Pain
Calculosis
� Visceral Pain Model, Kidney Stone Pain
CAMs
� Cellular Adhesion Molecules
Cancer PainZBIGNIEW ZYLICZ, MAŁGORZATA KRAJNIK
St. Elizabeth Hospice, Ipswich, Suffolk, [email protected]
Synonyms
Malignant pain; Pain Due to Cancer; oncological pain
Definition
’Cancer pain’ is a conglomerate name for all kinds ofpain symptoms experienced in the course of a malignantdisease. The common denominator of pain associatedwith cancer is that the suffering experienced by the pa-tient is a combination of many different kinds of pain,for example, other symptoms of the disease as well aspsychological, spiritual and existential factors.
Characteristics
Pain is experienced by 20–50% of cancer patients atthe time of diagnosis. This prevalence increases up to75% in the case of patients with advanced stages ofthe disease. Within these statistics half of the patientsnormally experience moderate or severe pain, whereas20–30% experience very severe or excruciating pain(Anonymous 1990).Usually, cancer patients experience pain of more thanone quality and in more than one location. Only 20% ofpatients experience one single location of pain. In onethird of patients there are three of more pain locations(Twycross et al. 1996).According to Grond et al. (1996) cancer pain may berelated to:
• tumor growth: 85%• tumor treatment: 17%• progressive debility:9%• concurrent disorder: 9%
Cancer pain may originate in many locations and havemultiple, inter-twined mechanisms. The top 10 painsamong 211 patients (Twycross 2003) with advancedcancer were:
• bone• visceral

C
Cancer Pain 195
• neuropathic• soft tissue• immobility• constipation• myofascial• cramp• esophagitis• degeneration of the spine
It therefore follows that careful evaluation and exami-nation is necessary to make a diagnosis of cancer pain.Evaluation of pain is based primarily on probability andpattern recognition. Factors that may be helpful in thediagnosis of cancer pain are:The natural history of the disease (e.g. breast canceroften causes bone metastases and � bone pain, ovariancancermay rarely causebrainmetastasesandheadache).A time course of the pain symptoms may be important.� Brachial or lumbal plexopathy that resulted in paineven before radiation therapy is probably caused by thegrowth of the tumor, but may be exacerbated by the ra-diation therapy. Lack of pain two or three weeks afterirradiation may be not related to the opioids adminis-tered, but to the radiation therapy.Plain radiographic imaging is helpful in discoveringthe origin of bone pain. Pain originating in soft tissuesand neural tissues needs more sophisticated techniques(MRI). Some types of pain (e.g. � neuropathic pain)may be “invisible” to radiographic imaging. Neuro-pathic pain may frequently be a component of anotherpain (Portenoy et al. 1999), it may be a complication oftherapy, but may also be a paraneoplastic symptom. Anevaluation of neurological deficit may frequently leadto better understanding and diagnosis of pain. � Spinalcord compression (SCC) occurs in 3% of all cancerpatients.� Nerve compression or entrapment usually gives a spe-cific syndrome (e.g. vertebral collapse may cause nerveroot compression).� Response to analgesics may often give a clue to thetype of pain (e.g. nociceptive pain responds readily toopioids, while neuropathic pain may be resistant to thistreatment). Full history of the pharmacological and non-pharmacological treatment of the pain should be taken.Emotional, socialandspiritual factorsmaymakethepre-cise diagnosis of pain difficult, and should be recognizedand addressed specifically.A distinction should be made between pain whilst at restand pain during movement. Pain may have a circadiandistribution. Many types of cancer pains are constant,but some may appear to have an exploding character(� breakthrough pain), even when the optimal analgesiais provided (Portenoy et al. 1999).Patients who describe their pain as throbbing, lancinat-ing and burning, and exacerbated by light touch duringexamination, may appear to have � mechanical allody-nia.
Cancer Pain, Table 1 The WHO analgesic ladder
Step 1 Step 2 Step 3
Non-opioids weak opioids strong opioids
paracetamol, variousNSAIDs
Codeine, tramadol,low dose oxycodone
morphine, fentanyl,oxycodone,methadone
Knowledge of the so called � referred pain syndromes(Giamberardino and Vecchiet 1995) can be helpful inestablishing diagnosis (e.g. unilateral facial or ear painmay be associated with mediastinal involvement bybronchial carcinoma or reflux esophagitis. Right shoul-der pain may be due to an enlarged liver. Metastases inthe lower lumbar region may result in pain localized inthe sacroiliacal joint.Most types of cancer pain respond readily to analgesics.Principles of cancer pain treatments were elaborated bythe WHO (1990). In specialist centers, 95–98% of painsymptoms can be successfully treated.Cancer pain is not usually the only symptom of the dis-ease. It is frequently accompanied by other symptomslike: � delirium, nausea and vomiting, weakness, fa-tigue, weight loss, dyspnea, dry mouth, constipation ordiarrhea, pruritus and probably many others. Treatmentof pain alone may decrease its intensity but increaseintensity of other symptoms. So cancer pain shouldalways be seen in the context of other symptoms and inthe context of the whole person.Cognitive failure progressing to delirium, but also someother adverse effects that emerge in the course of treat-ment, may compromise the patients quality of life moreseriously than pain. So the aim of the treatment is thebalanced control of all symptoms, not only pain control.Sometimes making pain and other symptoms bearable,but not alleviating them fully, is the only viable option.The principles of WHO are as follows:
• preferably give the medication by mouth• give the next dose of analgesics before the effect of
the previous dose ceases• give drugs according to the � analgesic ladder• use adjuvant drugs, either to alleviate the adverse
effects of analgesics or to enhance them, anal-gesia therapy should be individualized (Anony-mous 1990)
Cancer pain is usually a dynamic and complex phe-nomenon that should be assessed regularly. Prolongeduse of analgesics may induce plastic changes in thecentral nervous system which are similar to those in-duced by pain itself. Also, prolonged use of opioiddrugs for pain may induce tolerance, while the adverseeffects may increase. To prevent this, more and morecombinations of the various drugs are used. With properchoice of drugs, continuous assessment and adjustment

196 Cancer Pain, Animal Models
Cancer Pain, Table 2 Analgesic adjuvants
indication drugs used
insufficient analgesic effects ketamine
neuropathic pain amitryptyline, venlafaxine, gabapentin
nerve entrapment, compression dexamethasone, NSAIDs
reflux esophagitis proton pump inhibitors
abdominal cramp, bladder cramp butyl-scopolamine
muscle cramp benzodiazepine, baclofen
respiratory depression, breathlessness, sedation, tiredness methylphenidate
constipation lactulose and sennosides, or macrogol
nausea and vomiting metoclopramide, haloperidol, levomepromazine, cyclizine
dry mouth pilocarpine
pruritus paroxetine
of medication, it is possible to control pain with opti-mal preservation of alertness in most cancer patients.Controlling cancer pain is of importance for the dyingpatient, as well as for the family of the dying who needto carry on normal living insofar as that is possible, andto adapt to the loss of a loved one.� Cancer Pain Management, Treatment of Neuropathic
Components� Pain Treatment, Intracranial Ablative Procedures� Psychiatric Aspects of the Management of Cancer
Pain
References1. Anonymous (1990) Cancer Pain Relief and Palliative Care. Re-
port of a WHO Expert Committee. World Health Organ TechRep Ser 804:1–75
2. Giamberardino MA, Vecchiet L (1995) Visceral Pain, ReferredHyperalgesia and Outcome: New Concepts. Eur J AnaesthesiolSuppl 10:61–66
3. Grond S, Zech D, Diefenbach C et al. (1996) Assessment ofCancer Pain: A Prospective Evaluation in 2266 Cancer PatientsReferred to a Pain Service. Pain 64:107–114
4. Portenoy RK, Payne D, Jacobsen P (1999) BreakthroughPain: Characteristics and Impact in Patients with Cancer Pain.Pain 81:129–134
5. Twycross R (2003) Cancer Pain Syndromes. In: Sykes N, Fal-lon MT, Patt RB (eds) Clinical Pain Management. Cancer Pain.London, Arnold, pp 3–19
6. Twycross R, Harcourt J, Bergl S (1996) A Survey of Painin Patients with Advanced Cancer. J Pain Symptom Man-age 12:273–282
Cancer Pain, Animal ModelsMARY ANN C. SABINO, PATRICK W. MANTYH
Department Prevential Science, University ofMinnesota, Minneapolis, MN, [email protected]
Definition
Cancer pain, distinguished from non-malignant pain,arises from tumor cells which invade soft tissue and/orbony structures, or occur as a result of therapies usedto treat cancer.
Characteristics
Although there is significant variability in the type,severity and evolution of this pain, two major compo-nents are generally recognized. The first component,known as � ongoing pain, is most often the first topresent, described as a dull ache or throbbing in char-acter and usually increases in severity with diseaseprogression. A second component of bone cancer painfrequently emerges over time and is more acute innature. This second pain is known as � incident or� breakthrough pain, as it frequently occurs eitherspontaneously, with intermittent exacerbations of painor by movement of the cancerous bone (Mercadanteand Arcuri 1998). For many patients, pain is the firstsign of cancer and 30–50% of all cancer patients willexperience moderate to severe pain. Cancer-associatedpain can be present at any time during the course ofthe disease, but the frequency and intensity of cancerpain tends to increase with advancing stages of can-cer. 75–95% of patients with metastatic or advancedstage cancer will experience significant amounts ofcancer-induced pain (Portenoy et al. 1999).The first animal model of bone cancer pain involvedthe injection of murine osteolytic sarcoma cells into theintramedullary space of the murine femur (Fig. 1). Acritical component of this model is that the tumor cellsare confined within the marrow space of the injectedfemur, and the tumor cells do not invade adjacent softtissues (Schwei et al. 1999). Following tumor injec-tion, the fluorescent cancer cells proliferate, and both

C
Cancer Pain and Pain in HIV / AIDS 197
Cancer Pain and Pain in HIV / AIDSRUSSELL K. PORTENOY
Department of Pain Medicine and Palliative Care,Beth Israel Medical Center, New York, NY, [email protected]
Synonyms
Cancer-related pain; HIV / AIDS-related pain; Pain inHIV / AIDS
Definition
Theterms“cancerpain”and“pain inHIV/AIDS”referto the assessment and management of acute or chronicpain syndromes that are either directly related to a ma-lignant neoplasm or to HIV infection respectively or tothe treatments that are used to manage these diseases.
Introduction
Chronic pain, a highly prevalent symptom in popula-tions with cancer or HIV / AIDS, may be associatedwith loss of function, compromised quality of life andprofound suffering. Although there are important dif-ferencesbetween cancerand HIV/AIDS,and each dis-order itself is extraordinarily diverse, there are broadcommonalities in the approach to pain assessment andmanagement. The specific issues encountered in themanagement of HIV / AIDS are addressed in the es-say on � Pain in HIV / AIDS. The remaining essaysin this section, which focus on cancer pain may be un-derstood to apply to both the cancer and HIV / AIDSpopulations.
Epidemiology
Studies of cancer pain epidemiology reveal that ap-proximately 30–50% of patients undergoing antineo-plastic therapy and 75–90% of patients with advanceddiseasehavechronicpainsevereenoughtowarrantopi-oid therapy (Vainio and Auvinen 1996). Although theprevalenceofpaininHIV/AIDShasprobablydeclinedwith the advent of highly active anti-retroviral therapy,recent surveys suggest that chronic pain affects abouthalf of this population (Dobalian et al. 2004).It is widely accepted that a large majority of patientswith cancer pain can attain satisfactory relief withavailable therapies. Unfortunately, surveys indicate ahigh rateofundertreatment (Andersonetal. 2004).Un-dertreatment is a complex phenomenon that may resultfrom a variety of patient-related barriers and clinician-related barriers or from distortions in the health caresystem that limit access to treatment. Recent studiesunderscore the influence on these barriers of cultural
factors, and race and ethnicity (Anderson et al. 2004;Green et al. 2003). Education of patients, families andprofessional staff, and system level strategies such asquality improvement activities are needed to addressthe problem of undertreatment.
Models of Care
In populations with life-threatening illnesses, the man-agement of pain should be incorporated into a broadereffort toameliorate thephysical,psychosocialandspir-itual issues that undermine quality of life or worsensuffering for the patient or family. The therapeutic ap-proach thataddresses these issues isknownaspalliativecare. The relationship between cancer pain and pallia-tive care (see � Cancer Pain Management, InterfacebetweenCancerPainManagementandPalliativeCare)must be understood to optimize the care of these pa-tients, particularly those with advanced disease.Palliative care is a therapeutic approach to the care ofpatients with life-threatening illnesses and their fami-lies. It is focusedonmaintainingqualityof life through-out the course of the illness and addressing the chal-lenging needs of patients who are approaching the endof life. The goals of this model include control of painand other symptoms; management of psychologicaldistress, comorbid psychiatric disorders and spiritualdistress; support for effective communication and de-cision making; provision of practical help in the home;and ongoing support for the family and managementof the dying process in a manner that allows a comfort-able and dignified death and effective grieving on thepart of the family.Palliative care is now considered an approach thatshould be implemented at a generalist level by ev-ery physician who cares for those with serious med-ical illness. It should also be available at a special-ist level for those patients and families who warrantthis level of care. The need for specialist level pallia-tive care, which typically occurs in the setting of ad-vanced illness is being met in the United States bya growing number of institution-based palliative careprograms(www.nationalconsensusproject.org)andbymore than 3300 hospice programs providing palliativecare at the end of life. All of these programs are un-derutilized and poorly understood by patients, familiesand professional staff.
Evaluation of Pain
The goals � of pain assessment include characteriza-tion of the pain complaint, evaluation of the etiology,syndromeandputativemechanismssustaining thepainand the assessment of the impact of the pain and rele-vant comorbidities.

198 Cancer Pain and Pain in HIV / AIDS
Pain Characteristics
A comprehensive evaluation should begin with an as-sessment of the pain characteristics. The temporal fea-tures comprise onset, duration, course and fluctuation.Most patients with chronic pain related to a progres-sive illness experience pain that begins insidiously andfluctuates broadly, but gradually progresses. Periodicshort-lived flares of pain, or “� breakthrough pain”(Caraceni et al. 2004), are very common and shouldbe separately assessed.Topographic features include primary location and ra-diation. Pain may be referred from any structure, in-cluding nerve, bone, muscle, soft tissue and viscera,and knowledge of pain referral patterns is needed toguide the evaluation. For example, pain in the inguinalcrease may require evaluation of numerous structuresto identify the underlying lesion, including the pelvicbones and hip joint, pelvic sidewall, paraspinal gutterat an upper lumbar spinal level and intraspinal regionat the upper lumbar level.Measurement of pain intensity may be accomplishedusinganumericscale(0–10),verbalratingscale, (none,mild, moderate, severe) or a visual analogue scale. Pic-torial scalesareparticularly usefulwhenassessing painin the pediatric cancer (see � Cancer Pain, Assessmentin Children) population and pain in the cognitively im-paired (see � Cancer Pain, Assessment in the Cogni-tively Impaired). The particular scale is less importantthan its consistent use to monitor and document the sta-tus of a specific pain (e.g. “worst pain during the pastweek”) over time. In assessing pain intensity, it alsois important to obtain information about factors thatincrease or decrease the pain. The quality of the painis assessed using verbal descriptors, such as aching,sharp, throbbing, burning or stabbing. Combined withother information, these descriptors allow broad infer-ences about the type of pathophysiology that sustainsthe pain.
Inferred Pathophysiology, Etiology and Syndromes
Characterization of the pain complaint must be com-plemented by a physical examination and appropriatelaboratory testsand imaging toprovide the informationnecessary to elucidate the likely etiology of the pain,the pain syndrome and the inferred type of pathophys-iology sustaining the pain. In populations with canceror HIV / AIDS, the etiology often relates to an identi-fiable structural lesion, such as neoplastic invasion ofbone. Identification of the etiology often informs theoverall treatment of the patient by defining the extentof disease.Numerous pain syndromes have been characterized inthe cancer (Caraceni et al. 1999) and HIV / AIDS (He-witt et al. 1997) populations. Syndrome identification
helps to define the underlying etiology and prognosisand also may suggest the need for additional testing orspecific therapies.Although inferences about the type of pathophysiol-ogy sustaining the pain represent a simplification ofvery dynamic processes occurring in both the periph-ery and in the central nervous system, these inferenceshave been incorporated into clinical practice becausethey have utility when deciding on a treatment strate-gies. The labels that are applied to the pathophysiolog-ical categories include nociceptive, neuropathic, psy-chogenic and mixed.Nociceptive pain refers to pain that is believed to besustained by ongoing activation of pain sensitive pri-mary afferent neurons by injury to tissue. In the settingof cancer, nociceptive pain usually is due to direct in-vasion by the neoplasm (Caraceni et al. 1999). Whensomatic structures are involved, the pain is termed “so-matic pain” and the pain is typically aching, throbbing,stabbing and familiar. Bone pain is the most commontype. “Visceral pain” occurs when the nociceptive le-sion involves visceral structures; it is usually gnawingor crampy when arising from obstruction of a hollowviscus and aching or stabbing when arising from dam-age to organ capsules.Pain is labeled neuropathic if it is believed to be sus-tained by abnormal somatosensory processing in theperipheral or central nervous systems (CNS). Neuro-pathic mechanisms are involved in approximately 40%of cancer pain syndromes and may be caused by dis-ease or by treatment (Caraceni et al. 1999). Dysesthe-sia, or abnormal uncomfortable sensations that may bedescribed using words such as “burning”, “shock-like”or “electrical” are suggestive of neuropathic mecha-nisms, as is the presence of abnormal findings on thesensory examination, such as allodynia (pain inducedby non-painful stimuli) or hyperalgesia (increased per-ception of painful stimuli).The term “psychogenic pain” is a generic label re-ferring to pain that is believed to be sustained pre-dominantly by psychological factors. Pain of thistype may be more precisely characterized through thewidely accepted taxonomy of somatoform disordersproposed by the American Psychiatric Association(1994). These pains share an assessment that revealspositive evidence for the psychopathology that is be-lieved to causally related to the pain. Although psycho-logical influences are profoundly important in the pre-sentation of the pain and the patient’s ability to adaptand function, psychogenic pain itself appears to be dis-tinctly uncommon in the cancer and HIV / AIDS pop-ulations.Occasionally, pain occurs that defies clinical charac-terization according to a clear etiology or syndrome.In the absence of positive evidence for any distinctive

C
Cancer Pain and Pain in HIV / AIDS 199
type of pain, it is usually best to label the symptom as“idiopathic.” In the setting of progressive medical ill-nesses, idiopathic pains require regular reassessmentin the hope that an explanatory process will becomeclear over time.
Impact and Comorbidities
The pain evaluation also must include an assessmentof impact and relevant comorbidities (see � CancerPain, Evaluation of Relevant Comorbidities and Im-pact). The impact of the pain may be considered fromthe perspective of varied physical, psychosocial andspiritual domains. As appropriate, these domains andspecificmedicaland psychiatriccomorbiditiesmustbespecifically assessed to fully understand the targets fortreatment.
Pain Management
The overall treatment strategy (see � Cancer PainManagement, Overall Strategy) should proceed fromthe broader therapeutic perspective of palliative care.The multidimensional assessment guides treatmentthat is often multimodal and best implemented throughthe efforts of professionals in varied disciplines. Theimmediate goal of pain relief should be pursued in tan-dem with interventions that address other sources ofdistress.Analgesic approaches can be broadly divided into1) primary therapies directed against the etiology ofthe pain and 2) symptomatic therapies. Primary treat-ments for the pain include antineoplastic therapies –� radiotherapy,� chemotherapy, immunotherapyandsurgery (see � Palliative Surgery in Cancer Pain Man-agement) – and other interventions directed at struc-tural pathology. Orthopedic surgery interventions (see� Cancer Pain Management, Orthopedic Surgery) toaddress bony metastases exemplify the potential forprimary therapy directed at specific structural pathol-ogy. In the HIV / AIDS population, primary treatmentmay include anti-retroviral therapy and other interven-tions. If it is feasible and clinically appropriate to pro-vide a primary therapy that can effectively treat thesource of the pain, the analgesic consequences canbe profound. Most patients have pain that cannot beaddressed solely by a primary disease modifying ap-proach. The most important symptomatic therapy is anopioid-based analgesic drug regimen, which may becomplemented by a large number of other treatments.
Pharmacotherapy
Prospective trials indicate that more than 70% of pa-tients can achieve adequate relief of cancer pain usinga pharmacologic approach (Schug et al. 1990). Effec-tive pain management requires expertise in the use ofthe nonsteroidal anti-inflammatory drugs (NSAIDs),
opioid analgesics and adjuvant analgesics. The term“adjuvant analgesic” is applied to a diverse group ofdrugs, most of which have primary indications otherthan pain, but can be effective analgesics in specificdisorders such as neuropathic pain.There is a broad consensus in favor of an approach tocancer pain management that was developed by an ex-pert panel of the World Health Organization almosttwo decades ago and was termed the “analgesic lad-der” (1996). This approach has been highly influential,reinforcing the consensus view that persistent mod-erate to severe cancer pain should be treated with anopioid-based drug regimen. The details of the modelhave evolved over time, but it remains a useful as a toolfor educating clinicians and policymakers.According to the analgesic ladder approach, mild tomoderate cancer pain is first treated with a nonopioidanalgesic (see� CancerPainManagement,NonopioidAnalgesic), such as acetaminophen or a nonsteroidalanti-inflammatory drug (NSAID). This drug is com-bined with an adjuvant drug that can be selected eitherto provide additional analgesia (i.e. an adjuvant anal-gesic) or to treat a side effect of the analgesic or a coex-isting symptom. Patients who present with moderate tosevere pain or who do not achieve adequate relief aftera trial of a NSAID should be treated with an opioid,often combined with a NSAID or adjuvant drugs.
Nonsteroidal Anti-Inflammatory Drugs
NSAIDs appear to be especially useful in patients withbone pain or pain related to grossly inflammatory le-sions and relatively less useful in patients with neu-ropathic pain (Wallenstein and Portenoy 2002). Thesedrugs may have an opioid sparing effect that can limitthe potential for dose-related opioid side effects. Theuse of the NSAIDs may be limited by their toxicitiesand a maximal efficacy that is insufficient to addressmost cancer pain. All NSAIDs have the potential fornephrotoxicity, with effects that range from periph-eral edema to acute or chronic renal failure. All thesedrugs increase the risk of gastrointestinal ulcers andbleeding. The selective cyclo-oxygenase (COX)-2 in-hibitors have a relatively reduced risk of these out-comes and many clinicians recommend these drugsas first line therapy for all patients at relatively highrisk of ulcer, including the elderly, those concurrentlyreceiving a corticosteroid and those with a prior his-tory of peptic ulcer disease or NSAID-induced gastro-duodenopathy (Wallenstein and Portenoy 2002). Therisk is also reduced by co-administration of a protonpump inhibitor, the prostaglandin analogue misopros-tolandpossiblyhighdoseH2blockers.Recentdata thathave raised concerns about an increased risk of cardio-vascular events among those treated with the selective

200 Cancer Pain and Pain in HIV / AIDS
COX-2 inhibitors (Solomon et al. 2004), but the rela-tive risks and benefits compared to nonselective drugsin medically ill populations have yet to be defined.There are also no data in the medical ill from which tojudge the relative outcomes associated with adminis-tration of selective COX-2 inhibitors alone versus non-selective NSAIDs plus a gastroprotective agent. At thepresent time, the approach is a matter of clinical judg-ment.
Adjuvant Analgesics
The adjuvant analgesics comprise numerous drugs indiverse classes (Lussier and Portenoy 2004). Treat-ment with one of these drugs is generally considered ifan optimally administered opioid regimen fails to pro-vide a satisfactory balance between pain relief and sideeffects. These drugs are particularly useful in the treat-ment of neuropathic pain, bone pain and pain relatedto bowel obstruction.Corticosteroids are multipurpose adjuvant analgesicsand also are used to improve anorexia, nausea andfatigue. In populations with cancer pain or pain dueto HIV / AIDS, the first-line adjuvant analgesics forneuropathic pain (see � Adjuvant Analgesics in Man-agement of Cancer-Related Neuropathic Pain) are thecorticosteroids, anticonvulsants and antidepressants.Use of the anticonvulsants and antidepressants is sup-ported by numerous controlled trials in varied popula-tions (Lussier and Portenoy 2004).Otherdrugs consid-ered for neuropathic pain comprise the GABA agonistbaclofen, alpha-2 adrenergic agonists and various N-methyl-D-aspartate inhibitors. Topical agents, such asthe lidocainepatch, representanotherstrategyfor thesepain syndromes.The most commonly used adjuvant analgesics for bonepain (see � Adjuvant Analgesics in Management ofBone-Related Pain) are the bisphosphonates. Thesedrugs also have been demonstrated to reduce skeletalmorbidity, such as fractures. Other drugs used for bonepain include radiopharmaceuticals and calcitonin. Ad-juvant analgesics for bowel obstruction (see � CancerPain Management, Adjuvant Analgesics in Manage-ment of Pain Due to Bowel Obstruction) can often con-trol pain and other symptoms and obviate the need fordrainage procedures. Treatment usually involves thecombination of anticholinergic drugs, octreotide andcorticosteroids (Lussier and Portenoy 2004).
Opioid Analgesics
Opioid pharmacotherapy is the mainstay approach forthe management of moderate to severe pain in popula-tions with cancer or HIV / AIDS. Guidelines for opi-oid selection (see � Cancer Pain Management, Princi-ples of Opioid Therapy, Drug Selection) have evolvedfrom the WHO analgesic ladder approach, which orig-
inally labeled some opioids as “weak” (for moderatepain) and some as “strong” (for severe pain) (1996).This distinction is based on conventional practice andnot pharmacology. In the U.S., drugs typically admin-istered to address moderate pain in the opioid naïvepatient include codeine, hydrocodone (combined withacetaminophen or ibuprofen), dihydrocodeine (com-bined with aspirin), oxycodone (combined with as-pirin,acetaminophenor ibuprofen),propoxypheneandoccasionally, meperidine. Tramadol, a unique cen-trally acting analgesic with a mechanism that is partlyopioid is also generally included in this group. Thesedrugs are conventionally used for moderate pain eitherbecauseofdosedependent toxicityorbecause thecom-bination products contain a nonopioid analgesic witha maximum safe dose.Opioids conventionally selected for severe pain, par-ticularly when patients have already been exposed tothe short acting drugs on the first rung of the analgesicladder, include morphine, fentanyl, oxycodone (with-out acetaminophen or aspirin), hydromorphone, oxy-morphone, levorphanol and methadone. Historically,morphine was described as the preferred first line drug,but there is large variation in the response to differ-ent opioids and it is best to select an initial trial basedon the available formulations, cost and prior experi-ence. Although the role of methadone has expandedin recent years because of its low cost, long half lifeand unexpectedly high potency (presumably related tothe D-isomer in the racemate, which is a N-methyl-D-aspartate blocker), it poses challenges in dose se-lection, dose adjustment and monitoring that are notshared by the other pure mu agonist opioids. Experi-ence is needed to use this drug safely.Opioids may be delivered by any of numerous routesof administration (see � Opioid Therapy in CancerPain Management, Route of Administration). Long-term dosing is best accomplished by an oral or trans-dermal route. Numerous oral formulations are avail-able, including modified release forms of morphine,oxycodone or hydromorphone. Other drugs, such asoxymorphone may become available. The latter drugsprovide effective analgesia with a prolonged dosing in-terval, increasing convenience and potentially adher-ence to therapy. The transdermal route is available forfentanyl and offers a 48–72 h dosing interval. Othertransdermal formulations are in development. The oraltransmucosal form of fentanyl has been shown to besafe and efficacious when used to treat breakthroughpain in cancer patients (Christie et al. 1998).Rectal for-mulations of many opioids, such as oxymorphone,hy-dromorphone and morphine are available, but are sel-dom used for long-term administration.Long-term parenteral dosing is possible for patientswho are poor candidates for oral or transdermal for-

C
Cancer Pain and Pain in HIV / AIDS 201
mulations. Continuous subcutaneous infusion or con-tinuous intravenous infusion (if the patient has an in-dwelling centralvenousport) can be implementedwithany opioid available in an injectable formulation. Opi-oids and other drugs may also be delivered into theepidural or intrathecal spaces. The strongest indica-tion for neuraxial infusion is the presence of intoler-able somnolence or confusion during systemic opioidtherapy.The most important principle of opioid administrationis individualization of the dose (Jacox et al. 1994). Inall cases, the dose of an opioid should be gradually in-creased until acceptable analgesia is produced or un-manageable side effects supervene. The absolute doseof the opioid is immaterial as long as the balance be-tween analgesia and side effects remains acceptable tothe patient. Most patients achieve a favorable outcomeand remain on a stable dose until pain recurs as a resultof disease progression. Recurrent pain following a pe-riod of dose stability usually requires re-evaluation ofthe patient and another period of dose titration.Forpersistentor frequently recurringpain, thebestout-come is achieved by a fixed, around the clock dosingschedule. Long acting opioids are often used becauseof theconvenienceandthe likelihood that treatmentad-herence will be better than with frequent daily doses.Breakthroughpaincommonly ismanagedbycoadmin-istration of short acting, as needed, “rescue doses.”Dose titration usually yields a favorable balance be-tween analgesia and side effects. In some cases, how-ever, treatment-limiting side effects occur and ren-der the treatment ineffective. This scenario is knownas poor � opioid responsiveness, a phenomenon thatshould be viewed as individual to the patient, the drugand route and the moment in time.Patients with pain that is poorly responsive to the opi-oid therapy must undergo a change in treatment. Thereare no comparative trials to guide clinical practice.Four strategies should be considered and a specificapproach selected based on the assessment and clin-ical judgment. Given the individual variation in the re-sponse to different drugs, one strategy is to switch toan alternativeopioid, an approach called� opioid rota-tion. A second strategy is to co-administer one or moretreatments for the side effect that limits dose escala-tion. Sophisticated approaches are now available to ad-dress � cognitive dysfunction and gastrointestinal ef-fects (see � Cancer Pain Management, Gastrointesti-nal Dysfunction as Opioid Side Effects), the two mostcommon types of opioid-related toxicity. A third strat-egy involves the use of a pharmacological approachthat would potentially allow reduction in the require-ment for the systemic opioid. Coadministration of aNSAID or adjuvant analgesic or a trial of neuraxial in-fusion might be considered. Finally, a strategy using a
non-pharmacological approach that would potentiallyreduce the opioid requirement might be considered.This might involve an invasive therapy, such as neu-ral blockade or any of a variety of other approaches.Patients who are treated for a prolonged period withopioids must be continually reassessed for side effects.In addition to common toxicities, opioids may pro-duceavariety ofuncommon effects (see� CancerPainManagement, Opioid Side Effects, Uncommon SideEffects)oroutcomesthatareyetpoorlyrecognized.Forexample, endocrine changes (see � Cancer Pain Man-agement, Opioid Side Effects, Endocrine Changes andSexual Dysfunction) associated with opioid use, suchas hypogonadism may be associated with fatigue, sex-ual dysfunction or osteoporosis and should be assessedin some populations.Opioids are potentially abusable drugs and the clini-cians who prescribe them for chronic pain should befamiliar with the principles of addiction medicine. Al-though abuse and addiction during opioid therapy forpain are very uncommon in the population of cancerpatients with no prior history of substance abuse, theseoutcomesshouldalwaysbeassessedandaresignificantconcerns in subpopulations with substance use disor-ders. Understanding the special considerations posedby � opioid use in patients with substance use dis-orders (see � Opioid Therapy in Cancer Patiens withSubstance Abuse Disorders, Management) providesessential information that must be applied in the treat-ment of all patients.
Other Approaches in the Management of Chronic Pain
There are numerous alternative strategies that may beconsidered in the treatment of pain related to canceror HIV / AIDS. In almost every situation, the use ofthese approaches has been extrapolated from experi-ence in the populations with chronic non-cancer painsyndromes. Noninvasive analgesic strategies can bebroadly categorized into psychological interventions,rehabilitative treatments and complementary or alter-native medicine approaches. Specific psychologicalapproaches have been applied successfully in the man-agement of pain and related symptoms (Breitbart etal. 2004). Treatments include relaxation training, dis-traction, hypnosis and biofeedback. Although many ofthese techniques require experienced personnel to im-plement, several forms of relaxation training can betaught by the non-specialist. Behavioral interventions,like the use of an activities diary to improve physicalfunctioning haveachievedwideacceptance in theman-agement of non-cancer pain and are occasionally con-sidered for medically ill patients. A variety of psychoe-ducational and psychotherapeutic approaches may beimplemented in an effort to improve coping, adapta-tion, family integrity, functioning and quality of life.

202 Cancer Pain and Pain in HIV / AIDS
Rehabilitative therapies (see � Cancer Pain Manage-ment, Rehabilitative Therapies), such as therapeuticexercise, use of orthotics, and modalities such as heat,cold and electrical stimulation, may be useful in se-lected patients. Refractory, movement-induced pain,such as that related to bone metastases may be partiallyrelieved by bracing the painful part and a well fittingprosthesis may reduce stump pain. Therapeutic exer-cise may lessen pain associated with immobility, trig-ger points in muscle, and ankylosis. Although all therehabilitativeapproachesremain inadequatelystudied,clinical experience is favorable.Complementary and alternative medicine (CAM) ap-proaches are commonly pursued by medically ill pa-tients. Some of these interventions, such as meditationand other mind-body approaches, nutritional support,acupuncture and massage, are widely used for pain andare generally considered mainstream strategies (Pan etal. 2000). Others, such as homeopathy and naturopathyhave little scientific support. Clinicians should providewhatever data are available about these approaches andsupport informed decision-making.Invasive strategies for pain include neurosurgical in-terventions (see � Cancer Pain Management, Neuro-surgical Interventions), such ascordotomy; avariety ofinjection therapies, including neural blockade; and theimplantable therapies of neuraxial infusion and spinalcord stimulation. Although the injection therapies andimplants are sometimes described as anesthesiologicaltherapies (see � Cancer Pain Management, Anesthesi-ologic Interventions, Neural Blockade), they are nowperformedbypainspecialists inavarietyofdisciplines.� Neural Blockade includes a diverse group of pro-cedures that transiently or permanently block sympa-thetic nerves, somatic nerves or both (Swarm et al.2004). Injectionsmaybediagnostic,prognosticor ther-apeutic. The solutions injected may be local anesthet-ics, in which case the effects typically are short-livedonly or neurolytic substances. Neurolytic blockadegenerally is seldom employed and considered in thecontext of advanced illness. One exception is the celiacplexus blockade for pancreatic cancer, experience withwhich is sufficiently favorable to apply early in thetreatment of pain.In medically ill populations, neuraxial infusion andstimulation (see � Cancer Pain Management, Anes-thesiologic Interventions, Spinal Cord Stimulation,and Neuraxial Infusion) are seldom considered. Therole of neuraxial infusion may evolve as a result of acontrolled trial that demonstrated benefits of an im-planted pump for intrathecal drug delivery over con-ventional systemic opioid therapy in a population withcancer(Smithetal.2002).Other techniquesforneurax-ial infusion include a tunneled percutaneous epiduralcatheter and an implanted epidural catheter connected
to a subcutaneous portal. The latter techniques are usu-allypreferredforpatientswith lifeexpectanciesshorterthan 3 months.
Conclusion
Pain is a common complication of cancer andHIV / AIDS. Treatment of pain from a broader per-spective of palliative care is likely to yield the bestoutcomes. Relatively simple therapeutic approachescan provide effective pain relief in a large majorityof patients. Pain relief must be considered an aspectof best clinical practice for all clinicians who treatpatients with these illnesses.
References1. American Psychiatric Association (1994) Somatoform disor-
ders. In: Diagnostic and statistical manual of mental disorders(DSM-IV), 4th edn. American Psychiatric Association, Wash-ington, pp 445–471
2. Anderson KO, Mendoza TR, Payne R et al. (2004) Pain edu-cation for underserved minority cancer patients: a randomizedcontrolled trial. J Clin Oncol. 22:4918–4925
3. Breitbart W, Payne D, Passik S (2004) Psychological and psy-chiatric interventions in pain control. In: Doyle D, Hanks G,Cherny NI et al. (eds) Oxford Textbook of Palliative Medicine,3rd edn. Oxford University Press, Oxford, pp 424–438
4. Caraceni A, Portenoy RK, and a Working Group of the IASPTask Force on Cancer Pain (1999) An international survey ofcancer pain characteristics and syndromes. Pain 82:263–274
5. Caraceni A, Martini C, Zecca E et al. (2004) Breakthrough paincharacteristics and syndromes in patients with cancer pain. Aninternational survey. Palliat Med 18:177–183
6. Christie JM, Simmonds M, Patt R et al. (1998) A dose-titration,multicenter study of oral transmucosal fentanyl citrate (OTFC)for the treatment of breakthrough pain in cancer patients us-ing transdermal fentanyl for persistent pain. J Clin Oncol16:3238–3245
7. Dobalian A, Tsao JC, Duncan RP (2004) Pain and the use ofoutpatient services among persons with HIV: results from anationally representative survey. Med Care 42:129–138
8. Green CR, Anderson KO, Baker TA et al. (2003) The unequalburden of pain: confronting racial and ethnic disparities in pain.Pain Med 4:277–294
9. Hewitt DJ, McDonald M, Portenoy RK et al. (1997) Painsyndromes and etiologies in ambulatory AIDS patients. Pain70:117–124
10. Jacox A, Carr DB, Payne R et al. (1994) Management of Can-cer Pain. AHCPR Publication No. 94-0592: Clinical PracticeGuideline No. 9. Rockville, MD, U.S. Department of Healthand Human Services, Public Health Service
11. Lussier D, Portenoy RK (2004) Adjuvant analgesics. In: DoyleD, Hanks G, Cherny NI et al. (eds) Oxford Textbook of Pal-liative Medicine, 3rd edn. Oxford University Press, Oxford,pp 349–377
12. Pan CX, Morrison RS, Ness J et al. (2000) Complementary andalternative medicine in the management of pain, dyspnea, andnausea and vomiting near the end of life. A systematic review.J Pain Symptom Manage 20:374–387
13. Schug SA, Zech 0, Dorr U (1990) Cancer pain managementaccording to WHO analgesic guidelines. J Pain Symptom Man-age 5:27–32
14. Smith TJ, Staats PS, Stearns LJ et al. (2002) Randomized clin-ical trial of an implantable drug delivery system comparedwith comprehensive medical management for refractory can-cer pain: impact on pain, drug-related toxicity, and survival. JClin Oncol 19:4040–4049

C
Cancer Pain, Animal Models 203
15. Solomon DH, Schneeweiss S, Glynn RJ et al. (2004) Re-lationship between selective cyclooxygenase-2 inhibitorsand acute myocardial infarction in older adults. Circulation109:2068–2073
16. Swarm, RA, Karanikolas M, Cousins MJ (2004) Anaesthetictechniques for pain control In: Doyle D, Hanks G, Cherny NIet al. (eds) Oxford Textbook of Palliative Medicine, 3rd edn.Oxford University Press, Oxford, pp 378–395
17. Vainio A, Auvinen A (1996) Prevalence of symptoms amongpatients with advanced cancer: an international collaborativestudy. J Pain Symptom Manage 12:3–10
18. Wallenstein DJ, Portenoy RK (2002) Nonopioid and adjuvantanalgesics. In: Berger AM, Portenoy RK, Weissman DE (eds)Principles and Practice of Palliative Care and Supportive On-cology. Lippincott-Raven, Philadelphia, pp 84–97
19. World Health Organization (1996) Cancer pain relief, 2nd edn.World Health Organization, Geneva
20. www.nationalconsensusproject.org
Cancer Pain, Animal Models, Figure 1 Bone cancer pain animal model. (a) Radiograph of lower half of adult mouse demonstrating the femur throughwhich osteolytic fluorescent sarcoma cells were injected. Tumor cells are confined within the intramedullary space by placement of an amalgam plug(arrow). Two weeks later, femurs can be assessed at the whole bone level for extraosseous invasion (none noted in b), tumor burden (using excitationfilters to visualize green fluorescent protein expressed by tumor cells, (c) and bone destruction (high power radiographic imaging, arrow denotes extensivebone destruction, d).
ongoing and movement-evoked pain related behaviorsincrease in severity as the tumor develops. These painbehaviors correlate with the progressive tumor-inducedbone destruction that ensues, which appears to mimicthe condition seen in patients with primary or metastaticbone cancer. In this model, peripheral nerve destruc-tion as well as alterations in neurochemical markersimplicated in pain transmission has been observed(Fig. 2).
Cancer Pain, Animal Models,Figure 2 Neurochemical changesin the spinal cord and dorsal rootganglia (DRG) in bone cancer pain.(a) confocal imaging of glial fibrillaryacidic protein (GFAP) expressedby astrocytes in a spinal cordof a tumor-bearing mouse. Noteincreased expression only on sideipsilateral to tumorous limb. (b) Highpower magnification of spinal cordshowing hypertrophy of astrocytes(green) without changes in neuronalnumbers (red, stained with neuronalmarker, NeuN). (c) Confocal image ofdorsal root ganglia labeling injuredneurons labeled with activatingtranscription factor 3 (magenta,ATF-3). (d) Non-myelinating schwanncells (green, GFAP) and macrophageinfiltration (yellow, CD68) can alsobe seen.
Following the publication of the first animal model ofcancer pain, several rodent models of soft tissue andbone cancer pain have been described. A rat model ofbone cancer pain was developed (Medhurst et al. 2002)whereby MRMT-1 mammary carcinoma cells wereinjected into the tibiae of syngeneic rats. Morphine-reversible pain behaviors and � osteolysis were evident2–3 weeks following inoculation. Mouse models ofsoft tissue sarcoma (Wacnik et al. 2001) and rat models

204 Cancer Pain, Animal Models
of neuropathic cancer (Eliav et al. 2004) were alsodeveloped, and involved growth of tumor cells in softtissues surrounding bones and alongside sciatic nerves,respectively. Mechanical and thermal � hyperalgesia,demyelination, progressive tumor infiltration and nervedestruction were seen in these models.Given the development of animal models of cancer pain,significant advances have been made in understandingthe molecular and cellular mechanisms which drivecancer pain (Fig. 3). Cancer cells and tumor associatedmacrophages have both been shown to express high lev-elsofCOX–2, leading tohighlevelsof� prostaglandins.Prostaglandins have been shown to be involved in thesensitization and/or direct excitation of � nociceptors,by binding to several prostanoid receptors expressed bynociceptors that sensitize or directly excite nociceptors(Vasko 1995). Treatment of cancer animals with selec-tive COX–2 inhibitors resulted in significant attenuationof pain behaviors, as well as many of the neurochemicalchanges, suggestive of both � peripheral sensitizationand central sensitization (Medhurst et al. 2002; Sabinoet al. 2003).� Endothelins have been found in cancer patients (Nel-son et al. 1995) and in cancer-bearing mice (Wacnik2001), and their levels have been correlated with theseverity of pain (Nelson et al. 1995). Endothelins couldcontribute to cancer pain by directly sensitizing orexciting nociceptors, as a subset of small unmyeli-nated primary afferent neurons express endothelin Areceptors (Pomonis et al. 2001). Furthermore, directapplication of endothelin to peripheral nerves inducesactivation of primary afferent fibers and an induction ofpain behaviors (Davar et al. 1998). These findings indi-
Cancer Pain, Animal Models,Figure 3 Sensory neurons anddetection of noxious stimuli dueto tumor cells. Nociceptors usea diversity of signal transductionmechanisms to detect noxiousphysiological stimuli, and many ofthese mechanisms may be involvedin driving cancer pain. Thus, whennociceptors are exposed to productsof tumor cells, tissue injury orinflammation, their excitabilityis altered and this nociceptiveinformation is relayed to the spinalcord and then to higher centers of thebrain. Some of the mechanisms thatappear to be involved in generatingand maintaining cancer pain includeactivation of nociceptors by factorssuch as extracellular protons (+),endothelin-1 (ET-1), interleukins(ILs), prostaglandins (PG), and tumornecrosis factor (TNF).
cate endothelin antagonists may be useful in inhibitingcancer pain.� Osteoclasts, the body’s principal bone resorbing cell,play an essential role in cancer-induced bone loss, andcontribute to the etiology of bone cancer pain (Honoreet al. 2000; Luger et al. 2001; Sabino et al. 2002; Sev-cik 2004). Osteoprotegerin (OPG) is a secreted solublereceptor that prevents the activation and proliferation ofosteoclasts. Bisphosphonates induced osteoclast apop-tosis have been reported to reducepain in cancer patientsand in animal models of bone cancerpain (Sevcik 2004).Both anti-resorptive compounds were highly potent inreducing both cancer-induced bone destruction and thedevelopment of pain-related behaviors, suggesting animportant role for osteoclasts in the development andmaintenance of bone cancer pain.Cancer pain in advanced cancer patients is typicallyrecalcitrant to both non-steroidal anti-inflammatoryagentsandopioids,and typically requiresadjuvantssuchas gabapentin for adequate management. Gabapentin isalso commonly used to treat neuropathic pain patientswho are unresponsive to opioids. In several cancer painmodels, peripheral nerve destruction within skin (Cainet al. 2001) and bone (Peters et al. 2005) have been ob-served.Likewise, sensitization ofunmyelinatedprimaryafferent fibers and damage to small and medium sizedsensory neurons suggest that a neuropathic componentexists in cancer pain.Insights into the mechanisms that induce cancer painare now coming from animal models. These modelshave begun to provide a glimpse into the mechanisms bywhich tumors cause pain and how this sensory informa-tion is processed. Chemicals derived from tumor cells,

C
Cancer Pain, Assessment in Children 205
inflammatory cells and cells derived from bone appearto be simultaneously involved in driving this frequentlydifficult to control pain state. Understanding the mech-anisms involved in the pathophysiology of cancer painwill improve our ability to provide mechanism-basedtreatments and therapies, and improve the quality oflife of cancer patients. Insights such as this promiseto fundamentally change the way cancer pain is con-trolled.
References1. Cain DM, Wacnik PW, Turner M et al. (2001) Functional Inter-
actions between Tumor and Peripheral Nerve: Changes in Ex-citability and Morphology of Primary Afferent Fibers in a MurineModel of Cancer Pain. J Neurosci 21:9367–9376
2. Davar G, Hans G, Fareed MU et al. (1998) Behavioral Signsof Acute Pain Produced by Application of Endothelin–1 to RatSciatic Nerve. Neuroreport 9:2279–2283
3. Eliav E, Tal M, Benoliel R (2004) Experimental Malignancy inthe Rat Induces Early Hypersensitivity Indicative of Neuritis.Pain 110:727–737
4. Honore P, Luger, NM, Sabino MA et al. (2000) OsteoprotegerinBlocks Bone Cancer-Induced Skeletal Destruction, Skeletal Painand Pain-Related Neurochemical Reorganization of the SpinalCord. Nat Med 6:521–528
5. Luger NM, Honore P, Sabino MA et al. (2001) Osteoprote-gerin Diminishes Advanced Bone Cancer Pain. Cancer Res61:4038–4047
6. Medhurst SJ, Walker K, Bowes M et al. (2002) A Rat Model ofBone Cancer Pain. Pain 96:129–140
7. Mercadante S, Arcuri E (1998) Breakthrough Pain in CancerPatients: Pathophysiology and Treatment. Cancer Treat Rev24:425–432
8. Nelson, JB, Hedican SP, George DJ et al. (1995) Identificationof Endothelin–1 in the Pathophysiology of Metastatic Adeno-carcinoma of the Prostate. Nat Med 1:944–949
9. Peters C M, Ghilardi JR, Keyser CP et al. (2005) Tumor-InducedInjury of Primary Afferent Sensory Nerve Fibers in Bone CancerPain. Exp Neurol 193:85–100
10. Pomonis JD, Rogers SD Peters CM et al. (2001) Expressionand Localization of Endothelin Receptors: Implication for theInvolvement of Peripheral Glia in Nociception. J Neurosci21:999–1006
11. Portenoy RK, Payne D, Jacobsen P (1999) Breakthrough Pain:Characteristics and Impact in Patients with Cancer Pain. Pain81:129–134
12. Sabino MA, Ghilardi JR, Jongen JL et al. (2002) SimultaneousReduction in Cancer Pain, Bone Destruction, and Tumor Growthby Selective Inhibition of Cyclooxygenase–2. Cancer Res 62:7343–7349
13. Sabino MA, Luger NM, Mach DB et al. (2003) Different Tu-mors in Bone Each Give Rise to a Distinct Pattern of SkeletalDestruction, Bone Cancer-Related Pain Behaviors and Neuro-chemical Changes in the Central Nervous System. Int J Cancer104:550–558
14. Schwei MJ, Honore P, Rogers SD et al. (1999) Neurochemicaland Cellular Reorganization of the Spinal Cord in a Murine Modelof Bone Cancer Pain. J Neurosci: 19:10886–10897
15. Sevcik MA, Luger NM, Mach DB et al. (2004) Bone CancerPain: The Effects of the Bisphosphonate Alendronate on Pain,Skeletal Remodeling, Tumor Growth and Tumor Necrosis. Pain111:169–180
16. Vasko MR (1995) Prostaglandin-Induced Neuropeptide Releasefrom Spinal Cord. Prog Brain Res 104:367–380
17. Wacnik PW, Eikmeier LJ, Ruggles TR et al. (2001) Func-tional Interactions between Tumor and Peripheral Nerve:Morphology, Algogen Identification, and Behavioral Charac-terization of a New Murine Model of Cancer Pain. J Neurosci21:9355–9366
Cancer Pain, Assessment in ChildrenGARY A. WALCO
The David Center for Childrens Pain and PalliativeCare, University Medical Center Hackensack, NJ,[email protected]
Definition
Cancer pain in children is associated with three majoretiologies: (a) � procedural distress, (b) � iatrogenic ef-fects of treatment, and (c) disease-related pain. Chronicpain among long-term cancer survivors (see � cancersurvivorship) is increasingly recognized as surveillanceof thesepatientscontinues.Eachhasuniquecomponentsthat dictate the nature of the assessments to be made andtreatments that may ensue.
Characteristics
Procedural Distress
For many of the cancers most common in the pedi-atric population (e.g. leukemia, lymphoma), invasiveprocedures are integral to the diagnostic and treatmentprocess. Included here are bone marrow aspirations andbiopsies, for diagnostic purposes, and lumbar punc-tures, both for diagnostic purposes as well as to deliverintrathecal chemotherapy as prophylaxis against ortreatment for central nervous system disease (Balis etal. 2002). The latter occurs on a recurrent basis over thecourse of several months of treatment. Among survivorsof pediatric cancer, the trauma of undertreated procedu-ral distress is often the most disturbing element of theirentire cancer experience, sometimes severe enough toleave children and parents with post- traumatic stresssymptoms (Stuber et al. 1998). Interventions combiningsedating and analgesic agents along with preparatoryand cognitive-behavioral strategies (see � Cognitive-Behavioral Treatment of Pain) have greatly reduced thepain and anxiety associated with invasive procedures(Berde et al. 2002; Conte et al. 1999). Assessmentstrategies involve three modalities: self-report of thechild, behavioral observations, and physiological in-dicators of stress (Walco et al. 2005). As these do notnecessarily correlate with one another, it is imperative tospecify the target outcome(s) of the intervention (Walcoet al. 2005). Ultimately the goal would be to implementan algorithm optimizing the match between patientneeds and available interventions, so that comfort maybe assured while risk and cost are minimized.
Iatrogenic Effects
Treatments for cancer involve chemotherapy, radiation,surgery, and stem cell transplantation. Each poten-tially leads to iatrogenic pain problems (Collins andWeisman 2003). Symptoms resulting from chemother-apeutic and radiation treatment most commonly include

206 Cancer Pain, Assessment in Children
nausea and vomiting, fatigue, neutropenia and relatedvulnerability to infection, and pain. Common iatro-genic pain syndromes in pediatric cancer are related tomucositis, infectious process, and � neuropathic pain(from � peripheral neuropathy) associated with agentssuch as vincristine. Pain secondary to radiation is alsoseen in some instances. Painful sequelae of surgicalinterventions occur, including � phantom limb painrelated to amputations. Acute abdominal pain, severeenough to require administration of opioids, has beennoted among patients who have undergone allogeneicbone marrow transplantation. Finally, as follow-upprograms for long-term survivors of childhood cancerprovide data, it appears that chronic pain syndromesmay be of concern. For example, aseptic necrosis of thebone is a known long-term effect of high dose steroidusage, and does not manifest until well after the childhas completed standard treatment protocols.
Disease-Related Pain
Disease-related pain in pediatric cancer is not as com-mon as in neoplasms common in the adult population.Painmaybepresentat the timeofdiagnosis,aspain inthelong bones is associated with leukemia, severe headacheis a symptom of brain tumors, solid tumors may elicit so-matic pain in the focal area of tumor growth or infiltra-tion, and abdominal tumors may generate visceral pain.In contrast to adult patients with such tumors, childrenwith cancerusually experienceasignificant remission ofpain within two weeks of beginning treatment (Miser etal. 1987). Unfortunately, the other circumstance wherepain is problematic is in advanced illness, often in thecontextof end-of-lifecare. Thus,manyof thesame typesof syndromes seen at presentation, where pain is of highintensity and often unrelenting, recur in advanced illnessand should be addressed in service of maximizing qual-ity of life (Wolfe and Grier 2002).
Assessment Strategies
Specific pain assessment strategies depend on the ageor � developmental level of the child and the natureof the pain in question (McGrath and Gillespie 2001).Whenever possible, it is optimal to use patients’ verbalreports to assess their pain experience, skills that emergein children between the ages of 3 and 7 years (Ameri-can Academy of Pediatrics Committee on PsychosocialAspects of Child and Family Health, American PainSociety Task Force on Pain in Infants, Children, andAdolescents 2001). In preverbal children, pain is as-sessed through physiological indicators of distress(Sweet and McGrath 1998), through specific behav-ioral indicators (McGrath 1998; Lilley et al. 1997), orthrough some combination thereof (Franck et al. 2000).During the toddler and preschool years, as children be-gin to use language meaningfully, increased emphasismay be placed on verbal report, but one must take careto use language and terminology that is familiar to the
child. Parental ratings of pain may also be helpful inpreverbal children.For procedural distress, assessment strategies should in-clude two majorcomponents, anxiety andpain.The term“distress” is used as a way to represent the combinedeffect of these two factors, as they are separable onlyin concept, not in practice. Behavior rating instrumentstypically define specific behaviors, and frequency of oc-currence, duration, or intensity is scored during a spec-ified period. Typically, this includes a segment prior to,during, and after the procedure. Likewise, physiologi-cal indicators, including heart rate, blood pressure,vagaltone, and cortisol responses have been used as indicatorsof acute distress. Self-report measures focus on the sub-jective experience of the child and typically encompassconcernsaboutpain, anxiety,andperceivedself-efficacyin coping (Walco et al. 2005).For pain related to both disease and the iatrogenic effectsof treatment, self reportmeasureshelpascertain the loca-tion of pain, intensity, sensory, affective, and evaluativecomponents,aswellas the impactofpainonfunctioning.Especially when confronting pain that ismorechronicorrecurrent in nature, assessing the contextual factors as-sociated with the pain experience (developmental level,temperament,characteristicpainresponsiveness, familyissues, impact of pain, etc.) becomes very important.
References1. American Academy of Pediatrics Committee on Psychosocial
Aspects of Child and Family Health, American Pain Society TaskForce on Pain in Infants, Children, and Adolescents (2001) PolicyStatement: The Assessment and Management of Acute Pain in In-fants, Children and Adolescents (0793). Pediatrics 108:793–797
2. Balis FM, Holcenberg JS, Blaney SM (2002) General Principlesof Chemotherapy. In: Pizzo PA, Poplack DG (eds) Principles andPractice of Pediatric Oncology, 4th edn. Lippincott, Williams &Wilkins, Philadelphia, pp 237–308
3. Berde CB, Billett AL, Collins JJ (2002) Symptom Managementin Supportive Care. In: Pizzo PA, Poplack DG (eds) Principlesand Practice of Pediatric Oncology, 4th edn. Lippincott, Williams& Wilkins, Philadelphia, pp 1301–1332
4. Collins JJ, Weisman SJ (2003) Management of Pain in ChildhoodCancer. In: Schechter NL, Berde CB, Yaster M (eds) Pain inInfants, Children, and Adolescents, 2nd edn. Lippincott, Williams& Wilkins, Philadelphia, pp 517–538
5. Conte PM, Walco GA, Sterling CM et al. (1999) Procedural PainManagement in Pediatric Oncology: A Review of the Literature.Cancer Investigation 17:448–459
6. Franck LS, Greenberg CS, Stevens B (2000) Pain Assessmentin Infants and Children. Pediatric Clinics of North America47:487–512
7. Lilley CM, Craig KD, Grunau RE (1997) The Expression ofPain in Infants and Toddlers: Developmental Changes in FacialAction. Pain 72:161–70
8. McGrath PJ (1998) Behavioral Measures of Pain. In: Finley GA,McGrath PJ (eds) Measurement of Pain in Infants and Children.Progress in Pain Research and Management, vol 10. IASP Press,Seattle, Washington, pp 83–102
9. McGrath PA, Gillespie J (2001) Pain Assessment in Childrenand Adolescents. In: Turk DC, Melzack R (eds) Handbook ofPain Assessment, 2nd edn. Guilford, New York, pp 97–118
10. Miser A, Dothage J, Wesley R et al. (1987) The Prevalence ofPain in a Pediatric and Young Adult Cancer Population. Pain29:73–83

C
Cancer Pain, Assessment in the Cognitively Impaired 207
11. Stuber ML, Kazak AE, Meeske K et al. (1998) Is PosttraumaticStress a Viable Model for Understanding Responses to Child-hood Cancer? Child and Adolescent Psychiatric Clinics of NorthAmerica 7:169–182
12. Sweet SD, McGrath PJ (1998) Physiological Measures of Pain.In: Finley GA, McGrath PJ (eds) Measurement of Pain in Infantsand Children. Progress in Pain Research and Management, vol 10.IASP Press, Seattle, Washington, pp 59–81
13. Walco GA, Conte PM, Labay LE et al. (2005) Procedural distressin children with cancer: self-report, behavioral observations, andphysiological parameters. Clin J Pain 21:484–90
14. Wolfe J, Grier HE (2002) Care of the Dying Child. In: PizzoPA, Poplack DG (eds) Principles and Practice of Pediatric On-cology, 4th edn. Lippincott, Williams & Wilkins, Philadelphia,pp 1477–1493
Cancer Pain, Assessment in theCognitively Impaired
WENDY M. STEIN
San Diego Hospice and Palliative Care, UCSD, SanDiego, CA, [email protected]
Synonyms
Cognitive Impairment; dementia; delirium
Definition
Cognitive impairment or altered mental state is a changein the patient’s usual premorbid state of mind, which caninclude delirium and dementia as well as altered emo-tions and behaviors (8).
Characteristics
This section will focus on the challenging assess-ment of cancer pain in the communicative and non-communicative cognitively impaired patient. Acuteand subacute changes in mental status have been welldocumented in as many as 20–30% of medical inpa-tients and 50–90% of nursing home residents (Folsteinand Folstein 1994b), and can substantially impair apatient’s ability to participate actively in both the initialpain assessment and subsequent evaluation of treatmentefficacy. The initial step is to establish the patient’s pre-morbid mental status, and the nature and associationof any clinical changes that may have occurred. Visionand hearing impairments can further complicate boththe assessment and treatment of pain in the cognitivelyimpaired and need to be adequately compensated.Population-based studies of community dwelling el-derly have shown a two-fold increase in pain problemssignificant enough to impair daily function among thoseover age 60 (Crook et al. 1984). Older patients havea higher prevalence of a number of specific pain syn-dromes including most types of cancer, peripheral vas-cular disease, � temporal arteritis and � polymyalgiarheumatica, � peripheral neuropathies, � herpes zoster
and subsequent � postherpetic neuralgia. One mightthen reasonably expect that individuals suffering fromdementia and delirium would also be disproportion-ately affected by these syndromes, resulting in a largenumber of cognitively impaired elderly in desperateneed of aggressive and appropriate pain assessment andtreatment.In addition, older patients as a group are at high risk forundertreatment of cancer pain. Cleeland et al. showedthat those over the age of 70 were at higher risk of re-ceiving inadequate pain management (Cleeland 1998).Bernabei et al. documented significant numbers of nurs-ing home patients with cancer suffering from daily pain,and those over age 85 were at particular risk of havingno � analgesia at all (Bernabei et al. 1998).
Dementia versus Delirium
Folstein and Folstein define dementia as “a syndromecharacterized by a decline in multiple cognitive func-tions occurring in clear consciousness” (Folstein andFolstein 1994b). Dementia has been estimated in10–15% of elderly surgical patients, one-third of elderlymedical inpatients, and more than 50% of nursing homeresidents (Folstein and Folstein 1994b). Delirium, onthe other hand, is noted for its acute or subacute presen-tation with waxing and waning levels of consciousness,global cognitive impairment, and disorganized wake-sleep cycles. Delirium has been well described in themedical literature in patients with cancer (Derogatiset al. 1983); however, it also occurs commonly in theelderly, especially in those with underlying dementias.Rates of delirium have ranged as high as 50% in hos-pitalized patients with previously diagnosed dementia(Ouslander et al. 1997); in reality the figures may beeven larger, as in the community dementia is oftenwell hidden by well meaning family and friends whocompensate for gradually increasing mental deficitsover time.
Studies of Pain in the Communicative Cognitively Impaired
The reader should keep in mind that most pain studies ofassessment in the cognitively impaired have not focusedspecifically on cancer pain, but on all types of pain ingeneral.Parmaleeetal. (1996)studiedself-reportedpainin 758 elders with mild to moderate levels of cognitiveimpairment. This study showed that pain complaints de-creased with increasing levels of cognitive impairmentover time, i.e. that patients became less good at report-ing theirpain.However,whencognitively impaired indi-viduals reported pain, their pain complaints were no lessvalid. Ferrell et al. (1995) studied patients with moderateto severe degrees of cognitive impairment in 10 com-munity nursing homes. The researchers presented fivecommonly used pain scales in enlarged format and withadequate amounts of light, and with hearing augmenta-tion if required. Of those presented, the � Present PainIntensity Subscale (PPI) had the highest rate of comple-

208 Cancer Pain, Assessment in the Cognitively Impaired
tion (65%). Although only 32% could complete all fivescales presented, 83% of these patients with significantcognitive impairment could complete at least one of thescalespresented.Thesefindingsvalidate theutilityofof-fering a variety of scales when using standardized mea-sures with the cognitively impaired, and then continuingwith what works best for that patient.
Pain in Non-Communicative Cognitively Impaired Patients
Unfortunately, many early studies of pain assessmentin this population focused on the use of pediatric instru-ments, and specifically those developed for neonates,without first establishing data in this population. Thesetools were developed to measure acute, and often exter-nally induced procedure related pain. In the cognitivelyimpaired elderly, clinicians are most often evaluatingchronic, or acute on chronic pain, which is likely topresent differently. There have now been multiple stud-ies to validate the use of standardized tools specificallyadapted and/or developed for use in this population suchas the � Faces Pain Scale (Herr et al. 1998). However,global evaluations of a combination of nonverbal behav-ior, vocalizations, changes in function, and caregiverreports are most often used as indicators of pain in thenon-communicativecognitively impaired elderly (AGSPanel on Chronic Pain in Older Persons 2002). Marzin-ski (1991) studied 60 patients living in a dementia unit,of which 43% had potentially painful conditions basedon chart review. The most clinically interesting findingof this study was that the nursing staff could clearlyidentify what amounted to normative behavior for in-dividual patients, and once aberrations were identified,to act upon them.Several studies have sought to link assessment withinitiating pain interventions empirically in non-com-municative cognitively impaired elders. The mostcomprehensive project of this nature is that of Ko-vach et al. (1999). The research team worked with104 non-communicative demented elderly who hadsigns or symptoms of pain or discomfort at 32 nursinghomes. The nursing staffs were instructed in the use ofthe � Assessment of Discomfort in Dementia (ADD)Protocol if a patient displayed signs or symptoms ofdistress. After excluding common physical causes fordiscomfort such as occult infection, or impaction bythorough physical assessment, and review of historyincluding consultations with family and/or physicians,nonpharmacologic comfort interventions were un-dertaken. If unsuccessful, the nurses were educatedto administer ‘as needed’ non-opioid analgesics, andcontinue up the WHO ladder depending on responseand discussion with physicians. The sample populationdecreased behavioral symptoms associated discomfortfrom an average of 32.85–23.47 symptoms on protocol,which was a statistically significant change. Of notewas the fact that 88% of the staff felt that the protocolwas beneficial.
General Recommendations
The clinician needs to create an optimal environmentin order to adequately assess pain in the communica-tive cognitively impaired. Limited attention span maydemand dividing up the initial assessment into severalshorter sessions. Additional time should be allowed forthe patient to assimilate questions to allow for receptiveor expressive aphasia. Ensuring that large print cards,adequate lighting, and hearing aids or pocket amplifi-cation devices and refractive lenses are available is vi-tal. Qualitative descriptions of pain should bear equalweight and be encouraged. If using standardized tools,multiple tools should be presented upon initial assess-ment so as to discern which is easiest for that particularpatient,document this in theclinical record,andcommu-nicate this with the care team (Stein 1996). Copies of thistool can be made available (without identifying data onit) on the chart and at the bedside, ensuring that each sub-sequent assessment is performed exactly the same wayregardless of the team member asking the questions. Asthe cognitively impaired elderly are often unable to re-port on previous pain, assessment should be conductedmore frequently than would be necessary with a cogni-tively intact patient (Stein 2001). Family members andcaregivers can assist in this process by helping to jour-nal the patient’s pain when they visit, thus providing acomprehensive picture.Deviation from what is considered baseline or ‘nor-mal’ behavior for the non-communicative cogni-tively impaired patient remains the clinical imperative(Stein 2001). This should trigger a comprehensive bed-side physical examination coupled with laboratory andimaging studies, consistent with the benefits and bur-dens likely to be incurred and the patient and/or family’swishes. Physical examination should specifically focuson occult sources or atypical presentations of infectionsuch as pneumonia or urinary tract infection, as wellas fecal impaction. The clinical involvement of theentire interdisciplinary team should be sought to elicitalterations in sleeping, eating or elimination as sourcesof change in behavior. Chart review should excludechanges in medications, doses or dose intervals as po-tential causes. After all of the above have been carefullycompleted and reviewed with family members and staff,and informed consent obtained from involved familymembers, there may be a role for a well-defined empirictrial of short-acting pain medication with consistent andcontinual reassessment (Stein 2001).
References1. AGS Panel on Chronic Pain in Older Persons (2002) The Man-
agement of Chronic Pain in Older Persons. JAGS 50:1–202. Bernabei R, Gambassi G, Lapane K et al. (1998) Management
of Pain in Elderly Patients with Cancer. SAGE Study Group.Systematic Assessment of Geriatric Drug Use via Epidemiology.JAMA 279:1877–1882
3. Cleeland CS(1998) Undertreatment of Cancer Pain in the Elderly.JAMA 279:1914–1915

C
Cancer Pain, Assessment of Cultural Issues 209
4. Crook J, Rideout E, Browne G (1984) The Prevalence of PainComplaints among a General Population. Pain 18:299–314
5. Derogatis LR, Morrow GR, Fetting J et al. (1983) The Preva-lence of Psychiatric Disorders among Cancer Patients. JAMA249:751–757
6. Ferrell BA, Ferrell BR, Rivera L (1995) Pain in CognitivelyImpaired Nursing Home Patients. J Pain Symptom Manage10:591–598
7. Folstein MF, Folstein SE (1994a) Neuropsychiatric Assessmentof Syndromes of Altered Mental State. In: Hazzard WB, BiermanEL, Blass JP et al. (eds) Principles of Geriatric Medicine andGerontology. McGraw-Hill, pp 221–228
8. Folstein MF, Folstein SE (1994b) Syndromes of Altered Men-tal State. In: Hazzard WB, Bierman EL, Blass JP et al. (eds)Principles of Geriatric Medicine and Gerontology. McGraw-Hill,pp 1197–1204
9. Herr KA, Mobily PR, Kohout FJ et al. (1998) Evaluation of theFaces Pain Scale for Use with the Elderly. Clin J Pain 14:29–38
10. Kovach CR, Weissman DE, Griffi J et al. (1999) Assessment andTreatment of Discomfort for People with Late-Stage Dementia.J Pain Symptom Management 18:412–419
11. Marzinski LR (1991) The Tragedy of Dementia: Clinically As-sessingPain in theConfused, Nonverbal Elderly. JGerontologicalNursing 17:25–28
12. Ouslander JG, Osterweil D, Morley J (1997) Delirium and De-mentia. In: Medical Care in the Nursing Home. McGraw-Hill,pp 147–162
13. Parmalee PA (1996) Pain in Cognitively Impaired Older Persons.In: Ferrell BA, Saunders WB (eds) Clinics In Geriatric Medicine,pp 473–485
14. Stein WM (1996) Cancer Pain in the Elderly. In: Ferrell BR,Ferrell BA (eds) Pain in the Elderly. IASP Press, Seattle, pp 69–80
15. Stein WM (2001) Assessment of Symptoms in the CognitivelyImpaired. In: Topics in Palliative Care. Oxford University Press5:123–133
Cancer Pain, Assessment of CulturalIssues
TERRY ALTILIO
Department of Pain Medicine and Palliative Care, BethIsrael Medical Center, New York, NY, [email protected]
Definition
Culture is defined as learned values, beliefs, behaviorsand systems of meaning which guide a worldview andinform decisions. Culture is constantly redefined andnegotiated and respectful, comprehensive care requirescombining theoretical knowledge with a meaningfulexploration of the “patients unique history, familyconstellation and socioeconomic status” (Koenig andGates-Williams 1995).
Characteristics
Although knowledge of specific cultures can be instruc-tive, cultural identification alone is not predictive of spe-cific behaviors, values or beliefs. Intracultural variationemanating from such factors as gender, age, geographiclocation, ties to country of origin, � assimilation and� acculturation contribute to the dynamic nature of cul-ture. Culture infuses the experience of the patient and
family, and practitioners are more or less influencedby the culture of the health care system, the diseaseand the larger society. It is at this interface that under-standing, collaboration and negotiation needs to occur(Koenig and Gates-Williams 1995; Kagawa-Singer andBlackhall 2001; Kagawa-Singer 1996).Studies of the relationship of culture and pain dateback to 1950 and include both clinical and laboratoryresearch. Studies have focused on such varied aspectsas pain threshold, pain perception and description,attitudes and behaviors, undertreatment in minoritypatients, coping strategies, use of opioid medications,beliefs, ascribed meaning and outcomes (Edwards etal. 2001; Zatzick and Dimsdale 1990). As far back as1952, Zborowski studied the influence of � ethnicity onpain response patterns, attitudes, beliefs and meaning(Zborowski 1952). In 1966, Zola studied interethnic dif-ferences in the response and attitudes toward symptomssuch as pain (Zola 1966).Cultural aspects of pain such as meaning, attribution,description and health seeking behaviors become in-creasingly relevant as research points to the importanceof these factors on outcomes. For example, a study ofchest pain in a population from the Southern UnitedStates revealed that cultural differences resulted inatypical descriptions, which have the potential to mis-lead clinicians who depend on the description of thecharacter of chest pain as they triage for ischemic heartdisease (Summers et al. 1999). A study of indigenousand non-indigenous people with persistent chest pain inthe Northern Territory of Australia revealed that delaysin presentation affected both rural and urban indige-nous peoples, as well as rural non-indigenous people;these delays influence management options for acutemyocardial infarction (Ong and Weeramanthri 2000).Such information assists clinicians and health educatorsto know that signs and symptoms, and pain-related be-haviors, may not be the same for all cultural groups. Painrelated to a diagnosis of cancer becomes complicatedby the values and beliefs surrounding the disease itself,which may vary among optimism, hopelessness, shameor acceptance. These findings can provide direction toculturally informed assessment, education and outreachefforts.Within available research, there is considerable vari-ation in study populations, theoretical formulations,study design and findings. There is much opportunityfor ongoing research in this rich and complex topic.Assessment and study challenges include cross-culturalvalidity of behavioral cues to indicate pain level, cross-cultural validity of assessment tools, and expandingstudy designs to include variables such as intraculturaldifferences and influence of clinician culture on out-come. Assessment tools such as the Brief Pain Inventoryand McGill Pain Questionnaire have been validated andtranslated into languagesother than English. In addition,acceptance of unique cultures requires understanding

210 Cancer Pain, Assessment of Cultural Issues
that linear assessment tools may have little relevancein cultures where numbers have no relationship to painrating, or where narrative or pictures are essential tocommunication (Kagawa-Singer and Blackhall 2001,Hallenbeck and Goldstein 1999).Consideration of cultural issues in the health care settingmeans that practitioners have to reconcile the possibil-ity that their personal beliefs and values, and the valuesof the medical system, may not be shared by the patientand family (Hallenbeck 2002). Consequently, cliniciansneed to develop an awareness of the culture and tradi-tions of the population they treat. This awareness be-comes a hypothesis and serves only as background toguide inquiry and exploration. The subjective nature ofpain requires that each patient’s pain description, reportand behaviors be explored and understood in the contextofculturalvariationrelated topain.Cliniciansbringtheirown personal and professional cultural perspectives intothe medical setting and it is at this interface that the as-sessment of pain, clinical judgement and related treat-ment interventions take place. As early as 1977, Davitzet al. reported on the emergency room care of a 45-year-old male whose pain behaviors were observed by threenurses of different � ethnic group backgrounds (Davitzet al. 1977). Each nurse had different reactions and judg-ments of his expression of pain. A nurse from North-ern Europe described the patient as very emotional andoverreactive.A nurse from Puerto Rico felt the patient’soutbursts were understandable and an American nurseexpected that an adult male of his age and backgroundwould be stronger and more stoic. A follow-up studyfound that nurses from various countries differed in theirjudgments about the degree of patient suffering. Thesefindingsarean alert to alldisciplinesof the importanceofself awareness, as clinician beliefs and values can signif-icantly impact on attitudes and practice (Bonham 2001).Characteristics of pain assessment and managementmay be influenced by culture. While categorized asdiscrete aspects, these variables are integrated and over-lapping, and related to the larger historical/political,class and socioeconomic issues (Koenig and Gates-Williams 1995). For example, in some countries, theexperience of marginalization and discrimination ofminority patients creates an environment of mistrustand/or hopelessness, which requires clinicians to spendadditional time and ongoing effort to establish begin-ning rapport and credibility. The undertreatment ofpain, including cancer pain, in minority populationshas been identified in a variety of studies, and furtherwork is needed to isolate the multidimensional factorsthat influence these outcomes (Zborowsk 1969).
Expression and Language of Pain
Pain complaints can be conveyed using verbal, facial orbody language. For many, how one expresses and re-sponds to pain is learned through childhood experienceand either reinforced in adulthood or modified by other
experience, such as a diagnosis of a life threateningillness. Culture influences how, if and to whom thesubjective pain experience is expressed and whether itis described in direct, substitute or metaphoric terms.In cultures where control is valued, endurance andstoicism would be expected and outward expression ofpain viewed as a sign of weakness, possibly resulting inguilt or shame. Similar behaviors are not always basedin the same value system. For example, stoicism mayreflect a reluctance to impose or disrupt others ratherthan a sign of endurance. This is especially importantwith a diagnosis of cancer, where historically emphasishas been on curing the disease and pain, and quality oflife issues have been perceived as a distraction from thatprimary goal. Expressions of pain, such as crying, curs-ing or moaning, can be the learned and expected wayto express distress and seek care, and are not alwayscorrelated with the degree of pain. These behaviorsmay relate to feared consequences rather than the painitself (Mims 1989). In patients with cancer, emerging orincreasing pain may be interpreted as a sign of progress-ing disease, and the symbolic significance of the painbecomes a source of suffering and distress. Dramaticexpressions of pain can serve an important purpose insystems and situations where people have to competefor care, or where healthcare professional have mini-mized or challenged reports of pain. Cultures that valuepatience and choose not to disrupt others need outreachfrom health care staff to create an environment wherepatients feel their comfort to be an important focus ofcare. Another variable that influences the expression ofpain and related content is time orientation. In societiesthat are future-oriented, patients may project ahead,and rather than focus on the sensation of pain and relief,will anticipate and worry about the future impacts ofpain and disease (Mims 1989).
Meaning of Pain
The meaning of pain may have an important relationshipto response,behaviorsandcoping.Cultural traditionsof-ten prepare individuals to anticipatepain in certain situa-tions, which can increase feelings of control and lessenanxiety and distress related to the unknown. Pain thathas been experienced before has different meaning thanpain that is related to a life-threatening illness, or is un-expected, and all will be integrated in accordance withpersonal and cultural beliefs and values. The narrativesand descriptions not only reflect pain but also attempt tomake sense of it within a cultural context and within thecontext of a known diagnosis (Hallenbeck 2002; Davitzetal.1977;Lipsonetal.2000).Healthmaybeconsidereda gift from God or a reflection of internal equilibrium.Cancer and pain may be interpreted as a sign of inter-nal imbalance, divine displeasure, a curse, witchcraft,or perhaps, the result of transgressions in prior life. Ifpain is considered part of God’s plan, a test of faith or anopportunity for character building and redemption, then

C
Cancer Pain, Assessment of Cultural Issues 211
acceptance and the manner of coping may be a demon-stration of courage and faith. Where pain is an extensionof God’s will, or when suffering is felt to be an expectedpart of life, there may be a feeling of fatalism that re-sults in a feeling of powerlessness with no expectationor acceptance of treatment (Hallenbeck 2002; Davitz etal. 1977; Lipson et al. 2000).
Expectations of Health Care Professionals
The expectations of healthcare professionals are highlyinfluenced by cultural variables. Respect for cliniciansmay beexpressed by behaviors such asnotmakingdirecteye contact and not challenging or questioning practi-tioners. Many traditions support a hierarchical system,and patients do not expect a consultative model wherethey are asked for feedback and given options. Expect-ing to be guided by experts, patients may interpret theconsultative approach as a reflection of incompetence.Health care relationships are a reflection of the largerculture, which may be high or low-context. Low-contextculture, similar to Western biomedicine, places empha-sis on individuality and a more linear verbal communi-cation, whereas a high-context environment emphasizesthe relational aspects that are important to care, decisionmaking and inclusion of family and community (Hal-lenbeck 2002; Davitz et al. 1977). Consultation with ahealth care professional may follow the primary heal-ing efforts of family or healers. Acknowledging and in-tegrating these traditional interventions can be signs ofrespect for patients and their support systems and mayenhance outcome. In situations where the language ofpatient and clinician differ, perceptions of patient andfamily about the use of medical translators need to be ex-plored. Family members are untrained in the use of med-ical terminology and when acting as interpretersmay ex-perience role conflict and confusion (Zhou et al. 1993).Clinicians are in the unique position of being unaware ofthe actual content and accuracy of the communicationwhen family and friends translate throughtheirown cog-nitive and emotional filters.
Response to and Acceptance of Treatments
Treatment response is based on a range of values andbeliefs. In addition to the ongoing investigation of in-terethnic differences in drug response, culture impactsacceptance of medications, interventions and sideseffects. Sedation and cognitive impairment may bevery troubling to patients whose clarity of mind andcontact with others are essential to spiritual, emotionaland philosophical well being. Treatments that are in-ternal, such as pills or injections, may be preferred bysome, while external interventions, such as massageand salves, may be preferable to others. In cultureswhere acupuncture equates with positive outcome, thesensation of insertion of needles may have positiveassociation. Certain medications, such as morphine ormethadone, may have symbolic significance and be
associated with addiction or death. When medicationsare feared, patients may discontinue them quickly. Inhigh context cultures, treatment plans and options mayneed to be discussed with family and community, whichmay include healers, elders or clergy (Hallenbeck andGoldstein 1999).
Caregiver Responses
The responses of caregivers are multifaceted and oftenrelate to how care is provided to a sick family or com-munity member. The expected roles and responses ofpatients, parents, siblings, family and community mayevolve from an acute illness model. For some, a cancerdiagnosis may yield helplessness and passivity as the ac-ceptedandexpectedresponse toillnessandpain(Hallen-beck and Goldstein 1999). Transition to a chronic dis-ease state can challenge traditional beliefs and behav-iors, as the support must become long-term, and there isa need to accommodate to a person who receives ongo-ing treatments and may or may not be disabled (Lipsonet al. 2000). Traditional beliefs, which encourage restand dependence can be very responsive to situations ofpain in life threatening illness and less helpful in chronicsettings, where goals of care include recovering functionand encouraging participationbeyondtheroleofpatient.The convergence of culture, pain and the diagnosis ofcancer provides a rich and challenging opportunity forclinicians to individualize assessment and intervention,and maximize the support, comfort and continuity thatcomes from cultural beliefs and sustains patients andfamilies through medical and life transitions, crises andbeyond.
References1. Bonham VL (2001) Race, Ethnicity and Pain Treatment: Striving
to Understand the Causes and Solutions to the Disparities in PainTreatment. J Law Med Ethics 29:52–68
2. Davitz LL, Davitz JR, Higuchi Y (1977) Cross-Cultural In-ferences of Physical Pain and Psychological Distress. NursingTimes 73:521–558
3. Edwards CL, Fillingim RB, Keefe F (2001) Race, Ethnicity andPain – Topical Review. Pain 94:133–137
4. Groce NE, Zola IK (1993) Multiculturalism, Chronic Illness andDisability. Pediatrics 91:1048–1055
5. Hallenbeck JL (2002) Cross-Cultural Issues. In: Berger AM,Portenoy RK, Weissman DE (eds) Principles and Practiceof Palliative Care. Lippincott, Williams & Wilkins, Philadel-phia, pp 661–672
6. Hallenbeck JL, Goldstein MK (1999) Decisions at the End ofLife – Cultural Considerations beyond Medical Ethics. Gener-ations Spring:24–29
7. Koenig BA, Gates-Williams J (1995) Understanding Cul-tural Differences in Caring for Dying Patients. West JMed 163:244–249
8. Kagawa-Singer M (1996) Cultural Systems. In: McCorkle R,
Grant M, Frank-Stromborg M (eds) Cancer Nursing, 2nd edn.WB Saunders, Philadelphia, pp 38–52
9. Kagawa-Singer M, Blackhall LJ (2001) Negotiating Cross-Cultural Issues at the End of Life “You Got to Go Where heLives.” JAMA 286:2993–3001

212 Cancer Pain, Epidemiology
10. Lipson JG, Dibble SL, Minarik PA (eds) (2000). Culture &Nursing Care: A Pocket Guide. California: UCSF NursingPress, pp 3–4
11. Mims BC (1989) Sociologic and Cultural Aspects of Pain. In: Tol-lison CD (ed) Handbook of Chronic Pain Management. Williamsand Wilkins, Baltimore, pp 17–25
12. Ong MA, Weeramanthri TS (2000) Delay Times and Man-agement of Acute Myocardial Infarction in Indigenous andNon-Indigenous People in the Northern Territory. Med JAustralia 173:173–174
13. Summers RL, Cooper GJ, Carlton FB et al. (1999) Prevalenceof Chest Pain Descriptions in a Population from the SouthernUnited States. Amer J Medical Science 318:142–145
14. Zatzick DF, Dimsdale JE (1990) Cultural Variation in Responseto Painful Stimuli. Psychosom Med 52:544–557
15. Zborowski M (1952) Cultural Components in Responses to Pain.J Social Issues 8:16–30
16. Zborowski M (1969) People in Pain. Jossey-Bass, San Francisco,pp 30–41
17. Zhou HH, Sheller JR, Nu H et al. (1993) Ethnic Differences inResponse to Morphine. Clin Pharmacol Ther 54:507–513
18. Zola J (1966) Culture and Symptoms, an Analysis of PatientsPresenting Complaints. Am Sociol Rev 31:615
Cancer Pain, EpidemiologyCIELITO C. REYES-GIBBY,CHARLES S. CLEELAND
The University of Texas M. D., Anderson CancerCenter, Houston, TX, [email protected]
Definition
Epidemiology provides a framework for measuring theprevalence, incidence, and risks associated with pain incancer patients. Epidemiology provides research meth-ods that can be used to answer the following questions:What is the occurrence of pain in people with cancer? Atwhat stage of the disease does pain become a problem?Are cancer patients at a higher risk for pain comparedto patients with chronic conditions such as diabetes orcardiovascular disease? To what extent does the preva-lence of cancer pain vary by age, gender, or race? Whatfactors are associated with the prevalence or incidenceof pain? What proportion of patients receives adequatetreatment for pain?
Characteristics
Although many studies have attempted to answer thesebasic questions, consistent results have been difficultto obtain. Estimates of the number of cancer patientsexperiencing pain vary widely, mainly because of alack of uniformity (or standardization) in the defini-tions and assessment measures used (i.e. there is nogold standard) and the heterogeneity of pain conditions(nociceptive vs. neuropathic). Other factors contribut-ing to the wide variability of results include, but are notlimited to, the heterogeneity of cancer types (breast,lung, etc.), the stage of disease, and the type of treat-ment settings (outpatient vs. inpatient or palliative) in
which studies were conducted. In many instances, theissue of potential confounding factors has not been ad-equately addressed. There is also non-distinction on thevarious measures of disease occurrence and risk usedin measuring the distribution, determinants, and natu-ral history of pain. For example, prevalence measures(which quantify the proportion of a population witha condition at a given point in time (point prevalencerate), the proportion of persons affected by the condi-tion during a defined period of time (period prevalencerate), or the proportion of a population affected overtheir lifetime (lifetime prevalence rate)) are commonlyconfused with incidence measures (which quantifythe probability or rate of onset of a condition amongpersons with no prior history). A recent report of theNational Cancer Institute (Patrick et al. 2004), whileemphasizing the need for better symptom epidemio-logic studies, elaborates the methodological issues andchallenges facing researchers who study the epidemi-ology of pain. In this essay, we report on studies of theprevalence of pain among cancer patients and the riskfactors associated with pain and its undertreatment,and offer recommendations for future studies on theepidemiology of pain.
Prevalence of Cancer Pain
Pain is prevalent for large numbers of patients withcancer (Cleeland et al. 1997; Cleeland et al. 1994;Portenoy et al. 1994; Von Roenn et al. 1993). Approxi-mately 55% of outpatients with metastatic cancer havedisease-related pain, and 36% have pain of sufficientseverity to impair their functioning and quality of life.Significant pain is rarely a problem at diagnosis, but asdisease becomes metastatic, a majority of patients willhave pain (Daut and Cleeland 1982). Pain prevalenceand severity obviously varies with the adequacy ofpain management. However, despite the existence ofnational and international pain management guidelines,many patients with pain are not prescribed an analgesicappropriate to the severity of their pain. Multicenterstudies indicate that approximately 40% of patientswith cancer pain are not prescribed analgesics potentenough to manage their pain, with additional patientsreceiving insufficient doses of the analgesic prescribed.Studies of pain related to specific cancers show pain ashighly prevalent. For example, a study of breast cancerpatients (stages II, III, and IV breast cancer) showed47% had severe pain (Gaston-Johansson et al. 1999).In a study of pancreatic cancer patients, at least 44%were found to have severe pain (Brescia et al. 1992). Areview of studies of lung cancer patients document thatas many as 85% experienced severe pain (Potter andHigginson 2004).Studies of pain following surgical treatment show painas prevalent treatment sequelae. Despite the thousandsof cancer patients who are treated with curative surgery,very little is known about the prevalence, duration,

C
Cancer Pain, Epidemiology 213
and functional impact of pain in this patient popula-tion. Patients not only suffer from the side effects ofthe chemotherapy or radiotherapy before surgery fortheir cancer, but may also develop serious post-surgicalsymptoms.Among breast cancer patients, 41% of those who hadconservative breast surgery with radiotherapy reportedpain as a consequence of treatment. Pain generallystarted within three months after the completion oftherapy, was localized in the axillary region, and wasintermittent (Amichetti and Caffo 2003). The pain wasmainly described as aching (59%), tender (51%), andcramping (43%). In comparison to the patients who didnot experience pain, those who suffered from pain hadsignificantly worse scores in physical, psychological,and other quality-of-life measures.It is lessrecognized thatmanycancerpatientscontinue toexperience pain well after treatment has ended. Chaplinand Morton (1999) assessed 93 head and neck cancerpa-tients and found that 48% had head and neck pain whenfirstseen,and that25%and26%hadpain thatpersistedat12 and 24 months, respectively.Theprevalenceofshoul-der and arm pain was greater after treatment, increasingfrom 14% at diagnosis to 37% at 12 months and 26% at24 months. Any pain (pain in either the head and neck orshoulder and arm or both) at 24 months was strongly pre-dicted by earlier post-treatment pain (at three months orat 12 months). Shoulder and arm pain at 24 months wasstrongly correlated with surgical treatment of the neck,although no difference in pain experience was noted be-tween those who had radical neck dissections and thosewho had more conservative procedures.Studies have examined the prevalence of pain amongcancer patients in advanced stage. As part of the SUP-PORT studies, McCarthy et al. (2000) evaluated over1,000 cancer patients during the three days beforedeath, at one to three months before death, and threeto six months before death. As expected, as patientsprogressed toward death, their six-month prognosisdeteriorated significantly and the severity of theirdisease worsened. Cancer patients experienced signif-icantly more pain and confusion as death approached.Severe pain was common; more than one quarterof patients with cancer experienced significant painthree to six months before death, and more than 40%were in significant pain during their last three days oflife.While it is recognized that pain is prevalent for themajority of cancer patients, evidence suggests that theelderly and patients from minority groups may have aneven greater risk for pain and poor pain management(Cleeland et al. 1997; Anderson et al. 2000). Undertreat-ment of pain was shown to be higher among minoritypatients seen at clinics serving minority clients, withminority patients three times more likely to be un-dermedicated with analgesics than patients treated innon-minority community treatment settings (Cleeland
et al. 1994). Patients treated at university centers and atcenters seeing primarily African Americans, Hispanics,or both, were more likely to receive inadequate anal-gesia than patients treated in non-minority communitytreatment settings (77% vs. 52%, respectively). Minor-ity patients had the severity of their pain underestimatedby their physicians, reported that they needed strongerpain medication, and felt that they needed to take moreanalgesics than their doctors had prescribed. Assessingdifferences between minority groups, more Hispanicpatients reported lower levels of pain relief than didAfrican Americans.Although few disagree that painful conditions shouldbe treated regardless of age, studies document under-treatment of cancer pain in older populations. In a studyof 4,003 elderly cancer patients (24%, 29%, and 38%of those aged 85 years or older, 75–84 years, and 65–74years, respectively), Bernabei and colleagues (1998)found that more than a quarter (26%) of patients experi-encing daily pain received no analgesic agent. Patientsaged 85 years or older were less likely to receive mor-phine or other strong opiates than those aged 65–74years (13% vs. 38%, respectively), and were morelikely to receive no analgesia at all. African Americanelderly patients were also at a higher risk for under-treatment, suggesting the disparity in pain treatmentis compounded for elderly minority patients. A studythat looked at undertreatment of pain for ambulatorypatients with metastatic cancer (Cleeland et al. 1994)also showed that older age (70 years or older) was asignificant predictor of inadequate analgesia, accordingto the World Health Organization guidelines (WorldHealth Organization 1986) for treatment of patientswith cancer pain.
Factors Associated with Inadequate Treatment and Control ofPain
Undertreatment of pain is a major factor in the preva-lence and severity of pain. A number of factors predictpoor control or undertreatment of pain. Poor pain as-sessment remains the most salient barrier. Cleeland et al.(1994) found the degree of discrepancy between physi-cian estimate and patient report of pain severity was amajor predictor of undertreatment. However, althoughquantitative pain assessment has demonstrated its feasi-bility and validated pain assessment tools are available,data from a community-based oncology setting (Rhodeset al. 2001) show a virtual absence of documentation ofquantitative pain assessment (only 0–5% of medical andradiationoncologyphysicians’notescontainedanysuchdocumentation). Twenty-eight percent of patients withsignificantpain had no mention ofpain in thephysicians’notes, and 48% had no documented analgesic treatment.These findings point to the critical role of adequate as-sessmentandmonitoringfor thecontrolofpainandothersymptoms.

214 Cancer Pain, Epidemiology
Many cancer specialists recognize that pain control isoften suboptimal. Medical oncologists were surveyedabout their treatment of cancer pain in a study con-ducted by the Eastern Cooperative Oncology Group(ECOG) (Von Roenn et al. 1993). Only half of thephysicians surveyed indicated that cancer pain controlwas “good” or “very good” in their practice setting.Seventy-five percent of the physicians indicated thatthe most important barrier to cancer pain managementwas inadequate pain assessment. Over 60% reportedthat physicians’ reluctance to prescribe analgesics andpatient unwillingness to report pain or take opioidswere barriers to adequate pain treatment. Inadequateknowledge about cancer pain management was re-ported by over 50% of the ECOG physicians surveyed.The survey documents that a substandard level ofeducation about cancer pain management and a re-luctance to address it in practice existed at all levelsof professional health care. Cleeland and colleagues(2000) repeated the ECOG study format with physi-cian members of the Radiation Therapy OncologyGroup. Although there has been some improvementin the use of stronger analgesics, many barriers togood pain control remain, and poor pain assessmentis still seen as the major barrier to good pain manage-ment.
Improving Control of Cancer Pain
In spite of the recent concerns over symptom manage-ment, there is substantial evidence that symptoms thatcould, in principle, be well managed are nonetheless un-dertreated. Pain could be more adequately controlled ifwe systematically applied the knowledge that we nowhave about its management.There is at least preliminary evidence that improvingpain assessment can improve pain management, andmay improve the management of other symptoms aswell. Trowbridge et al. (1997) conducted a randomizedcontrolled trial of 320 patients and 13 oncologists.Patients were asked while in the clinic to completeassessments of their pain, their pain treatment regi-mens, and the degrees of relief received. Follow-upwas conducted four weeks later by mail-in survey. Theintervention group’s clinical charts contained a sum-mary of the completed pain scales, and the oncologistswho treated these patients were instructed to review thesummary sheet prior to an evaluation. This summarywas not available for the oncologists treating the pa-tients in the control group. Results showed a significantdifference (P = 0.016) in the physicians’ prescriptionpatterns. In the control group, prescriptions for 86%of the patients did not change, without any increasein analgesic prescriptions. In the intervention group,analgesic prescriptions changed for 25% of the patients,decreasing for 5% and increasing for 20%. A decreasein the incidence of pain described as “more than life’susual aches and pains” was found at follow-up for the
intervention group (P = 0.05). The findings from thisstudy suggest that standardized pain assessment leadsto improved cancer pain management.Beginning with the publication of the World HealthOrganization’s Cancer Pain Management guidelinesin 1986 (World Health Organization 1986), severalguidelines for the practice of cancer pain managementhave been issued. There is, however, only one publishedstudy that evaluates the effectiveness of adherence to apain management guideline for cancer pain (Du Pen etal. 1999). In this study, 81 cancer patients were enrolledin a prospective, longitudinal, randomized controlledstudy from 26 medical oncologist outpatient clinicsin western Washington. A multilevel treatment algo-rithm based on the AHRQ Guidelines for Cancer PainManagement was compared with standard–practice(control) therapies for pain and symptom managementused by community oncologists. Patients randomizedto the pain algorithm group achieved a statisticallysignificant reduction in pain intensity when comparedwith standard community practice.A recently completed Eastern Cooperative OncologyGroup study (Cleeland et al. 2005) found that the institu-tional use of a protocol for pain management improvedpain control in lung and prostate cancer patients, butfailed to improve the pain management of other patients(breast cancer and myeloma patients) in the same in-stitutions who were not specifically treated by the painprotocol. Forty-eight percent of patients with lung andprostate cancer in the institutions that used a protocolfor pain management reported a statistically significantreduction in moderate and severe pain (P < 0.02), com-pared with 15% of lung and prostate patients treated asusual in the control institutions.More recently, a system improvement approach wasused to improve pain management in a national health-care system (Cleeland et al. 2003), with some reportedsuccess. The focus of the project, a collaborative ini-tiative of the Veterans Health Administration and theInstitute for Healthcare Improvement (VHA-IHI), wasto achieve rapid improvements in pain management inthe clinical and operational areas in the national VHAsystem. An underlying premise was the spread of ex-isting knowledge to multiple sites. A total of 70 teamswere formed and were asked to identify their goalsand to implement changes in their practice setting.Importantly, faculty involved in the initiative developedthe attributes of an ideal pain management system.Changes that were implemented included the develop-ment of new assessment forms to increase the numberof patients with documented assessment and follow-upfor treatment plan; development of guidelines and/orprotocols; formation of one-on-one, group-provider, orcomputer-based educational methods to improve bothassessment and follow-up, and/or ways to effectivelylink provider education with other system changes suchas drug ordering or assessment processes; and develop-

C
Cancer Pain, Evaluation of Relevant Comorbidities and Impact 215
ment of innovative ways to link primary care physicianswith pain specialists.The following outcomes were reported: moderate orsevere pain on study units dropped from 24% to 17%;pain assessment increased from 75% to 85%; pain careplans for patients with at least mild pain increased from58% to 78%; and the number of patients provided withpain educational materials increased from 35% to 62%.The results of these studies, taken together, suggestthat improved assessment should improve symptommanagement for cancer patients.
Future Directions
Overall, studies of the incidence, prevalence, severity,and treatment of cancer-related pain have shortcomingsthat need to be addressed and remedied. Pain is oftenevaluated and reported without stratifying for hetero-geneity with respect to pain type, disease type and stage,disease treatment, and response to disease treatment.Although pain may endure for days, months, or years,assessments are often performed cross-sectionallyrather than longitudinally, thus failing to assess patternsand trajectories.Moreover, we need to explore whether pain and othersymptoms experienced by cancer patients differ quanti-tatively and qualitatively with those of non-cancer pop-ulations. Cohort studies that will provide clinicians withinformation regarding the incidence, severity, and dura-tion of thesesymptomsafter adiagnosisofcancer shouldalso be useful in determining the epidemiology of can-cer pain. Finally, we need to identify the current ade-quacy of care for these symptoms, including identifyingwhat factors (e.g. patient-related, clinician-related, andsystem-related) are predictive of poor symptom man-agement.
References1. Amichetti M, Caffo O (2003) Pain after quadrantectomy and
radiotherapy for early-stage breast cancer: incidence, character-istics and influence on quality of life. Results from a retrospectivestudy. Oncology 65:23–28
2. Anderson KO, Mendoza TR, Valero V et al. (2000) Minoritycancer patients and their providers: Pain management attitudesand practice. Cancer 88:1929–1938
3. Bernabei R, Gambassi G, Lapane K et al. (1998) Managementof pain in older adult patients with cancer. SAGE Study Group.Systematic Assessment of Geriatric Drug Use via Epidemiology.JAMA 279:1877–1882
4. Brescia FJ, Portenoy RK, Ryan M et al. (1992) Pain, opioid use,and survival in hospitalized patients with advanced cancer. J ClinOncol 10:149–155
5. Chaplin JM, Morton RP (1999) A prospective, longitudinal studyof pain in head and neck cancer patients. Head Neck 21:531–537
6. Cleeland CS, Gonin R, Baez L et al. (1997) Pain and treatment ofpain in minority patients with cancer. The Eastern CooperativeOncology Group Minority Outpatient Pain Study. Ann InternMed 127:813–816
7. Cleeland CS, Gonin R, Hatfield AK et al. (1994) Pain and itstreatment in outpatients with metastatic cancer. N Engl J Med330:592–596
8. Cleeland CS, Janjan NA, Scott CB et al. (2000) Cancer pain man-agement by radiotherapists: a survey of radiation therapy oncol-ogy group physicians. Int J Radiat Oncol Biol Phys 47:203–208
9. Cleeland CS, Portenoy RK, Rue M, et al. (2005) Does an oralanalgesic protocol improve pain control for patients with can-cer? An intergroup study coordinated by the Eastern CooperativeOncology group. Ann Oncol 16:972–980
10. Cleeland CS, Reyes-Gibby CC, Schall M et al. (2003) Rapid im-provement in pain management: the Veterans Health Administra-tion and the institute for healthcare improvement collaborative.Clin J Pain 19:298–305
11. Daut RL, Cleeland CS (1982) The prevalence and severity ofpain in cancer. Cancer 50:1913–1918
12. Du Pen SL, Du Pen AR, Polissar N et al. (1999) Implementingguidelines for cancer pain management: results of a randomizedcontrolled clinical trial. J Clin Oncol 17:361–370
13. Gaston-Johansson F, Fall-Dickson JM, Bakos AB et al. (1999)Fatigue, pain, and depression in pre-autotransplant breast cancerpatients. Cancer Pract 7:240–247
14. McCarthy EP, Phillips RS, Zhong Z et al. (2000) Dying withcancer: patients’ function, symptoms, and care preferences asdeath approaches. J Am Geriatr Soc 48:S110–S121
15. Patrick DL, Ferketich SL, Frame PS et al. (2004) National In-stitutes of Health State-of-the-Science Panel National Institutesof Health State-of-the-Science Conference Statement: Symptommanagement in cancer: pain, depression, and fatigue, July 15–17,2002. J Natl Cancer Inst Monogr 32:9–16
16. Portenoy RK, Thaler HT, Kornblith AB et al. (1994) Symptomprevalence, characteristics and distress in a cancer population.Qual Life Res 3:183–189
17. Potter J, Higginson IJ (2004) Pain experienced by lung cancerpatients: a review of prevalence, causes and pathophysiology.Lung Cancer 43:247–257
18. Rhodes DJ, Koshy RC, Waterfield WC et al. (2001) Feasibilityof quantitative pain assessment in outpatient oncology practice.J Clin Oncol 19:501–508
19. Trowbridge R, Dugan W, Jay SJ et al. (1997) Determining theeffectiveness of a clinical-practice intervention in improving thecontrol of pain in outpatients with cancer. Acad Med 72:798–800
20. Von Roenn JH, Cleeland CS, Gonin R et al. (1993) Physicianattitudes and practice in cancer pain management. A surveyfrom the Eastern Cooperative Oncology Group. Ann InternMed 119:121–126
21. World Health Organization (1986) Cancer pain relief. WorldHealth Organization, Geneva
Cancer Pain, Evaluation of RelevantComorbidities and Impact
MYRA GLAJCHEN
Department of Pain Medicine and Palliative Care, BethIsrael Medical Center, New York, NY, [email protected]
Definition
The assessment of patients with cancer pain often re-veals the existence of important physical or psychiatriccomorbidities.Thesecomorbiditiesmayormaynotcon-tribute to the pain. They often influence the selection ofpain therapy, and may be independent problems in needof management in the broad strategy to improve qualityof life.

216 Cancer Pain, Evaluation of Relevant Comorbidities and Impact
Characteristics
In some cases, a comorbid condition is both an inde-pendent medical issue and a potential etiology of thepain. For example, major depression may be expressed,in part, by persistent pain. Under these circumstances,treatment for the depression must be given priorityand included among the analgesic strategies pursued.In other circumstances, a comorbid condition may beunrelated to the pain itself, but may impair functionand negatively affect treatments intended to restorefunctioning. This is commonly encountered in thecancer patient with persistent gastrointestinal distressfollowing chemotherapy.A useful taxonomy for evaluating the impact of rele-vant comorbidities on cancer pain is listed below. Thecoexisting symptom or condition should be evaluatedfor its: direct contribution to the pain, predispositionto cause adverse treatment effects, compromise of re-habilitative efforts, ability to independently underminequality of life, and ability to increase risk of seriousadverse medical outcomes.Fatigue is a common comorbidity, affecting 14-96%of people with cancer (Cella et al. 2002; Vogelzanget al. 1997). Generally, fatigue is characterized by adecrease in energy, distress and decreased functionalstatus (Pickard-Holley 1991; Stone et al. 1998). Fatiguein cancer patients can result from the course of the dis-ease, preexisting physical or psychological conditions,effects of medication, or lack of exercise. Fatigue mayalso result from surgery, chemotherapy, and radiationtherapy. As fatigue can severely undermine the sense ofwell being, activities of daily living, relationships withfamily and friends, and treatment compliance, promptdiagnosis and treatment are recommended.Gastrointestinal complications (constipation, impac-tion, bowel obstruction, nausea, vomiting and diarrhea)are common in oncology patients. The growth andspread of cancer, as well as related treatment, contributeto these conditions. Despite advances in management,nausea and vomiting remain among the most distressingside effects for patients and families (Wickham 1999).In addition, gastrointestinal comorbidities underminequality of life and interfere with treatment (Pisters andKris 1998).Alterations in nutritional status begin at diagnosis, andmay proceed through treatment. � Protein-calorie mal-nutrition (PCM) is common and can lead to progressivewasting, weakness, and debilitation. Anorexia, the lossof appetite, is present in 15-25% of patients at diagnosisand may also occur as a treatment side effect (Vigano etal. 1994). Depression, loss of hope and anxiety areall as-sociatedwithanorexia(Ross1990).Anorexiacanhastenthe course of cachexia, a progressive wasting syndrome(Ross 1990) marked by weakness and progressive lossof body weight, fat, and muscle. Pain treatment in thecontext of anorexia and cachexia is complex.
About 44% of cancer patients report anxiety duringtreatment, while 23% report high anxiety (Nordin andGlimelius 1999; Pereira et al. 1997). Anxiety that isunusually intense or persistent may suggest an adjust-ment disorder or anxiety disorder in need of targetedtreatment. Factors that increase the likelihood of de-veloping adjustment disorders include pain, a historyof anxiety disorders, functional limitations, advancingdisease and absence of social support (Breitbar 1995;Schag and Heinrich 1989; Stark et al. 2002). Patientscan become immobilized by anxiety, and be unable tocomply with treatment. Therefore, prompt diagnosisand early intervention are optimal.Depression is a disabling condition affecting 15–25%of cancer patients (Breitbart et al. 2000; Nelson etal. 2002). While some sadness is normal in reaction tocancer, it is important to distinguish normal sadnessfrom an adjustment disorder with depressed mood ora depressive disorder (Block 2000). Clinicians shouldassess mood carefully and have a low threshold forinitiating therapies. Early intervention is indicated ifsymptoms persist or recur, or if patients present with ahistory of depression, poor social support, a poor prog-nosis and higher levels of disability. A combination ofpsychotherapy and antidepressant drugs represents themost effective strategy for pain-related depression. An-tidepressants with established analgesic effectivenessmay be preferred (Breitbart 1995).Delirium, agitation and cognitive impairment occurin 28-48% of patients with advanced cancer (Pereiraet al. 1997; Lawlor et al. 2000). The causes of delir-ium are multifactorial, and may include direct effectsof the disease on the CNS, metabolic or electrolytedisturbances, treatment and medications (Lawlor etal. 2000; Morita et al. 2002). The presence of deliriumposes a major barrier to doctor-patient communication,family distress and treatment adherence (Fainsinger etal. 1993). Prompt diagnosis and treatment are thereforeoptimal.Nearly one-third of the population of the United Stateshas used illicit drugs, and an estimated 6-27% have a� substanceabuseproblem of some type(see� aberrantdrug-related behaviors and � pseudoaddiction) (Col-liver and Kopstein 1991). Although problematic druguse is sometimes related to undertreatment (Weiss-man and Haddox 1989), primary abuse or � addictionmay be encountered in the oncology setting. A his-tory of substance abuse can increase the risk of mor-bidity or mortality among those with progressivelife-threatening disease, and undermine treatmentadherence. This can be mitigated by a therapeuticstrategy that addresses drug-taking behavior whileimplementing other therapies. Knowledge about thebasic concepts of addiction medicine and collab-oration with addiction specialists is needed (Sub-stance Abuse and Mental Health Services Administra-tion 2002).

C
Cancer Pain, Goals of a Comprehensive Assessment 217
Thegoalof acomprehensiveapproach to thepatientwithcancer pain is to organize a therapeutic strategy, whichcan enhance comfort and function and ameliorate co-morbidities – all in an effort to reduce suffering and im-prove quality of life.
References1. Block SD (2000) Assessing and Managing Depression in the
Terminally Ill Patient. ACP-ASIM End-of-Life Care ConsensusPanel. American College of Physicians – American Society ofInternal Medicine. Ann Intern Med 132: 209–218
2. Breitbart W (1995) Identifying Patients at Risk for, and TreatmentofMajorPsychiatricComplicationsof Cancer. Support Care Can-cer 3:45–60
3. Breitbart W, Rosenfeld B, Pessin H et al. (2000) Depression,Hopelessness, and Desire for Hastened Death in Terminally IllPatients with Cancer. JAMA 284:2907–2911
4. Cella D, Lai JS, Chang CH et al. (2002) Fatigue in Cancer PatientsCompared with Fatigue in the General United States Population.Cancer 94:528–538
5. Colliver JD, Kopstein AN (1991) Trends in Cocaine Abuse Re-flected in Emergency Room Episodes Reported to DAWN. PublicHealth Rep 10:59–68
6. Fainsinger RL, Tapper M, Breura E (1993) A Perspective on theManagement of Delirium in Terminally Ill Patients on a PalliativeCare Unit. J Palliat Care 9:4–8
7. Lawlor PG, Gagnon B, Mancini IL et al. (2000) Occurrence,Causes, and Outcome of Delirium in Patients with AdvancedCancer: A Prospective Study. Arch Intern Med 160:786–294
8. Morita T, Tei Y, Tsunoda J et al. (2002) Underlying Pathologiesand their Associations with Clinical Features in Terminal Delir-ium of Cancer Patients. J Pain Symptom Manage 23:107–113
9. Nelson CJ, Rosenfeld B, Breitbart W et al. (2002) Spirituality,Religion, and Depression in the Terminally Ill. Psychosomatics43:213–220
10. Nordin K, Glimelius B (1999) Predicting Delayed Anxiety andDepression in Patients with Gastrointestinal Cancer. Br J Cancer79:525–529
11. Pereira J, Hanson J, Bruera E (1997) The Frequency and Clin-ical Course of Cognitive Impairment in Patients with TerminalCancer. Cancer 79:835–842
12. Pickard-Holley S (1991) Fatigue in Cancer Patients. A Descrip-tive Study. Cancer Nurs 14:13–19
13. Pisters KM, Kris MG (1998) Treatment-Related Nausea andVomiting. In: Berger A, Portenoy RK, Weissman DE (eds) Prin-ciples and Practice of Supportive Oncology. Lippincott-RavenPublishers, Philadelphia, pp 165–178
14. Ross BT (1990) Cancer’s Impact on the Nutrition Status of Pa-tients. In: Bloch AS (ed) Nutrition Management of the CancerPatient. Aspen Publishers, Rockville, MD
15. Schag CA, Heinrich RL (1989) Anxiety in Medical Situations:Adult Cancer Patients. J Clin Psychol 45:20–27
16. Stark, D, Kiely M, Smith A et al. (2002) Anxiety Disordersin Cancer Patients: Their Nature, Associations, and Relation toQuality of Life. J Clin Oncol 20:3137–3148
17. Stone P, Richards M, Hardy J (1998) Fatigue in Patients withCancer. Eur J Cancer 34:1670–1676
18. Substance Abuse and Mental Health Services Administra-tion: Results From the 2001 National Household Survey onDrug Abuse: Volume I. Summary of National Findings (2002)SAMHSA, Office of Applied Studies, DHHS, Rockville, MD
19. Vigano A, Watanabe S, Bruera E (1994) Anorexia and Cachexiain Advanced Cancer Patients. Cancer Surv 21:99–115
20. Vogelzang NJ, Breitbart W, Cella D et al. (1997) Patient, Care-giver, and Oncologist Perceptions of Cancer-Related Fatigue:Results of a Tripart Assessment Survey. The Fatigue Coalition.Semin Hematol 34:4–12
21. Weissman DE, Haddox JD (1989) Opioid Pseudoaddiction – AnIatrogenic Syndrome. Pain 36:363–366
22. Wickham R (1999) Nausea and Vomiting. In: Yarbo CH, Frogge
MH, Goodman M (eds) Cancer Symptom Management, 2nd edn.Jones and Bartlett Publishers, Sudbury, MA, pp 228–263
Cancer Pain, Goals of a ComprehensiveAssessment
PAULINE LESAGE
Department of Pain Medicine and Palliative Care, BethIsrael Medical Center and Albert Einstein College ofMedicine, New York, NY, [email protected]
Definition
The assessment of cancer pain requires an understand-ing of the disease and its extent, in addition to its di-verse comorbidities, to clarify the nature of the pain andits physical, psychological, and social disturbances. Thelist below describes a stepwise assessment of patientswithcancerpain.Thisunderstandingwillguide the treat-ment plan, focused on providing comfort and improvingquality of life.
Step 1: Data Collection
• Pain-related history
– Other relevant history– Disease related– Other symptoms– Psychiatric history– Social resources
• Concurrent quality-of-life concerns
– Other symptoms– Concerns in physical, psychological, social, and
spiritual domains– Other concerns (e.g. financial)– Assessment of the family
• Available laboratory and imaging data
– Radiographs and scans– Tumor markers– Hematologic parameters– Biochemical parameters
Step 2: Interpret the Findings
• Pain-related constructs
– Etiology– Inferred pathophysiology– Syndrome identification
• Extent of disease

218 Cancer Pain, Goals of a Comprehensive Assessment
• Goals of care
– Prolonging survival– Optimizing function– Optimizing comfort
Step 3: Formulating a Treatment Strategy
• Further evaluation, if needed• Multimodality approach to the pain• Treatment of the pain etiology, if possible• Treatments for concurrent concerns• Patient/family education
Characteristics
The comprehensive assessment of pain characteris-tics should include information about: 1) temporalcharacteristics (onset and duration); 2) course (stable,improving, worsening, or widely fluctuating); 3) sever-ity (both average and worst); 4) location; 5) quality, and6) provocative and palliative factors.Acute pain usually has a well-defined onset and a read-ily identifiable cause (e.g. surgical incision). It may beassociated with anxiety, overt pain behaviors (moaningor grimacing), and signs of sympathetic hyperactivity(including tachycardia, hypertension, and diaphoresis).In contrast, chronic pain is usually characterized by anill-defined onset and association with persistent focusof pathology. The course of the pain may be linked tothe disease, and may change with the response to pri-mary antineoplastic therapies. With chronic pain, overtpain behaviors and sympathetic hyperactivity are typi-cally absent, and vegetative signs, including lassitude,sleep disturbance, and anorexia, may be present. A clin-ical depression evolves in some patients.Most patients with chronic cancer pain also experienceperiodicflaresofpain,orbreakthrough pain (Patt andEl-lison 1999). An important subtype of breakthrough painis known as � incident pain. Diagnosis of breakthroughpain may suggest specific interventions, such as the useof supplemental medication that specifically targets thecause.Pain may be focal, multifocal, referred or generalized.Pain may be referred from a lesion involving any of alarge group of structures, including nerve, bone, muscleor other soft tissue, and viscera (Ness and Gebhart 1990;Torebjork et al. 1984). Various subtypes of � referredpain can be distinguished. Pain may be referred any-where along the course of an injured peripheral nerve(such as pain in the thigh or knee from a lumbar plexuslesion) or nerve root (known as radicular pain). Painmay also be referred to a site remote from a nociceptivelesion and outside the dermatome affected by the lesion(e.g. shoulder pain from diaphragmatic irritation).Measurement of pain intensity is an essential element inthe pain assessment. Intensity may be monitored usinga numeric scale (0–10), verbal rating scale (none, mild,
moderate, severe), or a visual analogue scale. The par-ticular scale used is less important than its regular useto record the status of the pain over time.
Interpreting the Assessment
Thepainhistory,combinedwiththe informationgleanedfrom a physical examination and appropriate imagingand laboratory studies, usually provides sufficient datato generate meaningful conclusions concerning the eti-ology of the pain, its pathophysiology, and its definingsyndrome. The latter constructs are very useful in clari-fying the need for additional evaluation,prognosticatingoutcomes, and developing an efficient therapeutic strat-egy.
Etiology
The etiology of acute pain is usually clear-cut. Furtherevaluation to determine the underlying lesion is not in-dicated unless the course varies from the expected. Incontrast, the etiology of chronic cancer-related pain maybe more difficult to characterize. In most cases, pain isdue to direct invasion of pain-sensitive structures by theneoplasm (Cherny et al. 1994; Foley 1996). The struc-tures most often involved are bone and neural tissue, butpain can also occur when there is an obstruction of hol-lowviscus,distention oforgan capsules,distortionoroc-clusion of blood vessels, and infiltration of soft tissues.In about one-quarter of patients, the etiology relates toan antineoplastic treatment, and fewer than 10% havepainunrelated to theneoplasmor its treatment(Chernyetal. 1994; Foley 1996). Many patients, particularly thosewith advanced illness, have multiple etiologies and sev-eral sources of pain.Given the association between pain and the underlyingneoplasm, clarification of the specific relationship be-tween the pain and the disease is an essential element ofthe assessment. A survey of patients referred to a painservice in a major cancer hospital noted, that previouslyunsuspected lesions were identified in 63% of patients(Gonzalez et al. 1991). This outcome altered the knownextent of disease in virtually all patients, changed theprognosis for some, and provided an opportunity for aprimary antineoplastic therapy in approximately 15%.
Pathophysiology
Although inferences about the predominating mecha-nismsunderlyingpainarecertainlygrosssimplificationsof very complex and dynamic processes, and can neverbe proved in the clinical setting, this classification hasutility in treatment planning. Pain syndromes may be la-beled nociceptive, neuropathic, psychogenic and mixed(Merskey and Bogduk 1994).The quality of somatic � nociceptive pain is typicallydescribed as aching, stabbing, throbbing, or pressure-like. The quality of visceral nociceptive pain is usuallygnawing or crampy when related to obstruction of hol-

C
Cancer Pain, Goals of a Comprehensive Assessment 219
low viscus, and aching or stabbing when associated withinjury to other visceral structures.Neuropathic mechanisms are involved in approxi-mately 40% of cancer pain syndromes and can bedisease-related (e.g. tumor invasion of nerve plexus)or treatment-related (e.g. postmastectomy syndromeor chemotherapy-induced painful polyneuropathy)(Caraceni and Portenoy RK, and a working group ofthe IASP Task Force on Cancer Pain 1999). Amongthose with metastatic disease, � neuropathic pain usu-ally results from neoplastic injury to peripheral nerves(peripheral neuropathic pain). Other, less common,subtypes include: 1) those sustained by CNS processes(sometimes generically termed deafferentation pain);and 2) those in which the pain is believed to be main-tained by efferent activity in the sympathetic nervoussystem (so-called sympathetically-maintained pain)(Galer 1995).Neuropathic pain is diagnosed on the basis of the pa-tient’s verbal description of the pain, the findings onexamination, and evidence of nerve injury. If patientsdescribe pain in dysesthetic terms, such as “burning,”“shock-like,” or “electrical,” this is suggestive of neu-ropathic mechanisms (Grond et al. 1999). Likewise, theexistence of neuropathic pain may be inferred by thefindings of abnormal sensations on physical examina-tion, most notably � allodynia and � hyperalgesia.Pain may be labeled psychogenic if there is positive ev-idence from the assessment that psychological factorspredominate in sustaining the symptom. � Psychogenicpain may be more formally characterized according tothe widely-accepted taxonomy of the American Psychi-atric Association (one of the Somatoform Disorders de-scribed in the Diagnostic and Statistical Manual, 4th Re-vision). Although psychological factors commonly in-fluence the expression and severity of pain in the cancerpopulation, it is rare to identify a pain as psychogenic.If a credible pathophysiologic diagnosis is not apparent,and there is no strong evidence of a predominating psy-chological cause, it is best to label the pain idiopathic.
Assessment of Related Constructs
Chronic cancer-related pain is best addressed with con-sideration of a set of broader constructs, including suf-fering, quality of life, symptom distress, and the goals ofcare.Theseunderstandingscontinuallyinformdecision-making about interventions to manage pain.
Pain and Suffering
Suffering, a global construct intricately related to the ex-perience of pain (Fig. 1), has been described as a per-ceived threat to the integrity of the person, as a type of“total pain,” or as overall impairment in quality of life(Cassell 1982). Suffering may be primarily related tosymptoms such as pain or physical losses; to psychiatricdisorders such as depression or psychological processessuch as disturbed body image; to social issues such as
Cancer Pain, Goals of a Comprehensive Assessment,Figure 1 Distinctions and interactions between nociception, pain,and suffering. (Reproduced with permission from Portenoy RK (1992)Cancer pain: pathophysiology and syndromes. Lancet 339:1026).
loss of role functioning, familial disruption, or tensionin the relationship with a significant other; or to spiritualconcerns such as loss of faith. Other factors, such as fi-nancial concerns, may be prominent. Psychosocial andspiritual strengthsand weaknesses that longpredated thecancer may be important.Comprehensive pain assessment must address issues re-lated to suffering.An understanding of thephysical, psy-chological, social and spiritual issues important to thepatient is fundamental to this process. A therapeutic ap-proach focused only on pain may not meaningfully ben-efit a patient whose suffering is caused by other distur-bances.
Pain and Quality of Life
Quality of life is related to the construct of suffering buthasbeen more formally characterized fora researchcon-text. Numerous instruments have been created to mea-sure quality of life, and these have been developed fromtheperspectiveof two majorcharacteristics: subjectivityand multidimensionality (Skeel 2002).The inherent subjectivity of quality of life has impli-cations for assessment. Although clinicians commonlymake inferences about patients’ well-being, or rely onproxy evaluation by family or others, the likelihoodof inaccuracy in such appraisals must be appreciated(Grossman et al. 2001). For the evaluation of qualityof life, and each of its contributing concerns, includingpain, the “gold standard” of assessment is self-report.Like pain itself, quality of life is multidimensional.Although a single question can screen for overall well-being, a fuller understanding of the factors that must beaddressed to improve quality of life requires probingof issues related to physical, psychological, social, andspiritual functioning.
Pain and Symptom Distress
Most patients with chronic cancer pain experience othersymptoms concurrently. Studies have demonstrated thatpain, fatigue, and psychological distress are most preva-lent across populations with advanced cancer. Globalsymptom distress is a useful construct that characterizesoverall symptom burden (Portenoy et al. 1994).

220 Cancer Pain, Palliative Care in Children
Goals of Care
In developing a therapeutic approach to address pain andother quality-of-life concerns in patients with cancer, itis essential to clarify the goals of care. At any point intime, treatmentmay beguided by oneormoreoverridinggoals: 1) to cure or prolong life; 2) to maintain function;and 3) to provide comfort. These goals are strongly in-fluenced by many factors, including the status of the dis-ease, the availability and burdens of therapy, psychoso-cialcomorbidity,and thedegreeofspiritualorexistentialdistress. Goals are very dynamic, and often evolve overtime with the vagaries of the disease, the availability oftreatment and optimal palliative care. Current goals con-tinually influence therapeutic decision-making.
References1. Caraceni A, Portenoy RK, and a working group of the IASP Task
Force on Cancer Pain (1999) An international survey of cancerpain characteristics and syndromes. Pain 82:263–274
2. Cassell EJ (1982) The nature of suffering and the goals ofmedicine. N Engl J Med 306:639–645
3. Cherny NI, Coyle N, Foley KM (1994) Suffering in the advancedcancer patient: a definition and taxonomy. J Palliat Care 10:57–70
4. Foley KM (1996) Pain syndromes in patients with cancer. In:Portenoy RK, Kranner RM (eds) Pain management: Theory andpractice. FA Davis, Philadelphia, pp 191
5. Galer BS (1995) Neuropathic pain of peripheral origin: advancesin pharmacologic treatment. Neurology 45:S17–25
6. Gonzalez GR, Elliott KJ, Portenoy RK, Foley KM (1991) Theimpact of a comprehensive evaluation in the management of can-cer pain. Pain 47:141–144
7. Grond S, Radbruch L, Meuser T et al. (1999) Assessment andtreatment of neuropathic cancer pain following WHO guidelines.Pain 79:15–20
8. Grossman SA, Sheidler VR, Sweden K et al. (2001) Correlationof patient and caregiver ratings of cancer pain. J Pain SymptomManage 6:53–57
9. Merskey H, Bogduk N (1994) Classification of chronic pain:descriptions of chronic pain syndromes and definitions of painterms, 2nd edn. IASP Press, Seattle
10. Ness TJ, Gebhart GF (1990) Visceral pain: a review of experi-mental studies. Pain 41:167–234
11. Patt RB, Ellison N (1999) Breakthrough pain. In: Aronoff GM
(ed) Evaluation and treatment of chronic pain, 3rd edn. Williams& Wilkins, Baltimore, pp 377
12. Portenoy RK, Thaler HT, Kornblith AB et al. (1994) Patients withcancer: The Memorial Symptom Assessment Scale: an instru-ment for the evaluation of symptom prevalence, characteristicsand distress. Eur J Cancer 30A:1326–1336
13. Skeel RT (2002) Measurement of outcomes in supportive care:Quality of life. In: Berger AM, Portenoy RK, Weissman DE (eds)Principles and practice of palliative care and supportive oncology.Lippincott Williams & Wilkins, Philadelphia, pp 1107–1122
14. Torebjork HE, Ochoa JL, Schady W (1984) Referred pain fromintraneural stimulation of muscle fascicles in the median nerve.Pain 18:145–156
Cancer Pain, Palliative Care in ChildrenSTEPHEN C. BROWN
Department of Anesthesia, Divisional Centre of PainManagement and Pain Research, The Hospital for SickChildren, Toronto, ON, [email protected]
Synonyms
Pain Control in Children with Cancer; Palliative Care inChildren; End of Life Care; Dying Child
Definition
Pain control is an integral component of caring forall children with cancer. Children with cancer mayexperience many different types of pain from invasiveprocedures, the cumulative effects of toxic therapies,progressive disease or from psychological factors.While the goal in cancer care is to minimize morbidityon the road to cure, at times even with the best of care,we fail to achieve this goal and thus we also address theissue of palliative pain management. � Palliative careis the management of patients with active, progressive,far-advanced disease, for whom prognosis is limitedand the focus of care is the quality of life.
Characteristics
Pediatric cancer pain encompasses four broad etiologiccategories – procedural pain, the cumulative effectsof toxic therapies, progressive disease and psycholog-ical factors. Children’s cancer pain is often complexwith multiple sources, comprised of nociceptive andneuropathic components (Collins and Weisman 2003;McGrath and Brown 2004; Miaskowski et al. 2005;World Health Organization 1998). In addition, several� situational factors usually contribute to children’spain, distress and disability. Thus, to treat pain in thesechildren adequately, we must evaluate the primary painsources and also ascertain which situational factors arerelevant for which children and families. Treatmentemphasis should shift accordingly from an exclusivedisease-centered framework to a more child-centeredfocus.In 1993 the World Health Organization (WHO) and theInternational Association for the Study of Pain (IASP)invited experts in the fields of oncology, palliative care,anesthesiology, neurology, pediatrics, nursing, pal-liative care, psychiatry, psychology and pastoral careto write guidelines for the management of pediatriccancer pain and palliative care, resulting in the 1998publication “Cancer pain relief and palliative care inchildren”.A child-centered framework is required for understand-ing and controlling pain for these children. Pain controlshould include regular pain assessments, appropriateanalgesics administered at regular dosing intervals,adjunctive drug therapy for symptom and side effectscontrol and non-drug interventions to modify the situ-ational factors that can exacerbate pain and suffering.Parents concerned about medication centered on theirchildren’s comfort are calling for improved commu-nication, standardization of nursing procedures andtechniques and a guide for a clear understanding ofwhat to expect and from whom (Sobo et al. 2002).

C
Cancer Pain, Palliative Care in Children 221
Basic information on pathophysiology, pharmacology,analgesic guidelines for children and management ofprocedural pain is presented in other essays in thisEncyclopedic Reference of Pain. This essay provides acomplementary focus by describing the unique natureof children’s cancer pain including the primary factorsthat affect their pain and quality of life, providing ref-erences to guidelines for selecting and administeringdrug therapy in accordance with the nociceptive andneuropathic components and recommending practicalnon-drug therapies for integration within a hospital,home or hospice setting.
The Nature of a Child’s Cancer Pain
Throughout the last decade, we have gained an increas-ing appreciation of the � plasticity and complexity of achild’s pain. As with adults, a child’s pain is often ini-tiated by tissue damage caused by noxious stimulation,but the consequent pain is neither simply nor directly re-lated to the amount of tissue damage. Perhaps even morethan in adults, differing pain responses to the same tis-sue damage are noted. The eventual pain evoked by arelatively constant noxious stimulus can be different de-pending on children’s expectations, perceived control orthe significance that they attach to the pain. Children donot sustain tissue damage in an isolated manner, devoidof a particular context, but actively interpret the strengthand quality of any pain sensations, determine the rele-vance of any hurting and learn how to interpret the painby observing the general environment, especially thebe-havior of other people. Children’s perceptions of painare defined by their age and cognitive level, their previ-ous pain experiences against which they evaluate eachnew pain, the relevance of the pain or disease causingpain, their expectations for obtaining eventual recoveryand pain relief and their ability to control the pain them-selves. While plasticity and complexity are critical fea-tures for all pain perception, plasticity seems an evenmore important feature for controlling children’s pain.Much research has been conducted to identify thecritical factors responsible for the plasticity of painperception. Recent PET and functional MRI studieshave demonstrated that painful stimulation activatesdifferent cortical regions – depending on an individual’sexpectations and attention (Price and Bushnell 2004).Human studies evaluating the impact of environmentaland psychological factors on the perception of experi-mentally induced pain have been conducted primarily inadults. However, results from the few laboratory studiesconducted with children are consistent with those fromadult studies (see � Experimental Pain in Children). Inaddition, much compelling evidence about the powerfulmediating role of psychological factors in children’spain derives from clinical studies of acute, recurrentand chronic pain. These studies highlight the need torecognize and evaluate the mediating impact of thesefactors in order to optimally control children’s pain.
Certain child factors are stable such as gender, tem-perament and cultural background, while other factorschange progressively such as age, cognitive level, pre-vious pain experience and family learning. These childcharacteristics shape how children generally interpretand experience the various sensations caused by tis-sue damage. In contrast, various cognitive, behavioraland emotional factors are not stable. They represent aunique interaction between the child and the situationin which the pain is experienced. These situationalfactors can vary dynamically throughout the course of achild’s illness, depending on the specific circumstancesin which children experience pain. For example, a childreceiving treatment for cancer will have repeated injec-tions, central port access and lumbar punctures – all ofwhich may cause some pain (depending on the anal-gesics, anesthetics or sedatives used). Even though thetissue damage from these procedures is the same eachtime, the particular set of situational factors for eachtreatment is unique for a child – depending on a child’s(and parent’s) expectations, a child’s (and parent’sand staff’s) behaviors and on a child’s (and family’s)emotional state. Although the causal relationship be-tween an injury and a consequent pain seems direct andobvious, what children understand, what they do andhow they feel all affect their pain. Certain factors canintensify pain, exacerbate suffering or affect adverselya child’s quality of life. While parents and health careproviders may be unable to change the more stable childcharacteristics, they can modify situational factors anddramatically improve children’s pain and lives.
The Impact of Situational Factors on a Child’s Pain
Cognitive factors include children’s understandingabout the pain source, their ability to control whatwill happen, their expectations regarding the qualityand strength of pain sensations that they will experi-ence, their primary focus of attention (that is distractedaway from or focused primarily on the pain) and theirknowledge of pain control strategies. In general, chil-dren’s pain can be lessened by providing accurateage-appropriate information about pain, for exampleemphasizing the specific sensations that children willexperience (such as the stinging quality of an injection,rather than the general hurting aspects), by increasingtheir control and choices, by explaining the rationale forwhat can be done to reduce pain and by teaching themsome independent pain reducing strategies (Brownand McGrath 2005). Behavioral factors refer to thespecific behaviors of children, parents and staff whenchildren experience pain and also encompass parents’and children’s wider behaviors in response to a course ofrepeated painful treatments, chronic pain or progressiveillness. Common behavioral factors include children’sdistress or coping reactions (e.g. crying, using a paincontrol strategy, withdrawing from life) and parents’and health staff’s subsequent reactions to them (e.g. dis-

222 Cancer Pain, Palliative Care in Children
playing frustration, calmly providing encouragementfor children to use pain control strategies, engagingthem in conversation and activities). Emotional factorsinclude parents’ and children’s feelings in response topain and to the daily effects of the underlying illnessor condition. Children’s emotions affect their abilityto understand what is happening, their ability to copepositively, their behaviors and ultimately their pain.Therearedynamic interactionsamongcognitive,behav-ioralandemotional factors.Healthstaffcansignificantlylessen children’s pain, not only by administering potentanalgesics but also by increasing children’s understand-ing and control, by decreasing their emotional distressand by teaching children some simple physical, behav-ioral and cognitive methods to complement analgesicmedications and further reduce their pain.If the disease progresses and treatment emphasis shiftsfrom curative to palliative, cognitive and emotional fac-tors become the most salient situational factors that af-fect pain for children. Children probably have endured aprolonged period of intermittent pain, physical disabil-ity and multiple aversive treatments. Children receiv-ing curative therapies are more focused on the futureconsequencesof theirdisease.Their thoughts, behaviorsand feelings change if their care becomes palliative. Ifthis should happen, the type of support, information andguidance children require changes. While the impact ofpalliation is profound for all children and families, eachchild and family is unique with respect to their specificpsychological, medical, social and spiritual needs. Allfamilies experience anguish and grief, but they may alsoexperience denial, anxiety, anger, guilt, frustration anddepression. It is essential that health professionals listenattentively and observe carefully, not only to ensure thatall the needs of both the child and family are met, but alsoto resolve the myriad factors that can exacerbate chil-dren’s pain and suffering. The primary situational fac-tors in pediatric palliative care are listed (see below).
Situational Factors in Pediatric Palliative Care
Cognitive Factors
• Meaning of death• Inaccurate understanding: impact of situational fac-
tors on pain and quality of life• Course of disease• Palliative versus curative therapy• Little independent control over pain• Limited choices• Expectation for continuing pain and suffering• Misunderstanding of drug therapy: opioids
– dosing and administration– criteria for evaluating effectiveness
Behavioural Factors
• Social withdrawal• Physical inactivity
• Passive approach to pain control• Secondary gains: stress reduction
– emotional denial– parent or staff attention
• Inappropriate drug management: choice or mode ofdrug administration
• Failure to treat opioid-related side-effects aggres-sively
• Failure to evaluate pain sources and document painlevel
• Failure to use effective non-drug therapies
Emotional
• Anxiety about: dying and death
– suffering– meaning of life
• Fear of: separation
– inadequate pain control– increasing adverse symptoms– impact on family
• Anger• Sadness or depression• Distancing by staff and friends
A shift in care from curative to palliative therapies maysignify to some children and families that health profes-sionals are giving up on the child. Children and fami-lies must understand that stopping ineffective therapiesis not giving up, but represents a rational decision basedon children’s best interests. Pain control is an essentialcomponent of cancer care and of palliative care (Chaf-fee 2001; Galloway and Yaster 2000; Goldman 1998;Goldman et al. 2003). Children and parents should notfear that health professionals have given up on control-ling pain and aversive symptoms. Pain and all symptomsmustbe treated aggressively from thedualperspectiveoftargeting the primary source of tissue damage and modi-fying the secondary contributing factors. Although mostchildrenreceiveaccurate informationabout theirdiseaseand required treatments, few children or their parentsreceive concrete information about their pain, the fac-tors that can attenuate or exacerbate it, a rationale forthe interventions they receive and training in effectivenon-pharmacologicalpaincontrol techniques.Thelattermay be particularly important for children in palliativecare, who have diminishing control in their lives. Chil-dren and their parents do not know that prescribed paincontrol treatments may vary in efficacy at different timesthroughout their treatment due to variations in diseaseactivity or situational factors. Without this knowledge,their confidence in certain therapies can decrease, even

C
Cancer Pain, Palliative Care in Children 223
though these therapieswouldeffectively alleviatepainatanother time. The fear of inadequate pain control placesan enormous emotional burden on an already distressedchild and family and can create a situation in which theirpain and disability intensifies.Children seem to know intuitively, even when dying hasnot been discussed directly with them. They fear separa-tion and abandonment; some children may fear that theirillness is a punishment. Dying children may feel fright-ened, isolated and guilty unless they are able to openlyexpressand resolve their concerns.Manyobservershavenoted that children who are dying have a level of matu-rity far beyond their years. It is essential to acknowledgeand resolve their fears. Children should receive accurateinformation, consistent with their religious beliefs, pre-sented in a calm reassuring manner. They may need con-crete reassurance that they will not suffer when they die,that they will not be alone and that their families willremember them. Unresolved emotions add anguish andmay intensify their pain.
Treating a Child’s Pain
A treatment algorithm illustrating a practical approachfor treating a child’s pain is illustrated in Fig. 1. Painassessment is an integral component of diagnosis andtreatment. The differential diagnosis of a child’s pain isa dynamic process that guides clinical management. Weshould select specific therapies to target the responsiblecentral and peripheral mechanisms and to mitigate thepain-exacerbating impact of situational factors, recog-nizing that the multiple causes and contributing factorswill vary over time. Drug therapies – analgesics, adju-vant analgesics and anesthetics - are essential for paincontrol, but non-drug therapies – cognitive, physical andbehavioral - are also essential. As we monitor the child’simprovement in response to the therapies initiated, werefineourpain diagnosisand treatmentplanaccordingly.DrugtherapiesarecoveredintheessayAnalgesicGuide-lines for Children; anesthetic blocks are covered in theessay Post-operative Pain Control in Children and acuteprocedural pain is covered in the essay by Liossi.The optimal relief of pain in pediatric palliative carebegins with the recognition that you are assessing andtreating an individual child with pain, not managingpain as a symptom apart from the child. A thoroughmedical history, physical examination and assessmentof pain characteristics and contributing factors are nec-essary to establish a correct clinical diagnosis. Specificinterventions should be selected and administered tochildren as part of a comprehensive pain programme, inthe same manner as the most appropriate analgesics areselected and administered in adequate doses, at regulardosing intervals, through the most efficient routes.Children seem to possess an enhanced ability to absorbthemselves completely in a task, game or imaginedevent and thus might be more able than adults to triggerendogenous pain-inhibitory mechanisms. Even very
young children can easily learn to use a variety of practi-cal pain control methods to lessen their anxiety, distressand pain. The specific methods depend on the age of thechild, the type of pain experienced and the resourcesavailable. Deep breathing, alternately tightening andrelaxing their fists, squeezing their mother’s hand, lis-tening to stories or music and imagining that they arein a pleasant setting can be very effective for reducingprocedural-related pain, when used with appropriateanalgesics. Families should understand that what theythink, how they behave and how they feel affects theirchildren’s pain. Then they can begin to work inde-pendently and with staff to create additional non-drugpain control methods based on the child’s interest, thecultural setting and the availability of resources.
Summary
Optimal pain control for children with cancer and forchildren receiving palliative care requires an integratedtreatment plan with both drug and non-drug therapies(Frager 1997; Hooke et al. 2002; McGrath and Brown2004). Comprehensive care includes curative therapieswhen available, pain and symptom management andcompassionate support for children and their families. Itis essential to focus not only on the medical managementof children’s disease but also on the psychosocial andspiritual factors that affect children’s pain and suffering.Specific interventions must be selected after determi-nation of the primary and secondary sources of noxiousstimulation and after a thorough assessment of theunique situational, behavioral, emotional and familialfactors that affect a child’s pain. All analgesics shouldbe selected ‘by the ladder’ and administered ‘by theclock’, ‘by the child’ and by an effective and painlessroute. Dosing intervals should be frequent enough tocontrol pain adequately, so that children do not expe-rience an alternating cycle of pain, drowsy analgesia,pain, etc. Special problems in palliative pain controlmay arise when children die at home, unless parents andmedical and nursing teams communicate openly aboutthe availability of potent analgesics and the flexibilityof dosing routes and regimens. The choice for paincontrol is not merely ‘drug versus non-drug therapy’,but rather a therapy that mitigates both the causative andcontributing factors for pain. We have the knowledgeand thus the obligation to ensure that children receiveadequate pain control from the time that they are diag-nosed with cancer throughout their treatment protocol,including those cases that proceed to palliative care.
References1. Brown SC, McGrath PA (2005) Pain In Children. In: Pappagallo
M (ed) The Neurological Basis of Pain. McGraw-Hill, New York2. Chaffee S (2001) Pediatric palliative care. Prim Care 28:365–3903. Collin, JJ, Weisman SJ (2003) Management of pain in childhood
cancer. In: Schechter NL, Berde CB, Yaster M (eds) Pain in In-fants, Children, and Adolescents. Lippincott Williams & Wilkins,Philadelphia, pp 517–538

224 Cancer Pain Management
Cancer Pain, Palliative Care in Children, Figure 1 Treatment algorithm for pain management.
4. Doyle D, Hanks GWC, Cherny NI et al. (eds) (2004) Oxford Text-book of Palliative Medicine 3rd edn. Oxford University Press,Oxford, pp 775–789
5. Frager G (1997) Palliative care and terminal care of children.Child Adoles Clinic North Am 6:889–909
6. Galloway KS, Yaster M (2000) Pain and symptom control interminally ill children. Pediatr Clinic North Am 47:711–747
7. Goldman A (1998) ABC of palliative care. Special problems ofchildren. BMJ 316: 49–52
8. Goldman A, Frager G, Pomietto M (2003) Pain and PalliativeCare. In: Schechter NL, Berde CB, Yaster M (eds) Pain in In-fants, Children, and Adolescents. Lippincott Williams & Wilkins,Philadelphia, pp 539–562
9. Hooke C, Hellsten MB, Stutzer C et al. (2002) Pain managementfor the child with cancer in end-of-life care: APON position paper.J Pediatr Oncol Nurs 19:43–47
10. McGrath PA, Brown SC (2004) Paediatric palliative medicine –Pain control. In: Doyle D, Hanks G, Cherny N et al (eds) Ox-ford Textbook of Palliative Medicine, 3rd edn. Oxford UniversityPress, Oxford, pp 775–789
11. Miaskowski C, Cleary J, Burney J et al (2005) Guideline for theManagement of Cancer Pain in Adults and Children, APS Clin-
ical Practice Guidelines Series, No. 3. American Pain Society,Glenview, Illinois
12. Price DD, Bushnell MC (2004) Psychological Modulation ofPain: Integrating Basic Science and Clinical Perspectives. IASPPress, Seattle
13. Sobo EJ, Billman G, Lim L et al. (2002) A rapid interview pro-tocol supporting patient-centered quality improvement: hearingthe parent’s voice in a pediatric cancer unit. Jt Comm J QualImprov 28:498–509
14. World Health Organization (1998) Cancer pain relief and pal-liative care in children. World Health Organization, Geneva
Cancer Pain Management
Definition
Adisciplined approach to assessment, pharmacological,and nonpharmacological treatment aimed at reducing or

C
Cancer Pain Management, Adjuvant Analgesics in Management of Pain Due To Bowel Obstruction 225
eliminating pain in patients who have a diagnosis of can-cer.� Cancer Pain Management, Adjuvant Analgesics in
Management of Pain Due To Bowel Obstruction� Cancer Pain Management, Anesthesiologic Interven-
tions, Neural Blockade� Cancer Pain Management, Anesthesiologic Interven-
tions, Spinal Cord Stimulation, and Neuraxial Infu-sion
� Cancer Pain Management, Cancer-Related Break-through Pain, Therapy
� Cancer Pain Management, Chemotherapy� Cancer Pain Management, Gastrointestinal Dysfunc-
tion as Opioid Side Effects� Cancer Pain Management, Interface between Cancer
Pain Management and Palliative Care� Cancer Pain Management, Neurosurgical Interven-
tions� Cancer Pain Management, Nonopioid Analgesics� Cancer Pain Management, Opioid Side Effects, Cog-
nitive Dysfunction� Cancer Pain Management, Opioid Side Effects, En-
docrine Changes and Sexual Dysfunction� Cancer Pain Management, Opioid Side Effects, Un-
common Side Effects� Cancer Pain Management, Orthopedic Surgery� Cancer Pain Management, Overall Strategy� Cancer Pain Management, Palliation of Upper GICancer� Cancer Pain Management, Patient-Related Barriers� Cancer Pain Management, Principles of Opioid Ther-
apy, Dosing Guidelines� Cancer Pain Management, Principles of Opioid Ther-
apy, Drug Selection� Cancer Pain Management, Radiotherapy� Cancer Pain Management, Rehabilitative Therapies� Cancer Pain Management, Treatment of Neuropathic
Components� Cancer Pain Management, Undertreatment and
Clinician-Related Barriers� Pain Management, Cancer-Related Breakthrough
Pain Therapy
Cancer Pain Management, AdjuvantAnalgesics in Management of Pain Due ToBowel Obstruction
PAUL C. ROUSSEAU
VA Medical Center, Phoenix, AZ, [email protected]
Definition
Non-opioid analgesics utilized in the managementof pain and colic in malignant bowel obstruction.
Three types of medication are commonly used: 1) an-ticholinergics; 2) corticosteroids; and 3) the synthetic� somatostatin analogue octreotide.
Characteristics
The pharmacological management of pain associatedwith � malignant bowel obstruction addresses threecritical pathophysiological mechanisms: 1) intestinaldistention and resultant bowel ischemia; 2) paroxysmalintestinal hypermotility; and 3) increased intestinalsecretions that perpetuate a vicious cycle of distention-intestinal secretion-peristalsis (Basson et al. 1989;Rousseau 1998).Opioids are the mainstay of pain management in ma-lignant bowel obstruction, and frequently assuage thepain associated with intestinal distention and bowelischemia. The pain that occurs secondary to intesti-nal hypermotility is often referred to as colic, and isprecipitated by paroxysms of increased peristalsis thatthrust against the mechanical resistance of a malignantobstruction (Baines 1998). Colicky pain often requiresthe use of anticholinergic medications in addition toopioids to mitigate the excruciating discomfort of in-testinal hypermotility (Rousseau 1998; Baines 1998;Krouse et al. 2002; Lublin and Schwartzentruber 2002;Ripamonti et al. 2000; Ripamonti et al. 2001).Anticholinergic medications decrease peristalsis of thegastrointestinal tract through a competitive inhibitionof the muscarinic receptors of intestinal smooth muscle,and an impairment of ganglionic neural transmissionin the bowel wall (Mercadante 1997; Baines 1994). Al-though there are few well-controlled studies evaluatingtheir efficacy in reducing abdominal colic in malignantbowel obstruction, anecdotal experience supports theirability to relieve malignant colic, and they are com-monly used in the management of bowel obstruction.Recommended medications include glycopyrrolate,hyoscine butylbromide, scopolamine, hyoscyaminesulfate, and atropine. Glycopyrrolate, a quaternary am-monium anticholinergic, and hyoscine butylbromide(not available in the United States) both exhibit limitedlipid solubility (Rousseau 1998; Krouse et al. 2002;Davis and Furste 1999). They penetrate the blood-brainbarrier less than other anticholinergics, and as a result,reduce central nervous system side effects such as agi-tation and hallucinations (Rousseau 1998; Baines 1998;Mercadante 1997). Aside from agitation and halluci-nations, anticholinergic drugs can cause dry mouthand eyes, drowsiness, tachycardia, hypotension, andurinary retention; dry mouth can be reduced by suckingice cubes and drinking small sips of water, while dryeyes can be alleviated with physiologic eye drops.Corticosteroidshavebeen used empirically in malignantbowel obstruction to reduce peritumor and perineuralinflammatory edema (Rousseau 1998; Baines 1998;Krouse et al. 2002; Mercadante 1997), and therebyimprove gastrointestinal transport and colicky pain

226 Cancer Pain Management, Adjuvant Analgesics in Management of Pain Due To Bowel Obstruction
(Ripamont 1994). They act both as antiemetics andanalgesics, the latter ostensibly due to prostaglandininhibition, suppression of migration of polymorphonu-clear leukocytes, and reversal of increased capillarypermeability. In an inclusive meta-analysis of pub-lished articles and studies on the use of corticosteroidsin malignant bowel obstruction, secondary to advancedgynecological and gastrointestinal cancers, Feur andBroadley noted a trend for improvement in bowel ob-struction for patients treated with corticosteroids, butthis trend did not reach statistical significance. Althoughcorticosteroids did appear to improve the symptomsof bowel obstruction, Feur and Broadley did not ex-plicitly mention their ability to relieve pain (Feur andBroadley 1999). In another study on the benefits ofcorticosteroids in malignant bowel obstruction, 68%of patients without a nasogastric tube prescribed corti-costeroids, versus 33% without a nasogastric tube pre-scribed a placebo, achieved symptom relief (p = 0.047);however, in patients who already had a nasogastric tubein place, the results were less significant (60% versus33%, p = 0.080). Unfortunately, the sample size of thisstudy was small, and while the authors mentioned colicas a symptom in 62% of study participants, they did notspecify if colic was relieved with corticosteroids (Lavalet al. 2000). Side effects of corticosteroids are minimalwhen used in malignant bowel obstruction, with oralcandidiasis the most commonly reported adverse event(Mercadante 1997).Octreotide, a synthetic analogue of somatostatin, re-duces the gastrointestinal secretion of gastrin, vasoac-tive intestinal peptide (VIP), insulin, pepsin, glucagon,and pancreatic bicarbonate and enzymes; reducesmesenteric blood flow (Mercadante 1997, Pandha andWaxman 1996); exhibits a proabsorptive effect onwater and ions (Rousseau 1998); and inhibits intesti-nal motility (Rousseau 1998; Baines 1998; Krouseet al. 2002; Pandha and Waxman 1996). By reduc-ing intestinal secretions and inhibiting gastrointestinalmotility, octreotide positively modulates gastrointesti-nal function and controls emesis in 70–100% of patients(Baines 1998; Krouse et al. 2002). Abdominal disten-tion and colic are similarly controlled in a significantnumber of patients (Baines 1998). These statistics aresupported by a prospective randomized controlled trialcomparing the antisecretory effects of octreotide andhyoscine butylbromide in patients with inoperable ma-lignant bowel obstruction who have nasogastric tubes.In this study, octreotide was very effective in reducingthe amount of gastrointestinal secretions in patientswith nasogastric tubes, and as an implicit consequence,though not specifically stated, reducing colicky pain(Ripamonti et al. 2000). The toxicity and side effectprofile of octreotide is excellent (aside from discom-fort at the site of injection), with no major side effectsreported, even at a dose of 1.2 mg daily (Riley andFallon 1994).
Cancer Pain Management, Adjuvant Analgesics in Management ofPain Due To Bowel Obstruction, Table 1 � Adjuvant Analgesics in Ma-lignant Bowel Obstruction*
Drug Dose
glycopyrrolate** 1–2 mg tid-qid OR
0.1–0.2 mg tid-qid SC/IV
hyoscine butylbromide 40–120 mg daily SC/IV
Scopolamine 400–800 mcg OR every 4–6 h
1–2 TDP every 48–72 h
0.8–2 mg via CSI every 24 h
Atropine 1–2 drops ophthalmic solution SLevery 4 h
0.4 mg OR every 4 h
0.4 mg SC every 4 h
Dexamethasone 4–8 mg daily OR
2–8 mg every 6 h SC/IV
2–12 mg via CSI every 24 h
Prednisone 5–20 mg every 4–6 h
Octreotide 150 mcg tid SC
0.2–0.9 mg via CSI every 24 h
*List is not inclusive, dosages are suggested initial doses that may beprescribed as scheduled and/or prn doses, may need to be titrated to effectdependent upon patient’s clinical condition and expected life expectancy*Reduce dose in renal insufficiencyOR, oral; SC, subcutaneous; IV, intravenous; TDP, transdermal patch; SL,sublingual; CSI, continuous subcutaneous infusion; prn, as needed
References1. Baines M (1994) Intestinal Obstruction. In: Hanks GW (ed) Pal-
liative Medicine: Problem Areas in Pain and Symptom Man-agement. Cold Spring Harbor Laboratory Press, Plainview, NewYork, pp 147–156
2. Baines MJ (1998) The Pathophysiology and Management of Ma-lignant Intestinal Obstruction. In: Doyle D, Hanks GWC, Mac-Donald N (eds) Oxford Textbook of Palliative Medicine, 2nd edn.Oxford University Press, Oxford, pp 526–534
3. Basson MD et al. (1989) Does Vasoactive Intestinal PolypeptideMediate the Pathophysiology of Bowel Obstruction? Am J Surg157:109–115
4. Davis MP, Furste A (1999) Glycopyrrolate: A Useful Drug inthe Palliation of Mechanical Bowel Obstruction. J Pain SymptomManage 18:153–154
5. Feur DJ, Broadley KE (1999) Systematic Review and Met-Analysis of Corticosteroids for the Resolution of MalignantBowel Obstruction in Advanced Gynaecological and Gastroin-testinal Cancers. Ann Oncol 10:1035–1041
6. Krouse RS et al. (2002) When the Sun can Set on an UnoperatedBowel Obstruction: Management of Malignant Bowel Obstruc-tion. J Am Coll Surg 195:117–128
7. Laval G et al. (2000) The Use of Steroids in the Management ofInoperable Intestinal Obstruction in Terminal Cancer Patients:Do They Remove the Obstruction? Palliat Med 14:3–10
8. Lublin M, Schwartzentruber DJ (2002) Bowel Obstruction.In: Berger A, Portenoy RK, Weissman DE (eds) Principles &

C
Cancer Pain Management, Anesthesiologic Interventions 227
Practice of Palliative Care & Supportive Oncology. LippincottWilliams & Wilkins, Philadelphia, pp 250–263
9. Mercadante S (1997) Assessment and Management of Mechan-ical Bowel Obstruction. In: Portenoy RK, Bruera E (eds) Topicsin Palliative Care, vol 1. Oxford University Press, New York,pp 113–130
10. Pandha HS, Waxman J (1996) Octreotide in Malignant IntestinalObstruction. Anti-Cancer drugs 7:5–10
11. Riley J, Fallon MT (1994) Octreotide in Terminal Malignant Ob-struction of the Gastrointestinal Tract. Eur J Palliat Care 1:23–25
12. Ripamonti C (1994) Management of Bowel Obstruction in Ad-vanced Cancer Patients. J Pain Symptom Manage 9:193–200
13. Ripamonti C et al. (2000) Role of Octreotide, Scopolamine Butyl-bromide, and Hydration in Symptom Control of Patients with In-operable Bowel Obstruction and Nasogastric Tubes: A Prospec-tive Randomized Trial. J Pain Symptom Manage 19:23–34
14. Ripamonti C et al. (2001) Clinical-Practice Recommendationsfor the Management of Bowel Obstruction in Patients with End-Stage Cancer. Support Care Cancer 9:223–233
15. Rousseau PC (1998) Management of Malignant Bowel Obstruc-tion in Advanced Cancer: A Brief Review. J Palliat Med 1:65–72
Cancer Pain Management,Anesthesiologic Interventions
PAUL A. SLOAN
Department of Anesthesiology, University ofKentucky, Lexington, KY, [email protected]
Synonyms
Nerve block; anesthetic block
Definition
Information about noxious events is transmitted to thebrain via neurons of the peripheral and central nervoussystem. Blockade of this nerve conduction using appliedlocalanesthetics to temporarily block pain transmission,spinal medications (e.g. opioids) to modulate pain trans-mission, or neurolytic substances to destroy the pain-transmitting nerves is the domain of anesthesiologic in-terventions for cancer pain management.
Characteristics
Most patients with cancer pain can have their pain wellmanaged using standard opioidsandotheranalgesicsviathe oral or parenteral routes. However, approximately15% of cancer patients with pain will experience severepain resistant to traditional analgesic therapies (SloanandMelzack1999).For theseunfortunatepatients,anes-thesiologic techniques often provide welcome pain re-lief.Theuseofalcohol todestroynerve tissue in the treat-ment of painful conditions is almost 75 years old, and,along with phenol, became popular in the 1950’s and1960’s for the treatment of cancer pain (Maher 1955).With more recent acceptance and use of chronic opioidtherapy for cancer pain, the current role of neuroablativetechniques has chiefly been for patients with terminaldisease and pain unresponsive to traditional analgesics.
The use of local anesthetics and spinal opioids to modu-late pain transmission has gained popularity in the pastdecade, because of the low risk involved and the abilityto reverse the treatment course at any time.The use of local anesthetics to provide long-term painrelief for cancer patients has principally involved in-filtration around peripheral nerves, and � epidural or� intrathecal administration. Local anesthetics injectedclose to a peripheral nerve or the spinal cord will blocknerve impulses and provide degrees of nociceptive,sensory, or motor nerve blockade. Anesthesiologistshave searched for the correct combination of local anes-thetic concentration, infusion site, and rate of infusionto achieve analgesia without the significant side effectsof motor or sensory blockade. Two common sites ofperipheral nerve block with local anesthetic infusionare the brachial plexus (Fig. 1) and lumbar plexus.Tumors originating in lung, head and neck, or othersites may invade the brachial plexus, resulting in se-vere neuropathic pain, and pelvic tumors may similarlyinvade the lumbar plexus. The percutaneous insertionof catheters for the infusion of local anesthetics hasprovided excellent and long-term pain relief amongsuch cancer patients (Vranken et al. 2001; Douglas andBush 1999). A basal infusion may be physician pre-scribed, and augmented by the use of patient-controlledboluses for breakthrough pain. Portable infusion pumps(small enough to be worn on the body) allow the patientto return home for as long as possible. Typical localanesthetics used are bupivacaine (1–5 mg/ml), lido-caine (5–10 mg/ml) or ropivacaine (1–5 mg/ml), withinfusion rates of 3–8 ml/h.The spinal cord is bathed by cerebrospinal fluid (CSF)that is contained in a strong protective membrane, thedura mater. Local anesthetics applied outside the duramater (epidural) or within the CSF (intrathecal) havebeen used to control cancer pain (Fig. 2). A catheteris usually placed percutaneously into the epidural
Cancer Pain Management, Anesthesiologic Interventions,Figure 1 Interscalene approach to brachial plexus block.

228 Cancer Pain Management, Anesthesiologic Interventions
Cancer Pain Management,Anesthesiologic Interventions,Figure 2 Cross-section through alumbar vertebrae.
or intrathecal space for the chronic infusion of localanesthetics. The catheter may be tunneled under theskin and exit to an external portable pump, or remainburied and attached to an implanted pump. These pro-cedures are usually performed using local anesthesiaand intravenous sedatives. The pumps allow for theconstant infusion of local anesthetics such as bupiva-caine (Dahm et al. 2000). Cancer patients with lowerextremity or truncal pain to the waist are best suitedto these approaches. Possible complications includelocal anesthetic toxicity (uncommon), hypotension,tachyphylaxis, infection, and motor weakness. De-spite the side effect potential, most patients toleratechronic infusion of anesthetics without difficulty andcan be monitored at home. In addition to spinal ad-ministration, anesthetics have been infused chronicallyinto the pleural space via a percutaneous catheter forthe relief of refractory lung cancer pain (Aguilar etal. 1992).Spinal administration of opioids for pain relief was firstapplied to patients in 1979 (Behar et al. 1979), and hasbeen advocated for the relief of intractable cancer pain.Spinal opioids can be given by both the epidural andintrathecal routes of administration, with the epiduraldose being approximately 10 times the intrathecal dose.It is believed that spinally applied opioids modulate paintransmission by direct action on specific opioid recep-tors in the dorsal horn of the spinal cord (Bedder 1997).In this way, there may be fewer and/or less intense sys-temic opioid side effects and a better quality of analge-sia may be obtained. Many opioids have been used to
achieve successful analgesia, with morphine remainingthe most common. A single injection of spinal morphinewill provide 12–24 h of pain relief. However, a continu-ous infusion of opioid is often used and can be managedsafely at home (Samuelsson et al. 1995). The effectivedose is titrated to analgesia or intolerable side effects.A useful starting dose for epidural morphine is 20% ofthe current daily oral morphine dose, and the final dailyepiduraldosesreportedintheliteraturehaverangedfrom2 to over 1000 mg.The combination of opioids and local anesthetics ap-plied to the spinal cord in animals has resulted in asynergistic effect (Akerman et al. 1988), and led tothe clinical practice of combining spinal analgesics toachieve powerful analgesia with the fewest possibleside effects. The co-administration of these drugs hasgained widespread acceptance and has been shownto limit morphine dose progression during long-termspinal infusion (Dongen et al. 1999). Other spinaldrugs that have provided some analgesia include alpha-adrenergic agonists (clonidine, dexmedetomidine) andNMDA receptor antagonists (ketamine).Complications (10% of all patients) associated withspinal analgesics include local infection, CSF leak,pain on injection, mechanical problems with catheterfunction, headache, meningitis and epidural hematoma(Basta and Sloan 1999) or abscess (Fig. 3). Local in-fection can usually be managed with antibiotics andcatheters can remain in place for months. The typicalside effects of opioids may be seen, including nauseaand vomiting, sedation, urinary retention, and pruritus.

C
Cancer Pain Management, Anesthesiologic Interventions 229
Cancer Pain Management,Anesthesiologic Interventions,Figure 3 MRI of low thoracicepidural abscess in a patient treatedwith chronic epidural analgesics.
Patient accommodation to these side effects of opioidstypically occurs.The historic “nerve block” using neurolytic agents tophysically modify nerve tissue to produce analgesia hasnow become the least prevalent anesthesiologic proce-dure for the management of cancer pain. Nonetheless,among terminally ill patients with pain not well con-trolled by other measures, certain neurolytic injectionscan provide excellent pain relief with a minimum ofcomplications. The destruction of the celiac plexusin the upper abdomen is the most common neurolyticblock performed. Upper abdominal pain associated withcancer of the pancreas, distal esophagus, stomach orliver may be treated using a simple percutaneous tech-nique. Imaging studies (x-ray, CT scan, ultrasound)guide accurate needle placement, and the injectionof 25–50 ml of alcohol or phenol results in destruc-tion of nociceptive neurons passing through the celiacplexus, thus producing pain relief in the majority ofpatients that may last for many months (Rykowski andHilgier 2000). While significant complications (para-plegia, pneumothorax) are infrequent and have beenreduced by radiographic needle placement, they havenot been entirely eliminated. Common complicationsinclude postural hypotension and diarrhea.Additional neurolytic blocks occasionally used to treatcancer pain include lumbar sympathetic block for uro-logic pain, superior hypogastric block for pelvic pain,subarachnoid block for chest wall pain, subarachnoidsaddle block for perineal pain, and cranial nerve block
for head or neck pain. Noninvasive � gamma knifedestruction of the pituitary has also been tried forintractable bilateral cancer pain (Sloan et al. 1996).Other innovations may prove valuable in the future. Zi-conotide, a neuronal-specific calcium channel blocker,will be available for intrathecal use and has been shownto be an effective analgesic in controlled trials. The per-cutaneous injection of adrenal medullary allografts, ob-tained from organ donors, into the lumbar CSF presentsan exciting possibility for interventional management ofcancer pain. These cells produce met-enkephalin, andboth studies in animalsand small surveys inhumans(La-zorthes et al. 2000) have yielded positive findings.Anesthetic interventions for pain are well establishedand new therapies are evolving. The appropriate use ofanesthesiologic interventions to help manage acute andchronic pain among cancer patients will ensure pain re-lief and improved quality of life.
References1. Aguilar JL, Montes A, Samper D et al. (1992) Interpleural Anal-
gesia through a DuPen Catheter for Lung Cancer Pain. Cancer70:2621–2623
2. Akerman B, Arwestrom E, Post C (1988) Local AnestheticsPotentiate Spinal Morphine Antinociception. Anesth Analg67:943–948
3. Basta M, Sloan PA (1999) Epidural Hematoma following Epidu-ral Catheter Placement in a Patient with Chronic Renal Failure.Can J Anesth 46:271–274
4. Bedder MD (1997) Neuraxial Analgesic Blockade: Physiology,Pharmacology, and Complications. In: Parris WCV, Foster HW,Melzack R (eds) Cancer Pain Management: Principles and Prac-tice. Butterworth-Heinemann, Newton, MA, pp 171–180

230 Cancer Pain Management, Anesthesiologic Interventions, Neural Blockade
5. Behar M, Magora F, Olshwang D et al. (1979) Epidural Morphinein Treatment of Pain. Lancet 1:527–529
6. Dahm P, Lundborg C, Janson M et al. (2000) Comparison of 0.5%Intrathecal Bupivacaine with 0.5% Intrathecal Ropivacaine in theTreatment of Refractory Cancer and Noncancer Pain Conditions:Results from a Prospective, Crossover, Double-Blind, Random-ized Study. Reg Anesth Pain Med 25:480–487
7. Dongen RT van, Crul BJ, Egmond J van (1999) Intrathecal Coad-ministration of Bupivacaine Diminishes Morphine Dose Progres-sion during Long-Term Intrathecal Infusion in Cancer Patients.Clin J Pain 15:166–172
8. Douglas I, Bush D (1999) The Use of Patient-Controlled Bo-luses of Local Anaesthetic Via a Psoas Sheath Catheter in theManagement of Malignant Pain. Pain 82:105–107
9. Lazorthes Y, Sagen J, Sallerin B et al. (2000) Human ChromaffinCell Graft into the CSF for Cancer Pain Management: A Prospec-tive Phase II Clinical Study. Pain 87:19–32
10. Maher RM (1955) Relief of Pain in Incurable Cancer. Lancet1:18
11. Rykowski JJ, Hilgier M (2000) Efficacy of Neurolytic CeliacPlexus Block in Varying Locations of Pancreatic Cancer: Influ-ence on Pain Relief. Anesth 92:347–354
12. Samuelsson H, Malmberg F, Eriksson M et al. (1995) Outcomesof Epidural Morphine Treatment in Cancer Pain: Nine Years ofClinical Experience. J Pain Symptom Manage 10:105–112
13. Sloan PA, Hodes J, John W (1996) Radiosurgical Pituitary Ab-lation for Cancer Pain. J Palliat Care 12:51–53
14. Sloan PA, Melzack R (1999) Long-Term Patterns of MorphineDosage and Pain Intensity among Cancer Patients. Hospice J14:35–47
15. Vranken JH, Vegt MH van der, Zuurmond WW et al. (2001)Continuous Brachial Plexus Block at the Cervical Level using aPosterior Approach in the Management of Neuropathic CancerPain. Reg Anesth Pain Med 26:572–575
Cancer Pain Management,Anesthesiologic Interventions, NeuralBlockade
HARALD BREIVIK
Department of Anesthesiology, RikshospitaletUniversity Hospital, University of Oslo, Oslo, [email protected]
Synonyms
Anesthesiological Interventions; Neural Blockade
Definition
Anesthesiologic interventions are transient or long last-ing interruptions of pain impulse conduction in periph-eral nerves, nerve roots, or the spinal cord. This will hin-der the conscious perception of pain and lessen the suf-fering associated with cancer and its destruction of nor-mal tissues.
Characteristics
Anesthesiologic interventions may be performed with� local anesthetic drugs, which stop pain impulse con-duction along nerves for up to several hours, or with� neurolytic drugs, which block transmission for up toseveral months. These interventions will remove painfrom the locally anesthetized part of the body, which
may become numb and partly paralyzed. Interruptionsof pain impulses conducted through visceral nerves, e.g.the celiac plexus of the upper abdomen; do not causenumbness or skeletal muscle weakness. Severe forms ofcancer pain can be relieved effectively by skillfully ap-plied anesthesiologic interventions (Breivik 2000). Therisk of adverse effects exists and must be understoodwhen considering these approaches.
Reversible Blockade of Pain Impulses by Local AnestheticDrugs
Infiltration of a painful primary or metastatic tumor, orthe peripheral nerves innervating a painful cancerousgrowth, with a local anesthetic drug results in local orregional anesthesia and pain relief lasting from 1–12 h.The duration can be prolonged with repeated injectionsor infusion into � perineural catheters. Local anes-thetic infiltrations and � simple nerve blocks shouldbe used liberally (Twycross 1994). Relief of acute,overwhelmingly intense � breakthrough pain from apathological fracture or an acute tumor infarct can berelieved effectively with a � regional anesthetic block.Local anesthetic nerve blocks should not be used topredict the effect of neurolytic blocks or other neurode-structive treatment, such as � thermocoagulation or� surgical denervation (Hogan and Abrams 1997).
Spinal Cord Analgesia by Epidural or SubarachnoidCatheter Infusion of Drugs
Epidural Analgesia
Potent pain relief can occur when low concentrationsof a local anesthetic drug, an opioid, and an adrenergicdrug are administered epidurally (Breivik 2002a). Withan epidural catheter at the appropriate � spinal cord seg-mental level (cervical to the upper lumbar), a reliable in-fusion pump and trained nurses, analgesia can be main-tained for prolonged periods athome, in a hospice or pal-liative care institution. Stable and sterile drug mixturesare needed (Breivik 2002a). Details of epidural catheterplacement and maintenance, monitoring and preventionand management of complications are described in text-books (Breivik 2002a).
ProlongedInfusion intotheSpinalSubarachnoidSpace
Insertion of a catheter into the subarachnoid space al-lows infusion of a local anesthetic solution containingan opioid and donidine or adrenaline directly into the� cerebrospinal fluid. This may give satisfactory anal-gesia when most other methods have failed (Nitescu etal. 2002). Prolonged, effective, and safe pain relief ispossible,evenwhenthepatient is livingathome(Nitescuet al. 2002).
Inflammatory Pain Treated with Injections of LocalAnesthetic and Corticosteroid Drugs
Corticosteroids have analgesic effects when adminis-tered epidurally, perineurally or intralesionally. These

C
Cancer Pain Management, Anesthesiologic Interventions, Neural Blockade 231
are in part systemic effects, in part local effects on no-ciceptive nerve endings, and in part effects on inflam-matory or neurogenic pain mechanisms (Breivik 2000,Twycross 1994).Segmental epidural applications of local anestheticdrugs combined with methylprednisolone, dexametha-soneor triamcinolonemayrelieve� radicularnerve rootpain (Breivik 2000), including that caused by a tumorimpinging on spinal nerve roots (Twycross 1994). Per-ineural injections of a mixture of a local anesthetic anda corticosteroid may cause immediate and prolongedpain relief in nerves made hyperexcitable from localtrauma, infiltration of tumor or inflammatory reactions(Twycross 1994).Intralesional injection of local anesthetics and depotcorticosteroids similarly may cause immediate, and insome patients, prolonged pain relief, e.g. in multiplemyeloma lesions or metastases from breast cancer inribs (Twycross 1994).
Neurolytic Nerve Blocks with Ethanol or Phenol
The advantage of neurolytic blocks is apparent whena single intervention can replace or reduce the needfor daily administration of multiple drugs. However,a misplaced injection or injection of an inappropri-ate dose may cause severe complications. Durationof analgesia after a neurolytic block is limited. How-ever, some blocks can be repeated with success. Due tothe possibility of severe post-denervation neuropathicpain, neurolytic blocks of peripheral nerves should bereserved for patients with life expectancy of less thanabout one year. � Visceral sympathetic blocks may beconsidered in patients with longer life expectancy.
Celiac Plexus Block
Celiac plexus block relieves pain from cancer in theupper part of the abdomen (Breivik 2000). One double-blind, randomized, placebo-controlled study of intraop-erative celiac plexus neurolysis demonstrated improvedpain control, reduction in opioid analgesic consump-tion, and significantly prolonged survival (Lillemoet al. 1993). The block can be repeated with successif pain recurs after weeks to months. Pneumothoraxand shoulder pain from ethanol irritation of the di-aphragmatic peritoneum are short-lived side effects.The sympatholysis that results may cause � orthostatichypotension and diarrhea for a few days. However,paraplegia and intestinal infarction may result if theneurolytic solution is injected into arteries. Severelymisplaced epidural, paravertebral, and subarachnoidinjections have been reported, with tragic consequences(Breivik 2000).
Indications for Celiac Plexus Block
Cancer of the pancreas is the classic indication. How-ever, cancer of the stomach, duodenum, liver, gallblad-der, and choledocal duct causing visceral type pain in the
upperabdomenare indicationsaswell.Whenabdominalwall involvement occurs, pain impulses will also travelthrough somatic afferent nociceptor fibers of the inter-costal nerves. Neurolytic block of the visceral afferentnociceptor fibers passing through the celiac plexus willnot relieve this pain.
Techniques of Celiac Plexus and Splanchnic NerveBlockade
The celiac plexus is the prevertebral sympathetic plexusthat supplies the upper abdominal viscera with sympa-thetic innervations. It is located in the retroperitonealtissue space, anterior to the body of the first lumbarand twelfth thoracic vertebrae. The aorta lies behind,and the inferior vena cava and right renal vessels lie infront of the celiac plexus. The greater, the lesser, andthe least � splanchnic nerves connect the celiac plexusvia the spinal nerve roots to the thoracic spinal cord.These nerves can be interrupted by radiofrequencydenervation in the thoracic region, an approach favoredby some (Medicis and Leon-Casasola 2002).The celiac plexus can be injected intraoperatively whenthe surgeon has determined that the tumor is unre-sectable (Lillemo et al. 1993). However, the block hasmost often been performed with needles through theskin from the back, or with an anterior approach withneedle-guidance from computerized tomography scan-ning (CT) (Medicis and Leon-Casasola 2002). In thetraditional technique (Breivik 2000, Breivik 2002b)(Fig. 1), the patient is prone and a needle is inserted oneach side under the midpoint of the 12th rib. With localanesthetic infiltration, the needle is advanced towardsthe anterolateral corner of the body of the first lumbarvertebra. When this bone is contacted, the depth markeris moved 1.5–2 cm from the skin level towards the hubof the needle. The needle is now withdrawn to the sub-cutaneous tissue, redirected, and advanced 1.5–2 cmbeyond the anterolateral corner of the vertebral body. Ifthe aorta is punctured on the left side, or the vena cavaon the right side, the needle is withdrawn until bloodstops coming on aspiration. At this point, 5 ml of lido-caine 20 mg/ml is injected in each needle. The patientis soon able to tell whether his pain has disappeared.He will also be able to inform the anesthesiologist ofany signs of intraspinal or intravascular injection. Thisis sufficient information to be able to go ahead with aninjection of 50 ml of 50% ethanol (96% ethanol dilutedwith bupivacaine 2.5 mg/ml) in each of the two needles.It should be noted that radiographic imaging of the nee-dle position is no guarantee that the injected neurolyticagent will not cause somatic neurological deficit. Tworeported cases of paraplegia following celiac plexusblock in spite of radiographic needle control under-score this important point (Breivik 2000). If this blockis performed with the patient under general anesthesia,the indications of correct needle positioning from a testdose of a small, concentrated dose of local anesthetic

232 Cancer Pain Management, Anesthesiologic Interventions, Neural Blockade
are lost. Some of the reports of poor or short lastingpain relief from celiac plexus block may be due to aninsufficient injected volume or concentration of ethanol,which should not be less than 50 ml of 50%.
Side Effects of Celiac Plexus Block with Ethanol
An immediate side effect of celiac plexus block is adrop in blood pressure and also orthostatic hypotensionfor some time following the block. If this occurs, itmay be treated with ephedrine and intravenous colloid-containing fluids. Due to the sympathetic denervationof the major part of the gastrointestinal tract, diarrheamay also result, often a desirable effect in patients whohave been on oral opioids for some time. The patientshould be warned that transient shoulder pain may bea result of the ethanol reaching the diaphragm. Toorapid a discontinuation of morphine may cause with-drawal symptoms. Some patients may need a reduceddose of oral morphine for residual pain, or for painstemming from tumor invasion of the abdominal wall(Breivik 2000).
Superior Hypogastric Plexus Block and Bilateral Lum-bar Sympathetic Block
Phenol blocks of the superior hypogastric plexus or bi-lateral lumbar sympathetic block may relieve patientswith visceral pain from pelvic organs and sigmoid colon(Breivik 2000,Medicisand Leon-Casasola2002).Localpelvic infiltration of cervical or prostatic carcinoma cancause somatic nociceptive pains that limit the effective-ness of sympathetic blocks. The same is true for perinealpain, when mainly of somatic origin and pain impulsestravel via sacral and pudendal nerves.
Subarachnoid Spinal Nerve Root Neurolytic Block
Segmental, one-sided denervation of sacral nerve rootscan be obtained by spinal puncture close to the af-fected nerve roots, followed by subarachnoid injectionof 0.3–0.6 ml of hypobaric ethanol (96%) with thepatient’s painful side up, or hyperbaric phenol (5% inglycerol) with the painful side down. This techniqueis used less nowadays due to the dissatisfaction withthe degree and duration of relief, and because of risksof severe side effects (Breivik 2000, Twycross 1994).Continuous catheter infusion of local anesthetics withopioids is an alternative that is more effective and hasless risk of severe complications (Nitescu et al. 2002).However, under circumstances with very limited re-sources, where other pain relief is unavailable, thesimple methods of subarachnoid ethanol or phenolblock may still have a place. It can be performed at thebedside with a spinal needle and a syringe (Stovner andEndresen 1972). It is superior to no pain relief at allin a terminally ill cancer patient who is suffering fromexcruciating pain (Swerdlow 1983, Kuzucu et al. 1966,Drechsel 1984).
Subdural and Epidural Neurolytic Blockade with Phe-nol
These techniques have been used for cancer pain in thecervical and upper thoracic region where subarachnoidblock is less effective (Breivik 2000).
Neurolytic Blocks of Selected Peripheral and ParavertebralNerves (Hill 2002)
Trigeminal nerve block may be indicated for painfrom head and neck cancer with trigeminal nerve in-volvement. Less than 0.5 ml ethanol 96% is needed toanesthetize an appropriate branch (Swerdlow 1983).Glossopharyngeal nerve block may give good painrelief when pharmacological therapy fails in painfulconditions of the mouth and throat. Ethanol is injectedat the jugular foramen and may easily also block thevagus, accessory and hypoglossal nerves, causing dys-phagia if bilateral block is required (Montgomery andCousins 1972).Intercostal nerve block with 1.0 ml of ethanol 96% orphenol 5–6% often gives excellent pain relief, lasting upto a few weeks.
Paravertebral Spinal Nerve Blocks
For well-localized somatic pain, a paravertebral spinalnerve block can be performed, with needle insertion2–3 cm lateral to the spinous process (of the same ver-tebra in the lumbar region, but of the vertebra above thesegmental nerve to be blocked in the thoracic region).After contact with the transverse process, the needle isredirected below the transverse process, and 3–5 ml ofthe solution is injected. Pain relief may be good, butthe duration is unpredictable. The block can be consid-ered in debilitated and bedridden patients with severepain not responding well to pharmacological treatment.Unintended subarachnoid injection, or injection intoa radicular artery to the spinal cord, may cause severeneurological complications (Breivik 2000).
Sacral Nerve Blocks (Posterior Transsacral Blocks)
When pelvic metastases cause nerve compression painwhich is not well controlled by pharmacological means,sacral nerve blocks may be useful. The second sacralforamenlies1cmbelowandmedial totheposteriorsupe-rior iliac spine.Thefifth sacral foramen lies1 cm inferiorand lateral to the sacral cornua. The 3rd and 4th foram-ina lie on the line between the 1st and the 5th (Hill 2002).The needle is advanced 0.5–1.5 cm beyond the openingof the foramina and about 3 ml of the solution is injectedat each site.
References1. Breivik H (2000) Nerve Blocks – Simple Injections, Epidurals,
Spinals and More Complex Blocks. In: Simpson KH, Budd K(eds) Cancer Pain Management. A Comprehensive Approach.Oxford University Press, Oxford, pp 84–98
2. Breivik H (2002a) Epidural Analgesia. In: Breivik H, CampbellW, Eccleston C (eds) Clinical Pain Management. Practical Ap-plications and Procedures. Arnold, London, pp 409–416

C
Cancer Pain Management, Anesthesiologic Interventions, Spinal Cord Stimulation, and Neuraxial Infusion 233
3. Breivik H (2002b) Sympathetic Blocks. In: Breivik H, Camp-bell W, Eccleston C (eds) Clinical Pain Management. PracticalApplications and Procedures. Arnold, London, pp 233–246
4. Drechsel U (1984) Treatment of Cancer Pain with NeurolyticAgents. Recent Results of Cancer Research 89:137–147
5. Hill D (2002) Peripheral Nerve Blocks. In: Breivik H, Camp-bell W, Eccleston C (eds) Clinical Pain Management. PracticalApplications and Procedures. Arnold, London, pp 197–232
6. Hogan QH, Abrams SE (1997) Neural Blockade for Diagnosisand Prognosis: A Review. Anesthesiology 86:216–241
7. Kuzucu EY, Derrick WS, Wilber SA (1966) Control of In-tractable Pain with Subarachnoid Alcohol Block. J AmericanMed Ass 195:541–544
8. Lillemo KD, Cameron JL, Kaufman HS et al. (1993) Chemi-cal Splanchnicectomy in Patients with Unresectable PancreaticCancer. Annals of Surgery 217:447–457
9. Medicis E de, Leon-Casasola de O (2002) Neurolytic Blocks. In:Breivik H, Campbell W, Eccleston C (eds) Clinical Pain Manage-ment. Practical Applications and Procedures. Arnold, London,pp 247–254
10. Montgomery W, Cousins MJ (1972) Aspects of Management ofChronic Pain Illustrated by Ninth Nerve Block. British Journalof Anaesthesia 44: 383–385
11. Nitescu PV, Apelgren L, Curelaru IA (2002) Long-Term Intrathe-cal and Intracisternal Treatment of Malignant and NonmalignantPain Using External Pumps. In: Breivik H, Campbell W, Eccle-ston C (eds) Clinical Pain Management. Practical Applicationsand Procedures. Arnold, London, pp 285–306
12. Stovner J, Endresen R (1972) Intrathecal Phenol for Cancer Pain.Acta Anaesthesiol Scand 16:17–21
13. Swerdlow M (1983) Relief of Intractable Pain, 3rd edn. ExcerptaMedica, Amsterdam
14. Twycross R (1994) Pain Relief in Advanced Cancer. ChurchillLivingstone, Edinburgh
Cancer Pain Management,Anesthesiologic Interventions, SpinalCord Stimulation, and Neuraxial Infusion
MUTHUKUMAR VAIDYARAMAN, PETER S. STAATS
Division of Pain Medicine, The Johns HopkinsUniversity, Baltimore, MD, [email protected], [email protected]
Synonyms
Anesthesiological Interventions; spinal cord stimula-tion; neuraxial infusion
Definitions
Anesthesiologic interventions, � spinal cord stimula-tion and � neuraxial infusion are types of interventionaltherapies that may be used in the treatment of cancerpain.
Characteristics
Cancer is the second-most frequent cause of death in theUnited States. Cancer patients fear pain more than othersymptoms, and at least a thirdsufferpainat the timeofdi-agnosis (Jacox et al. 1994). Pain is heterogeneous (Bon-ica 1990), and the prevalence and complexity of pain in-creases in populations with advanced disease.
Humane treatment demands aggressive treatment ofcancer pain. To this end, the World Health Organization(World Health Organization 1990), and the Agency forHealth Care Policy and Research (Jacox et al. 1994)havepublished guidelineson themanagementofcancer-related pain. These guidelines, however, either fail tomention or minimize the importance of the role of in-terventional therapy. Although opioids continue to be amainstay of cancer pain treatment, patients frequentlyexperience side effects, such as sedation and consti-pation. Many experience only imperfect cancer painrelief.
The Role of Interventional Therapies
Interventional therapies include neural blockade, spinaldrug delivery, and spinal cord stimulation (Staats 1998).Clinicians should consider using these therapies in can-cer patients who suffer intractable opioid side effects,or in whom opioids provide inadequate relief. Alteringpain conduction with neural blockade techniques ordelivering lower doses of agents directly to the spinalcord can often improve the balance between analgesiaand side effects. Interventional therapies may also becost-effective (Erdine and Talu 1998); for example,long-term (more than three months) administrationof high-dose opioids delivered at home via patient-controlled-analgesia, is much more expensive on astrictly medical cost basis than implantable drug de-livery. In appropriate patients, interventional therapiescan make it possible to achieve the goal of decreasingpain and the side effects associated with higher dosesof systemic therapy while also reducing health care andassociated costs.
Neural Blockade
The effect of a nerve block can be short-term (using lo-cal anesthetics) or long-term (with chemical, thermal,or surgical applications). Nerve blocks can be periph-eral, visceral, or intraspinal. Intraspinal blocks are nowrarely performed because advances in spinal analgesiaoffer alternatives, and increased life expectancy in can-cer patients makes the risk of its associated complica-tions unacceptable.Short-acting local anesthetic blocks carry a very lowrisk and are usually diagnostic, guiding clinical de-cisions about the use of longer-acting methods. Forexample, the physician may anesthetize the painfulareas prior to a neurodestructive technique. This offersthe patient the opportunity to experience the feeling ofa permanent procedure. If anesthesia is not associatedwith pain relief, it also helps the physician prognosticatethe permanent neurolytic procedure. In some cases, aseries of blocks with local anesthetic (e.g. sympatheticblockade) can achieve lasting relief of neuropathic pain.Although clinicianscommonly refer toneurodestructiveblocks as permanent, the nerve may regenerate, leading

234 Cancer Pain Management, Anesthesiologic Interventions, Spinal Cord Stimulation, and Neuraxial Infusion
to a return of pain. Neurolysis typically provides threeto six months of relief.
Anatomic Location of Nerve Blocks
Among the many possible peripheral nerve blocks,clinicians most frequently block intercostal (Bolotin etal. 2000) and trigeminal nerves to treat somatic pain.A visceral nerve block can be performed to addressvisceral pain. The most common is the celiac plexusblock (Polati et al. 1998). The superior hypogastricplexus block is indicated for the visceral pain thatmay be prominent in patients with various pelvic or-gan cancers, even in advanced stages (Leon-Casasolaet al. 1993; Plancarte et al. 1997), and ganglion impar(Walther’s) blockade mitigates the burning visceral painin the perineal area and can have a beneficial impact onurgency (Plancarte et al. 1990).
Neuromodulation
Spinal Cord Stimulation (SCS)
SCS may be efficacious in patients whose pain has aneu-ropathic component (Grabow et al. 2003) and may ben-efit certain cancer patients, for example, those with post-thoracotomy pain, postherpetic neuralgia, and/or radic-ular lower extremity pain. With this approach, an elec-trical current is applied to the dorsal aspect of the spinalcord through an implanted wire. The current is createdeitherby an implanted generatoror an externalgeneratorthat transmits to an implanted antenna. There have beenno controlled trials of SCS in cancer patients, but anec-dotal experience has been favorable in carefully selectedpatients.
Neuraxial Infusion
Epidural delivery of morphine with an external pump iswidely used to treat cancer pain, especially in the post-operative setting. The timing of doses of epidural anal-gesia can be patient-controlled, and patients may con-tinue to use this method of pain control after they aredischarged from the hospital.Compared with epidural delivery, intrathecal delivery ofopioids has the advantages of providing analgesia witha much smaller dose of the drug, and a reduced chanceof infection with implanted systems. Intrathecal drugdelivery should be considered in those patients withchronic pain inadequately relieved by maximum medi-calmanagement,or relieved at theexpenseof intolerableside effects (Paice et al. 1996). Only preservative-freemorphine is approved to treat pain intrathecally. Ad-ditional widely-used agents include hydromorphone,fentanyl, clonidine, and bupivacaine. Ziconotide, anovel n-type calcium channel blocker, is under inves-tigation and has been demonstrated to be efficaciousin a controlled trial (Staats et al. 2004). Screening forintrathecal treatment includes assessment and treatmentof co-morbid psychological conditions (Olson 1992)and a trial with a single bolus dose, epidural delivery, or
intrathecal delivery of half of the oral opioid dose con-verted to its intrathecal equivalent. The remaining oraldose should be replaced with an equivalent intrathecaldose titrated over the next few days (Krames 1993).If the pain decreases by half with no intolerable sideeffects, the patient receives an external pump with apercutaneous catheter (for treatment duration of ≤three months) or an implanted constant flow-rate orprogrammable pump
Pain Treatment and Survival in Cancer Patients
Investigators are beginning to report findings of in-creased survival rates in cancer patients whose painis controlled in a manner that reduces side effects andimproves quality of life. In one study, patients withunresectable pancreatic cancer who received an alcoholceliac block survived longer than those who received aplacebo block (Staats et al. 2001). Another study thatcompared optimal medical management alone withoptimal medical management plus intrathecal drugdelivery, in a randomized trial involving 200 patientswith refractory cancer pain, intrathecal therapy reducedthe incidence of drug-related toxicity and reliance onsystemic analgesics while improving pain scores, qual-ity of life for patients and caregivers, and survival rates(Smith et al. 2002). The possibility that controlling painwill lengthen the life of terminally-ill patients is intrigu-ing, and should add to our urgency in promoting theconsideration of pain as a disease that must be treatedas aggressively as possible.
References1. Bolotin G, Lazarovici H, Uretzky G et al. (2000) The Efficacy
of Intraoperative Internal Intercostal Nerve Block during Video-Assisted Thoracic Surgery on Postoperative Pain. Ann ThoracSurg 70:1872–1875
2. Bonica JJ (1990) Cancer Pain. In: Bonica JJ (ed) The Manage-
ment of Pain, vol 1, 2nd edn. Lea and Febiger, Philadelphia,pp 200–460
3. Erdine S, Talu GK (1998). Cost Effectiveness of ImplantableDevices versus Tunneled Catheters. Current Review of Pain2:157–162
4. Grabow TS, Tella PK, Raja SN (2003) Spinal Cord Stimula-tion for Complex Regional Pain Syndrome: An Evidence-BasedMedicine Review of the Literature. Clin J Pain 19:371–383
5. Jacox A, Carr DB, Payne R (1994) New Clinical PracticeGuidelines for the Management of Cancer Pain. N Engl J Med330:169–173
6. Krames ES (1993). Intrathecal Infusion Therapies for IntractablePain: Patient Management Guidelines. J Pain Symptom Manage8:36
7. Leon-Casasola de OA, Kent E, Lema MJ (1993) Neurolytic Su-perior Hypogastric Plexus Block for Chronic Pelvic Pain Asso-ciated with Cancer. Pain 54:145–151
8. Olson K (1992) An Approach to Psychological Assessment ofChronic Pain Patients. NCS Assessments, Minneapolis
9. Paice JA, Penn RD, Shott S (1996) Intraspinal Morphine forChronic Pain: A Retrospective Multicenter Study. J Pain Symp-tom Manage 11:71
10. Plancarte R, Amescua C, Patt RB (1990) Presacral Blockadeof the Ganglion of Walther (Ganglion Impar). Anesthesiology73:A751

C
Cancer Pain Management, Cancer-Related Breakthrough Pain, Therapy 235
11. Plancarte R, de Leon-Casasola OA, El-Helaly M et al. (1997)Neurolytic Superior Hypogastric Plexus Block for Chronic PelvicPain Associated with Cancer. Reg Anesth 22:562–568
12. Polati E, Finco G, Gottin L et al. (1998) Prospective RandomizedDouble-Blind Trial of Neurolytic Celiac Plexus Block in Patientswith Pancreatic Cancer. Br J Surg 85:199–201
13. Smith TJ, Staats PS, Pool G et al. (2002) Randomized Clini-cal Trial of an Implantable Drug Delivery System Comparedto Comprehensive Medical Management for Refractory CancerPain: Impact on Pain, Drug-Related Toxicity, and Survival. J ClinOncol 20:4040–4049
14. Staats PS (1998) Cancer Pain: Beyond the Ladder. J Back Mus-culoskeletal Rehabilitation 10:69–80
15. Staats PS, Hekmat H, Sauter P, Lillemoe K (2001) The Effects ofAlcohol Celiac Plexus Block, Pain, and Mood on Longevity inPatients with Unresectable Pancreatic Cancer: A Double-Blind,Randomized, Placebo-Controlled Study. Pain Med 2:28–34
16. Staats PS, Yearwood T, Charapata S et al. (2004) IntrathecalZiconotide in the Treatment of Refractory Malignant Pain: AControlled Clinical Trial. JAMA 291:63–70
17. World Health Organization (1990) Cancer Pain Relief. WorldHealth Organization, Geneva
Cancer Pain Management,Cancer-Related Breakthrough Pain,Therapy
GIOVAMBATTISTA ZEPPETELLA
St. Clare Hospice, Hastingwood, [email protected]
Definition
Breakthrough pain is a transient increase in pain in-tensity over background pain. It occurs commonly incancer patients and is a heterogeneous phenomenonthat may be incapacitating or debilitating, or signifi-cantly impact quality of life. Breakthrough pain is adistinct component of cancer pain and requires specificmanagement.
Characteristics
People with cancer-related pain often report that theirpain varies during the course of the day. Two patternsof pain can be identified: continuous background pain,which may respond well to around-the-clock (ATC)� analgesics (Fig. 1), and transitory exacerbations ofpain, which break through the ATC analgesics (Fig. 2).Transient increases in pain in a cancer patient who hasstable persistent pain treated with � opioids may be de-fined as breakthrough pain (Portenoy and Hagen 1990).The definition of breakthrough pain has been the subjectof much discussion, with some investigators classifyingepisodic pains as breakthrough pain irrespective of theanalgesic regimen, and others classifying episodic painsin this way irrespective of whether background pain iscontrolled. Even the term ‘breakthrough’ is not one thatis universally accepted (Mercadante et al. 2002).Anumberof studieshaveevaluated thecharacteristicsofbreakthrough pain in patients attending cancer centers
or pain clinics, and in hospice inpatients or outpatients.These studies have varied in their sampling procedures,and in inclusion and exclusion criteria. Breakthroughpain is usually characterized according to its loca-tion, severity, temporal characteristics, relationship toregular � analgesia, precipitating factors, predictabil-ity, pathophysiology, etiology and palliative factors(Portenoy 1997). The reported prevalence of break-through pain has varied from 20 to 95% (Zeppetellaand Ribeiro 2003). Pain is typically of fast onset, shortduration and feels similar to background pain, exceptthat it may be more severe. Like background pain, thepathophysiology of breakthrough pain may be visceral,somatic or neuropathic, and the etiology may be relateddirectly to cancer or cancer treatment, or unrelated tothe cancer.Breakthrough pain is a heterogeneous phenomenon thatmaybedifferent foreachpatient;patientsmayhavemorethan one pain type. Two types of breakthrough pain havebeen described; incident pain, which is precipitated byvolitional factors such as movement or non-volitionalsuch as bladder spasm; and spontaneous pain, which oc-curs in the absence of a specific trigger. End-of-dose fail-ure is sometimes included as a breakthrough pain sub-type. It occurs either because the analgesic is describedatan inadequatedoseor the intervalbetweenadministra-tions is too long. As background pain is not controlled,end-of dose pain is not breakthrough pain.Despite the self-limiting nature of breakthrough pain,it can have a profound impact on both patients’ andcarers’ quality of life. Patients with breakthrough painare often less satisfied with their analgesic therapy, havedecreased functioning because of their pain and have anincreased level of anxiety and depression (Portenoy etal. 1999). Unrelieved breakthrough pain also increaseseconomic burden placed on the healthcare system (Fort-ner et al. 2002). Effective management is, therefore,essential and can only be achieved through meticu-lous assessment, good communication, and patientand caregiver participation. Failure to take these factorsinto account can lead to ineffective analgesia, unwantedadverse effects and poor adherence to therapy.Management of breakthrough pain should be part ofa holistic framework and appropriate to the stage ofthe patent’s disease. A combination of pharmacologi-cal and non-pharmacological treatment strategies maybe required. Three principles of management havebeen proposed (Portenoy 1997). First, implementationof primary therapies can lead to improvement in bothbackground and breakthrough pain. These interventionsinclude those that modify the pathological process (e.g.radiotherapy, chemotherapy, and surgery), and thosethat manage reversible problems (e.g. antitussives forcough, laxatives for constipation and antispasmodicsfor bladder spasm). Second, optimizing of the scheduledanalgesic regimen using the World Health Organizationanalgesic ladder as a basis for therapy (World Health

236 Cancer Pain Management, Cancer-Related Breakthrough Pain, Therapy
Cancer Pain Management, Cancer-Related Breakthrough Pain,Therapy, Figure 1 Backgroundpain. Successful managementof background pain with regularanalgesia and without seriousadverse effects.
Cancer Pain Management, Cancer-Related Breakthrough Pain,Therapy, Figure 2 Breakthroughpain. A transient increase overbackground pain that breaksthrough the regular analgesia; painmay vary in frequency, intensity andduration.
Organization 1996). Patients may require a combina-tion of opioid and non-opioid analgesics and, in somecases, � adjuvant analgesics such as antidepressants,anticonvulsants, bisphosphonates and corticosteroids.Third, use of specific non-pharmacological or phar-macological interventions for breakthrough pain. Non-pharmacological interventions include physiotherapy,cognitive techniques and orthopedic procedures. Phar-macological management is usually in the form ofsupplemental analgesia also known as rescue medica-tion. End-of dose failure responds best to increasingATC medication, whereas other breakthrough pain sub-types are usually managed with rescue medication, asincreasing the ATC medication to cover all incident and
spontaneous breakthrough pains can lead to adverseeffects.Successful use of rescue medication requires adequateanalgesia to be obtained without excessive adverse ef-fects. When using rescue medication, a number of is-suesshouldbeconsidered(Whatdowegive?Howmuch,when in relation to the pain? By what route and how fre-quently?). Rescue medication is best administered be-fore or soon after the onset of breakthrough pain. Asbreakthrough pain is typically of fast onset and short du-ration, rescue medication should ideally be potent, ab-sorbed and excreted rapidly, easy to administer and pro-duce minimal adverse effects (Fig. 3). Opioids are mostcommonly used, and the current approach involves giv-

C
Cancer Pain Management, Cancer-Related Breakthrough Pain, Therapy 237
Cancer Pain Management,Cancer-Related BreakthroughPain, Therapy, Figure 3 Idealrescue medication. The plasmalevel of medication follows theprofile of breakthrough pain withoutexcessive adverse effects.
inganadditionaldosebasedonthepatient’sATCanalge-sia. Opioids may be administered by several routes, in-cluding oral, oral transmucosal, rectal, intravenous, sub-cutaneousand intraspinal (intrathecalandepidural).Theroute of administration is important, as this can influ-ence the onset of analgesia and duration of effect. Oralmedication is generally used as it is convenient and of-ten the most acceptable (Walker et al. 2003). When us-ing morphineas rescuemedication, the ’normal-release’formulation (which has a four-hourly duration ofaction)is used; the current recommendation by the EuropeanAssociation for Palliative Care is to use the same as thefour-hourly dose of normal-release morphine (approx-imately 16% of the daily dose) when necessary (Hankset al. 2001). However, as breakthrough pain can vary inetiology, intensity and duration, the dose of rescue med-ication may also vary (Fig. 3).Patients with advanced disease may require more thanone route of drug administration due to difficulty inswallowing, nausea or other gastrointestinal problems(Coyle et al. 1990). Furthermore, the onset of effectwith most currently available opioids does not matchthe rapid onset of a typical breakthrough pain episode.Parenteral opioids (subcutaneous, intravenous or intra-muscular) achieve a peak effect more rapidly than oralopioids but are invasive, inconvenient, costly, and can beuncomfortable; the same is true of intraspinal opioids.Sublingualadministrationallowsrapidabsorptionandisconvenient, accessible, and generally well accepted, butabsorption can be poor or irregular. Rectal administra-tion, although generally safe, effective and inexpensive,may be inconvenient and unacceptable to some patients,and absorption can be unreliable. Oral transmucosaladministration provides a simple and convenient route,which offers the potential for more rapid absorption and
onset of action than the oral route and avoids hepaticfirstpassmetabolism. Oral transmucosal fentanylcitrate(OTFC) is a fentanyl-impregnated lozenge, specificallydeveloped for the management of breakthrough pain.OTFC is rapidly absorbed through the oral mucosa andin controlled studies has been shown to be safe andeffective (Coluzzi et al. 2001; Farrar et al. 1998). OTFCshould be individually titrated to a successful dose thatis not predicted from the ATC opioid dose.
References1. Coluzzi PH, Schwartzberg L, Conroy JD et al. (2001) Break-
through Cancer Pain: A Randomized Trial Comparing OralTransmucosal Fentanyl Citrate (OTFC) and Morphine SulphateImmediate Release (MSIR) Pain 91:123–130
2. Coyle N, Adelhardt J, Foley KM et al. (1990) Character of Ter-minal Illness in the Advanced Cancer Patient: Pain and OtherSymptoms during the Last Four Weeks of Life. J Pain SymptomManage 5:83–93
3. Farrar JT, Cleary J, Rauch R et al. (1998) Oral Transmucosal Fen-tanyl Citrate: Randomized, Double-Blind, Placebo-ControlledTrial for the Treatment of Breakthrough Pain in Cancer Patients.J Natl Cancer Inst 90:611–616
4. Fortner BV, Okon TA, Portenoy RK (2002) A Survey of Pain-Related Hospitalizations, Emergency Department Visits, andPhysician Office Visits Reported by Cancer Patients With andWithout History of Breakthrough Pain. J Pain 3:38–44
5. Hanks GW, De Conno F, Cherny N et al. (2001) Morphine andAlternative Opioids in Cancer Pain: The EAPC Recommenda-tions. Br J Cancer 84:587–93
6. Mercadante S, Radbruch L, Caraceni A et al. (2002) Episodic(Breakthrough) Pain: Consensus Conference of an Expert Work-ing Group of the European Association for Palliative Care. Can-cer 94:832–839
7. Portenoy RK (1993) A combination of pharmacological and non-pharmacological treatment strategies may be required and threeprinciples of management have been proposed
8. Portenoy RK (1997) Treatment of Temporal Variations inChronic Cancer Pain. Semin Oncol 24:S16-7–S16-12
9. Portenoy RK, Hagen NA (1990) Breakthrough Pain: Definition,Prevalence and Characteristics. Pain 41:273–281

238 Cancer Pain Management, Chemotherapy
10. Portenoy RK, Payne D, Jacobsen P (1999) BreakthroughPain: Characteristics and Impact in Patients with Cancer Pain.Pain 81:129–134
11. Walker G, Wilcock A, Manderson C et al. (2003) The Accept-ability of Different Routes of Administration of Analgesia forBreakthrough Pain. Palliat Med 17:219–221
12. World Health Organization (1996) Cancer Pain Relief. WHO,Geneva
13. Zeppetella G, Ribeiro MDC (2003) The Pharmacotherapy ofEpisodic Pain. Expert Opin Pharmacother 4:493–502
Cancer Pain Management, ChemotherapyRONALD H. BLUM
Beth Israel Medical Center, New York, NY, [email protected]
Synonyms
Chemotherapy
Definition
Chemotherapy, the use of chemicals as therapy, is, alongwith surgery and radiation, one of the most commontreatments for cancer. Chemotherapy is generally ad-ministered intravenously, but oral agents are becomingincreasingly available.
Characteristics
Over the last generation, chemotherapy has evolvedbased on the principles of cytotoxicity in cellular sys-tems, empiric observation in preclinical models, andincremental improvements achieved with clinical tri-als. Chemotherapeutic agents can be classified by theirpresumed mechanism of action, e.g. alkylator of DNA,antimetabolite, mitotic inhibitor, and repair enzymeinhibitor. Chemotherapy indications are based on clin-ical trials data, with the optimum therapeutic ratiodetermined by establishing the dose based on maxi-mum therapeutic benefit with acceptable toxicity. Manychemotherapeutic agents are schedule-dependent, bothfor efficacy and toxicity. Combination therapy usuallyhasa therapeuticadvantageoversingleagent treatments.Optimum benefit for cancer treatment is achieved witha basic understanding of the tumor site- specific clin-ical characteristics, including prognostic factors andpatterns of spread, coupled with knowledge of the roleand sequencing of the treatment modalities. Dependingon the tumor type and the presentation of the diseasein an individual patient, multidisciplinary planningresults in treatment that might involve a single modal-ity, such as surgery; the concurrent use of radiationand/or chemotherapy; or sequential treatments, suchas surgery followed by the addition of radiation and/orchemotherapy.Prospectiveclinical trials,oftenrandomized,haveestab-lished standardsofpractice.Therapeuticendpointsvary.
Inclinicalsituationswherecure is theexpectedoutcome,survival is conventionally used as the therapeutic end-point. In clinical situations where cure is a less likelyoutcome, then clinical endpoints such as progression-free survival, symptom-free interval, or overall survivalare commonly used. The � RECIST criteria have beenestablished as an objective reproducible measurementof reduction in tumor; these criteria generally correlatewith improvements in quality of life and survival.When the therapeutic intent is predominantly pallia-tive, then other therapeutic endpoints are used. Com-monly used palliative clinical trials endpoints include a> 50% decrease in pain score (measured using validatedmethodologies), > 50% decrease in opioid usage, andimprovement in performance scale, all lasting morethan four weeks.Cancer chemotherapy with established benefits is un-fortunately associated with what can be significanttoxicities. With the increasing availability of inter-ventions to manage symptoms, chemotherapy can bebetter tolerated. Fatigue is one of the most commonlyencountered chemotherapy-associated toxicities. Al-though often multifactorial, fatigue associated withchemotherapy is often caused by anemia. There is astrong body of evidence demonstrating the value of the� erythropoietins to increase the hemoglobin in patientsreceiving chemotherapy. This erythropoietin-inducedincrease in hemoglobin is correlated with improvementin quality of life and reversal of fatigue associated withthe cancer and cancer treatment.� Granulocytopenia is also a common chemother-apy toxicity. With the availability of recombinanthematopoietic growth factors, the associated morbidi-ties of fever, sepsis, and antibiotic use, which mayrequire hospitalization, are significantly reduced.Chemotherapy-induced nausea and vomiting, formerlya dose-limiting toxicity, is almost always preventableor at least greatly reduced by treatment. An array ofeffective antiemetic agents is now available, including� Serotonin Blockers, benzodiazepines, steroids, andthe recently available � NKδ1 blockers.In addition to these chemotherapy-associated toxici-ties, consideration needs to be given to the effects ofchemotherapy-associated organ damage. Examplesare the cumulative myocardial damage associated withanthracycline chemotherapy, the pulmonary toxicity as-sociated with bleomycin, the nephrotoxicity associatedwith the platinols, and the peripheral neuropathy asso-ciated with the vinca alkaloids. Other considerationsfor patients receiving chemotherapy revolve around theestablishment of safe and easy venous access for theadministration of chemotherapy and the maintenanceof nutrition.
Clinical Decision-Making
Given the reality that chemotherapy is often of limitedbenefitandassociatedwithsignificant toxicities,clinical

C
Cancer Pain Management, Chemotherapy 239
decision-making is critically important. The decisionwhether or not to use chemotherapy for palliative intentmust consider a number of important perspectives.Fromthe provider prospective, medical decisions are usuallybased on both evidence and the “expert” opinion of theprovider. The provider preferences are influenced bymany factors, including what could be globally definedas self-serving interests, practical issues, and issuessurrounding reimbursement. From the patient prospec-tive, preferences are influenced by the understandingand expectation of outcomes, by psychosocial issuesincluding developmental stage and beliefs, and by prac-tical and financial issues. Financial issues include notonly reimbursement for medical expenses, but what canbe burdensome, out-of-pocket expenses for such thingsas transportation and parking, and the loss of incomebecause of the patient or care partner not being ableto work. Clinical decision-making should be a sharedmedical decision-making process, which assumes thatboth provider and patient develop an understandingof the relative balance between the autonomy of thephysician and the preferences of the patient.A recent study (Koedoot et al. 2002) used clinical vi-gnettes to identify variables that influence providerpreference for “watchful waiting,” that is, deferringthe introduction of palliative chemotherapy. Based oninformation gathered from questionnaires administeredto more then 1000 oncologists, age was the strongestpredictor, followed by the patient’s wish to be treated,and the expected survival gain. One of the conclusionsof this study is that oncologists’ recommendations areconsistent and based on objective criteria (Koedoot etal. 2002).Probably the most important determinant of providerpreference is the available evidence of palliative ben-efit of chemotherapy for a specific cancer diagnosis.Although high level evidence from clinical trials islimited, these trials form the basis for the general as-sumption that chemotherapy can be a standard of carefor palliation of symptoms associated with most ma-lignancies. The risk/benefit determination of treatmentversus no treatment must be highly individualized andbased on the tumor type, the symptoms associated withthe tumor, overall clinical status and, of course, coupledwith patient preference.
Pancreatic Cancer
Perhaps the strongest argument for an evidence ba-sis for the palliative benefit of chemotherapy is forpancreatic cancer. In a landmark prospective studythat led to the licensing of gemcitabine, 126 symp-tomatic pancreas cancer patients were enrolled in astudy that began with a lead-in period during whichpatients were stabilized with analgesics. Patients werethen randomized to receive what was at that point theexperimental agent gemcitabine, or what was at thattime a standard of care, 5-fluorouracil. The primary
endpoints of the study were pain intensity and relatedanalgesic consumption, Karnofsky performance status,and weight. In order to meet the criteria of objectivebenefit, the required improvement in these symptomshad to be sustained for at least four weeks, withoutworsening of any symptom during the observationperiod. The symptom improvement was correlatedto objective tumor response, time to tumor progres-sion, and survival. There was evident clinical benefitin 24% of patients who received gemcitabine and 5%treated with 5-fluorouracil (P = 0.0022); median sur-vival durations were 6 vs. 4 months (P = 0.0025), andthe 12-month survival rate was 18% vs. 2% (Burris etal. 1997).
Colon Cancer
Patients with progressive metastatic colon cancer wererandomized to test supportive care with or withoutthe chemotherapeutic agent irinotecan. The primaryendpoint of survival demonstrated an improvementfrom 14% at one year to 36% (P = 0.001). Palliativebenefit was evident with demonstration in the sec-ondary endpoints, with a longer duration of pain-freesurvival, longer duration to any significant decrease inperformance status, and time to more than 5% weightloss. Corroborating data was evident in the results ofquality-of-life assessments (Cunningham et al. 1998).
Breast Cancer
The hypothesis that there is a relationship betweentumor shrinkage and improvement in disease-relatedsymptoms was evaluated in a prospective randomizedtrial of 300 women with metastatic breast cancer, dur-ing which symptoms were assessed for change overtime associated with the cancer chemotherapy (Geelset al. 2000). Utilizing established quality-of-life ques-tionnaires and what are now known as the � CommonToxicity Criteria, the authors were able to demonstratea clear correlation between patients’ symptoms andobjective tumor response.
Lung Cancer Chemotherapy
For non-small cell lung cancer, the benefits of palliativechemotherapy are evident from a meta-analysis of 52randomized clinical trials of chemotherapy. Compar-ing best supportive care to chemotherapy in a groupof patients who had not had prior chemotherapy formetastatic disease, there was a 10% absolute improve-ment and survival at one year with chemotherapy;expressed as a hazard ratio, this was equal to 0.73(Thongprasert et al. 1999). In a specific chemotherapytrial of docetaxel versus best supportive care in a groupof 103 patients who had had previous treatment withplatinum-based chemotherapy, there was a significantdifference between the two groups in their require-ment for opioid analgesics and other medications forsymptom management (Shepherd et al. 2000).

240 Cancer Pain Management, Gastrointestinal Dysfunction as Opioid Side Effects
Prostate
For prostate cancer, the best evidence is from a prospec-tive randomized trial of prednisone with or without thechemotherapeutic agent, mitoxantrone, in 161 men withmetastatic prostate cancer. The primary endpoints wereimprovement in health-related quality of life assessedby questionnaire. Both groups demonstrated improve-ment in quality of life, but the important parameters ofphysical functioning and pain were significantly betterin the mitoxantrone group, with longer duration of re-sponse compared to the prednisone alone group (Tan-nock et al. 1996).
Ovary Cancer
For ovarian cancer, the data are not as well established,but implied from objective response data. Among 27women, only seven achieved an objective response,and there were improvements in symptom endpoints(Doyle et al. 2001).
References1. Burris HA III, Moore MJ, Anderson J et al. (1997) Improvements
in Survival and Clinical Benefit with Gemcitabine as First LineTherapy for Patients with Advanced Pancreas Cancer: A Ran-domized Trial. J Clin Oncol 15:2403–2413
2. Cunningham D, Pyrohonen S, James RD et al. (1998) Ran-domised Trial of Irinotecan plus Supportive Care versusSupportive Care alone after Fluorouracil Failure for Patientswith Metastatic Colorectal Cancer. Lancet 352:1413–1418
3. Doyle C, Crump M, Pintilie M et al. (2001) Does PalliativeChemotherapy Palliate? Evaluation of Expectations, Outcomes,and Costs in Women Receiving Chemotherapy for AdvancedOvarian Cancer. J Clin Oncol 19:1266–1274
4. Geels P, Eisenhauer E, Bezjak A et al. (2000) Palliative Effect ofChemotherapy: Objective Tumor Response is Associated withSymptom Improvement in Patients with Metastatic Breast Can-cer. J Clin Oncol 18:2395–2405
5. Koedoot CG, Haes JC de, Heisterkamp SH et al. (2002) PalliativeChemotherapy or Watchful Waiting? A Vignettes Study amongOncologists. J Clin Oncol 20:3658–3664
6. Shepherd F, Dancey J, Ramlau R et al. (2000) Prospective Ran-domized Trial of Docetaxel versus Best Supportive Care in Pa-tients with Non-Small Cell Lung Cancer Previously Treated withPlatinum-Based Chemotherapy. J Clin Oncol 18:2095–2103
7. Tannock IF, Osoba D, Stockler MR et al. (1996) Chemother-apy with Mitoxantrone plus Prednisone or Prednisone Alonefor Symptomatic Hormone-Resistant Prostate Cancer: A Cana-dian Randomized Trial with Palliative End Points. J Clin Oncol14:1756–1764
8. Thongprasert S, Sanguanmitra P, Juthapan W et al. (1999) Re-lationship between Quality of Life and Clinical Outcomes inAdvanced Non-Small Cell Lung Cancer: Best Supportive Care(BSC) versus BSC plus Chemotherapy. Lung Cancer 24:17–24
Cancer Pain Management,Gastrointestinal Dysfunction as OpioidSide Effects
NIGEL P. SYKES
St. Christopher’s Hospice and King’s College,University of London, London, [email protected]
Synonyms
Opioid-Induced Bowel Dysfunction; opioid-relatedbowel dysfunction; Narcotic Bowel Syndrome
Definition
A constellation of symptoms resulting from the ef-fects of opioid analgesics on intestinal function. Themost common and enduring of these symptoms is con-stipation. The other principal symptoms referable toopioid-induced gastrointestinal dysfunction are nauseaand vomiting.
Characteristics
Gastrointestinal dysfunction due to opioids is importantbecause of the impact upon patients’ quality of life, animpact that is sometimes rated higher than that of pain it-self. Nausea affects up to 70% of patients with advancedcancer, and vomiting 10 to 30%. In advanced disease,opioids are probably the single most important identifi-able cause of constipation, but many other factors suchas impaired mobility and reductions or changes in di-etary intake are involved. Thus 63% of cancer patients’not taking opioids need laxatives, but with opioids thisrises to 87% (Sykes 1998).
Nausea and Vomiting
Opioids act in at least three ways to cause nausea andvomiting (Fig. 1):
• Detection by the chemoreceptor trigger area in the re-gion of the area postrema and nucleus tractus solitar-ius.
• Slowing of gastrointestinal transit and, in particular,gastric emptying
• Increase of vestibular sensitivity.
A first step in management is to ensure that the patientis actually vomiting rather than regurgitating, as thelatter will not be helped by antiemetics. Undigestedfood eaten in a current or immediately past meal, re-turned in small volumes with little or no prodromalnausea, suggests regurgitation. In any confirmed caseof nausea or vomiting, the existence of exacerbatingfactors such as strong smells, anxiety and, of course,constipation, must be considered and addressed. Atleast 30% of cancer patients receiving morphine donot need an antiemetic, but around 10% will need acombination of two or more antiemetics (Twycross andLack 1986). The logical choice of antiemetic dependson which of the three mechanisms of opioid-inducedemesis appears to be acting most strongly (Table 1). Inpractice, vestibular stimulation can be ignored unlessthe patient has to take a journey, as movement per se isnot usually the sole stimulus to nausea and vomiting inthis patient group.Delayed gastric emptying is suggested by large volumevomits, containing little or no bile, occurring suddenly

C
Cancer Pain Management, Gastrointestinal Dysfunction as Opioid Side Effects 241
Cancer Pain Management, Gastrointestinal Dysfunction as Opioid SideEffects, Figure 1 Receptor Activity of Commonly-Used Antiemetics
with little or no preceding nausea. There may be com-plaints of hiccups and heartburn, and there is often undi-gested food in the vomit from meals taken more than sixhourspreviously. In thissituation,metoclopramideis therational first choice of antiemetic because of its proki-netic action on the upper gut. Metoclopramide has been
Cancer Pain Management, Gastrointestinal Dysfunction as Opioid Side Effects, Table 1 Receptor Activity of Commonly-Used Antiemetics
D 2 ACh m H 1 5HT 3 5HT 4
Hyoscine - +++ - - -
Cyclizine - + +++ - -
Haloperidol +++ - - - -
Chlorpromazine ++ + ++ - -
Metoclopramide ++ - - + ++
Domperidone ++ - - - -
Ondansetron - - - +++ +
Levomepromazine ++ + + + -
Droperidol +++ - - - -
+++ indicates strong antagonism; - indicates little or no activity
showntoovercomeopioid-relateduppergutslowingandassociated vomiting (Stewart et al. 1976).The chemoreceptor areas involved in emetogenesis arerich in D2 � dopamine receptors. In the absence of ev-idence of gastric hold-up, it is appropriate to use a drugwithantidopaminergicactivity foropioid-relatednauseaor vomiting. The most potent and specific antidopamin-ergics are droperidol and haloperidol. Droperidol isshort-acting, but haloperidol has a half-life of about18 hours, rendering it suitable initially to be givenonce a day, usually in the evening because of its some-what sedative effect. A systematic review of the use ofhaloperidol as an antiemetic in palliative care foundevidence of effectiveness in nausea and vomiting dueto a variety of causes, including morphine (Critchleyet al. 2001). Extrapyramidal or Parkinsonian effects ofhaloperidol can be dose-limiting.Levomepromazine (methotrimeprazine) is a popu-lar antiemetic for use in advanced disease in Britain,because its broad spectrum of receptor actions cancover the mixed etiology of vomiting characteristic ofthis patient group. It is effective at much lower dosesthan previously assumed (from 6.25 mg/day orally, or2.5 mg/day subcutaneously), allowing the avoidanceof sedation. Extrapyramidal effects are less than withhaloperidol, but not absent.Cyclizine is an H1 antihistamine offering receptoractivity complementary to that of haloperidol. It hasbeen shown to have efficacy comparable with thatof droperidol in nausea and vomiting associated withpatient-controlled opioid analgesia (Walder and Aitken-head 1995). Its receptor activity suggests a role at vagallevel, which would be relevant where nausea was associ-ated with gut distension. The efficacy of any antiemeticin a vomiting patient is likely to be better if administeredby continuous subcutaneous infusion, and all the drugsmentioned can be administered in this way, alone or incombination with morphine.

242 Cancer Pain Management, Gastrointestinal Dysfunction as Opioid Side Effects
Among newer drugs, the place of 5HT3 antagonists inopioid-induced vomiting remains unclear. Moreover,clinical trials of NK1 receptor antagonists indicate pooreffectiveness in this indication (Loewen 2002).Public interest in non-drug approaches to anti-emesis,notably acupuncture and acupressure, is strong. Thereis controlled trial evidence that acupuncture or acupres-sure at the P6 point (just above the wrist) is effective fornausea and vomiting due to opioid premedication.
Constipation
Constipating effects of opioids on the bowel include:
• Reduction of peristalsis• Increase in sphincter tone• Increased water absorption• Impairment of rectal sensation
These actions are predominantly mediated through mu2receptors in the gut itself. Mu2 actions, such as delay-
ing of intestinal transit, show less tolerance than mu1mediatedanalgesia (Lingetal.1989). Incontrast tonau-
sea and vomiting caused by opioids, which usually sub-sides within 7 to 10 days, opioid-induced constipationis often persistent.In general, opioids differ little in their ability to con-stipate. Oxycodone has not shown constipating effectssignificantly different from those of morphine and nei-ther has hydromorphone. Reduction in laxative usehas been reported after changing from morphine tomethadone, but only on a case history basis (Daeninckand Bruera 1999). However, there is now good evidencethat transdermal fentanyl is significantly less constipat-ing than morphine (Radbruch et al. 2000), presumablybecause the gut is also exposed to relatively lower levelsof the drug.Functional definitions of constipation exist, but are un-helpful inpatientswhoseconstipation isrelated toopioiduse, where the condition’s importance is as a symptomnot a disease entity. Normal bowel habit is highly vari-able, and it is crucial to obtain a history of how bowelfunction has altered for the individual who is complain-ing of constipation. The most important differential di-agnosis is intestinal obstruction by tumor or adhesions.The distinction is important, as attempts to clear ’consti-pation’ which is actually obstruction by use of stimulantlaxatives can cause severe pain.It is better to prevent constipation rather than to treat itafter it has occurred. Potential prophylactic measures in-clude:
• Good general symptom control, without which noother measures are possible.
• Encouragement and facilitation of physical activity.• An adequate fluid intake.• Increased dietary fiber. However, fiber alone will not
correct severe constipation, and the priority remainsthat food should be as attractive as possible to the per-son who is expected to eat it.
• Awareness of which drugs are likely to cause con-stipation, e.g. vinca alkaloids and 5HT3 antagonistantiemetics, aswell asopioid analgesics. If avoidanceis impracticable, a laxative should be prescribed fromthe outset, without waiting until constipation is estab-lished.
• In institutions, ensure privacy for defecation.
Despite prophylaxis, most patients taking opioids willrequire a laxative. The basic division of laxatives is be-tween � stimulant s and � softener s (Fig. 2). This di-vision seems useful in clinical practice, although in factany drug that stimulates peristalsis will accelerate tran-sit, allow less time for water absorption and so producea softer stool. Similarly, softening the stool involves in-creasing its bulk, which will result in increased disten-sion of the intestinal wall, and a consequent stimulationof reflex enteric muscle contraction. Most trials of laxa-tive drugs have been carried out in gastroenterology or ingeriatrics. The results do not allow a clear recommenda-tionofoneagentoveranotherbecauseof thesmallsizeofthe studies, the number of different preparations, and thevarious endpoints and conditions involved. However:
• Systematic review evidence suggests that anykind of laxative can increase stool frequency byabout 1.4 bowel actions per week compared withplacebo (Pettigrew et al. 1997).
• A volunteer trial using loperamide as a source ofopioid-induced constipation, concluded that the op-timal combination of effectiveness with minimumadverse effects and medication burden was achievedby using a combination of stimulant and softeninglaxatives, rather than either alone (Sykes 1997).
• Laxative preparations vary significantly in price andphysical characteristics. Given the lack of major dif-ferences in efficacy, cost and individual patient ac-ceptability should both be strong influences in pre-scribing choice (NHS Center for Reviews and Dis-semination 2001).
Most patients prefer oral laxatives to rectal, so the use ofsuppositories and enemas should be minimized by opti-
Cancer Pain Management, Gastrointestinal Dysfunction as Opioid SideEffects, Figure 2 Cancer Pain Management, opioid side effects, gastroin-testinal dysfunction .

C
Cancer Pain Management, Interface between Cancer Pain Management and Palliative Care 243
mizing laxative treatmentby mouth.There is, however, aparticular role for enemas and suppositories in the reliefof fecal impaction and in bowel management in patientswhose neurological dysfunction is resulting in fecal in-continence. Evidence to guide their use is even scantierthan that for oral laxatives. Anything introduced into therectum can stimulate defecation via the anocolonic re-flex, but among rectal laxatives, only bisacodyl supposi-tories have a pharmacological stimulant action. Glycer-ine suppositories, and arachis or olive oil enemas, softenand lubricate the stool, as do proprietary mini-enemaswhich contain mixtures of surfactants.
References1. Critchley P, Plach N, Grantham M, Marshall D, Taniguchi A,
Latimer E (2001). Efficacy of Haloperidol in the Treatment ofNausea and Vomiting in the Palliative Patient: A Systematic Re-view. J Pain Symptom Manage 22:631–634
2. Daeninck PJ, Bruera E (1999) Reduction in Constipation andLaxative Requirements following Opioid Rotation to Methadone.J Pain Symptom Manage 18:303–309
3. Ling GS, Paul D, Simontov R, Pasternak GW (1989) DifferentialDevelopment of Acute Tolerance. Life Sciences 45:1627–1636
4. Loewen PS (2002) Anti-Emetics in Development. Expert Opin-ion on Investigational Drugs 11:801–805
5. NHS Center for Reviews and Dissemination (2001) Effectivenessof Laxatives in Adults. Effective Health Care 7:1–12
6. Petticrew M, Watt I, Sheldon T (1997) Systematic Review ofthe Effectiveness of Laxatives in the Elderly. Health TechnologyAssessment 1:1–52
7. Radbruch L, Sabatowski R, Loick G, Kulbe C, Kasper M, GrondS, Lehmann KA (2000) Constipation and the Use of Laxatives: AComparison between Transdermal Fentanyl and Oral Morphine.Palliative Medicine 14:111–119
8. Stewart JJ, Weisbrodt NW, Burko TF (1976) Intestinal ReversePeristalsis Associated with Morphine-Induced Vomiting. In:Kosterlitz HW (ed) Opiates and Endogenous Opioid Peptides.Elsevier, Amsterdam, pp 46–58
9. Sykes NP (1997) A Volunteer Model for the Comparison of Lax-atives in Opioid-Induced Constipation. J Pain Symptom Man-age 11:363–369
10. Sykes NP (1998) The Relationship between Opioid Use andLaxative Use in Terminally Ill Cancer Patients. PalliativeMedicine 12:375–382
11. Twycross RG, Lack SA. Control of Alimentary Symptoms in FarAdvanced Cancer. Churchill Livingstone, Edinburgh, pp 153
12. Walder AD, Aitkenhead AR (1995) A Comparison of Droperi-dol and Cyclizine in the Prevention of Postoperative Nausea andVomiting Associated with Patient-Controlled Analgesia. Anaes-thesia 50:654–656
Cancer Pain Management, Interfacebetween Cancer Pain Management andPalliative Care
PETER G. LAWLOR
Our Lady’s Hospice, Medical Department, Dublin,[email protected]
Synonyms
Hospice care; supportive care; Palliative Care and Can-cer Pain Management
Definition
The recently revised World Health Organization def-inition of palliative care reads: “Palliative care is anapproach that improves the � quality of life of patientsand their families facing the problems associated withlife-threatening illness, through the prevention andrelief of � suffering by means of early identificationand impeccable assessment and treatment of pain andother problems, physical, psychosocial and spiritual”(http://www.who.int/cancer/palliative/en/).
Characteristics
Cancer Pain and Palliative Care: A Global Perspective and In-troductory Outline
Cancer is one of those life-threatening illnesses re-ferred to in the WHO definition of palliative care.Approximately one-third of the population in devel-oped countries will be diagnosed with cancer. Theestimated worldwide number of new cases each yearis expected to rise from 10 million in the year 2000 to15 million in 2020. The number of annual worldwidecancer related deaths is expected to rise from 6 to 10 mil-lion over the same period (World Health Organizationand International Union against Cancer 2003). Muchof the projected increase in cancer mortality relatesto an increase in the elderly population, whose age isassociated with an increased risk of developing cancer,and who are likely to have multiple comorbidities andincreasing general care needs. Despite a survival rateof approximately 50% in developed countries for allcancers combined, about 70% of all cancer patientsare estimated to need palliative care. In developingcountries, this proportion rises to around 80% (WorldHealth Organization 2002). Hence, for the majorityof cancer patients, treatment with a curative outcomeproves to be either ultimately elusive or an unrealisticgoal from the time of diagnosis.Pain is present in 20–50% of cancer patients at diagno-sis and in at least 75% of those patients with advanceddisease, often in association with other distressingsymptoms such as fatigue and anorexia (Donnelly andWalsh 1995; World Health Organization 1997). A sur-vey of cancer patients suggested that pain was directlyrelated to the cancer in 85%, anti-cancer treatments suchas surgery, chemotherapy and radiotherapy in 17%, andother comorbidities in 9% (Grond et al. 1996).A consensus exists among pain management specialistsregarding the multidimensional nature of cancer pain,and scientific evidence supports the concept (WorldHealth Organization 1997; Lawlor 2003; Ahles etal. 1983; Portenoy and Lesage 1999). The ultimateexpression of pain intensity represents not only the per-ception of the basic physiological input from peripheralnociceptor activation but varying levels of multipleother inputs, which may relate to psychological state,cognitive status (the presence of delirium or dementia),

244 Cancer Pain Management, Interface between Cancer Pain Management and Palliative Care
the meaning of pain (for example, fears of disease pro-gression), cultural norms, and distress of an existentialand spiritual nature. The multidisciplinary palliativecare model with its broad holistic principles recognizesthese dimensions, and embodies a multidimensionalassessment approach as an integral part of cancer painmanagement (Lawlor 2003).To enable the reader to appreciate the special role ofpalliative care, and to assist in understanding interactiveroles in the interfaces of palliative care and cancer painmanagement, four broad aspects are described: firstly,the historical background of the palliative care modeland its interfaces; secondly, the fundamental practiceprinciples and service delivery levels of modern pallia-tive care; thirdly, issues in palliative care delivery in theinterface with other specialties and health care person-nel at the various locations and stages of cancer care;and fourthly, bridging strategies at the aforementionedinterfaces.
Palliative Care Interfaces: Historical Background
Palliative care originated from the hospice model of care(MacDonald 1993). Although the term “hospice” hasmedieval origins referring to a place of shelter or rest,its 19th century use referred mainly to a site of care, butin addition many of these sites also included “hospicefor the dying” as part of their name. Historically, “hos-pice” thereforehasastrong association with the terminalphase of illness, and the terms � hospice care and ter-minal care have been used interchangeably. Up to the20th century, most medical care interventions were notcurative but provided symptom relief, and as such wereessentially palliative. Medical advances in the first halfof the 20th century resulted in a shift to obtaining a cureand waging a “war” against cancer. The biomedical as-pects of care largely became the focus of care, often atthe cost of ignoring the total illness experience from thepatient and family perspective, an experience that in-variably generatessubstantialpsychosocialandspiritualneeds.Themoremodernhospicemovement, incorporat-ing the bulk of today’s palliative care principles, and typ-ified by St Christopher’s Hospice in London, was born inthe late 1960’s mainly to address these needs (MacDon-ald 1993). In the US, hospice care eligibility is restrictedby requirements for an estimated 6-monthprognosisandwillingness to forego life prolonging treatment. Gener-ally, palliative care is broader in its scope than eitherhospice or � supportive care, and is advocated earlierin the disease trajectory. � Palliative medicine now hasmedical specialty status in the UK, Australia, and Ire-land.
Practice Principles and Service Delivery Levels of Modern Pal-liative Care
The complex web of palliative care with its broad holis-tic purview is summarized through a schematic matrixin Fig. 1. For many patients with cancer pain, progres-
Cancer Pain Management, Interface between Cancer Pain Manage-ment and Palliative Care, Figure 1 Cancer pain and the multidisciplinarypalliative care approach (Adapted from reference 7).
sion of the disease process affects functioning in thephysical, psychological, spiritual, and social domains,thereby reducing overall quality of life (QOL). Exam-ples of problems in the QOL domains include: reducedmobility; loss of independence; depression; anger; fear;anxiety; guilt; anticipatory grieving; financial hardship;family stress and exhaustion. The palliative care ap-proach recognizes the distress generated in the mainQOL domains, and aims to support patients and fami-lies in coping with the burden of advancing disease, instriving to achieve optimal QOL, and in adjusting overtime to their inevitable demise. This recognition andintervention is especially important in the case of suf-fering (Cassell 1982) or � total pain (Kearney 1996),where the expression of pain is attributable only inpart to nociceptor activation, but perhaps in greaterproportion to psychosocial and spiritual distress.TheWHOdefinitionofpalliativecarestates that it is“ap-plicableearly in thecourseof illness, inconjunctionwithother therapies that are intended to prolong life, such aschemotherapy or radiation therapy, and includes thoseinvestigations needed to better understand and managedistressing clinical complications” (World Health Orga-nization 2002). This distinguishes the modern palliativecare approach as being active and not necessarily pas-sive. Nonetheless, the stigma of passivity often persists

C
Cancer Pain Management, Interface between Cancer Pain Management and Palliative Care 245
and probably reflects the more traditional origins of pal-liative care, especially hospice care.In developed countries, especially those where pallia-tive medicine is recognized as a specialty, palliative careservices are often tiered from level one to three on thebasis of the specialization level and expertise of the pro-fessionals delivering palliative care (National AdvisoryCommittee on Palliative Care 2001). Level one refersto the practice of the basic “palliative care approach”.This embodies a set of principles with which all healthcare professionals should be familiar and be capable ofadopting in their practice. Level two or generalist pallia-tive care refers to that delivered by professionals who arenot practicing full-time in palliative care, but who havesome additional training in palliative care. Level threerefers to � specialist palliative care. Patients with morecomplex and demanding care needs, for example thosepatients with neuropathic pain, substance abuse histo-ries, and features of “total pain” are referred to special-ist palliative care services (Bruera et al. 1995). Conse-quently, these services are more resource intensive, andare akin to secondary or tertiary healthcare services. Forthe healthcare professional, ease of access to specialistpalliative care advice as needed is essential. Healthcaredelivery models should ensure that patients have accessto the level of palliative care expertise most appropriateto their needs in a seamless and integrated fashion (Mac-Donald 1993; National Advisory Committee on Pallia-tive Care 2001).
Palliative Care and Cancer Pain Management: Clinical andOther Interface Issues
The interface between cancer pain management and pal-liativecare refers to theboundarieseither realornotionalbetween palliative care and the many locations of caredelivery, and the temporal changes in the degree of in-volvement of palliative care during thecourse of thecan-cer disease trajectory. The location or institutional in-terfaces are represented in an ideal, generic, developedworld model in Fig. 2, which shows each level of healthcare from primary to tertiary, and each with a direct linkto specialist palliative care services. In this model, someinternational or geographic differences may occur re-garding the level of interaction between and within var-ious levels, and also regarding the degree of provisionof specialist palliative care.The temporal interface of palliative care and diseasemodifying therapies, and their respective levels of usein the progressive disease trajectory (from diagnosis todeath) of a hypothetical cancer patient is represented inschematic form in Fig. 3. Disease modifying therapiessuch as surgery, chemotherapy, and radiation can beoffered depending on the relative burden/benefit associ-ated with the treatment. This is done with either curativeor palliative intent depending on the stage of disease.The curative intent phase for this patient is relativelybrief, is followed by a phase where there is modest use
Cancer Pain Management, Interface between Cancer Pain Manage-ment and Palliative Care, Figure 2 Interface of palliative care and spe-cific sites and levels of medical care during the cancer disease trajectory.
Cancer Pain Management, Interface between Cancer Pain Manage-ment and Palliative Care, Figure 3 Palliative care and its temporal in-volvement compared to other therapies in the cancer disease trajectory.
of palliative disease modifying interventions such asradiation therapy. This phase ends rather abruptly priorto a short terminal or hospice phase of care. The roleof palliative or supportive care progressively increasesin association with disease progression, and finally en-velopes the hospice contribution to the terminal phaseof care.

246 Cancer Pain Management, Interface between Cancer Pain Management and Palliative Care
Although the high level of need for palliative careis generally well recognized in advanced cancer, itsdelivery to patients and their families is often inade-quate. This shortfall may be associated with varioushealth service delivery factors of a political and/orfinancial nature, especially in the case of develop-ing countries, where palliative care services are oftenonly rudimentary or sometimes non-existent (WorldHealth Organization 2002). In developed countries,the shortfall in palliative care delivery may relate toprofessional factors such as lack of knowledge of painmanagement; multiple boundary issues such as thefear of losing or separating from the patient, or fearthat exposure to palliative care in itself will hastena patient’s demise, or concern that the patient couldfeel abandoned if palliative care are consulted; anda state of relative denial of disease progression. Thisdenial is often reflected by the relentless pursuit ofburdensome treatments, whose outcomes often have adeleterious effect on quality of life, and are perceivedas being unnecessarily aggressive by the palliative careprofessional. In addition, patient and caregiver denialmay result in varying degrees of reticence to acceptthe palliative care approach. Cultural norms may re-sult in a “conspiracy of silence” (denial reflected bynon discussion of disease status), or a “conspiracy ofwords” (denial reflected by limited discussion and useof euphemistic terms, for example, “spot” or “shadow”to evasively describe the presence of cancer). Thismust be sensitively recognized as a potential challengeto both the delivery and acceptance of palliative carein its most idealistic format (World Health Organiza-tion 1997).
Palliative Care and Cancer Pain Management: Interface Bridg-ing Strategies
A number of strategies can allow a functionally smoothand readily traversable interface between palliative careand other specialties in the management of cancer painand associated symptoms (MacDonald 1993).Firstly, the need for mutual appreciation of each othersroles is of pivotal importance, for example, the pallia-tive care physician needs to appreciate the potential pal-liative benefit associated with chemotherapy, radiationor surgery, and the oncologist or surgeon needs to ap-preciate the benefit of early palliative care involvementfor symptom control advice, support for adjustment todisease progression, and assistance with the planning ofcare, such as instituting palliative home care support ordiscussing hospice placement. Such a premise will oftenallow a shared care model, and thereby the shared goalof achieving optimal QOL for patients and their fami-lies rightly takes precedence over “patient ownership”or territorial concerns.Secondly, consistently good communication is essen-tial. The shared, systematic use of validated, low burdenassessment tools for pain and other symptoms through-
out all levels of health service delivery is of greatassistance in communication regarding cancer painmanagement (MacDonald 1993; Chang et al. 2000).Other ways to facilitate communication include personto person corridor conversations, joint rounds or jointclinics, and user friendly technology. For the purposeof maintaining continuity of care, both the mutual ap-preciation and enhanced communication paradigmsshould ensure that the patient’s general practitioner orfamily physician, and palliative home nurse are notdisenfranchised, especially in the case of patients whoare discharged to the community.Other valuable bridging strategies include mutuallyshared research agendas; mutually shared educationalrounds, ideally with some multidisciplinary input; inte-grated treatment sites; integrated administrative input,for example, shared participation in regional councilbodies that might advise on care delivery and its de-velopment; and shared use of resources. The benefitsfor the patient with cancer pain as a result of smoothnegotiation across the palliative care interfaces includeease of access to services, for example, fast-trackingof radiation oncology referrals; integration and conti-nuity of care, which diminishes the risk of a sense ofabandonment, a perception held by some patients whencurative therapy is no longer possible.
Summary and Conclusions
In conclusion, a multidimensional assessment of can-cer pain is paramount and constitutes an integral com-ponent of the palliative care approach. Optimal cancerpain management must recognize unique individual pa-tient and family care needs, whatever the location andwherever this may occur in the cancer disease trajectory.Although the need for specialist palliative care servicesvaries in relation to the temporal trajectory and locationof cancer care, the basic palliative care approach is afundamental requisite that essentially spans all stagesand sites of care. Although various political, cultural,geographical, administrative and financial factors willclearly influence the degree of development and supportof the palliative care model in different areas, healthcareplanning must aim to achieve a seamless integration ofthe different aspects of palliative care service deliveryand other areas of cancer care, and to offer flexibility forpatients to access the different levels of care (each levelwith a link to specialist palliative care services) as de-termined by their individual and specific needs.
References1. Ahles TA, Blanchard EB, Ruckdeschel JC (1983) The Multidi-
mensional Nature of Cancer-Related Pain. Pain 17:277–2882. Bruera E, Schoeller T, Wenk R et al. (1995) A Prospective Multi-
center Assessment of the Edmonton Staging System for CancerPain. J Pain Symptom Manage10:348–355
3. Cassell EJ (1982) The Nature of Suffering and the Goals ofMedicine. N Engl J Med 306:639–645

C
Cancer Pain Management, Neurosurgical Interventions 247
4. Chang VT, Hwang SS, Feuerman M (2000) Validation of theEdmonton Symptom Assessment Scale. Cancer 88:2164–2171
5. Donnelly S, Walsh D (1995) The Symptoms of Advanced Cancer.Semin Oncol 22:67–72
6. Grond S, Zech D, Diefenbach C et al. (1996) Assessment ofCancer Pain: A Prospective Evaluation in 2266 Cancer PatientsReferred to a Pain Service. Pain 64:107–114
7. http://www.who.int/cancer/palliative/en/ Accessed November
4th 20038. Kearney M (1996) Mortally Wounded. Stories of Soul Pain,
Death, and Healing. Scribner, New York9. Lawlor PG (2003) Multidimensional Assessment: Pain and Pal-
liative Care. In: Bruera E, Portenoy RK (eds) Cancer Pain. Cam-bridge University Press, New York, pp 67–88
10. MacDonald N (1993) The Interface between Oncology and Pal-liative Medicine In: Doyle D, Hanks GWC, MacDonald N (eds)Oxford Textbook of Palliative Medicine. Oxford UniversityPress, Oxford, pp 11–17
11. National Advisory Committee on Palliative Care (2001) Pallia-tive Care – An Overview. In: Report of the National AdvisoryCommittee on Palliative Care. Department of Health and Chil-dren, Dublin
12. Portenoy RK, Lesage P (1999) Management of Cancer Pain.Lancet 353:1695–1700
13. World Health Organization and International Union againstCancer (2003) Global Action against Cancer. WHO and UICC,Geneva, pp 1–24
14. World Health Organization (1997) Looking Forward to CancerPain Relief for All. International Consensus on the Managementof Cancer Pain. WHO, Oxford, pp 1–70
15. World Health Organization (2002) Pain Relief and PalliativeCare. WHO, Geneva, pp 83–91
Cancer Pain Management, NeurosurgicalInterventions
RICHARD B. NORTH1, SAMUEL J. HASSENBUSCH2
1The Johns Hopkins University, Baltimore, ML, USA2The University of Texas M. D. Anderson CancerCenter, Houston, TX, [email protected], [email protected]
Definition
Cancer pain arises from the presence, progression, ortreatment of cancer or from an unidentifiable source inpatients with cancer. Cancer pain may be nociceptive,neuropathic, or a mixture of both.A neurosurgical intervention uses an ablative, augmen-tative, or anatomic surgical technique, or a combinationof these techniques, to relieve pain.
Characteristics
Inhumans,cancerassumesmanyguises,canaffecteveryphysiologic system and tissue, and strikes with variousdegreesofvirulence.Cancerand its treatmentcausepainin most patients, with the severity and impact of this paindictated by a host of influences (Patt 2002).Medical management, which is often sufficient to treatcancerpain, sometimesfails toprovideadequaterelieforresults in side effects that substantially reduce the qual-ity of the patient’s life (nausea, constipation, vomiting,
incontinence, mood changes, sedation, diarrhea, confu-sion, etc.) (McNicol et al. 2003). It might seem reason-able to wait until medical management fails before pur-suing neurosurgical intervention, but in certain cases,for example when a patient foreseeably will need an im-planted device, neurosurgeons should intervene beforethe patient’s condition deteriorates too far to support theintervention.When neurosurgical techniques result in pain relief, theycan enhanceapatient’squality of lifeby increasing func-tional capacity and offering freedom from troublesomeside effects. Compared with medical management, neu-rosurgical techniques can improve continuity of relief,reduce the patient’s and physician’s time spent adjustingdosages, and minimize the development of tolerance oradverse effects from opioids. It is possible that, in somepatients, neurosurgical intervention for pain relief willprolong survival (Smith et al. 2002).
Patient Selection
Patient selection for neurosurgical intervention is basedon a consideration of the nature of the disease, the im-pact of the disease on the patient’s life, and the natureof the pain. One major factor in assessing disease im-pact and therapeutic options is the patient’s prognosis,which involves quantitative and qualitative factors, suchas age, life expectancy, type of cancer, the interven-tion’s cost effectiveness, risk/benefit ratio, duration ofeffect and the patient’s functional capacity, personalvalues/wishes, and living/family conditions. A multi-modal assessment will reveal if a patient has a good(expected to survival at least a year and to be activefor most of that time) or a poor prognosis (expected tosurvive less than six months and to be inactive). Paintype and severity are also important indicators of theappropriate intervention. Relative contraindications forinterventional pain therapy include the presence of anuntreated comorbid psychological disorder or currentdrug abuse (North 2002; Levy 2002).
Treatment Options
Interventional treatment options range from simpleinjections of short-acting local anesthetics (and, oc-casionally, of an adjuvant steroid or lytic agent) tocomplex anatomic, ablative, and augmentative neuro-surgical techniquesAnatomic procedures address structural problems caus-ing pain – for example, tumor removal or debulking.Spinal reconstructive surgery (decompression, stabi-lization) for metastatic disease is a common example. Tothe extent that this addresses the cause of pain directly,it has obvious appeal; but the cause of pain may not becompletely clear, and there may be alternatives (such asradiation therapy alone). Patients with advanced diseaseand limited life expectancy may not be candidates forreconstructive surgery.

248 Cancer Pain Management, Nonopioid Analgesics
Ablativeproceduresdestroyportionsof theperipheralorcentral nervous system to block pain transmission. Thismay be achieved through chemical (the direct applica-tion of alcohol or phenol), thermal (� cryoablation orradiofrequency, see � radiofrequency ablation), surgi-cal (cutting) or radiosurgical means.Peripheral ablative procedures are applicable to paingenerators in the distribution of specific peripheralnerves, if they may be sacrificed without incurringan unacceptable deficit. For example, a peripheral� neurectomy might relieve the pain in the distri-bution of the supra- or infraorbital nerve. Percuta-neous radiofrequency or open � dorsal rhizotomy hasa role in cases where a tumor involves the chest wall.� Sympathetic ganglionectomy involving several adja-cent levels will denervate somatic and/or visceral tissuein the trunk or abdomen or in a limb. All of these maybe emulated by reversible local anesthetic injections,to predict the results of a permanent procedure andthereby aid in patient selection.Intraspinal ablative techniques interrupt input or rostraltransmission of nociceptive signals in patients withsevere pain and a poor prognosis. These techniquesinclude open or percutaneous � anterolateral cordo-tomy for intermittent and/or evoked neuropathic painaffecting one, or sometimes, two limbs (Tasker 1995),and � midline commissural myelotomy for diffuselower body pain. Cordotomy is associated with sig-nificant risks, especially with bilateral application formidline or axial pain. Cordotomy is often ruled outwhen pain is above C5 or the patient suffers frompulmonary dysfunction. Myelotomy addresses bilat-eral and midline pain in a single procedure and isbest reserved for cancer patients with bladder, bowel,and sexual dysfunction. Most patients achieve nearlycomplete pain relief after cordotomy and myelo-tomy, but some experience recurrent pain monthslater.Intracranial ablative therapies interrupt or change theperception of pain transmission. � Stereotactic cingu-lotomy is appropriate for severe pain in diffuse areasof the body and provides at least three months relieffor most cancer patients (Hassenbusch 1996). Theless-frequently used � stereotactic medial thalamo-tomy relieves pain for as many as 50%of patients witha good or poor prognosis and severe, otherwise in-tractable, nociceptive pain that is widespread, midline,bilateral, or located in the head or neck; it also mayhelp approximately 30% with neuropathic pain (inter-mittent and evoked neuropathic pain responds morereadily than continuous pain). � Hypophysectomy isan appropriate treatment for diffuse pain associatedwith widespread cancer, and provides relief through anunknown mechanism of action in 45–95%of patients.These procedures may be performed not only by stereo-tactic probe placement but also by radiosurgery (see� stereotactic radiosurgery).
Augmentative procedures modulate activity in the intactnervous system by electrical stimulation or continuousdrug infusion to change pain perception. They have theadvantagesof reversibility, titration ofdose, andofa trialor test phase which emulates the definitiveprocedure ex-actly. This is not the case for anatomic or ablative pro-cedures. Due to the high initial expense, physicians re-serve implanted devices for patients expected to surviveat least three months.The usual indication for somatosensory stimulationis neuropathic pain restricted to a specific area, andthis stimulation can target the spinal cord, a peripheralnerve, or the thalamus (to treat continuous neuropathicpain, such as � post-radiation plexopathy). The goal ofsuch electrical stimulation is to induce a � paresthesiathat covers the painful area, effectively replacing thepain with a tolerable, non-noxious sensation. Noci-ceptive pain may also be treated by periaqueductal orperiventricular grey stimulation.The best-established indication for continuous drug in-fusion, in particular morphine, is diffuse midline or bi-lateralnociceptivecancerpain.The infusioncatheter en-ters the epidural, intrathecal, or intraventricular space,and the drug delivery system includes an implanted oran external pump (Staats and Luthardt 2004).
References1. Hassenbusch SI (1996) Intracranial Ablative Procedures for Pain.
In: Youmans JR (ed) Neurological Surgery, 4th edn. WB Saun-ders, Philadelphia, pp 3541–3551
2. Levy RM (2002) Intrathecal Opioids: Patient Selection. In:Burchiel K (ed) Surgical Management of Pain. Thieme, NewYork, pp 469–484
3. McNicol E, Horowicz-Mehler N, Fisk RA et al. American PainSociety (2003) Management of Opioid Side Effects in Cancer-Related and Chronic Noncancer Pain: A Systematic Review. JPain 4:231–256
4. North RB (2002) Spinal Cord Stimulation: Patient Selection. In:Burchiel K (ed) Surgical Management of Pain. Thieme, NewYork, pp 469–484
5. Patt RB (2002) Cancer Pain. In: Burchiel K (ed) Surgical Man-agement of Pain. Thieme, New York, pp 469–484
6. Smith TJ, Staats PS, Pool G et al. (2002) Randomized Clini-cal Trial of an Implantable Drug Delivery System Comparedto Comprehensive Medical Management for Refractory CancerPain: Impact on Pain, Drug-Related Toxicity, and Survival. J ClinOncol 20:4040–4049
7. Staats PS, Luthardt F (2004) Intrathecal Therapy for Cancer Pain.Just the Facts Pain Medicine. McGraw Hill, New York
8. Tasker RR (1995) Percutaneous Cordotomy. In: SchmidekHH, Sweet WH (eds) Operative Neurosurgical Techniques:Indications, Methods and Results. WB Saunders, Philadelphia,pp 1595–1611
Cancer Pain Management, NonopioidAnalgesics
ALISON MURRAY, JOSE PEREIRA
Foothills Medical Center, Calgary, AB, [email protected], [email protected]

C
Cancer Pain Management, Nonopioid Analgesics 249
Definition
Nonopioid analgesics comprise of all those medicationsprescribed for pain relief that do not fall into the opioidclass. These include paracetamol (acetaminophen),aspirin (acetylsalicylic acid), and the nonsteroidalanti-inflammatory drugs (NSAIDS). Paracetamol isan analgesic-antipyretic with weak anti-inflammatoryactivity. Aspirin is a derivative of salicylic acid and hasanalgesic, antipyretic and anti-inflammatory activity.Nonsteroidal anti-inflammatory drugs are a hetero-geneous group of compounds. They share the sametherapeutic action and side-effect profile as aspirin.Nonopioid analgesics are recommended for use in thecase of mild cancer pain, as described in Step I ofthe World Health Organization Analgesic Ladder forthe treatment of cancer pain (World Health Organiza-tion 1986). Nonopioids were used on 11% of treatmentdays in a large prospective study involving 2118 cancerpatients, while the so-called “weak opioids” (WHOStep II) were used on 31% of days and the so-called“strong” opioids (Step III) on 49% of treatment days(Zech et al. 1995). In another study, 52% of cancerpatients started on a nonopioid analgesic needed to beswitched to a weak or strong opioid because of escalat-ing pain (Ventafridda et al. 1987). Nonopioid analgesicsare also used as adjuvant medications to opioids for themanagement of moderate to severe pain (Step II and IIIof the � WHO Analgesic Ladder).
Characteristics
Paracetamol (Acetaminophen)
Mode of Action
Paracetamol has analgesic and antipyretic effects butonly weak anti-inflammatory effects. Its mechanismof action is unknown, although it is thought to actcentrally rather than peripherally (Flower et al. 1980).Paracetamol may be given orally or rectally.
Pharmacokinetics
It is metabolized by the liver.
Efficacy
Paracetamol is considered to be a weak analgesic with-out anti-inflammatory effects. There is little evidencesupporting the use of paracetamol alone in cancer pain,although there are some studies which support its usewhen combined with an opioid (codeine or oxycodone)(Carlson et al. 1990). Paracetamol 600 mg plus codeine60 mg has been found to be equivalent to ketorolac10 mg, and superior to placebo in reducing cancer painin a double-blind randomized controlled study.
Adverse Effects
Side effects include rash, urticaria and nausea. Parac-etamol may induce hepatotoxicity after acute ingestionof large doses (> 10 g) or chronic ingestion of dailydoses exceeding 4 g. Other serious but rare side effects
include: nephrotoxicity, blood dyscrasias, pancreatitisand angioedema. Caution should be used in patientswith impaired liver function/chronic alcohol use, orimpaired renal function (Flower et al. 1980). Most clin-icians will consider paracetamol safe to use in patientswith liver metastases on the condition that overt hepaticfailure is not present. There are no studies to support orrefute this practice.
Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
Mode of Action
NSAIDs inhibit peripheral prostaglandin synthesisthrough the inhibition of cyclo-oxygenase enzymes,COX-1 (found in normal cells) and COX-2 (inducedduring the inflammatory process). Inhibition of COX-2produces anti-inflammatory effects: decreased releaseof inflammatory mediators (such as substance P andcytokines), which leads to decreased stimulation ofperipheral � nociceptors (Jenkins and Bruera 1999).COX-1 inhibition can lead to many of the known sideeffects of NSAIDs, in particular gastrointestinal ul-ceration and inhibition of platelet aggregation. It hasalso been suggested that NSAIDs may have a centraleffect on pain perception by reducing NMDA-mediatedhyperalgesia (Jenkins and Bruera 1999).The older generation of NSAIDs (including aspirin) hasvariable effects on both COX-1 and COX-2. A new gen-eration of NSAIDs (etodolac, meloxicam, nabumetone,celecoxib, valdecoxib, and rofecoxib) show COX-2 se-lective inhibition (Jenkins and Bruera 1999), and thosecreated most recently (the coxibs celecoxib, valdecoxib,rofecoxib, and others in development)arehighly COX-2selective.
Pharmacokinetics
NSAIDS are given by the oral or the rectal route, withthe exception of ketorolac, which is also available ina parenteral preparation. NSAIDs are metabolized bythe liver and excreted in the urine and faeces (Floweret al. 1980).
Efficacy
In multiple dose trials, NSAIDs have been found to be aseffective as weak opioids or weak opioid/paracetamolpreparations (Goudasetal. 2001).No individualNSAIDor class of NSAID has been shown to be more effec-tive in the control of pain (Goudas et al. 2001; Mer-cadante 2001). NSAIDs appear to have a dose-responserelationship with respect to analgesic efficacy (Eisen-berg et al. 1994), and they also demonstrate a ceilingeffect (supramaximal doses do not demonstrate superi-ority over recommended doses) (Eisenberg et al. 1994).The efficacy of NSAIDs does not vary with the route ofadministration (Tramer et al 1998). It has been commonpractice to prescribe NSAIDs for certain cancer painsyndromes (in particular, metastatic bone pain), but the

250 Cancer Pain Management, Nonopioid Analgesics
evidence to support this is largely lacking (Goudas etal. 2001; Mercadante 2001; Eisenberg et al. 1994).There are no current trials available involving the useof COX-2 selective inhibitors in cancer pain. Data fromthe non-malignant pain literature (largely osteoarthritisand rheumatoid arthritis populations) demonstrate thatcoxibs are as effective as nonselective NSAIDs in termsof pain relief (Kuritzky and Weaver 2003).When NSAIDs are coadministered with opioids as� adjuvant analgesics, they produce an opioid sparingeffect, but there is no consistent reduction in side ef-fects (Jenkins and Bruera 1999; Goudas et al. 2001;Mercadante 2001). It is difficult to evaluate the opioidsparing effects of NSAIDs, given that they have anequally significant side effect profile of their own.
Side Effects
TheincidenceofsideeffectswithNSAIDsdemonstratesa dose-response relationship and rises significantly aftermultiple dosing over 7–10 days (Eisenberg et al. 1994).One of the major side effects of nonselective NSAIDsis gastrointestinal ulceration (resulting in clinically sig-nificant gastrointestinal bleeding) (Mercadante 2001).The majority of studies have been performed in noncancer populations. NSAID users have three timesthe risk of gastrointestinal ulceration compared tonon-users (Jenkins and Bruera 1999). Advanced age,history of peptic ulcer disease, and concurrent cor-ticosteroid or anticoagulant therapy are known riskfactors for NSAID-induced gastrointestinal bleedingand perforation (Hernandez-Diaz and Rodriguez 2000).Omeprazolehasbeen shown to decrease the incidenceofNSAID induced gastrointestinal ulceration. Eradicationof helicobacter pylori prior to NSAID administrationmay reduce the risk in the general population (Jenkinsand Bruera 1999). In uncontrolled studies of cancerpopulations, dyspepsia has been reported by 7–13%of users, and 5–20% of users discontinued NSAIDsdue to an adverse event (Goudas et al. 2001). In cancerpatients, advanced disease and the presence of liverdisease (primary cancer or metastases) have been as-sociated with a higher rate of gastrointestinal bleedingevents (Mercadante et al. 2000).Asecond sideeffect is impaired renal function.Acutere-nal dysfunction is usually reversible and improves afterdiscontinuation of the NSAID. It is caused by a decreaseinprostaglandindependent renalplasmaflow.Olderage,hypertension, concomitant use of diuretics, pre-existingrenal failure, diabetes and dehydration are risk factorsfor acute NSAID-induced renal failure (De Broe and El-seviers 1998). Chronic and permanent renal failure sec-ondary to NSAIDs is much rarer, and is probably due toacute tubular necrosis (Mercadante 2001).Other known side effects of NSAIDs include platelet in-hibition,blooddyscrasias,hepaticdamageandCNStox-icity (tinnitus, visual disturbances, dizziness etc.) (Mer-cadante 2001).
There are no trials comparing the side effects of COX-2 inhibitors compared to nonselective NSAIDs in can-cer populations (Goudas et al. 2001). The use of COX-2 inhibitors is associated with fewer endoscopic ulcersand fewer gastrointestinal events compared to nonselec-tive NSAIDs in the general population (Laine 2003), butthey have a similar rate of nephrotoxic events. Coxibsdo not inhibit platelet function as nonselective NSAIDsdo. There is controversy about whether coxibs are as-sociated with an increased risk of cardiovascular events(DeMaria and Weir 2003).
Dipyrone
Dipyrone has anti-inflammatory, anti-pyretic and anal-gesic effects. Its mechanism of action is unknown. It isused in Europe, but it is not available in North Amer-ica due to concerns about agranulocytosis (Flower etal. 1980).
References1. Carlson RW, Borrison RA, Sher HB et al. (1990) A Multi-
Institutional Evaluation of the Analgesic Efficacy and Safetyof Ketorolac Tromethamine, Acetaminophen plus Codeine, andPlacebo in Cancer Pain. Pharmacotherapy 10:211–216
2. De Broe ME, Elseviers MM (1998) Analgesic Nephropathy. NEngl J Med 338:446–452
3. DeMaria AN, Weir MR (2003) Coxibs – Beyond the GI tract: Re-nalandCardiovascular Issues. JPain Symptom Manage 25:41–49
4. Eisenberg E, Berkey CS, Carr D et al. (1994) Efficacy and Safetyof Nonsteroidal Anti-Inflammatory Drugs for Cancer Pain: AMeta-Analysis. J Clin Oncol 12:2756–2765
5. Flower RJ MS, Vane JR, Moncada S (1980) Analgesic-Antipyretics and Anti-Inflammatory Agents; Drugs Employedin the Treatment of Gout. In: Goodman and Gilman’s ThePharmacological Basis of Therapeutics, 6th edn. MacMillanpublishing Company Inc., New York
6. Goudas L, Carr DB, Bloch R et al. (2001) Management of CancerPain. Evid Rep Technol Assess 35:1–5
7. Hernandez-Diaz S, Rodriguez LA (2000) Association betweenNonsteroidal Anti-Inflammatory Drugs and Upper Gastrointesti-nal Tract Bleeding/Perforation: An Overview of EpidemiologicStudies Published in the 1990’s. Arch Intern Med 160:2093–2099
8. Jenkins CA, Bruera E (1999) Nonsteroidal Anti-InflammatoryDrugs as Adjuvant Analgesics in Cancer Patients. Palliat Med13:183–196
9. Kuritzky L, Weaver A (2003) Advances in Rheumatology: Cox-ibs and Beyond. J Pain Symptom Manage 25:6–20
10. Laine L (2003) Gastrointestinal Effects of NSAIDs and Coxibs.J Pain Symptom Manage 25:32–40
11. Mercadante S (2001) The Use of Anti-Inflammatory Drugs inCancer Pain. Cancer Treat Rev 27:51–61
12. MercadanteS, BarresiL, CassucioA et al. (2000)GastrointestinalBleeding in Advanced Cancer Patients. J Pain Symptom Manage19:160–162
13. Tramer MR, Williams JE, Carroll D et al. (1998) ComparingAnalgesic Efficacy of Non-Steroidal Anti-Inflammatory DrugsGiven by Different Routes in Acute and Chronic Pain: A Qual-itative Systematic Review. Acta Anaesthesiol Scand 42:71–79
14. Ventafridda V, Tamburini M, Caraceni A et al. (1987) A Valida-tion Study of the WHO Method for Cancer Pain Relief. Cancer59:850–856
15. World Health Organization (1986) Cancer Pain Relief. WorldHealth Organization, Geneva
16. Zech DF, Grond S, Lynch J et al. (1995). Validation of WorldHealth Organization Guidelines for Cancer Pain Relief: A 10-Year Prospective Trial. Pain 63:65–76

C
Cancer Pain Management, Opioid Side Effects, Cognitive Dysfunction 251
Cancer Pain Management, OpioidResponsiveness
� Opioid Responsiveness in Cancer Pain Management
Cancer Pain Management, Opioid SideEffects, Cognitive Dysfunction
S. YENNURAJALINGAM, EDUARDO BRUERA
Department of Palliative Care and RehabilitationMedicine, The University of Texas M. D. AndersonCancer Center, Houston, TX, [email protected]
Definition� Cognitive dysfunction refers to changes in conscious-ness, higher cortical functions, mood, or perception thatmay be induced by any of numerous neurological or sys-temic diseases, or by ingestion of substances, includingdrugs, that have the potential for central nervous systemtoxicity.
Characteristics
Painincancerpatientsisnotyettreatedeffectively.Manystudies have described undertreatment in this popula-tion. For example, a 1995 study of outpatients who hadmetastatic cancer found that pain occurred in 67% of thepatients, yet 42% had not been prescribed adequateanal-gesic therapy (Cleeland et al. 1994). Similarly, a 2000study found that 65% of minority patients with cancerreported severe pain despite having received analgesics(Anderson et al. 2000).Pain is multidimensional and can be described in termsof location, radiation, character, intensity, frequency,and syndromal presentation. Pain can also be describedin terms of its relationship to other symptoms. Preva-lence rates of the many symptoms reported by palliativecare patients vary: pain 41–76%, depression 33–40%,anxiety 57–68%, nausea 24–68%,constipation 65%, se-dation/confusion 46–60%, dyspnea 12–58%, anorexia85% and asthenia 90% (Cleeland et al. 1994; Andersonet al. 2000; Bruera 1998; Chang et al. 2000; Hopwoodand Stephens 2000).Due to the multidimensional nature of pain, health careprofessionals assessing a patient’s level of pain shouldkeep in mind the “production-perception-expression”-model of symptoms (Bruera 1998). This cascade modeladdresses the different levels of symptom developmentresulting inan individual ratingof thepatient’ssuffering.This model applies well to the symptoms of sedation,mental clouding, confusion or related phenomena.These cognitive disturbances characterize diverse typesof encephalopathy, including delirium and dementia
(Pereira et al. 1997; Manfredi et al. 2003; Farrell etal. 1996). Cognitive impairment may result from anyof numerous disorders, including drug toxicity. Opioidtherapy may cause cognitive disturbances that under-mine the positive effects of the drug, or render assess-ment of the pain more difficult. Since a patient’s expres-sion of distress requires cognition, a self-report by thepatient should not be requested if the degree of cognitiveimpairment is sufficient to compromisecommunication.
Management of Cancer Pain
Opioid-based pharmacotherapy is the mainstay in� cancer pain management and should be consid-ered for all cancer patients with moderate or severepain. Other approaches can be used in addition to theopioid-based pharmacotherapy, based on the goals ofcare. Pure opioid agonists used as a single agent arepreferred for treating pain in cancer patients. Partialagonists and mixed agonists-antagonists have limiteduse in the management of cancer pain due to mixedreceptor activity, side effects, and dose-related ceilingeffects. Once an opioid and route of delivery is selected,effective therapy depends on adjustment of the dose.There is no maximum recommended dose of opioids incancer pain management. The dose should be graduallyescalated until effects are favorable or side effects im-pose a maximum tolerated dose. Management of opioidside effects is an essential aspect of opioid therapy,which can allow opioid dose titration to effective levelsand directly improve the comfort of the patient.
Opioid-Induced Cognitive Dysfunction
Sedation
Opioid-induced sedation usually occurs when opioiddosing is initiated or when the dose is increased. Ap-proximately 7–10% of patients receiving strong opioidsfor cancer pain have persistent sedation related to opi-oid medication (Bruera et al. 1995). In some cases, thissedation is multifactorial; the opioid may contribute butmay not be the primary cause. Some patients, however,appear to have a very narrow or non-existing therapeu-tic window, and the persistent sedation can be ascribeddirectly to the drug.Persistent opioid-induced sedation can sometimes bemanaged by adding an opioid-sparing analgesic, ei-ther an NSAID or an adjuvant analgesic, such as acorticosteroid. Alternatively, psychostimulants, suchas dextroamphetamine, methyphenidate or modafinilmay help to counteract the effect. Patients who are notcandidates for psychostimulant therapy may be triedon an anticholinesterase inhibitor, such as donepezil(Slatkin et al. 2001). In patients with persistent sedation,a change of opioid may also be helpful.
Opioid-Induced Neurotoxicity
Opioid-induced neurotoxicity may take the form of asyndrome that may include, in addition to severe seda-

252 Cancer Pain Management, Opioid Side Effects, Endocrine Changes and Sexual Dysfunction
tion, cognitive impairment, hallucinosis, delirium, my-oclonus, and even seizures. Generalized � hyperalgesiaand � allodynia may also occur. This syndrome, whichmay occur in milder and partial forms, appears to bedose-related and also potentially associated with preex-isting cognitive impairment or delirium, or metabolicdisturbances such as dehydration or renal failure. Whenthese changes occur in morphine-treated patients,accumulation of morphine metabolites, specificallymorphine-3-glucuronide (M3G), may be causative.The management of severe neurotoxicity related to opi-oids incorporates the same strategies considered whenthe side effects are less severe. This begins with a de-tailed assessment to identify treatable causes.Therapeutic approaches include hydration, opioidswitching (� opioid rotation), opioid dose reduction,and discontinuation of contributing drugs like hyp-notics. Symptomatic treatment with haloperidol oranother neuroleptic may be needed.
References1. American Psychiatric Association (1994) Delirium, Dementia,
and Amnestic and Other Cognitive Disorders. In: American Psy-chiatric Association, Diagnostic and Statistical Manual of MentalDisorders, 4th edn. (DSM-IV) American Psychiatric Association,Washington DC, pp 123–133
2. Anderson KO, Mendoza TR, Valero V et al. (2000) MinorityCancer Patients and their Providers: Pain Management Attitudesand Practice. Cancer 88:1929–1938
3. Bruera E (1998) Research into Symptoms other than Pain. In:Doyle D, Hanks GW, MacDonald N (eds) Oxford Textbook ofPalliative Medicine, 2nd edn. Oxford University Press, New York:pp 179–185
4. Bruera E, Watanabe S, Faisinger RL et al. (1995) Custom-MadeCapsules and Suppositories of Methadone for Patients on HighDose Opioids for Cancer Pain. Pain 62:141–146
5. Chang VT, Hwang SS, Feuerman M (2000) Validation of theEdmonton Symptom Assessment Scale. Cancer 88:2164–2171
6. Cleeland CS, Gonin R, Hatfield AK et al. (1994) Pain and itsTreatment in Outpatients with Metastatic Cancer. N Engl J Med330:592–596
7. Farrell KR, Ganzini L (1995) Misdiagnosing Delirium as De-pression in Medically Ill Elderly Patients. Arch Intern Med155:2459–2464
8. Farrell MJ, Katz B, Helme RD (1996) The Impact of Dementiaon the Pain Experience. Pain 67:7–15
9. HopwoodP, StephensRJ (2000)Depression in Patientswith LungCancer: Prevalence and Risk Factors Derived from Quality-of-Life Data. J Clin Oncol 18:893–903
10. Lawlor PG, Bruera ED (2002) Delirium in Patients with Ad-vanced Cancer. Hematol Oncol Clin N Am 16:701–714
11. Manfredi PL, Breuer B, Meier DE et al. (2003) Pain Assessmentin Elderly Patients with Severe Dementia. J Pain Symptom Man-age 25:48–52
12. Mercadante S, Casuccio A, Fulfaro F et al. (2001) Switchingfrom Morphine to Methadone to Improve Analgesia and Toler-ability in Cancer Patients: A Prospective Study. J Clin Oncol19:2898–2904
13. Pereira J, Hanson J, Bruera E (1997) The Frequency and Clin-ical Course of Cognitive Impairment in Patients with TerminalCancer. Cancer 79:835–842
14. Ripamonti C, Bruera E (1991) Rectal, Buccal, and SublingualNarcotics for the Management of Cancer Pain. J Palliat Care7:30–35
15. Slatkin NE, Rhiner M, Maluso Bolton T (2001) Donepezil in theTreatment of Opioid-Induced Sedation: Report of Six Cases. JPain Symptom Manage 21:425–438
Cancer Pain Management, Opioid SideEffects, Endocrine Changes and SexualDysfunction
JUDITH A. PAICE
Division of Hematology-Oncology, NorthwesternUniversity; Feinberg School of Medicine, Chicago, IL,[email protected]
Definition
Endocrine changes associated with opioid use in-clude altered concentrations of sex hormones (e.g.� testosterone, � prolactin). These changes alter ovu-lation and menstruation patterns in women and causehypogonadism in men. The resultant sexual dysfunctionencompasses reduction in � libido (see also � sexualresponse) in both men and women, limited engorgementand subsequent excitation and orgasm in women, andinability to obtain and maintain erection and ejaculationin males.
Characteristics
Opioids alter libido and sexual performance in ani-mal models, individuals with addictive disease usingheroin, and persons in methadone maintenance pro-grams (Cicero et al. 1975; Wiesenfeld-Hallin andSdersten 1984). Opioids have also been shown to pro-duce � galactorrhea, inhibit ovulation, and trigger� amenorrhea in animal models and in women attend-ing methadone clinics (Johnson and Rosecrans 1980;Packman and Rothchild 1976; Pelosi et al. 1974). Littleattention has been given to these effects in personsprescribed opioids for the treatment of chronic pain.However, recent case reports document these reactions(i.e. diminished libido, sexual dysfunction, and amen-orrhea) in persons being treated with spinal or systemicopioids for chronic pain (Abs et al. 2000; Daniell 2002;Finch et al. 2000; Paice et al. 1994).Evidence that the sexual dysfunction is due to opi-oids, rather than psychological mechanisms commonin chronic pain, is provided by the reversibility of thisphenomenon when the antagonist naloxone is adminis-tered or when the opioid is discontinued (Packman andRothchild 1976). The underlying endocrine changesleading to sexual dysfunction appear to be multifacto-rial. Opioids significantly suppress plasma testosteronelevels in persons using heroin, methadone, or otheropioids (Finch et al. 2000; Paice et al. 1994; Mendel-son et al. 1975). These suppressed testosterone levels

C
Cancer Pain Management, Opioid Side Effects, Uncommon Side Effects 253
return to normal after stopping opioid therapy (Finchet al. 2000). Although pain may contribute to alteredtestosterone levels, Abs and colleagues compared theselevels with case-matched chronic pain patients not re-ceiving opioids and found that individuals treated withintraspinal opioids have lower testosterone levels (Abset al. 2000). These data provide additional support foropioids being the causative agent in sexual dysfunction,rather than chronic pain alone leading to changes intestosterone and performance.Reduced testosterone levels are likely to be a result ofincreased prolactin levels. Prolactin levels are increasedin heroin use (Ellingboe et al. 1980), in normal subjectsgiven intravenous injections of morphine (Delitala etal. 1983; Zis et al. 1984), and in cancer patients givenintraventricular injections of morphine (Su et al. 1987).Normally, the hypothalamus releases dopamine totonically suppress prolactin release from the anteriorpituitary. Opioids disinhibit this suppression, leadingto elevations in prolactin. Prolactin reduces levels ofluteinizing hormone (LH) and follicle stimulating hor-mone (FSH), which subsequently depress testosterone.In females, prolactin stimulates lactation, and reducesLH and FSH levels, leading to depressed libido andcessation of menses.Clinical experience suggests that testosterone replace-ment, either by injection, gel, or patch, may improvesexual function in persons treated with opioids whohave depressed serum testosterone (Abs et al. 2000). Inwomen with postmenopausal changes in libido, an oralcombination of estrogen and testosterone (Estratest) isbeing used “off label” to relieve sexual dysfunction, asis methyltestosterone gel applied to the vulva (Flemingand Paice 2001). Neither of these therapies has beensystematically evaluated in the relief of opioid-inducedsexual dysfunction.When decreased testosterone is also associated withincreased prolactin levels, testosterone replacementalone may not be sufficient to restore sexual function,as elevated prolactin levels prevent the body fromresponding normally to testosterone. Treatment forhyperprolactinemiawith bromocriptine (Parlodel), per-golide (Permax) or cabergoline (Dostinex) normalizesserum prolactin levels to restore normal sensitivity to thesexual effects of testosterone (Fleming and Paice 2001).However, the safety and efficacy of these drugs havenot been studied in persons with sexual dysfunction dueto opioids administered for pain and further research isneeded.� Sildenafil (Viagra) has been anecdotally described asbeing effective in relieving opioid-induced sexual dys-function in both men and women, although controlledtrialsarewarranted to establish efficacy and safety in thispopulation. Non-pharmacologic approaches, includingcognitive-behavioral techniques, may be useful to dis-tract attention from pain, theoretically allowing reduc-tions in opioid dose. Sex therapy may provide couples
with alternative positions that are less likely to elevatepain levels, as well as education to facilitate sexual plea-sure.Additional research is needed to determine the preva-lence of opioid-induced sexual dysfunction, as wellas the long-term effects of testosterone suppression.Suppression of testosterone may lead to chronic fatigueand osteoporosis, of particular concern to cancer sur-vivors and individuals with non-cancer pain who mightbe treated with opioids for extended periods. Finally,studies to confirm the safety and efficacy of androgenreplacement and other therapies designed to relievesexual dysfunction due to opioids are indicated.
References1. Abs R, Verhelst J, Maeyaert J et al. (2000) Endocrine Conse-
quences of Long-Term Intrathecal Administration of Opioids. JClin Endocrinol Metab 85:2215–2222
2. Cicero TH, Bell RD, Wiest WG et al. (1975) Function of theMale Sex Organs in Heroin and Methadone Users. N Engl J Med292:882–887
3. Daniell HW (2002) Hypogonadism in Men ConsumingSustained-Action Oral Opioids. J Pain 3:377–384
4. Delitala G, Grossman A, Besser GM (1983) The Participationof Hypothalamic Dopamine in Morphine-Induced Prolactin Re-lease in Man. Clin Endocrinol 19:437–444
5. Ellingboe J, Mendelson JH, Kuehnle JC (1980) Effects of Heroinand Naltrexone on Plasma Prolactin Levels in Man. PharmacolBiochem Behav 12:163–165
6. Finch PM, Roberts LJ, Price L et al. (2000) Hypogonadism in Pa-tients Treated with Intrathecal Morphine. Clin J Pain 16:251–254
7. Fleming MP, Paice JA (2001) Sexuality and Chronic Pain. J SexEduc Ther 26:204–214
8. Johnson JH, Rosecrans JA (1980) Blockade of Ovulation byMethadone in the Rat: A Central Nervous System-MediatedAcute Event. J Pharmacol Exp Ther 213:110–113
9. Mendelson JH, Meyer RE, Ellingboe J et al. (1975) Effects ofHeroin and Methadone on Plasma Cortisol and Testosterone. JPharmacol Exp Ther 195:296–302
10. Packman PM, Rothchild JA (1976) Morphine Inhibition of Ovu-lation: Reversal by Naloxone. Endocrinology 99:7–10
11. Paice JA, Penn RD, Ryan W (1994) Altered Sexual Function andDecreased Testosterone in Patients Receiving Intraspinal Opi-oids. J Pain Symptom Manage 9:126–131
12. Pelosi MA, Sama JC, Caterini H et al. (1974) Galactorrhea-Amenorrhea Syndrome Associated with Heroin Addiction. AmJ Obstet Gynecol 118:966–970
13. Su CF, Liu MY, Lin MT (1987) Intraventricular Morphine Pro-duces Pain Relief, Hypothermia, Hyperglycaemia and IncreasedProlactin and Growth Hormone Levels in Patients with CancerPain. J Neurol 235:105–108
14. Wiesenfeld-Hallin Z, Sdersten P (1984) Spinal Opiates AffectSexual Behavior in Rats. Nature 309:257–258
15. Zis AP, Haskett RF, Albala AA et al. (1984) Morphine InhibitsCortisol and Stimulates Prolactin Secretion in Man. Psychoneu-roimmunology 9:423–427
Cancer Pain Management, Opioid SideEffects, Uncommon Side Effects
CHRISTOPHER J. WATLING
The University of Western Ontario, London, Ontario,[email protected]

254 Cancer Pain Management, Opioid Side Effects, Uncommon Side Effects
Definition� Opioid analgesics are the mainstay of cancer paintreatment. Opioid analgesia is mediated by interactionwith specific receptors in the brain and spinal cord.In addition to the desired clinical effect of pain relief,opioids may also produce a variety of unwanted ad-verse effects that may compromise their usefulness.Common side effects, including constipation, nausea,vomiting, and sedation are well-recognized and pre-dictable. Other adverse effects, including respiratorydepression, pruritus, sweating, urinary retention, andheadache, are less common, but may occasionally haveimportant clinical implications in the cancer patientwith pain.
Characteristics
Respiratory Depression
All opioids in clinical use, given in sufficient doses, maydecrease respiratory rate, tidal volume, or both, as a re-sult of their direct depressant effects on brainstem res-piratory centers (Duthie and Nimmo 1987). Althoughperhaps the most feared of opioid side effects, clinicallysignificant respiratory depression is very rarely encoun-tered in practice, particularly in opioid-tolerant patients.Pain stimulates respiration, acting as a physiologic an-tagonist to therespiratorydepressanteffectsofopioids inan intensity-dependent fashion (Borgbjerg et al. 1996).Two situations may arise in cancer pain managementwhere the risk of respiratory depression is higher andmerits special caution. First, the neuraxial administra-tion of opioids (see � Neuraxial Infusion and � Spinal(Neuraxial) Opioid Analgesia), either epidural or in-trathecal, may be complicated by respiratory depressiondue to supraspinal migration of the drug. Although res-piratory depression may occur within minutes of spinalopioidadministration, itsappearancemaybedelayedforhours (Chaney 1995). Risk factors for clinically signif-icant respiratory depression after spinally administeredopioids include advanced age, coexisting medical orrespiratory problems, lack of opioid � tolerance, andconcurrent administration of parenteral opioids. Rarely,however, patients with no identifiable risk factors willdevelop life-threatening respiratory depression (Etcheset al. 1989). Careful monitoring of respiration and levelof consciousness is therefore necessary when initiatingtherapy with spinal opioids.Second, patients on long-term opioid treatment mayexperience respiratory depression following completerelief of pain by other methods. Opioid-treated cancerpatients undergoing neural blockade or � cordotomy,for example, are at risk of developing respiratory de-pression following the pain-relieving procedure (Wellset al. 1984). This effect, and the need to rapidly ad-just opioid dosing post-procedure, must be antici-pated.
Pruritus
Pruritus, when it occurs as an opioid side effect, is of-ten only a minor nuisance and may only be elicited bydirect questioning. For occasional patients, however, itis so severe that opioid therapy must be modified. Itchis considered an uncommon side effect of systemically-administeredopioids, thoughmayaffectupto17%ofpa-tients (Friedman et al. 2001). In contrast, itch is commonafter neuraxial opioid administration, with a reported in-cidence of 30–100% (Szarvas et al. 2003). Even withneuraxial opioid administration, however, severe pruri-tus is rare, probably affecting less than 1% of individuals(Chaney 1995). Itch is not generally associated with skinrash, which is distinctly uncommon with opioid admin-istration. Pruritus after systemic opioid administrationis generalized, while that after neuraxialopioid adminis-tration isoften localized to theface,neck,orupper thorax(Chaney 1995).The pathophysiology of opioid-induced pruritus is un-certain. Although opioids may induce histamine releasefrom mast cells in the periphery, it is not clear that thismechanism is important to the generation of pruritus.Rather, it is likely that a central mechanism is involved,a hypothesis supported by the reversibility of neuraxialopioid-induced pruritus with naloxone (Friedman andDello Buono 2001).In spite of the lack of evidence for histamine releasebeing an important etiologic factor in opioid-inducedpruritus, antihistamines may sometimes be an effectivetreatment, perhaps as a result of their sedative proper-ties. Infusions of the opioid antagonists � naloxone andnalbuphine may prevent or reduce itch with neuraxialopioids (Kendrick et al. 1996), while the oral opioidantagonist methylnaltrexone has been shown to reducepruritus when co-administered with morphine (Yuanet al. 1998). The long-term use of opioid antagonistsfor chronic opioid-induced pruritus has not been eval-uated. Other potential treatments for opioid-inducedpruritus include � NSAIDs, Survey (NSAIDs), the5-HT3 receptor antagonist ondansetron (Szarvas etal. 2003), and the opioid agonist-antagonist butor-phanol (Dunteman et al. 1996). Opioid rotation is also asimple and potentially effective strategy for managingopioid-induced pruritus (Katcher and Walsh 1999).
Sweating
Sweating may be a significant problem in some cancerpatients treated with opioids. Though the prevalence ofsweating has been reported to range from 14–28% inthis population, numerous non-opioid factors may alsobe causative, including effects of the neoplasm itself, co-existing infection, and other drugs (Mercadante 1998).As such, the incidence of true opioid-induced sweat-ing is difficult to estimate. Clearly, however, there areuncommon instances where intense sweating an occursecondary to opioid therapy, and has a significantlyadverse effect on quality of life. Numerous agents have

C
Cancer Pain Management, Orthopedic Surgery 255
been used to control sweating, including NSAIDs, cor-ticosteroids, benzodiazepines, H2-receptor blockers,thioridazine, and anticholinergic drugs such as hyoscinehydrobromide or butylbromide, with varying degreesof success (Mercadante 1998). Like many unwantedopioid side effects, the problem may also respond toopioid rotation.
Urinary Retention
Urinary retention is a frequent effect of spinally admin-istered opioids, but less commonly may be observed af-ter oral, parenteral, or transdermal opioid administra-tion. This effect is likely to be mediated by interactionwith opioid receptors in the lower spinal cord (Rawalet al. 1983). Caution should be exercised, however, inattributing urinary retention in a cancer patient to opi-oid therapy, particularly when the symptom appears in apatient on chronic, stable doses of opioid, as neoplasticinvolvement of the spinal cord or cauda equina may alsocompromise bladder emptying.
Headache
Occasionally cancer patients report that opioids causeheadaches, even as the pain for which the opioids areprescribed resolves. The etiology of this seeminglyparadoxical phenomenon is uncertain. Headache spe-cialists have long recognized drug-induced or analgesicrebound headaches, often resulting from the frequentuseofshort-actingopioids.Onecouldspeculate thatsus-ceptible patients prescribed opioids for cancer pain maydevelop such rebound headaches. The frequent use ofanalgesics may transform previously episodic headachesyndromes into chronic daily headaches (Silberstein etal. 1998), but it is possible that some individuals with-out a prior headache history may also develop reboundheadaches when exposed to frequent doses of opioidanalgesics. Whether the use of long-acting opioids isassociated with a lower risk of rebound headaches thanshort-acting opioids is not known. Headaches in thecancer setting may have many causes, of course, includ-ing brain or meningeal metastases, and should not beattributed to opioid therapy without diligent evaluationof other possibilities.
References1. Borgbjerg FM, Nielsen K, Franks J (1996) Experimental Pain
Stimulates Respiration and Attenuates Morphine-Induced Res-piratory Depression: A Controlled Study in Human Volunteers.Pain 64:123–128
2. Chaney MA (1995) Side Effects of Intrathecal and Epidural Opi-oids. Can J Anaesth 42:891–903
3. Dunteman E, Karanikolas M, Filos KS (1996) Transnasal Butor-phanol for the Treatment of Opioid-Induced Pruritus Unrespon-sive to Antihistamines. J Pain Symptom Manage 12:255–260
4. Duthie DJR, Nimmo WS (1987) Adverse Effects of Opioid Anal-gesic Drugs. Br J Anaesth 59:61–77
5. Etches RC, Sandler AN, Daley MD (1989) Respiratory Depres-sion and Spinal Opioids. Can J Anaesth 36:165–185
6. Friedman JD, Dello Buono FA (2001) Opioid Antagonists inthe Treatment of Opioid-Induced Constipation and Pruritus. AnnPharmacother 35:85–91
7. Katcher J, Walsh D (1999) Opioid-Induced Itching: MorphineSulfate and Hydromorphone Hydrochloride. J Pain SymptomManage 17:70–72
8. Kendrick WD, Woods AM, Daly MY et al. (1996) Naloxone ver-sus Nalbuphine Infusion for Prophylaxis of Epidural Morphine-Induced Pruritus. Anesth Analg 82:641–647
9. Mercadante S (1998) Hyoscine in Opioid-Induced Sweating. JPain Symptom Manage 15:214–215
10. Rawal N, Möllefors K, Axelsson K et al. (1983) An Experimen-tal Study of Urodynamic Effects of Epidural Morphine and ofNaloxone Reversal. Anesth Analg 62:641–647
11. Silberstein SD, Lipton RB, Goadsby PJ (1998) Headache in Clin-ical Practice. Isis Medical Media Ltd, Oxford, pp 106–107
12. Szarvas S, Harmon D, Murphy D (2003) Neuraxial Opioid-Induced Pruritus: A Review. J Clin Anesth 15:234–239
13. Wells CJ, Lipton S, Lahuerta J (1984) Respiratory Depressionafter Percutaneous Cervical Anterolateral Cordotomy in Patientson Slow-Release Oral Morphine. Lancet 1:739
14. Yuan CS, Foss JF, O’Connor M et al. (1998) Efficacy of OrallyAdministeredMethylnaltrexone in Decreasing Subjective Effectsafter Intravenous Morphine. Drug Alcohol Depend 52:161–165
Cancer Pain Management, OrthopedicSurgery
JOHN H. HEALEY
Memorial Sloan Kettering Cancer Center and WeillMedical College of Cornell University, New York, NY,[email protected]
Definition
Orthopedic cancer pain includes biologic or mechan-ical pain that affects the musculoskeletal system, andcompromises the function and independence of can-cer patients. Bone pain has a different neurochemicalbasis than either inflammatory or neuropathic pain. Itis often multifactorial in origin and requires treatmentof all contributing factors. Pain treatment includes thesurgical stabilization of fractured bones and often ofimpending fractures.
Characteristics
Bone pain can be multifactorial and requires a multi-pronged approach for accurate diagnosis and effectivetreatment. � Afferent signals come from stimuli that areinherently mechanical or biologic. Exclusion of remotecauses, such as referred and radicular pain, and otherdistant causes, must be done in each case to optimizetreatmentandavoidmissingconcomitantdiseasesuchasspinal cord compression. Comprehensive managementof bone pain requires specific treatment to address eachcause.One type of referred pain comes from an insult af-fecting the same dermatome. Typically, this comesfrom a lesion affecting the same bone proximal tothe symptomatic site. The most common example isdistal femur and knee pain due to a proximal femuror hip lesion. A careful physical examination is the

256 Cancer Pain Management, Orthopedic Surgery
best way to make the diagnosis clinically. The limpthat is due to a knee problem differs significantly fromthat of a hip problem, and should alert the clinicianto problems “upstream” from the reported site of thepain. Certain provocative tests have compelling diag-nostic value. For example, � passive � abduction or� active � adduction of the hip isolates the adductormusculature and its pubic origin as the source of pain.This can point away from intrinsic hip pathology andcan avoid an unnecessary hip replacement operation.Another common problem is an � avulsion fracture ofthe anterior inferior iliac spine. Since this is the originfor the rectus femoris, activities that stress it, such asstraight leg raising from a supine position, provokepain, whereas hip flexion from the seated position doesnot. Once again, identification of the pathologic paingenerator focuses treatment and prevents ill-advisedsurgical or medical treatment.Radicular pain is common from cervical tumors andcauses periscapular or arm pain that is often improperlyascribed to other sources. Similarly, lumbar tumorscause buttock or lower limb pain that may or may notbe associated with neurologic symptoms of a sensoryor motor nature.Alternative sources of pain must also be excluded.For example, degenerative arthritis of the hip, knee,spine, or shoulder is common in older cancer patients.Avascular necrosis, particularly of the hip or shoulder,may develop from steroids, chemotherapy, or radiationtherapy used to treat the underlying cancer. Simple ra-diographs are the best way to look for these traditional,non-oncologic causes of bone pain in the cancer patient.Occasionally, � paraneoplastic syndromes may causebone or joint pain and elude usual diagnostic tests. Thisproblem can occur from any cancer, but seems to bemost common in patients with small cell lung cancerand with HIV-related malignancies. In the midst ofchemotherapy, � granulocyte colony stimulating factor(GCSF) is commonly used and will produce localizedand diffuse bone pain. The cause is poorly defined, but itseems to be due to acute pressure developing in the bonemarrow from marrow expansion, and possibly from theevolution of nociceptors and cytokines in response tothe GCSF. Finally, infection must be excluded, partic-ularly in patients who have hematologic malignanciesor � treatment-related neutropenia.Mechanical pain characterizes orthopedic cancer pain.Excess force or weight bearing bends the mechanicallyinsufficient bone (strain). This stretches the periosteum,stimulates pain receptors, and produces pain. Beforefracture occurs, normal stimuli such as walking cantrigger lower extremity pain, and lifting or forcefulactivity cause upper extremity pain. In the extreme con-dition, these forces result in fractures that are associatedwith periosteal tears, hemorrhage and tissue trauma.Local cytokines are released and further stimulate thenociceptors.
Boneisweakestandmostlikelytofracturewhenstrainedin torque (twisting on a firmly planted foot, for exam-ple.) It is relatively stronger when the stress is axial andthe forces are in compression or distraction (tension).Metastases and erosions weaken the bone to well de-fined degrees. A 50% cortical defect in the femur causes60–90% reduction in bone strength. The fracture riskposed by a bone lesion can be characterized in differ-ent ways. Bone mineral density alone explains 80–90%of the fracture risk in cadaveric models of lytic bone le-sions of the femur (Michaeli et al. 1999). Usually, butnot always, these lesions are associated with pain. Con-versely, bone pain is usually associated with such a bonydefect. The presence of either a critical bone lesion ormechanical pain constitutes an impending fracture. Me-chanical treatment is mandatory for such a lesion. Thiscan comprise of external support (crutches) or internalreinforcement of the bone (implant). A common error isto treat the mechanical pain with antineoplastic agentsor radiation and analgesics, without addressing the me-chanical component.Plain radiographs remain the most efficient way to as-sess the global integrity of bone and determine whethersurgery is a consideration to treat the mechanical pain(Hipp et al. 1995). Three-dimensional imaging such asCT scans or MRI scans are occasionally needed to diag-noseoccult lesionsorplan surgeries, since they can iden-tify bony defects that must be bypassed. The mere pres-ence of a bone lesion or metastasis does not mean that isthe source of pain nor that it requires explicit treatment.Most bone lesions are asymptomatic. Rapidly growinglesions may evade diagnosis. Plain radiographs appearnormal until 30% of the mineral is lost, and bone scintig-raphy primarily identifies areas of bone reaction. If thehost bone has not had sufficient time to respond, thesestudies may yield false negative results, so a high indexof suspicion is needed.Biologically rapidly growing tumors raise intraosseouspressure by blocking venous blood return, expandingwithin a closed space, and releasing pain-mediatingsubstances. Many neural transmitters and nerve fibershave been identified within bone. They are involved innormal development and pathologic conditions (Sisasket al. 1995, Bergstrom et al. 2003). � Substance P,� calcitonin gene-related product (CGRP), vasoin-testinal peptide, and other compounds that stimulatenociceptors, augment local perfusion, and have directmetabolic effects on the bone contribute to the paingenerating milieu. Nerve fibers that stain for CGRPare widely distributed in bone, periosteum and marrow.They directly regulate local bone remodeling duringgrowth, and repair by elevating the CGRP concentra-tion in the microenvironment around bone cells (Irie etal. 2002). The connection between brain function andbone metabolism has recently been postulated to occurdue to leptin and mediated by noradrenaline acting onβ2adrenergic receptors on osteoblasts (Takeda et al. 2002).

C
Cancer Pain Management, Overall Strategy 257
Bone pain has a different profile of neurotransmittersthan either inflammatory or neuropathic pain (Clohisyand Mantyh 2003; Schwei et al. 1999). For exam-ple, substance P and calcitonin gene-related peptideare both � up-regulated in inflammatory pain, � down-regulated in neuropathic pain, and unchanged in modelsof bone metastasis (Honore et al. 2000a). On the otherhand, GFAP (glial fibrillary acidic protein) is mas-sively up-regulated in the spinal cord in bone cancerpain, but not in inflammatory or neuropathic pain. Sev-eral other changes occur in the spinal cord. There isup-regulation of c-FOS, reflecting increased neuronalactivity, dynorphin, and the development of astrocyto-sis. These chemical and morphologic changes indicatea central reorganization of the neural system in casesof orthopedic oncologic pain.Cancersencourage the recruitmentofosteoclasts that re-absorb bone. This bone resorption contributes to paindue to biologic and mechanical reasons. Blocking theosteoclastic action with agents such as osteoprotogeninprevents pain in animal models of bone cancer (Honoreet al. 2000b). Once the cortex is breached, the advanc-ingcancermechanicallyandbiologically irritates thepe-riosteum. Weak bone incurs greater strain, and pain en-sues.Prevention of bone resorption prevents bone painand improves patient quality of life. Clinical stud-ies have proven that � aminobisphosphonates reducebone resorption, pain, and the need for radiation ther-apy. Meta-analysis of 95 randomized studies withmore than six months follow up has shown that theseagents significantly reduced the odds ratio for fractures(vertebral 0.69, 95% confidence interval 0.57–0.84,P < 0.0001; non-vertebral 0.65, 0.54–0.79, P < 0.0001;combined 0.65, 0.55–0.78, P < 0.0001), radiother-apy (0.67, 0.57–0.79, P < 0.0001), and hypercalcemia(0.54, 0.36–0.81, P = 0.003) but not for orthopedicsurgery (0.70, 0.46–1.05, P = 0.086) or spinal cordcompression (0.71, 0.47–1.08, P = 0.113). The reduc-tion in orthopedic surgery was significant in studies thatlasted over a year 0.59, 0.39–0.88, P = 0.009) (Ross etal. 2003).Despite the clear benefits of optimal medical manage-ment, many patients will still have bone pain and sustainfractures. Mechanical pain responds to the relieving ofloads on the bone, externally or internally (Healey andBrown 2000). External support and protection comesfrom protected weight bearing with a walking aid (e.g.a cane, crutches, or walker) or brace (e.g. a lumbar sup-port or functional cast brace for the humerus). Internalfixation reinforces the bone with metal, bypassing thebony defect and sharing the stress with the intact bone.Fixation of an orthopedic implant in normal bone isneeded proximal and distal to the deficiency. When thedefect is close to the end of the bone and it is impossibleto meet the goal of rigid fixation through the metaph-ysis or epiphysis, the joint must be sacrificed and a
hemiarthroplasty replacement is needed. This surgeryis very successful in alleviating mechanical cancer painacutely. It works well long-term if antitumor therapiesprevent local bone destruction and destabilization ofthe implant.Treatment consists of reinforcing the bone, stopping thecancer progression, and preventing new sites of symp-tomatic disease involvement.
References1. Bergstrom J, Ahmed M, Kreicbergs A et al. (2003) Purifica-
tion and Quantification of Opioid Peptides in Bone and JointTissues – A Methodological Study in the Rat. J Orthop Res21:465–469
2. Clohisy D, Mantyh PW (2003) Bone Cancer Pain. Cancer97:866–873
3. HealeyJH, BrownHK(2000)ComplicationsofBoneMetastases:Surgical Management. Cancer 88:2940–2951
4. HippJA, SpringfieldDS, HayesWC(1995) PredictingPathologicFracture Risk in the Management of Metastatic Bone Defects.Clin Orthop 312:120–135
5. Honore P, Rogers SD, Schwei MG et al. (2000a) Murine Modelsof Inflammatory, Neuropathic and Cancer Pain Each Generate aUnique Set of Neurochemical Changes in the Spinal Cord andSensory Neurons. Neuroscience 98:585–598
6. Honore P, Luger NM, Sabino MA et al. (2000b) OsteoprotogeninBlocks Bone Cancer-Induced Skeletal Destruction, Skeletal Pain,and Pain Related to the Structural Reorganization of the SpinalCord. Nat Med 6:521–528
7. Irie K, Hara-Irie F, Ozawa H et al. (2002) Calcitonin Gene-Related Peptide (CGRP)-Containing Nerve Fibers in BoneTissue and their Involvement in Bone Remodeling. MicroscRes Tech 58:85–90
8. Michaeli DA, Inoue K, Hayes WC et al. (1999) Density Predictsthe Activity-Dependent Failure Load of Proximal Femora withDefects. Skeletal Radiol 28:90–95
9. Ross JR, Saunders Y, Edmonds PM et al. (2003) SystematicReview of Role of Bisphosphonates on Skeletal Morbidity inMetastatic Cancer. BMJ 327:469
10. Schwei MG, Honore P, Rogers SD et al. (1999) Neurochemicaland Cellular Reorganization of the Spinal Cord in a Murine Modelof Bone Cancer Pain. J Neurosci 19:10886–10897
11. Sisask G, Bjurholm A, Ahmed M et al. (1995) Ontogeny of Sen-sory Nerves in the Developing Skeleton. Anat Rec 243:234–240
12. Takeda S, Elefteriou F, Levasseur R et al. (2002) Leptin Regu-lates Bone Formation Via the Sympathetic Nervous System. Cell111:305–317
Cancer Pain Management, OverallStrategy
GILBERT J. FANCIULLO
Pain Management Center, Dartmouth-HitchcockMedical Center, Lebanon, NH, [email protected]
Definition
Pain isanexperienceuniquetoeach individualandbasedon perception, mood, and current and past experiences.Cancer pain, even more so than chronic or acute pain, ismultidimensional, and has emotional, social, and spiri-tual vectors that must be assessed and addressed. Given

258 Cancer Pain Management, Overall Strategy
the multidimensional nature of cancer pain, a team ormultidisciplinary approach geared towards assessmentand treatment is required to ensure the best care. Goodcancer pain treatment is labor intensive, requires highlyspecialized knowledge and skill, can change the lives ofcancer patients and their loved ones, and can be the mostfulfilling part of a pain clinicians practice.
Characteristics
Epidemiology and Impact
About half a million people in the United States andabout 6.6 million people worldwide die of cancer eachyear (American Cancer Society 2003; World HealthOrganization 1996). Lifetime probability of developingcancer is approximately 1 in 2 for men and 1 in 3 forwomen (American Cancer Society 2003). The survivalrate for adults is approximately 62% and for children is97% (American Cancer Society 2003). Roughly 40% ofnewly diagnosed cancer patients and 75% of advancedcancer patients suffer from pain (Sykes et al. 2003).The prevalence of pain varies with the type of cancer.Pain in patients with head and neck cancer, genitouri-nary, prostate, and esophageal cancer is far more com-mon than in patients with leukemia (Portenoy 1989;Sykes et al. 2003). Patients with metastatic diseasehave more frequent pain complaints than those withnonmetastatic cancer (Sykes et al. 2003). One-third ofpatients with advanced cancer have two sites of pain andtwo-thirds have three or more sites of pain (Grond etal. 1996). Seventeen percent of pain in patients with can-cer is treatment related and 9% is due to a concomitantdisease (Grond et al. 1996).The influence of uncontrolled cancer pain is dramatic.The severity and impact of pain caused by cancer isbelieved to be greater than pain in patients withoutcancer. Beliefs about the meaning of pain in cancer painpatients have been shown to increase the severity of painas well as levels of depression, anxiety, somatization,and hostility (Ahles et al. 1983). Severe, uncontrolledpain in patients with cancer is a major risk factor incancer related suicide (Chochinov and Breitbart 2000).Pain, depression, � delirium and lack of social supporthave all been associated with an increased desire for ahastened death in cancer patients (Chochinov and Bre-itbart 2000). Many of these symptoms can be treatedand pain can almost always be well controlled, oftenwith simple and noninvasive remedies. Psychologicaldistress is often lessened and psychiatric symptoms canresolve with good pain treatment and relief (Chochinovand Breitbart 2000).Special patient populations can be especially challeng-ing and includechildren and infants, elderly patients, pa-tients with concomitant preexisting personality or otherpsychiatric disorders, patients with preexisting chronicpain, patients who suffer from addiction, poverty, wholive in rural locations, are poorly educated or illiterate,
are non-English speaking, have no support network, orwho are in denial.
Characterization of Pain
Cancerpain can becaused by direct effectsof tumor, sideeffects of treatment, � paraneoplastic syndrome s, or berelated to a preexisting or concomitant condition. Paincan be characterized as neuropathic, somatic or visceral,or can be mixed. Diagnosis is based on history and phys-ical examination, and pharmacological treatment deci-sions will vary based on the characteristics and etiologyof the pain.Cancer pain related to direct effects of tumor canmanifest as somatic, visceral or � neuropathic painsyndromes. Boney, particularly vertebral body andrib metastases are common and often cause localized� somatic pain but can cause neuropathic symptomsparticularly with spinal cord, cauda equina, or nerveroot involvement or � Visceral Nociception and Painsyndromes such as pleuritic pain with rib metastases.Spinal cord compression occurs in approximately3% of all cancer patients (Kramer 1992). Thoracicradiculopathic pain patterns are common and may beeasily misdiagnosed. Brachial and lumbar plexopathy,meningeal carcinomatosis (� meningeal carcinoma-tous) and base of skull metastasis are frequent directtumor effect causes of neuropathic pain. Pleuritic pain,hepatic capsular stretch pain, and bowel obstructionpain are examples of visceral pain syndromes requiringspecial attention and skill to treat well.� Mucositis is an extremely prevalent, difficult to treat,and severe and debilitating pain syndrome caused bycancer treatment. Peripheral neuropathy pain can occuras a paraneoplastic syndrome in up to 5% of patientswith lung cancer, or can occur as often as 82% inpatients being treated with chemotherapy (Smith etal. 2002). Postthoracotomy pain syndrome can occur ingreater than 50% of patients undergoing thoracotomy(Perkins and Kehlet 2000). Fifty percent of womanundergoing breast surgery for cancer have pain oneyear after surgery, and 30–80% of patients undergoingamputation continue to suffer chronic pain (Perkins andKehlet 2000). Radiation � plexopathy or myelopathyare not uncommon pain syndromes in cancer survivors,nor is avascular necrosis secondary to corticosteroidtreatment.
Assessment
A pain history should incorporate questioning aboutmultiple sites of pain since this information is oftennot volunteered by the patient. Cancer patients arefrequently reluctant to report increasing pain, perhapsfearing progressive disease. The character, location, in-tensity, frequency and relationship of pain to activitiesshould all be investigated. Pain syndromes that existedprior to cancer diagnosis should be identified. Patientswith a long history of chronic pain, such as low back

C
Cancer Pain Management, Overall Strategy 259
pain or fibromyalgia, which has never been adequatelycontrolled even with long-term opioid treatment, maybe at risk of poorly-controlled pain as more aggressivetreatments for cancer pain are administered. At thesame time, it is not unusual for chronic pain syndromesto resolve or assume diminished importance within thecontext of a life threatening illness.A pain history should include an understanding of thecharacteristics of the cancer type, including diagnosis,histology, extent of disease, and prognosis. History ofantineoplastic treatment is important in order to assessperipheral neuropathy pain that might be secondary toa paraneoplastic syndrome, chemotherapy or radiationtreatment. Prognosis and treatment may vary based onetiology. Knowledge of specific cancer pain syndromescan help in diagnosis and in selecting treatments. For ex-ample, radiation therapy may be more effective in treat-ing intermittent pain due to bone metastasis than anal-gesics. A history of remote or concurrent alcoholism ordrug addiction can be important in prioritizing therapy.For example, an analgesic intrathecal infusion systemmay be selected for treatment earlier in the paradigm,rather than oral opioids. A social and emotional historyis an essential part of the cancer pain history. An assess-ment of cognitive ability, educational level, dementia ordelirium should all be part of the history.A thorough physical examination combined with a com-plete history will almost always provide sufficient infor-mation to formulate a good therapeutic plan. Review ofupcoming procedures is also important, because painfulprocedures in adults are too commonly overlooked as atreatablecomponentofcancerpain.Manycancercentershave “pain free” systems in place to ensure that infantsand children can undergo bone marrow biopsy, MRI ex-ams, and line and tube placement comfortably, but thesesame options are not typically available for adults. Clin-icians should offer analgesic guidance for proceduresto ensure that they are not painful and anticipated withdread and fear.Theability to reviewandinterpret laboratory tests, radio-graphs, MRI and CT scans, and to understand oncologicnomenclature, are important and useful skills when ad-dressing the problem of cancer pain.
Treatment
Cancer pain treatment can be divided into five strate-gies: drugs, interventional approaches (surgery andinjections), behavioral medicine approaches, phys-ical medicine approaches, and complementary andalternative approaches.Acetaminophen and nonsteroidal anti-inflammatorydrugs; opioids; and adjuvant analgesics, such as anti-convulsants, antidepressants, topical agents (e.g. lido-caine patch), and bisphosphonates are the backbone oftherapy and will be effective for the large majority ofpatients with cancer pain. The World Health Organi-zation ladder approach to treatment selection can be a
useful model upon which to guide therapy, but it mustbe remembered that cancer patients with severe painshould not be forced to fail treatment with NSAIDs be-fore having an opioid added to their regimen (Sykes etal. 2003). Patients with severe pain due to cancer shouldalmost always have therapy initiated with a single entity,pure mu agonist opioid at the time they are first seen.Routes of administration, such as intravenous, subcu-taneous, oral, rectal, buccal, and intranasal or inhaled,should be considered in special circumstances. Drugssuch as ketamine or local anesthetics can be infusedintravenously for refractory pain syndromes.The potential effectiveness of neural blockade in care-fully selected patients is exemplified by the neurolytic� celiac plexus block. This injection is still the mostuseful of injection therapies for cancer pain, and canprovide good to excellent analgesia in 85% of patientswith localized pain secondary to pancreatic carcinoma.It should be an early option for patients with pain fromthis disease or other intraabdominal cancer (Patt andCousins 1998). Epidural, intrathecal, and regional nerveblocks can be done using neurolytic agents such as al-cohol or phenol and can be individualized in specialcircumstances. Analgesia from neurolytic blocks willtypically last for 6 months.Patients with severe pain refractory to noninvasivetreatments should also be considered for treatment withintrathecal analgesics. Drugs routinely infused into theintrathecal space include morphine, hydromorphone,bupivacaine, and clonidine. Intrathecal infusions canbe successfully employed and should be considered inpatients with severe neuropathic pain, incident pain,or opioid tolerance or refractoriness. Patients with anestimated life expectancy of 3 months or less can havea percutaneous system connected to a mobile infusionpump. If life expectancy is greater than 6 months, aprogrammable, implanted pump can be used and willtypically need to be refilled only every 90 days. Anal-gesic infusion systems can be a useful option, and thereis now extensive experience supporting efficacy andsafety; these systems are labor intensive, however, andmay require frequent medication or rate adjustments.Neurosurgicalproceduressuchasanterolateral� cordo-tomy, medial � myelotomy, � dorsal root entry zone le-sioning, and other neurodestructive procedures are op-tions for carefully selected patients and can provide ex-cellent relief of pain in otherwise refractory situations.They, too, should be considered in cancer pain patientswhose pain does not respond to nondestructive remedies(Burchiel 2002).Behavioral interventions, such as coping skill trainingand pacing, learning about the differences betweenhurt and harm, reduction of catastophizing, relaxationtechniques, self-hypnosis, biofeedback and other psy-chological interventions are an essential component ofany cancer pain reduction plan. Patients should be as-sessed for denial, anger, and depression. When severe,

260 Cancer Pain Management, Palliation of Upper GI Cancer
these problems should be managed by a behavioralmedicine specialist. Astute pain medicine specialistsshould possess enough skill and knowledge in this areato enable them to provide this care to the majority ofcancer pain patients. Preexisting or concomitant psy-chiatric illness may make treating cancer pain morechallenging, but can also increase the rewards of suc-cessful therapy to the patient, his or her family, and allproviders involved.Physical medicine interventions should be consideredin all patients with cancer, but especially those withpain. Pain from immobility can be relieved with a pre-scribed regimen of physical activity, even if a patientis bed-bound or has advanced disease. Maintaining thehighest functional capacity possible will ensure thebest quality of life for the majority of patients withcancer pain. Modalities used for acute pain, such asfluidotherapy, heat, and massage, can be very useful inpatients suffering from cancer pain. Physical medicinespecialists with special skill in cancer rehabilitationshould be called upon early to help care for cancerpatients.Complementary and alternative pain managementstrategies should be employed whenever they mightbe useful. Thirty percent of cancer patients world-wide use complementary medicine approaches to helpmanage their cancer and complications (Ernst andCassileth 1998). A patient who specifically asks aboutacupuncture may be likely to find acupuncture a usefuladjunct, whether there is a true therapeutic effect orplacebo effect alone. Patient’s belief in efficacy of com-plementary and alternative treatments and their hightherapeutic index should not be overlooked.Attention to spirituality and cultural beliefs is extremelyimportant in managing patients with cancer pain. Spiri-tual beliefs may influence the patients understanding oftheir illness and suffering, and may affect treatment de-cision making. Spiritual beliefs may assist coping skills.Providers should respect the beliefs of their patients andappreciate the often profound importance of these be-liefs. This appreciation itself can be therapeutic, and en-able the provider to help his or her patient take full ad-vantage of the power of these beliefs (Bergeret al. 2002).
Summary
Pain in patients with cancer cannot be treated in a vac-uum, as a hard-wired nociceptive sensation. It is besttreated in context, taking advantage of the special skillsand knowledge of other professionals. Pain physicians’superior knowledge of the treatment of refractory can-cer pain can be enhanced by the palliative physicians’superior knowledge of communication skills; manage-ment of symptoms other than pain; ability to addresssocial, spiritual, and emotional conditions; and impor-tantly, ability to organize and prioritize the efforts ofoncologists, surgeons, primary providers, nurses andpain physicians. Good cancer pain medicine is more
than providing a paradigm for the administration ofmedications and procedures.Treatment of patients with cancer pain can be challeng-ing, requiresspecialskillsandknowledge, isbestaccom-plished in a multidisciplinary setting and can be extraor-dinarily rewarding. Attention to other symptoms and tothe social, emotional, and spiritual needs of cancer pa-tients should be a routine part of cancer pain manage-ment and can be addressed by pain specialists with in-terests and skill in those areas, or may require the specialtalents of palliative medicine providers working in con-junction with pain providers.
References1. Ahles TA, Blanchard EB, Ruckdeschel JC (1983) The Multidi-
mensional Nature of Cancer-Related Pain. Pain 17:277–2882. American Cancer Society (2003) http://www.cancer.org/docroot/
stt/stt\_0.asp3. Berger AM, Portenoy RK, Weissman, eds (2002) Principles and
Practice of Palliative Care and Supportive Oncology. LippincottWilliams & Wilkins, Philadelphia
4. Burchiel K (2002) Surgical Management of Pain. Thieme, NewYork
5. Chochinov HM, Breitbart W (2000) Handbook of Psychiatry inPalliative Medicine. Oxford University Press, Oxford, pp 57–58
6. Ernst E, Cassileth B (1998) The Prevalence of Complimen-tary/Alternative Medicine in Cancer. Cancer 83:777–782
7. Grond S, Zech D, Diefenbach et al. (1996) Assessment of CancerPain: A Prospective Evaluation in 2266 Cancer Patients Referredto a Pain Service. Pain 64:107–114
8. Kramer JA (1992) Spinal Cord Compression in Malignancy. Pal-liative Med 6:202–211
9. Smith EL, Whedon MB, Bookbinder M (2002) Quality Improve-ment of Painful Peripheral Neuropathy. Seminars in OncologyNursing 18:36–43
10. Patt RB, Cousins MJ (1998) Techniques for Neurolytic NeuralBlockade. In: Neural Blockade in Clinical Anesthesia and Man-agement of Pain (Cousins MJ, Bridenbaugh PO, Eds). Lippincott-Raven, Philadelphia. pp 1036–1037
11. Perkins FM, Kehlet H (2000) Chronic Pain as an Outcomeof Surgery. A Review of Predictive Factors. Anesthesiology93:1123–1133
12. Portenoy RK (1989) Cancer Pain: Epidemiology and Syndromes.Cancer 63:2298–2307
13. Sykes N, Fallon MT, Patt RB (2003) Cancer Pain. Arnold Pub-lishers, London, p 22
14. World Health Organization (1996) Cancer Pain Relief and Pal-
liative Care, 2nd edn. World Health Organization, Geneva
Cancer Pain Management, Palliation ofUpper GI Cancer
� Palliative Surgery in Cancer Pain Management
Cancer Pain Management,Patient-Related Barriers
CIELITO REYES-GIBBY
The University of Texas MD Anderson Cancer Center,Houston, TX, [email protected]

C
Cancer Pain Management, Patient-Related Barriers 261
Definition
Patient-related barriers refer to patients’ limited knowl-edge of, beliefs about, and attitudes towards pain andpain treatment that detract from optimal pain manage-ment.
Characteristics
Patients, as consumers of health care, play an importantrole in the successful management of pain. Critical com-ponents for the successful clinical management of paininclude the patients’ ability to communicate their needforpain control, provide feedbackontheeffectivenessoftreatment,andcompliancewith therequirementsof ther-apy.Patients’ limited knowledgeof,beliefsaboutandat-titudes towards pain and pain treatment may, therefore,detract from optimal pain management. Several barriers(Cleeland et al. 1997; Ward et al. 1993; Cleeland 1987)to the practice of good pain management havebeen iden-tified. They include those associated with patients (re-luctance to report pain and to take pain medications), thehealth care system (low priority given to pain control),and health care professionals (inadequate knowledge,reluctance to treat, fear of controlled-substance regula-tions).Among cancer patients, studies have shown that pa-tients’ reluctance to report pain is a primary reason forinadequate pain control. Von Roenn et al. (1993), Larsonet al. (1993), and Cleeland (1987) have demonstratedthat both oncologists and oncology nurses identifiedpatient reluctance to report pain as one of the majorbarriers to the adequate control of cancer pain.Patients are reluctant to report pain to their physiciansor nurses for many reasons. Fear of addiction and de-pendence is often rated as a number one concern is.Opioids are the cornerstone of cancer pain therapy.First described in the World Health Organization’sguidelines for cancer pain relief (World Health Organi-zation 1986), the protocol for pain treatment providessimple recommendations for the use of oral analgesicsand adjuvants: Non-opioids and adjuvants for mildpain; so-called “weak” opioids, often combined witha non-opioid and adjuvants, for moderate pain; andso-called “strong” opioids, combined with adjuvants,for moderate to severe pain. There is, however, a com-mon misconception among patients that opioids causeaddiction. Often, patients and their family caregiversmistake the signs of withdrawal for addiction ratherthan physical dependence, perpetuating the belief thataddiction is a sequela of taking opioids. Family mem-bers also fear that the patient will be thought of as anaddict, adding substantial pressure on the patient torefrain from taking opioids.The mistaken notion that pain medications taken earlywill not be effective when pain gets worse further com-pounds the problem. Some patients believe that if theytake pain medication they will become tolerant to the ef-
fects of analgesics when their disease progresses (Clee-land et al. 1997; Cleeland 1987). Due to this fear of drugtolerance, many withhold or “save” their medication un-til they can no longer tolerate their pain.Concern about side effects from pain medicines isanother commonly reported barrier to adequate painmanagement. Many believe that side effects from anal-gesics are even more bothersome than the pain itself. Ina study of underserved cancer patients, Anderson andcolleagues (Anderson et al. 2002) found that a majority(75%) reported problems with side effects from painmedicines. Commonly reported side effects includeconstipation, sedation, and nausea.Belief that increasing pain signifies disease progressioncauses patients who are unwilling to face this possibil-ity to deny their cancer pain. Patients are also afraid tobother their health care providers with symptoms theyconsider to be an expected part of their disease. Due tothe belief that pain is an inevitable part of cancer andthat nothing can be done about it, patients are willingto accept and endure pain. In a population-based sur-vey conducted several years ago (Levin et al. 1985), ap-proximately 50% of the respondents considered cancerto be an extremely painful disease. Approximately 40%believed that cancer treatment is extremely painful, and37% rated cancer treatment as moderately painful. Fur-thermore, over 70% thought that cancer pain could be sosevere that one would consider suicide, and more than60% believed that cancer patients usually die a painfuldeath. These findings document the misconceptions sur-rounding cancer pain.Patients also think that if they complain of symptoms,their health care providers will be distracted from theirefforts to cure the disease. A recent study specificallyinvestigated whether patients’ self-reports of pain varyby treatment setting (Reyes-Gibby et al. 2003), in thiscase an outpatient chemotherapy clinic and an outpa-tient breast clinic. Medical charts of patients seen duringthe same day in both the outpatient chemotherapy clinicand the outpatient breast clinic were reviewed and painratings were abstracted. Statistically significant differ-ences in patients’ self-reports of pain were observed inthe two treatment settings. Fifty-one percent of patients’self-reports of pain differed between the two treatmentsettings, with 38% reporting a pain score > 4 in the out-patient breast clinic, and 0 in the outpatient chemother-apy clinic. The authors suggested that the results mayindicate that patients were reluctant to report pain in thechemotherapy clinic to avoid delaying their treatment.Another possible explanation for this finding is that pa-tients may have believed that the chemotherapy clinicwas not set up for pain intervention (to contact a physi-cian for pain medication), and were thus reluctant to dis-tract the clinic heath care professionals from adminis-tering chemotherapy.Wanting to be labeled as “good patients” and not as“complainers” also influences patients’ reporting of

262 Cancer Pain Management, Patient-Related Barriers
pain. Many patients think that their behavior will influ-ence the quality of their care. Families may compoundthe problem by trying to work out with the patient whatis important to tell their physicians (Cleeland 1987).Not surprisingly, other frequently reported barriers areforgetting to take pain medications and the belief thatone should be able to tolerate pain without medication(Thomason et al. 1998).While most of the studies on patient-related barriers topain were conducted with non-Hispanic whites, studiesin recent years explored the influence of socioculturalfactors on patient-related barriers to adequate pain man-agement. There are many definitions of culture, but onethat is helpful for understanding the effects of culture onpain was offered by Hellman (1990). He defined cultureas “a set of guidelines (both explicit and implicit) that in-dividuals inherit as members of a particular society, thattells them how to view the world, how to experience itemotionally, and how to behave in it in relation to otherpeople, and to natural and supernatural forces.” Helmanoffered specific propositions as to the pervasive effectsof culture on pain: 1) Not all social or cultural groups re-spond to pain in the same way, 2) How people perceiveand respond to pain, both in themselves and in others,can be largely influenced by their cultural background,and3)How,andwhether,peoplecommunicate theirpainto health professionals and to others can also be influ-enced by cultural factors. These propositions underliethe commonly held assertion that there may be signifi-cant cultural and linguistic differences in the way peoplefeel, view, and report pain.Although recent research suggests that culture does notaffect pain thresholds or pain intensity ratings, cultureprobably does impact people’s behavioral responses topain and their interpretations of the meaning of pain. Astudy by Cleeland and colleagues (Cleeland et al. 1997)of Hispanics and African-Americans who attended mi-nority outpatientclinics, showed thatHispanics reportedmore concerns about taking too much pain medicationand more concerns about possible sideeffects from anal-gesics, as compared to African American patients.A recent study by Anderson and colleagues (Andersonet al. 2002) noted that, although the reasons for not tak-ing pain medications do not significantly vary amongAfrican-Americans and Hispanic patients, differencesexist between the two groups in terms of the meaningof cancer pain. African-Americans talked about the sen-sory component of pain, describing pain as “hurt” and aslimited activity and impaired function. In contrast, His-panics tended to focus more on the emotional compo-nentofpain,describing painas“emotional suffering.” Interms of patient-related barriers to cancer pain manage-ment, commonly stated barriers for both groups were:the need to be strong and not lean on pain medications;concern about addiction and the possible developmentof tolerance to pain medications; concern about side ef-fects; and family reactions to their use of pain medica-
tions. Another important finding of this study was that amajority of patients in both ethnic groups would wait un-til their pain severity was a 10 on a 10-point scale beforecalling their health care provider.Other studies have identified religious beliefs, folk heal-ers, non-drug interventions, and assistance from familymembers as important for pain management. A study ofpatients receiving analgesics from home health or hos-pice agencies, found that Hispanic patients were morelikely than Caucasian patients to report beliefs (e.g. takepain medicines only when pain is severe) that could hin-der effective pain management (Juarez et al. 1998a). Aqualitative study of Hispanic cancer patients receivinghome health or hospice care also found that many pa-tients believed that pain should be approached with sto-icism (Juarez et al. 1998b).While not directly related to patients’ attitudes and be-liefs,othernotablebarrierspatientsfaceincludesthecostand limited availability of analgesics. Difficulty with co-payments or incidental costs associated with obtainingtheir prescriptions is especially relevant for those wholack insurancecoverageorwhohavea limited income. Interms of availability, a study of pharmacies in New Yorkfound that only 25% of pharmacies in minority commu-nities stocked sufficient opioids for pain management,compared to 72% of pharmacies in non-minority com-munities (Morrison et al. 2000).When patients’ attitudes and beliefs interfere with ef-fective pain management, patients can benefit froma number of interventions. Educational interventionsthat provide accurate information about pain and paintreatments have shown some positive results. Rimerand colleagues (Rimer et al. 1987) used a randomizedSolomon Four-Group design to assess the effectivenessof a patient education intervention among 230 cancerpatients. The intervention consisted of nurse counselingand printed materials. Results showed that one monthlater, patients in the experimental group were morelikely to have taken their pain medicine on the correctschedule and to have taken the correct dosage. Theexperimental group was significantly less likely to havereported stopping the medicine when they felt better,and were significantly less worried about tolerance andaddiction to pain medicines as compared to the controlgroup. The results of this study provide support for theimportance of educational interventions, augmentedwith brief health care professional contact, in changingpain-related beliefs and improving pain management.
References1. Anderson KO, Richman SP, Hurley J et al. (2002) Cancer
Pain Management among Underserved Minority Outpatients:Perceived Needs and Barriers to Optimal Control. Cancer94:2295–2304
2. Cleeland CS (1987) Barriers to the Management of Cancer Pain.Oncology 1:19–26
3. Cleeland CS, Gonin R, Baez L et al. (1997) Pain and Treatment ofPain in Minority Patients with Cancer. The Eastern Cooperative

C
Cancer Pain Management, Principles of Opioid Therapy, Dosing Guidelines 263
Oncology Group Minority Outpatient Pain Study. Ann InternMed 127:813–816
4. Hellman C (1990) Culture, Health and Illness: An Introductionfor Health Professionals. Wright, London
5. Juarez G, Ferrell B, Borneman T (1998a) Influence of Cultureon Cancer Pain Management in Hispanic Patients. Cancer Pract6:262–269
6. Juarez G, Ferrell B, Borneman T (1998b) Perceptions of Qualityof Life in Hispanic Patients with Cancer. Cancer Pract 6:318–324
7. Larson PJ, Viele CS, Coleman S et al. (1993) Comparison ofPerceived Symptoms of Patients Undergoing Bone MarrowTransplant and the Nurses Caring for Them. Oncol Nurs Forum20:81–87
8. Levin DN, Cleeland CS, Dar R (1985) Public Attitudes towardCancer Pain. Cancer 56:2337–2339
9. Morrison RS, Wallenstein S, Natale DK et al. (2000) “WeDon’t Carry That"- Failure of Pharmacies in PredominantlyNon-White Neighborhoods to stock Opioid Analgesics. N EnglJ Med 342:1023–1026
10. Reyes-Gibby CC, McCrory LL, Cleeland CS (2003) Variationsin Patients’ Self-Report of Pain by Treatment Setting. J PainSymptom Manage 25:444–448
11. Rimer B, Levy MH, Keintz MK et al. (1987) Enhancing CancerPain Control Regimens through Patient Education. Patient EducCouns:267–277
12. Thomason TE, McCune JS, Bernard SA et al. (1998) CancerPain Survey: Patient-Centered Issues in Control. J Pain SymptomManage 15:275–284
13. Von Roenn JH, Cleeland CS, Gonin R et al. (1993) PhysicianAttitudes and Practice in Cancer Pain Management. A Surveyfrom the Eastern Cooperative Oncology Group. Ann Intern Med119:121–126
14. Ward SE, Goldberg N, Miller-McCauley et al. (1993) Patient-RelatedBarriers to Management ofCancer Pain. Pain52:319–324
15. World Health Organization (1986) Cancer Pain Relief. WHO,Geneva
Cancer Pain Management, Principles ofOpioid Therapy, Dosing Guidelines
JAMES F. CLEARY
University of Wisconsin Comprehensive CancerCenter, Madison, WI, [email protected]
Characteristics� Opioids are the mainstay of cancer pain manage-ment. All patients with moderate to severe cancer painshould have access to opioids (Cleary 2000). The pri-mary goal of opioid dosing is to establish pain reliefwith regular dosing within a therapeutic window, thedose that maximises pain control with minimal sideeffects. Opioids can be administered by various routes:oral (immediate-release or modified-release products);transdermal; transmucosal; intravenous; subcutaneousor intraspinal.
Initial Dosing
In most cases, the initial treatment with opioids beginswith short-acting formulations. This may be in theform of opioid-only products (codeine, oxycodone or
morphine) or oral combination products (e.g. hydro-codone/acetaminophen or oxycodone/acetaminophen).The dose-limiting factor in these combination productsis acetaminophen. The total daily dose should be limitedto 4 grams, placing a limitation of 8–12 tablets per day,depending on the dose of acetaminophen. Short-actingopioids are normally administered every 3–4 h, butproducts such as immediate-release oxycodone or mor-phine may be given as often as hourly in the situationof uncontrolled pain.Modified- or slow-release opioid products should beused cautiously as an initial opioid treatment, giventhe potential for side effects and the longer eliminationwith these compounds. This is particularly true withthe elderly and those with renal impairment, in whomopioid clearance may be decreased, causing increasedand prolonged side effects with low doses of theseproducts (Osborne et al. 1986).
Around-the-Clock Dosing
Theroutineadministration ofopioidsat regular intervalshas been an important part of cancer pain management(Saunders 1963). In registration studies, investigatorshave found analgesic equivalence between immediate-release products and modified-release products at iden-tical daily doses (Walsh et al. 1992). Improved patientcompliance, and, therefore, improved pain control, isanticipated with modified-release products. However,in the situation of limited resources, patients can beprescribed regularly-administered, immediate-releaseoral products with the anticipation of satisfactory paincontrol.Patients can be converted from immediate-releaseproducts to modified-release products. Some modified-release products have a biphasic release mechanismthat results in both immediate and more sustained painrelief. The dose of the modified-release formulationshould be calculated by converting the daily dose ofimmediate-release opioids (including those adminis-tered parenterally) to the modified-release formulation,which is then administered over the 24-h period accord-ing to the medication’s dosing schedule.There are now oral opioids approved for daily and twicedaily dosing. The transdermal fentanyl patch has a du-ration of 2–3 days. With modified-release compounds,dose escalation is usually best accomplished by increas-ing the dose rather than shortening the dosing interval.However, a careful history should be taken to explore theconcept of “end of dose failure.” Apatient may report ef-fectiveanalgesia for8–10 h following theadministrationof a modified-release opioid on a twice daily schedule.Rather than increasing the dose and therefore increasingthe risk of side effects, it may be preferable to decreasethe dosing interval to every 8 h. This also applies to oncedaily oral products, with which twice daily dosing maybe necessary. With the transdermal fentanyl patch, pa-tients may report only one good day out of three despite

264 Cancer Pain Management, Principles of Opioid Therapy, Drug Selection
increases in the dose delivered per hour. Changing thepatch every 48 hmayresult inmoreeffectivepain control(Payne et al. 1995)� Breakthrough pain can usually be managed by pro-viding a short-acting drug at a dose equal to 10–15% of24-h daily dosing (Portenoy and Hagen 1990). Experi-ence with oral transmucosal fentanyl citrate, however,suggests that there is not a clear correlation between thearound-the-clock opioid dose and the breakthrough paindose (Farrar et al. 1998).
Dose Escalation
If pain is not well controlled and side effects are not se-vere, the dose of opioid should be increased. The per-centage escalation should be based on the severity of thepain, the side effects, and other medical factors. If painis moderate, the increase should be 25–50% of the dailydose (Jacox et al. 1994). If pain is severe, a dose escala-tion of 50–100% of the daily dose should be made. Withmost oral products, this escalation can safely take placeevery 24 h. In the case of the transdermal fentanyl patch,dose escalation should not takeplacemoreoften than ev-ery 48 h, although in inpatient settingswith closeclinicalsupervision, dose increases have been safely made every24 h when needed (Payne et al. 1995).When opioid infu-sions are used in the treatment of pain, dose escalationsshouldtakeplacenomoreoftenthanthetimerequiredforfour half-lives, unless there is careful monitoring. In thecase of morphine, this is every 10–16 h. Escalating theinfusion rate more often than this may result in increaseddrug toxicity. Patients may use patient-controlled anal-gesia together with clinician-administered boluses to ef-fect better pain control, but it will still require 4–5 halflives to reach steady-state.
Pain Emergency
In the case of a pain emergency, a loading dose may bethe most effective way to treat the pain (Davis 2004).The loading dose should be established with frequentdosing administered either intravenously or subcuta-neously. Many clinicians commence an opioid infusionalone, but it will require 4–5 half-lives before maximalpain relief can be achieved. With the half life of mor-phine being 2.5–4 h, it would take 10–16 h to reachsteady state, and therefore potentially leave the patientwith uncontrolled pain. If a loading dose is added to anopioid infusion, the ongoing opioid dose should be thesum of the previous opioid regimen together with thatcalculated from the loading dose.
Dosing in Special Situations
In thepresenceof renal impairment(Osborneetal.1986)and in the elderly (Cleary and Carbone 1997), the clear-ance of either primary drug or metabolites may bedecreased. Therefore, both more cautious titration andlonger dosing intervals may be necessary. Near the end
of life, it may also be appropriate to decrease the doseof morphine administered to reduce the risk of toxicity.
References1. Cleary JF (2000) Cancer Pain Management Cancer Control
7:120–1312. Cleary JF, Carbone PP (1997) Palliative Medicine in the Elderly.
Cancer 80:1335–13473. Davis MP (2004) Acute Pain in Advanced Cancer: An Opi-
oid Dosing Strategy and Illustration. Am J Hosp Palliat Care21:47–50
4. Farrar JT, Cleary J, Rauck R et al. (1998) Oral Transmucosal Fen-tanyl Citrate: Randomized, Double-Blinded, Placebo-ControlledTrial for Treatment of Breakthrough Pain in Cancer Patients JNatl Cancer Inst 90: 611–616
5. Jacox A, Carr DB, Payne R et al. (1994) Management of CancerPain: Clinical Practice Guideline No 9. Agency for Health CarePolicy and Research. US Dept of Health and Human Services,Public Health Service AHCPr Publication 94-052
6. Osborne RJ, Joel SP, Slevin ML (1986) Morphine Intoxicationin Renal Failure: The Role of Morphine-6-Glucuronide. BMJ292:1548–1549
7. Payne R, Chandler S, Einhaus M (1995) Guidelines for the Clin-ical Use of Transdermal Fentanyl. Anticancer Drugs 6:50–53
8. Portenoy RK, Hagen NA (1990) Breakthrough Pain: Definition,Prevalence and Characteristics. Pain 41:273–281
9. Saunders C (1963) The Treatment of Intractable Pain in TerminalCancer. Proc R Soc Med 56:195–197
10. Walsh TD, MacDonald N, Bruera E et al. (1992) A ControlledStudy of Sustained-Release Morphine Sulfate Tablets in ChronicPain from Advanced Cancer. Am J Clin Oncol 15:268–272
Cancer Pain Management, Principles ofOpioid Therapy, Drug Selection
MARIE FALLON
Department of Oncology, Edinburgh Cancer Center,University of Edinburgh, Edinburgh, [email protected]
Definition� Opioid is a general term that includes naturally occur-ring, semisynthetic, and synthetic drugs that producetheir effects by combining with opioid receptors andare stereospecifically antagonized by naloxone. Opioiddrugs are the mainstay in the treatment of moderate tosevere cancer pain.
Characteristics
Although concurrent use of other approaches and inter-ventions may be appropriate in many patients, and nec-essary in some, analgesic drugs are needed in almost ev-ery patient with cancer pain.Thekeystone of cancerpainmanagement is a good assessment. Insight into the com-plexmultidimensionalfeaturesofcancerpain,andanap-preciationof thepatient’sclinicalandpsychosocialchar-acteristics, are fundamental for the success of any painmanagement strategy, pharmacological or otherwise.Drugs whose primary clinical action is the relief of painare conventionally classified on the basis of their activ-ity at opioid receptors, as either opioid or non-opioid

C
Cancer Pain Management, Principles of Opioid Therapy, Drug Selection 265
analgesics. A third class, � adjuvant analgesics, aredrugs with other primary indications that can be effec-tive analgesics in specific circumstances. The majorgroup of drugs used in cancer pain management are theopioid analgesics.Analgesic therapy with opioids, non-opioids and adju-vant analgesics is developed for the individual patientthrough a process of continuous evaluation, so thata favorable balance between pain relief and adversepharmacological effects is maintained. The WorldHealth Organization (WHO) structured approach todrug selection for cancer pain, known as the � WHOanalgesic ladder, when combined with appropriate dos-ing guidelines is capable of providing adequate relief to70–90% of patients (World Health Organization 1986;Ventafridda et al. 1987; Takeda 1990; Walker et al. 1983;Schug et al. 1990; Zech et al. 1995). This approach em-phasizes that the intensity of pain, rather than its specificetiology, should be the prime consideration in analgesicselection.The WHO ladder was never intended to be used inisolation. Rather, it should be integrated with otherapproaches to cancer pain management such as ra-diotherapy, chemotherapy, anesthetic interventions,physiotherapy and relaxation techniques.The WHO ladder approach advocates three basic steps(Fig. 1): Patients with mild cancer-related pain shouldbe treated with a non-opioid analgesic (also knownas a � simple analgesic), which should be combinedwith adjuvant drugs, if a specific indication for theseexists. For example, a patient with mild to moderate
Cancer Pain Management, Principles of Opioid Therapy, Drug Selec-tion, Figure 1 WHO analgesic ladder.
arm pain caused by radiation-induced brachial plex-opathy may benefit when a tricyclic antidepressant isadded to paracetamol (acetaminophen) (McQuay andMoore 1997; Kalso et al. 1998).Patients who are relatively non-tolerant and presentwith moderate pain, or who fail to achieve adequaterelief after a trial of a non-opioid analgesic, should betreated with an opioid conventionally used for mild tomoderate pain (formerly known as a “weak” opioid).This treatment is typically accomplished using a com-bination product containing a non-opioid (e.g. aspirinor paracetamol (acetaminophen)) and an opioid (suchas codeine, oxycodone or propoxyphene). This com-bination can also be coadministered with an adjuvantanalgesic. The doses of these combination products canbe increased until the maximum dose of the non-opioidanalgesic is attained (e.g. 4000–6000 mg paracetamol(acetaminophen)); beyond this dose, the opioid con-tained in the combination product could be increasedas a single agent, or the patient could be switched to anopioid conventionally used in Step 3.Patients who present with severe pain, or who fail toachieve adequate relief following appropriate admin-istration of drugs on the second step of the analgesicladder, should receive an opioid conventionally used formoderate to severe pain (formerly known as a “strong”opioid). This group includes morphine, diamorphine,fentanyl, oxycodone, phenazocine, hydromorphone,methadone, levorphanol, and oxymorphone. Thesedrugs may also be combined with a non-opioid anal-gesicoran adjuvantdrug.Clearly, theboundary betweenopioids used in the second and third steps of the anal-gesic ladder is somewhat artificial, since low doses ofmorphine or other opioids for severe pain can be lesseffective than high doses of codeine or propoxyphene.Accordingly, some debate surrounds the usefulnessof Step 2 of the WHO ladder. This is currently beingexamined in clinical studies.According to the WHO guidelines, a trial of opioidtherapy should be given to all patients with chronic painof moderate or greater severity. This approach has beensubject to criticism concerning its evidence base and itsuse over time. Much of the evidence is based on compo-nents of the ladder examined in nonmalignant pain, e.g.an opioid combined with a non-opioid is more effectivethan either alone, or systematic reviews of adjuvantanalgesics (which appear to suggest that the numberneeded-to-treat [NNT] for most of the commonly-useddrugs is about three (McQuay and Moore 1998)).Some of the criticism may be related to the commonmisconception that the WHO ladder is a ‘recipe’ forcancer pain management. In fact, it is a set of princi-ples that need to be applied appropriately with othernon-pharmacological treatments to each individualsituation.Themorphine-likeagonistdrugsarewidelyusedtoman-age cancer pain. Although they may differ from mor-

266 Cancer Pain Management, Principles of Opioid Therapy, Drug Selection
phine in quantitative characteristics, they qualitativelymimic the pharmacological profile of morphine, includ-ing both desirable and undesirable effects.Comparative trials of opioids in cancer pain are ex-tremely difficult to perform. While good quality ran-domized trials to provide evidence for pharmacother-apy of cancer pain are preferred, clinical decisions arecurrently based on limited trial evidence; basic pharma-cology of the opioid and particular properties relating torenal, hepatic and cognitive impairment; and progressin basic science which gives foundation to our beliefof genetic variability in response to opioid analgesia(Rossi et al. 1997). No strong evidence speaks for thesuperiority of one opioid over another. For this reason,the aforementioned factors, along with practical clinicalissues such as possible routes of drug administration,determine drug selection.Although most cancer pain is responsive to opioidanalgesia to some extent, the side effects experiencedby an individual are the practical limiting factors inwhat is termed “� opioid-responsiveness.” While pureopioid agonists have no pharmacological ceiling dose, a“� opioid pseudo-pharmacological ceiling dose existsin some situations because of dose-limiting side effects.The common side effects of all opioids are constipa-tion, dry mouth, sedation, nausea and vomiting. Thefirst two often persist, but tolerance usually developsto sedation, nausea and vomiting. Sedation, however,tends to be the common limiting factor during � opioiddose titration, particularly in genetically susceptibleindividuals, or in pain syndromes that usually requirelarger doses of opioid e.g. neuropathic pain (Portenoyet al. 1990).In individuals troubledwithsideeffects,especiallyseda-tion, with one opioid, a switch to an alternative opioidmay result in an improved balance between analgesiaand unwanted side-effects (Fallon 1997). It is impossi-ble to predict such an improvement, but clinical expe-rience with opioids makes this an acceptable strategy.In the case of neuropathic pain, use and titration of anappropriate adjuvant analgesic would seem another crit-ical step in improving thebalancebetween analgesiaandside effects.Thereareno good data thatexaminea route switch ratherthan an � opioid switch as a beneficial strategy in themanagement of � opioid adverse effects. Clinically, themain benefit in switch to the spinal route of delivery isthe possibility of adding drugs to manage neuropathicpain and incident pain, such as local anesthetic.The transdermal route can be useful in patients havingswallowing difficulties and in some cases of resistantconstipation with oral opioids. Studies with transdermalfentanyl show a trend towards less constipation (Wonget al. 1997).There is one randomized, controlled trial comparingoxycodone favorably with morphine with regard to hal-lucinations, however, the numbers are small and larger
trials would be needed to say there is good evidence forthe superiority of oxycodone (Kalso and Vainio 1990).Hydromorphone is another alternative to morphine iftoxicity or drowsiness is problematic, but again, thereis no high quality evidence suggesting that one drug issuperior to another.Methadone is a synthetic opioid with unusual qualitiesand different pharmacologicalproperties from the otheropioids used in cancer pain. Steady-state plasma con-centration is usually reached at one week, but may takeup to 28 days. Serious adverse effects are avoided if theinitialperiodofdosing isaccomplishedwith“asneeded”administration, which is not the usual recommendationin cancer pain dosing regimens. When steady-state hasbeen achieved, scheduled dose frequency should bedetermined by the duration of analgesia following eachdose.The � equianalgesic dose ratio of morphine to metha-done has been the subject of controversy. Recent datasuggest that the ratio correlates with the total opioiddose administered before switching to methadone.Among patients receiving low doses of morphine theratio is 4:1. In contrast, for patients receiving more than300 mg of oral morphine, the ratio is approximately10:1 or 12:1 (Ripamonti et al. 1998).The therapeutic armamentarium for opioids has ex-panded over time, and familiarity with a range of opioidagonists and with the use of equianalgesic tables toconvert doses if switching opioids, is necessary (Ta-ble 1). It is clear that patients are at risk of under- orover-dosing by virtue of individual sensitivities; hence,a logical, systematic approach to reassessment of theentire clinical situation is the key to managing opioidadverse effects and/or uncontrolled cancer pain, ratherthan an automatic switch to another opioid.
References1. Fallon MT (1997) Opioid Rotation – Does It Have a Role? Palliat
Med 11:176–1782. Kalso E, Tramer MR et al. (1998) Systemic Local Anaesthetic-
Type Drugs in Chronic Pain: A Systematic Review. Eur J Pain2:3–14
3. Kalso E, Vainio A (1990) Morphine and Oxycodone Hydrochlo-ride in the Management of Cancer Pain. Clin Pharmacol Ther47:639–646
4. McQuay HJ, Moore RA (1997) Antidepressants and ChronicPain. BMJ 314:763–764
5. McQuay H, Moore A (1998) An Evidence-Based Resource forPain Relief. Oxford Medical Publications, Oxford
6. Portenoy RK, Foley KM, Inturrisi CE (1990) The Nature of Opi-oid Responsiveness and its Implications for Neuropathic Pain:New Hypotheses Derived from Studies of Opioid Infusions. Pain43:273–286
7. Ripamonti C, De Conno F et al. (1998) Equianalgesic Dose/Ratiobetween Methadone and other Opioid Agonists in Cancer Pain:Comparison of Two Clinical Experiences. Ann Oncol 9:79–83
8. Rossi GC, Leventhal L, Pan YX et al. (1997) Antisense Map-ping of MOR-1 in Rats. Distinguishing between Morphine andMorphine-6 Beta-Glucuronide Antinociception. J PharmacolExp Ther 281:109–114

C
Cancer Pain Management, Principles of Opioid Therapy, Drug Selection 267
Cancer Pain Management, Principles of Opioid Therapy, Drug Selection, Table 1 Opioid analgesics (pure mu agonists) used for the treatment ofchronic pain
Morphine-like agonists
Equi-anal-gesicdosesa
Half-life(hr)
PeakEffect(hr)
Duration(hr)
Toxicity Comments OralBioavail-ability(%)
Activemetabolites
Morphine 10 s.c.20–60p.o.b
2–32–3
0.5–11.5–2
3–64–7
Constipation,nausea, sedationmost common;respiratorydepression rare incancer patients
Standard comparison foropioids; multiple routesavailable
20–30 M6G
Controlled-releasemorphine
20–60
p.o.b2–3 3–4 8–12 20–30 M6G
Sustained-releasemorphine
20–60
p.o.b2–3 4–6 24 Once-a-day morphine
approved in some countries20–30 M6G
Hydromorphone 1.5 s.c.7.5 p.o.
2–32–3
0.5–11–2
3–43–4
Same as morphine Used for multiple routes 35–80 No
Oxycodone 20–30 2–3 1 3–6 Same as morphine Combined with aspirinor acetaminophen, formoderate pain in USA;available orally withoutcoanalgesic for severe pain
60–90 oxymorphone
Controlled-releaseoxycodone
20–30 2–3 3–4 8–12 oxymorphone
Oxymorphone 1 s.c.10 p.r.
––
0.5–11.5–3
3–64–6
Same as morphine No oral formulation glucuronides
Meperidine(pethidine)
75 s.c. 2–3 0.5–1 3–4 Same asmorphine + CNSexcitation;contraindicated inthose on MAOinhibitors
Not used for cancer paindue to toxicity in higherdoses and short half-life
30–60 norpethidine
Diamorphine 5 s.c. 0.5 0.5–1 4–5 Same as morphine Analgesic action due tometabolites, predominantlymorphine; only available insome countries
Morphine
Levorphanol 2 s.c.4 p.o.
12–16 0.5–1 4–6 Same as morphine With long half-life,accumulation occurs afterbeginning or increasing dose
No
Methadonec 10 s.c.20 p.o.(seetext)
12 ≥150 0.5–1.5
4–8 Same as morphine Risk of delayed toxicity dueto accumulation; useful tostart dosing on p.r.n.
60–90 No
Codeine 130s.c.200p.o.
2–3 1.5–2 3–6 Same as morphine Usually combined withnon-opioid
60–90 morphine
PropoxypheneHCI (Dextro-propoxyphene)
– 12 1.5–2 3–6 Same as morphineplus seizures withoverdose
Toxic metaboliteaccumulates but notsignificant at doses usedclinically; usually combinedwith non-opioid
40 norpropoxy-phene
Propoxyphenenapsylate(Dextro-propoxyphene)
– 12 1.5–2 3–6 Same ashydrochloride
Same as hydrochloride 40 norpropoxy-phene
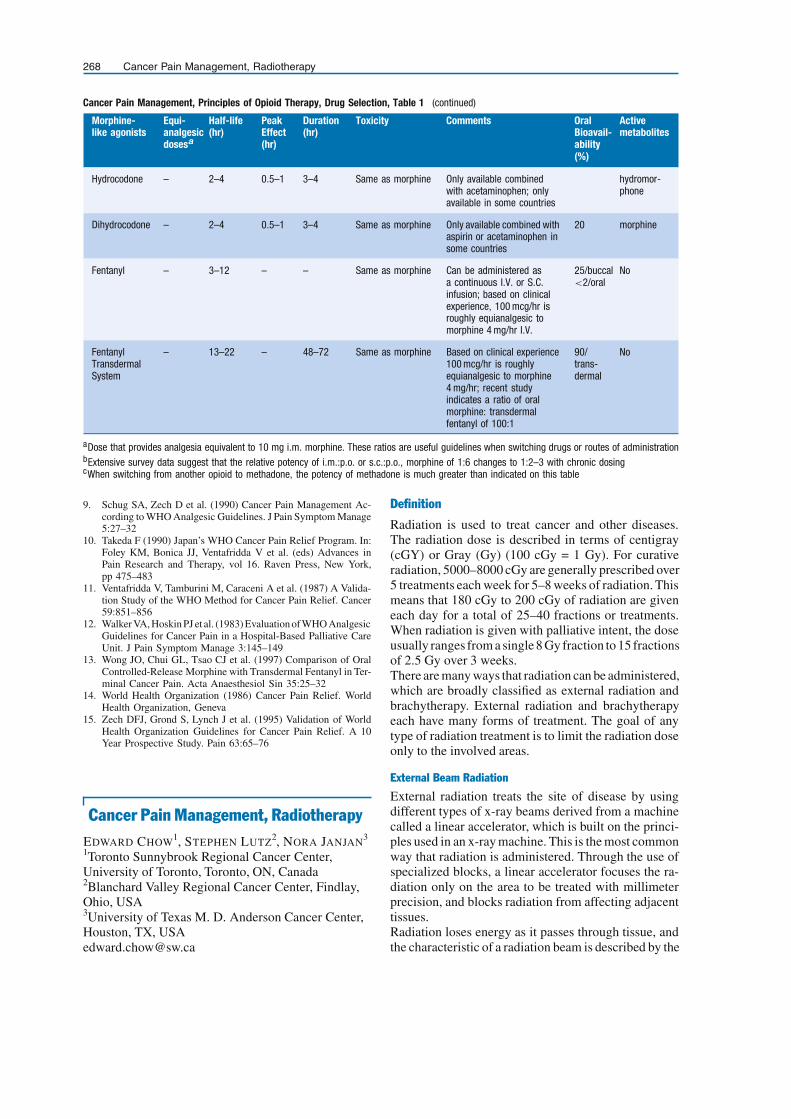
268 Cancer Pain Management, Radiotherapy
Cancer Pain Management, Principles of Opioid Therapy, Drug Selection, Table 1 (continued)
Morphine-like agonists
Equi-analgesicdosesa
Half-life(hr)
PeakEffect(hr)
Duration(hr)
Toxicity Comments OralBioavail-ability(%)
Activemetabolites
Hydrocodone – 2–4 0.5–1 3–4 Same as morphine Only available combinedwith acetaminophen; onlyavailable in some countries
hydromor-phone
Dihydrocodone – 2–4 0.5–1 3–4 Same as morphine Only available combined withaspirin or acetaminophen insome countries
20 morphine
Fentanyl – 3–12 – – Same as morphine Can be administered asa continuous I.V. or S.C.infusion; based on clinicalexperience, 100 mcg/hr isroughly equianalgesic tomorphine 4 mg/hr I.V.
25/buccal<2/oral
No
FentanylTransdermalSystem
– 13–22 – 48–72 Same as morphine Based on clinical experience100 mcg/hr is roughlyequianalgesic to morphine4 mg/hr; recent studyindicates a ratio of oralmorphine: transdermalfentanyl of 100:1
90/trans-dermal
No
aDose that provides analgesia equivalent to 10 mg i.m. morphine. These ratios are useful guidelines when switching drugs or routes of administrationbExtensive survey data suggest that the relative potency of i.m.:p.o. or s.c.:p.o., morphine of 1:6 changes to 1:2–3 with chronic dosingcWhen switching from another opioid to methadone, the potency of methadone is much greater than indicated on this table
9. Schug SA, Zech D et al. (1990) Cancer Pain Management Ac-cording to WHO Analgesic Guidelines. J Pain Symptom Manage5:27–32
10. Takeda F (1990) Japan’s WHO Cancer Pain Relief Program. In:Foley KM, Bonica JJ, Ventafridda V et al. (eds) Advances inPain Research and Therapy, vol 16. Raven Press, New York,pp 475–483
11. Ventafridda V, Tamburini M, Caraceni A et al. (1987) A Valida-tion Study of the WHO Method for Cancer Pain Relief. Cancer59:851–856
12. Walker VA, Hoskin PJ et al. (1983) Evaluation of WHO AnalgesicGuidelines for Cancer Pain in a Hospital-Based Palliative CareUnit. J Pain Symptom Manage 3:145–149
13. Wong JO, Chui GL, Tsao CJ et al. (1997) Comparison of OralControlled-Release Morphine with Transdermal Fentanyl in Ter-minal Cancer Pain. Acta Anaesthesiol Sin 35:25–32
14. World Health Organization (1986) Cancer Pain Relief. WorldHealth Organization, Geneva
15. Zech DFJ, Grond S, Lynch J et al. (1995) Validation of WorldHealth Organization Guidelines for Cancer Pain Relief. A 10Year Prospective Study. Pain 63:65–76
Cancer Pain Management, RadiotherapyEDWARD CHOW1, STEPHEN LUTZ2, NORA JANJAN3
1Toronto Sunnybrook Regional Cancer Center,University of Toronto, Toronto, ON, Canada2Blanchard Valley Regional Cancer Center, Findlay,Ohio, USA3University of Texas M. D. Anderson Cancer Center,Houston, TX, [email protected]
Definition
Radiation is used to treat cancer and other diseases.The radiation dose is described in terms of centigray(cGY) or Gray (Gy) (100 cGy = 1 Gy). For curativeradiation, 5000–8000 cGy are generally prescribed over5 treatments each week for 5–8 weeks of radiation. Thismeans that 180 cGy to 200 cGy of radiation are giveneach day for a total of 25–40 fractions or treatments.When radiation is given with palliative intent, the doseusually ranges from a single 8 Gy fraction to 15 fractionsof 2.5 Gy over 3 weeks.There are many ways that radiation can be administered,which are broadly classified as external radiation andbrachytherapy. External radiation and brachytherapyeach have many forms of treatment. The goal of anytype of radiation treatment is to limit the radiation doseonly to the involved areas.
External Beam Radiation
External radiation treats the site of disease by usingdifferent types of x-ray beams derived from a machinecalled a linear accelerator, which is built on the princi-ples used in an x-ray machine. This is the most commonway that radiation is administered. Through the use ofspecialized blocks, a linear accelerator focuses the ra-diation only on the area to be treated with millimeterprecision, and blocks radiation from affecting adjacenttissues.Radiation loses energy as it passes through tissue, andthe characteristic of a radiation beam is described by the

C
Cancer Pain Management, Radiotherapy 269
amount of energy that is lost as it passes through the tis-sue.ThetermDmax refers tothedepthofthe tissuewhere100% of the radiation dose is deposited. Only 50% of theprescribed radiation dose from a single beam may pene-trate to a tumor located 10 cm from the skin surface. Toovercome this, many beams of radiation are routinelyused to treat a tumor. The sum of the radiation doses atthe tumor gives a high total radiation dose.The choice of the type of radiation used in a radiationtreatment plan depends on the location of the tumor andcritical structures near the tumor. The concept of inte-gral dose is used to describe the selection of the type ofradiation in order to maximize the radiation dose in thetumor, yet minimize treatment of uninvolved adjacenttumors.Newer forms of radiation treatment planning, like three-dimensional conformal radiation therapy and intensitymodulated radiation therapy, apply the principles of in-tegral dose by targeting the tumor through multiple low-doseradiationbeams.All theradiationenergyfromthesebeams adds to give the tumor a very high radiation dose,but theradiationdosefromtheindividualbeamsisso lowthat there are minimal effects from the radiation in theadjacent normal tissues.There are many types of external beam radiation that arederived from a linear accelerator. These types of radia-tion include gamma rays and electron beam radiation.Gamma rays are used to treat tumors located deep inthebody,whileelectron beam radiation treats superficialcancers.
Gamma Rays
Gamma rays are penetrating forms of x-rays, and manyenergy levels of gamma rays are available for treatment(Tables 1 and 2). In general:
• High-energy gamma rays deeply penetrate the tissuesbut spare the skin from radiation reactions like ery-themaand moistdesquamation.This typeof radiationis used to treat deep-seated tumors in the abdominaland pelvic areas. Due to the characteristics of high-energy gamma rays, the skin receives little to no dose.
• An example of a high-energy gamma radiation beamis an 18 MV photon beam [a photon is a package ofenergy]. If 100 cGy is prescribed from one radiationbeam, 100 cGy is deposited 3.5 cm from the skin sur-face [Dmax] and 85% of the radiation dose [85 cGy]is deposited at 10 cm of tissue below the skin surface.
• Low-energy gamma rays do not penetrate the tissueswell and cause more skin reactions. This type of radi-ation is used to treat head and neck cancers and breastcancers where there may be tumor infiltration of theskin.
• An example of a low energy gamma radiation beam isa Cobalt-60 beam or a 6 MV photon beam. If 100 cGyis prescribed from one 6 MVradiation beam, 100 cGyis deposited 1.5 cm from theskin surface [Dmax], and
60% of the radiation dose [60 cGy] is deposited at10 cm of tissue below the skin surface.
Electron Beam Radiation
Electronbeamradiation isusedto treatcancers locatedinthe superficial tissues, like lymph nodes in the neck, thechest wall after a mastectomy, and skin cancers. It pro-vides an important alternative to gamma rays, becauseunderlying critical structures like the heart and spinalcord may not receive any radiation at all from electronbeam therapy.
• The depth of penetration in centimeters of tissue froman electron beam energy can be generalized by thefollowing rule (Table 1):
• 80%of the radiation dosewillbedeposited if theelec-tron beam energy is divided by three, and 95% of theradiation dose will be deposited if the electron beamenergy is divided by two.
– Forexample, a9 MeVelectron beam deposits80%of the dose 3 cm from the skin surface and 95% ofthe dose 4.5 cm from the skin surface.
External beam treatment planning involves the specificselection of radiation beams to target the tumor and min-imize treatment of adjacent normal tissues. Limiting thedose of radiation to adjacent tissues is critical to avoidside effects from radiation. These treatment-related sideeffects,especially those tomucosalsurfaces that result inmucositis, nausea and diarrhea, can significantly impacton the functional status of the patient. This is of particu-lar concern in patients who are already debilitated fromtheir disease.
Brachytherapy
Brachytherapy is the placement of radioactive sourcesin or adjacent to a tumor bed. These radioactive sourcescan be permanently implanted in a tumor or placed tem-porarily near the tumor location.Permanently implantedradiation sources are used to treat prostate cancer. Theradiation dose gradually decays until no further radi-ation is emitted. For lung cancer, radioactive sourcesthat are placed in a catheter are temporarily adjacent toa tumor blocking the bronchus for a prescribed amountof time to deliver a specific radiation dose. After theprescribed amount of time, the radiation sources areremoved. Brachytherapy also uses high-dose rate [avery strong radioactive source that gives radiation overa few minutes] and low-dose rate [a radioactive sourcethat gives a low-dose of radiation over several hours].The choice of brachytherapy used primarily depends onthe tumor location. The radiation dose is extremely lo-calized because of the Inverse Square Law [Radiationdose = 1/d2]. Applying this principle, the radiation dosedropsoffrapidlyasthedistancefromtheradiationsourceincreases. For example, the radioactive dose 2 cm awayfrom the radioactive source is only one-fourth the radia-

270 Cancer Pain Management, Radiotherapy
Cancer Pain Management, Radiotherapy, Table 1 Gamma Radiation – Prescribing 100 cGy for a tumor located 10 cm below the skin
Type of GammaBeam
Dmax [cm belowskin surface]
% Depth Dose at10 cm below theskin surface
Dose of radiation[cGy] needed togive 100 cGy @10 cm below theskin
Dose of radiationat Dmax with eachradiation fraction
Total dose ofradiation to theskin at Dmax [20radiation fractions]
Cobalt-60 0.5 cm 57% 175 cGy 175 cGy 3500 cGy ∼= 0.5 cm
6 MV photons 1.5 cm 65% 154 cGy 154 cGy 3080 cGy ∼= 1.5 cm
18 MV photons 3.5 cm 80% 125 cGy 125 cGy 2500 cGy ∼= 3.5 cm
Dmax is the depth in cm below the skin surface where 100% of the prescribed radiation dose is given. The % depth dose at 10 cm is the % of theprescribed radiation that penetrates to a tumor located 10 cm below the skin surface = 100 cGy/% depth dose. 2000 cGy will be given to the tumor[located 10 cm from the skin surface] from an anterior radiation field. Another 2000 cGy will be given to the tumor from a posterior radiation field. Thiswill deliver 4000 cGy to the tumor. Each radiation fraction will equal 200 cGy [100 cGy from the anterior and 100 cGy from the posterior field] and 20fractions will be required to give a total radiation dose of 4000 cGy. 18 MV photons are more effective in treating abdominal and pelvic tumors andthey cause little skin reaction. Cobalt-60 and 6 MV photons are effective in treating more superficial tumors like head and neck and breast cancersthat may have tumor infiltration of the skin; in this case a higher radiation dose to the skin is essential to control the tumor.
Cancer Pain Management, Radiotherapy, Table 2 Electron Beam Radiation - Radiation is deposited over a short distance from the skin’s surface
Type of Electron Beam Dmax [cm below skin surface] 80% of radiation dosedeposited within
95% of radiation dosedeposited within
6 MeV 1.5 cm 2 cm 3 cm
9 MeV 2.3 cm 3 cm 4.5 cm
12 MeV 3 cm 4 cm 6 cm
As an example, if a 100 cGy of radiation is administered with 6 MeV electron beam, 100 cGy would be given at 1.5 cm below the skin, only 20 cGy wouldbe delivered 2 cm below the skin surface [80% of the radiation dose deposited within 2 cm of the skin surface] and only 5 cGy would be delivered 3 cmbelow the skin surface [95% of the radiation dose delivered within 3 cm of the skin surface]. Therefore, 80% of the radiation dose is given between1.5 cm and 2 cm from the skin surface. Less than 5% of the radiation dose reaches structures more than 3 cm from the skin surface.
tion dose next to the source. Brachytherapy is an impor-tant option in palliative care,because it can deliver radia-tion over a few minutes to days instead of several weeks.As the radiation is well localized, brachytherapy can beused tore-irradiate tissues thathavepreviouslybeen irra-diated. Treatment-related side effects with brachyther-apy are limited.Radioactive isotopes, which have affinity to specificareas like the bone or thyroid, can also be injectedinto the blood stream and are a form of brachytherapy.The effects of the radiation are localized to the site ofdeposition and little radiation is administered to ad-jacent tissues. Like more conventional brachytherapy,� radioisotopes allow re-irradiation of previously irra-diated areas because the radiation dose is concentratedin the site of disease.Radiotherapy results in damage to cellular DNA. Ra-diotherapy causes both direct and indirect damage to thereproductive DNA material of the cell. Direct damagetakes place in the form of base deletions, single anddouble strand breaks in the DNA chain. Indirect damageoccurs by the interaction of radiotherapy with watermolecules in the cell, which releases toxic free radicals.
Mechanisms of Action� Palliative radiotherapy is well established for thetreatment of symptomatic � bone metastases. The ex-
act mechanism of its action is still uncertain, althoughtumor cell kill may be an important reason. However,the absence of a dose-response relationship, rapid re-sponses, and poor correlation of symptomatic reliefwith radiosensitivity suggest that an effect on hostmechanisms of � pain could also be important.Markers of bone remodeling have been shown to be sup-pressed by anti-resorptive therapy, and the response ofthese bone markers has been applied to monitoring ther-apy for bone metastases.In the recent UK Bone Pain Radiotherapy Trial (BonePain Trial Working Party 1999), 22 patients were en-tered into a supplementary study to establish the effectsof local radiotherapy for metastatic bone pain on mark-ers of osteoclast activity, particularly the pyridiniumcrosslinks pyridinoline and deoxypyridinoline, thelatter being specific for bone turnover. Urine sampleswere collected before and one month after radiotherapy.Patients were treated with either a single 8 Gy or 20 Gyin 5 daily fractions. Pain response was scored withvalidated pain charts completed by patients.Urinary pyridinium concentrations were correlatedwith pain response. In patients who did not respondto palliative radiation (non-responders), baseline con-centrations of both pyridinoline and deoxypyridinolinewere higher than those who responded (responders), androse further after treatment, whereas in responders, the

C
Cancer Pain Management, Radiotherapy 271
Cancer Pain Management,Radiotherapy, Figure 1 Effect ofRadiotherapy on Urinary Markersof Osteoclast Activity Related toPain Response. Total: 22 patients,8 with breast cancer and 14 withprostate cancer; 5 patients showedno response, 9 a partial responseand 8 a complete response.
mean values remained unchanged (Fig. 1). This resultedin significant differences between responders and non-responders for both indices after treatment (P = 0.027).The authors concluded that radiotherapy-mediated inhi-bition of bone resorption, and thus osteoclastic activity,could be a predictor for pain response. They also pro-posed that tumor cell killing reduces the production ofosteoclast-activating factors, or there is a direct effectupon osteoclasts within the radiation volume, distinctfrom tumor shrinkage. Their study supports the resultsfrom randomized trials that high dose radiotherapy isnot necessary for pain relief, and that single low-dosesof treatment are more than adequate for most patients(Hoskin et al. 2000).
Characteristics
External Beam Local Radiotherapy
Radiation therapy has long been employed in the man-agement of bone metastases, including relief of bonepain, prevention of impending fractures and promotionof healing in � pathological fractures. Stabilizationof bony destruction occurs in 80% and re-ossificationtakes place in 50% of patients after radiotherapy.Palliation of bone metastases comprises a significantworkload in the specialty of radiation oncology. Exter-nal beam radiation therapy is effectiveand cost-effectivein relieving symptomatic bone metastases. The mostcommonly employed schemes to treat bone metastases

272 Cancer Pain Management, Radiotherapy
include a single 8 Gy, 20 Gy in 5 daily fractions, 30 Gyin 10 daily fractions and 40 Gy in 20 daily fractions.Numerous randomized trials have been conducted ondose-fractionation schedules of palliative radiotherapy.Despite that, there is still no uniform consensus on theoptimal dose fractionation scheme.Retrospective series have documented prompt improve-ment in pain in 80–90% of patients with various dosefractionations, without causing significant hematolog-ical or gastrointestinal side effects. One of the firstrandomized studies on bone metastases was conductedby the Radiation Therapy Oncology Group (RTOG).The initial analysis of this trial (RTOG 74-02) concludedthat a low dose short-course schedule was as effectivein pain relief as more aggressive high-dose protractedschedules (Tong et al. 1982). However, this study wascriticized for using physician-based pain assessment.A re-analysis of the same set of data, grouping solitaryand multiple bone metastases, using the endpoint ofpain relief and taking into account analgesic intake andre-treatment, concluded that the number of radiationfractions was significantly associated with completepain relief. This conclusion was directly contrary tothe initial report (Blitzer 1985), making the choice ofendpoints very important in defining the outcome ofclinical trials (Chow et al. 2002).Several prospective randomized trials have subse-quently been performed that compared the efficacy ofdifferent dose-fractionation schedules. They includedthe recent large-scale multicenter trials comparing theefficacy of a single 8 Gy treatment against multipletreatments. The UK Bone Pain Working Party found nodifference in the degree and duration of pain relief ina study of 765 patients randomized to receive either asingle treatment or 5 fractionated treatments (Bone PainTrial Working Party 1999). The Dutch Bone MetastasesStudy included 1171 patients, and found no differencein pain relief or the quality of life following a single8 Gy or 24 Gy in 6 daily radiation treatments (Steenlandet al. 1999).One critical review on the subject of radiation dose-fractionation suggested that protracted fractionatedradiotherapy, given over 2–4 weeks, results in morecomplete and durable pain relief (Ratanatharathorn etal. 1999). This review was performed because of con-cerns regarding the influence of length of survival on thedurability of pain relief. It was unclear whether higherradiation doses were necessary for durable pain reliefin patients who survived longer. A recent meta-analysisshowed no significant difference in complete and overallpain relief between single and multi-fraction palliativeradiotherapy for bone metastases. No dose-responserelationship could be detected. The meta-analysis re-ported that the complete response rates (absence of painafter radiotherapy) were 33.4% and 32.3% after sin-gle and multi-fraction radiation treatment, respectively,while the overall response rates were 62.1% and 58.7%,
respectively. The latter became 72.7% and 72.5%, re-spectively, when the analysis was restricted to evaluatedpatients alone (Wu et al. 2002). Most patients will ex-perience pain relief in the first two to four weeks afterradiotherapy, be it single or multiple fractionations.How, then, are radiation oncologists to prescribe treat-ment? Despite the equivalence of single and multi-ple fractionations, recent surveys on the patterns ofpractice of radiation oncologists do not suggest theimplementation of employing single fractionation indaily practice (Ben-Josef et al. 1998; Chow et al. 2000;Roos 2000).There is no doubt that in patients with short life ex-pectancy, protracted schedules are a burden. However,in patientswith a longerexpected survival, such asbreastand prostate cancer patients with bone metastases only,other parameters need to be taken into account. Sincere-treatment rates are known to be higher following asingle versus multiple fractions, about 25% versus 10%respectively, patients with good performance status maywish to share the decision-making process. A recentsurvey of patients with bone metastases suggested thatpatients are not prepared to trade off long-term out-comes in favor of a shorter treatment course. Durabilityof pain relief was more important than short-term “con-venience” factors. Patients prefer multiple treatmentsupfront in hopes of avoiding re-treatment (Barton etal. 2001).However, theyneed to beawareof thepotentialphysician bias of more readiness to retreat after singlefraction, accounting for the difference in re-treatmentrates in the trials.The anatomic location to be treated may also influencethe radiation schedule that isused.Smallerdailydosesofradiation [250–300 cGy] are generally better toleratedwhen larger treatment fields are needed over mucosalsurfaces like those in the head and neck region, esoph-agus, abdomen and pelvis.
Re-Irradiation
As effective systemic treatment and better supportivecare result in improved survival, certain subsets of pa-tientswithbonemetastaseshavelonger lifeexpectanciesthan before. An increasing number of patients outlivethe duration of the benefits of initial palliative radio-therapy for symptomatic bone metastases, requiringre-irradiation of the previously treated sites. Addition-ally, some patients fail to respond initially but maybenefit from re-irradiation.Among the radiation trials comparing single versusmultiple fractionation schemes, re-irradiation rates var-ied from 11–42% following single fraction, and 0–24%following multiple-fraction schedules. There are atleast three scenarios of “failure” where re-irradiationmay be considered. Response to re-irradiation may bedifferent for each of these scenarios: 1) no pain relief orpain progression after initial radiotherapy; 2) partial re-sponse with initial radiotherapy and the hope to achieve

C
Cancer Pain Management, Radiotherapy 273
further pain reduction with more radiotherapy, and 3)partial or complete response with initial radiotherapybut subsequent recurrence of pain.Available data support the re-irradiation of sites ofmetastatic bone pain following initial irradiation, par-ticularly where this follows an initial period of response.There is also limited evidence that a proportion of non-responders would respond to re-irradiation. However,there remains a small group of patients who appear to benon-responsive to any amount of palliative radiother-apy. Although the data do support the clinical practiceof re-irradiation, the preferred dose-fractionation at thetime of re-irradiation is unknown.
Wide-Field/Half-Body External Beam Radiation (HBI)
Patients with bone metastases can have multiple sitesof disease and present with diffuse symptoms affectingseveral sites. � Wide-field radiation /half-body externalbeam radiation (HBI) has been used to treat patients withmultiple painful bone metastases. Single fraction HBIhas been shown to provide pain relief in 70–80% of pa-tients. Pain relief is apparent within 24–48 h. Toxici-ties include minor bone marrow suppression and gas-trointestinal side effects, such as nausea and vomiting inupper-abdominal radiation. Pulmonary toxicity is mini-mal provided the lung dose is limited to 6 Gy (correcteddose). Fractionated HBI was investigated in a phase IIstudy that compared a single fraction (n = 14) with frac-tionated HBI (25–30 Gy in a 9–10 fractions) (n = 15).Pain relief was achieved in over 94% of patients. At 1year, 70% in the fractionated and 15% in the single frac-tion group had pain control; re-treatment was requiredin 71% and 13% for the single and fractionated group,respectively. A randomized trial of 499 patients com-pared local radiation alone versus local radiation plus asingle fraction of HBI. The study documented a lowerincidence of new bone metastases (50% vs. 68%), andfewer patients requiring further local radiotherapy at 1year after HBI (60% vs. 76%) (Poulter et al. 1992).
Systemic Radiation – Radioisotopes
Analternativeapproachtothepalliationofmultiplebonemetastases is the administration of a bone seeking ra-dioactive isotope that is taken up at sites of bone metas-tases with osteoblastic activity. The isotopes deliver theradiation dose through the release of beta particles; theirrange of radiation is only a few millimeters, thereby con-centrating their dose within the bone metastases and de-livering little dose to the adjacent normal bone marrow.The radiation half-life is about 50 days in the metastasisand only 14 days in the normal bone marrow. Some ra-dioisotopes also have a gamma component, so that theuptake can be measured by conventional bone scan tech-niques.Systemic radiation using radioisotopes such as stron-tium, samarium and rhenium has been increasingly used
to palliate bone pain and improve the quality of life inthese patients. These agents are particularly usefulamong patients with multiple symptomatic metas-tases. As the radiation is localized to the metastases,radioisotopes can be used for re-irradiation when thereare concerns about normal tissue tolerance to furtherexternal beam radiation. Also, improved outcomesand cost-effectiveness have been demonstrated whenradioisotopes have been combined with external beamradiation. The Trans-Canada Study, comparing externalbeam radiation alone or in combination with Strontium-89 for bone metastases, demonstrated better pain reliefand a reduced need for external beam radiation to othersites in the latter group (Porter et al. 1993). Convenienceto the patient is the other key advantage, because ra-dioisotope therapy is administered as a single injection.With normal bone marrow parameters, re-treatmentwith radioisotope therapy is also possible because theadjacent normal tissues do not receive any radiationdose.A flare of pain, like that seen with hormonal therapyin breast cancer, may precede the relief of symptoms.It may take up to 1 to 2 months before there is reliefof symptoms. Due to this, patients should have a lifeexpectancy that allows the benefit of the relief of symp-toms. Contraindications to bone-seeking radioisotopesinclude compromised bone marrow tolerance definedas a platelet count < 60,000/mL, white blood cell count< 2.5 × 103/mL, disseminated intra-vascular coag-ulation, or myelo-suppressive chemotherapy withinprevious month. As bone-seeking radioisotopes do notpenetrate to soft tissues, they are also contraindicated fortreatment of soft tissue metastases or epidural extensionwith � spinal cord compression. As with external beamradiation, an impending pathological fracture shouldbe evaluated for surgical stabilization. Impending orestablished pathological fractures and cord compres-sions are acute emergencies to be managed by surgicalor radiation oncology teams. Once the fracture or com-pression is stabilized, radioisotopes may be appropriatetherapy for on-going palliation of pain.
Controlling Side Effects of Treatment
Radiation treatment planning is the most critical aspectof reducing radiation side effects. Management of theacute effects of radiotherapy requires attentive medicalmanagement that prevents expected side effect. Radia-tion side effects are specific to the area treated. No sideeffects are observed when a femoral bone metastasis istreated by radiation. Careful radiation treatment plan-ning that avoids critical structures like mucosal surfacescan prevent most side effects.Patients should be reassured that the unavoidable sideeffects that they experience will resolve following thecompletion of radiotherapy. Skin reactions are usuallyminimal during radiotherapy for bone metastases and

274 Cancer Pain Management, Radiotherapy
are limited only to the radiation portal. Nausea and vom-iting, resulting from a radiation portal that includes theabdomen, will usually respond to antiemetic therapy.Diarrhea, resulting from abdominopelvic radiation, willalso usually respond to treatment. Local irritation frommucositis of the oropharyngeal region may be relievedby soluble aspirin, analgesics or benzydamine mouth-washes. Secondary infections, like Candida, should betreated.The side effects of electron beam radiation are more lim-ited because they only treat superficial structures like theribs, skin lesions, and superficial lymph nodes. Underly-ing structures are spared with the selection of the properelectron beam energy. This characteristic is especiallyimportant with re-irradiation to avoid injury to criticalstructures like the spinal cord. The most prominent sideeffect of electron beam radiation is an erythematous skinreactionandpossiblemoistdesquamation.Othersideef-fects listed above do not occur with electron beam radi-ation because the radiation beam does not penetrate tothese structures.No side effects, other than a possible flare of pain in thefirst two weeks after administration, are observed withsystemic radioisotope therapy because all the radiationis localized to the bone. This is a significant considera-tion for patients who have symptoms of the disease orother treatments. Side effects from external beam radi-ation are also more severe when the radiation fields arelarge because more normal tissues are treated. Systemicradioisotopes can have significant advantage over largeexternal beam radiation fields by reducing the risk forside effects like nausea and diarrhea.
Radiotherapy for Complications of Bone Metastases
Pathological and Impending Fractures
Pathological fractures are handled with orthopedic sta-bilization whenever possible. Surgery rapidly controlspainandreturnsthepatienttomobility.Aselectiveortho-pedic stabilization has reportedly resulted in good painrelief and sustained mobility in up to 90% of patients,early identification ofpatientswith ahigh risk of fractureisespecially important.Prophylacticorthopedicfixationis often advised to avoid the trauma of a pathologicalfracture.The criteria often used to determine fracture risk in longbones include:
• Persistent or increasing local pain despite radiother-apy, particularly when aggravated by functional load-ing
• A solitary, well-defined lytic lesion greater than2.5 cm
• A solitary, well-defined lesion circumferentially in-volving more than 50% of the cortical bone
• Metastatic involvement of the proximal femur asso-ciated with a fracture of the lesser trochanter
Although radiotherapy provides pain relief and tumorcontrol, it does not restore bone stability. Postoperativeradiotherapy is usually recommended after surgical sta-bilization ofapathologicfracture.Patientswhoarewith-out visceral metastases and who have a relatively longexpected survival (e.g. > 3 months), are more likely tobenefit from post-op radiotherapy. As the entire bone isat risk for microscopic involvement and the procedureinvolved in rod placement may seed the bone at othersites, the length of the entire rod used for bone stabiliza-tion should be included in the radiation field. When theradiation fields are more limited, instability of the rod,resulting in pain and need for re-operation, can resultfrom recurrent osteolytic metastases outside the radia-tion portal.
Spinal Cord Compression and Cauda Equina Com-pression
Malignant spinal cord and cauda equina compressionis a devastating compression of advanced malignancy.Early diagnosis is essential. Presenting symptoms in-clude radicular pain, paresis, paralysis, paresthesiaand bowel/bladder dysfunction. Surgery, radiation andsteroids are the standard treatment options in this con-dition (Loblaw et al., Group at CCOPGIN-ODS 2003).Radiotherapy results in pain relief in over 75% ofpatients.Radiotherapy is indicated in patients without spinal in-stabilityorbonecompression,whensurgeryismedicallyhazardous or technically difficult, and in patients whorefuse surgery.Pre-existing co-morbidity, pre-treatment ambulatorystatus, the presence of bone compression and spinal in-stability, and patient preferences should be consideredin clinical decision making.The outcome of treatment depends mostly on the speedof diagnosis and neurological status at initiation of treat-ment. Over seventy percent of patients are still ambula-tory following radiation if they are ambulatory on pre-sentation. However, for those who are paralyzed whenthey present for treatment, less than 30%will regainneu-rologic function.
Conclusion
Many formsof radiation therapy arepossible in the treat-ment of bone metastases. Meeting the goal of palliativecare, suffering can be effectively and efficiently relievedwith the use of radiation. Ongoing trials continue to re-fine therapeutic approaches to determine the optimal ra-diation schedule and modalities used. Treatment-relatedside effects can be minimized through the use of radia-tion treatment planning, and anticipating and preventingknown side effects.Comparedtootherapproaches, likesystemicchemother-apy, hormonal therapy and bisphosphonates, that ad-minister treatment on an ongoing basis, all forms ofradiation therapy are completed within a day to several

C
Cancer Pain Management, Rehabilitative Therapies 275
weeks with durable control of symptoms. Cost-benefitanalyses demonstrate the benefit of radiation over otherforms of therapy for bone metastases. Furthermore,there is no evidence to support a survival benefit for theadministration of systemic chemotherapy, hormonaltherapy or bisphosphonates in metastatic disease. Con-sidering quality of life issuesof timespentunder therapy,toxicities of therapy and socioeconomic cost, radiother-apy continues to be under-utilized in the treatment ofbone metastases.
References1. Barton MB, Dawson R, Jacob S et al. (2001) Palliative Radiother-
apy of Bone Metastases: An Evaluation of Outcome Measures.J Eval Clin Pract 7:47–64
2. Ben-Josef E, Shamsa F, Williams A et al. (1998) Radiotherapeu-tic Management of Osseous Metastases: A Survey of CurrentPatterns of Care. Int J Radiat Oncol Phys 40:915–921
3. Blitzer P (1985) Reanalysis of the RTOG Study of the Palliationof Symptomatic Osseous Metastases. Cancer 55:1468–1472
4. Bone Pain Trial Working Party (1999) 8 Gy Single FractionRadiotherapy for the Treatment of Metastatic Skeletal Pain:Randomized Comparison with Multi-Fraction Schedule over12 Months of Patient Follow-Up. Radiother Oncol 52:111–121
5. Chow E, Danjoux C, Wong R et al. (2000) Palliation of BoneMetastases: A Survey of Patterns of Practice among CanadianRadiation Oncologists. Radiother Oncol 56:305–314
6. Chow E, Wu JS, Hoskin P et al. (2002) International Consensuson Palliative Radiotherapy Endpoints for Future Clinical Trialsin Bone Metastases. Radiother Oncol 64:275–280
7. Hoskin PJ, Stratford MRL, Folkes LK et al. (2000) Effect of LocalRadiotherapy for Bone Pain on Urinary Markers of OsteoclastActivity. The Lancet 355:1428–1429
8. Loblaw DA, Laperriere NJ, Chambers A et al., Groupat CCOPGIN-ODS (2003) Diagnosis and Managementof Malignant Epidural Spinal Cord Compression (Evi-dence Summary Report No. 9-9). Cancer Care Ontario;http://www.ccopebc.ca./neucpg.html. Accessed: April 4, 2003
9. Porter A, McEwan A, Powe J (1993) Results of a RandomizedPhase III Trial to Evaluate the Efficacy of Strontium-89 Adjuvantto Local Field External Beam Irradiation in the Managementof Endocrine Resistant Metastatic Prostate Cancer. Int J RadiatOncol Biol Phys 25:805–813
10. Poulter C, Cosmatos D, Rubin P et al. (1992) A Report of RTOG8206: A Phase III Study of Whether the Addition of Single DoseHemibody Irradiation to Standard Fractionated Local Field Irra-diation is More Effective than Local Field Irradiation Alone inthe Treatment of Symptomatic Osseous Metastases. Int J RadiatOncol Biol Phys 23:207–214
11. Ratanatharathorn V, Powers W, Moss W et al. (1999) Bone Metas-tasis: Review and Critical Analysis of Random Allocation Trialsof Local Field Treatment. Int J Radiat Oncol Biol Phys 44:1–18
12. Roos D (2000) Continuing Reluctance to use Single Fractionsof Radiotherapy for Metastatic Bone Pain: An Australian andNew Zealand Practice Survey and Literature Review. RadiotherOncol 56:315–322
13. Steenland E, Leer J, van Houwelingen H et al. (1999) The Effectof a Single Fraction Compared to Multiple Fractions on PainfulBone Metastases: A Global Analysis of the Dutch Bone Metas-tasis Study. Radiother Oncol 52:101–109
14. Tong D, Gillick L, Hendrickson F (1982) The Palliation of Symp-tomatic Osseous Metastases: Final Results of the Study by theRadiation Therapy Oncology Group. Cancer 50:893–899
15. Wu J, Wong R, Johnston M, Bezjak A, Whelan T (2002) Meta-Analysis of Dose-Fractionation Radiotherapy Trials for the Pal-liation of Painful Bone Metastases. Int J Radiat Oncol Biol Phys55:594–605
Cancer Pain Management, RehabilitativeTherapies
ANDREA CHEVILLE
Department of Rehabilitation Medicine, University ofPennsylvania School of Medicine, Philadelphia, PA,[email protected]
Definition
The potential role of rehabilitation in pain managementis often overlooked. Rehabilitative techniques includemodalities that can directly influence pain (e.g. topicalcold and desensitization techniques), and interventionsthatpreserveandrestorefunction.Thelatterare thefocusof this essay.
Characteristics
Rehabilitative Goal Setting in Pain Management
Aswithanyclinical intervention, the therapeuticgoalsofrehabilitation must be established prior to the initiationof therapy tofacilitate reassessmentat future timepoints.Dietz developed a structured approach to goal setting incancer rehabilitation that is extremely useful and appli-cable in pain management (Dietz 1985). He identifiedfour broad categories of rehabilitation goals that can beused to define the purpose of interventions and to guidetheir strategic integrationforoptimalresults.Asoutlinedin Table 1, these include: 1) preventative rehabilitationthat attempts to preclude or mitigate functional morbid-ity resulting from pain, the pathophysiological processdriving it, or its treatment; 2) restorative rehabilitationthat describes the effort to restore the patient to a pre-morbid level of function when little or no long-term im-pairment is anticipated; 3) supportive rehabilitation thatattempts to maximize function when long-term impair-ment, disability, and handicap result from the pain, itssource, or its treatment; and 4) palliative rehabilitation,which decreases dependency in mobility and self-care inassociation with the provision of comfort and emotionalsupport. Many interventions (e.g. resistive and aerobicexercise) may fall into more than one category, depend-ing on the motivation for their use. For example, resis-tive exercise can be used preventatively to avoid decon-ditioning, restoratively to reverse it, and supportively tominimize it. The specifics of the therapeutic prescrip-tionandanticipateddurationoftherapymayvarywidely,contingent on goal definition.The effort to precisely define how these four generaltypes of goals may apply to each patient is criticalfor a number of reasons. It ensures that potentiallybeneficial therapies will not be overlooked. It clarifiesfor both the clinician and the patient the purpose forwhich therapies are prescribed. This allows objectivefuture assessment of whether a therapy has been suc-cessful. If therapeutic goals have not been met after an

276 Cancer Pain Management, Rehabilitative Therapies
Cancer Pain Management, Rehabilitative Therapies, Table 1 Examples of goals and interventions that can be classified within the general therapeuticcategories of preventive, restorative, supportive, and palliative rehabilitation
Preventative Rehabilitation The effort to restore the patient to a premorbid level of function when little or no long-term impairmentis anticipated.
Goal Possible Intervention
Avoid development of secondary pain generators Normalize motor recruitment patterns
Minimize adverse effects of immobility
a.) deconditioning aerobic &resistive exercise
b.) contractures stretching, positioning
c.) osteopenia strategic loading of axial and appendicularstructures
Correct maladaptive biomechanical patterns posture &gait modification
Restorative Rehabilitation The effort to restore the patient to a premorbid level of function when little or no long-term impairmentis anticipated.
Goal Possible Intervention
Eliminate musculoskeletal pain generators Myofascial release techniques
Restore power postoperatively to compromisedmuscle groups
Progressive resistive exercises
Supportive Rehabilitation The attempt to maximize function when long-term impairment, disability, and handicap are anticipated.
Goal Possible Intervention
Optimize mobility status Provide patient with can, walker, etc.
Optimize ADL independence Instruction in compensatory strategies
Palliative Rehabilitation The effort to decrease dependency in mobility and self-care in association with the provision of comfortand support.
Goal Possible Intervention
Reduce dependency in toileting and grooming Provide appropriate ADL assistive devices
Preserve community integration Prescription of wheelchair or scooter
adequate trial, the rationale for discontinuation can bemade evident to the patient. Definition of goals is alsouseful in justifying therapy to third party payers, andin anticipating the duration of therapy. The profoundheterogeneity of presentation encountered in pain man-agement confounds a rigidly algorithmic approach tothe prescription of rehabilitative therapies. The fourbroad categories of clinical goals offer practitioners aflexible structure in which to develop a comprehensiveand integrated therapeutic plan for functional preserva-tion.
Rehabilitation, the Musculoskeletal System, and Pain
The musculoskeletal system is the primary focus ofvirtually all pain-oriented rehabilitation approaches.Dysfunction in the musculoskeletal system can: 1) pro-duce a primary pain generator; 2) function as a primarypain generator; 3) produce secondary pain generators;4) function as secondary pain generators; or 5) haveno role in the pain syndrome, but undermine patients’
functional status. Examples of the first four situationsare given in Table 2. It is important to note that manymusculoskeletal structures (e.g. the rotator cuff) canfunction in each of these categories. Rehabilitationis based on the fact that muscles, fascia, and bonesrespond to external forces that can be manipulatedwith therapeutic intent. For example, muscles can bestretched, strengthened, aerobically conditioned, orrendered more proprioceptively responsive, dependingon the therapeutic demands to which they are subjected.The correct choice of type, location and intensity ofpressure(s) requires accurate identification, not onlyof the involved anatomy and pathophysiological pro-cesses, but determination of precisely how these maybe contributing to a patient’s global pain experience andfunctional decline. It is critical that permissive factors(e.g. laxity, contractures, biomechanical malalignment)be identified and definitively addressed in order toprevent recurrence of the primary and development ofsecondary pain generators.

C
Cancer Pain Management, Rehabilitative Therapies 277
Cancer Pain Management, Rehabilitative Therapies, Table 2 Examples of musculoskeletal structures functioning as: 1) primary pain generators;2) contributors to primary pain generator; 3) secondary pain generators; and 4) contributors to secondary pain generators Effects of Inactivity
Primary pain generator Contributor to primary paingenerator
Secondary pain generator Contributor to secondary paingenerator
Structures that become painfuldue to trauma, overuse, orinflammation
Permissive factors (e.g. muscleweakness or tightness, ordysfunctional biomechanics) thatimpose stress on the primarypain generator.
Structures that become painfuldue to spasm, overuse orinflammation related to theprimary pain generator
Permissive biomechanical factorsthat arise consequent to theprimary pain generator
Rotator cuff tendonitis Weakness of scapular stabilizers Trazezius myofascial pain Premature upper trapeziusrecruitment
Osteoarthritis of the hip joint Flexibility deficits of hip muscles Greater trochanteric bursitis Iliotibial band tightness
Myofascial pain of scapular retrac-tors
Pectoralis muscle tightness Rotator cuff tendonitis Altered scapular biomechanics
Discogenic lumbar nerve rootcompression
Weakness of the abdominalmuscles
Lumbar paraspinal musclespasm
Lumbar hyperextension to reducepain
Pain, particularly if associated with movement, en-genders inactivity. The many adverse consequencesof inactivity have been well documented. They in-clude: reduced cardiovascular endurance, diminishedmuscle strength and stamina, osteopenia with reducedfracture threshold, reduced peri-articular distensi-bility, articular cartilage degeneration, compromiseof neural patterns required for coordinated activity,reduced plasma volume, diminished proprioceptiveacuity, and chemical alterations in connective tissue(e.g. ligaments, tendons) causing failure with reducedloading. Studies characterizing these physiologicalparameters have found that the rate of loss far ex-ceeds the rate of recovery once therapeutic activity hasbeen initiated (Saltin et al. 1968; Noyes et al. 1974;Beckman and Buchanan 1995). Some changes, partic-ularly those in articular cartilage, may be irreversible.As inactivity has such profound and widespread ad-verse effects, and because its consequences may beslow and difficult to reverse, it is essential that pa-tients preserve their activity levels within the limitsimposed by their pain. The prescription of preventa-tive rehabilitation strategies can greatly facilitate thisgoal.
Scope of Rehabilitation
Rehabilitative interventions encompass a broad andhighly varied collection of therapies. Most can be usedwith supportive, restorative, preventive, or palliativeintent. The overarching goal of rehabilitation is func-tional restoration and preservation. However, manyapproaches can be used to definitively address paingenerators, as with manual techniques for myofascialpain. Interventions can be grouped into the followingcategories: modalities, manual approaches, therapeuticexercise, provision of assistive devices, education incompensatory strategies, and orthotics.
Modalities
Although few blinded, prospective, randomized clinicaltrials have been conducted to establish the efficacy ofmost modalities, their routine integration into rehabili-tative programs is the current standard of care. A reviewof the few randomized controlled trials and the manyobservational studies (Philadelphia Panel 2001) foundevidence in support of a small, transient treatment effectfrom the application of heat. The delivery of therapeu-tic heat is often characterized by depth of penetration(superficial and deep), or mechanism of transmission(conduction, convection, radiation, evaporation, andconversion). Superficial heat increases the temperaturein skin and subcutaneous fat to a depth of approxi-mately 1 cm. Superficial modalities include hot packs,heating pads, fluidotherapy, and paraffin baths. Deepheating modalities increase temperature at a depth ofapproximately 3.5–7.0 cm and can, therefore, influencemuscles, tendons, ligaments, and bones, while sparingthe skin and subcutaneous fat. Although ultrasound isthe most commonly used deep heating modality, re-views offer little support of its efficacy, and its clinicalutility remains a subject of debate (Baker et al. 2001;Robertson and Baker 2001).Cryotherapy is a second modality used in the treat-ment of cancer pain (Lehmann 1990). The majority ofcryotherapeutic modalities use superficial conduction.Cold packs come in the form of ice packs, hydrocolla-tor packs, and endothermic packs that rely on chemicalreactions to lower temperature. Ice massage is theapplication of ice directly to the skin’s surface. Thephases of reaction are coolness, aching, hypesthesia,and analgesia. Cold (5–13˚C) water immersion is aconvection modality and vapocoolant sprays rely onevaporative cooling. Medical contraindications to coldtherapy include, but are not limited to, arterial insuffi-ciency, Raynaud’s phenomenon, cryoglobinemia, cold

278 Cancer Pain Management, Rehabilitative Therapies
hypersensitivity, and paroxysmal cold hemoglobin-uria.Hydrotherapy involves the external application of wa-ter of any temperature to achieve therapeutic goals. Hy-drotherapeutic modalities are often used for wound orskindebridementandcleansing,aswellasinthesupport-ive and palliative care of pain related to arthritis, chronicinflammatory states, and myofascial syndromes.Traction, the use of strategic displacing force to stretchsoft tissue and separate articular surfaces, has been usedfor nonmalignant conditions, particularly those associ-ated with nerve root impingement. Despite decades ofresearch regarding theclinicalbenefitsofspinal traction,there isnoconsensusregarding itsutility.Primarymalig-nancies of bone or spinal cord, osteomyelitis or discitis,unstable spinal fractures, end-stage osteoporosis, cen-tral disc herniations, carotid or vertebral artery disease,rheumatoid arthritis (cervical), and pregnancy (lumbar)are absolute contraindications to the use of traction.Functional electrical stimulation (FES) applies electri-cal stimulation via pad electrodes to depolarize motornerves, at either the axon or neuromuscular junction. Ithas been used in patients with potentially painful condi-tions such as spinal cord injury (SCI), peripheral nerveinjury, spasticity, and cardiopulmonary deconditioning.It has not been used in the management of cancer pain.Transcutaneous electrical nerve stimulation (TENS) in-fluences pain by stimulating large diameter, myelinatedAβ nerve fibers. There is a large clinical experience sug-gesting that a subgroup does benefit. Multiple electrodeand stimulation configurations must be tested to ensurean adequate trial. Studies of the technique have yieldedinconsistent results (Fargas-Babjak 2001). For theoret-ical reasons, patients are cautioned against stimulatingdirectly over tumors.Iontophoresis allows charged molecules to penetratecell membranes and enter tissue through the applica-tion of an electric field. Negative, positive and groundelectrodes are secured to the patient, and a 10–30 mcurrent is used to transfer medication from the electrodeinto the surrounding tissues. This modality creates thepotential for medication delivery in the treatment ofspasticity, chronic inflammatory states, and myofascialpain syndromes. There is no experience in the use ofthis approach in medically ill patients.Phonophoresis also facilitates the transdermal deliveryof topical medications, but uses ultrasound to facilitatemedicationdelivery.Thetechniquehasbeenused totreatsoft tissue inflammation. Again, there is no experiencein the cancer pain population.
Manual Therapies
Manual therapies refer to a vast array of hands ontechniques designed to normalize soft tissue and jointmobility. Types of manual therapies include everythingfrom massage to myofascial release, acupressure and
joint range of motion. Common manual techniquesinclude:
• Massage• Myofascial release• Soft tissue mobilization• Manual lymphatic drainage• Acupressure• Shiatsu• Rolfing• Reflexology• Craniosacral therapy• Osteopathic manipulation• Joint mobilization• Muscle energy techniques• Passive range of motion
The benefits of manual approaches are generally short-lived if patients do not comply with a concurrent stretch-ing, strengthening, and conditioning regimen. Physicaltherapists, osteopathic physicians, massage therapists,acupuncturists, as well as a host of complementary andalternative practitioners, use manual techniques for paincontrol.When chronic pain affects the musculoskeletal sys-tem, a pain-spasm cycle begins. Nociception causesreflexive muscle contraction, which in turn increasesnociception, and the cycle is set in motion leadingultimately to painful, chronic muscle hypertonicity.This results in muscle weakness, joint contractures,aberrant biomechanics, and dysfunctional kinestheticpatterns. As patients attempt to perform normal dailyactivities, the compromised system becomes overused,exacerbating the pain cycle and producing secondarypain generators. By normalizing joint and soft tissuephysiology, manual techniques can be used to breakthis pain cycle and reestablish function biomechanics.Ideally, patient referral for manual techniques shouldnot be delayed until the pain-muscle spasm cycle iswell established.Massage focuses on decreasing pain through increasedcirculation and mechanical movement of tissues. Tech-niques vary in the variety of hand strokes, appliedpressure, and direction of force. Many beneficial phys-iological effects have been associated with massage(Field 2002). In addition to its use in pain management,it has been adapted to the treatment of lymphedema andcontractures.Myosfascial release is a technique that purportedlyfacilitates normal movement within the fascial system.Fascia is the connective tissue that provides supportthroughout the body, and fascia that is injured or con-tracted could contribute to pain. Practitioners use vigor-ous “hands on” compression and stretching techniquesto alter the mobility of affected tissues.Several manual techniques are used to affect joint phys-iology and normalize accessory movement. The mostbasic technique is passive range of motion (PROM).

C
Cancer Pain Management, Rehabilitative Therapies 279
A practitioner using PROM will move a joint throughits physiologic range of motion in an effort to maintainand/or restore motion. In addition, PROM also stretchesthe soft tissues surrounding a joint and normalizes ac-cessory movements in a joint. By restoring normal jointmechanics on the accessory level, normal physiologicmotion can follow. There are five grades of joint mobi-lization based on the amplitude of movement throughthe full range of accessory movement. Grades I and IIprovide the smallest amount of movement. These tech-niques are used to prevent contractures and pain relief.Grades III and IV provide increased pressure withinthe joint’s range of normal motion. These techniquescan help to promote normal physiologic motion as wellas providing pain relief. Grade V joint mobilization isknown as a “manipulation.” Grade V manipulationsare performed at high velocity and intensity to theend of the accessory range of motion. Physical ther-apists, osteopathic physicians and chiropractors usejoint mobilization. In most cases, only chiropractorsuse manipulations.Muscle energy techniques (MET) are used to restorenormal joint and soft tissue movement through pa-tients’ own force. METs are based on the theory ofjoint mobilization to facilitate movement, but recruitpatients’ own muscular force. The practitioner placesthe patient in a specific position, the patient is asked topush against the practitioner’s counterforce in order tofacilitate movement in joints and soft tissues.Acupressure involves the strategic application of pres-sure to trigger points and derives from the theories ofacupuncture.Theuseofpressure to relieve triggerpointshas been incorporated into many soft tissue techniques.
Therapeutic Exercise
The strategic use of exercise to enhance strength, coordi-nation, stamina, and flexibility is perhaps the most pow-erful intervention in rehabilitation medicine. The factthat muscles and fascia respond predictably to imposedexternal demands underlies this therapeutic approach.Musclechangesthatcanbeachievedthroughtherapeuticexercise include: increased capillary density, enhancedneuromuscular responsiveness, normalization of mus-cle length-tensionrelationships,alteredrestingtone,andincreased elaboration of mitochondrial and sarcoplas-mic proteins (de Lateur 1996).For optimal benefit, the type, intensity, and frequency ofexercise must be rationally chosen following a compre-hensive clinical examination. The exercise prescriptionwill be determined by the presence, severity, and distri-bution of flexibility and strength deficits, the degree ofdeconditioning, and the presence abnormal segmentalbiomechanics. An exercise program combining stretch-ing, aerobic conditioning, and strengthening should betailored to each patient’s unique requirements.Patients may protest that the intensity of their painprecludes participation in an exercise program. Even
minimal resistive exercises, however, can lead to signif-icant improvements in strength and functional status.Brief isometric muscle contractions can be performedin bed or in a chair against gravity or with gravity elim-inated. One brief isometric contraction per day wasdemonstrated to prevent loss of strength in bed-riddenrheumatoid arthritis patients (Atha 1981).Stretching, or flexibility activities, can influence mus-cles by altering their length-tension relationships andresting tone. Stretching is an integral part of the treat-ment of myofascial pain (Travell and Simons 1983) andpain associated with muscle spasms. It is commonlyused to achieve adequate range of motion for perfor-mance of daily activities. Flexibility assessment mustconsider patients’ overall level of muscle tightness, theirrequired range of motion given their activity profile, andthe impact of contracture-related asymmetry on move-ment patterns. Two stretching techniques predominatein rehabilitation medicine: ballistic and static. Ballisticstretching involves repetitious bouncing movementsat the end-range of joint range. Static stretching, incontrast, involves slow, steady soft tissue distension,which is maintained for several seconds. Comparisonssuggest that static is superior to ballistic stretching,and that meaningful benefit can be achieved throughthree to five sessions per week (Sady et al. 1982). Painpatients require a slowly progressive approach to staticstretching. Ballistic stretching is indicated only in un-usual cases and should be performed under the care ofa physical medicine and rehabilitation specialist.Resistive exercise is used to strengthen selected musclesor muscle groups by forcing them to contract repeatedlyagainst resistance. Resistive training can beutilized withrestorative, supportive and/or preventative intent. Goalsmust consider patients’ current level of conditioning, theprognosis for their pain and related medical comorbidi-ties, their past fitness histories, and the rigor of their an-ticipated activity profile (e.g. vocational, avocational).To induce strength gains, an intensity of at least 60% ofthe one-repetition maximum must be used. Table 3 out-lines common parameters utilized in prescribing resis-tive exercise for generalized or focal weakness.Aerobic conditioning differs from resistive exercise initsemphasisoncontinuousrhythmiccontractionoflargemuscle groups. Jogging and cycling are common exam-ples. Aerobic training allows patients to perform dailyactivities with less effort, maintain greater indepen-dence, and enjoy an enhanced sense of well-being (NIHConsensus Developments Panel on Physical Activityand Cardiovascular Health 1996). If the medical condi-tion permits, regular physical activity may improve theability to perform physical activities and attenuate thepsychological morbidity associated with chronic pain.A prescription for exercise should consider baselinefitness levels, associated motor impairments and co-morbidities, and patient tolerance. For deconditionedpatients with chronic pain, the initial aerobic training

280 Cancer Pain Management, Rehabilitative Therapies
Cancer Pain Management, Rehabilitative Therapies, Table 3 Considerations in prescription of therapeutic resistive exercise
Exercise Parameter Considerations and Recommendations
Choice of exercise Exercises strength deficient muscle groups in multiple planes and across a range of length-tension relationships
Order of exercise Begin with large muscle group exercises. For circuit training start with legs
Number of sets Begin with one set and progress to three of more sets of each exercise
Rest between sets 3 min for heavy resistance, 2–3 for moderate resistance, 1–2 light resistance
Intensity 60% one repetition maximum, 6–15 repetitions
Rate of progression Increase 2.5–5% when level of resistance is perceived as “moderate”
Program variation Variations in intensity, positioning, order of exercises, choice of exercise should be adopted weekly to avoidovertraining
Speed specificity Intermediate velocity unless training goals involve rapid or slow velocity activities
Contraction specificity Isotonic training unless joint pain is prohibitive, then initiate training with isometric activities. Isometrics can beused to prevent loss of strength.
Joint angle specificity Loading should be maintained throughout entire functional range.
may entail walking slowly for 5–10 min. Exercise canalso be used to enhance coordination, posture, propri-oception, balance, and the performance of integratedmovement patterns. Much of the literature establishingthe value of exercise for these applications derives fromsports and performing arts medicine. Techniques toimprove proprioception include use of a tilt or wob-ble board, sideways walking or running, and agilitydrills. Balance enhancing activities include tossing andcatching a ball while standing on heels, toes, or oneleg. Therapy balls can be utilized to address deficitsin truncal stability. Generally, patients sit on the ballwhile shifting their weight in different directions orlifting their legs. There are many variations on balanceactivities. Their selection should consider the patients’deficits and desired activity profile. The adage that thebest training for an activity is the activity itself alsoholds true for coordination training.
Orthotics
Orthotics are braces designed to alter articular mechan-ics when their integrity has been compromised by pain,weak muscles, impaired sensation, or other anatomicaldisruption.Orthoticsmaybyused therapeutically topro-vide support, restore normal alignment, protect vulner-able structures, address soft-tissue contractures, substi-tute for weak muscles, or maintain joints in positions ofleast pain. Many orthotics are available pre-fabricated,“off-the-shelf.” While such braces often suffice,patientsmayrequiremoreexpensivecustomorthosesforoptimalbenefit.Orthoticscanbeusedtoaddresspathologyinvir-tually any articular structure.Theuseof thesedevices forpain patients must be tempered by concern for engender-ing long-term dependency and validating patients’ im-pairments. Orthotics are most often used in pain man-agement on a transient basis, to keep joints in a fixed
position, to allow resolution of local inflammation, orto rest painful muscles and/or tendons that act on thejoint. They also can be used preventatively, when jointsor osseous structures are at risk of injury or contracture,and patients are incapable, despite resistive exercise andproprioceptive enhancement, of protecting them. Suchcircumstances often arise in the context of systemic ill-ness. For example, spinal extension orthoses such as theJewitt or Cash brace limit spinal flexion, and therebyprevent excessive loading and compression fracture ofthe anterior vertebral bodies. Palliative splinting is usedto optimize comfort when function is no longer a pri-mary concern. An excellent example is the use of slingsto keep flaccid upper extremities tethered near the bodyand out of harm’s way. Referral to an orthotist or physi-calmedicineandrehabilitationspecialistwillensure thatpatients receive appropriate orthoses. However, many ofthese professionals lack experience with pain patients. Itis important to communicate the goals of treatment andtheprecise reason(s)why theorthotic isbeingprescribedto the rehabilitation professional. In this way, patientshave the best chance of receiving an orthotist suited totheir unique requirements.Many patients with chronic pain, particularly pain re-lated to chronic medical illness, require adaptive devicesto enhance their safety, comfort and autonomy whilemoving about the home or community. Ready access tosuch devices is essential if pain patients are to remainsocially integrated within their communities. Adaptiveequipment designed to augment mobility ranges fromprefabricated single-point canes to complex motorizedwheelchair systems. Hand-held assistive devices aregenerally variations on canes, crutches and walkers.Devices can be customized to distribute weight bearingonto intact structures to minimize the pain. Patientswith severe deconditioning, paresis, osseous instabil-

C
Cancer Pain Management, Treatment of Neuropathic Components 281
ity, or other sources of impaired mobility may requirea wheelchair or scooter. Even when deficits are pre-sumed transient, a wheelchair can sustain communityintegration and fragile social connections. Wheelchairtolerance and utilization depend on the prescription ofan appropriate model.Assistive devices have also been developed to maxi-mize patients’ independence and reduce pain duringperformance of activities of daily living (ADLs). De-pendence for self-care has been shown to erode qualityof life across many medical diagnoses. Devices areavailable to assist patients with independent dressing,grooming, toileting, as well as performance of morecomplex activities such as cooking and housekeeping.
Conclusion
Cliniciansmustbecomediscriminatingconsumersof re-habilitation services if they are to optimally benefit theirpatients. This need arises from the fact that the deliveryof rehabilitation services occurs within asocioeconomiccontext that imposes fiscal pressures upon its providers.It is essential that clinicians question patients regardingthe particulars of their treatment and relay any concernsto the treating therapist. Including specific requirementson the therapy prescription can also help to ensure thatpatients receive appropriate care.Clinicians must recog-nize that rehabilitation professionals vary widely in theirlevels of experience, biomechanical acumen, interper-sonal skill, and mastery of manual techniques. Ideally,clinicians should refer patients to therapists with whomthey are familiar and can readily enter into clinical di-alogue. Most therapists welcome guidance from physi-cians and nurses and are highly motivated to cultivatethe skills required to optimally serve pain patients.
References1. Atha J (1981) Strengthening Muscle. Exerc Sport Sci Rev 9:1–732. Baker K, Robertson V, Duck F (2001) A Review of Therapeutic
Ultrasound: Biophysical Effects. Phys Ther 81:1351–13583. Beckman S, Buchanan T (1995) Ankle Inversion Injury and Hy-
permobility: Effect on Hip and Ankle Muscle ElectromyographyOnset Latency. Arch Phys Med Rehabil 76:1138–1143
4. de Lateur BJ (1996) Therapeutic Exercise, pp 401–4195. Dietz JJ (1985) Rehabilitation of the Patient with Cancer. In:
Calabresi P, Schein PS, Rosenberg SA (eds) Medical oncology.Macmillan Publishing, New York, pp 1501–1522
6. Fargas-Babjak A (2001) Acupuncture, Transcutaneous ElectricalNerve Stimulation, and Laser Therapy in Chronic Pain. Clin JPain 17:105–113
7. Field T (2002) Massage Therapy. Med Clin North Am86:163–171
8. Lehmann JF (1990) Therapeutic Heat and Cold. Williams &Wilkins, Baltimore
9. NIH Consensus Developments Panel on Physical Activity andCardiovascular Health (1996) Physical Activity and Cardiovas-cular Health. JAMA 276:241–246
10. Noyes FR, Torvik PJ, Hyde WB et al. (1974) Biomechanicsof Ligament Failure II. An Analysis of Immobilization, Exer-cise, and Reconditioning Effects in Primates. J Bone Joint Surg56:1406–1418
11. Philadelphia Panel (2001) Philadelphia Panel Evidence-BasedClinical Practice Guidelines on Selected Rehabilitation for KneePain. Phys Ther 81:1675–1700
12. Robertson V, Baker K (2001) A Review of Therapeutic Ultra-sound: Effectiveness Studies. Phys Ther 81:1339–1350
13. Sady S, Wortman M, Blanke D (1982) Flexibility Training:Ballistic, Static or Propriospective Neuromuscular Facilitation?Arch Phys Med Rehabil 63:261–263
14. Saltin B, Blomqvist G, Mitchell JH et al. (1968) Response to Ex-ercise after Bed Rest and after Training: A Longitudinal Study ofAdaptive Changes in Oxygen Transport and Body Composition.Circulation 38:VII1–78
15. Travell J, Simons D (1983) Myofascial Pain and Dysfunction.The Trigger Point Manual. Williams and Wilkins, Baltimore
Cancer Pain Management, Treatment ofNeuropathic Components
PAUL W. WACNIK1, RICHARD L. BOORTZ-MARX2
1Department of Pharmacology, College of Medicine,University of Minnesota, Minneapolis, MN, USA2Department of Neurosciences, Gundersen LutheranHealth Care System, La Crosse, WI, [email protected],[email protected]
Definitions
Pain due to pathological functioning ofeither theperiph-eral nervous system (PNS) or the central nervous system(CNS) is classified as neuropathic. These processes maydirectly stimulate the pain system or damage nocicep-tive pathways to shift the balance between painful andnonpainful inputs to the CNS (Merskey and Bogduk1994). Neurological symptoms of � neuropathic painin cancer include continuous, burning, itching, achingand cramping or pain evoked by mechanical or thermalstimuli. Such symptoms can be accounted for by anintact, normally functioning nervous system sensing anoxious stimulus (in this case a � tumor) manifestingas � somatic pain or by a component of the nervoussystem damaged by the impact of previous antineo-plastic therapies, such as surgery, chemotherapeuticagents or radiation oncology or by progression of thedisease (Portnoy 1991). Distinguishing between thetwo etiologies is often problematic.
Characteristics
Pain is but one symptom of many experienced with can-cer. However, if uncontrolled, the pain can profoundlycompromise quality of life and may interfere with anti-neoplastic treatment (Portenoy and Lesage 1999). Painin cancer can be either constant or variable in character,owing to the inevitability that cancer will involve tumorgrowth and progression, changes in the tissue surround-ing the tumor and therapeutic interventions intended tocontrol tumor growth. Although no overall “cure” existsfor most cancers, advances in anti-neoplastic therapieshave allowed patients to live longer with their disease,

282 Cancer Pain Management, Treatment of Neuropathic Components
making long-term � cancer pain therapy a considera-tion of increasing importance. The incidence of cancerpain is high in patients with advanced disease as well asin patients undergoing active treatment for solid tumors(30–50% Portenoy and Lesage 1999). The intensity ofthis pain is often overwhelming. In a multi-site cancerpain study, two-thirds of patients rated their worst pain,using an 11 point numerical rating scale during a givenday, at 7 out of a maximum 10, with an average pain levelof 4.7 throughout the day, even though 91% of these pa-tients were receiving opioid analgesics (Caraceni andPortenoy 1999). This observation demonstrates thatmost patients, even those receiving analgesic therapy,live with moderate to severe daily pain. One compli-cation in understanding and treating cancer pain is itsvariable and complex nature (see Table 1). More than25% of patients have nerve injury that occurs in tandemwith damage to other structures and the pain has a mixedpathophysiology with more than one type of pain, mostfrequently somatic-nociceptive pain. � Nociceptivepain involves direct ongoing activation of intact noci-ceptors (pain sensitive neurons) in either somatic orvisceral tissue. In essence, this is the intact, normallyfunctioning nervous system sensing a noxious stimulus(in this case a tumor). On the other hand, pain due topathological function of either the peripheral or centralnervous system is classified as neuropathic. In this case,the presence of cancer induces a phenotypic changein the pain sensing system, increasing sensitivity ofnerves to normally innocuous stimuli or exaggeratingthe response to noxious stimuli.The findings of Boortz-Marx’s group in 2004 weresimilar with 15% of cancer patients having neuropathicpain, 25% showing somatic-nociceptive pain and 60%showing mixed pain characteristics. This outcomeunderscores the complexity of the alterations in pain
Cancer Pain Management, Treatment of Neuropathic Components,Table 1 A compilation of pain types due to cancer from a multi-site study(Adapted from Caraceni and Portenoy 1999)
Cancer pain pathophysiology % Occurrence
Somatic nociceptive only 32.2
Somatic and neuropathic 23.3
Visceral nociceptive only 15.2
Somatic and visceral 10.8
Neuropathic only 7.7
Somatic, visceral, and neuropathic 5.2
Visceral and neuropathic 3.6
Unknown only 1.7
Other with psychogenic 1.5
Psychogenic only 0.3
sensing systems in cancer. Although pain due to theneoplasm is the focus of much investigation and treat-ment, there are considerable instances of pain observedin cancer patients related to noxious interventions, in-cluding pain associated with diagnostic interventions,therapeutic interventions, lumbar puncture, analgesictechniques, � chemotherapy toxicity, hormonal ther-apy and radiotherapy as well as post-operative pain.The fact that cancer pain can evolve from one form toanother with progression of the disease implies thatanalgesic treatment regimens must also evolve to matcha changing etiology.
Diagnoses of Neuropathic Components of Cancer Pain
The diagnosis of neuropathic cancer pain is a clinicaldiagnosis. Based on the clinical presentation of thecharacter and quality of pain, one is led to a provisionaldiagnosis of neuropathic cancer pain, which appropri-ately initiates therapeutic options, possibly includinganti-neuropathic pharmacotherapy. Some types of neu-ropathic injury produce aching, stabbing or throbbingpain, but these syndromes often present with an unfa-miliar quality or sensory distortion. Burning, shootingand tingling are suggestive of nerve involvement, butnot sufficient to make the diagnosis. Accompanyingabnormal sensations are often found on examination,including hypesthesia (increased threshold), hyperes-thesia (decreased threshold), paresthesias (spontaneousnon-painful threshold), dysesthesia (spontaneous painthreshold), hyperpathia (prolonged stimulus response)and allodynia (pain from a normally innocuous stimu-lus). The presence of changes in small fibers on biopsyof the skin or peripheral nerves may be a useful confir-mation, but has proven largely unnecessary in severalclinical studies.
Pharmacological Treatment of Neuropathic Components ofCancer Pain
Traditionally opioids have been utilized in the treatmentof cancer pain. However, their efficacy for neuropathicpain states is controversial (McQuay 1999). The “mixedpain”state lends itself to effective treatmentwithopioids(several preparations of long- and short-acting opioidsto be administered by different routes). These routes ofadministration include oral, submucosal, subcutaneous,transdermal, rectal, parenteral, epidural and intrathecal.Undesirable side effects of opioids (cognitive impair-ment, somnolence, constipation, fatigue, hallucinationsand myoclonus) may present without adequate analge-sia being achieved.The adjuvant group of analgesics (pharmacotherapydesigned for other purposes, but producing analgesia incertain circumstances) has proved to be effective in thetreatment of neuropathic cancer pain. Traditionally, thetricyclic antidepressants (amitriptyline, nortriptyline,imipramine, desipramine and doxepin) have demon-strated efficacy in the treatment of neuropathic pain

C
Cancer Pain Management, Treatment of Neuropathic Components 283
states. The side effect profile of this group has ledindividuals not to consider these medications as firstline therapy. The predominance of anticholinergic sideeffects (dry mouth, somnolence, cognitive impairment,cardiac arrhythmias, urinary retention and constipation)is often dose related, but can have advantages in patientsafflicted with disrupted sleep architecture. Often dosesneeded for treatment of neuropathic pain states are muchlower than those needed for the treatment of depression.Other antidepressants such as the serotonin selectivereuptake inhibitors (SSRIs), atypical antidepressantsand monoamine oxidase inhibitors (MAOIs) have notproven efficacious unless predominant depression ac-companies the neuropathic pain state. Most recently,a selective norepinephrine reuptake inhibitor (SNRI)received approval for treatment of painful diabetic pe-ripheral neuropathy.One of the authors (RB-M) has notexperienced added benefit with this class of drugs inthe treatment of painful neuropathic pain states relatedto cancer.Several anticonvulsant medications constitute the main-stay in the treatment of most neuropathic pain states,including neuropathic pain accompanying cancer. Thetraditional anticonvulsants (phenytoin, carbamazepineand valproate) have fallen from favor because of theirtoxic side effects related to bone marrow suppression;this side effect is particularly unwelcome in a patientpopulation that has already received a toxic impactfrom chemotherapeutic agents used in the treatmentof their disease state. A newer class of anticonvul-sants has recently evolved that employs varying modesof activity relating to voltage gated channels (alpha-2/delta subunit of voltage gated calcium channels andvoltage gated sodium channels) and glutamate gatedchannels of the AMPA subtype. These agents includepregabalin and gabapentin, which target the calciumchannels, topiramate, tiagabine, levetiracetam, lamot-rigine, oxcarbazepine and zonisamide, which target thesodium channels and glutamate receptors. Drugs suchas gabapentin have few drug-drug interactions, are welltolerated (starting at a low dose and escalating slowly)and have produced favorable outcomes.Other adjuvant medications used or tested in the treat-ment of neuropathic cancer pain have included alpha-2adrenergic agonists (tizanidine and clonidine) ad-ministered orally, epidurally or intrathecally, localanesthetics (lidocaine, mexiletine, bupivacaine, ropiva-caine, tetracaine) administered perineurally (conductiveblock of major nerve trunks), parenterally, epidurally,intrathecally or orally, NMDA receptor antagonists(dextromethorphan and ketamine) administered orallyor parenterally or (ketamine only) intrathecally, GABAagonists (e.g. baclofen) or facilitators (e.g. diazepam)administered orally or intrathecally, corticosteroids(prednisone and dexamethasone) administered par-enterally or orally, topical agents (EMLA, gabapentin,morphine, lidocaine and capsaicin) and phenol or alco-
hol (chemical neurolysis in specific cases) administeredaround nerves or ganglia (Chong 1997; Eisenach 1995;Stubhaug 1997; Rowbotham 1994; Galer 1999; Watson1988).MostrecentlyBoortz-Marxandcolleaguespublishedre-sults of a multicenter study looking at the impact of in-trathecaldrugdeliveryoncancerpain(Smithetal.2002).Mixtures of drugs including opioid agonists, local anes-thetics and alpha-2 adrenergic agonists were applied asintrathecal preparations. Patients enrolled in this studyreported reduced pain, reduced toxic side effects, im-proved quality of life and a trend toward extended lifeexpectancy.
Non-Pharmacological Treatment of Neuropathic Componentsof Cancer Pain
Non-pharmacological treatment options serve as asuccessful adjunct in the treatment of neuropathiccancer pain. The International Association for theStudy of Pain (IASP) has characterized chronic painas a “bio-psycho-social-spiritual” process. Chronicpain affects all patients at all stages of their cancerdisease. Non-pharmacological strategies including pa-tient psychoeducation, supportive psychotherapy andcognitive-behavioral interventions have been demon-strated to be effective in the cancer pain patient. Thesetherapies lead to patient empowerment, improvedstress management and improved patient recognitionand modification of factors contributing to physical andemotional distress (Thomas and Weiss 2000). Other ma-jor non-pharmacological modalities that have demon-strated efficacy include therapeutic touch, massage,aromatherapy, reflexology, relaxation, guided imagery,visualization, meditation, biofeedback, acupunctureand music therapy (O’Callaghan 1996; Penson andFisher 1995).
Modeling Aspects of Persistent Cancer Pain
In order to understand the basic mechanisms involved incancer pain and ultimately to provide insight into mech-anism based therapies, several groups have developedrodent models of tumor induced hyperalgesia. The clas-sification of pain in cancer can be either neuropathic ornociceptive (somatic), but is often mixed (Caraceni andPortenoy 1999). This distinction is a familiar theme, notonly clinically, but also in pain models. � Neuropathicpain models in rodents have mostly focused on mechan-ical trauma to the sciatic or spinal nerves; similarly, inanimal models of cancer pain, the tumor mass itself mayimpose structural damage on nearby nerve bundles.
Neural Plasticity in Cancer Pain Models
Plasticity in pain processing within the CNS can leadto pathological pain states that manifest not only asincreased nociceptive sensitivity at the injury site, butalso as secondary hyperalgesia and referred pain. Inmodels of cancer pain, the potential for both peripheral

284 Cancer Pain Management, Treatment of Neuropathic Components
and central plasticity is likely, particularly when tumorcells are implanted into the distal femur, where hyper-algesia both at the tumor site (Schwei et al. 1999) andsecondarily in the paw (Wacnik et al. 2001) are measur-able. Schwei et al. (1999) and Shimoyama et al. (2005)found increased immunoreactivity for dynorphin andc-fos protein in the dorsal horn correlated with tumorgrowth, possibly signaling neuroplastic changes. In arat model of cancer pain where tumors are implantedin the tibia, Urch et al. (2003) demonstrated increasedresponses to mechanical, thermal and electrical (A beta,C-fiber and post-discharge evoked response) stimuliin wide dynamic range dorsal horn neurons in tumorbearing animals, but no changes in nociceptive specificneurons. Tumor induced peripheral neuropathies in-clude aberrant firing of peripheral nociceptors adjacentto the tumor, identified by spontaneous activity in 34%of cutaneous C-fibers and an increase in epidermalnerve branching concomitant with a decrease in theactual number of fibers in skin overlying the tumor(Cain et al. 2001). Furthermore, immunohistochemicalanalysis of tumors revealed innervation of tumors withCGRP-immunoreactive nerve fibers. The density ofthese tumor-nerve appositions was positively corre-lated with the level of hyperalgesia, whereas that ofblood vessels was inversely correlated (Wacnik et al.2005).
Models of Chemotherapy Induced Neuropathic Pain
In cancer patients, neuropathic pain is frequently as-sociated with direct tumor invasion of the peripheralnerve or spinal cord or secondarily caused by can-cer chemotherapy. Several rodent models have beendeveloped to model painful chemotherapy induced neu-ropathy, using for example, vincristine or paclitaxel. Inthe periphery, vincristine has been shown to enhanceC-fiber responsiveness and to induce structural changesto large diameter sensory neurons and myelinated axons(Topp et al. 2000). In the CNS, vincristine promotescentral sensitization in the dorsal horn of the spinalcord, as indicated by increased spontaneous activity,increased responsiveness to C- and Aδ-fiber activityand abnormal “wind-up” in response to afferent C-fiberactivity (Weng et al. 2003).
Conclusions
Pain categories say little about the actual underlyingmechanisms. Whether the category is neuropathic ornociceptive, the tumor or antecedent chemotherapy isultimately the genesis of the pain. Damage to severaldifferent tissue types is part of tumorigenesis, and thisdamage in turn may make different contributions tothe resulting pain. There is a high likelihood that atumor could damage the nerve through compression,stretching or infiltration (i.e. neuropathic), as well asby invading somatic or visceral structures and releasingmediators that activate nociceptive fibers (i.e. nocicep-
tive somatic/visceral). Although the malignant massbegins as a single entity, it may manifest pain via severalmeans and via complex interactions. Accordingly, worktowards a mechanistic classification of cancer pain musttake these various means and interactions into account.
References1. Bruera E, Roca E, Cedaro L (1985) Action of Oral Methylpred-
nisolone in Terminal Cancer Patients: A Perspective RandomizedDouble-blind Study. Cancer Treat Rep 69:751–754
2. Caraceni A, Portenoy R (1999) An international survey of cancerpain characteristics and syndromes. Pain 82:263–274
3. Chong SF, Bretsher ME, Mailliard JA, et al. (1997) Pilot StudyEvaluating Local Anesthetics Administered Systemically forTreatment of Pain in Patient with Advanced Cancer. J PainSymptom Manage 13:112–117
4. Cain DM, Wacnik PW, Turner M et al. (2001) Functional interac-tions between tumor and peripheral nerve: changes in excitabilityand morphology of primary afferent fibers in a murine model ofcancer pain. J Neurosci 21:9367–9376
5. Eisenach JC, DuPen S, Dubois M et al. (1995) Epidural ClonidineAnalgesia for Intractable Cancer Pain. The Epidural ClonidineStudy Group. Pain 61:391–399
6. Foley KM (2000) controlling cancer pain. Hosp Pract (Off Ed)35:101–108, 111–-102
7. Galer BS, Rowbotham MC, Pcrander J et al. (1999) Topical Li-docaine Patch Release Post-Herpetic Neuralgia More Effectivelythan a Vehicle Topical Patch: Results of an Enriched EnrollmentStudy. Pain 80:533–538
8. McQuay, H (1999) Opioids in Pain Management. Lancet353:2229–2232
9. Merskey H, Bogduk N (1994) Classification of Chronic Pain,2nd edn. IASP Press, Seattle
10. O’Collaghan CC (1996) Complimentary Therapies in TerminalCare: Pain, Music, Creativity, and Music Therapy in PalliativeCare. Am J Hospice Palliative Care 13:43–49
11. Penson J, Fisher R (1995) Complimentary Therapies in PalliativeCare for People with Cancer. Arnold, London, pp 233–245
12. Portenoy RK (1991) Cancer Pain General Design Issues. In: MaxM, Portenoy R, Laska E (eds) Advances in Pain Research andTherapy. Raven Press, New York, pp 233–266
13. Rowbotham MC (1994) Pharmacological Approaches to theTreatment of Chronic Pain: New Concepts in Critical Issues.IASP Press, Seattle
14. Schwei MJ, Honore P, Rogers SD et al (1999) Neurochemicaland cellular reorganization of the spinal cord in a murine modelof bone cancer pain. J Neurosci 19:10886–10897
15. Shimoyama M, Tatsuoka H, Ohtori S et al. (2005) Change ofdorsal horn neurochemistry in a mouse model of neuropathiccancer pain. Pain 114:221–230
16. Smith TJ, Staats PS, Pool G et al. (2002) An implantable drugdelivery system for refractory cancer pain improves pain control,drug-related toxicity, and survival compared to comprehensivemedical management. American Society of Clinical Oncology,May 2002. Proceedings of the American Society of Clinical On-cology 21:360a
17. Stubhaug A, Breivik H (1997) Long-term Treatment of ChronicNeuropathic Pain with NMDA (N-Methyl-D-Aspartate) Recep-tor Antagonists Ketamine. Acta Anaesthesiol Scand 41:329–331
18. Thomas EM, Weiss SM (2000) Non-pharmacological Inter-ventions with Chronic Cancer Pain in Adults. Cancer Control7:157–164
19. Urch CE, Donovan-Rodriguez T, Dickenson AH (2003) Alter-ations in dorsal horn neurones in a rat model of cancer-inducedbone pain. Pain 106:347–356
20. Wacnik PW, Eikmeier LJ, Ruggles TR et al. (2001) Functionalinteractions between tumor and peripheral nerve: morphology,algogen identification, and behavioral characterization of a newmurine model of cancer pain. J Neurosci 21:9355–9366
C
Cancer Pain Management, Undertreatment and Clinician-Related Barriers 285
21. Wacnik PW, Baker C, Blazar BR et al. (2005) Tumor-inducedmechanical hyperalgesia involves CGRP receptors and alteredinnervation and vascularization of DsRed2 fluorescent hindpawtumors. Pain 115:95–106
22. Weng HR, Cordella JV, Dougherty PM (2003) Changes in sen-sory processing in the spinal dorsal horn accompany vincristine-induced hyperalgesia and allodynia. Pain 103:131–138
Cancer Pain Management,Undertreatment and Clinician-RelatedBarriers
SEAN O’MAHONY
Montefiore Medical Center and Albert EinsteinCollege of Medicine, Bronx, New York, NY, [email protected]
Definitions
Cancerpain ispain thatcanbeattributed toamalignancy,or complication of a malignancy, or its treatment.
Characteristics
Cancer pain affects 17 million people worldwide (Coyleet al. 1990; Daut and Cleeland 1982). Prevalence rates of30–40% are reported for patients receiving active treat-ment, and 70–90% for patients with advanced cancer(Kelsen etal. 1995).Cancerpain occursatmultiple sites;in one study of 2266 cancer patients, 70% of patients hadpain at 2 or more sites (Zeppetella et al. 2000). The du-ration of cancer pain varies, but it can extend to severalmonths or years (Petzke et al. 1999). In the U.S., an East-ern Cooperative Oncology Group survey of 1308 am-bulatory cancer patients found that 67% reported recentpain, and 36% reported their pain severity as sufficientto interfere with their function (Von Roenn et al. 1994).
Undertreatment of Cancer Pain
Although reviews of the literature confirm that cancerpain may be relieved in 70–90% of patients, an increas-ing body of evidence suggests that cancer pain remainsundertreated internationally. Deficits in the treatmentof cancer pain extend across specialty and level ofexperience. A French national questionnaire study ofgeneral practitioners and specialists indicated that only10% of patients treated by general practitioners, and21% of patients treated by specialists, were receivingtreatment regimens appropriate to their pain severity(Vainio 1995). An analysis of the computerized medi-cal records of more than one million German patientsrevealed that only 1.9% of patients with cancer werereceiving prescriptions for strong opioid medications,and many patients with cancer were receiving medi-cations at inappropriate intervals and often on an “asneeded” basis (Zenz et al. 1995).Fear of addiction and respiratory depression appearto limit physician’s use of strong opioids. In a study
of 13,625 US nursing home residents with cancer anddaily pain, factors that were predictive of undertreat-ment included poor cognitive status, polypharmacy,and advanced age (age > 85) (Bernabei et al. 1998).Factors that were predictive of undertreatment of painin the ECOG study of ambulatory oncology patientsincluded minority status, discrepancy between patientand physician rating of pain severity, age, female sexand poor performance status.
Undertreatment of Cancer Pain in Special Populations
Elderly and Minority Patients
Undertreatment of cancer pain has been reported inminorities and the elderly in ambulatory patients, hos-pitalized patients and residents of nursing homes (VonRoenn et al. 1994; Bernabei et al. 1998). Elderly pa-tients with cancer pain often have comorbidities. Inconjunction with polypharmacy, this can account fora greater susceptibility of adverse drug events. Cog-nitive impairment and impaired communication alsorender some elderly patients with pain susceptible toundertreatment.Despite the high prevalence of cancer pain in the el-derly, they tend to be excluded from analgesic trials.Between 1987 and 1990, 83 randomized clinical trialsof anti-inflammatory drugs in 10,000 patients includedonly 203 patients over the age of 65. The occurrence ofcomplications of cancer pain in the elderly has not beenextensively studied, including gait disturbance, falls,delayed rehabilitation, malnutrition, polypharmacy andcognitive impairment.Ambulatory cancer patients treated at centers that pre-dominantly treat minority patients in the U.S., have beenreported to be three times less likely than patients treatedelsewhere to receive adequate cancer pain management(Von Roenn et al. 1994). Access to analgesic medicationis impaired by lower availability of opioid medicationsin pharmacies located in predominantly minority neigh-borhoods. Clinician adherence to racial stereotypes isimplicated in reports of disparities in morphine equiva-lent doses for different ethnic groups
Cancer Pain in the Developing World
It has been predicted that 10 of the 15 million new casesof cancer worldwide in the year 2015 will occur in theThird World; as many as 90% of these will continue topresent with advanced disease. The World Health Orga-nization assesses progress in cancer pain managementby national � per capita morphine consumption. Fiftypercent of countries use little or no morphine (U.N.� International Narcotics Control Board (United Na-tions International Narcotics Control Board 1992). Theten countries consuming 57% of all morphine in 1991have ranked highest in morphine consumption for manyyears. However, 100 of the poorest countries with themajority of the world’s population used just 14% ofall morphine. Many of these countries lack economic

286 Cancer Pain Management, Undertreatment and Clinician-Related Barriers
resources and medical infrastructure to produce anddistribute oral opioid medications. Restrictions exist onthe duration that a patient can receive oral morphine orthe locations where opioid medications can be received.When available orally, the available formulations ofmorphine (e.g. 10 mg controlled-release formulationsin the Philippines) may predispose to underdosing.
Barriers to Effective Pain Management
Clinician Educational Needs
Barriers to effective pain management are often con-ceptualized in terms of healthcare provider, patient,family, institutional and societal factors. About 50% ofphysicians are reported as having erroneous assump-tions about the use of opioids for cancer pain (Fifeet al. 1993). These misconceptions include concernsabout tolerance, addiction, the role of various routes ofadministration and the prevalence and management ofside effects. As many as 20% of physicians are reportedto regard cancer pain as inevitable and something thatcannot be effectively managed (Fife et al. 1993). Thesemisconceptions extend across disciplines and medicalspecialties. More than one-third of doctors and nursesin a U.S. survey of 971 clinicians believed that the useof opioid medications should be restricted based on thestage of a patient’s illness (Elliott and Elliott 1992).Knowledge deficits do not appear to correlate with thelevel of exposure to cancer pain and training in palliativecare. Despite their widespread availability, physicianscontinue to be reluctant to use validated assessmentinstruments.
Patient and Family Barriers
Many patients and families have unrealistic concernsabout the use of pain medications, and inadequateknowledge of cancer pain management. Patients oftenregard opioids as a last resort to be reserved for intol-erable pain, which they believe will be an inevitablesequela of their illness. Patient barriers are stronger inolder patients and in patients with lower educationaland income levels.
Economic Considerations
Internationally, reimbursement of patients for analgesicmedications is limited. Reimbursement by prevailingmedical payers also does not cover operational costsfor the provision of comprehensive cancer pain man-agement services. Palliative care is funded, in mostcountries, through a combination of public and privatefunding sources. However, there is heavy dependenceon philanthropy and community fund-raising. In anattempt to limit the impact on healthcare systems ofsoaring costs for medications, many health care insur-ance benefits limit coverage of medications or placerestrictions on the number of refills on prescriptions,the number of dosage units of a medication, or thenumber of medications that a patient can receive. An
unintentional effect of such policies may be the pre-mature admission of chronically ill patients to skilledlong term nursing care facilities (Soumerai et al. 1987).In many countries, oral opioids and long-acting for-mulations of opioid medications, in particular, areprohibitively expensive when consideration is given toaverage incomes.Even in wealthy countries, availability of inpatient pal-liative care beds is limited. In Germany, it was estimatedin 1996 that the national need for palliative care bedswas about 4000 beds. Only 230 were available, and atthe same time patients described spending an average of2 years with cancer pain prior to having access to a painclinic (Strumpf et al. 1996).Historically, in the U.S., healthcare insurance compa-nies have paid for procedures at the expense of compre-hensive medication coverage. Medicare, the prevailingcarrier for patients with chronic illness and for the el-derly, will pay for the cost of home infusions of opioidmedications at a cost of US $250–300 per day. However,the same medications administered orally are often notreimbursed (Witteveen et al. 1999).Inconsistent access to effective pain management re-sources commonly result in unnecessary hospital ad-missions for pain and symptom management. At onehospital alone, it was reported that 4% of the hospital’sadmissions were for uncontrolled pain, at an annual costof US $5.1 million. Little work exists on the impact of� cost shifting to patients and their families, in termsof family income or lost work days for cancer painmanagement in the community.The rising cost of opioid medications, for long-actingformulations in particular, may place severe strains onthe budgets of hospice organizations. Hospices mayalso be negatively impacted by requirements to destroyopioid medications after a patient dies. Recommendedchanges include alterations in federal guidelines toenable pharmacies to partially dispense if a patient isresident in a long-term care facility or has a documentedterminal illness.
References1. Bernabei R, Gambassi I, Lapane KF (1998) Pain Management
in Elderly Patients with Cancer. JAMA 279(23): 1877–18822. Coyle N, Adelhardt J, Foley KM et al. (1990) Character of Ter-
minal Illness in the Advanced Cancer Patient: Pain and OtherSymptoms in the Last 4 Weeks of Life. J Pain Symptom Manage5:83–93
3. Daut RL, Cleeland CS (1982) The Prevalence and Severity ofPain in Cancer. Cancer 50:13–18
4. Elliott TE, Elliott BA (1992) Physician Attitudes and Beliefsabout Use of Morphine for Cancer Pain. J Pain Symptom Manage7:141–148
5. Fife BL, Irick N, Painter JD (1993) A Comparative Study of theAttitudes of Physicians and Nurses towards the Management ofCancer Pain. J Pain Symptom Manage 8:132–139
6. Kelsen DP, Portenoy RK, Thaler HT et al. (1995) Pain and De-pression in Patients with Newly Diagnosed Pancreas Cancer JClin Oncol 13:748–755
7. Petzke F, Radbruch L, Zech D, Loick G, Grond S (1999) Tem-poral Presentation of Chronic Cancer Pain: Transitory Pains on

C
Cancer Pain Model, Bone Cancer Pain Model 287
Admission to a Multidisciplinary Pain Clinic. J Pain SymptomManage 17:391–401
8. Soumerai SB, Avorn J, Ross-Degnan D et al. (1987) Payment Re-strictions for Prescription Medications under Medicaid. N EnglJ Med 317:550–556
9. Strumpf M, Zenz M, Donner B (1996) Germany: Status of CancerPain and Palliative Care. J Pain Symptom Manage 12:109–111
10. United Nations International Narcotics Control Board (1992)Narcotic Drugs: Estimated World Requirements for 1993, Statis-tics for 1991. United Nations, Vienna
11. Vainio A (1995) Treatment of Terminal Cancer Pain in France:A Questionnaire Study. Pain 62:155–162
12. Von Roenn JH, Cleeland CS, Gonin R et al. (1994) Pain and itsTreatment in Outpatients with Metastatic Cancer. N Engl J Med330:592–596
13. Witteveen PO, Van Groenestijn MAC, Blijham GH et al. (1999)Use of Resources and Costs of Palliative Care with ParenteralFluids and Analgesics in the Home Setting for Patients with End-Stage Cancer. Annals Oncology 10:161–165
14. Zenz M, Zenz T, Tryba M et al. (1995) Severe Under-Treatmentof Cancer Pain: A 3 Year Survey of the German Situation. J PainSymptom Manage 10:187–190
15. Zeppetella G, O’Doherty CA, Collins S (2000) Prevalence andCharacteristics of Breakthrough Pain in Cancer Patients Admit-ted to a Hospice. J Pain Symptom Manage 20:87–95
Cancer Pain Model
Definition
A clinically relevant model used to study the mecha-nisms and neurobiology of cancer-induced pain. Often,but not exclusively, these models are developed inrodents or mammalians.� Cancer Pain, Animal Models� Cancer Pain Management, Treatment of Neuropathic
Components� Cancer Pain Model, Bone Cancer Pain Model
Cancer Pain Model, Bone Cancer PainModel
DARRYL T. HAMAMOTO, DONALD A. SIMONE
University of Minnesota, School of Dentistry, MoosTower, Minneapolis, MN, [email protected], [email protected]
Definition
Bone is the third most common site for tumor metas-tases (Rubens1998), and pain is themost frequent symp-tom for patients with metastatic bone cancer (Pecher-storfer and Vesely 2000). Bone cancer pain is often diffi-cult to treat (Mercadante 1997). Animal models have re-cently been developed to elucidate the underlying mech-anisms of bone cancer pain. A better understanding ofthese mechanisms may lead to the development of noveland more effective approaches to treating bone cancerpain.
Characteristics
Animal models of bone cancer pain have only been de-veloped in rodents (i.e. mice and rats). One advantage ofmurine models is that mice are commonly used to studycancer biology, so that many cancer cell lines are avail-able for use in mice. Many strains of mice have beengenetically modified, and these strains may be used todetermine the role of specific biochemicals in bone can-cer pain. The advantage of using rats in a model of bonecancer pain is that rats are commonly used in pain re-search, so their nociceptive systems have been well stud-ied. Many � nocifensive behavioral assays used to testrodents with bone cancer pain were initially developedin ratsand havebeen used in modelsof inflammatoryandneuropathicpain.Thus, comparisonsbetween themech-anisms underlying inflammatory, neuropathic, and bonecancer pain can be made more easily. Finally, because ofits larger size, it is easier to perform surgical procedureson a rat than a mouse.In these rodent models of bone cancer pain, tumor cellsare implanted into different bones. In three of the fourmodels, tumor cells are implanted into bones of thehind limb, specifically the femur, tibia, and calcaneousbones. Use of the hind limb is advantageous becausemany behavioral tests of � nociception apply the stim-ulus to the hind paw of rats, and thus the responses tothese stimuli have been well characterized. It is easierto apply stimuli to the hind paw than the forepaw inrodents because the hind paw is larger and away fromthe animal’s line of sight. The lumbar enlargementof the spinal cord is easier to access than the cervicalenlargement, and so it is easier to apply drugs to orrecord � electrophysiological activity from � dorsalhorn neurons. The lumbar and cervical enlargementsare where � primary afferents/neurons that innervatethe hind limb and forelimb terminate, respectively. Asa result, the electrophysiological responses and neuro-chemical characteristics of the dorsal horn neurons thathave receptive fields on the hind limb have been bettercharacterized than those innervating the forelimb. Asthe hind limb is longer than the forelimb in rodents,surgical preparation for electrophysiological record-ing from primary afferent fibers is easier. Thus, theelectrophysiological responses of the primary afferentfibers that innervate the hind paw, and the neurochem-ical characteristics of their associated � dorsal rootganglion neurons, have been better studied.
Femur Model
The first reported animal model of bone cancer painused NCTC 2472 cells, derived from a spontaneousconnective tissue tumor, which were implanted throughan arthrotomy in the knee joint into the medullary cavityof one femur of C3H/he mice (Schwei et al. 1999). Thehole in the articular surface of the distal femur, throughwhich the sarcoma cells are implanted, is sealed to

288 Cancer Pain Model, Bone Cancer Pain Model
keep the cells within the medullary cavity (Honoreet al. 2000a). Implantation of sarcoma cells producesan increase in both the number of osteoclasts and inosteoclast activation, which results in osteolytic lesionsin the implanted femur and invasion of the sarcomacells into the adjacent soft tissues (Clohisy et al. 1996).Micewithsarcomacells implanted intothefemurexhibitspontaneous guarding and flinches, movement-evokednocifensive behaviors during spontaneous or forced am-bulation, and mechanical � allodynia, as evidenced byflinching, guarding, fighting, and vocalization producedby normally non-noxious palpation of the affected limb(Schwei et al. 1999; Honore et al. 2000a; Luger et al.2001). The frequency of palpation-induced nocifensivebehaviorswascorrelated with theextentofbonedestruc-tion (Schwei et al. 1999).One feature of this model is that the sarcoma cells aresealed in the bone. This is similar to the clinical situa-tion in which tumor cells metastasize to the medullarycavity of a bone. Also, nociceptive stimuli are appliedto the distal femur, the location where the sarcoma cellserode through the bone, suggesting that the nociceptivebehaviors are due to excitation of nociceptors in the area.However, it isnotclearwhetherexcitationofnociceptorslocated in bone, muscle, or skin is responsible for evok-ing the nocifensive behaviors. Interestingly, implanta-tion of sarcoma cells into the femur also produced me-chanical allodynia at the plantar surface of the hind paw,as shown by a decrease in the threshold force requiredto evoke a hind paw withdrawal (Honore et al. 2000b).This finding suggests that the sarcoma cells may be in-juring nerve trunks passing through the area, resultingin a neuropathic pain condition as well as releasing po-tential algogens. Alternatively, excitation of nociceptorslocated near the sarcoma cells might produce sensitiza-tion of dorsal horn neurons (i.e. � central sensitization)that also have cutaneous receptive fields on the hind paw.
Tibia Model
A model of bone cancer pain in rats was developed inwhichmammaryglandcarcinomacells (MRMT-1)wereimplanted through an incision in the skin into the tibia,5 mm distal to the knee joint of one hind limb in fe-male (Medhurst et al. 2002) or male (Urch et al. 2003)Sprague-Dawley rats. The hole through which thebreastcarcinoma cells were implanted is sealed. Implantationof these breast carcinoma cells produces an increase inthe number of osteoclasts-like cells and time-dependentbone destruction. Tumor bearing rats exhibit mechani-cal � hyperalgesia (i.e. paw pressure) and allodynia (i.e.von Fey stimulation to the plantar surface of the hindpaw), cold allodynia (i.e. acetone applied to the plantarsurface of the hind paw), a decrease in weight bearingon the implanted limb, and ambulatory-evoked pain (i.e.limping and guarding on aRotarod treadmill) (Medhurstet al. 2002; Urch et al. 2003). Thus, this model of bonecancer pain in rats produces histological and behavioral
changes that were similar to those found in the femurmodel in mice.A murine model of bone cancer pain, produced byimplantation of NCTC 2472 sarcoma cells through askin incision into the tibia of C3H/he mice, has alsobeen reported (Menendez et al. 2003). The hole in thetibia through which the sarcoma cells are implanted isnot sealed. Implantation of sarcoma cells results in anincrease in the number of osteoclasts. At the time whenthe sarcoma cells erode through the bone and growinto the surrounding soft tissue, mice exhibit thermalhypoalgesia (i.e. increased paw withdrawal latencieswhen on a hot plate). As the tumor mass grows, andthe extent of bone destruction increases, mice exhibitthermal hyperalgesia.In both of these models, test stimuli are applied to thehind paw, a site distant from the location of the tumorcells. Increased responses to stimuli applied distant tothe site of implantation of the tumor cells suggesting aneuropathic injury or central sensitization may underliethese tumor-evoked behaviors.
Calcaneous Model
Implantation of NCTC 2472 sarcoma cells percuta-neously into and around the calcaneous bone of C3H/hemice produces osteolysis and evokes mechanical hyper-algesia (Wacnik et al. 2001). Mechanical hyperalgesiawas observed upon stimulation of the plantar surfaceof the ipsilateral hind paw with � von Frey monofil-aments. These mice also exhibited cold hyperalgesia(i.e. enhanced paw withdrawal responses when placedon a 5˚C plate). Histological examination shows thatsarcoma cells are found under the skin of the plantar sur-face of the hind paw, and that the number of nerve fibersin the epidermis (i.e. epidermal nerve fibers) above thetumor decreases (Cain et al. 2001). Interestingly, theproportion of neuropeptide containing primary afferentfibers increases suggesting that the sarcoma cells affectsubclasses of primary afferent fibers differently.One advantage of this model of bone cancer pain is thatthe effect of the sarcoma cells on the electrophysiologi-cal responses of primary afferent fibers innervating thetissue near the tumor can be determined. In fact, a pro-portion of nociceptive C-fibers innervating the plantarsurface of the hind paw exhibit spontaneous activity,which may produce central sensitization and contributeto the mechanical hyperalgesia observed (Cain et al.2001). Thus, interactions between the sarcoma cellsand primary afferent fibers can be examined using bothhistological and electrophysiological methods.This model differs from the models using the femur andtibia in that the sarcoma cells are not sealed in the bonebut are implanted both in and around the calcaneousbone. As a practical issue, the calcaneous bone in miceis small and the volume of its medullary cavity is low,making it difficult to keep the cell suspension withinthe medullary cavity. Additionally, sarcoma cells are

C
Cannabinoid 289
implanted without making an incision through the skin.To seal the hole would require an incision to expose thecalcaneous bone, which might produce inflammationand mechanical hyperalgesia. Moreover, implantationof sarcoma cells into the tissues around the calcaneousbone produced less mechanical and cold hyperalgesiathan when the sarcoma cells were implanted into thebone (Wacnik et al. 2001). These findings suggest thatinteraction of thesarcomacellswith thecalcaneousboneis important for full development of the mechanical andcold hyperalgesia observed in this model.
Humerus Model
Movement-related cancer pain is thought to be a pre-dictor of poor response to routine pharmacotherapy incancer patients (Mercadante et al. 1992). Thus, a modelof deep tissue cancer pain may be ideal for studyingthis specific characteristic of cancer pain. Implantationof NCTC 2472 sarcoma cells through the proximalend of each humerus bone in C3H/he mice producesmovement-related hyperalgesia, observed as a reduc-tion in forelimb � grip force (Wacnik et al. 2003) (see� Muscle Pain Model, Inflammatory Agents-Induced).This reduction in grip force can be attenuated withmorphine (Wacnik et al. 2003), and is possibly due tosensitization of nociceptors in the triceps muscles.Aninterestingadvantageofthehumerusmodelisthat theeffectiveness of an analgesic treatment is indicated by anincrease in response. That is, as the tumor grows, miceexhibit a decrease in grip force that is reversed by effec-tive analgesics. In other nocifensive behavioral tests, theanimal shows an increase in responsiveness with tissueinjury that is reversed by effective analgesic treatment.However, a decrease in paw withdrawal response or vo-calization could also be due to sedation or motor effectsof the test treatment. In the humerus model, sedation andmotor impairment would be likely to produce a decreasein grip force, resulting in the analgesic effects of a treat-ment being more easily separated from any sedative ef-fects or motor impairment.
References1. Cain DM, Wacnik PW, Turner M et al. (2001) Functional Inter-
actions between Tumor and Peripheral Nerve: Changes in Ex-citability and Morphology of Primary Afferent Fibers in a MurineModel of Cancer Pain. J Neurosci 21:9367–9376
2. Clohisy DR, Ogilvie CM, Carpenter RJ et al. (1996) Localized,Tumor-Associated Osteolysis Involves the Recruitment and Ac-tivation of Osteoclasts. J Orthop Res 14:2–6
3. Honore P, Luger NM, Sabino MA et al. (2000a) OsteoprotegerinBlocks Bone Cancer-Induced Skeletal Destruction, Skeletal Painand Pain-Related Neurochemical Reorganization of the SpinalCord. Nat Med 6:521–528
4. Honore P, Rogers SD, Schwei MJ et al. (2000b) Murine Modelsof Inflammatory, Neuropathic and Cancer Pain each Generatesa Unique Set of Neurochemical Changes in the Spinal Cord andSensory Neurons. Neuroscience 98:585–598
5. Luger NM, Honore P, Sabino MA et al. (2001) Osteoprote-gerin Diminishes Advanced Bone Cancer Pain. Cancer Res61:4038–4047
6. Medhurst SJ, Walker K, Bowes M et al. (2002) A Rat Model ofBone Cancer Pain. Pain 96:129–140
7. Menendez L, Lastra A, Fresno MF et al. (2003) Initial ThermalHeat Hypoalgesia and Delayed Hyperalgesia in a Murine Modelof Bone Cancer Pain. Brain Res 969:102–109
8. Mercadante S (1997) Malignant Bone Pain: Pathophysiology andTreatment. Pain 69:1–18
9. Mercadante S, Maddaloni S, Roccella S et al. (1992) PredictiveFactors in Advanced Cancer Pain Treated only by Analgesics.Pain 50:151–155
10. Pecherstorfer M, Vesely M (2000) Diagnosis and Monitoring ofBone Metastases: Clinical Means. In: Body J-J (ed) Tumor BoneDiseases and Osteoporosis in Cancer Patients. Marcel DekkerInc., New York, pp 97–129
11. Rubens RD (1998) Bone Metastases - The Clinical Problem. EurJ Cancer 34:210–213
12. Schwei MJ, Honore P, Rogers SD et al. (1999) Neurochemicaland Cellular Reorganization of the Spinal Cord in a Murine Modelof Bone Cancer Pain. J Neurosci 19:10886–10897
13. Urch CE, Donovan-Rodriguez T, Dickenson AH (2003) Alter-ations in Dorsal Horn Neurones in a Rat Model of Cancer-InducedBone Pain. Pain 106:347–356
14. Wacnik PW, Eikmeier LJ, Ruggles TR et al. (2001) FunctionalInteractions between Tumor and Peripheral Nerve: Morphology,Algogen Identification, and Behavioral Characterization of aNew Murine Model of Cancer Pain. J Neurosci 21:9355–9366
15. Wacnik PW, Kehl LJ, Trempe TM et al. (2003) Tumor Implanta-tion in Mouse Humerus Evokes Movement-Related Hyperalge-sia Exceeding that Evoked by Intramuscular Carrageenan. Pain101:175–186
Cancer Survivorship
Definition
The period of time during which an individual’s life isdefined from the moment of diagnosis with cancer untildeath. Often in pediatric oncology the focus is long-termsurvivorship, defined as a specified period of time aftertreatment during which the individual is disease free.� Cancer Pain, Assessment in Children
Cancer Therapy
Definition
Refers toanti-cancerchemotherapy,radiationtreatment,surgery or endocrine/hormonal treatment to cure or con-trol cancer and its progression.� Cancer Pain Management� Psychiatric Aspects of the Management of Cancer
Pain
Cannabinoid
Definition
Cannabinoids are derivatives of �9-tetrahydrocanna-binol (�9-THC), the constituent of marijuana that isresponsible for its psychoactive effects.� Evoked and Movement-related Neuropathic Pain

290 Cannabinoid Receptors
Cannabinoid Receptors
Definition
Receptors that are activated by the active constituent ofcannabis sativa, �9–tetrahydrocannabinol (�9–THC).These receptors can also be activated by endogenousligands such as anandamide (so-called „endocannabi-noids“).Two typesof receptorhavebeen identified,CB1and CB2, which are G-protein coupled. CB1 receptorsare found in several brain areas.� Nociceptive Neurotransmission in the Thalamus
Capacity
Definition
An individual’s ability to execute a task or an action, thehighest probable level of functioning that a person mayreach in a given domain, at a given moment.� Disability, Functional Capacity Evaluations
Capitated Care
Definition
A provider receives a set fee for each patient assigned tothe practice through an insurance carrier. The fee is oftencalled a per-member-per-month, and is independent ofthe care the patient requires.� Disability Management in Managed Care System
Capsaicin
Definition
The pungent ingredient of chili peppers (8-methyl N-vanillyl 6-nonenamide) from the capsicum family,which can be used to selectively activate nociceptivesensory neurones via its activation of a ligand-gatedcation channel TRPV1 (originally called the VR1channel, which can also be stimulated with heat andphysical abrasion, permits cations to pass), present onthese neurones. Stimulation of the cutaneous peripheralterminals of these nerve fibers with capsaicin can beused to produce neurogenic inflammation. It is alsoapplied to the skin in order to treat neuropathic painsuch as post herpetic neuralgia. Suggested mechanismof action is by activation of C fiber mechano-heat noci-coeptors, causing depletion of its neurotransmitters, e.g.substance P, thus stopping the function of the neuron.Plants produce the compound to deter predation. Cap-saicin is classified among the secondary metabolites.
The substance is widely used as an experimental modelof cutaneous hyperalgesia� Amygdala, Pain Processing and Behavior in Animals� Atypical Facial Pain, Etiology, Pathogenesis and
Management� Autologous Thrombocyte Injection as a Model of Cu-
taneous Pain� Exogenous Muscle Pain� Freezing Model of Cutaneous Hyperalgesia� Human Thalamic Response to Experimental Pain
(Neuroimaging)� Inflammation, Modulation by Peripheral Cannabi-
noid Receptors� Mechano-Insensitive C-Fibres, Biophysics� Muscle Pain Model, Ischemia-Induced and Hyper-
tonic Saline-Induced� Nociceptors in the Orofacial Region (Skin/Mucosa)� Opioid Modulation of Nociceptive Afferents In Vivo� PET and fMRI Imaging in Parietal Cortex (SI, SII, In-
ferior Parietal Cortex BA40)� Polymodal Nociceptors, Heat Transduction� Sensitization of Muscular and Articular Nociceptors� Species Differences in Skin Nociception� Spinothalamic Tract Neurons, Glutamatergic Input� Spinothalamic Tract Neurons, Role of Nitric Oxide� Sympathetically maintained Pain and Inflammation,
Human Experimentation� Toxic Neuropathies� TRPV1 Modulation by p2Y Receptors� TRPV1, Regulation by Nerve Growth Factor� TRPV1, Regulation by Protons
Capsaicin ReceptorANTONIO VICENTE FERRER-MONTIEL
Institute of Molecular and Cell Biology, UniversityMiguel Hernández de Elche, Alicante, [email protected]
Synonyms
TRPV1; vanilloid receptor subunit 1; Heat Sensor
Definition
The capsaicin receptor is a calcium permeable non-selective cation channel that is gated by noxious heat(≥ 42˚C), vanilloid compounds such as capsaicin andprotons. As a molecular sensor of painful stimuli atthe peripheral endings of nociceptive, primary sensoryneurons, the capsaicin receptor transduces noxiouschemical and thermal signals into action potentials.Thus, the capsaicin receptor is a key molecular compo-nent of the pain pathway.

C
Capsaicin Receptor 291
Characteristics
The capsaicin receptor is a member of the transientreceptor potential (TRP) mammalian gene superfam-ily (Caterina and Julius 2001). These channels areconsidered molecular gateways in sensory systems,since several of these proteins transduce chemical andphysical stimuli into neuronal activity, i.e. membranepotential changes. The capsaicin receptor gave its nameto the vanilloid subfamily (TRPV) of TRP channels.This sensory receptor is an integrator of noxious thermalstimuli as well as of irritant chemicals such as vanilloids,protons and pro-algesic substances (Caterina and Julius2001; Szallasi and Appendino 2004). Temperature gatesthe channel by shifting the voltage-dependent activa-tion towards the neuronal resting potential (Voets et al.2004). In contrast, chemical activators of the receptorsuch as capsaicinoid and vanilloid-like molecules andacidosis act as gating modifiers, reducing the temper-ature threshold of channel gating from 42˚C to belowbody temperature (36˚C). This is the underlying mech-anism for the characteristic pungency of capsaicin andrelated molecules.Molecularly, the functionalchannel isa tetramericmem-brane protein with four identical subunits assembledaround a central aqueous pore. Each receptor subunitdisplays a membrane domain composed of six trans-membrane segments (S1–S6) with an � amphipathicregion between the fifth and sixth segment that formsthe channel conductive pore (Caterina and Julius 2001;Ferrer-Montiel et al. 2004). The protein also has cyto-plasmic N- and C-termini (Fig. 1). In the N-terminus,TRPV1 channels exhibit three ankyrin domains thatmediate protein-protein interactions with cytosolic pro-teins and consensus sequences for protein kinases. Theprotein displays a cytosolic C-terminus domain contain-ing phosphoinositide, and calmodulin binding (CAM)domains, as well as phosphorylation sites (Caterinaand Julius 2001; Ferrer-Montiel et al. 2004; Nagy et al.2004). In addition, the C-end has a TRP-like motif thatfunctions as an association domain for receptor subunits(Garcia-Sanz et al. 2004). The receptor has two abun-dant single nucleotide � polymorphisms that produceamino acid substitutions, one in codon 315 (Met315 Ile)at the N-terminus domain and the other at amino acid585 (Ile585 Val) located in the fifth transmembrane seg-ment. Interestingly, gender, ethnicity and temperamentseem to contribute to individual variation in thermaland cold pain sensitivity by interactions in part withthese TRPV1 single nucleotide polymorphisms (Kimet al. 2004).The capsaicin receptor is widely expressed in neuronaland non-neuronal cells of both endodermal and meso-dermal origin, implying that the receptor is involvedin diverse physiological functions. These include ther-mosensory transduction, as well as chemical signallingpresumably mediated by � endovanilloid compounds.
In situ hybridisation, immunocytochemical analysis anddrug binding assays have shown TRPV1 expression in≈50% of dorsal root and trigeminal ganglion neurons,in the dorsal horn of the spinal cord and in the caudal nu-cleus of the spinal trigeminal complex. The majority ofTRPV1 positive neurons also colocalise with the nervegrowth factor (NGF) receptor trkA, the lectin IB4 andthe neuropeptides involved in nociceptive transmissionsuch as substance P (SP) and calcitonin gene relatedpeptide (CGRP) (Caterina and Julius 2001; Nagy et al.2004; Szallasi and Appendino 2004). Vanilloid sensi-tive nociceptors are peptidergic, small diameter neuronsthat give rise to unmyelinated C fibres, although someAδ fibres are responsive to vanilloid derivatives (Nagyet al. 2004; Szallasi and Appendino 2004). Somatic andvisceral primary afferents express TRPV1 at both thespinal and peripheral terminals. In addition to a subsetof nociceptors, the capsaicin receptor is present in neu-rons of the central nervous system and in non-neuronalcells. For instance, TRPV1 mRNA or protein is widelyexpressed in brain regions such as the olfactory nuclei,cerebral cortex, dentate gyrus, central amygdala, stria-tum, centromedian and paraventricular thalamic nuclei,hypothalamus, substantia nigra, reticular formation, lo-cus coeruleus, inferior olive and cerebellar cortex (Nagyet al. 2004). Furthermore, the receptor is expressed in avariety of epithelial tissues such as the skin, human hairfollicles, lungs, uroepithelium of the urinary bladder,the vascular system and the inner ear (Nagy et al. 2004).Taken together, all these observations underscore thenotion that TRPV1 is a widely expressed protein whosefunction is critical for diverse physiological conditions.The pivotal role of TRPV1 in nociceptive transduc-tion has suggested a contribution of the channel todiverse pathophysiological processes. In particular,cumulative evidence is substantiating the tenet that� nociceptor sensitisation by pro-inflammatory agentsis primarily achieved by the capsaicin receptor. Thisprotein is the endpoint target of intracellular signallingcascades triggered by inflammatory mediators thatlead to remarkable potentiation of its channel activ-ity which, in turn, promotes the hyperexcitability ofnociceptors (Planells-Cases et al. 2005; Julius andBasbaum 2001; Davis et al. 2000). Enhancement ofTRPV1 function by pro-algesic agents may be accom-plished either by direct activation of the channel orby its posttranslational modification by intracellularmetabolic cascades (Planells-Cases et al. 2005; Juliusand Basbaum 2001). Direct activation of TRPV1 re-sponses has been reported for lipid mediators such asarachidonic acid metabolites including anandamide, N-arachidonyl-dopamine (NADA) and N-oleyldopamine.Similarly, several eicosanoids, particularly those de-rived from the enzymatic action of 5-lipoxygenase or12-lipoxygenase, are capable of activating TRPV1.In particular, 12-(hyperoxy)eicosatetraenoic acid (12-HPETE) and leukotriene B4 (LTB4) have exhibited the

292 Capsaicin Receptor
Capsaicin Receptor, Figure 1 Molecular model of the capsaicin receptor subunit. The figure displays a membrane domain composed of six trans-membrane segments (S1–S6) with an amphipathic region between the fifth and sixth segment that forms the channel conductive pore, which alsocontains the glutamic acids (E600 and E648) responsible for the pH-induced channel gating. The protein also has cytoplasmic N- and C-termini. In theN-terminus, TRPV1 channels exhibit three ankyrin domains and consensus sequences for PKA and Src. The capsaicin-binding site is located at the N-endof the S3 segment, near S502, a serine residue phosphorylated by PKA, PKC and CaMKII. The protein displays a cytosolic C-terminus domain containingphosphoinositide (PIP2), and calmodulin binding (CAM) domains and phosphorylation sites for PKC (T704, S800) and CaMKII (T704). In addition, theC-end has a TRP domain that may contribute to the association of receptor subunits. The higher Ca2+permeability with respect to Na+and K+is alsodepicted.
most potent agonistic activity. In addition, the acidosisthat develops in inflamed tissues is also a direct activatorof the TRPV1 channel activity (van der Stelt and DiMarzo 2004). The potency and efficacy of each singularmediator is quite low but in inflammatory conditionsseveral of these modulators are simultaneously re-leased and act synergistically. Therefore, direct gatingof TRPV1 responses by inflammatory agents actingas channel agonists notably increases the excitabilityof nociceptors, resulting in a hyperalgesic condition.Prolonged activation of the receptor, leads to an intra-cellular [Ca2+] rise that, in turn, activates intracellularsignalling that triggers the release of pro-inflammatoryagents at peripheral terminals. This dual action furtherincreases the excitability of the nociceptors. In addi-tion, inflammation-evoked activation of intracellularprotein networks results in TRPV1 phosphorylation,release of tonically inhibited receptors and an incre-ment in the surface expression of functional channels,all being major events underlying the nociceptor ac-tivation and sensitisation that leads to � hyperalgesia(Planells-Cases et al. 2005). Indeed, TRPV1 expres-
sion is up-regulated in tissue samples from patientswith inflammatory bowel disease and Crohn’s diseaseand also in patients with rectal hypersensitivity, as wellas in those affected by vulvodynia (see ref. in Nagy etal. 2004; Szallasi and Appendino 2004; Planells-Caseset al. 2005). Thus, TRPV1 receptors are critical deter-minants of the sensitisation of primary afferents afterinjury or inflammation. The involvement of TRPV1in heat hypersensitivity is underscored by the reducedthermal hyperalgesia of TRPV1 null mice (Caterina etal. 2000), and by the attenuation of this inflammatory as-sociated phenomenon by non-competitive antagonistsof the TRPV1 channel (Garcia-Martinez et al. 2002).Accordingly, the important contribution of TRPV1receptor to the onset and maintenance of neurogenicinflammation has validated it as a therapeutic targetfor inflammatory pain management and a tremendouseffort is being carried out to develop clinically usefulmodulators of the receptor dysfunction characteristicof human diseases (Szallasi and Blumberg 1999).� Polymodal Nociceptors, Heat Transduction� TRPV1 Receptor, Species Variability

C
Carotid Arteries 293
� TRPV1, Regulation by Nerve Growth Factor� TRPV1, Regulation by Protons
References1. Caterina MJ, Julius D (2001) The vanilloid receptor: A molecular
gateway to the pain pathway. Annu Rev Neurosci 24:487–5172. Caterina MJ, Leffler A, Malmberg AB et al. (2000) Impaired
nociception and pain sensation in mice lacking the capsaicin re-ceptor. Science 288:306–313
3. Davis JB, Gray J, Gunthorpe MJ et al. (2000) Vanilloidreceptor-1 is essential for inflammatory thermal hyperalgesia.Nature 405:183–187
4. Ferrer-Montiel A, Garcia-Martinez C, Morenilla-Palao C et al.(2004) Molecular architecture of the vanilloid receptor. Insightsfor drug design. Eur J Biochem 271:1820–1826
5. García-Martínez C, Humet M, Planells-Cases R et al. (2002).Attenuation of thermal nociception and hyperalgesia by VR1blockers. Proc Natl Acad Sci USA 99:2374–2379
6. Garcia-Sanz N, Ferández-Carvajal A, Morenilla-Palao C et al.(2004) Identification of tetramerization domain in the C-terminusof the vanilloid receptor. J Neurosci 24:5306–5314
7. Julius D, Basbaum AI (2001) Molecular mechanisms of noci-ception. Nature 413:203–210
8. Kim H, Neubert JK, San Miguel A et al. (2004) Genetic influenceon variability in human acute experimental pain sensitivity as-sociated with gender, ethnicity and psychological temperament.Pain 109:488–496
9. Nagy I, Sántha P, Jancsó G et al. (2004) The role of the vanilloid(capsaicin) receptor (TRPV1) in physiology and pathology. EurJ Pharmacol 500:351–369
10. Planells-Cases R, García-Sanz N, Morenilla-Palao C et al. (2005)Functional aspects and mechanisms of TRPV1 involvement inneurogenic inflammation that leads to thermal hyperalgesia.Pflugers Arch Eur J Physiol 21 May, Epub ahead of print. PMID15909179
11. Stelt M van der, Di Marzo V (2004) Endovanilloids. Putativeendogenous ligands of transient receptor potential vanilloid 1channels. Eur J Biochem 271:1827–1834
12. Szallasi A, Appendino G (2004) Vanilloid receptor TRPV1 an-tagonists as the next generation of painkillers. Are we puttingthe cart before the horse? J Med Chem 47:1–7
13. Szallasi A, Blumberg PM (1999) Vanilloid (capsaicin) receptorsand mechanisms. Pharmacol Rev 51:159–211
14. Voets T, Droogmans G, Wissenbach U et al. (2004) The principleof temperature–dependent gating in cold- and heat-sensitive TRPchannels. Nature 430:748–754
Capsazepine
Definition
Capsazepine is a classical capsaicin antagonist, identi-fied by a combinatorial chemical screen. Interacts withTRPV1, the capsaicin receptor.� Capsaicin Receptors� TRPV1, Regulation by Protons
Carbenoxolone
Definition
Carbenoxolone is a gap junction decoupler. When ad-ministered over the spinal cord, it disrupts gap junctions
among astrocytes. In addition to decoupling gap junc-tions, carbenoxolone can also exert non-specific effects,including inhibition of11-beta-hydroxysteroid dehydro-genase, at higher doses. Peri-spinal administration ofcarbenoxolone blocks mirror-image pain.� Cord Glial Activation
Cardiac Stress Response
� Postoperative Pain, Pathophysiological Changes inCardiovascular Function in Response to Acute Pain
Cardiac Surgery
Definition
All cardiac surgical procedures performed with or with-out cardiopulmonary bypass.� Postoperative Pain, Thoracic and Cardiac Surgery
Career Assessment
� Vocational Assessment in Chronic Pain
Caregiver
Definition
Any person who assesses and provides care to the in-dividual experiencing pain (health care professionals,family member, friend). As it pertains to the newborninfants, the maternal caregiving relationship during in-fancy is considered a key mediator and moderator of riskfactors on infant development.� Pain Assessment in Neonates
Carotid Arteries
Definition
The common carotid artery divides into the internal andexternal carotid arteries in the neck. The former suppliesthe forebrain with blood and the latter supplies the faceand scalp.� Primary Cough Headache

294 Carotidynia
Carotidynia
Definition
A poorly defined syndrome with unilateral anterolateralcervical pain and local tenderness.� Headache due to Dissection
Carpal Tunnel Syndrome
Definition
Chronic compression of the median nerve as it passesthrough the carpal tunnel in the wrist. The pressureplaced on the median nerve could be caused by exces-sive pressure due to tendon or tissue inflammation andexcessive fluid in the wrist. The condition normallyresults in reduced nerve conduction velocity, and painand numbness in the thumb, index and middle fingers,sometimes the ring finger, but not the little finger. Withuse of the hand, these symptoms can become disturbingduring the daytime. Carpal tunnel syndrome has beenassociated with repetitive work and frequent forcefulexertions, as well as several systemic health conditionssuch as diabetes and pregnancy. The symptoms areover the palmar side of the hand, and not the dorsum.These include night-time awakening with numbness ortingling.� Carpal Tunnel Syndrome� Ergonomics Essay� Neuropathic Pain Model, Chronic Constriction Injury
Carpal Tunnel SyndromeA. LEE DELLON
Department of Plastic Surgery and Neurosurgery,Johns Hopkins University, Baltimore, MD, [email protected]
Synonyms
Median nerve compression at the wrist; EntrapmentNeuropathies, Carpal Tunnel Syndrome
Definition� Carpal tunnel syndrome is a combination of patientcomplaints related to chroniccompressionof themediannerve within the carpal tunnel. Since the carpal tunnel isat the wrist, the painful symptoms of which the patientcomplains are related to the small and large myelinatednerve fibers that supply the palmar, but not thenar, skinalong an axis that is radial to the longitudinal axis of thering finger, and thedistaldorsal tipsof the indexandmid-dle finger. The thenar skin is innervated by the palmarcutaneous branch of the median nerve,which arises 5 cm
proximal to the wrist, and therefore abnormal sensibil-ity of the thenar skin is not included in the definition ofcarpal tunnel syndrome. Motor symptoms include com-plaints of clumsiness in the use of the thumb, as the me-dian nerve’s motor branch innervates the abductor pol-licis brevis, the opponens pollicis, and the short headof the flexor pollicis brevis. When the wrist is flexed,pressure increases upon the median nerve, causing de-creased blood flow within the median nerve, and the re-sulting ischemia causes transmission of neural impulsesinterpreted asnumbnessor tingling(paresthesia), and, insome patients, actually as pain, causing them to awakenat night. Acute onset of pain in the distribution of the me-dian nerve is not included in the definition of carpal tun-nel syndrome, and indicates acute compression with ax-onal loss, rather than chronic compression and demyeli-nation.
Characteristics
Carpal tunnel syndrome is the most common example ofchronic nerve compression, with a prevalence of at least2% in the general population, 14% in diabetics withoutperipheral neuropathy, and 30% in diabetics with pe-ripheral neuropathy (Perkins et al. 2003). The physicalexamination findings required to confirm a diagnosis inthe first patient reported to have a carpal decompressionwere blisters on the tips of the thumb, index and mid-dle finger, due to anesthesia, and wasting of the thenarmuscles (Woltman 1941). The patient was an acrome-galic with hypertrophic neuropathy as the cause of thecompressionof themediannerve,andJamesLearmonth,a neurosurgeon at the Mayo Clinic, divided the trans-verse carpal ligament. In 1950, George Phalen, a sur-geon in Cleveland, described a series of patients withcarpal tunnel syndrome, which has become the classicdescription. Today a history of numbness or paresthe-sias in the thumb and index finger, associated with nighttimeawakening hasbecome theclassichistory.Theclas-sic physical examination findings are a positive Phalensign (symptoms provoked with wrist flexion for 1 min)or a positive Tinel sign (distally radiating sensory phe-nomenon when the median nerve is tapped at the wrist)(Mackinnon and Dellon 1988). It is unusual today fora patient to have sufficient chronicity of symptoms orseverity of compression to have thenar muscle wastingat the time or presentation.Documentation of carpal tunnel syndrome requires ei-ther� electrodiagnostictesting(EDT)or� neurosensorytesting (NST). EDT is objective, but remains with sig-nificant number of false negative findings, such that ameta-analysis done by the American Neurologic Asso-ciation (AAEM 1993) found that just 66% of patientsusing clinical symptoms and findings as the gold stan-dard had positive EDT. In contrast, quantitative sensorytesting has been demonstrated to be valid, reliable, cor-relate well with patient symptoms, and to be painless(Arezzo et al. 1993). Thermal threshold testing docu-

C
Carpal Tunnel Syndrome 295
ments the presence of small nerve fiber pathology, anddoes not become abnormal until late in the pathologyof carpal tunnel syndrome. Vibratory threshold testingdocuments the presence of large fiber pathology, but,because the stimulus is a wave, it can give ambiguousinformation when used to stimulate the index fingeror the thumb: these fingers are innervated by both theradial sensory and the median nerve, both of whichwill be stimulated by the waveform. NST is a formof quantitative sensory testing that measures the cuta-neous pressure threshold for one and two-point movingand static-touch. This testing found a clear distinctionbetween the 99% upper confidence limit in the nor-mal age-matched population, from those patients witheven a mild degree of carpal tunnel syndrome (Dellonand Keller 1997), suggesting that this methodologywould have a high sensitivity in evaluating patientswith chronic nerve compression. This was confirmedin a blinded, prospective study evaluating the ability ofEDT versus NST with the Pressure-Specified SensoryDevice to identify patients with carpal tunnel syndromefrom an asymptomatic population (Weber et al. 2000).That study found that the sensitivity of NST vs. EDTwas 92% vs. 81%, and the specificity of NST vs. EDTwas 82% vs. 77%. Since NST is painless, the patientis willing to have repeated studies in those clinicalsituations in which they may be necessary, e.g. whennon-operative treatment is first prescribed, or there isworkplace environment modification (ergonomics),treatment failure, or evaluation of impairment for adisability rating.Another indication for NST is the differential diag-nosis of failure to improve following carpal tunneldecompression, in which a proximal source of mediannerve compression, such as the pronator syndrome, isconsidered. EDT has a high false negative percentagewith this nerve compression, with up to 75% falsenegative in many studies, whereas NST, by measuringthe cutaneous pressure threshold of the thenar emi-nence, can document this proximal site of compression(Rosenberg et al. 2001). Evaluation of the cutaneouspressure threshold over the dorsoradial aspect of thehand can identify the presence of radial sensory nerveentrapment, another nerve compression to be con-sidered in the differential diagnosis of “failed carpaltunnel decompression”. In those patients in whom aC6 radiculopathy is being considered in the differentialdiagnosis, the electromyographic component of EDTis still the critical method required for documentation.The treatment of carpal tunnel syndrome is clearlydefined based upon staging the degree of compres-sion (Dellon 2001). Measurement of peripheral nervefunction permits a numerical grading system which in-corporates both the motor and sensory systems, and canbe applied to other upper extremity nerve compressionslike the ulnar nerve at the elbow, cubital tunnel syn-drome, or the lower extremity tibial nerve compression,
the tarsal tunnel syndrome. This numerical grading sys-tem permits statistical comparison of treatment optionsfor the wide range of clinical symptoms and findingsusually seen in carpal tunnel syndrome, or other nerveentrapment syndromes. For the mild degrees of com-pression, non-operative treatment is appropriate withsplinting of the wrist in a neutral position, non-steroidalanti-inflammatory medication, change of activities ofdaily living, and cortisone injection. Failure of thisapproach, manifested by persistence or progression ofsymptoms is an indication for surgical decompressionof the median nerve at the wrist. Another indication forsurgery is if more severe degrees of compression arepresent initially, such as the axonal loss associated withabnormal two-point discrimination or muscle atrophy.Randomized prospective studies (Gerritsen et al. 2001;Trumbleetal.2002), ingeneral,agreethat80–90%ofpa-tients can achieve good to excellent symptomatic reliefthrougheithera traditionalopenor thenewerendoscopicapproach. In experienced hands, the complications foreach procedure are similar. These complications includefailure of the procedure to achieve the desired result, in-jury to the median nerve or its branches, and a painful in-cision.Forcertainoccupations, theendoscopicapproachappears to permit a slightly earlier return to work.Based upon pre-operative staging, a routine intra-operative internal neurolysis does not improve results(Mackinnon et al. 1991), however, adding an internalmicrosurgical neurolysis based upon intra-operativepathology, has not been evaluated in a prospectivestudy. An � internal neurolysis may be indicated,therefore, and is utilized by this author, for intraneuralfibrosis typically identified in the setting or recurrentmedian nerve entrapment (Chang and Dellon 1993),or that observed in diabetics with superimposed nervecompression (Aszmann et al. 2000; Dellon 1992).Results of median nerve decompression in diabeticsgive excellent results in the majority of patients. In thepresence of neuropathy, EDT cannot reliably identifythe presence of carpal tunnel syndrome, and clinicaldecision making, based upon the presence of the Phalenand Tinel sign, is still considered valid (Perkins et al.2002).
References1. AAEM Quality Assurance Committee (1993) Literature Review
of the Usefulness of Nerve Conduction Studies and Electromyo-graphy for the Evaluation of Patients with Carpal Tunnel Syn-drome. Muscle Nerve 16:1392–1414
2. Arezzo JC, Bolton CF, Boulton A et al. (1993) Quantitative Sen-sory Testing: A Consensus Report from the Peripheral Neuropa-thy Association. Neurol 43:1050–1052
3. Aszmann OC, Kress K, Dellon AL (2002) Results of Decompres-sion of Peripheral Nerves in Diabetics: A Prospective, BlindedStudy Utilizing Computer-Assisted Sensorimotor Testing. PlastReconstr Surg 106:816–822
4. Chang B, Dellon AL (1993) Surgical Management of RecurrentCarpal Tunnel Syndrome. J Hand Surg 18:467–470

296 Carrageenan
5. Dellon AL (1992) Treatment of Symptoms of Diabetic Neuropa-thy by Peripheral Nerve Decompression. Plast Reconstr Surg89:689–697
6. Dellon AL (2001) Clinical Grading of Peripheral Nerve Prob-lems. Neurosurg Clinics N Amer 12:229–240
7. Dellon AL, Keller KM (1997) Computer-Assisted QuantitativeSensory Testing in Carpal and Cubital Tunnel Syndromes. AnnPlast Surg 38:493–502
8. Gerritsen AAM, Uitdehaag BMJ, Geldere D van et al. (2001)Systematic Review of Randomized Clinical Trials of SurgicalTreatment for Carpal Tunnel Syndrome. Br J Surg 88:1285–1295
9. Mackinnon SE, Dellon AL (1988) Carpal Tunnel Syndrome. In:Mackinnon and Dellon (eds) Surgery of the Peripheral Nerve.Thieme, New York, pp 149–170
10. Mackinnon SE, McCabe S, Murray JF et al. (1991) Internal Neu-rolysis Fails to Improve Results of Primary Carpal Tunnel De-compression. J Hand Surg 16:211–216
11. Perkins BA, Olaaleye D, Bril V (2002) Carpal Tunnel Syn-drome in Patients with Diabetic Polyneuropathy. Diabetes Care25:565–569
12. Rosenberg D, Conolley J, Dellon AL (2001) Thenar EminenceQuantitative Sensory Testing in Diagnosis of Proximal MedianNerve Compression. J Hand Therap 14:258–265
13. Trumble TE, Diao E, Abrams RA et al. (2002) Single-Portal En-doscopic Carpal Tunnel Release Compared with Open Release.J Bone Joint Surgery 84:1107–1115
14. Weber R, Weber RA, Schuchmann JA et al. (2000) A Prospec-tive Blinded Evaluation of Nerve Conduction Velocity versusPressure-Specified Sensory Testing in Carpal Tunnel Syndrome.Ann Plast Surg 45:252–257
15. Woltman HW (1941) Neuritis Associated with Acromegaly. ArchNeurol Psych 45:680–682
Carrageenan
Definition
A colloidal extract from carrageen seaweed and otherred algae, s. also Carrageenan Inflammation.� Amygdala, Pain Processing and Behavior in Animals
Carrageenan Inflammation
Definition
Carrageenan is an inflammatory irritant utilized tomimic inflammatory pain. Carrageenan can be injectedinto the paw, muscle or joint. Carrageenan inflammationis associated with heat and mechanical hyperalgesia.� ArthritisModel,Kaolin-CarrageenanInducedArthri-
tis (Knee)� TENS, Mechanisms of Action
Cartilage
Definition
Connective tissue that surrounds the ends of bones asthey meet to form a joint. The cartilage serves to forma smooth surface around the bones, providing for cush-ioning and allowing for smooth and easy movement of
the joint. Degradation of cartilage is a key characteristicof osteoarthritis.� Arthritis Model, Osteoarthritis
Case Control Study
Definition
A study that starts with the identification of persons withthe disease (or outcome variable) of interest, and a suit-able control (comparison) group of persons without thedisease (Last, 1988).� Prevalence of Chronic Pain Disorders in Children
Case Rate
Definition
Flat fee paid for a patient’s treatment, based on the di-agnosis and/or presenting problem.� Disability Management in Managed Care System
Caspases
Definition
Caspases are a family of cysteine proteases that cleaveproteins after aspartic acid residues. They are the mainexecutors of apoptosis or programmed cell death (PCD),and cause the characteristic morphological changes ofthe cell during apoptosis such as shrinkage, chromatincondensation and DNA fragmentation.� NSAIDs and Cancer
CAT Scan
� CT Scanning
Catabolism, Destructive Metabolism
� Postoperative Pain, Pathophysiological Changes inMetabolism in Response to Acute Pain
Catalogue
� Taxonomy

C
Catastrophizing 297
Catastrophic Cognitions
� Catastrophizing
Catastrophic Thinking
� Catastrophizing
CatastrophizingMICHAEL J.L. SULLIVAN, HEATHER ADAMS
Department of Psychology, University of Montreal,Montreal, QC, [email protected],[email protected]
Synonyms
Catastrophic thinking; catastrophic cognitions; mal-adaptive coping
Definition
Pain catastrophizing has been defined as an exagger-ated negative ‘mental set’ that is brought to bear duringan actual or anticipated pain experience (Sullivan etal. 2001). Pain catastrophizing is considered to be amultidimensional construct that includes elements of� rumination (i.e. excessive focus on pain sensations),� magnification (i.e. exaggerating the threat value ofpain sensations), and � helplessness (i.e. perceivingoneself as unable to cope with pain symptoms).
Characteristics
Catastrophizing, Pain and Disability
To date, approximately 200 studies have been publisheddocumenting a relation between catastrophizing andpain. A relation between catastrophizing and pain hasbeen observed in diverse clinical and experimental pop-ulations (Sullivan et al. 2001). Catastrophizing has beenassociated with increased pain and � pain behavior,increased use of health care services, longer hospi-tal stays, increased use of analgesic medication, andhigher rates of unemployment. In samples of chronicpain patients, catastrophizing has been associated withheightened disability, predicting the risk of chronicityand the severity of disability better than illness-relatedvariables or pain itself (Sullivan et al. 2001; Buer andLinton 2002; Picavet et al. 2002). A relation betweencatastrophizing and pain-related outcomes has been ob-served in children as young as 7 years (Gil et al. 1993).For a comprehensive review of current research andtheory on pain catastrophizing, the reader is referred toSullivan et al. (2001) and Vlaeyen and Linton (2000).
Most of the research demonstrating an association be-tween catastrophizing and pain has been correlational indesign, thus precluding the nature of causal inferencesthat can be drawn. However, a few studies have shownthat measures of catastrophizing prospectively predictpain outcomes. Keefe et al. (1989) assessed catastro-phizing and various pain-related outcomes in a sampleof patients with rheumatoid arthritis at two points intime, separated by a 6-month interval. Catastrophizingpredicted pain and functional disability even when con-trolling for initial pain and disability. In a sample of in-jured workers, Sullivan and Stanish (2003) showed thattreatment-related reductions in catastrophic thinkingwere associated with increased probability of returningto work. In several experimental studies, Sullivan andcolleagues showed that catastrophizing, measured in apain-free state, prospectively predicted pain responsesto painful procedures conducted as long as 6 weeks fol-lowing initial assessment of catastrophizing (Sullivanet al. 2001). Although these findings do not rule outthe possibility that catastrophizing may be reactive tovariations in pain experience, they do nevertheless high-light that the assessment of catastrophizing can permitprediction of future pain and pain-related disability.
Functions of Catastrophizing
Early conceptualizations of pain catastrophizing ap-pealed to cognitive constructs such as � appraisals,� cognitive errors and � schema activation to accountfor the relation between catastrophizing and pain (Sul-livan et al. 1995). It was suggested that, as a functionof a learning history characterized by heightened painexperience, catastrophizers may develop expectanciesabout the high threat value of painful stimuli (i.e. pri-mary appraisal), and about their inability to effectivelymanage the stress associated with painful experiences(i.e. secondary appraisal). Once activated, catastro-phizers’ ‘pain schema’ could influence emotional orcognitive functioning in a manner that contributed toheightened pain experience.More recently, it has been suggested that catastro-phizers might engage in exaggerated displays of theirpain-related distress as a means of coping with pain(Sullivan et al. 2001). This ‘communal coping’ modelof pain catastrophizing draws on recent theoreticaldiscussions of the interpersonal dimensions of coping,suggesting that individuals differ in the degree to whichthey adopt social or relational goals in their efforts tocope with stress. Catastrophizers’ expressive displaysof distress might be used, consciously or unconsciously,to maximize proximity, or to solicit assistance or em-pathic responses from others in their social environment(Sullivan et al. 2004a).
Mechanisms of Action: Catastrophizing and Pain
The role of attentional factors has been discussed as onemechanism through which castastrophic thinking might

298 Catastrophizing
exert its influence on the pain experience. For example,several investigations have shown the rumination sub-scaleof thePCSismorestronglycorrelated topain inten-sity ratings than the magnification or helplessness sub-scales (Sullivan et al. 2001). In other words, the endorse-ment of items, such as ‘I keep thinking about how muchit hurts’ and ‘I can’t seem to keep it out of my mind’ isassociated with higher pain ratings.Crombezetal. (1997) foundthat, inanticipation ofapainstimulus,catastrophizersshowedgreater interferenceonan attention-demanding task than non-catastrophizers.Heyneman et al. (1990) reported that pain catastrophiz-ers were unsuccessful in using attention diversion cop-ing strategies to reduce their pain. Other investigationshave provided data suggesting that catastrophizers maybe impaired in their ability to divert attention away frompain (Sullivan et al. 2001; Van Damme et al. 2002).
Mechanism of Action: Catastrophizing and Disability
The role of emotional factors, specifically fear, has beendiscussed asonemechanism through which catastrophicthinking might exert its influence on pain-related dis-ability. It has been suggested that following injury, indi-viduals who engage in catastrophic thinking are likelyto develop heightened fears of pain, movement and re-injury (Vlaeyen and Linton 2000). By contributing tothe development of pain-related fears, catastrophizingmight heighten the risk for different aspects of disabil-ity, such as activity discontinuation and activity avoid-ance (Picavet et al. 2002). Research suggests that pain-related fears do not mediate the relation between catas-trophizing and pain experience, but do mediate the re-lation between catastrophizing and disability (Sullivanet al. 2004b; Picavet et al. 2002).
Assessment
Several assessment instruments have been developed toassess pain catastrophizing. Considerable research oncatastrophizing has used the Coping Strategies Ques-tionnaire (CSQ) (Rosenstiel and Keefe 1983). The CSQconsists of 7 coping subscales, including a 6–item catas-trophizing subscale. Respondents are asked to rate thefrequencywithwhich theyuse thedifferentstrategiesde-scribed by scale items. The catastrophizing subscale ofthe CSQ contains items reflecting pessimism and help-lessness in relation to coping with pain (i.e. “It’s terribleand it’s never going to get any better”, “There’s nothingI can do to reduce the intensity of the pain”).The Pain Catastrophizing Scale (PCS) (Sullivan etal. 1995) is another commonly used measure of catas-trophizing that adopts a multidimensional view of theconstruct. The PCS is a 13–item self-report question-naire that assesses three dimensions of catastrophizing:rumination (“I can’t stop thinking about how much ithurts”), magnification (“I worry that something seriousmay happen”), and helplessness (“It’s awful and I feelthat it overwhelms me”).
Self-report measures have also been developed for as-sessing catastrophizing in children and adolescents (Gilet al. 1993; Crombez et al. 2003). Interview methodshave also been used; however, their application to clin-ical settings has been limited.
Treatment
The robust relation between catastrophizing and painhas prompted a growing number of clinicians and re-searchers to identify catastrophizing as a central factorin the clinical management of disabling pain condi-tions. Following multidisciplinary treatment for pain,reductions in catastrophizing are often noted (Burns etal. 2003). Recently, intervention programs have beendeveloped that specifically target catastrophic thinkingas a primary goal of treatment. Thorn et al. (2002)have described a 10–week, cognitive behavioral in-tervention designed to reduce catastrophic thinking inheadache sufferers. In this treatment program, thoughtrecording and � cognitive restructuring techniques areused as a means of monitoring and modifying catas-trophic thoughts. Sullivan and Stanish (2003) describeda 10–week, cognitive-behavioral program designed tofacilitate return-to-work following occupational injury.In the latter program, � activity mobilization strate-gies and cognitive restructuring are used to minimizecatastrophic thinking and facilitate progress towardoccupational re-integration.� Cognitive-Behavioral Perspective of Pain� Coping and Pain� Ethics of Pain, Culture and Ethnicity� Psychological Aspects of Pain in Women� Psychological Treatment in Acute Pain� Psychological Treatment of Headache
References1. Buer N, Linton SJ (2002) Fear-Avoidance Beliefs and Catastro-
phizing: Occurrence and Risk Factor in Back Pain and ADL inthe General Population. Pain 99:485–491
2. Burns JW, Kubilus A, Bruehl S, Harden RN, Lofland K (2003)Do Changes in Cognitive Factors Influence Outcome followingMultidisciplinary Treatment for Chronic Pain? A Cross-LaggedPanel Analysis. J Consult Clin Psychol 71:81–91
3. Crombez G, Bijttebier P, Eccleston E, Mascagni GM, Goubert L,Verstraeten K (2003) The Child Version of the Pain Catastrophiz-ing Scale (PCS-C): A Preliminary Validation. Pain 104:639–646
4. Crombez G, Eccleston C, Baeyens F, Eelen P (1997) When So-matic Information Threatens, Catastrophic Thinking EnhancesAttentional Interference. Pain 74:230–237
5. Gil KM, Thompson RJ, Keith BR, Tota-Faucette M, Noll S, Kin-ney TR (1993) Sickle Cell Disease Pain in Children and Ado-lescents: Change in Pain Frequency and Coping Strategies OverTime. J Ped Psychol 18:621–637
6. Heyneman NE, Fremouw WJ, Gano D, Kirkland F, Heiden L(1990) Individual Differences and the Effectiveness of DifferentCoping Strategies for Pain. Cog Ther Res 14:63–77
7. Keefe FJ, Brown GK, Wallston KA, Caldwell DS (1989) Cop-ing with Rheumatoid Arthritis: Catastrophizing as a MaladaptiveStrategy. Pain 37:51–56
8. Picavet HS, Vlaeyen JW, Schouten JS (2002) Pain Catastrophiz-ing and Kinesiophobia: Predictors of Chronic Low Back Pain.Am J Epidemiol 156:1028–1034

C
Causalgia 299
9. Rosenstiel AK, Keefe FJ (1983) The Use of Coping Strategies inChronic Low Back Pain Patients: Relationship to Patient Char-acteristics and Current Adjustment. Pain 17:33–44
10. Sullivan MJL, Adams H, Sullivan ME (2004a) CommunicativeDimensions of Pain Catastrophizing: Social Cueing Effects onPain Behaviour and Coping. Pain 107:220–226
11. Sullivan MJL, Bishop, SR, Pivik J (1995) The Pain Catastro-phizing Scale: Development and Validation. Psychological As-sessment 7:524–532
12. Sullivan MJL, Stanish WD (2003) Psychologically Based Occu-pational Rehabilitation: The Pain-Disability Prevention Program.Clin J Pain 19:97–104
13. Sullivan MJL, Thorn B, Haythornthwaite JA, Keefe FJ, Martin M,Bradley LA, Lefebvre JC (2001) Theoretical Perspectives on theRelation between Catastrophizing and Pain. Clin J Pain 17:52–64
14. Sullivan MJL, Thorn B, Rodgers W, Ward C (2004b) Path Modelof Psychological Antecedents of Pain Experience: Experimentaland Clinical Findings. Clin J Pain 20:164–173
15. Thorn BE, Boothy J, Sullivan MJL (2002) Targeted Treatmentof Catastrophizing in the Management of Chronic Pain. CognBehav Pract 9:127–138
16. Van Damme S, Crombez G, Eccleston C (2002) Retarded Disen-gagement from Pain Cues: The Effects of Pain Catastrophizingand Pain Expectancy. Pain 100:111–118
17. Vlaeyen JWS, Linton SJ (2000) Fear-Avoidance and its Conse-quences in Chronic Musculoskeletal Pain: A State of the Art.Pain 85:317–332
Categorization of Nociceptors
� Nociceptor, Categorization
Cauda Equina
Definition
A syndrome of fluctuating weakness and sensory losscaused by ischemia of the lumbosacral roots in a narrowspinal canal. It also refers to a collection of spinal rootsdescending from the lower spinal cord and occupyingthe vertebral canal below the cord.� Chronic Back Pain and Spinal Instability� Radiculopathies
Caudal Analgesia or Anesthesia
Definition
Regional anesthesia by injection of local anesthetic so-lution or other drugs into the epidural space via sacralhiatus.� Postoperative Pain, Epidural Infusions
Caudal Epidural Blocks
Definition
Sensory and motor block of the thoracic, lumbar orsacral nerves achieved by injecting local anesthetic(0.5-1 mg/kg) via needle or catheter inserted throughthe sacral hiatus into the epidural space.� Acute Pain in Children, Post-Operative
Caudal Epidural Steroids
� Epidural Steroid Injections
Caudal Injection
� Epidural Steroid Injections for Chronic Back Pain
Caudate Nucleus
Definition
One of the main nuclei of the basal ganglia; part of thestriatum connected principally with prefrontal and otherassociation areas of cortex.� Nociceptive Processing in the Nucleus Accumbens,
Neurophysiology and Behavioral Studies� Parafascicular Nucleus, Pain Modulation
Causalgia
Definition
A syndrome of sustained burning pain, allodynia, andhyperpathia after a traumatic nerve lesion, often com-bined with vasomotor and sudomotor dysfunction andlater trophic changes.� Causalgia, Assessment� Complex Regional Pain Syndrome and the Sympa-
thetic Nervous System� Complex Regional Pain Syndromes, General Aspects� Sympathetically Maintained Pain in CRPS II, Human
Experimentation

300 Causalgia, Assessment
Causalgia, AssessmentELLEN JØRUM
The Laboratory of Clinical Neurophysiology,Rikshospitalet University, Oslo, [email protected]
Definition� Causalgia is defined as “A syndrome of sustainedburning pain, � allodynia and � hyperpathia aftera traumatic � nerve lesion, often combined with� vasomotor and � sudomotor dysfunction and latertrophic changes.” (Classification of chronic pain 1994)This is an old term and causalgia will now be called� complex regional pain syndrome type 2 – CRPS–II(with nerve lesion).Causalgia, or complex regional pain syndrome, is asthe name implies a complex pain syndrome, beingcharacterized by the presence of � spontaneous pain,alterations in sensibility including allodynia and hy-perpathia, as well as symptoms and signs of autonomicdysfunction.Since this chapter will be dealing with “assessments”the complicated neurophysiological mechanisms willnot be mentioned. The aetiology is given, since we aretalking about a traumatic nerve lesion. This may occurin relation to all sorts of injuries.
Characteristics
Assessment of Nerve Lesion
This isapain syndromeoccurring after a traumaticnervelesion, and much emphasis will have to be put on theidentification of a specific nerve lesion.The best way to detect and to assess a peripheral nervelesion is to perform a detailed clinical neurologicalexamination of the patient, including investigation ofmotor and sensory function and myotatic reflexes. Sincepain may arise following either a sensory or a mixedmotor and sensory nerve, a detailed mapping of motorand sensory deficits is crucial. In most cases, therewill be a lesion of sensory nerve fibres, and a carefulstudy of the innervation territory of sensory deficit iswarranted. However, because of the involvement of cen-tral sensitization-mechanisms, the sensory deficit maysometimes exceed the innervation territory of the nerve;one may proceed by admitting the patient to a clinicalneurophysiologist for EMG (electromyography) andneurography. By neurography, measurements of con-duction velocities and other variables such as distaldelay, motor and sensory amplitudes and latency of latevolleys such as the H– and F– wave are measured. Nerveconduction studies play an important role in preciselydelineating the extent and distribution of a peripheralnerve lesion, and give some indication of nerve-rootpathology (by evaluation of late reflexes) (Jørum and
Arendt-Nielsen 2003). � Electrodiagnostic studies arecapable of demonstrating the peripheral nerve injury ofcausalgia or CRPS–II (Devor 1983). Neurography doesnot evaluate the function of thin nerve fibres such as Aδ mediating cold/sharp pain and C-fibres mediating thesensation of heat, heat pain and some forms of tactilepain. These nerve fibres may be evaluated by quantita-tive sensory testing (QST) (Gracely et al. 1996). It isimportant to note that the number of nerves available forneurography is restricted. Neurography will routinelybe performed on the major nerves of the upper extrem-ity (median, ulnar and radial nerves) and in the lowerextremity (peroneal, tibial and sural nerves); it is alsopossible, to some extent, to perform neurography of afew proximal sensory nerves in both upper and lowerextremity. EMG is also a helpful method in evaluatingneurogenic affection of muscles, and since it may beperformed in a large extent of muscles, more nervesmay hereby be examined.
Assessment of Clinical Pain
The pain in causalgia will have the same possible char-acteristics as pain following neuropathic pain in general,including the presence of spontaneous and evoked pain.Althoughpainfollowingnervelesionshasoftenbeende-scribed as burning, there are no pain descriptors whichare specific to neuropathic pain (and thereby to causal-gia).Pain in causalgia may be described by a large numberof adjectives, of which burning, throbbing, aching areonly a few examples. Spontaneous pain may be ongoingand/or paroxysmal, and the intensity may be evaluatedby a visual analogue score (0–10 cm) or (0–100 mm),where 0 represents no pain and 10 or100 the worst think-able pain. Pain intensity may spontaneously vary in in-tensity, but is often aggravated by physical activity andexposure to cold. Lightly touching the painful area will,in most cases, provoke a severe pain, but pain may alsobeevoked by thermal stimuli (frequently cold,not so fre-quently heat.)
Assessment of Allodynia/Hyperpathia
Since causalgia may be characterized by the presenceof allodynia and hyperpathia, an assessment of thesephenomena is important. Both are described elsewhere,but it is briefly repeated here that allodynia is defined as“pain due to a stimulus which does notnormally provokepain” and hyperpathia as “a painful syndrome charac-terized by an abnormally painful reaction to a stimulus,especially a repetitive stimulus, as well as an increasedthreshold” (Classification of chronic pain 1994). Al-lodynia and hyperpathia to both � tactile stimuli and� thermal stimuli may be tested. In clinical practice,allodynia to light touch is the easiest to perform. Onemay apply a cotton swab or a brush, gently moving itover the painful area, and record whether this normallynon-painful stimulus evokes pain or not. Hyperpathia

C
Causalgia, Assessment 301
to light touch may also be present, but in general thetwo phenomena may coexist. For the determination ofallodynia and hyperpathia to thermal stimuli, specialequipment is generally needed. One may obtain someindication of the presence or not of allodynia to coldor heat by applying thermorollers over the skin, rollerswhich are set at fixed temperatures, i.e. 25 and 40˚C.The rollers are first and foremost manufactured for test-ing reduced sensibility, and since heat pain is normallyperceived at temperatures around 42–43˚C, it may bedifficult to conclude with heat allodynia if pain is per-ceived at 40˚ C. Cold allodynia, on the other hand, maybe easier to demonstrate. In the upper extremity, coldpain will normally be seen at a threshold of 10–15˚C,while in the lower extremity, it will be below 10˚C. Formore accurate determinations of thresholds for coldallodynia or heat allodynia, quantitative sensory testing(QST) may be performed with the use of a thermotest.Cold allodynia will be the most prominent finding, andwill not be different from cold allodynia in other casesof neuropathic pain (Jørum et al. 2003).Heat allodynia may exist, but is seen less frequently. Hy-peralgesia/hyperpathia to pinprick may also be demon-strated, and as for allodynia to light touch, it may be ofvalue to map the area, by moving the von Frey hair or aneedle from normal skin centripetally towards the areaof hyperalgesia.
Assessment of Vasomotor and Sudomotor Dysfunction
The inclusion of possible vasomotor and sudomotordysfunction is essential for the diagnosis of CRPS–IIor causalgia. The clinician should look for signs likeoedema (Fig. 1), sweat dysregulation (usually increasedsweating, but also possibly reduced sweating), alter-ations in skin temperature (cooler or warmer) reflectingvasomotor changes, and trophic changes of the skin,hair and nails. The diagnosis of a full developed CRPSis not difficult. However, the diagnosis of milder casesmay prove difficult, especially since the patients’ clini-cal picture may change over time (vasodilatation at first,then vasoconstriction and finally dystrophic changes),
Causalgia, Assessment,Figure 1 Oedema in the right handin a patient with CRPS.
and the dynamic alterations may also include diurnalfluctuations. The evaluation of autonomic dysfunctionmay in most cases be performed by a clinical examina-tion, but laboratory tests may prove helpful. These canmeasure changes in autonomic function with highersensitivity and more objectivity. Most laboratory stud-ies of autonomic dysfunction in patients with CRPShave been conducted on patients with CRPS type 1(formerly reflex sympathetic dystrophy). One must addthat a general assumption is that CRPS–l or CRPS–II,do not differ in the changes believed to be dependenton the sympathetic nervous system (Stanton-Hicks etal. 1995). Various tests may be employed to assessthe function of the autonomic nervous system, bothwell validated routine tests as well as more experi-mental procedures. For the assessment of sudomotorfunction, sympathetic skin response and quantitativesudomotor axon reflex test (QSART) may be employed.Recordings of skin potentials from the foot or hand maybe made following a stimulus such as electric shock,a noise, a cough or an inspiratory gasp. The advan-tage of this method is that it is easy to perform in aroutine clinical neurophysiological laboratory. Thedisadvantage is its large variability, the tendency of theresponses to habituate, and that it has little sensitiv-ity, especially compared with the more sophisticatedQSART. In the latter test, the sweat output in responseto iontophoretic application of 10% acetylcholine isrecorded by a sudorometer. The major advantage is thatthe test is sensitive and reproducible in controls and inpatients with neuropathy (Low 2003). The disadvan-tage is that the equipment has only recently becomecommercially available and is not yet represented inmany laboratories. In a study of 102 patients withCRPS–I by Sandroni and co-workers (1998), theyfound that some of the indices that correlated mostreliably with clinical data, and with each other, wereQSART and skin temperature reductions. The authorscomputed the sudomotor index from the change insweat volume, latency and persistent sweat activity.QSART was positive at a single site if the affected side

302 Cawthorne and Cookseys’ Eye-Head Exercises
showed changes 50% greater than the non-affectedside.The assessment of vasomotor (vasoconstriction/vaso-dilatation) dysfunction may be performed by indi-rect methods, such as measuring of skin tempera-ture or thermography and by more sophisticated laserdoppler–examinations. The measurement of skin tem-perature is an easy but indirect way to detect changesin vasomotor function, where a difference between theaffected and non-affected extremity exceeding 1˚C willbe regarded as significant. Thermography is also easyto perform, but has the disadvantage that it will be re-garded as an indirect way of testing vasomotor function.Laser doppler investigations are also easy to perform,by measuring flow at a limited area or by scanning alarger area, but interpretations of data related to patho-physiology may be difficult. Elegant examinations areperformed with laser doppler examination, as describedin a paper by Weber et al. (2001), in combination withtrancutaneous electrical stimulation. They found thatthe vasodilatation as a response to electrical stimulationof the skin increased significantly (more pronouncedvasodilatation) in a group of mainly CRPS type 1 pa-tients compared to normal controls. There have beenmany critical comments to the IASP diagnostic criteriafor CRPS in general, and many authors have questionedthe specificity of the criteria.In a study by Bruehl and co-workers (1999) of 117 pa-tients meeting the IASP criteria for CRPS, and 43 pa-tients with neuropathic pain from diabetic neuropathy,they found that signs or symptoms of oedema versuscolour changes versus sweat dysregulation satisfiedthree criteria, and discriminated between the groups.Although diagnostic sensitivity was high at 98%, speci-ficity was poor at 36%. The diagnosis of CRPS waslikely to be correct in only 40% of the cases, and theresults of this study suggested that the criteria used byIASP had inadequate specificity and were likely to leadto over-diagnosis. However, it was again emphasizedthat this study was performed on patients with CRPSof both type 1 (approximately two thirds) and type 2.
References1. Bruehl S, Harden RN, Galer BS, Saltz S, Betram M, Backonja
M, Gayles R, Rudin N, Bhugra MK, Stanton-Hicks M (1999)External Validation of IASP Diagnostic Criteria for Complex Re-gional Pain Syndrome and Proposed Research Diagnostic Cri-teria. Pain 81:147–154
2. Merskey H, Bogduk N (1994) Classification of Chronic Pain.IASP Press, Seattle
3. Devor M (1983) Nerve Pathophysiology and Mechanisms of Painin Causalgia. J Autonom Nerv Syst 7:371–384
4. Gracely RH, Price DD, Rogers WJ, Bennett GJ (1996) Quanti-tative Sensory Testing in Patients with Complex Regional PainSyndrome (CRPS) l and ll. In: Jänig W, Stanton-Hicks M (eds)Reflex Sympathetic Dystrophy: A Reappraisal, Progress in PainResearch and Management, vol 6. IASP Press, Seattle, p 151
5. Jørum E, Arendt-Nielsen L (2002) Sensory Testing and Clin-ical Neurophysiology. In: Breivik H, Campell W, Eccleston C
(eds) Textbook of Clinical Pain Management. Arnold, London,pp 27–38
6. Jørum E, Warncke T, Stubhaug A (2003) Cold Allodyniaand Hyperalgesia in Neuropathic Pain: The Effect of N-methyl-D-aspartate (NMDA) Receptor Antagonist Ketamine:A Double-Blind, Cross-Over Comparison with Alfentanil andPlacebo. Pain 101:229–235
7. Low P (2003) Testing the Autonomic Nervous System. Seminarsin neurology 23:407–421
8. Sandroni P, Low PA, Ferrer T, Opfer-Gehrking T, WillnerC, Wilson PR (1998) Complex Regional Pain Syndrome(CRPS 1): Prospective Study and Laboratory Evaluation. ClinJ Pain 14:282–289
9. Stanton-Hicks M, Jänig W, Hassenbusch S et al. (1995) Re-flex Sympathetic Dystrophy: Changing Concepts and Taxonomy.Pain 63:127–133
10. Weber M, Birklein F, Neundörfer B, Schmelz M (2001) Facili-tated Neurogenic Inflammation in Complex Regional Pain Syn-drome. Pain 91:251–257
Cawthorne and Cookseys’ Eye-HeadExercises
� Coordination Exercises in the Treatment of CervicalDizziness
CBT
� Cognitive-Behavioral Therapy
CCI
� Chronic Constriction Injury� Chronic Constriction Injury Model� Neuropathic Pain Model, Chronic Constriction Injury
CCK
� Cholecystokinin
CDH
� Chronic Daily Headache in Children

C
Cell Therapy in the Treatment of Central Pain 303
Celiac Plexus Block
Definition
The celiac plexus is involved in nociceptive pain trans-mission from intraabdominal organs from the distalesophagus to the transverse, and sometimes to the de-scending colon. Interruption of nociceptive signals byinjection of phenol or alcohol onto the plexus mayprovide excellent and prolonged pain relief for pa-tients suffering particularly from gastric and pancreaticcarcinoma.� Cancer Pain Management, Anesthesiologic Interven-
tions, Neural Blockade� Cancer Pain Management, Overall Strategy
Cell Adhesion
Definition
An intercellular connection by which cells stick to othercells or non-cellular components of their environment.Cell adhesion generally requires special protein com-plexes at the surface of cells.� NSAIDs and Cancer
Cell Grafts
� Cell Therapy in the Treatment of Central Pain
Cell Minipumps
� Cell Therapy in the Treatment of Central Pain
Cell Therapy in the Treatment of CentralPain
MARY J. EATON
Miller School of Medicine at the University of Miami,Miami, FL, [email protected]
Synonyms
Cell Transplantation; Cell Grafts; Cell Minipumps
Definition
Cell therapy is the use of transplanted cells from pri-mary or immortalized sources to reverseor reducesymp-toms or causes of pain arising from injury to the cen-tral nervous system. Cell grafts used in this therapy canbe placed near the original injury, such as in or near thespinal cord, or further away, depending on the intendedmechanism to be targeted for therapeutic intervention.Primary cell sources are derived from a single cohortdonor and cannot be expanded or kept in vitro for ex-tended periods. Immortalized cell sources are derivedfrom any animal or human source, but have been engi-neered to be, or are naturally, expandable in vitro.
Characteristics
Even with continuous improvements in surgical man-agement, physical therapy and the availability of newerpharmacological agents, many patients following in-jury to the central nervous system continue to sufferfrom difficult to treat chronic pain. Newer treatmentsto modulate and reduce � central pain are likely to in-clude cell grafts that release antinociceptive moleculessynthesized by transplanted cells. Cell therapy to treatneuropathic pain after spinal cord injury (SCI) is inits infancy, but the development of cellular strategiesthat would replace or be used as an adjunct to currentpharmacological treatments for � neuropathic painhave progressed tremendously over the past 20 years.One strategy involves the placement of grafts in thespinal cord where a variety of antinociceptive sub-stances are released. Presumably, these cell grafts actas “cellular minipumps” that are able to release neu-roactive � antinociceptive molecules in the spinal cordand effect pain processing pathways. Cell lines, ratherthan primary cell grafts, can also offer a renewable andpossibly safe to use source of cells. Grafts of eitherprimary or immortalized sources could be expected toreduce or eliminate side effects associated with largedoses of pharmacological agents typically required forcentrally acting pain reducing agents, such as opioidsor antidepressants.The earliest studies using cell transplants for paintherapy were developed with the idea of mimicking de-scending or local spinal inhibitory � neurotransmittermodulation of sensory information. In these studiesagents released by cell grafts after injury resulted in� antinociception. A variety of neurotransmitters,peptides and more recently � neurotrophins, havebeen implicated in spinal inhibition. These includethe endogenous neurotransmitters serotonin (5-HT),noradrenaline and γ-aminobutyric acid (GABA), theendogenous opioid β-endorphin, enkephalins, endoge-nous peptides such galanin and neurotrophins such asbrain derived neurotrophic factor (BDNF). Many of thecommonly used pharmacological therapies target re-ceptors and re-uptake mechanisms of these substances

304 Cell Therapy in the Treatment of Central Pain
in order to increase or mimic their presence in acuteand chronic pain. In the early 1980’s it was recognizedthat these agents could be supplied by grafts of autolo-gous primary adrenal medullary chromaffin cells afternerve injury (� autologous graft). Chromaffin cellscontain a cocktail of antinociceptive agents, peptidesand neurotrophins (Wilson et al. 1981). To use chro-maffin cell therapy in humans, adrenal chromaffin cellgrafts were prepared from xenogenic bovine sourcesand tested for antinociception after nerve injury (Sagenet al. 1993). There have also been a number of animalstudies using primary medullary tissue or dissociatedchromaffin cultures placed in the � subarachnoid spaceto reduce behavioral hypersensitivity in models ofSCI-induced pain (Brewer and Yezierski 1998). Un-fortunately, non-human, xenogenic tissue sources arenot likely to be used clinically, even if they are moreabundant, given their increased risk of antigenicityand rapid rejection by the human host. Adult humanchromaffin tissue has been transplanted and tested inhumans for terminal cancer pain (Pappas et al. 1997),which is often neuropathic pain in nature. In thesestudies when the immune response in the human hostwas examined after graft placement, it was concludedthat further purification or � immunoisolation of graftswould be needed in order to use such tissues in multipletransplants, given the antigenicity of the diverse cellsources. Chromaffin cells from primary tissue sourcesare not likely to be homogeneous, since they are oftenobtained from multiple donors. The ability to use andmanipulate immortalized cell lines as a defined andstable source of cells will most probably permit theimplementation of cell therapy for pain in a clinicalsetting.A number of immortalized cell lines have been derivedfrom the rat brainstem to model how such cell linegrafts might function in models of pain after graftingnear the spinal cord. A common feature of these cells isthe expression of an oncogene, such as the temperaturesensitive � allele of large T antigen (tsTag) that con-fers � immortalization and allows for the expansionof cells at low temperatures in vitro. This oncogene isdown-regulated at higher transplant temperatures in theanimal. One of these rat neural precursor cell lines wasisolated from embryonic day 12.5 rat brainstem andimmortalized with the tsTag sequence. This cell line hasbeen made to synthesize and secrete the neurotrophinBDNF by the addition of the sequence for rat BDNFto its � genome, causing these cells to have improvedsurvival in vitro and in vivo and develop a permanentserotonergic phenotype. Since additional5-HTwas pos-tulated to have a beneficial effect on neuropathic pain,cells were placed in a lumbar subarachnoid space aftersciatic nerve injury. Grafts of these serotonergic cellsplaced 1 week after nerve injury and the developmentof severe hypersensitivity to thermal and tactile stimuliwere able to permanently reverse the symptoms of neu-
ropathic pain (Eaton et al. 1997). Transplants of similarmurine cell lines genetically engineered to synthesizeand secrete potentially antinociceptive molecules suchthe inhibitory peptide galanin, the neurotrophin BDNFand the inhibitory neurotransmitter GABA have beentested successfully in the same partial nerve injury painmodel (Eaton 2000).The same bioengineered rat serotonergic cell line men-tioned above has been successfully used to reduce neu-ropathic pain and improve locomotor function follow-ing SCI (Hains et al. 2001). Pain reduction requires thatcellsbeplaced in thesubarachnoidspace,where theycanaffect dorsal horn pathways and reduce spinal neuronalhyperexcitability (Hains et al. 2003), probably modu-lated throughspecific5-HTreceptors.Asimilarbioengi-neering approach was used to immortalize primary em-bryonic rat and bovine chromaffin cells, using the tsTagfor immortalization. Grafts of these cells placed in thesubarachnoid space in a model of neuropathic pain afternerve injury reduced pain without forming tumors in thehost animal (Eaton et al. 2000). For such an approach tobe completely safe as a clinical method for cell therapy,it will be necessary to remove the oncogene completelybefore grafting. The next advance in the creation of celllines for therapeutic use has been the development of re-versibly immortalized cell lines, as modeled by rat chro-maffin cell lines with an excisable oncogene.Studies exploiting site specific � DNA recombinationand Cre/lox excision have suggested that cells can betargeted in vitro and in vivo for removal of deleteri-ous genes, including the large T antigen. Reversibleimmortalization with Tag and Cre/lox technology wasfirst reported in human fibroblasts by Westerman andLeblouch (1996) and more recently in human myo-genic cells and hepatocytes (Kobayashi et al. 2000).Introduction of the gene for Cre recombinase into acell’s � genome allows for Cre to excise any recom-binant sequences present that are flanked by smallloxP sequences. Using this strategy, rat chromaffincells have been immortalized with an oncogenic tsTagconstruct, utilizing retroviral infection of these earlychromaffin precursors with the tsTag construct flankedby loxP sequences (floxed). Following isolation ofimmortalized cells, they were further infected with aretrovirus expressing the CrePR1 gene, which encodesfor a fusion protein that combines Cre activity with themutant human steroid receptor, hPRB891. After incu-bation of the cells with the synthetic steroid RU486,the fusion protein is translocated to the cell nucleus,allowing Cre to excise the tsTag oncogene and effec-tively dis-immortalize the cells in vitro. Such reversiblyimmortalized chromaffin cells, which express manyfeatures of the primary chromaffin cell, are able to re-verse neuropathic pain after spinal cord transplantationin a nerve injury model (Eaton et al. 2002). Such studiesmodel the use of reversibly immortalized cell lines inhumans.

C
Cellular Adhesion Molecules 305
An entirely differentapproach with cell lines is theuseofhuman neural lines that contain an oncogene that can bedown-regulated with agents such as retinoic acid (RA).An example of such a human neural cell line is the NT2line (Andrews 1984), which after � differentiation withRA for more than 2 weeks in vitro, differentiates into sta-blehuman neural cells thatnever formtumorsaftergraft-ing and have been used to ameliorate a variety of trau-maticandneurodegenerativeconditions(Trojanowskietal. 1997). Such cells represent immortalized stem cellsor neural progenitors that have been spontaneously im-mortalized and only differentiate after RA into the non-tumor, neural phenotype. These cells offer great poten-tial for the treatment of � central pain, since they appearsafe and can be easily used in the clinical setting, beingplaced via spinal tap into the subarachnoid space.Finally, there are no published successful methods fortreating human central pain with stem cells or precur-sors. The promise of this strategy lies in the future andwill probably require a degree of genetic or laboratorymanipulation. Regenerative medicine and the use of hu-man embryonic stem cells also currently engender eth-ical considerations. But, with rapid advances in knowl-edge about the basic biology of and ability to manipulateembryonic stem and precursor cells derived from CNSandother tissues, thefuturewillprobablyhaveaplaceforthe use of cell therapy. For example, adrenal chromaffinprogenitors can be kept proliferating by growth factorsinvitro (BesandSagen2002), suggesting that theymightprovide an alternative source for cell therapy, differentfrom bioengineered, immortalizedchromaffin cell lines.Thenear futurewillprobably providenewchallenges forthe implementation of cell therapy for those who suf-fer chronic pain. Some of the challenges common to allforms of cell transplantation include immune rejectionversus long-termsurvivalandefficacy in thehumanhost,dependable, well characterized cell sources for grafts,cells that can safely integrate into or near the CNS with-out danger of tumors or significant deleterious effects,ability to control theantinociceptiveoutputof cellgrafts,ideally increasing with the cyclic episodes of pain, andefficacy in a wide variety of pain causalities. Cell ther-apy for the treatment of pain offers much promise as a re-placement or adjunct to current clinical methodologies.The efficacy of this strategy will depend on a better un-derstanding of the mechanisms of pain, so that such bio-engineered cellular tools can be used appropriately.
References1. Andrews PW (1984) Retinoic acid induces neuronal differenti-
ation of a cloned human embryonal carcinoma cell line in vitro.Dev Biol 103:285–293
2. Bes JC, Sagen J (2002) Dissociated human embryonic and fetaladrenal glands in neural stem cell culture system: open fate forneuronal, nonneuronal, and chromaffin lineages? Ann N Y AcadSci 971:563–572
3. Brewer KL, Yezierski RP (1998) Effects of adrenal medullarytransplants on pain-related behaviors following excitotoxic spinalcord injury. Brain Res 798:83–92
4. Eaton MJ (2000) Emerging cell and molecular strategies for thestudy and treatment of painful peripheral neuropathies. J PeripherNerv Sys 5:59–74
5. Eaton MJ, Dancausse HR, Santiago DI et al. (1997) Lumbar trans-plants of immortalized serotonergic neurons alleviates chronicneuropathic pain. Pain 72:59–69
6. Eaton MJ, Martinez M, Frydel B et al. (2000) Initial characteriza-tion of the transplant of immortalized chromaffin cells for the at-tenuation of chronic neuropathic pain. Cell Transplant 9:637–656
7. Eaton MJ, Herman JP, Jullien N et al. (2002) Immortalized chro-maffin cells disimmortalized with Cre/lox site-directed recom-bination for use in cell therapy for pain. Exp Neurol 175:49–60
8. Hains BC, Johnson KM, McAdoo DJ et al. (2001) Engraftment ofimmortalized serotonergic neurons enhances locomotor functionand attenuates pain-like behavior following spinal hemisectioninjury in the rat. Exp Neurol 171:361–378
9. Hains BC, Johnson KM, Eaton MJ et al. (2003) Serotonergicneural precursor cell grafts attenuate bilateral hyperexcitabil-ity of dorsal horn neurons after spinal hemisection in rat. Neu-rosci 116:1097–1110
10. Kobayashi N, Miyazaki M, Fukaya K et al. (2000) Treatmentof surgically induced acute liver failure with transplantationof highly differentiated immortalized human hepatocytes. CellTransplant 9:733–735
11. Pappas GD, Lazorthes Y, Bes JC et al. (1997) Relief of intractablecancer pain by human chromaffin cell transplants: experience attwo medical centers. Neurol Res 19:71–77
12. Sagen J, Wang H, Tresco PA et al. (1993) Transplants ofimmunologically isolated xenogenic chromaffin cells providea long-term source of pain-reducing neuroactive substances. JNeurosci 13:2415–2423
13. Trojanowski JQ, Kleppner SR, Hartley RS et al. (1997) Trans-fectable and transplantable postmitotic human neurons: poten-tial “platform” for gene therapy of nervous system diseases. ExpNeurol 144:92–97
14. Westerman KA, Leboulch P (1996) Reversible immortalizationof mammalian cells mediated by retroviral transfer and site-specific recombination. Proc Nat Acad Sci USA 93:8971–8976
15. Wilson S, Chang K, Viveros O (1981) Opioid peptide synthe-sis in bovine and human adrenal chromaffin cells. Peptides 2Suppl:83–88
Cell Transplantation
� Cell Therapy in the Treatment of Central Pain
Cell-Mediated Immunity
Definition
An arm of the immune system that recognizes cell-associated antigens and consists of T-cells, phagocytesand NK cells as cellular effectors.� Viral Neuropathies
Cellular Adhesion Molecules
Synonyms
CAMs

306 Cellular Targets of Substance P
Definition
Cellular adhesion molecules (CAMs) are cell surfaceproteins involved in the binding of cells, usually leuko-cytes, to each other, to endothelial cells, or to extracel-lular matrix. Most of the CAMs characterized so far fallinto three general families of proteins: the immunoglob-ulin (Ig) superfamily, the integrin family, or the selectinfamily. The Ig superfamily of adhesion molecules,including ICAM–1, ICAM–2, ICAM–3, VCAM–1,and MadCAM–1, bind to integrins on leukocytes andmediate their flattening onto the blood vessel wall, withtheir subsequent extravasation into the surroundingtissue.� Cytokine Modulation of Opioid Action
Cellular Targets of Substance P
Definition
Possible sources of NK1 receptor stimulated NGFbiosynthesis including mast cells, which have beenreported to be prominent sources of skin NGF, althoughthe expression of NK1 receptors on these cells is unsure.There are only a few reports suggesting the presence ofNK1 receptors on mast cells. However, it has to be takeninto account that, depending on anatomic site, mast cellsshow variations in cell size, cytoplasmic granule ultra-structure, mediator content, sensitivity to stimulationby secretagogues, and in their susceptibility to variouspharmacological agents. Thus, it has been shown re-cently that functional NK1 receptors are induced byIL-4 and stem cell factor, suggesting that under certainconditions, like those accompanying inflammation,mast cells could gain increased responsiveness to NK1agonists. Keratinocytes have been shown to expressbeta adrenoceptors and to produce NGF in response tosubstance P. However, there are diverging reports as tothe type of tachykinin receptor primarily expressed bymurine keratinocytes. Other possible sources of NGFinclude macrophages/monocytes that express NK1 re-ceptors and can be stimulated by substance P to producecytokines.� NGF, Regulation during Inflammation
Cementum
Definition
Cementum is the mineralized tissue that covers the rootof a tooth. At the level where it abuts the enamel of thecrown it is very thin and often abraded, exposing the un-derlying sensitive dentin.� Dental Pain, Etiology, Pathogenesis and Management
Central Changes after Peripheral NerveInjury
MARSHALL DEVOR
Department of Cell and Animal Biology, Instituteof Life Sciences, and Center for Research on Pain,Hebrew University of Jerusalem, Jerusalem, [email protected]
Synonyms
Transsynaptic Changes after Peripheral Nerve Injury;central sensitization; central hyperexcitability state;Centralization; CNS Changes after Peripheral NerveInjury
Definition
Following nerve injury, including injury associated withchronic pain, numerous structural, neurochemical andelectrophysiological parameters are altered in the cen-tral nervous system (CNS), especially in the spinal cordand brainstem areas that receive direct primary afferentinput. This has led to the conviction that at least some ofthese central changes contribute to chronic neuropathicpain eitherdirectly,bygenerating ectopicpain-signalingimpulses, or indirectly, by amplifying orotherwise mod-ulating pain signals generated in the peripheral nervoussystem (PNS). In most instances we do not know withconfidence whether or not a particular central changeplays an important part in neuropathic pain.
Characteristics
Central Sensitization and Pain Centralization
“Centralsensitization”refers toanalteredstateofcentralneural processing in which nociceptive signals that enterthe CNS from the periphery are amplified, or in whichsignals carried centrally by low threshold mechanore-ceptorafferents(afferents thatnormallyprovokeasensa-tionof touch) insteadprovokeasensationofpain(Camp-bell et al. 1988; Devor et al. 1991; Woolf 1983). The con-cept that pain hypersensibility in inflamed tissue and inneuropathy may be due, at least in part, to abnormal sig-nal processing in the CNS, has a long history in neurol-ogy. The idea was promoted in particular by Hardy, Wolfand Goodell in the 1950s (Hardy et al. 1952), but wasmarginalized at the time, with most investigators favor-ing thealternativehypothesisofhyperexcitablenocicep-tive afferent endings in the periphery (Lewis 1942). Theconviction that the CNS makes an important contribu-tion was revived in the 1980s, partly under the influenceof Melzack and Wall’s “Gate control theory” and partlydue to theappearanceofagreatdealofnewdatabased onexperimental observations in humans and animal prepa-rations.When first introduced, the term central sensitizationreferred to a spinal pain hypersensitivity state triggered

C
Central Changes after Peripheral Nerve Injury 307
by afferent input entering the CNS on nociceptive C-afferents, and perhaps also nociceptive Aδ-afferents.This hypersensitivity state comes on rapidly followingonset of the nociceptive stimulus (seconds or minutes),and on cessation of the stimulus rapidly dissipates(minutes or hours). It can be maintained indefinitely,however, by continuous barrages of nociceptive inputsuch as may occur in chronic inflammatory conditionsand neuropathy. Thus, as originally conceived, centralsensitization is a labile, dynamic state dependent on anongoing barrage of nociceptive afferent input (Gracelyet al. 1992; Ji et al. 2003; Koltzenburg et al. 1994;Torebjork et al. 1992).Research into neural mechanisms that might underliecentral sensitization, however, revealed that a large va-riety of candidate processes are triggered by peripheralinflammation and neuropathy, and that some of these areneither transient and rapidly reversible, nor apparentlydependent on ongoing afferent input. The discovery ofsuch durable central changes coincided with the revivalof another classical concept, “� pain centralization”Be-lievers in pain centralization claim that persistent severepaincan“burn itself into” theCNS, in thesamewaythatatorrential stream can carve a canyon through solid rock.Persistent pain thus creates a central hyperexcitabilitystate thatbecomesindependentofafferent input fromtheperiphery. If true, this is an important matter, because itimplies that pain relief has a deadline; if it is not relievedsoon enough it centralizes and may become intractable,permanent (Kalso 1997).It is unlikely that pain, per se, can in fact cause perma-nent changes in central somatosensory processing. If itdid, then severe pain would persist after removal of aclearperipheral sourcesuchaspassageofakidneystone,childbirth, or replacement of an osteoarthritic hip. Pe-ripheral nerve injury, in contrast, may well induce per-manent CNS changes and intractable pain. In the con-text of neuropathy, the idea of durable centralization hasmergedwith theoriginaldynamicconceptofcentralsen-sitization. Thus, “central sensitization” has become anumbrella term that covers all peripherally evoked centralchanges that contribute to neuropathic pain, labile anddurable. This will be the use of the term in the presentessay. Note that central changes underlying neuropathicpain probably encompass someprocesses that are not in-volved in central sensitization evoked by acute noxiousevents, or by peripheral tissue inflammation.Central sensitization was originally conceived of asbeing regionally circumscribed. For example, follow-ing a localized burn, allodynia and hyperalgesia spreadsomewhat beyond the area of primary injury into asurrounding zone termed the area of “� secondary hy-peralgesia”. Likewise, if the precipitating injury is to aparticular nerve or sensory ganglion, central sensitiza-tion can cause the pain to extend into the distributionof neighboring nerves, or nearby dermatomes. Painextending beyond the triggering source is sometimes
given the dissonant name “extraterritorial pain” Theconcept can be extended still further. Pathology in oneorgan, for example, can cause hyperesthesia in neigh-boring ones, and meningeal inflammation in migrainecan cause tenderness on the scalp. Some authors havegone even further, positing that broad expanses of thecentral somatosensory representation can become per-sistently hyperexcitable. This is a popular explanationfor widely distributed global pain symptoms such as infibromyalgia (Banic et al. 2004; McDermid et al. 1996).
Varieties of Central Change
Numerous central changes have been documented in an-imal models of neuropathic (and inflammatory) pain. Inprinciple, it ought to be possible to determine the relativecontribution of each such change by spinal delivery ofagents that counter the changes, one at a time. Each suchagent should block a fraction of the neuropathic painsymptoms, and the appropriate combination of agentsshould block the pain entirely. In practice, however, thisapproach has not produced clear results. In many cases,appropriate blocking drugs are not available. In others,the application of drugs intended to reverse individualcentral changes has been claimed to eliminate neuro-pathic pain entirely. This suggests that experimental re-sults might have been exaggerated, or perhaps tested un-der highly specific, idiosyncratic circumstances. Alter-natively, pain symptoms may have a threshold such thatpartial suppression of many independent processes in-deed yields complete pain suppression.Anotherproblem iswith theagents themselves.Pharma-cological agents that show a high degree of specificitywhen tested under specific in vitro conditions, oftenprove to have unanticipated effects when tested in com-plex behavioral paradigms, in vivo. This also extendsto newer transgenic technologies. Finally, few authorscheck whether the agents they deliver to the spinal cordactually act there. Ectopic impulse discharge originat-ing in the � DRG is thought to play an important role inthe initiation and maintenance of central sensitization,particularly in animal models of neuropathy. Since theDRG shares the epidural and the intrathecal space withthe spinal cord, spinally delivered drugs access primarysensory neurons as well as CNS neurons. It is essentialto document that the spinally administered drug beingtested does not silence peripheral ectopia because thisalone would be expected to relieve pain symptoms,without regard to the central process being tested. Suchconfirmation is rarely done.What follows is a list of central changes induced by pe-ripheral nerve injury that might reasonably be predictedto affect pain processing. Most have been documentedin one, or only a few neuropathic pain models, or areinferred from models of inflammation, and are not nec-essarily universal. Some may appear paradoxical. Forexample, a priori one might presume that depletion ofan excitatory transmitter, or increased expression of an

308 Central Changes after Peripheral Nerve Injury
inhibitory one, is unlikely to cause pain. However, sincethesetransmittersmightbeactingoninhibitoryinterneu-rons in the spinal cord, a contribution to pain hypersensi-tivity by such changescannotbe ruledout.The listbelowis presented with a minimum of annotation (and withoutreferences due to editorial limitations imposed on all es-says in this volume). It is almost certainly incomplete atthe time of writing, and new changes are being identifiedat a rapid rate. Some changes may overlap, be redundant,or describe the same process using alternative functionalmarkers.
Changes in the Neurochemistry of Primary AfferentTerminals in the Spinal Cord after Peripheral NerveInjury
• Levels of the excitatory peptide neurotransmit-ter/neuromodulator � substance P (SP), and ex-pression of its precursor gene preprotachykinin, arereduced in small diameter nociceptive DRG neu-rons and their central terminals. However, there is aconcomitant increase in medium and large diameterDRG neurons.
• Expression of the excitatory peptide neurotransmit-ter/neuromodulator� CGRPisdecreased insmalldi-ameter DRG neurons and their central terminals.
• Expression of the inhibitory peptide neurotransmit-ter/neuromodulator galanin is increased.
• Cellular content of the excitatory peptide neurotrans-mitters/neuromodulators � neuropeptide Y (NPY)and vasoactive intestinal peptide (VIP) is increased,as is that of a variety of proinflammatory cytokines.
• Expression of the μ opioid morphine receptor gene(MOR) is reduced in DRG neurons and μ receptor isdepleted in afferent terminals
• The Ca 2+ channel subunitα2δ-1 is upregulated in ax-otomized primary afferent neurons, perhaps enhanc-ing synaptic release.
• Expression of the transducer/ion channels � TRPV1and P2X3 is depressed in afferent terminals
• Tissue plasminogen activator is induced in primaryafferent neurons by axotomy and released from theirterminal endings. This increases the excitability ofdorsal horn neurons.
• Expression of the � TTX -S Na+ channel Nav1.3 isupregulated in axotomized DRG neurons while thatof TTX-R Nav1.8 and Nav1.9 is downregulated. Allthree channels contribute to the membrane excitabil-ity of primary afferent neurons and their central ter-minals.
• The preceding are high-profile examples of changesin geneexpression in DRGneurons, and in geneprod-uct density in afferent terminals, following axotomy.Recent studies using � oligonucleotide arrays indi-cate thatmore than one thousand transcriptsareup-ordown-regulated in axotomized DRG neurons (Costi-gan et al. 2002; Xiao et al. 2002), and that “intact”neighboring neurons that have not been axotomized
also undergo changes in gene expression. All of theseare candidates, but few have been subjected to evenminimal functional analysis.
Changes in the Neurochemistry and Gene Expressionof CNS Neurons and Glia after Peripheral Nerve Injury
• A number of activity-regulated immediate earlygenes are upregulated in postsynaptic neurons in thedorsal horn including c-fos and jun-B. These tend tobe � transcription factors and hence probably affectthe expression of numerous other, still unidentified,downstream genes.
• Many transmembrane and intracellular signalingcascades in postsynaptic neurons are activated bythe phosphorylation of protein kinases such as ERK,MAPK, and CREB. More than 500 protein kinasegenes are present in the mammalian genome (Man-ning et al. 2002).
• Levels of cyclooxygenase (COX–1 and COX–2) inthedorsalhornarealteredwithconsequentchangesinarachidonic acid metabolites including (excitatory)prostanoids and leukotrienes.
• Expression of certain Na+ channel types is upregu-lated in postsynaptic spinal neurons following nerveinjury. Such changes are expected to increase the ex-citability of the affected neurons.
• A decrease in μ opiate receptors on postsynaptic dor-salhorn neurons following nerve injury mayoccasiondecreased intrinsic spinal inhibition.
• P2X4 receptors are upregulated in dorsal horn mi-croglia, potentially enhancing response to the exci-tatory neurotransmitter ATP.
• There is an increase in the spinal content of pro-inflammatory cytokines including IL1β, IL6, TNFα,but also in the anti-inflammatory cytokine IL10.These compounds are synthesized in activated as-trocytes and microglia and are released into theextracellular space. Some may also be producedin neurons. Proinflammatory cytokines can sensi-tize and directly excite postsynaptic dorsal hornneurons.
• There is an alteration in the content of many neu-rotransmitters in postsynaptic dorsal horn neurons,some inhibitory (e.g. 5-HT, NA, GABA, glycine)and some prohyperalgesic (e.g. dynorphin). Thereis also an increase in the spinal content of manybioactive molecules of uncertain function in painprocessing such as certain lectins and GAP43
• Increased nocistatin decreases spinal GABA inhibi-tion.
• As with primary sensory neurons, studies usingoligonucleotide arrays suggest that very large num-bers of transcripts are up- or down-regulated in thespinal cord as a consequence of nerve injury. Few ofthese have been subjected to even minimal functionalanalysis.

C
Central Changes after Peripheral Nerve Injury 309
Structural Changes in the CNS after Peripheral NerveInjury
• Central terminals of axotomized primary afferentneurons show a morphologically distinct “degen-eration atrophy”. The functional significance isuncertain, but the change might be associated withaltered synaptic release or even degeneration.
• There are reports that intraspinal terminals of lowthreshold mechanoreceptive Aβ afferents enter agrowth mode, extending sprouts dorsally into spinallaminae 1 and 2, where they may form ectopicsynaptic contacts with pain signaling spinal neu-rons. This finding is controversial, however, as itmight simply reflect axotomy-induced enhancementof the visualization of afferent connections presentnormally.
• There is a loss of neurons that immunolabel for the in-hibitory neurotransmitters glycine and GABA. Thismayreflectpermanentlossof inhibitoryinterneurons.
• Time-dependent loss of many functionally unidenti-fiedneuronsin thedorsalhornhasbeenreported(neu-rodegeneration), but the magnitude and significanceof this effect has been disputed.
• Transsynaptic atrophy and cell loss has been reportedin somatotopically appropriate supraspinal projec-tion systems including the primary somatosensorycortex (in long term amputees).
• Large numbers of astrocytes and microglia in thedorsal horn are “activated”, shortly after nerve injury,showing hypertrophy, increased numbers (hyperpla-sia), and altered expression of neuroactive moleculesincluding proinflammatory cytokines.
• Immune cells from the peripheral circulation, includ-ing macrophages and lymphocytes, invade the dor-sal horn grey matter. They may release excitatory cy-tokines and activate dorsal horn neurons.
• ATP, an excitatory neurotransmitter, is released fromastroglia activated following nerve injury.ATP is alsohydrolysedintotheinhibitoryneuroactivetransmitteradenosine.
Electrophysiological and Functional Changes in theCNS after Peripheral Nerve Injury
• The dorsal root potential (DRP) and primary affer-ent depolarization (PAD), two measures of spinal� presynaptic inhibition, are suppressed followingnerve injury. Reduced inhibition increases spinalresponse.
• Receptive fields (RF) of dorsal horn neurons expand,increasing the RF overlap between neighboring neu-rons. A given peripheral stimulus now activates morespinal cord neurons.
• The overall impulse volley that ascends in the spinalcord towards the brain upon electrical stimulation ofa peripheral nerve is reduced by about 50% beginning1–2 weeks following nerve injury. However, it is pos-
sible that some specific components of the ascendingvolley are enhanced.
• NMDA type glutamate receptors on postsynapticdorsal horn pain signaling neurons are normallyblocked and non-functional at resting membrane po-tential. Primary afferent nociceptive input producesa prolonged, shallow depolarization, probably due tothe release of SP (and other peptides) which relievesthe block, enables the NMDA-Rs, and enhancespostsynaptic response to Aβ touch input.
• Nociceptive afferent input induces PKC-dependentphorphorylation of NMDA-R subunits contributingto spinal pain hypersensitivity.
• There is also activation of non-NMDA glutamate re-ceptors (kainate receptors) in the spinal cord follow-ing nociceptive afferent input.
• Since the nociceptive mediators SP, NPY, and BDNFcome to be expressed in low threshold mechanore-ceptive Aβ afferents, activity in these afferents mightcome to directly activate pain signaling dorsal hornneurons.
• For the same reason, these afferents may acquire theability to trigger and maintain central sensitization.
• There is increased release of the excitatory neuro-transmitter glutamate in the dorsal horn.
• “Glycinespillover”facilitates theresponseofNMDAreceptors to glutamate, including glutamate releasedfrom Aβ touch afferents.
• Suppression of the Cl– pump, and the consequent de-polarizingshiftof theCl– reversalpotential, cancausethe normally inhibitory neurotransmitter GABA toyield excitation.
• Manysynapsespresentondorsalhornneuronsarerel-atively ineffective at driving the postsynaptic neuron(“silent synapses”). These can be strengthened by avariety of mechanisms, opening new functional path-ways including Aβ access to ascending nociceptivecircuitry.
• BDNF released from afferent terminals, and perhapssynthesized locally, sensitizes postsynaptic neuronsin the superficial dorsal horn.
• Elevatedbackgroundafferentactivity(ectopia)depo-larizes neurons, bringing them closer to spike thresh-old. This increases the level of spontaneous activitygenerated within thedorsalhorn, andenhances the re-sponse of dorsal horn neurons to weak residual inputsfrom the periphery.
• Repetitive stimulation at low frequency revealshomosynaptic facilitation ("windup"). This is aug-mented after nerve injury.
• Long term potentiation (LTP) is facilitated by nerveinjury.
• The duration of spinal postsynaptic potentiation isaugmented by nerve injury.
• Injury discharge triggered by acute transection ofprimary afferent axons may selectively damage in-hibitory spinal interneurons, perhaps by the sudden

310 Central Changes after Peripheral Nerve Injury
release of high levels of glutamate (excitotoxic celldeath).
• Nerve injury is associated with reduced GABA re-lease in the dorsal horn following electrical nervestimulation.
• Spontaneousdischarge,particularlyinaburstymode,is augmented in dorsal horn postsynaptic neurons andalso in supraspinal relays. Some of this activity maybe generated within the CNS, rather than reflectingelevated peripheral drive.
• Brainstem descending inhibition may be reduced fol-lowing nerve injury.
• Brainstem descending facilitation may be enhancedfollowing nerve injury.
• The gate control theory predicts that selective lossof large diameter low threshold afferent neurons willbias the spinal gate towards augmented nociception.
How Does Nerve Injury Trigger Central Change?
Little is know with confidence about how peripheralnerve injury triggers and maintains central sensitization.There are three fundamental possibilities:
Depolarization due to Impulse Traffic per se
The resting potential of postsynaptic neurons is deter-mined, in part, by the constant barrage of excitatoryand inhibitory postsynaptic potentials impinging ontheir dendritic arbor (spatial and temporal summa-tion). Ectopic afferent activity in neuropathy enhancesthe barrage, depolarizes the neuron, and brings rest-ing potential closer to firing threshold. This increasesspontaneous firing and response to normal and ectopicafferent input.
OtherActionsofTransmittersReleasedbyAfferentIm-pulse Traffic
Neurotransmitter and neuromodulator molecules re-leased from afferent terminals during spike activity mayhave postsynaptic effects beyond the moment to mo-ment modulation of the membrane potential. Couplingmay be via ligand-gated ion channels (and consequentmembrane depolarization), or transmembrane signalingpathways that are independent of membrane potential.
Trophic Interactions
More speculatively, nerve injury might bring aboutcentral changes completely independent of impulsetraffic and synaptic release. During embryonic de-velopment, the very survival of primary sensory andsecond order CNS neurons is dependent on mutualneurotrophic interactions. Beyond a critical period theneurons lose their acute dependence on neurotrophicsupport, but even in adulthood neuronal phenotype isaltered by changes in the provision of developmentalneurotrophins (Boucher et al. 2001). Both soluble andmembrane bound recognition molecules could be in-volved (neurotrophins, NCAMs, ephrin). Amounts of
these signaling molecules released or incorporated intothe membrane might be regulated by spike-evoked exo-cytosis, or perhaps by constitutive processes unrelatedto afferent impulse traffic (Battaglia et al. 2003; Fieldset al. 2001).
Perspective
Only a generation ago there was little concept of theprocesses that might underlie neuropathic pain. Thesituation has since reversed so that today we are awashwith candidate theories. It is a high priority to developstrategies for prioritizing central changes in terms oftheir relative contribution to pain symptomatology.Likewise, it is essential to establish the mechanism(s)by which nerve injury triggers CNS changes. If allor most central changes are due to abnormal primaryafferent input, it may be possible to prevent or reversethe central changes by controlling afferent input. Alter-natively, key central changes might offer opportunitiesfor direct therapeutic intervention.
Acknowledgements
Thanks to Linda Watkins and Zsuzsanna Wiesenfeld-Hallin for helpful comments on the manuscript. I wish toapologize to the numerous colleagues whose work wasnoted in this essay but not specifically cited because ofeditorial restrictionson thenumberof referencespermit-ted.
References1. Banic B, Petersen-Felix S, Andersen OK et al. (2004) Evidence
for Spinal Cord Hypersensitivity in Chronic Pain after WhiplashInjury and in Fibromyalgia. Pain 107:7–15
2. Battaglia AA, Sehayek K, Grist J et al. (2003) EphB Receptorsand Ephrin-B Ligands Regulate Spinal Sensory Connectivity andModulate Pain Processing. Nat Neurosci 6:339–340
3. Campbell JN, Raja SN, Meyer RA et al. (1988) Myelinated Af-ferents Signal the Hyperalgesia Associated with Nerve Injury.Pain 32:89–94
4. Costigan M, Befort K, Karchewski L et al. (2002) Replicate High-Density Rat Genome Oligonucleotide Microarrays Reveal Hun-dreds of Regulated Genes in the Dorsal Root Ganglion after Pe-ripheral Nerve Injury. BMC Neurosci 3:16–28
5. Devor M, Basbaum A, Bennett G et al. (1991) Mechanisms ofNeuropathic Pain following Peripheral Injury. In: Basbaum A,Besson J-M (eds) Towards a New Pharmacology of Pain, Chich-ester: Dahlem Konferenzen, Wiley, pp 417–440
6. Fields RD, Eshete F, Dudek S et al. (2001) Regulation of GeneExpression by Action Potentials: Dependence on Complexityin Cellular Information Processing. Novartis Found Symp239:160–172
7. Gracely R, Lynch S, Bennett G (1992) Painful Neuropathy: Al-tered Central Processing, Maintained Dynamically by PeripheralInput. Pain 51:175–194
8. Hardy JD, Wolf HG, Goodell H (1952) Pain Sensations and Re-actions. William and Wilkins, New York
9. Ji RR, Kohno T, Moore KA et al. (2003) Central Sensitization andLTP: Do Pain and Memory Share Similar Mechanisms? TrendsNeurosci 26:696–705
10. Kalso E (1997) Prevention of Chronicity. In: Jensen TS, Turner
JA, Wiesenfeld-Hallin ZH (eds), Proceedings of the 8th WorldCongress on Pain. Progress in Pain Research and Management,vol 8. IASP Press, Seattle, pp 215–230

C
Central Nervous System Stimulation for Pain 311
11. Koltzenburg M, Torebjork, H, Wahren L (1994) NociceptorModulated Central Sensitization Causes Mechanical Hyper-algesia in Acute Chemogenic and Chronic Neuropathic Pain.Brain 117:579–591
12. Lewis T (1942) Pain. MacMillan, New York13. Manning G, Whyte DB, Martinez R et al. (2002) The Pro-
tein Kinase Complement of the Human Genome. Science298:1912–1934
14. McDermid AJ, Rollman GB, McCain GA (1996) GeneralizedHypervigilance in Fibromyalgia: Evidence of Perceptual Ampli-fication. Pain 66:133–144
15. Torebjork H, Lundberg L, LaMotte R (1992) Central Changesin Processing of Mechanoreceptive Input in Capsaicin-InducedSecondary Hyperalgesia in Humans. J Physiol 448:765–780
16. Woolf CJ (1983) Evidence for a Central Component of Post-Injury Pain hypersensitivity. Nature 306:686–688
17. Xiao HS, Huang QH, Zhang FX et al. (2002) Identification ofGene Expression Profile of Dorsal Root Ganglion in the Rat Pe-ripheral Axotomy Model of Neuropathic Pain. Proc Nat AcadSci USA: 998360–998365
Central Gray/Central Grey
� Opioid Electrophysiology in PAG
Central Hyperexcitability
� Central Changes after Peripheral Nerve Injury� Visceral Pain Model, Esophageal Pain
Central Lateral Nucleus (CL)
Definition
The intralaminar complex is a group of thalamic nucleicomposed of neurons that are located within the internalmedullary lamina, a nerve fiber sheet that can be usedto subdivide different parts of the thalamus. The centrallateral nucleus is one of the rostral group of intralaminarnuclei of the primate thalamus. It receives input from thespinothalamic tract and projects broadly to the sensori-motor cortex, as well as to the striatum.� Spinothalamic Input, Cells of Origin (Monkey)� Spinothalamic Terminations, Core and Matrix� Thalamotomy for Human Pain Relief� Thalamus, Visceral Representation
Central Lobe
� Insular Cortex, Neurophysiology and FunctionalImaging of Nociceptive Processing
Central Medial Nucleus (CM)
Definition
A nucleus within the internal medullary lamina, locatedventrally to the central lateral nucleus and lateral to theparafascicular nucleus.� Thalamus, Visceral Representation
Central Nervous System Map
Definition
The organization of locations on or in the brain or spinalcord that represent the characteristics of a stimulus, suchas the receptive field, or of motor output, such as stim-ulation evoked movement.� Thalamus,ReceptiveFields,ProjectedFields,Human
Central Nervous System Portion of aCranial Nerve
Definition
The proximal portion of a cranial nerve over whichmyelin is associated with glial (oligodendroglial) cellsrather than with the Schwann cells, which are associatedwith myelin in the periphery.� Trigeminal, Glossopharyngeal, and Geniculate Neu-
ralgias
Central Nervous System Stimulation forPain
LUC JASMIN1, 2, PETER T. OHARA2, 3
1Department of Surgery, Division of Neurosurgery,University of Texas Medical Branch, Galveston, TX,USA2Department of Anatomy and,3the W.M. Keck Foundation Center for IntegrativeNeuroscience, University of California San Francisco,San Francisco, CA, [email protected], [email protected]
Synonyms
CNS Stimulation in Treatment of Neuropathic Pain

312 Central Nervous System Stimulation for Pain
Definition
Electrical stimulation of the central nervous system is anon-destructiveand reversible therapy for certain formsof difficult to treat chronic pain. Candidates have to fail atrial of the more conventional therapies. An electrode isplaced over the spinal cord, cerebral cortex or in the tha-lamus, hypothalamus or central gray matter. Analgesiais produced when a small current is delivered throughthis electrode and usually persists for some time afterthe current is turned off.
Characteristics
Both clinical and experimental studies have determinedthat electrical stimulation of the spinal cord or brainis analgesic. Considering the complexity of chronicpain, it is often perplexing that such a simple techniqueresults in relieving pain syndromes often deemed “in-tractable”, while complex pharmaceutical approaches,often because of their side effects, end in failure. Sincethe 1960s the technology associated with electricalstimulation for pain has remained essentially the same,although the quality of the components has improved.The two main components are the electrode and thecurrent generator, both of which are internalized (i.e.all inside the patient). The electrode (4 to 8 contacts) isusually placed over the dorsal aspect (dorsal columns)of the spinal cord, in the brain parenchyma (thalamus,hypothalamus or � periaqueductal gray matter [PAG]),or over the surface of the motor cortex. The currentgenerator, which is presently about the size of a pace-maker (4 cm × 4 cm × 1 cm), is concealed under the skinand connected to the electrode through subcutaneouswires. The current generator (including a rechargeablebattery) is programmed by telemetry using a handheldcomputer and an antenna laid over the appropriate skinarea. Voltage, frequency, pulse width and times of theday the system is on can be adjusted after the system isimplanted.
Spinal Cord Stimulation (SCS)
Spinal cord stimulation (SCS) was first performed in1967 and since then several hundred thousand patientshave received this treatment worldwide. About 10,000individuals will be implanted in the United States thisyear alone. While the mechanism remains to be fullyelucidated, a widely regarded explanation is the � gatecontrol theory. This theory, dating from the 1960s sug-gests that nociceptive information entering the CNSis reduced by the activity of innocuous (low thresholdlarge fibers) sensory afferents or brain activity. Theeffect of electrically stimulating neural pathways ca-pable of inhibiting nociceptive information is to “closethe gate” on the noxious input and result in analgesia.Accordingly, the electrode is positioned at the level ofthe spinal cord corresponding to the � dermatome or� viscerotome where the pain is felt. Interestingly, theanalgesia produced by stimulation often lasts long after
the cessation of the electric current (minutes to hours).This persistent analgesia is thought to depend not onlyon an effect on neurons adjacent to the stimulatingelectrode, but also on long neural loops linking thespinal cord to the brain. The result is the inhibition ofspinothalamic projection neurons (Gerhart et al. 1984).Clearly, when the underlying disease involves a lossof large fiber activity (as in multiple sclerosis or post-� cordotomy � dysesthesia), stimulation is less likelyto work. Another often cited mechanism is that spinalcord stimulation blocks sympathetic nervous systemfibers. This latter action would explain the favorableresults obtained in � complex regional pain syndrome(CRPS) and in angina pectoris. Other indications areneuropathic leg pain (not back pain) associated with� failed back syndrome, diabetic neuropathy, ischemicleg pain not treatable by vascular surgery, phantomlimb pain, post-herpetic neuralgia, spinal cord injurypain, � tabes dorsalis and spinal cord injury pain.Long term, moderate relief can be obtained in manypatients.In spite of the use of electrical stimulation to controlpain in large number of patients, there have been onlya few placebo-controlled evaluations of this treatment(Mailis-Gagnon et al. 2004). A significant placebo ef-fect might exist in patients utilizing SCS, and the reliefmight be related to the distraction of stimulation. Test-ing of this possibility is undermined by the difficultyin controlling for placebo response in a therapy thatdepends on the production of a sensory phenomenonto work (i.e. patients feel a tingling or paresthesia inthe stimulated area when the current generator is on).Although it is important to understand the exact mech-anism of pain relief, it will probably not matter to thepatient whether it is via placebo or some other mech-anism. While all agree that better clinical studies areneeded to confirm the effectiveness of SCS, especiallysince the benefits appear moderate, its continued useappears justified since it decreases the cost of treatingpain (Taylor et al. 2005).
Deep Brain Stimulation (DBS)
Deep brain stimulation (DBS) has been out of favorsince 1999 when Medtronic (Medtronic Inc. Min-neapolis, MN) decided not to pursue FDA approval forthis therapy due to the lack of conclusive clinical data(Coffey 2001). In spite of this, DBS is still used “off-label” here and in other countries for selected patients(Nandi and Aziz 2004). Electrodes are implanted inthe ventropostero-lateral thalamus, posterior limb ofthe internal capsule, periventricular gray including theposterior hypothalamus or PAG. Stimulation in theseareas is reported as fairly successful in patients withfailed back syndrome, trigeminal neuropathy otherthan tic douloureux, certain forms of � central pain(post-stroke pain), peripheral neuropathy, � anesthesiadolorosa and post-cordotomy dysesthesia.

C
Central Nervous System Stimulation for Pain 313
As with dorsal column stimulation, the neural mecha-nisms underlying DBS-induced analgesia are a matterof speculation. Marchand and colleagues (Marchandet al. 2003) studied the effect of placebo stimulationin patients with thalamic electrodes installed for paincontrol. Their key finding is that placebo analgesia is asignificant element of DBS and that this is reinforcedby the degree of paresthesia felt during the stimulation.The study of Marchand and colleague supports the con-tention that further controlled investigations are neededto understand the mechanisms by which stimulation ofthe central nervous system produces analgesia.Recently DBS has experienced a rebirth based on thefinding that stimulation of the hypothalamus can re-duce the occurrence of cluster headaches (Horton’sheadaches). Cluster headaches are a vascular type ofpain, occurring more commonly in males and charac-terized by unilateral headaches lasting 30 to 90 minutesand recurring 1 to 6 times a day for several weeks.Between attacks, patients can be asymptomatic formonths. The pain is reported as excruciating and char-acteristically located around the eye, which is visiblycongested and tearing. While some measures, such asavoiding alcohol and tobacco, reduce the frequency ofthe attacks, in many patients the prevention and treat-ment of cluster headaches presents a challenge. In 1998the positron emission tomography (PET) observationthat the symptomatic phase of cluster headaches wasaccompanied by the activation of a region of the ipsi-lateral medio-caudal hypothalamus led to the idea thatstimulation of this area might be of therapeutic value(Ekbom and Waldenlind 2004, Leone et al. 2004).Unilateral or bilateral electrodes and high frequencystimulation have been effective in reducing the occur-rence and duration of the attacks. PET imaging in clusterheadache has revealed that during hypothalamic stimu-lation, some pain activated areas such as the ipsilateralanterior cingulate, primary somatosensory cortices andthe insular cortex bilaterally are inactive (May et al.2003). While, DBS does not bring a cure to individualswith cluster headaches, for some it is the best treatmentavailable. For neuroscientists, it is a further indicationof the validity of electrical stimulation for pain and anincentive to purse basic research in this field as a meansof understanding pain mechanisms.
Motor Cortex Stimulation (MCS)
Motor cortex stimulation (MCS) has also yieldedpositive results in treating patients with central painfollowing ischemic brain or spinal injury and with� deafferentation pain in the trigeminal or spinal ter-ritories. Here an electrode is laid over the part of themotor cortex (usually over the dura rather than directlyon the pia mater) that corresponds to the area where thepain is felt on the opposite side of the body (accordingto the homunculus).
The rationale that guided surgeons to attempt corticalstimulation was based on the results of many decadesof experimentation, which demonstrated that electricalstimulation of the cerebral cortex affects spinal andtrigeminal afferent sensory transmission and that thiseffect is, in part, presynaptic on somatic afferents, in-cluding nociceptive afferents (Abdelmoumene et al.1970). The effect of stimulation of the cerebral cortexon spinothalamic neurons however, can be inhibitory,excitatory or both (Yezierski et al. 1983). Becausethe latency of excitation is significantly shorter thanthe latency of inhibition, inhibition could be polysy-naptic via inhibitory interneurons and/or presynapticprocesses on primary afferent terminals. Finally, ex-perimentation in cats has also shown that motor cortexstimulation blocks spontaneous burst activity inducedby spinothalamic deafferentation (Tsubokawa et al.1991).The most common indication for cortical stimulationis central pain syndrome. Dejerine recognized the syn-drome a century ago while an intern at the Salpêtrièrehospital in Paris. Because all of his patients with thispreviously unrecognized pain syndrome were found tohave strokes in the posterolateral thalamic area at au-topsy, Dejerine and Roussy, coined the term “thalamicsyndrome” A complete thalamic syndrome is uncom-mon and subsequently the term “thalamic pain” wasused forallpain conditions thatarose fromboth thalamicand non-thalamic CNS lesions. Since the majority ofcentral pain syndromes occur after an ischemic stroke,the designation ‘central post-stroke pain’ (CPSP) isoften employed. The current definition of central painhas become quite broad and accommodates etiologiesof central pain such as Parkinson’s disease or epilepsy,in which there is no thalamic lesion or interruption ofthalamic afferents. It should be noted that “central pain”differs from “centralized pain”, which is considered toresult from remodeling of the CNS as a consequence ofa peripheral injury. One example of centralized pain forwhich cortical stimulation has recently been shown tobe successful is trigeminal deafferentation pain (Brownand Pilitsis 2005).Although it is important to optimize patient selection formotor cortex stimulation, there is no unequivocal wayto separate the responders from the non-responders pre-operatively. Only patients with an intact motor cortexand corticospinal projections should be chosen. In pa-tients with large lesions of the motor cortex or pyramidaltracton thesideopposite to thesymptoms, stimulationofthe ipsilateral motor cortex has been shown to produceanalgesia. Stimulation is usually ineffective, however,in subjects with profound sensory loss. Imaging studieshave also been recommended prior to surgery in order toconfirm the presence of cortical hypoperfusion and as-certain thesiteof implantation, sincecorticalstimulationisassociated with acortical reperfusion.Finally,a trialofnon-invasive stimulation using a transcranial magnetic

314 Central Neuropathic Pain
coil over the motor cortex could also be a helpful wayof selecting the potential responders.
Vagal Nerve Stimulation (VNS)
Vagal nerve stimulation (VNS) acts indirectly to stim-ulate the CNS through sensory afferents to the caudalbrainstem. VNS is currently used to treat certain formsofepilepsy and isunder investigation aspossible therapyfordepression. Itmightalso becomeanaccepted methodfor treating cluster headaches and migraine (Mauskop2005) and possibly other pain disorders. Because it candecrease the nociceptive threshold in depressed individ-uals (Borckardt et al. 2005) and depression often accom-panies pain, patient selection for this technique will becritical.
Conclusion
Further clinical studies are needed to validate CNS stim-ulation as an effective treatment of pain, mainly becausemost of the evidence is anecdotal or retrospective. Basicresearch is critically needed to establish the mechanismof action and it is possible that stimulation induced anal-gesia might open the door to a new, unforeseen under-standing of the means by which pain operates. DBS iscurrently gaining popularity for the treatment of move-ment disorders, a field where much greater understand-ing of the neural circuitry has fostered unique cooper-ation between clinicians and basic scientists. The sametype of teamwork could benefit the development of newideas and advances in the field of pain.
References1. Abdelmoumene M, Besson JM, Aleonard P (1970) Cortical areas
exerting presynaptic inhibitory action on the spinal cord in catand monkey. Brain Res 20:327–329
2. Borckardt JJ, Kozel FA, Anderson B et al. (2005) Vagus nervestimulation affects pain perception in depressed adults. Pain ResManag 10:9–14
3. Brown JA, Pilitsis JG (2005) Motor cortex stimulation for centraland neuropathic facial pain: a prospective study of 10 patientsand observations of enhanced sensory and motor function duringstimulation. Neurosurgery 56:290–297; discussion 290–297
4. Coffey RJ (2001) Deep brain stimulation for chronic pain: re-sults of two multicenter trials and a structured review. Pain Med2:183–192
5. Ekbom K, Waldenlind E (2004) Cluster headache: the history ofthe Cluster Club and a review of recent clinical research. FunctNeurol 19:73–81
6. Gerhart KD, Yezierski RP, Wilcox TK et al. (1984) Inhibition ofprimate spinothalamic tract neurons by stimulation in periaque-ductal gray or adjacent midbrain reticular formation. J Neuro-physiol 51:450–466
7. Leone M, Franzini A, Broggi G et al. (2004) Long-term follow-up of bilateral hypothalamic stimulation for intractable clusterheadache. Brain 127:2259–2264
8. Mailis-Gagnon A, Furlan AD, Sandoval JA et al. (2004) Spinalcord stimulation for chronic pain. Cochrane Database SystRev:CD003783
9. Marchand S, Kupers RC, Bushnell MC et al. (2003) Analgesicand placebo effects of thalamic stimulation. Pain 105:481–488
10. Mauskop A (2005) Vagus nerve stimulation relieves chronic re-fractory migraine and cluster headaches. Cephalalgia 25:82–86
11. May A, Leone M, Boeker H et al. (2003) Deep brain stimulationin cluster headache: preventing intractable pain by activating thepain network. Cephalalgia 23:656
12. Nandi D, Aziz TZ (2004) Deep brain stimulation in the manage-ment of neuropathic pain and multiple sclerosis tremor. J ClinNeurophysiol 21:31–39
13. Taylor RS, Van Buyten JP, Buchser E (2005) Spinal cord stim-ulation for chronic back and leg pain and failed back surgerysyndrome: a systematic review and analysis of prognostic fac-tors. Spine 30:152–160
14. Tsubokawa T, Katayama Y, Yamamoto T et al. (1991) Treatmentof thalamic pain by chronic motor cortex stimulation. Pacing ClinElectrophysiol 14:131–134
15. Yezierski RP, Gerhart KD, Schrock BJ et al. (1983) A further ex-amination of effects of cortical stimulation on primate spinotha-lamic tract cells. J Neurophysiol 49:424–441
Central Neuropathic PainDAVID BOWSHER
Pain Research Institute, University Hospital Aintree,Liverpool, [email protected] or [email protected]
Synonyms
Dejerine and Roussy (1906) described three cases ofpain following strokes involving the thalamus, andnamed the condition “thalamic syndrome” – a namethat has, unfortunately, remained in the literature –because it was later shown that similar pain follows in-farction of other, non-thalamic, telencephalic areas suchas the cortex (Foix et al. 1927). Infarction in brainstemor the anterolateral medulla oblongata can also causepain in the condition known as Wallenberg’s syndrome(Ajuriaguerra 1937).The onset of pain following central lesions is notrestricted to supraspinal pathology. Central pain insyringomyelia has been reported by Spiller (1923)and was indistinguishable from central pain of cere-bral origin. Unfortunately, recognition of the fact thatcentral pains following spinal cord damage, such asanterolateral cordotomy (White and Sweet 1969), andof course spinal cord injury (SCI) are similar to thoseof supraspinal origin was slow to develop.
Definition
Leijon et al. (1989) proposed the name “Central Post-Stroke Pain” (CPSP) to cover all these contingencies –however, this name does not encompass cases caused byconditions other than stroke. The post-mortem anatom-ical pathology of eleven cases in which lesions of thecentral nervous system, including cortical lesions, twotumours and one multiple aneurysm, resulted in theonset of pain was described in detail by Davison andSchick (1935). Subarachnoid haemorrhage, multiplesclerosis, tumour, cerebral abscess, Behçet’s disease,Parkinson’s disease, and arteriovenous aneurysm haveall been implicated as causes of central pain. It is well-known that syringomyelia is associated with central

C
Central Neuropathic Pain 315
pain (Madsen et al. 1994), and central pain caused byspinal cord injury (SCI) has been described in a numberof reports (Yezierski 1996). Painful post-cordotomydysaesthesia was recognised by White and Sweet(1955), who stated that 20 % of patients undergoinganterolateral cordotomy and surviving for more thana year developed painful dysaesthesia. Siddal et al.(1999) concluded that 50 % of patients with spinal cordinjury (SCI) suffer central neuropathic pain, as do mostpatients with syringo/hydro-myelia.It can convincingly be argued that the seat of pathophys-iology in neuropathic pains due to insult of peripheralnerves (e.g. painful diabetic neuropathy, complex re-gional pain syndromes, and postherpetic neuralgia)is in the central nervous system; the symptomatologycertainly fulfils the criterion enunciated in the nextparagraph. However, they will not be dealt with in de-tail in this chapter. Thus, it would perhaps be better torecognise a category of central neuropathic pain (CNP),due to (unspecified) damage to any part of the neuraxis.That such pains be recognised as neuropathic requiresone more criterion: the pain occurs in an area of sensorychange (total or, much more frequently, partial deficit).
Incidence
While it has long been known that not all cases ofspinal cord injury or Wallenberg’s syndrome necessar-ily suffer spontaneous neuropathic pain, it is importantto emphasise the findings of Bogousslavsky and hiscolleagues (1988): only 25 % of patients with thalamicinfarcts involving the thalamic somatosensory relaynucleus (VPL, Vc) actually develop pain. In a prospec-tive study, Andersen et al. (1995) reported that about8 % of all surviving stroke patients develop CNP. In apopulation of 250 million (e.g. USA), there are 250,000strokes p.a., of whom about 170,000 survive. Thus, theannual incidence of CPSP is approximately 11,000 newcases. Since most patients with CPSP do not have verysevere or life-threatening motor impairment (only 8 %of 111 of our CPSP patients were plegic, and only 29 %paretic), the prevalence must be very much higher. Atleast 30 % of MS patients have central pain, and inspinal cord injury (SCI) CNP is present in about twothirds of patients. SCI pain has been subdivided intopain at, above, and below the level of injury in an at-tempt to develop a more meaningful taxonomy (Siddalland Loeser 2001). Thus, despite the fact that far fromall patients with injury to the CNS develops CNP, theoverall prevalence is very high – yet it is regarded asa rarity by most members of the medical and alliedprofessions.
Characteristics
Central pain is greatly influenced by autonomic factors.Seventy-nine CPSP patients were asked to identify fac-tors that exacerbated or alleviated their pain: 59 % foundtheir pain was exacerbated by cold and 57 % by emo-
tional stress; while 38 % were alleviated by relaxation(which is why most patients with CNP can fall asleepwithout difficulty, even though they may wake in pain)and 15 % by warmth (Bowsher 1996a). The most impor-tant feature of CNP, as noted above, is that it occurs in anarea of sensory change (partial or total deficit of one ormoresomatosensorymodalities); this is indeedanessen-tial criterion. The pain is experienced within the area ofsensory change, i.e. it is smaller than the area exhibit-ing sensory change. Of course patients do not presentwith sensory loss, but with pain; so this will be dealt withfirst. About 40 % of CPSP patients begin to experiencepain immediately after their stroke; the other 60 % havea later onset, which may be up to 2 years after stroke, butthe median is 3 months (Bowsher 1996a). In the case ofspinal cord injury, a similar pattern is observed: pain isimmediate in about a third of cases, with later onsets upto 2 years, but a median of 3 months (Widerström-Noga2003).Early descriptions emphasised burning pain as a promi-nent characteristic of central pain. Close interrogationreveals that this is most frequently paradoxical burning(ice-burn). While this type of pain, when it occurs, isindeed characteristic of central pain, and is much em-phasised because patients say “It’s like nothing I everexperienced before”, burning pain is not a sine qua nonof neuropathic pain. Only 47 % of 111 personal CPSPpatients complained of burning pain (Bowsher 1996a).Others experienced aching or throbbing pain (35 %) orshooting/stabbing pain (7 %); no type of pain was per-ceived to be more intense than any other (� Visual Ana-logue Scale, VAS). Background pain was exacerbatedby emotional stress or environmental cold in about halfof patients (28 % by both). Following spinal cord injury,burning and aching pain were found in almost equal pro-portions (Widerström-Noga 2002).
Sensory Change
Some somatosensory modalities may be entirely lost,while in others the sensation may still be present, butwith a raised threshold compared to the mirror-imagearea on the unaffected side. There is frequently disso-ciation between various somatosensory submodalities.From the point of view of spontaneous pain in CPSP, themodalities most concerned appear to be those subserv-ing innocuous thermal sensations (Bowsher 1996b)and sharpness discrimination (tested with weightedneedles); pain intensity correlated with thermal (partic-ularly warmth) and sharpness discrimination thresholdelevation. Patients with aching pain had a significantlyhigher perception threshold for tactile (von Frey) stim-uli than those with burning pain, while the latter hadmuch higher thresholds for innocuous warmth and cold(but not for painful heat). Both had higher thresholdsfor sharpness and innocuous thermal modalities thanpatients suffering from strokes with sensory loss butno pain; and additionally patients with burning pain,

316 Central Neuropathic Pain
but not those with aching pain, had a very much higherthreshold for warmth than did pain-free stroke patients(Bowsher 1996a).Eide et al. (1996) found that CNP in SCI patients wascorrelated with intensity of sensory deficit. Centralpain does not accompany loss of only Aβ modalities(touch, innocuous pressure, vibration), as those sub-served by smaller peripheral fibres (Aδ, C) are alsocompromised. It was noted that in cordotomised pa-tients with malignant disease, where non-neuropathicpain due to the neoplasm returned, pinprick (sharpness)threshold also returned towards that on the unaffectedside, while in those patients who developed neuro-pathic post-cordotomy pain, the deficit in sharpnesssensation remained (Lahuerta et al. 1994). Indeed, sofar as central pain is concerned, it is irrelevant whetheror not sensations subserved by Aβ fibres are affected.Contrarily, stroke patients with sensory deficits but nopain frequently have a very marked tactile deficit, butmuch less extensive thermal and sharpness deficits.� Allodynia is defined as pain produced by innocuousstimulation. As it only occurs in patients with peripheralor central neuropathic pain, it is pathognomonic whenfound. However, unfortunately for the diagnostician, itis found in only about half of patients with supraspinalCNP.Byfar thecommonest formofallodynia isdynamicmechanical or tactile: allodynia caused by a movingtactile stimulus, subserved by Aβ fibres. The provokingstimulus may be the movement of clothes across theskin or a breeze on the face. Other forms of stimulusthat may produce allodynia are thermal (particularlycold, which unlike other forms of allodynia is twiceas common in males as in females; warmth-provokedallodynia is rare). The threshold for innocuous warmthis significantly higher in CPSP patients with allodynia(all forms) than in those without. Movement relatedallodynia also occurs in CPSP, provoked by active orpassive movement, so presumably initiated from stretchreceptors.While the pain of allodynia usually occurs in the areastimulated, it may occur in a remote area, even onewhich itself is neither spontaneously painful nor allo-dynic. When somatosensory thresholds in patients withmechanical allodynia are compared with thresholds inpain-free stroke patients, it is found that the signifi-cance of the difference in thresholds between affectedand unaffected mirror-image areas between the twogroups is 0.02 for sharpness, 0.007 for warmth, 0.047for cold, and 0.004 for heat pain; but is non-significantfor mechanical modalities (Bowsher 1996a).
Treatment
The mainstay of treatment until recently has beenadrenergically-active � tricyclic antidepressants, i.e.principally ami- or nor- tryptiline, in relatively lowdoses (Leijon and Boivie 1989). Spontaneous recoveryundoubtedly occurs (usually unreported), sometimes
as a result of a further stroke (which may also suppressother neurogenic pains such as postherpetic neuralgia).Successful treatment with tricyclic antidepressants(TCAs) is time-dependent, as with several other neu-ropathic pains – i.e. if treatment is initiated within 6months of pain onset (NOT of stroke occurrence), 89 %of our patients gained relief; within 12 months, 67 %; butthereafter less than 50 %. Ami- and nor- tryptiline arepoorly tolerated, and produce disagreeable side-effects.Success has been reported with a more recent andless noxious antidepressant, venlafaxine. This is alsoadrenergically active; it should be noted that selectiveserotonergic reuptake inhibitors (SSRIs), which haveno SNRI activity, are ineffective in neuropathic pains(e.g. Max et al. 1992). Unlike peripheral neuropathicpain (PHN), the presence or absence of allodynia doesnot influence the therapeutic response to tricyclics.Older� Anticonvulsant(Agent),notablycarbamazepine,have proven themselves ineffective (Leijon and Boivie1989) in the treatment of central neuropathic pain.Membrane-stabilising drugs such as lignocaine (infu-sions) and mexiletine (Awerbuch and Sandyk (1990)have been effective; mexiletine added to a TCA hasbeen shown to be beneficial in CPSP (Bowsher 1995b)in some cases unresponsive to TCAs alone. Lignocaine(lidocaine) is a local anaesthetic that blocks sodiumchannels. Boas et al. (1982) reported its analgesic effectwhen given systemically (I.V.) in conditions with neu-ropathic pain. Among newer anticonvulsants, whichdo not block sodium channels, gabapentin monother-apy is now widely used, though no statistics are yetavailable. Lamotrigine has also shown promise, per-haps especially when added to a TCA. Of the opioids,dextromethorphan, in combination with gabapentin,is the most widely used; favourable claims have alsobeen made for methadone. NMDA receptor antagonists(a minor additional property of dextromethorphan andmethadone) are said to be effective, as shown by useof the short-acting ketamine; relief of CPSP by oralketamine has been reported (Vick and Lamer 2001),and there is a report of relief of syringomyelic pain byintravenous ketamine (Cohen and DeJesus 2004).Surgical treatment has varied from thalamic lesioningto the implantation of stimulating electrodes – thalamic,periaqueductal, or spinal; and more recently on the mo-tor cortex (Tsubokawa et al. 1993), which is the mostpromising of the stimulation methods, with a reportedsuccess rate of 60–70 %. Additional treatments of painassociated with spinal cord injury are dealt with in thevolume edited by Yezierski and Burchiel (2002). Re-laxation therapy, which has a known beneficial effect,should not be overlooked in all forms of CNP.
Possible Mechanisms of Neuropathic Pain
We have to explain a condition that differentially andvariably affects somatosensory submodalities and auto-nomic function; which follows insult to the central or pe-

C
Central Neuropathic Pain 317
ripheral nervous system, but not ineluctably – indeed, inonlyaminorityofcases;and inwhich thesensorychangemay or may not be accompanied by neuropathicpain (al-though, as discussed above, the presence or absence ofpain does appear to depend on the intensity of innocuousthermal loss, particularly for warmth).It strikes the present author that the cardinal fact aboutneuropathic pain (central or peripheral) is that only a mi-nority of individuals who suffer apparently appropriateinsult to thecentralorperipheralnervoussystemactuallydevelop neuropathic pain. This is equally true, it wouldseem, of nerve ligation experiments in animals, by nomeans all of which show signs or symptoms of neuro-pathic pain.It was suggested earlier (Bowsher 1995b) that the best-fit theoretical model for central pain would appear tobe one in which a widely-distributed transmitter/ligandin the central nervous system, and/or its specific recep-tors may become depleted; possible changes in recep-tor function were also mentioned by Siddall and Loeser(2001), specifically in relation tospinalcordinjury. Ithasbeen known for a long time that some transmitters, suchas serotonin, have both a global function, disturbanceof which may be reflected in some psychiatric disorders,and a specific one, disturbance of which is seen in partic-ular “focal” conditions such as migraine; enhanced painsensitivity following injury may be regulated by spinalNK1 receptor expressing neurons (Suzuki et al. 2002),while spinal 5HT3 receptors mediate descending excita-tory controls on spinal neurones activated in some neu-ropathic pain states (McCleane et al. 2003). Althoughwe still have little idea what the transmitter(s) or recep-tor(s) concerned with central pain may be, recent devel-opments in the field lend some support to this type of ar-gument. For example, it has been shown in the NMDAsystemthatpresynaptictransmittersandpostsynapticre-ceptors may be present in varying quantities (concentra-tions, densities) in the central nervous system (Yu andSalter 1999). Another relevant observation is that ubiq-uitinC-terminalhydrolase isupregulated inratswithsci-atic nerve constriction injuries (Moss et al. 2002). Wanget al. (2002) have described as many as 148 genes whichare up- or down-regulated in the dorsal root ganglia ofneuropathic rats.It may, therefore, be suggested that changes in trans-mitter concentration and/or receptor density, as eitherup- or down- regulation, may occur following nervoussystem injury. Following appropriate insult, transmit-ters and/or receptors may undergo sudden and massivedepletion, leading to immediate onset of CNP; or oneor other or both may deplete slowly, giving rise tolater onset of pain; they may recover their originallevels/concentrations/density, so that the pain “sponta-neously” disappears; fluctuant recovery may accountfor fluctuating degrees of CNP.However, if this hypothesis is even partly valid, there area number of unexplained phenomena, among which are:
a) Why, in what is apparently the same condition, doesone form of therapy succeed in some cases but fail inothers, in which another form of therapy (a differentdrug) iseffective?(e.g.TCAs,whichactonserotoner-gicand adrenergic systems,versusgabapentin,whichacts on subunits of voltage-dependentCa++ channels
b) It is fairly widely reported that patients with CPSPmay have their pain alleviated by a second stroke;we have also seen the pains of both post-herpeticand trigeminal neuralgias relieved by a subsequentstroke. Such events are hardly going to increaselevels of Transmitter X or densities of Receptor Y!
Although progress has been made in understandingthe mechanisms responsible for central pain, there areclearly additional questions to address, the answers towhich will hopefully provide new insights into moreeffective treatment strategies.� Spinal Cord Injury Pain Model, Hemisection Model
References1. Ajuriaguerra J de (1937) La Douleur dans les Affections du Sys-
tème Nerveux Central. Doin, Paris2. Andersen G (1995) Incidence of Central Post-Stroke Pain. Pain
61:187–1943. Awerbuch GI, Sandyk R (1990) Mexiletine for Thalamic Pain
Syndrome. Int J Neurosci 55:129–1334. Boas RA, Covino BG, Shanharian A (1982) Analgesic Response
to I. V. Lignocaine. Br J Anaesth 54:501–5055. Bogousslavsky J, Regli F, Uske A (1988) Thalamic Infarcts: Clin-
ical Syndromes, Etiology, and Prognosis. Neurol 38:837–8486. Bowsher (1995a) The management of central post-stroke pain.
Postgrad Med J 71:598-6047. Bowsher D (1995b) Central Pain. Pain Rev 2:175–1868. Bowsher D (1996a) Central Pain: Clinical and Physiological
Characteristics. J Neurol Neurosurg Psychiat 61:62–699. Bowsher, D (1996b) Central Pain of Spinal Origin. Spinal Cord
34:707–71010. Bowsher D, Leijon G, Thomas K-A (1998) Central Post-Stroke
Pain: Correlation of Magnetic Resonance Imaging with Clini-cal Pain Characteristics and Sensory Abnormalities. Neurology51:1352–1358
11. Cohen SP, DeJesus M (2004) Ketamine Patient-Controlled Anal-gesia for Dysesthetic Central Pain. Spinal Cord 42:425–428
12. Davison C, Schick W (1935) Spontaneous Pain and other SensoryDisturbances. Arch Neurol Psychiat (Chicago) 34:1204–1237
13. Dejerine J, Roussy J (1906) Le Syndrome Thalamique. Rev Neu-rol 14: 521–532
14. Eide PK, Jörum E, Stenejhem AE (1996) Somatosensory Find-ings in Spinal Cord Injury Patients with Central DysaesthesiaPain. J Neurol Neurosurg Psychiat 60:411–415
15. Foix C, Chavany J-A, Lévy M (1927) Syndrome pseudo-thalamique d’origine pariétale. Lésion de l’artère du silloninterpariétal (Pa P1P2 antérieures, petit territoire insulo-capsulaire). Rev Neurol (Paris) 35:68–76
16. Lahuerta J, Bowsher D, Buxton PH, Lipton S (1994) Percuta-neous cervical cordotomy: A review of 181 operations in 146patients, including a study on the location of “pain fibers” in thesecond cervical spinal cord segment of 29 cases. J Neurosurg80:975–985
17. Leijon G, Boivie J, Johansson I (1989) Central Post-Stroke Pain– A Study of the Mechanisms through Analyses of the SensoryAbnormalities. Pain 37:173–185
18. Madsen PW, Yezierski RP, Holets VR (1994) Syringomyelia:Clinical Observations and Experimental Studies. J Neurotrauma11:241–254

318 Central Neuropathic Pain from Spinal Cord Injury
19. Max M, Lynch SA, Muir J et al. (1992) Effects of Desipramine,Amitriptyline, and Fluoxetine on Pain in Diabetic Neuropathy.New Eng. J Med 326:1250–1256
20. McCleane GJ, Suzuki R, Dickenson AH (2003) Does a Single In-travenous Injection of 5HT3 Receptor Antagonist Ondansetronhave an Analgesic Effect in Neuropathic Pain? A Double-Blinded, Placebo-Controlled Cross-Over Study. Anesth Analg97:1474–1478
21. Moss A, Blackburn-Munro G, Garry EM et al. (2002) A Role ofthe Ubiquitin-Proteosome System in Neuropathic Pain. J Neu-rosci 22:1363–1372
22. Siddall PJ, Loeser JD (2001) Pain following Spinal Cord Injury.Spinal Cord 39:63–73
23. Siddall PJ, Taylor DA, McClelland JM et al. (1999) Pain Re-port and the Relationship of Pain to Physical Factors in the First6 Months following Spinal Cord Injury. Pain 81:187–197
24. Suzuki R, Morcuende S, Webber M et al. (2002) Superficial
NK1-Expressing Neurons Control Spinal Excitability throughActivation of Descending Pathways. Nat Neurosci 5:1319–1326
25. Taylor CP, Gee NS, Su T-Z et al. (1998) A Summary of Mech-anistic Hypotheses of Gabapentin Pharmacology. Epilepsy Res29:233–249
26. Tsubokawa T, Katayama Y, Yamamoto T, Hirayama T, Koyama S(1993) Chronic motor cortex stimulation in patients with thalamicpain. J Neurosurg 78:393–401
27. Vick PG, Lamer TJ (2003) Treatment of Central Post-Stroke Painwith Oral Ketamine. Pain 92:311–313
28. Wang H, Sun H, Della Penna K et al. (2002) Chronic NeuropathicPain is accompanied by Global Changes in Gene Expression andShares Pathobiology with Neurodegenerative Diseases. Neurosci114:529–546
29. White JC, Sweet WH (1955) Pain: Its Mechanisms and Neuro-surgical Control. CC Thomas, Springfield Ill
30. Widerström-Noga EG (2002) Evaluation of Clinical Characteris-tics of Pain and Psychosocial Factors after Spinal Cord Injury. In:Yezierski RP, Rurchiel KJ (eds) Spinal Cord Injury Pain: Assess-ment, Mechanisms, Management. IASP Press, Seattle, pp 53–82
31. Widerström-Noga EG (2003) Chronic Pain and Non-PainfulSensations following SCI: Is there a Relationship? Clin J Pain19:39–47
32. Yezierski RP (1996) Pain following Spinal Cord Injury: The Clin-ical Problem and Experimental Studies. Pain 73:115–119
33. Yezierski RP, Burchiel KJ (2002) Spinal Cord Injury Pain: As-sessment, Mechanisms, Management. IASP Press, Seattle
34. Yu X-M, Salter MW (1999) Src, A Molecular Switch GoverningGain Control of Synaptic Transmission Mediated by N-methyl-D-aspartate Receptors. Proc-Natl Acad Sci USA 96:7697–7704
Central Neuropathic Pain from SpinalCord Injury
PHILIP SIDDALL
Pain Management Research Institute, University ofSydney, Royal North Shore Hospital, Sydney, NSW,[email protected]
Definition
Central pain from spinal cord injury (SCI) refers to� neuropathic pain that occurs following traumatic oratraumatic injury to the spinal cord. It may be due to dys-function occurring at spinal and/or supraspinal levels.Twomain typesofcentralneuropathicpainaredescribedfollowing SCI. These are � at-level neuropathic painand� below-levelneuropathicpain(Siddall et al.2002).
Characteristics
Prevalence
The prevalence of central neuropathic pain followingSCI is relatively high. In the first six months followingSCI, it has been reported that 35 % of patients haveat-level neuropathic pain and 25 % of patients havebelow-level neuropathic pain. At five years followinginjury, there is little change in these numbers, with42 % having at-level neuropathic pain and 34 % havingbelow-level neuropathic pain (Siddall et al. 2003). Thisincrease in numbers of people reporting pain reflectsthe lack of success in alleviating the pain. It also reflectsthe late onset of neuropathic pain, even years follow-ing injury, in many people. The prospective study bySiddall et al. (2003) also indicates a strong correlationbetween the presence of both types of neuropathic painwithin six months and at five years following injury.This unfortunately suggests that if either of these paintypes is present at six months, then there is a stronglikelihood that it will be present at 5 years.
Diagnosis
A taxonomy of pain following SCI was proposed by theInternational Association for the Study of Pain (IASP)Task Force on SCI pain, and identifies five main typesof pain that occur following SCI (Siddall et al. 2002).Theseare:musculoskeletal, visceral, above-levelneuro-pathic,at-levelneuropathicandbelow-levelneuropathicpains. The presence of neuropathic pain is suggested bydescriptors such as electric, shooting and burning withpain located in or adjacent to a region of sensory loss.Central neuropathic pain will usually present at or be-low the level of injury and will therefore fall into the lasttwo groups. Above-level neuropathic pain usually refersto neuropathic pain arising from damage to peripheralnerves above the level of injury. Therefore, many typesof above-level neuropathic pain are peripheral in origin.However, some types of above-level neuropathic painmay be central in origin. For example, syringomyeliamay give rise to central neuropathic pain that is locatedin dermatomes above the level of injury.At-level neuropathic pain occurs as a band of pain in thedermatomes adjacent to the level of injury, and is there-fore sometimes referred to as segmental, end-zone orborder zone pain. It may be due to damage to nerve rootsand therefore be a form of peripheral neuropathic pain.However, animal models have clearly demonstrated thatat-level neuropathic pain may occur in the absence ofnerve root damage, and therefore it may be central inorigin.Below-level neuropathic pain occurs more diffusely, ina bilateral distribution below the level of the spinal cordlesion in the region of sensory disturbance, and is some-times referred to as central dysesthesia syndrome. It ismost likely due to changes in the spinal cord and brain

C
Central Neuropathic Pain from Spinal Cord Injury 319
following SCI. Therefore, below-level neuropathic painis generally regarded as a central neuropathic pain.
Mechanisms
At-level neuropathic pain may be due to nerve rootcompression. The mechanisms of pain associated withnerve root compression are similar to other forms ofperipheral neuropathic pain and are described else-where. However, at-level neuropathic pain may also bedue to changes within the spinal cord itself as a conse-quence of injury. The specific mechanisms underlyingboth at-level and below-level neuropathic pain are in-completely understood. However, there are a numberof secondary changes that occur as a consequence ofspinal cord damage, which may result in the generationor amplification of nociceptive signals (Vierck et al.2000, Yezierski 2003). These include:
1. Damage to the spinal cord may result in increasedlevels of glutamate which activates N-methyl D-aspartate (NMDA), non-NMDA and metabotropicglutamate receptors. This activation of glutamatereceptors results in activation of a cascade of sec-ondary processes within neurons, which ultimatelyresult in increased neuronal excitability.
2. Alternatively, increased neuronal excitability maybe a consequence of reduced inhibition within thespinal cord. Several mechanisms have been pro-posed, including reduced function of inhibitoryneurotransmitters and receptors such as γ aminobu-tyric acid (GABA) and glycine. This may occurthrough reduction in inputs from surrounding re-gions that normally exert an inhibitory action on theregion, which has lost inputs (inhibitory surround).Loss of inhibition may also occur through disruptionto inhibitory neurotransmitter production, releaseor uptake as a consequence of spinal cord damage.A reduction in inhibition may also be due to a de-crease in the levels of inhibitory controls exerted bydescending antinociceptive pathways.
3. Injury to the spinal cord will also initiate inflamma-tory and immune responses, which will have both di-rect and indirect effects on the long-term integrity ofspinal cord structures, as well as functional changesin sensory processing.
Both increased excitation and lossof inhibition maygiverise to a population of neurons close to the site of in-jury that have an increased responsiveness to peripheralstimulation and may even fire spontaneously. These al-terations in the properties of spinal neurons may giverise to the phenomenon of hyperaesthesia (� allodyniaand � hyperalgesia) and spontaneous pain, respectively.As well as alterations at a spinal level, alterations in thechemistry and firing properties of supraspinal neuronshavealso been demonstrated.Themain site thathasbeeninvestigated is the thalamus (Ralston et al. 2000; Oharaet al. 2002).
Treatment
There are relatively few studies that havespecifically ex-amined the effectiveness of treatments for pain follow-ing SCI, and in these situations subject numbers are gen-erally low. Therefore, there is little definitive evidenceto guide management. In the few randomized controlledtrials that have been done, many of the treatments wereno more effective than the placebo, and therefore ade-quatecontrolofcentralneuropathicSCIpainisgenerallydifficult (Finnerup et al. 2001). Principles of treatmentare derived largely from the treatment of other neuro-pathic pain conditions.It is traditionally stated that opioids are relatively inef-fective for the treatment of neuropathic pain. However,there is increasing evidence that they may be effectiveif an appropriate dose is used. A randomized controlledtrial of intravenous morphine (9–30 mg) found a signifi-cant reduction in brush-evoked allodynia, but no signif-icant effect on spontaneous neuropathic SCI pain (At-tal et al. 2002). Long term use of opioids may also bea problem because of side effects such as constipation,which may be more of an issue in individuals with SCI.Although there is little direct evidence in SCI pain, tra-madol may also be an option because of its serotonergicand noradrenergic effects, which may provide an advan-tage in the treatment of neuropathic pain.Intravenous or subcutaneous infusion of local anaes-thetics such as lidocaine (lignocaine), are also widelyused for the treatment of neuropathic pain and may beeffective for neuropathic SCI pain. One of the actionsof local anaesthetics is to produce sodium channelblockade. This reduces the amount of ectopic impulsesgenerated by activity at these receptors. Relativelylow concentrations of local anaesthetic are requiredto reduce ectopic neural activity in damaged nerves.There is evidence from a randomized controlled trialsupporting the efficacy of intravenous lidocaine in treat-ing neuropathic SCI pain (Attal et al. 2000). Althoughits mode of action is different from local anaesthetics,propofol is another agent that may be administeredsystemically and has been shown to provide effec-tive relief of neuropathic SCI pain (Canavero et al.1995).As mentioned above, SCI may result in an increased re-lease of glutamate and activation of NMDA receptors,resulting in central neuronal hyperexcitability. NMDAreceptor antagonists such as ketamine have been usedas a treatment for neuropathic pain following SCI (Eideet al. 1995). Administration is generally by infusion viathe intravenous or subcutaneous route. One of the mainproblems with the use of ketamine is the occurrence ofdisturbing side effects such as hallucinations, althoughbenzodiazepines may help reduce these symptoms. Al-though careful monitoring can help to minimize the rateof occurrence of these side effects, they can be distress-ing to the person when they do occur.

320 Central Pain
Oral rather than systemic administration of a number ofdrugs is also possible, and may be preferred. Unfortu-nately, most studies suggest that these oral agents areless effective than drugs used systemically. Most of theevidence for the effectiveness of opioids for the treat-mentofneuropathicpain comesfrom studiesusing acuteintravenous administration. Local anaesthetics are notavailable in oral form,and the localanaestheticcongenermexiletine does not appear to be as effective as lidocainein reducingneuropathicSCIpain(ChiouTanetal.1996).Similarly, ketamine is difficult to administer orally andother NMDA antagonists available for administrationvia the oral route, such as dextromethorphan, are alsonot as effective.Several agents that are used widely for the treatmentof persistent neuropathic pain are not available for sys-temic administration but are available in the oral form.These include the tricyclic antidepressants such asamitriptyline, prothiaden and nortriptyline and anticon-vulsants such as carbamazepine, valproate, lamotrigineand gabapentin. However, specific evidence of efficacyin the treatment of neuropathic SCI pain is limited.Randomised controlled trials of trazodone (Davidoffet al. 1987) and amitriptyline (Cardenas et al. 2002)both failed to find an effect greater than placebo, al-though numbers in the trazodone study were low andthe amitriptyline study contained subjects who hadboth musculoskeletal and neuropathic pains. A ran-domised controlled trial of sodium valproate also failedto demonstrate a significant analgesic effect (Dreweset al. 1994). Lamotrigine has been demonstrated tobe effective, but only for the evoked component ofneuropathic SCI pain (Finnerup et al. 2002).Consideration may be given to spinal administration ofdrugsiforalapproachesareunsuccessful. Intrathecalad-ministration of morphine and clonidine has been helpfulin some people with neuropathic SCI pain (Siddall et al.2000).Spinalcord injuryrequiresamajorpsychologicaladjust-ment.Awarenessof these issues is important intheevalu-ation of theperson with pain.Aswith any paincondition,psychological factors may contribute to the perceptionand expression of pain. Pain report may be an expressionof difficulty in adjustment, and therefore psychologicalapproaches that attempt to deal with these issues may behelpful. Utilisation of pain management strategies andcognitive behavioural therapy (CBT) may be helpful inachieving optimal pain management (Umlauf 1992).
References1. Attal N, Guirimand F, Brasseur L, Gaude V, Chauvin M, Bouhas-
sira D (2002) Effects of IV Morphine in Central Pain – A Ran-domized Placebo-Controlled Study. Neurology 58:554–563
2. Attal N, Gaudé V, Brasseur L et al. (2000) Intravenous Lido-caine in Central Pain: A Double-Blind, Placebo-Controlled, Psy-chophysical Study. Neurology 54:564–574
3. Canavero S, Bonicalzi V, Pagni CA et al. (1995) Propofol Analge-sia in Central Pain - Preliminary Clinical Observations. J Neurol242:561–567
4. Cardenas DD, Warms CA, Turner JA, Marshall H, Brooke MM,Loeser JD (2002) Efficacy of Amitriptyline for Relief of Pain inSpinal Cord Injury: Results of a Randomized Controlled Trial.Pain 96:365–373
5. Chiou Tan FY, Tuel SM, Johnson JC, Priebe MM, Hirsh DD,Strayer JR (1996) Effect of Mexiletine on Spinal Cord InjuryDysesthetic Pain. Am J Phys Med Rehabil 75:84–87
6. Davidoff G, Guarracini M, Roth E, Sliwa J, Yarkony G. (1987)Trazodone Hydrochloride in the Treatment of Dysesthetic Pain inTraumatic Myelopathy: A Randomized, Double-Blind, Placebo-Controlled Study. Pain 29:151–161
7. Eide PK, Stubhaug A, Stenehjem AE (1995) Central Dyses-thesia Pain after Traumatic Spinal Cord Injury is Dependenton N-methyl-D-aspartate Receptor Activation. Neurosurgery37:1080–1087
8. Finnerup NB, Yezierski RP, Sang CN, Burchiel KJ, Jensen TS(2001) Treatment of Spinal Cord Injury Pain. Pain Clinical Up-dates 9:1–6
9. Finnerup NB, Sindrup SH, Flemming WB, Johannesen IL, JensenTS (2002) Lamotrigine in Spinal Cord Injury Pain: A Random-ized Controlled Trial. Pain 96:375–383
10. OharaS, Garonzik I, HuaS, LenzFA(2002) Microelectrode Stud-ies of the Thalamus in Patients with Central Pain and in ControlPatients with Movement Disorders. In: Yezierski RP, Rurchiel KJ(eds) Spinal Cord Injury Pain: Assessment, Mechanisms, Man-agement. IASP Press, Seattle, pp 219–236
11. Siddall PJ, Molloy AR, Walker S, Mather LE, Rutkowski SB,Cousins MJ (2000) Efficacy of Intrathecal Morphine and Cloni-dine in the Treatment of Neuropathic Pain Following Spinal CordInjury. Anesth Analg 91:1493–1498
12. Siddall PJ, Yezierski RP, Loeser JD (2002) Taxonomy and Epi-demiology of Spinal Cord Injury Pain. In: Yezierski RP, RurchielKJ (eds) Spinal Cord Injury Pain: Assessment, Mechanisms,Management. IASP Press, Seattle, pp 9–24
13. Siddall PJ, McClelland JM, Rutkowski SB, Cousins MJ (2003)A Longitudinal Study of the Prevalence and Characteristics ofPain in the First 5 Years Following Spinal Cord Injury. Pain103:249–257
14. Ralston DD, Dougherty PM, Lenz FA, Weng HR, Vierck CJ,Ralston HJ (2000) Plasticity of the Inhibitory Circuitry of thePrimate Ventrobasal Thalamus Following Lesions of Somatosen-sory Pathways. In: Devor M, Rowbotham MC, Wiesenfeld-HallinZ (eds) Proceedings of the 9th World Congress on Pain, IASPPress, Seattle, pp 427–434
15. Umlauf RL (1992) Psychological Interventions for Chronic PainFollowing Spinal Cord Injury. Clin J Pain 8:111–118
16. Vierck CJ, Siddall PJ, Yezierski RP (2000) Pain FollowingSpinal Cord Injury: Animal Models and Mechanistic Studies.Pain 89:1–5
17. Yezierski RP (2002) Pathophysiology and Animal Models ofSpinal Cord Injury Pain. In: Yezierski RP, Rurchiel KJ (eds)Spinal Cord Injury Pain: Assessment, Mechanisms, Manage-ment. IASP Press, Seattle, pp 117–136
Central Pain
Definition
Central pain is defined by the International Associationfor the Study of Pain (IASP) as: „Regional pain causedby a primary lesion or dysfunction in the central nervoussystem, usually associated with abnormal sensibility totemperature and to noxious stimulation“.� Cell Therapy in the Treatment of Central Pain� Central Nervous System Stimulation for Pain� Central Pain, Diagnosis and Assessment of Clinical
Characteristics

C
Central Pain and Cancer 321
� Central Pain, Human Studies of Physiology� Central Pain in Multiple Sclerosis� Central Pain, Outcome Measures in Clinical Trials� Central Pain, Pharmacological Treatments� Central Pain Syndrome� Diagnosis and Assessment of Clinical Characteristics
of Central Pain� DREZ Procedures� Functional Changes in Sensory Neurons Following
Spinal Cord Injury in Central Pain� Pain Treatment, Motor Cortex Stimulation� Percutaneous Cordotomy� Post-Stroke Pain Model, Thalamic Pain (Lesion)� SecondarySomatosensoryCortex(S2)andInsula,Ef-
fecton Pain Related Behavior inAnimalsandHumans� Stimulation Treatments of Central Pain
Central Pain and CancerPAOLO L. MANFREDI
1, 2, GILBERT R. GONZALES1
1Department of Neurology, Memorial Sloan-KetteringCancer Center, New York, NY, USA2Essex Woodlands Health Ventures, New York, NY,[email protected], [email protected]
Definition
In order to be diagnosed with Central Pain (CP) asso-ciated with cancer, patients must have a lesion withinthe Central Nervous System (CNS) caused by cancer orits treatment, pain in a distribution compatible with theCNS lesion, and no other lesions that could potentiallycause pain in the same area (Casey 1991; Gonzales andCasey 2003; Gonzales et al. 2003).This definition includes pathology in the spinal cord,brainstem, or cerebral hemispheres. Lesions in theperipheral nervous system can produce CNS changes,but these are secondary CNS changes and are not cat-egorized as CP syndromes (Casey 1991; Gonzales andCasey 2003). The most common causes of CNS injuriesthat result in CP are stroke, spinal cord trauma and mul-tiple sclerosis (Casey 1991). However, cancer and itstreatment can also cause CP (Gonzales et al. 2003).
Characteristics
Although CP occurs infrequently, over 15% of patientswith systemic cancer have metastases to the brain orspinal cord (Clouston et al. 1992), making it possible forsome of these patients to go on and develop CP. Centralpain caused by cancer is mostly described through casereports, such as the study of thalamic tumors by Cheekand Taveras (Cheek et al. 1966). Pagni and Canavero(1993), and Gan and Choksey (2001) have reportedCP from extra-axial tumors such as meningiomas.Delattre and colleagues have reported CP caused by
leptomeningeal disease (Delatte et al. 1989). A morerecent study by Gonzales et al. described the prevalenceand causes of central pain in patients with cancer (Gon-zales et al. 2003). In this study conducted in a cancercenter, a relatively high number of general oncologypatients admitted to the Neurology Service (2%) orseen in consultation by the Pain Service (4%) werefound to have CP. It is important to underscore that theprevalence of central pain seen in these patients is notrepresentative of the true prevalence of central pain inhospitalized patients with cancer, as these patients wereselected by their referral to the pain service or admis-sion to the neurology ward. In this study, spinal cordlesions were by far more likely to cause CP comparedto brain and brainstem lesions, as is the case in patientswith non-cancer causes of central pain (Gonzales et al.2003).When a patient with cancer has radiological documen-tation of a lesion within the CNS, pain in a distributioncompatible with the CNS lesion, and no other lesionsthat could potentially cause pain in the same area, a di-agnosis of CPcan be made. In order to be classified as CPrelated to cancer the inciting CNS lesion must be causedby cancer or its treatment.PaindescriptorssuggestiveofCPsuchasburning,numb,cold, pins and needles, electric shock can also help withthe diagnosis.On physical examination it may be possible to elicit dif-ferent neurological abnormalities, depending on the lo-cation and size of the CNS lesion. The finding of alteredtemperature sensation in the painful area is consistentlyseen in all CP patients with cancer, as expected from theexperience with non-malignant causes of CP (Gonzalesand Casey 2003; Gonzales et al. 2003). A detailed sen-sory examination is therefore essential.Central pain may be delayed by days to years after CNSinjury (Gonzales 1995). In one cancer patient, CP wasfound to be delayed by up to 6 years after the diagnosisand treatment of the spinal cord tumor (Gonzales et al.2003). This is much longer than the delay usually seenin non-malignant causes of spinal cord CP.The treatment strategies in patients with cancer andCP may include anti-tumor therapies such as radiation,chemotherapy, surgical resection and steroids to de-crease edema. Aside from addressing the treatment ofthe tumor, the treatment of CP in patients with cancercan be approached as with non-malignant CP (Gonza-les and Casey 2003; Gonzales et al. 2003) and includeantidepressants, anticonvulsants, opioids, clonidine,baclofen, acetaminophen, and NSAIDs.
References1. Casey KL (1991) Pain and Central Nervous System Disease:
A Summary and Overview. In: Casey KL ed. Pain and CentralNervous System Disease: The Central Pain Syndromes. RavenPress, New York
2. Cheek WR, Taveras JM (1966) Thalamic Tumors. J Neurosurg24:505–513

322 Central Pain, Diagnosis
3. Clouston PD, DeAngelis LM, Posner J (1992) The Spectrumof Neurological Disease in Patients with Systemic Cancer. AnnNeurol 31:268–273
4. Delattre JY, Walker RW, Rosenblum MK (1989) LeptomeningealGliomatosis with Spinal Cord or Cauda Equina Compression: ACompletion of Supratentorial Gliomas in Adults. Acta NeurolScand 79:133–139
5. Gan YC, Choksey MS (2001) Parafalcine Meningioma Present-ing with Facial Pain: Evidence for Cortical Theory or Pain? BrJ Neurosurg 15:350–352
6. Gonzales GR (1995) Central Pain: Diagnosis and TreatmentStrategies. Neurology 45:11–16
7. Gonzales GR, Casey KL (2003) Central Pain Syndromes. In: RiceADS, Washeld CA, Justins D et al. (eds) Clinical Pain Manage-ment Chronic Pain. Arnold Press, London
8. Gonzales GR, Tuttle S, Thaler HT et al. (2003) Central Pain inPatients with Cancer. J Pain 4:351–354
9. Pagni CA, Canavero S (1993) Paroxysmal Perineal Pain Resem-bling Tic Doubureux, only Symptom of a Dorsal Meningioma.Ital J Neurol Sci 14:323–324
10. Tasker RR, DeCorvalho G, Dostrovosky JO (1991) The History ofCentral Pain Syndromes, with Observations Concerning Patho-physiology and Treatment. In: Casey KL (ed) Pain and CentralNervous System Disease: The Central Pain Syndromes. RavenPress, New York, pp 31–58
Central Pain, DiagnosisDAVID VIVIAN
Metro Spinal Clinic, Caulfield, VIC, [email protected]
Synonyms
Thalamic Pain; Dejerine-Roussy Syndrome; deaf-ferentation pain
Definition
Central pain is pain whose source lies in the central ner-voussystem, i.e. thebrain,brainstem,or spinalcord.Thecardinal defining feature is that the pain is not evoked byneural activity in peripheral nerves.
Characteristics
In terms of clinical features, central pain has particularcharacteristics. The pain is typically spontaneous andburning in quality, associated with abnormal sensations.The latter may include:
• hyperaesthesia (increased sensitivity to touch)• hyperalgesia (increased sensitivity to noxious stim-
uli)• allodynia (touch and brush are perceived as painful)• paraesthesiae (sensation of pins and needles)• formication (sensation of ants crawling on skin) and• diminished topoesthesia (ability to locate a sensation
somatotopically)
In these respects central pain resembles neuropathicpain, and the taxonomic distinction between the twoconditions is not always clear. Some forms of neuro-pathic pain are likely to be central in origin rather than
arising from the damaged peripheral nerve. The distinc-tion ismostclearwhen theprecipitating injury ofdiseaseis obviously in the central nervous system.In such casesthe term –central pain, applies unambiguously.
Examples
Classical examples of central pain are the pain ofbrachial plexus avulsion, spinal cord injury pain, painafter stroke, and pain due to infarction of � thalamicnuclei. The latter is known as thalamic pain syndromeor the Dejerine-Roussy syndrome. Complex regionalpain syndrome is the most florid example of centralpain.Others examples include postherpetic neuralgia,periph-eral nerve injury, and painful peripheral neuropathy. Thelatter, however, are contentious, for it is not always evi-dent theextent to which thepain iscentral inoriginordueto peripheral mechanisms such as neuroma, or ectopicimpulse generation in peripheral nerves or their� dorsalroot ganglia.
Mechanism
Central pain is believed to result from deafferentation:when neurons in thecentralnervoussystem lose their ac-customed afferent input, either from a peripheral nerveor from an ascending sensory tract. In particular, partialdeafferentation is considered most likely to be associ-ated with the development of central pain.Deafferentation seems to induce plastic changes in thecentral nervous system. Numerous theories describethese plastic changes in terms of: removal of local inhi-bition, changes in neuronal membrane excitability, andsynaptic reorganisation. These changes occur rapidlyafter central nervous system damage. However, it istypical for central pain to occur some time after suchan injury (days to weeks).Experiments in animals have been conducted in whichrecordings are established from dorsal horn neuronsthat respond to input from particular peripheral nerves.If those nerves are then severed, the dorsal horn neuronsno longer respond to peripheral stimuli but exhibit a va-riety of changes (Anderson et al. 1971; Macon 1979; 3).They become spontaneously active, and eventually nolonger become responsive to typical neurotransmitters.These features suggest that their membranes becomeunstable, and the neurons no longer maintain receptorswhen denied their accustomed input. The latter featureprobably underlies the notorious resistance of centralpain to pharmacological therapy.Spontaneousactivityhasbeenconfirmedinhumanswithcentral pain. When subjects with spinal cord injury painhave been explored with electrodes, spontaneously ac-tive neurons have been found in the spinal cord immedi-ately above the level of injury (Loeser et al. 1968). Sim-ilar activity has been recorded after experimental spinalcord injury in cats (Loeser and Ward 1967).

C
Central Pain, Diagnosis 323
Theabnormalsensationsassociatedwithcentralpainaremost likely due to disinhibition. Sensory perception isnormally subject to a variety of central excitatory andinhibitory controls. These are mediated by the dorsolat-eral tract and by tracts in the anterior funiculus of thespinal cord. When peripheral nerves are severed, the bal-ance between these central modulating influences is dis-turbed, sometimes with contrasting effects.Disinhibition results in sensitization of � Second OrderNeurons. Sensations mediated by intact nerves becomeexaggerated. This is manifest in the form of hyperaes-thesia, hyperalgesia, and allodynia.In experimental animals, the effects of sectioning thetrigeminal nerve (Denny-Brown et al. 1973), spinalnerves (Denny-Brown and Yanagisawa 1973) or thespinal cord (Denny-Brown 1979), can be modulatedpharmacologically and surgically. Discrete sectioningof the lateral portion of the dorsolateral tract resultsin shrinkage of the area of sensory nerve loss (Denny-Brown and Yanagisawa 1973; Denny-Brown et al.1973). Conversely, sectioning the medial portion ofthe dorsolateral tract increases the area (Denny-Brownand Yanagisawa 1973; Denny-Brown et al. 1973). Sec-tioning both anterior funiculi reverses the sensory losscaused by spinothalamic tractomy, but the restoredsensation is hyperaesthetic (Denny-Brown 1979). Ad-ministering L-dopa reduces sensory loss (Denny-Brownet al. 1973), as does a subconvulsive dose of strychnine:an antagonist of the inhibitory transmitter – glycine(Denny-Brown 1979; Denny-Brown and Yanagisawa1973; Denny-Brown et al. 1973.In humans who have undergone dorsal root section forpain but whose pain recurs, administration of L-dopa in-creases their pain but decreases the area of cutaneousanaesthesia (Hodge and King 1976). Reciprocally, ad-ministration of methyldopa decreases pain but increasesnumbness. Similarly, tryptophan – a serotonin precur-sor–reducespainbut increasesanaesthesia (King1980).These phenomenons indicate that the effects of deaf-ferentation are not fixed, but are subject to a complexvariety of controls. Release of these controls, followingperipheral nerve injury or central nervous injury, under-lies the varied appearance of pain and altered sensationsassociated with central pain.For the central pain of thalamic syndrome, a varietyof explanations have been advanced; but they, too, re-volve around deafferentation and disinhibition. Cellsin the ventroposterior thalamic nuclei become spon-taneously active, and produce pain in the area of thebody that they subtend (Lenz et al. 1987; Lenz et al.1989). Experimental stimulation of these cells evokespain in the deafferented region Lenz et al. 1988). Theabnormal activity is believed to arise because of lossof inhibition of medial thalamic nuclei by the reticularnucleus (Cesaro et al. 1991; Mauguiere and Desmedt1988). Damage to the spinothalamic tract seems to bethe precipitating factor for these changes.
Diagnosis
Thediagnosisofcentralpain rests largelyon therecogni-tion of the clinical features and history of the pain. Spon-taneous burning pain associated with abnormal, exag-gerated sensations implies a central mechanism. If thehistory indicates disease or injury to the central nervoussystem, the diagnosis is confirmed. The diagnosis is lesscertain if injury to the central nervous system is not ev-ident, or when the injury or disease affects peripheralnerves.A presumptive test for central pain is the administrationof lignocaine by systemic intravenous infusion.Such aninfusion is believed to suppress the spontaneous activityin the central nervous system believed to be responsiblefor central pain.
Treatment
Central pain is notoriously difficult to treat. Standardanalgesics seem to have little or no effect, which corre-lates with the lack of receptors found in animals withspontaneously active neurons after deafferentation.Agents that suppress ectopic activity, or which stabilizenerve-cell membranes, are more likely to relieve centralpain, provided that side-effects can be tolerated. Suchagents include local anaesthetic agents, administeredeither by systemic infusion or orally; and membrane-stabilizing agents such as gabapentin and lamotrigine.Otherwise, central pain can be treated, with reasonablesuccess, by neuroaugmentive surgical procedures suchas dorsal column stimulation, dorsal root entry zone le-sioning, and deep brain stimulation.
References1. Anderson LS, Black RG, Abraham J et al. (1971a) Neuronal Hy-
peractivity in Experimental Trigeminal Deafferentation. J Neu-rosurg 35:444–451
2. Anderson LS, Black RG, Abraham J et al. (1971b) Neuronal Hy-peractivity in Experimental Trigeminal Deafferentation. J Neu-rosurg 35:444–451
3. Cesaro P, Mann MW, Moretti JL et al. (1991) Central Pain andThalamic Hyperactivity: A Single Photon Emission Computer-ized Tomographic Study. Pain 47:329–336
4. Denny-Brown D (1979) The Enigma of Crossed Sensory Losswith Cord Hemisection. In: Bonica JJ et al. (eds) Advances in PainResearch and Therapy, vol 3. Raven Press, New York, pp 889–895
5. Denny-Brown D, Kirk EJ, Yanagisawa N (1973a) The Tractof Lissauer in Relation to Sensory Transmission in the DorsalHorn of Spinal Cord in the Macaque Monkey. J Comp Neurol151:175–199
6. Denny-Brown D, Yanagisawa N (1973b The Function of the De-scending Root of the Fifth Nerve. Brain 96:783–814
7. Hodge CJ, King RB (1976) Medical Modification of Sensation.J Neurosurg 44:21–28
8. King RB (1980) Pain and Tryptophan. J Neurosurg 53:44–529. Lenz FA, Tasker RR, Dostrovsky JO (1987) Abnormal Single
Unit Activity Recorded in the Somatosensory Thalamus of aQuadriplegic Patient with Central Pain. Pain 31:225–236
10. Lenz FA, Dostrovsky JO, Tasker RR et al. (1988) Single-UnitAnalysis of the Human Ventral Thalamic Nuclear Group: So-matosensory Responses. J Neurophysiol 59:299–316
11. Lenz FA, Kwan HC, Dostrovsky JO et al. (1989) Characteristicsof the Bursting Pattern of Action Potential that Occurs in theThalamus of Patients with Central Pain. Brain Res 496:375–360

324 Central Pain, Diagnosis and Assessment of Clinical Characteristics
12. Loeser JD, Ward AA (1967) Some Effects of Deafferentation onNeurons of the Cat spinal cord. Arch Neurol 17:629–636
13. Loeser JD, Ward AA, White LE (1968) Chronic Deafferentationof Human Spinal Cord Neurons. J Neurosurg 29:48–50
14. Macon JB (1979) Deafferentation Hyperactivity in the MonkeySpinal Trigeminal Nucleus: Neuronal Responses to Amino AcidIontophoresis. Brain Research 161:549–554
15. Mauguiere F, Desmedt JE (1988) Thalamic Pain Syndromeof Dejerine-Roussy: Differentiation of Four Subtypes As-sisted by Somatosensory Evoked Patients Data. Arch Neurol45:1312–1320
Central Pain, Diagnosis and Assessmentof Clinical Characteristics
� Diagnosis and Assessment of Clinical Characteristicsof Central Pain
Central Pain, Functional Changes inSensory Neurons Following Spinal CordInjury
� Functional Changes in Sensory Neurons FollowingSpinal Cord Injury in Central Pain
Central Pain, Human Studies ofPhysiology
A. TAGHVA, S.H. PATEL, A. FERNANDEZ,N. WEISS, FREDERICK A. LENZ
Department of Neurosurgery, Johns Hopkins Hospital,Baltimore, MD, [email protected]
Definition
Spontaneous thalamic cellular activity is often cate-gorized as either � bursting activity (� spike-bursts,bursting mode) or as � tonic firing mode (tonic mode)(Steriade et al. 1990). Many studies have suggestedthat increased spike-bursting occurs in the thalamus ofpatients with chronic neuropathic pain (Jeanmonod etal. 1994; Lenz et al. 1994, 1998; Rinaldi et al. 1991).Thalamic bursting has also been reported in monkeyswith interruption of the � spinothalamic tract (STT),which sometimes develop sensory abnormalities simi-lar to those seen in patients with similar lesions (Wenget al. 2000). This bursting is certainly associated withlesions of the somatic sensory pathways to thalamus,and is perhaps associated with the pain that developsfollowing such lesions.
Characteristics
The Thalamic Region of Vc and its Importance in Pain Process-ing
Several lines of evidence demonstrate that the ventralcaudal nucleus of the human sensory thalamus (Vc), thehuman analog of monkey ventral posterior (VP) nucleus(Hirai and Jones 1989), is an important component inhuman pain-signaling pathways. Studies of patients atautopsy following lesions of the STT show the densestSTT termination in the Vc region including: posteriorand inferior subnuclei of Vc, suprageniculate, and pos-terior subnuclei (Bowsher 1957; Mehler 1962; Walker1943). In monkeys, the STT originating in dorsal hornlamina I, in part, terminates in Vmpo (Craig et al. 1994;Graziano and Jones 2004). In humans, cells respondingto noxious and temperature stimuli can be located in allof these areas (Davis et al. 1999; Lee et al. 1999; Lenzet al. 1993). Thus, both anatomic and physiologic datademonstrates the presence of a distributed group of tha-lamic nuclei with pain related activity.
Is Thalamic Functional Mode Altered in Chronic Pain States?
Spike-bursting activity refers to a particular pattern of� interspike intervals (ISI) between action potentials,such that a spike-burst begins after a relatively long ISI,and is comprised of a series of action potentials with ashort ISI (typically < 6 ms) (Lenz et al. 1994; Steriadeet al. 1990). Thereafter, the ISIs progressively increasein length so that the cell’s firing decelerates throughoutthe spike-burst.In patients with spinal transection, the highest rate ofbursting occurs in cells thatdo nothaveperipheral recep-tive fields, and that are located in the thalamic represen-tation of the anesthetic part of the body. Since the pain isalso in the anesthetic part of the body, this bursting maybe due to loss of sensory input or be the cause of painor both. These cells also have the lowest firing rates inthe interval between bursts (principal event rate) (Lenzet al. 1994). The low firing rates suggest that these cellshave decreased tonic excitatory drive and are hyperpo-larized, perhaps due to loss of excitatory input from theSTT(Blomqvistetal.1996;Doughertyetal.1996;Eatonand Salt 1990). Therefore, the available evidence sug-gests that thalamic cells deafferentated by spinal tran-section (lesions) are dominated by spike-bursting andlow firing rates between bursts, consistent with mem-brane hyperpolarization (Lenz et al. 1998; Steriade etal. 1990).Spike-bursting activity is maximal in the region poste-riorand inferior to thecorenucleusofVc(Table4inLenzetal. 1994).Stimulation in thisareamayevokethesensa-tion of pain more frequently than does stimulation in thecore of Vc (Dostrovsky et al. 1991; Hassler 1970; Oharaand Lenz 2003). Thus, increased spike-bursting activitymay be correlated with some aspects of abnormal sensa-tions (e.g. dysesthesia or pain) that these patients expe-

C
Central Pain, Human Studies of Physiology 325
rience. However, in patients with spinal transection, thepainful area and the area of sensory loss overlap (Lenzet al. 1994). Thus, the bursting activity might be relatedto deafferentation of the thalamus from the input fromthe STT, rather than to pain.Thesefindingsabout spike-burstingactivity inspinalpa-tients have been called into question by a recent study inpatients with chronic pain (Radhakrishnan et al. 1999).It has been reported that the number of bursting cellsper trajectory in patients with movement disorders (con-trols) is not different from that in patients with chronicpain. However, there are significant differences betweenthe two studies (Lenz et al. 1994; Radhakrishnan et al.1999) in terms of: (1) patient population (spinal cord in-jury vs. mixed chronic pain); (2) location of cells stud-ied (Vc vs. anterior and posterior to Vc); and (3) analysismethods (incidence of bursting cells vs. bursting param-eters). Clearly, the increase in bursting activity demon-stratedintheearlierstudyismoreapplicabletotheregionof the principal somatic sensory nucleus in patients withcentral pain from spinal transection (Lenz et al. 1994).Further support for increased spike-bursts occurringin spinal cord injured patients is found in thalamicrecordings from monkeys with thoracic anterolateralcordotomies (Weng et al. 2000). Some of these animalsshowed increased responsiveness to electrocutaneousstimuli, and thus may represent a model of central pain(Vierck 1991). The most pronounced changes in firingpattern were found in thalamic multi-receptive cells,which respond to both cutaneous brushing and com-pressive stimuli, with activity that is not graded intothe noxious range. In comparison with normal controls,multi-receptive cells in monkeys with cordotomiesshowed significant increases in the number of burstsoccurring spontaneously or in response to brushing orcompressive stimuli. The changes in bursting behaviorwere widespread, occurring in the thalamic represen-tation of upper and lower extremities, both ipsilateraland contralateral to the cordotomy.Although there is an increase in spike-burst activity incentral pain secondary to spinal injury, there does notap-pear to be a direct relationship between spike-burst fir-ing and pain. Spike-bursts are also found in the thalamicrepresentation of the monkey upper extremity and of therepresentation of the arm and leg ipsilateral to the cor-dotomy. Pain is not typically experienced in these partsof the body in patients with thoracic spinal cord tran-section or cordotomy (Beric et al. 1988). Spike-burstsare increased in frequency during slow wave sleep anddrowsiness in all mammals studied (Steriade et al. 1990)including man in the absence of pain (Zirh et al. 1997).However, such bursting could cause pain if stimulationin the vicinity of the bursting cells produced the sensa-tion of pain. This finding has been reported in a studyof sensations evoked by stimulation of the region of Vcin patients with central pain, including those with spinalcord injuries (Lenz et al. 1998). Thus, there is evidence
from both human and animal studies for a correlationbetween central pain following spinal cord injury andan altered thalamic neuronal action potential firing pat-tern. It appears that there is an increase in spike-burstfiring in patients with pain following spinal injury. Theexact physiologic relationships which link the pattern ofthalamic firing to the human perception of pain in thiscondition are still unclear.
Acknowledgement
Supported by grants to FAL from the NIH: NS39498 andNS40059.
References1. Beric A, Dimitrijevic MR, Lindblom U (1988) Central Dysesthe-
sia Syndrome in Spinal Cord Injury Patients. Pain 34:109–1162. Blomqvist A, Ericson AC, Craig AD et al. (1996) Evidence for
Glutamate as a Neurotransmitter in Spinothalamic Tract Termi-nals in the Posterior Region of Owl Monkeys. Exp Brain Res108:33–44
3. Bowsher D (1957) Termination of the Central Pain Pathway inMan: The Conscious Appreciation of Pain. Brain 80:606–620
4. Craig AD, Bushnell MC, Zhang ET et al. (1994) A ThalamicNucleus Specific for Pain and Temperature Sensation. Nature372:770–773
5. Davis KD, Lozano AM, Manduch M et al. (1999) ThalamicRelay Site for Cold Perception in Humans. J. Neurophysiol81:1970–1973
6. Dostrovsky JO, Wells FEB, Tasker RR (1991) Pain Evoked byStimulation in Human Thalamus. In: Sjigenaga Y (ed) Interna-tional Symposium on Processing Nociceptive Information. El-sevier, Amsterdam, pp 115–120
7. Dougherty PM, Li YJ, Lenz FA et al. (1996) Evidence that Ex-citatory Amino Acids Mediate Afferent Input to the Primate So-matosensory Thalamus. Brain Res 278:267–273
8. Eaton SA, Salt TE (1990) Thalamic NMDA Receptors andNociceptive Sensory Synaptic Transmission. Neurosci Lett110:297–302
9. Graziano A, Jones EG (2004) Widespread Thalamic Termina-tions of Fibers Arising in the Superficial Medullary Dorsal Hornof Monkeys and their Telation to Calbindin Immunoreactivity.J Neurosci 24:248–256
10. Hassler R (1970) Dichotomy of Facial Pain Conduction in theDiencephalon. In: Walker AE (ed) Trigeminal Neuralgia. Saun-ders, Philadelphia, pp 123–138
11. Hirai T, Jones EG (1989) A New Parcellation of the Human Tha-lamus on the Basis of Histochemical Staining. Brain Res Rev14:1–34
12. Jeanmonod D, Magnin M, Morel A (1994) A Thalamic Conceptof Neurogenic Pain. In: Gebhart GF, Hammond DL, Jensen TS(eds) Proceedings of the 7th World Congress on Pain. Progressin Pain Research and Management, vol 2. IASP Press, Seattle,pp 767–787
13. Lee J-I, Antezanna D, Dougherty PM et al. (1999) Responses ofNeurons in the Region of the Thalamic Somatosensory Nucleus toMechanical and Thermal Stimuli Graded into the Painful Range.J Comp Neurol 410:541–555
14. Lenz FA, Gracely RH, Baker FH et al. (1998) Reorganization ofSensory Modalities Evoked by Stimulation in the Region of thePrincipal Sensory Nucleus (Ventral Caudal-Vc) in Patients withPain Secondary to Neural Injury. J Comp Neurol 399:125–138
15. Lenz FA, Kwan HC, Martin R et al. (1994) Characteristics ofSomatotopic Organization and Spontaneous Neuronal Activity inthe Region of the Thalamic Principal Sensory Nucleus in Patientswith Spinal Cord Transection. J.Neurophysiol 72:1570–1587
16. Lenz FA, Seike M, Lin YC et al. (1993) Neurons in the Area ofHuman Thalamic Nucleus Ventralis Caudalis Respond to PainfulHeat Stimuli. Brain Res 623:235–240

326 Central Pain in Multiple Sclerosis
17. Lenz FA, Zirh AT, Garonzik IM et al. (1998) Neuronal Activ-ity in the Region of the Principle Sensory Nucleus of HumanThalamus (Ventralis Caudalis) in Patients with Pain FollowingAmputations. Neurosci 86:1065–1081
18. Mehler WR (1962) The Anatomy of the So-Called “Pain Tract”in Man: An Analysis of the Course and Distribution of the As-cending Fibers of the Fasciculus Anterolateralis. In: French JD,Porter RW (eds) Basic Research in Paraplegia. Thomas, Spring-field, pp 26–55
19. Ohara S, Lenz FA (2003) Medial Lateral Extent of Thermal andPain Sensations Evoked by Microstimulation in Somatic SensoryNuclei of Human Thalamus. J Neurophysiol 90:2367–2377
20. Radhakrishnan V, Tsoukatos J, Davis KD et al. (1999) A Com-parison of the Burst Activity of Lateral Thalamic Neurons inChronic Pain and Non-Pain Patients. Pain 80:567–575
21. Rinaldi PC, Young RF, Albe-Fessard DG et al. (1991) Sponta-neous Neuronal Hyperactivity in the Medial and IntralaminarThalamic Nuclei in Patients with Deafferentation Pain. J Neu-rosurg 74:415–421
22. Steriade M, Jones EG, Llinas RR (1990) Thalamic Oscillationsand Signaling. Wiley, John & Sons, New York
23. Vierck CJ (1991) Can Mechanisms of Central Pain Syndromesbe Investigated in Animal Models? In: Casey KL (ed) Pain andCentral Nervous System Disease: the Central Pain Syndromes.Raven Press, New York, pp 129–141
24. Walker AE (1943) Central Representation of Pain. Res Publ As-soc Res Nerv Ment Dis 23:63–85
25. Weng HR, Lee J-I, Lenz FA et al. (2000) Functional Plasticityin Primate Somatosensory Thalamus Following Chronic Lesionof the Ventral Lateral Spinal Cord. Neurosci 101:393–401
26. Zirh AT, Lenz FA, Reich SG et al. (1997) Patterns of BurstingOccurring in Thalamic Cells during Parkinsonian Tremor. Neu-rosci 83:107–121
Central Pain in Multiple SclerosisJÖRGEN BOIVIE
Department of Neurology, University Hospital,Linköping, [email protected]
Synonyms
Central neuropathic pain in multiple sclerosis. Previ-ously equated with dysesthetic pain, since there was abelief that all central pain in multiple sclerosis (MS)was of dysesthetic quality, this has been shown to beincorrect.
Definition� Central pain (CP) is neuropathic pain caused by pri-mary lesions (e.g.MSlesions) in thecentralnervoussys-tem (CNS), either in the brain or spinal cord.
Characteristics
Epidemiology
Contrary to what was previously claimed in the liter-ature, several studies from the last two decades haveshown that many patients with MS have pain, and thatpain is a major problem for many MS patients. In theearly literature it was recognized that a small minority ofMS patients have � trigeminal neuralgia (TN) and evenfewer � painful tonic seizures. Furthermore, some MS
patients have pain caused by spasticity; while others re-port pain is not a common problem. According to recentresearch, however, 44%–79% of all MS patients haveproblems with pain (Ehde et al. 2003; Österberg 2005;Svendsen 2003), and about half of these patients havecentral pain, according to the only study in which cen-tral pain has been specifically investigated (Österberget al. 2005).In two postal surveys about pain, responses were re-ceived from 442 and 508 MS patients (Ehde et al.2003; Svendsen et al. 2003). In the American study44% reported persistent, bothersome pain as a result ofMS. Pain was of moderate to severe intensity in 63%,and interfered with life moderately or severely in 49%(Ehde et al. 2003). In the Danish study, no significantdifference in the total proportion of individuals withpain were found between MS patients and controls(79% and 75%), but when responses were analyzed itbecame clear that pain was more severe in MS patients(Svendsen et al. 2003). In this study the impact of painon daily life ranged from moderate to severe in 45% and7% of the patients, respectively. Results from studiesover the last twenty years in which neurologists haveinterviewed and examined MS with regard to pain pointin the same direction. Seven studies from the last 20years have shown the prevalence of pain in MS patientshas been found to be 54%–86% (Table 1).In a systematic study of central pain in MS, the preva-lence of CP in a population of 364 MS patients wasfound to be 27.5%, including 4.9% with TN (Österberget al. 2005). An additional 15 patients had possibleCP. If the patients with probable CP had been includedthe outcome would have been a prevalence of 31.6%.These figures compare well with results of previousstudies (Moulin et al. 1988; Moulin 1989; Vermonte etal. 1986).
Features of Central Pain
In the study by Österberg et al. (2005) many aspects ofCP in MS were investigated, including:
• The prevalence of CP increased with age and diseaseduration with peaks between 40 and 60 years-of-ageand 10–20 years of disease duration, but not with ahigher degree of disability. The prevalence of CP wasas high as 31% ten years after onset ofMS, and almostthe same after 11–20 years of disease, thereafter theprevalence of CP decreased to 14% – 18%. Thus, itappears that neither age nor duration of MS increasesthe risk of developing CP. This partly contradicts theresults of previous studies, where it was found thatthe pain prevalence increased with age (Clifford andTrotter1984;Moulinetal.1988;Stenageretal.1991),disease duration (Kassirer and Osterberg 1987) anddisability (Stenager et al. 1995). Prospective studiesare needed to give more reliable information on thesematters.

C
Central Pain in Multiple Sclerosis 327
Central Pain in Multiple Sclerosis, Table 1 Results from prevalence studies on pain in MS. Ages and durations in years. Prevalence in percent ofthe total population. The prevalence figures for central pain are estimates made from descriptions of pain, and were not calculated by the authorsthemselves.
Study Vermote1986
Kassirer1987
Moulin1988
Stenager1991
Indaco1994
Stenager1995
Österberg2005
Nr of pats 83 28 159 117 122 49 364
Mean age - 49 47 43 38 - 54
MS duration - 29 13 8 13 - 23
All pain 54 75 55 65 57 86 65
CP incl. TN 31 64* 29 - - - 28
TN 3,6 18** 5,9 3 9*** 14 4,9
Dysaesthetic pain - - 29 - 22 20 -
Pain in extremities 15 64 - 22 - 55 21
Spasm induced pain - 53 13 21 19 4 1
Non-trig. paroxysmal pain 4 - 5 7 5 41 2
Pain qualities BurningPrickingStabbingDull
BurningTingling
BurningTinglingAching
- - - AchingBurningPrickingStabbingSmartingSqueezing
TN=trigeminal neuralgia. *Neurogenic origin, **Including atypical facial pain, ***Neuralgic pain (face and head)
• There was a large span in the time interval betweenclinical onset of MS and the onset of CP, ranging from7 years before other symptoms to 25 years after othersymptoms. In 57% of patients with CP, pain startedwithin 5 years of onset of the disease, and after 10years the figure was 73%.
• In some patients, CP was the first symptom of MSbefore any other symptom, while in others CP ap-peared together with other symptoms. CP precededother symptoms in 6% of patients, and it was part ofthe onset symptoms in 20% of these patients and in5.5% of all MS patients.
• A large majority of patients experienced daily pain(88%);only30%hadpain-freemoments, lastingmin-utes to hours.
• The intensity of pain varied somewhat, and 44% ofpatientsexperienced aconstant intensity.Thisand theirritating quality of the pain, contribute to the fact thatpatients rate their pain as a heavy burden (Ehde et al.2003).
• More than one third of patients experienced CP in twoto four separate pain loci, often with differing modal-ity, time of onset and intensity (TN excluded).
• The most common location of CP was in the lowerextremities (87%)and in theupperextremities (31%).
• Half the patients experienced pain both superficiallyinskinandindeeperpartsof thebody,which issimilarto that found in central post-stroke pain (Leijon et al.1989).
• More than 80% of MS patients with CP experiencedtwo or more pain qualities, which is similar to thatfound by Leijon et al. (1989) for central post-strokepain.Themostcommonqualitieswereburning(40%)and aching (40%). Thus, no pain qualities or combi-nation of pain qualities are pathognomonic for CP inMS.
• Out of 364 patients only 2% had pain caused by spas-ticity. Instead, it was found that many patients withCP also have spasticity, but it was not the cause ofpain. This conclusion is shared by many clinicians.
As for other MS symptoms, CP can be one of severalsymptomsinarelapse,or theonlysymptom.CliffordandTrotter (1984) reported thisphenomenon, in twopatientswith temporary burning pain during a relapseofMS.Thedistribution of the three forms of MS in patients with CPdoes not generally differ among MS patients (relapsing-remitting, secondary progressive, primary progressive).From the literature it isknownthatemotionalstress, lighttouch, cold and physical activity can increaseCP(Boivie1999). This aspect has not been systematically studiedin MS, but it has been noted that many MS patients ex-perience worse pain after physical activity.Some patients with MS who have pareses, spasticity anddyscoordination of movement will develop nociceptivemusculoskeletal pain. In a recent study, 21% of MS pa-tients were found to have nociceptive pain (Österberget al. 2005), which is in the same range found in pre-

328 Central Pain in Multiple Sclerosis
vious studies (14%–39%; Kassirer and Osterberg 1987,Moulin 1989; Vermote et al. 1986).
Sensory Abnormalities
The most common neurological sign in patients withnon-trigeminal CP is sensory disturbance. Almost allpatients have at least one abnormal finding in the sen-sory examination, with a decrease in sensibility to coldoccurring more often than any other sub-modalities(Österberg and Boivie, in preparation). In this studyof 62 patients with non-trigeminal CP, both clinicaland quantitative methods were used to test sensibil-ity. There was a large variation between patients withregard to degree and submodality of abnormalities.Some patients had severe defects in all submodalities,whereas only one or two were affected in others. Inthe quantitative tests, all patients except two (97%)had abnormal sensibility to temperature and/or pain.Significant differences in abnormalities were foundbetween regions with CP and regions without CP forthe following perception thresholds: difference limen(i.e. innoxious temperature), warmth, cold, cold pain.No significant differences were found in the thresholdsfor heat pain.Among patients who did not perceive non-noxiouswarmth at all, but could feel heat pain, the burningsensation of heat struck patients suddenly and withhigh intensity as the temperature reached threshold.This was observed in 19% of patients. A correspondingsensation did not appear with cold. Eight patients hadnoxious cold evoked paradoxical heat pain. Non-painfuldysesthesias were commonly evoked by noxious heator cold.The results from the sensory tests indicate that most MSpatientswithCPhavelesionsaffectingthespinothalamo-cortical pathways (temperature and pain), but to a lesserdegree affect the medial lemniscal pathways (tactile,position sense and vibration).
Mechanisms
The cellular mechanisms underlying central pain in gen-eral, and definitely for MS, are largely unknown. Severalinvestigators have reported that CP develops as a resultof lesions affecting the spino- and quintothalamic path-ways, i.e. pathways most important for the sensibilityof pain and temperature. Furthermore, lesions of thesepathways can be located at any level of the neuraxis (forreferences see Boivie 1999). The results from examina-tion of the sensibility in MS patients with CP supportthis hypothesis. It has been proposed that the crucial le-sion isone thataffectsneospinothalamicprojections, i.e.projections to theventroposterior thalamic region (Bow-sher 1996). The effects of such a lesion involve neuronesof the spinothalamic pathway which become hyperex-citable due to reduced tonic inhibition.Based on results from experimental studies, Craig(1998) proposed a similar hypothesis about the mech-
anisms of central pain stating that “central pain is dueto the disruption of thermosensory integration and theloss of cold inhibition of burning pain”, which in turnis caused by a lesion of the spinothalamic projectionactivated by cold receptors in the periphery. The dis-rupted fibres are thought to tonically inhibit nociceptivethalamocortical neurones, increasing discharge andproducing pain. Like several other hypotheses, thismight be applicable in some patients, but not others,because of the location of the lesions and character ofthe pain.One can only speculate about the location of lesions re-sponsible for the development of CP in MS, because, asshown with MRI, practically all patients have dissemi-nated lesions in both the brain and spinal cord. However,based on clinical grounds, it is proposed that much of theCP located in the lower extremities is due to lesions inthe spinal cord. The bilateral nature of pain supports thisidea.
Treatment
The treatment of MS with interferons and similar sub-stances do not appear to have any symptomatic effect oncentral pain, or on any other symptom.Several treatment modalities are used in the manage-ment of CP in general, but almost no controlled clini-cal trials have been performed in MS, and only a fewin other forms of CP. The only exception is the study oforal cannabinoid dronabinol in 28 MS patients. A statis-tically significant, but weak effect was found (Svendsenet al. 2004).Treatments thatareused forCPare listedabove,butmostof them are based on clinical experience and tradition,rather than on results from controlled clinical trials. Thismeans that no evidence based recommendations can bemade for the management of CP in MS. Tricyclic an-tidepressants have been found to be effective for manypatients with central post-stroke pain (see essay on thispain condition), but the experience is that many MS pa-tients get severe side effects from these drugs.
Treatment Modalities Used for Central Pain
Among antidepressants and antiepileptics, the most fre-quently used are listed.
• Antidepressant drugs (AD)
– Amitriptyline– Desipramine– Doxepine– Imipramine– Nortriptyline
• Antiepileptic drugs (AED)
– Carbamazepine– Gabapentin– Lamotrigine

C
Central Pain, Outcome Measures in Clinical Trials 329
– Oxcarbazepine– Pregabalin
• Analgesics
– Morphine– Oxycontine– Codeine
• Sensory stimulation
– Transcutaneous electrical stimulation (TENS)– Spinal cord stimulation (SCS)– Deep brain stimulation (DBS)– Motor cortex stimulation (MCS)
Among the antiepileptic drugs, carbamazepine is ef-fective for trigeminal neuralgia associated with MS,but does not appear to relieve non-trigeminal centralpain (Österberg and Boivie, in preparation). Lamotrig-ine was shown to relieve CP in stroke, but it has notbeen tested in MS patients. Many neurologists havetried gabapentin with some success in non-trigeminalCP, but in the literature only case reports support itsuse.In one study with I.V. morphine, ten patients with CPfrom MS, and five patients from stroke were tested. Onlya trend to pain relief was found, and during the follow-ing 12 weeks open treatment period only three patientsexperienced a positive effect (Attal 2002). From clini-cal experience it appears that some MS patients obtainlong-term relief from weak opioids, but no systematicobservations support this. The experience with TENSfor CP is meagre and positive results have not been re-ported. The same is true for spinal cord stimulation anddeep brain stimulation.
References1. Boivie J (1999) Central Pain. In: Wall PD, Melzack R (ed)
Textbook of Pain 4th edn. Churchill Livingstone, Edinburgh,pp 879–914
2. Bowsher D (1996) Central Pain: Clinical and Physiological Char-acteristics. J Neurol Neurosurg Psychiat 61:62–69
3. Clifford DB, Trotter JL (1984) Pain in Multiple Sclerosis. Arch.Neurol 41:1270–1272
4. Craig AD (1998) A New Version of the Thalamic DisinhibitionHypothesis of Central Pain. Pain Forum 7:1–14
5. Ehde DM, Gibbons LE, Chwastiak L (2003) Chronic Pain in aLarge Community Sample of Persons with Multiple Sclerosis.Multiple Sclerosis 9:605–611
6. Indaco A, Iachetta C, Nappi C (1994) Chronic and Acute PainSyndromes in Patients with Multiple Sclerosis. Acta Neurol(Napoli) 16:97–102
7. Kassirer M, Osterberg D (1987) Pain in Chronic Multiple Scle-rosis. J Pain Symptom Manag 2:95–97
8. Moulin DE (1989) Pain in Multiple Sclerosis. Neurologic Clinics7:321–331
9. Österberg A, Boivie J, Thuomas K-Å (2005) Central Pain inMultiple Sclerosis – Prevalences, Clinical Characteristics andMechanisms. Eur J Pain 9:531–542
10. Stenager E, Knudsen L, Jensen K (1991) Acute and Chronic PainSyndromes in Multiple Sclerosis. Acta Neurol Scand 84:197–200
11. Stenager K, Knudsen L, Jensen K (1995) Acute and Chronic PainSyndromes in Multiple Sclerosis. A 5-Year Follow-Up Study. ItalJ Neurol Sci 16:629–632
12. Svendsen K, Jensen T, Bach F (2004) Does the CannabinoidDronabinol Reduce Central Pain in Multiple Sclerosis? Ran-domised Double Blind Controlled Crossover Trial. Br Med J329:253
13. Svendsen K, Jensen T, Overvald K (2003) Pain in Patients withMultiple Sclerosis: A Population-Based Study. Arch Neurol 60:1089–1094
14. Vermote R, Ketelaer P, Carton H (1986) Pain in Multiple SclerosisPatients. Clin Neurol Neurosurg 88: 87–93
Central Pain Mechanisms, MolecularContributions
� Molecular Contributions to the Mechanism of CentralPain
Central Pain Model
� Spinal Cord Injury Pain Model, Ischemia Model
Central Pain, Outcome Measures inClinical Trials
EVA WIDERSTRÖM-NOGA
The Miami Project to Cure Paralysis, Department ofNeurological Surgery University of Miami, VAMC,Miami, FL, [email protected]
Synonyms
Effectiveness Measure
Definition
An outcome measure is a performance indicator that as-sesses patient health status subsequent to, and resultingfrom, a health care treatment, procedure, or other ther-apeutic interventions.
Characteristics
Central neuropathic pain (CNP) is a result of traumaor neurological disease involving the central nervoussystem (CNS) (Bowsher et al. 1998). This type of paincan be a prominent feature in the complex clinicalpicture associated with disease or trauma involving theCNS, e.g. � stroke, � multiple sclerosis, � epilepsy,tumors, � syringomyelia, brain or spinal cord trauma,or � Parkinson’s disease (Boivie 2003). CNP is com-monly associated with both spontaneous non-painfulsensations and evoked pain (Widerström-Noga 2002),which further contribute to its unpleasant character.

330 Central Pain, Outcome Measures in Clinical Trials
Due to the refractory nature of CNP (Bowsher 1999),there is an obvious risk for a significantly decreasedhealth-related � quality of life (HRQOL). Therefore,� clinical trials examining treatments, or combina-tions of treatments, which may lead to more effectivestrategies for pain management in these patient popu-lations are urgently needed. Although CNP is commonin specific syndromes, the prevalence in the generalpopulation is relatively low (Boivie 2003). However,with increased awareness and more advanced diag-nostic procedures this number can be expected toincrease.The low numbers of people who experience CNP makeit difficult to obtain sufficient numbers of participantsfor definitive clinical trials. Consequently, few largescale, randomized, controlled clinical trials have beenconducted in persons with CNP. This further empha-sizes the need for clinical trial designs that permitcomparisons between trials. To achieve this goal, it isparticularly important to evaluate outcomes of treat-ments in a comprehensive and consistent manner. Theuse of standard sets of outcome measures in clinical tri-als involving people with CNP would greatly facilitatethe interpretation and application of research results tothe management of CNP.In a recent report, the Initiative on Methods, Measure-ment, and Pain Assessment in Clinical Trials (IMM-PACT) (Turk et al. 2003) recommended that clinicaltrials designed to evaluate the effectiveness of a therapyin relieving chronic pain, should consider including acore set of 6 outcome domains. The combination ofthese domains would generate more complete reports ofresults, and therefore facilitate the overall risk-benefitevaluation. The suggested domains include:
1. Pain2. Physical functioning3. Emotional functioning4. Participants ratings of improvement and satisfaction
with treatment5. Symptoms and adverse effects6. Participant disposition.
The authors emphasized those complementary mea-sures appropriate for specific patient populations shouldbe added as needed. Below is a brief description of thesix domains recommended to be included in the designof clinical trials for chronic pain.
Pain
Ratings of pain intensity, or pain severity by means of� numerical rating or � visual analogue scales, are themost widely used primary outcome measures in clinicalpain trials (Farrar et al. 2001). However, other clinicalfeatures of pain (i.e. location, quality temporal pattern)commonly evaluated in the � pain history (Wincent etal. 2003) may also be useful for the evaluation of treat-ment outcome. The differentiation of pain types is based
on a combination of clinical characteristics, and signsand symptoms of neurological dysfunction. This evalu-ation is particularly relevant for people who have CNP,since they frequently experience different types of painsimultaneously,with presumablydifferentmechanisms.Even though a clinical trial may be designed primarily totarget CNP, an improvement in physical and emotionalfunction may be caused by a decrease in the severity ofless refractory pain types, rather than a direct effect oncentral pain. Different types of pain may also influencepain-related impairment and function to various degrees(Marshall et al. 2002). Therefore, it is important to dif-ferentiate between the consequences of different paintypes to determine treatment effects on specific types ofpains.In central pain, the evaluation of neurological dysfunc-tion includes the quantification and determination ofsensory, motor, and autonomic function (Cruccu et al.2004). This evaluation is of primary importance for thediagnosis, and thus provides a basis for mechanism-based tailored treatments. However, the role of thesetypes of assessments as outcome measures in clinicaltrials is less clear. Specifically, more research is neededto establish reliability of the various ways of assessingand quantifying neurological dysfunction. In addition,the relationship between neurological dysfunction andimprovement in spontaneous neuropathic pain needs tobe further elucidated.
Physical Functioning
Because CNP is associated with neurological diseaseor trauma, physical functioning is often impaired. Al-though a general measure applicable to various painpopulations would allow for better comparisons, phys-ical functioning in chronic pain populations afflictedwith neurological disease or trauma may be influencedmore by the neurological impairment per se, than bychronic pain. One of the commonly used measures forthe evaluation of function in disabled populations isthe Functional Independence Measure (FIM). The FIMwas developed to provide a uniform measurement ofdisability (Granger 1998) and assesses independentperformance in self-care, sphincter control, transfers,locomotion, communication, and social cognition.However, the usefulness of this measure in CNP popu-lations needs to be determined. Moreover, the relativecontribution of CNP to the overall perceived disabilityin physically impaired central pain populations is notclear, and is also an important area for future research.Pain Interference measures may provide more usefulalternatives or complements to instruments that assessgeneral functional disability. For example, the extentto which pain hinders or interferes with daily activitiesmay provide more specific information in populationsafflicted with physical impairment (Widerström-Nogaet al. 2002). These measures can be used as comparisonsto samples of able-bodied chronic pain patients.

C
Central Pain, Outcome Measures in Clinical Trials 331
Emotional Functioning
Emotional distress (e.g. depressed mood, anxiety,anger, irritability) is intimately linked to the experienceof chronic pain, although no consistent causal rela-tionship has been proven. In neurological disease ortrauma, such as in traumatic brain injury (Jorge et al.2004), depression and anxiety levels are often elevated.Similar to physical functioning, it is not clear to whatextent pain itself contributes to affective distress in thecomplicated clinical syndromes associated with a neu-rological injury. Since affective distress is an importantfactor in the pain experience, this may have a significantimpact on HRQOL, and additional research in this areais warranted.
Participants Ratings of Global Improvement and Satisfactionwith Treatment
Related to the risk-benefit ratio, is the participant’spersonal estimation of how beneficial a treatment in-tervention is, namely, participants rating of globalimprovement and satisfaction with treatment. Althoughthis rating can be influenced by a variety of factors thatare difficult to control for (e.g. social desirability, recallbias, etc.), it still provides valuable and useful infor-mation (Farrar et al. 2001), incorporating the patient’sown unique view about the benefit and overall meaningof a treatment.
Symptoms and Adverse Effects
The assessment of adverse effects in a clinical trial aimsto determine the risk-benefit of the treatment. Adverseeffects can be directly caused by the treatment, or indi-rectly by worsening an underlying illnessorcompromis-ing previously impaired function. In people with CNP,the latter scenario may need special consideration, sinceadverse effects that have a relatively minor impact inable-bodied populations can cause significant problemswhen there are pre-existing impairments. For example,a decrease in cognitive function in a person with cogni-tive impairment due to a traumatic brain injury, or con-stipation in a person who has impaired bowel functiondue to spinal cord injury, may cause difficulties that hin-der adequate dosing as well as adherence to treatment.Therefore, it is important to monitor not only severity ofadverseeffects,butalso impactonpre-existingproblemsassociated with the neurological disease or trauma.
Participant Disposition
To adequately interpret the results of a trial and to deter-mine whether obtained results are representative and ap-plicable to larger population, details concerning partici-pants screened for enrollment (e.g. reasons for drop-outand non-compliance etc.) need to be provided (for de-tails see the� CONSORTstatement (Moheret al. 2001).This is particularly important in CNP populations, sincethe reasons for withdrawal and non-adherence may be
disease-specific and related to other sequela of neuro-logical disease and trauma.
Health Related Quality of Life
In CNP, complete remission of pain is unlikely to oc-cur either spontaneously or due to treatment (Bowsher1999). Therefore, measures that assess factors that mayinfluence HRQOL are of particular interest. HRQOL isa subjective concept, which is based on personal prefer-encesand valuesconcerningmultipledimensionsof life,including well-being and enjoyment of life. HRQOL indiverse populations has been categorized into the fol-lowing groups:
1. Physical functioning2. Social functioning3. Role limitations due to physical problems4. Role limitations due to emotional problems5. Mental health6. Vitality7. Bodily pain8. General Health (Ware and Sherbourne 1992).
The IMMPACT group (Turk et al. 2003) suggestedthat assessing some of these HRQOL dimensions (e.g.physical and emotional functioning and pain severity)would provide a basis for a multidimensional evaluationof pain. However, in CNP populations with physicalimpairments, the inclusion of additional dimensions(i.e. changed roles due to physical problems and gen-eral health) may be needed to determine the relativecontribution of CNP to the perception of HRQOL. Fur-thermore, increased understanding of the interactionbetween the various domains may improvemanagementof these complex pain syndromes.
Conclusion
The assessment domains recommended by the IMM-PACT appear to also be appropriate for CNP popu-lations. Due to the fact that people who have CNPfrequently have varying degrees of physical impair-ment, specific assessment of pain-related interferencewith physical and emotional functioning may be moreuseful than general measures of physical and emotionalfunction. A set of core outcome measures in combi-nation with more disease specific measures would beuseful for the purpose of comparison of clinical trialsin these populations. In the selection of specific instru-ments to be used as core outcome measures, not onlyvalidity and reliability must be considered, but alsowhether the instrument can be used with diverse CNPpopulations associated with a variety of diseases andtraumas.
References1. Boivie J (2003) Central Pain and the Role of Quantitative Sensory
Testing (QST) in Research and Diagnosis. Eur J Pain 7:339–343

332 Central Pain Pathways
2. Bowsher D, Leijon G, Thuomas KA (1998) Central PoststrokePain: Correlation of MRI with Clinical Pain Characteristics andSensory Abnormalities. Neurology 51:1352–1358
3. BowsherD(1999)CentralPain Following Spinal andSupraspinalLesions. Spinal Cord 37:235–238
4. Cruccu G, Anand P, Attal N et al. (2004) EFNS Guidelines onNeuropathic Pain Assessment. Eur J Neurol 11:153–162
5. Farrar JT, Young JP Jr, LaMoreaux Le et al. (2001) Clinical Im-portance of Changes in Chronic Pain Intensity Measured on an11-Point Numerical Pain Rating Scale. Pain 94:149–158
6. Granger CV (1998) The Emerging Science of Functional Assess-ment: Our Tool for Outcomes Analysis. Arch Phys Med Rehabil79:235–240
7. Jorge RE, Robinson RG, Moser D et al. (2004) Major Depres-sion Following Traumatic Brain Injury. Arch Gen Psychiatry61:42–50
8. Marshall HM, Jensen MP, Ehde DM et al. (2002) Pain Site andImpairment in Individuals with Amputation Pain. Arch Phys MedRehabil 83:1116–1119
9. Moher D, Schulz KF, Altman DG (2001) The CONSORTStatement: Revised Recommendations for Improving the Qual-ity of Reports of Parallel-Group Randomised Trials. Lancet357:1191–1194
10. Turk DC, Dworkin RH, Allen RR et al. (2003) Core OutcomeDomains for Chronic Pain Clinical Trials: IMMPACT Recom-mendations. Pain 106:337–345
11. Ware JE Jr, Sherbourne CD (1992) The MOS 36-Item Short-Form Health Survey (SF-36). I. Conceptual Framework and ItemSelection. Med Care 30:473–483
12. Widerström-Noga EG (2003) Chronic Pain and Nonpainful Sen-sations after Spinal Cord Injury: Is there a Relation? Clin J Pain19:39–47
13. Widerström-Noga EG, Duncan R, Felipe-Cuervo E et al. (2002)Assessment of the Impact of Pain and Impairments Associatedwith Spinal Cord Injuries. Arch Phys Med Rehabil 83:395–404
14. Wincent A, Liden Y, Arner S (2003) Pain Questionnaires in theAnalysis of Long Lasting (Chronic) Pain Conditions. Eur J Pain7:311–321
Central Pain Pathways
Definition
The pathways that carry information about noxiousstimuli to the brain, includes the spinalthalamic tractand trigeminal system.� Thalamic Nuclei Involved in Pain, Human and Mon-
key
Central Pain, PharmacologicalTreatments
NANNA BRIX FINNERUP1, SØREN HEIN SINDRUP2
1Department of Neurology and Danish Pain ResearchCentre, Aarhus University Hospital, Aarhus, Denmark2Department of Neurology, Odense UniversityHospital, Odense, [email protected], [email protected]
Definition� Central pain can be a consequence of different dis-eases and includes central post-stroke pain (CPSP),
central pain in spinal cord injury (SCI), multiple scle-rosis, perhaps Parkinson’s and Huntington’s disease,AIDS, and brain trauma. In spinal cord injury, centralneuropathic pain is experienced at and/or below thelevel of a lesion, and may be difficult to separate fromperipheral neuropathic pain components caused by rootlesions. Pain associated with this pathology is generallyfelt at the level of injury. Since different types of SCIpain are usually not separated, this review includes alltrials on the treatment of pain associated with spinalcord injury.Any lesion along thespinothalamocorticalpathway maylead to central pain, and � neuronal hyperexcitabilitycaused by increased excitation and/or decreased inhi-bition is an additional mechanism, which provides themechanistic basis for the use of drugs for neuropathicpain. Most pharmacological agents developed for treat-ment of this condition act by depressing neuronal activ-ity, modulating sodium or calcium channels, increasinginhibition with γ-aminobutyric acid (GABA), seroton-ergic, noradrenergic, or enkephalinergic agonists, or de-creasing activation via glutamate receptors, especiallythe N-methyl-D-aspartate (NMDA) receptor.
Characteristics
To suggestan evidence-based treatmentalgorithmbasedon � randomized � double-blind placebo-controlledtrials on central pain is difficult, considering the fact thatalthough new trials are emerging, there are still only afew, small sized studies on central pain (Table 1 and 2).� Number needed to treat (NNT) and number neededto harm (NNH) (in this text defined as treatment-relatedwithdrawals) are used to compare efficacy and harm ofindividual drugs.
Antidepressants
Tricyclic antidepressants block the reuptake of nore-pinephrine or serotonin, but activation on NMDAreceptors and sodium channels may also play a rolein their analgesic actions. The tricyclic antidepres-sant amitriptyline has been studied in two controlledtrials. In a three-way cross-over study, amitriptyline75 mg daily was effective in relieving pain (Leijonand Boivie 1989). The pain-relieving effect correlatedwell with total plasma concentration a with high num-ber of responders, b having plasma concentrationsexceeding 300 nmol/L. In patients with SCI, amitripty-line 10–125 mg daily had no effect on different types ofpain, including nociceptive pain (Cardenas et al. 2002),but the average amitriptyline dose was low, as wereserum concentrations (mean 92 ng/ml), i.e. below thelevel associated with response in CPSP. The hetero-cyclic antidepressant trazodone 150 mg daily had noeffect on neuropathic pain in spinal injury (Davidoffet al. 1987). The possibility of preventing CPSP wasstudied using amitriptyline (10 mg the first day after theonset of stroke was diagnosed, titrated to 75 mg within

C
Central Pain, Pharmacological Treatments 333
Central Pain, Pharmacological Treatments, Table 1 Randomized, double-blind, placebo-controlled trials on oral drugs in central pain
Active drug, daily dose Study Condition Design, no. ofpatients
Outcome NNT(95% CI)
NNH(95% CI)
Amitriptyline75 mg
Leijon and Boivie 1989 CPSP Cross-over15
Ami > pla 1.7(1.2–3.1)
∞
Amitriptyline10–125 mg
Cardenas et al. 2002 SCI pain Parallel84
Ami = pla - 9.2(4.2–∞)
Trazodone150 mg
Davidoff et al. 1987 SCI pain Parallel18
Tra = pla - NA
Carbamazepine800 mg
Leijon and Boivie 1989 CPSP Cross-over 15 Carb = pla - 15.0(5.2–∞)
Lamotrigine200 mg
Vestergaard etal. 2001
CPSP Cross-over 30 Ltg > pla NA 10.0(4.8–∞)
Lamotrigine200–400 mg
Finnerup et al. 2002 SCI pain Cross-over 22 Ltg = pla - ∞
Valproate 600–2400 mg Drewes et al. 1994 SCI pain Cross-over 20 Val = pla - ∞Gabapentinup to 1800 mg
Tai et al. 2002 SCI pain Cross-over 7 Gab = pla - 14.0 (4.8–∞)
Gabapentinup to 3600 mg
Levendoglu et al. 2004 SCI pain Cross-over 20 Gab > pla NA ∞
Mexiletine450 mg
Chiou-Tan et al. 1996 SCI pain Cross-over 11 Mex = pla - ∞
Dronabinol5–10 mg
Svendsen et al. 2004 Multiplesclerosis
Cross-over 24 Dro > pla 3.4(1.8–23.4)
∞
CPSP, central post-stroke pain; SCI, spinal cord injury; CI, confidence interval
three weeks) or placebo administered to 39 stroke pa-tients for one year (Lampl et al. 2002). Within this year,CPSP developed in three patients receiving amitripty-line (VAS 5.0), and in four receiving placebo (VAS 5.4).Two patients in the amitriptyline group and three pa-tients in the placebo group developed allodynia. Withan expected 8% incidence of CPSP, this sample size isprobably too small to detect an effect, but this was thefirst study of its kind and more are encouraged.
Antiepileptic Drugs
Antiepileptic drugs include a broad spectrum of drugsused in the management of epilepsy, and exert their anal-gesic actions through multiple mechanisms, by eitherreducing excitation and/or enhancing inhibition. Carba-mazepine blocks voltage dependent sodium channels,and may have minor effects on calcium channels andserotonergic systems. In a three-way cross-over study ofamitriptyline, carbamazepine 800 mg and placebo, car-bamazepine did not reduce CPSP compared to placebo(Leijon and Boivie 1989). However, both amitriptylineand carbamazepine treatments gave a 20% lower meanpain intensity score during the last week of treatment.Based on the relatively small number of patients in thisstudy,asignificanteffectofcarbamazepine inCPSPcan-not be excluded. Valproate has several pharmacologicaleffects, including GABAergic and anti-glutamatergic
actions. The effect of valproate 600–2400 mg dailywas examined in a cross-over study in patients withspinal injury (Drewes et al. 1994). Although a trendtoward improvement was observed, valproate was notsignificantly better than placebo in relieving pain. Lam-otrigine inhibits voltage dependent sodium channels tostabilize neuronal membranes and inhibits release ofexcitatory amino acids, principally glutamate. In CPSP,lamotrigine 200 mg daily reduced pain with a meanreduction of 30% (Vestergaard et al. 2001). Lamotriginealso reduced cold evoked � allodynia assessed by anacetone droplet. In spinal cord injury pain (SCIP), lam-otrigine 200–400 mg daily was not more effective thanplacebo in reducing pain, although a subgroup of pa-tients with incomplete injury and evoked pain reportedan effect on spontaneous pain (Finnerup et al. 2002).Gabapentin, which is thought to exert its analgesicactions by binding to an α2δ subunit of voltage gatedcalcium channels, has been studied in two cross-overtrials in SCIP. In a small study with seven patients,gabapentin up to 1800 mg had no significant effect onpain intensity (Tai et al. 2002). There was, however,a trend toward improvement, and a significant effecton unpleasant feeling. In another study, gabapentinup to 3600 mg reduced the intensity and frequency ofpain and several pain descriptors in 20 paraplegics withcomplete SCI (Levendoglu et al. 2004). Gabapentin in

334 Central Pain, Pharmacological Treatments
Central Pain, Pharmacological Treatments, Table 2 Randomized, double-blind, placebo-controlled trials on non-oral drugs in central pain
Active drug, dose administration Study Condition Design, no. ofpatients
Outcome
Lidocaine IV 5 mg/kg Attal et al. 2000 CPSP/SCI pain
Cross-over16
Lid > pla
Lidocaine IV 2.5 mg/kg Kvarnstrøm et al. 2004 SCI pain Cross-over10
Lid = pla
Lidocaine SA 50–100 mg Loubser and Donovan 1991 SCI pain Cross-over21
Lid > pla
Ketamine IV60 µg/kg +6 µg/kg/min
Eide et al. 1995 SCI pain Cross-over9
Ket > pla
Ketamine IV 0.4 mg/kg Kvarnstrøm et al. 2004 SCI pain Cross-over10
Ket > pla
Alfentanil IV 7 µg/kg +0.6 µg/kg/min
Eide et al. 1995 SCI pain Cross-over9
Alf > pla
Propofol IV 0,2 mg/kg Canavero and Bonicalzi 2004 CPSP/SCI pain
Cross-over44
Pro > pla
Morphine IV 9-30 mg Attal et al. 2002 CPSP/SCI pain
Cross-over15
Mor = pla
Morphine IT 0.2–1.5 mgClonidine IT 50–100 µgor 300–500 µg
Siddall et al. 2000 SCI pain Cross-over15
Mor = plaClo = plaMor + clo > pla
Naloxone IV up to 8 mg Bainton et al. 1992 CPSP Cross-over20
Nal = pla
Baclofen 50 µg Hermann et al. 1992 SCI pain Cross-over6
Bac > pla
CPSP, central post-stroke pain; SCI, spinal cord injury; IV, intravenous; SA, subarachoidal; IT, intrathecal
Central Pain, Pharmacological Treatments, Figure 1 L’Abbé plot ofcontrolled trials in central pain. Number of patients receiving active andplacebo treatments are indicated by circle sizes (lower right corner). Notethat the two trials showing a pain relieving effect of lamotrigine (Vestergaardet al. 2001) and gabapentin (Levendoglu et al. 2004) are not included inthe figure because dichotomized data were not provided.
combination with the NMDA antagonist dextromethor-phan was found to be superior to placebo, and to eithercomponent alone, in patients with neuropathic painfollowing spinal injury (Sang et al. 2001). Pregabalin
(similar mechanism as gabapentin) reduced SCIP ina large study which is not yet published (Siddall etal. 2005). Oxcarbazepine (similar mechanism as car-bamazepine), and other newer anticonvulsants such astiagabine, levetiracetam, and zonisamide, have not beentested in controlled trials in central pain.
Other Oral Drugs
Thecannabinoiddronabinol (asyntheticδ-9-tetrahydro-cannabinol) has been studied in 24 patients with cen-tral pain caused by multiple sclerosis. It significantly re-lieved central pain (Svendsen et al. 2004). Mexiletine,a sodium channel blocker, did not relieve pain in elevenpatients with SCIP in doses of 450 mg daily (Chiou-Tanet al. 1996).
Non-Oral Drugs
Sodium channel blockers may play a role in the treat-ment of central pain. Lidocaine in doses of 2.5 mg/kg,administered intravenously over40 minutes,had no painrelieving effect on pain in spinal cord injury patients(Kvarnstrom et al. 2004), while 5 mg/kg administeredintravenously over 30 minutes significantly decreasedspontaneous ongoing pain, brush-evoked allodynia,and static mechanical � hyperalgesia, but was no better

C
Central Pain, Pharmacological Treatments 335
than placebo against thermal allodynia and hyperalge-sia in patients with CPSP or SCIP (Attal et al. 2000). Itwas also found that lidocaine 5 mg/kg over 30 minutesrelieved spontaneous pain in spinal cord injury patientswith (n=12) and without (n=12) evoked pain, and thatlidocaine relieved pain felt at and below the level ofinjury (Finnerup et al. 2005). Subarachnoid infusion oflidocaine was significantly better than placebo in re-lieving SCIP (Loubser and Donovan 1991). Adequatespinal anesthesia, proximal to the level of spinal injury,seems important for a positive response to lidocaine,suggesting the existence of a ‘pain generator’ in thespinal cord of some patients.NMDA receptor antagonists given intravenously werereported to relieve SCIP in two studies (Eide et al. 1995;Kvarnstrom et al. 2004). Studies on opioids in centralpain trials have yielded diverging results. Intravenousmorphine was reported to have an effect on brush-evoked allodynia, but not on spontaneous pain in CPSPand SCIP patients (Attal et al. 2002), intravenous alfen-tanil was effective in relieving SCIP (Eide et al. 1995),and finally, morphine given intrathecally was effectivein SCIP patients, but only in combination with cloni-dine (an α2-adrenergic agonist) (Siddall et al. 2000).No effect of naloxone in CPSP was found (Baintonet al. 1992). Propofol, a GABAA-receptor agonist,injected as a single intravenous bolus of 0.2 mg/kg,relieved spontaneous pain and allodynia in 44 patientswith spinal cord injury and post-stroke pain (Canaveroand Bonicalzi 2004). Intrathecal baclofen, a GABABreceptor agonist, was also reported to relieve dyses-thesia in six patients with SCI or multiple sclerosis(Herman et al. 1992).
Conclusions
Tricyclic antidepressants, sodium channel blockers,NMDA antagonists, GABA agonists, calcium channelblockers, and cannabinoids, are shown to relieve centralpain. In randomized controlled trials on oral treatment,amitriptyline, lamotrigine, gabapentin, and dronabinolhave been effective in relieving pain, but large scalerandomized controlled studies are lacking, and the
Central Pain, Pharmacological Treatments, Table 3 First-line treatment options for central pain
Drug class and name Dosage Common side effects and cautions
Tricyclic antidepressants e.g.imipramine or amitriptyline
25 mg daily initially, increasing by 25 mg everytwo weeks, usually up to 150 mg daily in one totwo divided doses. Plasma drug levels should bemonitored (optimal plasma levels of imipramine plusdesipramine is 300–750 nM).
Dry mouth, constipation, and urinary retention,orthostatic hypotension, sedation, and increasedspasticity is reported. Contraindicated in patients withheart failure, cardiac conduction blocks (ECG beforestart) and epilepsy.
Gabapentin 300 mg daily initially, increasing by 300 mg everythird day, to 1800–4800 mg daily.
Dizziness, sedation, ataxia, and occasional peripheraledema. Renal impairment requires dosage adjustment.
Lamotrigine 25 mg daily initially, increasing the dose with 25 mgevery two weeks, later with 50 mg every week to400 mg daily
Dizziness, sedation, ataxia diplopia, and nausea. Riskof rash and potentially life-threatening hypersensitivityreactions requires slow dose escalation
treatment algorithm for central pain is still based oneffective treatments for peripheral neuropathic pain.Antidepressants and anticonvulsants (Table 3) are first-line drugs for central pain. In many cases, treatmentprovides only partial or no relief, and other types ofdrugs, combination therapy, intrathecal therapy, anddifferent non-pharmacological approaches may beconsidered in these cases.
References1. Attal N, Gaude V, Brasseur L, Dupuy M, Guirimand F, Parker F,
Bouhassira D (2000) Intravenous Lidocaine in Central Pain: ADouble-Blind, Placebo-Controlled, Psychophysical Study. Neu-rology 54:564–574
2. Attal N, Guirimand F, Brasseur L, Gaude V, Chauvin M, Bouhas-sira D (2002) Effects of IV Morphine in Central Pain: A Ran-domized Placebo-Controlled Study. Neurology 58:554–563
3. Bainton T, Fox M, Bowsher D, Wells C (1992) A Double-BlindTrial of Naloxone in Central Post-Stroke Pain. Pain 48:159–162
4. Canavero S, Bonicalzi V (2004) Intravenous Subhypnotic Propo-fol in Central Pain: A Double-Blind, Placebo-Controlled, Cross-over Study. Clin Neuropharm 27:182–186
5. Cardenas DD, Warms CA, Turner JA, Marshall H, Brooke MM,Loeser JD (2002) Efficacy of Amitriptyline for Relief of Pain inSpinal Cord Injury: Results of a Randomized Controlled Trial.Pain 96:365–373
6. Chiou-Tan FY, Tuel SM, Johnson JC, Priebe MM et al. (1996)Effect of Mexiletine on Spinal Cord Injury Dysesthetic Pain. AmJ Phys Med Rehabil 75:84–87
7. Davidoff G, Guarracini M, Roth E, Sliwa J, Yarkony G (1987)Trazodone Hydrochloride in the Treatment of Dysesthetic Pain inTraumatic Myelopathy: A Randomized, Double-Blind, Placebo-Controlled Study. Pain 29:151–161
8. Drewes AM, Andreasen A, Poulsen LH (1994) Valproate forTreatment of Chronic Central Pain after Spinal Cord Injury. Adouble-blind cross-over study. Paraplegia 32:565–569
9. Eide PK, Stubhaug A, Stenehjem AE (1995) Central Dyses-thesia Pain after Traumatic Spinal Cord Injury is Depen-dent on N-methyl-D-aspartate Receptor Activation. Neuro-surgery 37:1080–1087
10. Finnerup NB, Sindrup SH, Bach FW, Johannesen IL, Jensen TS(2002) Lamotrigine in Spinal Cord Injury Pain: A RandomizedControlled Trial. Pain 96:375–383
11. Finnerup NB, Biering-Sorensen F, Johannesen IL et al. (2005)Intravenous lidocaine relieves spinal cord injury pain: a random-ized controlled trial. Anesthesiology 102:1023–30
12. Herman RM, D’Luzansky SC, Ippolito R (1992) Intrathecal Ba-clofen Suppresses Central Pain in Patients with Spinal Lesions.A Pilot Study. Clin J Pain 8:338–345

336 Central Pain Syndrome
13. Kvarnstrøm A, Karlsten R, Quiding H, Gordh T (2004) The Anal-gesic Effect of Intravenous Ketamine and Lidocaine on Pain afterSpinal Cord Injury. Acta Anaesthesiol Scand 48:498–506
14. Lampl C, Yazdi K, Röper C (2002) Amitriptyline in the Prophy-laxis of Central Poststroke Pain. Stroke 33:3030–3032
15. Leijon G, Boivie J (1989) Central Post-Stroke Pain – A ControlledTrial of Amitriptyline and Carbamazepine. Pain 36:27–36
16. Levendoglu F, Ögün CÖ, Özerbil Ö, Ögun TC, Ugurlu H (2004)Gabapentin is a First Line Drug for the Treatment of NeuropathicPain in Spinal Cord Injury. Spine 29:743–751
17. Loubser PG, Donovan WH (1991) Diagnostic Spinal Anaesthesiain Chronic Spinal Cord Injury Pain. Paraplegia 29:25–36
18. Sang CN, Dobosh L, Miller V, Brown R (2001) CombinationTherapy for Refractory Pain following Spinal Cord Injury Us-ing the Low Affinity N-methyl-D-aspartate (NMDA) ReceptorAntagonist Dextromethorphan and Gabapentin. Abstract 20th
Annual Scientific Meeting APS. J Pain 2:1019. Siddall PJ, Molloy AR, Walker S, Rutkowski SB (2000) The
Efficacy of Intrathecal Morphine and Clonidine in the Treatmentof Pain after Spinal Cord Injury. Anesth Analg 91:1–6
20. Siddall PJ, Cousins M et al. (2005) Pregabalin safely and effec-tively treats chronic central neuropathic pain after spinal cordinjury. Abstr IASP 11th World Congress on Pain
21. Svendsen KB, Jensen TS, Bach F (2004) Does the cannabi-noid dronabinol reduce central pain in multiple sclerosis?Randomised double blind placebo controlled crossover trial.BMJ 329:253–258
22. Tai Q, Kirshblum S, Chen B, Millis S et al. (2002) Gabapentinin the Treatment of Neuropathic Pain after Spinal Cord Injury:A Prospective, Randomized, Double-Blind, Cross-over Trial. JSpinal Cord Med 25:100–105
23. Vestergaard K, Andersen G, Gottrup H, Kristensen BT, Jensen TS(2001) Lamotrigine for Central Poststroke Pain: A RandomizedControlled Trial. Neurology 56:184–190
Central Pain Syndrome
Definition
A neurological condition caused by damage to or dys-function of the central nervous system, most commonlyfollowing a thalamic stroke, s. also � Central Pain.� Lateral Thalamic Lesions, Pain Behavior in Animals
Central Pattern Generator
Definition
Cellular networks in the brainstem that are organized toinitiate and maintain motor activity through pattern gen-eration and rhythm generation.� Orofacial Pain, Movement Disorders
Central Sensitization
Definition
Central sensitization is an umbrella term for a numberof phenomena, all of which are characterized by anincrease in the responsiveness of nociceptive neuronsin the central nervous system, best characterized in
the spinal dorsal horn, to sensory stimulation. Cen-tral sensitization may be induced by conditioningnoxious stimulation such as trauma, inflammation,nerve injury or electrical stimulation of sensory nervesat C-fiber strength. It is considered to contribute toafferent-induced forms of hyperalgesia and allodynia.Proposed spinal mechanisms include reduced inhibi-tion, excessive primary afferent depolarization (PAD),and enhanced strength at excitatory synapses in painpathways (synaptic long-term potentiation: LTP).� ArthritisModel,Kaolin-CarrageenanInducedArthri-
tis (Knee)� Cancer Pain Model, Bone Cancer Pain Model� Central Changes after Peripheral Nerve Injury� Chronic Pelvic Pain, Musculoskeletal Syndromes� Drugs Targeting Voltage-Gated Sodium and Calcium
Channels� Exogenous Muscle Pain� Formalin Test� GABA Mechanisms and Descending Inhibitory
Mechanisms� Gynecological Pain, Neural Mechanisms� Hypersensitivity Maintained Pain� Long-Term Potentiation and Long-Term Depression
in the Spinal Cord� Metabotropic Glutamate Receptors in Spinal Noci-
ceptive Processing� Muscle Pain Model, Inflammatory Agents-Induced� Pain Modulatory Systems, History of Discovery� Postherpetic Neuralgia, Pharmacological and Non-
Pharmacological Treatment Options� Postoperative Pain, Acute Neuropathic Pain� Psychiatric Aspects of Pain and Dentistry� Psychological Treatment of Headache� Quantitative Sensory Testing� Referred Muscle Pain, Assessment� Restless Legs Syndrome� Spinothalamic Neuron� Spinothalamic Tract Neurons, Role of Nitric Oxide� Transition from Acute to Chronic Pain
Central Sulcus
Synonyms
Rolandic Sulcus
Definition
The convolutions of the cerebral cortex have a generalorganization that is similar for all humans. One constantand readily recognizable sulcus is the central sulcus (ofRolando),andmarksthedivisionbetweenthefrontalandparietal lobes.� Motor Cortex, Effect on Pain-Related Behavior

C
Cerebrospinal Fluid 337
Central Trigger Point
Synonyms
CTrP
Definition
Clinically, central trigger point is characteristicallya very tender, circumscribed nodule-like spot in themid-portion of a palpable taut band of skeletal musclefibers and it usually refers pain when compressed. Thistrigger point may be active or latent and can induceattachment trigger points.� Myofascial Trigger Points
Centralization
� Central Changes after Peripheral Nerve Injury
Central-Peripheral Distal Axonopathy
Definition
Peripheral nerve disorders beginning from degenerationof the most terminal parts of both central and periph-eral processes of neurons, the major pathology of toxicneuropathies; also dying-back neuropathy and distal ax-onopathy.� Toxic Neuropathies
Centrifugal Control of NociceptiveProcessing
� GABA Mechanisms and Descending InhibitoryMechanisms
� SpinothalamicTractNeurons,DescendingControlbyBrainstem Neurons
Centrifugal Control of Sensory Inputs
Definition
Regulation of the access of sensory information to thecentralnervoussystemiscarriedoutby theactionofneu-ral pathways that inhibit or facilitate sensory processing.Such regulatory pathways can be intrinsic to the spinalcord (and trigeminal nuclei) or can originate from a va-riety of structures in the brain.� SpinothalamicTractNeurons,DescendingControlby
Brainstem Neurons
Cephalalgia
� Headache
Ceramide
Definition
An intracellular signaling molecule liberated by activa-tion of the sphingomyelin pathway. This pathway is ac-tivated by NGF via its action on the p75 receptor.� Nerve Growth Factor, Sensitizing Action on Nocicep-
tors
Cerebellum
Definition
The cerebellum is located dorsal to the brainstem andpons, and inferior to the occipital lobe. It mainly servessensory-motor integration, by providing constant feed-back signals to adapt fine-tune movements according tomomentary muscle length and tone and body posture.� Functional Imaging of Cutaneous Pain
Cerebral Cortex
Definition
The cerebral cortex is the thin, convoluted surface layerof nerve cell bodies (also called gray matter) of the cere-bral hemispheres responsible for receiving and analyz-ing sensory information, for the execution of voluntarymuscle movement, thought, reasoning and memory.� Cingulate Cortex, Functional Imaging� Clinical Migraine with Aura� Descending Circuitry, Transmitters and Receptors� Nociceptive Processing in the Cingulate Cortex, Be-
havioral Studies in Humans� PET and fMRI Imaging in Parietal Cortex (SI, SII, In-
ferior Parietal Cortex BA40)
Cerebrospinal Fluid
Synonyms
CSF

338 Cervical Discogram
Definition
Fluid within the 4 brain ventricles, mainly producedby the choroid plexus. The average pressure (in lateralrecumbent position) is 150–250mmH2O, depending onCSF secretion & absorption, intracranial arterial andvenous pressure, hydrostatic pressure, brain bulk andstatus of surrounding coverings.� Cancer Pain Management, Anesthesiologic Interven-
tions, Neural Blockade� Headache due to Low Cerebrospinal Fluid Pressure
Cervical Discogram
� Cervical Discography
Cervical DiscographyDAVID DIAMANT
Neurological and Spinal Surgery, Lincoln, NE, [email protected]
Synonyms
Cervical Discogram; Provocation Discogram; provoca-tive discography
Definition
Cervicaldiscography isadiagnosticproceduredesignedto determine if a cervical intervertebral disc is the sourceof a patient’s neck pain. It involves injecting contrastmedium into the disc in an attempt to reproduce the pa-tient’s pain.
Characteristics
Principles
The cervical intervertebral discs are innervated by noci-ceptive fibers from the cervical sinuvertebral nerves, thevertebral nerves, and the cervical sympathetic trunks(Bogduk et al. 1989; Groen et al. 1990; Mendel etal. 1992). Being endowed with a nerve supply, thecervical discs are potentially a source of neck pain.There are no conventional means by which to determineif a patient’s neck pain arises from a cervical interverte-braldisc.Therearenosignson� musculoskeletalexam-ination by which this can be established, and no signs onmedical imaging. Abnormalities evident on � magneticresonance imaging (MRI) correlate poorly with whetherthe disc is painful or not (Parfenchuck and Janssen 1994;Schellhas et al. 1996). Furthermore, fissures that may bepresent across the posterior aspect of cervical discs area normal age change (Oda et al. 1988), and do not con-stitute a painful lesion (Parfenchuck and Janssen 1994;Schellhas et al. 1996).
Provocation discography is the only means by which totest if a cervical disc is painful or not. The procedure in-volves injecting contrast medium into the nucleus pul-posus of the disc, in an effort to reproduce the patient’spain. Although the contrast medium outlines the internalstructure of the disc, this is not seminal to the diagnosis.The critical component of the procedure is reproductionof the patient’s pain.Studies in normal volunteers and in patients havedemonstrated that cervical discs can produce neck pain,under experimental conditions (Schellhas et al. 1996;Cloward 1959; Grubb and Kelly 2000) Referred painpatterns encompass areas that are topographically sep-arated from the site of pathology. Furthermore, discsat particular segmental levels produce pain in fairlyconsistent regions (Schellhas et al. 1996; Grubb andKelly 2000) (Fig. 1). The C2–3 disc typically refers tothe occiput. The C3–4 disc typically refers to the areaof the C7 spinous process, with spread toward the sideof the neck. The C4–5 disc typically refers toward thesuperior angle of the scapula, but may spread from thebase of the neck to the top of the shoulder. The C5–6disc refers to the center of the scapular border, and theC6–7 disc refers to the inferior angle of the scapula,but both may spread over the entire scapula, across theshoulder and into the proximal upper limb. These painpatterns can be used to plan which segmental levelsshould be targeted for investigation.If stimulation of the disc reproduces the patient’s painpattern (concordant pain), it may be presumed that suchis their pain generator. If stimulating the disc is notpainful, or produces an atypical (non-concordant) painpattern, thisdisc ispresumed not to be thepaingenerator.
Cervical Discography, Figure 1 Patterns of distribution of pain afterstimulation of cervical intervertebral discs at the segments indicated. Re-produced courtesy of the International Spinal Intervention Society.

C
Cervical Discography 339
Cervical Discography, Figure 2 Radiographs showing needles placed into cervical intervertebral discs in preparation for discography. (a) Anteriorview. (b) Lateral view. Reproduced courtesy of the International Spinal Intervention Society.
Cervical Discography, Figure 3 Radiographs of cervical discography after injecting of contrast medium. (a) Anterior view. (b) Lateral view. Reproducedcourtesy of the International Spinal Intervention Society.
TechniqueThe patient lies supine and the neck is prepared for anaseptic procedure. The operator inserts a needle throughthe skin of the neck and into the anterolateral aspect of
the target disc, until it reaches the centre of the nucleus(Fig. 2). Thereupon, contrast medium is injected, bothto verify correct placement (Fig. 3), and to test for re-production of pain. The nucleus pulposus of a typical

340 Cervical Discography
cervical intervertebral disc will admit 0.2–0.4cc of in-jectate (Kambin et al. 1980). Whether the patient devel-ops concordant pain or not is the critical component ofthe procedure.
Validity
In order to be valid, the International Association forthe Study of Pain (Merskey and Bogduk 1994) recom-mends thatcervicaldiscography besubjected to anatom-ical controls. Not only does provocation of the interver-tebral disc need to reproduce the individual’s pain con-cordantly, but also provocation at adjacent levels mustnot reproduce such pain. Additional criteria have beenrecommended by the International Spinal InterventionSociety (2004) pertaining to the intensity of the pain pro-duced during disc stimulation, and the potential role ofother structures in the generation of pain.Cervical discs in normal, asymptomatic volunteers canbe made to hurt by discography (Schellhas et al. 1996).However, in such individuals the evoked pain is notsevere. They rate the pain as typically less than 6 on a10–point scale. In contrast, patients with disc pain reportreproduction of moderate or severe pain, which theytypically rate as greater than 7, Schellhas et al. 1996).Accordingly, it is recommended that for cervical discstimulation to be considered positive, the evoked painmust have an intensity of 7 or greater (InternationalSpinal Intervention Society 2004). This criterion servesto prevent minor pain from an asymptomatic disc, beingconsidered positive.Provocation of the intervertebral disc may elicit con-cordant pain, yet other sources of such pain can be theactual pain generator. As such, the issue of diagnosticspecificity of this procedure is questionable. As theyshare a similar segmental innervation, the cervical zy-gapophysial joints can refer pain to similar regions asthe intervertebral discs (Bogduk and Aprill 1993). Con-sequently, cervical discography can be false-positive inpatients whose pain originates from the zygapophysialjoints at the same segment as the disc stimulated. Some40% of patients with positive responses to discogra-phy have their pain relieved by blocks of the cervicalzygapophysial joints (see � Cervical Medial BranchBlocks), which is not compatible with the disc beingthe primary source of their pain. Accordingly, it hasbeen recommended that cervical discography be under-taken only when the cervical zygapophysial joints, atthe areas of concern, have been excluded as the sourceof the patient’s pain (International Spinal InterventionSociety 2004).Additionally, there are other pitfalls that may compro-mise the validity of cervical discography. Technical er-rors will compromise the diagnostic validity of cervi-cal discography. The needle tip must be in the nucleuspulposus—otherwise, stimulation of the anulus fibrosuswill be likely to yield a painful response, regardless ofwhether that disc is the pain generator or not.
Applications
The primary purpose of cervical discography is to de-termine if cervical discs are the source of patient’s neckpain. It is indicated, therefore, in patients whose causeof pain cannot be established by other means, who havenot benefited from conservative therapy, and for whoma diagnosis is desired or required.A secondary purpose of cervical discography is to helpphysicians plan interventional management. One treat-ment option is anterior cervical discectomy and fusion.For this procedure, surgeons are not only interested inif a disc hurts, but also if other discs hurt. The greaterthenumbersofdiscs thatappearpainful, the less inclinedsurgeonsare toundertakesurgery.Notonlyismulti-levelfusionmore technicallydemandingfor thesurgeons,andmore hazardous to the patient, its outcomes are less fa-vorable than fusion at a single level.
Utility
Cervical discography was originally developed with theprospect of finding one, or perhaps only two, discs thatwere painful, so that fusion might be undertaken to re-lieve the patient’s pain. Accordingly, cervical discogra-phy was expected to have positive predictive value. Sub-sequent studies, however, have thwarted this aspiration.It has become evident thatcervical discs are infrequentlysymptomatic at single levels (Grubb and Kelly 2000).More commonly, discs at three levels, and even four ormore levels, are symptomatic. This pattern essentiallyprecludes surgical therapy. Consequently, in practice,cervical discography has more of a negative predictivevalue. It serves far more often to prevent surgery than toencourage it. Indeed, in one series, only 10% of patientsproceeded to surgery in the light of their responses tocervical discography (Grubb and Kelly 2000).
References1. Bogduk N, Aprill C (1993) On the Nature of Neck Pain, Discogra-
phy and Cervical Zygapophysial Joint Blocks. Pain 54:213–2172. Bogduk N, Windsor M, Inglis A (1989) The Innervation of the
Cervical Intervertebral Discs. Spine 13:2–83. Cloward RB (1959) Cervical Diskography. A Contribution to the
Aetiology and Mechanism of Neck, Shoulder and Arm Pain. AnnSurg 130:1052–1064
4. Groen GJ, Baljet B, Drukker J (1990) Nerves and Nerve Plexusesof the Human Vertebral Column. Am J Anat 188: 282–296
5. Grubb SA, Kelly CK (2000) Cervical Discography: Clinical Im-plications from 12 Years of Experience. Spine 25:1382–1389
6. International Spinal Intervention Society (2004). CervicalDiscography. In: Bogduk N (ed) Practice Guidelines for SpinalDiagnostic and Treatment Procedures (2004) InternationalSpinal Intervention Society, San Francisco
7. Kambin P, Abda S, Kurpicki F (1980) Intradiskal Pressure andVolume Recording: Evaluation of Normal and Abnormal Cervi-cal Disks. Clin Orthop 146: 144–147
8. Mendel T, Wink CS, Zimny ML (1992) Neural Elements in Hu-man Cervical Intervertebral Discs. Spine 17:132– 135
9. Merskey H, Bogduk N (1994) Classification of Chronic Pain.Descriptions of Chronic Pain Syndromes and Definition of PainTerms, 2nd ed. IASP Press Seattle, p 108

C
Cervical Medial Branch Blocks 341
10. Oda J, Tanaka H, Tsuzuki N (1988) Intervertebral Disc Changeswith Aging of Human Cervical Vertebra from the Neonate to theEighties. Spine 13:1205–1211
11. Parfenchuck TA, Janssen ME (1994) A Correlation of Cervi-cal Magnetic Resonance Imaging and Discography/ComputedTomographic Discograms. Spine 19:2819–2825
12. Schellhas KP, Smith MD, Gundry CR, Pollei SR (1996) CervicalDiscogenic Pain. Prospective Correlation of Magnetic ResonanceImaging and Discography in Asymptomatic Subjects and PainSufferers. Spine 21:300–312
Cervical Facet Blocks
� Cervical Medial Branch Blocks
Cervical Facet Denervation
� Cervical Medial Branch Neurotomy
Cervical MBBs
� Cervical Medial Branch Blocks
Cervical Medial Branch BlocksJAYANTILAL GOVIND
Department of Anaesthesia, Pain Clinic, LiverpoolHospital, University of New South Wales, Sydney,NSW, [email protected]
Synonyms
Cervical Zygapophysial Joint Blocks; Cervical FacetBlocks; Cervical MBBs; Z Joint Blocks
Definition
Cervical medial branch blocks (MBBs) are a diagnostictest to determine if a patient’s neck pain is mediated byone or more of the medial branches of the cervical dorsalrami. This is achieved by anaesthetising the target nervewith aminutevolumeof localanaesthetic. In theabsenceof evidence to the contrary, a positive response to MBBsimplies that thepatient’spainstemsfromthezygapophy-seal joint innervated by the nerves anaesthetised.
Cervical Medial Branch Blocks, Figure 1 A lateral radiograph of the cer-vical spine. The course of the third occipital nerve and the medial branchesof the C3 to C7 dorsal rami across the articular pillars is indicated withdotted lines.
Characteristics
Rationale
At typical cervical levels, the medial branches of the cer-vical dorsal rami pass across the waist of the ipsiseg-mental articular pillar (Fig. 1). They innervate the zy-gapophysial joints above and below, before supplyingthe posterior muscles of the neck (Bogduk 1982). Thethird occipital nerve and the C7 medial branch cross thejoint that they supply.The zygapophysial (“Z”) joints are the only structuressupplied by these nerves that are affected by disordersthat can be a source of chronic pain (Barnsley and Bog-duk 1993).Thesedisorderscannotbediagnosedbymus-culoskeletal examination or by medical imaging. Diag-nostic blocks are the only validated means by which theZ joints can be implicated or excluded as the source ofpain. In order to anaesthetise a given joint, both nervesthat innervate it must be blocked.
Technique
Theblocksareperformedwith thepatient lying inacom-fortable position, prone, supine, or on their side. Underfluoroscopic guidance, a fine needle is inserted throughthe skin and muscles of the neck and onto the articularpillar where the target nerve lies (Fig. 2). The nerve canbe anaesthetised with as little as 0.3 ml of local anaes-thetic.
Principles
The primary objective of cervical MBBs is to establishif anaesthetising the target nerves relieves the patient’spain. If the pain is not relieved, the targeted joint can be

342 Cervical Medial Branch Blocks
Cervical Medial Branch Blocks, Figure 2 A lateral radiograph of a cer-vical spine, showing a needle in position for a C5 medial branch block.
excluded as the source of pain, and a new source con-sidered, such as a joint at another segmental level, or anintervertebral disc. If pain is relieved, the response con-stitutes prima facie evidence that the targeted nerves aremediating the patient’s pain, and that it arises from thejoint that they supply.In order to bepositive, theblocksmustproducecompletereliefofpain.Partial reductionofpaindoesnotconstitutea positive response.In some patients, however, their pain may arise frommore than one joint. They may experience pain fromboth joints at the same segment, from consecutivejoints on the same side, or from joints at separate anddisplaced segments. Typical patterns are: C5–6 onboth sides, C5–6 and C6–7 ipsilaterally, and C5–6 andC2–3 on the same side.In such patients, anaesthetising one joint will not relieveall of their pain. However, blocking that joint will com-pletely relieve pain in the particular region to which thatjoint refers its pain. Similarly, blocking the other jointwill relievepain in theremainingarea.Thesubtletyofthediagnostic criterion is that the patient obtains completerelief of pain in a particular topographical distribution.This is not the same as the patient obtaining partial reliefof their pain overall (International Spinal InterventionSociety 2004).
Validity
Cervical MBBs are target-specific, and the use ofminutevolumes of local anaesthetic precludes other structuresbeing anaesthetised (Barnsley and Bogduk 1993). Toavoid false-positive responses, the blocks must be con-
trolled. Single diagnostic blocks are associated withan unacceptably high rate of false-positive responses(Barnsley et al. 1993a). Although placebo controlscan be used, these may not be practical under conven-tional circumstances, but comparative local anaestheticblocks can be used (International Spinal InterventionSociety 2004; Barnsley et al. 1993b; Lord et al. 1995).On separate occasions, the same block is repeated usinglocal anaesthetics with different durations of action. Thetest is negative if the repeat block fails to relieve pain. Ifboth blocks relieve the pain, the relief may be concor-dant or discordant, and can be either prolonged or not(Barnsley et al. 1993b).Concordant relief is short-lasting relief when a short-acting agent is used and long-lasting relief when a long-acting agent is used. When relief is longerafter theshort-acting agent is used, the response is classed as discor-dant. If the relief substantially outlasts the expected du-ration of action of either agent, the response is classedas prolonged. Discordant and prolonged responses areprobably due to local anaesthetics, particularly ligno-caine, acting on “open” sodium channels (Butterworthand Strichartz 1990).Concordant responses are the ideal. They have a sensi-tivity of 54% and specificity of 88% (Lord et al. 1995).Thehighspecificitymeansthatconcordantresponsesarevery unlikely to be false. The low sensitivity, however,means that not all patients with zygapophysial joint painwill be detected.If discordant responses are accepted as positive, thesensitivity rises to 100% but the specificity dropsto 65% (Lord et al. 1995). Thus, all patients with zy-gapophysial joint pain will be detected, but some willbe false-positive.
Epidemiology
The zygapophysial joints are the single-most commonsource of chronic neck pain. They are the source of painin at least 50% (Barnsley et al. 1995; Lord et al. 1996a),and up to 88% (Gibson et al. 2000), of patients with neckpain after whiplash. In 53% of patients with headacheafter whiplash, the pain can be traced to the C2–3 joint(Lord et al. 1994).
Indications
Neckpainforwhichadiagnosis is requiredis theprimaryindication for cervical MBBs. To date, they have beenused only for the investigation of patients with chronicneck pain, but their judicious application in patients withsub-acutepain would beworthy ofexploration. Isolatingthe source of pain and instituting appropriate treatmentexpeditiously could serve to prevent chronicity.
Patient Selection
Studies in normal volunteers (Dwyer et al. 1990) and inpatients (Fukui et al. 1996) have shown that the cervi-cal zygapophysial joints generate somatic referred pain

C
Cervical Medial Branch Blocks 343
Cervical Medial Branch Blocks, Figure 3 A map of the referred painpatterns from cervical zygapophysial joints at the segments indicated.
in characteristic regions, specific to the segmental loca-tion of the joint stimulated (Fig. 3). These patterns canbe used to select the joints and nerves most likely to re-spond to blocks (International Spinal Intervention So-ciety 2004; Aprill et al. 1990).To optimise their efficiency, MBBs should be performedin patients with discrete areas of neck pain, which cor-respond to one or more of these areas of referred pain.Patients with more diffuse patterns of pain are less likelyto have identifiable joints as the source of pain.
Contraindications
Absolute contraindications include localised or sys-temic infection, a bleeding diathesis, and possiblepregnancy. Relative contraindications may include anallergy to contrast media or local anaesthetics, the con-current treatment with non-steroidal anti-inflammatorymedication including aspirin and neurological signs.� Radicular pain and chronic neck pain may co-exist.Whilst cervical medial branch blocks may alleviateneck pain and any � somatic referred pain, they willnot relieve radicular pain.
Evaluation
The value of diagnostic blocks lies in the informationthat they provide (International Spinal Intervention So-ciety 2004). For the blocks to be valid, the patient mustbe able to cooperate fully. They must understand that theprocedure is a diagnostic one, and it is neither designednor intended to be therapeutic. When multiple sourcesof pain are suspected, patients should understand that re-lief may occur in only a particular topographic area; andthey must be able to determine if they obtain relief in adiscrete area. They should also understand the use of avisual analogue scale or numerical pain rating scale.
Blocks should not be performed when the patient’s painis minimal, lest they be unable to distinguish the effectsof a block from natural fluctuations in pain. CervicalMBBs are not recommended in patients whose typicalpain is less than 40 on a 100 mm scale.The response to diagnostic blocks should be evaluatedimmediately after the procedure and for some time after-wards, at the location at which the block was performed,and by an independent observer using validated and ob-jective instruments and tools. Doing so avoids potentialerrors such as observer bias, patient or operator’s expec-tations, and recall bias. For a response to be judged posi-tive, relief of pain should be accompanied by restorationof activities that are normally limited by pain.
Utility
Cervical MBBs have diagnostic utility, in that they canpinpoint the source of the patient’s pain. Establishing afirm diagnosis prevents the futile pursuit of a diagnosisby other means. MBBs also have therapeutic utility.A positive response to blocks predicts a favourableoutcome from � radiofrequency neurotomy (Lord etal. 1996b).
References1. Aprill C, Dwyer A, Bogduk N (1990) Cervical Zygapophyseal
Joint Pain Patterns – II: A Clinical Evaluation. Spine 15:458–4612. Barnsley L, Bogduk N (1993) Medial Branch Blocks are Specific
for the Diagnosis of Cervical Zygapophyseal Joint Pain. RegAnaesth 18:343–350
3. Barnsley L, Lord S, Wallis B, Bogduk N (1993a) False-Positive Rates of Cervical Zygapophysial Joint Blocks. Clin JPain 9:124–130
4. Barnsley L, Lord S, Bogduk N (1993b) Comparative LocalAnaesthetic Blocks in the Diagnosis of Cervical ZygapophysealJoint. Pain 55:99–106
5. Barnsley L, Lord SM, Wallis BJ, Bogduk N (1995) The Preva-lence of Chronic Cervical Zygapophyseal Joint Pain afterWhiplash. Spine 20:20–26
6. Bogduk N (1982) The Clinical Anatomy of the Cervical DorsalRami. Spine 7:319–330
7. Butterworth JF, Strichartz GR (1990) Molecular Mechanisms ofLocal Anesthesia: A Review. Anesthesiology 72:711–734
8. Dwyer A, Aprill C, Bogduk N (1990) Cervical Zygapophy-seal Joint Pain Patterns – I: A Study in Normal Volunteers.Spine 15:453–457
9. Fukui S, Ohseto K, Shiotani M et al. (1996) Referred Pain Dis-tribution of the Cervical Zygapophyseal Joints and the CervicalDorsal Rami. Pain 68:79–83
10. Gibson T, Bogduk N, MacPherson J, McIntosh A (2000) CrashCharacteristics of Whiplash Associated Chronic Neck Pain. JMusculoskeletal Pain 8:87–95
11. International Spinal Intervention Society (2004) Cervical MedialBranch Blocks. In: Bogduk N (ed) Practice Guidelines for SpinalDiagnostic and Treatment Procedures. International Spinal In-tervention Society, San Francisco
12. Lord SM, Barnsley L, Bogduk N (1995) The Utility of Compara-tive Local Anaesthetic Blocks versus Placebo Controlled Blocksfor the Diagnosis of Cervical Zygapophyseal Joint Pain. Clin JPain 11:208–213
13. Lord S, Barnsley L, Wallis B, Bogduk N (1994) Third OccipitalNerve Headache: A Prevalent Study. J Neurol Neurosurg Psy-chiatry 57:1187–1190
14. Lord S, Barnsley L, Wallis BJ, Bogduk N (1996a) Chronic Cervi-cal Zygapophyseal Joint Pain after Whiplash: Placebo ControlledPrevalence Study. Spine 21:1737–1745

344 Cervical Medial Branch Neurotomy
15. Lord SM, Barnsley L, Wallis BJ, McDonald GJ, Bogduk N(1996b) Percutaneous Radiofrequency Neurotomy for ChronicCervical Zygapophyseal Joint Pain. N Eng J Med 335:1721–1726
Cervical Medial Branch NeurotomyJAYANTILAL GOVIND
Department of Anaesthesia, Pain Clinic, LiverpoolHospital, University of New South Wales, Sydney,NSW, [email protected]
Synonyms
Cervical Facet Denervation; Cervical RadiofrequencyNeurotomy
Definition
Cervical medial branch neurotomy is a treatment forneck pain or headache, stemming from one or more ofthe zygapophysial joints of thecervical spine. It involvescoagulating the nerves that innervate the painful joint,or joints, with an electrode inserted onto the nervesthrough the skin and muscles of the back of the neck.
Characteristics
Mechanism
Medial branch neurotomy achieves relief of pain byinterrupting the transmission of nociceptive informa-tion from a painful zygapophysial joint, by generatinga heat lesion in the nerves that mediate the pain (see� Electrophysiological Principles of RadiofrequencyNeurotomy).
Indications
Cervical medial branch neurotomy is not a treatmentfor any form of neck pain. It is explicitly and solelydesigned to relieve pain from the zygapophysial joints.Therefore, the singular indication for the procedure iscomplete, or near complete, relief of pain followingcontrolled, � diagnostic blocks of the nerves from thepainful joint or joints, i.e. � cervical medial branchblocks. These blocks must be controlled, because thefalse-positive rate of uncontrolled blocks is such thatresponses to single blocks will be false in up to 30%of patients, and those patients will not benefit from thedenervation procedure (Barnsley et al. 1993; Bogdukand Holmes 2000).
Technique
A detailed protocol has been produced by the Interna-tional Spinal Injection Society (International Spinal In-tervention Society 2004). In essence, the procedure isperformed under local anaesthesia, in a room equippedwith a fluoroscope and the necessary equipment to gen-
Cervical Medial Branch Neurotomy, Figure 1 A sketch of a top view ofthe course of a cervical medial branch. As the nerve follows a curved patharound the articular pillar, electrodes must be introduced along a sagittalplane and along a 30o oblique plane.
erate the lesions. Sedation should be avoided so that thepatient can be alert to any problems thatmight occurdur-ing the procedure, and which threaten their safety. Theobjective is to make a lesion as long as possible along thecourse of the target nerve. In order to capture the curvedcourseofeachcervicalmedialbranch, theelectrodemustbe introduced in both of two ways (Fig. 1). An obliquepass, about 30o lateral from the sagittal plane is used toreach the proximal part of the nerve, where it lays an-terolaterally to the articular pillar (or anterolaterally tothe C2/3 zygapophysial joint, in the case of the third oc-cipital nerve). The second pass is along the sagittal planeto reach the nerve where it lies laterally to the articularpillar.Along both the oblique pass and the sagittal pass, theelectrode is introduced through the skin and muscles ofthe posterior neck, so that its tip lies parallel to the targetnerve and against the articular pillar (or the C2–3 joint).At typical cervical levels, this requires inserting theelec-trode upwards from below the target level, for the nervescourse downwards as well as backwards (Fig. 2). Thethird occipital nerve runs transversely and so, can be ap-proached along a transverse plane instead of an inclinedone (Fig. 3).At each target point, two or three lesions need to bemade, in order to accommodate possible variations inthe course of the nerve (International Spinal Interven-tion Society 2004; Lord et al. 1998). Each lesion ismade by increasing the heating current gradually byabout 1˚C per second. Raising the temperature slowlyprovides time for both the patient and the physician toreact if any untoward sensations arise, either becausethe electrode has dislodged or because the target site hasnot been adequately anaesthetized; and for the physi-cian to respond before any injury occurs to the patient.Once a temperature of 80˚–85˚C has been achieved, it

C
Cervical Medial Branch Neurotomy 345
Cervical Medial Branch Neurotomy, Figure 2 Lateral radiograph of anelectrode, inserted along a sagittal path, in position to coagulate a C5 medialbranch. The course of the nerve is depicted by a dotted line.
Cervical Medial Branch Neurotomy, Figure 3 Lateral radiograph of anelectrode, inserted along a sagittal path, in position to coagulate the thirdoccipital nerve. The course of the nerve is depicted by a dotted line.
is maintained for about 90 seconds to ensure adequatecoagulation of the nerve.The procedure is repeated for all nerves that were anaes-thetized, inorder toproducereliefofpainduringthepriorconduct of diagnostic cervical medial branch blocks.
Variants
The optimal technique requires that the electrode beplaced parallel to the target nerves, and that multiple le-sions be made to accommodate variations in the courseof the nerve (International Spinal Intervention Society
2004; Lord et al. 1998; Lord et al. 1996a; McDonaldet al. 1999). Only this technique has been tested andshown to produce complete and lasting relief of pain.Variants are used by some operators, ostensibly in thebelief that the procedure is faster or easier. These vari-ants, however, have not been tested; and their efficacy isnot known (Bogduk 2002).
Efficacy
A controlled trial has shown that the effects of cervi-cal medial branch neurotomy cannot be attributed to aplacebo response (Lord et al. 1996a). When correctlyperformed, the efficacy of cervical medial branch neu-rotomy is genuine.Provided that patients are correctly selected using con-trolled cervical medial branch blocks, and provided thatthe optimal technique is used, good outcome can be ex-pected from cervical medial branch neurotomy. All pa-tients should obtain relief of their pain, which shouldbe evident as soon as the anaesthesia for the procedurewears off, and any postoperative pain abates. If such im-mediate relief is not evident, an error will have occurredeither during the diagnostic blocks or in the conduct ofthe procedure; both of which should then be reviewed.When neck pain is the target complaint, and joints belowC2/3 are treated, some 70% of patients obtain completerelief of their pain (Lord et al. 1998; Lord et al. 1996a;McDonaldetal.1999).Whenheadacheisthetargetcom-plaint,and the thirdoccipitalnerve is targeted, some85%of patients obtain complete relief (Govind et al. 2003).The cardinal reasons for initial failures are suboptimalplacement of electrodes or failure, during the conduct ofdiagnostic blocks, to recognize a source of pain from anadjacent joint.If complete relief of pain is achieved, it is attended byrestoration of activities of normal living, and no needfor other health care for the pain (Lord et al. 1998;Lord et al. 1996a; McDonald et al. 1999; Govind etal. 2003). Furthermore, it is associated with completeresolution of psychological distress, without any needfor psychological treatment (Wallis et al. 1997). Theprocedure is equally effective in patients who havecompensation claims as those who do not (McDonaldet al. 1999; Bogduk 2002; Govind et al. 2003; Sapir andGorup 2001).Relief of pain is not permanent. In time, the coagulatednerves regenerate and may again transmit nociceptiveinformation from the painful joint or joints. The timethat it takes for this regeneration to occur, depends onhow accurately and how thoroughly the nerves werecoagulated. After medial branch neurotomy at typicalcervical levels, patients can expect complete relief ofpain for at least 9 months, and up to 12 months orlonger (Lord et al. 1998; Lord et al. 1996a; McDonaldet al. 1999). The duration of relief after third occipitalneurotomy for headache is, on the average, slightlyshorter; some patients may maintain relief for only

346 Cervical Periradicular Epidural Steroid Injection
6 months, although durations longer than 12 monthshave been reported (Govind et al. 2003).Pain usually returns gradually; although it may not re-turn to its former intensity. If pain recurs and becomessufficiently intense again as to warrant treatment, cervi-cal medial branch neurotomy can be repeated in orderto reinstate relief. Patients can have multiple repetitionswithoutprejudicing their response(Lordetal.1998;Mc-Donald et al. 1999; Govind et al. 2003).
Complications
Provided that the correct technique is used, no compli-cations are associated with this procedure. Side-effectsare uncommon when the procedure is performed at typ-ical cervical levels (Lord et al. 1998); but are more com-mon when the third occipital nerve is coagulated. Theyinclude dysaesthesiae when medial branches with cuta-neous distributions are coagulated; and ataxia when thethirdoccipitalnerve iscoagulated.Thedysaesthesiaeareself-limiting and do not require treatment, as a rule. Theataxia is accommodated by the patient relying on visualcues for balance; and is readily tolerated in exchange forthe relief from headache.Whereas it may be believed by some that denervat-ing a joint will create a neuropathic joint (Charcot’sarthropathy), there is no evidence that this occurs, andno grounds for believing that it would occur (Lordand Bogduk 1997). Charcot’s arthropathy occurs inlimbs that have been completely denervated, in whichpotentially unstable joints are not protected by mus-cle activity. In contrast, the zygapophysial joints areintrinsically stable; they are stabilized further by theintervertebral disc, and most of the muscles that act onthe affected segment remain functional.
Utility
Cervical medial branch neurotomy is the singular meansby which pain from cervical zygapophysial joints canbe eliminated. No other forms of treatment have beenshown to be as effective for the treatment of proven cer-vical zygapophysial joint pain. No other form of treat-ment has been shown to consistently provide completerelief of neck pain or cervicogenic headache.Given that the prevalence of cervical zygapophysialjoint pain is in excess of 50% in patients with chronicneck pain after whiplash (Lord et al. 1994; Barnsley etal. 1995; Lord et al. 1996b; Gibson et al. 2000), andgiven that no other form of treatment has been shown tobe effective for these patients, cervical medial branchneurotomy has a potentially enormous application inpractice.
References1. Barnsley L, Lord S, Wallis B, Bogduk N (1993) False-
Positive Rates of Cervical Zygapophysial Joint Blocks. Clin JPain 9:124–130
2. Barnsley L, Lord SM, Wallis BJ, Bogduk N (1995) The Preva-lence of Chronic Cervical Zygapophysial Joint Pain afterWhiplash. Spine 20:20–26
3. Bogduk N (2002) Radiofrequency Treatment in Australia. PainPractice 2:180–182
4. Bogduk N, Holmes S (2000) Controlled Zygapophysial JointBlocks: The Travesty of Cost-Effectiveness. Pain Med 1:25–34
5. Gibson T, Bogduk N, Macpherson J, McIntosh A (2000) CrashCharacteristics of Whiplash Associated Chronic Neck Pain. JMusculoskeletal Pain 8:87–95
6. Govind J, King W, Bailey B, Bogduk N (2003) RadiofrequencyNeurotomy for the Treatment of Third Occipital Headache. JNeurol Neurosurg Psychiatry 74:88–93
7. International Spinal Intervention Society (2004) Cervical Me-dial Branch Neurotomy. In: Bogduk N (ed). Practice Guidelinesfor Spinal Diagnostic and Treatment Procedures. InternationalSpinal Intervention Society, San Francisco
8. Lord S, Barnsley L, Wallis B, Bogduk N (1994) Third Occip-ital Nerve Headache: A Prevalence Study. J Neurol NeurosurgPsychiatry 57:1187–1190
9. Lord S, Barnsley L, Wallis BJ, Bogduk N (1996b) ChronicCervical Zygapophysial Joint Pain after Whiplash: A Placebo-Controlled Prevalence Study. Spine 21:1737–1745
10. Lord SM, Barnsley L, Wallis B, McDonald GM, Bogduk N(1996a) Percutaneous Radio–Frequency Neurotomy for ChronicCervical Zygapophyseal Joint Pain. N Eng J Med 335:1721–1726
11. Lord SM, Bogduk N (1997) Treatment of Chronic Cervical Zy-gapophysial Joint Pain. N Engl J Med 336:1531
12. Lord SM, McDonald GJ, Bogduk N (1998) Percutaneous Ra-diofrequency Neurotomy of the Cervical Medial Branches: AValidated Treatment for Cervical Zygapophyseal Joint Pain. Neu-rosurgery Quarterly 8:288–308
13. McDonald GJ, Lord SM, Bogduk N (1999) Long Term Follow-Up of Patients Treated with Cervical Radiofrequency Neurotomyfor Chronic Neck Pain. Neurosurgery 45:61–68
14. Sapir DA, Gorup JM (2001) Radiofrequency Medial BranchNeurotomy in Litigant and Non-Litigant Patients with CervicalWhiplash. Spine 26:E268–E273
15. Wallis BJ, Lord SM, Bogduk N (1997) Resolution of Psycho-logical Distress of Whiplash Patients following Treatment byRadiofrequency Neurotomy: A Randomised, Double-Blind,Placebo-Controlled Trial. Pain 73:15û22
Cervical Periradicular Epidural SteroidInjection
� Cervical Transforaminal Injection of Steroids
Cervical Radiofrequency Neurotomy
� Cervical Medial Branch Neurotomy
Cervical Root Avulsion
Definition
Traumatic lesion of ventral and/or dorsal root, at the cer-vical level, consisting of detachment of the constitutingrootlets of the root from the spinal cord; main mecha-nism is stretching.� BrachialPlexusAvulsion and DorsalRootEntryZone

C
Cervical Transforaminal Injection of Steroids 347
Cervical Selective Nerve Root Injection
� Cervical Transforaminal Injection of Steroids
Cervical Transforaminal Injection ofCorticosteroids
Definition
The directed deposition of corticosteroid into the cervi-cal intervertebral neuroforamen.� Cervical Transforaminal Injection of Steroids
Cervical Transforaminal Injection ofSteroids
TIMOTHY R. LAIR, JAMES P. RATHMELL
Department of Anesthesiology, University of VermontCollege of Medicine, Burlington, VT, [email protected]
Synonyms
Cervical Periradicular Epidural Steroid Injection; Cer-vical Selective Nerve Root Injection
Definition� Cervical transforaminal injection of corticosteroids isa treatment for cervical � radicular pain in which cor-ticosteroids are delivered into a cervical intervertebralneuroforamen.
Characteristics
Cervical radicular pain affects about one personper 1,000 of population, per year (Radhakrishnan etal. 1994), and is most often caused by a disc herniationor foraminal stenosis. Its natural history can be favor-able (Bogduk et al. 1999), but not all patients recovernaturally. For relieving cervical radicular pain, conser-vative therapy, typically including graduated exerciseand oral analgesics, is supported only by observationalstudies, which have not controlled for natural history ornon-specific effects of treatment. The controlled studiesthat have been conducted have shown no significantbenefit for traction or exercises (British Association ofPhysical Medicine 1966; Goldie and Landquist 1970;Klaber et al. 1990). Surgery is the mainstay of treat-ment if conservative therapy fails (Chestnut et al. 1992;Ahlgren and Garfin 1996). Surgery, however, is notwithout risks, and constitutes a major undertaking forpatients.CTFIS constitutes an option for treatment, instead ofsurgery, when conservative therapy does not result inresolution of symptoms, and pain is the sole indicationfor treatment.
Rationale
The rationale for injecting steroids is that they suppressinflammation of the nerve, which is believed to be thebasis for radicular pain. The rationale for using a trans-foraminal route of injection, rather than an interlaminarroute, is that the injectate is delivered directly onto thetarget nerve. This ensures that the medication reachesthe target area in maximum concentration at the site ofthe suspected pathology.
Indications
Cervical radicular pain is the only indication for cervi-cal transforaminal injection of steroids. Radicular painis recognized by its dynatomal distribution, which isdistinctly different from the � dermatomes of the samenerve (Slipman et al. 1998). Confidence in the diagno-sis is enhanced if the patient also has � radiculopathy,although this may not always be evident. Paraesthesiae,segmental numbness, weakness, and loss of reflexesare reliable and valid signs of radiculopathy that allowthe diagnosis to be made clinically, without recourse toinvestigations. Disc protrusion and foraminal stenosisare the most common causes, but diagnostic imaging isrequired to exclude tumors and other infrequent causessuch as infection, trauma, or inflammatory arthritides(Boyce and Wang 2003).
Anatomy
The C3-C8 spinal nerves lie in the lower half of theirrespective intervertebral foramina. These foramina faceanterolaterally. The vertebral artery lies just anterior tothe exiting nerve (Fig. 1). Radicular branches from the
Cervical Transforaminal Injection of Steroids, Figure 1 A drawing of anaxial view of the cervical intervertebral foramen and adjacent structures atthe level of C6, with a needle inserted parallel to the axis of the foramen alongits posterior wall. Note the proximity of adjacent structures, IJV, internaljugular vein; CA, common carotid artery; VA, vertebral artery; C6, vertebralbody of C6; ScA, anterior scalene muscle, ScM, middle scalene muscle;sap, superior articular process of C5–6 zygapophysial joint. (Reproducedwith permission from Rathmell et al. 2004).

348 Cervical Transforaminal Injection of Steroids
Cervical Transforaminal Injection of Steroids, Figure 2 A sketch show-ing patient position and fluoroscope orientation to obtain an oblique viewof the cervical intervertebral foramina.
vertebral artery lie adjacent to the spinal nerve and itsroots to the spinal cord.
Technique (Rathmell et al. 2004)
The patient lies supine, and a correct oblique view of thetarget foramen is obtained with a fluoroscope (Fig. 2).The correct oblique view is critical because, in lessoblique views, the vertebral artery may lie along thecourse of the needle.Through a puncture point overlying the posterior halfof the target foramen, a 25 gauge, 2½ – 3½ inch nee-dle is passed into the neck, and then carefully readjustedto enter the foramen immediately in front of the ante-rior aspect of the superior articular process, at the mid-point of the foramen (Fig. 3a). Above this level, the nee-
Cervical Transforaminal Injection of Steroids, Figure 3 Right anterior oblique radiograph demonstrating a needle in position along the posterior aspectof the right C6–7 intervertebral foramen. Inset of mid portion of image with bony structures labeled: SAP, Superior Articular Process; La, Lamina; Ped,Pedicle; IAP, Inferior Articular Process; SpP, Spinous Process; C6, C6 vertebral body; C7, C7 vertebral body. (b) Anteroposterior radiograph demonstratingneedle in final position within the right C6–7 intervertebral foramen. The needle lies halfway between the medial and lateral borders of the articularpillars. Inset of mid portion of image with bony structures labeled: SpP, Spinous Processes of C5, C6, and C7; Facets, medial and lateral aspect of thefacet column; TrP (T1), Transverse Process of T1. (Reproduced with permission from Rathmell et al. 2004).
dle may encounter veins; below it, the needle may en-counter the spinal nerve and its arteries. The needle muststay in contact with the posterior wall to avoid the verte-bral artery. On anteroposterior view, the tip of the needleshould not be advanced past the midpoint of the articularpillar (Fig. 3b). Insertion beyond this depth risks punc-turing the dural sleeve or thecal sac.Under direct, real-time fluoroscopy, a small volume ofnon-ionic contrast medium (1.0 ml or less) is injected.The solution should outline the proximal end of thespinal nerve and spread centrally toward the epiduralspace (Fig. 4). Real-time fluoroscopy is essential tocheck for inadvertent intra-arterial injection, whichmay occur even if the needle is correctly placed. Intra-arterial injection is manifested by very rapid clearanceof the injected contrast material. In a vertebral artery,the contrast material will streak in a cephalized di-rection. In a radicular artery, it will blush briefly in atransverse direction medially towards the spinal cord.In either instance, the needle should be withdrawn andthe procedure should be postponed until after a periodlong enough for the puncture to have healed.Sometimes the contrast medium may fill epiradicularveins. These are recognized by the slow clearance of thecontrast medium, characteristic of venous flow. In thatevent, the needle should be adjusted by either slightlywithdrawing the needle, or redirecting it to a positionslightly lower on the posterior wall of the foramen.Only a small volume of contrast medium (1.0 ml or less)is required to outline the dural sleeve of the spinal nerve.As it spreads onto the thecal sac, the contrast mediumwill assume a linear configuration (Fig. 4). Rapid di-lution of the contrast medium implies subarachnoid

C
Cervical Transforaminal Injection of Steroids 349
Cervical Transforaminal Injection of Steroids,Figure 4 Anteroposterior radiograph demonstrating needle in fi-nal position within the right C6–7 intervertebral foramen after injectionof 1 ml of radiographic contrast medium (iohexol 180 mg/ml). Contrastoutlines the spinal nerve and extends along the lateral aspect of theepidural space above the foramen (arrows). (Reproduced with permissionfrom Rathmell et al. 2004).
spread, which may occur if the needle has puncturedthe thecal sac or a lateral dilatation of the dural rootsleeve into the � intervertebral foramen. In that event,the procedure should be abandoned and rescheduledto avoid potential subarachnoid deposition of localanesthetic or steroid. Once the target nerve has beencorrectly outlined, a small volume of a short-actinglocal anesthetic (lidocaine 1%, 0.5 to 1.5 ml) is injectedin order to anaesthetize the target nerve. While ensur-ing that the needle has not displaced, the procedure iscompleted by injecting a small dose of corticosteroid(betamethasone, 3 – 6 mg, or triamcinolone 20 – 40 mg).
Complications
A case report has detailed fatal spinal cord infarctionfollowing CTFIS (Brouwers et al. 2001). Another re-port referred to several unpublished cases in Australia,Europe, and the USA in which patients suffered severeneurologic sequelae (Rathmell et al. 2004). Injectionof corticosteroid into a radicular artery is one plausiblemechanism for neurologic injury to occur (Baker Ret al. 2002). Meticulous attention to real-time fluoro-scopic imaging is required to avoid such complications(Rathmell et al. 2004; Baker et al. 2002).
Outcomes
There are no randomized controlled trials comparingCTFIS to placebo or other treatments. The literature islimited to three small observational studies.
Bush and Hillier (1996) treated patients with three dif-ferent forms of injection therapy: cervical or brachialplexus block, CTFIS, and x-ray guided, interlaminarepidural steroid injection. They reported that 76% ofpatients achieved complete relief of arm pain, but it isnot possible from their report to derive what proportionresponded to transforaminal injections.Slipman et al. (2000) reported good or excellent results,at 12–45 month follow-up, in 60% of 20 patients treatedwith an average of 2.2 injections. They did not, however,provide separate results for each category of outcome.Vallee et al. (2001) studied 34 patients with cervi-cal radiculopathy with refractory symptoms after twomonths of medical management. Good or excellentresults were reported in 53% of 32 patients at sixmonths, after an average of 1.3 injections. At threemonths, 29% of patients had complete relief of pain.This proportion persisted at six months, but diminishedto 20% at 12 months.These studies appear to paint an encouraging picture oftheroleforCTFIS.However, thissentimentmustbe tem-peredbytherelatively lowlevelofevidencethesestudiesprovide.
Caveats
CTFIS is an emerging therapy whose efficacy has notbeen corroborated by controlled studies. Yet it is asso-ciated with seriouscomplicationswhose incidence isnotproperly known. Although a possible option for cervicalradicular pain, it should only be undertaken by operatorsfamiliar with the relevant anatomy, with sufficient expe-rience and skill to maximize the safety of the procedure.
References1. Ahlgren BR, Garfin SR (1996) Cervical Radiculopathy. Orthop
Clin North Am 27:253–2632. Baker R, Dreyfuss P, Mercer S, Bogduk N (2002) Cervical Trans-
foraminal Injection of Corticosteroids into a Radicular Artery: APossible Mechanism for Spinal Cord Injury. Pain 103:211–215
3. Bogduk N (1999) Medical Management of Acute Cervical Radic-ular Pain. An Evidence-Based Approach. Newcastle Bone andJoint Institute, Newcastle Australia
4. Boyce BH, Wang JC (2003) Evaluation of Neck Pain, Radicu-lopathy, and Myelopathy: Imaging, Conservative Treatment, andSurgical Indications. Instr Course Lect 52:489–95
5. British Association of Physical Medicine (1966) Pain in the Neckand Arm: A Multicentre Trial of the Effects of Physiotherapy.Brit Med J 1:253–258
6. Brouwers PJAM, Kottnik EJBL, Simon MAM, Prevo RL (2001)A Cervical Anterior Spinal Artery Syndrome after DiagnosticBlockade of the Right C6-Nerve Root. Pain 91:397–399
7. Bush K, Hillier S (1996) Outcome of Cervical RadiculopathyTreated with Periradicular/Epidural Corticosteroid Injections: AProspective Study with Independent Clinical Review. Eur SpineJ 5:319–325
8. ChestnutRM, AbitholJJ, GarfinSR (1992)Surgical Managementof Cervical Radiculopathy. Orthop Clin North Am 23:461–474
9. Goldie I, Landquist A (1970) Evaluation of the Effects of Dif-ferent Forms of Physiotherapy in Cervical Pain. Scand J RehabMed 2–3:117–121
10. Klaber Moffett JA, Hughes GI, Griffiths P (1990) An Investiga-tion of the Effects of Cervical Traction. Part 1: Clinical Effec-tiveness. Clin Rehab 4:205–211

350 Cervical Zygapophysial Joint Blocks
11. Radhakrishnan K, Litchy WJ, O’Fallon WM, Kurland LT (1994)Epidemiology of Cervical Radiculopathy. A Population-BasedStudy of Rochester, Minnesota, 1976 – 1990. Brain 117:325–335
12. Rathmell JP, Aprill C, Bogduk N (2004) Cervical TransforaminalInjection of Steroids. Anesthesiology 100:1595–1600
13. Slipman CW, Lipetz JS, Jackson HB, Rogers DP, Vresilovic EJ(2000). Therapeutic Selective Nerve Root Block in the Non-Surgical Treatment of Atraumatic Cervical Spondylotic Radic-ular Pain: A Retrospective Analysis with Independent ClinicalReview. Arch Phys Med Rehabil 81:741–746
14. Slipman CW, Plastaras CT, Palmitier RA, Huston CW, SterenfeldEB (1998) Symptom Provocation of Fluoroscopically GuidedCervical Nerve Root Stimulation. Are Dynatomal Maps Identicalto Dermatomal Maps? Spine 23:2235–42
15. Vallee JN, Feydy A, Carlier RY, Mutschler C, MompointD, Vallee CA (2001) Chronic Cervical Radiculopathy: Lat-eral Approach Periradicular Corticosteroid Injection. Radiol-ogy 218:886–892
Cervical Zygapophysial Joint Blocks
� Cervical Medial Branch Blocks
CFA
Synonyms
Complete Freund’s Adjuvant
Definition
Complete Freund’s Adjuvant is used in animal experi-ments to induce inflammation.� Complete Freund’s Adjuvant� Substance P Regulation in Inflammation
C Fiber
� C Afferent Axons/Fibers
c-Fos
Definition
A gene that codes for a transcription factor (Fos). c-foscan be switched on rapidly as a result of various stimuli,and its product regulates the expression of various othergenes in the cell. Fos protein, which can be detected byimmunocytochemistry, can be used to demonstrate thata neuron has been activated, and, is therefore used as amarker tomapneuronal recruitment tostimuli, includingnoxious stimuli. In addition, c-Fos may play a role inactivating ’late response’ genes.� Alternative Medicine in Neuropathic Pain� c-Fos Immediate-Early Gene Expression
� Freezing Model of Cutaneous Hyperalgesia� Nociceptive Processing in the Hippocampus and
Entorhinal Cortex, Neurophysiology and Pharma-cology
� Opioid Receptors at Postsynaptic Sites� Spinothalamic Tract Neurons, Role of Nitric Oxide
c-Fos Immediate-Early Gene Expression
Definition
c-Fos is one of a family of genes, called „immediate-early genes,“ which are expressed very soon after asalient environmental event (e.g. pain). The proteinsencoded by immediate-early genes act as transcriptionfactors to affect the expression of other genes. By usingimmunohistochemistry for Fos, the protein product ofc-fos, one can identify with single cell resolution thoseneurons that „responded“ to the noxious stimulus, s.also c-Fos.� c-Fos� Heritability of Inflammatory Nociception
CFS
� Cutaneous Field Stimulation
CGRP
� Calcitonin Gene Related Peptide� Calcitonin Gene-Related Peptide and Migraine
Headaches� CGRP and Spinal Cord Nociception
CGRP and Spinal Cord NociceptionANDREA EBERSBERGER
Department of Physiology, Friedrich SchillerUniversity of Jena, Jena, [email protected]
Synonym
Calcitoningene-relatedpeptideandspinalcordnocicep-tion; Spinal Cord Nociception and CGRP

C
CGRP and Spinal Cord Nociception 351
Definition� Calcitonin gene-related peptide (CGRP) isa37 aminoacid peptide of the calcitonin family with two isoforms,α andβCGRP, with similar biological functions (Poyner1992). The neuropeptide is synthesized in up to 50% ofthe small- and medium-sized dorsal root ganglion neu-rons (DRGs) and is transported along the axon to the pe-ripheral endings (Donnerer et al. 1992) and to the cen-tral endings of the neuron in the dorsal horn of the spinalcord. In addition to its role in nociception, CGRP is in-volved in a number of other functions including vasodi-lation.
Characteristics
Localization of Spinal CGRP
Fibers showing CGRP-immunoreactivity are locatedin the dorsal horn of the spinal cord in laminae I andII at high density and in lamina V at lower density(Wiesenfeld-Hallin et al. 1984). CGRP-like immunore-activity and CGRP mRNA are also localized in mo-toneurons of the ventral horn.
Localization of CGRP Receptors
The density of CGRP receptors is highest in the superfi-cial and deep dorsal horn, but there are also receptors inthe ventral horn. The distribution of CGRP binding sitesis thus similar to the distribution of CGRP positive fibersbut they may even be located at sites where no CGRP-containing fibers are terminating. These receptors mightbe reached by the neuropeptide by diffusion within thetissue.Immunostaining of RCP, an essential component of theCGRP receptor complex, corroborated the distributionof CGRP receptors in the spinal cord. The distributionof the CGRP receptor subtypes, CGRP1-receptor (cor-responding to CRLR/RAMP1) and CGRP2-receptor inthe spinal cord has not been investigated.Under pathophysiological conditions such as peripheralinflammation, increases and decreases in binding sitesfor CGRP have been observed (Galeazza et al. 1992).Notonlythereceptorbutalsoitsaccessoryprotein(RCP)can be regulated in inflammatory or neuropathic painstates (Ma et al. 2003).
Release of CGRP
There is a high basal release of CGRP from centralendings of afferents in the spinal cord, which wasshown with antibody-coated microprobes (Schaible etal. 1994; Morton and Hutchison 1989). This release isnot influenced by activating peripheral afferents withinnocuous stimuli or motor activity in the physiologicalrange. Noxious mechanical stimuli, however, increasethis basal release (Morton and Hutchison 1989). Thesituation changes during peripheral inflammation. Dur-ing acute knee inflammation, mechanical stimuli ofinnocuous intensity to the knee induce spinal CGRPrelease (Schaible et al. 1994). This is probably caused
by a sensitization of the afferents to mechanical stimuli.Additionally basal release is much higher in inflamedthan in normal animals (Collin et al. 1993). This mayresult from an up-regulation of the synthesis of CGRPthat has been observed in the acute and chronic stageof inflammation.
CGRP Receptor Agonists and Antagonists
There are two CGRP receptor subtypes, namely CGRP1and CRGP2, which both bind the endogenous ligandsCGRPα and CGRPβ. The subtypes are characterized bythe abilities of the fragment CGRP8 – 37 to antagonizethe effect of CGRP (CGRP1) and the linear agonisticanalog [Cys(ACN)2,7 ]hCGRPα to mimic the effect ofCGRP (CGRP2). BIBN4096BS, the first potent non-peptide antagonist preferentially binds to the CGRP2receptor (Watling 2001).
Effect of Spinal CGRP
Released CGRP can exert its action directly by bindingto CGRP receptors. However, it also interacts with therelease and metabolism of substance P. CGRP can fa-cilitate release of substance P and, in addition, CGRPcontrols the amount of substance P by inhibiting the en-zymaticdegradationofsubstanceP(Dugganetal.1992).Behavioral ExperimentsIn behavioral experiments, intrathecally applied CGRPfacilitated the responses to noxious stimulation (e.g.Wiesenfeld-Hallin et al. 1984) and antagonization ofendogenous CGRP with CGRP8-37, a CGRP1 recep-tor antagonist, was antinociceptive. CGRP was alsoshown to support the generation and maintenance of� mechanical allodynia and � hyperalgesia in rats.CGRP8-37 alleviated mechanical and � thermal allo-dynia in chronic central pain. Thus CGRP has a role innormal nociception but it is also involved in pain states(reviewed by Schaible et al. 2004).
Effect on Neuronal Activity
Application of CGRP in the vicinity of spinal cordneurons caused no, or only weak, excitation of theneurons (Ryu et al. 1988). But CGRP has a facilitatoryeffect on evoked activity in spinal cord neurons, e.g.activities evoked by innocuous or noxious mechanicalstimulation or substance P (Biella et al. 1991). CRGPis also involved in the development and maintenanceof spinal hyperexcitability. This effect was shown in amodel of knee joint inflammation where CGRP or theantagonist CGRP8-37 had been ionophoretically appliedin the vicinity of spinal cord neurons that responded tomechanical stimulation of the leg (Fig. 1).Since � glutamate receptors are of major importance inthe excitation of spinal nociceptive neurons, a possibleinteraction between the responses of spinal cord neu-rons to CGRP and � NMDA or � AMPA was investi-gated.Coadministration ofCGRPand AMPAorNMDAenhanced the responses to the excitatory amino acids

352 Channel Inactivation
CGRP and Spinal Cord Nociception, Figure 1 The development of kneejoint inflammation is paralleled by the development of spinal hyperexcitabil-ity measured as an increase in neuronal responses to repetitive noxiouspressure applied to the knee joint (upper trace). When CGRP8−37wasionophoretically applied during and 90 min after induction of inflammationin the vicinity of the recorded neurons the development of spinal hyper-excitability was prevented (Neugebauer et al. 1996).
(Ebersberger et al. 2000). Thus one explanation for thespinaleffectofCGRPis its influenceon� glutamatergicneuronal transmission.
References1. Biella G, Panara C, Pecile A, Sotgiu ML (1991) Facilitatory role
of calcitonin gene-related peptide (CGRP) on excitation inducedby substance P (SP) and noxious stimuli in rat spinal dorsal hornneurons. Brain Res 559:352–356
2. Donnerer J, Schuligoi R, Stein C (1992) Increased content andtransport of substance P and calcitonin gene-related peptide insensory nerves innervatin inflamed tissue: evidence for a reg-ulatory function of nerve growth factor in vivo. Neuroscience49:693–698
3. Duggan AW, Schaible HG, Hope PJ, Lang CW (1992) Effect ofpeptidase inhibition on the pattern of intraspinally released im-munoreactive substance P detected with antibody microprobes.Brain Res. 579:261–269
4. Ebersberger A, Charbel Issa P, Venegas H, Schaible HG (2000)Differential effects of calcitonin gene-related peptide andcalcitonin gene-related peptide8-37 responses to N-methyl-D-aspartate or (R,S)-α-amino-3-hydroxy-5-methylisoxazole-4-propionate in spinal nociceptive neurons with knee joint inputin the rat. Neuroscience 99:171–178
5. Galeazza MT, Stucky CL, Seybold VS (1992) Changes in125IhCGRP binding sites in rat spinal cord in an experimentalmodel of acute, peripheral inflammation. Brain Res 591:198–208
6. Ma W, Chabot J-G, Powell KJ et al. (2003) Localization andmodulation of calcitonin gene-related peptide-receptor compo-nent protein-immunoreactive cells in the rat central and periph-eral nervous system. Neuroscience 120:677–694
7. Morton CR, Hutchison WD (1989) Release of sensory neuropep-tides in the spinal cord: studies with calcitonin-gene related pep-tide and galanin. Neuroscience 31:807–815
8. Neugebauer V, Rümenapp P, Schaible H-G (1996) Calcitoningene related peptide is involved in the generation and mainte-nance of hyperexcitability of dorsal horn neurons observed during
development of acute inflammation in rat’s knee joint. Neuro-science 71: 1095–1109
9. Poyner DR (1992) Calcitonin gene related peptide: multiple ac-tions, multiple receptors. Pharmac Ther 56:23–51
10. Ryu PD, Gerber G, Murase K, Randic M (1988) Actions of cal-citonin gene-related peptid on rat spinal dorsal horn neurons.Brain Res. 441:357–361
11. Schaible H-G, Freudenberger U, Neugebauer V et al. (1994) In-traspinal release of immunoreactive calcitonin gene-related pep-tide during development of inflammation in the joint in vivo –a study with antibody microprobes in cat and rat. Neuroscience62:1293–1304
12. Schaible H-G et al. (2004) Involvement of CGRP in nociceptiveprocessing and hyperalgesia: Effects of CGRP on spinal and dor-sal root ganglion neurons. In: Brune K, Handwerker HO (eds)Hyperalgesia: Molecular Mechanisms and Clinical Implications.Progress in Brain Resarch and Management, vol 30. IASP Press,Seattle, pp 201–227
13. Watling KJ (2001) The Sigma-RBI handbook of receptor classi-fication and signal transduction. Sigma-RBI, Natick, pp 82–83
14. Wiesenfeld-Hallin S, Hökfelt T, Lundberg JM et al. (1984) Im-munoreactive calcitonin-gene related peptide and substance Pcoexist in sensory neurons in the spinal cord and interact in spinalbehavioral responses of the rat. Neurosci Lett 52:199–204
Channel Inactivation
Definition
A period of silencing (due to the inability to re-open)after an ion channel opens and then closes.� Painful Channelopathies
Channelopathies
Definition
Channelopathies are disorders in which absence of ionchannels, abnormal function of ion channels, or deploy-ment of an aberrant of ensemble of ion channels produceclinical symptoms.� Migraine, Pathophysiology� Painful Channelopathies
Charcot-Marie-Tooth Disease
Synonyms
CMT
Definition
CMT is any inherited neuropathy that is not part of asyndrome.� Hereditary Neuropathies
C-Heat Receptor
� Polymodal Nociceptors, Heat Transduction

C
Chemotactic Cytokines 353
Chemesthesis
Definition
Sensitivity to all chemicals thatproducesensationsotherthan (or in addition to) taste or smell.� Nociception in Nose and Oral Mucosa
Chemical Lesion
Definition
Selective lesion of neuronal cell bodies of the CNS. Itconsists of injecting a concentrated solution of an exci-tatory amino-acid that can normally excite the neuronsat high concentration. At high concentration, the aminoacid (glutamic, kainic, quisqualic, ibotenic acids) canproduce selective neuronal death (cell bodies only spar-ing nerve fibers) by excitotoxicity.� Thalamotomy, Pain Behavior in Animals
Chemical Sympathectomy
� Sympathetic Blocks
Chemical Transmitter
� Nociceptive Neurotransmission in the Thalamus
Chemoattractants
Definition
Chemoattractants have been divided into two cate-gories. One category is represented by the classicalchemoattractants like platelet activating factor (PAF),leukotriene B4 (LTB4), formyl-methionyl-leucyl-phenylalanine (FMLP), and complement protein C5a.The second category consists of compounds belong-ing to the chemokine group. Both classical chemoat-tractants and chemokines act on target cells throughseven-transmembrane domain receptors that are cou-pled to heteromeric G-proteins and elicit chemotacticresponses.� Neutrophils in Inflammatory Pain
Chemokines
Synonyms
Chemotactic Cytokines
Definition
Chemokines are cytokines with chemoattractant prop-erties, inducing cells with the appropriate receptors tomigrate towards the source of the chemokines, whichincludes the family of proinflammatory activation-inducible cytokines. These proteins are mainly chemo-tactic for different cell types. Based on chromoso-mal locations of individual genes, two different sub-families of chemokines are distinguished as CXC-chemokines (CXCL; also known as alpha-chemokinesor 4q chemokine family) and CC-chemokines (CCL;also known as beta-chemokines or 17q chemokine fam-ily). In the earliest phases of inflammation, chemokinesare released and induce direct chemotaxis in nearbyresponsive cells. Together with intercellular adhesionmolecules, chemokines and their receptors serve tolocalize and enhance the inflammatory reaction at thesite of tissue damage.� Cytokines as Targets in the Treatment of Neuropathic
Pain� Cytokines, Effects on Nociceptors� Cytokine Modulation of Opioid Action� Neutrophils in Inflammatory Pain
Chemosensation
Definition
Sensations initiated through chemicals, e.g. gustatoryor olfactory mediated sensations or sensations mediatedthrough the intranasal trigeminal nerves.� Nociception in Nose and Oral Mucosa
Chemosensitive Sympathetic AfferentFibers
Definition
Afferentfibers that transmit informationresultingfromavariety of chemicals that are released during myocardialischemia.
Chemotactic
Definition
Achemical (sodiummorrhuate)used inprolotherapyso-lutions, which acts by attracting inflammatory cells.� Prolotherapy
Chemotactic Cytokines
� Chemokines

354 Chemotherapy
Chemotherapy
Definition
Treatment with drugs that kill cancer cells that may begiven by oneormoreof the followingmethods:orally,byvenous or arterial injection (through a catheter or port),or topically.� Cancer Pain Management, Chemotherapy� Cancer Pain Management, Treatment of Neuropathic
Components
Chemotherapy-Induced Neuropathy
Definition
A group of drugs used in chemotherapy are associatedwith a peripheral neuropathy. Vincristine was the firstdrug in thisgroup.Themostcommonly used chemother-apy agents that produce a painful neuropathy, which isalso associated with a sensory loss, are Cisplatin (andCarboplatin) and Taxol. These two drugs bind to tubulinin theaxoplasm and reduce theanterogradeslowcompo-nent of axoplasmic transport. This makes the nerves sus-ceptible to chronic compression, which can be helped bydecompression of the involved nerves. The most recentdrug to be used for chemotherapy that has an associatedneuropathy is Thalidomide.� Ulceration, Prevention by Nerve Decompression
Chest Pain
Definition
Chest pain is often caused by coronary artery disease,but can originate from non-cardiac structures such as theesophagus. The most prominent feelings are pressure,squeezing and/or crushing on the chest.� Visceral Pain Model, Angina Pain
Chiari Type I Malformation
Definition
This is a protrusion of the cerebellar tonsils, below theforamen magnum, which can cause a valve-like obstruc-tion to the flow of cerebrospinal fluid.� Primary Cough Headache
Childhood Migraine
� Migraine, Childhood Syndromes
Childhood Sexual Abuse
Definition
Any child below the age of consent may be deemed tohave been sexually abused when another sexually ma-ture person has, by design or by neglect of their usual so-cietal or specific responsibilities in relation to that child,engaged or permitted the engagement of that person inany activity of a sexual nature that is intended to lead tothe sexual gratification of the sexually mature person.This definition pertains whether or not it involves geni-tal contact or physical contact, and whether or not thereis discernible harmful outcome in the short-term.� Chronic Pelvic Pain, Physical and Sexual Abuse
Chiropractic
Definition
Therapeutic manipulation of the spine to treat a wide va-riety of conditions by correcting dysfunction in spinalalignment.� Alternative Medicine in Neuropathic Pain� Spinal Manipulation, Characteristics� Spinal Manipulation, Pain Management
Chloride Transporter
Synonyms
Cl– Transporter
Definition
A chloride transporter is a membrane protein that assistsin the movement of ions across the surface membraneof a neuron. The result can be a greater concentration ofchloride ions on one or the other side of the membrane.� GABA Mechanisms and Descending Inhibitory
Mechanisms
Chloro-phenyl-2-methylaminocyclohexanone-hydrochloride
� Postoperative Pain, Ketamine
Cholecystokinin
Synonyms
CCK

C
Chronic Back Pain and Spinal Instability 355
Definition
An eight amino acid peptide present in the gastroin-testinal tract and in the nervous system that modulatespain sensation as well as other neuronal processes. Itwas named for its effects on the gall bladder, but alsothought to have pro-nociceptive effects in the spinalcord.� Alternative Medicine in Neuropathic Pain� Pain Modulatory Systems, History of Discovery� Peptides in Neuropathic Pain States� Placebo Analgesia and Descending Opioid Modula-
tion
Chondrocytes
Definition
Chondrocytes are cells that produce cartilage by secre-tion of the cartilaginous matrix. The secretion of thematrix by chondrocytes leads to their encapsulation inthis matrix where they eventually undergo programmedcell death, or apoptosis. As a consequence, new chon-drocytes constantly arise from their precursor cells.Chondrocytes arise from chondroblasts, which arisefrom mesenchymal cells.� Arthritis Model, Osteoarthritis
Chromosomes
Definition
Chromosomes contain the cell’s genetic information,and are structured as compact intertwined molecules ofDNA located in the nucleus of cells.� NSAIDs, Pharmacogenetics
Chronic Abdominal Pain of Childhood
� Recurrent Abdominal Pain in Children
Chronic Back Pain and Spinal InstabilityKENE UGOKWE
1, AJIT KRISHNANEY1,
MICHAEL STEINMETZ1, EDWARD BENZEL1, 2
1The Cleveland Clinic Foundation, Department ofNeurosurgery, Cleveland, OH, USA2The Cleveland Clinic Foundation, Cleveland ClinicSpine Institute, Cleveland, OH, [email protected]
Synonyms
Dysfunctional Segmental Motion; Mechanical LowBack Pain; Lumbago; Back Pain; Myofacial pain syn-drome; Muscle Spasm; Discogenic pain; Painful DiscSyndrome
Definition
Chronic back pain is defined as pain in the dorsal aspectof the trunk (from the neck to the pelvis) that persistsfor more than twelve weeks (Gatchel 1986). It may berelated to degenerative, neoplastic, traumatic or infec-tious conditions. Chronic back pain may also be relatedto spinal � instability. Spinal instability is defined as theinability of the spine to limit patterns of movement ordisplacement that may lead to deformity or pain. Otherentities that are particularly worthy of definition are me-chanical back pain and myofacial pain syndrome, disco-genic pain, pain of soft tissue injury origin and pain ofbony tissue injury origin:
• Mechanical back pain – a deep and agonizing painthat increases with activity, such as the assumptionof the upright posture (loading) and decreases withinactivity, such as assuming the supine position (un-loading).
• Myofacialpain syndrome–synonymouswithmusclespasm or strain. It is usually self-limiting. There oftenexists an underlying cause.
• Discogenic low back pain – pain that originates fromthe intervertebral disc and the disc space.
• Pain of soft tissue injury origin – such pain originatesfrom the damage or destruction of richly innervatedsoft tissue. It may occur after surgery and is also seenwith muscle tear.
• Pain of bony tissue destruction origin – pain that isassociated with bony distortion. It is usually associ-ated with weakened bone, as may be seen with tumor,infection, or trauma.
Characteristics
Chronic back pain is common. Eighty five percent ofcases are idiopathic. Potential anatomical sources ofback pain include muscle, ligaments, tendons, bones,� facet joints and discs. In many cases, it is difficultto determine the exact cause of back pain because ofsignificant overlap in the nerve supply to the aforemen-tioned structures. Approximately 80% of Americansexperience clinically-significant back pain. Eighty toninety percent of the attacks resolve within 6 weeks(Bigos 1994). It is the second most common reason forwhich people seek medical attention (Cypress 1983).Back pain accounts for 15% of all sick leave and it isthe most common cause of disability for people lessthan 45 years of age (Cunningham 1984).Spinal instability is a common cause of back pain. Someof the causes of spinal instability include age related

356 Chronic Back Pain and Spinal Instability
degenerative changes, prior spinal surgery, physicallydependent occupations, sedentary lifestyles, obesity,poor posture and certain sporting activities. In a pa-tient with chronic back pain, a diagnosis to consider isspinal tumor. Pain at night that is relieved by aspirinmay be suggestive of an osteoid osteoma or a benign� osteoblastoma. Infections such as discitis (an infec-tion of the disc space between the vertebral bodies)must also be ruled out. Spinal � compression fracturesmay also be the source of severe back pain, particularlyin the elderly. Other potential etiologies of chronic backpain include:
Degenerative Conditions
• Degenerative spondylolisthesis: slippage of one ver-tebral body over another (Pearcy 1983).
• � Spinal stenosis• Lateral recesssyndrome: the lateral recess is thechan-
nel alongside the pedicle where the exiting nerve rootresides.
Spondyloarthropathies
• Paget’s disease: this is a condition characterized byareas of abnormal bone growth and an increased rateof bone resorption.
• Ankylosing spondylitis: this is a connective tissuedisease characterized by inflammation of the spineand joints resulting in pain and stiffness.
It is important to note that all of the aforementioned con-ditions contribute to or cause spinal instability. Certainpatients, however,havenoorganicdiseaseand theirbackpain is � psychogenic in nature. This may be as a resultof secondary gain, i.e. financial or emotional gain (Wad-dell 1980).
Spinal Instability
There are two categories of spinal instability: (1) Acutespinal instability, and (2) Chronic spinal instability.Acute spinal instability may be further divided intoovert and limited instability, while chronic instability issubcategorized into glacial instability and dysfunctionalsegmental motion (Benzel 2001). Denis described thethree-column concept of identifying criteria for insta-bility of the spine (Denis 1983).
The Three Column Concept of Spinal Integrity and Stability
The spine is divided into three columns.
• Anterior column – composed of the ventral half ofthe disc and the vertebral body, including the anteriorlongitudinal ligament.
• Middle column – composed of the dorsal half of thedisc and vertebral body and the posterior longitudinalligament
• Posterior column – the dorsal bony complex (poste-rior arch) and the dorsal ligamentous complex, in-
Chronic Back Pain and Spinal Instability, Table 1 Quantitation of AcuteInstability for Subaxial Cervical, Thoracic, and Lumbar Injuries (The PointSystem)
Condition Points Assigned
Loss of integrity of anterior and middle column 2
Loss of integrity of posterior columns 2
Acute resting translational deformity 2
Acute resting angulation deformity 2
Acute dynamic translation deformityexaggeration
2
Acute dynamic angulation deformityexaggeration
2
Neural element injury 3
Acute disc narrowing at the level of suspectedpathology
1
Dangerous loading anticipated 1
(Panjabi 1994; White 1990)
cluding the supraspinous and interspinous ligamentsand the ligamentum flavum.
Many authors have used a point system approach toquantify the extent of acute instability. White and Pan-jabi described the accumulation of 5 or more pointsas being indicative of spinal instability (Panjabi 1994;White 1990) (Table 1). They also described a stretch testin which the progressive addition of cervical tractionweight was accompanied by clinical assessments andradiographs. The test was positive for instability whena disc interspace separation of greater than 1.7 mm, ora change in angle greater than 7.5 degrees between preand post stretch measurements, was observed. Mostclinicians do not employ this method due to the risksinvolved and its cumbersome nature. Flexion and ex-tension radiographs or MRI (Dvorak 1991) may alsobe helpful in determining the degree of instability.
Acute Instability
Overt Instability
Overt instability is defined as the inability of the spine tosupport the torso during normal activity. This is usuallyacute in nature, e.g. after a trauma. It also has a chroniccomponent, and may also occur in the setting of tumor,infection, or � degenerative disease. It is characterizedby circumferential loss of spinal integrity. Treatmentmay involve surgical stabilization, with or without de-compression. The back pain experienced with overtinstability is usually associated with soft tissue injuryand muscle spasms (Fig. 1a).
Limited Instability
Limited instability is characterized by loss of either ven-tral or dorsal spinal integrity. Posterior column disrup-tion is not always associated with instability, unless the
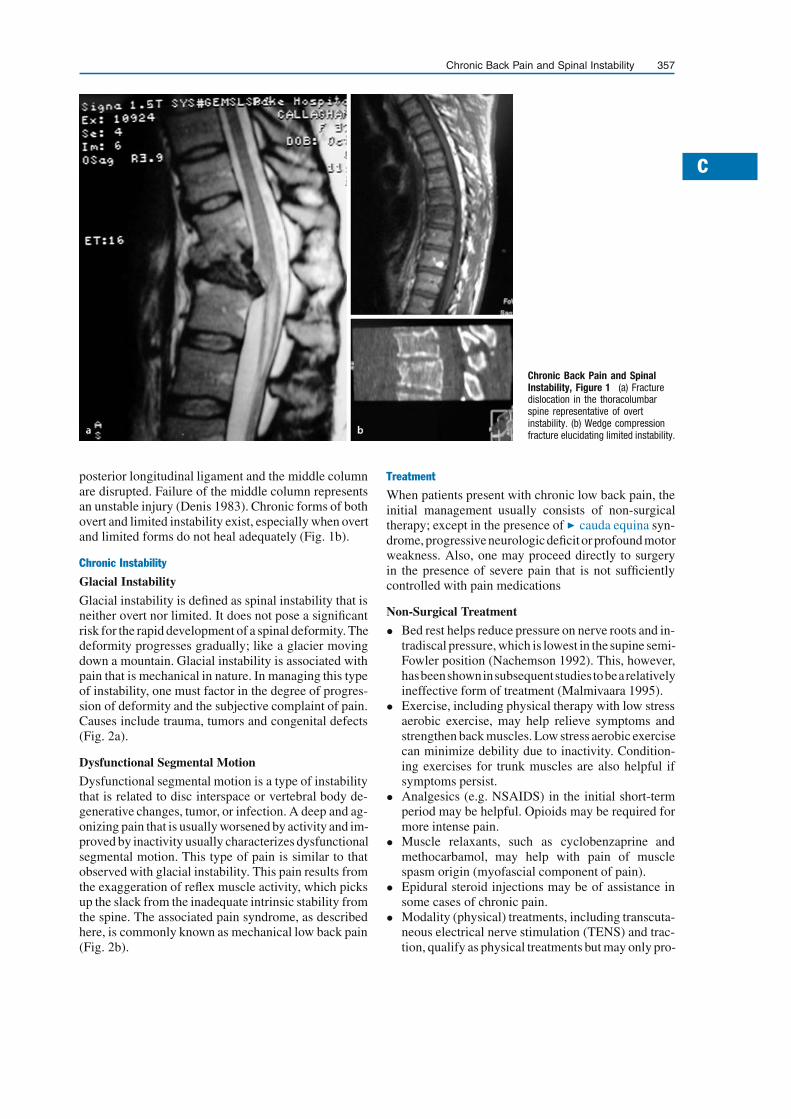
C
Chronic Back Pain and Spinal Instability 357
Chronic Back Pain and SpinalInstability, Figure 1 (a) Fracturedislocation in the thoracolumbarspine representative of overtinstability. (b) Wedge compressionfracture elucidating limited instability.
posterior longitudinal ligament and the middle columnare disrupted. Failure of the middle column representsan unstable injury (Denis 1983). Chronic forms of bothovert and limited instability exist, especially when overtand limited forms do not heal adequately (Fig. 1b).
Chronic Instability
Glacial Instability
Glacial instability is defined as spinal instability that isneither overt nor limited. It does not pose a significantrisk for the rapid development of a spinal deformity. Thedeformity progresses gradually; like a glacier movingdown a mountain. Glacial instability is associated withpain that is mechanical in nature. In managing this typeof instability, one must factor in the degree of progres-sion of deformity and the subjective complaint of pain.Causes include trauma, tumors and congenital defects(Fig. 2a).
Dysfunctional Segmental Motion
Dysfunctional segmental motion is a type of instabilitythat is related to disc interspace or vertebral body de-generative changes, tumor, or infection. A deep and ag-onizing pain that is usually worsened by activity and im-proved by inactivity usually characterizes dysfunctionalsegmental motion. This type of pain is similar to thatobserved with glacial instability. This pain results fromthe exaggeration of reflex muscle activity, which picksup the slack from the inadequate intrinsic stability fromthe spine. The associated pain syndrome, as describedhere, is commonly known as mechanical low back pain(Fig. 2b).
Treatment
When patients present with chronic low back pain, theinitial management usually consists of non-surgicaltherapy; except in the presence of � cauda equina syn-drome,progressiveneurologicdeficitorprofound motorweakness. Also, one may proceed directly to surgeryin the presence of severe pain that is not sufficientlycontrolled with pain medications
Non-Surgical Treatment
• Bed rest helps reduce pressure on nerve roots and in-tradiscal pressure, which is lowest in the supine semi-Fowler position (Nachemson 1992). This, however,hasbeenshowninsubsequentstudiestobearelativelyineffective form of treatment (Malmivaara 1995).
• Exercise, including physical therapy with low stressaerobic exercise, may help relieve symptoms andstrengthen back muscles. Low stress aerobic exercisecan minimize debility due to inactivity. Condition-ing exercises for trunk muscles are also helpful ifsymptoms persist.
• Analgesics (e.g. NSAIDS) in the initial short-termperiod may be helpful. Opioids may be required formore intense pain.
• Muscle relaxants, such as cyclobenzaprine andmethocarbamol, may help with pain of musclespasm origin (myofascial component of pain).
• Epidural steroid injections may be of assistance insome cases of chronic pain.
• Modality (physical) treatments, including transcuta-neous electrical nerve stimulation (TENS) and trac-tion, qualify as physical treatments but may only pro-

358 Chronic Central Pain Models
Chronic Back Pain and Spinal Instability, Figure 2 (a) Spondylolisthesis in the lumbar spine which is an example of glacial instability. (b) Lumbarcanal stenosis and degenerative disc disease showing dysfunctional segmental motion.
vide minor relief for some patients. � Biofeedbackhas been advocated for chronic low back pain (Bush1985).
• Injection therapy, including trigger point and liga-ment injections,arecontroversialandareofequivocalefficacy. Acupuncture has been studied in random-ized clinical trials for chronic low back pain. Thestudies have been mostly contradictory. This, how-ever, should not discount the fact that they may beeffective for a subset of people.
Surgical Treatment
In patients with compressive lesions, surgery (decom-pression; e.g. � laminectomy) is the next step whenconservative therapy fails (Holdsworth 1963). Fusioninstrumentation is appropriate in the refractory patientwith mechanical low back pain. The goal of surgicalintervention for mechanical low back pain is stabiliza-tion of unstable spinal segments. Spinal fusion is anaccepted therapy for fracture/dislocation or acute in-stability that may result from tumor or infection. It alsomay be used in selected patients with glacial instabilityor dysfunctional segmental motion. It is important tonote that the use of spinal instrumentation increasesthe fusion rate (Lorenz 1991), but not necessarily theclinical outcome.
References1. Benzel EC (2001) Biomechanics of Spine Stabilization: Stability
and Instability of the Spine. AANS Press, pp 29–432. Bigos S, Bowyer O, Braen G et al. (1994) Acute Low Back Prob-
lems in Adults. Clinical Practice Guideline 14. AHCPR Publica-tion No. 95-0642. Agency for Healthcare Policy and Research,Public Health Service, U.S. Department of Health and HumanServices, Rockville, MD
3. Bush C, Ditto B, Feuerstein M (1985) A Controlled Evaluationof Paraspinal EMG Biofeedback in the Treatment of ChronicLow Back Pain. Health Psychol 4:307–321
4. Cunningham LS, Kelsey JL (1984) Epidemiology of Muscu-loskeletal Impairments and Associated Disability. Am J PublicHealth 74:574–579
5. Cypress BK (1983) Characteristics of Physician Visits for BackSymptoms: A National Perspective. Am Journal of Public Health73:389–395
6. Denis F (1983) The Three Column Spine and its Significance inthe Classification of Acute Thoracolumbar Spine Injuries. Spine8:817–831
7. Dvorak J, Panjabi MM (1991) Functional Radiographic Diagno-sis of the Lumbar Spine: Flexion-Extension and Lateral Bending.Spine 16:562–571
8. Gatchel RJ, Mayer TG, Capra P et al. (1986) Quantification ofLumbar Function, VI: The Use of Psychological Measures inGuiding Physical Functional Restoration. Spine 11:36–42
9. Holdsworth FW (1963) Fractures, Dislocations, and Fracture-Dislocations of the Spine. J Bone Joint Surg 45B:6–20
10. Lorenz M, Zindrick M (1991) A Comparison of Single LevelFusion With and Without Hardware. Spine 16:455–458
11. Malmivaara A, Hakkinen U, Aro T (1995) The Treatment ofAcute Low Back Pain – Bed Rest, Exercises, or Ordinary Ac-tivity? N Engl J Med 322:351–355
12. Nachemson AL (1992) Newest Knowledge of Low Back Pain.A Critical Look. Clin Orthop 279:8–20
13. Panjabi MM, Lydon C (1994) On the Understanding of ClinicalInstability. Spine 19:2642–2650
14. Pearcy M, Shepherd J (1983) Is there Instability in Spondylolis-thesis? Spine10:461–473
15. Waddell G, McCulloch JA, Kummel E et al. (1980) Non-organicPhysical Signs in Low Back Pain. Spine 5:117–25
16. White AA, Panjabi MM (1990) Clinical Biomechanics of the
Spine, 2nd edn. Lippincott, Philadelphia, pp 30–342
Chronic Central Pain Models
� Spinal Cord Injury Pain Model, Hemisection Model

C
Chronic Daily Headache in Children 359
Chronic Constriction Injury Model
Synonyms
CCI Model
Definition
This is a nerve injury model of persistent pain. It consistof a partial nerve injury, mostly used in rodents, that isproduced by tying several ligatures around a nerve, suchthat these ligatures slightly constrict the nerve. This in-duces an incomplete nerve injury that entails behavioralsigns of hyperalgesia in the animals.� Neuropathic Pain Model, ChronicConstriction Injury� Neuropathic Pain Model, Partial Sciatic Nerve Liga-
tion Model� Nociceptive Processing in the Hippocampus and En-
torhinal Cortex, Neurophysiology and Pharmacology� Peptides in Neuropathic Pain States� Purine Receptor Targets in the Treatment of Neuro-
pathic Pain
Chronic Daily Headache
� New Daily Persistent Headache
Chronic Daily Headache in ChildrenPATRICIA A. MCGRATH
The Hospital for Sick Children and University ofToronto, Toronto, ON, [email protected]
Synonyms
Headache; CDH; Transformed Migraine
Definition
Chronic daily headache (CDH) is an almost continualheadache in the absence of organic pathology (Holdenet al. 1994). This relatively new diagnostic category wascreated to characterize individuals who did not meet thecriteria for episodic tension or migraine headaches, butinstead presented with chronic daily pain.
Characteristics
In 1994, Silberstein and colleagues proposed a new setof diagnostic criteria for chronic daily headache thatincluded 4 types seen in clinical practice, � transformedmigraine headache, � chronic tension type headache,� new daily persistent headache and � hemicraniacontinua headache, as defined below (Silberstein et al.1994). Gladstein and Holden (1996) evaluated whetherthese new criteria were adequate for diagnosing a clin-ical sample of 37 children with CDH. Almost half the
children (45%) did not fit within the four types of CDH.Instead, these children had a pattern of intermittentmigraines with an underlying daily tension headache,thus leading the authors to propose a fifth diagnosticcategory of � comorbid headache.
Proposed Diagnostic Classification for Pediatric Chronic DailyHeadache
Transformed Migraine
A chronic daily (or near daily) headache that developedgradually over time from a pre-existing, well-definedmigraine headache. Headache is longer than 4 h perday, can include a mixture of autonomic and tension-type symptoms and symptoms have progressed withincreasing frequency and decreasing severity over atleast 3 months.
Chronic Tension-type
Very frequent headaches (>180 episodes per year) thatdeveloped gradually over at least 3 months from pre-existing tension-type headache. Pain has pressing orsqueezing quality, bilateral location and there is a rela-tive absence of autonomic nervous system symptoms.
New Daily Persistent
Abrupt onset of head pain that continues on a daily basis,with no history of pre-existing migraine or tension-typeheadache. Pain episodes last longer than 4 h per day andhave been present for greater than one month.
Hemicrania Continua
Daily unilateral headache for at least 1 month. Pain iscontinuous but fluctuating, moderately severe, lacksprecipitating triggers and responds positively to in-domethacin.
Comorbid Headache
Daily tension-type headache, accompanied by intermit-tent and less frequent episodes of well-defined migraineheadache.Large descriptive studies should be conducted for chil-dren to establish age and sex-related data on the clinicalfeatures of CDH in children. At present, our knowledgeof CDH in children is derived primarily from a few caseseries (Esposito and Gherpelli 2004; Gladstein et al.1993; Hershey et al. 2001). Such studies indicate thatCDH typically has a bifrontal, rather than uni-laterallocation. Children and adolescents often describe theheadache as diffuse, e.g. “All over, or around my head”,instead of a specific region. Headache episodes varywidely in length from lasting only a few minutes to al-most continuously. In my clinical experience, childrenusually report that the headache “lasts all day”. They donot know exactly when they first notice the headachein the morning – some children describing noticingit when they first open their eyes in bed, while otherchildren notice the headache when they are brushingtheir teeth, eating breakfast, or dressing for school.

360 Chronic Daily Headache in Children
Children have similar difficulty in determining exactlywhen the headache ends each day – often noting that itis present until they fall asleep. Children rarely reportthat the headache disturbs their sleep at night.Headache intensity also varies considerably amongchildren. Some children report a consistently mild pain,whileother children describeasevereand incapacitatingheadache. Some children report that the pain intensityvaries throughout the day, while other children reportthat the pain is constant, regardless of the time of dayor their activities. Some of the children, who rate theirheadache as very strong, do not appear distressed bytheir continual pain – almost exhibiting “� la belle in-difference”. They explain that the pain does not botherthem because they have learned to adjust to it.
Prevalence of CDH in Children
Prevalence estimates of headache in children range from1.4–27% for migraine headache and from 6.3–49%for other types of headache (McGrath 2001). Theseestimates differ widely due to differences among epi-demiological studies in the sampling method used toidentify children, the age and sex of children studied,the diagnostic criteria used to classify headache, thecountry of origin and the presentation and analysis ofdata.At present, we do not know the prevalence of CDHfor children and adolescents in the general populationaccording to age, gender and the diagnostic categorieslisted above. The overall rate of CDH has been estimatedas low (<1%) in community samples (Abu-Arefeh andRussell 1994; Sillanpää et al. 1991), but this rate mayunderestimate the actual prevalence because most epi-demiological studies of childhood headache have notdetermined prevalence by headache frequency (Mc-Grath 2001). The prevalence of CDH for children whoseek treatment at specialized pediatric clinics is notknown, although in my experience approximately 15%of children with headache have CDH with half of thesechildren experiencing an associated emotional prob-lem. Rossi and colleagues (1992) describe a prevalencerate of 4.6% for children with daily headache andpsychological problems in their clinical sample.
Pathophysiology
Many questions remain about the pathophysiologyof recurrent headache in children, especially CDH(Holden et al. 2001). As noted previously in the sec-tion on diagnostic classification, CDH has differentexpressions in children and adults and the differentexpressions may reflect several different etiologies or adevelopmental continuum. Most childhood headaches,including CDH, are not caused by an underlying diseaseor disorder. While a positive family history predisposeschildren to develop headache, many environmental,biological and psychological processes are relevant.Despite widely held beliefs that many environmental
and physical stimuli (e.g. foods, weather conditions andactivities) can trigger recurrent headache attacks, theevidence base for these presumed triggers is negligible.Heredity is important, but certain cognitive, behavioraland emotional factors are critical for triggering attacks,increasing pain, prolonging disability or maintaining acycle of almost daily headache (McGrath and Hillier2001).While CDH in children probably involves both centraland peripheral nervous systems, the specific interplayof systems is not known. Similarly, the extent to whichvascular and muscular components are involved is un-known and may differ according to the type of CDH. Todate, no studies have examined the pathophysiology ofCDH in children, so that our understanding is presumedrather than documented and based primarily on extrapo-lation from adult studies. For some cases with migrainefeatures, presumed mechanisms include a neurogenicinflammatory cascade, vascular reactivity and serotonin(5-HT), while for other cases, mechanisms may includepericranial muscle tenderness or musculoskeletal ab-normalities as noted recently for adults (Holden et al.2001; Lipchik et al. 1996). Serotonergic dysregulationhas been postulated as a common point of neurotrans-mitter abnormality in anxiety, depression and migraine(Rossi et al. 1992). In view of the association betweenCDH and features of depression and anxiety in a subsetof children, serotonin dysfunction may also play a rolein CDH.
Risk Factors and Impact
Almost all studies of childhood headache evaluatedemographic and psychosocial factors in an effort toidentify potential risk factors that may predispose chil-dren to develop headache. However, only a few studieshave focused on CDH. Holden and colleagues (1994)compared 3 groups of children (CDH, migraine andboth CDH and migraine) with respect to the impact ofheadache, children’s coping and headache disability.Children with CDH had higher rates of concurrentpsychiatric diagnoses, missed more school days andtended more to blame others as a coping mechanism incomparison to children with migraine headache.Galli and colleagues (2004) noted psychiatric disordersin approximately 64% of children with CDH, espe-cially sleep and anxiety disorders. From my clinicalexperience, a subset of children with CDH also havelong-standing emotional problems suggestive of mooddisorders, anxiety disorders and somatoform disorders.Many of these children satisfy the existing IHS diagnos-tic criteria outlined for chronic tension-type headacheunassociated with disorder of pericranial muscles (pre-viously described as chronic psychogenic headache),even though these children do not necessarily satisfy thecriteria for a DSM-IV diagnosis (as required for codinganxiety, etc. as a causative factor). At present, we donot know whether this subset of CDH is associated with

C
Chronic Daily Headache in Children 361
a particular one (or more) of the diagnostic categorieslisted above.
Management of CDS
Drug Therapy
Drug therapies for treating children’s headache includeanalgesics, ergot derivatives, serotonin receptor ago-nists, antiemetics, β-blockers, serotonin antagonists,tricyclic antidepressants, antihistamines, calcium chan-nel blockers and antiepileptics (Levin 2001). Yet theirefficacy has generally been accepted on the basis ofstudies with adults rather than demonstrated in con-trolled trials with children and adolescents. At present,we lack data about which drugs are best for childrenwith CDH or its subtypes.Dosing guidelines for prophylactic medication for chil-dren with CDH are based on their use for children withfrequent migraine. Holden and colleagues (2001) rec-ommend that only those children with severe headachewho exhibited significant functional disability shouldbe considered for prophylaxis. Rothner (2001) recom-mends that if effective, children should use prophylacticmedication for 4–6 months and then be weaned. If noteffective, the medication should be discontinued after6–10 weeks and another medication tried. The dosingguidelines for the common prophylactic medicationsused for childhood headache are listed in Table 1.Randomized controlled trials are needed to evaluatethe efficacy of the varied drug therapies for treatingCDH in children and adolescents. In my clinical experi-ence, many children benefit from a combined drug andnon-drug protocol, including a low dose schedule ofamitriptyline, a tricyclic antidepressant, combined witha cognitive-behavioral pain management program.
Nondrug Therapy
A diverse array of nondrug therapies are used to treatchildren’s headache, including counseling, guidedimagery, hypnosis, biofeedback, behavioral manage-ment,acupuncture,massage,chiropracticmanipulation,homeopathic remedies, naturopathic approaches andherbal medicines (McGrath and Hillier 2001).
Cognitive-behavioral Therapies
Cognitive therapy, designed to modify an individual’sbeliefs, expectations and coping abilities, is an intrin-sic component of all headache treatment. Health careproviders educate families about the circumstancesthat cause headache, often counseling them about howthey can alter those circumstances (e.g., lifestyle man-agement, diet, sleep, exercise). In addition, childrenmay learn specialized stress management techniques aspart of a treatment program and families may receiveguidance about how to minimize headache related dis-ability. In some programs, therapists teach childrenhow to use individual cognitive pain control methods,
such as attention and distraction, guided imagery andhypnosis to lessen their pain.Behavior therapy, often used in combination with cog-nitive therapy, is targeted either for children themselvesor for the adults who respond to them when they expe-rience headache. At the initial consultation, health careproviders may assess whether children’s behaviors orthose of key adults (parents, teachers or coaches) areinfluencing the pattern and severity of headache attacks.If so, they recommend how they should change theirbehaviors to improve pain control and lessen disability.Strong and consistent evidence supports the efficacy ofmost cognitive and behavioral therapies for relievingchildren’s headache. However, all studies have focusedon either migraine or general recurrent headache, sothat we lack definitive evidence about the efficacy ofthese cognitive-behavioral therapies specifically forCDH. Alternatively, psychologists and therapists coun-sel families about the impact of their behaviors andassist families to make required changes using operantconditioning programs.Many of these cognitive-behavioral therapies share acommon “child-centered” focus, addressing the uniquecausative and contributing factors for each child’sheadache. Although the evidence base supporting theirefficacy for relieving childhood headache is strong,there are no controlled trials evaluating their efficacyfor children with CDH.
Physical Techniques
Physical techniques include thermal stimulation, visualmodulation, transcutaneous nerve stimulation (TENS),acupuncture, massage and chiropractic or osteopathicmanipulation. Although each technique has been used totreat headache in children, almost no studies have beenconducted to evaluate their efficacy objectively. Instead,physical techniques are recommended primarily on thebasis of clinical experience and anecdotal information.
Summary
CDH is a relatively new diagnostic category that de-scribes an almost continual headache in the absenceof organic pathology. The management of CDH inchildren is exceptionally challenging. The current prin-ciples guiding our management of CDH in children andadolescents are extrapolated from the existing literatureon childhood headache, CDH in adults and our clinicalexperience.A child-centered focus is particularly important in thetreatment of CDH because it is not caused by an under-lying disease or disorder. Optimal treatment of CDHbegins with the differential diagnosis and a compre-hensive pain assessment to identify relevant causativeand contributing factors. These factors may vary amongchildren, even children presenting with seemingly iden-tical headache symptoms. In our experience, childrenbenefit from a combined drug and nondrug regimen.

362 Chronic Daily Headache in Children
Chronic Daily Headache in Children, Table 1 Drugs used in the prophylaxis of childhood headache
Drug Dosage _Comments
Beta-blockers
Propranolol 1–3 mg kg−1 day−1 as b.i.d. Side effects: fatigue, bradycardia, hypotension, depression.Contraindications: asthma, heart block, bradyarrhythmias, diabetes,congestive heart failure. Avoid abrupt withdrawal.
Tricyclic antidepressants
Amitriptyline 0.2–2.0 mg kg−1 day−1 as t.i.d. dose Side effects: weight gain, drowsiness, anticholinergic effects.Contraindication: cardiac disease.
Serotonin antagonists
Pizotifen 0.5 mg t.i.d. (may use0.5–1.5 mg kg−1 as t.i.d. dose)
Side effects: sedation, weight gain. Start small dose at night andincrease at weekly intervals to t.i.d. dose.
Methysergide 2–6 mg day−1 Side effects: retroperitoneal fibrosis. Discontinue for 1 month every3–6 months. Use in adolescents only.
Calcium channel blockers
Flunarizine 5 mg day−1 Side effects: bradycardia, hypotension, weight gain, drowsiness.Contraindications: depression, extrapyramidal disorders.
Antihistamines
Cyproheptadine Age 2–6 yr: 2 mg q8 –12 h
(max 12 mg day−1)Age 7–14 yr: 4 mg q8–12 h(max 16 mg day−1)
Side effect: drowsiness
Antiepileptics
Valproate 10–50 mg kg−1 day−1 as b.i.d. dose Side effects: hepatoxicity, thrombocytopenia. Start at low dose andincrease at weekly intervals.
Gabapentin 300–400 mg t.i.d. Start at 100 mg t.i.d. and increase daily by 100 mg t.i.d. to maximumdose.
Abbreviations: b.i.d., twice a day; t.i.d., three times a day; q 8–12 h, every 8–12 h (Levin 2001)
Although the specific drug(s) are selected in accordancewith the needs of individual children, our clinical ex-perience has led us to begin treatment with a combinedprotocol of amitriptyline concurrent with a cognitive-behavioral pain management program. Children learnspecific nondrug pain strategies to complement thedrug therapy, while a therapist assists them to identifyand address any contributing factors (e.g. unresolvedsituation-specific stressors, excessive disability andemotional problems). Some children may also receivea formal psychiatric evaluation.Although special effort should be expended towardsstudying children and adolescents with CDH, a dualchallenge for the future is to integrate a child-centeredapproach more efficiently into clinicalpractice. We needto evaluate therapies according to individual children,beginning by identifying which children respond opti-mally (i.e. immediately or with a major improvement) todrug, nondrug and multimodal therapies. Future studiesshould be designed to identify the child characteristicsthat should enable us to better match treatments toindividual children, as well as to headache type.
References1. Abu-Arefeh I, Russell G (1994) Prevalence of headache and mi-
graine in schoolchildren. Bmj 309:765–7692. EspositoSB, Gherpelli JL (2004)Chronic daily headaches inchil-
dren and adolescents: a study of clinical characteristics. Cepha-lalgia 24:476–482
3. Galli F, Patron L, Russo PM et al. (2004) Chronic daily headachein childhood and adolescence: clinical aspects and a 4-yearfollow-up. Cephalalgia 24:850–858
4. Gladstein J, Holden EW (1996) Chronic daily headache inchildren and adolescents: a 2-year prospective study. Headache36:349–351
5. Gladstein J, Holden EW, Peralta L et al. (1993) Diagnoses andsymptom patterns in children presenting to a pediatric headacheclinic. Headache 33 497–500
6. Hershey AD, Powers SW, Bentti AL et al. (2001) Characteriza-tion of chronic daily headaches in children in a multidisciplinaryheadache center. Neurology 56:1032–1037
7. Holden EW, Gladstein,J, Trulsen M et al. (1994) Chronic dailyheadache in children and adolescents. Headache 34:508–514
8. Holden EW, Bachanas P, Kullgren K et al. (2001) Chronic DailyHeadache in Children and Adolescents. In: McGrath PA, HillierLM (eds) The Child with Headache: Diagnosis and Treatment.IASP Press, Seattle, pp 221–241
9. Levin SD (2001) Drug Therapies for Childhood Headache. In:McGrath PA, Hillier LM (eds) The Child with Headache: Diag-nosis and Treatment. IASP Press, Seattle, pp 109–127

C
Chronic Gynaecological Pain, Doctor-Patient Interaction 363
10. Lipchik GL, Holroyd KA, France CR et al. (1996) Central andperipheral mechanisms in chronic tension-type headache. Pain64:467–475
11. McGrath PA, Hillier LM (2001) The Child with Headache: Di-agnosis and Treatment. IASP Press, Seattle
12. Rossi LN, Cortinovis I, Bellettini G et al. (1992) Diagnostic crite-ria for migraine and psychogenic headache in children. Dev.MedChild Neurol 34:516–523
13. Rothner AD (2001) Differential Diagnosis of Headaches in Chil-dren and Adolescents. In: McGrath PA, Hillier LM (eds) TheChild with Headache: Diagnosis and Treatment. IASP Press,Seattle, pp 57–76
14. Silberstein SD, Lipton RB, Solomon S et al. (1994) Classifica-tion of daily and near-daily headaches in the headache clinic.Proposed revision to the International Headache Society crite-ria. In: Olesen J (ed) Frontiers in Headache Research: HeadacheClassification and Epidemiology, vol 4. Raven Press, New York,pp 117–126
15. Sillanpää M, Piekkala P, Kero P (1991) Prevalence of headacheat preschool age in an unselected child population. Cephalalgia11:239–242
Chronic Gynaecological Pain,Doctor-Patient Interaction
R. WILLIAM STONES
Princess Anne Hospital, University of Southampton,Southampton, [email protected]
Synonyms
Doctor-Patient Communication; Therapeutic Relation-ships
Definition
The proposition that patient outcomes in � chronicpelvic pain are influenced by the quality of interactionbetween patient and doctor.
Characteristics
While it is a truism that across the spectrum of illnessand disease, patients link their outcomes to experi-ences in consultations with particular doctors, thereare specific factors to consider in the case of chronicgynaecological pain. The nature of the condition andassociated symptoms mean that women are often dis-tressed and anxious about associated issues such asfertility and sexuality. Women frequently report unsat-isfactory and dismissive attitudes during consultationsfor pain (Grace 1995) and this has been ascribed toinappropriately persistent mechanistic views of paincausation (Grace 1998). Gynaecologists trained into atechnical diagnostic and therapeutic role experience adissonance between patient expectations for explana-tion and support and their own approach of detectingdisease and disengaging once its apparent absence isestablished, despite patients’ ongoing symptoms ofpain.
What Do Doctors Think About Women with Pelvic Pain? (Selfeet al. 1998a)
To obtain primary data on medical attitudes, focus groupdiscussionswereconducted with groupsofgeneralprac-titioners, gynaecologists and patients. Themes commonto all groups were expression of the need to find a patho-logical cause for the pain, something that would providea diagnosis. Issues relating to time were discussed byall groups and this was particularly related by hospitalgynaecologists and GPs to aspects of communication.Both groups of doctors were aware of the possible stressrelated and psychological influences of pain, althoughpatients seemed to avoid direct discussion of psycholog-ical factors which may have been related to their pain.Themes particular to general practitioners were diagno-sis by exclusion, especially with respect to � irritablebowel syndrome (IBS) and � pelvic inflammatory dis-ease (PID). They stated that the lack of a firm diagnosismeant that dealing with patients with CPP could be diffi-cult, particularly those patients who have experienced a’negative’ laparoscopy. If no visible pathology was seenat laparoscopy to account for the pain, GPs found it dif-ficult to know how to proceed with persistent patients.A provisional diagnosis, even if it was considered im-precise, could provide a label by which to justify thepatient’s symptoms. This applied especially to IBS and“pelvic congestion”GPs recognised the value of effective communication,but acknowledged that a good rapport with a patient wasunlikely to develop after one short visit. GPs also com-mented on the complexity of a complaint in which it wasnecessary to sort out “the emotional components of theproblem”Hospital gynaecologists implied that identifying pathol-ogy would somehow validate the pain as ’real’. Whenvisible pathology had been excluded by previous refer-rals to other specialities such as gastroenterology, com-ments included “some patients are going to be afraid thatyou’re going to think it’s a psychological problem” and“they [the patients] come in and they say, I’m not madyou know” There was a clear awareness that an anxiouspatientmay makediagnosisdifficult and thatpatientsarealarmed by the suggestion of a psychological diagnosis,because they will be ’labelled’. Hospital gynaecologistswere acutely aware of the time sometimes necessary todealeffectively with patients suffering from CPP.Devel-opment of rapport was found to be “difficult to establishin one outpatient session” If needed, consultation timewas extended, but doctors were concerned that “you’refilling up the waiting room” and there was anxiety that if,for example, a patient starts to divulge adverse psycho-sexual experiences, it may well become a lengthy con-sultation; the doctor thinks “Oh hell! I’ve got three pa-tients in the waiting room” After a negative laparoscopyhospital gynaecologists felt the need to look for othercauses, asking the question “Have I missed something"?

364 Chronic Gynaecological Pain, Doctor-Patient Interaction
They recognised this as problematic, as the patient is dis-heartened by not having a diagnosis, a ’label’ by whichto define her problem.It was hypothesised that a propensity to inwardly di-rected � hostility might underlie some of the difficultyexperienced by some patients in establishing rapport(Fry and Stones 1996). However, further work high-lighted the importance of the individual clinician andconsultation in influencing outcomes. Disease factorsare of course also important; in statistical models theinteraction between disease states and the consultationsetting was identified. In women referred to a hospi-tal gynaecology department for symptoms present forat least 6 months, continuing pain 6 months after aninitial consultation was predicted by the presence ofendometriosis, but also by the patient’s initial reportof pain interfering with exercise, her rating of the ini-tial medical consultation as less satisfactory and theindividual clinician undertaking the consultation. Inter-estingly, the outcomes were not affected by the doctor’sgrade or gender (Selfe et al. 1998b), although there hasbeen much attention in women’s health literature tothe gender imbalance among gynaecologists and themismatch with women’s preference to see a femaledoctor in many countries. In this study there was aninteraction between the impact of pain on exercise andthe extent to which the patient’s rating of the qualityof the consultation was associated with probability ofpain resolution. For the group where exercise was notimpaired, there was a significant association, whereasthis was not the case among those in whom exercisewas impaired by pain (Fig. 1). It may be that those with
Chronic Gynaecological Pain,Doctor-Patient Interaction,Figure 1 Fitted probabilities of painresolution and women’s rating ofinitial consultation, with and withoutexercise impairment. (Reproducedwith permission from Selfe et al.1998b).
less impairment are more amenable to the therapeuticeffect of a good consultation.
Lasting Influences of Consultations
The dimensions within which women recalled consul-tations 6 months later were examined. Lasting impres-sions of the doctor-patient interaction that had takenplace could be characterised in terms of the constructs“affect”, “expectation” and “cognition” (Stones et al.2006). The first describes social interaction and theemotional response felt by the patient. It relates towhether the doctor is recalled as approachable andexpressing a friendly interest in and concern for thepatient. Opposite recollections would not necessarilymean that the doctor had been unpleasant or rude to thepatient, but may simply reflect a businesslike manner,a hurried consultation or the use of technical jargon.The construct “cognition” relates to memory and un-derstanding, a pre-requisite for adherence to treatment.Often patients do not understand what they have beentold, are afraid to ask questions and forget much of whathas been said during a consultation. Under such circum-stances it is not unreasonable that patients who weregiven little information or could not remember much ofthe detail of the encounter would find it unsatisfactory.The items loading to the subscale denoted “expectation”relate to the patient’s wish to understand her problemand what the implications may be for the future. Womenexpected to be given a diagnosis and as a result a cure.If this expectation was not fulfilled, patients describedthe situation as ‘disappointing’ or felt that they had been‘fobbed off’. In the present study, the item “I have re-

C
Chronic Low Back Pain, Definitions and Diagnosis 365
ceived enough information about my condition” loadedto “expectation” rather than to “cognition”. This sug-gests that, rather than the quantity, the appropriatenessof information given in relation to expectations is im-portant in determining satisfaction.Lower current levels of pain at follow up were associ-ated with highly significantly more favourable recall ofthe original consultation in terms of the “expectation”subscale. However, the impact of an initial consultationrated positively by the patient on the subscales “affect”and “expectation”, but not “cognition”, was still evidentafter controlling for current pain intensity. Thus, the ex-perience of the initial consultation appeared to have aninfluence on the patient 6 months later irrespective ofpain outcome. It is concluded that the doctor’s affect andthe extent to which expectations were met rather thansimple information provision are the elements of com-munication through which this influence is mediated.
Reassurance
Relief of symptoms by provision of reassurance is likelyto be one of the doctor’s aims following negative investi-gations such as laparoscopy, but can also arise from ex-planation of normal findings at an initial consultation,for example where a careful history and physical exam-ination indicates a minimal likelihood of infection or en-dometriosis. However, there are mixed findings from re-search on the impact of assessment as therapy. In a ran-domised trial design, an ultrasound scan used as a basisfor counselling about normal findings was found to behelpful in relieving symptoms (Ghaly 1994). The reas-suring effect of laparoscopy has been reviewed (Priceand Blake 1999). However, this approach can be coun-terproductive, as shown in a study where women wereshown photographs of laparoscopic findings in order toreinforce counselling, where no benefit was seen (On-wude et al. 2004).In conclusion, doctors need to be aware of the impor-tance of establishing a therapeutic relationship througheffective consulting behaviour that meets patients’ ex-pectations and exploits opportunities for provision of re-assurance and support.
References1. Fry RPW, Stones RW (1996) Hostility and doctor-patient interac-
tion in chronic pelvic pain. Psychother Psychosom 65:253–2572. Ghaly AFF (1994) The psychological and physical benefits of
pelvic ultrasonography in patients with chronic pelvic pain andnegative laparoscopy. A random allocation trial. J Obstet Gy-naecol 14:269–271
3. Grace VM (1995) Problems of communication, diagnosis, andtreatment experienced by women using the New Zealand healthservices for chronic pelvic pain: a quantitative analysis. HealthCare Women Int 16:521–535
4. Grace VM (1998) Mind / body dualism in medicine: The case ofchronic pelvic pain without organic pathology –A critical reviewof the literature. Int J Health Serv 28:127–151
5. Onwude JL, Thornton JG, Morley S et al. (2004) A randomisedtrial of photographic reinforcement during postoperative coun-selling after diagnostic laparoscopy for pelvic pain. Eur J ObstetGynecol Reprod Biol 112:89–94
6. Price JR, Blake F (1999) Chronic pelvic pain: The assessmentas therapy. J Psychosom Res 46:7–14
7. Selfe SA, van Vugt M, Stones RW (1998a) Chronic gynaecolog-ical pain: an exploration of medical attitudes. Pain 77:215–225
8. Selfe SA, Matthews Z, Stones RW (1998b) Factors influenc-ing outcome in consultations for chronic pelvic pain. J WomensHealth 7:1041–1048
9. Stones RW, Lawrence WT, Selfe SA (2006) Lasting impressions:influence ot the initial hospital consultation for chronic pelvicpain on dimensions of patient satisfaction at follow-up. J Psy-chosom Res 60:163–167
Chronic Illness Problem Inventory
Definition
The Chronic Illness Problem Inventory is a 65-item in-strumentdeveloped tomeasurepatient functioningin theareas of physical limitations, psychosocial functioning,health care behaviors, and marital adjustment.� Pain Inventories
Chronic Inflammatory DemyelinatingPolyneuropathy
Synonym
CIDP; chronic relapsing polyneuropathy
Definition
Chronic inflammatory demyelinating polyneuropathy iscaused by demyelination due to an immune reaction. Itis characterized by progressive weakness and impairedsensoryfunction in thearmsandlegs. It is related toGuil-laim Barré syndrome, and is sometimes considered to bethe chronic version of that disease.� Inflammatory Neuritis
Chronic Low Back Pain, Definitions andDiagnosis
CHRISTOPHER J. WINFREE
Deptartment of Neurological Surgery, NeurologicalInstitute, Columbia University, New York, NY, [email protected]
Synonyms
Ankylosing spondylitis; Chronic pain; CT myelogra-phy; Diagnostic block; Discogenic pain; Facet joint;Fibromyalgia; Internal disc disruption; Intervertebraldisc; Low back pain; Paget’s disease; Pathologicalfracture; Provocative discography; Reiter’s syndrome;Sacroiliac joint; Spondyloarthropathy;Spondylolisthe-sis; Zygapophyseal joint

366 Chronic Low Back Pain, Definitions and Diagnosis
Definition
Chronic � low back pain is defined as pain localized tothe region bordered by L1 above, S1 below, and the erec-tor spinae muscles laterally (Merskey 1994), which lastsfor more than 3 months (Merskey 1986). Chronic lowback pain is often associated with pain radiating to thebuttock or legs; however, it is useful to distinguish be-tweenthesedistinctpainsyndromes,astheyaretypicallytreated differently.
Characteristics
General
Men and women are affected equally, most commonlyduring the 4–6th decades (Deyo 2001). Chronic lowback pain is the most costly of the work-related disabil-ities (Andersson 1999). The lumbar spine is a complexanatomical region, with a number of structures that mayserve as pain generators to be discussed below.
History
The initial assessment of the chronic low back pain pa-tient includesacarefulmedicalhistory.Theduration andseverity of symptoms, predisposing factors, exacerbat-ing factors, alleviating factors, and treatments may allbe explored in the patient interview. Information regard-ing occupationalhistory,disability, litigation,psychoso-cial influences, and secondary gain may also be gleanedduring the initial discussion. It is important to inquireabout neurological function, such as weakness, boweland bladder function, and sexual function, to establishwhether neurological compromise is present, as treat-ment of these patients will likely proceed in a more ur-gent manner. It is also important to document a baselinelevel of pain upon which to judge efficacy of interven-tions, if any.
Physical Exam
The physical exam is generally helpful but not typicallysensitive or specific in the setting of chronic low backpain. The astute observer may discern peculiar move-ments or postures characteristic of the back pain patient.For example, these patients sometimes sit bent forwardat thewaist, ashyperextensionoftenaggravates lowbacksymptoms. Some patients fail to get comfortable, andspend the time during the interview switching positions,or alternating standing and sitting.
Imaging
Conventional roentgenography is rapid, inexpensive,and best suited for inspection of the osseous structures.Vertebral fracture, osteoporosis, loss of disc height, endplate changes, facet hypertrophy, and alignment defor-mityareall readilyseenonconventionalX-rays.Charac-teristic bony changes of selected spondyloarthropathiesare also readily identifiable with this modality. Thetypical static images include anteroposterior and laterallumbar and sacral views, left and right lateral lumbar
oblique (for inspection of the neural foraminae), and acone down lateral sacral view. Dynamic images to assistin the evaluation of spinal stability include lateral flex-ion and extension views. Magnetic resonance imagingis the best modality available for evaluation of the softtissue structures of the spine. The � intervertebral discs,ligaments, neural structures, and osseous structures areall well seen. Typically, non-contrast imaging is allthat is required; however, the use of contrast may beuseful in the setting of tumor, malignancy, or previoussurgery. Caution must be exercised in the interpretationof positive findings on MRI, as over half of asymp-tomatic subjects will have at least one abnormalityon MR imaging (Jensen 1994). CT scanning is a vitalpart of � provocative discography, providing detailedanatomical data on the morphology of the interverte-bral discs in question. � CT myelography provides theoptimum contrast between neural and non-neural struc-tures. Subtle nerve root compression or spinal canalencroachment invisible on MRI may be obvious on CTmyelography. Bone scanning has limited but specificuses in the imaging of chronic back pain. It may be use-ful in the evaluation of suspected pseudoarthrosis at aprevious fusion site, or also of malignancy or infection.
Discogenic Pain� Discogenic pain is defined as pain from the disc itselfandnotsurroundingstructurescompressedbythedisc. Itis probably the most common cause of chronic low backpain, with � internal disc disruption present in approxi-mately 40% of cases (Schwarzer 1995a). These patientsoften describe pain localized to the low back, often ac-companied by pain referred to the hip, buttock, or groin.Pain that radiates to the lower extremities may be patchyor “sclerotomal” in nature rather that dermatomal, asseen in herniated discs. These patients typically reportthat their pain is aggravated by standing or sitting andrelieved by lying down, presumably since this positiontakes the pressure off the intervertebral discs. The in-tervertebral disc receives innervation along at least theouter third of the annulus (Coppes 1997). The disc maybecome painful when it undergoes disruption; however,nonspecific degenerative changes are not thought tobe specifically painful (Moneta 1994). These changesmay be obvious on conventional imaging studies, andinclude loss of height, rupture, end plate changes, anddehydration. Other, subtler changes, such as internaldisc disruption (IDD), may only be revealed as smallradial fissures on CT imaging following discography(Vanharanta 1988). Provocative discography consistsof both physiologic and radiographic assessment, andis used to establish whether a degenerated disc is apain generator in the chronic low back pain patient. Itinvolves the fluoroscopic placement of a needle into theintervertebral disc of the awake patient, and subsequentinjection of contrast dye. Intradiscal insertion and in-jection pressures are measured. A positive discogram

C
Chronic Low Back Pain, Definitions and Diagnosis 367
occurs when the patient’s back pain is reproduced whendye is injected into a particular disc at modest pressures.A negative discogram occurs when the pain on injectiononly occurs at extremely high pressures, or does notmatch the patient’s normal pain. A complete discogramalways includes the injection of a normal control disc,to exclude the possibility of non-specific patient painresponses to injection. Once the procedure is complete,high resolution CT scanning is performed to illustratethe morphology of the injected discs. Typically, positivediscs show some evidence of internal disruption, withextravasation of contrast beyond the inner confines ofthe annulus. The key diagnostic criteria are the presenceof concordant pain in a radiographically demonstrateddegenerated disc. When careful technique is performedusing these rigid criteria, the false positive rate forprovocative discography approaches 0% (Walsh 1990).
Zygapophyseal Joint Pain
The lumbar � facet joints, or � zygapophyseal joints,are synovial joints that receive their segmental inner-vation from the medial facet branch of the posteriordivision of the respective spinal nerve (Bogduk 1979).The role of facet joint arthropathy in the pathogenesisof low back pain was recognized early in the 20th Cen-tury (Ghormley 1933). These patients typically havelow back pain that may radiate across the buttock orthigh. One estimate of its incidence in a low back painpopulation was 15%, based upon diagnostic blockade(Schwarzer 1994). As in other forms of low back pain,there are no reliable, reproducible diagnostic criteria(Jackson 1988; Schwarzer 1994). Injection of the jointor its innervating fibers using a double block techniqueto help reduce the influence of the placebo effect, andto increase the sensitivity and specificity, may representthe most reliable diagnostic method (Schwarzer 1994).This technique involves the injection of facet joint (orthe medial facet branch) on one visit, followed by asecond confirmatory injection at a separate visit. Apositive response occurs when the patient reports >50%relief with both blocks.
Sacroiliac Joint Pain
The � sacroiliac joint is a diarthrodial joint with limitedmobility, receiving its innervation from the lumbosacralroots. Thought to be an important contributor to chroniclow back pain, one estimate of its incidence in a se-lected population of low back pain was 19% (Maigne1996). Pain may be located across the low back withradiation to the buttock or groin, as in other forms oflow back pain. Some patients have tenderness over thesacroiliac joint. Despite the myriad of specific physicalmaneuvers designed to provoke a positive response inpatients with sacroiliac joint pain, no test alone or incombination with others is reliable when comparedwith diagnostic blockade of the joint itself (Dreyfuss
1996). Radiographic imaging is likewise unhelpful(Schwarzer 1995b).
Spinal Instability� Spondylolisthesis consists of facet joint arthropathycombined with disc degeneration, resulting in one ver-tebral body subluxing over another (Mardjetko 1994).Common at L4-5 and L5-S1, such movement may bedue to trauma,degenerativechanges, congenitaldefects,or � pathological fracture. X-rays readily demonstratespondylolisthesis, and may further show movement ofthe vertebral bodies in relation to each other on dynamicviews.
Other Causes
Thespondyloarthropathiesareagroup of rheumatologicdiseases that typically generate chronic low back painthat isworstupon awakening, and improveswithactivity(McCowin 1991). � Ankylosing spondylitis commonlyaffects young adult males, causes low back pain, de-creased spinal range of motion, and has characteristicbony changes on spine imaging. � Reiter’s syndrome,another common cause of arthritis and low back painin men, consists of the triad of arthritis, conjunctivitis,and urethritis. � Paget’s disease is a common cause ofback pain in the elderly (Mazanec 1999). Characteristicfindings on history are deep, arthritic pain, and on imag-ing are localized bony overgrowths. � Fibromyalgiais a common disorder causing back pain, associatedwith other conditions such as headache and irritablebowel syndrome. Radiographic investigations are typi-cally normal. Diagnosis is based upon the symptoms ofwidespread pain and discreet trigger points (Mazanec1999).� Disability, Fear of Movements
References1. Andersson GBJ (1999) Epidemiologic Features of Chronic Low
Back Pain. Lancet 354:581–5852. Bogduk N, Long DM (1979) The Anatomy of the so-called “Ar-
ticular Nerves” and their Relationship to Facet Denervation inthe Treatment of Low-Back Pain. J Neurosurg 51:172–177
3. Coppes MH, Tamaki T, Hayashi N et al. (1997) Innervation of“Painful” Lumbar Discs. Spine 22:2342–2350
4. Deyo RA, Weinstein JN (2001) Low Back Pain. N Engl J Med344:363–370
5. Dreyfuss et al. (1996) The Value of Medical History and Phys-ical Examination in Diagnosing Sacroiliac Joint Pain. Spine21:2594–2602
6. Ghormley RK (1933) Low Back Pain: With Special Reference tothe Articular Facets, with Presentation of an Operative Procedure.JAMA 101:1773–1777
7. Jackson RP, Jacobs RR, Montesano PX (1988) Facet Joint In-jection in Low-Back Pain: A Prospective Statistical Study. Spine13:966–971
8. Jensen MC, Brant-Zawadzki MN, Obuchowski N et al. (1994)Magnetic Resonance Imaging of the Lumbar Spine in Peoplewithout Back Pain. N Engl J Med 331:69–73
9. Maigne J-Y, Aivaliklis A, Pfefer F (1996) Results of SacroiliacJoint Double Block and Value of Sacroiliac Pain ProvocationTests in 54 Patients with Low Back Pain. Spine 21:1889–1892

368 Chronic Migraine
10. Mardjetko SM, Connolly PJ, Shott S (1994) DegenerativeLumbar Spondylolisthesis: A Meta-Analysis of Literature1970–1993. Spine 19:2256–2265
11. Mazanec DJ (1999) Evaluating Back Pain in the Elderly. ClevClin J Med 66:89–99
12. McCowin PR, Borenstein D, Wiesel SW (1991) The CurrentApproach to the Medical Diagnosis of Low Back Pain. OrthoClin North Am 22:315–325
13. Merskey H (1986) Classification of Chronic Pain: Descriptionsof Chronic Pain Syndromes and Definitions of Pain Terms. Pain3:1–225
14. Merskey H, Bogduk N (1994) Classification of Chronic Pain:Descriptions of Chronic Pain Syndromes and Definitions of PainTerms, 2nd edn. IASP Press, Seattle, pp 11–36
15. Moneta GB, Videman T, Kaivanto K et al. (1994) Reported Painduring Lumbar Discography as a Function of Annular Rupturesand Disc Degeneration: A Re-Analysis of 833 Discograms. Spine19:1968–1974
16. Schwarzer AC, Aprill CN, Derby R et al. (1994) Clinical Featuresof Patients with Pain Stemming from the Lumbar ZygapophysialJoints: Is the Lumbar Facet Syndrome a Clinical Entity? Spine19:1132–1137
17. Schwarzer AC et al. (1995a) The Prevalence and Clinical Featuresof Internal Disc Disruption in Patients with Chronic Low BackPain. Spine 20:1878–1883
18. Schwarzer AC, Aprill CN, Bogduk N (1995b) The SacroiliacJoint in Chronic Low Back Pain. Spine 20:31–37
19. Vanharanta H, Sachs BL, Spivey M et al. (1988) A Comparison ofCT/Discography, Pain Response and Radiographic Disc Height.Spine 13:321–324
20. Walsh TR, Weinstein JN, Spratt KF et al. (1990) Lumbar Discog-raphy in Normal Subjects: A Controlled, Prospective Study. JBone Joint Surg Am 72A:1081–1088
Chronic Migraine
Definition
Migraine headache occurring more than 15 days permonth. Typically, a patient has a remote history ofepisodic migraine which slowly increases in frequencyover time to a near daily headache with migrainefeatures. In many instances the patient is overusinganalgesics.� New Daily Persistent Headache
Chronic Neural Sensitization
� Visceral Pain Model, Irritable Bowel SyndromeModel
Chronic Neuropathic Pain
Definition
Chronic pain caused by dysfunction of or damage to thenervous system.� Pain Treatment, Implantable Pumps for Drug Deliv-
ery
Chronic Pain
Definition
Pain that persists on a constant basis for three monthsor more. Some researchers and clinicians use a timelineof six months or more. Chronic pain rarely has a knowncause, and may behard to localize in thebody. Treatmentis usually limited to general measures of pain control.Emotive symptoms are commonly an important compo-nent of the suffering associated with chronic pain. Thecharacter of a chronic pain signal is often misinterpretedor grossly distorted. There is often a measurable imbal-ance between pronociceptive and antinociceptive forcesconsistent with the perception of pain. No definition ofchronic pain exists for newborns, but prolonged pain hasbeen defined as that lasting several hours or days.� Acute Pain, Subacute Pain and Chronic Pain� Amygdala, Pain Processing and Behavior in Animals� Assessment of Pain Behaviors� Chronic Low Back Pain, Definitions and Diagnosis� Depression and Pain� ImpactofFamilialFactorsonChildren’sChronicPain� Muscle Pain, Fibromyalgia Syndrome (Primary, Sec-
ondary)� Pain Assessment in Neonates� Pain in theWorkplace,Risk factors forChronicity, Job
Demands� Pain Inventories� Pain Treatment, Intracranial Ablative Procedures� Pain Treatment, Motor Cortex Stimulation� Physical Exercise� Postoperative Pain, Persistent Acute Pain� Prevalence of Chronic Pain Disorders in Children� Psychiatric Aspects of Pain and Dentistry� Psychological Treatment of Chronic Pain, Prediction
of Outcome� Thalamus, Clinical Pain, Human Imaging
Chronic Pain Disorder Prevalence inChildren
� Prevalence of Chronic Pain Disorders in Children
Chronic Pain in Children, PhysicalMedicine and Rehabilitation
JOYCE M. ENGEL1, DEBORAH A. O’ROURKE2
1Department of Rehabilitation Medicine, University ofWashington, Seattle, WA, USA2College of Nursing and Health Sciences, Universityof Vermont, Burlington, VT, USA

C
Chronic Pain in Children, Physical Medicine and Rehabilitation 369
[email protected],[email protected]
Synonyms
Pediatric Physical Therapy; Occupational Therapy inChildren; Pediatric Physiotherapy
Definition
Physical medicine and rehabilitation are core compo-nents of current multimodal and multidisciplinary ap-proaches to chronic pain management and include thedisciplinesofphysical therapyandoccupationaltherapy.Physical therapists apply a wide range of physical andbehavioral interventions to reduce pain, prevent impair-ment and disability as well as to promote function. Oc-cupational therapists are primarily concerned with thepsychosocial and environmental factors that contributeto pain and have an impact on an individual’s daily ac-tivities and participation (Engel and Kartin 2004; Inter-national Association for the Study of Pain ad hoc Sub-committee forOccupationalTherapy /PhysicalTherapyCurriculum 1994).
Characteristics
Physical therapists and occupational therapists are pri-marily, although not exclusively, involved in rehabilita-tion programs for children with chronic musculoskeletalpain. Many diseases, injuries and disabling conditionsare associated with chronic musculoskeletal pain (En-gel and Kartin 2004).These includepain associated withphysical diseases (e.g. arthritis), pain that is secondaryto a physical disability (e.g. cerebral palsy (CP) and painthat may occur without an identifiable cause (e.g. com-plex regional pain syndrome).
Rehabilitation Conceptual Models
Rehabilitation interventions are based on the biopsy-chosocial model of health, functioning and pain. Asan example, Loeser and Fordyce’s biopsychosocialmodel (1983) of pain is conceptualized into four do-mains, nociception, pain, suffering and pain behavior.A child may experience some, but not all, domains.Some children with chronic pain may experience painand suffering and demonstrate pain behaviors in theabsence of nociception. Developmental aspects arealso critical to consider for the clinical assessment andmanagement of chronic pain in children. The ability todescribe and self-report pain and suffering is limitedin young children and in children with cognitive orcommunication impairments, so that it is important toevaluate and monitor a child’s overt pain behaviors.For some children with physical disabilities (e.g. CP),the range of potential pain behaviors may also be re-duced secondary to paralysis, muscle � contractures,� joint deformities and communication impairments.In this situation, family members and caregivers helpto identify and interpret pain behaviors.
The World Health Organization (WHO) InternationalClassification of Functioning, Disability, and Health(ICF; 2001) classification system uses a biopsychoso-cial framework to describe functioning at three levels,the body, the individual and the individual within abroad social context. Biological aspects include bodystructures and body functions, while individual aspectsincludeparticipating indailyactivitiesandsocialaspectsencompass overall functioning in society. Pain relateddisability and optimal functioning are not simply linkedto particular pain conditions. Instead, they depend oninteractions among the specific child characteristics,the specific pain condition and the environmental orcontextual factors in which the child experiences pain.According to this model, chronic pain impairs bodyfunction due to various health conditions that oftenresult in additional impairments, activity limitationsand participation restrictions (i.e., secondary disabili-ties). The child’s environment (family, physical, social,cultural) and their personal characteristics interact withand determine functioning and disability in a dynamicway. A comprehensive assessment of the child’s impair-ments, activities, participation and contextual factorsis needed to guide intervention. Clarity about the goalsof rehabilitation, the levels of intervention, the spe-cific treatment techniques or modalities and expectedoutcomes is essential.
Interventions
Interventions for children with chronic pain are typi-cally multimodal. Physical therapists and occupationaltherapists follow the principles of � family-centeredcare when developing a treatment plan. In collaborationwith the child, family and other health care providers,they carefully identify all impairments, activity limi-tations and participation restrictions, pain frequency,pain intensity and the child’s stage in development.Rehabilitation interventions reduce impairments at thebody structure and function level, promote activity andparticipation level functioning, and address environ-mental or personal barriers to health and functioning.At the body structure and function level, interventionsinclude electrotherapy modalities and physical agents.Electrotherapy modalities (e.g. � transcutaneous elec-trical nerve stimulation (TENS) and � physical agents(e.g. � cryotherapy, hydrotherapy, � manual therapy,massage, therapeutic exercise) are not widely used torelieve chronic pain in children, but may have a place,especially in preparing the child for physical retraining.Possible clinical indications for TENS in children mayinclude chronic low back pain, arthritis, inflammatorydisorders of soft tissues and procedural pain (McCarthyet al. 2003). Cryotherapy has been used successfully inreducing chronic muscle spasm and inflammation as-sociated with arthritis (Bell and Prentice 2002). Carefulmonitoring of the child’s skin is necessary with both ofthese interventions. � Hydrotherapy (e.g. whirlpool)

370 Chronic Pain in Children, Physical Medicine and Rehabilitation
promotes muscle relaxation and can be a medium forexercise. Manual therapy techniques such as therapeuticmassage and � mobilization can induce muscle relax-ation, help lessen muscle spasm and increase range ofmotion.� Therapeutic exercise is a primary component of re-habilitation of adults and children with chronic pain(Eccleston and Eccleston 2004). Children with chronicpain do not move or exercise as much as their healthypeers and this can result in decreased aerobic capacity,muscle strength, and flexibility. This pattern of inactiv-ity can result in a vicious cycle of additional inactivity,greater deconditioning and further reductions in musclestrength and flexibility (Anthony and Schanberg 2003).Aerobic conditioning exercises can lessen chronic painin children with arthritis (Klepper 1999) and in childrenwith complex regional pain syndrome (CRPS) (Sherryet al. 1999). For children with CRPS, exercise andother forms of physical activity play an important rolein recovery of function (Lee et al. 2002). Research isneeded to determine the frequency, type and duration ofexercise in combination with other forms of treatmentrequired to achieve optimum outcomes in this group ofchildren (Berde 2005). Clearly, exercises for childrenwith chronic pain must be developmentally appropriateand as enjoyable as possible.Exercises to improve muscle strength and flexibility areanother important component of therapeutic exercise.Muscle strengthening exercises appear to increase phys-ical functioning in children with and without disabilities(Damiano et al. 2002). Research is needed to examinewhether muscle-strengthening exercises reduce pain.Flexibility exercises such as passive range of motionand stretching exercise must be individualized to eachchild to address potential biomechanical limitations andother constraints. A recent study reported that childrenwith significant physical disabilities demonstrated painbehaviors during passive stretching exercises (Haddenand von Baeyer 2002). In contrast, this particular formof therapeutic exercise has been advocated as a painreducing intervention in children with musculoskeletalpain associated with other diagnoses. Meticulous at-tention to assessment findings and family knowledgeof pain triggers is essential when therapists are work-ing with children who are nonverbal. For children whohave the ability to self-report, muscle strengthening andstretching exercises can be progressed in an incrementalmanner to tolerance. Other forms of therapeutic exer-cise include activities to improve posture and increasebalance and coordination. Often these exercises can beaddressed through games and age-appropriate physicalactivities.Activity and participation level interventions are es-sential components in rehabilitation. Interventions atthis level include graded tasks, mobility training, self-care training and education. For example, childrenwith chronic musculoskeletal pain often demonstrate
problems walking and may benefit from rehabilitationinterventions to correct gait deviations and increasewalking capabilities. Chronic pain may also compro-mise the child’s usual level of participation in socialinteractions, school participation and community recre-ation and play or leisure activities. Physical therapistsand occupational therapists use a variety of develop-mentally appropriate strategies to promote the child’scapacity to resume their typical activities and participa-tion. For example, therapists often work in collaborationwith school personnel to identify activities that are in-teresting and socially engaging for a child with chronicpain.Attention to contextual factors is also an essential com-ponent of physical rehabilitation. An assessment ofthe child’s environment may yield information aboutphysical or social factors that can be modified to reducechronic pain in addition to impairment and associateddisability. Interventions at this level include productsand technology as well as social support systems. Forexample, for children with limited mobility due to sig-nificant physical disability, modification of the physicalenvironment is important and may include the pre-scription of postural support systems, mobility devicesand � adaptive equipment to promote comfort and im-prove access to and interaction with the environment.Assessment of the social environment is critical andinterventions may be warranted at home, at school andin the community to address assumptions, attitudesand beliefs about chronic pain, its impact and its man-agement. Education and counseling are often required.Finally, personal factors represent the second contex-tual factor and these characteristics are prominent indetermining appropriate rehabilitation interventions.The child’s age, cognitive skills and communicationcapabilities will determine whether physical therapistsand occupational therapists can incorporate cogni-tive and behavioral strategies along with rehabilitativeinterventions. For young children and children withsignificant cognitive and communication impairments,this might not be possible.The occupational therapist and physical therapist mayuse cognitive behavioral strategies as adjuncts to theabove-described interventions. Personal factors treat-ments consist of relaxation training, distraction andcontingency management. Relaxation techniques mayconsist of diaphragmatic breathing, autogenic training,progressive muscle relaxation or guided imagery. Thebenefits of relaxation techniques include alleviation ofskeletal muscle tension, lessening of fatigue, distrac-tion and enhancement of other pain relief measures.Numerous studies support the use of relaxation anddistraction in the treatment of arthritic pain, headachedisorders and burn wound care (McGrath et al. 2003).An infrequent and mild side effect of relaxation train-ing is a child feeling out of control when relaxationoccurs. Relaxation training may be done in conjunction

C
Chronic Pain, Patient-Therapist Interaction 371
with � biofeedback. Some research supports the useof biofeedback in children with arthritis and childrenwith headaches (Engel and Kartin 2004). Distrac-tion has been effective in reducing pain and distressin youths with burn injuries (Hoffman et al. 2000).� Contingency management procedures for the treat-ment of children with recurrent abdominal pain, burninjuries or headaches have resulted in increased activitylevels and participation, in addition to reduced painfrequency and pain behaviors (Engel and Kartin 2004).In summary, the roles of the physical therapist and oc-cupational therapist on the pediatric pain managementteam are emerging. Physical therapists and occupationaltherapists use their knowledge of anatomy, physiology,kinesiology, psychology and human development andfunction to develop and implement comprehensive eval-uations and interventions for the child with chronic pain.A variety of activity-based and family-centered inter-ventions are available. Evidence to support these inter-ventions, however, is greatly needed.
References1. Ad Hoc Committee OT / PT Pain Curriculum (1994) Pain cur-
riculum for students in occupational therapy or physical therapy.IASP Newsletter, International Association for the Study of Pain,Seattle
2. Anthony KK, Schanberg LE (2003) Pain in children with arthritis:a review of the current literature. Arthritis Rheum 49:272–279
3. Bell GW, Prentice WE. (2002) Therapeutic modalities for phys-ical therapists, 2nd edn. McGraw-Hill, New York
4. Berde CB, Lebel A (2005) Complex regional pain syndromes inchildren and adolescents. Anesthesiology 102:252–255
5. Damiano DL, Dodd K, Taylor NF (2002) Should we be testingand training muscle strength in cerebral palsy? Dev Med ChildNeurol 44:68–72
6. Eccleston Z, Eccleston C (2004) Interdisciplinary managementof adolescent chronic pain: developing the role of physiotherapy.Physiotherapy 90:77–81
7. Engel JM, Kartin D (2004) Pain in youth: a primer for current
practice. Critical Reviews™ in Physical and RehabilitationMedicine 16:53–76
8. Hadden KL, von Baeyer CL (2002) Pain in children withcerebral palsy: Common triggers and expressive behaviors. Pain99:281–288
9. Hoffman HG, Doctor JN, Patterson DR et al. (2000) Virtual re-ality as an adjunctive pain control in wound care in adolescentpatients. Pain 85:305–309
10. Klepper SE (1999) Effects of an eight-week physical condition-ing program on disease signs and symptoms in children withchronic arthritis. Arthritis Care Res 12:52–60
11. Lee BH, Scharff L, Sethna NF et al. (2002) Physical therapy andcognitive-behavioral treatment for complex regional pain syn-dromes. J Pediatr 141:135–140
12. Loeser JD, Fordyce WE (1983) Chronic pain. In: Carr JE, Den-gerink HA (eds) Behavioral science in the practice of medicine.Elsevier, New York
13. McCarthy CF, Shea AM, Sullivan P (2003) Physical therapy man-agement of pain in children. In: Schechter NL, Berde CB, YasterM (eds) Pain in Infants, Children and Adolescents, 2nd edn. Lip-pincott Williams and Wilkins, Philadelphia, pp 434–448
14. McGrath PA, Hiller LM (2003) Modifying the psychologicalfactors that intensify children’s pain and prolong disability. In:Schechter NL, Berde CB, Yaster M (eds) Pain in Infants, Chil-dren, andAdolescents2nd edn. Lippincott, Williamsand Wilkins,Philadelphia, pp 85–104
15. Sherry DD, Wallace CA, Kelley C et al. (1999) Short and long-term outcomes of children with complex regional pain syndrometype I treated with exercise therapy. Clin J Pain 15:218–223
16. World Health Organization (2001) International Classification ofFunctioning Disability and Health. World Health Organization,Geneva, pp 3–20
Chronic Pain, Patient-TherapistInteraction
MARK P. JENSEN
Department of Rehabilitation Medicine, University ofWashington, Seattle, WA, [email protected]
Synonyms
Relationship; Therapeutic Alliance
Definition� Patient-therapist interaction refers to the verbal andnonverbalinteractionsbetweenhealthcareprovidersandtheir patients or clients. These interactions may include,but are not necessarily limited to, communication andnegotiations concerning the patient’s history, diagnosis,and clinical care.
Characteristics
Patient-Therapist Interaction and Pain Treatment Satisfaction
Research shows that pain intensity has only a weak tomoderate association with pain treatment satisfaction,due primarily to the fact that patients tend to report rela-tively high levels of satisfaction with pain managementcare, regardless of pain severity levels (Miaskowski etal. 1994; Ward and Gordon 1996; Dawson et al. 2002).On the other hand, factors related to the interactionsbetween patients and clinicians show consistent asso-ciations with treatment satisfaction across measuresand samples. For example, Sherwood and colleagues(Sherwood et al. 2000) found that treatment satisfactionwith pain treatment was higher when patients felt thattheir pain was addressed with the patient as an informedpartner, and was lower when the providers appeareduncaring, were slow to respond to pain complaints, orwere perceived to lack knowledge and skills. Similarly,Dawson and colleagues (Dawson et al. 2002) foundthat many patients who reported severe pain, and whostill reported that they were satisfied with pain care,attributed their satisfaction to their belief that theirhealthcare provider was making efforts to provide painrelief. Riley and colleagues (Riley et al. 2001) foundthat patient-perceived quality of caregiver communi-cation predicted satisfaction with individualized paintreatment plans in a sample of 107 patients seen inan orofacial pain clinic. McCracken and colleagues(McCracken et al. 1997) identified confidence and trustin the treatment provider, pain reduction, and time

372 Chronic Pain, Patient-Therapist Interaction
spent waiting in the clinic as predictors of satisfactionwith chronic pain treatment. In short, patients who aresatisfied with their pain care seem to be those who seethemselves as having a collaborative relationship witha treatment provider who works collaboratively withthe patient to address the pain problem. While painreduction may be associated with treatment satisfactionin some instances, pain reduction does not appear to benecessary for patients to be satisfied with their care.
Patient-Therapist Interaction and Treatment Adherence andOutcomes
Research also shows that � treatment adherence is re-lated to patient-therapist interactions; in particular, theexistence of a collaborative relationship between thepatient and clinician. While very little of this researchhas been performed in samples of persons with chronicpain (for an exception, see discussion of Alamo et al.2002, below), this finding is consistent across a widevariety of patient populations and treatments (Cruz andPincus 2002). For example, Gavin et al. (2002) showedthat a measure of � treatment alliance (measuring theextent to which patients and clinicians agree on treat-ment goals and hold each other in positive regard) wasassociated with medication adherence and treatmentoutcome in a sample of adolescents with severe asthma.Weiss et al.(2002) similarly found that a measure of� working alliance (which assessed patient-therapistagreement of treatment goals and the tasks to be used towork toward these goals, and the degree to which a bondexists between the therapist and patient) was associatedwith future medication adherence and treatment out-come in a sample of patients with psychotic disorders.In a sample of patients with schizophrenia, Frank andGunderson (1990) found that patients who were ableto form a good treatment alliance with their therapistswithin the first six months of treatment, adhered more totheir medication regimen and achieved better outcomesafter two years (with less medication) than patients whodid not form a good treatment alliance.Alamo and colleagues (Alamo et al. 2002) found evi-dence for the efficacy of a � patient-centered approachin a sample of patients with chronic pain. In this study,a group of family physicians were trained in the use ofa patient-centered approach to pain treatment, whichincluded the following components, among others:listening to the patient without interrupting in the firstmoments of the consultation, being supportive and� empathic, allowing and encouraging patients to askquestions, trying to reach an agreement about the na-ture of the problem, and trying to find common groundabout the management plan. Patients of the physicianswho were trained in and used the patient-centered ap-proach reported significantly greater improvementsafter one year in psychological distress and number oftender points, than the patients of family physicians nottrained in the patient-centered approach. Although not
statistically significant, there was also a trend for pa-tients in the patient-centered condition to report greaterdecreases in pain intensity than patients who receivedusual care.
Implications for Improving Pain Management Care
The findings briefly reviewed above support the conclu-sion that patient-therapist interaction factors play a roleinpatienttreatmentsatisfactionandadherence,aswellasin long-term treatmentoutcome.Clinicianswould there-fore be wise to make any appropriate changes in the waythey interact with patients to maximize therapeutic al-liance. Attention to three specific areas may be partic-ularly useful: (1) communicate efforts to manage pain;(2) make an effort to build and maintain rapport; (3) en-courage a collaborative relationship.
Communicate Efforts to Manage Pain
Most patients come to realize, by the time their pain be-comes chronic, that there is no quick fix for their painproblem. However, these patients may still hope that anew treatment will be discovered that will provide painrelief. Also, there exist many treatments for pain thatsubgroups of patients may find effective, even if thesetreatments are not necessarily effective for the major-ity of patients (Engel et al. 2002). Clinicians could im-prove their relationships with patients, and increase pa-tient treatment satisfaction, if they communicated that(1) they are vigilant in their efforts to identify effectivepain treatments as these treatments are reported in theresearch literature and (2) they are willing to work withthe patient to find the specific combination of treatmentsand approaches that are most effective for each individ-ual patient.
Make an Effort to Build and Maintain Rapport
One of the most effective ways to build rapport is to in-corporate � reflective listening in interactions with pa-tients. Reflective listening involves making statementsthat indicate that you understand what the patient is say-ing.Such statementsdiffer substantially from usualclin-ician responses, such as questions that call for or requirea response or statements that merely provide informa-tion (Miller and Rollnick 2002; Rollnick et al. 1999).Examples of reflective responses to the statement, “I amsick and tired of this pain” would include, “You are frus-trated that it is taking so long for us to find an approachthat effectively reduces your pain” or “You are ready totry something new to get this pain under better control.”The immediate concern of some clinicians, when theyconsider using reflective listening during a patient en-counter, is that such statements might open a Pandora’sBox of patient talking, which may then use up the (lim-ited) time devoted to the encounter. However, cliniciansneed not make every statement a reflective one. More-over, encounters that include reflective listening can ac-tually be more efficient than encounters that do not, be-

C
Chronic Paroxysmal Hemicrania 373
cause once patients feel understood, they may feel lesscompelled to interrupt and ask questions. In support ofthis, one study found that being responsive to patientconcerns (as opposed to ignoring patient concerns) wasassociated with a decrease in the time of the encounter(Levinson et al. 2000).
Encourage a Collaborative Relationship
For the most part, adequate management of chronicpain involves active patient participation and involve-ment, and good long-term adjustment depends muchmore on what patients do, than on what is done to them(Jensen et al. 2003). As reviewed above, patients aremore likely to actively participate in treatment andadhere to treatment recommendations when there is agood therapeutic alliance and when there is a collab-orative patient-therapist relationship. Developing andmaintaining a collaborative relationship with patientsdoes not have to involve any special skills, other than awillingness to avoid lecturing patients or telling themwhat to do, and a willingness to provide the patient withoptions and choices.Lecturing patients can create resentment and � resis-tance (Miller and Rollnick 2002). It is more effective toprovide guidance, options, and advice, while at the sametime communicating the expectation that the patient candecide which parts of the recommended treatment planhe or she will follow. As choice increases adherence, thecollaborative clinician offers patients choices wheneverpossible (Miller and Rollnick 2002). For example, ifboth the clinician and patient decide that a graduatedexercise program is worth trying, the patient shouldthen be offered different methods for starting and main-taining such a program. The patient could be offeredsessions with a physical therapist who could help themto develop a home program. Another option would beto allow the patient to develop a simple reactivationprogram at home, under the guidance of his or herphysician, without the need to visit a physical therapist.The home program could be highly structured, with aseries of specific exercises that the patient decides toengage in on a daily basis; or it could be less structured,with the patient setting goals to increase general ac-tivity levels by a certain percent every week. As thereare so many paths that may be taken to reach any onetreatment goal, a treatment plan can, and should, bedeveloped that is tailored to the patient’s own situa-tion, goals, and interests, and that is developed in closecollaboration with the patient. Such collaboration willincrease the chances that the patient will adhere to thetreatment plan, and ultimately increase the chances ofa successful treatment outcome.
References1. Cruz M, Pincus HA (2002) Research on the Influence that Com-
munication in Psychiatric Encounters has on Treatment. Psychi-atr Serv 53:1253–1265
2. Dawson R, Spross JA, Jablonski ES et al. (2002) Probing theParadox of Patients’ Satisfaction with Inadequate Pain Manage-ment. J Pain Symptom Manage 23:211–220
3. Engel JM, Kartin D, Jensen MP (2002) Pain Treatment and HealthCare in Persons with Cerebral Palsy: Frequency and Helpfulness.Am J Phys Med Rehabil 81:291–296
4. Frank AF, Gunderson JG (1990) The Role of the TherapeuticAlliance in the Treatment of Schizophrenia. Arch Gen Psychiatry47:228–236
5. Gavin LA, Wamboldt MZ, Sorokin N et al. (1999) TreatmentAlliance and its Association with Family Functioning, Adher-ence, and Medical Outcome in Adolescents with Severe, ChronicAsthma. J Pediatr Psychol 24:355–365
6. Jensen MP, Nielson WR, Kerns RD (2003) Toward the Develop-ment of a Motivational Model of Pain Self-Management. J Pain4:477–492
7. Levinson W, Gorawara-Bhat R, Lamb J (2000) A Study of PatientClues and Physician Responses in Primary Care and SurgicalSettings. JAMA 284:1021–1027
8. McCracken LM, Klock PA, Mingay DJ et al. (1997) Assessmentof Satisfaction with Treatment for Chronic Pain. J Pain SymptomManage 14:292–299
9. Miaskowski C, Nichols R, Brody R et al. (1994) Assessment ofPatient Satisfaction Utilizing the American Pain Society’s Qual-ity Assurance Standards on Acute and Cancer-Related Pain. JPain Symptom Manage 9:5–11
10. Miller W, Rollnick S (2002) Motivational Interviewing: Prepar-
ing People to Change, 2nd edn. Guilford Press, New York11. Riley JL, Meyers CD, Robinson ME, Bulcourf B et al. (2001)
Factors Predicting Orofacial Pain Patient Satisfaction with Im-provement. J Orofac Pain 15:29–35
12. Rollnick S, Mason P, Butler C (1999) Health Behavior Change:A Guide for Practitioners. Churchill Livingstone, Edinburgh
13. Sherwood G, Adams-McNeill J, Starck PL et al. (2000) Qualita-tive Assessment of Hospitalized Patients’ Satisfaction with PainManagement. Res Nurs Health 23:486–495
14. Ward SE, Gordon DB (1996) Patient Satisfaction and Pain Sever-ity as Outcomes in Pain Management: A Longitudinal View ofone Settings’ Experience. J Pain Symptom Manage 11:242–251
15. Weiss KA, Smith TE, Hull JW et al. (2002) Predictors of Riskof Non-Adherence in Outpatients with Schizophrenia and OtherPsychotic Disorders. Schizophr Bull 28:341–349
Chronic Pain, Thalamic Plasticity
� Thalamic Plasticity and Chronic Pain
Chronic Paroxysmal Hemicrania
Synonyms
CPH
Definition
Chronic paroxysmal hemicrania is a trigemino-auto-nomic syndrome with frequent repeated facial pains,each lasting for 3 minutes or more. Attacks can re-cur over >1 year without remission periods or withremission periods lasting <1 month.� Paroxysmal Hemicrania� Primary Stabbing Headache

374 Chronic Pelvic Inflammatory Disease
Chronic Pelvic Inflammatory Disease
� Chronic Pelvic Pain, Pelvic Inflammatory Diseaseand Adhesions
Chronic Pelvic Pain
Definition
In woman, chronic pelvic pain is intermittent or constantpain in the lower abdomen or pelvis of at least 6 months’duration,notoccurring exclusively with menstruationorintercourse and not associated with pregnancy.� Chronic Gynaecological Pain, Doctor-Patient Inter-
action� Chronic Pelvic Pain, Physical and Sexual Abuse� Gynecological Pain and Sexual Functioning� Gynecological Pain, Neural Mechanisms
Chronic Pelvic Pain, EndometriosisFRED M. HOWARD
University of Rochester, Rochester, NY, [email protected]
Synonyms
Endometriosis Externa
Definition
Endometriosis is the presence of ectopic endometrialglands and stroma, that is endometrium located outsidethe endometrial cavity (Fig. 1). Occasionally only en-dometrial glands are present in cases of endometriosis.Hemosiderin-laden macrophages may be present also,but their solitary presence without endometrial glandsor stroma does not confirm endometriosis. Sampsonfirst applied the name “endometriosis” to ectopic en-dometrium in 1921 (Sampson 1921).
Characteristics
Endometriosis is most often found within the peritonealcavity in the pelvis, but may also occur in numerousother, even remote, locations (Table 1). There is still agreat deal about it that is unclear and controversial andit remains an enigmatic disorder in that the etiology, thenatural history and the precise mechanisms by whichit causes pain are not completely understood. In somepatients it behaves almost like a malignancy, spreadingrapidly and widely, yet in others it is a seemingly irrel-evant, insignificant, incidental histological diagnosis.Grossly, endometriosis has a variety of appearances; itmay be red, purple, blue, white, yellow, brown, clear orblack lesions, peritoneal pockets or windows, adhesions
Chronic Pelvic Pain, Endometriosis, Figure 1 Endometriosis of thepelvic peritoneum.
Chronic Pelvic Pain, Endometriosis, Table 1 Possible sites of en-dometriosis
Common sites Less common or rare sites
Ovaries Umbilicus
Round ligaments Laparotomy scars
Broad ligaments Hernial sacs
Uterosacral ligaments Small intestine
Rectovaginal septum Rectum
Appendix Sigmoid
Pelvic peritoneum Ureters
Bladder Vulva
Pelvic lymph nodes Extremities
Cervix Pleural cavity
Vagina Lung
Fallopian tubes Nasal mucosa
or chocolate cysts. Endometriosis is primarily a diseaseof women of reproductive age.
Prevalence
As endometriosis is accurately diagnosed only by sur-gical biopsy with histological confirmation, accurateprevalence is difficult to determine, but is estimated tobe about 7% (Barbieri 1990). In women who undergoa laparoscopy to evaluate chronic pelvic pain (CPP)the prevalence of endometriosis is about 33% (Howard1993). In patients undergoing laparoscopy for infertilitythe prevalence is about 40%. Additionally it appears thatabout 70% of women with endometriosis have sometype of pelvic pain symptoms. It has been observed thatthe severity of pain frequently does not correlate withthe severity of endometriosis (Vercellini 1991).

C
Chronic Pelvic Pain, Endometriosis 375
Etiology
None of several theories of etiology alone explainthe protean manifestations of endometriosis or thepredilection of some women but not others to developsymptomatic endometriosis. Sampson’s theory is thatendometriosis is due to retrograde flow of menstrualeffluent through the fallopian tubes into the peritonealcavity. However, most women experience some de-gree of retrograde menstruation, so there is more tothe development of endometriosis than just retrogradeflow. Metaplasia of coelomic epithelium, the epitheliumfrom which the mullerian duct is derived, can resultin endometrium. Metaplasia needs an induction phe-nomenon or factor, which might be menstrual debris,estrogen or progesterone. The theory of lymphatic andvascular metastases is invoked to explain the occur-rence of endometriosis in remote locations such as thepleura, nose and spinal column. It has been reportedthat endometriosis is present in pelvic lymph nodes in30% of women with pelvic endometriosis, which sup-ports this theory. A defect of the immunological systemis supported by a good deal of research and helps toexplain why not all women develop endometriosis sec-ondary to retrograde menstruation. It also ties into thetheory of genetic predisposition, as an immunologicdisorder may be inherited. Finally, recent research hasfocused on the endometrial cells that are present inendometriosis and found a number of abnormalitiesthat may contribute either to initiation or developmentof endometriosis. For example, endometriosis cellshave been found to have abnormal production of aro-matase cytochrome P450, an enzyme that is not presentin normal endometrium and is integral to the conversionof androstenedione and testosterone to estrogen. Thisability to produce estrogen locally may directly stim-ulate the growth of endometrial cells of endometrioticlesions. Endometriosis cells have also been observed tohave increased amounts of vascular endothelial growthfactor and interleukin-6.It is worthwhile to especially note the role of estrogen, asthere are several clinical observations that suggest thatthe development and persistence of endometriosis areestrogen dependent. First, endometriosis is rare beforepuberty or after menopause unless the woman is on es-trogen replacement therapy.Second,bilateraloophorec-tomy typically results in regression of endometriotic le-sions. Third, decreased levels of estradiol via GnRH ag-onist treatment results in regression of endometriosis.Fourth, endometriosis can develop in the prostatic utri-cle of a male with DES treatment for prostatic cancer.Finally, immunohistochemical studiesshowvirtually allendometriosis lesions contain estrogen receptors.The etiology of symptoms in some women but not inothers is also not understood. Endometriosis mightproduce symptoms due to swelling of the tissue withhormonal stimulation, plus extravasation of blood and
menstrual debris into surrounding tissues, with produc-tion of prostaglandins as possible chemical mediatorsof pain and inflammation. It is also hypothesized thatlesions produce prostaglandins and cause functionalpain symptoms, like dysmenorrhea, via direct produc-tion of prostaglandins (Vernon 1985). Finally, it hasbeen suggested that lesions cause pain via nociceptorstimulation by mechanical pressure or by stretchingtissue. Such a mechanism would predict that largerlesions and more deeply infiltrating lesions wouldcause more frequent or more severe pain (Cornillie1990).
Symptoms and Signs
Classically the woman with endometriosis presentswith one or more of the following, an adnexal mass(endometrioma), infertility, pelvic pain or dysmen-orrhea. Estimates are that up to 40% of women withendometriosis have chronic pelvic pain. Pelvic painmost often starts as dysmenorrhea and at least 75% ofwomen with endometriosis-associated pelvic pain havedysmenorrhea as an initial component of their pain.Dyspareunia with deep penetration is also a frequentcomponent of endometriosis-associated pain, occur-ring in about 33% of cases. Although CPP, dyspareuniaand dysmenorrhea are significantly more commonin women with endometriosis than in women with anormal pelvis, these pain symptoms are not as spe-cific nor diagnostic for endometriosis as is commonlythought and by themselves do not justify a diagnosis ofendometriosis.Intestinal involvement, usually of the appendix, rec-tosigmoid or anterior rectum, may cause abdominalpain, dyspareunia, tenesmus, dyschezia, constipation,diarrhea, low back pain and, rarely, hematochezia orsymptoms of bowel obstruction. Urinary tract involve-ment, most often at the bladder peritoneum and anteriorcul-de-sac, may cause frequency, pressure, dysuria orhematuria. Involvement of the distal one-third of theureter may lead in rare cases to symptoms of ureteralobstruction. With lung involvement, endometriosismay rarely cause dyspnea on exertion, pleural effusionand lung collapse. Catamenial hemothorax has been re-ported. A cyclically bleeding or a cyclically tender massin an incisional scar may also occur with endometriosis.The physical examination is often normal, but thereis tenderness, especially during the menses, in manywomen with endometriosis-associated pelvic pain. Afixed retroverted uterus with posterior tenderness is par-ticularly suggestive of endometriosis. Tender nodularityof the uterosacral ligaments and cul-de-sac is a classi-cally described finding with endometriosis. Narrowingof the posterior vaginal fornix or lateral deviation of theposition of the cervix may rarely be present. In patientswith endometriomas a tender adnexal mass may benoted.

376 Chronic Pelvic Pain, Endometriosis
Diagnostic Studies
At the present time an accurate diagnosis can only bemade by surgical and histological confirmation. Beforethe introduction of diagnostic laparoscopy, this requiredan exploratory laparotomy. Laparoscopy is a much lessinvasiveprocedureand iscurrently therecommended di-agnostic procedure for any patient suspected of havingendometriosis.A preoperative ultrasound is worthwhile as 15–20% ofwomen with endometriosis have endometriomas. Thesegenerally range from 3 to 8 cm in size and are not al-ways palpable by physical examination. Measurementof serum Ca-125 levels has a low sensitivity and speci-ficity, although it is more reliable for advanced stage dis-ease (Lanzone 1991). Ca-125 levels are also elevatedwith cancers of the ovary, endometrium,gastrointestinaltract, fallopian tube and breast as well as pelvic inflam-matory disease, pregnancy, menses and leiomyomata.Adolescents with endometriosis should be evaluated forobstructive anomalies of the reproductive system usingmagnetic resonance imaging, ultrasound and hysterog-raphy. About 10% will have such an anomaly.In patients in whom intestinal endometriosis is sus-pected, evaluation of the intestinal tract is usuallynormal, as most patients have involvement of the serosaor muscularis, not the mucosa. Sigmoidoscopy mayshow a bluish submucosal mass in some of these cases.Mucosal lesions may be diagnosed by sigmoidoscopy,colonoscopy or barium enema studies, but these evalu-ations are certainly not necessary on a routine basis.In patients with suspected urinary tract involvement,cystoscopy and intravenous pyelography or comput-erized tomography of the kidney, ureters and bladdermay be indicated.
Medical Treatment
There are many options for medical and surgical treat-ment of endometriosis-associated pelvic pain (see listbelow).
General treatment options for women with endometri-osis-associated pelvic pain
• Observation with palliative treatment• Conservative surgery• Hormonal suppression• Combined medical and surgical treatments• Definitive extirpative surgery (radical surgery)
Danazol, a 17-ethinyl-testosterone derivative, was ap-proved by the FDA for treatment of endometriosis in1976 (Greenblatt et al. 1971). It is mildly androgenicand anabolic, properties that account for many of itsside effects. Side effects include acne, edema, weightgain, hirsutism, voice changes, hot flushes, abnormaluterine bleeding, decreased breast size, decreased li-bido, vaginal dryness, nausea, weakness and musclecramps. Danazol does not significantly affect LH and
FSH levels in premenopausal women, but lowers es-trogen levels by directly inhibiting steroidogenesis atthe ovarian and adrenal levels. Sixty to 83% of patientsobtain significant relief of pelvic pain with danazoltherapy and the number needed to treat is 1.7 (Barbieriet al. 1982). Danazol is contraindicated in patients withabnormal uterine bleeding, pregnancy, breastfeeding orimpaired renal, cardiac or hepatic function.Gonadotropin releasing hormone (GnRH) agonistsare analogues of naturally occurring gonadotropin-releasing hormone and are the most commonly pre-scribed medical treatment for endometriosis in theU.S.A. Examples of GnRH agonists are nafarelin,leuprolide and goserelin. They all work at the hypo-thalamic-pituitary level to shut down LH and FSHproduction and release, resulting in a dramatic declinein estradiol levels. Pain relief with GnRH agonists isabout the same as with danazol. Side effects of theGnRH agonists are loss of bone density, hot flashes,vaginal dryness, decreased libido, headaches, emo-tional lability, acne and reduced breast size (Bergqvistet al. 1998; Kennedy et al. 1990; Wheeler et al. 1992).Because of concerns about loss of bone density, add-back therapy with 5 mg day-1 of norethindrone acetate,with or without 0.625 conjugated equine estrogen, isrecommended for up to 1 year of treatment (Hornsteinet al. 1998). After discontinuation of treatment, symp-toms tend to recur in most patients, with mean time torecurrence between 8 to 11 months.A number of progestagens, particularly medroxypro-gesterone acetate and norethindroneacetate, are used totreat endometriosis. Breakthrough bleeding, prolongedamenorrhea, mood changes, depression, weight gainand irritability are common side effects. Gestrinone,a 19-nortestosterone derivative with mostly progesta-genic and low androgenic activity, has also been usedto treat endometriosis (not available in the US) (TheGestrinone Italian Study Group 1996).Oral contraceptives are commonly used to treat en-dometriosis. They appear to be less effective than GnRHagonists in relieving dysmenorrhea and dyspareunia,but comparable in relief of non-menstrual pelvic pain(Vercellini et al. 1993). Side effects are weight gain,breast tenderness, nausea, chloasma, abnormal uterinebleeding, enlargement of myomas, thrombophlebitisand thromboembolism, increased appetite, irritabil-ity, depression, edema, hypertension and increasedvaginal discharge. They are contraindicated in womenwith a history of or high risk of thrombosis or a his-tory of breast cancer and relatively contraindicatedwith diabetes, collagen vascular disease or hyperten-sion.
Surgical Treatment
Surgical treatment of endometriosis may be conser-vative (i.e. without extirpation of the uterus, tubes orovaries) or radical (i.e. with extirpation of the uterus

C
Chronic Pelvic Pain, Endometriosis 377
or one or both ovaries). Radical surgery appears to bemore effective in achieving pain relief, but conserva-tive surgery is more appropriate in younger women,especially if preservation of reproductive potential isimportant. Also, conservative surgery can be done atthe time of laparoscopic diagnosis (Howard 1994). Thecore of either conservative or radical surgical treat-ment is the removal or destruction of all endometrioticlesions. A randomized clinical trial of conservativesurgery for endometriosis shows that on average thereis a 50% decrease of pain 6 months postoperativelyand the number needed to treat is 2.5 (Sutton et al.1994).Both presacral neurectomy (resection of the supe-rior hypogastric plexus) and uterosacral neurectomy(transection of the uterosacral ligament) have beenrecommended for relief of CPP associated with en-dometriosis, but results of randomized clinical trialsshow efficacy only for presacral neurectomy, (Candianiet al. 1992; Zullo et al. 2003) not uterosacral neurectomy(Sutton et al. 2001; Vercellini et al. 2003). Presacralneurectomy is most effective for the treatment specif-ically of midline dysmenorrhea. There appears to bea small effect, if any, on non-menstrual pelvic pain ordyspareunia.If fertility is not desired, then hysterectomy, with orwithout bilateral salpingo-oophorectomy, is often rec-ommended for endometriosis-associated pelvic pain.There is no consensus as to the advisability of removalof both ovaries if one or both are not directly involved byendometriosis, but recurrence of pain when one or bothovaries are preserved has been reported to be increased(relative risk for pain recurrence of 6.1, confidenceinterval 2.5 to 14.6) (Namnoum et al. 1995). Althoughuncommon, endometriosis has been reported to recuraf-ter hysterectomy and bilateral salpingo-oophorectomy,with and without estrogen replacement therapy. Finally,currently available data do not allow a conclusion asto whether medical or conservative surgical treatmentis more effective in the treatment of endometriosisassociated pelvic pain.
Combined Medical and Surgical Treatment
There are no clinical trials of preoperative medicaltreatment. There are however, at least three random-ized, placebo-controlled clinical trials of postoperativemedical treatment (Hornstein et al. 1997; Parazziniet al. 1994; Telimaa et al. 1987). These trials suggestthat pain is decreased with postoperative medical treat-ment while patients are on the medications, but within6–12 months after discontinuation of medications painlevels are similar in postoperative patients whether ornot they received medical treatment. A reasonable wayto apply these data is to initiate medical treatment afterconservative surgical debulking therapy if patients havepersistent or recurrent pain, rather than treat all patientspostoperatively.
References
1. Barbieri RL (1990) Etiology and epidemiology of endometriosis.Am J Obstet Gynecol 162:565–567
2. Barbieri RL, Evans S, Kistner RW (1982) Danazol in the treat-ment of endometriosis: analysis of 100 cases with 4-year follow-up. Fertil Steril 37:737–746
3. Bergqvist A, Bergh T, Hogstrom L et al. (1998) Effects of trip-torelin versus placebo on the symptoms of endometriosis. FertilSteril 69:702–708
4. Candiani GB, Fedele L, Vercellini P et al. (1992) Presacralneurectomy for the treatment of pelvic pain associated withendometriosis: a controlled study. Am J Obstet Gynecol167:100–103
5. Cornillie FJ, Oosterlynck D, Lauweryns JM et al. (1990) Deeplyinfiltrating pelvic endometriosis: Histology and clinical signifi-cance. Fertil Steril 53:978–983
6. Greenblatt RB, Dmowski WP, Mahesh VB et al. (1971) Clin-ical studies with an antigonadotropin – danazol. Fertil Steril22:102–112
7. Hornstein MD, Hemmings R, Yuzpe AA et al. (1997) Use ofnafarelin versus placebo after reductive laparoscopic surgery forendometriosis. Fertil Steril 68:860–864
8. Hornstein MD, Surrey ES, Weisberg GW et al. for the LupronAdd-Back Study Group (1998) Leuprolide acetate depot and hor-monal add-back in endometriosis: a 12-month study. Obstet Gy-necol 91:16–24
9. Howard FM (1993) The role of laparoscopy in chronic pelvicpain: promise and pitfalls. Obstet Gynecol Survey 48:357–387
10. Howard FM (1994) Laparoscopic evaluation and treatment ofwomenwithchronicpelvicpain. JAmer Assoc Gynecol Laparosc1:325–331
11. Kennedy SH, Williams IA, Brodribb et al. (1990) A comparisonof nafarelin acetate and danazol in the treatment of endometriosis.Fertil Steril 53:998–1003
12. Lanzone A, Marane R, Muscatello R et al. (1991) Serum Ca-125 levels in the diagnosis and management of endometriosis.J Reprod Med 36:603
13. Namnoum AB, Hickman TN, Goodman SB et al. (1995) Inci-dence of symptom recurrence after hysterectomy for endometrio-sis. Fertil Steril 64:898–902
14. Parazzini F, Fedele L, Busacca M et al. (1994) Postsurgical medi-cal treatment of advanced endometriosis: results of a randomizedclinical trial. Am J Obstet Gynecol 171:1205–1207
15. Sampson JA (1921) Perforating hemorrhagic (chocolate) cystsof the ovary. Arch Surg 3:245
16. Sutton CJG, Ewen SP, Whitelaw N et al. (1994) Prospective,randomized, double-blind trial of laser laparoscopy in the treat-ment of pelvic pain associated with minimal, mild, and moderateendometriosis. Fertil Steril 62:696–700
17. Sutton C, Pooley AS, Jones KD et al. (2001) A prospective, ran-domized, double-blind controlled trial of laparoscopic uterinenerve ablation in the treatment of pelvic pain associated withendometriosis. Gynaecol Endoscopy 10:217–222
18. Telimaa S, Ronnberg L, Kauppila A (1987) Placebo-controlledcomparison of danazol and high-dose medroxyprogesterone ac-etate in the treatment of endometriosis after conservative surgery.Gynecol Endocrinol 1:363–371
19. The Gestrinone Italian Study Group (1996) Gestrinone versusa gonadotropin-releasing hormone agonist for the treatment ofpelvic pain associated with endometriosis: a multicenter, ran-domized, double-blind study. Fertil Steril 66:911–919
20. Vercellini P, Bocciolone L, Vendola N et al. (1991) Peritonealendometriosis: morphologic appearance in women with chronicpelvic pain. J Reprod Med 36:533
21. VercelliniP, TrespidiL, ColomboAetal. (1993) Agonadotrophin-releasing hormone agonist versus a low-dose oral contraceptivefor pelvic pain associated with endometriosis. Fertil Steril60:75–79
22. Vercellini P, Aimi G, Busacca M et al. (2003) Laparoscopicuterosacral ligament resection for dysmenorrhea associated

378 Chronic Pelvic Pain, Epidemiology
with endometriosis: results of a randomized, controlled trial.Fertil Steril 80:310–319
23. Vernon MW, Beard JS, Graves K et al. (1985) Classification ofendometriotic implants by morphological appearance and capac-ity to synthesize prostaglandin F. Fertil Steril 46:801–806
24. Wheeler JM, Knittle JD, Miller JD (1992) Depot leuprolideversus danazol in treatment of women with symptomaticendometriosis. I. Efficacy results. Am J Obstet Gynecol167:1367–1371
25. Zullo F, Palomba S, Zupi E et al. (2003) Effectiveness of pre-sacral neurectomy in women with severe dysmenorrhea causedby endometriosis who were treated with laparoscopic conserva-tive surgery: A 1-year prospective randomized double-blind trial.Am J Obstet Gynecol 189:5–10
Chronic Pelvic Pain, Epidemiology
� Epidemiology of Chronic Pelvic Pain
Chronic Pelvic Pain, Interstitial Cystis
� Interstitial Cystitis and Chronic Pelvic Pain
Chronic Pelvic Pain, Laparoscopic PainMapping
FRED M. HOWARD
Department of Obstetrics and Gynecology, Universityof Rochester, Rochester, NY, [email protected]
Synonyms
Conscious Laparoscopic Pain Mapping; Pain Map-ping; Conscious Pain Mapping; Patient Assisted La-paroscopy; Laparoscopy (for Pain) under Local Anes-thesia; Laparoscopic Pain Mapping
Definition
Laparoscopic pain mapping is a diagnostic laparoscopyunder local anesthesia, with or without conscious seda-tion, performed with the goal of identifying sources orgenerators of pain in women with chronic pelvic pain. Ithas been suggested that laparoscopic pain mapping canlead to the treatment of subtle or atypical areas of dis-ease that might have been overlooked if the procedurehad been done under general anesthesia (Almeida andVal-Gallas 1997). Also, it may help to avoid surgical in-terventions when there are no surgically treatable paingenerators present. However, there are limited data con-firming these potential benefits (Demco 1997).Laparoscopy under local anesthesia is not new, but itsuse as a diagnostic modality to localize areas of ten-derness potentially responsible for chronic pelvic painis a relatively new technique. It was first described in1996 in a series of eleven patients with pelvic pain, ten
Chronic Pelvic Pain, Laparoscopic Pain Mapping, Table 1 Visual ana-logue scores (VAS) of various anatomic structures at the time of laparoscopicpain mapping
Anatomic Structure Median VAS WhenStructure is NotSite of Pain
Median VAS WhenStructure is Site ofPain
Uterus 2 9
Ovaries 3 8
Fallopian Tubes 2 -
Round Ligaments 1 -
UterosacralLigaments &Cul-de-sac
1 9
Intestines 1 -
Unpublished data courtesy of P. Reginald
of whom were found to have diffuse visceroperitoneal� tenderness (Palter and Olive 1996). It has also beenused to evaluate women with endometriosis-associatedpelvic pain (Demco 1998).The technique used to map the pelvis is a gentle probingor tractioning of tissues and organs with a blunt probe orforceps passed through a secondary cannula site. Duringa systematic evaluation of the entire pelvis, the patient isasked to note the presence or absence of tenderness andpain and to rate its severity when present. In particular,the patient is to note if there is replication of her usualor presenting pain. Diagnosis of an etiologic lesion ororgan should be based on the severity and quality ofpain elicited, especially reproduction of the patient’spresenting pain. It has been suggested that applying orinjecting local anesthetic to sites of focal tendernessmay block the pain response and possibly improve thepredictability that surgical excision will be therapeutic.Also, � superior hypogastric plexus block can be doneat the time of laparoscopic pain mapping and may helpto predict the efficacy of presacral neurectomy (Steege1998).It has been shown that when laparoscopy is done underlocal anesthesia in women without pelvic pain, there isno significant pain or tenderness to probing of theuterus,ovaries, omentum or bowel (Zupi et al. 1999). Table 1summarizes the pain levels of viscera in women withchronic pelvic pain in one unpublished series of laparo-scopies under local anesthesia.
Characteristics
Not all women with chronic pelvic pain are candidatesfor laparoscopic pain mapping. Patients who are mor-bidly obese (BMI greater than 30), have significantanesthesia risk, have anxiety disorders or psychiatricdisease or are known or suspected to have severe adhe-sive disease are not ideal candidates for the procedure.Counseling and preparation of the patient is also cru-

C
Chronic Pelvic Pain, Laparoscopic Pain Mapping 379
cial, because chronic pelvic pain patients experiencegreater pain with laparoscopy under local anesthesiathan non-pain patients. Intolerable pain is the mostcommon reason for failures with laparoscopic painmapping. Other reasons for failures may include adhe-sions that obliterate the visual field, inability to accessthe peritoneal cavity and inability to visualize the entirepelvis. Published success rates range from 70–100%.As with traditional diagnostic laparoscopy, endometrio-sis and adhesions are the most common diagnoses madewith laparoscopic pain mapping; i.e. they are the lesionsthatmost frequently elicitpain and tendernessat the timeof pain mapping. However, even in patients with tenderendometriosis or adhesions, other endometriotic lesionsor adhesions may not be tender to probing at the time oflaparoscopic pain mapping.Other less common lesions found to map pain at the timeof laparoscopic pain mapping include sciatic hernia,leiomyoma, hernia repair site, postoperative peritonealcyst, colon carcinoma, chronic ileal disease, staple at theureter, pseudo stone secondary to gallbladder spillage,peritoneal puckering, two with ovary, herniorrhaphysite and peritoneal scarring. Individual pelvic viscerahave also been mapped as painful, including the uterus,ovary, fallopian tube, round ligament, appendix, bladderand vaginal apex.
Endometriosis
In one published series there were 15 cases with suc-cessful conscious pain mapping and a visual diagnosisof endometriosis and in these cases endometrioticlesions were mapped as painful sites in seven. In allseven of these cases there was histological confirmationof the diagnosis. In the remaining eight successfullymapped cases in which endometriotic lesions did notmap positively, there was histological confirmation ofthe diagnosis in only two cases. Thus seven of nine caseswith histologically confirmed endometriosis mappedpain to endometriotic lesions, versus none of six casesin which the visual diagnosis of endometriosis wasnot histologically confirmed (P = 0.007, Fischer’s ex-act test). These findings emphasize the importance ofthe histologically confirmed presence of endometrialglands and stroma to generation of pain by suspectedendometriotic lesions. Another published series cor-relating the appearance of endometriotic lesions withtenderness showed that 84% of red lesions, 76% of clearlesions, 44% of white scar lesions and 22% of blacklesions are painful (Demco 1998). Findings at laparo-scopic pain mapping have also suggested that up to asmuch as a 3 cm area of normal-appearing peritoneumsurrounding endometriotic lesions may be tender.
Adhesions
Whether adhesions can produce pain is controversial.All of the published series of conscious pain mappinghave shown that adhesions can be tender and that their
stimulation can reproduce a patient’s pain. This stronglysupports the hypothesis that some adhesions cause ab-dominopelvic pain. As appears to be the case with en-dometriosis, these data also suggest that adhesions arenotalwaysasourceofpain in womenwith chronicpelvicpain and adhesions.
Chronic Visceral Pain
Laparoscopicpain mapping not infrequently showsgen-eralized pelvic visceral and peritoneal hypersensitivity,suggesting such patients may have chronic visceral painsyndrome of visceral neuropathic etiology. We believethat our finding of patients with diffuse pelvic visceraland peritoneal tenderness may represent a way to con-firm the diagnosis of chronic visceral pain syndrome,a diagnosis that has been suggested for chronic painsyndromes believed to be of visceral origin (Wesselman1999). Unpublished data suggest that reproductive vis-cera tend to be tenderer than peritoneum or intestinesat the time of laparoscopic pain mapping. It may bethat many of the patients with no apparent diagnosisat the time of diagnostic laparoscopy under generalanesthesia may have chronic visceral pain syndrome.Clearly further evaluations are needed to confirm theseproposals.
Summary
Chronic pelvic pain is a multifactorial and complicateddisorder. It is premature to assume that the findings withlaparoscopic pain mapping translate directly into causeandcure.Forexample,comparingseriesofpatientsfromour center who were evaluated with traditional diagnos-tic laparoscopyto thoseevaluatedwithlaparoscopicpainmapping showed similar prevalences of endometrio-sis and adhesions in both groups (endometriosis in38% versus 40% and adhesions in 34% versus 54%,respectively) (Howard 1994). Treatment based on thefindings at the time of laparoscopic pain mapping didnot change the outcomes however, compared to theoutcomes based on traditional diagnostic laparoscopy.With laparoscopic evaluation and treatment withoutpain mapping, 78% of patients had decreased pain and45% were pain-free. With laparoscopic pain mapping,44% had decreased pain and 16% were pain-free. Thepatients in the two groups were not identical, as onlyone-half of the patients in the traditional diagnosticlaparoscopy series had undergone prior evaluations andtreatments for chronic pelvic pain, compared to all ofthe patients evaluated by laparoscopic pain mapping.The clinical value of conscious pain mapping bothdiagnostically and therapeutically cannot be stated yet,as only observational studies are available. Current datasuggest it does help to avoid unnecessary operativelaparoscopies in some cases. Whether it improves out-comes in women with chronic pelvic pain by leading tomore specific medical and surgical treatments requires

380 Chronic Pelvic Pain Model
more study and probably a prospective, randomizedtrial.
References1. Almeida Jr OD, Val-Gallas JM (1997) Conscious pain mapping.
J Am Assoc Gynecol Laparosc 4:587–5902. Demco LA (1997) Effect on negative laparoscopy rate in chronic
pelvic pain patients using patient assisted laparoscopy. J Soc La-paroendosc Surg 1:319–321
3. Demco LA (1998) Mapping the source and character of pain dueto endometriosis by patient-assisted laparoscopy. J Am AssocGynecol Laparosc 5:241–245
4. Howard FM (1994) Laparoscopic evaluation and treatment ofwomenwithchronicpelvic pain. J AmerAssoc Gynecol Laparosc1:325–31
5. Metha PV (1989) A total of 250,136 laparoscopic sterilizationsby a single operator. Br J Obstet Gynaecol 96:1024–1034
6. Palter SF, Olive DL (1996) Office microlaparoscopy under localanesthesia for chronic pelvic pain. J Am Assoc Gynecol Laparosc3:359–364
7. Steege JF (1998) Superior hypogastric block during microlaparo-scopic pain mapping. J Am Assoc Gynecol Laparosc 5:265–267
8. Wesselman U (1999) A call for recognizing, legitimizing,and treating chronic visceral pain syndromes. Pain Forum8:146–150
9. Zupi E, Sbracia M, Marconi D et al. (1999) Pain mapping duringminilaparoscopy in infertile patients without pathology. J AmAssoc Gynecol Laparosc 6:51–54
Chronic Pelvic Pain Model
� Visceral Pain Models, Female Reproductive OrganPain
Chronic Pelvic Pain, MusculoskeletalSyndromes
ROBERT D. GERWIN
Department of Neurology, Johns Hopkins University,Bethesda, MD, [email protected]
Synonyms
Viscerosomatic pain syndromes; myofascial pain syn-dromes; myofascial trigger points.
Definition
Chronic pelvic pain syndromes (CPPS) and even acutepelvic pain syndromes (APPS) can have both visceraland a body wall (somatic) representations, referred to asviscerosomatic and musculoskeletal or myofascial painsyndromes respectively.
Characteristics
Pain can arise from a disorder of a visceral organ, as ininflammatory bowel disease or endometriosis, ureteralcalculus or interstitial cystitis. The presenting complaint
however, can be � somatic pain, such as lower abdom-inal wall pain in irritable bowel syndrome, celiac dis-ease or colitis, flank pain in renal colic and pelvic flooror pelvic region � myofascial pain syndromes in inter-stitial cystitis or endometriosis. The visceral componentcan be difficult to identify or can be overlooked, becausevisceral pain is diffuse and poorly localized. One musthave a high degree of suspicion in order to identify thevisceral component of pain when the complaint is so-matic pain like a myofascial pelvic floor muscle painsyndrome. The visceral syndromes that are common inwomen include endometriosis and interstitial cystitis, ir-ritable bowel syndrome and irritable bladder syndrome,whereas prostatitis or � prostadynia, interstitial cystitisand irritable bowel syndrome are common in men (Vec-chiet et al. 1992; Wesselmann 1999; Lukban et al. 2001;Verne et al. 2001; Nadler 2002).Myofascial pain syndromes can also refer pain to a re-gion where visceral pain is common, either as local oras referred pain. The attendant trigger point formationand the referred pain can cause or aggravate visceral or-gan dysfunction. This is readily seen in bladder or boweldysfunction in the presence of trigger points in the lev-ator ani and other pelvic floor muscles. Abdominal walland pelvic floor trigger points can persist long after aninitiating visceral insult has passed. This is seen verystrikinglywhenabdominalwall� triggerpointsform(inthe abdominal oblique muscles) in response to ureteralcolic and persist for weeks after the stone has passed,or recur weeks or months later like renal colic, when infact there is only somatic trigger point pain. Treatmentof the trigger points eliminates the local and the referredpain.
Visceral Pain� Visceral Nociception and Pain can result from suchnon-tissue injuring mechanisms as distention or in-creased capsular pressure or from inflammation, is-chemia or obstruction. Thus, visceral pain can arisefrom conditions that produce or threaten tissue de-struction or from conditions that are benign. Interstitialcystitis, irritable bowel syndrome, chronic prostatitisand endometriosis are common causes of pelvic painwith pelvic region muscular pain representation. Asmany as 20–30% of cases of chronic prostatic relatedpain conditionsarenotdue to inflammatory or infectiouscauses (Krieger et al. 2002; Schaeffer et al. 2002) andcould be called prostadynia, a condition largely relatedto pelvic floor myofascial pain syndromes. Vulvadyniaand vulvar vestibulitis are not visceral pain syndromes,in the strict sense that they do not arise from hollowviscera, but they are non-muscular sources of chronicpelvic pain that are associated with musculoskeletalpain syndromes.Pain from pelvic region visceral and genital structuresis transmitted to the central nervous system throughthe visceral afferent sensory fibers of both sympathetic

C
Chronic Pelvic Pain, Musculoskeletal Syndromes 381
nerves (the splanchnic nerves) and parasympatheticnerves (the pelvic nerve), involving both the parasym-pathetic and sympathetic nerves in the superior andinferior hypogastric plexuses. Transmission of pelvicregion pain is by both the dorsal spinal column to thethalamus, and via the lateral columns to the medullarylateral reticular nucleus (Ness 2000). Pseudoaffectiveresponses associated with heart rate and blood pressurechanges are mediated via the lateral column.In addition to direct � nociceptive pathways from vis-ceral organs as well as from muscle to thespinal cord andbrain, there are psychophysiological responses as well.These responses are associated with central and perhapsperipheral sensitization. They are not uniformly foundin all hollow viscera. Rectal distention does not resultin an accelerated response with repeated stimulation asis found in the colon or in the urinary bladder. Repeatedstimulation of the urinary bladder by a distending stim-ulus results in lowering of the pressure threshold neededto evoke sensory responses and an acceleration of auto-nomic responses (Ness et al. 1998). The same effect hasbeen noted following repeated distention of the colon.Moreover, the area of sensitization or the region of thebody where discomfort is experienced widens with suc-cessive stimulation.
Referred Pain from Viscera
Studiesof subjectsexposed to repeateddistentionofhol-loworgans (colon,urinary bladder)haveshown thatpainfrom visceral organs is experienced in the body wall. Re-ferred pain from the gall bladder to the right shoulderarea, esophageal pain to the chest and cardiac pain tothe neck and arm are well known, as are prostatic andlabor pains referred to the perineum. Visceral organs ingeneral have both a somatic representation and a cuta-neous representation. These representations are relatedto the local spread of incoming nociceptive stimulationto the spinal cord. Thus, referred pain from genitouri-nary structures is felt in pelvic region musculoskeletalstructures rather than thoracic or lower extremity struc-tures.The mechanisms underlying central sensitization havebeen well studied over the past quarter century. Cuta-neous pain and somatic referred pain are both clinicallyexperienced. Pelvic floor pain, lower abdominal andflank pain and proximal thigh pain are all examples ofmyofascial referred pain syndromes. There is an interac-tion between primary visceral pain, primary myofascialpain and referred pain to and from these regions. Painthat originates as a myofascial pain syndrome fromnon-visceral causes can be experienced as visceral painwith symptoms characteristic of interstitial cystitis,irritable bowel syndrome or genital dysfunction. Asdiscussed above, visceral pain can result in muscularpain. In other words, the symptoms of referred pain goin both directions, visceral to somatic and somatic tovisceral (Gerwin 2002). Both the visceral and somatic
(muscular) pain syndromes need to be treated in orderto produce a positive outcome.The mechanisms of visceral induced hypersensitiza-tion include both peripheral nerve and central nervoussystem activation. Sensitization lowers the pain thresh-old, magnifies pain and results in a larger area of thebody being perceived to be painful. An example of amechanism resulting in peripheral sensitization is theincrease in rectal nerve fibers that are immunoreactiveto the heat and capsaicin receptor vanilloid receptor 1(Chan et al. 2003). � Central sensitization results in partthrough activation of the dorsal horn neuron by suchmeans as N-methyl D-aspartate receptor activation orby the convergence of two afferent nociceptive nervefibers on one dorsal horn neuron. A recently discoveredmechanism of central hypersensitization is the increasein the number of spinal lamina 1 neurons that expresssubstance P receptor, seen in both non-inflamed dis-tended rat colon and in the inflamed rat colon (Honoréet al. 2002). Visceral inflammation markedly increasedthe number and the rostro-caudal extent of lamina 1substance P receptor neurons that were activated bynormally non-noxious and noxious distention of thecolon. Neuroplastic changes in the central nervous sys-tem take place very rapidly in response to nociceptiveafferent input from viscera and from muscle, resultingin � hypersensitivity, � allodynia and an increase inthe receptive fields of individual dorsal horn neurons.Tenderness develops in response to non-nociceptivestimulation, increased perceived pain in response tonociceptive stimulation and this is perhaps part of thebasis for referred pain.Another phenomenon that is important for pain referredfrom viscera to somatic tissues and from abdominal andpelvic myofascial trigger points to viscera is the extentof spread of afferent input in the spinal cord. Spinal cordspread of non-nociceptive sensory afferent fibers in theclassical sensory system is over about 4 segments, 2 seg-ments upwards and 2 segments downward. Spinal cordspread of nociceptive sensory afferent fibers is 7–10 seg-ments in extent. The more extensive spread of nocicep-tive sensory afferent fibers increases the possibility ofreferred pain at a greater distance from the source of thenociceptivestimulus.Nociceptiveneuronalactivation inthe dorsal horn spreads from neuron to neuron throughthe excitation of cell surface receptors and the unmask-ing and activation of inactive or non-functional affer-ent connections from normally non-functional receptivefields. Activating these quiescent afferent connectionsresults in a given dorsal horn neuron responding to stim-ulation of receptive fields that normally belong to otherdorsal horn neurons. Thus, chronic painful stimulationfrom either pelvic region viscera or from abdominal andpelvic region myofascial trigger points results in pain re-ferral either to the somatic muscles or to visceral struc-tures or regions respectively. Viscerosomatic pain refer-ral is segmental and is most common locally. Thus, pain

382 Chronic Pelvic Pain, Musculoskeletal Syndromes
from interstitial cystitis is most often felt in the pubic re-gion and in the ventral portion of the pelvic floor mus-cles, like the levator ani muscle. Pain from endometrio-sis is often felt in the suprapubic and pubic region and inthe low back. Pain in irritable bowel syndrome is oftenfelt in the dorsal or posterior portion of the levator aniand other pelvic floor muscles like the piriformis mus-cles. Trophic changes can also be seen in the region ofreferred pain from visceral trigger points. Neurogenicplasmaextravasationcausingcutaneousedemawasseenin the region of referred pain in the rat in which uter-ine inflammation was produced (Wesselmann and Lai1997).
Abdominal and Pelvic Floor Myofascial Pain Syndromes
Myofascial trigger points are painful areas within mus-cle that are composed of tender regions or zones ontight or taut bands of muscle that can be palpated inaccessible muscles (Simons et al. 1999). The triggerzones within the muscle can be quiescent and notpainful until the muscle is activated by use or they canbe spontaneously painful even at rest. A property ofmyofascial trigger points that arises from central sensi-tization of dorsal horn neurons in the spinal cord is thedevelopment of referred pain zones in a predominantlylocalized, segmental manner, similar to the segmentalspread of referred pain from viscera. Trigger points inthe muscles discussed below are relevant to chronicpelvic pain syndromes when stimulation of the triggerpoints reproduces symptoms commonly experiencedby the patient. Visceral dysfunction, such as bladder orbowel irritability or dyspareunia, can occur as a result ofmyofascial trigger points. The classical chronic pelvicpain triad of endometriosis or prostadynia together withinterstitial cystitis and irritable bowel syndrome is usu-ally accompanied by abdominal and pelvic floor muscletrigger points that serve to perpetuate and aggravate thepelvic visceral syndromes.The following muscle trigger point referred patterns areof importance in pelvic visceral pain syndromes.
1. Lateral abdominal wall myofascial trigger pointsrefer pain to the lower abdominal quadrant and to thegroin. These muscles are affected by chronic colitis,Crohn’s disease and renal and ureteral chronic painconditions and can be associated with abdominalcramping pain, diarrhea or constipation.
2. Thoracolumbar paraspinal muscle trigger points,especially the lower thoracic, lumbar and multi-fidi muscle trigger points, refer pain to the buttock,sacral and coccygeal region and are associated withboth rectal-colonic dysfunction and genitourinarydysfunction.
3. Pelvic floor muscles, including the pubococcygeousand iliococcygeous muscles of the levator ani, are as-sociated with pelvic organ dysfunction, the anterioror ventral portion with genitourinary dysfunction, the
posterior or dorsal portion with colon and rectal/analdysfunction.Thebulbospongiosus, ischiocavernosusand transverse perinei muscles develop trigger pointsin association with genital dysfunction and give riseto � dyspareunia in women and penile, scrotal andprostatic pain in men.
4. Obturator internus trigger points often accompanychronic pelvic pain conditions involving bowel, blad-der and genital organs, but are particularly associatedwith rectal pain.
5. The gluteal muscles, including the gluteus maximus,gluteus medius, gluteus minimis and the piriformismuscle, give rise to trigger points in association withpain from any of the pelvic organs.
6. Adductor magnus medial thigh muscle trigger pointsreferpaindeepwithin thepelvisandcansimulategen-ital, bladder or rectal pain.
Diagnosis of these myofascial pain syndromes is madeby palpation of the appropriate muscles for hardened ortaut bands within the muscle. These bands generally runfrom one tendinis insertion to the other, will be tender topalpation and may refer pain to areas commonly experi-enced as painful by the patient. Referred pain phenom-ena usually take about 5–10 seconds of firm pressure todevelop.
Treatment
Treatment is directed towards inactivating the myofas-cial trigger points and preventing their return. Inactiva-tion of triggerpoints requires reducing oreliminating thepain from the trigger point and restoring normal lengthto the shortened, contracted, taut or hard band of mus-cle that harbors the trigger point. This can be done man-ually through the use of trigger point compression, lo-cal stretching and then stretching the entire muscle. Inchronic pelvic pain conditions, this may involve work-ing within the pelvis through the vagina or the rectum,even though the majority of manual work can be doneexternally.Trigger points can be reduced and pain relieved by phys-ical therapy modalities such as electrical stimulation,including percutaneous electrical stimulation. Ultra-sound may release superficial trigger points, but doesnot penetrate far enough to be effective in most deeptrigger points. Trigger point injection with local anes-thetic or needling the trigger zone with an acupunctureneedle without instilling local anesthetic is a highlyeffective way of inactivating trigger points. A localtwitch response elicited from the trigger zone (whichis followed by partial or complete relaxation of thetaut or hardened band and a reduction in trigger pointtenderness) is the confirmatory sign that the triggerzone has actually been entered and injected. There isno evidence to support the injection of substances otherthan local anesthetics, such as steroids, cyanocobal-amin or ketorolac. Injection or dry needling can be

C
Chronic Pelvic Pain, Pelvic Inflammatory Disease and Adhesions 383
done diagnostically to see if a trigger point is indeedcausing a problem, to treat acute pain and to facilitatephysical therapy. Trigger point injections in the pelvicregion can almost always be done externally, includinginjections of the levator ani, piriformis and obturatorinternus muscles. Only rarely is it actually necessary toinject vaginally.Conditions that create or perpetuate pelvic pain andpelvic region myofascial trigger points must be ad-dressed and corrected. Thus, vulvar vestibulitis, in-terstitial cystitis and structural factors such as pelvictorsion, pubic symphysis shear and sacroiliac joint dys-function must be treated and corrected. Muscle energytechniques are often adequate for the correction of thestructural perpetuating factors. Treatment of triggerpoints in the muscles that refer pain to the pelvis willoften result in dramatic improvement of chronic pelvicpain states and of pelvic organ dysfunction.
References1. Chan CHL, Facer P, Davis JB et al. (2003) Sensory fibres ex-
pressing capsaicin receptor TRPV1 in patients with rectal hy-persensitivity and faecal urgency. Lancet 361:385–391
2. Gerwin RD (2002) Myofascial and visceral pain syndromes:visceral-somatic pain representations. J Musculoskel Pain10:165–175
3. Honoré P, Kamp EH, Rogers SD, Gebhart GF, Mantyh PW (2002)Activation of lamina 1 spinal cord neurons that express the sub-stance P receptor in visceral nociception and hyperalgesia. J Pain3:3–11
4. Krieger JN, Ross SO, Deutsch L et al. (2002) The NIH Consen-sus concept of chronic prostatitis/chronic pelvic pain syndromecompared with traditional concepts of nonbacterial prostatitis andprostatodynia. Curr Urol Rep 3:301–306
5. Lukban JC, Parkin JV, Holzberg AS et al. (2001) Interstitial cys-titis and pelvic floor dysfunction: a comprehensive review. PainMedicine 2:60–71
6. Nadler RB (2002) Bladder training biofeedback and pelvic floormyalgia. Urology 60 (S6):42–43
7. Ness TJ (2000) Evidence for ascending visceral nociceptiveinformation in the dorsal midline and lateral spinal cord. Pain87:83–88
8. Ness TJ, Richter HE, Varner RE et al. (1998) A psychophysio-logical study of discomfort produced by repeated filling of theurinary bladder. Pain 76:61–69
9. Schaeffer AJ, Knauss JS, Landis JR et al. (2002) Chronic Pro-statitis Collaborative Research Network Study Group. Leukocyteand bacterial counts do not correlate with severity of symptomsin men with chronic prostatitis: the National Institutes of HealthChronic Prostatitis Cohort Study. J Urology 168:1048–1053
10. Simons DG, Travell JG, Simons LS (1999) Myofascial Pain andDysfunction: The trigger point manual, 2nd edn. Williams andWilkins, Baltimore, pp 11–93
11. Vecchiet L, Giamberardino MA, de Bigontina (1992) ReferredPain from Viscera. In: Sicuteri F, Tenenius L, Vecchiet L et al.(eds) Pain versus Man, Advances in Pain Research and Therapy,vol 20. Raven Press, New York, pp 101–110
12. Verne GN, Robinson ME, Price DD (2001) Hypersensitivity tovisceral and cutaneous pain in the irritable bowel syndrome. Pain93:7–14
13. Wesselmann U (1999) Pain - the neglected aspect of visceraldisease. Eur J Pain 3:189–191
14. Wesselmann U, Lai J (1997) Mechanisms of referred visceralpain: uterine inflammation in the adult virgin rat results in neu-rogenic plasma extravasation in the skin. Pain 73:309–317
Chronic Pelvic Pain, Pelvic InflammatoryDisease and Adhesions
FRED M. HOWARD
Department of Obstetrics and Gynecology, Universityof Rochester, Rochester, NY, [email protected]
Synonyms
Acute Salpingitis; Salpingitis-Oophoritis-Peritonitis;Chronic Pelvic Inflammatory Disease; Tubo-OvarianComplex; pelvic inflammatory disease
Definition
Pelvic inflammatory disease (PID) comprises a spec-trum of inflammatory disorders of the upper femalegenital tract, including any combination of endometri-tis, salpingitis, tuboovarian abscess and pelvic peri-tonitis (Centers for Disease Control 1998). Chronicabdominopelvic pain (CPP) and adhesive disease aresignificant sequelae of pelvic inflammatory disease(Safrin et al. 1992).PID is most often due to ascent of organisms from thevagina and cervix, but it may also be from contiguousspread of organisms (e.g. from appendicitis) or fromlymphatic or hematogenous spread (e.g. tuberculo-sis). PID may be iatrogenic after invasive diagnosticor therapeutic procedures, but more often it is sponta-neously associate with sexual activity. Infection withgonococcus or chlamydia increases the risk of PID.In the United States there are an estimated 1.2 millionvisits per year to physicians’ offices (Curran 1980) andabout 280,000 women per year are hospitalized forPID (Jones 1980; Washington 1984). In addition, anestimated 150,000 surgical procedures are performedannually for complications of salpingitis. The estimatedincidence of PID is 14.2 per 100 women.
Characteristics
Etiology
PID is a polymicrobial infection. Microorganisms thathave been recovered from the upper genital tracts ofwomen with PID include N. gonorrhoeae, C. trachoma-tis, mycoplasmas, anaerobic and aerobic bacteria fromthe endogenous vaginal floor such as Bacteroides, Pep-tostreptococcus, Gardnerella vaginalis, Escherichiacoli, Haemophilus influenza and aerobic Streptocci(Eschenbach et al. 1975; Monif et al. 1976). PID is of-ten precipitated by gonococcal or chlamydial infectionsof the cervix.Chronic pelvic pain develops in 18–36% of women sub-sequent to PID and may occur in up to 67% after three ormore episodes of PID (Haggerty 2003; Westrom 1980).(The etiology of CPP after PID is not known, but is gen-erally thought to be due to adhesive disease and to in-jury of the fallopian tubes and ovaries by the infection

384 Chronic Pelvic Pain, Pelvic Inflammatory Disease and Adhesions
Chronic Pelvic Pain, Pelvic Inflammatory Disease and Adhesions,Table 1 Peritubal adhesions and distal tubal pathology among PID patientwith chronic pain
Women withchronic pain
Total women Number Rate ( % )
ADHESIONS
None 57 5 9
Slight 23 3 13
Moderate 40 25 63
Extensive 32 29 91
FIMBRIATED ENDS
Normal 74 23 31
Phimotic 18 8 44
Clubbed 41 23 56
(Westrom1988)).OnepossiblemechanismforCPPmaybe related to chronic inflammation due to host immuno-logical responses to the acute infection. Another maybe recurrent infections due to repeated infectious expo-sures and weakened host defenses secondary to previ-ous damage (Moller et al. 1995; Patton et al. 1983). Atsecond-look laparoscopy, 88% of post-PID women withCPP had morphological changes in the fallopian tubesor ovaries or both and the severity of chronic pelvic painwas highly correlated with the extensiveness of pelvicadhesions (Table 1) (Westrom 1992).
Signs and Symptoms
PID is difficult to diagnosis because of wide variationin symptoms and signs. Overall, the clinical diagnosisof symptomatic PID has a positive predictive value of65 to 90%, yet many patients with mild symptoms maygo unrecognized. Even though PID is an infectious dis-ease, 30–50% of patients are afebrile. Lower abdomi-nal and pelvic pain are usually present and of less than2 weeks duration. Physical examination usually showsbilateral lower abdominal tenderness, bilateral adnexaltenderness and cervical motion tenderness. Abnormalcervical or vaginal discharge is characteristic. Labora-tory testing may show elevated erythrocyte sedimenta-tion rate, elevated C-reactive protein, leukocytosis andpositive cultures for N. gonorrhoeae or C. trachomatis.There is a strong correlation between exposure to sex-ually transmitted organisms and PID.Laparoscopy is the current gold standard for the di-agnosis of acute PID. However, routine laparoscopyis logistically and economically impractical for allpatients suspected of having acute PID. Other usefulstudies for diagnosing acute PID include histopatho-logical evidence of endometritis on endometrial biopsy(Paavonen et al. 1985) and transvaginal sonographyor other imaging techniques showing thickened fluid
filled tubes with or without pelvic fluid or tubo-ovariancomplex (Cacciatore et al. 1992).CPP associated with prior PID is generally thought to bedue to adhesionsor tubaldisease,butusually therearenospecific findings on examination that allow a diagnosisof adhesions or tubal damage. Occasionally with denseuterine adhesions the uterus is found in a fixed, immo-bile retroverted position. With hydrosalpinges or tubo-ovarian complexes, a tender adnexal mass may be palpa-ble. Laparoscopy for CPP may show fallopian tubes thatare tortuous, clubbed or phimotic and may show tubo-ovarian adhesions in women with prior PID. In manypatients laparoscopic findings may be normal.
Treatment
Acute PID should be treated empirically with broad-spectrum antibiotics to cover thevariety of likely aerobicand anaerobic pathogens. Oral versus parenteral treat-ment does not appear to alter outcomes nor change thelikelihood of developing CPP. Hospitalization shouldoccur if the diagnosis is uncertain and the patient seemsill, the patient is pregnant, the patient does not respondclinically to oral antimicrobial therapy, the patient isunable to follow or tolerate an outpatient oral regimen,the patient has severe illness, nausea and vomiting orhigh fever, the patient has a tubo-ovarian abscess or thepatient is immunodeficient.The ideal treatment of women with CPP secondary toPID is not known. Empirical antibiotic therapy is oftentried in women with CPP in whom prior, chronic orrecurrent PID is suspected. Unfortunately there are nostudies supporting efficacy for this approach. Surgicaltreatment by adhesiolysis or even removal of severelydamaged organs, such as hydrosalpinges, is utilized forconservative management, but only observational andanecdotal data are available to support this approach.Hysterectomy with bilateral salpingo-oophorectomyis commonly performed for CPP with pelvic findingssuggestive of prior PID, although there is not muchpublished information documenting efficacy for reliefof CPP.
References1. Cacciatore B, Leminen A, Ingman-Friberg S et al. (1992)
Transvaginal sonographic findings in ambulatory patients withsuspected PID. Obstet Gynecol 80:912–916
2. Centers for Disease Control (1997) 1998 guidelines for treat-ment of sexually transmitted diseases. MMWR Recomm Rep47:79–86
3. Curran JW (1980) Economic consequences of pelvic inflam-matory disease in the United States. Am J Obstet Gynecol1080:138–905
4. Eschenbach DA, Buchanan T, Pollock HM et al. (1975) Polymi-crobial etiology of acute pelvic inflammatory disease. N Engl JMed 293:166
5. Haggerty CL, Schulz R, Ness RB (2003) Lower Quality of LifeAmong Women With Chronic Pelvic Pain After Pelvic Inflam-matory Disease. Obstet Gynecol 102:934–939
6. Jones OG, Saida AA, St John RK (1980) Frequency and distribu-tion of salpingitis and pelvic inflammatory disease in short stayin hospitals in the United States. Am J Obstet Gynecol 138–905

C
Chronic Pelvic Pain, Physical and Sexual Abuse 385
7. Moller BR, Krostiansen FV, Thorsen P et al. (1995) Sterility ofthe uterine cavity. Acta Obstet Gynecol Scand 74:216–219
8. Monif GRG, Welkos SL, Baer H et al. (1976) Cul-de-sac iso-lates from patients with endometritis, salpingitis, peritonitis andgonococcal endocervicitis. Am J Obstet Gynecol 126:158
9. Paavonen J, Aine R, Teisala K et al. (1985) Comparison ofendometrial biopsy and peritoneal fluid cytology with la-paroscopy in the diagnosis of acute PID. Am J Obstet Gynecol151:645–650
10. Patton DL, Halbert SA, Kuo CC et al. (1983) Host response toChlamydia trachomatis infection of the fallopian tube in pig-tailed monkeys. Fertil Steril 40:829–840
11. Safrin S, Schachter J, Dahrouge D et al. (1992) Long-term se-quelae of acute PID. Am J Obstet Gynecol 166:1300–1305
12. Washington AE, Cates W, Sadi AA (1984) Hospitalizations forpelvic inflammatory disease. Epidemiology and trends in theUnited States 1975 and 1981. JAMA 251:2529–2533
13. Westrom L (1980) Incidence, prevalence and trends of acutepelvic inflammatory disease and its consequences in industri-alized countries. Am J Obstet Gynecol 138:880–892
14. Westrom L (1988) Chronic pain after acute PID. In: Belfort P,Piatti JA, Eskes TKAB, (eds) Advances in gynecology and obstet-rics. Proc XIIth World Congress Gynecol Obstet. Rio de Janeiro,October 1988, vol 6, pp 265–272
15. Westrom LV, Berger GS (1992) In: Berger GS, Westrom LV (eds)Consequences of pelvic inflammatory disease. Raven Press, NewYork, pp 101–114
Chronic Pelvic Pain, Physical and SexualAbuse
BEVERLY J. COLLETT, CHRISTINE CORDLE
University Hospitals of Leicester, Leicester, [email protected]
Definition
Physical Abuse
Hitting, shaking, throwing, poisoning, burning or scald-ing, drowning, suffocating, or otherwise causing phys-ical harm to another person (DoH 2000a).
Sexual Abuse
Forcing or enticing another person to take part in sexualactivities, whether or not they are aware of what ishappening. The activities may involve physical con-tact, including penetrative (e.g. rape or buggery) andnon-penetrative acts. They may include non-contactactivities, such as involving another person in look-ing at, or in the production of, pornographic materialor watching sexual activities or encouraging anotherperson to behave in sexually inappropriate ways (DoH2000a).The issue of defining sexual abuse in practice is bothcomplex and problematical.
Characteristics
The role of abusive experiences in � chronic pelvic painbegan to be the focus of investigation in the early 1980’s.Since then, there has been growing documentation ofprevalence rates for sexual and � physical abuse during
childhood and adulthood, in patients presenting with avariety of chronic medical conditions including chronicpelvic pain. Much of the published research comes fromNorth America, and how well these findings generaliseto other countries is not clear.More attention has been given to � sexual abuse thanphysical abuse in the literature. Reported prevalencerates for sexual abuse in patients with chronic pelvicpain range from 26% to 64% (Collett et al. 1998; Reiterand Gambone 1990; Toomey et al. 1993; Walker etal. 1988; Walling et al. 1994), and from 11% to 50%for physical abuse (Rapkin et al. 1990; Toomey et al.1993). This wide range is a reflection of the significantmethodological problems characterising this area ofresearch. One of the main problems is with definitions.Sexual abuse is defined in various ways by differentinvestigators. Some studies have only included con-tact sexual abuse, whereas others have used a widerdefinition of sexual abuse and have included episodesof threatened or attempted abuse without any directgenital contact. Other studies have excluded isolatedincidents of abuse. Some have distinguished betweenchildhood abuse (usually below the age of 14 years)and abuse in adulthood, whereas others have not madethis distinction.Similar problems exist with definitions of physicalabuse. Some studies only include life threatening abuse,where there is intent to seriously harm or kill, whereasothers have defined it as any pattern of physical dis-cipline or punishment, performed by a more powerfulother individual to a person aged under 18 years, re-sulting in physical injury such as marks, bruises andwelts.It is clearly important for investigators to define sexualand physical abuse in a more uniform way, taking intoaccount the age at the time of abuse, the nature, the rangeand duration of the abuse, and the relationship of theperpetrator to the abused person. There are also prob-lems with defining chronic pelvic pain,which representsa very heterogeneous group of patients. It has been sug-gested that certain subgroups of patients with chronicpelvic pain have a higher prevalence of sexual trauma(Reiter et al. 1991).The other factor known to influence reported prevalencerates is the method of data collection. Most data is col-lectedusingface-to-face interviewsorself-administeredquestionnaires. It has been suggested that lengthy inter-views carried out in a certain style are more likely to re-sult in abuse disclosure (Wyatt and Peters 1986).Many of the early studies did not include control groups,and although this has been addressed in more recentresearch, there is still lack of agreement over whatconstitutes an appropriate control group. Groups arerarely matched for such factors as chronicity of painand age. Age may have a role in abuse reporting. Brierefound that older women reported less sexual abusethan younger women, and this was attributed to the

386 Chronic Pelvic Pain, Physical and Sexual Abuse
older woman’s discomfort with speaking about sexu-ality (Briere 1992). Many studies are limited by smallsample sizes and are based on a population of patientsreferred to speciality pain clinics. The findings fromsuch clinics may not be generalisable to patients seenin routine gynaecology clinics or in the primary caresetting. There is a need for prospective studies withlarger sample groups, although these are very difficultto carry out. The methodological problems in this areaof research make it difficult to draw conclusions fromthe data presented.A number of controlled studies, comparing women withchronic pelvic pain with women with pain in a differentsite and women with no pain, have demonstrated anincreased prevalence of lifetime sexual abuse in thechronic pelvic pain group (Collett et al. 1998). In onestudy, this association only held for women who hadbeen abused as an adult, whether or not they had alsobeen abused as a child (Jamieson 1997). She also foundthat recent abuse was more likely to be associated withpain syndromes.There is much less information about physical abuse andchronic pelvic pain. One often quoted study by Rapkin(1990), found that women with chronic pelvic pain weresignificantly more likely to report a history of childhoodphysical abuse than women receiving routine gynaecol-ogy care or women with pain in another site. This find-ing has not been replicated, although other workers havesuggested that a history of physical abuse may be morerelevant than a history of sexual abuse in women withchronic pelvic pain (Walling et al. 1994).There has been considerable speculation in the literatureas to thepossiblemechanismslinkingabusewithchronicpelvic pain. It has been suggested by several workersthat any type of childhood trauma, including violence,separations, illnesses and neglect, would be a predictorfor pain proneness in adulthood. It is argued that trau-matised individuals are more likely to feel vulnerableabout their body and their health. Some psychologistsconceptualise the pain amongst victims of sexual abuseas a defence against the overwhelming emotions con-nected to the traumatic experience. Linton (1996) sug-gested an indirect relationship in that abuse may affectpain by altering perception and ones ability to cope withpain. Support for this model comes from the knowledgethat abused patients have higher levels of depression andaffective distress, and lower levels of perceived control,compared to non abused patients. It may be that womenwith an abuse history have a tendency to report moresymptomsofany kind asa function ofpsychologicaldis-turbance. Although the data are consistent with the ideathat abuse may be instrumental in the development ofchronic pain problems, we do not understand the mech-anisms involved with this. It has been pointed out thatabuse may be a correlate rather than a causal variable,since abuse may be related to many lifestyle risk factors(Fry 1993).
A recent prospective investigation of childhood sexualandphysicalabuseandneglect foundnoassociationwithadult pain symptoms. However,unexplained pain symp-toms were found to be associated with retrospectiveself-reports of all types of childhood victimisation. Perhapspatientswhorecallchildhoodabuseandneglectperceivethemselves to be trapped by a history that they cannotundo, and this in turn leads to helplessness and passivity(Raphael 2001).In view of the high prevalence of lifetime abuse inwomen with chronic pelvic pain, it has been arguedthat such women should be routinely asked about anyabuse history as part of their assessment. A number ofstudies have shown that women with chronic pelvicpain are rarely asked about assault, and only a smallminority of women volunteer this information to agynaecologist or physician. When women were askedwhether they thought they should be asked, 90 per centanswered in the affirmative (Robohm and Buttenheim1996). In addition to asking about any past abuse his-tory, it is important to ensure that the women are notinvolved in any ongoing abuse. Interpersonal sensitiv-ity in treating these women is particularly important.Concerns about trust in the doctor-patient relationshipare common, and women with a history of � childhoodsexual abuse report more anxiety, embarrassment andvulnerability associated with a gynaecological exam-ination than other women (Robohm and Buttenheim1996).Linton found that more than 85 percent of the womenin his sample did not believe that their history of abuseaffected their pain or their sex lives. Interventions, there-fore, oriented directly towards abuse may be difficult toincorporate into general pain treatment. Specific ther-apy for the abuse may be the best way to deal with theproblem if the patient has unresolved issues around theabuse, which are affecting her current functioning.In summary, there are complex interactions betweenchild and adult abuse, depression, stressful life eventsand the occurrence of chronic pelvic pain, and cliniciansneed to take these psychosocial factors into considera-tion when assessing and treating women with chronicpelvic pain.Little research into physical and sexual abuse amongstpatients with chronic vulvar pain syndromes or � vulvo-dynia has been undertaken. However, studies that havebeen undertaken show that there is a significantly higherincidence of sexual abuse and psychological distressin chronic pelvic pain patients, compared to womenwith chronic vulvar pain and to gynaecological controls(Bodden-Heidrich et al. 1999, Reed et al 2000).
References1. Bodden-Heidrich R, Kuppers V, Beckmann MW, Rechenberger
I, Bender HG (1999) Chronic Pelvic Pain Syndrome (CPPS) andChronic Vulvar Pain Syndrome (CVPS): Evaluation of Psycho-somatic Aspects. J Psychosom Obstet Gynecol 20:145–151

C
Chronic Pelvic Pain, Physical Therapy Approaches and Myofascial Abnormalities 387
2. Briere J (1992) Child Abuse Trauma. Theory and Treatment ofthe Lasting Effects. SAGE Publications, London
3. Collett BJ, Cordle CJ, Stewart CR, Jagger C (1998) A Compar-ative Study of Women with Chronic Pelvic Pain, Chronic Non-Pelvic Pain and Those with no History of Pain Attending GeneralPractitioners. Br J Obstetrics Gynaecology 105:87–92
4. Department of Health (2000a) Working Together to SafeguardChildren in Need and Their Families. The Stationary Office, Lon-don, p 5
5. Fry RP, Crisp AH, Beard RW, McGuigan S (1993) PsychosocialAspects of Chronic Pelvic Pain with Special Reference to SexualAbuse. A study of 164 women. Postgrad Med J 69:566–574
6. Glaser D & Frosch S (1988) Child Sexual Abuse. Macmillan,London, p 5
7. Jamieson DJ, Steege JF (1997) The Association of Sexual Abusewith Pelvic Pain Complaints in a Primary Care Population. AmJ Obstet Gynecol 177:1408–1412
8. Linton SJ, Larden M, Gillow AM (1996) Sexual Abuse andChronic Musculoskeletal Pain: Prevalence and PsychologicalFactors. Clinical Journal of Pain 12:215–221
9. Raphael KG, Widom CS, Lange G (2001) Childhood Victimiza-tion and Pain in Adulthood: A Prospective Investigation. Pain92:283–293
10. Rapkin AJ, Kames LD, Darke LL, Stampler FM, Nabiloff BD(1990) History of Physical and Sexual Abuse in Women withChronic Pelvic Pain. Obstet Gynecol 76:92–95
11. Reed BD, Haefner HK, Punch MR, Roth RS, Gorenflo DW,Gillespie BW (2000) Psychosocial and Sexual Functioning inWomen with Vulvodynia and Chronic Pelvic Pain. J Reprod Med45:624–632
12. Reiter RC, Gambone JC (1990) Demographic and Historic Vari-ables in Women with Idiopathic Chronic Pelvic Pain. Obstet Gy-necol 75:428–432
13. Reiter RC, Shakerin LR, Gambone JC, Milburn AR (1991) Cor-relation Between Sexual Abuse and Somatisation in Women withSomatic and Nonsomatic Chronic Pelvic Pain. Am J Obstet Gy-necol 165:104–109
14. Robohm JS, Buttenheim M (1996) The Gynaecological Care Ex-periences of Adult Survivors of Childhood Sexual Abuse: A Pre-liminary Investigation. Women Health 24:59–75
15. Toomey TC, Hernandez JT, Gittelman DF, Hulka JF (1993) Rela-tionship of Sexual and Physical Abuse to Pain and PsychologicalAssessment Variables in Chronic Pelvic Pain. Pain 53:105–109
16. Walker E, Katon W, Harrop-Griffiths J, Holm L, Russo J, HickokLR (1988) Relationship of Chronic Pelvic Pain to PsychiatricDiagnoses and Childhood Sexual Abuse. Am J Psychiatry145:75–80
17. Walling MK, Reiter RC, O’Hara MW, Milburn AK, Lilly G,Vincent SD (1994) Abuse History and Chronic Pain in Women:Prevalence of Sexual Abuse and Physical Abuse. Obstet Gy-naecol 84:193–199
18. Wyatt GE, Peters SD (1986) Methodological Considerations inResearch on the Prevalence of Child Sexual Abuse. Child AbuseNegl 10:241–251
Chronic Pelvic Pain, Physical TherapyApproaches and MyofascialAbnormalities
RHONDA K. KOTARINOS
Long Grove, IL, [email protected]
Synonyms
Myofascial trigger point; myofascial pain syndrome
Definition
A � myofascial trigger point is a hyper-irritable spotwithin a taut band of skeletal muscle or muscle fas-cia which is painful on compression and gives rise tocharacteristic referral pain patterns, tenderness andautonomic phenomena. (Travell and Simons 1983)� Myofascial pain syndrome has had various defini-tions over the years. An early definition identifies it asa regional muscle pain disorder that is characterizedby tender spots in taut bands of muscle that refer painto areas overlying or distant to the tenderness. (Travell1990) The sensory, motor and autonomic phenomenoncaused by myofascial trigger points is the currentlyacceptable definition. (Simons et al. 1999) In diagnos-ing a myofascial pain syndrome, the specific muscle ormuscle group must be specified.
Characteristics
Chronic pelvic pain has many definitions. At this time,there is not a universally accepted definition of chronicpelvic pain, which mirrors the problems with defin-ing myofascial pain syndrome. In 1989, the AmericanCollege of Obstetricians and Gynecologists definedchronic pelvic pain as pain that had persisted for sixmonths or longer and of such severity that it signifi-cantly impacted the ability to function and relationships.(Steege 1989) Six common characteristics associatedwith chronic pelvic pain were: duration of 6 months orlonger, incomplete relief by most previous treatments,significantly impaired function at home or work, signsof depression, pain out of proportion to pathology andaltered family roles” (Steege 1989). Over time, definingchronic pelvic pain evolved to be based on the duration,the anatomical and physical basis or psychologicalcharacteristics of the pain. (Steege et al. 1993) Chronicpelvic pain in the absence of obvious pathology is de-fined by the International Association for the Study ofPain as chronic or recurrent pelvic pain that appearsto have a gynecologic origin but without a definitivelesion or cause (Mersky and Bogduk 1994).Many pain syndromes are included within the domainof chronic pelvic pain. Vulvodynia, vulvar vestibulitis,urethral syndrome, interstitial cystitis, penile pain, or-chialgia, perineal pain, chronic prostatitis, prostadynia,proctalgia fugax, are a few of the pain syndromes asso-ciated with chronic pelvic pain.Confusion in defining chronic pelvic pain has not beenlimited to medical management of the female. In 1995,the National Institutes of Health (NIH) proposed thatthe definition of Chronic Pelvic Pain Syndrome in menwould be based on “the presence of genito urinary painand the absence of uropathogenic bacteria by standardmicrobiological methodology.” (Kreiger et al. 1999)ChronicAbacterialProstatitis /ChronicPelvicPainSyn-drome is a new category (Category III) established byNIH. The specific definition being discomfort of pain

388 Chronic Pelvic Pain, Physical Therapy Approaches and Myofascial Abnormalities
in the pelvic region (for at least three months, variablevoiding and sexual symptoms with no demonstrable in-fection).Chronic pelvic pain in both sexes continues to be a diag-nostic and therapeutic challenge. Musculoskeletal dys-function is emerging as a common denominator in themanifestation of chronic pelvic pain in both men andwomen.Two major categories of musculoskeletal dysfunctionassociated with chronic pelvic pain are myofascialdysfunction and � somatic dysfunction (Grunman1989). Several studies have investigated the most com-mon components of the somatic dysfunction. Somaticdysfunction describes dysfunction within the mus-culoskeletal system that is characterized by skeletalasymmetry, altered articular mobility and tissue textureabnormality. In a retrospective study performed at theUniversity of Tennessee, 75 % of 132 patients werefound to have a “typical pelvic pain posture.” (King etal. 1991) A lordosis of the lumbar spine with an anteriorpelvic tilt were the common components of the typicalpelvic pain posture. Other common musculoskeletaldysfunctions identified in the typical pelvic pain posturepatients included decreased iliopsoas length, decreasedrange of motion of lumbar spine flexion, decreasedrange of motion of hip rotation and increased pelvicfloor muscle tone.Individualized physical therapy treatment plans weredeveloped and executed for each patient. Physical ther-apy treatment included active and passive stretching,active and passive lumbar flexion exercises, abdominalmuscle strengthening, and joint mobilization. Otherphysical therapy modalities included massage, externalsupports, moist heat and electrotherapy. Education as toproper posturing for lifestyle factors was included in thephysical therapy management. Complete or significantrelief was achieved in 70 % of the chronic pelvic painpatients that received physical therapy treatment. Adlerinvestigated musculoskeletal structure as sources ofundiagnosed pelvic and / or abdominal pain. (Adler2003) Twenty women that had continued pain afterhysterectomy for pelvic / abdominal pain were referredto physical therapy, primarily for concomittent lowback pain. During the comprehensive orthopedic phys-ical therapy evaluation, the subjects were to inform thetherapist if their chief complaint could be reproducedby palpation of various musculoskeletal structures. Apositive result was documented when their pain wasreproduced to a level of 80 % or higher.Seventeen of the twenty subjects (85 %) reported thattheir pain was reproduced during the physical therapyevaluation. Mechanical dysfunctions, poor posturalhabits and myofascial trigger points were musculoske-tal factors that were determined to be elements of pelvicand / or abdominal pain.Two major categories of musculoskeletal dysfunctionassociated with chronic pelvic pain, myofascial disor-
ders and skeletal malalignment, have been described.(Punch et al. 1994) Within each category the specificdiagnostic criteria, typical muscle groups implicatedfor each category and the therapeutic treatment plan forthe dysfunction was delineated. (Table 1)Punch et al. found that 35 women of 160 that were re-ferred to their university hospital clinic had a muscu-loskeletal cause for their chronic pelvic pain. Physicaltherapy management as described (Table 1) and triggerpoint injections, being determined on an individual ba-sis, was administered to the subjects. Sixty-nine percentreported total or significant pain relief.Pelvic floor dysfunction is well established as being afactor in many of the syndromes associated with chronicpelvic pain. Weiss performed a retrospective study of52 patients that presented to him with a diagnosis of ei-ther interstitial cystitis or urgency-frequency syndrome.(Weiss 2001) Manual physical therapy to the pelvic floorincludes trigger point release techniques with and with-out injections, active and passive stretching, and neuro-muscular reeducation. Eighty-three percent of the pa-tients with urgency-frequency syndrome had moderatetocomplete resolutionof their symptoms.Of thepatientswith a diagnosis of interstitial cystitis, 70 % had markedor moderate improvement.Another retrospective study investigated musculoskele-tal pelvic pain in a pediatric and adolescent gynecologysetting. (Schroeder et al. 2000) To be included in thestudy, the subject had to have a diagnosis of pelvic painnot explained by a standard gynecologic work up or noresponse to standard treatments for known endometrio-sis. Of the sixty three patients who met the inclusion cri-teria, 50 % had a final diagnosis of musculoskeletal painwith 10 % having trigger points as a causative factor.Physical therapy management resulted in complete res-olution in 20 / 21 (95.24 %) who completed treatment.Fivesubjectsunderwenttriggerpointinjectionswith4/5(80 %) responding positively.In thepast,pelvicpaincomplaints inmostmenhavebeenattributed to prostate pathology, even when no pathol-ogy could be demonstrated. More recent studies are nowdemonstrating that there is a high incidence of muscu-loskeletal dysfunction in men who present with chronicpain syndrome type III A and III B. (Hetrick et al. 2003)This study compared pelvic muscle function in 62 menwith chronic pelvic pain syndrome III to 89 healthy menwithoutpelvicpain. Increased pelvicmuscle tenderness,increased pelvic floor muscle tone, greater incidence ofpelvicfloormuscle spasm and agreater incidenceofsub-stitution of other muscles when an isolated pelvic floorcontractionwasattemptedwasfoundin thesubjectswitha diagnosis of chronic pelvic pain syndrome III A & IIIB.Musculoskeletal dysfunction is slowly, but surely, be-ing established as one of many contributing factors as-sociated with chronic pelvic pain in men and women. Si-multaneously, health care professionals are learning that

C
Chronic Pelvic Pain, Physical Therapy Approaches and Myofascial Abnormalities 389
Chronic Pelvic Pain, Physical Therapy Approaches and Myofascial Abnormalities, Table 1 Assessment of Musculoskeletal Dysfunction (Punchet al 1994).
1. Typical Muscle Groups Affecting Pelvic Function (most common muscles emphasized)
Pelvic Floor Levator Ani
Coccygeous
Anterior Action Abdominal Wall
Iliopsoas
Rectus Fermoris
Sartorius
Quadratus Femoris
Gracilis
Posterior Action Gluteus Maximus
Hamstrings
Quadratus Lumborum
Piriformis
Lateral Rotators
Medial Action Adductor Magnus
Adductor Longus
Adductor Brevis
Pectineus
Lateral Action Tensor Fascia Latae
Gluteus Medius
Gluteus Minimus
2. Articular Dysfunctions Relevant to Pelvic Pain
Pubic Symphysis
Sacroiliac Joints
Lumbosacral Junction
Lumbar Spine
3. Screening for Musculoskeletal Dysfunctions
Clinical Picture Exacerbated by Movement, Postures or Positioning
Stiffness
Poorly Localized
Deep Ache, Tightness or Burning
May become more Diffuse Over Time
4. Treatment of Musculoskeletal Dysfunction
Restore ROM for involved muscles with Stretching protocol emphasizingTwice Daily Home Exercises and Duration of Stretch (15–30 Seconds)
Modalities to facilitate ROM Ice
Heat
Fluorimethane Spray
Ultrasound
Trigger Point Injections
Post Re-education
Progressive Strengthening Program

390 Chronic Postoperative Pain
a multidisciplinary approach is more likely to be effec-tive in managing chronic pelvic pain. (Wesselman 1998)A comprehensive multidisciplinary pain clinic shouldinclude representation from gynecologists, urogynecol-ogists, urologists, anesthesiologists, gastroenterologist,colorectal surgeons, physical therapists and various al-ternative medicine disciplines.Physical therapy is developing into an essential servicein treating chronic pelvic pain. All patients should beevaluated for musculoskeletal dysfunction and thenmanaged with an individualized treatment plan that ad-dresses the skeletal and myofascial dysfunctions noted.A comprehensive physical therapy evaluation wouldinclude a postural evaluation, gait analysis, musclestrength assessment, articular range of motion of thetrunk and extremities, and muscle length.A soft tissue evaluation should also be done. The tissuesto be assessed with this evaluation are the connective,muscle and neural tissues. Neural tissue assessmentwould be looking for � adverse neural tension. Painsymptoms can develop from neural tissue that hasimpaired movement and elasticity. (Butler 1991) Thephysical therapist should also perform a thorough pelvicfloor exam. An internal exam would include a localizedsoft tissue assessment, as well as assessment of thepelvic floor strength and range of motion. An instru-mented evaluation of the pelvic floor with EMG orpressure biofeedback can be useful, but is not required.The individualized treatment plan would address alldysfunctions noted. Treatment could include posturalcorrective exercise, active and passive stretching, neu-romuscular reeducation, progressive strengthening, andjoint mobilization. Manual therapy techniques would beemployed to address the soft tissue dysfunctions. Theycould include� myofascialmanipulation,� connectivetissue manipulation, neural mobilization / stretching,muscle energy techniques, and � myofascial release.Adjunctive management with modalities of physicaltherapy could include ice, heat, ultrasound, diathermy,electrical stimulation (TENS, high volt pulsed gal-vanic, interferential, etc.), biofeedback, and triggerpoint injections.
References1. Adler T, Personius W, Lamb R et al. (2003) Abstract Presentation.
Musculoskeletal Symptoms Mimicking Pathological Pelvic Painin Women. The International Pelvic Pain Society 10th ScientificMeeting on Chronic Pelvic Pain
2. Butler D (1991) Mobilization of the Nervous System. ChurchillLivingstone, Melbourne, p vii
3. Greenman P (1989) Principles of Manual Medicine. Williams& Wilkins, Baltimore
4. Hetrick D, Ciol M, Rothman I et al. (2003) Musculoskeletal Dys-function in Men with Chronic Pelvic Pain Syndrome Type III:A Case Control Study. J Urol 170:828–831
5. King P, Myers L, Ling F et al. (1991) Journal of Psychosomatics,Obstetrics and Gynecology 12:87–98
6. Kreiger JN, Nyberg L, Nickel J (1999) NIH Consensus Definitionand Classification of Prostatitis. Journal of American MedicalAssociation
7. Mersky H, Bogduk N (1994) Classification of Chronic Pain. IASPPress
8. Punch MR, Roth RS, Pominville L (1994) Musculoskeletal Ori-gins of Chronic Pelvic Pain in Women. American Society forPsychosomatic Obstetrics and Gynecology, 22nd Annual Meet-ing. San Diego, California. Poster Presentation
9. Shroeder B, Sanfilippo J, Hertweck S (2000) MusculoskeletalPelvic Pain in a Pediatric and Adolescent Gynecology Practice.Journal of Pediatric and Adolescent Gynecology 13:90
10. Simons D, Travell J, Simons L (1999) Myofascial Pain and Dys-
function: The Trigger Point Manual, vol 1, 2nd edn11. Steege J (1989) Chronic Pelvic Pain. ACOG Technical Bulletin
129:1–612. Steege J, Stout A, Somkuti S (1993) Chronic Pelvic Pain in
Women: Toward and Integrated Model. Obstetric and Gynecol-ogy Survey 48:95–110
13. Travell J, Simons D (1983) Myofascial Pain and Dysfunction:The Trigger Point Manual, vol 1, 1st edn
14. Travell JG (1990) Chronic Myofascial Pain Syndromes Advancesin Pain Research and Therapy 17:129–137
15. Weiss J (2001) Pelvic Floor Myofascial Trigger Points: Man-ual Therapy for Interstitial Cystitis and the Urgency-FrequencySyndrome. J Urol 166: 2226–2231
16. Wesselmann U (1998) Management of Chronic Pelvic Pain.In: Arnoff G (ed) Evaluation and Treatment of Chronic Pain.Williams & Wilkens, Baltimore, pp 269–279
Chronic Postoperative Pain
� Iatrogenic Causes of Neuropathy
Chronic Post-Surgical Neuralgia
� Iatrogenic Causes of Neuropathy
Chronic Post-Surgical Pain Syndromes
Definition
A pain lasting more than three months, persisting afterhealing from a surgical procedure. Chronic post surgi-cal pain syndromes are most often the consequence of aperipheral nerve injury directly or indirectly caused bythe surgical intervention. Proper identification of the in-jured nerve is crucial for adequate pain management.� Iatrogenic Causes of Neuropathy
Chronic Relapsing Polyneuropathy
� Chronic Inflammatory Demyelinating Polyneuropa-thy

C
Chronicity, Prevention 391
Chronic Tension-Type Headache
Definition
Classification of International Headache Society de-scribing a subtype of chronic daily headache as veryfrequent headaches (≥ 15 days per month for at least3 months, ≥ 180 days per year). Pain has 2 of the fol-lowing characteristics: pressing or tightening quality,mild or moderate intensity, bilateral location, and notaggravated by routine physical activity. Headache hasonly one of the following: photophobia, phonophobiaor nausea and does not have moderate or severe nauseaand no vomiting. Headache is not attributed to anotherdisorder, an individual’s use of analgesics or other acutemedication, and is ≤ 10 days per month.� Chronic Daily Headache in Children� New Daily Persistent Headache
Chronic Vulvar Pain
� Gynecological Pain and Sexual Functioning
Chronic Widespread Allodynia
Definition
The fibromyalgia syndrome can now be viewed phys-iologically as the classical human model for chronic,widespread allodynia.� Allodynia� Muscle Pain, Fibromyalgia Syndrome (Primary, Sec-
ondary)
Chronic Widespread Pain
Synonyms
CWP
Definition
Chronic widespread pain refers to pain in the left side ofthe body, pain in the right side of thebody, pain above thewaist, and pain below the waist. In addition, axial pain(cervical, thoracic or low back) must be present and painmust have persisted for at least three months (Wolfe F,Smythe H, Yunus M, et al. 1990).� Physical Exercise� Fibromyalgia
Reference
Wolfe F, Smythe H, Yunus M, et al. (1990) The Ameri-canCollegeofRheumatology.Criteriafor theClassifica-tion of Fibromyalgia. Report of the Multicenter CriteriaCommittee. Arthritis Rheum 33:160-172
Chronicity, PreventionMICHAEL K. NICHOLAS
University of Sydney, Royal North Shore Hospital, St.Leonards, NSW, [email protected]
Synonyms
Secondary Prevention
Definition
Interventions aimed at reducing the risk of a recently in-jured person developing chronic pain and disability.
Characteristics
The natural history of pain following injury, especiallynon-specific injuries like low back pain, is that such paintypically eases to minimal levels within 1–12 weeks. Ifpain persists beyond 12 weeks it has been reclassified as‘chronic’ (Merskey and Bogduk 1994) and may last forprolonged periods. However, recurrences of low backpain, once it has settled, are common. A systematic re-view of published evidence by Pengel et al. (2003) foundthat recurrences of low back pain in the first year afterinitial onset were in the region of 70%. Epidemiologi-cal findings of chronic pain, using the 3–month defini-tion, indicate that around 20% of adults in western in-dustrialisedcountriesreportexperiencingsuchpain(e.g.Blyth et al. 2001). Importantly, however, at least half ofthis group report that persisting pain was having littleimpact on their lives, indicating that having persistingpain does not, by itself, mean that the person will be dis-abled by it. In contrast, the remaining half of those withpersisting pain reported that it was interfering in theirlives to some degree, a proportion reporting substantialimpact on their lifestyles due to pain.Given the evidence that the transition from acute tochronic pain, and the concurrent development of dis-ability, can be modulated by psychological and envi-ronmental (or social) factors, a number of studies havedescribed attempts to modify these psychosocial fac-tors to prevent the development of secondary disability.Some interventions have addressed psychological riskfactors, such as beliefs, fears, coping strategies, andavoidance and escape behaviours. Other interventionshave addressed environmental or social risk factors,such as workplace arrangements, or compensation

392 Chronicity, Prevention
factors. A number of controlled treatment studies, ad-dressing these risk factors in people with acute andsub-acute musculoskeletal pain conditions, have nowbeen reported.Waddell and Burton (2000), in their systematic reviewofthe treatment literature for acute and sub-acute low backpain, concluded that there is strong evidence that adviceto continueordinary activitiesofdaily livingasnormallyas possible despite the pain, can give equivalent or fastersymptomatic recovery from acute symptoms, and leadsto shorter periods of work loss, fewer recurrences andless work loss the following year than “traditional” med-ical treatment. Specifically, they reported that interven-tions containing education (aimed at managing pain anddisability, as opposed to simply anatomy/physiology),reassurance and advice (to stay active), progressive fit-ness exercises, and pain management advice (using be-havioural principles) were likely to reduce the risks ofdeveloping chronic, disabling pain. Waddell and Burtonalso found that there was moderate evidence that suchapproaches were more effective, if they were combinedwith organisational (workplace) arrangements aimed atfacilitating return to work.Since that review, a number of randomised controlledstudies have provided further evidence that interven-tions aimed at psychosocial risk factors were effectiveat preventing the development of chronic disability. Forexample, Linton and Anderson (2001) demonstratedthat a brief (six 2–hour group sessions) cognitive-behavioural pain management (conducted by a clinicalpsychologist) intervention, for workers (who were stillworking but increasingly missing days at work due toback pain) with sub-acute low back pain (defined bythem as 6–8 months), was more effective than standardrehabilitation and information provision (via booklets)in terms of lost sick days and reduced use of healthcare.These effects were still present a year later, and therewas a 9–fold advantage for the cognitive-behaviouralapproach over the alternative interventions in terms oflost work days.Haldorsen et al. (2002) compared three different treat-ment modalities with a large sample of injured workerswith a range of musculoskeletal conditions who stillhad jobs, but had been sick-listed for at least 8–weeks inthe previous 2–years. The patients were first classifiedaccording to three prognostic categories for likely re-turn to work (based on a combination of questionnaireevaluation of psychosocial factors and physiotherapyassessment). Patients in each category were then ran-domly assigned to one of the different treatments. Thetreatments consisted of ‘ordinary treatment’ (referralto a general practitioner combined with some phys-iotherapy); ‘light multidisciplinary treatment’ (like alight mobilisation program or encouragement to resumenormal activities, similar to that reported by Indahl etal. 1995); and ‘extensive multidisciplinary treatment’(4–weeks of an intensive program similar to that de-
scribed by Bendix et al. 1998). Patients were followedup 14–months post-treatment.The results reported by Haldorsen et al. indicated thatinjured workers assessed to have a good prognosis ofreturn to work achieved good outcomes, regardless ofwhichever level of intervention they received. Whilethose with only medium prognostic profiles benefitedequally from the light and intensive multidisciplinaryprograms,butnotfrom‘standardorordinary’care.How-ever, those assessed to have a poor prognosis respondedbest to the intensive multidisciplinary treatment, withsignificantly better return to work rates up to 14–monthspost-treatment than light mobilisation (55 vs. 37%).Recently, Schonstein et al. (2003) reported the resultsof a systematic review of randomised and controlledphysiotherapy exercise programs for injured workers.This review concluded that there is evidence that theprograms “that include a cognitive-behavioural ap-proach can reduce the number of sick days lost forworkers with chronic back pain” (p. 5). They also con-cluded that “there is no evidence for or against specificexercises which are not accompanied by a cognitive-behavioural approach being effective” (p. 5) (in termsof sick days lost, for both acute and chronic back paincases). Thus, there is strong evidence that encourage-ment to resume normal activities or exercises, usingcognitive-behavioural methods, such as goal setting,consistent reinforcement for progress, and graduated in-crements in activities and exercises can limit secondarydisability due to persisting musculoskeletal pain.
References1. Bendix BT, Bendix A, Labriola M, Boekgaard P (1998) Func-
tional Restoration for Chronic Low Back Pain. Two Year Follow-Up of Two Randomized Clinical Trials. Spine 23:717–725
2. Blyth FM, March LM, Brnabic AJM, Jorm LR, Williamson M,Cousins MJ (2001) Chronic Pain in Australia: A PrevalenceStudy. Pain 89:127–134
3. Haldorsen EM, Grasdal AL, Skouen JS, Risa AE, Kronholm K,Ursin H (2002) Is There a Right Treatment for a Particular Pa-tient Group? Comparison of Ordinary Treatment, Light Multi-disciplinary Treatment, and Extensive Multidisciplinary Treat-ment for Long-Term Sick-Listed Employees with Musculoskele-tal Pain. Pain 95:49–63
4. Indahl A, Velund L, Reikeraas O (1995) Good Prognosis for LowBack Pain when Left Untampered: A Randomized Clinical Trial.Spine 20:473–477
5. Linton SJ, Andersson T (2000) Can Chronic Disability be Pre-vented? A Randomized Trial of a Cognitive-Behavioral Inter-vention and Two Forms of Information for Spinal Pain Patients.Spine 25:2825–2831
6. Merskey H, Bogduk N (1994) Classification of Chronic Pain.Descriptions of Chronic pain Syndromes and Definitions of PainTerms, 2nd edn. IASP Press, Seattle
7. Pengel LH, Herbert R, Maher CG, Refshauge KM (2003)Acute Low Back Pain: Systematic Review of its Prognosis.BMJ 327:323–327
8. Schonstein E, Kenny DT, Keating J, Koes BW (2003) Work Con-ditioning, Work Hardening and Functional Restoration for Work-ers with Back and Neck Pain. Meta-Analysis. Cochrane Databaseof Systematic Reviews (1)
9. Waddell G, Burton K (2000) Evidence Review. In: Carter JT, Bir-rell LN (eds) Occupational Health Guidelines for the Manage-

C
Cingulate Cortex, Functional Imaging 393
ment of Low Back Pain at Work – Principal Recommendations.Faculty of Occupational Medicine, London
Chung Model
� Animal Models and Experimental Tests to Study No-ciception and Pain
� Neuropathic Pain Model, Spinal Nerve LigationModel
� Retrograde Cellular Changes after Nerve Injury� Spinal Nerve Ligation Model
CIDP
� Chronic Inflammatory Demyelinating Polyneuropa-thy
Cingulate Cortex
Definition
Cortical tissue also referred to as Limbic Cortex or Cin-gulate Gyrus that encircles the hippocampus and otherstructures of the limbic region. It is sometimes inter-rupted as treatment for obsessive compulsive disorderor pain.� Cingulate Cortex, Nociceptive Processing, Behav-
ioral Studies in Animals� Pain Treatment, Intracranial Ablative Procedures
Cingulate Cortex, Effect on Pain-RelatedBehavior in Humans
� Pain Processing in the Cingulate Cortex, BehavioralStudies in Humans
Cingulate Cortex, Functional ImagingPIERRE RAINVILLE
Department of Stomatology, Faculty of DentalMedicine, University of Montreal, Montreal, QC,[email protected]
Definition
The cingulate cortex is a part of the medial frontaland parietal � cerebral cortices situated immediatelyabove the � corpus callosum and curving around itsmost anterior part. The human cingulate cortex canbe subdivided into several sub-regions as shown inFig. 1. Histologically, the anterior cingulate cortex
Cingulate Cortex, Functional Imaging, Figure 1 Anatomy of the humancingulate cortex. The cingulate cortex is delimited ventrally by the corpuscallosum. The full line corresponds to its approximate anterior, posteriorand dorsal borders. The sub-regions of the cingulate cortex are delimitedby dotted lines according to the corresponding Brodmann areas identifiedby numbers. Regions of the cingulate cortex can also be divided basedon their location relative to the body of the corpus callosum (dorsal =supracallosal; ventral = subcallosal) and to the anterior (rost = rostrumand genu) or posterior (spl = splenium) parts of the corpus callosum. Thesubgenual area corresponds to BA25, the perigenual area corresponds toBA33 and to the anterior part of BA24 and BA32 and the retrosplenial areacorresponds to BA26, BA29 and BA30.
(ACC) comprises � Brodmann area 25 (BA25) belowthe rostrum of the corpus callosum and BA24, BA32and BA33 above the body and curving around the genuof the corpus callosum. The posterior region of the cin-gulate gyrus corresponds to BA23, BA31, BA30, BA29and BA26. Traditionally, the cingulate cortex is consid-ered part of the � limbic system, which is associatedwith emotions. Furthermore, functional brain imagingstudies have shown that sub-regions of the cingulatecortex, in particular within the anterior cingulate cortex(ACC), are activated in response to painful stimuli andtherefore may be involved in pain related functions.Seeking to explain these findings, several theoreticalmodels have placed the cingulate cortex at the interfaceof the sensory, affective, cognitive, skeletomotor andvisceromotor systems (e.g. Vogt 2005).
Characteristics
Nociceptive Activation of the Cingulate Cortex
Almost all functional brain-imaging studies of painusing � positron emission tomography (PET) or� functional magnetic resonance imaging (fMRI) havefound pain related activation of the ACC (Apkarian etal. 2005). In these studies, experimental pain is pro-duced using noxious thermal, mechanical, electrical orchemical stimuli applied to the skin or viscera of normalhuman volunteers. Peaks of activation are found mostreliably in the caudal part of the supracallosal ACC andoccasionally in the perigenual area. This activation isconsistent with the projection of nociceptive neuronsfrom the medial and intralaminar nuclei of the thalamusto BA24 (Vogt 2005).

394 Cingulate Cortex, Functional Imaging
Functional Role of the ACC in Pain and Pain Modulation
Pain isacomplexexperiencedescribedalong� sensory-discriminativeand� affective-motivationaldimensionsinfluenced by cognitive processes and associated withsomato-motor and viscero-motor responses. The ACCmay contribute to each of these aspects. Levels ofactivation in the supracallosal ACC have been corre-lated with the subjective reports of pain (Coghill etal. 2003). More specifically, activity in certain regionsof the ACC may reflect the � affective-motivationaldimension of pain, as the modulation of pain unpleas-antness, independently of pain intensity, changes ACCactivity (Rainville 2002). Furthermore, the affective-motivational dimension of pain is strongly influencedby cognitive-evaluative processes shown to be highlydependent upon the function of the ACC (Price 2000).The supracallosal ACC is part of higher order systemsinvolved in the voluntary regulation of behavioral andmotor responses. Therefore, pain related activation inthis area probably reflects motivational aspects of painbehaviors and conscious processes involved in pain re-lated responses. Similarly, the perigenual region of theACC is involved in physiological arousal, a fundamentalaspect of emotion and a critical component of pain re-lated affective responses. Changes in activity within theperigenual area have been associated with physiologicalarousal during emotional experiences, the performanceof motor and cognitive tasks and the anticipation of pain(see Rainville 2002). However, the precise nature of therelationshipbetweenpainrelatedactivityin theACCandphysiological arousal remains to be demonstrated. Fi-nally,posterior regionsof thecingulatecortexmay be in-volved in the representation of viscerosomatic changes,but the functional role of this area in pain is unclear.The ACC is also critically involved in cognitive pro-cesses, as demonstrated by innumerable brain imagingstudies showing activation in this area during the perfor-mance of cognitive tasks (see Rainville 2002). However,this activation is typically observed in a more dorsalregion, within BA32, whereas pain related activationis more ventral, in BA24. Nonetheless, regions of theACC involved in cognitive processes may be involvedin the modulation of pain. Studies investigating themodulation of pain by hypnosis (Rainville et al. 1999),placebo analgesia (Petrovic et al. 2002; Wager et al.2004) and distraction (Valet et al. 2004) have in factshown some activation in the dorsal anterior region ofthe ACC (typically in BA32). This activation is associ-ated with a decrease in the response to painful stimuliin other pain related areas such as the somatosensorycortices and is consistent with a reduction in the painreported by subjects. In some of these studies, activa-tion of the ACC has also been found to correlate withactivity in the brain stem, consistent with the activationof the periaqueductal grey area (PAG), a key structureof descending pain inhibitory mechanisms.
A role for the ACC in pain modulation is also supportedby studies investigating the opioid system. Theμ-opioidreceptor is found in many brain areas including theACC.In a PET study, the systemic administration of the μ-opioid agonist fentanyl increased activity in theACCin acontrol condition without pain and reduced pain evokedactivity within the thalamusand cortical areas, includingtheACC(Caseyetal.2000).Thisdecrease inpainrelatedACC activity was associated with a decrease in reportedpain intensity and pain unpleasantness, as well as withpain related heart rate responses. Endogenous activationof the μ-opioid system in the ACC and other areas hasalso been associated with decreased affective ratings ofpain (Zubietaet al. 2001)and suggested asan underlyingmechanism of placebo analgesia (Petrovic et al. 2002).
Beyond Nociception: the ACC and the Mental Representationof Pain
In addition to its roles in the experience of pain and in themodulation of pain, the ACC may also be activated in thecontextofpain, intheabsenceofanoxiousstimulus.Thishas been suggested by studies showing that ACC activa-tion may occur during the anticipation of pain, prior tothe presentation of a painful stimulus (Rainville 2002).However, pain related activation of the ACC may also beobserved when the subject is merely thinking about, butnot expecting or anticipating, an actual painful stimulusto the self. For example, ACC activity has been reportedin response to visual stimuli depicting a hand or foot re-ceiving apainful stimulus (Morrison etal. 2004; Jacksonet al. 2005), videos showing apatient displaying pain be-haviors (Botvinick et al. 2005) or cues indicating that aloved one is receiving a painful stimulus (Singer et al.2004). ACC activation during both pain experiences andin response to cues signaling impending pain in the selfor pain in others may reflect a general involvement ofthis structure in the mental representation of pain.
A Multifunctional and Integrative Role for the ACC in Pain
From this brief overview of brain imaging studies, it isclear that the role of the ACC in pain is multifaceted.The ACC receives ascending nociceptive input and is inan excellent position to integrate this information withsignals related to the motivational, emotional and under-lying viscerosomatic state of the organism. The ACC isalso well positioned to modify cognitive and behavioralprioritiesbasedonthebiologicalsignificanceofpainsig-nals. In addition, theACCmay contribute to higherorderprocesses involved in pain modulation. Finally, theACCmay play a critical role in the mental representation ofpain in self and in others. This may provide a fundamen-tal neurobiological basis for social interactions and painempathy.
References1. Apkarian AV, Bushnell MC, Treede RD, Zubieta JK (2005) Hu-
man brain mechanisms of pain perception and regulation in healthand disease. Eur J Pain 9(4):463–484

C
Cingulate Cortex, Nociceptive Processing, Behavioral Studies in Animals 395
2. Botvinick M, Jha AP, Bylsma LM et al. (2005) Viewing facialexpressions of pain engages cortical areas involved in the directexperience of pain. Neuroimage 25:312–319
3. Casey KL, Svensson P, Morrow TJ et al. (2000) Selective opi-ate modulation of nociceptive processing in the human brain. JNeurophysiol 84:525–533
4. Coghill RC, McHaffie JG, Yen YF (2003) Neural correlates ofinterindividual differences in the subjective experience of pain.Proc Natl Acad Sci USA 100:8538–8542
5. Jackson PL, Meltzoff, AN, Decety J (2005) How do we perceivethe pain of others? A window into the neural processes involvedin empathy. Neuroimage 24:771–779
6. Morrison I, Lloyd D, di Pellegrino G et al. (2004) Vicariousresponses to pain in anterior cingulate cortex: is empathy a mul-tisensory issue? Cogn Affect Behav Neurosci 4:270–278
7. Petrovic P, Kalso E, Petersson KM et al. (2002) Placeboand opioid analgesia– imaging a shared neuronal network.Science 295:1737–1740
8. Price DD (2000) Psychological and neural mechanisms of theaffective dimension of pain. Science 288:1769–1772
9. Rainville P (2002) Brain mechanisms of pain affect and painmodulation. Curr Opin Neurobiol 12:195–204
10. Rainville P, Hofbauer RK, Paus T et al. (1999) Cerebralmechanisms of hypnotic induction and suggestion. J CognNeurosci 11:110–125
11. Singer T, Seymour B, O’Doherty J et al. (2004) Empathy forpain involves the affective but not sensory components of pain.Science 303:1157–1162
12. Valet M, Sprenger T, Boecker H et al. (2004) Distraction modu-lates connectivity of the cingulo-frontal cortex and the midbrainduring pain–an fMRI analysis. Pain 109:399–408
13. Vogt BA (2005) Pain and emotion interactions in subregions ofthe cingulate gyrus. Nat Rev Neurosci 6:533–544
14. Wager TD, Rilling JK, Smith EE et al. (2004) Placebo-inducedchanges in FMRI in the anticipation and experience of pain. Sci-ence 303:1162–1167
15. Zubieta JK, Smith YR, Bueller JA et al. (2001) Regional muopioid receptor regulation of sensory and affective dimensionsof pain. Science 293:311–315
Cingulate Cortex, NociceptiveProcessing, Behavioral Studies in Animals
PERRY N. FUCHS, VERNE C. COX
Department of Psychology, University of Texas atArlington, Arlington, TX, [email protected]
Synonyms
Anterior cingulate cortex; pain affect; Nociceptive Pro-cessing in the Cingulate Cortex, Behavioral Studies inAnimals
Definition
Nociceptive processing in the � cingulate cortex is be-lieved to reflect the affective component of pain and isprobably a critical structure in the neural network thatcontributes to the suffering that accompanies persistentpain states. Behavioral studies in animals have utilizedparadigms that measure escape and / or avoidance of anoxious stimulus. It is assumed that escape / avoidancebehavior isevidence thatanimalsfind thenoxiousstimu-lus aversive. With the use of these paradigms, the precise
natureof theneuroanatomicalandneurochemicalmech-anisms underlying the processing of higher order painprocessing in rodents is beginning to be understood.
Characteristics
The experience of pain consists of affective and sensorycomponents. It is the affective component that under-lies the suffering that accompanies many persistent painstates. An understanding of the neural substrates medi-ating the affective processing of nociceptive stimulationis essential for the development of successful pain thera-pies. The � anterior cingulate cortex (ACC) is one brainregion that has been implicated in the affective compo-nent of pain with relatively little involvement in sensoryprocessing (Vogt 1985). For instance, ACC neuronal ac-tivity increases in direct response to and / or anticipa-tion of noxious, but not nonnoxious chemical, mechan-ical and thermal stimuli (Hutchison et al. 1999; Koyamaet al. 2001). Surgical cingulotomy and cingulectomy, ortransection of the cingulum bundle and cingulate cortexrespectively, decrease the affective response to noxiousstimuli but do not alter ability to localize the unpleas-ant stimulus. Brain imaging studies consistently reportincreased ACC neuronal activity preceding and duringthe presentation of an acute noxious stimulus or duringpersistent pain conditions. Hypnotic suggestions to se-lectively decreasepain affectprior to and during noxiousstimulationresultedindecreasedratingsofpainunpleas-antness but not pain intensity (Rainville et al. 1997). Ma-nipulating pain unpleasantness by hypnotic suggestionalso changed the regional cerebral blood flow (rCBF) inthe ACC but not in the somatosensory cortex, providingevidence that the ACC is involved in the processing ofpain-related affect but not in the sensory processing ofnoxious stimulation (Rainville et al. 1997).Most of the studies that have examined supraspinalfocal brain stimulation or � microinjection of drugsinto discrete nuclei have measured reflexive behav-ioral response to acute noxious stimulation. Indeed,activation of various subcortical, brainstem and spinalcord systems produces antinociception, as revealedby an increase in the threshold or latency to respondto noxious stimulation. In most studies, it is assumedthat manipulations of limbic system structures alterpain processing through selective modulation of painaffect (Donahue et al. 2001). However, the majority ofpast and current behavioral paradigms cannot providedefinitive information about the aversive and unpleas-ant qualities of a persistent pain condition. Thus, it hasbeen difficult to examine the affective / motivational andsensory / discriminative components of pain processingin animal models. In addition, any study that attemptsto examine higher order processing of noxious input inanimals must address the exact nature of pain affect. Forinstance, the affective (i.e. worrisome, cruel, fearful,terrifying, etc.) nature of chronic pain in humans isdissociable from the sensory (i.e. shooting, stabbing,

396 Cingulate Cortex, Nociceptive Processing, Behavioral Studies in Animals
pinching, cramping, etc.) nature of the condition by thedescriptors that patients select on the � McGill PainQuestionnaire. In animal studies, the precise nature ofpain affect is more difficult to define. Affect, as it relatesto noxious input, is most certainly a negative hedonicstate that can be identified in one way as aversion to anoxious stimulus.With this in mind, a number of investigators have devel-oped new behavioral methodologies to study the com-plexity of nociceptive processing in the ACC of animals.Theunderlying featureof thesemethodologies is that es-capeand/oravoidanceofanoxiousstimulusareclear in-dications that animals find the stimulus aversive (Fuchs2000). For instance, Johansen et al. (2001) utilized the� formalin test with the place-conditioning paradigm.In this paradigm, formalin injection elicits an acute no-ciceptive response and induces conditioned place avoid-ance (F-CPA) to the compartment of the apparatus thatis associated with the formalin injection. Another recentparadigm utilizes place escape / avoidance in which an-imals must associate the application of the mechanicalstimulus to the hyperalgesic paw with the preferred darkarea of the test chamber (LaBuda and Fuchs 2000). Es-cape / avoidance behavior is measured as a shift fromthe preferred dark area of the chamber to increased timespent within the non-preferred light area of the chamber.In both instances, damage to the ACC, by either neu-rotoxic or electrolytic procedures, decreases behavioralevidence that the noxious stimulus is aversive (Johansenet al. 2001; LaGraize et al. 2004). At this time, the mostparsimoniousexplanationof thebehavioralstudies in ro-dents is that the ACC is involved in the modulation andprocessing of pain affect and that manipulations of theACC decrease the affective component of pain process-ing.Behavioral paradigms that permit the separate assess-ment of affective and sensory components of the painexperience have led to examination of the underlyingneurochemical processes that might be involved in mod-ulating pain affect. One possible mechanism of actionby which the ACC selectively modulates pain affect isvia the mu-opioid receptor system. The ACC has a highdensity of opioid receptors and activation of the ACCmu-opioid receptor system during sustained pain is neg-atively correlated with McGillPain Questionnaireaffec-tive scores (Zubieta et al. 2001). In animals, morphinemicroinjection into the ACC produces a selective de-crease inescape/avoidance tomechanicalstimulationofthe hyperalgesic paw (LaGraize et al., 2006). Additionalcontributions of the NMDA (Lei et al. 2004), cholecys-tokinin (Erel et al. 2004), and glutamatergic (Johansenet al. 2004) systems have been reported.It is unlikely that the above findings can be attributed tothe role of the ACC in learning and memory processes,that is the possibility that ACC manipulation interfereswith acquisition and retention of an escape / avoidanceresponse rather than a change in the negative hedonic
value of the mechanical stimulus. Morphine has beenfound to impair performance in various tests of memorysuch as the � Morris water maze and the � radial armmaze. However, the effect of morphine on the radial armmaze requires chronic high dose administration (up to40 mg / kg) that almost certainly is associated with se-dation and impairment in task performance rather thanwith interference in memory. Other investigators reportbiphasic results in rats such that lowerdosesofmorphineenhance, while higher doses impair, memory. Anatom-ically, impairment of learning and memory function istypically associated with manipulations to the more pos-terior regions of the cingulate cortex.It is inappropriate to examine the role of the ACCin nociceptive processing in animals with the use ofreflexive behaviors to examine the aversive nature ofpersistent pain conditions. Experiments using onlyquantified mechanical thresholds or acute formalin in-jection behaviors can lead to the erroneous conclusionthat the ACC does not effect supraspinal pain process-ing. Clearly, functional alterations of the ACC by lesionand neurochemical methods reduce the avoidance ofnoxious mechanical hind paw stimulation as measuredusing the place escape / avoidance paradigm and the for-malin conditioned place avoidance paradigm. Sensorymechanisms of pain processing are clearly importantbut fail to highlight the mechanisms underlying theaffect that accompanies many persistent pain condi-tions. Clinically, the sensation of pain can be treated byreducing the sensory input as well as by manipulatingaffective-motivational and cognitive factors (Melzackand Casey 1968). Therefore, an understanding of theneural substrates mediating the affective processing ofnociceptive stimulation should advance our knowledgeof pain processing and contribute to advances in thera-peutic interventions to reduce the affective componentof pain that accounts for the suffering so frequentlyseen in clinical conditions.
References1. Donahue RR, LaGraize SC, Fuchs PN (2001) Electrolytic lesion
of the anterior cingulate cortex decreases inflammatory, but notneuropathic pain in rats. Brain Res 897:131–138
2. Erel U, Arborelius L, Brodin E (2004) Increased cholecystokininrelease in the rat anterior cingulate cortex during carrageenan-induced arthritis. Brain Res 1022:39–46
3. Fuchs PN (2000) Beyond reflexive measures to examine higherorder pain processing in rats. Pain Res Manag 5:215–219
4. Hutchinson WD, Davis KD, Lozano AM et al. (1999) Pain-related neurons in human cingulate cortex. Nat Neurosci2:403–405
5. Johansen JP, Fields HL (2004) Glutamatergic activation of an-terior cingulate cortex produces an aversive teaching signal. NatNeurosci 7:398–403
6. Johansen JP, Fields HL, Manning BH (2001) The affective com-ponent of pain in rodents: direct evidence for a contribution of theanterior cingulate cortex. Proc Natl Acad Sci USA 98:8077–8082
7. Koyama T, Kato K, Tanaka YZ et al. (2001) Anterior cingu-late activity during pain-avoidance and reward tasks in monkeys.Neurosci Res 39:421–430

C
Classification 397
8. LaBuda CJ, Fuchs PN (2000) A behavioral test paradigm to mea-sure the aversive quality of inflammatory and neuropathic painin rats. Exp Neurol 163:490–494
9. LaGraize SC, LaBuda CJ, Rutledge MA et al. (2004) Differentialeffect of anterior cingulate cortex lesion on mechanical hyper-sensitivity and escape / avoidance behavior in an animal modelof neuropathic pain. Exp Neurol 188:139–148
10. LaGraize SC, Borzan J, Peng YB et al. (2006) Selective regulationof pain affect following activation of the opioid anterior cingulatecortex system. Exp Neurol 197:22–30
11. Lei L-G, Sun S, Gao Y-J et al. (2004) NMDA receptors in the an-terior cingulate cortex mediate pain-related aversion. Exp Neurol189:413–421
12. Melzack R, Casey KL (1968) Sensory, motivational, and centralcontrol determinants of pain. In: Kenshalo DR (ed) The SkinSenses. CC Thomas, Springfield, pp 423–439
13. Rainville P, Duncan GH, Price DD et al. (1997) Pain affect en-coded in human anterior cingulate but not somatosensory cortex.Science 277:968–971
14. Vogt BA (1985) Cingulate cortex, In: Peters A, Johns EG (eds)Cerebral Cortex. Plenum Publishing Corporation, New York,pp 80–149
15. Zubieta J-K, Smith YR, Bueller JA et al. (2001) Regional muopioid receptor regulation of sensory and affective dimensionsof pain. Science 293:311–315
Cingulotomy
Definition
The creation of lesions in the cingulate gyrus, usuallyfor the relief of intractable pain and in the treatment ofpsychiatric disorders and addiction.� Pain Processing in the Cingulate Cortex, Behavioral
Studies in Humans� Pain Treatment, Intracranial Ablative Procedures
CIPA
� Congenital Insensitivity to Pain with Anhidrosis
Circadian Rhythms/Variations
Definition
Rhythms of parameters with a frequency close to, butnot exactly, 24–hr.� Diurnal Variations of Pain in Humans
Circadian Variations in Pain Level
� Diurnal Variations of Pain in Humans
Circumventricular Brain Structures
Definition
Specific regions within the brain where the blood brainbarrier is weak or absent.� Proinflammatory Cytokines
Cl– Transporter
� Chloride Transporter
Classical Conditioning
Synonyms
Pavlovian conditioning; respondent conditioning
Definition
Also called “Pavlovian conditioning” or “respondentconditioning” it is a type of learning that results from theassociation of stimuli with reflex responses, whereby aneutral stimulus (usually called the conditioned stimu-lus, CS) acquires the response eliciting properties of apreviously potent stimulus (the unconditioned stimulus,US). Through repeated pairings of the CS (e.g. tone)with the US (e.g. shock) stimulus, the CS can be usedto elicit the same or similar response, the conditionedresponse (CR, e.g. withdrawal) as the US.� Amygdala, Functional Imaging� Amygdala, Pain Processing and Behavior in Animals� Behavioral Therapies to Reduce Disability� Muscle Pain, Fear-Avoidance Model� Pavlovian Conditioning� Psychology of Pain and Psychological Treatment� Respondent Conditioning of Chronic Pain
Classical Massage
� Massage and Pain Relief Prospects
Classical Migraine
� Clinical Migraine with Aura
Classification
� Taxonomy

398 Claudication
Claudication
Definition
Claudication is characterized by leg pain and weaknessbrought on by walking, with the disappearance of thesymptoms following a brief rest.� Vascular Neuropathies
Clearance
Definition
The clearance describes the hypotheticalvolume of fluidthat is cleared from the unchanged drug per unit of timebyanyeliminationpathway.Theclearancecanbefurthercategorized as the total clearance (CL) (all eliminationpathways) or the organic clearance (e.g. renal clearance(CLR), hepatic clearance (CLH), etc.).� NSAIDs, Pharmacokinetics
Clinical Migraine With AuraF. MICHAEL CUTRER
Department of Neurology, Mayo Clinic, Rochester,MN, [email protected]
Synonyms
Classical Migraine; classic migraine; Complex Mi-graine; Complicated Migraine; Migraine Accompa-gnee; Migraine Ophthalmic; Migraine With Aura;Migraine Optical; Migraine Hemiparesthetic; MigraineAphasic; Migraine Hemiplegic
Definition
Migraine aura is a disorder during which episodes oftransient focal neurological symptoms develop over aperiod of 5–20 minutes and resolve within 60 minutes(IHS 2004). Most commonly, these symptoms occurwithin 60 minutes of the onset of a migraine headache(i.e. unilateral throbbing headache of moderate to se-vere intensity, lasting 4–72 hours and associated withnausea, vomiting, � photophobia, � phonophobia andworsening with routine exertion). Less commonly, theaura may occur during the course of a headache, inassociation with a headache which does not have all ofthe features of a migraine headache or in the absenceof headache altogether. The aura is distinct from theterm “prodrome” which refers to often vague symptomsthat occur hours to a day prior to the onset of headacheand which include both vegetative symptoms such asfatigue, pallor, yawning, � anorexia, nausea, light or
sound sensitivity or neck stiffness or affective symp-toms namely depression, euphoria and concentrationdifficulties.
Characteristics
General Characteristics
It has been estimated that migraine with aura occursin about 4% of the general population each year (Ras-mussen and Stewart 2000) suggesting that it occurs inup to one third of migraine sufferers. Many patients whohave attacks of migraine with aura also have attacksof migraine without aura. Aura symptoms are clini-cally localizable to the � cerebral cortex or brainstemand resolve fully in between attacks. In addition, nostatic changes in conventional anatomical neuroimag-ing occur as a result of the migraine aura. Althoughthe duration of a single migraine aura is limited to60 minutes, an individual patient may within a singleattack have more than one type of aura. When the aurasoccur in sequence, their total time may extend beyond60 minutes up to as much as 60 minutes for each auratype and still be considered aura. When the aura typesoccur in sequence, the most common order is visual,then sensory followed by language or motor symptomsalthough the order may vary. There are two generalcharacteristics of the aura that seem to distinguish itfrom ischemia. 1. There is a tendency for the symptomsto spread or migrate slowly with time and 2. there isbimodal progression in which positive symptoms (tin-gling or visual shimmering) are followed by negativesymptoms (numbness or visual scotoma).
Aura Types
Traditionally, four types of migraine aura have beenrecognized. These include visual, sensory, language andmotor.However, themost recent InternationalHeadacheSociety (IHS 2004) diagnostic criteria consider motoraura a separate migraine subtype, as recent genetic datasuggest the possibility of a distinct pathophysiologyin motor aura. The three remaining aura types, visual,sensory and language auras are collectively termed“typical aura”.
Visual Aura
Visual aura consists of episodes of visual disturbance,which although frequently stereotypical within a givenindividual, may differ from on individual to another. Inthe classical progression, the aura begins as a small areaof visual disturbance often just lateral to central fixation.This visual phenomenon, generally described as eithera shimmering or sparkling light or as a crawling geo-metric or zigzagging pattern, is very characteristic of theaura of migraine. Within a few minutes of onset, the areaof visual dysfunction begins to expand from its originalcentral location slowly outward often in a crescent-likepattern to involveasmuchasaquarterorhalfof thevisualfield in both eyes. The expanding shimmering margin of
C
Clinical Migraine With Aura 399
the aura leaves in its wake an area in which there is noimage. This area is termed a � scotoma. The scotoma isusually not a particular color but has been likened to theblind spot left in the visual field after having looked at aflashing light. The rate of the shimmering or flickeringobserved by the patient during aura seems to increase asthe aura spreads toward the periphery. Gradually visionis restored, first centrally and then in areas of peripheralvision as the aura moves out of the visual field.The spread is usually quite slow taking from 40–60 min-utes, but may be much more rapid, sometimes beingcompleted in less than 15 minutes. Fragments of theaura (scotoma with shimmering or vice versa) mayberecalled as well as differences in the direction of expan-sion implying variability from one patient to another orwithin the same patient from one attack to another. Theshimmering component of the aura is usually seen whenthe eyes are closed and passive movement of the eyeballthrough the eyelid does not change the position of theaura, implying that the abnormality occurs outside theeyeball itself. The visual aura is by far the most commonform of migraine aura.
Sensory Aura
Sensory aura is the second most common aura type andgenerally first manifests as a tingling sensation or pares-thesiaononesideof thefaceor inanarmor leg. Justas thevisual aura expands or migrates, the sensory disturbancemay march along the arm or leg only to jump upward toaffect theface,graduallymovingacross itandthen insidethe mouth to affect the gums and/or tongue on one side.The involvement of half the tongue is quite suggestiveof migraine and not typical for ischemia. Also indica-tive of migraine is the sensory aura’s bimodal wave ofparesthesias, which leaves in its wake a mild to moderatenumbness that persists for up to an hour.
Language Aura
Language aura is the least common of the typical auraforms but can be quite disturbing to patients when theyfirst experience it. This aura type is actually a dysfunc-tion of language, which makes it difficult for the patientto choose the correct words or speak them in a coher-ent fashion. The language aura may also disrupt readingor writing. It is clearly distinct from slurring of speech,which may occur with sensory aura if half the tongueis numb. Because thought is generally in conducted ina given language, patients are often distressed by an in-ability to think clearly.
Motor Aura
Motor aura is now considered as a separate entity by theInternationalHeadacheSocietybecausesinglegenemu-tations have been identified as the cause of hemiplegicmigraine in several families. Patients with hemiplegicmigraine report unilateral weakness involving the faceand/or an extremity. The duration of the motor aura dif-
fers from other typical aura types in that it is sometimeslonger than 1 hour and may actually persist after reso-lution of the headache. This would argue for a distinctpathophysiology. However, most patients who experi-ence hemiplegic migraine also report other aura typesthat may occur within the same attack.
Pathophysiology
The slow spreading nature of the scintillating distur-bance in migraine visual aura led to early speculationthat aura may be caused by the phenomenon of corti-cal spreading depression (CSD) (Lashley 1941). CSDis an electrically measurable wave of neuro-glial ex-citation that causes a brief disruption in local ionic� homeostasis and is followed by a resultant depres-sion of activity (Leao 1944). The wave appears andthen migrates over the cortex in experimental animalsat a slow rate of 3–4 mm per minute after mechanicalor chemical perturbation. Functional magnetic reso-nance imaging (fMRI) techniques including perfusionweighted (Cutrer et al. 1998) and blood oxygen leveldependent (BOLD) imaging (Hadjikhani et al. 2001)applied during spontaneous migraine visual auras in hu-mans have shown that CSD and visual aura share manycharacteristics. 1. Both CSD and the migraine visualaura are characterized by an initial � hyperemia lasting3–4.5 minutes. 2. The hyperemia signal spreads acrossthe affected cortex at a slow rate (2–5 mm/min) 3. Thehyperemia in both CSDand migraineaura is followed bymild hypoperfusion lasting 1–2 hours. 4. Evoked visualresponses during CSD and during aura are suppressedand take about 15 minutes to recover. 5. The BOLDsignal complexes during both aura and induced CSD inanimals halt at major � sulci. 6. In CSD and migraineaura, the first affected area is the first to recover normalresponse to standard visual stimuli. Thus far, factorsthat render over 25% of migraineurs vulnerable to aCSD-like phenomenon are poorly understood and maybe genetically determined. One recent report found thatprolonged visual symptoms associated with migraineheadaches are not associated with the perfusion defectsseen in typical migraine visual aura. (Jager et al. 2005)At this point, the relationship between the aura and mi-graine headache is incompletely understood. There isexperimental evidence that events intrinsic to the cere-bral cortex such as CSD are capable of exerting effectson trigeminal perivascular nociceptive neurons, therebyactivating headache. Immunohistochemical studies inrodents have shown that CSD is capable of activatingthe expression of the immediate early gene c-fos, a non-specific marker of neuronal activation within the nucleiof neurons of the superficial laminae of the trigeminalnucleus caudalis (second order nociceptive neurons)(Moskowitz et al. 1993). In addition, � laser speckleimaging studies (Bolay et al. 2002) recently demon-strated that CSD could initiate long lasting dilationwithin pain sensitive middle meningeal artery branches

400 Clinical Migraine Without Aura
by a brainstem reflex dependent on intact trigeminalprimary afferent and parasympathetic efferent neurons.It may well be that the aura represents one of severalmechanisms by which the headache is activated, as it isclear that migraine headache may occur without auraand the aura may occasionally occur with activation ofheadache.
References1. Bolay H, Reuter U, Dunn AK et al. (2002) Intrinsic brain activity
triggers trigeminal meningeal afferents in a migraine model. NatMed 8:136–142
2. Cutrer FM, Sorensen AG, Weisskoff RM et al. (1998) Perfusion-Weighted Imaging Defects During Spontaneous MigrainousAura. Ann Neurol 43:25–31
3. Hadjikhani N, Sanchez Del Rio M, Wu O et al. (2001) Mech-anisms of migraine aura revealed by functional MRI in humanvisual cortex. Proc Natl Acad Sci USA 10;98:4687–4692
4. Headache Classification Subcommittee of the InternationalHeadache Society (2004) The International Classification ofHeadache Disorders, 2nd edn. Cephalalgia 24:24–30
5. Jager HR, Taylor MN, Theodossy T et al. (2005) MR imaging-guided interstitial photodynamic laser therapy for advanced headand neck tumors. Am J Neuroradiol 26:1193–200
6. Lashley KS (1941) Patterns of cerebral integration indicated bythe scotomas of migraine. Archives of Neurology and Psychiatry(Chicago) 46:331
7. Leao AAP (1944) Spreading depression of activity in the cerebralcortex. J Neurophysiol 7:359–390
8. Moskowitz MA, Nozaki K, Kraig RP (1993) Neocortical spread-ing depression provokes the expression of c-fos protein-like im-munoreactivity within trigeminal nucleus caudalis via trigemi-novascular mechanisms. J Neurosci 13:1167–1177
9. Rasmussen BK and Stewart WF (2000) Epidemiology of Mi-graine. In: Olesen J, Tfelt-Hansen P, Welch KMA (eds) TheHeadaches, 2nd edn. Lippincott Williams & Wilkins, Philadel-phia, pp 231–232
Clinical Migraine Without Aura
� Migraine Without Aura
Clinical Pain
Definition
„Physiological”pain ispainfelt in theintact,non-injuredorganism. „Clinical“ pain is pain felt after a tissue injuryhas induced sensitization of the peripheral and centralnervous system.� Postoperative Pain, Pre-Emptive or Preventive Anal-
gesia
Clinical Signs
Definition
Clinical signs are abnormal responses elicited by clini-cians during the physical examination.� Hypoalgesia, Assessment
Clinical Trial
Definition
A clinical trial is a research study designed to test thesafety and/or effectivenessofdrugs,devices, treatments,or preventive measures in humans. Clinical trials canusually be divided into four categories or “phases”� Central Pain, Outcome Measures in Clinical Trials
Clitoral PainALLAN GORDON
Wasser Pain Management Centre, Mount SinaiHospital, University of Toronto, Toronto, ON, [email protected]
Characteristics
Introduction
“Why is it that the very places in my body that shouldgive me pleasure give me pain”Quote from a woman with a painful clitoris and painfulnipples (The PNPC Syndrome).
Description of the Clitoris
The best place to find out about the clitoris is the web-site www.the-clitoris.com. Here the clitoris is describedin clear terms with excellent graphics. The major partsare the � prepuce or hood, the � glans, the body andthe crura (O’Connell et al. 1998; www.the-clitoris.com)(see Fig. 1). The major function is sexual pleasure andorgasm. The clitoris has up to 8000 nerve endings mak-ing it extremely sensitive (www.the-clitoris.com).
Clitoral Pain, Figure 1 The Clitoris.

C
Clitoral Pain 401
The clitoris is innervated by the dorsal nerve of the cli-toris off the pudendal nerve. That transmits somatic sen-sation including pain, temperature, vibration, and pro-prioception. The clitoris also receives sympathetic andparasympathetic fibers for sexual function.
What is Clitoral Pain?
Clitoral pain is pain either present at rest and/or inducedby touch or pressure on the glans, � body of the clitorisor � crura of the clitoris. Occasionally pain is felt in ornext to the clitoral hood or just posterior to the glans andbody. It may be there on its own or morecommonly asso-ciated with vulvar pain or urethral pain and also deepermuscular pain. The pain may be referred into the urethrafrom other sites e.g. the urethra.One definition is a “specific subset of vulvodynia pro-duced by neuralgia of the anterior division of the puden-dal nerve” (Perry 2004). However, that may be too ex-clusive a definition since there is such a variety of causespossible.Many women with genital pain including vulvodyniaand vulvar vestibulitis, may not mention their cli-toral pain unless they have been so involved with thehealthcare system that they lose their reserve. Moreimportantly, many practitioners do not ask or examinefor it. For instance, many women with fibromyalgia orirritable bowel may also have vulvar pain and/or clitoralpain, but do not volunteer it or are not asked about it.This is certainly the case in our pain clinic where suchpain is described mainly upon direct questioning.Some women have a ‘sensitive’ clitoris that is uncom-fortable at rest or to touch but it does not interfere withsexual activity. Others may have a true pain in the cli-toris, enough so that they do not like it touched. Theseterms need to be better defined in further populationhealth studies.In an internet survey of423 womenwith vulvarpainonly3.3% had clitoral pain, and none had it alone (Gordonet al. 2003).
Literature and Internet Search
Wesselman and Burnett (Wesselmann and Burnett1999) refer to very few cases and talk mainly about painpost- ritualistic clitoral excision. It is not mentioned in“Chronic Pelvic Pain: An Integrated approach” (Steegeet al. 1998).The International Pelvic Pain Society website http://www.pelvicpain.org (Perry 2004) contains an articleon Clitoral Pain that was also published in a text-book (Perry 2000) and in the Fall 2000 edition of theNational Vulvodynia Association Newsletter. Perrymentions metabolic (e.g. diabetes), violent stimulation,tight clothing, or laser vaporization as known causes ofclitoral painA Pub Med search for key words “Clitoris Pain” yieldsarticles on FGM (female genital mutilation) (Okonofy etal. 2002), painful priapism (Medina 2002), clitoral neu-
roma (Fernandes-Aguilar and Noel 2003), hair tourni-quet (Kuo et al. 2002), and phimosis (Munarriz et al.2002) as well as various tumors. The author’s paper in2002 represents the only significant collection of cases(Gordon 2002), which reports the clinical features of 21women with clitoral pain.An Internet search, however, will pick up information onchat line discussions, sex information sites and/or sitesthat appear pornographic.
My Patient Population
In our paper (Gordon 2002) we reported on 21 individ-uals, 7 from my own practice and 14 who had contactedthe author online through various sources. We haveadded to the numbers and are in the process of reportinga larger group of 26 patients, and more than 40 whosought and supplied information via the internet. Somepatients were followed for up to 4 years. The NationalVulvodynia Association also referred women patients.Thefollowingrepresents informationfromthepaperandpersonal observations and communication.
Clinical Points
• The rest pain is often described as mild to severe andto be burning, stinging or aching. All our examinedclinic patients have rest pain.
• There is pain on touching or contacting the clitoris,and the pain is moderate to severe in intensity. Thewomen examined may have � allodynia, hyperalge-sia or pain on firmer touch or pressure. The allodyniaandhyperalgesiasuggestsaneuropathicpainprocess.
• Allodynia of the clitoris and introitus often coexist aswell as periurethral touch induced pain.
• Intercourse is almost always painfuleven with the useof techniques to avoid touching the clitoris. This in-terferes greatly with intimate relations.
• � Primary anorgasmia is relatively uncommon (Gor-don 2002), and secondary anorgasmia may occur be-cause of the pain and unwillingness to try because ofpain.Mostcontinue tobeorgasmic, somealsoachiev-ing orgasm through a vaginal approach.
• Many women avoid intercourse or sexual activity be-cause of the pain. Sexual desire may not be decreaseddespite the pain but more commonly desire is sup-pressed. Non-penetrative sex may also be painful.
• The pain may be part of established diseases includ-ing � Lichen Sclerosus. Our article describes 5 suchpatients (Gordon 2002).
• Some patients have had it for 10 or more years, up to18 years in practice and 25 years online.
• In others it was much shorter in duration, sometimesjust months.
• Relapse and remissions may occur and spontaneousrecovery may also occur.
• We know of at least 4 women who had remission withpregnancy, with the remission persisting in four postpartum. Another one worsened after pregnancy.

402 Clitoral Pain
• We had at least 10 women who complained of painfulor very highly sensitive nipples associated with theclitoral pain (Gordon 2000, 2002). The reason for thisassociation is unclear.
• Clitoral pain may be associated with vulvar pain,vaginismus, urethral pain, and occasionally analpain as well as interstitial cystitis, painful urethralsyndromes and � urethral dyssynergia.
• There is often a fruitless search for infections.• Other c-morbidities include endometriosis, fi-
bromyalgia, anorexia, and back pain includingspondylolisthesis. Depression was common in atleast 14 of our own patients.
• Painful clitoral priapism was seen in 2 of our patients.• Clitoral pain may rarely be associated with a constant
state of arousal.• Clitoral pain may be the presenting feature in some,
and themostdisconcerting,butmorecommonlythereare other genital pain issues.
• Women with clitoral pain can be desperate for ex-planations and relief, are concerned about beinglabeled as psychogenic, and look back in regret toevents, particularly traumatic or surgical events thatmay have precipitated or aggravated their condi-tion.
Causes of Clitoral Pain in our Groups
1. Direct ‘sexual’ trauma (e.g. vigorous masturbation;vigorous cunnilingus; a slipped’ vibrator; vigoroussexual intercourse were all reported to us)
2. Direct ‘non sexual’ trauma (e.g. doing the splits on abeam while doing gymnastics; injury during car ac-cident from direct trauma)
3. Injury to lumbar spine and/or coccyx and possiblelower sacral root irritation
4. Pelvic fracture and indirect trauma5. Multiple Sclerosis with other urogenital complaints
of pain, altered libido and voiding dysfunction due tocentral plaques
6. Post-hysterectomy especially with vascular misad-venture (2 with recurrent engorgement)
7. Post spinal fusion procedure with insertion of a cage8. Peripheral polyneuropathy9. Part of a unilateral or bilateral � pudendal neuralgia
syndrome10.Associated with Lichen Sclerosis with deforming tis-
sue destruction11.Following explained or unexplained infection, such
as yeast, vaginosis, or herpes12.Primary clitoral pain of unknown cause13.Part of unexplained genital pain syndrome involving
clitoris, urethra, vulva, and anus14.Part of a severe chronic pelvic pain disorder with dif-
fuse muscle and genital pain15.Related to sexual abuse16.A feature of vulvodynia
Common Mechanism
While yeast or other infections might suggest an acutenociceptive mechanism, most patients have evidence ofa chronic neuropathic pain. There is clitoral allodyniaand at times hyperalgesia. While documented or un-documented pudendal nerve entrapment may presentin some in � Alcock’s canal, this would not explainpain seen in direct trauma. Clitoral pain seems to be anexample of neuropathic pain and seen in central pain(MS), polyneuropathy or Lichen Sclerosis. Ultimately,whatever the insult, there must be peripheral and centralsensitization. Clitoral pain deserves more study as anexample of neuropathic pain derived from many basiccauses, be it post-infectious, post-traumatic, iatrogenic,direct injury, or chronic nerve entrapment
Clinical Evaluation
This must include:
• Clinical history• Sexual History• Psychosocial history and evaluation• Alcohol, addiction and abuse history• Treatments tried• Neurological, musculoskeletal and gynecological
exam• Detailed vulvar exam including Q tip and pain and
temperature and retraction of prepuce• Pelvic and rectal exam checking for deeper pain and
anal pain• Pelvic and spinal imaging when clinically appropri-
ate with ultrasound, CT scan or magnetic resonancescan
• Pudendal nerve latencies if available• Quantitative sensory testing of genital area• Cultures of vulva, vagina and urine• Urogynecological evaluation if urinary symptoms
Treatment
The treatment depends upon clinical diagnosis andco-morbidity. There are no published clinical trialsand even very few anecdotal reports on clitoral pain.Awareness of the condition, asking the right questionsin the right way, and validating the patients pain arekey, and a detailed multidisciplinary or transdisciplinaryexamination is necessary: Management is best in a mul-tidisciplinary pain clinic where chronic pelvic regionpain is regularly treated.
Treatments to Try and Comments
1. Oral tricyclic antidepressants such as amitriptyline.Occasionally effective
2. Oral anticonvulsants such as gabapentin. Variable re-sults
3. Topical medications such as amitriptyline, gabapen-tin, ketamine and even capsaicin (which burns). More

C
Cluster Analysis 403
studies needed with these agents. Clinical trials areneeded
4. Opiates. They are often tried because of other co-morbid pain conditions, and experience suggeststhat they are not particularly effective in clitoral pain
5. Topical cocaine. Usually associated with addictivebehavior
6. Anesthetic block of dorsal nerve of clitoris. No liter-ature studies (Perry 2004)
7. Pudendal nerve block. Of diagnostic value in puden-dal neuralgia and no specific studies for clitoral pain.
8. Pudendal nerve decompression. Must be well docu-mented and in experienced hands only.
9. Physical therapy May have through therapy of spine,internal and external muscle.
10.Specific treatment of underlying, associated or co-morbid conditions such as vulvodynia, Lichen Scle-rosis and depression.
11.Psychological therapies including cognitive behav-ioral therapy.
12.Pelvic floor surface EMG. Only if evidence of pelvicfloor disturbance and probe does not hurt.
13.Sexualtherapies.Assistsindevelopingalternatetech-niques and exploring attitudes, preferences and expe-riences.
14.Cannabis: No trials but anecdotal reports from pa-tients does suggest some benefit
Conclusion
Clinical trials will clearly be necessary in order to un-derstand what really works. In the meantime, conserva-tive multimodal treatments should be considered. Therelative rarity of clitoral pain, the many associated con-ditions, and the fact that most practitioners are not pre-pared to evaluate these patients has meant that trials arenot carried out. However, it is also clear that we needto know more about the clinical and natural history ofclitoralpain, aswell asunderstand moreabout thepatho-physiology and the various associated and/or co-morbidfeatures. That can be achieved by detailed study includ-ing the use of neurophysiologic techniques and the cre-ation of an observational database.Clitoral pain is reframed as an example of neuropathicpain, and studied in the same way as other forms of neu-ropathic pain.
References1. Fernandes-Aguilar S, Noel JC (2003) Neuroma of the Clitoris
after Female Genital Cutting Obstet Gynecol 101:1053–10542. Gordon AS (2000) The PNPC Syndrome. Platform presentation
at PUGO Special Interest Group meeting (Sept 23, 2000) Ham-burg, Germany
3. Gordon AS (2002) Clitoral Pain: The Great Unexplored Pain inWomen. J Sex Marital Ther 28:181–185
4. Gordon AS, Panahian-Jand M, McComb F et al. (2003) Char-acteristics of Women with Vulvar Pain Disorders: Response toa Web Based Survey. J Sex Marital Ther 29:25.58
5. Kuo JH, Smith LM, Berkowitz CD (2002) A Hair TourniquetResulting in Strangulation and Amputation of the Clitoris. ObstetGynecol 99:939–941
6. Medina CA (2002) Clitoral Priapism: A Rare Condition Present-ing as a Cause of Vulvar Pain. Obstet Gynecol 100:1089–1091
7. Munarriz R, Talakoub L, Kuohung W et al. (2002) The Prevalenceof Phimosis of the Clitoris in Women Presenting to the SexualDysfunction Clinic: Lack of Correlation to Disorders of Desire,Arousal and Orgasm. J Sex Marital Ther 28:181–185
8. O’Connell HM, Hutson JM, Anderson CR et al. (1998)Anatomical Relationship between Urethra and Clitoris. JUrol 159:1892–1897
9. Okonofy FE, Larsen U, Oronsaye F et al. (2002) The Associ-ation between Female Genital Cutting and Correlates of Sex-ual and Gynecological Morbidity in Edo State, Nigeria. BJOG109:1089–1096
10. Perry CP (2000) Vulvodynia. In: Howard FM, Perry CP, Carter JEet al. (eds) Pelvic Pain: Diagnosis and Management. LippincottWilliams & Wilkins, Philadelphia, pp 204–210
11. Perry CP (2004) Clitoral Pain. http://www.pelvicpain.org/12. Steege JF, Metzger DA, Levy BS (eds) (1998) Chronic Pelvic
Pain: An Integrated Approach. WB Saunders Company, Philadel-phia
13. Wesselmann U, Burnett AL (1999) Genitourinary Pain. In: Wall
P, Melzack R (eds) Textbook of Pain, 4th edn. Churchill Living-stone, Edinburgh, pp 689–709
14. www.the-clitoris.com, Copyright 1998–2004 Fox Internet Ser-vices
Clofazimine
Definition
Clofazimine is a substituted iminophenazine dye withantibacterial properties, which is used in the treatmentof leprosy; it is administered orally.� Hansen’s Disease
Clonidine
Definition
Clonidine isaprototypicalα2-adrenoceptoragonistwithpotent sympatholytic effects. It activates neuronal cellmembrane potassium channels causing hyperpolariza-tion, reducing the rate of neuronal firing. It also inhibitsneurotransmitter release by inhibiting calcium conduc-tance through N-typecalcium channels.Clinically, it hasantihypertensive, sedative, anxiolytic and analgesic ac-tions, which may also be useful in the management ofcomplex pain states.� Acute Pain in Children, Post-Operative� Alpha(α) 2-Adrenergic Agonists in Pain Treatment� Postoperative Pain, Appropriate Management
Cluster Analysis
� Multidimensional Scaling and Cluster Analysis Ap-plication for Assessment of Pain

404 Cluster Headache
� Pain Measurement by Questionnaires, Psychophysi-cal Procedures and Multivariate Analysis
Cluster Headache
Definition
An uncommon headache disorder with a striking malepredilection. They are called cluster headaches becauseattacks occur in a group or “cluster” during which timepatients suffer from 1–8 headaches daily. Individualheadaches last between 20–180 minutes each, are ex-cruciatingly severe, and are associated with one ormore autonomic features such as conjuntival injection,lacrimation, nasal congestion, rhinorrhea, forehead andfacial sweating, miosis, ptosis, eyelid edema. Clustercycles last 2–8 weeks each and are followed by remis-sion periods of 6–12 months, during which time patientsare pain-free. Attacks are strictly unilateral orbitally,supraorbitally and/or temporally.� Hemicrania Continua� Human Thalamic Response to Experimental Pain
(Neuroimaging)� Paroxysmal Hemicrania
Clustering
� Trafficking and Localization of Ion Channels
C-Mechanoheat Receptor
� Polymodal Nociceptors, Heat Transduction
C-Mechanoreceptor
� Mechanonociceptors
CM-PF Complex
� Parafascicular Nucleus, Pain Modulation
CMT
� Charcot-Marie-Tooth Disease
CNS Changes after Peripheral NerveInjury
� Central Changes after Peripheral Nerve Injury
CNS Stimulation in Treatment ofNeuropathic Pain
� Central Nervous System Stimulation for Pain
CNV
� Contingent Negative Variation
CO Staining
� Cytochrome Oxidase Staining
CO2 Laser
Definition
CO2 laser is frequently used as a pain (heat) stimulator.Since it is a heat beam, tactile receptors are not excited,and the time-lock is extremely good.� Magnetoencephalography in Assessment of Pain in
Humans
Cochlea
Definition
The cochlea is the coiled structure within the inner earwhere vibrations caused by sound are transduced intoneural impulses by the Organ of Corti.� Perireceptor Elements
Cognition
Definition
Cognition is the mental act or process by which knowl-edge may be acquired or analyzed. A distinction is typi-cally made between the content of cognition such as be-liefs,attitudes,ormemories;andtheprocessofcognitioninvolving acts such as perception, interpretation, infer-ence, retrieval, or problem solving.� Pain Assessment in the Elderly

C
Cognitive-Behavioral Perspective of Pain 405
� Psychology of Pain, Assessment of Cognitive Vari-ables
Cognitive
Definition
Pertaining to the internal thoughts, images and con-structs of the individual.� Pain as a Cause of Psychiatric Illness� Psychological Treatment in Acute Pain
Cognitive Appraisal
Definition
Cognitive appraisal is an evaluation of environmentalstimuli. Resources available to cope with a potentialstressor, and their ability to offset the threatening stim-uli, determines the degree and intensity of the stressresponse.� Stress and Pain
Cognitive Aspect of Pain
Definition
Perceptual component of pain perception includingpain-related learning and memory and the recognitionof the painful nature of the stimulus.� Primary Somatosensory Cortex (S1), Effect on Pain-
Related Behavior in Humans
Cognitive Assessment
� Psychology of Pain, Assessment of Cognitive Vari-ables
Cognitive-Behavior Modification
� Cognitive-Behavioral Treatment of Pain
Cognitive-Behavioral Model
Definition
In the context of bodily sensations, this model states that(mis)interpretations (cognitions) of bodily sensationshave a profound impact upon how patients perceivetheir body, cope and behave. Often a vicious circle isassumed between bodily sensations, cognitions andbehavior.� Muscle Pain, Fear-Avoidance Model
Cognitive-Behavioral Model of ChronicLow Back Pain
Definition
Cognitive behavioral models of chronic low back painstate that catastrophic misinterpretations in response toacute pain lead to fear of movement/(re)injury. As a con-sequence, a vicious cycle develops in which subsequentavoidance of activities and hypervigilance lead to an in-crease of functional disability, pain, depression and adecrease of physical fitness, thereby further advancingchronicity.� Disability, Fear of Movement� Fear and Pain
Cognitive-Behavioral Perspective of PainDENNIS C. TURK
Department of Anesthesiology, University ofWashington, Seattle, WA, [email protected]
Synonyms
Cognitive Model of Pain; Behavioral/Cognitive Per-spective
Definition
The Cognitive-Behavioral (CB) model of pain incorpo-rates pain sufferers’ fear avoidance and � contingenciesof reinforcement, but suggests that � cognitive factors,in particular, and expectations rather than conditioningfactors are of central importance. Thus, the model is ahyphenated one – CB. It does not ignore the importantrole of contextual factors and principles of learning the-ory, but rather incorporates them within an integratedperspective on pain sufferers and pain management. TheCB model proposes that so-called conditioned reactionsare largely self-activated on the basis of learned expecta-tions rather than automatically evoked. The critical fac-tor for the CB model, therefore, is not that events oc-cur together in time or are operantly reinforced, but that

406 Cognitive-Behavioral Perspective of Pain
people learn to predict them based on experiences andinformation processing. They filter information thoughtheir preexisting knowledge, and organized representa-tions of knowledge (Turk and Salovey 1985), and reactaccordingly. Their responses, consequently, are basednot on objective reality but their idiosyncratic interpre-tations of reality. As interaction with the environmentis not a static process, attention is given to the ongoingreciprocal relationships among physical, cognitive, af-fective, social, and behavioral factors.
Characteristic
According to the CB model then, it is the pain sufferer’sperspective, based on their idiosyncratic attitudes, be-liefs, appraisals, and expectations that filter and interactreciprocally with emotional factors, social influences,behavioral responses, as well as sensory phenomena.Moreover, patients’ behaviors elicit responses fromsignificant others (including health care professionals)that can reinforce both adaptive and maladaptive modesof thinking, feeling, and behaving.There are five central assumptions that characterize theCB perspective on pain (Turk and Okifuji 1999). Thefirst assumption is that all people are active processors ofinformation rather than passive reactors to environmen-tal contingencies. People attempt to make sense of stim-uli from the external environment by filtering informa-tion through organized schema derived from their priorlearning histories, and by general strategies that guidethe processing of information. People’s responses (overtas well as covert) are based on appraisals and subsequentexpectations and are not totally dependent on the actualconsequences of their behaviors (i.e. positive and nega-tive reinforcements and punishments). Thus, from thisperspective, anticipated consequences are as importantin guiding behavior as actual consequences.A second assumption is that one’s thoughts (e.g. ap-praisals, attributions, expectancies) can elicit or mod-ulate affect and physiological arousal, both of whichmay serve as impetuses for behavior. Conversely, af-fect, physiology, and behavior can instigate or influenceone’s thinking processes. Thus, the causal priority isdependent upon where in the cycle one chooses to begin.Causal priority may be less of a concern than the viewof an interactive process that extends over time.Unlike orthodox behavioral models (operant and re-spondent conditioning) that emphasize the influenceof the environment on behavior, the CB perspectivefocuses on the reciprocal effects of the person on theenvironment, as well as the influence of environmenton behavior. The third assumption of the CB perspec-tive, therefore, is that both the environment and theindividual reciprocally determine behavior. People notonly passively respond to their environment but elicitenvironmental responses by their behavior. In a veryreal sense, people create their environments. The personwho becomes aware of physical events (symptoms) and
decides the symptom requires attention from a healthcare provider, initiates a set of circumstances differentfrom the person with the same symptom who choosesto self–manage (� self-management).A fourth assumption is that if people have learned mal-adaptive ways of thinking, feeling, and responding,then successful interventions designed to alter behaviorshould focus on maladaptive thoughts, feelings, physi-ology, and behaviors, and not one to the exclusion of theothers. There is no expectancy that changing thoughts,feelings, or behaviors will necessarily result in the othertwo following suit.The final assumption of the CB perspective is that inthe same way as people are instrumental in develop-ing and maintaining maladaptive thoughts, feelings,and behaviors, they can, are, and should be consideredactive agents of change of their maladaptive modes ofresponding. People with chronic pain, no matter howsevere, despite their common beliefs to the contrary,are not helpless pawns of fate. They can and shouldbecome instrumental in learning and carrying out moreeffective modes of responding to their environment andtheir plight.From the CB perspective, people with pain are viewed ashaving negative expectations about their own ability tocontrolcertain motor skillswithoutpain.Moreover,painpatients tend to believe they have limited ability to ex-ert any control over their pain. Such negative, maladap-tive appraisals about the situation and personal efficacymay reinforce the experience of demoralization, inactiv-ity, and overreaction to nociceptive stimulation. Thesecognitive appraisals and expectations are postulated ashaving an effect on behavior, leading to reduced effortsand activity that may contribute to increased psycholog-ical distress (� helplessness) and subsequently physicallimitations. If we accept that pain is a complex, subjec-tive phenomenon that is uniquely experienced by eachperson, then knowledge about idiosyncratiCBeliefs, ap-praisals, and � coping repertoire s become critical foroptimal treatment planning, and for accurately evaluat-ing treatment outcome (Turk et al. 1983).Biomedical factors that may have initiated the originalreport of pain play less and less of a role in disability overtime, although secondary problems associated with de-conditioning may exacerbate and serve to maintain theproblem. Inactivity leads to increased focus on and pre-occupation with the body and pain, and these cognitive-attentional changes increase the likelihood of misinter-preting symptoms, overemphasis on symptoms, and theperception of oneself as being disabled.Reduction of ac-tivity, fear of re-injury, pain, loss of compensation, andan environment that, perhaps, unwittingly supports thepain-patient role can each impede alleviation of pain,successful rehabilitation, reduction ofdisability, and im-provement in adjustment. As has been noted, cognitivefactors may not only affect the patient’s behavior and in-directly their pain, but may actually have a direct effect

C
Cognitive-Behavioral Perspective of Pain 407
of physiological factors believed to be associated withthe experience of pain (e.g. Flor et al. 1985).People respond to medical conditions in part based ontheir subjective representations of illness and symp-toms (� cognitive schemata). When confronted withnew stimuli, the person engages in a meaning anal-ysis that is guided by the schemata that best matchthe attributes of the stimulus. It is on the basis of theperson’s idiosyncratic schema that incoming stimuliare interpreted, labeled, and acted on.People build fairly elaborate representations of theirphysical state, and these representations provide thebasis for action plans and coping. Beliefs about themeaning of pain and one’s ability to function de-spite discomfort are important aspects of the cogni-tive schemata of pain. These representations are usedto construct causal, co-variational, and consequentialinformation from their symptoms. For example, a cog-nitive schema that one has a very serious, debilitating,condition, that disability is a necessary aspect of pain,that activity is dangerous, and that pain is an accept-able excuse for neglecting responsibilities will likelyresult in maladaptive responses. Similarly, if patientsbelieve they have a serious condition that is quite fragileand a high risk for re-injury, they may fear engagingin physical activities. Through a process of stimulusgeneralization, patients may avoid more and more ac-tivities, become more physically deconditioned, andmore disabled.People’s beliefs, appraisals, and expectations aboutpain, their ability to cope, social supports, their disor-der, the medicolegal system, the health care system,and their employers are all important as they may facil-itate or disrupt the patient’s � sense of control. Thesefactors also influence patients’ investment in treatment,acceptance of responsibility, perceptions of disability,support from significant others, expectancies for treat-ment, acceptance of treatment rationale, and adherenceto treatment.Cognitive interpretations will also affect how patientspresent symptoms to significant others, including healthcare providers and employers. Overt communication ofpain, suffering, and distress will enlist responses thatmay reinforce pain behaviors and impressions about theseriousness, severity, and uncontrollability of the pain.That is, reports of pain may lead physicians to prescribemore potent medications, order additional diagnostictests, and, in some cases perform surgery. Family mem-bers may express sympathy, excuse the patient fromusual responsibilities, and encourage passivity therebyfostering further � physical deconditioning. It shouldbe obvious that the CB perspective integrates the op-erant conditioning emphasis on external reinforcementand the respondent’s view of learned avoidance withinthe framework of information processing.People with persistent pain often have negative expecta-tions about their own ability and responsibility to exert
any control over their pain, and they avoid activities thatthey believe will exacerbate their pain or contribute toadditional injury (Vlaeyen et al. 1995). Moreover, theyoften view themselves as helpless. Such negative, mal-adaptive appraisals about their condition, situation, andtheir personal efficacy in controlling their pain and prob-lems associated with pain serve to reinforce their over-reaction to nociceptive stimulation, inactivity, and expe-rience of demoralization. These cognitive appraisals areposed ashaving an effectonbehavior; leading to reducedeffort, reduced perseverance in the face of difficulty andactivities and increased psychological distress.The specific thoughts and feelings that patients experi-ence prior to exacerbations of pain, during an exacerba-tion or intenseepisodeofpain, aswell as followingapainepisode can greatly influence the experience of pain andsubsequent pain episodes (e.g. Jensen et al. 1994; Turkand Okifuji 2002). Moreover, the methods patients useto control their emotional arousal and symptoms are im-portant predictors of both cognitive and behavioral re-sponses.TheCBperspectiveonpainmanagementfocusesonpro-viding patients with a repertoire of techniques to helpthem gain a sense of control over the effects of pain ontheir lives, as well as actually modifying the affective,behavioral, cognitive, and sensory facets of the experi-ence. Behavioral experiences help to show patients thatthey are capable of more than they assumed, increas-ing their sense of personal competence. Cognitive tech-niques (e.g. problem solving and coping skills training)help to place affective, behavioral, cognitive, and sen-sory responses under the patient’s control. The assump-tion is that long-termmaintenanceofbehavioralchangeswill only occur if the patient has learned to attribute suc-cess to his or her own efforts. There are suggestions thatthese treatments can result in changes of beliefs aboutpain, coping style, and reported pain severity, as well asdirect behavior changes. Further, treatment that resultsin increases in perceived controloverpain and decreased� catastrophizing also are associated with decreases inpain severity ratings and functional disability (Sullivanet al. 2001; Turner and Aaron 2001). The most importantfactor in poor coping may be the presence of catastro-phizing, rather than differences in the nature of specificadaptive coping strategies (Jensen et al. 1999; Jensen etal. 1994).In summary, people have prior learning histories thatprecede the development of their current pain. Basedon these experiences, they have developed cognitiveschema that consist of all information acquired overtheir lifetime. These cognitive schemata serve as thefilters through which all subsequent experiences areperceived and to which they are responded. Thus, itis essential that people with chronic pain be viewedas integrated wholes, not body parts that are damagedand requiring repair. Failure to attend to cognitiveand affective influences either by a narrow focus on

408 Cognitive-Behavioral Programs
physiology and anatomy, as is the case in the tradi-tional medical model, or exclusively on environmentalinfluences, as is emphasized in operant models, willprove to be inadequate. People are more than physicalparameters or pawns of reinforcement contingences.Rather, they observe, anticipate, and interpret internaland external stimuli. Moreover, people exist in a so-cial environment and contextual factors also play animportant role in the pain experience. Since chronicpain is by virtue of its sole defining characteristicchronic, and since there is no cure, it is essential thattreatment focuses on their adaptation to the symptomsand accompanying problems and not just the symp-toms.
References1. Flor H, Turk DC, Birbaumer N (1985) Assessment of Stress-
Related Psychophysiological Responses in Chronic Back PainPatients. J Consult Clin Psychology 54:354–364
2. Jensen MP, Romano JM, Turner JA et al. (1999). Patient BeliefsPredict Patient Functioning: Further Support for a Cognitive-Behavioral Model of Chronic Pain. Pain 81:95–104
3. Jensen MP, Turner JA, Romano RM et al. (1994) Relationshipof Pain-Specific Beliefs to Chronic Pain Adjustment. Pain57:301–309
4. Sullivan MJL, Thorn B, Haythornthwaite JA et al. (2001) The-oretical Perspectives on the Relation between Catastrophizingand Pain. Clin J Pain 17:52–64
5. Turk DC, Meichenbaum D, Genest M (1983) Pain and Behav-ioral Medicine: A Cognitive-Behavioral Perspective. New York,Guilford, 1983
6. Turk DC, Okifuji A (1999) A Cognitive-Behavioral Approachto Pain Management. In: Wall PD, and Melzack R (eds)Textbook of Pain, 4th edn. Churchill-Livingstone, London,pp 1431–1444
7. Turk DC, Okifuji A (2002) Psychological Factors in ChronicPain: Evolution and Revolution. J Consult Clin Psychol70:678–690
8. Turk DC, Salovey P (1985) Cognitive Structures, Cognitive Pro-cesses, and Cognitive-Behavioral Modification: I. Client Issues.Cogn Ther Res 9:1–17
9. Turner JA, Aaron LA (2001) Pain-Related Catastrophizing: WhatIs It? Clin J Pain 17:65–71
10. Vlaeyen JWS, Kole-Snijders A, Boeren R et al. (1995) Fear ofMovement/(Re) Injury in Chronic Low Back Pain and its Relationto Behavioral Performance. Pain 62:363–372
Cognitive-Behavioral Programs
� Interdisciplinary Pain Rehabilitation
Cognitive-Behavioral Theories
Definition
Cognitive-behavioral theories of the relationship be-tween pain and depression suggest that a persons’
negative cognitive appraisals of pain may contribute tothe development of depression.� Depression and Pain
Cognitive-Behavioral Therapy
Synonyms
CBT
Definition
Cognitive behavioral therapy refers to a class of psy-chotherapy incorporating a wide range of techniques,and which is capable of addressing a range of psycho-logical problems including chronic pain e.g. anxiety, de-pression, specific symptoms of psychosis. A central as-sumption of CBT is that a person’s emotional and be-havioral reactions to adverse circumstances are deter-mined by their cognitive representation of the circum-stances, and their appraisal of them, thus being able toinfluence a person’s mood orbehaviour. Themain aim oftherapy is therefore to change the way in which the indi-vidual represents the circumstance and their appraisals.This is achieved through active elicitation of a person’sthoughts and beliefs, and active behavioral and cogni-tive tasks that are designed to enable the person to re-evaluate their circumstances in a manner that is likelyto be beneficial for them.� Cognitive-Behavioral Perspective of Pain� Cognitive-Behavioral Treatment of Pain� Coping and Pain� Dyspareunia and Vaginismus� ImpactofFamilialFactorsonChildren’sChronicPain� Premenstrual Syndrome� Psychiatric Aspects of Visceral Pain� Psychological Treatment in Acute Pain� Psychological Treatment of Headache� Psychological Treatment of Pain in Children� Psychology of Pain, Efficacy� Recurrent Abdominal Pain in Children� Relaxation in the Treatment of Pain
Cognitive-Behavioral TransactionalModel of Family Functioning
Definition
Cognitive-behavioral transactional model of familyfunctioning emphasizes the role of cognitions and be-liefs in the appraisal of pain and pain-related behavioralinteractions.� Spouse, Role in Chronic Pain

C
Cognitive-Behavioral Treatment of Pain 409
Cognitive-Behavioral Treatment of PainDENNIS C. TURK
Department of Anesthesiology, University ofWashington, Seattle, WA, [email protected]
Synonyms
Cognitive-Behavioral Therapy (CBT); Cognitive-Be-havior Modification; Cognitive Therapy
Definition
Cognitive-Behavioral Therapy (CBT) or cognitive-behavior modification (CBM) are generic terms thatincorporate a wide-range of treatment modalities (e.g.stress management, distraction, relaxation, problem-solving, cognitive restructuring), all of which are de-signed to enhance coping, facilitate self-management,and improve emotional and physical functioning. Theprimary goals are to help patients understand the effectsthat thoughts, feelings, and behaviors have on pain, thepotential of patients to exert some control over theirsymptoms, and education and practice in the use ofcognitive and behavioral coping skills.
Characteristics
The cognitive-behavioral (CB) approach to pain man-agement evolved from research on a number of mentalhealth problems (e.g. anxiety, depression and pho-bias). Following the initial empirical research on CBtechniques in the early 1970s, there have been a largenumber of research and clinical applications. The com-mon denominators across different CB approachesinclude:
1. Interest in the nature and modification of a patient’sthoughts, feelings and beliefs, as well as behaviors;
2. Some commitment to behavior therapy procedures inpromoting change (such as graded practice, home-work assignments, relaxation, relapse preventiontraining, social skills training) (Turk et al. 1983).
In general, the CB therapist is concerned with usingenvironmental manipulations, as are behavior (operantconditioning) therapists, but for the CB therapist suchmanipulations represent informational feedback trialsthat provide an opportunity for the patient to question,reappraise, and acquire self-control over maladaptivethoughts, feelings, behaviors and physiological re-sponses. Although the CB approach was originallydeveloped for the treatment of mental health disorders,the perspective has much in common with the multidi-mensional conceptualizations of pain, which emphasizethe contributions of cognitive and affective, as well assensory phenomena (Melzack and Wall 1965). The CBperspective emphasizes the important contribution of
psychological variables such as the perception of con-trol, the meaning of pain to the patient, and dysphoricaffect (Turk and Flor 1999).It is important to differentiate the CB perspective fromCB treatments. The CB perspective is based on fivecentral assumptions, and can be superimposed uponany treatment approach used with chronic pain patients:
• People are active processors of information and notpassive reactors
• Thoughts (e.g. appraisals, expectancies, beliefs) canelicit and influence mood, affect physiological pro-cesses, have social consequences and can also serveas an impetus for behavior; conversely, mood, physi-ology, environmental factors, and behavior can influ-ence the nature and content of thought processes
• Behavior is reciprocally determined by both the in-dividual and environmental factors
• Peoplecan learnmoreadaptivewaysofthinking,feel-ing, and behaving
• Peopleshouldbeactivecollaborativeagentsinchang-ing their maladaptive thoughts, feelings, and behav-iors
In many cases, the perspective is as important as the con-tent of the therapeutic modalities employed, somatic aswell as psychological (Turk 1997).The application of the CB perspective to the treatmentof chronic pain involves a complex clinical interactionand makes use of a wide range of tactics and techniques.Despite the specific techniques used, all CB treatmentapproaches are characterized by being present, focused,active, time limited, and structured. Therapists are notsimply conveyers of information acting on passive pa-tients, but serveaseducators, coaches, and trainers.Theywork in concert with the patient (and sometimes familymembers) to achieve mutually agreed upon goals.A growing body of research has demonstrated the im-portant roles that cognitive factors (appraisals, beliefs,expectancies) play in exacerbating pain and suffering,contributing to disability and influencing response totreatment (Turk and Rudy 1992). Thus, CB interven-tions are designed to help patients identify maladaptivepatterns and acquire, develop and practice more adap-tive ways of responding. Patients are encouraged tobecome aware of, and monitor, the impact that negativepain-engendering thoughts and feelings play in themaintenance of maladaptive overt and covert behav-iors. Additionally, patients are taught to recognize theconnections linking cognitions, affective, behavioral,and physiological responses together with their jointconsequences. Finally, patients are encouraged to un-dertake ‘personal experiments’, and to test the effectsof their appraisals, expectations, and beliefs by meansof selected homework assignments.The CB therapist is concerned not only with the role thatpatients’ thoughts play in contributing to their disordersbut, equally important, with the nature and adequacy

410 Cognitive-Behavioral Treatment of Pain
of the patients’ behavioral repertoire, since this affectsresultant intrapersonal and interpersonal situations. ACB treatment program for pain patients is multifaceted.Treatment may be conducted for individuals or groupson an inpatient or outpatient basis.The CB perspective should be considered not merelyas a set of methods designed to address the psycho-logical components of pain and disability, but as anorganizing strategy for more comprehensive rehabili-tation (Turk 1997). For example, patients’ difficultiesarising during physical therapy may be associated notonly with physical limitations, but also with the fearengendered by anticipation of increased pain or con-cern about injury. Therefore, from a CB perspective,physical therapists need to address not only the pa-tient’s performance of physical therapy exercises andthe accompanying attention to body mechanics, butalso the patient’s expectancies and fears as they willaffect the amount of effort, perseverance in the faceof difficulties and adherence with the treatment plan(Meichenbaum and Turk 1987). These cognitive andaffective processes, including self-management con-cerns, may be impediments to rehabilitation and thusneed to be considered and addressed, along with tradi-tional instructions regarding the proper performance ofexercise. The attention paid to the individual’s thoughtsand expectancies by a psychologist should be adoptedby all members of the interdisciplinary treatment team.In short, CB treatment should not be viewed as totallyscripted. Therapists must realize that flexibility andclinical skills have to be brought to bear throughout thetreatment program.The CB treatment consists of five overlapping phases:
1. Initial assessment2. Collaborative reconceptualization of the patient’s
views of pain3. Skills acquisition and skills consolidation, including
cognitive and behavioral rehearsal4. Generalization, maintenance, and relapse prevention5. Booster sessions and follow-up
Although the five treatment phases are listed separately,it is important to appreciate that they overlap. The dis-tinction between phases is designed to highlight the dif-ferent components of the multidimensional treatment.Moreover, although the treatment, as presented, followsa logical sequence, it should be implemented in a flex-ible, individually tailored fashion. Patients proceed atvarying paces and the therapist must be sensitive to theseindividual differences.The CB treatment is not designed to eliminate patients’pain per se, although the intensity and frequency of theirpain may be reduced as a result of increased activity,physical reconditioning achieved during physical ther-apy, and the acquisition of various cognitive and behav-ioral coping skills. Rather, the treatment is designed tohelp patients learn to live more effective and satisfying
lives, despite the presence of varying levels of discom-fort that may persist. Other goals include the reductionof excessive reliance on the healthcare system, reduceddependence on analgesic medications, increased func-tionalcapacityand,whenever feasible, returntoemploy-ment or usual household activities. The primary objec-tives of CB treatment are:
• To combat demoralization by assisting patients tochange their view of their pain and suffering fromoverwhelming to manageable
• To teach patients that there are coping techniques andskills that can be used to help them to adapt and re-spond to pain and the resultant problems
• To assist patients to reconceptualize their view ofthemselves from being passive, reactive and helplessto being active, resourceful and competent
• To help patients learn the associations betweenthoughts, feelings and their behavior, and subse-quently to identify and alter automatic, maladaptivepatterns
• To teach patients specific coping skills and, more-over, when and how to utilize these more adaptiveresponses
• To bolster self-confidence and to encourage patientsto attribute successful outcomes to their own efforts
• To help patients anticipate problems proactively andgenerate solutions, thereby facilitating maintenanceand generalization
The over-riding message of the CB approach is that peo-ple are not helpless in dealing with their pain, nor needthey view pain as an all-encompassing determinant oftheir lives. Rather, a variety of resources are availablefor confronting pain, and pain will come to be viewedby patients in a more differentiated manner. The treat-ment encourages patients to maintain a problem-solvingorientation and to develop a sense of resourcefulness, in-stead of the feelings of helplessness and withdrawal thatrevolve around bed, physicians, and pharmacists.The CB approach offers promise for use with a varietyof chronic pain syndromes across all developmental lev-els (Turk and Okifuji 1999). CB approaches have beenevaluated in a number of clinical pain studies. The re-sults tend to support the effectiveness of CB therapy inreducing pain and improving functional activities (Mor-ley et al. 1999). The American Psychological Associa-tion Task Force on Treatment Efficacy designated CBTfor chronic pain as one of 20 applications of psycholog-ical treatments for which there was significant empiri-cal support. CBT is frequently used as a complement toother treatment modalities including information, exer-cise, and medication in the treatment of FMS patients,and is incorporated within interdisciplinary and multi-disciplinary programs (Flor et al. 1992).Taken as an aggregate, the available evidence suggeststhat the CB approach has a good deal of potential as atreatment approach by itself and in conjunction with

C
Cognitive Schemata 411
other treatments. The CB perspective is a reasonableway forhealthcareproviders to think aboutanddealwiththeir patients, regardless of the therapeutic modalitiesutilized.
References1. Flor H, Fydrich T, Turk DC 1992 Efficacy of Multidisci-
plinary Pain Treatment Centers: A Meta-Analytic Review. Pain49:221–230
2. Meichenbaum D, Turk DC (1987) Facilitating Treatment Adher-ence: A Practitioner’s Guidebook. Plenum Press, New York
3. Melzack R, Wall PD (1965) Pain Mechanisms: A New Theory.Science 150:971–979
4. Morley S, Eccleston C, Williams AC de (1999) Systematic Re-view and Meta-Analysis of Randomized Controlled Trials ofCognitive Behavior Therapy and Behavior Therapy for ChronicPain in Adults, Excluding Headache. Pain 80:1–13
5. Turk DC (1997) Psychological Aspects of Pain. In: Bakule P(ed) Expert Pain Management. Springhouse, pp 124–178
6. Turk DC, Rudy TE (1992) Cognitive Factors and Persistent Pain:A Glimpse into Pandora’s Box. Cognitive Therapy and Research16:99–122
7. Turk DC, Flor H (1999) Chronic Pain: A Biobehavioral Perspec-tive. In: Gatchel RJ, Turk DC (eds) Psychosocial Factors in Pain.Guilford Press, New York, pp 18–34
8. Turk DC, Okifuji (1999) A Cognitive-Behavioral Approach toPain Management. In: Wall PD, Melzack R (eds). Textbook ofPain, 4th edn. Churchill Livingstone, London, pp 1431–1444
9. Turk DC, Meichenbaum D, Genest M (1983) Pain and BehavioralMedicine: A Cognitive-Behavioral Perspective. Guilford Press,New York
Cognitive Coping Training
Definition
CognitiveCopingTraining includes,but isnot limited to,attention diversion strategies, reinterpreting pain sensa-tions, calming self-statements, and imagery techniques.� Psychological Treatment of Headache
Cognitive Dysfunction
Definition
Changes in consciousness, higher cortical functions,mood, or perception that may be induced by any ofnumerous neurological or systemic diseases, or by in-gestion of substances, including drugs, that have thepotential for central nervous system toxicity.� Cancer Pain Management, Opioid Side Effects, Cog-
nitive Dysfunction
Cognitive Error
Definition
A discrepancy between actual and perceived aspects ofa particular situation.� Catastrophizing
Cognitive Factors
Definition
Cognitive factors are the beliefs, appraisals, expecta-tions, and meaning through which individuals filterinformation. These cognitive factors will have an in-fluence on emotional and physiological arousal andbehavior.� Cognitive-Behavioral Perspective of Pain� Psychological Assessment of Pain
Cognitive Impairment
� Cancer Pain, Assessment in the Cognitively Impaired
Cognitive Model of Pain
� Cognitive-Behavioral Perspective of Pain
Cognitive Modulation of Pain
� Descending Circuits in the Forebrain, Imaging
Cognitive Restructuring
Definition
Cognitive restructuring isaprocesswhereby patientsaretaught tomonitor their thoughtsandfeelings,andtoeval-uate whether these are appropriate in light of the circum-stances and evidence available. Patients are encouragedtobecomeawareof theirautomatic responsesand tocon-sider the accuracy of the assumptions on which these re-sponses are based. They are instructed to evaluate theassumptions that result in specific behaviors and to con-sider alternatives that may be more adaptive.� Catastrophizing� Multidisciplinary Pain Centers, Rehabilitation� Psychological Treatment of Headache
Cognitive Schemata
Definition
Cognitive schemata are models that people create toassist them to structure and make sense of life circum-stances, constructs, and categories. These are efficienttemplates thathelp peoplenavigate in theirworld and fil-ter new information. Newly acquired information mustbe assimilated into these existing cognitive structures

412 Cognitive Tasks
or will contribute to a modification (accommodation)ofthe schemata to incorporate the new data of experience.� Cognitive-Behavioral Perspective of Pain
Cognitive Tasks
Definition
Procedures used to engage participants in a particularcognitive activity. These include (but are not restrictedto) tasks such as the retrieval of words or memories, re-action times to identify specific stimulus features or tocomplete different mental operations, or the interpreta-tion ofambiguousstimuli.Theoperationof specificcog-nitive processes is typically inferred on the basis of dif-ferent patterns of cognitive task performance.� Psychology of Pain, Assessment of Cognitive Vari-
ables
Cognitive Therapy
� Cognitive-Behavioral Treatment of Pain
Cohort
Definition
Cohort refers to a group, band, or body of people whoare followed over time.� Prevalence of Chronic Pain Disorders in Children
Cohort Study
Longitudinal Study� Longitudinal Study
Coital Pain
� Dyspareunia and Vaginismus
Cold Allodynia
Definition
Pain produced by a normally non-painfulcold stimulus.� Neuropathic Pain Model, Partial Sciatic Nerve Liga-
tion Model� Neuropathic Pain Model, Tail Nerve Transection
Model
Cold Allodynia Test
Definition
One or two drops of acetone are thrown on the plantaraspect of the leg. In rats, this procedure does not pro-duce a significant reaction (score <0.5), however, in ratswith mononeuropathya vigorous reaction is induced byacetone-drops for a period up to 20 s.� Allodynia Test, Mechanical and Cold Allodynia� Thalamotomy, Pain Behavior in Animals
Cold Hyperalgesia
Definition
Pain induced abnormally, or exacerbated, by low tem-perature.Acommon symptom in manyneuropathicpainpatients.� Nociceptors, Cold Thermotransduction
Cold Nociception
� Nociceptors, Cold Thermotransduction
Cold NociceptorsDONALD A. SIMONE
Department of Diagnostic and Biological Sciences,University of Minnesota, School of Dentistry,Minneapolis, MN, [email protected]
Definition
Nociceptors are sensory receptors located on peripheralnerveendingsthatareexcitedbynoxiousorpainfulstim-uli. Subgroups of nociceptors are excited by cold andencode the intensity of cold stimuli.
Characteristics
In humans, reduction of skin temperature to approxi-mately 15˚C or less evokes a sensation of pain. Interest-ingly, pain from noxious cold can have different qual-ities, including cold, burning, pricking and aching, de-pendingonthe intensity,duration, rateofstimulationandlocation of the cold stimulus (Chery-Croz 1983; Davisand Pope 2002; Kunkle 1949). This suggests that differ-ent classes of nociceptors are excited by noxious coldstimuli.Early studies documented that a portion of cutaneousAδ and C nociceptors that are responsive to mechanicalstimuli are excited by noxious cold (Bessou and Perl1969; Burgess and Perl 1967; Georgopoulos 1976;

C
Cold Pressor Test 413
LaMotte and Thalhammer 1982; Saumet et al. 1985).Many of the nociceptors excited by cold are also ex-cited by heat, and are considered to be polymodalnociceptors. However, the exact proportion of Aδ andC nociceptors excited by cold varied among the studiesbecause stimulus temperatures and species used varied.For example, nociceptors in monkeys were not excitedby stimuli to 15˚C (Perl 1968), whereas 78% of Aδ
and C nociceptors were excited by the application ofice to the skin (LaMotte and Thalhammer 1982). Inan extensive study of the response properties of thevarious subtypes of nociceptors in rats, Leem et al.(1993) found that approximately 10% or less of Aδ
and C nociceptors were excited by cold. Using stim-ulus temperatures between 27 and 12˚C, they foundresponse thresholds of nociceptors were between 22and 12˚C. However, when a wider range of stimulustemperatures was used, it was found that nearly allmechanosensitive nociceptors in rat hairy skin wereexcited by noxious cold (Simone and Kajander 1996;Simone and Kajander 1997). Response thresholds forAδ nociceptors ranged from 14 to -18˚C; 79% of Aδ
nociceptors had cold response thresholds at or below0˚C. Most C nociceptors exhibited response thresh-olds above 0˚C and thresholds ranged from 12 to -6˚C.A wide range of cold response thresholds was alsoobserved for nociceptors in mouse skin (Cain et al.2001).Sensitivityofnociceptors tocoldhasalsobeendescribedin humans (Campero et al. 1996; Torebjrk 1974). Usingstimulus intensities between 19 and 0˚C, it was foundthat 40% of C nociceptors that were sensitive to mechan-ical and heat stimuli were also excited by noxious coldstimuli.A few studies have examined the intensity encodingpropertiesofnociceptors fornoxiouscold stimuli (Geor-gopoulos 1977; Simone and Kajander 1996; Simoneand Kajander 1997). Using a range of stimulus temper-atures from 20 to -12˚C (or sometimes to -12˚C), eachfor a duration of 10 seconds, it was found that responsesof Aδ and C nociceptors in rats increased as stimulustemperature decreased (Simone and Kajander 1996;Simone and Kajander 1997). The number of evokedimpulses, the average discharge rate and the peak dis-charge rate each increased as stimulus temperaturedecreased. Discharge rates evoked by stimulus temper-atures greater than 0˚C were typically low (less than 1impulse per second) and increased with colder temper-atures. Power functions were generated to determinethe stimulus-response relationship for Aδ nociceptorsand the slopes of the power functions ranged from 0.12to 2.28.In summary, the majority of cutaneous nociceptors thatare excited by mechanical stimuli, including polymodalnociceptors, are excited by noxious cold stimuli. Cuta-neous nociceptors exhibit a wide range of cold responsethresholds and encode stimulus intensity.
References1. Bessou P, Perl ER (1969) Response of cutaneous sensory units
with unmyelinated fibers to noxious stimuli. J Neurophys-iol 32:1025–1043
2. Burgess PR, Perl ER (1967) Myelinated afferent fibres re-sponding specifically to noxious stimulation of the skin. JPhysiol 190:541–562
3. Cain DM, Khasabov SG, Simone DA (2001) Response propertiesof mechanoreceptors and nociceptors in mouse glabrous skin:an in vivo study. J Neurophysiol 85:1561–1574
4. Campero M, Serra J, Ochoa JL (1996) C-polymodal nociceptorsactivated by noxious low temperature in human skin. J Phys-iol 497:565–572
5. Chéry-Croze S (1983) Painful sensation induced by a thermalcutaneous stimulus. Pain 17:109–137
6. Davis KD, Pope GE (2002) Noxious cold evokes multiple sen-sations with distinct time courses. Pain 98:179–185
7. Georgopoulos A (1977) Stimulus-response relations in high-threshold mechanothermal fibers innervating primate glabrousskin. Brain Res 128:547–552
8. Kunkle EC (1949) Phasic pains induced by cold. J App Phys-iol 1:811–824
9. LaMotte RH, Thalhammer JG (1982) Response properties ofhigh-threshold cutaneous cold receptors in the primate. BrainResearch 244:279–287
10. Leem JW, Willis WD, Chung JM (1993) Cutaneous sensory re-ceptors in the rat foot. J Neurophysiol 69:1684–1699
11. Perl ER (1968) Myelinated afferent fibers innervating theprimate skin and their response to noxious stimuli. J Physiol(Lond) 197:593–615
12. Saumet J-L, Chéry-Croze S, Duclaux R (1985) Response of catskin mechanothermal nociceptors to cold stimulation. Brain ResBull 15:529–532
13. Simone DA, Kajander KC (1996) Excitation of rat cutaneousnociceptors by noxious cold. Neurosci Lett 213:53–56
14. Simone DA, Kajander KC (1997) Responses of cutaneous A-fibernociceptors in noxious cold. J Neurophysiol 77:2049–2060
15. Torebjrk HE (1974) Afferent C units responding to mechanical,thermal and chemical stimuli in human non-glabrous skin. ActaPhysiol Scand 92:374–390
Cold Pressor Test
Definition
The cold pressor test is a widely used experimental painprocedure to determine a person’s pain threshold andpain tolerance. Subjects are asked to immerse their rightor left lower arm (up to the elbow) or foot into a basinof water, which is kept at a constant given temperaturebetween 0˚C and 10˚C. Pain threshold is defined asthe elapsed time between arm immersion and the firstreport of a pain sensation. Pain tolerance is defined asthe elapsed time until voluntary withdrawal of the hand.Since the cold pressor test induces pronounced sym-pathetic activation and vasoconstriction, the maximumduration of limb immersion is typically restricted bythe experimenter in order to prevent vascular problems.� Experimental Pain in Children� Modeling, Social Learning in Pain� Pain in Humans, Thermal Stimulation (Skin, Muscle,
Viscera), Laser, Peltier, Cold (Cold Pressure), Radi-ant, Contact
� Pain in Humans, Thresholds

414 Cold Therapy
� Psychological Aspects of Pain in Women� Psychology of Pain, Self-Efficacy
Cold Therapy
� Therapeutic Heat, Microwaves and Cold
Cold Thermoreceptor
Definition
In biophysical terms, a cold thermoreceptor is a nerveending excited only, or preferentially, by a cold tempera-ture stimulus.They should bedistinguishedfrom „spuri-ous“ thermoreceptors like slowly adapting mechanore-ceptors that also respond to thermal stimulation.� Cold Nociceptors� Nociceptors, Cold Thermotransduction
Cold Thermotransduction
� Cold Nociceptors� Nociceptors, Cold Thermotransduction
Cold-Induced Hyperalgesia
� Freezing Model of Cutaneous Hyperalgesia
Colitis
Definition
Inflammation of the large intestine, or colon, oftencaused by a primary disease, irritation of the bowel, an-tibiotic use, or ulceration. Acute colitis can be producedexperimentally by the introduction of an irritant, suchas mustard oi1, zymosan or capsaicin into the lumen ofthe colon. Symptoms may include abdominal pain orbloating, diarrhea, dehydration, and increased intestinalgas.� Amygdala, Pain Processing and Behavior in Animals� Animal Models of Inflammatory Bowel Disease� Visceral Pain Model, Lower Gastrointestinal Tract
Pain
Collateral Sprouting
Definition
Induction of new axonal sprouts from an intact nerve bynerve growth factor. The sprouts grow into an area of anadjacent, injured, degenerating, peripheral nerve. Corti-cal sensations related to this phenomenon can be relatedto either the injury itself, or the response to dividing theinjured peripheral nerve to treat a painful neuroma. Col-lateral sprouting pain can be misinterpreted as failure ofthe original treatment for the painful scar or painful neu-roma.� Painful Scars
Colorectal Distension
Synonyms
CRD
Definition
Controlled innocuous or noxious visceral stimulus ap-plied by distension of a balloon placed in the lumen ofthe descending colon and rectum. In humans under nor-mal conditions, distension pressures below 40 mmHgare felt as non-painful, whereas distension pressuresgreater than 40 mmHg are felt as painful.� Descending Modulation of Visceral Pain� Postsynaptic Dorsal Column Neurons, Responses to
Visceral Input� Spinal Dorsal Horn Pathways, Dorsal Column (Vis-
ceral)� Visceral Pain Model, Lower Gastrointestinal Tract
Pain
Colposcopy
Definition
Colposcopy is a diagnostic tool aimed at verifying thecause of abnormalities found in Pap smears. It involves avisual examination of the cervix, genitals, and vagina aswell as theapplication ofaceticacid to identifyabnormalcells.� Dyspareunia and Vaginismus
Combined Spinal Epidural (CSE)Technique
Definition
An anesthetic technique where both spinal and epidu-ral anesthesia is administered to the same patient as one

C
Complete Freund’s Adjuvant 415
technique. It offers the advantages of a spinal anesthetic(intense analgesia) with the advantages of an epiduralanesthetic (flexibility and long duration of action).� Analgesia During Labor and Delivery
Common Fears
Definition
More specific fears directed at an apparent object (suchas spider phobia, agoraphobia, fear of pain). They ariseas the result of an interaction between the fundamentalfears and learning experiences, and can thus be logicallyderived from these three fundamental fears.� Fear and Pain
Common Migraine
� Migraine Without Aura
Common Toxicity Criteria
Definition
WHOand NationalCancer Institutemethodofassessingthe morbidity associated with cancer and cancer treat-ment by organ system.� Cancer Pain Management, Chemotherapy
Communication Limitations orNeurological Impairment
� Pain in Children with Disabilities
Comorbid Headache
Definition
Classification proposed by Gladstein and Holden(1996), describing a subtype of chronic daily headachein children as a daily tension-type headache, accom-panied by intermittent and less frequent episodes ofwell-defined migraine headache.� Chronic Daily Headache in Children
Reference
Gladstein J, Holden EW (1996) Chronic daily headachein children and adolescents: a 2-year prospective study.Headache 36:349-351
Comorbidity
Definition
Comorbiditydefinesanassociationbetweentwoormoredisorders or diagnoses at one time that are more thancoincidental.� Migraine, Preventive Therapy� Psychiatric Aspects of the Epidemiology of Pain
Compartmental Syndrome
� Postoperative Pain, Compartment Syndrome
Competitive Agonist or Antagonist
Definition
Compound that interacts with the endogenous ligand-binding site of the receptor.� NociceptiveProcessing in theAmygdala,Neurophys-
iology and Neuropharmacology� Spinal Cord Nociception, Glutamate Receptor(Metabotropic)
Complement
Definition
Non-specific mediator of humoral immunity. Manyagents (antigens) trigger the complement cascade,which may ultimately result in the generation of mem-brane attack complex and lysis of cells presenting thetriggering agent.� Inflammatory Neuritis
Complementary Medicine
� Alternative Medicine in Neuropathic Pain
Complementary Therapies
� Alternative Medicine in Neuropathic Pain
Complete Freund’s Adjuvant
Synonyms
CFA

416 Compensation, Disability, and Pain in the Workplace
Compensation, Disability, and Pain inthe Workplace
JAMES P. ROBINSON, DENNIS C. TURK
Department of Anesthesiology, University ofWashington School of Medicine, Seattle, WA, [email protected],[email protected]
Introduction
Pain is the epitome of a private experience. Only theperson with pain has direct access to the experience.At the same time however, pain has a public face, be-cause people in pain communicate their suffering toothers either verbally or by non-verbal behavior andoften request assistance. Observers of someone in painare challenged because they are not able to experiencethe other’s pain directly. Thus, they are forced to makeinferencesand may wellhavedifficulty interpreting thecommunications of the pain sufferer.Social interactions related to pain occur in both for-mal and informal settings. As an example of the latter,a person with pain will communicate his or her suffer-ing tofamilymembers.Researchhasdemonstratedthatthe family members, in turn, respond to the pain suf-ferer in fairly predictable ways (Romano et al. 1995).But not only family members respond to the behaviorof those who experience pain. Co-workers and super-visors and health care providers are also asked to re-spond by making work place accommodations in thecase of the former and prescribing treatment in the lat-ter. Health care providers are also frequently asked tomake recommendations regarding the impairments ofindividuals who report incapacitation because of pain.These may serve as the basis for financial compen-sation and accommodations on the job. The presentfield of this volume addresses social interactions re-lated to pain that occur in a formal context – in partic-ular, it addresses interactions between pain sufferersand 1) health care providers who offer treatment andmake decisions about disability and 2) societal agen-cies that provide benefits for work disability.Examplesof such societal agencies include workers’ compensa-tion programs (which compensate individuals only iftheir medical problems were caused by work) and pro-gramssuchastheUnitedStatesSocialSecurityAdmin-istration (which compensate disabled people regard-less of the cause of their disability).The problems of impairment and disability (these 2inter-related concepts are defined and differentiatedbelow) secondary to pain are elusive and yield con-flicts and contradictions at multiple levels of analy-sis. The central problem relates to the fact that thereis currently no objective measure of pain. As a con-
sequence, decisions regarding the presence and im-pact of pain are based on inferences derived from priorexperience and assumptions related to the amount ofpain that might be expected given objective indica-tions of pathology or disease. At a clinical level, con-flicts and distrust frequently develop between disabil-ity applicants and the health care provider and disabil-ity adjudicators who are involved in their claims. In-dependent medical examiners and attorneys often be-come participants in these conflicts. People experienc-ing pain often feel that physicians and others discounttheir reports; physicians and adjudicators may experi-ence doubt or outright skepticism about reports of painin the absence of corroborating physical findings. Theessay � Ethics of Pain-Related Disability Evaluationsexplores ethical and conceptual issues related to thetask ofmaking inferencesabout thepainofanotherper-son.
Disability Systems
Communities frequently provide assistance to peoplewho are incapacitated. This type of helping behaviorcan be seen not only in modern societies, but also inprimitive ones and even in communities of infrahumanprimates (Fabrega 1997). Tolerance toward and careof the sick, infirm, injured and disabled appears to bea fundamental feature of society dating back to pre-historic times (Ranavaya and Rondinelli 2000). For-mal disability compensation systems were recorded asmany as 4000 years ago by the Babylonians, who pro-vided compensation for loss of life or a body part in-curred in the service of the state. During the time of theancient Egyptians and Greeks, the state provided com-pensation for injuries caused by a wrongful act or oc-curring in the context of military service, respectively.Contemporary approaches to the issue of assistance forincapacitated people can be traced back to social insur-ance programs instituted in Germany in the late 19th
century (Ritter 1983).The social insurance programs that are most relevantto the present field of this volume are those that pro-vide income maintenance benefits (also referred to as“wage replacement” or “time loss” benefits) for per-sons who are incapacitated from work. As noted in acomprehensive survey of social insurance programs in138 countries and territories, programs to assist citi-zens who are incapacitated exist in most countries (So-cialSecurity Administration,OfficeofResearch,Eval-uation and Statistics 1999). Several of these are dis-cussed as illustrations in the essays � impairment rat-ing, ambiguity; � impairment rating, ambiguity, IA-IABC system; � disability evaluation in the social se-curity administration and � rating impairment due topain in a workers’ compensation system.

C
Compensation, Disability, and Pain in the Workplace 417
Among income maintenance programs, a basic dis-tinction can be made between work injury (or work-ers’ compensation)programs and disability programs.Workers’ compensation programs provide benefits forindividuals who are disabled because they have sus-tained injuries or developed diseases “out of and in thecourse of employment” (p. 10) (Williams 1991). Dis-ability programs in contrast provide benefits for peo-ple who are incapable of working for any reason. Thus,both workers’ compensation programs and disabilityprograms provide income maintenance only if an indi-vidual is judged to be unable to work because of a med-ical condition, but workers’ compensation programsimpose an additional criterion – that the medical con-dition was caused by the person’s work activities.A central thesis of this field in the Encyclopedic Ref-erence of Pain is that important problems and signif-icant ambiguities emerge as individuals with painfuldisorders interactwithagencies thatadminister incomemaintenance programs. A corollary of this thesis is thatthe problems that emerge in these interactions will de-pend on specific features of disability programs. It isbeyond the scope of this essay to discuss the complexi-ties of disability programs, but even a cursory review ofthem revealsenormousvariation from country to coun-try in the manner in which programs are financed andintegrated into a network of social security programs,and in the eligibility criteria and procedures they useto evaluateapplicants (SocialSecurity Administration,Office of Research, Evaluation and Statistics 1999).Some of the essays (e.g. the ones on patient credibilityand pain behavior; see � credibility, assessment and� nonorganic symptoms and signs) are relevant to anysystem of income maintenance for persons who allegework incapacity because of pain. However, many ofthe other essays discuss attempts by specific disabil-ity agencies to address problems presented by pain re-lated incapacitation. These essays should be viewed asproviding examples of ways in which specific disabil-ity agencies have addressed problems associated withpain, rather than as comprehensive discussions of theways in which these problems might be addressed.At an administrative level, bureaucracies that havespecific imperatives operate disability programs. Forexample, the Social Security Administration in theUnited States, which operates the 2 largest disabil-ity programs, strives for uniformity, objectivity andcostcontainment in itsdisability evaluationprocedures(Derthick1990).Oneof theessays,� impairment,painrelated, points out that however sensible these goals arefrom a bureaucratic standpoint, they are often at oddswith the clinical realities of patients with chronic pain(Osterweis et al. 1987; Robinson et al. 2004).At a societal level, additional concerns and perspec-tives emerge. As noted previously, disability programs
reflect an ethical commitment to support citizens whoare incapableofworking. If aprogramis too restrictive,it may consign needy and worthy applicants to poverty;if it is too lax, it may encourage disability applicationsfrom peoplewho areactually capableofworking.Evenif a program is meeting its ethical mandate quite well,it may strain the financial resources of the payer to thebreaking point.This isprecisely theconcern that isnowbeing voiced about many of the programs run by theSocial Security Administration in the United States.At a scientific level, issues related to disability areusually unanswerable, because the research underpin-nings for “disability evaluation science” are so mea-ger. Moreover, the search for scientifically valid con-clusions about disability may be compromised by theadversarial settings in which disability evaluations areconducted, and the enormous financial stakes involved(see � independent medical examinations).Finally, at a philosophical level, the problem of disabil-ity evaluation in chronic pain rests on an epistemolog-ical dilemma – the information available to an individ-ual suffering pain is fundamentally different from theinformation available to any external observer who at-tempts to assess the pain. Scarry succinctly capturedthis dilemma when she asserted: “To have great painis to have certainty; to hear that another person has painis to have doubt.”(p. 7) (Scarry 1985).In clinical situations, patients frequently communicatethe sense that they are severely incapacitated by painand ask health care providers to support their claims.Typically, the health care providers who evaluate thesepatients cannot identify tissue damage or organ pathol-ogy that makes the limitations communicated by thepatient seem inevitable, proportional or even plausible.The health care provider then has the dilemma of inte-grating thepatient’ssubjectivereportwiththeobjectiveevidence of tissue damage and organ pathology to es-tablish some final judgment about the extent to whichthe patient really is incapacitated. At one extreme, ahealth care provider might simply ignore a patient’sself-assessments and make a disability determinationbased strictly on objective findings of tissue damage ororgan pathology. At the opposite extreme, the healthcare provider might accept the patient’s descriptionof the situation, and provide a disability rating that iscongruent with the patient’s self-assessment. Adjudi-cators at disability agencies face the same dilemmawhen they decide whether or not to award benefitsto disability applicants. It has proved extremely diffi-cult to find some intermediate position in which bothobjective evidence and self-assessments by patientscan be incorporated into disability evaluations (see� impairment rating, ambiguity; � impairment rat-ing, ambiguity, IAIABC system; � impairment, pain-related and � independent medical examinations).

418 Compensation, Disability, and Pain in the Workplace
The issues discussed in this field are particularlyrelevant to 5 groups of professionals: 1) clinicianswho treat patients with chronic pain, 2) physicianswho conduct independent medical examinations (see� independent medical examinations), 3) allied pro-fessionals who participate in disability mitigation pro-grams (e.g. vocational � rehabilitation counselors) 4)individuals involved in disability policy and 5) psy-chologists interested in the study of interpersonal per-ception and the ways in which social interactions in-fluence pain.
Definitions: Disability and Impairment
“Disability” and “impairment” are fundamental con-cepts that provide the conceptual cornerstones for dis-ability programs. Disability can be informally definedas the inability to carry out certain activities becauseof a medical problem (an abnormality in the structureor function of an organ or body part). There are differ-ent kinds of disability, since there are different types ofactivities that might be affected by a physical disorder.For example, a person might be disabled in the senseof being unable to work, in the sense of being unableto manage his or her personal finances or in the senseof being unable to perform activities of daily living in-dependently. The current field focuses specifically onwork disability – the inability to engage in substantial,gainful employment.Unfortunately, there is no unique formal definition ofwork disability, since various agencies that adminis-ter disability programs define the term slightly differ-ently. These differences reflect a fundamental realityabout disability agencies and the criteria used for mak-ing decisions. For a disability agency, definitions servethe practical function of identifying the criteria that ap-plicants must meet in order to be eligible for benefits.Thus, agencies have different definitions, because theyhave different mandates and different eligibility crite-ria.The United States Social Security Administration de-fines disability as: “the inability to engage in any sub-stantialgainfulactivity...byreasonofanymedicallyde-terminable physical or mental impairment that can beexpected to result in death or that has lasted or can beexpected to last for a continuous period of not less than12 months” (p. 2) (SSA Publication 1994). This def-inition reflects 3 facts about eligibility criteria for theSocialSecurity Disability InsuranceandSupplementalSecurity Income programs: 1) applicants must be to-tally disabled from work; 2) the work disability mustbe “permanent” (or at least long-term); 3) causation isirrelevant – that is, an individual is eligible for benefitsregardless of how or why he or she became disabled. Incontrast, the American Medical Association’s Guidesto theEvaluation ofPermanent Impairment,5thedition
(AMA Guides) defines disability as “an alteration ofan individual’s capacity to meet personal, social or oc-cupational demands or statutory or regulatory require-ments because of an impairment” (p. 8) (Cocchiarellaand Andersson 2001). This very broad definition re-flects the fact that the AMA Guides describe an evalu-ation system that is relevant to many kinds of disability(rather than just work disability) and that permits gra-dations in disability to be identified (rather than just the2 categories of totally disabled vs. non-disabled.)An impairment can best be understood as a deficiencyin the functioning of an organ or body part that leads toincapacitation or disadvantage in various arenas (suchas inability to work or inability to do routine activitiesat home). “Impairment” is defined in a similar way bydifferent disability agencies and expert panels. As anexample, the formal definition of impairment given inthe AMA Guides is: “a loss, loss of use or derange-ment of any body part, organ system ororgan function”(p. 2) (Cocchiarella and Andersson 2001). Thus, onemight say: “Mr. Jones’ heart has been impaired sincehe suffered a myocardial infarction” or “Mrs. Brown’sright hand is impaired because of her carpal tunnelsyndrome.” The essay � impairment, pain-related ad-dressesproblemsthatarisewhentheAMAGuidescon-struct of impairment is applied to individuals who re-port incapacitation because of pain. Additional discus-sions of the definitions and the relationships amongbody function and structures, activities and participa-tion as conceptualized by the World Health Organiza-tion are included in the essays � disability and impair-ment definitions and � WHO system on impairmentand disability.Disability agencies assume significant linkages be-tween impairment and disability. First, they construeimpairment as a necessary condition for disability. Thelogic underlying this requirement is simple. Disabilityprograms are designed to assist people who are inca-pable of competing in the workplace because of a med-ical condition. In essence, disability programs attemptto partition persons who fail in the workplace into 2large groups, ones who fail because of a medical con-dition and ones who fail for other reasons (e.g. lackof demand for their skills). Therefore, disability pro-grams require evidence that an applicant actually has amedical problem underlying his or her workplace fail-ure. Impairmentprovides thenecessaryevidence,sinceit can be viewed as a marker that an individual has amedical problem that diminishes his or her capability.Conversely, if a person has no apparent impairment,this means that he or she does not have limitations dueto a medical condition.Disability agencies typically assume that the severityof a person’s impairment is highly correlated with theseverity (or probability) of his or her being disabled

C
Compensation, Disability, and Pain in the Workplace 419
from work. Thus, even when an agency grants awardsonly on the basis of work disability, the agency willoften seek information about a person’s impairmentin order to rationalize its decision about whether ornot to award disability benefits. Studies have shown,however, that the association between physical impair-ments and work disability is far from perfect (Waddell1987). As the above discussion suggests, the practi-cal question facing a disability agency is to determinewhetherornotan applicant is sufficiently incapacitatedto be eligible for disability benefits. Impairment evalu-ation should be viewed as an intermediate step in mak-ing this determination. Many of the essays in the fieldof compensation, disability and pain in the workplacefocus on disability and disability determination.
When Should a Disorder Be Construed as a Pain Prob-lem?
Pain occurs in a wide range of medical disorders. It isusually conceptualized as a “component” of a disor-der that is typically inextricably interwoven with othermanifestations of disease or injury. From this perspec-tive, it is somewhat arbitrary to abstract pain from othermanifestationsofdisorders, justas itwouldbearbitraryto isolate fevers from malaria or shortness of breathfrom myocardial infarction.A related point is that many painful disorders aretreated by specialists of an affected organ system ratherthan by pain specialists. For example, chest pain is acardinal symptom of cardiac ischemia, but a patientwith chest pain of cardiac origin is much more likely tobe treated by a cardiologist or a thoracic surgeon ratherthan by a pain specialist. Specialists in organ pathol-ogy typically view pain as a symptom of a biologicalabnormality that is important as a guide to appropri-ate diagnosis and treatment. In this model, symptomsand signs are used to diagnose disorders and treatmentis directed toward the abnormal pathophysiology thatcomprises a disorder, rather than toward the symptomsof the disorder per se. The assumption is that once theunderlying biological abnormality has been corrected,the symptoms – including pain – will abate.The discussion in the previous paragraph raises a prac-tical question. When should disorders that occur in theworkplace be construed as pain problems? Two relatedcriteria are suggested. A disorder is appropriately con-strued as a pain problem when either 1) patients reportpain, but do not demonstrate structural or functionalabnormalities that unequivocally explain their pain or2) patients demonstrate limitations in activities that arenot inevitable consequences of biological abnormali-ties, but rather appear to be consequences of pain thatthepatientsexperienceas theyengageinactivities.Oneor both of these circumstances occur sufficiently fre-
quently to warrant a thorough discussion of pain in theworkplace.
Basic Problems Involving the Interface between Dis-ability Systems and Injured Workers with Chronic Pain
Objective Factors
Disability agencies strive to use disability evaluationprocedures that are based on objective findings of in-capacitation. This administrative objective seems in-nocuous enough; however, it has profound implica-tions. In essence, disability agencies must make signif-icant simplifying assumptions about disability in orderto achieve their administrative goal. The most funda-mental simplifying assumption is that impairment anddisability should be “transparent” to an experiencedphysician,namely thatactivity limitationsasdescribedordemonstratedbypatientsshouldbehighlycorrelatedwith evidence of tissue damage or organ dysfunctionthatcan beobjectively assessed by aphysician.Thisas-sumption underlies the routine demand that disabilityadjudicators make for physicians to rely on “objectivefindings” when they proffer conclusions about activitylimitations of claimants.The assumption that impairment and disability can beobjectively assessed is so pervasive that most physi-cians – and essentially all disability adjudicators – ac-cept it without question. The assumption is valid forcertain medical conditions. For example, physicianshave tools to quantify impairment stemming from am-putations or complete spinal cord injuries. However,in many medical conditions – including most chronicpain syndromes – physicians cannot objectively iden-tifyimpairmentsthatrationalizetheactivitylimitationsthat patients report. In a monograph on the disabilityprograms administered by the Social Security Admin-istration in the United States, Osterweis et al. (1987)summarize the problem as follows.The notion that all impairments should be verifiable byobjective evidence is administratively necessary for anentitlement program. Yet this notion is fundamentallyat odds with a realistic understanding of how diseaseand injury operate to incapacitate people. Except for avery few conditions, such as the loss of a limb, blind-ness, deafness, paralysis or coma, most diseases andinjuries do not prevent people from working by me-chanical failure. Rather, people are incapacitated by avariety of unbearable sensations when they try to work(p. 28).In essence, this statement indicates that in many medi-cal disorders disability is related to subjective factors –especially pain – rather than to objectively measurable“mechanical failure” of body parts or organs. As dis-cussed in several essays (� impairment rating, ambi-guity� impairmentrating,ambiguity, IAIABCsystem

420 Compensation, Disability, and Pain in the Workplace
� disability evaluation in the social security adminis-tration� disability, effectofphysiciancommunication� rating impairment due to pain in a workers’ com-pensation system), disability agencies have developeddifferent solutions to theproblem of reconciling thead-ministrative imperative of basing disability determina-tions on objective findings with the reality that subjec-tive factors are the proximate cause of work incapac-itation for many patients.
Credibility
Many disability agencies have at least implicitly ac-cepted the premise that determinations about eligibil-ity for disability benefits should rely, at least in part,on claimants’ reports about pain and other subjectiveexperiences. To the extent that disability determina-tion relies on subjective reports by claimants about thedifficulties they have when working, agencies must beconcerned about how to assess the integrity of these re-ports. In the extreme case, it is possible for malingerersto simulate incapacitation and receive disability bene-fitswhentheyhaveessentiallynowork limitations.Theproblem of malingering is addressed in � malingering,primary and secondary gain.A more common scenario is that claimants report dra-matic activity restrictions because of pain, and demon-strate severe functional limitations during physical ex-amination. Examining physicians and disability agen-cies face a quandary when evaluating these patients,since, as noted above, it is often not possible to iden-tify evidence of organ damage that makes the allegedactivity restrictions seem inevitable, proportional oreven plausible. The essay � credibility, assessment ad-dresses general problems in the assessment of credibil-ity and veracity among patients with chronic pain. In� nonorganic symptoms and signs, the assessment of“non-organic signs” on physical examination is specif-ically addressed, namely the assessment of examina-tion findings that indicate something other than well-described organic pathology.
Severity of Impairment and Disability
As discussed, disability agencies attempt to base de-cisions on objective evidence of organ or body partdysfunction. The assessment of disability secondary topain is in conflict with this administrative imperative.People with chronic pain typically attribute their painand activity limitations to dysfunction of an organ orbody part. But these subjective reports are difficult toassess precisely because examination of the involvedorganorbodypartoftendoesnot identifyabnormalitiesthat make the pain reports inevitable (Robinson et al.2004). It often appears to an examiner that the affectedorgan or body part is capable of functioning, but thatthe claimant does not use it normally because of pain.Thus, the examiner has the challenge of determining
how much weight to place on the claimant’s subjec-tivereports,asopposed toobjectivefindingsoforganorbody part dysfunction (see � impairment, pain-relatedand � disability evaluation in the social security ad-ministration for discussions of attempts to integratedsubjective reports with objective evidence in impair-ment / disability determination).A comparison between rheumatoid arthritis (RA) andfibromyalgia syndrome (FMS) provides a dramaticexample of the difficulty of assessing severity ofimpairment-disability in a person with chronic pain.People with RA and FMS typically report compara-bly severe activity limitations. However, the formertypically have observable evidence of joint inflamma-tion or destruction, whereas physical and laboratoryexaminations for the latter are often completely nor-mal (except for tenderness to palpation). The questionfor a disability agency is should the activity limitationsreported by people diagnosed with FMS be given asmuch weight as those reported by people with RA forpurposes of awarding disability benefits? This type ofdilemma occurs routinely when claimants allege in-capacitation secondary to pain. Three essays in thisfield cover specific examples of syndromes in whichpatients complain of severe pain, but have little or noevidence of tissue pathology that rationalizes the com-plaints – low back pain (� epidemiology of work dis-ability, back pain), FMS (� disability in fibromyalgiapatients), and upper extremity injuries (� disability,upper extremity).
Causation
Causation is important when a person is seeking dis-ability benefits from an agency that is responsible onlyfor medical conditions that arise in certain circum-stances. In particular, workers’ compensation carriersare responsible only for conditions that arise out ofemployment. The assessment of causation is thorny atboth the conceptual (Kramer and Lane 1992; Lakoffand Johnson 1999) and practical levels. The difficultyin determining whether a medical condition has beencaused by work is by no means limited to painful con-ditions. For example, controversy rages about whetherand when hearing loss should be construed as workrelated (Dembe 1996). However, issues of causationare often particularly vexing for painful conditionsthat are commonly attributed to work. The difficultystems in part from the fact that many disorders that arecommonly attributed to work (e.g. non-radicular lowback pain) often reflect a combination of degenerativechanges and inciting physical loads. As a result, it isdifficult to weigh the influence of work exposures withnon-work exposures. But another reason for the dif-ficulty is that an examiner typically has no objectivemethod for determining the severity of incapacitation

C
Compensation, Disability, and Pain in the Workplace 421
in a patient with LBP. The claimant may allege that hisLBP started or became worse during the course of ac-tivitiesatwork,but theexaminerwillnotbeable to con-firm or deny such a statement on the basis of objectivemedical information. Thus, the problem of determin-ing causation in people with chronic pain overlaps withthe problem of determining severity of disability – inboth instances, the examiner must decide how muchweight to assign to claimants’ reports.Disability agencies differ significantly in the standardthey set for establishing causation. Some agencies fol-low the principle that in order for an index injury tobe accepted as the cause of a claimant’s impairment,the injury must be the significant factor contributingto the impairment. Others adopt a much lower stan-dard of causation that has been described as “lightingup”. When this standard applies, an index injury maybe viewed as the cause of an impairment even when theinjury is minor and impairment is severe. For example,consider a person with a multiply operated knee whofalls at work, develops an effusion in the knee and istold by an orthopedist thatheneedsa totalknee replace-ment. If the individual’s workers’ compensation car-rier operated under the “lighting up” standard of cau-sation, thisperson’skneesymptomsand needfora totalkneereplacementwouldbeviewedascausedbyhisslipand fall. The differences between disability agenciesin the criteria required for establishing causation high-light the general point that the rules and regulations ofdifferent disability agencies vary greatly.
Iatrogenesis
Most clinicians who treat injured workers believe thatsome of them report symptoms that are not explainedbiologically, but rather reflect influences of the dis-ability system as filtered by psychological tendencies.The term “disability syndrome” is often used to de-scribe these people. A disability syndrome is concep-tualized as a set of dysfunctional attitudes and beliefsthat evolves over time following an injury (Robinson etal. 1997). One probable contributor to a disability syn-drome is the injured worker’s adaptation to non-workroles; for example, an injured worker might take overchildcare duties, while his wife enters the work force tomake up for family income losses. Another likely con-tributor is thedysfunctional interactions thatmayoccurbetween an injured worker and a disability agency.As Hadler (1996) has pointed out, injured workers whoclaim ongoing work disability must run a gauntlet ofchallengesby theirclaimsmanager, threats totheirben-efits and independent medical examinations. In thesesituations, they must convincingly portray themselvesas incapacitated in order to maintain their benefits.Hadler argues that after trying so hard to convince oth-ersof their incapacity, injuredworkersarelikelytohavedifficulty conceptualizing themselves as fit for work or
toapproachreturn toworkwithconfidence. Inaddition,workers may develop resentment toward the disabilityagency with which they interact and thereby becomemore resistant to rehabilitation.The disability syndrome construct is difficult to proveempirically. For example, it is possible that injuredworkerswho fail to recover ina timely wayhadmedicalor psychosocial risk factors that existed at the time oftheir injury, but were recognized only after the workersshowed a delayed recovery (Mustard and Hertzmann2001). However, the construct provides a plausible ex-planation for the common observation that an injuredworker, who seems straightforward and highly moti-vated just after an injury, often becomes more resistantto rehabilitation at a later point.The possibility that disability policies and agencies in-advertently promote disability is a cause for great con-cern. The concern is similar to that expressed by crit-ics of welfare programs in the United States during the1990s.Thecriticism of thoseprogramswas thatby pro-viding long-term financial support for unemployed, in-digent members of the society, welfare programs ac-tually promoted continued indigence and unemploy-ment.
Epidemiology of Pain in the Workplace
As discussed above, there is ambiguity about the cir-cumstances in which it is appropriate to label a medicaldisorder as a pain disorder. This ambiguity clouds theinterpretation of data on the epidemiology of pain inthe workplace. The ambiguity is increased further bythe fact that the databases of workers’ compensationsystems and disability agencies generally do not pro-vide data in a manner that highlights the role that painplays in various injuries.However, a few simplifying assumptions make it pos-sible to obtain at least approximate data regarding thefrequency of work related disorders in which pain is amajor problem, but objective evidence of biological in-jury is either minimal or bears an equivocal relation tothepain that injuredworkersreport.First,manymuscu-loskeletal disorders meet these criteria. The discussionbelow will focus on these disorders, and in particularon 2 types of musculoskeletal problems – LBP and up-per extremity disorders associated with repetitive mo-tion (see � epidemiology of work disability, back painand � disability, upper extremity). Second, althoughsprains can be associated with unequivocal evidence ofa� structural lesion (e.g. acomplete tearof theanteriorcruciate ligament would be coded as a sprain), work-ers’ compensation carriers routinely use the designa-tion sprain / strain to describe musculoskeletal com-plaints in the absence of definite evidence of a signif-icant structural lesion. Thus, the designation “sprainor strain” in a workers’ compensation database can be

422 Compensation, Disability, and Pain in the Workplace
taken as a proxy for a disorder characterized primar-ily by musculoskeletal pain in the absence of a definitestructural lesion. Third, many of the disorders coded asupper extremity repetitive motion disorders meet theabove criteria, since they are not associated with defi-nite evidence of structural lesions (Miller and Topliss1988).
Common Work Injuries and Illness
Workers’ compensation carriers generally distinguishbetween work injuries and occupational illnesses(Blessmann 1991). Conceptually, an injury involvesa single event, whereas an illness arises gradually asa consequence of repeated work exposures. The dis-tinction between a work injury and an occupationalillness is obvious if a logger who is crushed by a treeis compared to a carpenter who develops a mesothe-lioma after years of exposure to asbestos. However, thedistinction becomes opaque when it is applied to mus-culoskeletal disorders. For example, episodes of LBPare coded as injuries, whereas carpal tunnel syndromeand other upper extremity disorders associated withrepetitive motion are coded as occupational illnesses.Tables 1 and 2 provide unpublished data about injuriesthat occurred among workers covered by the Depart-mentofLaborandIndustries inWashingtonStateof theUnited States in 1988. Table 1 provides a break downof injuries according to the mechanism of injury. Col-umn 1 indicates that the largest proportion of injurieswereclassifiedascontusions,bruises,cuts, lacerations,punctures, scratches or abrasions. The second largest
Compensation, Disability, and Pain in the Workplace, Table 1 1988 Washington State injury profile by nature of injury
Nature of injury IAll Claims (% of total claims)
II% of Claims in Column 1 thatlead to time loss > 120 days
III# of Claims with time loss> 120 days (% of total claimswith time loss > 120 days)
Contusions, Bruises, Cuts,Lacerations, Punctures,Scratches, Abrasions
75,713 (47.6%) 0.8% 644 (9.6%)
Sprains, Strains 59,729 (37.6%) 7.5% 4456 (66.1%)
Fractures 7,424 (4.7%) 11.9% 882 (13.1%)
Burns 5,777 (3.6%) 0.6% 38 (0.6%)
Multiple Injuries 2,689 (1.7%) 10.2% 273 (4.0%)
Dislocations 1,483 (0.9%) 19.0% 282 (4.2%)
Amputations 237 (0.1%) 18.1% 43 (0.6%)
Other 5,918 (3.7%) 2.1% 123 (1.8%
Totals 158,970 (100%) – 6,741 (100%)
Washington State Department of Labor and Industries (unpublished)
group consisted of sprains and strains. Table 2 providesa breakdown of conditions (injuries and illnesses com-bined) according to the body part affected. The mostcommonly affected body part is the hand or fingers.However, over 27,000 injuries involved the back, withan additional 8,427 involving the back and neck. Ap-proximately 90% of the back injuries were diagnosedas sprains or strains.Data from the Bureau of Labor Statistics in the UnitedStates (U.S. Department of Labor 1995) indicate thatapproximately 7% of all claims filed during 1992 werefor occupational illnesses rather than injuries. Approx-imately 60% of the claims for illnesses involved repet-itive trauma, usually of the upper extremity. (Carpaltunnel syndrome is a subset of upper extremity ill-nesses caused by repetitive trauma.) The second andthird largest groups are skin disorders (14%) and res-piratory conditions due to toxic agents (5%). The mostfrequent types of repetitive activities associated withoccupational illnesses are repetitive grasping or mov-ing of objects (other than tools) and repetitive use oftools. As one would expect from the types of repeti-tive activities that produce occupational illnesses, theoverwhelming majority of them occur in manufactur-ing jobs. In fact, the 25 industries with the highest ratesof repetitive trauma occupational illnesses are all inthemanufacturing sector,with meatpacking plantsandmanufacturers of motor vehicles leading the way. TheBureau of Labor Statistics also identifies keyboardingas a significant cause of repetitive trauma induced oc-cupational illnesses, but it is much less important thanrepetitive grasping or repetitive use of tools.

C
Compensation, Disability, and Pain in the Workplace 423
Compensation, Disability, and Pain in the Workplace, Table 2 1988 Washinton State injury and illness profile by body part
Body part IAll Claims (% of total claims)
II% of Claims in Column 1 thatlead to time loss > 120 days
III# of Claims with time loss> 120 days (% of total claimswith time loss > 120 days)
Finger 29,721 (17.7%) 0.7% 207 (2.8%)
Back 27,196 (16.2%) 9.6% 2598 (34.6%)
Eyes 17,981 (10.7%) 0.1% 19 (0.2%)
Hand / Wrist 17,444 (10.4%) 3.7% 643 (8.5%)
Back &Neck 8427 (5.0%) 8.7% 734 (9.8%)
Knee 7478 (4.4%) 8.1% 609 (8.1%)
Foot 6611 (3.9%) 2.6% 173 (2.3%)
Multiple 5583 (3.3%) 10.2% 571 (7.6%)
Other 47,616 (28.3%) 4.1% 1945 (25.9%)
Totals 168,057 (100%) – 7499 (100%)
Washington State Department of Labor and Industries (unpublished)
The Effect of Work Place Factors
An enormous amount of research has been conductedto determinework place factors thataffect theprobabil-ity that workers will become injured. The essay � painin the workplace, risk factors for chronicity, workplacefactorsreviewsmanyof theworkplacefactors thathavebeen investigated. The essay � ergonomics provides ahistorical overview of the field of ergonomics and sum-marizes research on risk factors for upper extremitywork related musculoskeletal disorders and LBP. Thisresearch has supported the conclusion that the risk ofupper extremity musculoskeletal disorders is increaseswhen jobs require forceful, repetitive motions, espe-cially when workers are also subjected to vibration andhave to maintain awkward positions. Research has alsofound 4 factors associated with an increased risk ofLBP, 1) lifting and forceful movements, 2) awkwardpostures, 3) heavy physical work and 4) whole bodyvibration.The essay � Pain in the workplace, risk factors forchronicity, job demands also addresses work place fac-tors that influence the frequency of work injuries. Itconsiders ergonomic factors briefly and also reviewsseveral psychosocial work place factors that influenceinjury rates, including monotonous work, lack of per-sonal control and job dissatisfaction.
Conditions Associated with Prolonged Time Off Work
Bureau of Labor Statistics data (U.S. Department ofLabor1995) in theUnitedStates indicate that66%ofallworkers who filed injury or occupational illness claimsin 1992 did not miss time from work. Among claims
that are associated with work disability, it is importantto distinguish ones associated with short periods offwork vs. ones associated with prolonged time loss. Al-though any injured worker who reports that he or sheis unable to work must be viewed with concern, mostinjuries involving time off work end uneventfully withthe worker returning to his or her job after a short timeperiod. For example, among workers in 1992 who wentoff work because of a back injury, the median time offwork was 7 days (U.S. Department of Labor 1995).As far as long term work disability is concerned, Col-umn 1 of Table 1 shows that contusions, bruises, cuts,lacerations, punctures, scratches and abrasions rep-resented the largest category of industrial injuries inWashington State during 1988, but Column 2 indicatesthat only 0.8% of patients with these conditions lostmore than 120 days from work. As a result, these pa-tients represented only 9.6% of the total of patientswith time loss of more than 120 days (column 3). Fur-ther examination of Columns 2 and 3 reveals that theprobability of protracted time loss is high for disloca-tions, amputations, fractures and multiple injuries. Itis moderately high for sprains and strains. However,since sprains and strains are relatively common to be-gin with, patients with these conditions represent 66%of the total number of patients with time loss greaterthan 120 days.Columns 2 and 3 of Table 2 provide similar informa-tion for industrial conditions in Washington State as afunctionofaffectedbodypart (injuriesand illnessesarecombined in this table). Inspection reveals that 9.6%of patients with back disorders remain off work morethan 120 days. Since back problems occur frequently,

424 Compensation, Disability, and Pain in the Workplace
fully 34.6% of the group who miss more than 120 daysfrom work do so because of back problems.
Skewed Recovery Curves
A major problem is that the recovery curves for someof the most important industrial conditions are highlyskewed.Forexample,althoughmostworkerswithLBPreturn toworkwithinseveraldays(if theygooffworkatall), a small proportion go on to very extended or evenpermanent work incapacity. In a representative study,Cheadle et al. (1994) examined 28,473 claims amongWashington State workers between 1987 and 1989.Allworkers with claims involving more than 3 days offwork were included. Approximately 86% of the backpain claimants returned to work within 4 months of in-jury. After that, however, the recovery curve flattenedout, so that only about 5% of patients returned to workduring months 5–8 following injury. Similar resultshave been reported by Spitzer et al. (1987) and others(Clinical Standards Advisory Group (1994).A few points about the skewed recovery curve deserveemphasis. First, the curve is by no means descriptiveonly of LBP. In fact, Cheadle et al. (1994) found simi-larly skewed curves for carpal tunnel syndrome, frac-tures and unspecified other industrial injuries. Second,the costs of claims with delayed recoveries are stagger-ing. In Washington State, almost 80% of work injuriesdo not lead to any time off work. Of people who gooff work because of injuries, more than three-fourthsreturn to their jobs within 120 days. Thus, injuries as-sociated with the loss of more than 120 days from workrepresent less than 5% of the total number of injuries.However, fully 84% of the total payments made to in-jured workers are paid to this small group (WashingtonStateDepartmentofLaborandIndustries1994).Third,the flattening of the recovery curve demonstrated byCheadle et al. and other investigators (Waddell 1987)indicates that a worker who has been on disability for aprolonged time is at great risk of continuing on disabil-ity indefinitely. Inarecent literaturesynthesis, theClin-ical Standards Advisory Group (1994) constructed anestimated long-termrecoverycurveforLBPpatients. Itindicates that the probability of ever returning to workis about 25% for a person who has been off work 1 yearand about 10% for a person who has been off work2 years.
Predictors of Delayed Recovery
Data provided above indicate that prevalent muscu-loskeletal conditions, particularly LBP and carpal tun-nel syndrome, are sometimes associated with the pro-tracted disability. But the data are only of limited value,because of the enormous variation in outcomes amonginjured workers with these conditions. The clinician’sjob would be much easier if he or she could identify
factors that permitted predictions to be made aboutwhich workers are most likely to become chronicallydisabled. Research directed toward several of the fac-tors that have been investigated is briefly summarizedhere. Specifically, the essays � Pain in the workplace,risk factors for chronicity, demographics � Pain inthe workplace, risk factors for chronicity, psychoso-cial factors � Pain in the workplace, risk factors forchronicity, workplace factors, and � Pain in the Work-place, Compensation and Disability Management dis-cuss the roles of demographic, sychosocial, and work-place factors in predictingprolongeddisability.Amoreextended discussion can be found a recent review byKrause et al. (2001a).
Severity of Injury
At the extremes, the expected relation between injuryseverity and duration of disability has been demon-strated. For example, Cheadle et al. found that injuredworkers with “catastrophic injuries” (i.e., ones hospi-talized within 28 days of injury) were off work about2.5 times as long as ones without catastrophic injuries(Cheadleetal. 1994). However,only 6%of theworkersin their samplehadcatastrophic injuries.Thus, thefind-ing that patients with catastrophic injuries are disabledfor prolonged time periods does little to help the physi-cian make predictions among the much larger group ofpeople who do not sustain catastrophic injuries.
Diagnosis
Statisticsclearly demonstrate that the risk ofprotracteddisability is much greater for some types of injuriesthan for others. For example, workers with lacera-tionsorabrasionsonlyrarelyhaveprotracteddisability,whereas ones with sprains or strains account for fully66% of claims with more than 120 days of time loss(Table 1). In particular, since back strains have a highincidence rate and a moderately high associated proba-bility of protracted time loss, they account for approxi-mately 35% of all protracted time loss claims (Cheadleet al. 1994).
Specific Diagnosis Within an Injury Category
It is a difficult task to predict the duration of disabil-ity among patients with a common problem such asLBP. Making predictions within LBP patients is im-portant for an obvious reason. Since the outcomes ofinjuriesarehighlyvariable,aphysicianwhocanpredictwhich patients are likely to become chronic can focuson rehabilitating them (see � epidemiology of workdisability, back pain).Unfortunately,predictionsbasedon detailed medical information have been only mod-estly successful. Several studies have shown that pa-tientswith sciaticahavemoreprolonged disability thanones only with low back pain (Andersson et al. 1983).

C
Compensation, Disability, and Pain in the Workplace 425
Also, there isevidence that injuredworkersgivenaspe-cific diagnosis within 1 week of injury (such as sciat-ica, disc injury or facet joint syndrome) are more likelyto demonstrate prolonged disability than ones given anon-specific diagnosis such as lumbar strain (Aben-haim et al. 1995). This suggests that physicians canidentifysomehigh-riskpatientson thebasisofahistoryand physical examination. However, since only 8.9%of thepatients inAbenhaimetal.’sstudyreceivedaspe-cific diagnosis, the study is not helpful in identifyingpredictors among the remaining 91% of patients whowere given non-specific diagnoses. In a similar vein,Franklin et al. (1994) studied injured workers who un-derwent lumbarspinal fusions.Althoughthesepatientsended up having very protracted disability, most ofthem were initially given non-specific diagnoses suchas lumbar strain.
Age
Data from the Bureau of Labor Statistics indicate thatolder workers are less likely than younger ones to sus-tain work related injuries, but are at greater risk forprotracted disability if they do sustain an injury. Sev-eral studies have confirmed the fact that among pa-tients who sustain disabling injuries, older ones aremore likely to experience prolonged disability (Chea-dle et al. 1994; Rossignol et al. 1988). See the essay� Pain in the workplace, risk factors for chronicity, de-mographics for a more extended discussion of age aswell as other demographic factors in predicting pro-longed disability.
The Effect of Work Place Factors
Multiple factors associated with the work place affectthe duration of work injuries, which is considered inthe essay � Pain in the Workplace, Compensation andDisability Management. At the level of the physicaldemands of work, there is good evidence that work-ers who do physically demanding work are more likelyto demonstrate protracted disability after a back injurythanoneswith lighterwork(Krauseetal.2001b).How-ever, as pointed out in � Pain in the Workplace, Com-pensation and Disability Management, psychosocialaspects of the work environment – including the ex-tent to which employers invest resources to encouragereturn to work – also affect the duration of work in-juries.
Disability Evaluation –General
The Biopsychosocial Model
Virtually all experts agree that one must use a biopsy-chosocial model (Waddell 1987; Waddell 1998) toevaluate disabling musculoskeletal disorders in theworkplace. Within this model, it is appropriate to dis-tinguish among 3 broad groups of factors that might
contribute to disability. All of them need to be includedin acomprehensive reviewofpain in theworkplaceandin a comprehensive evaluation of an individual injuredworker.
Medical Factors
These, of course, vary with the specific disorder un-der consideration. Several essays (� disability assess-ment, psychological / psychiatric evaluation; � yellowflags; � ethics of pain-related disability evaluations)state (or imply) that medical factors are not as im-portant as psychosocial factors in determining whichworkers become disabled by musculoskeletal injuriesA few general observations on this issue are worth-while. First, the role of medical factors in the outcomeof a musculoskeletal injury depends on the severityof the injury. Severe musculoskeletal injuries (frac-tures, amputations and any injuries requiring immedi-ate hospitalization) are associated with a high risk ofprotracted work disability. However, the bulk of lowback injuries and upper extremity disorders that leadto disability are not associated with obvious markersof severe biological dysfunction. As a consequence, ananalysis that attempts to predict length of disability onthe basis of severity of biological injury is hamperedby restriction in the range of the independent variable.Second, most of the painful disorders that occur in theworkplace can be construed as making it more diffi-cult for an individual to continue working,but notcom-pletely precluding work.The relation between pain severity and strength of mo-tivation to avoid or discontinue activity limitation is il-lustrated in Fig. 1. As the figure indicates, people withno or minimal pain are described as being in an unre-stricted zone as far as activities are concerned, whereasas ones with extremely severe pain are described as be-ing inacompulsoryzone,such that it isvirtually impos-sible for them to continue with normal activities. Butmost people with musculoskeletal pain are in what isdescribed as a discretionary zone – they can continue
Compensation, Disability, and Pain in the Workplace,Figure 1 Motivational consequences of activity-related pain.

426 Compensation, Disability, and Pain in the Workplace
to engage in important activities, but only with signif-icant effort. The behavior of patients with pain in thediscretionary zone will depend on psychological fac-tors such as their resourcefulness in finding alternativeways to accomplish tasks and their ability to manageemotional distress provoked by pain.
Psychological Factors
As discussed in the essays on � disability assessment,psychological / psychiatric evaluation � yellow flags,and � Psychological assessment of pain, individualswith psychological vulnerabilities are relatively likelyto succumb to disability following musculoskeletal in-jury. In particular, the risk of disability has been foundto be elevated among individuals with anxiety dis-orders, depressive disorders, personality disorders orproblems with chemical dependency. In addition, per-sons who are somatically focused (as manifested, forexample, by elevated scores on the hypochondriasisscale of the Minnesota multiphasic personality inven-tory [MMPI]) are at risk, even if they do not warrant apsychiatric diagnosis.
Situational and Social Factors
Another theme that emerges from several of the es-says in this field (e.g. � Pain in the workplace, riskfactors for chronicity, psychosocial factors and � Painin the Workplace, Compensation and Disability Man-agement) is that the likelihood of prolonged disabilityamong injured workers is affected by their satisfactionwith their jobsand theefforts that theiremployersmaketo reintegrate them into the work force.
Assessing Credibility
As indicated, disability assessment in painful condi-tions poses a challenge because an examiner must relyontheverbalandnonverbalpainbehaviorsofaninjuredworker inorder toassess theextenttowhichpainaffectsthe worker’s ability to function. Some disability agen-cies attempt to finesse this dilemma by mandating thatdecisions about disability should rely almost entirelyon objective findings. However, if an agency permitssubjective data from injured workers to be consideredin disability evaluations, it must immediately confrontthe issue of assessing the credibility of patients withpain problems. Issues related to patient credibility areoften poorly formulated and emotionally tinged.As a point of departure in clarifying these issues, it isworth considering the type of presentation by a patientthat an examiner would find highly credible. The tablelisted below lists a set of findings that would convincemost examiners that an examinee was highly credible(see Characteristics associated with high patient cred-ibility). The areas mentioned cover a wide range – in-cluding thenatureof the injury, thebiologicresponseof
claimants, claimants’ current symptoms and reportedactivity limitations, their physical findings on a singlephysical examination, the consistency of their findingsover repeated examinations, the presence or absenceof acute or chronic psychiatric conditions, their appar-ent motivation to return to productivity and various in-centives or disincentives for continued disability. As ametaphor, we can visualize very high claimant credi-bility asanalogous to amountaintop,withvariouspath-ways leading “downward” to questionable credibility.An assumption in discussions of credibility is that, in ahighly credible patient, there is a relatively direct pathfrom injury through tissue damage to present signs,symptoms and reported activity limitations. Anotherway to state the assumption is that the presentation ofa highly credible patient is determined almost exclu-sively by abnormal biology. In contrast, the factors thatcompromise patient credibility are usually construedas being in the psychosocial sphere. The question thenbecomes what are the psychological processes that un-derlie the behavior of claimants whose credibility issuspect? Some investigators have emphasized the roleof somatic anxiety as a factor underlying claimants’verbal statements about their abilities and their behav-iorduringaphysicalexamination(see� disability, fearof movement). For example, if claimants are extremelyanxious about hurting themselves during a physical ex-amination, they might well demonstrate exaggeratedpain behaviors such as guarding and pain-inhibitedweakness.Another possibility is that claimants exaggerate theirreports about their incapacity and demonstrate limita-tions on examination as a deliberate strategy to max-imize the disability payments they are awarded. Thatis, they are malingerers. A more subtle analysis posits“secondary gain” as a determinant of a patient’s behav-ior. In effect, this analysis indicates that money acts as areinforcer that influences a claimant’s behavior. How-ever, it allows for the possibility that the influence oc-cursatanunconsciouslevel,namely that theclaimant isnot necessarily maliciously and deliberately mislead-ing an examiner (as occurs in the case of malingering).The essay � malingering, primary and secondary gaindeals specifically with the issues of secondary gain andmalingering and adds an important concept to the lexi-con related to patientcredibilitywhenitdiscusses“sec-ondary losses” (i.e., the types of reinforcers that a per-son is less likely to receive ifhe isseverelydisabled).Aspointed out in � malingering, primary and secondarygain, formost injured workers thefinancial lossesasso-ciated with protracted disability far outweigh the gainsassociated with disability payments (Reno et al. 1997;Reville et al. 2000).In principle, information bearing on the credibility ofclaimants can be gleaned from several sources, includ-

C
Compensation, Disability, and Pain in the Workplace 427
Compensation, Disability, and Pain in the Workplace, Table 3 Characteristics Associated with High Patient Credibility (Robinson JP “Psycho-logical Aspects of Disability.” Presented to Employer Advisory Group, Valley Medical Center, Renton WA, June, 1997)
Characteristics Associated with High Patient Credibility
No pre-existing condition
No medical co-morbidities
Definite stimulus – e.g. crushed by a tree
Definite tissue damage – e.g. fracture
Symptoms, signs, activity limitations – fit expectations for the medical problem
Consistent findings over repeated examinations
No exaggerated pain behavior
No inconsistencies between symptoms / signs noted in MD’s office and behavior outside the office
No chronic psychiatric disorders or long-term psychosocial risk factors
No reactive psychiatric problems – e.g. anxiety disorder, depression
Patient motivated to return to productivity
Job opportunities exist
No incentives for disability
ing information about the individual’s injury, examina-tion of records of health practitioners who have seenhim in the past, statements by the patient about his cur-rent symptoms and activity restrictions and observa-tion of claimants’ behavior during a physical exami-nation. The essay � credibility, assessment discussesthe significance of these types of data.The essay � nonorganic symptoms and signs dealswith aspecific issue related to credibility – thebehaviorof a patient during a physical examination. In particu-lar, a set of “non-organic” signs have been developedthat can sometimes be observed by an examiner duringthe physical examination of a patient with LBP. Exten-sive research on the “Waddell signs” suggests that theyare primarily indicators of somatic anxiety on the partof patients with LBP.The interpretation of Waddell signs is far from obvious(see � malingering, primary and secondary gain). Al-though Waddelldescribed themas“non-organic”signsin his initial publication on them, recent research sug-gests that they could be manifestations of altered ner-vous system functioning in response to pain (Banic etal. 2004; Curatolo et al. 2004). That is, they might beconstrued as manifestations of a genuine medical dis-order rather than solely as indicators of psychologicaldysfunction (see � dysfunctional pain and the interna-tional classification of function.)
Rehabilitation of Pain Related Disability
During the interval shortly after a worker sustains adisabling injury, the focus of attention is typically onmedical or surgical treatment of his injury. If disabil-ity persists, various evaluations and interventions may-
be performed to manage the worker’s disability (i.e.to foster return to work). If the worker’s disability be-comes protracted, the focus of evaluations subtly shiftstoward issues related to the extent of permanent im-pairment and disability and the financial liability of aninsurer or disability agency in the event of permanentwork disability. Sometimes an evaluation can serve adual purpose, namely, it can be used either to facilitatereturn to work or to establish the severity of disabilityforpurposesof long-term compensation.The� Pain inthe Workplace, Compensation and Disability Manage-ment; � ethics of pain-related disability evaluationsand � impairment, pain-related essays deal with eval-uations and interventions that are often used to managedisability by facilitating return to work. One crucial el-ement in disability management is the assessment ofa worker’s risk for long-term disability. The essay on� yellow flags addresses this important issue.Another crucial issue for a worker who is unlikely toreturn fully to his pre-injury status is the assessmentof his residual physical capacities. Although disabil-ity agencies routinely ask treating physicians to pro-vide detailed information about a patient’s activity tol-erances and activity restrictions, the examinations thata physician conducts in an office setting generally donot provide relevant data to make such judgments. Asdiscussed in the essay � disability, functional capacityevaluations, physical capacities evaluations can pro-vide detailed data about the ability of a patient to per-formarangeofphysical tasksoverperiodsoftimerang-ing from a few hours to a few days.Anothercrucial input fordisability management isare-alistic assessment of the workers’ vocational options,especially if the probability is high that they will not

428 Compensation, Disability, and Pain in the Workplace
be able to return to the job they had when they wereinjured. As discussed in � vocational assessment inchronic Pain, the role of the vocational rehabilitationcounselor is to identify vocational options and to facili-tate communication among physicians, employers andthe worker to maximize the probability that the workerwill be able to return to gainful employment.As far as treatment of disability is concerned, the� disability, effect of physician communication essayhighlights the importance of communication betweenphysicians and injured workers. Effective communica-tion that enables patients to cope with their injuries isnotusually thoughtofasa treatment,butexpertopinionand at least some empirical evidence (Catchlove andCohen 1982; Hall et al. 1994) support the conclusionthat such communication can substantially influencethe outcome of work injuries.Manyworkersreceivephysical therapyasacomponentof the treatment they receive for their work injuries. Al-though such treatment is often helpful, workers whoare sliding into protracted disability often report lackof benefit from physical therapy. Ineffective physicaltherapycanoccur foravarietyof reasons.Onecommonproblem is that physical therapists sometimes focusexcessively on passive treatments such as diathermyor massage, rather than on active functional restora-tion. Even when progressive exercise is emphasized inphysical therapy, patients may fail to benefit becausethey are fearful that physical activity will cause rein-jury or will delay their recovery (see � disability, fearof movement). As discussed in � physical condition-ingprograms,structuredphysicalconditioningorworkhardening programs may be helpful in this situation.These programs are structured in the sense that theyemphasize progressive exercise and that they requirepatients to attend treatment sessions several times perweek.It is noteworthy that a recent extensive review of litera-ture on structured physical conditioning programs re-vealed that such programs were reliably effective onlywhen they were combined with psychosocial support(Schonstein et al. 2002) (see � physical conditioningprograms and � multidisciplinary pain centers). Thisfinding supports the logic underlying the most aggres-sive rehabilitation programs for workers with chronic,disabling pain – multidisciplinary pain center or func-tional restoration treatments. As discussed by Turk inhis essay � multidisciplinary pain centers, these pro-grams have demonstrated efficacy in the treatment ofselected injured workers. However, there is often re-luctance by third party payers to provide coverage andreimbursement for these treatments.Managed care organizations in the United States haveparticular difficulties when it comes to treatment ofpeople they cover that experience work related disabil-
ities. The essay � disability management in managedcare system describes the interaction between man-aged care organizations and injured workers.Finally, as discussed � Pain in the Workplace, Com-pensation and Disability Management, there is persua-sive evidence that initiatives by employers can reducethe incidence of work injury claims and the durationof disability for claims that are filed. These initiativesinclude programs for rotating activity schedules forworkers and promoting early return to modified workfollowing a work injury. The essay � Pain in the Work-place, Compensation and Disability Management alsocites data supporting the importance of programs topromote a positive psychosocial environment in theworkplace. In particular, it describes research demon-strating that workers are relatively likely to return toworkquicklyfollowing injuryif theyhavegoodrapportwith their supervisors and if their supervisors expressconcern about them following an injury.
Assessing Permanent Impairment / Disability Associ-ated with Pain
As noted previously, if a worker fails to recover fullyfrom an injury, the agencies involved with his claimneed to make some determination regarding his per-manent impairment and his ability to work. Decisionsregarding these issues determine the agencies’ finan-cial obligations to the worker. Logically, the startingpoint for a system to evaluate impairment and disabil-ity in an injured worker is a set of concepts that linksthe many interacting factors that contribute to disabil-ity following a work injury. The essays � disabilityand impairment definitions and � WHO system on im-pairment and disability describe the current WHO con-ceptual system. Key concepts in it are body functions,body structures, impairments, activity-activity limita-tions, participation-participation limitations and dis-ability.Theessay� dysfunctionalpain and the interna-tional classification of function describes how sensorychangesthatarepostulated tooccur inchronicpainsyn-dromes can be conceptualized within the WHO frame-work.At a practical level, the essay � impairment rating, am-biguity describesseveral issues thatmakeitdifficult foragencies to evaluate impairment and disability in anefficient, equitable manner. The essays are not limitedto the evaluation of painful conditions, but emphasizethedifficultyofdeterminingimpairmentordisability insuch conditions. The companion essay � impairmentrating, ambiguity, IAIABC system describes the re-centlydevelopedimpairmentratingsystemoftheInter-nationalAssociation of IndustrialAccidentBoardsandCommissions. For the most part, this system does notspecifically address impairment secondary to chronic

C
Compensation, Disability, and Pain in the Workplace 429
pain, but does do so in selected disorders (such as phan-tom limb pain).Essays on � disability evaluation in the social secu-rity administration � rating impairment due to pain ina workers’ compensation system and � impairment,pain-related describe the approaches to the assessmentof impairment-disability associated with chronic paintaken by the Social Security Administration, the Wash-ington State workers’ compensation system, the Cal-ifornia workers’ compensation system and the AMAGuides. The Social Security Administration systememphasizes the potential importance of pain to disabil-ity and provides fairly specific guidelines for adjudi-cators to follow as they gather information from ap-plicants regarding their pain. The California systemalso emphasizes thepotential importanceofpain to dis-ability, but does not give specific guidelines regardingits assessment. The AMA Guides devote a chapter tothe assessment of pain-related impairment, but fail tointegrate the concepts elaborated in the chapter intothe overall impairment assessment system and containmultiple inconsistencies related to the assessment ofimpairment secondary to pain. The Washington Statesystem specifically excludes chronic pain as a basis forimpairment. These essays are presented as representa-tive; however, there are wide variations in compensa-tion systems within and between countries. The onlyconclusion one can reach with confidence from read-ing the essays � disability evaluation in the social se-curity administration � rating impairment due to painin a workers’ compensation system and � impairment,pain-related is that there is a striking lack of consen-sus about how to incorporate pain into impairment anddisability evaluations.
Paradigm Shifts; Systemic Changes
It is safe to say that no system has solved the problemsof how to assess, rehabilitate and compensate peoplewho report chronicpainfollowingwork injuries. In thisunsatisfactory situation, it is appropriate to considerstrategies for improving the ways in which disabilityagencies conceptualize and evaluate chronic pain anddisability. Two essays in this field discuss conceptsthat need to be considered in any systemic change inworkers’ compensation systems or disability systemsin general. � Disability incentives addresses the influ-ences of incentives and “moral hazards” on the behav-ior of both injured workers and the health professionalswho treat them. It does not propose specific changes incurrent disability systems, but it strongly suggests thata successful disability system needs to be based on acareful consideration of incentives and disincentives todisability. The essay � disability prevention reviews awealth ofdataon factorsassociated with long-term dis-
ability following non-traumatic work injuries. Itmakesa convincing case that we have sufficient data to craftprogramsthat focusondisabilitypreventionrather thantreatment and long-term wage replacement followingthe development of disability. � Disability preventionaddresses protracted disability in general rather thanchronic pain specifically. However, it is highly relevantto an understanding of work related chronic pain, sincechronic pain is a major cause of protracted disabilityfollowing a work injury.The essay � back pain in the workplace describes amonograph about work related low back pain. Themonograph, entitled Back Pain in the Workplace(Fordyce 1995) focuses on problems associated withour current concepts regarding low back pain and workdisability. In essence, the authors argue that impair-ment cannot be assessed validly in nonspecific LBP,because 1) an examiner’s assessment of impairmentfrom LBP depends on the performance of a patientduring an examination and 2) a back pain patient’sperformance during an examination is determined notonly by the severity of the anatomic and physiolog-ical functional loss he or she has sustained, but alsoby a variety of psychosocial factors. In the authors’words: “Not all potential impairments can be con-firmed by verifiable measures of their presence in-dependent of performance by the person purportedto be impaired. Because performance is also “effort-related” as well as related to anatomical or physiolog-icalcapabilities, it is inevitably linked toandinfluencedby such factors as attitudes, motivation and personal-ity”(p. 28).The authors of the Back Pain in the Workplace reportgo on to promote the idea that people with nonspecificLBP should be classified as “unemployed” rather thandisabled if they “persist... in activity intolerance be-yond the allotted time for medical treatment and tem-porary disability status” (p. 59). Thus, people with per-sistent nonspecific LBP would, for benefits purposes,be classified with healthy people who are unable to findwork.It is important to note that Back Pain in the Workplacemakes recommendations for disability policy only inrelation to nonspecific LBP; they do not consider anyother chronic pain conditions. Also, although their rec-ommendations about disability policy rest on their pes-simistic view of the ability of physicians to determineimpairment in patients with nonspecific LBP, they donot provide any data to buttress this view. In essence,their monograph is a consensus document rather than apresentation of empirical data. However, in view of theeminence of its authors, Back Pain in the Workplaceis a provocative work that has been read widely and,as documented in � back pain in the workplace, hasgenerated a heated debate.

430 Compensation, Disability, and Pain in the Workplace
Summary
Many vexing and inter-related issues are associatedwith the assessment and compensation of individu-als who develop painful conditions in the workplace.The essays included in this field were designed to beevocativeand to offer insightfulperspectiveson the im-portant nuances that come into play when judgmentsare made about such individuals. Some of the essaysdescribe efforts that selected disability agencies havemade to address problems associated with the assess-ment of impairment and disability in injured workerswith painfulconditions.But rather than providingclearand definitive answers to the difficult issues surround-ing pain in the workplace, the essays should sensitizereaders to thecomplexitiesand ambiguities in thisarea.
References1. Abenhaim L, Rossignol M, Gobeille D et al. (1995) The prog-
nostic consequences in the making of the initial medical diag-nosis of work-related back injuries. Spine 20:791–795
2. Andersson GB, Svensson HO, Oden A (1983) The intensityof work recovery in low back pain. Spine 8:880–884
3. Banic B, Petersen-Felix S, Andersen OK et al. (2004) Evidencefor spinal cord hypersensitivity in chronic pain after whiplashinjury and in fibromyalgia. Pain 107:7–15
4. Blessman JE (1991) Differential treatment of occupational dis-ease v occupational injury by workers’ compensation in Wash-ington State. J Occup Med 33:121–126
5. Catchlove R, Cohen K (1982) Effects of a directive return towork approach in the treatment of workman’s compensationpatients with chronic pain. Pain 14:181–191
6. Cheadle A, Franklin G, Wolfhagen C et al. (1994) Factors in-fluencing the duration of work-related disability: a population-based study of Washington state workers’ compensation. AmJ Publ Health 84:190–196
7. Clinical Standards Advisory Group (1994) Back Pain. HMSO,London
8. Cocchiarella L, Andersson GBJ (2001) Guides to the Evalua-tion of Permanent Impairment, 5th edn. AMA Press, Chicago
9. Curatolo M, Arendt-Nielsen L, Petersen-Felix S (2004) Ev-idence, mechanisms, and clinical implications of central hy-persensitivity in chronic pain after whiplash injury. Clin J Pain20:469–476
10. Dembe AE (1996) Occupation and Disease. Yale UniversityPress, New Haven
11. Derthick M (1990) Agency under stress. The Brookings Insti-tution, Washington, DC
12. Fabrega HJ (1997) Evolution of Sickness and Healing. Uni-versity of California Press, Berkeley
13. Fordyce WE (1995) Back Pain in the Workplace. IASP Press,Seattle
14. Franklin GM, Haug J, Heyer NJ et al. (1994) Outcome of lum-bar fusion in Washington state workers’ compensation. Spine19:1897–1904
15. Hadler NM (1996) If you have to prove you are ill, you can’t getwell. The object lesson of fibromyalgia. Spine 21:2397–2400
16. Hall H, McIntosh G, Melles T et al. (1994) Effect of dischargerecommendations on outcome. Spine 19:2033–2037
17. Kramer MS, Lane DA (1992) Causal propositions in clinicalresearch and practice. J Clin Epidemiol 45:639–649
18. Krause N, Frank JW, Dasinger LK et al. (2001a) Determinantsof duration of disability and return-to-work after work-related
injury and illness; challenges for future research. Am J Ind Med40:464–484
19. Krause N, Dasinger LK, Deegan LJ et al. (2001b) Psychoso-cial job factors and return-to-work after compensated low backinjury: a disability phase-specific analysis. Am J Ind Med40:374–392
20. Lakoff G, Johnson M (1999) Philosophy in the Flesh. BasicBooks, New York
21. Miller MH, Topliss DJ (1988) Chronic upper limb pain syn-drome (repetitive strain injury) in the Australian workforce:a systematic cross sectional rheumatological study of 229 pa-tients. J Rheumatol 11:1705–1712
22. Mustard C, Hertzman C (2001) Relationship between healthservices outcomes and social and economic outcomes in work-place injury and disease: data sources and methods. Am J IndMed 40:335–343
23. Osterweis M, Kleinman A, Mechanic D (eds) (1987) Pain andDisability. National Academy Press, Washington, DC
24. Ranavaya MI, Rondinelli RD (2000) The Major U.S. Disabilityand Compensation Systems: Origins and Historical Overview.In:Rondinelli RD, Katz RT (eds) Impairment Rating and Dis-ability Evaluation. WB Saunders, Philadelphia, pp 3–16
25. Reno VP, Mashaw JL, Gradison B (1997) Disability. NationalAcademy of Social Insurance, Washington, DC
26. Reville RT, Polich S, Seabury S, Gidens E (2000) Perma-nent disability at private, self-insured firms. (MR-1268-ICJ).RAND, Santa Monica
27. Ritter GA (1983) Social Welfare in Germany and Britain. Berg,New York
28. Robinson JP, Rondinelli RD, Scheer SJ (1997) Industrial reha-bilitation medicine 1: Why is industrial rehabilitation medicineunique? Arch Phys Med Rehabil 78:3–9
29. Robinson JP, Turk DC, Loeser JD (2004) Pain, impairment, anddisability in the AMA Guides. J Law Med Ethics 32:315–326
30. Romano JM, Turner JA, Jensen MP et al. (1995) Chronic painpatient-spouse behavioral interactions predict patient disabil-ity. Pain 63:353–360
31. Rossignol M, Suissa S, Abenhaim L (1988) Working disabilitydue to occupational back pain: Three-year follow-up of 2,300compensated workers in Quebec. J Occup Med 30:502–505
32. Scarry E (1985) The Body in Pain. Oxford University Press,New York
33. Schonstein E, Kenny DT, Keating J et al. (2002) Work condi-tioning, work hardening and functional restoration for work-ers with back and neck pain. The Cochrane Database of Sys-tematic Reviews 2002, issue 4. Art No.: CD001822. DOI:10.1002/14651858. CD001822
34. Social Security Administration, Office of Research, Evaluationand Statistics (1999) Social security programs throughout theworld –1999. (SSA Publication no. 13-11805). GovernmentPrinting Office, Washington, DC
35. Spitzer WO et al. (1987) Scientific approach to the assessmentand management of activity-related spinal disorders. Spine12:1–57
36. SSA Publication No. 64-039 (1994) Disability evaluation un-der social security. Government Printing Office, Washington,DC
37. U.S. Department of Labor, Bureau of Labor Statistics (1995)Occupational Injuries and Illnesses: Counts, Rates, and Char-acteristics, 1992. Government Printing Office, Washington, DC
38. Waddell G (1987) Volvo award in clinical sciences. A new clini-cal model for the treatment of low-back pain. Spine 12:632–644
39. Waddell G (1998) The back pain revolution. Churchill Living-stone, Philadelphia
40. Washington State Department of Labor and Industries (1994)Long-term disability prevention pilots. Annual Report to theLegislature
41. Williams CA (1991) An International Comparison of Workers’Compensation. Kluwer, Boston

C
Complex Chronic Pain in Children, Interdisciplinary Treatment 431
Definition
An oil emulsion thatcontainsadeadmycobacterium thatelicitsan inflammatory and immuneresponse in vivo. In-jection of CFA into the skin of the hind paw is frequentlyused as an experimental model of peripheral inflamma-tion in mice or rats.� CFA� IB4-Positive Neurons, Role in Inflammatory Pain� NerveGrowthFactorOverexpressingMiceasModels
of Inflammatory Pain
Complex Adaptive System
Definition
A complex adaptive system is a large set of units thatinteract with each other, and with an external environ-ment, to produce overall patterns that are significantlymore complex than the behaviors of the individual en-tities comprising the system.� Consciousness and Pain
Complex Chronic Pain in Children,Interdisciplinary Treatment
JENNIFER N. STINSON
The Hospital for Sick Children and The University ofToronto, Toronto, ON, [email protected]
Synonyms
Multidisciplinary treatment; Paediatric Chronic PainManagement; Pain-Related Disability
Definition
Chronic pain in children is defined as any recurring (e.g.headaches, abdominal and limb pain) or persistent pain(e.g. back pain, cancer pain, � complex regional painsyndrome) that lasts a minimum of 3 months (McGrath1999). While most children with chronic pain functionquite well, some develop more complex chronic painconditions with associated distress and disability (Mc-Grath and Finley 1999).Thesechildren typically presentwith subjective ratings of pain out of proportion to theobjective physical findings and are more disabled thanone would expect.The pain adversely affects all aspects of children’slives. They stop going to school, refrain from exercis-ing or playing sports for fear of increasing the pain andwithdraw from their peers. These children often haveimpaired sleep, suffer from anxiety and or depressionand have disrupted family relationships (Bursch et al1998; Dahlquist and Switkin 2003). The pain becomesthe focus of the children’s lives and a vicious cycle
of pain and disability develops. Furthermore, manyfactors such the how the child thinks, feels and behavesin response to the pain can intensify the pain and dis-tress and prolong the disability. Some of the commonsituational and child factors that intensify pain andprolong disability are outlined in Fig. 1 (McGrath andHillier 2003). These children also tend to have compo-nents of � nociceptive (normal pain) and � neuropathic(nerve pain), which make them more difficult to treat.Therefore, � interdisciplinary chronic pain teams arenecessary to treat complex chronic pain conditionsadequately in order to ensure that assessments and in-terventions are child-centred (e.g. tailored to the needsof the individual child) rather than just focused on theunderlying disease or condition.
Characteristics
Given that these complex chronic pain conditions havemultiple causes, children must be treated from an inter-disciplinary, � multimodal, rehabilitation perspective.Drug, physical and psychological therapies should beincorporated into a flexible, child-friendly programwith particular attention to the cognitive, behaviouraland emotional factors contributing to the underlyingproblem. Because of the complexity of chronic pain,no single discipline has the expertise to assess andmanage it independently. Therefore, specialised inter-disciplinary chronic pain teams are now considered thestandard of care for children with complex chronic painconditions.
Composition of Interdisciplinary Pain Teams
Chronic pain teams for children generally includespecialised physicians (e.g. anaesthesiologists, neu-rologists, psychiatrists), nurses, psychologists andphysical therapists. More recently, teams may alsoinclude complementary and alternative therapists (e.g.acupuncturists, massage therapists). The specific teammembers involved in any one case depend on the indi-vidual needs of the child and family. A child’s initialconsultation includes either a joint team interview andphysical examination or separate interviews with eachhealthcare professional. Comprehensive physical andpsychosocial assessment may typically last a few hoursto a full day, depending on the child’s previous diag-nostic tests and the team’s core assessment battery (i.e.standardised sensory testing, questionnaires). The teamthen meets to formulate the child’s pain diagnosis andtreatment plan. The treatment plan should include: thediagnosis (underlying causes and contributing factors),rationale for a rehabilitative approach with a cleardescription of the specific treatment options and anopportunity for the family to help fine-tune the plan. Itis essential to educate children and their families aboutthe nature of chronic pain (e.g. different from acute painwhere there is a single cause and a single treatment) andthe factors that intensify it, as well as the drug and non-

432 Complex Chronic Pain in Children, Interdisciplinary Treatment
Complex Chronic Pain in Children, Interdisciplinary Treatment, Figure 1 Model of situational and child factors that modify pain and disability.
drug strategies they can use to control the pain. Somechildren’s clinics also offer inpatient, day or residentialtreatment programs (Berde and Solodiuk 2003).
Goals of Interdisciplinary Chronic Pain Treatment
Interdisciplinary chronic pain programs use a rehabili-tative approach where children’s pain is treated with themostappropriatedrugtherapyandwheretheteamassistschildren and their parents to improve children’s functiondespite their pain. In some instances, teams work withfamilies to help them understand that their child’s painmight not be eradicated fully, so that efforts are directedtowards improving function and quality of life. Interdis-ciplinary treatment goals include:
• Comprehensive physical and psychosocial assess-mentof thechildwithpainandtheir family toevaluateaetiology and contributing factors.
• Design and implementation of a flexible child-centredtreatmentapproachthataddressesallcausativefactors.
• The treatment plan typically including pharmaco-logical, psychological and physical therapies and insome cases medical (e.g. nerve blocks) intervention.
• The specific goals of the treatment plan including: (a)increasing independent function in terms of activitiesof daily living, school, social and physical activity;(b) facilitating adaptive problem solving, communi-cation and coping skills; (c) treating specific prob-lems identified from the comprehensive assessment(e.g.depression,anxiety)and(d)helpingchildrenandtheir families tounderstand thenatureofpain, thepaincondition and its treatment from a holistic perspec-tive.
• Ongoing assessment and re-evaluation of the treat-ment plan. One way to monitor children with chronicpain is through the use of electronic pain diaries. Stin-son and colleagues (2005; 2006) have developed andare testing a new electronic (PDA-based) multidi-mensional chronic pain measure for children calledthe e-Ouch.

C
Complex Chronic Pain in Children, Interdisciplinary Treatment 433
Pharmacological Therapies
Pharmacologic methods are an important component ofan integrated, flexible approach that combines psycho-logical and physical strategies.Thechoiceofmedicationdepends in part on the source of pain (e.g. nociceptive,neuropathic or mixed). Pain medications are tailored tothe individual needs of each child based on the results oftheirassessment.Drug therapiesaredividedbroadly intoanalgesics and adjuvant medication. Analgesics are ad-ministered in astepwiseapproach and are recommendedfor pain conditions with characteristics of nociceptive ormixed pain. Simple analgesics, such as acetaminophenand non-steroidal anti-inflammatory drugs (e.g. ibupro-fen) in adequate doses, are effective for some children.Opioids may be added to the analgesics regimen whenthese mild analgesics do not alleviate the pain. In con-trast, pain conditions with characteristics of neuropathicpain areoften resistant to drug therapies that typically re-lievenociceptivepain(e.g.opioids).Therefore,adjuvantpain medications such as anti-convulsants and tricyclicanti-depressants are used. Gabapentin is the most com-monly used anti-convulsant, as it is safe and well toler-ated. Amitriptyline is the most commonly used tricyclicanti-depressant and is often recommended for childrenwhose sleep is disturbed. Antidepressants are also help-ful for children who have chronic pain and who are de-pressed (Sethna 1999) (see � Analgesic guidelines forinfants and children).
Psychological Therapies
Many psychological therapies are available to treatchronic pain in children. These treatments includecounselling, � relaxation therapy, � biofeedback,� behavioural modification and cognitive strategiesincluding � hypnosis and � psychotherapy (McGrathet al. 2003). Often these therapies are integrated intoa comprehensive cognitive-behavioural therapy (CBT)program that is directed at identifying and amelioratingthe thinking, behaving and feeling factors that affect achild’s pain and disability. A recent systematic reviewdocumented the efficacy of CBT for chronic headacheand abdominal pain in children (Eccleston et al. 2002).CBT is often organized into a program of therapy that isdelivered by various members of the chronic pain team.The content of the programs varies across clinics butusually includes teaching children specific pain and lifecoping skills, encouraging positive family responses forresuming typical activities, reframing or changing thefamily’s beliefs that may impede rehabilitation, exercisetherapy, education and self-management strategies. Thegoal of these psychological therapies is to help childrenregain their lives and take back control from the pain.Finally, there is strong evidence that these psychologi-cal treatments can be effective without a therapist beingphysically present, using alternative models of servicedelivery such as the Internet (Elgar and McGrath 2003).We are currently developing a web-enabled distance
treatment program for children with chronic pain. Thesetypes of programs might help to overcome some of thetraditional barriers to treatment (e.g. stigma associatedwith these therapies, acceptability and accessibility).
Physical Therapies
Chronic pain often leads a child to avoid physical activ-ity due to fear of re-injury or because it exacerbates thepain. Lack of muscle use leads to loss ofmuscle strength,flexibility and endurance and overall deconditioning.Therefore,physical therapiesarean integral component,and in certain instances the cornerstone, of treatment forchildren with complex chronic pain problems. Exercisetherapy, physiotherapy, thermal (heat and cold) andsensory (� desensitization, � transcutaneous electricalnerve stimulation or TENS) stimulation and massageare the most commonly used physical modalities. Theyare frequently used in combination. Regular exercise(e.g. 20 min 3 × per week) should help improve sleep,mood, self-esteem and energy levels. However, main-taining normal daily activities such as school, sportsand play are often as effective as a formal exerciseprogram. Some children will benefit from intensivephysiotherapy. Physiotherapy is usually administeredon an outpatient basis with the ultimate goal of teachingthe child to execute the program at home. A program thechild enjoys (e.g. swimming) and one where the amountof time spent in the activity is gradually increased isone the child is more likely to continue with (McCarthyet al. 2003).
Summary
In summary, children with complex chronic pain con-ditions experience prolonged suffering and disability.The pain adversely impacts all aspects of children’slives in terms of physical, psychological, social androle functioning. Many sensory, cognitive, behaviouraland emotional factors may intensify the pain and pro-long pain related disability. Moreover, these complexpain conditions tend to have components of nociceptiveand neuropathic pain, which makes them more difficultto treat. Given this complexity, unidisciplinary andunimodal treatments are rarely successful. Therefore,children with complex chronic pain conditions must betreated from an interdisciplinary, multi-modal, reha-bilitation perspective. Pharmacological, physical andpsychological therapies should be incorporated into aflexible, child-centred program.
References1. Berde CB, Solodiuk J (2003) Multidisciplinary programs for
management of acute and chronic pain in children. In: SchechterNL, Berde CB, Yaster M (eds) Pain in Infants, Children andAdolescents. Lippincott Williams and Wilkens, Philadelphia,pp 471–486
2. Bursch B, Walco GA, Zeltzer L (1998) Clinical assessment andmanagement of chronic pain and pain-associated disability syn-drome. Dev Behav Pediatr 19:45–53

434 Complex Migraine
3. Dahlquist LM, Switkin MC (2003) Chronic and recurrent pain.In: Schechter NL, Berde CB, Yaster M (eds) Pain in Infants,Children and Adolescents. Lippincott Williams and Wilkens,Philadelphia, pp 198–215
4. Eccleston C, Morley S, Williams A et al. (2002) Systematic re-view of randomised controlled trials of psychological therapyfor chronic pain in children and adolescents, with a subset meta-analysis of pain relief. Pain 99:157–165
5. Elgar FJ, McGrath PJ (2003) Self-administered psychosocialtreatments for children and families. J Clin Psychol 59:321–339
6. McGrath PA (1999) Chronic pain in children. In: Crombie IK(ed) Epidemiology of Pain. IASP Press, Seattle, pp 81–101
7. McGrath PJ, Finley GA (1999) Chronic and recurrent pain in chil-dren and adolescents. In: McGrath PJ, Finley GA (eds) Chronicand recurrent pain in children and adolescents. Progress in PainResearch and Management, vol 13. IASP Press, Seattle, pp 1–4
8. McGrath PA, Hillier LM (2003) Modifying the psychologicalfactors that intensify children’s pain and prolong disability. In:Schechter NL, Berde CB, Yaster M (eds) Pain in Infants, Childrenand Adolescents. Lippincott Williams and Wilkens, Philadelphia,pp 85–104
9. McGrath PJ, Dick B, Unruh AM (2003) Psychologic andbehavioural treatment in pain in children and adolescents.In: Schechter NL, Berde CB, Yaster M (eds) Pain in Infants,Children and Adolescents. Lippincott Williams and Wilkens,Philadelphia, pp 303–328
10. McCarthy CF, Shea AM, Sullivan P (2003) Physical therapy man-agement of pain in children. In: Schechter NL, Berde CB, YasterM (eds) Pain in Infants, Children and Adolescents. LippincottWilliams and Wilkens, Philadelphia, pp 434–448
11. Sethna NF (1999) Pharmacotherapy in long-term pain: Currentexperience and future direction. In: McGrath PJ, Finley GA(eds) Chronic and Recurrent Pain in Children and Adolescents.Progress in Pain Research and Management, vol 13. IASP Press,Seattle, pp 243–264
12. Stinson J Petroz G, Stevens B et al. (2005) e-Ouch electronicpain diary for adolescents with arthritis: A pilot test. InternationalAssociation for the Study of Pain 11th World Congress, SydneyAustralia, August 21–26
13. Stinson J, Petroz G, Tait G et al. (2006) e-Ouch: Usability testingof an electronic chronic pain diary for adolescents with arthritis.Clin J Pain 22:295–305
Complex Migraine
� Clinical Migraine with Aura
Complex Regional Pain Syndrome
Synonymss
CRPS; Complex Regional Pain Syndrome Type I(CRPS I)
Definition
CRPS is a medical syndrome characterized by chronicregionalized STP, edema, blood flow changes, sudomo-tor changes, dysfunction, and bone turnover dispropor-tionate in response to what is often a recognized nox-ious inciting event. TheCRPSdesignation isanewnamefor this kind of disorder. The name applies to CRPS–1,which was formerly known as sympathetic dystrophywithout nerve injury, and to CRPS–2, formerly known
as causalgia. Whether it exists in the facial region is stilla matter of debate.� Adrenergic Agonist� Atypical Facial Pain, Etiology, Pathogenesis and
Management� Causalgia, Assessment� Central Nervous System Stimulation for Pain� Complex Chronic Pain In Children, Interdisciplinary
Treatment� Complex Regional Pain Syndrome and the Sympa-
thetic Nervous System� Complex Regional Pain Syndromes, General Aspects� CRPS-1 in Children� Muscle Pain, Fibromyalgia Syndrome (Primary, Sec-
ondary)� Sympathetically maintained Pain and Inflammation,
Human Experimentation� Sympathetically Maintained Pain, Clinical Pharma-
cological Tests� Sympathetically Maintained Pain in CRPS I, Human
Experimentation� Sympathetically Maintained Pain in CRPS II, Human
Experimentation
Complex Regional Pain Syndrome and theSympathetic Nervous System
JAMES N. CAMPBELL
Johns Hopkins University School of Medicine,Baltimore, MD, [email protected]
Synonyms
Reflex Sympathetic Dystrophy; Sympathetically-maintained pain; Causalgia
Definition� Sympathetically maintained pain (SMP) refers topain that is dependent on neural activity in the sympa-thetic nervous system and is present in some patientswith � complex regional pain syndrome (CRPS).
Characteristics
Activity in nociceptors induces an increase in sympa-thetic discharge. It is in this way, in part, that noxious(painful) stimuli inducea rise in blood pressure.Usually,theconverse isnot true:sympatheticactivitydoesnot im-pact the discharge of nociceptive neurons. In certain pa-tients with pain, however, nociceptors acquire sensitiv-ity to norepinephrine released by sympathetic efferents.Pain dependent on activity in the sympathetic nervoussystem is referred to as sympathetically maintained pain(SMP).This linkage with the sympathetic nervous system may,in some patients, be a dominant mechanism for pain.

C
Complex Regional Pain Syndrome and the Sympathetic Nervous System 435
SMP, in particular, is noted in many cases of complexregional pain syndrome (CRPS). CRPS typically occursafter trauma that may or may not result in nerve injury.The distal extremities, areas rich in sympathetic inner-vation, are usually affected. The patients present withedema (at least in the early stages) and striking hyper-algesia. Patients with CRPS often have motor disabilitywith difficulty moving the affected painful body parts,regardless of an intact sensory/motor pathway. The skinmay be very cool and sweaty, or sometimes very warmcompared to the opposite normal side. The disorder ap-pears to spread in some patients from distal to proximalparts of the extremity, and may in fact spread to otherextremities as well.
SMP is a Receptor Disorder
The dramatic relief of pain that occurs with selectiveblockage of the sympathetic nervous system definesSMP. Three general ideas have been advanced to ex-plain this phenomenon: 1) the anesthetic blocks “pain”fibers that course with the sympathetic efferent fibers;2) the sympathetic nervous system is overactive andthus induces pain; 3) the sympathetic nervous systemacquires the capacity to activate nociceptors and henceinduce pain. Evidence from both human and animalstudies supports the latter hypothesis.Stimulation of the sympathetic chain induces pain in pa-tients with causalgia (Walker and Nulson 1948; Whiteand Sweet 1969), even when the sympathetic chainis disconnected from the spinal cord. Thus, efferentactions of the sympathetic nervous system account forSMP. Injection of noradrenaline around stump neu-romas or skin in patients with postherpetic neuralgiainduces an increase in spontaneous pain (Chabal et al.1992; Raja et al. 1998; Choi and Rowbotham 1997).In patients relieved of pain after a sympathetic block,intradermal injection of norepinephrine into the previ-ously hyperalgesic area in physiological concentrationsinduces pain (Ali et al. 2000). Norepinephrine injectedinto normal subjects evokes little or no pain. This evi-dence strongly suggests that SMP does not arise from anexcess of epinephrine, but rather from the presence ofadrenergic receptors coupled to cutaneous nociceptors.Therefore, in SMP, norepinephrine that is normallyreleased from the sympathetic terminals acquires thecapacity to evoke pain by activating nociceptors.
Nerve Injury Induces Catechol Sensitization in Nociceptors
In a primate model, the L6 root was lesioned leavingthe dorsum of the foot partly dennervated (Ali et al.1999). Intact nociceptors from adjacent uninjured rootsdeveloped spontaneous activity and a response to anα1-adrenergic agonist, phenylephrine, applied to thereceptive field. In monkeys where no spinal nerve lesionwas applied, little or no catechol sensitivity and sponta-neous activity was present. Using a somewhat differentmodel, studies in rats have also demonstrated catechol
sensitization of intact nociceptors after nerve injuryof companion fibers (Sato and Perl 1991). C-fibersending in a neuroma also display adrenergic sensitivity(Devor and Jänig 1981; Häbler et al. 1987; Wall andGutnick 1974; Scadding 1981). These data indicate thatSMP is likely to arise from expression of α1-adrenergicreceptors on the terminals of nociceptors.
Phentolamine Infusion as a Test for SMP
The gold standard for diagnosing SMP has been deter-mination of the response to blockade of the appropriatelevel of the sympathetic chain with local anesthetic.Phentolamine, given systemically, has proven to besafe and is now considered (by some at least) to be amore specific way to diagnose SMP. After infusion ofsaline to hydrate the patient, and after administrationof 1–2 mg of propranalol to block the development ofreflex tachycardia, phentolamine in a dose of 1 mg/kg isgiven over 10 minutes. Skin temperature is monitored.If the skin temperature does not rise, then a higher doseof phentolamine may have to be given. The test canbe blinded, such that the patient does not know whenthe drug is given. A positive result is the finding thatsystemic phentolamine and α-adrenergic antagonistrelieve pain when given to patients with SMP (Raja etal. 1991; Arner 1991).
Alpha 1 or Alpha 2 Adrenergic Receptors
To sort out the adrenergic mechanisms in humans,further investigators have applied topical clonidine, anα2-adrenergic agonist, to the painful skin in patientswith SMP. Relief of hyperalgesia in the painful area re-sulted (Davis et al. 1991). Activation of α2-adrenergicreceptors, located on sympathetic terminals, blocksnorepinephrine release. Thus, clonidine appears to re-lieve pain by blocking norepinephrine release. Whenphenylephrine, a selective α1-adrenergic agonist, wasapplied to the clonidine-treated area, pain was rekindledin patients with SMP (Davis et al. 1991). Thus, clinicaldata, as with the primate physiological data, suggest thatthe α1-adrenergic receptor plays a pivotal role in SMP.Whether a phenotypic change or other change explainsthis nociceptor chemical sensitization is unanswered. Itis of interest that the density of α1-adrenoceptors in theepidermis of hyperalgesic skin of patients with complexregional pain syndrome is increased (Drummond et al.1996).
Treatment of Sympathetically Maintained Pain
By definition, SMP is relieved by performance of asympathetic block. It has been frequently observed,that in some patients the pain relief outlives the phar-macological action of the anesthetic block. A similarlong-lasting pain relief has also been reported followingsystemic phentolamine infusion (Galer et al. 1992). Aseries of sympathetic blocks may lead to successfulresolution of the pain problem.

436 Complex Regional Pain Syndrome Type I
In cases where sympathetic blockade fails to provideenduring pain relief other strategies are needed. Surgi-cal � sympathectomy provides permanent sympatheticdenervation and offers lasting pain relief (Singh et al.2003). In the case of the upper extremity, the T2, 3,4 ganglia are removed. The stellate ganglion providesno innervation of the hand, and injury of this ganglion isavoided in order to prevent development of a Horner’ssyndrome. The thoraco-endoscopic approach affordsexcellent visualization of the sympathetic chain, andprovides a minimally invasive technique by which toachieve a thoracic sympathectomy.For the lumbar area,it is necessary to remove the sympathetic chain fromL1 to L5. Typically, at least three ganglia are removed,and the length of the excised chain is 10 cm.Signs of sympathetic innervation to the foot may returnafter weeks or months. This may be due to crossed in-nervation. In other words, sympathetic fibers from thecontralateral side may reach the foot and provide suffi-cient innervation that the SMP returns. The test for this isto perform a contralateral sympathetic block. The blockshould lead to a striking increase in temperature in thecontralateral foot (this does not occur customarily), andbe associated with pain relief for at least the duration oftheblock. In thiscase, acontralateral lumbarsympathec-tomy may be performed, which will provide enduringpain relief.Complications of sympathectomy include new pain at-tributable to the surgery. These patients appear to havea vulnerability to develop new pain with trauma. Com-pensatory hyperhidrosis may develop, but this is moreof a problem in patients in whom the sympathectomy isdone to treat hyperhidrosis.Spinal cord electrical stimulation is an alternative treat-ment for SMP (Kemler et al. 2000). Of course � spinalcord stimulation may be effective for treatment of sym-pathetically independent pain as well. The advantage ofthis technique is that the morbidity is low. The disad-vantage is that continued stimulation and maintenanceof the device is required to maintain the therapeutic ef-fect. Notably, use of one modality does not preclude thelater use of the other modality.
References1. Ali Z, Raja S N, Wesselmann U et al. (2000) Intradermal Injection
of Norepinephrine Evokes Pain in Patients with SympatheticallyMaintained Pain. Pain 88:161–168
2. Ali Z, Ringkamp M, Hartke T V et al. (1999) Uninjured C-FiberNociceptors Develop Spontaneous Activity and Alpha Adrener-gic Sensitivity Following L6 Spinal Nerve Ligation in the Mon-key. J Neurophysiol 81:455–466
3. Arner S (1991) Intravenous Phentolamine Test: Diagnostic andPrognostic use in Reflex Sympathetic Dystrophy. Pain 46:17-22
4. Chabal C, Jacobson L, Russell L C et al. (1992) Pain Responseto Perineuromal Injection of Normal Saline, Epinephrine, andLidocaine in Humans. Pain 49:9–12
5. Choi B, Rowbotham M C (1997) Effect of Adrenergic ReceptorActivation on Post-Herpetic Neuralgia Pain and Sensory Distur-bances. Pain 69:55–63
6. Davis K D, Treede R-D, Raja S N et al. (1991) Topical Ap-plication of Clonidine Relieves Hyperalgesia in Patients withSympathetically Maintained Pain. Pain 47:309–317
7. Devor M, Jänig W (1981) Activation of Myelinated AfferentsEnding in a Neuroma by Stimulation of the Sympathetic Supplyin the Rat. Neurosci Lett 24:43–47
8. Drummond P D, Skipworth S, Finch P M (1996) Alpha1-Adrenoceptors in Normal and Hyperalgesic Human Skin.Clin Sci (Colch) 91:73–77
9. Galer B S, Rowbotham M C, Von Miller K et al. (1992) Treatmentof Inflammatory, Neuropathic and Sympathetically MaintainedPain in a Patient with Sjögren’s Syndrome. Pain 50:205–208
10. Häbler H-J, Jänig W, Koltzenburg M (1988) A Novel Type of Un-myelinated Chemosensitive Nociceptor in the Acutely InflamedUrinary Bladder. Agents Actions 25:219–221
11. Kemler M A, Barendse G A, van Kleef M et al. (2000) SpinalCord Stimulation in Patients with Chronic Reflex SympatheticDystrophy. N Engl J Med 343:618–624
12. Raja S N, Abatzis V, Frank S (1998) Role of α-Adrenoceptorsin Neuroma Pain in Amputees. American Society of Anesthe-siologists Abstracts
13. Raja S N, Treede R-D, Davis K D et al. (1991) SystemicAlpha-Adrenergic Blockade with Phentolamine: A DiagnosticTest for Sympathetically Maintained Pain. Anesthesiology74:691–698
14. Sato J, Perl E R (1991) Adrenergic Excitation of CutaneousPain Receptors Induced by Peripheral Nerve Injury. Science251:1608–1610
15. Scadding J W (1981) Development of Ongoing Activity,Mechanosensitivity and Adrenaline Sensitivity in SeveredPeripheral Nerve Axons. Experimental Neurology 73:345–364
16. Singh B, Moodley J, Shaik A S et al. (2003) Sympathectomyfor Complex Regional Pain Syndrome. J Vasc Surg 37:508–511
17. Walker A E and Nulson F (1948) Electrical Stimulation of the Up-per Thoracic Portion of the Sympathetic Chain in Man. Archivesof Neurology and Psychiatry 59:559–560
18. Wall P D and Gutnick M (1974) Ongoing Activity in PeripheralNerves: The Physiology and Pharmacology of Impulses Origi-nating from a Neuroma. Experimental Neurology 43:580–593
19. White J C, Sweet W H (1969) Pain and the Neurosurgeon: AForty Year Experience. Charles C. Thomas, Springfield
Complex Regional Pain Syndrome Type I
� Sympathetically Maintained Pain in CRPS I, HumanExperimentation
Complex Regional Pain Syndrome Type I(CRPS I) and Type II (CRPS II)
� Complex Regional Pain Syndrome
Complex Regional Pain Syndromes,General Aspects
KOK E. KHOR
Department of Pain Management, Prince of WalesHospital, Randwick, NSW, [email protected]

C
Complex Regional Pain Syndromes, General Aspects 437
Synonyms
CRPSCRPS Type 1: Reflex sympathetic dystrophy; algo-dystrophy; Sudeck’s Atrophy; Traumatic Angiospasm;Shoulder-Hand Syndrome; Post-Infarction Sclero-dactylyCRPS Type 2: Causalgia
Definition
CRPSType1isasyndromethatusuallydevelopsafteraninitiating noxious event. It consists of spontaneous painor allodynia/hyperalgesia, in a regional distribution notlimited to the territory of a single peripheral nerve, anddisproportionate in severity to the inciting event, asso-ciated at some point with evidence of oedema, changesin skin blood flow or abnormal sudomotor activity in theregionofpain(Complexregionalpainsyndromes1994).CRPS Type 2 is the same as Type 1, but the syndromedevelops in association with a partial nerve injury (Com-plex regional pain syndromes 1994).
Characteristics
Clinical Manifestations
CRPS can be initiated by events ranging from minorinjuries to surgical lesions, visceral diseases (e.g. my-ocardial infarction) and central neurological disorders(e.g. acute stroke). Various stages of CRPS have beenproposed, but have not been corroborated in populationstudies (Veldman et al. 1993).Pain is the essential feature and is disproportionateto the severity of the injury (Complex regional painsyndromes 1994). It can be burning, aching, prick-ling, shooting or tearing, and felt distally, diffuselyand deeply in the affected region. It can be sponta-neous or evoked by light touch, thermal stimulation,dependent position, palpation and joint movements(Walker and Cousins 1997; Birklein et al. 2000; Rib-bers et al. 1995; Bogduk 2001). If the pain is relieved by� Sympathetic Nerve Block or � intravenous infusionsof an α–adrenoceptor antagonist, it is considered tobe sympathetically maintained pain (SMP) (Complexregional pain syndromes 1994). If not so relieved, itis considered to be sympathetically independent pain(SIP).Skin changes range from warm and red to cold and cyan-otic, and are associated with swelling and increased ordecreased sweating (Walkerand Cousins1997).Trophicchanges include increased or decreased nail and hairgrowth, thin shiny skin, muscle wasting and fibrosis, andosteoporosis (Walker and Cousins 1997). Motor impair-ments include weakness, tremor, dystonia, myoclonicjerks, joint stiffness, and difficulty initiating movements(Walker and Cousins 1997;, Ribbers et al. 1995). Thesevasomotor, sudomotor, and trophic changes distinguishCRPS from other painful conditions due to neuropathy,musculoskeletal injury or visceral diseases (Fig. 1).
Complex Regional Pain Syndromes, General Aspects, Figure 1 Patientwith complex regional pain syndrome (CRPS). The patient developed CRPSfollowing a crush injury to the right foot.
Somatization, anxiety, depression and fear avoidancebehaviours found in patients with CRPS are identicalto those of patients with chronic pain, and are a result,rather than a cause, of pain (Walker and Cousins 1997).The diagnosis of CRPS is based solely on clinical crite-ria. Investigations are used only to confirm clinical im-pressions about autonomic, sensory and motor dysfunc-tion. These include bone scintigraphy, quantitative sen-sory testing and tests for autonomic function (Baron andWasner 2001).
Demographics
CRPS affects women more often (66%), and most oftenthe upper limb (73%) (Birklein et al. 2000). The meanage of patients is 50.4 years, but CRPS also occurs inchildren–mainly adolescent females and affecting lowerlimbs–but carries a more favourable prognosis (Walkerand Cousins 1997). CRPS 1 is 5 times more commonthan CRPS 2.CRPS occurs in 2–5% patients with peripheral nerveinjuries, and in 1–2% of patients who sustain fractures,although the incidence is higher following Colles’ frac-

438 Complex Regional Pain Syndromes, General Aspects
ture (Walker and Cousins 1997). In 10–26% of patientsno significant precipitant cause is found (Ribbers etal. 1995). A genetic predisposition to CRPS had alsobeen suggested (Walker and Cousins 1997).
Natural History
Symptoms tend to improve in about two-thirds of pa-tients. After Colles’ fracture, although most patients im-prove rapidly, pain and swelling persist in some 20–30%patients at 6 months (Walker and Cousins 1997). In pa-tientswho areunresponsive to treatmentduring theacutestage, pain may become refractory and associated withsignificant impairment in activities ofdaily living, recre-ational activities, work and mood (Ribbers et al. 1995).Recurrence or spread to another region occurs in 10%of patients.
Mechanisms
As the features of CRPS 1 and CRPS 2 are identical, itis likely that CRPS 1 involves an undetected nerve in-jury. CRPS is thus a form of � neuropathic pain (Baronand Wasner 2001; Bennett 1999). The underlying mech-anism of CRPS has not been explicitly elucidated (Bog-duk 2001). Multiple mechanisms appear to be involved,with somatosensory dysfunctions interacting with thesympathetic nervous system and peripheral inflamma-tory reactions (Bogduk 2001; Bennett 1999). Peripheraland central mechanisms for pain generation have beeninvoked (Bennett 1999).Injury of a peripheral nerve may result in a neuromaformation or constriction of the nerve. These can gen-erate ectopic activity in the Aδ and C fibres, whichexcites nociceptive neurons in the dorsal horn, result-ing in central hyperexcitability (Bogduk 2001; Ben-nett 1999). This becomes the basis for neurogenic pain,mechanical hyperalgesia, and allodynia. Sprouting ofsympathetic efferent fibres onto dorsal root ganglia(DRG), and production of α–adrenoreceptors in theDRG and nerve terminals, renders the affected nervesmore responsive to noradrenaline (NA) and sympatheticstimulation (Bogduk 2001; Baron and Wasner 2001;Bennett 1999).Deafferentation following peripheral nerve injury canresult in disinhibition of dorsal horn neurons, and conse-quent spontaneous activity and facilitation of nocicep-tive neurons (Bogduk 2001). CRPS following lesions inthe central nervous system might also be due to disinhi-bition of central nociceptive pathways (Bogduk 2001).It remainsuncertain if the so-calledsympathetic featuresare caused by abnormalities in sympathetic nerve activ-ity, by inflammatory changes, or a combination of both,at different phases of CRPS.In the early phase, central sympathetic activity is func-tionally reduced,with reducedreleaseofNAandrelativevasodilatation. Antidromic activity in C fibres may lib-erate inflammatory mediators and enhance vasodilata-tion. In the advanced phase, central sympathetic activity
returns but vasoconstrictor innervation disappears, be-cause some sympathetic postganglionicneurons degen-erate. Blood vessels develop denervation hypersensitiv-ity with increased α–adrenoceptor density, leading to in-creased vasoconstriction with manifestation of chroni-cally cold, bluish limbs (Bogduk 2001; Baron and Was-ner 2001; Bennett 1999).Inflammatory responses, with proliferation of immunecell infiltrates and liberation of proinflammatory cy-tokines, accompany nerve injury. These chemicals cansensitise sensory neurones, resulting in mechanicalallodynia and hyperalgesia (Bennett 1999). The exces-sive production of free oxygen radicals by activatedphagocytes in inflamed tissues may also play a role(Baron and Wasner 2001; Veldman 1999).
Treatment
Although CRPS has attracted treatment with a varietyof agents and interventions, used alone or in combina-tion, systematic and pragmatic reviews have shown thatfew interventions have been vindicated by controlled tri-als (Kingery 1997; Robinson 2002; Hord and Oaklan-der 2003). The management of CRPS, therefore, restslargely on recommendations (Stanton-Hicks et al. 1998)rather than strong evidence.Early recognition and treatment are associated with thebestchanceofagoodoutcome.Comprehensivemanage-ment entails physical therapy and functional restoration,coupled with behavioural therapy, and drugs or injec-tions to reduce pain (Stanton-Hicks et al. 1998).Recommended, but unproven, interventions includedynamic splinting, exercises, and stress-loading pro-grams in order to maintain limb function and min-imise secondary effects due to disuse (Walker andCousins 1997; Hord and Oaklander 2003). Althoughcognitive behavioural therapy may be effective forchronic pain in general (Walker and Cousins 1997;Hord and Oaklander 2003), its efficacy for CRPS hasnot been demonstrated.� Sympathetic nerve blocks have been a traditionalintervention for CRPS, but a systematic review showedthat the response rates were no better than what couldbe expected from a placebo effect (Cepeda et al. 2002).� Sympathetic blocks or � epidural infusions may beused to facilitate physical therapy, but their utility re-mains unproven. Bretylium and ketanserinedelivered as� regional intravenous infusions have been vindicatedin controlled trials, but phentolamine and guanethidinehave effects no greater than placebo (Robinson 2002;Hord and Oaklander 2003). Clonidine may be effectiveby intravenous, transdermal, or epidural application(Hord and Oaklander 2003). Nifedipine and phenoxy-benzamine may be effective in recent onset CRPS (Hordand Oaklander 2003).There is some evidence that oral corticosteroids may beeffective (Kingery 1997; Hord and Oaklander 2003).There is emerging evidence that � bisphosphonates can

C
Complex Regional Pain Syndromes, Clinical Aspects 439
relieve the pain of CRPS (Robinson 2002; Hord andOaklander 2003). Topical dimethylsulfoxide cream,which acts as a free radical scavenger, may reduce thesigns of CRPS (Veldman 1999).Gabapentin, lamotrigine, subcutaneous and transder-mal lignocaine appear to be effective in open label trials,but there have been no published trials of oral opioids,anticonvulsants, mexiletine, ketamine, or amitripty-line (Robinson 2002; Hord and Oaklander 2003). Theefficacy of NSAIDs (Baron and Wasner 2001) andacupuncture (Hord and Oaklander 2003) has not beendemonstrated. Amitriptyline and � TENS appear to beeffective in children (Hord and Oaklander 2003).For intractable CRPS, some authorities advocate neuro-modulation with peripheral nerve stimulator and epidu-ral spinal cord stimulator (Hord and Oaklander 2003;Stanton-Hicks et al. 1998), but a controlled trial showedthat although spinal cord stimulation did relieve pain, itdid not improve function (Kemleret al. 2000).Fordysto-nia associated with CRPS, intrathecal baclofen has beeneffective(HordandOaklander2003). Intrathecaladmin-istration of morphine can also be considered, althoughefficacy has only been reported in case series (Hord andOaklander 2003).
References1. Baron R, Wasner G (2001) Complex Regional Pain Syndromes.
Curr Pain Headache Rep 5:114–1232. Bennett G (1999) Scientific Basis for the Evaluation and Treat-
ment of RSD/CRPS Syndromes: Laboratory Studies in Animalsand Man. In: Max M (ed) Pain 1999 – An updated review. Re-fresher Course Syllabus. IASP Press, Seattle, pp 331–337
3. Birklein F, Riedl N, Sieweke N et al. (2000) Neurological Find-ings in Complex Regional Pain Syndromes – Analysis of 145Cases. Acta Neurol Scand 101:262–269
4. Bogduk N (2001) Mechanisms of Complex Regional Pain Syn-dromes. Aust Musculoskeletal Med 6:88–102
5. Cepeda MS, Lau J, Carr B (2002) Defining the Therapeutic Roleof Local Anesthetic Sympathetic Blockade in Complex RegionalPain Syndrome: A Narrative and Systematic Review. Clin J Pain18:216–233
6. Complex Regional Pain Syndromes (1994) In: Merskey H,Bogduk N (eds) Classification of Chronic Pain: Descriptionsof Chronic Pain Syndromes and Definition of Pain Terms, 2ndedn. IASP Press, Seattle, pp 40–43
7. Hord E, Oaklander A (2003) Complex Regional Pain Syndrome:A Review of Evidence-Supported Treatment Options. Curr PainHeadache Rep 7:188–196
8. Kemler MA, Barendse GAM, van Kleef M, de Vet HCW, RijksCPM, Furnee CA, van den Wildenberg FAJM (2000). SpinalCord Stimulation in Patients with Chronic Reflex SympatheticDystrophy. New Engl J Med 343:618–624
9. Kingery WS (1997) A Critical Review of Controlled ClinicalTrials for Peripheral Neuropathic Pain and Complex RegionalPain Syndromes. Pain 73:123–139
10. Ribbers G, Geurts A, Mulder T (1995) The Reflex Sympa-thetic Dystrophy Syndrome: A Review with Special Referenceto Chronic Pain and Motor Impairments. Int J Rehab Res18:277–295
11. Robinson J (2002) The Treatment of Complex Regional PainSyndrome Type 1. Aust Musculoskeletal Med 7:101–105
12. Stanton-Hicks M, Baron R, Boas R, Gordh T, Harden N, HendlerN, Koltzenburg M, Raj P, Wilder R (1998) Complex RegionalPain Syndromes: Guidelines for Therapy. Clin J Pain14:155–166
13. Veldman P (1999) Inflammatory Aspects of RSD. In: Max M(ed) Pain 1999 – An Updated Review. Refresher Course Syllabus.IASP Press, Seattle, pp 343–345
14. Veldman P, Reynen H, Arntz E et al. (1993) Signs and Symp-toms of Reflex Sympathetic Dystrophy: Prospective Study of 829Patients. Lancet 342:1012–1016
15. Walker S, Cousins M (1997) Complex Regional Pain Syndromes:Including “Reflex Sympathetic Dystrophy” and “Causalgia”.Anaesth Intens Care 25: 113–125
Complex Regional Pain Syndromes,Clinical Aspects
RALF BARON
Clinic for Neurology, Christian Albrechts UniversityKiel, Kiel, [email protected]
Synonyms
CRPS; reflex sympatheticdystrophy;causalgia;MorbusSudeck; algodystrophy
Definition
The “IASP classification of chronic pain” redefinedpain syndromes formerly known as reflex sympatheticdystrophy and causalgia. The term Complex RegionalPain Syndrome describes, “a variety of painful condi-tions following injury which appear regionally havinga distal predominance of abnormal findings, exceedingin both magnitude and duration the expected clinicalcourse of the inciting event often resulting in significantimpairment of motor function, and showing variableprogression over time”. These chronic pain syndromescomprise of different additional clinical features includ-ing � spontaneous pain, � allodynia, � hyperalgesia,oedema, autonomic abnormalities and trophic signs. In� CRPS type I (reflex sympathetic dystrophy), minorinjuries or fractures of a limb precede the onset of symp-toms. � CRPS type II (causalgia) develops after injuryto a major peripheral nerve (Merskey and Bogduk 1995;Harden et al. 2001; Janig and Baron 2003).
Characteristics
CRPS Type I (Reflex Sympathetic Dystrophy)
The most common precipitating event is a trauma affect-ing the distal part of an extremity (65 %), especially frac-tures, postsurgical conditions, contusions and strain orsprain. Less common occurrences are central nervoussystem lesions, like spinal cord injuries and cerebrovas-cular accidents as well as cardiac ischemia (Allen et al.1999).CRPS I patients develop asymmetrical distal extremitypain and swelling without presenting with a demon-strable nerve lesion. These patients often report aspontaneous burning pain felt in the distal part of theaffected extremity. Characteristically, the pain is dis-proportionate in intensity to the inciting event. The pain

440 Complex Regional Pain Syndromes, Clinical Aspects
usually increases when the extremity is in a dependentposition. Stimulus-evoked pains are a striking clini-cal feature; they include � mechanical allodynia and� thermal allodynia and/or hyperalgesia. These sensoryabnormalities often appear early, are most pronounceddistally, and have no consistent spatial relationship toindividual nerve territories or to the site of the incitinglesion (Sieweke et al. 1999). Movement of, and pressureon, the joints (deep somatic allodynia) can elicit pain,even if the inciting lesion does not directly affect these.Autonomic abnormalities include swelling and changesin sweating and skin blood flow (Chelimsky et al. 1995;Birklein et al. 1998; Wasner et al. 2002; Wasner et al.2001). In the acute stages of CRPS I, the affected limbis often warmer than thecontralateral limb.Sweating ab-normalities, either hypohidrosis or, more frequently, hy-perhidrosis are present in nearly all CRPS I patients. Theacute distal swelling of the affected limb depends verycritically on aggravating stimuli. Since it diminishes af-ter sympathetic blocks, it is likely that it is maintainedby sympathetic activity.Trophic changes such as abnormal nail growth, in-creased or decreased hair growth, fibrosis, thin glossyskin and osteoporosis may be present, particularly inchronic stages. Restrictions of passive movement areoften present in long-standing cases, and may be re-lated to both functional motor disturbances and trophicchanges of joints and tendons.Weakness of all muscles of the affected distal ex-tremity is often present. Small accurate movementsare characteristically impaired. Nerve conduction andelectromyography studies are normal, except in patientsin very chronic and advanced stages. About half of thepatients have a postural or action tremor representing anincreased physiological tremor (Deuschl et al. 1991).In about 10 % of cases, dystonia of the affected hand orfoot develops (Bhatia et al. 1993).
CRPS Type II (Causalgia)
The symptoms of CRPS II are similar to those of CRPS I.The only exception is that a lesion of peripheral nervestructures and subsequent focal deficits are mandatoryfor the diagnosis. The symptoms and signs spread be-yond the innervation territory of the injured peripheralnerveandoftenoccurremotefromthesiteof injury,how-ever, a restriction to the territory is not in conflict withthe current definition.
Sympathetically Maintained Pain (SMP)
On the basis of experience and recent clinical stud-ies the term � sympathetically maintained pain wasre-defined: Neuropathic pain patients presenting withsimilar clinical signs and symptoms can clearly be di-vided into two groups, by the negative or positive effectof selective sympathetic blockade, selective activationof sympathetic activity or antagonism of alpha adreno-ceptor mechanisms (Raja et al. 1991; Baron et al. 2002).
The pain component that is relieved by specific sym-patholytic procedures is considered ”sympatheticallymaintained pain” (SMP). Thus, SMP is now defined tobe a symptom or the underlying mechanism in a subsetof patients with neuropathic disorders and not a clinicalentity. The positive effect of a sympathetic blockade isnot essential for the diagnosis. On the other hand, theonly possibility of differentiating between SMP and”sympathetically independent pain” (SIP) is the effi-cacy of a correctly applied sympatholytic intervention(Stanton-Hicks et al. 1995).
Diagnostic Procedure
The diagnosis of CRPS I and II follows the IASP clinicalcriteria (Stanton-Hicks and Jänig 1996). If two clinicalsigns are joined by “or”, if either sign is present or both,the condition of the statement is satisfied.
CRPS Type I
TypeI isa syndrome thatdevelopsafteran initiatingnox-ious event.Spontaneous pain or allodynia/hyperalgesia occurs, isnot limited to the territory of a single peripheral nerve,and is disproportionate to the inciting event.There is or has been evidence of oedema, skin blood flowabnormality, or abnormal sudomotor activity in the re-gion of the pain since the inciting event.This diagnosis is excluded by theexistenceofconditionsthat would otherwise account for the degree of pain anddysfunction.
CRPS Type II
Type II is a syndrome that develops after nerve injury.Spontaneous pain or allodynia/hyperalgesia occurs andis not necessarily limited to the territory of the injurednerve.There is or has been evidence of oedema, skin blood flowabnormality, or abnormal sudomotor activity in the re-gion of the pain since the inciting event.This diagnosis is excluded by theexistenceofconditionsthat would otherwise account for the degree of pain anddysfunction.Pain is essential for the diagnosis, whereby ‘sponta-neous‘ indicates pain without external cause. Motorsymptoms and findings are not included in this classi-fication, although they are common, and can includetremor, dystonia and weakness.Possible inciting events of CRPS include:
CRPS I
• Peripheral tissues
– fractures and dislocations– soft-tissue injury– fasciitis– tendonitis– bursitis– ligamentous strain

C
Complex Regional Pain Syndromes, Clinical Aspects 441
– arthritis– mastectomy– deep vein thrombosis– immobilization
• Idiopathic
CRPS often follows minor trauma that could not be re-membered by the patient. Also some patients negate anyinciting event
• Viscera
– abdominal disease– myocardial infarction
• Central nervous system
– spinal cord lesions– head injury– cerebral infarction– cerebral tumor
CRPS II
• Peripheral nerve and dorsal root
– peripheral nerve trauma– brachial plexus lesions– root lesions
Treatment Algorithm
Treatment should be immediate and most importantlydirected towardrestorationoffullfunctionoftheextrem-ity. This objective is best attained in a comprehensive in-terdisciplinary setting, with particular emphasis on painmanagement and functional restoration (treatment algo-rithm see (Stanton-Hicks et al. 1998)). The pain special-ists should include neurologists, anesthesiologists, or-thopedics, physiotherapists, psychologists and the gen-eral practicioner.Destructive surgery on the peripheral or central afferentnervous system in cases of CRPS always implicates fur-ther deafferentation, and thereby provides an increasedrisk for persistent deafferentation type of pain.The severity of the disease determines the therapeuticalregime. The reduction of pain is the precondition thatall other interventions have to comply with. At the acutestage of CRPS, when the patients still suffer from severepain, it is often impossible to carry out intensive activetherapy. Painful interventions, and in particular vigor-ous physical therapy, at this stage leads to deterioration.Therefore, immobilization of the affected extremityand careful contralateral physical therapy should be theacute treatment of choice and pain treatment shouldbe initiated immediately. There are only a few con-trolled treatment studies on CRPS. The first choiceanalgesic drugs, in which efficacy has been shown by
clinical studies on other neuropathic pain syndromes,include opioids, tricyclic antidepressants, gabapentin,pregabalin and carbamazepine. Additionally, systemiccorticosteroids treatment is frequently used. Calcium-regulating agents (calcitonin, bisphosphonates) areused in case of refractory pain. Sympatholytic proce-dures for SMP testing, preferably sympathetic ganglionblocks, are used if no or an insufficient pain relief isachieved and should be perpetuated in case of efficacy.If resting pain subsides, first passive physical therapy,later active isometric followed by active isotonic train-ing should be performed in combination with sensorydesensitization programmes until restitution of com-plete motor function. Psychological treatment has toflank the regime to strengthen coping strategies anddiscover contributing factors. In refractory cases spinalcord stimulation could be considered. If refractory dys-tonia develops intrathecal baclofen application is worthconsidering.
References1. Allen G, Galer BS, Schwartz L (1999) Epidemiology of Complex
Regional Pain Syndrome: A Retrospective Chart Review of 134Patients. Pain 80:539–544
2. Baron R, Schattschneider J, Binder A, Siebrecht D, WasnerG (2002) Relation Between Sympathetic Vasoconstrictor Ac-tivity and Pain and Hyperalgesia in Complex Regional PainSyndromes: A Case-Control Study. Lancet 359:1655–1660
3. Bhatia KP, Bhatt MH, Marsden CD (1993) The Causalgia-Dystonia Syndrome. Brain 116(Pt 4):843–851
4. Birklein F, Riedl B, Neundörfer B, Handwerker HO (1998) Sym-pathetic Vasoconstrictor Reflex Pattern in Patients with ComplexRegional Pain Syndrome. Pain 75:93–100
5. Chelimsky TC, Low PA, Naessens JM, Wilson PR, Amadio PC,Ot’Brien PC (1995) Value of Autonomic Testing in Reflex Sym-pathetic Dystrophy. Mayo Clin Proc 70:1029–1040
6. Deuschl G, Blumberg H, Lücking CH (1991) Tremor in ReflexSympathetic Dystrophy. Arch Neurol 48:1247–1252
7. Harden RN, Baron R, Jänig W (2001) Complex Regional PainSyndrome. IASP Press, Seattle
8. Janig W, Baron R (2003) Complex Regional Pain Syndrome:Mystery Explained? Lancet Neurol 2:687–697
9. Merskey H, Bogduk N (1995) Classification of Chronic Pain De-scriptions of Chronic Pain Syndromes and Definition of Terms.IASP press, Seattle
10. Raja SN, Treede RD, Davis KD, Campbell JN (1991) SystemicAlpha-Adrenergic Blockade with Phentolamine: A DiagnosticTest for Sympathetically Maintained Pain. Anesthesiology74:691–698
11. Sieweke N, Birklein F, Riedl B, Neundorfer B, Handwerker HO(1999) Patterns of Hyperalgesia in Complex Regional Pain Syn-drome. Pain 80:171–177
12. Stanton-Hicks M, Janig W, Hassenbusch S, Haddox JD, BoasR, Wilson P (1995) Reflex Sympathetic Dystrophy: ChangingConcepts and Taxonomy. Pain 63:127–133
13. Stanton-Hicks M, Jänig W (1996) Reflex Sympathetic Dystro-phy: A Reappraisal. IASP Press, Seattle, pp 1–249
14. Stanton-Hicks M, Baron R, Boas R, Gordh T, Harden N, HendlerN, Koltzenburg M, Raj P, Wilder R (1998) Complex RegionalPain Syndromes: Guidelines for Therapy. Clin J Pain 14:155–166
15. Wasner G, Schattschneider J, Baron R (2002) Skin TemperatureSide Differences – A Diagnostic Tool for CRPS? Pain 98:19–26
16. Wasner G, Schattschneider J, Heckmann K, Maier C, BaronR (2001) Vascular Abnormalities in Reflex Sympathetic Dys-trophy (CRPS I): Mechanisms and Diagnostic Value. Brain124:587–599

442 Compliance
Compliance
Definition
The extent to which patients are obedient and follow theinstructions and prescriptions of a health care provider.� Multidisciplinary Pain Centers, Rehabilitation
Complicated Migraine
� Clinical Migraine with Aura
Comprehensive Assessment
� Multiaxial Assessment of Pain
Compression Fracture
Definition
Compression failure of the anterior column of the spinewith an intact middle and posterior column.� Chronic Back Pain and Spinal Instability
Computed Radiography
� Plain Radiography
Computerised Axial Tomography
� CT Scanning
Conditioned Analgesia
Definition
Conditioned Analgesia is a learned activation of pain-inhibitory systems.� Pain Modulatory Systems, History of Discovery
Conditioned Place Avoidance
Definition
In this paradigm, the animal received aversive footshockin one chamber (shock chamber) of a two chamber ap-paratus (Selden et al. 1991). On a subsequent day, theanimal was placed in the non-shock (safe) chamber andthe time spent in this chamber was recorded. Hippocam-pus lesioned animals spent less time in the safe chamberas compared to control animals.� Nociceptive Processing in the Hippocampus and En-
torhinal Cortex, Neurophysiology and Pharmacology
Conditioning
Definition
Mechanism through which repeated associations be-tween two stimuli induces a new learned response. Inparticular, by pairing a neutral stimulus (conditionedstimulus) with an unconditioned stimulus (that inducesa physiological response) many times, the neutral stim-ulus alone will be capable of producing a conditionedphysiological response.� Operant Perspective of Pain� Placebo Analgesia and Descending Opioid Modula-
tion
Conductance
Definition
Passage of ions such as Na+, K+, Cl– or Ca++ throughchannels in the plasma membrane. Entry of positivelycharged ions depolarizes a neuron and leads to the gen-eration of action potentials, whereas their exit can causehyperpolarization andasuppressionofactionpotentials.Conductances may be activated by ligands binding totheir receptor, such as in thecaseofγ-aminobutyricacid,or by changes in resting membrane potential.� Descending Circuitry, Opioids
Conduction Velocity
Definition
Speed ofpropagation ofan actionpotential alonganervefiber.� Nociceptor, Categorization

C
Congenital Insensitivity to Pain with Anhidrosis 443
Confidence in Coping Abilities
� Psychology of Pain, Self-Efficacy
Confusional Migraine
Definition
An unusual migraine aura that consists of a suddenonset of agitation, confusion and disorientation. It maybe associated with dysarthria or aphasia. The episodelasts from a few minutes to an hour and is followedby headache consistent with migraine. The individ-ual is usually amnestic for the period of confusion.It often occurs in teenagers, and may be triggered bymild head trauma or can occur spontaneously. Thedifferential diagnosis includes complex partial seizure,intoxication/drug ingestion and encephalitis.� Migraine, Childhood Syndromes
Congener
Definition
Acongener isoneof two ormore thingsof thesamekind,as of animal or plant, with respect to classification.� Headache Attributed to a Substance or its Withdrawal
Congenital Hypomyelinating Neuropathy
� Hereditary Neuropathies
Congenital Insensitivity to Pain withAnhidrosis
MAX J. HILZ
University of Erlangen-Nuernberg,Erlangen, [email protected]
Synonyms
Hereditary Sensory and Autonomic Neuropathy TypeIV, HSAN IV, HSAN 4; CIPA; Congenital Sensory Neu-ropathy with Anhidrosis; Familial Dysautonomia TypeII
Definition
Congenital Insensitivity to pain with anhidrosis (CIPA)is a rare autosomal recessive disorder characterized bya lack of pain sensation, recurrent episodes of high,unexplained fever, anhidrosis, i.e. absence of sweating,self-mutilating behavior and mental retardation (Swan-son 1963; Pinsky and DiGeorge 1966; Dyck 1993;Axelrod 2002; Hilz et al. 1999)
Characteristics
CIPAis thesecond most frequentamong thefiveHSANsclassified by Ohta and Dyck (Dyck 1993). The combi-nation of distinctive anhidrosis and insensitivity to deepas well as superficial pain, with manifestation already inearly childhood, is among the most prominent findingsdifferentiating CIPA from the other HSANs, in particu-lar from the most common of the five disorders, HSANIII, also called Riley-Day-syndrome or familial dysau-tonomia. Familial dysautonomia is characterized by ex-cessive sweating during autonomic crises and by signif-icantly impaired perception of superficial pain but pre-served deep pain perception (Axelrod 2002).CIPA manifests in infancy or early childhood with fre-quent bouts of extreme, at first sight unexplained, feverand heat intolerance.Anhidrosis is present on the trunk and upper extremi-ties in all CIPA patients while other body parts may bevariably affected. Particularly with high environmentaltemperatures, anhidrosis induces hyperpyrexia, whichin turn can lead to recurrent febrile convulsions and hasbeen reported to account for death within the first threeyears in up to 20 percent of CIPA children (Axelrod2002; Indo 2002).Anhidrosis also contributes to the development of a cal-loused, thickenedskinwith lichenification, i.e.aleatheryinduration and thickening of the epidermis with exag-geration of normal skin lines, giving it a bark-like ap-pearance and hyperkeratosis particularly at palms andsoles (Fig. 1) (Indo 2002). The skin is dry and warm andfrequently shows deep and persistent ulcers at the heels(Fig. 2), nails are dystrophic (Axelrod 2002; Indo 2002;Pinsky and DiGeorge 1966).Initially insensitivity to pain may not be apparent. Yetwith increasing mobility, children sustain severe, fre-quently unrecognized injuries without complaint. Theyincur repeated bruises or inadvertently self-inflictedburn injuries and cuts and multiple scars. Insensitivityto pain also accounts for, often self-inflicted cornealscarring with opacities and even perforation of thecornea (Axelrod 2002, Indo 2002). With dentition, chil-dren start to bite their tongue, lips and fingers, leading toa mutilated, bifid tongue with decubital ulcers or absenttip of the tongue, mutilated lips (Fig. 3), jaw malforma-tion with edentate areas due to self-extraction of teeth(Bodner et al. 2002), or to amputated finger tips. Openwounds with poor healing, continuous self-mutilation

444 Congenital Insensitivity to Pain with Anhidrosis
Congenital Insensitivity to Pain with Anhidrosis,Figure 1 Hyperkeratosis and leathery induration of the skin withexaggeration of normal skin lines in the palm of a CIPA patient.Fingernails are dystrophic. Fingertips show signs of chronic inflammationdue to repeated self-mutilation.
Congenital Insensitivity to Pain with Anhidrosis, Figure 2 Deep per-sistent ulcer and chronic inflammation at the area of the heel in a CIPApatient.
and frequent, often unnoticed fractures and joint injurieslead to osteomyelitis and - over the years - to grotesquejoint deformities with neurogenic arthropathy (Fig. 3)or amputations (Axelrod 2002). Even with active orpassive movement of fractured joints or bones, there isno tenderness or discomfort (Swanson 1963). Radio-grams frequently show numerous fractures, particularlyof the weight-bearing bones with neuropathic Charcotjoints (Indo 2002).
Congenital Insensitivity to Pain with Anhidrosis, Figure 3 Neuropathicankle joint (Charcot joint) due to repetitive fractures. Tissue swelling asa result of chronic inflammation and osteomyelitis. Chronic ulcer at thebottom of the heel. Mutilation of lower left lip due to repeated lip biting.
Chronic inflammation may lead to secondary amyloido-sis (Axelrod 2002; Indo 2002). Local and systemic in-fections often induce sepsis, which accounted for 20%fatalities in one patient group (Shorer et al. 2001).Most CIPA children are mentally retarded and havelearning problems. 50 % show irritability, hyperactivityand a tendency to rages and tantrums (Axelrod 2002).Clinical examination confirms the absence of responsesto superficial or deep, visceral pain, e.g. with electricalshock during neurophysiologic examination, intramus-cular injection or urinary catheterization (Swanson1963), Moreover, temperature perception and dis-crimination between hot and cold stimuli is impaired(Indo 2002). Similarly, discrimination of sharp and dullstimuli is compromised while light touch, vibrationand position senses are normal. Deep tendon reflexesare preserved and there are no pathological reflexes.Corneal reflexes may be inconsistent. In contrast toHSAN III, emotional tear flow and fungiform papillaeof the tongue are present (Axelrod 2002).Motorandsensorynerveconduction,somatosensory,vi-sual or brainstem evoked potentials are usually normal,while quantitative sensory testing of warm, cold or heatperception is highly abnormal. The � sympathetic skinresponse (SSR) is abnormal in all CIPA patients (Hilzet al. 1999; Shorer et al. 2001).Intradermal injection of diluted histamine does notinduce the typical � triple response of a C-nerve fiberaxon reflex mediated vasodilatation with diffuse ery-thema and itching pain, but only results in a circumscriptwheal at the site of injection (Axelrod 2002; Indo 2002).Similarly, local sweating cannot be induced by injectionof pilocarpine or methacholine (Pinsky and DiGeorge1966).Apart from anhidrosis, autonomic dysfunction is nota predominant characteristic of CIPA, though present.There may be orthostatic hypotension with preservedreflex tachycardia, and supersensitivity to exogenous

C
Connective Tissue Disease 445
vasopressor drugs (Pinsky and DiGeorge 1966). Pupil-lary responses to cocaine are absent, yet preservedwith epinephrine instillation into the conjunctival sac,also suggesting sympathetic denervation (Indo 2002).Subcutaneous injection of cholinergic methacholine orneostigmine in a dosage that would normally inducetearing does not result in lacrimation in CIPA patientsalthough emotional tearing is preserved (Pinsky andDiGeorge 1966).Thedeficiency in pain and temperatureperception and insweating can be explained by the bioptic findings of ab-senceofsmallmyelinatedandunmyelinatednervefibersin the cutaneous branch of the radial nerve and a sig-nificant reduction of these fibers in the sural nerve (forreview see Indo 2002).Skin biopsies show preserved sweat glands but absentinnervation with loss of unmyelinated sudomotor fibers(for review see Indo 2002).Absence of intradermal C- and A-delta fibers appears tobe the morphological basis of insensitivity to pain andanhidrosis (for review see Indo 2002).Verzé et al. found no nerve branches or endings in theepidermis and only a few nerve fibers in deeper layersof the dermis (for review see Indo 2002).Autopsy of one CIPA patient showed absence of smallneurons in dorsal root ganglia, absence of small nervefibers in the dorsal roots, absence of Lissauer’s tract andpaucity of small fibers in thespinal tractof the trigeminalnerve (Swanson et al. 1965), i.e. lack of afferent pain andtemperature mediating structures (Swanson 1963).The genetic basis for CIPA are not mutations in thegenes encoding � neurotrophins, but mutations in thegene encoding the � tyrosine kinase A receptor (TRKA/NTRK1) located on chromosome 1 (1q21-q22) (Indo etal. 1996).So far, 37 mutations have been identified in CIPA pa-tients of various ethnicities (Indo 2002).The similarities of anatomical and clinical changes inTrkA knockout mice and in CIPA patients led Indo andco-workers to the discovery that mutations of the trkA(NTRK1) gene are the genetic basis of CIPA. DefectNGF signal transduction at the trkA receptor causesfailure to survive and probably apoptosis of developingsmall nerve fiber neurons (Indo et al. 1996; Indo 2002).The only tool for prenatal diagnosis of CIPA is the iden-tification of trkA (NTRK1) mutations (Indo 2002) butthere are numerous mutations which prevents simpleDNA diagnosis of the disease (Axelrod 2002).There is no specific therapy, but treatment remains sup-portive and attempts to control hyperthermia, to preventinjuries, self-mutilation and orthopedic or dental com-plications and to modify behavioral problems such ashyperactivity or rages (Axelrod 2002).
References1. Axelrod FB (2002) Hereditary sensory and autonomic neu-
ropathies. Familial dysautonomia and other HSANs. Clin AutonRes 12 Suppl 1:I/2–I/14
2. Bodner L, Woldenberg Y, Pinsk V et al. (2002) Orofacial man-ifestations of congenital insensitivity to pain with anhidrosis: areport of 24 cases. ASDC J Dent Child 69:293–296
3. Dyck PJ (1993) Neuronal atrophy and degeneration predomi-nantly affecting peripheral sensory and autonomic neurons. In:Dyck PJ, Griffin PK, Low PA et al. (eds) Peripheral Neuropathy.WB Saunders, Philadelphia, pp 1065–1093
4. Hilz MJ (2002) Assessment and evaluation of hereditary sensoryand autonomic neuropathies with autonomic and neurophysio-logical examinations. Clin Auton Res 12 Suppl 1:I33–I43
5. Hilz MJ, Stemper B, Axelrod FB (1999) Sympathetic skin re-sponse differentiates hereditary sensory autonomic neuropathiesIII and IV. Neurology 52:1652–1657
6. Indo Y (2002) Genetics of congenital insensitivity to pain with an-hidrosis (CIPA) or hereditary sensory and autonomic neuropathytype IV. Clinical, biological and molecular aspects of mutationsin TRKA (NTRK1) gene encoding the receptor tyrosine kinasefor nerve growth factor. Clin Auton Res 12 Suppl 1:I20–I32
7. Indo Y, Tsuruta M, Hayashida Y et al. (1996) Mutations in theTRKA/NGF receptor gene in patients with congenital insensitiv-ity to pain with anhidrosis. Nat Genet 13:485–488
8. Pinsky L, DiGeorge AM (1966) Congenital familial sensory neu-ropathy with anhidrosis. J Pediatr 68:1–13
9. Shorer Z, Moses SW, Hershkovitz E et al. (2001) Neurophysio-logic studies in congenital insensitivity to pain with anhidrosis.Pediatr Neurol 25:397–400
10. Swanson AG (1963) Congenital insensitivity to pain with an-hidrosis. Arch Neurol 8:299–306
11. Swanson AG, Buchan GC, Alvord EC (1965) Anatomic changesin congenital insensitivity to pain. Arch Neurol 12:12–18
Congenital Sensory Neuropathy withAnhidrosis
� Congenital Insensitivity to Pain with Anhidrosis
Conjunctival Injection
Definition
Redness of the conjunctiva (white) of the eye.� Hemicrania Continua
Connective Tissue Disease
Definition
The autoimmune disease is characterized by an abnor-mal structure or function of one or more of the elementsof connective tissue, i.e. collagen, elastin, or the mu-copolysaccharides, including, for example, rheumatoidarthritis, systemic lupus erythematosus, scleroderma.� Vascular Neuropathies

446 Connective Tissue Manipulation
Connective Tissue Manipulation
Definition
A superficial form of myofascial manipulation is thesimple definition of connective manipulation. It in-volves manipulating the skin and superficial connectivetissues above muscle to achieve reflex and local effects,which is believed to be based on a viscerocutaneous re-flex. Reflex reactions include vasodilatation and diffuseor localized increase in sudomotor activity.� Chronic Pelvic Pain, Physical Therapy Approaches
and Myofascial Abnormalities
Conscious Laparoscopic Pain Mapping
� Chronic Pelvic Pain, Laparoscopic Pain Mapping
Conscious Pain Mapping
� Chronic Pelvic Pain, Laparoscopic Pain Mapping
Consciousness and PainC. RICHARD CHAPMAN, YOSHIO NAKAMURA
Pain Research Center, Department of Anesthesiology,University of Utah School of Medicine, Salt Lake City,UT, [email protected]
Synonym
Awareness
Definitions
Pain as Conscious Experience
Pain is the unique meaning of a tissue injury event thatthe brain, as a � complex adaptive system, constructs.Pain emerges from large scale patterns of brain activitythat reflect sensory, emotional and cognitive processing.As it is an aspect of consciousness, pain is distinct from� nociception.
Consciousness
Consciousness is an emergent, self-organizing featureof brain activity that makes complex, adaptive interac-tions with the internal and external environments andself-reference in thoseenvironmentspossible (Chapmanand Nakamura 2003).
Complex Adaptive System
A complex adaptive system is a large set of units thatinteract with each other and with an external environ-ment, to produce overall patterns that are significantlymore complex than the behaviors of the individual en-tities comprising the system. A complex adaptive sys-tem changes according to three key principles: order isemergent as opposed to predetermined, thesystem’s his-tory is irreversible, and the system’s future is often un-predictable. Simpler complex systems nest within moreelaborate complex systems (Morowitz and Singer 1995;Dooley 1996).The essence of a complex adaptive system is that itorganizes itself to optimize its adaptation to its envi-ronment. Its dynamic instability gives it the flexibilityit needs to accommodate quickly to environmentalchange. Complex adaptive systems are dynamic in thatthey constantly change and adjust to disturbances. Sucha system does not always undergo linear changes whenit reorganizes to accommodate a disturbance; instead,it may demonstrate abrupt transitions in organizationalpatterns known as state transitions.
Self-Organization� Self-organization is a process whereby a pattern atthe global level of a system emerges solely from inter-actions among lower-level components of the system.The global pattern is an emergent property of the sys-tem itself. A self-organizing, adaptive system tendsto take on life-like qualities such as self-directedness,self-correction, self-preservation, and intelligence (Ca-mazine et al. 2001).
Emergence� Emergence is the process by which a system ofinteracting elements spontaneously acquires a qualita-tively new pattern and structure, which is unpredictablefrom knowledge of the individual elements (Camazine,et al. 2001). For example, combining hydrogen andoxygen gases at room temperature produces liquidity.
Intentionality
A complex adaptive system has � intentionality when itexhibits directedness toward some future state or goal.Intentcomprises theendogenousinitiation, constructionand direction of perception, action and goal-directed be-havior (Freeman 1995; 2000).
Schemata
A � schema is a perceptual hypothesis that serves asthe fundamental unit for constructing awareness (Mar-cel 1983). � Schemata are fuzzy, preconscious anddynamical patterns, roughly related to dynamically sta-ble patterns in neural networks (Rumelhart et al. 1986).The brain, as a complex adaptive system, adapts to theworld and the body in which it dwells, by constantlyforming, evaluating, and refining these global percep-tual hypotheses. Ongoing awareness of the body and the

C
Consciousness and Pain 447
world depends upon a continual process of reconstruc-tion based on schemata. Simpler schemata nest withinmore complex schemata (for review see Martin 1994).
Characteristics
Pain and Nociception
Pain is an unpleasant, compelling aspect of somaticawareness. Like other aspects of consciousness, it isemergent, dynamic, intentional and constructed. Also,likeother aspectsof consciousness,pain is theproductofthe brain operating as a pattern forming, self-organizedcomplex adaptive system.Nociceptive traffic within the nervous system has manyconsequences (Willis and Westlund 1997; Craig 2003).Nociception is a reflexive motor stimulus and a triggerfor autonomic arousal. In addition to activating sensoryprocesses, nociceptive traffic activates the limbic brainvia multiple pathways. Functional brain imaging stud-ies reveal that complex patterns of processing occurin mesencephalic, limbic and cortical structures dur-ing the emergence of pain as a conscious experience.These processes appear to be complex, dynamic self-organization that makes the construction of subjectiveexperience possible (Kelso and Fuchs 1995). Nocicep-tion is normally necessary, but not sufficient, for pain,which as an aspect of consciousness is an emergentfeature of brain activity.Properties of consciousness in general are also proper-tiesofpain.Theseproperties include thefollowing.Con-sciousness:
• Is personal, with a necessarily limited point of view;• Has mental contents that are stable for short periods
and vary over longer intervals;• Has mental contents that are unified at any one mo-
ment and continuous over time;• Is selective, with a foreground and background, and
has a limited capacity at a given moment;• Is intentional because it is directed at the world or the
body.
Pain and the Construction of Consciousness
The brain deals, not with reality as the physical sci-ences study it, but rather with an internal, autonomousrepresentation of reality that it builds and revises frommoment to moment, using sensory information andschemata that involve networks of association inmemory. Subjective reality undergoes constant self-organized revision, which integrates sensory infor-mation, emotion, ratiocination and other aspects ofcognition to produce meaning. Therefore, brain rep-resentations of external objects and bodily events aredynamic constructions, not replications, of the externalworld or the body (Mountcastle 1998). Pain is not astatic entity that an individual possesses, but rather adynamic construction of bodily awareness, typicallybased on nociception.
The construction of consciousness, at any given mo-ment, proceeds in response to the intentional and situa-tional imperatives of each person. The intentionality ofthe person perceiving, feeling and emoting constrainsand drives the construction of consciousness (Free-man 2000). This process involves integrating sensorysignals, memory and prior experience, expectations, andimmediate and long-term goals and plans. It weaves allof these into a coherent, stable macro-emergent-patternthat seems to underlie awareness of the world and one’sself. Far from being a passive entity that merely registersinformation coming in from various sensory channels,the brain is an active, adaptive system that constantlymodels the world and the body in which it dwells.This modeling can change gradually from moment tomoment or in abrupt state transitions.
Acute versus Chronic Pain
In the consciousness studies framework, pain is a state ofthe brain. Nociceptive signaling from acute tissue injurycan perturb the complex adaptive system and force non-stable reorganization. It tends to provoke a state transi-tion from ordinary purposeful activity focused on im-mediate goals or needs, to somatic preoccupation andprotection. However, the system will tend to return toits normal, habitual patterns when the nociception de-creases or terminates.When pain becomes chronic, the complex adaptive sys-tem undergoes reorganization to a stable, global statecharacterized by low dynamic instability that makes thesystem resistant to change. The stable state is a complexadaptation to the physical health of the body, the socialenvironment and role expectations, interpersonal rela-tionships, and mood. Patients tend to demonstrate so-matic preoccupation, conservation ofenergy, and illnessbehavior.The consciousness studies perspective holds thatchronic pain is difficult to treat, because an effectiveintervention must do more than eliminate the elementof nociceptive signaling. It must disturb the complexadaptive system sufficiently to permit adaptive reorga-nization to a stable state of well-being, normal functionand optimal somatic awareness. The termination ofnociceptive activity often fails to disturb the systemsufficiently to enable reorganization in the desired di-rection. Psychological intervention, social adjustmentsand increased physical activity are often necessaryadjuncts for chronic pain therapy, because the syner-gistic effect of these combined has a better chance ofperturbing the complex adaptive system than a singleintervention alone.
Individual Differences
Individuals differ markedly from one another in thepain they experience in response to virtually identicaltissue trauma. Although this stems in part from ge-netic factors that influence nociceptive transduction

448 Consolidated Standards of Reporting Trials Statement
and/or transmission, most inter-individual variance re-flects each individual’s unique construction of the painexperience. Personal past experience and personal in-terpretation of the immediate situation generate highlyvaried schemata, and these in turn construct highly in-dividual personal experiences of pain. Put more simply,pain is the unique meaning of a tissue injury event thatthe brain, as a complex adaptive system, constructs.Different people construct different meanings in highlysimilar tissue injury situations.
Culture and Pain
Conscious experience is subject to cultural influencesbecause the brain, as a complex adaptive system, is em-bedded within larger social and cultural complex adap-tive systems. Consequently, cultural meaning systemsmay determine the possible range of states of conscious-ness.Someculturesmay predispose those they influenceto experience pain differently than others in a particularsituation.
Pain Measurement
As pain is a personal experience, subjective report is theonly way to access it.Conventional� pain measurementpractice assumes that patients and research subjects canexercise introspection to gauge the magnitude of somefeature of pain, assign numbers accordingly, and reportsuch numbers without bias. In principle, different peo-ple reporting pain should use a common scale. From theconsciousness studies perspective, pain is the meaningof an injury event that the brain constructs. In contrivedresearch contexts, pain reports behave more or less asconventional practice requires, albeit with substantialmeasurement error. It is less clear if clinical pain states,as personal meanings, possess the assumed feature ofnumerical scalability. Future progress in pain measure-ment must reexamine conventional assumptions aboutpain measurement, recognize the uniqueness of con-scious individual experience as meaning, and evolveimproved methods for pain assessment (Nakamura andChapman 2002).
References1. Camazine S, Deneubourg J, Franks NR, Sneyd J, Theraulaz G,
Bonabeau E (2001) Self-Organization in Biological Systems.Princeton Univ Press
2. Chapman CR, Nakamura Y (2003) Feeling Pain: A Construc-tivist Perspective. In: Kalso E, Estlander A, Klockars M (eds)Psyche, Soma and Pain. The Signe and Ane Gyllenberg Foun-dation, Helsinki, Finland, pp 115–123
3. Craig AD (2003) Interoception: The Sense of the PhysiologicalCondition of the Body. Cur Opin Neurobiol 13:500–505
4. Dooley K (1996) A Nominal Definition of Complex AdaptiveSystems. The Chaos Network 8:2–3
5. Freeman WJ (1995) Societies of Brains: A Study in the Neuro-science of Love and Hate. Erlbaum L (ed) Hillsdale, New Jersey.
6. Freeman WJ (2000) How Brains Make Up Their Minds.Columbia University Press, New York
7. Kelso JAS (1995) Dynamic Patterns: The Self-Organization ofBrain and Behavior. MIT Press, Cambridge, MA
8. Marcel A (1983) Conscious and Unconscious Perception: Ex-periments on Visual Masking and Word Recognition. CognitivePsychology 15:197–237
9. Martin B (1994) The Schema. In: Cowan G, Pines D, MeltzerD (eds) Complexity: Metaphors, Models and Reality. Addison-Wesley, Reading, MA, pp 263–285
10. Morowitz HJ Singer JL (1995) The Mind, the Brain, and ComplexAdaptive Systems. Morowitz H, Singer JL (eds) Addison-WesleyPub. Co., Reading, Mass, p 237
11. Mountcastle VB (1998) Brain Science at the Century’s Ebb.Daedalus vol 127:1–36
12. Nakamura Y, Chapman CR (2002) Measuring Pain: An Intro-spective Look at Introspection. Conscious Cognition 11:582–592
13. Rumelhart DD, Smolensky P, McClelland JL, Hinton GE (1986)Schemata and Sequential Thought Processes in PDP Models. In:McCleeland JL, Rumelhart DE (eds) Parallel Distributed Pro-cessing: Explorations in the Microstructure of Cognition, vol 2:Psychological and Biological Models. MIT press, Cambridge,MA, pp 7–57
14. Willis WD, Westlund KN (1997) Neuroanatomy of the Pain Sys-tem and the Pathways that Modulate Pain. J Clin Neurophys-iol 14:2–31
Consolidated Standards of ReportingTrials Statement
� CONSORT Statement
CONSORT Statement
Synonyms
Consolidated standards of reporting trials statement
Definition
A group of scientists and editors developed the CON-SORT (Consolidated Standards of Reporting Trials)statement to improve the quality of reporting of clinicaltrials. The statement consists of a checklist and flowdiagram that authors can use for reporting a trial. Manyleading medical journals and major international edito-rial groups have adopted the CONSORT statement. TheCONSORT statement facilitates critical appraisal andinterpretation of trials by providing guidance to authorsabout how to improve the reporting of their trials.� Central Pain, Outcome Measures in Clinical Trials
Constitutive Gene
Definition
A gene that is continuously expressed without regula-tion, i.e. the transcription can be neither suppressed norencouraged. Constitutive genes often encode proteinswith housekeeping functions.� COX-1 and COX-2 in Pain� NSAIDs, Adverse Effects

C
Contingent Negative Variation 449
Construction of Consciousness
Definition
The construction of consciousness, at any given mo-ment, proceeds in response to the intentional and situa-tional imperatives of each person. The intentionality ofthe person perceiving, feeling and emoting constrainsand drives the construction of consciousness. Thisprocess involves integrating sensory signals, memoryand prior experience, expectations, and immediate andlong-term goals and plans. Far from being a passiveentity that merely registers information coming in fromvarious sensory channels, the brain is an active, adaptivesystem that constantly models the world and the bodyin which it dwells.� Consciousness and Pain
Contact Stimulator
Definition
The most commonly used heat/cold contact stimulatorsrely on the Peltier principle (a thermoelectric effect inwhich passage of an electric current through a junctionbetween two different solids causes heat to be producedor absorbed at that junction, according to the directionof current).� Pain in Humans, Thermal Stimulation (Skin, Muscle,
Viscera), Laser, Peltier, Cold (Cold Pressure), Radi-ant, Contact
Contemplation
Definition
A readiness to change stage, in which a person recog-nizes the potential importance of making a change in be-havior, but has not yet made a commitment to changingbehavior.� Motivational Aspects of Pain
Contextual Factors
Definition
Contextual factors consist of two components: Environ-mental factors and personal factors. Contextual factorsare factors that together constitute the complete contextof an individual’s life, and in particular the backgroundagainst which health states are classified in ICF.� Disability and Impairment Definitions
Contingencies
Definition
Contingencies are events that occur in response to be-havior. According to the operant model, contingenciescan be reinforcing, punishing, or neutral with respectto their effects on behavior. Reinforcing contingenciesstrengthen (increases the probability of future occur-rence of) behavior, punishing contingencies weakenbehavior, and neutral contingencies have no impact onthe future occurrence of behavior.� Cognitive-Behavioral Perspective of Pain� Motivational Aspects of Pain
Contingencies of Reinforcement
Definition
The nature of the responses that the behaviors of indi-viduals elicit from significant people in their environ-ment. Patterns of reinforcementwill influence theoccur-rence or nonoccurrence of behaviours, with reinforce-ment leading to an increase in the behaviors and punish-ment contributing to a reduction in behaviors. The prox-imity, strength, desirability, and frequency of responsesby others will influence the behaviors.� Cognitive-Behavioral Perspective of Pain� Motivational Aspects of Pain
Contingency Management
Definition
A system in which an individual’s successful task com-pletion is consistently rewarded.� Chronic Pain in Children, Physical Medicine and Re-
habilitation� Training by Quotas
Contingent Negative Variation
Synonyms
CNV
Definition
The CNV is a negative slow cortical potential that is typ-ically observed between a warning signal and a follow-ing imperative signal requiring a response. The CNV re-flects attention, arousal, expectancy and response prepa-ration. For time intervals between the warning and theimperative signal that exceed 3 sec, an early CNV com-ponent during the first 500 ms after the warning signal,

450 Continuous Video-Tape Recordings
and a late CNV component starting at about 1 sec priorto the imperative signal, can be distinguished. The earlyCNV component presumably reflects an orienting re-sponse and contingency processing, while the late CNVis closely related to response preparation. In migraine,an enhanced CNV amplitude and an impaired habitu-ation of the CNV have been observed, which has beeninterpreted as evidence for abnormal cortical informa-tion processing in migraine.� Modeling, Social Learning in Pain� Psychological Treatment of Pain in Children
Continuous Video-Tape Recordings
Definition
Non-stop recordings of animals’ spontaneous behaviorvia a telecamera connected to a time-lapse videotapewith a wide range (3-960 hr/tape) of recording/readingspeeds. This system allows a detailed analysis of ani-mals’ movements. An infrared lighting system permitsfilming during the dark phase (8:00 p.m. – 8:00 a.m.)(Giamberardino et al. 1995)� Visceral Pain Model, Kidney Stone Pain
Contract-Release
Definition
Contract-release isamanual techniqueused for the treat-ment of myofascial trigger points that can serve as a pa-tient self-treatment. It is a repeated series of brief (2 or3 seconds), gentle (10% of maximum effort), voluntarycontractions of the muscle harboring the trigger point.This is followed immediately by either passive or activestretching of the same muscle.� Myofascial Trigger Points
Contracture
Definition
Involuntary muscle contractions are called contrac-ture. There are three types of contractures: antalgiccontractures, painful contractures and myotactic con-tractures. Antalgic contractures mainly consist of acompensating phenomenon, related to a polysynapticreflex, secondary to pain (for example the contractureof paraspinal muscles due to discal herniation), andusually last from several days to weeks. By contrast,painful contractures (also called contractures) includevarious types of cramps.
� Chronic Pain in Children, Physical Medicine and Re-habilitation
� Muscular Cramps
Contralateral
Definition
On or relating to the opposite side of the body.The output of the primary motor cortex is principallyto the opposite side of the body. Thus, to relieve painrestricted to one side of the motor cortex, the oppositeside is stimulated.� Motor Cortex, Effect on Pain-Related Behavior� Opioid Receptor Trafficking in Pain States� PET and fMRI Imaging in Parietal Cortex (SI, SII, In-
ferior Parietal Cortex BA40)� Spinothalamocortical Projections from SM
Controlled Trial
Definition
A clinical trial that compares the effect of the drug tobe tested with either a standard treatment or a placebotreatment.� Antidepressants in Neuropathic Pain
Contusion
Definition
A hematoma or bruise.� Spinal Cord Injury Pain Model, Contusion Injury
Model
Conus medularis DREZ
� DREZ Procedures
Conventional TENS
Definition
The delivery of TENS to stimulate selectively large di-ameter non-noxious cutaneous afferents, without con-currentlyactivatingsmalldiameternociceptiveafferentsor muscle efferents. This is achieved by high frequency(50 – 120 Hz), low (sensory) intensity pulsed currentsto generate a ’strong but comfortable’ non-painful elec-trical paresthesia.

C
Coordination Exercises in the Treatment of Cervical Dizziness 451
� Transcutaneous Electrical Nerve Stimulation Out-comes
� TranscutaneousElectricalNerveStimulation(TENS)in Treatment of Muscle Pain
Convergent
Definition
Characteristic of the receptive field size increase at eachsynaptic relay level, because ascending projections con-verge onto a single neuron in the subsequent synaptic re-lay. Like a single ganglion cell receives input from sev-eral primary afferents.� Postsynaptic Dorsal Column Projection, Functional
Characteristics
Conversion Disorder
Definition
One or more symptoms occur, involving voluntary mo-tor or sensory functions that suggest a neurological orgeneral medical condition (e.g. inability to move an armor leg). The beginning or worsening of the symptomsmust be linked to a psychological stressor. In children,pseudoseizures are the most common conversion dis-order manifestation. Conversion Disorders occur morefrequently in girls than boys, and more frequently post-puberty than pre-puberty.Unlikeadultswith ConversionDisorderwho showLaBelle Indifference,childrenshowconcern for their symptoms.� Somatization and Pain Disorders in Children
Coordination Exercises in the Treatmentof Cervical Dizziness
KJERSTI WILHELMSEN, ANNE E. LJUNGGREN
Section for Physiotherapy Science, Department ofPublic Health and Primary Health Care, Faculty ofMedicine, University of Bergen, Bergen, [email protected],[email protected]
Synonyms
Vestibular rehabilitation; Cawthorne and Cookseys’Eye-Head Exercises; vestibular compensation; vestibu-lar adaptation exercises;vestibularhabituationexercises
Definitions� Vestibular rehabilitation (VR) is a physiotherapyprogram for persons with symptomatic lesions ofthe vestibular system (Foster 1994). The program isdesigned to decrease � dizziness, improve balancefunction and increase activity level. It is based on ex-ercises to promote central � vestibular compensation(Herdman and Whitney 2000).� Vertigo is an illusory sensation of motion (rotational,translational or tilting of the visual environment) ofeither the self or the surroundings (Wrisley et al. 2000).Dizziness is a non-specific term that describes an alteredorientation in space, reflecting a discrepancy betweeninternal sensation and external reality, creating sensoryconflicts. The conflicts can occur between any of thevestibular, visual or somatosensory systems, or dizzi-ness may be caused by central problems involving theintegration and weighting of the different modalitiesand their relation to memory (Berthoz and Viaud-Delmon 1999). Dizziness may include sensations oflight-headedness, faintness, giddiness, unsteadiness,imbalance, falling, waving or floating (Wrisley et al.2000).Cervical vertigo can be defined as a syndrome of imbal-ance arising from disturbance of the cervical joint recep-tors and associated with a sensation of dizziness (Brown1992). Cervical dizziness is a non-specific sensation ofaltered orientation in space and disequilibrium originat-ing from abnormal afferent activities in the neck (Wris-ley et al. 2000).
Characteristics
Cervical Vertigo
A large number of patients seek physiotherapy for neck-associated disorders (Clendaniel 2000). Different syn-onyms exist, but commonly used terms are cervical ver-tigo and cervical dizziness. According to the definitionsgiven, the two concepts seem to reflect the same type offunctional problems from the patient’s point of view.Cervical vertigo is described as a condition of dizzinessfollowing neck trauma, usually caused by flexion-extension movement of the neck (cf. whiplash trauma).Neck pain is associated with the injury and precedesall other symptoms (Brown 1992; Wrisley et al. 2000).True vertigo, which is found in patients with acutevestibular conditions, is rare in patients with cervicalvertigo (Brown 1992). The sensation of dizziness isvague and non-specific in character; the same type ofdizziness is often described by patients with chronicvestibular deficits and by patients with neurologicaldisorders (Clendaniel 2000). Patients may use wordslike light-headedness, faintness, giddiness, unsteadi-ness, imbalance, falling, waving and floating. Othersymptoms are disequilibrium, ataxia, limited rangeof motion in the cervical region (Clendaniel 2000)and disturbance of vision (Tjell 2001). It is a common

452 Coordination Exercises in the Treatment of Cervical Dizziness
experience to find that head movements and / or move-ments in the environment, aggravate the visual problem.Headache and tinnitus as well as hearing loss may alsobe present (Brown 1992; Clendaniel 2000). Accord-ing to some authors, cervical vertigo is classified as acentral vestibular disorder (Whitney and Rossi 2000).There is dispute as to whether the condition exists asan independent diagnosis; no definite diagnostic test isavailable (Wrisley et al. 2000). Diagnosis is inferredfrom the patient’s history in conjunction with exclusionof other causes.The cause of cervical vertigo is still debated (Clen-daniel 2000). It has been proposed to be a subset ofpost-concussion syndrome (Brown 1992). Patientswith cervical dizziness usually have normal responseson vestibular function tests, with the exception of pos-turography (Clendaniel 2000; Wrisley et al. 2000).There seems to be consensus regarding the neck’scontribution to postural control and balance (Brown1992; Clendaniel 2000; Karlberg et al. 1996), but con-troversies as to whether cervical mechano-receptordysfunction contributes to dizziness and influences thefunction of the vestibular system (Brown 1992; Clen-daniel 2000). Neck receptors have a role in eye-headco-ordination through the cervico-ocular reflex and inthe perception of balance, according to Brown (1992).Focus on dizziness and balance may therefore be ofinterest for patients with cervical vertigo.Traditionally, treatment of cervical vertigo has beendirected towards relieving pain and consequences ofpain (Furman and Whitney 2000). Karlberg et al (1996)have shown that an intervention consisting of traditionalphysiotherapy aimed at reducing cervical discomfort,also managed to decrease the frequency and intensity ofdizziness. Exercises intended to reduce dizziness mayenhance these effects.
Vestibular Rehabilitation (VR)
VRwasdevelopedinEnglandinthe1940sbyCawthorneand Cooksey. Patients with post-concussion syndromeand vestibular deficiencies were introduced to exercisesdesigned to train the eyes, muscle and joint sense tocompensate for vestibular dysfunction and to restorebalance (Cooksey 1946). The program incorporatedhead and neck exercises, which the patient practiced indifferent starting positions (Dix 1974).Today’s approaches can be traced back to the treatmentprinciples developed in England. Increased knowl-edge of the brain’s ability to compensate for deficientstructures, along with development of theories of motorcontrol and learning, have given rise to an understandingof the vestibular compensatory mechanisms as learningprocesses. Vestibular compensation is the process bywhich vestibular symptoms are brought to resolution.The patient may take advantage of different strategies inthe compensatory process. The overall goal of the pro-cess is to achieve stability of gaze and postural control,
in static as well as more challenging dynamic situa-tions. Complete recovery depends on the restoration ofsymmetry between the incoming signals to the differentcomponents constituting the balance system, i.e. vision,somatosensory and vestibular systems (Luxon 1997).The central compensatory process seems to involveboth physical and chemical changes in the brain. It canbe divided into acute and chronic stages (Herdman andWhitney 2000). Four neurophysiological mechanismsare described. � Tonic rebalancing (spontaneous, phys-iological process by which the system tries to restoresymmetry at the level of the vestibular nuclei) is themost important process in the acute stage. Vestibu-lar adaptation (the long-term adjustments in the basicvestibulo-ocular and vestibulo-spinal reflexes) andvestibular habituation (the long-term reduction in theneurological responses to a noxious stimulus) (Shepardand Telian 1996) are compensatory processes in thechronic phase. Vestibular adaptation and habituation arefacilitated by error signals, i.e. dizziness, which can bebrought on in different ways. The facilitating stimulusin adaptation is termed � retinal slips, i.e. movementsof images across the retina. The error signal is broughton by a combination of visual fixation and head move-ments. The brain tries to minimize the error signalby increasing the gain of the vestibulo-ocular reflexes(Herdman and Whitney 2000). With habituation, dizzi-ness is provoked by repeated exposure to movementsprovoking it, that is performance of certain movementswill produce dizziness (Shepard and Telian 1996). Thelast mechanism described is substitution, i.e. alterna-tive strategies are chosen to compensate for deficientvestibular functions. The latter mechanism comes intoaction when optimal compensation is lacking.In the acute phase, compensation (the tonic rebalancingprocess) is a pathophysiological process occurring in-dependently of the patient’s activities. In the so-calledchronic phase, activities and exposure to visual input arenecessary pre-requisites in order to keep up the recoveryprocess. For some patients, a systematic and structuredprogram of exercises often referred to as vestibular re-habilitation (VR), may be required to enhance the com-pensatory process in the chronic stages. Based on theunderlying neurophysiological understanding of com-pensatory processes, two majorapproaches to VRcanbeidentified. The exercise strategies are founded on eitheradaptation or habituation, but in clinical practice therearenoclear-cutbordersbetweenthe twoapproaches.Ba-sically, if there is a visually provoked vertigo, exercisesthat promote adaptation might be choice number one,whilehabituationmaybeusedwithpatientswhosedizzi-ness primarily is produced by a change in head and / orbodily positions.Examples of gaze adaptation exercises are: Exercise 1:look at a stationary target placed on the wall. Move thehead from side to side as fast as possible, keeping the tar-get in focus. Repeat after a short rest, moving the head up

C
Coping 453
and down, and Exercise 2: hold a card in the hand at arm-length. Move the head and card in opposite directions,again keeping the target in focus. Exercise 1 can alsobe performed holding a card in the hand. This reducesthe distance between the eyes and target and stresses an-other part of the visual-vestibular system. Varying thetasks with regards to tempo, starting-positions and sur-roundings are ways to progress, the guiding lines shouldalways be the patient’s ability to keep the visual targetin focus (Herdman and Whitney 2000).A program of habituation exercises involves exposingthe patient to positional changes that cause dizziness.Systematic assessment of various positional changesshould be carried out and movements provoking thedizziness make up the program. If, in lying, turningfrom supine and on to the side provokes dizziness, thismovement should be included in the patient’s program.The actual number of movements included should notexceed 3–4 at the time (see Shepard and Telian 1996).There seem to be only a few articles describing the useof VR in the treatment of cervical vertigo. Wrisley et al.(2000) present the successful treatment of two patientswith cervical dizziness having used a combination oftraditional physiotherapy (such as ice treatment, mas-sage, mobilisation and exercises) to decrease pain andincrease the range of movement, VR in the form of adap-tation (exercises 1 and 2 as presented above)and balanceexercises. Tjell (2001) uses a habituation approach inthe treatment of whiplash-associated disorders. Theprogram comprises gaze and walk-gaze exercises andprogression is based on the patient’s experience of painfollowing each treatment session. It is a slow process,but improvement in pain and dizziness is reported. Aprogram with special focus on eye-neck coordinationwas administered to a group of patients with chronicneck pain (Revel et al. 1994). The aim of the programwas to improve neck proprioception and to decreasepain and discomfort. The program included passive andactive movements of eye and head, gaze stability andcervical repositioning exercises. The exercises wereperformed in different starting positions over a periodof 8 weeks. The authors suggest that the program couldbe useful for patients with cervical vertigo.It is our experience that a comprehensive approach isneeded in the rehabilitation of patients with cervicalvertigo. Reports from patients indicate optimal com-pensation in situations with few challenges, i.e. settingswhere the head and thus vision can be kept stable. Inmore dynamic and thus demanding surroundings, theimpression of a condition of disablement still exists andmany patients choose a sedentary lifestyle to avoid thedizziness. A rehabilitation program should thereforechallenge dizziness through specific as well as gen-eral activity. Our program consists of group treatmentbased on a cognitive behavioural approach promotingdirect and indirect learning processes (Bandura 1986).Adaptation, habituation and balance exercises as well
as relaxation techniques are included. Every-day activi-ties that provoke dizziness are emphasised as importantand necessary premises for compensation. The signifi-cance of having a focus on body awareness as describedelsewhere in this volume (see � Body Awareness Ther-apies), is stressed throughout the program. Alterationin body alignment in general as well as specifically inthe cervical region might be a pre-requisite for allowingchanges in the other systems responsible for balance.
References1. Bandura A (1986) Models of human nature and causality. So-
cial foundation of thought and action, a social cognitive theory.Prentice-Hall, New Jersey, pp 1–46
2. Berthoz A, Viaud-Delmon I (1999) Multisensory integration inspatial orientation. Curr Opin Neurobiol 9:708–712
3. Brown JJ (1992) Cervical contribution to balance: cervical ver-tigo. In: Berthoz W, Graf P, Vidal P (eds) The head-neck sensorymotor system. Oxford University Press, New York, pp 644–647
4. Clendaniel RA (2000) Cervical vertigo. In: Herdman SJ (ed)Vestibular rehabilitation. F.A. Davies, Philadelphia, pp 494–509
5. Cooksey FS (1946) Rehabilitation in vestibular injuries. Proc RSoc Med 39:273–277
6. Dix MR (1974) Treatment of vertigo. Physiotherapy 60:380–3847. Foster CA (1994) Vestibular rehabilitation. Baillieres Clin Neurol
3:577–5928. Furman JM, Whitney SL (2000) Central causes of dizziness. Phys
Ther 80:179–1879. Herdman SJ, Whitney SL (2000) Treatment of vestibular hy-
pofunction. In: Herdman SJ (ed) Vestibular rehabilitation. F.A.Davies, Philadelphia, pp 387–423
10. Karlberg M, Magnusson M, Malmstrom EM et al. (1996) Postu-ral and symptomatic improvement after physiotherapy in patientswith dizziness of suspected cervical origin. Arch Phys Med Re-habil 77: 874–882
11. Luxon L (1997) Vestibular compensation. In: Luxon L, Davies R(eds) Handbook of vestibular rehabilitation. Singular PublishingGroup, San Diego, pp 17–29
12. Revel M, Minguet M, Gregoy P et al. (1994) Changes in cervico-cephalic kinesthesia after a proprioceptive rehabilitation programin patients with neck pain: a randomized controlled study. ArchPhys Med Rehabil 75:895–899
13. Shepard NT, Telian SA (1996) Vestibular rehabilitation pro-grams. In: Shepard NT, Telian SA (eds) Practical managementof the balance disorder patient. Singular, San Diego, pp 169–185
14. Tjell C (2001) Cervicogenic vertigo: with special emphasis onwhiplash-associated disorder. In: Vernon H (ed) The cranio-cervical syndrome Mechanisms, assessment and treatment.Butterworth-Heinemann, Oxford, pp 231–243
15. Whitney SL, Rossi MM (2000) Efficacy of vestibular rehabili-tation. Otolaryngol Clin North Am 33:659–672
16. Wrisley DM, Sparto PJ, Whitney SL et al. (2000) Cervicogenicdizziness: a review of diagnosis and treatment. J Orthop SportsPhys Ther 30:755–766
Coping
Definition
Psychological or behavioral strategies invoked in orderto minimize the impact of specific stressors on an indi-vidual’ physical or emotional well-being.� Catastrophizing� Coping and Pain

454 Coping and Pain
� Psychological Assessment of Pain� Psychology of Pain, Assessment of Cognitive Vari-
ables
Coping and PainJENNIFER A. HAYTHORNTHWAITE
Johns Hopkins University, Baltimore, MD, [email protected]
Synonyms
Adaptation; coping strategies; coping style
Definition
Cognitive and behavioral efforts to manage pain or pain-related experiences, such as disability or negative mood.
Characteristics
How individuals cope with pain is a consistent predictorof various aspects of pain, including physical functionand psychological adaptation, with � catastrophizingbeing by far the most consistent correlate of pain-relatedphenomena. Much of the pain coping literature has astrong theoretical foundation in the larger literatureexamining how individuals cope with stress. Copingis usually defined as “constantly changing cognitiveand behavioral efforts to manage specific externaland/or internal demands that are appraised as taxingor exceeding the resources of the person” (Lazarusand Folkman 1984, p 141). Note that this definitionsuggests that intention underlies the efforts made by theindividual, and emphasizes a process that may or maynot be successful. Complex issues arise in determiningthe “adaptive” or “maladaptive” nature of any copingstrategy used to manage pain, and, when pain becomeschronic, coping attempts necessarily broaden to en-compass not only pain itself but also negative emotions,social connectedness, and pain-related disability acrossmultiple domains of function. A seemingly maladaptivecoping strategy at one point in time may be adaptiveat another time; similarly, an adaptive strategy in onedomain (e.g. physical function) may be maladaptive inanother domain (e.g. social function). For example, theperson with low back pain who spends the weekend inbed during a pain flare may experience less pain in theshort run, but may also become de-conditioned if thisuse of rest persists across weeks or months. Time spentin bed may reduce pain, but may endanger employmentor social relationships.
Style vs. Strategy
Specific coping styles – assimilative (active attempts toalter the situation to accomplish personal goals) vs. ac-commodative (revision of personal goals to accommo-date limitations or losses) – can interact with pain cop-
ing strategies and moderate important outcomes such asdisability and depression (Schmitz et al. 1996). In addi-tion to these clearly dispositional processes, much of theexisting literature uses measures of pain coping strate-gies that encompass an indeterminate time frame, andthereby measure general use of a strategy-style – as op-posed to specific use of a coping strategy at a given pointin time. While this approach has provided valuable dataon stylistic use of pain coping strategies, the loss of in-formation about the dynamic process of coping may ex-plain the inconsistencies in the literature. Recent tech-nologicaldevelopmentshaveoffered improvedmethodsfor assessing specific use of pain coping strategies withthedistinctpossibilityofdeterminingshort-termimpact.Since coping is inherently a dynamic process, daily di-aries (Keefeetal. 1997), and more recently electronicdi-aries(Petersetal.2000),arejuststartingtoyieldvaluableinformation about the interplay of coping, pain, mood,and disability over time. This technology also offers thepotential for identifying social interactions and environ-mental characteristics that influence these evolving pro-cesses.
Active vs. Passive Coping
Early conceptualizations of pain coping in rheuma-toid arthritis distinguished between active and passivecoping. Active coping strategies are strategies used todirectly control pain or pain-related dysfunction (e.g.distracting one’s attention), whereas passive strategiesrelinquish control to others or limit activities (Brownand Nicassio 1987; e.g. the use of rest). Althoughoriginally conceptualized as adaptive (active) vs. mal-adaptive (passive), more recent work has refined thischaracterization to include more detailed coping strate-gies that are associated with both positive and negativeadjustment, although the distinction between active andpassive coping remains valuable (Jensen et al. 2001).
Specific Pain Coping Strategies
Distraction, Ignoring Pain, or Distancing
Distraction – directing attention to something other thanpain – may be more useful for managing acute pain thanchronicpain (Boothby etal. 1999).Evenwith acutepain,however, distraction may not relieve the severe levelsof pain often seen in clinical settings (Haythornthwaiteet al. 2001). Although some studies indicate distractioncan improve function and well-being, others suggestdistraction correlates with greater pain, pain-relatedinterference and distress. Ignoring pain is conceptuallysimilar to distraction but focuses more on blocking outthe pain; it has been associated with lower ratings ofpain and improved pain-related functioning (Boothbyet al. 1999), as well as with perceptions that pain iscontrollable (Haythornthwaite et al. 1998). Ignoringpain is reported more frequently in individuals with

C
Coping and Pain 455
a longer duration of chronic pain (Peters et al. 2000),suggesting that this strategy may be one that increases asindividuals gain experience dealing with the challengesof chronic pain. Distancing includes thinking of thepain as outside one’s body (Robinson et al. 1997) andoverlaps with reinterpreting pain as another sensation(e.g. numbness). Although inconsistently related topositive outcomes, distancing may contribute to theperception that pain is controllable (Haythornthwaiteet al. 1998). Increases in the use of these strategies asseen following multidisciplinary treatment (Jensen etal. 2001), are consistent with the cognitive-behavioralformulation that these strategies are generally adaptive,and contribute to the individual’s perception that painis controllable.
Positive Coping Statements
Coping self-statements refers to the positive, encour-aging thoughts people use to manage pain. Certainstudies have found positive self-statements to be as-sociated with the perception that pain is controllable(Haythornthwaite et al. 1998); however, the positiveimpact of coping self-statements is not consistent acrossstudies. Recent reviews have concluded that positivecoping self-statements do not generally show a con-sistent relationship with reduced pain or improvedfunctioning (Boothby et al. 1999). However, thesecoping self-statements are an integral component ofmost psychological interventions for pain manage-ment, and show changes with treatment (Jensen etal. 2001).
Spirituality/Religiosity
Although spiritual beliefs and religious activities areoften used to cope with stress and painful chronic ill-nesses, this domain has generally received surprisinglylittle attention in the pain literature. Historically, theprimary method of measuring this domain has reliedon a subscale of the Coping Strategies Questionnaire(Rosenstiel and Keefe 1983) that assesses passiveprayerand hope. Higher scores on this scale are consistentlyassociated with greater pain severity, disability, anddistress across a number of studies. The measurementof praying and hoping has been empirically linked tocatastrophizing, probably due to the shared passivequality of these scales. Since this strategy may be aresponse to difficult times, longitudinal or diary studiesare needed to confirm its “maladaptive” function. Infact, more detailed assessments of day-to-day spiritual-ity as a coping strategy, have found that daily spiritualexperiences and positive spiritual coping are associ-ated with greater positive mood and lower negativemood, but this coping strategy does not impact on painreports (Keefe et al. 2001). Further research investigat-ing the spiritual dimensions of coping may discoverthat actively seeking spiritual experiences forms a keydimension of accepting pain.
Social Support
When social interactions, including some expressionsof pain, are intended to elicit help in managing pain orpain-related difficulties, these social interactions areconceptualized as coping strategies. The measurementof social support usually focuses on the individual’soverall perceptions of support, typically incorporatingtwo primary domains: instrumental support – the per-ception that the social environment provides resourcesor information, completes tasks to help the individual,or facilitates problem-solving; and emotional sup-port – the perception that the social network providessympathy, distraction, and sources of positive affect. Asis the case with other coping strategies, the beneficialand/or harmful effects of social support may differacross domains of functioning and may interact withother coping strategies, such as catastrophizing. Re-cent prospective analyses have indicated that perceivedsocial support predicted reductions in pain-relateddisability and depression over 5 months following alimb amputation (Jensen et al. 2002). Diary analysesprovid further details about the process by which thesechanges may transpire. Provision of social support is as-sociated with lower same-day negative mood and lowernext-day pain (Feldman et al. 1999). In the contextof high pain, social support reduced depressed moodon the next day, suggesting a buffering role for socialsupport. Very little research has examined what hap-pens during these supportive exchanges, but qualitativeinformation suggests that the sources of support areaffirming their commitment to help, encouraging activecoping – coping self-statements in particular – and dis-couraging helplessness and catastrophizing (Feldmanet al. 1999). These responses contrast with more generalsocial responses to pain that derive from the operantliterature and are conceptualized as negative, or punish-ing, responses to pain expression (i.e., anger, irritationor ignoring) from a significant other, or attentive andsolicitous responses (i.e., encouraging rest or takingover responsibilities), the latter being associated withpoorer adaptation following a limb amputation (Jensenet al. 2002).
Rest
Resting in response to pain is a pain coping strategy thatderives largely from the operant pain literature, and hasbeen consistently related to poorer outcomes (Jensen etal. 1991) when studied in heterogenous samples of pa-tients, typically seen in multidisciplinary specialty clin-ics. Most of the studies examining the deleterious effectsof rest on pain-related interference and mood are cross-sectional (Jensen et al. 2002). Although use of rest fol-lowing a limb amputation is not prospectively associ-ated with poorer function (Jensen et al. 2002), reduc-tions in rest are seen following multidisciplinary treat-ment and remain an important target for these interven-tions (Jensen et al. 2001).

456 Coping Repertoire
To date, coping research has focused on pain copingstrategies that influence pain and pain-related outcomes.Little attention, however, has been paid to the possibilitythat strategies for managing pain-related disability ornegative mood are likely to differ from strategies formanaging pain, or that people suffering from chronicpain may not report use of these strategies when ori-ented to describe how they cope with pain. Recentdata indicating that the use of pain coping strategiesdiffers by pain duration (Peters et al. 2000) and site ofpain (Heinberg et al. 2004), highlight the difficulties ofsummarizing this complex literature across these, andother yet to be identified, dimensions.
References1. Boothby JL, Thorn BE, Stroud MW, Jensen MP (1999) Coping
with Pain. In: Gatchel RJ, Turk DC (eds) Psychosocial Factorsin Pain. Guilford Press, New York, pp 343–359
2. Brown GK, Nicassio PM (1987) Development of a Questionnairefor the Assessment of Active and Passive Coping Strategies inChronic Pain Patients. Pain 31:53–64
3. Feldman SI, Downey G, Schaffer-Neitz R (1999) Pain, Nega-tive Mood, and Perceived Support in Chronic Pain Patients: ADaily Diary Study of People with Reflex Sympathetic DystrophySyndrome. J Consult Clin Psychol 67:776–785
4. Haythornthwaite JA, Lawrence JW, Fauerbach JA (2001)Brief Cognitive Interventions for Burn Pain. Ann BehavMed 23:42–49
5. Haythornthwaite JA, Menefee LA, Heinberg LJ, Clark MR(1998) Pain Coping Strategies Predict Perceived Control OverPain. Pain 77:33–39
6. Heinberg LJ, Fisher BJ, Wesselmann U, Reed J, HaythornthwaiteJA (2004) Psychological Factors in Pelvic/Urogenital Pain: TheInfluence of Site of Pain versus Sex. Pain 108:88–94
7. Jensen MP, Ehde DM, Hoffman AJ, Patterson DR, CzernieckiJM, Robinson LR (2002) Cognitions, Coping and SocialEnvironment Predict Adjustment to Phantom Limb Pain.Pain 95:133–142
8. Jensen MP, Turner JA, Romano JM (2001) Changes in Beliefs,Catastrophizing, and Coping are Associated with Improve-ment in Multidisciplinary Pain Treatment. J Consult ClinPsychol 69:655–662
9. Jensen MP, Turner JA, Romano JM, Karoly P (1991) Cop-ing with Chronic Pain: A Critical Review of the Literature.Pain 47:249–283
10. Keefe FJ, Affleck G, Lefebvre J, Underwood L, Caldwell DS,Drew J, Egert J, Gibson J, Pargament K (2001) Living withRheumatoid Arthritis: The Role of Daily Spirituality and DailyReligious and Spiritual Coping. J Pain 2:101–110
11. Keefe FJ, Affleck G, Lefebvre JC, Starr K, Caldwell DS, Ten-nen H (1997) Pain Coping Strategies and Coping Efficacy inRheumatoid Arthritis: A Daily Process Analysis. Pain 69:35–42
12. Lazarus RS, Folkman S (1984) Stress, Appraisal, and Coping.Springer Publishing Company, New York
13. Peters ML, Sorbi MJ, Kruise DA, Kerssens JJ, Verhaak PF, Bens-ing JM (2000) Electronic Diary Assessment of Pain, Disabilityand Psychological Adaptation in Patients Differing in Durationof Pain. Pain 84:181–192
14. Robinson ME, Riley JL, III, Myers CD, Sadler IJ, Kvaal SA,Geisser ME, Keefe FJ (1997) The Coping Strategies Ques-tionnaire: A Large Sample, Item Level Factor Analysis. Clin JPain 13:43–49
15. Rosenstiel AK, Keefe FJ (1983) The Use of Coping Strategies inChronic Low Back Pain Patients: Relationship to Patient Char-acteristics and Current Adjustment. Pain 3:1–8
16. Schmitz U, Saile H, Nilges P (1996) Coping with Chronic Pain:Flexible Goal Adjustment as an Interactive Buffer Against Pain-Related Distress. Pain 67:41–51
Coping Repertoire
Definition
Resources that individuals have for responding to prob-lems and sources of stress and distress. These consistof methods to change the situation, adjust to emotionalarousal and uncontrollable circumstances, and accep-tance of limitations. The coping repertoire includes theinternal resources, the external supports that are avail-able, and the instrumental means that facilitate responsesuch as financial means to assist in accommodation.� Cognitive-Behavioral Perspective of Pain
Coping Strategy/Style
Definition
A cognitive-behavioral response to a stressor (e.g. prob-lem solving, recruiting social support) that mediates aperson’s response to a stressor and can impact the stress-pain relationship.� Coping and Pain� Stress and Pain
Coprevalence
Definition
Coprevalence refers to the rates of co-occurrenceof twospecific disorders or clinical problems.� Depression and Pain
Cord Glial ActivationJULIE WIESELER-FRANK, ERIN D. MILLIGAN,STEVEN F. MAIER, LINDA R. WATKINS
Department of Psychology and Center forNeuroscience, University of Colorado at Boulder,Boulder, CO, [email protected]
Synonyms
Spinal Cord Astrocyte; Microglia Activation
Definition
Cord glial activation refers to the activation of dorsalspinal cord � microglia and � astrocytes, which in-duces exaggerated pain via the release of substancesthat excite nocisponsive neurons (reviewed in Watkinset al. 2001). Activation is evidenced by upregulation ofimmunohistochemically-detectable cell-type specificactivation markers, and increased release of neuroactive

C
Cord Glial Activation 457
glial products including � proinflammatory cytokines,� excitatory amino acids (EAA), � nitric oxide (NO),adenosine triphosphate (ATP), and prostaglandins.These released substances then act on neurons, therebyamplifying the pain response. Some evidence points tothe activation of microglia leading to the activation ofastrocytes (Raghavendra et al. 2003).
Characteristics
Glia are non-neuronal cells traditionally thought ofas “supportive cells” for neurons(Araque et al. 1999).Many of their functions involve the release of growthfactors, protecting neurons from excitotoxicity, regu-lating extracellular ion concentrations, and removal ofcellular debris (Fig. 1).As discussed here, the term glia refers to astrocytes andmicroglia. While these are distinct cell types, most stud-ies investigating exaggerated pain andgliaarenotable toisolate the individual contribution of the two cell types.The glia in the dorsal spinal cord differ from glia in otherregions of the central nervous system (CNS). Severallines of evidence point to astriking heterogeneity amongglial cells, which is influenced by the regional biochemi-cal milieu. That is, spinal cord glia express receptors notfoundongliaderivedfromvariousbrain regionsandviceversa. For example, spinal cord is one of the few CNSregions in which glia express receptors for substance P(Beaujouan 1990). Differences have also been reportedbetween dorsal spinal cord and ventral spinal cord, andeven between superficial dorsal horn and the remainderof the gray matter (Ochalski et al. 1997).
Cord Glial Activation, Figure 1 Glia are activated by three sources: 1)bacteria and viruses which bind specific activation receptors expressed bymicroglia and astrocytes, 2) substance P, excitatory amino acids (EAAs), andadenosine triphosphate (ATP) released by either A-delta or C fiber presy-naptic terminals or by brain to spinal cord pain enhancement pathways,and 3) nitric oxide (NO), prostaglandins (PGs), and fractalkine released frompain transmission neurons. Following activation, microglia and astrocytescause pain transmission neuron hyperexcitability and exaggerated releaseof substance P and EAAs from presynaptic terminals. These changes arecreated by the glial release of NO, EAAs, PGs, reactive oxygen species (ROS),and proinflammatory cytokines. Reprinted with permission from Watkinset al. 2001.
Glia, specifically astrocytes, are intimately entangledwith neurons insofar as they encapsulate neuronalsynapses, as well as wrap their processes around neu-ronal somas, axons and dendrites (Araque et al. 1999).This proximity puts astrocytes in a unique position tomodulate the activity of nocisponsive neurons. Garrisonet al. were the first to investigate the relationship be-tween exaggerated pain and � glial activation (1994).Using the sciatic chronic constriction injury (CCI)model, they compared the expression of CCI-inducedhyperalgesia and immunohistochemical markers ofastrocyte activation (Garrison et al. 1991). In addition,they evaluated whether CCI-induced astrocyte activa-tion would be affected by an � N-methyl-D-aspartate(NMDA) receptor antagonist (MK801), known to in-hibit CCI-induced hyperalgesia (Garrison et al. 1994).They found that 1) hyperalgesia induced by CCI isassociated with astrocyte activation, and 2) this glialactivation (like CCI-induced hyperalgesia) is inhibitedby MK801. Thus, these studies revealed a predictiverelationship between glial activation and exaggeratedpain. Since then, positive correlations between exag-gerated pain and activation of spinal cord microglia (seecaption of Fig. 2 for discussion) and astrocytes havebeen revealed by diverse animal models of exaggeratedpain, including those induced by inflammation and/ortrauma to tissues, peripheral nerves, spinal roots, and/or spinal cord (DeLeo and Colburn 1999; Watkins etal. 2001). Such data naturally raise the question ofwhether glial activation is necessary and/or sufficientfor induction and maintenance of exaggerated pain.That glial activation plays a prominent role in the induc-tion of exaggerated pain has been demonstrated usingglial inhibitors. � Fluorocitrate selectively blocks glialmetabolic activity by inhibiting aconitase, a Krebs cycleenzyme (Paulsen et al. 1987; Hassel 1992). Blockingthe activation of spinal cord glial cells with fluorocitrateblocks exaggerated pain states, including thermal andmechanical hyperalgesia and mechanical allodynia(Meller et al. 1994; Milligan et al. 2000). Recently,a similar pattern has also been observed with the mi-croglia specific inhibitor, � minocycline. Minocyclineselectively inhibits the release of several neuroexcita-tory substances from microglia, including inflammatorymediators. Administration of minocycline attenuatesthe development of mechanical allodynia and thermalhyperalgesia in response to spinal nerve transection,peripheral nerve inflammation, or spinal cord inflam-mation (Raghavendra et al. 2003). Thus microglialactivation plays a significant role in the developmentof exaggerated pain. Intriguingly, minocycline failed toreverse, or minimally reversed, these exaggerated painstates once they were fully expressed. These data, sup-ported by parallel analyses of glial activation markers,revealing upregulation of GFAP (astrocyte activationmarker), suggest that microglial activation may lead toastrocyte activation. Astrocytes may then play a more

458 Cord Glial Activation
Cord Glial Activation, Figure 2 Example of microglial activation in response to a stimulus that creates exaggerated pain states. Peri-spinal administrationof HIV-1 envelope glycoprotein gp120 creates exaggerated responses to both thermal and touch/pressure stimuli. Disruption of glial activation abolishesthe pain changes. Furthermore, these pain changes are correlated with anatomical evidence of activation of both astrocytes and microglia. An exampleof such microglial activation is illustrated here. Panel A illustrates the dorsal horn of a rat injected peri-spinally with vehicle. Panel B is identical exceptthat the rat received peri-spinal HIV-1 gp120 at a dose that creates exaggerated pain states. These photomicrographs are from the tissues collected foranalysis reported in Milligan et al. 2001. Activation of microglia induces these cells to upregulate their expression of complement type 3 receptors. Thusenzyme labeled antibodies directed against complement receptor type 3 (OX-42 monoclonal antibodies) can be used to detect microglial activation bylight microscopy. In the photomicrographs shown here, the bound enzyme labeled antibodies catalyzed a reaction leading to precipitation of a coloredreaction product. Thus, more antibodies bound (and hence more colored reaction product produced) reflects upregulation of the complement receptortype 3 microglial activation marker. By this method, activated microglia appear darker and more densely stained in accordance with their increasedexpression of OX-42 antibody bound receptors. Scale bar, 25 μm in (a) and (b). (Reproduced from Milligan et al. 2001 with permission).
significant role in the maintenance of the pain facili-tatory process. Taken together, these data suggest thatglial activation is important for both the induction andmaintenance of exaggerated pain.It is important to note another key finding from studiesof minocycline and fluorocitrate. That is, glia are not in-volved in normal pain processing (Milligan et al. 2000).Normally, glia are quiescent, releasing nothing that en-hances pain. However, in situations leading to exagger-ated pain states, glia become activated. Once activated,theybeginreleasingsubstances thatcontribute to theam-plification of pain. Therefore the involvement of glia inpain is determined by their state of activation.The data strongly suggest the glial activation is im-portant for the expression of exaggerated pain, but isit sufficient? To assess this question, glia alone needto be directly activated. While glia can be activated byclassical pain neurotransmitters, including EAA, NO,prostaglandins and extracellular ATP, these substancesalso activate neurons. To activate spinal cord glia with-out activating neurons, the portions of bacteria andviruses that bind to and activate the immune-like glialcells have been used. Administration of these substancesinduces mechanical allodynia and thermal hyperalgesia(Meller et al. 1994; Milligan et al. 2000). Thus, takentogether, spinal cord glial activation is implicated inboth the creation and maintenance pain facilitation.
Bidirectional Neuron-Glia Communication
The discussion above describes glia as integral to thecreation and maintenance of exaggerated pain. Thequestion remains as to what signal from the periph-ery induces glial activation in the dorsal horn of thespinal cord, thereby inducing exaggerated pain. Asdescribed, one way is via the release of classical painneurotransmitters/ neuromodulators including EAA,
substance P, prostaglandins, ATP, and NO among oth-ers, by incoming sensory neurons and/or by intrinsicdorsal horn neurons in proximity to glia. While each ofthese substances excites spinal cord neurons in the painpathway, they also activate astrocytes and microglia.Thus these traditional neuronal mediators may exerttheir pain modulating effects, at least in part, via glialactivationOnce glia are activated, the question becomes whatsignal(s) maintains the persistent glial activation. Onepossible answer is that the signal is something releasedfrom dying or degenerating neurons associated withsome models of chronic pain (Sugimoto et al. 1990;Coggeshall et al. 2001; Moore et al. 2002). It is wellknown that neuronal injury and degeneration activateglia via different pathways. Degenerating neurons haveporous membranes, through which proteins such asheat-shock proteins can pass. These proteins may serveas signals of dying cells, thereby activating glia. Addi-tionally, neurons inhibit glial activation via cell-to-cellcontact (Chang et al. 2001; Neumann 2001). When aneuron dies, this contact is disrupted leading to glialactivation. Thus it seems possible that persistent glialactivation may be the end result.There are a number of peripheral signals that may po-tentially trigger glial activation, such as altered neuronalactivity, transported molecules from sensory neurons,or the removal of tonic inhibitory signals. However,little is know about the signal resulting in glial activa-tion. One signal currently being explored is the putativeneuron-to-glia signal � fractalkine, a protein expressedon the extracellular surface of sensory neurons as well asdorsal horn neurons. Fractalkine is tethered to neuronalmembranes by a mucin stalk (Chapman 2000). Whenneurons are sufficiently activated, the mucin stalksbreak, releasing fractalkine into the extracellular fluid.

C
Cord Glial Activation 459
Cord Glial Activation, Figure 3 Mixed astrocyte and microglia culture from neonatal rat pups showing selectivity of fractalkine for microglia. (a)Astrocytes labeled with glial fibrillary acidic protein (GFAP) visualized by a fluorescent antibody conjugated to Alexa 488. GFAP is a cytoskeletal proteinthat is highly specific to astrocytes. Note, that despite these astrocytes being in a mixed culture containing microglia, no microglia are labeled for GFAP.(b) Microglia labeled with fractalkine, which is directly conjugated to the Cy3b fluorochrome. In the dorsal spinal cord, fractalkine receptors are foundexclusively on microglia. Note that, despite these microglia being in a culture containing astrocytes, no astrocytes are labeled by fractalkine. (c) Overlayof (a) and (b) to provide the true picture of the mixed culture.
Within the spinal cord, only microglia express receptorsfor fractalkine, supporting the concept of fractalkine asa neuron-to-glia signal (Fig. 3).Spinal administration of fractalkine induces mechanicalallodynia and thermal hyperalgesia, while spinal ad-ministration of a fractalkine receptor antagonist blocksexaggerated pain, including neuropathic pain (Watkinsand Maier 2003). Whether fractalkine-induced mi-croglial activation leads, in turn, to astrocyte activationis a question that remains to be explored.These neuron-to-glia signals point to a means by whichsensory nocisponsive neurons and dorsal horn neuronscommunicate to glia, thereby inducing activation. In re-sponse to neuron-to-glia signals, glia release substancesthat then excite other glia and neurons. For example, mi-croglial binding of fractalkine rapidly induces the re-lease of the neuro- and glial-excitatory substances (in-cluding interleukin-1beta and nitric oxide) from dorsalspinal cord (Watkins and Maier 2003). The release ofthese excitatory substances induces exaggerated pain.As � immunocompetent cells, activated glia releaseclassical immune products in response to neuronal sig-nals. These include proinflammatory cytokines such asinterleukin-1beta, interleukin-6, and � tumor necrosisfactor alpha (TNF-α) reduced. In their role as classicalimmune signals, these cytokines are “proinflammatory”because they orchestrate the early immune responseto infection and damage by recruiting immune cellsto the site and activating them. In spinal cord, theseproinflammatory cytokines are signal molecules thatactivate neurons as well as glia, via binding to specificreceptors on these cells. This is one means by whichglia can signal neurons. Proinflammatory cytokinesare not constitutively released in the spinal cord, and
pharmacologically blocking their activity does not al-ter normal pain responsivity. However, in conditionsleading to exaggerated pain, including CCI, sciaticinflammatory neuropathy (SIN), and spinal nerve tran-section, blocking proinflammatory cytokine activity inspinal cord blocks mechanical allodynia and thermalhyperalgesia (reviewed in DeLeo and Colburn 1999).Proinflammatory cytokines are,therefore, necessary forthese exaggerated pain states. Mechanical allodynia andmechanical and thermal hyperalgesia are induced byspinal administration of proinflammatory cytokines (re-viewed in Watkins et al. 2001). Thus, proinflammatorycytokines are sufficient for exaggerated pain.In addition to released signals acting on glia, astrocytesare also able to communicate with other astrocytes via� gap junctions. This spread of excitation leads to theactivation of distant glia (Fig. 4) and their release of neu-roexcitatory substances (Araque et al. 1999).The importance of this type of astrocyte-to-astrocytecommunication, causing excitation of distant glia, raisesthe question of whether gap junctions may potentiallyprovide an explanation for the spread of human painbeyond the original site of trauma; that is, mirror imagepain and extraterritorial pain. Such a communicationnetwork could, theoretically at least, lead to releaseof pain enhancing substances by newly activated gliadistant from the initial site of gap junctional activation.While no data yet exist in humans, the spread of painin animal models is indeed blocked by spinal adminis-tration of the gap junction decoupler � carbenoxolone.Carbenoxolone blocks the spread of mechanical allody-nia in CCI and SIN (Spataro et al. 2003). Control studies,using glycyrrhetinic acid, verify that carbenoxolone-induced disruption of CCI and SIN-induced mirror

460 Cord Glial Activation
Cord Glial Activation,Figure 4 Illustration of the spreadof a calcium wave among astrocytes.Astrocytes are electrically coupledby gap junctions into vast networks.These electrical couplings allowastrocytes to rapidly communicatewith one another over widespreadareas. These images show asequence of time-lapse photographicimages, illustrating the rapid spreadof excitation that occurs after theactivation of a single glial cell attime 0. These newly activated,distant cells can then releasepain-enhancing substances, therebyactivating nearby pain neurons.Such gap junctional spread ofexcitation has recently been linkedto pain facilitation, especially tomirror-image pain. (Modified fromAraque et al. 1999. Reprinted withpermission.)
image pains are indeed due to its disruption of gapjunctions. This is the first example of gap junctions,most likely of glial origin, being implicated in pain.Thus, gap junctional communication among astrocytesprovides an intriguing and novel explanation for painthat arises in otherwise healthy body parts.In summary, cord glial activation is integrally involvedin diverse exaggerated pain phenomena. The powerfulrole that glia play in pain facilitation suggests that drugstargeting this non-neuronal cell type may hold promisefor effective clinical pain control.
References1. Araque A, Parpura V, Sanzgiri RP, Haydon PG (1999) Tripartite
Synapses: Glia, The Unacknowledged Partner. Trends in Neu-rosci 22:208–215
2. Beaujouan JC, DaguetdeMontety MC, Torrens Y, Saffroy M,Dietl M, Glowinski J (1990) Marked Regional Heterogeneityof 125I-Bolton Hunter Substance P Binding and Substance P-Induced Activation of Phospholipase C in Astrocyte Culturesfrom the Embryonic or Newborn Rat. J Neurochem 54:669–675
3. Chang RC, Chen W, Hudson P, Wilson B, Han DS, HongJS (2001) Neurons Reduce Glial Responses to Lipopolysac-charide (LPS) and Prevent Injury of Microglial Cells fromOver-Activation by LPS. J Neurochem 76:1042–1049
4. Chapman GA, Moores K, Harrison D, Campbell CA, StewardBR, Strijbos PJLM (2000) Fractalkine Cleavage from NeuronalMembranes Represents an Acute Event in the Inflammatory Re-sponse to Excitotoxic Brain Damage. Journal of Neuroscience20: RC87 pp 81–85
5. Coggeshall RE, Lekan HA, White FA, Woolf CJ (2001) A-FiberSensory Input Induces Neuronal Cell Death in the Dorsal Hornof the Adult Rat Spinal Cord. J Comp Neurol 435:276–282
6. DeLeo JA, Colburn RW (1999) Proinflammatory Cytokines andGlial Cells: Their Role in Neuropathic Pain. In: Watkins L (ed)Cytokines and Pain. Birkhauser, Basel, pp 159–182
7. Garrison CJ, Dougherty PM, Carlton SM (1994) GFAP Expres-sion in Lumbar Spinal Cord of Naive and Neuropathic RatsTreated with MK-801. Exp Neurol 129:237–243
8. Garrison CJ, Dougherty PM, Kajander KC, Carlton SM (1991)Staining of Glial Fibrillary Acidic Protein (GFAP) in Lumbar
Spinal Cord Increases Following a Sciatic Nerve ConstrictionInjury. Brain Res 565:1–7
9. Hassel B, Paulsen RE, Johnson A, & Fonnum F (1992) SelectiveInhibition of Glial Cell Metabolism by Fluorocitrate. Brain Res249:120–124
10. Meller ST, Dykstra C, Grzybycki D, Murphy S, Gebhart GF(1994) The Possible Role of Glia in Nociceptive Processing andHyperalgesia in the Spinal Cord of the Rat. Neuropharmacology33:1471–1478
11. Milligan ED, Mehmert KK, Hinde JL, Harvey LO, Martin D,Tracey KJ, Maier SF, Watkins LR (2000) Thermal Hyperalgesiaand Mechanical Allodynia Produced by Intrathecal Administra-tion of the Human Immunodeficiency Virus-1 (HIV-1) EnvelopeGlycoprotein, gp120. Brain Res 861:105–116
12. Moore KA, Kohno T, Karchewski LA, Scholz J, Baba H, WoolfCJ (2002) Partial Peripheral Nerve Injury Promotes a SelectiveLoss of GABAergic Inhibition in the Superficial Dorsal Horn ofthe Spinal Cord. J Neurosci 22:6724–6731
13. Neumann H (2001) Control of Glial Immune Function by Neu-rons. Glia 36:191-199
14. Ochalski PA, Frankenstein UN, Hertzberg EL, Nagy JI (1997)Connexin-43 in Rat Spinal Cord: Localization in Astrocytes andIdentification of Heterotypic Astro-Oligodendrocytic Gap Junc-tions. Neuroscience 76:931–945
15. Paulsen RE, Contestabile A, Villani L, Fonnum F (1987) An InVivo Model for Studying Function of Brain Tissue TemporarilyDevoid of Glial Cell Metabolism: The Use of Fluorocitrate. JNeurochem 48:1377–1385
16. Raghavendra V, Tanga F, DeLeo JA (2003) Inhibition of Mi-croglial Activation Attenuates the Development but not ExistingHypersensitivity in a Rat Model of Neuropathy. J Pharmacol ExpTher 306:624–630
17. Spataro LE, Sloane E, Milligan ED, Maier SF, Wieseler-Frank J,Schoeniger D, Jekrich BM, Barrientos RM, Watkins LR (2004)Spinal gap junctions: potential involvement in pain facilitation.J Pain 5:392–405
18. Sugimoto T, Bennett GJ, Kajander KC (1990) Transsynaptic De-generation in the Superficial Dorsal Horn after Sciatic Nerve In-jury: Effects of a Chronic Constriction Injury, Transection, andStrychnine. Pain 42:205–213
19. Watkins LR, Maier SF (2003) Glia: A Novel Drug Discovery Tar-get for Clinical Pain. Nature Reviews Drug Discovery 2:973–985
20. Watkins LR, Milligan ED, Maier SF (2001) Glial Activa-tion: A Driving Force for Pathological Pain. Trends Neurosci24:450–455

C
Cordotomy Effects on Humans and Animal Models 461
Cordotomy
Definition
Originally anterolateral chordotomy, referring to thegeometric term “chord” to indicate interruption of whitematter. Cordotomy was developed as a surgical proce-dure, to sever the spinothalamic tract at a spinal levelabove dermatomes to which extreme chronic pain wasreferred. It is generally performed percutaneously atthe cervical level, which interrupts the ascending lateralspinothalamic tract. Cordotomy is most useful in themanagement of intractable, unilateral lower extremitycancer pain. Cordotomy tends to be more effectivefor nociceptive pain syndromes than for neuropathicsyndromes. Unilateral pain is a better indication thanbilateral pain, and midline pain tends to respond poorlyeven to bilateral cordotomy.� Cancer Pain Management, Opioid Side Effects, Un-
common Side Effects� Cancer Pain Management, Overall Strategy� Central Nervous System Stimulation for Pain� Postherpetic Neuralgia, Pharmacological and Non-
Pharmacological Treatment Options� Spinal Cord Injury Pain Model, Cordotomy Model� Thalamus, Receptive Fields, Perceptive Fields, Hu-
man
Cordotomy Effects on Humans and AnimalModels
CHARLES J. VIERCK1, ALAN R. LIGHT2
1Department of Neuroscience, McKnight BrainInstitute, University of Florida College of Medicine,Gainesville, FL, USA2Department of Anesthesiology, University of Utah,Salt Lake City, UT, [email protected]
Definition
Cordotomy is a surgical procedure introduced in theearly 1900s for reduction of chronic intractable painin humans. An anterolateral column of spinal whitematter is cut or coagulated at a spinal level above andcontralateral to a source of clinical pain, intention-ally interrupting the � spinothalamic tract. For weeks,months or years after successful interruption of as-cending pathways in the anterolateral column, pain andtemperature sensations are diminished contralaterallyover dermatomes beginning several segments below(caudal) to the lesion. The reduction of pain is apparentfor clinical pain and for nociceptive stimulation of hu-mans, other primates and mammals (Vierck et al. 1986;Vierck et al. 1995; White and Sweet 1969).
Characteristics
The intent of surgical section of anterolateral spinalwhite matter is to interrupt axons of the spinothalamictract that originate predominantly in the contralateralgray matter in spinal segments below the lesion. Thetargeted projection cells receive input from nocicep-tive peripheral afferents selectively sensitive to stimulithat elicit pain or temperature sensations, and someare excited by non-nociceptive afferents. Other axonssituated posteriorly in the spinal white matter, ipsilat-eral to their cells of origin, convey non-nociceptiveinformation that subserves sensations of touch and� proprioception. Therefore, cordotomy reduces painand temperature sensitivity withoutproducing clinicallyrelevant deficits of touch or proprioception. Sensationsreported to be lost or diminished by cordotomy arepain, itch, discrimination of sharpness with or without apainful quality, wetness, cold, warmth and voluptuoussensations elicited by genital stimulation (Vierck et al.1986). It is important to recognize that these effects ofcordotomy probably result from combined interruptionof ascending pathways to cerebral sites that includenumerous thalamus nuclei, the hypothalamus and theamygdaloid complex (Giesler et al. 1994).Often chronic clinical pain is referred to deep tissuesand appears to be particularly attenuated by cordotomy(Nathan and Smith 1979). The upper segmental levelsfor reduction of clinical pain and of pain from deep pres-sure stimulation have been reported to be well correlatedand lower than the upper level of � hypoalgesia for cu-taneous stimulation. Similarly, visceral pain is reportedto be well controlled by cordotomy (White and Sweet1969), but the upper level of visceral pain reduction candiffer from the upper level of diminished pain elicited bycutaneous pin prick testing. These differences in “sen-sory level” for deep and superficial pain are probablybased on different entry levels for visceral and somaticafferents and on a more extensive rostrocaudal disper-sioninthespinalcordofafferentinputfromdeepsomaticstructures. The effectiveness of anterolateral cordotomyfor attenuation of visceral pain is surprising in view ofevidence that interruption of a pathway located in thedorsal spinal columns can attenuate visceral pain (Nautaet al. 2000). It appears that different aspects (qualitativefeatures?) of visceral sensation depend on rostral con-duction by dorsal and ventral spinal pathways.The dorsoventral and mediolateral extents of lateral andventral column damage are important determinants ofthe sensory effects of cordotomy. A somatotopic orga-nization exists dorsoventrally, with sacral dermatomesdorsal and rostral dermatomes ventral. Accordinglyrestriction of cordotomy to the anterolateral columncan miss the most dorsal spinothalamic axons and resultin sacral sparing. In addition, there are differences indorsoventral distribution of rostrally projecting axonswith distinguishable origins. For example, spinotha-

462 Cordotomy Effects on Humans and Animal Models
lamic axons originating in the deep dorsal horn aremore ventrally located in the anterolateral and ventralcolumn, relative to cells from the superficial dorsalhorn (Zhang et al. 2000). This appears to be the case ingeneral for cells originating in the superficial and deepdorsal horn, which have overlapping, but differential,functional properties and projections to targets in thebrain stem and thalamus (e.g. Craig 1998). These re-lationships could influence the long-term effects of acordotomy.For the mediolateral dimension of the anterolateralcolumn, clinical investigators have postulated thatpain from mechanical stimulation of the skin dependsupon peripherally located axonal projections, whiletemperature sensations and pain from stimulation ofdeep tissues depend upon more medially located ax-ons (Walker 1940). These suppositions encouraged aclinical strategy involving medially extensive antero-lateral cordotomy, in order to maximally attenuate painfrom deep tissues. Given this surgical approach, theexpectation is that a successful unilateral cordotomywould produce contralateral analgesia, particularly forcutaneous stimulation. However, human and animalstudies involving nociceptive cutaneous stimulationwithin dermatomes maximally affected by cordotomyindicate that pain sensitivity is not eliminated (King1957; Vierck et al. 1990; Vierck et al. 1995; Vierck andLuck 1979).Not only is pain sensitivity partially preserved contralat-erally, but chronic pain returns and pain sensitivity in-creases over time for some but not all cases after an ini-tially successful cordotomy. Early on, the explanationfor this was that the anterolateral lesion for cases of re-covery was incomplete dorsally, ventrally or medially.However this possibility is contradicted by human andanimal studies with histological confirmation of highlyrestricted lesions (superficially located in the anterolat-eral column) that produced very long-term hypoalgesia(Nathan and Smith 1979; Vierck and Luck 1979). Directcomparisons of cordotomy effects in monkeys indicatethat recovery of pain sensitivity over time is more sub-stantial for extensive lesions (primarily medially) thanfor superficial lesions (Vierck et al. 1990). Explanationsfor these results may be 1) that all spinothalamic axonsshift laterally with ascension of the spinal cord (Zhanget al. 2000) and 2) that the more extensive lesions par-tially damage spinal projection systems other than thespinothalamic tract (Fig. 1) (see � Spinal Cord InjuryPain Model, Cordotomy Model).When chronic pain returns after cordotomy, it appearsto be qualitatively distinct from that experienced beforesurgery. Discrimination between qualitative features ofchronic pain is difficult, but recovered pain can be morediffuse in character and bilaterally distributed (Whiteand Sweet 1969). Several possible mechanisms for thisare related to 1) � deafferentation of neurons normallyreceiving input from rostrally projecting axons sec-
tioned by cordotomy, and 2) enhanced transmission ofnociception by diffusely projecting ascending pathwaysspared by cordotomy.Return of clinical pain and of painful sensations elicitedby stimulation after cordotomy is consistent with devel-opment of chronic pain that can occur following strokesthat produce deficits of elicited pain and temperaturesensations and, by implication, damage the spinotha-lamic tract at some level of the neuraxis (Boivie etal. 1989). Numerous human studies involving thalamicrecording have demonstrated abnormal spontaneous ac-tivity in regions deafferented by these and other lesions(Lenz 1992). The presence of abnormally high levels ofactivity among populations of neurons that previouslyreceived nociceptive input can potentially be interpretedas pain. If this occurs, the distribution of pain would beexpected to involve much of the deafferented region,rather than the more restricted site of pain experiencedbefore cordotomy. Furthermore, recordings from thethalamus of monkeys after medially extensive cordo-tomy have shown that abnormal spontaneous activity isnot restricted to the region of primary deafferentationwithin the nucleus ventralis posterolateralis (Weng etal. 2000). That is, the effects of deafferentation canextend beyond the somatotopically appropriate regionof a principal target of spinothalamic projections to thethalamus.Other clues relevant to an eventual return of clinicalpain and pain sensitivity are offered by the stimulicapable of eliciting pain sensations after cordotomy.Thresholds for elicitation of pain are clearly elevated,but strong suprathreshold stimulation is perceived aspainful (King 1957). This is apparent for electricalstimulation of the skin or a peripheral nerve, whichprogressively activates A-delta and C afferents as no-ciceptive stimulus intensity increases. A cordotomythat eliminates pain elicited by stimulation of A-deltaafferents can preserve pain from electrical stimulationat intensities sufficient to excite C nociceptors (Collinset al. 1960). Similarly, pain elicited by the standardpinprick test involving single stimuli can be eliminatedby a cordotomy, but repetitive pinprick stimulation atthe same location produces pain (Nathan and Smith1979; Walker 1940), presumably because of temporalsummation. Temporal summation by repetitive stimu-lation has been shown to depend upon stimulation of Cnociceptors (e.g. Vierck et al. 1997). Also, when painfrom application of focal pressure to deep tissues iseliminated by cordotomy, pain from muscular crampscan be perceived (White 1968). In this example, spatialsummation from simultaneous stimulation of many Cnociceptors may be responsible for break through pain.The varieties of pain retained after cordotomy suggestthat pathways of rostral projection outside the contralat-eral lateral column are particularly sensitive to C noci-ceptor input. The following evidence indicates that thisconduction system is diffusely distributed in the antero-

C
Cordotomy Effects on Humans and Animal Models 463
Cordotomy Effects on Humans and Animal Models, Figure 1 (a) Diagrams of 4 unilateral cervical cordotomies in humans that produced enduringreductions of chronic clinical pain and sensitivity to nociceptive stimulation. Note that the lesions are restricted to the peripheral portions of the anterolateralwhite matter (after Nathan and Smith, 1979). (b) Plots of the uniformly peripheral distribution of anterolateral axons (at the C2 segment of monkeys) thatproject to the ipsilateral thalamus from cells of origin in the contralateral gray matter. Upper diagram: solid circles: axons from cells in the superficialdorsal horn; open circles: axons from cells in the deep dorsal horn. Overall, axons from superficial cells are distributed more dorsally, especially atthoracic levels (not shown). Lower diagram: cells with input from different populations of peripheral afferents: solid circles: wide dynamic range neurons;open circles: low threshold neurons; stars: high threshold neurons (from Zhang et al. 2000).
lateral and ventral spinal cord and is responsible for re-turn of pain sensitivity after cordotomy. Bilateral cor-dotomy does not prevent recovery of pain or eliminatepain that has developed after interruption of one antero-lateral column (White and Sweet 1969). Therefore, it isunlikely that sparing of spinothalamic axons underliesthe return of pain after cordotomy. Also, secondary le-sions of dorsal spinal pathways in monkeys do not atten-uate pain sensitivity that has returned after cordotomy(Vierck and Luck 1979). However, complete interrup-tion of both ventral spinal quadrants (ventral hemisec-tion) appears to eliminate pain sensitivity without recov-ery (Vierck and Luck 1979). Obvious candidates for dif-fuserostralpain transmissionare thespinoreticularpath-ways, with bilateral relays to cerebral systems involvedin pain coding and modulation(e.g. spinomesencephalicand spinoreticulothalamic).In summary, clinical and laboratory animal studies withhistologicalverificationofspinal lesionsindicate that in-terruption of spinothalamic axons located superficiallyin the anterolateral spinal column effectively reduceschronic pain and pain sensitivity, long term. However,partial interruption of diffuse ventral spinal projectionsystems by more extensive lesions can initiate a re-covery process with adverse effects on pain sensitivity.Complete interruption of the bilateral ventral projectionsystem and the spinothalamic tract produces analgesia,in contrast to the hypoalgesia produced by anterolat-eral cordotomy. Unfortunately, ventral hemisectionalso produces profound motor deficits by interruptinga number of descending spinal pathways. Therefore,when employment of spinal surgery is considered for
alleviation of chronic, intractable pain, available ev-idence favors interruption of superficial axons in theanterolateral column.
References1. Boivie J, Leijon G, Johansson I (1989) Central post-stroke pain
- a study of the mechanisms through analyses of the sensoryabnormalities. Pain 37:173–185
2. Collins W, Nulsen F, Randt C (1960) Relation of peripheral nervefibre size and sensation in man. Arch Neurol 5:381–385
3. Craig, AD (1998) A new version of the thalamic disinhibitionhypothesis of central pain. Pain Forum 7:1–14
4. Giesler GJ Jr, Katter JT, Dado RJ (1994) Direct spinal pathways tothe limbic system for nociceptive information. TINS 17:244–250
5. King RB (1957) Postchordotomy studies of pain threshold. Neu-rology 7:610–614
6. Lenz FA (1992) The ventral posterior nucleus of thalamus isinvolved in thegeneration of central pain syndromes. APSJournal1:42–51
7. Nathan PW, Smith MC (1979) Clinico-anatomical correlation inanterolateral cordotomy. Adv Pain Res Ther 3:921–926
8. Nauta HJW, Soukup VM, Fabian RH et al (2000) Punctate mid-line myelotomy for the relief of visceral cancer pain. J Neursurg92:125–130
9. Vierck CJ Jr, Luck MM (1979) Loss and recovery of reactivity tonoxious stimuli in monkeys with primary spinothalamic chordo-tomies, followed by secondary and tertiary lesions of other cordsectors. Brain 102:233–248
10. Vierck CJ Jr, Greenspan JD, Ritz LA et al (1986) The spinalpathways contributing to the ascending conduction and the de-scending modulation of pain sensations and reactions. In: YakshTL (ed) Spinal systems of afferent processing. Plenum Press,New York, pp 275–329
11. Vierck CJ Jr, Greenspan JD, Ritz LA (1990) Long term changesin purposive and reflexive responses to nociceptive stimulationin monkeys following anterolateral chordotomy. J Neurosci10:2077–2095

464 Core and Matrix
12. Vierck CJ Jr, Lee CL, Willcockson HH et al. (1995) Effects ofanterolateral spinal lesions on escape responses of rats to hindpawstimulation. Somatosens Motor Res 12:163–174
13. Vierck CJ Jr, Cannon RL, Fry G et al. (1997) Characteristics oftemporal summation of second pain sensations elicited by briefcontact of glabrous skin by a preheated thermode. J Neurophysiol78:992–1002
14. Walker AE (1940) The spinothalmic tract in man. Arch NeurolPsychiat 43:284–298
15. Weng H-R, Lee J, Lenz F et al. (2000) Functional plasticity inprimate somatosensory thalamus following chronic lesion of theventral lateral spinal cord. Neurosci 101:393–401
16. White JC, Sweet WH (1969) Pain and the neurosurgeon: A forty-year experience. Thomas CC, Springfield
17. White J (1968) Operations for the relief of pain in the torso andextremities: Evaluation of their effectiveness over long periods.In: Soulairac A, Cahn J, Charpentier J (eds) Pain. Academic Press,New York, pp 503–519
18. Zhang X, Honda C, Giesler GJ Jr (2000) Position of spinotha-lamic tract axons in upper cervical spinal cord of monkeys. JNeurophysiol 84:1180–1185
Core and Matrix
� Spinothalamic Terminations, Core and Matrix
Coronary Artery Disease
� Visceral Pain Model, Angina Pain
Coronary Insufficiency
� Visceral Pain Model, Angina Pain
Corpus Callosum
Definition
The largest bundle of fibers connecting the two hemi-spheres. The corpus callosum is subdivided into foursub-regions with the splenium located in the mostposterior region, the body extending anterior from thesplenium, the genu consisting in the most anterior part,and the rostrum below the genu. Each region of thecorpus callosum connects specific regions of one hemi-sphere of the cerebral cortex to the homologous area inthe other hemisphere.� Cingulate Cortex, Functional Imaging� Nociceptive Processing in the Cingulate Cortex, Be-
havioral Studies in Humans� Pain Processing in the Cingulate Cortex, Behavioral
Studies in Humans
Correct Rejection
Definition
Correct rejection is theprobabilityof response„B“whenevent B has occurred.� Statistical Decision Theory Application in Pain As-
sessment
Correlation
Definition
The degree to which variables change together.� Pain in theWorkplace,Risk factors forChronicity, Job
Demands
Cortex and Pain
Definition
Cortical areas (anterior cingulate, parietal operculum,insula, primary somatic sensory cortex) that show pain-related activity, usually based on imaging studies.� Pain Treatment, Motor Cortex Stimulation
Cortical Feedback
Definition
Back projections from cortical regions that receive for-ward projections from the thalamus.� Thalamic Plasticity and Chronic Pain
Cortical Information Flow
� Thalamocortical Loops and Information Processing
Cortical Plasticity
Definition
Flexible organization of the cortical textures and circuitsadapting to input variability and regulated by ’experi-ence’, i.e. preferential use increase/reduction of definitepathways. At the synaptic level, strengthening or weak-ening of the synaptic connections depending on a cor-relation principle.� Deafferentation Pain

C
Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior 465
Cortical and Limbic MechanismsMediating Pain and Pain-RelatedBehavior
KENNETH L. CASEY
Department of Neurology, Department ofMolecular and Integrative Physiology, University ofMichigan, and Consultant in Neurology, VeteransAdministration Medical Center, Ann Arbor, MI,[email protected]
Scope of This Review
This article will briefly review pain related functionsof the cerebral cortex and limbic system. For the pur-poses of this review, the limbic system is defined asthe medial and orbital portions of the frontal, parietaland temporal lobes that form a ring around the upperbrainstem and diencephalon. The cingulate gyrus is adefining structure of the limbic system, the major com-ponents of which have direct or oligosynaptic connec-tionswithcingulatecortex(seealso� cingulatecortex,functional imaging; � pain processing in the cingulatecortex, behavioral studies in humans; � cingulate cor-tex, nociceptive processing, behavioral studies in ani-mals) and with the hypothalamus (MacLean 1955; Pa-pez 1937). The subcortical limbic structures such asthe amygdala (see also � amygdala, functional imag-ing; � nociceptive processing in the amygdala, neu-rophysiology and neuropharmacology), which is cov-ered thoroughly in the essay in this Section by VolkerNeugebaurer,willnotbediscussed.Modulatorymech-anismsmediatedbypathwaysdescendingfromthecor-tex and brainstem are discussed elsewhere in this vol-ume and will not be discussed here.Theneurobiological response to injurycomplicates theanalysis of cortical function during pain. Peripheral orcentral nervous system injuries trigger complex bio-chemical mechanisms that result in varying degrees ofanatomical and functional reorganization of the cere-bral cortex (Kaas et al. 1997). In this review, corticalfunctionswillbeconsideredonlyasmediatednormallyin the absence of clinically significant reorganization.
Conceptual Issues
“Function” refers to the mix of psychological, be-havioral and physiological manifestations of cere-bral cortical activity, including somatic and auto-nomic responses that may be independent of thefully developed sensation of pain and the sensory,affective-motivational and cognitive components ofpain(MelzackandCasey1968;Price1988;Price1999)as recognized by the International Association for theStudy of Pain (IASP) (Merskey and Bogduk 1994) and
in recent reviews of the cerebral cortical mechanismsmediating pain (Treede et al. 1999).
Spatial Distribution of Function
The clinical observation that pain can be relieved, atleast partially, by spinothalamic tractotomy (Spillerand Martin 1912) supports the concept of an anatom-ically distinct pain pathway, but subsequent clinicalandneurosurgicalexperiencehasemphasized the long-term unpredictability of the results obtained follow-ing most ablative procedures, especially those involv-ing cerebral structures (Sweet 1982). Current meth-ods of analyzing brain function show that all corti-cal and limbic functions are mediated by networksof interconnected cortical areas, each with a specific,although incompletely characterized, neuronal func-tion. This concept is in accord with the results of cur-rent functional imaging studies of pain (Casey 1999;Casey 2000; Davis 2000; Derbyshire 2000; Peyron etal. 2000) and the contemporary view that distributedparallel systems mediate cortical functions (Mesulam1990).
Temporal Distribution of Function
Cortical and limbic functions are also distributed overtime. This concept is important for considering corti-cal functions as they affect both acute and chronicallypainful conditions. How cortical functions influencethe perception of pain and pain related behavior maychange with time from injury or, in the experimentalsetting, with time following a noxious stimulus. Sometemporal variance may be due to the sequential acti-vation of different cortical areas. Imaging studies ofpain, for example, show that changes in the cortical re-sponse to noxious stimulation occur over a time spanof approximately 45 s (Casey et al. 2001). Other tem-poral variation in cortical influence may occur simplybecause an injury or the context surrounding the injuryhas changed over time, so that the perceptual and be-havioral impact of that function changes. All corticalareas are active to some degree throughout all time pe-riods during which pain is experienced. Neurophysio-logical and functional brain imaging studies (cited be-low) show that each of thecortical structures listed hereis active within milliseconds following a noxious stim-ulus.However, theclinically relevant impactofspecificcortical structures on pain and pain behaviors deservesemphasis within particular time frames. Figure 1 is in-tended to summarize thishypothesized temporaldistri-butionof the influenceandimpactofcorticalandlimbicfunctions over time. Unfortunately, information aboutcortical and limbic function over periods ranging fromhours to years is available only in the clinical settingand only when long-term follow-up is available.

466 Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior
Cortical and Limbic Mechanisms Mediating Pain and Pain-RelatedBehavior, Figure 1 Relative influence of cortical function on pain andpain-related behavior. The figure summarizes the distribution of the in-fluence of cerebral cortical and limbic functions on pain perception andpain related behavior over time. All structures listed in the left columnhave some influence on pain and behavior throughout the experienceof pain, but the degree of this influence and its clinical and behavioralimpact varies over time as indicated by the size and boldness of theX marks. The sensory-discriminative function (blue) is largely limited tothe primary (S1) somatosensory cortex. Affective function is indicatedby shades of red and cognitive function by green. Hippocampal (andentorhinal cortex) function is a mixture of affective and cognitive ele-ments. S1, primary somatosensory cortex; S2, secondary somatosensorycortex; AI, anterior insula; ACC, anterior cingulate cortex; PCC, posteriorcingulate cortex; IPL, inferior parietal lobule; Pr.Mot., premotor cortex; PI,posterior insula; MPC, medial prefrontal cortex; OFC, orbitofrontal cortex;HIPP, hippocampus and entorhinal cortex; DLPFC, dorsolateral prefrontalcortex.
Early Cortical and Limbic Processing (Milliseconds)
Primary Somatosensory Cortex (S1)
TheS1cortex(seealso� PrimarySomatosensoryCor-tex (S1), Effect on Pain-Related Behavior in Humans)within the postcentral gyrus is composed of Brodmannareas 1, 2, 3a and 3b, the latter two areas lying in thedepths of the central sulcus and generally consideredto be the major recipient of spatially refined cutaneoussomatosensory input.
Lesions
There is evidence from clinical, neurophysiologicaland functional brain imaging that the S1 cortex is amajor site for identifying noxious stimuli along thetemporo-spatial and intensity domains. Early clini-cal analysis based on wartime missile wounds sug-gested thatsmall lesionswithin theS1cortexcouldpro-duce a somatotopically restricted hypoalgesia along
with an impairment of somesthetic spatial and tempo-ral discriminative functions (Marshall 1951; Russell1945). However, direct anatomical corroboration wasnot available at the time and subsequent studies haveshown that even relatively modest impact trauma to thecortex can result in otherwise unrecognized and clini-cally significant subcortical lesions thatcould interruptdeep nociceptive pathways (Lighthall 1988; Lighthallet al. 1989).Selective surgical lesions of S1 cortex for the reliefof clinical pain have produced poor results over time(Sweet 1982). Furthermore, infarctions limited to theterritoryof thepostcentralgyrusandsuperior-posteriorparietal region produce a somatotopically limited im-pairment of tactile and kinesthetic discriminative func-tions with sparing of pain and temperature sensations(Bassetti et al. 1993). This suggests that the S1 cortexis not essential for mediating the perceptual aspects ofclinically relevant chronic pain states.
Stimulation
Despite the strong evidence for nociceptive informa-tion reaching the S1 cortex (see below), electrical stim-ulation of the postcentral gyrus rarely, if ever, evokespain in the conscious or partially sedated human (Nii etal. 1996; Sweet 1982). However, these stimuli do nottypically activateneurons in thesulcaldepthsofS1 cor-tex, where nociresponsive neurons may be located.
Electrophysiology
The detailed somatotopic organization of neurons re-sponding to tactile stimuli (Whitsel et al. 1971) hasbeen confirmed in numerous investigations (Kaas etal. 1979; Kaas 1993). Single cell recordings fromthe monkey reveal that there are nociceptive neuronswithin S1 cortex and that these have restricted re-ceptive fields and responses that could mediate ther-mal nociceptive discrimination in the monkey (Ken-shalo and Isensee 1983; Kenshalo et al. 1988; Ken-shalo et al. 2000). In humans, the earliest nocicep-tive information to reach the cerebral cortex, as de-termined by magnetoencephalographic (MEG) (seealso � Insular Cortex, Neurophysiology and Func-tional Imaging of Nociceptive Processing) and evokedpotential (EP) (see also � insular cortex, neurophys-iology and functional imaging of nocicepetive pro-cessing, � nociceptive processing in the hippocampusand entorhinal cortex, neurophysiology and pharma-cology) studies with noxious laser or brief mechan-ical stimulation, arrives nearly simultaneously in theprimary somatosensory (S1), secondary somatosen-sory (S2) (see also � secondary somatosensory cor-tex (S2) and insula, effect on pain related behavior inanimals and humans), anterior insular (AI) (see also

C
Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior 467
� insular cortex, neurophysiology and functionalimaging of nocicepetive processing) and the rostralanterior cingulate cortex (ACC) (see also � cingulatecortex, nociceptive processing, behavioral studies inanimals, � pain processing in the cingulate cortex, be-havioral studies in humans, � cingulate cortex, func-tional imaging) (Arendt-Nielsen et al. 1999; Kakigiet al. 1995; Ploner et al. 1999; Schnitzler and Ploner2000). Kanda and colleagues used recordings from thescalp and from implanted subdural electrodes to showthat painful infrared laser stimulation evokes a poten-tial with a peak latency of 220 ms in human S1 cortex(Kanda et al. 2000). A recent MEG study with laserevoked selective stimulation of C fibers found nearlysimultaneous responses within approximately 750 msin both the S1 and S2 cortices (Tran et al. 2002).
Functional Imaging
Functional imaging studies support the concept thattheS1 cortex participates in thesensory-discriminativeaspect of pain although cognitive variables modifythe intensity of the response significantly (Bushnell etal. 1999; Hofbauer et al. 2001). High-resolution op-tical imaging studies show unique and possibly spe-cific responses to noxious heating in subdivisions ofarea 3a (Tommerdahl et al. 1996). However, functionalmagnetic resonance imaging (fMRI) studies (see also� PET and fMRI imaging in parietal cortex (Si, Sii,inferior parietal cortex BA40)) show that responses tonoxious stimuli are also likely to be obtained from area1 of the S1 cortex (Gelnar et al. 1999), a finding in gen-eral agreement with the results of cellular recording(Kenshalo and Isensee 1983; Kenshalo et al. 1988).In summary, the weight of evidence from a variety ofsourcesfavors theviewthatS1corticalneuronsarespe-cialized to engage in the earliest processes mediatingthediscriminativeaspectsofsomaticsensation, includ-ing pain. Clinical observations suggest that these neu-rons are essential for nociceptive discriminative func-tions, but are less likely to be essential for mediating ormodulating the affective or cognitive aspects of chron-ically painful conditions.
Secondary Somatosensory Cortex (S2)
The S2 cortex occupies the posterior parietal oper-culum over the lateral (Sylvian) fissure and is adja-cent to the posterior insula (see also � insular cor-tex, neurophysiology and functional imaging of noci-cepetive processing, � secondary somatosensory cor-tex (s2) and insula, effect on pain related behavior inanimals and humans, � nociceptive processing in thesecondary somatosensory cortex). Because the S2 cor-tex receives input via the spinothalamic tract (Stevenset al. 1993) and has strong projections to the insula, itis in a position to transmit nociceptive information tolimbic cortical structures, such as the cingulate, medial
prefrontal(seealso� prefrontalcortex,effectsonpain-related behavior) and orbital frontal cortices, via insu-lar connections (Mesulam and Mufson 1982a; Mesu-lam and Mufson 1982b).
Lesions
Lesions involving the human S2 cortex or the adjacentsubcortical white matter have been associated with acentral pain syndrome and a clinically detectable con-tralateral hypalgesia (Horiuchi et al. 1996; Schmah-mann and Leifer 1992), but a contributing effect of in-jury to the insular cortex could not be completely elim-inated. Greenspan and colleagues (1999) found thatlesions involving the posterior opercular (S2) cortexwere associated with a clinically detectable elevationofpain threshold inhumans,whilepatientswith lesionssparing S2 cortex had normal heat pain thresholds evenwhen the lesion also involved the insula (Greenspan etal. 1999).
Stimulation
Recent studies using imaging methods to confirm thelocation of implanted depth electrodes have not thusfar reported pain sensations or pain related behaviorduring direct stimulation of the S2 cortex in humans(Ostrowsky et al. 2000; Ostrowsky et al. 2002). How-ever, these investigations were focused on stimulationof the insular cortex, so a more definitive assessmentawaitsasystematicexplorationof thehumanS2cortex.
Electrophysiology
Cellular recordings from S2 cortex in anesthetized pri-mates reveal very few neurons that respond to noxiousstimuli. The somatotopic organization of primate S2is quite coarse compared to that of S1 cortex and thereceptive fields are typically large - often bilateral orcovering most of a single limb (Burton et al. 1995). Incontrast with the observations in recordings from ani-mals, noxious stimulation regularly evokes distinctiveelectrical and magnetic responses in human S2 cortex(Arendt-Nielsen etal. 1999;Bromm 2001;Kakigiet al.2000; Ploner et al. 2002). Nociceptive information ar-rivesnearlysimultaneouslyat thehumanS2andS1cor-tex (approximately 150–200msto peak)but, followinga brief stimulus, the duration of neuronal activity is sig-nificantly longer in S2 than in the S1 cortex (Inui et al.2003; Kanda et al. 2000; Ploner et al. 2002). SelectiveC fiber stimulation also evokes MEG and EP responsesin S2 cortex (Opsommer et al. 2001; Tran et al. 2002).Frot and colleagues (2001) revealed differences in thelatency and amplitude of S2 cortical responses to in-nocuous electrical and noxious (laser) stimulation dur-ing depth electrode recording in humans, suggestingthat this cortex integrates both tactile and nociceptiveinputs (Frot et al. 2001).

468 Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior
Functional Imaging
The S2 cortex is one of the most consistently activatedstructures in positron emission tomographic (PET)and fMRI studies (see also � PET and fMRI imag-ing in parietal cortex (SI, SII, inferior parietal cor-tex BA40))designed to distinguish among responsesto noxious and innocuous stimuli (Burton et al. 1993;Casey 1999; Davis 2000; Derbyshire 2003; Peyron etal. 2000). An fMRI study revealed a coarse somato-topic organization within the S2 cortex (Ruben et al.2001). However, Peyron and colleagues (2002), us-ing a multi-modality approach involving PET, fMRI,and scalp LEP recording with dipole localization in thesame subjects, could not determine whether the painrelated activations they obtained were localized to theS2 cortex, the insula or both structures. Their resultsled the authors to suggest the term “operculoinsular”cortex to refer to responses within the S2-insular re-gion (Peyron et al. 2002). However, the recent resultsobtained from detailed depth recording favor the inter-pretation that both the S2 and insular cortices are in-dependent generators of responses to noxious stimuli(Frot and Mauguiere 2003).In summary, theevidencesupports theviewthathumanS2cortex isacriticalcomponentof thecorticalnetworkmediating pain. Although there is a crude somatotopicorganization within this cortex, it seems unlikely thatit is critical for spatial discrimination. Rather, the S2cortex appears to be involved in the early identificationof noxious events that are combined with the localizinginformation provided through the S1 cortex and trans-mitted to other cortical areas for further analysis.
Anterior Insula
The anterior insula (see also � insular cortex, neu-rophysiology and functional imaging of nocicepetiveprocessing, � secondary somatosensory cortex (s2)and insula, effect on pain related behavior in ani-mals and humans, � nociceptive processing in the sec-ondary somatosensory cortex) lies rostral to the mostlateral point of the central sulcus, which also approx-imately defines the vertical plane extending throughthe anterior commissure perpendicular to the sagittalplane. The cortex of the anteroventral part of the in-sula is agranular, receives input from entorhinal cortex(see also � nociceptive processing in the hippocampusand entorhinal cortex, neurophysiology and pharma-cology, � hippocampus and entorhinal complex, func-tional imaging)and sendsprojections to limbiccorticalstructures such as the entorhinal, periamygdaloid andanterior cingulate cortices (Augustine 1996).
Lesions
There are no studies of the effects of localized an-terior insular lesions specifically on pain perception.
Greenspan and colleagues, however, identified 2 pa-tients with lesions involving the anterior insula, bothof whom had normal heat pain thresholds. Their 3 pa-tients with anterior insular sparing and involvement ofboth S2 and posterior insula however,had contralateralelevated thresholds for heat or mechanically inducedpain (Greenspan et al. 1999). These observations sug-gest that the anterior insula is not an essential compo-nent of the cortical network mediating pain.
Stimulation
In a study confirming the site of stimulation in con-scious humans, stimulation of the anterior insula pro-duced visceral sensory experiences and visceral mo-tor responses, but not reports of pain (Ostrowsky et al.2000).
Electrophysiology
A neurophysiological study directed specifically at theanterior (granular) portion of the primate insula foundthat all responsive neurons had large receptive fieldsand were excited by innocuous somatic stimuli; how-ever, the investigators searched for responses only withinnocuous stimuli (Schneider et al. 1993).
Functional Imaging
PET imaging shows that the anterior insula is activeduring the early phase of a series of repetitive noxiousheat stimuli, but not after the stimulation continues for45 s (Casey et al. 2001). This is consistent with thefindings of Ploghaus and colleagues who showed, us-ing fMRI, that the anterior insula was active specifi-cally during theanticipation ofexperimentally inducedpain rather than during the experience of pain itself(Ploghaus et al. 1999). However, Porro and colleaguesshowedthatactivity in theanterior insula, togetherwiththe S1, anterior cingulate, and medial prefrontal cor-tices, increases during the anticipation of pain and isalso correlated with perceived pain intensity (Porro etal. 2002). Nonetheless, a recent fMRI study revealsthat the anterior insula is among the frontal and tempo-ral brain structures responding specifically to stimulusnovelty (Downaretal.2002).Theseresultsconfirmandelaborate on earlier imaging studies showing pain re-lated activity in the anterior insula (Casey et al. 1996;Coghill et al. 1994; Davis et al. 1998; Hsieh et al. 1994;Svensson et al. 1997).In summary, the results suggest that the anterior insulais an essential component of the cortical network me-diating some early aspects of pain perception includ-ing the anticipation of pain. Because anticipation im-plies the influence of past experience with pain, theanatomical connections of the anterior insula with lim-bic structures, such as the entorhinal cortex of the tem-poral lobe (see also � hippocampus and entorhinal

C
Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior 469
� complex, functional imaging � nociceptive pro-cessing in thehippocampusand entorhinalcortex:neu-rophysiology and pharmacology) are likely to be ofcritical importance in mediating this function.
Cingulate Cortex
Based on clinical observations and recent experimen-tal studies, Vogt and colleagues have proposed that theanterior cingulate cortex (ACC; rostral to the plane ofthe anterior commissure) mediates primarily executivefunctions related to the emotional control of visceral,skeletal and endocrine outflow; the posterior cingulatecortex (PCC) (see also � cingulate cortex, nocicep-tive processing, behavioral studies in animals, � painprocessing in the cingulate cortex, behavioral studiesin humans, � cingulate cortex, functional imaging),however, is thought to subserve evaluative functionssuch as monitoring sensory events and personal be-havior in relation to spatial orientation and memory(Vogt et al. 1992). The results of a more recent PETstudy suggested further that increased responses (acti-vation) in subdivisions of the ACC signal participationin response selection and affective elaboration, whilereduced responses (deactivation) in the PCC may re-flect disengagement from visually guided processes(Vogt et al. 1996). However, other studies have shownstrong neurovascular (Gelnar et al. 1999) and laserevoked responses (� insular cortex, neurophysiologyand functional imaging of nocicepetive processing,� nociceptive processing in the secondary somatosen-sory cortex) in the PCC (Bentley et al. 2003).Anatomical data shows that sectors of the ACC and amid-cingulate area just below the supplementary mo-tor area are strongly connected to the ventral horns ofthe spinal cord, thus providing direct access to motormechanisms and the direct modulation of voluntaryresponses to noxious stimuli (Dum and Strick 1993;Hutchins et al. 1988).
Anterior Cingulate Cortex (ACC)
Lesions
Anteriorcingulate lesionsdonot interferewith theabil-ity of humans to recognize or respond to acute nox-ious stimuli. This is most clearly demonstrated in clin-ical cases. There are very few studies in which the lo-cation and extent of the lesion is known to be con-fined to the anterior cingulate cortex and the responseto pain is tested specifically. However, Cohen and col-leagues (Cohen et al. 1999) examined 12 patients,all with normal neurological examinations except forperipheral findings related to their pain syndrome.Each underwent cingulotomy (see also � cingulatecortex, nociceptive processing, behavioral studies inanimals, � pain processing in the cingulate cortex, be-havioral studies in humans, � cingulate cortex, func-
tional imaging) for intractable pain and was examinedpre- and post-operatively. The lesions were limited tothesupracallosalmid-anterior cingulatecortex.There-sponse to acuteexperimentalpain wasnot tested.How-ever, the patients reported only a modest relief of theintensity of their clinical pain but a significant reduc-tion in the degree to which the pain interfered with theirdaily behavior and social functionAnimal studies of rostral ACC lesions reveal deficitsin avoidance learning and nociceptively conditionedplace avoidance, but the normal response to acute painappearsunimpaired (Gabrielet al.1991; Johansenetal.2001). Lesions involving the rodent mid-anterior, butnot the pregenual cingulate cortex however, impair theexecution of escape responses to gradually increasingheat, while sparing other nocifensive behaviors (Pas-toriza et al. 1996).Overall, the results show that different sectors of theACC participate in the acquisition of learned responsesto noxious stimuli, the association of negative hedo-nic attributes with acute noxious stimuli and the exe-cution ofmotor responses to acutenoxiousstimuli.Thelonger-term effects of ACC lesions will be consideredin subsequent sections of this review.
Stimulation
The most consistent responses during electrical stim-ulation in humans are visceromotor changes associ-ated with nausea, sensations of fullness, changes inblood pressure and heart rate and cutaneous flushing(Talairach et al. 1973). Unpleasant emotional reactionsare occasionally reported (Laitinen 1979;von Cramonand Jurgens 1983). In the rodent, biochemical stim-ulation of the rostral ACC (see also � cingulate cor-tex, nociceptive processing, behavioral studies in ani-mals, � pain processing in the cingulate cortex, behav-ioral studies in humans, � cingulate cortex, functionalimaging) produced conditioned avoidance and bio-chemical suppression of the same site impairs condi-tioned avoidance learning (Johansen and Fields 2004).Overall, the results suggest a negative affective statethat must be associated with noxious stimuli for thenormal experience of pain.
Electrophysiology
Severalevokedpotentialandsinglecell recordingstud-ies showthatnoxiousstimuli evokeneuronal responseswithin the rostral and mid-anterior sectors of the ACCofhumansandexperimentalanimals. In thehuman,no-ciceptive responses appear within 300 ms of a noxiouslaser stimulus (Inui et al. 2003; Kakigi et al. 2000; Lenzet al. 1998). Neurophysiological studies show that theACC becomes active nearly simultaneously with theS1 and S2 cortices, indicating that spatio-temporal andintensity analysis begins in parallel with the process-

470 Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior
ing of affective related information (Ploner et al. 2002;Schnitzler and Ploner 2000). The early parallel pro-cessing of affective and sensory information is consis-tent with the concept that noxious stimuli have an in-trinsic, primary unpleasantness (Fields 1999; Melzackand Casey 1968; Price 2000).The limited sample of cellular recordings from humansubjects shows that some mid-anterior ACC neuronsresponded only to noxious thermal (heat or cold) stim-uli but also responded in anticipation of noxious stim-ulation (Hutchison et al. 1999); the receptive field sizecould not be determined. In experimental animals, no-ciceptively responding cells had large receptive fields(Sikes and Vogt 1992; Yamamura et al. 1996). In theconscious monkey, neurons in the ACC and in theanatomically associated caudate nucleus respondedduring the anticipation of pain in a pain avoidance task(Koyama et al. 1998; Koyama et al. 2000, 2001).
Functional Imaging
Reviews of functional imaging studies show that eitherthe rostral or mid-anterior or both sectors of the ACCare activated consistently during pain (Bushnell et al.1999; Casey 1999; Derbyshire 2000, 2003). Davis andcolleagues showed that a sector of the ACC rostral tothat responding during pain is activated specifically bya pain independent attention-demanding task (Davis etal. 1997). Rainville and colleagues (1997) showed thatan anterior, supragenual area of this cortex participatesspecifically in the affective coding of pain (Rainville2002; Rainville et al. 1997). During prolonged, repeti-tive heat stimulation, the most rostral sectorof theACCisactiveonly during theearly phase,whileactivation ofthemorecaudalpartof theACCappearsduringthelaterphase (Casey et al. 2001). This result is in accord withthe observation that the most rostral sector of the ACCis associated with the anticipation of pain (Ploghaus etal. 1999).
Posterior Cingulate Cortex (PCC)
Nociceptive information arrives at the PCC within ap-proximately 200–250 ms of the application of a nox-ious laser stimulus (Bentley et al. 2003; Bromm 2001),so, like the ACC, it is involved in the earliest stagesof nociceptive analysis. As noted above in the generaldiscussion of the cingulate cortex, there is neurophys-iological and functional imaging (Gelnar et al. 1999)evidence that the PCC participates in both the sensoryand behavioral aspects of pain processing.
Intermediate Cortical and Limbic Processing (Millisec-onds–Minutes)
As the nociceptive identification process is sustained,it leads to the allocation of attentional resources andthe distraction from competing stimuli. Ward and col-
leagues presented evidence that, in the visual system,the application of attentional mechanisms requires upto 500 ms (Ward et al. 1996). Following this very earlystage, there is an elaboration of the identity of the stim-ulus so that its location, physical property and affec-tive qualities are recognized more clearly and begin toform the basis for further analysis and response. Thisearly identificationof theaffectivecomponentofanox-ious stimulus is probably identical to the “primary un-pleasantness” of Fields (Fields 1999) and the “imme-diate pain unpleasantness” of Price (Price 2000) and isclosely tied to perceived stimulus intensity.Somatic, visceral and autonomic responses may be re-flexive and preconscious at the earliest stages of cor-tical engagement, but may be facilitated or prolongedby the action of specific cortical mechanisms. Immedi-ate withdrawal from the stimulus and the facilitation offlexion reflexes is an example of an early somatomotorresponse that may be modified quickly to include moreelaborate voluntary escape maneuvers. Early cogni-tive reactions at this stage may include the recogni-tion of tissue injury, the experience of fear or angerand the development of immediate defensive actions.Cortical connections with the amygdala are importantfor these affective and autonomic responses (LeDoux2000; Neugebauer et al. 2004).
Inferior Parietal Lobule (B40)
Lesions involving the inferiorparietal lobule (IPL)(seealso � PET and fMRI imaging in parietal cortex (SI,SII, inferior parietal cortex BA40)), particularly of theright hemisphere, are associated classically with hemi-body neglect syndromes (Adams and Victor 1993; De-Jong 1979; Mesulam 1990). In humans, lesions in-volving this cortical area, which includes the poste-rior parietal operculum and Brodmann’s area 40, haveclinically obvious deficits in detecting and respondingto noxious stimuli (Bassetti et al. 1993). Neurons re-sponding to noxious stimulation or the visual threat ofnoxious stimulation have been recorded from the pos-terior parietal (7b) cortex of monkeys and a lesion inthis same area was associated with contralateral hy-palgesia (Dong et al. 1994, 1996). Functional imagingstudies have frequently revealed activity in this lateralposterior parietal cortex during pain, particularly whenthe task involves attending specifically to the painfulstimulation (Coghill et al. 2001; Duncan and Albanese2003; Peyron et al. 1999; Peyron et al. 2000; Svens-son et al. 1997) or during simulated pathological painstates (Baron et al. 1999; Hsieh et al. 1994; Hsieh etal. 1995a). However, Karnath (Karnath 2001; Karnathet al. 2001) has presented and summarized evidencethat pure spatial neglect follows lesions of the superiortemporalgyrus(STG)andthatlesionsinvolvingthehu-man IPL are more likely to reflect deficits in organizing

C
Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior 471
movements directed within extrapersonal, body ori-ented hemispace. Downar and colleagues showed thatactivation of the cortex at the temporo-parietal junc-tion, which includes the inferior parietal lobule and su-perior temporal gyrus, is associated with the perceivedsalience of both painful and painless stimuli (Downaret al. 2002; Downar et al. 2003). In summary, there issubstantial evidence that the cortex in the area of thetemporo-parietal junction, including the IPL(B40)andSTG, participates in attentional mechanisms that arelikely to be critical for the normal perception of andattention to injurious stimuli. This interpretation is ofinterest in view of the strong connections between thiscortex and the premotor cortical areas (see below).
Premotor Cortex (B6)
The premotor cortex (see also � prefrontal cortex, ef-fects on pain-related behavior) is active during pain asshown in many functional imaging studies of normalhumansubjects(Casey1999;Caseyetal.2001;Coghillet al. 1999; Ladabaum et al. 2000; Tracey et al. 2000),including those focused on the related sensation of itch(Drzezga et al. 2001; Hsieh et al. 1994). Fibromyal-gia patients who show a high degree of catastrophizingabout their pain have an increased response in the me-dial premotor cortex (B6) to somatic pressure stimuli(Gracely et al. 2004).There is a strong anatomical and functional relation-ship between the parietal and frontal motor (see also� prefrontal cortex, effects on pain-related behavior,� PET and fMRI imaging in parietal cortex (SI,SII, in-ferior parietal cortex BA40)) areas of the monkey andhuman brain (Rizzolatti et al. 1998). The circuits con-necting predominantly somatosensory posterior pari-etal association areas with the dorsal and ventral pre-motor cortex are important for nociceptive processingin the cortex. For example, a component of the dorsalpremotor circuit is involved in motor planning basedprimarily on somatosensory information (Rizzolatti etal. 1998). A functional imaging study has now shownthat theboth theventral and dorsalpremotorcortexpar-ticipate in the development of the sense of ownershipof a body part (Ehrsson et al. 2004). Therefore, it ispossible that the premotor cortex contributes to stim-ulus recognition and identification in addition to par-ticipating in the development of a motor response to astimulus.
Posterior Insula
Lesions
The recent observations by Greenspan and colleaguesshow that lesions involving the posterior insula maynot attenuate pain threshold but are associated with asignificant increase in pain tolerance as assessed bythe cold pressor test (Greenspan et al. 1999). Clini-
cal observations also show that lesions involving thedeep parasylvian cortex are associated with significanthypalgesia (Bassetti et al. 1993; Davison and Schick1935; Greenspan and Winfield 1992; Horiuchi et al.1996; Schmahmann and Leifer 1992). Involvement ofthe insula also leads to the clinical phenomenon of painasymbolia, in which the patient fails to recognize or re-spond to the threat of noxious stimuli (Berthier et al.1988).
Stimulation
Ostrowsky and colleagues (Ostrowsky et al. 2000,2002) explored the insular cortex in 43 patients under-going evaluation for epilepsy surgery and were able toverify the location of the stimulating electrodes withMR imaging. Stimulation within the posterior insulaevoked painful sensations in theupperposterior insularcortexat17of93(18.2%)insularstimulationsites in14patients. The patients described the stimulus-evokedsensations as burning, stinging or disabling, locatedeither contralaterally or bilaterally and rarely outlast-ing thestimulation.Non-painful somatosensorysensa-tions, described as warmth, cold or tingling, were alsoevoked in 21 of these 93 insular sites (37.2%). The painrelated region shows a striking overlap with the dorsalposterior insular site activated by heat pain (Craig et al.2000). Although these electrical stimuli did not evokeafter-discharge, it is likely thatother corticalareaswereactivated during the insular stimulation and may haveparticipated in the elaboration of the sensory experi-ences.
Electrophysiology
A small number of neurons responding to noxiousstimuli have been recorded from the posterior insula(Robinson and Burton 1980). Zhang and colleaguesrecorded single insular neurons that responded to bothinnocuous and noxious somatic stimuli; some of thesecells were localized to the more posterior granular areaand also responded to baroreceptor stimulation (Zhanget al. 1999). In addition, numerous electrophysiolog-ical studies in humans have shown insular responsesto painful cutaneous stimulation (Kakigi et al. 2000;Kakigi et al. 2003; Treede et al. 2000).
Functional Imaging
The anterior insula is activated early in the course ofrepetitive stimulation with noxious heat, but this re-sponse is replaced by a shift of the peak activity cau-dally to the mid-posterior insulaas thestimulation con-tinues (Casey et al. 2001). The mid- and posterior-insula is among the most regularly responsive regionsfound among a variety of functional imaging studies(Casey 1999; Craig et al. 2000; Peyron et al. 2000;Peyron et al. 2002). Derbyshire (2003) has reviewed

472 Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior
evidence showing that visceral distention activatesboth the anterior and posterior insula, but the intensity,timing and duration of stimulation varied across stud-ies (Derbyshire 2003).
Anterior and Posterior Cingulate Cortex
The more rostral perigenual sectors of the ACC are ac-tive only early in the course of prolonged repetitiveheat stimulation. Such stimulation is followed by sus-tained activity more caudally within Brodmann area24 (Casey et al. 2001). Both attentional mechanismsand the perception of pain activate adjacent but sep-arate sectors of the ACC (Davis et al. 1997). Gelnarand colleagues showed that the posterior cingulate cor-tex, which receives input from thalamic targets of thespinothalamic tract (Apkarian and Shi 1997), respondsspecifically during painful heat stimulation (Gelnaret al. 1999); the PCC also participates in identifyingthe salience of prolonged (1 minute) noxious stimuli(Downar et al. 2003).
Long-Term Cortical and Limbic Processes (Minutes—Years)
Unlike the preceding responses, which generally occurover periods of seconds or less, a more detailed eval-uation of an injury proceeds over time periods rang-ing from minutes to years and, especially in the caseof chronic pain, may change over time. The qualita-tive evaluation includes mnemonic processes such asa comparison of present and past experiences with in-jurious physical stimuli such as heat, mechanical dis-tortions and chemical changes in the tissue. Most crit-ically, a global assessment of the environment and thecontext in which the noxious event occurred is an im-portant determinant of the perceived severity of thenoxiousstimulation or injury.Theaffectivecomponentof the experience may vary over time but is fully devel-oped at this stage; it is probably related to what Fieldshas called “secondary unpleasantness” (Fields 1999)and Price refers to as “secondary pain unpleasantness”(Price 2000). Cognitive mechanisms are engaged atthis stage and these may include mnemonic functions,adjustments to daily living and planning for the future.Overall, this aspect of pain related cortical function isclosely related to the concept of pain as a “need-state”(Wall 1979) or a homeostatic function (Craig 2002).
Anterior Cingulate Cortex
Patients with lesions specifically confined to the ACChave an attenuation of the affective component of painthat is sustained for many months and, where informa-tion is available, for years (Cohen et al. 1999; Hurt andBallantine 1973). Unfortunately, these patients mayalso show impairment of sustained attention and spon-taneous behavioral responses (Cohen et al. 1999). A
patient with a surgical lesion confined to the right mid-anterior cingulate gyrus had impaired executive con-trol of manual but not verbal responses; responses tonoxious stimuli were not tested (Turken and Swick1999).Surgical lesionswithin themore rostral,pregen-ual (“affective”) sector of the ACC are associated withaffective blunting and a reduction of concern aboutclinical pain, but the responses to acute experimentallyinducedpainaregenerallynotdescribedindetail (Foltzand White 1962; Hornak et al. 2003; Hurt and Bal-lantine 1973); the same is true of an extensively an-alyzed case of medial prefrontal damage (Damasio etal. 1994).There is insufficientdata towarrantcommenton the long-term pain related effects of posterior cin-gulate lesions in humans.
Medial Prefrontal Cortex (B9, 10, 11)
Although the medial prefrontal cortex participates inthe elaboration of emotional and high order cognitivestates that are independent of noxious somatic and vis-ceral stimuli (Ramnani and Owen 2004; Simpson etal. 2001; Wager et al. 2003), a significant minority offunctional imaging studies have shown that this cor-tex is active during experimental somatic or visceralpain (Derbyshire 2003; Peyron et al. 2000; Wager etal. 2004) or simulated pathological states (Hsieh et al.1995b; Iadarola et al. 1998). Extensive lesions of thehuman mesial prefrontal cortex extending rostral to thecingulate gyrus (see also � cingulate cortex, nocicep-tive processing, behavioral studies in animals, � painprocessing in the cingulate cortex, behavioral stud-ies in humans, � cingulate cortex, functional imaging)are associated with profound and lasting neurologicaldeficits ranging from blunting of emotional responses(abulia) to the syndrome of akinetic mutism and mo-tor neglect (Damasio et al. 1994; Mochizuki and Saito1990; Kumral et al. 2002; Minagar and David 1999;Mochizuki and Saito 1990). Although extensive dam-age to this cortex precludes an unbiased examinationof pain sensations, it is likely that it participates in thelong-term evaluation of the emotional impact of painand the need to apply cognitive strategies to adapt ac-cordingly.
Orbitofrontal Cortex (OFC)
The orbitofrontal cortex (see also � hypothalamus andnociceptive pathways, � prefrontal cortex, effects onpain-related behavior) is the major cortical output tothe hypothalamus (see also � hypothalamus and no-ciceptive pathways) and also has direct efferent con-nections to the amygdala and periaqueductal gray mat-ter (Ongur et al. 1998). Functional imaging studies ofpain show OFC activation during experimental painstudies of heat (Craig et al. 2000), visceral stimulation(Derbyshire 2003) and simulated pathological pain

C
Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior 473
states (Lorenz et al. 2002). Other imaging investiga-tions show that the OFC plays a critical role in assign-ing affective valence to sensory information and in es-tablishing the rewarding or punishing value of experi-ences including pain (Rolls et al. 2003), which in turnguide behavioral responses (Rolls 2000). In studying43 patients with a variety of prefrontal cortical lesions,Hornack and colleagues (Hornak et al. 2003) identi-fied 6 patients with bilateral circumscribed surgical le-sions involving the OFC. These patients had difficultyidentifying emotions and impairments in their subjec-tive emotional states. Therefore, the greatest long-termclinical significance of OFC participation in pain re-lated behavior may be a sustained impairment of theability to recognizepain asaprimary reinforcer,which,in turn, leads to adaptive behaviors and emotional re-sponses to injury (Kringelbach and Rolls 2004).
Dorsolateral Prefrontal Cortex (DLPFC; B9, 46)
The DLPFC (see also � prefrontal cortex, effects onpain-related behavior) is active during executive pro-cesses involving shifts of attention between or amongtasks (Smith and Jonides 1999). Cortical activationsthat include the DLPFC are observed in a majorityof neuroimaging studies of pain (Peyron et al. 2000).However, as Peyron and colleagues have shown, theactivation appears to be due to the participation of at-tentional and executive processes involved in attempt-ing to attend to or ignore the painful stimulation, ratherthan an analysis of the sensory or affective dimensionsof the stimulus (Peyron et al. 1999). Thus, during thepain of heat allodynia (Lorenz et al. 2002), a high levelof activation intensity in the left DLPFC is correlatedwith reduced pain unpleasantness and reduced func-tional connectivity between the midbrain and medialthalamus; right DLPFC activity however, is associatedwith a reduced correlation of anterior insular activitywith both pain unpleasantness and intensity (Lorenz etal.2003).TheDLPFCalsoappears tobeanactiveagentin mediating placebo analgesia, because the intensityof DLPFC activity correlates with and predicts the in-tensity of expected pain relief in the placebo condition(Wager et al. 2004). The DLPFC thus participates inmediating acute pain, but the current author suggeststhat the sustained pain modulatory effects of DLPFCactivity are most strongly engaged following the ini-tial sensory and hedonic analysis of injuries and dur-ing chronicpain states,where the impairmentof frontallobe function would have clinically significant impacton the recruitment of pain coping strategies (Stuss andBenson 1986).
Hippocampus and Entorhinal Cortex
The hippocampus (see � nociceptive processing in thehippocampus and entorhinal cortex, neurophysiology
and pharmacology) and its major input, the entorhi-nal cortex, are part of a cortical network, includingthe DLPFC and anatomically related frontal cortices,for the encoding, storage and retrieval of polymodalsensory information emanating from parietal associa-tion areas (Sakai 2003; Simons and Spiers 2003). Inthe rodent, the synaptic excitability of hippocampalpyramidal neurons undergoes a prolonged, choliner-gically dependent depression following noxious stim-ulation; this evoked depression shows a marked habit-uation to repeated stimulation (Khanna and Sinclair1989; Khanna and Sinclair1992).Noxious stimuli alsoactivate immediate early genes in neurons within thesame hippocampal sector (Khanna et al. 2004), furthersuggesting a role in mnemonic circuitry. Prolonged in-creases in neuronal activity are also seen in the rodententorhinal cortex (Frank and Brown 2003). Hippocam-pal or entorhinal activation or deactivation is rarelyseen in most neuroimaging studies, but appears in stud-ies in which the stimulus intensity increases during thescan period (Derbyshire et al. 1997) or when painful,but not painless, stimulation is unexpected (Ploghauset al. 2000). When the expectation of a noxious stim-ulus is manipulated so as to produce anxiety, there isan anxiety related increase in pain and in the pain re-sponse in the entorhinal cortex (Ploghaus et al. 2001).Together, these findings show that these medial tempo-ral lobe structures participate in elaborating the experi-ence of pain based on emotional state, expectation andpast experience. The author suggests that this elabora-tion follows the earlier sensory identification and af-fective labeling of the noxious stimulation and that itssustained clinical impact is on the ability of patients tointerpret the long-term significance of internal states,including clinically painful conditions. A well-studiedexample of this rare but important condition has beenpresented by Hebben and colleagues (Hebben et al.1985).
References1. Adams RD, Victor M (1993) Principles of Neurology, 5th edn.
McGraw-Hill, New York2. Apkarian AV, Shi T (1997) Thalamocortical connections of the
cingulate and insula in relation to nociceptive inputs to the cor-tex. In: Ayrapetian S, Apkarian AV (eds) Pain Mechanisms andManagement. IOS Press, Amsterdam, pp 212–220
3. Arendt-Nielsen L, Yamasaki H, Nielse, J et al. (1999) Mag-netoencephalographic responses to painful impact stimulation.Brain Res 839:203–208
4. Augustine JR (1996) Circuitry and functional aspects of theinsular lobe in primates including humans. Brain Res Rev22:229–244
5. Baron R, Baron Y, Disbrow E et al. (1999) Brain processing ofcapsaicin-induced secondary hyperalgesia: A functional MRIstudy. Neurol 53:548
6. Bassetti C, Bogousslavsky J Regli F (1993) Sensory syndromesin parietal stroke. Neurology 43:1942–1949

474 Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior
7. Bentley DE, Derbyshire SWG, Youell PD et al. (2003) Cau-dal cingulate cortex involvement in pain processing: an inter-individual laser evoked potential source localisation study usingrealistic head models. Pain 102:265–271
8. Berthier M, Starkstein S, Leiguarda R (1988) Asymobolia forpain: A sensory-limbic disconnection syndrome. Annals Neu-rol 24:41–49
9. Bromm B (2001) Brain Images of Pain. News Physiol Sci16:244–249
10. Burton H, Videen TO, Raichle ME (1993) Tactile-vibration-activated foci in insular and parietal-opercular cortex studiedwith positron emission tomography: Mapping the second so-matosensory area in humans. Somatosen Mot Res10:297–308
11. Burton H, Fabri M, Alloway K (1995) Cortical areas within thelateral sulcus connected to cutaneous representations in areas3b and 1: A revised interpretation of the second somatosensoryarea in macaque monkeys. J Comparative Neurol 355:539–562
12. Bushnell MC, Duncan GH, Hofbauer RK et al. (1999) Painperception: Is there a role for primary somatosensory cortex?Proc Natl Acad Sci USA 96:7705–7709
13. Casey KL (1999) Forebrain mechanisms of nociception andpain: Analysis through imaging. Proc Natl Acad Sci USA96:7668–7674
14. Casey KL (2000) The Imaging of Pain: Background and Ra-tionale. In: Casey KL, Bushnel MC (eds) Pain Imaging. IASPPress, Seattle, pp 1–29
15. Casey KL, Minoshima S, Morrow TJ et al. (1996) Comparisonof human cerebral activation patterns during cutaneous warmth,heat pain, and deep cold pain. J Neurophysiol 76:571–581
16. Casey KL, Morrow TJ, Lorenz J et al. (2001) Temporal andspatial dynamics of human forebrain activity during heat pain:analysis by positron emission tomography. J Neurophysiol85:951–959
17. Coghill RC, Talbot JD, Evans AC et al. (1994) Distributed pro-cessing of pain and vibration by the human brain. J Neurosci14:4095–4108
18. Coghill RC, Sang CN, Maisog JH et al. (1999) Pain inten-sity processing within the human brain: A bilateral, distributedmechanism. J Neurophysiol 82:1934–1943
19. Coghill RC, Gilron I, Iadarola MJ (2001) Hemisphericlateralization of somatosensory processing. J Neurophysiol85:2602–2612
20. Cohen RA, Kaplan RF, Moser DJ et al. (1999) Impairmentsof attention after cingulotomy. Neurology 53:p 819
21. Craig AD (2002) How do you feel? Interoception: the senseof the physiological condition of the body. Nat Rev Neurosci3:655–666
22. Craig AD, Chen K, Bandy D et al. (2000) Thermosensory ac-tivation of insular cortex. Nature Neurosci 3:184–190
23. Damasio H, Grabowski T, Frank R et al. (1994) The return ofPhineas Gage: Clues about the brain from the skull of a famouspatient. Science 264:1102–1105
24. Davis KD (2000) The neural circuitry of pain as explored withfunctional MRI. Neurological Res 22:313–317
25. Davis KD, Taylor SJ, Crawley AP et al. (1997) Functional MRIof pain- and attention-related activations in the human cingulatecortex. J Neurophysiol 77:3370–3380
26. Davis KD, Kwan CL. Crawley AP et al. (1998) Functional MRIstudy of thalamic and cortical activations evoked by cutaneousheat, cold, and tactile stimuli. J Neurophysiol 80:1533–1546
27. Davison C, Schick W (1935) Spontaneous pain and othersubjective sensory disturbances. AMA Arch Neurol Psychiat34:1204–1237
28. DeJong RN (1979) The Neurologic Examination, 4th edn.Harper and Row, Hagerstown
29. Derbyshire SW (2000) Exploring the pain “neuromatrix” CurrRev Pain 4:467–477
30. Derbyshire SWG (2003) A systematic review of neuroimag-ing data during visceral stimulation. Am J Gastroenterol98:12–20
31. Derbyshire SW, Jones AK, Gyulai F et al. (1997) Pain pro-cessing during three levels of noxious stimulation producesdifferential patterns of central activity. Pain 73:431–445
32. Dong WK, Chudler EH, Sugiyama K et al. (1994) Somatosen-sory, multisensory, and task-related neurons in cortical area 7b(PF) of unanesthetized monkeys. J Neurophysiol 72:542–564
33. Dong WK, Hayashi T, Roberts VJ et al. (1996) Behavioral out-come of posterior parietal cortex injury in the monkey. Pain64:579–587
34. Downar JD, Crawley AP, Mikulis DJ et al. (2002) A corti-cal network sensitive to stimulus salience in a neutral behav-ioral context across multiple sensory modalities. J Neurophys-iol 87:615–620
35. Downar J, Mikulis DJ, Davis KD. (2003) Neural correlatesof the prolonged salience of painful stimulation. Neuroimage20:1540–1551
36. Drzezga A, Darsow U, Treede RD et al. (2001) Central activa-tion by histamine-induced itch: analogies to pain processing: acorrelational analysis of O-15 H2O positron emission tomog-raphy studies. Pain 92:295–305
37. Dum RP, Strick PL (1993) Cingulate Motor Areas. In: VogtBA, Gabriel M (eds) Neurobiology of Cingulate Cortex andLimbic Thalamus: A Comprehensive Handbook. Birkhauser,Boston
38. Duncan GH, Albanese MC (2003) Is there a role for the parietallobes in the perception of pain? Adv Neurol 93:69–86
39. Ehrsson HH, Spence C, Passingham RE (2004) That’s MyHand! Activity in Premotor Cortex Reflects Feeling of Own-ership of a Limb. Science 305:875–877
40. Fields HL (1999) Pain: an unpleasant topic. Pain 6: 61–6941. Foltz EL, White LE (1962) Pain “relief” by frontal cingulu-
motomy. J Neurosurgery 19:89–10042. Frank LM, Brown EN (2003) Persistent activity and memory
in the entorhinal cortex. Trends in Neurosci 26:400–40143. Frot M, Mauguiere F (2003) Dual representation of pain in the
operculo-insular cortex in humans. Brain 126:438–45044. Frot M, Garcia-Larrea L, Guenot M et al. (2001) Responses
of the supra-sylvian (SII) cortex in humans to painful and in-nocuous stimuli: A study using intra-cerebral recordings. Pain94:65–73
45. Gabriel,M, Kubota Y, Sparenborg S et al. (1991) Effects ofcingulate cortical lesions on avoidance learning and training-induced unit activity in rabbits. Experimental Brain Res86:585–600
46. Gelnar PA, Krauss BR, Sheehe PR et al. (1999) A Compar-ative fMRI Study of Cortical Representations for ThermalPainful, Vibrotactile, and Motor Performance Tasks. Neuroim-age 10:460–482
47. Gracely RH, Geisser ME Giesecke T et al. (2004) Pain catas-trophizing and neural responses to pain among persons withfibromyalgia. Brain 127:835–843
48. Greenspan JD, Winfield JA (1992) Reversible pain and tac-tile deficits associated with a cerebral tumor compressing theposterior insula and parietal operculum. Pain 50:29–39
49. Greenspan JD, Lee RR, Lenz FA (1999) Pain sensitivity alter-ations as a function of lesion location in the parasylvian cortex.Pain 81:273–282
50. Hebben N, Corkin S, Eichenbaum H et al. (1985) Dimin-ished ability to interpret and report internal states after bilat-eral medial temporal resection: case H.M. Behavioral Neurosci99:1031–1039
51. Hofbauer RK, Rainville P, Duncan GH et al. (2001) Corticalrepresentation of the sensory dimension of pain. J Neurophysiol86:402–411
52. Horiuchi T, Unoki T, Yokoh A et al. (1996) Pure sensory strokecaused by cortical infarction associated with the secondary so-matosensory area. J Neurol Neurosurg Psychiatry 60:588–589
53. Hornak J, Bramham J, Rolls ET et al. (2003) Changes in emo-tion after circumscribed surgical lesions of the orbitofrontaland cingulate cortices. Brain 126:1691–1712

C
Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior 475
54. Hsieh J-C, Hagermark O, Stahle-Backdahl M et al. (1994) Urgeto scratch represented in the human cerebral cortex during itch.J Neurophysiol 72:3004–3008
55. Hsieh J-C, Belfrage M, Stone-Elander S et al. (1995a) Centralrepresentation of chronic ongoing neuropathic pain studied bypositron emission tomography. Pain 63:225–336
56. Hsieh J-C, Belfrage M, Stone-Elander S et al. (1995b) Centralrepresentation of chronic ongoing neuropathic pain studied bypositron emission tomography. Pain 63:225–236
57. Hurt RW, Ballantine HT (1973) Stereotactic anterior cingulatelesions for persistent pain: A report on 68 cases. Clin Neurosurg21:334–351
58. Hutchins KD, Martino AM, Strick PL (1988) Corticospinal pro-jections from the medial wall of the hemisphere. ExperimentalBrain Res 71:667–672
59. Hutchison WD, Davis KD, Lozano AM et al. (1999) Pain-related neurons in the human cingulate cortex. Nat Neurosci2:403–405
60. Iadarola MJ, Berman KF, Zeffiro TA et al. (1998) Neural activa-tion during acute capsaicin-evoked pain and allodynia assessedwith PET. Brain 121:931–947
61. Inui K, Tran TD, Qiu Y et al. (2003) A comparative mag-netoencephalographic study of cortical activations evoked bynoxious and innocuous somatosensory stimulations. Neurosci120:235–248
62. Johansen JP, Fields HL (2004) Glutamatergic activation of an-terior cingulate cortex produces an aversive teaching signal.Nat Neurosci 7:398–403
63. Johansen JP Fields HL, Manning BH (2001) The affectivecomponent of pain in rodents: Direct evidence for a contribu-tion of the anterior cingulate cortex. Proc Natl Acad Sci USA98:8077–8082
64. Kaas JH (1993) The functional organization of somatosensorycortex in primates. Ann.Anat 175:509–518
65. Kaas JH, Nelson RJ, Sur M et al. (1979) Multiple representa-tions of the body within the primary somatosensory cortex ofprimates. Science 204:521–523
66. Kaas JH, Florence SL, Neeraj J (1997) Reorganization ofsensory systems of primates after injury. The Neuroscientist3:123–130
67. Kakigi R, Koyama S, Hoshiyama M et al. (1995) Pain-relatedmagnetic fields following painful CO2 laser stimulation in man.Neurosci Letters 192:45–48
68. Kakigi R, Watanabe S, Yamasaki H (2000) Pain-Relatedsomatosensory evoked potentials. J Clinical Neurophysiol17:295–308
69. Kakigi R Tran TD, Qiu Y et al. (2003) Cerebral responsesfollowing stimulation of unmyelinated C-fibers in humans:electro- and magneto-encephalographic study. Neurosci Res45:255–275
70. Kanda M, Nagamine T, Ikeda A et al. (2000) Primary so-matosensory cortex is actively involved in pain processing inhuman. Brain Research 853:282–289
71. Karnath HO (2001) New insights into the functions of the su-perior temporal cortex. Nat Rev Neurosci 2:568–576
72. Karnath HO, Ferber S, Himmelbach M (2001) Spatial aware-ness is a function of the temporal not the posterior parietal lobe.Nature 411:950–953
73. Kenshalo DR, Isensee O (1983) Responses of primate S1 corti-cal neurons to noxious stimuli. J Neurophysiol 50:1479–1496
74. Kenshalo DR, Chudler EH, Anton F et al. (1988) SI nociceptiveneurons participate in the encoding process by which monkeysperceive the intensity of noxious thermal stimulation. Brain Res454:378–382
75. Kenshalo DR, Iwata K, Sholas M et al. (2000), Response prop-erties and organization of nociceptive neurons in Area 1 of mon-key primary somatosensory cortex. J Neurophysiol 84:719–729
76. Khanna S, Sinclair JG (1989) Noxious stimuli produce pro-longed changes in the CA1 region f the rat hippocampus. Pain39:337–343
77. Khanna S, Sinclair JG (1992) Responses in the CA1 regionof the rat hippocampus to a noxious stimulus. Exp Neurol117:28–35
78. Khanna S, Seong Chang L, Jiang F et al. (2004) Nociception-driven decreased induction of Fos protein in ventral hippocam-pus field CA1 of the rat. Brain Res 1004:167–176
79. Koyama T, Tanaka YZ, Mikami A (1998) Nociceptive neuronsin the macaque anterior cingulate activate during anticipationof pain. Neuroreport 9:2663–2667
80. Koyama T, Kato K, Mikami A (2000) During pain-avoidanceneurons activated in the macaque anterior cingulate and cau-date. Neurosci Letters 283:17–20
81. Koyama T, Kato K, Tanaka YZ et al. (2001) Anterior cingulateactivity during pain-avoidance and reward tasks in monkeys.Neurosci Res 39:421–430
82. Kringelbach ML, Rolls ET (2004) The functional neu-roanatomy of the human orbitofrontal cortex: evidencefrom neuroimaging and neuropsychology. Prog Neurobiol72:341–372
83. Kumral E, Bayulkem G, Evyapan D et al. (2002) Spectrum ofanterior cerebral artery territory infarction: clinical and MRIfindings. Eur J Neurol 9:615–624
84. Ladabaum U, Minoshima S, Owyang C (2000) Pathobiologyof visceral pain: Molecular mechanisms and therapeutic impli-cations v. Central nervous system processing of somatic andvisceral sensory signals. Am J Physiol Gastrointest Liver Phys-iol 279:1–6
85. Laitinen LV (1979) Emotional responses to subcortical electri-cal stimulation in psychiatric patients. Clin Neurol Neurosurg81:148–157
86. LeDoux JE (2000) Emotion circuits in the brain. Ann Rev Neu-rosci 23:155–184
87. Lenz FA, Rios M, Zirh A et al. (1998) Painful stimuli evokepotentials recorded over the human anterior cingulate gyrus. JNeurophysiol 79:2231–2234
88. Lighthall JW (1988) Controlled cortical impact: a new exper-imental brain injury model. J Neurotrauma 5:1–15
89. Lighthall JW, Dixon CE, Anderson TE (1989) Experimentalmodels of brain injury. J Neurotrauma 6:83–97
90. Lorenz J, Cross D, Minoshima S et al. (2002) A uniquerepresentation of heat allodynia in the human brain. Neuron35:383–393
91. Lorenz J, Minoshima S, Casey KL (2003) Keeping pain outof mind: the role of the dorsolateral prefrontal cortex in painmodulation. Brain 126:1079–1091
92. MacLean PD (1955) The limbic system ("visceral brain") inrelation to the central gray and reticulum of the brain stem.Psychosom Med 17:355–366
93. Marshall J (1951) Sensory disturbances in cortical woundswith special reference to pain. J Neurol Neurosurg Psychiat14:187–204
94. Melzack R, Casey KL (1968) Sensory, Motivationaland Cen-tral Control Determinants of Pain. In: Kenshalo DR (ed) TheSkin Senses. CC Thomas, Springfield, pp 423–439
95. Merskey H, Bogduk N (1994) Classification of Chronic Pain:Descriptions of Chronic Pain Syndromes and Definitions ofPain Terms, 2nd edn. IASP Press, Seattle
96. Mesulam MM (1990) Large-scale neurocognitive networks anddistributed processing for attention, language, and memory.Ann Neurol 28:597–613
97. Mesulam MM, Mufson EJ (1982a) Insula of the old world mon-key. II. Afferent cortical input and comments on the claustrum.J Comparative Neurol 212:23–37
98. Mesulam MM, Mufson EJ (1982b) Insula of the old world mon-key: III. Efferent cortical input and comments on function. JComparative Neurol 212:38–52
99. Minagar A, David NJ (1999) Bilateral infarction in the territoryof the anterior cerebral arteries. Neurol 52:886–888

476 Cortical and Limbic Mechanisms Mediating Pain and Pain-Related Behavior
100.Mochizuki H, Saito H (1990) Mesial frontal lobe syndromes:correlations between neurological deficits and radiological lo-calizations. Tohoku J Exp Med 161:231–239
101.Neugebauer V, Li,W, Bird GC et al. (2004) The Amygdala andPersistent Pain. The Neuroscientist
102.Nii Y, Uematsu S, Lesser RP et al1996) Does the central sulcusdivide motor and sensory functions? Cortical mapping of hu-man hand areas as revealed by electrical stimulation throughsubdural grid electrodes. Neurol 46:360–367
103.Ongur D, An X, Price JL (1998) Prefrontal cortical projec-tions to the hypothalamus in macaque monkeys. J Comp Neurol401:480–505
104.Opsommer E, Weiss T, Plaghki L et al. (2001) Dipole analysisof ultralate (C-fibres) evoked potentials after laser stimulationof tiny cutaneous surface areas in humans. Neurosci Letters298:41–44
105.Ostrowsky K, Isnard J, Ryvlin P et al. (2000) Functional map-ping of the insular cortex: clinical implication in temporal lobeepilepsy. Epilepsia 41:681–686
106.Ostrowsky K, Magnin M, Ryvlin P et al. (2002) Representationof Pain and Somatic Sensation in the Human Insula: a Study ofResponses to Direct Electrical Cortical Stimulation. CerebralCortex 12:376–385
107.Papez JW (1937) A proposed mechanism of emotion. Archivesof Neurological Psychiatry 38:725–743
108.Pastoriza LN, Morrow TJ, Casey KL (1996) Medial frontal cor-tex lesions selectively attenuate the hot plate response: possiblenocifensive apraxia in the rat. Pain 64:11–17
109.Peyron R, Garcia-Larrea L, Gregoire MC et al. (1999) Haemo-dynamic brain responses to acute pain in humans: sensory andattentional networks. Brain 122:1765–1780
110.Peyron R, Laurent B, Garcia-Larrea L (2000) Functional imag-ing of brain responses to pain. A review and meta-analysis.Neurophysiol Clin 30:263–288
111.Peyron R, Frot M, Schneider F et al. (2002) Role of Opercu-loinsular Cortices in Human Pain Processing: Converging Ev-idence from PET, fMRI, Dipole Modeling, and IntracerebralRecordings of Evoked Potentials. Neuroimage 17:1336–1346
112.Ploghaus A, Narain C, Beckmann CF et al. (2001) Exacerbationof pain by anxiety is associated with activity in a hippocampalnetwork. J Neurosci 21:9896–9903
113.Ploghaus A, Tracey I, Gati JS et al. (1999) Dissociat-ing pain from its anticipation in the human brain. Science284:1979–1981
114.Ploghaus A, Trace, I, Clare S et al. (2000) Learning about pain:the neural substrate of the prediction error for aversive events.Proc Natl Acad Sci USA 97:9281–9286
115.Ploner M, Schmitz F, Freund HJ et al. (1999) Parallel activa-tion of primary and secondary somatosensory cortices in humanpain processing. J Neurophysiol 81:3100–3104
116.Ploner M, Gross J, Timmermann L et al. (2002) Cortical rep-resentation of first and second pain sensation in humans. ProcNatl Acad Sci USA 99:12444–12448
117.Porro CA, Baraldi P, Pagnoni G et al. (2002) Does Anticipa-tion of Pain Affect Cortical Nociceptive Systems? J Neurosci22:3206–3214
118.Price DD (1988) Psychological and Neural Mechanisms ofPain. Raven Press, New York
119.Price DD (1999) Psychological Mechanisms of Pain and Anal-gesia. IASP Press, Seattle
120.Price DD (2000) Psychological and Neural Mechanisms of theAffective Dimension of Pain. Science 288:1769–1772
121.Rainville P (2002) Brain mechanisms of pain affect and painmodulation. Curr Opin Neurobiol 12:195–204
122.Rainville P, Duncan GH, Price DD et al. (1997) Pain affectencoded in human anterior cingulate but not somatosensorycortex. Science 277:968–971
123.Ramnani N, Owen AM (2004) Anterior Prefrontal Cortex: In-sights into Function from Anatomy and Neuroimaging. NatRev Neurosci 5:184–194
124.Rizzolatti G, Luppino G, Matelli M (1998) The organization ofthe cortical motor system: new concepts. ElectroencephalogrClin Neurophysiol 106:283–296
125.Robinson CJ, Burton H (1980) Organization of somatosen-sory receptive fields in cortical areas 7b, retroinsula, postau-ditory and granular insula of M. fascicularis. J Comp Neurol192:69–92
126.Rolls ET (2000) The orbitofrontal cortex and reward. CerebCortex 10:284–294
127.Rolls ET, O’Doherty J, Kringelbach ML et al. (2003) Repre-sentations of Pleasant and Painful Touch in the Human Or-bitofrontal and Cingulate Cortices. Cereb Cortex 13:308–317
128.Ruben J, Schwiemann J, Deuchert M, et al. (2001) Somato-topic organization of human secondary somatosensory cortex.Cereb Cortex 11:463–473
129.Russell WR (1945) Transient disturbances following gunshotwounds of the head. Brain 68:79–97
130.Sakai K (2003) Reactivation of memory: role of medial tem-poral lobe and prefrontal cortex. Rev Neurosci 14:241–252
131.Schmahmann JD, Leifer D (1992) Parietal pseudothalamic painsyndrome: Clinical features and anatomic correlates. Arch Neu-rol 49:1032–1037
132.Schneider RJ, Friedman DP, Mishkin M (1993) A modality-specific somatosensory area within the insula of the rhesus mon-key. Brain Res 621:116–120
133.Schnitzler A, Ploner M (2000) Neurophysiology and func-tional neuroanatomy of pain perception. J Clin Neurophysiol17:592–603
134.Sikes RW, Vogt BA (1992) Nociceptive neurons in area 24 ofrabbit cingulate cortex. J Neurophysiol 68:1720–1732
135.Simons JS, Spiers HJ (2003) Prefrontal and medial tempo-ral lobe interactions in long-term memory. Nat Rev Neurosci4:637–648
136.Simpson JR Jr, Drevets WC, Snyder AZ et al. (2001) Emotion-induced changes in human medial prefrontal cortex: II. Duringanticipatory anxiety. Proc Natl Acad Sci USA 98:688–693
137.Smith EE, Jonides J (1999) Storage and Executive Processesin the Frontal Lobes. Science 283:1657–1661
138.Spiller WG, Martin E (1912) The treatment of persistent painof organic origin in the lower part of the body by division of theanterolateral column of the spiinal cord. J Am Med Association58:1489–1492
139.Stevens RT, London SM, Apkarian AV (1993) Spinothalam-ocortical projections to the secondary somatosensory cortex(SII) in squirrel monkey. Brain Res 631:241–246
140.Stuss DT, Benson DF (1986) The Frontal Lobes. Raven, NewYork
141.Svensson P, Minoshima S, Beydoun A et al. (1997) Cerebralprocessing of acute skin and muscle pain in humans. J Neu-rophysiol 78:450–460
142.Sweet, WH (1982) Cerebral localization of pain. In: ThompsonRA, Green JR (eds) New Perspectives in Cerebral Localization.Raven Press, New York, pp 205–242
143.Talairach J, Bancaud J, Geier S et al. (1973) The cingulate gyrusand human behaviour. Electroencephalogr Clin Neurophysiol34:45–52
144.Tommerdahl M, Delemos KA, Vierck CJ Jr et al. (1996) Ante-rior parietal cortical response to tactile and skin-heating stimuliapplied to the same skin site. J Neurophysiol 75:2662–2670
145.Tracey I, Becerra L, Chang I et al. (2000) Noxious hot and coldstimulation produce common patterns of brain activation in hu-mans: a functional magnetic resonance imaging study. NeuroscLett 288:159–162
146.Tran TD, Inui K, Hoshiyama M et al. (2002) Cerebral ac-tivation by the signals ascending through unmyelinated C-fibers in humans: a magnetoencephalographic study. Neuro-sciece 113:375–386
147.Treede RD, Kenshalo DR, Gracely RH et al. (1999) The corticalrepresentation of pain. Pain 79:105–111

C
Corticosteroid Injections 477
148.Treede RD, Apkarian AV, Bromm B et al. (2000) Cortical rep-resentation of pain: functional characterization of nociceptiveareas near the lateral sulcus. Pain 87:113–119
149.Turken, A. U. and Swick, D. (1999) Response selec-tion in the human anterior cingulate cortex. Nat Neurosci2:920–924
150.Vogt BA, Derbyshire S, Jones AKP et al. (1996) Pain pro-cessing in four regions of human cingulate cortex localizedwith co-registered PET and MR imaging. Eur J Neurosci8:1461–1473
151.Vogt BA, Finch DM, Olson CR (1992) Functional heterogene-ity in cingulate cortex: the anterior executive and posterior eval-uative regions. Cereb Cortex 2:435–443
152.von Cramon D, Jurgens U (1983) The anterior cingulate cor-tex and the phonatory control in monkey and man. NeurosciBiobehav Rev 7:423–425
153.Wager TD, Phan KL, Liberzon I et al. (2003) Valence, gen-der, and lateralization of functional brain anatomy in emotion:
a meta-analysis of findings from neuroimaging. Neuroimage19:513–531
154.Wager TD, Rilling JK, Smith EE et al. (2004) Placebo-inducedchanges in fMRI in the anticipation and experience of pain.Science 303:1162–1167
155.Wall PD (1979) On the relation of injury to pain the John J.Bonica Lecture. Pain 6:253–264
156.Ward R, Duncan J, Shapiro K (1996) The Slow Time-Courseof Visual Attention. Cog Psychol 30:79–109
157.Whitsel BL, Dreyer DA, Roppolo JR (1971) Determinants ofbody representation in postcentral gyrus of macaques. J Neu-rophysiol 34:1018–1034
158.Yamamura H, Iwata K, Tsuboi Y et al. (1996) Morphologicaland electrophysiological properties of ACC nociceptive neu-rons in rats. Brain Res 735:83–92
159.Zhang ZH, Dougherty PM, Oppenheimer SM (1999) Monkeyinsular cortex neurons respond to baroreceptive and somatosen-sory convergent inputs. Neurosci 94:351–360
Cortical Projections
� Corticothalamic and Thalamocortical Interactions
Cortical Reorganization
Definition
A functional or structural change in the primary sensori-motor areas of the cortex that can also occur in the adultnervous system but was long thought possible only inthe developing organism.� Phantom Limb Pain, Treatment
Cortical Spreading Depression
Definition
Awaveofactivationfollowedbydeactivationthatmovesacross the surface of the brain typically at 2–6 mm/min.It is widely considered to be the animal equivalent ofmigraine aura.� Migraine, Pathophysiology
Cortical Stimulation for Relief of Pain
� Pain Treatment, Motor Cortex Stimulation
Corticolimbic Circuits
Definition
Pathway through parietal opercular cortex, includingSII, and insula cortex to the medial temporal lobeincluding amygdala and hippocampus� Angina Pectoris, Neurophysiology and Psycho-
physics
Corticortical Pathways
� Thalamocortical Loops and Information Processing
Corticospinal Tract
Definition
A motor pathway originating in the motorcortex and ter-minating in brainstem and spinal motor nuclei. Injury ofthis pathway can lead to paresis of the ipsilateral lowerlimb.� Percutaneous Cordotomy
Corticosteroid Injections
� Steroid Injections

478 Corticothalamic and Thalamocortical Interactions
Corticothalamic and ThalamocorticalInteractions
EDWARD JONES
Center for Neuroscience, University of California,Davies, CA, [email protected]
Synonyms
Bursting activity; 40 Hz oscillations; Reticular NucleusInputs from Cortex; Cortical Projections; Thalamic Pro-jections; Thalamocortical and Corticothalamic Interac-tions
Definition
Cortical projections to dorsal thalamic nuclei andto thalamic reticular nucleus, together with projec-tions from the thalamus to the cortex form the basicthalamocortical- corticothalamic loop. Neuronal con-nectivity in these loops, involved neurotransmitters andsynaptic mechanisms define distinct dynamical statesof this network.
Characteristics� Corticothalamic fibers arise in every area of the cere-bral cortex and every dorsal thalamic nucleus receivesthe terminations of corticothalamic fibers. The cells oforigin of these fibers form two distinct classes. Bothare a form of � pyramidal neuron, with spiny dendritesand utilize glutamate as the transmitter. One class, withsoma located in layer VI is characterized by small size,a thin ascending apical dendrite that devolves into a tuftof branches in layer IV where it receives monosynap-tic inputs from thalamic fibers and strongly recurrent,columnar axon collaterals (Fig. 1). The thin primaryaxon of these cells returns to the thalamic nucleus fromwhich the cortical area in which it lies receives thalamicinput, giving off collateral branches to the � thalamicreticular nucleus en route (Fig. 2). A second class, withsoma located in layer V is larger, with an apical dendritethat ascends to layer I, ending there in a tuft of spinybranches and a set of lengthy horizontal axon collater-als that connect extensive stretches of layers III and V(Fig. 1). The relatively thick primary axon of these cellsdescends and sends branches to multiple subcorticalsites, such as the spinal cord, brainstem, tectum, basalganglia and thalamus. The thalamic branches traversethe reticular nucleus without giving off collaterals andend primarily in nuclei other than the primary sensorynuclei, especially in those characterized by a high den-sity of matrix cells (see � Spinothalamic terminations,core ans matrix) (Fig. 2).The reticular nucleus, which is innervated by the collat-eralsof the layerVIcorticothalamiccells, occupiesakeyplace in the circuitry connecting thalamus and cortex; itisalso innervatedbycollateralsof thalamocorticalaxons
arising in the underlying dorsal thalamus. Because of thedifferences in the diameters of the corticothalamic and� thalamocortical fibers that provide collateral inputsto the reticular nucleus, it is possible physiologically toidentify the two kinds of collateral synapse. A brief elec-trical stimulus applied to the cerebral cortex or underly-ing white matter elicits short latency � EPSCs in retic-ular nucleus cells due to � antidromic invasion of tha-lamocortical collaterals and longer latency EPSCs dueto � orthodromic activation of the slower corticothala-mic fibers (Golshani et al. 2001; Liu et al. 2001). EPSCsattributable to collateral corticothalamic synapses havea consistent amplitude, reflecting their small size and asingle vesicle release site, but a wide range of rise times,reflecting their wide distribution over the dendritic treeof reticular nucleus cells (Liu et al. 2001). Unitary EP-SCs attributable to collateral thalamocortical synapsestend to have large, although more variable amplitudes,reflecting their large size and multiple release sites, butvery consistent rise times, reflecting their proximal lo-cation on the dendritic tree.In the dorsal thalamus, more than 40% of the synapseson a thalamic relay cell are derived from layer VI cor-ticothalamic fibers and are concentrated on secondaryand especially on tertiary dendrites (Liu et al. 1995a).Less than 20% are derived from medial lemniscal or op-tic tract or other subcortical fibers and are concentratedonproximaldendrites.These terminals tendtohavemul-tiple points of synaptic contact, including on dendriticprotrusions and the parent shafts. The remaining 40% ofsynapses are inhibitory and tend to be concentrated onproximal and second order dendrites and on the soma.Themajorityof these terminalsarederivedfromaxonsofthe reticular nucleus (Liu et al. 1995b). A lesser numberare derived from the presynaptic dendrites of intrinsicinterneurons in animals that possess these neurons. Theterminals of layer V-originating corticothalamic fibersend in large terminals concentrated proximally, in num-bers that have not yet been quantified.The glutamatergic nature of corticothalamic synapses isevidencedbytheability to record� NMDA-,� AMPA-and � metabotropic glutamate receptor-based EPSCs inrelay cells and in reticular nucleus cells under appropri-ate conditions (McCormick and Von Krosigk 1992; Kaoand Coulter 1997; Turner and Salt 1998, 1999; Golshanietal.1998;ZhangandJones2004).However,corticotha-lamic stimulation can also engendera powerful disynap-tic, feed-forward inhibition of relay cells, resulting fromco-activation of the reticular nucleus. The importanceof this corticothalamic-induced inhibition of the relaycells is that it drives them towards the burst-firing mode.As they recover from this inhibition, the � low thresh-old calcium conductance, I T, is de-inactivated and thecells fire a burst of action potentials. This has the ef-fect of re-exciting, via the collaterals of thalamocorti-cal fibers, the reticular nucleus cells, which then fire anew burst of action potentials. These re-inhibit the relay

C
Corticothalamic and Thalamocortical Interactions 479
Corticothalamic and Thalamocortical Interactions, Figure 1 Schematic view of the background matrix (left) of the ventral posterior complex, withits input from the spinothalamic and spinal trigeminothalamic systems and widespread projection to superficial layers of the cerebral cortex, contrastedwith the core, restricted to the VPM and VPL nuclei, with its input from the lemniscal system and topographically-organized projection to middle layersof the primary somatosensory cortex. Based on Jones (2006). Abbreviations: VMb, basal ventral medial nucleus; VPI, ventral posterior inferior nucleus;VPL, ventral posterior lateral nucleus; VPM, ventral posterior medial nucleus.
cells, which burst again on recovering and so the cyclecontinues at 7–14 Hz, the spindle frequency. Recordingsmade simultaneously from reticular nucleus and relaycells in the underlying dorsal thalamus clearly demon-strate synchrony of their discharges at spindle frequen-cies, a result of the synaptic interplay between the twosets of cells.Apart from causing repetitive burst firing in relay cells,a reticular nucleus cell, by reason of the widespreadterminations of its axon within the dorsal thalamus,has the effect of distributing the disynaptic inhibitoryeffects of corticothalamic stimulation across many relaycells, thus helping to promote synchrony throughoutthe whole thalamo-cortico-thalamicnetwork. Spread ofcorticothalamic effects across many reticular nucleuscells and recruitment of others by collateral inputs fromthe thalamocortical axons of bursting relay cells willalso serve to spread spindle oscillations across mostof the thalamus and cortex. The simultaneous onsetof spindles throughout cortex and thalamus impliesrapid diffusion of reticular nucleus effects on relay cellsand equally rapid collateral excitation of widespread
sections of the reticular nucleus by bursting relay cells(Steriade and Amzica 1996). Although the corticothala-mic system is particularly powerful in inducing spindleoscillations, it is the reticular nucleus that is the primemover in synchronizing the oscillations of virtually allcells in the network. Its capacity to do this is enhancedwhen the weak inhibitory effects ofone reticular nucleuscell on another are removed (Sohal et al. 2000).The power of the corticothalamic projection to induce� low frequency oscillations in the spindle range clearlydepends upon the capacity of the disynaptic inhibitoryeffect of the reticular nucleus to overcome the direct,monosynaptic excitatory effect of corticothalamic fibersupon the relay cells of the dorsal thalamus. To effectthis, the strength of the corticothalamic input to thereticular nucleus is stronger than that to the relay cells.Corticothalamic EPSCs in the reticular nucleus cells arenearly three times larger than in relay cells (Golshani etal 2001). The basis for this difference in AMPA-receptorbased synaptic strength depends upon the presence ofnearly three times as many GluR4 receptor subunits atthe corticothalamic synapses on the reticular nucleus

480 Corticothalamic and Thalamocortical Interactions
Corticothalamic and Thalamocortical Interactions, Figure 2 Photomicrographs of adjacent frontal sections through the thalamus of a macaquemonkey, showing the parvalbumin immunoreactive core of the ventral posterior nucleus (a) and the calbindin immunoreactive matrix (b). Bar 500 μm.s, enhanced matrix region of VPM; CL, central lateral nucleus; CM, centre median nucleus; other abbreviations as in Fig 1. Arrow indicates region ofparvalbumin and calbindin overlap in medial VPM. From Jones (2005).
Corticothalamic and Thalamocortical Interactions, Figure 3 Laminar and areal projections of neurons in the ventral posterior nucleus of monkeys.Core regions (gray) receiving inputs from different classes of peripheral mechanoreceptors project to middle layers of specific cortical fields. Matrixregions (crosses) receiving inputs fro the spinothalamic and spinal trigeminothalamic systems project to superficial layers of all fields. From Jones (2006).
cells than at corticothalamic synapses on relay cells(Liu et al. 2001). Increases in channel opening timeconsequent upon this enrichment should account forthe larger EPSCs in the reticular nucleus cells.
Unlike the corticothalamic synapses at which GluR4 re-ceptor subunits are enriched in comparison with otherAMPA receptor subunits, notably GluR3 , the larger col-lateral thalamocortical synapses in the reticular nucleus

C
Cost Shifting 481
possess GluR4 and GluR3 subunits in equal propor-tions. The collateral thalamocortical synapses providethe capacity for the powerful � re-entrant excitation ofthe reticular nucleus cells by bursts of action potentialsin relay cells during the course of spindle oscillations.When thalamic relay cells are relatively depolarized, asin the alert attentive state, they tend to display intrin-sic membrane oscillations at 20–50 Hz (Pedroarena andLlinás, 1997). Under these circumstances, with the disy-naptic inhibition of the reticular nucleus rendered lesseffective, corticothalamic stimulation tends to promoteoscillatory activity at ~40 Hz in the connected thalamo-cortico-thalamic network. � Forty Hz Oscillations is anaccompaniment of attention, perception and higher cog-nitive states.In cooperation with the corticothalamic system, thecells of the thalamic matrix form a basis for dispersionof activity across larger areas of cortex than those ofthe core with their focused projections to an individualarea. Within an area, the terminations of matrix cellaxons on distal dendrites in superficial layers and ofmatrix cell axons on more proximal dendrites in middlelayers should serve as a coincidence detection circuitleading to a high degree of temporal integration (Llinásand Paré 1997) (Fig. 3). This in turn should promotesynchronous activity in the cells of individual corti-cal columns and in a group of columns activated bythe same stimulus. Oscillatory activity in these corticalcolumns should be fed back by layer VI corticothalamiccells to the thalamic nucleus from which they receiveinput, serving to reinforce the synchrony. Synchronousactivity would be spread across other cortical columnsin the same cortical area and in adjacent cortical areasby the diffuse projections of matrix cells in the thalamicnucleus. However, other thalamic nuclei and, throughtheir matrix cells, other cortical areas should also berecruited into large scale coherent activity by the diffuseintracortical and corticothalamic projections of layerV corticothalamic neurons. This is thought to be a keyto the binding together of the various elements of acognitive event.
References1. Golshani P, Warren RA, Jones EG (1998) Progression of change
in NMDA, non-NMDA, and metabotropic glutamate receptorfunction at the developing corticothalamic synapse. J Neurophys-iol 80:143–154
2. Golshani P, Liu X-B, Jones EG (2001) Differences in quantalamplitude reflect GluR4- subunit number at corticothalamicsynapses on two populations of thalamic neurons. Proc NatlAcad Sci USA 98:4172–4177
3. Jones, EG (2005) The Thalamus – Revisited. Cambridge Uni-versity Press, Cambridge
4. Kao CQ, Coulter DA (1997) Physiology and pharmacology ofcorticothalamic stimulation- evoked responses in rat somatosen-sory thalamic neurons in vitro. J Neurophysiol 77:2661–2676
5. Liu X-B, Warren RA, Jones EG (1995a) Synaptic distributionof afferents from reticular nucleus in ventroposterior nucleus ofcat thalamus. J Comp Neurol 352:187–202
6. Liu X-B, Honda CN, Jones EG (1995b) Distribution of fourtypes of synapse on physiologically identified relay neurons in
the ventral posterior thalamic nucleus of the cat. J Comp Neurol352:69–91
7. Liu X-B, Bolea S, Golshani P et al. (2001) Differentiation of cor-ticothalamic and thalamocortical collateral synapses on mousereticular nucleus neurons by EPSC amplitude and AMPA recep-tor subunit composition. Thalamus Related Systems 1:15–29
8. Llinás R, Paré D (1997) Coherent oscillations in specific and non-specific thalamocortical networks and their role in cognition. In:Steriade M, Jones EG, McCormick DA (eds) Thalamus VolumeII Experimental and Clinical Aspects. Elsevier, Amsterdam, pp501-516
9. McCormick DA, von Krosigk M (1992) Corticothalamic activa-tion modulates thalamic firing through glutamate “metabotropic”receptors. Proc Natl Acad Sci USA 89:2774–2778
10. Pedroarena C, Llinás R (1997) Dendritic calcium conductancesgenerate high-frequency oscillation in thalamocortical neurons.Proc Natl Acad Sci USA 94:724–728
11. Sohal VS, Huntsman MM, Huguenard JR (2000) Reciprocal in-hibitory connections regulate the spatiotemporal properties ofintrathalamic oscillations. J Neurosci 20:1735–1745
12. Steriade M, Amzica F (1996) Intracortical and corticothalamiccoherency of fast spontaneous oscillations. Proc Natl Acad SciUSA 93:2533–2538
13. Turner JP, Salt TE (1998) Characterization of sensory and corti-cothalamic excitatory inputs to rat thalamocortical neurones invitro. J Physiol 510:829–843
14. Turner JP, Salt TE (1999) Group III metabotropic glutamate re-ceptors control corticothalamic synaptic transmission in the ratthalamus in vitro. J Physiol 519:481–491
15. Zhang L, Jones EG (2004) Corticothalamic inhibition in the tha-lamic reticular nucleus. J Neurophysiol 91:759–766
Corticothalamic Fibers
Definition
Axons with cell bodies located in the cortex with termi-nations in the thalamus.� Corticothalamic and Thalamocortical Interactions
Cortisol
Definition
Hormone released by the adrenal glands. It is regulatedby many endogenous substances, e.g. the serotonin 5-HT1receptors,whichinduceabiphasicresponse.Infact,5-HT1 agonists first induce a cortisol increase, followedby a decrease.� Placebo Analgesia and Descending Opioid Modula-
tion
Cost Shifting
Definition
Cost shifting can be said to occur in health care whenchanges in the reimbursement for the delivery of healthservices, or alterations in the parameters of healthbenefits displace part of the cost of health care expendi-tures from one sphere of healthcare to another, or from

482 Costoclavicular Syndrome
healthcare institutions to patients and/or their fami-lies. Examples of this would include attempts by stategovernments to attempt to restrict reimbursement formedications to cheaper non-brand name medications,or to limit access to categories of medications such asthe Cox B anti-inflammatory medications. This costis displaced onto underinsured consumers. Often asa result of inability to absorb such costs, patients arehospitalized or placed in skilled nursing facilities.� Cancer Pain Management, Undertreatment and Clini-
cian-Related Barriers
Costoclavicular Syndrome
� Thoracic Outlet Syndrome
Co-Transmission
Definition
Many neurons synthesize two different types of neu-rotransmitters. Small molecule neurotransmitters suchas glutamate and acetylcholine, are recycled or syn-thesized at the level of the nerve terminal and storedin small synaptic vesicles. Peptidergic transmittersare synthesized as part of large precursor proteins onthe rough endoplasmic reticulum in the cell body andtransported into the Golgi apparatus where they arepackaged into large, dense-core vesicles that are trans-ported to the nerve terminal. Transmitters releasedfrom small clear vesicles generate rapid synaptic re-sponses, because small vesicles are located closest tothe voltage-dependent Ca2+ channels that provide theinflux of Ca2+ that activates the release process, andsmall molecule transmitters in synaptic vesicles acti-vate ionotropic receptors. As large, dense-core vesiclesare located at a greater distance from the site of Ca2+
influx, higher firing frequencies are required to initiaterelease of transmitter from these vesicles. Peptidergictransmitters activate metabotropic receptors that coupleto intracellular signaling pathways. Thus, peptidergictransmission is capable of modulating neurotransmis-sion of small molecule transmitters.� Spinothalamic Tract Neurons, Peptidergic Input
Cotrimoxazol
Definition
Treatment of choice in the limited stage of WG (combi-nation of 2 x 800 mg sulfamethoxazol and 2 x 160 mgtrimethoprime).� Headache Due to Arteritis
Cotunnius Disease
� Sciatica
Counterirritation
Definition
The mechanisms by which any kind of intense and nox-ious stimulus elicits an analgesic effect distant from thesite of the pain producing effect.� Acupuncture Mechanisms� Tourniquet Test
Coupling Media of Ultrasound
Definition
Coupling media are mineral oil or several commerciallyavailable coupling gels. They have similar transmissivi-ties to the reference standard of distilled degassed water.� Ultrasound Therapy ofPain from theMusculoskeletal
System
Coupling of Sympathetic PostganglionicNeurons onto Primary Afferent NerveFibers
� Sympathetic-AfferentCoupling in theAfferentNerveFiber, Neurophysiological Experiments
COX
� Cyclooxygenases� Cyclooxygenases in Biology and Disease� NSAIDs, COX-Independent Actions� NSAIDs, Mode of Action� COX-1 and COX-2 in Pain
COX Isozymes
Definition
Are subsets of the cycloxygenaseenzymes that catalyzethe conversion of arachidonic acid to prostaglandins andother products involved in pain signaling.� Drugs with Mixed Action and Combinations, Empha-
sis on Tramadol

C
COX-1 and COX-2 in Pain 483
COX-1
� COX-1 and COX-2 in Pain
COX-1 and COX-2 in PainIRMGARD TEGEDER
Center of Pharmacology, University Clinic Frankfurt,Frankfurt, [email protected]
Synonyms
Cyclooxygenase-1; Cyclooxygenase-2; COX-1; COX-1; PGHS-1; PGHS-2; prostaglandin endoperoxide syn-thase 1; prostaglandin endoperoxide synthase 2; Ptgs1;Ptgs2
Definition
The isoenzymes � Cyclooxygenases -1 and -2 (COX-1and COX-2) catalyze the conversion of arachidonic acid(AA) to prostaglandin H2 (PGH2) which is the rate lim-iting step in thebiosynthesisofvarious� prostaglandinsand � thromboxanes. The subsequent specificstep is ac-complished by various prostaglandin synthases whichconvert PGH2 to PGE2, PGD2, PGF2alpha, PGI2 andTXA2.ProstaglandinE2(PGE2)playsaparticularly im-portant role in pain signaling (Fig. 1).
Characteristics
COX-1 and COX-2 are the key enzymes in the prosta-glandin and thromboxane biosynthetic pathway. Al-though the structure and enzymatic activity of bothenzymes are very similar, COX-1 and COX-2 performdifferent tasks which is allowed for by a different local-ization and regulation. COX-1 is expressed in all tissuesin certain cell types, and produces prostaglandins andthromboxanes that are needed for the maintenance ofphysiological functions such as regulation of bloodflow, platelet aggregation and mucus production in thestomach. On the other hand, COX-2 is not normallyexpressed in “healthy” tissue but only occurs follow-ing adequate stimulation, which may be any kind oftissue damage such as trauma, ischemia, infection orinflammation. Such stimuli result in activation of COX-2 regulating � transcription factors including nuclearfactor kappa B (NFkappaB), activator protein-1 (AP-1), CCAAT Enhancer-binding protein-1 (C/EBPbeta)and cAMP response element binding protein (CREB),which translate the stimulus into COX-2 � upregulationand excessive prostaglandin production. PGE2 is par-ticularly involved in the activation and � sensitizationof the nociceptive system. This effect is mediated bystimulation of � nociceptors in the periphery, anddirect � depolarization of postsynaptic nociceptive
neurons in the spinal cord, which is mediated throughprostaglandin E (EP2) receptors (Baba et al. 2001). Inaddition, PGE2 causes a dys-inhibition of nociceptiveneurons by suppressing inhibitory glycinergic synaptictransmission in the spinal cord (Ahmadi et al. 2002).Enhanced or mal-controlled PGE2 release results inspontaneous pain and � hyperalgesia, i.e. increasedsensitivity to painful stimuli. The functional disparityof COX-1 and COX-2 has encouraged the developmentof COX-2 selective inhibitors. These drugs are supposedto inhibit only the “pain"-related PG synthesis with-out affecting physiological prostaglandins. Multipleclinical trials have demonstrated that COX-2 selectiveinhibitors cause somewhat less gastrointestinal toxic-ity than unselective agents, and are equally effectivein the treatment of arthritis (pain and function) andpostoperative pain in clinical studies. However, thereare some exceptions from the COX-1/COX-2 rule, inthat COX-2 is also constitutively expressed in sometissues and COX-1 might contribute to pain-associatedPG-release.
Contribution of COX-1 Derived Prostaglandins to Nociception
Some experimental studies suggest that COX-1 is in-volved in the “injury"-induced immediate release ofPGE2 in the spinal cord and periphery, and therebycontributes to the activation and sensitization of noci-ceptive neurons (Tegeder et al. 2001a; Wallace et al.1998). However, this is contradicted by others (Ghilardiet al. 2004; Yaksh et al. 2001). The debate is primarilyfuelled by a controversy about the exact localization ofconstitutive COX-2 and the time needed for its upreg-ulation. For example, constitutive COX-2 expressionwas observed in motor neurons of the ventral horn, butneither in dorsal horn sensory neurons nor glial cells(Maihofner et al. 2000). In line with the lack of baselineexpression of COX-2 in nociceptive neurons, celecoxib(COX-2 inhibitor, injected i.p.) had no antinocicep-tive effect in a model of acute nociception, whereas aCOX-1 inhibitor was effective (Tegeder et al. 2001a).Another study, however, reported a constitutive ex-pression of COX-2 in dorsal horn sensory neurons andradial glial cells (Ghilardi et al. 2004). In this study, theCOX-2 inhibitor reduced acute nociceptive behaviorand the COX-1 inhibitor was ineffective (Ghilardi etal. 2004). In this study, the drugs were delivered ontothe lumbar spinal cord via a chronically implantedspinal catheter. The catheter may by itself cause anactivation of radial glia and COX-2 upregulation in thedorsal horn. Hence, the nociceptive system might havebeen pre-activated in this study, which would explainthe antinociceptive effect of the COX-2 inhibitor. Thestudies generally agree upon the COX-2 upregulationin dorsal horn neurons following inflammatory or no-ciceptive stimulation (Beiche et al. 1996; Dolan et al.2003; Ghilardi et al. 2004; Samad et al. 2001; Tegederet al. 2001b).

484 COX-1 and COX-2 in Pain
COX-1 and COX-2 in Pain, Figure 1 Synthesis of prostaglandins and thromboxanes.
COX-1 and COX-2 in Clinical Pain
In clinical studies, COX-2 inhibitors were generallyas effective as traditional NSAIDs in the treatmentof arthritis, postoperative pain, gout, migraine, dentalpain, dental surgery and dysmenorrhea. Thus, selectiveCOX-2 inhibitors not only reduce chronic inflamma-tory pain caused, for example, by chronic arthritis, butalso “acute” pain, although COX-2 is not constitutivelyexpressed in most peripheral human tissues or in hu-man sensory neurons in the spinal cord (Maihofner etal. 2003). Hence, the potential contribution of COX-1derived prostaglandins to “acute” clinical pain is ap-parently of minor importance. This is explained by thefact that even “acute” pain (such as postoperative pain,acute gout, dental pain, dysmenorrhea) that requirestreatment with non-opioid analgesics lasts for at leastseveral hours, and hence, COX-2 is going to be upreg-ulated in the course of the affection and contributesto PG-production. The onset of effects will probablydepend more on pharmacokinetic issues than on thespeed of COX-2 upregulation.
COX-2 in Higher Brain Regions
Results of some clinical studies, however, cannot besatisfactorily explained by COX-2 upregulation. Forexample, preemptive treatment with a COX-2 inhibitorbefore starting surgery resulted in a reduction of postop-erative pain, although the time from the skin incision tothe first pain assessment was very short and no pain wasreportedbeforesurgery.Thissuggeststhatprostaglandinrelease from constitutively expressed COX-2 in higherbrain regions also contributes to nociception. This ideais supported by experimental data showing that COX-2derived prostaglandins in the pre-optic hypothalamusmediate lipopolysaccharide (LPS) induced hyperalge-sia in rats (Abe et al. 2001). An experimental pain studyin humans also suggests an involvement of constitutivebrain COX-2 (Koppert et al. 2004).This study employedelectrically evoked non-inflammatory pain, where theelectrical current directly stimulated axons withoutaffecting the nociceptive nerve terminals. Intravenousparecoxib (prodrug of valdecoxib) reduced secondaryhyperalgesia and allodynia within 30 min after starting

C
COX-2 Inhibitor 485
the stimulation, so that COX-2 upregulation at any sitewas highly unlikely. The analgesic effects are thereforeprobably caused by inhibition of constitutive COX-2 inhigher brain regions such as hypothalamus or cortex.
Peripheral versus Central Effects in Humans
In light of the growing evidence for central effects ofCOX-inhibitors, it is interesting to dissect the relativecontributions of peripheral and central effects, particu-larly because NSAID gels and creams that only provideCOX inhibition in the skin and directly underlying tis-sue are very popular in some countries. A recent clinicalstudy has addressed this question, employing local andsystemicdiclofenac in the� freeze lesionmodel (Burianet al. 2003). In this study, diclofenac gel significantly re-duced mechanical hyperalgesia. However, overall painrelief with systemic diclofenac was stronger with equaltissue concentrations. Thus, both peripheral and centraleffects do contribute to the analgesic efficacy in this in-flammatory model. The relative contribution of periph-eral versus central effects, however, may vary dependingon the type and source of pain.
Neuropathic Pain
The role of prostaglandins in � neuropathic pain ishighly controversial and depends on the model used. Ithas recently been suggested that COX-1 plays a signif-icant role because an increase of its expression in thespinal cord was observed. However,COX-1 is expressedin microglial cells in the spinal cord. These cells pro-liferate in response to a peripheral nerve injury. Thus,the observed COX-1 “upregulation” is probably causedby an increase in the number of microglial cells, ratherthan an increase of its transcription in the individualcell. The role of microglia proliferation for neuropathicpain is still elusive. COX-2 is not upregulated in thespinal cord in response to a peripheral nerve injury,suggesting that its contribution, if any, to neuropathicpain is of minor importance. In support, inhibitors ofcyclooxygenase activity (traditional NSAIDs and se-lective COX-2 inhibitors) are generally considered tobe ineffective in reducing neuropathic pain in clinicalpractice.
References1. Abe M, Oka T, Hori T et al. (2001) Prostanoids in the Preoptic Hy-
pothalamus Mediate Systemic Lipopolysaccharide-Induced Hy-peralgesia in Rats. Brain Res 916:41–49
2. Ahmadi S, Lippross S, Neuhuber WL et al. (2002) PGE(2) Se-lectively Blocks Inhibitory Glycinergic Neurotransmission ontoRat Superficial Dorsal Horn Neurons. Nat Neurosci 5:34–40
3. Baba H, Kohno T, Moore KA et al. (2001) Direct Activation ofRat Spinal Dorsal Horn Neurons by Prostaglandin E2. J Neurosci21:1750–1756
4. Beiche F, Scheuerer S, Brune K et al. (1996) Up-Regulation ofCyclooxygenase-2 mRNA in the Rat Spinal Cord following Pe-ripheral Inflammation. FEBS Lett 390:165–169
5. BurianM, Tegeder I, SeegelM et al. (2003) Peripheral and CentralAntihyperalgesic Effects of Diclofenac in a Model of HumanInflammatory Pain. Clin Pharmacol Ther 74:113–120
6. Dolan S, Kelly JG, Huan M et al. (2003) Transient Up-Regulationof Spinal Cyclooxygenase-2 and Neuronal Nitric Oxide Synthasefollowing Surgical Inflammation. Anesthesiology 98:170–180
7. Ghilardi JR, Svensson CI, Rogers SD et al. (2004) ConstitutiveSpinal Cyclooxygenase-2 Participates in the Initiation of TissueInjury-Induced Hyperalgesia. J Neurosci 24:2727–2732
8. Koppert W, Wehrfritz A, Korber N et al. (2004) The Cyclooxy-genase Isozyme Inhibitors Parecoxib and Paracetamol ReduceCentral Hyperalgesia in Humans. Pain 108:148–153
9. Maihofner C, Probst-Cousin S, Bergmann M et al. (2003) Ex-pression and Localization of Cyclooxygenase-1 and -2 in Hu-man Sporadic Amyotrophic Lateral Sclerosis. Eur J Neurosci18:1527–1534
10. Maihofner C, Tegeder I, Euchenhofer C et al. (2000) Local-ization and Regulation of Cyclooxygenase-1 and -2 and Neu-ronal Nitric Oxide Synthase in Mouse Spinal Cord. Neuroscience101:1093–1108
11. Samad TA, Moore KA, Sapirstein A et al. (2001) Interleukin-1beta-Mediated Induction of Cox-2 in the CNS Contributes toInflammatory Pain Hypersensitivity. Nature 410:471–475
12. Tegeder I, Niederberger E, Vetter G et al. (2001a) Effects of Selec-tive COX-1 and -2 Inhibition on Formalin-Evoked NociceptiveBehaviour and Prostaglandin E(2) Release in the Spinal Cord.J Neurochem 79:777–786
13. Tegeder I, Niederberger E, Israr E et al. (2001b) Inhibition ofNF-{kappa}B and AP-1 Activation by R- and S-flurbiprofen.FASEB J 15:2–4
14. Wallace JL, Bak A, McKnight W et al. (1998) Cyclooxygenase-1 Contributes to Inflammatory Responses in Rats and Mice:Implications for Gastrointestinal Toxicity. Gastroenterology115:101–109
15. Yaksh TL, Dirig DM, Conway CM et al. (2001) The Acute Anti-hyperalgesic Action of Nonsteroidal, Anti-Inflammatory Drugsand Release of Spinal Prostaglandin E2 is Mediated by the In-hibition of Constitutive Spinal Cyclooxygenase-2 (COX-2) butnot COX-1. J Neurosci 21:5847–5853
COX-1 Inhibitor
Definition
A drug that inhibits type 1 of the enzyme cyclo-oxidase,which takes part in production of prostaglandins thatcause inflammation and pain, cause blood platelets tobecome sticky and stop bleeding, protect the gastricmucosal cells (and also have many other physiologicfunctions).� COX-1 and COX-2 in Pain� Postoperative Pain, Acute Pain Management, Princi-
ples
COX-2
� COX-1 and COX-2 in Pain
COX-2 Inhibitor
Synonyms
Coxib; NSAIDs

486 Coxibs
Definition
Non-steroidal anti-inflammatory drugs (NSAIDs) areincreasingly used for postoperative analgesia. Whilelacking some of the troublesome adverse effects ofopioids, non-selective NSAIDs may cause bleeding,gastric ulceration, and renal injury as a result of theirinhibitory effects on cyclo-oxygenase–1 (COX–1).Cyclo-oxygenase–2 (COX–2) is normally present insmall concentrations, but is induced peripherally un-der conditions of inflammation. Cyclo-oxygenase–2(COX–2) is constitutively expressed in the brain andspinal cord and is further up-regulated after persistentnoxious inputs. Spinal COX–2 inhibition may be animportant mechanism for reducing post-injury hyper-algesia. For this reason, COX–2-selective inhibitors(COXIBS) could uncouple the therapeutic and adverseeffects of the non-selective NSAIDs. COX–2-selectiveinhibitors are effective for the treatment of preoperativeand postoperative pain and reduce post-surgical require-ments for opioids. They have similar analgesic efficacyto the non-selective NSAIDs. Data from large multi-centre, multi-dose comparative studies are needed toestablish whether COX–2-selective inhibitors are moreefficacious, cost-effective and safe compared to thenon-selective NSAIDs with respect to gastric, renal andcoagulation problems, and whether COX–2-selectiveinhibitors confer greater cardiovascular risk in theperioperative setting.� Multimodal Analgesia in Postoperative Pain� Postoperative Pain, Acute Pain Management, Princi-
ples� Postoperative Pain, Cox-2 Inhibitors
Coxibs
Definition
Structural heterogenous class of compounds inhibitingCOX–2, more or less selectively.� COX–2 Inhibitor NSAIDs� COX–1 and COX–2 in Pain� COX-2 Inhibitor� Coxibs and Novel Compounds, Chemistry� NSAIDs, Chemical Structure and Molecular Mode of
Action� Postoperative Pain, COX-2 Inhibitors
Coxibs and Novel Compounds, ChemistrySTEFAN A. LAUFER
Institute of Pharmacy, Eberhard-Karls University ofTuebingen, Tuebingen, [email protected]
Synonyms
NSAIDs and Coxibs; Cyclooxygenase Inhibitors,Chemistry
Definition
As most � NSAID s are believed to act via a substrateanalogue of � arachidonic acid mechanism at the ac-tive site of the molecular target, � Cyclooxygenases(COX), chemical structure and biological activity areclosely linked. Acidic groups and π-electron systemsof NSAIDs mimic key structural features of the genuinesubstrate, arachidonic acid. COX-1/COX-2 selectiv-ity is mainly determined by different conformationalrequirements rather than specific interactions.
Characteristics
Unselective COX Inhibitors
Structure and Metabolic Function of COX-1
COX-1 is a 70 kD enzyme, catalyzing the reaction ofarachidonic acid to PGG2 (cyclooxygenase reaction)and consecutively PGG2 to PGH2 (peroxidase reaction)as outlined in Fig. 1.Therearedistinct activesites for thecyclooxygenaseandperoxidase reactions (Fig. 2).
Inhibitors
Differentchemicalclassescanprovide thestructural fea-tures necessary to mimic arachidonic acid at the activesite. The substrate, arachidonic acid is a C20 carboxylicacid with 4 isolated double bonds at positions 5, 8, 11and 14. For the enzyme reaction, arachidonic acid mustadapt to a “folded” conformation, allowing the oxygento insert between C9 and C11 and the ring closure be-tween C8 and C12 (Fig. 3). To fix arachidonic acid insuch a conformation, several interactions to the activesite of the enzyme are necessary, e.g. ionic interaction(a salt bridge) between the carboxylic group and argi-nine 120, π-π interactions between the double bonds ofarachidonic acid and aromatic amino acids and numer-ous hydrophobic interactions (Fig. 4).All these structural features can be identified in manyNSAIDs. Most acidic NSAIDs are therefore believed tomimic arachidonic acid in its folded conformation at theactive site of COX. The structure activity relationshipfollows these structural constrictions closely. The activ-ity against COX-1 clearly correlates with torsion anglesaroundtheπ-electronsystemsandtheoverall lipophilic-ity of the molecule (Moser at al. 1990).Two classesofcompoundshoweverhaveadistinctly dif-ferent molecular mode of action,
• ASS irreversibly acetylates Ser 530 at the active siteof the enzyme
• Theoxicamesarebelieved to interferewith theperox-idase active site, which also explains their structuraldifference.

C
Coxibs and Novel Compounds, Chemistry 487
Coxibs and Novel Compounds,Chemistry, Figure 1 Reactionscatalyzed by COX enzymes.
Coxibs and Novel Compounds, Chemistry, Figure 2 A ribbon represen-tation of the Co3+-oPGHS-1 monomer with AA bound in the COX channel.The EGF domain, MBD and catalytic domain are shown in green, orangeand blue, respectively; Co3+-protoporphyrin IX is depicted in red, disul-fide bonds (Cys36-Cys47, Cys37-Cys159, Cys41−Cys57, Cys59-Cys69and Cys569-Cys575) in dark blue and side chain atoms for COX chan-nel residues Arg120, Tyr355 and Tyr385 in magenta (from Malkowski etal. (2000)).
Coxibs and Novel Compounds,Chemistry, Figure 3 Mechanisticsequence for converting AA to PGG2.Abstraction of the 13-proS hydrogenby the tyrosyl radical leads to themigration of the radical to C-11 onAA. An attack of molecular oxygen,coming from the base of the COXchannel, occurs on the side interfacialto the hydrogen abstraction. As the11R-peroxyl radical swings over C-8for an R-side attack on C-9 to formthe endoperoxide bridge, C-12 isbrought closer to C-8 via rotationabout the C-10/C-11 bond, allowingthe formation of the cyclopentanering. The movement of C-12 alsopositions C-15 optimally for additionof a second molecule of oxygen,formation of PGG2 and the migrationof the radical back to Tyr385 (fromMalkowski et al. (2000)).
Most of the currently used NSAIDs, including di-clofenac, ibuprofen, naproxen, piroxicam and in-domethacin for instance, may produce full inhibition ofboth COX-1 and COX-2 with relatively poor selectiv-ity under therapeutic conditions (Warner et al. 1999).Acidic NSAIDs like diclofenac accumulate particularlyin blood, liver, milt and bone marrow, but also in tissueswith acidic extracellular pH values. Such tissues aremainly inflamed tissues, such as gastric tissue and themanifolds of the kidney. In inflamed tissue, NSAIDs in-hibit the pathological overproduction of prostaglandins.In contrast neutral NSAIDs (paracetamol) and weaklyacidic NSAIDs (metamizol) distribute themselvesquickly and homogeneously in the organism. They alsopenetrate the blood-brain-barrier.
Fenamate Group
The core structure is 2-aminobenzoic acid (anthranilicacid). The 2-amino group is substituted with aromaticresidues.
• flufenamic acid• mefenamic acid• meclofenamic acid• nifluminic acid (core structure, 2-amino-pyridyl-
3-carboxylic acid). For topical application, the

488 Coxibs and Novel Compounds, Chemistry
Coxibs and Novel Compounds,Chemistry, Figure 4 A schematicof interactions between AA and COXchannel residues. Carbon atoms ofAA are yellow, oxygen atoms redand the 13proS hydrogen blue. Alldashed lines represent interactionswithin 4.0 Å between the specificside chain atom of the protein andAA (from Malkowski et al. (2000)).
carboxylic acid group is esterified with diethyleneg-lycol
• etofenamate
Fenac Group
The core structure is 2-aminophenylacetic acid. The 2-amino group is substituted with aromatic residues.
• diclofenac• felbinac (only used topically)
Heteroaryl Acetic Acid Group
• indomethacin• acemetacine• proglumetacine• tolmetin (and its ring closed analog ketorolac)• ionazolac
Profene Group
Core structure: 2-arylpropionic acid
• ibuprofen• ketoprofen• thiaprofen• naproxen• ketorolac (can be seen formally as a ring closed pro-
fene)
Oxicame Group
Core structure: 1,2-benzothiazine
• piroxicam• tenoxicam
Coxibs and Novel Compounds, Chemistry, Figure 5 Comparison of theactive sites of COX-1 (PGHS-1) and COX-2 (PGHS-2) (from Wong et al.(1997).

C
Coxibs and Novel Compounds, Chemistry 489
Coxibs and Novel Compounds,Chemistry, Figure 6 Chemicalstructures of NSAIDs and coxibs.

490 CPH
• lornoxicam• droxicam• cinoxicam• sudoxicam• meloxicam
Pyrazolone Group
The mode of action of the pyrazolones remains un-clear. It is thought that they may not be involved inthe inhibition of COX-1 or COX-2. The compounds ofthe pyrazol-3-on series at least are neutral moleculeswith no acidity. A central mode of action is suggested.They also act antispasmodically and they are effectiveagainst visceral pain. In the past, pyrazolones wereamong the nonsteroidal anti-inflammatory drugs usedvery frequently. They show a high plasma protein bind-ing and therefore have a high rate of interaction withother pharmaceuticals. Agranulocytosis is a rare butsevere side effect.The core structure is 3H-pyrazol-3-on
• propyphenazone• metamizol-Na• phenazone
Pyrazolidindione
The core structure is pyrazolidin-3,5-dion
• phenylbutazone• mofebutazone
COX-2 Selective Inhibitors
Isoform 2 of the COX enzyme catalyzes the identicalreaction, AA to PGG2; the active site however is slightlydifferent from that of COX-1 (Fig. 5).Isoleucine 523 is replaced by valine 509, making the ac-tive site of COX-2 more “spacious”. This difference canbe used to generate COX-2 selective inhibitors, as thisactive site tolerates more bulky molecules. Celecoxibis capable of producing full inhibition of COX-1 andCOX-2. However it shows a preferential selectivity to-ward COX-2 (>5 fold). The newer coxibs like rofecoxibstrongly inhibit COX-2 with only weak activity againstCOX-1 (Warner et al. 1999).A common pharmacophore cannot be identified; how-ever vicinal diaryl systems (celecoxib, rofecoxib, valde-coxib) and sulfone or sulphonamide groups seem to beadvantageous (Dannhardt and Laufer 2000). Lumira-coxib is an excellent example of the fact that spatialdemanding substituents (bulky groups) alone are suffi-cient to generate selectivity, even with a diclofenac-likepharmacophore.
Structural Features of Selective COX-2 Inhibitors
Sulfonamide Structure
• celecoxib• valdecoxib
Methylsulfone Structure
• rofecoxib• etoricoxib
Aryl Acetic Acid
• lumiracoxib
Others:
• parecoxib (water soluble prodrug for parenteral ap-plication, rapidly metabolized to valdecoxib)
References1. Dannhardt G, Laufer S (2000) Structural approaches to explain
the selectivity of COX-2 inhibitors: Is there a common pharma-cophore? Current Med Chem 7:1101–1112
2. Malkowski M, Ginell SL, Smith WL, Garavito RM (2000)The Productive Conformation of Arachidonic Acid Bound toProstaglandin Synthase. Science 289:1933–1937
3. Moser P, Sallmann A, Wiesenberg L (1990) Synthesis and quan-titative structure-activity relationships of diclofenac analogues.J Med Chem 33:2358–2368
4. Warner T, Giuliano F, Vojnovic I et al. (1999) Nonsteroid drugselectivities for cyclo-oxygenase-1 rather than cyclo-oxygenase2 are associated with human gastrointestinal toxicity: A full invitro analysis. Proc. Natl Acad Sci USA 96:7563–7568
5. Wong E, Bayly E, Waterman HL et al. (1997) Conversion ofprostaglandin G/H synthase-1 into an enzyme sensitive to PGHS-2-selective inhibitors by a double His513→Arg and Ile523→Valmutation. J Biol Chem 272:9280–9286
CPH
� Chronic Paroxysmal Hemicrania
Cranial Arteritis
� Headache Due to Arteritis� Temporal Arteritis
Cranial Nerve Neuralgia
Definition
A family of chronic neuropathic pain states associatedwith injury or dysfunction of a cranial nerve, most oftenin the trigeminal or glossopharyngeal nerve. Ongoingpain and/or hypersensibility is felt primarily in the dis-tribution of the injured nerve.� Tic and Cranial Neuralgias

C
Credibility, Assessment 491
Cranial Nerves
Definition
The 12 pairs of nerves originating from the brain thatprovide motor, sensory, and autonomic function to thestructures of the head and neck. The N. vagus (X) alsoinnervates the viscera.� Diabetic Neuropathies
Cranial Neuralgias
� Tic and Cranial Neuralgias
Craniomandibular Disorders
� Temporomandibular Joint Disorders
Cranium
Definition
The skull and its associated soft tissues.� Orofacial Pain, Taxonomy/Classification
CRD
� Colorectal Distension
CREB
� Cyclic Adenosine Monophosphate-Responsive Ele-ment-Binding Protein
Credibility Finding
Definition
An adjudicative finding of the extent to which a person’sstatements about the intensity, persistence, and func-tional effects of his or her symptoms can be believedand accepted as true. The credibility finding takes intoconsideration the objective medical evidence and theother evidence in the case record, to include the person’sstatements, the statements and other evidence providedby physicians and psychologists who have treated orexamined the person, evidence from other health careprofessionals, and statements from other persons, to in-clude the person’s spouse, family members, neighbors,friends, co-workers, etc.
� Disability Evaluation in the Social Security Admin-istration
Credibility, AssessmentKENNETH D. CRAIG
University of British Columbia, Vancouver, BC,[email protected]
University of British Columbia, Vancouver,BC, CanadaSynonyms
Deception; malingering
Definition
Pain reports and disability are regularly subjected toscrutiny to establish their veracity, with contextualfactors, self-report, nonverbal behavior, the reports ofsignificant others, and medical information variablyuseful as determinants of judgments.
Characteristics
Pain enmeshes people in complex social transactions,with the credibility of complaints invariably subjected tocareful appraisal by others. A substantial range of care-giving resourcesmay beavailable,whethermotivatedbysympathy, professional responsibility, contractual obli-gation (e.g. disability insurance), legislated entitlement(e.g. workers’ compensation benefits) or court order. Inall instances, optimal caregiving and prudent steward-ship of resources require judgmentsabout the legitimacyof the representations of the person in distress. In health-care settings, it would be ideal if norms of trust were toprevail, and negotiation of care did not require patientsto persuade health care practitioners of the legitimacyof their concerns. However, patients sometimes warrantand often encounter distrust, particularly when physicalpathology is not manifestly obvious. Patients are likelyto be scrutinized to discover whether financial incen-tives, efforts to obtain illicit drugs, or avoidance of oner-ous responsibilities are involved. Werner and Malterud(2003)describewomen with medically unexplained dis-orders encountering skepticism, lack ofcomprehension,rejection,beingblamedfor theircondition,andsufferingfeelings of being ignored or belittled.The real incidence and costs of various forms of decep-tion is unknown, because people work hard to avoid dis-covery of dishonesty (Craig et al 1999). Denial of painto avoid noxious treatments or imposition of sick rolesis an often ignored but widespread form of deception,because its immediate effects do not usually inflict de-mandson others, despite thepotential forcollapseofper-sonal health and long-term medical costs. Opportunis-tic feigning or exaggeration of minor pain is relativelycommon and may be approved by others (e.g. sick days),despite substantial costs (e.g. to employers). Flagrant,

492 Credibility, Assessment
planned fraud isgenerally estimated to be rare;neverthe-less systems costs to employers, health care providers,insurance companies, and social service could mountdramatically.Decisions that another is malingering require a judg-ment of intentional production of false symptoms toobtain financial incentives or other privileges. Manyclinicians eschew providing reports on credibility be-cause they perceive them inconsistent with their role aspatient advocate. Challenging patients is also fraughtwith a substantial risk of reprisal and angry, emotionalconfrontations. Patients reasonably perceive seriousconsequences, including denial of treatment, loss ofincome, or criminal investigations.Regrettably, universally acceptable and valid measuresof neither pain nor deception are available, and judg-ments require inferences based upon information thathasdemonstrable limitations.Efforts to detectdeceptiongenerally appear not to be particularly effective. Thereare considerable individual differences in detecting de-ception.Hill and Craig (2004) reported that success ratesin accurately differentiating genuine and faked or sup-pressed facial expressions of pain varied across individ-uals between 18 and 63%.
Strategies for Assessing Credibility
Useful information often emerges during pain assess-ments, when listening to complaints, symptoms, andpersonal histories, observing nonverbal manifestationsof distress and disability, examining standardized ques-tionnaires and physical examinations, and studyingarchival documents and reports of significant others,including reports of laboratory tests. Assessors usuallylook at matches between their personal conceptions asto how one should behave and the actual behavior of theindividual, with inconsistencies indicative of deception.We know more about cues that have “illusory correla-tions” with deception than about sensitive and specificcues to honest or dishonest representations. Erroneouscues to deception, not unique to pain, include signs ofnervousness, clearing the throat, faltering speech, andbiting the lips (Porter et al 2002). Concerning pain, peo-ple who respond to placebos have been misconstrued asnot experiencing “real” pain, despite clear evidence thatplacebos can dramatically reduce pain instigated by in-jury and surgery.
Contextual Analysis
The contexts in which people present themselves to bein pain are important. Sometimes a discrete, precipitat-ing event may be required to legitimize work-related in-juries, or engineering reports must describe substantialphysical forces in motor vehicle accidents, but these arecontroversial as pain onset can occur without trauma.Analyses of the settings in which people lead their livesmay disclose circumstances leading to deception, forexample, work dissatisfaction or domestic distress. Of
course, disincentives for assuming the life of a per-son with persistent pain also must be considered (e.g.loss of employment or impaired family and friendshiprelationships). The American Psychiatric Associationdiagnostic manual (2000) implicates malingering whenthere is a medicolegal context, a strong discrepancybetween claimed stress and disability and objectivefindings, or limited cooperation with assessment orlack of compliance in treatment. However, these arecommonplace and their use can cast inappropriateaspersions on people.
Use of Self-Report
Capitalizing on the unique capacity of humans to use so-phisticated language to describe subjective states, self-report has been favored as a communication medium forthe measurement of pain. Guidelines on pain manage-ment often assert, “Pain is what the patient says it is.”But self-report is also a prime medium for dissemblingpain. Distrust of self-report in reality is widespread.Scarry (1985) captures the suspicion in the observationthat, “To have great pain is to have certainty, to hear thatanother person has pain is to have doubt”. Nevertheless,analyses of the content of verbal statements can discloseuseful information. Mendelson and Mendelson (2004)reviewed questionnaire studies contrasting people gen-uinely in pain with people coached to pretend they werein pain, finding that simulators exaggerated the genuinepattern of response. However, cutting scores yieldedsubstantial numbers of misidentified false positivesand negatives. A review of the MMPI-2 (Arbisi andButcher 2004) concluded that it is useful in detectinginconsistent and inaccurate self-report responding, un-cooperative responding, unusually positive or virtuousself-presentation, and general defensiveness.
Biomedical Approaches
The biomedical model of pain requires physical lesionsto account for pain complaints. The model persistsbecause it is adequate for painful conditions arisingfrom serious injury or surgery, provided there is someallowance for variability related to the individual and thesituation. However, patients encounter medical distrustand resistance when physicians cannot find evidenceof physical pathology. The reality is that medicallyunexplained pain is common and a serious health careproblem. Some patients do not receive adequate med-ical examinations or expert use of diagnostic tests, buteven when used properly these are not as reliable andvalid as might be expected (Hunt et al 2001). Controlleddiagnostic blocks serve as useful diagnostic tools whena specific source of pain can be posited and is subject tobeing anaesthetized (e.g. spinal pain) (Bogduk 2004).
Nonverbal Cues
Nonverbal information weighs heavily when peoplemake judgments about others’ reports of pain, includ-

C
Creep 493
ing their credibility. Painful distress can be manifest infacial expression, qualities of speech, guarded posture,protective movements, and other actions as people en-gage their daily lives. Reflexive, automatic reactionsare less subject to ongoing self-monitoring and per-sonal control than voluntary actions. The latter providethe basis for misrepresenting pain, but require ongo-ing careful scrutiny. Inconsistencies with self-reportand failure to match the reflexive pattern can disclosemisrepresentation (Hill and Craig 2002).Several illustrationsof spurioususeofcuespresumedin-dicative of deception are available. Evidence that painbehavior can be controlled by social consequences (e.g.release from responsibilities, potentmedication, sympa-thy) has been taken to suggest, incorrectly, that the be-havior represented voluntary dishonesty or efforts to se-cure incentives. However, environmental contingenciescan operate on behavior without consciousnessTherehavebeen similarmisinterpretationsofdiagnosticsigns related to low back pain that could not have a basisin physicalpathology,asweunderstandcurrentanatomyand physiology (e.g. nonanatomic or superficial tender-ness).MainandWaddell (1998)andFishbainetal (2004)concluded that there was little evidenceofan associationbetween these signs and secondary gain or malingering.Main and Waddell (1998) warn that these signs “are noton their own a test of credibility or faking” and considerinferences based on that supposition to be misuse, bothclinically and medico-legally.Other measures have pursued observations that peoplewho sincerely exercise effort in strength testing appearless likely to be misrepresenting themselves. Displaysof weakness and decreased range and velocity of mo-tion have been interpreted as conscious attempts to de-ceive. Investigations of a variety of indices of this typeled Robinson and Dannecker (2004) to conclude “thatthe current ‘state of the art’, while promising in someinstances, does not warrant the clinical application ofmuscle testing as a means of sincerity of effort”. Prob-lems arise because performance is also influenced byfear of injury, pain, medications and other motivationaland cognitive factors, and discriminating maximal andsubmaximal effort remains a problem.
Reports of Significant Others
Reports of family members, friends, colleagues andothers can provide valuable collateral information ableto confirm or disconfirm patient self-report. Collusionwould be possible, but contradiction seems more likely,unless there has been very careful grooming. Unobtru-sive behavioral observation can be undertaken usingcovert surveillance, to provide photographic or videorecords of people claiming to have severely disablingpain engaging in vigorous physical activity. While thisappears to represent flagrant abuse, careful analysisoften suggests the need for income or commitments to
family and others can lead people to engage in vigorousactivities, despite severe immediate or delayed pain.
Conclusion
Assessment of credibility is an evolving process. Thosewho would deceive can be well motivated and well tu-tored by priorpersonalexperience,or instructionalmod-els in their families. In turn, those interested in assessingcredibilitymustuseabroadrangeof informationsourcesthat will hopefully improve in sensitivity and specificityto deceptive behavior. Sequential, progressive evalua-tion seems the best strategy, using broad screening ap-proaches to trigger suspicion, followed by progressivelymore rigorous methods.
References1. American Psychiatric Association (2000) Diagnostic and Statis-
tical Manual of Mental Disorders. Fourth edition. Text revision.Washington, DC
2. Arbisi PA and Butcher JN (2004) Psychometric Perspectives onDetection of Malingering of Pain: Use of the MMPI-2. Clin JPain 20:383–391
3. Bogduk N (2004) Diagnostic blocks: A Truth Serum for Malin-gering. Clin J Pain 20:409–414
4. Craig KD, Hill ML, McMurtry B. Detecting Deception and Ma-lingering. In A.R. Block AR, Kramer EF, Fernandez E (1999)Handbook of Chronic Pain Syndromes: Biopsychosocial Per-spectives. Mahwah NJ: Lawrence Erlbaum Associates, pp 41–58
5. Fishbain DA, Cutler RB, Rosomoff HL, Rosomoff RS (2004). IsThere a Relationship Between Non-Organic Physical Findings(Waddell Signs) and Secondary Gain/Malingering? Clin J Pain20:399–408
6. Hill ML, Craig KD (2002) Detecting Deception in Pain Expres-sions: The Structure of Genuine and Deceptive Facial Displays.Pain 98:135–144
7. Hill ML, Craig KD (2004) Detecting Deception in Facial Expres-sions of Pain: Accuracy and Training. Clin J Pain 20:415–422
8. Hunt DG, Zuberbier OA, Kozlowski A, Robinson J, Berkowitz J,Schultz IZ, Milner RA, Crook JM, Turk DC (2001) Reliability ofthe Lumbar Flexion, Lumbar Extension and Passive Straight LegRaise Test in Normal Populations Embedded within a CompletePhysical Examination. Spine 26:2714–2718
9. Main CJ, Waddell G (1998) Behavioral Responses to Examina-tion: A Reappraisal of the Interpretation of “Nonorganic Signs.Spine 23:2367–2371
10. Mendelson G, Mendelson D (2004) Malingering Pain in theMedico-Legal Context. Clin J Pain 20:423–432
11. Porter S, Campbell MA, Stapleton J, Birt AR (2002) The In-fluence of Judge, Target, and Stimulus Characteristics on theAccuracy of Detecting Deceit. Can J Behav Sci 34:172–185
12. Robinson ME, and Dannecker EA (2004) Critical Issues in theUse of Muscle Testing for the Determination of Sincerity of Ef-fort. Clin J Pain 20:392–398
13. Scarry E (1985) The Body in Pain. Oxford University Press, NewYork
14. Werner A and Malterud K (2003) It is Hard Work Behaving as aCredible Patient: Encounters between Women with Chronic Painand their Doctors. Social Science and Medicine 57:1409–1419
Creep
Definition
Creep is a physiologic property of collagenous tissue. Inresponse to the application of a constant force, collagen

494 Criterion-Referenced Assessment
starts to deform (stretch). However, this deformation isnot directly proportional to time. Initially, the deforma-tion is small, but the longer the constant force is applied,the more rapidly collagen will deform (and weaken),even if the magnitude of the force remains constant.This phenomenon is defined as creep and may lead tocomplete failure of the collagen fibre.� Ergonomic Counseling
Criterion-Referenced Assessment
Definition
In criterion-referenced assessment, the critical aspectsof a job are analyzed to determine standards essentialfor the for the worker’s adequate performances of a job.The results are stated in terms of skills mastered, e.g.Method Time Methods (MTM) (the time it would takethe average, well-trained worker to complete the worksample tasks if they were carried out over the eight-hourwork day in a typical industrial context), and the WorkerQualification Profiles given in Jist’s Enhanced DOT.� Vocational Counselling
Crohn’s Disease
� Animal Models of Inflammatory Bowel Disease
Cross Excitation
Definition
Electrophysiologicalphenomenonwherebyneurotrans-mittermolecules,andprobablyalsoK+ions,arereleasedinto the extracellular space from active neurons. Thesediffuse towards neighboring neurons and excite them.Cross excitation occurs within sensory ganglia and atsites of nerve injury.� Pain Paroxysms
Cross Sectional Study
Definition
A research methodology that examines relationships be-tween variables at one point in time.� Pain in theWorkplace,Risk factors forChronicity, Job
Demands
Cross-Excitatory Discharge
Definition
Excitation evoked within the dorsal root ganglion be-tween repetitively discharging neurons and their passiveneighbors. This excitatory interaction between neuronsis believed to be chemically and not electrically medi-ated.� Ectopia, Spontaneous
Cross-System Viscero-VisceralInteractions
� Gynecological Pain, Neural Mechanisms
Cross-System Viscero-Visceral orViscero-Somatic Convergence
Definition
A connective situation in which neurons in the CNS re-ceive converging input from different organs (viscero-visceral),sometimesindifferentfunctionalsystems(e.g.reproductive and urinary), and from different types ofstructures such as skin, muscle, and internal organs (vis-cerosomatic).� Gynecological Pain, Neural Mechanisms
CRPS
� Complex Regional Pain Syndrome� Complex Regional Pain Syndromes, Clinical Aspects� Complex Regional Pain Syndromes, General Aspects� Sympathetically Maintained Pain, Clinical Pharma-
cological Tests
CRPS, Evidence-Based TreatmentANNE LOUISE OAKLANDER
Nerve Injury Unit, Departments of Anesthesiology,Neurology, and Neuropathology, MassachusettsGeneral Hospital, Harvard Medical School, Boston,MA, [email protected]
Synonyms
• Complex regional pain syndrome (CRPS): term des-ignated by International Association for the Study ofPain (IASP) in 1994

C
CRPS, Evidence-Based Treatment 495
• Reflex sympathetic dystrophy (RSD): term first usedby Evans in 1946
• Algodystrophy: most common designation in Europe• Shoulder-hand syndrome: refers specifically to
CRPS originating in hand, spreading to shoulder• Causalgia: from Greek, causos = heat; algia = pain
(OxfordEnglishDictionaryfirstuse:S.WeirMitchell1872)
• Sudeck’s atrophy (1901)• Major or minor causalgia• Post-traumatic dystrophy• Pourfour du Petit syndrome• Postinfarctional sclerodactylia• Traumatic angiospasm• Peripheral acute trophoneurosis• Post-traumatic neuralgia
Definition
Because the biological cause of CRPS is unknown,the definition is currently based on the presence ofvarious non-specific symptoms. Many investigatorscreate their own definitions, hampering comparisonof study results. The International Association for theStudy of Pain (IASP) formulated consensus defini-tions in 1994 (see below) (Merskey and Bogduk 1994).“Type I” classifies patients without diagnosed nerveinjury; “type II” classifies those with known neuralinjuries. This dichotomy depends more on the skill ofthe examiner than the patient and contributes to theconfusion. Although flawed, the use of IASP criteria isencouraged until a better definition is developed.More rigorous definitions proposed for research userequire visual confirmation of autonomic dysfunction.This improves specificity, but at the cost of reducingsensitivity. Rigorous diagnostic criteria may limit studyto severely affected patients, who do not represent theoverall population and who may be least likely to im-prove in clinical trials. This author suggests adoptingthe hierarchy of definitions used for other neurologicalresearch (definite CRPS, probable CRPS and possi-ble CRPS) to permit greater or less sensitivity andspecificity for use in individual research projects.
IASP Diagnostic Criteria for CRPS-I (Reflex Sympathetic Dys-trophy)
1. The presence of an initiating noxious event or a causeof immobilization.
2. Continuing pain, � allodynia, or � hyperalgesia inwhich the pain is disproportionate to any incitingevent.
3. Evidence at some time of edema, changes in skinblood flow or abnormal sudomotor activity in theregion of the pain.
4. This diagnosis is excluded by the existence of con-ditions that would otherwise account for the degree
of pain and dysfunction. Note: Criteria 2–4 must besatisfied (Merskey and Bogduk 1994)
IASP Diagnostic Criteria for CRPS-II (Causalgia)
1. The presence of continuing pain, allodynia or hyper-algesia after a nerve injury, not necessarily limited tothe distribution of the injured nerve.
2. Evidence at some time of edema, changes in skinblood flow or abnormal sudomotor activity in theregion of the pain.
3. This diagnosis is excluded by the existence of con-ditions that would otherwise account for the degreeof pain and dysfunction. Note: All three criteria mustbe satisfied (Merskey and Bogduk 1994)
Characteristics
CRPS is a “pain plus” syndrome comprising regionalneuralgia plus additional symptoms. Most cases followtrauma, but symptoms persist after apparent healingof injuries. Autonomic dysregulation (hyperhidrosis,vasomotor instability causing edema, abnormal skincolor or temperature) is part of the definition. Motor ab-normalities are common and increasingly recognized.Some patients have mild or transient symptoms; othersare chronically disabled. CRPS was first characterizedin Weir Mitchell’s astute descriptions of Civil War sol-diers with � causalgia after penetrating wounds. It is notknown why rare nerve injury patients develop CRPS-IIand why identical symptoms develop without obviouscause in CRPS-I. The fundamental lesion in CRPS-Iappears to involve specific peripheral axons, the smalldiameter unmyelinated and thinly myelinated axonsthat subserve pain and some autonomic functions (vander Laan et al. 1998; Albrecht et al. 2006; Oaklanderet al. 2006). Relative sparing of motor and large fibersensory axons can preserve enough function to givesome patients a misleadingly normal appearance.
Treatments for Recent Onset CRPS
Early on, medications must be secondary to and sup-portive of efforts to mobilize the affected limb andto restore its function. Several trials have evaluatedtreatments for CRPS symptoms present for less than6 months. Inflammation and remodeling from the orig-inal trauma may still be present and the final effects ofinjury on the CNS may not yet have occurred, making itpossible to find treatments to modify the disease course(provide permanent cure or improvement) rather thanmerely alleviate symptoms. It has not been examinedwhether these early treatments are also effective forchronic CRPS, and their mechanisms are completelyunknown. Two small, unblinded trials (Braus et al.1994) support the use of oral corticosteroids. Sys-tematic meta-analysis (Perez et al. 2001) of severalplacebo controlled randomized controlled trials (RCT)of intranasal calcitonin (100–400 IU) support its use.

496 CRPS, Evidence-Based Treatment
Calcitonin is a neuropeptide with direct antihyperal-gesic effects independent of its effects on bone (Braga1994). Use of bisphosphonates, which also inhibitosteoclast mediated bone resorption, is supported byseveral small RCT (Varenna et al. 2000). One studyfound pamidronate (30 mg daily for 3 days) effective in35 patients with acute or chronic CRPS. Single RCTssupport the efficacy of topical dimethylsulfoxide, andof oral vitamin C in CRPS-I. The alpha-adrenergicantagonist phenoxybenzamine was effective in smalltrials in early CRPS (Muizelaar et al. 1997) and variousneuralgias including CRPS-II.
Conservative Treatments for Established CRPS
Rehabilitation is essential. In addition to preventingsecondary problems including deconditioning, con-tractures, weight gain and depression, it now appearsthat abnormal cortical reorganization in CRPS maybe ameliorated by aggressive restoration of function.Psychotherapy and/or psychotropic medications areindicated for many patients who develop reactive de-pression or other psychological difficulties caused bytheir chronic pain and disability. The limited evidencesuggests that acupuncture, magnets, and other alterna-tive treatments are ineffective.
Medical Treatments for Established CRPS
Pharmacotherapy becomes the major treatment forpatients whose symptoms do not improve substantiallydespite aggressive rehabilitation. Few pharmaceuticalcompanies consider CRPS a suitable condition for clin-ical trials and so there are no strong drug trials in chronicCRPS. Clinicians must currently extrapolate from theresults of well-designed and conclusive trials for relatedconditions (primarily painful diabetic neuropathy andpostherpetic � neuralgia (PHN)). No medication hasa U.S. Food and Drug Administration indication forCRPS. Regardless, most chronic CRPS patients takemedications, of necessity “off label”.Randomized, controlled, clinical trials studying thetreatment of neuralgia have established the efficacyand safety of four classes of medication. There are notenough data to support the use of one class over anotherand efficacy data must be tempered with considerationof possible adverse effects and cost. Standard princi-ples should be applied, namely selection of medicationbased not only on the patient’s symptoms, but also ontheir overall medical, social and financial situations.Each medication should be tried in an adequate doseand for long enough (1 to 2 months for tricyclics).If ineffective or ill tolerated, a medication should betapered, discontinued and then replaced with the nextchoice. Multiple medications are indicated only wheneach provides added benefit and there are no adverseinteractions. Usually, a selection of medications fromdifferent classes is required. Polytherapy is common inCRPS because pain relief is often elusive.
Topical Local Anesthetics
The most important characteristic of topically appliedmedications (whose active ingredient remains in theskin) is the low incidence of adverse effects. These areavailable in various forms including gels, creams andsprays. The 5% lidocaine patch is probably the mostcommonly topical medication prescribed for CRPS.The patch itself protects allodynic skin from contactand the local anesthetics within reduce hyperalgesia.An RCT of 40 patients with focal � neuropathic painincluding CRPS documents its efficacy (Meier et al.2003), as does an earlier uncontrolled open label addon study of six CRPS patients.
Tricyclic Antidepressants (TCA)
TCAs that augment noradrenergic neurotransmis-sion are perhaps the most effective option for treatingneuralgia. Generic forms are available. TCAs haveseveral mechanisms that contribute to efficacy, includ-ing potentiation of descending inhibitory pathways todecrease dorsal horn hyperactivity, μ-opioid receptoractivation and cation channel blockade. There are nostudies specifically documenting the efficacy of TCAsin CRPS, but their efficacy in neuralgias including di-abetic neuropathy (Max et al. 1992) and PHN is betterdocumented than for any other medications. TCAsthat increase norepinephrine are effective; those withserotonergic effects only are not, whereas those thatincrease both may work best. Adverse effects, whichlimit TCA use, are more common with amitriptylinethan nortriptyline (Watson et al. 1998) or desipramine(Max et al. 1992). CRPS patients are often younger thanother neuralgia patients and thus may tolerate TCAsbetter.
Antiepileptic Drugs (AED)
AEDs decrease central neuronal hyperexcitability totreat neuralgic pain as well as seizures. Gabapentin,well studied in PHN and diabetic neuropathy, is a pri-mary option. It binds to the α2δ subunit of voltage gatedcalcium channels and decreases calcium-mediated re-lease of excitatory neurotransmitters. Gabapentin hasno drug interactions and serum levels do not usuallyneed to be monitored. Serious adverse effects appear tobe less common than with TCAs, though this may notbe true for minor ones. In CRPS, gabapentin was usefulin an open label uncontrolled study of nine adult pa-tients given 600 mg/day (a lower dose than is now used)(Mellick and Mellick 1997) and in a single pediatriccase. Carbamazepine, FDA-approved for trigeminalneuralgia, is supported by a single small, uncontrolledstudy adding it to spinal cord stimuation (Harke et al.2001).
Opioids
Reluctance to prescribe is common, though some CRPSpatients do benefit from opioid treatment and remain on

C
CRPS, Evidence-Based Treatment 497
stable doses. Like other options, opioids help some butnot all sufferers and usually provide only partial relief.Physical � dependence or � tolerance do not always de-velop and can usually be managed by avoiding dose es-calation and sudden withdrawal. There are inadequatedata to support preference for any particular opioid, al-though methadone is attractive because of its low cost.Direct evidence from CRPS patients is almost nil; therationale for use is based largely on the results of well-designed studies in other neuralgic conditions (Raja etal. 2002). An add-on study of morphine in CRPS pa-tients with spinal cord stimulators did not demonstrateefficacy, but the subjects were too unique to generalizeits conclusions. Current or former substance abuse is themajor contraindication to opioid use, although they cansometimes be prescribed for abusers with severe pain ifthey are rigorously monitored.
Other Medications to Consider
Systemic local anesthetics are sometimes efficaciousbut require invasive or subcutaneous administration.Such use was supported by the results of a small RCTin 16 patients with CRPS-I and -II (Raja et al. 2002)and a case series. Administration must be carefullymonitored to prevent seizures or cardiac arrest. Theevidence supporting clonidine is weak. A case series offour CRPS patients screened by regional and system-atic sympathetic blocks found that the antihyperalgesiceffect was restricted to skin directly under the clonidinepatch (Davis et al. 1991). Thalidomide, which inhibitsrelease of TNF-alpha, is under evaluation.
Surgical Treatments for Established CRPS
If medications have not provided significant relief afteradequate trials, two surgical options deserve consider-ation and one does not, namely cutting nerves or neu-ral structures transmitting pain sensations from the af-fected areas. Ablative neurosurgery has a simplistic ap-peal and occasionally provides a pain-free interval toterminal patients; it is not indicated for most CRPS pa-tients who have largely preserved motor function andlong life expectancy. Limb amputation is still occasion-ally performed and may very rarely be indicated for se-rious complications such as gangrene, but it should notbe performed for pain control. CRPS pain is almost cer-tainly maintained by CNS abnormalities not addressedby peripheral ablation.In contrast, the possibility of nerve entrapment or com-pression should more often be considered. Surgicaldecompression can provide dramatic cures in these sit-uations (Thimineur and Saberski 1996). Occasionally,unexpected causes of CRPS such as leprosy, tumorsor vascular malformations are diagnosable only byexploratory surgery. The single most powerful treat-ment for severe established CRPS is implantation of abipolar neural stimulator. Properly selected patients canachieve dramatic pain relief permitting discontinuation
of medications and major functional gains. Experi-enced clinicians have noted that, unlike medications,stimulators can have disease modifying effects, such aspain relief that persists for longer and longer periodsafter the stimulator is turned off. Similar propertieshave also been documented after CNS stimulation inother diseases. Stimulation of the dorsal column is themost common procedure, because the electrode canbe placed percutaneously. Although device trials aredifficult to control for, there is at least one well-designedstudy (Kemler et al. 2000) and several case series thatdemonstrate efficacy in about half of implanted CRPSpatients. Expense and not infrequent complications arethe major limitations. For patients whose CRPS is dueto single nerve damage, surgically implanted peripheralnerve stimulators have had even higher efficacy in aprospective trial (Hassenbusch et al. 1996).
References1. Albrecht PJ, Hines S, Eisenberg E et al. (2006) Pathologic al-
terations of cutaneous innervation and vasculature in affectedlimbs from patients with complex regional pain syndrome. Pain120:244–266
2. Braga PC (1994) Calcitonin and its antinociceptive activity:animal and human investigations 1975–1992. Agents Actions41:121–131
3. Braus DF, Krauss JK, Strobel J (1994) The shoulder-handsyndrome after stroke: a prospective clinical trial. Ann Neu-rol 36:728–733
4. Davis KD, Treede RD, Raja SN et al. (1991) Topical applicationof clonidine relieves hyperalgesia in patients with sympatheti-cally maintained pain. Pain 47:309–317
5. Harke H, Gretenkort P, Ladleif HU et al. (2001) The response ofneuropathic pain and pain in complex regional pain syndromeI to carbamazepine and sustained-release morphine in patientspretreated with spinal cord stimulation: a double-blinded ran-domized study. Anesth Analg 92:488–495
6. Hassenbusch SJ, Schoppa D, Walsh JG et al. (1996) Long-termresults of peripheral nerve stimulation for reflex sympathetic dys-trophy. J Neurosurg 84:415–423
7. Kemler MA, Barendse GA, van Kleef M et al. (2000) Spinal cordstimulation in patients with chronic reflex sympathetic dystrophy.N Engl J Med 343:618–624
8. Max MB, Lynch SA, Muir J et al. (1992) Effects of desipramine,amitriptyline, and fluoxetine on pain in diabetic neuropathy. NEngl J Med 326:250–1256
9. Meier T, Wasner G, Faust M et al. (2003) Efficacy of lidocainepatch 5 % in the treatment of focal peripheral neuropathic painsyndromes: a randomized, double-blind, placebo-controlledstudy. Pain 106:151–158
10. Mellick GA, Mellick LB (1997) Reflex sympathetic dystrophytreated with gabapentin. Arch Phys Med Rehabil 78:98–105
11. Merskey H, Bogduk N (1994) Classification of chronic pain:Descriptions of chronic pain syndromes and definitions of painterms, 2nd edn. IASP Press, Seattle
12. Muizelaar JP, Kleyer M, Hertogs IA et al. (1997) Complex re-gional pain syndrome (reflex sympathetic dystrophy and causal-gia): management with the calcium channel blocker nifedipineand/or the alpha-sympathetic blocker phenoxybenzamine in 59patients. Clin Neurol Neurosurg 99:26–30
13. Oaklander AL, Rissmiller JG, Gelman LB et al. (2006) Evidenceof focal small-fiber axonal degeneration in complex regional painsyndrome-I (reflex sympathetic dystrophy). Pain 120:235–243
14. Perez RS, Kwakkel G, Zuurmond WW et al. (2001) Treatmentof reflex sympathetic dystrophy (CRPS type 1): a research syn-thesis of 21 randomized clinical trials. J Pain Symptom Man-age 21:511–526

498 CRPS Type-I
15. Raja SN, Haythornthwaite JA, Pappagallo M et al. (2002) Opioidsversus antidepressants in postherpetic neuralgia: a randomized,placebo-controlled trial. Neurology 59:1015–1021
16. Thimineur MA, Saberski L (1996) Complex regional pain syn-drome type I (RSD) or peripheral mononeuropathy: A discussionof three cases. Clin J Pain 12:145–150
17. van der Laan L, ter Laak HJ, Gabreels-Festen A et al. (1998)Complex regional pain syndrome type I (RSD): pathology ofskeletal muscle and peripheral nerve. Neurology 51:20–25
18. Varenna M, Zucchi F, Ghiringhelli D et al. (2000) Intravenousclodronate in the treatment of reflex sympathetic dystrophy syn-drome. A randomized, double blind, placebo controlled study.J Rheumatol 27:1477–1483
19. Watson CPN, Vernich L, Chipman M et al. (1998) Nortriptylineversus amitriptyline in postherpetic neuralgia: a randomized trial.Neurology 51:1166–1171
CRPS Type-I
Definition
Pain syndrome that develops after minor injuries or frac-tures of a limb� Complex Regional Pain Syndromes, Clinical Aspects� Postoperative Pain, Acute Presentation of Complex
Regional Pain Syndrome� Sympathetically Maintained Pain in CRPS I, Human
Experimentation
CRPS Type-II
Definition
Complex regional pain syndrome type 2, previouslycalled causalgia. A pain syndrome that develops afterinjury to a major peripheral nerve.� Complex Regional Pain Syndromes, Clinical Aspects� Postoperative Pain, Acute Presentation of Complex
Regional Pain Syndrome� Sympathetically Maintained Pain in CRPS II, Human
Experimentation
CRPS-1 in ChildrenGUNNAR L. OLSSON
Pain Treatment Services, Astrid Lindgren Children’sHospital/Karolinksa Hospital, Stockholm, [email protected]
Synonyms
Complex regional pain syndrome; Reflex SympatheticDystrophy; RSD
Definition
The diagnostic criteria for � CRPS -1 were establishedin 1995 (Stanton-Hicks et al. 1995):
1. An eliciting event, but no demonstrable injury to aperipheral nerve
2. Pain, spontaneous or evoked, often with evidence of� allodynia in a limb
3. � Dysautonomic signs4. No other explanations for the pain
CRPS occurs more frequently in girls, than boys. Themostcommon ageofonset isapproximately 10–14yearsof age. The site of CRPS-1 is predominantly in the lowerextremities. The cause is unknown but children have of-ten had a history of psychosocial stress, such as bullyinginschool.However, themostcommonstressfactor is thatchildren have atypically high expectations for achieve-ment in school and / or sports.Harden et al. performed a factor analysis of symptomsand signs associated with CRPS-1 and proposed an-other diagnostic classification: 1. pain, 2. vasomotordisturbances, 3. oedema and sweating changes, 4. motorchanges (Harden et al. 1999; Wilson et al. 2005). Theysuggested that the criteria of an eliciting event should bedropped because no eliciting trauma could be identifiedin 8% of the cases in a large case series in adults.
Characteristics
Age and Gender
CRPS-1 is much more common in girls; approximately85% of affected children are girls (Bernstein et al. 1978;Olsson etal. 1997;Wilder et al. 1992;Sherry etal. 1999).It is most commonly reported for children in the pre-teen or early teen years (11–14 years of age), althoughthere are case reports on children as young as 3 years old(Kozin et al. 1977).
Localisation
The foot is the most commonly affected site, followedby other parts of the leg and then the upper extremities,including hands, elbows and shoulders. Although the di-agnosis of CRPS-1 in other regions is controversial, Ihave treated a girl with CRPS-1 in the forehead.
Dysautonomic Signs
For adults with CRPS-1, the skin temperature often in-creases initially so that the affected region feels warm;later a cold dystrophic phase ensues. In contrast, chil-dren usually first experience a lower temperature inthe affected region. An infrared skin thermometer isof great value in the clinical setting for temperaturedetermination. Discoloration is usually bluish, blueand red or pale and appears intermittently rather thanconsistently. Oedema may be very soft and subcuta-neous and may also recur intermittently. Many childrenhave had a MRI before their referral to the pain clinic.In several of our cases the radiologist has described a

C
CRPS-1 in Children 499
CRPS-1 in Children, Figure 1 An11 year old girl with a severe CRPS-1including contractures of knee andhip. She was successfully treatedwith spinal stimulation.
bone marrow oedema, but its relevance is not known. Inthe more classic cases of CRPS-1 the child’s extremityis continuously cold, swollen, blue-reddish and veryallodynic (Fig. 1).
Motor Disturbances
Some motor weakness and even paresthesias may beattributed to reflexes associated with pain. However,even active motor disturbances are sometimes involun-tary movements and contractures due to predominanceof flexors or extensors.
Psychosocial Stress
Certain chronic pain syndromes in children are associ-ated with high levels of psychosocial stress. Child abuseand bullying in school is not uncommon among girlswithCRPS.Howeverthemosttypicalstressfactorseemsto be a child’s unrealistically high expectations of per-formance in school and athletics.
Diagnosis
First, physicians must determine whether the painarises from a known cause. This determination is oftendifficult. CRPS-1 is classified as a neurogenic painsyndrome. Although there is no identified lesion in thenervous system, there is a dysfunction of the sympa-thetic nervous system and pain transmission. CRPS-1does not respond to traditional analgesics, even to opi-oids in normal doses. Thus, pharmacological testing isa valuable diagnostic tool to investigate the presencesof ongoing noxious stimulation. We often administera course of oral NSAIDs in a reasonably high dose,e.g. diclofenac or ibuprofen, for 1 week where chil-dren have not had any analgesics. . We assess painby self-report 3 × a day and note the time of day whenchildren experience their worst pain. Sometimes we per-
form an intravenous � alfentanil test in a standardiseddouble blind manner. CRPS-1 children who typicallyexperience spontaneous pain do not experience relief,while children with nociceptive pain usually experiencecomplete pain relief.According to the criteria from 1995, a history of dysau-tonomia was sufficient for a CRPS-1 diagnosis when achild had pain without any other explanation. Dysauto-nomic signs may also prevail in connection with acutetrauma. However, such signs usually resolve whenwounds and fractures have healed. An updated reviewof CRPS in adults and children has recently been pub-lished as a proceeding from a meeting of the SpecialInterest Group on Pain and the Sympathetic Nervoussystem in Budapest August 2003 (Wilson et al. 2005).
Treatment
Children and families require reassurance that the painis not a sign of continuing damage and that the pain is nota symptom of correlating injury. Many children requirepsychological counselling in order to be able to resumetheir previous activities.
Physiotherapy
Physiotherapy (PT) is a mainstay in the treatment ofCRPS-1. Bernstein and colleagues described the firstcase series in children; they treated the children as inpa-tients with intensive physiotherapy including massageand “towelling” (Bernstein 1978).More recently,Sherryadvocated 6 h daily PT, including desensitisation andtouching allodynic areas, for a large case series of 103children. However, in the only randomized controlledtrial evaluating PT for children with CRPS-1, Lee et al.(2002) used a more intense PT treatment (3 × weekly)that was not more effective than a weekly program. Thepositive effect of PT is probably due to the increased

500 CRPS-1 in Children
activity of affected extremities (i.e. increasing normalsensory input) and to the increased overall activity ofthe children (i.e. resuming normal social and physicalactivities), rather than avoiding activity due to fear ofpain and further injury.
Drugs
Analgesics do not relieve pain associated with CRPS-1. There are no published studies evaluating the effectof other drugs in childhood CRPS, despite clinical prac-tice in which tricyclic antidepressants (TCA) are widelyused and effective in certain cases (Olsson 2003). How-ever TCA’s may have adverse effects, the drug must bevery slowly titrated and the child must be closely mon-itored to ensure compliance. Common side effects in-cludesedation,drymouth,nightmares,dizzinessandoc-casional nausea. The effective dose is not known, withsome physicians prescribing a maximum dose of 10 mg.In our centre, we slowly increase the dose from 10 mguntil the child benefits or there are adverse effects, to amaximum of 100 mg. There are no published studies in-dicating effects of other drugs used for neurogenic painsuch as gabapentin or other antiepileptic drugs in chil-dren.
Sympathetic Blocks
Some children obtain pain relief by a sympathetic block(Olsson 1990; Olsson 2003). In Europe, this block isoften performed as an intravenous regional block us-ing guanethidine. Paravertebral blocks using localanaesthetics seldom have long-lasting effects. Epidu-ral analgesia with an indwelling catheter may providelonger relief in severe cases. The long-term effect ofthis treatment is not well documented. Sympathectomyshould not be used in children due to the nature of theprocedure and the tendency to improve non-surgically.
Dorsal Column Stimulation
Neurogenic pain can often be treated with spinal stimu-lation. In our centre, we have applied � dorsal columnstimulation to seven children with severe CRPS (Olsson2003) and achieved good pain relief for most children.However, this therapy is very invasive, expensive andusually performed on conscious patients, so it should beconsidered only in very special, severe, selected cases.
Psychological Treatment
Psychological treatmentsarean importantcomponent inthe treatment of CRPS-1. Specific therapies range fromreassurance and education to sophisticated programs ofcognitive behavioural therapy. There are no publishedstudies proving the efficacy of CBT in CRPS althoughit is included in the treatment program in many studies(Lee et al. 2002; Wilder et al. 1992). In our centre, weuse a well-defined form of CBT called acceptance andcommitment therapy (Robinson et al. 2004)based on ac-ceptance, fear / avoidance, activation and exposure tovalued life.
Prognosis
The long-term prognosis for CRPS in children is un-known and studies to date yield contradictory informa-tion. CRPS-1 in childhood seems to be milder, with lessatrophy and with a good short-term prognosis, in com-parison to CRPS-1 in adults. Veldman and Goris (1997)reported 118 cases of recurrence in 1183 consecutivepatients, in a predominantly adult sample. Recurrencesoccurred especially in younger patients, often not onlyin the originally affected limb. In a 5 year follow upat our centre, 25% of children continued to experiencepain (Olsson et al. 1991). Only 50% of 70 children withCRPS in the Boston series were free from pain (Wilderet al. 1992). In a series of 1006 RSD patients aged10–84 years, 7% developed severe complications suchas infection, ulcers, chronic oedema, dystonia and / ormyoclonus. Patients affected were younger and moreoften female. The skin temperature at onset was in thesepatients lower than in non-complicated cases (van derLaan et al.1998). The long-term prognosis has to befurther evaluated in children.
References1. Bernstein BH, Singsen BH, Kent JT et al. (1978) Reflex neu-
rovascular dystrophy in childhood. J Pediatr 93:211–2152. Harden RN, Bruehl S, Galer BS et al. (1999) Complex regional
pain syndrome: are the IASP diagnostic criteria valid and suffi-ciently comprehensive? Pain 83:211–219
3. Kozin F, Haughton V, Ryan L (1977) The reflex sympatheticdystrophy syndrome in a child. J Pediatr 90:417–419
4. Lee BH, Scharff L, Sethna NF et al. (2002) Physical therapy andcognitive-behavioral treatment for complex regional pain syn-dromes. J Pediatr 141:135–140
5. Olsson GL (2003) The effect of i.v. regional sympathetic blockin children with CRPS-1. SIG Pain in Childhood ISPP2003, Syd-ney
6. Olsson GL, Arnér S, Hirsch G (1991) Reflex sympatheticdystrophy in children. Advances in Pain research and theraphy15:323–331
7. Olsson GL, Linderoth B, Meyerson B (2003) Spinal cord stimu-lation as a treatment option in severe cases of complex regionalpain syndrome. SIG Pain in Childhood ISPP2003, Sydney
8. Robinson P, Wicksell R, Olsson GL (2004) ACT with chronicpain patients. In: Hayes S, Strosahl KD (eds) A practical guideto acceptance and commitment therapy. Springer New York
9. Sherry DD, Wallace CA, Kelley C et al. (1999) Short- and long-term outcomes of children with complex regional pain syndrometype I treated with exercise therapy. Clin J Pain 15:218–23
10. Stanton-Hicks M, Janig W, Hassenbusch S et al. (1995) Reflexsympathetic dystrophy: changing concepts and taxonomy. Pain63:127–33
11. van der Laan L, Veldman PH, Goris RJ (1998) Severe complica-tions of reflex sympathetic dystrophy: infection, ulcers, chronicedema, dystonia, and myoclonus. Arch Phys Med Rehabil79:424–429
12. Veldman PH, Goris RJ (1997) Multiple reflex sympathetic dys-trophy. Which patients are at risk for developing a recurrence ofreflex sympathetic dystrophy in the same or another limb. Pain71:207–208
13. Wilder RT, Berde CB, Wolohan M et al. (1992) Reflex sympa-thetic dystrophy in children. Clinical characteristics and follow-up of seventy patients. J Bone Joint Surg Am 74:910–919
14. Wilson PR, Stanton-Hicks M, Harden RN (2005) CRPS: Currentdiagnosis and therapy. IASP Press, Seattle

C
CT Scanning 501
Crura of Clitoris
Definition
The crura or bulbs extend posteriorly and horizontallyas two cylinders of erectile tissue arising from the bodyof the clitoris where it meets the pubic bone for up to 9cm.� Clitoral Pain
Cryoablation
Definition
The use of sub-zero temperatures to destroy tissue.� Cancer Pain Management, Neurosurgical Interven-
tions
Cryoglobulinemia
Definition
Conditionwhereincryoglobulins,aclassof immunoglob-ulins that precipitate when cooled and re-dissolve whenheated, are present in the blood.� Viral Neuropathies
Cryotherapy
Definition
Application of cold to body surfaces.� Chronic Pain in Children, Physical Medicine and Re-
habilitation
CSF
� Cerebrospinal Fluid
CSF Examination
Definition
Shows pleocytosis, elevation of protein, or oligoclonalbanding in Neuro-Behcet, collagene vascular disease,systemic vasculitides and the isolated angiitis of the cen-tral nervous system.� Headache Due to Arteritis
CSF Leak
� Spontaneous Cerebrospinal Fluid (CSF) Leak
CT Myelography
Definition
Imaging of the spinal cord using computerized analysisof cross-sectional scans (tomograms) after injection ofa contrast agent into the spinal fluid.� Chronic Low Back Pain, Definitions and Diagnosis
CT ScanningPETER LAU
Department of Clinical Research, Royal NewcastleHospital, University of Newcastle, Newcastle, NSW,[email protected]
Synonyms
CAT Scan; Helical CT; Spiral CT; Multichannel CT;Computerised Axial Tomography
Definition
Computerised axial tomography (CATor CT) is a meansby which images of the internal structure of the body canbe obtained in selected planes and at selected depths.
Characteristics
Principles
In CT scanning, a computer is used to synthesise im-ages based on X-ray absorption data. The object to bescanned isplacedat thecentreofacirculargantry,aroundwhich an X-ray camera and its receiver rotate. As thecamera rotates, X-rays are beamed through the objectalong multiple, selected diameters. Along each diame-ter the X-ray shadows (see � Plain Radiography) of theobject and its internal structure are transmitted to the re-ceiver and stored by a computer. Using an iterative pro-gram, the computer then analyses the stored informationto generate a synthetic image of what the internal, three-dimensional structure of the object must be, in order toaccount for all of the different patterns of X-ray absorp-tion obtained along each of the diameters across whichthe object was viewed.The plane across which the object is studied is typicallytransverse to the long axis of the object; but this planecan be varied by tilting the gantry. Also, the object canbe translated relative to the gantry so that it can be stud-ied across multiple, selected sections, also referred to as“slices”. By scanning across its entire length, images of

502 CT Scanning
CT Scanning, Figure 1 SagittalCT scans of the cervical spine inwhich the vertebrae C4 to C7 havebeen fused with interbody grafts andan anterior metal plate. (a) Midlinesection. (b) 3-D reconstruction.Reproduced courtesy of ToshibaMedical.
the entire object can be synthesized. By using specialcomputer programs, images can be synthesized to viewthe object from any angle or perspective, at any depth.The images can be planar, i.e. depicting the appearanceof a single, selected slice through the object (Fig. 1a)or they can be simulated, three-dimensional reconstruc-tions of the internal structure of the object (Fig. 1b).
Capabilities
The first generation scanner took about 7 min to performa single scan. Since then, the technology involved hasbeen improved greatly, through at least five generationsof development. Today, with multi-slice or multichan-nel, slip-ring CT systems, which allow continuousscanner gantry motion, coupled with synchronous tablefeed provide the basis for so-called helical or spiralCT scanning (Fox et al. 1998). Ultra-fast scanners arecapable of performing as many as 32 scans in half asecond which is the time taken per rotation of the gantry.This is achieved by unique design of detectors, isotropicscanning and fast reconstruction. Sub-millimetre thinand ultra-thin slices can be obtained. There is nowcommercially available CT scanner capable of morethan 64 slices per half a second.In the past, using slow scanners, CT provided imagesof all but the smallest of soft tissues. Today with sub-millimetre, micro-voxel scanning (Pretorius and Fish-man 1999), the smallest structures in the body, particu-larly small bony structures such as those of the middleand inner ear, can be well demonstrated (Fig. 2). Thecardinal advantage of CT is that it allows observers to“see inside” cavities such as the chest, abdomen, skulland vertebral canal (Fig. 3). The ability to demonstratesoft tissues allows CT to detect displacement and distor-
CT Scanning, Figure 2 A CT scan through the temporal bone, showing theexternal ear and contents of the middle and internal ear. (a) Transversesection showing the ossicles of the middle ear. (b) Transverse sectionshowing the cochlea and semicircular canals.
tion of thesestructuresby tumours, infiltration, infectionandinflammation(Fig.4).Ofparticularrelevancetopainmedicine is the ability of CT to demonstrate intracranialpathology in patients with headaches and the relation-ship between spinal nerves and the vertebral column inpatients with radicular pain.However, CT still relies on detecting the X-ray shad-ows of internal structures. Consequently, although CTcan demonstrate the location, shape and density of tis-sues it cannot reveal their internal architecture, althoughhollow or permeable structures can be indirectly visu-

C
CT Scanning 503
CT Scanning, Figure 3 Sagittal CT scan of the abdomen showing internalviscera and vessels. a aorta. l liver. m superior mesenteric artery. c colon.s small intestine. Reproduced courtesy of Toshiba Medical.
CT Scanning, Figure 4 Axial CT scan of the thoracic spine showing os-teomyelitis of a vertebral body.
alised by injection or infusion of radio-opaque agents,which localise in targeted tissues. Thus, injection ofcon-trastmedium willoutline the lumenofholloworgansandblood vessels, joint cavities and the subarachnoid space(Fig. 5). The internal structure of the intervertebral disc
can bevisualised by injection ofcontrast into thenucleus(Fig. 6) and intravenous infusion of a rapidly excretedcontrastmedium will enhance thestructureof thekidneyand urinary tract.Multichannel techniques have had a significant impacton the style and quality of spine CT. Coverage is nolonger limited by practical problems. Lumbar studiesroutinely extend from T12 to S1 and cervical spinestudies from C2 to T2. With a 64-channel scanner, thefull spine scan may be obtained in the duration of onebreath-hold, which is easier for patients to tolerate thanMRI scans.
Applications
Microvoxel volumetric acquisition techniques provide asignificant boost in spatial and contrast resolution. Theycan be used to create exquisite sagittal images of the in-tervertebral foramina in patients with radicular pain, es-pecially in those with persisting pain after surgery, whenmissed foraminal stenosis is a major source of chronicpain.With the advent of fine, sub-millimetre technology, CTis becoming the modality of choice for the assessmentof failed back surgery syndrome. Artifacts from inter-vertebral metal cages or pedicular screws can be min-imised, which allows for assessment of failure of spinalfixation hardware by loosening or metal fracture and fa-tigue.CT can demonstrate the progress of healing in the skele-tal system and can detect pseudoarthrosis in the spine af-terattemptedarthrodesis.Similar techniquescanbeusedfor the assessment of joint replacement in the hip, shoul-der and knee. Microvoxel scan techniques minimise par-tial volume artefact and allow evaluation of the state ofbone surrounding hardware implants, as well as evalua-tionofpossible looseningandmigrationoftheprosthesisas a chronic source of pain.With the advent of 32 and 64 slice scanners, dynamic,real-time imaging of joint movements and spinal move-ment in order to assess biomechanical abnormalities ispossible.Real time fluoroscopy-CT is used to perform pain in-terventional procedures. It enables drugs to be injectedaccurately and safely. It enables the accurate and safede-livery of ablation devices, such as radio-frequencyelec-trodes, todeepsites thatwereconsidereddifficult,unsafeand inaccurate in the past. This opens up a new arena ofoncological pain management by using radiofrequencyablation to destroy pain-producing tumours that have in-vaded nerve plexuses e.g. metastatic carcinoma of therectum with invasion of the lumbo-sacral plexus. Abla-tion of painful bone tumours, such as osteoid osteoma,is another avenue of application of CT in pain manage-ment.High-contrast resolution and the seamless multi-planarcapability of the latest multi-channel CT imagers havetheir greatest application in musculoskeletal pain after

504 CT Scanning
CT Scanning, Figure 5 Parasagittaland sagittal CT scans of the entirespine. Contrast medium has beeninjected into the subarachnoid space,which appears white (sa), andoutlines the spinal cord (sc), whichappears dark. Reproduced courtesyof Toshiba Medical.
CT Scanning, Figure 6 An axial CT scan of a lumbar intervertebral disc.Contrast medium fills the nucleus pulposus (NP), a left posterolateral radialfissure (1) that extends into the annulus fibrosus and a right posterolateralfissure (2) that has a circumferential extension (3).
trauma. Fractures are now delineated easily in any planewhile the patient is situated comfortably on the table.Positioning during the scan is not critical, as any planecan be created from the volumetric data. Trauma seriesare typically performed in less than 30 s, minimizing thelikelihood of patient motion (Tanenbaum 2003). Treat-ment can be better planned when CT demonstrates the
CT Scanning, Figure 7 A sagittal CT scan of the ankle, showing an obliquefracture (arrow) through the posterior tibia, extending into the talocruraljoint. Reproduced courtesy of Toshiba Medical.
presence and extent of subtle cortical fractures, fracturefragments, intra-articular loose bodies and articular sur-face offset / depression; this was not possible by plainradiography (Fig. 7).Whereas magnetic resonance imaging is superior for thedelineation of the extent of tumours in medullary bone,CT is better able to delineate cortical bone, calcifications

C
Cuban Neuropathy Fabry’s Disease 505
in the matrix of lesions and periosteal new bone forma-tion.
Utility
The utility of CT emerges from a tension between whatcan be seen with CT and what is relevant and valid. Al-though CT can provide detailed images of the internalstructure of the body, abnormalities demonstrated by CTare not necessarily the cause of a patient’s pain. In thecontext of pain medicine, CT is useful as a diagnostictest only if and when it reliably shows the cause of pain.
Reliability
For major and obvious lesions, the reliability of radiol-ogists using CT has not been questioned. Such lesions,however,arerarelypertinenttopainmedicine.Ofgreaterrelevanceareminorabnormalities thatare sometimes re-ported in scans of patients with pain.Conspicuously, re-liability data are largely lacking in the radiology litera-ture. There has been a tradition to assume that all radi-ologists agree on what they report. When this has beenstudied, however, the converse emerges.In reading CT scans of the lumbar spine, radiologists failto agree on the presence of such features as spinal steno-sis, degenerative joint disease and even herniated nu-cleus pulposus (Wiesel et al. 1986). Unfortunately, datahave not been presented in a manner from which kappascores can be calculated.
Validity
In the joints of the appendicular skeleton, CT can showabnormalities of joint space, subchondral bone and eveninternal and external ligaments. However, there are nodata that incriminate these abnormalities as the cause ofpain (Bogduk 2003).In CT scans of the lumbar spine, abnormalities, such asdegenerative joint disease, disc bulges and disc herni-ations are the most commonly encountered abnormali-ties. These abnormalities, however, also frequently oc-cur in asymptomatic individuals (Wiesel et al. 1986).Indeed, some 20–30% of asymptomatic individuals ex-hibitherniated lumbar intervertebraldiscs.Thesefigureswarn that finding such abnormalities in symptomatic pa-tients does not necessarily prove that they are the causeof pain.Tumours and infections are assumed to be valid causesof pain but they are rare causes of either acute orchronic pain. The same applies for conditions, suchas osteonecrosis. For most patients with pain, thereis nothing demonstrable by CT that has actually beenproven to be a cause of pain. Even pseudoarthrosisfollowing spine surgery has not been validated as acause of pain.
Future Trends
Improvements in the technology of CT are likely to con-tinue. There is an urgent need, however, for clinical sci-ence to catch up with the technology. Urgently needed
are studies in which the presence and absence of mor-phological abnormalities are correlated with the pres-ence and absence of pain. Such studies are necessary lestabnormalities simply be assumed to be relevant to the di-agnosis of pain.Another opportunity lies in the fusion of morpho-logical CT technology with physiological imagingtechniques such � as positron emission tomography(PET) (Erickson 2003). Already PET-CT can producethe physiological properties of certain neoplasms com-bined with anatomical imaging. In the same way, itmay become possible to demonstrate the physiology oflesions, seen on CT, that are suspected of being causesof pain.
References1. Bogduk N (2003) Diagnostic procedures in chronic pain. In:
Jensen TS, Wilson PR, Rice ASC (eds) Clinical Pain Manage-ment: Chronic Pain. Arnold, London, pp 125–144
2. Erickson JE (2003) TRIP 3-Possible Future Technologies. Paper
presented at the 89th Annual Meeting of the Radiological Societyof North America. Chicago, Illinois, November 2003
3. Fox SH, Tanenbaum LN, Ackelsberg S et al. (1998) Future di-rections in CT technology. Neuroimaging Clin N Am 8:497–513
4. Pretorius ES, Fishman EK (1999) Volume-rendered three-dimensional spiral CT: musculoskeletal application. Radio-graphics19:1143–1160
5. Tanenbaum LN (2003) Multichannel helical CT of the muscu-loskeletal system. Appl Radiol 32:15–22
6. Wiesel SW, Tsourmas N, Feffer HL et al. (1986) A study ofcomputer-assisted tomography. 1. The incidence of positive CATscans in an asymptomatic group of patients. Spine 9:549–551
CT Scans
Definition
CT (computed tomography), sometimes called CATscan (computed axial tomography), uses x-ray imagestaken at different angles around the body, and then bycomputer processing of the information produces two-or three-dimensional slice images.� Motor Cortex, Effect on Pain-Related Behavior
CTDs
� Disability, Upper Extremity
CTrP
� Central Trigger Point
Cuban Neuropathy Fabry’s Disease
� Metabolic and Nutritional Neuropathies

506 Cumulative Trauma Disorders
Cumulative Trauma Disorders
Definition
A descriptive term used to label pain associated withrepetitive activities.� Disability, Upper Extremity
Cuneate Nucleus
Definition
A nucleus at the upper cervical spinal cord where thefirst synapse of the dorsal columns occurs. Discrimina-tive sensory information from cutaneous regions fromthe upper half of the body is relayed to this nucleus.� Brainstem Subnucleus Reticularis Dorsalis Neuron� Postsynaptic Dorsal Column Projection, Anatomical
Organization
Cutaneous
Definition
Relating to, or affecting, the skin.� Psychiatric Aspects of Visceral Pain
Cutaneous Allodynia
Definition
Pain elicited by a non-noxious stimulus that is not nor-mally painful.� Migraine Without Aura
Cutaneous Field StimulationJENS SCHOUENBORG
Section for Neurophysiology, Department ofPhysiological Sciences, Lund University, Lund,[email protected]
Synonyms
CFS
Definition
Cutaneous field stimulation (CFS) allows topograph-ically restricted and tolerable electrical stimulation ofthin (Aδ and C) cutaneous fibers for the symptomaticrelief of � itch and pain.
Characteristics
The CFS technology is based on the organization of en-dogenous intermodality interactions and allows tolera-ble stimulation of cutaneous Aδ and C afferent fibers(McMahon and Koltzenburg 1992; Ward et al. 1996).For example, mechanical stimulation inhibits ongoingpain (Bromm et al. 1995; Sjölund et al. 1990; Wall andCronly-Dillon 1960; Ward et al. 1996). In fact, particu-larly strong interactions are found between submodali-ties of the nociceptive system (here including itch), e.g.low frequency electrical stimulation of Aδ fibers maycause a durable depression of nociceptive C fiber trans-mission both in vivo (Sjölund 1985; Sjölund 1988) andin vitro spinal preparations (Sandkühler et al. 1997) andnoxious mechanical stimulation, such as scratching, re-duces itch. These interactions occur at several levels inthe somatosensory system, the dorsal horn of the spinalcord (Cervero et al. 1979; Melzack and Wall 1965), thedorsal column nuclei (Saade et al. 1985) and the thala-mus (Olausson et al. 1994)and are often topographicallywell organized. To use these interactions for the symp-tomatic relief of itch and pain, a new technique, termedcutaneousfieldstimulation(CFS),wasintroduced(Nils-son et al. 1997). CFS allows topographically restrictedand tolerable electrical stimulation of thin (Aδ and C)cutaneous fibers.CFS uses a flexible rubber plate with multiarray needle-like electrodes regularly fixed at 2 cm intervals (Fig. 1).Each electrode is surrounded by a “stop-device” 2.0 mmin diameter that protrudes 2.0 mm from the plate. Theelectrode tip protrudes 0.3 mm from the stop-device.When the electrode plate is gently pressed against theskin, the electrode tips are introduced close to the recep-tors in the epidermis and the superficial part of dermis.Since the electrodes traverse the electrically isolatinghorny layer of the epidermis and the current densityis high near the sharp electrode tips, the voltage andcurrent necessary to stimulate cutaneous nerve fibersare small, typically less than 10 V and up to 0.8 mA,respectively. As the current density decreases rapidlywith distance, localized stimulation is achieved. Theelectrodes are stimulated consecutively with a constantcurrent stimulator (64 pulses / s), each electrode witha frequency of 1–10 Hz (pulse duration 1.0 ms). Treat-ment duration is 5–45 min. A self-adhesive surface(TENS) electrode serves as anode and is placed about5–30 cm away from the needle electrode plate.Several pieces of evidence demonstrate that CFS actsvia stimulation of nociceptive Aδ and C fibers (Nilssonet al. 1997; Nilsson et al. 2003). 1) The needle-likeelectrodes of the CFS plate are introduced close to thedermo-epidermal junction, known to be richly inner-vated by thin afferent fibers (Fundin et al. 1994; Krugeret al. 1985), 2) CFS evokes a sensation of prickingand slightly burning pain of weak / moderate intensity,indicating an activation of nociceptive Aδ- and / or

C
Cutaneous Field Stimulation 507
Cutaneous Field Stimulation, Figure 1 (a) Schematic of CFS apparatus with electrodes. (b) The needle-like electrodes are inserted into the dermo-epidermal junction, permitting stimulation of thin nerve fibers with low electrical voltage and current.
C-fibers, respectively (Bromm and Treede 1987), 3)during a selective blockade of the impulse conduction inA fibers, CFS still produces a burning sensation, knownto be due to heat sensitive nociceptive C fibers and 4)a flare, known to be caused by nociceptive C fibers(Kenins 1981), develops around the CFS electrodes. Itshould be noted that while Aβ-fibers are presumablyalso activated by CFS due to their low electrical thresh-old, the stimulation frequencies used for CFS are verylow for Aβ fibers (but relatively high for C fibers).CFS acts preferentially on nociceptive senses, sincehomo- but not hetero-topical (with respect to testing
sites) CFS, abolishes itch evoked by histamine in normalhumans and reduces CO2-laser evoked Aδ- and C-fibermediated heat pain and pinch evoked pain (Nilsson andSchouenborg 1999) but has no effect on fabric evokedprickle (assumed to be mediated by high thresholdmechanoreceptive Aδ and C fibers; Garnsworthy et al.1988) (Fig. 2). The relative potency of CFS on noci-ceptive skin senses is thus, in a descending order, itch,secondary heat pain, primary heat pain, pinch-evokedpain and prickle. Regarding innocuous senses, CFSincreases the warm and cold thresholds somewhat buthas no effect on tactile sensibility.

508 Cutaneous Field Stimulation
Cutaneous Field Stimulation, Figure 2 Differential effect on differentsensory qualities of nociception after CFS (n = 10 subjects except for itchwhere n = 7 subjects) and lack of effect after conventional high frequencyTENS (n = 10 subjects except for itch where n = 7 subjects). The condi-tioning stimulations and all sensory testings were performed on the rightvolar forearm. The mean magnitude of sensation after CFS (black bars) orTENS (hatched bars) is indicated as percentage of control (unfilled bars).Top diagram shows effects after CFS, bottom diagram shows effects af-ter TENS. Statistical comparisons (Wilcoxons signed ranks test, 2-tailed)were made both between control values and values obtained after condi-tioning stimulation and also between values obtained after CFS and TENSrespectively. Normalized visual analogue scale (VAS) on the vertical axes. *P<0.05, ** P<0.01, *** P<0.001; ns, non-significant. Error bars indicate+S.E.M. (From Nilsson et al. 1997, 1999).
CFS causes a dramatic reduction in histamine-induceditch. In fact, all subjects tested have reported a completeor near complete inhibition of itch evoked by histamine.This inhibitory effect lasts 4–8 h and extends 10–20 cmalong the same dermatome, but appears to be more re-stricted in a direction across dermatomal borders (Nils-son et al. 1997). Maximal effects are reached already af-ter 8–10 min and more prolonged CFS stimulation (upto 45 min tested) does not appear to add to the inhibitoryeffect (Nilsson et al. 2003). The optimal stimulation fre-
quency appears to be around 4 Hz per electrode (Nilssonet al. 2003). Notably, the effective stimulation parame-ters are similar to those known to cause long-term de-pression(LTD)(Sandkuhleretal.1997)–amemory-likemechanism – in the spinal cord and elsewhere.Figure 3 shows the results from a randomized controlledclinical study on chronic itch due to localized atopic der-matitis (n = 27; Nilsson et al. 2004). As can be seen, CFSdepresses itch significantly for more than 7 h. Peak in-hibitory effect (down to about 25% of control) is reachedbetween 1 and 5 h postconditioning. Similar results haverecently been reached for chronic itch due to neuroder-matitis (n = 30; Bäck et al, in preparation). In the latter
Cutaneous Field Stimulation, Figure 3 Effects of CFS (top diagram) andTENS (bottom diagram) on chronic itch due to atopic dermatitis. For com-parison, the mean VAS values were normalized with respect to control(unfilled bars). The mean sensory intensities after CFS (black bars, n = 15)and TENS (hatched bars, n = 12) are shown. ANOVA repeated measureswith Dunnet’s post hoc test was applied for matched comparisons withina group, whereas the Mann-Whitney U test was used when comparingeffects of the two treatments; ns, non-significant, * p<0.05, ** p<0.01.Error bars indicate + S.E.M. (From Nilsson et al. 2004).

C
Cutaneous Hyperalgesia 509
single-blind study, CFS was compared to conventionalTENSovera treatmentperiodof2weeks(twotreatmentsa day). It was found that CFS provided effective reliefof itch in practically all patients and also markedly im-proved the skin condition. The improvement of the skincondition may be due to a reduced urge to scratch theskin (or care not to scratch the treated skin), thus stop-ping the vicious itch –scratch circle that may sustain thistype of condition. Other workers have reported similarfindings on the relief of chronic itch by CFS in variousdermatoses (Wallengren 2002; Wallengren and Sundler2001) In addition, a normalized innervation of the skinmay result from CFS (Wallengren and Sundler 2001).No adverse effects of CFS have been reported (Wallen-gren 2002).CFS not only affects cutaneous nociception but alsomusculoskeletal nociception. In a recent study on 142TENS resistant patients with chronic musculoskeletalpain (i.e. a group of patients that received no pain re-lief from established treatments of electrostimulation),30% received clinically relevant pain relief from CFS(Martinsson and Sjölund, in preparation). The groupstudied consisted of 91 patients with nociceptive painand 51 patients with neuropathic pain according toestablished criteria. 33 / 91 patients with nociceptivepain and 10 / 51 with neuropathic pain got clinicallyrelevant pain relief from CFS for more than 3 months.In conclusion, CFS preferentially affects nociceptivesenses via endogenous inhibitory memory-like mecha-nisms and has no significant adverse side effects. Thefindings that CFS causes a strong inhibitory effect onitch and that skin conditions improve considerably andthe lack of adverse side effects demonstrate that CFS isa useful itch therapy. Moreover, CFS is clearly worthtrying for the treatment of chronic musculoskeletalpain.
References1. Bäck O, Svensson Å, Thelin I et al. (2004) Chronic itch in neu-
rodermatitis is dramatically reduced by Cutaneous Field Stim-ulation (CFS). In manuscript
2. Bromm B, Scharein E, Darsow U et al. (1995) Effects of mentholand cold on histamine-induced itch and skin reactions in man.Neurosci Lett 187:157–160
3. Bromm B, Treede R-D (1987) Human cerebral potentials evokedby CO2 laser stimuli causing pain. Exp Brain Res 67:153-162
4. Cervero F, Iggo A, Molony V (1979) An electrophysiologicalstudy of neurones in the substantia gelatinosa rolandi of the cat’sspinal cord. Quart J Exp Physiol 64:297–314
5. Fundin BT, Rice FL, Pfaller K et al. (1994) The innervation ofthe mystacial pad in the adult rat studied by anterograde transportof HRP-conjugates. Exp Brain Res 99:233–246
6. Garnsworthy RK, Gully PL, Kenins P et al. (1988) Identificationof the physical stimulus and the neural basis of fabric-evokedprickle. J Neurophysiol 59:1083–1097
7. Kenins P (1981) Identification of the unmyelinated sensorynerves which evoke plasma extravasation in response to an-tidromic stimulation. Neurosci Lett 25:137–141
8. Kruger L, Sampogna SL, Rodin BE et al. (1985) Thin-fiber cuta-neous innervation and its intraepidermal contribution studied bylabelling methods and neurotoxin treatment in rats. SomatosensRes 2:335–356
9. Martinsson K, Sjölund BH (2004) Cutaneous field stimulation(CFS) in TENS-resistant chronic pain. In manuscript
10. McMahon SB, Koltzenburg M (1992) Itching for an explanation.Trends in Neurosci 15 / 12:497–501
11. Melzack R (1975) Prolonged relief of pain by brief, intense tran-scutaneous somatic stimulation. Pain 1:357–373
12. Melzack R, Wall PD (1965) Pain mechanisms: a new theory. Agate control system modulates sensory input from the skin beforeit evokes pain perception and response. Science 150:971–979
13. Nilsson H-J, Schouenborg J (1999) Differential inhibitory effecton human nociceptive skin senses induced by local stimulationof thin cutaneous fibers. Pain 80:103–112
14. Nilsson H-J, Levinsson A, Schouenborg J (1997) Cutaneous FieldStimulation (CFS) – a new powerful method to combat itch. Pain71:49–55
15. Nilsson H-J, Psouni E, Schouenborg J (2003) Long term de-pression of human nociceptive skin senses induced by thin fibrestimulation. Eur J Pain 7:225–233
16. Nilsson H-J, Psouni E, Carstam R et al. (2004) Profound inhi-bition of chronic itch induced by stimulation of thin cutaneousnerve fibres. J Eur Acad Dermatol Venereol 18:37–43
17. Olausson B, Xu Z-Q, Shyu B-C (1994) Dorsal column inhibitionof nociceptive thalamic cells mediated by gamma-aminobutyricacid mechanisms in the cat. Acta Physiol Scand 152: 239–247
18. Saade NE, Dajani BM, Atweh SF et al. (1985) Inhibition ofdorsal column nuclei by stimulation of trigeminal afferents indecerebrate-decerebellate cats. Brain Res 348:405–407
19. Sandkühler J, Chen JG, Cheng G et al. (1997) Low-frequencystimulation of afferent Aδ-fibers induces long-term depressionat primary afferent synapses with substantia gelatinosa neuronsin the rat. J Neurosci 17:6483–6491
20. Sjölund B H (1985) Peripheral nerve stimulation suppressionof C-fiber-evoked flexion reflex in rats. Part 1: parameters ofcontinuous stimulation. J Neurosurg 63:612–616
21. Sjölund B H (1988) Peripheral nerve stimulation suppressionof C-fiber-evoked flexion reflex in rats. Part 2: parameters oflow-rate train stimulation of skin and muscle afferent nerves. J.Neurosurg. 68:279–283
22. Sjölund BH, Eriksson M, Loeser JD (1990) Transcutaneous andimplanted electric stimulation of peripheral nerves. In: Bonica J(ed), Management of Pain, 2nd edn. Lea & Fegiber, Philadelphia,pp 1852–1861
23. Wall PD, Cronly-Dillon JR (1960) Pain, itch, and vibration,A.M.A. Archives of Neurology 2:365–375
24. Wallengren J, Sundler F (2001) Cutaneous field stimulation inthe treatment of severe itch. Arch Dermatol 137:1323–1325
25. Wallengren J (2002) Cutaneous field stimulation of sensory nervefibers reduces itch without affecting contact dermatitis. Allergy57:1195–1199
26. Ward L, Wright E, McMahon SB (1996) A comparison of the ef-fects of noxious and innocuous counterstimuli on experimentallyinduced itch and pain. Pain 64:129–138
Cutaneous Freeze Trauma
� Freezing Model of Cutaneous Hyperalgesia
Cutaneous Hyperalgesia
� Freezing Model of Cutaneous Hyperalgesia

510 Cutaneous Mechanoreception
Cutaneous Mechanoreception
Definition
Neuronal responses to mechanical stimuli applied to theskin are transduced by specialized receptive endings ofafferent nerve fibers.� Postsynaptic Dorsal Column Projection, Anatomical
Organization
Cutaneous Pain Model
� Autologous Thrombocyte Injection as a Model of Cu-taneous Pain
Cutaneous Stimulation
Definition
Chemical, thermal, or mechanical input delivered to theskin to activate one or more superficial or cutaneous sen-sory receptor types.� Postsynaptic Dorsal Column Projection, Functional
Characteristics
CWP
� Chronic Widespread Pain
Cyclic AdenosineMonophosphate-ResponsiveElement-Binding Protein
Synonyms
CREB
Definition
CREB is a transcription factor that is activated by thecAMP signal transduction pathway. It is phosphorylatedby protein kinase A, enters the nucleus of a neuron andcan alter gene expression.� Spinothalamic Tract Neurons, Role of Nitric Oxide
Cyclic Alternating Pattern
Definition
Repetition of micro-arousal every 20–60 s as a sentinelthat allows for a „reset“ of physiological functions (e.g.heart rate, respiration,muscle tone),orprepares thebodyfor an appropriate response if an event could be poten-tially disrupting.� Orofacial Pain, Sleep Disturbance
Cyclic Pain
Definition
Cyclic pain occurs with definite association to the men-strual cycle, generally 1–2 days prior to the onset of orduring menses.� Dyspareunia and Vaginismus
Cyclooxygenase Inhibitors
� NSAIDs, Adverse Effects� NSAIDs and Cancer� NSAIDs and Cardio-Vascular Effects� Postoperative Pain, Non Steroidal Anti-Inflammatory
Drugs
Cyclooxygenase Inhibitors, Chemistry
� Coxibs and Novel Compounds, Chemistry
Cyclooxygenase-2 Inhibitors
Definition
A class of drugs related to non-steroidal anti-inflam-matory drugs (NSAIDs) that prevent the synthesisof prostaglandins by the enzyme cyclooxygenase–2.These drugs are relatively new additions to the stan-dard treatment regimen of osteoarthritis, and includeCelebrex® and Vioxx®.� Arthritis Model, Osteoarthritis� Postoperative Pain, COX-2 Inhibitors
Cyclooxygenases
Synonyms
COX

C
Cyclooxygenases in Biology and Disease 511
Definition
COX is a 70–72 kD enzyme, catalyzing the reaction ofArachidonic acid to PGG2 (cyclooxygenase reaction)and consecutively PGG2 to PGH2 (peroxidase reac-tion). Prostaglandin H2 (PGH2) is further convertedinto various prostaglandins and thromboxanes There isa distinct active site for both cyclooxygenase and per-oxidase reaction. There are at least 3 isoforms, COX1,COX2 and COX3, which are also slightly differentat the active site, explaining particular selectivitiesof inhibitors. Prostaglandins are involved in pain, in-flammation and fever, but also in cytoprotection inthe stomach and blood flow regulation in the kidneys.NSAIDS (non steroidal anti-inflammatory drugs) aretherapeutic agents that block this enzyme and thus actas pain killers, antipyretic and anti-inflammatory drugs.� COX-1 and COX-2 in Pain� Coxibs and Novel Compounds, Chemistry� Cyclooxygenases in Biology and Disease� NSAIDs, Adverse Effects� NSAIDs and Cancer� NSAIDs, Chemical Structure and Molecular Mode of
Action� NSAIDs, COX-Independent Actions� NSAIDs, Mode of Action� Wind-Up of Spinal Cord Neurons
Cyclooxygenases in Biology and DiseaseREGINA M. BOTTING
The William Harvey Research Institute, The John VaneScience Centre, Queen Mary University of London, StBartholomew’s and the London School of Medicineand Dentistry, Charterhouse Square, London, [email protected]
Synonyms
Cyclooxygenase; COX; Prostaglandin EndoperoxideSynthase; Ptgs
Definition
Cyclooxygenases are enzymes which synthesiseprostaglandins.
Characteristics
Three isoenzymes of cyclooxygenase have been charac-terised:cyclooxygenase–1 (COX–1;Ptgs–1),cyclooxy-genase–2 (COX–2; Ptgs–2) and a putative cyclooxyge-nase–3 (COX–3; Ptgs–3), which is currently under in-vestigation.
Cyclooxygenase–1
In the 1930s, Goldblatt in England (Goldblatt 1935) andvonEuler inSweden(vonEuler1934)foundthatseminal
fluid contained activity that contracted uterine smoothmuscle, and also caused a fall in blood pressure. VonEuler identified the active principle as a lipid-solubleacid, which he named ‘prostaglandin’ (PG) becausehe thought it originated from the prostate gland. In the1960’s, technical advances allowed the characterisa-tion of the PGs as a family of lipid compounds with aunique structure. They proved to be 20–carbon unsat-urated carboxylic acids with a cyclopentane ring, andin 1964, PGE2 was synthesised using � arachidonicacid and an enzyme preparation from ram seminalvesicles (Bergström et al. 1964). Prostaglandins andrelated compounds are some of the most prevalent ofautocoids and can be released from every tissue exceptred blood cells. As local hormones, they produce, inminute concentrations, an incredibly broad spectrumof effects that modulate almost every biological func-tion. They derive mostly from the 20–carbon fatty acid,arachidonic acid (C20:4ω6), and almost 100 differentderivatives have been identified, including lipoxins andisoprostanes. Prostaglandins are important to inflamma-tory processes, as evidenced by the anti-inflammatoryeffects of drugs that interfere with their synthesis, suchas the steroid and non-steroid anti-inflammatory drugs(NSAIDs). The discovery 15 years ago of a secondcyclooxygenase (COX–2), inducible by cytokines, hasled to an important clarification of the roles of PGsas mediators of inflammation. COX–2 is induced ininflammation and makes PGs locally, whereas COX–1is a ‘housekeeping’ enzyme involved in the modulationof physiological events.Cyclooxygenase had long been studied in preparationsfrom ram seminal vesicles and a homogeneous, enzy-matically active prostaglandin endoperoxide synthasewas isolated in 1976 (Hemler et al. 1976), and clonedin 1988 (DeWitt and Smith 1988). This membrane-bound haemo– and glycoprotein, with a molecularweight of 71kDA, is found in greatest amounts in theendoplasmic reticulum of prostanoid-forming cells.It both cyclizes arachidonic acid and adds the 15-hydroperoxy group to form PGG2. The hydroperoxygroup of PGG2, is reduced to the hydroxy group ofPGH2, by a peroxidase (in the same enzyme protein)that utilizes a wide variety of compounds to providethe requisite pair of electrons. The � hydroperoxidesalso drive the cyclooxygenase reaction by maintain-ing a ‘hydroperoxide tone’. The three dimensionalstructure of COX–1 was determined in 1994 (Picot etal. 1994). This enzyme consists of three independentfolding units: an epidermal growth factor-like domain,a membrane-binding section and an enzymatic domain.The sites for peroxidase and cyclooxygenase activityare adjacent but spatially distinct. Three of the helicesof the COX–1 structure form an entrance channel to theactive site, which is a long, hydrophobic channel. Sincethe enzyme integrates into only a single leaflet of themembrane lipid bilayer, the position of the cyclooxy-

512 Cyclooxygenases in Biology and Disease
Cyclooxygenases in Biology and Disease, Figure 1 The arachidonic acid cascade. Cyclooxygenase-1 (COX-1) and cyclooxygenase-2 (COX-2) utilisearachidonic acid to form the unstable endoperoxide intermediates, prostaglandin G2 (PGG2) and prostaglandin H2 (PGH2). From these intermediatesthe more stable prostaglandins are synthesised by individual synthases. Prostaglandin E2 (PGE2) is mostly involved in pain, fever and inflammation,prostaglandin F2 α (PGF2 α) in labour and parturition and prostaglandin D2 (PGD2) is a mediator in brain and mast cells. Prostacyclin (PGI2) with ahalf life of 3 minutes, protects the stomach mucosa from damage and prevents aggregation of blood platelets. It breaks down spontaneously to inactive6-keto-PGF1 α. Thromboxane A2 is mainly found in blood platelets and promotes clotting of blood by inducing platelet aggregation. It has a half life of30 seconds and breaks down to inactive thromboxane B2. The activity of COX-1 and COX-2 is inhibited by aspirin and similar drugs, the non steroidanti-inflammatory drugs (NSAIDs), thereby preventing formation of prostanoids.
genase channel allows arachidonic acid to gain accessto the active site from the interior of the bilayer.Most NSAIDs compete with arachidonic acid for bind-ing to the active site (Fig. 1). � Flurbiprofen, for exam-ple, inhibits COX–1 by excluding arachidonic acid fromthe upper portion of the channel, and blocking its accessto tyrosine (Tyr) 385 and serine (Ser) 530 at the apexof the long active site. Uniquely, aspirin irreversibly in-hibits COX–1 by acetylation of (Ser) 530, thereby ex-cluding access for the arachidonic acid to (Tyr) 385 bysteric hindrance.Before 1971, many biochemical effects of the NSAIDshad been reported, and there were many hypothesesabout the mechanism of action of these drugs. How-ever, in 1971, John Vane elegantly demonstrated thataspirin, salicylate and indomethacin inhibited COX ofguinea pig lung homogenates, and thus prevented theformation of PGs (Vane 1971). Two other reports fromthe same laboratory, that aspirin prevented the releaseof prostanoids from aggregating human platelets andthat NSAIDs blocked PG release from the perfusedisolated spleen of the dog, lent support to and extendedhis finding.COX–1 is constitutively expressed in most tissues,and performs a ‘housekeeping’ function to synthesizePGs which regulate normal cell activity (Fig. 2). ThePGs produced are therefore protective to the organ-
ism. The concentration of the enzyme remains largelystable, but small 2– to 4–fold increases can occur inresponse to stimulation with hormones or growth fac-tors. COX–1 has clear physiological functions (Vaneand Botting 2001). Its activation leads, for instance,to the production of prostacyclin (PGI2), which whenreleased by endothelial cells is antithrombogenic, andwhen released by the gastric mucosa, is cytoprotective.However, it is likely that in humans endothelial PGI2 isalso synthesised by COX–2, induced by � Shear Stresson endothelial cells. Release of PGI2 and PGE2 madeby COX–1 also sensitises nociceptors on peripheralsensory nerve terminals and thus acutely amplifies� painful stimulation. Since COX–2 is induced by in-flammatory stimuli and by cytokines in migratory andother cells, it appears likely that the anti-inflammatoryactions of NSAIDs are due to the inhibition of COX–2,whereas the unwanted side effects such as irritationof the stomach lining are due to the inhibition of theconstitutive enzyme, COX–1.The inhibition of PG synthesis explains all the actionsof the NSAIDs. They prevent the pathological over-production of PGs by COX–2 which contribute to theinflammatory process (therapeutic effects), and preventthe physiological formation of prostanoids by COX–1(side effects). For instance, the ulcerogenic activityof aspirin arises from the inhibition of prostacyclin
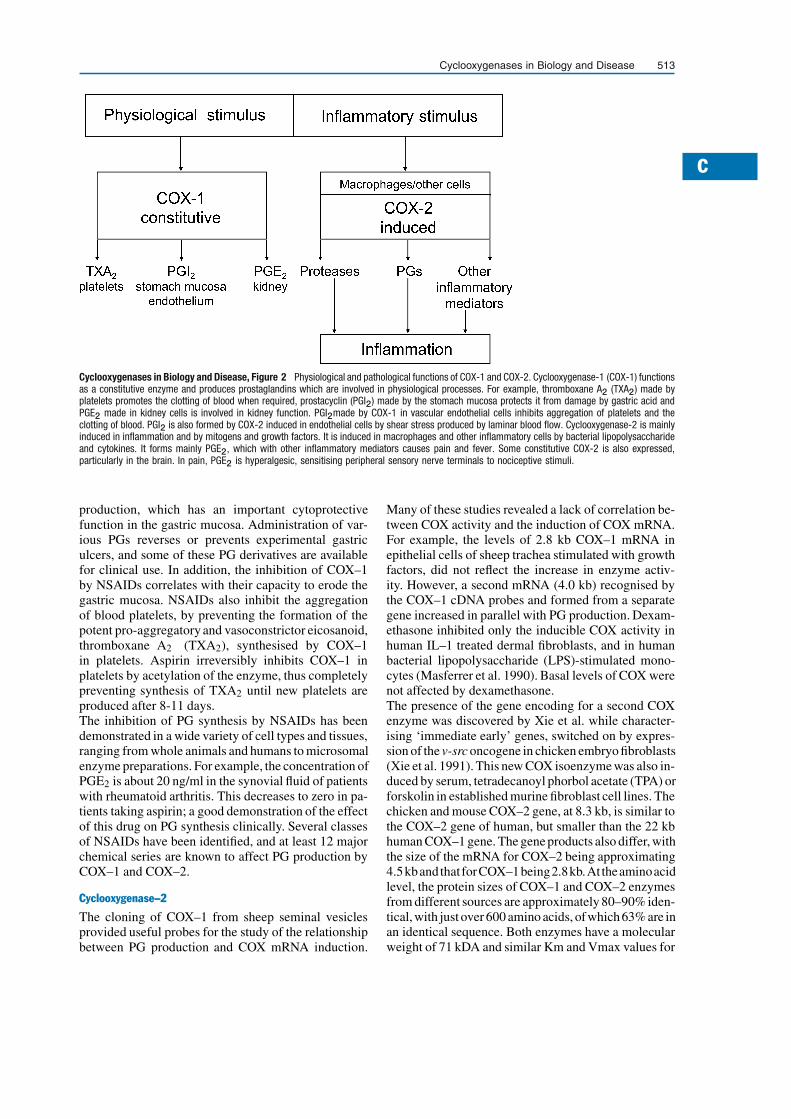
C
Cyclooxygenases in Biology and Disease 513
Cyclooxygenases in Biology and Disease, Figure 2 Physiological and pathological functions of COX-1 and COX-2. Cyclooxygenase-1 (COX-1) functionsas a constitutive enzyme and produces prostaglandins which are involved in physiological processes. For example, thromboxane A2 (TXA2) made byplatelets promotes the clotting of blood when required, prostacyclin (PGI2) made by the stomach mucosa protects it from damage by gastric acid andPGE2 made in kidney cells is involved in kidney function. PGI2made by COX-1 in vascular endothelial cells inhibits aggregation of platelets and theclotting of blood. PGI2 is also formed by COX-2 induced in endothelial cells by shear stress produced by laminar blood flow. Cyclooxygenase-2 is mainlyinduced in inflammation and by mitogens and growth factors. It is induced in macrophages and other inflammatory cells by bacterial lipopolysaccharideand cytokines. It forms mainly PGE2, which with other inflammatory mediators causes pain and fever. Some constitutive COX-2 is also expressed,particularly in the brain. In pain, PGE2 is hyperalgesic, sensitising peripheral sensory nerve terminals to nociceptive stimuli.
production, which has an important cytoprotectivefunction in the gastric mucosa. Administration of var-ious PGs reverses or prevents experimental gastriculcers, and some of these PG derivatives are availablefor clinical use. In addition, the inhibition of COX–1by NSAIDs correlates with their capacity to erode thegastric mucosa. NSAIDs also inhibit the aggregationof blood platelets, by preventing the formation of thepotent pro-aggregatory and vasoconstrictor eicosanoid,thromboxane A2 (TXA2), synthesised by COX–1in platelets. Aspirin irreversibly inhibits COX–1 inplatelets by acetylation of the enzyme, thus completelypreventing synthesis of TXA2 until new platelets areproduced after 8-11 days.The inhibition of PG synthesis by NSAIDs has beendemonstrated in a wide variety of cell types and tissues,ranging from whole animals and humans to microsomalenzyme preparations. For example, the concentration ofPGE2 is about 20 ng/ml in the synovial fluid of patientswith rheumatoid arthritis. This decreases to zero in pa-tients taking aspirin; a good demonstration of the effectof this drug on PG synthesis clinically. Several classesof NSAIDs have been identified, and at least 12 majorchemical series are known to affect PG production byCOX–1 and COX–2.
Cyclooxygenase–2
The cloning of COX–1 from sheep seminal vesiclesprovided useful probes for the study of the relationshipbetween PG production and COX mRNA induction.
Many of these studies revealed a lack of correlation be-tween COX activity and the induction of COX mRNA.For example, the levels of 2.8 kb COX–1 mRNA inepithelial cells of sheep trachea stimulated with growthfactors, did not reflect the increase in enzyme activ-ity. However, a second mRNA (4.0 kb) recognised bythe COX–1 cDNA probes and formed from a separategene increased in parallel with PG production. Dexam-ethasone inhibited only the inducible COX activity inhuman IL–1 treated dermal fibroblasts, and in humanbacterial lipopolysaccharide (LPS)-stimulated mono-cytes (Masferrer et al. 1990). Basal levels of COX werenot affected by dexamethasone.The presence of the gene encoding for a second COXenzyme was discovered by Xie et al. while character-ising ‘immediate early’ genes, switched on by expres-sion of the v-src oncogene in chicken embryo fibroblasts(Xie et al. 1991). This new COX isoenzyme was also in-duced by serum, tetradecanoyl phorbol acetate (TPA) orforskolin in established murine fibroblast cell lines. Thechicken and mouse COX–2 gene, at 8.3 kb, is similar tothe COX–2 gene of human, but smaller than the 22 kbhuman COX–1 gene. The gene products also differ, withthe size of the mRNA for COX–2 being approximating4.5kbandthat forCOX–1being2.8kb.At theaminoacidlevel, the protein sizes of COX–1 and COX–2 enzymesfrom different sources are approximately 80–90% iden-tical, with just over 600 amino acids, ofwhich 63% are inan identical sequence. Both enzymes have a molecularweight of 71 kDA and similar Km and Vmax values for

514 Cyclooxygenases in Biology and Disease
metabolismofarachidonicacid.Bothenzymesalsohavesimilar activesites for theattachmentofarachidonicacidor NSAIDs, although the active site of COX–2 is largerthan thatofCOX–1andcanacceptawider rangeofstruc-tures as substrates.The residues that form the substrate binding channel, thecatalytic sites, and the residues immediately adjacentareall identical in COX–1 and COX–2 except for two smallvariations.Theprimary sequencedifference in theactivesite itself is the valine 523 side chain in COX–2, whichis smaller by a single methyl group than the isoleucineside chain that it replaces in COX–1. This opens up ac-cess to a side pocket off the main substrate channel inCOX–2, allowing an enzyme inhibitor to react with argi-nine 513, which replaces histidine in COX–1. Anothersequence difference is situated outside, but close to, theactivesite, and can indirectly influence itsconformation.The large residue, phenylalanine 503, in COX–1 is re-placed by the smaller leucine in COX–2. This allowsleucine 384, which borders the active site, to re-orientateits methyl side chain out of the active site, and thus leavemore space available for a larger inhibitor molecule inCOX–2 than in COX–1.The importanceof thediscovery of the inducibleCOX–2is highlighted by the differences in pharmacology ofthe two enzymes (Warner et al. 1999). Aspirin, in-domethacin and ibuprofen are much less active againstCOX–2 than against COX–1. Indeed, the strongestinhibitors of COX–1 such as aspirin, indomethacin andpiroxicam are the NSAIDs which cause the most dam-age to the stomach. The spectrum of activities of someten standard NSAIDs against the two enzymes rangesfrom a high selectivity towards COX–1 (166-fold foraspirin), through to equiactivity on both (for example,diclofenac). The range of activities of NSAIDs againstCOX–1 compared with COX–2 explains the variationsin the side effects of NSAIDs at their anti-inflammatorydoses. Drugs which have a high potency against COX–2and a low COX–2/COX–1 activity ratio will have po-tent anti-inflammatory activity with few side effectson the stomach and kidney. Published epidemiologicaldata on the side effects of NSAIDs reported that pirox-icam and indomethacin in anti-inflammatory dosesshowed high gastrointestinal toxicity. These drugs havea much higher potency against COX–1 than againstCOX–2.The discovery of COX–2, induced by inflammatorystimuli and cytokines in migratory and other cells,stimulated several laboratories to develop highly selec-tive inhibitors of this enzyme (Fig. 2). Monsanto/Searle(now Pfizer) are marketing celecoxib and its successor,� valdecoxib, whereas Merck and Company developedthe selective COX–2 inhibitors, rofecoxib and etori-coxib. Early trials of celecoxib (Silverstein et al. 2000)and of rofecoxib (Bombardier et al. 2000) demon-strated good analgesia and anti-inflammatory activity,with less adverse effects on the stomach mucosa than
comparator drugs. Millions of arthritic patients werethen prescribed these drugs. However, the rofecoxibtrial revealed that 4 times as many patients receiv-ing rofecoxib suffered a myocardial infarction thanthose treated with naproxen. This was interpreted asa protective effect of naproxen, which would inhibitaggregation of platelets and therefore prevent heartattacks. Following these initial trials, Merck and Pfizerbegan large scale trials of rofecoxib and celecoxib inpatients with recurrent neoplastic � polyps of the largebowel, a precancerous condition preceding colorectalneoplasia. These trials were instituted since cancercells have high levels of COX–2, while surroundinghealthy colon cells have none. In these anti-cancertrials, the effects of rofecoxib and celecoxib were com-pared with patients receiving placebo treatment. Bothtrials were terminated after eighteen months, whenit became clear that the incidence of adverse cardio-vascular events, primarily myocardial infarctions andischemic cerebrovascular events, was greater in thepatients receiving selective COX–2 inhibitors. At thisstage, Merck decided to withdraw rofecoxib from themarket. The most plausible explanation for this increasein heart attacks is that selective COX–2 inhibitors pre-vent synthesis of anti-aggregatory prostacyclin in thevascular endothelium. Since these drugs do not affectTXA2 synthesis by COX–1 in blood platelets, theaggregatory action of TXA2 progresses unopposed andthrombotic emboli form to cause myocardial infarc-tions.
Cyclooxygenase–3� Paracetamol (acetaminophen) has potent analgesicand antipyretic actions but very little anti-inflammatoryactivity. Its mechanism of action has remained a mys-tery for many years, since it is only a weak inhibitor ofPG biosynthesis by either COX–1 or COX–2 in vitro,but inhibits PG biosynthesis in vivo. Reduction of PGbiosynthesis by paracetamol varies in different tissues,and COX activity in brain is particularly sensitive toinhibition (Flower and Vane 1972). In 2002, Simmonsand colleagues cloned, characterised and expressed avariant of COX–1 from dog and human brain, whichthey named COX–3 (Chandrasekharan et al. 2002).This enzyme, expressed in insect cells, was sensitiveto inhibition with low concentrations of paracetamoland other related antipyretic analgesic drugs, such asantipyrine and aminopyrine. However, significantlyincreased concentrations of paracetamol were neededto inhibit COX–1 and COX–2 under the same ex-perimental conditions. COX–3 was also sensitive toinhibition with low concentrations of non-selectiveNSAIDs, which may explain the antipyretic action ofthese drugs.Similarly to COX–1 and COX–2, COX–3 was shownto possess COX and peroxidase active sites and to havethe same cellular localisation. COX–3 was also shown

C
Cytochrome Oxidase Staining 515
to be glycosylated and to have the capacity to metabolisearachidonic acid, leading to the formation of PGE2. Themajor difference between COX–3 and COX–1 is thatat the mRNA level, COX–3 retains intron–1, which en-codes a 30aa sequence inserted into the N-terminal hy-drophobic signal peptide of the enzyme. Although in ca-nine COX–3 mRNA, intron–1 is within frame, in the hu-man there is a frameshift in intron–1 of the COX–3 tran-script. The conversion of COX–3 mRNA into enzymeprotein in humans requires further investigation.
References1. Bergström S, Danielsson H, Samuelsson B (1964) The En-
zymatic Formation of Prostaglandin E2 from ArachidonicAcid. Prostaglandins and related factors 32. Biochim BiophysActa 90:207–210
2. Bombardier C, Laine L, Reicin A, Shapiro D, Burgos-VargasR, Davis B et al. (2000) Comparison of Upper GastrointestinalToxicity of Rofecoxib and Naproxen in Patients with RheumatoidArthritis. N Engl J Med 343:1520û1528
3. Chandrasekharan NV, Dai H, Roos KLT, Evanson NK, TomsikJ, Elton TS, Simmons DL (2002) COX–3, A Cyclooxyge-nase–1 Variant Inhibited by Acetaminophen and Other Anal-gesic/Antipyretic Drugs: Cloning, Structure and Expression.Proc Natl Acad Sci USA 99:13926–13931
4. DeWitt DL, Smith WL (1988) Primary Structure of ProstaglandinG/H Synthase from Sheep Vesicular Gland Determined fromthe Complementary DNA Sequence. Proc Natl Acad SciUSA 85:1412–1416
5. Flower RJ, Vane JR (1972) Inhibition of Prostaglandin Syn-thetase in Brain Explains the Antipyretic Activity of Paracetamol(4–acetamidophenol). Nature 240:410–411
6. Goldblatt MW (1935) Properties of Human Seminal Plasma. JPhysiol (Lond) 84:208–218
7. Hemler M, Lands WEM, Smith WL (1976) Purification of the Cy-cloxygenase that Forms Prostaglandins: Demonstration of TwoForms of Iron in the Holoenzyme. J Biol Chem 251:5575–5579
8. Masferrer JL, Zweifel BS, Seibert K, Needleman P (1990) Se-lective Regulation of Cellular Cyclooxygenase and Endotoxinin Mice. J Clin Invest 86:1375–1379
9. Picot D, Loll PJ, Garavito RM (1994) The X-ray Crystal Struc-ture of the Membrane Protein Prostaglandin H2 Synthase–1. Na-ture 367:243–249
10. Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus T,Whelton A et al. (2000) Gastrointestinal Toxicity with Celecoxibvs. Nonsteroidal Anti-Inflammatory Drugs for Osteoarthritisand Rheumatoid Arthritis: The CLASS Study: A RandomisedControlled Trial. Celecoxib Long-term Arthritis Safety Study.J Am Med Assoc 284:1247–1255
11. Vane JR (1971) Inhibition of Prostaglandin Synthesis as a Mech-anism of Action for the Aspirin-Like Drugs. Nature 231:232–235
12. Vane JR, Botting RM (2001) Formation and Actions ofProstaglandins and Inhibition of their Synthesis. In: VaneJR, Botting RM (eds) Therapeutic Roles of Selective COX–2Inhibitors. William Harvey Press, London, pp 1–47
13. von Euler US (1934) Zur Kenntnis der PharmakologischenWirkung von Nativsekreten und Extracten Männlicher Acces-sorischer Geschlechtsdrüsen. Arch Exp Path Pharmak 175:78–84
14. Warner TD, Giuliano F, Vojnovic I, Bukasa A, Mitchell JA, VaneJR (1999) Nonsteroid Drug Selectivities for Cyclooxygenase–1Rather than Cyclooxygenase–2 are Associated with Human Gas-trointestinal Toxicity: A Full In Vitro Analysis. Proc Natl AcadSci USA 96:7563–7568
15. Xie W, Chipman JG, Robertson DL, Erikson RL, Simmons DL(1991) Expression of a Mitogen-Responsive Gene EncodingProstaglandin Synthase is Regulated by mRNA Splicing. ProcNatl Acad Sci USA 88:2692–2696
Cyclophosphamide
Definition
An alkylating agent frequently used as immunosup-pressant. The treatment of choice, in combination withsteroids, in systemic vasculitides like WG.� Headache Due to Arteritis� Vascular Neuropathies
Cyclosporin, Methotrexate
Definition
Drugs used to suppress immune functions in organ-transplanted patients and in patients with diseases withdisturbances in immune functions, e.g. rheumatoidarthritis, psoriasis.� Postoperative Pain, Acute Pain Management, Princi-
ples
Cystitis Models
� Visceral Pain Model, Urinary Bladder Pain (Irritantsor Distension)
Cytoarchitectural
Definition
Pertaining to the cellular composition of bodily struc-ture.� Pain Processing in the Cingulate Cortex, Behavioral
Studies in Humans
Cytochrome Oxidase Staining
Synonyms
CO staining
Definition
Type of staining that reflects mitochondrial activity inneurons.� Spinothalamic Terminations, Core and Matrix� Thalamus,ReceptiveFields,ProjectedFields,Human

516 Cytokine Modulation of Opioid Action
Cytokine Modulation of Opioid ActionVASUDEVA RAGHAVENDRA1, JOYCE A. DELEO2
1Algos Therapeutics Inc., Saint Paul, MN, USA2Dartmouth Hitchcock Medical Center, DartmouthMedical School, Lebanon, NH, [email protected],[email protected]
Synonyms
Opioid Modulation by Cytokines
Definition
A conceptual framework has recently emerged to sup-port the hypothesis that an � opioid may, in fact, bebroadly defined as a � cytokine. This is due to thepresence of opioid receptors on immune cells, and theability of opioids to mediate interactions between cellsand regulate processes in the extracellular environment.In addition, it has been demonstrated that a bidirectionalinteraction exists among endogenous opioids and clas-sically defined cytokines. In the central nervous system(CNS), cytokines appear to be modulated by endoge-nous opioids, and the neural effects of opioids alteredby cytokines. In particular, cytokines modulate opioidregulation of neuronal activity, sensory motor func-tion, body temperature, food intake and regulation ofhypothalamic-pituitary-adrenocortical axis functions.Recently, the role of cytokines in modulating opioid� analgesia, tolerance and � hyperalgesia has also beenreported.
Characteristics
Opioids are a class of the most effective analgesicsfor treating many forms of acute and chronic pain. Inaddition to the known adverse effects, the clinical utilityof opioid analgesics is often hampered by the develop-ment of analgesic tolerance, hyperalgesia and physicaldependence. A wide range of neurotransmitters andneuromodulators play a role in the development oftolerance and dependence to opioids. Recent studieshave demonstrated that cytokines are also capable ofmodulating opioid-induced analgesia, and play a rolein the development of opioid tolerance and withdrawal-induced hyperalgesia.
Cytokines
Cytokines, e.g. IL–1β, IL–6, IL–10, interferons, andchemokines have the ability to modulate the analgesicaction of opioids. For example, the proinflammatory cy-tokine, IL–1β directly attenuates opioid analgesia (Gulet al. 2000). IL–1β also plays a role in the anti-analgesicactivity of dynorphin and ligands of the peripheral ben-zodiazepine receptor (Laughlin et al. 2000; Rady andFujimoto 2001). The role of IL–6 in modulating opioidanalgesia is more complicated. Although IL–6 is known
to induce hyperalgesia in animals, IL–6 knock-out miceshowed reduced morphine analgesia and an early devel-opment of morphine tolerance (Bianchi et al. 1999). Wehave shown that neutralizing or blocking IL–6, IL–1β
and TNF–α spared the analgesic action of morphinein rats following a peripheral nerve injury (Raghaven-dra et al. 2002). A sickness-inducing agent such aslipopolysaccharide or lithium chloride, which inducesproinflammatory cytokine release, reduces morphineanalgesia (Johnston and Westbrook 2003). Proinflam-matory cytokines also play a role in the development ofmorphine tolerance and withdrawal-induced hyperal-gesia. Chronic administration of heroin or morphine tomice or rats resulted in increased peripheral and centralexpression of proinflammatory cytokines (Raghavendraet al. 2002; Jolan et al. 2003). The central expressionof proinflammatory cytokines after chronic morphinetreatment, exhibited a temporal correlation with thedevelopment of analgesic tolerance and withdrawal-induced hyperalgesia in rats (Raghavendra et al. 2002).Conversely, IL–10, an anti-inflammatory cytokine,spared the analgesic actions of opioids in dynorphintreated rats (Laughlin et al. 2000). Interferon-alpha(IFN–α), which exhibits structural and functional simi-larities to endorphins, induces opioid receptor-mediatedanalgesia and prevents the development of tolerance toopioids (Dafny 1984).
Chemokines� Chemokines (chemotactic cytokines) also influ-ence the perception of pain by interacting with G-protein-coupled opioid receptors. Recent studies haveshown that cross-desensitization between opioid andchemokine receptors has significant implications inthe regulation of leukocyte trafficking, progressionof inflammatory disease and regulation of opioidreceptor function in the CNS (Steele et al. 2002).The direct administration of chemokines, particu-larly CXCL12 and CCL5, into the periaqueductal graymatter, inhibited opioid-induced analgesia by crossdesensitizing μ opioid receptors (Szabo et al. 2002).Opioid enhancement of chemokine up-regulation is alsoresponsible for enhanced HIV infection and progressionto AIDS in opioid abusers (Peterson et al. 1998).
Glial Component
Major sources of proinflammatory cytokines andchemokines in the CNS are activated � glial cells. Thepresence of opioid receptors on microglia and astro-cytes is well documented, and priming these cells withopioids induces enhanced secretion of proinflammatorycytokines and chemokines (Peterson et al. 1998). Acti-vation of spinal proinflammatory cytokines by chronicopioid treatment may be caused by its interaction withglial cells (Raghavendraetal. 2002).Attenuationofglialactivation using the methylxanthine, propentofylline,restored opioid analgesia, prevented the development of

C
Cytokine Modulation of Opioid Action 517
morphine tolerance and morphine withdrawal-inducedhyperalgesia, and opioid-induced neuroimmune acti-vation (Raghavendra and DeLeo 2004). This reductionin neuroimmune activation by propentofylline includeddecreased microglial, astrocytic activation and cytokineexpression in the lumbar spinal cord following mor-phine administration in a peripheral nerve injury in arat model of neuropathy.
Intracellular Signaling Cascades
Mitogen-activated protein (MAP) kinase or proteinkinase C (PKC) pathways may be involved in opioid-induced activation of proinflammatory immune re-sponses. MAP kinase and PKC are intriguing, becausethey are key players in the intracellular signaling cas-cade leading to the development of morphine toleranceand production of proinflammatory immune activa-tion (Raghavendra et al. 2002). Since proinflammatorycytokines and chemokines induce hyperalgesia in an-imals, it is possible that activation of pro-nociceptivepathways by these mediators could counteract opioidanalgesia.
Cellular Adhesion Molecules
The immune system has the capacity to modulate paindirectly at the site of tissue injury by liberating opioidpeptides from immune cells. In an inflammatory painmodel, the peripheral analgesic activity of opioids ismodulated by � selectins and intracellular adhesionmolecule–1 (ICAM–1). ICAM–1, expressed on vas-cular endothelium, recruits immunocytes containingopioids to promote the local control of inflammatorypain. Anti-selectin or anti-ICAM–1 treatment stronglyreduces endogenous peripheral opioid analgesia, ap-parently by blocking the extravasation of immunecells containing β–endorphin, and by the consequentdecrease of the β–endorphin level in the inflamed tis-sue (Machelska et al. 1998; Machelska et al. 2002).Therefore, the immune control of opioid action maydemonstrate a dichotomous action in the periphery ascompared with the central nervous system.
Clinical Relevance
One of the reasons for decreased opioid analgesia inneuropathic pain conditions may be an enhanced ex-pression of proinflammatory cytokines and chemokinesin the CNS, which is evoked following peripheral nerveinjury. It is well-established that exaggerated painstates occur as a part of an inflammatory stress reaction.Pre-clinical studies demonstrated that neutralizing pro-inflammatory cytokines restored the analgesic actionof opioids in neuropathic conditions, induced eitherby experimental diabetes or by L5 nerve transectionin rats (Gul et al. 2000; Raghavendra et al. 2002).Pathological pain is the result of a dynamic interplaybetween hyperalgesic and analgesic mediators. Duringtissue injury or inflammation, both hyperalgesic and
anti-hyperalgesic/analgesic mediators are produced byactivated immune cells. Hyperalgesic mediators, suchas proinflammatory cytokines and chemokines, andanti-hyperalgesic mediators, such as anti-inflammatorycytokines and adhesion molecules, modulate opioidanalgesia. Drugs such as immunosuppressants that in-fluence this interplay may also modulate endogenousor exogenously administered opioid analgesia.
Conclusions
Of particular clinical interest, the glial modulatingagent, propentofylline, was shown to prevent opioidtolerance and hyperalgesia in a rat model of neuropa-thy (Raghavendra and DeLeo 2004; Raghavendra etal. 2003). Together, these data offer a novel clinicaltherapy for the prevention or delay of opioid toleranceand hyperalgesia: the co-administration of cytokineinhibitors and/or glial modulators with opioids. Rec-ognizing that opioids remain the gold standard for thetreatment of acute pain, improvement of their untowardside-effect profile would enhance their clinical efficacy.
References1. Bianchi M, Maggi R, Pimpinelli F, Rubino T, Parolaro D, Poli
V, Ciliberto G, Panerai AE, Sacerdote P (1999) Presence of aReduced Opioid Response in Interleukin–6 Knock-Out Mice.Eur J Neurosci 11:1501–1507
2. Dafny N (1984) Interferon: A Candidate as the Endogenous Sub-stance Preventing Tolerance Dependence to Brain Opioids. ProgNeuropsychopharmacol 8:351–357
3. Gul H, Yildiz O, Dogrul A, Yesilyurt O, Isimer A (2000) TheInteraction between IL–1β and Morphine: Possible Mechanismof the Deficiency of Morphine-Induced Analgesia in DiabeticMice. Pain 89:39–45
4. Holan V, Zajikova A, Krulova M, Blahoutova V, Wilczek H(2003) Augmented Production of Proinflammatory Cytokinesand Accelerated Allotransplantation Reaction in Heroin-TreatedMice. Clin Exp Immunol 132:40–45
5. Johnston IN, Westbrook RF (2003) Acute and Conditioned Sick-ness Reduces Morphine Analgesia. Behav Brain Res 142:89–97
6. Laughlin TM, Bethea JR, Yezierski RP, Wilcox GL (2000)Cytokine Involvement in Dynorphin-Induced Allodynia.Pain 84:159–167
7. Machelska H, Cabot, PJ, Mousa SA, Zhang Q. Stein C (1998)Pain Control in Inflammation Governed by Selectins. NatMed 4:1425–1428
8. Machelska H, Mousa,SA, Brack A, Schopohl JK, RittnerHL, Schafer M, Stein C (2002) Opioid Control of Inflamma-tory Pain Regulated by Intracellular Adhesion Molecule–1. JNeurosci 22:5588–5596
9. Peterson PK, Molitor TW, Chao CC (1998) The Opioid-CytokineConnection. J Neuroimmunol 83:63–69
10. Rady JJ, Fujimoto JM (2001) Confluence of Antianalgesic Ac-tion of Diverse Agents through Brain Interleukin1 β in Mice. JPharmacol Exp Ther 299:659–665
11. Raghavendra V, DeLeo JA (2004) The Role of Astrocytes andMicroglia in Persistent Pain. In: Hertz L (eds) Non-NeuronalCells in the Nervous System: Function and Dysfunction. Elsevier,Amsterdam, pp 951–966
12. Raghavendra V, Rutkowski MD, DeLeo JA (2002) TheRole of Spinal Neuroimmune Activation in Morphine Tol-erance/Hyperalgesia in Neuropathic and Sham Operated Rats.J Neurosci 22:9980–9989
13. Raghavendra V, Tanga F, Rutkowski MD, DeLeo JA (2003)Anti-Hyperalgesic and Morphine-Sparing Actions of Propento-fylline following Peripheral Nerve Injury in Rats: Mechanistic

518 Cytokines
Implications of Spinal Glia and Proinflammatory Cytokines.Pain 104:657–665
14. Steele AD, Szabo I, Bednar F, Rogers TJ (2002) Interaction be-tween Opioid and Chemokine Receptors: Heterologous Desen-sitization. Cytokine Growth Factor Rev 13:209–222
15. Szabo I, Chen XH, Xin L, Adler MW, Howard OM, OppenheimJJ, Rogers TJ (2002) Heterologous Desensitization of OpioidReceptors by Chemokines Inhibits Chemotaxis and Enhances thePerception of Pain. Proc Natl Acad Sci USA 99:10276–10281
Cytokines
Definition
Any of several small regulatory proteins (25 kDa), suchas the interleukins and lymphokines, that are released bycells of the immune system and act as intercellular me-diators in the generation of immune and inflammatoryresponses. They can act in an autocrine, paracrine, andendocrine manner. Interleukins, interferons and tumornecrosis factor (TNF) alpha are typical members of thecytokine family.� Adjuvant Analgesics in Management of Cancer-
Rated Bone Pain� Animal Models of Inflammatory Bowel Disease� Cytokines as Targets in the Treatment of Neuropathic
Pain� Cytokine Modulation of Opioid Action� Cytokines, Regulation in Inflammation� Inflammatory Neuritis� Muscle Pain in Systemic Inflammation (Polymyalgia
Rheumatica, Giant Cell Arteritis, Rheumatoid Arthri-tis)
� Neutrophils in Inflammatory Pain� Vascular Neuropathies� Wallerian Degeneration
Cytokines as Targets in the Treatment ofNeuropathic Pain
CLAUDIA SOMMER1, LINDA S. SORKIN2
1Department of Neurology, University of Würzburg,Würzburg, Germany2Anesthesiology Research, University of California,San Diego, CA, [email protected], [email protected]
Synonyms
NA; interleukins; Lymphokines; chemokines
Definition
Extracellular signaling proteins within the immune sys-tem and between the immune system and nervous sys-tem.
Characteristics
Cytokines� Cytokines are a heterogeneous group of proteinsthat were originally found to mediate activation of theimmune system and inflammatory responses. They areproduced by white blood cells and a variety of other cellsincluding neurons, Schwann cells and other glial cells.Most cytokines act on a variety of tissues, includingthe peripheral and central nervous systems. Cytokinesare extracellular signaling proteins that form part ofa bi-directional circuit between the immune systemand the nervous system, acting at hormonal concen-trations through high-affinity receptors, and producingendocrine, paracrine and autocrine effects. In contrastto circulating hormones, they exert their effects overshort distances onto nearby cells. In vivo concentra-tions are in the range of a few pg to ng per ml. Dueto local cytokine effects at low concentrations, serumlevels may not reliably reflect activity. Cytokines arecalled ‘pleiotropic’, due to a broad range of redundant,frequently overlapping functions. Their activation ordysregulation is implied in a variety of disease stateslike sepsis, rheumatoid arthritis, Crohn’s disease, mul-tiple sclerosis, skin diseases, and many more. Somecytokines are labeled ‘pro-inflammatory’ or ‘Th1’,others ‘anti-inflammatory’or ‘Th2’, depending on theireffects on immune cells, in particular on lymphocytes.
Cytokines and Pain
Evidence from Experimental Studies
Numerous experimental studies provide evidence thatproinflammatory cytokines induce or facilitate inflam-matory as well as neuropathic pain and hyperalgesia.Di-rect receptor-mediated actions of cytokines on afferentnerve fibers have been reported, as well as cytokine ef-fects involving downstream mediators. The first indica-tions of a hyperalgesic effect of cytokines came fromstudies using intraplantar cytokine injections in the rat;interleukin-1β (� IL-1beta)and� tumornecrosisfactoralpha (TNF-α) reduced mechanical nociceptive thresh-olds in a cyclooxygenase-dependent process. Cytokineantagonists reduced hyperalgesia in this animal model,indicating that the cytokines were activated in a classicalsequence (TNF⇒IL-1⇒� IL-6), and that activation ofthis pro-inflammatory cytokine cascade is an importantstep in thedevelopmentof inflammatorypain(for reviewsee Poole et al. 1999).After nerve injury, cytokine production in the injurednerve is upregulated, and blockade of the proinflamma-tory cytokinesTNFαand IL-1β reducesbehavioral signsof hyperalgesia in experimental animals (for review seeSommer 2001). The mechanisms by which proinflam-matory cytokines induce hyperalgesia have not yet beenfully elucidated.IL-1β, among its other actions involving secondary pro-ductionofnitricoxide,bradykininorprostaglandins,has

C
Cytokines as Targets in the Treatment of Neuropathic Pain 519
a direct excitatory action on nociceptive fibers, whichare activated within one minute by IL-1β application(Fukuoka et al. 1994). In a skin-nerve in vitro prepara-tion, brief exposure of the corium to IL-1β results in afacilitation of heat-evoked calcitonin gene-related pep-tide release from peptidergic neurons (Opree and Kress2000). The short latency of the effect, and the absenceof the neuronal cell soma in the preparation, indicatethat the heat sensitization is independent of changes ingene expression or receptor up-regulation. Further ex-periments showed that IL-1β can act directly on sensoryneurons to increase their sensitivity to noxious heat viaa mechanism involving IL-1 receptor I, tyrosine kinaseand protein kinase C (Obreja et al. 2002).TNFα has been shown to lower mechanical activationthresholds in C nociceptors of the rat sural nerve wheninjected subcutaneously (Junger and Sorkin 2000).While mechanisms of this action are unknown, the acuteTNF-induced decrease in K+ conductance may play animportant role (Diem et al. 2001). In vitro perfusionof TNFα to dorsal root ganglia (DRG) elicits neuronaldischarges in both A and C-fibers. Firing frequencyis markedly higher and the discharge longer-lastingafter nerve injury, indicating an increased sensitivity ofinjured afferent neurons to TNFα (Schäfers et al. 2003).Furthermore, DRG neurons with injured afferents, andneighboring neurons attached to intact afferents runningwithin the same peripheral nerve, have an increasedimmunoreactivity to TNFα (probable increased TNFα
protein), and both display increased sensitivity to TNFα
(Schäfers et al. 2003, 2003a). Injection or perfusion ofTNFα into/onto rat DRGs in vivo induces allodynia.Subthreshold quantities of TNFα, injected into a DRGat the same time that its spinal nerve was ligated resultedin a synergy that manifests as faster onset of allodyniaand increased spontaneous pain behavior (Schäferset al. 2003). Thus, there is strong in vivo and in vitroevidence that injury results in increased endogenousTNFα, and that injured nerve fibers are sensitized to theexcitatory effects of TNFα.� Nucleus pulposus, the material within the verte-bral discs, is highly enriched with a variety of pro-inflammatory cytokines. Subsequent to disc herniation,it is likely that this material comes into contact withthe dorsal roots. Application of autologous nucleuspulposus to dorsal roots, or experimental disc herni-ation in animals, results in pain behavior as well asboth ongoing and enhanced evoked activity in spinalnociceptive neurons (Onda et al. 2003). Animals treatedwith either neutralizing antibodies to TNFα directlyon the nerve root or with systemic TNFα antagonists,showed a marked reduction of both the neuronal activity(Onda et al. 2003) and the pain behavior, implicating arole for TNFα in the process.Increased spinal cord expression of TNFα, IL-1β, or IL-6 is associated with pain. Protein and mRNA levels ofall three cytokines increase in the spinal cord following
nerve injury in animal models (Winkelstein et al. 2001).Spinal administration of exogenous TNFα and IL-1β
produces pain behavior and neuronal sensitization invivo, with IL-1 being the more effective (Reeve et al.2000). In animals with nerve injury and pain behavior,spinal administration of TNFα antagonists prevents orreduces allodynia and hyperalgesia. Whereas spinalIL-1β antagonists alone are seemingly without effectin nerve injury models, they synergize with TNFα
antagonists causing a further reduction of allodynia.Interestingly, while this combination treatment reducesthe spinal cord expression of the pro-inflammatory cy-tokine IL-6, spinal expression of the anti-inflammatorycytokine � IL-10 was unaffected.Anti-inflammatory cytokines like � IL-4 and IL-10seem to have anti-hyperalgesic actions in animal mod-els of pain (Wagner et al. 1998). IL-10 pretreatmentreduces the hyperalgesic responses to intraplantar in-jections of carrageenan, IL-1β, IL-6 and TNFα (Pooleet al. 1999). Systemic IL-10 down-regulates local lev-els of IL-1β, TNFα, and nerve growth factor (NGF)after endotoxin injection into the hindpaw, and reducesthermal and mechanical hyperalgesia. IL-4, deliveredby a viral vector, reduces behavioral signs of pain in ananimal model of neuropathic pain.
Clinical Applications
The most striking correlation between cytokine lev-els and neuropathic pain comes from leprosy, wherea subgroup of patients has elevated serum levels ofTNFα and IL-1; these patients suffer from excruciat-ing pain. Treatment with thalidomide reduces TNFα
secretion in peripheral blood mononuclear cells by>90% and greatly reduces pain in the patients (Barneset al. 1992). In other human neuropathies, prelimi-nary data also point to a correlation between cytokineexpression and pain. Not all patients with elevated cy-tokine levels in their sural nerve biopsy had pain, butcytokine levels were increased more often in patientswith painful neuropathies (Lindenlaub and Sommer2003), indicating that at least a subgroup of patientswith painful neuropathies might benefit from cytokineinhibition. Occasionally, inflammatory neuropathieshave been treated with TNFα inhibitors, but data onpain are lacking in these reports. One remarkable casereport describes remission of long standing complexregional pain syndrome (CRPS) after treatment withthalidomide for Behçet’s disease (Ching et al. 2003).Anti-TNFα strategies have been used in various non-neuropathic painful conditions like AIDS-associatedproctitis, rheumatoid arthritis, and HIV-associated aph-thous ulcers. Many other reports have followed sincethe advent of � etanercept and � infliximab : for ex-ample, a controlled trial showing a beneficial effect ofetanercept in ankylosing spondylitis, and a prospectivestudy with historical controls using infliximab in lowback pain.

520 Cytokines, Effects on Nociceptors
Several studies have reported increased levels of cy-tokines in the vicinity of herniated discs and a correla-tion of their presence to sciatica (Brisby et al. 2002).Inhibitors of TNFα have been used successfully forpatients with chronic nerve root pain, but up to nowonly data from case reports and uncontrolled studieshave been available.In summary, evidence from numerous preclinical stud-ies and preliminary data in humans point to a possiblebeneficial role of cytokine inhibition in patients withpainful neuropathy or radiculopathy. Randomized con-trolled trials are needed to determine whether cytokineinhibitors have a role in the treatment of neuropathicpain.
References1. Barnes PF, Chatterjee D, Brennan et al. (1992) Tumor Necro-
sis Factor Production in Patients with Leprosy. Infec Immun60:1441–1446
2. Brisby H, Olmarker K, Larsson K et al. (2002) ProinflammatoryCytokines in Cerebrospinal Fluid and Serum in Patients withDisc Herniation and Sciatica. Eur Spine J 11:62–66
3. Ching DWT, McClintock A, Beswick F (2003) Successful Treat-mentwithLow-DoseThalidomide in aPatient with BothBehcet‘sDisease and Complex Regional Pain Syndrome Type I. J ClinRheumatology 9:96–98
4. Diem R, Meyer R, Weishaupt JH et al. (2001) Reduction of Potas-sium Currents and Phosphatidylinositol 3-Kinase-DependentAKT Phosphorylation by Tumor Necrosis Factor-(alpha) Res-cues Axotomized Retinal Ganglion Cells from Retrograde CellDeath In Vivo. J Neurosci 21:2058–2066
5. Fukuoka H, Kawatani M, Hisamitsu T et al. (1994) CutaneousHyperalgesia Induced by Peripheral Injection of Interleukin-1β
in the Rat. Brain Res 657:133–1406. Junger H, Sorkin LS (2000) Nociceptive and Inflammatory Ef-
fects of Subcutaneous TNFalpha. Pain 85:145–1517. Lindenlaub T, Sommer C (2003) Cytokines in Sural Nerve Biop-
sies from Inflammatory and Non-Inflammatory Neuropathies.Acta Neuropathol 105:593–602
8. Obreja O, Rathee PK, Lips KS et al. (2002) IL-1 Beta Potenti-ates Heat-Activated Currents in Rat Sensory Neurons: Involve-ment of IL-1RI, Tyrosine Kinase, and Protein Kinase C. FASEBJ 16:1497–1503
9. Olmarker K, Nutu M, Storkson R (2003) Changes in Spon-taneous Behavior in Rats Exposed to Experimental DiscHerniation are Blocked by Selective TNF-Alpha Inhibition.Spine 28:1635–1641
10. Onda A, Yabuki S, Kikuchi S (2003) Effects of Neutralizing An-tibodies to Tumor Necrosis Factor-Alpha on Nucleus Pulposus-Induced Abnormal Nociresponses in Rat Dorsal Horn Neurons.Spine 28:967–972
11. Opree A, Kress M (2000) Involvement of the ProinflammatoryCytokines Tumor Necrosis Factor-Alpha, IL-1Beta, and IL-6 butnot IL-8 in the Development of Heat Hyperalgesia: Effects onHeat-Evoked Calcitonin Gene-Related Peptide Release from RatSkin. J Neurosci 20:6289–6293
12. Poole S, Cunha FQ, Ferreira SH (1999) Hyperalgesia from Sub-cutaneous Cytokines. In: Watkins LR, Maier SF (eds) Cytokinesand Pain. Birkhäuser, Basel, pp 59–87
13. Reeve AJ, Patel S, Fox A et al. (2000) Intrathecally Adminis-tered Endotoxin or Cytokines Produce Allodynia, Hyperalgesiaand Changes in Spinal Cord Neuronal Responses to NociceptiveStimuli in the Rat. Eur J Pain 4:247–257
14. Schäfers M, Geis C, Svensson CI et al. (2003) Selective Increaseof Tumour Necrosis Factor-Alpha in Injured and Spared Myeli-nated Primary Afferents after Chronic Constrictive Injury of RatSciatic Nerve. Eur J Neurosci 17:791–804
15. Schäfers M, Lee DH, Brors D et al. (2003a) Increased Sensitivityof Injured and Adjacent Uninjured Rat Primary Sensory Neuronsto Exogenous Tumor Necrosis Factor-Alpha after Spinal NerveLigation. J Neurosci 23:3028–3038
16. Sommer C (2001) Cytokines and Neuropathic Pain. In: HanssonP, Fields H, Hill R et al. (eds) Neuropathic Pain: Pathophysiologyand Treatment. IASP Press, Seattle, pp 37–62
17. Wagner R, Janjigian M, Myers RR (1998) Anti-InflammatoryInterleukin-10 Therapy in CCI Neuropathy Decreases ThermalHyperalgesia, Macrophage Recruitment, and Endoneurial TNF-Alpha Expression. Pain 74:35–42
18. WinkelsteinBA, Rutkowski MD, SweitzerSM et al. (2001) NerveInjury Proximal or Distal to the DRG Induces Similar SpinalGlial Activation and Selective Cytokine Expression but Differen-tial Behavioral Responses to Pharmacologic Treatment. J CompNeurol 439:127–139
Cytokines, Effects on NociceptorsVICTORIA C. J. WALLACE
Department of Anaesthetics, Pain Medicine andIntensive Care, Chelsea and Westminster HospitalCampus, London, [email protected]
Synonyms
Immunocytokines
Definition
Cytokinesarea family ofgrowth factorproteinssecretedprimarily from � leukocytes as part of the immune andinflammatory response.
Characteristics
Interactions with Peripheral Nociceptive Terminals
Proinflammatory cytokines, such as IL-1, TNF-α andIL-6, as well as other inflammatory mediators that cy-tokines influence as part of the inflammatory response,can directly stimulate and sensitise peripheral terminalsof small diameter � nociceptors (C-fibres) influencingtransduction and transmission of the nociceptive sig-nal contributing to � peripheral sensitisation (Fig 1a).For example, a subcutaneous injection of IL-1, TNF-αor IL-6 has been shown to directly excite peripheralnociceptive fibres (Poole et al. 1999). Also, TNF-α,which causes the subsequent release of IL-1, producesthermal hyperalgesia and mechanical allodynia, as wellas endoneurial inflammation, demyelination, and ax-onal degeneration whilst lowering C-fibre thresholdsand inducing ectopic activity in single primary afferentnociceptive fibers (Junger 2000). Such stimulation ofnociceptors not only results in signalling to the spinalcord, leading to sensation/perception of pain, but also toa local axon reflex. Importantly,SP acts directly via sur-face expressed NK1 receptors, to degranulate mast cellscausing release of histamine, which further sensitisenociceptive terminals, and proinflammatory cytokines,thus inducing a SP-cytokine positive-feedback loop.

C
Cytokines, Effects on Nociceptors 521
Cytokines, Effects on Nociceptors, Figure 1 (a) Interactions of cytokines with nociceptors at their peripheral terminals and in the DRG. Injurious stimuliinduce immune and inflammatory cells to release cytokines and chemokines, which stimulate further release of cytokines and non-cytokine inflammatorymediators such as prostaglandins (PGs), NGF and nitric oxide (NO) from various tissue cells. Cytokines and various inflammatory mediators such ashistamine (Hist) and bradykinin (BK) can activate nociceptor terminals to release neurotransmitters such as SP leading to neurogenic inflammation.Retrogradely transported signal proteins cause the release of cytokines and other factors from blood, neurones and glia (G) into the DRG which canactivate intracellular cascades (see 1b) regulating gene transcription, cell phenotype and excitability and therefore sensory transmission to the spinalcord. (b) Highlighted region in (1a) (dashed line) representing examples of some of the intracellular mechanisms of proinflammatory cytokine-inducedcell change. IL-1 via the IL-1R activates a number of protein kinase cascades including; protein tyrosine kinase (PTK), and protein kinase C (PKC)inducing intracellular Ca++ increase and phosphorylation of ion channels such as TRPV1 and others inducing changes in Na+ and Ca++ currents.Early events in all cascades involve MyD88, IL-1 receptor-associated kinase (IRAK-1) and a TNF receptor-associated factor (TRAF). Ras activation ofp38 MAP kinase (MAPK) and Rac mediated transactivation of gene expression by NFkB regulation also occur. The IL-6/IL-6R complex activates; JAKwhich recruits STAT3 to the phosphorylated receptor, gp130, and activates the Ras/MAP kinase pathway via the SHP-2 pathway ultimately affectingnuclear transcription factors such as CREB, c-fos, and c-jun. In contrast to such kinase signalling, the TNF/TNFR complex is regulated by intracellularadaptor proteins (TRADD and TRAF), via which it activates the IKK complex to phosphorylate IkB, liberating NFkB to the nucleus (see Hanada et al.2002; Obreja et al. 2002; Heinrich et al. 2003).
Proinflammatory cytokines can also modulate nocicep-tors indirectly, by stimulating the release of a variety ofpronociceptive inflammatory mediators such as; BK,which directly stimulates nociceptor terminals via BK
receptors (Dray 1997), also upregulated by proinflam-matory cytokines; prostaglandins, such as PGE2, whichcan be produced by almost all types of cells and is awell known key player in the inflammatory cascade and

522 Cytokines, Effects on Nociceptors
inflammatory hyperalgesia (Samad et al. 2002); and� chemokines (small chemottractant cytokines) suchas IL-8 (CXCL8) which in turn stimulate the produc-tion of � sympathomimetic amines capable of directlysensitising nociceptors (Sachs et al. 2001).Another major pronociceptive target of cytokine func-tion is NGF, which is released by a variety of cells at thesite of infection/inflammation in response to proinflam-matory cytokines, and plays a role in exaggerated painstates (Woolf et al. 1994) via direct (binding to TrκA re-ceptors on nociceptive fibers) and indirect (via cytokine-like actions, causing immune cells to accumulate and re-lease their cellular contents exciting nociceptive fibers)actions on the nociceptive function.Peripheral stimulation of nociceptive afferents canalso produce an axon reflex, in which � prodromicnerve impulses travelling up the sensory axon initiate� antidromic impulses in neighbouring axons. This re-sults in a release of � neuropeptides and � neurogenicinflammation at sites distant from the original stimuliincreasing the area of sensitivity.Such cytokine driven, neurogenic inflammatory loopsstimulate and sensitise nociceptors in the absence of fur-ther peripheral stimulation, which could, in theory, cre-ateenough ‘drive’ tocreateandmaintain spinalcordsen-sitisation, resulting in persisting pain.
Influences in the DRG
Cytokinescan also havedirect and indirect effectson no-ciceptor function, at the level of the DRG, resulting inexcitability and phenotypic changes. This contributes toaltered synaptic transmission in the spinal cord (centralsensitisation) involved in the development of hyperalge-sia and persistent pain (Fig. 1a). Levels of cytokines canincrease in the DRG following inflammation and nervedamage in response to signal proteins produced at thesite of damage, such as the cytokines LIF and IL-6 aswell as cytokine induced NGF, which are retrogradelytransported by both intact and injured axons (Watkinsand Maier 2000). Such signals can initiate the recruit-ment of immune cells to the DRG and induce prolifer-ation and activation of satellite (glial) cells, resulting inthe release of a variety of growth factors, including cy-tokines, into the extracellular fluid of the DRG wherethey modulate sensory neuron, and/or glial cell functionvia differentially expressed cytokine receptors. For ex-ample, the proinflammatory cytokines IL-1 and TNF-αbind directly to neuronally expressed receptors inducingrapid increases in sensory neuronal excitation, facilitat-ing pain transmission to the spinal cord. On the otherhand, the primary receptor for IL-6 (IL6-R) is predom-inantly expressed by glial cells and therefore IL-6, al-though produced by DRG neurons, likely affects noci-ceptor function indirectly (such as via Schwann cell re-lease of IL-1 and TNF-α), although receptor expressionis likely to change under pathological conditions (DeJongh 2003). In fact, even in the absence of nerve dam-
age or of any action at receptors expressed by peripheralnerveterminals,proinflammatorycytokinesactingintheDRG can rapidly induce aberrant responses in periph-eral nociceptors (Sorkin et al. 1997, Watkins and Meier2000).Retrogradely transported signals can also induce phe-notypic changes in primary sensory neurons, such as in-creased expression of BDNF, TRPV1, NAv1.8, CGRP,SP, and galanin (Watkins and Meier 2002), all of whichcan change the properties of nociceptive neurons.In the DRG, � G-protein coupled, chemokine � recep-tors are expressed by small diameter nociceptors,suggesting a direct involvement of chemokines in no-ciceptive signal transduction and the pathogenesis ofpain. This is supported by the fact that endogenouschemokines such as SDF1α/CXCL12, MDC/CCL22and RANTES/CCL5 or exogenous factors such as theHIV-1 coat protein gp120, which is a ligand at thechemokine receptors CXCR4 and CCR5, have beenshown to produce powerful excitatory effects on sen-sory neurons via increased calcium mobilization andthe lowering of the threshold for action potential gen-eration (Oh et al. 2001). Chemokine receptors are alsoexpressed by glial cells, the activation of which en-hances the release of neuroactive substances, includingNGF, NO, glutamate and other chemokines, whichcan further affect nociceptor activity and even lead toneurotoxicity.
Intracellular Mechanisms
Cytokines modulate nociceptor activity contributingto � neural plasticity and pain, via the initiation ofintracellular cascades of phosphorylation of constitu-tively expressed signal proteins involved in nociceptionand pain such as PKC, MAP kinase, Ras/Raf c-jun,c-fos and STAT (Fig 1b). As a result there are alter-ations to the transcription rate and/or posttranslationalchanges in proteins involved in the pain pathway,which ultimately lead to a modification of transduction,conduction and transmission functionality of theseneurons. For example, IL-1 binds to the specific cellsurface receptors, IL-1RI and IL-1RII; members ofthe Toll-like receptor superfamily of which IL-1R1 areexpressed by nociceptive neurons. IL-1RI-mediatedmechanisms, involving activation of tyrosine kinasesand PKC associated phosphorylation, lead to long last-ing increases in voltage-sensitive sodium and calciumchannel conductance, increasing excitability of thecell as well as changes in specific receptor function(Obreja et al. 2002). In nociceptors, this may includephopshorylation of heat-transducing vanilloid recep-tors; TRPV1 or TRPVL-1, supported by evidence thatIL-1β directly sensitises rat sensory neurons to heat.Downstream pathways of IL-1Rs and TNF-α recep-tors (TNFRI and TFNRII) ultimately activate NFκB,which modulates the expression of a variety of pro-teins implicated in nociceptor sensitivity and pain,

C
Cytokines, Regulation in Inflammation 523
including growth factors and inducible enzymes suchas cyclooxygenase 2 (COX2) and inducible nitric oxidesynthase (iNOS) (Hanada 2002). NFκB also promotesfurther proinflammatory cytokine and chemokine pro-duction, potentiating cytokine-mediated mechanismsof nociceptor excitability and signalling. In additionto receptor function, the TNF-α molecule itself maycause changes in neuronal excitability due to pH facil-itated insertion into lipid membranes, to form a centralpore-like region forming voltage-dependent sodiumchannels, which may not only be associated with thegeneration of neuronal hyperexcitability, but may inter-act with endogenous sodium and calcium channels toincrease membrane conductance (Kagan et al. 1992).In contrast, IL-6 signalling occurs via binding to theα-subunit non-signalling receptor IL-6R (gp80), whichleads to homodimerisation of the transmembranoussignalling transducer receptor gp130, which signalsintracellularly via the JAK/STAT pathways to influencegene expression via MAPK (Heinrich et al. 2003).IL-6R and gp130 are expressed predominantly on glialcells; however, although peripheral nociceptors lackIL-6R subunits under normal physiological conditions,they do express gp130 molecules, and the expressionpatterns of each have been reported to change followingnerve damage (De Jongh et al. 2003).
Antinociceptive Functions
In addition to the anti-inflammatory and antinocicep-tive function of cytokines, such as IL-10, IL-4 andIL-13 (Vale et al. 2003), there is evidence of the directinteraction of cytokines with nociceptors in an antinoci-ceptive manner. For example, IL-2 induces peripheral� antinociception via the IL-2R specific receptor,whichis expressed in small and medium (i. e. nociceptive)primary sensory neurons of DRG, and is transported tothe peripheral axon terminals (Song et al. 2000). Themechanism underlying cytokine-induced antinocicep-tion may include inhibition of neurotransmitter release,due to Ca2+ channel blocking properties decreasingnociceptor activity.
References1. De Jongh RF, Vissers KC, Meert TF, Booij LH, De Deyne CS,
Heylen RJ (2003) The Role of Interleukin-6 in Nociception andPain. Anesth Analg 96:1096–103
2. Dray A (1997) Kinins and their Receptors in Hyperalgesia. CanJ Physiol Pharmacol 75:704–712
3. Hanada T, Yoshimura A (2002) Regulation of Cytokine Signalingand Inflammation. Cytokine Growth Factor Rev 13:413–421
4. Heinrich PC, Behrmann I, Haan S, Hermanns HM, Muller-Newen G, Schaper F (2003) Principles of Interleukin (IL)-6-typeCytokine Signalling and its Regulation. Biochem J 374:1–20
5. Junger H, Sorkin LS (2000) Nociceptive and Inflammatory Ef-fects of Subcutaneous TNF-alpha. Pain 85:145–151
6. Kagan BL, Baldwin RL, Munoz D, Wisnieski BJ (1992) For-mation of Ion-Permeable Channels by Tumor Necrosis Factor-Alpha. Science 255:1427–1430
7. Obreja O, Rathee PK, Lips KS, Distler C, Kress M (2002) IL-1Beta Potentiates Heat-Activated Currents in Rat Sensory Neu-
rons: Involvement of IL-1RI, Tyrosine Kinase and Protein KinaseC. FASEB J 16:1497–1503
8. Oh SB, Tran PB, Gillard SE, Hurley RW, Hammond DL, MillerRJ (2001) Chemokines and Glycoprotein120 Produce Pain Hy-persensitivity by Directly Exciting Primary Nociceptive Neu-rons. J Neurosci 21:5027–5035
9. Poole S, Cunha FDQ, Ferreira SH (1999) Hyperalgesia from Sub-cutaneous Cytokines. In: Watkins LR, Maier SF (eds) Cytokinesand Pain. Birkhauser, Basel, pp 59–88
10. Samad TA, Sapirstein A, Woolf CJ (2002) Prostanoids and Pain:Unraveling Mechanisms and Revealing Therapeutic Targets.Trends Mol Med 8:390–396
11. Song J, Jang YY, Shin YK, Lee C, Chung S (2000) N-Ethylmaleimide Modulation of Tetrodotoxin-Sensitive andTetrodotoxin-Resistant Sodium Channels in Rat Dorsal RootGanglion Neurons. Brain Res 855:267–273
12. Sorkin LS, Xiao WH, Wagner R, Myers RR (1997) TumourNecrosis Factor-Alpha Induces Ectopic Activity in NociceptivePrimary Afferent Fibres. Neuroscience 81:255–262
13. Watkins LR, Maier SF (2000) The Pain of Being Sick: Impli-cations of Immune-to-Brain Communication for UnderstandingPain. Annu Rev Psychol 51:29–57
14. Watkins LR, Maier SF (2002) Beyond Neurons: Evidence thatImmune and Glial Cells Contribute to Pathological Pain States.Physiol Rev 82:981–1011
15. Woolf CJ, Safieh-Garabedian B, Ma QP, Crilly P, Winter J (1994)Nerve Growth Factor Contributes to the Generation of Inflam-matory Sensory Hypersensitivity. Neuroscience 62:327–331
Cytokines, Regulation in InflammationVICTORIA WALLACE
Department of Anaesthetics, Pain Medicine andIntensive Care, Chelsea and Westminster HospitalCampus, London, [email protected]
Synonyms
Immunocytokines
Definition� Cytokines are a large family of growth factor proteins(MW 8-30 kD) secreted primarily from leukocytes (aswell as a variety of cells) as part of the immune and in-flammatory response.
Characteristics
Over 150 cytokines have been cloned, which may begrouped into various sub-families, based upon func-tional properties and receptor utilisation, althoughnomenclature is somewhat confusing and arbitrary(Vilcek 1998). Cytokines that are particularly in-volved in regulation of inflammation are termed the� proinflammatory cytokines (which can also encom-pass the inflammatory chemokines) and the � antiinflammatory cytokines.
Proinflammatory Cytokines
The major proinflammatory cytokines include tumournecrosis factor-α (TNF-α), interleukin-1α and β (IL-1α

524 Cytokines, Regulation in Inflammation
and β) and interleukin-6 (IL-6), which are secreted ina sequential cascade (TNF-α>IL-1>IL-6), by a varietyof immune and inflammatory cells, in response to in-flammation. A wealth of literature supports a role forproinflammatory cytokines in the production of inflam-mation associated pain and hyperalgesia. For example,pain associated with signs of inflammation after periph-eral nerve injury in rodents correlates with the number ofproinflammatory cytokine-producing cells at the injurysite; and thermal hyperalgesia and mechanical allody-nia can be reduced via the blockade of IL-1 or TNF-α(Watkins and Meier 2000). Furthermore, an intraplantarinjection of TNF-α results in hyperalgesia, which lastsfor several hours and can be associated with a cascade ofcytokine involvement, including IL-1 followed by IL-6,as well as the activation of IL-8 (Junger et al. 2000).TNF-α, a member of the TNF family of cytokinesis produced primarily by macrophages, and acts viathe TNFRI and TNFRII receptors (Orlinick and Chao1998). Binding of TNF-α triggers intracellular sig-nalling cascades to induce changes in gene expression,mainly via the activation of NFκB. Effects can in-clude the upregulation of; proinflammatory cytokines,adhesion molecules, chemokines, growth factors, in-ducible enzymes such as cyclooxygenase 2 (COX2)and inducible nitric oxide synthase (iNOS) (Hanada2002), all of which can have effects on mechanisms ofnociception. Importantly, TNF-α induces productionof IL-1, a member of the interleukin family, which isproduced in two molecular forms (α and β) by manycell types including mononuclear cells, fibroblasts,synoviocytes, macrophages, keratinocytes, mast cells,glial cells, and neurons (Bianchi 1998). Additionally,the inactive precursor of IL-1 (pro-IL-1) is constantlyproduced by keratinocytes and fibroblasts in the skin,and in increasing amounts following tissue damage,during which degranulation of mast cells releases theenzyme, chymase, which cleaves the IL-1 precursor toits active form. IL-1 binds to the specific cell surfacereceptors, IL-1RI and IL-1RII, which are membersof the Toll-like receptor superfamily. Like TNF-α, theproinflammatory and pronociceptive actions of IL-1 aremediated via complex intracellular signalling cascadesthat ultimately activate NFκB. In the context of pain,IL-1 is likely to be the most important proinflammatorycytokine, with many outcomes of other proinflamma-tory cytokine actions occurring via IL-1 release. In mostcell types, IL-1 and TNF-α induce the release of IL-6, amember of the neuropoetic cytokine family. IL-6 playsa minimal role in inducing inflammatory mediatorsor other inflammatory cytokines in tissues, althoughmay play a role in inducing chemokine production.IL-6 binds to the α-subunit non-signalling receptor,IL-6R (gap80), leading to homodimerisation of thetransmembranous signal transducer receptor, gp130,and an intracellulular cascade of phosphorylation (DeJongh 2003). This affects cell activity and initiates the
release of many cell specific � neuroactive substancesand inflammatory substances.In general, proinflammatory cytokines act to increasevascular endothelial membrane permeability, and in-duce upregulation of endothelial adhesion moleculesand thus leukocyte adhesion, migration and extrava-sation. Due to a self-promoting cytokine loop, thereis a rapid accumulation of proinflammatory cytokinesat the site of damage, ensuring a rapid onset of theinflammatory response (Fig. 1).In the context of pain, which is a key component ofthe inflammatory response designed to prevent fur-ther insult to the damaged site, it is important to notethat proinflammatory cytokines are released from andact upon neurones and glial cell, via which they sig-nal to the brain that infection or injury has occurred(Watkins and Maier 2000; Watkins and Maier 2002).This � neuroimmune interaction can influence mech-anisms implicated in the development of hyperalgesiaand persistent pain, which are associated with many in-flammatory conditions. For example, cytokines releasedin damaged tissue can activate peripheral terminals ofprimary sensory neurones either directly, via neuronallyexpressed cytokine receptors, or indirectly via the stim-ulation of other substances that have relevance to theproduction of pain such as prostaglandins, nitric oxideand nerve growth factor (NGF) (see � cytokines, effectson nociceptors ). Such activation enhances the releaseof neuroactive transmitters, such as � substance P (SP),enhancing neurogenic inflammation leading to sensi-tisation and increased excitability of sensory primaryafferents (Fig. 1) (Black 2002). Inflammation of, ordamage to, the peripheral nerve itself causes the activa-tion of recruited and resident macrophages, fibroblasts,mast cells, dendritic cells, and endothelial cells, all ofwhich can release proinflammatory cytokines which,due to their induction of oedema-associated disruptionof the � blood nerve barrier, can lead to further immuneinvasion of the nervous system. Furthermore, activatedSchwann cells, which myelinate peripheral nerves, re-lease proinflammatory cytokines (as well as many otherdamaging substances such as NO, ROS, PGs and ATP).This can damage myelin, with resulting demyelinationand/or nerve degeneration (� Wallerian degeneration),all of which can be associated with the development ofpain.
Chemokines
Chemokines are a family of small chemoattractantcytokines (MW 8-10kDa) that have potent leukocyteactivation and/or chemotactic activity. Over 50 havebeen identified so far, the majority of which are classedinto the CC group or CXC group based in their cys-teine residues. Via actions on their specific G-proteincoupled receptors, chemokines are intimately involvedin the orchestration of inflammatory responses, by in-ducing cell migration across a concentration gradient.

C
Cytokines, Regulation in Inflammation 525
Cytokines, Regulation in Inflammation, Figure 1 A representation of the network of cytokine production in tissue, following typical injurious stimuli.Degranulation of local and infiltrating mast cells releases proinflammatory cytokines which stimulate further cytokine release from macrophages (Mac)attracted to the site of injury to phagocytose pathogens (* ), a process which in itself triggers cytokine production. Cytokines act to increase vascularpermeability inducing leukocyte extravasation and further stimulating release of cytokines and non-cytokine inflammatory mediators such as PGs, growthfactors and NO from various tissue cells (TC). IL-1 is also formed from its precursor pro-IL1 and chemokines are secreted enhancing further leukocytemigration from the bloodstream. Cytokines and various inflammatory mediators such as histamine and BK can activate primary sensory neurones torelease neurotransmitters such as SP. Activation of Schwann cells causes further cytokine and chemokine release which can cause demyelination anddegeneration of 1y afferents.
Although most pain research related to neuroimmunefunction has focussed on proinflammatory cytokines,the involvement of chemokines in inflammatory painand hyperalgesia has become more apparent (Boddeke2001). In addition to immune cells, many nervous sys-tem cells (neuronaland glial) arecapableof synthesisingchemokines and express a variety of chemokine recep-tors, suggesting that chemokines act as messengersbetween peripheral immune cells and sensory afferentneuronsfrominflamedsites.Evidencesupportsarolefora number of chemokines in inflammation and pain suchas IL-8/CXCL8 (Bodekke 2001), SDF1α/CXCL12,MDC/CCL22 and RANTES/CCL5 (Oh et al. 2001),which may act to increase intracellular calcium and,therefore, cell excitability and release.
Limiting Actions of Cytokines
Since cytokines are potent mediators of potentiallydamaging tissue responses, several mechanisms existto ensure that the effects of these cytokines are re-stricted, thereby limiting the inflammatory response.
For example, the IL-1 receptor antagonist (IL-1ra),a member of the interleukin cytokine family, is up-regulated during inflammation and prevents bindingof IL-1 to its receptors (Hopkins 2003). Additionally,the cellular receptors for both IL-1 and TNF-α existin soluble forms, and are able to bind and neutralisetheir cytokine ligands after being cleaved from the cellsurface. Some cytokines, such as IL-10, IL-4 (Hamiltonet al. 2002) and LIF (see Gadient and Patterson 1999),have anti-inflammatory activity and are able to down-regulate expression of pro-inflammatory cytokines. Theactual role of LIF is however controversial, and has beenimplicated as a proinflammatory cytokine (McKenzieet al. 1996) and as an anti-inflammatory and analgesiccytokine (Banner et al. 1997). It is likely that the in-creased activation of leukocytes and, therefore, releaseof proinflammatory cytokines, characteristic of chronicinflammation and associated persistent pain, involvesa dysfunction of these negative regulatory mechanismsleading to sustained positive feedback cytokine-neuralinteractions.

526 Cytoprotection
References
1. Banner LR, Patterson PH, Allchorne A, Poole S, Woolf CJ (1998)Leukemia Inhibitory Factor is an Anti-Inflammatory and Anal-gesic Cytokine. J Neurosci 18:5456–5462
2. Bianchi M, Dib B, Panerai AE (1998) Interleukin-1 and Noci-ception in the Rat. J Neurosci Res 53:645–650
3. Black PH (2002) Stress and the Inflammatory Response: AReview of Neurogenic Inflammation. Brain Behav Immun16:622–653
4. Boddeke EW (2001) Involvement of Chemokines in Pain. EurJ Pharmacol 429:115–119
5. De Jongh RF, Vissers KC, Meert TF, Booij LH, De Deyne CS,Heylen RJ (2003) The Role of Interleukin-6 in Nociception andPain. Anesth Analg 96:1096–103
6. Gadient RA, Patterson PH (1999) Leukemia Inhibitory Factor,Interleukin 6, and Other Cytokines Using the GP130 Trans-ducing Receptor: Roles in Inflammation and Injury. Stem Cells17:127–137
7. Hamilton TA, Ohmori Y, Tebo J (2002) Regulation of ChemokineExpression by Anti-Inflammatory Cytokines. Immunol Res25:229–245
8. Hanada T, Yoshimura A (2002) Regulation of Cytokine Signalingand Inflammation. Cytokine Growth Factor Rev 13:413–421
9. Hopkins SJ (2003) The Pathophysiological Role of Cytokines.Leg Med (Tokyo) 5 Suppl 1:S45–S57
10. Junger H, Sorkin LS (2000) Nociceptive and Inflammatory Ef-fects of Subcutaneous TNFalpha. Pain 85:145–151
11. Oh SB, Tran PB, Gillard SE, Hurley RW, Hammond DL, MillerRJ (2001) Chemokines and Glycoprotein120 Produce Pain Hy-persensitivity by Directly Exciting Primary Nociceptive Neu-rons. J Neurosci 21:5027–5035
12. Orlinick JR, Chao MV (1998) TNF-Related Ligands and TheirReceptors. Cell Signal 10:543–551
13. Vilcek J (1998). The cytokines: an overview. In: Thomson A (ed)The Cytokine Handbook, 3rd edn. Academic Press, San Diego,pp 1–20
14. Watkins LR, Maier SF (2000) The Pain of Being Sick: Impli-cations of Immune-to-Brain Communication for UnderstandingPain. Annu Rev Psychol 51:29–57
15. Watkins LR, Maier SF (2002) Beyond Neurons: Evidence thatImmune and Glial Cells Contribute to Pathological Pain States.Physiol Rev 82:981–1011
Cytoprotection
Definition
As applied to the gastrointestinal tract, cytoprotectionindicates the development of mechanisms that protectthe tract from damage from the digestive enzymes and,in the stomach and duodenum, from the acidic contents.� NSAIDs and their Indications
Cytoskeleton
Definition
Thescaffold structuresofcells, alsocytoskeletal system.� Toxic Neuropathies




















