
BRAC Maternity Centers Report (2015), by Natasha Merali
21
BRAC MATERNITY CENTERS REPORT – MANOSHI PROGRAMME MATERNAL, NEONATAL & CHILD HEALTH DIVISION Under BRAC’s Maternal, Neonatal and Child Health department, Manoshi was founded in 2007 with the financial assistance of the Bill & Melinda Gates Foundation as a five-year pilot program. The program strives to aid Bangladesh in achieving the Millennium Development Goals of reducing maternal, neonatal, and child mortality rates by the year 2015. The objective of the Manoshi Project in particular is to promote reproductive health education within urban slums through integrated maternity centers and community health workers, and to reduce overall illness and preventable deaths in mothers, newborns, and children across the country. The Strategic Partnership Agreement (SPA) now primarily funds Manoshi. The program was created as a result of the high maternal, neonatal and child mortality and morbidity, in consonance with rising migration and population growth in urban slums. In 2007, 86% of births were home-deliveries, and only 8% of expectant mothers received at least four sessions of antenatal care. If and when complications occur at home, there is no emergency call services currently available, leaving women unable to receive professional help. With previously inadequate access to skilled human resources and functional health facilities, the need for demographic and community- specific care was evident. Consequently, Manoshi operates through capacity and human resources development, and delivery of an integrated community-based package of essential health services. The primary aim of this holistic approach is to ultimately engage underserved populations in a previously isolated healthcare system, empowering women and families to make educated decisions regarding their health and that of their children. Along with an elaborate referral system between households, delivery centers, and hospitals, Manoshi provides basic primary healthcare to mothers and children until the age of five, as well as links local communities with various governmental and non-governmental organizations to further their goals. To increase access to reproductive health resources in Bangladesh, BRAC’s Manoshi Project opened multiple Delivery Centers in 2007 across urban slums, which serve to offer 24/7 women centric, culturally appropriate, and safe delivery care whilst ensuring cleanliness, privacy, and dignity. These centers are regarded as an intermediate between home and hospital deliveries to allow for the comfort of being in an intimate, yet safe environment. Through an array of community health workers who work through both household visits and birth monitoring at centers, the Delivery Centers seek to educate and provide women with fundamental antenatal, pregnancy, and postnatal care. Today, each delivery center covers approximately 10,000 people, reaching about 6.9 million in 11 city districts across Bangladesh. While the Delivery Centers are situated within close proximity of the slum community households, the birth attendants and community health workers present are often unequipped to handle complicated cases, leading to high rates of hospital referrals. Accordingly, 5 pilot “upgraded delivery centers” called BRAC Maternity Centers (BMCs), were established in the later months of 2011, to provide a better set up with more options for mothers and households. At these updated and more spacious centers, antenatal and postnatal check-ups occur on-site, and with more trained and specialized health workers, the centers are able to better manage complications and thus reduce referral rates. Out of the 357 Delivery Centers, 27 have currently been upgraded to BRAC Maternity Centers. OVERVIEW
Transcript of BRAC Maternity Centers Report (2015), by Natasha Merali

BRAC MATERNITY CENTERS REPORT – MANOSHI PROGRAMME MATERNAL, NEONATAL & CHILD HEALTH DIVISION
Under BRAC’s Maternal, Neonatal and Child Health department, Manoshi was founded in 2007
with the financial assistance of the Bill & Melinda Gates Foundation as a five-year pilot program. The program strives to aid Bangladesh in achieving the Millennium Development Goals of reducing maternal, neonatal, and child mortality rates by the year 2015. The objective of the Manoshi Project in particular is to promote reproductive health education within urban slums through integrated maternity centers and community health workers, and to reduce overall illness and preventable deaths in mothers, newborns, and children across the country. The Strategic Partnership Agreement (SPA) now primarily funds Manoshi.
The program was created as a result of the high maternal, neonatal and child mortality and morbidity, in consonance with rising migration and population growth in urban slums. In 2007, 86% of births were home-deliveries, and only 8% of expectant mothers received at least four sessions of antenatal care. If and when complications occur at home, there is no emergency call services currently available, leaving women unable to receive professional help. With previously inadequate access to skilled human resources and functional health facilities, the need for demographic and community-specific care was evident. Consequently, Manoshi operates through capacity and human resources development, and delivery of an integrated community-based package of essential health services. The primary aim of this holistic approach is to ultimately engage underserved populations in a previously isolated healthcare system, empowering women and families to make educated decisions regarding their health and that of their children. Along with an elaborate referral system between households, delivery centers, and hospitals, Manoshi provides basic primary healthcare to mothers and children until the age of five, as well as links local communities with various governmental and non-governmental organizations to further their goals.
To increase access to reproductive health resources in Bangladesh, BRAC’s Manoshi Project opened multiple Delivery Centers in 2007 across urban slums, which serve to offer 24/7 women centric, culturally appropriate, and safe delivery care whilst ensuring cleanliness, privacy, and dignity. These centers are regarded as an intermediate between home and hospital deliveries to allow for the comfort of being in an intimate, yet safe environment. Through an array of community health workers who work through both household visits and birth monitoring at centers, the Delivery Centers seek to educate and provide women with fundamental antenatal, pregnancy, and postnatal care. Today, each delivery center covers approximately 10,000 people, reaching about 6.9 million in 11 city districts across Bangladesh.
While the Delivery Centers are situated within close proximity of the slum community
households, the birth attendants and community health workers present are often unequipped to handle complicated cases, leading to high rates of hospital referrals. Accordingly, 5 pilot “upgraded delivery centers” called BRAC Maternity Centers (BMCs), were established in the later months of 2011, to provide a better set up with more options for mothers and households. At these updated and more spacious centers, antenatal and postnatal check-ups occur on-site, and with more trained and specialized health workers, the centers are able to better manage complications and thus reduce referral rates. Out of the 357 Delivery Centers, 27 have currently been upgraded to BRAC Maternity Centers.
OVERVIEW

Why Upgrade? “To establish a maternity center through a community approach and deliver integrated qualitative, and cost effective health services for improving maternal and neonatal health while reducing mortality and morbidity.”
The need to upgrade from Delivery Centers to BMCs came at request from the Maternal, Neonatal & Child Health Committee (a group consisting of 9 to 11 local respected community members such as NGO workers, BRAC volunteers, local elites, business professionals, and teachers). This community-driven demand arose from the desire for “a better set up with more options” for women and their children, to increase skilled deliveries by health workers, and to extend the acceptability and popularity of BRAC reproductive services among the local urban slum communities and those who are not already Manoshi beneficiaries.
As previous Delivery Centers offered limited or no space for pre-delivery waiting, support groups meetings, family reception area, and regular check-ups, both staff and attending women mandated centers with the appropriate resources capable of catering to more comprehensive needs and services. In order to meet these new standards, larger spaces were attained, and higher skilled and more specialized health professionals were placed and trained to recognize and manage various maternal and neonatal complications, thus also abating the need to unnecessarily refer cases to hospitals, where quality care is not always guaranteed and access to transportation services is not readily available. So as to promote continued financial sustainability, BMCs operate on a fee-for-service basis, further outlined below. Overall, the introduction and maintenance of BRAC Maternity Centers has led to increased number of successful deliveries at the center, reduction of referrals, decreased sepsis occurrence, improved management of cases, better awareness and educational services throughout the duration of pregnancy and until the child is five years of age.
Enhanced characteristics of new BRAC Maternity Centers (BMCs): 1. Pregnancy and Labor Complication Management – Due to the low number of skilled medical
workers at the Delivery center, a high amount of referrals would take place for all complicated cases. At the BMCs, the medical officer and MMWs are able to handle a range of complications including post-partum hemorrhage, early management of Eclampsia, provision of Episiotomy, repair of second degree perineal tear, decreased oxygen levels, urinary catheterization for urinary retention, and birth Asphyxia management. This increase in skill level has decreased the need for high-referral rates, and hospital referrals are only made when necessary.
MMWs are BRAC project staff, and are trained paramedics or nurses. Prior to beginning work at Manoshi, they are required to complete basic EoC training from Azimpur Maternity and LAMB Hospital for 8 weeks. They also have a mandatory skills-based training for 15 days prior to their work start date at BMCs. While Manoshi Midwives (MMWs) were available during the daytime to assist in deliveries and related activities at the delivery centers, there were only 2-3 MMWs per branch. Given the 24/7-operation schedule of the centers, it was difficult for MMWs to contribute in a maximum capacity. In branches that have updated Maternity Centers under their
SERVICE DELIVERY

jurisdiction, there are now 4 MMW that operate on a rotation – three MMWs are always staffed in the centers, while the other midwife makes rounds in the field to provide support and assistance to families who may not come to the center.
Medical Officers (MOs): The existing Manoshi regional MOs perform medical check-ups to patients once a week at the BMCs. MMWs are able to consult medical officers on the management of complications, and other gestational, antenatal and postnatal matters.
2. Spatial Improvements – The Centers have adequate space (at least four rooms), allowing for better privacy, comfort, and individualized care of mothers and newborns. Manoshi aims to have at least one BMC in each regional branch. When selecting Maternity Center, it must be situated within close distance of other delivery centers and referral locations, ensuring easy communication and transportation within slum and surrounding area.
BMCs are well equipped and are regularly cleaned to maintain a hygienic and safe environment. (Urban Birthing Attendants assist with daily cleaning of the centers).
Located in a well maintained building, and situated conveniently in the middle of the respective slum area, promoting easy access and quick referral times.
4 different rooms (reception, pre and post-labor observation room, check-up room, labor room with two areas for traditional birth and a table with stirrups for complications, as well as a small kitchen with space for hand-washing). These separations ensure privacy, while also allowing multiple activities to take place simultaneously.
BMCs have sterilized and more tools, kept sanitized by the autoclave. BMC staff are trained to use autoclave and keep area hygienic and safe.
3. Fee-for-service – In keeping with the need for a sustainable and cost-effective model of BRAC Maternity Centers, BMCs operate on a fee-for-service basis. Not everyone who comes to the center is required to pay if they do not have the financial ability to do so, but most patients are able to afford the BRAC subsidized prices. Attending support groups are currently free, to encourage participation and attendance.
Currently, approximately 90% of patients pay for the services provided by the BMC. Not only does this approach promote cost recovery, but it also empowers women and families by
allowing them to save and pay for the services they receive. Rather than being entirely dependent on BRAC and the affiliated centers for paying for their services, families are encouraged and supported in financial planning prior to deliveries to ensure they have enough money well in advance of the birth.
The prices for the basic standard services are outline below:
Service Price (Tk): Price (USD): Natural Delivery 1000 Tk $12 ANC/PNC visit 40 Tk $0.50 Complication 1200 Tk $15

Continued Delivery Center & BMC Strategies: 1. Behavior Change Communication – This means of intervention aims to raise awareness and
generate sustainable healthy behavior changes based on BRAC-developed messages. The current Behavior Change Communication tools are:
Face-to-face counseling for targeted program participants by community health volunteers and workers during visits to maternity centers to build support system and trust of health professionals.
Pamphlets, posters, and stickers are distributed to raise awareness of maternal, neonatal, and child health risks and disease prevention. Topics include: pregnancy and post-partum danger signs, proper breastfeeding techniques, child infection/cold/fever recognition, pneumonia and remedies, management of diarrhea, etc.
Spouse Forum: Targets the men in the community and households with the goal of involving and educating husbands to assist in pregnancy process, and post-delivery care.
EDD Meeting: A support group conducted by Midwives, in the presence of SS and SK for women in their last trimester who are nearing their delivery date. Discussions involve financial planning for delivery or complications, arrangement of location and transport, deciding who will be present during birth, as well as the education of proper newborn care and feeding.
2. Culturally Sensitive Material and Interactions – Discussions regarding pregnancy and reproductive health are often considered stigmatized topics in regions such as Bangladesh’s urban slums. Through education and adaptation, Manoshi staff and community health workers aim to bring women’s health issues to the surface while being respectful of cultural and religious traditions.
On visits to households by SSs and SKs, they would provide expectant mothers with posters that outlined pregnancy tips and risks, neonatal care, and important phone numbers. However, due to the sensitive nature of the material and pictures, it was found that family members did not feel comfortable putting such posters on the walls of the home in view of others.
In order to address this issue SKs, and MMWs, now provide a “Maternal & Child Health” (MCH) Handbook. In addition to important phone numbers on the cover, educational information and pictures, the handbook allows for space to input educational information, personal history, immunization, and services provided to mothers and their children – in other words, it stands as their “Health Passport.”
3. Management of Health Workers – Through an interdisciplinary team of BRAC officials, health
professionals, and local volunteers, the Maternity Centers are able to link slum households to effective healthcare, education, and support prior, during, and after deliveries. The key roles taken on by the community health workers are as follows:
Shasthya Shebikas (SS): Frontline community health workers from the local area responsible for visiting approximately 200 households, taking note of expectant mothers, newborns, and children under five-years of age.
o Their role is primarily to encourage pregnant women to deliver at Maternity or Delivery Center for safety and hygiene purposes, and attend ANC and PNC sessions at BMC.
o Also responsible for: couple follow up, providing Misoprostol to reduce post-partum hemorrhage, arrange for referral of complicated cases, be present during child birth and provide essential newborn care, supervise local birthing attendant, motivate for immunization and Vitamin A.
o They are authorized to sell delivery kits, sanitary napkins, and basic vitamin and mineral supplements. SSs are also trained to recognize ten common deficiencies and diseases, such as birth asphyxia, neonatal sepsis, ARI, and diarrhea.
Shasthya Kormis (SK): Each SK supervises 10 SSs, covering a total of 2000 households. She conducts home visits according to SS’s gathered information, registers expectant mothers, and provides antenatal care. SKs must be educated to at least a grade 10 level, and receive training for Antenatal and Postnatal Care.
o In addition to reiterating the responsibilities of the SS, they help to provide fundamental health education to expectant mothers, birth weight measurement and monitoring, local birthing attendant management, ensure referral for complications, and supportive assistance to SSs.
o SKs receive quarterly three-day refresher trainings on technical issues conducted by Medical Officers.
Urban Birth Attendants (UBA): Although BMCs do not encourage traditional birthing methods that occur at home, without engaging UBAs and including them in the delivery environment, it is unlikely that women would feel comfortable in coming to the Delivery Centers. In order to prevent malpractice of UBAs during delivery, they are taught “Do’s and Don’ts” of delivering a newborn.
o At the BMC, where assisting in births is primarily the role of MMWs and medical officers, the UBAs are responsible for keeping the centers neat and clean, to manage waste, and clean the instruments after use (those that do not need to be autoclaved).
Manoshi Midwives (MMW): MMWs are a critical component to ensuring the safety of the pregnancy, delivery, and post-delivery care. Four MMWs per branch are assigned to a rotation schedule at the BMC and field. Midwives must be previously trained as a paramedic or nurse, and are assigned a salary according to their skills and educational background.
o Their responsibilities include handling deliveries, providing ANC and PNC at BMC, managing UBAs, holding support groups and Expected Delivery Date (EDD) meetings, use of medicines when appropriate, reduce complications, recording patient visits and services in MCH Handbook. In the field, MMWs also provide follow-up visits at regular intervals, and inform and encourage family planning methods.

Organization:
4. Antenatal and Postnatal Care – Manoshi places a strong emphasis on the provision of antenatal care (ANC) and postnatal care (PNC) through household visits. While SSs and SKs are able to visit individual families within the local communities, part of their role includes encouragement of women to attend at least four ANC sessions. SSs and SKs also help with scheduling of visits to maintain regularity and continuum of care for. Visits are recorded in their MCH handbook, which they are given when they first register at their nearest center.
Antenatal Care: The SKs provide four mandatory ANC sessions through household visits. MMWs and Medical Officers provide regular medical check-ups, and women support groups at the BMC, along with various other services:
o Physical examinations, education on healthy, hygienic and risk-free practices, counseling on gestational nutrition (such as iron-folic acid supplementation), immunization (such as Tetanus Toxoid), financial planning, education on recognition and management of danger signs, birth and emergency preparedness (such as blood grouping, planning transportation arrangements, and deciding who will be present during the delivery).
o SSs can also sell pre-packaged “Delivery Kits,” which contain basic supplements and information for the birthing process. However, if women come to the Delivery Center or BMC, they receive it for free.
o SKs perform examination of blood pressure, detection of anemia, edema and jaundice, and external abdominal examination to measure the fundal height as well as observe the presentation status of the fetus.
Central Level Management [Director, Program Coordinator, Program Manager]
Field Level Management [1 Medical Officer per region, 1 Regional Manager per 7-8 Branches, 1 Branch Manager per 3-4 Program Organizer]
Community Health Workers
Program Organizer (PO) [1 PO per 4-5 SK]
Manoshi Midwife (MMW) [2-3 MMW per Branch, 4 per Branch with BMC]
Shasthya Kormi (SK) [1 SK per 10 SS]
Shasthya Shebika (SS) [1 SK per 200 Households]
Urban Birth Attendant (UBA) [1 per Delivery Center, 1 per BMC]

Postnatal Care: PNC visits are scheduled days 1, 3, 7, 28, and 42 days post-partum with special visit on day 14 for babies who demonstrate low-birth weight. Mothers are also strongly encouraged to stay at BMCs for up to 12 hours after giving birth for observation and monitoring vitals of both new mother and child. PNC care includes the following:
o Immediate care: Mothers are given misoprostol tablets (400 micrograms) during the third stage of labor after the delivery of the baby and prior to the delivery of the placenta to reduce postpartum blood loss. They are taught to keep the baby warm, and to identify and report and danger signs during the neonatal period, and UBA will weigh newborns.
o Post-Immediate care: MMWs and MOs are trained to help with management of birth asphyxia, sepsis management. Immunization planning is provided, and vitamin A supplementation is also given. Mothers receive health education on newborn care, motivation for exclusive breastfeeding, and at later ages, complimentary feeding.
o For babies and children who are underweight, quarterly visits ensure proper nutrition is provided, and mothers are taught how to make suitable and easy-to-make food for baby given available resources.
Family Planning: Family planning allows individuals and couples to anticipate and attain their desired number of children through safe practices and contraceptive methods. It has been shown that a women’s ability to space and limit her pregnancies has a direct impact on her health and well-being, as well as on the outcome of each pregnancy (WHO).
o During daily household visits, the SSs meet with eligible couples within their respective regions and discuss with them the importance of family planning. They motivate couples to use contraceptive methods, and sell condoms or pills according to their preference.
o SKs follow up with contraceptive users through regular household visits, and encourage eligible couples to consider a gradual transition from short-term to long-term/permanent family planning methods.
5. Extensive Referral System – Manoshi has established an integrative referral system that spans from
the frontline community workers, BRAC staff, delivery and maternity centers, to various health facilities with which BRAC holds a Memorandum of Understanding (MoU). An outline of the referral process is shown in the figure below.
Incentives: In order to encourage continuum of care through the referral system, SSs are offered incentives at all levels of the scheme. This includes when she informs her SK about household news, when she brings a woman to the delivery or maternity centers, when she attends support groups, and when she is present for a birth. Not only does this allow for decreased home deliveries and increased usage of maternity centers, but it allows encourages SSs to learn about the health and care for mothers and neonates.
Reducing Delays: In order to guarantee timely management and care of expectant mothers prior to and during delivery, Manoshi has set up methods to address delays at three different stages.
o 1st Delay – Ensuring early recognition of labor and complications: Teaching women and families how to identify danger signs and reduce risk-factors, giving women numbers for Delivery Center/BMC staff including SS, SK, MMW, and PO (Program Organizer) for emergency communication, and providing community support network and educational information.

o 2nd Delay – Organized and swift transport to Health Professionals or Hospital: Prior arrangement of transportation services, and who will accompany expectant mother to Delivery Center/BMC/Hospital, building MoUs with private ambulance providers.
o 3rd Delay – Efficient management of mother at destination: MoU with private and NGO clinics and/or hospitals, coordination with public facilities, referral program organizers, arranging physical and financial support.
Hospital Complication Management: For complicated cases that do need to be managed in a better-equipped hospital setting, expectant mothers, Delivery Centers, and BMCs are given the referral phone numbers. If a phone call is received, the BRAC staff will arrange pick-up and transportation to the nearest hospital – if ambulances are not available, they will take expectant mother and accompanying relative to the hospital by motor rickshaw.
o Once at the hospital, patients may not be familiar with the environment and there are usually long waits, delaying treatment of pregnancy complications. For this reason, the referral PO will assist the woman through her hospital process and ensure medical professionals are there to attend to her needs.
Maternal Deaths: Over seven years of intervention, Manoshi has been able to reduce maternal mortality rates significantly (294 per 100,000 live births in 2008, to 132 per 100,000 live births in 2012). For the maternal deaths to do occur, death audits take place to evaluate each deceased individual and provide further insight on how to avert similar deaths.
o Following the death of a mother or newborn, SS/SK/MMW/MO will call and immediately notify PO or Branch Manager. PO will arrive at site of death to collect basic information of the deceased (name, age, time and date of death, and management provided by care provider, probably cause of death, who was involved in assisting the individual before death, etc.). POs will pass along information to Regional Manager through the Branch Manager via SMS. The message is then sent to the Head office for death notification.
o Head Office staff performs social autopsy in the presence of MNCH committee at house of the deceased within 3-5 of death. This allows the community members to understand what steps will be taken in the future to prevent cause of death. Within 7-10 days, Manoshi Medical Officers perform verbal autopsy, and interview with the family members using a standard verbal autopsy questionnaire. All death audits are then analyzed to establish actual cause of death, and whether it was due to a medical cause or programmatic gap.
o Most common causes of maternal death between 2008-2012 [n=600] were Hemorrhage (30.6%) and Eclampsia (20.5%). The majority of maternal deaths occur in governmental facilities or hospitals, because cases that referred to these facilities are usually the most complicated or at-risk patients (Manoshi 2008-2012 Report).

Overview of Referral Model:
6. Community Engagement Groups – Various support groups allow for coordination and integration between Slum Households and BMC professionals. These committees include:
MNCH Committee: Consists of 9 to 11 members such as ward commissioner, teachers, local elites, NGO workers, BRAC volunteers, SS and SK. This group meets bimonthly to discuss relevant issues, and responsibilities.
Women Support Group: A 7 to 9 member group hosted by locally influential women to engage and encourage women to practice safe and hygienic pregnancies and deliveries.
7. Scaling Up of Successful Approaches – Today, the Manoshi Project has expanded to serve 6.9 million people in 11 city corporations throughout Bangladesh by means of the development and delivery of community-based packages of essential health services, collaboration with local stakeholders, government facilitation, as well as mobilization and empowerment of women’s groups.
Gradually, the BRAC Delivery Centers around Bangladesh will be closed and replaced by Maternity Centers. Due to the larger size of BMCs, a fewer number of centers will be able to serve a larger population while conserving financial and human resources.
Manoshi will continue to expand upon the success of BMCs cost sustainability model, skilled delivery, and better management of complications during childbirth.

1. Total Deliveries – The following graph shows number and local of deliveries in the Dhaka City Corporation that occurred under Manoshi from January to December 2014. Facilities include government hospitals, private hospitals/clinics, UPHCP, and BRAC health center. Number of deliveries at facilities came to a total of 39,039; number of deliveries at BDCs was 11,212; at home 6,404; and at BMCs it was 5,841. Currently, it is expected that the number of births that occur at BMCs are relatively lower because there are not as many Maternity Centers as Delivery Centers. Ideally, births that occur at BDCs and at home should be absorbed by BMCs as they scale up in abundance.
2. Referral Rates – While BRAC Delivery Centers strive to train its midwives to better manage complications during pregnancy and labor, such as malpresentation, fetal distress, ecalmpsia, premature rupture of membrane, and hemorrhaging, risk of improper or incomplete treatment remains a significant hurdle in decreasing maternal and neonatal mortality rates. Through the introduction of Medical Officers, who are present on rotation in BRAC Maternity Centers, the need to refer complicated cases to hospitals has been reduced from 30% at BDCs to 20% at BMCs.
3. 4. 5. 6. 7. 8. 9. 10. 11.
0 5000 10000 15000 20000 25000 30000 35000 40000 45000
Facilities BDC Home BMC
Number and Location of Deliveries (2014) Number of Deliveries - Dhaka City Corp.
IMPACT & ANALYTICS
0%
5%
10%
15%
20%
25%
30%
35%
BDC BMC
Referral Rates in Delivery Centres and Maternity Centers (2013)
30%
20%
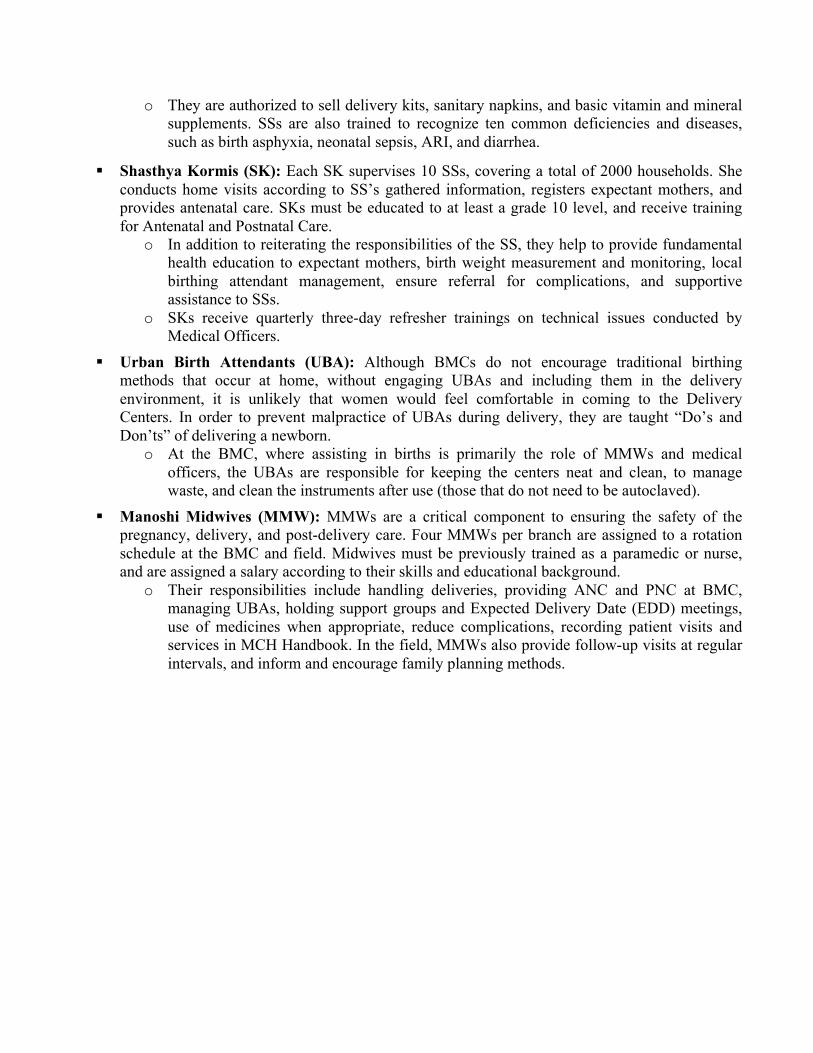
3. Neonatal Mortality Rates – The following graph shows a slight decline in neonatal mortality rates from BDCs to BMC (10 per 1000 to 7 per 1000). While the difference does not appear to be substantial, in reality BDCs refer patients or their newborns to hospitals if any slight complication occurs, making the neonatal mortality rate at hospitals higher. At BMCs, more skilled MMWs and Medical Officers are able to tend to newborns that may present with complications, though it may not always be treated in time.
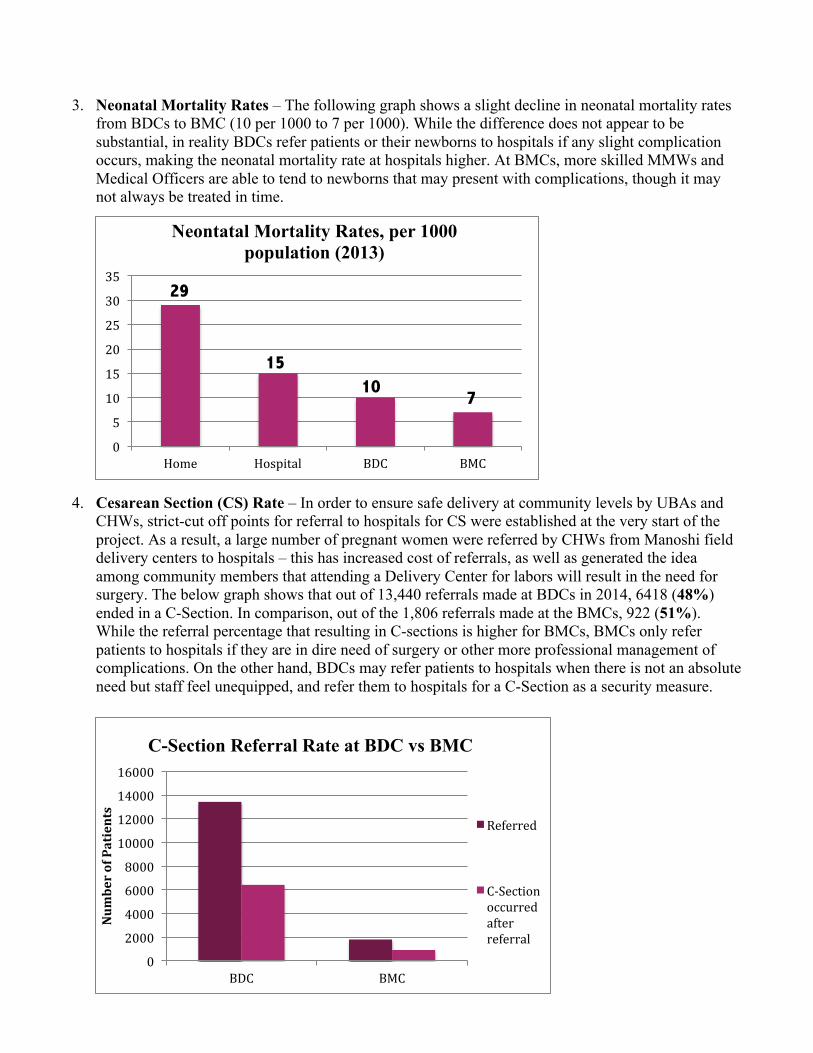
4. Cesarean Section (CS) Rate – In order to ensure safe delivery at community levels by UBAs and CHWs, strict-cut off points for referral to hospitals for CS were established at the very start of the project. As a result, a large number of pregnant women were referred by CHWs from Manoshi field delivery centers to hospitals – this has increased cost of referrals, as well as generated the idea among community members that attending a Delivery Center for labors will result in the need for surgery. The below graph shows that out of 13,440 referrals made at BDCs in 2014, 6418 (48%) ended in a C-Section. In comparison, out of the 1,806 referrals made at the BMCs, 922 (51%). While the referral percentage that resulting in C-sections is higher for BMCs, BMCs only refer patients to hospitals if they are in dire need of surgery or other more professional management of complications. On the other hand, BDCs may refer patients to hospitals when there is not an absolute need but staff feel unequipped, and refer them to hospitals for a C-Section as a security measure.
0
5
10
15
20
25
30
35
Home Hospital BDC BMC
Neontatal Mortality Rates, per 1000 population (2013)
29
15 10
7
0
2000
4000
6000
8000
10000
12000
14000
16000
BDC BMC
Num
ber of Patients
C-Section Referral Rate at BDC vs BMC
Referred
C-‐Section occurred after referral

5. Sepsis Occurrence – Sepsis rates in 2014 show a significant different between percentages of sepsis occurrence in BDCs versus BMCs. Out of 5875 complications that occurred at BDCs, 397 (6.8%) were due to Sepsis. By contrast, out of the 173 complications that occurred at BRAC Maternity Centers, 2 (1.2%) were due to Sepsis. Maternal Sepsis can occur due to prolonged or obstructed labor, ruptured membranes, infection following vaginal delivery, or induced abortions. Though BMCs demonstrate improved sepsis rates, the difference could in part be based on indirect factors affecting the patient, and not necessarily due to location of birth, such as viral or bacterial illnesses previously carried by the mother, pneumonia, or urinary tract infections. More information would be needed to assess cause of sepsis in these cases.
6. Mode of Vaginal Delivery (2014) – When evaluating the mode of vaginal delivery (NVD – normal
vaginal delivery, or Episiotomy) between BRAC Delivery and Maternity Centers, there appears to be no significant difference between the percentages of episiotomies performed. Out of 80,765 vaginal deliveries at BDCs, 59,297 (73%) were NVDs, and 21,468 (27%) were Episiotomies. Similarly, out of 12,984 vaginal deliveries at BMCs, 9,573 (74%) were NVDs, and 3,411 (26%) were Episiotomies. Given the presence of more skilled MMWs and MOs at BMCs, there should be fewer Episiotomies performed. According to Mayo Clinic, Obstetricians used to do Episiotomies routinely to speed delivery and prevent the perineum from tearing spontaneously, but many studies over the past 20 years show that Episiotomies can actually be more harmful than beneficial. Episiotomies tend to result in more hemorrhaging during delivery, more pain during recovery, higher risk of infection, and increased risk of complications during the next birth. Unless the baby is very large, or needs to be delivered as quickly as possible to save the baby, Episiotomies should not be performed regularly. Further research needs to be done to examine reasons for Episiotomies in BDCs and BMCs.
0
1000
2000
3000
4000
5000
6000
BDC BMC
Num
ber of Cases
Sepsis Occurrence (2014)
Complications
Sepsis
0% 10% 20% 30% 40% 50% 60% 70% 80%
NVD Episiotomy NVD Episiotomy
BDC BMC
Mode of Vaginal Delivery (2014)

1. Urban Slum Population Growth – Bangladesh faces unabated population growth, especially in
urban areas, as an estimated 400,000 individuals from rural districts migrate to the capital city each year in search of better financial, educational, and professional prospects. Dhaka’s population, specifically, is expected to reach 20 million by 2050 (PBS). While the volume of urban residents continues to swell, the city’s existing infrastructure is strained by inadequate resources, forcing people into informal settlements or slum communities – due to this rapid urbanization, approximately 60% of Bangladesh’s urban population lives in slums (UNDP). Moreover, this issue is exacerbated by the fact that slums are not recognized by the government, leaving little investment in such communities, and available healthcare facilities remain limited in number and difficult to access.
Thanks to the innovation and progress of Manoshi, slum-dwellers can seek out maternal and child healthcare services within their local communities; however, the underlying primary care services in these regions are still largely non-existent.
Additionally, slum residents also face the constant threat of eviction and demolition of homes. Though BRAC has established numerous Delivery and Maternity Centers across slums, residents may be forced to relocate to areas where such facilities and services are no longer available.
As urban slum population growth increases, the density of residents living in a constrained area also escalates. As a result, the number of individuals living in close proximity to each other leads to an unhygienic environment, diminished access to sufficient nutrition and sanitized water, and a higher probability of the transmission of communicable diseases. These factors have the potential to cause higher maternal and child mortality rates when combined with the lack of access to appropriate healthcare and treatment.
2. Cultural Restrictions – In Bangladesh, especially in urban slum areas, female reproductive and maternal health is often seen as a highly sensitive and culturally stigmatized subject. Sexual health, in both developed and developing regions, is considered a private matter; therefore, its discussion outside of the immediate family has not been widely encouraged, and many are uncomfortable bringing up reproductive health issues with health professionals. It is for this reason that Manoshi aims to provide culturally-appropriate services by employing local women to be trained as community health workers – individuals who can competently educate expectant mothers while being knowledgeable and aware of their social, religious, and cultural norms. Even so, such traditions and norms in slum communities present as obstacles to healthcare delivery of BRAC Delivery and Maternity Centers.
Historically, women in urban slums have been prone to give birth at home, usually alongside their mother-in-law and a traditional birth attendant, both of whom often do not have health risk management skills and frequently employ malpractices. These practices include pulling the baby out too early, and tying a string around the belly to rush delivery. Additionally, if complications occur at home, there is no emergency phone and transport service. or easily accessible hospital. Manoshi continues to create solutions to these obstacles by training birthing attendants, encouraging deliveries at equipped centers, and building a referral system.
CHALLENGES
There still exists an expectation for girls to marry at a younger age, and therefore pregnancies during teenage years or early adulthood remain prevalent across Bangladesh. The United Nations Population Fund (UNFPA) highlights Bangladesh among the ten top countries with the highest child marriage rate, with an average of 66% of girls getting married before age 18, and 10% of girls who give birth to their first child prior to the age of 15 in 2007. It is commonly believed that arranging marriage for a girl at a young age will protect her honor and value within her community. Following the lack of familiarity and usage of contraception, early-age pregnancy and childbirth are a common, and can result in multiple complications due to the underdeveloped female reproductive system. It is for this reason, SSs and SKs seek to introduce and explore family planning services in their respective communities.
Regular check-ups are essential to maintain good sexual health, and allow for early diagnosis of any abnormalities, infections, or cancerous tissue. However, since early age pregnancy and childbirth is frequent, girls and their parents see little need to seek gynecological check-ups prior to pregnancy. In the predominantly conservative atmosphere of Bangladesh, it may also be conceived that seeing a reproductive health specialist prior to marriage or pregnancy is shameful and denotes promiscuity.
When it comes to household responsibility, women in Bangladesh are not often seen as primary-decision makers – this role usually lies with the husband or mother-in-law. While women are the primary caretaker of children, nutrition, and housework, their ability to provide care is controlled by more dominant household figures. These decisions affect maternal and child health when women are restricted from visiting BRAC Delivery and Maternity Centers, or other healthcare facilities and professionals.
At the Manoshi centers, post-partum mothers are strongly encouraged to stay up to 12 hours after delivery for emergency observation. However, during observation, it was found that women “did not want to stay long in the center because of their responsibilities to household work.” (icddr,b – 2012)
3. Educational Impediments – Access to education, especially for young girls and women, remains a substantial hurdle across Bangladesh and urban slums. When children lack the opportunity to learn fundamental reading and writing skills, as adults they are unable benefit from the advances in literary, educational, and health-related teaching materials. The literacy rate for women in Bangladesh is currently 85.8%, however the literacy rate of women in slums or below poverty line is expected to less than 69% (BRAC, 2013).
Manoshi, for example, provides local families and expectant mothers with posters and handbooks with information on pregnancy, birth, risk management, and overall reproductive health education. While these educational tools have numerous visual aids, key information is often overlooked or misinterpreted due to low literacy rates. Moreover, when sensitive reproductive information is displayed graphically on posters, families feel uncomfortable places such posters on the walls of their home.
While there is a slow growth in he number of children in urban slums able to attend primary schools and secondary education, there is currently no sexual health education or workshops integrated into the curriculum. In order for both men and women to become familiar and comfortable with discussing sexual and reproductive health issues, basic concepts and risk management needs to be introduced at an early age.
In order to provide community-specific and sustainable maternal care, BRAC takes the initiative to ensure comprehensive training of MMWs. However, it has been found that the

midwives have a tendency to leave following training, to seek better paid jobs elsewhere. While being a MMW is emotionally rewarding, it is not provide sufficient financial stability local women seek. Additionally, since MMWs are BRAC project staff, there exists a continuous sense of job insecurity, because if Manoshi stops then the midwives will no longer be employed. In regards to SSs and SKs, it is estimated that 50% Manoshi community health workers drop out within six months of employment, 76% within nine months, 90% within the first year (icddr,b – 2012). This creates a burden on BRAC for replacements, and increased training costs.
4. Manoshi Logistics – The foundation of the Manoshi project is built on an elaborate infrastructure of collaboration and effective communication. Due to the multi-level system and integration of local community households, health workers, BRAC staff, Delivery and Maternity centers, as well as hospitals across Bangladesh, if there fails to be efficient coordination between these units, the Manoshi infrastructure becomes destabilized.
When making household visits, SSs and SKs record house numbers and family’s names to ensure regular checkups and surveillance. In the urban slum areas, however, the doors of houses are changed and/or families are relocated. If Manoshi community health workers lose track of family residences, they are no longer able to maintain communication, and the referral system is compromised. Manoshi’s recent initiative of Mobile Health (eHealth), has allowed for some improvement in this area, by leveraging technology to enhance and maintain constant communication and management.
In interviews with Delivery Center and BMC staff, a concern expressed was safety of women at night. As one MMW and Urban Birthing Attendant must be on-call during the night shift, they feel insecure without security for protection, and fear that if men with ill intentions enter the centers at night, they are not prepared to defend themselves.
The BRAC Manoshi Programme continues to facilitate the scaling up of successful approaches,
as well as work to overcome challenges of the Maternity and Delivery Centers throughout the urban slum community. In conjunction with existing Manoshi staff, facilities, and various local governmental and non-governmental organizations, BRAC seeks to implement the following future steps to help advance our goal of reducing maternal and infant mortality rates across Bangladesh.
1. More Reproductive Health Services – Manoshi seeks to increase its number of sexual and
reproductive services for antenatal, labor, and postnatal stages, to provide more holistic preventative measures and treatments that will improve the health and well-being of women across urban slums. Additionally, BRAC Maternity Centers hopes to further expand the demographic served to include young girls or women who are not yet pregnant, in order to address sexual health risks and family planning early on. The following services are anticipated to be added in due time:
Clinical Screening for Breast Carcinoma, Cervical, and Ovarian Cancer – Early cancer detection is crucial to preventing the spread of malignant tissue, organ failure, and death. If detected early, breast, cervical, and ovarian cancer can be cured through chemotherapy and/or surgery to remove cancerous cells.
o Examples of testing include breast cancer screening using mammography, and cervical cancer screening using cytology methods, including pap smears and VIA
FUTURE STEPS & SUGGESTIONS

Tests (WHO). Currently, BRAC is sending health professionals to India to learn how to administer screenings, and perform VIA Tests at BMCs or clinics, as pap smears are relatively expensive.
o Screening programs should be undertaken only when their effectiveness has been demonstrated, when facilities exist for confirming diagnosis, and treating abnormal test results. The prevalence of the disease should also be high enough to justify the effort and costs of the screening.
o Efforts should therefore be taken, in collaboration with other governmental or non-governmental organizations, to gauge prevalence of breast, cervical, and ovarian cancer in women within urban slums. As cancer screening in these regions have not previously been done, this will be a long-term endeavor, and should be encouraged along with the awareness that cancer can be cured.
Sexually Transmitted Infections (STI) Testing – STI testing currently exists as part of the comprehensive antenatal package provided by Manoshi when a pregnancy is confirmed. However, in order for STI testing to be more effective, it has to occur regularly if a woman is sexually active, even before pregnancy may occur.
o Pre-pregnancy testing is especially important because many STIs do not always have obvious signs or symptoms, and therefore can be transmitted to a sexual partner unknowingly. This testing can occur through annual gynecological check-ups, starting from the time a woman is sexually active.
o Screening should be used to detect Chlamydia, Gonorrhea, Genital Herpes, HIV, Syphilis, Hepatitis, and HPV. An HPV vaccine, such as Gardasil, should be administered during a girl’s teenage years regardless of previous sexual activity. This vaccine can prevent occurrence of certain types of vaginal cancers (Mayo Clinic).
o As previously highlighted, early testing prior to marriage or pregnancy may be conceived as shameful and denotes promiscuity in the more conservative atmosphere of Bangladesh. For this reason, parents should be encouraged by SSs and SKs to send their children who are girls, for a standard gynecological testing at the age of 16.
Preventing and Treating Obstetric Fistulas – The most common type of fistula is a vesicovaginal fistula, in which the woman’s vagina is connected to the urinary bladder. This causes leakage of urine from the vagina, and can result in frequent vaginal and bladder infections. Fistulas can also develop between the vagina and the large intestine or rectum. This results in feces leakage from the vagina, leading to further infection. Fistulas can occur after difficult labor or childbirth, especially in very young girls (Cornell Urology).
According to a situation analysis of obstetric fistula carried out by the NGO in 2003, Engender Health in collaboration with the UNFP, over 400,000 women in Bangladesh suffered from vesicovaginal fistulas, and over 16,000 women were shown to have rectovaginal fistulas. These numbers are expected to be higher due to the fact that not all cases of vaginal or rectal fistulas were recorded, or treated in a hospital. – [UNFP]
o Women who suffer from Fistulas are often considered social outcasts, leading them to be disowned by their family, unable to find employment, and prone to both physiological and physical stress.
o As Fistulas are usually treated through surgery to repair the opening, BRAC can explore possible partnerships with UNFP, EngenderHealth, and the “Fistula
Foundation,” all of which operate in Bangladesh and may have staff to provide a MoU to send at-risk mothers to their facilities.
o Manoshi and BMCs are already addressing the prevention of Fistulas through the 3-tiered delay reduction system, as well as through the increase in skilled MMWs and MOs.
Further Encouragement for LAPM – Long-acting, and permanent methods for contraception, or LAPM, include IUDs, implants, Tubectomies, or Vasectomies. The Bangladesh government provides incentive in the form of a one-time financial remuneration, a sari or lungi, if Tubectomies/vasectomies are performed at hospitals. During their household visits, SSs and SKs also educate and encourage long-term family planning methods, but their popularity is not widespread.
In the Manoshi 2007-2012 Report, it was found that out of 656,693 surveyed couples in 2012 the most commonly used contraceptive method was oral pills (52%), followed by injectables (26%), and condoms (14%). The use of long-term contraceptive methods was considerably lower, with IUD and implant usage at 3%, Tubectomy at 5%, and Vasectomy at 1%. – [BRAC, 2012]
o The advantage of using LAPM is that couples do not have to sustain the usage and monitoring of short-acting methods such as pills, injectables, and condoms. They can also reduce the number of unplanned or unwanted pregnancies, as well as abortions. LAPMs can also aid in abating the challenge of over-population in Bangladesh urban slum areas.
o In addition to having SSs and SKs promote the use of LAPM, it may be more effective for women who have already undergone a LAPM procedure, or are currently using an implant or IUD. If this occurs during EDD meetings, or in separate community group sessions for woman prior to pregnancy, it would give local women an opportunity to ask another person about their personal experience and perspective with LAPM.
Addressing Postpartum Depression (PPD) and Other Mental Health Illness – Postpartum depression occurs commonly following childbirth, and can result in severe mood wings, anxiety, sadness, irritability, insomnia, difficulty bonding with your baby, withdrawal from family and friends, loss of appetite, and in extreme cases, thoughts of harming yourself or your baby (Mayo Clinic). Thus, the prevalence of postpartum depression, thoughts of self-harm, abuse and neglect in the slums of urban Bangladesh thus require further investigation and availability of treatment.
The rate of postpartum depression at 6-8 weeks after delivery in rural Bangladesh has previously been reported as 22%. Among the risk factors identified were a poor relationship with the mother’s mother-in-law and either the mother or her husband leaving home after a dispute. Regarding antepartum depression, a history of physical intimate partner violence had the strongest association for antepartum depression (at 34-35 weeks) among rural Bangladeshi women; additionally, 14% of the depressed women admitted to thoughts of self-harm during the pregnancy. – [Icddr,b, 2012]
o In EDD meetings or following each delivery, MMWs and/or Medical Officers should take the time to go through the signs and symptoms of PPD, ideally in the presence of spouses or mother in laws. It is often difficult for a mother herself to recognize the difference between “baby blues” and PPD – having a knowledgeable husband or

mother-in-law who are able to notice differences in behavior and well-being would be able to suggest the mother to seek further assistance.
o Topics addressed during these private or group counseling sessions should include: a) Mothers need breaks too! It can be common for a new mother to believe that
if she loves her baby enough, she should be with him/her all the time. A mother’s own needs can be forgetting in the midst of caring for the baby. Taking breaks, engaging in relaxing activities, and maintaining good nutrition and hygiene, are all essential factors to promote well-being and good health of the mother and family.
b) Reaching out and asking for help is important – with husbands normally at work, participation of spouses in the care of the newborn is not frequent. Mothers should be encouraged to not try and take all the responsibility on their own; involve older children, family members, or neighbors in the care of the newborn.
c) There may be an expectation for having a baby to be among the happiest and most joyous occasions in one’s life. While introducing a baby to a family can bring pleasure to everyone at home, it is also a big adjustment that comes with both ups and downs. No one is perfect, and it’s a learning process for everyone!
o BMC staff should have a guide or wellness strategy to follow if a mother presents with symptoms of PPD, and schedule regular follow-up visits at the Maternity Centers or in households.
2. Improved Outreach Strategies – Marketing and social mobilization is a pivotal component of
advancing the popularity, acceptability, and usage of BMCs. Currently, BRAC has various publicity and marketing programs in place to generate awareness of Manoshi services. These include: posters, pamphlets, radio, TV spots, YouTube channel, Facebook, street performances and theatre, word-of-mouth, and field visits by local and international NGOs. The issue with these strategies, is that most are geared toward the awareness of Manoshi services outside of the population and demographic actually served by BMCs. Most individuals, especially women, in urban slum areas are illiterate, and some families do not have access to TVs and/or Internet. It would be beneficial for BMC popularity, as well as overall population health, if outreach methods were to include women who are not pregnant.
Monthly Presentations at BMCs – In addition to the antenatal and EDD sessions, BMC should advertise and hold monthly presentations, each on a different topic relating to women’s reproductive health.
o Such topics can include: Cancer of the female reproductive organs, mental health issues susceptible to women, teen or unwanted pregnancies, sexual and domestic violence, HIV/AIDS, Endometriosis, irregular menstruation and/or introduction to puberty for teenage girls, infertility, family planning, Obstetric Fistulas, Nutrition, and Hygiene. Each session should end with a question and answer session, as well as advertisement of current available local resources and contact information. All age ranges encouraged.
o Incentives can be offered such as food/tea, micronutrient packages, mini hand sanitizer, small bags of milk powder/sugar/rice. OR, during an individual’s first session, they will be given a “punch/stamp” card, and once a person attends and receives four stamps at the BMC, they get a free delivery, for example.

Leveraging International Women’s Day [March 8th] – On this day, or throughout the week, BRAC and Manoshi can organize special camps for screening and treatment within each city district urban slum areas with established BDCs or BMCs. These can also occur on 28th May, for Safe Motherhood Day.
o These reproductive and sexual health screenings should include preventative tests for breast and cervical cancer, sexually transmitted infections, HIV/AIDS, Rh incompatibility, gestational diabetes, mental health illness, anemia, vitamin deficiencies, domestic or dating violence, and sexual assault.
o In addition to screenings, medical officers can be on site to provide various contraceptive methods such as IUDs and implants. Immunizations can also be administered. If possible, HPV vaccines should be highly recommended, if not mandatory for all young women to reduce the prevalence of cervical cancer.
o The camps or health assemblies can take place at local community centers or schools, and should include a series of talks and group sessions to highlight reproductive health risks, which are not limited to those that occur during pregnancy or childbirth, but those that can occur at any stage of a women’s life.
o SSs and SKs should include the advertising of International Women’s Day activities and their locations during household visits in the month leading up to the event. They can also create and hand out calendars, with pre-marked important dates such as International Women’s Day, BMC Monthly Presentation Sessions, as well as the patient’s individual scheduled EDD meetings, expected delivery date, check-ups at BMCs, and household visits.
3. Adolescent Sexual Health Education Program – According to a report by the James P Grant
School of Public Health at BRAC University on adolescent reproductive and sexual health interventions in South Asia, adolescents represent almost one quarter of the total Bangladesh population. Furthermore, they are generally discouraged from discussing their sexual health and rights with their guardians or superiors due to cultural conservative norms.
This constraint has led to a range of health issues including, early fertility, transmission of STIs and HIV, and sexual abuse. The ICDDR,B outlined that the fertility rate among female adolescents aged 15-19 is 144 births per 1,000 population, and approximately 40% of urban males are reported to be engaging in sexual activity prior to the age of 19. Therefore, young adults need to be educated in both a formal and non-formal setting regarding their reproductive health to increase their understanding and prevention of various health risks, as well as promote respect for one’s sexual health rights. – [Icddr,b, 2012]
Partner with existing BRAC schools in urban slum areas, and have CHWs, MMWs, and/or medical officers teach sexual and reproductive health to both girls and boys as part of their mandatory school curriculum.
Sessions can be presented through general lectures, workshops, and peer sessions, and include topics of basic anatomy, mensuration, risks of early pregnancy and childbirth, STIs and HIV transmission, family planning, preventing sexual assault and child marriage, associated mental health challenges, and promoting health rights. These sessions should take place in a safe, judgment-free, and encouraging environment.
There should be a session in which parents are taught by Manoshi staff, to understand sexual health risks as well as understand how to best approach their children regarding these sensitive issues.

Adolescent girls with irregular menstruation cycles, and/or who are engaging in sexual activity should be encouraged to come to BMCs for regular gynecological check-ups and family planning, with or without parental knowledge.
4. eHealth – In partnership with mPower Social Inc., Manoshi has employed various technological and
mobile health (eHealth) solutions to strengthen responses to pregnancies, birth complications, and maternal and child illness in urban slum areas of Bangladesh. Firstly, it will remodel the patient management and care system. Secondly, it will implement an emergency management system and finally, expand the monitoring and reporting process.
CHW are equipped with basic mobile phones to record demographic and medical information of the patients in their respective areas. It is expected that the information feeds into a comprehensive medical database, which can be used for Manoshi research and evaluation. BRAC Manoshi staff should regularly review data and provide targeted instructions to community health workers.
Current challenges include technical failures, beneficiary migration, CHW dropouts, under-utilization, and improper use of hotlines.
A type of “Triage System” should be incorporated into mobile patient history, with risk of mother and/or neonate rated on a scale of 1-3. This way, CHWs and medical officers will be able to visit and treat high-risk patients with more attentiveness.
Automatic reminders should be set on mobiles to alert CHWs of pre-natal and post-natal visit schedule, to ensure routine check-ups occur.
5. Monitoring and Evaluation: It is early years, Manoshi programs used to be evaluated by ICDDR,B
through research and working papers. Currently, the work is being monitored through a two-tiered system. Firstly, need-based research is conducted on required selected data through BRAC’s health research and evaluation department. Secondly, information collected from the field on a monthly basis. The Management Information System (MIS) is outlined below:
Monthly Reports – After each household visit, SKs will register every individual in their respective regions on paper. On an assigned day each month, SKs under a single region meet to collaborate data together and submit it to their PO. Once a PO has received amalgamated household data from the (approximately 6) SKs under their supervision, the POs of each region will meet and submit their compiled information to the branch manager. Branch managers will then electronically submit their branch data to the BRAC MNCH division.
Bi-Yearly Household Survey – Outreach should not be limited in the direction of BMC to local communities, but also local communities should be able to express their concerns and challenges with BMCs and Manoshi. These surveys enable BRAC staff and BMCs to keep up to date, and tailor their services to better fit the current needs of each region.
o Questions should focus on financial, health, or family related challenges, as well as assess their prior knowledge of the location and services provided by BMCs. No names will be recorded to maintain anonymity and confidentiality.
Challenges – Since the introduction and scaling up of upgraded BRAC Maternity Centers, the ability to effectively and accurately compare statistics from BDCs with BMCs has become a hurdle. The services offered by both types of centers are different, some regions have only BDCs, and comparisons made across regions do not present the same type of patient demographics. The following suggestions may help address such challenges:

o Evaluate BDCs that have been upgraded to BMCs 12 months pre-upgrade and 12 months post-upgrade– factors of measurement should include number of deliveries at center, maternal mortality rate, neonatal mortality rate, and referral rate.
o Introduction of post-BMC service survey: What service did you receive? Were you satisfied with your service today? Would you come back again? Would you recommend us to other women?
o New measurement statistics: number of months seen by SS/SK (complete 9 months, or less?), average age of mother at delivery (in order to gauge what age Manoshi should target their programs at), in regions where there are both BDC and BMC evaluate reason why an individual attends BDC over BMC (% too far, financial reasons, familiarity, etc.)
Report by: Natasha Merali, BRAC Intern Under the supervision of: Dr. Tamjida Hanfi, HNP Senior Manager April 2015




















