
Boone County Health Department
10
Permit #: Confirmation #: New # of Bedrooms: Public Repair Private Tank Only # of Employees: Gallons per day: Address: Property Owner: City/Zip Code: Mailing Address: Subdivision: City/Zip: Lot #: Phone #: Parcel #: Email: Applicant: Contractor: Address: Address: City/Zip Code: City/Zip Code: Phone #: Phone #: Email: Email: State License: yes no #: County License: yes no Scale: Filter Brand: Soil Bores Used: Filter Size: Pump Estimated Gallons: Distribution Box: yes no Even Dosing Tank Brand: Low Pressure Tank Gallons: Trench System N/A IL ID#: Rock & Pipe Field Distribution ATU Serial #: Chamber Serial Loading Rate: EZFlow Level Surface Area: Other Gravelless Combination Linear Feet: Other: Tank Distribution Residential Type of Permit Septic Permit Application Septic Plan Information Property Information Application & Contractor Information Commerical Water Supply Boone County Health Department 1204 Logan Avenue, Belvidere, Illinois 61008 Main Office 815.544.2951 Clinic 815.544.9730 Fax 815.544.2050 www.boonehealth.org MIN. TANK _____________ / _____________ _______________g/day ÷ ____________g/ft 2 /day = ______________sq. ft W/ GARBAGE DISP / NO GARBAGE DISP (EST. WASTE STREAM) (EST. LOAD RATE) (MIN. TRENCH AREA) SURFACE AREA REQUIRED _______________________ LINEAL FEET REQUIRED _______________________
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Boone County Health Department
Permit #:Confirmation #:
New # of Bedrooms: Public
Repair Private
Tank Only # of Employees:
Gallons per day:
Address: Property Owner:
City/Zip Code: Mailing Address:
Subdivision: City/Zip:
Lot #: Phone #:
Parcel #: Email:
Applicant: Contractor:
Address: Address:
City/Zip Code: City/Zip Code:
Phone #: Phone #:
Email: Email:
State License: yes no #:
County License: yes no
Scale: Filter Brand:
Soil Bores Used: Filter Size: Pump
Estimated Gallons: Distribution Box: yes no Even Dosing
Tank Brand: Low Pressure
Tank Gallons: Trench System N/A
IL ID#: Rock & Pipe Field Distribution
ATU Serial #: Chamber Serial
Loading Rate: EZFlow Level
Surface Area: Other Gravelless Combination
Linear Feet: Other:
Tank Distribution
ResidentialType of Permit
Septic Permit Application
Septic Plan Information
Property Information
Application & Contractor Information
Commerical
Water Supply
Boone CountyHealth Department1204 Logan Avenue, Belvidere, Illinois 61008
Main Office 815.544.2951 Clinic 815.544.9730 Fax 815.544.2050www.boonehealth.org
MIN. TANK _____________ / _____________ _______________g/day ÷ ____________g/ft2 /day = ______________sq. ftW/ GARBAGE DISP / NO GARBAGE DISP (EST. WASTE STREAM) (EST. LOAD RATE) (MIN. TRENCH AREA)
SURFACE AREA REQUIRED _______________________ LINEAL FEET REQUIRED _______________________
Conventional 260.00$ Revised Plan Review 75.00$
Mechanical 340.00$ Unlicensed Installer 175.00$
Tank Only 220.00$ Installer Education 80.00$
Additional Lines 15.00$ Homeowner Install 175.00$
Site Verification 125.00$ 175.00$
Soil Bores Report Plan Checklist
Wastestream Information Sheet Elevations Sheet
Owner Sign Off - Maintenance Agreement ATU Operator Permit
Proposed Site Plan Alteration Agreement
Permit Receipt #:
Revised Plan Review Receipt #:
Receipt #:
Proposed Septic System:
Approved Date:
Rejected Date:
Revised Plan Approved Date:
Revised Plan Rejected Date:
County Building Department Property Owner
Assessor's Office Contractor
Com Ed Noitification Township Supervisor
*** OFFICIAL USE ONLY ***
Unlicensed Installer
Inspection
Type of Permit
Other:
Plan Approval & Status
Notification
Other:
Other:
Date:
Required Documentation
Payment
Date:
Date:
Final Approval Stamp Here:
Total Amount: $
V:\Env Programs\private sewage\Forms-Lists\admin forms\Wastestream and Homeowner Install Signoff_feb2020.docx
WASTESTREAM INFORMATION SHEET
Property Address: __________________________________________________________________________
□ Residential *
Number of bedrooms: □ 2 bedrooms □ 3 bedrooms □ 4 bedrooms □5 bedrooms □ Other: ___________
Garbage disposal: □ Yes, there will be a garbage disposal installed
□ No, there will not be a garbage disposal installed
Water Softener: □ NSF Standard 44 (high efficiency) unit is/will be installed. No change in sizing of septic
field will be required and the discharge will be connected indirectly to the main building
drain.
□ The water softener is/will not be a high efficiency unit. The septic field will be increased
in size to accommodate the discharge or the softener unit will discharge to a separate field
sized to accommodate said discharge. If discharging to the main septic system, the discharge
line will bypass the septic tank.
□ No water softener will be installed (for the life of the septic system).
Hot tub/Jacuzzi: □ Yes, there will be a hot tub/jacuzzi or similar fixture (of greater than 100 gallons)
(draining to the Volume:___________ gallons
septic system) □ No, there will not be a hot tub/jacuzzi or similar fixture (of greater than 100 gallons)
□ Commercial/Other
Type of establishment: ______________________________________________________________________
Hours of operation: ____Hours/day ____Days/week
Number and type of employees: □___Full time □___Part time
Number and type of fixtures: □ #___Toilets □ #___Urinals □ #___Sinks □ #___Showers □ #___Washing machines
Water Softener: □ NSF Standard 44 (high efficiency) unit will be installed. No change in sizing of septic field
will be required and the discharge will be connected indirectly to the main building drain.
□ The water softener will not be a high efficiency unit. The septic field will be increased in
size to accommodate the discharge or the softener unit will discharge to a separate field sized
to accommodate said discharge. If discharging to the main septic system, the discharge line
will bypass the septic tank.
□ No water softener will be installed (for the life of the septic system).
Estimated number of customers or residents per day: ________
Estimated square footage of floor area (shopping center): ________
Number of beds (hospitals/hotels) or spaces (mobile home parks or campgrounds): _____
Restaurants: □ No bar & Cocktail □ With bar & Cocktail □ Number of meals served each day: ______
Other notes (ex. chemical disposal): ________________________________________________
_________________________________________ ___________________
Property Owner Signature Date
*NOTE: IF THE SEPTIC IS FOR A SINGLE FAMILY RESIDENCE & IS GOING TO BE INSTALLED BY
THE HOMEOWNER, PLEASE SIGN ON THE BACK OF THIS FORM.
The mission of the Boone County Health Department is to serve our community by
preventing the spread of disease, promoting optimal wellness & protecting the public’s health.
Boone County Health Department
1204 Logan Avenue, Belvidere, Illinois 61008
Main Office 815.544.2951 Clinic 815.544.9730 Fax 815.544.2050 www.boonehealth.org
V:\Env Programs\private sewage\Forms-Lists\admin forms\Wastestream and Homeowner Install Signoff_feb2020.docx
NOTICE FOR HOMEOWNER INSTALLATIONS
I, , the property owner of ______________________________,
Name Property Address
plan to install the septic system at this property as allowed by the following county code.
Sec. 66-28. License requirements.
(a) On and after the effective date of the ordinance from which this article is derived, no person, except for a private
sewage disposal system contractor licensed by the health authority, may construct or alter a private sewage disposal
system. Resident owners or intended resident owners who can demonstrate that they are able to perform the installation
or alteration in conformance with this chapter may install or alter a system for their own single-family residence,
provided such resident owner or intended resident owner pays the applicable unlicensed installer permit fee and complies
with two additional mandatory inspections at times as set forth by the health authority.
I understand that, as the property owner, I am assuming the role and responsibility of the licensed septic system contractor
for this installation. The physical installation of the septic system and its components may not be done by anyone other
than the actual single family resident property owner/s or a licensed septic installer. I understand that I may NOT hire an
unlicensed installer, such as another family member personal friend, etc. to install the septic system. I further understand
that Homeowner Installations require two additional compliance inspections, the cost of which adds $175.00 to the permit
fee. The total of 3 compliance inspections shall consist of:
1) inspection of tank placement
2) inspection of first installed line
3) final inspection of all lines/field
Before each of these inspections a 48 Hour Notice must be given to Boone County Health Department for scheduling
purposes. There is also an optional homeowner septic system installation education available for $80.00 / hour.
I understand and concur that I am assuming the role of a licensed septic system contractor for this installation. I must be
present during all of the installation construction. I agree to hold myself responsible for compliance with any and all
applicable local and state regulations. Failure to abide by this agreement will invoke legal action according to Sec. 66-30
of the Boone County Sewers and Sewage Disposal Code.
____________________________________ _______________________
Property Owner Signature Date
The mission of the Boone County Health Department is to serve our community by
preventing the spread of disease, promoting optimal wellness & protecting the public’s health.
Boone County Health Department
1204 Logan Avenue, Belvidere, Illinois 61008
Main Office 815.544.2951 Clinic 815.544.9730 Fax 815.544.2050 www.boonehealth.org
V:\Env Programs\private sewage\Forms-Lists\admin forms\Maintenance agreement for private sewage disposal systems PHAB rev
2017_05_19.docm
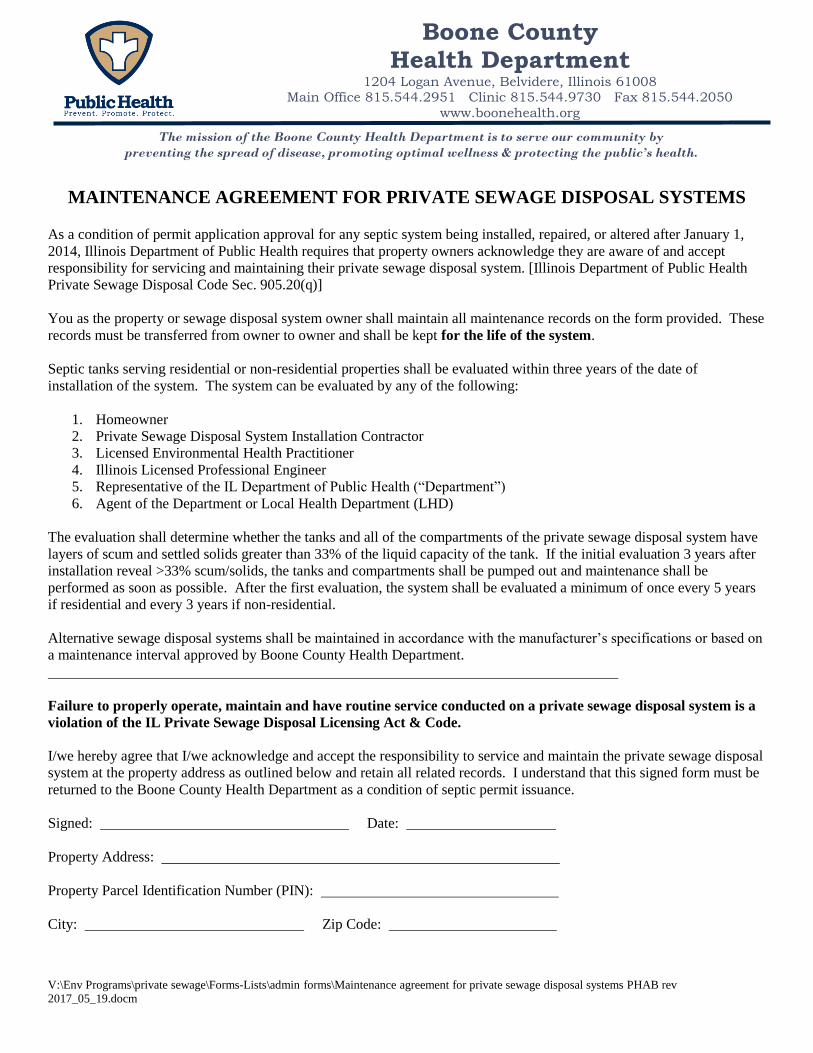
MAINTENANCE AGREEMENT FOR PRIVATE SEWAGE DISPOSAL SYSTEMS
As a condition of permit application approval for any septic system being installed, repaired, or altered after January 1,
2014, Illinois Department of Public Health requires that property owners acknowledge they are aware of and accept
responsibility for servicing and maintaining their private sewage disposal system. [Illinois Department of Public Health
Private Sewage Disposal Code Sec. 905.20(q)]
You as the property or sewage disposal system owner shall maintain all maintenance records on the form provided. These
records must be transferred from owner to owner and shall be kept for the life of the system.
Septic tanks serving residential or non-residential properties shall be evaluated within three years of the date of
installation of the system. The system can be evaluated by any of the following:
1. Homeowner
2. Private Sewage Disposal System Installation Contractor
3. Licensed Environmental Health Practitioner
4. Illinois Licensed Professional Engineer
5. Representative of the IL Department of Public Health (“Department”)
6. Agent of the Department or Local Health Department (LHD)
The evaluation shall determine whether the tanks and all of the compartments of the private sewage disposal system have
layers of scum and settled solids greater than 33% of the liquid capacity of the tank. If the initial evaluation 3 years after
installation reveal >33% scum/solids, the tanks and compartments shall be pumped out and maintenance shall be
performed as soon as possible. After the first evaluation, the system shall be evaluated a minimum of once every 5 years
if residential and every 3 years if non-residential.
Alternative sewage disposal systems shall be maintained in accordance with the manufacturer’s specifications or based on
a maintenance interval approved by Boone County Health Department.
Failure to properly operate, maintain and have routine service conducted on a private sewage disposal system is a
violation of the IL Private Sewage Disposal Licensing Act & Code.
I/we hereby agree that I/we acknowledge and accept the responsibility to service and maintain the private sewage disposal
system at the property address as outlined below and retain all related records. I understand that this signed form must be
returned to the Boone County Health Department as a condition of septic permit issuance.
Signed: Date:
Property Address:
Property Parcel Identification Number (PIN):
City: Zip Code:
The mission of the Boone County Health Department is to serve our community by
preventing the spread of disease, promoting optimal wellness & protecting the public’s health.
Boone County Health Department
1204 Logan Avenue, Belvidere, Illinois 61008 Main Office 815.544.2951 Clinic 815.544.9730 Fax 815.544.2050
www.boonehealth.org
V:\Env Programs\private sewage\Forms-Lists\admin forms\Maintenance agreement for private sewage disposal systems PHAB rev
2017_05_19.docm
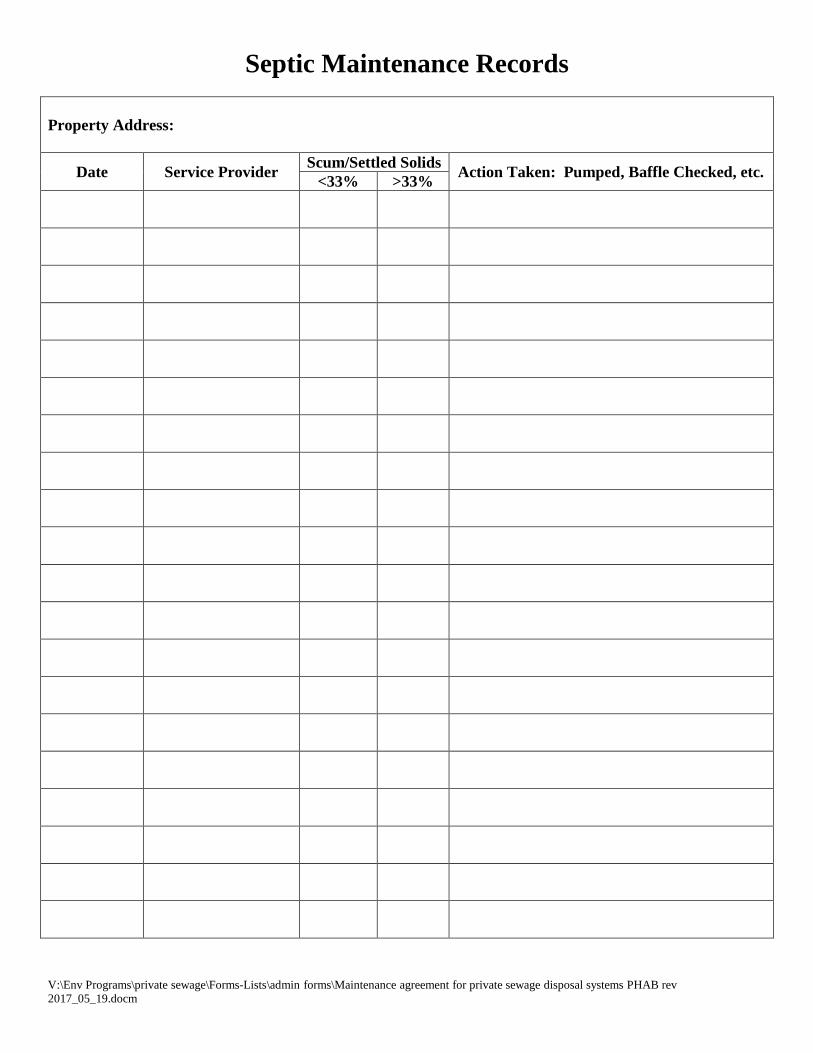
Septic Maintenance Records
Property Address:
Date Service Provider Scum/Settled Solids
Action Taken: Pumped, Baffle Checked, etc. <33% >33%
V:\Env Programs\private sewage\Forms-Lists\admin forms\ATU Owner signoff REV March 2018.docx
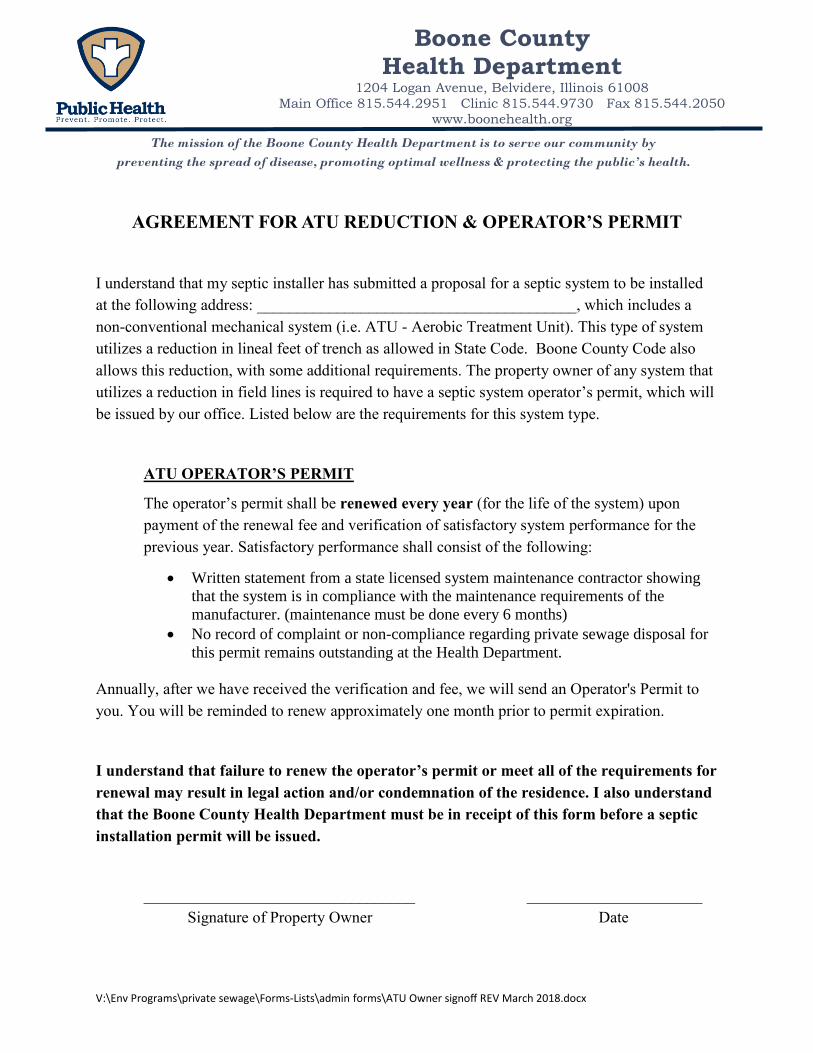
AGREEMENT FOR ATU REDUCTION & OPERATOR’S PERMIT
I understand that my septic installer has submitted a proposal for a septic system to be installed
at the following address: ________________________________________, which includes a
non-conventional mechanical system (i.e. ATU - Aerobic Treatment Unit). This type of system
utilizes a reduction in lineal feet of trench as allowed in State Code. Boone County Code also
allows this reduction, with some additional requirements. The property owner of any system that
utilizes a reduction in field lines is required to have a septic system operator’s permit, which will
be issued by our office. Listed below are the requirements for this system type.
ATU OPERATOR’S PERMIT
The operator’s permit shall be renewed every year (for the life of the system) upon
payment of the renewal fee and verification of satisfactory system performance for the
previous year. Satisfactory performance shall consist of the following:
Written statement from a state licensed system maintenance contractor showing
that the system is in compliance with the maintenance requirements of the
manufacturer. (maintenance must be done every 6 months)
No record of complaint or non-compliance regarding private sewage disposal for
this permit remains outstanding at the Health Department.
Annually, after we have received the verification and fee, we will send an Operator's Permit to
you. You will be reminded to renew approximately one month prior to permit expiration.
I understand that failure to renew the operator’s permit or meet all of the requirements for
renewal may result in legal action and/or condemnation of the residence. I also understand
that the Boone County Health Department must be in receipt of this form before a septic
installation permit will be issued.
__________________________________ ______________________
Signature of Property Owner Date
The mission of the Boone County Health Department is to serve our community by
preventing the spread of disease, promoting optimal wellness & protecting the public’s health.
Boone County Health Department
1204 Logan Avenue, Belvidere, Illinois 61008
Main Office 815.544.2951 Clinic 815.544.9730 Fax 815.544.2050
www.boonehealth.org
V:\Env Programs\private sewage\Forms-Lists\admin forms\septic alteration agreement_feb2020.docx
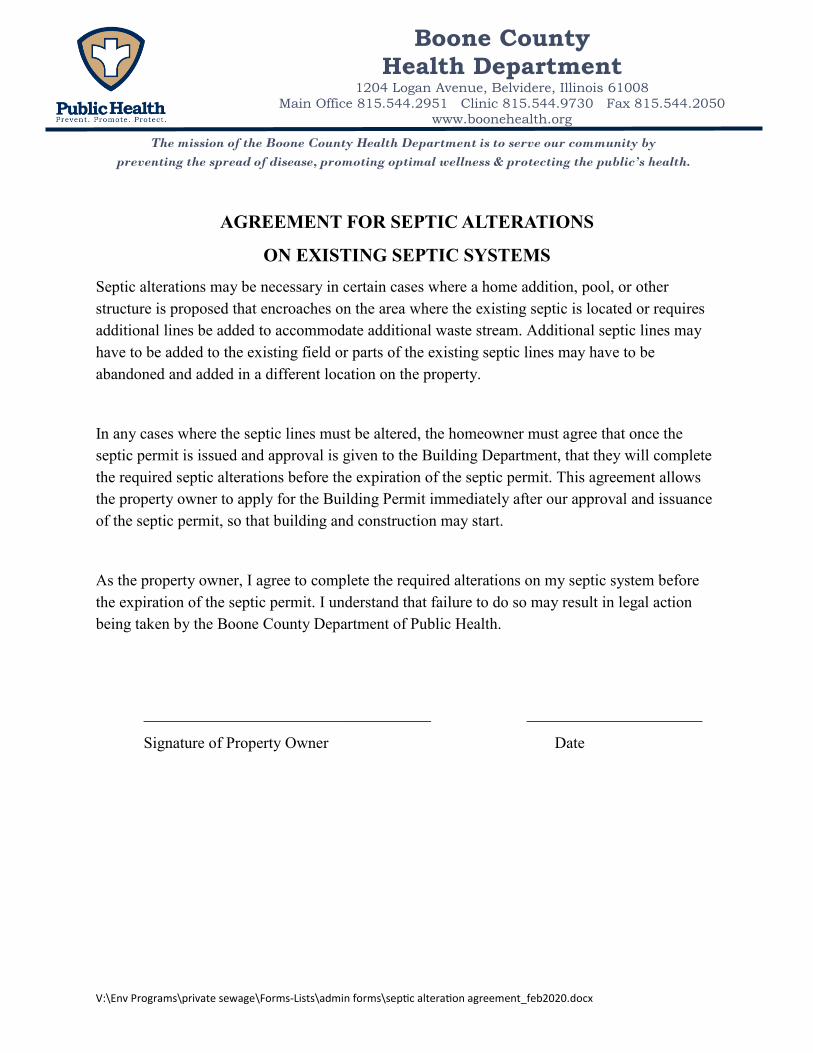
AGREEMENT FOR SEPTIC ALTERATIONS
ON EXISTING SEPTIC SYSTEMS
Septic alterations may be necessary in certain cases where a home addition, pool, or other
structure is proposed that encroaches on the area where the existing septic is located or requires
additional lines be added to accommodate additional waste stream. Additional septic lines may
have to be added to the existing field or parts of the existing septic lines may have to be
abandoned and added in a different location on the property.
In any cases where the septic lines must be altered, the homeowner must agree that once the
septic permit is issued and approval is given to the Building Department, that they will complete
the required septic alterations before the expiration of the septic permit. This agreement allows
the property owner to apply for the Building Permit immediately after our approval and issuance
of the septic permit, so that building and construction may start.
As the property owner, I agree to complete the required alterations on my septic system before
the expiration of the septic permit. I understand that failure to do so may result in legal action
being taken by the Boone County Department of Public Health.
____________________________________ ______________________
Signature of Property Owner Date
The mission of the Boone County Health Department is to serve our community by
preventing the spread of disease, promoting optimal wellness & protecting the public’s health.
Boone County Health Department
1204 Logan Avenue, Belvidere, Illinois 61008
Main Office 815.544.2951 Clinic 815.544.9730 Fax 815.544.2050
www.boonehealth.org
Permit application fee must accompany septic plan. The plan will be reviewed and
approved or disapproved within 7 working days and you will be notified by phone. If
approved, a septic permit will be mailed. If disapproved, a written response and
explanation will be mailed.
SEPTIC PLAN CHECKLIST
ADDRESS: _______________________________________________________
CONVENTIONAL SOIL PLANS SHOWS ALL OF THE FOLLOWING:
(Check each box to verify the requirements of the plan have been provided)
Lot dimensions
North orientation
Suitable soils area
Contours
Length of lines/size of tank/approved filter make, size and location
Number of bedrooms in home
All field tile issues (if applicable)
All house/buildings, driveways, pools, easements, drainage areas, etc., which may impact
the septic system or its orientation
Site plan and septic plan are both drawn to an approved scale and the scale is indicated
Existing grade elevations from on-site investigation on at least 4 corners of septic field &
are relative to system profile elevations on the completed profile elevation form
Elevations are consistent throughout the system profile information form
Variance requests must be submitted in writing by the septic contractor and include
acknowledgement from the homeowner
NON-CONVENTIONAL SOIL PLANS MUST ALSO SUBMIT THE FOLLOWING: Aerobic treatment unit specifications, i.e.: make/model
Ground surface contours on at least 5 ft. intervals
Soil bores located on plan
Soil bore information, including limitation types & elevations
REPAIR PLANS MUST ALSO CHECK THE FOLLOWING:
Include the location, depth and elevation detail of the old septic tank and field
As the contractor, I confirm that the information checked above and as presented on the plan are
accurate representations of on-site observations. In addition, I have verified that municipal sewer
is more than 200 ft. from this property. Note: Plan will not be approved if it lacks any of the
above items. Each additional septic plan review is $75.00.
_______________________________ __________________ _________________
Septic Contractor Signature Date Phone Number
The mission of the Boone County Health Department is to serve our community by
preventing the spread of disease, promoting optimal wellness & protecting the public’s health.
Boone County Health Department
1204 Logan Avenue, Belvidere, Illinois 61008
Main Office 815.544.2951 Clinic 815.544.9730 Fax 815.544.2050
www.boonehealth.org
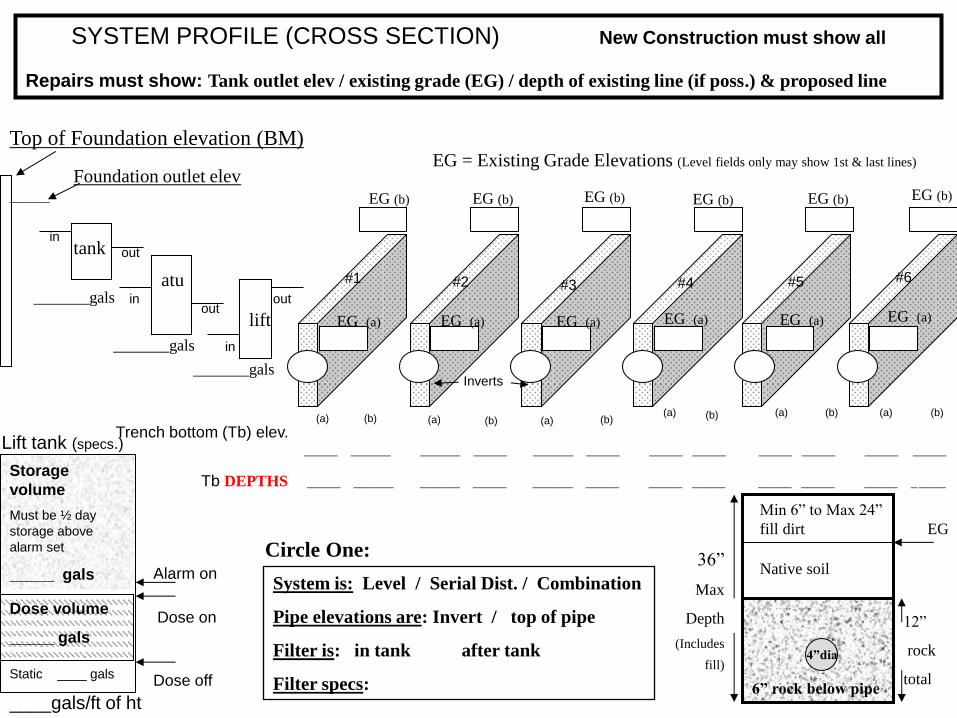
4”dia
6” rock below pipe
12”
rock
total
36”
Max
Depth
(Includes
fill)
Top of Foundation elevation (BM)
Foundation outlet elev
SYSTEM PROFILE (CROSS SECTION) New Construction must show all
Repairs must show: Tank outlet elev / existing grade (EG) / depth of existing line (if poss.) & proposed line
tank
______
System is: Level / Serial Dist. / Combination
Pipe elevations are: Invert / top of pipe
Filter is: in tank after tank
Filter specs:
Min 6” to Max 24”
fill dirt
EG = Existing Grade Elevations (Level fields only may show 1st & last lines)
Trench bottom (Tb) elev. _____ ______ ______ _____ ______ _____ _____ _____ _____ _____ _____ _____
Circle One:
Tb DEPTHS
EG (b)
_______gals atu
lift
_______gals
_______gals
EG (a)
Inverts
in
out
in
in
out out
Native soil
EG
____gals/ft of ht
Dose volume
_____ gals
Alarm on
Dose on
Dose off
Storage
volume
Must be ½ day
storage above
alarm set
_____ gals
Lift tank (specs.)
#1 #2 #5 #4 #3 #6
EG (a) EG (a) EG (a) EG (a) EG (a)
_____ ______ ______ _____ ______ _____ _____ _____ _____ _____ _____ _____
EG (b) EG (b) EG (b) EG (b) EG (b)
(a) (b) (a) (a) (a) (a) (a)
(b) (b) (b) (b) (b)
Static ____ gals




















