Blood Bank Review - ASCLS-Michigan
18
1 Blood Bank Review Mary Burroughs Blood Bank Technical Specialist Mercy Health Saint Mary’s Case #1 – ABO/Rh Forward Grouping Reverse Grouping Anti-A Anti-B Anti-D A1 cells B cells 0 0 3+ 4+ 4+ 2 • Is the ABO grouping discrepant? No • Interpretation: O positive Case #1 – Antibody Screen 3 Screening Cell AHG Reaction I 0 II 4+ • Antibody Screen is Positive • Next Step: Antibody Identification
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Blood Bank Review - ASCLS-Michigan
1
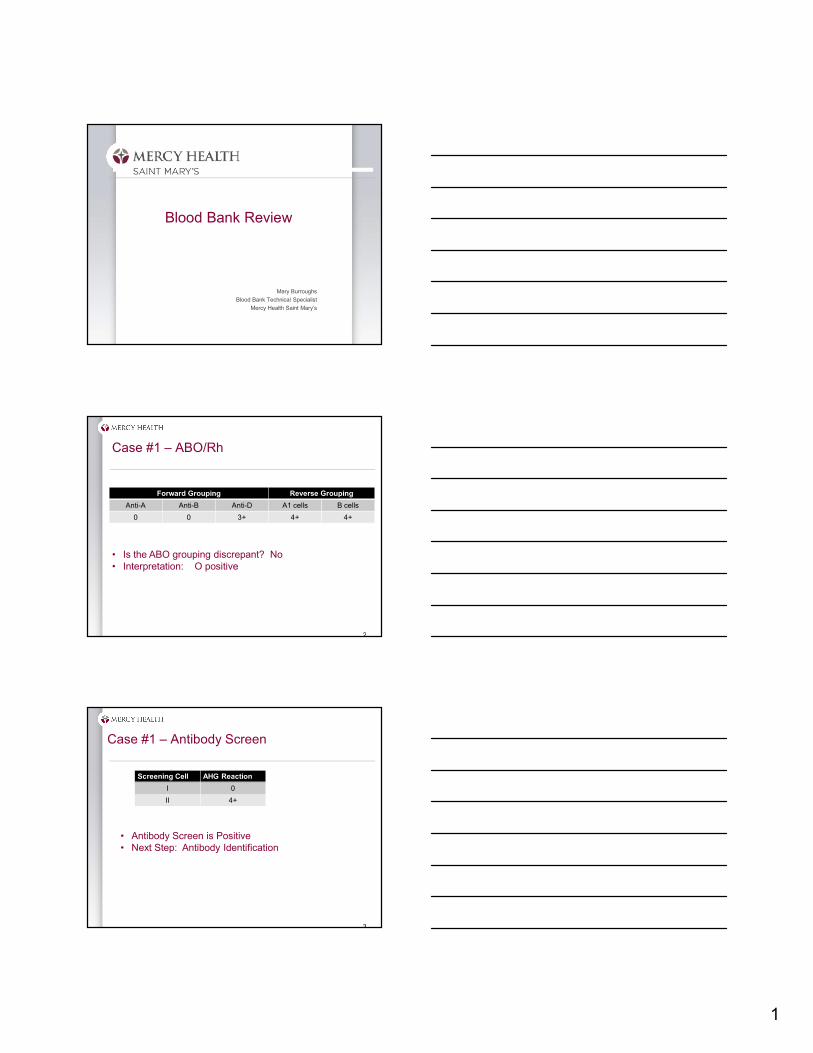
Blood Bank Review
Mary Burroughs
Blood Bank Technical Specialist
Mercy Health Saint Mary’s
Case #1 – ABO/Rh
Forward Grouping Reverse Grouping
Anti-A Anti-B Anti-D A1 cells B cells
0 0 3+ 4+ 4+
2
• Is the ABO grouping discrepant? No• Interpretation: O positive
Case #1 – Antibody Screen
3
Screening Cell AHG Reaction
I 0
II 4+
• Antibody Screen is Positive• Next Step: Antibody Identification
2
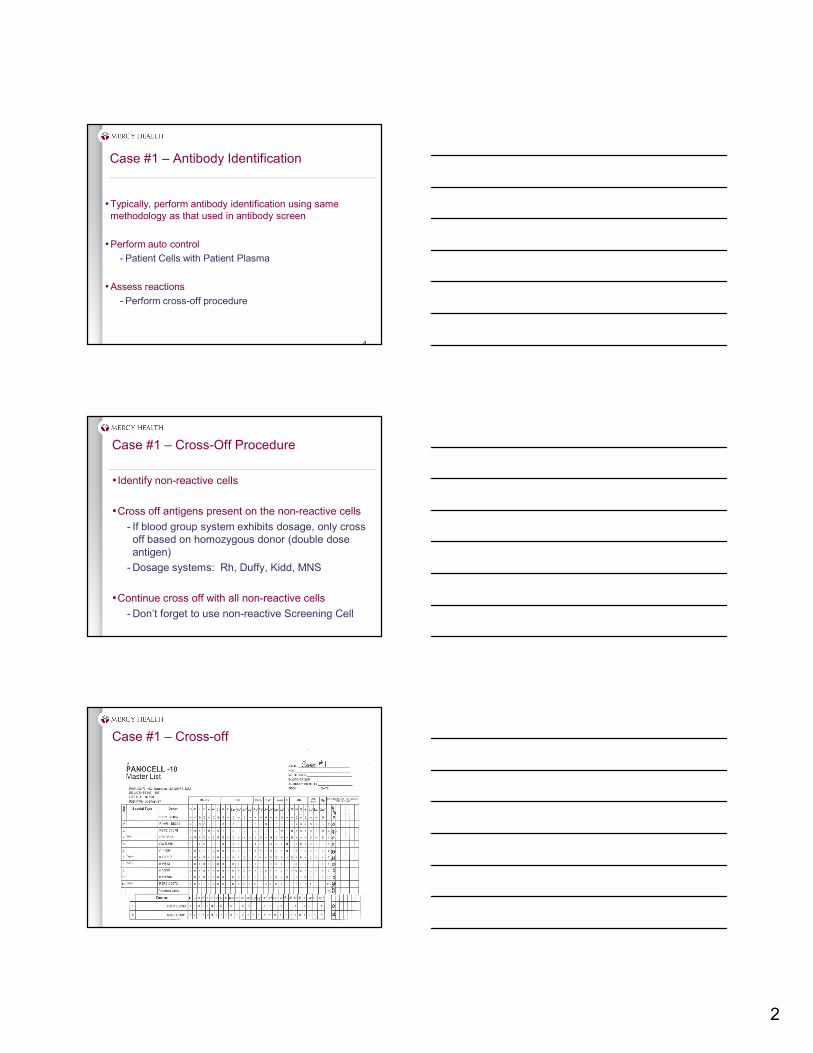
Case #1 – Antibody Identification
•Typically, perform antibody identification using same methodology as that used in antibody screen
•Perform auto control
- Patient Cells with Patient Plasma
•Assess reactions
- Perform cross-off procedure
4
Case #1 – Cross-Off Procedure
• Identify non-reactive cells
•Cross off antigens present on the non-reactive cells
- If blood group system exhibits dosage, only cross off based on homozygous donor (double dose antigen)
- Dosage systems: Rh, Duffy, Kidd, MNS
•Continue cross off with all non-reactive cells
- Don’t forget to use non-reactive Screening Cell
Case #1 – Cross-off
3
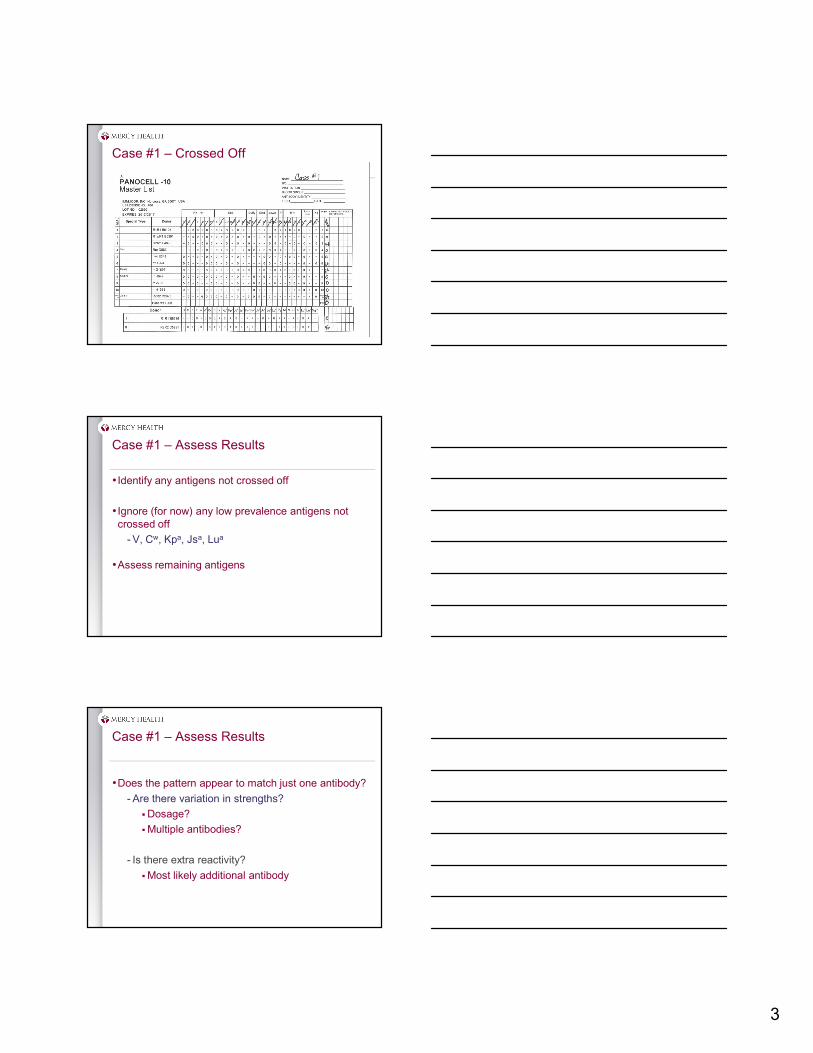
Case #1 – Crossed Off
Case #1 – Assess Results
• Identify any antigens not crossed off
• Ignore (for now) any low prevalence antigens not crossed off
- V, Cw, Kpa, Jsa, Lua
•Assess remaining antigens
Case #1 – Assess Results
•Does the pattern appear to match just one antibody?
- Are there variation in strengths?
Dosage?
Multiple antibodies?
- Is there extra reactivity?
Most likely additional antibody
4
Case #1 – Assess results
•Assess for satisfaction of Rule of Three
- Three reactive cells where antigen is present
- Three non-reactive cells where antigen is absent
- If multiple antibodies – satisfy the Rule of Three independently for each antibody
- Gives 95% certainty that antibody identification is correct.
Case #1 – Further Work?
•Are all non-suspect antigens ruled out?
- Yes
•Have we satisfied the Rule of Three?
- Do we have 3 E+K- cells that reacted?
No – need one more
- Do we have 3 E-K+ cells that reacted?
No – we need two more
- Do we have 3 E-K- cells that failed to react?
Yes
Case #1 – Further Work
•Find additional cells that will fit the phenotype needed
•Run cells using same methodology
•Reassess for expected reactivity
5
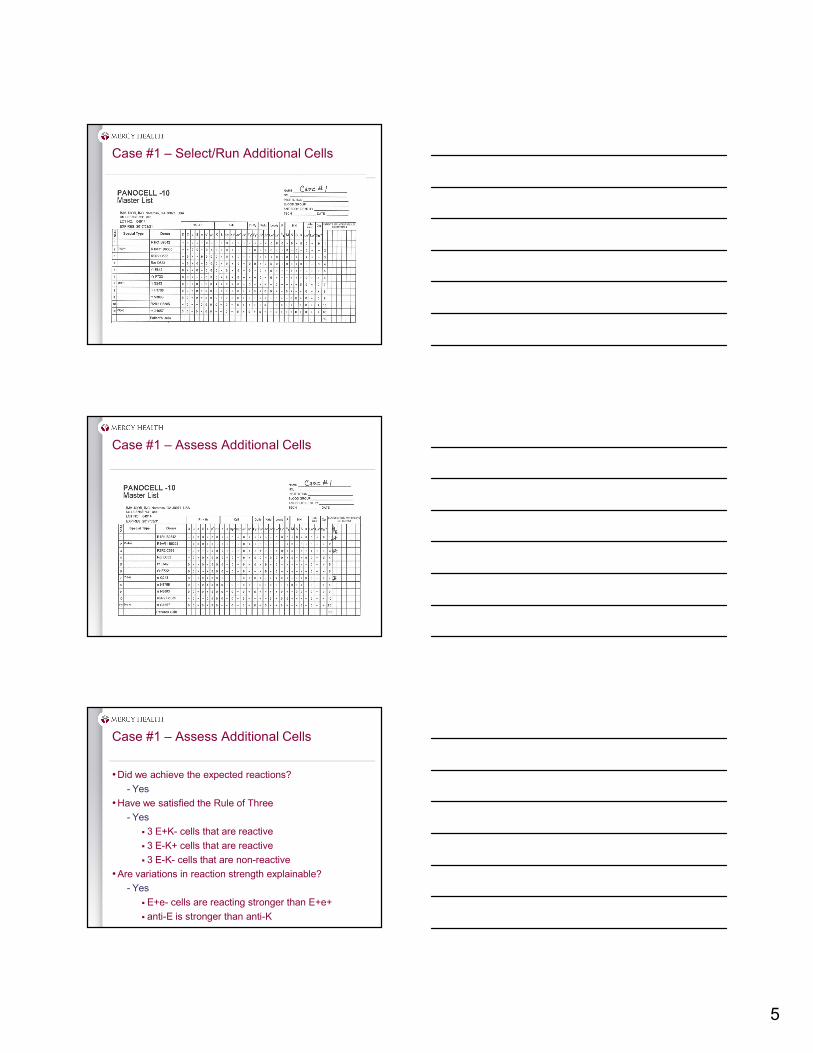
Case #1 – Select/Run Additional Cells
Case #1 – Assess Additional Cells
Case #1 – Assess Additional Cells
•Did we achieve the expected reactions?
- Yes
•Have we satisfied the Rule of Three
- Yes
3 E+K- cells that are reactive
3 E-K+ cells that are reactive
3 E-K- cells that are non-reactive
•Are variations in reaction strength explainable?
- Yes
E+e- cells are reacting stronger than E+e+
anti-E is stronger than anti-K
6
Case #1 - Transfusion
• If this patient needs an RBC Transfusion
- Must supply E-K- unit
- Must perform serologic AHG crossmatch
- If units are incompatible – look for additional antibody (ies)
Case #2 – ABO/Rh
Forward Grouping Reverse Grouping
Anti-A Anti-B Anti-D A1 cells B cells
4+ 0 4+ 3+ 4+
17
• Is the ABO grouping discrepant? Yes• Interpretation: ??
Case #2 – Saline Replacement
•Saline Replacement Technique
- Spin reverse grouping tubes
- Remove plasma with pipette
- Replace removed plasma with 2 drops of saline
- Shake out tubes
- True agglutination will remain but rouleaux will disperse
Reverse Grouping beforeSaline Replacement
A1 cells B cells
3+ 4+
Reverse Grouping afterSaline Replacement
A1 cells B cells
3+ 4+
7
Case #2 – Antibody Screen Gel Card
Causes for Mixed Field in Gel
• Patient Reacting to pre-diluted cells
- Most common reason we see mixed field in gel in our lab
- Resolve by diluting 3% cells to 0.8% and repeating in gel
- BUT – in this case we also have the ABO discrepancy
• Rouleaux
- Already attempted saline replacement in ABO discrepancy without resolution
• Actual two cell population
- Would not be seen in antibody screen since commercial cells are from non-transfused donors
• IgM antibodies
- Start our investigation here.
Case #2 – Antibody Screen
21
Screening Cell AHG Reaction
I mf
II 0
• Antibody Screen is Invalid
• Next Step: Antibody Identification –Alternate Method
8
Case #2 – Original Panel – LISS/Tube
Case #2 – Cross-Off Procedure
• Identify non-reactive cells in all 3 phases
•Cross off antigens present on the non-reactive cells
- If blood group system exhibits dosage, only cross off based on homozygous donor (double dose antigen)
- Dosage systems: Rh, Duffy, Kidd, MNS
•Continue cross off with all non-reactive cells
Case #2 – Assess Results
• Identify any antigens not crossed off
• Ignore (for now) any low prevalence antigens not crossed off
- V, Cw, Kpa, Jsa, Lua
•Assess remaining antigens
9
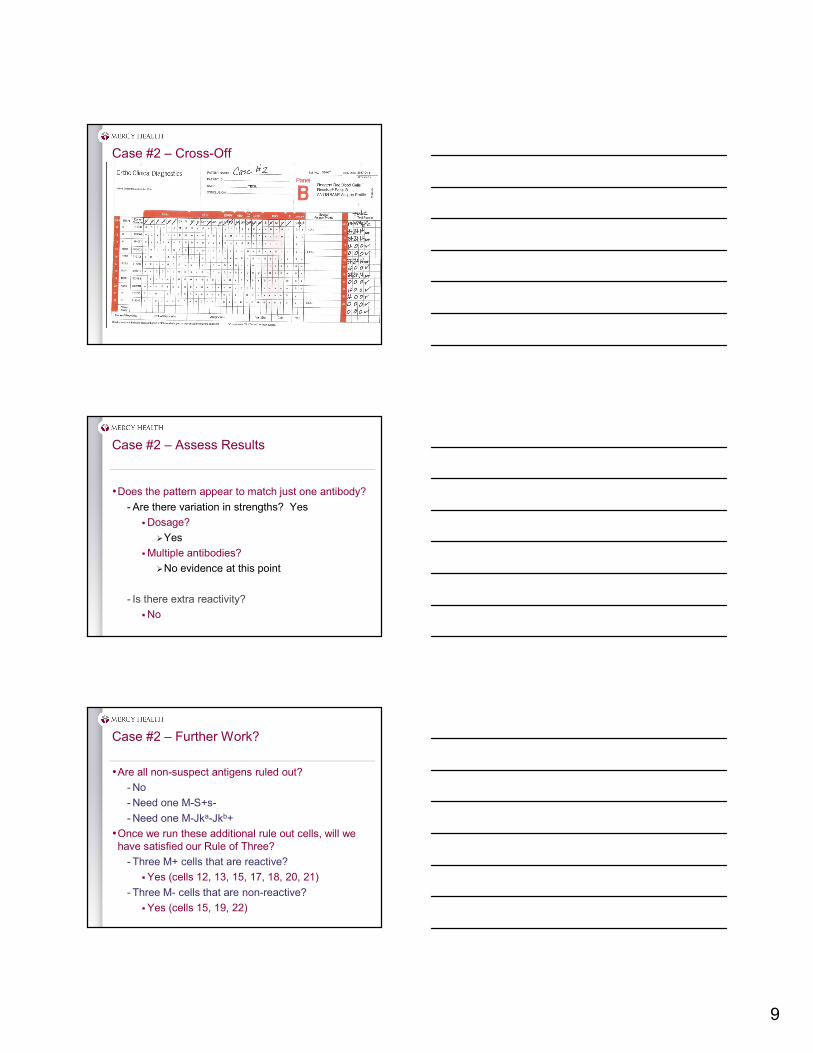
Case #2 – Cross-Off
Case #2 – Assess Results
•Does the pattern appear to match just one antibody?
- Are there variation in strengths? Yes
Dosage?
Yes
Multiple antibodies?
No evidence at this point
- Is there extra reactivity?
No
Case #2 – Further Work?
•Are all non-suspect antigens ruled out?
- No
- Need one M-S+s-
- Need one M-Jka-Jkb+
•Once we run these additional rule out cells, will we have satisfied our Rule of Three?
- Three M+ cells that are reactive?
Yes (cells 12, 13, 15, 17, 18, 20, 21)
- Three M- cells that are non-reactive?
Yes (cells 15, 19, 22)
10
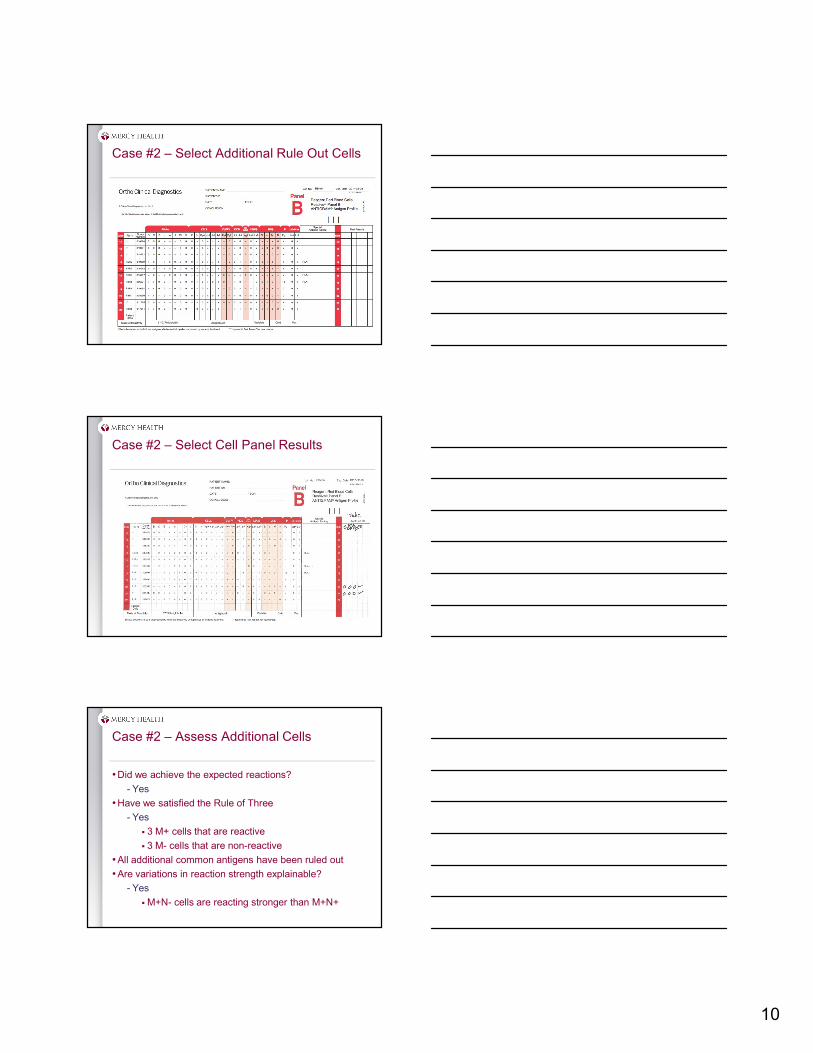
Case #2 – Select Additional Rule Out Cells
Case #2 – Select Cell Panel Results
Case #2 – Assess Additional Cells
•Did we achieve the expected reactions?
- Yes
•Have we satisfied the Rule of Three
- Yes
3 M+ cells that are reactive
3 M- cells that are non-reactive
•All additional common antigens have been ruled out
•Are variations in reaction strength explainable?
- Yes
M+N- cells are reacting stronger than M+N+
11
Alternate Method for Rule Outs
•M-S+s- is a rare cell. What if not available?
- Antigen Type the patient
Cannot be transfused in past three months
If antigen positive – patient cannot make corresponding allo antibody
Saves from having to rule out in the future
Patient cannot have positive DAT if commercial antisera utilizes an AHG reaction.
Cells are already coated with antibody and will give possible false positive reaction at AHG.
What about our ABO Discrepancy?
•Commercial A1 and B cells are a pool of donors
- Most likely several of those donors are M+
- Type commercial cells for M
- Perform reverse grouping using known M- reverse grouping cells to resolve discrepancy
- Patient is A positive
Forward Grouping Reverse Grouping
Anti-A Anti-B Anti-D M- A1 cells M- B cells
4+ 0 4+ 0 4+
Case #2 - Transfusion
• If this patient needs an RBC Transfusion
- Refer to institutional policy
- Options:
Supply AHG xm compatible, M- units
Supply AHG xm compatible units
Treat as non clinically significant and don’t perform AHG crossmatch
12
Case #3
•43yo Female with bowel obstruction
•Hgb 8.5 g/dl
•Scheduled for colectomy on 2/15/17
Case #3 – ABO/Rh
• Is the ABO grouping discrepant? No
• Interpretation: B positive
Forward Grouping Reverse Grouping
Anti-A Anti-B Anti-D A1 cells B cells
0 4+ 4+ 4+ 0
Case #3 – Antibody Screen
Screening Cell AHG Reaction
I 0
II 4+
• Antibody Screen is Positive• Next Step: Antibody Identification
13
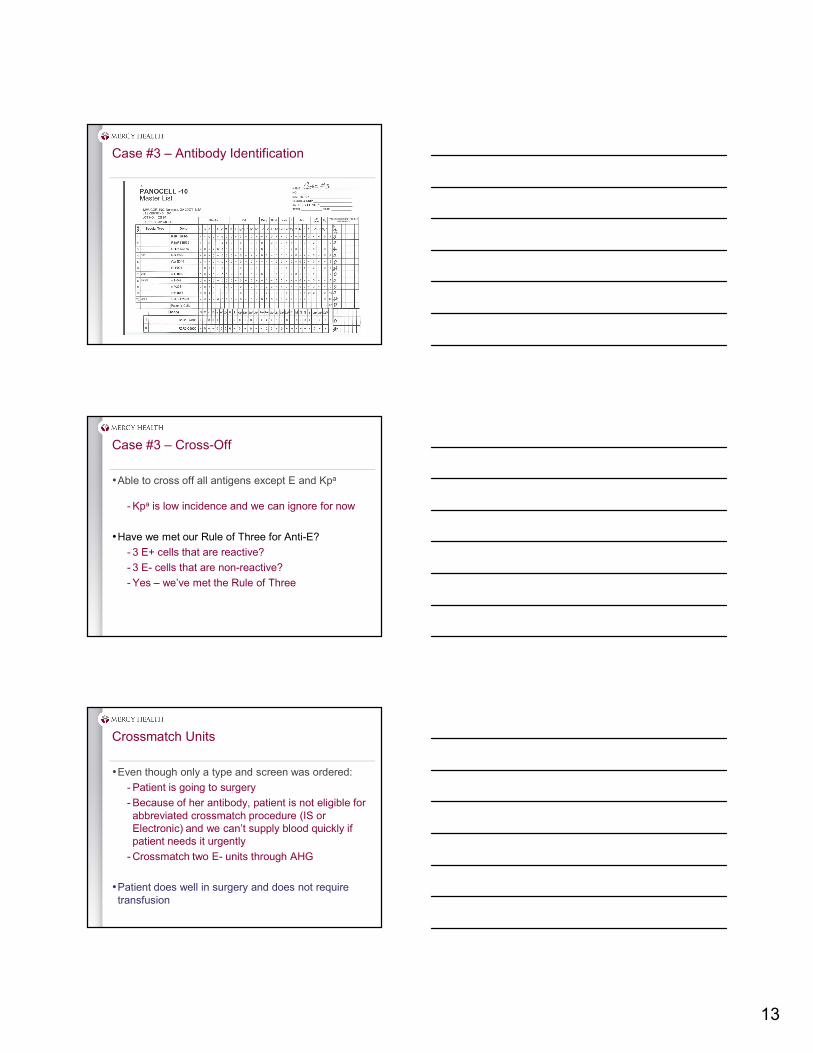
Case #3 – Antibody Identification
Case #3 – Cross-Off
•Able to cross off all antigens except E and Kpa
- Kpa is low incidence and we can ignore for now
•Have we met our Rule of Three for Anti-E?
- 3 E+ cells that are reactive?
- 3 E- cells that are non-reactive?
- Yes – we’ve met the Rule of Three
Crossmatch Units
•Even though only a type and screen was ordered:
- Patient is going to surgery
- Because of her antibody, patient is not eligible for abbreviated crossmatch procedure (IS or Electronic) and we can’t supply blood quickly if patient needs it urgently
- Crossmatch two E- units through AHG
•Patient does well in surgery and does not require transfusion
14
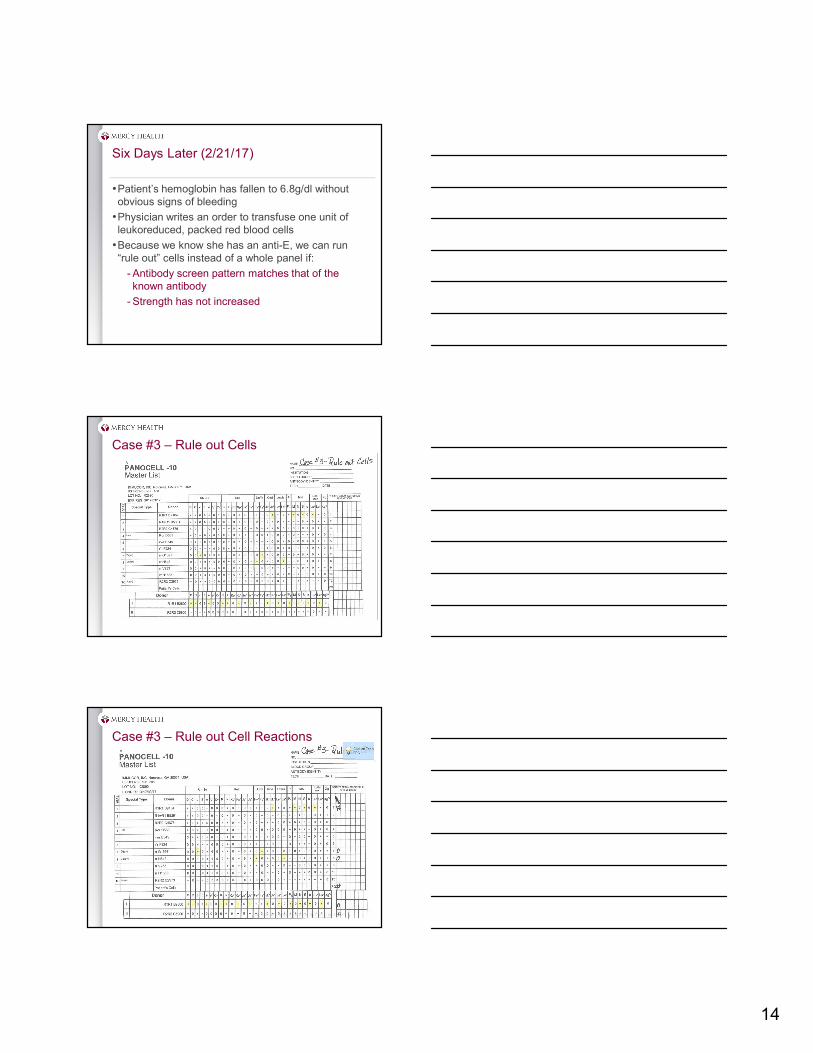
Six Days Later (2/21/17)
•Patient’s hemoglobin has fallen to 6.8g/dl without obvious signs of bleeding
•Physician writes an order to transfuse one unit of leukoreduced, packed red blood cells
•Because we know she has an anti-E, we can run “rule out” cells instead of a whole panel if:
- Antibody screen pattern matches that of the known antibody
- Strength has not increased
Case #3 – Rule out Cells
Case #3 – Rule out Cell Reactions
15
Case #3 – Full Panel Results
Case #3 – Cross-Off
Case #3 – Panel Assessment
•Other than the anti-E; what additional antibody appears to be present?
- Kpa, Jkb, S, and Lua remain after cross-off
- Ignore low incidence for now: Kpa, Lua
- Looking at the E- cells, does the pattern fit Jkb or S perfectly?
Yes – perfect Jkb pattern showing dosage
16
Case #3 – Additional Work
•Need to rule out anti-S with E-, Jkb-, S+s- cell
•Have we satisfied the Rule of Three?
- We have 3 Jkb+ cells that are reactive
- We have 3 E-, Jkb- cells that are non-reactive
- We only have 1 E+, Jkb- cell that is reactive
Refer to institutional policy regarding previously identified antibodies
•What about the positive Auto Control?
- Need to perform an elution and identify that antibody
Case #3 – Rule out S
Elution
•Dissociate antibody from the cell for purposes of phenotyping the red cell
- Acid/Glycine EDTA or Chloroquine
•Dissociate antibody from the cell leaving the antibody in usable form for identification
- Heat or Freeze/Thaw – used for ABO HDN investigations
- Acid or organic solvents
17
Case #3 – Eluate Results
Case # 3 - Interpretation
•Anti-E and anti-Jkb
•Anti- Jkb is also coating the patient cells
- Where did this come from?
Not present 6 days ago
Patient had remained hospitalized and not received blood
- Communication with patient revealed prior medical history in Florida and also a transfusion at a different hospital in Grand Rapids.
Case #3 – Medical History Investigation
•Called other Grand Rapids hospital
- Positive antibody screen – identified anti-E
- Transfused two E- RBC on 2/14/17 (day before admission to our hospital)
•Called Florida hospital
- Patient had been seen in previous years
- Anti-E and anti-Jkb identified!!!!!!
18
Case #3 - Conclusion
•Previous history of anti-E, anti-Jkb
•Anti-Jkb had fallen to undetectable levels
•Both of the units given at neighboring GR hospital had been Jkb +
•Patient suffered Delayed Hemolytic Transfusion Reaction
- Low grade fever
- Hemoglobin fell from 8.5 g/dl to 6.8 g/dl in 7 days
- Bilirubin rose from 0.5 mg/dl to 2.3 mg/dl
- No “pre” LDH – but post LDH was 430 IU/L
•Thank you for your attention today
•Good luck to the students taking the national certification exam
•Remember: Antibodies are what make blood banking fun!