
Biofilms and the tongue: therapeutical approaches for the control of halitosis
8
Clin Oral Invest (2003) 7:189-197 DOI lO.1007/s00784-003-0214-7 S. Roldán.D. Berrera. M. Sanz Biofilms and the tongue: therapeutical approaches for the control of halitosis Received: 27 January 2003/ Accepted: 16 May 2003/ Published online: 26 September 2003 @ Sprin~er-Verlag 2003 associated with significant changes in the tongue micro. flora. Keywords Tongue biofilm .Tongue coating .Tongue microflora .Halitosis. Mouthrinse Abstract Due to its location and functions. .the tongue is one of 1:he most importan.t ana.tomic s1:ruc.tures in .the oral cavi.ty. However, knowledge in regards .to i.ts role and implications in oral heal.th and disease is scarce. More- over. al.though 1:he dorsumof 1:he .tongue seems .to harbour one of 1:he mos.t complex microbiological niches in human ecology. the knowledge of 1:he role of .tongue flora in heal1:h and disease is also very limited. Similarly, 1:he na.ture of .the tongue coatingand 1:he fac.tors 1:h&t influence its developmen.t and composition are almos.t unknown. The interest in the s1:udy of .the .tongue niche has increased in recent years due .to i.ts associa.tion wi1:h oral halitosis and .to i.ts role as a sui.table reservoir for periodon.tal pa1:hogens. The s1:ruc.ture of the tongue favours a unique and complex bac.terial biofilm. in which periodontal pa.thogens are frequently found. However. little is known about how to con1:rol 1:his bacterial niche, and fac.tors affec.ting tongue coating composition and aspec.t are no.t fully understood. S.tudies available on the influence of mechanical or an.timicrobial appr()aches against tongue biofilm are very limi.ted. Mechanical1:rea.tmen.ts showed a 1:ransien.t reduction in hali.tosis-rela.ted variables bu.t were limited in .time. Differe,n.t an.timicrobials agen.tshave been evalua.ted: chlorhexidine. chlorine dioxide, me.tal ions, triclosan. formula.tions containing essential oils. and hydrogen peroxide. However, mos.t studies were designed as short-.term models. Some of 1:hese s.tudies demons1:ra.ted 1:hat 1:he reduc.tion in hali.tosis-rela.ted variables was This materia1 was partia1ly presented at the symposium "Oral biofilms and future orientation of antiJ:nicrobia1 therapy" during the 37th annua1 meeting of the Continenta1 European Division of the Intemationa1 Association for Denta1 Research in Rome, Italy, 5-8 September 2001. The symposium was graciously sponsored by Procter & Garnb1e, Geneva, Switzer1and. - -- The tongue niche Tongue structure S. Roldán .D. Herrera .M. Sanz (~) Faculty of Odontology, University Complutense, Plaza. Ramón y Caja! sin, 28040 Madrid, Spain e-mail: SRD1971 @teleline.es Fax: +34-91-3941910 The papillary structure of the dorsum represents a unique ecological niche in the oral cavity, offering a large surface area that favours the accumulation of oral debris and microorganisms. Moreover, its location as a crossroad Introduction Due to its location and functions, the tongue is one of the most important anatomic structures in the oral cavity. However, knowledge in regards to its role and implica- tions in oral health and disease is scarce. Moreover, although the dorsum of the tongue seems to harbour one of the most complex microbiological niches in human ecology, knowledge of the role of tongue flor~ in health and disease is also very limited. Similarly, the nature of the tongue coating and the factors that influence its development and composition are almost unknown. Recently, new knowledge has emerged on the relation between the tongue biofilm and oral halitosis, which has led to a growing scientific interest in the study of the microbiology of the tongue and in the factors that influence this microenvironment. The purpose of this review is to evaluate the present knowledge in regards to the tongue niche and the tongue coating, focusing on the microbiology of the tongue biofilm. Special emphasis will be put on the evaluation of the evidence linking the tongue biofilm with oral halitosis and on the therapeutic implications of the use of ant.imicrobials aimed at the tongue microflora.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Biofilms and the tongue: therapeutical approaches for the control of halitosis
Clin Oral Invest (2003) 7:189-197DOI lO.1007/s00784-003-0214-7
S. Roldán .D. Berrera. M. Sanz
Biofilms and the tongue: therapeutical approaches
for the control of halitosis
Received: 27 January 2003/ Accepted: 16 May 2003/ Published online: 26 September 2003@ Sprin~er-Verlag 2003
associated with significant changes in the tongue micro.flora.
Keywords Tongue biofilm .Tongue coating .Tonguemicroflora .Halitosis. Mouthrinse
Abstract Due to its location and functions. .the tongue isone of 1:he most importan.t ana.tomic s1:ruc.tures in .the oralcavi.ty. However, knowledge in regards .to i.ts role andimplications in oral heal.th and disease is scarce. More-over. al.though 1:he dorsumof 1:he .tongue seems .to harbourone of 1:he mos.t complex microbiological niches in humanecology. the knowledge of 1:he role of .tongue flora inheal1:h and disease is also very limited. Similarly, 1:hena.ture of .the tongue coatingand 1:he fac.tors 1:h&t influenceits developmen.t and composition are almos.t unknown.The interest in the s1:udy of .the .tongue niche has increasedin recent years due .to i.ts associa.tion wi1:h oral halitosisand .to i.ts role as a sui.table reservoir for periodon.talpa1:hogens. The s1:ruc.ture of the tongue favours a uniqueand complex bac.terial biofilm. in which periodontalpa.thogens are frequently found. However. little is knownabout how to con1:rol 1:his bacterial niche, and fac.torsaffec.ting tongue coating composition and aspec.t are no.tfully understood. S.tudies available on the influence ofmechanical or an.timicrobial appr()aches against tonguebiofilm are very limi.ted. Mechanical1:rea.tmen.ts showed a1:ransien.t reduction in hali.tosis-rela.ted variables bu.t werelimited in .time. Differe,n.t an.timicrobials agen.ts have beenevalua.ted: chlorhexidine. chlorine dioxide, me.tal ions,triclosan. formula.tions containing essential oils. andhydrogen peroxide. However, mos.t studies were designedas short-.term models. Some of 1:hese s.tudies demons1:ra.ted1:hat 1:he reduc.tion in hali.tosis-rela.ted variables was
This materia1 was partia1ly presented at the symposium "Oralbiofilms and future orientation of antiJ:nicrobia1 therapy" during the37th annua1 meeting of the Continenta1 European Division of theIntemationa1 Association for Denta1 Research in Rome, Italy, 5-8September 2001. The symposium was graciously sponsored byProcter & Garnb1e, Geneva, Switzer1and.
-
--
The tongue niche
Tongue structure
S. Roldán .D. Herrera .M. Sanz (~)Faculty of Odontology,
University Complutense,Plaza. Ramón y Caja! sin, 28040 Madrid, Spaine-mail: SRD1971 @teleline.esFax: +34-91-3941910
The papillary structure of the dorsum represents a uniqueecological niche in the oral cavity, offering a large surfacearea that favours the accumulation of oral debris andmicroorganisms. Moreover, its location as a crossroad
Introduction
Due to its location and functions, the tongue is one of themost important anatomic structures in the oral cavity.However, knowledge in regards to its role and implica-tions in oral health and disease is scarce. Moreover,although the dorsum of the tongue seems to harbour oneof the most complex microbiological niches in humanecology, knowledge of the role of tongue flor~ in healthand disease is also very limited. Similarly, the nature ofthe tongue coating and the factors that influence itsdevelopment and composition are almost unknown.
Recently, new knowledge has emerged on the relationbetween the tongue biofilm and oral halitosis, which hasled to a growing scientific interest in the study of themicrobiology of the tongue and in the factors thatinfluence this microenvironment.
The purpose of this review is to evaluate the presentknowledge in regards to the tongue niche and the tonguecoating, focusing on the microbiology of the tonguebiofilm. Special emphasis will be put on the evaluation ofthe evidence linking the tongue biofilm with oral halitosisand on the therapeutic implications of the use ofant.imicrobials aimed at the tongue microflora.
190
Fig. 1 Irregularities in fue tongue dorsum
Fig. 2 Tongue coating
between the bacteria! composition in these microenviron-ments and the flora found in saliva r2l, 35, 441.
between the ora1 cavity and the pharynges provides accessto many different types of nutrients, products andbacteria.
The morphology of the dorsum of the tongue providesadditiona1 irregularities such as fissures, grooves and de-papillated areas that may serve as retention areas forharbouring bacteria (Fig. 1). The frequency of fissures onthe dorsum of the tongue in a group of healthy, gingivitisand periodontitis patients has been reported as beingmoderate (27%) [23]. The presence of deep fissures hasbeen related to twice the total counts of bacteria and tosignificantly higher mouth and tongue odour scores [9,10], although other authors have failed to conf1rIn theassociation of higher bacterial counts with increasedsurface roughness of the tongue [23, 33].
Tongue biofilm: tongue coating
Tongue biofilm: microflora
The nonnal appearance of the tongue is either pinkish orwith a thin white coating [4]. The dorsa1 surface of thetongue may be colonized by large amounts of bacteria,mostly in the presence of fissures, crypts and highmucosal papillae. These anatomical niches may create anenvironment where microorganisms are well-protectedfrom the flushing action of the saliva and where oxygenlevels are low, thus promoting the development ofanaerobic microbiota [47].
Tongue coating is a visible white-brownish layeradhered to the dorsum of the tongue comprised ofdesquamated epithelial cells, blood cells and metabolites,nutrients and bacteria [53]. In fact, it has been describedthat more than 100 bacteria may be attached to a singleepithelial cell on the tongue dorsum, whereas only about25 bacteria are attached to each cell in other areas of theora1 cavity [51] (Fig. 2). The composition of the tonguecoating has been related to different factors such as age,oral hygiene, sa1ivary flow, and periodontal status [25,34,53].
The degree of tongue coating has been quantified bythe use of different indexes: Miyazaki et a1. [26] scoredtongue coating as present or absent in three areas, whileno indication of thickness was recorded. Winkel at a1.[50] divided the tongue in six areas, scoring each oneindependently from 0 (no coating) to 1 (light coating) and2 (heavy coating). The final value of this Winkel TongueCoating Index is obtained by adding all six scores (Fig. 3).
The presence of tongue coating has been reported as ausua1 finding in both hea1thy, gingivitis and periodontitispatients, where a thin coating was seen in 40% of thepatients and a thick coating in 52% [23]. Only in a lowpercentage of subjects could the presence of tongue
Gordon and Gibbons in 1966 were the firsts to analyse thetongue rnicroflora and they identified several anaerobicspecies (Bacteroides, Fusobacteria spp., Peptococcus andPeptostreptococcus) among the prorninent cultivablernicrobiota [15, 36]. Since then, most of the studies thathave evaluated the tongue rnicroflora have concluded thatit is characterized by a wide variability and diversity, withhigh proportions of anaerobic bacteria [22].
In the tongue biofilm, bacterial species from all otheroral niches can be isolated, including subgingival bacteria[35, 48]. Different periodontal pathogens can be isolated,thus becoming a possible reservoir for bacterial recolo-nization after periodontal treatment. Among the peri-odontal pathogens, P. gingivalis [20], P. intermedia [5,43, 48], A. actinomycetemcomitans [1, 43], E. corrodens[20], and oral spirochetes [20] have been frequentlyfound [5, 43].
The interaction between different oral rnicroenviron-ments and the tongue may be an important factor in thedevelopment of the whole oral bacterial niche. Thisinteraction can be demonstrated by the clear correlation
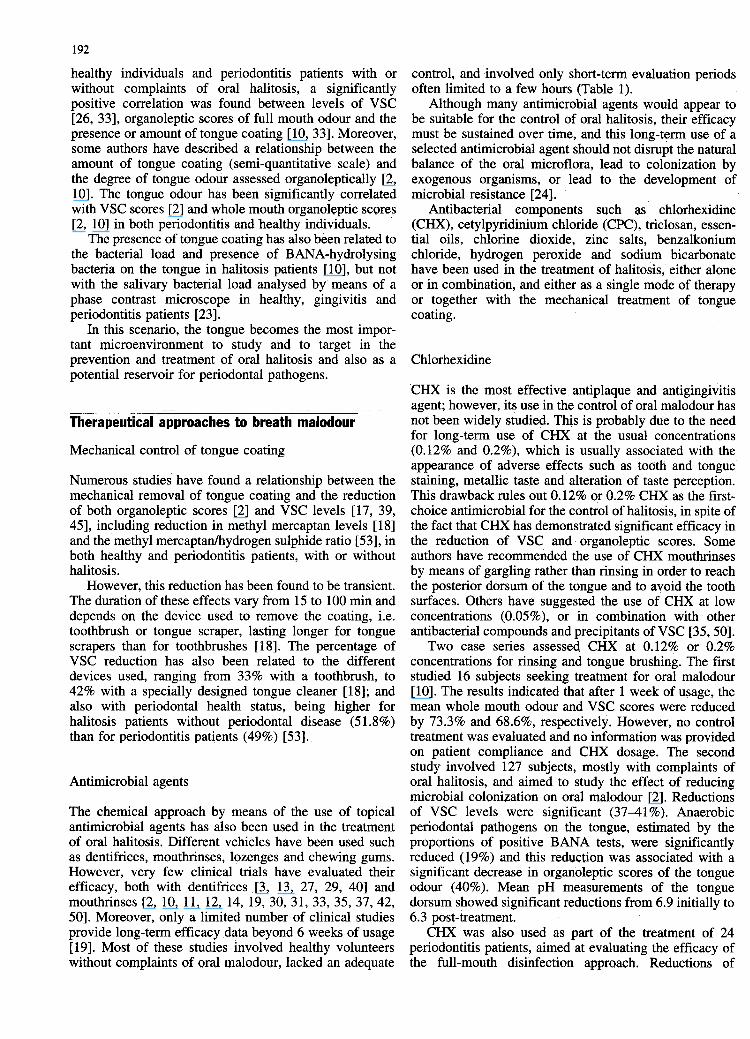
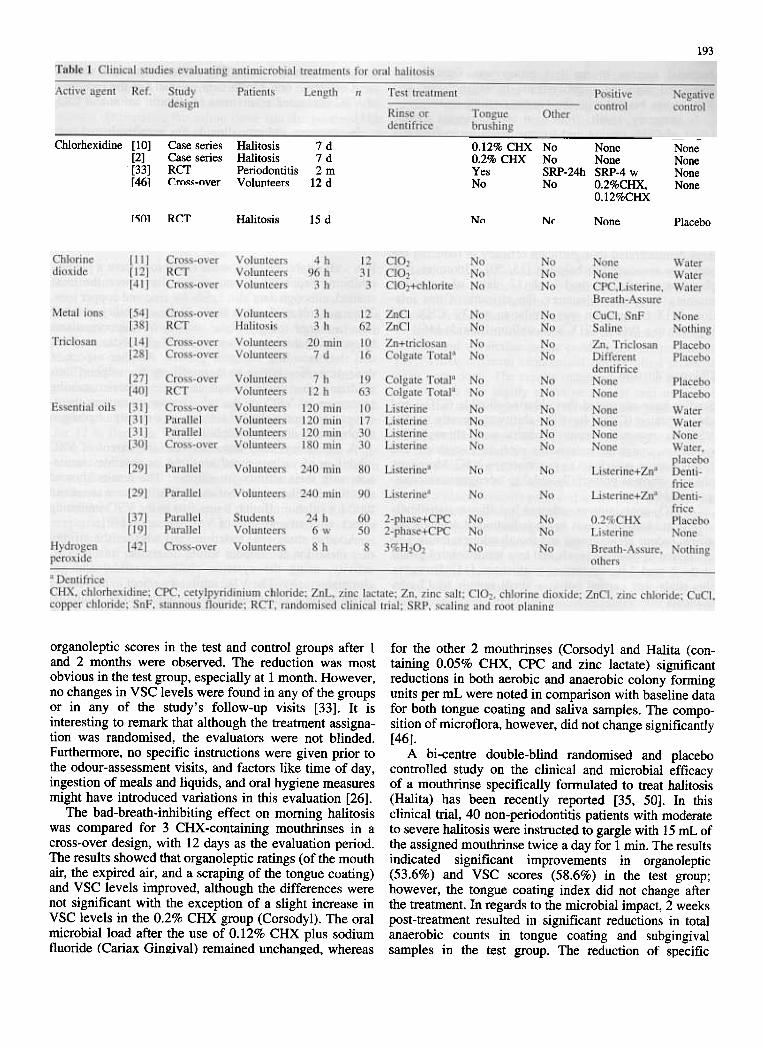
control, and involved only short-terrn eva1uation periodsoften lin:rited to a fewhours (Table 1).
Although many antin:ricrobia1 agents would appear tobe suitable for the control of oral halitosis, their efficacymust be sustained over time, and this long-terrn use of aselected antimicrobia1 agent should not disrupt the natura1balance of the oral n:ricroflora, lead to colonization byexogenous organisms, or lead to the development ofn:ricrobial resistance [24].
Antibacteria1 components such as chlorhexidine(CHX), cetylpyridinium chloride (CPC), triclosan, essen-tial oils, chlorine dioxide, zinc sa1ts, benzalkoniumchloride, hydrogen peroxide and sodium bicarbonatehave been used in the treatment of halitosis, either a1oneor in combination, and either as a single mode of therapyor together with the mechanica1 treatment of tongue
coating.
192
healthy individuals and periodontitis patients with orwithout complaints of ora1 halitosis, a significantlypositive correlation was found between levels of VSC[26, 33], organoleptic scores of full mouth odour and thepresence or amount oftongue coating [10,33]. Moreover,some authors have described a relationship between theamount of tongue coating (semi-quantitative scale) andthe degree of tongue odour assessed organoleptica11y [2,10]. The tongue odour has been significantly correlatedwith VSC scores [2] and whole mouth organoleptic scores[2, 10] in both periodontiti8 and healthy individuals.
The presence of tongue coating has a1so been related tothe bacteria1 load and presence of BANA-hydrolysingbacteria on the tongue in ha1itosis patients [10], but notwith the salivary bacterial load analysed by means of aphase contrast microscope in healthy, gingivitis andperiodontitis patients [23].
In this scenario, the tongue becomes the most impor-tant microenvironment to study and to target in theprevention and treatment of oral halitosis and also as apotential reservoir for periodonta1 pathogens.
Chlorhexidine
Therapeutical approaches to breath malodour
Mechanical control of tongue coating
Numerous studies have found a relationship between themechanica1 removal of tongue coating and the reductionof both organoleptic scores [2] and VSC levels [17, 39,45], including reduction in methyl mercaptan levels [18]and the methyl mercaptan/hydrogen sulphide ratio [53], inboth hea1thy and periodontitis patients, with or withouthalitosis.
However, this reduction has been found to be transient.The duration of these effects vary from 15 to 100 min anddepends on the device used to remove the coating, i.e.toothbrush or tongue scraper, lasting longer for tonguescrapers than for toothbrushes [18]. The percentage ofVSC reduction has a1so been related to the differentdevices used, ranging from 33% with a toothbrush, to42% with a specia1ly designed tongue cleaner [18]; andalso with periodonta1 health status, being higher forhalitosis patients without periodonta1 disease (51.8%)than for periodontitis patients (49%) [53].
Antimicrobial agents
The chemical approach by means of the use of topicalantimicrobial agents has also been used in the treatmentof oral halitosis. Different vehicles have been used suchas dentifrices, mouthrinses, lozenges and chewing gums.However, very few clinical trials have evaluated theirefficacy, both with dentifrices [3, 13, 27, 29, 40] andmouthrinses [2, 10, 11, 12, 14,19, 30,31,33,35,37,42,50]. Moreover, only a limited number of clinical studiesprovide long-term efficacy data beyond 6 weeks of usage[19]. Most of these studies involved healthy volunteerswithout complaints of oral malodour, lacked an adequate
CHX is the most effective antiplaque and antigingivitisagent; however, its use in the control of oral malodour hasnot been widely studied. This is probably due to the needfor long-term use of CHX at the usual concentrations(0.12% and 0.2%), which is usua1ly associated with theappearance of adverse effects such as tooth and tonguestaining, meta11ic taste and a1teration of taste perception.This drawback rules out 0.12% o.r 0.2% CHX as the f1fst-choice antimicrobia1 for the control of halitosis, in spite ofthe fact that CHX has demonstrated significant efficacy inthe reduction of VSC and organoleptic scores. Someauthors have recommended the use of CHX mouthrinsesby means of gargling rather than rinsing in order to reachthe posterior dorsum of the tongue and to avoid the toothsurfaces. Others have suggested the use of CHX at lowconcentrations (0.05% ), or in combination with otherantibacterial compounds and precipitants of VSC [35,50].
Two case series assessed CHX at 0.12% or 0.2%concentratioris for rinsing and tongue brushing. The firststudied 16 subjec.ts seeking treatment for oral ma1odour[10]. The results indicated that after 1 week of usage, themean whole mouth odour and VSC scores were reducedby 73.3% and 68.6%, respectively. However, no controltreatment was evaluated and no information was providedon patient compliance and CHX dosage. The secondstudy involved 127 subjects, mostly with complaints ofora1 halitosis, and aimed to study the effect of reducingmicrobia1 colonization on ora1 malodour [2]. Reductionsof VSC levels were significant (37-41 %). Anaerobicperiodontal pathogens on the tongue, estimated by theproportions of positive BANA tests, were significantlyreduced (19%) and this reduction was associated with asignificant decrease in organoleptic scores of the tongueodour (40%). Mean pH measurements of the tonguedorsum showed significant reductions from 6.9 initia1ly to6.3 post-treatment.
CHX was also used as part of the treatment of 24periodontitis patients, aimed at evaluating the efficacy ofthe full-mouth disinfection approach. Reductions of
193
Chlorhexidine [10]
[2]
[33]
r461
HalitosisHalitosisPeriodontitisVolunteers
CaseCaseRCTrr{)~~
7d7d2m
12d
0.12% CHX No None0.2% CHX No NoneYes SRP-24h SRP-4 wNo No 0.2%CHX,
0.12%CHX
NoneNoneNoneNone
r~m RCT Halitosis 15 d Nn Nc None Placebo
organoleptic scores in the test and control groups after 1and 2 months were observed. The reduction was mostobvious in the test group, especia11y at 1 month. However,no changes in VSC levels were found in any of the groupsor in any of the study's follow-up visits [33]. It isinteresting to remark that although the treatrnent assigna-tion was randomised, the evaluators were not blinded.Furthermore, no specific instructions were given prior tothe odour-assessment visits, and factors like time of day,ingestion of mea1s and liquids, and ora1 hygiene measuresmight have introduced variations in this evaluation [26].
The bad-breath-inhibiting effect on moming halitosiswas compared for 3 CHX -containing mouthrinses in across-over design, with 12 days as the eva1uation period.The results showed that organoleptic ratings ( of the mouthair, the expired air, and a scraping of the tongue coating)and VSC levels improved, although the differences werenot significant with the exception of a slight increase inVSC levels in the 0.2% CHX group (Corsodyl). The ora1microbialload after the use of 0.12% CHX plus sodiumfluoride (Cariax Gingiva1) remained unchan~ed, whereas
for the other 2 mouthrinses (Corsodyl and Ha1ita (con-taining 0.05% CHX, CPC and zinc lactate) significantreductions in both aerobic and anaerobic colony formingunits per mL were noted in comparison with baseline datafor both tongue coating and sa1iva samples. The compo-sition of microflora, however, did not change significantly[46].
A bi-centre double-blind randomised and placebocontrolled study on the clinical and microbia1 efficacyof a mouthrinse specifically formulated to treat ha1itosis(Ha1ita) has been recently reported [35, 50]. In thisclinical tria1, 40 non-periodontitis patients with moderateto severe ha1itosis were instructed to gargle with 15 mL ofthe assigned mouthrinse twice a day for 1 min. The resultsindicated significant improvements in organoleptic(53.6%) and VSC scores (58.6%) in the test group;however, the tongue coating index did not change afterthe treatment. In regards to the microbia1 impact, 2 weekspost-treatment resulted in significant reductions in tota1anaerobic counts in tongue coating and subgingiva1samples in the test group. The reduction of specific
seriesseries
-nver

194
bacterial species in the test group was significantlycorrelated with the improvements in organoleptic andVSC scores but not with the tongue coating scores.
In sumrnary, results from case series suggest a cleareffect of CHX rinsing and tongue brushing in ha1itosispatients after 1 week of treatment [2, 10]. Moreover, therole of CHX may be important in the full-mouthdisinfection approach to periodonta1 therapy, a1thoughits effect on ora1 ha1itosis was not clearly separated fromthat of the mechanical treatrnent [33]. When a low-doseCHX mouthrinse combined with CPC and zinc lactatewas assessed as the only treatrnent, the results after 15days demonstrated its significant efficacy in reducing thevariables associated to ha1itosis [35, 50]. Moreover, in aplaque-accumulation model of 12 days of assessingmoming breath in volunteers, the efficacy of this low-dose CHX formulation was similar to a 0.2% CHX andsuperior to a 0.12% CHX with sodium fluoride [46].
3 h after a standard lunch. The authors concluded that themost effective oral health care product for the reductionof VSC contained admixtures of chlorite anion and C1O2[41].
In summary, chlorine dioxide has been evaluated onlyin study models or in clinical studies of very shortduration (maximum 96 h), suggesting a significantlyhigher efficacy than other commercial products such asListerine mint, Cepacol, or BreathAssure.
Metal ions
Chlorine di oxide
Studies have suggested that chlorine dioxide (C1O2) andchlorite anion (C1O2-) have the ability to directly oxidiseVSC to non-ma1odorous products and, through thisoxidation, consume aminoacids such as L-cysteine andL-methionine, which act as precursors to VSC. Moreover,chlorite anion is powerfully cidal to odorigenic microor-
ganisms[4l].A C1O2-containing mouthrinse has shown statistica1ly
significant improvements in the reduction of organolepticscores (odour pleasantness and mouth odour intensity), ascompared to baseline levels and to a water control group,at the 2- and 4-h post-rinsing evaluations [11]. However,this study was carried out in a sma1l sample of 12 non-ha1itosis subjects.
Another study [12], tested the efficacy of a C1O2-containing mouthrinse at different time points for a totalof 96 h post-rinse. The results showed that the testedmouthrinse obtained a statistica1ly significant improve-ment in organoleptic ratings (odour pleasantness andmouth odour intensity) and VSC levels compared to thewater control at 2 h post-rinse. The mean VSC concen-tration in the test group reached its minimum level at 8 hpost rinse.
The relative effectiveness and duration of action of 6different mouthrinse formulations [three chlorine-diox-ide- and chlorite-anion-containing mouthrinses (Re-tarDEX, Profresh and Oxyfresh), one phenol-thymol-containing mouthrinse (Listerine mint), one CPC-con-taining mouthrinse (Scope ), and Breath Assure capsulesand water as the placebo control] were tested for thereduction of VSC concentrations (Halimeter). With theexception of Breath Assure, each product tested wasfound to reduce reproducibly VSC concentrations within20 min of treatment. Subsequently, VSC concentrationslowly retumed to the baseline va1ues at around 2.5 h,with the exception of RetarDEX, which effectivelyretained VSC concentrations significantly below thebaseline va1ue and only retumed to the baseline scores
It is well established that some metal ions have a plaque-inhibiting capability. Stannous ions have been the moststudied, although data also exists for zinc and copper ions.The mechanism of action involves the capability of metalions to reduce the glycolytic activity of microorganismsby oxidating thiols groups in essential glycolytic enzymesand thus retarding bacterial growth. Another aspect oftheir properties is due to their affinity for sulphur, thusoxidizing the thiols groups in the sulphur-containingprecursors of VSC, or the odoriferous substances them-selves, to non-volatile substances, mainly hydrogensulphide and dimethyl sulphide [49].
A laboratory study tested in vitro the extent of VSCinhibition of various metal ions and its possible correla-tion with their affinity for sulphur. The results showedthat this correlation did not exist. While zinc was rankedthird for sulphur affinity, it was first in the VSC-inhibitingeffect, with around 35% of VSC reduction [49].
Another study [54] tested in vivo whether the affinityof a metal ion for sulphur would determine its anti- VSCactivity, using the cysteine challenge model and gaschromatography. The VSC inhibitory effect in decreasingorder were: CuC12>SnF2>ZnC12; with CuC12 inhibitingVSC production close to 100% at 1, 2 and 3 h. ZnC12solution gave a more variable response between testsubjects than the other 2 solutions and was also signif -icantly less effective in inhibiting H2S production at allevaluation points.
Another in vitro experiment [54] was carried out to testthe VSC-inhibiting efficacy of metal ions. Stimulatedsaliva samples from 30 healthy volunteers were co11ectedand mixed with 10-.uL aliquots of different metal saltsolutions. Mter 24-30 h of incubation the saliva head-space was analysed for VSC directly in the gas chro-matograph. The 3 metal ions, Hg2+, Cd2+ and CU2+,resulted in an almost complete inhibition of VSC
production.A single-blind parallel study [38] was carried out in
subjects with a baseline organoleptic rating score ~ 1 ( ona 0-3 scale). Subjects were randomly assigned to receiveeither a test mouthrinse, a saline rinse or no treatment.The results showed that the levels of organoleptic odourscores and VSC after rinsing with the test mouthrinsewere significantly lower than the baseline levels at 60,120 and 180 min post-treatment, and significantly lowerthan the effects observed for the saline rinse and the no-treatment groups at the 3 post-treatment time periods.
195
Saline rinse obtained a significant reduction in organo-leptic scores at 1 has compared with the baseline scores,likely due to the mechanica1 effect associated withrinsing. Otherwise, the saline rinse and the no-treatmenthad no significant effect either on the organoleptic orVSC scores at any of the 3 post-treatment time periods.
In summary , different meta1 ions have been testedmostly through in vitro or in short-term clinica1 studies.Zinc chloride demonstrated a slight activity in a 3-hdesign study, although in other studies its VSC inhibitingeffectivity was inferior when compared to other metalsa1ts.
their teeth with the assigned dentifrice, and they wereagain evaluated after 12 h. Subjects in both treatmentgroups presented statistical1y significantly lower meanbreath-odour scores than those observed at baseline;however, test dentifrice achieved a significantly higherreduction in odour scores than the control.
In summary , triclosan, when combined with either zincor copolymer, has demonstrated anti-halitosis activity, butonly on a short-term basis.
Mouthrinses containing essential oils
TriclosanEssential oils have been included in different formulationsof antiseptic products due to their antimicrobial activity.One of these formulations, Listerine, has clearly demon-strated its antiplaque and antigingivitis activity.
Listerine has been evaluated for its efficacy to reducetongue and crevicular odour-producing microorganisms[31]. Three different randomised double-blind protocolshave been done. The results indicated that the antisepticmouthwash was highly effective against oral malodour,crevicular and tongpe odorigenous microorganisms. Theeffect was statistically significant for at least 2 h aftertreatment. The water control showed no significant effect.
The same research group tested the relative contribu-tions of masking malodour and antisepsis to the overallanti-odour effect of an antiseptic mouthwash, comparingit with a placebo mouthwash and water [30]. Organolepticwhole mouth odour, levels of methanethiol and hydrogensulphide (gas chromatograph), and odorigens in tongueand crevicular samples were registered at different timeintervals up to180 min. The results indicated that theeffect of the mouthwash significantly depressed the levelof all oral malodour parameters, except for the methylmercaptan level, at 30 min (mouthwash vs. placebo) Theeffect of the mouthwash was significantly greater thanthat of water and placebo.
Listerine has also been formulated as dentifrice. Twoclinical trials [29] were carried out to assess its efficacy inthe reduction of moming breath by the use of a singlesupervised brushing with an essential oil-containingdentifrice, with an essential oil-containing dentifrice plus1% of zinc citrate, or with a negative control dentifrice.The results showed that both essential oil-containingdentifrices were significantly more effective than thecontrol dentifrice in reducing oral malodour, throughout120 min in the case of the essential oil-containingdentifrice, and throughout 90 min in the case of theessential oil-containing dentifrice plus 1% of zinc citrate.
Another study [37] tested the short-term efficacy of a2-phase mouthwash containing CPC and a mixture ofolive oil and essential oils in reducing malodour andbacterial counts, compared with a placebo rinse, and a0.2% CHX mouthrinse. Baseline measurements of VSCand organoleptic scores were registered and approximate-ly 8 h later individuals rinsed for two consecutive 30-speriods, directly before bedtime on day 1 and again earlythe next moming of day 2. Post-rinsing measurementswere performed in the late aftemoon of day 2, about 8-
Triclosan is an antimicrobial agent widely used as anantiseptic agent. Its activity and substantivity is increasedwhen combined either with zinc salts or with a copoly-mer.
The effects of 4 mouthrinses containing zinc, zinc+tri-closan, triclosan and placebo were evaluated on VSCformation after cysteine rinsing [~4]. Assessments witheach mouthrinse were made after avoiding oral hygienefor 12 h. Baseline VSC values were registered and then,after two sequential cysteine challenges and the use of thetested mouthrinse, VSC values were monitored againevery 2 min for 20 min. Rinsing with zinc or zinc-plus-triclosan mouthrinses produced an immediate 60% re-duction of VSC, and prevented the occurrence of a VSCresponse after the successive cysteine challenges. Theeffect of zinc plus triclosan was superior to zinc alone.Neither the placebo nor the triclosan mouthrinses pro-duced any effect on VSC.
Different studies have tested a dentifrice containingtriclosan and copolymer (Colgate Total): The effect onbreath odour was compared to a similar placebo dentifriceand to a negative control dentifrice, each used for 7 days[28]. Measurements of VSC (hydrogen sulphide, methylmercaptan and dimethyl sulphide) with a gas chromato-graph showed a significant 45% reduction in VSC for thetested dentifrice when compared to the placebo andnegative control.
The effectiveness of this triclosan-copolymer denti-frice in the reduction of moming breath odour wascompared with a placebo dentifrice not containingtriclosan or a copolymer [27]. On the morning after eachtreatment period, duplicate measurements of VSC with agas chromatograph were registered. Directly followingthis, subjects brushed their teeth, ate and drank normally,and reported once again to the clinical facility at 7 h post-tooth brushing for another breath.odour assessment. Thetwo dentifrices exhibited statistically significant differ-ences with respect to both moming breath odour and 7-h-post-toothbrushing breath odour.
Colgate Total was also tested and compared to aplacebo dentifrice for the control of breath odour 12 hafter toothbrushing [40]. Following a baseline evaluationof breath odour, subjects were stratified by score andrandomised into two treatment groups. Subiects brushed

persist or increase slightly over the ensuing 7 h. Brushingthe teeth or ingestion of Breath Assure had no apparentinfluence on the sulphur gases. Ingestion of breakfast andtongue brushing resulted in a strong tendency towarddecreased methanethiol. Hydrogen peroxide significantlyreduced the sulphur gas concentrations of the threeeva1uated gases for 8 h.
Conclusions
The tongue biofilm seems to be directly involved in theproduction of oral halitosis and may have an importantrole in the success of periodontitis therapy since it is apotential reservoir for periodontal pathogens.
Mechanical and antimicrobial approaches to reduce thetongue microflora have been evaluated, and their effectshave been studied by assessing halitosis-related outcomes.In spite of the scarcity of well-designed clinical trials, thelimited data available suggests the use of mouthrinseformulations based on chlorhexidine, essential oils andtriclosan for the treatment of halitosis derived from thetongue microflora.
References
196
10 h fol1owing the last rinsing. Bacterial counts wereestimated using the Oratest. The results indicated that thedecrease in sulphide levels after rinsing was statisticallysignificant in both 2-phase and CHX mouthrinses ascompared to the placebo; however, no significant differ-ence was found between both active mouthrinses. Inrelation to the Oratest results, the overall changes ofboth the 2-phase and the CHX group were significantlyincreased with respect to the placebo group. The increasein Oratest scores (higher values indicate lower microbiallevels and correspond to lower plaque and gingiva1scores) was statistica1ly significantly in the CHX group asopposed to the 2-phase group.
A reformulation of the 2-phas.e mouthrinse (notexplained by the authors) was compared with Listerineon its efficacy in controlling oral malodour, plaque, andgingivitis over a 6-week period in 50 volunteers [19]. Thedifference from the previous study was that instead ofrinsing, patients were asked to mix the rinse in the mouthvigorously and then to gargle with the rinse for 30 s twicea day (moming and night). The results indicated that, after6 weeks of use, the mean whole mouth, anterior dorsumof the tongue, and posterior dorsum of the tongue odourswere reduced by 80%, 79%, and 70%, respectively, in theexperimental group, as compared to corresponding meanreductions of 70%, 77%, and 59% in the control group. Inrelation to mean VSC, they were reduced by 40% in theexperimental group after 6 weeks of use and by 29% inthe control group, but this difference was not significant.However, it is interesting to remark that patients wereasked to refrain from eating, drinking or chewing gum for2 h prior to examination.
In summary , essentia1 oils have been evaluated as a 2-phase mouthwash combined with CPC and as a well-known commercial formulation (Listerine ), both asmouthrinse and as dentifrice. The results from studieseva1uating the 2-phase mouthrinse showed effectivenesson a short-term basis, similar to the outcomes obtainedwith Listerine in a 6-week period. However, Listerine hasonly been compared with negative controls and placebo inshort-term models. The same was true regarding Listerineformulated as a dentifrice.
Hydrogen peroxide
There is only one comparative study evaluating hydrogenperoxide on moming breath using gas chromatography[42]. Upon awakening in the moming, oral gas sampleswere collected, both before and 8 h after six differenttreatment regimes: 1) no treatrnent, 2) brushing the teethwith toothpaste, 3) brushing the tongue, 4) rinsing with 5mL of 3% hydrogen peroxide, 5) breakfast ingestion, or 6)swa11owing two BreathAssure capsu1es. Baseline co1lec-tions usually contained three sulphur gases: hydrogensulphide, methanethiol, and dimethy1sulphide. In theabsence of any intervention, the concentration of eachof the gases tended to decline over the first hour after"llhip~t" ¡¡W()k-P ¡¡nil thp fir"t -h ...()n...pntr",tirln tpnilpil trl
1. Asikainen S, A1a1uusua S, Saxen L (1991) Recovery of A.actinomycetemcomitans from teeth, tongue, and sa1iva. JPeriodontol 62:203-206
2. Bosy A, Kulkarni GV, Rosenberg M, McCulloch G (1994)Relationship of ora1 malodor to periodontitis: evidence ofindependence in discrete subpopulations. J Periodontol 65:37-46
3. Brunette DM, Proskin HM, Nelson BJ (1998) The effects ofdentifrice systems on oral malodor. J Clin Dent 9:76-82
4. Chen ZL (1987) Brief history of tongue inspection. Chin Med J100:38-44
5. Danser, M. (1996) The preva1ence of periodonta1 bacteriacolonizing the oral mucous membranes. Thesis, ACTA, Ams-terdam
6. Danser MM, Timmerman MF, van Winkelhoff AJ, van derVelden U (1996) The effect of periodonta1 treatment onperiodontal bacteria on the oral mucous membranes. JPeriodonto167:478-485
7. Danser MM, van Winkelhoff AJ, De Graaff J, Loos BG, vander Velden U (1994) Short-term effect of full-mouth extractionon periodontal pathogens colonizing the ora1 mucous mem-branes. J Clin Periodontol 21:484-489
8. Danser MM, van Winkelhoff AJ, De Graaff J, van der VeldenU(1995) Putative periodontal pathogens colonizing ora1 mucousmembranes in denture-wearing subjects with a past history ofperiodontitis. J Clin Periodontol 22:854-859
9. De Boever, EH, De Uzeda, M, Loesche, WJ (1995) Role oftongue surface characteristics and tongue flora in halitosis. JDent Res 74:127.
10. De Boever EH, Loesche WJ (1995) Assessing the contributionof anaerobic microflora of the tongue to ora1 malodor. JADA126:1384-1392
11. Frascella J, Gilbert R, Fernandez P (1998) Odor reductionpotentia1 of a chlorine dioxide mouthrinse. J Clin Dent 9:39-42
12. Frascella J, Gilbert RD, Fernandez P, Hendler J (2000) Efficacyof a chlorine dioxide-containing mouthrinse in ora1 malodor.Compend Contin Educ Dent 21:241-248
13. Gerlach RW, Hyde m, Poore CL, Stevens DP, Witt JJ (1998)Breath effects of three marketed dentifrices: a comnarative

197
study eva1uating single and cumulative use. J Clin Dent 9:83- 35. Roldán S, Winkel EG, Herrera D, Sanz M, van Winkelhoff AJ88 (2003) The effects of a new mouthrinse containing chlorhex-
14. Giani PL, Abbate M, Kanapka J, Codipilly M, and Kleinberg I idine, cetylpyridinium chloride and zinc lactate on the micro-(1996) VSC inhibiting activity of experimenta1 mouthwashes. J flora of oral halitosis patients. A dua1-centre, double-blindDent Res 75:195. placebo-controlled study. J Clin Periodontol 30:427-434.
15. Goldberg S, Cardash H, Browning H, Sahly H, Rosenberg M 36. Rosenberg M (1997) Bad breath: research perspectives. Ramot(1997) Isolation of Enterobacteriaceae from the Mouth and Publishing- Tel Aviv University, Ramat AvivPotentia1 Association with Ma1odor. J Dent Res 76:l770-l775 37. Rosenberg M, Gelernter I, Barki M, Bar-Ness R (1992) Day-
16. Greenstein G (2002) Full-mouth therapy versus individua1 long reduction of ora1 ma1odor by a two-phase oil:waterquadrant root planning: a critical commentary .J Periodontol mouthrinse as compared to chlorhexidine and placebo rinses. J73:797-812 Periodontol 63:39-43
17. Hoshi K, van Steenberghe D (1996) The effect of tongue 38. Schrnidt NF, Tarbet WJ (1978) The effect of ora1 rinses onbrushing or toothpaste application on ora1 ma1odor reduction. organoleptic mouth odor ratings and levels of volatile sulfurIn: van Steenberghe D, Rosenberg M (eds) Bad breath. A compounds. Ora1 Surg Ora1 Med Oral Pathol 45:876-883multidisciplinary approach. Leuven University Press, Leuven, 39. Seemann R, Kison A, Bizhang M, Zimmer S (2001) Effective-pp 255-264 ness of mechanica1 tongue cleaning on oral levels of volatile
18. Kaizu T, Tsunoda M, Aoki H, Kimura K (1978) Ana1ysis of su1fur compounds. JADA 132:1263-1267volatile sulphur compounds in mouth air by gas chromatogra- 40. Sharma NC, Ga1ustians HJ, Qaquish J, Ga1ustians A, Rustogiphy. Bull Tokyo Dent Coll19:43-52 KN, Petrone ME, Chaknis P, Garcia L, Volpe AR, Proskin HM
19. Kozlovsky A, Goldberg S, Natour I, Rogatky-Gat A, Gelernter (1999) The clinica1 effectiveness of a dentifrice containingI, Rosenberg M (1996) Efficacy of a 2-phase oil:water triclosan and a copolymer for controlling breath odor measuredmouthrinse in controlling oral ma1odor, gingivitis, and plaque. organoleptica11y twelve hours after toothbrushing. J Clin DentJ Periodontol 67:577-582 10:131-134
20. Lee KH, Tanner ACR, Maiden MFJ, Weber HP (1999) Pre- and 41. Silwood CJL, Grootveld MC, Maiden MFJ (2001) A multifac-Post-implantation rnicrobiota of the tongue, teeth, and newly- torial investigation of the ability of ora1 hea1th care productsplaced implants. J Clin Periodontol 26:822-832 (OHCPs) to a11eviate ora1 ma1odour. J Clin Periodontol 28:634-
21. Lindquist B, Ernilson CG, Wennerholm K (1989) Relationship 641between mutans streptococci in sa1iva and their colonization of 42. Suarez FL, Furne JK, Springfield J, Levitt MD (2000) Morningthe tooth surfaces. Oral Microbiol Immunol 4:71-76 breath odor: influence of treatrnents on sulfur gases. J Dent Res
22. Loesche WJ, Kazor C (2002) Microbiology and treatrnent of 79:l773-l777ha1itosis. Periodontol 200028:256-279 43. Timmerman MF, van der Weijden GA, Armand S, Abbas F,
23. Mantilla-G6mez S, Danser MM, Sipos PM, Rowshani B, Van Winkel EG, van Winkelhoff AJ, van d, V (1998) Untreatedder Velden U, van der Weijden GA (2001) Tongue coating and periodonta1 disease in Indonesian adolescents. Clinica1 andsa1ivary bacterial counts in hea1thy/gingivitis subjects and rnicrobiologica1 baseline data. J Clin Periodontol 25:215-224periodontitis patients. J Clin Periodontol 28:978 44. Togelius J, Kristoffersson K, Anderson H, Brattha11 D (1984)
24. Marsh PD (1992) Microbiologica1 aspects of the chernica1 Streptococcus mutans in sa1iva: intraindividual variations andcontrol of plaque and gingivitis. J Dent Res 71:1431-1438 relation to the number of colonized sites. Acta Odontol Scand
25. Massler M (1980) Geriatric nutrition: the role of taste and smell 42: 157-163in appetite. J Prosthet Dent 43:247-250 45. Tonzetich J, Ng SK (1976) Reduction of ma1odor by oral
26. Miyazaki H, Sakao S, Katoh Y, Takehara T (1995) Correlation cleansing procedures. Ora1 Surg Ora1 Med Ora1 Patho142:172-between volatile sulphur compounds and certain ora1 hea1th 181measurements in the genera1 population. J Periodonto166:679- 46. van Steenberghe D, Avontroodt P, Peeters W, Pauwels M,684 Coucke W, Lijnen A, Quirynen M (2001) Effect of different
27. Niles HP, Vazquez J, Rustogi KN, Williams M, Gaffar A, mouthrinses on morning breath. J Periodonto172:1183-1191Proskin HM (1999) The clinical effectiveness of a dentifrice 47. van Steenberghe D, Rosenberg M (1996) Bad Breath: Acontaining triclosan and a copolymer for providing long-term multidisciplinary approach. Leuven University Press, Leuvencontrol of breath odor measured chromatographically. J Clin 48. van Winkelhoff AJ, Van der Velden U, Winkel EG, De Graaf JDent 10:135-138 (1986) Black-pigmenting bacteroides and motile organisms on
28. Niles, HP (1995) Long-lasting breath protection with a oral mucosal surfaces in individuals with and without peri-triclosan/copolymer/NaF dentifrice. J Dent Res 74:209. odonta1 breakdown. J Periodont Res 21:434-439
29. Olshan AM, Kohut BE, Vincent JW, Borden LC, Delgado N, 49. Wa1er SM (1997) The effect of some meta1 ions on volatileQaquish J, Sharma NC, McGuire JA (2000) Clinica1 effective- sulfur-containing compounds originating from the ora1 cavity.ness of essentia1 oil-containing dentifrices in controlling oral Acta Odontol Scand 55:261-264ma1odor. Am J Dent 13:18C-22C 50. Winkel EG, Roldán S, van Winkelhoff AJ, Herrera D, Sanz M
30. Pitts G, Brogdon C, Hu L, Masurat T, Pianotti R, Schumann P (2003) The clinica1 effects of a new mouthrinse containing(1983) Mechanism of action of an antiseptic, anti-odor chlorhexidine, cetylpyridinium chloride and zinc lactate on ora1mouthwash. J Dent Res 62:738-742 ha1itosis. A dua1-center, double-blind placebo-controlled study.
31. Pitts G, Pianotti R, Feary TW, McGuiness J, Masurat T (1981) J Clin Periodontol 30:300-306The in vivo effects of an antiseptic mouthwash on odor- 51. Yaegaki K, Coil JM (2000) Exarnination, classification andproducing microorganisms. J Dent Res 60:1891-1896 treatrnent of ha1itosis; clinical perspectives. J Can Dent Assoc
32. Quirynen M, De Soete M, Dierickx K, van Steenberghe D 66:257-261(2001) The intraoral translocation of periodontopathogens 52. Yaegaki K, Sanada K (1992) Biochernical and clinica1 factorsjeopardises the outcome of periodonta1 therapy. A review of influencing ora1 ma1odor in periodonta1 patients. J Periodontolthe literature. J Clin Periodontol 28:499-507 63:783-789
33. Quirynen M, Mongardini C, van Steenberghe D (1998) The 53. Yaegaki K, Sanada K (1992) Volatile sulfur compounds ineffect of a l-stage full-mouth disinfection on ora1 malodor and mouth air from clinica11y hea1thy subjects and patients withmicrobia1 colonization ofthe tongue in periodontitis patients. A periodonta1 disease. J Periodont Res 27:233-238pilot study. J Periodonto169:374-382 54. Young A, Jonski G, Rolla G, Waler SM (2001) Effects ofmeta1
34. Ra1ph WJ (1987) Hygiene of the tongue. Gerodontics 3:169- salts on the ora1 production of volatile sulfur-containing170 compounds (VSC). J Clin Periodontol 28:776-77




















